User login
High-dose folic acid during pregnancy tied to cancer risk in children
new data from a Scandinavian registry of more than 3 million pregnancies suggests.
The increased risk for cancer did not change after considering other factors that could explain the risk, such as use of antiseizure medication (ASM).
There was no increased risk for cancer in children of mothers without epilepsy who used high-dose folic acid.
The results of this study “should be considered when the risks and benefits of folic acid supplements for women with epilepsy are discussed and before decisions about optimal dose recommendations are made,” the authors write.
“Although we believe that the association between prescription fills for high-dose folic acid and cancer in children born to mothers with epilepsy is robust, it is important to underline that these are the findings of one study only,” first author Håkon Magne Vegrim, MD, with University of Bergen (Norway) told this news organization.
The study was published online in JAMA Neurology.
Risks and benefits
Women with epilepsy are advised to take high doses of folic acid before and during pregnancy owing to the risk for congenital malformations associated with ASM. Whether high-dose folic acid is associated with increases in the risk for childhood cancer is unknown.
To investigate, the researchers analyzed registry data from Denmark, Norway, and Sweden for 3.3 million children followed to a median age of 7.3 years.
Among the 27,784 children born to mothers with epilepsy, 5,934 (21.4%) were exposed to high-dose folic acid (mean dose, 4.3 mg), with a cancer incidence rate of 42.5 per 100,000 person-years in 18 exposed cancer cases compared with 18.4 per 100,000 person-years in 29 unexposed cancer cases – yielding an adjusted hazard ratio of 2.7 (95% confidence interval, 1.2-6.3).
The absolute risk with exposure was 1.5% (95% CI, 0.5%-3.5%) in children of mothers with epilepsy compared with 0.6% (95% CI, 0.3%-1.1%) in children of mothers with epilepsy who were not exposed high-dose folic acid.
Prenatal exposure to high-dose folic acid was not associated with an increased risk for cancer in children of mothers without epilepsy.
In children of mothers without epilepsy, 46,646 (1.4%) were exposed to high-dose folic acid (mean dose, 2.9 mg). There were 69 exposed and 4,927 unexposed cancer cases and an aHR for cancer of 1.1 (95% CI, 0.9-1.4) and absolute risk for cancer of 0.4% (95% CI, 0.3%-0.5%).
There was no association between any specific ASM and childhood cancer.
“Removing mothers with any prescription fills for carbamazepine and valproate was not associated with the point estimate. Hence, these two ASMs were not important effect modifiers for the cancer association,” the investigators note in their study.
They also note that the most common childhood cancer types in children among mothers with epilepsy who took high-dose folic acid did not differ from the distribution in the general population.
“We need to get more knowledge about the potential mechanisms behind high-dose folic acid and childhood cancer, and it is important to identify the optimal dose to balance risks and benefits – and whether folic acid supplementation should be more individualized, based on factors like the serum level of folate and what type of antiseizure medication that is being used,” said Dr. Vegrim.
Practice changing?
Weighing in on the study, Elizabeth E. Gerard, MD, director of the Women with Epilepsy Program and associate professor of neurology at Northwestern University in Chicago, said, “There are known benefits of folic acid supplementation during pregnancy including a decreased risk of neural tube defects in the general population and improved neurodevelopmental outcomes in children born to mothers with and without epilepsy.”
“However, despite some expert guidelines recommending high-dose folic acid supplementation, there is a lack of certainty surrounding the ‘just right’ dose for patients with epilepsy who may become pregnant,” said Dr. Gerard, who wasn’t involved in the study.
Dr. Gerard, a member of the American Epilepsy Society, noted that other epidemiologic studies of folic acid supplementation and cancer have had “contradictory results, thus further research on this association will be needed. Additionally, differences in maternal/fetal folate metabolism and blood levels may be an important factor to study in the future.
“That said, this study definitely should cause us to pause and reevaluate the common practice of high-dose folic acid supplementation for patients with epilepsy who are considering pregnancy,” said Dr. Gerard.
The study was supported by the NordForsk Nordic Program on Health and Welfare. Dr. Vegrim and Dr. Gerard report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new data from a Scandinavian registry of more than 3 million pregnancies suggests.
The increased risk for cancer did not change after considering other factors that could explain the risk, such as use of antiseizure medication (ASM).
There was no increased risk for cancer in children of mothers without epilepsy who used high-dose folic acid.
The results of this study “should be considered when the risks and benefits of folic acid supplements for women with epilepsy are discussed and before decisions about optimal dose recommendations are made,” the authors write.
“Although we believe that the association between prescription fills for high-dose folic acid and cancer in children born to mothers with epilepsy is robust, it is important to underline that these are the findings of one study only,” first author Håkon Magne Vegrim, MD, with University of Bergen (Norway) told this news organization.
The study was published online in JAMA Neurology.
Risks and benefits
Women with epilepsy are advised to take high doses of folic acid before and during pregnancy owing to the risk for congenital malformations associated with ASM. Whether high-dose folic acid is associated with increases in the risk for childhood cancer is unknown.
To investigate, the researchers analyzed registry data from Denmark, Norway, and Sweden for 3.3 million children followed to a median age of 7.3 years.
Among the 27,784 children born to mothers with epilepsy, 5,934 (21.4%) were exposed to high-dose folic acid (mean dose, 4.3 mg), with a cancer incidence rate of 42.5 per 100,000 person-years in 18 exposed cancer cases compared with 18.4 per 100,000 person-years in 29 unexposed cancer cases – yielding an adjusted hazard ratio of 2.7 (95% confidence interval, 1.2-6.3).
The absolute risk with exposure was 1.5% (95% CI, 0.5%-3.5%) in children of mothers with epilepsy compared with 0.6% (95% CI, 0.3%-1.1%) in children of mothers with epilepsy who were not exposed high-dose folic acid.
Prenatal exposure to high-dose folic acid was not associated with an increased risk for cancer in children of mothers without epilepsy.
In children of mothers without epilepsy, 46,646 (1.4%) were exposed to high-dose folic acid (mean dose, 2.9 mg). There were 69 exposed and 4,927 unexposed cancer cases and an aHR for cancer of 1.1 (95% CI, 0.9-1.4) and absolute risk for cancer of 0.4% (95% CI, 0.3%-0.5%).
There was no association between any specific ASM and childhood cancer.
“Removing mothers with any prescription fills for carbamazepine and valproate was not associated with the point estimate. Hence, these two ASMs were not important effect modifiers for the cancer association,” the investigators note in their study.
They also note that the most common childhood cancer types in children among mothers with epilepsy who took high-dose folic acid did not differ from the distribution in the general population.
“We need to get more knowledge about the potential mechanisms behind high-dose folic acid and childhood cancer, and it is important to identify the optimal dose to balance risks and benefits – and whether folic acid supplementation should be more individualized, based on factors like the serum level of folate and what type of antiseizure medication that is being used,” said Dr. Vegrim.
Practice changing?
Weighing in on the study, Elizabeth E. Gerard, MD, director of the Women with Epilepsy Program and associate professor of neurology at Northwestern University in Chicago, said, “There are known benefits of folic acid supplementation during pregnancy including a decreased risk of neural tube defects in the general population and improved neurodevelopmental outcomes in children born to mothers with and without epilepsy.”
“However, despite some expert guidelines recommending high-dose folic acid supplementation, there is a lack of certainty surrounding the ‘just right’ dose for patients with epilepsy who may become pregnant,” said Dr. Gerard, who wasn’t involved in the study.
Dr. Gerard, a member of the American Epilepsy Society, noted that other epidemiologic studies of folic acid supplementation and cancer have had “contradictory results, thus further research on this association will be needed. Additionally, differences in maternal/fetal folate metabolism and blood levels may be an important factor to study in the future.
“That said, this study definitely should cause us to pause and reevaluate the common practice of high-dose folic acid supplementation for patients with epilepsy who are considering pregnancy,” said Dr. Gerard.
The study was supported by the NordForsk Nordic Program on Health and Welfare. Dr. Vegrim and Dr. Gerard report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new data from a Scandinavian registry of more than 3 million pregnancies suggests.
The increased risk for cancer did not change after considering other factors that could explain the risk, such as use of antiseizure medication (ASM).
There was no increased risk for cancer in children of mothers without epilepsy who used high-dose folic acid.
The results of this study “should be considered when the risks and benefits of folic acid supplements for women with epilepsy are discussed and before decisions about optimal dose recommendations are made,” the authors write.
“Although we believe that the association between prescription fills for high-dose folic acid and cancer in children born to mothers with epilepsy is robust, it is important to underline that these are the findings of one study only,” first author Håkon Magne Vegrim, MD, with University of Bergen (Norway) told this news organization.
The study was published online in JAMA Neurology.
Risks and benefits
Women with epilepsy are advised to take high doses of folic acid before and during pregnancy owing to the risk for congenital malformations associated with ASM. Whether high-dose folic acid is associated with increases in the risk for childhood cancer is unknown.
To investigate, the researchers analyzed registry data from Denmark, Norway, and Sweden for 3.3 million children followed to a median age of 7.3 years.
Among the 27,784 children born to mothers with epilepsy, 5,934 (21.4%) were exposed to high-dose folic acid (mean dose, 4.3 mg), with a cancer incidence rate of 42.5 per 100,000 person-years in 18 exposed cancer cases compared with 18.4 per 100,000 person-years in 29 unexposed cancer cases – yielding an adjusted hazard ratio of 2.7 (95% confidence interval, 1.2-6.3).
The absolute risk with exposure was 1.5% (95% CI, 0.5%-3.5%) in children of mothers with epilepsy compared with 0.6% (95% CI, 0.3%-1.1%) in children of mothers with epilepsy who were not exposed high-dose folic acid.
Prenatal exposure to high-dose folic acid was not associated with an increased risk for cancer in children of mothers without epilepsy.
In children of mothers without epilepsy, 46,646 (1.4%) were exposed to high-dose folic acid (mean dose, 2.9 mg). There were 69 exposed and 4,927 unexposed cancer cases and an aHR for cancer of 1.1 (95% CI, 0.9-1.4) and absolute risk for cancer of 0.4% (95% CI, 0.3%-0.5%).
There was no association between any specific ASM and childhood cancer.
“Removing mothers with any prescription fills for carbamazepine and valproate was not associated with the point estimate. Hence, these two ASMs were not important effect modifiers for the cancer association,” the investigators note in their study.
They also note that the most common childhood cancer types in children among mothers with epilepsy who took high-dose folic acid did not differ from the distribution in the general population.
“We need to get more knowledge about the potential mechanisms behind high-dose folic acid and childhood cancer, and it is important to identify the optimal dose to balance risks and benefits – and whether folic acid supplementation should be more individualized, based on factors like the serum level of folate and what type of antiseizure medication that is being used,” said Dr. Vegrim.
Practice changing?
Weighing in on the study, Elizabeth E. Gerard, MD, director of the Women with Epilepsy Program and associate professor of neurology at Northwestern University in Chicago, said, “There are known benefits of folic acid supplementation during pregnancy including a decreased risk of neural tube defects in the general population and improved neurodevelopmental outcomes in children born to mothers with and without epilepsy.”
“However, despite some expert guidelines recommending high-dose folic acid supplementation, there is a lack of certainty surrounding the ‘just right’ dose for patients with epilepsy who may become pregnant,” said Dr. Gerard, who wasn’t involved in the study.
Dr. Gerard, a member of the American Epilepsy Society, noted that other epidemiologic studies of folic acid supplementation and cancer have had “contradictory results, thus further research on this association will be needed. Additionally, differences in maternal/fetal folate metabolism and blood levels may be an important factor to study in the future.
“That said, this study definitely should cause us to pause and reevaluate the common practice of high-dose folic acid supplementation for patients with epilepsy who are considering pregnancy,” said Dr. Gerard.
The study was supported by the NordForsk Nordic Program on Health and Welfare. Dr. Vegrim and Dr. Gerard report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NEUROLOGY
Not just a bad dream: Nightmares may predict dementia
Results from a large cohort study showed that healthy middle-aged adults who had bad dreams at least once a week were four times more likely to experience cognitive decline over the following decade, and older adults were twice as likely to be diagnosed with dementia, compared with peers who never had bad dreams.
Frequent nightmares may “identify people who are at high risk of developing dementia in the future, several years or decades before the characteristic memory and thinking problems emerge,” study investigator Abidemi Otaiku, BMBS, University of Birmingham, England, said in an interview.
“This would be the optimum time for doctors to intervene to try and slow down or prevent dementia from developing,” Dr. Otaiku said.
The findings were published online in The Lancet journal eClinicalMedicine).
Distressing dreams
Distressing dreams have been previously associated with faster cognitive decline and increased dementia risk in patients with Parkinson’s disease (PD), but whether the same holds for individuals from the general population without PD is unknown.
To investigate, Dr. Otaiku examined data from three community-based cohorts in the United States. This included 605 middle-aged adults (aged 35-64 years) who were followed for up to 13 years and 2,600 adults aged 79 and older who were followed for up to 7 years. All were considered cognitively normal at baseline.
The prevalence of frequent distressing dreams, defined as occurring “once a week or more,” was higher in the older cohort compared with the middle-aged cohort (6.9% vs. 6.0%, respectively).
This is in line with other research that showed distressing dreams remain relatively stable throughout early adulthood and then progressively increase in prevalence from middle to older adulthood.
After adjustment for all covariates, a higher frequency of distressing dreams was linearly and statistically significantly associated with a higher risk for cognitive decline in middle-aged adults (P = .016) and a higher risk for dementia in older adults (P = .001).
In the fully adjusted model, compared with middle-aged adults who never had bad dreams, those who reported having one or more bad dreams weekly had a fourfold risk for cognitive decline (adjusted odds ratio [aOR], 3.99; 95% confidence interval [CI], 1.07-14.85).
Older adults who had one or more bad dreams weekly had a greater than twofold increased risk for developing dementia (aOR, 2.21; 95% CI, 1.35-3.62).
Early days
In sex-stratified analyses, distressing dreams were strongly and statistically significantly associated with cognitive decline and dementia in men, but were only weakly and nonsignificantly associated with cognitive decline and dementia in women.
Dr. Otaiku said he suspects some individuals in the preclinical phase of dementia have “subtle neurodegeneration occurring over time in the right frontal lobe: the area of the brain that helps to downregulate negative emotions whilst we are awake, and also whilst we are dreaming.”
This could result in “depression and anxiety in the day, and nightmares and bad dreams during the night,” he said.
It is possible that treatment for frequent nightmares may help to slow cognitive decline and delay or prevent dementia, Dr. Otaiku added.
He noted that prazosin is used to treat nightmares and has been shown to prevent memory decline and reduce amyloid B generation in preclinical studies of Alzheimer’s disease.
“This is an exciting prospect [but] it is still early days and we will need research to see whether treating nightmares might help to reduce dementia risk down the line,” Dr. Otaiku said.
Credible research
In an interview regarding these findings, Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, said: “This is credible research consistent with the idea that sleep disturbances may be a risk factor or warning sign of cognitive decline.”
She added that “what’s novel here” is the researchers examined distressing dreams – not more physical sleep disturbances and disorders such as insomnia or apnea.
“However, nightmares can disturb sleep in the same way these disorders do by waking people up in the middle of the night,” said Dr. Carrillo, who was not involved with the study.
“Previous research has pointed to nightmares being indicative of potential changes in the brain that can precede other dementias like Parkinson’s disease. More research is needed to tease out what exactly is happening in the brain during nightmares that may be contributing to this increased risk,” she said.
Dr. Carrillo noted that “getting good sleep” is important for overall health, which includes brain health.
“The good news is there are treatments – both drug and nondrug – that can help address sleep disturbances,” she added.
This study received no external funding. Dr. Otaiku and Dr. Carrillo have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results from a large cohort study showed that healthy middle-aged adults who had bad dreams at least once a week were four times more likely to experience cognitive decline over the following decade, and older adults were twice as likely to be diagnosed with dementia, compared with peers who never had bad dreams.
Frequent nightmares may “identify people who are at high risk of developing dementia in the future, several years or decades before the characteristic memory and thinking problems emerge,” study investigator Abidemi Otaiku, BMBS, University of Birmingham, England, said in an interview.
“This would be the optimum time for doctors to intervene to try and slow down or prevent dementia from developing,” Dr. Otaiku said.
The findings were published online in The Lancet journal eClinicalMedicine).
Distressing dreams
Distressing dreams have been previously associated with faster cognitive decline and increased dementia risk in patients with Parkinson’s disease (PD), but whether the same holds for individuals from the general population without PD is unknown.
To investigate, Dr. Otaiku examined data from three community-based cohorts in the United States. This included 605 middle-aged adults (aged 35-64 years) who were followed for up to 13 years and 2,600 adults aged 79 and older who were followed for up to 7 years. All were considered cognitively normal at baseline.
The prevalence of frequent distressing dreams, defined as occurring “once a week or more,” was higher in the older cohort compared with the middle-aged cohort (6.9% vs. 6.0%, respectively).
This is in line with other research that showed distressing dreams remain relatively stable throughout early adulthood and then progressively increase in prevalence from middle to older adulthood.
After adjustment for all covariates, a higher frequency of distressing dreams was linearly and statistically significantly associated with a higher risk for cognitive decline in middle-aged adults (P = .016) and a higher risk for dementia in older adults (P = .001).
In the fully adjusted model, compared with middle-aged adults who never had bad dreams, those who reported having one or more bad dreams weekly had a fourfold risk for cognitive decline (adjusted odds ratio [aOR], 3.99; 95% confidence interval [CI], 1.07-14.85).
Older adults who had one or more bad dreams weekly had a greater than twofold increased risk for developing dementia (aOR, 2.21; 95% CI, 1.35-3.62).
Early days
In sex-stratified analyses, distressing dreams were strongly and statistically significantly associated with cognitive decline and dementia in men, but were only weakly and nonsignificantly associated with cognitive decline and dementia in women.
Dr. Otaiku said he suspects some individuals in the preclinical phase of dementia have “subtle neurodegeneration occurring over time in the right frontal lobe: the area of the brain that helps to downregulate negative emotions whilst we are awake, and also whilst we are dreaming.”
This could result in “depression and anxiety in the day, and nightmares and bad dreams during the night,” he said.
It is possible that treatment for frequent nightmares may help to slow cognitive decline and delay or prevent dementia, Dr. Otaiku added.
He noted that prazosin is used to treat nightmares and has been shown to prevent memory decline and reduce amyloid B generation in preclinical studies of Alzheimer’s disease.
“This is an exciting prospect [but] it is still early days and we will need research to see whether treating nightmares might help to reduce dementia risk down the line,” Dr. Otaiku said.
Credible research
In an interview regarding these findings, Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, said: “This is credible research consistent with the idea that sleep disturbances may be a risk factor or warning sign of cognitive decline.”
She added that “what’s novel here” is the researchers examined distressing dreams – not more physical sleep disturbances and disorders such as insomnia or apnea.
“However, nightmares can disturb sleep in the same way these disorders do by waking people up in the middle of the night,” said Dr. Carrillo, who was not involved with the study.
“Previous research has pointed to nightmares being indicative of potential changes in the brain that can precede other dementias like Parkinson’s disease. More research is needed to tease out what exactly is happening in the brain during nightmares that may be contributing to this increased risk,” she said.
Dr. Carrillo noted that “getting good sleep” is important for overall health, which includes brain health.
“The good news is there are treatments – both drug and nondrug – that can help address sleep disturbances,” she added.
This study received no external funding. Dr. Otaiku and Dr. Carrillo have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results from a large cohort study showed that healthy middle-aged adults who had bad dreams at least once a week were four times more likely to experience cognitive decline over the following decade, and older adults were twice as likely to be diagnosed with dementia, compared with peers who never had bad dreams.
Frequent nightmares may “identify people who are at high risk of developing dementia in the future, several years or decades before the characteristic memory and thinking problems emerge,” study investigator Abidemi Otaiku, BMBS, University of Birmingham, England, said in an interview.
“This would be the optimum time for doctors to intervene to try and slow down or prevent dementia from developing,” Dr. Otaiku said.
The findings were published online in The Lancet journal eClinicalMedicine).
Distressing dreams
Distressing dreams have been previously associated with faster cognitive decline and increased dementia risk in patients with Parkinson’s disease (PD), but whether the same holds for individuals from the general population without PD is unknown.
To investigate, Dr. Otaiku examined data from three community-based cohorts in the United States. This included 605 middle-aged adults (aged 35-64 years) who were followed for up to 13 years and 2,600 adults aged 79 and older who were followed for up to 7 years. All were considered cognitively normal at baseline.
The prevalence of frequent distressing dreams, defined as occurring “once a week or more,” was higher in the older cohort compared with the middle-aged cohort (6.9% vs. 6.0%, respectively).
This is in line with other research that showed distressing dreams remain relatively stable throughout early adulthood and then progressively increase in prevalence from middle to older adulthood.
After adjustment for all covariates, a higher frequency of distressing dreams was linearly and statistically significantly associated with a higher risk for cognitive decline in middle-aged adults (P = .016) and a higher risk for dementia in older adults (P = .001).
In the fully adjusted model, compared with middle-aged adults who never had bad dreams, those who reported having one or more bad dreams weekly had a fourfold risk for cognitive decline (adjusted odds ratio [aOR], 3.99; 95% confidence interval [CI], 1.07-14.85).
Older adults who had one or more bad dreams weekly had a greater than twofold increased risk for developing dementia (aOR, 2.21; 95% CI, 1.35-3.62).
Early days
In sex-stratified analyses, distressing dreams were strongly and statistically significantly associated with cognitive decline and dementia in men, but were only weakly and nonsignificantly associated with cognitive decline and dementia in women.
Dr. Otaiku said he suspects some individuals in the preclinical phase of dementia have “subtle neurodegeneration occurring over time in the right frontal lobe: the area of the brain that helps to downregulate negative emotions whilst we are awake, and also whilst we are dreaming.”
This could result in “depression and anxiety in the day, and nightmares and bad dreams during the night,” he said.
It is possible that treatment for frequent nightmares may help to slow cognitive decline and delay or prevent dementia, Dr. Otaiku added.
He noted that prazosin is used to treat nightmares and has been shown to prevent memory decline and reduce amyloid B generation in preclinical studies of Alzheimer’s disease.
“This is an exciting prospect [but] it is still early days and we will need research to see whether treating nightmares might help to reduce dementia risk down the line,” Dr. Otaiku said.
Credible research
In an interview regarding these findings, Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, said: “This is credible research consistent with the idea that sleep disturbances may be a risk factor or warning sign of cognitive decline.”
She added that “what’s novel here” is the researchers examined distressing dreams – not more physical sleep disturbances and disorders such as insomnia or apnea.
“However, nightmares can disturb sleep in the same way these disorders do by waking people up in the middle of the night,” said Dr. Carrillo, who was not involved with the study.
“Previous research has pointed to nightmares being indicative of potential changes in the brain that can precede other dementias like Parkinson’s disease. More research is needed to tease out what exactly is happening in the brain during nightmares that may be contributing to this increased risk,” she said.
Dr. Carrillo noted that “getting good sleep” is important for overall health, which includes brain health.
“The good news is there are treatments – both drug and nondrug – that can help address sleep disturbances,” she added.
This study received no external funding. Dr. Otaiku and Dr. Carrillo have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ECLINICALMEDICINE
WHO releases six ‘action steps’ to combat global disparities in Parkinson’s disease
Since 2000, Parkinson’s disease has increased 81% and related deaths have increased 100% globally. In addition, many patients affected by Parkinson’s disease live in low- and middle-income countries and experience large inequalities in access to neurologic care and essential medicines.
To address these issues, the Brain Health Unit at the WHO developed six “action steps” it says are urgently required to combat global disparities in Parkinson’s disease.
The need for action is great, said lead author Nicoline Schiess, MD, MPH, a neurologist and technical officer in the WHO’s Brain Health Unit in Geneva.
“In adults, disorders of the nervous system are the leading cause of disability adjusted life years, or DALYs, and the second leading cause of death globally, accounting for 9 million deaths per year,” Dr. Schiess said.
The WHO’s recommendations were published online recently as a “Special Communication” in JAMA Neurology.
Serious public health challenge
Parkinson’s disease is the fastest growing disorder in terms of death and disability, and it is estimated that it caused 329,000 deaths in 2019 – an increase of more than 100% since 2000.
“The rise in cases is thought to be multifactorial and is likely affected by factors such as aging populations and environmental exposures, such as certain pesticides. With these rapidly increasing numbers, compounded by a lack of specialists and medicines in low- and middle-income countries, Parkinson’s disease presents a serious public health challenge,” Dr. Schiess said.
The publication of the six action steps is targeted toward clinicians and researchers who work in Parkinson’s disease, she added. The steps address the following areas:
- 1. Disease burden
- 2. Advocacy and awareness
- 3. Prevention and risk reduction
- 4. Diagnosis, treatment, and care
- 5. Caregiver support
- 6. Research
Dr. Schiess noted that data on disease burden are lacking in certain areas of the world, such as low- and middle-income countries, and information “based on race and ethnicity are inconsistent. Studies are needed to establish more representative epidemiological data.”
She said that advocacy and awareness are particularly important since young people may not be aware they can also develop Parkinson’s disease, and sex and race differences can factor in to the potential for delays in diagnosis and care. “This is often due to the incorrect perception that Parkinson’s disease only affects older people,” she noted.
In addition, “a substantial need exists to identify risks for Parkinson’s disease – in particular the risks we can mitigate,” said Dr. Schiess, citing pesticide exposure as one example. “The evidence linking pesticide exposure, for example paraquat and chlorpyrifos, with the risk of developing Parkinson’s disease is substantial. And yet in many countries, these products are still being used.”
Under the heading of diagnosis, treatment, and care, Dr. Schiess noted that patients with Parkinson’s disease in “low resource settings” and low- to middle-income countries are unable to obtain “even the most basic medications” to treat Parkinson’s disease.
“Strengthening health and social systems, and building capacity to improve medical care, including rehabilitation and palliative care and medication access, are vital. Also, education and training of primary health care professionals, growing the neurological workforce, and increasing the use of digital technology such as telemedicine, are key mechanisms to improving diagnosis and sustainability of care,” she said.
For caregiver support, Dr. Schiess pointed out that the progressive nature of the disease and timing of onset are contributors to increased caregiver burden. Other contributors, as the disease advances in a patient, include the development of cognitive impairment, psychiatric manifestations, and sleep disruption.
“Solutions that could decrease the burden on caregivers include providing an accurate and timely diagnosis and training and education to caregivers, such as the WHO iSUPPORT program, as well as psychosocial, financial, and community-based support,” said Dr. Schiess.
For research, she noted that the amount of studies in the field of Parkinson’s disease has grown because of increased funding and a greater number of initiatives over the past 2 decades.
“Continuing to build on this momentum is important in order to generate new treatment options, better care, and research capacity, especially in low- and middle-income countries,” she said.
Dr. Schiess emphasized the urgency for adopting these measures as cases of Parkinson’s disease continue to rise.
“The take-away message for clinicians is that Parkinson disease is a growing global public health issue. There is a pressing need for a global public health response to address health and social requirements for people with Parkinson’s disease,” she said.
Dr. Schiess reports having received grants from the Edmond J. Safra Foundation paid to her institution during the conduct of the study.
A version of this article first appeared on Medscape.com.
Since 2000, Parkinson’s disease has increased 81% and related deaths have increased 100% globally. In addition, many patients affected by Parkinson’s disease live in low- and middle-income countries and experience large inequalities in access to neurologic care and essential medicines.
To address these issues, the Brain Health Unit at the WHO developed six “action steps” it says are urgently required to combat global disparities in Parkinson’s disease.
The need for action is great, said lead author Nicoline Schiess, MD, MPH, a neurologist and technical officer in the WHO’s Brain Health Unit in Geneva.
“In adults, disorders of the nervous system are the leading cause of disability adjusted life years, or DALYs, and the second leading cause of death globally, accounting for 9 million deaths per year,” Dr. Schiess said.
The WHO’s recommendations were published online recently as a “Special Communication” in JAMA Neurology.
Serious public health challenge
Parkinson’s disease is the fastest growing disorder in terms of death and disability, and it is estimated that it caused 329,000 deaths in 2019 – an increase of more than 100% since 2000.
“The rise in cases is thought to be multifactorial and is likely affected by factors such as aging populations and environmental exposures, such as certain pesticides. With these rapidly increasing numbers, compounded by a lack of specialists and medicines in low- and middle-income countries, Parkinson’s disease presents a serious public health challenge,” Dr. Schiess said.
The publication of the six action steps is targeted toward clinicians and researchers who work in Parkinson’s disease, she added. The steps address the following areas:
- 1. Disease burden
- 2. Advocacy and awareness
- 3. Prevention and risk reduction
- 4. Diagnosis, treatment, and care
- 5. Caregiver support
- 6. Research
Dr. Schiess noted that data on disease burden are lacking in certain areas of the world, such as low- and middle-income countries, and information “based on race and ethnicity are inconsistent. Studies are needed to establish more representative epidemiological data.”
She said that advocacy and awareness are particularly important since young people may not be aware they can also develop Parkinson’s disease, and sex and race differences can factor in to the potential for delays in diagnosis and care. “This is often due to the incorrect perception that Parkinson’s disease only affects older people,” she noted.
In addition, “a substantial need exists to identify risks for Parkinson’s disease – in particular the risks we can mitigate,” said Dr. Schiess, citing pesticide exposure as one example. “The evidence linking pesticide exposure, for example paraquat and chlorpyrifos, with the risk of developing Parkinson’s disease is substantial. And yet in many countries, these products are still being used.”
Under the heading of diagnosis, treatment, and care, Dr. Schiess noted that patients with Parkinson’s disease in “low resource settings” and low- to middle-income countries are unable to obtain “even the most basic medications” to treat Parkinson’s disease.
“Strengthening health and social systems, and building capacity to improve medical care, including rehabilitation and palliative care and medication access, are vital. Also, education and training of primary health care professionals, growing the neurological workforce, and increasing the use of digital technology such as telemedicine, are key mechanisms to improving diagnosis and sustainability of care,” she said.
For caregiver support, Dr. Schiess pointed out that the progressive nature of the disease and timing of onset are contributors to increased caregiver burden. Other contributors, as the disease advances in a patient, include the development of cognitive impairment, psychiatric manifestations, and sleep disruption.
“Solutions that could decrease the burden on caregivers include providing an accurate and timely diagnosis and training and education to caregivers, such as the WHO iSUPPORT program, as well as psychosocial, financial, and community-based support,” said Dr. Schiess.
For research, she noted that the amount of studies in the field of Parkinson’s disease has grown because of increased funding and a greater number of initiatives over the past 2 decades.
“Continuing to build on this momentum is important in order to generate new treatment options, better care, and research capacity, especially in low- and middle-income countries,” she said.
Dr. Schiess emphasized the urgency for adopting these measures as cases of Parkinson’s disease continue to rise.
“The take-away message for clinicians is that Parkinson disease is a growing global public health issue. There is a pressing need for a global public health response to address health and social requirements for people with Parkinson’s disease,” she said.
Dr. Schiess reports having received grants from the Edmond J. Safra Foundation paid to her institution during the conduct of the study.
A version of this article first appeared on Medscape.com.
Since 2000, Parkinson’s disease has increased 81% and related deaths have increased 100% globally. In addition, many patients affected by Parkinson’s disease live in low- and middle-income countries and experience large inequalities in access to neurologic care and essential medicines.
To address these issues, the Brain Health Unit at the WHO developed six “action steps” it says are urgently required to combat global disparities in Parkinson’s disease.
The need for action is great, said lead author Nicoline Schiess, MD, MPH, a neurologist and technical officer in the WHO’s Brain Health Unit in Geneva.
“In adults, disorders of the nervous system are the leading cause of disability adjusted life years, or DALYs, and the second leading cause of death globally, accounting for 9 million deaths per year,” Dr. Schiess said.
The WHO’s recommendations were published online recently as a “Special Communication” in JAMA Neurology.
Serious public health challenge
Parkinson’s disease is the fastest growing disorder in terms of death and disability, and it is estimated that it caused 329,000 deaths in 2019 – an increase of more than 100% since 2000.
“The rise in cases is thought to be multifactorial and is likely affected by factors such as aging populations and environmental exposures, such as certain pesticides. With these rapidly increasing numbers, compounded by a lack of specialists and medicines in low- and middle-income countries, Parkinson’s disease presents a serious public health challenge,” Dr. Schiess said.
The publication of the six action steps is targeted toward clinicians and researchers who work in Parkinson’s disease, she added. The steps address the following areas:
- 1. Disease burden
- 2. Advocacy and awareness
- 3. Prevention and risk reduction
- 4. Diagnosis, treatment, and care
- 5. Caregiver support
- 6. Research
Dr. Schiess noted that data on disease burden are lacking in certain areas of the world, such as low- and middle-income countries, and information “based on race and ethnicity are inconsistent. Studies are needed to establish more representative epidemiological data.”
She said that advocacy and awareness are particularly important since young people may not be aware they can also develop Parkinson’s disease, and sex and race differences can factor in to the potential for delays in diagnosis and care. “This is often due to the incorrect perception that Parkinson’s disease only affects older people,” she noted.
In addition, “a substantial need exists to identify risks for Parkinson’s disease – in particular the risks we can mitigate,” said Dr. Schiess, citing pesticide exposure as one example. “The evidence linking pesticide exposure, for example paraquat and chlorpyrifos, with the risk of developing Parkinson’s disease is substantial. And yet in many countries, these products are still being used.”
Under the heading of diagnosis, treatment, and care, Dr. Schiess noted that patients with Parkinson’s disease in “low resource settings” and low- to middle-income countries are unable to obtain “even the most basic medications” to treat Parkinson’s disease.
“Strengthening health and social systems, and building capacity to improve medical care, including rehabilitation and palliative care and medication access, are vital. Also, education and training of primary health care professionals, growing the neurological workforce, and increasing the use of digital technology such as telemedicine, are key mechanisms to improving diagnosis and sustainability of care,” she said.
For caregiver support, Dr. Schiess pointed out that the progressive nature of the disease and timing of onset are contributors to increased caregiver burden. Other contributors, as the disease advances in a patient, include the development of cognitive impairment, psychiatric manifestations, and sleep disruption.
“Solutions that could decrease the burden on caregivers include providing an accurate and timely diagnosis and training and education to caregivers, such as the WHO iSUPPORT program, as well as psychosocial, financial, and community-based support,” said Dr. Schiess.
For research, she noted that the amount of studies in the field of Parkinson’s disease has grown because of increased funding and a greater number of initiatives over the past 2 decades.
“Continuing to build on this momentum is important in order to generate new treatment options, better care, and research capacity, especially in low- and middle-income countries,” she said.
Dr. Schiess emphasized the urgency for adopting these measures as cases of Parkinson’s disease continue to rise.
“The take-away message for clinicians is that Parkinson disease is a growing global public health issue. There is a pressing need for a global public health response to address health and social requirements for people with Parkinson’s disease,” she said.
Dr. Schiess reports having received grants from the Edmond J. Safra Foundation paid to her institution during the conduct of the study.
A version of this article first appeared on Medscape.com.
COVID-19 linked to increased Alzheimer’s risk
The study of more than 6 million people aged 65 years or older found a 50%-80% increased risk for AD in the year after COVID-19; the risk was especially high for women older than 85 years.
However, the investigators were quick to point out that the observational retrospective study offers no evidence that COVID-19 causes AD. There could be a viral etiology at play, or the connection could be related to inflammation in neural tissue from the SARS-CoV-2 infection. Or it could simply be that exposure to the health care system for COVID-19 increased the odds of detection of existing undiagnosed AD cases.
Whatever the case, these findings point to a potential spike in AD cases, which is a cause for concern, study investigator Pamela Davis, MD, PhD, a professor in the Center for Community Health Integration at Case Western Reserve University, Cleveland, said in an interview.
“COVID may be giving us a legacy of ongoing medical difficulties,” Dr. Davis said. “We were already concerned about having a very large care burden and cost burden from Alzheimer’s disease. If this is another burden that’s increased by COVID, this is something we’re really going to have to prepare for.”
The findings were published online in Journal of Alzheimer’s Disease.
Increased risk
Earlier research points to a potential link between COVID-19 and increased risk for AD and Parkinson’s disease.
For the current study, researchers analyzed anonymous electronic health records of 6.2 million adults aged 65 years or older who received medical treatment between February 2020 and May 2021 and had no prior diagnosis of AD. The database includes information on almost 30% of the entire U.S. population.
Overall, there were 410,748 cases of COVID-19 during the study period.
The overall risk for new diagnosis of AD in the COVID-19 cohort was close to double that of those who did not have COVID-19 (0.68% vs. 0.35%, respectively).
After propensity-score matching, those who have had COVID-19 had a significantly higher risk for an AD diagnosis compared with those who were not infected (hazard ratio [HR], 1.69; 95% confidence interval [CI],1.53-1.72).
Risk for AD was elevated in all age groups, regardless of gender or ethnicity. Researchers did not collect data on COVID-19 severity, and the medical codes for long COVID were not published until after the study had ended.
Those with the highest risk were individuals older than 85 years (HR, 1.89; 95% CI, 1.73-2.07) and women (HR, 1.82; 95% CI, 1.69-1.97).
“We expected to see some impact, but I was surprised that it was as potent as it was,” Dr. Davis said.
Association, not causation
Heather Snyder, PhD, Alzheimer’s Association vice president of medical and scientific relations, who commented on the findings for this article, called the study interesting but emphasized caution in interpreting the results.
“Because this study only showed an association through medical records, we cannot know what the underlying mechanisms driving this association are without more research,” Dr. Snyder said. “If you have had COVID-19, it doesn’t mean you’re going to get dementia. But if you have had COVID-19 and are experiencing long-term symptoms including cognitive difficulties, talk to your doctor.”
Dr. Davis agreed, noting that this type of study offers information on association, but not causation. “I do think that this makes it imperative that we continue to follow the population for what’s going on in various neurodegenerative diseases,” Dr. Davis said.
The study was funded by the National Institute of Aging, National Institute on Alcohol Abuse and Alcoholism, the Clinical and Translational Science Collaborative of Cleveland, and the National Cancer Institute. Dr. Synder reports no relevant financial conflicts.
A version of this article first appeared on Medscape.com.
The study of more than 6 million people aged 65 years or older found a 50%-80% increased risk for AD in the year after COVID-19; the risk was especially high for women older than 85 years.
However, the investigators were quick to point out that the observational retrospective study offers no evidence that COVID-19 causes AD. There could be a viral etiology at play, or the connection could be related to inflammation in neural tissue from the SARS-CoV-2 infection. Or it could simply be that exposure to the health care system for COVID-19 increased the odds of detection of existing undiagnosed AD cases.
Whatever the case, these findings point to a potential spike in AD cases, which is a cause for concern, study investigator Pamela Davis, MD, PhD, a professor in the Center for Community Health Integration at Case Western Reserve University, Cleveland, said in an interview.
“COVID may be giving us a legacy of ongoing medical difficulties,” Dr. Davis said. “We were already concerned about having a very large care burden and cost burden from Alzheimer’s disease. If this is another burden that’s increased by COVID, this is something we’re really going to have to prepare for.”
The findings were published online in Journal of Alzheimer’s Disease.
Increased risk
Earlier research points to a potential link between COVID-19 and increased risk for AD and Parkinson’s disease.
For the current study, researchers analyzed anonymous electronic health records of 6.2 million adults aged 65 years or older who received medical treatment between February 2020 and May 2021 and had no prior diagnosis of AD. The database includes information on almost 30% of the entire U.S. population.
Overall, there were 410,748 cases of COVID-19 during the study period.
The overall risk for new diagnosis of AD in the COVID-19 cohort was close to double that of those who did not have COVID-19 (0.68% vs. 0.35%, respectively).
After propensity-score matching, those who have had COVID-19 had a significantly higher risk for an AD diagnosis compared with those who were not infected (hazard ratio [HR], 1.69; 95% confidence interval [CI],1.53-1.72).
Risk for AD was elevated in all age groups, regardless of gender or ethnicity. Researchers did not collect data on COVID-19 severity, and the medical codes for long COVID were not published until after the study had ended.
Those with the highest risk were individuals older than 85 years (HR, 1.89; 95% CI, 1.73-2.07) and women (HR, 1.82; 95% CI, 1.69-1.97).
“We expected to see some impact, but I was surprised that it was as potent as it was,” Dr. Davis said.
Association, not causation
Heather Snyder, PhD, Alzheimer’s Association vice president of medical and scientific relations, who commented on the findings for this article, called the study interesting but emphasized caution in interpreting the results.
“Because this study only showed an association through medical records, we cannot know what the underlying mechanisms driving this association are without more research,” Dr. Snyder said. “If you have had COVID-19, it doesn’t mean you’re going to get dementia. But if you have had COVID-19 and are experiencing long-term symptoms including cognitive difficulties, talk to your doctor.”
Dr. Davis agreed, noting that this type of study offers information on association, but not causation. “I do think that this makes it imperative that we continue to follow the population for what’s going on in various neurodegenerative diseases,” Dr. Davis said.
The study was funded by the National Institute of Aging, National Institute on Alcohol Abuse and Alcoholism, the Clinical and Translational Science Collaborative of Cleveland, and the National Cancer Institute. Dr. Synder reports no relevant financial conflicts.
A version of this article first appeared on Medscape.com.
The study of more than 6 million people aged 65 years or older found a 50%-80% increased risk for AD in the year after COVID-19; the risk was especially high for women older than 85 years.
However, the investigators were quick to point out that the observational retrospective study offers no evidence that COVID-19 causes AD. There could be a viral etiology at play, or the connection could be related to inflammation in neural tissue from the SARS-CoV-2 infection. Or it could simply be that exposure to the health care system for COVID-19 increased the odds of detection of existing undiagnosed AD cases.
Whatever the case, these findings point to a potential spike in AD cases, which is a cause for concern, study investigator Pamela Davis, MD, PhD, a professor in the Center for Community Health Integration at Case Western Reserve University, Cleveland, said in an interview.
“COVID may be giving us a legacy of ongoing medical difficulties,” Dr. Davis said. “We were already concerned about having a very large care burden and cost burden from Alzheimer’s disease. If this is another burden that’s increased by COVID, this is something we’re really going to have to prepare for.”
The findings were published online in Journal of Alzheimer’s Disease.
Increased risk
Earlier research points to a potential link between COVID-19 and increased risk for AD and Parkinson’s disease.
For the current study, researchers analyzed anonymous electronic health records of 6.2 million adults aged 65 years or older who received medical treatment between February 2020 and May 2021 and had no prior diagnosis of AD. The database includes information on almost 30% of the entire U.S. population.
Overall, there were 410,748 cases of COVID-19 during the study period.
The overall risk for new diagnosis of AD in the COVID-19 cohort was close to double that of those who did not have COVID-19 (0.68% vs. 0.35%, respectively).
After propensity-score matching, those who have had COVID-19 had a significantly higher risk for an AD diagnosis compared with those who were not infected (hazard ratio [HR], 1.69; 95% confidence interval [CI],1.53-1.72).
Risk for AD was elevated in all age groups, regardless of gender or ethnicity. Researchers did not collect data on COVID-19 severity, and the medical codes for long COVID were not published until after the study had ended.
Those with the highest risk were individuals older than 85 years (HR, 1.89; 95% CI, 1.73-2.07) and women (HR, 1.82; 95% CI, 1.69-1.97).
“We expected to see some impact, but I was surprised that it was as potent as it was,” Dr. Davis said.
Association, not causation
Heather Snyder, PhD, Alzheimer’s Association vice president of medical and scientific relations, who commented on the findings for this article, called the study interesting but emphasized caution in interpreting the results.
“Because this study only showed an association through medical records, we cannot know what the underlying mechanisms driving this association are without more research,” Dr. Snyder said. “If you have had COVID-19, it doesn’t mean you’re going to get dementia. But if you have had COVID-19 and are experiencing long-term symptoms including cognitive difficulties, talk to your doctor.”
Dr. Davis agreed, noting that this type of study offers information on association, but not causation. “I do think that this makes it imperative that we continue to follow the population for what’s going on in various neurodegenerative diseases,” Dr. Davis said.
The study was funded by the National Institute of Aging, National Institute on Alcohol Abuse and Alcoholism, the Clinical and Translational Science Collaborative of Cleveland, and the National Cancer Institute. Dr. Synder reports no relevant financial conflicts.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF ALZHEIMER’S DISEASE
Vitamins or cocoa: Which preserves cognition?
Unexpected results from a phase 3 trial exploring the effect of multivitamins and cognition have now been published.
Originally presented last November at the 14th Clinical Trials on Alzheimer’s Disease (CTAD) conference, this is the first large-scale, long-term randomized controlled trial to examine the effects of cocoa extract and multivitamins on global cognition. The trial’s primary focus was on cocoa extract, which earlier studies suggest may preserve cognitive function. Analyzing the effect of multivitamins was a secondary outcome.
Showing vitamins, but not cocoa, were beneficial is the exact opposite of what researchers expected. Still, the results offer an interesting new direction for future study, lead investigator Laura D. Baker, PhD, professor of gerontology and geriatric medicine at Wake Forest University, Winston-Salem, N.C., said in an interview.
“This study made us take notice of a pathway for possible cognitive protection,” Dr. Baker said. “Without this study, we would never have looked down that road.”
The full results were published online in Alzheimer’s and Dementia.
Unexpected effect
The COSMOS-Mind study is a substudy to a larger parent trial called COSMOS. It investigated the effects of cocoa extract and a standard multivitamin-mineral on cardiovascular and cancer outcomes in more than 21,000 older participants.
In COSMOS-Mind, researchers tested whether daily intake of cocoa extract vs. placebo and a multivitamin-mineral vs. placebo improved cognition in older adults.
More than 2,200 participants aged 65 and older were enrolled and followed for 3 years. They completed tests over the telephone at baseline and annually to evaluate memory and other cognitive abilities.
Results showed cocoa extract had no effect on global cognition compared with placebo (mean z-score, 0.03; P = .28). Daily multivitamin use, however, did show significant benefits on global cognition vs. placebo (mean z, 0.07, P = .007).
The beneficial effect was most pronounced in participants with a history of cardiovascular disease (no history 0.06 vs. history 0.14; P = .01).
Researchers found similar protective effects for memory and executive function.
Dr. Baker suggested one possible explanation for the positive effects of multivitamins may be the boost in micronutrients and essential minerals they provided.
“With nutrient-deficient diets plus a high prevalence of cardiovascular disease, diabetes, and other medical comorbidities that we know impact the bioavailability of these nutrients, we are possibly dealing with older adults who are at below optimum in terms of their essential micronutrients and minerals,” she said.
“Even suboptimum levels of micronutrients and essential minerals can have significant consequences for brain health,” she added.
More research needed
Intriguing as the results may be, more work is needed before the findings could affect nutritional guidance, according to Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association.
“While the Alzheimer’s Association is encouraged by these results, we are not ready to recommend widespread use of a multivitamin supplement to reduce risk of cognitive decline in older adults,” Dr. Carrillo said in a statement.
“For now, and until there is more data, people should talk with their health care providers about the benefits and risks of all dietary supplements, including multivitamins,” she added.
Dr. Baker agreed, noting that the study was not designed to measure multivitamin use as a primary outcome. In addition, nearly 90% of the participants were non-Hispanic White, which is not representative of the overall population demographics.
The investigators are now designing another, larger trial that would include a more diverse participant pool. It will be aimed specifically at learning more about how and why multivitamins seem to offer a protective effect on cognition, Dr. Baker noted.
The study was funded by the National Institute on Aging of the National Institutes of Health. Dr. Baker and Dr. Carrillo report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unexpected results from a phase 3 trial exploring the effect of multivitamins and cognition have now been published.
Originally presented last November at the 14th Clinical Trials on Alzheimer’s Disease (CTAD) conference, this is the first large-scale, long-term randomized controlled trial to examine the effects of cocoa extract and multivitamins on global cognition. The trial’s primary focus was on cocoa extract, which earlier studies suggest may preserve cognitive function. Analyzing the effect of multivitamins was a secondary outcome.
Showing vitamins, but not cocoa, were beneficial is the exact opposite of what researchers expected. Still, the results offer an interesting new direction for future study, lead investigator Laura D. Baker, PhD, professor of gerontology and geriatric medicine at Wake Forest University, Winston-Salem, N.C., said in an interview.
“This study made us take notice of a pathway for possible cognitive protection,” Dr. Baker said. “Without this study, we would never have looked down that road.”
The full results were published online in Alzheimer’s and Dementia.
Unexpected effect
The COSMOS-Mind study is a substudy to a larger parent trial called COSMOS. It investigated the effects of cocoa extract and a standard multivitamin-mineral on cardiovascular and cancer outcomes in more than 21,000 older participants.
In COSMOS-Mind, researchers tested whether daily intake of cocoa extract vs. placebo and a multivitamin-mineral vs. placebo improved cognition in older adults.
More than 2,200 participants aged 65 and older were enrolled and followed for 3 years. They completed tests over the telephone at baseline and annually to evaluate memory and other cognitive abilities.
Results showed cocoa extract had no effect on global cognition compared with placebo (mean z-score, 0.03; P = .28). Daily multivitamin use, however, did show significant benefits on global cognition vs. placebo (mean z, 0.07, P = .007).
The beneficial effect was most pronounced in participants with a history of cardiovascular disease (no history 0.06 vs. history 0.14; P = .01).
Researchers found similar protective effects for memory and executive function.
Dr. Baker suggested one possible explanation for the positive effects of multivitamins may be the boost in micronutrients and essential minerals they provided.
“With nutrient-deficient diets plus a high prevalence of cardiovascular disease, diabetes, and other medical comorbidities that we know impact the bioavailability of these nutrients, we are possibly dealing with older adults who are at below optimum in terms of their essential micronutrients and minerals,” she said.
“Even suboptimum levels of micronutrients and essential minerals can have significant consequences for brain health,” she added.
More research needed
Intriguing as the results may be, more work is needed before the findings could affect nutritional guidance, according to Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association.
“While the Alzheimer’s Association is encouraged by these results, we are not ready to recommend widespread use of a multivitamin supplement to reduce risk of cognitive decline in older adults,” Dr. Carrillo said in a statement.
“For now, and until there is more data, people should talk with their health care providers about the benefits and risks of all dietary supplements, including multivitamins,” she added.
Dr. Baker agreed, noting that the study was not designed to measure multivitamin use as a primary outcome. In addition, nearly 90% of the participants were non-Hispanic White, which is not representative of the overall population demographics.
The investigators are now designing another, larger trial that would include a more diverse participant pool. It will be aimed specifically at learning more about how and why multivitamins seem to offer a protective effect on cognition, Dr. Baker noted.
The study was funded by the National Institute on Aging of the National Institutes of Health. Dr. Baker and Dr. Carrillo report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unexpected results from a phase 3 trial exploring the effect of multivitamins and cognition have now been published.
Originally presented last November at the 14th Clinical Trials on Alzheimer’s Disease (CTAD) conference, this is the first large-scale, long-term randomized controlled trial to examine the effects of cocoa extract and multivitamins on global cognition. The trial’s primary focus was on cocoa extract, which earlier studies suggest may preserve cognitive function. Analyzing the effect of multivitamins was a secondary outcome.
Showing vitamins, but not cocoa, were beneficial is the exact opposite of what researchers expected. Still, the results offer an interesting new direction for future study, lead investigator Laura D. Baker, PhD, professor of gerontology and geriatric medicine at Wake Forest University, Winston-Salem, N.C., said in an interview.
“This study made us take notice of a pathway for possible cognitive protection,” Dr. Baker said. “Without this study, we would never have looked down that road.”
The full results were published online in Alzheimer’s and Dementia.
Unexpected effect
The COSMOS-Mind study is a substudy to a larger parent trial called COSMOS. It investigated the effects of cocoa extract and a standard multivitamin-mineral on cardiovascular and cancer outcomes in more than 21,000 older participants.
In COSMOS-Mind, researchers tested whether daily intake of cocoa extract vs. placebo and a multivitamin-mineral vs. placebo improved cognition in older adults.
More than 2,200 participants aged 65 and older were enrolled and followed for 3 years. They completed tests over the telephone at baseline and annually to evaluate memory and other cognitive abilities.
Results showed cocoa extract had no effect on global cognition compared with placebo (mean z-score, 0.03; P = .28). Daily multivitamin use, however, did show significant benefits on global cognition vs. placebo (mean z, 0.07, P = .007).
The beneficial effect was most pronounced in participants with a history of cardiovascular disease (no history 0.06 vs. history 0.14; P = .01).
Researchers found similar protective effects for memory and executive function.
Dr. Baker suggested one possible explanation for the positive effects of multivitamins may be the boost in micronutrients and essential minerals they provided.
“With nutrient-deficient diets plus a high prevalence of cardiovascular disease, diabetes, and other medical comorbidities that we know impact the bioavailability of these nutrients, we are possibly dealing with older adults who are at below optimum in terms of their essential micronutrients and minerals,” she said.
“Even suboptimum levels of micronutrients and essential minerals can have significant consequences for brain health,” she added.
More research needed
Intriguing as the results may be, more work is needed before the findings could affect nutritional guidance, according to Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association.
“While the Alzheimer’s Association is encouraged by these results, we are not ready to recommend widespread use of a multivitamin supplement to reduce risk of cognitive decline in older adults,” Dr. Carrillo said in a statement.
“For now, and until there is more data, people should talk with their health care providers about the benefits and risks of all dietary supplements, including multivitamins,” she added.
Dr. Baker agreed, noting that the study was not designed to measure multivitamin use as a primary outcome. In addition, nearly 90% of the participants were non-Hispanic White, which is not representative of the overall population demographics.
The investigators are now designing another, larger trial that would include a more diverse participant pool. It will be aimed specifically at learning more about how and why multivitamins seem to offer a protective effect on cognition, Dr. Baker noted.
The study was funded by the National Institute on Aging of the National Institutes of Health. Dr. Baker and Dr. Carrillo report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ALZHEIMER’S AND DEMENTIA
One in three MS patients reports chronic itch
, according to investigators.
Itch is historically underrecognized as a symptom of MS, but physicians should know that it is common and may negatively impact quality of life, reported lead author Giuseppe Ingrasci, MD, a dermatology research fellow at the University of Miami, Miller School of Medicine, and colleagues.

While previous publications suggest that pruritus occurs in just 2%-6% of patients with MS, principal author Gil Yosipovitch, MD, professor, Stiefel Chair of Medical Dermatology, and director of the Miami Itch Center in the Dr. Phillip Frost department of dermatology and cutaneous surgery at the University of Miami Miller School of Medicine, encountered itch in enough patients with MS that he presented his observations to a group of neurologists.
Most of them dismissed him, he recalled in an interview: “The neurologists said, ‘Very interesting, but we don’t really see it.’ ”
One of those neurologists, however, decided to take a closer look.
Andrew Brown, MD, assistant professor of clinical neurology and chief of the general neurology division at the University of Miami, Miller School of Medicine, began asking his patients with MS if they were experiencing itch and soon found that it was “a very common problem,” according to Dr. Yosipovitch.
Dr. Yosipovitch, who was the first to report pruritus in patients with psoriasis, launched the present investigation with Dr. Brown to determine if itch is also a blind spot in the world of MS. Their results, and their uphill battle to publication, suggest that it very well could be.
After being rejected from six neurology journals, with one editor suggesting that itch is “not relevant at all to neurology,” their findings were published in the Journal of the European Academy of Dermatology & Venereology.
A common problem that may indicate more severe disease
At the Multiple Sclerosis Center of Excellence in Miami, 27 out of 79 outpatients with MS (35%) reported pruritus, with an average severity of 5.42 out of 10. Among those with itch, the extremities were affected in about half of the patients, while the face, scalp, and trunk were affected in about one-third of the patients. Many described paroxysmal itch that was aggravated by heat, and about half experienced itch on a weekly basis.
Further investigation showed that itch was associated with more severe MS. Compared with patients not experiencing itch, those with itch were significantly more likely to report fatigue (77% vs. 44%), anxiety or depression (48% vs. 16%), and cognitive impairment (62% vs. 26%).
MRI findings backed up these clinical results. Compared with patients not experiencing itch, patients with itch had significantly more T2 hyperintensities in the posterior cervical cord (74.1% vs. 46.0%) and anterior pons/ventromedial medulla (62% vs. 26%). These hyperintensities in the medulla were also associated with an 11-fold increased rate of itch on the face or scalp (odds ratio, 11.3; 95% confidence interval, 1.6-78.6, P = 0.025).
“Health care providers should be aware of episodes of localized, neuropathic itch in MS patients, as they appear to be more prevalent than previously thought and may impair these patients’ quality of life,” the investigators concluded.
Challenges with symptom characterization, management
“This is an important study for both patients and clinicians,” said Justin Abbatemarco, MD, of Cleveland Clinic’s Mellen Center for Multiple Sclerosis, in a written comment. “As the authors mention, many of our patients experience transient symptoms, including many different types of sensory disturbance (that is, pins & needles, burning, electrical shocks, and itching). These symptoms can be really distressing for patients and their caregivers.”
While Dr. Abbatemarco has encountered severe itching in “several patients” with MS, he maintained that it is “relatively uncommon” and noted that MS symptomatology is an inherently cloudy subject.

“I think it is difficult to be definite in any opinion on this topic,” Dr. Abbatemarco said. “How patients experience these symptoms is very subjective and can be difficult to describe/characterize.”
Dr. Abbatemarco emphasized that transient symptoms “do not usually represent MS relapse/flare or new inflammatory disease activity. Instead, we believe these symptoms are related to old areas of injury or demyelination.”
Symptom management can be challenging, he added. He recommended setting realistic expectations, and in the case of pruritus, asking dermatologists to rule out other causes of itch, and to offer “unique treatment approaches.”
Cool the itch?
Noting how heat appears to aggravate itch in patients with MS, Dr. Yosipovitch suggested that one of those unique – and simple – treatment approaches may be cooling itchy areas. Alternatively, clinicians may consider oral agents, like gabapentin to dampen neural transmission, or compounded formulations applied to the skin to reduce neural sensitivity, such as topical ketamine. Finally, Dr. Yosipovitch speculated that newer antibody agents for MS could potentially reduce itch.
All these treatment suggestions are purely hypothetical, he said, and require further investigation before they can be recommended with confidence.
The investigators disclosed relationships with Galderma, Pfizer, Novartis, and others. Dr. Abbatemarco disclosed no conflicts of interest.
Correction, 9/19/22: An earlier version of this article misidentified the photo of Dr. Justin Abbatemarco.
, according to investigators.
Itch is historically underrecognized as a symptom of MS, but physicians should know that it is common and may negatively impact quality of life, reported lead author Giuseppe Ingrasci, MD, a dermatology research fellow at the University of Miami, Miller School of Medicine, and colleagues.
While previous publications suggest that pruritus occurs in just 2%-6% of patients with MS, principal author Gil Yosipovitch, MD, professor, Stiefel Chair of Medical Dermatology, and director of the Miami Itch Center in the Dr. Phillip Frost department of dermatology and cutaneous surgery at the University of Miami Miller School of Medicine, encountered itch in enough patients with MS that he presented his observations to a group of neurologists.
Most of them dismissed him, he recalled in an interview: “The neurologists said, ‘Very interesting, but we don’t really see it.’ ”
One of those neurologists, however, decided to take a closer look.
Andrew Brown, MD, assistant professor of clinical neurology and chief of the general neurology division at the University of Miami, Miller School of Medicine, began asking his patients with MS if they were experiencing itch and soon found that it was “a very common problem,” according to Dr. Yosipovitch.
Dr. Yosipovitch, who was the first to report pruritus in patients with psoriasis, launched the present investigation with Dr. Brown to determine if itch is also a blind spot in the world of MS. Their results, and their uphill battle to publication, suggest that it very well could be.
After being rejected from six neurology journals, with one editor suggesting that itch is “not relevant at all to neurology,” their findings were published in the Journal of the European Academy of Dermatology & Venereology.
A common problem that may indicate more severe disease
At the Multiple Sclerosis Center of Excellence in Miami, 27 out of 79 outpatients with MS (35%) reported pruritus, with an average severity of 5.42 out of 10. Among those with itch, the extremities were affected in about half of the patients, while the face, scalp, and trunk were affected in about one-third of the patients. Many described paroxysmal itch that was aggravated by heat, and about half experienced itch on a weekly basis.
Further investigation showed that itch was associated with more severe MS. Compared with patients not experiencing itch, those with itch were significantly more likely to report fatigue (77% vs. 44%), anxiety or depression (48% vs. 16%), and cognitive impairment (62% vs. 26%).
MRI findings backed up these clinical results. Compared with patients not experiencing itch, patients with itch had significantly more T2 hyperintensities in the posterior cervical cord (74.1% vs. 46.0%) and anterior pons/ventromedial medulla (62% vs. 26%). These hyperintensities in the medulla were also associated with an 11-fold increased rate of itch on the face or scalp (odds ratio, 11.3; 95% confidence interval, 1.6-78.6, P = 0.025).
“Health care providers should be aware of episodes of localized, neuropathic itch in MS patients, as they appear to be more prevalent than previously thought and may impair these patients’ quality of life,” the investigators concluded.
Challenges with symptom characterization, management
“This is an important study for both patients and clinicians,” said Justin Abbatemarco, MD, of Cleveland Clinic’s Mellen Center for Multiple Sclerosis, in a written comment. “As the authors mention, many of our patients experience transient symptoms, including many different types of sensory disturbance (that is, pins & needles, burning, electrical shocks, and itching). These symptoms can be really distressing for patients and their caregivers.”
While Dr. Abbatemarco has encountered severe itching in “several patients” with MS, he maintained that it is “relatively uncommon” and noted that MS symptomatology is an inherently cloudy subject.
“I think it is difficult to be definite in any opinion on this topic,” Dr. Abbatemarco said. “How patients experience these symptoms is very subjective and can be difficult to describe/characterize.”
Dr. Abbatemarco emphasized that transient symptoms “do not usually represent MS relapse/flare or new inflammatory disease activity. Instead, we believe these symptoms are related to old areas of injury or demyelination.”
Symptom management can be challenging, he added. He recommended setting realistic expectations, and in the case of pruritus, asking dermatologists to rule out other causes of itch, and to offer “unique treatment approaches.”
Cool the itch?
Noting how heat appears to aggravate itch in patients with MS, Dr. Yosipovitch suggested that one of those unique – and simple – treatment approaches may be cooling itchy areas. Alternatively, clinicians may consider oral agents, like gabapentin to dampen neural transmission, or compounded formulations applied to the skin to reduce neural sensitivity, such as topical ketamine. Finally, Dr. Yosipovitch speculated that newer antibody agents for MS could potentially reduce itch.
All these treatment suggestions are purely hypothetical, he said, and require further investigation before they can be recommended with confidence.
The investigators disclosed relationships with Galderma, Pfizer, Novartis, and others. Dr. Abbatemarco disclosed no conflicts of interest.
Correction, 9/19/22: An earlier version of this article misidentified the photo of Dr. Justin Abbatemarco.
, according to investigators.
Itch is historically underrecognized as a symptom of MS, but physicians should know that it is common and may negatively impact quality of life, reported lead author Giuseppe Ingrasci, MD, a dermatology research fellow at the University of Miami, Miller School of Medicine, and colleagues.
While previous publications suggest that pruritus occurs in just 2%-6% of patients with MS, principal author Gil Yosipovitch, MD, professor, Stiefel Chair of Medical Dermatology, and director of the Miami Itch Center in the Dr. Phillip Frost department of dermatology and cutaneous surgery at the University of Miami Miller School of Medicine, encountered itch in enough patients with MS that he presented his observations to a group of neurologists.
Most of them dismissed him, he recalled in an interview: “The neurologists said, ‘Very interesting, but we don’t really see it.’ ”
One of those neurologists, however, decided to take a closer look.
Andrew Brown, MD, assistant professor of clinical neurology and chief of the general neurology division at the University of Miami, Miller School of Medicine, began asking his patients with MS if they were experiencing itch and soon found that it was “a very common problem,” according to Dr. Yosipovitch.
Dr. Yosipovitch, who was the first to report pruritus in patients with psoriasis, launched the present investigation with Dr. Brown to determine if itch is also a blind spot in the world of MS. Their results, and their uphill battle to publication, suggest that it very well could be.
After being rejected from six neurology journals, with one editor suggesting that itch is “not relevant at all to neurology,” their findings were published in the Journal of the European Academy of Dermatology & Venereology.
A common problem that may indicate more severe disease
At the Multiple Sclerosis Center of Excellence in Miami, 27 out of 79 outpatients with MS (35%) reported pruritus, with an average severity of 5.42 out of 10. Among those with itch, the extremities were affected in about half of the patients, while the face, scalp, and trunk were affected in about one-third of the patients. Many described paroxysmal itch that was aggravated by heat, and about half experienced itch on a weekly basis.
Further investigation showed that itch was associated with more severe MS. Compared with patients not experiencing itch, those with itch were significantly more likely to report fatigue (77% vs. 44%), anxiety or depression (48% vs. 16%), and cognitive impairment (62% vs. 26%).
MRI findings backed up these clinical results. Compared with patients not experiencing itch, patients with itch had significantly more T2 hyperintensities in the posterior cervical cord (74.1% vs. 46.0%) and anterior pons/ventromedial medulla (62% vs. 26%). These hyperintensities in the medulla were also associated with an 11-fold increased rate of itch on the face or scalp (odds ratio, 11.3; 95% confidence interval, 1.6-78.6, P = 0.025).
“Health care providers should be aware of episodes of localized, neuropathic itch in MS patients, as they appear to be more prevalent than previously thought and may impair these patients’ quality of life,” the investigators concluded.
Challenges with symptom characterization, management
“This is an important study for both patients and clinicians,” said Justin Abbatemarco, MD, of Cleveland Clinic’s Mellen Center for Multiple Sclerosis, in a written comment. “As the authors mention, many of our patients experience transient symptoms, including many different types of sensory disturbance (that is, pins & needles, burning, electrical shocks, and itching). These symptoms can be really distressing for patients and their caregivers.”
While Dr. Abbatemarco has encountered severe itching in “several patients” with MS, he maintained that it is “relatively uncommon” and noted that MS symptomatology is an inherently cloudy subject.
“I think it is difficult to be definite in any opinion on this topic,” Dr. Abbatemarco said. “How patients experience these symptoms is very subjective and can be difficult to describe/characterize.”
Dr. Abbatemarco emphasized that transient symptoms “do not usually represent MS relapse/flare or new inflammatory disease activity. Instead, we believe these symptoms are related to old areas of injury or demyelination.”
Symptom management can be challenging, he added. He recommended setting realistic expectations, and in the case of pruritus, asking dermatologists to rule out other causes of itch, and to offer “unique treatment approaches.”
Cool the itch?
Noting how heat appears to aggravate itch in patients with MS, Dr. Yosipovitch suggested that one of those unique – and simple – treatment approaches may be cooling itchy areas. Alternatively, clinicians may consider oral agents, like gabapentin to dampen neural transmission, or compounded formulations applied to the skin to reduce neural sensitivity, such as topical ketamine. Finally, Dr. Yosipovitch speculated that newer antibody agents for MS could potentially reduce itch.
All these treatment suggestions are purely hypothetical, he said, and require further investigation before they can be recommended with confidence.
The investigators disclosed relationships with Galderma, Pfizer, Novartis, and others. Dr. Abbatemarco disclosed no conflicts of interest.
Correction, 9/19/22: An earlier version of this article misidentified the photo of Dr. Justin Abbatemarco.
FROM THE JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY & VENEREOLOGY
TBI is an unrecognized risk factor for cardiovascular disease
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
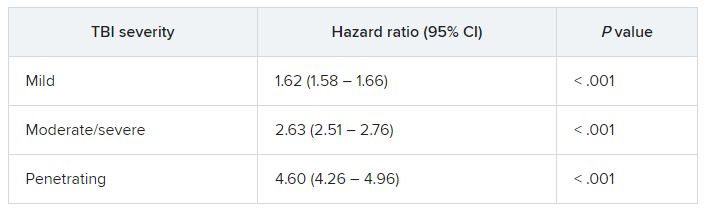
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Blood type linked to higher risk for early onset stroke
Conversely, results from a meta-analysis of nearly 17,000 cases of ischemic stroke in adults younger than 60 years showed that having type O blood reduced the risk for EOS by 12%.
In addition, the associations with risk were significantly stronger in EOS than in those with late-onset stroke (LOS), pointing to a stronger role for prothrombotic factors in younger patients, the researchers noted.
“What this is telling us is that maybe what makes you susceptible to stroke as a young adult is the blood type, which is really giving you a much higher risk of clotting and stroke compared to later onset,” coinvestigator Braxton Mitchell, PhD, professor of medicine and epidemiology and public health at the University of Maryland, Baltimore, said in an interview.
The findings were published online in Neurology.
Strong association
The genome-wide association study (GWAS) was done as part of the Genetics of Early Onset Ischemic Stroke Consortium, a collaboration of 48 different studies across North America, Europe, Japan, Pakistan, and Australia. It assessed early onset ischemic stroke in patients aged 18-59 years.
Researchers included data from 16,927 patients with stroke. Of these, 5,825 had a stroke before age 60, defined as early onset. GWAS results were also examined for nearly 600,000 individuals without stroke.
Results showed two genetic variants tied to blood types A and O emerged as highly associated with risk for early stroke.
Researchers found that the protective effects of type O were significantly stronger with EOS vs. LOS (odds ratio [OR], 0.88 vs. 0.96, respectively; P = .001). Likewise, the association between type A and increased EOS risk was significantly stronger than that found in LOS (OR, 1.16 vs. 1.05; P = .005).
Using polygenic risk scores, the investigators also found that the greater genetic risk for venous thromboembolism, another prothrombotic condition, was more strongly associated with EOS compared with LOS (P = .008).
Previous studies have shown a link between stroke risk and variants of the ABO gene, which determines blood type. The new analysis suggests that type A and O gene variants represent nearly all of those genetically linked with early stroke, the researchers noted.
While the findings point to blood type as a risk factor for stroke in younger people, Dr. Mitchell cautions that “at the moment, blood group does not have implications for preventive care.”
“The risk of stroke due to blood type is smaller than other risk factors that we know about, like smoking and hypertension,” he said. “I would be much more worried about these other risk factors, especially because those may be modifiable.”
He noted the next step in the study is to assess how blood type interacts with other known risk factors to raise stroke risk.
“There may be a subset of people where, if you have blood type A and you have some of these other risk factors, it’s possible that you may be at particularly high risk,” Dr. Mitchell said.
More research needed on younger patients
In an accompanying editorial, Jennifer Juhl Majersik, MD, associate professor of neurology at the University of Utah, Salt Lake City, and Paul Lacaze, PhD, associate professor and head of the public health genomics program at Monash University, Australia, noted that the study fills a gap in stroke research, which often focuses mostly on older individuals.
“In approximately 40% of people with EOS, the stroke is cryptogenic, and there is scant data from clinical trials to guide the selection of preventative strategies in this population, as people with EOS are often excluded from trials,” Dr. Majersik and Dr. Lacaze wrote.
“This work has deepened our understanding of EOS pathophysiology,” they added.
The editorialists noted that future research can build on the results from this analysis, “with the goal of a more precise understanding of stroke pathophysiology, leading to targeted preventative treatments for EOS and a reduction in disability in patients’ most productive years.”
Dr. Mitchell echoed the call for greater inclusion of young patients with stroke in clinical trials.
“As we’re learning, stroke in older folks isn’t the same as stroke in younger people,” he said. “There are many shared risk factors but there are also some that are different ... so there really is a need to include younger people.”
A version of this article first appeared on Medscape.com.
Conversely, results from a meta-analysis of nearly 17,000 cases of ischemic stroke in adults younger than 60 years showed that having type O blood reduced the risk for EOS by 12%.
In addition, the associations with risk were significantly stronger in EOS than in those with late-onset stroke (LOS), pointing to a stronger role for prothrombotic factors in younger patients, the researchers noted.
“What this is telling us is that maybe what makes you susceptible to stroke as a young adult is the blood type, which is really giving you a much higher risk of clotting and stroke compared to later onset,” coinvestigator Braxton Mitchell, PhD, professor of medicine and epidemiology and public health at the University of Maryland, Baltimore, said in an interview.
The findings were published online in Neurology.
Strong association
The genome-wide association study (GWAS) was done as part of the Genetics of Early Onset Ischemic Stroke Consortium, a collaboration of 48 different studies across North America, Europe, Japan, Pakistan, and Australia. It assessed early onset ischemic stroke in patients aged 18-59 years.
Researchers included data from 16,927 patients with stroke. Of these, 5,825 had a stroke before age 60, defined as early onset. GWAS results were also examined for nearly 600,000 individuals without stroke.
Results showed two genetic variants tied to blood types A and O emerged as highly associated with risk for early stroke.
Researchers found that the protective effects of type O were significantly stronger with EOS vs. LOS (odds ratio [OR], 0.88 vs. 0.96, respectively; P = .001). Likewise, the association between type A and increased EOS risk was significantly stronger than that found in LOS (OR, 1.16 vs. 1.05; P = .005).
Using polygenic risk scores, the investigators also found that the greater genetic risk for venous thromboembolism, another prothrombotic condition, was more strongly associated with EOS compared with LOS (P = .008).
Previous studies have shown a link between stroke risk and variants of the ABO gene, which determines blood type. The new analysis suggests that type A and O gene variants represent nearly all of those genetically linked with early stroke, the researchers noted.
While the findings point to blood type as a risk factor for stroke in younger people, Dr. Mitchell cautions that “at the moment, blood group does not have implications for preventive care.”
“The risk of stroke due to blood type is smaller than other risk factors that we know about, like smoking and hypertension,” he said. “I would be much more worried about these other risk factors, especially because those may be modifiable.”
He noted the next step in the study is to assess how blood type interacts with other known risk factors to raise stroke risk.
“There may be a subset of people where, if you have blood type A and you have some of these other risk factors, it’s possible that you may be at particularly high risk,” Dr. Mitchell said.
More research needed on younger patients
In an accompanying editorial, Jennifer Juhl Majersik, MD, associate professor of neurology at the University of Utah, Salt Lake City, and Paul Lacaze, PhD, associate professor and head of the public health genomics program at Monash University, Australia, noted that the study fills a gap in stroke research, which often focuses mostly on older individuals.
“In approximately 40% of people with EOS, the stroke is cryptogenic, and there is scant data from clinical trials to guide the selection of preventative strategies in this population, as people with EOS are often excluded from trials,” Dr. Majersik and Dr. Lacaze wrote.
“This work has deepened our understanding of EOS pathophysiology,” they added.
The editorialists noted that future research can build on the results from this analysis, “with the goal of a more precise understanding of stroke pathophysiology, leading to targeted preventative treatments for EOS and a reduction in disability in patients’ most productive years.”
Dr. Mitchell echoed the call for greater inclusion of young patients with stroke in clinical trials.
“As we’re learning, stroke in older folks isn’t the same as stroke in younger people,” he said. “There are many shared risk factors but there are also some that are different ... so there really is a need to include younger people.”
A version of this article first appeared on Medscape.com.
Conversely, results from a meta-analysis of nearly 17,000 cases of ischemic stroke in adults younger than 60 years showed that having type O blood reduced the risk for EOS by 12%.
In addition, the associations with risk were significantly stronger in EOS than in those with late-onset stroke (LOS), pointing to a stronger role for prothrombotic factors in younger patients, the researchers noted.
“What this is telling us is that maybe what makes you susceptible to stroke as a young adult is the blood type, which is really giving you a much higher risk of clotting and stroke compared to later onset,” coinvestigator Braxton Mitchell, PhD, professor of medicine and epidemiology and public health at the University of Maryland, Baltimore, said in an interview.
The findings were published online in Neurology.
Strong association
The genome-wide association study (GWAS) was done as part of the Genetics of Early Onset Ischemic Stroke Consortium, a collaboration of 48 different studies across North America, Europe, Japan, Pakistan, and Australia. It assessed early onset ischemic stroke in patients aged 18-59 years.
Researchers included data from 16,927 patients with stroke. Of these, 5,825 had a stroke before age 60, defined as early onset. GWAS results were also examined for nearly 600,000 individuals without stroke.
Results showed two genetic variants tied to blood types A and O emerged as highly associated with risk for early stroke.
Researchers found that the protective effects of type O were significantly stronger with EOS vs. LOS (odds ratio [OR], 0.88 vs. 0.96, respectively; P = .001). Likewise, the association between type A and increased EOS risk was significantly stronger than that found in LOS (OR, 1.16 vs. 1.05; P = .005).
Using polygenic risk scores, the investigators also found that the greater genetic risk for venous thromboembolism, another prothrombotic condition, was more strongly associated with EOS compared with LOS (P = .008).
Previous studies have shown a link between stroke risk and variants of the ABO gene, which determines blood type. The new analysis suggests that type A and O gene variants represent nearly all of those genetically linked with early stroke, the researchers noted.
While the findings point to blood type as a risk factor for stroke in younger people, Dr. Mitchell cautions that “at the moment, blood group does not have implications for preventive care.”
“The risk of stroke due to blood type is smaller than other risk factors that we know about, like smoking and hypertension,” he said. “I would be much more worried about these other risk factors, especially because those may be modifiable.”
He noted the next step in the study is to assess how blood type interacts with other known risk factors to raise stroke risk.
“There may be a subset of people where, if you have blood type A and you have some of these other risk factors, it’s possible that you may be at particularly high risk,” Dr. Mitchell said.
More research needed on younger patients
In an accompanying editorial, Jennifer Juhl Majersik, MD, associate professor of neurology at the University of Utah, Salt Lake City, and Paul Lacaze, PhD, associate professor and head of the public health genomics program at Monash University, Australia, noted that the study fills a gap in stroke research, which often focuses mostly on older individuals.
“In approximately 40% of people with EOS, the stroke is cryptogenic, and there is scant data from clinical trials to guide the selection of preventative strategies in this population, as people with EOS are often excluded from trials,” Dr. Majersik and Dr. Lacaze wrote.
“This work has deepened our understanding of EOS pathophysiology,” they added.
The editorialists noted that future research can build on the results from this analysis, “with the goal of a more precise understanding of stroke pathophysiology, leading to targeted preventative treatments for EOS and a reduction in disability in patients’ most productive years.”
Dr. Mitchell echoed the call for greater inclusion of young patients with stroke in clinical trials.
“As we’re learning, stroke in older folks isn’t the same as stroke in younger people,” he said. “There are many shared risk factors but there are also some that are different ... so there really is a need to include younger people.”
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Ublituximab bests teriflunomide in head-to-head clinical trials
Study shows ublituximab’s superiority over teriflunomide in suppressing MS relapses and MRI lesions.
Patients with relapsing multiple sclerosis (MS) treated with intravenous ublituximab had fewer relapses and brain lesions compared with those treated with oral teriflunomide, although both therapies resulted in similar rates of worsening disability, according to results of the two identical phase 3 ULTIMATE I and II trials.
“In these two 96-week trials involving participants with MS, annualized relapse rates were lower with intravenous ublituximab than with oral teriflunomide. Ublituximab was associated with infusion-related reactions. Larger and longer trials are required to determine the efficacy and safety of ublituximab in patients with relapsing MS, including comparison with other disease-modifying treatments such as existing anti-CD20 monoclonal antibodies,” noted lead author Lawrence Steinman, MD, professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) University, and colleagues.

The results, published in the New England Journal of Medicine, pave the way for ublituximab’s approval as the third high-efficacy anti-CD20 monoclonal antibody to treat relapsing forms of MS, predicted Patricia Coyle, MD, director of the MS Comprehensive Care Center, and professor of neurology, at Stony Brook (N.Y.) Neurosciences Institute, who was not involved in the research. Ublituximab will “widen the anti-CD20 monoclonal choices for MS, and should directly compete with ocrelizumab and ofatumumab,” she said.
Two trials
The double-blind, double-dummy ULTIMATE I and II trials enrolled 549 and 545 participants respectively, with a median follow-up of 95 weeks. Subjects, aged between 18 and 55 years, were randomized to receive either oral placebo and intravenous ublituximab (150 mg on day 1, followed by 450 mg on day 15 and at weeks 24, 48, and 72), or oral teriflunomide (14 mg once daily) and intravenous placebo. The primary endpoint was the annualized relapse rate, defined as the number of confirmed MS relapses per participant-year, with a range of secondary end points including number of lesions on magnetic resonance imaging (MRI) by 96 weeks, and worsening of disability confirmed at 12 weeks.
Prevention and management of infusion-related reactions was with oral antihistamine and dexamethasone, administered 30 to 60 minutes before each intravenous dose of ublituximab or placebo, as well as reductions in infusion flow rates and discretionary acetaminophen.
Results for the primary endpoint in ULTIMATE I showed the adjusted annualized relapse rate over a period of 96 weeks was 0.08 in the ublituximab group and 0.19 in the teriflunomide group (rate ratio, 0.41; P < .001). Corresponding rates for ULTIMATE II were 0.09 and 0.18 (rate ratio, 0.51; P = .002).
The mean number of lesions in both ublituximab arms of the trials was 0.02 and 0.01 compared with 0.49 and 0.25 in the teriflunomide arms (rate ratios 0.03 and 0.04 respectively; P < .001 for both).
Similar disability worsening in both groups
A pooled analysis of the two trials showed worsening disability in 5.2% of the ublituximab group, and 5.9% of the teriflunomide group (hazard ratio, 0.84; P = 0.51). “In both trials, teriflunomide was associated with a numerically lower rate of worsening of disability than that reported in previous studies with this drug, but no conclusions can be drawn from these comparisons,” noted the authors.
Infusion-related reactions occurred in 47.7% of the participants in the ublituximab group, consisting mainly of mild to moderate pyrexia, headache, chills, and influenza-like illness. “The reactions may have been related to cytokine release from immune cells (B and NK cells) on interaction of the Fc antibody domain with Fc gamma receptors on effector cells,” they suggested.
Although no opportunistic infections occurred, a higher frequency of infections, including serious infections, was observed with ublituximab (5.0%) than with teriflunomide (2.9%).
While the ULTIMATE trials showed no difference between ublituximab and teriflunomide in confirmed worsening of disability, only a small percentage of participants in either arm showed deterioration, Dr. Coyle remarked. “In a relatively short trial (96 weeks), in a relapsing population on active treatment, this result was not surprising … If the study was bigger, or longer it would increase the chances of seeing a progressive slow worsening component to affect the EDSS [Expanded Disability Status Scale],” she added.
Equivalent efficacy
Ultimately, “it appears likely” that ublituximab is “equivalent in efficacy” to the earlier anti-CD20 agents ocrelizumab and ofatumumab, Dr. Coyle said. While all three agents target B-cells, “ublituximab targets a novel CD20 binding site, and is bioengineered to have a particularly potent antibody dependent cell cytotoxicity lysis mechanism,” she added. “It has been touted to ultimately allow a short infusion of 1 hour.”
Although the serious infection rate is slightly higher with ublituximab (5.0% vs. 2.5% for ofatumumab, and 1.3% for ocrelizumab), “it is still low,” and infusion-related reactions are also higher with ublituximab, she added (47.7% vs. 20.2% and 34.3%, respectively). She suggested factors that might influence which treatment is chosen for a given patient might include cost, convenience, whether it is more or less likely to cause low IgG, interference with vaccination, or influence on cancer or COVID risk.
The trials were supported by TG Therapeutics.
Dr. Coyle has received consulting fees from Accordant, Biogen, Bristol Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio and grant funding from Actelion, Alkermes, Bristol Myers Squibb, CorEvitas LLD, Genentech/Roche, Sanofi Genzyme, MedDay, NINDS, and Novartis.
Study shows ublituximab’s superiority over teriflunomide in suppressing MS relapses and MRI lesions.
Study shows ublituximab’s superiority over teriflunomide in suppressing MS relapses and MRI lesions.
Patients with relapsing multiple sclerosis (MS) treated with intravenous ublituximab had fewer relapses and brain lesions compared with those treated with oral teriflunomide, although both therapies resulted in similar rates of worsening disability, according to results of the two identical phase 3 ULTIMATE I and II trials.
“In these two 96-week trials involving participants with MS, annualized relapse rates were lower with intravenous ublituximab than with oral teriflunomide. Ublituximab was associated with infusion-related reactions. Larger and longer trials are required to determine the efficacy and safety of ublituximab in patients with relapsing MS, including comparison with other disease-modifying treatments such as existing anti-CD20 monoclonal antibodies,” noted lead author Lawrence Steinman, MD, professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) University, and colleagues.
The results, published in the New England Journal of Medicine, pave the way for ublituximab’s approval as the third high-efficacy anti-CD20 monoclonal antibody to treat relapsing forms of MS, predicted Patricia Coyle, MD, director of the MS Comprehensive Care Center, and professor of neurology, at Stony Brook (N.Y.) Neurosciences Institute, who was not involved in the research. Ublituximab will “widen the anti-CD20 monoclonal choices for MS, and should directly compete with ocrelizumab and ofatumumab,” she said.
Two trials
The double-blind, double-dummy ULTIMATE I and II trials enrolled 549 and 545 participants respectively, with a median follow-up of 95 weeks. Subjects, aged between 18 and 55 years, were randomized to receive either oral placebo and intravenous ublituximab (150 mg on day 1, followed by 450 mg on day 15 and at weeks 24, 48, and 72), or oral teriflunomide (14 mg once daily) and intravenous placebo. The primary endpoint was the annualized relapse rate, defined as the number of confirmed MS relapses per participant-year, with a range of secondary end points including number of lesions on magnetic resonance imaging (MRI) by 96 weeks, and worsening of disability confirmed at 12 weeks.
Prevention and management of infusion-related reactions was with oral antihistamine and dexamethasone, administered 30 to 60 minutes before each intravenous dose of ublituximab or placebo, as well as reductions in infusion flow rates and discretionary acetaminophen.
Results for the primary endpoint in ULTIMATE I showed the adjusted annualized relapse rate over a period of 96 weeks was 0.08 in the ublituximab group and 0.19 in the teriflunomide group (rate ratio, 0.41; P < .001). Corresponding rates for ULTIMATE II were 0.09 and 0.18 (rate ratio, 0.51; P = .002).
The mean number of lesions in both ublituximab arms of the trials was 0.02 and 0.01 compared with 0.49 and 0.25 in the teriflunomide arms (rate ratios 0.03 and 0.04 respectively; P < .001 for both).
Similar disability worsening in both groups
A pooled analysis of the two trials showed worsening disability in 5.2% of the ublituximab group, and 5.9% of the teriflunomide group (hazard ratio, 0.84; P = 0.51). “In both trials, teriflunomide was associated with a numerically lower rate of worsening of disability than that reported in previous studies with this drug, but no conclusions can be drawn from these comparisons,” noted the authors.
Infusion-related reactions occurred in 47.7% of the participants in the ublituximab group, consisting mainly of mild to moderate pyrexia, headache, chills, and influenza-like illness. “The reactions may have been related to cytokine release from immune cells (B and NK cells) on interaction of the Fc antibody domain with Fc gamma receptors on effector cells,” they suggested.
Although no opportunistic infections occurred, a higher frequency of infections, including serious infections, was observed with ublituximab (5.0%) than with teriflunomide (2.9%).
While the ULTIMATE trials showed no difference between ublituximab and teriflunomide in confirmed worsening of disability, only a small percentage of participants in either arm showed deterioration, Dr. Coyle remarked. “In a relatively short trial (96 weeks), in a relapsing population on active treatment, this result was not surprising … If the study was bigger, or longer it would increase the chances of seeing a progressive slow worsening component to affect the EDSS [Expanded Disability Status Scale],” she added.
Equivalent efficacy
Ultimately, “it appears likely” that ublituximab is “equivalent in efficacy” to the earlier anti-CD20 agents ocrelizumab and ofatumumab, Dr. Coyle said. While all three agents target B-cells, “ublituximab targets a novel CD20 binding site, and is bioengineered to have a particularly potent antibody dependent cell cytotoxicity lysis mechanism,” she added. “It has been touted to ultimately allow a short infusion of 1 hour.”
Although the serious infection rate is slightly higher with ublituximab (5.0% vs. 2.5% for ofatumumab, and 1.3% for ocrelizumab), “it is still low,” and infusion-related reactions are also higher with ublituximab, she added (47.7% vs. 20.2% and 34.3%, respectively). She suggested factors that might influence which treatment is chosen for a given patient might include cost, convenience, whether it is more or less likely to cause low IgG, interference with vaccination, or influence on cancer or COVID risk.
The trials were supported by TG Therapeutics.
Dr. Coyle has received consulting fees from Accordant, Biogen, Bristol Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio and grant funding from Actelion, Alkermes, Bristol Myers Squibb, CorEvitas LLD, Genentech/Roche, Sanofi Genzyme, MedDay, NINDS, and Novartis.
Patients with relapsing multiple sclerosis (MS) treated with intravenous ublituximab had fewer relapses and brain lesions compared with those treated with oral teriflunomide, although both therapies resulted in similar rates of worsening disability, according to results of the two identical phase 3 ULTIMATE I and II trials.
“In these two 96-week trials involving participants with MS, annualized relapse rates were lower with intravenous ublituximab than with oral teriflunomide. Ublituximab was associated with infusion-related reactions. Larger and longer trials are required to determine the efficacy and safety of ublituximab in patients with relapsing MS, including comparison with other disease-modifying treatments such as existing anti-CD20 monoclonal antibodies,” noted lead author Lawrence Steinman, MD, professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) University, and colleagues.
The results, published in the New England Journal of Medicine, pave the way for ublituximab’s approval as the third high-efficacy anti-CD20 monoclonal antibody to treat relapsing forms of MS, predicted Patricia Coyle, MD, director of the MS Comprehensive Care Center, and professor of neurology, at Stony Brook (N.Y.) Neurosciences Institute, who was not involved in the research. Ublituximab will “widen the anti-CD20 monoclonal choices for MS, and should directly compete with ocrelizumab and ofatumumab,” she said.
Two trials
The double-blind, double-dummy ULTIMATE I and II trials enrolled 549 and 545 participants respectively, with a median follow-up of 95 weeks. Subjects, aged between 18 and 55 years, were randomized to receive either oral placebo and intravenous ublituximab (150 mg on day 1, followed by 450 mg on day 15 and at weeks 24, 48, and 72), or oral teriflunomide (14 mg once daily) and intravenous placebo. The primary endpoint was the annualized relapse rate, defined as the number of confirmed MS relapses per participant-year, with a range of secondary end points including number of lesions on magnetic resonance imaging (MRI) by 96 weeks, and worsening of disability confirmed at 12 weeks.
Prevention and management of infusion-related reactions was with oral antihistamine and dexamethasone, administered 30 to 60 minutes before each intravenous dose of ublituximab or placebo, as well as reductions in infusion flow rates and discretionary acetaminophen.
Results for the primary endpoint in ULTIMATE I showed the adjusted annualized relapse rate over a period of 96 weeks was 0.08 in the ublituximab group and 0.19 in the teriflunomide group (rate ratio, 0.41; P < .001). Corresponding rates for ULTIMATE II were 0.09 and 0.18 (rate ratio, 0.51; P = .002).
The mean number of lesions in both ublituximab arms of the trials was 0.02 and 0.01 compared with 0.49 and 0.25 in the teriflunomide arms (rate ratios 0.03 and 0.04 respectively; P < .001 for both).
Similar disability worsening in both groups
A pooled analysis of the two trials showed worsening disability in 5.2% of the ublituximab group, and 5.9% of the teriflunomide group (hazard ratio, 0.84; P = 0.51). “In both trials, teriflunomide was associated with a numerically lower rate of worsening of disability than that reported in previous studies with this drug, but no conclusions can be drawn from these comparisons,” noted the authors.
Infusion-related reactions occurred in 47.7% of the participants in the ublituximab group, consisting mainly of mild to moderate pyrexia, headache, chills, and influenza-like illness. “The reactions may have been related to cytokine release from immune cells (B and NK cells) on interaction of the Fc antibody domain with Fc gamma receptors on effector cells,” they suggested.
Although no opportunistic infections occurred, a higher frequency of infections, including serious infections, was observed with ublituximab (5.0%) than with teriflunomide (2.9%).
While the ULTIMATE trials showed no difference between ublituximab and teriflunomide in confirmed worsening of disability, only a small percentage of participants in either arm showed deterioration, Dr. Coyle remarked. “In a relatively short trial (96 weeks), in a relapsing population on active treatment, this result was not surprising … If the study was bigger, or longer it would increase the chances of seeing a progressive slow worsening component to affect the EDSS [Expanded Disability Status Scale],” she added.
Equivalent efficacy
Ultimately, “it appears likely” that ublituximab is “equivalent in efficacy” to the earlier anti-CD20 agents ocrelizumab and ofatumumab, Dr. Coyle said. While all three agents target B-cells, “ublituximab targets a novel CD20 binding site, and is bioengineered to have a particularly potent antibody dependent cell cytotoxicity lysis mechanism,” she added. “It has been touted to ultimately allow a short infusion of 1 hour.”
Although the serious infection rate is slightly higher with ublituximab (5.0% vs. 2.5% for ofatumumab, and 1.3% for ocrelizumab), “it is still low,” and infusion-related reactions are also higher with ublituximab, she added (47.7% vs. 20.2% and 34.3%, respectively). She suggested factors that might influence which treatment is chosen for a given patient might include cost, convenience, whether it is more or less likely to cause low IgG, interference with vaccination, or influence on cancer or COVID risk.
The trials were supported by TG Therapeutics.
Dr. Coyle has received consulting fees from Accordant, Biogen, Bristol Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio and grant funding from Actelion, Alkermes, Bristol Myers Squibb, CorEvitas LLD, Genentech/Roche, Sanofi Genzyme, MedDay, NINDS, and Novartis.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Large genetic study links 72 genes to autism spectrum disorders
according to a study published in Nature Genetics. The findings, based on analysis of more than 150,000 people’s genetics, arose from a collaboration of five research groups whose work included comparisons of ASD cohorts with separate cohorts of individuals with developmental delay or schizophrenia.
“We know that many genes, when mutated, contribute to autism,” and this study brought together “multiple types of mutations in a wide array of samples to get a much richer sense of the genes and genetic architecture involved in autism and other neurodevelopmental conditions,” co–senior author Joseph D. Buxbaum, PhD, director of the Seaver Autism Center for Research and Treatment at Mount Sinai and a professor at the Icahn School of Medicine at Mount Sinai, both in New York, said in a prepared statement. “This is significant in that we now have more insights as to the biology of the brain changes that underlie autism and more potential targets for treatment.”
Glen Elliott, PhD, MD, a clinical professor of psychiatry at Stanford (Calif.) University who was not involved in the study, said the paper is important paper for informing clinicians of where the basic research is headed. “We’re still in for a long road” before it bears fruit in terms of therapeutics. The value of studies like these, that investigate which genes are most associated with ASD, is that they may lead toward understanding the pathways in the brain that give rise to certain symptoms of ASD, which can then become therapeutic targets, Dr. Elliott said.
Investigating large cohorts
The researchers analyzed genetic exome sequencing data from 33 ASD cohorts with a total of 63,237 people and then compared these data with another cohort of people with developmental delay and a cohort of people with schizophrenia. The combined ASD cohorts included 15,036 individuals with ASD, 28,522 parents, and 5,492 unaffected siblings. The remaining participants were 5,591 people with ASD and 8,597 matched controls from case control studies.
In the ASD cohorts, the researchers identified 72 genes that were associated with ASD. De novo variants were eight times more likely in cases (4%) than in controls (0.5%). Ten genes occurred at least twice in ASD cases but never occurred in unaffected siblings.
Then the researchers integrated these ASD genetic data with a cohort of 91,605 people that included 31,058 people with developmental delay and their parents. Substantial overlap with gene mutations existed between these two cohorts: 70.1% of the genes related to developmental delay appeared linked to risk for ASD, and 86.6% of genes associated with ASD risk also had associations with developmental delay. Overall, the researchers identified 373 genes strongly associated with ASD and/or developmental delay and 664 genes with a likely association.
“Isolating genes that exert a greater effect on ASD than they do on other developmental delays has remained challenging due to the frequent comorbidity of these phenotypes,” wrote lead author Jack M. Fu, of Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues. “Still, an estimated 13.4% of the transmission and de novo association–ASD genes show little evidence for association in the developmental delay cohort.”
ASD, developmental delay, and schizophrenia
When the researchers compared the cells where the genetic mutations occurred in fetal brains, they found that genes associated with developmental delay more often occurred in less differentiated cell types – less mature cells in the developmental process. Gene mutations associated with ASD, on the other hand, occurred in more mature cell types, particularly in maturing excitatory neurons and related cells.
”Our results are consistent with developmental delay-predominant genes being expressed earlier in development and in less differentiated cells than ASD-predominant genes,” they wrote.
The researchers also compared the specific gene mutations found in these two cohorts with a previously published set of 244 genes associated with schizophrenia. Of these, 234 genes are among those with a transmission and de novo association to ASD and/or developmental delay. Of the 72 genes linked to ASD, eight appear in the set of genes linked to schizophrenia, and 61 were associated with developmental delay, though these two subsets do not overlap each other much.
“The ASD-schizophrenia overlap was significantly enriched, while the developmental delay-schizophrenia overlap was not,” they reported. ”Together, these data suggest that one subset of ASD risk genes may overlap developmental delay while a different subset overlaps schizophrenia.”
Chasing therapy targets by backtracking through genes
The findings are a substantial step forward in understanding the potential genetic contribution to ASD, but they also highlight the challenges of eventually trying to use this information in a clinically meaningful way.
“Given the substantial overlap between the genes implicated in neurodevelopmental disorders writ large and those implicated directly in ASD, disentangling the relative impact of individual genes on neurodevelopment and phenotypic spectra is a daunting yet important challenge,” the researchers wrote. “To identify the key neurobiological features of ASD will likely require convergence of evidence from many ASD genes and studies.”
Dr. Elliott said the biggest takeaway from this study is a better understanding of how the paradigm has shifted away from finding “one gene” for autism or a cure based on genetics and more toward understanding the pathophysiology of symptoms that can point to therapies for better management of the condition.
“Basic researchers have completely changed the strategy for trying to understand the biology of major disorders,” including, in this case, autism, Dr. Elliott said. “The intent is to try to find the underlying systems [in the brain] by backtracking through genes. Meanwhile, given that scientists have made substantial progress in identifying genes that have specific effects on brain development, “the hope is that will mesh with this kind of research, to begin to identify systems that might ultimately be targets for treating.”
The end goal is to be able to offer targeted approaches, based on the pathways causing a symptom, which can be linked backward to a gene.
”So this is not going to offer an immediate cure – it’s probably not going to offer a cure at all – but it may actually lead to much more targeted medications than we currently have for specific types of symptoms within the autism spectrum,” Dr. Elliott said. “What they’re trying to do, ultimately, is to say, when this system is really badly affected because of a genetic abnormality, even though that genetic abnormality is very rare, it leads to these specific kinds of symptoms. If we can find out the neuroregulators underlying that change, then that would be the target, even if that gene were not present.”
The research was funded by the Simons Foundation for Autism Research Initiative, the SPARK project, the National Human Genome Research Institute Home, the National Institute of Mental Health, the National Institute of Child Health and Development, AMED, and the Beatrice and Samuel Seaver Foundation. Five authors reported financial disclosures linked to Desitin, Roche, BioMarin, BrigeBio Pharma, Illumina, Levo Therapeutics, and Microsoft.
according to a study published in Nature Genetics. The findings, based on analysis of more than 150,000 people’s genetics, arose from a collaboration of five research groups whose work included comparisons of ASD cohorts with separate cohorts of individuals with developmental delay or schizophrenia.
“We know that many genes, when mutated, contribute to autism,” and this study brought together “multiple types of mutations in a wide array of samples to get a much richer sense of the genes and genetic architecture involved in autism and other neurodevelopmental conditions,” co–senior author Joseph D. Buxbaum, PhD, director of the Seaver Autism Center for Research and Treatment at Mount Sinai and a professor at the Icahn School of Medicine at Mount Sinai, both in New York, said in a prepared statement. “This is significant in that we now have more insights as to the biology of the brain changes that underlie autism and more potential targets for treatment.”
Glen Elliott, PhD, MD, a clinical professor of psychiatry at Stanford (Calif.) University who was not involved in the study, said the paper is important paper for informing clinicians of where the basic research is headed. “We’re still in for a long road” before it bears fruit in terms of therapeutics. The value of studies like these, that investigate which genes are most associated with ASD, is that they may lead toward understanding the pathways in the brain that give rise to certain symptoms of ASD, which can then become therapeutic targets, Dr. Elliott said.
Investigating large cohorts
The researchers analyzed genetic exome sequencing data from 33 ASD cohorts with a total of 63,237 people and then compared these data with another cohort of people with developmental delay and a cohort of people with schizophrenia. The combined ASD cohorts included 15,036 individuals with ASD, 28,522 parents, and 5,492 unaffected siblings. The remaining participants were 5,591 people with ASD and 8,597 matched controls from case control studies.
In the ASD cohorts, the researchers identified 72 genes that were associated with ASD. De novo variants were eight times more likely in cases (4%) than in controls (0.5%). Ten genes occurred at least twice in ASD cases but never occurred in unaffected siblings.
Then the researchers integrated these ASD genetic data with a cohort of 91,605 people that included 31,058 people with developmental delay and their parents. Substantial overlap with gene mutations existed between these two cohorts: 70.1% of the genes related to developmental delay appeared linked to risk for ASD, and 86.6% of genes associated with ASD risk also had associations with developmental delay. Overall, the researchers identified 373 genes strongly associated with ASD and/or developmental delay and 664 genes with a likely association.
“Isolating genes that exert a greater effect on ASD than they do on other developmental delays has remained challenging due to the frequent comorbidity of these phenotypes,” wrote lead author Jack M. Fu, of Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues. “Still, an estimated 13.4% of the transmission and de novo association–ASD genes show little evidence for association in the developmental delay cohort.”
ASD, developmental delay, and schizophrenia
When the researchers compared the cells where the genetic mutations occurred in fetal brains, they found that genes associated with developmental delay more often occurred in less differentiated cell types – less mature cells in the developmental process. Gene mutations associated with ASD, on the other hand, occurred in more mature cell types, particularly in maturing excitatory neurons and related cells.
”Our results are consistent with developmental delay-predominant genes being expressed earlier in development and in less differentiated cells than ASD-predominant genes,” they wrote.
The researchers also compared the specific gene mutations found in these two cohorts with a previously published set of 244 genes associated with schizophrenia. Of these, 234 genes are among those with a transmission and de novo association to ASD and/or developmental delay. Of the 72 genes linked to ASD, eight appear in the set of genes linked to schizophrenia, and 61 were associated with developmental delay, though these two subsets do not overlap each other much.
“The ASD-schizophrenia overlap was significantly enriched, while the developmental delay-schizophrenia overlap was not,” they reported. ”Together, these data suggest that one subset of ASD risk genes may overlap developmental delay while a different subset overlaps schizophrenia.”
Chasing therapy targets by backtracking through genes
The findings are a substantial step forward in understanding the potential genetic contribution to ASD, but they also highlight the challenges of eventually trying to use this information in a clinically meaningful way.
“Given the substantial overlap between the genes implicated in neurodevelopmental disorders writ large and those implicated directly in ASD, disentangling the relative impact of individual genes on neurodevelopment and phenotypic spectra is a daunting yet important challenge,” the researchers wrote. “To identify the key neurobiological features of ASD will likely require convergence of evidence from many ASD genes and studies.”
Dr. Elliott said the biggest takeaway from this study is a better understanding of how the paradigm has shifted away from finding “one gene” for autism or a cure based on genetics and more toward understanding the pathophysiology of symptoms that can point to therapies for better management of the condition.
“Basic researchers have completely changed the strategy for trying to understand the biology of major disorders,” including, in this case, autism, Dr. Elliott said. “The intent is to try to find the underlying systems [in the brain] by backtracking through genes. Meanwhile, given that scientists have made substantial progress in identifying genes that have specific effects on brain development, “the hope is that will mesh with this kind of research, to begin to identify systems that might ultimately be targets for treating.”
The end goal is to be able to offer targeted approaches, based on the pathways causing a symptom, which can be linked backward to a gene.
”So this is not going to offer an immediate cure – it’s probably not going to offer a cure at all – but it may actually lead to much more targeted medications than we currently have for specific types of symptoms within the autism spectrum,” Dr. Elliott said. “What they’re trying to do, ultimately, is to say, when this system is really badly affected because of a genetic abnormality, even though that genetic abnormality is very rare, it leads to these specific kinds of symptoms. If we can find out the neuroregulators underlying that change, then that would be the target, even if that gene were not present.”
The research was funded by the Simons Foundation for Autism Research Initiative, the SPARK project, the National Human Genome Research Institute Home, the National Institute of Mental Health, the National Institute of Child Health and Development, AMED, and the Beatrice and Samuel Seaver Foundation. Five authors reported financial disclosures linked to Desitin, Roche, BioMarin, BrigeBio Pharma, Illumina, Levo Therapeutics, and Microsoft.
according to a study published in Nature Genetics. The findings, based on analysis of more than 150,000 people’s genetics, arose from a collaboration of five research groups whose work included comparisons of ASD cohorts with separate cohorts of individuals with developmental delay or schizophrenia.
“We know that many genes, when mutated, contribute to autism,” and this study brought together “multiple types of mutations in a wide array of samples to get a much richer sense of the genes and genetic architecture involved in autism and other neurodevelopmental conditions,” co–senior author Joseph D. Buxbaum, PhD, director of the Seaver Autism Center for Research and Treatment at Mount Sinai and a professor at the Icahn School of Medicine at Mount Sinai, both in New York, said in a prepared statement. “This is significant in that we now have more insights as to the biology of the brain changes that underlie autism and more potential targets for treatment.”
Glen Elliott, PhD, MD, a clinical professor of psychiatry at Stanford (Calif.) University who was not involved in the study, said the paper is important paper for informing clinicians of where the basic research is headed. “We’re still in for a long road” before it bears fruit in terms of therapeutics. The value of studies like these, that investigate which genes are most associated with ASD, is that they may lead toward understanding the pathways in the brain that give rise to certain symptoms of ASD, which can then become therapeutic targets, Dr. Elliott said.
Investigating large cohorts
The researchers analyzed genetic exome sequencing data from 33 ASD cohorts with a total of 63,237 people and then compared these data with another cohort of people with developmental delay and a cohort of people with schizophrenia. The combined ASD cohorts included 15,036 individuals with ASD, 28,522 parents, and 5,492 unaffected siblings. The remaining participants were 5,591 people with ASD and 8,597 matched controls from case control studies.
In the ASD cohorts, the researchers identified 72 genes that were associated with ASD. De novo variants were eight times more likely in cases (4%) than in controls (0.5%). Ten genes occurred at least twice in ASD cases but never occurred in unaffected siblings.
Then the researchers integrated these ASD genetic data with a cohort of 91,605 people that included 31,058 people with developmental delay and their parents. Substantial overlap with gene mutations existed between these two cohorts: 70.1% of the genes related to developmental delay appeared linked to risk for ASD, and 86.6% of genes associated with ASD risk also had associations with developmental delay. Overall, the researchers identified 373 genes strongly associated with ASD and/or developmental delay and 664 genes with a likely association.
“Isolating genes that exert a greater effect on ASD than they do on other developmental delays has remained challenging due to the frequent comorbidity of these phenotypes,” wrote lead author Jack M. Fu, of Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues. “Still, an estimated 13.4% of the transmission and de novo association–ASD genes show little evidence for association in the developmental delay cohort.”
ASD, developmental delay, and schizophrenia
When the researchers compared the cells where the genetic mutations occurred in fetal brains, they found that genes associated with developmental delay more often occurred in less differentiated cell types – less mature cells in the developmental process. Gene mutations associated with ASD, on the other hand, occurred in more mature cell types, particularly in maturing excitatory neurons and related cells.
”Our results are consistent with developmental delay-predominant genes being expressed earlier in development and in less differentiated cells than ASD-predominant genes,” they wrote.
The researchers also compared the specific gene mutations found in these two cohorts with a previously published set of 244 genes associated with schizophrenia. Of these, 234 genes are among those with a transmission and de novo association to ASD and/or developmental delay. Of the 72 genes linked to ASD, eight appear in the set of genes linked to schizophrenia, and 61 were associated with developmental delay, though these two subsets do not overlap each other much.
“The ASD-schizophrenia overlap was significantly enriched, while the developmental delay-schizophrenia overlap was not,” they reported. ”Together, these data suggest that one subset of ASD risk genes may overlap developmental delay while a different subset overlaps schizophrenia.”
Chasing therapy targets by backtracking through genes
The findings are a substantial step forward in understanding the potential genetic contribution to ASD, but they also highlight the challenges of eventually trying to use this information in a clinically meaningful way.
“Given the substantial overlap between the genes implicated in neurodevelopmental disorders writ large and those implicated directly in ASD, disentangling the relative impact of individual genes on neurodevelopment and phenotypic spectra is a daunting yet important challenge,” the researchers wrote. “To identify the key neurobiological features of ASD will likely require convergence of evidence from many ASD genes and studies.”
Dr. Elliott said the biggest takeaway from this study is a better understanding of how the paradigm has shifted away from finding “one gene” for autism or a cure based on genetics and more toward understanding the pathophysiology of symptoms that can point to therapies for better management of the condition.
“Basic researchers have completely changed the strategy for trying to understand the biology of major disorders,” including, in this case, autism, Dr. Elliott said. “The intent is to try to find the underlying systems [in the brain] by backtracking through genes. Meanwhile, given that scientists have made substantial progress in identifying genes that have specific effects on brain development, “the hope is that will mesh with this kind of research, to begin to identify systems that might ultimately be targets for treating.”
The end goal is to be able to offer targeted approaches, based on the pathways causing a symptom, which can be linked backward to a gene.
”So this is not going to offer an immediate cure – it’s probably not going to offer a cure at all – but it may actually lead to much more targeted medications than we currently have for specific types of symptoms within the autism spectrum,” Dr. Elliott said. “What they’re trying to do, ultimately, is to say, when this system is really badly affected because of a genetic abnormality, even though that genetic abnormality is very rare, it leads to these specific kinds of symptoms. If we can find out the neuroregulators underlying that change, then that would be the target, even if that gene were not present.”
The research was funded by the Simons Foundation for Autism Research Initiative, the SPARK project, the National Human Genome Research Institute Home, the National Institute of Mental Health, the National Institute of Child Health and Development, AMED, and the Beatrice and Samuel Seaver Foundation. Five authors reported financial disclosures linked to Desitin, Roche, BioMarin, BrigeBio Pharma, Illumina, Levo Therapeutics, and Microsoft.
FROM NATURE GENETICS