User login
Coffee’s ‘Sweet Spot’: Daily Consumption and Cardiometabolic Risk
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.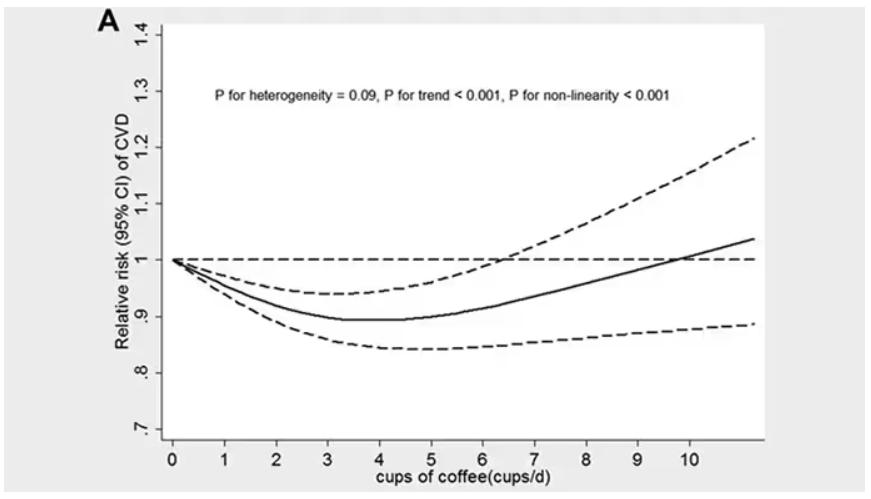
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.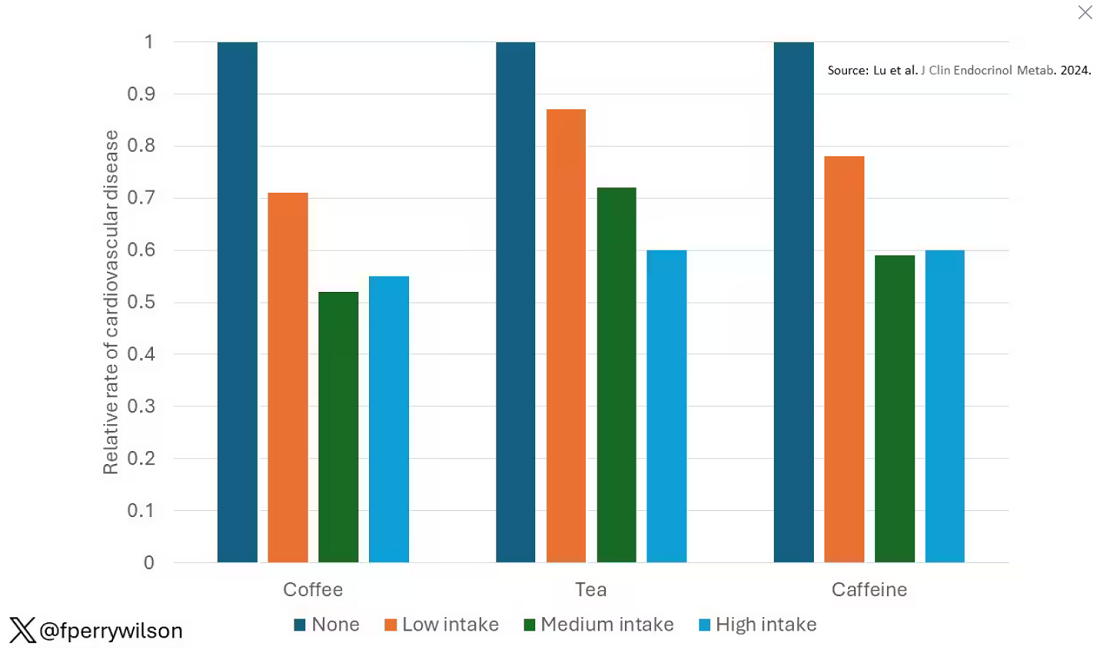
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine. 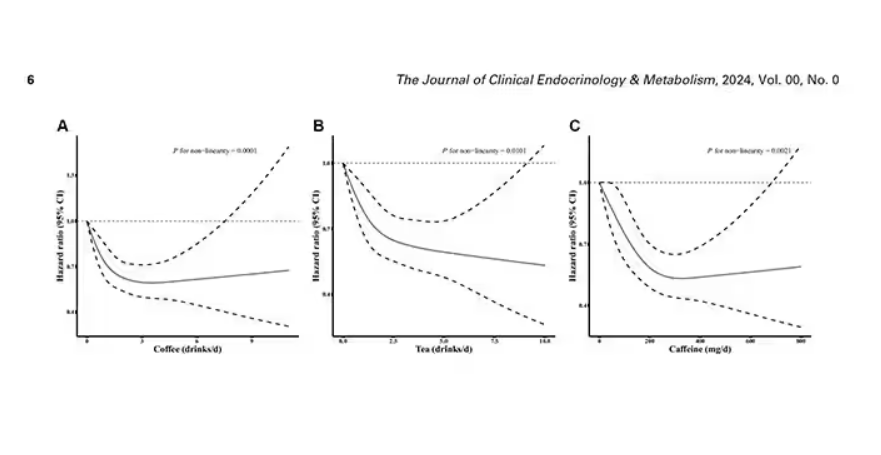
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated. 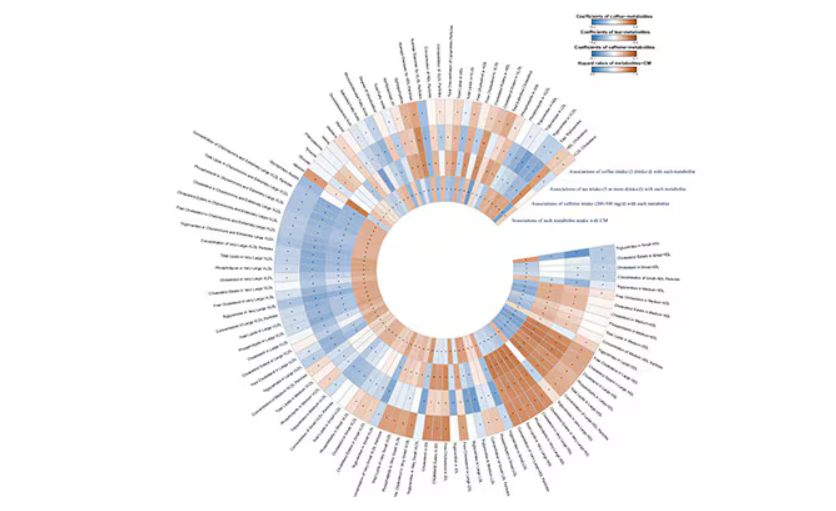
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.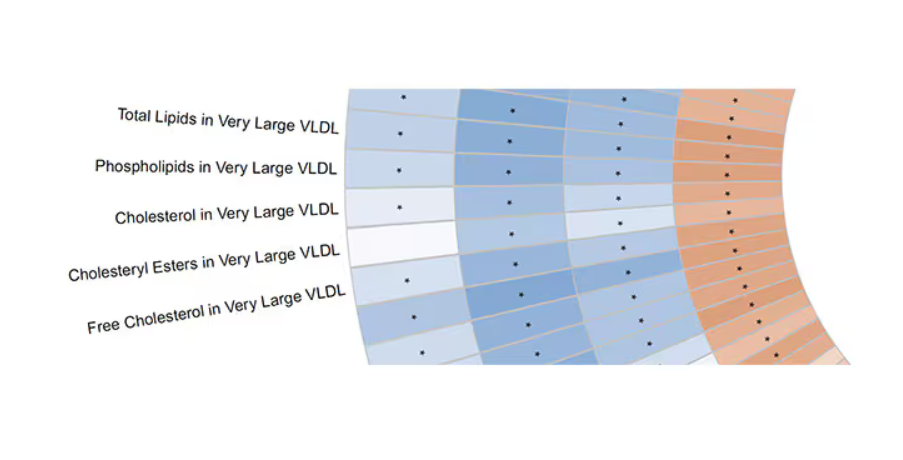
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.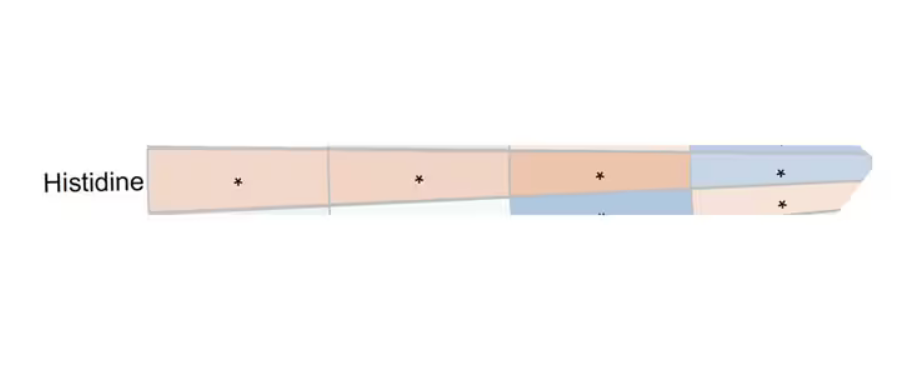
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Can AI Improve Cardiomyopathy Detection in Pregnant Women?
TOPLINE:
Artificial intelligence (AI)–guided screening using digital stethoscopes doubled the detection of left ventricular systolic dysfunction (LVSD) in pregnant and postpartum women in Nigeria. Cardiomyopathy during pregnancy and post partum is challenging to diagnose because of symptom overlap with normal pregnancy changes. AI-guided screening showed a significant improvement in diagnosis rates, compared with usual care.
METHODOLOGY:
- Researchers conducted an open-label, randomized clinical trial involving 1232 pregnant and postpartum women in Nigeria.
- Participants were randomized to either AI-guided screening using digital stethoscopes and 12-lead ECGs or usual care.
- The primary outcome was the identification of LVSD confirmed by echocardiography.
- Secondary outcomes were AI model performance across subgroups and the effectiveness of AI in identifying various levels of LVSD.
TAKEAWAY:
- AI-guided screening using digital stethoscopes detected LVSD in 4.1% of participants, compared with 2.0% of controls (P = .032).
- The 12-lead AI-ECG model detected LVSD in 3.4% of participants in the intervention arm, compared with 2.0% of those in the control arm (P = .125).
- No serious adverse events related to study participation were reported.
- The study highlighted the potential of AI-guided screening to improve the diagnosis of pregnancy-related cardiomyopathy.
IN PRACTICE:
“Delays in the diagnosis of cardiomyopathy during the peripartum period is associated with poorer outcomes as such, it is imperative that we are able to identify cardiac dysfunction early so that appropriate care can be initiated to reduce associated adverse maternal and infant outcomes,” wrote the authors of the study.
SOURCE:
This study was led by Demilade A. Adedinsewo, MBchB, Mayo Clinic in Jacksonville, Florida. It was published online in Nature Medicine.
LIMITATIONS:
The study’s pragmatic design and enrollment at teaching hospitals with echocardiography capabilities limited generalizability. Two thirds of participants were in the third trimester or postpartum at study entry, which limited follow-up visits. The study did not require completion of all seven visits, which led to potential attrition bias. The selected cutoff for LVSD (left ventricular ejection fraction < 50%) did not match the original model specifications, which potentially affected results.
DISCLOSURES:
Dr. Adedinsewo disclosed receiving grants from the Mayo Clinic BIRCWH program funded by the National Institutes of Health. Two coauthors reported holding patents for AI algorithms licensed to Anumana, AliveCor, and Eko Health. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Artificial intelligence (AI)–guided screening using digital stethoscopes doubled the detection of left ventricular systolic dysfunction (LVSD) in pregnant and postpartum women in Nigeria. Cardiomyopathy during pregnancy and post partum is challenging to diagnose because of symptom overlap with normal pregnancy changes. AI-guided screening showed a significant improvement in diagnosis rates, compared with usual care.
METHODOLOGY:
- Researchers conducted an open-label, randomized clinical trial involving 1232 pregnant and postpartum women in Nigeria.
- Participants were randomized to either AI-guided screening using digital stethoscopes and 12-lead ECGs or usual care.
- The primary outcome was the identification of LVSD confirmed by echocardiography.
- Secondary outcomes were AI model performance across subgroups and the effectiveness of AI in identifying various levels of LVSD.
TAKEAWAY:
- AI-guided screening using digital stethoscopes detected LVSD in 4.1% of participants, compared with 2.0% of controls (P = .032).
- The 12-lead AI-ECG model detected LVSD in 3.4% of participants in the intervention arm, compared with 2.0% of those in the control arm (P = .125).
- No serious adverse events related to study participation were reported.
- The study highlighted the potential of AI-guided screening to improve the diagnosis of pregnancy-related cardiomyopathy.
IN PRACTICE:
“Delays in the diagnosis of cardiomyopathy during the peripartum period is associated with poorer outcomes as such, it is imperative that we are able to identify cardiac dysfunction early so that appropriate care can be initiated to reduce associated adverse maternal and infant outcomes,” wrote the authors of the study.
SOURCE:
This study was led by Demilade A. Adedinsewo, MBchB, Mayo Clinic in Jacksonville, Florida. It was published online in Nature Medicine.
LIMITATIONS:
The study’s pragmatic design and enrollment at teaching hospitals with echocardiography capabilities limited generalizability. Two thirds of participants were in the third trimester or postpartum at study entry, which limited follow-up visits. The study did not require completion of all seven visits, which led to potential attrition bias. The selected cutoff for LVSD (left ventricular ejection fraction < 50%) did not match the original model specifications, which potentially affected results.
DISCLOSURES:
Dr. Adedinsewo disclosed receiving grants from the Mayo Clinic BIRCWH program funded by the National Institutes of Health. Two coauthors reported holding patents for AI algorithms licensed to Anumana, AliveCor, and Eko Health. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Artificial intelligence (AI)–guided screening using digital stethoscopes doubled the detection of left ventricular systolic dysfunction (LVSD) in pregnant and postpartum women in Nigeria. Cardiomyopathy during pregnancy and post partum is challenging to diagnose because of symptom overlap with normal pregnancy changes. AI-guided screening showed a significant improvement in diagnosis rates, compared with usual care.
METHODOLOGY:
- Researchers conducted an open-label, randomized clinical trial involving 1232 pregnant and postpartum women in Nigeria.
- Participants were randomized to either AI-guided screening using digital stethoscopes and 12-lead ECGs or usual care.
- The primary outcome was the identification of LVSD confirmed by echocardiography.
- Secondary outcomes were AI model performance across subgroups and the effectiveness of AI in identifying various levels of LVSD.
TAKEAWAY:
- AI-guided screening using digital stethoscopes detected LVSD in 4.1% of participants, compared with 2.0% of controls (P = .032).
- The 12-lead AI-ECG model detected LVSD in 3.4% of participants in the intervention arm, compared with 2.0% of those in the control arm (P = .125).
- No serious adverse events related to study participation were reported.
- The study highlighted the potential of AI-guided screening to improve the diagnosis of pregnancy-related cardiomyopathy.
IN PRACTICE:
“Delays in the diagnosis of cardiomyopathy during the peripartum period is associated with poorer outcomes as such, it is imperative that we are able to identify cardiac dysfunction early so that appropriate care can be initiated to reduce associated adverse maternal and infant outcomes,” wrote the authors of the study.
SOURCE:
This study was led by Demilade A. Adedinsewo, MBchB, Mayo Clinic in Jacksonville, Florida. It was published online in Nature Medicine.
LIMITATIONS:
The study’s pragmatic design and enrollment at teaching hospitals with echocardiography capabilities limited generalizability. Two thirds of participants were in the third trimester or postpartum at study entry, which limited follow-up visits. The study did not require completion of all seven visits, which led to potential attrition bias. The selected cutoff for LVSD (left ventricular ejection fraction < 50%) did not match the original model specifications, which potentially affected results.
DISCLOSURES:
Dr. Adedinsewo disclosed receiving grants from the Mayo Clinic BIRCWH program funded by the National Institutes of Health. Two coauthors reported holding patents for AI algorithms licensed to Anumana, AliveCor, and Eko Health. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Beyond Weight Loss, Limited Bariatric Surgery Benefits in Older Adults
TOPLINE:
For older adults with obesity, bariatric surgery does not appear to significantly reduce the risk for obesity-related cancer and cardiovascular disease (CVD), as it does in younger adults.
METHODOLOGY:
- Bariatric surgery has been shown to decrease the risk for obesity-related cancer and CVD but is typically reserved for patients aged < 60 years. Whether the same holds for patients who undergo surgery at older ages is unclear.
- Researchers analyzed nationwide data from three countries (Denmark, Finland, and Sweden) to compare patients with no history of cancer or CVD and age ≥ 60 years who underwent bariatric surgery against matched controls who received nonoperative treatment for obesity.
- The main outcome was obesity-related cancer, defined as a composite outcome of breast, endometrial, esophageal, colorectal, and kidney cancer. The secondary outcome was CVD, defined as a composite of myocardial infarction, ischemic stroke, and cerebral hemorrhage.
- Analyses were adjusted for diabetes, hypertension, peripheral vascular disease, chronic obstructive pulmonary disease, kidney disease, and frailty.
TAKEAWAY:
- Of the 15,300 patients (66.4% women) included, 2550 underwent bariatric surgery (including gastric bypass in 1930) and 12,750 matched controls received nonoperative treatment for obesity.
- During a median 5.8 years of follow-up, 658 (4.3%) people developed obesity-related cancer and 1436 (9.4%) developed CVD.
- Bariatric surgery in adults aged ≥ 60 years was not associated with a reduced risk for obesity-related cancer (hazard ratio [HR], 0.81) or CVD (HR, 0.86) compared with matched nonoperative controls.
- Bariatric surgery appeared to be associated with a decreased risk for obesity-related cancer in women (HR, 0.76).
- There was a decreased risk for both obesity-related cancer (HR, 0.74) and CVD (HR, 0.82) in patients who underwent gastric bypass.
IN PRACTICE:
“The findings from this study suggest a limited role of bariatric surgery in older patients for the prevention of obesity-related cancer or cardiovascular disease,” the authors wrote, noting that this “may be explained by the poorer weight loss and resolution of comorbidities observed in patients who underwent surgery at an older age.”
SOURCE:
The study, with first author Peter Gerber, MD, PhD, Department of Surgery, Capio St Göran’s Hospital, Stockholm, Sweden, was published online in JAMA Network Open.
LIMITATIONS:
Data on smoking status and body mass index were not available. The observational design limited the ability to draw causal inferences. The null association between bariatric surgery and outcomes may be due to limited power.
DISCLOSURES:
The study was funded by the Swedish Society of Medicine. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
For older adults with obesity, bariatric surgery does not appear to significantly reduce the risk for obesity-related cancer and cardiovascular disease (CVD), as it does in younger adults.
METHODOLOGY:
- Bariatric surgery has been shown to decrease the risk for obesity-related cancer and CVD but is typically reserved for patients aged < 60 years. Whether the same holds for patients who undergo surgery at older ages is unclear.
- Researchers analyzed nationwide data from three countries (Denmark, Finland, and Sweden) to compare patients with no history of cancer or CVD and age ≥ 60 years who underwent bariatric surgery against matched controls who received nonoperative treatment for obesity.
- The main outcome was obesity-related cancer, defined as a composite outcome of breast, endometrial, esophageal, colorectal, and kidney cancer. The secondary outcome was CVD, defined as a composite of myocardial infarction, ischemic stroke, and cerebral hemorrhage.
- Analyses were adjusted for diabetes, hypertension, peripheral vascular disease, chronic obstructive pulmonary disease, kidney disease, and frailty.
TAKEAWAY:
- Of the 15,300 patients (66.4% women) included, 2550 underwent bariatric surgery (including gastric bypass in 1930) and 12,750 matched controls received nonoperative treatment for obesity.
- During a median 5.8 years of follow-up, 658 (4.3%) people developed obesity-related cancer and 1436 (9.4%) developed CVD.
- Bariatric surgery in adults aged ≥ 60 years was not associated with a reduced risk for obesity-related cancer (hazard ratio [HR], 0.81) or CVD (HR, 0.86) compared with matched nonoperative controls.
- Bariatric surgery appeared to be associated with a decreased risk for obesity-related cancer in women (HR, 0.76).
- There was a decreased risk for both obesity-related cancer (HR, 0.74) and CVD (HR, 0.82) in patients who underwent gastric bypass.
IN PRACTICE:
“The findings from this study suggest a limited role of bariatric surgery in older patients for the prevention of obesity-related cancer or cardiovascular disease,” the authors wrote, noting that this “may be explained by the poorer weight loss and resolution of comorbidities observed in patients who underwent surgery at an older age.”
SOURCE:
The study, with first author Peter Gerber, MD, PhD, Department of Surgery, Capio St Göran’s Hospital, Stockholm, Sweden, was published online in JAMA Network Open.
LIMITATIONS:
Data on smoking status and body mass index were not available. The observational design limited the ability to draw causal inferences. The null association between bariatric surgery and outcomes may be due to limited power.
DISCLOSURES:
The study was funded by the Swedish Society of Medicine. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
For older adults with obesity, bariatric surgery does not appear to significantly reduce the risk for obesity-related cancer and cardiovascular disease (CVD), as it does in younger adults.
METHODOLOGY:
- Bariatric surgery has been shown to decrease the risk for obesity-related cancer and CVD but is typically reserved for patients aged < 60 years. Whether the same holds for patients who undergo surgery at older ages is unclear.
- Researchers analyzed nationwide data from three countries (Denmark, Finland, and Sweden) to compare patients with no history of cancer or CVD and age ≥ 60 years who underwent bariatric surgery against matched controls who received nonoperative treatment for obesity.
- The main outcome was obesity-related cancer, defined as a composite outcome of breast, endometrial, esophageal, colorectal, and kidney cancer. The secondary outcome was CVD, defined as a composite of myocardial infarction, ischemic stroke, and cerebral hemorrhage.
- Analyses were adjusted for diabetes, hypertension, peripheral vascular disease, chronic obstructive pulmonary disease, kidney disease, and frailty.
TAKEAWAY:
- Of the 15,300 patients (66.4% women) included, 2550 underwent bariatric surgery (including gastric bypass in 1930) and 12,750 matched controls received nonoperative treatment for obesity.
- During a median 5.8 years of follow-up, 658 (4.3%) people developed obesity-related cancer and 1436 (9.4%) developed CVD.
- Bariatric surgery in adults aged ≥ 60 years was not associated with a reduced risk for obesity-related cancer (hazard ratio [HR], 0.81) or CVD (HR, 0.86) compared with matched nonoperative controls.
- Bariatric surgery appeared to be associated with a decreased risk for obesity-related cancer in women (HR, 0.76).
- There was a decreased risk for both obesity-related cancer (HR, 0.74) and CVD (HR, 0.82) in patients who underwent gastric bypass.
IN PRACTICE:
“The findings from this study suggest a limited role of bariatric surgery in older patients for the prevention of obesity-related cancer or cardiovascular disease,” the authors wrote, noting that this “may be explained by the poorer weight loss and resolution of comorbidities observed in patients who underwent surgery at an older age.”
SOURCE:
The study, with first author Peter Gerber, MD, PhD, Department of Surgery, Capio St Göran’s Hospital, Stockholm, Sweden, was published online in JAMA Network Open.
LIMITATIONS:
Data on smoking status and body mass index were not available. The observational design limited the ability to draw causal inferences. The null association between bariatric surgery and outcomes may be due to limited power.
DISCLOSURES:
The study was funded by the Swedish Society of Medicine. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Old, Frail Patients: Study More, Intervene Less?
Lessons From SENIOR-RITA
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lessons From SENIOR-RITA
Lessons From SENIOR-RITA
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Variation in Cardiovascular Risk Assessment Status in Patients Receiving Oral Anti-Cancer Therapies: A Focus on Equity throughout VISN (Veteran Integrated Service Network) 12
Background
Oral anti-cancer therapies have quickly moved to the forefront of cancer treatment for several oncologic disease states. While these treatments have led to improvements in prognosis and ease of administration, many of these agents carry the risk of serious short- and long-term toxicities affecting the cardiovascular system. This prompted the Journal of the American Heart Association (JAHA) to release special guidance focused on cardiovascular monitoring strategies for anti-cancer agents. The primary objective of this retrospective review was to evaluate compliance with cardiovascular monitoring based on JAHA cardio-oncologic guidelines. The secondary objective was to assess disparities in cardiovascular monitoring based on markers of equity such as race/ ethnicity, rurality, socioeconomic status and gender.
Methods
Patients who initiated pazopanib, cabozantinib, lenvatinib, axitinib, regorafenib, nilotinib, ibrutinib, sorafenib, sunitinib, ponatinib or everolimus between January 1, 2019 and December 31, 2022 at a VHA VISN 12 site with oncology services were followed forward until treatment discontinuation or 12 months of therapy had been completed. Data was acquired utilizing the VA Informatics and Computing Infrastructure (VINCI) and the Corporate Data Warehouse (CDW). The following cardiovascular monitoring markers were recorded at baseline and months 3, 6, 9 and 12 after initiation anti-cancer therapy: blood pressure, blood glucose, cholesterol, ECG and echocardiogram. Descriptive statistics were used to examine all continuous variables, while frequencies were used to examine categorical variables. Univariate statistics were performed on all items respectively.
Results
A total of 219 patients were identified initiating pre-specified oral anti-cancer therapies during the study time period. Of these, a total of n=145 met study inclusion criteria. 97% were male (n=141), 80% (n=116) had a racial background of white, 36% (n=52) live in rural or highly rural locations and 23% (n=34) lived in a high poverty area. Based on the primary endpoint, the mean compliance with recommended cardiovascular monitoring was 44.95% [IQR 12]. There was no statistically significant difference in cardiovascular monitoring based on equity.
Conclusions
Overall uptake of cardiovascular monitoring markers recommended by JAHA guidance is low. We plan to evaluate methods to increase these measures, utilizing clinical pharmacy provider support throughout VISN 12.
Background
Oral anti-cancer therapies have quickly moved to the forefront of cancer treatment for several oncologic disease states. While these treatments have led to improvements in prognosis and ease of administration, many of these agents carry the risk of serious short- and long-term toxicities affecting the cardiovascular system. This prompted the Journal of the American Heart Association (JAHA) to release special guidance focused on cardiovascular monitoring strategies for anti-cancer agents. The primary objective of this retrospective review was to evaluate compliance with cardiovascular monitoring based on JAHA cardio-oncologic guidelines. The secondary objective was to assess disparities in cardiovascular monitoring based on markers of equity such as race/ ethnicity, rurality, socioeconomic status and gender.
Methods
Patients who initiated pazopanib, cabozantinib, lenvatinib, axitinib, regorafenib, nilotinib, ibrutinib, sorafenib, sunitinib, ponatinib or everolimus between January 1, 2019 and December 31, 2022 at a VHA VISN 12 site with oncology services were followed forward until treatment discontinuation or 12 months of therapy had been completed. Data was acquired utilizing the VA Informatics and Computing Infrastructure (VINCI) and the Corporate Data Warehouse (CDW). The following cardiovascular monitoring markers were recorded at baseline and months 3, 6, 9 and 12 after initiation anti-cancer therapy: blood pressure, blood glucose, cholesterol, ECG and echocardiogram. Descriptive statistics were used to examine all continuous variables, while frequencies were used to examine categorical variables. Univariate statistics were performed on all items respectively.
Results
A total of 219 patients were identified initiating pre-specified oral anti-cancer therapies during the study time period. Of these, a total of n=145 met study inclusion criteria. 97% were male (n=141), 80% (n=116) had a racial background of white, 36% (n=52) live in rural or highly rural locations and 23% (n=34) lived in a high poverty area. Based on the primary endpoint, the mean compliance with recommended cardiovascular monitoring was 44.95% [IQR 12]. There was no statistically significant difference in cardiovascular monitoring based on equity.
Conclusions
Overall uptake of cardiovascular monitoring markers recommended by JAHA guidance is low. We plan to evaluate methods to increase these measures, utilizing clinical pharmacy provider support throughout VISN 12.
Background
Oral anti-cancer therapies have quickly moved to the forefront of cancer treatment for several oncologic disease states. While these treatments have led to improvements in prognosis and ease of administration, many of these agents carry the risk of serious short- and long-term toxicities affecting the cardiovascular system. This prompted the Journal of the American Heart Association (JAHA) to release special guidance focused on cardiovascular monitoring strategies for anti-cancer agents. The primary objective of this retrospective review was to evaluate compliance with cardiovascular monitoring based on JAHA cardio-oncologic guidelines. The secondary objective was to assess disparities in cardiovascular monitoring based on markers of equity such as race/ ethnicity, rurality, socioeconomic status and gender.
Methods
Patients who initiated pazopanib, cabozantinib, lenvatinib, axitinib, regorafenib, nilotinib, ibrutinib, sorafenib, sunitinib, ponatinib or everolimus between January 1, 2019 and December 31, 2022 at a VHA VISN 12 site with oncology services were followed forward until treatment discontinuation or 12 months of therapy had been completed. Data was acquired utilizing the VA Informatics and Computing Infrastructure (VINCI) and the Corporate Data Warehouse (CDW). The following cardiovascular monitoring markers were recorded at baseline and months 3, 6, 9 and 12 after initiation anti-cancer therapy: blood pressure, blood glucose, cholesterol, ECG and echocardiogram. Descriptive statistics were used to examine all continuous variables, while frequencies were used to examine categorical variables. Univariate statistics were performed on all items respectively.
Results
A total of 219 patients were identified initiating pre-specified oral anti-cancer therapies during the study time period. Of these, a total of n=145 met study inclusion criteria. 97% were male (n=141), 80% (n=116) had a racial background of white, 36% (n=52) live in rural or highly rural locations and 23% (n=34) lived in a high poverty area. Based on the primary endpoint, the mean compliance with recommended cardiovascular monitoring was 44.95% [IQR 12]. There was no statistically significant difference in cardiovascular monitoring based on equity.
Conclusions
Overall uptake of cardiovascular monitoring markers recommended by JAHA guidance is low. We plan to evaluate methods to increase these measures, utilizing clinical pharmacy provider support throughout VISN 12.
Eating the Right Fats May Help Patients Live Longer
These are the results of a study published in JAMA Internal Medicine that followed more than 600,000 participants over 2 decades.
Bin Zhao, PhD, of the National Clinical Research Center for Metabolic Diseases at the Key Laboratory of Diabetes Immunology in Changsha, China, and colleagues concluded from these data that consuming plant-based fats instead of animal fats could be beneficial for health and improve survival.
It may not be so simple, however. “We are one step ahead of the publication: We no longer just distinguish between animal and plant fats but mainly consider the composition,” said Stefan Lorkowski, PhD, chair of biochemistry and physiology of nutrition at the Institute of Nutritional Sciences at the University of Jena in Germany, in response to inquiries from this news organization.
What’s in a Fat?
Although Dr. Zhao and colleagues studied the effect of different plant and animal fat sources (eg, grains, nuts, legumes, plant oils, red and white meat, dairy, eggs, and fish), they did not consider the composition of the fatty acids that they contained. “It matters which dairy products, which plant oils, and which fish are consumed,” said Dr. Lorkowski.
The data analyzed in the Chinese study come from a prospective cohort study (NIH-AARP Diet and Health Study) conducted in the United States from 1995 to 2019. At the beginning, the 407,531 study participants (average age, 61 years) filled out dietary questionnaires once. They were then followed for up to 24 years for total and cardiovascular mortality.
During this period, 185,111 study participants died, including 58,526 from cardiovascular diseases. Participants who consumed the most plant-based fats, according to the dietary questionnaires filled out in 1995, had a lower risk for death than those who consumed the least plant-based fats. Their overall mortality risk was 9% lower, and their cardiovascular mortality risk was 14% lower. This finding was especially noticeable when it came to plant fats from grains or plant oils.
Animal Fat and Mortality
In contrast, a higher intake of animal fat was associated with both a higher overall mortality risk (16%) and a higher cardiovascular mortality risk (14%). This was especially true for fat from dairy products and eggs.
A trend towards a reduced overall and cardiovascular mortality risk was observed for fat from fish. “The fact that only a trend towards fish consumption was observed may be due to the study having many more meat eaters than fish eaters,” said Dr. Lorkowski.
Another imbalance limits the significance of the study, he added. The two groups, those who primarily consumed plant fats and those who primarily consumed animal fats, were already distinct at the beginning of the study. Those who consumed more plant fats were more likely to have diabetes, a higher body mass index (BMI), higher energy intake, and higher alcohol consumption but consumed more fiber, fruits, and vegetables and were more physically active. “They may have been trying to live healthier because they were sicker,” said Dr. Lorkowski.
Potential Confounding
Dr. Zhao and his team adjusted the results for various potential confounding factors, including age, gender, BMI, ethnicity, smoking, physical activity, education, marital status, diabetes, health status, vitamin intake, protein, carbohydrates, fiber, trans fats, cholesterol intake, and alcohol consumption. However, according to Dr. Lorkowski, “statistical adjustment is always incomplete, and confounding cannot be completely ruled out.”
Nevertheless, these results provide relevant insights for dietary recommendations that could help improve health and related outcomes, according to the authors. “Replacement of 5% energy from animal fat with 5% energy from plant fat, particularly fat from grains or vegetable oils, was associated with a lower risk for mortality: 4%-24% reduction in overall mortality and 5%-30% reduction in cardiovascular disease mortality.”
Fat Composition Matters
Animal fat, however, should not simply be replaced with plant fat, said Dr. Lorkowski. “Cold-water fish, which provides important long-chain omega-3 fatty acids, is also considered animal fat. And palm and coconut fat, while plant-based, contain unhealthy long-chain saturated fats. And the type of plant oils also makes a difference, whether one uses corn germ or sunflower oil rich in omega-6 fatty acids or flaxseed or rapeseed oil rich in omega-3 fatty acids.
“A diet rich in unsaturated fats, with sufficient and balanced intake of omega-3 and omega-6 fatty acids, that is also abundant in fiber-rich carbohydrate sources and plant-based protein, is always better than too much fat from animal sources.”
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
These are the results of a study published in JAMA Internal Medicine that followed more than 600,000 participants over 2 decades.
Bin Zhao, PhD, of the National Clinical Research Center for Metabolic Diseases at the Key Laboratory of Diabetes Immunology in Changsha, China, and colleagues concluded from these data that consuming plant-based fats instead of animal fats could be beneficial for health and improve survival.
It may not be so simple, however. “We are one step ahead of the publication: We no longer just distinguish between animal and plant fats but mainly consider the composition,” said Stefan Lorkowski, PhD, chair of biochemistry and physiology of nutrition at the Institute of Nutritional Sciences at the University of Jena in Germany, in response to inquiries from this news organization.
What’s in a Fat?
Although Dr. Zhao and colleagues studied the effect of different plant and animal fat sources (eg, grains, nuts, legumes, plant oils, red and white meat, dairy, eggs, and fish), they did not consider the composition of the fatty acids that they contained. “It matters which dairy products, which plant oils, and which fish are consumed,” said Dr. Lorkowski.
The data analyzed in the Chinese study come from a prospective cohort study (NIH-AARP Diet and Health Study) conducted in the United States from 1995 to 2019. At the beginning, the 407,531 study participants (average age, 61 years) filled out dietary questionnaires once. They were then followed for up to 24 years for total and cardiovascular mortality.
During this period, 185,111 study participants died, including 58,526 from cardiovascular diseases. Participants who consumed the most plant-based fats, according to the dietary questionnaires filled out in 1995, had a lower risk for death than those who consumed the least plant-based fats. Their overall mortality risk was 9% lower, and their cardiovascular mortality risk was 14% lower. This finding was especially noticeable when it came to plant fats from grains or plant oils.
Animal Fat and Mortality
In contrast, a higher intake of animal fat was associated with both a higher overall mortality risk (16%) and a higher cardiovascular mortality risk (14%). This was especially true for fat from dairy products and eggs.
A trend towards a reduced overall and cardiovascular mortality risk was observed for fat from fish. “The fact that only a trend towards fish consumption was observed may be due to the study having many more meat eaters than fish eaters,” said Dr. Lorkowski.
Another imbalance limits the significance of the study, he added. The two groups, those who primarily consumed plant fats and those who primarily consumed animal fats, were already distinct at the beginning of the study. Those who consumed more plant fats were more likely to have diabetes, a higher body mass index (BMI), higher energy intake, and higher alcohol consumption but consumed more fiber, fruits, and vegetables and were more physically active. “They may have been trying to live healthier because they were sicker,” said Dr. Lorkowski.
Potential Confounding
Dr. Zhao and his team adjusted the results for various potential confounding factors, including age, gender, BMI, ethnicity, smoking, physical activity, education, marital status, diabetes, health status, vitamin intake, protein, carbohydrates, fiber, trans fats, cholesterol intake, and alcohol consumption. However, according to Dr. Lorkowski, “statistical adjustment is always incomplete, and confounding cannot be completely ruled out.”
Nevertheless, these results provide relevant insights for dietary recommendations that could help improve health and related outcomes, according to the authors. “Replacement of 5% energy from animal fat with 5% energy from plant fat, particularly fat from grains or vegetable oils, was associated with a lower risk for mortality: 4%-24% reduction in overall mortality and 5%-30% reduction in cardiovascular disease mortality.”
Fat Composition Matters
Animal fat, however, should not simply be replaced with plant fat, said Dr. Lorkowski. “Cold-water fish, which provides important long-chain omega-3 fatty acids, is also considered animal fat. And palm and coconut fat, while plant-based, contain unhealthy long-chain saturated fats. And the type of plant oils also makes a difference, whether one uses corn germ or sunflower oil rich in omega-6 fatty acids or flaxseed or rapeseed oil rich in omega-3 fatty acids.
“A diet rich in unsaturated fats, with sufficient and balanced intake of omega-3 and omega-6 fatty acids, that is also abundant in fiber-rich carbohydrate sources and plant-based protein, is always better than too much fat from animal sources.”
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
These are the results of a study published in JAMA Internal Medicine that followed more than 600,000 participants over 2 decades.
Bin Zhao, PhD, of the National Clinical Research Center for Metabolic Diseases at the Key Laboratory of Diabetes Immunology in Changsha, China, and colleagues concluded from these data that consuming plant-based fats instead of animal fats could be beneficial for health and improve survival.
It may not be so simple, however. “We are one step ahead of the publication: We no longer just distinguish between animal and plant fats but mainly consider the composition,” said Stefan Lorkowski, PhD, chair of biochemistry and physiology of nutrition at the Institute of Nutritional Sciences at the University of Jena in Germany, in response to inquiries from this news organization.
What’s in a Fat?
Although Dr. Zhao and colleagues studied the effect of different plant and animal fat sources (eg, grains, nuts, legumes, plant oils, red and white meat, dairy, eggs, and fish), they did not consider the composition of the fatty acids that they contained. “It matters which dairy products, which plant oils, and which fish are consumed,” said Dr. Lorkowski.
The data analyzed in the Chinese study come from a prospective cohort study (NIH-AARP Diet and Health Study) conducted in the United States from 1995 to 2019. At the beginning, the 407,531 study participants (average age, 61 years) filled out dietary questionnaires once. They were then followed for up to 24 years for total and cardiovascular mortality.
During this period, 185,111 study participants died, including 58,526 from cardiovascular diseases. Participants who consumed the most plant-based fats, according to the dietary questionnaires filled out in 1995, had a lower risk for death than those who consumed the least plant-based fats. Their overall mortality risk was 9% lower, and their cardiovascular mortality risk was 14% lower. This finding was especially noticeable when it came to plant fats from grains or plant oils.
Animal Fat and Mortality
In contrast, a higher intake of animal fat was associated with both a higher overall mortality risk (16%) and a higher cardiovascular mortality risk (14%). This was especially true for fat from dairy products and eggs.
A trend towards a reduced overall and cardiovascular mortality risk was observed for fat from fish. “The fact that only a trend towards fish consumption was observed may be due to the study having many more meat eaters than fish eaters,” said Dr. Lorkowski.
Another imbalance limits the significance of the study, he added. The two groups, those who primarily consumed plant fats and those who primarily consumed animal fats, were already distinct at the beginning of the study. Those who consumed more plant fats were more likely to have diabetes, a higher body mass index (BMI), higher energy intake, and higher alcohol consumption but consumed more fiber, fruits, and vegetables and were more physically active. “They may have been trying to live healthier because they were sicker,” said Dr. Lorkowski.
Potential Confounding
Dr. Zhao and his team adjusted the results for various potential confounding factors, including age, gender, BMI, ethnicity, smoking, physical activity, education, marital status, diabetes, health status, vitamin intake, protein, carbohydrates, fiber, trans fats, cholesterol intake, and alcohol consumption. However, according to Dr. Lorkowski, “statistical adjustment is always incomplete, and confounding cannot be completely ruled out.”
Nevertheless, these results provide relevant insights for dietary recommendations that could help improve health and related outcomes, according to the authors. “Replacement of 5% energy from animal fat with 5% energy from plant fat, particularly fat from grains or vegetable oils, was associated with a lower risk for mortality: 4%-24% reduction in overall mortality and 5%-30% reduction in cardiovascular disease mortality.”
Fat Composition Matters
Animal fat, however, should not simply be replaced with plant fat, said Dr. Lorkowski. “Cold-water fish, which provides important long-chain omega-3 fatty acids, is also considered animal fat. And palm and coconut fat, while plant-based, contain unhealthy long-chain saturated fats. And the type of plant oils also makes a difference, whether one uses corn germ or sunflower oil rich in omega-6 fatty acids or flaxseed or rapeseed oil rich in omega-3 fatty acids.
“A diet rich in unsaturated fats, with sufficient and balanced intake of omega-3 and omega-6 fatty acids, that is also abundant in fiber-rich carbohydrate sources and plant-based protein, is always better than too much fat from animal sources.”
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
FROM JAMA INTERNAL MEDICINE
Not Kidding: Yellow Dye 5 May Lead to Invisibility
Applying the dye to lab mice made their skin temporarily transparent, allowing Stanford University researchers to observe the rodents’ digestive system, muscle fibers, and blood vessels, according to a study published in Science.
“It’s a stunning result,” said senior author Guosong Hong, PhD, who is assistant professor of materials science and engineering at Stanford University in California. “If the same technique could be applied to humans, it could offer a variety of benefits in biology, diagnostics, and even cosmetics.”
The work drew upon optical concepts first described in the early 20th century to form a surprising theory: Applying a light-absorbing substance could render skin transparent by reducing the chaotic scattering of light as it strikes proteins, fats, and water in tissue.
A search for a suitable light absorber led to FD&C Yellow 5, also called tartrazine, a synthetic color additive certified by the Food and Drug Administration (FDA) for use in foods, cosmetics, and medications.
Rubbed on live mice (after areas of fur were removed using a drugstore depilatory cream), tartrazine rendered skin on their bellies, hind legs, and heads transparent within 5 minutes. With the naked eye, the researchers watched a mouse’s intestines, bladder, and liver at work. Using a microscope, they observed muscle fibers and saw blood vessels in a living mouse’s brain — all without making incisions. Transparency faded quickly when the dye was washed off.
Someday, the concept could be used in doctors’ offices and hospitals, Dr. Hong said.
“Instead of relying on invasive biopsies, doctors might be able to diagnose deep-seated tumors by simply examining a person’s tissue without the need for invasive surgical removal,” he said. “This technique could potentially make blood draws less painful by helping phlebotomists easily locate veins under the skin. It could also enhance procedures like laser tattoo removal by allowing more precise targeting of the pigment beneath the skin.”
From Cake Frosting to Groundbreaking Research
Yellow 5 food dye can be found in everything from cereal, soda, spices, and cake frosting to lipstick, mouthwash, shampoo, dietary supplements, and house paint. Although it’s in some topical medications, more research is needed before it could be used in human diagnostics, said Christopher J. Rowlands, PhD, a senior lecturer in the Department of Bioengineering at Imperial College London, England, where he studies biophotonic instrumentation — ways to image structures inside the body more quickly and clearly.
But the finding could prove useful in research. In a commentary published in Science, Dr. Rowlands and his colleague Jon Gorecki, PhD, an experimental optical physicist also at Imperial College London, noted that the dye could be an alternative to other optical clearing agents currently used in lab studies, such as glycerol, fructose, or acetic acid. Advantages are the effect is reversible and works at lower concentrations with fewer side effects. This could broaden the types of studies possible in lab animals, so researchers don’t have to rely on naturally transparent creatures like nematodes and zebrafish.
The dye could also be paired with imaging techniques such as MRI or electron microscopy.
“Imaging techniques all have pros and cons,” Dr. Rowlands said. “MRI can see all the way through the body albeit with limited resolution and contrast. Electron microscopy has excellent resolution but limited compatibility with live tissue and penetration depth. Optical microscopy has subcellular resolution, the ability to label things, excellent biocompatibility but less than 1 millimeter of penetration depth. This clearing method will give a substantial boost to optical imaging for medicine and biology.”
The discovery could improve the depth imaging equipment can achieve by tenfold, according to the commentary.
Brain research especially stands to benefit. “Neurobiology in particular will have great use for combinations of multiphoton, optogenetics, and tissue clearing to record and control neural activity over (potentially) the whole mouse brain,” he said.
Refraction, Absorption, and The Invisible Man
The dye discovery has distant echoes in H.G. Wells’ 1897 novel The Invisible Man, Dr. Rowlands noted. In the book, a serum makes the main character invisible by changing the light scattering — or refractive index (RI) — of his cells to match the air around him.
The Stanford engineers looked to the past for inspiration, but not to fiction. They turned to a concept first described in the 1920s called the Kramers-Kronig relations, a mathematical principle that can be applied to relationships between the way light is refracted and absorbed in different materials. They also read up on Lorentz oscillation, which describes how electrons and atoms inside molecules react to light.
They reasoned that light-absorbing compounds could equalize the differences between the light-scattering properties of proteins, lipids, and water that make skin opaque.
With that, the search was on. The study’s first author, postdoctoral researcher Zihao Ou, PhD, began testing strong dyes to find a candidate. Tartrazine was a front-runner.
“We found that dye molecules are more efficient in raising the refractive index of water than conventional RI-matching agents, thus resulting in transparency at a much lower concentration,” Dr. Hong said. “The underlying physics, explained by the Lorentz oscillator model and Kramers-Kronig relations, reveals that conventional RI matching agents like fructose are not as efficient because they are not ‘colored’ enough.”
What’s Next
Though the dye is already in products that people consume and apply to their skin, medical use is years away. In some people, tartrazine can cause skin or respiratory reactions.
The National Science Foundation (NSF), which helped fund the research, posted a home or classroom activity related to the work on its website. It involves painting a tartrazine solution on a thin slice of raw chicken breast, making it transparent. The experiment should only be done while wearing a mask, eye protection, lab coat, and lab-quality nitrile gloves for protection, according to the NSF.
Meanwhile, Dr. Hong said his lab is looking for new compounds that will improve visibility through transparent skin, removing a red tone seen in the current experiments. And they’re looking for ways to induce cells to make their own “see-through” compounds.
“We are exploring methods for cells to express intensely absorbing molecules endogenously, enabling genetically encoded tissue transparency in live animals,” he said.
A version of this article first appeared on Medscape.com.
Applying the dye to lab mice made their skin temporarily transparent, allowing Stanford University researchers to observe the rodents’ digestive system, muscle fibers, and blood vessels, according to a study published in Science.
“It’s a stunning result,” said senior author Guosong Hong, PhD, who is assistant professor of materials science and engineering at Stanford University in California. “If the same technique could be applied to humans, it could offer a variety of benefits in biology, diagnostics, and even cosmetics.”
The work drew upon optical concepts first described in the early 20th century to form a surprising theory: Applying a light-absorbing substance could render skin transparent by reducing the chaotic scattering of light as it strikes proteins, fats, and water in tissue.
A search for a suitable light absorber led to FD&C Yellow 5, also called tartrazine, a synthetic color additive certified by the Food and Drug Administration (FDA) for use in foods, cosmetics, and medications.
Rubbed on live mice (after areas of fur were removed using a drugstore depilatory cream), tartrazine rendered skin on their bellies, hind legs, and heads transparent within 5 minutes. With the naked eye, the researchers watched a mouse’s intestines, bladder, and liver at work. Using a microscope, they observed muscle fibers and saw blood vessels in a living mouse’s brain — all without making incisions. Transparency faded quickly when the dye was washed off.
Someday, the concept could be used in doctors’ offices and hospitals, Dr. Hong said.
“Instead of relying on invasive biopsies, doctors might be able to diagnose deep-seated tumors by simply examining a person’s tissue without the need for invasive surgical removal,” he said. “This technique could potentially make blood draws less painful by helping phlebotomists easily locate veins under the skin. It could also enhance procedures like laser tattoo removal by allowing more precise targeting of the pigment beneath the skin.”
From Cake Frosting to Groundbreaking Research
Yellow 5 food dye can be found in everything from cereal, soda, spices, and cake frosting to lipstick, mouthwash, shampoo, dietary supplements, and house paint. Although it’s in some topical medications, more research is needed before it could be used in human diagnostics, said Christopher J. Rowlands, PhD, a senior lecturer in the Department of Bioengineering at Imperial College London, England, where he studies biophotonic instrumentation — ways to image structures inside the body more quickly and clearly.
But the finding could prove useful in research. In a commentary published in Science, Dr. Rowlands and his colleague Jon Gorecki, PhD, an experimental optical physicist also at Imperial College London, noted that the dye could be an alternative to other optical clearing agents currently used in lab studies, such as glycerol, fructose, or acetic acid. Advantages are the effect is reversible and works at lower concentrations with fewer side effects. This could broaden the types of studies possible in lab animals, so researchers don’t have to rely on naturally transparent creatures like nematodes and zebrafish.
The dye could also be paired with imaging techniques such as MRI or electron microscopy.
“Imaging techniques all have pros and cons,” Dr. Rowlands said. “MRI can see all the way through the body albeit with limited resolution and contrast. Electron microscopy has excellent resolution but limited compatibility with live tissue and penetration depth. Optical microscopy has subcellular resolution, the ability to label things, excellent biocompatibility but less than 1 millimeter of penetration depth. This clearing method will give a substantial boost to optical imaging for medicine and biology.”
The discovery could improve the depth imaging equipment can achieve by tenfold, according to the commentary.
Brain research especially stands to benefit. “Neurobiology in particular will have great use for combinations of multiphoton, optogenetics, and tissue clearing to record and control neural activity over (potentially) the whole mouse brain,” he said.
Refraction, Absorption, and The Invisible Man
The dye discovery has distant echoes in H.G. Wells’ 1897 novel The Invisible Man, Dr. Rowlands noted. In the book, a serum makes the main character invisible by changing the light scattering — or refractive index (RI) — of his cells to match the air around him.
The Stanford engineers looked to the past for inspiration, but not to fiction. They turned to a concept first described in the 1920s called the Kramers-Kronig relations, a mathematical principle that can be applied to relationships between the way light is refracted and absorbed in different materials. They also read up on Lorentz oscillation, which describes how electrons and atoms inside molecules react to light.
They reasoned that light-absorbing compounds could equalize the differences between the light-scattering properties of proteins, lipids, and water that make skin opaque.
With that, the search was on. The study’s first author, postdoctoral researcher Zihao Ou, PhD, began testing strong dyes to find a candidate. Tartrazine was a front-runner.
“We found that dye molecules are more efficient in raising the refractive index of water than conventional RI-matching agents, thus resulting in transparency at a much lower concentration,” Dr. Hong said. “The underlying physics, explained by the Lorentz oscillator model and Kramers-Kronig relations, reveals that conventional RI matching agents like fructose are not as efficient because they are not ‘colored’ enough.”
What’s Next
Though the dye is already in products that people consume and apply to their skin, medical use is years away. In some people, tartrazine can cause skin or respiratory reactions.
The National Science Foundation (NSF), which helped fund the research, posted a home or classroom activity related to the work on its website. It involves painting a tartrazine solution on a thin slice of raw chicken breast, making it transparent. The experiment should only be done while wearing a mask, eye protection, lab coat, and lab-quality nitrile gloves for protection, according to the NSF.
Meanwhile, Dr. Hong said his lab is looking for new compounds that will improve visibility through transparent skin, removing a red tone seen in the current experiments. And they’re looking for ways to induce cells to make their own “see-through” compounds.
“We are exploring methods for cells to express intensely absorbing molecules endogenously, enabling genetically encoded tissue transparency in live animals,” he said.
A version of this article first appeared on Medscape.com.
Applying the dye to lab mice made their skin temporarily transparent, allowing Stanford University researchers to observe the rodents’ digestive system, muscle fibers, and blood vessels, according to a study published in Science.
“It’s a stunning result,” said senior author Guosong Hong, PhD, who is assistant professor of materials science and engineering at Stanford University in California. “If the same technique could be applied to humans, it could offer a variety of benefits in biology, diagnostics, and even cosmetics.”
The work drew upon optical concepts first described in the early 20th century to form a surprising theory: Applying a light-absorbing substance could render skin transparent by reducing the chaotic scattering of light as it strikes proteins, fats, and water in tissue.
A search for a suitable light absorber led to FD&C Yellow 5, also called tartrazine, a synthetic color additive certified by the Food and Drug Administration (FDA) for use in foods, cosmetics, and medications.
Rubbed on live mice (after areas of fur were removed using a drugstore depilatory cream), tartrazine rendered skin on their bellies, hind legs, and heads transparent within 5 minutes. With the naked eye, the researchers watched a mouse’s intestines, bladder, and liver at work. Using a microscope, they observed muscle fibers and saw blood vessels in a living mouse’s brain — all without making incisions. Transparency faded quickly when the dye was washed off.
Someday, the concept could be used in doctors’ offices and hospitals, Dr. Hong said.
“Instead of relying on invasive biopsies, doctors might be able to diagnose deep-seated tumors by simply examining a person’s tissue without the need for invasive surgical removal,” he said. “This technique could potentially make blood draws less painful by helping phlebotomists easily locate veins under the skin. It could also enhance procedures like laser tattoo removal by allowing more precise targeting of the pigment beneath the skin.”
From Cake Frosting to Groundbreaking Research
Yellow 5 food dye can be found in everything from cereal, soda, spices, and cake frosting to lipstick, mouthwash, shampoo, dietary supplements, and house paint. Although it’s in some topical medications, more research is needed before it could be used in human diagnostics, said Christopher J. Rowlands, PhD, a senior lecturer in the Department of Bioengineering at Imperial College London, England, where he studies biophotonic instrumentation — ways to image structures inside the body more quickly and clearly.
But the finding could prove useful in research. In a commentary published in Science, Dr. Rowlands and his colleague Jon Gorecki, PhD, an experimental optical physicist also at Imperial College London, noted that the dye could be an alternative to other optical clearing agents currently used in lab studies, such as glycerol, fructose, or acetic acid. Advantages are the effect is reversible and works at lower concentrations with fewer side effects. This could broaden the types of studies possible in lab animals, so researchers don’t have to rely on naturally transparent creatures like nematodes and zebrafish.
The dye could also be paired with imaging techniques such as MRI or electron microscopy.
“Imaging techniques all have pros and cons,” Dr. Rowlands said. “MRI can see all the way through the body albeit with limited resolution and contrast. Electron microscopy has excellent resolution but limited compatibility with live tissue and penetration depth. Optical microscopy has subcellular resolution, the ability to label things, excellent biocompatibility but less than 1 millimeter of penetration depth. This clearing method will give a substantial boost to optical imaging for medicine and biology.”
The discovery could improve the depth imaging equipment can achieve by tenfold, according to the commentary.
Brain research especially stands to benefit. “Neurobiology in particular will have great use for combinations of multiphoton, optogenetics, and tissue clearing to record and control neural activity over (potentially) the whole mouse brain,” he said.
Refraction, Absorption, and The Invisible Man
The dye discovery has distant echoes in H.G. Wells’ 1897 novel The Invisible Man, Dr. Rowlands noted. In the book, a serum makes the main character invisible by changing the light scattering — or refractive index (RI) — of his cells to match the air around him.
The Stanford engineers looked to the past for inspiration, but not to fiction. They turned to a concept first described in the 1920s called the Kramers-Kronig relations, a mathematical principle that can be applied to relationships between the way light is refracted and absorbed in different materials. They also read up on Lorentz oscillation, which describes how electrons and atoms inside molecules react to light.
They reasoned that light-absorbing compounds could equalize the differences between the light-scattering properties of proteins, lipids, and water that make skin opaque.
With that, the search was on. The study’s first author, postdoctoral researcher Zihao Ou, PhD, began testing strong dyes to find a candidate. Tartrazine was a front-runner.
“We found that dye molecules are more efficient in raising the refractive index of water than conventional RI-matching agents, thus resulting in transparency at a much lower concentration,” Dr. Hong said. “The underlying physics, explained by the Lorentz oscillator model and Kramers-Kronig relations, reveals that conventional RI matching agents like fructose are not as efficient because they are not ‘colored’ enough.”
What’s Next
Though the dye is already in products that people consume and apply to their skin, medical use is years away. In some people, tartrazine can cause skin or respiratory reactions.
The National Science Foundation (NSF), which helped fund the research, posted a home or classroom activity related to the work on its website. It involves painting a tartrazine solution on a thin slice of raw chicken breast, making it transparent. The experiment should only be done while wearing a mask, eye protection, lab coat, and lab-quality nitrile gloves for protection, according to the NSF.
Meanwhile, Dr. Hong said his lab is looking for new compounds that will improve visibility through transparent skin, removing a red tone seen in the current experiments. And they’re looking for ways to induce cells to make their own “see-through” compounds.
“We are exploring methods for cells to express intensely absorbing molecules endogenously, enabling genetically encoded tissue transparency in live animals,” he said.
A version of this article first appeared on Medscape.com.
FROM SCIENCE
Analysis of Colchicine’s Drug-Drug Interactions Finds Little Risk
TOPLINE:
The presence of an operational classification of drug interactions (ORCA) class 3 or 4 drug-drug interactions (DDIs) did not increase the risk for colchicine-related gastrointestinal adverse events or modify the effect of colchicine on death or hospitalization caused by COVID-19 infection in ambulatory patients.
METHODOLOGY:
- This secondary analysis of the COLCORONA trial aimed to evaluate if a potential DDI of colchicine was associated with changes in its pharmacokinetics or modified its clinical safety and efficacy in patients with COVID-19.
- Overall, 4432 ambulatory patients with COVID-19 (median age, 54 years; 54% women) were randomly assigned to receive colchicine 0.5 mg twice daily for 3 days and then 0.5 mg once daily for 27 days (n = 2205) or a placebo (n = 2227).
- All the participants had at least one high-risk criterion such as age ≥ 70 years, diabetes, heart failure, systolic blood pressure ≥ 150 mm Hg, respiratory disease, coronary disease, body temperature ≥ 38.4 °C within the last 48 hours, dyspnea, bicytopenia, pancytopenia, or high neutrophil count with low lymphocyte count.
- The medications that could interact with colchicine were determined and categorized under ORCA classes 1 (contraindicated), 2 (provisionally contraindicated), 3 (conditional use), or 4 (minimal risk).
- The primary outcome was any gastrointestinal adverse event assessed over a 30-day follow-up period.
TAKEAWAY:
- Among all the participants, 1% received medications with an ORCA class 2 interaction, 14% with a class 3 interaction, and 13% with a class 4 interaction; rosuvastatin (12%) and atorvastatin (10%) were the most common interacting medications.
- The odds of any gastrointestinal adverse event were 1.80 times and 1.68 times higher in the colchicine arm than in the placebo arm among those without and with a DDI, respectively, with the effect of colchicine being consistent regardless of the presence of drug interactions (P = .69 for interaction).
- Similarly, DDIs did not influence the effect of colchicine on combined risk for COVID-19 hospitalization or mortality (P = .80 for interaction).
IN PRACTICE:
“Once potential DDIs have been identified through screening, they must be tested,” Hemalkumar B. Mehta, PhD, and G. Caleb Alexander, MD, of the Johns Hopkins Bloomberg School of Public Health, Baltimore, wrote in an invited commentary published online in JAMA Network Open. “Theoretical DDIs may not translate into real-world harms,” they added.
SOURCE:
The study was led by Lama S. Alfehaid, PharmD, of Brigham and Women’s Hospital, Boston. It was published online in JAMA Network Open.
LIMITATIONS:
This study focused on the medications used by participants at baseline, which may not have captured all potential DDIs. The findings did not provide information on rare adverse events, such as rhabdomyolysis, which usually occur months after initiating drug therapy. Furthermore, all the study participants had confirmed SARS-CoV-2 infection, which may have increased their susceptibility to adverse reactions associated with the use of colchicine.
DISCLOSURES:
Some authors were supported by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute, American Heart Association, and other sources. The authors also declared serving on advisory boards or on the board of directors; receiving personal fees, grants, research support, or speaking fees; or having other ties with many pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The presence of an operational classification of drug interactions (ORCA) class 3 or 4 drug-drug interactions (DDIs) did not increase the risk for colchicine-related gastrointestinal adverse events or modify the effect of colchicine on death or hospitalization caused by COVID-19 infection in ambulatory patients.
METHODOLOGY:
- This secondary analysis of the COLCORONA trial aimed to evaluate if a potential DDI of colchicine was associated with changes in its pharmacokinetics or modified its clinical safety and efficacy in patients with COVID-19.
- Overall, 4432 ambulatory patients with COVID-19 (median age, 54 years; 54% women) were randomly assigned to receive colchicine 0.5 mg twice daily for 3 days and then 0.5 mg once daily for 27 days (n = 2205) or a placebo (n = 2227).
- All the participants had at least one high-risk criterion such as age ≥ 70 years, diabetes, heart failure, systolic blood pressure ≥ 150 mm Hg, respiratory disease, coronary disease, body temperature ≥ 38.4 °C within the last 48 hours, dyspnea, bicytopenia, pancytopenia, or high neutrophil count with low lymphocyte count.
- The medications that could interact with colchicine were determined and categorized under ORCA classes 1 (contraindicated), 2 (provisionally contraindicated), 3 (conditional use), or 4 (minimal risk).
- The primary outcome was any gastrointestinal adverse event assessed over a 30-day follow-up period.
TAKEAWAY:
- Among all the participants, 1% received medications with an ORCA class 2 interaction, 14% with a class 3 interaction, and 13% with a class 4 interaction; rosuvastatin (12%) and atorvastatin (10%) were the most common interacting medications.
- The odds of any gastrointestinal adverse event were 1.80 times and 1.68 times higher in the colchicine arm than in the placebo arm among those without and with a DDI, respectively, with the effect of colchicine being consistent regardless of the presence of drug interactions (P = .69 for interaction).
- Similarly, DDIs did not influence the effect of colchicine on combined risk for COVID-19 hospitalization or mortality (P = .80 for interaction).
IN PRACTICE:
“Once potential DDIs have been identified through screening, they must be tested,” Hemalkumar B. Mehta, PhD, and G. Caleb Alexander, MD, of the Johns Hopkins Bloomberg School of Public Health, Baltimore, wrote in an invited commentary published online in JAMA Network Open. “Theoretical DDIs may not translate into real-world harms,” they added.
SOURCE:
The study was led by Lama S. Alfehaid, PharmD, of Brigham and Women’s Hospital, Boston. It was published online in JAMA Network Open.
LIMITATIONS:
This study focused on the medications used by participants at baseline, which may not have captured all potential DDIs. The findings did not provide information on rare adverse events, such as rhabdomyolysis, which usually occur months after initiating drug therapy. Furthermore, all the study participants had confirmed SARS-CoV-2 infection, which may have increased their susceptibility to adverse reactions associated with the use of colchicine.
DISCLOSURES:
Some authors were supported by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute, American Heart Association, and other sources. The authors also declared serving on advisory boards or on the board of directors; receiving personal fees, grants, research support, or speaking fees; or having other ties with many pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The presence of an operational classification of drug interactions (ORCA) class 3 or 4 drug-drug interactions (DDIs) did not increase the risk for colchicine-related gastrointestinal adverse events or modify the effect of colchicine on death or hospitalization caused by COVID-19 infection in ambulatory patients.
METHODOLOGY:
- This secondary analysis of the COLCORONA trial aimed to evaluate if a potential DDI of colchicine was associated with changes in its pharmacokinetics or modified its clinical safety and efficacy in patients with COVID-19.
- Overall, 4432 ambulatory patients with COVID-19 (median age, 54 years; 54% women) were randomly assigned to receive colchicine 0.5 mg twice daily for 3 days and then 0.5 mg once daily for 27 days (n = 2205) or a placebo (n = 2227).
- All the participants had at least one high-risk criterion such as age ≥ 70 years, diabetes, heart failure, systolic blood pressure ≥ 150 mm Hg, respiratory disease, coronary disease, body temperature ≥ 38.4 °C within the last 48 hours, dyspnea, bicytopenia, pancytopenia, or high neutrophil count with low lymphocyte count.
- The medications that could interact with colchicine were determined and categorized under ORCA classes 1 (contraindicated), 2 (provisionally contraindicated), 3 (conditional use), or 4 (minimal risk).
- The primary outcome was any gastrointestinal adverse event assessed over a 30-day follow-up period.
TAKEAWAY:
- Among all the participants, 1% received medications with an ORCA class 2 interaction, 14% with a class 3 interaction, and 13% with a class 4 interaction; rosuvastatin (12%) and atorvastatin (10%) were the most common interacting medications.
- The odds of any gastrointestinal adverse event were 1.80 times and 1.68 times higher in the colchicine arm than in the placebo arm among those without and with a DDI, respectively, with the effect of colchicine being consistent regardless of the presence of drug interactions (P = .69 for interaction).
- Similarly, DDIs did not influence the effect of colchicine on combined risk for COVID-19 hospitalization or mortality (P = .80 for interaction).
IN PRACTICE:
“Once potential DDIs have been identified through screening, they must be tested,” Hemalkumar B. Mehta, PhD, and G. Caleb Alexander, MD, of the Johns Hopkins Bloomberg School of Public Health, Baltimore, wrote in an invited commentary published online in JAMA Network Open. “Theoretical DDIs may not translate into real-world harms,” they added.
SOURCE:
The study was led by Lama S. Alfehaid, PharmD, of Brigham and Women’s Hospital, Boston. It was published online in JAMA Network Open.
LIMITATIONS:
This study focused on the medications used by participants at baseline, which may not have captured all potential DDIs. The findings did not provide information on rare adverse events, such as rhabdomyolysis, which usually occur months after initiating drug therapy. Furthermore, all the study participants had confirmed SARS-CoV-2 infection, which may have increased their susceptibility to adverse reactions associated with the use of colchicine.
DISCLOSURES:
Some authors were supported by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute, American Heart Association, and other sources. The authors also declared serving on advisory boards or on the board of directors; receiving personal fees, grants, research support, or speaking fees; or having other ties with many pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Cell Phone Use Linked to Higher Heart Disease Risk
“We found that a poor sleep pattern, psychological distress, and neuroticism significantly mediated the positive association between weekly mobile phone usage time and the risk for incident CVD, with a mediating proportion of 5.11%, 11.50%, and 2.25%, respectively,” said principal investigator Xianhui Qin, MD, professor of nephrology at Southern Medical University, Guangzhou, China.
Poor sleep patterns and poor mental health could disrupt circadian rhythms and endocrine and metabolic functions, as well as increase inflammation, he explained.
In addition, chronic exposure to radiofrequency electromagnetic fields (RF-EMF) emitted from cell phones could lead to oxidative stress and an inflammatory response. Combined with smoking and diabetes, this exposure “may have a synergistic effect in increasing CVD risk,” Dr. Qin suggested.
The study was published online in the Canadian Journal of Cardiology.
Risk Underestimated?
The researchers aimed to examine the association of regular cell phone use with incident CVD and explore the mediating effects of sleep and mental health using linked hospital and mortality records.
Their analysis included 444,027 participants (mean age, 56 years; 44% men) without a history of CVD from the UK Biobank. A total of 378,161 participants were regular cell phone users.
Regular cell phone use was defined as at least one call per week. Weekly use was self-reported as the average time of calls per week during the previous 3 months.
The primary outcome was incident CVD. Secondary outcomes were each component of CVD (ie, coronary heart disease, stroke, atrial fibrillation, and heart failure) and increased carotid intima media thickness (CIMT).
Compared with nonregular cell phone users, regular users were younger, had higher proportions of current smokers and urban residents, and had lower proportions of history of hypertension and diabetes. They also had higher income, Townsend deprivation index, and body mass index, and lower education levels.
During a median follow-up of 12.3 years, 56,181 participants developed incident CVD. Compared with nonregular cell phone users, regular users had a significantly higher risk for incident CVD (hazard ratio, 1.04) and increased CIMT (odds ratio, 1.11).
Among regular cell phone users, the duration of cell phone use and hands-free device/speakerphone use during calls was not significantly associated with incident CVD. Yet a significant and positive dose-response relationship was seen between weekly cell phone usage time and the risk for CVD. The positive association was stronger in current vs noncurrent smokers and people with vs without diabetes.
To different extents, sleep patterns (5.11%), psychologic distress (11.5%), and neuroticism (2.25%) mediated the relationship between weekly cell phone usage time and the risk for incident CVD.
“Our study suggests that despite the advantages of mobile phone use, we should also pay attention to the potential harm of mobile phone use to cardiovascular health,” Dr. Qin said. “Future studies to assess the risk-benefit balance will help promote mobile phone use patterns that are conducive to cardiovascular health.”
Meanwhile, he added, “We encourage measures to reduce time spent on mobile phones to promote the primary prevention of CVD. On the other hand, improving sleep and mental health status may help reduce the higher risk of CVD associated with mobile phone use.”
There are several limitations to the study in addition to its observational nature, which cannot show cause and effect. The questionnaires on cell phone use were restricted to phone calls; other use patterns of cell phones (eg, messaging, watching videos, and browsing the web) were not considered. Although the researchers adjusted for many potential confounders, unmeasured confounding bias (eg, the type of cell phone used and other sources of RF-EMF) cannot be eliminated.
Weak Link?
In a comment, Nicholas Grubic, MSc, a PhD student in epidemiology at the University of Toronto, Ontario, Canada, and coauthor of a related editorial, said, “I found it interesting that there was a connection observed between mobile phone use and CVD. However, it is crucial to understand that this link appeared to be much weaker compared with other well-known cardiovascular risk factors, such as smoking, diabetes, and high blood pressure. For now, mobile phone use should not be a major concern for most people.”
Nevertheless, clinicians should encourage patients to practice healthy habits around their screen time, he advised. “This could include limiting mobile phone use before bedtime and taking regular breaks to engage in activities that promote heart health, such as exercising or spending time outdoors.
“For the time being, we probably won’t see mobile phone use included in standard assessments for cardiovascular risk or as a focal point of cardiovascular health promotion initiatives,” he added. Instead, clinicians should “focus on established risk factors that have a stronger impact on patients’ cardiovascular health.”
Nieca Goldberg, MD, a clinical associate professor of medicine at NYU Grossman School of Medicine in New York City and American Heart Association volunteer expert, had a similar message. “You don’t have to go back to using a landline,” she said. “Instead, patients should be more mindful of how much phone use is taking away from their physical activity, keeping them from sleeping, and causing them stress.” Clinicians should also remember to counsel smokers on smoking cessation.
“It would be important for future studies to look at time spent on the phone and the type of activities patients are doing on their phones, such as social media, calls, texts, movies, or streaming TV shows,” she said. “It would be important to see how phone use is leading to a sedentary lifestyle” and what that means for a larger, more diverse population.
The study was supported by the National Key R&D Program, the National Natural Science Foundation of China, and the Outstanding Youth Development Scheme of Nanfang Hospital, Southern Medical University. Dr. Qin, Dr. Grubic, and Dr. Goldberg reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We found that a poor sleep pattern, psychological distress, and neuroticism significantly mediated the positive association between weekly mobile phone usage time and the risk for incident CVD, with a mediating proportion of 5.11%, 11.50%, and 2.25%, respectively,” said principal investigator Xianhui Qin, MD, professor of nephrology at Southern Medical University, Guangzhou, China.
Poor sleep patterns and poor mental health could disrupt circadian rhythms and endocrine and metabolic functions, as well as increase inflammation, he explained.
In addition, chronic exposure to radiofrequency electromagnetic fields (RF-EMF) emitted from cell phones could lead to oxidative stress and an inflammatory response. Combined with smoking and diabetes, this exposure “may have a synergistic effect in increasing CVD risk,” Dr. Qin suggested.
The study was published online in the Canadian Journal of Cardiology.
Risk Underestimated?
The researchers aimed to examine the association of regular cell phone use with incident CVD and explore the mediating effects of sleep and mental health using linked hospital and mortality records.
Their analysis included 444,027 participants (mean age, 56 years; 44% men) without a history of CVD from the UK Biobank. A total of 378,161 participants were regular cell phone users.
Regular cell phone use was defined as at least one call per week. Weekly use was self-reported as the average time of calls per week during the previous 3 months.
The primary outcome was incident CVD. Secondary outcomes were each component of CVD (ie, coronary heart disease, stroke, atrial fibrillation, and heart failure) and increased carotid intima media thickness (CIMT).
Compared with nonregular cell phone users, regular users were younger, had higher proportions of current smokers and urban residents, and had lower proportions of history of hypertension and diabetes. They also had higher income, Townsend deprivation index, and body mass index, and lower education levels.
During a median follow-up of 12.3 years, 56,181 participants developed incident CVD. Compared with nonregular cell phone users, regular users had a significantly higher risk for incident CVD (hazard ratio, 1.04) and increased CIMT (odds ratio, 1.11).
Among regular cell phone users, the duration of cell phone use and hands-free device/speakerphone use during calls was not significantly associated with incident CVD. Yet a significant and positive dose-response relationship was seen between weekly cell phone usage time and the risk for CVD. The positive association was stronger in current vs noncurrent smokers and people with vs without diabetes.
To different extents, sleep patterns (5.11%), psychologic distress (11.5%), and neuroticism (2.25%) mediated the relationship between weekly cell phone usage time and the risk for incident CVD.
“Our study suggests that despite the advantages of mobile phone use, we should also pay attention to the potential harm of mobile phone use to cardiovascular health,” Dr. Qin said. “Future studies to assess the risk-benefit balance will help promote mobile phone use patterns that are conducive to cardiovascular health.”
Meanwhile, he added, “We encourage measures to reduce time spent on mobile phones to promote the primary prevention of CVD. On the other hand, improving sleep and mental health status may help reduce the higher risk of CVD associated with mobile phone use.”
There are several limitations to the study in addition to its observational nature, which cannot show cause and effect. The questionnaires on cell phone use were restricted to phone calls; other use patterns of cell phones (eg, messaging, watching videos, and browsing the web) were not considered. Although the researchers adjusted for many potential confounders, unmeasured confounding bias (eg, the type of cell phone used and other sources of RF-EMF) cannot be eliminated.
Weak Link?
In a comment, Nicholas Grubic, MSc, a PhD student in epidemiology at the University of Toronto, Ontario, Canada, and coauthor of a related editorial, said, “I found it interesting that there was a connection observed between mobile phone use and CVD. However, it is crucial to understand that this link appeared to be much weaker compared with other well-known cardiovascular risk factors, such as smoking, diabetes, and high blood pressure. For now, mobile phone use should not be a major concern for most people.”
Nevertheless, clinicians should encourage patients to practice healthy habits around their screen time, he advised. “This could include limiting mobile phone use before bedtime and taking regular breaks to engage in activities that promote heart health, such as exercising or spending time outdoors.
“For the time being, we probably won’t see mobile phone use included in standard assessments for cardiovascular risk or as a focal point of cardiovascular health promotion initiatives,” he added. Instead, clinicians should “focus on established risk factors that have a stronger impact on patients’ cardiovascular health.”
Nieca Goldberg, MD, a clinical associate professor of medicine at NYU Grossman School of Medicine in New York City and American Heart Association volunteer expert, had a similar message. “You don’t have to go back to using a landline,” she said. “Instead, patients should be more mindful of how much phone use is taking away from their physical activity, keeping them from sleeping, and causing them stress.” Clinicians should also remember to counsel smokers on smoking cessation.
“It would be important for future studies to look at time spent on the phone and the type of activities patients are doing on their phones, such as social media, calls, texts, movies, or streaming TV shows,” she said. “It would be important to see how phone use is leading to a sedentary lifestyle” and what that means for a larger, more diverse population.
The study was supported by the National Key R&D Program, the National Natural Science Foundation of China, and the Outstanding Youth Development Scheme of Nanfang Hospital, Southern Medical University. Dr. Qin, Dr. Grubic, and Dr. Goldberg reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We found that a poor sleep pattern, psychological distress, and neuroticism significantly mediated the positive association between weekly mobile phone usage time and the risk for incident CVD, with a mediating proportion of 5.11%, 11.50%, and 2.25%, respectively,” said principal investigator Xianhui Qin, MD, professor of nephrology at Southern Medical University, Guangzhou, China.
Poor sleep patterns and poor mental health could disrupt circadian rhythms and endocrine and metabolic functions, as well as increase inflammation, he explained.
In addition, chronic exposure to radiofrequency electromagnetic fields (RF-EMF) emitted from cell phones could lead to oxidative stress and an inflammatory response. Combined with smoking and diabetes, this exposure “may have a synergistic effect in increasing CVD risk,” Dr. Qin suggested.
The study was published online in the Canadian Journal of Cardiology.
Risk Underestimated?
The researchers aimed to examine the association of regular cell phone use with incident CVD and explore the mediating effects of sleep and mental health using linked hospital and mortality records.
Their analysis included 444,027 participants (mean age, 56 years; 44% men) without a history of CVD from the UK Biobank. A total of 378,161 participants were regular cell phone users.
Regular cell phone use was defined as at least one call per week. Weekly use was self-reported as the average time of calls per week during the previous 3 months.
The primary outcome was incident CVD. Secondary outcomes were each component of CVD (ie, coronary heart disease, stroke, atrial fibrillation, and heart failure) and increased carotid intima media thickness (CIMT).
Compared with nonregular cell phone users, regular users were younger, had higher proportions of current smokers and urban residents, and had lower proportions of history of hypertension and diabetes. They also had higher income, Townsend deprivation index, and body mass index, and lower education levels.
During a median follow-up of 12.3 years, 56,181 participants developed incident CVD. Compared with nonregular cell phone users, regular users had a significantly higher risk for incident CVD (hazard ratio, 1.04) and increased CIMT (odds ratio, 1.11).
Among regular cell phone users, the duration of cell phone use and hands-free device/speakerphone use during calls was not significantly associated with incident CVD. Yet a significant and positive dose-response relationship was seen between weekly cell phone usage time and the risk for CVD. The positive association was stronger in current vs noncurrent smokers and people with vs without diabetes.
To different extents, sleep patterns (5.11%), psychologic distress (11.5%), and neuroticism (2.25%) mediated the relationship between weekly cell phone usage time and the risk for incident CVD.
“Our study suggests that despite the advantages of mobile phone use, we should also pay attention to the potential harm of mobile phone use to cardiovascular health,” Dr. Qin said. “Future studies to assess the risk-benefit balance will help promote mobile phone use patterns that are conducive to cardiovascular health.”
Meanwhile, he added, “We encourage measures to reduce time spent on mobile phones to promote the primary prevention of CVD. On the other hand, improving sleep and mental health status may help reduce the higher risk of CVD associated with mobile phone use.”
There are several limitations to the study in addition to its observational nature, which cannot show cause and effect. The questionnaires on cell phone use were restricted to phone calls; other use patterns of cell phones (eg, messaging, watching videos, and browsing the web) were not considered. Although the researchers adjusted for many potential confounders, unmeasured confounding bias (eg, the type of cell phone used and other sources of RF-EMF) cannot be eliminated.
Weak Link?
In a comment, Nicholas Grubic, MSc, a PhD student in epidemiology at the University of Toronto, Ontario, Canada, and coauthor of a related editorial, said, “I found it interesting that there was a connection observed between mobile phone use and CVD. However, it is crucial to understand that this link appeared to be much weaker compared with other well-known cardiovascular risk factors, such as smoking, diabetes, and high blood pressure. For now, mobile phone use should not be a major concern for most people.”
Nevertheless, clinicians should encourage patients to practice healthy habits around their screen time, he advised. “This could include limiting mobile phone use before bedtime and taking regular breaks to engage in activities that promote heart health, such as exercising or spending time outdoors.
“For the time being, we probably won’t see mobile phone use included in standard assessments for cardiovascular risk or as a focal point of cardiovascular health promotion initiatives,” he added. Instead, clinicians should “focus on established risk factors that have a stronger impact on patients’ cardiovascular health.”
Nieca Goldberg, MD, a clinical associate professor of medicine at NYU Grossman School of Medicine in New York City and American Heart Association volunteer expert, had a similar message. “You don’t have to go back to using a landline,” she said. “Instead, patients should be more mindful of how much phone use is taking away from their physical activity, keeping them from sleeping, and causing them stress.” Clinicians should also remember to counsel smokers on smoking cessation.
“It would be important for future studies to look at time spent on the phone and the type of activities patients are doing on their phones, such as social media, calls, texts, movies, or streaming TV shows,” she said. “It would be important to see how phone use is leading to a sedentary lifestyle” and what that means for a larger, more diverse population.
The study was supported by the National Key R&D Program, the National Natural Science Foundation of China, and the Outstanding Youth Development Scheme of Nanfang Hospital, Southern Medical University. Dr. Qin, Dr. Grubic, and Dr. Goldberg reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE CANADIAN JOURNAL OF CARDIOLOGY
Skip Potassium After Cardiac Surgery
LONDON —
“The widespread practice of giving patients potassium after bypass heart surgery even though their blood levels are within the normal range can be abandoned,” said Benjamin O’Brien, MD, PhD, director of the Clinic for Cardioanesthesiology and Intensive Care Medicine at Charité Hospital in Berlin, Germany.
Results from the randomized TIGHT-K trial that assessed two levels of potassium supplementation were presented at the annual congress of the European Society of Cardiology.
In the tight-control group, supplementation was provided to maintain high-normal levels of potassium (> 4.5 mEq/L). In the relaxed-control group, supplementation was provided only when potassium levels fell below the low-normal threshold (< 3.6 mEq/L).
Trial Upending Popular Practice
The multinational trial involved 23 centers in Germany and the United Kingdom. All 1690 participants enrolled were scheduled to undergo a coronary artery bypass graft procedure, but Dr. O’Brien said he considers the results of TIGHT-K to be broadly applicable.
“There is no physiological basis to expect a different result in patients undergoing different types of cardiac surgery,” he said.
The primary endpoint was clinically and electrocardiography confirmed new-onset atrial fibrillation that occurred in the 5 days after the bypass procedure.
For the primary atrial fibrillation endpoint, event rates were similar in the tight-control and the relaxed-control groups (26.2% vs 27.8%); the 1.7% difference did not approach statistical significance (P = .44). The difference in dysrhythmias other than atrial fibrillation, although numerically lower in the tight-control group, was also not significant (19.1% vs 21.1%; P = .26).
There were no significant differences in several secondary endpoints, including length of hospital stay and in-patient mortality, but cost, a prespecified secondary endpoint, was approximately $120 lower per patient in the relaxed-control group than in the tight-control group (P < .001).
Lowering Cost Across Cardiac Surgeries
During the 5-day follow-up, median potassium levels were higher in the tight-control group. Levels in both groups fell gradually, but essentially in parallel, over the study period, so median potassium levels were always higher in the tight-control group than in the relaxed-control group. At the end of the observation period, mean potassium levels were 4.34 mEq/L in the tight-control group and 4.08 mEq/L in the relaxed-control group.
Prior to the development of atrial fibrillation, participants in the tight-control group received a medium of seven potassium administrations (range, 4-12), whereas those in the relaxed-control group received a medium of zero.
There were no significant differences in episodes in any subgroup evaluated, including those divided by age, sex, baseline left ventricular ejection fraction, and the absence or presence of beta blockers or loop diuretics. A per-protocol analysis also failed to show any advantage for tight potassium control.
Atrial fibrillation occurs in about one third of patients after bypass surgery, as it does after many types of cardiac surgery. Institutions often have strategies in place to reduce the risk after cardiac surgery, and potassium supplementation is one of the most common, despite the lack of supportive evidence, Dr. O’Brien said.
Narrow Window for Optimal Potassium Levels
The difference in potassium levels between the tight-control group and the relaxed-control group were modest in this study, said Subodh Verma, MD, a cardiac surgeon at St Michael’s Hospital and professor at the University of Toronto, Ontario, Canada.
However, this is unavoidable and central to the question being posed, Dr. O’Brien pointed out. Because of the risks for both hypokalemia and hyperkalemia, the window for safe supplementation is short. Current practice is to achieve high-normal levels to reduce atrial fibrillation, but TIGHT-K demonstrates this has no benefit.
The conclusion of TIGHT-K is appropriate, said Faiez Zannad, MD, PhD, professor of therapeutics in the Division of Cardiology at the University of Lorraine in Nancy, France, who praised the design and conduct of the study.
He acknowledged an unmet need for effective methods to reduce the risk for atrial fibrillation after cardiac surgery, but the ESC invited discussant said it is now necessary to look at other strategies. Several are under current evaluation, such as supplementary magnesium and the use of sodium-glucose transporter-2 inhibitors.
Although Dr. Zannad encouraged more studies of methods to reduce atrial fibrillation risk after cardiac surgery, he said that TIGHT-K has answered the question of whether potassium supplementation is beneficial.
Potassium supplementation should no longer be offered, he said, which will “reduce healthcare costs and decrease patient risk from an unnecessary intervention.”
A version of this article first appeared on Medscape.com.
LONDON —
“The widespread practice of giving patients potassium after bypass heart surgery even though their blood levels are within the normal range can be abandoned,” said Benjamin O’Brien, MD, PhD, director of the Clinic for Cardioanesthesiology and Intensive Care Medicine at Charité Hospital in Berlin, Germany.
Results from the randomized TIGHT-K trial that assessed two levels of potassium supplementation were presented at the annual congress of the European Society of Cardiology.
In the tight-control group, supplementation was provided to maintain high-normal levels of potassium (> 4.5 mEq/L). In the relaxed-control group, supplementation was provided only when potassium levels fell below the low-normal threshold (< 3.6 mEq/L).
Trial Upending Popular Practice
The multinational trial involved 23 centers in Germany and the United Kingdom. All 1690 participants enrolled were scheduled to undergo a coronary artery bypass graft procedure, but Dr. O’Brien said he considers the results of TIGHT-K to be broadly applicable.
“There is no physiological basis to expect a different result in patients undergoing different types of cardiac surgery,” he said.
The primary endpoint was clinically and electrocardiography confirmed new-onset atrial fibrillation that occurred in the 5 days after the bypass procedure.
For the primary atrial fibrillation endpoint, event rates were similar in the tight-control and the relaxed-control groups (26.2% vs 27.8%); the 1.7% difference did not approach statistical significance (P = .44). The difference in dysrhythmias other than atrial fibrillation, although numerically lower in the tight-control group, was also not significant (19.1% vs 21.1%; P = .26).
There were no significant differences in several secondary endpoints, including length of hospital stay and in-patient mortality, but cost, a prespecified secondary endpoint, was approximately $120 lower per patient in the relaxed-control group than in the tight-control group (P < .001).
Lowering Cost Across Cardiac Surgeries
During the 5-day follow-up, median potassium levels were higher in the tight-control group. Levels in both groups fell gradually, but essentially in parallel, over the study period, so median potassium levels were always higher in the tight-control group than in the relaxed-control group. At the end of the observation period, mean potassium levels were 4.34 mEq/L in the tight-control group and 4.08 mEq/L in the relaxed-control group.
Prior to the development of atrial fibrillation, participants in the tight-control group received a medium of seven potassium administrations (range, 4-12), whereas those in the relaxed-control group received a medium of zero.
There were no significant differences in episodes in any subgroup evaluated, including those divided by age, sex, baseline left ventricular ejection fraction, and the absence or presence of beta blockers or loop diuretics. A per-protocol analysis also failed to show any advantage for tight potassium control.
Atrial fibrillation occurs in about one third of patients after bypass surgery, as it does after many types of cardiac surgery. Institutions often have strategies in place to reduce the risk after cardiac surgery, and potassium supplementation is one of the most common, despite the lack of supportive evidence, Dr. O’Brien said.
Narrow Window for Optimal Potassium Levels
The difference in potassium levels between the tight-control group and the relaxed-control group were modest in this study, said Subodh Verma, MD, a cardiac surgeon at St Michael’s Hospital and professor at the University of Toronto, Ontario, Canada.
However, this is unavoidable and central to the question being posed, Dr. O’Brien pointed out. Because of the risks for both hypokalemia and hyperkalemia, the window for safe supplementation is short. Current practice is to achieve high-normal levels to reduce atrial fibrillation, but TIGHT-K demonstrates this has no benefit.
The conclusion of TIGHT-K is appropriate, said Faiez Zannad, MD, PhD, professor of therapeutics in the Division of Cardiology at the University of Lorraine in Nancy, France, who praised the design and conduct of the study.
He acknowledged an unmet need for effective methods to reduce the risk for atrial fibrillation after cardiac surgery, but the ESC invited discussant said it is now necessary to look at other strategies. Several are under current evaluation, such as supplementary magnesium and the use of sodium-glucose transporter-2 inhibitors.
Although Dr. Zannad encouraged more studies of methods to reduce atrial fibrillation risk after cardiac surgery, he said that TIGHT-K has answered the question of whether potassium supplementation is beneficial.
Potassium supplementation should no longer be offered, he said, which will “reduce healthcare costs and decrease patient risk from an unnecessary intervention.”
A version of this article first appeared on Medscape.com.
LONDON —
“The widespread practice of giving patients potassium after bypass heart surgery even though their blood levels are within the normal range can be abandoned,” said Benjamin O’Brien, MD, PhD, director of the Clinic for Cardioanesthesiology and Intensive Care Medicine at Charité Hospital in Berlin, Germany.
Results from the randomized TIGHT-K trial that assessed two levels of potassium supplementation were presented at the annual congress of the European Society of Cardiology.
In the tight-control group, supplementation was provided to maintain high-normal levels of potassium (> 4.5 mEq/L). In the relaxed-control group, supplementation was provided only when potassium levels fell below the low-normal threshold (< 3.6 mEq/L).
Trial Upending Popular Practice
The multinational trial involved 23 centers in Germany and the United Kingdom. All 1690 participants enrolled were scheduled to undergo a coronary artery bypass graft procedure, but Dr. O’Brien said he considers the results of TIGHT-K to be broadly applicable.
“There is no physiological basis to expect a different result in patients undergoing different types of cardiac surgery,” he said.
The primary endpoint was clinically and electrocardiography confirmed new-onset atrial fibrillation that occurred in the 5 days after the bypass procedure.
For the primary atrial fibrillation endpoint, event rates were similar in the tight-control and the relaxed-control groups (26.2% vs 27.8%); the 1.7% difference did not approach statistical significance (P = .44). The difference in dysrhythmias other than atrial fibrillation, although numerically lower in the tight-control group, was also not significant (19.1% vs 21.1%; P = .26).
There were no significant differences in several secondary endpoints, including length of hospital stay and in-patient mortality, but cost, a prespecified secondary endpoint, was approximately $120 lower per patient in the relaxed-control group than in the tight-control group (P < .001).
Lowering Cost Across Cardiac Surgeries
During the 5-day follow-up, median potassium levels were higher in the tight-control group. Levels in both groups fell gradually, but essentially in parallel, over the study period, so median potassium levels were always higher in the tight-control group than in the relaxed-control group. At the end of the observation period, mean potassium levels were 4.34 mEq/L in the tight-control group and 4.08 mEq/L in the relaxed-control group.
Prior to the development of atrial fibrillation, participants in the tight-control group received a medium of seven potassium administrations (range, 4-12), whereas those in the relaxed-control group received a medium of zero.
There were no significant differences in episodes in any subgroup evaluated, including those divided by age, sex, baseline left ventricular ejection fraction, and the absence or presence of beta blockers or loop diuretics. A per-protocol analysis also failed to show any advantage for tight potassium control.
Atrial fibrillation occurs in about one third of patients after bypass surgery, as it does after many types of cardiac surgery. Institutions often have strategies in place to reduce the risk after cardiac surgery, and potassium supplementation is one of the most common, despite the lack of supportive evidence, Dr. O’Brien said.
Narrow Window for Optimal Potassium Levels
The difference in potassium levels between the tight-control group and the relaxed-control group were modest in this study, said Subodh Verma, MD, a cardiac surgeon at St Michael’s Hospital and professor at the University of Toronto, Ontario, Canada.
However, this is unavoidable and central to the question being posed, Dr. O’Brien pointed out. Because of the risks for both hypokalemia and hyperkalemia, the window for safe supplementation is short. Current practice is to achieve high-normal levels to reduce atrial fibrillation, but TIGHT-K demonstrates this has no benefit.
The conclusion of TIGHT-K is appropriate, said Faiez Zannad, MD, PhD, professor of therapeutics in the Division of Cardiology at the University of Lorraine in Nancy, France, who praised the design and conduct of the study.
He acknowledged an unmet need for effective methods to reduce the risk for atrial fibrillation after cardiac surgery, but the ESC invited discussant said it is now necessary to look at other strategies. Several are under current evaluation, such as supplementary magnesium and the use of sodium-glucose transporter-2 inhibitors.
Although Dr. Zannad encouraged more studies of methods to reduce atrial fibrillation risk after cardiac surgery, he said that TIGHT-K has answered the question of whether potassium supplementation is beneficial.
Potassium supplementation should no longer be offered, he said, which will “reduce healthcare costs and decrease patient risk from an unnecessary intervention.”
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2024