User login
VIDEO: Updating the rule of threes for melanoma gene testing
ORLANDO – The rule of threes that has been used to identify patients at risk of hereditary melanoma who may be candidates for genetic testing may be modified soon, according to Sancy Leachman, MD, PhD, professor and chair of the department of dermatology, Oregon Health and Science University, Portland.
Dr. Leachman was the author of a 2009 study that listed three factors as criteria for identifying melanoma: a personal history of at least three invasive melanomas, a combination of at least three melanomas in the individual and in first-degree and second-degree blood relatives – or, in first- or second-degree relatives, a total of at least three diagnoses of melanoma or pancreatic cancer or astrocytoma, which also have been associated with a known susceptibility gene, p16 (J Am Acad Dermatol. 2009 Oct;61[4]:677.e1-14).
But with more genetic testing, it is becoming clear that there are other cancers associated with an increased risk of hereditary melanoma, she explained in a video interview at the annual meeting of the American Academy of Dermatology. “The genes are a little bit different, but if you could identify those patients, you could potentially then screen them for those other cancers,” said Dr. Leachman, who is also director of the melanoma research program at Knight Cancer Institute at OHSU.
In the interview, she discussed a soon-to-be-published literature review that builds upon the rule of threes and suggests a strategy for deciding which patients should be considered for genetic testing, and includes “a suggested list of genes” that should be used in these different subsets of patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Leachman had no relevant disclosures.
ORLANDO – The rule of threes that has been used to identify patients at risk of hereditary melanoma who may be candidates for genetic testing may be modified soon, according to Sancy Leachman, MD, PhD, professor and chair of the department of dermatology, Oregon Health and Science University, Portland.
Dr. Leachman was the author of a 2009 study that listed three factors as criteria for identifying melanoma: a personal history of at least three invasive melanomas, a combination of at least three melanomas in the individual and in first-degree and second-degree blood relatives – or, in first- or second-degree relatives, a total of at least three diagnoses of melanoma or pancreatic cancer or astrocytoma, which also have been associated with a known susceptibility gene, p16 (J Am Acad Dermatol. 2009 Oct;61[4]:677.e1-14).
But with more genetic testing, it is becoming clear that there are other cancers associated with an increased risk of hereditary melanoma, she explained in a video interview at the annual meeting of the American Academy of Dermatology. “The genes are a little bit different, but if you could identify those patients, you could potentially then screen them for those other cancers,” said Dr. Leachman, who is also director of the melanoma research program at Knight Cancer Institute at OHSU.
In the interview, she discussed a soon-to-be-published literature review that builds upon the rule of threes and suggests a strategy for deciding which patients should be considered for genetic testing, and includes “a suggested list of genes” that should be used in these different subsets of patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Leachman had no relevant disclosures.
ORLANDO – The rule of threes that has been used to identify patients at risk of hereditary melanoma who may be candidates for genetic testing may be modified soon, according to Sancy Leachman, MD, PhD, professor and chair of the department of dermatology, Oregon Health and Science University, Portland.
Dr. Leachman was the author of a 2009 study that listed three factors as criteria for identifying melanoma: a personal history of at least three invasive melanomas, a combination of at least three melanomas in the individual and in first-degree and second-degree blood relatives – or, in first- or second-degree relatives, a total of at least three diagnoses of melanoma or pancreatic cancer or astrocytoma, which also have been associated with a known susceptibility gene, p16 (J Am Acad Dermatol. 2009 Oct;61[4]:677.e1-14).
But with more genetic testing, it is becoming clear that there are other cancers associated with an increased risk of hereditary melanoma, she explained in a video interview at the annual meeting of the American Academy of Dermatology. “The genes are a little bit different, but if you could identify those patients, you could potentially then screen them for those other cancers,” said Dr. Leachman, who is also director of the melanoma research program at Knight Cancer Institute at OHSU.
In the interview, she discussed a soon-to-be-published literature review that builds upon the rule of threes and suggests a strategy for deciding which patients should be considered for genetic testing, and includes “a suggested list of genes” that should be used in these different subsets of patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Leachman had no relevant disclosures.
AT AAD 17

Connective tissue diseases reported in patients receiving immune checkpoint inhibitors
For the first time, new-onset connective tissue disease has been reported in patients who were treated with anti-PD1/PDL-1 agents, according to findings published in the Annals of the Rheumatic Diseases.
In a cohort of 447 cancer patients who received therapy with immune checkpoint inhibitors (ICIs), Sébastien Le Burel, MD, of the Bicêtre Hospital in Le Kremlin-Bicêtre, France, and his colleagues described four patients who developed a connective tissue disease (CTD). There were two cases of Sjögren’s syndrome in patients taking an anti–programmed cell death 1 (anti-PD1) drug, one case of cryoglobulinemic vasculitis as a complication of suspected Sjögren’s syndrome in a patient taking an anti–programmed cell death ligand 1 (PDL-1) agent, and a case of a patient with antinuclear antibody positive myositis who was taking an anti-PDL-1 drug (Ann Rheum Dis. 2017 Feb 27. doi: 10.1136/annrheumdis-2016-210820).
“While the onset of systemic autoimmune disease after ICI treatment remains uncommon, greater awareness of these conditions should enable physicians to provide more effective patient care,” the investigators wrote. “This underlines the need for close collaboration within a network of oncologists and other specialist physicians in the new era of immunotherapy.”
The investigators discovered the cases by screening the French prospective, multicenter, academic REISAMIC registry for reports of CTD among patients being treated with anti-PD1 or anti-PDL-1 agents.
All four of the patients who developed a CTD had metastatic cancer, and their mean age was 62 years. Two patients had been treated with anti-PD1 agents and two with anti-PDL-1 agents. None of the four patients had presented with symptoms of CTD before they began treatment.
The mean time interval between the first treatment dose and the first symptom of CTD was 60 days (range, 24-72), and the mean time interval between the first symptom and subsequent diagnosis of CTD was 40 days (range, 10-74).
Three patients discontinued the ICI agent, and two patients were treated with steroids (1 mg/kg/day).
The estimated prevalence of CTD was 0.7% in the REISAMIC registry, and the authors emphasize that the high proportion of cases of Sjögren’s syndrome is noteworthy, with two of the patients fulfilling the recent American College of Rheumatology/European League Against Rheumatism criteria for Sjögren’s syndrome.
A limitation of the study is that some patients presenting with milder symptoms might not have been investigated by their oncologist.
The findings raise the question of whether asymptomatic patients taking ICIs who are at risk for immune-related adverse events should be screened and monitored closely, the authors explained.
One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
For the first time, new-onset connective tissue disease has been reported in patients who were treated with anti-PD1/PDL-1 agents, according to findings published in the Annals of the Rheumatic Diseases.
In a cohort of 447 cancer patients who received therapy with immune checkpoint inhibitors (ICIs), Sébastien Le Burel, MD, of the Bicêtre Hospital in Le Kremlin-Bicêtre, France, and his colleagues described four patients who developed a connective tissue disease (CTD). There were two cases of Sjögren’s syndrome in patients taking an anti–programmed cell death 1 (anti-PD1) drug, one case of cryoglobulinemic vasculitis as a complication of suspected Sjögren’s syndrome in a patient taking an anti–programmed cell death ligand 1 (PDL-1) agent, and a case of a patient with antinuclear antibody positive myositis who was taking an anti-PDL-1 drug (Ann Rheum Dis. 2017 Feb 27. doi: 10.1136/annrheumdis-2016-210820).
“While the onset of systemic autoimmune disease after ICI treatment remains uncommon, greater awareness of these conditions should enable physicians to provide more effective patient care,” the investigators wrote. “This underlines the need for close collaboration within a network of oncologists and other specialist physicians in the new era of immunotherapy.”
The investigators discovered the cases by screening the French prospective, multicenter, academic REISAMIC registry for reports of CTD among patients being treated with anti-PD1 or anti-PDL-1 agents.
All four of the patients who developed a CTD had metastatic cancer, and their mean age was 62 years. Two patients had been treated with anti-PD1 agents and two with anti-PDL-1 agents. None of the four patients had presented with symptoms of CTD before they began treatment.
The mean time interval between the first treatment dose and the first symptom of CTD was 60 days (range, 24-72), and the mean time interval between the first symptom and subsequent diagnosis of CTD was 40 days (range, 10-74).
Three patients discontinued the ICI agent, and two patients were treated with steroids (1 mg/kg/day).
The estimated prevalence of CTD was 0.7% in the REISAMIC registry, and the authors emphasize that the high proportion of cases of Sjögren’s syndrome is noteworthy, with two of the patients fulfilling the recent American College of Rheumatology/European League Against Rheumatism criteria for Sjögren’s syndrome.
A limitation of the study is that some patients presenting with milder symptoms might not have been investigated by their oncologist.
The findings raise the question of whether asymptomatic patients taking ICIs who are at risk for immune-related adverse events should be screened and monitored closely, the authors explained.
One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
For the first time, new-onset connective tissue disease has been reported in patients who were treated with anti-PD1/PDL-1 agents, according to findings published in the Annals of the Rheumatic Diseases.
In a cohort of 447 cancer patients who received therapy with immune checkpoint inhibitors (ICIs), Sébastien Le Burel, MD, of the Bicêtre Hospital in Le Kremlin-Bicêtre, France, and his colleagues described four patients who developed a connective tissue disease (CTD). There were two cases of Sjögren’s syndrome in patients taking an anti–programmed cell death 1 (anti-PD1) drug, one case of cryoglobulinemic vasculitis as a complication of suspected Sjögren’s syndrome in a patient taking an anti–programmed cell death ligand 1 (PDL-1) agent, and a case of a patient with antinuclear antibody positive myositis who was taking an anti-PDL-1 drug (Ann Rheum Dis. 2017 Feb 27. doi: 10.1136/annrheumdis-2016-210820).
“While the onset of systemic autoimmune disease after ICI treatment remains uncommon, greater awareness of these conditions should enable physicians to provide more effective patient care,” the investigators wrote. “This underlines the need for close collaboration within a network of oncologists and other specialist physicians in the new era of immunotherapy.”
The investigators discovered the cases by screening the French prospective, multicenter, academic REISAMIC registry for reports of CTD among patients being treated with anti-PD1 or anti-PDL-1 agents.
All four of the patients who developed a CTD had metastatic cancer, and their mean age was 62 years. Two patients had been treated with anti-PD1 agents and two with anti-PDL-1 agents. None of the four patients had presented with symptoms of CTD before they began treatment.
The mean time interval between the first treatment dose and the first symptom of CTD was 60 days (range, 24-72), and the mean time interval between the first symptom and subsequent diagnosis of CTD was 40 days (range, 10-74).
Three patients discontinued the ICI agent, and two patients were treated with steroids (1 mg/kg/day).
The estimated prevalence of CTD was 0.7% in the REISAMIC registry, and the authors emphasize that the high proportion of cases of Sjögren’s syndrome is noteworthy, with two of the patients fulfilling the recent American College of Rheumatology/European League Against Rheumatism criteria for Sjögren’s syndrome.
A limitation of the study is that some patients presenting with milder symptoms might not have been investigated by their oncologist.
The findings raise the question of whether asymptomatic patients taking ICIs who are at risk for immune-related adverse events should be screened and monitored closely, the authors explained.
One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
Key clinical point:
Major finding: In a cohort of 447 patients, 4 with metastatic cancer developed connective tissue disease following anti-PD-1/PDL-1 treatment.
Data source: A prospective, multicenter, academic registry was screened for reports of CTD among patients being treated with anti-PD1/PDL-1 agents.
Disclosures: One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
Soluble PD-L1 correlates with melanoma outcomes
ORLANDO – Patients with metastatic melanoma who have high blood levels of the soluble form of the programmed death-ligand 1 (sPD-L1) have poor clinical outcomes, decreased overall survival, and disease that is resistant to PD-L1 checkpoint inhibitors, compared with patients with low levels of sPD-L1, investigators have found.
High sPD-L1 levels are also associated with an immunosuppressive disease phenotype and with higher levels of pro-inflammatory cytokines, said Roxana S. Dronca, MD, from the Mayo Clinic in Rochester, Minn.
Tumor-induced immune suppression
Membrane-bound, tumor associated PD-L1 has been shown to play a key role in tumor-induced immunosuppression in melanoma and many other malignancies. Expression of PD-L1 on tumors has been shown to be associated with more aggressive tumor biology and with decreased survival in various tumor types, and it was previously thought to be prognostic, she said.
“However, other investigators more recently have found that expression of PD-L1, for instance in metastatic melanoma, is associated with improved survival, possibly reflective of endogenous anti-tumor immunity. So, therefore, the prognostic role of tumor associated PD-L1 is unclear. And also, PD-L1 has been found to be a suboptimal predictive biomarker for response to PD-1 blockade, likely due to heterogeneous and dynamic expression in the tumor tissues, which really cannot be captured with a single-time-point, random tumor biopsy,” she added.
In 2011, Mayo investigators reported on the presence of sPD-L1 (then called B7-H1) in the sera of patients with advanced renal-cell carcinoma and that it was associated with advanced tumor stage and negative clinicopathologic tumor characteristics.
“It seems that the molecule is biologically able to engage PD-1 on circulating T cells, and therefore, it may represent an unanticipated contributing factor to immune homeostasis beyond the tumor microenvironment,” Dr. Dronca said.
Higher levels correlate with outcomes
To see whether sPD-L1 levels are related to outcome and response to immune checkpoint inhibitor therapy in patients with metastatic melanoma, the investigators collected baseline peripheral blood samples from 276 patients with advanced melanoma prior to enrollment in nonimmunotherapy clinical trials, as well as samples from 36 healthy blood donors at their center.
They also evaluated samples from 80 patients who were undergoing anti-PD-1 based immunotherapy, with peripheral blood collected at baseline and each subsequent radiographic tumor evaluation, and serial monthly blood samples from healthy pregnant women (number not specified), with samples taken at 2 hours and at 6 weeks post delivery. Levels of PD-L1 were measured by enzyme-linked immunosorbent assay.
The investigators first observed that sPD-L1 levels rose steadily during pregnancy then fell sharply after delivery, showing the presence of PD-L1 levels in healthy subjects and in a normal model of immune tolerance (that is, pregnancy). This finding is not especially surprising given that PD-L1 was first cloned from human placentas, where it is present in abundant levels and forms a barrier at the fetal-maternal interface, Dr. Dronca said.
They also found that sPD-L1 was significantly higher among melanoma patients than among controls, with a mean level of 1.73 ng/mL, compared with 0.77 ng/mL in controls.
Using receiver operating characteristic analysis, the researchers determined a cutoff value of 0.239 ng/mL to distinguish between low and high levels of sPD-L1.
They found that melanoma patients with levels above 0.293 ng/mL had a median overall survival of 11.3 months, compared with 14.8 months for those with levels of 0.293 ng/mL or lower (P = .04).
They also found that high sPD-L1 levels were associated with resistance to anti-PD-1 therapy. Patients who had complete or partial objective responses had a mean level of 0.3 ng/mL, whereas patients who had unequivocal disease progression at 12 weeks had levels 7.5 times higher.
“Interestingly, at 12 weeks the levels were actually quite stable, both in responders and progressors, suggesting that, maybe, soluble PD-L1 is not only a direct reflection of the tumor load, but as mentioned, it can be released by other immune cells and is possibly a more global marker of immune dysfunction,” Dr. Dronca said.
‘A little bit curious’
Douglas G. McNeel, MD, PhD, from the University of Wisconsin–Madison, the invited discussant, commended the authors for their study and noted that it raises important questions about the role of PD-L1 in healthy and malignant cells.

He added that it’s still unclear, but worth pursuing, whether measuring sPD-L1 levels can identify patients who may benefit from anti-PD1 monotherapy versus combinatorial strategies and agrees with the authors’ conclusion that larger studies are needed to establish whether sPD-L1 can be a prognostic or predictive biomarker.
The study was supported by grants from the National Institutes of Health, Mayo Clinic, and Fraternal Order of Eagles Cancer Research Fund. Dr. Dronca disclosed institution research funding from Merck Sharp & Dohme, and other financial relationship with Elsevier. Dr. McNeel disclosed leadership, stock ownership, and consulting with Madison Vaccines, and consulting and/or institutional research funding from Bristol-Myers Squibb, Dendreon, Janssen, Madison Vaccines, and Medivation.
ORLANDO – Patients with metastatic melanoma who have high blood levels of the soluble form of the programmed death-ligand 1 (sPD-L1) have poor clinical outcomes, decreased overall survival, and disease that is resistant to PD-L1 checkpoint inhibitors, compared with patients with low levels of sPD-L1, investigators have found.
High sPD-L1 levels are also associated with an immunosuppressive disease phenotype and with higher levels of pro-inflammatory cytokines, said Roxana S. Dronca, MD, from the Mayo Clinic in Rochester, Minn.
Tumor-induced immune suppression
Membrane-bound, tumor associated PD-L1 has been shown to play a key role in tumor-induced immunosuppression in melanoma and many other malignancies. Expression of PD-L1 on tumors has been shown to be associated with more aggressive tumor biology and with decreased survival in various tumor types, and it was previously thought to be prognostic, she said.
“However, other investigators more recently have found that expression of PD-L1, for instance in metastatic melanoma, is associated with improved survival, possibly reflective of endogenous anti-tumor immunity. So, therefore, the prognostic role of tumor associated PD-L1 is unclear. And also, PD-L1 has been found to be a suboptimal predictive biomarker for response to PD-1 blockade, likely due to heterogeneous and dynamic expression in the tumor tissues, which really cannot be captured with a single-time-point, random tumor biopsy,” she added.
In 2011, Mayo investigators reported on the presence of sPD-L1 (then called B7-H1) in the sera of patients with advanced renal-cell carcinoma and that it was associated with advanced tumor stage and negative clinicopathologic tumor characteristics.
“It seems that the molecule is biologically able to engage PD-1 on circulating T cells, and therefore, it may represent an unanticipated contributing factor to immune homeostasis beyond the tumor microenvironment,” Dr. Dronca said.
Higher levels correlate with outcomes
To see whether sPD-L1 levels are related to outcome and response to immune checkpoint inhibitor therapy in patients with metastatic melanoma, the investigators collected baseline peripheral blood samples from 276 patients with advanced melanoma prior to enrollment in nonimmunotherapy clinical trials, as well as samples from 36 healthy blood donors at their center.
They also evaluated samples from 80 patients who were undergoing anti-PD-1 based immunotherapy, with peripheral blood collected at baseline and each subsequent radiographic tumor evaluation, and serial monthly blood samples from healthy pregnant women (number not specified), with samples taken at 2 hours and at 6 weeks post delivery. Levels of PD-L1 were measured by enzyme-linked immunosorbent assay.
The investigators first observed that sPD-L1 levels rose steadily during pregnancy then fell sharply after delivery, showing the presence of PD-L1 levels in healthy subjects and in a normal model of immune tolerance (that is, pregnancy). This finding is not especially surprising given that PD-L1 was first cloned from human placentas, where it is present in abundant levels and forms a barrier at the fetal-maternal interface, Dr. Dronca said.
They also found that sPD-L1 was significantly higher among melanoma patients than among controls, with a mean level of 1.73 ng/mL, compared with 0.77 ng/mL in controls.
Using receiver operating characteristic analysis, the researchers determined a cutoff value of 0.239 ng/mL to distinguish between low and high levels of sPD-L1.
They found that melanoma patients with levels above 0.293 ng/mL had a median overall survival of 11.3 months, compared with 14.8 months for those with levels of 0.293 ng/mL or lower (P = .04).
They also found that high sPD-L1 levels were associated with resistance to anti-PD-1 therapy. Patients who had complete or partial objective responses had a mean level of 0.3 ng/mL, whereas patients who had unequivocal disease progression at 12 weeks had levels 7.5 times higher.
“Interestingly, at 12 weeks the levels were actually quite stable, both in responders and progressors, suggesting that, maybe, soluble PD-L1 is not only a direct reflection of the tumor load, but as mentioned, it can be released by other immune cells and is possibly a more global marker of immune dysfunction,” Dr. Dronca said.
‘A little bit curious’
Douglas G. McNeel, MD, PhD, from the University of Wisconsin–Madison, the invited discussant, commended the authors for their study and noted that it raises important questions about the role of PD-L1 in healthy and malignant cells.
He added that it’s still unclear, but worth pursuing, whether measuring sPD-L1 levels can identify patients who may benefit from anti-PD1 monotherapy versus combinatorial strategies and agrees with the authors’ conclusion that larger studies are needed to establish whether sPD-L1 can be a prognostic or predictive biomarker.
The study was supported by grants from the National Institutes of Health, Mayo Clinic, and Fraternal Order of Eagles Cancer Research Fund. Dr. Dronca disclosed institution research funding from Merck Sharp & Dohme, and other financial relationship with Elsevier. Dr. McNeel disclosed leadership, stock ownership, and consulting with Madison Vaccines, and consulting and/or institutional research funding from Bristol-Myers Squibb, Dendreon, Janssen, Madison Vaccines, and Medivation.
ORLANDO – Patients with metastatic melanoma who have high blood levels of the soluble form of the programmed death-ligand 1 (sPD-L1) have poor clinical outcomes, decreased overall survival, and disease that is resistant to PD-L1 checkpoint inhibitors, compared with patients with low levels of sPD-L1, investigators have found.
High sPD-L1 levels are also associated with an immunosuppressive disease phenotype and with higher levels of pro-inflammatory cytokines, said Roxana S. Dronca, MD, from the Mayo Clinic in Rochester, Minn.
Tumor-induced immune suppression
Membrane-bound, tumor associated PD-L1 has been shown to play a key role in tumor-induced immunosuppression in melanoma and many other malignancies. Expression of PD-L1 on tumors has been shown to be associated with more aggressive tumor biology and with decreased survival in various tumor types, and it was previously thought to be prognostic, she said.
“However, other investigators more recently have found that expression of PD-L1, for instance in metastatic melanoma, is associated with improved survival, possibly reflective of endogenous anti-tumor immunity. So, therefore, the prognostic role of tumor associated PD-L1 is unclear. And also, PD-L1 has been found to be a suboptimal predictive biomarker for response to PD-1 blockade, likely due to heterogeneous and dynamic expression in the tumor tissues, which really cannot be captured with a single-time-point, random tumor biopsy,” she added.
In 2011, Mayo investigators reported on the presence of sPD-L1 (then called B7-H1) in the sera of patients with advanced renal-cell carcinoma and that it was associated with advanced tumor stage and negative clinicopathologic tumor characteristics.
“It seems that the molecule is biologically able to engage PD-1 on circulating T cells, and therefore, it may represent an unanticipated contributing factor to immune homeostasis beyond the tumor microenvironment,” Dr. Dronca said.
Higher levels correlate with outcomes
To see whether sPD-L1 levels are related to outcome and response to immune checkpoint inhibitor therapy in patients with metastatic melanoma, the investigators collected baseline peripheral blood samples from 276 patients with advanced melanoma prior to enrollment in nonimmunotherapy clinical trials, as well as samples from 36 healthy blood donors at their center.
They also evaluated samples from 80 patients who were undergoing anti-PD-1 based immunotherapy, with peripheral blood collected at baseline and each subsequent radiographic tumor evaluation, and serial monthly blood samples from healthy pregnant women (number not specified), with samples taken at 2 hours and at 6 weeks post delivery. Levels of PD-L1 were measured by enzyme-linked immunosorbent assay.
The investigators first observed that sPD-L1 levels rose steadily during pregnancy then fell sharply after delivery, showing the presence of PD-L1 levels in healthy subjects and in a normal model of immune tolerance (that is, pregnancy). This finding is not especially surprising given that PD-L1 was first cloned from human placentas, where it is present in abundant levels and forms a barrier at the fetal-maternal interface, Dr. Dronca said.
They also found that sPD-L1 was significantly higher among melanoma patients than among controls, with a mean level of 1.73 ng/mL, compared with 0.77 ng/mL in controls.
Using receiver operating characteristic analysis, the researchers determined a cutoff value of 0.239 ng/mL to distinguish between low and high levels of sPD-L1.
They found that melanoma patients with levels above 0.293 ng/mL had a median overall survival of 11.3 months, compared with 14.8 months for those with levels of 0.293 ng/mL or lower (P = .04).
They also found that high sPD-L1 levels were associated with resistance to anti-PD-1 therapy. Patients who had complete or partial objective responses had a mean level of 0.3 ng/mL, whereas patients who had unequivocal disease progression at 12 weeks had levels 7.5 times higher.
“Interestingly, at 12 weeks the levels were actually quite stable, both in responders and progressors, suggesting that, maybe, soluble PD-L1 is not only a direct reflection of the tumor load, but as mentioned, it can be released by other immune cells and is possibly a more global marker of immune dysfunction,” Dr. Dronca said.
‘A little bit curious’
Douglas G. McNeel, MD, PhD, from the University of Wisconsin–Madison, the invited discussant, commended the authors for their study and noted that it raises important questions about the role of PD-L1 in healthy and malignant cells.
He added that it’s still unclear, but worth pursuing, whether measuring sPD-L1 levels can identify patients who may benefit from anti-PD1 monotherapy versus combinatorial strategies and agrees with the authors’ conclusion that larger studies are needed to establish whether sPD-L1 can be a prognostic or predictive biomarker.
The study was supported by grants from the National Institutes of Health, Mayo Clinic, and Fraternal Order of Eagles Cancer Research Fund. Dr. Dronca disclosed institution research funding from Merck Sharp & Dohme, and other financial relationship with Elsevier. Dr. McNeel disclosed leadership, stock ownership, and consulting with Madison Vaccines, and consulting and/or institutional research funding from Bristol-Myers Squibb, Dendreon, Janssen, Madison Vaccines, and Medivation.
Key clinical point: Soluble PD-L1 may be a predictive or prognostic biomarker for malignant melanoma outcomes.
Major finding: Patients with high levels of sPD-L1 had a median overall survival of 11.3 months, compared with 14.8 months for those with levels below a specified cutoff.
Data source: Prospective study of sPD-L1 in 276 patients with metastatic melanoma, 36 healthy volunteers, and 80 patients who were undergoing anti-PD-1 based immunotherapy.
Disclosures: The study was supported by grants from the National Institutes of Health, Mayo Clinic, and Fraternal Order of Eagles Cancer Research Fund. Dr. Dronca disclosed institution research funding from Merck Sharp & Dohme and another financial relationship with Elsevier. Dr. McNeel disclosed leadership, stock ownership, and consulting with Madison Vaccines and consulting and/or institutional research funding from Bristol-Myers Squibb, Dendreon, Janssen, Madison Vaccines, and Medivation.
Teen indoor tanning drops, but schools fall short on sun safety
Indoor tanning among adolescents in the United States has dropped significantly, but fewer than half of schools in the United States reported sun safety practices to help minimize students’ UV exposure in the school setting, based on data from two studies presented at the annual meeting of the American Academy of Dermatology and published simultaneously in JAMA Dermatology.
“Data suggest that intermittent, recreational exposure (vs. chronic exposure, as with outdoor workers) more often leads to sunburn,” wrote Sherry Everett Jones, PhD, MPH, and Gery P. Guy Jr, PhD, MPH, of the Centers for Disease Control and Prevention. “Although a small proportion of school districts and schools have adopted policies to address sun safety, most have not, even though it is common for students to be outside during the midday hours or after school when the sun is still at peak intensity.”
To characterize sun safety practices at schools, the researchers reviewed data from the 2014 School Health Policies and Practices Study Healthy and Safe School Environment questionnaire including 577 elementary, middle, and high schools (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2016.6274).
Overall, 48% of schools reported that teachers allowed students time to apply sunscreen at school (the most frequent sun safety practice). However, only 13% made sunscreen available, 16% asked parents to ensure sunscreen application before school, and 15% made an effort to avoid scheduling outdoor activities during times of peak sun intensity. High schools were less likely than elementary or middle schools to follow sun safety practices.
“None of the sun safety policies or practices were statistically significantly associated with metropolitan status,” the researchers noted. However, the findings were limited by the cross-sectional nature of the study and lack of data about natural shade and man made shade structures in outdoor areas of the schools.
“Interventions driven by the public health and medical community educating school leadership and policy makers about the importance of sun safety are needed regardless of level, location, size, and poverty concentration of the school. These efforts could be instrumental in increasing the adoption of sun safety practices among schools,” Dr. Jones and Dr. Guy emphasized.
However, data from another study showed a significant reduction in the prevalence of indoor tanning among adolescents.
In particular, indoor tanning among non-Hispanic white females (the group at highest risk for skin cancer) dropped from 37% in 2009 to 15% in 2015. CDC researchers led by Dr. Guy pooled data from the 2009, 2011, 2013, and 2015 national Youth Risk Behavior Surveillance System Surveys (JAMA Dermatol. 2017. doi:10.1001/jamadermatol.2016.6273). Overall, the prevalence of indoor tanning among U.S. high school students decreased from 16% in 2009 to 7% in 2015.
“Despite declines in indoor tanning, continued efforts are needed,” the researchers wrote. “Public health efforts could help address the misconception that indoor tanning protects against sunburn. The medical community also can play a key role in counseling adolescents and young adults in accordance with the U.S. Preventive Services Task Force guidelines.”
The findings were limited by several factors including the use of self-reports and the inability to control for skin type, the researchers wrote. However, “Reducing the proportion of youth who engage in indoor tanning and experience sunburns presents an important cancer prevention opportunity.”
None of the researchers on either study had relevant financial conflicts to disclose.
Explore best practices for public education campaigns “For more than 10 years, much effort has been made to educate the public on sun-safety practices, including warnings about the harmful effects of indoor tanning on those at higher risk, such as young adults and children. In this issue of JAMA Dermatology, 2 important articles describe the progress made toward sun safety,” wrote Henry W. Lim, MD, and Samantha L. Schneider, MD, in the accompanying editorial.
Data from a study of indoor tanning showed a significant decrease in prevalence of indoor tanning among adolescents, from 16% in 2009 to 7% in 2015. Although these results are encouraging, public education is needed for further improvement, they said. “One myth is that UV radiation prevents vitamin D deficiency; however, oral vitamin D supplementation is known to be a safer alternative. Another myth is that obtaining a baseline tan before the summer or a vacation reduces the risk of sunburn. However, as Guy and colleagues observed, those who tanned indoors were more likely to develop sunburn than students who did not engage in indoor tanning.”

“Clearly, both the dermatology and medical communities need to continue public awareness campaigns regarding photoprotection, including sun-safety practices such as seeking shade when outdoors and wearing photoprotective clothing, wide-brimmed hats, and sunglasses,” they emphasized.
In addition, “A highly effective means of public education may be to identify a campaign, such as Portugal’s sugar packet initiative, that makes sun-safety awareness and practice a part of everyone’s daily routine,” they said (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2016.6272).
Dr. Lim and Dr. Schneider are affiliated with the department of dermatology at Henry Ford Hospital in Detroit. Dr Lim disclosed serving as an investigator or coinvestigator on clinical research projects for Ferndale Pharma, Estée Lauder, and Allergan. Dr. Schneider had no relevant conflicts to disclose.
Explore best practices for public education campaigns “For more than 10 years, much effort has been made to educate the public on sun-safety practices, including warnings about the harmful effects of indoor tanning on those at higher risk, such as young adults and children. In this issue of JAMA Dermatology, 2 important articles describe the progress made toward sun safety,” wrote Henry W. Lim, MD, and Samantha L. Schneider, MD, in the accompanying editorial.
Data from a study of indoor tanning showed a significant decrease in prevalence of indoor tanning among adolescents, from 16% in 2009 to 7% in 2015. Although these results are encouraging, public education is needed for further improvement, they said. “One myth is that UV radiation prevents vitamin D deficiency; however, oral vitamin D supplementation is known to be a safer alternative. Another myth is that obtaining a baseline tan before the summer or a vacation reduces the risk of sunburn. However, as Guy and colleagues observed, those who tanned indoors were more likely to develop sunburn than students who did not engage in indoor tanning.”
“Clearly, both the dermatology and medical communities need to continue public awareness campaigns regarding photoprotection, including sun-safety practices such as seeking shade when outdoors and wearing photoprotective clothing, wide-brimmed hats, and sunglasses,” they emphasized.
In addition, “A highly effective means of public education may be to identify a campaign, such as Portugal’s sugar packet initiative, that makes sun-safety awareness and practice a part of everyone’s daily routine,” they said (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2016.6272).
Dr. Lim and Dr. Schneider are affiliated with the department of dermatology at Henry Ford Hospital in Detroit. Dr Lim disclosed serving as an investigator or coinvestigator on clinical research projects for Ferndale Pharma, Estée Lauder, and Allergan. Dr. Schneider had no relevant conflicts to disclose.
Explore best practices for public education campaigns “For more than 10 years, much effort has been made to educate the public on sun-safety practices, including warnings about the harmful effects of indoor tanning on those at higher risk, such as young adults and children. In this issue of JAMA Dermatology, 2 important articles describe the progress made toward sun safety,” wrote Henry W. Lim, MD, and Samantha L. Schneider, MD, in the accompanying editorial.
Data from a study of indoor tanning showed a significant decrease in prevalence of indoor tanning among adolescents, from 16% in 2009 to 7% in 2015. Although these results are encouraging, public education is needed for further improvement, they said. “One myth is that UV radiation prevents vitamin D deficiency; however, oral vitamin D supplementation is known to be a safer alternative. Another myth is that obtaining a baseline tan before the summer or a vacation reduces the risk of sunburn. However, as Guy and colleagues observed, those who tanned indoors were more likely to develop sunburn than students who did not engage in indoor tanning.”
“Clearly, both the dermatology and medical communities need to continue public awareness campaigns regarding photoprotection, including sun-safety practices such as seeking shade when outdoors and wearing photoprotective clothing, wide-brimmed hats, and sunglasses,” they emphasized.
In addition, “A highly effective means of public education may be to identify a campaign, such as Portugal’s sugar packet initiative, that makes sun-safety awareness and practice a part of everyone’s daily routine,” they said (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2016.6272).
Dr. Lim and Dr. Schneider are affiliated with the department of dermatology at Henry Ford Hospital in Detroit. Dr Lim disclosed serving as an investigator or coinvestigator on clinical research projects for Ferndale Pharma, Estée Lauder, and Allergan. Dr. Schneider had no relevant conflicts to disclose.
Indoor tanning among adolescents in the United States has dropped significantly, but fewer than half of schools in the United States reported sun safety practices to help minimize students’ UV exposure in the school setting, based on data from two studies presented at the annual meeting of the American Academy of Dermatology and published simultaneously in JAMA Dermatology.
“Data suggest that intermittent, recreational exposure (vs. chronic exposure, as with outdoor workers) more often leads to sunburn,” wrote Sherry Everett Jones, PhD, MPH, and Gery P. Guy Jr, PhD, MPH, of the Centers for Disease Control and Prevention. “Although a small proportion of school districts and schools have adopted policies to address sun safety, most have not, even though it is common for students to be outside during the midday hours or after school when the sun is still at peak intensity.”
To characterize sun safety practices at schools, the researchers reviewed data from the 2014 School Health Policies and Practices Study Healthy and Safe School Environment questionnaire including 577 elementary, middle, and high schools (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2016.6274).
Overall, 48% of schools reported that teachers allowed students time to apply sunscreen at school (the most frequent sun safety practice). However, only 13% made sunscreen available, 16% asked parents to ensure sunscreen application before school, and 15% made an effort to avoid scheduling outdoor activities during times of peak sun intensity. High schools were less likely than elementary or middle schools to follow sun safety practices.
“None of the sun safety policies or practices were statistically significantly associated with metropolitan status,” the researchers noted. However, the findings were limited by the cross-sectional nature of the study and lack of data about natural shade and man made shade structures in outdoor areas of the schools.
“Interventions driven by the public health and medical community educating school leadership and policy makers about the importance of sun safety are needed regardless of level, location, size, and poverty concentration of the school. These efforts could be instrumental in increasing the adoption of sun safety practices among schools,” Dr. Jones and Dr. Guy emphasized.
However, data from another study showed a significant reduction in the prevalence of indoor tanning among adolescents.
In particular, indoor tanning among non-Hispanic white females (the group at highest risk for skin cancer) dropped from 37% in 2009 to 15% in 2015. CDC researchers led by Dr. Guy pooled data from the 2009, 2011, 2013, and 2015 national Youth Risk Behavior Surveillance System Surveys (JAMA Dermatol. 2017. doi:10.1001/jamadermatol.2016.6273). Overall, the prevalence of indoor tanning among U.S. high school students decreased from 16% in 2009 to 7% in 2015.
“Despite declines in indoor tanning, continued efforts are needed,” the researchers wrote. “Public health efforts could help address the misconception that indoor tanning protects against sunburn. The medical community also can play a key role in counseling adolescents and young adults in accordance with the U.S. Preventive Services Task Force guidelines.”
The findings were limited by several factors including the use of self-reports and the inability to control for skin type, the researchers wrote. However, “Reducing the proportion of youth who engage in indoor tanning and experience sunburns presents an important cancer prevention opportunity.”
None of the researchers on either study had relevant financial conflicts to disclose.
Indoor tanning among adolescents in the United States has dropped significantly, but fewer than half of schools in the United States reported sun safety practices to help minimize students’ UV exposure in the school setting, based on data from two studies presented at the annual meeting of the American Academy of Dermatology and published simultaneously in JAMA Dermatology.
“Data suggest that intermittent, recreational exposure (vs. chronic exposure, as with outdoor workers) more often leads to sunburn,” wrote Sherry Everett Jones, PhD, MPH, and Gery P. Guy Jr, PhD, MPH, of the Centers for Disease Control and Prevention. “Although a small proportion of school districts and schools have adopted policies to address sun safety, most have not, even though it is common for students to be outside during the midday hours or after school when the sun is still at peak intensity.”
To characterize sun safety practices at schools, the researchers reviewed data from the 2014 School Health Policies and Practices Study Healthy and Safe School Environment questionnaire including 577 elementary, middle, and high schools (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2016.6274).
Overall, 48% of schools reported that teachers allowed students time to apply sunscreen at school (the most frequent sun safety practice). However, only 13% made sunscreen available, 16% asked parents to ensure sunscreen application before school, and 15% made an effort to avoid scheduling outdoor activities during times of peak sun intensity. High schools were less likely than elementary or middle schools to follow sun safety practices.
“None of the sun safety policies or practices were statistically significantly associated with metropolitan status,” the researchers noted. However, the findings were limited by the cross-sectional nature of the study and lack of data about natural shade and man made shade structures in outdoor areas of the schools.
“Interventions driven by the public health and medical community educating school leadership and policy makers about the importance of sun safety are needed regardless of level, location, size, and poverty concentration of the school. These efforts could be instrumental in increasing the adoption of sun safety practices among schools,” Dr. Jones and Dr. Guy emphasized.
However, data from another study showed a significant reduction in the prevalence of indoor tanning among adolescents.
In particular, indoor tanning among non-Hispanic white females (the group at highest risk for skin cancer) dropped from 37% in 2009 to 15% in 2015. CDC researchers led by Dr. Guy pooled data from the 2009, 2011, 2013, and 2015 national Youth Risk Behavior Surveillance System Surveys (JAMA Dermatol. 2017. doi:10.1001/jamadermatol.2016.6273). Overall, the prevalence of indoor tanning among U.S. high school students decreased from 16% in 2009 to 7% in 2015.
“Despite declines in indoor tanning, continued efforts are needed,” the researchers wrote. “Public health efforts could help address the misconception that indoor tanning protects against sunburn. The medical community also can play a key role in counseling adolescents and young adults in accordance with the U.S. Preventive Services Task Force guidelines.”
The findings were limited by several factors including the use of self-reports and the inability to control for skin type, the researchers wrote. However, “Reducing the proportion of youth who engage in indoor tanning and experience sunburns presents an important cancer prevention opportunity.”
None of the researchers on either study had relevant financial conflicts to disclose.
FROM AAD 2017
Key clinical point:
Major finding: Fewer than half (48%) of schools in the United States allowed time for sunscreen application, and fewer than 15% provided sunscreen. However, overall prevalence of indoor tanning among U.S. adolescents dropped from 16% in 2009 to 7% in 2015.
Data source: Data were taken from the 2014 School Health Policies and Practices Study in the first study and from the 2009, 2011, 2013, and 2015 national Youth Risk Behavior Surveys in the second.
Disclosures: The researchers had no financial conflicts to disclose.
Pigmented skin lesions lightened during melanoma immunotherapy
Treatment with pembrolizumab, a humanized antibody used in cancer immunotherapy, may affect the pigmentation of some benign skin lesions, according to a case study in British Journal of Dermatology.
Pembrolizumab works by targeting the programmed cell death-1 (PD-1) receptor and is used in the treatment of metastatic melanoma and some other cancers.
The case report, by Zachary J. Wolner, MD, of Memorial Sloan Kettering Cancer Center in New York, and his colleagues, describes a male patient in his 60s with HRAS mutant metastatic melanoma who was treated with pembrolizumab 2 mg/kg every 3 weeks for 13 months, and had received no previous systematic treatment. At 4 months after starting pembrolizumab, the patient experienced whitening of eyebrows and eyelashes, along with scalp and body hair, followed by lighter overall skin pigmentation and the fading of pigmented skin lesions. Baseline (pre-pembrolizumab) and 1-year follow-up skin photography confirmed lightening or disappearance of solar lentigines, seborrheic keratoses, and melanocytic nevi along with overall lightening of the skin (Br J. Dermatol. 2017 doi: 10.1111/bjd.15354).
Dr. Wolner and his colleagues noted that while changing skin lesions have not been reported in clinical trials of anti-PD-1 therapies, one study in patients treated with an anti-PD-1 therapy for metastatic melanoma found changes to nevi in 6 of 34 (18%) patients. Patients using a melanoma website also have self-reported disappearing nevi after immunotherapy treatment, the authors noted.
Expression of the coinhibitory molecule PD-L1 “is not limited to malignant tumors,” the researchers wrote, adding that previous studies have identified PD-L1 expression in melanocytes of benign melanocytic nevi. “Therefore it is biologically plausible that PD-1 inhibition may affect the natural history of benign melanocytic neoplasms.”
Also, they wrote, “the co-occurrence of vitiligo and poliosis in our patient suggests a role for autoimmunity in the fading/disappearance of his pigmented lesions.” The investigators cited a recent study in 67 patients with metastatic melanoma receiving pembrolizumab, which found that 25% developed vitiligo. Response to treatment also was significantly associated with occurrence of vitiligo (JAMA Dermatol. 2016;152[1]:45-51).
Dr. Wolner and his colleagues cautioned that their findings were limited to a single case report, and also by “lack of histological sampling and molecular characterization of fading/disappearing nevi.” An alternative explanation for the observed changes “includes fading/disappearance not related to PD-1 inhibition or due to chance alone.”
A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
Treatment with pembrolizumab, a humanized antibody used in cancer immunotherapy, may affect the pigmentation of some benign skin lesions, according to a case study in British Journal of Dermatology.
Pembrolizumab works by targeting the programmed cell death-1 (PD-1) receptor and is used in the treatment of metastatic melanoma and some other cancers.
The case report, by Zachary J. Wolner, MD, of Memorial Sloan Kettering Cancer Center in New York, and his colleagues, describes a male patient in his 60s with HRAS mutant metastatic melanoma who was treated with pembrolizumab 2 mg/kg every 3 weeks for 13 months, and had received no previous systematic treatment. At 4 months after starting pembrolizumab, the patient experienced whitening of eyebrows and eyelashes, along with scalp and body hair, followed by lighter overall skin pigmentation and the fading of pigmented skin lesions. Baseline (pre-pembrolizumab) and 1-year follow-up skin photography confirmed lightening or disappearance of solar lentigines, seborrheic keratoses, and melanocytic nevi along with overall lightening of the skin (Br J. Dermatol. 2017 doi: 10.1111/bjd.15354).
Dr. Wolner and his colleagues noted that while changing skin lesions have not been reported in clinical trials of anti-PD-1 therapies, one study in patients treated with an anti-PD-1 therapy for metastatic melanoma found changes to nevi in 6 of 34 (18%) patients. Patients using a melanoma website also have self-reported disappearing nevi after immunotherapy treatment, the authors noted.
Expression of the coinhibitory molecule PD-L1 “is not limited to malignant tumors,” the researchers wrote, adding that previous studies have identified PD-L1 expression in melanocytes of benign melanocytic nevi. “Therefore it is biologically plausible that PD-1 inhibition may affect the natural history of benign melanocytic neoplasms.”
Also, they wrote, “the co-occurrence of vitiligo and poliosis in our patient suggests a role for autoimmunity in the fading/disappearance of his pigmented lesions.” The investigators cited a recent study in 67 patients with metastatic melanoma receiving pembrolizumab, which found that 25% developed vitiligo. Response to treatment also was significantly associated with occurrence of vitiligo (JAMA Dermatol. 2016;152[1]:45-51).
Dr. Wolner and his colleagues cautioned that their findings were limited to a single case report, and also by “lack of histological sampling and molecular characterization of fading/disappearing nevi.” An alternative explanation for the observed changes “includes fading/disappearance not related to PD-1 inhibition or due to chance alone.”
A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
Treatment with pembrolizumab, a humanized antibody used in cancer immunotherapy, may affect the pigmentation of some benign skin lesions, according to a case study in British Journal of Dermatology.
Pembrolizumab works by targeting the programmed cell death-1 (PD-1) receptor and is used in the treatment of metastatic melanoma and some other cancers.
The case report, by Zachary J. Wolner, MD, of Memorial Sloan Kettering Cancer Center in New York, and his colleagues, describes a male patient in his 60s with HRAS mutant metastatic melanoma who was treated with pembrolizumab 2 mg/kg every 3 weeks for 13 months, and had received no previous systematic treatment. At 4 months after starting pembrolizumab, the patient experienced whitening of eyebrows and eyelashes, along with scalp and body hair, followed by lighter overall skin pigmentation and the fading of pigmented skin lesions. Baseline (pre-pembrolizumab) and 1-year follow-up skin photography confirmed lightening or disappearance of solar lentigines, seborrheic keratoses, and melanocytic nevi along with overall lightening of the skin (Br J. Dermatol. 2017 doi: 10.1111/bjd.15354).
Dr. Wolner and his colleagues noted that while changing skin lesions have not been reported in clinical trials of anti-PD-1 therapies, one study in patients treated with an anti-PD-1 therapy for metastatic melanoma found changes to nevi in 6 of 34 (18%) patients. Patients using a melanoma website also have self-reported disappearing nevi after immunotherapy treatment, the authors noted.
Expression of the coinhibitory molecule PD-L1 “is not limited to malignant tumors,” the researchers wrote, adding that previous studies have identified PD-L1 expression in melanocytes of benign melanocytic nevi. “Therefore it is biologically plausible that PD-1 inhibition may affect the natural history of benign melanocytic neoplasms.”
Also, they wrote, “the co-occurrence of vitiligo and poliosis in our patient suggests a role for autoimmunity in the fading/disappearance of his pigmented lesions.” The investigators cited a recent study in 67 patients with metastatic melanoma receiving pembrolizumab, which found that 25% developed vitiligo. Response to treatment also was significantly associated with occurrence of vitiligo (JAMA Dermatol. 2016;152[1]:45-51).
Dr. Wolner and his colleagues cautioned that their findings were limited to a single case report, and also by “lack of histological sampling and molecular characterization of fading/disappearing nevi.” An alternative explanation for the observed changes “includes fading/disappearance not related to PD-1 inhibition or due to chance alone.”
A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
Key clinical point:
Major finding: Pembrolizumab and other PD-1 inhibitors may affect benign pigmented lesions.
Data source: A single-center, single-patient case report.
Disclosures: A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
Use of IHC stains on rise in melanoma diagnosis
While there is little consensus on the ideal role of immunohistochemical (IHC) stains in the diagnosis of melanoma, their use increased dramatically over a 15-year period, according to results from a study.
Randie H. Kim, MD, PhD, and Shane A. Meehan, MD, of New York University, reviewed nearly 6,300 pathology reports from patients with melanomas, all referred (along with tissue samples) to their center from other institutions during 2001-2015. One or more IHC stains were used diagnostically in 871 cases during the study period, with use increasing from 5% of patients in 2001 to 25% in 2015 (P less than .0001). Usage increased gradually over time, although the number of stains used per case did not increase significantly (J Cutan Pathol. 2017 Mar;44[3]:221-7).
IHC stain use was associated with melanomas occurring on the head or neck (odds ratio = 1.6; 95% confidence interval, 1.4-1.9), acral melanomas (OR = 1.5; 95% CI 1.1-2.0) and melanomas thicker than 4 mm (OR = 2.5; 95% CI 1.7-3.6). The most common stain used in the study was Melan-A/MART-1 (melanoma antigen recognized by T cells), the most specific of the IHC markers available and the one “largely responsible for the increased incidence in overall immunostain use in our study,” the researchers wrote. “The perception that melanocytic markers, such as Melan-A, can more accurately stage melanomas, is a potential explanation for its increased usage over the duration of the study period.”
The higher use of immunostains in thicker melanomas may be because these “exhibit greater morphological heterogeneity, such as nodular, spindled and desmoplastic subtypes, that lead to additional confirmational testing,” Dr. Kim and Dr. Meehan noted. However, they cautioned that extrinsic factors, including reimbursement fees and concerns about malpractice claims, could also influence the use of IHC stains in the diagnosis of melanomas.
“While Melan-A/MART-1 is a useful adjunct for determining melanocytic density or the presence of invasion in difficult cases, its routine use on melanomas has not been validated,” the researchers wrote in their analysis. “A consensus conference delineating the appropriate use of IHC in the diagnosis of melanoma may be of value in this regard.”
Dr. Kim and Dr. Meehan also noted that while a greater proportion of the melanomas seen in the study were thick (greater than 4 mm) compared with most population-based studies, this may reflect patient management practices in which thinner melanomas are treated in outpatient centers while thicker ones get referred to tertiary care centers such as theirs.
The researchers disclosed no outside funding or conflicts of interest.
While there is little consensus on the ideal role of immunohistochemical (IHC) stains in the diagnosis of melanoma, their use increased dramatically over a 15-year period, according to results from a study.
Randie H. Kim, MD, PhD, and Shane A. Meehan, MD, of New York University, reviewed nearly 6,300 pathology reports from patients with melanomas, all referred (along with tissue samples) to their center from other institutions during 2001-2015. One or more IHC stains were used diagnostically in 871 cases during the study period, with use increasing from 5% of patients in 2001 to 25% in 2015 (P less than .0001). Usage increased gradually over time, although the number of stains used per case did not increase significantly (J Cutan Pathol. 2017 Mar;44[3]:221-7).
IHC stain use was associated with melanomas occurring on the head or neck (odds ratio = 1.6; 95% confidence interval, 1.4-1.9), acral melanomas (OR = 1.5; 95% CI 1.1-2.0) and melanomas thicker than 4 mm (OR = 2.5; 95% CI 1.7-3.6). The most common stain used in the study was Melan-A/MART-1 (melanoma antigen recognized by T cells), the most specific of the IHC markers available and the one “largely responsible for the increased incidence in overall immunostain use in our study,” the researchers wrote. “The perception that melanocytic markers, such as Melan-A, can more accurately stage melanomas, is a potential explanation for its increased usage over the duration of the study period.”
The higher use of immunostains in thicker melanomas may be because these “exhibit greater morphological heterogeneity, such as nodular, spindled and desmoplastic subtypes, that lead to additional confirmational testing,” Dr. Kim and Dr. Meehan noted. However, they cautioned that extrinsic factors, including reimbursement fees and concerns about malpractice claims, could also influence the use of IHC stains in the diagnosis of melanomas.
“While Melan-A/MART-1 is a useful adjunct for determining melanocytic density or the presence of invasion in difficult cases, its routine use on melanomas has not been validated,” the researchers wrote in their analysis. “A consensus conference delineating the appropriate use of IHC in the diagnosis of melanoma may be of value in this regard.”
Dr. Kim and Dr. Meehan also noted that while a greater proportion of the melanomas seen in the study were thick (greater than 4 mm) compared with most population-based studies, this may reflect patient management practices in which thinner melanomas are treated in outpatient centers while thicker ones get referred to tertiary care centers such as theirs.
The researchers disclosed no outside funding or conflicts of interest.
While there is little consensus on the ideal role of immunohistochemical (IHC) stains in the diagnosis of melanoma, their use increased dramatically over a 15-year period, according to results from a study.
Randie H. Kim, MD, PhD, and Shane A. Meehan, MD, of New York University, reviewed nearly 6,300 pathology reports from patients with melanomas, all referred (along with tissue samples) to their center from other institutions during 2001-2015. One or more IHC stains were used diagnostically in 871 cases during the study period, with use increasing from 5% of patients in 2001 to 25% in 2015 (P less than .0001). Usage increased gradually over time, although the number of stains used per case did not increase significantly (J Cutan Pathol. 2017 Mar;44[3]:221-7).
IHC stain use was associated with melanomas occurring on the head or neck (odds ratio = 1.6; 95% confidence interval, 1.4-1.9), acral melanomas (OR = 1.5; 95% CI 1.1-2.0) and melanomas thicker than 4 mm (OR = 2.5; 95% CI 1.7-3.6). The most common stain used in the study was Melan-A/MART-1 (melanoma antigen recognized by T cells), the most specific of the IHC markers available and the one “largely responsible for the increased incidence in overall immunostain use in our study,” the researchers wrote. “The perception that melanocytic markers, such as Melan-A, can more accurately stage melanomas, is a potential explanation for its increased usage over the duration of the study period.”
The higher use of immunostains in thicker melanomas may be because these “exhibit greater morphological heterogeneity, such as nodular, spindled and desmoplastic subtypes, that lead to additional confirmational testing,” Dr. Kim and Dr. Meehan noted. However, they cautioned that extrinsic factors, including reimbursement fees and concerns about malpractice claims, could also influence the use of IHC stains in the diagnosis of melanomas.
“While Melan-A/MART-1 is a useful adjunct for determining melanocytic density or the presence of invasion in difficult cases, its routine use on melanomas has not been validated,” the researchers wrote in their analysis. “A consensus conference delineating the appropriate use of IHC in the diagnosis of melanoma may be of value in this regard.”
Dr. Kim and Dr. Meehan also noted that while a greater proportion of the melanomas seen in the study were thick (greater than 4 mm) compared with most population-based studies, this may reflect patient management practices in which thinner melanomas are treated in outpatient centers while thicker ones get referred to tertiary care centers such as theirs.
The researchers disclosed no outside funding or conflicts of interest.
FROM THE JOURNAL OF CUTANEOUS PATHOLOGY
Key clinical point:
Major finding: One or more stains was used diagnostically in 5% of melanoma cases in 2001, compared with 25% in 2015 (P less than .0001).
Data source: A retrospective review of more than 6,000 case records referred after diagnosis to a tertiary care center during 2001-2015.
Disclosures: The researchers disclosed no outside funding or conflicts of interest.
Redefine dysplastic nevi to stratify cancer risk
WAILEA, HAWAII – It is time for a new system of classifying nevi, according to Ashfaq Marghoob, MD, of Memorial Sloan Kettering Cancer Center, New York.
“It was known for the last 30 or 40 years that we do need to subclassify nevi into groups, so as to better stratify for melanoma risk,” identifying groups of individuals who would benefit most from targeted screening, Dr. Marghoob said in a video interview at the meeting, provided by Global Academy for Medical Education/Skin Disease Education Foundation. But it has been clear that there are many flaws in the current classification system, he added.
This is beginning to change as new data emerge about gene mutations and other science that can better stratify “or segregate” the nevi into subsets, and “the hope is we will be better able to predict which subsets are associated with melanoma risk either within the lesion itself or poses an increased risk to the patient,” he explained.
“As our understanding grows, we will start to come out with subsets of nevi that have a certain clinical and dermoscopic morphology,” to help predict which patients would benefit most from being monitored very closely, with the aim of detecting – and curing – melanomas early, said Dr. Marghoob, director of Memorial Sloan Kettering’s regional skin cancer clinic in Hauppauge, N.Y.
He had no financial conflicts to disclose.
SDEF and this news organization are owned by the same parent organization.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – It is time for a new system of classifying nevi, according to Ashfaq Marghoob, MD, of Memorial Sloan Kettering Cancer Center, New York.
“It was known for the last 30 or 40 years that we do need to subclassify nevi into groups, so as to better stratify for melanoma risk,” identifying groups of individuals who would benefit most from targeted screening, Dr. Marghoob said in a video interview at the meeting, provided by Global Academy for Medical Education/Skin Disease Education Foundation. But it has been clear that there are many flaws in the current classification system, he added.
This is beginning to change as new data emerge about gene mutations and other science that can better stratify “or segregate” the nevi into subsets, and “the hope is we will be better able to predict which subsets are associated with melanoma risk either within the lesion itself or poses an increased risk to the patient,” he explained.
“As our understanding grows, we will start to come out with subsets of nevi that have a certain clinical and dermoscopic morphology,” to help predict which patients would benefit most from being monitored very closely, with the aim of detecting – and curing – melanomas early, said Dr. Marghoob, director of Memorial Sloan Kettering’s regional skin cancer clinic in Hauppauge, N.Y.
He had no financial conflicts to disclose.
SDEF and this news organization are owned by the same parent organization.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – It is time for a new system of classifying nevi, according to Ashfaq Marghoob, MD, of Memorial Sloan Kettering Cancer Center, New York.
“It was known for the last 30 or 40 years that we do need to subclassify nevi into groups, so as to better stratify for melanoma risk,” identifying groups of individuals who would benefit most from targeted screening, Dr. Marghoob said in a video interview at the meeting, provided by Global Academy for Medical Education/Skin Disease Education Foundation. But it has been clear that there are many flaws in the current classification system, he added.
This is beginning to change as new data emerge about gene mutations and other science that can better stratify “or segregate” the nevi into subsets, and “the hope is we will be better able to predict which subsets are associated with melanoma risk either within the lesion itself or poses an increased risk to the patient,” he explained.
“As our understanding grows, we will start to come out with subsets of nevi that have a certain clinical and dermoscopic morphology,” to help predict which patients would benefit most from being monitored very closely, with the aim of detecting – and curing – melanomas early, said Dr. Marghoob, director of Memorial Sloan Kettering’s regional skin cancer clinic in Hauppauge, N.Y.
He had no financial conflicts to disclose.
SDEF and this news organization are owned by the same parent organization.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF HAWAII DERMATOLOGY SEMINAR
VIDEO: Molecular testing helps pinpoint ambiguous lesions
WAILEA, HAWAII – In a video interview, Pedram Gerami, MD, professor of dermatology, pathology, and pediatrics, Northwestern University, Chicago, discusses the use of molecular testing for melanoma and suspicious lesions.
Molecular tests are available for various components of diagnosis and prognosis of melanoma, and one of the most popular scenarios for their use is to confirm a diagnosis if a lesion is biopsied and the histopathologist “feels that the diagnosis is ambiguous by standard pathology methods,” Dr. Gerami said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, between 1% and 5% of cases of suspicious lesions may need molecular testing to confirm the diagnosis, he noted. Of the available options for molecular testing, FISH (fluorescence in situ hybridization) testing is the most validated in the setting of ambiguous histology, he said.
Dr. Gerami disclosed serving as a consultant and researcher for Castle Biosciences, Myriad Genetics, and DermTech.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – In a video interview, Pedram Gerami, MD, professor of dermatology, pathology, and pediatrics, Northwestern University, Chicago, discusses the use of molecular testing for melanoma and suspicious lesions.
Molecular tests are available for various components of diagnosis and prognosis of melanoma, and one of the most popular scenarios for their use is to confirm a diagnosis if a lesion is biopsied and the histopathologist “feels that the diagnosis is ambiguous by standard pathology methods,” Dr. Gerami said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, between 1% and 5% of cases of suspicious lesions may need molecular testing to confirm the diagnosis, he noted. Of the available options for molecular testing, FISH (fluorescence in situ hybridization) testing is the most validated in the setting of ambiguous histology, he said.
Dr. Gerami disclosed serving as a consultant and researcher for Castle Biosciences, Myriad Genetics, and DermTech.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – In a video interview, Pedram Gerami, MD, professor of dermatology, pathology, and pediatrics, Northwestern University, Chicago, discusses the use of molecular testing for melanoma and suspicious lesions.
Molecular tests are available for various components of diagnosis and prognosis of melanoma, and one of the most popular scenarios for their use is to confirm a diagnosis if a lesion is biopsied and the histopathologist “feels that the diagnosis is ambiguous by standard pathology methods,” Dr. Gerami said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, between 1% and 5% of cases of suspicious lesions may need molecular testing to confirm the diagnosis, he noted. Of the available options for molecular testing, FISH (fluorescence in situ hybridization) testing is the most validated in the setting of ambiguous histology, he said.
Dr. Gerami disclosed serving as a consultant and researcher for Castle Biosciences, Myriad Genetics, and DermTech.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF HAWAII DERMATOLOGY SEMINAR

Immunotherapy in Melanoma
Immunotherapies have brought rapid and momentous advances—and at the same time, tricky management challenges, say clinicians from Boston Medical Center in Massachusetts. They report on a patient’s case that “underscores the complexity” of interpreting and managing the common and uncommon adverse effects of therapies.
Their patient, a 65-year-old man with metastatic melanoma, was started on ipilimumab and nivolumab. Two weeks after the first cycle, the patient came back to the hospital with symptoms of generalized fatigue and right upper quadrant abdominal pain; he was diagnosed with new ascites, leucocytosis, and normocytic anemia that required 2 transfusions. Magnetic resonance cholangiopancreatography showed a significant increase in tumor burden and mild left hepatic ductal dilation.
Related: NRAS mutations predict immunotherapy outcomes in melanoma patients
Because of the worsening severity of the hepatic tumor load, the patient was switched to dabrafenib and trametinib. He improved clinically, and his liver function tests improved, but by day 5, the patient had developed disseminated intravascular coagulation and pancytopenia. Clinically, however, he seemed well, with stable haemodynamics and no signs of infection.
The patient was started on high-dose steroids, and continued on dabrafenib and trametinib. The next several days saw “dramatic improvement in all parameters,” according to his clinicians. The steroids were tapered, and the patient was discharged to a rehabilitation facility. The following week at an outpatient visit he had no symptoms or significant abnormalities in his laboratory values.
The clinicians note that their patient brings to life several of the management challenges of immunotherapies. Notably, in addition to the immune-related adverse events common to immunotherapies—including life-threatening effects—clinicians may be faced with pseudoprogression: an initial increase in the size of tumor lesions with subsequent improvement.
Related: SU2C announces researcher-industry collaboration on immunotherapy
Other challenges, the clinicians note, are deciding how to sequence new immunotherapies and when is the right time to treat with high-dose steroids. So far, they say, no studies have delineated the best sequence of treatment, particularly in combination with other targeted agents, such as BRAF inhibitors like dabrafenib.
The exciting new hope offered by the new therapeutic options, the clinicians conclude, is tempered by the need to resolve these and other questions. In the meantime, the unique management challenges require “vigilance and ongoing research.”
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
Source:
Tran A, Sarosiek S, Ko NY. BMJ Case Rep. 2016; pii: bcr2016216681.
doi: 10.1136/bcr-2016-216681.
Immunotherapies have brought rapid and momentous advances—and at the same time, tricky management challenges, say clinicians from Boston Medical Center in Massachusetts. They report on a patient’s case that “underscores the complexity” of interpreting and managing the common and uncommon adverse effects of therapies.
Their patient, a 65-year-old man with metastatic melanoma, was started on ipilimumab and nivolumab. Two weeks after the first cycle, the patient came back to the hospital with symptoms of generalized fatigue and right upper quadrant abdominal pain; he was diagnosed with new ascites, leucocytosis, and normocytic anemia that required 2 transfusions. Magnetic resonance cholangiopancreatography showed a significant increase in tumor burden and mild left hepatic ductal dilation.
Related: NRAS mutations predict immunotherapy outcomes in melanoma patients
Because of the worsening severity of the hepatic tumor load, the patient was switched to dabrafenib and trametinib. He improved clinically, and his liver function tests improved, but by day 5, the patient had developed disseminated intravascular coagulation and pancytopenia. Clinically, however, he seemed well, with stable haemodynamics and no signs of infection.
The patient was started on high-dose steroids, and continued on dabrafenib and trametinib. The next several days saw “dramatic improvement in all parameters,” according to his clinicians. The steroids were tapered, and the patient was discharged to a rehabilitation facility. The following week at an outpatient visit he had no symptoms or significant abnormalities in his laboratory values.
The clinicians note that their patient brings to life several of the management challenges of immunotherapies. Notably, in addition to the immune-related adverse events common to immunotherapies—including life-threatening effects—clinicians may be faced with pseudoprogression: an initial increase in the size of tumor lesions with subsequent improvement.
Related: SU2C announces researcher-industry collaboration on immunotherapy
Other challenges, the clinicians note, are deciding how to sequence new immunotherapies and when is the right time to treat with high-dose steroids. So far, they say, no studies have delineated the best sequence of treatment, particularly in combination with other targeted agents, such as BRAF inhibitors like dabrafenib.
The exciting new hope offered by the new therapeutic options, the clinicians conclude, is tempered by the need to resolve these and other questions. In the meantime, the unique management challenges require “vigilance and ongoing research.”
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
Source:
Tran A, Sarosiek S, Ko NY. BMJ Case Rep. 2016; pii: bcr2016216681.
doi: 10.1136/bcr-2016-216681.
Immunotherapies have brought rapid and momentous advances—and at the same time, tricky management challenges, say clinicians from Boston Medical Center in Massachusetts. They report on a patient’s case that “underscores the complexity” of interpreting and managing the common and uncommon adverse effects of therapies.
Their patient, a 65-year-old man with metastatic melanoma, was started on ipilimumab and nivolumab. Two weeks after the first cycle, the patient came back to the hospital with symptoms of generalized fatigue and right upper quadrant abdominal pain; he was diagnosed with new ascites, leucocytosis, and normocytic anemia that required 2 transfusions. Magnetic resonance cholangiopancreatography showed a significant increase in tumor burden and mild left hepatic ductal dilation.
Related: NRAS mutations predict immunotherapy outcomes in melanoma patients
Because of the worsening severity of the hepatic tumor load, the patient was switched to dabrafenib and trametinib. He improved clinically, and his liver function tests improved, but by day 5, the patient had developed disseminated intravascular coagulation and pancytopenia. Clinically, however, he seemed well, with stable haemodynamics and no signs of infection.
The patient was started on high-dose steroids, and continued on dabrafenib and trametinib. The next several days saw “dramatic improvement in all parameters,” according to his clinicians. The steroids were tapered, and the patient was discharged to a rehabilitation facility. The following week at an outpatient visit he had no symptoms or significant abnormalities in his laboratory values.
The clinicians note that their patient brings to life several of the management challenges of immunotherapies. Notably, in addition to the immune-related adverse events common to immunotherapies—including life-threatening effects—clinicians may be faced with pseudoprogression: an initial increase in the size of tumor lesions with subsequent improvement.
Related: SU2C announces researcher-industry collaboration on immunotherapy
Other challenges, the clinicians note, are deciding how to sequence new immunotherapies and when is the right time to treat with high-dose steroids. So far, they say, no studies have delineated the best sequence of treatment, particularly in combination with other targeted agents, such as BRAF inhibitors like dabrafenib.
The exciting new hope offered by the new therapeutic options, the clinicians conclude, is tempered by the need to resolve these and other questions. In the meantime, the unique management challenges require “vigilance and ongoing research.”
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
Source:
Tran A, Sarosiek S, Ko NY. BMJ Case Rep. 2016; pii: bcr2016216681.
doi: 10.1136/bcr-2016-216681.
Online Patient-Reported Reviews of Mohs Micrographic Surgery: Qualitative Analysis of Positive and Negative Experiences
Mohs micrographic surgery (MMS) remains the gold standard for the removal of skin cancers in high-risk areas of the body while offering an excellent safety profile and sparing tissue.1 In the current health care environment, online patient reviews have grown in popularity and influence. More than 60% of consumers consult social media before making health care decisions.2 A recent analysis of online patient reviews of general dermatology practices demonstrated the perceived importance of physician empathy, thoroughness, and cognizance of cost in relation to patient-reported satisfaction.3 Because MMS is a well-recognized and unique outpatient-based surgical procedure, a review and analysis of online patient reviews specific to MMS can provide useful practice insights.
Materials and Methods
This study was conducted using an online platform (RealSelf [http://www.realself.com]) that connects patients and providers offering aesthetically oriented procedures; the site has 35 million unique visitors yearly.4 The community’s directory was used to identify and analyze all cumulative patient reviews from 2006 to December 20, 2015, using the search terms Mohs surgery or Mohs micrographic surgery. The study was exempt by the Northwestern University (Chicago, Illinois) institutional review board.
A standardized qualitative coding methodology was created and applied to all available comments regarding MMS. A broad list of positive and negative patient experiences was first created and agreed upon by all 3 investigators. Each individual comment was then attributed to 1 or more of these positive or negative themes. Of these comments, 10% were coded by 2 investigators (S.X. and Z.A.) to ensure internal validity; 1 investigator coded the remaining statements by patients (Z.A.). Patient-reported satisfaction ratings categorized as “worth it” or “not worth it” (as used by RealSelf to describe the patient-perceived value and utility of a given procedure) as well as cost of MMS were gathered. Cumulative patient ratings were collected for the procedure overall, physician’s bedside manner, answered questions, aftercare follow-up, time spent with patients, telephone/email responsiveness, staff professionalism/courtesy, payment process, and wait times. Patient-reported characteristics of MMS also were evaluated including physician specialty, lesion location, type of skin cancer, and type of closure. For lesion location, we graded whether the location represented a high-risk area as defined by the American Academy of Dermatology, American College of Mohs Surgery, and American Society for Dermatologic Surgery.5
Results
A total of 219 reviews related to MMS were collected as of December 20, 2015. Overall, MMS was considered “worth it” by 89% of patients (Table 1). Only 2% of patients described MMS as “not worth it.” There was a wide range reported for the cost of the procedure ($1–$100,000 [median, $1800]). Of those patients who reported their sex, females were 2.5-times more likely to post a review compared to males (51% vs 20%); however, 30% of reviewers did not report their sex. The mean (standard deviation) overall satisfaction rating was 4.8 (0.8). With regard to category-specific ratings (eg, bedside manner, aftercare follow-up, time spent with patients), the mean scores were all 4.7 or greater (Table 2).
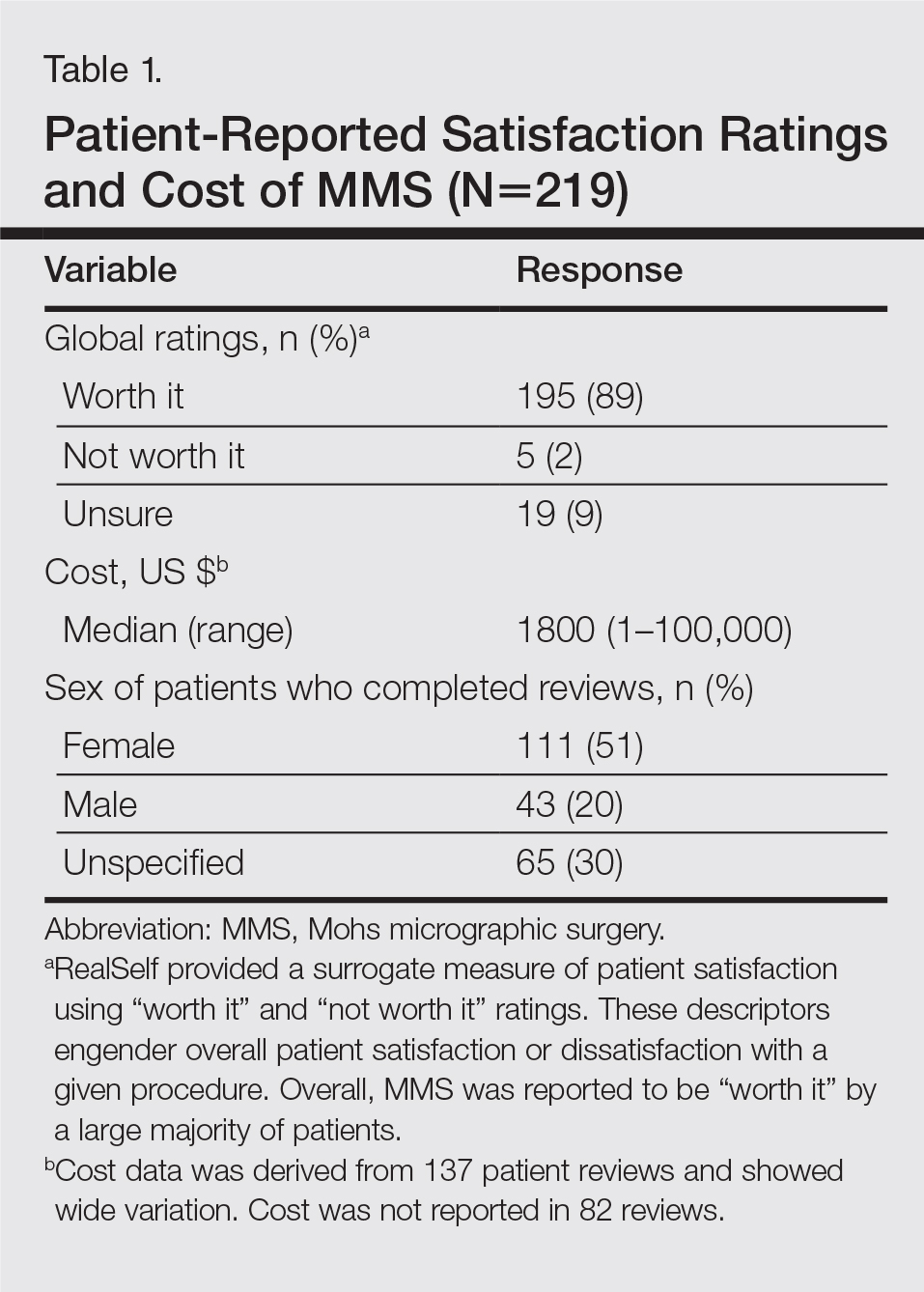

Regarding the surgical aspects of the procedure, the majority of patients reported that the excision of the lesion was performed by a dermatologist (62%). However, a notable portion of patients reported that the excision was performed by a plastic surgeon (21%). Physician specialty was not reported in 16% of the reviews. For the lesion closure, the patient-reported specialty of the physician was only slightly higher for dermatologists versus plastic surgeons (46% vs 44%)(Table 3).

The majority of patients who reported the location of the lesion treated with MMS identified a high-risk location (45%), a medium-risk location (18%), or an unspecified region of the face (15%), according to the appropriate-use criteria for MMS (Table 3).5 Patients did not specify the site of surgery 17% of the time. Only 5% of reported procedures were performed on low-risk areas.
Basal cell carcinomas were the most commonly reported lesions removed by MMS (38%), though 48% of reviews did not specify the type of tumor being treated (Table 3). A large majority (76%) did not specify the type of closure performed. When specified, secondary intention was used 10% of the time, followed by either a flap (6%) or skin graft (6%). Only 5% of patients reported an estimated size of the primary lesion in our study (data not shown).
The qualitative analysis demonstrated variance in themes for positive and negative characteristics (Table 4). Surgeon characteristics encompassed the 3 most commonly cited themes of positive remarks, including bedside manner (78%), communication skills (74%), and perceived expertise (58%). Specific to MMS, the tissue-sparing nature of the technique was cited by 14% of reviews as a positive theme. The most commonly cited themes of negative remarks were intraoperative and postoperative concerns, including postoperative disfigurement (16%), large scar (9%), healing time (9%), and procedural or postoperative pain (8%). A subtheme analysis of postoperative disfigurement revealed that eyelid or eyebrow distortion was the most common concern (29%), followed by redness and swelling (23%), an open wound (14%), and nostril/nose distortion (14%)(data not shown). Themes not commonly cited as either positive or negative included office environment, cost, and procedure time (data not shown).
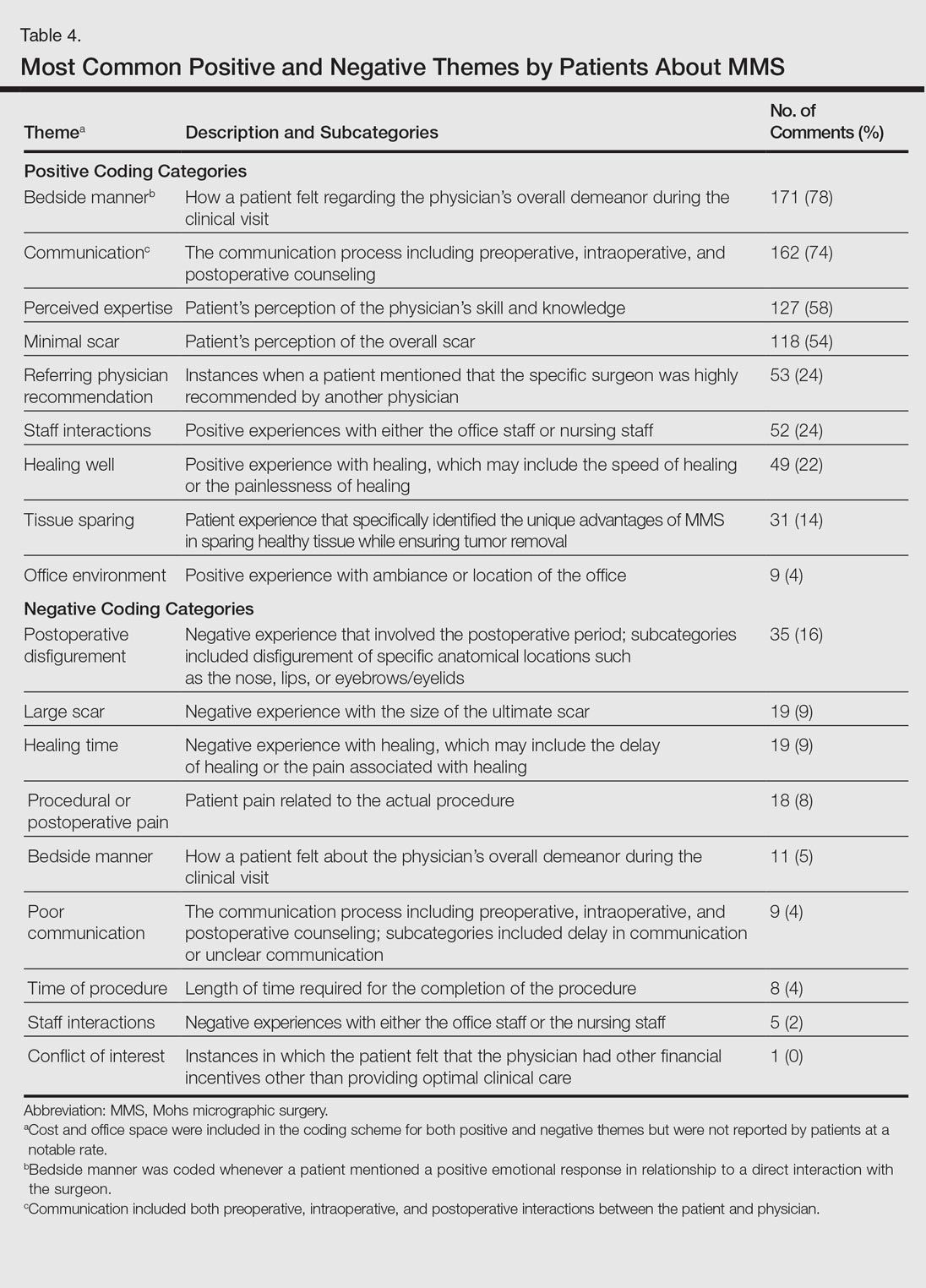
Comment
The overall satisfaction with MMS (89%) was one of the highest for any procedure on this online patient review site, albeit based on fewer reviews compared to other common aesthetic surgical procedures. In comparison, 78% of 13,500 reviewers rated breast augmentation as “worth it,” while 60% of 6800 reviewers rated rhinoplasty as “worth it” (as of December 2015). Overall, the online patient reviews evaluated in this study were consistent with a previously published structured data report on patient satisfaction with MMS.6
The results show a greater than expected proportion of both the MMS excision and closure being performed by plastic surgeons compared to dermatologists. In reality, the majority of MMS excisions are performed by dermatologists. Based on a survey of American College of Mohs Surgery (ACMS) members, only 6% of procedures were sent to other specialties for closure.7 Our results may reflect reporting bias or patients misconstruing true MMS with an excision and standard frozen sections, techniques that have lower cure rates. If so, there may be a need to educate patients regarding the specifics of MMS. Other possible explanations for the discrepancy between the online patient reviews and ACMS data include misinterpretation by patients on the exact definition of MMS or that a higher than expected number of procedures were performed by non-ACMS Mohs surgeons.
Our qualitative analysis revealed that patients most frequently commented on the interpersonal skills of their surgeons (eg, bedside manner, communication) as positive themes during MMS, similar to prior analyses of general dermatology practices.3 In comparison to a recent study assessing patient satisfaction with rhinoplasty on RealSelf, the final appearance of the nose represented the most common positive- and negative-cited theme.8 Mohs micrographic surgery procedures typically are done under local anesthesia, which may explain the greater importance of bedside manner and communication intraoperatively in comparison to final surgical outcomes for patient satisfaction. For negative themes, 3 of 4 most common concerns were directly related to the intraoperative and postoperative periods. Providers may be able to improve patient satisfaction by explaining the postoperative course, such as healing time and temporary physical restrictions, as well as possible sequelae in greater detail, which may be particularly pertinent for MMS involving the nose or near the eyes.
The global ratings for MMS are high, as shown in our data set of patient reviews; however, patient reviews are highly susceptible to reporting bias, recall bias, and missing information. Prior work using this online patient review website to investigate laser and light procedures also demonstrated the risk for imperfect information associated with patient reviews.9 Even so, the data does provide a glimpse into what is considered important to patients. Surgeon interpersonal skills and communication were the most frequently cited positive themes for MMS. The best surgical aspects of MMS focused on the unique tissue-sparing nature of the procedure and the removal of a cancerous lesion. Potential areas for improvement include a more thorough explanation of the intraoperative and postoperative process, specifically potential asymmetry related to the nose or the eyes, healing time, and scarring. These patient reviews underscore the importance of setting appropriate patient expectations. As patients become more connected and utilize online platforms to report their experiences, Mohs surgeons can take insights derived from online patient reviews for their own practice or geographic area to improve satisfaction and manage expectations.
- Alam M, Ibrahim O, Nodzenski M, et al. Adverse events associated with Mohs micrographic surgery: multicenter prospective cohort study of 20,821 cases at 23 centers. JAMA Dermatol. 2013;149:1378-1385.
- Fox S. The social life of health information. Pew Research Center website. http://www.pewresearch.org/fact-tank/2014/01/15/the-social-life-of-health-information/. Published January 15, 2014. Accessed February 11, 2017.
- Smith RJ, Lipoff JB. Evaluation of dermatology practice online reviews: lessons from qualitative analysis. JAMA Dermatol. 2016;152:153-157.
- Schlichte MJ, Karimkhani C, Jones T, et al. Patient use of social media to evaluate cosmetic treatments and procedures. Dermatol Online J. 2015;21. pii:13030/qt88z6r65x.
- American Academy of Dermatology; American College of Mohs Surgery; American Society for Dermatologic Surgery Association; American Society for Mohs Surgery; Ad Hoc Task Force, Connolly SM, Baker DR, Coldiron BM, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery [published online September 7, 2012]. Dermatol Surg. 2012;38:1582-1603.
- Asgari MM, Bertenthal D, Sen S, et al. Patient satisfaction after treatment of nonmelanoma skin cancer. Derm Surg. 2009;35:1041-1049.
- Campbell RM, Perlis CS, Malik MK, et al. Characteristics of Mohs practices in the United States: a recall survey of ACMS surgeons. Dermatol Surg. 2007;33:1413-1418; discussion, 1418.
- Khansa I, Khansa L, Pearson GD. Patient satisfaction after rhinoplasty: a social media analysis. Aesthet Surg J. 2016;36:NP1-5.
- Xu S, Walter J, Bhatia A. Patient-reported online satisfaction for laser and light procedures: need for caution. Dermatol Surg. 2017;43:154-158.
Mohs micrographic surgery (MMS) remains the gold standard for the removal of skin cancers in high-risk areas of the body while offering an excellent safety profile and sparing tissue.1 In the current health care environment, online patient reviews have grown in popularity and influence. More than 60% of consumers consult social media before making health care decisions.2 A recent analysis of online patient reviews of general dermatology practices demonstrated the perceived importance of physician empathy, thoroughness, and cognizance of cost in relation to patient-reported satisfaction.3 Because MMS is a well-recognized and unique outpatient-based surgical procedure, a review and analysis of online patient reviews specific to MMS can provide useful practice insights.
Materials and Methods
This study was conducted using an online platform (RealSelf [http://www.realself.com]) that connects patients and providers offering aesthetically oriented procedures; the site has 35 million unique visitors yearly.4 The community’s directory was used to identify and analyze all cumulative patient reviews from 2006 to December 20, 2015, using the search terms Mohs surgery or Mohs micrographic surgery. The study was exempt by the Northwestern University (Chicago, Illinois) institutional review board.
A standardized qualitative coding methodology was created and applied to all available comments regarding MMS. A broad list of positive and negative patient experiences was first created and agreed upon by all 3 investigators. Each individual comment was then attributed to 1 or more of these positive or negative themes. Of these comments, 10% were coded by 2 investigators (S.X. and Z.A.) to ensure internal validity; 1 investigator coded the remaining statements by patients (Z.A.). Patient-reported satisfaction ratings categorized as “worth it” or “not worth it” (as used by RealSelf to describe the patient-perceived value and utility of a given procedure) as well as cost of MMS were gathered. Cumulative patient ratings were collected for the procedure overall, physician’s bedside manner, answered questions, aftercare follow-up, time spent with patients, telephone/email responsiveness, staff professionalism/courtesy, payment process, and wait times. Patient-reported characteristics of MMS also were evaluated including physician specialty, lesion location, type of skin cancer, and type of closure. For lesion location, we graded whether the location represented a high-risk area as defined by the American Academy of Dermatology, American College of Mohs Surgery, and American Society for Dermatologic Surgery.5
Results
A total of 219 reviews related to MMS were collected as of December 20, 2015. Overall, MMS was considered “worth it” by 89% of patients (Table 1). Only 2% of patients described MMS as “not worth it.” There was a wide range reported for the cost of the procedure ($1–$100,000 [median, $1800]). Of those patients who reported their sex, females were 2.5-times more likely to post a review compared to males (51% vs 20%); however, 30% of reviewers did not report their sex. The mean (standard deviation) overall satisfaction rating was 4.8 (0.8). With regard to category-specific ratings (eg, bedside manner, aftercare follow-up, time spent with patients), the mean scores were all 4.7 or greater (Table 2).
Regarding the surgical aspects of the procedure, the majority of patients reported that the excision of the lesion was performed by a dermatologist (62%). However, a notable portion of patients reported that the excision was performed by a plastic surgeon (21%). Physician specialty was not reported in 16% of the reviews. For the lesion closure, the patient-reported specialty of the physician was only slightly higher for dermatologists versus plastic surgeons (46% vs 44%)(Table 3).
The majority of patients who reported the location of the lesion treated with MMS identified a high-risk location (45%), a medium-risk location (18%), or an unspecified region of the face (15%), according to the appropriate-use criteria for MMS (Table 3).5 Patients did not specify the site of surgery 17% of the time. Only 5% of reported procedures were performed on low-risk areas.
Basal cell carcinomas were the most commonly reported lesions removed by MMS (38%), though 48% of reviews did not specify the type of tumor being treated (Table 3). A large majority (76%) did not specify the type of closure performed. When specified, secondary intention was used 10% of the time, followed by either a flap (6%) or skin graft (6%). Only 5% of patients reported an estimated size of the primary lesion in our study (data not shown).
The qualitative analysis demonstrated variance in themes for positive and negative characteristics (Table 4). Surgeon characteristics encompassed the 3 most commonly cited themes of positive remarks, including bedside manner (78%), communication skills (74%), and perceived expertise (58%). Specific to MMS, the tissue-sparing nature of the technique was cited by 14% of reviews as a positive theme. The most commonly cited themes of negative remarks were intraoperative and postoperative concerns, including postoperative disfigurement (16%), large scar (9%), healing time (9%), and procedural or postoperative pain (8%). A subtheme analysis of postoperative disfigurement revealed that eyelid or eyebrow distortion was the most common concern (29%), followed by redness and swelling (23%), an open wound (14%), and nostril/nose distortion (14%)(data not shown). Themes not commonly cited as either positive or negative included office environment, cost, and procedure time (data not shown).
Comment
The overall satisfaction with MMS (89%) was one of the highest for any procedure on this online patient review site, albeit based on fewer reviews compared to other common aesthetic surgical procedures. In comparison, 78% of 13,500 reviewers rated breast augmentation as “worth it,” while 60% of 6800 reviewers rated rhinoplasty as “worth it” (as of December 2015). Overall, the online patient reviews evaluated in this study were consistent with a previously published structured data report on patient satisfaction with MMS.6
The results show a greater than expected proportion of both the MMS excision and closure being performed by plastic surgeons compared to dermatologists. In reality, the majority of MMS excisions are performed by dermatologists. Based on a survey of American College of Mohs Surgery (ACMS) members, only 6% of procedures were sent to other specialties for closure.7 Our results may reflect reporting bias or patients misconstruing true MMS with an excision and standard frozen sections, techniques that have lower cure rates. If so, there may be a need to educate patients regarding the specifics of MMS. Other possible explanations for the discrepancy between the online patient reviews and ACMS data include misinterpretation by patients on the exact definition of MMS or that a higher than expected number of procedures were performed by non-ACMS Mohs surgeons.
Our qualitative analysis revealed that patients most frequently commented on the interpersonal skills of their surgeons (eg, bedside manner, communication) as positive themes during MMS, similar to prior analyses of general dermatology practices.3 In comparison to a recent study assessing patient satisfaction with rhinoplasty on RealSelf, the final appearance of the nose represented the most common positive- and negative-cited theme.8 Mohs micrographic surgery procedures typically are done under local anesthesia, which may explain the greater importance of bedside manner and communication intraoperatively in comparison to final surgical outcomes for patient satisfaction. For negative themes, 3 of 4 most common concerns were directly related to the intraoperative and postoperative periods. Providers may be able to improve patient satisfaction by explaining the postoperative course, such as healing time and temporary physical restrictions, as well as possible sequelae in greater detail, which may be particularly pertinent for MMS involving the nose or near the eyes.
The global ratings for MMS are high, as shown in our data set of patient reviews; however, patient reviews are highly susceptible to reporting bias, recall bias, and missing information. Prior work using this online patient review website to investigate laser and light procedures also demonstrated the risk for imperfect information associated with patient reviews.9 Even so, the data does provide a glimpse into what is considered important to patients. Surgeon interpersonal skills and communication were the most frequently cited positive themes for MMS. The best surgical aspects of MMS focused on the unique tissue-sparing nature of the procedure and the removal of a cancerous lesion. Potential areas for improvement include a more thorough explanation of the intraoperative and postoperative process, specifically potential asymmetry related to the nose or the eyes, healing time, and scarring. These patient reviews underscore the importance of setting appropriate patient expectations. As patients become more connected and utilize online platforms to report their experiences, Mohs surgeons can take insights derived from online patient reviews for their own practice or geographic area to improve satisfaction and manage expectations.
Mohs micrographic surgery (MMS) remains the gold standard for the removal of skin cancers in high-risk areas of the body while offering an excellent safety profile and sparing tissue.1 In the current health care environment, online patient reviews have grown in popularity and influence. More than 60% of consumers consult social media before making health care decisions.2 A recent analysis of online patient reviews of general dermatology practices demonstrated the perceived importance of physician empathy, thoroughness, and cognizance of cost in relation to patient-reported satisfaction.3 Because MMS is a well-recognized and unique outpatient-based surgical procedure, a review and analysis of online patient reviews specific to MMS can provide useful practice insights.
Materials and Methods
This study was conducted using an online platform (RealSelf [http://www.realself.com]) that connects patients and providers offering aesthetically oriented procedures; the site has 35 million unique visitors yearly.4 The community’s directory was used to identify and analyze all cumulative patient reviews from 2006 to December 20, 2015, using the search terms Mohs surgery or Mohs micrographic surgery. The study was exempt by the Northwestern University (Chicago, Illinois) institutional review board.
A standardized qualitative coding methodology was created and applied to all available comments regarding MMS. A broad list of positive and negative patient experiences was first created and agreed upon by all 3 investigators. Each individual comment was then attributed to 1 or more of these positive or negative themes. Of these comments, 10% were coded by 2 investigators (S.X. and Z.A.) to ensure internal validity; 1 investigator coded the remaining statements by patients (Z.A.). Patient-reported satisfaction ratings categorized as “worth it” or “not worth it” (as used by RealSelf to describe the patient-perceived value and utility of a given procedure) as well as cost of MMS were gathered. Cumulative patient ratings were collected for the procedure overall, physician’s bedside manner, answered questions, aftercare follow-up, time spent with patients, telephone/email responsiveness, staff professionalism/courtesy, payment process, and wait times. Patient-reported characteristics of MMS also were evaluated including physician specialty, lesion location, type of skin cancer, and type of closure. For lesion location, we graded whether the location represented a high-risk area as defined by the American Academy of Dermatology, American College of Mohs Surgery, and American Society for Dermatologic Surgery.5
Results
A total of 219 reviews related to MMS were collected as of December 20, 2015. Overall, MMS was considered “worth it” by 89% of patients (Table 1). Only 2% of patients described MMS as “not worth it.” There was a wide range reported for the cost of the procedure ($1–$100,000 [median, $1800]). Of those patients who reported their sex, females were 2.5-times more likely to post a review compared to males (51% vs 20%); however, 30% of reviewers did not report their sex. The mean (standard deviation) overall satisfaction rating was 4.8 (0.8). With regard to category-specific ratings (eg, bedside manner, aftercare follow-up, time spent with patients), the mean scores were all 4.7 or greater (Table 2).
Regarding the surgical aspects of the procedure, the majority of patients reported that the excision of the lesion was performed by a dermatologist (62%). However, a notable portion of patients reported that the excision was performed by a plastic surgeon (21%). Physician specialty was not reported in 16% of the reviews. For the lesion closure, the patient-reported specialty of the physician was only slightly higher for dermatologists versus plastic surgeons (46% vs 44%)(Table 3).
The majority of patients who reported the location of the lesion treated with MMS identified a high-risk location (45%), a medium-risk location (18%), or an unspecified region of the face (15%), according to the appropriate-use criteria for MMS (Table 3).5 Patients did not specify the site of surgery 17% of the time. Only 5% of reported procedures were performed on low-risk areas.
Basal cell carcinomas were the most commonly reported lesions removed by MMS (38%), though 48% of reviews did not specify the type of tumor being treated (Table 3). A large majority (76%) did not specify the type of closure performed. When specified, secondary intention was used 10% of the time, followed by either a flap (6%) or skin graft (6%). Only 5% of patients reported an estimated size of the primary lesion in our study (data not shown).
The qualitative analysis demonstrated variance in themes for positive and negative characteristics (Table 4). Surgeon characteristics encompassed the 3 most commonly cited themes of positive remarks, including bedside manner (78%), communication skills (74%), and perceived expertise (58%). Specific to MMS, the tissue-sparing nature of the technique was cited by 14% of reviews as a positive theme. The most commonly cited themes of negative remarks were intraoperative and postoperative concerns, including postoperative disfigurement (16%), large scar (9%), healing time (9%), and procedural or postoperative pain (8%). A subtheme analysis of postoperative disfigurement revealed that eyelid or eyebrow distortion was the most common concern (29%), followed by redness and swelling (23%), an open wound (14%), and nostril/nose distortion (14%)(data not shown). Themes not commonly cited as either positive or negative included office environment, cost, and procedure time (data not shown).
Comment
The overall satisfaction with MMS (89%) was one of the highest for any procedure on this online patient review site, albeit based on fewer reviews compared to other common aesthetic surgical procedures. In comparison, 78% of 13,500 reviewers rated breast augmentation as “worth it,” while 60% of 6800 reviewers rated rhinoplasty as “worth it” (as of December 2015). Overall, the online patient reviews evaluated in this study were consistent with a previously published structured data report on patient satisfaction with MMS.6
The results show a greater than expected proportion of both the MMS excision and closure being performed by plastic surgeons compared to dermatologists. In reality, the majority of MMS excisions are performed by dermatologists. Based on a survey of American College of Mohs Surgery (ACMS) members, only 6% of procedures were sent to other specialties for closure.7 Our results may reflect reporting bias or patients misconstruing true MMS with an excision and standard frozen sections, techniques that have lower cure rates. If so, there may be a need to educate patients regarding the specifics of MMS. Other possible explanations for the discrepancy between the online patient reviews and ACMS data include misinterpretation by patients on the exact definition of MMS or that a higher than expected number of procedures were performed by non-ACMS Mohs surgeons.
Our qualitative analysis revealed that patients most frequently commented on the interpersonal skills of their surgeons (eg, bedside manner, communication) as positive themes during MMS, similar to prior analyses of general dermatology practices.3 In comparison to a recent study assessing patient satisfaction with rhinoplasty on RealSelf, the final appearance of the nose represented the most common positive- and negative-cited theme.8 Mohs micrographic surgery procedures typically are done under local anesthesia, which may explain the greater importance of bedside manner and communication intraoperatively in comparison to final surgical outcomes for patient satisfaction. For negative themes, 3 of 4 most common concerns were directly related to the intraoperative and postoperative periods. Providers may be able to improve patient satisfaction by explaining the postoperative course, such as healing time and temporary physical restrictions, as well as possible sequelae in greater detail, which may be particularly pertinent for MMS involving the nose or near the eyes.
The global ratings for MMS are high, as shown in our data set of patient reviews; however, patient reviews are highly susceptible to reporting bias, recall bias, and missing information. Prior work using this online patient review website to investigate laser and light procedures also demonstrated the risk for imperfect information associated with patient reviews.9 Even so, the data does provide a glimpse into what is considered important to patients. Surgeon interpersonal skills and communication were the most frequently cited positive themes for MMS. The best surgical aspects of MMS focused on the unique tissue-sparing nature of the procedure and the removal of a cancerous lesion. Potential areas for improvement include a more thorough explanation of the intraoperative and postoperative process, specifically potential asymmetry related to the nose or the eyes, healing time, and scarring. These patient reviews underscore the importance of setting appropriate patient expectations. As patients become more connected and utilize online platforms to report their experiences, Mohs surgeons can take insights derived from online patient reviews for their own practice or geographic area to improve satisfaction and manage expectations.
- Alam M, Ibrahim O, Nodzenski M, et al. Adverse events associated with Mohs micrographic surgery: multicenter prospective cohort study of 20,821 cases at 23 centers. JAMA Dermatol. 2013;149:1378-1385.
- Fox S. The social life of health information. Pew Research Center website. http://www.pewresearch.org/fact-tank/2014/01/15/the-social-life-of-health-information/. Published January 15, 2014. Accessed February 11, 2017.
- Smith RJ, Lipoff JB. Evaluation of dermatology practice online reviews: lessons from qualitative analysis. JAMA Dermatol. 2016;152:153-157.
- Schlichte MJ, Karimkhani C, Jones T, et al. Patient use of social media to evaluate cosmetic treatments and procedures. Dermatol Online J. 2015;21. pii:13030/qt88z6r65x.
- American Academy of Dermatology; American College of Mohs Surgery; American Society for Dermatologic Surgery Association; American Society for Mohs Surgery; Ad Hoc Task Force, Connolly SM, Baker DR, Coldiron BM, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery [published online September 7, 2012]. Dermatol Surg. 2012;38:1582-1603.
- Asgari MM, Bertenthal D, Sen S, et al. Patient satisfaction after treatment of nonmelanoma skin cancer. Derm Surg. 2009;35:1041-1049.
- Campbell RM, Perlis CS, Malik MK, et al. Characteristics of Mohs practices in the United States: a recall survey of ACMS surgeons. Dermatol Surg. 2007;33:1413-1418; discussion, 1418.
- Khansa I, Khansa L, Pearson GD. Patient satisfaction after rhinoplasty: a social media analysis. Aesthet Surg J. 2016;36:NP1-5.
- Xu S, Walter J, Bhatia A. Patient-reported online satisfaction for laser and light procedures: need for caution. Dermatol Surg. 2017;43:154-158.
- Alam M, Ibrahim O, Nodzenski M, et al. Adverse events associated with Mohs micrographic surgery: multicenter prospective cohort study of 20,821 cases at 23 centers. JAMA Dermatol. 2013;149:1378-1385.
- Fox S. The social life of health information. Pew Research Center website. http://www.pewresearch.org/fact-tank/2014/01/15/the-social-life-of-health-information/. Published January 15, 2014. Accessed February 11, 2017.
- Smith RJ, Lipoff JB. Evaluation of dermatology practice online reviews: lessons from qualitative analysis. JAMA Dermatol. 2016;152:153-157.
- Schlichte MJ, Karimkhani C, Jones T, et al. Patient use of social media to evaluate cosmetic treatments and procedures. Dermatol Online J. 2015;21. pii:13030/qt88z6r65x.
- American Academy of Dermatology; American College of Mohs Surgery; American Society for Dermatologic Surgery Association; American Society for Mohs Surgery; Ad Hoc Task Force, Connolly SM, Baker DR, Coldiron BM, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery [published online September 7, 2012]. Dermatol Surg. 2012;38:1582-1603.
- Asgari MM, Bertenthal D, Sen S, et al. Patient satisfaction after treatment of nonmelanoma skin cancer. Derm Surg. 2009;35:1041-1049.
- Campbell RM, Perlis CS, Malik MK, et al. Characteristics of Mohs practices in the United States: a recall survey of ACMS surgeons. Dermatol Surg. 2007;33:1413-1418; discussion, 1418.
- Khansa I, Khansa L, Pearson GD. Patient satisfaction after rhinoplasty: a social media analysis. Aesthet Surg J. 2016;36:NP1-5.
- Xu S, Walter J, Bhatia A. Patient-reported online satisfaction for laser and light procedures: need for caution. Dermatol Surg. 2017;43:154-158.
Resident Pearl
Patients are posting reviews online now more than ever regarding their experiences with dermatologic surgical procedures. Mohs micrographic surgery is rated highly by patients but suspect to missing information and a higher than expected attribution of the procedure to plastic surgeons.