User login
Dietary flavonol intake linked to reduced risk of Alzheimer’s

Onset of Alzheimer’s disease (AD) was inversely associated with intake of flavonols, a subclass of flavonoids with antioxidant and anti-inflammatory properties, according to the study authors.
The rate of developing AD was reduced by 50% among individuals reporting high intake of kaempferol, a flavonol plentiful in leafy green vegetables, and by 38% for high intake of the flavonols myricetin and isorhamnetin, researchers said in a report published in Neurology.
The findings are from the Rush Memory and Aging Project (MAP), a large, prospective study of older individuals in retirement communities and public housing in the Chicago area that has been ongoing since 1997.
“Although there is more work to be done, the associations that we observed are promising and deserve further study,” said Thomas M. Holland, MD, of the Rush Institute for Healthy Aging in Chicago, and coauthors.
Those associations between flavonol intake and AD help set the stage for U.S. POINTER and other randomized, controlled trials that seek to evaluate the effects of dietary interventions in a more rigorous way, according to Laura D. Baker, PhD, associate professor of internal medicine at Wake Forest University, Winston-Salem, N.C.
“This kind of data helps us feel like we are looking in the right direction in the randomized, controlled trials,” Dr. Baker said in an interview.
Dr. Baker is an investigator in the U.S. POINTER study, which will in part evaluate the impact of the MIND diet, which has been shown to slow cognitive decline with age in a previously published MAP study.
However, in the absence of randomized, controlled trial data, Dr. Baker cautioned against “prematurely advocating” for specific dietary approaches when speaking to patients and caregivers now.
“What I say is, we know for sure that the standard American Heart Association diet has been shown in clinical trials to reduce the risk of heart disease, and in terms of brain health, if you can reduce risk of heart disease, you are protecting your brain,” she said in the interview.
The present MAP study linking a reduced rate of AD to flavonol consumption is believed to be the first of its kind, though two previous studies from the early 2000s did find inverse associations between incident AD and intake of flavonoids, of which flavonoids are just one subclass, said Dr. Holland and coinvestigators in their report.
Moreover, in a MAP study published in 2018, Martha Clare Morris, ScD, and coauthors concluded that consuming about a serving per day of green leafy vegetables and foods rich in kaempferol, among other nutrients and bioactive compounds, may help slow cognitive decline associated with aging.
To more specifically study the relationship between kaempferol and other flavonols and the development of AD, Dr. Holland and colleagues evaluated data for MAP participants who had completed a comprehensive food frequency questionnaire and underwent at least two evaluations to assess incidence of disease.
The mean age of the 921 individuals in the present analysis was 81 years, three-quarters were female, and over approximately 6 years of follow-up, 220 developed AD.
The rate of developing AD was 48% lower among participants reporting the highest total dietary intake of flavonols, compared with those reporting the lowest intake, Dr. Holland and coauthors reported.
Intake of the specific flavonols kaempferol, myricetin, and isorhamnetin were associated with incident AD reductions of 50%, 38%, and 38%, respectively. Another flavonol, quercetin, was by contrast not inversely associated with incident AD, according to the report.
Kaempferol was independently associated with AD in subsequent analyses, while there was no such independent association for myricetin, isorhamnetin, or quercetin, according to Dr. Holland and coinvestigators.
Further analyses of the data suggested the linkages between flavonols and AD were independent of lifestyle factors, dietary intakes, or cardiovascular conditions, they said in their report.
“Confirmation of these findings is warranted through other longitudinal epidemiologic studies and clinical trials, in addition to further elucidation of the biologic mechanisms,” they concluded.
The study was funded by grants from the National Institutes of Health and the USDA Agricultural Research Service. Dr. Holland and coauthors said that they had no disclosures relevant to their report.
SOURCE: Holland TM et al. Neurology. 2020 Jan 29. doi: 10.1212/WNL.0000000000008981.
Onset of Alzheimer’s disease (AD) was inversely associated with intake of flavonols, a subclass of flavonoids with antioxidant and anti-inflammatory properties, according to the study authors.
The rate of developing AD was reduced by 50% among individuals reporting high intake of kaempferol, a flavonol plentiful in leafy green vegetables, and by 38% for high intake of the flavonols myricetin and isorhamnetin, researchers said in a report published in Neurology.
The findings are from the Rush Memory and Aging Project (MAP), a large, prospective study of older individuals in retirement communities and public housing in the Chicago area that has been ongoing since 1997.
“Although there is more work to be done, the associations that we observed are promising and deserve further study,” said Thomas M. Holland, MD, of the Rush Institute for Healthy Aging in Chicago, and coauthors.
Those associations between flavonol intake and AD help set the stage for U.S. POINTER and other randomized, controlled trials that seek to evaluate the effects of dietary interventions in a more rigorous way, according to Laura D. Baker, PhD, associate professor of internal medicine at Wake Forest University, Winston-Salem, N.C.
“This kind of data helps us feel like we are looking in the right direction in the randomized, controlled trials,” Dr. Baker said in an interview.
Dr. Baker is an investigator in the U.S. POINTER study, which will in part evaluate the impact of the MIND diet, which has been shown to slow cognitive decline with age in a previously published MAP study.
However, in the absence of randomized, controlled trial data, Dr. Baker cautioned against “prematurely advocating” for specific dietary approaches when speaking to patients and caregivers now.
“What I say is, we know for sure that the standard American Heart Association diet has been shown in clinical trials to reduce the risk of heart disease, and in terms of brain health, if you can reduce risk of heart disease, you are protecting your brain,” she said in the interview.
The present MAP study linking a reduced rate of AD to flavonol consumption is believed to be the first of its kind, though two previous studies from the early 2000s did find inverse associations between incident AD and intake of flavonoids, of which flavonoids are just one subclass, said Dr. Holland and coinvestigators in their report.
Moreover, in a MAP study published in 2018, Martha Clare Morris, ScD, and coauthors concluded that consuming about a serving per day of green leafy vegetables and foods rich in kaempferol, among other nutrients and bioactive compounds, may help slow cognitive decline associated with aging.
To more specifically study the relationship between kaempferol and other flavonols and the development of AD, Dr. Holland and colleagues evaluated data for MAP participants who had completed a comprehensive food frequency questionnaire and underwent at least two evaluations to assess incidence of disease.
The mean age of the 921 individuals in the present analysis was 81 years, three-quarters were female, and over approximately 6 years of follow-up, 220 developed AD.
The rate of developing AD was 48% lower among participants reporting the highest total dietary intake of flavonols, compared with those reporting the lowest intake, Dr. Holland and coauthors reported.
Intake of the specific flavonols kaempferol, myricetin, and isorhamnetin were associated with incident AD reductions of 50%, 38%, and 38%, respectively. Another flavonol, quercetin, was by contrast not inversely associated with incident AD, according to the report.
Kaempferol was independently associated with AD in subsequent analyses, while there was no such independent association for myricetin, isorhamnetin, or quercetin, according to Dr. Holland and coinvestigators.
Further analyses of the data suggested the linkages between flavonols and AD were independent of lifestyle factors, dietary intakes, or cardiovascular conditions, they said in their report.
“Confirmation of these findings is warranted through other longitudinal epidemiologic studies and clinical trials, in addition to further elucidation of the biologic mechanisms,” they concluded.
The study was funded by grants from the National Institutes of Health and the USDA Agricultural Research Service. Dr. Holland and coauthors said that they had no disclosures relevant to their report.
SOURCE: Holland TM et al. Neurology. 2020 Jan 29. doi: 10.1212/WNL.0000000000008981.
Onset of Alzheimer’s disease (AD) was inversely associated with intake of flavonols, a subclass of flavonoids with antioxidant and anti-inflammatory properties, according to the study authors.
The rate of developing AD was reduced by 50% among individuals reporting high intake of kaempferol, a flavonol plentiful in leafy green vegetables, and by 38% for high intake of the flavonols myricetin and isorhamnetin, researchers said in a report published in Neurology.
The findings are from the Rush Memory and Aging Project (MAP), a large, prospective study of older individuals in retirement communities and public housing in the Chicago area that has been ongoing since 1997.
“Although there is more work to be done, the associations that we observed are promising and deserve further study,” said Thomas M. Holland, MD, of the Rush Institute for Healthy Aging in Chicago, and coauthors.
Those associations between flavonol intake and AD help set the stage for U.S. POINTER and other randomized, controlled trials that seek to evaluate the effects of dietary interventions in a more rigorous way, according to Laura D. Baker, PhD, associate professor of internal medicine at Wake Forest University, Winston-Salem, N.C.
“This kind of data helps us feel like we are looking in the right direction in the randomized, controlled trials,” Dr. Baker said in an interview.
Dr. Baker is an investigator in the U.S. POINTER study, which will in part evaluate the impact of the MIND diet, which has been shown to slow cognitive decline with age in a previously published MAP study.
However, in the absence of randomized, controlled trial data, Dr. Baker cautioned against “prematurely advocating” for specific dietary approaches when speaking to patients and caregivers now.
“What I say is, we know for sure that the standard American Heart Association diet has been shown in clinical trials to reduce the risk of heart disease, and in terms of brain health, if you can reduce risk of heart disease, you are protecting your brain,” she said in the interview.
The present MAP study linking a reduced rate of AD to flavonol consumption is believed to be the first of its kind, though two previous studies from the early 2000s did find inverse associations between incident AD and intake of flavonoids, of which flavonoids are just one subclass, said Dr. Holland and coinvestigators in their report.
Moreover, in a MAP study published in 2018, Martha Clare Morris, ScD, and coauthors concluded that consuming about a serving per day of green leafy vegetables and foods rich in kaempferol, among other nutrients and bioactive compounds, may help slow cognitive decline associated with aging.
To more specifically study the relationship between kaempferol and other flavonols and the development of AD, Dr. Holland and colleagues evaluated data for MAP participants who had completed a comprehensive food frequency questionnaire and underwent at least two evaluations to assess incidence of disease.
The mean age of the 921 individuals in the present analysis was 81 years, three-quarters were female, and over approximately 6 years of follow-up, 220 developed AD.
The rate of developing AD was 48% lower among participants reporting the highest total dietary intake of flavonols, compared with those reporting the lowest intake, Dr. Holland and coauthors reported.
Intake of the specific flavonols kaempferol, myricetin, and isorhamnetin were associated with incident AD reductions of 50%, 38%, and 38%, respectively. Another flavonol, quercetin, was by contrast not inversely associated with incident AD, according to the report.
Kaempferol was independently associated with AD in subsequent analyses, while there was no such independent association for myricetin, isorhamnetin, or quercetin, according to Dr. Holland and coinvestigators.
Further analyses of the data suggested the linkages between flavonols and AD were independent of lifestyle factors, dietary intakes, or cardiovascular conditions, they said in their report.
“Confirmation of these findings is warranted through other longitudinal epidemiologic studies and clinical trials, in addition to further elucidation of the biologic mechanisms,” they concluded.
The study was funded by grants from the National Institutes of Health and the USDA Agricultural Research Service. Dr. Holland and coauthors said that they had no disclosures relevant to their report.
SOURCE: Holland TM et al. Neurology. 2020 Jan 29. doi: 10.1212/WNL.0000000000008981.
FROM NEUROLOGY
BP levels during endovascular stroke therapy affect neurologic outcomes
For patients with acute ischemic stroke, prolonged durations of blood pressure above or below certain thresholds during endovascular therapy may be linked to poor functional outcome, results of a retrospective study suggest.
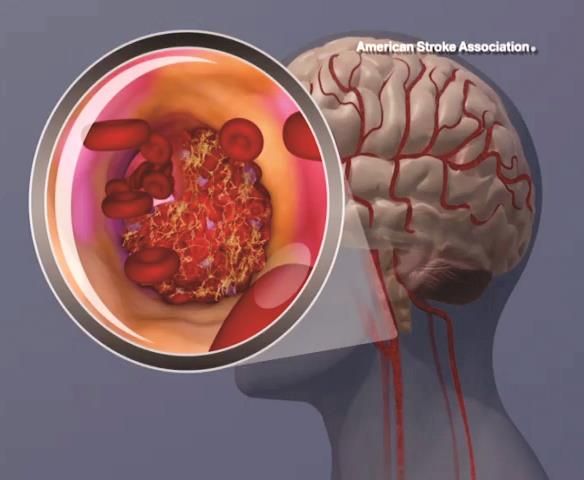
Mean arterial blood pressure (MABP) lower than 70 mm Hg for 10 minutes or more, or higher than 90 mm Hg for 45 minutes or more, represented “critical thresholds” associated with worse neurologic outcomes, the study authors wrote in JAMA Neurology.
“These results suggest MABP may be a modifiable therapeutic target to prevent or reduce poor functional outcome in patients undergoing endovascular therapy for acute ischemic stroke, and that MABP should possibly be maintained within such narrow limits, wrote the authors, led by Mads Rasmussen, MD, PhD, of the department of anesthesia at Aarhus (Denmark) University Hospital.
The findings come from an analysis of BP data from 365 patients with acute ischemic stroke enrolled in three randomized trials evaluating different strategies for anesthesia. Among those patients, the mean age was approximately 71 years, and about 45% were women.
The investigators looked at a variety of BP-related variables during endovascular therapy to assess their impact on functional outcome, based on modified Rankin Scale (mRS) scores at 90 days.
Having an MABP below 70 mm Hg for a cumulative time of at least 10 minutes substantially increased odds of higher 90-day mRS scores (odds ratio, 1.51; 95% confidence interval, 1.02-2.22), according to Dr. Rasmussen and colleagues. The number needed to harm (NNH) at this threshold was 10; in other words, to harm 1 patient, 10 patients are needed with procedural MABP below 70 mm Hg for at least 10 minutes.
Likewise, having an MABP above 90 mm Hg for a cumulated time of at least 45 minutes significantly increased odds of higher 90-day mRS scores, with an OR of 1.49 (95% CI, 1.11-2.02) and a number needed to harm of 10.
Odds of shifting toward a worse neurologic outcome increased by 62% for every continuous 10 minutes of MABP below 70 mm Hg, and by 8% for every continuous 10 minutes above 90 mm Hg.
The maximum MABP during the procedure was significantly associated with neurologic outcomes in the study, while by contrast, maximum procedural systolic BP was not, according to the investigators.
In general, the study findings suggest that MABP is “more sensitive” than systolic BP when assessing hypotension and hypertension in these patients. However, these findings are subject to a number of limitations, the investigators wrote, including the retrospective nature of the analysis and the selected group of patients enrolled in studies designed to evaluate anesthesia strategies, not hemodynamic management.
“Randomized studies are needed to determine the optimal blood pressure management strategy during endovascular therapy,” the investigators wrote.
Dr. Rasmussen reported grant support from the Health Research Foundation of Central Denmark Region and the National Helicopter Emergency Medical Service Foundation. Coauthors reported receiving grant support from the Novo Nordisk Foundation; a research award from the Patient-Centered Outcomes Research Institute; and personal fees from Abbott Medical Sweden, I4L Innovation for Life, Boehringer Ingelheim, Medtronic, and Zoll.
SOURCE: Rasmussen M et al. JAMA Neurol. 2020 Jan 27. doi: 10.1001/jamaneurol.2019.4838.
For patients with acute ischemic stroke, prolonged durations of blood pressure above or below certain thresholds during endovascular therapy may be linked to poor functional outcome, results of a retrospective study suggest.
Mean arterial blood pressure (MABP) lower than 70 mm Hg for 10 minutes or more, or higher than 90 mm Hg for 45 minutes or more, represented “critical thresholds” associated with worse neurologic outcomes, the study authors wrote in JAMA Neurology.
“These results suggest MABP may be a modifiable therapeutic target to prevent or reduce poor functional outcome in patients undergoing endovascular therapy for acute ischemic stroke, and that MABP should possibly be maintained within such narrow limits, wrote the authors, led by Mads Rasmussen, MD, PhD, of the department of anesthesia at Aarhus (Denmark) University Hospital.
The findings come from an analysis of BP data from 365 patients with acute ischemic stroke enrolled in three randomized trials evaluating different strategies for anesthesia. Among those patients, the mean age was approximately 71 years, and about 45% were women.
The investigators looked at a variety of BP-related variables during endovascular therapy to assess their impact on functional outcome, based on modified Rankin Scale (mRS) scores at 90 days.
Having an MABP below 70 mm Hg for a cumulative time of at least 10 minutes substantially increased odds of higher 90-day mRS scores (odds ratio, 1.51; 95% confidence interval, 1.02-2.22), according to Dr. Rasmussen and colleagues. The number needed to harm (NNH) at this threshold was 10; in other words, to harm 1 patient, 10 patients are needed with procedural MABP below 70 mm Hg for at least 10 minutes.
Likewise, having an MABP above 90 mm Hg for a cumulated time of at least 45 minutes significantly increased odds of higher 90-day mRS scores, with an OR of 1.49 (95% CI, 1.11-2.02) and a number needed to harm of 10.
Odds of shifting toward a worse neurologic outcome increased by 62% for every continuous 10 minutes of MABP below 70 mm Hg, and by 8% for every continuous 10 minutes above 90 mm Hg.
The maximum MABP during the procedure was significantly associated with neurologic outcomes in the study, while by contrast, maximum procedural systolic BP was not, according to the investigators.
In general, the study findings suggest that MABP is “more sensitive” than systolic BP when assessing hypotension and hypertension in these patients. However, these findings are subject to a number of limitations, the investigators wrote, including the retrospective nature of the analysis and the selected group of patients enrolled in studies designed to evaluate anesthesia strategies, not hemodynamic management.
“Randomized studies are needed to determine the optimal blood pressure management strategy during endovascular therapy,” the investigators wrote.
Dr. Rasmussen reported grant support from the Health Research Foundation of Central Denmark Region and the National Helicopter Emergency Medical Service Foundation. Coauthors reported receiving grant support from the Novo Nordisk Foundation; a research award from the Patient-Centered Outcomes Research Institute; and personal fees from Abbott Medical Sweden, I4L Innovation for Life, Boehringer Ingelheim, Medtronic, and Zoll.
SOURCE: Rasmussen M et al. JAMA Neurol. 2020 Jan 27. doi: 10.1001/jamaneurol.2019.4838.
For patients with acute ischemic stroke, prolonged durations of blood pressure above or below certain thresholds during endovascular therapy may be linked to poor functional outcome, results of a retrospective study suggest.
Mean arterial blood pressure (MABP) lower than 70 mm Hg for 10 minutes or more, or higher than 90 mm Hg for 45 minutes or more, represented “critical thresholds” associated with worse neurologic outcomes, the study authors wrote in JAMA Neurology.
“These results suggest MABP may be a modifiable therapeutic target to prevent or reduce poor functional outcome in patients undergoing endovascular therapy for acute ischemic stroke, and that MABP should possibly be maintained within such narrow limits, wrote the authors, led by Mads Rasmussen, MD, PhD, of the department of anesthesia at Aarhus (Denmark) University Hospital.
The findings come from an analysis of BP data from 365 patients with acute ischemic stroke enrolled in three randomized trials evaluating different strategies for anesthesia. Among those patients, the mean age was approximately 71 years, and about 45% were women.
The investigators looked at a variety of BP-related variables during endovascular therapy to assess their impact on functional outcome, based on modified Rankin Scale (mRS) scores at 90 days.
Having an MABP below 70 mm Hg for a cumulative time of at least 10 minutes substantially increased odds of higher 90-day mRS scores (odds ratio, 1.51; 95% confidence interval, 1.02-2.22), according to Dr. Rasmussen and colleagues. The number needed to harm (NNH) at this threshold was 10; in other words, to harm 1 patient, 10 patients are needed with procedural MABP below 70 mm Hg for at least 10 minutes.
Likewise, having an MABP above 90 mm Hg for a cumulated time of at least 45 minutes significantly increased odds of higher 90-day mRS scores, with an OR of 1.49 (95% CI, 1.11-2.02) and a number needed to harm of 10.
Odds of shifting toward a worse neurologic outcome increased by 62% for every continuous 10 minutes of MABP below 70 mm Hg, and by 8% for every continuous 10 minutes above 90 mm Hg.
The maximum MABP during the procedure was significantly associated with neurologic outcomes in the study, while by contrast, maximum procedural systolic BP was not, according to the investigators.
In general, the study findings suggest that MABP is “more sensitive” than systolic BP when assessing hypotension and hypertension in these patients. However, these findings are subject to a number of limitations, the investigators wrote, including the retrospective nature of the analysis and the selected group of patients enrolled in studies designed to evaluate anesthesia strategies, not hemodynamic management.
“Randomized studies are needed to determine the optimal blood pressure management strategy during endovascular therapy,” the investigators wrote.
Dr. Rasmussen reported grant support from the Health Research Foundation of Central Denmark Region and the National Helicopter Emergency Medical Service Foundation. Coauthors reported receiving grant support from the Novo Nordisk Foundation; a research award from the Patient-Centered Outcomes Research Institute; and personal fees from Abbott Medical Sweden, I4L Innovation for Life, Boehringer Ingelheim, Medtronic, and Zoll.
SOURCE: Rasmussen M et al. JAMA Neurol. 2020 Jan 27. doi: 10.1001/jamaneurol.2019.4838.
FROM JAMA NEUROLOGY
Cognitive screening of older physicians: What’s fair?
Cognitive screening of 141 clinicians 70 years or older at Yale New Haven (Conn.) Hospital identified 18 with cognitive deficits likely to impair their ability to practice medicine. Six retired and 12 agreed to limit their practice to closely proctored environments, according to a report in JAMA.
It was part of a program to screen all practitioners 70 years or older who apply for reappointment to the medical staff, and every 2 years thereafter, due to “concerns about the potentially compromised ability of older clinicians,” said the authors, Yale rheumatologist and geriatrician Leo M. Cooney Jr., MD, and Thomas Balcezak, MD, Yale New Haven’s chief medical officer.
Yale is not alone. Intermountain Healthcare, Stanford Hospitals and Clinics, Scripps Health Care, Penn Medicine, and the University of California, San Diego, are among the institutions with similar programs.
The move is being driven by the aging of the medical community. About 15% of U.S. physicians are over 65 years old, a tripling from 23,000 in 1980 to 73,000 in 2012-2016, and the number is growing, according to an editorial by Jeffrey L. Saver, MD, professor of neurology and senior associate vice president of neurology at the University of California, Los Angeles.
Given the trend, “it is not surprising that the issue of screening aging physicians for cognitive deficits has gained attention over the last decade,” Katrina Armstrong, MD, chair of the department of medicine at Massachusetts General Hospital, Boston, and Eileen E. Reynolds, MD, associate professor of medicine at Beth Israel Deaconess Medical Center, Boston, noted in a second editorial.
“Cognitive decline often accompanies aging, and the prevalence of dementia increases rapidly after age 70 years,” they said.
The data on whether older clinicians pose a risk to patients is limited and somewhat mixed. An analysis of 736,537 Medicare hospitalizations found no association between physician age and 30-day patient mortality among physicians 60 years or older with more than 201 admissions per year, but higher mortality among older physicians with lower volumes.
A meta-analysis of 62 studies showed that “older physicians have less factual knowledge, are less likely to adhere to appropriate standards of care, and may also have poorer patient outcomes.”
The new Yale data, meanwhile, suggests that “approximately 13% [18 of 141] of physicians and other clinicians older than 70 years should not be practicing independently,” Dr. Armstrong and Dr. Reynolds said in their editorial.
There is support for screening efforts. “As a profession that deals with human life, medical practitioners must obviously have the cognitive capacity to safely practice medicine. I applaud the approach taken by Yale New Haven Hospital in that cognitive abilities themselves, and not simply funds of knowledge, are assessed,” said Richard J. Caselli, MD, professor of neurology at the Mayo Clinic Arizona, Scottsdale, and a leader of the Alzheimer’s disease program there.

However, it’s not hard to imagine highly competent but older physicians taking umbrage at cognitive screening, and there’s been pushback. Stanford was considering a Yale-like approach but opted instead for peer review after opposition. Objections from the Utah Medical Association led Utah to enact a law banning age-based physician screening. In 2015, the American Medical Association issued a report calling for the development of guidelines and standards for assessing competency in aging physicians, but the AMA House of Delegates shelved it pending further study.
There are concerns about age discrimination, discounting the accumulated wisdom of long-practicing physicians, and misclassifying competent physicians, particularly those who provide quality care in rural and other underserved areas. Indeed, 8 of 14 clinicians who screened positive at Yale and underwent more extensive testing were allowed to recredential, “suggesting that the false-positive screening rate could be as high as 57%,” Dr. Armstrong and Dr. Reynolds noted.
The consensus seems to be that there probably is a need for some sort of screening, but it must be both sound and fair. Rather than a piecemeal institutional approach, perhaps there is “an important opportunity for other groups, including specialty boards and state licensing boards” to standardize the process, they said.
Among other things, assessments could focus less on test scores and more on the practice of medicine. For instance, fine motor skill/motor planning assessments for surgeons, and intermediate results could trigger a more extensive assessment of actual clinical performance, perhaps even direct observation, Dr. Saver said in his editorial.
As far as clinical performance goes, none of the 18 clinicians at Yale had previous performance problems. “Was this a failure of the system to report impaired physicians or were these physicians compensating sufficiently to avoid detection?” In either case, “cognitive testing should be a red flag that triggers other clinical assessments,” said Carl I. Cohen, MD, professor and director of the division of geriatric psychiatry at the State University of New York, Brooklyn.
The original plan at Yale was for neurologic and ophthalmologic examinations beginning at age 70, but ultimately it was decided to go with a battery of 16 tests to assess visual scanning and psychomotor efficiency, processing speed under pressure, concentration, and working memory, among other things. Testing takes about 50-90 minutes, and is graded by single neuropsychologist to ensure consistency. Results were compared with normative scores from both older and younger clinicians.
To prevent clinicians from preparing for it, Yale isn’t releasing its test battery.
Suboptimal performance triggered additional evaluations, including in-depth assessment of intellectual, memory, and executive function. Final reviews and recommendations were made by a committee that included a geriatrician, the clinician’s section or department chair, and current and past chief medical officers.

Among the 18 providers who demonstrated deficits impairing their ability to practice medicine, 5 were 70-74 years old; 4 were 75-79; and 9 were 80 years or older. Minor abnormalities were found in 34 other candidates (24.1%); they were allowed to recredential but were scheduled for rescreening at 1-year intervals, instead of every 2 years.
The mean age among the 141 screened clinicians was 74.3 years and ranged from 69 to 92 years; 86% were men. Applicants included 125 physicians (88.7%) as well as 5 advanced practice registered nurses; 4 dentists; 3 psychologists; 2 podiatrists; 1 physician associate; and 1 midwife.
The authors had no relevant disclosures.
SOURCE: Cooney L et al. JAMA. 2020 Jan 14;323(2):179-80.
Cognitive screening of 141 clinicians 70 years or older at Yale New Haven (Conn.) Hospital identified 18 with cognitive deficits likely to impair their ability to practice medicine. Six retired and 12 agreed to limit their practice to closely proctored environments, according to a report in JAMA.
It was part of a program to screen all practitioners 70 years or older who apply for reappointment to the medical staff, and every 2 years thereafter, due to “concerns about the potentially compromised ability of older clinicians,” said the authors, Yale rheumatologist and geriatrician Leo M. Cooney Jr., MD, and Thomas Balcezak, MD, Yale New Haven’s chief medical officer.
Yale is not alone. Intermountain Healthcare, Stanford Hospitals and Clinics, Scripps Health Care, Penn Medicine, and the University of California, San Diego, are among the institutions with similar programs.
The move is being driven by the aging of the medical community. About 15% of U.S. physicians are over 65 years old, a tripling from 23,000 in 1980 to 73,000 in 2012-2016, and the number is growing, according to an editorial by Jeffrey L. Saver, MD, professor of neurology and senior associate vice president of neurology at the University of California, Los Angeles.
Given the trend, “it is not surprising that the issue of screening aging physicians for cognitive deficits has gained attention over the last decade,” Katrina Armstrong, MD, chair of the department of medicine at Massachusetts General Hospital, Boston, and Eileen E. Reynolds, MD, associate professor of medicine at Beth Israel Deaconess Medical Center, Boston, noted in a second editorial.
“Cognitive decline often accompanies aging, and the prevalence of dementia increases rapidly after age 70 years,” they said.
The data on whether older clinicians pose a risk to patients is limited and somewhat mixed. An analysis of 736,537 Medicare hospitalizations found no association between physician age and 30-day patient mortality among physicians 60 years or older with more than 201 admissions per year, but higher mortality among older physicians with lower volumes.
A meta-analysis of 62 studies showed that “older physicians have less factual knowledge, are less likely to adhere to appropriate standards of care, and may also have poorer patient outcomes.”
The new Yale data, meanwhile, suggests that “approximately 13% [18 of 141] of physicians and other clinicians older than 70 years should not be practicing independently,” Dr. Armstrong and Dr. Reynolds said in their editorial.
There is support for screening efforts. “As a profession that deals with human life, medical practitioners must obviously have the cognitive capacity to safely practice medicine. I applaud the approach taken by Yale New Haven Hospital in that cognitive abilities themselves, and not simply funds of knowledge, are assessed,” said Richard J. Caselli, MD, professor of neurology at the Mayo Clinic Arizona, Scottsdale, and a leader of the Alzheimer’s disease program there.
However, it’s not hard to imagine highly competent but older physicians taking umbrage at cognitive screening, and there’s been pushback. Stanford was considering a Yale-like approach but opted instead for peer review after opposition. Objections from the Utah Medical Association led Utah to enact a law banning age-based physician screening. In 2015, the American Medical Association issued a report calling for the development of guidelines and standards for assessing competency in aging physicians, but the AMA House of Delegates shelved it pending further study.
There are concerns about age discrimination, discounting the accumulated wisdom of long-practicing physicians, and misclassifying competent physicians, particularly those who provide quality care in rural and other underserved areas. Indeed, 8 of 14 clinicians who screened positive at Yale and underwent more extensive testing were allowed to recredential, “suggesting that the false-positive screening rate could be as high as 57%,” Dr. Armstrong and Dr. Reynolds noted.
The consensus seems to be that there probably is a need for some sort of screening, but it must be both sound and fair. Rather than a piecemeal institutional approach, perhaps there is “an important opportunity for other groups, including specialty boards and state licensing boards” to standardize the process, they said.
Among other things, assessments could focus less on test scores and more on the practice of medicine. For instance, fine motor skill/motor planning assessments for surgeons, and intermediate results could trigger a more extensive assessment of actual clinical performance, perhaps even direct observation, Dr. Saver said in his editorial.
As far as clinical performance goes, none of the 18 clinicians at Yale had previous performance problems. “Was this a failure of the system to report impaired physicians or were these physicians compensating sufficiently to avoid detection?” In either case, “cognitive testing should be a red flag that triggers other clinical assessments,” said Carl I. Cohen, MD, professor and director of the division of geriatric psychiatry at the State University of New York, Brooklyn.
The original plan at Yale was for neurologic and ophthalmologic examinations beginning at age 70, but ultimately it was decided to go with a battery of 16 tests to assess visual scanning and psychomotor efficiency, processing speed under pressure, concentration, and working memory, among other things. Testing takes about 50-90 minutes, and is graded by single neuropsychologist to ensure consistency. Results were compared with normative scores from both older and younger clinicians.
To prevent clinicians from preparing for it, Yale isn’t releasing its test battery.
Suboptimal performance triggered additional evaluations, including in-depth assessment of intellectual, memory, and executive function. Final reviews and recommendations were made by a committee that included a geriatrician, the clinician’s section or department chair, and current and past chief medical officers.
Among the 18 providers who demonstrated deficits impairing their ability to practice medicine, 5 were 70-74 years old; 4 were 75-79; and 9 were 80 years or older. Minor abnormalities were found in 34 other candidates (24.1%); they were allowed to recredential but were scheduled for rescreening at 1-year intervals, instead of every 2 years.
The mean age among the 141 screened clinicians was 74.3 years and ranged from 69 to 92 years; 86% were men. Applicants included 125 physicians (88.7%) as well as 5 advanced practice registered nurses; 4 dentists; 3 psychologists; 2 podiatrists; 1 physician associate; and 1 midwife.
The authors had no relevant disclosures.
SOURCE: Cooney L et al. JAMA. 2020 Jan 14;323(2):179-80.
Cognitive screening of 141 clinicians 70 years or older at Yale New Haven (Conn.) Hospital identified 18 with cognitive deficits likely to impair their ability to practice medicine. Six retired and 12 agreed to limit their practice to closely proctored environments, according to a report in JAMA.
It was part of a program to screen all practitioners 70 years or older who apply for reappointment to the medical staff, and every 2 years thereafter, due to “concerns about the potentially compromised ability of older clinicians,” said the authors, Yale rheumatologist and geriatrician Leo M. Cooney Jr., MD, and Thomas Balcezak, MD, Yale New Haven’s chief medical officer.
Yale is not alone. Intermountain Healthcare, Stanford Hospitals and Clinics, Scripps Health Care, Penn Medicine, and the University of California, San Diego, are among the institutions with similar programs.
The move is being driven by the aging of the medical community. About 15% of U.S. physicians are over 65 years old, a tripling from 23,000 in 1980 to 73,000 in 2012-2016, and the number is growing, according to an editorial by Jeffrey L. Saver, MD, professor of neurology and senior associate vice president of neurology at the University of California, Los Angeles.
Given the trend, “it is not surprising that the issue of screening aging physicians for cognitive deficits has gained attention over the last decade,” Katrina Armstrong, MD, chair of the department of medicine at Massachusetts General Hospital, Boston, and Eileen E. Reynolds, MD, associate professor of medicine at Beth Israel Deaconess Medical Center, Boston, noted in a second editorial.
“Cognitive decline often accompanies aging, and the prevalence of dementia increases rapidly after age 70 years,” they said.
The data on whether older clinicians pose a risk to patients is limited and somewhat mixed. An analysis of 736,537 Medicare hospitalizations found no association between physician age and 30-day patient mortality among physicians 60 years or older with more than 201 admissions per year, but higher mortality among older physicians with lower volumes.
A meta-analysis of 62 studies showed that “older physicians have less factual knowledge, are less likely to adhere to appropriate standards of care, and may also have poorer patient outcomes.”
The new Yale data, meanwhile, suggests that “approximately 13% [18 of 141] of physicians and other clinicians older than 70 years should not be practicing independently,” Dr. Armstrong and Dr. Reynolds said in their editorial.
There is support for screening efforts. “As a profession that deals with human life, medical practitioners must obviously have the cognitive capacity to safely practice medicine. I applaud the approach taken by Yale New Haven Hospital in that cognitive abilities themselves, and not simply funds of knowledge, are assessed,” said Richard J. Caselli, MD, professor of neurology at the Mayo Clinic Arizona, Scottsdale, and a leader of the Alzheimer’s disease program there.
However, it’s not hard to imagine highly competent but older physicians taking umbrage at cognitive screening, and there’s been pushback. Stanford was considering a Yale-like approach but opted instead for peer review after opposition. Objections from the Utah Medical Association led Utah to enact a law banning age-based physician screening. In 2015, the American Medical Association issued a report calling for the development of guidelines and standards for assessing competency in aging physicians, but the AMA House of Delegates shelved it pending further study.
There are concerns about age discrimination, discounting the accumulated wisdom of long-practicing physicians, and misclassifying competent physicians, particularly those who provide quality care in rural and other underserved areas. Indeed, 8 of 14 clinicians who screened positive at Yale and underwent more extensive testing were allowed to recredential, “suggesting that the false-positive screening rate could be as high as 57%,” Dr. Armstrong and Dr. Reynolds noted.
The consensus seems to be that there probably is a need for some sort of screening, but it must be both sound and fair. Rather than a piecemeal institutional approach, perhaps there is “an important opportunity for other groups, including specialty boards and state licensing boards” to standardize the process, they said.
Among other things, assessments could focus less on test scores and more on the practice of medicine. For instance, fine motor skill/motor planning assessments for surgeons, and intermediate results could trigger a more extensive assessment of actual clinical performance, perhaps even direct observation, Dr. Saver said in his editorial.
As far as clinical performance goes, none of the 18 clinicians at Yale had previous performance problems. “Was this a failure of the system to report impaired physicians or were these physicians compensating sufficiently to avoid detection?” In either case, “cognitive testing should be a red flag that triggers other clinical assessments,” said Carl I. Cohen, MD, professor and director of the division of geriatric psychiatry at the State University of New York, Brooklyn.
The original plan at Yale was for neurologic and ophthalmologic examinations beginning at age 70, but ultimately it was decided to go with a battery of 16 tests to assess visual scanning and psychomotor efficiency, processing speed under pressure, concentration, and working memory, among other things. Testing takes about 50-90 minutes, and is graded by single neuropsychologist to ensure consistency. Results were compared with normative scores from both older and younger clinicians.
To prevent clinicians from preparing for it, Yale isn’t releasing its test battery.
Suboptimal performance triggered additional evaluations, including in-depth assessment of intellectual, memory, and executive function. Final reviews and recommendations were made by a committee that included a geriatrician, the clinician’s section or department chair, and current and past chief medical officers.
Among the 18 providers who demonstrated deficits impairing their ability to practice medicine, 5 were 70-74 years old; 4 were 75-79; and 9 were 80 years or older. Minor abnormalities were found in 34 other candidates (24.1%); they were allowed to recredential but were scheduled for rescreening at 1-year intervals, instead of every 2 years.
The mean age among the 141 screened clinicians was 74.3 years and ranged from 69 to 92 years; 86% were men. Applicants included 125 physicians (88.7%) as well as 5 advanced practice registered nurses; 4 dentists; 3 psychologists; 2 podiatrists; 1 physician associate; and 1 midwife.
The authors had no relevant disclosures.
SOURCE: Cooney L et al. JAMA. 2020 Jan 14;323(2):179-80.
FROM JAMA
Sarcopenia associated with increased cardiometabolic risk
LOS ANGELES –

“Loss of lean body mass and function with aging decreases the amount of metabolically active tissue, which can lead to insulin resistance,” Elena Volpi, MD, said at the World Congress on Insulin Resistance, Diabetes and Cardiovascular Disease. “Insulin resistance reduces muscle protein anabolism and accelerates sarcopenia, perpetuating a vicious cycle.”
Sarcopenia, the involuntary loss of muscle mass and function that occurs with aging, is an ICD-10 codable condition that can be diagnosed by measuring muscle strength and quality, said Dr. Volpi, director of the Sealy Center on Aging at the University of Texas Medical Branch at Galveston. In the Health, Aging and Body Composition Study (Health ABC), researchers followed 2,292 relatively healthy adults aged 70-79 years for an average of 4.9 years (J Gerontol A Biol Sci Med. 2006;61[1]:72-7). The researchers used isokinetic dynamometry to measure knee extension strength, isometric dynamometry to measure grip strength, CT scan to measure thigh muscle area, and dual X-ray absorptiometry to determine leg and arm lean soft-tissue mass. “Those individuals who started with the highest levels of muscle strength had the greatest survival, while those who had the lowest levels of muscle strength died earlier,” said Dr. Volpi, who was not affiliated with the study. “That was true for both men and women.”
More recently, researchers conducted a pooled analysis of nine cohort studies involving 34,485 community-dwelling older individuals who were tested with gait speed and followed for 6-21 years (JAMA. 2011;305[1]:50-8). They found that a higher gait speed was associated with higher survival at 5 and 10 years (P less than .001). “Muscle mass also appears to be associated in part with mortality and survival, although the association is not as strong as measures of strength and gait speed,” Dr. Volpi said.
Data from the 2009 Korea National Health and Nutrition Examination Survey of 1,537 participants, aged 65 years and older, found that sarcopenia is independently associated with cardiovascular disease (PLoS One. 2013 Mar 22. doi: 10.1371/journal.pone.0060119). Most of the risk factors for cardiovascular disease – such as age, waist circumference, body mass index, fasting plasma glucose, and total cholesterol – showed significant negative correlations with the ratio between appendicular skeletal muscle mass and body weight. Multiple logistic regression analysis demonstrated that sarcopenia was associated with cardiovascular disease, independent of other well-documented risk factors, renal function, and medications (odds ratio, 1.77; P = .025).
In addition, data from the British Regional Heart Study, which followed 4,252 older men for a mean of 11.3 years, found an association of sarcopenia and adiposity with cardiovascular mortality and all-cause mortality (J Am Geriatr Soc. 2014;62[2]:253-60). Specifically, all-cause mortality risk was significantly greater in men in the sarcopenic and obese groups (HRs, 1.41 and 1.21, respectively), compared with those in the optimal reference group, with the highest risk in sarcopenic obese individuals (HR, 1.72) after adjustment for lifestyle characteristics.
“Diabetes also accelerates loss of lean body mass in older adults,” added Dr. Volpi. “Data from the Health ABC study showed that individuals who did not have diabetes at the beginning of the 6-year observation period ... lost the least amount of muscle, compared with those who had undiagnosed or already diagnosed diabetes.”
The precise way in which sarcopenia is linked to metabolic disease remains elusive, she continued, but current evidence suggests that sarcopenia is characterized by a reduction in the protein synthetic response to metabolic stimulation by amino acids, exercise, and insulin in skeletal muscle. “This reduction in the anabolic response to protein synthesis is called anabolic resistance of aging, and it is mediated by reduced acute activation of mTORC1 [mTOR complex 1] signaling,” Dr. Volpi said. “There’s another step upstream of the mTORC1, in which the amino acids and insulin have to cross the blood-muscle barrier. Amino acids need to be transported into the muscle actively, like glucose. That is an important unexplored area that may contribute to sarcopenia.”
Dr. Volpi went on to note that endothelial dysfunction underlies muscle anabolic resistance and cardiovascular risk and is likely to be a fundamental cause of both problems. Recent studies have shown that increased levels of physical activity improve endothelial function, enhance insulin sensitivity and anabolic sensitivity to nutrients, and reduce cardiovascular risk.
For example, in a cohort of 45 nonfrail older adults with a mean age of 72 years, Dr. Volpi and colleagues carried out a phase 1, double-blind, placebo-controlled, randomized clinical trial to determine if chronic essential amino acid supplementation, aerobic exercise training, or a combination of the two interventions could improve muscle mass and function by stimulating muscle protein synthesis over the course of 24 weeks (J Gerontol A Biol Sci Med Sci. 2019;74[10]:1598-604). “We found that exercise supervised three times per week on a treadmill for 6 months improved physical function in both groups randomized to exercise,” Dr. Volpi said. “Disappointingly, there was no change in total lean mass with any of the interventions. There was a decrease in fat mass with exercise alone, and no change with exercise and amino acids. [Of note is that] the individuals who were randomized to the amino acids plus exercise group had a significant increase in leg strength, whereas the others did not.”
Preliminary findings from ongoing work by Dr. Volpi and colleagues suggest that, in diabetes, muscle protein synthesis and blood flow really “are not different in response to insulin in healthy older adults and diabetic older adults because they don’t change at all. However, we did find alterations in amino acid trafficking in diabetes. We found that older individuals with type 2 diabetes had a reduction of amino acid transport and a higher intracellular amino acid concentration, compared with age-matched, healthier individuals. The intracellular amino acid clearance improved in the healthy, nondiabetic older adults with hyperinsulinemia, whereas it did not change in diabetic older adults. As a result, the net muscle protein balance improved a little in the nondiabetic patients, but did not change in the diabetic patients.”
The researchers are evaluating older patients with type 2 diabetes to see whether there are alterations in vascular reactivity and protein synthesis and whether those can be overcome by resistance-exercise training. “Preliminary results show that flow-mediated dilation can actually increase in an older diabetic patient with resistance exercise training three times a week for 3 months,” she said. “Exercise can improve both endothelial dysfunction and sarcopenia and therefore improve physical function and reduce cardiovascular risk.”
Dr. Volpi reported having no relevant disclosures.
LOS ANGELES –
“Loss of lean body mass and function with aging decreases the amount of metabolically active tissue, which can lead to insulin resistance,” Elena Volpi, MD, said at the World Congress on Insulin Resistance, Diabetes and Cardiovascular Disease. “Insulin resistance reduces muscle protein anabolism and accelerates sarcopenia, perpetuating a vicious cycle.”
Sarcopenia, the involuntary loss of muscle mass and function that occurs with aging, is an ICD-10 codable condition that can be diagnosed by measuring muscle strength and quality, said Dr. Volpi, director of the Sealy Center on Aging at the University of Texas Medical Branch at Galveston. In the Health, Aging and Body Composition Study (Health ABC), researchers followed 2,292 relatively healthy adults aged 70-79 years for an average of 4.9 years (J Gerontol A Biol Sci Med. 2006;61[1]:72-7). The researchers used isokinetic dynamometry to measure knee extension strength, isometric dynamometry to measure grip strength, CT scan to measure thigh muscle area, and dual X-ray absorptiometry to determine leg and arm lean soft-tissue mass. “Those individuals who started with the highest levels of muscle strength had the greatest survival, while those who had the lowest levels of muscle strength died earlier,” said Dr. Volpi, who was not affiliated with the study. “That was true for both men and women.”
More recently, researchers conducted a pooled analysis of nine cohort studies involving 34,485 community-dwelling older individuals who were tested with gait speed and followed for 6-21 years (JAMA. 2011;305[1]:50-8). They found that a higher gait speed was associated with higher survival at 5 and 10 years (P less than .001). “Muscle mass also appears to be associated in part with mortality and survival, although the association is not as strong as measures of strength and gait speed,” Dr. Volpi said.
Data from the 2009 Korea National Health and Nutrition Examination Survey of 1,537 participants, aged 65 years and older, found that sarcopenia is independently associated with cardiovascular disease (PLoS One. 2013 Mar 22. doi: 10.1371/journal.pone.0060119). Most of the risk factors for cardiovascular disease – such as age, waist circumference, body mass index, fasting plasma glucose, and total cholesterol – showed significant negative correlations with the ratio between appendicular skeletal muscle mass and body weight. Multiple logistic regression analysis demonstrated that sarcopenia was associated with cardiovascular disease, independent of other well-documented risk factors, renal function, and medications (odds ratio, 1.77; P = .025).
In addition, data from the British Regional Heart Study, which followed 4,252 older men for a mean of 11.3 years, found an association of sarcopenia and adiposity with cardiovascular mortality and all-cause mortality (J Am Geriatr Soc. 2014;62[2]:253-60). Specifically, all-cause mortality risk was significantly greater in men in the sarcopenic and obese groups (HRs, 1.41 and 1.21, respectively), compared with those in the optimal reference group, with the highest risk in sarcopenic obese individuals (HR, 1.72) after adjustment for lifestyle characteristics.
“Diabetes also accelerates loss of lean body mass in older adults,” added Dr. Volpi. “Data from the Health ABC study showed that individuals who did not have diabetes at the beginning of the 6-year observation period ... lost the least amount of muscle, compared with those who had undiagnosed or already diagnosed diabetes.”
The precise way in which sarcopenia is linked to metabolic disease remains elusive, she continued, but current evidence suggests that sarcopenia is characterized by a reduction in the protein synthetic response to metabolic stimulation by amino acids, exercise, and insulin in skeletal muscle. “This reduction in the anabolic response to protein synthesis is called anabolic resistance of aging, and it is mediated by reduced acute activation of mTORC1 [mTOR complex 1] signaling,” Dr. Volpi said. “There’s another step upstream of the mTORC1, in which the amino acids and insulin have to cross the blood-muscle barrier. Amino acids need to be transported into the muscle actively, like glucose. That is an important unexplored area that may contribute to sarcopenia.”
Dr. Volpi went on to note that endothelial dysfunction underlies muscle anabolic resistance and cardiovascular risk and is likely to be a fundamental cause of both problems. Recent studies have shown that increased levels of physical activity improve endothelial function, enhance insulin sensitivity and anabolic sensitivity to nutrients, and reduce cardiovascular risk.
For example, in a cohort of 45 nonfrail older adults with a mean age of 72 years, Dr. Volpi and colleagues carried out a phase 1, double-blind, placebo-controlled, randomized clinical trial to determine if chronic essential amino acid supplementation, aerobic exercise training, or a combination of the two interventions could improve muscle mass and function by stimulating muscle protein synthesis over the course of 24 weeks (J Gerontol A Biol Sci Med Sci. 2019;74[10]:1598-604). “We found that exercise supervised three times per week on a treadmill for 6 months improved physical function in both groups randomized to exercise,” Dr. Volpi said. “Disappointingly, there was no change in total lean mass with any of the interventions. There was a decrease in fat mass with exercise alone, and no change with exercise and amino acids. [Of note is that] the individuals who were randomized to the amino acids plus exercise group had a significant increase in leg strength, whereas the others did not.”
Preliminary findings from ongoing work by Dr. Volpi and colleagues suggest that, in diabetes, muscle protein synthesis and blood flow really “are not different in response to insulin in healthy older adults and diabetic older adults because they don’t change at all. However, we did find alterations in amino acid trafficking in diabetes. We found that older individuals with type 2 diabetes had a reduction of amino acid transport and a higher intracellular amino acid concentration, compared with age-matched, healthier individuals. The intracellular amino acid clearance improved in the healthy, nondiabetic older adults with hyperinsulinemia, whereas it did not change in diabetic older adults. As a result, the net muscle protein balance improved a little in the nondiabetic patients, but did not change in the diabetic patients.”
The researchers are evaluating older patients with type 2 diabetes to see whether there are alterations in vascular reactivity and protein synthesis and whether those can be overcome by resistance-exercise training. “Preliminary results show that flow-mediated dilation can actually increase in an older diabetic patient with resistance exercise training three times a week for 3 months,” she said. “Exercise can improve both endothelial dysfunction and sarcopenia and therefore improve physical function and reduce cardiovascular risk.”
Dr. Volpi reported having no relevant disclosures.
LOS ANGELES –
“Loss of lean body mass and function with aging decreases the amount of metabolically active tissue, which can lead to insulin resistance,” Elena Volpi, MD, said at the World Congress on Insulin Resistance, Diabetes and Cardiovascular Disease. “Insulin resistance reduces muscle protein anabolism and accelerates sarcopenia, perpetuating a vicious cycle.”
Sarcopenia, the involuntary loss of muscle mass and function that occurs with aging, is an ICD-10 codable condition that can be diagnosed by measuring muscle strength and quality, said Dr. Volpi, director of the Sealy Center on Aging at the University of Texas Medical Branch at Galveston. In the Health, Aging and Body Composition Study (Health ABC), researchers followed 2,292 relatively healthy adults aged 70-79 years for an average of 4.9 years (J Gerontol A Biol Sci Med. 2006;61[1]:72-7). The researchers used isokinetic dynamometry to measure knee extension strength, isometric dynamometry to measure grip strength, CT scan to measure thigh muscle area, and dual X-ray absorptiometry to determine leg and arm lean soft-tissue mass. “Those individuals who started with the highest levels of muscle strength had the greatest survival, while those who had the lowest levels of muscle strength died earlier,” said Dr. Volpi, who was not affiliated with the study. “That was true for both men and women.”
More recently, researchers conducted a pooled analysis of nine cohort studies involving 34,485 community-dwelling older individuals who were tested with gait speed and followed for 6-21 years (JAMA. 2011;305[1]:50-8). They found that a higher gait speed was associated with higher survival at 5 and 10 years (P less than .001). “Muscle mass also appears to be associated in part with mortality and survival, although the association is not as strong as measures of strength and gait speed,” Dr. Volpi said.
Data from the 2009 Korea National Health and Nutrition Examination Survey of 1,537 participants, aged 65 years and older, found that sarcopenia is independently associated with cardiovascular disease (PLoS One. 2013 Mar 22. doi: 10.1371/journal.pone.0060119). Most of the risk factors for cardiovascular disease – such as age, waist circumference, body mass index, fasting plasma glucose, and total cholesterol – showed significant negative correlations with the ratio between appendicular skeletal muscle mass and body weight. Multiple logistic regression analysis demonstrated that sarcopenia was associated with cardiovascular disease, independent of other well-documented risk factors, renal function, and medications (odds ratio, 1.77; P = .025).
In addition, data from the British Regional Heart Study, which followed 4,252 older men for a mean of 11.3 years, found an association of sarcopenia and adiposity with cardiovascular mortality and all-cause mortality (J Am Geriatr Soc. 2014;62[2]:253-60). Specifically, all-cause mortality risk was significantly greater in men in the sarcopenic and obese groups (HRs, 1.41 and 1.21, respectively), compared with those in the optimal reference group, with the highest risk in sarcopenic obese individuals (HR, 1.72) after adjustment for lifestyle characteristics.
“Diabetes also accelerates loss of lean body mass in older adults,” added Dr. Volpi. “Data from the Health ABC study showed that individuals who did not have diabetes at the beginning of the 6-year observation period ... lost the least amount of muscle, compared with those who had undiagnosed or already diagnosed diabetes.”
The precise way in which sarcopenia is linked to metabolic disease remains elusive, she continued, but current evidence suggests that sarcopenia is characterized by a reduction in the protein synthetic response to metabolic stimulation by amino acids, exercise, and insulin in skeletal muscle. “This reduction in the anabolic response to protein synthesis is called anabolic resistance of aging, and it is mediated by reduced acute activation of mTORC1 [mTOR complex 1] signaling,” Dr. Volpi said. “There’s another step upstream of the mTORC1, in which the amino acids and insulin have to cross the blood-muscle barrier. Amino acids need to be transported into the muscle actively, like glucose. That is an important unexplored area that may contribute to sarcopenia.”
Dr. Volpi went on to note that endothelial dysfunction underlies muscle anabolic resistance and cardiovascular risk and is likely to be a fundamental cause of both problems. Recent studies have shown that increased levels of physical activity improve endothelial function, enhance insulin sensitivity and anabolic sensitivity to nutrients, and reduce cardiovascular risk.
For example, in a cohort of 45 nonfrail older adults with a mean age of 72 years, Dr. Volpi and colleagues carried out a phase 1, double-blind, placebo-controlled, randomized clinical trial to determine if chronic essential amino acid supplementation, aerobic exercise training, or a combination of the two interventions could improve muscle mass and function by stimulating muscle protein synthesis over the course of 24 weeks (J Gerontol A Biol Sci Med Sci. 2019;74[10]:1598-604). “We found that exercise supervised three times per week on a treadmill for 6 months improved physical function in both groups randomized to exercise,” Dr. Volpi said. “Disappointingly, there was no change in total lean mass with any of the interventions. There was a decrease in fat mass with exercise alone, and no change with exercise and amino acids. [Of note is that] the individuals who were randomized to the amino acids plus exercise group had a significant increase in leg strength, whereas the others did not.”
Preliminary findings from ongoing work by Dr. Volpi and colleagues suggest that, in diabetes, muscle protein synthesis and blood flow really “are not different in response to insulin in healthy older adults and diabetic older adults because they don’t change at all. However, we did find alterations in amino acid trafficking in diabetes. We found that older individuals with type 2 diabetes had a reduction of amino acid transport and a higher intracellular amino acid concentration, compared with age-matched, healthier individuals. The intracellular amino acid clearance improved in the healthy, nondiabetic older adults with hyperinsulinemia, whereas it did not change in diabetic older adults. As a result, the net muscle protein balance improved a little in the nondiabetic patients, but did not change in the diabetic patients.”
The researchers are evaluating older patients with type 2 diabetes to see whether there are alterations in vascular reactivity and protein synthesis and whether those can be overcome by resistance-exercise training. “Preliminary results show that flow-mediated dilation can actually increase in an older diabetic patient with resistance exercise training three times a week for 3 months,” she said. “Exercise can improve both endothelial dysfunction and sarcopenia and therefore improve physical function and reduce cardiovascular risk.”
Dr. Volpi reported having no relevant disclosures.
EXPERT ANALYSIS FROM WCIRDC 2019
Hip fracture patients with dementia benefit from increased rehab intensity
according to a recent Japanese study in the Archives of Physical Medicine and Rehabilitation.

Looking at 43,506 patients cared for at 1,053 hospitals, Kazuaki Uda, MPH, and colleagues of the University of Tokyo found that scores on the Barthel Index, a measure of functional status, climbed significantly as the frequency and duration of postoperative rehabilitation increased. There was also a statistically significant, but small, association with improved functional status and early initiation of rehabilitation.
“Our results suggest that additional days of rehabilitation or an additional 20 minutes for each daily rehabilitation session in acute-care hospitals may provide better functional outcomes for patients with dementia,” concluded Mr. Uda and coinvestigators.
The Barthel Index (BI) measures independence in performing 10 activities of daily living (ADLs), including feeding, bathing, grooming, and dressing; bowel, bladder, and toileting; and transfers, mobility, and stair use. Each ADL is rate 0, 5, 10, or, for some, 15 points, and higher scores indicate more independence.
Compared with patients who received 3 days or fewer of rehabilitation weekly, patients receiving 3-4 days of rehabilitation saw an improvement of 2.62 on the BI. For those receiving 4-5 days, 5-6 days, and 6 or more days of rehabilitation, BI scores were higher by 5.83, 7.56, and 9.16, respectively. The results were statistically significant for all but the 3-4 day rehabilitation group.
Similarly, patients who received longer periods of rehabilitation saw more improvement in functional status. Compared with those who received 20-39 minutes per day of rehabilitation, those who received 40-59 minutes of therapy saw an increase of 4.37 on the BI, and those receiving an hour or more of therapy saw BI scores rise by 6.60 – both significant increases.
These results included a multivariable analysis that accounted for a number of patient characteristics such as comorbidities and body mass index, as well as fracture, fixation, and anesthesia type, and the interval from injury to surgery.
Representing the data in another way, the investigators found that “each increase in the average units of rehabilitation (units per day) was associated with a 5.46 increase in the BI.”
This retrospective cohort study, when placed in the context of previous work, suggests that “patients with cognitive impairment may benefit from rehabilitation for functional gains after hip fracture surgery in both acute and postacute settings,” the investigators wrote. They noted, however, that patients with dementia have often been excluded from larger outcome studies of hip fracture rehabilitation.
Patients in this study had a median 21-day inpatient stay after admission for their hip fracture, so much of the rehabilitation included as inpatient care in the Japanese schema would be delivered in the outpatient setting in the United States, where the mean inpatient length of stay after hip fracture is about 5 days.
Patients aged 65 years and older were included in the study if they had a prefracture diagnosis of dementia and sustained a hip fracture that was surgically repaired. Patients with multiple fracture sites, those with incomplete data, and those who didn’t undergo surgery or died in the hospital were excluded from the study. Almost two-thirds of patients (65.7%) were aged 85 years or older, and about a third (36.6%) were living in nursing facilities at the time of fracture. About 60% of patients were assessed as having mild dementia – a classification requiring little assistance with ADLs – before admission.
The authors noted that their study broke out timing, duration, and frequency of rehabilitation separately, unlike some previous work. They posited that longer or more frequent rounds of rehabilitation may be particularly effective in patients with dementia, who may face some communication barriers and require reteaching.
The study was unrandomized by design, and unmeasured confounders may have affected the results, they noted. Also, the study wasn’t designed to detect whether patient factors such as premorbid functional status, level of dementia, or living situation affected the timing, duration, and intensity of rehabilitation they were provided. The investigators recommended randomized studies to validate the effect of early, intensive rehabilitation for hip fracture surgery in patients with dementia.
The study was funded by the Japanese Ministry of Health, Labor, and Welfare. The authors reported that they have no relevant conflicts of interest.
SOURCE: Uda K et al. Arch Phys Med Rehabil. 2019;100:2301-7.
according to a recent Japanese study in the Archives of Physical Medicine and Rehabilitation.
Looking at 43,506 patients cared for at 1,053 hospitals, Kazuaki Uda, MPH, and colleagues of the University of Tokyo found that scores on the Barthel Index, a measure of functional status, climbed significantly as the frequency and duration of postoperative rehabilitation increased. There was also a statistically significant, but small, association with improved functional status and early initiation of rehabilitation.
“Our results suggest that additional days of rehabilitation or an additional 20 minutes for each daily rehabilitation session in acute-care hospitals may provide better functional outcomes for patients with dementia,” concluded Mr. Uda and coinvestigators.
The Barthel Index (BI) measures independence in performing 10 activities of daily living (ADLs), including feeding, bathing, grooming, and dressing; bowel, bladder, and toileting; and transfers, mobility, and stair use. Each ADL is rate 0, 5, 10, or, for some, 15 points, and higher scores indicate more independence.
Compared with patients who received 3 days or fewer of rehabilitation weekly, patients receiving 3-4 days of rehabilitation saw an improvement of 2.62 on the BI. For those receiving 4-5 days, 5-6 days, and 6 or more days of rehabilitation, BI scores were higher by 5.83, 7.56, and 9.16, respectively. The results were statistically significant for all but the 3-4 day rehabilitation group.
Similarly, patients who received longer periods of rehabilitation saw more improvement in functional status. Compared with those who received 20-39 minutes per day of rehabilitation, those who received 40-59 minutes of therapy saw an increase of 4.37 on the BI, and those receiving an hour or more of therapy saw BI scores rise by 6.60 – both significant increases.
These results included a multivariable analysis that accounted for a number of patient characteristics such as comorbidities and body mass index, as well as fracture, fixation, and anesthesia type, and the interval from injury to surgery.
Representing the data in another way, the investigators found that “each increase in the average units of rehabilitation (units per day) was associated with a 5.46 increase in the BI.”
This retrospective cohort study, when placed in the context of previous work, suggests that “patients with cognitive impairment may benefit from rehabilitation for functional gains after hip fracture surgery in both acute and postacute settings,” the investigators wrote. They noted, however, that patients with dementia have often been excluded from larger outcome studies of hip fracture rehabilitation.
Patients in this study had a median 21-day inpatient stay after admission for their hip fracture, so much of the rehabilitation included as inpatient care in the Japanese schema would be delivered in the outpatient setting in the United States, where the mean inpatient length of stay after hip fracture is about 5 days.
Patients aged 65 years and older were included in the study if they had a prefracture diagnosis of dementia and sustained a hip fracture that was surgically repaired. Patients with multiple fracture sites, those with incomplete data, and those who didn’t undergo surgery or died in the hospital were excluded from the study. Almost two-thirds of patients (65.7%) were aged 85 years or older, and about a third (36.6%) were living in nursing facilities at the time of fracture. About 60% of patients were assessed as having mild dementia – a classification requiring little assistance with ADLs – before admission.
The authors noted that their study broke out timing, duration, and frequency of rehabilitation separately, unlike some previous work. They posited that longer or more frequent rounds of rehabilitation may be particularly effective in patients with dementia, who may face some communication barriers and require reteaching.
The study was unrandomized by design, and unmeasured confounders may have affected the results, they noted. Also, the study wasn’t designed to detect whether patient factors such as premorbid functional status, level of dementia, or living situation affected the timing, duration, and intensity of rehabilitation they were provided. The investigators recommended randomized studies to validate the effect of early, intensive rehabilitation for hip fracture surgery in patients with dementia.
The study was funded by the Japanese Ministry of Health, Labor, and Welfare. The authors reported that they have no relevant conflicts of interest.
SOURCE: Uda K et al. Arch Phys Med Rehabil. 2019;100:2301-7.
according to a recent Japanese study in the Archives of Physical Medicine and Rehabilitation.
Looking at 43,506 patients cared for at 1,053 hospitals, Kazuaki Uda, MPH, and colleagues of the University of Tokyo found that scores on the Barthel Index, a measure of functional status, climbed significantly as the frequency and duration of postoperative rehabilitation increased. There was also a statistically significant, but small, association with improved functional status and early initiation of rehabilitation.
“Our results suggest that additional days of rehabilitation or an additional 20 minutes for each daily rehabilitation session in acute-care hospitals may provide better functional outcomes for patients with dementia,” concluded Mr. Uda and coinvestigators.
The Barthel Index (BI) measures independence in performing 10 activities of daily living (ADLs), including feeding, bathing, grooming, and dressing; bowel, bladder, and toileting; and transfers, mobility, and stair use. Each ADL is rate 0, 5, 10, or, for some, 15 points, and higher scores indicate more independence.
Compared with patients who received 3 days or fewer of rehabilitation weekly, patients receiving 3-4 days of rehabilitation saw an improvement of 2.62 on the BI. For those receiving 4-5 days, 5-6 days, and 6 or more days of rehabilitation, BI scores were higher by 5.83, 7.56, and 9.16, respectively. The results were statistically significant for all but the 3-4 day rehabilitation group.
Similarly, patients who received longer periods of rehabilitation saw more improvement in functional status. Compared with those who received 20-39 minutes per day of rehabilitation, those who received 40-59 minutes of therapy saw an increase of 4.37 on the BI, and those receiving an hour or more of therapy saw BI scores rise by 6.60 – both significant increases.
These results included a multivariable analysis that accounted for a number of patient characteristics such as comorbidities and body mass index, as well as fracture, fixation, and anesthesia type, and the interval from injury to surgery.
Representing the data in another way, the investigators found that “each increase in the average units of rehabilitation (units per day) was associated with a 5.46 increase in the BI.”
This retrospective cohort study, when placed in the context of previous work, suggests that “patients with cognitive impairment may benefit from rehabilitation for functional gains after hip fracture surgery in both acute and postacute settings,” the investigators wrote. They noted, however, that patients with dementia have often been excluded from larger outcome studies of hip fracture rehabilitation.
Patients in this study had a median 21-day inpatient stay after admission for their hip fracture, so much of the rehabilitation included as inpatient care in the Japanese schema would be delivered in the outpatient setting in the United States, where the mean inpatient length of stay after hip fracture is about 5 days.
Patients aged 65 years and older were included in the study if they had a prefracture diagnosis of dementia and sustained a hip fracture that was surgically repaired. Patients with multiple fracture sites, those with incomplete data, and those who didn’t undergo surgery or died in the hospital were excluded from the study. Almost two-thirds of patients (65.7%) were aged 85 years or older, and about a third (36.6%) were living in nursing facilities at the time of fracture. About 60% of patients were assessed as having mild dementia – a classification requiring little assistance with ADLs – before admission.
The authors noted that their study broke out timing, duration, and frequency of rehabilitation separately, unlike some previous work. They posited that longer or more frequent rounds of rehabilitation may be particularly effective in patients with dementia, who may face some communication barriers and require reteaching.
The study was unrandomized by design, and unmeasured confounders may have affected the results, they noted. Also, the study wasn’t designed to detect whether patient factors such as premorbid functional status, level of dementia, or living situation affected the timing, duration, and intensity of rehabilitation they were provided. The investigators recommended randomized studies to validate the effect of early, intensive rehabilitation for hip fracture surgery in patients with dementia.
The study was funded by the Japanese Ministry of Health, Labor, and Welfare. The authors reported that they have no relevant conflicts of interest.
SOURCE: Uda K et al. Arch Phys Med Rehabil. 2019;100:2301-7.
REPORTING FROM THE ARCHIVES OF PHYSICAL MEDICINE AND REHABILITATION
Delayed hospital admission after hip fracture raises mortality risk
a retrospective, observational study suggests.
Among 867 elderly patients who underwent hip fracture surgery at a university hospital in China and who were available for follow-up, the proportion hospitalized on the day of injury was 25.4%, and the proportion hospitalized on days 1, 2, and 7 after injury were 54.7%, 66.3%, and 12.6%, respectively, reported Wei He, MD, of the Second Affiliated Hospital of Zhejiang University, Hangzhou, China, and colleagues in the World Journal of Emergency Medicine.
The mean time from admission to surgery was 5.2 days. Mortality rates at 1 year, 3 months, and 1 month after surgery were 10.5%, 5.4%, and 3.3%, respectively. Hospitalization at 7 or more days after injury was an independent risk factor for 1-year mortality (odds ratio, 1.76), the authors found.
Although the influence of surgical delay on mortality and morbidity among hip fracture patients has been widely studied, most data focus on surgery timing among hospitalized patients and fail to consider preadmission waiting time, they noted.
The current study aimed to assess outcomes based on “actual preadmission waiting time” through an analysis of data and surgical outcomes from a hospital electronic medical record system and from postoperative telephone interviews. Study subjects were patients aged over 65 years who underwent hip fracture surgery between Jan. 1, 2014, and Dec. 31, 2017. The mean age was 81.4 years, 74.7% of the patients were women, 67.1% had femoral neck fracture, and 56.1% had hip replacement surgery.
The findings, though limited by the retrospective nature of the study and the single-center design, suggest that, under the current conditions in China, admission delay may increase 1-year mortality, they wrote, concluding that “[i]n addition to early surgery highlighted in the guidelines, we also advocate early admission.”
The authors reported having no disclosures.
SOURCE: He W et al. World J Emerg Med. 2020;11(1):27-32.
a retrospective, observational study suggests.
Among 867 elderly patients who underwent hip fracture surgery at a university hospital in China and who were available for follow-up, the proportion hospitalized on the day of injury was 25.4%, and the proportion hospitalized on days 1, 2, and 7 after injury were 54.7%, 66.3%, and 12.6%, respectively, reported Wei He, MD, of the Second Affiliated Hospital of Zhejiang University, Hangzhou, China, and colleagues in the World Journal of Emergency Medicine.
The mean time from admission to surgery was 5.2 days. Mortality rates at 1 year, 3 months, and 1 month after surgery were 10.5%, 5.4%, and 3.3%, respectively. Hospitalization at 7 or more days after injury was an independent risk factor for 1-year mortality (odds ratio, 1.76), the authors found.
Although the influence of surgical delay on mortality and morbidity among hip fracture patients has been widely studied, most data focus on surgery timing among hospitalized patients and fail to consider preadmission waiting time, they noted.
The current study aimed to assess outcomes based on “actual preadmission waiting time” through an analysis of data and surgical outcomes from a hospital electronic medical record system and from postoperative telephone interviews. Study subjects were patients aged over 65 years who underwent hip fracture surgery between Jan. 1, 2014, and Dec. 31, 2017. The mean age was 81.4 years, 74.7% of the patients were women, 67.1% had femoral neck fracture, and 56.1% had hip replacement surgery.
The findings, though limited by the retrospective nature of the study and the single-center design, suggest that, under the current conditions in China, admission delay may increase 1-year mortality, they wrote, concluding that “[i]n addition to early surgery highlighted in the guidelines, we also advocate early admission.”
The authors reported having no disclosures.
SOURCE: He W et al. World J Emerg Med. 2020;11(1):27-32.
a retrospective, observational study suggests.
Among 867 elderly patients who underwent hip fracture surgery at a university hospital in China and who were available for follow-up, the proportion hospitalized on the day of injury was 25.4%, and the proportion hospitalized on days 1, 2, and 7 after injury were 54.7%, 66.3%, and 12.6%, respectively, reported Wei He, MD, of the Second Affiliated Hospital of Zhejiang University, Hangzhou, China, and colleagues in the World Journal of Emergency Medicine.
The mean time from admission to surgery was 5.2 days. Mortality rates at 1 year, 3 months, and 1 month after surgery were 10.5%, 5.4%, and 3.3%, respectively. Hospitalization at 7 or more days after injury was an independent risk factor for 1-year mortality (odds ratio, 1.76), the authors found.
Although the influence of surgical delay on mortality and morbidity among hip fracture patients has been widely studied, most data focus on surgery timing among hospitalized patients and fail to consider preadmission waiting time, they noted.
The current study aimed to assess outcomes based on “actual preadmission waiting time” through an analysis of data and surgical outcomes from a hospital electronic medical record system and from postoperative telephone interviews. Study subjects were patients aged over 65 years who underwent hip fracture surgery between Jan. 1, 2014, and Dec. 31, 2017. The mean age was 81.4 years, 74.7% of the patients were women, 67.1% had femoral neck fracture, and 56.1% had hip replacement surgery.
The findings, though limited by the retrospective nature of the study and the single-center design, suggest that, under the current conditions in China, admission delay may increase 1-year mortality, they wrote, concluding that “[i]n addition to early surgery highlighted in the guidelines, we also advocate early admission.”
The authors reported having no disclosures.
SOURCE: He W et al. World J Emerg Med. 2020;11(1):27-32.
FROM THE WORLD JOURNAL OF EMERGENCY MEDICINE
Food Insecurity Among Veterans: Resources to Screen and Intervene
Nearly 1 in 8 households—and 1 in 6 households with children—experienced food insecurity in 2017, defined as limited or uncertain availability of nutritionally adequate and safe foods.1 Food insecurity is often even more pronounced among households with individuals with acute or chronic medical conditions.2-6 Moreover, food insecurity is independently associated with a range of adverse health outcomes, including poorer control of diabetes mellitus, hypertension, depression and other major psychiatric disorders, HIV, and chronic lung and kidney disease, as well as poorer overall health status.7-14 Food insecurity also has been associated with increased health care costs and acute care utilization as well as increased probability of delayed or missed care.15-19
The relationship between food insecurity and poor health outcomes is a complex and often cyclic phenomenon (Figure 1). Poor nutritional status is fueled by limited access to healthful foods as well as increased reliance on calorie-dense and nutrient-poor “junk” foods, which are less expensive and often more readily available in low-income neighborhoods.5,20-24 These compensatory dietary patterns place individuals at higher risk for developing cardiometabolic conditions and for poor control of these conditions.5,8,9,12,25,26 Additionally, the physiological and psychological stressors of food insecurity may precipitate depression and anxiety or worsen existing mental health conditions, resulting in feelings of overwhelm and decreased self-management capacity.5,8,27-31 Food insecurity has further been associated with poor sleep, declines in cognitive function, and increased falls, particularly among the frail and elderly.32-34
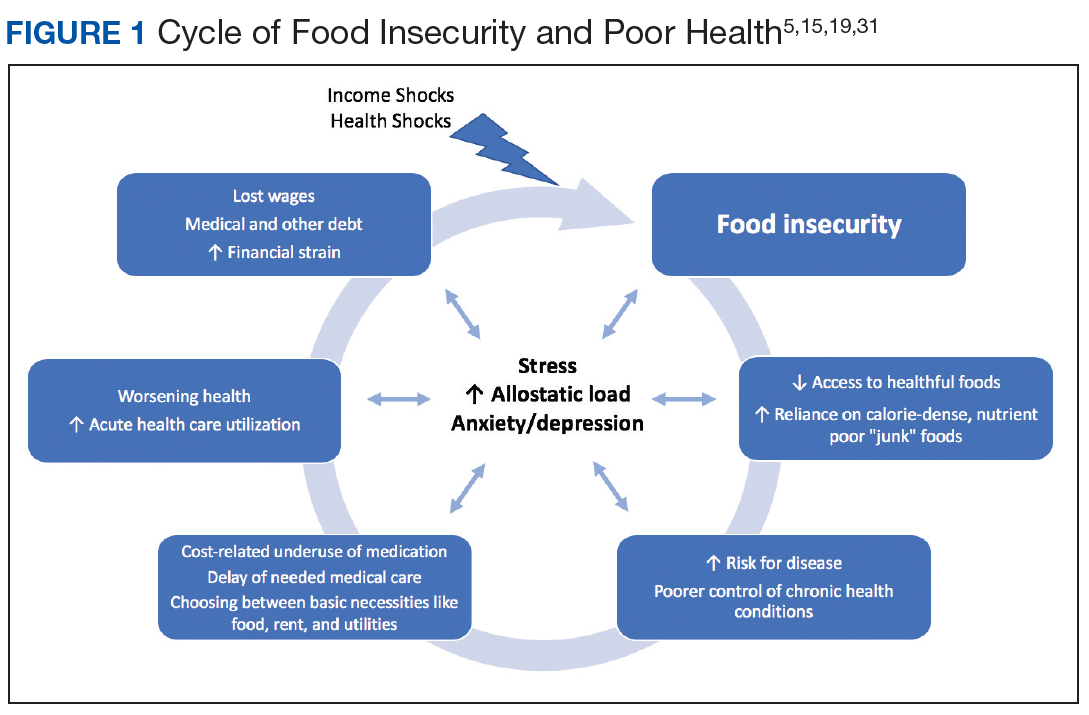
Individuals experiencing food insecurity often report having to make trade-offs between food and other necessities, such as paying rent or utilities. Additional strategies to stretch limited resources include cost-related underuse of medication and delays in needed medical care.4,17,31,35 In a nationally representative survey among adults with at least 1 chronic medical condition, 1 in 3 reported having to choose between food and medicine; 11% were unable to afford either.3 Furthermore, the inability to reliably adhere to medication regimens that need to be taken with food can result in potentially life-threatening hypoglycemia (as can lack of food regardless of medication use).5,26,36 In addition to the more obvious risks of glucose-lowering medications, such as insulin and long-acting sulfonylureas in patients experiencing food insecurity, many drugs commonly used among nondiabetic adults such as ACE-inhibitors, β blockers, quinolones, and salicylates can also precipitate hypoglycemia, and food insecurity has been associated with experiences of hypoglycemia even among individuals without diabetes mellitus.32,37 In one study the risk for hospital admissions for hypoglycemia among low-income populations increased by 27% at the end of the month when food budgets were more likely to be exhausted.38 Worsening health status and increased emergency department visits and hospitalizations may then result in lost wages and mounting medical bills, contributing to further financial strain and worsening food insecurity.
Prevalence and Importance of Food Insecurity Among US Veterans
Nearly 1.5 million veterans in the US are living below the federal poverty level (FPL).39 An additional 2.4 million veterans are living paycheck to paycheck at < 200% of the FPL.40 Veterans living in poverty are at even higher risk than nonveterans for food insecurity, homelessness, and other material hardship.41
Estimates of food insecurity among veterans vary widely, ranging from 6% to 24%—nearly twice that of the general US population.8,42-45 Higher rates of food insecurity have been reported among certain high-risk subgroups, including veterans who served in Iraq and Afghanistan (27%), female veterans (28%), homeless and formerly homeless veterans (49%), and veterans with serious mental illness (35%).6,32,43,46 Additional risk factors for food insecurity specific to veteran populations include younger age, having recently left active-duty military service, and lower final military paygrade.42,45-47 As in the general population, veteran food insecurity is associated with a range of adverse health outcomes, including poorer overall health status as well as increased probability of delayed or missed care.6,8,32,42-44,46
Even among veterans enrolled in federal food assistance programs, many still struggle to afford nutritionally adequate foods. As one example, in a study of mostly male homeless and formerly homeless veterans, O’Toole and colleagues found that nearly half of those reporting food insecurity were already receiving federal food assistance benefits, and 22% relied on emergency food resources.32 Of households served by Feeding America food pantries and meal programs, 20% have a member who has served in the US military.48
Federal Programs To Address Food Insecurity
There are several important federal food assistance programs designed to help alleviate food insecurity. The Supplemental Nutrition Assistance Program (SNAP, formerly the Food Stamp program) is the largest federal food assistance program and provides low-income Americans with cash benefits to purchase food. SNAP has been shown to substantially reduce food insecurity.7,49 The program also is associated with significant decreases in cost-related medication nonadherence as well as reductions in health care costs and both acute care and nursing home utilization.16,50-54 Although nearly 1.4 million veterans live in SNAP-enrolled households, 59% of eligible veterans are not enrolled.43,55 Closing this SNAP eligibility-enrollment gap, has been a focus of recent efforts to improve long-term food security among veterans. There also are several federal food assistance programs for households with children, including the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and school meals programs. Among federal nutrition programs for seniors, the Older American’s Act contains designated funding to support nutrition services for older adults, including congregate meal programs in community settings like senior centers, places of worship, and housing communities, and home-delivered meals through programs like Meals on Wheels.56
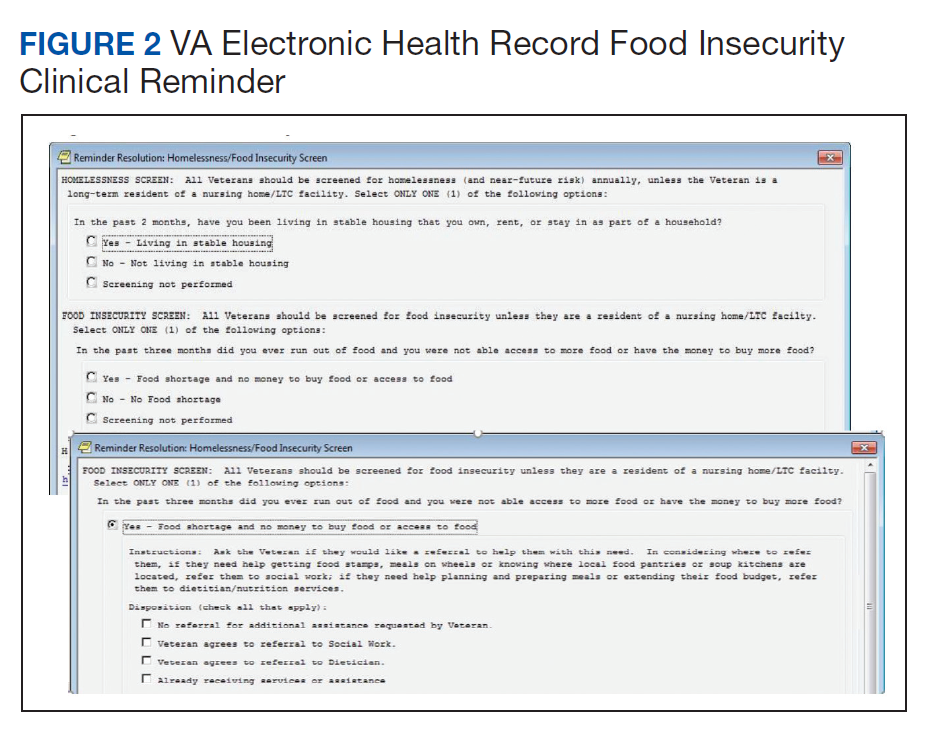
VHA Response to Food Insecurity
The Veterans Health Administration (VHA) is the country’s largest integrated, federally funded health care system.57 In November 2015, congressional briefings on veteran food insecurity organized by the national non-profit organization MAZON: A Jewish Response to Hunger and hosted with bipartisan support were provided to the US House and Senate. As a result of these briefings, VHA chartered the national Ensuring Veteran Food Security Workgroup with a mandate to partner with governmental and nonprofit agencies to “focus on the issue of food insecurity, the identification of veterans at risk, the needed training of VHA staff and the coordination of resources and initiatives to support the veterans for whom we care.” Building off a pilot in US Department of Veterans Affairs (VA) Homeless Patient Aligned Care Teams (H-PACTs),32 VHA subsequently integrated a single-item food insecurity screening tool into the VA electronic health record (EHR) clinical reminder system (Figure 2). The clinical reminder, which was rolled out across VA medical centers nationally in October 2017, provides an alert to screen all noninstitutionalized veterans for food insecurity. To date, nearly 5 million veterans have been screened. When a veteran endorses food insecurity based on the initial screening question, a prompt appears to offer the veteran a referral to a social worker and/or dietitian. Positive screening results also should be communicated to the patient’s primary care provider. Depending on site-specific clinical flow, the reminders are typically completed in the outpatient setting either by nurses or medical assistants during intake or by providers as part of the clinical visit. However, any member of the health care team can complete the clinical reminder at any time. As of September 2019, approximately 74,000 veterans have been identified as food insecure.58
Addressing Food Insecurity
VHA has been a recognized leader in addressing homelessness and other social determinants of health through its integrated care and PACT delivery models.59-61 The food insecurity clinical reminder was designed to facilitate a tailored, interdisciplinary approach to identify and address food insecurity. Interdisciplinary care team members—including medical assistants, clinicians, social workers, registered dietitians, nurse care managers, occupational or physical therapists, and pharmacists—are uniquely positioned to identify veterans impacted by food insecurity, assess for associated clinical and/or social risk factors, and offer appropriate medical and nutrition interventions and resource referrals.
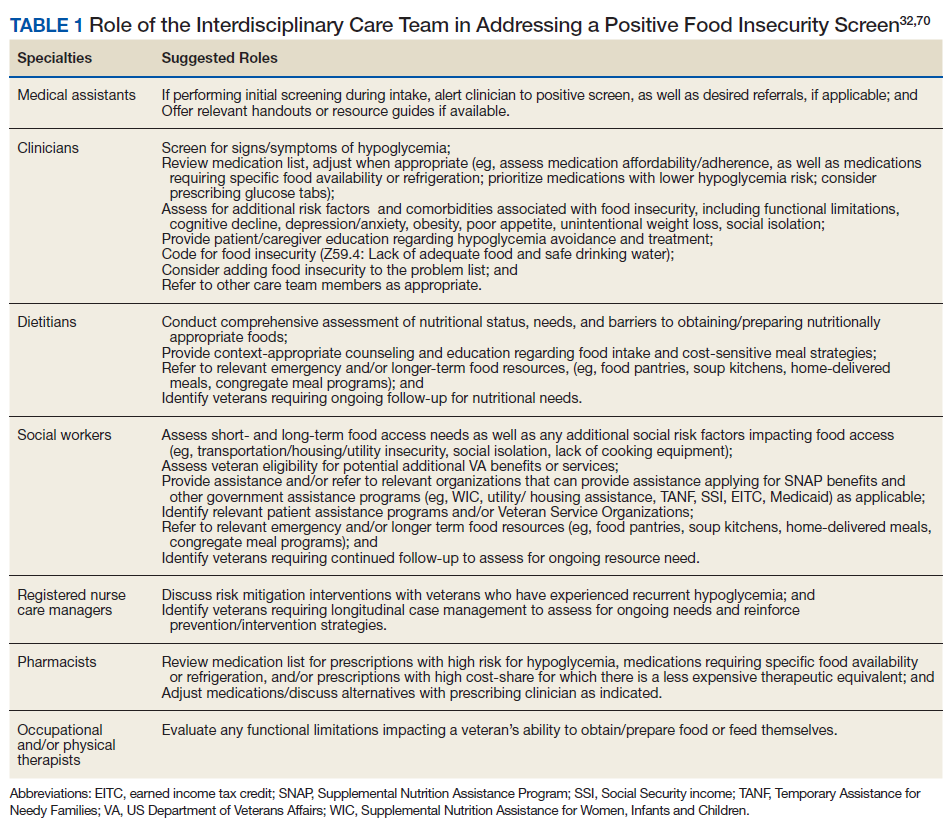
This interdisciplinary team-based model is essential given the range of potential drivers underlying veteran experiences of food insecurity and subsequent health outcomes. It is critically important for clinicians to review the medication list with veterans screening positive for food insecurity to assess for risk of hypoglycemia and/or cost-related nonadherence, make any necessary adjustments to therapeutic regimens, and assess for additional risk factors associated with food insecurity. Examples of tailored nutrition counseling that clinical dietitians may provide include meal preparation strategies for veterans who only have access to a microwave or hotplate, or recommendations for how veterans on medically restricted diets can best navigate food selection at soup kitchens or food pantries. Resource referrals provided by social workers or other care team members may include both emergency food resources to address immediate shortages (eg, food pantries, soup kitchens, or vouchers for free lunch) as well as resources focused on improving longer term food security (eg, federal food assistance programs or home delivered meal programs). Importantly, although providing a list of food resources may be helpful for some patients, such lists are often insufficient.62,63 Many patients require active assistance with program enrollment either onsite the day of their clinic visit or through connection with a partnering community-based organization that can, in turn, identify appropriate resources and facilitate program enrollment.63,64 Planned follow-up is also crucial to determine whether referrals are successful and to assess for ongoing need. Proposed roles for interdisciplinary care team members in addressing a positive food insecurity screen are outlined in Table 1.
VHA-Community Partnerships
In addition to services offered within VA, public and private sector partnerships can greatly enhance the range of resources available to food insecure veterans. Several VA facilities have developed formal community partnerships, such as the Veterans Pantry Pilot (VPP) program, a national partnership between Feeding America food banks and VA medical centers to establish onsite or mobile food pantries. There are currently 17 active Feeding America VPP sites, with a number of additional sites under development. Several of the VPP sites also include other “wraparound services,” such as SNAP application assistance.65,66
State Veterans Affairs offices67 and Veterans Service Organizations (VSOs)68 also can serve as valuable partners for connecting veterans with needed resources. VSOs offer a range of services, including assistancewith benefit claims, employment and housing assistance, emergency food assistance, and transportation to medical appointments. Some VSOs also have established local affiliations with Meals on Wheels focused on veteran outreach and providing hot meals for low-income, homebound, and disabled veterans.
Additional Resources
Although resources vary by regional setting, several key governmental and community-based food assistance programs are summarized in Table 2. Local community partners and online/phone-based directories, such as United Way’s 2-1-1 can help identify additional local resources. For older adults and individuals with disabilities, local Aging and Disability Resources Centers can provide information and assistance connecting to needed resources.69 Finally, there are a number of online resources available for clinicians interested in learning more about the impact of food insecurity on health and tools to use in the clinical setting (Table 3).
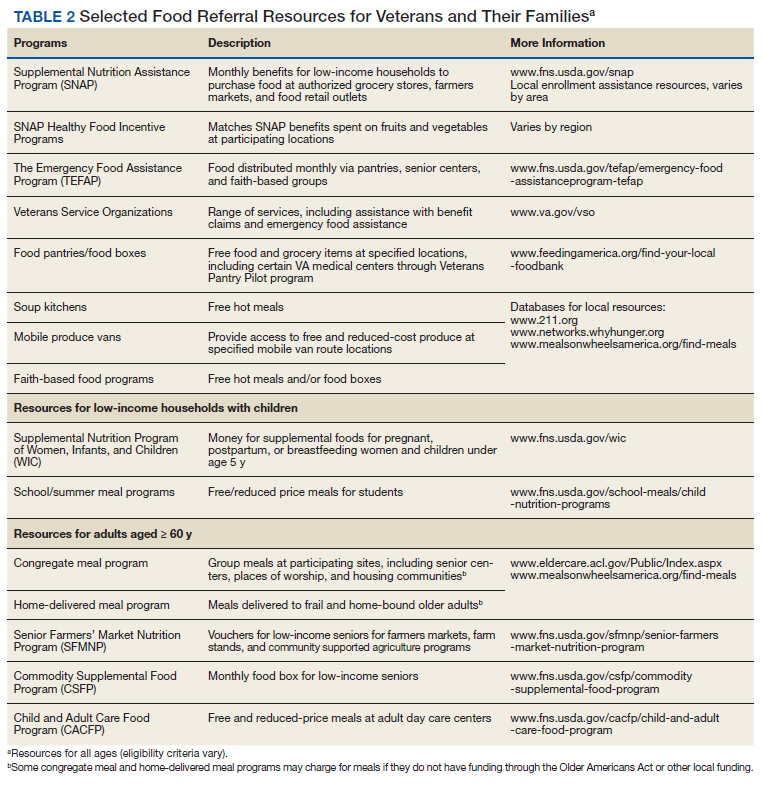
Conclusion
The VA has recognized food insecurity as a critical concern for the well-being of our nation’s veterans. Use of the EHR clinical reminder represents a crucial first step toward increasing provider awareness about veteran food insecurity and improving clinical efforts to address food insecurity once identified. Through the reminder, health care teams can connect veterans to needed resources and create both the individual and population-level data necessary to inform VHA and community efforts to address veteran food insecurity. Clinical reminder data are currently being used for local quality improvement efforts and have established the need nationally for formalized partnerships between VHA Social Work Services and Nutrition and Food Services to connect veterans with food and provide them with strategies to best use available food resources.
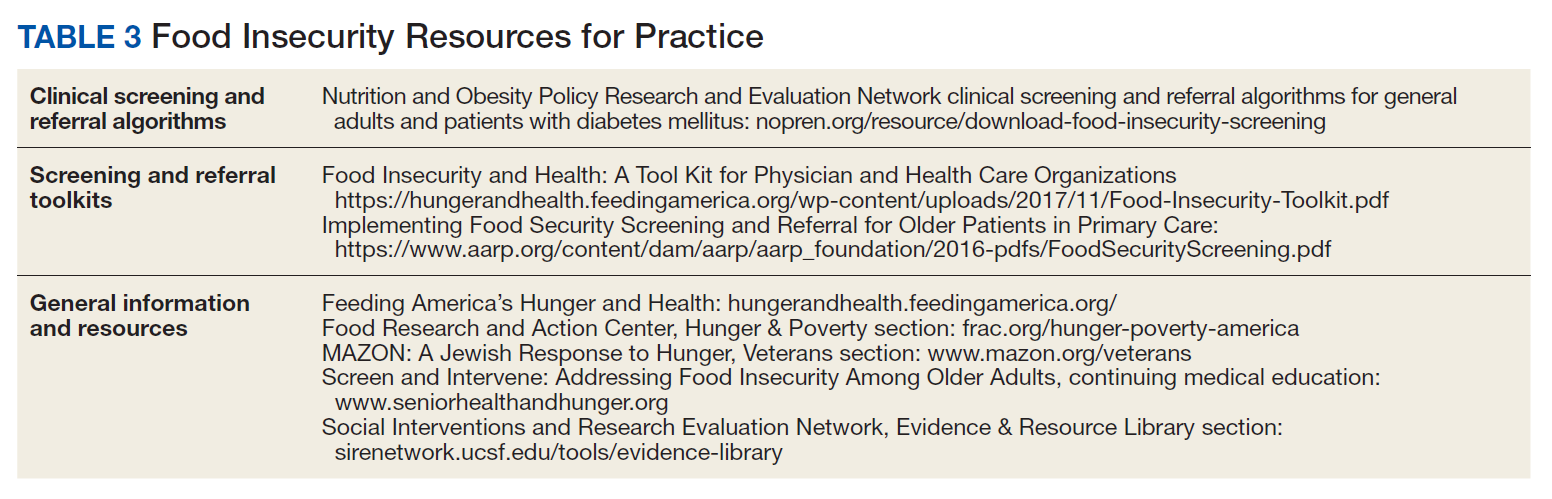
Moving forward, the Ensuring Veteran Food Security Workgroup continues to work with agencies and organizations across the country to improve food insecure veterans’ access to needed services. In addition to existing VA partnerships with Feeding America for the VPP, memorandums of understanding are currently underway to formalize partnerships with both the Food Research and Action Center (FRAC) and MAZON. Additional research is needed both to formally validate the current food insecurity clinical reminder screening question and to identify best practices and potential models for how to most effectively use VHA-community partnerships to address the unique needs of the veteran population.
Ensuring the food security of our nation’s veterans is essential to VA’s commitment to providing integrated, veteran-centered, whole person care. Toward that goal, VA health care teams are urged to use the clinical reminder and help connect food insecure veterans with relevant resources both within and outside of the VA health care system.
1. Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. Household food security in the United States in 2017. http://www.ers.usda.gov/publications/pub-details/?pubid=90022. Published September 2018. Accessed December 9, 2019.
2. Berkowitz SA, Meigs JB, DeWalt D, et al. Material need insecurities, control of diabetes mellitus, and use of health care resources: results of the Measuring Economic Insecurity in Diabetes study. JAMA Intern Med. 2015;175(2):257-265.
3. Berkowitz SA, Seligman HK, Choudhry NK. Treat or eat: food insecurity, cost-related medication underuse, and unmet needs. Am J Med. 2014;127(4):303-310.e3.
4. Lyles CR, Seligman HK, Parker MM, et al. Financial strain and medication adherence among diabetes patients in an integrated health care delivery system: The Diabetes Study of Northern California (DISTANCE). Health Serv Res. 2016;51(2):610-624.
5. Seligman HK, Schillinger D. Hunger and socioeconomic disparities in chronic disease. N Engl J Med. 2010;363(1):6-9.
6. Narain K, Bean-Mayberry B, Washington DL, Canelo IA, Darling JE, Yano EM. Access to care and health outcomes among women veterans using veterans administration health care: association with food insufficiency. Womens Health Issues. 2018;28(3):267-272.
7. Gundersen C, Ziliak JP. Food insecurity and health outcomes. Health Aff. 2015;34(11):1830-1839.
8. Wang EA, McGinnis KA, Goulet J, et al; Veterans Aging Cohort Study Project Team. Food insecurity and health: data from the Veterans Aging Cohort Study. Public Health Rep. 2015;130(3):261-268.
9. Berkowitz SA, Berkowitz TSZ, Meigs JB, Wexler DJ. Trends in food insecurity for adults with cardiometabolic disease in the United States: 2005-2012. PloS One. 2017;12(6):e0179172.
10. Seligman HK, Laraia BA, Kushel MB. Food insecurity is associated with chronic disease among low-income NHANES participants. J Nutr. 2010;140(2):304-310.
11. Berkowitz SA, Baggett TP, Wexler DJ, Huskey KW, Wee CC. Food insecurity and metabolic control among U.S. adults with diabetes. Diabetes Care. 2013;36(10):3093-3099.
12. Seligman HK, Jacobs EA, López A, Tschann J, Fernandez A. Food insecurity and glycemic control among low-income patients with type 2 diabetes. Diabetes Care. 2012;35(2):233-238.
13. Banerjee T, Crews DC, Wesson DE, et al; CDC CKD Surveillance Team. Food insecurity, CKD, and subsequent ESRD in US adults. Am J Kidney Dis. 2017;70(1):38-47.
14. Bruening M, Dinour LM, Chavez JBR. Food insecurity and emotional health in the USA: a systematic narrative review of longitudinal research. Public Health Nutr. 2017;20(17):3200-3208.
15. Berkowitz SA, Basu S, Meigs JB, Seligman HK. Food insecurity and health care expenditures in the United States, 2011-2013. Health Serv Res. 2018;53(3):1600-1620.
16. Berkowitz SA, Seligman HK, Basu S. Impact of food insecurity and SNAP participation on healthcare utilization and expenditures. http://www.ukcpr.org/research/discussion-papers. Published 2017. Accessed December 9, 2019.
17. Kushel MB, Gupta R, Gee L, Haas JS. Housing instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med. 2006;21(1):71-77.
18. Garcia SP, Haddix A, Barnett K. Incremental health care costs associated with food insecurity and chronic conditions among older adults. Chronic Dis. 2018;15:180058.
19. Berkowitz SA, Seligman HK, Meigs JB, Basu S. Food insecurity, healthcare utilization, and high cost: a longitudinal cohort study. Am J Manag Care. 2018;24(9):399-404.
20. Larson NI, Story MT, Nelson MC. Neighborhood environments: disparities in access to healthy foods in the U.S. Am J Prev Med. 2009;36(1):74-81.
21. Darmon N, Drewnowski A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: a systematic review and analysis. Nutr Rev. 2015;73(10):643-660.
22. Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87(5):1107-1117.
23. Drewnowski A. The cost of US foods as related to their nutritive value. Am J Clin Nutr. 2010;92(5):1181-1188.
24. Lucan SC, Maroko AR, Seitchik JL, Yoon DH, Sperry LE, Schechter CB. Unexpected neighborhood sources of food and drink: implications for research and community health. Am J Prev Med. 2018;55(2):e29-e38.
25. Castillo DC, Ramsey NL, Yu SS, Ricks M, Courville AB, Sumner AE. Inconsistent access to food and cardiometabolic disease: the effect of food insecurity. Curr Cardiovasc Risk Rep. 2012;6(3):245-250.
26. Seligman HK, Davis TC, Schillinger D, Wolf MS. Food insecurity is associated with hypoglycemia and poor diabetes self-management in a low-income sample with diabetes. J Health Care Poor Underserved. 2010;21(4):1227-1233.
27. Siefert K, Heflin CM, Corcoran ME, Williams DR. Food insufficiency and physical and mental health in a longitudinal survey of welfare recipients. J Health Soc Behav. 2004;45(2):171-186.
28. Mangurian C, Sreshta N, Seligman H. Food insecurity among adults with severe mental illness. Psychiatr Serv. 2013;64(9):931-932.
29. Melchior M, Caspi A, Howard LM, et al. Mental health context of food insecurity: a representative cohort of families with young children. Pediatrics. 2009;124(4):e564-e572.
30. Brostow DP, Gunzburger E, Abbate LM, Brenner LA, Thomas KS. Mental illness, not obesity status, is associated with food insecurity among the elderly in the health and retirement study. J Nutr Gerontol Geriatr. 2019;38(2):149-172.
31. Higashi RT, Craddock Lee SJ, Pezzia C, Quirk L, Leonard T, Pruitt SL. Family and social context contributes to the interplay of economic insecurity, food insecurity, and health. Ann Anthropol Pract. 2017;41(2):67-77.
32. O’Toole TP, Roberts CB, Johnson EE. Screening for food insecurity in six Veterans Administration clinics for the homeless, June-December 2015. Prev Chronic Dis. 2017;14:160375.
33. Feil DG, Pogach LM. Cognitive impairment is a major risk factor for serious hypoglycaemia; public health intervention is warranted. Evid Based Med. 2014;19(2):77.
34. Frith E, Loprinzi PD. Food insecurity and cognitive function in older adults: Brief report. Clin Nutr. 2018;37(5):1765-1768.
35. Herman D, Afulani P, Coleman-Jensen A, Harrison GG. Food insecurity and cost-related medication underuse among nonelderly adults in a nationally representative sample. Am J Public Health. 2015;105(10):e48-e59.
36. Tseng C-L, Soroka O, Maney M, Aron DC, Pogach LM. Assessing potential glycemic overtreatment in persons at hypoglycemic risk. JAMA Intern Med. 2014;174(2):259-268.
37. Vue MH, Setter SM. Drug-induced glucose alterations part 1: drug-induced hypoglycemia. Diabetes Spectr. 2011;24(3):171-177.
38. Seligman HK, Bolger AF, Guzman D, López A, Bibbins-Domingo K. Exhaustion of food budgets at month’s end and hospital admissions for hypoglycemia. Health Aff (Millwood). 2014;33(1):116-123.
39. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Veteran poverty trends. https://www.va.gov/vetdata/docs/specialreports/veteran_poverty_trends.pdf. Published May 2015. Accessed December 9, 2019.
40. Robbins KG, Ravi A. Veterans living paycheck to paycheck are under threat during budget debates. https://www.americanprogress.org/issues/poverty/news/2017/09/19/439023/veterans-living-paycheck-paycheck-threat-budget-debates. Published September 19, 2017. Accessed December 9, 2019.
41. Wilmoth JM, London AS, Heflin CM. Economic well-being among older-adult households: variation by veteran and disability status. J Gerontol Soc Work. 2015;58(4):399-419.
42. Brostow DP, Gunzburger E, Thomas KS. Food insecurity among veterans: findings from the health and retirement study. J Nutr Health Aging. 2017;21(10):1358-1364.
43. Pooler J, Mian P, Srinivasan M, Miller Z. Veterans and food insecurity. https://www.impaqint.com/sites/default/files/issue-briefs/VeteransFoodInsecurity_IssueBrief_V1.3.pdf. Published November 2018. Accessed December 9, 2019.
44. Schure MB, Katon JG, Wong E, Liu C-F. Food and housing insecurity and health status among U.S. adults with and without prior military service. SSM Popul Health. 2016;29(2):244-248.
45. Miller DP, Larson MJ, Byrne T, DeVoe E. Food insecurity in veteran households: findings from nationally representative data. Public Health Nutr. 2016;19(10):1731-1740.
46. Widome R, Jensen A, Bangerter A, Fu SS. Food insecurity among veterans of the US wars in Iraq and Afghanistan. Public Health Nutr. 2015;18(5):844-849.
47. London AS, Heflin CM. Supplemental Nutrition Assistance Program (SNAP) use among active-duty military personnel, veterans, and reservists. Popul Res Policy Rev. 2015;34(6):805-826.
48. Weinfield NS, Mills G, Borger C, et al. Hunger in America 2014. Natl rep prepared for Feeding America. https://www.feedingamerica.org/research/hunger-in-america. Published 2014. Accessed December 9, 2019.
49. Mabli J, Ohls J, Dragoset L, Castner L, Santos B. Measuring the Effect of Supplemental Nutrition Assistance Program (SNAP) Participation on Food Security. Washington, DC: US Department of Agriculture, Food and Nutrition Service; 2013.
50. Srinivasan M, Pooler JA. Cost-related medication nonadherence for older adults participating in SNAP, 2013–2015. Am J Public Health. 2017;108(2):224-230.
51. Heflin C, Hodges L, Mueser P. Supplemental Nutrition Assistance Progam benefits and emergency room visits for hypoglycaemia. Public Health Nutr. 2017;20(7):1314-1321.
52. Samuel LJ, Szanton SL, Cahill R, et al. Does the Supplemental Nutrition Assistance Program affect hospital utilization among older adults? The case of Maryland. Popul Health Manag. 2018;21(2):88-95.
53. Szanton SL, Samuel LJ, Cahill R, et al. Food assistance is associated with decreased nursing home admissions for Maryland’s dually eligible older adults. BMC Geriatr. 2017;17(1):162.
54. Carlson S, Keith-Jennings B. SNAP is linked with improved nutritional outcomes and lower health care costs. https://www.cbpp.org/research/food-assistance/snap-is-linked-with-improved-nutritional-outcomes-and-lower-health-care. Published January 17, 2018. Accessed December 10, 2019.
55. Keith-Jennings B, Cai L. SNAP helps almost 1.4 million low-income veterans, including thousands in every state. https://www.cbpp.org/research/food-assistance/snap-helps-almost-14-million-low-income-veterans-including-thousands-in. Updated November 8, 2018. Accessed December 10, 2019.
56. US Department of Health and Human Services. Older Americans Act nutrition programs. https://acl.gov/sites/default/files/news%202017-03/OAA-Nutrition_Programs_Fact_Sheet.pdf. Accessed December 10, 2019.
57. US Department of Veterans Affairs. About VHA. https://www.va.gov/health/aboutvha.asp. Accessed December 10, 2019.
58. US Department of Veterans Affairs. VA Corporate Data Warehouse.
59. Yano EM, Bair MJ, Carrasquillo O, Krein SL, Rubenstein LV. Patient aligned care teams (PACT): VA’s journey to implement patient-centered medical homes. J Gen Intern Med. 2014;29(suppl 2):S547-s549.
60. O’Toole TP, Pape L. Innovative efforts to address homelessness among veterans. N C Med J. 2015;76(5):311-314.
61. O’Toole TP, Johnson EE, Aiello R, Kane V, Pape L. Tailoring care to vulnerable populations by incorporating social determinants of health: the Veterans Health Administration’s “Homeless Patient Aligned Care Team” Program. Prev Chronic Dis. 2016;13:150567.
62. Marpadga S, Fernandez A, Leung J, Tang A, Seligman H, Murphy EJ. Challenges and successes with food resource referrals for food-insecure patients with diabetes. Perm J. 2019;23.
63. Stenmark SH, Steiner JF, Marpadga S, Debor M, Underhill K, Seligman H. Lessons learned from implementation of the food insecurity screening and referral program at Kaiser Permanente Colorado. Perm J. 2018;22.
64. Martel ML, Klein LR, Hager KA, Cutts DB. Emergency department experience with novel electronic medical record order for referral to food resources. West J Emerg Med. 2018;19(2):232-237.
65. Going C, Cohen AJ, Bares M, Christensen M. Interdisciplinary approaches to addressing the food insecure veteran. Veterans Health Administration Employee Education System webinar; October 30, 2018.
66. Feeding America Announces New Partnership With U.S. Department Of Veterans Affairs. https://www.prnewswire.com/news-releases/feeding-america-announces-new-partnership-with-us-department-of-veterans-affairs-300481891.html. Published June 29, 2017. Accessed December 10, 2019.
67. US Department of Veterans Affairs. State Veterans Affairs offices. https://www.va.gov/statedva.htm. Updated March 20, 2019. Accessed December 10, 2019.
68. US Department of Veterans Affairs. Directory of veterans service organizations. https://www.va.gov/vso. Updated December 24, 2013. Accessed December 10, 2019.
69. ACL Administration for Community Living. Aging and disability resource centers. https://acl.gov/programs/aging-and-disability-networks/aging-and-disability-resource-centers. Updated December 13, 2017. Accessed December 10, 2019.
70. Nutrition and Obesity Policy Research and Evaluation Network (NOPREN). Clinical screening algorithms. https://nopren.org/resource/download-food-insecurity-screening-and-referral-algorithms-for-adults-patients-living-with-diabetes-and-pediatric-patients. Accessed December 10, 2019.
Nearly 1 in 8 households—and 1 in 6 households with children—experienced food insecurity in 2017, defined as limited or uncertain availability of nutritionally adequate and safe foods.1 Food insecurity is often even more pronounced among households with individuals with acute or chronic medical conditions.2-6 Moreover, food insecurity is independently associated with a range of adverse health outcomes, including poorer control of diabetes mellitus, hypertension, depression and other major psychiatric disorders, HIV, and chronic lung and kidney disease, as well as poorer overall health status.7-14 Food insecurity also has been associated with increased health care costs and acute care utilization as well as increased probability of delayed or missed care.15-19
The relationship between food insecurity and poor health outcomes is a complex and often cyclic phenomenon (Figure 1). Poor nutritional status is fueled by limited access to healthful foods as well as increased reliance on calorie-dense and nutrient-poor “junk” foods, which are less expensive and often more readily available in low-income neighborhoods.5,20-24 These compensatory dietary patterns place individuals at higher risk for developing cardiometabolic conditions and for poor control of these conditions.5,8,9,12,25,26 Additionally, the physiological and psychological stressors of food insecurity may precipitate depression and anxiety or worsen existing mental health conditions, resulting in feelings of overwhelm and decreased self-management capacity.5,8,27-31 Food insecurity has further been associated with poor sleep, declines in cognitive function, and increased falls, particularly among the frail and elderly.32-34
Individuals experiencing food insecurity often report having to make trade-offs between food and other necessities, such as paying rent or utilities. Additional strategies to stretch limited resources include cost-related underuse of medication and delays in needed medical care.4,17,31,35 In a nationally representative survey among adults with at least 1 chronic medical condition, 1 in 3 reported having to choose between food and medicine; 11% were unable to afford either.3 Furthermore, the inability to reliably adhere to medication regimens that need to be taken with food can result in potentially life-threatening hypoglycemia (as can lack of food regardless of medication use).5,26,36 In addition to the more obvious risks of glucose-lowering medications, such as insulin and long-acting sulfonylureas in patients experiencing food insecurity, many drugs commonly used among nondiabetic adults such as ACE-inhibitors, β blockers, quinolones, and salicylates can also precipitate hypoglycemia, and food insecurity has been associated with experiences of hypoglycemia even among individuals without diabetes mellitus.32,37 In one study the risk for hospital admissions for hypoglycemia among low-income populations increased by 27% at the end of the month when food budgets were more likely to be exhausted.38 Worsening health status and increased emergency department visits and hospitalizations may then result in lost wages and mounting medical bills, contributing to further financial strain and worsening food insecurity.
Prevalence and Importance of Food Insecurity Among US Veterans
Nearly 1.5 million veterans in the US are living below the federal poverty level (FPL).39 An additional 2.4 million veterans are living paycheck to paycheck at < 200% of the FPL.40 Veterans living in poverty are at even higher risk than nonveterans for food insecurity, homelessness, and other material hardship.41
Estimates of food insecurity among veterans vary widely, ranging from 6% to 24%—nearly twice that of the general US population.8,42-45 Higher rates of food insecurity have been reported among certain high-risk subgroups, including veterans who served in Iraq and Afghanistan (27%), female veterans (28%), homeless and formerly homeless veterans (49%), and veterans with serious mental illness (35%).6,32,43,46 Additional risk factors for food insecurity specific to veteran populations include younger age, having recently left active-duty military service, and lower final military paygrade.42,45-47 As in the general population, veteran food insecurity is associated with a range of adverse health outcomes, including poorer overall health status as well as increased probability of delayed or missed care.6,8,32,42-44,46
Even among veterans enrolled in federal food assistance programs, many still struggle to afford nutritionally adequate foods. As one example, in a study of mostly male homeless and formerly homeless veterans, O’Toole and colleagues found that nearly half of those reporting food insecurity were already receiving federal food assistance benefits, and 22% relied on emergency food resources.32 Of households served by Feeding America food pantries and meal programs, 20% have a member who has served in the US military.48
Federal Programs To Address Food Insecurity
There are several important federal food assistance programs designed to help alleviate food insecurity. The Supplemental Nutrition Assistance Program (SNAP, formerly the Food Stamp program) is the largest federal food assistance program and provides low-income Americans with cash benefits to purchase food. SNAP has been shown to substantially reduce food insecurity.7,49 The program also is associated with significant decreases in cost-related medication nonadherence as well as reductions in health care costs and both acute care and nursing home utilization.16,50-54 Although nearly 1.4 million veterans live in SNAP-enrolled households, 59% of eligible veterans are not enrolled.43,55 Closing this SNAP eligibility-enrollment gap, has been a focus of recent efforts to improve long-term food security among veterans. There also are several federal food assistance programs for households with children, including the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and school meals programs. Among federal nutrition programs for seniors, the Older American’s Act contains designated funding to support nutrition services for older adults, including congregate meal programs in community settings like senior centers, places of worship, and housing communities, and home-delivered meals through programs like Meals on Wheels.56
VHA Response to Food Insecurity
The Veterans Health Administration (VHA) is the country’s largest integrated, federally funded health care system.57 In November 2015, congressional briefings on veteran food insecurity organized by the national non-profit organization MAZON: A Jewish Response to Hunger and hosted with bipartisan support were provided to the US House and Senate. As a result of these briefings, VHA chartered the national Ensuring Veteran Food Security Workgroup with a mandate to partner with governmental and nonprofit agencies to “focus on the issue of food insecurity, the identification of veterans at risk, the needed training of VHA staff and the coordination of resources and initiatives to support the veterans for whom we care.” Building off a pilot in US Department of Veterans Affairs (VA) Homeless Patient Aligned Care Teams (H-PACTs),32 VHA subsequently integrated a single-item food insecurity screening tool into the VA electronic health record (EHR) clinical reminder system (Figure 2). The clinical reminder, which was rolled out across VA medical centers nationally in October 2017, provides an alert to screen all noninstitutionalized veterans for food insecurity. To date, nearly 5 million veterans have been screened. When a veteran endorses food insecurity based on the initial screening question, a prompt appears to offer the veteran a referral to a social worker and/or dietitian. Positive screening results also should be communicated to the patient’s primary care provider. Depending on site-specific clinical flow, the reminders are typically completed in the outpatient setting either by nurses or medical assistants during intake or by providers as part of the clinical visit. However, any member of the health care team can complete the clinical reminder at any time. As of September 2019, approximately 74,000 veterans have been identified as food insecure.58
Addressing Food Insecurity
VHA has been a recognized leader in addressing homelessness and other social determinants of health through its integrated care and PACT delivery models.59-61 The food insecurity clinical reminder was designed to facilitate a tailored, interdisciplinary approach to identify and address food insecurity. Interdisciplinary care team members—including medical assistants, clinicians, social workers, registered dietitians, nurse care managers, occupational or physical therapists, and pharmacists—are uniquely positioned to identify veterans impacted by food insecurity, assess for associated clinical and/or social risk factors, and offer appropriate medical and nutrition interventions and resource referrals.
This interdisciplinary team-based model is essential given the range of potential drivers underlying veteran experiences of food insecurity and subsequent health outcomes. It is critically important for clinicians to review the medication list with veterans screening positive for food insecurity to assess for risk of hypoglycemia and/or cost-related nonadherence, make any necessary adjustments to therapeutic regimens, and assess for additional risk factors associated with food insecurity. Examples of tailored nutrition counseling that clinical dietitians may provide include meal preparation strategies for veterans who only have access to a microwave or hotplate, or recommendations for how veterans on medically restricted diets can best navigate food selection at soup kitchens or food pantries. Resource referrals provided by social workers or other care team members may include both emergency food resources to address immediate shortages (eg, food pantries, soup kitchens, or vouchers for free lunch) as well as resources focused on improving longer term food security (eg, federal food assistance programs or home delivered meal programs). Importantly, although providing a list of food resources may be helpful for some patients, such lists are often insufficient.62,63 Many patients require active assistance with program enrollment either onsite the day of their clinic visit or through connection with a partnering community-based organization that can, in turn, identify appropriate resources and facilitate program enrollment.63,64 Planned follow-up is also crucial to determine whether referrals are successful and to assess for ongoing need. Proposed roles for interdisciplinary care team members in addressing a positive food insecurity screen are outlined in Table 1.
VHA-Community Partnerships
In addition to services offered within VA, public and private sector partnerships can greatly enhance the range of resources available to food insecure veterans. Several VA facilities have developed formal community partnerships, such as the Veterans Pantry Pilot (VPP) program, a national partnership between Feeding America food banks and VA medical centers to establish onsite or mobile food pantries. There are currently 17 active Feeding America VPP sites, with a number of additional sites under development. Several of the VPP sites also include other “wraparound services,” such as SNAP application assistance.65,66
State Veterans Affairs offices67 and Veterans Service Organizations (VSOs)68 also can serve as valuable partners for connecting veterans with needed resources. VSOs offer a range of services, including assistancewith benefit claims, employment and housing assistance, emergency food assistance, and transportation to medical appointments. Some VSOs also have established local affiliations with Meals on Wheels focused on veteran outreach and providing hot meals for low-income, homebound, and disabled veterans.
Additional Resources
Although resources vary by regional setting, several key governmental and community-based food assistance programs are summarized in Table 2. Local community partners and online/phone-based directories, such as United Way’s 2-1-1 can help identify additional local resources. For older adults and individuals with disabilities, local Aging and Disability Resources Centers can provide information and assistance connecting to needed resources.69 Finally, there are a number of online resources available for clinicians interested in learning more about the impact of food insecurity on health and tools to use in the clinical setting (Table 3).
Conclusion
The VA has recognized food insecurity as a critical concern for the well-being of our nation’s veterans. Use of the EHR clinical reminder represents a crucial first step toward increasing provider awareness about veteran food insecurity and improving clinical efforts to address food insecurity once identified. Through the reminder, health care teams can connect veterans to needed resources and create both the individual and population-level data necessary to inform VHA and community efforts to address veteran food insecurity. Clinical reminder data are currently being used for local quality improvement efforts and have established the need nationally for formalized partnerships between VHA Social Work Services and Nutrition and Food Services to connect veterans with food and provide them with strategies to best use available food resources.
Moving forward, the Ensuring Veteran Food Security Workgroup continues to work with agencies and organizations across the country to improve food insecure veterans’ access to needed services. In addition to existing VA partnerships with Feeding America for the VPP, memorandums of understanding are currently underway to formalize partnerships with both the Food Research and Action Center (FRAC) and MAZON. Additional research is needed both to formally validate the current food insecurity clinical reminder screening question and to identify best practices and potential models for how to most effectively use VHA-community partnerships to address the unique needs of the veteran population.
Ensuring the food security of our nation’s veterans is essential to VA’s commitment to providing integrated, veteran-centered, whole person care. Toward that goal, VA health care teams are urged to use the clinical reminder and help connect food insecure veterans with relevant resources both within and outside of the VA health care system.
Nearly 1 in 8 households—and 1 in 6 households with children—experienced food insecurity in 2017, defined as limited or uncertain availability of nutritionally adequate and safe foods.1 Food insecurity is often even more pronounced among households with individuals with acute or chronic medical conditions.2-6 Moreover, food insecurity is independently associated with a range of adverse health outcomes, including poorer control of diabetes mellitus, hypertension, depression and other major psychiatric disorders, HIV, and chronic lung and kidney disease, as well as poorer overall health status.7-14 Food insecurity also has been associated with increased health care costs and acute care utilization as well as increased probability of delayed or missed care.15-19
The relationship between food insecurity and poor health outcomes is a complex and often cyclic phenomenon (Figure 1). Poor nutritional status is fueled by limited access to healthful foods as well as increased reliance on calorie-dense and nutrient-poor “junk” foods, which are less expensive and often more readily available in low-income neighborhoods.5,20-24 These compensatory dietary patterns place individuals at higher risk for developing cardiometabolic conditions and for poor control of these conditions.5,8,9,12,25,26 Additionally, the physiological and psychological stressors of food insecurity may precipitate depression and anxiety or worsen existing mental health conditions, resulting in feelings of overwhelm and decreased self-management capacity.5,8,27-31 Food insecurity has further been associated with poor sleep, declines in cognitive function, and increased falls, particularly among the frail and elderly.32-34
Individuals experiencing food insecurity often report having to make trade-offs between food and other necessities, such as paying rent or utilities. Additional strategies to stretch limited resources include cost-related underuse of medication and delays in needed medical care.4,17,31,35 In a nationally representative survey among adults with at least 1 chronic medical condition, 1 in 3 reported having to choose between food and medicine; 11% were unable to afford either.3 Furthermore, the inability to reliably adhere to medication regimens that need to be taken with food can result in potentially life-threatening hypoglycemia (as can lack of food regardless of medication use).5,26,36 In addition to the more obvious risks of glucose-lowering medications, such as insulin and long-acting sulfonylureas in patients experiencing food insecurity, many drugs commonly used among nondiabetic adults such as ACE-inhibitors, β blockers, quinolones, and salicylates can also precipitate hypoglycemia, and food insecurity has been associated with experiences of hypoglycemia even among individuals without diabetes mellitus.32,37 In one study the risk for hospital admissions for hypoglycemia among low-income populations increased by 27% at the end of the month when food budgets were more likely to be exhausted.38 Worsening health status and increased emergency department visits and hospitalizations may then result in lost wages and mounting medical bills, contributing to further financial strain and worsening food insecurity.
Prevalence and Importance of Food Insecurity Among US Veterans
Nearly 1.5 million veterans in the US are living below the federal poverty level (FPL).39 An additional 2.4 million veterans are living paycheck to paycheck at < 200% of the FPL.40 Veterans living in poverty are at even higher risk than nonveterans for food insecurity, homelessness, and other material hardship.41
Estimates of food insecurity among veterans vary widely, ranging from 6% to 24%—nearly twice that of the general US population.8,42-45 Higher rates of food insecurity have been reported among certain high-risk subgroups, including veterans who served in Iraq and Afghanistan (27%), female veterans (28%), homeless and formerly homeless veterans (49%), and veterans with serious mental illness (35%).6,32,43,46 Additional risk factors for food insecurity specific to veteran populations include younger age, having recently left active-duty military service, and lower final military paygrade.42,45-47 As in the general population, veteran food insecurity is associated with a range of adverse health outcomes, including poorer overall health status as well as increased probability of delayed or missed care.6,8,32,42-44,46
Even among veterans enrolled in federal food assistance programs, many still struggle to afford nutritionally adequate foods. As one example, in a study of mostly male homeless and formerly homeless veterans, O’Toole and colleagues found that nearly half of those reporting food insecurity were already receiving federal food assistance benefits, and 22% relied on emergency food resources.32 Of households served by Feeding America food pantries and meal programs, 20% have a member who has served in the US military.48
Federal Programs To Address Food Insecurity
There are several important federal food assistance programs designed to help alleviate food insecurity. The Supplemental Nutrition Assistance Program (SNAP, formerly the Food Stamp program) is the largest federal food assistance program and provides low-income Americans with cash benefits to purchase food. SNAP has been shown to substantially reduce food insecurity.7,49 The program also is associated with significant decreases in cost-related medication nonadherence as well as reductions in health care costs and both acute care and nursing home utilization.16,50-54 Although nearly 1.4 million veterans live in SNAP-enrolled households, 59% of eligible veterans are not enrolled.43,55 Closing this SNAP eligibility-enrollment gap, has been a focus of recent efforts to improve long-term food security among veterans. There also are several federal food assistance programs for households with children, including the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and school meals programs. Among federal nutrition programs for seniors, the Older American’s Act contains designated funding to support nutrition services for older adults, including congregate meal programs in community settings like senior centers, places of worship, and housing communities, and home-delivered meals through programs like Meals on Wheels.56
VHA Response to Food Insecurity
The Veterans Health Administration (VHA) is the country’s largest integrated, federally funded health care system.57 In November 2015, congressional briefings on veteran food insecurity organized by the national non-profit organization MAZON: A Jewish Response to Hunger and hosted with bipartisan support were provided to the US House and Senate. As a result of these briefings, VHA chartered the national Ensuring Veteran Food Security Workgroup with a mandate to partner with governmental and nonprofit agencies to “focus on the issue of food insecurity, the identification of veterans at risk, the needed training of VHA staff and the coordination of resources and initiatives to support the veterans for whom we care.” Building off a pilot in US Department of Veterans Affairs (VA) Homeless Patient Aligned Care Teams (H-PACTs),32 VHA subsequently integrated a single-item food insecurity screening tool into the VA electronic health record (EHR) clinical reminder system (Figure 2). The clinical reminder, which was rolled out across VA medical centers nationally in October 2017, provides an alert to screen all noninstitutionalized veterans for food insecurity. To date, nearly 5 million veterans have been screened. When a veteran endorses food insecurity based on the initial screening question, a prompt appears to offer the veteran a referral to a social worker and/or dietitian. Positive screening results also should be communicated to the patient’s primary care provider. Depending on site-specific clinical flow, the reminders are typically completed in the outpatient setting either by nurses or medical assistants during intake or by providers as part of the clinical visit. However, any member of the health care team can complete the clinical reminder at any time. As of September 2019, approximately 74,000 veterans have been identified as food insecure.58
Addressing Food Insecurity
VHA has been a recognized leader in addressing homelessness and other social determinants of health through its integrated care and PACT delivery models.59-61 The food insecurity clinical reminder was designed to facilitate a tailored, interdisciplinary approach to identify and address food insecurity. Interdisciplinary care team members—including medical assistants, clinicians, social workers, registered dietitians, nurse care managers, occupational or physical therapists, and pharmacists—are uniquely positioned to identify veterans impacted by food insecurity, assess for associated clinical and/or social risk factors, and offer appropriate medical and nutrition interventions and resource referrals.
This interdisciplinary team-based model is essential given the range of potential drivers underlying veteran experiences of food insecurity and subsequent health outcomes. It is critically important for clinicians to review the medication list with veterans screening positive for food insecurity to assess for risk of hypoglycemia and/or cost-related nonadherence, make any necessary adjustments to therapeutic regimens, and assess for additional risk factors associated with food insecurity. Examples of tailored nutrition counseling that clinical dietitians may provide include meal preparation strategies for veterans who only have access to a microwave or hotplate, or recommendations for how veterans on medically restricted diets can best navigate food selection at soup kitchens or food pantries. Resource referrals provided by social workers or other care team members may include both emergency food resources to address immediate shortages (eg, food pantries, soup kitchens, or vouchers for free lunch) as well as resources focused on improving longer term food security (eg, federal food assistance programs or home delivered meal programs). Importantly, although providing a list of food resources may be helpful for some patients, such lists are often insufficient.62,63 Many patients require active assistance with program enrollment either onsite the day of their clinic visit or through connection with a partnering community-based organization that can, in turn, identify appropriate resources and facilitate program enrollment.63,64 Planned follow-up is also crucial to determine whether referrals are successful and to assess for ongoing need. Proposed roles for interdisciplinary care team members in addressing a positive food insecurity screen are outlined in Table 1.
VHA-Community Partnerships
In addition to services offered within VA, public and private sector partnerships can greatly enhance the range of resources available to food insecure veterans. Several VA facilities have developed formal community partnerships, such as the Veterans Pantry Pilot (VPP) program, a national partnership between Feeding America food banks and VA medical centers to establish onsite or mobile food pantries. There are currently 17 active Feeding America VPP sites, with a number of additional sites under development. Several of the VPP sites also include other “wraparound services,” such as SNAP application assistance.65,66
State Veterans Affairs offices67 and Veterans Service Organizations (VSOs)68 also can serve as valuable partners for connecting veterans with needed resources. VSOs offer a range of services, including assistancewith benefit claims, employment and housing assistance, emergency food assistance, and transportation to medical appointments. Some VSOs also have established local affiliations with Meals on Wheels focused on veteran outreach and providing hot meals for low-income, homebound, and disabled veterans.
Additional Resources
Although resources vary by regional setting, several key governmental and community-based food assistance programs are summarized in Table 2. Local community partners and online/phone-based directories, such as United Way’s 2-1-1 can help identify additional local resources. For older adults and individuals with disabilities, local Aging and Disability Resources Centers can provide information and assistance connecting to needed resources.69 Finally, there are a number of online resources available for clinicians interested in learning more about the impact of food insecurity on health and tools to use in the clinical setting (Table 3).
Conclusion
The VA has recognized food insecurity as a critical concern for the well-being of our nation’s veterans. Use of the EHR clinical reminder represents a crucial first step toward increasing provider awareness about veteran food insecurity and improving clinical efforts to address food insecurity once identified. Through the reminder, health care teams can connect veterans to needed resources and create both the individual and population-level data necessary to inform VHA and community efforts to address veteran food insecurity. Clinical reminder data are currently being used for local quality improvement efforts and have established the need nationally for formalized partnerships between VHA Social Work Services and Nutrition and Food Services to connect veterans with food and provide them with strategies to best use available food resources.
Moving forward, the Ensuring Veteran Food Security Workgroup continues to work with agencies and organizations across the country to improve food insecure veterans’ access to needed services. In addition to existing VA partnerships with Feeding America for the VPP, memorandums of understanding are currently underway to formalize partnerships with both the Food Research and Action Center (FRAC) and MAZON. Additional research is needed both to formally validate the current food insecurity clinical reminder screening question and to identify best practices and potential models for how to most effectively use VHA-community partnerships to address the unique needs of the veteran population.
Ensuring the food security of our nation’s veterans is essential to VA’s commitment to providing integrated, veteran-centered, whole person care. Toward that goal, VA health care teams are urged to use the clinical reminder and help connect food insecure veterans with relevant resources both within and outside of the VA health care system.
1. Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. Household food security in the United States in 2017. http://www.ers.usda.gov/publications/pub-details/?pubid=90022. Published September 2018. Accessed December 9, 2019.
2. Berkowitz SA, Meigs JB, DeWalt D, et al. Material need insecurities, control of diabetes mellitus, and use of health care resources: results of the Measuring Economic Insecurity in Diabetes study. JAMA Intern Med. 2015;175(2):257-265.
3. Berkowitz SA, Seligman HK, Choudhry NK. Treat or eat: food insecurity, cost-related medication underuse, and unmet needs. Am J Med. 2014;127(4):303-310.e3.
4. Lyles CR, Seligman HK, Parker MM, et al. Financial strain and medication adherence among diabetes patients in an integrated health care delivery system: The Diabetes Study of Northern California (DISTANCE). Health Serv Res. 2016;51(2):610-624.
5. Seligman HK, Schillinger D. Hunger and socioeconomic disparities in chronic disease. N Engl J Med. 2010;363(1):6-9.
6. Narain K, Bean-Mayberry B, Washington DL, Canelo IA, Darling JE, Yano EM. Access to care and health outcomes among women veterans using veterans administration health care: association with food insufficiency. Womens Health Issues. 2018;28(3):267-272.
7. Gundersen C, Ziliak JP. Food insecurity and health outcomes. Health Aff. 2015;34(11):1830-1839.
8. Wang EA, McGinnis KA, Goulet J, et al; Veterans Aging Cohort Study Project Team. Food insecurity and health: data from the Veterans Aging Cohort Study. Public Health Rep. 2015;130(3):261-268.
9. Berkowitz SA, Berkowitz TSZ, Meigs JB, Wexler DJ. Trends in food insecurity for adults with cardiometabolic disease in the United States: 2005-2012. PloS One. 2017;12(6):e0179172.
10. Seligman HK, Laraia BA, Kushel MB. Food insecurity is associated with chronic disease among low-income NHANES participants. J Nutr. 2010;140(2):304-310.
11. Berkowitz SA, Baggett TP, Wexler DJ, Huskey KW, Wee CC. Food insecurity and metabolic control among U.S. adults with diabetes. Diabetes Care. 2013;36(10):3093-3099.
12. Seligman HK, Jacobs EA, López A, Tschann J, Fernandez A. Food insecurity and glycemic control among low-income patients with type 2 diabetes. Diabetes Care. 2012;35(2):233-238.
13. Banerjee T, Crews DC, Wesson DE, et al; CDC CKD Surveillance Team. Food insecurity, CKD, and subsequent ESRD in US adults. Am J Kidney Dis. 2017;70(1):38-47.
14. Bruening M, Dinour LM, Chavez JBR. Food insecurity and emotional health in the USA: a systematic narrative review of longitudinal research. Public Health Nutr. 2017;20(17):3200-3208.
15. Berkowitz SA, Basu S, Meigs JB, Seligman HK. Food insecurity and health care expenditures in the United States, 2011-2013. Health Serv Res. 2018;53(3):1600-1620.
16. Berkowitz SA, Seligman HK, Basu S. Impact of food insecurity and SNAP participation on healthcare utilization and expenditures. http://www.ukcpr.org/research/discussion-papers. Published 2017. Accessed December 9, 2019.
17. Kushel MB, Gupta R, Gee L, Haas JS. Housing instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med. 2006;21(1):71-77.
18. Garcia SP, Haddix A, Barnett K. Incremental health care costs associated with food insecurity and chronic conditions among older adults. Chronic Dis. 2018;15:180058.
19. Berkowitz SA, Seligman HK, Meigs JB, Basu S. Food insecurity, healthcare utilization, and high cost: a longitudinal cohort study. Am J Manag Care. 2018;24(9):399-404.
20. Larson NI, Story MT, Nelson MC. Neighborhood environments: disparities in access to healthy foods in the U.S. Am J Prev Med. 2009;36(1):74-81.
21. Darmon N, Drewnowski A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: a systematic review and analysis. Nutr Rev. 2015;73(10):643-660.
22. Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87(5):1107-1117.
23. Drewnowski A. The cost of US foods as related to their nutritive value. Am J Clin Nutr. 2010;92(5):1181-1188.
24. Lucan SC, Maroko AR, Seitchik JL, Yoon DH, Sperry LE, Schechter CB. Unexpected neighborhood sources of food and drink: implications for research and community health. Am J Prev Med. 2018;55(2):e29-e38.
25. Castillo DC, Ramsey NL, Yu SS, Ricks M, Courville AB, Sumner AE. Inconsistent access to food and cardiometabolic disease: the effect of food insecurity. Curr Cardiovasc Risk Rep. 2012;6(3):245-250.
26. Seligman HK, Davis TC, Schillinger D, Wolf MS. Food insecurity is associated with hypoglycemia and poor diabetes self-management in a low-income sample with diabetes. J Health Care Poor Underserved. 2010;21(4):1227-1233.
27. Siefert K, Heflin CM, Corcoran ME, Williams DR. Food insufficiency and physical and mental health in a longitudinal survey of welfare recipients. J Health Soc Behav. 2004;45(2):171-186.
28. Mangurian C, Sreshta N, Seligman H. Food insecurity among adults with severe mental illness. Psychiatr Serv. 2013;64(9):931-932.
29. Melchior M, Caspi A, Howard LM, et al. Mental health context of food insecurity: a representative cohort of families with young children. Pediatrics. 2009;124(4):e564-e572.
30. Brostow DP, Gunzburger E, Abbate LM, Brenner LA, Thomas KS. Mental illness, not obesity status, is associated with food insecurity among the elderly in the health and retirement study. J Nutr Gerontol Geriatr. 2019;38(2):149-172.
31. Higashi RT, Craddock Lee SJ, Pezzia C, Quirk L, Leonard T, Pruitt SL. Family and social context contributes to the interplay of economic insecurity, food insecurity, and health. Ann Anthropol Pract. 2017;41(2):67-77.
32. O’Toole TP, Roberts CB, Johnson EE. Screening for food insecurity in six Veterans Administration clinics for the homeless, June-December 2015. Prev Chronic Dis. 2017;14:160375.
33. Feil DG, Pogach LM. Cognitive impairment is a major risk factor for serious hypoglycaemia; public health intervention is warranted. Evid Based Med. 2014;19(2):77.
34. Frith E, Loprinzi PD. Food insecurity and cognitive function in older adults: Brief report. Clin Nutr. 2018;37(5):1765-1768.
35. Herman D, Afulani P, Coleman-Jensen A, Harrison GG. Food insecurity and cost-related medication underuse among nonelderly adults in a nationally representative sample. Am J Public Health. 2015;105(10):e48-e59.
36. Tseng C-L, Soroka O, Maney M, Aron DC, Pogach LM. Assessing potential glycemic overtreatment in persons at hypoglycemic risk. JAMA Intern Med. 2014;174(2):259-268.
37. Vue MH, Setter SM. Drug-induced glucose alterations part 1: drug-induced hypoglycemia. Diabetes Spectr. 2011;24(3):171-177.
38. Seligman HK, Bolger AF, Guzman D, López A, Bibbins-Domingo K. Exhaustion of food budgets at month’s end and hospital admissions for hypoglycemia. Health Aff (Millwood). 2014;33(1):116-123.
39. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Veteran poverty trends. https://www.va.gov/vetdata/docs/specialreports/veteran_poverty_trends.pdf. Published May 2015. Accessed December 9, 2019.
40. Robbins KG, Ravi A. Veterans living paycheck to paycheck are under threat during budget debates. https://www.americanprogress.org/issues/poverty/news/2017/09/19/439023/veterans-living-paycheck-paycheck-threat-budget-debates. Published September 19, 2017. Accessed December 9, 2019.
41. Wilmoth JM, London AS, Heflin CM. Economic well-being among older-adult households: variation by veteran and disability status. J Gerontol Soc Work. 2015;58(4):399-419.
42. Brostow DP, Gunzburger E, Thomas KS. Food insecurity among veterans: findings from the health and retirement study. J Nutr Health Aging. 2017;21(10):1358-1364.
43. Pooler J, Mian P, Srinivasan M, Miller Z. Veterans and food insecurity. https://www.impaqint.com/sites/default/files/issue-briefs/VeteransFoodInsecurity_IssueBrief_V1.3.pdf. Published November 2018. Accessed December 9, 2019.
44. Schure MB, Katon JG, Wong E, Liu C-F. Food and housing insecurity and health status among U.S. adults with and without prior military service. SSM Popul Health. 2016;29(2):244-248.
45. Miller DP, Larson MJ, Byrne T, DeVoe E. Food insecurity in veteran households: findings from nationally representative data. Public Health Nutr. 2016;19(10):1731-1740.
46. Widome R, Jensen A, Bangerter A, Fu SS. Food insecurity among veterans of the US wars in Iraq and Afghanistan. Public Health Nutr. 2015;18(5):844-849.
47. London AS, Heflin CM. Supplemental Nutrition Assistance Program (SNAP) use among active-duty military personnel, veterans, and reservists. Popul Res Policy Rev. 2015;34(6):805-826.
48. Weinfield NS, Mills G, Borger C, et al. Hunger in America 2014. Natl rep prepared for Feeding America. https://www.feedingamerica.org/research/hunger-in-america. Published 2014. Accessed December 9, 2019.
49. Mabli J, Ohls J, Dragoset L, Castner L, Santos B. Measuring the Effect of Supplemental Nutrition Assistance Program (SNAP) Participation on Food Security. Washington, DC: US Department of Agriculture, Food and Nutrition Service; 2013.
50. Srinivasan M, Pooler JA. Cost-related medication nonadherence for older adults participating in SNAP, 2013–2015. Am J Public Health. 2017;108(2):224-230.
51. Heflin C, Hodges L, Mueser P. Supplemental Nutrition Assistance Progam benefits and emergency room visits for hypoglycaemia. Public Health Nutr. 2017;20(7):1314-1321.
52. Samuel LJ, Szanton SL, Cahill R, et al. Does the Supplemental Nutrition Assistance Program affect hospital utilization among older adults? The case of Maryland. Popul Health Manag. 2018;21(2):88-95.
53. Szanton SL, Samuel LJ, Cahill R, et al. Food assistance is associated with decreased nursing home admissions for Maryland’s dually eligible older adults. BMC Geriatr. 2017;17(1):162.
54. Carlson S, Keith-Jennings B. SNAP is linked with improved nutritional outcomes and lower health care costs. https://www.cbpp.org/research/food-assistance/snap-is-linked-with-improved-nutritional-outcomes-and-lower-health-care. Published January 17, 2018. Accessed December 10, 2019.
55. Keith-Jennings B, Cai L. SNAP helps almost 1.4 million low-income veterans, including thousands in every state. https://www.cbpp.org/research/food-assistance/snap-helps-almost-14-million-low-income-veterans-including-thousands-in. Updated November 8, 2018. Accessed December 10, 2019.
56. US Department of Health and Human Services. Older Americans Act nutrition programs. https://acl.gov/sites/default/files/news%202017-03/OAA-Nutrition_Programs_Fact_Sheet.pdf. Accessed December 10, 2019.
57. US Department of Veterans Affairs. About VHA. https://www.va.gov/health/aboutvha.asp. Accessed December 10, 2019.
58. US Department of Veterans Affairs. VA Corporate Data Warehouse.
59. Yano EM, Bair MJ, Carrasquillo O, Krein SL, Rubenstein LV. Patient aligned care teams (PACT): VA’s journey to implement patient-centered medical homes. J Gen Intern Med. 2014;29(suppl 2):S547-s549.
60. O’Toole TP, Pape L. Innovative efforts to address homelessness among veterans. N C Med J. 2015;76(5):311-314.
61. O’Toole TP, Johnson EE, Aiello R, Kane V, Pape L. Tailoring care to vulnerable populations by incorporating social determinants of health: the Veterans Health Administration’s “Homeless Patient Aligned Care Team” Program. Prev Chronic Dis. 2016;13:150567.
62. Marpadga S, Fernandez A, Leung J, Tang A, Seligman H, Murphy EJ. Challenges and successes with food resource referrals for food-insecure patients with diabetes. Perm J. 2019;23.
63. Stenmark SH, Steiner JF, Marpadga S, Debor M, Underhill K, Seligman H. Lessons learned from implementation of the food insecurity screening and referral program at Kaiser Permanente Colorado. Perm J. 2018;22.
64. Martel ML, Klein LR, Hager KA, Cutts DB. Emergency department experience with novel electronic medical record order for referral to food resources. West J Emerg Med. 2018;19(2):232-237.
65. Going C, Cohen AJ, Bares M, Christensen M. Interdisciplinary approaches to addressing the food insecure veteran. Veterans Health Administration Employee Education System webinar; October 30, 2018.
66. Feeding America Announces New Partnership With U.S. Department Of Veterans Affairs. https://www.prnewswire.com/news-releases/feeding-america-announces-new-partnership-with-us-department-of-veterans-affairs-300481891.html. Published June 29, 2017. Accessed December 10, 2019.
67. US Department of Veterans Affairs. State Veterans Affairs offices. https://www.va.gov/statedva.htm. Updated March 20, 2019. Accessed December 10, 2019.
68. US Department of Veterans Affairs. Directory of veterans service organizations. https://www.va.gov/vso. Updated December 24, 2013. Accessed December 10, 2019.
69. ACL Administration for Community Living. Aging and disability resource centers. https://acl.gov/programs/aging-and-disability-networks/aging-and-disability-resource-centers. Updated December 13, 2017. Accessed December 10, 2019.
70. Nutrition and Obesity Policy Research and Evaluation Network (NOPREN). Clinical screening algorithms. https://nopren.org/resource/download-food-insecurity-screening-and-referral-algorithms-for-adults-patients-living-with-diabetes-and-pediatric-patients. Accessed December 10, 2019.
1. Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. Household food security in the United States in 2017. http://www.ers.usda.gov/publications/pub-details/?pubid=90022. Published September 2018. Accessed December 9, 2019.
2. Berkowitz SA, Meigs JB, DeWalt D, et al. Material need insecurities, control of diabetes mellitus, and use of health care resources: results of the Measuring Economic Insecurity in Diabetes study. JAMA Intern Med. 2015;175(2):257-265.
3. Berkowitz SA, Seligman HK, Choudhry NK. Treat or eat: food insecurity, cost-related medication underuse, and unmet needs. Am J Med. 2014;127(4):303-310.e3.
4. Lyles CR, Seligman HK, Parker MM, et al. Financial strain and medication adherence among diabetes patients in an integrated health care delivery system: The Diabetes Study of Northern California (DISTANCE). Health Serv Res. 2016;51(2):610-624.
5. Seligman HK, Schillinger D. Hunger and socioeconomic disparities in chronic disease. N Engl J Med. 2010;363(1):6-9.
6. Narain K, Bean-Mayberry B, Washington DL, Canelo IA, Darling JE, Yano EM. Access to care and health outcomes among women veterans using veterans administration health care: association with food insufficiency. Womens Health Issues. 2018;28(3):267-272.
7. Gundersen C, Ziliak JP. Food insecurity and health outcomes. Health Aff. 2015;34(11):1830-1839.
8. Wang EA, McGinnis KA, Goulet J, et al; Veterans Aging Cohort Study Project Team. Food insecurity and health: data from the Veterans Aging Cohort Study. Public Health Rep. 2015;130(3):261-268.
9. Berkowitz SA, Berkowitz TSZ, Meigs JB, Wexler DJ. Trends in food insecurity for adults with cardiometabolic disease in the United States: 2005-2012. PloS One. 2017;12(6):e0179172.
10. Seligman HK, Laraia BA, Kushel MB. Food insecurity is associated with chronic disease among low-income NHANES participants. J Nutr. 2010;140(2):304-310.
11. Berkowitz SA, Baggett TP, Wexler DJ, Huskey KW, Wee CC. Food insecurity and metabolic control among U.S. adults with diabetes. Diabetes Care. 2013;36(10):3093-3099.
12. Seligman HK, Jacobs EA, López A, Tschann J, Fernandez A. Food insecurity and glycemic control among low-income patients with type 2 diabetes. Diabetes Care. 2012;35(2):233-238.
13. Banerjee T, Crews DC, Wesson DE, et al; CDC CKD Surveillance Team. Food insecurity, CKD, and subsequent ESRD in US adults. Am J Kidney Dis. 2017;70(1):38-47.
14. Bruening M, Dinour LM, Chavez JBR. Food insecurity and emotional health in the USA: a systematic narrative review of longitudinal research. Public Health Nutr. 2017;20(17):3200-3208.
15. Berkowitz SA, Basu S, Meigs JB, Seligman HK. Food insecurity and health care expenditures in the United States, 2011-2013. Health Serv Res. 2018;53(3):1600-1620.
16. Berkowitz SA, Seligman HK, Basu S. Impact of food insecurity and SNAP participation on healthcare utilization and expenditures. http://www.ukcpr.org/research/discussion-papers. Published 2017. Accessed December 9, 2019.
17. Kushel MB, Gupta R, Gee L, Haas JS. Housing instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med. 2006;21(1):71-77.
18. Garcia SP, Haddix A, Barnett K. Incremental health care costs associated with food insecurity and chronic conditions among older adults. Chronic Dis. 2018;15:180058.
19. Berkowitz SA, Seligman HK, Meigs JB, Basu S. Food insecurity, healthcare utilization, and high cost: a longitudinal cohort study. Am J Manag Care. 2018;24(9):399-404.
20. Larson NI, Story MT, Nelson MC. Neighborhood environments: disparities in access to healthy foods in the U.S. Am J Prev Med. 2009;36(1):74-81.
21. Darmon N, Drewnowski A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: a systematic review and analysis. Nutr Rev. 2015;73(10):643-660.
22. Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87(5):1107-1117.
23. Drewnowski A. The cost of US foods as related to their nutritive value. Am J Clin Nutr. 2010;92(5):1181-1188.
24. Lucan SC, Maroko AR, Seitchik JL, Yoon DH, Sperry LE, Schechter CB. Unexpected neighborhood sources of food and drink: implications for research and community health. Am J Prev Med. 2018;55(2):e29-e38.
25. Castillo DC, Ramsey NL, Yu SS, Ricks M, Courville AB, Sumner AE. Inconsistent access to food and cardiometabolic disease: the effect of food insecurity. Curr Cardiovasc Risk Rep. 2012;6(3):245-250.
26. Seligman HK, Davis TC, Schillinger D, Wolf MS. Food insecurity is associated with hypoglycemia and poor diabetes self-management in a low-income sample with diabetes. J Health Care Poor Underserved. 2010;21(4):1227-1233.
27. Siefert K, Heflin CM, Corcoran ME, Williams DR. Food insufficiency and physical and mental health in a longitudinal survey of welfare recipients. J Health Soc Behav. 2004;45(2):171-186.
28. Mangurian C, Sreshta N, Seligman H. Food insecurity among adults with severe mental illness. Psychiatr Serv. 2013;64(9):931-932.
29. Melchior M, Caspi A, Howard LM, et al. Mental health context of food insecurity: a representative cohort of families with young children. Pediatrics. 2009;124(4):e564-e572.
30. Brostow DP, Gunzburger E, Abbate LM, Brenner LA, Thomas KS. Mental illness, not obesity status, is associated with food insecurity among the elderly in the health and retirement study. J Nutr Gerontol Geriatr. 2019;38(2):149-172.
31. Higashi RT, Craddock Lee SJ, Pezzia C, Quirk L, Leonard T, Pruitt SL. Family and social context contributes to the interplay of economic insecurity, food insecurity, and health. Ann Anthropol Pract. 2017;41(2):67-77.
32. O’Toole TP, Roberts CB, Johnson EE. Screening for food insecurity in six Veterans Administration clinics for the homeless, June-December 2015. Prev Chronic Dis. 2017;14:160375.
33. Feil DG, Pogach LM. Cognitive impairment is a major risk factor for serious hypoglycaemia; public health intervention is warranted. Evid Based Med. 2014;19(2):77.
34. Frith E, Loprinzi PD. Food insecurity and cognitive function in older adults: Brief report. Clin Nutr. 2018;37(5):1765-1768.
35. Herman D, Afulani P, Coleman-Jensen A, Harrison GG. Food insecurity and cost-related medication underuse among nonelderly adults in a nationally representative sample. Am J Public Health. 2015;105(10):e48-e59.
36. Tseng C-L, Soroka O, Maney M, Aron DC, Pogach LM. Assessing potential glycemic overtreatment in persons at hypoglycemic risk. JAMA Intern Med. 2014;174(2):259-268.
37. Vue MH, Setter SM. Drug-induced glucose alterations part 1: drug-induced hypoglycemia. Diabetes Spectr. 2011;24(3):171-177.
38. Seligman HK, Bolger AF, Guzman D, López A, Bibbins-Domingo K. Exhaustion of food budgets at month’s end and hospital admissions for hypoglycemia. Health Aff (Millwood). 2014;33(1):116-123.
39. US Department of Veterans Affairs, National Center for Veterans Analysis and Statistics. Veteran poverty trends. https://www.va.gov/vetdata/docs/specialreports/veteran_poverty_trends.pdf. Published May 2015. Accessed December 9, 2019.
40. Robbins KG, Ravi A. Veterans living paycheck to paycheck are under threat during budget debates. https://www.americanprogress.org/issues/poverty/news/2017/09/19/439023/veterans-living-paycheck-paycheck-threat-budget-debates. Published September 19, 2017. Accessed December 9, 2019.
41. Wilmoth JM, London AS, Heflin CM. Economic well-being among older-adult households: variation by veteran and disability status. J Gerontol Soc Work. 2015;58(4):399-419.
42. Brostow DP, Gunzburger E, Thomas KS. Food insecurity among veterans: findings from the health and retirement study. J Nutr Health Aging. 2017;21(10):1358-1364.
43. Pooler J, Mian P, Srinivasan M, Miller Z. Veterans and food insecurity. https://www.impaqint.com/sites/default/files/issue-briefs/VeteransFoodInsecurity_IssueBrief_V1.3.pdf. Published November 2018. Accessed December 9, 2019.
44. Schure MB, Katon JG, Wong E, Liu C-F. Food and housing insecurity and health status among U.S. adults with and without prior military service. SSM Popul Health. 2016;29(2):244-248.
45. Miller DP, Larson MJ, Byrne T, DeVoe E. Food insecurity in veteran households: findings from nationally representative data. Public Health Nutr. 2016;19(10):1731-1740.
46. Widome R, Jensen A, Bangerter A, Fu SS. Food insecurity among veterans of the US wars in Iraq and Afghanistan. Public Health Nutr. 2015;18(5):844-849.
47. London AS, Heflin CM. Supplemental Nutrition Assistance Program (SNAP) use among active-duty military personnel, veterans, and reservists. Popul Res Policy Rev. 2015;34(6):805-826.
48. Weinfield NS, Mills G, Borger C, et al. Hunger in America 2014. Natl rep prepared for Feeding America. https://www.feedingamerica.org/research/hunger-in-america. Published 2014. Accessed December 9, 2019.
49. Mabli J, Ohls J, Dragoset L, Castner L, Santos B. Measuring the Effect of Supplemental Nutrition Assistance Program (SNAP) Participation on Food Security. Washington, DC: US Department of Agriculture, Food and Nutrition Service; 2013.
50. Srinivasan M, Pooler JA. Cost-related medication nonadherence for older adults participating in SNAP, 2013–2015. Am J Public Health. 2017;108(2):224-230.
51. Heflin C, Hodges L, Mueser P. Supplemental Nutrition Assistance Progam benefits and emergency room visits for hypoglycaemia. Public Health Nutr. 2017;20(7):1314-1321.
52. Samuel LJ, Szanton SL, Cahill R, et al. Does the Supplemental Nutrition Assistance Program affect hospital utilization among older adults? The case of Maryland. Popul Health Manag. 2018;21(2):88-95.
53. Szanton SL, Samuel LJ, Cahill R, et al. Food assistance is associated with decreased nursing home admissions for Maryland’s dually eligible older adults. BMC Geriatr. 2017;17(1):162.
54. Carlson S, Keith-Jennings B. SNAP is linked with improved nutritional outcomes and lower health care costs. https://www.cbpp.org/research/food-assistance/snap-is-linked-with-improved-nutritional-outcomes-and-lower-health-care. Published January 17, 2018. Accessed December 10, 2019.
55. Keith-Jennings B, Cai L. SNAP helps almost 1.4 million low-income veterans, including thousands in every state. https://www.cbpp.org/research/food-assistance/snap-helps-almost-14-million-low-income-veterans-including-thousands-in. Updated November 8, 2018. Accessed December 10, 2019.
56. US Department of Health and Human Services. Older Americans Act nutrition programs. https://acl.gov/sites/default/files/news%202017-03/OAA-Nutrition_Programs_Fact_Sheet.pdf. Accessed December 10, 2019.
57. US Department of Veterans Affairs. About VHA. https://www.va.gov/health/aboutvha.asp. Accessed December 10, 2019.
58. US Department of Veterans Affairs. VA Corporate Data Warehouse.
59. Yano EM, Bair MJ, Carrasquillo O, Krein SL, Rubenstein LV. Patient aligned care teams (PACT): VA’s journey to implement patient-centered medical homes. J Gen Intern Med. 2014;29(suppl 2):S547-s549.
60. O’Toole TP, Pape L. Innovative efforts to address homelessness among veterans. N C Med J. 2015;76(5):311-314.
61. O’Toole TP, Johnson EE, Aiello R, Kane V, Pape L. Tailoring care to vulnerable populations by incorporating social determinants of health: the Veterans Health Administration’s “Homeless Patient Aligned Care Team” Program. Prev Chronic Dis. 2016;13:150567.
62. Marpadga S, Fernandez A, Leung J, Tang A, Seligman H, Murphy EJ. Challenges and successes with food resource referrals for food-insecure patients with diabetes. Perm J. 2019;23.
63. Stenmark SH, Steiner JF, Marpadga S, Debor M, Underhill K, Seligman H. Lessons learned from implementation of the food insecurity screening and referral program at Kaiser Permanente Colorado. Perm J. 2018;22.
64. Martel ML, Klein LR, Hager KA, Cutts DB. Emergency department experience with novel electronic medical record order for referral to food resources. West J Emerg Med. 2018;19(2):232-237.
65. Going C, Cohen AJ, Bares M, Christensen M. Interdisciplinary approaches to addressing the food insecure veteran. Veterans Health Administration Employee Education System webinar; October 30, 2018.
66. Feeding America Announces New Partnership With U.S. Department Of Veterans Affairs. https://www.prnewswire.com/news-releases/feeding-america-announces-new-partnership-with-us-department-of-veterans-affairs-300481891.html. Published June 29, 2017. Accessed December 10, 2019.
67. US Department of Veterans Affairs. State Veterans Affairs offices. https://www.va.gov/statedva.htm. Updated March 20, 2019. Accessed December 10, 2019.
68. US Department of Veterans Affairs. Directory of veterans service organizations. https://www.va.gov/vso. Updated December 24, 2013. Accessed December 10, 2019.
69. ACL Administration for Community Living. Aging and disability resource centers. https://acl.gov/programs/aging-and-disability-networks/aging-and-disability-resource-centers. Updated December 13, 2017. Accessed December 10, 2019.
70. Nutrition and Obesity Policy Research and Evaluation Network (NOPREN). Clinical screening algorithms. https://nopren.org/resource/download-food-insecurity-screening-and-referral-algorithms-for-adults-patients-living-with-diabetes-and-pediatric-patients. Accessed December 10, 2019.
Biofeedback corrects dyssynergic constipation in elderly
SAN ANTONIO – Biofeedback for treatment of dyssynergic constipation is highly effective in the elderly, just as it is in younger patients, Samantha Spilman, MD, reported at the annual meeting of the American College of Gastroenterology.

“I think the main point of this study is that older adults have a profound burden of constipation with dyssynergic defecation, and we propose that biofeedback be given strong consideration as first-line therapy for this population, in whom overall we’re trying to reduce medication use,” said Dr. Spilman, a gastroenterology fellow at the University of California, San Diego.
The prevalence of constipation in older patients is estimated to be up to 40%. Yet few prior studies have scrutinized how well older patients with constipation actually respond to biofeedback. It’s a legitimate question, since biofeedback training involves operant conditioning and requires learning new techniques. For this reason, she and her coinvestigators conducted a retrospective analysis of 58 patients over age 65 referred from the university’s gastrointestinal motility and physiology program to the biofeedback program for treatment of dyssynergic defection. The patients’ mean age was 74 years, with a 9.5-year history of constipation. The oldest patient was 88. Most of the subjects were high school graduates. Thirteen of the 58 carried a diagnosis of irritable bowel syndrome.
Numerous studies have demonstrated that 70%-80% of younger adults with dyssynergic constipation experience marked improvement in response to biofeedback training, which typically utilizes an inflated rectal balloon to simulate retained stool. The key finding in Dr. Spilman’s study was that the elderly patients did comparably well in terms of both self-reported outcomes and objective high-resolution anorectal manometric parameters upon completing an average of three biofeedback sessions.
Mean global bowel satisfaction on a 1-10 scale nearly doubled from 2.77 at baseline to 5.01 with biofeedback. Moreover, 79% of seniors demonstrated resolution of their dyssynergia on high-resolution anorectal manometry performed with sensors in the rectum and anal canal. The proportion of patients who reported a feeling of incomplete evacuation after stooling – a sensation individuals with constipation find highly bothersome – improved from 95% to 24% with biofeedback.
The strongest response in terms of the defecation index was observed in older patients with type 2 dyssynergia, characterized by defective propulsion coupled with a paradoxical contraction of the sphincter muscles during defecation. Their defecation index score, derived by dividing intrarectal pressure by residual intra-anal pressure during simulated defection, showed a robust improvement from 0.307 at baseline to 0.793. Patients with types 1 and 3 dyssynergia showed lesser improvements on this objective measure.
Dr. Spilman noted as a study limitation that baseline cognitive status wasn’t formally assessed, so the investigators don’t know how many of the older patients had minimal cognitive impairment. However, baseline quality of life assessment via the Short Form-36 indicated that patients scored average or above for physical and social functioning as well as emotional well-being.
Dr. Spilman reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Spilman S. ACG 2019. Abstract 45.
SAN ANTONIO – Biofeedback for treatment of dyssynergic constipation is highly effective in the elderly, just as it is in younger patients, Samantha Spilman, MD, reported at the annual meeting of the American College of Gastroenterology.
“I think the main point of this study is that older adults have a profound burden of constipation with dyssynergic defecation, and we propose that biofeedback be given strong consideration as first-line therapy for this population, in whom overall we’re trying to reduce medication use,” said Dr. Spilman, a gastroenterology fellow at the University of California, San Diego.
The prevalence of constipation in older patients is estimated to be up to 40%. Yet few prior studies have scrutinized how well older patients with constipation actually respond to biofeedback. It’s a legitimate question, since biofeedback training involves operant conditioning and requires learning new techniques. For this reason, she and her coinvestigators conducted a retrospective analysis of 58 patients over age 65 referred from the university’s gastrointestinal motility and physiology program to the biofeedback program for treatment of dyssynergic defection. The patients’ mean age was 74 years, with a 9.5-year history of constipation. The oldest patient was 88. Most of the subjects were high school graduates. Thirteen of the 58 carried a diagnosis of irritable bowel syndrome.
Numerous studies have demonstrated that 70%-80% of younger adults with dyssynergic constipation experience marked improvement in response to biofeedback training, which typically utilizes an inflated rectal balloon to simulate retained stool. The key finding in Dr. Spilman’s study was that the elderly patients did comparably well in terms of both self-reported outcomes and objective high-resolution anorectal manometric parameters upon completing an average of three biofeedback sessions.
Mean global bowel satisfaction on a 1-10 scale nearly doubled from 2.77 at baseline to 5.01 with biofeedback. Moreover, 79% of seniors demonstrated resolution of their dyssynergia on high-resolution anorectal manometry performed with sensors in the rectum and anal canal. The proportion of patients who reported a feeling of incomplete evacuation after stooling – a sensation individuals with constipation find highly bothersome – improved from 95% to 24% with biofeedback.
The strongest response in terms of the defecation index was observed in older patients with type 2 dyssynergia, characterized by defective propulsion coupled with a paradoxical contraction of the sphincter muscles during defecation. Their defecation index score, derived by dividing intrarectal pressure by residual intra-anal pressure during simulated defection, showed a robust improvement from 0.307 at baseline to 0.793. Patients with types 1 and 3 dyssynergia showed lesser improvements on this objective measure.
Dr. Spilman noted as a study limitation that baseline cognitive status wasn’t formally assessed, so the investigators don’t know how many of the older patients had minimal cognitive impairment. However, baseline quality of life assessment via the Short Form-36 indicated that patients scored average or above for physical and social functioning as well as emotional well-being.
Dr. Spilman reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Spilman S. ACG 2019. Abstract 45.
SAN ANTONIO – Biofeedback for treatment of dyssynergic constipation is highly effective in the elderly, just as it is in younger patients, Samantha Spilman, MD, reported at the annual meeting of the American College of Gastroenterology.
“I think the main point of this study is that older adults have a profound burden of constipation with dyssynergic defecation, and we propose that biofeedback be given strong consideration as first-line therapy for this population, in whom overall we’re trying to reduce medication use,” said Dr. Spilman, a gastroenterology fellow at the University of California, San Diego.
The prevalence of constipation in older patients is estimated to be up to 40%. Yet few prior studies have scrutinized how well older patients with constipation actually respond to biofeedback. It’s a legitimate question, since biofeedback training involves operant conditioning and requires learning new techniques. For this reason, she and her coinvestigators conducted a retrospective analysis of 58 patients over age 65 referred from the university’s gastrointestinal motility and physiology program to the biofeedback program for treatment of dyssynergic defection. The patients’ mean age was 74 years, with a 9.5-year history of constipation. The oldest patient was 88. Most of the subjects were high school graduates. Thirteen of the 58 carried a diagnosis of irritable bowel syndrome.
Numerous studies have demonstrated that 70%-80% of younger adults with dyssynergic constipation experience marked improvement in response to biofeedback training, which typically utilizes an inflated rectal balloon to simulate retained stool. The key finding in Dr. Spilman’s study was that the elderly patients did comparably well in terms of both self-reported outcomes and objective high-resolution anorectal manometric parameters upon completing an average of three biofeedback sessions.
Mean global bowel satisfaction on a 1-10 scale nearly doubled from 2.77 at baseline to 5.01 with biofeedback. Moreover, 79% of seniors demonstrated resolution of their dyssynergia on high-resolution anorectal manometry performed with sensors in the rectum and anal canal. The proportion of patients who reported a feeling of incomplete evacuation after stooling – a sensation individuals with constipation find highly bothersome – improved from 95% to 24% with biofeedback.
The strongest response in terms of the defecation index was observed in older patients with type 2 dyssynergia, characterized by defective propulsion coupled with a paradoxical contraction of the sphincter muscles during defecation. Their defecation index score, derived by dividing intrarectal pressure by residual intra-anal pressure during simulated defection, showed a robust improvement from 0.307 at baseline to 0.793. Patients with types 1 and 3 dyssynergia showed lesser improvements on this objective measure.
Dr. Spilman noted as a study limitation that baseline cognitive status wasn’t formally assessed, so the investigators don’t know how many of the older patients had minimal cognitive impairment. However, baseline quality of life assessment via the Short Form-36 indicated that patients scored average or above for physical and social functioning as well as emotional well-being.
Dr. Spilman reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Spilman S. ACG 2019. Abstract 45.
REPORTING FROM ACG 2019
Could preventing dementia be as simple as following your mom’s advice?
SAN DIEGO – To prevent dementia, follow Mom’s advice: Get up off the couch, go play with your friends, and eat your vegetables.
After 15 years of disappointing drug trials, strong new evidence says the best way to attack Alzheimer’s disease is not to treat it once it develops, but to prevent it in the first place, Laura D. Baker, PhD, said at the Clinical Trials on Alzheimer’s Disease conference. Studies of exercise, cognitive and social stimulation, and diet show that each one can reduce the risk of dementia, and that a combination of all three may have even a more powerful and synergistic effect.
“We have become absolutely phobic of exercise,” said Dr. Baker of Wake Forest University, Winston-Salem, N.C. And it’s not just structured exercise we shirk. “We take the closest parking space, sit for hours on end, don’t even take the stairs. Yet we know from years of work that exercise has a powerful benefit on cardiovascular disease, lipid profiles, metabolic disease, stress, and mood. Now we are seeing that exercise also promotes brain health in normal aging and protects against cognitive decline and prevention.”
Get off the couch
The general benefits of exercise – chiefly aerobic exercise – are myriad, Dr. Baker said.
“Exercise increases effective neurorepair. It reduces oxidative stress. It improves insulin sensitivity and helps with maintaining normal weight. It reduces inflammation and increases normal clearance of amyloid-beta.”
A 2017 meta-analysis reviewed some of these findings. “The current review [of 16 studies] suggests that aerobic exercise may have positive effects on the right hippocampus and potentially beneficial effects on the overall and other parts of the hippocampus, the cingulate cortex, and the medial temporal areas. ... Moreover, aerobic exercise may increase functional connectivity or activation in the hippocampus, cingulate cortex, and parahippocampal gyrus regions,” wrote Mo-yi Li, PhD, of Fujian University of Traditional Chinese Medicine, Fuzhou, China, and colleagues.
Exercise increases brain-derived neurotrophic factor (BDNF), which in turn increases neuronal potentiation and synaptic plasticity. BDNF is also important in hippocampal neurogenesis; mice, after just one aerobic session, showed dramatic boosts in BDNF. A 2018 review elaborates on these findings.
Eat right
Diet mediates dementia risk through less direct, but very effective, pathways, Dr. Baker said. Diets rich in vegetables, berries, nuts, fish, lean proteins, and healthy fats improves virtually all metabolic measures. These, in turn, reduce the risk cerebrovascular disease – an important driver of vascular dementias and a contributor to Alzheimer’s disease risk as well.
The MIND diet study (Mediterranean-DASH Diet Intervention for Neurodegenerative Delay), reported in 2015 was a very successful demonstration of this concept. A combination of the Mediterranean diet and the DASH diet (Dietary Approaches to Stop Hypertension), the MIND diet stresses frequent consumption of vegetables – especially leafy greens – as well as nuts, berries, whole grains, fish, poultry, and wine or grape juice. In the large, nearly 5-year study of 923 subjects aged 58-98 years, the MIND diet was associated with significant gains in cognition – equivalent to a 7-year reversal of age. After 4.5 years, those who strictly adhered to the diet had a 53% reduction in risk for Alzheimer’s disease, and those who adhered moderately had a 35% reduction. And in a more recent Australian longitudinal study, the MIND diet was associated with a 53% reduced risk of cognitive impairment over 12 years.
Ketogenic diets also may exert a benefit. Theoretically, a state of ketosis forces the brain to burn ketones as an alternative fuel to glucose, thus boosting brain function in glucose-starved brains. A small pilot study with exploratory cognitive endpoints determined that diet-compliant subjects with mild to moderate Alzheimer’s experienced a mean 5-point improvement in the Alzheimer’s Disease Assessment Score–Cognition. They reverted to baseline scores within a month of ending the study.
Recent initial work into the gut microbiome provides some additional speculative, but interesting, data. A dysregulated microbiome can shift microbial populations toward a more inflammatory profile. Some work suggests that inflammatory cytokines then travel to the brain and induce a hyperresponse of neuron-damaging immune cells. A comprehensive review article discusses the complicated mechanisms that may be in play.
Play with your friends
Cognitive stimulation and social interaction also appear to modify dementia risk, although the data are a little more limited. But personal interaction is a key element of Dr. Baker’s ongoing EXERT trial.
The ongoing phase 3 trial randomized 300 adults with amnestic mild cognitive impairment to moderate to high intensity aerobic exercise plus one-on-one support at local YMCA gyms or a low-intensity stretching, balance, and range of motion program. In additional to cognitive testing, the trial includes brain imaging, cerebrospinal fluid sampling for biomarkers of Alzheimer’s disease, and a sleep study.
A key component is personal interaction with a trainer. “They spend a lot of one-on-one time with each person,” Dr. Baker said. “For me, that’s the crucial ingredient – that personal touch. It’s what helps people move from Point A to Point B in their behaviors.”
Virtual cognitive stimulation is also a burgeoning area of dementia prevention research right now. Numerous studies are ongoing to test whether virtual reality or other computer-based games might keep the mind sharp or even improve cognition in people at risk.
The power of three
If one lifestyle change can reduce dementia risk, what happens when all three work together?
That’s the newest question, first successfully explored in the mid-2000s, with the FINGER study (Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability). In FINGER, the triad of exercise, personal support at the gym, and a modified Mediterranean diet reduced Alzheimer’s disease risk and improved cognition relative to the control group.
FINGER showed that the intervention was feasible and that it was associated with cognitive preservation and reduced Alzheimer’s disease risk in a group of at-risk subjects. The active group also had a 25% greater improvement on a neuropsychological test battery relative to the control group. They also performed 150% better in processing speed, 83% better in executive function, and 40% better in short-term memory. They showed no increased risk of cognitive decline relative to the control group, which experienced a 30% increase in risk, according to lead investigator Miia Kivipelto, PhD, of the Karolinska Institute, Stockholm.
So successful was FINGER that it launched a global consortium of related studies called World Wide FINGERS. Active in six countries now, including the United States, the studies aim to discover whether such combinations of lifestyle interventions are workable across countries and cultures. World Wide FINGERS is largely supported by the Alzheimer’s Association.
Global enthusiasm for lifestyle interventions
In recognition of the importance of lifestyle changes for dementia prevention, the World Health Organization recently published “Risk reduction of cognitive decline and dementia.” The document reviews many studies and makes recommendations regarding not only exercise, diet, and cognitive stimulation, but also smoking and alcohol.
Research interest in these areas is surging, Dr. Baker said. “The [U.S.] National Institute on Aging now has 29 ongoing trials. There’s a strong commitment to investigations into how lifestyle interventions could protect brain health as we get older. Certainly, many fit and healthy people do develop Alzheimer’s. But for some, it could be medicine.”
But no matter how compliant people are, lifestyle changes will never completely rid the world of Alzheimer’s and other dementias. The view of Dr. Baker – and most other Alzheimer’s researchers – is to employ lifestyle changes to reduce risk as much as possible and not to stop when cognitive problems do present.
“We need to understand how lifestyle interventions might work in combination with pharmaceuticals,” she said. “If we can support the health of the body and the health of the mind, lifestyle interventions can be the fertilizer that would help drug therapy have its maximum effect.”
SAN DIEGO – To prevent dementia, follow Mom’s advice: Get up off the couch, go play with your friends, and eat your vegetables.
After 15 years of disappointing drug trials, strong new evidence says the best way to attack Alzheimer’s disease is not to treat it once it develops, but to prevent it in the first place, Laura D. Baker, PhD, said at the Clinical Trials on Alzheimer’s Disease conference. Studies of exercise, cognitive and social stimulation, and diet show that each one can reduce the risk of dementia, and that a combination of all three may have even a more powerful and synergistic effect.
“We have become absolutely phobic of exercise,” said Dr. Baker of Wake Forest University, Winston-Salem, N.C. And it’s not just structured exercise we shirk. “We take the closest parking space, sit for hours on end, don’t even take the stairs. Yet we know from years of work that exercise has a powerful benefit on cardiovascular disease, lipid profiles, metabolic disease, stress, and mood. Now we are seeing that exercise also promotes brain health in normal aging and protects against cognitive decline and prevention.”
Get off the couch
The general benefits of exercise – chiefly aerobic exercise – are myriad, Dr. Baker said.
“Exercise increases effective neurorepair. It reduces oxidative stress. It improves insulin sensitivity and helps with maintaining normal weight. It reduces inflammation and increases normal clearance of amyloid-beta.”
A 2017 meta-analysis reviewed some of these findings. “The current review [of 16 studies] suggests that aerobic exercise may have positive effects on the right hippocampus and potentially beneficial effects on the overall and other parts of the hippocampus, the cingulate cortex, and the medial temporal areas. ... Moreover, aerobic exercise may increase functional connectivity or activation in the hippocampus, cingulate cortex, and parahippocampal gyrus regions,” wrote Mo-yi Li, PhD, of Fujian University of Traditional Chinese Medicine, Fuzhou, China, and colleagues.
Exercise increases brain-derived neurotrophic factor (BDNF), which in turn increases neuronal potentiation and synaptic plasticity. BDNF is also important in hippocampal neurogenesis; mice, after just one aerobic session, showed dramatic boosts in BDNF. A 2018 review elaborates on these findings.
Eat right
Diet mediates dementia risk through less direct, but very effective, pathways, Dr. Baker said. Diets rich in vegetables, berries, nuts, fish, lean proteins, and healthy fats improves virtually all metabolic measures. These, in turn, reduce the risk cerebrovascular disease – an important driver of vascular dementias and a contributor to Alzheimer’s disease risk as well.
The MIND diet study (Mediterranean-DASH Diet Intervention for Neurodegenerative Delay), reported in 2015 was a very successful demonstration of this concept. A combination of the Mediterranean diet and the DASH diet (Dietary Approaches to Stop Hypertension), the MIND diet stresses frequent consumption of vegetables – especially leafy greens – as well as nuts, berries, whole grains, fish, poultry, and wine or grape juice. In the large, nearly 5-year study of 923 subjects aged 58-98 years, the MIND diet was associated with significant gains in cognition – equivalent to a 7-year reversal of age. After 4.5 years, those who strictly adhered to the diet had a 53% reduction in risk for Alzheimer’s disease, and those who adhered moderately had a 35% reduction. And in a more recent Australian longitudinal study, the MIND diet was associated with a 53% reduced risk of cognitive impairment over 12 years.
Ketogenic diets also may exert a benefit. Theoretically, a state of ketosis forces the brain to burn ketones as an alternative fuel to glucose, thus boosting brain function in glucose-starved brains. A small pilot study with exploratory cognitive endpoints determined that diet-compliant subjects with mild to moderate Alzheimer’s experienced a mean 5-point improvement in the Alzheimer’s Disease Assessment Score–Cognition. They reverted to baseline scores within a month of ending the study.
Recent initial work into the gut microbiome provides some additional speculative, but interesting, data. A dysregulated microbiome can shift microbial populations toward a more inflammatory profile. Some work suggests that inflammatory cytokines then travel to the brain and induce a hyperresponse of neuron-damaging immune cells. A comprehensive review article discusses the complicated mechanisms that may be in play.
Play with your friends
Cognitive stimulation and social interaction also appear to modify dementia risk, although the data are a little more limited. But personal interaction is a key element of Dr. Baker’s ongoing EXERT trial.
The ongoing phase 3 trial randomized 300 adults with amnestic mild cognitive impairment to moderate to high intensity aerobic exercise plus one-on-one support at local YMCA gyms or a low-intensity stretching, balance, and range of motion program. In additional to cognitive testing, the trial includes brain imaging, cerebrospinal fluid sampling for biomarkers of Alzheimer’s disease, and a sleep study.
A key component is personal interaction with a trainer. “They spend a lot of one-on-one time with each person,” Dr. Baker said. “For me, that’s the crucial ingredient – that personal touch. It’s what helps people move from Point A to Point B in their behaviors.”
Virtual cognitive stimulation is also a burgeoning area of dementia prevention research right now. Numerous studies are ongoing to test whether virtual reality or other computer-based games might keep the mind sharp or even improve cognition in people at risk.
The power of three
If one lifestyle change can reduce dementia risk, what happens when all three work together?
That’s the newest question, first successfully explored in the mid-2000s, with the FINGER study (Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability). In FINGER, the triad of exercise, personal support at the gym, and a modified Mediterranean diet reduced Alzheimer’s disease risk and improved cognition relative to the control group.
FINGER showed that the intervention was feasible and that it was associated with cognitive preservation and reduced Alzheimer’s disease risk in a group of at-risk subjects. The active group also had a 25% greater improvement on a neuropsychological test battery relative to the control group. They also performed 150% better in processing speed, 83% better in executive function, and 40% better in short-term memory. They showed no increased risk of cognitive decline relative to the control group, which experienced a 30% increase in risk, according to lead investigator Miia Kivipelto, PhD, of the Karolinska Institute, Stockholm.
So successful was FINGER that it launched a global consortium of related studies called World Wide FINGERS. Active in six countries now, including the United States, the studies aim to discover whether such combinations of lifestyle interventions are workable across countries and cultures. World Wide FINGERS is largely supported by the Alzheimer’s Association.
Global enthusiasm for lifestyle interventions
In recognition of the importance of lifestyle changes for dementia prevention, the World Health Organization recently published “Risk reduction of cognitive decline and dementia.” The document reviews many studies and makes recommendations regarding not only exercise, diet, and cognitive stimulation, but also smoking and alcohol.
Research interest in these areas is surging, Dr. Baker said. “The [U.S.] National Institute on Aging now has 29 ongoing trials. There’s a strong commitment to investigations into how lifestyle interventions could protect brain health as we get older. Certainly, many fit and healthy people do develop Alzheimer’s. But for some, it could be medicine.”
But no matter how compliant people are, lifestyle changes will never completely rid the world of Alzheimer’s and other dementias. The view of Dr. Baker – and most other Alzheimer’s researchers – is to employ lifestyle changes to reduce risk as much as possible and not to stop when cognitive problems do present.
“We need to understand how lifestyle interventions might work in combination with pharmaceuticals,” she said. “If we can support the health of the body and the health of the mind, lifestyle interventions can be the fertilizer that would help drug therapy have its maximum effect.”
SAN DIEGO – To prevent dementia, follow Mom’s advice: Get up off the couch, go play with your friends, and eat your vegetables.
After 15 years of disappointing drug trials, strong new evidence says the best way to attack Alzheimer’s disease is not to treat it once it develops, but to prevent it in the first place, Laura D. Baker, PhD, said at the Clinical Trials on Alzheimer’s Disease conference. Studies of exercise, cognitive and social stimulation, and diet show that each one can reduce the risk of dementia, and that a combination of all three may have even a more powerful and synergistic effect.
“We have become absolutely phobic of exercise,” said Dr. Baker of Wake Forest University, Winston-Salem, N.C. And it’s not just structured exercise we shirk. “We take the closest parking space, sit for hours on end, don’t even take the stairs. Yet we know from years of work that exercise has a powerful benefit on cardiovascular disease, lipid profiles, metabolic disease, stress, and mood. Now we are seeing that exercise also promotes brain health in normal aging and protects against cognitive decline and prevention.”
Get off the couch
The general benefits of exercise – chiefly aerobic exercise – are myriad, Dr. Baker said.
“Exercise increases effective neurorepair. It reduces oxidative stress. It improves insulin sensitivity and helps with maintaining normal weight. It reduces inflammation and increases normal clearance of amyloid-beta.”
A 2017 meta-analysis reviewed some of these findings. “The current review [of 16 studies] suggests that aerobic exercise may have positive effects on the right hippocampus and potentially beneficial effects on the overall and other parts of the hippocampus, the cingulate cortex, and the medial temporal areas. ... Moreover, aerobic exercise may increase functional connectivity or activation in the hippocampus, cingulate cortex, and parahippocampal gyrus regions,” wrote Mo-yi Li, PhD, of Fujian University of Traditional Chinese Medicine, Fuzhou, China, and colleagues.
Exercise increases brain-derived neurotrophic factor (BDNF), which in turn increases neuronal potentiation and synaptic plasticity. BDNF is also important in hippocampal neurogenesis; mice, after just one aerobic session, showed dramatic boosts in BDNF. A 2018 review elaborates on these findings.
Eat right
Diet mediates dementia risk through less direct, but very effective, pathways, Dr. Baker said. Diets rich in vegetables, berries, nuts, fish, lean proteins, and healthy fats improves virtually all metabolic measures. These, in turn, reduce the risk cerebrovascular disease – an important driver of vascular dementias and a contributor to Alzheimer’s disease risk as well.
The MIND diet study (Mediterranean-DASH Diet Intervention for Neurodegenerative Delay), reported in 2015 was a very successful demonstration of this concept. A combination of the Mediterranean diet and the DASH diet (Dietary Approaches to Stop Hypertension), the MIND diet stresses frequent consumption of vegetables – especially leafy greens – as well as nuts, berries, whole grains, fish, poultry, and wine or grape juice. In the large, nearly 5-year study of 923 subjects aged 58-98 years, the MIND diet was associated with significant gains in cognition – equivalent to a 7-year reversal of age. After 4.5 years, those who strictly adhered to the diet had a 53% reduction in risk for Alzheimer’s disease, and those who adhered moderately had a 35% reduction. And in a more recent Australian longitudinal study, the MIND diet was associated with a 53% reduced risk of cognitive impairment over 12 years.
Ketogenic diets also may exert a benefit. Theoretically, a state of ketosis forces the brain to burn ketones as an alternative fuel to glucose, thus boosting brain function in glucose-starved brains. A small pilot study with exploratory cognitive endpoints determined that diet-compliant subjects with mild to moderate Alzheimer’s experienced a mean 5-point improvement in the Alzheimer’s Disease Assessment Score–Cognition. They reverted to baseline scores within a month of ending the study.
Recent initial work into the gut microbiome provides some additional speculative, but interesting, data. A dysregulated microbiome can shift microbial populations toward a more inflammatory profile. Some work suggests that inflammatory cytokines then travel to the brain and induce a hyperresponse of neuron-damaging immune cells. A comprehensive review article discusses the complicated mechanisms that may be in play.
Play with your friends
Cognitive stimulation and social interaction also appear to modify dementia risk, although the data are a little more limited. But personal interaction is a key element of Dr. Baker’s ongoing EXERT trial.
The ongoing phase 3 trial randomized 300 adults with amnestic mild cognitive impairment to moderate to high intensity aerobic exercise plus one-on-one support at local YMCA gyms or a low-intensity stretching, balance, and range of motion program. In additional to cognitive testing, the trial includes brain imaging, cerebrospinal fluid sampling for biomarkers of Alzheimer’s disease, and a sleep study.
A key component is personal interaction with a trainer. “They spend a lot of one-on-one time with each person,” Dr. Baker said. “For me, that’s the crucial ingredient – that personal touch. It’s what helps people move from Point A to Point B in their behaviors.”
Virtual cognitive stimulation is also a burgeoning area of dementia prevention research right now. Numerous studies are ongoing to test whether virtual reality or other computer-based games might keep the mind sharp or even improve cognition in people at risk.
The power of three
If one lifestyle change can reduce dementia risk, what happens when all three work together?
That’s the newest question, first successfully explored in the mid-2000s, with the FINGER study (Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability). In FINGER, the triad of exercise, personal support at the gym, and a modified Mediterranean diet reduced Alzheimer’s disease risk and improved cognition relative to the control group.
FINGER showed that the intervention was feasible and that it was associated with cognitive preservation and reduced Alzheimer’s disease risk in a group of at-risk subjects. The active group also had a 25% greater improvement on a neuropsychological test battery relative to the control group. They also performed 150% better in processing speed, 83% better in executive function, and 40% better in short-term memory. They showed no increased risk of cognitive decline relative to the control group, which experienced a 30% increase in risk, according to lead investigator Miia Kivipelto, PhD, of the Karolinska Institute, Stockholm.
So successful was FINGER that it launched a global consortium of related studies called World Wide FINGERS. Active in six countries now, including the United States, the studies aim to discover whether such combinations of lifestyle interventions are workable across countries and cultures. World Wide FINGERS is largely supported by the Alzheimer’s Association.
Global enthusiasm for lifestyle interventions
In recognition of the importance of lifestyle changes for dementia prevention, the World Health Organization recently published “Risk reduction of cognitive decline and dementia.” The document reviews many studies and makes recommendations regarding not only exercise, diet, and cognitive stimulation, but also smoking and alcohol.
Research interest in these areas is surging, Dr. Baker said. “The [U.S.] National Institute on Aging now has 29 ongoing trials. There’s a strong commitment to investigations into how lifestyle interventions could protect brain health as we get older. Certainly, many fit and healthy people do develop Alzheimer’s. But for some, it could be medicine.”
But no matter how compliant people are, lifestyle changes will never completely rid the world of Alzheimer’s and other dementias. The view of Dr. Baker – and most other Alzheimer’s researchers – is to employ lifestyle changes to reduce risk as much as possible and not to stop when cognitive problems do present.
“We need to understand how lifestyle interventions might work in combination with pharmaceuticals,” she said. “If we can support the health of the body and the health of the mind, lifestyle interventions can be the fertilizer that would help drug therapy have its maximum effect.”
EXPERT ANALYSIS FROM CTAD 2019
Positive functional results reported for aducanumab in a pooled, post hoc analysis
SAN DIEGO – Positive findings from a post hoc subanalysis of two unsuccessful studies represent “a major step forward in Alzheimer’s disease research” and could set the antiamyloid antibody up as a “foothold” in slowing disease progression, study investigators said at the Clinical Trials on Alzheimer’s Disease conference.

After full follow-up of 78 weeks, patients with mild Alzheimer’s disease (AD) who took the highest 10-mg/kg dose for a full 14 doses experienced up to a 53% slowing of functional decline on the Clinical Dementia Rating–Sum of Boxes (CDR-SB) in one study and a 48% slowing in the other study – relative to placebo – a result that might give them “an extra year or 2” of independence; they might perhaps retain the ability to drive and even stay employed, said Sharon Cohen, MD, a panelist at the meeting’s aducanumab presentation session and a clinical investigator in EMERGE, one of two phase 3 studies from which the data were derived.
Samantha Budd Haeberlein, PhD, Biogen’s vice president and head of late-stage clinical development in Alzheimer’s disease, presented the new data. They “are complex” and require much more study before investigators, clinicians, and federal regulators can fully embrace them, said the panelists who discussed the results. Nevertheless, Biogen, which is codeveloping the antibody with partner Eisai, said in October it will put aducanumab forward to the Food and Drug Administration in a new drug application for the first-ever AD disease-modifying agent. FDA regulators have said they will review the data.
The new subanalysis comprised 570 of 3,285 patients in two identical studies with negative primary endpoint results. One, ENGAGE, failed to reach both its primary and secondary endpoints; the other, EMERGE, was halted last spring after a futility analysis determined that aducanumab was unlikely to confer significant benefit. The post hoc subanalysis looked at a combined subset of those who received the highest 10-mg/kg dose for the full 78 weeks of each trial. The statistically significant functional endpoints occurred in this group, comprised largely of apolipoprotein E epsilon-4 (APOE4) allele carriers.
“The futility analysis of EMERGE was highly unfortunate,” said panelist Paul Aisen, MD, founding director of the Alzheimer’s Therapeutic Research Institute at the University of Southern California, Los Angeles. “Clearly in the final analysis, EMERGE was positive in the primary endpoints, and now the secondary analysis of both studies is positive and consistent.” The diverging trajectory of placebo and treatment groups continued to the end of follow-up in both studies, a finding that at least suggests continuing improvement, he added.
Biogen undertook the pooled analysis after ENGAGE’s futility analysis. Early in the development program, concern about amyloid-related imaging abnormalities (ARIA) in APOE4 carriers led Biogen to stratify doses in that group.
“When we started [creating aducanumab trials], we stratified the dose so that e4 carriers had the lowest dose, but in PRIME [the phase 1b study], we saw the best result from the 10-mg/kg dose, so we believed that was important for efficacy. However, we didn’t have sufficient evidence to believe that it was safe to put carriers on that dose. In EMERGE, we saw that carriers could safely take it until the end of the study.”
Since the trials were running almost synchronously, a new version of randomization ensued. This allowed more e4 carriers to go forward on the 10-mg/kg dose.
“I would not normally recommend changing dose in the middle of a phase 3 trial, but it did have a real impact in the high-dose group,” Dr. Haeberlein said. Additionally, by the time of data lock after the futility analysis, more patients had completed the entire 78 weeks at the 10-mg/kg dose. Cumulative dosing ended up being quite different in the APOE4 carriers after this new version ensued. Before, the median cumulative dose for both carriers and noncarriers was 116 mg/kg. After the change, the median cumulative dose was 153 mg/kg. And before the alteration, 21% in EMERGE and 15% in ENGAGE received the full 14 possible 10-mg/kg doses. After the change, 51% in EMERGE and 47% in ENGAGE received the full 14 doses of 10 mg/kg.
The pooled analysis comprised this combined group, which was then largely composed of APOE4 carriers.
Imaging confirmed such dose-driven reductions in both brain amyloid plaques and phosphorylated tau. Although amyloid reduction has never been tied to cognitive or functional benefits, tau reduction has been associated with nonsignificant cognitive benefits in prior studies.
In the primary analysis of ENGAGE, aducanumab conferred no cognitive or functional benefit. In EMERGE, there were significant cognitive improvements on both the Mini Mental State Exam score (an 18% slowing of decline relative to placebo) and the Alzheimer’s Disease Assessment Scale cognitive portion (a 27% slowing).
However, the functional improvements seen in the pooled post hoc data “are a big deal,” and probably more meaningful to patients and families than the memory improvements, Dr. Cohen said.
“Those of us who know this disease well know what it means to lose yourself slice by slice, and anything you can hang onto is a triumph,” said Dr. Cohen, medical director and principal investigator of the Toronto Memory Program, an independent medical facility for dementia care and research. “I am pleased with a 27% slowing of cognitive decline, but a 40% slowing of functional decline is what will be really meaningful to patients. This is a long, slow disease, and if we can slow it at all, we’re winning out.”
Safety endpoints, especially ARIA, were not unexpected considering past studies. ARIA occurred in 41% of patients treated with the high aducanumab dose in EMERGE and in 40% in ENGAGE. It was largely asymptomatic (80% in EMERGE and 71% in ENGAGE). Headache was the next most common adverse event, followed by dizziness, visual disturbance, and nausea and vomiting. ARIA generally resolved within 4-6 weeks, and most patients continued their 10-mg/kg dose.
Biogen intends to begin a new study, an open-label nonrandomized trial that will offer the 10-mg/kg dose to all patients in both trials, including those who took placebo. This may provide interesting data regarding redosing patients who were off their successful 10-mg/kg dose for an extended period of time, said Laurie Ryan, PhD, chief of the Dementias of Aging Branch in the Division of Neuroscience at the National Institute on Aging.
“If those in the high-dose group had a regression of their improvements and then improved again when restarted, that would certainly tell us something,” she said in an interview. Likewise, researchers will be carefully looking at any placebo group response. “But we have to remember that this will not be a randomized study,” and will bring with it all the issues that such a study typically carries.
“I agree it’s unfortunate that they had to stop the EMERGE trial,” she said. “It really did complicate the results, even though they are certainly trending in the right way. But we have had a number of post hoc analyses that show APOE4-positive benefiting, or e4-negative benefiting, and these haven’t panned out.”
SAN DIEGO – Positive findings from a post hoc subanalysis of two unsuccessful studies represent “a major step forward in Alzheimer’s disease research” and could set the antiamyloid antibody up as a “foothold” in slowing disease progression, study investigators said at the Clinical Trials on Alzheimer’s Disease conference.
After full follow-up of 78 weeks, patients with mild Alzheimer’s disease (AD) who took the highest 10-mg/kg dose for a full 14 doses experienced up to a 53% slowing of functional decline on the Clinical Dementia Rating–Sum of Boxes (CDR-SB) in one study and a 48% slowing in the other study – relative to placebo – a result that might give them “an extra year or 2” of independence; they might perhaps retain the ability to drive and even stay employed, said Sharon Cohen, MD, a panelist at the meeting’s aducanumab presentation session and a clinical investigator in EMERGE, one of two phase 3 studies from which the data were derived.
Samantha Budd Haeberlein, PhD, Biogen’s vice president and head of late-stage clinical development in Alzheimer’s disease, presented the new data. They “are complex” and require much more study before investigators, clinicians, and federal regulators can fully embrace them, said the panelists who discussed the results. Nevertheless, Biogen, which is codeveloping the antibody with partner Eisai, said in October it will put aducanumab forward to the Food and Drug Administration in a new drug application for the first-ever AD disease-modifying agent. FDA regulators have said they will review the data.
The new subanalysis comprised 570 of 3,285 patients in two identical studies with negative primary endpoint results. One, ENGAGE, failed to reach both its primary and secondary endpoints; the other, EMERGE, was halted last spring after a futility analysis determined that aducanumab was unlikely to confer significant benefit. The post hoc subanalysis looked at a combined subset of those who received the highest 10-mg/kg dose for the full 78 weeks of each trial. The statistically significant functional endpoints occurred in this group, comprised largely of apolipoprotein E epsilon-4 (APOE4) allele carriers.
“The futility analysis of EMERGE was highly unfortunate,” said panelist Paul Aisen, MD, founding director of the Alzheimer’s Therapeutic Research Institute at the University of Southern California, Los Angeles. “Clearly in the final analysis, EMERGE was positive in the primary endpoints, and now the secondary analysis of both studies is positive and consistent.” The diverging trajectory of placebo and treatment groups continued to the end of follow-up in both studies, a finding that at least suggests continuing improvement, he added.
Biogen undertook the pooled analysis after ENGAGE’s futility analysis. Early in the development program, concern about amyloid-related imaging abnormalities (ARIA) in APOE4 carriers led Biogen to stratify doses in that group.
“When we started [creating aducanumab trials], we stratified the dose so that e4 carriers had the lowest dose, but in PRIME [the phase 1b study], we saw the best result from the 10-mg/kg dose, so we believed that was important for efficacy. However, we didn’t have sufficient evidence to believe that it was safe to put carriers on that dose. In EMERGE, we saw that carriers could safely take it until the end of the study.”
Since the trials were running almost synchronously, a new version of randomization ensued. This allowed more e4 carriers to go forward on the 10-mg/kg dose.
“I would not normally recommend changing dose in the middle of a phase 3 trial, but it did have a real impact in the high-dose group,” Dr. Haeberlein said. Additionally, by the time of data lock after the futility analysis, more patients had completed the entire 78 weeks at the 10-mg/kg dose. Cumulative dosing ended up being quite different in the APOE4 carriers after this new version ensued. Before, the median cumulative dose for both carriers and noncarriers was 116 mg/kg. After the change, the median cumulative dose was 153 mg/kg. And before the alteration, 21% in EMERGE and 15% in ENGAGE received the full 14 possible 10-mg/kg doses. After the change, 51% in EMERGE and 47% in ENGAGE received the full 14 doses of 10 mg/kg.
The pooled analysis comprised this combined group, which was then largely composed of APOE4 carriers.
Imaging confirmed such dose-driven reductions in both brain amyloid plaques and phosphorylated tau. Although amyloid reduction has never been tied to cognitive or functional benefits, tau reduction has been associated with nonsignificant cognitive benefits in prior studies.
In the primary analysis of ENGAGE, aducanumab conferred no cognitive or functional benefit. In EMERGE, there were significant cognitive improvements on both the Mini Mental State Exam score (an 18% slowing of decline relative to placebo) and the Alzheimer’s Disease Assessment Scale cognitive portion (a 27% slowing).
However, the functional improvements seen in the pooled post hoc data “are a big deal,” and probably more meaningful to patients and families than the memory improvements, Dr. Cohen said.
“Those of us who know this disease well know what it means to lose yourself slice by slice, and anything you can hang onto is a triumph,” said Dr. Cohen, medical director and principal investigator of the Toronto Memory Program, an independent medical facility for dementia care and research. “I am pleased with a 27% slowing of cognitive decline, but a 40% slowing of functional decline is what will be really meaningful to patients. This is a long, slow disease, and if we can slow it at all, we’re winning out.”
Safety endpoints, especially ARIA, were not unexpected considering past studies. ARIA occurred in 41% of patients treated with the high aducanumab dose in EMERGE and in 40% in ENGAGE. It was largely asymptomatic (80% in EMERGE and 71% in ENGAGE). Headache was the next most common adverse event, followed by dizziness, visual disturbance, and nausea and vomiting. ARIA generally resolved within 4-6 weeks, and most patients continued their 10-mg/kg dose.
Biogen intends to begin a new study, an open-label nonrandomized trial that will offer the 10-mg/kg dose to all patients in both trials, including those who took placebo. This may provide interesting data regarding redosing patients who were off their successful 10-mg/kg dose for an extended period of time, said Laurie Ryan, PhD, chief of the Dementias of Aging Branch in the Division of Neuroscience at the National Institute on Aging.
“If those in the high-dose group had a regression of their improvements and then improved again when restarted, that would certainly tell us something,” she said in an interview. Likewise, researchers will be carefully looking at any placebo group response. “But we have to remember that this will not be a randomized study,” and will bring with it all the issues that such a study typically carries.
“I agree it’s unfortunate that they had to stop the EMERGE trial,” she said. “It really did complicate the results, even though they are certainly trending in the right way. But we have had a number of post hoc analyses that show APOE4-positive benefiting, or e4-negative benefiting, and these haven’t panned out.”
SAN DIEGO – Positive findings from a post hoc subanalysis of two unsuccessful studies represent “a major step forward in Alzheimer’s disease research” and could set the antiamyloid antibody up as a “foothold” in slowing disease progression, study investigators said at the Clinical Trials on Alzheimer’s Disease conference.
After full follow-up of 78 weeks, patients with mild Alzheimer’s disease (AD) who took the highest 10-mg/kg dose for a full 14 doses experienced up to a 53% slowing of functional decline on the Clinical Dementia Rating–Sum of Boxes (CDR-SB) in one study and a 48% slowing in the other study – relative to placebo – a result that might give them “an extra year or 2” of independence; they might perhaps retain the ability to drive and even stay employed, said Sharon Cohen, MD, a panelist at the meeting’s aducanumab presentation session and a clinical investigator in EMERGE, one of two phase 3 studies from which the data were derived.
Samantha Budd Haeberlein, PhD, Biogen’s vice president and head of late-stage clinical development in Alzheimer’s disease, presented the new data. They “are complex” and require much more study before investigators, clinicians, and federal regulators can fully embrace them, said the panelists who discussed the results. Nevertheless, Biogen, which is codeveloping the antibody with partner Eisai, said in October it will put aducanumab forward to the Food and Drug Administration in a new drug application for the first-ever AD disease-modifying agent. FDA regulators have said they will review the data.
The new subanalysis comprised 570 of 3,285 patients in two identical studies with negative primary endpoint results. One, ENGAGE, failed to reach both its primary and secondary endpoints; the other, EMERGE, was halted last spring after a futility analysis determined that aducanumab was unlikely to confer significant benefit. The post hoc subanalysis looked at a combined subset of those who received the highest 10-mg/kg dose for the full 78 weeks of each trial. The statistically significant functional endpoints occurred in this group, comprised largely of apolipoprotein E epsilon-4 (APOE4) allele carriers.
“The futility analysis of EMERGE was highly unfortunate,” said panelist Paul Aisen, MD, founding director of the Alzheimer’s Therapeutic Research Institute at the University of Southern California, Los Angeles. “Clearly in the final analysis, EMERGE was positive in the primary endpoints, and now the secondary analysis of both studies is positive and consistent.” The diverging trajectory of placebo and treatment groups continued to the end of follow-up in both studies, a finding that at least suggests continuing improvement, he added.
Biogen undertook the pooled analysis after ENGAGE’s futility analysis. Early in the development program, concern about amyloid-related imaging abnormalities (ARIA) in APOE4 carriers led Biogen to stratify doses in that group.
“When we started [creating aducanumab trials], we stratified the dose so that e4 carriers had the lowest dose, but in PRIME [the phase 1b study], we saw the best result from the 10-mg/kg dose, so we believed that was important for efficacy. However, we didn’t have sufficient evidence to believe that it was safe to put carriers on that dose. In EMERGE, we saw that carriers could safely take it until the end of the study.”
Since the trials were running almost synchronously, a new version of randomization ensued. This allowed more e4 carriers to go forward on the 10-mg/kg dose.
“I would not normally recommend changing dose in the middle of a phase 3 trial, but it did have a real impact in the high-dose group,” Dr. Haeberlein said. Additionally, by the time of data lock after the futility analysis, more patients had completed the entire 78 weeks at the 10-mg/kg dose. Cumulative dosing ended up being quite different in the APOE4 carriers after this new version ensued. Before, the median cumulative dose for both carriers and noncarriers was 116 mg/kg. After the change, the median cumulative dose was 153 mg/kg. And before the alteration, 21% in EMERGE and 15% in ENGAGE received the full 14 possible 10-mg/kg doses. After the change, 51% in EMERGE and 47% in ENGAGE received the full 14 doses of 10 mg/kg.
The pooled analysis comprised this combined group, which was then largely composed of APOE4 carriers.
Imaging confirmed such dose-driven reductions in both brain amyloid plaques and phosphorylated tau. Although amyloid reduction has never been tied to cognitive or functional benefits, tau reduction has been associated with nonsignificant cognitive benefits in prior studies.
In the primary analysis of ENGAGE, aducanumab conferred no cognitive or functional benefit. In EMERGE, there were significant cognitive improvements on both the Mini Mental State Exam score (an 18% slowing of decline relative to placebo) and the Alzheimer’s Disease Assessment Scale cognitive portion (a 27% slowing).
However, the functional improvements seen in the pooled post hoc data “are a big deal,” and probably more meaningful to patients and families than the memory improvements, Dr. Cohen said.
“Those of us who know this disease well know what it means to lose yourself slice by slice, and anything you can hang onto is a triumph,” said Dr. Cohen, medical director and principal investigator of the Toronto Memory Program, an independent medical facility for dementia care and research. “I am pleased with a 27% slowing of cognitive decline, but a 40% slowing of functional decline is what will be really meaningful to patients. This is a long, slow disease, and if we can slow it at all, we’re winning out.”
Safety endpoints, especially ARIA, were not unexpected considering past studies. ARIA occurred in 41% of patients treated with the high aducanumab dose in EMERGE and in 40% in ENGAGE. It was largely asymptomatic (80% in EMERGE and 71% in ENGAGE). Headache was the next most common adverse event, followed by dizziness, visual disturbance, and nausea and vomiting. ARIA generally resolved within 4-6 weeks, and most patients continued their 10-mg/kg dose.
Biogen intends to begin a new study, an open-label nonrandomized trial that will offer the 10-mg/kg dose to all patients in both trials, including those who took placebo. This may provide interesting data regarding redosing patients who were off their successful 10-mg/kg dose for an extended period of time, said Laurie Ryan, PhD, chief of the Dementias of Aging Branch in the Division of Neuroscience at the National Institute on Aging.
“If those in the high-dose group had a regression of their improvements and then improved again when restarted, that would certainly tell us something,” she said in an interview. Likewise, researchers will be carefully looking at any placebo group response. “But we have to remember that this will not be a randomized study,” and will bring with it all the issues that such a study typically carries.
“I agree it’s unfortunate that they had to stop the EMERGE trial,” she said. “It really did complicate the results, even though they are certainly trending in the right way. But we have had a number of post hoc analyses that show APOE4-positive benefiting, or e4-negative benefiting, and these haven’t panned out.”
REPORTING FROM CTAD 2019
Key clinical point: A pooled posthoc subanalysis of two unsuccessful phase 3 trials, found that the antiamyloid antibody aducanumab conferred significant functional benefits in patients with mild Alzheimer’s disease who took the highest 10-mg/kg dose for a full 78 weeks.
Major finding: Aducanumab conferred a 53% slowing of functional decline on the Clinical Dementia Rating–Sum of Boxes (CDR-SB) in one study, ENGAGE, and a 48% slowing in the other, EMERGE, relative to placebo.
Study details: The pooled group comprised 570 of 3,285 patients in the two identical ENGAGE and EMERGE studies.
Disclosures: Biogen and Eisai sponsored the studies and are codeveloping aducanumab.
Source: Budd SH et al. CTAD 2019, OC 1-4.