User login
Romosozumab reduces fracture risk out to 36 months, with no signs of cardiovascular problems
DENVER – in an extended analysis of the FRAME study.
The combination had already proven effective at 12 months and 24 months (N Engl J Med. 2016 Oct 20;375[16]:1532-43).
Romosozumab binds sclerostin, leading to both increased bone formation and decreased bone resorption, though its activity favors formation, leading it to be classified as an anabolic agent. Denosumab is an antibody that targets receptor-activated nuclear factor–kappaB ligand (RANKL), interfering with osteoclast formation and the accompanied breakdown of bone.
In the FRAME study, women aged 55-90 years with a T score of –2.5 or less in the total hip or femoral neck received romosozumab or placebo for 12 months, and then all patients were switched to denosumab at 12 months to 24 months. At 24 months, women who initially received romosozumab had a 75% relative risk reduction in new vertebral fractures and a 33% reduction in clinical fractures, compared with those who began with placebo, Dr. Lewiecki said at the annual meeting of the American Society for Bone and Mineral Research.
Of 7,180 women initially enrolled, 5,743 (80%) completed the study out to 36 months, when women who initially received 12 months of romosozumab had lower rates of new vertebral fractures than did the placebo group (1.0% vs. 2.8%; P less than .001), clinical fractures (4.0% vs. 5.5%; P = .004), and nonvertebral fractures (3.9% vs. 4.9%; P = .039).
Bone mineral density also continued to improve at month 36, with an increase of 18.1% in the lumbar spine and 9.4% in the total hip in the romosozumab group, compared with 7.5% and 4.2%, respectively, in the group that initially received placebo.
Both the placebo and romosozumab groups had similar rates of adverse events. At month 24, there were two cases of osteonecrosis of the jaw and one case of atypical femoral fracture. No new cases of either condition were observed in months 24-36.
Notably, there was no difference in risk for cardiovascular disease, with rates of 3.6% in the romosozumab patients and 3.5% in the placebo patients at 36 months. The development of romosozumab ran into a snag earlier this year when researchers found an increased risk of cardiovascular disease in the romosozumab arm of the ARCH study, in which patients received either romosozumab or alendronate for the first 12 months and then switched to alendronate (N Engl J Med. 2017 Sep 11. doi: 10.1056/NEJMoa1708322). At the end of the first year, patients in the romosozumab group had a higher rate of cardiovascular events (2.5% vs. 1.9%). That finding led the Food and Drug Administration to reject the application. Amgen and UCB are refiling in hopes of a 2018 approval.
As to romosozumab’s place in a treatment landscape that already includes teriparatide and abaloparatide, Dr. Lewiecki said, “I think it will depend on the product label. It’s not a self-administered subcutaneous injection like teriparatide and abaloparatide: The patient would present to a doctor’s office once a month for a year to get an injection – and that may be preferable to some patients,” he said.
The study was sponsored by Amgen and UCB. Dr. Lewiecki has consulted for Amgen.
DENVER – in an extended analysis of the FRAME study.
The combination had already proven effective at 12 months and 24 months (N Engl J Med. 2016 Oct 20;375[16]:1532-43).
Romosozumab binds sclerostin, leading to both increased bone formation and decreased bone resorption, though its activity favors formation, leading it to be classified as an anabolic agent. Denosumab is an antibody that targets receptor-activated nuclear factor–kappaB ligand (RANKL), interfering with osteoclast formation and the accompanied breakdown of bone.
In the FRAME study, women aged 55-90 years with a T score of –2.5 or less in the total hip or femoral neck received romosozumab or placebo for 12 months, and then all patients were switched to denosumab at 12 months to 24 months. At 24 months, women who initially received romosozumab had a 75% relative risk reduction in new vertebral fractures and a 33% reduction in clinical fractures, compared with those who began with placebo, Dr. Lewiecki said at the annual meeting of the American Society for Bone and Mineral Research.
Of 7,180 women initially enrolled, 5,743 (80%) completed the study out to 36 months, when women who initially received 12 months of romosozumab had lower rates of new vertebral fractures than did the placebo group (1.0% vs. 2.8%; P less than .001), clinical fractures (4.0% vs. 5.5%; P = .004), and nonvertebral fractures (3.9% vs. 4.9%; P = .039).
Bone mineral density also continued to improve at month 36, with an increase of 18.1% in the lumbar spine and 9.4% in the total hip in the romosozumab group, compared with 7.5% and 4.2%, respectively, in the group that initially received placebo.
Both the placebo and romosozumab groups had similar rates of adverse events. At month 24, there were two cases of osteonecrosis of the jaw and one case of atypical femoral fracture. No new cases of either condition were observed in months 24-36.
Notably, there was no difference in risk for cardiovascular disease, with rates of 3.6% in the romosozumab patients and 3.5% in the placebo patients at 36 months. The development of romosozumab ran into a snag earlier this year when researchers found an increased risk of cardiovascular disease in the romosozumab arm of the ARCH study, in which patients received either romosozumab or alendronate for the first 12 months and then switched to alendronate (N Engl J Med. 2017 Sep 11. doi: 10.1056/NEJMoa1708322). At the end of the first year, patients in the romosozumab group had a higher rate of cardiovascular events (2.5% vs. 1.9%). That finding led the Food and Drug Administration to reject the application. Amgen and UCB are refiling in hopes of a 2018 approval.
As to romosozumab’s place in a treatment landscape that already includes teriparatide and abaloparatide, Dr. Lewiecki said, “I think it will depend on the product label. It’s not a self-administered subcutaneous injection like teriparatide and abaloparatide: The patient would present to a doctor’s office once a month for a year to get an injection – and that may be preferable to some patients,” he said.
The study was sponsored by Amgen and UCB. Dr. Lewiecki has consulted for Amgen.
DENVER – in an extended analysis of the FRAME study.
The combination had already proven effective at 12 months and 24 months (N Engl J Med. 2016 Oct 20;375[16]:1532-43).
Romosozumab binds sclerostin, leading to both increased bone formation and decreased bone resorption, though its activity favors formation, leading it to be classified as an anabolic agent. Denosumab is an antibody that targets receptor-activated nuclear factor–kappaB ligand (RANKL), interfering with osteoclast formation and the accompanied breakdown of bone.
In the FRAME study, women aged 55-90 years with a T score of –2.5 or less in the total hip or femoral neck received romosozumab or placebo for 12 months, and then all patients were switched to denosumab at 12 months to 24 months. At 24 months, women who initially received romosozumab had a 75% relative risk reduction in new vertebral fractures and a 33% reduction in clinical fractures, compared with those who began with placebo, Dr. Lewiecki said at the annual meeting of the American Society for Bone and Mineral Research.
Of 7,180 women initially enrolled, 5,743 (80%) completed the study out to 36 months, when women who initially received 12 months of romosozumab had lower rates of new vertebral fractures than did the placebo group (1.0% vs. 2.8%; P less than .001), clinical fractures (4.0% vs. 5.5%; P = .004), and nonvertebral fractures (3.9% vs. 4.9%; P = .039).
Bone mineral density also continued to improve at month 36, with an increase of 18.1% in the lumbar spine and 9.4% in the total hip in the romosozumab group, compared with 7.5% and 4.2%, respectively, in the group that initially received placebo.
Both the placebo and romosozumab groups had similar rates of adverse events. At month 24, there were two cases of osteonecrosis of the jaw and one case of atypical femoral fracture. No new cases of either condition were observed in months 24-36.
Notably, there was no difference in risk for cardiovascular disease, with rates of 3.6% in the romosozumab patients and 3.5% in the placebo patients at 36 months. The development of romosozumab ran into a snag earlier this year when researchers found an increased risk of cardiovascular disease in the romosozumab arm of the ARCH study, in which patients received either romosozumab or alendronate for the first 12 months and then switched to alendronate (N Engl J Med. 2017 Sep 11. doi: 10.1056/NEJMoa1708322). At the end of the first year, patients in the romosozumab group had a higher rate of cardiovascular events (2.5% vs. 1.9%). That finding led the Food and Drug Administration to reject the application. Amgen and UCB are refiling in hopes of a 2018 approval.
As to romosozumab’s place in a treatment landscape that already includes teriparatide and abaloparatide, Dr. Lewiecki said, “I think it will depend on the product label. It’s not a self-administered subcutaneous injection like teriparatide and abaloparatide: The patient would present to a doctor’s office once a month for a year to get an injection – and that may be preferable to some patients,” he said.
The study was sponsored by Amgen and UCB. Dr. Lewiecki has consulted for Amgen.
AT ASBMR
Key clinical point: Romosozumab followed by denosumab significantly reduced fracture risk, compared with placebo followed by denosumab.
Major finding: 1.0% of patients on romosozumab had new vertebral fractures, compared with 2.8% of those in the placebo group.
Data source: A randomized, controlled trial of 7,180 postmenopausal women with osteoporosis.
Disclosures: The study was sponsored by Amgen and UCB. Dr. Lewiecki has consulted for Amgen.
How to Interpret the Results of Clinical Trials
BOSTON—The interpretation of clinical trial results can stray from the data in many ways. Creating spin (ie, stressing an experimental treatment’s advantages) may or may not be the intention of the researchers or of people who write press releases, but clinicians evaluating the results should not be distracted from the key characteristics of a meaningful trial. They can use several strategies to keep the facts in focus, according to a researcher.
“Here are some words that should put you on alert: ‘revolutionary,’ ‘groundbreaking,’ and ‘first-line.’ It is time to be cautious when you are hearing the spin and the results at the same time,” said Elizabeth W. Loder, MD, MPH, Professor of Neurology at Harvard Medical School in Boston. At the 59th Annual Scientific Meeting of the American Headache Society, Dr. Loder spoke about migraine prevention trials, but she allowed that her remarks are relevant to any clinical trial. 
Guidelines Aim to Increase Objectivity
The potential for overinterpretation, misinterpretation, or misleading interpretation of trial results was reduced greatly in 2005. At that time, the International Committee of Medical Journal Editors agreed that trials accepted for publication should first be registered and have their methodology defined before study initiation. Establishing the trial design and primary end points in advance makes selective reporting and data manipulation more difficult. The approach, however, does not eliminate the potential for spin, said Dr. Loder. “The trial registrations on sites like ClinicalTrials.gov are easy to find, and it is worth looking back to compare what was registered to what was reported. There can be some surprises,” Dr. Loder explained.
One potential surprise may be a discrepancy between the prespecified outcomes and the outcomes that the researchers stress at the conclusion of the study. The peer-review process of a high-quality journal limits claims based on secondary outcomes, but press releases do not have similar constraints. In addition, favorable reporting on outcomes that did not appear in the trial registration should arouse suspicion. “It is fair to include data on outcomes that were not prespecified, but they should be flagged. These are hypothesis-generating and should not be given the same weight as those prespecified,” Dr. Loder explained.
Guidelines to improve the objectivity of data gathered and reported for trials are growing increasingly rigorous, according to Dr. Loder. For headache prevention trials, the International Headache Society has issued specific recommendations about trial conduct and the measurement of end points. Although Dr. Loder conceded that strict constraints may make reports of trial results formulaic or tedious, the consistency of the formula, which progresses from an introduction through methods, results, discussion, and conclusions, makes the findings easier to interpret and to place into context.
Data Should Guide Interpretation of Results
A paper’s discussion section may cloud the reader’s understanding of the trial’s findings, Dr. Loder cautioned. In a properly reported study, the results section confines itself to the facts. In the discussion section, interpretation of the facts varies with perspective, according to Dr. Loder. The authors’ perception of relative benefit following a favorable outcome or of the burden of an adverse event is subjective. The potential for intentional or unintentional spin is substantial.
“Examples of spin include focusing on an outcome [that] the trial was not designed to study, focusing on subgroups rather than [on] the overall population, and downplaying adverse safety data,” explained Dr. Loder. Dr. Loder cited several studies that compared reader reaction to abstracts with and without spin. The studies showed that spin was persuasive. Moreover, Dr. Loder noted that spin in abstracts is typically passed on in press releases, news stories, and other accounts of the studies.
One strategy for remaining circumspect about new data is to consult one of many watchdog organizations that monitor clinical data and evaluate data collection and analysis. One such organization is HealthNewsReview.org, which has an editorial team that routinely critiques claims made about drugs, devices, vitamins, and surgical procedures. According to Dr. Loder, the website has examined migraine therapies and provided a perspective that was fully independent of the trials’ sponsors, their authors, and sometimes of the prevailing view.
Pure objectivity may not be appealing for those who want to draw attention to their research, and spin is hard to resist in the desire to develop an engaging narrative. Whether or not those who focus on the most favorable findings of a trial are conscious of their disservice to scientific inquiry, spin has been found repeatedly in systematic reviews of study data. Dr. Loder cited one study that found spin in 47% of 498 press releases on scientific articles.
“There were various types of spin, but 19% of the press releases failed to acknowledge that the primary end point was not statistically significant,” Dr. Loder noted. When abstracts that provided the basis for the press releases were analyzed, 40% were found to contain spin.
The Value of Common Sense
Randomized controlled trials are considered the gold standard for objectively evaluating most treatment strategies, but Dr. Loder cautioned that this design by itself is not enough to ensure reproducible results. The results of the study should include not only how many patients were randomized, but also how many patients received treatment and how many were followed to the trial’s end. Low enrollment or high dropout rates are red flags. These problems can be detected by critical thinking.
“There really is no substitute for common sense,” Dr. Loder said. She suggested that studies that include all of the standard points of discussion, such as the generalizability of results, the limitations of the design, the statistical significance of the findings, and a fair interpretation of benefits and hazards, establish credibility and are generally recognizable with a discerning eye.
“For clinicians considering how to interpret results, one question to ask is whether the patients enrolled are representative of the ones that are in front of you,” Dr. Loder suggested.
A critical view of new data helps to avoid the fads that some critics have observed in the treatment of headaches and in clinical medicine overall. Typically, excessive enthusiasm about positive trial results is followed by a period of disillusionment until clinicians finally arrive at a realistic perspective of the strengths and weaknesses of a new therapeutic option. Warning of a coming brace of headache trial results, which will include studies of devices, apps, and new drugs, Dr. Loder urged clinicians to read the studies rather than the press releases, applying the criteria that define a well designed and fairly reported trial.
—Theodore Bosworth
Suggested Reading
Tfelt-Hansen P, Pascual J, Ramadan N, et al. Guidelines for controlled trials of drugs in migraine: third edition. A guide for investigators. Cephalalgia. 2012;32(1):6-38.
Yavchitz A, Boutron I, Bafeta A, et al. Misrepresentation of randomized controlled trials in press releases and news coverage: a cohort study. PLoS Med. 2012;9(9):e1001308.
BOSTON—The interpretation of clinical trial results can stray from the data in many ways. Creating spin (ie, stressing an experimental treatment’s advantages) may or may not be the intention of the researchers or of people who write press releases, but clinicians evaluating the results should not be distracted from the key characteristics of a meaningful trial. They can use several strategies to keep the facts in focus, according to a researcher.
“Here are some words that should put you on alert: ‘revolutionary,’ ‘groundbreaking,’ and ‘first-line.’ It is time to be cautious when you are hearing the spin and the results at the same time,” said Elizabeth W. Loder, MD, MPH, Professor of Neurology at Harvard Medical School in Boston. At the 59th Annual Scientific Meeting of the American Headache Society, Dr. Loder spoke about migraine prevention trials, but she allowed that her remarks are relevant to any clinical trial.
Guidelines Aim to Increase Objectivity
The potential for overinterpretation, misinterpretation, or misleading interpretation of trial results was reduced greatly in 2005. At that time, the International Committee of Medical Journal Editors agreed that trials accepted for publication should first be registered and have their methodology defined before study initiation. Establishing the trial design and primary end points in advance makes selective reporting and data manipulation more difficult. The approach, however, does not eliminate the potential for spin, said Dr. Loder. “The trial registrations on sites like ClinicalTrials.gov are easy to find, and it is worth looking back to compare what was registered to what was reported. There can be some surprises,” Dr. Loder explained.
One potential surprise may be a discrepancy between the prespecified outcomes and the outcomes that the researchers stress at the conclusion of the study. The peer-review process of a high-quality journal limits claims based on secondary outcomes, but press releases do not have similar constraints. In addition, favorable reporting on outcomes that did not appear in the trial registration should arouse suspicion. “It is fair to include data on outcomes that were not prespecified, but they should be flagged. These are hypothesis-generating and should not be given the same weight as those prespecified,” Dr. Loder explained.
Guidelines to improve the objectivity of data gathered and reported for trials are growing increasingly rigorous, according to Dr. Loder. For headache prevention trials, the International Headache Society has issued specific recommendations about trial conduct and the measurement of end points. Although Dr. Loder conceded that strict constraints may make reports of trial results formulaic or tedious, the consistency of the formula, which progresses from an introduction through methods, results, discussion, and conclusions, makes the findings easier to interpret and to place into context.
Data Should Guide Interpretation of Results
A paper’s discussion section may cloud the reader’s understanding of the trial’s findings, Dr. Loder cautioned. In a properly reported study, the results section confines itself to the facts. In the discussion section, interpretation of the facts varies with perspective, according to Dr. Loder. The authors’ perception of relative benefit following a favorable outcome or of the burden of an adverse event is subjective. The potential for intentional or unintentional spin is substantial.
“Examples of spin include focusing on an outcome [that] the trial was not designed to study, focusing on subgroups rather than [on] the overall population, and downplaying adverse safety data,” explained Dr. Loder. Dr. Loder cited several studies that compared reader reaction to abstracts with and without spin. The studies showed that spin was persuasive. Moreover, Dr. Loder noted that spin in abstracts is typically passed on in press releases, news stories, and other accounts of the studies.
One strategy for remaining circumspect about new data is to consult one of many watchdog organizations that monitor clinical data and evaluate data collection and analysis. One such organization is HealthNewsReview.org, which has an editorial team that routinely critiques claims made about drugs, devices, vitamins, and surgical procedures. According to Dr. Loder, the website has examined migraine therapies and provided a perspective that was fully independent of the trials’ sponsors, their authors, and sometimes of the prevailing view.
Pure objectivity may not be appealing for those who want to draw attention to their research, and spin is hard to resist in the desire to develop an engaging narrative. Whether or not those who focus on the most favorable findings of a trial are conscious of their disservice to scientific inquiry, spin has been found repeatedly in systematic reviews of study data. Dr. Loder cited one study that found spin in 47% of 498 press releases on scientific articles.
“There were various types of spin, but 19% of the press releases failed to acknowledge that the primary end point was not statistically significant,” Dr. Loder noted. When abstracts that provided the basis for the press releases were analyzed, 40% were found to contain spin.
The Value of Common Sense
Randomized controlled trials are considered the gold standard for objectively evaluating most treatment strategies, but Dr. Loder cautioned that this design by itself is not enough to ensure reproducible results. The results of the study should include not only how many patients were randomized, but also how many patients received treatment and how many were followed to the trial’s end. Low enrollment or high dropout rates are red flags. These problems can be detected by critical thinking.
“There really is no substitute for common sense,” Dr. Loder said. She suggested that studies that include all of the standard points of discussion, such as the generalizability of results, the limitations of the design, the statistical significance of the findings, and a fair interpretation of benefits and hazards, establish credibility and are generally recognizable with a discerning eye.
“For clinicians considering how to interpret results, one question to ask is whether the patients enrolled are representative of the ones that are in front of you,” Dr. Loder suggested.
A critical view of new data helps to avoid the fads that some critics have observed in the treatment of headaches and in clinical medicine overall. Typically, excessive enthusiasm about positive trial results is followed by a period of disillusionment until clinicians finally arrive at a realistic perspective of the strengths and weaknesses of a new therapeutic option. Warning of a coming brace of headache trial results, which will include studies of devices, apps, and new drugs, Dr. Loder urged clinicians to read the studies rather than the press releases, applying the criteria that define a well designed and fairly reported trial.
—Theodore Bosworth
Suggested Reading
Tfelt-Hansen P, Pascual J, Ramadan N, et al. Guidelines for controlled trials of drugs in migraine: third edition. A guide for investigators. Cephalalgia. 2012;32(1):6-38.
Yavchitz A, Boutron I, Bafeta A, et al. Misrepresentation of randomized controlled trials in press releases and news coverage: a cohort study. PLoS Med. 2012;9(9):e1001308.
BOSTON—The interpretation of clinical trial results can stray from the data in many ways. Creating spin (ie, stressing an experimental treatment’s advantages) may or may not be the intention of the researchers or of people who write press releases, but clinicians evaluating the results should not be distracted from the key characteristics of a meaningful trial. They can use several strategies to keep the facts in focus, according to a researcher.
“Here are some words that should put you on alert: ‘revolutionary,’ ‘groundbreaking,’ and ‘first-line.’ It is time to be cautious when you are hearing the spin and the results at the same time,” said Elizabeth W. Loder, MD, MPH, Professor of Neurology at Harvard Medical School in Boston. At the 59th Annual Scientific Meeting of the American Headache Society, Dr. Loder spoke about migraine prevention trials, but she allowed that her remarks are relevant to any clinical trial.
Guidelines Aim to Increase Objectivity
The potential for overinterpretation, misinterpretation, or misleading interpretation of trial results was reduced greatly in 2005. At that time, the International Committee of Medical Journal Editors agreed that trials accepted for publication should first be registered and have their methodology defined before study initiation. Establishing the trial design and primary end points in advance makes selective reporting and data manipulation more difficult. The approach, however, does not eliminate the potential for spin, said Dr. Loder. “The trial registrations on sites like ClinicalTrials.gov are easy to find, and it is worth looking back to compare what was registered to what was reported. There can be some surprises,” Dr. Loder explained.
One potential surprise may be a discrepancy between the prespecified outcomes and the outcomes that the researchers stress at the conclusion of the study. The peer-review process of a high-quality journal limits claims based on secondary outcomes, but press releases do not have similar constraints. In addition, favorable reporting on outcomes that did not appear in the trial registration should arouse suspicion. “It is fair to include data on outcomes that were not prespecified, but they should be flagged. These are hypothesis-generating and should not be given the same weight as those prespecified,” Dr. Loder explained.
Guidelines to improve the objectivity of data gathered and reported for trials are growing increasingly rigorous, according to Dr. Loder. For headache prevention trials, the International Headache Society has issued specific recommendations about trial conduct and the measurement of end points. Although Dr. Loder conceded that strict constraints may make reports of trial results formulaic or tedious, the consistency of the formula, which progresses from an introduction through methods, results, discussion, and conclusions, makes the findings easier to interpret and to place into context.
Data Should Guide Interpretation of Results
A paper’s discussion section may cloud the reader’s understanding of the trial’s findings, Dr. Loder cautioned. In a properly reported study, the results section confines itself to the facts. In the discussion section, interpretation of the facts varies with perspective, according to Dr. Loder. The authors’ perception of relative benefit following a favorable outcome or of the burden of an adverse event is subjective. The potential for intentional or unintentional spin is substantial.
“Examples of spin include focusing on an outcome [that] the trial was not designed to study, focusing on subgroups rather than [on] the overall population, and downplaying adverse safety data,” explained Dr. Loder. Dr. Loder cited several studies that compared reader reaction to abstracts with and without spin. The studies showed that spin was persuasive. Moreover, Dr. Loder noted that spin in abstracts is typically passed on in press releases, news stories, and other accounts of the studies.
One strategy for remaining circumspect about new data is to consult one of many watchdog organizations that monitor clinical data and evaluate data collection and analysis. One such organization is HealthNewsReview.org, which has an editorial team that routinely critiques claims made about drugs, devices, vitamins, and surgical procedures. According to Dr. Loder, the website has examined migraine therapies and provided a perspective that was fully independent of the trials’ sponsors, their authors, and sometimes of the prevailing view.
Pure objectivity may not be appealing for those who want to draw attention to their research, and spin is hard to resist in the desire to develop an engaging narrative. Whether or not those who focus on the most favorable findings of a trial are conscious of their disservice to scientific inquiry, spin has been found repeatedly in systematic reviews of study data. Dr. Loder cited one study that found spin in 47% of 498 press releases on scientific articles.
“There were various types of spin, but 19% of the press releases failed to acknowledge that the primary end point was not statistically significant,” Dr. Loder noted. When abstracts that provided the basis for the press releases were analyzed, 40% were found to contain spin.
The Value of Common Sense
Randomized controlled trials are considered the gold standard for objectively evaluating most treatment strategies, but Dr. Loder cautioned that this design by itself is not enough to ensure reproducible results. The results of the study should include not only how many patients were randomized, but also how many patients received treatment and how many were followed to the trial’s end. Low enrollment or high dropout rates are red flags. These problems can be detected by critical thinking.
“There really is no substitute for common sense,” Dr. Loder said. She suggested that studies that include all of the standard points of discussion, such as the generalizability of results, the limitations of the design, the statistical significance of the findings, and a fair interpretation of benefits and hazards, establish credibility and are generally recognizable with a discerning eye.
“For clinicians considering how to interpret results, one question to ask is whether the patients enrolled are representative of the ones that are in front of you,” Dr. Loder suggested.
A critical view of new data helps to avoid the fads that some critics have observed in the treatment of headaches and in clinical medicine overall. Typically, excessive enthusiasm about positive trial results is followed by a period of disillusionment until clinicians finally arrive at a realistic perspective of the strengths and weaknesses of a new therapeutic option. Warning of a coming brace of headache trial results, which will include studies of devices, apps, and new drugs, Dr. Loder urged clinicians to read the studies rather than the press releases, applying the criteria that define a well designed and fairly reported trial.
—Theodore Bosworth
Suggested Reading
Tfelt-Hansen P, Pascual J, Ramadan N, et al. Guidelines for controlled trials of drugs in migraine: third edition. A guide for investigators. Cephalalgia. 2012;32(1):6-38.
Yavchitz A, Boutron I, Bafeta A, et al. Misrepresentation of randomized controlled trials in press releases and news coverage: a cohort study. PLoS Med. 2012;9(9):e1001308.
Stop using codeine, oxycodone, hydrocodone, tramadol, and aspirin in women who are breastfeeding
In 2015 more than 30,000 deaths from opioid overdose were reported (FIGURE).1 More than 50% of the deaths were due to prescription opioids. The opioid crisis is a public health emergency and clinicians are diligently working to reduce both the number of opioid prescriptions and the doses prescribed per prescription.

In obstetrics, there is growing concern that narcotics used for the treatment of pain in women who are breastfeeding may increase the risk of adverse effects in newborns, including excessive sedation and respiratory depression. The American Academy of Pediatrics (AAP), the US Food and Drug Administration (FDA) and the American College of Obstetricians and Gynecologists (ACOG) recommend against the use of codeine and tramadol in women who are breastfeeding because their newborns may have adverse reactions, including excessive sleepiness, difficulty breathing, and potentially fatal breathing problems.2–4 In addition, there is growing concern that the use of oxycodone and hydrocodone should also be limited in women who are breastfeeding. In this article, I discuss the rationale for these recommendations.
Related article:
Landmark women’s health care remains law of the land
Codeine
Codeine is metabolized to morphine by CYP2D6 and CYP2D7. Both codeine and morphine are excreted into breast milk. Some women are ultrarapid metabolizers of codeine because of high levels of CYP2D6, resulting in higher concentrations of morphine in their breast milk and their breast fed newborn.2,5 In many women who are ultra-rapid metabolizers of codeine, CYP2D6 gene duplication or multiplication is the cause of the increased enzyme activity.6 Genotyping can identify some women who are ultrarapid metabolizers, but it is not currently utilized widely in clinical practice.
In the United States approximately 5% of women express high levels of CYP2D6 and are ultra-rapid metabolizers of codeine.4 In Ethiopia as many as 29% of women are ultrarapid metabolizers.7 Newborn central nervous system (CNS) depression is the most common adverse effect of fetal ingestion of excessive codeine and mor-phine from breast milk and may present as sedation, apnea, bradycardia, or cyanosis.8 Multiple newborn fatalities have been re-ported in the literature when lactating mothers who were ultrarapid metabolizers took co-deine. The FDA and ACOG recommend against the use of codeine in lactating women.
Hydrocodone
Hydrocodone, a hydrogenated ketone derivative of codeine, is metabolized by CYP2D6 to hydromorphone. Both hydrocodone and hydromorphone are present in breast milk. In lactating mothers taking hydrocodone, up to 9% of the dose may be ingested by the breastfeeding newborn.9 There is concern that hydrocodone use by women who are breastfeeding and are ultrarapid metabolizers may cause increased fetal consumption of hydromorphone resulting in adverse outcomes in the newborn. The AAP cautions against the use of hydrocodone.2
Oxycodone
Oxycodone is metabolized by CYP2D6 to oxymorphone and is concentrated into breast milk.10 Oxymorphone is more than 10 times more potent than oxycodone. In one study of lactating women taking oxycodone, codeine, or acetaminophen, the rates of neonate CNS depression were 20%, 17%, and 0.5%, respectively.11 The authors concluded that for mothers who are breastfeeding oxycodone was no safer than codeine because both medications were associated with a high rate of depression in the neonate. Newborns who develop CNS depression from exposure to oxycodone in breast milk will respond to naloxone treatment.12 The AAP recommends against prescribing oxycodone for women who are breastfeeding their infants.2
In a recent communication, the Society for Obstetric Anesthesia and Perinatology (SOAP) observed that in the United States, following cesarean delivery the majority of women receive oxycodone or hydrocodone.13 SOAP disagreed with the AAP recommendation against the use of oxycodone or hydrocodone in breastfeeding women. SOAP noted that all narcotics can produce adverse effects in newborns of breastfeeding women and that there are no good data that the prescription of oxycodone or hydrocodone is more risky than morphine or hydromorphone. However, based on their assessment of risk and benefit, pediatricians prioritize the use of acetaminophen and morphine and seldom use oxycodone or hydrocodone to treat moderate to severe pain in babies and children.
Tramadol
Tramadol is metabolized by CYP2D6 to O-desmethyltramadol. Both tramadol and O-desmethyltramadol are excreted into breast milk. In ultrarapid metabolizers, a greater concentration of O-desmethyltramadol is excreted into breast milk. The FDA reported that they identified no serious neonatal adverse events in the literature due to the use of tramadol by women who are breastfeeding. However, given that tramadol and its CYP2D6 metabolite enter breast milk and the potential for life-threatening respiratory de-pression in the infant, the FDA included tramadol in its warning about codeine.3
Codeine, hydrocodone, oxycodone, and tramadol are all metabolized to more potent metabolites by the CYP2D6 enzyme. Individuals with low CYP2D6 activity, representing about 5% of the US population, cannot fully activate these narcotics. Hence they may not get adequate pain relief when treated with codeine, oxycodone, hydrocodone, or tramadol. Given their resistance to these medications they may first be placed on a higher dose of the narcotic and then switched from a high ineffective dose of one of the agents activated by CYP2D6 to a high dose of morphine or hydromorphone. This can be dangerous because they may then receive an excessive dose of narcotic and develop respiratory depression.14
Read about how other pain medications affect breast milk.
Aspirin
There are very little high quality data about the use of aspirin in women breastfeeding and the effect on the neonate. If a mother takes aspirin, the drug will enter breast milk. It is estimated that the nursing baby receives about 4% to 8% of the mother’s dose. The World Health Organization recommends that aspirin is compatible with breastfeeding in occasional small doses, but repeated administration of aspirin in normal doses should be avoided in women who are breastfeeding. If chronic or high-dose aspirin therapy is recommended, the infant should be monitored for side effects including metabolic acidosis15 and coagulation disorders.16 The National Reye’s Syndrome Foundation recommends against the use of aspirin in women who are breastfeeding because of the theoretical risk of triggering Reye syndrome.17 Acetaminophen and ibuprofen are recommended by the WHO for chronic treatment of pain during breastfeeding.16
Acetaminophen and ibuprofen
For the medication treatment of pain in women who are breastfeeding, the WHO recommends the use of acetaminophen and ibuprofen.16 Acetaminophen is transferred from the maternal circulation into breast milk, but it is estimated that the dose to the nursing neonate is <0.3% of the maternal dose.18 In mothers taking ibuprofen 1600 mg daily, the concentration of ibuprofen in breast milk was below the level of laboratory detection (<1 mg/L).19 Ibuprofen treatment is thought to be safe for women who are breastfeeding because of its short half-life (2 hours), low excretion into milk, and few reported adverse effects in infants.
Morphine
Morphine is not metabolized by CYP2D6 and is excreted into breast milk. Many experts believe that women who are breastfeeding may take standard doses of oral morphine with few adverse effects in the newborn.20,21 For the treatment of moderate to severe pain in opioid-naive adults, morphine doses in the range of 10 mg orally every 4 hours up to 30 mg orally every 4 hours are prescribed. When using a solution of morphine, standard doses are 10 mg to 20 mg every 4 hours, as needed to treat pain. When using morphine tablets, standard doses are 15 mg to 30 mg every 4 hours. The WHO states that occasional doses of morphine are usually safe for women breastfeeding their newborn.16 The AAP recommends the use of morphine and hydromorphone when narcotic agents are needed to treat pain in breastfeeding women.2
Hydromorphone
Hydromorphone, a hydrogenated ketone derivative of morphine, is not metabolized by CYP2D6 and is excreted into breast milk. There are limited data on the safety of hydromorphone during breastfeeding. Breast milk concentrations of hydromorphone are low, and an occasional dose is likely associated with few adverse effects in the breastfeeding newborn.22 For the treatment of moderate to severe pain in opioid-naive adults, hydromorphone doses in the range of 2 mg orally every 4 hours up to 4 mg orally every 4 hours are prescribed. Like all narcotics, hydromorphone can result in central nervous system depression. If a mother ingests sufficient quantities of hydromorphone, respiratory depression in the breastfeeding newborn can occur. In one case report, a nursing mother was taking hydromorphone 4 mg every 4 hours for pain following a cesarean delivery. On day 6 following birth, her newborn was lethargic and she brought the infant to an emergency room. In the emergency room the infant became apneic and was successfully treated with naloxone, suggesting anarcotic overdose due to the presence of hydromorphone in breast milk.23 Hydromorphone should only be used at the lowest effective dose and for the shortest time possible.
Related article:
Should coffee consumption be added as an adjunct to the postoperative care of gynecologic oncology patients?
The bottom line
Pediatricians seldom prescribe codeine, oxycodone, hydrocodone, or tramadol for the treatment of pain in newborns or children. Pediatricians generally use acetaminophen and morphine for the treatment of pain in newborns. Although data from large, high quality clinical trials are not available, expert opinion recommends that acetaminophen and ibuprofen should be prescribed as first-line medications for the treatment of pain in women who are breastfeeding. Use of narcotics that are metabolized by CYP2D6 should be minimized or avoided in women who are breastfeeding. If narcotic medication is necessary, the lowest effective dose of morphine or hy-dromorphone should be prescribed for the shortest time possible. If morphine is prescribed to wo-men who are breastfeeding, they should be advised to observe their baby for signs of narcotic excess, including drowsiness, poor nursing, slow breathing, or low heart rate.
The goal of reducing morbidity and mortality from opioid use is a top public health priority. Obstetrician-gynecologists can contribute through the optimal use of opioid analgesics. Reducing the number of opioid prescriptions and the quantity of medication prescribed per prescription is an important first step in our effort to reduce opioid-related deaths.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- National Overdose Deaths—Number of Deaths from Opioid Drugs. National Institute on Drug Abuse website. . Update January 2017. Accessed September 14, 2017.
- Sachs HC; Committee on Drugs. The transfer of drugs and therapeutics into human breast milk: an update on selected topics. Pediatrics. 2013;132(3):e796–e809.
- US Food and Drug Administration. FDA Drug Safety Communication. FDA restricts use of prescription codeine pain and cough medicines and tramadol pain medicines in children; recommends against use in breastfeeding women. Silver Spring, MD: US Food and Drug Administration. https://www.fda.gov/Drugs/DrugSafety/ucm118113.htm. Published April 2017. Accessed September 12, 2017.
- Practice advisory on codeine and tramadol for breast feeding women. American College of Obstetricians and Gynecologists website. https://www.acog.org/About-ACOG/News-Room/Practice-Advisories/Practice-Advisory-on-Codeine-and-Tramadol-for-Breastfeeding-Women. Published April 27, 2017. Accessed September 12, 2017.
- Madadi P, Shirazi F, Walter FG, Koren G. Establishing causality of CNS depression in breastfed infants following maternal codeine use. Paediatr Drugs. 2008;10(6):399–404.
- Langaee T, Hamadeh I, Chapman AB, Gums JG, Johnson JA. A novel simple method for determining CYP2D6 gene copy number and identifying allele(s) with duplication/multiplication. PLoS One. 2015;10(1):e0113808.
- Cascorbi I. Pharmacogenetics of cytochrome p4502D6: genetic background and clinical implication. Eur J Clin Invest. 2003;33(suppl 2):17–22.
- Naumburg EG, Meny RG. Breast milk opioids and neonatal apnea. Am J Dis Child. 1988;142(1):11–12.
- Sauberan JB, Anderson PO, Lane JR, et al. Breast milk hydrocodone and hydromorphone levels in mothers using hydrocodone for postpartum pain. Obstet Gynecol. 2011;117(3):611–617.
- Seaton S, Reeves M, McLean S. Oxycodone as a component of multimodal analgesia for lactating mothers after Cesarean section: relationships between maternal plasma, breast milk and neonatal plasma levels. Aust N Z J Obstet Gynaecol. 2007;47(3):181–185.
- Lam J, Kelly L, Ciszkowski C, et al. Central nervous system depression of neonates breastfed by mothers receiving oxycodone for postpartum analgesia. J Pediatr. 2012;160(1):33–37.e2.
- Timm NL. Maternal use of oxycodone resulting in opioid intoxication in her breastfed neonate. J Pediatr. 2013;162(2):421–422.
- The Society for Obstetric Anesthesia and Perinatology. Comments in response to the ACOG/SMFM Practice Advisory on Codeine and Tramadol for Breastfeeding Women. The Society for Obstetric Anesthesia and Perinatology website. https://soap.org/soap-response-acog-smfm-advisory.pdf. Published June 10, 2017. Accessed August 28, 2017.
- Banning AM. Respiratory depression following medication change from tramadol to morphine [article in Danish]. Ugeskr Laeger. 1999;161(47):6500–6501.
- Clark JH, Wilson WG. A 16-day old breast-fed infant with metabolic acidosis caused by salicylate. Clin Pediatr (Phila). 1981;20(1):53–54.
- World Health Organization. Breastfeeding and maternal medication. Recommendations for drugs in the 11th WHO model list of essential drugs. http://apps.who.int/iris/bitstream/10665/62435/1/55732.pdf. Published 2002. Accessed September 12, 2017.
- Reye’s syndrome. National Reye’s Syndrome Foundation website. http://www.reyessyndrome.org. Accessed September 12, 2017.
- Berline CM Jr, Yaffe SJ, Ragni M. Disposition of acetaminophen in milk, saliva, and plasma of lactating women. Pediatr Pharmacol (New York). 1980;1(2):135–141.
- Townsend RJ, Benedetti TJ, Erickson SH, et al. Excretion of ibuprofen into breast milk. Am J Obstet Gynecol. 1984;149(2):184–186.
- Spigset O, Hägg S. Analgesics and breast-feeding: safety considerations. Paediatr Drugs. 2000;2(3):223–238.
- Bar-OZ B, Bulkowstein M, Benyamini L, et al. Use of antibiotic and analgesic drugs during lactation. Drug Saf. 2003;26(13):925–935.
- Edwards JE, Rudy AC, Wermeling DP, Desai N, McNamara PJ. Hydromorphone transfer into breast milk after intranasal administration. Pharmacotherapy. 2003;23(2):153–158.
- Schultz ML, Kostic M, Kharasch S. A case of toxic breast-feeding [published online ahead of print January 6, 2017]. Pediatr Emerg Care. doi:10.1097/PEC.0000000000001009.

Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri reports no financial relationships relevant to this article.
In 2015 more than 30,000 deaths from opioid overdose were reported (FIGURE).1 More than 50% of the deaths were due to prescription opioids. The opioid crisis is a public health emergency and clinicians are diligently working to reduce both the number of opioid prescriptions and the doses prescribed per prescription.
In obstetrics, there is growing concern that narcotics used for the treatment of pain in women who are breastfeeding may increase the risk of adverse effects in newborns, including excessive sedation and respiratory depression. The American Academy of Pediatrics (AAP), the US Food and Drug Administration (FDA) and the American College of Obstetricians and Gynecologists (ACOG) recommend against the use of codeine and tramadol in women who are breastfeeding because their newborns may have adverse reactions, including excessive sleepiness, difficulty breathing, and potentially fatal breathing problems.2–4 In addition, there is growing concern that the use of oxycodone and hydrocodone should also be limited in women who are breastfeeding. In this article, I discuss the rationale for these recommendations.
Related article:
Landmark women’s health care remains law of the land
Codeine
Codeine is metabolized to morphine by CYP2D6 and CYP2D7. Both codeine and morphine are excreted into breast milk. Some women are ultrarapid metabolizers of codeine because of high levels of CYP2D6, resulting in higher concentrations of morphine in their breast milk and their breast fed newborn.2,5 In many women who are ultra-rapid metabolizers of codeine, CYP2D6 gene duplication or multiplication is the cause of the increased enzyme activity.6 Genotyping can identify some women who are ultrarapid metabolizers, but it is not currently utilized widely in clinical practice.
In the United States approximately 5% of women express high levels of CYP2D6 and are ultra-rapid metabolizers of codeine.4 In Ethiopia as many as 29% of women are ultrarapid metabolizers.7 Newborn central nervous system (CNS) depression is the most common adverse effect of fetal ingestion of excessive codeine and mor-phine from breast milk and may present as sedation, apnea, bradycardia, or cyanosis.8 Multiple newborn fatalities have been re-ported in the literature when lactating mothers who were ultrarapid metabolizers took co-deine. The FDA and ACOG recommend against the use of codeine in lactating women.
Hydrocodone
Hydrocodone, a hydrogenated ketone derivative of codeine, is metabolized by CYP2D6 to hydromorphone. Both hydrocodone and hydromorphone are present in breast milk. In lactating mothers taking hydrocodone, up to 9% of the dose may be ingested by the breastfeeding newborn.9 There is concern that hydrocodone use by women who are breastfeeding and are ultrarapid metabolizers may cause increased fetal consumption of hydromorphone resulting in adverse outcomes in the newborn. The AAP cautions against the use of hydrocodone.2
Oxycodone
Oxycodone is metabolized by CYP2D6 to oxymorphone and is concentrated into breast milk.10 Oxymorphone is more than 10 times more potent than oxycodone. In one study of lactating women taking oxycodone, codeine, or acetaminophen, the rates of neonate CNS depression were 20%, 17%, and 0.5%, respectively.11 The authors concluded that for mothers who are breastfeeding oxycodone was no safer than codeine because both medications were associated with a high rate of depression in the neonate. Newborns who develop CNS depression from exposure to oxycodone in breast milk will respond to naloxone treatment.12 The AAP recommends against prescribing oxycodone for women who are breastfeeding their infants.2
In a recent communication, the Society for Obstetric Anesthesia and Perinatology (SOAP) observed that in the United States, following cesarean delivery the majority of women receive oxycodone or hydrocodone.13 SOAP disagreed with the AAP recommendation against the use of oxycodone or hydrocodone in breastfeeding women. SOAP noted that all narcotics can produce adverse effects in newborns of breastfeeding women and that there are no good data that the prescription of oxycodone or hydrocodone is more risky than morphine or hydromorphone. However, based on their assessment of risk and benefit, pediatricians prioritize the use of acetaminophen and morphine and seldom use oxycodone or hydrocodone to treat moderate to severe pain in babies and children.
Tramadol
Tramadol is metabolized by CYP2D6 to O-desmethyltramadol. Both tramadol and O-desmethyltramadol are excreted into breast milk. In ultrarapid metabolizers, a greater concentration of O-desmethyltramadol is excreted into breast milk. The FDA reported that they identified no serious neonatal adverse events in the literature due to the use of tramadol by women who are breastfeeding. However, given that tramadol and its CYP2D6 metabolite enter breast milk and the potential for life-threatening respiratory de-pression in the infant, the FDA included tramadol in its warning about codeine.3
Codeine, hydrocodone, oxycodone, and tramadol are all metabolized to more potent metabolites by the CYP2D6 enzyme. Individuals with low CYP2D6 activity, representing about 5% of the US population, cannot fully activate these narcotics. Hence they may not get adequate pain relief when treated with codeine, oxycodone, hydrocodone, or tramadol. Given their resistance to these medications they may first be placed on a higher dose of the narcotic and then switched from a high ineffective dose of one of the agents activated by CYP2D6 to a high dose of morphine or hydromorphone. This can be dangerous because they may then receive an excessive dose of narcotic and develop respiratory depression.14
Read about how other pain medications affect breast milk.
Aspirin
There are very little high quality data about the use of aspirin in women breastfeeding and the effect on the neonate. If a mother takes aspirin, the drug will enter breast milk. It is estimated that the nursing baby receives about 4% to 8% of the mother’s dose. The World Health Organization recommends that aspirin is compatible with breastfeeding in occasional small doses, but repeated administration of aspirin in normal doses should be avoided in women who are breastfeeding. If chronic or high-dose aspirin therapy is recommended, the infant should be monitored for side effects including metabolic acidosis15 and coagulation disorders.16 The National Reye’s Syndrome Foundation recommends against the use of aspirin in women who are breastfeeding because of the theoretical risk of triggering Reye syndrome.17 Acetaminophen and ibuprofen are recommended by the WHO for chronic treatment of pain during breastfeeding.16
Acetaminophen and ibuprofen
For the medication treatment of pain in women who are breastfeeding, the WHO recommends the use of acetaminophen and ibuprofen.16 Acetaminophen is transferred from the maternal circulation into breast milk, but it is estimated that the dose to the nursing neonate is <0.3% of the maternal dose.18 In mothers taking ibuprofen 1600 mg daily, the concentration of ibuprofen in breast milk was below the level of laboratory detection (<1 mg/L).19 Ibuprofen treatment is thought to be safe for women who are breastfeeding because of its short half-life (2 hours), low excretion into milk, and few reported adverse effects in infants.
Morphine
Morphine is not metabolized by CYP2D6 and is excreted into breast milk. Many experts believe that women who are breastfeeding may take standard doses of oral morphine with few adverse effects in the newborn.20,21 For the treatment of moderate to severe pain in opioid-naive adults, morphine doses in the range of 10 mg orally every 4 hours up to 30 mg orally every 4 hours are prescribed. When using a solution of morphine, standard doses are 10 mg to 20 mg every 4 hours, as needed to treat pain. When using morphine tablets, standard doses are 15 mg to 30 mg every 4 hours. The WHO states that occasional doses of morphine are usually safe for women breastfeeding their newborn.16 The AAP recommends the use of morphine and hydromorphone when narcotic agents are needed to treat pain in breastfeeding women.2
Hydromorphone
Hydromorphone, a hydrogenated ketone derivative of morphine, is not metabolized by CYP2D6 and is excreted into breast milk. There are limited data on the safety of hydromorphone during breastfeeding. Breast milk concentrations of hydromorphone are low, and an occasional dose is likely associated with few adverse effects in the breastfeeding newborn.22 For the treatment of moderate to severe pain in opioid-naive adults, hydromorphone doses in the range of 2 mg orally every 4 hours up to 4 mg orally every 4 hours are prescribed. Like all narcotics, hydromorphone can result in central nervous system depression. If a mother ingests sufficient quantities of hydromorphone, respiratory depression in the breastfeeding newborn can occur. In one case report, a nursing mother was taking hydromorphone 4 mg every 4 hours for pain following a cesarean delivery. On day 6 following birth, her newborn was lethargic and she brought the infant to an emergency room. In the emergency room the infant became apneic and was successfully treated with naloxone, suggesting anarcotic overdose due to the presence of hydromorphone in breast milk.23 Hydromorphone should only be used at the lowest effective dose and for the shortest time possible.
Related article:
Should coffee consumption be added as an adjunct to the postoperative care of gynecologic oncology patients?
The bottom line
Pediatricians seldom prescribe codeine, oxycodone, hydrocodone, or tramadol for the treatment of pain in newborns or children. Pediatricians generally use acetaminophen and morphine for the treatment of pain in newborns. Although data from large, high quality clinical trials are not available, expert opinion recommends that acetaminophen and ibuprofen should be prescribed as first-line medications for the treatment of pain in women who are breastfeeding. Use of narcotics that are metabolized by CYP2D6 should be minimized or avoided in women who are breastfeeding. If narcotic medication is necessary, the lowest effective dose of morphine or hy-dromorphone should be prescribed for the shortest time possible. If morphine is prescribed to wo-men who are breastfeeding, they should be advised to observe their baby for signs of narcotic excess, including drowsiness, poor nursing, slow breathing, or low heart rate.
The goal of reducing morbidity and mortality from opioid use is a top public health priority. Obstetrician-gynecologists can contribute through the optimal use of opioid analgesics. Reducing the number of opioid prescriptions and the quantity of medication prescribed per prescription is an important first step in our effort to reduce opioid-related deaths.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
In 2015 more than 30,000 deaths from opioid overdose were reported (FIGURE).1 More than 50% of the deaths were due to prescription opioids. The opioid crisis is a public health emergency and clinicians are diligently working to reduce both the number of opioid prescriptions and the doses prescribed per prescription.
In obstetrics, there is growing concern that narcotics used for the treatment of pain in women who are breastfeeding may increase the risk of adverse effects in newborns, including excessive sedation and respiratory depression. The American Academy of Pediatrics (AAP), the US Food and Drug Administration (FDA) and the American College of Obstetricians and Gynecologists (ACOG) recommend against the use of codeine and tramadol in women who are breastfeeding because their newborns may have adverse reactions, including excessive sleepiness, difficulty breathing, and potentially fatal breathing problems.2–4 In addition, there is growing concern that the use of oxycodone and hydrocodone should also be limited in women who are breastfeeding. In this article, I discuss the rationale for these recommendations.
Related article:
Landmark women’s health care remains law of the land
Codeine
Codeine is metabolized to morphine by CYP2D6 and CYP2D7. Both codeine and morphine are excreted into breast milk. Some women are ultrarapid metabolizers of codeine because of high levels of CYP2D6, resulting in higher concentrations of morphine in their breast milk and their breast fed newborn.2,5 In many women who are ultra-rapid metabolizers of codeine, CYP2D6 gene duplication or multiplication is the cause of the increased enzyme activity.6 Genotyping can identify some women who are ultrarapid metabolizers, but it is not currently utilized widely in clinical practice.
In the United States approximately 5% of women express high levels of CYP2D6 and are ultra-rapid metabolizers of codeine.4 In Ethiopia as many as 29% of women are ultrarapid metabolizers.7 Newborn central nervous system (CNS) depression is the most common adverse effect of fetal ingestion of excessive codeine and mor-phine from breast milk and may present as sedation, apnea, bradycardia, or cyanosis.8 Multiple newborn fatalities have been re-ported in the literature when lactating mothers who were ultrarapid metabolizers took co-deine. The FDA and ACOG recommend against the use of codeine in lactating women.
Hydrocodone
Hydrocodone, a hydrogenated ketone derivative of codeine, is metabolized by CYP2D6 to hydromorphone. Both hydrocodone and hydromorphone are present in breast milk. In lactating mothers taking hydrocodone, up to 9% of the dose may be ingested by the breastfeeding newborn.9 There is concern that hydrocodone use by women who are breastfeeding and are ultrarapid metabolizers may cause increased fetal consumption of hydromorphone resulting in adverse outcomes in the newborn. The AAP cautions against the use of hydrocodone.2
Oxycodone
Oxycodone is metabolized by CYP2D6 to oxymorphone and is concentrated into breast milk.10 Oxymorphone is more than 10 times more potent than oxycodone. In one study of lactating women taking oxycodone, codeine, or acetaminophen, the rates of neonate CNS depression were 20%, 17%, and 0.5%, respectively.11 The authors concluded that for mothers who are breastfeeding oxycodone was no safer than codeine because both medications were associated with a high rate of depression in the neonate. Newborns who develop CNS depression from exposure to oxycodone in breast milk will respond to naloxone treatment.12 The AAP recommends against prescribing oxycodone for women who are breastfeeding their infants.2
In a recent communication, the Society for Obstetric Anesthesia and Perinatology (SOAP) observed that in the United States, following cesarean delivery the majority of women receive oxycodone or hydrocodone.13 SOAP disagreed with the AAP recommendation against the use of oxycodone or hydrocodone in breastfeeding women. SOAP noted that all narcotics can produce adverse effects in newborns of breastfeeding women and that there are no good data that the prescription of oxycodone or hydrocodone is more risky than morphine or hydromorphone. However, based on their assessment of risk and benefit, pediatricians prioritize the use of acetaminophen and morphine and seldom use oxycodone or hydrocodone to treat moderate to severe pain in babies and children.
Tramadol
Tramadol is metabolized by CYP2D6 to O-desmethyltramadol. Both tramadol and O-desmethyltramadol are excreted into breast milk. In ultrarapid metabolizers, a greater concentration of O-desmethyltramadol is excreted into breast milk. The FDA reported that they identified no serious neonatal adverse events in the literature due to the use of tramadol by women who are breastfeeding. However, given that tramadol and its CYP2D6 metabolite enter breast milk and the potential for life-threatening respiratory de-pression in the infant, the FDA included tramadol in its warning about codeine.3
Codeine, hydrocodone, oxycodone, and tramadol are all metabolized to more potent metabolites by the CYP2D6 enzyme. Individuals with low CYP2D6 activity, representing about 5% of the US population, cannot fully activate these narcotics. Hence they may not get adequate pain relief when treated with codeine, oxycodone, hydrocodone, or tramadol. Given their resistance to these medications they may first be placed on a higher dose of the narcotic and then switched from a high ineffective dose of one of the agents activated by CYP2D6 to a high dose of morphine or hydromorphone. This can be dangerous because they may then receive an excessive dose of narcotic and develop respiratory depression.14
Read about how other pain medications affect breast milk.
Aspirin
There are very little high quality data about the use of aspirin in women breastfeeding and the effect on the neonate. If a mother takes aspirin, the drug will enter breast milk. It is estimated that the nursing baby receives about 4% to 8% of the mother’s dose. The World Health Organization recommends that aspirin is compatible with breastfeeding in occasional small doses, but repeated administration of aspirin in normal doses should be avoided in women who are breastfeeding. If chronic or high-dose aspirin therapy is recommended, the infant should be monitored for side effects including metabolic acidosis15 and coagulation disorders.16 The National Reye’s Syndrome Foundation recommends against the use of aspirin in women who are breastfeeding because of the theoretical risk of triggering Reye syndrome.17 Acetaminophen and ibuprofen are recommended by the WHO for chronic treatment of pain during breastfeeding.16
Acetaminophen and ibuprofen
For the medication treatment of pain in women who are breastfeeding, the WHO recommends the use of acetaminophen and ibuprofen.16 Acetaminophen is transferred from the maternal circulation into breast milk, but it is estimated that the dose to the nursing neonate is <0.3% of the maternal dose.18 In mothers taking ibuprofen 1600 mg daily, the concentration of ibuprofen in breast milk was below the level of laboratory detection (<1 mg/L).19 Ibuprofen treatment is thought to be safe for women who are breastfeeding because of its short half-life (2 hours), low excretion into milk, and few reported adverse effects in infants.
Morphine
Morphine is not metabolized by CYP2D6 and is excreted into breast milk. Many experts believe that women who are breastfeeding may take standard doses of oral morphine with few adverse effects in the newborn.20,21 For the treatment of moderate to severe pain in opioid-naive adults, morphine doses in the range of 10 mg orally every 4 hours up to 30 mg orally every 4 hours are prescribed. When using a solution of morphine, standard doses are 10 mg to 20 mg every 4 hours, as needed to treat pain. When using morphine tablets, standard doses are 15 mg to 30 mg every 4 hours. The WHO states that occasional doses of morphine are usually safe for women breastfeeding their newborn.16 The AAP recommends the use of morphine and hydromorphone when narcotic agents are needed to treat pain in breastfeeding women.2
Hydromorphone
Hydromorphone, a hydrogenated ketone derivative of morphine, is not metabolized by CYP2D6 and is excreted into breast milk. There are limited data on the safety of hydromorphone during breastfeeding. Breast milk concentrations of hydromorphone are low, and an occasional dose is likely associated with few adverse effects in the breastfeeding newborn.22 For the treatment of moderate to severe pain in opioid-naive adults, hydromorphone doses in the range of 2 mg orally every 4 hours up to 4 mg orally every 4 hours are prescribed. Like all narcotics, hydromorphone can result in central nervous system depression. If a mother ingests sufficient quantities of hydromorphone, respiratory depression in the breastfeeding newborn can occur. In one case report, a nursing mother was taking hydromorphone 4 mg every 4 hours for pain following a cesarean delivery. On day 6 following birth, her newborn was lethargic and she brought the infant to an emergency room. In the emergency room the infant became apneic and was successfully treated with naloxone, suggesting anarcotic overdose due to the presence of hydromorphone in breast milk.23 Hydromorphone should only be used at the lowest effective dose and for the shortest time possible.
Related article:
Should coffee consumption be added as an adjunct to the postoperative care of gynecologic oncology patients?
The bottom line
Pediatricians seldom prescribe codeine, oxycodone, hydrocodone, or tramadol for the treatment of pain in newborns or children. Pediatricians generally use acetaminophen and morphine for the treatment of pain in newborns. Although data from large, high quality clinical trials are not available, expert opinion recommends that acetaminophen and ibuprofen should be prescribed as first-line medications for the treatment of pain in women who are breastfeeding. Use of narcotics that are metabolized by CYP2D6 should be minimized or avoided in women who are breastfeeding. If narcotic medication is necessary, the lowest effective dose of morphine or hy-dromorphone should be prescribed for the shortest time possible. If morphine is prescribed to wo-men who are breastfeeding, they should be advised to observe their baby for signs of narcotic excess, including drowsiness, poor nursing, slow breathing, or low heart rate.
The goal of reducing morbidity and mortality from opioid use is a top public health priority. Obstetrician-gynecologists can contribute through the optimal use of opioid analgesics. Reducing the number of opioid prescriptions and the quantity of medication prescribed per prescription is an important first step in our effort to reduce opioid-related deaths.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- National Overdose Deaths—Number of Deaths from Opioid Drugs. National Institute on Drug Abuse website. . Update January 2017. Accessed September 14, 2017.
- Sachs HC; Committee on Drugs. The transfer of drugs and therapeutics into human breast milk: an update on selected topics. Pediatrics. 2013;132(3):e796–e809.
- US Food and Drug Administration. FDA Drug Safety Communication. FDA restricts use of prescription codeine pain and cough medicines and tramadol pain medicines in children; recommends against use in breastfeeding women. Silver Spring, MD: US Food and Drug Administration. https://www.fda.gov/Drugs/DrugSafety/ucm118113.htm. Published April 2017. Accessed September 12, 2017.
- Practice advisory on codeine and tramadol for breast feeding women. American College of Obstetricians and Gynecologists website. https://www.acog.org/About-ACOG/News-Room/Practice-Advisories/Practice-Advisory-on-Codeine-and-Tramadol-for-Breastfeeding-Women. Published April 27, 2017. Accessed September 12, 2017.
- Madadi P, Shirazi F, Walter FG, Koren G. Establishing causality of CNS depression in breastfed infants following maternal codeine use. Paediatr Drugs. 2008;10(6):399–404.
- Langaee T, Hamadeh I, Chapman AB, Gums JG, Johnson JA. A novel simple method for determining CYP2D6 gene copy number and identifying allele(s) with duplication/multiplication. PLoS One. 2015;10(1):e0113808.
- Cascorbi I. Pharmacogenetics of cytochrome p4502D6: genetic background and clinical implication. Eur J Clin Invest. 2003;33(suppl 2):17–22.
- Naumburg EG, Meny RG. Breast milk opioids and neonatal apnea. Am J Dis Child. 1988;142(1):11–12.
- Sauberan JB, Anderson PO, Lane JR, et al. Breast milk hydrocodone and hydromorphone levels in mothers using hydrocodone for postpartum pain. Obstet Gynecol. 2011;117(3):611–617.
- Seaton S, Reeves M, McLean S. Oxycodone as a component of multimodal analgesia for lactating mothers after Cesarean section: relationships between maternal plasma, breast milk and neonatal plasma levels. Aust N Z J Obstet Gynaecol. 2007;47(3):181–185.
- Lam J, Kelly L, Ciszkowski C, et al. Central nervous system depression of neonates breastfed by mothers receiving oxycodone for postpartum analgesia. J Pediatr. 2012;160(1):33–37.e2.
- Timm NL. Maternal use of oxycodone resulting in opioid intoxication in her breastfed neonate. J Pediatr. 2013;162(2):421–422.
- The Society for Obstetric Anesthesia and Perinatology. Comments in response to the ACOG/SMFM Practice Advisory on Codeine and Tramadol for Breastfeeding Women. The Society for Obstetric Anesthesia and Perinatology website. https://soap.org/soap-response-acog-smfm-advisory.pdf. Published June 10, 2017. Accessed August 28, 2017.
- Banning AM. Respiratory depression following medication change from tramadol to morphine [article in Danish]. Ugeskr Laeger. 1999;161(47):6500–6501.
- Clark JH, Wilson WG. A 16-day old breast-fed infant with metabolic acidosis caused by salicylate. Clin Pediatr (Phila). 1981;20(1):53–54.
- World Health Organization. Breastfeeding and maternal medication. Recommendations for drugs in the 11th WHO model list of essential drugs. http://apps.who.int/iris/bitstream/10665/62435/1/55732.pdf. Published 2002. Accessed September 12, 2017.
- Reye’s syndrome. National Reye’s Syndrome Foundation website. http://www.reyessyndrome.org. Accessed September 12, 2017.
- Berline CM Jr, Yaffe SJ, Ragni M. Disposition of acetaminophen in milk, saliva, and plasma of lactating women. Pediatr Pharmacol (New York). 1980;1(2):135–141.
- Townsend RJ, Benedetti TJ, Erickson SH, et al. Excretion of ibuprofen into breast milk. Am J Obstet Gynecol. 1984;149(2):184–186.
- Spigset O, Hägg S. Analgesics and breast-feeding: safety considerations. Paediatr Drugs. 2000;2(3):223–238.
- Bar-OZ B, Bulkowstein M, Benyamini L, et al. Use of antibiotic and analgesic drugs during lactation. Drug Saf. 2003;26(13):925–935.
- Edwards JE, Rudy AC, Wermeling DP, Desai N, McNamara PJ. Hydromorphone transfer into breast milk after intranasal administration. Pharmacotherapy. 2003;23(2):153–158.
- Schultz ML, Kostic M, Kharasch S. A case of toxic breast-feeding [published online ahead of print January 6, 2017]. Pediatr Emerg Care. doi:10.1097/PEC.0000000000001009.
- National Overdose Deaths—Number of Deaths from Opioid Drugs. National Institute on Drug Abuse website. . Update January 2017. Accessed September 14, 2017.
- Sachs HC; Committee on Drugs. The transfer of drugs and therapeutics into human breast milk: an update on selected topics. Pediatrics. 2013;132(3):e796–e809.
- US Food and Drug Administration. FDA Drug Safety Communication. FDA restricts use of prescription codeine pain and cough medicines and tramadol pain medicines in children; recommends against use in breastfeeding women. Silver Spring, MD: US Food and Drug Administration. https://www.fda.gov/Drugs/DrugSafety/ucm118113.htm. Published April 2017. Accessed September 12, 2017.
- Practice advisory on codeine and tramadol for breast feeding women. American College of Obstetricians and Gynecologists website. https://www.acog.org/About-ACOG/News-Room/Practice-Advisories/Practice-Advisory-on-Codeine-and-Tramadol-for-Breastfeeding-Women. Published April 27, 2017. Accessed September 12, 2017.
- Madadi P, Shirazi F, Walter FG, Koren G. Establishing causality of CNS depression in breastfed infants following maternal codeine use. Paediatr Drugs. 2008;10(6):399–404.
- Langaee T, Hamadeh I, Chapman AB, Gums JG, Johnson JA. A novel simple method for determining CYP2D6 gene copy number and identifying allele(s) with duplication/multiplication. PLoS One. 2015;10(1):e0113808.
- Cascorbi I. Pharmacogenetics of cytochrome p4502D6: genetic background and clinical implication. Eur J Clin Invest. 2003;33(suppl 2):17–22.
- Naumburg EG, Meny RG. Breast milk opioids and neonatal apnea. Am J Dis Child. 1988;142(1):11–12.
- Sauberan JB, Anderson PO, Lane JR, et al. Breast milk hydrocodone and hydromorphone levels in mothers using hydrocodone for postpartum pain. Obstet Gynecol. 2011;117(3):611–617.
- Seaton S, Reeves M, McLean S. Oxycodone as a component of multimodal analgesia for lactating mothers after Cesarean section: relationships between maternal plasma, breast milk and neonatal plasma levels. Aust N Z J Obstet Gynaecol. 2007;47(3):181–185.
- Lam J, Kelly L, Ciszkowski C, et al. Central nervous system depression of neonates breastfed by mothers receiving oxycodone for postpartum analgesia. J Pediatr. 2012;160(1):33–37.e2.
- Timm NL. Maternal use of oxycodone resulting in opioid intoxication in her breastfed neonate. J Pediatr. 2013;162(2):421–422.
- The Society for Obstetric Anesthesia and Perinatology. Comments in response to the ACOG/SMFM Practice Advisory on Codeine and Tramadol for Breastfeeding Women. The Society for Obstetric Anesthesia and Perinatology website. https://soap.org/soap-response-acog-smfm-advisory.pdf. Published June 10, 2017. Accessed August 28, 2017.
- Banning AM. Respiratory depression following medication change from tramadol to morphine [article in Danish]. Ugeskr Laeger. 1999;161(47):6500–6501.
- Clark JH, Wilson WG. A 16-day old breast-fed infant with metabolic acidosis caused by salicylate. Clin Pediatr (Phila). 1981;20(1):53–54.
- World Health Organization. Breastfeeding and maternal medication. Recommendations for drugs in the 11th WHO model list of essential drugs. http://apps.who.int/iris/bitstream/10665/62435/1/55732.pdf. Published 2002. Accessed September 12, 2017.
- Reye’s syndrome. National Reye’s Syndrome Foundation website. http://www.reyessyndrome.org. Accessed September 12, 2017.
- Berline CM Jr, Yaffe SJ, Ragni M. Disposition of acetaminophen in milk, saliva, and plasma of lactating women. Pediatr Pharmacol (New York). 1980;1(2):135–141.
- Townsend RJ, Benedetti TJ, Erickson SH, et al. Excretion of ibuprofen into breast milk. Am J Obstet Gynecol. 1984;149(2):184–186.
- Spigset O, Hägg S. Analgesics and breast-feeding: safety considerations. Paediatr Drugs. 2000;2(3):223–238.
- Bar-OZ B, Bulkowstein M, Benyamini L, et al. Use of antibiotic and analgesic drugs during lactation. Drug Saf. 2003;26(13):925–935.
- Edwards JE, Rudy AC, Wermeling DP, Desai N, McNamara PJ. Hydromorphone transfer into breast milk after intranasal administration. Pharmacotherapy. 2003;23(2):153–158.
- Schultz ML, Kostic M, Kharasch S. A case of toxic breast-feeding [published online ahead of print January 6, 2017]. Pediatr Emerg Care. doi:10.1097/PEC.0000000000001009.

Where should a baby sleep after delivery?

Many hospitals across the country have received designation as “Baby Friendly”; many other hospitals are in the process of seeking this designation. In order to be Baby Friendly, a hospital or birth center must prove they have implemented a set of 10 rules to encourage breastfeeding. As Baby Friendly USA puts it in their byline, it has become the gold standard of care.
Importantly, Baby Friendly fails to recognize that there is another equally crucial participant in any childbirth experience—the woman. Although childbirth is natural and usually healthy, it is not easy. Women commonly lose up to 1 L of blood during childbirth.1 Labor can take 18 to 24 hours for a first-timer and about 12 to 18 hours for an encore performance, often disrupting at least1 entire night of sleep. The minimally invasive cesarean delivery continues to elude us, and women undergoing cesarean delivery must contend with a sizable incision and the additional pain and associated recovery.
Hospitals adopting the Baby Friendly rules must not allow formula, must prohibit pacifier use, and must go to great lengths to encourage rooming-in. Rooming-in means that the baby shares the same room as the new mother around-the-clock, which is reported to help the new mother distinguish sounds that indicate “feed me” from those that indicate a cool breeze. Rooming-in has been shown to be associated with a modest increase in breastfeeding2; however, women who are committed to breastfeeding likely room-in more often than women less committed to breastfeeding. Whether or not forcing the woman who is less committed to breastfeeding or the woman highly committed to breastfeeding who just wants a good night’s rest to room-in with her baby has a meaningful impact on breastfeeding remains unknown.
- Have written breastfeeding policy that is routinely communicated to all health care staff.
- Train all health care staff in skills necessary to implement this policy.
- Inform all pregnant women about benefits and management of breastfeeding.
- Help mothers initiate breastfeeding within 1 hour of birth.
- Show mothers how to breastfeed and how to maintain lactation, even if separated from their infants.
- Give infants no food or drink other than breast milk, unless medically indicated.
- Practice rooming in--allow mothers and infants to remain together 24 hours per day.
- Encourage breastfeeding on demand.
- Give no pacifiers or artificial nipples to breastfeeding infants.
- Foster the establishment of breastfeeding support groups and refer mothers to them on discharge.
Reference
- The ten steps to successful breastfeeding. Baby Friendly USA website. https://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative/the-ten-steps. Accessed September 14, 2017.
Are we violating ethics rules?
When hospitals adopt the Baby Friendly rules—policies that limit women’s choices for themselves and for their baby—we violate medical ethics principles regarding respect for autonomy, beneficence, and truthfulness. For instance, women are told that if they breastfeed their babies will be smarter, healthier, and have stronger emotional bonds. However, when research studies control for factors such as mothers’ education level or the amount of time spent talking to the baby, the effect of breastfeeding on intelligence “washes out.”3 Babies who are formula-fed but cuddled experience the same degree of bonding with their mothers as breast-fed babies.4,5
Although breast is best, the reported benefits that underlie Baby Friendly are overblown and oversold. When we explain to a woman why her newborn cannot spend a few hours in the nursery or why we cannot allow a pacifier, we are denying her the right to parent and make choices for herself and her baby, not acting in the best interest of the woman. We are in fact misrepresenting the truth. We are also acting paternalistic, propagating the long tradition of telling women that we know better about their reproductive health and choices.
Related article:
Women’s Preventive Services Initiative Guidelines provide consensus for practicing ObGyns
Breastfeeding still not fully accepted outside the hospital
The Baby Friendly rules restrict autonomy and prod women to breastfeed for the few days that they remain in the hospital postpartum. However, these women go home to societal and institutional systems that are deeply unsupportive of breastfeeding. In addition to being the birthplace for 98% of babies born in the United States, the health care industry is the single largest employer of US women.6,7 There are 5 academic hospitals in the Boston area. After contacting the human resources department at each, I found that only 1 has a policy for their breastfeeding employees.
Women should not be forced to choose between breastfeeding and working, between taking a longer maternity leave (often unpaid and professionally detrimental) and shelving the breast pump. What we invest in reveals our values. When we require women to room-in without respecting their choices or needs, and when workplaces fail to provide reasonable flexibility and private space for breast-pumping employees, our values as a society are revealed.
Women and men, hospital users and hospital employees, need to insist that the principles of autonomy, respect for persons, truthfulness, and justice guide breastfeeding policy both within our hospitals and within our workplaces. We need to respect women and the choices that they make for themselves and their families. We need to allow women to decide to recover from their delivery without their baby constantly in arms’ reach. We need to ensure that our counseling and our policies are rooted in sound science and not influenced by passionate but biased perspectives.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Guidelines for perinatal care, 8th ed. AAP; Washington, DC: American College of Obstetricians and Gynecologists; 2017:272.
- Jaafar SH, Ho JJ, Lee KS. Rooming-in for new mother and infant versus separate care for increasing the duration of breastfeeding. Cochrane Database Syst Rev. 2016;(8):CD006641.
- Jain A, Concato J, Leventhal JM. How good is the evidence linking breastfeeding and intelligence? Pediatrics. 2002;109(6):1044-1053.
- Britton JR, Britton HL, Gronwaldt V. Breastfeeding, sensitivity, and attachment. Pediatrics. 2006;118(5):e1436-e1443.
- Jansen J, de Weerth C, Riksen-Walraven JM. Breastfeeding and the mother-infant relationship--a review. Dev Rev. 2008;28(4):503-521.
- MacDorman MF, Mathews TJ, Declercq E. Trends in out-of-hospital births in the United States, 1990-2012. CDC National Center for Health Statistics. https://www.cdc.gov/nchs/products/databriefs/db144.htm. Published March 4, 2014. Accessed September 11, 2017.
- US Bureau of Labor Statistics. Women in the labor force: a databook. BLS Reports. https://www.bls.gov/opub/reports/womens-databook/2016/home.htm. Published April 2017. Accessed September 11, 2017.
Dr. Baecher-Lind is Director, Division of General Obstetrics & Gynecology, Tufts Medical Center, and Clerkship Director, Obstetrics & Gynecology Clerkship, Tufts University School of Medicine.
The author reports no financial relationships relevant to this article.
Dr. Baecher-Lind is Director, Division of General Obstetrics & Gynecology, Tufts Medical Center, and Clerkship Director, Obstetrics & Gynecology Clerkship, Tufts University School of Medicine.
The author reports no financial relationships relevant to this article.
Dr. Baecher-Lind is Director, Division of General Obstetrics & Gynecology, Tufts Medical Center, and Clerkship Director, Obstetrics & Gynecology Clerkship, Tufts University School of Medicine.
The author reports no financial relationships relevant to this article.
Many hospitals across the country have received designation as “Baby Friendly”; many other hospitals are in the process of seeking this designation. In order to be Baby Friendly, a hospital or birth center must prove they have implemented a set of 10 rules to encourage breastfeeding. As Baby Friendly USA puts it in their byline, it has become the gold standard of care.
Importantly, Baby Friendly fails to recognize that there is another equally crucial participant in any childbirth experience—the woman. Although childbirth is natural and usually healthy, it is not easy. Women commonly lose up to 1 L of blood during childbirth.1 Labor can take 18 to 24 hours for a first-timer and about 12 to 18 hours for an encore performance, often disrupting at least1 entire night of sleep. The minimally invasive cesarean delivery continues to elude us, and women undergoing cesarean delivery must contend with a sizable incision and the additional pain and associated recovery.
Hospitals adopting the Baby Friendly rules must not allow formula, must prohibit pacifier use, and must go to great lengths to encourage rooming-in. Rooming-in means that the baby shares the same room as the new mother around-the-clock, which is reported to help the new mother distinguish sounds that indicate “feed me” from those that indicate a cool breeze. Rooming-in has been shown to be associated with a modest increase in breastfeeding2; however, women who are committed to breastfeeding likely room-in more often than women less committed to breastfeeding. Whether or not forcing the woman who is less committed to breastfeeding or the woman highly committed to breastfeeding who just wants a good night’s rest to room-in with her baby has a meaningful impact on breastfeeding remains unknown.
- Have written breastfeeding policy that is routinely communicated to all health care staff.
- Train all health care staff in skills necessary to implement this policy.
- Inform all pregnant women about benefits and management of breastfeeding.
- Help mothers initiate breastfeeding within 1 hour of birth.
- Show mothers how to breastfeed and how to maintain lactation, even if separated from their infants.
- Give infants no food or drink other than breast milk, unless medically indicated.
- Practice rooming in--allow mothers and infants to remain together 24 hours per day.
- Encourage breastfeeding on demand.
- Give no pacifiers or artificial nipples to breastfeeding infants.
- Foster the establishment of breastfeeding support groups and refer mothers to them on discharge.
Reference
- The ten steps to successful breastfeeding. Baby Friendly USA website. https://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative/the-ten-steps. Accessed September 14, 2017.
Are we violating ethics rules?
When hospitals adopt the Baby Friendly rules—policies that limit women’s choices for themselves and for their baby—we violate medical ethics principles regarding respect for autonomy, beneficence, and truthfulness. For instance, women are told that if they breastfeed their babies will be smarter, healthier, and have stronger emotional bonds. However, when research studies control for factors such as mothers’ education level or the amount of time spent talking to the baby, the effect of breastfeeding on intelligence “washes out.”3 Babies who are formula-fed but cuddled experience the same degree of bonding with their mothers as breast-fed babies.4,5
Although breast is best, the reported benefits that underlie Baby Friendly are overblown and oversold. When we explain to a woman why her newborn cannot spend a few hours in the nursery or why we cannot allow a pacifier, we are denying her the right to parent and make choices for herself and her baby, not acting in the best interest of the woman. We are in fact misrepresenting the truth. We are also acting paternalistic, propagating the long tradition of telling women that we know better about their reproductive health and choices.
Related article:
Women’s Preventive Services Initiative Guidelines provide consensus for practicing ObGyns
Breastfeeding still not fully accepted outside the hospital
The Baby Friendly rules restrict autonomy and prod women to breastfeed for the few days that they remain in the hospital postpartum. However, these women go home to societal and institutional systems that are deeply unsupportive of breastfeeding. In addition to being the birthplace for 98% of babies born in the United States, the health care industry is the single largest employer of US women.6,7 There are 5 academic hospitals in the Boston area. After contacting the human resources department at each, I found that only 1 has a policy for their breastfeeding employees.
Women should not be forced to choose between breastfeeding and working, between taking a longer maternity leave (often unpaid and professionally detrimental) and shelving the breast pump. What we invest in reveals our values. When we require women to room-in without respecting their choices or needs, and when workplaces fail to provide reasonable flexibility and private space for breast-pumping employees, our values as a society are revealed.
Women and men, hospital users and hospital employees, need to insist that the principles of autonomy, respect for persons, truthfulness, and justice guide breastfeeding policy both within our hospitals and within our workplaces. We need to respect women and the choices that they make for themselves and their families. We need to allow women to decide to recover from their delivery without their baby constantly in arms’ reach. We need to ensure that our counseling and our policies are rooted in sound science and not influenced by passionate but biased perspectives.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Many hospitals across the country have received designation as “Baby Friendly”; many other hospitals are in the process of seeking this designation. In order to be Baby Friendly, a hospital or birth center must prove they have implemented a set of 10 rules to encourage breastfeeding. As Baby Friendly USA puts it in their byline, it has become the gold standard of care.
Importantly, Baby Friendly fails to recognize that there is another equally crucial participant in any childbirth experience—the woman. Although childbirth is natural and usually healthy, it is not easy. Women commonly lose up to 1 L of blood during childbirth.1 Labor can take 18 to 24 hours for a first-timer and about 12 to 18 hours for an encore performance, often disrupting at least1 entire night of sleep. The minimally invasive cesarean delivery continues to elude us, and women undergoing cesarean delivery must contend with a sizable incision and the additional pain and associated recovery.
Hospitals adopting the Baby Friendly rules must not allow formula, must prohibit pacifier use, and must go to great lengths to encourage rooming-in. Rooming-in means that the baby shares the same room as the new mother around-the-clock, which is reported to help the new mother distinguish sounds that indicate “feed me” from those that indicate a cool breeze. Rooming-in has been shown to be associated with a modest increase in breastfeeding2; however, women who are committed to breastfeeding likely room-in more often than women less committed to breastfeeding. Whether or not forcing the woman who is less committed to breastfeeding or the woman highly committed to breastfeeding who just wants a good night’s rest to room-in with her baby has a meaningful impact on breastfeeding remains unknown.
- Have written breastfeeding policy that is routinely communicated to all health care staff.
- Train all health care staff in skills necessary to implement this policy.
- Inform all pregnant women about benefits and management of breastfeeding.
- Help mothers initiate breastfeeding within 1 hour of birth.
- Show mothers how to breastfeed and how to maintain lactation, even if separated from their infants.
- Give infants no food or drink other than breast milk, unless medically indicated.
- Practice rooming in--allow mothers and infants to remain together 24 hours per day.
- Encourage breastfeeding on demand.
- Give no pacifiers or artificial nipples to breastfeeding infants.
- Foster the establishment of breastfeeding support groups and refer mothers to them on discharge.
Reference
- The ten steps to successful breastfeeding. Baby Friendly USA website. https://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative/the-ten-steps. Accessed September 14, 2017.
Are we violating ethics rules?
When hospitals adopt the Baby Friendly rules—policies that limit women’s choices for themselves and for their baby—we violate medical ethics principles regarding respect for autonomy, beneficence, and truthfulness. For instance, women are told that if they breastfeed their babies will be smarter, healthier, and have stronger emotional bonds. However, when research studies control for factors such as mothers’ education level or the amount of time spent talking to the baby, the effect of breastfeeding on intelligence “washes out.”3 Babies who are formula-fed but cuddled experience the same degree of bonding with their mothers as breast-fed babies.4,5
Although breast is best, the reported benefits that underlie Baby Friendly are overblown and oversold. When we explain to a woman why her newborn cannot spend a few hours in the nursery or why we cannot allow a pacifier, we are denying her the right to parent and make choices for herself and her baby, not acting in the best interest of the woman. We are in fact misrepresenting the truth. We are also acting paternalistic, propagating the long tradition of telling women that we know better about their reproductive health and choices.
Related article:
Women’s Preventive Services Initiative Guidelines provide consensus for practicing ObGyns
Breastfeeding still not fully accepted outside the hospital
The Baby Friendly rules restrict autonomy and prod women to breastfeed for the few days that they remain in the hospital postpartum. However, these women go home to societal and institutional systems that are deeply unsupportive of breastfeeding. In addition to being the birthplace for 98% of babies born in the United States, the health care industry is the single largest employer of US women.6,7 There are 5 academic hospitals in the Boston area. After contacting the human resources department at each, I found that only 1 has a policy for their breastfeeding employees.
Women should not be forced to choose between breastfeeding and working, between taking a longer maternity leave (often unpaid and professionally detrimental) and shelving the breast pump. What we invest in reveals our values. When we require women to room-in without respecting their choices or needs, and when workplaces fail to provide reasonable flexibility and private space for breast-pumping employees, our values as a society are revealed.
Women and men, hospital users and hospital employees, need to insist that the principles of autonomy, respect for persons, truthfulness, and justice guide breastfeeding policy both within our hospitals and within our workplaces. We need to respect women and the choices that they make for themselves and their families. We need to allow women to decide to recover from their delivery without their baby constantly in arms’ reach. We need to ensure that our counseling and our policies are rooted in sound science and not influenced by passionate but biased perspectives.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Guidelines for perinatal care, 8th ed. AAP; Washington, DC: American College of Obstetricians and Gynecologists; 2017:272.
- Jaafar SH, Ho JJ, Lee KS. Rooming-in for new mother and infant versus separate care for increasing the duration of breastfeeding. Cochrane Database Syst Rev. 2016;(8):CD006641.
- Jain A, Concato J, Leventhal JM. How good is the evidence linking breastfeeding and intelligence? Pediatrics. 2002;109(6):1044-1053.
- Britton JR, Britton HL, Gronwaldt V. Breastfeeding, sensitivity, and attachment. Pediatrics. 2006;118(5):e1436-e1443.
- Jansen J, de Weerth C, Riksen-Walraven JM. Breastfeeding and the mother-infant relationship--a review. Dev Rev. 2008;28(4):503-521.
- MacDorman MF, Mathews TJ, Declercq E. Trends in out-of-hospital births in the United States, 1990-2012. CDC National Center for Health Statistics. https://www.cdc.gov/nchs/products/databriefs/db144.htm. Published March 4, 2014. Accessed September 11, 2017.
- US Bureau of Labor Statistics. Women in the labor force: a databook. BLS Reports. https://www.bls.gov/opub/reports/womens-databook/2016/home.htm. Published April 2017. Accessed September 11, 2017.
- American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Guidelines for perinatal care, 8th ed. AAP; Washington, DC: American College of Obstetricians and Gynecologists; 2017:272.
- Jaafar SH, Ho JJ, Lee KS. Rooming-in for new mother and infant versus separate care for increasing the duration of breastfeeding. Cochrane Database Syst Rev. 2016;(8):CD006641.
- Jain A, Concato J, Leventhal JM. How good is the evidence linking breastfeeding and intelligence? Pediatrics. 2002;109(6):1044-1053.
- Britton JR, Britton HL, Gronwaldt V. Breastfeeding, sensitivity, and attachment. Pediatrics. 2006;118(5):e1436-e1443.
- Jansen J, de Weerth C, Riksen-Walraven JM. Breastfeeding and the mother-infant relationship--a review. Dev Rev. 2008;28(4):503-521.
- MacDorman MF, Mathews TJ, Declercq E. Trends in out-of-hospital births in the United States, 1990-2012. CDC National Center for Health Statistics. https://www.cdc.gov/nchs/products/databriefs/db144.htm. Published March 4, 2014. Accessed September 11, 2017.
- US Bureau of Labor Statistics. Women in the labor force: a databook. BLS Reports. https://www.bls.gov/opub/reports/womens-databook/2016/home.htm. Published April 2017. Accessed September 11, 2017.

‘Multimorbidities’ in RA make impact on treatment efficacy, disease activity
While clinicians are accustomed to managing patients with rheumatoid arthritis and comorbidities, RA patients more frequently have “multimorbidities” – the simultaneous presence of two or more chronic conditions.
“For anyone who sees patients, this is the reality of our lives,” said Jeffrey R. Curtis, MD, at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education. Some conditions are “bystanders” that don’t impact RA, some are risk factors for RA, and some can be caused by RA treatments, said Dr. Curtis, professor of medicine and William J. Koopman Professor in Rheumatology and Immunology at the University of Alabama at Birmingham. He discussed several comorbid conditions and their interactions with RA.
Obesity’s toll on disease activity
It’s long been recognized that obesity along with RA makes things worse for patients, he said: “If you have a patient who is obese, with a BMI [body mass index] over 30-35, they’re less likely clinically to achieve low disease activity or remission.”

Obesity also affects biomarkers, he said. The multibiomarker disease activity test, marketed as Vectra DA, incorporates several adipokines in its score, but given any level of RA disease, that score is roughly 5 units higher if someone is obese (Sem Arthritis Rheum. 2017 Aug 2. doi: 10.1016/j.semarthrit.2017.07.010). “The company that manufactures the test is working on an adjustment factor to optimize the role of obesity and what those adipokines are doing to better predict x-ray progression to take this influence into account,” he said. “How we measure obesity and how we’re measuring RA are probably very much affected by this issue.”
RA and the somatization comorbidity phenotype
A second common co-occurrence is what Dr. Curtis calls a somatization comorbidity phenotype (SCP), defined as RA with several other ailments such as fibromyalgia, depression, anxiety, sleep apnea, or neuropathy. “The troubling thing about this is I could cure this patient’s RA tomorrow, but they actually wouldn’t feel better in their overall health because of other things dragging down their function,” he said, noting patients are more concerned about their fatigue and pain than their swollen joint count or DAS28 score.
Dr. Curtis and his colleagues completed a recent analysis that’s in press in Arthritis Research & Therapy of about 800 RA patients in the United States starting certolizumab pegol (Cimzia) to look for how well patients with this phenotype responded to a tumor necrosis factor (TNF) inhibitor. The percentage of patients with RA plus SCP who achieved American College of Rheumatology (ACR) 20/50/70 scores were all about 10% lower than for patients with RA alone, and about 15% fewer patients achieved remission using a score of less than 2.6 on the DAS28, based on erythrocyte sedimentation rate. There was about a 10% higher withdrawal rate among the RA plus SCP group, compared with those with RA alone, mainly for lack of efficacy, and the RA plus SCP patients had three times the rate of serious infections and twice the rate of nonserious infections of typical RA patients.
Impact on choice of therapy
Clinicians have questioned whether multimorbidities should affect the choice of RA therapy, Dr. Curtis said. One of the most vexing scenarios has been in patients with a history of cancer, he noted. There have been five studies worldwide looking at RA therapy in this population. One from Sweden (Ann Rheum Dis. 2015 Dec;74[12]:2137-43), of 240 breast cancer survivors, found no difference in the occurrence or hazard ratio of recurrent breast cancer between those treated with TNF inhibitors versus those who were not. Another study coauthored by Dr. Curtis found similar results (Arthritis Rheumatol. 2016 Dec;68[10]:2403–11).
According to the ACR’s 2015 treatment guidelines, “If your RA patient has a previously treated, solid organ malignancy, there’s no restrictions on what you and I should use,” he said. “Basically, treat them like they hadn’t had a history of cancer.” The exception is for patients with previously treated nonmelanoma skin cancer or melanoma, in whom conventional synthetic DMARDs are preferred over biologics or tofacitinib (Xeljanz). In addition, patients with previously treated lymphoproliferative disorders should be given rituximab (Rituxan) – or DMARDs, abatacept (Orencia), or tocilizumab (Actemra) – over TNF inhibitors. “This is good news,” Dr. Curtis said. “It really expands the range of options for patients, now supported by data, who have a history of cancer and bad RA.”
Global Academy for Medical Education and this news organization are owned by the same parent company. Dr. Curtis receives research support or serves as a consultant for Amgen, Bristol-Myers Squibb, Corrona, Lilly, Janssen, Myriad, Pfizer, and Sanofi/Regeneron.
While clinicians are accustomed to managing patients with rheumatoid arthritis and comorbidities, RA patients more frequently have “multimorbidities” – the simultaneous presence of two or more chronic conditions.
“For anyone who sees patients, this is the reality of our lives,” said Jeffrey R. Curtis, MD, at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education. Some conditions are “bystanders” that don’t impact RA, some are risk factors for RA, and some can be caused by RA treatments, said Dr. Curtis, professor of medicine and William J. Koopman Professor in Rheumatology and Immunology at the University of Alabama at Birmingham. He discussed several comorbid conditions and their interactions with RA.
Obesity’s toll on disease activity
It’s long been recognized that obesity along with RA makes things worse for patients, he said: “If you have a patient who is obese, with a BMI [body mass index] over 30-35, they’re less likely clinically to achieve low disease activity or remission.”
Obesity also affects biomarkers, he said. The multibiomarker disease activity test, marketed as Vectra DA, incorporates several adipokines in its score, but given any level of RA disease, that score is roughly 5 units higher if someone is obese (Sem Arthritis Rheum. 2017 Aug 2. doi: 10.1016/j.semarthrit.2017.07.010). “The company that manufactures the test is working on an adjustment factor to optimize the role of obesity and what those adipokines are doing to better predict x-ray progression to take this influence into account,” he said. “How we measure obesity and how we’re measuring RA are probably very much affected by this issue.”
RA and the somatization comorbidity phenotype
A second common co-occurrence is what Dr. Curtis calls a somatization comorbidity phenotype (SCP), defined as RA with several other ailments such as fibromyalgia, depression, anxiety, sleep apnea, or neuropathy. “The troubling thing about this is I could cure this patient’s RA tomorrow, but they actually wouldn’t feel better in their overall health because of other things dragging down their function,” he said, noting patients are more concerned about their fatigue and pain than their swollen joint count or DAS28 score.
Dr. Curtis and his colleagues completed a recent analysis that’s in press in Arthritis Research & Therapy of about 800 RA patients in the United States starting certolizumab pegol (Cimzia) to look for how well patients with this phenotype responded to a tumor necrosis factor (TNF) inhibitor. The percentage of patients with RA plus SCP who achieved American College of Rheumatology (ACR) 20/50/70 scores were all about 10% lower than for patients with RA alone, and about 15% fewer patients achieved remission using a score of less than 2.6 on the DAS28, based on erythrocyte sedimentation rate. There was about a 10% higher withdrawal rate among the RA plus SCP group, compared with those with RA alone, mainly for lack of efficacy, and the RA plus SCP patients had three times the rate of serious infections and twice the rate of nonserious infections of typical RA patients.
Impact on choice of therapy
Clinicians have questioned whether multimorbidities should affect the choice of RA therapy, Dr. Curtis said. One of the most vexing scenarios has been in patients with a history of cancer, he noted. There have been five studies worldwide looking at RA therapy in this population. One from Sweden (Ann Rheum Dis. 2015 Dec;74[12]:2137-43), of 240 breast cancer survivors, found no difference in the occurrence or hazard ratio of recurrent breast cancer between those treated with TNF inhibitors versus those who were not. Another study coauthored by Dr. Curtis found similar results (Arthritis Rheumatol. 2016 Dec;68[10]:2403–11).
According to the ACR’s 2015 treatment guidelines, “If your RA patient has a previously treated, solid organ malignancy, there’s no restrictions on what you and I should use,” he said. “Basically, treat them like they hadn’t had a history of cancer.” The exception is for patients with previously treated nonmelanoma skin cancer or melanoma, in whom conventional synthetic DMARDs are preferred over biologics or tofacitinib (Xeljanz). In addition, patients with previously treated lymphoproliferative disorders should be given rituximab (Rituxan) – or DMARDs, abatacept (Orencia), or tocilizumab (Actemra) – over TNF inhibitors. “This is good news,” Dr. Curtis said. “It really expands the range of options for patients, now supported by data, who have a history of cancer and bad RA.”
Global Academy for Medical Education and this news organization are owned by the same parent company. Dr. Curtis receives research support or serves as a consultant for Amgen, Bristol-Myers Squibb, Corrona, Lilly, Janssen, Myriad, Pfizer, and Sanofi/Regeneron.
While clinicians are accustomed to managing patients with rheumatoid arthritis and comorbidities, RA patients more frequently have “multimorbidities” – the simultaneous presence of two or more chronic conditions.
“For anyone who sees patients, this is the reality of our lives,” said Jeffrey R. Curtis, MD, at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education. Some conditions are “bystanders” that don’t impact RA, some are risk factors for RA, and some can be caused by RA treatments, said Dr. Curtis, professor of medicine and William J. Koopman Professor in Rheumatology and Immunology at the University of Alabama at Birmingham. He discussed several comorbid conditions and their interactions with RA.
Obesity’s toll on disease activity
It’s long been recognized that obesity along with RA makes things worse for patients, he said: “If you have a patient who is obese, with a BMI [body mass index] over 30-35, they’re less likely clinically to achieve low disease activity or remission.”
Obesity also affects biomarkers, he said. The multibiomarker disease activity test, marketed as Vectra DA, incorporates several adipokines in its score, but given any level of RA disease, that score is roughly 5 units higher if someone is obese (Sem Arthritis Rheum. 2017 Aug 2. doi: 10.1016/j.semarthrit.2017.07.010). “The company that manufactures the test is working on an adjustment factor to optimize the role of obesity and what those adipokines are doing to better predict x-ray progression to take this influence into account,” he said. “How we measure obesity and how we’re measuring RA are probably very much affected by this issue.”
RA and the somatization comorbidity phenotype
A second common co-occurrence is what Dr. Curtis calls a somatization comorbidity phenotype (SCP), defined as RA with several other ailments such as fibromyalgia, depression, anxiety, sleep apnea, or neuropathy. “The troubling thing about this is I could cure this patient’s RA tomorrow, but they actually wouldn’t feel better in their overall health because of other things dragging down their function,” he said, noting patients are more concerned about their fatigue and pain than their swollen joint count or DAS28 score.
Dr. Curtis and his colleagues completed a recent analysis that’s in press in Arthritis Research & Therapy of about 800 RA patients in the United States starting certolizumab pegol (Cimzia) to look for how well patients with this phenotype responded to a tumor necrosis factor (TNF) inhibitor. The percentage of patients with RA plus SCP who achieved American College of Rheumatology (ACR) 20/50/70 scores were all about 10% lower than for patients with RA alone, and about 15% fewer patients achieved remission using a score of less than 2.6 on the DAS28, based on erythrocyte sedimentation rate. There was about a 10% higher withdrawal rate among the RA plus SCP group, compared with those with RA alone, mainly for lack of efficacy, and the RA plus SCP patients had three times the rate of serious infections and twice the rate of nonserious infections of typical RA patients.
Impact on choice of therapy
Clinicians have questioned whether multimorbidities should affect the choice of RA therapy, Dr. Curtis said. One of the most vexing scenarios has been in patients with a history of cancer, he noted. There have been five studies worldwide looking at RA therapy in this population. One from Sweden (Ann Rheum Dis. 2015 Dec;74[12]:2137-43), of 240 breast cancer survivors, found no difference in the occurrence or hazard ratio of recurrent breast cancer between those treated with TNF inhibitors versus those who were not. Another study coauthored by Dr. Curtis found similar results (Arthritis Rheumatol. 2016 Dec;68[10]:2403–11).
According to the ACR’s 2015 treatment guidelines, “If your RA patient has a previously treated, solid organ malignancy, there’s no restrictions on what you and I should use,” he said. “Basically, treat them like they hadn’t had a history of cancer.” The exception is for patients with previously treated nonmelanoma skin cancer or melanoma, in whom conventional synthetic DMARDs are preferred over biologics or tofacitinib (Xeljanz). In addition, patients with previously treated lymphoproliferative disorders should be given rituximab (Rituxan) – or DMARDs, abatacept (Orencia), or tocilizumab (Actemra) – over TNF inhibitors. “This is good news,” Dr. Curtis said. “It really expands the range of options for patients, now supported by data, who have a history of cancer and bad RA.”
Global Academy for Medical Education and this news organization are owned by the same parent company. Dr. Curtis receives research support or serves as a consultant for Amgen, Bristol-Myers Squibb, Corrona, Lilly, Janssen, Myriad, Pfizer, and Sanofi/Regeneron.
EXPERT ANALYSIS FROM THE ANNUAL PERSPECTIVES IN RHEUMATIC DISEASES
Inclusive sexual health counseling and care
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.

Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.
Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.
Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.
Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
Sexual health screening and counseling is an important part of wellness care for all adolescents, and transgender and gender nonconforming (TGNC) youth are no exception. TGNC youth may avoid routine health visits and sexual health conversations because they fear discrimination in the health care setting and feel uncomfortable about physical exams.1 Providers should be aware of the potential anxiety patients may feel during health care visits and work to establish an environment of respect and inclusiveness. Below are some tips to help provide care that is inclusive of the diverse gender and sexual identities of the patients we see.
Obtaining a sexual history
1. Clearly explain the reasons for asking sexually explicit questions.
TGNC youth experiencing dysphoria may have heightened levels of anxiety when discussing sexuality. Before asking these questions, acknowledge the sensitivity of this topic and explain that this information is important for providers to know so that they can provide appropriate counseling and screening recommendations. This may alleviate some of their discomfort.
2. Ensure confidentiality.
When obtaining sexual health histories, it is crucial to ensure confidential patient encounters, as described by the American Academy of Pediatrics and Society for Adolescent Health and Medicine.2,3 The Guttmacher Institute provides information about minors’ consent law in each state.4
3. Do not assume identity equals behavior.
Here are some sexual health questions you need to ask:
- Who are you attracted to? What is/are the gender(s) of your partner(s)?
- Have you ever had anal, genital, or oral sex? If yes:
Do you give, receive, or both?
When was the last time you had sex?
How many partners have you had in past 6 months?
Do you use barrier protection most of the time, some of the time, always, or never?
Do you have symptoms of an infection, such as burning when you pee, abnormal genital discharge, pain with sex, or irregular bleeding?
- Have you ever been forced/coerced into having sex?
Starting with open-ended questions about attraction can give patients an opportunity to describe their pattern of attraction. If needed, patients can be prompted with more specific questions about their partners’ genders. It is important to ask explicitly about genital, oral, and anal sex because patients sometimes do not realize that the term sex includes oral and anal sex. Patients also may not be aware that it is possible to spread infections through oral and anal sex.
4. Anatomy and behavior may change over time, and it is important to reassess sexually transmitted infection risk at each visit
Studies suggest that, as gender dysphoria decreases, sexual desires may increase; this is true for all adolescents but of particular interest with TGNC youth. This may affect behaviors.5 For youth on hormone therapy, testosterone can increase libido, whereas estrogen may decrease libido and affect sexual function.6
Physical exam
Dysphoria related to primary and secondary sex characteristics may make exams particularly distressing. Providers should clearly explain reasons for performing various parts of the physical exam. When performing the physical exam, providers should use a gender-affirming approach. This includes using the patient’s identified name and pronouns throughout the visit and asking patients preference for terminology when discussing body parts (some patients may prefer the use of the term “front hole” to vagina).1,7,8 The exam and evaluation may need to be modified based on comfort. If a patient refuses a speculum exam after the need for the its use has been discussed, consider offering an external genital exam and bimanual exam instead. If a patient refuses to allow a provider to obtain a rectal or vaginal swab, consider allowing patients to self-swab. Providers also should consider whether genital exams can be deferred to subsequent visits. These techniques offer an opportunity to build trust and rapport with patients so that they remain engaged in care and may become comfortable with the necessary tests and procedures at future visits.
Sexual health counseling
Sexual health counseling should address reducing risk and optimizing physical and emotional satisfaction in relationships and encounters.9 In addition to assessing risky behaviors and screening for sexually transmitted infections, providers also should provide counseling on safer-sex practices. This includes the use of lubrication to reduce trauma to genital tissues, which can potentiate the spread of infections, and the use of barrier protection, such as external condoms (often referred to as male condoms), internal condoms (often referred to as female condoms), dental dams during oral sex, and gloves for digital penetration. Patients at risk for pregnancy should receive comprehensive contraceptive counseling. TGNC patients may be at increased risk of sexual victimization, and honest discussions about safety in relationships is important. The goal of sexual health counseling should be to promote safe, satisfying experiences for all patients.
Email her at pdnews@frontlinemedcom.com.
References
1. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, in Center of Excellence for Transgender Health, Department of Family and Community Medicine, 2nd ed. (San Francisco: University of California, 2016).
2. Pediatrics. 2008. doi: 10.1542/peds.2008-0694.
3. J Adol Health. 2004;35:160-7.
4. An Overview of Minors’ Consent Law: State Laws and Policies. 2017, by the Guttmacher Institute.
5. Eur J Endocrinol. 2011 Aug;165(2):331-7.
6. J Clin Endocrinol Metab. 2009 Sep;94(9):3132-54.
7. Sex Roles. 2013 Jun 1;68(11-12):675-89.
8. J Midwifery Womens Health. 2008 Jul-Aug;53(4):331-7.
9. “The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health,” 2nd ed. (Philadelphia: American College of Physicians Press, 2008).
New AAP policy recommends flu vaccination regardless of egg allergy
CHICAGO – The American Academy of Pediatrics has released a new policy statement that in part suggests that physicians can administer influenza vaccine to children and teenagers with egg allergies without any special precautions beyond those that apply to other vaccines.
This is some “egg-citing news,” said Mary Ann Jackson, MD. “In 28 studies with 4,315 egg allergic subjects, 656 of whom had severe allergies, there were no serious allergic reactions.” In other words, there was no respiratory distress or hypotension observed after participants received the influenza vaccine in these studies, she added.
Officially, the policy statement from the academy’s Committee on Infectious Diseases reads: “All children with egg allergy of any severity can receive influenza vaccine without any additional precautions beyond those recommended for any vaccine. Special precautions for egg-allergic recipients of IIV [inactivated influenza vaccine] are not warranted, as the rate of anaphylaxis after IIV administration is no greater in egg-allergic than non–egg-allergic recipients or from other universally recommended vaccines. Standard vaccination practice for all vaccines in children should include the ability to respond to rare acute hypersensitivity reactions.” The full policy statement was published online in the journal Pediatrics (2017 Sep. 6; doi: 10.1542/peds.2017-2550.)
This new policy “makes your life so much easier … and allows you to continue to recommend the vaccine strongly,” said Dr. Jackson, division director of infectious diseases at Children’s Mercy Hospital and professor of pediatrics at the University of Missouri at Kansas City.
Other reasons to recommend flu vaccination
Dr. Jackson also gave an overview of influenza epidemiology and why ongoing education of patients and families remains essential. “It’s almost flu season now. It’s inevitable – like RSV [respiratory syncytial virus] is inevitable – but when the seasons starts is unknown,” she said. “How severe and long the season will be is also unpredictable.” Which viruses are spread and whether there is a good match between circulating virus and the vaccine are additional unknowns each year.

Patient and family education are important for these reasons, and because “it’s the most likely vaccine to be opted out of by the otherwise fully immunized,” she noted.
The lowest covered population are individuals between 18 years and 49 years, Dr. Jackson said. “My young adult son did not think he needed to worry about flu for himself; he said he was healthy and well. But it’s a bummer when your mom is an ID doctor who likes vaccines, because I made it happen for him.”
Dr. Jackson had no relevant financial disclosures.
CHICAGO – The American Academy of Pediatrics has released a new policy statement that in part suggests that physicians can administer influenza vaccine to children and teenagers with egg allergies without any special precautions beyond those that apply to other vaccines.
This is some “egg-citing news,” said Mary Ann Jackson, MD. “In 28 studies with 4,315 egg allergic subjects, 656 of whom had severe allergies, there were no serious allergic reactions.” In other words, there was no respiratory distress or hypotension observed after participants received the influenza vaccine in these studies, she added.
Officially, the policy statement from the academy’s Committee on Infectious Diseases reads: “All children with egg allergy of any severity can receive influenza vaccine without any additional precautions beyond those recommended for any vaccine. Special precautions for egg-allergic recipients of IIV [inactivated influenza vaccine] are not warranted, as the rate of anaphylaxis after IIV administration is no greater in egg-allergic than non–egg-allergic recipients or from other universally recommended vaccines. Standard vaccination practice for all vaccines in children should include the ability to respond to rare acute hypersensitivity reactions.” The full policy statement was published online in the journal Pediatrics (2017 Sep. 6; doi: 10.1542/peds.2017-2550.)
This new policy “makes your life so much easier … and allows you to continue to recommend the vaccine strongly,” said Dr. Jackson, division director of infectious diseases at Children’s Mercy Hospital and professor of pediatrics at the University of Missouri at Kansas City.
Other reasons to recommend flu vaccination
Dr. Jackson also gave an overview of influenza epidemiology and why ongoing education of patients and families remains essential. “It’s almost flu season now. It’s inevitable – like RSV [respiratory syncytial virus] is inevitable – but when the seasons starts is unknown,” she said. “How severe and long the season will be is also unpredictable.” Which viruses are spread and whether there is a good match between circulating virus and the vaccine are additional unknowns each year.
Patient and family education are important for these reasons, and because “it’s the most likely vaccine to be opted out of by the otherwise fully immunized,” she noted.
The lowest covered population are individuals between 18 years and 49 years, Dr. Jackson said. “My young adult son did not think he needed to worry about flu for himself; he said he was healthy and well. But it’s a bummer when your mom is an ID doctor who likes vaccines, because I made it happen for him.”
Dr. Jackson had no relevant financial disclosures.
CHICAGO – The American Academy of Pediatrics has released a new policy statement that in part suggests that physicians can administer influenza vaccine to children and teenagers with egg allergies without any special precautions beyond those that apply to other vaccines.
This is some “egg-citing news,” said Mary Ann Jackson, MD. “In 28 studies with 4,315 egg allergic subjects, 656 of whom had severe allergies, there were no serious allergic reactions.” In other words, there was no respiratory distress or hypotension observed after participants received the influenza vaccine in these studies, she added.
Officially, the policy statement from the academy’s Committee on Infectious Diseases reads: “All children with egg allergy of any severity can receive influenza vaccine without any additional precautions beyond those recommended for any vaccine. Special precautions for egg-allergic recipients of IIV [inactivated influenza vaccine] are not warranted, as the rate of anaphylaxis after IIV administration is no greater in egg-allergic than non–egg-allergic recipients or from other universally recommended vaccines. Standard vaccination practice for all vaccines in children should include the ability to respond to rare acute hypersensitivity reactions.” The full policy statement was published online in the journal Pediatrics (2017 Sep. 6; doi: 10.1542/peds.2017-2550.)
This new policy “makes your life so much easier … and allows you to continue to recommend the vaccine strongly,” said Dr. Jackson, division director of infectious diseases at Children’s Mercy Hospital and professor of pediatrics at the University of Missouri at Kansas City.
Other reasons to recommend flu vaccination
Dr. Jackson also gave an overview of influenza epidemiology and why ongoing education of patients and families remains essential. “It’s almost flu season now. It’s inevitable – like RSV [respiratory syncytial virus] is inevitable – but when the seasons starts is unknown,” she said. “How severe and long the season will be is also unpredictable.” Which viruses are spread and whether there is a good match between circulating virus and the vaccine are additional unknowns each year.
Patient and family education are important for these reasons, and because “it’s the most likely vaccine to be opted out of by the otherwise fully immunized,” she noted.
The lowest covered population are individuals between 18 years and 49 years, Dr. Jackson said. “My young adult son did not think he needed to worry about flu for himself; he said he was healthy and well. But it’s a bummer when your mom is an ID doctor who likes vaccines, because I made it happen for him.”
Dr. Jackson had no relevant financial disclosures.
AT AAP 2017
Retrospective review: No difference in PFS, OS with radiation before PD-1/PD-L1 inhibition
CHICAGO – Exposure to radiation therapy prior to PD-1/PD-L1 therapy was not associated with improved outcomes in a retrospective review of 66 lung cancer patients.
The patients had stage IIIB or IV non–small cell lung cancer, median age of 64 years, received at least 6 weeks of single-agent anti-PD-1/PD-L1 therapy in the second-line setting or beyond, and had survived at least 8 weeks from immunotherapy initiation. Compared with 13 patients who received no radiation therapy, the 53 who received any prior radiation therapy – including 44 with extracranial radiation and 22 with intracranial radiation – did not differ significantly with respect to progression-free survival (median 4-5 months; hazard ratio, 0.83), or overall survival (median of about 12 months in both groups; HR, 0.96), Christopher Strouse, MD, of the University of Iowa, Iowa City, reported at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
There also were no significant differences in the outcomes between those who had extracranial radiation and those who had intracranial radiation (HRs for PFS and OS, respectively, 0.91 and 1.19), or (on univariate analysis), between those receiving any vs. no intracranial radiation therapy (HRs for PFS and OS, respectively, 0.92 and 0.98), Dr. Strouse said.
The patients who received extracranial radiation therapy had lower lymphocyte counts at the time of anti-PD-1/PD-L1 therapy initiation vs. those who received only radiation therapy (mean lymphocyte count, 809 vs. 1,519), and those who received intracranial radiation therapy were younger than those who did not (median age, 59 vs. 65 years), but the groups were similar with respect to other variables, including gender, histology, performance status, smoking history, KRAS mutation, and number of prior lines of systemic therapies. Anti-PD-1/PD-L1 therapies are promising treatment options for metastatic non–small cell lung cancer, and combining these agents with other immune-modulating therapies may enhance their efficacy and lead to a greater proportion of patients with responses to these treatments, Dr. Strouse noted.
“It’s known that immune response depends on a lot of steps, even beyond the PD-1/PD-L1 axis, and one possible explanation for some of these patients [not responding] may be that there is some failure along the way in some other step,” he said. “Our hypothesis was that radiation therapy would be helpful in overcoming some of these barriers.”
However, in this study, which is limited by small sample size and single-institution retrospective design, no such effect was identified.
The findings conflict with some larger studies, including the recently-reported PACIFIC study, which showed a significant PFS benefit in lung cancer patients who received chemoradiation therapy followed by treatment with the PD-L1 inhibitor durvalumab.
Dr. Strouse said he looks forward to seeing further reports looking into the effects of radiation therapy at different doses and timing.
Invited discussant Heather Wakelee, MD, of Stanford (Calif.) University, also stressed the limitations of the University of Iowa study, and noted that while there are many unanswered questions, findings such as those from the PACIFIC trial show that radiation and PD-L1 inhibition is here to stay.
“It appears safe; there will be more coming,” she said.
Dr. Strouse reported having no disclosures. Dr. Wakelee has been the institutional principal investigator for studies of nivolumab, tocilizumab, and other agents. She has consulted for Peregrine, ACEA, Pfizer, Helsinn, Genentech/Roche, Clovis, and Lilly, and received research/grant support from Clovis, Exelixis, AstraZeneca/Medimmune, Genentech/Roche, BMS, Gilead, Novartis, Xcovery, Pfizer, Celgene, Gilead, Pharmacyclics, and Lilly.
CHICAGO – Exposure to radiation therapy prior to PD-1/PD-L1 therapy was not associated with improved outcomes in a retrospective review of 66 lung cancer patients.
The patients had stage IIIB or IV non–small cell lung cancer, median age of 64 years, received at least 6 weeks of single-agent anti-PD-1/PD-L1 therapy in the second-line setting or beyond, and had survived at least 8 weeks from immunotherapy initiation. Compared with 13 patients who received no radiation therapy, the 53 who received any prior radiation therapy – including 44 with extracranial radiation and 22 with intracranial radiation – did not differ significantly with respect to progression-free survival (median 4-5 months; hazard ratio, 0.83), or overall survival (median of about 12 months in both groups; HR, 0.96), Christopher Strouse, MD, of the University of Iowa, Iowa City, reported at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
There also were no significant differences in the outcomes between those who had extracranial radiation and those who had intracranial radiation (HRs for PFS and OS, respectively, 0.91 and 1.19), or (on univariate analysis), between those receiving any vs. no intracranial radiation therapy (HRs for PFS and OS, respectively, 0.92 and 0.98), Dr. Strouse said.
The patients who received extracranial radiation therapy had lower lymphocyte counts at the time of anti-PD-1/PD-L1 therapy initiation vs. those who received only radiation therapy (mean lymphocyte count, 809 vs. 1,519), and those who received intracranial radiation therapy were younger than those who did not (median age, 59 vs. 65 years), but the groups were similar with respect to other variables, including gender, histology, performance status, smoking history, KRAS mutation, and number of prior lines of systemic therapies. Anti-PD-1/PD-L1 therapies are promising treatment options for metastatic non–small cell lung cancer, and combining these agents with other immune-modulating therapies may enhance their efficacy and lead to a greater proportion of patients with responses to these treatments, Dr. Strouse noted.
“It’s known that immune response depends on a lot of steps, even beyond the PD-1/PD-L1 axis, and one possible explanation for some of these patients [not responding] may be that there is some failure along the way in some other step,” he said. “Our hypothesis was that radiation therapy would be helpful in overcoming some of these barriers.”
However, in this study, which is limited by small sample size and single-institution retrospective design, no such effect was identified.
The findings conflict with some larger studies, including the recently-reported PACIFIC study, which showed a significant PFS benefit in lung cancer patients who received chemoradiation therapy followed by treatment with the PD-L1 inhibitor durvalumab.
Dr. Strouse said he looks forward to seeing further reports looking into the effects of radiation therapy at different doses and timing.
Invited discussant Heather Wakelee, MD, of Stanford (Calif.) University, also stressed the limitations of the University of Iowa study, and noted that while there are many unanswered questions, findings such as those from the PACIFIC trial show that radiation and PD-L1 inhibition is here to stay.
“It appears safe; there will be more coming,” she said.
Dr. Strouse reported having no disclosures. Dr. Wakelee has been the institutional principal investigator for studies of nivolumab, tocilizumab, and other agents. She has consulted for Peregrine, ACEA, Pfizer, Helsinn, Genentech/Roche, Clovis, and Lilly, and received research/grant support from Clovis, Exelixis, AstraZeneca/Medimmune, Genentech/Roche, BMS, Gilead, Novartis, Xcovery, Pfizer, Celgene, Gilead, Pharmacyclics, and Lilly.
CHICAGO – Exposure to radiation therapy prior to PD-1/PD-L1 therapy was not associated with improved outcomes in a retrospective review of 66 lung cancer patients.
The patients had stage IIIB or IV non–small cell lung cancer, median age of 64 years, received at least 6 weeks of single-agent anti-PD-1/PD-L1 therapy in the second-line setting or beyond, and had survived at least 8 weeks from immunotherapy initiation. Compared with 13 patients who received no radiation therapy, the 53 who received any prior radiation therapy – including 44 with extracranial radiation and 22 with intracranial radiation – did not differ significantly with respect to progression-free survival (median 4-5 months; hazard ratio, 0.83), or overall survival (median of about 12 months in both groups; HR, 0.96), Christopher Strouse, MD, of the University of Iowa, Iowa City, reported at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
There also were no significant differences in the outcomes between those who had extracranial radiation and those who had intracranial radiation (HRs for PFS and OS, respectively, 0.91 and 1.19), or (on univariate analysis), between those receiving any vs. no intracranial radiation therapy (HRs for PFS and OS, respectively, 0.92 and 0.98), Dr. Strouse said.
The patients who received extracranial radiation therapy had lower lymphocyte counts at the time of anti-PD-1/PD-L1 therapy initiation vs. those who received only radiation therapy (mean lymphocyte count, 809 vs. 1,519), and those who received intracranial radiation therapy were younger than those who did not (median age, 59 vs. 65 years), but the groups were similar with respect to other variables, including gender, histology, performance status, smoking history, KRAS mutation, and number of prior lines of systemic therapies. Anti-PD-1/PD-L1 therapies are promising treatment options for metastatic non–small cell lung cancer, and combining these agents with other immune-modulating therapies may enhance their efficacy and lead to a greater proportion of patients with responses to these treatments, Dr. Strouse noted.
“It’s known that immune response depends on a lot of steps, even beyond the PD-1/PD-L1 axis, and one possible explanation for some of these patients [not responding] may be that there is some failure along the way in some other step,” he said. “Our hypothesis was that radiation therapy would be helpful in overcoming some of these barriers.”
However, in this study, which is limited by small sample size and single-institution retrospective design, no such effect was identified.
The findings conflict with some larger studies, including the recently-reported PACIFIC study, which showed a significant PFS benefit in lung cancer patients who received chemoradiation therapy followed by treatment with the PD-L1 inhibitor durvalumab.
Dr. Strouse said he looks forward to seeing further reports looking into the effects of radiation therapy at different doses and timing.
Invited discussant Heather Wakelee, MD, of Stanford (Calif.) University, also stressed the limitations of the University of Iowa study, and noted that while there are many unanswered questions, findings such as those from the PACIFIC trial show that radiation and PD-L1 inhibition is here to stay.
“It appears safe; there will be more coming,” she said.
Dr. Strouse reported having no disclosures. Dr. Wakelee has been the institutional principal investigator for studies of nivolumab, tocilizumab, and other agents. She has consulted for Peregrine, ACEA, Pfizer, Helsinn, Genentech/Roche, Clovis, and Lilly, and received research/grant support from Clovis, Exelixis, AstraZeneca/Medimmune, Genentech/Roche, BMS, Gilead, Novartis, Xcovery, Pfizer, Celgene, Gilead, Pharmacyclics, and Lilly.
AT A SYMPOSIUM IN THORACIC ONCOLOGY
Key clinical point:
Major finding: PFS and OS did not differ significantly between patients who did and did not receive prior radiation therapy (HRs for PFS and OS, respectively, 0.83 and 0.96).
Data source: A retrospective review of 66 patients.
Disclosures: Dr. Strouse reported having no disclosures. Dr. Wakelee has been the institutional principal investigator for studies of nivolumab, tocilizumab, and other agents. She has consulted for Peregrine, ACEA, Pfizer, Helsinn, Genentech/Roche, Clovis, and Lilly, and received research/grant support from Clovis, Exelixis, AstraZeneca/Medimmune, Genentech/Roche, BMS, Gilead, Novartis, Xcovery, Pfizer, Celgene, Gilead, Pharmacyclics, and Lilly.
2017 Update on pelvic floor dysfunction
The International Continence Society (ICS) defines overactive bladder (OAB) as a syndrome of "urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence (UUI), in the absence of urinary tract infection [UTI] or obvious pathology."1 The Agency for Healthcare Research and Quality (AHRQ) reported OAB prevalence to be 15% in US women, with 11% reporting UUI.2 OAB represents a significant health care burden that impacts nearly every aspect of life, including physical, emotional, and psychological domains.3,4 The economic impact is notable; the projected cost is estimated to reach $82.6 billion annually by 2020.5
The American Urological Association (AUA) and the Society for Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction (SUFU) have endorsed an algorithm for use in the evaluation of idiopathic OAB (FIGURE).6 If the patient's symptoms are certain, minimal evaluation is needed and it is reasonable to proceed with first-line therapy, which includes fluid management (decreasing caffeine intake and limiting evening fluid intake), bladder retraining drills such as timed voiding, and improving pelvic floor muscles with the use of biofeedback and functional electrical stimulation.6,7 Pelvic floor muscle training can be facilitated with a referral to a physical therapist trained in pelvic floor muscle education.
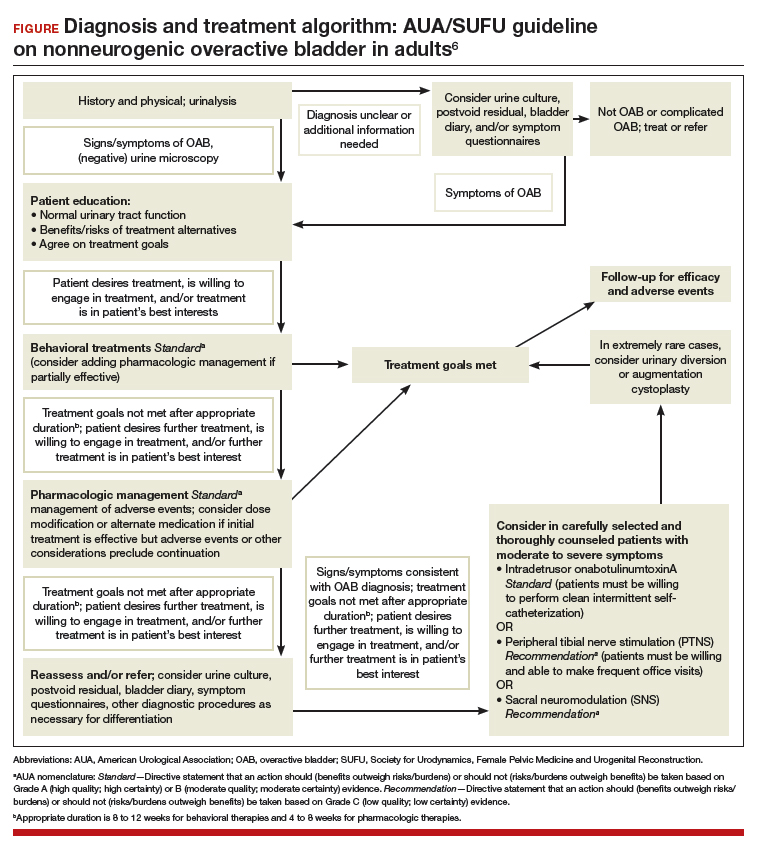
If treatment goals are not met with first-line strategies, second-line therapy may be initiated with anticholinergic or β3-adrenergic receptor agonist medications. If symptoms persist after 4 to 8 weeks of pharmacologic therapy, clinicians are encouraged to reassess or refer the patient to a specialist. Further evaluation may include a bladder diary in which the patient documents voided volumes, voiding frequency, and number of incontinent episodes; symptom-specific questionnaires; and/or urodynamic testing.
Related article:
The latest treatments for urinary and fecal incontinence: Which hold water?
Based on that evaluation, the patient may be a candidate for third-line therapy with either intradetrusor onabotulinumtoxinA, posterior tibial nerve stimulation (PTNS), or sacral neuromodulation.
There is a paucity of information comparing third-line therapies. In this Update, we focus on 4 randomized clinical trials that compare third-line treatment options for idiopathic OAB.
Read about how anticholinergic medication and onabotulinumtoxinA compare for treating UUI.
Anticholinergic therapy and onabotulinumtoxinA produce equivalent reductions in the frequency of daily UUI episodes
Visco AG, Brubaker L, Richter HE, et al; for the Pelvic Floor Disorders Network. Anticholinergic therapy vs onabotulinumtoxinA for urgency urinary incontinence. N Engl J Med. 2012;367(19):1803-1813.
In a double-blind, double-placebo-controlled randomized trial, Visco and colleagues compared anticholinergic medication with onabotulinumtoxinA 100 U for the treatment of women with UUI.
Details of the study
Two hundred forty-one women with moderate to severe UUI received either 6 months of oral anticholinergic therapy (solifenacin 5 mg daily with the option of dose escalation to 10 mg daily or change to trospium XR 60 mg daily based on the Patient Global Symptom Control score) plus a single intradetrusor injection of saline, or a single intradetrusor injection of onabotulinumtoxinA 100 U plus a 6-month oral placebo regimen.
Inclusion criteria were 5 or more UUI episodes on a 3-day diary, insufficient resolution of symptoms after 2 medications, or being drug naive. Exclusions included a postvoid residual (PVR) urine volume greater than 150 mL or previous therapy with onabotulinumtoxinA.
Participants were scheduled for follow up every 2 to 6 months post randomization, at which time all study medications were discontinued. The primary outcome was reduction from baseline in the mean number of UUI episodes per day over the 6-month period, as recorded in the monthly 3-day bladder diaries. Secondary outcomes included the proportion of participants with complete resolution of UUI, the proportion of participants with 75% or more reduction in UUI episodes, Overactive Bladder Questionnaire Short Form (OABq-SF) scores, other symptom-specific questionnaire scores, and adverse events.
Related article:
Which treatments for pelvic floor disorders are backed by evidence?
Both treatments significantly reduced UUI episodes
At baseline, participants reported a mean (SD) of 5.0 (2.7) UUI episodes per day, and 41% of participants were drug naive. Both treatment groups experienced significant reductions compared with baseline in mean UUI episodes, and the reductions were similar between the 2 groups (reduction of 3.4 episodes per day in the anticholinergic group, reduction of 3.3 episodes in the onabotulinumtoxinA group; P = .81). Complete resolution of UUI was more common in the onabotulinumtoxinA group (27%) as compared with the anticholinergic group (13%) (P = .003). There were no differences in improvement in OABq-SF scores (37.05 in the anticholinergic group vs 37.13 in the onabotulinumtoxinA group; P = .98) or other quality-of-life measures.
Adverse events. The anticholinergic group experienced a higher rate of dry mouth compared with the onabotulinumtoxinA group (46% vs 31%; P = .02) but had lower rates of intermittent catheterization use at 2 months (0% vs 5%, P = .01) and UTIs (13% vs 33%, P<.001).
Strengths and limitations. This was a well-designed, multicenter, randomized double-blind, double placebo-controlled trial. The study design allowed for dose escalation and change to another medication for inadequate symptom control and included drug-naive participants, which increases the generalizability of the results. However, current guidelines recommend reserving onabotulinumtoxinA therapy for third-line therapy, thus deterring this treatment's use in the drug-naive population. Additionally, the lack of a pure placebo arm makes it difficult to interpret the extent to which a placebo effect contributed to observed improvements in clinical symptoms.
Through 6 months, both a single intradetrusor injection of onabotulinumtoxinA 100 U and anticholinergic therapy reduce UUI episodes and improve quality-of-life measures in women who have failed medications or are drug naive. Use of onabotulinumtoxinA, however, more likely will lead to complete resolution of UUI, although with an increased risk of transient urinary retention and UTI. Even given the study findings supporting the use of onabotulinumtoxinA over anticholinergic therapy for complete resolution of UUI, it is most appropriate to align with current practice, which includes a trial of pharmacotherapy before proceeding with third-line onabotulinumtoxinA.
Read: onabotulinumtoxinA vs PTNS for OAB.
OnabotulinumtoxinA has greater 9-month durability for OAB symptoms compared with12 weeks of PTNS
Sherif H, Khalil M, Omar R. Management of refractory idiopathic overactive bladder: intradetrusor injection of botulinum toxin type A versus posterior tibial nerve stimulation. Can J Urol. 2017;24(3):8838-8846.
In this randomized clinical trial, Sherif and colleagues compared the safety and efficacy of a single intradetrusor injection of onabotulinumtoxinA 100 U with that of PTNS for OAB.
Details of the study
Sixty adult men and women with OAB who did not respond to medical therapy were randomly assigned to treatment with either onabotulinumtoxinA 100 U or PTNS. Criteria for exclusion were current UTI, PVR urine volume of more than 150 mL, previous radiation therapy or chemotherapy, previous incontinence surgery or bladder malignancy, or presence of mixed urinary incontinence.
At baseline, participants completed a 3-day bladder diary, an OAB symptom score (OABSS) questionnaire, and urodynamic testing. The OABSS questionnaire included 7 questions (scoring range, 0-28), with higher scores indicating worse symptoms, and included subscales for urgency and quality-of-life measures. Total OABSS, urgency score, quality-of-life score, bladder diary records, and urodynamic testing parameters were assessed at 6, 12, 24, and 36 weeks, along with adverse events.
OnabotulinumtoxinA injections were performed under spinal anesthesia. If PVR urine volume was greater than 200 mL at any follow-up visit, participants were instructed to begin clean intermittent self-catheterization. PTNS was administered as weekly 30-minute sessions for 12 consecutive weeks.
Participants' baseline demographics and symptoms were similar. Average age was 45 years. Averages (SD) for duration of anticholinergic use was 13 (0.8) weeks, UUI episode score was 4.5 (1) on 3-day bladder diary, and OABSS was 22 (2.7). Nine-month data were available for 29 participants in the onabotulinumtoxinA group and for 8 in the PTNS group.
Related article:
Update on pelvic floor dysfunction: Focus on urinary incontinence
OnabotulinumtoxinA treatment benefits sustained for 9 months
Through 6 months, compared with baseline assessments, both treatment groups had significant improvements in clinical symptoms and OABSS total score, as well as urgency and quality-of-life subscales. At 3 months, urodynamic study parameters were similarly improved from baseline in both groups.
At 9 months, however, only the onabotulinumtoxinA group, compared with the PTNS group, maintained the significant improvement from baseline in 3-day bladder diary voiding episodes (average [SD], 10.7 [1.01] vs 11.6 [1.09]; P = .009), 3-day bladder diary nocturia episodes (average [SD], 3.8 [1.09] vs 4.4 [0.8]; P = .02), and average [SD] UUI episodes over 3 days (3.5 [1.2] vs 4.2 [1.04]; P = .02). Similarly, onabotulinumtoxinA-treated participants, compared with those treated with PTNS, maintained improvements at 9 months in average (SD): OABSS total score (19.2 [2.4] vs 20.4 [1.7]; P = .03), urgency scores (10.9 [1.3] vs 11.8 [1.4]; P = .009), urine volume at first desire (177.8 [9.2] vs 171.8 [7.7]), maximum cystometric capacity (304 [17.6] vs 290 [13.1]), and Qmax (mL/sec) (20.7 [1.6] vs 22.2 [1.2]).
Adverse events. Average PVR urine volumes were higher in the onabotulinumtoxinA group compared with the PTNS group (36.8 [2.7] vs 32.4 [3.03]; P = .0001) at all time points, and self-catheterization was required in 6.6% of onabotulinumtoxinA-treated participants. Urinary tract infection occurred in 6.6% of participants in the onabotulinumtoxinA group and in none of the PTNS group. In the PTNS group, few experienced pain and minor bleeding at the needle site.
Strengths and limitations. This randomized, open-label trial comparing treatment with onabotulinumtoxinA 100 U and PTNS included both men and women with idiopathic OAB symptoms. The participants were assessed at regular intervals with various measures, and follow-up adherence was good. The sample size was small, so the study may not have been powered to see differences prior to 9 months.
Although at 9 months only the onabotulinumtoxinA group maintained significant improvement over baseline levels, the improvement was diminished, and therefore the clinical meaningfulness is uncertain. Further, participants in the PTNS group did not undergo monthly maintenance therapy after 3 months, which is recommended for those with a 12-week therapeutic response; this may have affected 9-month outcomes in this group. Since the one-time onabotulinumtoxinA 100 U injection was performed under spinal anesthesia, cost comparisons should be considered, since future onabotulinumtoxinA injections would be necessary.
A one-time onabotulinumtoxinA 100 U injection and 12 weeks of PTNS therapy are reasonable short-term options for symptomatic OAB relief after unsuccessful therapy with medications. OnabotulinumtoxinA injection may provide more durable OAB symptom control at 9 months but with a risk of UTI and need for self-catheterization.
Read about using different doses of onabotulinumtoxinA for OAB.
OnabotulinumtoxinA 200-U injection provides longer OAB symptom improvement than 100-U injection
Abdelwahab O, Sherif H, Soliman T, Elbarky I, Eshazly A. Efficacy of botulinum toxin type A 100 units versus 200 units for treatment of refractory idiopathic overactive bladder. Int Braz J Urol. 2015;41(6):1132-1140.
Abdelwahab and colleagues conducted a single-center, randomized clinical trial to investigate the safety and efficacy of a single injection of intradetrusor onabotulinumtoxinA in 2 different doses (100 U and 200 U) for treatment of OAB.
Details of the study
Eighty adults (63 women, 17 men) who did not benefit from anticholinergic medication during the previous 3 months were randomly assigned to receive either a 100-U (n = 40) or a 200-U (n = 40) injection of onabotulinumtoxinA. Exclusion criteria were PVR urine volume greater than 150 mL and previous radiation therapy or chemotherapy.
Initial assessments -- completed at baseline and at 1, 3, 6, and 9 months -- included the health-related quality-of-life (HR-QOL) questionnaire (maximum score, 100; higher score indicates better quality of life), an abbreviated OABSS questionnaire (4 questions; score range, 0-15; higher score indicates more severe symptoms), and urodynamic evaluation. Outcomes included OABSS, HR-QOL score, and urodynamic parameters at the various time points.
Related article:
Is there a link between impaired mobility and urinary incontinence in elderly, community-dwelling women?
Higher dose, greater symptom improvement and higher adverse event rate
At baseline, participants (average age, 31 years) had an average (SD) OABSS of 1.7 (1.6). OnabotulinumtoxinA treatment with both a 100-U and a 200-U dose resulted in significant improvements (compared with baseline levels) in frequency, nocturia, UUI episodes, OABSS, and urodynamic parameters throughout the 9 months. At 9 months, however, the group treated with the 200-U dose had greater improvements, compared with the group who received a 100-U dose, in urinary frequency symptom scores (mean [SD], 0.32 [0.47] vs 1.1 [0.51]; P<.05), nocturia symptom scores (mean [SD], 0.13 [0.34] vs 0.36 [0.49]; P<.05), UUI symptom scores (mean [SD], 0.68 [0.16] vs 1.26 [1.1]; P<.05), and mean (SD) total OABSS (2.6 [2.31] vs 5.3 [2.11]; P<.05). Similarly, at 9 months the 200-U dose resulted in greater improvements in volume at first desire (mean [SD], 291.8 [42.8] vs 246.8 [53.8] mL; P<.05), volume at strong desire (mean [SD], 392.1 [37.3] vs 313.1 [67.4] mL; P<.05), detrusor pressure (mean [SD], 10.4 [4.0] vs 19.2 [7.8] cm H2O; P<.05), and maximum cystometric capacity (mean [SD], 430.5 [34.2] vs 350 [69.1] mL; P<.05) compared with the 100-U dose.
Adverse events. No participant had a PVR urine volume greater than 100 mL at any follow-up visit. Postoperative hematuria occurred in 23% of the group treated with onabotulinumtoxinA 200 U versus in 15% of those treated with a 100-U dose. Similarly, UTIs occurred in 17.5% of the 200-U dose group and in 7.5% of the 100-U dose group. Dysuria was reported in 37.5% and 15% of the 200-U and 100-U dose groups, respectively.
Strengths and limitations. This randomized, open-label trial comparing a single injection of 100 U versus 200 U of onabotulinumtoxinA included mostly women. OAB symptoms and urodynamic parameters improved after treatment with both dose levels, but a longer duration of improvement was seen with the 200-U dose. The cohort had a low baseline OAB severity, based on the OABSS questionnaire, and a young average age of participants, which limits the generalizability of the study results to a population with refractory OAB. The 0% rate of clean intermittent self-catheterization postinjection might be based on the study's criteria for requiring clean intermittent catheterization. In addition, the initial postinjection visit occurred at 1 month, possibly missing participants who had symptoms of retention soon after injection.
Two dose levels (100 U and 200 U) of a single injection of onabotulinumtoxinA are associated with comparable OAB symptom and urodyanamic improvements. The benefits of a longer duration of effect with the 200-U dose must be weighed against the possible higher risks of transient hematuria, dysuria, and UTI.
Read: onabotulinumtoxinA vs sacral neuromodulation therapy for UUI.
Treatment with onabotulinumtoxinA may control UUI symptoms better than sacral neuromodulation therapy
Amundsen CL, Richter HE, Menefee SA, et al; Pelvic Floor Disorders Network. OnabotulinumtoxinA vs sacral neuromodulation on refractory urgency urinary incontinence in women: a randomized clinical trial. JAMA. 2016;316(13):1366-1374.
In this multicenter open-label randomized trial, Amundsen and colleagues compared the efficacy and safety of onabotulinumtoxinA 200 U with that of sacral neuromodulation.
Details of the study
Three hundred sixty-four women with UUI had data available for primary analysis at 6 months. Women were considered eligible for the study if they had 6 or more UUI episodes on a 3-day bladder diary, persistent symptoms despite anticholinergic therapy, a PVR urine volume of less than 150 mL, and had never previously received either study treatment.
There were no differences in baseline characteristics of the participants. The average (SD) age of the study population was 63 (11.6) years, with an average (SD) daily number of UUI episodes of 5.3 (2.8). The average (SD) body mass index was 32 (8) kg/m2.
Participants were randomly assigned to undergo either sacral neuromodulation (n = 174) or intradetrusor injection of onabotulinumtoxinA 200 U (n = 190). The primary outcome was change from baseline in mean number of daily UUI episodes averaged over 6 months as recorded on a monthly 3-day bladder diary. Secondary outcomes included complete resolution of urgency incontinence, 75% or more reduction in UUI episodes, the Overactive Bladder Questionnaire Short Form (SF) score (range, 0-100; higher score indicates higher symptom severity), the Overactive Bladder Satisfaction of Treatment questionnaire (range, 0-100; higher score indicates better satisfaction), other quality-of-life measures, and adverse events.
Related article:
2015 Update on pelvic floor dysfunction: Bladder pain syndrome
Greater symptom bother improvement, treatment satisfaction with onabotulinumtoxinA 200 U
Participants treated with onabotulinumtoxinA had a greater mean reduction of 3.9 UUI episodes per day than the sacral neuromodulation group's reduction of 3.3 UUI episodes per day (mean difference, 0.63; 95% confidence interval [CI], 0.13-1.14; P = .01). In addition, complete UUI resolution was higher in the onabotulinumtoxinA group as compared with the sacral neuromodulation group (20% vs 4%; P<.001). The onabotulinumtoxinA group also had higher rates of 75% or more reduction of UUI episodes compared with the sacral neuromodulation group (46% vs 26%; P<.001). Over 6 months, both groups had improvements in all quality-of-life measures, but the onabotulinumtoxinA group had greater improvement in symptom bother compared with the sacral neuromodulation group (-46.7 vs -38.6; mean difference, 8.1; 95% CI, 3.0-13.3; P = .002). Furthermore, the onabotulinumtoxinA group had greater treatment satisfaction compared with the sacral neuromodulation group (mean difference, 7.8; 95% CI, 1.6-14.1; P = .01).
Adverse events. Six women (3%) underwent sacral neuromodulation device revision or removal. Approximately 8% of onabotulinumtoxinA-treated participants required intermittent self-catheterization at 1 month, 4% at 3 months, and 2% at 6 months. The risk of UTI was higher in the onabotulinumtoxinA group compared with the sacral neuromodulation group (35% vs 11%; risk difference, 23%; 95% CI, -33% to -13%; P<.001).
Strengths and limitations. This is a well-designed randomized clinical trial comparing clinical outcomes and adverse events after treatment with onabotulinumtoxinA 200-U versus sacral neuromodulation. The interventions were standardized across investigators at multiple sites, and the study design required close follow-up to assess efficacy and adverse events. The study used a 200-U dose based on reported durability of effect at that time and findings of equivalency between onabotulinumtoxinA 100 U and anticholinergic therapy. The US Food and Drug Administration's recommendation to use a 100-U dose in all patients with idiopathic OAB might dissuade clinicians from considering the higher dose of onabotulinumtoxinA. The study was limited by the lack of a placebo group.
Both onabotulinumtoxinA 200 U and sacral neuromodulation provide significant improvement in UUI episodes and quality of life over 6 months. However, while treatment with onabotulinumtoxinA has a likelihood of complete UUI resolution, greater improvements in symptom bother and treatment satisfaction, these benefits must be weighed against the risks of transient catheterization and UTI.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Haylen BT, de Ridder D, Freeman RM, et al; International Urogynecological Association; International Continence Society. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4-20.
- Hartmann KE, McPheeters ML, Biller DH, et al. Treatment of overactive bladder in women. Evid Rep Technol Assess (Full Rep). 2009;187:1-120.
- Reynolds,WS, Fowke J, Dmochowski, R. The burden of overactive bladder on US public health. Curr Bladder Dysfunct Rep. 2016;11(1):8-13.
- Willis-Gray MG, Dieter AA, Geller EJ. Evaluation and management of overactive bladder: strategies for optimizing care. Res Rep Urol. 2016;8:113-122.
- Ganz ML, Smalarz AM, Krupski TL, et al. Economic costs of overactive bladder in the United States. Urology. 2010;75(3):526-532.
- Gormley EA, Lightner DJ, Faraday M, Vasavada SP; American Urological Association; Society of Urodyndamics, Female Pelvic Medicine. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline amendment. J Urol. 2015; 193(5):1572-1580.
- Gormley EA, Lightner DJ, Burgio KL, et al; American Urological Association; Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. J Urol. 2012;188(6 suppl):2455-2463.
Dr. Vaughan is a Fellow, Division of Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, Duke University Medical Center, Durham, North Carolina.

Dr. Amundsen is Roy T. Parker Professor in Obstetrics and Gynecology, Urogynecology and Reconstructive Pelvic Surgery; Associate Professor of Surgery, Division of Urology; Program Director of the Female Pelvic Medicine and Reconstructive Surgery Fellowship; Program Director of K12 Multidisciplinary Urologic Research Scholars Program, Duke University Medical Center, Durham, North Carolina.
The authors report no financial relationships relevant to this article.
Dr. Vaughan is a Fellow, Division of Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, Duke University Medical Center, Durham, North Carolina.
Dr. Amundsen is Roy T. Parker Professor in Obstetrics and Gynecology, Urogynecology and Reconstructive Pelvic Surgery; Associate Professor of Surgery, Division of Urology; Program Director of the Female Pelvic Medicine and Reconstructive Surgery Fellowship; Program Director of K12 Multidisciplinary Urologic Research Scholars Program, Duke University Medical Center, Durham, North Carolina.
The authors report no financial relationships relevant to this article.
Dr. Vaughan is a Fellow, Division of Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, Duke University Medical Center, Durham, North Carolina.
Dr. Amundsen is Roy T. Parker Professor in Obstetrics and Gynecology, Urogynecology and Reconstructive Pelvic Surgery; Associate Professor of Surgery, Division of Urology; Program Director of the Female Pelvic Medicine and Reconstructive Surgery Fellowship; Program Director of K12 Multidisciplinary Urologic Research Scholars Program, Duke University Medical Center, Durham, North Carolina.
The authors report no financial relationships relevant to this article.
The International Continence Society (ICS) defines overactive bladder (OAB) as a syndrome of "urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence (UUI), in the absence of urinary tract infection [UTI] or obvious pathology."1 The Agency for Healthcare Research and Quality (AHRQ) reported OAB prevalence to be 15% in US women, with 11% reporting UUI.2 OAB represents a significant health care burden that impacts nearly every aspect of life, including physical, emotional, and psychological domains.3,4 The economic impact is notable; the projected cost is estimated to reach $82.6 billion annually by 2020.5
The American Urological Association (AUA) and the Society for Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction (SUFU) have endorsed an algorithm for use in the evaluation of idiopathic OAB (FIGURE).6 If the patient's symptoms are certain, minimal evaluation is needed and it is reasonable to proceed with first-line therapy, which includes fluid management (decreasing caffeine intake and limiting evening fluid intake), bladder retraining drills such as timed voiding, and improving pelvic floor muscles with the use of biofeedback and functional electrical stimulation.6,7 Pelvic floor muscle training can be facilitated with a referral to a physical therapist trained in pelvic floor muscle education.
If treatment goals are not met with first-line strategies, second-line therapy may be initiated with anticholinergic or β3-adrenergic receptor agonist medications. If symptoms persist after 4 to 8 weeks of pharmacologic therapy, clinicians are encouraged to reassess or refer the patient to a specialist. Further evaluation may include a bladder diary in which the patient documents voided volumes, voiding frequency, and number of incontinent episodes; symptom-specific questionnaires; and/or urodynamic testing.
Related article:
The latest treatments for urinary and fecal incontinence: Which hold water?
Based on that evaluation, the patient may be a candidate for third-line therapy with either intradetrusor onabotulinumtoxinA, posterior tibial nerve stimulation (PTNS), or sacral neuromodulation.
There is a paucity of information comparing third-line therapies. In this Update, we focus on 4 randomized clinical trials that compare third-line treatment options for idiopathic OAB.
Read about how anticholinergic medication and onabotulinumtoxinA compare for treating UUI.
Anticholinergic therapy and onabotulinumtoxinA produce equivalent reductions in the frequency of daily UUI episodes
Visco AG, Brubaker L, Richter HE, et al; for the Pelvic Floor Disorders Network. Anticholinergic therapy vs onabotulinumtoxinA for urgency urinary incontinence. N Engl J Med. 2012;367(19):1803-1813.
In a double-blind, double-placebo-controlled randomized trial, Visco and colleagues compared anticholinergic medication with onabotulinumtoxinA 100 U for the treatment of women with UUI.
Details of the study
Two hundred forty-one women with moderate to severe UUI received either 6 months of oral anticholinergic therapy (solifenacin 5 mg daily with the option of dose escalation to 10 mg daily or change to trospium XR 60 mg daily based on the Patient Global Symptom Control score) plus a single intradetrusor injection of saline, or a single intradetrusor injection of onabotulinumtoxinA 100 U plus a 6-month oral placebo regimen.
Inclusion criteria were 5 or more UUI episodes on a 3-day diary, insufficient resolution of symptoms after 2 medications, or being drug naive. Exclusions included a postvoid residual (PVR) urine volume greater than 150 mL or previous therapy with onabotulinumtoxinA.
Participants were scheduled for follow up every 2 to 6 months post randomization, at which time all study medications were discontinued. The primary outcome was reduction from baseline in the mean number of UUI episodes per day over the 6-month period, as recorded in the monthly 3-day bladder diaries. Secondary outcomes included the proportion of participants with complete resolution of UUI, the proportion of participants with 75% or more reduction in UUI episodes, Overactive Bladder Questionnaire Short Form (OABq-SF) scores, other symptom-specific questionnaire scores, and adverse events.
Related article:
Which treatments for pelvic floor disorders are backed by evidence?
Both treatments significantly reduced UUI episodes
At baseline, participants reported a mean (SD) of 5.0 (2.7) UUI episodes per day, and 41% of participants were drug naive. Both treatment groups experienced significant reductions compared with baseline in mean UUI episodes, and the reductions were similar between the 2 groups (reduction of 3.4 episodes per day in the anticholinergic group, reduction of 3.3 episodes in the onabotulinumtoxinA group; P = .81). Complete resolution of UUI was more common in the onabotulinumtoxinA group (27%) as compared with the anticholinergic group (13%) (P = .003). There were no differences in improvement in OABq-SF scores (37.05 in the anticholinergic group vs 37.13 in the onabotulinumtoxinA group; P = .98) or other quality-of-life measures.
Adverse events. The anticholinergic group experienced a higher rate of dry mouth compared with the onabotulinumtoxinA group (46% vs 31%; P = .02) but had lower rates of intermittent catheterization use at 2 months (0% vs 5%, P = .01) and UTIs (13% vs 33%, P<.001).
Strengths and limitations. This was a well-designed, multicenter, randomized double-blind, double placebo-controlled trial. The study design allowed for dose escalation and change to another medication for inadequate symptom control and included drug-naive participants, which increases the generalizability of the results. However, current guidelines recommend reserving onabotulinumtoxinA therapy for third-line therapy, thus deterring this treatment's use in the drug-naive population. Additionally, the lack of a pure placebo arm makes it difficult to interpret the extent to which a placebo effect contributed to observed improvements in clinical symptoms.
Through 6 months, both a single intradetrusor injection of onabotulinumtoxinA 100 U and anticholinergic therapy reduce UUI episodes and improve quality-of-life measures in women who have failed medications or are drug naive. Use of onabotulinumtoxinA, however, more likely will lead to complete resolution of UUI, although with an increased risk of transient urinary retention and UTI. Even given the study findings supporting the use of onabotulinumtoxinA over anticholinergic therapy for complete resolution of UUI, it is most appropriate to align with current practice, which includes a trial of pharmacotherapy before proceeding with third-line onabotulinumtoxinA.
Read: onabotulinumtoxinA vs PTNS for OAB.
OnabotulinumtoxinA has greater 9-month durability for OAB symptoms compared with12 weeks of PTNS
Sherif H, Khalil M, Omar R. Management of refractory idiopathic overactive bladder: intradetrusor injection of botulinum toxin type A versus posterior tibial nerve stimulation. Can J Urol. 2017;24(3):8838-8846.
In this randomized clinical trial, Sherif and colleagues compared the safety and efficacy of a single intradetrusor injection of onabotulinumtoxinA 100 U with that of PTNS for OAB.
Details of the study
Sixty adult men and women with OAB who did not respond to medical therapy were randomly assigned to treatment with either onabotulinumtoxinA 100 U or PTNS. Criteria for exclusion were current UTI, PVR urine volume of more than 150 mL, previous radiation therapy or chemotherapy, previous incontinence surgery or bladder malignancy, or presence of mixed urinary incontinence.
At baseline, participants completed a 3-day bladder diary, an OAB symptom score (OABSS) questionnaire, and urodynamic testing. The OABSS questionnaire included 7 questions (scoring range, 0-28), with higher scores indicating worse symptoms, and included subscales for urgency and quality-of-life measures. Total OABSS, urgency score, quality-of-life score, bladder diary records, and urodynamic testing parameters were assessed at 6, 12, 24, and 36 weeks, along with adverse events.
OnabotulinumtoxinA injections were performed under spinal anesthesia. If PVR urine volume was greater than 200 mL at any follow-up visit, participants were instructed to begin clean intermittent self-catheterization. PTNS was administered as weekly 30-minute sessions for 12 consecutive weeks.
Participants' baseline demographics and symptoms were similar. Average age was 45 years. Averages (SD) for duration of anticholinergic use was 13 (0.8) weeks, UUI episode score was 4.5 (1) on 3-day bladder diary, and OABSS was 22 (2.7). Nine-month data were available for 29 participants in the onabotulinumtoxinA group and for 8 in the PTNS group.
Related article:
Update on pelvic floor dysfunction: Focus on urinary incontinence
OnabotulinumtoxinA treatment benefits sustained for 9 months
Through 6 months, compared with baseline assessments, both treatment groups had significant improvements in clinical symptoms and OABSS total score, as well as urgency and quality-of-life subscales. At 3 months, urodynamic study parameters were similarly improved from baseline in both groups.
At 9 months, however, only the onabotulinumtoxinA group, compared with the PTNS group, maintained the significant improvement from baseline in 3-day bladder diary voiding episodes (average [SD], 10.7 [1.01] vs 11.6 [1.09]; P = .009), 3-day bladder diary nocturia episodes (average [SD], 3.8 [1.09] vs 4.4 [0.8]; P = .02), and average [SD] UUI episodes over 3 days (3.5 [1.2] vs 4.2 [1.04]; P = .02). Similarly, onabotulinumtoxinA-treated participants, compared with those treated with PTNS, maintained improvements at 9 months in average (SD): OABSS total score (19.2 [2.4] vs 20.4 [1.7]; P = .03), urgency scores (10.9 [1.3] vs 11.8 [1.4]; P = .009), urine volume at first desire (177.8 [9.2] vs 171.8 [7.7]), maximum cystometric capacity (304 [17.6] vs 290 [13.1]), and Qmax (mL/sec) (20.7 [1.6] vs 22.2 [1.2]).
Adverse events. Average PVR urine volumes were higher in the onabotulinumtoxinA group compared with the PTNS group (36.8 [2.7] vs 32.4 [3.03]; P = .0001) at all time points, and self-catheterization was required in 6.6% of onabotulinumtoxinA-treated participants. Urinary tract infection occurred in 6.6% of participants in the onabotulinumtoxinA group and in none of the PTNS group. In the PTNS group, few experienced pain and minor bleeding at the needle site.
Strengths and limitations. This randomized, open-label trial comparing treatment with onabotulinumtoxinA 100 U and PTNS included both men and women with idiopathic OAB symptoms. The participants were assessed at regular intervals with various measures, and follow-up adherence was good. The sample size was small, so the study may not have been powered to see differences prior to 9 months.
Although at 9 months only the onabotulinumtoxinA group maintained significant improvement over baseline levels, the improvement was diminished, and therefore the clinical meaningfulness is uncertain. Further, participants in the PTNS group did not undergo monthly maintenance therapy after 3 months, which is recommended for those with a 12-week therapeutic response; this may have affected 9-month outcomes in this group. Since the one-time onabotulinumtoxinA 100 U injection was performed under spinal anesthesia, cost comparisons should be considered, since future onabotulinumtoxinA injections would be necessary.
A one-time onabotulinumtoxinA 100 U injection and 12 weeks of PTNS therapy are reasonable short-term options for symptomatic OAB relief after unsuccessful therapy with medications. OnabotulinumtoxinA injection may provide more durable OAB symptom control at 9 months but with a risk of UTI and need for self-catheterization.
Read about using different doses of onabotulinumtoxinA for OAB.
OnabotulinumtoxinA 200-U injection provides longer OAB symptom improvement than 100-U injection
Abdelwahab O, Sherif H, Soliman T, Elbarky I, Eshazly A. Efficacy of botulinum toxin type A 100 units versus 200 units for treatment of refractory idiopathic overactive bladder. Int Braz J Urol. 2015;41(6):1132-1140.
Abdelwahab and colleagues conducted a single-center, randomized clinical trial to investigate the safety and efficacy of a single injection of intradetrusor onabotulinumtoxinA in 2 different doses (100 U and 200 U) for treatment of OAB.
Details of the study
Eighty adults (63 women, 17 men) who did not benefit from anticholinergic medication during the previous 3 months were randomly assigned to receive either a 100-U (n = 40) or a 200-U (n = 40) injection of onabotulinumtoxinA. Exclusion criteria were PVR urine volume greater than 150 mL and previous radiation therapy or chemotherapy.
Initial assessments -- completed at baseline and at 1, 3, 6, and 9 months -- included the health-related quality-of-life (HR-QOL) questionnaire (maximum score, 100; higher score indicates better quality of life), an abbreviated OABSS questionnaire (4 questions; score range, 0-15; higher score indicates more severe symptoms), and urodynamic evaluation. Outcomes included OABSS, HR-QOL score, and urodynamic parameters at the various time points.
Related article:
Is there a link between impaired mobility and urinary incontinence in elderly, community-dwelling women?
Higher dose, greater symptom improvement and higher adverse event rate
At baseline, participants (average age, 31 years) had an average (SD) OABSS of 1.7 (1.6). OnabotulinumtoxinA treatment with both a 100-U and a 200-U dose resulted in significant improvements (compared with baseline levels) in frequency, nocturia, UUI episodes, OABSS, and urodynamic parameters throughout the 9 months. At 9 months, however, the group treated with the 200-U dose had greater improvements, compared with the group who received a 100-U dose, in urinary frequency symptom scores (mean [SD], 0.32 [0.47] vs 1.1 [0.51]; P<.05), nocturia symptom scores (mean [SD], 0.13 [0.34] vs 0.36 [0.49]; P<.05), UUI symptom scores (mean [SD], 0.68 [0.16] vs 1.26 [1.1]; P<.05), and mean (SD) total OABSS (2.6 [2.31] vs 5.3 [2.11]; P<.05). Similarly, at 9 months the 200-U dose resulted in greater improvements in volume at first desire (mean [SD], 291.8 [42.8] vs 246.8 [53.8] mL; P<.05), volume at strong desire (mean [SD], 392.1 [37.3] vs 313.1 [67.4] mL; P<.05), detrusor pressure (mean [SD], 10.4 [4.0] vs 19.2 [7.8] cm H2O; P<.05), and maximum cystometric capacity (mean [SD], 430.5 [34.2] vs 350 [69.1] mL; P<.05) compared with the 100-U dose.
Adverse events. No participant had a PVR urine volume greater than 100 mL at any follow-up visit. Postoperative hematuria occurred in 23% of the group treated with onabotulinumtoxinA 200 U versus in 15% of those treated with a 100-U dose. Similarly, UTIs occurred in 17.5% of the 200-U dose group and in 7.5% of the 100-U dose group. Dysuria was reported in 37.5% and 15% of the 200-U and 100-U dose groups, respectively.
Strengths and limitations. This randomized, open-label trial comparing a single injection of 100 U versus 200 U of onabotulinumtoxinA included mostly women. OAB symptoms and urodynamic parameters improved after treatment with both dose levels, but a longer duration of improvement was seen with the 200-U dose. The cohort had a low baseline OAB severity, based on the OABSS questionnaire, and a young average age of participants, which limits the generalizability of the study results to a population with refractory OAB. The 0% rate of clean intermittent self-catheterization postinjection might be based on the study's criteria for requiring clean intermittent catheterization. In addition, the initial postinjection visit occurred at 1 month, possibly missing participants who had symptoms of retention soon after injection.
Two dose levels (100 U and 200 U) of a single injection of onabotulinumtoxinA are associated with comparable OAB symptom and urodyanamic improvements. The benefits of a longer duration of effect with the 200-U dose must be weighed against the possible higher risks of transient hematuria, dysuria, and UTI.
Read: onabotulinumtoxinA vs sacral neuromodulation therapy for UUI.
Treatment with onabotulinumtoxinA may control UUI symptoms better than sacral neuromodulation therapy
Amundsen CL, Richter HE, Menefee SA, et al; Pelvic Floor Disorders Network. OnabotulinumtoxinA vs sacral neuromodulation on refractory urgency urinary incontinence in women: a randomized clinical trial. JAMA. 2016;316(13):1366-1374.
In this multicenter open-label randomized trial, Amundsen and colleagues compared the efficacy and safety of onabotulinumtoxinA 200 U with that of sacral neuromodulation.
Details of the study
Three hundred sixty-four women with UUI had data available for primary analysis at 6 months. Women were considered eligible for the study if they had 6 or more UUI episodes on a 3-day bladder diary, persistent symptoms despite anticholinergic therapy, a PVR urine volume of less than 150 mL, and had never previously received either study treatment.
There were no differences in baseline characteristics of the participants. The average (SD) age of the study population was 63 (11.6) years, with an average (SD) daily number of UUI episodes of 5.3 (2.8). The average (SD) body mass index was 32 (8) kg/m2.
Participants were randomly assigned to undergo either sacral neuromodulation (n = 174) or intradetrusor injection of onabotulinumtoxinA 200 U (n = 190). The primary outcome was change from baseline in mean number of daily UUI episodes averaged over 6 months as recorded on a monthly 3-day bladder diary. Secondary outcomes included complete resolution of urgency incontinence, 75% or more reduction in UUI episodes, the Overactive Bladder Questionnaire Short Form (SF) score (range, 0-100; higher score indicates higher symptom severity), the Overactive Bladder Satisfaction of Treatment questionnaire (range, 0-100; higher score indicates better satisfaction), other quality-of-life measures, and adverse events.
Related article:
2015 Update on pelvic floor dysfunction: Bladder pain syndrome
Greater symptom bother improvement, treatment satisfaction with onabotulinumtoxinA 200 U
Participants treated with onabotulinumtoxinA had a greater mean reduction of 3.9 UUI episodes per day than the sacral neuromodulation group's reduction of 3.3 UUI episodes per day (mean difference, 0.63; 95% confidence interval [CI], 0.13-1.14; P = .01). In addition, complete UUI resolution was higher in the onabotulinumtoxinA group as compared with the sacral neuromodulation group (20% vs 4%; P<.001). The onabotulinumtoxinA group also had higher rates of 75% or more reduction of UUI episodes compared with the sacral neuromodulation group (46% vs 26%; P<.001). Over 6 months, both groups had improvements in all quality-of-life measures, but the onabotulinumtoxinA group had greater improvement in symptom bother compared with the sacral neuromodulation group (-46.7 vs -38.6; mean difference, 8.1; 95% CI, 3.0-13.3; P = .002). Furthermore, the onabotulinumtoxinA group had greater treatment satisfaction compared with the sacral neuromodulation group (mean difference, 7.8; 95% CI, 1.6-14.1; P = .01).
Adverse events. Six women (3%) underwent sacral neuromodulation device revision or removal. Approximately 8% of onabotulinumtoxinA-treated participants required intermittent self-catheterization at 1 month, 4% at 3 months, and 2% at 6 months. The risk of UTI was higher in the onabotulinumtoxinA group compared with the sacral neuromodulation group (35% vs 11%; risk difference, 23%; 95% CI, -33% to -13%; P<.001).
Strengths and limitations. This is a well-designed randomized clinical trial comparing clinical outcomes and adverse events after treatment with onabotulinumtoxinA 200-U versus sacral neuromodulation. The interventions were standardized across investigators at multiple sites, and the study design required close follow-up to assess efficacy and adverse events. The study used a 200-U dose based on reported durability of effect at that time and findings of equivalency between onabotulinumtoxinA 100 U and anticholinergic therapy. The US Food and Drug Administration's recommendation to use a 100-U dose in all patients with idiopathic OAB might dissuade clinicians from considering the higher dose of onabotulinumtoxinA. The study was limited by the lack of a placebo group.
Both onabotulinumtoxinA 200 U and sacral neuromodulation provide significant improvement in UUI episodes and quality of life over 6 months. However, while treatment with onabotulinumtoxinA has a likelihood of complete UUI resolution, greater improvements in symptom bother and treatment satisfaction, these benefits must be weighed against the risks of transient catheterization and UTI.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The International Continence Society (ICS) defines overactive bladder (OAB) as a syndrome of "urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence (UUI), in the absence of urinary tract infection [UTI] or obvious pathology."1 The Agency for Healthcare Research and Quality (AHRQ) reported OAB prevalence to be 15% in US women, with 11% reporting UUI.2 OAB represents a significant health care burden that impacts nearly every aspect of life, including physical, emotional, and psychological domains.3,4 The economic impact is notable; the projected cost is estimated to reach $82.6 billion annually by 2020.5
The American Urological Association (AUA) and the Society for Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction (SUFU) have endorsed an algorithm for use in the evaluation of idiopathic OAB (FIGURE).6 If the patient's symptoms are certain, minimal evaluation is needed and it is reasonable to proceed with first-line therapy, which includes fluid management (decreasing caffeine intake and limiting evening fluid intake), bladder retraining drills such as timed voiding, and improving pelvic floor muscles with the use of biofeedback and functional electrical stimulation.6,7 Pelvic floor muscle training can be facilitated with a referral to a physical therapist trained in pelvic floor muscle education.
If treatment goals are not met with first-line strategies, second-line therapy may be initiated with anticholinergic or β3-adrenergic receptor agonist medications. If symptoms persist after 4 to 8 weeks of pharmacologic therapy, clinicians are encouraged to reassess or refer the patient to a specialist. Further evaluation may include a bladder diary in which the patient documents voided volumes, voiding frequency, and number of incontinent episodes; symptom-specific questionnaires; and/or urodynamic testing.
Related article:
The latest treatments for urinary and fecal incontinence: Which hold water?
Based on that evaluation, the patient may be a candidate for third-line therapy with either intradetrusor onabotulinumtoxinA, posterior tibial nerve stimulation (PTNS), or sacral neuromodulation.
There is a paucity of information comparing third-line therapies. In this Update, we focus on 4 randomized clinical trials that compare third-line treatment options for idiopathic OAB.
Read about how anticholinergic medication and onabotulinumtoxinA compare for treating UUI.
Anticholinergic therapy and onabotulinumtoxinA produce equivalent reductions in the frequency of daily UUI episodes
Visco AG, Brubaker L, Richter HE, et al; for the Pelvic Floor Disorders Network. Anticholinergic therapy vs onabotulinumtoxinA for urgency urinary incontinence. N Engl J Med. 2012;367(19):1803-1813.
In a double-blind, double-placebo-controlled randomized trial, Visco and colleagues compared anticholinergic medication with onabotulinumtoxinA 100 U for the treatment of women with UUI.
Details of the study
Two hundred forty-one women with moderate to severe UUI received either 6 months of oral anticholinergic therapy (solifenacin 5 mg daily with the option of dose escalation to 10 mg daily or change to trospium XR 60 mg daily based on the Patient Global Symptom Control score) plus a single intradetrusor injection of saline, or a single intradetrusor injection of onabotulinumtoxinA 100 U plus a 6-month oral placebo regimen.
Inclusion criteria were 5 or more UUI episodes on a 3-day diary, insufficient resolution of symptoms after 2 medications, or being drug naive. Exclusions included a postvoid residual (PVR) urine volume greater than 150 mL or previous therapy with onabotulinumtoxinA.
Participants were scheduled for follow up every 2 to 6 months post randomization, at which time all study medications were discontinued. The primary outcome was reduction from baseline in the mean number of UUI episodes per day over the 6-month period, as recorded in the monthly 3-day bladder diaries. Secondary outcomes included the proportion of participants with complete resolution of UUI, the proportion of participants with 75% or more reduction in UUI episodes, Overactive Bladder Questionnaire Short Form (OABq-SF) scores, other symptom-specific questionnaire scores, and adverse events.
Related article:
Which treatments for pelvic floor disorders are backed by evidence?
Both treatments significantly reduced UUI episodes
At baseline, participants reported a mean (SD) of 5.0 (2.7) UUI episodes per day, and 41% of participants were drug naive. Both treatment groups experienced significant reductions compared with baseline in mean UUI episodes, and the reductions were similar between the 2 groups (reduction of 3.4 episodes per day in the anticholinergic group, reduction of 3.3 episodes in the onabotulinumtoxinA group; P = .81). Complete resolution of UUI was more common in the onabotulinumtoxinA group (27%) as compared with the anticholinergic group (13%) (P = .003). There were no differences in improvement in OABq-SF scores (37.05 in the anticholinergic group vs 37.13 in the onabotulinumtoxinA group; P = .98) or other quality-of-life measures.
Adverse events. The anticholinergic group experienced a higher rate of dry mouth compared with the onabotulinumtoxinA group (46% vs 31%; P = .02) but had lower rates of intermittent catheterization use at 2 months (0% vs 5%, P = .01) and UTIs (13% vs 33%, P<.001).
Strengths and limitations. This was a well-designed, multicenter, randomized double-blind, double placebo-controlled trial. The study design allowed for dose escalation and change to another medication for inadequate symptom control and included drug-naive participants, which increases the generalizability of the results. However, current guidelines recommend reserving onabotulinumtoxinA therapy for third-line therapy, thus deterring this treatment's use in the drug-naive population. Additionally, the lack of a pure placebo arm makes it difficult to interpret the extent to which a placebo effect contributed to observed improvements in clinical symptoms.
Through 6 months, both a single intradetrusor injection of onabotulinumtoxinA 100 U and anticholinergic therapy reduce UUI episodes and improve quality-of-life measures in women who have failed medications or are drug naive. Use of onabotulinumtoxinA, however, more likely will lead to complete resolution of UUI, although with an increased risk of transient urinary retention and UTI. Even given the study findings supporting the use of onabotulinumtoxinA over anticholinergic therapy for complete resolution of UUI, it is most appropriate to align with current practice, which includes a trial of pharmacotherapy before proceeding with third-line onabotulinumtoxinA.
Read: onabotulinumtoxinA vs PTNS for OAB.
OnabotulinumtoxinA has greater 9-month durability for OAB symptoms compared with12 weeks of PTNS
Sherif H, Khalil M, Omar R. Management of refractory idiopathic overactive bladder: intradetrusor injection of botulinum toxin type A versus posterior tibial nerve stimulation. Can J Urol. 2017;24(3):8838-8846.
In this randomized clinical trial, Sherif and colleagues compared the safety and efficacy of a single intradetrusor injection of onabotulinumtoxinA 100 U with that of PTNS for OAB.
Details of the study
Sixty adult men and women with OAB who did not respond to medical therapy were randomly assigned to treatment with either onabotulinumtoxinA 100 U or PTNS. Criteria for exclusion were current UTI, PVR urine volume of more than 150 mL, previous radiation therapy or chemotherapy, previous incontinence surgery or bladder malignancy, or presence of mixed urinary incontinence.
At baseline, participants completed a 3-day bladder diary, an OAB symptom score (OABSS) questionnaire, and urodynamic testing. The OABSS questionnaire included 7 questions (scoring range, 0-28), with higher scores indicating worse symptoms, and included subscales for urgency and quality-of-life measures. Total OABSS, urgency score, quality-of-life score, bladder diary records, and urodynamic testing parameters were assessed at 6, 12, 24, and 36 weeks, along with adverse events.
OnabotulinumtoxinA injections were performed under spinal anesthesia. If PVR urine volume was greater than 200 mL at any follow-up visit, participants were instructed to begin clean intermittent self-catheterization. PTNS was administered as weekly 30-minute sessions for 12 consecutive weeks.
Participants' baseline demographics and symptoms were similar. Average age was 45 years. Averages (SD) for duration of anticholinergic use was 13 (0.8) weeks, UUI episode score was 4.5 (1) on 3-day bladder diary, and OABSS was 22 (2.7). Nine-month data were available for 29 participants in the onabotulinumtoxinA group and for 8 in the PTNS group.
Related article:
Update on pelvic floor dysfunction: Focus on urinary incontinence
OnabotulinumtoxinA treatment benefits sustained for 9 months
Through 6 months, compared with baseline assessments, both treatment groups had significant improvements in clinical symptoms and OABSS total score, as well as urgency and quality-of-life subscales. At 3 months, urodynamic study parameters were similarly improved from baseline in both groups.
At 9 months, however, only the onabotulinumtoxinA group, compared with the PTNS group, maintained the significant improvement from baseline in 3-day bladder diary voiding episodes (average [SD], 10.7 [1.01] vs 11.6 [1.09]; P = .009), 3-day bladder diary nocturia episodes (average [SD], 3.8 [1.09] vs 4.4 [0.8]; P = .02), and average [SD] UUI episodes over 3 days (3.5 [1.2] vs 4.2 [1.04]; P = .02). Similarly, onabotulinumtoxinA-treated participants, compared with those treated with PTNS, maintained improvements at 9 months in average (SD): OABSS total score (19.2 [2.4] vs 20.4 [1.7]; P = .03), urgency scores (10.9 [1.3] vs 11.8 [1.4]; P = .009), urine volume at first desire (177.8 [9.2] vs 171.8 [7.7]), maximum cystometric capacity (304 [17.6] vs 290 [13.1]), and Qmax (mL/sec) (20.7 [1.6] vs 22.2 [1.2]).
Adverse events. Average PVR urine volumes were higher in the onabotulinumtoxinA group compared with the PTNS group (36.8 [2.7] vs 32.4 [3.03]; P = .0001) at all time points, and self-catheterization was required in 6.6% of onabotulinumtoxinA-treated participants. Urinary tract infection occurred in 6.6% of participants in the onabotulinumtoxinA group and in none of the PTNS group. In the PTNS group, few experienced pain and minor bleeding at the needle site.
Strengths and limitations. This randomized, open-label trial comparing treatment with onabotulinumtoxinA 100 U and PTNS included both men and women with idiopathic OAB symptoms. The participants were assessed at regular intervals with various measures, and follow-up adherence was good. The sample size was small, so the study may not have been powered to see differences prior to 9 months.
Although at 9 months only the onabotulinumtoxinA group maintained significant improvement over baseline levels, the improvement was diminished, and therefore the clinical meaningfulness is uncertain. Further, participants in the PTNS group did not undergo monthly maintenance therapy after 3 months, which is recommended for those with a 12-week therapeutic response; this may have affected 9-month outcomes in this group. Since the one-time onabotulinumtoxinA 100 U injection was performed under spinal anesthesia, cost comparisons should be considered, since future onabotulinumtoxinA injections would be necessary.
A one-time onabotulinumtoxinA 100 U injection and 12 weeks of PTNS therapy are reasonable short-term options for symptomatic OAB relief after unsuccessful therapy with medications. OnabotulinumtoxinA injection may provide more durable OAB symptom control at 9 months but with a risk of UTI and need for self-catheterization.
Read about using different doses of onabotulinumtoxinA for OAB.
OnabotulinumtoxinA 200-U injection provides longer OAB symptom improvement than 100-U injection
Abdelwahab O, Sherif H, Soliman T, Elbarky I, Eshazly A. Efficacy of botulinum toxin type A 100 units versus 200 units for treatment of refractory idiopathic overactive bladder. Int Braz J Urol. 2015;41(6):1132-1140.
Abdelwahab and colleagues conducted a single-center, randomized clinical trial to investigate the safety and efficacy of a single injection of intradetrusor onabotulinumtoxinA in 2 different doses (100 U and 200 U) for treatment of OAB.
Details of the study
Eighty adults (63 women, 17 men) who did not benefit from anticholinergic medication during the previous 3 months were randomly assigned to receive either a 100-U (n = 40) or a 200-U (n = 40) injection of onabotulinumtoxinA. Exclusion criteria were PVR urine volume greater than 150 mL and previous radiation therapy or chemotherapy.
Initial assessments -- completed at baseline and at 1, 3, 6, and 9 months -- included the health-related quality-of-life (HR-QOL) questionnaire (maximum score, 100; higher score indicates better quality of life), an abbreviated OABSS questionnaire (4 questions; score range, 0-15; higher score indicates more severe symptoms), and urodynamic evaluation. Outcomes included OABSS, HR-QOL score, and urodynamic parameters at the various time points.
Related article:
Is there a link between impaired mobility and urinary incontinence in elderly, community-dwelling women?
Higher dose, greater symptom improvement and higher adverse event rate
At baseline, participants (average age, 31 years) had an average (SD) OABSS of 1.7 (1.6). OnabotulinumtoxinA treatment with both a 100-U and a 200-U dose resulted in significant improvements (compared with baseline levels) in frequency, nocturia, UUI episodes, OABSS, and urodynamic parameters throughout the 9 months. At 9 months, however, the group treated with the 200-U dose had greater improvements, compared with the group who received a 100-U dose, in urinary frequency symptom scores (mean [SD], 0.32 [0.47] vs 1.1 [0.51]; P<.05), nocturia symptom scores (mean [SD], 0.13 [0.34] vs 0.36 [0.49]; P<.05), UUI symptom scores (mean [SD], 0.68 [0.16] vs 1.26 [1.1]; P<.05), and mean (SD) total OABSS (2.6 [2.31] vs 5.3 [2.11]; P<.05). Similarly, at 9 months the 200-U dose resulted in greater improvements in volume at first desire (mean [SD], 291.8 [42.8] vs 246.8 [53.8] mL; P<.05), volume at strong desire (mean [SD], 392.1 [37.3] vs 313.1 [67.4] mL; P<.05), detrusor pressure (mean [SD], 10.4 [4.0] vs 19.2 [7.8] cm H2O; P<.05), and maximum cystometric capacity (mean [SD], 430.5 [34.2] vs 350 [69.1] mL; P<.05) compared with the 100-U dose.
Adverse events. No participant had a PVR urine volume greater than 100 mL at any follow-up visit. Postoperative hematuria occurred in 23% of the group treated with onabotulinumtoxinA 200 U versus in 15% of those treated with a 100-U dose. Similarly, UTIs occurred in 17.5% of the 200-U dose group and in 7.5% of the 100-U dose group. Dysuria was reported in 37.5% and 15% of the 200-U and 100-U dose groups, respectively.
Strengths and limitations. This randomized, open-label trial comparing a single injection of 100 U versus 200 U of onabotulinumtoxinA included mostly women. OAB symptoms and urodynamic parameters improved after treatment with both dose levels, but a longer duration of improvement was seen with the 200-U dose. The cohort had a low baseline OAB severity, based on the OABSS questionnaire, and a young average age of participants, which limits the generalizability of the study results to a population with refractory OAB. The 0% rate of clean intermittent self-catheterization postinjection might be based on the study's criteria for requiring clean intermittent catheterization. In addition, the initial postinjection visit occurred at 1 month, possibly missing participants who had symptoms of retention soon after injection.
Two dose levels (100 U and 200 U) of a single injection of onabotulinumtoxinA are associated with comparable OAB symptom and urodyanamic improvements. The benefits of a longer duration of effect with the 200-U dose must be weighed against the possible higher risks of transient hematuria, dysuria, and UTI.
Read: onabotulinumtoxinA vs sacral neuromodulation therapy for UUI.
Treatment with onabotulinumtoxinA may control UUI symptoms better than sacral neuromodulation therapy
Amundsen CL, Richter HE, Menefee SA, et al; Pelvic Floor Disorders Network. OnabotulinumtoxinA vs sacral neuromodulation on refractory urgency urinary incontinence in women: a randomized clinical trial. JAMA. 2016;316(13):1366-1374.
In this multicenter open-label randomized trial, Amundsen and colleagues compared the efficacy and safety of onabotulinumtoxinA 200 U with that of sacral neuromodulation.
Details of the study
Three hundred sixty-four women with UUI had data available for primary analysis at 6 months. Women were considered eligible for the study if they had 6 or more UUI episodes on a 3-day bladder diary, persistent symptoms despite anticholinergic therapy, a PVR urine volume of less than 150 mL, and had never previously received either study treatment.
There were no differences in baseline characteristics of the participants. The average (SD) age of the study population was 63 (11.6) years, with an average (SD) daily number of UUI episodes of 5.3 (2.8). The average (SD) body mass index was 32 (8) kg/m2.
Participants were randomly assigned to undergo either sacral neuromodulation (n = 174) or intradetrusor injection of onabotulinumtoxinA 200 U (n = 190). The primary outcome was change from baseline in mean number of daily UUI episodes averaged over 6 months as recorded on a monthly 3-day bladder diary. Secondary outcomes included complete resolution of urgency incontinence, 75% or more reduction in UUI episodes, the Overactive Bladder Questionnaire Short Form (SF) score (range, 0-100; higher score indicates higher symptom severity), the Overactive Bladder Satisfaction of Treatment questionnaire (range, 0-100; higher score indicates better satisfaction), other quality-of-life measures, and adverse events.
Related article:
2015 Update on pelvic floor dysfunction: Bladder pain syndrome
Greater symptom bother improvement, treatment satisfaction with onabotulinumtoxinA 200 U
Participants treated with onabotulinumtoxinA had a greater mean reduction of 3.9 UUI episodes per day than the sacral neuromodulation group's reduction of 3.3 UUI episodes per day (mean difference, 0.63; 95% confidence interval [CI], 0.13-1.14; P = .01). In addition, complete UUI resolution was higher in the onabotulinumtoxinA group as compared with the sacral neuromodulation group (20% vs 4%; P<.001). The onabotulinumtoxinA group also had higher rates of 75% or more reduction of UUI episodes compared with the sacral neuromodulation group (46% vs 26%; P<.001). Over 6 months, both groups had improvements in all quality-of-life measures, but the onabotulinumtoxinA group had greater improvement in symptom bother compared with the sacral neuromodulation group (-46.7 vs -38.6; mean difference, 8.1; 95% CI, 3.0-13.3; P = .002). Furthermore, the onabotulinumtoxinA group had greater treatment satisfaction compared with the sacral neuromodulation group (mean difference, 7.8; 95% CI, 1.6-14.1; P = .01).
Adverse events. Six women (3%) underwent sacral neuromodulation device revision or removal. Approximately 8% of onabotulinumtoxinA-treated participants required intermittent self-catheterization at 1 month, 4% at 3 months, and 2% at 6 months. The risk of UTI was higher in the onabotulinumtoxinA group compared with the sacral neuromodulation group (35% vs 11%; risk difference, 23%; 95% CI, -33% to -13%; P<.001).
Strengths and limitations. This is a well-designed randomized clinical trial comparing clinical outcomes and adverse events after treatment with onabotulinumtoxinA 200-U versus sacral neuromodulation. The interventions were standardized across investigators at multiple sites, and the study design required close follow-up to assess efficacy and adverse events. The study used a 200-U dose based on reported durability of effect at that time and findings of equivalency between onabotulinumtoxinA 100 U and anticholinergic therapy. The US Food and Drug Administration's recommendation to use a 100-U dose in all patients with idiopathic OAB might dissuade clinicians from considering the higher dose of onabotulinumtoxinA. The study was limited by the lack of a placebo group.
Both onabotulinumtoxinA 200 U and sacral neuromodulation provide significant improvement in UUI episodes and quality of life over 6 months. However, while treatment with onabotulinumtoxinA has a likelihood of complete UUI resolution, greater improvements in symptom bother and treatment satisfaction, these benefits must be weighed against the risks of transient catheterization and UTI.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Haylen BT, de Ridder D, Freeman RM, et al; International Urogynecological Association; International Continence Society. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4-20.
- Hartmann KE, McPheeters ML, Biller DH, et al. Treatment of overactive bladder in women. Evid Rep Technol Assess (Full Rep). 2009;187:1-120.
- Reynolds,WS, Fowke J, Dmochowski, R. The burden of overactive bladder on US public health. Curr Bladder Dysfunct Rep. 2016;11(1):8-13.
- Willis-Gray MG, Dieter AA, Geller EJ. Evaluation and management of overactive bladder: strategies for optimizing care. Res Rep Urol. 2016;8:113-122.
- Ganz ML, Smalarz AM, Krupski TL, et al. Economic costs of overactive bladder in the United States. Urology. 2010;75(3):526-532.
- Gormley EA, Lightner DJ, Faraday M, Vasavada SP; American Urological Association; Society of Urodyndamics, Female Pelvic Medicine. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline amendment. J Urol. 2015; 193(5):1572-1580.
- Gormley EA, Lightner DJ, Burgio KL, et al; American Urological Association; Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. J Urol. 2012;188(6 suppl):2455-2463.
- Haylen BT, de Ridder D, Freeman RM, et al; International Urogynecological Association; International Continence Society. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4-20.
- Hartmann KE, McPheeters ML, Biller DH, et al. Treatment of overactive bladder in women. Evid Rep Technol Assess (Full Rep). 2009;187:1-120.
- Reynolds,WS, Fowke J, Dmochowski, R. The burden of overactive bladder on US public health. Curr Bladder Dysfunct Rep. 2016;11(1):8-13.
- Willis-Gray MG, Dieter AA, Geller EJ. Evaluation and management of overactive bladder: strategies for optimizing care. Res Rep Urol. 2016;8:113-122.
- Ganz ML, Smalarz AM, Krupski TL, et al. Economic costs of overactive bladder in the United States. Urology. 2010;75(3):526-532.
- Gormley EA, Lightner DJ, Faraday M, Vasavada SP; American Urological Association; Society of Urodyndamics, Female Pelvic Medicine. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline amendment. J Urol. 2015; 193(5):1572-1580.
- Gormley EA, Lightner DJ, Burgio KL, et al; American Urological Association; Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. J Urol. 2012;188(6 suppl):2455-2463.
Bringing up the rear: Disorders of the rectum and colon
The final session of the course opened with Uri Ladabaum, MD, entertaining the question “Colon cancer screening and surveillance: who, when, and how?” Dr. Ladabaum pointed out that there is consensus that colorectal cancer screening for average-risk individuals should begin at age 50 with a choice of modalities and that surveillance depends on the findings on each colonoscopy. He reviewed the evidence for screening modalities and for surveillance and offered perspectives on the role of the gastroenterologist/colonoscopist in the quality of colonsocopy. Douglas K. Rex, MD, AGAF followed by asking “Does every big polyp need EMR?” Dr. Rex discussed the available approaches to the large colonic polyp, including endoscopic mucosal resection, endoscopic submucosal dissection, and surgery. He provided evidence for the advantages and expanded use of EMR, with the conclusion that almost every large benign polyp needs EMR.

Jennifer A. Christie, MD, then spoke on “Pelvic floor dysfunction and constipation.” Dr. Christie stressed the importance of a good history and the digital rectal exam in diagnosis of pelvic floor dysfunction. When over-the-counter or prescribed medications are not effective, the work-up should include anorectal manometry, balloon expulsion, and colonic transit testing. Attempts should be made to remove all potential offending agents, such as anticholinergics, narcotics, calcium channel blockers, and beta-blockers. Biofeedback is a safe and effective treatment for pelvic floor dysfunction. Lin Chang, MD, AGAF, continued with a talk on irritable bowel syndrome, which can be considered a combination of disorders, with clusters of symptoms and subgroups. There must be recurrent abdominal pain or discomfort at least 1 day/week for the prior 3 months, associated with 2 or more of the following: a relationship to defecation, change in stool frequency, or stool form/appearance. Risk includes genetic and environmental factors, stress/abuse, and acute gastroenteritis. After a structured evaluation, a graded treatment response is undertaken, ranging from diet/lifestyle counseling to pharmacotherapy to psychological therapies.
Neil Hyman, MD, concluded the session with a talk entitled “Disorders of the anorectum,” also stressing that the history is key to the diagnosis, with an emphasis on asking the right questions. Pain may be related to fissures, thrombosed hemorrhoids, abscesses, and proctalgia/levator spasm. New technologies, and pharmacological and surgical approaches were discussed.
This is a summary provided by the moderator of one of the AGA Postgraduate Courses held at DDW 2017. Dr. Cohen is the chief of the division of gastroenterology and hepatology in the Weill department of medicine, New York–Presbyterian Hospital Center, New York.
The final session of the course opened with Uri Ladabaum, MD, entertaining the question “Colon cancer screening and surveillance: who, when, and how?” Dr. Ladabaum pointed out that there is consensus that colorectal cancer screening for average-risk individuals should begin at age 50 with a choice of modalities and that surveillance depends on the findings on each colonoscopy. He reviewed the evidence for screening modalities and for surveillance and offered perspectives on the role of the gastroenterologist/colonoscopist in the quality of colonsocopy. Douglas K. Rex, MD, AGAF followed by asking “Does every big polyp need EMR?” Dr. Rex discussed the available approaches to the large colonic polyp, including endoscopic mucosal resection, endoscopic submucosal dissection, and surgery. He provided evidence for the advantages and expanded use of EMR, with the conclusion that almost every large benign polyp needs EMR.
Jennifer A. Christie, MD, then spoke on “Pelvic floor dysfunction and constipation.” Dr. Christie stressed the importance of a good history and the digital rectal exam in diagnosis of pelvic floor dysfunction. When over-the-counter or prescribed medications are not effective, the work-up should include anorectal manometry, balloon expulsion, and colonic transit testing. Attempts should be made to remove all potential offending agents, such as anticholinergics, narcotics, calcium channel blockers, and beta-blockers. Biofeedback is a safe and effective treatment for pelvic floor dysfunction. Lin Chang, MD, AGAF, continued with a talk on irritable bowel syndrome, which can be considered a combination of disorders, with clusters of symptoms and subgroups. There must be recurrent abdominal pain or discomfort at least 1 day/week for the prior 3 months, associated with 2 or more of the following: a relationship to defecation, change in stool frequency, or stool form/appearance. Risk includes genetic and environmental factors, stress/abuse, and acute gastroenteritis. After a structured evaluation, a graded treatment response is undertaken, ranging from diet/lifestyle counseling to pharmacotherapy to psychological therapies.
Neil Hyman, MD, concluded the session with a talk entitled “Disorders of the anorectum,” also stressing that the history is key to the diagnosis, with an emphasis on asking the right questions. Pain may be related to fissures, thrombosed hemorrhoids, abscesses, and proctalgia/levator spasm. New technologies, and pharmacological and surgical approaches were discussed.
This is a summary provided by the moderator of one of the AGA Postgraduate Courses held at DDW 2017. Dr. Cohen is the chief of the division of gastroenterology and hepatology in the Weill department of medicine, New York–Presbyterian Hospital Center, New York.
The final session of the course opened with Uri Ladabaum, MD, entertaining the question “Colon cancer screening and surveillance: who, when, and how?” Dr. Ladabaum pointed out that there is consensus that colorectal cancer screening for average-risk individuals should begin at age 50 with a choice of modalities and that surveillance depends on the findings on each colonoscopy. He reviewed the evidence for screening modalities and for surveillance and offered perspectives on the role of the gastroenterologist/colonoscopist in the quality of colonsocopy. Douglas K. Rex, MD, AGAF followed by asking “Does every big polyp need EMR?” Dr. Rex discussed the available approaches to the large colonic polyp, including endoscopic mucosal resection, endoscopic submucosal dissection, and surgery. He provided evidence for the advantages and expanded use of EMR, with the conclusion that almost every large benign polyp needs EMR.
Jennifer A. Christie, MD, then spoke on “Pelvic floor dysfunction and constipation.” Dr. Christie stressed the importance of a good history and the digital rectal exam in diagnosis of pelvic floor dysfunction. When over-the-counter or prescribed medications are not effective, the work-up should include anorectal manometry, balloon expulsion, and colonic transit testing. Attempts should be made to remove all potential offending agents, such as anticholinergics, narcotics, calcium channel blockers, and beta-blockers. Biofeedback is a safe and effective treatment for pelvic floor dysfunction. Lin Chang, MD, AGAF, continued with a talk on irritable bowel syndrome, which can be considered a combination of disorders, with clusters of symptoms and subgroups. There must be recurrent abdominal pain or discomfort at least 1 day/week for the prior 3 months, associated with 2 or more of the following: a relationship to defecation, change in stool frequency, or stool form/appearance. Risk includes genetic and environmental factors, stress/abuse, and acute gastroenteritis. After a structured evaluation, a graded treatment response is undertaken, ranging from diet/lifestyle counseling to pharmacotherapy to psychological therapies.
Neil Hyman, MD, concluded the session with a talk entitled “Disorders of the anorectum,” also stressing that the history is key to the diagnosis, with an emphasis on asking the right questions. Pain may be related to fissures, thrombosed hemorrhoids, abscesses, and proctalgia/levator spasm. New technologies, and pharmacological and surgical approaches were discussed.
This is a summary provided by the moderator of one of the AGA Postgraduate Courses held at DDW 2017. Dr. Cohen is the chief of the division of gastroenterology and hepatology in the Weill department of medicine, New York–Presbyterian Hospital Center, New York.
