User login
Consumers Union Joins Hospital Safety Ratings Game
A new hospital patient-safety ranking system was released in July by Consumers Union (CU), an independent consumer advocacy organization in Yonkers, N.Y., and published in the August issue of its magazine Consumer Reports.1 CU rated 1,155 hospitals in six categories, including hospital-acquired infections, readmissions, and the quality of communication by physicians and nurses to patients. The highest-scoring hospital: Billings Clinic in Montana, which received a 72 on CU’s 100-point safety score.
“The new Consumer Reports hospital safety ratings add to a growing list of publicly reported performance rating schemes,” says SHM president Shaun Frost, MD, SFHM, FACP, associate medical director for care-delivery systems at HealthPartners in Minneapolis. Hospitalists should be aware of these ratings and review them “with an eye toward identifying improvement opportunities that are within their scope of influence....Hospitalists must embrace these issues as theirs to own and improve upon, as the ability to demonstrably improve the safety and care quality in the hospitals in which we practice is dependent on us.”
Reference
A new hospital patient-safety ranking system was released in July by Consumers Union (CU), an independent consumer advocacy organization in Yonkers, N.Y., and published in the August issue of its magazine Consumer Reports.1 CU rated 1,155 hospitals in six categories, including hospital-acquired infections, readmissions, and the quality of communication by physicians and nurses to patients. The highest-scoring hospital: Billings Clinic in Montana, which received a 72 on CU’s 100-point safety score.
“The new Consumer Reports hospital safety ratings add to a growing list of publicly reported performance rating schemes,” says SHM president Shaun Frost, MD, SFHM, FACP, associate medical director for care-delivery systems at HealthPartners in Minneapolis. Hospitalists should be aware of these ratings and review them “with an eye toward identifying improvement opportunities that are within their scope of influence....Hospitalists must embrace these issues as theirs to own and improve upon, as the ability to demonstrably improve the safety and care quality in the hospitals in which we practice is dependent on us.”
Reference
A new hospital patient-safety ranking system was released in July by Consumers Union (CU), an independent consumer advocacy organization in Yonkers, N.Y., and published in the August issue of its magazine Consumer Reports.1 CU rated 1,155 hospitals in six categories, including hospital-acquired infections, readmissions, and the quality of communication by physicians and nurses to patients. The highest-scoring hospital: Billings Clinic in Montana, which received a 72 on CU’s 100-point safety score.
“The new Consumer Reports hospital safety ratings add to a growing list of publicly reported performance rating schemes,” says SHM president Shaun Frost, MD, SFHM, FACP, associate medical director for care-delivery systems at HealthPartners in Minneapolis. Hospitalists should be aware of these ratings and review them “with an eye toward identifying improvement opportunities that are within their scope of influence....Hospitalists must embrace these issues as theirs to own and improve upon, as the ability to demonstrably improve the safety and care quality in the hospitals in which we practice is dependent on us.”
Reference
Ultrasound Joins Stethoscope as Portable Diagnostic Tool for Hospitalists
Prairie Business Magazine recently reported that hospitalist Neville Alberto, MD, FACP, of Sanford Health in Fargo, N.D., carries on his rounds not a stethoscope but “a portable ultrasound draped around his neck.”1 The article illustrates ultrasound’s increased portability, wider application at the hospital bedside, and increased use by trained hospitalists. It’s a topic also discussed in a recent post by Robert Wachter, MD, MHM, author of the blog Wachter’s World, professor, and chief of the division of hospital medicine at the University of California at San Francisco (UCSF). Dr. Wachter says “the time has come to—carefully and thoughtfully—add hospitalists” to the growing list of medical specialties that have staked a claim to a procedure previously reserved for radiologists.2
“The one I carry on me is no larger than my smartphone,” Dr. Alberto explains. “It’s well-placed, so nobody notices.”
A hospitalist since 2001, Dr. Alberto is often on the move in his seven-story hospital building. He uses the device to assist in determining whether a patient needs more fluids, or to examine an elderly patient’s bladder for urinary retention when a urinary tract infection is suspected. Only a few colleagues in Dr. Alberto’s 22-member hospitalist group are as comfortable with ultrasound technology, he says, but he has helped develop a curriculum to teach ultrasound techniques to physicians, residents, and medical students.
Diane Sliwka, MD, a UCSF hospitalist and advocate for more widespread ultrasound use by hospitalists, says most physicians have yet to adopt the technology as fully as Dr. Alberto has. “But they’ve seen it and they want it,” she adds.
Hospitalists first utilized portable ultrasound to guide such procedures as thoracentesis or paracentesis. Increasingly, it is being used to assess, for example, cardiac function, fluid buildup around the heart, or the location of a blood clot—“when decisions are needed quickly about what’s going on and how to treat it,” she says. Other growing targets include lung pathologies (pneumothorax) and differentiating between COPD and pulmonary edema, or pneumonia and gallstones, she says.
The technology is advancing faster than the speed of light, with an iPad/tablet application in the works, according to a recent Technology Review blog post from the Massachusetts Institute of Technology.3
References
- Doctors use technology to better diagnose and treat illnesses in a less invasive manner. Prairie Business website. Available at: www.prairiebizmag.com. Accessed July 31, 2012.
- Wachter RM. Bedside ultrasound for hospitalists: our time has come. Wachter’s World website. Available at: http://community.the-hospitalist.org/2012/05/16/bedside-ultrasound-for-hospitalists-our-time-has-come. Accessed July 31, 2012.
- Mims C. Patent hints at iPad-powered portable ultrasound machine. Technology Review website. Available at: www.technologyreview.com/view/427600/patent-hints-at-ipad-powered-portable-ultrasound. Accessed July 29, 2012.
Prairie Business Magazine recently reported that hospitalist Neville Alberto, MD, FACP, of Sanford Health in Fargo, N.D., carries on his rounds not a stethoscope but “a portable ultrasound draped around his neck.”1 The article illustrates ultrasound’s increased portability, wider application at the hospital bedside, and increased use by trained hospitalists. It’s a topic also discussed in a recent post by Robert Wachter, MD, MHM, author of the blog Wachter’s World, professor, and chief of the division of hospital medicine at the University of California at San Francisco (UCSF). Dr. Wachter says “the time has come to—carefully and thoughtfully—add hospitalists” to the growing list of medical specialties that have staked a claim to a procedure previously reserved for radiologists.2
“The one I carry on me is no larger than my smartphone,” Dr. Alberto explains. “It’s well-placed, so nobody notices.”
A hospitalist since 2001, Dr. Alberto is often on the move in his seven-story hospital building. He uses the device to assist in determining whether a patient needs more fluids, or to examine an elderly patient’s bladder for urinary retention when a urinary tract infection is suspected. Only a few colleagues in Dr. Alberto’s 22-member hospitalist group are as comfortable with ultrasound technology, he says, but he has helped develop a curriculum to teach ultrasound techniques to physicians, residents, and medical students.
Diane Sliwka, MD, a UCSF hospitalist and advocate for more widespread ultrasound use by hospitalists, says most physicians have yet to adopt the technology as fully as Dr. Alberto has. “But they’ve seen it and they want it,” she adds.
Hospitalists first utilized portable ultrasound to guide such procedures as thoracentesis or paracentesis. Increasingly, it is being used to assess, for example, cardiac function, fluid buildup around the heart, or the location of a blood clot—“when decisions are needed quickly about what’s going on and how to treat it,” she says. Other growing targets include lung pathologies (pneumothorax) and differentiating between COPD and pulmonary edema, or pneumonia and gallstones, she says.
The technology is advancing faster than the speed of light, with an iPad/tablet application in the works, according to a recent Technology Review blog post from the Massachusetts Institute of Technology.3
References
- Doctors use technology to better diagnose and treat illnesses in a less invasive manner. Prairie Business website. Available at: www.prairiebizmag.com. Accessed July 31, 2012.
- Wachter RM. Bedside ultrasound for hospitalists: our time has come. Wachter’s World website. Available at: http://community.the-hospitalist.org/2012/05/16/bedside-ultrasound-for-hospitalists-our-time-has-come. Accessed July 31, 2012.
- Mims C. Patent hints at iPad-powered portable ultrasound machine. Technology Review website. Available at: www.technologyreview.com/view/427600/patent-hints-at-ipad-powered-portable-ultrasound. Accessed July 29, 2012.
Prairie Business Magazine recently reported that hospitalist Neville Alberto, MD, FACP, of Sanford Health in Fargo, N.D., carries on his rounds not a stethoscope but “a portable ultrasound draped around his neck.”1 The article illustrates ultrasound’s increased portability, wider application at the hospital bedside, and increased use by trained hospitalists. It’s a topic also discussed in a recent post by Robert Wachter, MD, MHM, author of the blog Wachter’s World, professor, and chief of the division of hospital medicine at the University of California at San Francisco (UCSF). Dr. Wachter says “the time has come to—carefully and thoughtfully—add hospitalists” to the growing list of medical specialties that have staked a claim to a procedure previously reserved for radiologists.2
“The one I carry on me is no larger than my smartphone,” Dr. Alberto explains. “It’s well-placed, so nobody notices.”
A hospitalist since 2001, Dr. Alberto is often on the move in his seven-story hospital building. He uses the device to assist in determining whether a patient needs more fluids, or to examine an elderly patient’s bladder for urinary retention when a urinary tract infection is suspected. Only a few colleagues in Dr. Alberto’s 22-member hospitalist group are as comfortable with ultrasound technology, he says, but he has helped develop a curriculum to teach ultrasound techniques to physicians, residents, and medical students.
Diane Sliwka, MD, a UCSF hospitalist and advocate for more widespread ultrasound use by hospitalists, says most physicians have yet to adopt the technology as fully as Dr. Alberto has. “But they’ve seen it and they want it,” she adds.
Hospitalists first utilized portable ultrasound to guide such procedures as thoracentesis or paracentesis. Increasingly, it is being used to assess, for example, cardiac function, fluid buildup around the heart, or the location of a blood clot—“when decisions are needed quickly about what’s going on and how to treat it,” she says. Other growing targets include lung pathologies (pneumothorax) and differentiating between COPD and pulmonary edema, or pneumonia and gallstones, she says.
The technology is advancing faster than the speed of light, with an iPad/tablet application in the works, according to a recent Technology Review blog post from the Massachusetts Institute of Technology.3
References
- Doctors use technology to better diagnose and treat illnesses in a less invasive manner. Prairie Business website. Available at: www.prairiebizmag.com. Accessed July 31, 2012.
- Wachter RM. Bedside ultrasound for hospitalists: our time has come. Wachter’s World website. Available at: http://community.the-hospitalist.org/2012/05/16/bedside-ultrasound-for-hospitalists-our-time-has-come. Accessed July 31, 2012.
- Mims C. Patent hints at iPad-powered portable ultrasound machine. Technology Review website. Available at: www.technologyreview.com/view/427600/patent-hints-at-ipad-powered-portable-ultrasound. Accessed July 29, 2012.
By the Numbers: 1%
Share of physician job-search assignments conducted by Irving, Texas-based physician recruiting firm Merritt Hawkins from April 1, 2011, and March 31, 2012, that featured openings for independent, solo practitioners; the share was 17% in 2006.1 Merritt Hawkins’ 2012 Review of Physician Recruiting Incentives report concludes “the recruitment of physicians into solo practice settings has almost abated.” Conversely, 63% of the firm’s job searches were with hospitals, up from 56% the year before.
Reference
Share of physician job-search assignments conducted by Irving, Texas-based physician recruiting firm Merritt Hawkins from April 1, 2011, and March 31, 2012, that featured openings for independent, solo practitioners; the share was 17% in 2006.1 Merritt Hawkins’ 2012 Review of Physician Recruiting Incentives report concludes “the recruitment of physicians into solo practice settings has almost abated.” Conversely, 63% of the firm’s job searches were with hospitals, up from 56% the year before.
Reference
Share of physician job-search assignments conducted by Irving, Texas-based physician recruiting firm Merritt Hawkins from April 1, 2011, and March 31, 2012, that featured openings for independent, solo practitioners; the share was 17% in 2006.1 Merritt Hawkins’ 2012 Review of Physician Recruiting Incentives report concludes “the recruitment of physicians into solo practice settings has almost abated.” Conversely, 63% of the firm’s job searches were with hospitals, up from 56% the year before.
Reference
Interactive Quality, Leadership Lessons for Residents
An interactive program to teach quality and leadership skills to internal-medicine residents at Mount Sinai School of Medicine in New York City—described in an Research, Innovations and Clinical Vignettes (RIV) poster presented at HM12 in San Diego—found that medical trainees are eager and willing to learn the skills that will be required from hospitalists in a reformed healthcare system.1 Lead author Brian Markoff, MD, SFHM, associate chief of hospital medicine at Mount Sinai, says the Healthcare Leadership Track’s elective, one-month block in quality improvement (QI) and patient safety was established with four second-year residents in 2011-2012.
Along with didactic presentations, participants were offered novel structured learning exercises that included:
- Teaching a care-transitions module to interns;
- Proposing a new clinical pathway;
- Leading a conference on QI;
- Examining a hospital readmission for what went wrong;
- Pairing with a ward medical director;
- Conducting a mentored QI research project; and
- Participating in a book club.
All four participants from the first year “strongly agree that the block was highly relevant to their current and future careers,” Dr. Markoff says.
In their third year, the residents will have the opportunity to participate in one-month electives for leadership, teaching, and the business of medicine.
Six new second-year residents are joining the program, and longitudinal components span the program’s two years. “Most institutions that train residents have a lot of this activity going on,” he says. “Why not get house staff involved in experiential learning in these areas?”
Reference
An interactive program to teach quality and leadership skills to internal-medicine residents at Mount Sinai School of Medicine in New York City—described in an Research, Innovations and Clinical Vignettes (RIV) poster presented at HM12 in San Diego—found that medical trainees are eager and willing to learn the skills that will be required from hospitalists in a reformed healthcare system.1 Lead author Brian Markoff, MD, SFHM, associate chief of hospital medicine at Mount Sinai, says the Healthcare Leadership Track’s elective, one-month block in quality improvement (QI) and patient safety was established with four second-year residents in 2011-2012.
Along with didactic presentations, participants were offered novel structured learning exercises that included:
- Teaching a care-transitions module to interns;
- Proposing a new clinical pathway;
- Leading a conference on QI;
- Examining a hospital readmission for what went wrong;
- Pairing with a ward medical director;
- Conducting a mentored QI research project; and
- Participating in a book club.
All four participants from the first year “strongly agree that the block was highly relevant to their current and future careers,” Dr. Markoff says.
In their third year, the residents will have the opportunity to participate in one-month electives for leadership, teaching, and the business of medicine.
Six new second-year residents are joining the program, and longitudinal components span the program’s two years. “Most institutions that train residents have a lot of this activity going on,” he says. “Why not get house staff involved in experiential learning in these areas?”
Reference
An interactive program to teach quality and leadership skills to internal-medicine residents at Mount Sinai School of Medicine in New York City—described in an Research, Innovations and Clinical Vignettes (RIV) poster presented at HM12 in San Diego—found that medical trainees are eager and willing to learn the skills that will be required from hospitalists in a reformed healthcare system.1 Lead author Brian Markoff, MD, SFHM, associate chief of hospital medicine at Mount Sinai, says the Healthcare Leadership Track’s elective, one-month block in quality improvement (QI) and patient safety was established with four second-year residents in 2011-2012.
Along with didactic presentations, participants were offered novel structured learning exercises that included:
- Teaching a care-transitions module to interns;
- Proposing a new clinical pathway;
- Leading a conference on QI;
- Examining a hospital readmission for what went wrong;
- Pairing with a ward medical director;
- Conducting a mentored QI research project; and
- Participating in a book club.
All four participants from the first year “strongly agree that the block was highly relevant to their current and future careers,” Dr. Markoff says.
In their third year, the residents will have the opportunity to participate in one-month electives for leadership, teaching, and the business of medicine.
Six new second-year residents are joining the program, and longitudinal components span the program’s two years. “Most institutions that train residents have a lot of this activity going on,” he says. “Why not get house staff involved in experiential learning in these areas?”
Reference
Win Whitcomb: Inflexible, Big-Box EHRs Endanger the QI Movement

In “The Lean Startup,” author Eric Ries notes that in its early stages, his gaming company would routinely issue new versions of their software application several times each day. Continuous deployment—the process Ries’ company used—leveraged such Lean principles as reduced batch size and continuous learning based on end-user feedback to achieve rapid improvements in their product.
Ries says companies that learn the quickest about what the customer wants, and can incorporate that information into products more efficiently, stand the greatest chance of succeeding. A software engineer by trade, Ries uses many examples of companies that have succeeded with this approach, none of which are from healthcare.
In stark relief, the chief technology hospitalists interface with daily is the electronic health record (EHR), widely recognized as a system that fails to consider the end-user experience, that is unable to interoperate with other software, and is incapable of using data for quality improvement (QI). The PDSA (“plan, do, study, act”) cycle is the foundation of QI activities and relies on rapidly incorporating observations made by those performing the work to create novel workflows and processes based on learning. EHRs, by digitizing health information, theoretically provide the ideal tool for supporting QI.
The reality is that EHRs have been a colossal disappointment with regard to QI efforts. The space in and around EHR effectively represents “dead zones” for innovation and improvement. Mandl and Kohane note:
EHR companies have followed a business model whereby they control all data, rather than liberating the data for use in innovative applications in clinical care.
Conducting a Google-style search of an EHR database usually requires involvement of a clinician’s information services department and often the specialized knowledge and cooperation of the vendor’s technical teams.
Greg Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement, recently provided testimony to the Office of the National Coordinator for Health Information Technology about the challenges current EHRs present to QI efforts and what features EHRs need to incorporate to better serve the needs of patients and clinicians. Dr. Maynard answered a few questions for The Hospitalist:
Q: What is it about current EHRs that make continuous improvement so difficult?
A: EHRs were built for fiscal and administrative purposes, not for quality improvement and safety. The administrative/fiscal roots of today’s IT systems lead to poor availability of clinical, quality, and safety data. In many medical centers and practices, the great majority of information available is months-old administrative data, which does not lend itself to rapid cycle improvement.
Q: Why is the PDSA cycle endangered in most systems?
A: EHRs often do not facilitate rapid-cycle, PDSA-style improvements on a small pilot scale. Most improvement teams get one shot to get the clinical decision support and data-capture tools correct after months of waiting in queue and development time. Any request for revisions and refinements is treated as a failure of the improvement team, and it is often difficult or impossible to pilot new tools in a limited setting.
Q: What features would you like to see in EHRs that would facilitate QI?
A: We need a user-friendly interface for clinicians and for data analysts/reporters. Other industries have common data formats to allow for sharing of information across disparate systems. We need the same capability for clinical information in healthcare. Also, a change in architecture of EHRs and other health IT tools that allows for not just interoperability but substitutable options is required. In the more “app”-like environment, innovation and flexibility would be the rule. An underlying architecture could have different plug-and-play modules for different functions. Some companies are overcoming the current barriers to provide wonderful, easy-to-generate and useful reports, but most are stymied by proprietary systems.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
In “The Lean Startup,” author Eric Ries notes that in its early stages, his gaming company would routinely issue new versions of their software application several times each day. Continuous deployment—the process Ries’ company used—leveraged such Lean principles as reduced batch size and continuous learning based on end-user feedback to achieve rapid improvements in their product.
Ries says companies that learn the quickest about what the customer wants, and can incorporate that information into products more efficiently, stand the greatest chance of succeeding. A software engineer by trade, Ries uses many examples of companies that have succeeded with this approach, none of which are from healthcare.
In stark relief, the chief technology hospitalists interface with daily is the electronic health record (EHR), widely recognized as a system that fails to consider the end-user experience, that is unable to interoperate with other software, and is incapable of using data for quality improvement (QI). The PDSA (“plan, do, study, act”) cycle is the foundation of QI activities and relies on rapidly incorporating observations made by those performing the work to create novel workflows and processes based on learning. EHRs, by digitizing health information, theoretically provide the ideal tool for supporting QI.
The reality is that EHRs have been a colossal disappointment with regard to QI efforts. The space in and around EHR effectively represents “dead zones” for innovation and improvement. Mandl and Kohane note:
EHR companies have followed a business model whereby they control all data, rather than liberating the data for use in innovative applications in clinical care.
Conducting a Google-style search of an EHR database usually requires involvement of a clinician’s information services department and often the specialized knowledge and cooperation of the vendor’s technical teams.
Greg Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement, recently provided testimony to the Office of the National Coordinator for Health Information Technology about the challenges current EHRs present to QI efforts and what features EHRs need to incorporate to better serve the needs of patients and clinicians. Dr. Maynard answered a few questions for The Hospitalist:
Q: What is it about current EHRs that make continuous improvement so difficult?
A: EHRs were built for fiscal and administrative purposes, not for quality improvement and safety. The administrative/fiscal roots of today’s IT systems lead to poor availability of clinical, quality, and safety data. In many medical centers and practices, the great majority of information available is months-old administrative data, which does not lend itself to rapid cycle improvement.
Q: Why is the PDSA cycle endangered in most systems?
A: EHRs often do not facilitate rapid-cycle, PDSA-style improvements on a small pilot scale. Most improvement teams get one shot to get the clinical decision support and data-capture tools correct after months of waiting in queue and development time. Any request for revisions and refinements is treated as a failure of the improvement team, and it is often difficult or impossible to pilot new tools in a limited setting.
Q: What features would you like to see in EHRs that would facilitate QI?
A: We need a user-friendly interface for clinicians and for data analysts/reporters. Other industries have common data formats to allow for sharing of information across disparate systems. We need the same capability for clinical information in healthcare. Also, a change in architecture of EHRs and other health IT tools that allows for not just interoperability but substitutable options is required. In the more “app”-like environment, innovation and flexibility would be the rule. An underlying architecture could have different plug-and-play modules for different functions. Some companies are overcoming the current barriers to provide wonderful, easy-to-generate and useful reports, but most are stymied by proprietary systems.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
In “The Lean Startup,” author Eric Ries notes that in its early stages, his gaming company would routinely issue new versions of their software application several times each day. Continuous deployment—the process Ries’ company used—leveraged such Lean principles as reduced batch size and continuous learning based on end-user feedback to achieve rapid improvements in their product.
Ries says companies that learn the quickest about what the customer wants, and can incorporate that information into products more efficiently, stand the greatest chance of succeeding. A software engineer by trade, Ries uses many examples of companies that have succeeded with this approach, none of which are from healthcare.
In stark relief, the chief technology hospitalists interface with daily is the electronic health record (EHR), widely recognized as a system that fails to consider the end-user experience, that is unable to interoperate with other software, and is incapable of using data for quality improvement (QI). The PDSA (“plan, do, study, act”) cycle is the foundation of QI activities and relies on rapidly incorporating observations made by those performing the work to create novel workflows and processes based on learning. EHRs, by digitizing health information, theoretically provide the ideal tool for supporting QI.
The reality is that EHRs have been a colossal disappointment with regard to QI efforts. The space in and around EHR effectively represents “dead zones” for innovation and improvement. Mandl and Kohane note:
EHR companies have followed a business model whereby they control all data, rather than liberating the data for use in innovative applications in clinical care.
Conducting a Google-style search of an EHR database usually requires involvement of a clinician’s information services department and often the specialized knowledge and cooperation of the vendor’s technical teams.
Greg Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement, recently provided testimony to the Office of the National Coordinator for Health Information Technology about the challenges current EHRs present to QI efforts and what features EHRs need to incorporate to better serve the needs of patients and clinicians. Dr. Maynard answered a few questions for The Hospitalist:
Q: What is it about current EHRs that make continuous improvement so difficult?
A: EHRs were built for fiscal and administrative purposes, not for quality improvement and safety. The administrative/fiscal roots of today’s IT systems lead to poor availability of clinical, quality, and safety data. In many medical centers and practices, the great majority of information available is months-old administrative data, which does not lend itself to rapid cycle improvement.
Q: Why is the PDSA cycle endangered in most systems?
A: EHRs often do not facilitate rapid-cycle, PDSA-style improvements on a small pilot scale. Most improvement teams get one shot to get the clinical decision support and data-capture tools correct after months of waiting in queue and development time. Any request for revisions and refinements is treated as a failure of the improvement team, and it is often difficult or impossible to pilot new tools in a limited setting.
Q: What features would you like to see in EHRs that would facilitate QI?
A: We need a user-friendly interface for clinicians and for data analysts/reporters. Other industries have common data formats to allow for sharing of information across disparate systems. We need the same capability for clinical information in healthcare. Also, a change in architecture of EHRs and other health IT tools that allows for not just interoperability but substitutable options is required. In the more “app”-like environment, innovation and flexibility would be the rule. An underlying architecture could have different plug-and-play modules for different functions. Some companies are overcoming the current barriers to provide wonderful, easy-to-generate and useful reports, but most are stymied by proprietary systems.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Teach Back Communication Strategy Helps Healthcare Providers Help Their Patients
“Do you understand what I just told you?”
Hospitalists who are experts on communicating with patients say that this kind of simple, yes/no question can engender all sorts of confusion. This kind of query often results in unrealistic discharge plans, failed post-discharge treatments, and unnecessary rehospitalizations. And they happen all the time in hospitals across the country.
“Yes/no questions, unless they are very concrete—such as ‘Do you have a headache?’—have little relation to assessing a patient’s understanding of essential healthcare information,” says Jeffrey Greenwald, MD, SFHM, hospitalist and educator at Massachusetts General Hospital in Boston. Many times, he adds, patients say “yes” just to please the doctor or nurse, or to avoid looking ignorant.
A better approach to patient-provider communication, one that successfully addresses communication gaps, is teach-back, a strategy in which providers ask patients to repeat (or “teach back”), in their own words, what they have just learned about their medical condition, treatments, and self-care. For example, a physician using the teach-back method could ask, “Mr. Smith, can you tell me why you are in the hospital?”
The approach is an integral part of SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) care-transitions quality initiative, says Dr. Greenwald, a BOOST coinvestigator. But too often, hospitalists fail to embrace the mandate of effective communication, he says, leaving responsibility to clarify the patient’s understanding to nurses and other members of the care team.
“Having taught this skill all over the country, I continue to find members of my own profession who feel that it is not their job to assess if patients understand self-care and medication instructions. To me, there’s no question that physicians have a role to play as teachers. We educate patients, whether we think we do or not,” Dr. Greenwald says, adding that some hospitalists do so with greater effectiveness than others.
In an era of accountable-care organizations, patient-centered care, and shared decision-making, hospitalists need to provide their patients the same core messages as the rest of the care team does. According to a recent report by the University of California San Francisco (UCSF) Center for Vulnerable Populations at San Francisco General Hospital, 77 million Americans have difficulty understanding even basic healthcare information.1
In addition to widespread language barriers, the Institute of Medicine in a 2004 report concluded that 90 million U.S. adults have literacy skills that test below the high-school level.2 As most hospitalists know, many inpatients go to great lengths to mask these limitations—appearing knowledgeable while failing to grasp essential health concepts. Medical jargon, acronyms, and instructions can be confusing, even for patients with a high level of education.
“First and foremost, we have to be able to communicate with our patients—to make sure that we understand their goals and that they understand our approach to treatment and the therapeutic goals we are proposing,” Dr. Greenwald says. “This process also helps to achieve true informed consent. We want to ensure that their questions are being answered, and that the options we are discussing are in line with their goals of care so that they are more likely to actually undertake them when they go home. And if they can’t, we need to know that in advance, so that we can intervene in other ways.”
Embracing the Method
One health system that has embraced teach-back as a patient-education strategy is the Lehigh Valley Health Network (LVHN), a 988-bed, three-hospital system based in Allentown, Pa. In an HM12 workshop, the Lehigh Valley team explained how its teach-back initiative grew out of quality initiatives to target patient flow and readmissions. Lehigh joined an Institute for Healthcare Improvement quality collaborative, implemented “Lean” quality-improvement (QI) methodologies, and adopted a patient-coaching program.3
“This process has shined a stark spotlight on how poorly we as physicians communicate with patients overall,” says Michael Pistoria, DO, SFHM, former hospitalist and president of medical staff at LVHN who was a member of the teach-back team.
“I’d like to think I’m a little above averagein this regard, but it has made me realize how much better I could be in checking in with patients, gauging their health literacy, and engaging them with the care plan. As hospitalists, we all have to rethink how we talk to patients and families.”
A multidisciplinary team, originally created to analyze care transitions, was divided into four work groups. One group, which focused on patient/family understanding of the disease process, quickly learned that care-team members often failed to identify the patient’s “key learner”—the patient, a family member, or someone else. If the information is given to the wrong person, breakdowns can result. Such breakdowns usually lead to readmissions. One instrumental change that came as a result of the QI team’s efforts is that LVHN care-team members now recognize it is their responsibility to ask who the key learner is and to put that person’s name on a whiteboard in the patient’s room.
In the workshop in at SHM’s annual meeting in San Diego, Kim Jordan, MHA, BSN, RN, NE-BC, LVHN’s administrator of patient-care services, described teach-back as an effective, easy-to-use communication strategy that improves patient learning outcomes. “We created a standard work process using teach-back strategies across the healthcare system,” with training offered to all professionals who provide education to patients and families, she said.
Starting with heart failure, prompts were written into the electronic health record (EHR) to provide four scripted teach-back questions, each focused on the patient’s knowledge, attitudes, and behavior, to be asked consecutively over three days. Information was “chunked” into manageable pieces, emphasizing what was most important for the patient to learn on that day.
Results from one of the pilot units showed 30-day readmission rates for heart failure patients were cut in half, from 28% to 14%.4 Teach-back scripts also are being developed for the anticoagulant clinic and for patients with stroke, myocardial infarction, chronic obstructive pulmonary disease (COPD), community-acquired pneumonia, and diabetes.
“Continued analysis continues to show reduced rehospitalizations, and we even find that for those who are readmitted, their second admissions have been shorter,” Dr. Pistoria says, noting LVHN nurses have reported higher satisfaction. “They say, ‘This is wonderful. This is what I love about nursing—I get to teach the patients.’”
A Quality Mandate
The importance of effective communication with hospitalized patients is recognized in the federal Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)5 quality ratings and, more recently, by Consumers Union’s new hospital safety ratings,6 which include communication in its six categories of patient-safety measures. And a recent study from the University of Washington says patients place high value on verbal communication about their discharge care plans and how to improve their health, and personal communication between their inpatient and outpatient providers.7
Large volumes of important information often are “dumped” on hospitalized patients, and many times patients are provided insufficient time to assimilate the information or ask questions about it.8 Such situations are especially common at discharge. And although physicians and other care-team members might feel they can’t afford the time to assure themselves that the patient understands what they are saying, the alternative is a lot more time spent dealing with preventable crises, misunderstandings—and preventable readmissions.
“People say, ‘I don’t have time for this,’” says Laura Vento, MSN, RN, clinical nurse leader on an acute-care medical unit at the University of California at San Diego medical center, who spearheaded teach-back at her hospital. “I did some observations around discharge visits, and it took an average of six minutes. After we implemented teach-back, it took eight to nine minutes. Nurses and patients were both very satisfied with the results. I say to staff: ‘Give it a try, and see what a difference an extra two minutes can make.’”
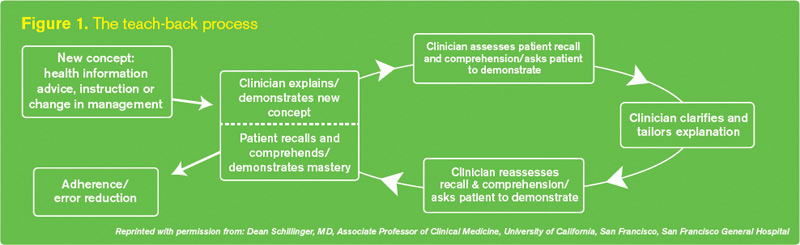
Dr. Pistoria describes teach-back as “humble inquiry...the simple need and ability to ask patients, ‘I know I’ve been throwing a lot of information at you. Can you tell me what I just said?’ Then, shut up and listen.” The goal is to have patients confirm that they understand fully what the provider thinks they need to know. The technique is presented as a test not of the patient’s learning ability, but of the provider’s communication effectiveness and success in explaining the information (see Figure 1). If the message has not been transmitted successfully, the professional reteaches, corrects misconceptions, and again asks the patient to teach back.
The theory is that physicians will then avoid the closed-ended questions (“Do you understand what I just told you?”) that make patients uncomfortable or inhibit the communication that needs to happen between patient and provider.
“We didn’t invent teach-back, which long predated Project BOOST,” Dr. Greenwald says. “But we use it and endorse it strongly, and believe it is an important part of communication with patients, particularly around care transitions.”
Dr. Greenwald thinks teach-back “is not a big stretch for hospitalists.” But he says it requires meaningful training and practice, ideally in a multidisciplinary team context. Participating Project BOOST (BOOST@hospitalmedicine.org) and Electronic Quality Improvement Programs (eQUIPS) sites receive a two-year license to post the “train-the-trainer” curriculum on their intranet systems.8 An instructional webinar, and the trainer curriculum and video, are available in the SHM store (www.hospitalmedicine.org/store). SHM also provides on-site training sessions for health systems or learning collaboratives (contact tbudnitz@hospitalmedicine.org).
‘Teach-Back on Steroids’
Teach-back, while a useful approach for improving patients’ understanding about hospital discharges, post-discharge care plans, and patient self-care, is just one of many teaching models that hospitalist groups can use to improve provider-to-patient communication. HM groups should assess health literacy in their regions and physician communication skills before deciding on one or more improvement tools.
LVHN, for example, has incorporated brief motivational interviewing techniques to its teach-back system, and the results are now being studied, says Paula Robinson, MSN, RN, BC, LVHN’s manager of patient, family, and consumer education.
“A lot of research out there emphasizes how patient education and knowledge alone don’t make a difference in adherence or compliance to treatment plans, even if they are getting the knowledge right 100% of the time,” Robinson says. “You also need to give patients permission to explore their feelings.”
One of Robinson’s colleagues, patient-care specialist Debra Peters, MSN, RN, BC, CMSRN, remembers using teach-back with a heart failure patient with recurrent rehospitalizations, exploring why it was important to control his salt intake. “The patient said, ‘Honey, I salt my ham, and I have no intention of changing that.’ This issue would not have come up if we had just addressed the knowledge component and told him: ‘You need to reduce your salt intake.’”
There might not be easy solutions to that kind of patient attitude, although in this case Peters made a referral to a dietitian who worked with the patient on food substitutions and other tools for managing his salt intake. “I don’t know if we made a big difference, but I haven’t seen him back in the hospital,” she says.
Motivational interviewing is a directive, client-centered counseling style for eliciting behavioral changes by helping clients to explore and resolve their ambivalence about making changes.9 Robinson calls it “the next step in our journey, with teach-back as a jumping-off place. We’ve worked on open-ended questions, getting patients to tell their stories, and our own reflective listening skills. I look at teach-back as a great communication tool and strategy—and motivational interviewing as ‘teach-back on steroids.’”
A number of similar, comparable, or complementary techniques and systems, with names like “Teach-to-Goal” and often paired with such resources as written materials, can help advance the same ends (visit the-hospitalist.org to learn about a technique for communicating bad news to patients).
The Flinders Program, developed at Flinders University in Adelaide, Australia, is a four-part structured motivational interview that asks patients to identify what they see as the biggest problem they face.10 LVHN medical educator Krista Hirschmann, MA, PhD, says this method was taught at LVHN by Australian experts and is now being used by its home-care department. “It is truly a patient-centered approach, and could be used by anybody in the health system,” she says.
Project RED (Re-Engineered Discharge), a care-transitions strategy developed by Brian Jack, MD, and colleagues at Boston University School of Medicine, was used to create a “virtual discharge advocate,” a computer avatar that simulates the face-to-face interaction between a patient and a nurse at the bedside.11 Patients interact with the avatar, named Louise, through a touch-screen display to review their after-hospital care packet and to answer her questions, confirming their understanding without being rushed for time.
Ultimately, Dr. Greenwald says, it doesn’t matter if physicians use teach-back or some other system to improve health literacy. “What matters is whether your patients understand what they need to know in order to go home and take care of themselves,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Brach C, Keller D, Hernandez LM, et al. Ten attributes of health literate health care organizations. Institute of Medicine of the National Academies website. Available at: http://iom.edu/Global/Perspectives/2012/HealthLitAttributes.aspx. Accessed Aug. 9, 2012.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds., Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington: Institute of Medicine; 2004.
- Care Transitions Program; University of Colorado School of Medicine, Division of Health Care Policy and Research. Available at: www.caretransitions.org. Accessed July 28, 2012.
- Healthcare Benchmarks and Quality Improvement. Teach-back program reduces readmissions. HighBeam Research website. Available at: http://www.highbeam.com/doc/1G1-269890846.html. Accessed Aug. 9, 2012.
- Hospital Consumer Assessment of Healthcare Providers and Systems. Centers for Medicare & Medicaid Services website. Available at: www.hcahpsonline.org. Accessed July 23, 2012.
- Consumer Reports. How safe is your hospital? Our new ratings find that some are riskier than others. Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/2012/08/how-safe-is-your-hospital/index.htm. Accessed Aug. 1, 2012.
- Shoeb M, Merel SE, Jackson MB, Anawalt BD. “Can’t we just stop and talk?” Patients value verbal communication about discharge care plans. J Hosp Med. 2012;7(6):504-7.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163:83-90.
- Borrelli B, Riekert KA, Weinstein W, Rathier L. Brief motivational interviewing as a clinical strategy to promote asthma medication adherence. J Allergy Clinical Immunol. 2007;120(5):1023-30.
- eQUIPS (Electronic Quality Improvement Programs). Society of Hospital Medicine website. Available at: http:// www.hospitalmedicine.org/equips. Accessed Aug. 1, 2012.
- Kelly J, Kubina N. Navigating self-management: a practical approach for Australian health agencies. Flinders University, Adelaide, Australia. Available at: www.flinders.edu.au/medicine/sites/fhbhru/self-management.cfm. Accessed Aug. 1, 2012.
- Project RED (Re-Engineered Discharge). Boston University Medical Center website. Available at: http:// www.bu.edu/fammed/projectred/publications.html. Accessed Aug. 1, 2012.
“Do you understand what I just told you?”
Hospitalists who are experts on communicating with patients say that this kind of simple, yes/no question can engender all sorts of confusion. This kind of query often results in unrealistic discharge plans, failed post-discharge treatments, and unnecessary rehospitalizations. And they happen all the time in hospitals across the country.
“Yes/no questions, unless they are very concrete—such as ‘Do you have a headache?’—have little relation to assessing a patient’s understanding of essential healthcare information,” says Jeffrey Greenwald, MD, SFHM, hospitalist and educator at Massachusetts General Hospital in Boston. Many times, he adds, patients say “yes” just to please the doctor or nurse, or to avoid looking ignorant.
A better approach to patient-provider communication, one that successfully addresses communication gaps, is teach-back, a strategy in which providers ask patients to repeat (or “teach back”), in their own words, what they have just learned about their medical condition, treatments, and self-care. For example, a physician using the teach-back method could ask, “Mr. Smith, can you tell me why you are in the hospital?”
The approach is an integral part of SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) care-transitions quality initiative, says Dr. Greenwald, a BOOST coinvestigator. But too often, hospitalists fail to embrace the mandate of effective communication, he says, leaving responsibility to clarify the patient’s understanding to nurses and other members of the care team.
“Having taught this skill all over the country, I continue to find members of my own profession who feel that it is not their job to assess if patients understand self-care and medication instructions. To me, there’s no question that physicians have a role to play as teachers. We educate patients, whether we think we do or not,” Dr. Greenwald says, adding that some hospitalists do so with greater effectiveness than others.
In an era of accountable-care organizations, patient-centered care, and shared decision-making, hospitalists need to provide their patients the same core messages as the rest of the care team does. According to a recent report by the University of California San Francisco (UCSF) Center for Vulnerable Populations at San Francisco General Hospital, 77 million Americans have difficulty understanding even basic healthcare information.1
In addition to widespread language barriers, the Institute of Medicine in a 2004 report concluded that 90 million U.S. adults have literacy skills that test below the high-school level.2 As most hospitalists know, many inpatients go to great lengths to mask these limitations—appearing knowledgeable while failing to grasp essential health concepts. Medical jargon, acronyms, and instructions can be confusing, even for patients with a high level of education.
“First and foremost, we have to be able to communicate with our patients—to make sure that we understand their goals and that they understand our approach to treatment and the therapeutic goals we are proposing,” Dr. Greenwald says. “This process also helps to achieve true informed consent. We want to ensure that their questions are being answered, and that the options we are discussing are in line with their goals of care so that they are more likely to actually undertake them when they go home. And if they can’t, we need to know that in advance, so that we can intervene in other ways.”
Embracing the Method
One health system that has embraced teach-back as a patient-education strategy is the Lehigh Valley Health Network (LVHN), a 988-bed, three-hospital system based in Allentown, Pa. In an HM12 workshop, the Lehigh Valley team explained how its teach-back initiative grew out of quality initiatives to target patient flow and readmissions. Lehigh joined an Institute for Healthcare Improvement quality collaborative, implemented “Lean” quality-improvement (QI) methodologies, and adopted a patient-coaching program.3
“This process has shined a stark spotlight on how poorly we as physicians communicate with patients overall,” says Michael Pistoria, DO, SFHM, former hospitalist and president of medical staff at LVHN who was a member of the teach-back team.
“I’d like to think I’m a little above averagein this regard, but it has made me realize how much better I could be in checking in with patients, gauging their health literacy, and engaging them with the care plan. As hospitalists, we all have to rethink how we talk to patients and families.”
A multidisciplinary team, originally created to analyze care transitions, was divided into four work groups. One group, which focused on patient/family understanding of the disease process, quickly learned that care-team members often failed to identify the patient’s “key learner”—the patient, a family member, or someone else. If the information is given to the wrong person, breakdowns can result. Such breakdowns usually lead to readmissions. One instrumental change that came as a result of the QI team’s efforts is that LVHN care-team members now recognize it is their responsibility to ask who the key learner is and to put that person’s name on a whiteboard in the patient’s room.
In the workshop in at SHM’s annual meeting in San Diego, Kim Jordan, MHA, BSN, RN, NE-BC, LVHN’s administrator of patient-care services, described teach-back as an effective, easy-to-use communication strategy that improves patient learning outcomes. “We created a standard work process using teach-back strategies across the healthcare system,” with training offered to all professionals who provide education to patients and families, she said.
Starting with heart failure, prompts were written into the electronic health record (EHR) to provide four scripted teach-back questions, each focused on the patient’s knowledge, attitudes, and behavior, to be asked consecutively over three days. Information was “chunked” into manageable pieces, emphasizing what was most important for the patient to learn on that day.
Results from one of the pilot units showed 30-day readmission rates for heart failure patients were cut in half, from 28% to 14%.4 Teach-back scripts also are being developed for the anticoagulant clinic and for patients with stroke, myocardial infarction, chronic obstructive pulmonary disease (COPD), community-acquired pneumonia, and diabetes.
“Continued analysis continues to show reduced rehospitalizations, and we even find that for those who are readmitted, their second admissions have been shorter,” Dr. Pistoria says, noting LVHN nurses have reported higher satisfaction. “They say, ‘This is wonderful. This is what I love about nursing—I get to teach the patients.’”
A Quality Mandate
The importance of effective communication with hospitalized patients is recognized in the federal Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)5 quality ratings and, more recently, by Consumers Union’s new hospital safety ratings,6 which include communication in its six categories of patient-safety measures. And a recent study from the University of Washington says patients place high value on verbal communication about their discharge care plans and how to improve their health, and personal communication between their inpatient and outpatient providers.7
Large volumes of important information often are “dumped” on hospitalized patients, and many times patients are provided insufficient time to assimilate the information or ask questions about it.8 Such situations are especially common at discharge. And although physicians and other care-team members might feel they can’t afford the time to assure themselves that the patient understands what they are saying, the alternative is a lot more time spent dealing with preventable crises, misunderstandings—and preventable readmissions.
“People say, ‘I don’t have time for this,’” says Laura Vento, MSN, RN, clinical nurse leader on an acute-care medical unit at the University of California at San Diego medical center, who spearheaded teach-back at her hospital. “I did some observations around discharge visits, and it took an average of six minutes. After we implemented teach-back, it took eight to nine minutes. Nurses and patients were both very satisfied with the results. I say to staff: ‘Give it a try, and see what a difference an extra two minutes can make.’”
Dr. Pistoria describes teach-back as “humble inquiry...the simple need and ability to ask patients, ‘I know I’ve been throwing a lot of information at you. Can you tell me what I just said?’ Then, shut up and listen.” The goal is to have patients confirm that they understand fully what the provider thinks they need to know. The technique is presented as a test not of the patient’s learning ability, but of the provider’s communication effectiveness and success in explaining the information (see Figure 1). If the message has not been transmitted successfully, the professional reteaches, corrects misconceptions, and again asks the patient to teach back.
The theory is that physicians will then avoid the closed-ended questions (“Do you understand what I just told you?”) that make patients uncomfortable or inhibit the communication that needs to happen between patient and provider.
“We didn’t invent teach-back, which long predated Project BOOST,” Dr. Greenwald says. “But we use it and endorse it strongly, and believe it is an important part of communication with patients, particularly around care transitions.”
Dr. Greenwald thinks teach-back “is not a big stretch for hospitalists.” But he says it requires meaningful training and practice, ideally in a multidisciplinary team context. Participating Project BOOST (BOOST@hospitalmedicine.org) and Electronic Quality Improvement Programs (eQUIPS) sites receive a two-year license to post the “train-the-trainer” curriculum on their intranet systems.8 An instructional webinar, and the trainer curriculum and video, are available in the SHM store (www.hospitalmedicine.org/store). SHM also provides on-site training sessions for health systems or learning collaboratives (contact tbudnitz@hospitalmedicine.org).
‘Teach-Back on Steroids’
Teach-back, while a useful approach for improving patients’ understanding about hospital discharges, post-discharge care plans, and patient self-care, is just one of many teaching models that hospitalist groups can use to improve provider-to-patient communication. HM groups should assess health literacy in their regions and physician communication skills before deciding on one or more improvement tools.
LVHN, for example, has incorporated brief motivational interviewing techniques to its teach-back system, and the results are now being studied, says Paula Robinson, MSN, RN, BC, LVHN’s manager of patient, family, and consumer education.
“A lot of research out there emphasizes how patient education and knowledge alone don’t make a difference in adherence or compliance to treatment plans, even if they are getting the knowledge right 100% of the time,” Robinson says. “You also need to give patients permission to explore their feelings.”
One of Robinson’s colleagues, patient-care specialist Debra Peters, MSN, RN, BC, CMSRN, remembers using teach-back with a heart failure patient with recurrent rehospitalizations, exploring why it was important to control his salt intake. “The patient said, ‘Honey, I salt my ham, and I have no intention of changing that.’ This issue would not have come up if we had just addressed the knowledge component and told him: ‘You need to reduce your salt intake.’”
There might not be easy solutions to that kind of patient attitude, although in this case Peters made a referral to a dietitian who worked with the patient on food substitutions and other tools for managing his salt intake. “I don’t know if we made a big difference, but I haven’t seen him back in the hospital,” she says.
Motivational interviewing is a directive, client-centered counseling style for eliciting behavioral changes by helping clients to explore and resolve their ambivalence about making changes.9 Robinson calls it “the next step in our journey, with teach-back as a jumping-off place. We’ve worked on open-ended questions, getting patients to tell their stories, and our own reflective listening skills. I look at teach-back as a great communication tool and strategy—and motivational interviewing as ‘teach-back on steroids.’”
A number of similar, comparable, or complementary techniques and systems, with names like “Teach-to-Goal” and often paired with such resources as written materials, can help advance the same ends (visit the-hospitalist.org to learn about a technique for communicating bad news to patients).
The Flinders Program, developed at Flinders University in Adelaide, Australia, is a four-part structured motivational interview that asks patients to identify what they see as the biggest problem they face.10 LVHN medical educator Krista Hirschmann, MA, PhD, says this method was taught at LVHN by Australian experts and is now being used by its home-care department. “It is truly a patient-centered approach, and could be used by anybody in the health system,” she says.
Project RED (Re-Engineered Discharge), a care-transitions strategy developed by Brian Jack, MD, and colleagues at Boston University School of Medicine, was used to create a “virtual discharge advocate,” a computer avatar that simulates the face-to-face interaction between a patient and a nurse at the bedside.11 Patients interact with the avatar, named Louise, through a touch-screen display to review their after-hospital care packet and to answer her questions, confirming their understanding without being rushed for time.
Ultimately, Dr. Greenwald says, it doesn’t matter if physicians use teach-back or some other system to improve health literacy. “What matters is whether your patients understand what they need to know in order to go home and take care of themselves,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Brach C, Keller D, Hernandez LM, et al. Ten attributes of health literate health care organizations. Institute of Medicine of the National Academies website. Available at: http://iom.edu/Global/Perspectives/2012/HealthLitAttributes.aspx. Accessed Aug. 9, 2012.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds., Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington: Institute of Medicine; 2004.
- Care Transitions Program; University of Colorado School of Medicine, Division of Health Care Policy and Research. Available at: www.caretransitions.org. Accessed July 28, 2012.
- Healthcare Benchmarks and Quality Improvement. Teach-back program reduces readmissions. HighBeam Research website. Available at: http://www.highbeam.com/doc/1G1-269890846.html. Accessed Aug. 9, 2012.
- Hospital Consumer Assessment of Healthcare Providers and Systems. Centers for Medicare & Medicaid Services website. Available at: www.hcahpsonline.org. Accessed July 23, 2012.
- Consumer Reports. How safe is your hospital? Our new ratings find that some are riskier than others. Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/2012/08/how-safe-is-your-hospital/index.htm. Accessed Aug. 1, 2012.
- Shoeb M, Merel SE, Jackson MB, Anawalt BD. “Can’t we just stop and talk?” Patients value verbal communication about discharge care plans. J Hosp Med. 2012;7(6):504-7.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163:83-90.
- Borrelli B, Riekert KA, Weinstein W, Rathier L. Brief motivational interviewing as a clinical strategy to promote asthma medication adherence. J Allergy Clinical Immunol. 2007;120(5):1023-30.
- eQUIPS (Electronic Quality Improvement Programs). Society of Hospital Medicine website. Available at: http:// www.hospitalmedicine.org/equips. Accessed Aug. 1, 2012.
- Kelly J, Kubina N. Navigating self-management: a practical approach for Australian health agencies. Flinders University, Adelaide, Australia. Available at: www.flinders.edu.au/medicine/sites/fhbhru/self-management.cfm. Accessed Aug. 1, 2012.
- Project RED (Re-Engineered Discharge). Boston University Medical Center website. Available at: http:// www.bu.edu/fammed/projectred/publications.html. Accessed Aug. 1, 2012.
“Do you understand what I just told you?”
Hospitalists who are experts on communicating with patients say that this kind of simple, yes/no question can engender all sorts of confusion. This kind of query often results in unrealistic discharge plans, failed post-discharge treatments, and unnecessary rehospitalizations. And they happen all the time in hospitals across the country.
“Yes/no questions, unless they are very concrete—such as ‘Do you have a headache?’—have little relation to assessing a patient’s understanding of essential healthcare information,” says Jeffrey Greenwald, MD, SFHM, hospitalist and educator at Massachusetts General Hospital in Boston. Many times, he adds, patients say “yes” just to please the doctor or nurse, or to avoid looking ignorant.
A better approach to patient-provider communication, one that successfully addresses communication gaps, is teach-back, a strategy in which providers ask patients to repeat (or “teach back”), in their own words, what they have just learned about their medical condition, treatments, and self-care. For example, a physician using the teach-back method could ask, “Mr. Smith, can you tell me why you are in the hospital?”
The approach is an integral part of SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) care-transitions quality initiative, says Dr. Greenwald, a BOOST coinvestigator. But too often, hospitalists fail to embrace the mandate of effective communication, he says, leaving responsibility to clarify the patient’s understanding to nurses and other members of the care team.
“Having taught this skill all over the country, I continue to find members of my own profession who feel that it is not their job to assess if patients understand self-care and medication instructions. To me, there’s no question that physicians have a role to play as teachers. We educate patients, whether we think we do or not,” Dr. Greenwald says, adding that some hospitalists do so with greater effectiveness than others.
In an era of accountable-care organizations, patient-centered care, and shared decision-making, hospitalists need to provide their patients the same core messages as the rest of the care team does. According to a recent report by the University of California San Francisco (UCSF) Center for Vulnerable Populations at San Francisco General Hospital, 77 million Americans have difficulty understanding even basic healthcare information.1
In addition to widespread language barriers, the Institute of Medicine in a 2004 report concluded that 90 million U.S. adults have literacy skills that test below the high-school level.2 As most hospitalists know, many inpatients go to great lengths to mask these limitations—appearing knowledgeable while failing to grasp essential health concepts. Medical jargon, acronyms, and instructions can be confusing, even for patients with a high level of education.
“First and foremost, we have to be able to communicate with our patients—to make sure that we understand their goals and that they understand our approach to treatment and the therapeutic goals we are proposing,” Dr. Greenwald says. “This process also helps to achieve true informed consent. We want to ensure that their questions are being answered, and that the options we are discussing are in line with their goals of care so that they are more likely to actually undertake them when they go home. And if they can’t, we need to know that in advance, so that we can intervene in other ways.”
Embracing the Method
One health system that has embraced teach-back as a patient-education strategy is the Lehigh Valley Health Network (LVHN), a 988-bed, three-hospital system based in Allentown, Pa. In an HM12 workshop, the Lehigh Valley team explained how its teach-back initiative grew out of quality initiatives to target patient flow and readmissions. Lehigh joined an Institute for Healthcare Improvement quality collaborative, implemented “Lean” quality-improvement (QI) methodologies, and adopted a patient-coaching program.3
“This process has shined a stark spotlight on how poorly we as physicians communicate with patients overall,” says Michael Pistoria, DO, SFHM, former hospitalist and president of medical staff at LVHN who was a member of the teach-back team.
“I’d like to think I’m a little above averagein this regard, but it has made me realize how much better I could be in checking in with patients, gauging their health literacy, and engaging them with the care plan. As hospitalists, we all have to rethink how we talk to patients and families.”
A multidisciplinary team, originally created to analyze care transitions, was divided into four work groups. One group, which focused on patient/family understanding of the disease process, quickly learned that care-team members often failed to identify the patient’s “key learner”—the patient, a family member, or someone else. If the information is given to the wrong person, breakdowns can result. Such breakdowns usually lead to readmissions. One instrumental change that came as a result of the QI team’s efforts is that LVHN care-team members now recognize it is their responsibility to ask who the key learner is and to put that person’s name on a whiteboard in the patient’s room.
In the workshop in at SHM’s annual meeting in San Diego, Kim Jordan, MHA, BSN, RN, NE-BC, LVHN’s administrator of patient-care services, described teach-back as an effective, easy-to-use communication strategy that improves patient learning outcomes. “We created a standard work process using teach-back strategies across the healthcare system,” with training offered to all professionals who provide education to patients and families, she said.
Starting with heart failure, prompts were written into the electronic health record (EHR) to provide four scripted teach-back questions, each focused on the patient’s knowledge, attitudes, and behavior, to be asked consecutively over three days. Information was “chunked” into manageable pieces, emphasizing what was most important for the patient to learn on that day.
Results from one of the pilot units showed 30-day readmission rates for heart failure patients were cut in half, from 28% to 14%.4 Teach-back scripts also are being developed for the anticoagulant clinic and for patients with stroke, myocardial infarction, chronic obstructive pulmonary disease (COPD), community-acquired pneumonia, and diabetes.
“Continued analysis continues to show reduced rehospitalizations, and we even find that for those who are readmitted, their second admissions have been shorter,” Dr. Pistoria says, noting LVHN nurses have reported higher satisfaction. “They say, ‘This is wonderful. This is what I love about nursing—I get to teach the patients.’”
A Quality Mandate
The importance of effective communication with hospitalized patients is recognized in the federal Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)5 quality ratings and, more recently, by Consumers Union’s new hospital safety ratings,6 which include communication in its six categories of patient-safety measures. And a recent study from the University of Washington says patients place high value on verbal communication about their discharge care plans and how to improve their health, and personal communication between their inpatient and outpatient providers.7
Large volumes of important information often are “dumped” on hospitalized patients, and many times patients are provided insufficient time to assimilate the information or ask questions about it.8 Such situations are especially common at discharge. And although physicians and other care-team members might feel they can’t afford the time to assure themselves that the patient understands what they are saying, the alternative is a lot more time spent dealing with preventable crises, misunderstandings—and preventable readmissions.
“People say, ‘I don’t have time for this,’” says Laura Vento, MSN, RN, clinical nurse leader on an acute-care medical unit at the University of California at San Diego medical center, who spearheaded teach-back at her hospital. “I did some observations around discharge visits, and it took an average of six minutes. After we implemented teach-back, it took eight to nine minutes. Nurses and patients were both very satisfied with the results. I say to staff: ‘Give it a try, and see what a difference an extra two minutes can make.’”
Dr. Pistoria describes teach-back as “humble inquiry...the simple need and ability to ask patients, ‘I know I’ve been throwing a lot of information at you. Can you tell me what I just said?’ Then, shut up and listen.” The goal is to have patients confirm that they understand fully what the provider thinks they need to know. The technique is presented as a test not of the patient’s learning ability, but of the provider’s communication effectiveness and success in explaining the information (see Figure 1). If the message has not been transmitted successfully, the professional reteaches, corrects misconceptions, and again asks the patient to teach back.
The theory is that physicians will then avoid the closed-ended questions (“Do you understand what I just told you?”) that make patients uncomfortable or inhibit the communication that needs to happen between patient and provider.
“We didn’t invent teach-back, which long predated Project BOOST,” Dr. Greenwald says. “But we use it and endorse it strongly, and believe it is an important part of communication with patients, particularly around care transitions.”
Dr. Greenwald thinks teach-back “is not a big stretch for hospitalists.” But he says it requires meaningful training and practice, ideally in a multidisciplinary team context. Participating Project BOOST (BOOST@hospitalmedicine.org) and Electronic Quality Improvement Programs (eQUIPS) sites receive a two-year license to post the “train-the-trainer” curriculum on their intranet systems.8 An instructional webinar, and the trainer curriculum and video, are available in the SHM store (www.hospitalmedicine.org/store). SHM also provides on-site training sessions for health systems or learning collaboratives (contact tbudnitz@hospitalmedicine.org).
‘Teach-Back on Steroids’
Teach-back, while a useful approach for improving patients’ understanding about hospital discharges, post-discharge care plans, and patient self-care, is just one of many teaching models that hospitalist groups can use to improve provider-to-patient communication. HM groups should assess health literacy in their regions and physician communication skills before deciding on one or more improvement tools.
LVHN, for example, has incorporated brief motivational interviewing techniques to its teach-back system, and the results are now being studied, says Paula Robinson, MSN, RN, BC, LVHN’s manager of patient, family, and consumer education.
“A lot of research out there emphasizes how patient education and knowledge alone don’t make a difference in adherence or compliance to treatment plans, even if they are getting the knowledge right 100% of the time,” Robinson says. “You also need to give patients permission to explore their feelings.”
One of Robinson’s colleagues, patient-care specialist Debra Peters, MSN, RN, BC, CMSRN, remembers using teach-back with a heart failure patient with recurrent rehospitalizations, exploring why it was important to control his salt intake. “The patient said, ‘Honey, I salt my ham, and I have no intention of changing that.’ This issue would not have come up if we had just addressed the knowledge component and told him: ‘You need to reduce your salt intake.’”
There might not be easy solutions to that kind of patient attitude, although in this case Peters made a referral to a dietitian who worked with the patient on food substitutions and other tools for managing his salt intake. “I don’t know if we made a big difference, but I haven’t seen him back in the hospital,” she says.
Motivational interviewing is a directive, client-centered counseling style for eliciting behavioral changes by helping clients to explore and resolve their ambivalence about making changes.9 Robinson calls it “the next step in our journey, with teach-back as a jumping-off place. We’ve worked on open-ended questions, getting patients to tell their stories, and our own reflective listening skills. I look at teach-back as a great communication tool and strategy—and motivational interviewing as ‘teach-back on steroids.’”
A number of similar, comparable, or complementary techniques and systems, with names like “Teach-to-Goal” and often paired with such resources as written materials, can help advance the same ends (visit the-hospitalist.org to learn about a technique for communicating bad news to patients).
The Flinders Program, developed at Flinders University in Adelaide, Australia, is a four-part structured motivational interview that asks patients to identify what they see as the biggest problem they face.10 LVHN medical educator Krista Hirschmann, MA, PhD, says this method was taught at LVHN by Australian experts and is now being used by its home-care department. “It is truly a patient-centered approach, and could be used by anybody in the health system,” she says.
Project RED (Re-Engineered Discharge), a care-transitions strategy developed by Brian Jack, MD, and colleagues at Boston University School of Medicine, was used to create a “virtual discharge advocate,” a computer avatar that simulates the face-to-face interaction between a patient and a nurse at the bedside.11 Patients interact with the avatar, named Louise, through a touch-screen display to review their after-hospital care packet and to answer her questions, confirming their understanding without being rushed for time.
Ultimately, Dr. Greenwald says, it doesn’t matter if physicians use teach-back or some other system to improve health literacy. “What matters is whether your patients understand what they need to know in order to go home and take care of themselves,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Brach C, Keller D, Hernandez LM, et al. Ten attributes of health literate health care organizations. Institute of Medicine of the National Academies website. Available at: http://iom.edu/Global/Perspectives/2012/HealthLitAttributes.aspx. Accessed Aug. 9, 2012.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds., Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington: Institute of Medicine; 2004.
- Care Transitions Program; University of Colorado School of Medicine, Division of Health Care Policy and Research. Available at: www.caretransitions.org. Accessed July 28, 2012.
- Healthcare Benchmarks and Quality Improvement. Teach-back program reduces readmissions. HighBeam Research website. Available at: http://www.highbeam.com/doc/1G1-269890846.html. Accessed Aug. 9, 2012.
- Hospital Consumer Assessment of Healthcare Providers and Systems. Centers for Medicare & Medicaid Services website. Available at: www.hcahpsonline.org. Accessed July 23, 2012.
- Consumer Reports. How safe is your hospital? Our new ratings find that some are riskier than others. Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/2012/08/how-safe-is-your-hospital/index.htm. Accessed Aug. 1, 2012.
- Shoeb M, Merel SE, Jackson MB, Anawalt BD. “Can’t we just stop and talk?” Patients value verbal communication about discharge care plans. J Hosp Med. 2012;7(6):504-7.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163:83-90.
- Borrelli B, Riekert KA, Weinstein W, Rathier L. Brief motivational interviewing as a clinical strategy to promote asthma medication adherence. J Allergy Clinical Immunol. 2007;120(5):1023-30.
- eQUIPS (Electronic Quality Improvement Programs). Society of Hospital Medicine website. Available at: http:// www.hospitalmedicine.org/equips. Accessed Aug. 1, 2012.
- Kelly J, Kubina N. Navigating self-management: a practical approach for Australian health agencies. Flinders University, Adelaide, Australia. Available at: www.flinders.edu.au/medicine/sites/fhbhru/self-management.cfm. Accessed Aug. 1, 2012.
- Project RED (Re-Engineered Discharge). Boston University Medical Center website. Available at: http:// www.bu.edu/fammed/projectred/publications.html. Accessed Aug. 1, 2012.
HM Leaders Highlight Benefits of Specialty Hospitalist Programs
Safer patients, improved quality of care, innovative uses of resources, increased job satisfaction: Those themes threaded their way through presentation after presentation at “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” a one-day meeting of hospitalist leaders and hospital administrators following the annual Health Forum/AHA Leadership Summit on July 21 in San Francisco.
The five-hour presentation to about 80 hospital CEOs, chief financial officers, and chief medical officers focused on the ever-expanding roles of subspecialty hospitalists and how subspecialty hospitalist programs can help administrators solve multiple challenges in an era of healthcare reform.
“When I started in 2007, I could only identify 15 hospitals in the United States with OB hospitalist programs. And now we know of 169, and the nation is adding one or two new programs a month,” says Rob Olson, MD, an OB/GYN hospitalistor “laborist”at PeaceHealth St. Joseph Medical Center in Bellingham, Wash., and editor of ObGynHospitalist.com. “If you think about it, if you can make it safer for women in labor, then duh! Why wouldn’t you want to do that?
“The finances work best at a hospital that delivers more than 2,000 babies a year. But many small hospitals, like those doing 800 or 1,000 deliveries a year, have programs because it makes it safer for women in labor,” he says. “Therefore, even though it might be more expensive at those lower numbers, it’s worth it. It’s the right thing to do.”
The July meeting was the second time SHM gathered stakeholders to discuss the growth of specialty hospitalists; a similar panel of experts convened last November in Las Vegas. Most at the San Francisco meeting recognized the upward trend in such HM-focused subspecialties as neurology, orthopedics, obstetrics, and general surgery, according to John Nelson, MD, MHM, organizer of the focused-practice meetings.
“Most people in healthcare feel like this is going to continue and intensify,” says Dr. Nelson, cofounder and past president of SHM, medical director of the hospitalist practice at Overlake Hospital Medical Center, Bellevue, Wash., and practice-management columnist for The Hospitalist. “There is consensus that each specialty can learn from the other about how they organize their practice and approach their work. There was consensus that we don’t have a lot of research data about what this means for things like cost of care, quality of care, patient experience, physician career longevity. So we need to encourage people to begin to study those things, and what this means for the stakeholders in healthcare.”


Four subspecialty hospitalists—neurohospitalist David Likosky, MD, SFHM, surgicalist John Maa, MD, orthopedic hospitalist Kurt Ehlert, MD, and Dr. Olson, the laborist—took part in a 90-minute panel discussion in which they explained their practice models and fielded questions from the audience.
“My message was that there are a large number of people doing this now—we estimate there are between 600 and 700 neurohospitalists nationally—and that the model holds a lot of promise. There’s not a huge amount of data right now on outcomes and other metrics, but we’re starting to see that data,” said Dr. Likosky, medical director of the Evergreen Neuroscience Institute in Kirkland, Wash., and co-founder of the Neurohospitalist Society (neurohospitalistsociety.org). “The neurohospitalist model is a good solution to many of the problems that hospitals are facing now.”
—Kurt Ehlert, MD, medical director, Orthopedic Hospitalists of New Bern, national director for orthopedic services, Delphi Healthcare Partners, Morrisville, N.C.
Dr. Ehlert, director of orthopaedic services, Orthopeadic Hospitalists of New Bern (N.C.), and national orthopaedic medical director of Delphi of TEAMHealth, says subspecialty HM programs offer hospitals a “great chance of improving quality and patient safety over what they have currently, even if they have their emergency room covered.”
“I think hospitalists who are subspecialists in trauma can provide a bump up in productivity, safety, reliability,” he says. “Results will be better. I think it will be less expensive. [I told them] that there is an option out there that can benefit them in all of the various key ways that groups are looking at right now.”
Dr. Ehlert’s ortho-hospitalist group formed when the 300-bed hospital in New Bern encountered a manpower issue not unfamiliar to hospitals across the country. The bylaws of the medical staff allowed subspecialists to stop taking call when they turned 55, and four of the seven orthopedists aged out.
“Three doctors taking all the call is not really sustainable for them in their private practices,” Dr. Ehlert said. “So they looked at various options, came to us, and we started in December of 2009. It has been very successful, according to the administration. They love us being there. The emergency room is very happy with our responsiveness. I think our results have been very good.”
The new arrangement is a win-win, Dr. Ehlert says. The orthopedists are focused on their elective practices, and “they’re very happy with that. So their life is much better; their elective practice has actually gotten busier because they’re not having to leave space open for all the trauma from the ER. So I think all around it’s been very successful.”
The hospital has added a general surgery hospitalist program, which is doing well, too. “They’re much busier,” he says. “They’re really taking a load off the general surgeons in town.”
Dr. Maa, assistant professor and director of the surgical hospitalist program at University of California San Francisco Medical Center, says growth in his field is fueled by the ever-growing crises in emergency departments.
“Most hospitals critically depend on a general surgical service,” he said. “If you can’t keep a panel of general surgeons to take call, you’re probably going to have to close your emergency room.”
Dr. Maa, who founded UCSF’s surgical hospitalist program in 2005, explained how the terms “surgicalist” and “acute-care surgeon” have come to represent the concept of a dedicated emergency surgeon, whether it be in trauma or in general surgery. “It really does parallel the medical hospitalist model,” he says, adding that his field has had to overcome doubts about scheduling and patient safety.
“The danger in each of these specialty programs is to become too much of the silo mentality, to focus on their own discipline,” he adds. “We need to work across specialties, we need to collaborate, we need to find ways of utilizing the precious existing resources for emergency care, and make certain that the needs of society are met. Society places trust in doctors, hospital leaders, to build a system that will care for them when they need it. It’s our ethical obligation to design the safest, best system, with the resources that we have.”
Jason Carris is editor of The Hospitalist.
Safer patients, improved quality of care, innovative uses of resources, increased job satisfaction: Those themes threaded their way through presentation after presentation at “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” a one-day meeting of hospitalist leaders and hospital administrators following the annual Health Forum/AHA Leadership Summit on July 21 in San Francisco.
The five-hour presentation to about 80 hospital CEOs, chief financial officers, and chief medical officers focused on the ever-expanding roles of subspecialty hospitalists and how subspecialty hospitalist programs can help administrators solve multiple challenges in an era of healthcare reform.
“When I started in 2007, I could only identify 15 hospitals in the United States with OB hospitalist programs. And now we know of 169, and the nation is adding one or two new programs a month,” says Rob Olson, MD, an OB/GYN hospitalistor “laborist”at PeaceHealth St. Joseph Medical Center in Bellingham, Wash., and editor of ObGynHospitalist.com. “If you think about it, if you can make it safer for women in labor, then duh! Why wouldn’t you want to do that?
“The finances work best at a hospital that delivers more than 2,000 babies a year. But many small hospitals, like those doing 800 or 1,000 deliveries a year, have programs because it makes it safer for women in labor,” he says. “Therefore, even though it might be more expensive at those lower numbers, it’s worth it. It’s the right thing to do.”
The July meeting was the second time SHM gathered stakeholders to discuss the growth of specialty hospitalists; a similar panel of experts convened last November in Las Vegas. Most at the San Francisco meeting recognized the upward trend in such HM-focused subspecialties as neurology, orthopedics, obstetrics, and general surgery, according to John Nelson, MD, MHM, organizer of the focused-practice meetings.
“Most people in healthcare feel like this is going to continue and intensify,” says Dr. Nelson, cofounder and past president of SHM, medical director of the hospitalist practice at Overlake Hospital Medical Center, Bellevue, Wash., and practice-management columnist for The Hospitalist. “There is consensus that each specialty can learn from the other about how they organize their practice and approach their work. There was consensus that we don’t have a lot of research data about what this means for things like cost of care, quality of care, patient experience, physician career longevity. So we need to encourage people to begin to study those things, and what this means for the stakeholders in healthcare.”
Four subspecialty hospitalists—neurohospitalist David Likosky, MD, SFHM, surgicalist John Maa, MD, orthopedic hospitalist Kurt Ehlert, MD, and Dr. Olson, the laborist—took part in a 90-minute panel discussion in which they explained their practice models and fielded questions from the audience.
“My message was that there are a large number of people doing this now—we estimate there are between 600 and 700 neurohospitalists nationally—and that the model holds a lot of promise. There’s not a huge amount of data right now on outcomes and other metrics, but we’re starting to see that data,” said Dr. Likosky, medical director of the Evergreen Neuroscience Institute in Kirkland, Wash., and co-founder of the Neurohospitalist Society (neurohospitalistsociety.org). “The neurohospitalist model is a good solution to many of the problems that hospitals are facing now.”
—Kurt Ehlert, MD, medical director, Orthopedic Hospitalists of New Bern, national director for orthopedic services, Delphi Healthcare Partners, Morrisville, N.C.
Dr. Ehlert, director of orthopaedic services, Orthopeadic Hospitalists of New Bern (N.C.), and national orthopaedic medical director of Delphi of TEAMHealth, says subspecialty HM programs offer hospitals a “great chance of improving quality and patient safety over what they have currently, even if they have their emergency room covered.”
“I think hospitalists who are subspecialists in trauma can provide a bump up in productivity, safety, reliability,” he says. “Results will be better. I think it will be less expensive. [I told them] that there is an option out there that can benefit them in all of the various key ways that groups are looking at right now.”
Dr. Ehlert’s ortho-hospitalist group formed when the 300-bed hospital in New Bern encountered a manpower issue not unfamiliar to hospitals across the country. The bylaws of the medical staff allowed subspecialists to stop taking call when they turned 55, and four of the seven orthopedists aged out.
“Three doctors taking all the call is not really sustainable for them in their private practices,” Dr. Ehlert said. “So they looked at various options, came to us, and we started in December of 2009. It has been very successful, according to the administration. They love us being there. The emergency room is very happy with our responsiveness. I think our results have been very good.”
The new arrangement is a win-win, Dr. Ehlert says. The orthopedists are focused on their elective practices, and “they’re very happy with that. So their life is much better; their elective practice has actually gotten busier because they’re not having to leave space open for all the trauma from the ER. So I think all around it’s been very successful.”
The hospital has added a general surgery hospitalist program, which is doing well, too. “They’re much busier,” he says. “They’re really taking a load off the general surgeons in town.”
Dr. Maa, assistant professor and director of the surgical hospitalist program at University of California San Francisco Medical Center, says growth in his field is fueled by the ever-growing crises in emergency departments.
“Most hospitals critically depend on a general surgical service,” he said. “If you can’t keep a panel of general surgeons to take call, you’re probably going to have to close your emergency room.”
Dr. Maa, who founded UCSF’s surgical hospitalist program in 2005, explained how the terms “surgicalist” and “acute-care surgeon” have come to represent the concept of a dedicated emergency surgeon, whether it be in trauma or in general surgery. “It really does parallel the medical hospitalist model,” he says, adding that his field has had to overcome doubts about scheduling and patient safety.
“The danger in each of these specialty programs is to become too much of the silo mentality, to focus on their own discipline,” he adds. “We need to work across specialties, we need to collaborate, we need to find ways of utilizing the precious existing resources for emergency care, and make certain that the needs of society are met. Society places trust in doctors, hospital leaders, to build a system that will care for them when they need it. It’s our ethical obligation to design the safest, best system, with the resources that we have.”
Jason Carris is editor of The Hospitalist.
Safer patients, improved quality of care, innovative uses of resources, increased job satisfaction: Those themes threaded their way through presentation after presentation at “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” a one-day meeting of hospitalist leaders and hospital administrators following the annual Health Forum/AHA Leadership Summit on July 21 in San Francisco.
The five-hour presentation to about 80 hospital CEOs, chief financial officers, and chief medical officers focused on the ever-expanding roles of subspecialty hospitalists and how subspecialty hospitalist programs can help administrators solve multiple challenges in an era of healthcare reform.
“When I started in 2007, I could only identify 15 hospitals in the United States with OB hospitalist programs. And now we know of 169, and the nation is adding one or two new programs a month,” says Rob Olson, MD, an OB/GYN hospitalistor “laborist”at PeaceHealth St. Joseph Medical Center in Bellingham, Wash., and editor of ObGynHospitalist.com. “If you think about it, if you can make it safer for women in labor, then duh! Why wouldn’t you want to do that?
“The finances work best at a hospital that delivers more than 2,000 babies a year. But many small hospitals, like those doing 800 or 1,000 deliveries a year, have programs because it makes it safer for women in labor,” he says. “Therefore, even though it might be more expensive at those lower numbers, it’s worth it. It’s the right thing to do.”
The July meeting was the second time SHM gathered stakeholders to discuss the growth of specialty hospitalists; a similar panel of experts convened last November in Las Vegas. Most at the San Francisco meeting recognized the upward trend in such HM-focused subspecialties as neurology, orthopedics, obstetrics, and general surgery, according to John Nelson, MD, MHM, organizer of the focused-practice meetings.
“Most people in healthcare feel like this is going to continue and intensify,” says Dr. Nelson, cofounder and past president of SHM, medical director of the hospitalist practice at Overlake Hospital Medical Center, Bellevue, Wash., and practice-management columnist for The Hospitalist. “There is consensus that each specialty can learn from the other about how they organize their practice and approach their work. There was consensus that we don’t have a lot of research data about what this means for things like cost of care, quality of care, patient experience, physician career longevity. So we need to encourage people to begin to study those things, and what this means for the stakeholders in healthcare.”
Four subspecialty hospitalists—neurohospitalist David Likosky, MD, SFHM, surgicalist John Maa, MD, orthopedic hospitalist Kurt Ehlert, MD, and Dr. Olson, the laborist—took part in a 90-minute panel discussion in which they explained their practice models and fielded questions from the audience.
“My message was that there are a large number of people doing this now—we estimate there are between 600 and 700 neurohospitalists nationally—and that the model holds a lot of promise. There’s not a huge amount of data right now on outcomes and other metrics, but we’re starting to see that data,” said Dr. Likosky, medical director of the Evergreen Neuroscience Institute in Kirkland, Wash., and co-founder of the Neurohospitalist Society (neurohospitalistsociety.org). “The neurohospitalist model is a good solution to many of the problems that hospitals are facing now.”
—Kurt Ehlert, MD, medical director, Orthopedic Hospitalists of New Bern, national director for orthopedic services, Delphi Healthcare Partners, Morrisville, N.C.
Dr. Ehlert, director of orthopaedic services, Orthopeadic Hospitalists of New Bern (N.C.), and national orthopaedic medical director of Delphi of TEAMHealth, says subspecialty HM programs offer hospitals a “great chance of improving quality and patient safety over what they have currently, even if they have their emergency room covered.”
“I think hospitalists who are subspecialists in trauma can provide a bump up in productivity, safety, reliability,” he says. “Results will be better. I think it will be less expensive. [I told them] that there is an option out there that can benefit them in all of the various key ways that groups are looking at right now.”
Dr. Ehlert’s ortho-hospitalist group formed when the 300-bed hospital in New Bern encountered a manpower issue not unfamiliar to hospitals across the country. The bylaws of the medical staff allowed subspecialists to stop taking call when they turned 55, and four of the seven orthopedists aged out.
“Three doctors taking all the call is not really sustainable for them in their private practices,” Dr. Ehlert said. “So they looked at various options, came to us, and we started in December of 2009. It has been very successful, according to the administration. They love us being there. The emergency room is very happy with our responsiveness. I think our results have been very good.”
The new arrangement is a win-win, Dr. Ehlert says. The orthopedists are focused on their elective practices, and “they’re very happy with that. So their life is much better; their elective practice has actually gotten busier because they’re not having to leave space open for all the trauma from the ER. So I think all around it’s been very successful.”
The hospital has added a general surgery hospitalist program, which is doing well, too. “They’re much busier,” he says. “They’re really taking a load off the general surgeons in town.”
Dr. Maa, assistant professor and director of the surgical hospitalist program at University of California San Francisco Medical Center, says growth in his field is fueled by the ever-growing crises in emergency departments.
“Most hospitals critically depend on a general surgical service,” he said. “If you can’t keep a panel of general surgeons to take call, you’re probably going to have to close your emergency room.”
Dr. Maa, who founded UCSF’s surgical hospitalist program in 2005, explained how the terms “surgicalist” and “acute-care surgeon” have come to represent the concept of a dedicated emergency surgeon, whether it be in trauma or in general surgery. “It really does parallel the medical hospitalist model,” he says, adding that his field has had to overcome doubts about scheduling and patient safety.
“The danger in each of these specialty programs is to become too much of the silo mentality, to focus on their own discipline,” he adds. “We need to work across specialties, we need to collaborate, we need to find ways of utilizing the precious existing resources for emergency care, and make certain that the needs of society are met. Society places trust in doctors, hospital leaders, to build a system that will care for them when they need it. It’s our ethical obligation to design the safest, best system, with the resources that we have.”
Jason Carris is editor of The Hospitalist.
Shaun Frost: High-Value Healthcare

In my previous column, we considered a comprehensive and practical definition of accountability advanced by Connors, Smith, and Hickman in their well-written book “The Oz Principle.”1 In order to apply these concepts successfully to HM practice, it is useful to conceive of accountability as a process that should be approached in a step-wise manner. In this month’s column, we will explore the “process of accountability” by considering how “The Oz Principle” can further assist hospitalists in accomplishing what is expected of them as agents of high-quality, cost-effective healthcare delivery.
The Process
Recall that Connors and colleagues define accountability as “a personal choice to rise above one’s circumstances, and demonstrate ownership necessary for achieving results.” Such a definition empowers us to anticipate the future by proactively avoiding problems versus retrospectively explaining why problems occurred. To apply this definition in our daily lives, we must contemplate how to proactively avoid problems. This can be accomplished by following a process described as the four-step approach: “see it, own it, solve it, and do it.”
Step No. 1 on the road to accountability requires that hospitalists be aware of issues in their external environments that affect their practice, and is referred to by Connors et al as “seeing it.” As it concerns healthcare reform, Step 1 requires that hospitalists educate themselves about such keystone reform initiatives as value-based purchasing and the public reporting of performance. Initiatives such as these are centerpieces of care delivery reform, and will occur irrespective of the fate of such legislation as the Affordable Care Act. Clinicians thus must understand the features of these initiatives, and appreciate how policies and programs emanating from them will necessitate changes in medical practice.
There are innumerable resources available to assist with understanding these concepts. If you have yet to do so, I encourage you to explore the hospital value-based purchasing (HVBP) toolkit on SHM’s website (www.hospitalmedicine.org/hvbp). Additionally, in order to appreciate the power of public performance reporting, please review the Hospital Compare and Physician Compare pages on the Centers for Medicare & Medicaid Services (CMS) website. Knowledge is power, and in this situation it is essential to ensure your continued professional success. “The Oz Principle” admonishes that “if changes are inevitable, then those who resist them will inevitably fail.” Please ensure that failure is not an option by seeking first to understand how healthcare reform will impact your practice.
Step No. 2 on the road to accountability requires that hospitalists sincerely accept healthcare challenges as theirs to personally embrace. Connors et al define this step as “owning it.” In order to truly own our country’s problem of substandard healthcare delivery, “The Oz Principle” suggests that the profession of medicine must “accept ownership of past and present behaviors that keep it mired in current circumstances, (as this is the only way it can) hope to improve its future situation.”
This is challenging for hospitalists, as most HM practitioners are only a few years removed from completion of clinical training. It is thus tempting for young hospitalists to refuse ownership of healthcare system problems as ones that they personally created. Although this position is understandable, we should not accept it. It might be true that a single physician’s practice contributed little to our current overall healthcare challenges; however, we are all members of the same profession, and a collective identity when it comes to ownership of healthcare system problems is essential to our ability to eventually solve these problems. Complaining that our predecessors are responsible for our present maladies will stifle improvement efforts by creating a culture of victimization. According to “The Oz Principle,” “owning our circumstances gives us the strength to overcome the powerlessness that comes from being a victim, and allows us to move forward and achieve more satisfying results.”
Step No. 3 mandates that hospitalists capitalize on reform opportunities by designing process-improvement strategies through critical analysis and innovative thinking. Connors and colleagues define this step as “solving it.” Contributing to “solving it” is a fundamental job responsibility of every hospitalist, and not the exclusive province of hospitalist leaders. HM clinicians focusing primarily on bedside care must actively participate in the process of solving the problems that currently plague our healthcare system.
To do so should not necessitate an overly burdensome time commitment. It is often sufficient to simply attend and actively participate in your team and hospital staff meetings. At other times, it might be necessary for you to volunteer an hour or so once a month in service to a hospital committee or a team activity. Contributing your observations and thoughts in these forums is essential to creating effective solutions. Although you might not be the ultimate decision-maker, you have an obligation to build a broad collective understanding of the issues through the voicing of your opinions.
According to “The Oz Principle,” “solving it is not an extra activity, but part of the job.” Each of us has a professional obligation to identify better methods to deliver high-value healthcare. Doing so necessitates that we each identify improvement opportunities by critically evaluating the success of our current situations. We must then, at a minimum, share our thoughts with the decision-makers responsible for enacting improvement strategies.
The fourth and final step on the road to accountability requires that hospitalists successfully implement solutions and ensure that the desired results are achieved. Connors and colleagues define this step as “doing it.” Successfully “doing it” to enhance healthcare quality and efficiency necessitates hard work, because rarely is it sufficient to simply implement a healthcare improvement project. In order to achieve true results, projects must be actively managed after initial deployment, tweaked to become better, then redeployed and reanalyzed to ensure effectiveness.
In healthcare, it is tempting to become satisfied with simply deploying processes, as much of the healthcare reform work done to date has focused on payment for process improvements. This, however, will change in the near future. For example, Medicare’s hospital value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” January 2012, p. 1) will incorporate outcome measures as soon as 2014. We must, therefore, get into the habit of aggressively managing the processes that we operate through diligent data collection and subsequent decision-making that is informed by actionable information.
Conclusion
Holding ourselves accountable for enacting healthcare reform initiatives to improve the care of our patients will be difficult. The task is made easier by employing a process to guide our efforts. “The Oz Principle” teaches us a succinct, four-step approach. Applying this approach to changes mandated by healthcare reform will make it easier for hospitalists to transcend their current dysfunctional situations and achieve demonstrable healthcare system improvements for the betterment of patient care.
Dr. Frost is president of SHM.
Reference
In my previous column, we considered a comprehensive and practical definition of accountability advanced by Connors, Smith, and Hickman in their well-written book “The Oz Principle.”1 In order to apply these concepts successfully to HM practice, it is useful to conceive of accountability as a process that should be approached in a step-wise manner. In this month’s column, we will explore the “process of accountability” by considering how “The Oz Principle” can further assist hospitalists in accomplishing what is expected of them as agents of high-quality, cost-effective healthcare delivery.
The Process
Recall that Connors and colleagues define accountability as “a personal choice to rise above one’s circumstances, and demonstrate ownership necessary for achieving results.” Such a definition empowers us to anticipate the future by proactively avoiding problems versus retrospectively explaining why problems occurred. To apply this definition in our daily lives, we must contemplate how to proactively avoid problems. This can be accomplished by following a process described as the four-step approach: “see it, own it, solve it, and do it.”
Step No. 1 on the road to accountability requires that hospitalists be aware of issues in their external environments that affect their practice, and is referred to by Connors et al as “seeing it.” As it concerns healthcare reform, Step 1 requires that hospitalists educate themselves about such keystone reform initiatives as value-based purchasing and the public reporting of performance. Initiatives such as these are centerpieces of care delivery reform, and will occur irrespective of the fate of such legislation as the Affordable Care Act. Clinicians thus must understand the features of these initiatives, and appreciate how policies and programs emanating from them will necessitate changes in medical practice.
There are innumerable resources available to assist with understanding these concepts. If you have yet to do so, I encourage you to explore the hospital value-based purchasing (HVBP) toolkit on SHM’s website (www.hospitalmedicine.org/hvbp). Additionally, in order to appreciate the power of public performance reporting, please review the Hospital Compare and Physician Compare pages on the Centers for Medicare & Medicaid Services (CMS) website. Knowledge is power, and in this situation it is essential to ensure your continued professional success. “The Oz Principle” admonishes that “if changes are inevitable, then those who resist them will inevitably fail.” Please ensure that failure is not an option by seeking first to understand how healthcare reform will impact your practice.
Step No. 2 on the road to accountability requires that hospitalists sincerely accept healthcare challenges as theirs to personally embrace. Connors et al define this step as “owning it.” In order to truly own our country’s problem of substandard healthcare delivery, “The Oz Principle” suggests that the profession of medicine must “accept ownership of past and present behaviors that keep it mired in current circumstances, (as this is the only way it can) hope to improve its future situation.”
This is challenging for hospitalists, as most HM practitioners are only a few years removed from completion of clinical training. It is thus tempting for young hospitalists to refuse ownership of healthcare system problems as ones that they personally created. Although this position is understandable, we should not accept it. It might be true that a single physician’s practice contributed little to our current overall healthcare challenges; however, we are all members of the same profession, and a collective identity when it comes to ownership of healthcare system problems is essential to our ability to eventually solve these problems. Complaining that our predecessors are responsible for our present maladies will stifle improvement efforts by creating a culture of victimization. According to “The Oz Principle,” “owning our circumstances gives us the strength to overcome the powerlessness that comes from being a victim, and allows us to move forward and achieve more satisfying results.”
Step No. 3 mandates that hospitalists capitalize on reform opportunities by designing process-improvement strategies through critical analysis and innovative thinking. Connors and colleagues define this step as “solving it.” Contributing to “solving it” is a fundamental job responsibility of every hospitalist, and not the exclusive province of hospitalist leaders. HM clinicians focusing primarily on bedside care must actively participate in the process of solving the problems that currently plague our healthcare system.
To do so should not necessitate an overly burdensome time commitment. It is often sufficient to simply attend and actively participate in your team and hospital staff meetings. At other times, it might be necessary for you to volunteer an hour or so once a month in service to a hospital committee or a team activity. Contributing your observations and thoughts in these forums is essential to creating effective solutions. Although you might not be the ultimate decision-maker, you have an obligation to build a broad collective understanding of the issues through the voicing of your opinions.
According to “The Oz Principle,” “solving it is not an extra activity, but part of the job.” Each of us has a professional obligation to identify better methods to deliver high-value healthcare. Doing so necessitates that we each identify improvement opportunities by critically evaluating the success of our current situations. We must then, at a minimum, share our thoughts with the decision-makers responsible for enacting improvement strategies.
The fourth and final step on the road to accountability requires that hospitalists successfully implement solutions and ensure that the desired results are achieved. Connors and colleagues define this step as “doing it.” Successfully “doing it” to enhance healthcare quality and efficiency necessitates hard work, because rarely is it sufficient to simply implement a healthcare improvement project. In order to achieve true results, projects must be actively managed after initial deployment, tweaked to become better, then redeployed and reanalyzed to ensure effectiveness.
In healthcare, it is tempting to become satisfied with simply deploying processes, as much of the healthcare reform work done to date has focused on payment for process improvements. This, however, will change in the near future. For example, Medicare’s hospital value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” January 2012, p. 1) will incorporate outcome measures as soon as 2014. We must, therefore, get into the habit of aggressively managing the processes that we operate through diligent data collection and subsequent decision-making that is informed by actionable information.
Conclusion
Holding ourselves accountable for enacting healthcare reform initiatives to improve the care of our patients will be difficult. The task is made easier by employing a process to guide our efforts. “The Oz Principle” teaches us a succinct, four-step approach. Applying this approach to changes mandated by healthcare reform will make it easier for hospitalists to transcend their current dysfunctional situations and achieve demonstrable healthcare system improvements for the betterment of patient care.
Dr. Frost is president of SHM.
Reference
In my previous column, we considered a comprehensive and practical definition of accountability advanced by Connors, Smith, and Hickman in their well-written book “The Oz Principle.”1 In order to apply these concepts successfully to HM practice, it is useful to conceive of accountability as a process that should be approached in a step-wise manner. In this month’s column, we will explore the “process of accountability” by considering how “The Oz Principle” can further assist hospitalists in accomplishing what is expected of them as agents of high-quality, cost-effective healthcare delivery.
The Process
Recall that Connors and colleagues define accountability as “a personal choice to rise above one’s circumstances, and demonstrate ownership necessary for achieving results.” Such a definition empowers us to anticipate the future by proactively avoiding problems versus retrospectively explaining why problems occurred. To apply this definition in our daily lives, we must contemplate how to proactively avoid problems. This can be accomplished by following a process described as the four-step approach: “see it, own it, solve it, and do it.”
Step No. 1 on the road to accountability requires that hospitalists be aware of issues in their external environments that affect their practice, and is referred to by Connors et al as “seeing it.” As it concerns healthcare reform, Step 1 requires that hospitalists educate themselves about such keystone reform initiatives as value-based purchasing and the public reporting of performance. Initiatives such as these are centerpieces of care delivery reform, and will occur irrespective of the fate of such legislation as the Affordable Care Act. Clinicians thus must understand the features of these initiatives, and appreciate how policies and programs emanating from them will necessitate changes in medical practice.
There are innumerable resources available to assist with understanding these concepts. If you have yet to do so, I encourage you to explore the hospital value-based purchasing (HVBP) toolkit on SHM’s website (www.hospitalmedicine.org/hvbp). Additionally, in order to appreciate the power of public performance reporting, please review the Hospital Compare and Physician Compare pages on the Centers for Medicare & Medicaid Services (CMS) website. Knowledge is power, and in this situation it is essential to ensure your continued professional success. “The Oz Principle” admonishes that “if changes are inevitable, then those who resist them will inevitably fail.” Please ensure that failure is not an option by seeking first to understand how healthcare reform will impact your practice.
Step No. 2 on the road to accountability requires that hospitalists sincerely accept healthcare challenges as theirs to personally embrace. Connors et al define this step as “owning it.” In order to truly own our country’s problem of substandard healthcare delivery, “The Oz Principle” suggests that the profession of medicine must “accept ownership of past and present behaviors that keep it mired in current circumstances, (as this is the only way it can) hope to improve its future situation.”
This is challenging for hospitalists, as most HM practitioners are only a few years removed from completion of clinical training. It is thus tempting for young hospitalists to refuse ownership of healthcare system problems as ones that they personally created. Although this position is understandable, we should not accept it. It might be true that a single physician’s practice contributed little to our current overall healthcare challenges; however, we are all members of the same profession, and a collective identity when it comes to ownership of healthcare system problems is essential to our ability to eventually solve these problems. Complaining that our predecessors are responsible for our present maladies will stifle improvement efforts by creating a culture of victimization. According to “The Oz Principle,” “owning our circumstances gives us the strength to overcome the powerlessness that comes from being a victim, and allows us to move forward and achieve more satisfying results.”
Step No. 3 mandates that hospitalists capitalize on reform opportunities by designing process-improvement strategies through critical analysis and innovative thinking. Connors and colleagues define this step as “solving it.” Contributing to “solving it” is a fundamental job responsibility of every hospitalist, and not the exclusive province of hospitalist leaders. HM clinicians focusing primarily on bedside care must actively participate in the process of solving the problems that currently plague our healthcare system.
To do so should not necessitate an overly burdensome time commitment. It is often sufficient to simply attend and actively participate in your team and hospital staff meetings. At other times, it might be necessary for you to volunteer an hour or so once a month in service to a hospital committee or a team activity. Contributing your observations and thoughts in these forums is essential to creating effective solutions. Although you might not be the ultimate decision-maker, you have an obligation to build a broad collective understanding of the issues through the voicing of your opinions.
According to “The Oz Principle,” “solving it is not an extra activity, but part of the job.” Each of us has a professional obligation to identify better methods to deliver high-value healthcare. Doing so necessitates that we each identify improvement opportunities by critically evaluating the success of our current situations. We must then, at a minimum, share our thoughts with the decision-makers responsible for enacting improvement strategies.
The fourth and final step on the road to accountability requires that hospitalists successfully implement solutions and ensure that the desired results are achieved. Connors and colleagues define this step as “doing it.” Successfully “doing it” to enhance healthcare quality and efficiency necessitates hard work, because rarely is it sufficient to simply implement a healthcare improvement project. In order to achieve true results, projects must be actively managed after initial deployment, tweaked to become better, then redeployed and reanalyzed to ensure effectiveness.
In healthcare, it is tempting to become satisfied with simply deploying processes, as much of the healthcare reform work done to date has focused on payment for process improvements. This, however, will change in the near future. For example, Medicare’s hospital value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” January 2012, p. 1) will incorporate outcome measures as soon as 2014. We must, therefore, get into the habit of aggressively managing the processes that we operate through diligent data collection and subsequent decision-making that is informed by actionable information.
Conclusion
Holding ourselves accountable for enacting healthcare reform initiatives to improve the care of our patients will be difficult. The task is made easier by employing a process to guide our efforts. “The Oz Principle” teaches us a succinct, four-step approach. Applying this approach to changes mandated by healthcare reform will make it easier for hospitalists to transcend their current dysfunctional situations and achieve demonstrable healthcare system improvements for the betterment of patient care.
Dr. Frost is president of SHM.
Reference
John Nelson: Post-Discharge Calls

There are lots of places to learn methods to improve patient satisfaction, including my thoughts from the January 2009 issue. Run an Internet search on “improve patient satisfaction” to get a huge number of articles, many of which have useful information and inspiration.
If you’re in a high-functioning hospitalist group, you’ve already read a lot on the topic, listened to presentations by someone at your hospital and elsewhere, and reliably reported and analyzed satisfaction survey results including HCAHPS questions and others. Maybe you’ve even engaged a consultant to help.
You might already have in place a number of strategies, such as reliably providing a business card with your photo, always sitting down in the patient’s room, asking “Is there anything else I can do?” before ending your time with a patient, etc. You’re doing all these things and more, but perhaps you’ve barely moved the needle on your satisfaction scores.
Despite your efforts, I bet your hospitalist group’s aggregate score is among the lowest of any physician group at your hospital.
You’re not alone.
What can you do about this?
High-Value Strategy: Phoning Patients after Discharge
I’m lucky enough to practice with some of the smartest, most professional, and most personable hospitalists you could ever meet. Yet our satisfaction scores are among the lowest for physicians at our hospital. Despite all of the improvement strategies we put in place over the last few years, our scores have barely budged. But that all changed once we instituted a formal program of phoning patients after discharge. That produced the largest uptick in our scores we’ve ever seen.
I can’t guarantee that our results are generalizable. But I have all the anecdotal information I need to be willing to invest the resources to make the calls. They improve scores. Likely more than any other single strategy. And they seem to have a positive effect on all survey questions, from how well the doctor explained things (nearly always the lowest of the HCAHPS scores for hospitalists) to the patient’s opinion of the hospital food.
Though initially resistant to expending the time and energy to make the calls, most in our group have said that they regularly feel really gratified by the response they get from patients or families. I think it is much better if a hospitalist who cared for the patient makes the calls, and I suspect (I have no proof) that calls made by a nurse or clerk are much less effective at improving patient satisfaction. And the call can serve as a valuable clinical encounter to briefly troubleshoot a problem or review a test result that was pending at discharge.
Simple Strategies
- More than 80% of these calls should last less than three minutes. Most patients or family members will report things are going OK and thank you profusely for the call. “No doctor has ever called before,” many will say. “Can we get you the next time Mom is hospitalized?”
- You could reduce the number of calls needed if you limit them to patients eligible for a survey; this typically is only about half of a hospitalist’s patient census. For example, patients on observation status and those discharged somewhere other than to home (e.g. to a skilled-nursing facility) are not eligible for a survey.
- It’s usually best not to tell a patient or family to expect the call. Surprising them makes them more delighted when you do call, and a patient told to expect a call but doesn’t get one will be less satisfied than if never told to expect it. Best if no one at the hospital knows you’re making the calls, because someone might brag about you and tell the patient to expect the call.
- For patients seen by several hospitalists, decide ahead of time which doctor makes the call. The doctor who discharged the patient is probably the simplest protocol.
- Develop a system to track patients who have been discharged. Every morning, we get a printout of all patients discharged the prior day. We try to call all patients the day after discharge to ensure that we reach them before they’ve had a chance to complete a satisfaction survey and before the discharging doctor rotates off.
- Develop a protocol to document the calls. Calls that lead to any new advice or therapies (e.g. see your primary-care physician sooner than planned) must be documented in the medical record, e.g., by dictating an addendum to the discharge summary. Don’t let the system get too complicated or keep you from making the calls.
- Use your judgment about whether to call the patient or just call a family member directly; it’s often better to do the latter.
- If you reach a voicemail (about 50% of the calls I make), leave a message and don’t keep calling back to reach a person.
Sample Scripts
Here are some simple scripts to use for post-discharge calls. If you reach the patient or family member:
- “This is Dr. X from Superior Hospital. I was just thinking about you/your mother/your father and wanted to know how things have gone since you/she/he left the hospital.”
- Ask about something related to the reason for their stay. “How is your appetite?” or “You haven’t had any more fever, have you?” or “Have you made your appointment with Dr. PCP yet?”
- “I hope things go really well for you, but if you ever need the hospital again, we’d be happy to care for you at Superior Hospital.”
If you get a voicemail:
- “This is Dr. X from Superior Hospital. I’ve been thinking about you/your mother/father since you/she/he left the hospital, and I am calling just to check on how things are going.” (For HIPPA reasons, don’t use the patient’s name when leaving a voicemail.)
- Mention some medical concern specific to the patient, e.g., “Your culture test turned out OK and I hope you’ve been able to get the antibiotic I prescribed.”
- “You don’t need to call me back, but if you have questions or want to provide an update, I can be reached at 555-123-4567.” (It’s very important to include this last sentence and a number where you can be reached. If omitted, many patients/families will think you must have called to convey something really important and will be distressed until able to reach you.)
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
There are lots of places to learn methods to improve patient satisfaction, including my thoughts from the January 2009 issue. Run an Internet search on “improve patient satisfaction” to get a huge number of articles, many of which have useful information and inspiration.
If you’re in a high-functioning hospitalist group, you’ve already read a lot on the topic, listened to presentations by someone at your hospital and elsewhere, and reliably reported and analyzed satisfaction survey results including HCAHPS questions and others. Maybe you’ve even engaged a consultant to help.
You might already have in place a number of strategies, such as reliably providing a business card with your photo, always sitting down in the patient’s room, asking “Is there anything else I can do?” before ending your time with a patient, etc. You’re doing all these things and more, but perhaps you’ve barely moved the needle on your satisfaction scores.
Despite your efforts, I bet your hospitalist group’s aggregate score is among the lowest of any physician group at your hospital.
You’re not alone.
What can you do about this?
High-Value Strategy: Phoning Patients after Discharge
I’m lucky enough to practice with some of the smartest, most professional, and most personable hospitalists you could ever meet. Yet our satisfaction scores are among the lowest for physicians at our hospital. Despite all of the improvement strategies we put in place over the last few years, our scores have barely budged. But that all changed once we instituted a formal program of phoning patients after discharge. That produced the largest uptick in our scores we’ve ever seen.
I can’t guarantee that our results are generalizable. But I have all the anecdotal information I need to be willing to invest the resources to make the calls. They improve scores. Likely more than any other single strategy. And they seem to have a positive effect on all survey questions, from how well the doctor explained things (nearly always the lowest of the HCAHPS scores for hospitalists) to the patient’s opinion of the hospital food.
Though initially resistant to expending the time and energy to make the calls, most in our group have said that they regularly feel really gratified by the response they get from patients or families. I think it is much better if a hospitalist who cared for the patient makes the calls, and I suspect (I have no proof) that calls made by a nurse or clerk are much less effective at improving patient satisfaction. And the call can serve as a valuable clinical encounter to briefly troubleshoot a problem or review a test result that was pending at discharge.
Simple Strategies
- More than 80% of these calls should last less than three minutes. Most patients or family members will report things are going OK and thank you profusely for the call. “No doctor has ever called before,” many will say. “Can we get you the next time Mom is hospitalized?”
- You could reduce the number of calls needed if you limit them to patients eligible for a survey; this typically is only about half of a hospitalist’s patient census. For example, patients on observation status and those discharged somewhere other than to home (e.g. to a skilled-nursing facility) are not eligible for a survey.
- It’s usually best not to tell a patient or family to expect the call. Surprising them makes them more delighted when you do call, and a patient told to expect a call but doesn’t get one will be less satisfied than if never told to expect it. Best if no one at the hospital knows you’re making the calls, because someone might brag about you and tell the patient to expect the call.
- For patients seen by several hospitalists, decide ahead of time which doctor makes the call. The doctor who discharged the patient is probably the simplest protocol.
- Develop a system to track patients who have been discharged. Every morning, we get a printout of all patients discharged the prior day. We try to call all patients the day after discharge to ensure that we reach them before they’ve had a chance to complete a satisfaction survey and before the discharging doctor rotates off.
- Develop a protocol to document the calls. Calls that lead to any new advice or therapies (e.g. see your primary-care physician sooner than planned) must be documented in the medical record, e.g., by dictating an addendum to the discharge summary. Don’t let the system get too complicated or keep you from making the calls.
- Use your judgment about whether to call the patient or just call a family member directly; it’s often better to do the latter.
- If you reach a voicemail (about 50% of the calls I make), leave a message and don’t keep calling back to reach a person.
Sample Scripts
Here are some simple scripts to use for post-discharge calls. If you reach the patient or family member:
- “This is Dr. X from Superior Hospital. I was just thinking about you/your mother/your father and wanted to know how things have gone since you/she/he left the hospital.”
- Ask about something related to the reason for their stay. “How is your appetite?” or “You haven’t had any more fever, have you?” or “Have you made your appointment with Dr. PCP yet?”
- “I hope things go really well for you, but if you ever need the hospital again, we’d be happy to care for you at Superior Hospital.”
If you get a voicemail:
- “This is Dr. X from Superior Hospital. I’ve been thinking about you/your mother/father since you/she/he left the hospital, and I am calling just to check on how things are going.” (For HIPPA reasons, don’t use the patient’s name when leaving a voicemail.)
- Mention some medical concern specific to the patient, e.g., “Your culture test turned out OK and I hope you’ve been able to get the antibiotic I prescribed.”
- “You don’t need to call me back, but if you have questions or want to provide an update, I can be reached at 555-123-4567.” (It’s very important to include this last sentence and a number where you can be reached. If omitted, many patients/families will think you must have called to convey something really important and will be distressed until able to reach you.)
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
There are lots of places to learn methods to improve patient satisfaction, including my thoughts from the January 2009 issue. Run an Internet search on “improve patient satisfaction” to get a huge number of articles, many of which have useful information and inspiration.
If you’re in a high-functioning hospitalist group, you’ve already read a lot on the topic, listened to presentations by someone at your hospital and elsewhere, and reliably reported and analyzed satisfaction survey results including HCAHPS questions and others. Maybe you’ve even engaged a consultant to help.
You might already have in place a number of strategies, such as reliably providing a business card with your photo, always sitting down in the patient’s room, asking “Is there anything else I can do?” before ending your time with a patient, etc. You’re doing all these things and more, but perhaps you’ve barely moved the needle on your satisfaction scores.
Despite your efforts, I bet your hospitalist group’s aggregate score is among the lowest of any physician group at your hospital.
You’re not alone.
What can you do about this?
High-Value Strategy: Phoning Patients after Discharge
I’m lucky enough to practice with some of the smartest, most professional, and most personable hospitalists you could ever meet. Yet our satisfaction scores are among the lowest for physicians at our hospital. Despite all of the improvement strategies we put in place over the last few years, our scores have barely budged. But that all changed once we instituted a formal program of phoning patients after discharge. That produced the largest uptick in our scores we’ve ever seen.
I can’t guarantee that our results are generalizable. But I have all the anecdotal information I need to be willing to invest the resources to make the calls. They improve scores. Likely more than any other single strategy. And they seem to have a positive effect on all survey questions, from how well the doctor explained things (nearly always the lowest of the HCAHPS scores for hospitalists) to the patient’s opinion of the hospital food.
Though initially resistant to expending the time and energy to make the calls, most in our group have said that they regularly feel really gratified by the response they get from patients or families. I think it is much better if a hospitalist who cared for the patient makes the calls, and I suspect (I have no proof) that calls made by a nurse or clerk are much less effective at improving patient satisfaction. And the call can serve as a valuable clinical encounter to briefly troubleshoot a problem or review a test result that was pending at discharge.
Simple Strategies
- More than 80% of these calls should last less than three minutes. Most patients or family members will report things are going OK and thank you profusely for the call. “No doctor has ever called before,” many will say. “Can we get you the next time Mom is hospitalized?”
- You could reduce the number of calls needed if you limit them to patients eligible for a survey; this typically is only about half of a hospitalist’s patient census. For example, patients on observation status and those discharged somewhere other than to home (e.g. to a skilled-nursing facility) are not eligible for a survey.
- It’s usually best not to tell a patient or family to expect the call. Surprising them makes them more delighted when you do call, and a patient told to expect a call but doesn’t get one will be less satisfied than if never told to expect it. Best if no one at the hospital knows you’re making the calls, because someone might brag about you and tell the patient to expect the call.
- For patients seen by several hospitalists, decide ahead of time which doctor makes the call. The doctor who discharged the patient is probably the simplest protocol.
- Develop a system to track patients who have been discharged. Every morning, we get a printout of all patients discharged the prior day. We try to call all patients the day after discharge to ensure that we reach them before they’ve had a chance to complete a satisfaction survey and before the discharging doctor rotates off.
- Develop a protocol to document the calls. Calls that lead to any new advice or therapies (e.g. see your primary-care physician sooner than planned) must be documented in the medical record, e.g., by dictating an addendum to the discharge summary. Don’t let the system get too complicated or keep you from making the calls.
- Use your judgment about whether to call the patient or just call a family member directly; it’s often better to do the latter.
- If you reach a voicemail (about 50% of the calls I make), leave a message and don’t keep calling back to reach a person.
Sample Scripts
Here are some simple scripts to use for post-discharge calls. If you reach the patient or family member:
- “This is Dr. X from Superior Hospital. I was just thinking about you/your mother/your father and wanted to know how things have gone since you/she/he left the hospital.”
- Ask about something related to the reason for their stay. “How is your appetite?” or “You haven’t had any more fever, have you?” or “Have you made your appointment with Dr. PCP yet?”
- “I hope things go really well for you, but if you ever need the hospital again, we’d be happy to care for you at Superior Hospital.”
If you get a voicemail:
- “This is Dr. X from Superior Hospital. I’ve been thinking about you/your mother/father since you/she/he left the hospital, and I am calling just to check on how things are going.” (For HIPPA reasons, don’t use the patient’s name when leaving a voicemail.)
- Mention some medical concern specific to the patient, e.g., “Your culture test turned out OK and I hope you’ve been able to get the antibiotic I prescribed.”
- “You don’t need to call me back, but if you have questions or want to provide an update, I can be reached at 555-123-4567.” (It’s very important to include this last sentence and a number where you can be reached. If omitted, many patients/families will think you must have called to convey something really important and will be distressed until able to reach you.)
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
Establish Rules of Engagement before Covering Ortho Inpatients

One of our providers wants to use adult hospitalists for coverage of inpatient orthopedic surgery patients. Is this acceptable practice? Are there qualifiers?
—Libby Gardner
Dr. Hospitalist responds:
Let’s see how far we can tackle this open-ended question. There has been lots of discussion on the topic of comanagement in the past by people eminently more qualified than I am. Still, it never hurts to take a fresh look at things.
For one, on the subject of admissions, I am a firm believer that hospitalists should admit all adult hip fractures. The overwhelming majority of the time, these patients are elderly with comorbid conditions. Sure, they are going to get their hip fixed, because the alternative usually is unacceptable, but some thought needs to go into the process.
The orthopedic surgeon sees a hip that needs fixing and not much else. When such issues as renal failure, afib, congestive heart failure, prior DVT, dementia, and all the other common conditions are present, we as adult hospitalists should take charge of the case. That is the best way to ensure that the patient receives optimal medical care and the documentation that goes along with it. I love our orthopedic surgeons, but I don’t want them primarily admitting, managing, and discharging my elderly patients. Let the surgeon do what they do best—operate—and leave the rest to us as hospitalists.
On the subject of orthopedic trauma, I take the exact opposite approach—this is not something where we have daily expertise. A young, healthy patient with trauma should be admitted by the orthopedic service; that patient population’s complications are much more likely to be directly related to their trauma.
When it comes to elective surgery when the admitting surgeon (orthopedic or otherwise) wants the help of a hospitalist, then I think it is of paramount importance to establish clear “rules of engagement” (see “The Comanagement Conundrum,” April 2011, p. 1). I think with good expectations, you can have a fantastic relationship with your surgeons. Without them, it becomes a nightmare. As a real-life example, here are my HM group’s rules for elective orthopedic surgery:
- Orthopedics handles all pain medications and VTE prophylaxis, including discharge prescriptions;
- Medicine does the admission and medication reconciliation (“med rec”) at discharge;
- There is shared discussion on the need for transfusion; and
- There is shared discussion on the need for VTE prophylaxis when a patient already is on chronic anticoagulation.
We do not vary from this protocol. I never adjust a patient’s pain medications—even the floor nurses know this. Because I’m doing the admit and med rec, it also means that the patient doesn’t have their HCTZ continued after 600cc of EBL and spinal anesthesia. It works because the rules are clear and the communication is consistent.
This does not mean that we cover the orthopedic service at night; they are equally responsible for their patients under the items outlined above. In my view—and this might sound simplistic—the surgeon caused the post-op pain, so they should be responsible for managing it. With regard to VTE prophylaxis, I might take a more nuanced view, but for our surgeons, they own the wound and the post-op follow-up, so they get the choice on what agent to use.
Would I accept an arrangement in which I covered all the orthopedic issues out of regular hours? Nope—not when they have primary responsibility for the case; they should always be directly available to the nurse. I think that anything else would be a system ripe for abuse.
Our exact rules will not work for every situation, but I would strongly encourage the two basic tenets from above: No. 1, the hospitalist should primarily admit and manage elderly hip fractures, and No. 2, there should be clear rules of engagement with your orthopedic or surgery group. It’s a discussion worth having during daylight hours, because trying to figure out the rules at 3 in the morning rarely ends well.
One of our providers wants to use adult hospitalists for coverage of inpatient orthopedic surgery patients. Is this acceptable practice? Are there qualifiers?
—Libby Gardner
Dr. Hospitalist responds:
Let’s see how far we can tackle this open-ended question. There has been lots of discussion on the topic of comanagement in the past by people eminently more qualified than I am. Still, it never hurts to take a fresh look at things.
For one, on the subject of admissions, I am a firm believer that hospitalists should admit all adult hip fractures. The overwhelming majority of the time, these patients are elderly with comorbid conditions. Sure, they are going to get their hip fixed, because the alternative usually is unacceptable, but some thought needs to go into the process.
The orthopedic surgeon sees a hip that needs fixing and not much else. When such issues as renal failure, afib, congestive heart failure, prior DVT, dementia, and all the other common conditions are present, we as adult hospitalists should take charge of the case. That is the best way to ensure that the patient receives optimal medical care and the documentation that goes along with it. I love our orthopedic surgeons, but I don’t want them primarily admitting, managing, and discharging my elderly patients. Let the surgeon do what they do best—operate—and leave the rest to us as hospitalists.
On the subject of orthopedic trauma, I take the exact opposite approach—this is not something where we have daily expertise. A young, healthy patient with trauma should be admitted by the orthopedic service; that patient population’s complications are much more likely to be directly related to their trauma.
When it comes to elective surgery when the admitting surgeon (orthopedic or otherwise) wants the help of a hospitalist, then I think it is of paramount importance to establish clear “rules of engagement” (see “The Comanagement Conundrum,” April 2011, p. 1). I think with good expectations, you can have a fantastic relationship with your surgeons. Without them, it becomes a nightmare. As a real-life example, here are my HM group’s rules for elective orthopedic surgery:
- Orthopedics handles all pain medications and VTE prophylaxis, including discharge prescriptions;
- Medicine does the admission and medication reconciliation (“med rec”) at discharge;
- There is shared discussion on the need for transfusion; and
- There is shared discussion on the need for VTE prophylaxis when a patient already is on chronic anticoagulation.
We do not vary from this protocol. I never adjust a patient’s pain medications—even the floor nurses know this. Because I’m doing the admit and med rec, it also means that the patient doesn’t have their HCTZ continued after 600cc of EBL and spinal anesthesia. It works because the rules are clear and the communication is consistent.
This does not mean that we cover the orthopedic service at night; they are equally responsible for their patients under the items outlined above. In my view—and this might sound simplistic—the surgeon caused the post-op pain, so they should be responsible for managing it. With regard to VTE prophylaxis, I might take a more nuanced view, but for our surgeons, they own the wound and the post-op follow-up, so they get the choice on what agent to use.
Would I accept an arrangement in which I covered all the orthopedic issues out of regular hours? Nope—not when they have primary responsibility for the case; they should always be directly available to the nurse. I think that anything else would be a system ripe for abuse.
Our exact rules will not work for every situation, but I would strongly encourage the two basic tenets from above: No. 1, the hospitalist should primarily admit and manage elderly hip fractures, and No. 2, there should be clear rules of engagement with your orthopedic or surgery group. It’s a discussion worth having during daylight hours, because trying to figure out the rules at 3 in the morning rarely ends well.
One of our providers wants to use adult hospitalists for coverage of inpatient orthopedic surgery patients. Is this acceptable practice? Are there qualifiers?
—Libby Gardner
Dr. Hospitalist responds:
Let’s see how far we can tackle this open-ended question. There has been lots of discussion on the topic of comanagement in the past by people eminently more qualified than I am. Still, it never hurts to take a fresh look at things.
For one, on the subject of admissions, I am a firm believer that hospitalists should admit all adult hip fractures. The overwhelming majority of the time, these patients are elderly with comorbid conditions. Sure, they are going to get their hip fixed, because the alternative usually is unacceptable, but some thought needs to go into the process.
The orthopedic surgeon sees a hip that needs fixing and not much else. When such issues as renal failure, afib, congestive heart failure, prior DVT, dementia, and all the other common conditions are present, we as adult hospitalists should take charge of the case. That is the best way to ensure that the patient receives optimal medical care and the documentation that goes along with it. I love our orthopedic surgeons, but I don’t want them primarily admitting, managing, and discharging my elderly patients. Let the surgeon do what they do best—operate—and leave the rest to us as hospitalists.
On the subject of orthopedic trauma, I take the exact opposite approach—this is not something where we have daily expertise. A young, healthy patient with trauma should be admitted by the orthopedic service; that patient population’s complications are much more likely to be directly related to their trauma.
When it comes to elective surgery when the admitting surgeon (orthopedic or otherwise) wants the help of a hospitalist, then I think it is of paramount importance to establish clear “rules of engagement” (see “The Comanagement Conundrum,” April 2011, p. 1). I think with good expectations, you can have a fantastic relationship with your surgeons. Without them, it becomes a nightmare. As a real-life example, here are my HM group’s rules for elective orthopedic surgery:
- Orthopedics handles all pain medications and VTE prophylaxis, including discharge prescriptions;
- Medicine does the admission and medication reconciliation (“med rec”) at discharge;
- There is shared discussion on the need for transfusion; and
- There is shared discussion on the need for VTE prophylaxis when a patient already is on chronic anticoagulation.
We do not vary from this protocol. I never adjust a patient’s pain medications—even the floor nurses know this. Because I’m doing the admit and med rec, it also means that the patient doesn’t have their HCTZ continued after 600cc of EBL and spinal anesthesia. It works because the rules are clear and the communication is consistent.
This does not mean that we cover the orthopedic service at night; they are equally responsible for their patients under the items outlined above. In my view—and this might sound simplistic—the surgeon caused the post-op pain, so they should be responsible for managing it. With regard to VTE prophylaxis, I might take a more nuanced view, but for our surgeons, they own the wound and the post-op follow-up, so they get the choice on what agent to use.
Would I accept an arrangement in which I covered all the orthopedic issues out of regular hours? Nope—not when they have primary responsibility for the case; they should always be directly available to the nurse. I think that anything else would be a system ripe for abuse.
Our exact rules will not work for every situation, but I would strongly encourage the two basic tenets from above: No. 1, the hospitalist should primarily admit and manage elderly hip fractures, and No. 2, there should be clear rules of engagement with your orthopedic or surgery group. It’s a discussion worth having during daylight hours, because trying to figure out the rules at 3 in the morning rarely ends well.