User login
How to Use Hospitalist Productivity, Compensation Survey Data
The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.

The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.
The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.
Focus on cervical biopsy
Are multiple lesion-directed biopsies better than one at detecting cervical cancer precursors?
Yes. In this observational study of 690 women referred to colposcopy for abnormal cervical screening results, the sensitivity of biopsy in the detection of high-grade squamous intraepithelial lesions (HSIL) increased from 60.6% (95% confidence interval [CI], 54.8–66.6) for a single biopsy to 95.6% (95% CI, 91.3–99.2) for three biopsies.
Wentsensen N, Walker JL, Gold MA, et al. Multiple biopsies and detection of cervical cancer precursors at colposcopy [published online ahead of print November 24, 2014]. J Clin Oncol. pii:JCO.2014.55.9948.
Recent updates of cervical cancer screening protocols have altered the way we screen women but have not changed colposcopic practices, which vary widely in the United States. Investigators funded by the National Cancer Institute studied 690 women (median age, 26 years; range, 18–67 years) who underwent as many as four directed biopsies of distinct acetowhite lesions. HSIL (which included cervical intraepithelial neoplasia [CIN] 2 and 3 and invasive cancer) represented the gold standard for the sensitivity of the cervical biopsies.
Colposcopists performed a median of one, three, and four biopsies in women with no observed lesions, acetowhite lesions only, and low- or high-grade colposcopic impressions, respectively. More than 95% of HSIL was found in women noted to have a colposcopic impression of at least low-grade disease.
Although multiple biopsies increased the diagnostic yield in all groups, the greatest increase in yield was observed in women with HSIL cytology, positivity for HPV 16, and a colposcopic impression suggesting HSIL. Similar trends were observed for each of the six colposcopists (all well trained and highly experienced), each of whom performed at least 60 colposcopies in the study population.
What this evidence means for practice
When HSIL is missed at colposcopy, the patient is subjected to delayed treatment and repeat assessment. Although multiple biopsies can increase patient discomfort and costs, these findings add to other published data underscoring their value. Instead of biopsying only the worst-appearing lesion, obtain at least two or three biopsies when distinct lesions, including acetowhite areas, are noted.
—Andrew M. Kaunitz, MD
How useful is random biopsy when no lesions are seen?
Useful. It identifies approximately 20% of otherwise undetected cases of CIN 2, CIN 3, or worse. The absolute risks of disease associated with the random biopsy were higher for women positive for HPV 16 or 18, according to this large post hoc analysis.
Huh WK, Sideri M, Stoler M, Zhang G, Feldman R, Behrens CM. Relevance of random biopsy at the transformation zone when colposcopy is negative. Obstet Gynecol. 2014;124(4):670–678.
When performing colposcopy for abnormal cytology results or high-risk HPV, clinicians often are faced with an absence of visible lesions. This situation prompts the question: Is a random biopsy warranted?
Details of the study
In a multicenter US study of more than 47,000 women—conducted to assess HPV diagnostics between May 2008 and August 2009—nonpregnant women aged 25 or older with an intact uterus underwent colposcopy after a finding of atypical squamous cells of undetermined significance or higher-grade cytology results or high-risk HPV. Patients and colposcopists were blinded to the results. In women who had satisfactory colposcopy results but no visible lesions, one random biopsy of the squamocolumnar junction was obtained.
Among 2,796 women (mean age, 39.5 years) who underwent random biopsy, the findings were normal, CIN 1, CIN 2, and CIN 3 in 90.0%, 5.7%, 1.3%, and 1.4%, respectively. Among all participants aged 25 and older, random biopsies accounted for 20.9% and 18.9% of the CIN 2 or worse and CIN 3 or worse cases, respectively.
Among women positive for HPV 16 or 18, the likelihood of the random biopsy detecting CIN 2 or worse was 24.7% and 8.6% for those with abnormal cytology or normal cytology, respectively.
What this evidence means for practice
This post hoc analysis underscores the limitations of colposcopy, as have other reports. Just as the findings of Wentsensen and colleagues demonstrate that two or more lesion-directed biopsies increase the diagnostic yield over a single sample, this large study points out the substantial benefit of random biopsy of the squamocolumnar junction when no colposcopic lesions are identified.
—Andrew M. Kaunitz, MD
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Are multiple lesion-directed biopsies better than one at detecting cervical cancer precursors?
Yes. In this observational study of 690 women referred to colposcopy for abnormal cervical screening results, the sensitivity of biopsy in the detection of high-grade squamous intraepithelial lesions (HSIL) increased from 60.6% (95% confidence interval [CI], 54.8–66.6) for a single biopsy to 95.6% (95% CI, 91.3–99.2) for three biopsies.
Wentsensen N, Walker JL, Gold MA, et al. Multiple biopsies and detection of cervical cancer precursors at colposcopy [published online ahead of print November 24, 2014]. J Clin Oncol. pii:JCO.2014.55.9948.
Recent updates of cervical cancer screening protocols have altered the way we screen women but have not changed colposcopic practices, which vary widely in the United States. Investigators funded by the National Cancer Institute studied 690 women (median age, 26 years; range, 18–67 years) who underwent as many as four directed biopsies of distinct acetowhite lesions. HSIL (which included cervical intraepithelial neoplasia [CIN] 2 and 3 and invasive cancer) represented the gold standard for the sensitivity of the cervical biopsies.
Colposcopists performed a median of one, three, and four biopsies in women with no observed lesions, acetowhite lesions only, and low- or high-grade colposcopic impressions, respectively. More than 95% of HSIL was found in women noted to have a colposcopic impression of at least low-grade disease.
Although multiple biopsies increased the diagnostic yield in all groups, the greatest increase in yield was observed in women with HSIL cytology, positivity for HPV 16, and a colposcopic impression suggesting HSIL. Similar trends were observed for each of the six colposcopists (all well trained and highly experienced), each of whom performed at least 60 colposcopies in the study population.
What this evidence means for practice
When HSIL is missed at colposcopy, the patient is subjected to delayed treatment and repeat assessment. Although multiple biopsies can increase patient discomfort and costs, these findings add to other published data underscoring their value. Instead of biopsying only the worst-appearing lesion, obtain at least two or three biopsies when distinct lesions, including acetowhite areas, are noted.
—Andrew M. Kaunitz, MD
How useful is random biopsy when no lesions are seen?
Useful. It identifies approximately 20% of otherwise undetected cases of CIN 2, CIN 3, or worse. The absolute risks of disease associated with the random biopsy were higher for women positive for HPV 16 or 18, according to this large post hoc analysis.
Huh WK, Sideri M, Stoler M, Zhang G, Feldman R, Behrens CM. Relevance of random biopsy at the transformation zone when colposcopy is negative. Obstet Gynecol. 2014;124(4):670–678.
When performing colposcopy for abnormal cytology results or high-risk HPV, clinicians often are faced with an absence of visible lesions. This situation prompts the question: Is a random biopsy warranted?
Details of the study
In a multicenter US study of more than 47,000 women—conducted to assess HPV diagnostics between May 2008 and August 2009—nonpregnant women aged 25 or older with an intact uterus underwent colposcopy after a finding of atypical squamous cells of undetermined significance or higher-grade cytology results or high-risk HPV. Patients and colposcopists were blinded to the results. In women who had satisfactory colposcopy results but no visible lesions, one random biopsy of the squamocolumnar junction was obtained.
Among 2,796 women (mean age, 39.5 years) who underwent random biopsy, the findings were normal, CIN 1, CIN 2, and CIN 3 in 90.0%, 5.7%, 1.3%, and 1.4%, respectively. Among all participants aged 25 and older, random biopsies accounted for 20.9% and 18.9% of the CIN 2 or worse and CIN 3 or worse cases, respectively.
Among women positive for HPV 16 or 18, the likelihood of the random biopsy detecting CIN 2 or worse was 24.7% and 8.6% for those with abnormal cytology or normal cytology, respectively.
What this evidence means for practice
This post hoc analysis underscores the limitations of colposcopy, as have other reports. Just as the findings of Wentsensen and colleagues demonstrate that two or more lesion-directed biopsies increase the diagnostic yield over a single sample, this large study points out the substantial benefit of random biopsy of the squamocolumnar junction when no colposcopic lesions are identified.
—Andrew M. Kaunitz, MD
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Are multiple lesion-directed biopsies better than one at detecting cervical cancer precursors?
Yes. In this observational study of 690 women referred to colposcopy for abnormal cervical screening results, the sensitivity of biopsy in the detection of high-grade squamous intraepithelial lesions (HSIL) increased from 60.6% (95% confidence interval [CI], 54.8–66.6) for a single biopsy to 95.6% (95% CI, 91.3–99.2) for three biopsies.
Wentsensen N, Walker JL, Gold MA, et al. Multiple biopsies and detection of cervical cancer precursors at colposcopy [published online ahead of print November 24, 2014]. J Clin Oncol. pii:JCO.2014.55.9948.
Recent updates of cervical cancer screening protocols have altered the way we screen women but have not changed colposcopic practices, which vary widely in the United States. Investigators funded by the National Cancer Institute studied 690 women (median age, 26 years; range, 18–67 years) who underwent as many as four directed biopsies of distinct acetowhite lesions. HSIL (which included cervical intraepithelial neoplasia [CIN] 2 and 3 and invasive cancer) represented the gold standard for the sensitivity of the cervical biopsies.
Colposcopists performed a median of one, three, and four biopsies in women with no observed lesions, acetowhite lesions only, and low- or high-grade colposcopic impressions, respectively. More than 95% of HSIL was found in women noted to have a colposcopic impression of at least low-grade disease.
Although multiple biopsies increased the diagnostic yield in all groups, the greatest increase in yield was observed in women with HSIL cytology, positivity for HPV 16, and a colposcopic impression suggesting HSIL. Similar trends were observed for each of the six colposcopists (all well trained and highly experienced), each of whom performed at least 60 colposcopies in the study population.
What this evidence means for practice
When HSIL is missed at colposcopy, the patient is subjected to delayed treatment and repeat assessment. Although multiple biopsies can increase patient discomfort and costs, these findings add to other published data underscoring their value. Instead of biopsying only the worst-appearing lesion, obtain at least two or three biopsies when distinct lesions, including acetowhite areas, are noted.
—Andrew M. Kaunitz, MD
How useful is random biopsy when no lesions are seen?
Useful. It identifies approximately 20% of otherwise undetected cases of CIN 2, CIN 3, or worse. The absolute risks of disease associated with the random biopsy were higher for women positive for HPV 16 or 18, according to this large post hoc analysis.
Huh WK, Sideri M, Stoler M, Zhang G, Feldman R, Behrens CM. Relevance of random biopsy at the transformation zone when colposcopy is negative. Obstet Gynecol. 2014;124(4):670–678.
When performing colposcopy for abnormal cytology results or high-risk HPV, clinicians often are faced with an absence of visible lesions. This situation prompts the question: Is a random biopsy warranted?
Details of the study
In a multicenter US study of more than 47,000 women—conducted to assess HPV diagnostics between May 2008 and August 2009—nonpregnant women aged 25 or older with an intact uterus underwent colposcopy after a finding of atypical squamous cells of undetermined significance or higher-grade cytology results or high-risk HPV. Patients and colposcopists were blinded to the results. In women who had satisfactory colposcopy results but no visible lesions, one random biopsy of the squamocolumnar junction was obtained.
Among 2,796 women (mean age, 39.5 years) who underwent random biopsy, the findings were normal, CIN 1, CIN 2, and CIN 3 in 90.0%, 5.7%, 1.3%, and 1.4%, respectively. Among all participants aged 25 and older, random biopsies accounted for 20.9% and 18.9% of the CIN 2 or worse and CIN 3 or worse cases, respectively.
Among women positive for HPV 16 or 18, the likelihood of the random biopsy detecting CIN 2 or worse was 24.7% and 8.6% for those with abnormal cytology or normal cytology, respectively.
What this evidence means for practice
This post hoc analysis underscores the limitations of colposcopy, as have other reports. Just as the findings of Wentsensen and colleagues demonstrate that two or more lesion-directed biopsies increase the diagnostic yield over a single sample, this large study points out the substantial benefit of random biopsy of the squamocolumnar junction when no colposcopic lesions are identified.
—Andrew M. Kaunitz, MD
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.

Recent NCCI edits have significantly impacted billing and reimbursement for vaginal hysterectomy

The Centers for Medicare and Medicaid Services (CMS) developed the National Correct Coding Initiative (NCCI) to promote national correct coding methodologies and to control what it considers to be duplicative and improper coding of multiple procedures performed in a single setting in Part B claims.
Since 1996, Medicare has used NCCI edits to limit additional payments for two procedures that were thought to be similar because of anatomic and temporal considerations. For example, billing for both lysis of adhesions and total abdominal hysterectomy in the same operation has long been denied, as preoperative and postoperative care typically are the same and the intraservice times are not appreciably different. Both require opening and closing of the same incision, and so on.
The most recent set of NCCI edits, effective October 1, 2014, “bundles” procedures for high uterosacral vaginal vault suspension (also known as vaginal colpopexy—intraperitoneal approach—CPT code 57283) and combined colporrhaphy (code 57260) when they are performed at the same time as a vaginal hysterectomy. Previously, these procedures could be billed together and separately paid for by Medicare, although the additional procedures were subjected to a -51 modifier, designating multiple procedures, which reduced the payment for them by approximately 50%.
How the NCCI makes its determinations
The NCCI develops coding policies, or “edits,” by analyzing coding conventions and reviewing standard medical and surgical practices. It reviews current coding practices and guidelines developed by national societies, such as the American College of Obstetricians and Gynecologists (ACOG), but the NCCI has the power to decide what surgical procedures get “bundled” with other procedures that commonly are performed in the same setting. As a general rule, the NCCI feels that procedures performed through the same incision, in close anatomic proximity, and by the same surgeon should not be billed separately. The NCCI develops and implements its coding edits on a quarterly basis, after notifying the medical societies most likely to be affected by the new bundles and soliciting feedback.
As gynecologic surgeons, we are familiar with the multitude of bundles that already exist for abdominal and laparoscopic procedures—lysis of adhesions, ureterolysis, abdominal enterocele repair, removal of both tubes and ovaries (as opposed to unilateral salpingo-oophorectomy)—which have been around for decades. However, until recently, vaginal surgical procedures were not bundled but were billed “a la carte.”
Because the October 1 edits deny separate payment when combined colporrhaphy and high uterosacral vaginal vault suspension are performed alongside vaginal hysterectomy, gynecologic surgeons now get paid only for the vaginal hysterectomy. These edits are likely to have a profound impact on practicing vaginal surgeons, especially subspecialists in female pelvic medicine and reconstructive surgery.
Procedures that can no longer be billed when performed at the same time as a vaginal hysterectomy include:
- combined anterior and posterior colporrhaphy (code 57260)
- abdominal sacrocolpopexy (57280)
- extraperitoneal vaginal colpopexy (eg, sacrospinous ligament suspension, or SSLS, 57282)
- intraperitoneal vaginal colpopexy (eg, high uterosacral ligament suspension, 57283)
- abdominal paravaginal repair (57284).
For a full version of current edits, see the CMS Web site at www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/NCCI-Coding-Edits.html.
AUGS, ACOG, and others respond to the edits
Since implementation of the October 1 edits, both ACOG and the American Urogynecologic Society (AUGS) have received numerous complaints and protests from members. Both societies reviewed and strongly disagreed with the proposed edits before their implementation, but NCCI ultimately decided to implement them.
In cooperation with ACOG and several other national medical societies, such as the Society for Gynecologic Surgeons and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction, AUGS formed a task force that already has engaged CMS in a series of communications focused on changing or reversing some of these edits.
This task force, under the leadership of AUGS, believes that CMS and NCCI do not fully understand the complexity of vaginal reconstruction performed for advanced pelvic organ prolapse, or the fact that vaginal hysterectomy is an extirpative procedure that often is required to facilitate the more time-consuming reconstructive procedures. Furthermore, the reconstructive procedures require separate entry and closure of different surgical spaces (eg, rectovaginal, vesicovaginal). In addition, the surgical risks and postoperative care often are more complex than they are when a simple vaginal hysterectomy is performed for benign gynecologic indications other than pelvic organ prolapse.
Thus far, both NCCI and CMS have listened to our objections, indicated that they understand them, and agreed to reexamine the appropriateness of the bundles. As of press time, however, CMS has not announced any plans to change or reverse any of these edits.
The October 1 edits are not the only ones that adversely affect the gynecologic surgeon. As of January 1, 2015, NCCI and CMS implemented another set of edits that no longer allow separate billing and reimbursement for cystoscopy (52000) performed at the time of pelvic surgery, when the purpose of the procedure is to assure the surgeon that the ureters and urinary bladder are free of injury. However, cystoscopy may be billed separately when the primary purpose differs from that scenario.
ACOG and AUGS intend to stay in discussion with CMS regarding the appropriateness of the most recent edits. If any edits are reversed, the decision will be retroactive to the October 1, 2014, date. Stay tuned for the final decision.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Marc R. Toglia, MD

Dr. Toglia is a board-certified subspecialist in Female Pelvic Medicine and Reconstructive Surgery who serves as vice chair of the Coding Committee for the American Urogynecologic Society. He is Associate Professor of Obstetrics and Gynecology at Sidney Kimmel Medical College (formerly Jefferson Medical College) and practices at Main Line Health System in the Philadelphia, Pennsylvania, suburbs.
The author reports no financial relationships relevant to this article.
Marc R. Toglia, MD
Dr. Toglia is a board-certified subspecialist in Female Pelvic Medicine and Reconstructive Surgery who serves as vice chair of the Coding Committee for the American Urogynecologic Society. He is Associate Professor of Obstetrics and Gynecology at Sidney Kimmel Medical College (formerly Jefferson Medical College) and practices at Main Line Health System in the Philadelphia, Pennsylvania, suburbs.
The author reports no financial relationships relevant to this article.
Marc R. Toglia, MD
Dr. Toglia is a board-certified subspecialist in Female Pelvic Medicine and Reconstructive Surgery who serves as vice chair of the Coding Committee for the American Urogynecologic Society. He is Associate Professor of Obstetrics and Gynecology at Sidney Kimmel Medical College (formerly Jefferson Medical College) and practices at Main Line Health System in the Philadelphia, Pennsylvania, suburbs.
The author reports no financial relationships relevant to this article.
The Centers for Medicare and Medicaid Services (CMS) developed the National Correct Coding Initiative (NCCI) to promote national correct coding methodologies and to control what it considers to be duplicative and improper coding of multiple procedures performed in a single setting in Part B claims.
Since 1996, Medicare has used NCCI edits to limit additional payments for two procedures that were thought to be similar because of anatomic and temporal considerations. For example, billing for both lysis of adhesions and total abdominal hysterectomy in the same operation has long been denied, as preoperative and postoperative care typically are the same and the intraservice times are not appreciably different. Both require opening and closing of the same incision, and so on.
The most recent set of NCCI edits, effective October 1, 2014, “bundles” procedures for high uterosacral vaginal vault suspension (also known as vaginal colpopexy—intraperitoneal approach—CPT code 57283) and combined colporrhaphy (code 57260) when they are performed at the same time as a vaginal hysterectomy. Previously, these procedures could be billed together and separately paid for by Medicare, although the additional procedures were subjected to a -51 modifier, designating multiple procedures, which reduced the payment for them by approximately 50%.
How the NCCI makes its determinations
The NCCI develops coding policies, or “edits,” by analyzing coding conventions and reviewing standard medical and surgical practices. It reviews current coding practices and guidelines developed by national societies, such as the American College of Obstetricians and Gynecologists (ACOG), but the NCCI has the power to decide what surgical procedures get “bundled” with other procedures that commonly are performed in the same setting. As a general rule, the NCCI feels that procedures performed through the same incision, in close anatomic proximity, and by the same surgeon should not be billed separately. The NCCI develops and implements its coding edits on a quarterly basis, after notifying the medical societies most likely to be affected by the new bundles and soliciting feedback.
As gynecologic surgeons, we are familiar with the multitude of bundles that already exist for abdominal and laparoscopic procedures—lysis of adhesions, ureterolysis, abdominal enterocele repair, removal of both tubes and ovaries (as opposed to unilateral salpingo-oophorectomy)—which have been around for decades. However, until recently, vaginal surgical procedures were not bundled but were billed “a la carte.”
Because the October 1 edits deny separate payment when combined colporrhaphy and high uterosacral vaginal vault suspension are performed alongside vaginal hysterectomy, gynecologic surgeons now get paid only for the vaginal hysterectomy. These edits are likely to have a profound impact on practicing vaginal surgeons, especially subspecialists in female pelvic medicine and reconstructive surgery.
Procedures that can no longer be billed when performed at the same time as a vaginal hysterectomy include:
- combined anterior and posterior colporrhaphy (code 57260)
- abdominal sacrocolpopexy (57280)
- extraperitoneal vaginal colpopexy (eg, sacrospinous ligament suspension, or SSLS, 57282)
- intraperitoneal vaginal colpopexy (eg, high uterosacral ligament suspension, 57283)
- abdominal paravaginal repair (57284).
For a full version of current edits, see the CMS Web site at www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/NCCI-Coding-Edits.html.
AUGS, ACOG, and others respond to the edits
Since implementation of the October 1 edits, both ACOG and the American Urogynecologic Society (AUGS) have received numerous complaints and protests from members. Both societies reviewed and strongly disagreed with the proposed edits before their implementation, but NCCI ultimately decided to implement them.
In cooperation with ACOG and several other national medical societies, such as the Society for Gynecologic Surgeons and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction, AUGS formed a task force that already has engaged CMS in a series of communications focused on changing or reversing some of these edits.
This task force, under the leadership of AUGS, believes that CMS and NCCI do not fully understand the complexity of vaginal reconstruction performed for advanced pelvic organ prolapse, or the fact that vaginal hysterectomy is an extirpative procedure that often is required to facilitate the more time-consuming reconstructive procedures. Furthermore, the reconstructive procedures require separate entry and closure of different surgical spaces (eg, rectovaginal, vesicovaginal). In addition, the surgical risks and postoperative care often are more complex than they are when a simple vaginal hysterectomy is performed for benign gynecologic indications other than pelvic organ prolapse.
Thus far, both NCCI and CMS have listened to our objections, indicated that they understand them, and agreed to reexamine the appropriateness of the bundles. As of press time, however, CMS has not announced any plans to change or reverse any of these edits.
The October 1 edits are not the only ones that adversely affect the gynecologic surgeon. As of January 1, 2015, NCCI and CMS implemented another set of edits that no longer allow separate billing and reimbursement for cystoscopy (52000) performed at the time of pelvic surgery, when the purpose of the procedure is to assure the surgeon that the ureters and urinary bladder are free of injury. However, cystoscopy may be billed separately when the primary purpose differs from that scenario.
ACOG and AUGS intend to stay in discussion with CMS regarding the appropriateness of the most recent edits. If any edits are reversed, the decision will be retroactive to the October 1, 2014, date. Stay tuned for the final decision.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The Centers for Medicare and Medicaid Services (CMS) developed the National Correct Coding Initiative (NCCI) to promote national correct coding methodologies and to control what it considers to be duplicative and improper coding of multiple procedures performed in a single setting in Part B claims.
Since 1996, Medicare has used NCCI edits to limit additional payments for two procedures that were thought to be similar because of anatomic and temporal considerations. For example, billing for both lysis of adhesions and total abdominal hysterectomy in the same operation has long been denied, as preoperative and postoperative care typically are the same and the intraservice times are not appreciably different. Both require opening and closing of the same incision, and so on.
The most recent set of NCCI edits, effective October 1, 2014, “bundles” procedures for high uterosacral vaginal vault suspension (also known as vaginal colpopexy—intraperitoneal approach—CPT code 57283) and combined colporrhaphy (code 57260) when they are performed at the same time as a vaginal hysterectomy. Previously, these procedures could be billed together and separately paid for by Medicare, although the additional procedures were subjected to a -51 modifier, designating multiple procedures, which reduced the payment for them by approximately 50%.
How the NCCI makes its determinations
The NCCI develops coding policies, or “edits,” by analyzing coding conventions and reviewing standard medical and surgical practices. It reviews current coding practices and guidelines developed by national societies, such as the American College of Obstetricians and Gynecologists (ACOG), but the NCCI has the power to decide what surgical procedures get “bundled” with other procedures that commonly are performed in the same setting. As a general rule, the NCCI feels that procedures performed through the same incision, in close anatomic proximity, and by the same surgeon should not be billed separately. The NCCI develops and implements its coding edits on a quarterly basis, after notifying the medical societies most likely to be affected by the new bundles and soliciting feedback.
As gynecologic surgeons, we are familiar with the multitude of bundles that already exist for abdominal and laparoscopic procedures—lysis of adhesions, ureterolysis, abdominal enterocele repair, removal of both tubes and ovaries (as opposed to unilateral salpingo-oophorectomy)—which have been around for decades. However, until recently, vaginal surgical procedures were not bundled but were billed “a la carte.”
Because the October 1 edits deny separate payment when combined colporrhaphy and high uterosacral vaginal vault suspension are performed alongside vaginal hysterectomy, gynecologic surgeons now get paid only for the vaginal hysterectomy. These edits are likely to have a profound impact on practicing vaginal surgeons, especially subspecialists in female pelvic medicine and reconstructive surgery.
Procedures that can no longer be billed when performed at the same time as a vaginal hysterectomy include:
- combined anterior and posterior colporrhaphy (code 57260)
- abdominal sacrocolpopexy (57280)
- extraperitoneal vaginal colpopexy (eg, sacrospinous ligament suspension, or SSLS, 57282)
- intraperitoneal vaginal colpopexy (eg, high uterosacral ligament suspension, 57283)
- abdominal paravaginal repair (57284).
For a full version of current edits, see the CMS Web site at www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/NCCI-Coding-Edits.html.
AUGS, ACOG, and others respond to the edits
Since implementation of the October 1 edits, both ACOG and the American Urogynecologic Society (AUGS) have received numerous complaints and protests from members. Both societies reviewed and strongly disagreed with the proposed edits before their implementation, but NCCI ultimately decided to implement them.
In cooperation with ACOG and several other national medical societies, such as the Society for Gynecologic Surgeons and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction, AUGS formed a task force that already has engaged CMS in a series of communications focused on changing or reversing some of these edits.
This task force, under the leadership of AUGS, believes that CMS and NCCI do not fully understand the complexity of vaginal reconstruction performed for advanced pelvic organ prolapse, or the fact that vaginal hysterectomy is an extirpative procedure that often is required to facilitate the more time-consuming reconstructive procedures. Furthermore, the reconstructive procedures require separate entry and closure of different surgical spaces (eg, rectovaginal, vesicovaginal). In addition, the surgical risks and postoperative care often are more complex than they are when a simple vaginal hysterectomy is performed for benign gynecologic indications other than pelvic organ prolapse.
Thus far, both NCCI and CMS have listened to our objections, indicated that they understand them, and agreed to reexamine the appropriateness of the bundles. As of press time, however, CMS has not announced any plans to change or reverse any of these edits.
The October 1 edits are not the only ones that adversely affect the gynecologic surgeon. As of January 1, 2015, NCCI and CMS implemented another set of edits that no longer allow separate billing and reimbursement for cystoscopy (52000) performed at the time of pelvic surgery, when the purpose of the procedure is to assure the surgeon that the ureters and urinary bladder are free of injury. However, cystoscopy may be billed separately when the primary purpose differs from that scenario.
ACOG and AUGS intend to stay in discussion with CMS regarding the appropriateness of the most recent edits. If any edits are reversed, the decision will be retroactive to the October 1, 2014, date. Stay tuned for the final decision.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.

Sorting out optimal TB testing can be tricky
LAS VEGAS – In the clinical opinion of Dr. Andi L. Shane, tuberculin skin testing and interferon gamma release assay diagnostics and surveillance for Mycobacterium tuberculosis infection are game-changers in the ongoing effort to reduce the rates of TB infection nationwide.
“From 1982 to 2013, we’ve had a very nice decline in the number of TB cases. However, we still have quite a bit of work to do,” Dr. Shane said at a pediatric update sponsored by the American Academy of Pediatrics California District 9.

Reported case rates are especially high in California, Nevada, Texas, Florida, New York, Washington, New Jersey, and the District of Columbia. By age group, those under 5 years old and those aged 15-24 years are more likely to be affected.
“It’s really important to identify TB as soon as possible, especially in children,” said Dr. Shane of the department of pediatrics, division of infectious diseases, Emory University, Atlanta. “An interferon gamma release assay (IGRA) or a tuberculin skin test (TST) may be used in situation where assessment for MTB [M. tuberculosis] exposure is indicated. IGRA is preferred in persons who received BCG vaccine and who have low rates of test completion, while TST is preferred for testing of children younger than age 5.”
TB disease in people younger than age 15 years is a marker for transmission of TB, usually from an adult. “So when we identify a case of TB in children, that requires a contact investigation,” she said. “We’re more concerned with children under the age of 5 with TB because they are more likely to have disseminated disease.”
Latent TB means that the patient has been exposed to the disease but that his or her body has been able to control the infection; no systemic manifestations of infection are present. “It’s very important to identify the difference between latent tuberculosis infection (LTBI) and actual tuberculosis disease,” she said. “This is one of the most challenging aspects to explain to families when you’re giving your diagnosis. The reason this is important is that children or adults who have LTBI are not infectious to other people, whereas someone who has pulmonary or laryngeal TB is considered to be an infectious risk to other individuals.”
Dr. Shane went on to discuss limitations of the TST in diagnosing TB. For one, the test may be placed incorrectly, resulting in an inflammatory response or no response, “and there is reader variability,” she said. “The other issue is that the reading needs to occur 48-72 hours after placement of the test. So, if you place it on a Thursday, that means you really are not going to read it at the optimal time unless the child comes to you on a weekend or the test is read by somebody else.”
As an alternative, two IGRAs have been developed that measure how the immune system reacts to MTB. One is QuantiFERON, which is widely used in the United States; the other is the T-SPOT.TB test, which is widely used in Europe. A positive result on either test indicates that there has been interaction with MTB bacteria but it does not differentiate between LTBI and active TB disease.
“A negative IGRA tells you there is no reaction to the test and MTB is not likely, while an indeterminate result is when you’re unable to interpret the result due to low positive [mitogen] or increased negative control [nil] compared to TB response,” Dr. Shane said. “This usually indicates that there’s some problem with the assay itself. It can also indicate that the individual may not have an immune system that can respond to and produce the interferon gamma that’s needed.”
Assessment of IGRA accuracy is challenged by a lack of a standard for the diagnosis of LTBI and active TB, especially in children. “The reason is, we just don’t have a lot of good data from resource-endowed settings,” Dr. Shane explained. “We have good data from areas where TB is prevalent.” According to the Centers for Disease Control and Prevention and the AAP, IGRAs are probably reliable in children over the age of 5 years, but a TST is still recommended in children under the age of 5.
“The nice thing about the IGRAs is that their specificity is much higher” than TSTs, Dr. Shane said. “However, in some cases a TST might be more sensitive for detecting more remote MTB infections than an IGRA, but IGRAs may be better at detecting a recent infection. Like the TST, an IGRA also shows that if you’re infected with TB you have 5-10% chance of developing active TB in your lifetime.”
She also pointed out that a significant amount of blood is required to perform an IGRA. “That might not always be optimal, especially in a young child,” Dr. Shane said. “Low CD4 counts and other immunodeficiencies have also been associated with false-negative TST and indeterminate/false-negative IGRA results.”
For contact investigations, IGRAs offer increased specificity, are completed during a single visit, and their response is not boosted if an additional evaluation is needed 8-10 weeks after exposure. For periodic screening of health care workers, IGRA offers “technical and logistical advantages, and two-step testing is not required,” she said.
If the TST or IGRA is positive, additional diagnostic efforts are needed “to differentiate between LTBI and active MTB,” said Dr. Shane, who recommended the Curry International Tuberculosis Center as a resource for clinicians. “Your clinical history, chest radiography, [and results of] sputum/gastric aspirates will help,” she added.
If the TST or IGRA is negative, “it’s not sufficient to exclude MTB infection. If you have a discordant TST and IGRA result, consider history and epidemiologic risk factors. Treat with clinical suspicion or risk of a poor outcome (those younger than age 5 and those infected with HIV).”
Dr. Shane reported having no relevant financial disclosures.
On Twitter @dougbrunk
LAS VEGAS – In the clinical opinion of Dr. Andi L. Shane, tuberculin skin testing and interferon gamma release assay diagnostics and surveillance for Mycobacterium tuberculosis infection are game-changers in the ongoing effort to reduce the rates of TB infection nationwide.
“From 1982 to 2013, we’ve had a very nice decline in the number of TB cases. However, we still have quite a bit of work to do,” Dr. Shane said at a pediatric update sponsored by the American Academy of Pediatrics California District 9.
Reported case rates are especially high in California, Nevada, Texas, Florida, New York, Washington, New Jersey, and the District of Columbia. By age group, those under 5 years old and those aged 15-24 years are more likely to be affected.
“It’s really important to identify TB as soon as possible, especially in children,” said Dr. Shane of the department of pediatrics, division of infectious diseases, Emory University, Atlanta. “An interferon gamma release assay (IGRA) or a tuberculin skin test (TST) may be used in situation where assessment for MTB [M. tuberculosis] exposure is indicated. IGRA is preferred in persons who received BCG vaccine and who have low rates of test completion, while TST is preferred for testing of children younger than age 5.”
TB disease in people younger than age 15 years is a marker for transmission of TB, usually from an adult. “So when we identify a case of TB in children, that requires a contact investigation,” she said. “We’re more concerned with children under the age of 5 with TB because they are more likely to have disseminated disease.”
Latent TB means that the patient has been exposed to the disease but that his or her body has been able to control the infection; no systemic manifestations of infection are present. “It’s very important to identify the difference between latent tuberculosis infection (LTBI) and actual tuberculosis disease,” she said. “This is one of the most challenging aspects to explain to families when you’re giving your diagnosis. The reason this is important is that children or adults who have LTBI are not infectious to other people, whereas someone who has pulmonary or laryngeal TB is considered to be an infectious risk to other individuals.”
Dr. Shane went on to discuss limitations of the TST in diagnosing TB. For one, the test may be placed incorrectly, resulting in an inflammatory response or no response, “and there is reader variability,” she said. “The other issue is that the reading needs to occur 48-72 hours after placement of the test. So, if you place it on a Thursday, that means you really are not going to read it at the optimal time unless the child comes to you on a weekend or the test is read by somebody else.”
As an alternative, two IGRAs have been developed that measure how the immune system reacts to MTB. One is QuantiFERON, which is widely used in the United States; the other is the T-SPOT.TB test, which is widely used in Europe. A positive result on either test indicates that there has been interaction with MTB bacteria but it does not differentiate between LTBI and active TB disease.
“A negative IGRA tells you there is no reaction to the test and MTB is not likely, while an indeterminate result is when you’re unable to interpret the result due to low positive [mitogen] or increased negative control [nil] compared to TB response,” Dr. Shane said. “This usually indicates that there’s some problem with the assay itself. It can also indicate that the individual may not have an immune system that can respond to and produce the interferon gamma that’s needed.”
Assessment of IGRA accuracy is challenged by a lack of a standard for the diagnosis of LTBI and active TB, especially in children. “The reason is, we just don’t have a lot of good data from resource-endowed settings,” Dr. Shane explained. “We have good data from areas where TB is prevalent.” According to the Centers for Disease Control and Prevention and the AAP, IGRAs are probably reliable in children over the age of 5 years, but a TST is still recommended in children under the age of 5.
“The nice thing about the IGRAs is that their specificity is much higher” than TSTs, Dr. Shane said. “However, in some cases a TST might be more sensitive for detecting more remote MTB infections than an IGRA, but IGRAs may be better at detecting a recent infection. Like the TST, an IGRA also shows that if you’re infected with TB you have 5-10% chance of developing active TB in your lifetime.”
She also pointed out that a significant amount of blood is required to perform an IGRA. “That might not always be optimal, especially in a young child,” Dr. Shane said. “Low CD4 counts and other immunodeficiencies have also been associated with false-negative TST and indeterminate/false-negative IGRA results.”
For contact investigations, IGRAs offer increased specificity, are completed during a single visit, and their response is not boosted if an additional evaluation is needed 8-10 weeks after exposure. For periodic screening of health care workers, IGRA offers “technical and logistical advantages, and two-step testing is not required,” she said.
If the TST or IGRA is positive, additional diagnostic efforts are needed “to differentiate between LTBI and active MTB,” said Dr. Shane, who recommended the Curry International Tuberculosis Center as a resource for clinicians. “Your clinical history, chest radiography, [and results of] sputum/gastric aspirates will help,” she added.
If the TST or IGRA is negative, “it’s not sufficient to exclude MTB infection. If you have a discordant TST and IGRA result, consider history and epidemiologic risk factors. Treat with clinical suspicion or risk of a poor outcome (those younger than age 5 and those infected with HIV).”
Dr. Shane reported having no relevant financial disclosures.
On Twitter @dougbrunk
LAS VEGAS – In the clinical opinion of Dr. Andi L. Shane, tuberculin skin testing and interferon gamma release assay diagnostics and surveillance for Mycobacterium tuberculosis infection are game-changers in the ongoing effort to reduce the rates of TB infection nationwide.
“From 1982 to 2013, we’ve had a very nice decline in the number of TB cases. However, we still have quite a bit of work to do,” Dr. Shane said at a pediatric update sponsored by the American Academy of Pediatrics California District 9.
Reported case rates are especially high in California, Nevada, Texas, Florida, New York, Washington, New Jersey, and the District of Columbia. By age group, those under 5 years old and those aged 15-24 years are more likely to be affected.
“It’s really important to identify TB as soon as possible, especially in children,” said Dr. Shane of the department of pediatrics, division of infectious diseases, Emory University, Atlanta. “An interferon gamma release assay (IGRA) or a tuberculin skin test (TST) may be used in situation where assessment for MTB [M. tuberculosis] exposure is indicated. IGRA is preferred in persons who received BCG vaccine and who have low rates of test completion, while TST is preferred for testing of children younger than age 5.”
TB disease in people younger than age 15 years is a marker for transmission of TB, usually from an adult. “So when we identify a case of TB in children, that requires a contact investigation,” she said. “We’re more concerned with children under the age of 5 with TB because they are more likely to have disseminated disease.”
Latent TB means that the patient has been exposed to the disease but that his or her body has been able to control the infection; no systemic manifestations of infection are present. “It’s very important to identify the difference between latent tuberculosis infection (LTBI) and actual tuberculosis disease,” she said. “This is one of the most challenging aspects to explain to families when you’re giving your diagnosis. The reason this is important is that children or adults who have LTBI are not infectious to other people, whereas someone who has pulmonary or laryngeal TB is considered to be an infectious risk to other individuals.”
Dr. Shane went on to discuss limitations of the TST in diagnosing TB. For one, the test may be placed incorrectly, resulting in an inflammatory response or no response, “and there is reader variability,” she said. “The other issue is that the reading needs to occur 48-72 hours after placement of the test. So, if you place it on a Thursday, that means you really are not going to read it at the optimal time unless the child comes to you on a weekend or the test is read by somebody else.”
As an alternative, two IGRAs have been developed that measure how the immune system reacts to MTB. One is QuantiFERON, which is widely used in the United States; the other is the T-SPOT.TB test, which is widely used in Europe. A positive result on either test indicates that there has been interaction with MTB bacteria but it does not differentiate between LTBI and active TB disease.
“A negative IGRA tells you there is no reaction to the test and MTB is not likely, while an indeterminate result is when you’re unable to interpret the result due to low positive [mitogen] or increased negative control [nil] compared to TB response,” Dr. Shane said. “This usually indicates that there’s some problem with the assay itself. It can also indicate that the individual may not have an immune system that can respond to and produce the interferon gamma that’s needed.”
Assessment of IGRA accuracy is challenged by a lack of a standard for the diagnosis of LTBI and active TB, especially in children. “The reason is, we just don’t have a lot of good data from resource-endowed settings,” Dr. Shane explained. “We have good data from areas where TB is prevalent.” According to the Centers for Disease Control and Prevention and the AAP, IGRAs are probably reliable in children over the age of 5 years, but a TST is still recommended in children under the age of 5.
“The nice thing about the IGRAs is that their specificity is much higher” than TSTs, Dr. Shane said. “However, in some cases a TST might be more sensitive for detecting more remote MTB infections than an IGRA, but IGRAs may be better at detecting a recent infection. Like the TST, an IGRA also shows that if you’re infected with TB you have 5-10% chance of developing active TB in your lifetime.”
She also pointed out that a significant amount of blood is required to perform an IGRA. “That might not always be optimal, especially in a young child,” Dr. Shane said. “Low CD4 counts and other immunodeficiencies have also been associated with false-negative TST and indeterminate/false-negative IGRA results.”
For contact investigations, IGRAs offer increased specificity, are completed during a single visit, and their response is not boosted if an additional evaluation is needed 8-10 weeks after exposure. For periodic screening of health care workers, IGRA offers “technical and logistical advantages, and two-step testing is not required,” she said.
If the TST or IGRA is positive, additional diagnostic efforts are needed “to differentiate between LTBI and active MTB,” said Dr. Shane, who recommended the Curry International Tuberculosis Center as a resource for clinicians. “Your clinical history, chest radiography, [and results of] sputum/gastric aspirates will help,” she added.
If the TST or IGRA is negative, “it’s not sufficient to exclude MTB infection. If you have a discordant TST and IGRA result, consider history and epidemiologic risk factors. Treat with clinical suspicion or risk of a poor outcome (those younger than age 5 and those infected with HIV).”
Dr. Shane reported having no relevant financial disclosures.
On Twitter @dougbrunk
EXPERT ANALYSIS FROM A PEDIATRIC UPDATE

VIDEO: Focused cardiac ultrasound aids acute heart failure patients
VIENNA – Bedside echocardiography has become a key part of quickly assessing patients with acute heart failure to decide the best management strategy.
But bedside echo images often are challenging to interpret, so physicians performing an initial work-up of an acute heart failure patient need training in a basic echocardiography examination, Dr. Nuno Cardim said in an interview during the annual meeting of the European Association of Cardiovascular Imaging.
Known as Focused Cardiac Ultrasound (FoCUS), this triage-level exam is distinct from a comprehensive echocardiography assessment. Instead, FoCUS addresses some basic, yes-or-no, present-or-absent questions regarding systolic function, hypovolemia, tamponade, pleural effusion, and pulmonary embolus.
In a position paper and then in practice recommendations issued in 2014, the European Association of Cardiovascular Imaging acknowledged that use of FoCUS in acute heart failure patients was “irreversible,” said Dr. Cardim, professor and director of echocardiography and cardiac imaging at Hospital da Luz in Lisbon.
Cardiologists and echocardiography specialists need to make sure that FoCUS training is available to all physicians who might see suspected acute heart failure patients in emergency medicine settings, Dr. Cardim said.
Dr. Cardim had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
VIENNA – Bedside echocardiography has become a key part of quickly assessing patients with acute heart failure to decide the best management strategy.
But bedside echo images often are challenging to interpret, so physicians performing an initial work-up of an acute heart failure patient need training in a basic echocardiography examination, Dr. Nuno Cardim said in an interview during the annual meeting of the European Association of Cardiovascular Imaging.
Known as Focused Cardiac Ultrasound (FoCUS), this triage-level exam is distinct from a comprehensive echocardiography assessment. Instead, FoCUS addresses some basic, yes-or-no, present-or-absent questions regarding systolic function, hypovolemia, tamponade, pleural effusion, and pulmonary embolus.
In a position paper and then in practice recommendations issued in 2014, the European Association of Cardiovascular Imaging acknowledged that use of FoCUS in acute heart failure patients was “irreversible,” said Dr. Cardim, professor and director of echocardiography and cardiac imaging at Hospital da Luz in Lisbon.
Cardiologists and echocardiography specialists need to make sure that FoCUS training is available to all physicians who might see suspected acute heart failure patients in emergency medicine settings, Dr. Cardim said.
Dr. Cardim had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
VIENNA – Bedside echocardiography has become a key part of quickly assessing patients with acute heart failure to decide the best management strategy.
But bedside echo images often are challenging to interpret, so physicians performing an initial work-up of an acute heart failure patient need training in a basic echocardiography examination, Dr. Nuno Cardim said in an interview during the annual meeting of the European Association of Cardiovascular Imaging.
Known as Focused Cardiac Ultrasound (FoCUS), this triage-level exam is distinct from a comprehensive echocardiography assessment. Instead, FoCUS addresses some basic, yes-or-no, present-or-absent questions regarding systolic function, hypovolemia, tamponade, pleural effusion, and pulmonary embolus.
In a position paper and then in practice recommendations issued in 2014, the European Association of Cardiovascular Imaging acknowledged that use of FoCUS in acute heart failure patients was “irreversible,” said Dr. Cardim, professor and director of echocardiography and cardiac imaging at Hospital da Luz in Lisbon.
Cardiologists and echocardiography specialists need to make sure that FoCUS training is available to all physicians who might see suspected acute heart failure patients in emergency medicine settings, Dr. Cardim said.
Dr. Cardim had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
AT EUROECHO-IMAGING 2014

Don’t think tendinitis in kids, but apophysitis instead
LAS VEGAS – Beware the diagnosis of tendinitis in children and adolescents who present with varying degrees of knee or foot pain.
“If you make the diagnosis of tendinitis, you’re probably wrong,” Dr. Sally S. Harris said at a pediatric update sponsored by the American Academy of Pediatrics California District 9. “Tendinitis rarely occurs in the pediatric and adolescent age group because tendinitis is a degenerative condition. So think of other things, especially apophysitis.”

An apophysis is a secondary center of ossification that contributes to the peripheral prominences around bones, such as around the ankles, elbows, pelvis, and knees: “The bumps, so to speak,” said Dr. Harris, who practices in the departments of sports medicine and pediatrics at Palo Alto (Calif.) Medical Foundation. “It’s a bone-related pain, an inflammation of that softer cartilage turning to bone that isn’t completely formed.”
Osgood-Schlatter disease ranks as the most-common apophysitis injury. This occurs during midpuberty and is marked by a prominent swollen bump on the front of the knee, just below the knee cap, where the patellar tendon attaches to the tibial tubercle, explained Dr. Harris, who founded the AAP section on sports medicine. “It’s a secondary center of ossification that appears at ages 10-12 years and fuses at ages 14-18.” Telltale signs are tenderness with or without swelling at the tibial tubercle that worsens with running, jumping, or impact activities. “If you ask [patients] to extend their knee against the resistance of your hand, you’ll probably reproduce the pain,” she said.
X-rays usually are not required. “You might do it to confirm the presence of an open apophysitis or to rule out other pathology, but other pathology is almost always unheard of at that area.”
Recommended treatment involves decreasing running and jumping activity as needed to keep symptoms manageable, and decreasing inflammation with ice and possibly nonsteroidal anti-inflammatory drugs. Wearing protective knee pads also can help. “Anytime the bump gets hit, kicked, or kneeled on, it will be more irritated,” she said. “Stretching quadriceps and especially hamstrings can help offload this problem.”.
Dr. Harris described the condition as self-limited although it can last 2-3 years. Potential complications considered minor include enlargement of the tibial tubercle, ununited ossicles in the patellar tendon, and avulsion of the tibial tubercle (rare). “Generally, Osgood-Schlatter is a harmless condition that you just want to manage,” she said.
Another common injury is Sinding-Larsen-Johansson syndrome, which is an apophysitis of the inferior pole of the patella that occurs in prepubescent boys and girls. “This is going to be knee pain, but there won’t be anything obvious for you to see or for them to point at,” Dr. Harris said. “You will focus on the inferior pole of the patella and palpate where the patellar tendon attaches to the knee cap. It’s analogous to jumper’s knee in adults.”
Lateral x-rays will reveal a small ossific fragment at the distal portion of the patella. Sinding-Larsen-Johansson disease typically resolves within 1 year. “It rarely interferes with activity; they just need an explanation of what’s going on,” she said.
Severs disease, which occurs in early puberty, is an apophysitis injury that affects the heels of children who participate in soccer and gymnastics. It’s marked by a traction/impact apophysitis at the site of insertion of the Achilles’ tendon at the posterior calcaneus. “At times, it can last for 2-3 years, but it is a self-limited condition,” Dr. Harris said. “Nothing ever bad comes from this other than the ups and downs of the pain. It’s pain at the base of the heel, not the Achilles’ tendon area, but patients will come in and some of them have been told they have Achilles’ tendinitis.”
Telltale signs include pain with heel walking and positive lateral squeeze test of the posterior calcaneus. “That reproduces the symptoms,” she said. “If they’re not symptomatic when you see them in the office, you can ask them to try this test after their next [sports] practice, and this will confirm the diagnosis. X-rays are not needed.”
Treatment involves modifying physical activity to keep symptoms manageable. Insertion of silicone heel cups can help, as can wearing shoes with good padding.
If a child of pubertal age presents with pain localized to the inner side of the arching foot, think tarsal navicular bone apophysitis, which is due to the presence of accessory navicular or open apophysitis. “It doesn’t really matter what the anatomy is; it’s all treated the same way, which is to support pronation with arch support,” Dr. Harris said. “If this doesn’t alleviate symptoms well enough, they need custom orthotics made.”
The final injury Dr. Harris discussed was Iselin’s disease, which is a secondary center of ossification at the site of insertion of the peroneal tendon at the base of the 5th metatarsal. Pain in the region is exacerbated by excessive lateral ankle movement. “On an x-ray, this looks like a small crescent of bone growing that hasn’t completely fused yet,” she said. “It’s often misread as a fracture, but it’s normal development.” Treatment consists of activity modification, icing, and NSAIDs as needed, and an ankle brace to provide lateral ankle support. She described Iselin’s as “harmless and short lived, from 6-10 months at the most.”
Dr. Harris reported having no financial disclosures.
On Twitter @dougbrunk
LAS VEGAS – Beware the diagnosis of tendinitis in children and adolescents who present with varying degrees of knee or foot pain.
“If you make the diagnosis of tendinitis, you’re probably wrong,” Dr. Sally S. Harris said at a pediatric update sponsored by the American Academy of Pediatrics California District 9. “Tendinitis rarely occurs in the pediatric and adolescent age group because tendinitis is a degenerative condition. So think of other things, especially apophysitis.”
An apophysis is a secondary center of ossification that contributes to the peripheral prominences around bones, such as around the ankles, elbows, pelvis, and knees: “The bumps, so to speak,” said Dr. Harris, who practices in the departments of sports medicine and pediatrics at Palo Alto (Calif.) Medical Foundation. “It’s a bone-related pain, an inflammation of that softer cartilage turning to bone that isn’t completely formed.”
Osgood-Schlatter disease ranks as the most-common apophysitis injury. This occurs during midpuberty and is marked by a prominent swollen bump on the front of the knee, just below the knee cap, where the patellar tendon attaches to the tibial tubercle, explained Dr. Harris, who founded the AAP section on sports medicine. “It’s a secondary center of ossification that appears at ages 10-12 years and fuses at ages 14-18.” Telltale signs are tenderness with or without swelling at the tibial tubercle that worsens with running, jumping, or impact activities. “If you ask [patients] to extend their knee against the resistance of your hand, you’ll probably reproduce the pain,” she said.
X-rays usually are not required. “You might do it to confirm the presence of an open apophysitis or to rule out other pathology, but other pathology is almost always unheard of at that area.”
Recommended treatment involves decreasing running and jumping activity as needed to keep symptoms manageable, and decreasing inflammation with ice and possibly nonsteroidal anti-inflammatory drugs. Wearing protective knee pads also can help. “Anytime the bump gets hit, kicked, or kneeled on, it will be more irritated,” she said. “Stretching quadriceps and especially hamstrings can help offload this problem.”.
Dr. Harris described the condition as self-limited although it can last 2-3 years. Potential complications considered minor include enlargement of the tibial tubercle, ununited ossicles in the patellar tendon, and avulsion of the tibial tubercle (rare). “Generally, Osgood-Schlatter is a harmless condition that you just want to manage,” she said.
Another common injury is Sinding-Larsen-Johansson syndrome, which is an apophysitis of the inferior pole of the patella that occurs in prepubescent boys and girls. “This is going to be knee pain, but there won’t be anything obvious for you to see or for them to point at,” Dr. Harris said. “You will focus on the inferior pole of the patella and palpate where the patellar tendon attaches to the knee cap. It’s analogous to jumper’s knee in adults.”
Lateral x-rays will reveal a small ossific fragment at the distal portion of the patella. Sinding-Larsen-Johansson disease typically resolves within 1 year. “It rarely interferes with activity; they just need an explanation of what’s going on,” she said.
Severs disease, which occurs in early puberty, is an apophysitis injury that affects the heels of children who participate in soccer and gymnastics. It’s marked by a traction/impact apophysitis at the site of insertion of the Achilles’ tendon at the posterior calcaneus. “At times, it can last for 2-3 years, but it is a self-limited condition,” Dr. Harris said. “Nothing ever bad comes from this other than the ups and downs of the pain. It’s pain at the base of the heel, not the Achilles’ tendon area, but patients will come in and some of them have been told they have Achilles’ tendinitis.”
Telltale signs include pain with heel walking and positive lateral squeeze test of the posterior calcaneus. “That reproduces the symptoms,” she said. “If they’re not symptomatic when you see them in the office, you can ask them to try this test after their next [sports] practice, and this will confirm the diagnosis. X-rays are not needed.”
Treatment involves modifying physical activity to keep symptoms manageable. Insertion of silicone heel cups can help, as can wearing shoes with good padding.
If a child of pubertal age presents with pain localized to the inner side of the arching foot, think tarsal navicular bone apophysitis, which is due to the presence of accessory navicular or open apophysitis. “It doesn’t really matter what the anatomy is; it’s all treated the same way, which is to support pronation with arch support,” Dr. Harris said. “If this doesn’t alleviate symptoms well enough, they need custom orthotics made.”
The final injury Dr. Harris discussed was Iselin’s disease, which is a secondary center of ossification at the site of insertion of the peroneal tendon at the base of the 5th metatarsal. Pain in the region is exacerbated by excessive lateral ankle movement. “On an x-ray, this looks like a small crescent of bone growing that hasn’t completely fused yet,” she said. “It’s often misread as a fracture, but it’s normal development.” Treatment consists of activity modification, icing, and NSAIDs as needed, and an ankle brace to provide lateral ankle support. She described Iselin’s as “harmless and short lived, from 6-10 months at the most.”
Dr. Harris reported having no financial disclosures.
On Twitter @dougbrunk
LAS VEGAS – Beware the diagnosis of tendinitis in children and adolescents who present with varying degrees of knee or foot pain.
“If you make the diagnosis of tendinitis, you’re probably wrong,” Dr. Sally S. Harris said at a pediatric update sponsored by the American Academy of Pediatrics California District 9. “Tendinitis rarely occurs in the pediatric and adolescent age group because tendinitis is a degenerative condition. So think of other things, especially apophysitis.”
An apophysis is a secondary center of ossification that contributes to the peripheral prominences around bones, such as around the ankles, elbows, pelvis, and knees: “The bumps, so to speak,” said Dr. Harris, who practices in the departments of sports medicine and pediatrics at Palo Alto (Calif.) Medical Foundation. “It’s a bone-related pain, an inflammation of that softer cartilage turning to bone that isn’t completely formed.”
Osgood-Schlatter disease ranks as the most-common apophysitis injury. This occurs during midpuberty and is marked by a prominent swollen bump on the front of the knee, just below the knee cap, where the patellar tendon attaches to the tibial tubercle, explained Dr. Harris, who founded the AAP section on sports medicine. “It’s a secondary center of ossification that appears at ages 10-12 years and fuses at ages 14-18.” Telltale signs are tenderness with or without swelling at the tibial tubercle that worsens with running, jumping, or impact activities. “If you ask [patients] to extend their knee against the resistance of your hand, you’ll probably reproduce the pain,” she said.
X-rays usually are not required. “You might do it to confirm the presence of an open apophysitis or to rule out other pathology, but other pathology is almost always unheard of at that area.”
Recommended treatment involves decreasing running and jumping activity as needed to keep symptoms manageable, and decreasing inflammation with ice and possibly nonsteroidal anti-inflammatory drugs. Wearing protective knee pads also can help. “Anytime the bump gets hit, kicked, or kneeled on, it will be more irritated,” she said. “Stretching quadriceps and especially hamstrings can help offload this problem.”.
Dr. Harris described the condition as self-limited although it can last 2-3 years. Potential complications considered minor include enlargement of the tibial tubercle, ununited ossicles in the patellar tendon, and avulsion of the tibial tubercle (rare). “Generally, Osgood-Schlatter is a harmless condition that you just want to manage,” she said.
Another common injury is Sinding-Larsen-Johansson syndrome, which is an apophysitis of the inferior pole of the patella that occurs in prepubescent boys and girls. “This is going to be knee pain, but there won’t be anything obvious for you to see or for them to point at,” Dr. Harris said. “You will focus on the inferior pole of the patella and palpate where the patellar tendon attaches to the knee cap. It’s analogous to jumper’s knee in adults.”
Lateral x-rays will reveal a small ossific fragment at the distal portion of the patella. Sinding-Larsen-Johansson disease typically resolves within 1 year. “It rarely interferes with activity; they just need an explanation of what’s going on,” she said.
Severs disease, which occurs in early puberty, is an apophysitis injury that affects the heels of children who participate in soccer and gymnastics. It’s marked by a traction/impact apophysitis at the site of insertion of the Achilles’ tendon at the posterior calcaneus. “At times, it can last for 2-3 years, but it is a self-limited condition,” Dr. Harris said. “Nothing ever bad comes from this other than the ups and downs of the pain. It’s pain at the base of the heel, not the Achilles’ tendon area, but patients will come in and some of them have been told they have Achilles’ tendinitis.”
Telltale signs include pain with heel walking and positive lateral squeeze test of the posterior calcaneus. “That reproduces the symptoms,” she said. “If they’re not symptomatic when you see them in the office, you can ask them to try this test after their next [sports] practice, and this will confirm the diagnosis. X-rays are not needed.”
Treatment involves modifying physical activity to keep symptoms manageable. Insertion of silicone heel cups can help, as can wearing shoes with good padding.
If a child of pubertal age presents with pain localized to the inner side of the arching foot, think tarsal navicular bone apophysitis, which is due to the presence of accessory navicular or open apophysitis. “It doesn’t really matter what the anatomy is; it’s all treated the same way, which is to support pronation with arch support,” Dr. Harris said. “If this doesn’t alleviate symptoms well enough, they need custom orthotics made.”
The final injury Dr. Harris discussed was Iselin’s disease, which is a secondary center of ossification at the site of insertion of the peroneal tendon at the base of the 5th metatarsal. Pain in the region is exacerbated by excessive lateral ankle movement. “On an x-ray, this looks like a small crescent of bone growing that hasn’t completely fused yet,” she said. “It’s often misread as a fracture, but it’s normal development.” Treatment consists of activity modification, icing, and NSAIDs as needed, and an ankle brace to provide lateral ankle support. She described Iselin’s as “harmless and short lived, from 6-10 months at the most.”
Dr. Harris reported having no financial disclosures.
On Twitter @dougbrunk
EXPERT ANALYSIS AT PEDIATRIC UPDATE

It’s a Republican majority following midterm election results. How will that affect the ACA and women’s health?
Does this new evidence for noninvasive prenatal testing to detect fetal aneuploidy move NIPT closer to universal use in pregnancy?
The introduction of cell-free fetal DNA (cfDNA) testing has had a tremendous impact on prenatal care. Numerous series reporting near-diagnostic accuracy for trisomy 21 detection have been reported,1 and several commercial laboratories offer clinical testing. Many patients now take advantage of these tests, and the very low false-positive rates have resulted in a marked decrease in the rate of invasive diagnostic testing.2 At present, most professional societies suggest that these tests be reserved for women at high risk for fetal aneuploidy.3
Details of the study
In this recent article by Porreco and colleagues, the researchers reported on a large cohort study of patients who had made the decision to undergo invasive diagnostic testing with chorionic villus sampling or amniocentesis prior to undergoing noninvasive testing, in order to validate the clinical performance of massively parallel genomic sequencing of cfDNA. As in several prior reports, the study authors found that the detection rate of cfDNA for trisomy 21 was 100%, and somewhat less for trisomy 18 (92%) and trisomy 13 (87%). The false-positive rate was very low, with only three false-positive results (all for trisomy 21) in 3,430 patients. Testing for fetal sex chromosomes reported 7 out of 3,322 errors in fetal sex and 100% detection of sex chromosomal aneuploidies, with 16 out of 3,200 false-positive results.
Study limitations
As in prior reports, limitations to the test were not clearly presented. Patients with “complex chromosomal abnormalities” not detectable by cfDNA were excluded from the reported cohort. Considering these cases, fewer of the total chromosomal abnormalities in the cohort were detected.
Also, adequate fetal DNA is necessary for accurate results, and patients with less than 4% fetal DNA were excluded. Low fetal DNA is associated with an increased risk of trisomy.4,5 Therefore, excluding such cases will bias results toward a higher detection rate.
The outcomes for cases of low fetal DNA were not included in this study, but in another recent paper 22% of cases of low fetal DNA had aneuploidy, and 16% of common aneuploidies were not detected because of failed testing.4
What this evidence means for practice
Cell-free fetal DNA is an exciting technology, and this study adds to the existing literature in the field. However, use of the test requires careful patient counseling regarding the limitations in detecting abnormalities other than trisomy 21, which comprises just 50% of all aneuploidies. Women who desire a comprehensive prenatal genetic assessment may prefer invasive diagnostic testing and should be counseled appropriately. Patients in whom the test fails should be informed that they are at high risk for a chromosomal abnormality.
Considering these outcomes, the benefits of prenatal screening with cfDNA over current testing alternatives, with serum analytes and/or invasive diagnostic testing, become less clear and the options more complex. Of primary importance is that patients understand the risks and benefits of alternative tests.
—Mary E. Norton, MD
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Gil MM, Akolekar R, Quezada MS, Bregant B, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: meta-analysis. Fetal Diagn Ther. 2014;35(3):156−173.
2. Wax JR, Cartin A, Chard R, Lucas FL, Pinette MG. Noninvasive prenatal testing: Impact on genetic counseling, invasive prenatal diagnosis, and trisomy 21 detection [published online ahead of print October 9, 2014]. J Clin Ultrasound. doi:`10.1002/jcu.22243. [Epub ahead of print]
3. American College of Obstetricians and Gynecologists Committee on Genetics. Committee Opinion No. 545: Noninvasive prenatal testing for fetal aneuploidy. Obstet Gynecol. 2012;120(6):1532−1534.
4. Pergament E, Cuckle H, Zimmermann B, et al. Single-nucleotide polymorphism-based noninvasive prenatal screening in a high-risk and low-risk cohort. Obstet Gynecol. 2014;124(2 pt 1):210−218.
5. Rava RP, Srinivasan A, Sehnert AJ, Bianchi DW. Circulating fetal cell-free DNA fractions differ in autosomal aneuploidies and monosomy X. Clin Chem. 2014;60(1):243−250.
The introduction of cell-free fetal DNA (cfDNA) testing has had a tremendous impact on prenatal care. Numerous series reporting near-diagnostic accuracy for trisomy 21 detection have been reported,1 and several commercial laboratories offer clinical testing. Many patients now take advantage of these tests, and the very low false-positive rates have resulted in a marked decrease in the rate of invasive diagnostic testing.2 At present, most professional societies suggest that these tests be reserved for women at high risk for fetal aneuploidy.3
Details of the study
In this recent article by Porreco and colleagues, the researchers reported on a large cohort study of patients who had made the decision to undergo invasive diagnostic testing with chorionic villus sampling or amniocentesis prior to undergoing noninvasive testing, in order to validate the clinical performance of massively parallel genomic sequencing of cfDNA. As in several prior reports, the study authors found that the detection rate of cfDNA for trisomy 21 was 100%, and somewhat less for trisomy 18 (92%) and trisomy 13 (87%). The false-positive rate was very low, with only three false-positive results (all for trisomy 21) in 3,430 patients. Testing for fetal sex chromosomes reported 7 out of 3,322 errors in fetal sex and 100% detection of sex chromosomal aneuploidies, with 16 out of 3,200 false-positive results.
Study limitations
As in prior reports, limitations to the test were not clearly presented. Patients with “complex chromosomal abnormalities” not detectable by cfDNA were excluded from the reported cohort. Considering these cases, fewer of the total chromosomal abnormalities in the cohort were detected.
Also, adequate fetal DNA is necessary for accurate results, and patients with less than 4% fetal DNA were excluded. Low fetal DNA is associated with an increased risk of trisomy.4,5 Therefore, excluding such cases will bias results toward a higher detection rate.
The outcomes for cases of low fetal DNA were not included in this study, but in another recent paper 22% of cases of low fetal DNA had aneuploidy, and 16% of common aneuploidies were not detected because of failed testing.4
What this evidence means for practice
Cell-free fetal DNA is an exciting technology, and this study adds to the existing literature in the field. However, use of the test requires careful patient counseling regarding the limitations in detecting abnormalities other than trisomy 21, which comprises just 50% of all aneuploidies. Women who desire a comprehensive prenatal genetic assessment may prefer invasive diagnostic testing and should be counseled appropriately. Patients in whom the test fails should be informed that they are at high risk for a chromosomal abnormality.
Considering these outcomes, the benefits of prenatal screening with cfDNA over current testing alternatives, with serum analytes and/or invasive diagnostic testing, become less clear and the options more complex. Of primary importance is that patients understand the risks and benefits of alternative tests.
—Mary E. Norton, MD
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The introduction of cell-free fetal DNA (cfDNA) testing has had a tremendous impact on prenatal care. Numerous series reporting near-diagnostic accuracy for trisomy 21 detection have been reported,1 and several commercial laboratories offer clinical testing. Many patients now take advantage of these tests, and the very low false-positive rates have resulted in a marked decrease in the rate of invasive diagnostic testing.2 At present, most professional societies suggest that these tests be reserved for women at high risk for fetal aneuploidy.3
Details of the study
In this recent article by Porreco and colleagues, the researchers reported on a large cohort study of patients who had made the decision to undergo invasive diagnostic testing with chorionic villus sampling or amniocentesis prior to undergoing noninvasive testing, in order to validate the clinical performance of massively parallel genomic sequencing of cfDNA. As in several prior reports, the study authors found that the detection rate of cfDNA for trisomy 21 was 100%, and somewhat less for trisomy 18 (92%) and trisomy 13 (87%). The false-positive rate was very low, with only three false-positive results (all for trisomy 21) in 3,430 patients. Testing for fetal sex chromosomes reported 7 out of 3,322 errors in fetal sex and 100% detection of sex chromosomal aneuploidies, with 16 out of 3,200 false-positive results.
Study limitations
As in prior reports, limitations to the test were not clearly presented. Patients with “complex chromosomal abnormalities” not detectable by cfDNA were excluded from the reported cohort. Considering these cases, fewer of the total chromosomal abnormalities in the cohort were detected.
Also, adequate fetal DNA is necessary for accurate results, and patients with less than 4% fetal DNA were excluded. Low fetal DNA is associated with an increased risk of trisomy.4,5 Therefore, excluding such cases will bias results toward a higher detection rate.
The outcomes for cases of low fetal DNA were not included in this study, but in another recent paper 22% of cases of low fetal DNA had aneuploidy, and 16% of common aneuploidies were not detected because of failed testing.4
What this evidence means for practice
Cell-free fetal DNA is an exciting technology, and this study adds to the existing literature in the field. However, use of the test requires careful patient counseling regarding the limitations in detecting abnormalities other than trisomy 21, which comprises just 50% of all aneuploidies. Women who desire a comprehensive prenatal genetic assessment may prefer invasive diagnostic testing and should be counseled appropriately. Patients in whom the test fails should be informed that they are at high risk for a chromosomal abnormality.
Considering these outcomes, the benefits of prenatal screening with cfDNA over current testing alternatives, with serum analytes and/or invasive diagnostic testing, become less clear and the options more complex. Of primary importance is that patients understand the risks and benefits of alternative tests.
—Mary E. Norton, MD
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Gil MM, Akolekar R, Quezada MS, Bregant B, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: meta-analysis. Fetal Diagn Ther. 2014;35(3):156−173.
2. Wax JR, Cartin A, Chard R, Lucas FL, Pinette MG. Noninvasive prenatal testing: Impact on genetic counseling, invasive prenatal diagnosis, and trisomy 21 detection [published online ahead of print October 9, 2014]. J Clin Ultrasound. doi:`10.1002/jcu.22243. [Epub ahead of print]
3. American College of Obstetricians and Gynecologists Committee on Genetics. Committee Opinion No. 545: Noninvasive prenatal testing for fetal aneuploidy. Obstet Gynecol. 2012;120(6):1532−1534.
4. Pergament E, Cuckle H, Zimmermann B, et al. Single-nucleotide polymorphism-based noninvasive prenatal screening in a high-risk and low-risk cohort. Obstet Gynecol. 2014;124(2 pt 1):210−218.
5. Rava RP, Srinivasan A, Sehnert AJ, Bianchi DW. Circulating fetal cell-free DNA fractions differ in autosomal aneuploidies and monosomy X. Clin Chem. 2014;60(1):243−250.
1. Gil MM, Akolekar R, Quezada MS, Bregant B, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: meta-analysis. Fetal Diagn Ther. 2014;35(3):156−173.
2. Wax JR, Cartin A, Chard R, Lucas FL, Pinette MG. Noninvasive prenatal testing: Impact on genetic counseling, invasive prenatal diagnosis, and trisomy 21 detection [published online ahead of print October 9, 2014]. J Clin Ultrasound. doi:`10.1002/jcu.22243. [Epub ahead of print]
3. American College of Obstetricians and Gynecologists Committee on Genetics. Committee Opinion No. 545: Noninvasive prenatal testing for fetal aneuploidy. Obstet Gynecol. 2012;120(6):1532−1534.
4. Pergament E, Cuckle H, Zimmermann B, et al. Single-nucleotide polymorphism-based noninvasive prenatal screening in a high-risk and low-risk cohort. Obstet Gynecol. 2014;124(2 pt 1):210−218.
5. Rava RP, Srinivasan A, Sehnert AJ, Bianchi DW. Circulating fetal cell-free DNA fractions differ in autosomal aneuploidies and monosomy X. Clin Chem. 2014;60(1):243−250.
A Practice Resolution
In the heart of the holiday season’s gluttony (and the challenges of staffing the holidays), we need something to get us excited for 2015. Let me suggest that you resolve to use “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” to trim those holiday pounds and make your hospitalist group (HMG) fitter than ever.1
When we published the “Key Principles and Characteristics” in the Journal of Hospital Medicine in February, we intended it to be “aspirational, helping to raise the bar for the specialty of hospital medicine.”1 The author group’s intent was to provide a framework for quality improvement at the HMG level. One can use the 10 principles and 47 characteristics as a basis for self-assessment within the cycle of quality improvement. I will provide an illustration of how a group might utilize the guide to improve its performance using an example and W. Edward Deming’s classic plan-do-study-act (PDSA) cycle.
Principle 6: The HMG supports care coordination across settings.
Characteristic 6.1: The HMG has systems in place to ensure effective and reliable communication with the patient’s primary care provider and/or other providers involved in the patient’s care in the nonacute care setting.
Plan
This phase involves identifying a goal, setting success metrics, and putting a plan into action.
Example: 90% of primary care providers (PCPs) will receive a discharge summary within 24 hours of discharge.
Do
Here the key components of the plan are implemented.
Example: All referring PCPs’ preferred methods of communication and contact information are documented. The HMG has the ability to utilize such communication, e.g. electronic health record (EHR) e-mail or electronic fax. All hospitalists prepare a discharge summary in real time.
Study
In this phase, outcomes are assessed for success and barriers.
Example: Although 97% of discharge summaries are transmitted according to the PCPs’ preferred communication, PCPs state that they received it only 78% of the time.
Act
This is where the lessons learned throughout the process are integrated to adjust the methods, the goal, or the approach in general. Then the entire cycle is repeated.
Example: Even though most PCPs are on the same EHR system as the hospitalists, they don’t check their EHR e-mail (even though during the Plan phase they said they did). Their office staff uses electronic fax, so that will be the method of communication for the PCPs who do not check their EHR e-mail inbox.
In this example, the next time the PDSA cycle is completed, the new approach—using electronic fax for PCPs who don’t check their EHR e-mail while using e-mail for those who check it—will be employed, measured, and further improved in iterative cycles.
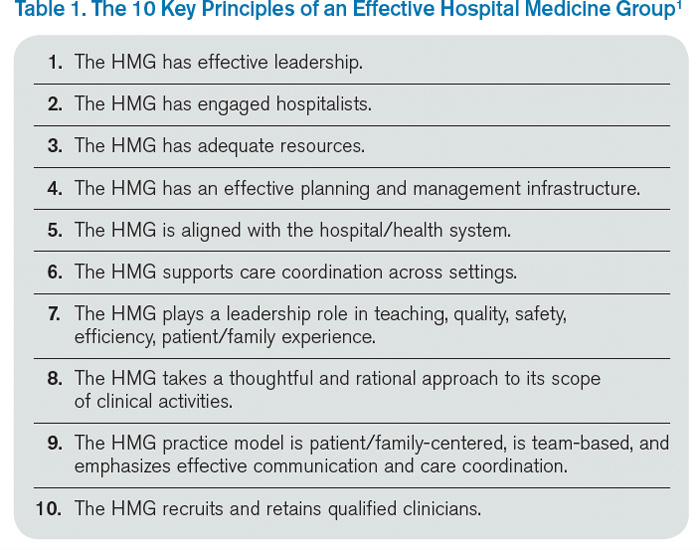
Gap Analysis
Another way you can use the “Key Principles and Characteristics” is to do a gap analysis of your HMG. You can assess the current state of your HMG against the “Key Principles and Characteristics,” which can be viewed as an ideal state. The gap between the current and the ideal state can be a roadmap to improvement for your HMG.
For an example of a large HMG’s gap analysis, see “TeamHealth Hospital Medicine Shares Performance Stats” in the August 2014 issue of The Hospitalist.
Strategic Planning
You may be thinking about taking a block of time to devote to your group’s strategic planning. The “Key Principles and Characteristics” is the ideal framework for such planning. You can use the document as a backdrop to your SWOT (strengths, weaknesses, opportunities, and threats) analysis, which forms the basis of your HMG strategic planning activities.
Keep Your Resolution
One of the best ways to maintain your new habit in the New Year is to let others know of your resolution. In the case of your “Key Principles and Characteristics” resolution, announce your plans at the next monthly meeting of your HMG, and find a way to involve other group members in the project. You might assign a single principle or characteristic to each group member, who is tasked with doing a QI project and reporting on the results at a future date. Or, group members can engage in a portion of a gap analysis or SWOT analysis.
No matter how you use the “Key Principles and Characteristics,” I hope they will guide your HMG to a happy, healthy, and effective 2015!

Reference
In the heart of the holiday season’s gluttony (and the challenges of staffing the holidays), we need something to get us excited for 2015. Let me suggest that you resolve to use “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” to trim those holiday pounds and make your hospitalist group (HMG) fitter than ever.1
When we published the “Key Principles and Characteristics” in the Journal of Hospital Medicine in February, we intended it to be “aspirational, helping to raise the bar for the specialty of hospital medicine.”1 The author group’s intent was to provide a framework for quality improvement at the HMG level. One can use the 10 principles and 47 characteristics as a basis for self-assessment within the cycle of quality improvement. I will provide an illustration of how a group might utilize the guide to improve its performance using an example and W. Edward Deming’s classic plan-do-study-act (PDSA) cycle.
Principle 6: The HMG supports care coordination across settings.
Characteristic 6.1: The HMG has systems in place to ensure effective and reliable communication with the patient’s primary care provider and/or other providers involved in the patient’s care in the nonacute care setting.
Plan
This phase involves identifying a goal, setting success metrics, and putting a plan into action.
Example: 90% of primary care providers (PCPs) will receive a discharge summary within 24 hours of discharge.
Do
Here the key components of the plan are implemented.
Example: All referring PCPs’ preferred methods of communication and contact information are documented. The HMG has the ability to utilize such communication, e.g. electronic health record (EHR) e-mail or electronic fax. All hospitalists prepare a discharge summary in real time.
Study
In this phase, outcomes are assessed for success and barriers.
Example: Although 97% of discharge summaries are transmitted according to the PCPs’ preferred communication, PCPs state that they received it only 78% of the time.
Act
This is where the lessons learned throughout the process are integrated to adjust the methods, the goal, or the approach in general. Then the entire cycle is repeated.
Example: Even though most PCPs are on the same EHR system as the hospitalists, they don’t check their EHR e-mail (even though during the Plan phase they said they did). Their office staff uses electronic fax, so that will be the method of communication for the PCPs who do not check their EHR e-mail inbox.
In this example, the next time the PDSA cycle is completed, the new approach—using electronic fax for PCPs who don’t check their EHR e-mail while using e-mail for those who check it—will be employed, measured, and further improved in iterative cycles.
Gap Analysis
Another way you can use the “Key Principles and Characteristics” is to do a gap analysis of your HMG. You can assess the current state of your HMG against the “Key Principles and Characteristics,” which can be viewed as an ideal state. The gap between the current and the ideal state can be a roadmap to improvement for your HMG.
For an example of a large HMG’s gap analysis, see “TeamHealth Hospital Medicine Shares Performance Stats” in the August 2014 issue of The Hospitalist.
Strategic Planning
You may be thinking about taking a block of time to devote to your group’s strategic planning. The “Key Principles and Characteristics” is the ideal framework for such planning. You can use the document as a backdrop to your SWOT (strengths, weaknesses, opportunities, and threats) analysis, which forms the basis of your HMG strategic planning activities.
Keep Your Resolution
One of the best ways to maintain your new habit in the New Year is to let others know of your resolution. In the case of your “Key Principles and Characteristics” resolution, announce your plans at the next monthly meeting of your HMG, and find a way to involve other group members in the project. You might assign a single principle or characteristic to each group member, who is tasked with doing a QI project and reporting on the results at a future date. Or, group members can engage in a portion of a gap analysis or SWOT analysis.
No matter how you use the “Key Principles and Characteristics,” I hope they will guide your HMG to a happy, healthy, and effective 2015!
Reference
In the heart of the holiday season’s gluttony (and the challenges of staffing the holidays), we need something to get us excited for 2015. Let me suggest that you resolve to use “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” to trim those holiday pounds and make your hospitalist group (HMG) fitter than ever.1
When we published the “Key Principles and Characteristics” in the Journal of Hospital Medicine in February, we intended it to be “aspirational, helping to raise the bar for the specialty of hospital medicine.”1 The author group’s intent was to provide a framework for quality improvement at the HMG level. One can use the 10 principles and 47 characteristics as a basis for self-assessment within the cycle of quality improvement. I will provide an illustration of how a group might utilize the guide to improve its performance using an example and W. Edward Deming’s classic plan-do-study-act (PDSA) cycle.
Principle 6: The HMG supports care coordination across settings.
Characteristic 6.1: The HMG has systems in place to ensure effective and reliable communication with the patient’s primary care provider and/or other providers involved in the patient’s care in the nonacute care setting.
Plan
This phase involves identifying a goal, setting success metrics, and putting a plan into action.
Example: 90% of primary care providers (PCPs) will receive a discharge summary within 24 hours of discharge.
Do
Here the key components of the plan are implemented.
Example: All referring PCPs’ preferred methods of communication and contact information are documented. The HMG has the ability to utilize such communication, e.g. electronic health record (EHR) e-mail or electronic fax. All hospitalists prepare a discharge summary in real time.
Study
In this phase, outcomes are assessed for success and barriers.
Example: Although 97% of discharge summaries are transmitted according to the PCPs’ preferred communication, PCPs state that they received it only 78% of the time.
Act
This is where the lessons learned throughout the process are integrated to adjust the methods, the goal, or the approach in general. Then the entire cycle is repeated.
Example: Even though most PCPs are on the same EHR system as the hospitalists, they don’t check their EHR e-mail (even though during the Plan phase they said they did). Their office staff uses electronic fax, so that will be the method of communication for the PCPs who do not check their EHR e-mail inbox.
In this example, the next time the PDSA cycle is completed, the new approach—using electronic fax for PCPs who don’t check their EHR e-mail while using e-mail for those who check it—will be employed, measured, and further improved in iterative cycles.
Gap Analysis
Another way you can use the “Key Principles and Characteristics” is to do a gap analysis of your HMG. You can assess the current state of your HMG against the “Key Principles and Characteristics,” which can be viewed as an ideal state. The gap between the current and the ideal state can be a roadmap to improvement for your HMG.
For an example of a large HMG’s gap analysis, see “TeamHealth Hospital Medicine Shares Performance Stats” in the August 2014 issue of The Hospitalist.
Strategic Planning
You may be thinking about taking a block of time to devote to your group’s strategic planning. The “Key Principles and Characteristics” is the ideal framework for such planning. You can use the document as a backdrop to your SWOT (strengths, weaknesses, opportunities, and threats) analysis, which forms the basis of your HMG strategic planning activities.
Keep Your Resolution
One of the best ways to maintain your new habit in the New Year is to let others know of your resolution. In the case of your “Key Principles and Characteristics” resolution, announce your plans at the next monthly meeting of your HMG, and find a way to involve other group members in the project. You might assign a single principle or characteristic to each group member, who is tasked with doing a QI project and reporting on the results at a future date. Or, group members can engage in a portion of a gap analysis or SWOT analysis.
No matter how you use the “Key Principles and Characteristics,” I hope they will guide your HMG to a happy, healthy, and effective 2015!