User login
Diagnosis and treatment of uterine isthmocele
In recent years, uterine isthmocele has increasingly been included as part of the differential in women with a history of a cesarean section who present with postmenstrual bleeding, pelvic pain, or secondary infertility.
The defect appears as a fluid-filled, pouch-like abnormality in the anterior uterine wall at the site of a prior cesarean section. The best method for diagnosis is usually a saline-infused sonogram. It can be treated in various ways, depending on the patient’s symptoms and desire for future fertility. Although we have treated isthmoceles with hysteroscopic desiccation, or resection, our best success has occurred with laparoscopic resection and reapproximation of normal tissue in a small series of patients.
There is no standard definition of the defect that fully describes its size, depth, and other characteristics. Many words and phrases have been used to describe the defect: It is commonly referred to as an isthmocele, because of its usual location at the uterine isthmus, but others have referred to it as a cesarean scar defect or niche, as the defect may be found at the endocervical canal or in the lower uterine segment. In any case, while diagnoses appear to be increasing, the incidence of the defect is unknown.

More research on risk factors and treatment is needed, but the literature, as well as our own experience, has demonstrated that this treatable defect should be considered in the differential diagnosis for women who have undergone cesarean section and subsequently have abnormal bleeding or staining, pelvic pain, or secondary infertility, especially when fluid is clearly visible in the cesarean section defect.
Diagnosis, symptoms
An isthmocele forms in the first place, it is thought, after an incision scar forms and causes retraction and dilation in the thinner, lower segment of the anterior wall and a thickening in the upper portion. There is a deficient scar, in other words, with disparate wound healing on the sides of the incision site.
The defect and its consequences were described in 1995 by Dr. Hugh Morris, who studied hysterectomy specimens in 51 women with a history of cesarean section (in most cases, more than one). Dr. Morris concluded that scar tissue in these patients contributed to significant pathological changes and anatomical abnormalities that, in turn, gave rise to a variety of clinical symptoms including menorrhagia, dysmenorrhea, dyspareunia, and lower abdominal pain refractory to medical management.
Distortion and widening of the lower uterine segment and “free” red blood cells in endometrial stroma of the scar were the most frequently identified pathological changes, followed by fragmentation and breakdown of the endometrium of the scar, and iatrogenic adenomyosis (Int. J. Gynecol. Pathol.1995;14:16-20).
Several small reports and case series published in the late 1990s offered additional support for a cause-and-effect correlation between cesarean scar defects and abnormal vaginal bleeding. Several years later, the link was strengthened as more investigators reported connections between the defects and various symptoms. These reports were followed by published comparisons of imaging techniques for the diagnosis of isthmoceles.
Diagnosis of the defects can be made with transvaginal ultrasound (TVUS), saline infused sonohysterogram (SIS), hysterosalpingogram, hysteroscopy, and magnetic resonance imaging (MRI). With any modality, imaging is best performed in the early proliferative phase, right after the menstrual cycle has ended.

Comparisons of unenhanced TVUS and SIS – both of which may be easily performed in the office and at a much lower cost than MRI – have shown the latter technique to be superior for evaluating isthmoceles. Distension of the endometrial cavity makes the borders of the defects easier to delineate, which enables detection of more subtle defects and improves our ability to measure the size of defects.
This advantage was described by in 2010 by Dr. O. Vikhareva Osser and colleagues, who performed both TVUS and SIS in 108 women with a history of one or more cesarean sections. They identified more scar defects with SIS than with TVUS (Ultrasound Obstet. Gynecol. 2010;35:75-83).
Another benefit of SIS over TVUS and hysterosalpingogram is that one can measure the thickness of the remaining myometrium overlying the isthmocele, which is especially important knowledge for patients considering another pregnancy. As a result, we have relied on this technique to diagnose every case within our practice. I will perform SIS in a patient who has a history of one or multiple cesarean sections and symptoms of abnormal bleeding, pelvic pain, or secondary infertility as part of the basic work-up.
Similarly, an observational prospective cohort study of 225 women who had undergone a cesarean section 6-12 months prior compared TVUS and gel-infused sonohysterogram (GIS), and found that the prevalence of a niche – defined as an anechoic area at the site of the cesarean scar, with a depth of at least 1 mm on GIS – was 24% with TVUS and 56% with GIS (Ultrasound Obstet. Gynecol. 2011;37:93-9).
The abnormal bleeding is often described by patients as spotting or bleeding that continues for days or weeks after menstrual flow has ended; it is believed to result from an accumulation of blood in the defect and a lack of coordinated muscle contractions, which leads to continued accumulation of blood and menstrual debris. Dysmenorrhea and chronic pelvic pain are thought to be associated with iatrogenic adenomyosis and/or a chronic inflammatory state created when accumulated blood and mucus are intermittently expelled. Secondary infertility can occur, it is believed, as accumulated fluid and blood interfere with the endocervical and even the endometrial environment and disrupt sperm transport, sperm quality, and embryo implantation. Difficulty in embryo transfer may also occur because of the distortion caused to the endometrial cavity. Many of the isthmoceles that we and others have diagnosed have been in patients undergoing invitro fertilization. The patients are often found to have an accumulation of fluid in the endometrial canal and isthmocele during stimulation for either a fresh or frozen embryo transfer, thus necessitating the cancellation of their cycle.
Treatment
The choice of treatment depends upon the patient’s symptoms and desire for future fertility, but it can include hormonal treatment, hysteroscopic resection, transvaginal repair, a laparoscopic or robot-assisted approach, and hysterectomy.
Little has been published on nonsurgical treatment, but this may be considered for patients whose primary symptoms are bleeding or pain and who desire the least invasive option. In a small observational study of women with an isthmocele and bleeding, symptoms were eliminated with several cycles of oral contraceptive pills (Fertil. Steril. 2006;86: 477-9).

Hysteroscopic isthmocele correction or resection are the surgical techniques most frequently described in the literature, but, as with other surgical approaches, studies are small. Hysteroscopic repair has typically involved the use of electrical energy to desiccate or cauterize abnormal tissue and eliminate the outpouching in which blood and fluid accumulate. Hysteroscopic resection is another technique that has also been championed.
However, for patients who desire future pregnancy, we do not recommend a hysteroscopic approach because it does not reinforce the often-thinning myometrium covering the defect. We are concerned that if this area is simply desiccated or resected, and not reapproximated, the patient will be at greater risk of pregnancy-related complications, including cesarean scar ectopic pregnancy with potential uterine dehiscence.
Laparoscopic repair was first described by Dr. Olivier Donnez, who rightly pointed out that the laparoscopic approach offers an optimal view from above during dissection of the vesico-vaginal space. Dr. Donnez used a CO2 laser to excise fibrotic tissue, followed by laparoscopic closure (Fertil. Steril. 2008;89:974-80).
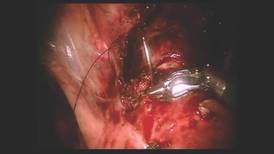
We have had success with a laparoscopic approach that uses concomitant hysteroscopy. The vesico-uterine peritoneum is incised over the anterior uterine wall, and the bladder is backfilled so that its boundaries may be identified prior to further dissection. With the area exposed, we perform a hysteroscopy to determine the exact location of the isthmocele. As the hysteroscope enters the thinned out isthmocele, the light will be more visible via laparoscopic visualization.
When performing conventional laparoscopy, the isthmocele is excised with an ultrasonic curved blade. We use this instrument because it has no opposing arm and because it enables precise tissue dissection in multiple planes. With harmonic energy, we can limit tissue dessication and destruction, lowering the risk of future pregnancy-related complications. Monopolar scissors are best when a robotic approach is used.
Once the isthmocele is resected, the clean edges are sutured together in two layers. The first layer is sutured in an interrupted mattress-style fashion, to prevent tissue strangulation and necrosis. We use a monofilament nonbarbed delayed-absorbable 3-0 PDS suture on a CT-1 needle – a choice that limits tissue trauma and postoperative inflammation.
Sutures are initially placed at each angle with one or two sutures placed between. These sutures must be placed deep to close the bottom of the defect. A second layer of suture is then placed to imbricate over the initial layer of closure. We utilize 3-0 PDS in a running or mattress style, or a running 3-0 V-Loc suture. Our patients return after 1-3 months for a postoperative image, and are instructed to wait at least 3 months after surgery before attempting conception.
In our experience, of more than 10 patients, symptoms ceased in all patients whose surgery was performed for the indication of abnormal uterine bleeding. The follow-up on our series of patients who underwent the procedure for secondary infertility is ongoing, but the preliminary results are very positive, with resolution of intrauterine fluid in all of the patients, as well as several successful pregnancy outcomes.
A recent systematic review of minimally invasive therapy for symptoms related to an isthmocele shows good outcomes across the 12 included studies but does not offer evidence to favor one treatment over another. The studies show significant reductions in abnormal uterine bleeding and pain, as well as a high rate of satisfaction in most patients after hysteroscopic niche resection or vaginal or laparoscopic niche repair, with a low complication rate (BJOG 2014;121:145-6).
Pregnancies were reported after treatment, but sample sizes and follow-up were insufficient to draw conclusions on pregnancy and delivery outcomes, according to the review. As the reviewers wrote, following patients through their next delivery in larger, higher-quality studies will help provide more guidance for selecting the best isthmocele treatments and implementing these treatments into practice.
Dr. Sasaki reported having no financial disclosures relevant to this Master Class.
In recent years, uterine isthmocele has increasingly been included as part of the differential in women with a history of a cesarean section who present with postmenstrual bleeding, pelvic pain, or secondary infertility.
The defect appears as a fluid-filled, pouch-like abnormality in the anterior uterine wall at the site of a prior cesarean section. The best method for diagnosis is usually a saline-infused sonogram. It can be treated in various ways, depending on the patient’s symptoms and desire for future fertility. Although we have treated isthmoceles with hysteroscopic desiccation, or resection, our best success has occurred with laparoscopic resection and reapproximation of normal tissue in a small series of patients.
There is no standard definition of the defect that fully describes its size, depth, and other characteristics. Many words and phrases have been used to describe the defect: It is commonly referred to as an isthmocele, because of its usual location at the uterine isthmus, but others have referred to it as a cesarean scar defect or niche, as the defect may be found at the endocervical canal or in the lower uterine segment. In any case, while diagnoses appear to be increasing, the incidence of the defect is unknown.
More research on risk factors and treatment is needed, but the literature, as well as our own experience, has demonstrated that this treatable defect should be considered in the differential diagnosis for women who have undergone cesarean section and subsequently have abnormal bleeding or staining, pelvic pain, or secondary infertility, especially when fluid is clearly visible in the cesarean section defect.
Diagnosis, symptoms
An isthmocele forms in the first place, it is thought, after an incision scar forms and causes retraction and dilation in the thinner, lower segment of the anterior wall and a thickening in the upper portion. There is a deficient scar, in other words, with disparate wound healing on the sides of the incision site.
The defect and its consequences were described in 1995 by Dr. Hugh Morris, who studied hysterectomy specimens in 51 women with a history of cesarean section (in most cases, more than one). Dr. Morris concluded that scar tissue in these patients contributed to significant pathological changes and anatomical abnormalities that, in turn, gave rise to a variety of clinical symptoms including menorrhagia, dysmenorrhea, dyspareunia, and lower abdominal pain refractory to medical management.
Distortion and widening of the lower uterine segment and “free” red blood cells in endometrial stroma of the scar were the most frequently identified pathological changes, followed by fragmentation and breakdown of the endometrium of the scar, and iatrogenic adenomyosis (Int. J. Gynecol. Pathol.1995;14:16-20).
Several small reports and case series published in the late 1990s offered additional support for a cause-and-effect correlation between cesarean scar defects and abnormal vaginal bleeding. Several years later, the link was strengthened as more investigators reported connections between the defects and various symptoms. These reports were followed by published comparisons of imaging techniques for the diagnosis of isthmoceles.
Diagnosis of the defects can be made with transvaginal ultrasound (TVUS), saline infused sonohysterogram (SIS), hysterosalpingogram, hysteroscopy, and magnetic resonance imaging (MRI). With any modality, imaging is best performed in the early proliferative phase, right after the menstrual cycle has ended.
Comparisons of unenhanced TVUS and SIS – both of which may be easily performed in the office and at a much lower cost than MRI – have shown the latter technique to be superior for evaluating isthmoceles. Distension of the endometrial cavity makes the borders of the defects easier to delineate, which enables detection of more subtle defects and improves our ability to measure the size of defects.
This advantage was described by in 2010 by Dr. O. Vikhareva Osser and colleagues, who performed both TVUS and SIS in 108 women with a history of one or more cesarean sections. They identified more scar defects with SIS than with TVUS (Ultrasound Obstet. Gynecol. 2010;35:75-83).
Another benefit of SIS over TVUS and hysterosalpingogram is that one can measure the thickness of the remaining myometrium overlying the isthmocele, which is especially important knowledge for patients considering another pregnancy. As a result, we have relied on this technique to diagnose every case within our practice. I will perform SIS in a patient who has a history of one or multiple cesarean sections and symptoms of abnormal bleeding, pelvic pain, or secondary infertility as part of the basic work-up.
Similarly, an observational prospective cohort study of 225 women who had undergone a cesarean section 6-12 months prior compared TVUS and gel-infused sonohysterogram (GIS), and found that the prevalence of a niche – defined as an anechoic area at the site of the cesarean scar, with a depth of at least 1 mm on GIS – was 24% with TVUS and 56% with GIS (Ultrasound Obstet. Gynecol. 2011;37:93-9).
The abnormal bleeding is often described by patients as spotting or bleeding that continues for days or weeks after menstrual flow has ended; it is believed to result from an accumulation of blood in the defect and a lack of coordinated muscle contractions, which leads to continued accumulation of blood and menstrual debris. Dysmenorrhea and chronic pelvic pain are thought to be associated with iatrogenic adenomyosis and/or a chronic inflammatory state created when accumulated blood and mucus are intermittently expelled. Secondary infertility can occur, it is believed, as accumulated fluid and blood interfere with the endocervical and even the endometrial environment and disrupt sperm transport, sperm quality, and embryo implantation. Difficulty in embryo transfer may also occur because of the distortion caused to the endometrial cavity. Many of the isthmoceles that we and others have diagnosed have been in patients undergoing invitro fertilization. The patients are often found to have an accumulation of fluid in the endometrial canal and isthmocele during stimulation for either a fresh or frozen embryo transfer, thus necessitating the cancellation of their cycle.
Treatment
The choice of treatment depends upon the patient’s symptoms and desire for future fertility, but it can include hormonal treatment, hysteroscopic resection, transvaginal repair, a laparoscopic or robot-assisted approach, and hysterectomy.
Little has been published on nonsurgical treatment, but this may be considered for patients whose primary symptoms are bleeding or pain and who desire the least invasive option. In a small observational study of women with an isthmocele and bleeding, symptoms were eliminated with several cycles of oral contraceptive pills (Fertil. Steril. 2006;86: 477-9).
Hysteroscopic isthmocele correction or resection are the surgical techniques most frequently described in the literature, but, as with other surgical approaches, studies are small. Hysteroscopic repair has typically involved the use of electrical energy to desiccate or cauterize abnormal tissue and eliminate the outpouching in which blood and fluid accumulate. Hysteroscopic resection is another technique that has also been championed.
However, for patients who desire future pregnancy, we do not recommend a hysteroscopic approach because it does not reinforce the often-thinning myometrium covering the defect. We are concerned that if this area is simply desiccated or resected, and not reapproximated, the patient will be at greater risk of pregnancy-related complications, including cesarean scar ectopic pregnancy with potential uterine dehiscence.
Laparoscopic repair was first described by Dr. Olivier Donnez, who rightly pointed out that the laparoscopic approach offers an optimal view from above during dissection of the vesico-vaginal space. Dr. Donnez used a CO2 laser to excise fibrotic tissue, followed by laparoscopic closure (Fertil. Steril. 2008;89:974-80).
We have had success with a laparoscopic approach that uses concomitant hysteroscopy. The vesico-uterine peritoneum is incised over the anterior uterine wall, and the bladder is backfilled so that its boundaries may be identified prior to further dissection. With the area exposed, we perform a hysteroscopy to determine the exact location of the isthmocele. As the hysteroscope enters the thinned out isthmocele, the light will be more visible via laparoscopic visualization.
When performing conventional laparoscopy, the isthmocele is excised with an ultrasonic curved blade. We use this instrument because it has no opposing arm and because it enables precise tissue dissection in multiple planes. With harmonic energy, we can limit tissue dessication and destruction, lowering the risk of future pregnancy-related complications. Monopolar scissors are best when a robotic approach is used.
Once the isthmocele is resected, the clean edges are sutured together in two layers. The first layer is sutured in an interrupted mattress-style fashion, to prevent tissue strangulation and necrosis. We use a monofilament nonbarbed delayed-absorbable 3-0 PDS suture on a CT-1 needle – a choice that limits tissue trauma and postoperative inflammation.
Sutures are initially placed at each angle with one or two sutures placed between. These sutures must be placed deep to close the bottom of the defect. A second layer of suture is then placed to imbricate over the initial layer of closure. We utilize 3-0 PDS in a running or mattress style, or a running 3-0 V-Loc suture. Our patients return after 1-3 months for a postoperative image, and are instructed to wait at least 3 months after surgery before attempting conception.
In our experience, of more than 10 patients, symptoms ceased in all patients whose surgery was performed for the indication of abnormal uterine bleeding. The follow-up on our series of patients who underwent the procedure for secondary infertility is ongoing, but the preliminary results are very positive, with resolution of intrauterine fluid in all of the patients, as well as several successful pregnancy outcomes.
A recent systematic review of minimally invasive therapy for symptoms related to an isthmocele shows good outcomes across the 12 included studies but does not offer evidence to favor one treatment over another. The studies show significant reductions in abnormal uterine bleeding and pain, as well as a high rate of satisfaction in most patients after hysteroscopic niche resection or vaginal or laparoscopic niche repair, with a low complication rate (BJOG 2014;121:145-6).
Pregnancies were reported after treatment, but sample sizes and follow-up were insufficient to draw conclusions on pregnancy and delivery outcomes, according to the review. As the reviewers wrote, following patients through their next delivery in larger, higher-quality studies will help provide more guidance for selecting the best isthmocele treatments and implementing these treatments into practice.
Dr. Sasaki reported having no financial disclosures relevant to this Master Class.
In recent years, uterine isthmocele has increasingly been included as part of the differential in women with a history of a cesarean section who present with postmenstrual bleeding, pelvic pain, or secondary infertility.
The defect appears as a fluid-filled, pouch-like abnormality in the anterior uterine wall at the site of a prior cesarean section. The best method for diagnosis is usually a saline-infused sonogram. It can be treated in various ways, depending on the patient’s symptoms and desire for future fertility. Although we have treated isthmoceles with hysteroscopic desiccation, or resection, our best success has occurred with laparoscopic resection and reapproximation of normal tissue in a small series of patients.
There is no standard definition of the defect that fully describes its size, depth, and other characteristics. Many words and phrases have been used to describe the defect: It is commonly referred to as an isthmocele, because of its usual location at the uterine isthmus, but others have referred to it as a cesarean scar defect or niche, as the defect may be found at the endocervical canal or in the lower uterine segment. In any case, while diagnoses appear to be increasing, the incidence of the defect is unknown.
More research on risk factors and treatment is needed, but the literature, as well as our own experience, has demonstrated that this treatable defect should be considered in the differential diagnosis for women who have undergone cesarean section and subsequently have abnormal bleeding or staining, pelvic pain, or secondary infertility, especially when fluid is clearly visible in the cesarean section defect.
Diagnosis, symptoms
An isthmocele forms in the first place, it is thought, after an incision scar forms and causes retraction and dilation in the thinner, lower segment of the anterior wall and a thickening in the upper portion. There is a deficient scar, in other words, with disparate wound healing on the sides of the incision site.
The defect and its consequences were described in 1995 by Dr. Hugh Morris, who studied hysterectomy specimens in 51 women with a history of cesarean section (in most cases, more than one). Dr. Morris concluded that scar tissue in these patients contributed to significant pathological changes and anatomical abnormalities that, in turn, gave rise to a variety of clinical symptoms including menorrhagia, dysmenorrhea, dyspareunia, and lower abdominal pain refractory to medical management.
Distortion and widening of the lower uterine segment and “free” red blood cells in endometrial stroma of the scar were the most frequently identified pathological changes, followed by fragmentation and breakdown of the endometrium of the scar, and iatrogenic adenomyosis (Int. J. Gynecol. Pathol.1995;14:16-20).
Several small reports and case series published in the late 1990s offered additional support for a cause-and-effect correlation between cesarean scar defects and abnormal vaginal bleeding. Several years later, the link was strengthened as more investigators reported connections between the defects and various symptoms. These reports were followed by published comparisons of imaging techniques for the diagnosis of isthmoceles.
Diagnosis of the defects can be made with transvaginal ultrasound (TVUS), saline infused sonohysterogram (SIS), hysterosalpingogram, hysteroscopy, and magnetic resonance imaging (MRI). With any modality, imaging is best performed in the early proliferative phase, right after the menstrual cycle has ended.
Comparisons of unenhanced TVUS and SIS – both of which may be easily performed in the office and at a much lower cost than MRI – have shown the latter technique to be superior for evaluating isthmoceles. Distension of the endometrial cavity makes the borders of the defects easier to delineate, which enables detection of more subtle defects and improves our ability to measure the size of defects.
This advantage was described by in 2010 by Dr. O. Vikhareva Osser and colleagues, who performed both TVUS and SIS in 108 women with a history of one or more cesarean sections. They identified more scar defects with SIS than with TVUS (Ultrasound Obstet. Gynecol. 2010;35:75-83).
Another benefit of SIS over TVUS and hysterosalpingogram is that one can measure the thickness of the remaining myometrium overlying the isthmocele, which is especially important knowledge for patients considering another pregnancy. As a result, we have relied on this technique to diagnose every case within our practice. I will perform SIS in a patient who has a history of one or multiple cesarean sections and symptoms of abnormal bleeding, pelvic pain, or secondary infertility as part of the basic work-up.
Similarly, an observational prospective cohort study of 225 women who had undergone a cesarean section 6-12 months prior compared TVUS and gel-infused sonohysterogram (GIS), and found that the prevalence of a niche – defined as an anechoic area at the site of the cesarean scar, with a depth of at least 1 mm on GIS – was 24% with TVUS and 56% with GIS (Ultrasound Obstet. Gynecol. 2011;37:93-9).
The abnormal bleeding is often described by patients as spotting or bleeding that continues for days or weeks after menstrual flow has ended; it is believed to result from an accumulation of blood in the defect and a lack of coordinated muscle contractions, which leads to continued accumulation of blood and menstrual debris. Dysmenorrhea and chronic pelvic pain are thought to be associated with iatrogenic adenomyosis and/or a chronic inflammatory state created when accumulated blood and mucus are intermittently expelled. Secondary infertility can occur, it is believed, as accumulated fluid and blood interfere with the endocervical and even the endometrial environment and disrupt sperm transport, sperm quality, and embryo implantation. Difficulty in embryo transfer may also occur because of the distortion caused to the endometrial cavity. Many of the isthmoceles that we and others have diagnosed have been in patients undergoing invitro fertilization. The patients are often found to have an accumulation of fluid in the endometrial canal and isthmocele during stimulation for either a fresh or frozen embryo transfer, thus necessitating the cancellation of their cycle.
Treatment
The choice of treatment depends upon the patient’s symptoms and desire for future fertility, but it can include hormonal treatment, hysteroscopic resection, transvaginal repair, a laparoscopic or robot-assisted approach, and hysterectomy.
Little has been published on nonsurgical treatment, but this may be considered for patients whose primary symptoms are bleeding or pain and who desire the least invasive option. In a small observational study of women with an isthmocele and bleeding, symptoms were eliminated with several cycles of oral contraceptive pills (Fertil. Steril. 2006;86: 477-9).
Hysteroscopic isthmocele correction or resection are the surgical techniques most frequently described in the literature, but, as with other surgical approaches, studies are small. Hysteroscopic repair has typically involved the use of electrical energy to desiccate or cauterize abnormal tissue and eliminate the outpouching in which blood and fluid accumulate. Hysteroscopic resection is another technique that has also been championed.
However, for patients who desire future pregnancy, we do not recommend a hysteroscopic approach because it does not reinforce the often-thinning myometrium covering the defect. We are concerned that if this area is simply desiccated or resected, and not reapproximated, the patient will be at greater risk of pregnancy-related complications, including cesarean scar ectopic pregnancy with potential uterine dehiscence.
Laparoscopic repair was first described by Dr. Olivier Donnez, who rightly pointed out that the laparoscopic approach offers an optimal view from above during dissection of the vesico-vaginal space. Dr. Donnez used a CO2 laser to excise fibrotic tissue, followed by laparoscopic closure (Fertil. Steril. 2008;89:974-80).
We have had success with a laparoscopic approach that uses concomitant hysteroscopy. The vesico-uterine peritoneum is incised over the anterior uterine wall, and the bladder is backfilled so that its boundaries may be identified prior to further dissection. With the area exposed, we perform a hysteroscopy to determine the exact location of the isthmocele. As the hysteroscope enters the thinned out isthmocele, the light will be more visible via laparoscopic visualization.
When performing conventional laparoscopy, the isthmocele is excised with an ultrasonic curved blade. We use this instrument because it has no opposing arm and because it enables precise tissue dissection in multiple planes. With harmonic energy, we can limit tissue dessication and destruction, lowering the risk of future pregnancy-related complications. Monopolar scissors are best when a robotic approach is used.
Once the isthmocele is resected, the clean edges are sutured together in two layers. The first layer is sutured in an interrupted mattress-style fashion, to prevent tissue strangulation and necrosis. We use a monofilament nonbarbed delayed-absorbable 3-0 PDS suture on a CT-1 needle – a choice that limits tissue trauma and postoperative inflammation.
Sutures are initially placed at each angle with one or two sutures placed between. These sutures must be placed deep to close the bottom of the defect. A second layer of suture is then placed to imbricate over the initial layer of closure. We utilize 3-0 PDS in a running or mattress style, or a running 3-0 V-Loc suture. Our patients return after 1-3 months for a postoperative image, and are instructed to wait at least 3 months after surgery before attempting conception.
In our experience, of more than 10 patients, symptoms ceased in all patients whose surgery was performed for the indication of abnormal uterine bleeding. The follow-up on our series of patients who underwent the procedure for secondary infertility is ongoing, but the preliminary results are very positive, with resolution of intrauterine fluid in all of the patients, as well as several successful pregnancy outcomes.
A recent systematic review of minimally invasive therapy for symptoms related to an isthmocele shows good outcomes across the 12 included studies but does not offer evidence to favor one treatment over another. The studies show significant reductions in abnormal uterine bleeding and pain, as well as a high rate of satisfaction in most patients after hysteroscopic niche resection or vaginal or laparoscopic niche repair, with a low complication rate (BJOG 2014;121:145-6).
Pregnancies were reported after treatment, but sample sizes and follow-up were insufficient to draw conclusions on pregnancy and delivery outcomes, according to the review. As the reviewers wrote, following patients through their next delivery in larger, higher-quality studies will help provide more guidance for selecting the best isthmocele treatments and implementing these treatments into practice.
Dr. Sasaki reported having no financial disclosures relevant to this Master Class.

DDW: Menopausal hormone therapy increases major GI bleed risk
Menopausal hormone therapy is associated with an increased risk of major gastrointestinal bleeding, particularly in the lower gastrointestinal tract, that is associated with duration of use, a study has found.
Analysis of data from 73,863 women enrolled in the Nurses’ Health Study II in 1989 showed that current users of menopausal hormone therapy had a 46% increase in the risk of a major gastrointestinal bleed and a more than twofold increase in the risk of a lower GI bleed or ischemic colitis, compared with never users, said Dr. Prashant Singh of Massachusetts General Hospital, Boston.
Past users showed a much smaller increase risk of bleeding, while increasing duration of hormone therapy was significantly associated with increasing risk of major and low gastrointestinal bleeding.
“Although our findings show that menopausal hormone therapy may increase the risk of major GI bleeding, especially in the lower GI tract, it is important for these patients to know that this therapy is still an effective treatment; however, both clinician and patient should be more cautious in using this therapy in some cases, such as with patients who have a history of ischemic colitis,” Dr. Singh said at the annual Digestive Disease Week.
Dr. Singh does not have any relevant financial or other relationship with any manufacturer or provider of commercial products or services that he discussed during the presentation.
Menopausal hormone therapy is associated with an increased risk of major gastrointestinal bleeding, particularly in the lower gastrointestinal tract, that is associated with duration of use, a study has found.
Analysis of data from 73,863 women enrolled in the Nurses’ Health Study II in 1989 showed that current users of menopausal hormone therapy had a 46% increase in the risk of a major gastrointestinal bleed and a more than twofold increase in the risk of a lower GI bleed or ischemic colitis, compared with never users, said Dr. Prashant Singh of Massachusetts General Hospital, Boston.
Past users showed a much smaller increase risk of bleeding, while increasing duration of hormone therapy was significantly associated with increasing risk of major and low gastrointestinal bleeding.
“Although our findings show that menopausal hormone therapy may increase the risk of major GI bleeding, especially in the lower GI tract, it is important for these patients to know that this therapy is still an effective treatment; however, both clinician and patient should be more cautious in using this therapy in some cases, such as with patients who have a history of ischemic colitis,” Dr. Singh said at the annual Digestive Disease Week.
Dr. Singh does not have any relevant financial or other relationship with any manufacturer or provider of commercial products or services that he discussed during the presentation.
Menopausal hormone therapy is associated with an increased risk of major gastrointestinal bleeding, particularly in the lower gastrointestinal tract, that is associated with duration of use, a study has found.
Analysis of data from 73,863 women enrolled in the Nurses’ Health Study II in 1989 showed that current users of menopausal hormone therapy had a 46% increase in the risk of a major gastrointestinal bleed and a more than twofold increase in the risk of a lower GI bleed or ischemic colitis, compared with never users, said Dr. Prashant Singh of Massachusetts General Hospital, Boston.
Past users showed a much smaller increase risk of bleeding, while increasing duration of hormone therapy was significantly associated with increasing risk of major and low gastrointestinal bleeding.
“Although our findings show that menopausal hormone therapy may increase the risk of major GI bleeding, especially in the lower GI tract, it is important for these patients to know that this therapy is still an effective treatment; however, both clinician and patient should be more cautious in using this therapy in some cases, such as with patients who have a history of ischemic colitis,” Dr. Singh said at the annual Digestive Disease Week.
Dr. Singh does not have any relevant financial or other relationship with any manufacturer or provider of commercial products or services that he discussed during the presentation.
FROM DDW 2015
Key clinical point: Menopausal hormone therapy is associated with an increased risk of major gastrointestinal bleeding, particularly in the lower gastrointestinal tract.
Major finding: Current users of menopausal hormone therapy had a 46% increase in the risk of a major gastrointestinal bleed and a more than twofold increase in the risk of a lower GI bleed or ischemic colitis.
Data source: Analysis of data from 73,863 women enrolled in the Nurses’ Health Study II.
Disclosures: No conflicts of interest were disclosed.
NASPAG: Obesity raises unique contraceptive concerns in teens
ORLANDO – The data with respect to the effects of obesity on the efficacy of contraceptives in adolescents are limited, but the general consensus is that if efficacy is reduced, it isn’t by enough to make a real difference, according to Dr. Alene Toulany.
The effect of obesity is likely to be very small, and studies that have looked at pharmacokinetics in obesity have estimated that body weight accounts for only about 10%-20% of the variability of hormone levels, Dr. Toulany said at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
“We know that this is within the normal range for individuals who are not obese, she said.

The concerns regarding efficacy in obese patients are understandable, as obesity increases the metabolic rate, increases clearance of hepatically metabolized drugs, increases circulating blood volume, and affects the absorption of contraceptive steroids through the adipose tissue, she said, adding that “it makes sense that the serum drug levels may be insufficient to maintain contraceptive effects, but the data are very limited and inconsistent.”
That’s not to say obesity isn’t a concern, added Dr. Toulany, an adolescent medicine specialist at the Hospital for Sick Children, Toronto, and the University of Toronto.
“Without fail, all of us will be seeing patients with obesity,” she said. The rate of adolescent obesity has quadrupled in the last 3 decades, increasing from 5% among those aged 12-19 years in 1980 to more than 20% now. A third are currently overweight or obese.
Further, sexually active obese women, regardless of age, are significantly less likely to use contraception, and obese teens are more likely to engage in risky sexual behaviors than are nonobese teens.
For these reasons, it is important to find the most effective contraceptive method, taking into account other risk factors and the likelihood of compliance, she said, noting that obesity is an independent risk factor for venous thromboembolism (VTE) and that studies suggest the risk is additive in users of estrogen-containing contraceptives.
However, she said, the benefits outweigh the risks of pregnancy in obesity – especially of unintended pregnancy.
The absolute risk of VTE in healthy women of reproductive age is small, and in adolescents it’s even smaller, she explained.
“The presence of risk factors for VTE should be taken into account when we see these youth in our clinics, but we can and should offer estrogen-containing contraceptives as long as there are no other risk factors,” she said.
Contraceptive options in young obese patients include:
• Intrauterine devices. There is no evidence that either copper IUDs or progestin-releasing IUDs have reduced efficacy in obese adolescents.
• Implants. These are highly effective in obese women, and even though the concentrations may be 30%-60% lower in obese women, they do remain above the contraceptive threshold for at least the first 3 years, Dr. Toulany said.
• Depot medroxyprogesterone acetate. There is some concern about weight gain with this injectable progestin-only contraceptive, particularly in those who are already obese, but it remains an option, as the levels do remain above what is needed to prevent ovulation. Interestingly, the persistence of ovulation suppression following discontinuation is different in obese women, and may be prolonged, compared with nonobese women; it is important to counsel patients about this, she said.
“So although randomized, controlled trials report no significant weight gain, we do agree with these observational studies that show that overweight and obese teens gain more weight with Depo-Provera than with oral contraceptives or with no contraceptives,” she said.
• Oral contraceptive pills. Although these may be less effective in obese adolescents, they remain an option and may be the best option in a given patient. Combined oral contraceptives are believed to be generally effective for pregnancy prevention, but “may be less forgiving of imperfect use,” and thus may not be the best choice in those who may have problems with adherence, for example.
The contraceptive patch is probably not a good option, because efficacy may be diminished as a result of absorption through the adipose tissues in those weighing more than 90 kg, Dr .Toulany said. Evidence is insufficient regarding the use of contraceptive rings in obese patients.
Bariatric surgery is increasingly being performed in adolescents, and this raises unique concerns with respect to contraception, Dr. Toulany said.
“We recommend discontinuing estrogen-containing contraceptives 1 month before surgery to reduce the risk of VTE postoperatively,” she said.
After bariatric surgery, those who undergo a restrictive procedure such as gastric banding or a gastric sleeve procedure that reduces the volume of the stomach can use oral contraceptives, but postsurgery vomiting and diarrhea could increase the risk of complications. In those who undergo surgery using a technique that involves a significant malabsorption component, such as Roux-en-Y gastric bypass, nonoral contraceptives are the best option.
“Most patients going for bariatric surgery have an IUD inserted at the time of surgery, and that’s what we would recommend,” Dr. Toulany said.
She reported having no relevant financial disclosures.
ORLANDO – The data with respect to the effects of obesity on the efficacy of contraceptives in adolescents are limited, but the general consensus is that if efficacy is reduced, it isn’t by enough to make a real difference, according to Dr. Alene Toulany.
The effect of obesity is likely to be very small, and studies that have looked at pharmacokinetics in obesity have estimated that body weight accounts for only about 10%-20% of the variability of hormone levels, Dr. Toulany said at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
“We know that this is within the normal range for individuals who are not obese, she said.
The concerns regarding efficacy in obese patients are understandable, as obesity increases the metabolic rate, increases clearance of hepatically metabolized drugs, increases circulating blood volume, and affects the absorption of contraceptive steroids through the adipose tissue, she said, adding that “it makes sense that the serum drug levels may be insufficient to maintain contraceptive effects, but the data are very limited and inconsistent.”
That’s not to say obesity isn’t a concern, added Dr. Toulany, an adolescent medicine specialist at the Hospital for Sick Children, Toronto, and the University of Toronto.
“Without fail, all of us will be seeing patients with obesity,” she said. The rate of adolescent obesity has quadrupled in the last 3 decades, increasing from 5% among those aged 12-19 years in 1980 to more than 20% now. A third are currently overweight or obese.
Further, sexually active obese women, regardless of age, are significantly less likely to use contraception, and obese teens are more likely to engage in risky sexual behaviors than are nonobese teens.
For these reasons, it is important to find the most effective contraceptive method, taking into account other risk factors and the likelihood of compliance, she said, noting that obesity is an independent risk factor for venous thromboembolism (VTE) and that studies suggest the risk is additive in users of estrogen-containing contraceptives.
However, she said, the benefits outweigh the risks of pregnancy in obesity – especially of unintended pregnancy.
The absolute risk of VTE in healthy women of reproductive age is small, and in adolescents it’s even smaller, she explained.
“The presence of risk factors for VTE should be taken into account when we see these youth in our clinics, but we can and should offer estrogen-containing contraceptives as long as there are no other risk factors,” she said.
Contraceptive options in young obese patients include:
• Intrauterine devices. There is no evidence that either copper IUDs or progestin-releasing IUDs have reduced efficacy in obese adolescents.
• Implants. These are highly effective in obese women, and even though the concentrations may be 30%-60% lower in obese women, they do remain above the contraceptive threshold for at least the first 3 years, Dr. Toulany said.
• Depot medroxyprogesterone acetate. There is some concern about weight gain with this injectable progestin-only contraceptive, particularly in those who are already obese, but it remains an option, as the levels do remain above what is needed to prevent ovulation. Interestingly, the persistence of ovulation suppression following discontinuation is different in obese women, and may be prolonged, compared with nonobese women; it is important to counsel patients about this, she said.
“So although randomized, controlled trials report no significant weight gain, we do agree with these observational studies that show that overweight and obese teens gain more weight with Depo-Provera than with oral contraceptives or with no contraceptives,” she said.
• Oral contraceptive pills. Although these may be less effective in obese adolescents, they remain an option and may be the best option in a given patient. Combined oral contraceptives are believed to be generally effective for pregnancy prevention, but “may be less forgiving of imperfect use,” and thus may not be the best choice in those who may have problems with adherence, for example.
The contraceptive patch is probably not a good option, because efficacy may be diminished as a result of absorption through the adipose tissues in those weighing more than 90 kg, Dr .Toulany said. Evidence is insufficient regarding the use of contraceptive rings in obese patients.
Bariatric surgery is increasingly being performed in adolescents, and this raises unique concerns with respect to contraception, Dr. Toulany said.
“We recommend discontinuing estrogen-containing contraceptives 1 month before surgery to reduce the risk of VTE postoperatively,” she said.
After bariatric surgery, those who undergo a restrictive procedure such as gastric banding or a gastric sleeve procedure that reduces the volume of the stomach can use oral contraceptives, but postsurgery vomiting and diarrhea could increase the risk of complications. In those who undergo surgery using a technique that involves a significant malabsorption component, such as Roux-en-Y gastric bypass, nonoral contraceptives are the best option.
“Most patients going for bariatric surgery have an IUD inserted at the time of surgery, and that’s what we would recommend,” Dr. Toulany said.
She reported having no relevant financial disclosures.
ORLANDO – The data with respect to the effects of obesity on the efficacy of contraceptives in adolescents are limited, but the general consensus is that if efficacy is reduced, it isn’t by enough to make a real difference, according to Dr. Alene Toulany.
The effect of obesity is likely to be very small, and studies that have looked at pharmacokinetics in obesity have estimated that body weight accounts for only about 10%-20% of the variability of hormone levels, Dr. Toulany said at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
“We know that this is within the normal range for individuals who are not obese, she said.
The concerns regarding efficacy in obese patients are understandable, as obesity increases the metabolic rate, increases clearance of hepatically metabolized drugs, increases circulating blood volume, and affects the absorption of contraceptive steroids through the adipose tissue, she said, adding that “it makes sense that the serum drug levels may be insufficient to maintain contraceptive effects, but the data are very limited and inconsistent.”
That’s not to say obesity isn’t a concern, added Dr. Toulany, an adolescent medicine specialist at the Hospital for Sick Children, Toronto, and the University of Toronto.
“Without fail, all of us will be seeing patients with obesity,” she said. The rate of adolescent obesity has quadrupled in the last 3 decades, increasing from 5% among those aged 12-19 years in 1980 to more than 20% now. A third are currently overweight or obese.
Further, sexually active obese women, regardless of age, are significantly less likely to use contraception, and obese teens are more likely to engage in risky sexual behaviors than are nonobese teens.
For these reasons, it is important to find the most effective contraceptive method, taking into account other risk factors and the likelihood of compliance, she said, noting that obesity is an independent risk factor for venous thromboembolism (VTE) and that studies suggest the risk is additive in users of estrogen-containing contraceptives.
However, she said, the benefits outweigh the risks of pregnancy in obesity – especially of unintended pregnancy.
The absolute risk of VTE in healthy women of reproductive age is small, and in adolescents it’s even smaller, she explained.
“The presence of risk factors for VTE should be taken into account when we see these youth in our clinics, but we can and should offer estrogen-containing contraceptives as long as there are no other risk factors,” she said.
Contraceptive options in young obese patients include:
• Intrauterine devices. There is no evidence that either copper IUDs or progestin-releasing IUDs have reduced efficacy in obese adolescents.
• Implants. These are highly effective in obese women, and even though the concentrations may be 30%-60% lower in obese women, they do remain above the contraceptive threshold for at least the first 3 years, Dr. Toulany said.
• Depot medroxyprogesterone acetate. There is some concern about weight gain with this injectable progestin-only contraceptive, particularly in those who are already obese, but it remains an option, as the levels do remain above what is needed to prevent ovulation. Interestingly, the persistence of ovulation suppression following discontinuation is different in obese women, and may be prolonged, compared with nonobese women; it is important to counsel patients about this, she said.
“So although randomized, controlled trials report no significant weight gain, we do agree with these observational studies that show that overweight and obese teens gain more weight with Depo-Provera than with oral contraceptives or with no contraceptives,” she said.
• Oral contraceptive pills. Although these may be less effective in obese adolescents, they remain an option and may be the best option in a given patient. Combined oral contraceptives are believed to be generally effective for pregnancy prevention, but “may be less forgiving of imperfect use,” and thus may not be the best choice in those who may have problems with adherence, for example.
The contraceptive patch is probably not a good option, because efficacy may be diminished as a result of absorption through the adipose tissues in those weighing more than 90 kg, Dr .Toulany said. Evidence is insufficient regarding the use of contraceptive rings in obese patients.
Bariatric surgery is increasingly being performed in adolescents, and this raises unique concerns with respect to contraception, Dr. Toulany said.
“We recommend discontinuing estrogen-containing contraceptives 1 month before surgery to reduce the risk of VTE postoperatively,” she said.
After bariatric surgery, those who undergo a restrictive procedure such as gastric banding or a gastric sleeve procedure that reduces the volume of the stomach can use oral contraceptives, but postsurgery vomiting and diarrhea could increase the risk of complications. In those who undergo surgery using a technique that involves a significant malabsorption component, such as Roux-en-Y gastric bypass, nonoral contraceptives are the best option.
“Most patients going for bariatric surgery have an IUD inserted at the time of surgery, and that’s what we would recommend,” Dr. Toulany said.
She reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM THE NASPAG ANNUAL MEETING

Allis clamp, nitrous oxide improve patient experience during IUD insertion
SAN FRANCISCO – A suitable and effective method for relieving pain among women undergoing intrauterine device insertion has eluded investigators, but the search has not been in vain.
Findings from two studies presented at the annual meeting of the American College of Obstetricians and Gynecologists may have failed to demonstrate clearcut improvements in pain management, but they did show improvement in other aspects of the patient experience.
In one randomized controlled study, use of an Allis clamp to stabilize the uterus during device placement failed to improve pain when compared with the use of a single-tooth tenaculum, but Allis clamp use was associated with a reduced risk of bleeding requiring intervention, Dr. Lee Taylor Johnson reported at the meeting.

Pain scores at the time of placement as measured using a 100-mm visual analog scale were 23.5 mm in 38 patients randomized to undergo placement using an Allis clamp, and 31.5 mm in 40 patients who underwent placement using the tenaculum. The scores at 10 minutes were 4.5 mm and 9 mm, respectively. The scores did not differ significantly between the groups.
However, the tenaculum group required more interventions to stop bleeding with pressure or cauterization (15 patients vs. 1 patient in the Allis clamp group), said Dr. Johnson, who conducted the research with colleagues at the Carilion Clinic Residency Gynecology Clinic in Roanoke, Va. She is now at the Tuba City Healthcare Corporation in Tuba City, Ariz.
Patients included in the study were at least 18 years old and were enrolled between September 2012 and November 2013. The study is the first to compare the effects of different instruments on pain during IUD placement, although multiple studies have looked at other ways to reduce pain, she noted.
“They have looked at NSAIDs, paracervical blocks, lidocaine gel, misoprostol, and nitroglycerin. In 2009 a Cochrane Database Review noted that no interventions that have been properly evaluated reduce pain during or after IUD insertion,” Dr. Johnson said.
Based on the current findings, providers should consider using an Allis clamp during IUD placement to decrease the risk of cervical bleeding following the procedure, she said.
In another study, Dr. Lauren D. Thaxton, of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, found that the use of nitrous oxide improved satisfaction with pain management.

The mean pain score among 40 women in the randomized double-blind study who were treated with 50/50 nitrous oxide and oxygen at the time of IUD insertion was 54 mm on a 100 mm visual analog scale, which was not significantly different from the mean of 55 mm in women who received only oxygen. However, satisfaction with pain management, as measured on a 5-point Likert scale, was significantly greater in the nitrous oxide group, she said.
The study included nulliparous women aged 13-45 years.
Nitrous oxide is relatively inexpensive and has few side effects, which are rapidly reversible with 100% oxygen, making it a feasible approach to improving the experience of IUD insertion for many women, according to Dr. Thaxton.
In fact, women in the study reported being willing to pay $20 to $50 out of pocket for nitrous oxide administration at the time of IUD insertion, Dr. Thaxton said.
In a video interview, she speculated that the amnestic and anxiolytic effects of nitrous oxide may play a role in the higher satisfaction scores, and that higher dosing could contribute to better pain relief.
Dr. Rameet H. Singh, also of the University of New Mexico and the principle investigator for the study, said that it only takes about 1 minute to administer 50/50 nitrous oxide and oxygen, and about 90 seconds to achieve 70/30 concentration, so the process doesn’t substantially prolong the insertion process.
Both Dr. Johnson and Dr. Thaxton reported having no financial disclosures. Dr. Singh reported receiving an honorarium for authoring an article on long-acting reversible contraception.
SAN FRANCISCO – A suitable and effective method for relieving pain among women undergoing intrauterine device insertion has eluded investigators, but the search has not been in vain.
Findings from two studies presented at the annual meeting of the American College of Obstetricians and Gynecologists may have failed to demonstrate clearcut improvements in pain management, but they did show improvement in other aspects of the patient experience.
In one randomized controlled study, use of an Allis clamp to stabilize the uterus during device placement failed to improve pain when compared with the use of a single-tooth tenaculum, but Allis clamp use was associated with a reduced risk of bleeding requiring intervention, Dr. Lee Taylor Johnson reported at the meeting.
Pain scores at the time of placement as measured using a 100-mm visual analog scale were 23.5 mm in 38 patients randomized to undergo placement using an Allis clamp, and 31.5 mm in 40 patients who underwent placement using the tenaculum. The scores at 10 minutes were 4.5 mm and 9 mm, respectively. The scores did not differ significantly between the groups.
However, the tenaculum group required more interventions to stop bleeding with pressure or cauterization (15 patients vs. 1 patient in the Allis clamp group), said Dr. Johnson, who conducted the research with colleagues at the Carilion Clinic Residency Gynecology Clinic in Roanoke, Va. She is now at the Tuba City Healthcare Corporation in Tuba City, Ariz.
Patients included in the study were at least 18 years old and were enrolled between September 2012 and November 2013. The study is the first to compare the effects of different instruments on pain during IUD placement, although multiple studies have looked at other ways to reduce pain, she noted.
“They have looked at NSAIDs, paracervical blocks, lidocaine gel, misoprostol, and nitroglycerin. In 2009 a Cochrane Database Review noted that no interventions that have been properly evaluated reduce pain during or after IUD insertion,” Dr. Johnson said.
Based on the current findings, providers should consider using an Allis clamp during IUD placement to decrease the risk of cervical bleeding following the procedure, she said.
In another study, Dr. Lauren D. Thaxton, of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, found that the use of nitrous oxide improved satisfaction with pain management.
The mean pain score among 40 women in the randomized double-blind study who were treated with 50/50 nitrous oxide and oxygen at the time of IUD insertion was 54 mm on a 100 mm visual analog scale, which was not significantly different from the mean of 55 mm in women who received only oxygen. However, satisfaction with pain management, as measured on a 5-point Likert scale, was significantly greater in the nitrous oxide group, she said.
The study included nulliparous women aged 13-45 years.
Nitrous oxide is relatively inexpensive and has few side effects, which are rapidly reversible with 100% oxygen, making it a feasible approach to improving the experience of IUD insertion for many women, according to Dr. Thaxton.
In fact, women in the study reported being willing to pay $20 to $50 out of pocket for nitrous oxide administration at the time of IUD insertion, Dr. Thaxton said.
In a video interview, she speculated that the amnestic and anxiolytic effects of nitrous oxide may play a role in the higher satisfaction scores, and that higher dosing could contribute to better pain relief.
Dr. Rameet H. Singh, also of the University of New Mexico and the principle investigator for the study, said that it only takes about 1 minute to administer 50/50 nitrous oxide and oxygen, and about 90 seconds to achieve 70/30 concentration, so the process doesn’t substantially prolong the insertion process.
Both Dr. Johnson and Dr. Thaxton reported having no financial disclosures. Dr. Singh reported receiving an honorarium for authoring an article on long-acting reversible contraception.
SAN FRANCISCO – A suitable and effective method for relieving pain among women undergoing intrauterine device insertion has eluded investigators, but the search has not been in vain.
Findings from two studies presented at the annual meeting of the American College of Obstetricians and Gynecologists may have failed to demonstrate clearcut improvements in pain management, but they did show improvement in other aspects of the patient experience.
In one randomized controlled study, use of an Allis clamp to stabilize the uterus during device placement failed to improve pain when compared with the use of a single-tooth tenaculum, but Allis clamp use was associated with a reduced risk of bleeding requiring intervention, Dr. Lee Taylor Johnson reported at the meeting.
Pain scores at the time of placement as measured using a 100-mm visual analog scale were 23.5 mm in 38 patients randomized to undergo placement using an Allis clamp, and 31.5 mm in 40 patients who underwent placement using the tenaculum. The scores at 10 minutes were 4.5 mm and 9 mm, respectively. The scores did not differ significantly between the groups.
However, the tenaculum group required more interventions to stop bleeding with pressure or cauterization (15 patients vs. 1 patient in the Allis clamp group), said Dr. Johnson, who conducted the research with colleagues at the Carilion Clinic Residency Gynecology Clinic in Roanoke, Va. She is now at the Tuba City Healthcare Corporation in Tuba City, Ariz.
Patients included in the study were at least 18 years old and were enrolled between September 2012 and November 2013. The study is the first to compare the effects of different instruments on pain during IUD placement, although multiple studies have looked at other ways to reduce pain, she noted.
“They have looked at NSAIDs, paracervical blocks, lidocaine gel, misoprostol, and nitroglycerin. In 2009 a Cochrane Database Review noted that no interventions that have been properly evaluated reduce pain during or after IUD insertion,” Dr. Johnson said.
Based on the current findings, providers should consider using an Allis clamp during IUD placement to decrease the risk of cervical bleeding following the procedure, she said.
In another study, Dr. Lauren D. Thaxton, of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, found that the use of nitrous oxide improved satisfaction with pain management.
The mean pain score among 40 women in the randomized double-blind study who were treated with 50/50 nitrous oxide and oxygen at the time of IUD insertion was 54 mm on a 100 mm visual analog scale, which was not significantly different from the mean of 55 mm in women who received only oxygen. However, satisfaction with pain management, as measured on a 5-point Likert scale, was significantly greater in the nitrous oxide group, she said.
The study included nulliparous women aged 13-45 years.
Nitrous oxide is relatively inexpensive and has few side effects, which are rapidly reversible with 100% oxygen, making it a feasible approach to improving the experience of IUD insertion for many women, according to Dr. Thaxton.
In fact, women in the study reported being willing to pay $20 to $50 out of pocket for nitrous oxide administration at the time of IUD insertion, Dr. Thaxton said.
In a video interview, she speculated that the amnestic and anxiolytic effects of nitrous oxide may play a role in the higher satisfaction scores, and that higher dosing could contribute to better pain relief.
Dr. Rameet H. Singh, also of the University of New Mexico and the principle investigator for the study, said that it only takes about 1 minute to administer 50/50 nitrous oxide and oxygen, and about 90 seconds to achieve 70/30 concentration, so the process doesn’t substantially prolong the insertion process.
Both Dr. Johnson and Dr. Thaxton reported having no financial disclosures. Dr. Singh reported receiving an honorarium for authoring an article on long-acting reversible contraception.
AT THE ACOG ANNUAL CLINICAL MEETING

FDA proposes 1-year blood donor deferral for gay and bisexual men
Men who have sex with men, and women who have sexual relations with them, will be permitted to donate blood if a year has elapsed between the last such sexual encounter and the time of donation, the Food and Drug Administration has recommended.
The agency’s draft guidance follows that of the federal Advisory Committee on Blood and Tissue Safety and Availability. In November 2014, the group voted 16-2 to support a 1-year deferral policy for these populations. Any deferral decision made at a donor site would be based on donor self-identification and self-report, the draft guidance noted. Clinicians should “use their own discretion” with regard to deferring a donation from a person who self-identifies as transgender.
The document would supplant prior guidance, issued in 1985, which recommended permanent deferral for men who have sex with men (MSM) and women who had sex with them.
Should it be adopted, the new policy “will better align the deferral period with that of other men and women at increased risk for HIV infection,” then FDA Commissioner Dr. Margaret A. Hamburg said in a press statement last December. Safety and blood surveillance measures already in place will be enough to detect any HIV-contaminated blood that might enter the donor pool, she said.
The national blood surveillance system will help the agency monitor the effect of any policy change and further ensure the continued safety of the blood supply. This, along with a donor education program, has reduced the risk of an HIV infection from donated blood to about 1/1.47 million transfusions, according to the draft document.
The proposal was based on the committee’s evidence review, during which data from a similar change in deferral status in Australia weighed in favor of the recommendations. During the 5 years before and after a change from lifetime deferral to the 1-year deferral for MSM, there was no change in the risk of HIV-contaminated blood entering the donor pool or the proportion of HIV-positive donors.
Despite being “a step in the right direction,” the proposed 1-year deferral still discriminates against MSM, according to David Stacy, government affairs director for the Human Rights Campaign, the nation’s largest lesbian, gay, bisexual, and transgender civil rights organization.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply,” he said in a press statement. “It simply cannot be justified in light of current scientific research and updated blood screening technology.”
The draft guidance is not binding. It will be published on the Federal Register, which at that time will announce the deadline for comment.
On Twitter @alz_gal
Men who have sex with men, and women who have sexual relations with them, will be permitted to donate blood if a year has elapsed between the last such sexual encounter and the time of donation, the Food and Drug Administration has recommended.
The agency’s draft guidance follows that of the federal Advisory Committee on Blood and Tissue Safety and Availability. In November 2014, the group voted 16-2 to support a 1-year deferral policy for these populations. Any deferral decision made at a donor site would be based on donor self-identification and self-report, the draft guidance noted. Clinicians should “use their own discretion” with regard to deferring a donation from a person who self-identifies as transgender.
The document would supplant prior guidance, issued in 1985, which recommended permanent deferral for men who have sex with men (MSM) and women who had sex with them.
Should it be adopted, the new policy “will better align the deferral period with that of other men and women at increased risk for HIV infection,” then FDA Commissioner Dr. Margaret A. Hamburg said in a press statement last December. Safety and blood surveillance measures already in place will be enough to detect any HIV-contaminated blood that might enter the donor pool, she said.
The national blood surveillance system will help the agency monitor the effect of any policy change and further ensure the continued safety of the blood supply. This, along with a donor education program, has reduced the risk of an HIV infection from donated blood to about 1/1.47 million transfusions, according to the draft document.
The proposal was based on the committee’s evidence review, during which data from a similar change in deferral status in Australia weighed in favor of the recommendations. During the 5 years before and after a change from lifetime deferral to the 1-year deferral for MSM, there was no change in the risk of HIV-contaminated blood entering the donor pool or the proportion of HIV-positive donors.
Despite being “a step in the right direction,” the proposed 1-year deferral still discriminates against MSM, according to David Stacy, government affairs director for the Human Rights Campaign, the nation’s largest lesbian, gay, bisexual, and transgender civil rights organization.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply,” he said in a press statement. “It simply cannot be justified in light of current scientific research and updated blood screening technology.”
The draft guidance is not binding. It will be published on the Federal Register, which at that time will announce the deadline for comment.
On Twitter @alz_gal
Men who have sex with men, and women who have sexual relations with them, will be permitted to donate blood if a year has elapsed between the last such sexual encounter and the time of donation, the Food and Drug Administration has recommended.
The agency’s draft guidance follows that of the federal Advisory Committee on Blood and Tissue Safety and Availability. In November 2014, the group voted 16-2 to support a 1-year deferral policy for these populations. Any deferral decision made at a donor site would be based on donor self-identification and self-report, the draft guidance noted. Clinicians should “use their own discretion” with regard to deferring a donation from a person who self-identifies as transgender.
The document would supplant prior guidance, issued in 1985, which recommended permanent deferral for men who have sex with men (MSM) and women who had sex with them.
Should it be adopted, the new policy “will better align the deferral period with that of other men and women at increased risk for HIV infection,” then FDA Commissioner Dr. Margaret A. Hamburg said in a press statement last December. Safety and blood surveillance measures already in place will be enough to detect any HIV-contaminated blood that might enter the donor pool, she said.
The national blood surveillance system will help the agency monitor the effect of any policy change and further ensure the continued safety of the blood supply. This, along with a donor education program, has reduced the risk of an HIV infection from donated blood to about 1/1.47 million transfusions, according to the draft document.
The proposal was based on the committee’s evidence review, during which data from a similar change in deferral status in Australia weighed in favor of the recommendations. During the 5 years before and after a change from lifetime deferral to the 1-year deferral for MSM, there was no change in the risk of HIV-contaminated blood entering the donor pool or the proportion of HIV-positive donors.
Despite being “a step in the right direction,” the proposed 1-year deferral still discriminates against MSM, according to David Stacy, government affairs director for the Human Rights Campaign, the nation’s largest lesbian, gay, bisexual, and transgender civil rights organization.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply,” he said in a press statement. “It simply cannot be justified in light of current scientific research and updated blood screening technology.”
The draft guidance is not binding. It will be published on the Federal Register, which at that time will announce the deadline for comment.
On Twitter @alz_gal
ACOG: Practice and referral patterns may affect occult uterine sarcoma risk post hysterectomy
SAN FRANCISCO – Occult uterine sarcoma occurred in less than 0.1% of more than 10,000 hysterectomies performed at a large hospital system between 2000 and 2014 for presumed benign gynecologic indications.
Of 10,083 patients who underwent such hysterectomies at University of Texas Southwestern Medical Center hospitals during the study period, 9 were found to have uterine sarcoma (overall rate of 8.9 per 10,000), including 5 with leiomyosarcoma (rate of 4.96 per 10,000) and 2 each with endometrial stromal sarcoma and uterine adenosarcoma (rate of 1.98 per 10,000 for each) Dr. Ken Yu Lin reported at the annual meeting of the American College of Obstetricians and Gynecologists.
The patients’ median age at diagnosis was 39 years, and their median body mass index was 27 kg/m2. Six had prior hormonal therapy, and three reported responding to leuprolide, including two who experienced decreased bleeding, and one who experienced uterine mass size reduction. None had a history of tamoxifen use or pelvic radiation exposure, and one had rapid uterine enlargement and was found to have leiomyosarcoma.
At a median follow-up of 48 months, one had died, one had a recurrence of endometrial stromal sarcoma, and seven were alive with no evidence of disease, Dr. Lin said.
Leiomyomas were associated with significantly larger uterine size (mean weight of 3,500 g), compared with endometrial stromal sarcoma and adenosarcoma, he noted.
Four of five patients with leiomyoma underwent a biopsy prior to surgery, and the results were normal. One underwent manual morcellation during abdominal hysterectomy because of large mass size, but power morcellation was not used in any patient.
The 0.1% frequency of uterine sarcoma in patients undergoing hysterectomy for a benign condition was lower than the frequency in previously reported studies and pooled analyses, Dr. Lin said.
The patients were women who underwent hysterectomy for benign conditions – abnormal bleeding in 78% of cases and leiomyoma in 56% of cases. Five underwent total abdominal hysterectomy, three had a total vaginal hysterectomy, and one had a supracervical hysterectomy.
Occult uterine sarcoma was defined as uterine sarcoma on pathology postoperatively in those with no preoperative suspicion of malignancy, Dr. Lin said.
Hysterectomy is one of the most common surgical procedures in the United States, and outcomes have improved thanks to minimally invasive procedures that require only small incisions.
However, small incisions lead to challenges with respect to the removal of large specimens, Dr. Lin said, adding that morcellation, which has been used to facilitate the removal of tissue in cases involving minimally invasive surgery, has come under scrutiny because of concerns about its role in the dissemination of occult gynecologic malignancies, and particularly uterine sarcoma.
Central to this discussion is the question of the prevalence of occult sarcoma in the setting of hysterectomy for benign indications, he said, noting that the prevalence of occult sarcoma in women undergoing surgery for presumed uterine fibroids has been reported to be as high as 1 in 350 by some authors.
The findings suggest that “clinical practices and regional referral patterns may impact local rates of occult uterine sarcoma and should be considered during patient counseling and when developing clinical recommendations,” Dr Lin concluded.
Dr. Lin reported having no relevant disclosures.
SAN FRANCISCO – Occult uterine sarcoma occurred in less than 0.1% of more than 10,000 hysterectomies performed at a large hospital system between 2000 and 2014 for presumed benign gynecologic indications.
Of 10,083 patients who underwent such hysterectomies at University of Texas Southwestern Medical Center hospitals during the study period, 9 were found to have uterine sarcoma (overall rate of 8.9 per 10,000), including 5 with leiomyosarcoma (rate of 4.96 per 10,000) and 2 each with endometrial stromal sarcoma and uterine adenosarcoma (rate of 1.98 per 10,000 for each) Dr. Ken Yu Lin reported at the annual meeting of the American College of Obstetricians and Gynecologists.
The patients’ median age at diagnosis was 39 years, and their median body mass index was 27 kg/m2. Six had prior hormonal therapy, and three reported responding to leuprolide, including two who experienced decreased bleeding, and one who experienced uterine mass size reduction. None had a history of tamoxifen use or pelvic radiation exposure, and one had rapid uterine enlargement and was found to have leiomyosarcoma.
At a median follow-up of 48 months, one had died, one had a recurrence of endometrial stromal sarcoma, and seven were alive with no evidence of disease, Dr. Lin said.
Leiomyomas were associated with significantly larger uterine size (mean weight of 3,500 g), compared with endometrial stromal sarcoma and adenosarcoma, he noted.
Four of five patients with leiomyoma underwent a biopsy prior to surgery, and the results were normal. One underwent manual morcellation during abdominal hysterectomy because of large mass size, but power morcellation was not used in any patient.
The 0.1% frequency of uterine sarcoma in patients undergoing hysterectomy for a benign condition was lower than the frequency in previously reported studies and pooled analyses, Dr. Lin said.
The patients were women who underwent hysterectomy for benign conditions – abnormal bleeding in 78% of cases and leiomyoma in 56% of cases. Five underwent total abdominal hysterectomy, three had a total vaginal hysterectomy, and one had a supracervical hysterectomy.
Occult uterine sarcoma was defined as uterine sarcoma on pathology postoperatively in those with no preoperative suspicion of malignancy, Dr. Lin said.
Hysterectomy is one of the most common surgical procedures in the United States, and outcomes have improved thanks to minimally invasive procedures that require only small incisions.
However, small incisions lead to challenges with respect to the removal of large specimens, Dr. Lin said, adding that morcellation, which has been used to facilitate the removal of tissue in cases involving minimally invasive surgery, has come under scrutiny because of concerns about its role in the dissemination of occult gynecologic malignancies, and particularly uterine sarcoma.
Central to this discussion is the question of the prevalence of occult sarcoma in the setting of hysterectomy for benign indications, he said, noting that the prevalence of occult sarcoma in women undergoing surgery for presumed uterine fibroids has been reported to be as high as 1 in 350 by some authors.
The findings suggest that “clinical practices and regional referral patterns may impact local rates of occult uterine sarcoma and should be considered during patient counseling and when developing clinical recommendations,” Dr Lin concluded.
Dr. Lin reported having no relevant disclosures.
SAN FRANCISCO – Occult uterine sarcoma occurred in less than 0.1% of more than 10,000 hysterectomies performed at a large hospital system between 2000 and 2014 for presumed benign gynecologic indications.
Of 10,083 patients who underwent such hysterectomies at University of Texas Southwestern Medical Center hospitals during the study period, 9 were found to have uterine sarcoma (overall rate of 8.9 per 10,000), including 5 with leiomyosarcoma (rate of 4.96 per 10,000) and 2 each with endometrial stromal sarcoma and uterine adenosarcoma (rate of 1.98 per 10,000 for each) Dr. Ken Yu Lin reported at the annual meeting of the American College of Obstetricians and Gynecologists.
The patients’ median age at diagnosis was 39 years, and their median body mass index was 27 kg/m2. Six had prior hormonal therapy, and three reported responding to leuprolide, including two who experienced decreased bleeding, and one who experienced uterine mass size reduction. None had a history of tamoxifen use or pelvic radiation exposure, and one had rapid uterine enlargement and was found to have leiomyosarcoma.
At a median follow-up of 48 months, one had died, one had a recurrence of endometrial stromal sarcoma, and seven were alive with no evidence of disease, Dr. Lin said.
Leiomyomas were associated with significantly larger uterine size (mean weight of 3,500 g), compared with endometrial stromal sarcoma and adenosarcoma, he noted.
Four of five patients with leiomyoma underwent a biopsy prior to surgery, and the results were normal. One underwent manual morcellation during abdominal hysterectomy because of large mass size, but power morcellation was not used in any patient.
The 0.1% frequency of uterine sarcoma in patients undergoing hysterectomy for a benign condition was lower than the frequency in previously reported studies and pooled analyses, Dr. Lin said.
The patients were women who underwent hysterectomy for benign conditions – abnormal bleeding in 78% of cases and leiomyoma in 56% of cases. Five underwent total abdominal hysterectomy, three had a total vaginal hysterectomy, and one had a supracervical hysterectomy.
Occult uterine sarcoma was defined as uterine sarcoma on pathology postoperatively in those with no preoperative suspicion of malignancy, Dr. Lin said.
Hysterectomy is one of the most common surgical procedures in the United States, and outcomes have improved thanks to minimally invasive procedures that require only small incisions.
However, small incisions lead to challenges with respect to the removal of large specimens, Dr. Lin said, adding that morcellation, which has been used to facilitate the removal of tissue in cases involving minimally invasive surgery, has come under scrutiny because of concerns about its role in the dissemination of occult gynecologic malignancies, and particularly uterine sarcoma.
Central to this discussion is the question of the prevalence of occult sarcoma in the setting of hysterectomy for benign indications, he said, noting that the prevalence of occult sarcoma in women undergoing surgery for presumed uterine fibroids has been reported to be as high as 1 in 350 by some authors.
The findings suggest that “clinical practices and regional referral patterns may impact local rates of occult uterine sarcoma and should be considered during patient counseling and when developing clinical recommendations,” Dr Lin concluded.
Dr. Lin reported having no relevant disclosures.
AT THE ACOG ANNUAL CLINICAL MEETING
Key clinical point: Consider local clinical practice and referral patterns when counseling patients about occult uterine sarcoma risk.
Major finding: Occult uterine sarcoma occurred in 0.1% of women undergoing hysterectomy for benign conditions.
Data source: A retrospective review of 10,083 hysterectomies.
Disclosures: Dr. Lin reported having no relevant disclosures.
Liletta intrauterine system shows high 3-year safety, efficacy
The newly approved 52-mg levonorgestrel intrauterine contraceptive (LNG20) system demonstrated safety and efficacy for 3 years for a range of women, regardless of weight or parity, according to a study of 1,750 women recently published in Contraception.
In February, the Food and Drug Administration approved the new hormonal intrauterine contraceptive system, which is now being marketed in the United States as Liletta (LNG20) by the Dublin-based pharmaceutical company Actavis and the nonprofit women’s health pharmaceutical company Medicines360. The LNG20 is a flexible, plastic T-frame measuring 32 mm × 32 mm with a release rate–controlling membrane over a reservoir containing 52 mg levonorgestrel. The system is indicated to prevent pregnancy for up to 3 years.

The newly published data include 3 years of results from the ACCESS IUS study (A Comprehensive Contraceptive Efficacy and Safety Study of an IUS). The multicenter study is ongoing and will evaluate the safety and effectiveness of the system for up to 7 years of use.
Dr. Mitchell Creinin of the University of California, Davis, and colleagues recruited 1,600 U.S. women aged 16-35 years and 151 women aged 36-45 years.
Overall, the pregnancy rate (as measured by the Pearl Index) was 0.15 (95% confidence interval, 0.02-0.55) per 100 women-years through the first year of the study. Through year 2, the Pearl Index was 0.26 (95% CI, 0.10-0.57), and 0.22 (95% CI, 0.08-0.49) through year 3. The cumulative life-table pregnancy rate was 0.55 (95% CI, 0.24-1.23) through 3 years (Contraception 2015 [doi:10.1016/j.contraception.2015.04.006]).
The researchers reported a total of six pregnancies in the study cohort, four of which were ectopic. Four of the six pregnancies occurred in parous women.
Expulsion of the device leading to discontinuation occurred in 3.5% of women (n = 62), mostly in the first year of use and more frequently among subjects who had previously given birth. Other adverse effects leading to discontinuation of use included bleeding, acne, and mood swings.
Symptomatic ovarian cysts developed in 3.4% of the cohort, though only five patients discontinued for this reason. Pelvic infection (including endometriosis) occurred in 10 women, with seven cases of pelvic inflammatory disease and three cases of endometritis.
Of the 68 women followed for fertility outcomes after discontinuing the device, 70.6% conceived spontaneously within 6 months and 86.8% within a year, with a median time to conception of 4 months.
Based on the safety and effectiveness findings, the researchers concluded that the LNG20 system meets the criteria defined by the Centers for Disease Control and Prevention and the World Health Organization for highly effective contraceptive methods.
The study, conducted exclusively in the United States, is notable because a quarter of the cohort had a body mass index of 30 or greater, with 5% of study participants having a BMI of 40 or greater; nearly 60% of the study participants were nulliparous.
It was conducted at 29 sites including public, private, and university clinics and enrolled 13.3% African American, 14.7% Hispanic, and 78.4% white subjects, in keeping with the expected racial, age, and weight characteristics of women likely to use this method of contraception, the researchers noted.
The study enrolled “a substantial number of nulliparous participants, representing 57.7% of the study efficacy population,” the researchers wrote. “This number was not a result of targeted recruitment and thus may represent the interest of nulliparous U.S. women in using highly effective contraceptives such as an IUS.”
Despite the high number of nulliparous subjects, 98.7% of placement attempts were successful.
Although IUDs have been available in the United States for decades, adoption remains low, with less than 8% of U.S. women using them as their preferred method of contraception. The new contraceptive system “will address some of the barriers that have previously limited full access to intrauterine contraceptives,” the researchers wrote.
The study was sponsored by Medicines360. The researchers reported having no financial disclosures.
The newly approved 52-mg levonorgestrel intrauterine contraceptive (LNG20) system demonstrated safety and efficacy for 3 years for a range of women, regardless of weight or parity, according to a study of 1,750 women recently published in Contraception.
In February, the Food and Drug Administration approved the new hormonal intrauterine contraceptive system, which is now being marketed in the United States as Liletta (LNG20) by the Dublin-based pharmaceutical company Actavis and the nonprofit women’s health pharmaceutical company Medicines360. The LNG20 is a flexible, plastic T-frame measuring 32 mm × 32 mm with a release rate–controlling membrane over a reservoir containing 52 mg levonorgestrel. The system is indicated to prevent pregnancy for up to 3 years.
The newly published data include 3 years of results from the ACCESS IUS study (A Comprehensive Contraceptive Efficacy and Safety Study of an IUS). The multicenter study is ongoing and will evaluate the safety and effectiveness of the system for up to 7 years of use.
Dr. Mitchell Creinin of the University of California, Davis, and colleagues recruited 1,600 U.S. women aged 16-35 years and 151 women aged 36-45 years.
Overall, the pregnancy rate (as measured by the Pearl Index) was 0.15 (95% confidence interval, 0.02-0.55) per 100 women-years through the first year of the study. Through year 2, the Pearl Index was 0.26 (95% CI, 0.10-0.57), and 0.22 (95% CI, 0.08-0.49) through year 3. The cumulative life-table pregnancy rate was 0.55 (95% CI, 0.24-1.23) through 3 years (Contraception 2015 [doi:10.1016/j.contraception.2015.04.006]).
The researchers reported a total of six pregnancies in the study cohort, four of which were ectopic. Four of the six pregnancies occurred in parous women.
Expulsion of the device leading to discontinuation occurred in 3.5% of women (n = 62), mostly in the first year of use and more frequently among subjects who had previously given birth. Other adverse effects leading to discontinuation of use included bleeding, acne, and mood swings.
Symptomatic ovarian cysts developed in 3.4% of the cohort, though only five patients discontinued for this reason. Pelvic infection (including endometriosis) occurred in 10 women, with seven cases of pelvic inflammatory disease and three cases of endometritis.
Of the 68 women followed for fertility outcomes after discontinuing the device, 70.6% conceived spontaneously within 6 months and 86.8% within a year, with a median time to conception of 4 months.
Based on the safety and effectiveness findings, the researchers concluded that the LNG20 system meets the criteria defined by the Centers for Disease Control and Prevention and the World Health Organization for highly effective contraceptive methods.
The study, conducted exclusively in the United States, is notable because a quarter of the cohort had a body mass index of 30 or greater, with 5% of study participants having a BMI of 40 or greater; nearly 60% of the study participants were nulliparous.
It was conducted at 29 sites including public, private, and university clinics and enrolled 13.3% African American, 14.7% Hispanic, and 78.4% white subjects, in keeping with the expected racial, age, and weight characteristics of women likely to use this method of contraception, the researchers noted.
The study enrolled “a substantial number of nulliparous participants, representing 57.7% of the study efficacy population,” the researchers wrote. “This number was not a result of targeted recruitment and thus may represent the interest of nulliparous U.S. women in using highly effective contraceptives such as an IUS.”
Despite the high number of nulliparous subjects, 98.7% of placement attempts were successful.
Although IUDs have been available in the United States for decades, adoption remains low, with less than 8% of U.S. women using them as their preferred method of contraception. The new contraceptive system “will address some of the barriers that have previously limited full access to intrauterine contraceptives,” the researchers wrote.
The study was sponsored by Medicines360. The researchers reported having no financial disclosures.
The newly approved 52-mg levonorgestrel intrauterine contraceptive (LNG20) system demonstrated safety and efficacy for 3 years for a range of women, regardless of weight or parity, according to a study of 1,750 women recently published in Contraception.
In February, the Food and Drug Administration approved the new hormonal intrauterine contraceptive system, which is now being marketed in the United States as Liletta (LNG20) by the Dublin-based pharmaceutical company Actavis and the nonprofit women’s health pharmaceutical company Medicines360. The LNG20 is a flexible, plastic T-frame measuring 32 mm × 32 mm with a release rate–controlling membrane over a reservoir containing 52 mg levonorgestrel. The system is indicated to prevent pregnancy for up to 3 years.
The newly published data include 3 years of results from the ACCESS IUS study (A Comprehensive Contraceptive Efficacy and Safety Study of an IUS). The multicenter study is ongoing and will evaluate the safety and effectiveness of the system for up to 7 years of use.
Dr. Mitchell Creinin of the University of California, Davis, and colleagues recruited 1,600 U.S. women aged 16-35 years and 151 women aged 36-45 years.
Overall, the pregnancy rate (as measured by the Pearl Index) was 0.15 (95% confidence interval, 0.02-0.55) per 100 women-years through the first year of the study. Through year 2, the Pearl Index was 0.26 (95% CI, 0.10-0.57), and 0.22 (95% CI, 0.08-0.49) through year 3. The cumulative life-table pregnancy rate was 0.55 (95% CI, 0.24-1.23) through 3 years (Contraception 2015 [doi:10.1016/j.contraception.2015.04.006]).
The researchers reported a total of six pregnancies in the study cohort, four of which were ectopic. Four of the six pregnancies occurred in parous women.
Expulsion of the device leading to discontinuation occurred in 3.5% of women (n = 62), mostly in the first year of use and more frequently among subjects who had previously given birth. Other adverse effects leading to discontinuation of use included bleeding, acne, and mood swings.
Symptomatic ovarian cysts developed in 3.4% of the cohort, though only five patients discontinued for this reason. Pelvic infection (including endometriosis) occurred in 10 women, with seven cases of pelvic inflammatory disease and three cases of endometritis.
Of the 68 women followed for fertility outcomes after discontinuing the device, 70.6% conceived spontaneously within 6 months and 86.8% within a year, with a median time to conception of 4 months.
Based on the safety and effectiveness findings, the researchers concluded that the LNG20 system meets the criteria defined by the Centers for Disease Control and Prevention and the World Health Organization for highly effective contraceptive methods.
The study, conducted exclusively in the United States, is notable because a quarter of the cohort had a body mass index of 30 or greater, with 5% of study participants having a BMI of 40 or greater; nearly 60% of the study participants were nulliparous.
It was conducted at 29 sites including public, private, and university clinics and enrolled 13.3% African American, 14.7% Hispanic, and 78.4% white subjects, in keeping with the expected racial, age, and weight characteristics of women likely to use this method of contraception, the researchers noted.
The study enrolled “a substantial number of nulliparous participants, representing 57.7% of the study efficacy population,” the researchers wrote. “This number was not a result of targeted recruitment and thus may represent the interest of nulliparous U.S. women in using highly effective contraceptives such as an IUS.”
Despite the high number of nulliparous subjects, 98.7% of placement attempts were successful.
Although IUDs have been available in the United States for decades, adoption remains low, with less than 8% of U.S. women using them as their preferred method of contraception. The new contraceptive system “will address some of the barriers that have previously limited full access to intrauterine contraceptives,” the researchers wrote.
The study was sponsored by Medicines360. The researchers reported having no financial disclosures.
FROM CONTRACEPTION
Key clinical point: A recently approved hormonal intrauterine system (LNG20) is highly effective and safe for up to 3 years of use in parous and nulliparous women, as well as obese women.
Major finding: The Pearl Index for LNG20 was 0.15 (95% CI, 0.02-0.55) through year 1, 0.26 (95% CI, 0.10-0.57) through year 2, and 0.22 (95% CI, 0.08-0.49) through year 3, with an expulsion rate of 3.5%. Conception occurred within 12 months in 87% of patients who discontinued to become pregnant.
Data source: Prospective efficacy and safety cohort study of 1,600 sexually active U.S. women aged 16-35 years and 151 women aged 36-45 years recruited from 29 public, private, and university centers.
Disclosures: Sponsored by Medicines 360, a nonprofit women’s health pharmaceutical company. The researchers reported having no financial disclosures.
ACOG: Few physicians follow IUD placement recommendations
SAN FRANCISCO – Few physicians in a recent survey regarding levonorgestrel intrauterine device placement follow the manufacturer’s placement instructions provided on the product insert.
Only 7.5% of 132 respondents said they always perform every recommended placement technique, Dr. Todd R. Jenkins of the University of Alabama at Birmingham (UAB), reported at the annual meeting of the American College of Obstetricians and Gynecologists.
During a brief introduction of the study, Dr. Jenkins, who presented the findings on behalf of his colleague and lead investigator, Dr. Sabrina N. Wyatt, also of UAB, explained that the study was initiated as a result of a system-wide standardization effort.
“We tried to standardize all our residents’ and faculty members’ intrauterine device insertion technique and placement. That resulted in quite the debacle and debate,” he said, adding that a subsequent search of the literature revealed that “there are no studies on the best ways to place an IUD.”
A proposal to conduct a study to determine the best approach to IUD placement was denied by the university’s institutional review board, which deemed such a study unethical because the product insert provides detailed placement instructions.

“So therefore, we decided to survey obstetrician-gynecologists to see how many people actually follow those guidelines,” Dr. Jenkins said.
Members of the Society for Academic Specialists in General Obstetrics and Gynecology and directors of Ryan Residency Training Program were invited to participate. Respondents practiced throughout the United States, and their length of experience ranged from 0-5 years to 21 years or more. Most respondents (81%) were women.
The respondents were divided with respect to premedication of women undergoing IUD placement, with 67% saying they rarely or never premedicate patients, and 33% reporting that they always or frequently premedicate.
Tenaculum use and use of uterine sound for cavity depth were recommended steps eliminated by 30% and 20% of respondents, respectively. Further, 64% of respondents reported eliminating the step of changing from non-sterile to sterile gloves prior to device handling. Few respondents used ultrasound in any capacity, including during, immediately after, or at a later date; 98% said they rarely or never used ultrasound.
No significant relationships were found between the number of years in practice and any of the responses, but there was a significant relationship between practice region and changing into sterile gloves prior to device handling, and having the patient return to the clinic for a string check, the investigators said.
For example, about 70% of those practicing in the Southeast reported changing into sterile gloves, compared with about 20% of those practicing in the Northeast. And about 80% of those practicing in the Midwest reported having patients return for a string check, compared with about 25% of those in the West.
Long-acting reversible contraception (LARC) methods, such as the levonorgestrel IUD, have higher continuation and efficacy rates than do other reversible methods, but barriers to use remain, including cost, patient anticipation of discomfort, and concern for complications, the investigators explained.
Prior studies have demonstrated that variations in practice exist, they said, noting that it is possible that variations and/or reductions in instrumentation could result in decreased discomfort for patients, as well as in decreased time and cost – all of which could increase LARC uptake.
“Our survey confirmed that variations in practice patterns exist among obstetrician-gynecologists in the United States. While some of these variations may be attributed to not practicing in an evidence-based fashion, other variations exist in the absence of evidence,” they wrote, noting that further investigation to determine best practices among these variations is warranted.
Based on the findings of the current study, the UAB’s institutional review board has relented and agreed to allow studies comparing different practice patterns to help determine the most effective and comfortable experience for patients, Dr. Jenkins said.
The researchers reported having no financial disclosures.
SAN FRANCISCO – Few physicians in a recent survey regarding levonorgestrel intrauterine device placement follow the manufacturer’s placement instructions provided on the product insert.
Only 7.5% of 132 respondents said they always perform every recommended placement technique, Dr. Todd R. Jenkins of the University of Alabama at Birmingham (UAB), reported at the annual meeting of the American College of Obstetricians and Gynecologists.
During a brief introduction of the study, Dr. Jenkins, who presented the findings on behalf of his colleague and lead investigator, Dr. Sabrina N. Wyatt, also of UAB, explained that the study was initiated as a result of a system-wide standardization effort.
“We tried to standardize all our residents’ and faculty members’ intrauterine device insertion technique and placement. That resulted in quite the debacle and debate,” he said, adding that a subsequent search of the literature revealed that “there are no studies on the best ways to place an IUD.”
A proposal to conduct a study to determine the best approach to IUD placement was denied by the university’s institutional review board, which deemed such a study unethical because the product insert provides detailed placement instructions.
“So therefore, we decided to survey obstetrician-gynecologists to see how many people actually follow those guidelines,” Dr. Jenkins said.
Members of the Society for Academic Specialists in General Obstetrics and Gynecology and directors of Ryan Residency Training Program were invited to participate. Respondents practiced throughout the United States, and their length of experience ranged from 0-5 years to 21 years or more. Most respondents (81%) were women.
The respondents were divided with respect to premedication of women undergoing IUD placement, with 67% saying they rarely or never premedicate patients, and 33% reporting that they always or frequently premedicate.
Tenaculum use and use of uterine sound for cavity depth were recommended steps eliminated by 30% and 20% of respondents, respectively. Further, 64% of respondents reported eliminating the step of changing from non-sterile to sterile gloves prior to device handling. Few respondents used ultrasound in any capacity, including during, immediately after, or at a later date; 98% said they rarely or never used ultrasound.
No significant relationships were found between the number of years in practice and any of the responses, but there was a significant relationship between practice region and changing into sterile gloves prior to device handling, and having the patient return to the clinic for a string check, the investigators said.
For example, about 70% of those practicing in the Southeast reported changing into sterile gloves, compared with about 20% of those practicing in the Northeast. And about 80% of those practicing in the Midwest reported having patients return for a string check, compared with about 25% of those in the West.
Long-acting reversible contraception (LARC) methods, such as the levonorgestrel IUD, have higher continuation and efficacy rates than do other reversible methods, but barriers to use remain, including cost, patient anticipation of discomfort, and concern for complications, the investigators explained.
Prior studies have demonstrated that variations in practice exist, they said, noting that it is possible that variations and/or reductions in instrumentation could result in decreased discomfort for patients, as well as in decreased time and cost – all of which could increase LARC uptake.
“Our survey confirmed that variations in practice patterns exist among obstetrician-gynecologists in the United States. While some of these variations may be attributed to not practicing in an evidence-based fashion, other variations exist in the absence of evidence,” they wrote, noting that further investigation to determine best practices among these variations is warranted.
Based on the findings of the current study, the UAB’s institutional review board has relented and agreed to allow studies comparing different practice patterns to help determine the most effective and comfortable experience for patients, Dr. Jenkins said.
The researchers reported having no financial disclosures.
SAN FRANCISCO – Few physicians in a recent survey regarding levonorgestrel intrauterine device placement follow the manufacturer’s placement instructions provided on the product insert.
Only 7.5% of 132 respondents said they always perform every recommended placement technique, Dr. Todd R. Jenkins of the University of Alabama at Birmingham (UAB), reported at the annual meeting of the American College of Obstetricians and Gynecologists.
During a brief introduction of the study, Dr. Jenkins, who presented the findings on behalf of his colleague and lead investigator, Dr. Sabrina N. Wyatt, also of UAB, explained that the study was initiated as a result of a system-wide standardization effort.
“We tried to standardize all our residents’ and faculty members’ intrauterine device insertion technique and placement. That resulted in quite the debacle and debate,” he said, adding that a subsequent search of the literature revealed that “there are no studies on the best ways to place an IUD.”
A proposal to conduct a study to determine the best approach to IUD placement was denied by the university’s institutional review board, which deemed such a study unethical because the product insert provides detailed placement instructions.
“So therefore, we decided to survey obstetrician-gynecologists to see how many people actually follow those guidelines,” Dr. Jenkins said.
Members of the Society for Academic Specialists in General Obstetrics and Gynecology and directors of Ryan Residency Training Program were invited to participate. Respondents practiced throughout the United States, and their length of experience ranged from 0-5 years to 21 years or more. Most respondents (81%) were women.
The respondents were divided with respect to premedication of women undergoing IUD placement, with 67% saying they rarely or never premedicate patients, and 33% reporting that they always or frequently premedicate.
Tenaculum use and use of uterine sound for cavity depth were recommended steps eliminated by 30% and 20% of respondents, respectively. Further, 64% of respondents reported eliminating the step of changing from non-sterile to sterile gloves prior to device handling. Few respondents used ultrasound in any capacity, including during, immediately after, or at a later date; 98% said they rarely or never used ultrasound.
No significant relationships were found between the number of years in practice and any of the responses, but there was a significant relationship between practice region and changing into sterile gloves prior to device handling, and having the patient return to the clinic for a string check, the investigators said.
For example, about 70% of those practicing in the Southeast reported changing into sterile gloves, compared with about 20% of those practicing in the Northeast. And about 80% of those practicing in the Midwest reported having patients return for a string check, compared with about 25% of those in the West.
Long-acting reversible contraception (LARC) methods, such as the levonorgestrel IUD, have higher continuation and efficacy rates than do other reversible methods, but barriers to use remain, including cost, patient anticipation of discomfort, and concern for complications, the investigators explained.
Prior studies have demonstrated that variations in practice exist, they said, noting that it is possible that variations and/or reductions in instrumentation could result in decreased discomfort for patients, as well as in decreased time and cost – all of which could increase LARC uptake.
“Our survey confirmed that variations in practice patterns exist among obstetrician-gynecologists in the United States. While some of these variations may be attributed to not practicing in an evidence-based fashion, other variations exist in the absence of evidence,” they wrote, noting that further investigation to determine best practices among these variations is warranted.
Based on the findings of the current study, the UAB’s institutional review board has relented and agreed to allow studies comparing different practice patterns to help determine the most effective and comfortable experience for patients, Dr. Jenkins said.
The researchers reported having no financial disclosures.
AT THE ACOG ANNUAL CLINICAL MEETING
Key clinical point: In the absence of data on the best approach to IUD placement, practice patterns vary widely.
Major finding: Only 7.5% of respondents said they always perform every recommended placement technique,
Data source: A survey of 132 physicians.
Disclosures: The researchers reported having no financial disclosures.

Viral illness often precedes genital aphthous ulcers in adolescents
ORLANDO – Infectious processes, such as those associated with vulvar abscesses and aphthous ulcers, are among the more common culprits in young patients who present to the emergency department with pelvic pain, according to Dr. Heather Appelbaum.
Vulvar abscesses should be distinguished from Bartholin’s gland abscesses and cysts (which tend to occur more medially) and should be treated to cover for methicillin-resistant Staphylococcus aureus; Bactrim and clindamycin are good choices, Dr. Appelbaum, director of the division of pediatric and adolescent gynecology at Long Island Jewish Medical Center, New Hyde Park, N.Y., said during a workshop on pediatric gynecologic emergencies at the annual meeting of the North American Society for Pediatric and Adolescent Gynecology.
Similarly, aphthous ulcers of the vulva should not be confused with herpes. These ulcers are deep, with irregular borders. They usually occur in non–sexually active individuals and are exquisitely tender, she said.
They look different than herpes and have “a totally different history associated with them,” she said, adding that even in girls who don’t seem to be giving an honest history, keep in mind that aphthous ulcers don’t look anything like herpes.
Aphthous ulcers are usually associated with a viral syndrome. A good history will typically reveal a preceding viral-type illness or sore throat. Parvovirus, Epstein-Barr virus, and cytomegalovirus all can be associated with aphthous ulcers, but in most cases the virus is unknown.
“In any case, recognizing this is very important, and for a primary lesion like this, it is important to look for ulcers in other locations,” she said.
Ulcers in the mouth, for example, also can be associated with a viral syndrome, but could be a sign of Behçet’s disease, Crohn’s disease, or some other autoimmune disorder, especially if the ulcers are recurrent, she noted.
Treatment for aphthous ulcers of the vulva is generally supportive. The lesions can weep and become necrotic. They often are associated with a lot of discharge and are purulent.
“They scare mom, they scare the kid, and they scare the clinician, but they really just need to be treated with supportive therapy, because they generally go away in 7-10 days,” Dr Appelbaum said, adding that because the lesions are exquisitely tender, she recommends that patients sit in a warm bath multiple times daily.
Warm baths are really the most soothing thing for these patients, she added, noting that topical lidocaine can be used, but sometimes it burns and doesn’t help much.
“But Percocet does, Tylenol does, and sitting in that warm bath frequently really does. And a lot of hand holding of parents is obviously essential. But it does go away and it resolves without any structural defect or, typically, any long-term sequelae or recurrence,” she said.
The characteristics of genital ulcers were further explored in an unrelated study presented in a poster at the meeting. Dr. Amy Sass and her colleagues from the University of Colorado and Children’s Hospital Colorado, Aurora, reviewed a series of 110 cases of acute genital ulcers (AGUs) in adolescents presenting between March 2002 and August 2014.
None tested positive for bacterial infection, herpes simplex virus, or cytomegalovirus, and six were positive for Epstein-Barr virus (EBV). An additional 18 had a past EBV infection; 34 tested negative for EBV.
Symptoms included vulvar pain and painful urination in all patients, fever in 89%, pharyngitis in 67%, cough in 63%, and headache in 57%.
Nine patients experienced one recurrence, nine had two recurrences, two had three recurrences, and one had five recurrences; 73% of the 38 recurrences occurred in the setting of viral illness, and 27% occurred in the setting of physical exhaustion or emotional stress. The timing of recurrence ranged from 2 weeks to 7 years after the initial episode.
Case patients had a mean age of 13.6 years, and 48% were postmenarcheal, 29% were premenarcheal, and menarcheal status was unknown in 33%. The vast majority (99%) were not sexually active, 36% had a history of oral aphthous ulcers, and 10 had concurrent oral aphthous ulcers at the time of diagnosis.
The mean number of days before AGU onset following prodromal illness was 3 days, and the mean number of days to AGU resolution was 13 days.
Treatment was most often oral NSAIDS, topical lidocaine jelly or lidocaine-epinephrine-tetracaine gel, and sitz baths.
“Acute genital ulcers in sexually inexperienced adolescent are painful and distressing,”the investigators wrote, noting that the differential diagnosis for AGUs includes sexually transmitted infections, autoimmune disease, genital manifestations of systemic illness, and drug reactions.
“Unfortunately, a causative etiology is often not identified, they added.
The investigators designed the study to shed some light on AGUs, as the available literature is limited, and many providers may not be familiar with the evaluation and management of patients with AGUs, they said.
The findings demonstrate that AGUs occur most often in postmenarcheal adolescents vs. premenarcheal adolescents. Most cases in this series were preceded by 3 days of febrile viral illness and were associated with elevated inflammatory markers. Only six had an infectious etiology identified, and those patients had acute mononucleosis infection.
Of note, two patients developed complications of labial fusion during healing requiring surgical separation.
A third had a past history of oral aphthous ulcers, and 10 had concurrent oral aphthous ulcers, suggesting a diagnosis of complex aphthosis, they said.
Recurrences most often occurred in the setting of febrile viral illness, physical exhaustion, or emotional stress.
The authors reported having no relevant financial disclosures.
ORLANDO – Infectious processes, such as those associated with vulvar abscesses and aphthous ulcers, are among the more common culprits in young patients who present to the emergency department with pelvic pain, according to Dr. Heather Appelbaum.
Vulvar abscesses should be distinguished from Bartholin’s gland abscesses and cysts (which tend to occur more medially) and should be treated to cover for methicillin-resistant Staphylococcus aureus; Bactrim and clindamycin are good choices, Dr. Appelbaum, director of the division of pediatric and adolescent gynecology at Long Island Jewish Medical Center, New Hyde Park, N.Y., said during a workshop on pediatric gynecologic emergencies at the annual meeting of the North American Society for Pediatric and Adolescent Gynecology.
Similarly, aphthous ulcers of the vulva should not be confused with herpes. These ulcers are deep, with irregular borders. They usually occur in non–sexually active individuals and are exquisitely tender, she said.
They look different than herpes and have “a totally different history associated with them,” she said, adding that even in girls who don’t seem to be giving an honest history, keep in mind that aphthous ulcers don’t look anything like herpes.
Aphthous ulcers are usually associated with a viral syndrome. A good history will typically reveal a preceding viral-type illness or sore throat. Parvovirus, Epstein-Barr virus, and cytomegalovirus all can be associated with aphthous ulcers, but in most cases the virus is unknown.
“In any case, recognizing this is very important, and for a primary lesion like this, it is important to look for ulcers in other locations,” she said.
Ulcers in the mouth, for example, also can be associated with a viral syndrome, but could be a sign of Behçet’s disease, Crohn’s disease, or some other autoimmune disorder, especially if the ulcers are recurrent, she noted.
Treatment for aphthous ulcers of the vulva is generally supportive. The lesions can weep and become necrotic. They often are associated with a lot of discharge and are purulent.
“They scare mom, they scare the kid, and they scare the clinician, but they really just need to be treated with supportive therapy, because they generally go away in 7-10 days,” Dr Appelbaum said, adding that because the lesions are exquisitely tender, she recommends that patients sit in a warm bath multiple times daily.
Warm baths are really the most soothing thing for these patients, she added, noting that topical lidocaine can be used, but sometimes it burns and doesn’t help much.
“But Percocet does, Tylenol does, and sitting in that warm bath frequently really does. And a lot of hand holding of parents is obviously essential. But it does go away and it resolves without any structural defect or, typically, any long-term sequelae or recurrence,” she said.
The characteristics of genital ulcers were further explored in an unrelated study presented in a poster at the meeting. Dr. Amy Sass and her colleagues from the University of Colorado and Children’s Hospital Colorado, Aurora, reviewed a series of 110 cases of acute genital ulcers (AGUs) in adolescents presenting between March 2002 and August 2014.
None tested positive for bacterial infection, herpes simplex virus, or cytomegalovirus, and six were positive for Epstein-Barr virus (EBV). An additional 18 had a past EBV infection; 34 tested negative for EBV.
Symptoms included vulvar pain and painful urination in all patients, fever in 89%, pharyngitis in 67%, cough in 63%, and headache in 57%.
Nine patients experienced one recurrence, nine had two recurrences, two had three recurrences, and one had five recurrences; 73% of the 38 recurrences occurred in the setting of viral illness, and 27% occurred in the setting of physical exhaustion or emotional stress. The timing of recurrence ranged from 2 weeks to 7 years after the initial episode.
Case patients had a mean age of 13.6 years, and 48% were postmenarcheal, 29% were premenarcheal, and menarcheal status was unknown in 33%. The vast majority (99%) were not sexually active, 36% had a history of oral aphthous ulcers, and 10 had concurrent oral aphthous ulcers at the time of diagnosis.
The mean number of days before AGU onset following prodromal illness was 3 days, and the mean number of days to AGU resolution was 13 days.
Treatment was most often oral NSAIDS, topical lidocaine jelly or lidocaine-epinephrine-tetracaine gel, and sitz baths.
“Acute genital ulcers in sexually inexperienced adolescent are painful and distressing,”the investigators wrote, noting that the differential diagnosis for AGUs includes sexually transmitted infections, autoimmune disease, genital manifestations of systemic illness, and drug reactions.
“Unfortunately, a causative etiology is often not identified, they added.
The investigators designed the study to shed some light on AGUs, as the available literature is limited, and many providers may not be familiar with the evaluation and management of patients with AGUs, they said.
The findings demonstrate that AGUs occur most often in postmenarcheal adolescents vs. premenarcheal adolescents. Most cases in this series were preceded by 3 days of febrile viral illness and were associated with elevated inflammatory markers. Only six had an infectious etiology identified, and those patients had acute mononucleosis infection.
Of note, two patients developed complications of labial fusion during healing requiring surgical separation.
A third had a past history of oral aphthous ulcers, and 10 had concurrent oral aphthous ulcers, suggesting a diagnosis of complex aphthosis, they said.
Recurrences most often occurred in the setting of febrile viral illness, physical exhaustion, or emotional stress.
The authors reported having no relevant financial disclosures.
ORLANDO – Infectious processes, such as those associated with vulvar abscesses and aphthous ulcers, are among the more common culprits in young patients who present to the emergency department with pelvic pain, according to Dr. Heather Appelbaum.
Vulvar abscesses should be distinguished from Bartholin’s gland abscesses and cysts (which tend to occur more medially) and should be treated to cover for methicillin-resistant Staphylococcus aureus; Bactrim and clindamycin are good choices, Dr. Appelbaum, director of the division of pediatric and adolescent gynecology at Long Island Jewish Medical Center, New Hyde Park, N.Y., said during a workshop on pediatric gynecologic emergencies at the annual meeting of the North American Society for Pediatric and Adolescent Gynecology.
Similarly, aphthous ulcers of the vulva should not be confused with herpes. These ulcers are deep, with irregular borders. They usually occur in non–sexually active individuals and are exquisitely tender, she said.
They look different than herpes and have “a totally different history associated with them,” she said, adding that even in girls who don’t seem to be giving an honest history, keep in mind that aphthous ulcers don’t look anything like herpes.
Aphthous ulcers are usually associated with a viral syndrome. A good history will typically reveal a preceding viral-type illness or sore throat. Parvovirus, Epstein-Barr virus, and cytomegalovirus all can be associated with aphthous ulcers, but in most cases the virus is unknown.
“In any case, recognizing this is very important, and for a primary lesion like this, it is important to look for ulcers in other locations,” she said.
Ulcers in the mouth, for example, also can be associated with a viral syndrome, but could be a sign of Behçet’s disease, Crohn’s disease, or some other autoimmune disorder, especially if the ulcers are recurrent, she noted.
Treatment for aphthous ulcers of the vulva is generally supportive. The lesions can weep and become necrotic. They often are associated with a lot of discharge and are purulent.
“They scare mom, they scare the kid, and they scare the clinician, but they really just need to be treated with supportive therapy, because they generally go away in 7-10 days,” Dr Appelbaum said, adding that because the lesions are exquisitely tender, she recommends that patients sit in a warm bath multiple times daily.
Warm baths are really the most soothing thing for these patients, she added, noting that topical lidocaine can be used, but sometimes it burns and doesn’t help much.
“But Percocet does, Tylenol does, and sitting in that warm bath frequently really does. And a lot of hand holding of parents is obviously essential. But it does go away and it resolves without any structural defect or, typically, any long-term sequelae or recurrence,” she said.
The characteristics of genital ulcers were further explored in an unrelated study presented in a poster at the meeting. Dr. Amy Sass and her colleagues from the University of Colorado and Children’s Hospital Colorado, Aurora, reviewed a series of 110 cases of acute genital ulcers (AGUs) in adolescents presenting between March 2002 and August 2014.
None tested positive for bacterial infection, herpes simplex virus, or cytomegalovirus, and six were positive for Epstein-Barr virus (EBV). An additional 18 had a past EBV infection; 34 tested negative for EBV.
Symptoms included vulvar pain and painful urination in all patients, fever in 89%, pharyngitis in 67%, cough in 63%, and headache in 57%.
Nine patients experienced one recurrence, nine had two recurrences, two had three recurrences, and one had five recurrences; 73% of the 38 recurrences occurred in the setting of viral illness, and 27% occurred in the setting of physical exhaustion or emotional stress. The timing of recurrence ranged from 2 weeks to 7 years after the initial episode.
Case patients had a mean age of 13.6 years, and 48% were postmenarcheal, 29% were premenarcheal, and menarcheal status was unknown in 33%. The vast majority (99%) were not sexually active, 36% had a history of oral aphthous ulcers, and 10 had concurrent oral aphthous ulcers at the time of diagnosis.
The mean number of days before AGU onset following prodromal illness was 3 days, and the mean number of days to AGU resolution was 13 days.
Treatment was most often oral NSAIDS, topical lidocaine jelly or lidocaine-epinephrine-tetracaine gel, and sitz baths.
“Acute genital ulcers in sexually inexperienced adolescent are painful and distressing,”the investigators wrote, noting that the differential diagnosis for AGUs includes sexually transmitted infections, autoimmune disease, genital manifestations of systemic illness, and drug reactions.
“Unfortunately, a causative etiology is often not identified, they added.
The investigators designed the study to shed some light on AGUs, as the available literature is limited, and many providers may not be familiar with the evaluation and management of patients with AGUs, they said.
The findings demonstrate that AGUs occur most often in postmenarcheal adolescents vs. premenarcheal adolescents. Most cases in this series were preceded by 3 days of febrile viral illness and were associated with elevated inflammatory markers. Only six had an infectious etiology identified, and those patients had acute mononucleosis infection.
Of note, two patients developed complications of labial fusion during healing requiring surgical separation.
A third had a past history of oral aphthous ulcers, and 10 had concurrent oral aphthous ulcers, suggesting a diagnosis of complex aphthosis, they said.
Recurrences most often occurred in the setting of febrile viral illness, physical exhaustion, or emotional stress.
The authors reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM THE NASPAG ANNUAL MEETING
VIDEO: Nitrous oxide for IUD insertion improves patient satisfaction
SAN FRANCISCO – Intrauterine device insertion can be a painful experience, especially for nulliparous women, but the quest for an intervention to reduce pain has yielded disappointing results.
A new study, however, suggests that nitrous oxide improves women’s satisfaction with respect to pain management during the procedure.
In a video interview at the annual meeting of the American College of Obstetricians and Gynecologists, Dr. Lauren D. Thaxton of the University of New Mexico, Albuquerque, discusses the results of her randomized, controlled, double-blind trial comparing nitrous oxide and oxygen with oxygen alone in 80 women aged 13-45 years. Women receiving nitrous oxide didn’t have lower visual analog scale pain scores than those receiving oxygen, but did report significantly greater satisfaction with pain management, she said.
Dr. Thaxton reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN FRANCISCO – Intrauterine device insertion can be a painful experience, especially for nulliparous women, but the quest for an intervention to reduce pain has yielded disappointing results.
A new study, however, suggests that nitrous oxide improves women’s satisfaction with respect to pain management during the procedure.
In a video interview at the annual meeting of the American College of Obstetricians and Gynecologists, Dr. Lauren D. Thaxton of the University of New Mexico, Albuquerque, discusses the results of her randomized, controlled, double-blind trial comparing nitrous oxide and oxygen with oxygen alone in 80 women aged 13-45 years. Women receiving nitrous oxide didn’t have lower visual analog scale pain scores than those receiving oxygen, but did report significantly greater satisfaction with pain management, she said.
Dr. Thaxton reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN FRANCISCO – Intrauterine device insertion can be a painful experience, especially for nulliparous women, but the quest for an intervention to reduce pain has yielded disappointing results.
A new study, however, suggests that nitrous oxide improves women’s satisfaction with respect to pain management during the procedure.
In a video interview at the annual meeting of the American College of Obstetricians and Gynecologists, Dr. Lauren D. Thaxton of the University of New Mexico, Albuquerque, discusses the results of her randomized, controlled, double-blind trial comparing nitrous oxide and oxygen with oxygen alone in 80 women aged 13-45 years. Women receiving nitrous oxide didn’t have lower visual analog scale pain scores than those receiving oxygen, but did report significantly greater satisfaction with pain management, she said.
Dr. Thaxton reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ACOG ANNUAL CLINICAL MEETING
