User login
Early endovenous ablation speeds venous ulcer healing
Intervening early with endovenous ablation in patients with venous leg ulcers could significantly improve ulcer healing times and delay their recurrence, new research has found.
A randomized study presented at the International Charing Cross Symposium and published simultaneously in the April 24 issue of the New England Journal of Medicine compared the effects of early endovenous ablation with those of deferred ablation in 450 patients with venous leg ulcers, all of whom also received compression therapy.
The study showed that patients who received endovenous ablation within 2 weeks of randomization had significantly shorter healing times, compared with patients whose ablation was deferred for 6 months or until after the ulcer healed.
In the early-treatment group, the median time to ulcer healing was 56 days, while in the deferred-treatment group, it was 82 days. By 12 months, 93.8% of the early-intervention group had healed ulcers, compared with 85.8% in the deferred-intervention group.
Even after adjustment for factors such as patient age, ulcer size, ulcer duration, and recruitment center, patients who received early endovenous ablation were 38% more likely to have healed by 12 months, compared with the deferred-intervention group.
Researchers also saw significantly higher healing rates at 12 weeks in the early-intervention group, compared with the deferred-intervention group (63.5% vs. 51.6%, respectively).
“Observational studies have suggested that endovenous treatment of varicose veins – a treatment that may be particularly appropriate for the elderly population with venous leg ulcers – may improve ulcer healing,” wrote Manjit S. Gohel, MD, from the Cambridge (United Kingdom) University Hospitals NHS Foundation Trust and from Imperial College London and his coauthors. “In the current trial, we found that faster ulcer healing can be attained if an endovenous intervention is performed promptly.”
Early endovenous ablation also was associated with a delay in the recurrence of ulcers. The rate of recurrence was 11.4% among patients in the early-intervention group whose ulcers had healed and 16.5% among those in the delayed-intervention group whose ulcers had healed.
Patients who received the early endovenous ablation had a median ulcer-free time of 306 days, compared with 278 days in the delayed-intervention group, a significant difference.
The authors noted that all patients in the study also received high-quality compression therapy, which may account for the good healing rates seen in both groups that might not otherwise be observed in a real-world clinical setting.
“Accordingly, the improvement in ulcer healing with early endovenous intervention is likely to be greater in clinical practice than was observed in this trial,” the authors wrote. “Because endovenous intervention is usually performed as a single procedure, the clinical benefits are likely to be less dependent on ongoing patient adherence than they would be with compression therapy.”
The most common method for endovenous ablation used in this multicenter study was ultrasound-guided foam sclerotherapy, a minimally-invasive procedure the authors said had versatility and acceptability.
However, they commented that some previous, large randomized trials have suggested that the rates of complete venous occlusion are lower with foam sclerotherapy than with thermal ablation.
The main complications seen with endovenous ablation were pain and deep vein thrombosis.
The authors pointed out that two limitations of their trial were that patients with a leg ulcer that had been present for more than 6 months were excluded from patient selection and that the 450 patients enrolled had been selected from a larger group of around 6,500.
The study was supported by a grant from the National Institute for Health Research Health Technology Assessment Program. One author declared grants from a pharmaceutical company outside the submitted work, and seven declared funding from the NIHR as part of the conduct of the study. No other conflicts of interest were declared.
SOURCE: Gohel MS et al. NEJM. 2018 April 24. doi: 10.1056/NEJMoa1801214
Finally! A randomized controlled trial (RCT) which proves what we all kind of expected but which until now was unsupported by available literature. That is that endovenous ablation (EVA) in the presence of a concomitant venous ulcer not only decreases ulcer recurrence rates and increases ulcer-free time, it also significantly hastens ulcer healing times. I don’t know about you, but it always made sense to me that treatment of an incompetent saphenous vein, a known cause of ulceration, could be a factor in the time to ulcer healing.
But that’s what a whole host of retrospective and or nonrandomized studies seemed to suggest: Garbage in, garbage out. Enter the RCT – Issue resolved? Yes, with some caveats, and maybe no.
First, as the authors readily admit, the compression therapy which was applied to patients in both arms of the study was of “high quality” and would not likely be reproduced in real world practice. The authors also suggest that, in a real-world, clinical practice, the benefits of early EVA may prove to be even more pronounced because of poor patient compliance with compression. Not sure about that. In fact, if – in a real-world setting – the rate of compliance with compression in both groups turned out to be less than optimal, particularly in the patients who had EVA, the benefits of early ablation with respect to ulcer healing times might disappear.
In other words, we do not know from this study whether there would be the same advantages to early saphenous vein intervention without the addition of compression as compared with compression alone. This might explain why shorter ulcer healing times of EVA have been difficult to prove in non-RCT, more real-world studies. Perhaps a randomized trial comparing ulcer healing times with early EVA without compression versus compression therapy only? Hmmm.
Also, would the outcomes of the current study be similar on this side of the pond? Only 31.7% of limbs were treated with endothermal ablation only, by far the most common form of ablation performed in the United States. Almost 65% of limbs in the study were ablated with either foamed sclerotherapy alone or in conjunction with endothermal or mechanical modalities – not a common form of treatment here in the colonies. Inexplicably, the authors do not indicate whether outcomes were in any way influenced by the type of ablation performed. I am going to assume for now that it did not.
In summary, this study does not answer all the questions related to the use of EVA for the treatment of venous ulcers, but it comes pretty close. My take away is that there is no downside (or none that I can think of) to the use of EVA early on in the treatment of venous ulcers but a whole lot of potential upside for the patient. Now I, and probably you, have proof that what we were already doing really does have some increased benefit. Finally!
Alan M Dietzek, MD, is the Linda and Stephen R. Cohen Chair in Vascular Surgery at Danbury (Conn.) Hospital and a clinical professor of surgery at the University of Vermont, Burlington. He is also an associate medical editor for Vascular Specialist.
Finally! A randomized controlled trial (RCT) which proves what we all kind of expected but which until now was unsupported by available literature. That is that endovenous ablation (EVA) in the presence of a concomitant venous ulcer not only decreases ulcer recurrence rates and increases ulcer-free time, it also significantly hastens ulcer healing times. I don’t know about you, but it always made sense to me that treatment of an incompetent saphenous vein, a known cause of ulceration, could be a factor in the time to ulcer healing.
But that’s what a whole host of retrospective and or nonrandomized studies seemed to suggest: Garbage in, garbage out. Enter the RCT – Issue resolved? Yes, with some caveats, and maybe no.
First, as the authors readily admit, the compression therapy which was applied to patients in both arms of the study was of “high quality” and would not likely be reproduced in real world practice. The authors also suggest that, in a real-world, clinical practice, the benefits of early EVA may prove to be even more pronounced because of poor patient compliance with compression. Not sure about that. In fact, if – in a real-world setting – the rate of compliance with compression in both groups turned out to be less than optimal, particularly in the patients who had EVA, the benefits of early ablation with respect to ulcer healing times might disappear.
In other words, we do not know from this study whether there would be the same advantages to early saphenous vein intervention without the addition of compression as compared with compression alone. This might explain why shorter ulcer healing times of EVA have been difficult to prove in non-RCT, more real-world studies. Perhaps a randomized trial comparing ulcer healing times with early EVA without compression versus compression therapy only? Hmmm.
Also, would the outcomes of the current study be similar on this side of the pond? Only 31.7% of limbs were treated with endothermal ablation only, by far the most common form of ablation performed in the United States. Almost 65% of limbs in the study were ablated with either foamed sclerotherapy alone or in conjunction with endothermal or mechanical modalities – not a common form of treatment here in the colonies. Inexplicably, the authors do not indicate whether outcomes were in any way influenced by the type of ablation performed. I am going to assume for now that it did not.
In summary, this study does not answer all the questions related to the use of EVA for the treatment of venous ulcers, but it comes pretty close. My take away is that there is no downside (or none that I can think of) to the use of EVA early on in the treatment of venous ulcers but a whole lot of potential upside for the patient. Now I, and probably you, have proof that what we were already doing really does have some increased benefit. Finally!
Alan M Dietzek, MD, is the Linda and Stephen R. Cohen Chair in Vascular Surgery at Danbury (Conn.) Hospital and a clinical professor of surgery at the University of Vermont, Burlington. He is also an associate medical editor for Vascular Specialist.
Finally! A randomized controlled trial (RCT) which proves what we all kind of expected but which until now was unsupported by available literature. That is that endovenous ablation (EVA) in the presence of a concomitant venous ulcer not only decreases ulcer recurrence rates and increases ulcer-free time, it also significantly hastens ulcer healing times. I don’t know about you, but it always made sense to me that treatment of an incompetent saphenous vein, a known cause of ulceration, could be a factor in the time to ulcer healing.
But that’s what a whole host of retrospective and or nonrandomized studies seemed to suggest: Garbage in, garbage out. Enter the RCT – Issue resolved? Yes, with some caveats, and maybe no.
First, as the authors readily admit, the compression therapy which was applied to patients in both arms of the study was of “high quality” and would not likely be reproduced in real world practice. The authors also suggest that, in a real-world, clinical practice, the benefits of early EVA may prove to be even more pronounced because of poor patient compliance with compression. Not sure about that. In fact, if – in a real-world setting – the rate of compliance with compression in both groups turned out to be less than optimal, particularly in the patients who had EVA, the benefits of early ablation with respect to ulcer healing times might disappear.
In other words, we do not know from this study whether there would be the same advantages to early saphenous vein intervention without the addition of compression as compared with compression alone. This might explain why shorter ulcer healing times of EVA have been difficult to prove in non-RCT, more real-world studies. Perhaps a randomized trial comparing ulcer healing times with early EVA without compression versus compression therapy only? Hmmm.
Also, would the outcomes of the current study be similar on this side of the pond? Only 31.7% of limbs were treated with endothermal ablation only, by far the most common form of ablation performed in the United States. Almost 65% of limbs in the study were ablated with either foamed sclerotherapy alone or in conjunction with endothermal or mechanical modalities – not a common form of treatment here in the colonies. Inexplicably, the authors do not indicate whether outcomes were in any way influenced by the type of ablation performed. I am going to assume for now that it did not.
In summary, this study does not answer all the questions related to the use of EVA for the treatment of venous ulcers, but it comes pretty close. My take away is that there is no downside (or none that I can think of) to the use of EVA early on in the treatment of venous ulcers but a whole lot of potential upside for the patient. Now I, and probably you, have proof that what we were already doing really does have some increased benefit. Finally!
Alan M Dietzek, MD, is the Linda and Stephen R. Cohen Chair in Vascular Surgery at Danbury (Conn.) Hospital and a clinical professor of surgery at the University of Vermont, Burlington. He is also an associate medical editor for Vascular Specialist.
Intervening early with endovenous ablation in patients with venous leg ulcers could significantly improve ulcer healing times and delay their recurrence, new research has found.
A randomized study presented at the International Charing Cross Symposium and published simultaneously in the April 24 issue of the New England Journal of Medicine compared the effects of early endovenous ablation with those of deferred ablation in 450 patients with venous leg ulcers, all of whom also received compression therapy.
The study showed that patients who received endovenous ablation within 2 weeks of randomization had significantly shorter healing times, compared with patients whose ablation was deferred for 6 months or until after the ulcer healed.
In the early-treatment group, the median time to ulcer healing was 56 days, while in the deferred-treatment group, it was 82 days. By 12 months, 93.8% of the early-intervention group had healed ulcers, compared with 85.8% in the deferred-intervention group.
Even after adjustment for factors such as patient age, ulcer size, ulcer duration, and recruitment center, patients who received early endovenous ablation were 38% more likely to have healed by 12 months, compared with the deferred-intervention group.
Researchers also saw significantly higher healing rates at 12 weeks in the early-intervention group, compared with the deferred-intervention group (63.5% vs. 51.6%, respectively).
“Observational studies have suggested that endovenous treatment of varicose veins – a treatment that may be particularly appropriate for the elderly population with venous leg ulcers – may improve ulcer healing,” wrote Manjit S. Gohel, MD, from the Cambridge (United Kingdom) University Hospitals NHS Foundation Trust and from Imperial College London and his coauthors. “In the current trial, we found that faster ulcer healing can be attained if an endovenous intervention is performed promptly.”
Early endovenous ablation also was associated with a delay in the recurrence of ulcers. The rate of recurrence was 11.4% among patients in the early-intervention group whose ulcers had healed and 16.5% among those in the delayed-intervention group whose ulcers had healed.
Patients who received the early endovenous ablation had a median ulcer-free time of 306 days, compared with 278 days in the delayed-intervention group, a significant difference.
The authors noted that all patients in the study also received high-quality compression therapy, which may account for the good healing rates seen in both groups that might not otherwise be observed in a real-world clinical setting.
“Accordingly, the improvement in ulcer healing with early endovenous intervention is likely to be greater in clinical practice than was observed in this trial,” the authors wrote. “Because endovenous intervention is usually performed as a single procedure, the clinical benefits are likely to be less dependent on ongoing patient adherence than they would be with compression therapy.”
The most common method for endovenous ablation used in this multicenter study was ultrasound-guided foam sclerotherapy, a minimally-invasive procedure the authors said had versatility and acceptability.
However, they commented that some previous, large randomized trials have suggested that the rates of complete venous occlusion are lower with foam sclerotherapy than with thermal ablation.
The main complications seen with endovenous ablation were pain and deep vein thrombosis.
The authors pointed out that two limitations of their trial were that patients with a leg ulcer that had been present for more than 6 months were excluded from patient selection and that the 450 patients enrolled had been selected from a larger group of around 6,500.
The study was supported by a grant from the National Institute for Health Research Health Technology Assessment Program. One author declared grants from a pharmaceutical company outside the submitted work, and seven declared funding from the NIHR as part of the conduct of the study. No other conflicts of interest were declared.
SOURCE: Gohel MS et al. NEJM. 2018 April 24. doi: 10.1056/NEJMoa1801214
Intervening early with endovenous ablation in patients with venous leg ulcers could significantly improve ulcer healing times and delay their recurrence, new research has found.
A randomized study presented at the International Charing Cross Symposium and published simultaneously in the April 24 issue of the New England Journal of Medicine compared the effects of early endovenous ablation with those of deferred ablation in 450 patients with venous leg ulcers, all of whom also received compression therapy.
The study showed that patients who received endovenous ablation within 2 weeks of randomization had significantly shorter healing times, compared with patients whose ablation was deferred for 6 months or until after the ulcer healed.
In the early-treatment group, the median time to ulcer healing was 56 days, while in the deferred-treatment group, it was 82 days. By 12 months, 93.8% of the early-intervention group had healed ulcers, compared with 85.8% in the deferred-intervention group.
Even after adjustment for factors such as patient age, ulcer size, ulcer duration, and recruitment center, patients who received early endovenous ablation were 38% more likely to have healed by 12 months, compared with the deferred-intervention group.
Researchers also saw significantly higher healing rates at 12 weeks in the early-intervention group, compared with the deferred-intervention group (63.5% vs. 51.6%, respectively).
“Observational studies have suggested that endovenous treatment of varicose veins – a treatment that may be particularly appropriate for the elderly population with venous leg ulcers – may improve ulcer healing,” wrote Manjit S. Gohel, MD, from the Cambridge (United Kingdom) University Hospitals NHS Foundation Trust and from Imperial College London and his coauthors. “In the current trial, we found that faster ulcer healing can be attained if an endovenous intervention is performed promptly.”
Early endovenous ablation also was associated with a delay in the recurrence of ulcers. The rate of recurrence was 11.4% among patients in the early-intervention group whose ulcers had healed and 16.5% among those in the delayed-intervention group whose ulcers had healed.
Patients who received the early endovenous ablation had a median ulcer-free time of 306 days, compared with 278 days in the delayed-intervention group, a significant difference.
The authors noted that all patients in the study also received high-quality compression therapy, which may account for the good healing rates seen in both groups that might not otherwise be observed in a real-world clinical setting.
“Accordingly, the improvement in ulcer healing with early endovenous intervention is likely to be greater in clinical practice than was observed in this trial,” the authors wrote. “Because endovenous intervention is usually performed as a single procedure, the clinical benefits are likely to be less dependent on ongoing patient adherence than they would be with compression therapy.”
The most common method for endovenous ablation used in this multicenter study was ultrasound-guided foam sclerotherapy, a minimally-invasive procedure the authors said had versatility and acceptability.
However, they commented that some previous, large randomized trials have suggested that the rates of complete venous occlusion are lower with foam sclerotherapy than with thermal ablation.
The main complications seen with endovenous ablation were pain and deep vein thrombosis.
The authors pointed out that two limitations of their trial were that patients with a leg ulcer that had been present for more than 6 months were excluded from patient selection and that the 450 patients enrolled had been selected from a larger group of around 6,500.
The study was supported by a grant from the National Institute for Health Research Health Technology Assessment Program. One author declared grants from a pharmaceutical company outside the submitted work, and seven declared funding from the NIHR as part of the conduct of the study. No other conflicts of interest were declared.
SOURCE: Gohel MS et al. NEJM. 2018 April 24. doi: 10.1056/NEJMoa1801214
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Early endovenous ablation can speed healing of venous ulcers.
Major finding: Median ulcer healing time was 56 days with early venous ablation, compared with 82 days with deferred ablation.
Study details: Randomized controlled trial in 450 patients with venous leg ulcers.
Disclosures: The study was supported by a grant from the National Institute for Health Research Health Technology Assessment Program. One author declared grants from a pharmaceutical company outside the submitted work, and seven declared funding from the NIHR as part of the conduct of the study. No other conflicts of interest were declared.
Source: Gohel M et al. NEJM. 2018 April 24. doi: 10.1056/NEJMoa1801214
Pregnancy and safety rates evaluated for Liletta at 5 years of use
Liletta, a levonorgestrel 52 mg contraceptive intrauterine system (IUS) (Allergan), is currently approved by the US Food and Drug Administration for up to 4 years of use. A multicenter trial is continuing to measure Liletta’s efficacy and safety for a total of 8 years of use.1
Meanwhile, investigators led by Stephanie B. Teal, MD, from the University of Colorado, Aurora, have evaluated the 5-year data for Liletta. Resea
Study details
A total of 1,714 women aged 16−45 years were enrolled in the multicenter study for 5 years after successful IUS placement. This included 146 women aged 36−45 years who received the IUS for safety evaluation only, and 1,568 women aged 16−35 years who were evaluated for both safety and efficacy.1
Results of the study
The 16−35-year-old participants included 1,011 (57.7%) nulliparous and 438 (25.1%) obese women. Among these participants, 9 pregnancies occurred, including 4 in nulliparous women and 1 in an obese woman. In this age group, 1 pregnancy occurred after perforation and 1 following expulsion. Six (67%) of the pregnancies were ectopic.1
The Pearl Index in the first year was .15 (95% confidence interval [CI], .02−.55). Cumulative life-table pregnancy rates at the end of years 3 and 5 were .59 (95% CI, .28−1.25) and .92 (95% CI, .46–1.82), respectively.1
Of the total participants, perforation occurred in 2 (0.1%) women, both within the first year. Expulsion occurred in 63 participants (3.7%), most (50 [80.6%]) during the first year. Eleven patients (0.6%) were found to have a pelvic infection. Thirty-nine women (2.3%) discontinued use of Liletta due to bleeding complaints, primarily (n = 29 [74.3%]) in the first year.1
Conclusion
The researchers concluded that Liletta is highly effective and has an excellent safety profile over 5 years of use. Most adverse effects, including expulsion and discontinuation for bleeding, occurred during the first year.1
- Teal SB, Turok DK, Jensen JT, Chen BA, Kimble TD, Creinin MD. Five-year efficacy and safety of the Liletta® Levonorgestrel Intrauterine System. Obstet Gynecol. 2018;131(5 suppl):66S−67S.
Liletta, a levonorgestrel 52 mg contraceptive intrauterine system (IUS) (Allergan), is currently approved by the US Food and Drug Administration for up to 4 years of use. A multicenter trial is continuing to measure Liletta’s efficacy and safety for a total of 8 years of use.1
Meanwhile, investigators led by Stephanie B. Teal, MD, from the University of Colorado, Aurora, have evaluated the 5-year data for Liletta. Resea
Study details
A total of 1,714 women aged 16−45 years were enrolled in the multicenter study for 5 years after successful IUS placement. This included 146 women aged 36−45 years who received the IUS for safety evaluation only, and 1,568 women aged 16−35 years who were evaluated for both safety and efficacy.1
Results of the study
The 16−35-year-old participants included 1,011 (57.7%) nulliparous and 438 (25.1%) obese women. Among these participants, 9 pregnancies occurred, including 4 in nulliparous women and 1 in an obese woman. In this age group, 1 pregnancy occurred after perforation and 1 following expulsion. Six (67%) of the pregnancies were ectopic.1
The Pearl Index in the first year was .15 (95% confidence interval [CI], .02−.55). Cumulative life-table pregnancy rates at the end of years 3 and 5 were .59 (95% CI, .28−1.25) and .92 (95% CI, .46–1.82), respectively.1
Of the total participants, perforation occurred in 2 (0.1%) women, both within the first year. Expulsion occurred in 63 participants (3.7%), most (50 [80.6%]) during the first year. Eleven patients (0.6%) were found to have a pelvic infection. Thirty-nine women (2.3%) discontinued use of Liletta due to bleeding complaints, primarily (n = 29 [74.3%]) in the first year.1
Conclusion
The researchers concluded that Liletta is highly effective and has an excellent safety profile over 5 years of use. Most adverse effects, including expulsion and discontinuation for bleeding, occurred during the first year.1
Liletta, a levonorgestrel 52 mg contraceptive intrauterine system (IUS) (Allergan), is currently approved by the US Food and Drug Administration for up to 4 years of use. A multicenter trial is continuing to measure Liletta’s efficacy and safety for a total of 8 years of use.1
Meanwhile, investigators led by Stephanie B. Teal, MD, from the University of Colorado, Aurora, have evaluated the 5-year data for Liletta. Resea
Study details
A total of 1,714 women aged 16−45 years were enrolled in the multicenter study for 5 years after successful IUS placement. This included 146 women aged 36−45 years who received the IUS for safety evaluation only, and 1,568 women aged 16−35 years who were evaluated for both safety and efficacy.1
Results of the study
The 16−35-year-old participants included 1,011 (57.7%) nulliparous and 438 (25.1%) obese women. Among these participants, 9 pregnancies occurred, including 4 in nulliparous women and 1 in an obese woman. In this age group, 1 pregnancy occurred after perforation and 1 following expulsion. Six (67%) of the pregnancies were ectopic.1
The Pearl Index in the first year was .15 (95% confidence interval [CI], .02−.55). Cumulative life-table pregnancy rates at the end of years 3 and 5 were .59 (95% CI, .28−1.25) and .92 (95% CI, .46–1.82), respectively.1
Of the total participants, perforation occurred in 2 (0.1%) women, both within the first year. Expulsion occurred in 63 participants (3.7%), most (50 [80.6%]) during the first year. Eleven patients (0.6%) were found to have a pelvic infection. Thirty-nine women (2.3%) discontinued use of Liletta due to bleeding complaints, primarily (n = 29 [74.3%]) in the first year.1
Conclusion
The researchers concluded that Liletta is highly effective and has an excellent safety profile over 5 years of use. Most adverse effects, including expulsion and discontinuation for bleeding, occurred during the first year.1
- Teal SB, Turok DK, Jensen JT, Chen BA, Kimble TD, Creinin MD. Five-year efficacy and safety of the Liletta® Levonorgestrel Intrauterine System. Obstet Gynecol. 2018;131(5 suppl):66S−67S.
- Teal SB, Turok DK, Jensen JT, Chen BA, Kimble TD, Creinin MD. Five-year efficacy and safety of the Liletta® Levonorgestrel Intrauterine System. Obstet Gynecol. 2018;131(5 suppl):66S−67S.
New single-dose treatment for bacterial vaginosis
What Are the Consequences of Changing Antiepileptic Drug Regimens as Part of Pregnancy Planning?
WASHINGTON, DC—Women with epilepsy of reproductive age have a high likelihood of successfully changing their antiepi
Mitigating Risk to Offspring
Studies have found that certain AEDs increase the risk of structural and neurodevelopmental teratogenicity. “Women with epilepsy of childbearing age require careful reconsideration of their AED type and dose, given that the maternal benefits of treatment during potential future pregnancies should be weighed against adverse effects on the developing fetus,” said P. Emanuela Voinescu, MD, PhD, and colleagues. “Too often, not switching AEDs leads to exposing future offspring to undue risk.” Neurologists may be hesitant to change an AED regimen due to concerns about worsening seizures, however, and data to predict the risk of seizure worsening with an AED regimen change are lacking, the researchers said. Dr. Voinescu is an Instructor in Neurology at Harvard University and a neurologist at Brigham and Woman’s Hospital in Boston. 
Dr. Voinescu and colleagues conducted a retrospective study to quantify the risk of failure when altering an AED regimen for reproductive safety, and to identify the causes of failure. The study included 40 women with epilepsy between ages 16 and 45 who had been on a stable AED regimen for more than six months and whose AED regimen was changed to improve the outcome of a future pregnancy. Changes included AED switch, AED dose reduction, AED number reduction, and complete discontinuation of AEDs.
The researchers excluded patients with psychogenic nonepileptic seizures, history of substance abuse, history of nonadherence to medications or scheduled visits, progressive cerebral disease or lesion, or other major medical illness. The patients’ AED regimen changes occurred between 2005 and 2017.
The investigators conducted a retrospective chart review for seizure frequency during the six months prior to the AED regimen change, during the transition interval, and in the six months after achieving the final regimen. They also collected demographic and epilepsy history details and reviewed patients’ most recent neurology clinic notes to assess long-term prognosis.
An AED regimen change was considered successful if the new regimen was continued without additional alterations. Otherwise, the change was considered a failure, and researchers documented the reason for continued alterations and the final outcome.
Most Changes Were Successful
The initial AED regimen change was successful for 75% of patients (n = 30). After taking into account patients whose regimens underwent a second change, 90% of patients (n = 36) had a successful change.
“A failed first change is not a predictor of failure for a subsequent alteration,” the researchers said. Half of the failed first changes occurred because of medication side effects. In those cases, a trial of another medication or complete AED discontinuation were successful strategies. Seven out of nine patients (78%) who initially were on valproic acid discontinued it successfully.
Persistent seizure worsening occurred in two patients with medically refractory epilepsy. Patients rarely and only transiently lost seizure-free status. Potential covariates (eg, epilepsy and seizure types, seizure freedom status, AED type, and type of alteration) did not seem to significantly affect outcomes.
To further study AED regimen changes for reproductive safety, the researchers are conducting a prospective, observational, parallel-group, switch-control study.
—Jake Remaly
WASHINGTON, DC—Women with epilepsy of reproductive age have a high likelihood of successfully changing their antiepi
Mitigating Risk to Offspring
Studies have found that certain AEDs increase the risk of structural and neurodevelopmental teratogenicity. “Women with epilepsy of childbearing age require careful reconsideration of their AED type and dose, given that the maternal benefits of treatment during potential future pregnancies should be weighed against adverse effects on the developing fetus,” said P. Emanuela Voinescu, MD, PhD, and colleagues. “Too often, not switching AEDs leads to exposing future offspring to undue risk.” Neurologists may be hesitant to change an AED regimen due to concerns about worsening seizures, however, and data to predict the risk of seizure worsening with an AED regimen change are lacking, the researchers said. Dr. Voinescu is an Instructor in Neurology at Harvard University and a neurologist at Brigham and Woman’s Hospital in Boston.
Dr. Voinescu and colleagues conducted a retrospective study to quantify the risk of failure when altering an AED regimen for reproductive safety, and to identify the causes of failure. The study included 40 women with epilepsy between ages 16 and 45 who had been on a stable AED regimen for more than six months and whose AED regimen was changed to improve the outcome of a future pregnancy. Changes included AED switch, AED dose reduction, AED number reduction, and complete discontinuation of AEDs.
The researchers excluded patients with psychogenic nonepileptic seizures, history of substance abuse, history of nonadherence to medications or scheduled visits, progressive cerebral disease or lesion, or other major medical illness. The patients’ AED regimen changes occurred between 2005 and 2017.
The investigators conducted a retrospective chart review for seizure frequency during the six months prior to the AED regimen change, during the transition interval, and in the six months after achieving the final regimen. They also collected demographic and epilepsy history details and reviewed patients’ most recent neurology clinic notes to assess long-term prognosis.
An AED regimen change was considered successful if the new regimen was continued without additional alterations. Otherwise, the change was considered a failure, and researchers documented the reason for continued alterations and the final outcome.
Most Changes Were Successful
The initial AED regimen change was successful for 75% of patients (n = 30). After taking into account patients whose regimens underwent a second change, 90% of patients (n = 36) had a successful change.
“A failed first change is not a predictor of failure for a subsequent alteration,” the researchers said. Half of the failed first changes occurred because of medication side effects. In those cases, a trial of another medication or complete AED discontinuation were successful strategies. Seven out of nine patients (78%) who initially were on valproic acid discontinued it successfully.
Persistent seizure worsening occurred in two patients with medically refractory epilepsy. Patients rarely and only transiently lost seizure-free status. Potential covariates (eg, epilepsy and seizure types, seizure freedom status, AED type, and type of alteration) did not seem to significantly affect outcomes.
To further study AED regimen changes for reproductive safety, the researchers are conducting a prospective, observational, parallel-group, switch-control study.
—Jake Remaly
WASHINGTON, DC—Women with epilepsy of reproductive age have a high likelihood of successfully changing their antiepi
Mitigating Risk to Offspring
Studies have found that certain AEDs increase the risk of structural and neurodevelopmental teratogenicity. “Women with epilepsy of childbearing age require careful reconsideration of their AED type and dose, given that the maternal benefits of treatment during potential future pregnancies should be weighed against adverse effects on the developing fetus,” said P. Emanuela Voinescu, MD, PhD, and colleagues. “Too often, not switching AEDs leads to exposing future offspring to undue risk.” Neurologists may be hesitant to change an AED regimen due to concerns about worsening seizures, however, and data to predict the risk of seizure worsening with an AED regimen change are lacking, the researchers said. Dr. Voinescu is an Instructor in Neurology at Harvard University and a neurologist at Brigham and Woman’s Hospital in Boston.
Dr. Voinescu and colleagues conducted a retrospective study to quantify the risk of failure when altering an AED regimen for reproductive safety, and to identify the causes of failure. The study included 40 women with epilepsy between ages 16 and 45 who had been on a stable AED regimen for more than six months and whose AED regimen was changed to improve the outcome of a future pregnancy. Changes included AED switch, AED dose reduction, AED number reduction, and complete discontinuation of AEDs.
The researchers excluded patients with psychogenic nonepileptic seizures, history of substance abuse, history of nonadherence to medications or scheduled visits, progressive cerebral disease or lesion, or other major medical illness. The patients’ AED regimen changes occurred between 2005 and 2017.
The investigators conducted a retrospective chart review for seizure frequency during the six months prior to the AED regimen change, during the transition interval, and in the six months after achieving the final regimen. They also collected demographic and epilepsy history details and reviewed patients’ most recent neurology clinic notes to assess long-term prognosis.
An AED regimen change was considered successful if the new regimen was continued without additional alterations. Otherwise, the change was considered a failure, and researchers documented the reason for continued alterations and the final outcome.
Most Changes Were Successful
The initial AED regimen change was successful for 75% of patients (n = 30). After taking into account patients whose regimens underwent a second change, 90% of patients (n = 36) had a successful change.
“A failed first change is not a predictor of failure for a subsequent alteration,” the researchers said. Half of the failed first changes occurred because of medication side effects. In those cases, a trial of another medication or complete AED discontinuation were successful strategies. Seven out of nine patients (78%) who initially were on valproic acid discontinued it successfully.
Persistent seizure worsening occurred in two patients with medically refractory epilepsy. Patients rarely and only transiently lost seizure-free status. Potential covariates (eg, epilepsy and seizure types, seizure freedom status, AED type, and type of alteration) did not seem to significantly affect outcomes.
To further study AED regimen changes for reproductive safety, the researchers are conducting a prospective, observational, parallel-group, switch-control study.
—Jake Remaly
Aim for remission, not low disease activity, in rheumatoid arthritis
LIVERPOOL, ENGLAND – , according to the conclusion of a study presented at the British Society for Rheumatology annual conference.
The study showed clear differences in functional and quality of life outcomes over time when comparing patients who achieved remission with those who achieved low disease activity.
Indeed, from baseline assessments to 12 months follow-up, HAQ scores fell from an average of about 0.8 for those in remission and 0.9 for those with a low disease activity index to approximately 0.4 and 0.6, respectively.
The physical component score of the SF-36 also improved from around 35 and 30 at baseline in the remission and low disease activity groups to just above 40 and just under 35, respectively, at 12 months.
Baseline SF-36 mental component scores were around 51 and 49 in each group, respectively, at baseline but improved to around 55 with remission and remained steady in the low disease activity group at 12 months.
“This is something you often don’t see,” observed Sam Norton, PhD, who presented the findings on behalf of the lead author Elena Nikiphorou, MD. Dr. Norton is a senior lecturer in the department of health psychology at King’s College London whose research interests lie in studying the psychological well-being and illness outcomes in rheumatoid arthritis and other chronic physical illnesses.
“Of course, there could be a bit of reverse causality with people with good mental health being more likely to hit remission, which is why you can see there is a gap at baseline as well,” Dr. Norton suggested.
The researchers used data on 2,701 patients who were enrolled in the Early Rheumatoid Arthritis Network (ERAN) and Early Rheumatoid Arthritis Study (ERAS) cohorts. The research question was whether achieving low disease activity was an acceptable target in rheumatoid arthritis, and if disease outcomes made a difference to those who achieved remission.
The mean age of participants was 55 years in ERAS and 57 years in ERAN, with a similar percentage of female participants (67%), and slightly better baseline HAQ and Disease Activity Scale scores in the ERAN cohort, which is to be expected, Dr. Norton said, as this was a later-recruited population of patients (2002-2013 vs. 1986-2000 for ERAS).
Disease activity was categorized in three ways: firstly, remission or low disease activity over 1-5 years were defined as mean DAS28 score of less than 2.6 and a score of 2.6-3.2, respectively. Secondly, sustained low disease activity or remission was considered over 1-2 years, and thirdly, Boolean remission over 1-2 years, which are strict criteria of remission to meet.
Overall, 23.4% of patients achieved remission and 13.7% achieved low disease activity, and a respective 10.3% and 13.7% met criteria for sustained remission or sustained low disease activity. Just 3.4% met Boolean criteria for remission.
“The key messages are: There is a really important difference between remission and low disease activity score categories and that treating people to a remission target means they will do better in terms of quality of life outcomes over time compared to just stopping at a low disease activity,” Dr. Norton noted.
There was an important caveat to stating that remission should be the primary treat-to-target goal, in that there will likely be a relatively small proportion of patients that will achieve the strictest definition of remission, he added. Perhaps different targets need to be set for those with comorbidities or who are older.
“So, while remission should be a primary target there should be other targets considered alongside that,” he proposed.
Dr. Norton and his coauthors had nothing to disclose.
SOURCE: Nikiphorou E et al. Rheumatology. 2018;57[Suppl. 3]:key075.189.
LIVERPOOL, ENGLAND – , according to the conclusion of a study presented at the British Society for Rheumatology annual conference.
The study showed clear differences in functional and quality of life outcomes over time when comparing patients who achieved remission with those who achieved low disease activity.
Indeed, from baseline assessments to 12 months follow-up, HAQ scores fell from an average of about 0.8 for those in remission and 0.9 for those with a low disease activity index to approximately 0.4 and 0.6, respectively.
The physical component score of the SF-36 also improved from around 35 and 30 at baseline in the remission and low disease activity groups to just above 40 and just under 35, respectively, at 12 months.
Baseline SF-36 mental component scores were around 51 and 49 in each group, respectively, at baseline but improved to around 55 with remission and remained steady in the low disease activity group at 12 months.
“This is something you often don’t see,” observed Sam Norton, PhD, who presented the findings on behalf of the lead author Elena Nikiphorou, MD. Dr. Norton is a senior lecturer in the department of health psychology at King’s College London whose research interests lie in studying the psychological well-being and illness outcomes in rheumatoid arthritis and other chronic physical illnesses.
“Of course, there could be a bit of reverse causality with people with good mental health being more likely to hit remission, which is why you can see there is a gap at baseline as well,” Dr. Norton suggested.
The researchers used data on 2,701 patients who were enrolled in the Early Rheumatoid Arthritis Network (ERAN) and Early Rheumatoid Arthritis Study (ERAS) cohorts. The research question was whether achieving low disease activity was an acceptable target in rheumatoid arthritis, and if disease outcomes made a difference to those who achieved remission.
The mean age of participants was 55 years in ERAS and 57 years in ERAN, with a similar percentage of female participants (67%), and slightly better baseline HAQ and Disease Activity Scale scores in the ERAN cohort, which is to be expected, Dr. Norton said, as this was a later-recruited population of patients (2002-2013 vs. 1986-2000 for ERAS).
Disease activity was categorized in three ways: firstly, remission or low disease activity over 1-5 years were defined as mean DAS28 score of less than 2.6 and a score of 2.6-3.2, respectively. Secondly, sustained low disease activity or remission was considered over 1-2 years, and thirdly, Boolean remission over 1-2 years, which are strict criteria of remission to meet.
Overall, 23.4% of patients achieved remission and 13.7% achieved low disease activity, and a respective 10.3% and 13.7% met criteria for sustained remission or sustained low disease activity. Just 3.4% met Boolean criteria for remission.
“The key messages are: There is a really important difference between remission and low disease activity score categories and that treating people to a remission target means they will do better in terms of quality of life outcomes over time compared to just stopping at a low disease activity,” Dr. Norton noted.
There was an important caveat to stating that remission should be the primary treat-to-target goal, in that there will likely be a relatively small proportion of patients that will achieve the strictest definition of remission, he added. Perhaps different targets need to be set for those with comorbidities or who are older.
“So, while remission should be a primary target there should be other targets considered alongside that,” he proposed.
Dr. Norton and his coauthors had nothing to disclose.
SOURCE: Nikiphorou E et al. Rheumatology. 2018;57[Suppl. 3]:key075.189.
LIVERPOOL, ENGLAND – , according to the conclusion of a study presented at the British Society for Rheumatology annual conference.
The study showed clear differences in functional and quality of life outcomes over time when comparing patients who achieved remission with those who achieved low disease activity.
Indeed, from baseline assessments to 12 months follow-up, HAQ scores fell from an average of about 0.8 for those in remission and 0.9 for those with a low disease activity index to approximately 0.4 and 0.6, respectively.
The physical component score of the SF-36 also improved from around 35 and 30 at baseline in the remission and low disease activity groups to just above 40 and just under 35, respectively, at 12 months.
Baseline SF-36 mental component scores were around 51 and 49 in each group, respectively, at baseline but improved to around 55 with remission and remained steady in the low disease activity group at 12 months.
“This is something you often don’t see,” observed Sam Norton, PhD, who presented the findings on behalf of the lead author Elena Nikiphorou, MD. Dr. Norton is a senior lecturer in the department of health psychology at King’s College London whose research interests lie in studying the psychological well-being and illness outcomes in rheumatoid arthritis and other chronic physical illnesses.
“Of course, there could be a bit of reverse causality with people with good mental health being more likely to hit remission, which is why you can see there is a gap at baseline as well,” Dr. Norton suggested.
The researchers used data on 2,701 patients who were enrolled in the Early Rheumatoid Arthritis Network (ERAN) and Early Rheumatoid Arthritis Study (ERAS) cohorts. The research question was whether achieving low disease activity was an acceptable target in rheumatoid arthritis, and if disease outcomes made a difference to those who achieved remission.
The mean age of participants was 55 years in ERAS and 57 years in ERAN, with a similar percentage of female participants (67%), and slightly better baseline HAQ and Disease Activity Scale scores in the ERAN cohort, which is to be expected, Dr. Norton said, as this was a later-recruited population of patients (2002-2013 vs. 1986-2000 for ERAS).
Disease activity was categorized in three ways: firstly, remission or low disease activity over 1-5 years were defined as mean DAS28 score of less than 2.6 and a score of 2.6-3.2, respectively. Secondly, sustained low disease activity or remission was considered over 1-2 years, and thirdly, Boolean remission over 1-2 years, which are strict criteria of remission to meet.
Overall, 23.4% of patients achieved remission and 13.7% achieved low disease activity, and a respective 10.3% and 13.7% met criteria for sustained remission or sustained low disease activity. Just 3.4% met Boolean criteria for remission.
“The key messages are: There is a really important difference between remission and low disease activity score categories and that treating people to a remission target means they will do better in terms of quality of life outcomes over time compared to just stopping at a low disease activity,” Dr. Norton noted.
There was an important caveat to stating that remission should be the primary treat-to-target goal, in that there will likely be a relatively small proportion of patients that will achieve the strictest definition of remission, he added. Perhaps different targets need to be set for those with comorbidities or who are older.
“So, while remission should be a primary target there should be other targets considered alongside that,” he proposed.
Dr. Norton and his coauthors had nothing to disclose.
SOURCE: Nikiphorou E et al. Rheumatology. 2018;57[Suppl. 3]:key075.189.
REPORTING FROM RHEUMATOLOGY 2018
Key clinical point: Better outcomes were achieved if patients with rheumatoid arthritis met criteria for remission rather than low disease activity.
Major finding: The study showed clear differences in functional and quality of life outcomes over time when comparing patients who achieved remission with those who achieved low disease activity.
Study details: A prospective study of 2,701 patients enrolled in two early rheumatoid arthritis cohorts.
Disclosures: Dr. Norton and his coauthors had nothing to disclose.
Source: Nikiphorou E et al. Rheumatology. 2018;57[Suppl. 3]:key075.189.

Cost-effectiveness battle: FFR vs. iFR in DEFINE-FLAIR trial
ORLANDO – The use of an instantaneous wave-free ratio (iFR)–guided strategy to identify physiologically significant coronary stenoses that warrant revascularization proved substantially more cost effective than did a fractional flow reserve (FFR)–based strategy in a prespecified secondary analysis of the randomized DEFINE-FLAIR trial, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.
The difference in total health care costs over the course of a year of follow-up was $896 per patient in favor of the instantaneous wave-free ratio (iFR) approach, said Dr. Patel, a professor of medicine, the chief of the division of cardiology, and the chief of the division of clinical pharmacology at Duke University in Durham, N.C.
DEFINE-FLAIR was a multicenter study in which 2,492 patients with coronary artery disease were randomized to undergo either iFR- or FFR-guided coronary revascularization. It had previously been established that decision making regarding coronary revascularization or deferral that was guided by FFR leads to better patient outcomes than decision making guided by angiography alone.
DEFINE-FLAIR showed that iFR provides clinical benefits similar to those of FFR. The 1-year primary endpoint, a composite of all-cause mortality, nonfatal MI, or unplanned revascularization, occurred in 6.8% of the iFR group and 7.0% of the FFR group, while the revascularization rate was significantly lower in the iFR group, by a margin of 47.5% to 53.4% (N Engl J Med. 2017 May 11;376(19):1824-34).
Dr. Patel presented a formal study of total health care costs and quality of life in the two study arms through 1 year of follow-up. The cost of coronary physiologic assessment by iFR was lower because, unlike FFR, iFR doesn’t use adenosine for vasodilation. Plus, median procedural time was 4.5 minutes shorter in the iFR group, resulting in lower costs for staff time. After investigators added up the costs of balloons, stents, laboratory testing, and a year’s worth of primary care visits, specialty consults, and unplanned revascularization procedures, the total cost per patient was $7,442.23 in 2017 U.S. dollars in the iFR group and $8,243.39 in the FFR group.
Session cochair Christopher Granger, MD, was favorably impressed.
“With equal clinical outcomes, the iFR – in not using adenosine and by identifying fewer patients needing referral for coronary artery bypass surgery or percutaneous coronary intervention – had a better cost effectiveness by about $900. That’s pretty good,” commented Dr. Granger, a professor of medicine at Duke University.
“At the moment, there is a longer track record for FFR data than iFR data for outcomes, but this is a fairly strong finding in a large population in a well-conducted study, and it shows very positive favorable economic results,” the cardiologist added. “There is no doubt that this [iFR] does have streamlined work flow, lower cost, and the same outcomes. So I think this is actually quite a positive effect.”
Dr. Patel, in acknowledging that there is a spirited ongoing debate among some interventional cardiologists as to which coronary physiology assessment tool should be used, declared, “We should stop arguing about which one to use and just use more of it, first and foremost.”
“I couldn’t agree more,” Dr. Granger said. “Coronary physiology for best decision making, whichever index you decide to choose, will lead to better outcomes and lower cost.”
Dr. Patel estimated that, worldwide, coronary physiology assessment is used in cardiac catheterization laboratories in fewer than 20% of patients. Achieving a substantial increase in that number is a matter of physician education perhaps coupled with payer requirements that interventional cardiologists must demonstrate evidence of ischemia before performing percutaneous coronary intervention on a given coronary lesion. Also, the American College of Cardiology/American Heart Association guidelines, which at present give a Class IIa recommendation for the use of FFR in patients with an intermediate stenosis, probably need to be revisited in light of DEFINE-FLAIR.
“One might argue that the recommendation could be a little stronger. And we have other proven technologies now besides FFR,” he observed.
Dr. Patel reported receiving research grants from Philips Volcano, sponsor of the DEFINE-FLAIR trial, as well as from AstraZeneca, Bayer, Janssen, ProCyrion, and the National Heart, Lung, and Blood Institute. He serves as a consultant to AstraZeneca, Bayer, Janssen, and Medscape.
SOURCE: Patel MR et al. ACC 18, Abstract 402-09.
ORLANDO – The use of an instantaneous wave-free ratio (iFR)–guided strategy to identify physiologically significant coronary stenoses that warrant revascularization proved substantially more cost effective than did a fractional flow reserve (FFR)–based strategy in a prespecified secondary analysis of the randomized DEFINE-FLAIR trial, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.
The difference in total health care costs over the course of a year of follow-up was $896 per patient in favor of the instantaneous wave-free ratio (iFR) approach, said Dr. Patel, a professor of medicine, the chief of the division of cardiology, and the chief of the division of clinical pharmacology at Duke University in Durham, N.C.
DEFINE-FLAIR was a multicenter study in which 2,492 patients with coronary artery disease were randomized to undergo either iFR- or FFR-guided coronary revascularization. It had previously been established that decision making regarding coronary revascularization or deferral that was guided by FFR leads to better patient outcomes than decision making guided by angiography alone.
DEFINE-FLAIR showed that iFR provides clinical benefits similar to those of FFR. The 1-year primary endpoint, a composite of all-cause mortality, nonfatal MI, or unplanned revascularization, occurred in 6.8% of the iFR group and 7.0% of the FFR group, while the revascularization rate was significantly lower in the iFR group, by a margin of 47.5% to 53.4% (N Engl J Med. 2017 May 11;376(19):1824-34).
Dr. Patel presented a formal study of total health care costs and quality of life in the two study arms through 1 year of follow-up. The cost of coronary physiologic assessment by iFR was lower because, unlike FFR, iFR doesn’t use adenosine for vasodilation. Plus, median procedural time was 4.5 minutes shorter in the iFR group, resulting in lower costs for staff time. After investigators added up the costs of balloons, stents, laboratory testing, and a year’s worth of primary care visits, specialty consults, and unplanned revascularization procedures, the total cost per patient was $7,442.23 in 2017 U.S. dollars in the iFR group and $8,243.39 in the FFR group.
Session cochair Christopher Granger, MD, was favorably impressed.
“With equal clinical outcomes, the iFR – in not using adenosine and by identifying fewer patients needing referral for coronary artery bypass surgery or percutaneous coronary intervention – had a better cost effectiveness by about $900. That’s pretty good,” commented Dr. Granger, a professor of medicine at Duke University.
“At the moment, there is a longer track record for FFR data than iFR data for outcomes, but this is a fairly strong finding in a large population in a well-conducted study, and it shows very positive favorable economic results,” the cardiologist added. “There is no doubt that this [iFR] does have streamlined work flow, lower cost, and the same outcomes. So I think this is actually quite a positive effect.”
Dr. Patel, in acknowledging that there is a spirited ongoing debate among some interventional cardiologists as to which coronary physiology assessment tool should be used, declared, “We should stop arguing about which one to use and just use more of it, first and foremost.”
“I couldn’t agree more,” Dr. Granger said. “Coronary physiology for best decision making, whichever index you decide to choose, will lead to better outcomes and lower cost.”
Dr. Patel estimated that, worldwide, coronary physiology assessment is used in cardiac catheterization laboratories in fewer than 20% of patients. Achieving a substantial increase in that number is a matter of physician education perhaps coupled with payer requirements that interventional cardiologists must demonstrate evidence of ischemia before performing percutaneous coronary intervention on a given coronary lesion. Also, the American College of Cardiology/American Heart Association guidelines, which at present give a Class IIa recommendation for the use of FFR in patients with an intermediate stenosis, probably need to be revisited in light of DEFINE-FLAIR.
“One might argue that the recommendation could be a little stronger. And we have other proven technologies now besides FFR,” he observed.
Dr. Patel reported receiving research grants from Philips Volcano, sponsor of the DEFINE-FLAIR trial, as well as from AstraZeneca, Bayer, Janssen, ProCyrion, and the National Heart, Lung, and Blood Institute. He serves as a consultant to AstraZeneca, Bayer, Janssen, and Medscape.
SOURCE: Patel MR et al. ACC 18, Abstract 402-09.
ORLANDO – The use of an instantaneous wave-free ratio (iFR)–guided strategy to identify physiologically significant coronary stenoses that warrant revascularization proved substantially more cost effective than did a fractional flow reserve (FFR)–based strategy in a prespecified secondary analysis of the randomized DEFINE-FLAIR trial, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.
The difference in total health care costs over the course of a year of follow-up was $896 per patient in favor of the instantaneous wave-free ratio (iFR) approach, said Dr. Patel, a professor of medicine, the chief of the division of cardiology, and the chief of the division of clinical pharmacology at Duke University in Durham, N.C.
DEFINE-FLAIR was a multicenter study in which 2,492 patients with coronary artery disease were randomized to undergo either iFR- or FFR-guided coronary revascularization. It had previously been established that decision making regarding coronary revascularization or deferral that was guided by FFR leads to better patient outcomes than decision making guided by angiography alone.
DEFINE-FLAIR showed that iFR provides clinical benefits similar to those of FFR. The 1-year primary endpoint, a composite of all-cause mortality, nonfatal MI, or unplanned revascularization, occurred in 6.8% of the iFR group and 7.0% of the FFR group, while the revascularization rate was significantly lower in the iFR group, by a margin of 47.5% to 53.4% (N Engl J Med. 2017 May 11;376(19):1824-34).
Dr. Patel presented a formal study of total health care costs and quality of life in the two study arms through 1 year of follow-up. The cost of coronary physiologic assessment by iFR was lower because, unlike FFR, iFR doesn’t use adenosine for vasodilation. Plus, median procedural time was 4.5 minutes shorter in the iFR group, resulting in lower costs for staff time. After investigators added up the costs of balloons, stents, laboratory testing, and a year’s worth of primary care visits, specialty consults, and unplanned revascularization procedures, the total cost per patient was $7,442.23 in 2017 U.S. dollars in the iFR group and $8,243.39 in the FFR group.
Session cochair Christopher Granger, MD, was favorably impressed.
“With equal clinical outcomes, the iFR – in not using adenosine and by identifying fewer patients needing referral for coronary artery bypass surgery or percutaneous coronary intervention – had a better cost effectiveness by about $900. That’s pretty good,” commented Dr. Granger, a professor of medicine at Duke University.
“At the moment, there is a longer track record for FFR data than iFR data for outcomes, but this is a fairly strong finding in a large population in a well-conducted study, and it shows very positive favorable economic results,” the cardiologist added. “There is no doubt that this [iFR] does have streamlined work flow, lower cost, and the same outcomes. So I think this is actually quite a positive effect.”
Dr. Patel, in acknowledging that there is a spirited ongoing debate among some interventional cardiologists as to which coronary physiology assessment tool should be used, declared, “We should stop arguing about which one to use and just use more of it, first and foremost.”
“I couldn’t agree more,” Dr. Granger said. “Coronary physiology for best decision making, whichever index you decide to choose, will lead to better outcomes and lower cost.”
Dr. Patel estimated that, worldwide, coronary physiology assessment is used in cardiac catheterization laboratories in fewer than 20% of patients. Achieving a substantial increase in that number is a matter of physician education perhaps coupled with payer requirements that interventional cardiologists must demonstrate evidence of ischemia before performing percutaneous coronary intervention on a given coronary lesion. Also, the American College of Cardiology/American Heart Association guidelines, which at present give a Class IIa recommendation for the use of FFR in patients with an intermediate stenosis, probably need to be revisited in light of DEFINE-FLAIR.
“One might argue that the recommendation could be a little stronger. And we have other proven technologies now besides FFR,” he observed.
Dr. Patel reported receiving research grants from Philips Volcano, sponsor of the DEFINE-FLAIR trial, as well as from AstraZeneca, Bayer, Janssen, ProCyrion, and the National Heart, Lung, and Blood Institute. He serves as a consultant to AstraZeneca, Bayer, Janssen, and Medscape.
SOURCE: Patel MR et al. ACC 18, Abstract 402-09.
REPORTING FROM ACC 2018
Key clinical point:
Major finding: A coronary revascularization strategy guided by physiologic information provided by instantaneous wave-free ratio resulted in $896 less in health care costs per patient over 1 year of follow-up than a fractional flow reserve–guided strategy had.
Study details: This was a prespecified analysis of all health care costs during 1 year of follow-up in the 2,492-patient randomized DEFINE-FLAIR study.
Disclosures: The study presenter reported receiving a research grant from Philips Volcano, sponsor of the DEFINE-FLAIR trial.
Source: Patel MR et al. ACC 18, Abstract 402-09.
Challenging dogma: Postop fever
The dogma
During our medical school and residency years, many of us learned the “Rule of W” as a helpful mnemonic for causes of postoperative fever: Wind (pulmonary causes, including atelectasis), Water (urinary tract infection), Wound (infection), Walking (deep venous thrombosis), and Wonder Drugs (drug fever). Classic teaching has been that noninfectious causes predominate during the first 48 hours post op, with infectious diseases taking over after that. Atelectasis is also very common in the immediate postoperative period, seen in up to 90% of patients by postoperative day 3, and is often taught as the primary cause of fever in the immediate postoperative period.1,2 But is this backed up by the evidence?
The evidence
A 2011 systematic review looked at the association between atelectasis and fever. Eight studies involving 998 postoperative patients were included, with the majority of cases being postcardiac or abdominal surgeries. Seven of the eight studies failed to show a significant association between early postoperative fever (EPF) and atelectasis; in the one “positive” study, atelectasis was assessed only once on postop day 4. The authors of the review concluded that “there is no clinical evidence suggesting that atelectasis is a major cause of early EPF”.3 A subsequent study of postoperative fever in pediatric patients showed similar negative results.4 This begs the question – does atelectasis cause fever at all? Likely not. In an animal study from 1963, experimentally induced atelectasis resulted in fever, but the fever appeared secondary to infectious causes (i.e. pneumonia in the affected lung) and resolved with antibiotic administration.5 It seems more likely that EPF is due to other factors, such as the increase in pyrogenic cytokines seen in the postoperative period.3

Takeaway
Atelectasis and early postoperative fever are both commonly seen after surgery, but the relationship appears to be simply an association, not causal. The “Rule of W” can be an effective mnemonic for the causes of postop fever – just make sure you use the updated version.
Dr. Sehgal is clinical associate professor of medicine, division of hospital medicine, South Texas Veterans Health Care System and University of Texas Health Sciences Center at San Antonio. He is a member of the editorial advisory board for The Hospitalist.
References
1. Carter AR, et al. Thoracic Alterations After Cardiac Surgery. AJR. 1983;140(3):475-81.
2. Chu DI, Agarwal S. Postoperative Complications. In: Doherty GM. eds. CURRENT Diagnosis & Treatment: Surgery, 14e New York, NY: McGraw-Hill; 2014.
3. Mavros MN, Velmahos GC, Falagas ME. Atelectasis as a Cause of Postoperative Fever. Chest. 2011;140(2):418-24. doi: 10.1378/chest.11-0127.
4. Kane JM, Friedman M, Mitchell JB, Wang D, Huang Z, Backer CL. Association Between Postoperative Fever and Atelectasis in Pediatric Patients. World J Pediatr Congenit Heart Surg. 2011;2(3):359-63. doi: 10.1177/2150135111403778.
5. Lansing AM, Jamieson WG. Mechanisms of fever in pulmonary atelectasis. Arch Surg. 1963;87:168-74.
6. Hyder JA, Wakeam E, Arora V, Hevelone ND, Lipsitz SR, Nguyen LL. Investigating the “Rule of W,” a Mnemonic for Teaching on Postoperative Complications. J Surg Educ. 2015;72(3):430-7. doi: 10.1016/j.jsurg.2014.11.004.
The dogma
During our medical school and residency years, many of us learned the “Rule of W” as a helpful mnemonic for causes of postoperative fever: Wind (pulmonary causes, including atelectasis), Water (urinary tract infection), Wound (infection), Walking (deep venous thrombosis), and Wonder Drugs (drug fever). Classic teaching has been that noninfectious causes predominate during the first 48 hours post op, with infectious diseases taking over after that. Atelectasis is also very common in the immediate postoperative period, seen in up to 90% of patients by postoperative day 3, and is often taught as the primary cause of fever in the immediate postoperative period.1,2 But is this backed up by the evidence?
The evidence
A 2011 systematic review looked at the association between atelectasis and fever. Eight studies involving 998 postoperative patients were included, with the majority of cases being postcardiac or abdominal surgeries. Seven of the eight studies failed to show a significant association between early postoperative fever (EPF) and atelectasis; in the one “positive” study, atelectasis was assessed only once on postop day 4. The authors of the review concluded that “there is no clinical evidence suggesting that atelectasis is a major cause of early EPF”.3 A subsequent study of postoperative fever in pediatric patients showed similar negative results.4 This begs the question – does atelectasis cause fever at all? Likely not. In an animal study from 1963, experimentally induced atelectasis resulted in fever, but the fever appeared secondary to infectious causes (i.e. pneumonia in the affected lung) and resolved with antibiotic administration.5 It seems more likely that EPF is due to other factors, such as the increase in pyrogenic cytokines seen in the postoperative period.3
Takeaway
Atelectasis and early postoperative fever are both commonly seen after surgery, but the relationship appears to be simply an association, not causal. The “Rule of W” can be an effective mnemonic for the causes of postop fever – just make sure you use the updated version.
Dr. Sehgal is clinical associate professor of medicine, division of hospital medicine, South Texas Veterans Health Care System and University of Texas Health Sciences Center at San Antonio. He is a member of the editorial advisory board for The Hospitalist.
References
1. Carter AR, et al. Thoracic Alterations After Cardiac Surgery. AJR. 1983;140(3):475-81.
2. Chu DI, Agarwal S. Postoperative Complications. In: Doherty GM. eds. CURRENT Diagnosis & Treatment: Surgery, 14e New York, NY: McGraw-Hill; 2014.
3. Mavros MN, Velmahos GC, Falagas ME. Atelectasis as a Cause of Postoperative Fever. Chest. 2011;140(2):418-24. doi: 10.1378/chest.11-0127.
4. Kane JM, Friedman M, Mitchell JB, Wang D, Huang Z, Backer CL. Association Between Postoperative Fever and Atelectasis in Pediatric Patients. World J Pediatr Congenit Heart Surg. 2011;2(3):359-63. doi: 10.1177/2150135111403778.
5. Lansing AM, Jamieson WG. Mechanisms of fever in pulmonary atelectasis. Arch Surg. 1963;87:168-74.
6. Hyder JA, Wakeam E, Arora V, Hevelone ND, Lipsitz SR, Nguyen LL. Investigating the “Rule of W,” a Mnemonic for Teaching on Postoperative Complications. J Surg Educ. 2015;72(3):430-7. doi: 10.1016/j.jsurg.2014.11.004.
The dogma
During our medical school and residency years, many of us learned the “Rule of W” as a helpful mnemonic for causes of postoperative fever: Wind (pulmonary causes, including atelectasis), Water (urinary tract infection), Wound (infection), Walking (deep venous thrombosis), and Wonder Drugs (drug fever). Classic teaching has been that noninfectious causes predominate during the first 48 hours post op, with infectious diseases taking over after that. Atelectasis is also very common in the immediate postoperative period, seen in up to 90% of patients by postoperative day 3, and is often taught as the primary cause of fever in the immediate postoperative period.1,2 But is this backed up by the evidence?
The evidence
A 2011 systematic review looked at the association between atelectasis and fever. Eight studies involving 998 postoperative patients were included, with the majority of cases being postcardiac or abdominal surgeries. Seven of the eight studies failed to show a significant association between early postoperative fever (EPF) and atelectasis; in the one “positive” study, atelectasis was assessed only once on postop day 4. The authors of the review concluded that “there is no clinical evidence suggesting that atelectasis is a major cause of early EPF”.3 A subsequent study of postoperative fever in pediatric patients showed similar negative results.4 This begs the question – does atelectasis cause fever at all? Likely not. In an animal study from 1963, experimentally induced atelectasis resulted in fever, but the fever appeared secondary to infectious causes (i.e. pneumonia in the affected lung) and resolved with antibiotic administration.5 It seems more likely that EPF is due to other factors, such as the increase in pyrogenic cytokines seen in the postoperative period.3
Takeaway
Atelectasis and early postoperative fever are both commonly seen after surgery, but the relationship appears to be simply an association, not causal. The “Rule of W” can be an effective mnemonic for the causes of postop fever – just make sure you use the updated version.
Dr. Sehgal is clinical associate professor of medicine, division of hospital medicine, South Texas Veterans Health Care System and University of Texas Health Sciences Center at San Antonio. He is a member of the editorial advisory board for The Hospitalist.
References
1. Carter AR, et al. Thoracic Alterations After Cardiac Surgery. AJR. 1983;140(3):475-81.
2. Chu DI, Agarwal S. Postoperative Complications. In: Doherty GM. eds. CURRENT Diagnosis & Treatment: Surgery, 14e New York, NY: McGraw-Hill; 2014.
3. Mavros MN, Velmahos GC, Falagas ME. Atelectasis as a Cause of Postoperative Fever. Chest. 2011;140(2):418-24. doi: 10.1378/chest.11-0127.
4. Kane JM, Friedman M, Mitchell JB, Wang D, Huang Z, Backer CL. Association Between Postoperative Fever and Atelectasis in Pediatric Patients. World J Pediatr Congenit Heart Surg. 2011;2(3):359-63. doi: 10.1177/2150135111403778.
5. Lansing AM, Jamieson WG. Mechanisms of fever in pulmonary atelectasis. Arch Surg. 1963;87:168-74.
6. Hyder JA, Wakeam E, Arora V, Hevelone ND, Lipsitz SR, Nguyen LL. Investigating the “Rule of W,” a Mnemonic for Teaching on Postoperative Complications. J Surg Educ. 2015;72(3):430-7. doi: 10.1016/j.jsurg.2014.11.004.
Treatment of HCV in special populations
MAUI, HAWAII – Treatment of acute rather than chronic hepatitis C infection is well worth considering in selected circumstances, Norah Terrault, MD, asserted at the Gastroenterology Updates, IBD, Liver Disease meeting.
This is not at present guideline-recommended therapy. Current American Association for the Study of Liver Disease/Infectious Diseases Society of America guidance states that while there is emerging data to support treatment of acute hepatitis C, the evidence isn’t yet sufficiently robust to support a particular regimen or duration. The guidelines currently recommend waiting 6 months to see if the acute infection resolves spontaneously, as happens in a minority of cases, or becomes chronic, at which point it becomes guideline-directed treatment time. But Dr. Terrault believes persuasive evidence to back treatment of acute hepatitis C infection (HCV) is forthcoming, and she noted that the guidelines leave the door ajar by stating, “There are instances wherein a clinician may decide that the benefits of early treatment outweigh waiting for possible spontaneous clearance.”
Treatment of acute HCV
Dr. Terrault deems treatment of acute HCV warranted in circumstances in which there is significant danger of transmission from the acutely infected individual to others. For example, health care providers with a needlestick HCV infection, injecting drug users, and men with acute HCV/HIV coinfection. She also treats acute HCV in patients with underlying chronic liver disease.
“Clearly, I wouldn’t want those individuals to have any worsening of their liver function, so I would treat them acutely,” explained Dr. Terrault, professor of medicine and director of the Viral Hepatitis Center at the University of California, San Francisco.
She cited as particularly impressive the results of the SWIFT-C trial presented by Suzanna Naggie, MD, of Duke University, Durham, N.C., at the 2017 AASLD annual meeting. In this modest-size, National Institutes of Health–sponsored, multicenter study of HIV-infected men with acute HCV coinfection, the sustained viral response (SVR) rate with 8 weeks of ledipasvir/sofosbuvir (Harvoni) was 100%, regardless of their baseline HCV RNA level.
“I think this is remarkable. They cleared virus quite late and yet they went on to achieve HCV eradication. It highlights how little we really know about the treatment of individuals in this phase and that relying on HCV RNA levels may not tell the whole story. I think this is important data to suggest maybe when we treat acute hepatitis C we can use a shorter duration of treatment for that population. There are also other small studies testing 8 weeks of treatment in non–HIV-infected individuals with acute hepatitis C in which they also showed very high SVR rates,” the hepatologist said.
Copanelist Steven L. Flamm, MD, said that when he encounters a patient with acute HCV he, too, is prepared to offer treatment – he finds the available supporting evidence sufficiently compelling – but he often encounters a problem.
“Sometimes I’m blocked by insurance companies because this isn’t officially approved,” noted Dr. Flamm, professor of medicine and chief of the hepatology program at Northwestern University, Chicago.
“You’re right,” Dr. Terrault commented, “we have to make a pretty compelling argument to the insurer as to why we’re treating. But ‘treat to prevent transmission to others’ usually is successful in our hands.”
HCV in patients with end-stage renal disease
The product labeling for sofosbuvir (Sovaldi) says the drug’s safety and efficacy haven’t been established in patients with severe renal impairment or end-stage renal disease. However, a small multicenter study presented at the 2017 AASLD meeting demonstrated that 12 weeks of ledipasvir/sofosbuvir achieved a 100% SVR rate in patients with genotype 1 HCV and severe renal impairment, including some on dialysis, with no clinically meaningful change in estimated glomerular filtration rate or any signal of cardiac arrhythmia.
“The serum drug levels went up significantly, but reassuringly they saw no meaningful safety signals,” according to Dr. Terrault. “This, I think, is initial reassuring information that we were all very much waiting for.”
Still, as the AASLD/IDSA guidelines point out, ledipasvir/sofosbuvir is not a recommended option for HCV treatment in end-stage renal disease.
“In general, I think glecapravir/pibrentasvir [Mavyret] has become the go-to drug for patients who have renal dysfunction because it’s a pangenic regimen, it doesn’t require use of sofosbuvir, and there’s no dose adjustment. But I would say you could encounter situations where you might want to use sofosbuvir, and for me that situation is typically those direct-acting, antiviral-experienced patients who have failed other therapies and you really need to use sofosbuvir/velpatasvir/voxilaprevir [Vosevi] as your last or rescue therapy,” the hepatologist continued.
HCV in liver transplant recipients
“In the years before the direct-acting antivirals, treating transplant patients was always very challenging,” Dr. Terrault recalled. “They had very low response rates to therapy. That’s all gone away. Now we can say that liver transplant recipients who require treatment have response rates that are the same as in individuals who have not had a transplant. These patients are now being treated earlier and earlier after their transplant because you can do it safely.”
She pointed to a study presented at the 2017 AASLD meeting by Kosh Agarwal, MD, of Kings College London. It involved 79 adults with recurrent genotypes 1-4 HCV infection post–liver transplant who were treated with sofosbuvir/velpatasvir (Epclusa) for 12 weeks with a total SVR rate of 96%.
“The nice thing about sofosbuvir/velpatasvir is there are no drug-drug interactions with immunosuppressive drugs. Now it’s very easy to take care of these patients. The SVR rates are excellent,” Dr. Terrault observed.
The other combination that’s been studied specifically in liver transplant recipients, and in kidney transplant recipients as well, is glecapravir/pibrentasvir. In the MAGELLAN-2 study of 100 such patients with genotypes 1-6 HCV, the SVR rate was 99% with no drug-related adverse events leading to discontinuation.
Persons who inject drugs
The Centers for Disease Control and Prevention and the World Health Organization want HCV eradicated by 2030. If that’s going to happen, physicians will have to become more comfortable treating the disease in injectable drug users, a population with a high prevalence of HCV. Several studies have now shown that very high SVR rates can be achieved with direct-acting antiviral regimens as short as 8 weeks in these individuals, even if they are concurrently injecting drugs.
“There is increasing evidence that we should be doing more treatment in persons who inject drugs. Many of these individuals have very early disease and their response rates are excellent,” according to Dr. Terrault.
Moreover, their reinfection rates “are not outrageous,” she said: 1% or less in individuals who stopped injecting drugs decades prior to anti-HCV treatment, 5%-10% over the course of 3-5 years in those who continue injecting drugs after achieving SVR, and about 2% in those on methadone substitution therapy.
“These are very acceptable levels of reinfection if our goal is to move toward elimination of hepatitis C in this population,” she said.
She reported having no financial conflicts regarding her presentation.
MAUI, HAWAII – Treatment of acute rather than chronic hepatitis C infection is well worth considering in selected circumstances, Norah Terrault, MD, asserted at the Gastroenterology Updates, IBD, Liver Disease meeting.
This is not at present guideline-recommended therapy. Current American Association for the Study of Liver Disease/Infectious Diseases Society of America guidance states that while there is emerging data to support treatment of acute hepatitis C, the evidence isn’t yet sufficiently robust to support a particular regimen or duration. The guidelines currently recommend waiting 6 months to see if the acute infection resolves spontaneously, as happens in a minority of cases, or becomes chronic, at which point it becomes guideline-directed treatment time. But Dr. Terrault believes persuasive evidence to back treatment of acute hepatitis C infection (HCV) is forthcoming, and she noted that the guidelines leave the door ajar by stating, “There are instances wherein a clinician may decide that the benefits of early treatment outweigh waiting for possible spontaneous clearance.”
Treatment of acute HCV
Dr. Terrault deems treatment of acute HCV warranted in circumstances in which there is significant danger of transmission from the acutely infected individual to others. For example, health care providers with a needlestick HCV infection, injecting drug users, and men with acute HCV/HIV coinfection. She also treats acute HCV in patients with underlying chronic liver disease.
“Clearly, I wouldn’t want those individuals to have any worsening of their liver function, so I would treat them acutely,” explained Dr. Terrault, professor of medicine and director of the Viral Hepatitis Center at the University of California, San Francisco.
She cited as particularly impressive the results of the SWIFT-C trial presented by Suzanna Naggie, MD, of Duke University, Durham, N.C., at the 2017 AASLD annual meeting. In this modest-size, National Institutes of Health–sponsored, multicenter study of HIV-infected men with acute HCV coinfection, the sustained viral response (SVR) rate with 8 weeks of ledipasvir/sofosbuvir (Harvoni) was 100%, regardless of their baseline HCV RNA level.
“I think this is remarkable. They cleared virus quite late and yet they went on to achieve HCV eradication. It highlights how little we really know about the treatment of individuals in this phase and that relying on HCV RNA levels may not tell the whole story. I think this is important data to suggest maybe when we treat acute hepatitis C we can use a shorter duration of treatment for that population. There are also other small studies testing 8 weeks of treatment in non–HIV-infected individuals with acute hepatitis C in which they also showed very high SVR rates,” the hepatologist said.
Copanelist Steven L. Flamm, MD, said that when he encounters a patient with acute HCV he, too, is prepared to offer treatment – he finds the available supporting evidence sufficiently compelling – but he often encounters a problem.
“Sometimes I’m blocked by insurance companies because this isn’t officially approved,” noted Dr. Flamm, professor of medicine and chief of the hepatology program at Northwestern University, Chicago.
“You’re right,” Dr. Terrault commented, “we have to make a pretty compelling argument to the insurer as to why we’re treating. But ‘treat to prevent transmission to others’ usually is successful in our hands.”
HCV in patients with end-stage renal disease
The product labeling for sofosbuvir (Sovaldi) says the drug’s safety and efficacy haven’t been established in patients with severe renal impairment or end-stage renal disease. However, a small multicenter study presented at the 2017 AASLD meeting demonstrated that 12 weeks of ledipasvir/sofosbuvir achieved a 100% SVR rate in patients with genotype 1 HCV and severe renal impairment, including some on dialysis, with no clinically meaningful change in estimated glomerular filtration rate or any signal of cardiac arrhythmia.
“The serum drug levels went up significantly, but reassuringly they saw no meaningful safety signals,” according to Dr. Terrault. “This, I think, is initial reassuring information that we were all very much waiting for.”
Still, as the AASLD/IDSA guidelines point out, ledipasvir/sofosbuvir is not a recommended option for HCV treatment in end-stage renal disease.
“In general, I think glecapravir/pibrentasvir [Mavyret] has become the go-to drug for patients who have renal dysfunction because it’s a pangenic regimen, it doesn’t require use of sofosbuvir, and there’s no dose adjustment. But I would say you could encounter situations where you might want to use sofosbuvir, and for me that situation is typically those direct-acting, antiviral-experienced patients who have failed other therapies and you really need to use sofosbuvir/velpatasvir/voxilaprevir [Vosevi] as your last or rescue therapy,” the hepatologist continued.
HCV in liver transplant recipients
“In the years before the direct-acting antivirals, treating transplant patients was always very challenging,” Dr. Terrault recalled. “They had very low response rates to therapy. That’s all gone away. Now we can say that liver transplant recipients who require treatment have response rates that are the same as in individuals who have not had a transplant. These patients are now being treated earlier and earlier after their transplant because you can do it safely.”
She pointed to a study presented at the 2017 AASLD meeting by Kosh Agarwal, MD, of Kings College London. It involved 79 adults with recurrent genotypes 1-4 HCV infection post–liver transplant who were treated with sofosbuvir/velpatasvir (Epclusa) for 12 weeks with a total SVR rate of 96%.
“The nice thing about sofosbuvir/velpatasvir is there are no drug-drug interactions with immunosuppressive drugs. Now it’s very easy to take care of these patients. The SVR rates are excellent,” Dr. Terrault observed.
The other combination that’s been studied specifically in liver transplant recipients, and in kidney transplant recipients as well, is glecapravir/pibrentasvir. In the MAGELLAN-2 study of 100 such patients with genotypes 1-6 HCV, the SVR rate was 99% with no drug-related adverse events leading to discontinuation.
Persons who inject drugs
The Centers for Disease Control and Prevention and the World Health Organization want HCV eradicated by 2030. If that’s going to happen, physicians will have to become more comfortable treating the disease in injectable drug users, a population with a high prevalence of HCV. Several studies have now shown that very high SVR rates can be achieved with direct-acting antiviral regimens as short as 8 weeks in these individuals, even if they are concurrently injecting drugs.
“There is increasing evidence that we should be doing more treatment in persons who inject drugs. Many of these individuals have very early disease and their response rates are excellent,” according to Dr. Terrault.
Moreover, their reinfection rates “are not outrageous,” she said: 1% or less in individuals who stopped injecting drugs decades prior to anti-HCV treatment, 5%-10% over the course of 3-5 years in those who continue injecting drugs after achieving SVR, and about 2% in those on methadone substitution therapy.
“These are very acceptable levels of reinfection if our goal is to move toward elimination of hepatitis C in this population,” she said.
She reported having no financial conflicts regarding her presentation.
MAUI, HAWAII – Treatment of acute rather than chronic hepatitis C infection is well worth considering in selected circumstances, Norah Terrault, MD, asserted at the Gastroenterology Updates, IBD, Liver Disease meeting.
This is not at present guideline-recommended therapy. Current American Association for the Study of Liver Disease/Infectious Diseases Society of America guidance states that while there is emerging data to support treatment of acute hepatitis C, the evidence isn’t yet sufficiently robust to support a particular regimen or duration. The guidelines currently recommend waiting 6 months to see if the acute infection resolves spontaneously, as happens in a minority of cases, or becomes chronic, at which point it becomes guideline-directed treatment time. But Dr. Terrault believes persuasive evidence to back treatment of acute hepatitis C infection (HCV) is forthcoming, and she noted that the guidelines leave the door ajar by stating, “There are instances wherein a clinician may decide that the benefits of early treatment outweigh waiting for possible spontaneous clearance.”
Treatment of acute HCV
Dr. Terrault deems treatment of acute HCV warranted in circumstances in which there is significant danger of transmission from the acutely infected individual to others. For example, health care providers with a needlestick HCV infection, injecting drug users, and men with acute HCV/HIV coinfection. She also treats acute HCV in patients with underlying chronic liver disease.
“Clearly, I wouldn’t want those individuals to have any worsening of their liver function, so I would treat them acutely,” explained Dr. Terrault, professor of medicine and director of the Viral Hepatitis Center at the University of California, San Francisco.
She cited as particularly impressive the results of the SWIFT-C trial presented by Suzanna Naggie, MD, of Duke University, Durham, N.C., at the 2017 AASLD annual meeting. In this modest-size, National Institutes of Health–sponsored, multicenter study of HIV-infected men with acute HCV coinfection, the sustained viral response (SVR) rate with 8 weeks of ledipasvir/sofosbuvir (Harvoni) was 100%, regardless of their baseline HCV RNA level.
“I think this is remarkable. They cleared virus quite late and yet they went on to achieve HCV eradication. It highlights how little we really know about the treatment of individuals in this phase and that relying on HCV RNA levels may not tell the whole story. I think this is important data to suggest maybe when we treat acute hepatitis C we can use a shorter duration of treatment for that population. There are also other small studies testing 8 weeks of treatment in non–HIV-infected individuals with acute hepatitis C in which they also showed very high SVR rates,” the hepatologist said.
Copanelist Steven L. Flamm, MD, said that when he encounters a patient with acute HCV he, too, is prepared to offer treatment – he finds the available supporting evidence sufficiently compelling – but he often encounters a problem.
“Sometimes I’m blocked by insurance companies because this isn’t officially approved,” noted Dr. Flamm, professor of medicine and chief of the hepatology program at Northwestern University, Chicago.
“You’re right,” Dr. Terrault commented, “we have to make a pretty compelling argument to the insurer as to why we’re treating. But ‘treat to prevent transmission to others’ usually is successful in our hands.”
HCV in patients with end-stage renal disease
The product labeling for sofosbuvir (Sovaldi) says the drug’s safety and efficacy haven’t been established in patients with severe renal impairment or end-stage renal disease. However, a small multicenter study presented at the 2017 AASLD meeting demonstrated that 12 weeks of ledipasvir/sofosbuvir achieved a 100% SVR rate in patients with genotype 1 HCV and severe renal impairment, including some on dialysis, with no clinically meaningful change in estimated glomerular filtration rate or any signal of cardiac arrhythmia.
“The serum drug levels went up significantly, but reassuringly they saw no meaningful safety signals,” according to Dr. Terrault. “This, I think, is initial reassuring information that we were all very much waiting for.”
Still, as the AASLD/IDSA guidelines point out, ledipasvir/sofosbuvir is not a recommended option for HCV treatment in end-stage renal disease.
“In general, I think glecapravir/pibrentasvir [Mavyret] has become the go-to drug for patients who have renal dysfunction because it’s a pangenic regimen, it doesn’t require use of sofosbuvir, and there’s no dose adjustment. But I would say you could encounter situations where you might want to use sofosbuvir, and for me that situation is typically those direct-acting, antiviral-experienced patients who have failed other therapies and you really need to use sofosbuvir/velpatasvir/voxilaprevir [Vosevi] as your last or rescue therapy,” the hepatologist continued.
HCV in liver transplant recipients
“In the years before the direct-acting antivirals, treating transplant patients was always very challenging,” Dr. Terrault recalled. “They had very low response rates to therapy. That’s all gone away. Now we can say that liver transplant recipients who require treatment have response rates that are the same as in individuals who have not had a transplant. These patients are now being treated earlier and earlier after their transplant because you can do it safely.”
She pointed to a study presented at the 2017 AASLD meeting by Kosh Agarwal, MD, of Kings College London. It involved 79 adults with recurrent genotypes 1-4 HCV infection post–liver transplant who were treated with sofosbuvir/velpatasvir (Epclusa) for 12 weeks with a total SVR rate of 96%.
“The nice thing about sofosbuvir/velpatasvir is there are no drug-drug interactions with immunosuppressive drugs. Now it’s very easy to take care of these patients. The SVR rates are excellent,” Dr. Terrault observed.
The other combination that’s been studied specifically in liver transplant recipients, and in kidney transplant recipients as well, is glecapravir/pibrentasvir. In the MAGELLAN-2 study of 100 such patients with genotypes 1-6 HCV, the SVR rate was 99% with no drug-related adverse events leading to discontinuation.
Persons who inject drugs
The Centers for Disease Control and Prevention and the World Health Organization want HCV eradicated by 2030. If that’s going to happen, physicians will have to become more comfortable treating the disease in injectable drug users, a population with a high prevalence of HCV. Several studies have now shown that very high SVR rates can be achieved with direct-acting antiviral regimens as short as 8 weeks in these individuals, even if they are concurrently injecting drugs.
“There is increasing evidence that we should be doing more treatment in persons who inject drugs. Many of these individuals have very early disease and their response rates are excellent,” according to Dr. Terrault.
Moreover, their reinfection rates “are not outrageous,” she said: 1% or less in individuals who stopped injecting drugs decades prior to anti-HCV treatment, 5%-10% over the course of 3-5 years in those who continue injecting drugs after achieving SVR, and about 2% in those on methadone substitution therapy.
“These are very acceptable levels of reinfection if our goal is to move toward elimination of hepatitis C in this population,” she said.
She reported having no financial conflicts regarding her presentation.
EXPERT ANALYSIS FROM GUILD 2018
Inhaled nitrous oxide for labor analgesia: Pearls from clinical experience
Nitrous oxide, a colorless, odorless gas, has long been used for labor analgesia in many countries, including the United Kingdom, Canada, throughout Europe, Australia, and New Zealand. Recently, interest in its use in the United States has increased, since the US Food and Drug Administration (FDA) approval in 2012 of simple devices for administration of nitrous oxide in a variety of locations. Being able to offer an alternative technique, other than parenteral opioids, for women who may not wish to or who cannot have regional analgesia, and for women who have delivered and need analgesia for postdelivery repair, conveys significant benefits. Risks to its use are very low, although the quality of pain relief is inferior to that offered by regional analgesic techniques. Our experience with its use since 2014 at Brigham and Women’s Hospital in Boston, Massachusetts, corroborates that reported in the literature and leads us to continue offering inhaled nitrous oxide and advocating that others do as well.1–7 When using nitrous oxide in your labor and delivery unit, or if considering its use, keep the following points in mind.
A successful inhaled nitrous oxide program requires proper patient selection
Inhaled nitrous oxide is not an epidural (TABLE).8 The pain relief is clearly inferior to that of an epidural. Inhaled nitrous oxide will not replace epidurals or even have any effect on the epidural rate at a particular institution.6 However, the use of inhaled nitrous oxide for labor analgesia has a long track record of safety (albeit with moderate efficacy for selected patients) for many years in many countries around the world. Inhaled nitrous oxide is a valuable addition to the options we can offer patients:
- who are poor responders to opioid medication or who have high opioid tolerance
- with certain disorders of coagulation
- with chronic pain or anxiety
- who for other reasons need to consider alternatives or adjuncts to neuraxial analgesia.
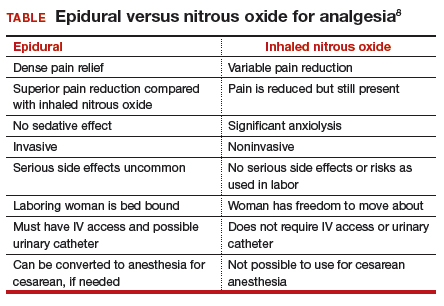
Although it is important to be realistic regarding the expectations of analgesia quality offered by this agent,7 compared with other agents we have tried, it has less adverse effects, is economically reasonable, and has no proven impact on neonatal outcomes.
No significant complications with inhaled nitrous oxide have been reported
Systematic reviews did not report any significant complications to either mother or newborn.1,2 Our personal experiences corroborate this, as no complications have been associated with its frequent use at Brigham and Women’s Hospital. Reported adverse effects are mild. The incidence of nausea is 13%, dizziness is 3% to 5%, and drowsiness is 4%; these rates are hard to detect over the baseline rates of those side effects associated with labor and delivery alone.1 Many other centers have now adopted the use of this agent, with several hundred locations now offering inhaled nitrous oxide for labor analgesia in the United States.
Practical use of inhaled nitrous oxide is relatively simple
Several vendors offer portable, user-friendly, cost-effective equipment that is appropriate for labor and delivery use. All devices are structured in demand-valve modality, meaning that the patient must initiate a breath in order to open a valve that allows gas to flow. Cessation of the inspiratory effort closes the valve, thus preventing the free flow of gas into the ambient atmosphere of the room. The devices generally include a tank with nitrous oxide as well as a source of oxygen. Most devices designed for labor and delivery provide a fixed mixture of 50% nitrous oxide and 50% oxygen, with fail-safe mechanisms to allow increased oxygen delivery in the event of failure or depletion of the nitrous supply. All modern, FDA–approved devices include effective scavenging systems, such that expired gases are vented outside (generally via room suction), which prevents occupational exposure to low levels of nitrous oxide.
Inhaled nitrous oxide for labor pain must be patient controlled
An essential feature of the use of inhaled nitrous oxide for labor analgesia is that it must be considered a patient-controlled system. Patients have an option to use either a mask or a mouthpiece, according to their preferences and comfort. The patient must hold the mask or mouthpiece herself; it is neither appropriate nor safe for anyone else, such as a nurse, family member, or labor support personnel, to assist with this task.
Some coordination with the nurse is essential for optimal timing of administration. Onset of a therapeutic level of pain relief is generally 30 to 60 seconds after inhalation has begun, with rapid resolution after cessation of the inhalation. The patient should thus initiate the inspiration of the gas at the earliest signs of onset of a contraction, so as to achieve maximal analgesia at the peak of the contraction. Waiting until the peak of the contraction to initiate inhalation of the nitrous oxide will not provide effective analgesia, yet will result in sedation after the contraction has ended.
Read about patient satisfaction with inhaled nitrous oxide.
No oversight by an anesthesiologist is required
The Centers for Medicare and Medicaid Services (CMS) produced a clarification statement for definitions of “anesthesia services” (42 CFR 482.52)9 that may be offered by a hospital, based on American Society of Anesthesiologists (ASA) definitions. CMS, consistent with ASA guidelines, does not define moderate or conscious sedation as “anesthesia,” thus direct oversight by an anesthesiologist is not required. Furthermore, the definition of “minimal sedation,” which is where 50% concentration delivery of inhaled nitrous oxide would be categorized, also does not meet this requirement by CMS.

Women who use inhaled nitrous oxide for labor pain typically are satisfied with its use
The use of analog pain scale measurements may not be appropriate in a setting where dissociation from pain might be the primary beneficial effect. Measurements of maternal satisfaction with their analgesic experience support this. The experiences at Vanderbilt University and Brigham and Women’s Hospital show that, while pain relief is limited, like reported in systematic reviews, maternal satisfaction scores for labor analgesia are not different among women who receive inhaled nitrous oxide analgesia, neuraxial analgesia, and those who transition from nitrous to neuraxial analgesia. In fact, published evidence supports extraordinarily high satisfaction in women who plan to use inhaled nitrous oxide, and actually successfully do so, despite only limited degrees of pain relief.10,11 Work to identify the characteristics of women who report success with inhaled nitrous oxide use needs to be performed so that patients can be better selected and informed when making analgesic choices.
Animal research on inhaled nitrous oxide may not translate well to human neonates
A very recent task force convened by the European Society of Anaesthesiology (ESA) addressed some of the potential concerns about inhaled nitrous oxide analgesia.12 Per their report:
“the potential teratogenic effect of N2O observed in experimental models cannot be extrapolated to humans. There is a lack of evidence for an association between N2O and reproductive toxicity. The incidence of health hazards and abortion was not shown to be higher in women exposed to, or spouses of men exposed to N2O than those who were not so exposed. Moreover, the incidence of congenital malformations was not higher among women who received N2O for anaesthesia during the first trimester of pregnancy nor during anaesthesia management for cervical cerclage, nor for surgery in the first two trimesters of pregnancy.”
There is a theoretical concern of an increase in neuronal apoptosis in neonates, demonstrated in laboratory animals in anesthetic concentrations, but the human relevance of this is not clear, since the data on animal developmental neurotoxicity is generally combined with data wherein potent inhalational anesthetic agents were also used, not nitrous oxide alone.13 The analgesic doses and time of exposure of inhaled nitrous oxide administered for labor analgesia are well below those required for these changes, as subanesthetic doses are associated with minimal changes, if any, in laboratory animals.
No labor analgesic is without the potential for fetal effects, and alternative labor analgesics such as systemic opioids in higher doses also may have potential adverse effects on the fetus, such as fetal heart rate effects or early tone, alertness, and breastfeeding difficulties. The low solubility and short half-life of inhaled nitrous oxide contribute to low absorption by tissues, thus contributing to the safety of this agent. Nitrous oxide via inhalation for sedation during elective cesarean has been reported to show no adverse effects on neonatal Apgar scores.14
Modern equipment keeps occupational exposure to nitrous oxide safe
One retrospective review of women exposed to high concentrations of inhaled nitrous oxide reported reduced fertility.15 However, the only effects on fertility were seen when nitrous was used without scavenging equipment, and in high concentrations. Moreover, that study examined dental offices, where nitrous was free flowing during procedures—quite a different setting than the intermittent inhalation, demand-valve modality as is used during labor—and when using appropriate modern, FDA-approved equipment, and scavenging devices. Per the recent ESA task force12:
“Members of the task force agreed that, despite theoretical concerns and laboratory data, there is no evidence indicating that the use of N2O in a clinically relevant setting would increase health risk in patients or providers exposed to this drug. With the ubiquitous availability of scavenging systems in the modern operating room, the health concern for medical staff has decreased dramatically. Properly operating scavenging systems reduce N2O concentrations by more than 70%, thereby efficiently keeping ambient N2O levels well below official limits.”
The ESA task force concludes: “An extensive amount of clinical evidence indicates that N2O can be used safely for procedural pain management, for labour pain, and for anxiolysis and sedation in dentistry.”12
Two important reminders
Inhaled nitrous oxide has been a central component of the labor pain relief menu in most of the rest of the world for decades, and the safety record is impeccable. This agent has now had extensive and growing experience in American maternity units. Remember 2 critical points: 1) patient selection is key, 2) analgesia is not like that provided by regional anesthetic techniques such as an epidural.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Likis FE, Andrews JC, Collins MR, et al. Nitrous oxide for the management of labor pain: a systematic review. Anesth Analg. 2014;118(1):153-167.
- Rosen MA. Nitrous oxide for relief of labor pain: a systematic review. Am J Obstet Gynecol. 2002;186(5 suppl nature):S110-S126.
- Angle P, Landy CK, Charles C. Phase 1 development of an index to measure the quality of neuraxial labour analgesia: exploring the perspectives of childbearing women. Can J Anaesth. 2010;57(5):468-478.
- Migliaccio L, Lawton R, Leeman L, Holbrook A. Initiating intrapartum nitrous oxide in an academic hospital: considerations and challenges. J Midwifery Womens Health. 2017;62(3):358-362.
- Markley JC, Rollins MD. Non-neuraxial labor analgesia: options. Clin Obstet Gynecol. 2017;60(2);350-364.
- Bobb LE, Farber MK, McGovern C, Camann W. Does nitrous oxide labor analgesia influence the pattern of neuraxial analgesia usage? An impact study at an academic medical center. J Clin Anesth. 2016;35:54-57.
- Sutton CD, Butwick AJ, Riley ET, Carvalho B. Nitrous oxide for labor analgesia: utilization and predictors of conversion to neuraxial analgesia. J Clin Anesth. 2017;40:40-45.
- Collins MR, Starr SA, Bishop JT, Baysinger CL. Nitrous oxide for labor analgesia: expanding analgesic options for women in the United States. Rev Obstet Gynecol. 2012;5(3-4):e126-e131.
- 42 CFR 482.52 - Condition of participation: Anesthesia services. US Government Publishing Office website. https://www.gpo.gov/fdsys/granule/CFR-2011-title42-vol5/CFR-2011-title42-vol5-sec482-52. Accessed April 16, 2018.
- Richardson MG, Lopez BM, Baysinger CL, Shotwell MS, Chestnut DH. Nitrous oxide during labor: maternal satisfaction does not depend exclusively on analgesic effectiveness. Anesth Analg. 2017;124(2):548-553.
- Camann W. Pain, pain relief, satisfaction, and excellence in obstetric anesthesia: a surprisingly complex relationship. Anesth Analg. 2017;124(2):383-385.
- European Society of Anaesthesiology Task Force on Use of Nitrous Oxide in Clinical Anaesthetic Practice. The current place of nitrous oxide in clinical practice: an expert opinion-based task force consensus statement of the European Society of Anaesthesiology. Eur J Anaesthesiol. 2015;32(8):517-520.
- Rappaport B, Mellon RD, Simone A, Woodcock J. Defining safe use of anesthesia in children. N Engl J Med. 2011;364(15):1387-1390.
- Vallejo MC, Phelps AL, Shepherd CJ, Kaul B, Mandell GL, Ramanathan S. Nitrous oxide anxiolysis for elective cesarean section. J Clin Anesth. 2005;17(7):543-548.
- Rowland AS, Baird DD, Weinberg CR, et al. Reduced fertility among women employed as dental assistants exposed to high levels of nitrous oxide. N Engl J Med. 1992;327(14):993-997.

Dr. Camann is Associate Professor of Anesthesia, Harvard Medical School, and Director Emeritus, Obstetric Anesthesiology, Brigham and Women’s Hospital, Boston, Massachusetts.
The author reports no financial relationships relevant to this article.
Dr. Camann is Associate Professor of Anesthesia, Harvard Medical School, and Director Emeritus, Obstetric Anesthesiology, Brigham and Women’s Hospital, Boston, Massachusetts.
The author reports no financial relationships relevant to this article.
Dr. Camann is Associate Professor of Anesthesia, Harvard Medical School, and Director Emeritus, Obstetric Anesthesiology, Brigham and Women’s Hospital, Boston, Massachusetts.
The author reports no financial relationships relevant to this article.
Nitrous oxide, a colorless, odorless gas, has long been used for labor analgesia in many countries, including the United Kingdom, Canada, throughout Europe, Australia, and New Zealand. Recently, interest in its use in the United States has increased, since the US Food and Drug Administration (FDA) approval in 2012 of simple devices for administration of nitrous oxide in a variety of locations. Being able to offer an alternative technique, other than parenteral opioids, for women who may not wish to or who cannot have regional analgesia, and for women who have delivered and need analgesia for postdelivery repair, conveys significant benefits. Risks to its use are very low, although the quality of pain relief is inferior to that offered by regional analgesic techniques. Our experience with its use since 2014 at Brigham and Women’s Hospital in Boston, Massachusetts, corroborates that reported in the literature and leads us to continue offering inhaled nitrous oxide and advocating that others do as well.1–7 When using nitrous oxide in your labor and delivery unit, or if considering its use, keep the following points in mind.
A successful inhaled nitrous oxide program requires proper patient selection
Inhaled nitrous oxide is not an epidural (TABLE).8 The pain relief is clearly inferior to that of an epidural. Inhaled nitrous oxide will not replace epidurals or even have any effect on the epidural rate at a particular institution.6 However, the use of inhaled nitrous oxide for labor analgesia has a long track record of safety (albeit with moderate efficacy for selected patients) for many years in many countries around the world. Inhaled nitrous oxide is a valuable addition to the options we can offer patients:
- who are poor responders to opioid medication or who have high opioid tolerance
- with certain disorders of coagulation
- with chronic pain or anxiety
- who for other reasons need to consider alternatives or adjuncts to neuraxial analgesia.
Although it is important to be realistic regarding the expectations of analgesia quality offered by this agent,7 compared with other agents we have tried, it has less adverse effects, is economically reasonable, and has no proven impact on neonatal outcomes.
No significant complications with inhaled nitrous oxide have been reported
Systematic reviews did not report any significant complications to either mother or newborn.1,2 Our personal experiences corroborate this, as no complications have been associated with its frequent use at Brigham and Women’s Hospital. Reported adverse effects are mild. The incidence of nausea is 13%, dizziness is 3% to 5%, and drowsiness is 4%; these rates are hard to detect over the baseline rates of those side effects associated with labor and delivery alone.1 Many other centers have now adopted the use of this agent, with several hundred locations now offering inhaled nitrous oxide for labor analgesia in the United States.
Practical use of inhaled nitrous oxide is relatively simple
Several vendors offer portable, user-friendly, cost-effective equipment that is appropriate for labor and delivery use. All devices are structured in demand-valve modality, meaning that the patient must initiate a breath in order to open a valve that allows gas to flow. Cessation of the inspiratory effort closes the valve, thus preventing the free flow of gas into the ambient atmosphere of the room. The devices generally include a tank with nitrous oxide as well as a source of oxygen. Most devices designed for labor and delivery provide a fixed mixture of 50% nitrous oxide and 50% oxygen, with fail-safe mechanisms to allow increased oxygen delivery in the event of failure or depletion of the nitrous supply. All modern, FDA–approved devices include effective scavenging systems, such that expired gases are vented outside (generally via room suction), which prevents occupational exposure to low levels of nitrous oxide.
Inhaled nitrous oxide for labor pain must be patient controlled
An essential feature of the use of inhaled nitrous oxide for labor analgesia is that it must be considered a patient-controlled system. Patients have an option to use either a mask or a mouthpiece, according to their preferences and comfort. The patient must hold the mask or mouthpiece herself; it is neither appropriate nor safe for anyone else, such as a nurse, family member, or labor support personnel, to assist with this task.
Some coordination with the nurse is essential for optimal timing of administration. Onset of a therapeutic level of pain relief is generally 30 to 60 seconds after inhalation has begun, with rapid resolution after cessation of the inhalation. The patient should thus initiate the inspiration of the gas at the earliest signs of onset of a contraction, so as to achieve maximal analgesia at the peak of the contraction. Waiting until the peak of the contraction to initiate inhalation of the nitrous oxide will not provide effective analgesia, yet will result in sedation after the contraction has ended.
Read about patient satisfaction with inhaled nitrous oxide.
No oversight by an anesthesiologist is required
The Centers for Medicare and Medicaid Services (CMS) produced a clarification statement for definitions of “anesthesia services” (42 CFR 482.52)9 that may be offered by a hospital, based on American Society of Anesthesiologists (ASA) definitions. CMS, consistent with ASA guidelines, does not define moderate or conscious sedation as “anesthesia,” thus direct oversight by an anesthesiologist is not required. Furthermore, the definition of “minimal sedation,” which is where 50% concentration delivery of inhaled nitrous oxide would be categorized, also does not meet this requirement by CMS.
Women who use inhaled nitrous oxide for labor pain typically are satisfied with its use
The use of analog pain scale measurements may not be appropriate in a setting where dissociation from pain might be the primary beneficial effect. Measurements of maternal satisfaction with their analgesic experience support this. The experiences at Vanderbilt University and Brigham and Women’s Hospital show that, while pain relief is limited, like reported in systematic reviews, maternal satisfaction scores for labor analgesia are not different among women who receive inhaled nitrous oxide analgesia, neuraxial analgesia, and those who transition from nitrous to neuraxial analgesia. In fact, published evidence supports extraordinarily high satisfaction in women who plan to use inhaled nitrous oxide, and actually successfully do so, despite only limited degrees of pain relief.10,11 Work to identify the characteristics of women who report success with inhaled nitrous oxide use needs to be performed so that patients can be better selected and informed when making analgesic choices.
Animal research on inhaled nitrous oxide may not translate well to human neonates
A very recent task force convened by the European Society of Anaesthesiology (ESA) addressed some of the potential concerns about inhaled nitrous oxide analgesia.12 Per their report:
“the potential teratogenic effect of N2O observed in experimental models cannot be extrapolated to humans. There is a lack of evidence for an association between N2O and reproductive toxicity. The incidence of health hazards and abortion was not shown to be higher in women exposed to, or spouses of men exposed to N2O than those who were not so exposed. Moreover, the incidence of congenital malformations was not higher among women who received N2O for anaesthesia during the first trimester of pregnancy nor during anaesthesia management for cervical cerclage, nor for surgery in the first two trimesters of pregnancy.”
There is a theoretical concern of an increase in neuronal apoptosis in neonates, demonstrated in laboratory animals in anesthetic concentrations, but the human relevance of this is not clear, since the data on animal developmental neurotoxicity is generally combined with data wherein potent inhalational anesthetic agents were also used, not nitrous oxide alone.13 The analgesic doses and time of exposure of inhaled nitrous oxide administered for labor analgesia are well below those required for these changes, as subanesthetic doses are associated with minimal changes, if any, in laboratory animals.
No labor analgesic is without the potential for fetal effects, and alternative labor analgesics such as systemic opioids in higher doses also may have potential adverse effects on the fetus, such as fetal heart rate effects or early tone, alertness, and breastfeeding difficulties. The low solubility and short half-life of inhaled nitrous oxide contribute to low absorption by tissues, thus contributing to the safety of this agent. Nitrous oxide via inhalation for sedation during elective cesarean has been reported to show no adverse effects on neonatal Apgar scores.14
Modern equipment keeps occupational exposure to nitrous oxide safe
One retrospective review of women exposed to high concentrations of inhaled nitrous oxide reported reduced fertility.15 However, the only effects on fertility were seen when nitrous was used without scavenging equipment, and in high concentrations. Moreover, that study examined dental offices, where nitrous was free flowing during procedures—quite a different setting than the intermittent inhalation, demand-valve modality as is used during labor—and when using appropriate modern, FDA-approved equipment, and scavenging devices. Per the recent ESA task force12:
“Members of the task force agreed that, despite theoretical concerns and laboratory data, there is no evidence indicating that the use of N2O in a clinically relevant setting would increase health risk in patients or providers exposed to this drug. With the ubiquitous availability of scavenging systems in the modern operating room, the health concern for medical staff has decreased dramatically. Properly operating scavenging systems reduce N2O concentrations by more than 70%, thereby efficiently keeping ambient N2O levels well below official limits.”
The ESA task force concludes: “An extensive amount of clinical evidence indicates that N2O can be used safely for procedural pain management, for labour pain, and for anxiolysis and sedation in dentistry.”12
Two important reminders
Inhaled nitrous oxide has been a central component of the labor pain relief menu in most of the rest of the world for decades, and the safety record is impeccable. This agent has now had extensive and growing experience in American maternity units. Remember 2 critical points: 1) patient selection is key, 2) analgesia is not like that provided by regional anesthetic techniques such as an epidural.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
Nitrous oxide, a colorless, odorless gas, has long been used for labor analgesia in many countries, including the United Kingdom, Canada, throughout Europe, Australia, and New Zealand. Recently, interest in its use in the United States has increased, since the US Food and Drug Administration (FDA) approval in 2012 of simple devices for administration of nitrous oxide in a variety of locations. Being able to offer an alternative technique, other than parenteral opioids, for women who may not wish to or who cannot have regional analgesia, and for women who have delivered and need analgesia for postdelivery repair, conveys significant benefits. Risks to its use are very low, although the quality of pain relief is inferior to that offered by regional analgesic techniques. Our experience with its use since 2014 at Brigham and Women’s Hospital in Boston, Massachusetts, corroborates that reported in the literature and leads us to continue offering inhaled nitrous oxide and advocating that others do as well.1–7 When using nitrous oxide in your labor and delivery unit, or if considering its use, keep the following points in mind.
A successful inhaled nitrous oxide program requires proper patient selection
Inhaled nitrous oxide is not an epidural (TABLE).8 The pain relief is clearly inferior to that of an epidural. Inhaled nitrous oxide will not replace epidurals or even have any effect on the epidural rate at a particular institution.6 However, the use of inhaled nitrous oxide for labor analgesia has a long track record of safety (albeit with moderate efficacy for selected patients) for many years in many countries around the world. Inhaled nitrous oxide is a valuable addition to the options we can offer patients:
- who are poor responders to opioid medication or who have high opioid tolerance
- with certain disorders of coagulation
- with chronic pain or anxiety
- who for other reasons need to consider alternatives or adjuncts to neuraxial analgesia.
Although it is important to be realistic regarding the expectations of analgesia quality offered by this agent,7 compared with other agents we have tried, it has less adverse effects, is economically reasonable, and has no proven impact on neonatal outcomes.
No significant complications with inhaled nitrous oxide have been reported
Systematic reviews did not report any significant complications to either mother or newborn.1,2 Our personal experiences corroborate this, as no complications have been associated with its frequent use at Brigham and Women’s Hospital. Reported adverse effects are mild. The incidence of nausea is 13%, dizziness is 3% to 5%, and drowsiness is 4%; these rates are hard to detect over the baseline rates of those side effects associated with labor and delivery alone.1 Many other centers have now adopted the use of this agent, with several hundred locations now offering inhaled nitrous oxide for labor analgesia in the United States.
Practical use of inhaled nitrous oxide is relatively simple
Several vendors offer portable, user-friendly, cost-effective equipment that is appropriate for labor and delivery use. All devices are structured in demand-valve modality, meaning that the patient must initiate a breath in order to open a valve that allows gas to flow. Cessation of the inspiratory effort closes the valve, thus preventing the free flow of gas into the ambient atmosphere of the room. The devices generally include a tank with nitrous oxide as well as a source of oxygen. Most devices designed for labor and delivery provide a fixed mixture of 50% nitrous oxide and 50% oxygen, with fail-safe mechanisms to allow increased oxygen delivery in the event of failure or depletion of the nitrous supply. All modern, FDA–approved devices include effective scavenging systems, such that expired gases are vented outside (generally via room suction), which prevents occupational exposure to low levels of nitrous oxide.
Inhaled nitrous oxide for labor pain must be patient controlled
An essential feature of the use of inhaled nitrous oxide for labor analgesia is that it must be considered a patient-controlled system. Patients have an option to use either a mask or a mouthpiece, according to their preferences and comfort. The patient must hold the mask or mouthpiece herself; it is neither appropriate nor safe for anyone else, such as a nurse, family member, or labor support personnel, to assist with this task.
Some coordination with the nurse is essential for optimal timing of administration. Onset of a therapeutic level of pain relief is generally 30 to 60 seconds after inhalation has begun, with rapid resolution after cessation of the inhalation. The patient should thus initiate the inspiration of the gas at the earliest signs of onset of a contraction, so as to achieve maximal analgesia at the peak of the contraction. Waiting until the peak of the contraction to initiate inhalation of the nitrous oxide will not provide effective analgesia, yet will result in sedation after the contraction has ended.
Read about patient satisfaction with inhaled nitrous oxide.
No oversight by an anesthesiologist is required
The Centers for Medicare and Medicaid Services (CMS) produced a clarification statement for definitions of “anesthesia services” (42 CFR 482.52)9 that may be offered by a hospital, based on American Society of Anesthesiologists (ASA) definitions. CMS, consistent with ASA guidelines, does not define moderate or conscious sedation as “anesthesia,” thus direct oversight by an anesthesiologist is not required. Furthermore, the definition of “minimal sedation,” which is where 50% concentration delivery of inhaled nitrous oxide would be categorized, also does not meet this requirement by CMS.
Women who use inhaled nitrous oxide for labor pain typically are satisfied with its use
The use of analog pain scale measurements may not be appropriate in a setting where dissociation from pain might be the primary beneficial effect. Measurements of maternal satisfaction with their analgesic experience support this. The experiences at Vanderbilt University and Brigham and Women’s Hospital show that, while pain relief is limited, like reported in systematic reviews, maternal satisfaction scores for labor analgesia are not different among women who receive inhaled nitrous oxide analgesia, neuraxial analgesia, and those who transition from nitrous to neuraxial analgesia. In fact, published evidence supports extraordinarily high satisfaction in women who plan to use inhaled nitrous oxide, and actually successfully do so, despite only limited degrees of pain relief.10,11 Work to identify the characteristics of women who report success with inhaled nitrous oxide use needs to be performed so that patients can be better selected and informed when making analgesic choices.
Animal research on inhaled nitrous oxide may not translate well to human neonates
A very recent task force convened by the European Society of Anaesthesiology (ESA) addressed some of the potential concerns about inhaled nitrous oxide analgesia.12 Per their report:
“the potential teratogenic effect of N2O observed in experimental models cannot be extrapolated to humans. There is a lack of evidence for an association between N2O and reproductive toxicity. The incidence of health hazards and abortion was not shown to be higher in women exposed to, or spouses of men exposed to N2O than those who were not so exposed. Moreover, the incidence of congenital malformations was not higher among women who received N2O for anaesthesia during the first trimester of pregnancy nor during anaesthesia management for cervical cerclage, nor for surgery in the first two trimesters of pregnancy.”
There is a theoretical concern of an increase in neuronal apoptosis in neonates, demonstrated in laboratory animals in anesthetic concentrations, but the human relevance of this is not clear, since the data on animal developmental neurotoxicity is generally combined with data wherein potent inhalational anesthetic agents were also used, not nitrous oxide alone.13 The analgesic doses and time of exposure of inhaled nitrous oxide administered for labor analgesia are well below those required for these changes, as subanesthetic doses are associated with minimal changes, if any, in laboratory animals.
No labor analgesic is without the potential for fetal effects, and alternative labor analgesics such as systemic opioids in higher doses also may have potential adverse effects on the fetus, such as fetal heart rate effects or early tone, alertness, and breastfeeding difficulties. The low solubility and short half-life of inhaled nitrous oxide contribute to low absorption by tissues, thus contributing to the safety of this agent. Nitrous oxide via inhalation for sedation during elective cesarean has been reported to show no adverse effects on neonatal Apgar scores.14
Modern equipment keeps occupational exposure to nitrous oxide safe
One retrospective review of women exposed to high concentrations of inhaled nitrous oxide reported reduced fertility.15 However, the only effects on fertility were seen when nitrous was used without scavenging equipment, and in high concentrations. Moreover, that study examined dental offices, where nitrous was free flowing during procedures—quite a different setting than the intermittent inhalation, demand-valve modality as is used during labor—and when using appropriate modern, FDA-approved equipment, and scavenging devices. Per the recent ESA task force12:
“Members of the task force agreed that, despite theoretical concerns and laboratory data, there is no evidence indicating that the use of N2O in a clinically relevant setting would increase health risk in patients or providers exposed to this drug. With the ubiquitous availability of scavenging systems in the modern operating room, the health concern for medical staff has decreased dramatically. Properly operating scavenging systems reduce N2O concentrations by more than 70%, thereby efficiently keeping ambient N2O levels well below official limits.”
The ESA task force concludes: “An extensive amount of clinical evidence indicates that N2O can be used safely for procedural pain management, for labour pain, and for anxiolysis and sedation in dentistry.”12
Two important reminders
Inhaled nitrous oxide has been a central component of the labor pain relief menu in most of the rest of the world for decades, and the safety record is impeccable. This agent has now had extensive and growing experience in American maternity units. Remember 2 critical points: 1) patient selection is key, 2) analgesia is not like that provided by regional anesthetic techniques such as an epidural.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Likis FE, Andrews JC, Collins MR, et al. Nitrous oxide for the management of labor pain: a systematic review. Anesth Analg. 2014;118(1):153-167.
- Rosen MA. Nitrous oxide for relief of labor pain: a systematic review. Am J Obstet Gynecol. 2002;186(5 suppl nature):S110-S126.
- Angle P, Landy CK, Charles C. Phase 1 development of an index to measure the quality of neuraxial labour analgesia: exploring the perspectives of childbearing women. Can J Anaesth. 2010;57(5):468-478.
- Migliaccio L, Lawton R, Leeman L, Holbrook A. Initiating intrapartum nitrous oxide in an academic hospital: considerations and challenges. J Midwifery Womens Health. 2017;62(3):358-362.
- Markley JC, Rollins MD. Non-neuraxial labor analgesia: options. Clin Obstet Gynecol. 2017;60(2);350-364.
- Bobb LE, Farber MK, McGovern C, Camann W. Does nitrous oxide labor analgesia influence the pattern of neuraxial analgesia usage? An impact study at an academic medical center. J Clin Anesth. 2016;35:54-57.
- Sutton CD, Butwick AJ, Riley ET, Carvalho B. Nitrous oxide for labor analgesia: utilization and predictors of conversion to neuraxial analgesia. J Clin Anesth. 2017;40:40-45.
- Collins MR, Starr SA, Bishop JT, Baysinger CL. Nitrous oxide for labor analgesia: expanding analgesic options for women in the United States. Rev Obstet Gynecol. 2012;5(3-4):e126-e131.
- 42 CFR 482.52 - Condition of participation: Anesthesia services. US Government Publishing Office website. https://www.gpo.gov/fdsys/granule/CFR-2011-title42-vol5/CFR-2011-title42-vol5-sec482-52. Accessed April 16, 2018.
- Richardson MG, Lopez BM, Baysinger CL, Shotwell MS, Chestnut DH. Nitrous oxide during labor: maternal satisfaction does not depend exclusively on analgesic effectiveness. Anesth Analg. 2017;124(2):548-553.
- Camann W. Pain, pain relief, satisfaction, and excellence in obstetric anesthesia: a surprisingly complex relationship. Anesth Analg. 2017;124(2):383-385.
- European Society of Anaesthesiology Task Force on Use of Nitrous Oxide in Clinical Anaesthetic Practice. The current place of nitrous oxide in clinical practice: an expert opinion-based task force consensus statement of the European Society of Anaesthesiology. Eur J Anaesthesiol. 2015;32(8):517-520.
- Rappaport B, Mellon RD, Simone A, Woodcock J. Defining safe use of anesthesia in children. N Engl J Med. 2011;364(15):1387-1390.
- Vallejo MC, Phelps AL, Shepherd CJ, Kaul B, Mandell GL, Ramanathan S. Nitrous oxide anxiolysis for elective cesarean section. J Clin Anesth. 2005;17(7):543-548.
- Rowland AS, Baird DD, Weinberg CR, et al. Reduced fertility among women employed as dental assistants exposed to high levels of nitrous oxide. N Engl J Med. 1992;327(14):993-997.
- Likis FE, Andrews JC, Collins MR, et al. Nitrous oxide for the management of labor pain: a systematic review. Anesth Analg. 2014;118(1):153-167.
- Rosen MA. Nitrous oxide for relief of labor pain: a systematic review. Am J Obstet Gynecol. 2002;186(5 suppl nature):S110-S126.
- Angle P, Landy CK, Charles C. Phase 1 development of an index to measure the quality of neuraxial labour analgesia: exploring the perspectives of childbearing women. Can J Anaesth. 2010;57(5):468-478.
- Migliaccio L, Lawton R, Leeman L, Holbrook A. Initiating intrapartum nitrous oxide in an academic hospital: considerations and challenges. J Midwifery Womens Health. 2017;62(3):358-362.
- Markley JC, Rollins MD. Non-neuraxial labor analgesia: options. Clin Obstet Gynecol. 2017;60(2);350-364.
- Bobb LE, Farber MK, McGovern C, Camann W. Does nitrous oxide labor analgesia influence the pattern of neuraxial analgesia usage? An impact study at an academic medical center. J Clin Anesth. 2016;35:54-57.
- Sutton CD, Butwick AJ, Riley ET, Carvalho B. Nitrous oxide for labor analgesia: utilization and predictors of conversion to neuraxial analgesia. J Clin Anesth. 2017;40:40-45.
- Collins MR, Starr SA, Bishop JT, Baysinger CL. Nitrous oxide for labor analgesia: expanding analgesic options for women in the United States. Rev Obstet Gynecol. 2012;5(3-4):e126-e131.
- 42 CFR 482.52 - Condition of participation: Anesthesia services. US Government Publishing Office website. https://www.gpo.gov/fdsys/granule/CFR-2011-title42-vol5/CFR-2011-title42-vol5-sec482-52. Accessed April 16, 2018.
- Richardson MG, Lopez BM, Baysinger CL, Shotwell MS, Chestnut DH. Nitrous oxide during labor: maternal satisfaction does not depend exclusively on analgesic effectiveness. Anesth Analg. 2017;124(2):548-553.
- Camann W. Pain, pain relief, satisfaction, and excellence in obstetric anesthesia: a surprisingly complex relationship. Anesth Analg. 2017;124(2):383-385.
- European Society of Anaesthesiology Task Force on Use of Nitrous Oxide in Clinical Anaesthetic Practice. The current place of nitrous oxide in clinical practice: an expert opinion-based task force consensus statement of the European Society of Anaesthesiology. Eur J Anaesthesiol. 2015;32(8):517-520.
- Rappaport B, Mellon RD, Simone A, Woodcock J. Defining safe use of anesthesia in children. N Engl J Med. 2011;364(15):1387-1390.
- Vallejo MC, Phelps AL, Shepherd CJ, Kaul B, Mandell GL, Ramanathan S. Nitrous oxide anxiolysis for elective cesarean section. J Clin Anesth. 2005;17(7):543-548.
- Rowland AS, Baird DD, Weinberg CR, et al. Reduced fertility among women employed as dental assistants exposed to high levels of nitrous oxide. N Engl J Med. 1992;327(14):993-997.

What’s Eating You? Ixodes Tick and Related Diseases, Part 3: Coinfection and Tick-Bite Prevention
Tick-borne diseases are increasing in prevalence, likely due to climate change in combination with human movement into tick habitats.1-3 The Ixodes genus of hard ticks is a common vector for the transmission of pathogenic viruses, bacteria, parasites, and toxins. Among these, Lyme disease, which is caused by Borrelia burgdorferi, is the most prevalent, followed by babesiosis and human granulocytic anaplasmosis (HGA), respectively.4 In Europe, tick-borne encephalitis is commonly encountered. More recently identified diseases transmitted by Ixodes ticks include Powassan virus and Borrelia miyamotoi infection; however, these diseases are less frequently encountered than other tick-borne diseases.5,6
As tick-borne diseases become more prevalent, the likelihood of coinfection with more than one Ixodes-transmitted pathogen is increasing.7 Therefore, it is important for physicians who practice in endemic areas to be aware of the possibility of coinfection, which can alter clinical presentation, disease severity, and treatment response in tick-borne diseases. Additionally, public education on tick-bite prevention and prompt tick removal is necessary to combat the rising prevalence of these diseases.
Coinfection
Risk of coinfection with more than one tick-borne disease is contingent on the geographic distribution of the tick species as well as the particular pathogen’s prevalence within reservoir hosts in a given area (Figure). Most coinfections occur with B. burgdorferi and an additional pathogen, usually Anaplasma phagocytophilum (which causes human granulocytic anaplasmosis [HGA]) or Babesia microti (which causes babesiosis). In Europe, coinfection with tick-borne encephalitis virus may occur. There is limited evidence of human coinfection with B miyamotoi or Powassan virus, as isolated infection with either of these pathogens is rare.
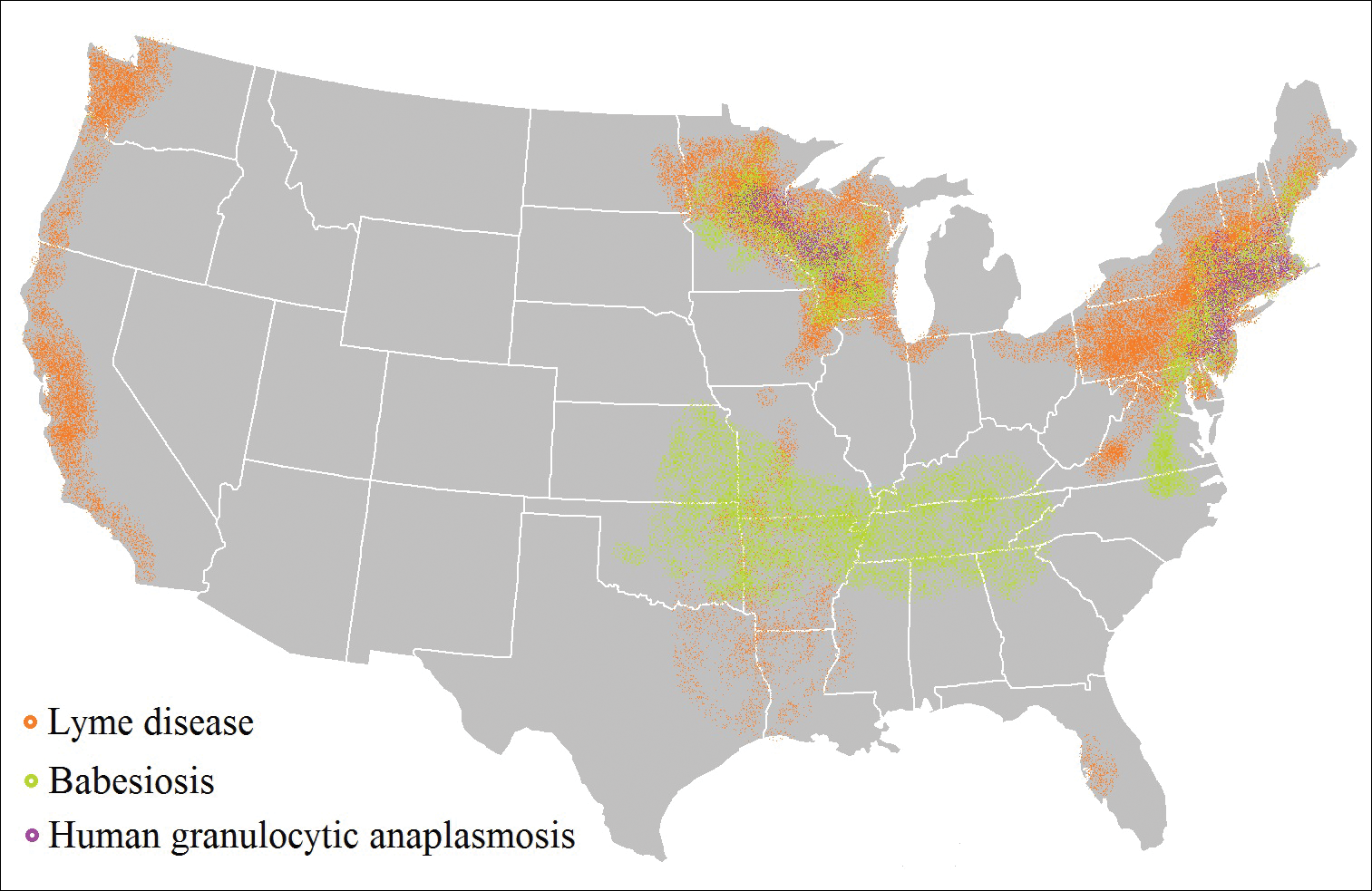
In patients with Lyme disease, as many as 35% may have concurrent babesiosis, and as many as 12% may have concurrent HGA in endemic areas (eg, northeast and northern central United States).7-9 Concurrent HGA and babesiosis in the absence of Lyme disease also has been documented.7-9 Coinfection generally increases the diversity of presenting symptoms, often obscuring the primary diagnosis. In addition, these patients may have more severe and prolonged illness.8,10,11
In endemic areas, coinfection with B burgdorferi and an additional pathogen should be suspected if a patient presents with typical symptoms of early Lyme disease, especially erythema migrans, along with (1) combination of fever, chills, and headache; (2) prolonged viral-like illness, particularly 48 hours after appropriate antibiotic treatment; and (3) unexplained blood dyscrasia.7,11,12 When a patient presents with erythema migrans, it is unnecessary to test for HGA, as treatment of Lyme disease with doxycycline also is adequate for treating HGA; however, if systemic symptoms persist despite treatment, testing for babesiosis and other tick-borne illnesses should be considered, as babesiosis requires treatment with atovaquone plus azithromycin or clindamycin plus quinine.13
A complete blood count and peripheral blood smear can aid in the diagnosis of coinfection. The complete blood count may reveal leukopenia, anemia, or thrombocytopenia associated with HGA or babesiosis. The peripheral blood smear can reveal inclusions of intra-erythrocytic ring forms and tetrads (the “Maltese cross” appearance) in babesiosis and intragranulocytic morulae in HGA.12 The most sensitive diagnostic tests for tick-borne diseases are organism-specific IgM and IgG serology for Lyme disease, babesiosis, and HGA and polymerase chain reaction for babesiosis and HGA.7
Prevention Strategies
The most effective means of controlling tick-borne disease is avoiding tick bites altogether. One method is to avoid spending time in high-risk areas that may be infested with ticks, particularly low-lying brush, where ticks are likely to hide.14 For individuals traveling in environments with a high risk of tick exposure, behavioral methods of avoidance are indicated, including wearing long pants and a shirt with long sleeves, tucking the shirt into the pants, and wearing closed-toe shoes. Wearing light-colored clothing may aid in tick identification and prompt removal prior to attachment. Permethrin-impregnated clothing has been proven to decrease the likelihood of tick bites in adults working outdoors.15-17
Topical repellents also play a role in the prevention of tick-borne diseases. The most effective and safe synthetic repellents are N,N-diethyl-meta-toluamide (DEET); picaridin; p-menthane-3,8-diol; and insect repellent 3535 (IR3535)(ethyl butylacetylaminopropionate).16-19 Plant-based repellents also are available, but their efficacy is strongly influenced by the surrounding environment (eg, temperature, humidity, organic matter).20-22 Individuals also may be exposed to ticks following contact with domesticated animals and pets.23,24 Tick prevention in pets with the use of ectoparasiticides should be directed by a qualified veterinarian.25
Tick Removal
Following a bite, the tick should be removed promptly to avoid transmission of pathogens. Numerous commercial and in-home methods of tick removal are available, but not all are equally effective. Detachment techniques include removal with a card or commercially available radiofrequency device, lassoing, or freezing.26,27 However, the most effective method is simple removal with tweezers. The tick should be grasped close to the skin surface and pulled upward with an even pressure. Commercially available tick-removal devices have not been shown to produce better outcomes than removal of the tick with tweezers.28
Conclusion
When patients do not respond to therapy for presumed tick-borne infection, the diagnosis should be reconsidered. One important consideration is coinfection with a second organism. Prompt identification and removal of ticks can prevent disease transmission.
- McMichael C, Barnett J, McMichael AJ. An ill wind? climate change, migration, and health. Environ Health Perspect. 2012;120:646-654.
- Ostfeld RS, Brunner JL. Climate change and Ixodes tick-borne diseases of humans. Philos Trans R Soc Lond B Biol Sci. 2015;370:20140051.
- Ogden NH, Bigras-Poulin M, O’Callaghan CJ, et al. Vector seasonality, host infection dynamics and fitness of pathogens transmitted by the tick Ixodes scapularis. Parasitology. 2007;134(pt 2):209-227.
- Tickborne diseases of the United States. Centers for Disease Control and Prevention website. http://www.cdc.gov/ticks/diseases/index.html. Updated July 25, 2017. Accessed April 10, 2018.
- Hinten SR, Beckett GA, Gensheimer KF, et al. Increased recognition of Powassan encephalitis in the United States, 1999-2005. Vector Borne Zoonotic Dis. 2008;8:733-740.
- Platonov AE, Karan LS, Kolyasnikova NM, et al. Humans infected with relapsing fever spirochete Borrelia miyamotoi, Russia. Emerg Infect Dis. 2011;17:1816-1823.
- Krause PJ, McKay K, Thompson CA, et al; Deer-Associated Infection Study Group. Disease-specific diagnosis of coinfecting tickborne zoonoses: babesiosis, human granulocytic ehrlichiosis, and Lyme disease. Clin Infect Dis. 2002;34:1184-1191.
- Krause PJ, Telford SR 3rd, Spielman A, et al. Concurrent Lyme disease and babesiosis. evidence for increased severity and duration of illness. JAMA. 1996;275:1657-1660.
- Belongia EA, Reed KD, Mitchell PD, et al. Clinical and epidemiological features of early Lyme disease and human granulocytic ehrlichiosis in Wisconsin. Clin Infect Dis. 1999;29:1472-1477.
- Sweeny CJ, Ghassemi M, Agger WA, et al. Coinfection with Babesia microti and Borrelia burgdorferi in a western Wisconsin resident. Mayo Clin Proc.1998;73:338-341.
- Nadelman RB, Horowitz HW, Hsieh TC, et al. Simultaneous human granulocytic ehrlichiosis and Lyme borreliosis. N Engl J Med. 1997;337:27-30.
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1089-1134.
- Swanson SJ, Neitzel D, Reed DK, et al. Coinfections acquired from Ixodes ticks. Clin Microbiol Rev. 2006;19:708-727.
- Hayes EB, Piesman J. How can we prevent Lyme disease? N Engl J Med. 2003;348:2424-2430.
- Vaughn MF, Funkhouser SW, Lin FC, et al. Long-lasting permethrin impregnated uniforms: a randomized-controlled trial for tick bite prevention. Am J Prev Med. 2014;46:473-480.
- Miller NJ, Rainone EE, Dyer MC, et al. Tick bite protection with permethrin-treated summer-weight clothing. J Med Entomol. 2011;48:327-333.
- Richards SL, Balanay JAG, Harris JW. Effectiveness of permethrin-treated clothing to prevent tick exposure in foresters in the central Appalachian region of the USA. Int J Environ Health Res. 2015;25:453-462.
- Pages F, Dautel H, Duvallet G, et al. Tick repellents for human use: prevention of tick bites and tick-borne diseases. Vector Borne Zoonotic Dis. 2014;14:85-93.
- Büchel K, Bendin J, Gharbi A, et al. Repellent efficacy of DEET, icaridin, and EBAAP against Ixodes ricinus and Ixodes scapularis nymphs (Acari, Ixodidae). Ticks Tick Borne Dis. 2015;6:494-498.
- Schwantes U, Dautel H, Jung G. Prevention of infectious tick-borne diseases in humans: comparative studies of the repellency of different dodecanoic acid-formulations against Ixodes ricinus ticks (Acari: Ixodidae). Parasit Vectors. 2008;8:1-8.
- Bissinger BW, Apperson CS, Sonenshine DE, et al. Efficacy of the new repellent BioUD against three species of ixodid ticks. Exp Appl Acarol. 2009;48:239-250.
- Feaster JE, Scialdone MA, Todd RG, et al. Dihydronepetalactones deter feeding activity by mosquitoes, stable flies, and deer ticks. J Med Entomol. 2009;46:832-840.
- Jennett AL, Smith FD, Wall R. Tick infestation risk for dogs in a peri-urban park. Parasit Vectors. 2013;6:358.
- Rand PW, Smith RP Jr, Lacombe EH. Canine seroprevalence and the distribution of Ixodes dammini in an area of emerging Lyme disease. Am J Public Health. 1991;81:1331-1334.
- Baneth G, Bourdeau P, Bourdoiseau G, et al; CVBD World Forum. Vector-borne diseases—constant challenge for practicing veterinarians: recommendations from the CVBD World Forum. Parasit Vectors. 2012;5:55.
- Akin Belli A, Dervis E, Kar S, et al. Revisiting detachment techniques in human-biting ticks. J Am Acad Dermatol. 2016;75:393-397.
- Ashique KT, Kaliyadan F. Radiofrequency device for tick removal. J Am Acad Dermatol. 2015;72:155-156.
- Due C, Fox W, Medlock JM, et al. Tick bite prevention and tick removal. BMJ. 2013;347:f7123.
Tick-borne diseases are increasing in prevalence, likely due to climate change in combination with human movement into tick habitats.1-3 The Ixodes genus of hard ticks is a common vector for the transmission of pathogenic viruses, bacteria, parasites, and toxins. Among these, Lyme disease, which is caused by Borrelia burgdorferi, is the most prevalent, followed by babesiosis and human granulocytic anaplasmosis (HGA), respectively.4 In Europe, tick-borne encephalitis is commonly encountered. More recently identified diseases transmitted by Ixodes ticks include Powassan virus and Borrelia miyamotoi infection; however, these diseases are less frequently encountered than other tick-borne diseases.5,6
As tick-borne diseases become more prevalent, the likelihood of coinfection with more than one Ixodes-transmitted pathogen is increasing.7 Therefore, it is important for physicians who practice in endemic areas to be aware of the possibility of coinfection, which can alter clinical presentation, disease severity, and treatment response in tick-borne diseases. Additionally, public education on tick-bite prevention and prompt tick removal is necessary to combat the rising prevalence of these diseases.
Coinfection
Risk of coinfection with more than one tick-borne disease is contingent on the geographic distribution of the tick species as well as the particular pathogen’s prevalence within reservoir hosts in a given area (Figure). Most coinfections occur with B. burgdorferi and an additional pathogen, usually Anaplasma phagocytophilum (which causes human granulocytic anaplasmosis [HGA]) or Babesia microti (which causes babesiosis). In Europe, coinfection with tick-borne encephalitis virus may occur. There is limited evidence of human coinfection with B miyamotoi or Powassan virus, as isolated infection with either of these pathogens is rare.
In patients with Lyme disease, as many as 35% may have concurrent babesiosis, and as many as 12% may have concurrent HGA in endemic areas (eg, northeast and northern central United States).7-9 Concurrent HGA and babesiosis in the absence of Lyme disease also has been documented.7-9 Coinfection generally increases the diversity of presenting symptoms, often obscuring the primary diagnosis. In addition, these patients may have more severe and prolonged illness.8,10,11
In endemic areas, coinfection with B burgdorferi and an additional pathogen should be suspected if a patient presents with typical symptoms of early Lyme disease, especially erythema migrans, along with (1) combination of fever, chills, and headache; (2) prolonged viral-like illness, particularly 48 hours after appropriate antibiotic treatment; and (3) unexplained blood dyscrasia.7,11,12 When a patient presents with erythema migrans, it is unnecessary to test for HGA, as treatment of Lyme disease with doxycycline also is adequate for treating HGA; however, if systemic symptoms persist despite treatment, testing for babesiosis and other tick-borne illnesses should be considered, as babesiosis requires treatment with atovaquone plus azithromycin or clindamycin plus quinine.13
A complete blood count and peripheral blood smear can aid in the diagnosis of coinfection. The complete blood count may reveal leukopenia, anemia, or thrombocytopenia associated with HGA or babesiosis. The peripheral blood smear can reveal inclusions of intra-erythrocytic ring forms and tetrads (the “Maltese cross” appearance) in babesiosis and intragranulocytic morulae in HGA.12 The most sensitive diagnostic tests for tick-borne diseases are organism-specific IgM and IgG serology for Lyme disease, babesiosis, and HGA and polymerase chain reaction for babesiosis and HGA.7
Prevention Strategies
The most effective means of controlling tick-borne disease is avoiding tick bites altogether. One method is to avoid spending time in high-risk areas that may be infested with ticks, particularly low-lying brush, where ticks are likely to hide.14 For individuals traveling in environments with a high risk of tick exposure, behavioral methods of avoidance are indicated, including wearing long pants and a shirt with long sleeves, tucking the shirt into the pants, and wearing closed-toe shoes. Wearing light-colored clothing may aid in tick identification and prompt removal prior to attachment. Permethrin-impregnated clothing has been proven to decrease the likelihood of tick bites in adults working outdoors.15-17
Topical repellents also play a role in the prevention of tick-borne diseases. The most effective and safe synthetic repellents are N,N-diethyl-meta-toluamide (DEET); picaridin; p-menthane-3,8-diol; and insect repellent 3535 (IR3535)(ethyl butylacetylaminopropionate).16-19 Plant-based repellents also are available, but their efficacy is strongly influenced by the surrounding environment (eg, temperature, humidity, organic matter).20-22 Individuals also may be exposed to ticks following contact with domesticated animals and pets.23,24 Tick prevention in pets with the use of ectoparasiticides should be directed by a qualified veterinarian.25
Tick Removal
Following a bite, the tick should be removed promptly to avoid transmission of pathogens. Numerous commercial and in-home methods of tick removal are available, but not all are equally effective. Detachment techniques include removal with a card or commercially available radiofrequency device, lassoing, or freezing.26,27 However, the most effective method is simple removal with tweezers. The tick should be grasped close to the skin surface and pulled upward with an even pressure. Commercially available tick-removal devices have not been shown to produce better outcomes than removal of the tick with tweezers.28
Conclusion
When patients do not respond to therapy for presumed tick-borne infection, the diagnosis should be reconsidered. One important consideration is coinfection with a second organism. Prompt identification and removal of ticks can prevent disease transmission.
Tick-borne diseases are increasing in prevalence, likely due to climate change in combination with human movement into tick habitats.1-3 The Ixodes genus of hard ticks is a common vector for the transmission of pathogenic viruses, bacteria, parasites, and toxins. Among these, Lyme disease, which is caused by Borrelia burgdorferi, is the most prevalent, followed by babesiosis and human granulocytic anaplasmosis (HGA), respectively.4 In Europe, tick-borne encephalitis is commonly encountered. More recently identified diseases transmitted by Ixodes ticks include Powassan virus and Borrelia miyamotoi infection; however, these diseases are less frequently encountered than other tick-borne diseases.5,6
As tick-borne diseases become more prevalent, the likelihood of coinfection with more than one Ixodes-transmitted pathogen is increasing.7 Therefore, it is important for physicians who practice in endemic areas to be aware of the possibility of coinfection, which can alter clinical presentation, disease severity, and treatment response in tick-borne diseases. Additionally, public education on tick-bite prevention and prompt tick removal is necessary to combat the rising prevalence of these diseases.
Coinfection
Risk of coinfection with more than one tick-borne disease is contingent on the geographic distribution of the tick species as well as the particular pathogen’s prevalence within reservoir hosts in a given area (Figure). Most coinfections occur with B. burgdorferi and an additional pathogen, usually Anaplasma phagocytophilum (which causes human granulocytic anaplasmosis [HGA]) or Babesia microti (which causes babesiosis). In Europe, coinfection with tick-borne encephalitis virus may occur. There is limited evidence of human coinfection with B miyamotoi or Powassan virus, as isolated infection with either of these pathogens is rare.
In patients with Lyme disease, as many as 35% may have concurrent babesiosis, and as many as 12% may have concurrent HGA in endemic areas (eg, northeast and northern central United States).7-9 Concurrent HGA and babesiosis in the absence of Lyme disease also has been documented.7-9 Coinfection generally increases the diversity of presenting symptoms, often obscuring the primary diagnosis. In addition, these patients may have more severe and prolonged illness.8,10,11
In endemic areas, coinfection with B burgdorferi and an additional pathogen should be suspected if a patient presents with typical symptoms of early Lyme disease, especially erythema migrans, along with (1) combination of fever, chills, and headache; (2) prolonged viral-like illness, particularly 48 hours after appropriate antibiotic treatment; and (3) unexplained blood dyscrasia.7,11,12 When a patient presents with erythema migrans, it is unnecessary to test for HGA, as treatment of Lyme disease with doxycycline also is adequate for treating HGA; however, if systemic symptoms persist despite treatment, testing for babesiosis and other tick-borne illnesses should be considered, as babesiosis requires treatment with atovaquone plus azithromycin or clindamycin plus quinine.13
A complete blood count and peripheral blood smear can aid in the diagnosis of coinfection. The complete blood count may reveal leukopenia, anemia, or thrombocytopenia associated with HGA or babesiosis. The peripheral blood smear can reveal inclusions of intra-erythrocytic ring forms and tetrads (the “Maltese cross” appearance) in babesiosis and intragranulocytic morulae in HGA.12 The most sensitive diagnostic tests for tick-borne diseases are organism-specific IgM and IgG serology for Lyme disease, babesiosis, and HGA and polymerase chain reaction for babesiosis and HGA.7
Prevention Strategies
The most effective means of controlling tick-borne disease is avoiding tick bites altogether. One method is to avoid spending time in high-risk areas that may be infested with ticks, particularly low-lying brush, where ticks are likely to hide.14 For individuals traveling in environments with a high risk of tick exposure, behavioral methods of avoidance are indicated, including wearing long pants and a shirt with long sleeves, tucking the shirt into the pants, and wearing closed-toe shoes. Wearing light-colored clothing may aid in tick identification and prompt removal prior to attachment. Permethrin-impregnated clothing has been proven to decrease the likelihood of tick bites in adults working outdoors.15-17
Topical repellents also play a role in the prevention of tick-borne diseases. The most effective and safe synthetic repellents are N,N-diethyl-meta-toluamide (DEET); picaridin; p-menthane-3,8-diol; and insect repellent 3535 (IR3535)(ethyl butylacetylaminopropionate).16-19 Plant-based repellents also are available, but their efficacy is strongly influenced by the surrounding environment (eg, temperature, humidity, organic matter).20-22 Individuals also may be exposed to ticks following contact with domesticated animals and pets.23,24 Tick prevention in pets with the use of ectoparasiticides should be directed by a qualified veterinarian.25
Tick Removal
Following a bite, the tick should be removed promptly to avoid transmission of pathogens. Numerous commercial and in-home methods of tick removal are available, but not all are equally effective. Detachment techniques include removal with a card or commercially available radiofrequency device, lassoing, or freezing.26,27 However, the most effective method is simple removal with tweezers. The tick should be grasped close to the skin surface and pulled upward with an even pressure. Commercially available tick-removal devices have not been shown to produce better outcomes than removal of the tick with tweezers.28
Conclusion
When patients do not respond to therapy for presumed tick-borne infection, the diagnosis should be reconsidered. One important consideration is coinfection with a second organism. Prompt identification and removal of ticks can prevent disease transmission.
- McMichael C, Barnett J, McMichael AJ. An ill wind? climate change, migration, and health. Environ Health Perspect. 2012;120:646-654.
- Ostfeld RS, Brunner JL. Climate change and Ixodes tick-borne diseases of humans. Philos Trans R Soc Lond B Biol Sci. 2015;370:20140051.
- Ogden NH, Bigras-Poulin M, O’Callaghan CJ, et al. Vector seasonality, host infection dynamics and fitness of pathogens transmitted by the tick Ixodes scapularis. Parasitology. 2007;134(pt 2):209-227.
- Tickborne diseases of the United States. Centers for Disease Control and Prevention website. http://www.cdc.gov/ticks/diseases/index.html. Updated July 25, 2017. Accessed April 10, 2018.
- Hinten SR, Beckett GA, Gensheimer KF, et al. Increased recognition of Powassan encephalitis in the United States, 1999-2005. Vector Borne Zoonotic Dis. 2008;8:733-740.
- Platonov AE, Karan LS, Kolyasnikova NM, et al. Humans infected with relapsing fever spirochete Borrelia miyamotoi, Russia. Emerg Infect Dis. 2011;17:1816-1823.
- Krause PJ, McKay K, Thompson CA, et al; Deer-Associated Infection Study Group. Disease-specific diagnosis of coinfecting tickborne zoonoses: babesiosis, human granulocytic ehrlichiosis, and Lyme disease. Clin Infect Dis. 2002;34:1184-1191.
- Krause PJ, Telford SR 3rd, Spielman A, et al. Concurrent Lyme disease and babesiosis. evidence for increased severity and duration of illness. JAMA. 1996;275:1657-1660.
- Belongia EA, Reed KD, Mitchell PD, et al. Clinical and epidemiological features of early Lyme disease and human granulocytic ehrlichiosis in Wisconsin. Clin Infect Dis. 1999;29:1472-1477.
- Sweeny CJ, Ghassemi M, Agger WA, et al. Coinfection with Babesia microti and Borrelia burgdorferi in a western Wisconsin resident. Mayo Clin Proc.1998;73:338-341.
- Nadelman RB, Horowitz HW, Hsieh TC, et al. Simultaneous human granulocytic ehrlichiosis and Lyme borreliosis. N Engl J Med. 1997;337:27-30.
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1089-1134.
- Swanson SJ, Neitzel D, Reed DK, et al. Coinfections acquired from Ixodes ticks. Clin Microbiol Rev. 2006;19:708-727.
- Hayes EB, Piesman J. How can we prevent Lyme disease? N Engl J Med. 2003;348:2424-2430.
- Vaughn MF, Funkhouser SW, Lin FC, et al. Long-lasting permethrin impregnated uniforms: a randomized-controlled trial for tick bite prevention. Am J Prev Med. 2014;46:473-480.
- Miller NJ, Rainone EE, Dyer MC, et al. Tick bite protection with permethrin-treated summer-weight clothing. J Med Entomol. 2011;48:327-333.
- Richards SL, Balanay JAG, Harris JW. Effectiveness of permethrin-treated clothing to prevent tick exposure in foresters in the central Appalachian region of the USA. Int J Environ Health Res. 2015;25:453-462.
- Pages F, Dautel H, Duvallet G, et al. Tick repellents for human use: prevention of tick bites and tick-borne diseases. Vector Borne Zoonotic Dis. 2014;14:85-93.
- Büchel K, Bendin J, Gharbi A, et al. Repellent efficacy of DEET, icaridin, and EBAAP against Ixodes ricinus and Ixodes scapularis nymphs (Acari, Ixodidae). Ticks Tick Borne Dis. 2015;6:494-498.
- Schwantes U, Dautel H, Jung G. Prevention of infectious tick-borne diseases in humans: comparative studies of the repellency of different dodecanoic acid-formulations against Ixodes ricinus ticks (Acari: Ixodidae). Parasit Vectors. 2008;8:1-8.
- Bissinger BW, Apperson CS, Sonenshine DE, et al. Efficacy of the new repellent BioUD against three species of ixodid ticks. Exp Appl Acarol. 2009;48:239-250.
- Feaster JE, Scialdone MA, Todd RG, et al. Dihydronepetalactones deter feeding activity by mosquitoes, stable flies, and deer ticks. J Med Entomol. 2009;46:832-840.
- Jennett AL, Smith FD, Wall R. Tick infestation risk for dogs in a peri-urban park. Parasit Vectors. 2013;6:358.
- Rand PW, Smith RP Jr, Lacombe EH. Canine seroprevalence and the distribution of Ixodes dammini in an area of emerging Lyme disease. Am J Public Health. 1991;81:1331-1334.
- Baneth G, Bourdeau P, Bourdoiseau G, et al; CVBD World Forum. Vector-borne diseases—constant challenge for practicing veterinarians: recommendations from the CVBD World Forum. Parasit Vectors. 2012;5:55.
- Akin Belli A, Dervis E, Kar S, et al. Revisiting detachment techniques in human-biting ticks. J Am Acad Dermatol. 2016;75:393-397.
- Ashique KT, Kaliyadan F. Radiofrequency device for tick removal. J Am Acad Dermatol. 2015;72:155-156.
- Due C, Fox W, Medlock JM, et al. Tick bite prevention and tick removal. BMJ. 2013;347:f7123.
- McMichael C, Barnett J, McMichael AJ. An ill wind? climate change, migration, and health. Environ Health Perspect. 2012;120:646-654.
- Ostfeld RS, Brunner JL. Climate change and Ixodes tick-borne diseases of humans. Philos Trans R Soc Lond B Biol Sci. 2015;370:20140051.
- Ogden NH, Bigras-Poulin M, O’Callaghan CJ, et al. Vector seasonality, host infection dynamics and fitness of pathogens transmitted by the tick Ixodes scapularis. Parasitology. 2007;134(pt 2):209-227.
- Tickborne diseases of the United States. Centers for Disease Control and Prevention website. http://www.cdc.gov/ticks/diseases/index.html. Updated July 25, 2017. Accessed April 10, 2018.
- Hinten SR, Beckett GA, Gensheimer KF, et al. Increased recognition of Powassan encephalitis in the United States, 1999-2005. Vector Borne Zoonotic Dis. 2008;8:733-740.
- Platonov AE, Karan LS, Kolyasnikova NM, et al. Humans infected with relapsing fever spirochete Borrelia miyamotoi, Russia. Emerg Infect Dis. 2011;17:1816-1823.
- Krause PJ, McKay K, Thompson CA, et al; Deer-Associated Infection Study Group. Disease-specific diagnosis of coinfecting tickborne zoonoses: babesiosis, human granulocytic ehrlichiosis, and Lyme disease. Clin Infect Dis. 2002;34:1184-1191.
- Krause PJ, Telford SR 3rd, Spielman A, et al. Concurrent Lyme disease and babesiosis. evidence for increased severity and duration of illness. JAMA. 1996;275:1657-1660.
- Belongia EA, Reed KD, Mitchell PD, et al. Clinical and epidemiological features of early Lyme disease and human granulocytic ehrlichiosis in Wisconsin. Clin Infect Dis. 1999;29:1472-1477.
- Sweeny CJ, Ghassemi M, Agger WA, et al. Coinfection with Babesia microti and Borrelia burgdorferi in a western Wisconsin resident. Mayo Clin Proc.1998;73:338-341.
- Nadelman RB, Horowitz HW, Hsieh TC, et al. Simultaneous human granulocytic ehrlichiosis and Lyme borreliosis. N Engl J Med. 1997;337:27-30.
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1089-1134.
- Swanson SJ, Neitzel D, Reed DK, et al. Coinfections acquired from Ixodes ticks. Clin Microbiol Rev. 2006;19:708-727.
- Hayes EB, Piesman J. How can we prevent Lyme disease? N Engl J Med. 2003;348:2424-2430.
- Vaughn MF, Funkhouser SW, Lin FC, et al. Long-lasting permethrin impregnated uniforms: a randomized-controlled trial for tick bite prevention. Am J Prev Med. 2014;46:473-480.
- Miller NJ, Rainone EE, Dyer MC, et al. Tick bite protection with permethrin-treated summer-weight clothing. J Med Entomol. 2011;48:327-333.
- Richards SL, Balanay JAG, Harris JW. Effectiveness of permethrin-treated clothing to prevent tick exposure in foresters in the central Appalachian region of the USA. Int J Environ Health Res. 2015;25:453-462.
- Pages F, Dautel H, Duvallet G, et al. Tick repellents for human use: prevention of tick bites and tick-borne diseases. Vector Borne Zoonotic Dis. 2014;14:85-93.
- Büchel K, Bendin J, Gharbi A, et al. Repellent efficacy of DEET, icaridin, and EBAAP against Ixodes ricinus and Ixodes scapularis nymphs (Acari, Ixodidae). Ticks Tick Borne Dis. 2015;6:494-498.
- Schwantes U, Dautel H, Jung G. Prevention of infectious tick-borne diseases in humans: comparative studies of the repellency of different dodecanoic acid-formulations against Ixodes ricinus ticks (Acari: Ixodidae). Parasit Vectors. 2008;8:1-8.
- Bissinger BW, Apperson CS, Sonenshine DE, et al. Efficacy of the new repellent BioUD against three species of ixodid ticks. Exp Appl Acarol. 2009;48:239-250.
- Feaster JE, Scialdone MA, Todd RG, et al. Dihydronepetalactones deter feeding activity by mosquitoes, stable flies, and deer ticks. J Med Entomol. 2009;46:832-840.
- Jennett AL, Smith FD, Wall R. Tick infestation risk for dogs in a peri-urban park. Parasit Vectors. 2013;6:358.
- Rand PW, Smith RP Jr, Lacombe EH. Canine seroprevalence and the distribution of Ixodes dammini in an area of emerging Lyme disease. Am J Public Health. 1991;81:1331-1334.
- Baneth G, Bourdeau P, Bourdoiseau G, et al; CVBD World Forum. Vector-borne diseases—constant challenge for practicing veterinarians: recommendations from the CVBD World Forum. Parasit Vectors. 2012;5:55.
- Akin Belli A, Dervis E, Kar S, et al. Revisiting detachment techniques in human-biting ticks. J Am Acad Dermatol. 2016;75:393-397.
- Ashique KT, Kaliyadan F. Radiofrequency device for tick removal. J Am Acad Dermatol. 2015;72:155-156.
- Due C, Fox W, Medlock JM, et al. Tick bite prevention and tick removal. BMJ. 2013;347:f7123.
Practice Points
- As tick-borne diseases become more prevalent, the likelihood of coinfection with more than one Ixodes-transmitted pathogen is increasing, particularly in endemic areas.
- Coinfection generally increases the diversity of presenting symptoms, obscuring the primary diagnosis. The disease course also may be prolonged and more severe.
- Prevention of tick attachment and prompt tick removal are critical to combating the rising prevalence of tick-borne diseases.