User login
Tirzepatide Reduces Sleep Interruptions, Halting Almost Half of CPAP Use
ORLANDO, FLA. — The diabetes and weight loss drug tirzepatide (Mounjaro for type 2 diabetes; Zepbound for obesity) was so effective at reducing sleep disruptions in patients with obesity and obstructive sleep apnea (OSA) that 40%-50% no longer needed to use a continuous positive airway pressure (CPAP) device, according to two new studies.
Tirzepatide, a long-acting glucose-dependent insulinotropic polypeptide (GIP) receptor agonist and glucagon-like peptide 1 (GLP-1) receptor agonist, also lowered C-reactive protein levels and systolic blood pressure. And patients taking the medication lost 18%-20% of their body weight.
said lead author Atul Malhotra, MD, professor of medicine at the University of California, San Diego, and director of sleep medicine at UC San Diego Health.
The two double-blind, randomized, controlled trials in patients with obesity and moderate to severe OSA were conducted at 60 sites in nine countries. The results were presented at the American Diabetes Association (ADA) 84th Scientific Sessions and simultaneously published online in the New England Journal of Medicine.
OSA affects 1 billion people worldwide and 30 million American adults, many of whom are undiagnosed. Obesity is a common risk factor. According to the ADA, 40% of those with obesity have OSA and 70% of those with OSA have obesity.
CPAP is an effective and the most-used intervention for OSA, but many patients refuse to use the device, stop using it, or cannot use it. Should tirzepatide eventually gain Food and Drug Administration approval for OSA, it would be the first drug approved for the condition.
“This new drug treatment offers a more accessible alternative for individuals who cannot tolerate or adhere to existing therapies,” said Dr. Malhotra.
Huge Reduction in Episodes, Severity
For the two studies, patients were enrolled who had moderate to severe OSA, defined as more than 15 events per hour (using the apnea-hypopnea index [AHI]) and a body mass index of 30 kg/m2 or greater. Those not using a CPAP device were enrolled in study 1, and those using a CPAP device were enrolled in study 2.
Participants received either the maximum tolerated dose of tirzepatide (10 or 15 mg by once-weekly injection) or placebo for 1 year. In study 1, 114 individuals received tirzepatide and 120 received placebo. For study 2, 119 patients received tirzepatide and 114 received placebo. All participants received regular lifestyle counseling sessions about nutrition and were instructed to reduce food intake by 500 kcal/day and to engage in at least 150 min/week of physical activity.
Enrollment was limited to 70% men to ensure adequate representation of women.
At baseline, 65%-70% of participants had severe OSA, with more than 30 events/hour on the AHI scale and a mean of 51.5 events/hour.
By 1 year, patients taking tirzepatide had 27-30 fewer events/hour, compared with 4-6 fewer events/hour for those taking placebo.
Up to half of those who received tirzepatide in both trials had less than 5 events/hour or 5-14 AHI events/hour and an Epworth Sleepiness Scale score of 10 or less. Those thresholds “represent a level at which CPAP therapy may not be recommended,” wrote the authors.
Patients in the tirzepatide group also had a decrease in systolic blood pressure from baseline of 9.7 mm Hg in study 1 and 7.6 mm Hg in study 2 at week 48.
The most common adverse events were diarrhea, nausea, and vomiting, which occurred in approximately a quarter of patients taking tirzepatide. There were two adjudicated-confirmed cases of acute pancreatitis in those taking tirzepatide in study 2.
Patients who received tirzepatide also reported fewer daytime and nighttime disturbances, as measured using the Patient-Reported Outcomes Measurement Information System Short Form scale for Sleep-Related Impairment and Sleep Disturbance.
Tirzepatide Plus CPAP Are Best
Writing in an accompanying editorial, Sanjay R. Patel, MD, noted that, although clinical guidelines have recommended that weight loss strategies be incorporated as part of OSA treatment, “the integration of obesity management into the approaches to care for obstructive sleep apnea has lagged.”
As many as half of patients abandon CPAP therapy within 3 years, wrote Dr. Patel, who is professor of medicine and epidemiology at the University of Pittsburgh, Pittsburgh, Pennsylvania, and medical director of the UPMC Comprehensive Sleep Disorders program. “An effective medication to treat obesity is thus an obvious avenue to pursue.”
Dr. Patel noted the large reductions in the number of events on the AHI scale. He wrote that the improvement in systolic blood pressure “was substantially larger than effects seen with CPAP therapy alone and indicate that tirzepatide may be an attractive option for those patients who seek to reduce their cardiovascular risk.”
Dr. Patel raised concerns about whether patients outside of a trial would stick with therapy, noting studies have shown high rates of discontinuation of GLP-1 receptor agonists.
And, he wrote, “racial disparities in the use of GLP-1 receptor agonists among patients with diabetes arouse concern that the addition of tirzepatide as a treatment option for obstructive sleep apnea without directly addressing policies relative to coverage of care will only further exacerbate already pervasive disparities in clinical care for obstructive sleep apnea.”
Commenting on the study during the presentation of the results, Louis Aronne, MD, said he believes the trials demonstrate “the treatment of obesity with tirzepatide plus CPAP is really the optimal treatment for obstructive sleep apnea and obesity-related cardiometabolic risks.” Dr. Aronne is the Sanford I. Weill professor of metabolic research at Weill Cornell Medical College, New York City.
Dr. Aronne added there is still much to learn. It is still not clear whether tirzepatide had an independent effect in the OSA trial — as has been seen in other studies where the drug clearly reduced cardiovascular risk — or whether the positive results were primarily caused by weight loss.
“I believe that over time we’ll see that this particular effect in sleep apnea is related to weight,” he said.
The study was supported by Eli Lilly. Dr. Malhotra has reported being a paid consultant for Lilly and ZOLL Medical and a cofounder of Healcisio.
A version of this article appeared on Medscape.com.
ORLANDO, FLA. — The diabetes and weight loss drug tirzepatide (Mounjaro for type 2 diabetes; Zepbound for obesity) was so effective at reducing sleep disruptions in patients with obesity and obstructive sleep apnea (OSA) that 40%-50% no longer needed to use a continuous positive airway pressure (CPAP) device, according to two new studies.
Tirzepatide, a long-acting glucose-dependent insulinotropic polypeptide (GIP) receptor agonist and glucagon-like peptide 1 (GLP-1) receptor agonist, also lowered C-reactive protein levels and systolic blood pressure. And patients taking the medication lost 18%-20% of their body weight.
said lead author Atul Malhotra, MD, professor of medicine at the University of California, San Diego, and director of sleep medicine at UC San Diego Health.
The two double-blind, randomized, controlled trials in patients with obesity and moderate to severe OSA were conducted at 60 sites in nine countries. The results were presented at the American Diabetes Association (ADA) 84th Scientific Sessions and simultaneously published online in the New England Journal of Medicine.
OSA affects 1 billion people worldwide and 30 million American adults, many of whom are undiagnosed. Obesity is a common risk factor. According to the ADA, 40% of those with obesity have OSA and 70% of those with OSA have obesity.
CPAP is an effective and the most-used intervention for OSA, but many patients refuse to use the device, stop using it, or cannot use it. Should tirzepatide eventually gain Food and Drug Administration approval for OSA, it would be the first drug approved for the condition.
“This new drug treatment offers a more accessible alternative for individuals who cannot tolerate or adhere to existing therapies,” said Dr. Malhotra.
Huge Reduction in Episodes, Severity
For the two studies, patients were enrolled who had moderate to severe OSA, defined as more than 15 events per hour (using the apnea-hypopnea index [AHI]) and a body mass index of 30 kg/m2 or greater. Those not using a CPAP device were enrolled in study 1, and those using a CPAP device were enrolled in study 2.
Participants received either the maximum tolerated dose of tirzepatide (10 or 15 mg by once-weekly injection) or placebo for 1 year. In study 1, 114 individuals received tirzepatide and 120 received placebo. For study 2, 119 patients received tirzepatide and 114 received placebo. All participants received regular lifestyle counseling sessions about nutrition and were instructed to reduce food intake by 500 kcal/day and to engage in at least 150 min/week of physical activity.
Enrollment was limited to 70% men to ensure adequate representation of women.
At baseline, 65%-70% of participants had severe OSA, with more than 30 events/hour on the AHI scale and a mean of 51.5 events/hour.
By 1 year, patients taking tirzepatide had 27-30 fewer events/hour, compared with 4-6 fewer events/hour for those taking placebo.
Up to half of those who received tirzepatide in both trials had less than 5 events/hour or 5-14 AHI events/hour and an Epworth Sleepiness Scale score of 10 or less. Those thresholds “represent a level at which CPAP therapy may not be recommended,” wrote the authors.
Patients in the tirzepatide group also had a decrease in systolic blood pressure from baseline of 9.7 mm Hg in study 1 and 7.6 mm Hg in study 2 at week 48.
The most common adverse events were diarrhea, nausea, and vomiting, which occurred in approximately a quarter of patients taking tirzepatide. There were two adjudicated-confirmed cases of acute pancreatitis in those taking tirzepatide in study 2.
Patients who received tirzepatide also reported fewer daytime and nighttime disturbances, as measured using the Patient-Reported Outcomes Measurement Information System Short Form scale for Sleep-Related Impairment and Sleep Disturbance.
Tirzepatide Plus CPAP Are Best
Writing in an accompanying editorial, Sanjay R. Patel, MD, noted that, although clinical guidelines have recommended that weight loss strategies be incorporated as part of OSA treatment, “the integration of obesity management into the approaches to care for obstructive sleep apnea has lagged.”
As many as half of patients abandon CPAP therapy within 3 years, wrote Dr. Patel, who is professor of medicine and epidemiology at the University of Pittsburgh, Pittsburgh, Pennsylvania, and medical director of the UPMC Comprehensive Sleep Disorders program. “An effective medication to treat obesity is thus an obvious avenue to pursue.”
Dr. Patel noted the large reductions in the number of events on the AHI scale. He wrote that the improvement in systolic blood pressure “was substantially larger than effects seen with CPAP therapy alone and indicate that tirzepatide may be an attractive option for those patients who seek to reduce their cardiovascular risk.”
Dr. Patel raised concerns about whether patients outside of a trial would stick with therapy, noting studies have shown high rates of discontinuation of GLP-1 receptor agonists.
And, he wrote, “racial disparities in the use of GLP-1 receptor agonists among patients with diabetes arouse concern that the addition of tirzepatide as a treatment option for obstructive sleep apnea without directly addressing policies relative to coverage of care will only further exacerbate already pervasive disparities in clinical care for obstructive sleep apnea.”
Commenting on the study during the presentation of the results, Louis Aronne, MD, said he believes the trials demonstrate “the treatment of obesity with tirzepatide plus CPAP is really the optimal treatment for obstructive sleep apnea and obesity-related cardiometabolic risks.” Dr. Aronne is the Sanford I. Weill professor of metabolic research at Weill Cornell Medical College, New York City.
Dr. Aronne added there is still much to learn. It is still not clear whether tirzepatide had an independent effect in the OSA trial — as has been seen in other studies where the drug clearly reduced cardiovascular risk — or whether the positive results were primarily caused by weight loss.
“I believe that over time we’ll see that this particular effect in sleep apnea is related to weight,” he said.
The study was supported by Eli Lilly. Dr. Malhotra has reported being a paid consultant for Lilly and ZOLL Medical and a cofounder of Healcisio.
A version of this article appeared on Medscape.com.
ORLANDO, FLA. — The diabetes and weight loss drug tirzepatide (Mounjaro for type 2 diabetes; Zepbound for obesity) was so effective at reducing sleep disruptions in patients with obesity and obstructive sleep apnea (OSA) that 40%-50% no longer needed to use a continuous positive airway pressure (CPAP) device, according to two new studies.
Tirzepatide, a long-acting glucose-dependent insulinotropic polypeptide (GIP) receptor agonist and glucagon-like peptide 1 (GLP-1) receptor agonist, also lowered C-reactive protein levels and systolic blood pressure. And patients taking the medication lost 18%-20% of their body weight.
said lead author Atul Malhotra, MD, professor of medicine at the University of California, San Diego, and director of sleep medicine at UC San Diego Health.
The two double-blind, randomized, controlled trials in patients with obesity and moderate to severe OSA were conducted at 60 sites in nine countries. The results were presented at the American Diabetes Association (ADA) 84th Scientific Sessions and simultaneously published online in the New England Journal of Medicine.
OSA affects 1 billion people worldwide and 30 million American adults, many of whom are undiagnosed. Obesity is a common risk factor. According to the ADA, 40% of those with obesity have OSA and 70% of those with OSA have obesity.
CPAP is an effective and the most-used intervention for OSA, but many patients refuse to use the device, stop using it, or cannot use it. Should tirzepatide eventually gain Food and Drug Administration approval for OSA, it would be the first drug approved for the condition.
“This new drug treatment offers a more accessible alternative for individuals who cannot tolerate or adhere to existing therapies,” said Dr. Malhotra.
Huge Reduction in Episodes, Severity
For the two studies, patients were enrolled who had moderate to severe OSA, defined as more than 15 events per hour (using the apnea-hypopnea index [AHI]) and a body mass index of 30 kg/m2 or greater. Those not using a CPAP device were enrolled in study 1, and those using a CPAP device were enrolled in study 2.
Participants received either the maximum tolerated dose of tirzepatide (10 or 15 mg by once-weekly injection) or placebo for 1 year. In study 1, 114 individuals received tirzepatide and 120 received placebo. For study 2, 119 patients received tirzepatide and 114 received placebo. All participants received regular lifestyle counseling sessions about nutrition and were instructed to reduce food intake by 500 kcal/day and to engage in at least 150 min/week of physical activity.
Enrollment was limited to 70% men to ensure adequate representation of women.
At baseline, 65%-70% of participants had severe OSA, with more than 30 events/hour on the AHI scale and a mean of 51.5 events/hour.
By 1 year, patients taking tirzepatide had 27-30 fewer events/hour, compared with 4-6 fewer events/hour for those taking placebo.
Up to half of those who received tirzepatide in both trials had less than 5 events/hour or 5-14 AHI events/hour and an Epworth Sleepiness Scale score of 10 or less. Those thresholds “represent a level at which CPAP therapy may not be recommended,” wrote the authors.
Patients in the tirzepatide group also had a decrease in systolic blood pressure from baseline of 9.7 mm Hg in study 1 and 7.6 mm Hg in study 2 at week 48.
The most common adverse events were diarrhea, nausea, and vomiting, which occurred in approximately a quarter of patients taking tirzepatide. There were two adjudicated-confirmed cases of acute pancreatitis in those taking tirzepatide in study 2.
Patients who received tirzepatide also reported fewer daytime and nighttime disturbances, as measured using the Patient-Reported Outcomes Measurement Information System Short Form scale for Sleep-Related Impairment and Sleep Disturbance.
Tirzepatide Plus CPAP Are Best
Writing in an accompanying editorial, Sanjay R. Patel, MD, noted that, although clinical guidelines have recommended that weight loss strategies be incorporated as part of OSA treatment, “the integration of obesity management into the approaches to care for obstructive sleep apnea has lagged.”
As many as half of patients abandon CPAP therapy within 3 years, wrote Dr. Patel, who is professor of medicine and epidemiology at the University of Pittsburgh, Pittsburgh, Pennsylvania, and medical director of the UPMC Comprehensive Sleep Disorders program. “An effective medication to treat obesity is thus an obvious avenue to pursue.”
Dr. Patel noted the large reductions in the number of events on the AHI scale. He wrote that the improvement in systolic blood pressure “was substantially larger than effects seen with CPAP therapy alone and indicate that tirzepatide may be an attractive option for those patients who seek to reduce their cardiovascular risk.”
Dr. Patel raised concerns about whether patients outside of a trial would stick with therapy, noting studies have shown high rates of discontinuation of GLP-1 receptor agonists.
And, he wrote, “racial disparities in the use of GLP-1 receptor agonists among patients with diabetes arouse concern that the addition of tirzepatide as a treatment option for obstructive sleep apnea without directly addressing policies relative to coverage of care will only further exacerbate already pervasive disparities in clinical care for obstructive sleep apnea.”
Commenting on the study during the presentation of the results, Louis Aronne, MD, said he believes the trials demonstrate “the treatment of obesity with tirzepatide plus CPAP is really the optimal treatment for obstructive sleep apnea and obesity-related cardiometabolic risks.” Dr. Aronne is the Sanford I. Weill professor of metabolic research at Weill Cornell Medical College, New York City.
Dr. Aronne added there is still much to learn. It is still not clear whether tirzepatide had an independent effect in the OSA trial — as has been seen in other studies where the drug clearly reduced cardiovascular risk — or whether the positive results were primarily caused by weight loss.
“I believe that over time we’ll see that this particular effect in sleep apnea is related to weight,” he said.
The study was supported by Eli Lilly. Dr. Malhotra has reported being a paid consultant for Lilly and ZOLL Medical and a cofounder of Healcisio.
A version of this article appeared on Medscape.com.
FROM ADA 2024
Urgent Need for Better Care, New Policies to Lower Insomnia Burden
HOUSTON — A new analysis highlights the high burden of insomnia across the Americas, with about 17% of adults suffering from this chronic sleep disorder.
“Our findings underscore the urgent need for enhanced clinical care pathways and policy interventions to effectively diagnose and treat insomnia. It is crucial to foster greater awareness of the critical role that sleep plays in overall health,” lead investigator Adam Benjafield, PhD, vice president for medical affairs at ResMed, Sydney, Australia, said in an interview.
“Insomnia not only affects individuals’ health and quality of life but also has broader implications for public health systems. Developing comprehensive care strategies and promoting education about sleep health could significantly improve outcomes for individuals suffering from insomnia disorder,” Dr. Benjafield said.
The findings were presented at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies.
Underdiagnosed, Undertreated
Sleep disruptions contribute to various medical problems, including cognitive impairment, reduced immune function, metabolic imbalance, and exacerbation of psychiatric conditions. While the prevalence of insomnia in developed countries like the United States and Canada is known, there is limited epidemiologic evidence, and no reliable estimate for the disorder across the Americas — especially in low- and middle-income countries.
The researchers used published nation-specific data to estimate the prevalence of adult insomnia disorder across the 55 countries defined by the United Nations as comprising the Americas.
Based on the available data, the researchers estimated that about 123 million adults across the Americas have insomnia disorder (16.8%) — with greater prevalence in women (73 million, 19.5%) than in men (50 million, 14%).
The nations with the greatest burden of insomnia disorder are the United States (37 million), Brazil (29 million), and Mexico (16 million).
“While our study did not specifically investigate trends over time due to its scope, evidence from other research suggests that insomnia is becoming more prevalent over the long term. This growing trend highlights the increasing need for awareness and intervention in managing sleep health,” Dr. Benjafield said.
Insomnia is underdiagnosed and undertreated partly because of general lack of awareness about the importance of addressing sleep disorders and the fact that cognitive-behavioral therapy for insomnia (CBT-I), which is recommended as first-line treatment, is not widely accessible because of a shortage of trained CBT-I practitioners.
“Many individuals with insomnia struggle to find and receive this effective nonpharmacological treatment. Consequently, there is an overreliance on pharmaceutical solutions, which are ideally used for short-term management but are often extended due to the lack of alternatives. These medications can lead to dependency and other side effects,” Dr. Benjafield said.
Ask About Sleep
Insomnia symptoms are a “common presenting complaint in doctors’ offices in the United States. The percentages in this poster show that insomnia disorder has a similar, high percent prevalence across countries in the Americas,” Boris Gilyadov, MD, assistant professor of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai in New York City, said in an interview.
“During preventive care visits and general physical exams, patients should be asked about the quality of their sleep. Patients may benefit from a referral to the sleep medicine clinic when appropriate,” said Dr. Gilyadov, who wasn’t involved in the study.
“CBT-I is the first-line treatment for chronic insomnia disorder and can be an effective treatment for most patients. An alternative to CBT-I, when it is not available, is digital CBT-I,” Dr. Gilyadov said.
“There are also behavioral therapies called BBT-I [brief behavioral treatment for insomnia] and ACT [acceptance and commitment therapy]. These are therapies that may be offered by psychologists who specialize in the treatment of chronic insomnia disorder,” Dr. Gilyadov noted.
The study was conducted in collaboration with medXcloud and funded by ResMed. Dr. Benjafield is an employee of ResMed. Dr. Gilyadov had no relevant disclosures.
A version of this article first appeared on Medscape.com.
HOUSTON — A new analysis highlights the high burden of insomnia across the Americas, with about 17% of adults suffering from this chronic sleep disorder.
“Our findings underscore the urgent need for enhanced clinical care pathways and policy interventions to effectively diagnose and treat insomnia. It is crucial to foster greater awareness of the critical role that sleep plays in overall health,” lead investigator Adam Benjafield, PhD, vice president for medical affairs at ResMed, Sydney, Australia, said in an interview.
“Insomnia not only affects individuals’ health and quality of life but also has broader implications for public health systems. Developing comprehensive care strategies and promoting education about sleep health could significantly improve outcomes for individuals suffering from insomnia disorder,” Dr. Benjafield said.
The findings were presented at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies.
Underdiagnosed, Undertreated
Sleep disruptions contribute to various medical problems, including cognitive impairment, reduced immune function, metabolic imbalance, and exacerbation of psychiatric conditions. While the prevalence of insomnia in developed countries like the United States and Canada is known, there is limited epidemiologic evidence, and no reliable estimate for the disorder across the Americas — especially in low- and middle-income countries.
The researchers used published nation-specific data to estimate the prevalence of adult insomnia disorder across the 55 countries defined by the United Nations as comprising the Americas.
Based on the available data, the researchers estimated that about 123 million adults across the Americas have insomnia disorder (16.8%) — with greater prevalence in women (73 million, 19.5%) than in men (50 million, 14%).
The nations with the greatest burden of insomnia disorder are the United States (37 million), Brazil (29 million), and Mexico (16 million).
“While our study did not specifically investigate trends over time due to its scope, evidence from other research suggests that insomnia is becoming more prevalent over the long term. This growing trend highlights the increasing need for awareness and intervention in managing sleep health,” Dr. Benjafield said.
Insomnia is underdiagnosed and undertreated partly because of general lack of awareness about the importance of addressing sleep disorders and the fact that cognitive-behavioral therapy for insomnia (CBT-I), which is recommended as first-line treatment, is not widely accessible because of a shortage of trained CBT-I practitioners.
“Many individuals with insomnia struggle to find and receive this effective nonpharmacological treatment. Consequently, there is an overreliance on pharmaceutical solutions, which are ideally used for short-term management but are often extended due to the lack of alternatives. These medications can lead to dependency and other side effects,” Dr. Benjafield said.
Ask About Sleep
Insomnia symptoms are a “common presenting complaint in doctors’ offices in the United States. The percentages in this poster show that insomnia disorder has a similar, high percent prevalence across countries in the Americas,” Boris Gilyadov, MD, assistant professor of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai in New York City, said in an interview.
“During preventive care visits and general physical exams, patients should be asked about the quality of their sleep. Patients may benefit from a referral to the sleep medicine clinic when appropriate,” said Dr. Gilyadov, who wasn’t involved in the study.
“CBT-I is the first-line treatment for chronic insomnia disorder and can be an effective treatment for most patients. An alternative to CBT-I, when it is not available, is digital CBT-I,” Dr. Gilyadov said.
“There are also behavioral therapies called BBT-I [brief behavioral treatment for insomnia] and ACT [acceptance and commitment therapy]. These are therapies that may be offered by psychologists who specialize in the treatment of chronic insomnia disorder,” Dr. Gilyadov noted.
The study was conducted in collaboration with medXcloud and funded by ResMed. Dr. Benjafield is an employee of ResMed. Dr. Gilyadov had no relevant disclosures.
A version of this article first appeared on Medscape.com.
HOUSTON — A new analysis highlights the high burden of insomnia across the Americas, with about 17% of adults suffering from this chronic sleep disorder.
“Our findings underscore the urgent need for enhanced clinical care pathways and policy interventions to effectively diagnose and treat insomnia. It is crucial to foster greater awareness of the critical role that sleep plays in overall health,” lead investigator Adam Benjafield, PhD, vice president for medical affairs at ResMed, Sydney, Australia, said in an interview.
“Insomnia not only affects individuals’ health and quality of life but also has broader implications for public health systems. Developing comprehensive care strategies and promoting education about sleep health could significantly improve outcomes for individuals suffering from insomnia disorder,” Dr. Benjafield said.
The findings were presented at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies.
Underdiagnosed, Undertreated
Sleep disruptions contribute to various medical problems, including cognitive impairment, reduced immune function, metabolic imbalance, and exacerbation of psychiatric conditions. While the prevalence of insomnia in developed countries like the United States and Canada is known, there is limited epidemiologic evidence, and no reliable estimate for the disorder across the Americas — especially in low- and middle-income countries.
The researchers used published nation-specific data to estimate the prevalence of adult insomnia disorder across the 55 countries defined by the United Nations as comprising the Americas.
Based on the available data, the researchers estimated that about 123 million adults across the Americas have insomnia disorder (16.8%) — with greater prevalence in women (73 million, 19.5%) than in men (50 million, 14%).
The nations with the greatest burden of insomnia disorder are the United States (37 million), Brazil (29 million), and Mexico (16 million).
“While our study did not specifically investigate trends over time due to its scope, evidence from other research suggests that insomnia is becoming more prevalent over the long term. This growing trend highlights the increasing need for awareness and intervention in managing sleep health,” Dr. Benjafield said.
Insomnia is underdiagnosed and undertreated partly because of general lack of awareness about the importance of addressing sleep disorders and the fact that cognitive-behavioral therapy for insomnia (CBT-I), which is recommended as first-line treatment, is not widely accessible because of a shortage of trained CBT-I practitioners.
“Many individuals with insomnia struggle to find and receive this effective nonpharmacological treatment. Consequently, there is an overreliance on pharmaceutical solutions, which are ideally used for short-term management but are often extended due to the lack of alternatives. These medications can lead to dependency and other side effects,” Dr. Benjafield said.
Ask About Sleep
Insomnia symptoms are a “common presenting complaint in doctors’ offices in the United States. The percentages in this poster show that insomnia disorder has a similar, high percent prevalence across countries in the Americas,” Boris Gilyadov, MD, assistant professor of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai in New York City, said in an interview.
“During preventive care visits and general physical exams, patients should be asked about the quality of their sleep. Patients may benefit from a referral to the sleep medicine clinic when appropriate,” said Dr. Gilyadov, who wasn’t involved in the study.
“CBT-I is the first-line treatment for chronic insomnia disorder and can be an effective treatment for most patients. An alternative to CBT-I, when it is not available, is digital CBT-I,” Dr. Gilyadov said.
“There are also behavioral therapies called BBT-I [brief behavioral treatment for insomnia] and ACT [acceptance and commitment therapy]. These are therapies that may be offered by psychologists who specialize in the treatment of chronic insomnia disorder,” Dr. Gilyadov noted.
The study was conducted in collaboration with medXcloud and funded by ResMed. Dr. Benjafield is an employee of ResMed. Dr. Gilyadov had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2024
Better Sleep Tied to Less Loneliness
HOUSTON — Sleep may have a role in driving down rates of loneliness, especially among younger adults.
A study of nearly 2300 participants showed that better sleep health is associated with significantly lower levels of loneliness across ages and that the association is particularly strong in younger individuals.
The US Surgeon General has identified loneliness as “a major public health concern, linked to high rates of negative physical and mental health outcomes,” lead researcher Joseph Dzierzewski, PhD, vice president for research and scientific affairs at the National Sleep Foundation, told this news organization.
“Loneliness is an urgent public health crisis, and there is a pressing need for providers to better understand and treat it,” Dr. Dzierzewski said in a statement.
“Better sleep health might be connected to lower feelings of loneliness by empowering people to engage in social activities, reducing feelings of negative emotions and increasing the likelihood that people interpret interactions in a positive way,” he added.
The findings were presented at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies and recently published in an online supplement of the journal Sleep.
Rested, Connected
An American Psychiatric Association poll conducted earlier this year showed 30% of US adults reported feelings of loneliness at least once a week over the past year, and 10% reported feeling lonely every day.
Younger people are more likely to report feeling lonely, with 30% of Americans, aged 18-34 years, feeling lonely every day or several times a week.
While there is growing research identifying a relationship between loneliness and poor sleep in different age groups, few studies have explored ties between social and emotional loneliness and sleep health across the adult lifespan.
In the current study led by Dr. Dzierzewski, 2297 adults (mean age, 44 years; 51% male) completed a validated sleep health questionnaire and loneliness scale.
Linear regression analyses were used to examine the direct associations between sleep health, age, and loneliness. Moderation analyses tested whether the link between sleep health and loneliness differed by age.
On average, the total sleep score was 7.7 (range, 0-12), with higher scores indicating better multidimensional sleep health, and total loneliness scale score was 8.9 (out of 11), indicating moderate levels of loneliness.
Better sleep health and younger age were associated with significantly lower loneliness total scores and social and emotional loneliness subscale scores (all P < .001).
Age significantly moderated the association between sleep health and total (P < .001) and emotional loneliness scores (P < .001) but did not moderate the association between sleep health and social loneliness (P = .034). Better sleep health was associated with lower loneliness across ages, and this association was stronger at younger ages.
“Why younger adults might experience more sleep-related benefits to loneliness than older adults is unknown and intriguing — certainly worth further investigation,” Dr. Dzierzewski said in a conference statement.
Untapped Avenue
Promoting sleep health may be an “untapped avenue” to support efforts and programs that aim to reduce loneliness and increase engagement in all age groups but especially in younger ages, the researchers noted.
Future research should consider monitoring sleep health in programs or interventions that address loneliness, they added.
“Healthcare providers should be aware of the important link between sleep health and loneliness as both sleep and social connections are essential to health and well-being. When sitting across from patients, asking about both sleep health and loneliness might yield important insights into avenues for health promotion,” said Dr. Dzierzewski.
Michael Breus, PhD, clinical psychologist and founder of SleepDoctor.com, who wasn’t involved in the study, is not surprised by the results.
It makes sense that better sleep would lead to less feelings of loneliness, he told this news organization.
Research has shown that when someone is not sleeping well, they “give others a sense of unhappiness, which socially deflects new encounters or even encounters with friends. So social awareness and social initiation would appear to both be affected by sleep quality, therefore potentially leading, at least in part, to loneliness,” he said.
Support for the study was provided by the National Institute on Aging. Dr. Dzierzewski and Dr. Breus had no relevant disclosures.
A version of this article first appeared on Medscape.com.
HOUSTON — Sleep may have a role in driving down rates of loneliness, especially among younger adults.
A study of nearly 2300 participants showed that better sleep health is associated with significantly lower levels of loneliness across ages and that the association is particularly strong in younger individuals.
The US Surgeon General has identified loneliness as “a major public health concern, linked to high rates of negative physical and mental health outcomes,” lead researcher Joseph Dzierzewski, PhD, vice president for research and scientific affairs at the National Sleep Foundation, told this news organization.
“Loneliness is an urgent public health crisis, and there is a pressing need for providers to better understand and treat it,” Dr. Dzierzewski said in a statement.
“Better sleep health might be connected to lower feelings of loneliness by empowering people to engage in social activities, reducing feelings of negative emotions and increasing the likelihood that people interpret interactions in a positive way,” he added.
The findings were presented at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies and recently published in an online supplement of the journal Sleep.
Rested, Connected
An American Psychiatric Association poll conducted earlier this year showed 30% of US adults reported feelings of loneliness at least once a week over the past year, and 10% reported feeling lonely every day.
Younger people are more likely to report feeling lonely, with 30% of Americans, aged 18-34 years, feeling lonely every day or several times a week.
While there is growing research identifying a relationship between loneliness and poor sleep in different age groups, few studies have explored ties between social and emotional loneliness and sleep health across the adult lifespan.
In the current study led by Dr. Dzierzewski, 2297 adults (mean age, 44 years; 51% male) completed a validated sleep health questionnaire and loneliness scale.
Linear regression analyses were used to examine the direct associations between sleep health, age, and loneliness. Moderation analyses tested whether the link between sleep health and loneliness differed by age.
On average, the total sleep score was 7.7 (range, 0-12), with higher scores indicating better multidimensional sleep health, and total loneliness scale score was 8.9 (out of 11), indicating moderate levels of loneliness.
Better sleep health and younger age were associated with significantly lower loneliness total scores and social and emotional loneliness subscale scores (all P < .001).
Age significantly moderated the association between sleep health and total (P < .001) and emotional loneliness scores (P < .001) but did not moderate the association between sleep health and social loneliness (P = .034). Better sleep health was associated with lower loneliness across ages, and this association was stronger at younger ages.
“Why younger adults might experience more sleep-related benefits to loneliness than older adults is unknown and intriguing — certainly worth further investigation,” Dr. Dzierzewski said in a conference statement.
Untapped Avenue
Promoting sleep health may be an “untapped avenue” to support efforts and programs that aim to reduce loneliness and increase engagement in all age groups but especially in younger ages, the researchers noted.
Future research should consider monitoring sleep health in programs or interventions that address loneliness, they added.
“Healthcare providers should be aware of the important link between sleep health and loneliness as both sleep and social connections are essential to health and well-being. When sitting across from patients, asking about both sleep health and loneliness might yield important insights into avenues for health promotion,” said Dr. Dzierzewski.
Michael Breus, PhD, clinical psychologist and founder of SleepDoctor.com, who wasn’t involved in the study, is not surprised by the results.
It makes sense that better sleep would lead to less feelings of loneliness, he told this news organization.
Research has shown that when someone is not sleeping well, they “give others a sense of unhappiness, which socially deflects new encounters or even encounters with friends. So social awareness and social initiation would appear to both be affected by sleep quality, therefore potentially leading, at least in part, to loneliness,” he said.
Support for the study was provided by the National Institute on Aging. Dr. Dzierzewski and Dr. Breus had no relevant disclosures.
A version of this article first appeared on Medscape.com.
HOUSTON — Sleep may have a role in driving down rates of loneliness, especially among younger adults.
A study of nearly 2300 participants showed that better sleep health is associated with significantly lower levels of loneliness across ages and that the association is particularly strong in younger individuals.
The US Surgeon General has identified loneliness as “a major public health concern, linked to high rates of negative physical and mental health outcomes,” lead researcher Joseph Dzierzewski, PhD, vice president for research and scientific affairs at the National Sleep Foundation, told this news organization.
“Loneliness is an urgent public health crisis, and there is a pressing need for providers to better understand and treat it,” Dr. Dzierzewski said in a statement.
“Better sleep health might be connected to lower feelings of loneliness by empowering people to engage in social activities, reducing feelings of negative emotions and increasing the likelihood that people interpret interactions in a positive way,” he added.
The findings were presented at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies and recently published in an online supplement of the journal Sleep.
Rested, Connected
An American Psychiatric Association poll conducted earlier this year showed 30% of US adults reported feelings of loneliness at least once a week over the past year, and 10% reported feeling lonely every day.
Younger people are more likely to report feeling lonely, with 30% of Americans, aged 18-34 years, feeling lonely every day or several times a week.
While there is growing research identifying a relationship between loneliness and poor sleep in different age groups, few studies have explored ties between social and emotional loneliness and sleep health across the adult lifespan.
In the current study led by Dr. Dzierzewski, 2297 adults (mean age, 44 years; 51% male) completed a validated sleep health questionnaire and loneliness scale.
Linear regression analyses were used to examine the direct associations between sleep health, age, and loneliness. Moderation analyses tested whether the link between sleep health and loneliness differed by age.
On average, the total sleep score was 7.7 (range, 0-12), with higher scores indicating better multidimensional sleep health, and total loneliness scale score was 8.9 (out of 11), indicating moderate levels of loneliness.
Better sleep health and younger age were associated with significantly lower loneliness total scores and social and emotional loneliness subscale scores (all P < .001).
Age significantly moderated the association between sleep health and total (P < .001) and emotional loneliness scores (P < .001) but did not moderate the association between sleep health and social loneliness (P = .034). Better sleep health was associated with lower loneliness across ages, and this association was stronger at younger ages.
“Why younger adults might experience more sleep-related benefits to loneliness than older adults is unknown and intriguing — certainly worth further investigation,” Dr. Dzierzewski said in a conference statement.
Untapped Avenue
Promoting sleep health may be an “untapped avenue” to support efforts and programs that aim to reduce loneliness and increase engagement in all age groups but especially in younger ages, the researchers noted.
Future research should consider monitoring sleep health in programs or interventions that address loneliness, they added.
“Healthcare providers should be aware of the important link between sleep health and loneliness as both sleep and social connections are essential to health and well-being. When sitting across from patients, asking about both sleep health and loneliness might yield important insights into avenues for health promotion,” said Dr. Dzierzewski.
Michael Breus, PhD, clinical psychologist and founder of SleepDoctor.com, who wasn’t involved in the study, is not surprised by the results.
It makes sense that better sleep would lead to less feelings of loneliness, he told this news organization.
Research has shown that when someone is not sleeping well, they “give others a sense of unhappiness, which socially deflects new encounters or even encounters with friends. So social awareness and social initiation would appear to both be affected by sleep quality, therefore potentially leading, at least in part, to loneliness,” he said.
Support for the study was provided by the National Institute on Aging. Dr. Dzierzewski and Dr. Breus had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2024
Solving Restless Legs: Largest Genetic Study to Date May Help
For decades, scientists have been trying to unravel the mysteries of restless legs syndrome (RLS), a poorly understood and underdiagnosed neurological disorder causing itching, crawling, and aching sensations in the limbs that can only be relieved with movement.
A sweeping new genetic study, coauthored by an international team of 70 — including the world’s leading RLS experts — marks a significant advance in that pursuit. Published in Nature Genetics, it is the largest genetic study of the disease to date.
“It’s a huge step forward for patients as well as the scientific community,” said lead author Juliane Winkelmann, MD, a neurologist and geneticist with the Technical University of Munich, Munich, Germany, who’s been studying and treating patients with RLS for 30 years. “We believe it will allow us to better predict the likelihood of developing RLS and investigate new ways to prevent and modify it.”
The common condition, affecting about 1 in 10 adults, was first described centuries ago — by English physician Thomas Willis in the late 1600s. And while we know a lot more about it today — it’s familial in about half of all patients and has been linked to iron deficiency, among other conditions — its exact cause remains unknown.
With preferred drugs long prescribed to quell symptoms shown in recent years to actually worsen the disorder over time, doctors and patients are hungry for alternatives to treat or prevent the sleep-sabotaging condition.
“The main treatments that everybody continues to use are actually making people worse,” said Andrew Berkowski, MD, a Michigan-based neurologist and RLS specialist not involved in the study. These drugs — dopamine agonists such as levodopa and pramipexole — can also potentially cause drug dependence, Dr. Berkowski said.
How This Could Lead to New Treatments
In the new study, the group analyzed three genome-wide association studies, collectively including genetic information from 116,647 patients with RLS and more than 1.5 million people without it.
They identified 161 gene regions believed to contribute to RLS, about a dozen of which are already targets for existing drugs for other conditions. Previously, scientists knew of only 22 associated genes.
“It’s useful in that it identifies new genes we haven’t looked at yet and reinforces the science behind some of the older genes,” said Dr. Berkowski. “It’s given us some ideas for different things we should look into more closely.”
Among the top candidates are genes that influence glutamate — a key chemical messenger that helps move signals between nerve cells in the brain.
Several anticonvulsant and antiseizure drugs, including perampanel, lamotrigine, and gabapentin, target glutamate receptors. And at least one small study has shown perampanel prescribed off-label can improve RLS symptoms.
“Compared to starting at the beginning and developing an entirely new chemical entity, we could run clinical trials using these alternatives in RLS patients,” said the study’s first author, Steven Bell, PhD, an epidemiologist with the University of Cambridge, Cambridge, England.
The study also confirmed the MIES1 gene, which is related to dopamine expression and iron homeostasis, as a key genetic contributor to RLS risk. Low levels of iron in the blood have long been thought to trigger RLS.
The Role of Gene-Environment Interactions
Through additional data analysis, the team confirmed that many of the genes associated with RLS play a role in development of the central nervous system.
“This strongly supports the hypothesis that restless legs syndrome is a neurodevelopmental disorder that develops during the embryo stage but doesn’t clinically manifest until later in life,” said Dr. Winkelmann.
About half of people with RLS report some family history of it.
But not all with a genetic predisposition will develop symptoms.
For instance, the study found that while the same gene regions seem to be associated with risk in both men and women, in practice, RLS is twice as common among women. This suggests that something about women’s lives — menstruation, childbirth, metabolism — may switch a preexisting risk into a reality.
“We know that genetic factors play an important role in making people susceptible to the disease,” said Dr. Winkelmann, “but in the end, it is the interaction between genetic and environmental factors that may lead to its manifestation.”
The study also found associations between RLS and depression and suggests that RLS may increase the risk for type 2 diabetes.
Improving RLS Care
A potentially useful tool coming out of the study was a “polygenic risk score,” which the researchers developed based on the genes identified. When they tested how accurately the score could predict whether someone would develop RLS within the next 5 years, the model got it right about 90% of the time.
Dr. Winkelmann imagines a day when someone could use such a polygenic risk score to flag the high risk for RLS early enough to take action to try to prevent it. More research is necessary to determine precisely what that action would be.
As for treatments, Dr. Berkowski thinks it’s unlikely that doctors will suddenly begin using existing, glutamate-targeting drugs off-label to treat RLS, as many are prohibitively expensive and wouldn’t be covered by insurance. But he’s optimistic that the study can spawn new research that could ultimately help fill the treatment gap.
Shalini Paruthi, MD, an adjunct professor at Saint Louis University, St. Louis, Missouri, and chair of the Restless Legs Syndrome Foundation’s board of directors, sees another benefit.
“The associations found in this study between RLS and other medical disorders may help patients and their physicians take RLS more seriously,” Dr. Paruthi said, “as treating RLS can lead to multiple other downstream improvements in their health.”
A version of this article appeared on Medscape.com.
For decades, scientists have been trying to unravel the mysteries of restless legs syndrome (RLS), a poorly understood and underdiagnosed neurological disorder causing itching, crawling, and aching sensations in the limbs that can only be relieved with movement.
A sweeping new genetic study, coauthored by an international team of 70 — including the world’s leading RLS experts — marks a significant advance in that pursuit. Published in Nature Genetics, it is the largest genetic study of the disease to date.
“It’s a huge step forward for patients as well as the scientific community,” said lead author Juliane Winkelmann, MD, a neurologist and geneticist with the Technical University of Munich, Munich, Germany, who’s been studying and treating patients with RLS for 30 years. “We believe it will allow us to better predict the likelihood of developing RLS and investigate new ways to prevent and modify it.”
The common condition, affecting about 1 in 10 adults, was first described centuries ago — by English physician Thomas Willis in the late 1600s. And while we know a lot more about it today — it’s familial in about half of all patients and has been linked to iron deficiency, among other conditions — its exact cause remains unknown.
With preferred drugs long prescribed to quell symptoms shown in recent years to actually worsen the disorder over time, doctors and patients are hungry for alternatives to treat or prevent the sleep-sabotaging condition.
“The main treatments that everybody continues to use are actually making people worse,” said Andrew Berkowski, MD, a Michigan-based neurologist and RLS specialist not involved in the study. These drugs — dopamine agonists such as levodopa and pramipexole — can also potentially cause drug dependence, Dr. Berkowski said.
How This Could Lead to New Treatments
In the new study, the group analyzed three genome-wide association studies, collectively including genetic information from 116,647 patients with RLS and more than 1.5 million people without it.
They identified 161 gene regions believed to contribute to RLS, about a dozen of which are already targets for existing drugs for other conditions. Previously, scientists knew of only 22 associated genes.
“It’s useful in that it identifies new genes we haven’t looked at yet and reinforces the science behind some of the older genes,” said Dr. Berkowski. “It’s given us some ideas for different things we should look into more closely.”
Among the top candidates are genes that influence glutamate — a key chemical messenger that helps move signals between nerve cells in the brain.
Several anticonvulsant and antiseizure drugs, including perampanel, lamotrigine, and gabapentin, target glutamate receptors. And at least one small study has shown perampanel prescribed off-label can improve RLS symptoms.
“Compared to starting at the beginning and developing an entirely new chemical entity, we could run clinical trials using these alternatives in RLS patients,” said the study’s first author, Steven Bell, PhD, an epidemiologist with the University of Cambridge, Cambridge, England.
The study also confirmed the MIES1 gene, which is related to dopamine expression and iron homeostasis, as a key genetic contributor to RLS risk. Low levels of iron in the blood have long been thought to trigger RLS.
The Role of Gene-Environment Interactions
Through additional data analysis, the team confirmed that many of the genes associated with RLS play a role in development of the central nervous system.
“This strongly supports the hypothesis that restless legs syndrome is a neurodevelopmental disorder that develops during the embryo stage but doesn’t clinically manifest until later in life,” said Dr. Winkelmann.
About half of people with RLS report some family history of it.
But not all with a genetic predisposition will develop symptoms.
For instance, the study found that while the same gene regions seem to be associated with risk in both men and women, in practice, RLS is twice as common among women. This suggests that something about women’s lives — menstruation, childbirth, metabolism — may switch a preexisting risk into a reality.
“We know that genetic factors play an important role in making people susceptible to the disease,” said Dr. Winkelmann, “but in the end, it is the interaction between genetic and environmental factors that may lead to its manifestation.”
The study also found associations between RLS and depression and suggests that RLS may increase the risk for type 2 diabetes.
Improving RLS Care
A potentially useful tool coming out of the study was a “polygenic risk score,” which the researchers developed based on the genes identified. When they tested how accurately the score could predict whether someone would develop RLS within the next 5 years, the model got it right about 90% of the time.
Dr. Winkelmann imagines a day when someone could use such a polygenic risk score to flag the high risk for RLS early enough to take action to try to prevent it. More research is necessary to determine precisely what that action would be.
As for treatments, Dr. Berkowski thinks it’s unlikely that doctors will suddenly begin using existing, glutamate-targeting drugs off-label to treat RLS, as many are prohibitively expensive and wouldn’t be covered by insurance. But he’s optimistic that the study can spawn new research that could ultimately help fill the treatment gap.
Shalini Paruthi, MD, an adjunct professor at Saint Louis University, St. Louis, Missouri, and chair of the Restless Legs Syndrome Foundation’s board of directors, sees another benefit.
“The associations found in this study between RLS and other medical disorders may help patients and their physicians take RLS more seriously,” Dr. Paruthi said, “as treating RLS can lead to multiple other downstream improvements in their health.”
A version of this article appeared on Medscape.com.
For decades, scientists have been trying to unravel the mysteries of restless legs syndrome (RLS), a poorly understood and underdiagnosed neurological disorder causing itching, crawling, and aching sensations in the limbs that can only be relieved with movement.
A sweeping new genetic study, coauthored by an international team of 70 — including the world’s leading RLS experts — marks a significant advance in that pursuit. Published in Nature Genetics, it is the largest genetic study of the disease to date.
“It’s a huge step forward for patients as well as the scientific community,” said lead author Juliane Winkelmann, MD, a neurologist and geneticist with the Technical University of Munich, Munich, Germany, who’s been studying and treating patients with RLS for 30 years. “We believe it will allow us to better predict the likelihood of developing RLS and investigate new ways to prevent and modify it.”
The common condition, affecting about 1 in 10 adults, was first described centuries ago — by English physician Thomas Willis in the late 1600s. And while we know a lot more about it today — it’s familial in about half of all patients and has been linked to iron deficiency, among other conditions — its exact cause remains unknown.
With preferred drugs long prescribed to quell symptoms shown in recent years to actually worsen the disorder over time, doctors and patients are hungry for alternatives to treat or prevent the sleep-sabotaging condition.
“The main treatments that everybody continues to use are actually making people worse,” said Andrew Berkowski, MD, a Michigan-based neurologist and RLS specialist not involved in the study. These drugs — dopamine agonists such as levodopa and pramipexole — can also potentially cause drug dependence, Dr. Berkowski said.
How This Could Lead to New Treatments
In the new study, the group analyzed three genome-wide association studies, collectively including genetic information from 116,647 patients with RLS and more than 1.5 million people without it.
They identified 161 gene regions believed to contribute to RLS, about a dozen of which are already targets for existing drugs for other conditions. Previously, scientists knew of only 22 associated genes.
“It’s useful in that it identifies new genes we haven’t looked at yet and reinforces the science behind some of the older genes,” said Dr. Berkowski. “It’s given us some ideas for different things we should look into more closely.”
Among the top candidates are genes that influence glutamate — a key chemical messenger that helps move signals between nerve cells in the brain.
Several anticonvulsant and antiseizure drugs, including perampanel, lamotrigine, and gabapentin, target glutamate receptors. And at least one small study has shown perampanel prescribed off-label can improve RLS symptoms.
“Compared to starting at the beginning and developing an entirely new chemical entity, we could run clinical trials using these alternatives in RLS patients,” said the study’s first author, Steven Bell, PhD, an epidemiologist with the University of Cambridge, Cambridge, England.
The study also confirmed the MIES1 gene, which is related to dopamine expression and iron homeostasis, as a key genetic contributor to RLS risk. Low levels of iron in the blood have long been thought to trigger RLS.
The Role of Gene-Environment Interactions
Through additional data analysis, the team confirmed that many of the genes associated with RLS play a role in development of the central nervous system.
“This strongly supports the hypothesis that restless legs syndrome is a neurodevelopmental disorder that develops during the embryo stage but doesn’t clinically manifest until later in life,” said Dr. Winkelmann.
About half of people with RLS report some family history of it.
But not all with a genetic predisposition will develop symptoms.
For instance, the study found that while the same gene regions seem to be associated with risk in both men and women, in practice, RLS is twice as common among women. This suggests that something about women’s lives — menstruation, childbirth, metabolism — may switch a preexisting risk into a reality.
“We know that genetic factors play an important role in making people susceptible to the disease,” said Dr. Winkelmann, “but in the end, it is the interaction between genetic and environmental factors that may lead to its manifestation.”
The study also found associations between RLS and depression and suggests that RLS may increase the risk for type 2 diabetes.
Improving RLS Care
A potentially useful tool coming out of the study was a “polygenic risk score,” which the researchers developed based on the genes identified. When they tested how accurately the score could predict whether someone would develop RLS within the next 5 years, the model got it right about 90% of the time.
Dr. Winkelmann imagines a day when someone could use such a polygenic risk score to flag the high risk for RLS early enough to take action to try to prevent it. More research is necessary to determine precisely what that action would be.
As for treatments, Dr. Berkowski thinks it’s unlikely that doctors will suddenly begin using existing, glutamate-targeting drugs off-label to treat RLS, as many are prohibitively expensive and wouldn’t be covered by insurance. But he’s optimistic that the study can spawn new research that could ultimately help fill the treatment gap.
Shalini Paruthi, MD, an adjunct professor at Saint Louis University, St. Louis, Missouri, and chair of the Restless Legs Syndrome Foundation’s board of directors, sees another benefit.
“The associations found in this study between RLS and other medical disorders may help patients and their physicians take RLS more seriously,” Dr. Paruthi said, “as treating RLS can lead to multiple other downstream improvements in their health.”
A version of this article appeared on Medscape.com.
Narcolepsy an Independent Cardiovascular Disease Risk Factor
HOUSTON — Narcolepsy is associated with a significantly increased risk for cardiovascular disease (CVD) and major adverse cardiac events (MACEs), independent of common comorbid conditions and medications commonly used to treat the chronic sleep disorder, according to two new studies.
A nationwide analysis revealed that people with narcolepsy had a 77% higher risk for CVD and an 82% higher risk for MACE than those without the disorder.
“These findings indicate that it is important for clinicians to regularly monitor patients for cardiovascular disease and take this into consideration when recommending specific treatments for narcolepsy,” study investigators Christopher Kaufmann, PhD; Munaza Riaz, PharmD, MPhil; and Rakesh Bhattacharjee, MD, told this news organization.
“Additionally, physicians should consider monitoring the presence of other health conditions as contributing factors to the risk of CVD,” they said. Dr. Kaufmann and Dr. Riaz are with the University of Florida, Gainesville, Florida, and Dr. Bhattacharjee is with the University of California, San Diego.
They presented their research at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies.
Independent Risk Factor
The National Institute of Neurological Disorders and Stroke reports an estimated 125,000 to 200,000 people in the United States live with narcolepsy. The condition often coexists with other common health conditions including obstructive sleep apnea (OSA), diabetes, and other comorbidities, which can all contribute to the risk for CVD.
This raises doubt as to whether narcolepsy itself directly leads to CVD or if it is the result of these comorbid health conditions. Additionally, some medications used to treat narcolepsy carry their own cardiovascular risks.
Using the IBM MarketScan Commercial and Medicare supplemental databases, the researchers identified 34,562 adults with a diagnosis of narcolepsy and a propensity-matched comparison cohort of 100,405 adults without narcolepsy. The patients had a mean age of 40 years, and 62% were women.
Compared with adults without narcolepsy, those with the chronic sleep disorder that causes overwhelming daytime drowsiness had a 77% increased risk for any CVD (hazard ratio [HR], 1.77) and an 82% increased risk for MACE (HR, 1.82).
They also had an increased risk for stroke (HR, 2.04), heart failure or myocardial infarction (MI; HR, 1.64), and atrial fibrillation (HR, 1.58).
The results were similar in a separate analysis of the same population that also controlled for baseline use of stimulants, oxybates, and wake-promoting agents — medications commonly used to treat excessive daytime sleepiness associated with narcolepsy.
In this analysis, narcolepsy was associated with an 89% higher risk for CVD (HR, 1.89) and a 95% increased risk for MACE (HR, 1.95). The risk for any stroke (HR, 2.06), heart failure (HR, 1.90), atrial fibrillation (HR, 1.66), and MI (HR, 1.93) was also higher in those with narcolepsy.
“Our study found that even after considering the presence of health conditions like obstructive sleep apnea, diabetes, hypertension, hyperlipidemia, and even depression, as well as medication use, there still appears to be an independent relationship between narcolepsy and CVD,” the investigators said.
They cautioned that the mechanisms explaining the link between CVD and narcolepsy are unclear and warrant further study.
“Sleep fragmentation is a hallmark of narcolepsy, and it is speculated that this fragmentation, which may trigger disturbances in autonomic function, predisposes individuals to CVD. In rodent models, a possible link has been observed between hypocretin — a central neurotransmitter that is reduced or deficient in patients with narcolepsy — and atherosclerosis.
“However, it remains uncertain whether this is the primary mechanism related to CVD,” they commented.
Compelling Evidence for Higher CVD
Commenting on the findings for this news organization, Shaheen Lakhan, MD, a neurologist and researcher based in Miami, Florida, called for narcolepsy to be recognized as a significant contributor to higher CVD risk.
“Given the compelling evidence linking narcolepsy to a higher incidence of cardiovascular disease, it is crucial that narcolepsy be included in clinical guidelines and risk assessment tools alongside other known risk factors,” said Dr. Lakhan, who was not involved in this research.
“Physicians and health care providers should proactively address the increased cardiovascular risk associated with narcolepsy by incorporating preventive strategies and interventions into the management of patients with this condition,” Dr. Lakhan suggested.
Regular CVD screening, a healthier lifestyle, and targeted therapies could all decrease cardiac risk, Dr. Lakhan added.
“Ultimately, novel disease-modifying therapies for narcolepsy should target the core mechanisms driving the increased cardiovascular risk associated with this condition. By elucidating the specific biological pathways and developing targeted therapies that address the unique challenges faced by narcolepsy patients, we can effectively mitigate the risk,” Dr. Lakhan said.
The studies were funded by the Sleep Research Society Foundation. The authors and Dr. Lakhan had no relevant disclosures.
A version of this article appeared on Medscape.com.
HOUSTON — Narcolepsy is associated with a significantly increased risk for cardiovascular disease (CVD) and major adverse cardiac events (MACEs), independent of common comorbid conditions and medications commonly used to treat the chronic sleep disorder, according to two new studies.
A nationwide analysis revealed that people with narcolepsy had a 77% higher risk for CVD and an 82% higher risk for MACE than those without the disorder.
“These findings indicate that it is important for clinicians to regularly monitor patients for cardiovascular disease and take this into consideration when recommending specific treatments for narcolepsy,” study investigators Christopher Kaufmann, PhD; Munaza Riaz, PharmD, MPhil; and Rakesh Bhattacharjee, MD, told this news organization.
“Additionally, physicians should consider monitoring the presence of other health conditions as contributing factors to the risk of CVD,” they said. Dr. Kaufmann and Dr. Riaz are with the University of Florida, Gainesville, Florida, and Dr. Bhattacharjee is with the University of California, San Diego.
They presented their research at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies.
Independent Risk Factor
The National Institute of Neurological Disorders and Stroke reports an estimated 125,000 to 200,000 people in the United States live with narcolepsy. The condition often coexists with other common health conditions including obstructive sleep apnea (OSA), diabetes, and other comorbidities, which can all contribute to the risk for CVD.
This raises doubt as to whether narcolepsy itself directly leads to CVD or if it is the result of these comorbid health conditions. Additionally, some medications used to treat narcolepsy carry their own cardiovascular risks.
Using the IBM MarketScan Commercial and Medicare supplemental databases, the researchers identified 34,562 adults with a diagnosis of narcolepsy and a propensity-matched comparison cohort of 100,405 adults without narcolepsy. The patients had a mean age of 40 years, and 62% were women.
Compared with adults without narcolepsy, those with the chronic sleep disorder that causes overwhelming daytime drowsiness had a 77% increased risk for any CVD (hazard ratio [HR], 1.77) and an 82% increased risk for MACE (HR, 1.82).
They also had an increased risk for stroke (HR, 2.04), heart failure or myocardial infarction (MI; HR, 1.64), and atrial fibrillation (HR, 1.58).
The results were similar in a separate analysis of the same population that also controlled for baseline use of stimulants, oxybates, and wake-promoting agents — medications commonly used to treat excessive daytime sleepiness associated with narcolepsy.
In this analysis, narcolepsy was associated with an 89% higher risk for CVD (HR, 1.89) and a 95% increased risk for MACE (HR, 1.95). The risk for any stroke (HR, 2.06), heart failure (HR, 1.90), atrial fibrillation (HR, 1.66), and MI (HR, 1.93) was also higher in those with narcolepsy.
“Our study found that even after considering the presence of health conditions like obstructive sleep apnea, diabetes, hypertension, hyperlipidemia, and even depression, as well as medication use, there still appears to be an independent relationship between narcolepsy and CVD,” the investigators said.
They cautioned that the mechanisms explaining the link between CVD and narcolepsy are unclear and warrant further study.
“Sleep fragmentation is a hallmark of narcolepsy, and it is speculated that this fragmentation, which may trigger disturbances in autonomic function, predisposes individuals to CVD. In rodent models, a possible link has been observed between hypocretin — a central neurotransmitter that is reduced or deficient in patients with narcolepsy — and atherosclerosis.
“However, it remains uncertain whether this is the primary mechanism related to CVD,” they commented.
Compelling Evidence for Higher CVD
Commenting on the findings for this news organization, Shaheen Lakhan, MD, a neurologist and researcher based in Miami, Florida, called for narcolepsy to be recognized as a significant contributor to higher CVD risk.
“Given the compelling evidence linking narcolepsy to a higher incidence of cardiovascular disease, it is crucial that narcolepsy be included in clinical guidelines and risk assessment tools alongside other known risk factors,” said Dr. Lakhan, who was not involved in this research.
“Physicians and health care providers should proactively address the increased cardiovascular risk associated with narcolepsy by incorporating preventive strategies and interventions into the management of patients with this condition,” Dr. Lakhan suggested.
Regular CVD screening, a healthier lifestyle, and targeted therapies could all decrease cardiac risk, Dr. Lakhan added.
“Ultimately, novel disease-modifying therapies for narcolepsy should target the core mechanisms driving the increased cardiovascular risk associated with this condition. By elucidating the specific biological pathways and developing targeted therapies that address the unique challenges faced by narcolepsy patients, we can effectively mitigate the risk,” Dr. Lakhan said.
The studies were funded by the Sleep Research Society Foundation. The authors and Dr. Lakhan had no relevant disclosures.
A version of this article appeared on Medscape.com.
HOUSTON — Narcolepsy is associated with a significantly increased risk for cardiovascular disease (CVD) and major adverse cardiac events (MACEs), independent of common comorbid conditions and medications commonly used to treat the chronic sleep disorder, according to two new studies.
A nationwide analysis revealed that people with narcolepsy had a 77% higher risk for CVD and an 82% higher risk for MACE than those without the disorder.
“These findings indicate that it is important for clinicians to regularly monitor patients for cardiovascular disease and take this into consideration when recommending specific treatments for narcolepsy,” study investigators Christopher Kaufmann, PhD; Munaza Riaz, PharmD, MPhil; and Rakesh Bhattacharjee, MD, told this news organization.
“Additionally, physicians should consider monitoring the presence of other health conditions as contributing factors to the risk of CVD,” they said. Dr. Kaufmann and Dr. Riaz are with the University of Florida, Gainesville, Florida, and Dr. Bhattacharjee is with the University of California, San Diego.
They presented their research at SLEEP 2024: 38th Annual Meeting of the Associated Professional Sleep Societies.
Independent Risk Factor
The National Institute of Neurological Disorders and Stroke reports an estimated 125,000 to 200,000 people in the United States live with narcolepsy. The condition often coexists with other common health conditions including obstructive sleep apnea (OSA), diabetes, and other comorbidities, which can all contribute to the risk for CVD.
This raises doubt as to whether narcolepsy itself directly leads to CVD or if it is the result of these comorbid health conditions. Additionally, some medications used to treat narcolepsy carry their own cardiovascular risks.
Using the IBM MarketScan Commercial and Medicare supplemental databases, the researchers identified 34,562 adults with a diagnosis of narcolepsy and a propensity-matched comparison cohort of 100,405 adults without narcolepsy. The patients had a mean age of 40 years, and 62% were women.
Compared with adults without narcolepsy, those with the chronic sleep disorder that causes overwhelming daytime drowsiness had a 77% increased risk for any CVD (hazard ratio [HR], 1.77) and an 82% increased risk for MACE (HR, 1.82).
They also had an increased risk for stroke (HR, 2.04), heart failure or myocardial infarction (MI; HR, 1.64), and atrial fibrillation (HR, 1.58).
The results were similar in a separate analysis of the same population that also controlled for baseline use of stimulants, oxybates, and wake-promoting agents — medications commonly used to treat excessive daytime sleepiness associated with narcolepsy.
In this analysis, narcolepsy was associated with an 89% higher risk for CVD (HR, 1.89) and a 95% increased risk for MACE (HR, 1.95). The risk for any stroke (HR, 2.06), heart failure (HR, 1.90), atrial fibrillation (HR, 1.66), and MI (HR, 1.93) was also higher in those with narcolepsy.
“Our study found that even after considering the presence of health conditions like obstructive sleep apnea, diabetes, hypertension, hyperlipidemia, and even depression, as well as medication use, there still appears to be an independent relationship between narcolepsy and CVD,” the investigators said.
They cautioned that the mechanisms explaining the link between CVD and narcolepsy are unclear and warrant further study.
“Sleep fragmentation is a hallmark of narcolepsy, and it is speculated that this fragmentation, which may trigger disturbances in autonomic function, predisposes individuals to CVD. In rodent models, a possible link has been observed between hypocretin — a central neurotransmitter that is reduced or deficient in patients with narcolepsy — and atherosclerosis.
“However, it remains uncertain whether this is the primary mechanism related to CVD,” they commented.
Compelling Evidence for Higher CVD
Commenting on the findings for this news organization, Shaheen Lakhan, MD, a neurologist and researcher based in Miami, Florida, called for narcolepsy to be recognized as a significant contributor to higher CVD risk.
“Given the compelling evidence linking narcolepsy to a higher incidence of cardiovascular disease, it is crucial that narcolepsy be included in clinical guidelines and risk assessment tools alongside other known risk factors,” said Dr. Lakhan, who was not involved in this research.
“Physicians and health care providers should proactively address the increased cardiovascular risk associated with narcolepsy by incorporating preventive strategies and interventions into the management of patients with this condition,” Dr. Lakhan suggested.
Regular CVD screening, a healthier lifestyle, and targeted therapies could all decrease cardiac risk, Dr. Lakhan added.
“Ultimately, novel disease-modifying therapies for narcolepsy should target the core mechanisms driving the increased cardiovascular risk associated with this condition. By elucidating the specific biological pathways and developing targeted therapies that address the unique challenges faced by narcolepsy patients, we can effectively mitigate the risk,” Dr. Lakhan said.
The studies were funded by the Sleep Research Society Foundation. The authors and Dr. Lakhan had no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM SLEEP 2024
Chronotherapy: Why Timing Drugs to Our Body Clocks May Work
Do drugs work better if taken by the clock?
A new analysis published in The Lancet journal’s eClinicalMedicine suggests: Yes, they do — if you consider the patient’s individual body clock. The study is the first to find that timing blood pressure drugs to a person’s personal “chronotype” — that is, whether they are a night owl or an early bird — may reduce the risk for a heart attack.
The findings represent a significant advance in the field of circadian medicine or “chronotherapy” — timing drug administration to circadian rhythms. A growing stack of research suggests this approach could reduce side effects and improve the effectiveness of a wide range of therapies, including vaccines, cancer treatments, and drugs for depression, glaucoma, pain, seizures, and other conditions. Still, despite decades of research, time of day is rarely considered in writing prescriptions.
“We are really just at the beginning of an exciting new way of looking at patient care,” said Kenneth A. Dyar, PhD, whose lab at Helmholtz Zentrum München’s Institute for Diabetes and Cancer focuses on metabolic physiology. Dr. Dyar is co-lead author of the new blood pressure analysis.
“Chronotherapy is a rapidly growing field,” he said, “and I suspect we are soon going to see more and more studies focused on ‘personalized chronotherapy,’ not only in hypertension but also potentially in other clinical areas.”
The ‘Missing Piece’ in Chronotherapy Research
Blood pressure drugs have long been chronotherapy’s battleground. After all, blood pressure follows a circadian rhythm, peaking in the morning and dropping at night.
That healthy overnight dip can disappear in people with diabetes, kidney disease, and obstructive sleep apnea. Some physicians have suggested a bed-time dose to restore that dip. But studies have had mixed results, so “take at bedtime” has become a less common recommendation in recent years.
But the debate continued. After a large 2019 Spanish study found that bedtime doses had benefits so big that the results drew questions, an even larger, 2022 randomized, controlled trial from the University of Dundee in Dundee, Scotland — called the TIME study — aimed to settle the question.
Researchers assigned over 21,000 people to take morning or night hypertension drugs for several years and found no difference in cardiovascular outcomes.
“We did this study thinking nocturnal blood pressure tablets might be better,” said Thomas MacDonald, MD, professor emeritus of clinical pharmacology and pharmacoepidemiology at the University of Dundee and principal investigator for the TIME study and the recent chronotype analysis. “But there was no difference for heart attacks, strokes, or vascular death.”
So, the researchers then looked at participants’ chronotypes, sorting outcomes based on whether the participants were late-to-bed, late-to-rise “night owls” or early-to-bed, early-to-rise “morning larks.”
Their analysis of these 5358 TIME participants found the following results: Risk for hospitalization for a heart attack was at least 34% lower for “owls” who took their drugs at bedtime. By contrast, owls’ heart attack risk was at least 62% higher with morning doses. For “larks,” the opposite was true. Morning doses were associated with an 11% lower heart attack risk and night doses with an 11% higher risk, according to supplemental data.
The personalized approach could explain why some previous chronotherapy studies have failed to show a benefit. Those studies did not individualize drug timing as this one did. But personalization could be key to circadian medicine’s success.
“Our ‘internal personal time’ appears to be an important variable to consider when dosing antihypertensives,” said co-lead author Filippo Pigazzani, MD, PhD, clinical senior lecturer and honorary consultant cardiologist at the University of Dundee School of Medicine. “Chronotherapy research has been going on for decades. We knew there was something important with time of day. But researchers haven’t considered the internal time of individual people. I think that is the missing piece.”
The analysis has several important limitations, the researchers said. A total of 95% of participants were White. And it was an observational study, not a true randomized comparison. “We started it late in the original TIME study,” Dr. MacDonald said. “You could argue we were reporting on those who survived long enough to get into the analysis.” More research is needed, they concluded.
Looking Beyond Blood Pressure
What about the rest of the body? “Almost all the cells of our body contain ‘circadian clocks’ that are synchronized by daily environmental cues, including light-dark, activity-rest, and feeding-fasting cycles,” said Dr. Dyar.
An estimated 50% of prescription drugs hit targets in the body that have circadian patterns. So, experts suspect that syncing a drug with a person’s body clock might increase effectiveness of many drugs.
A handful of US Food and Drug Administration–approved drugs already have time-of-day recommendations on the label for effectiveness or to limit side effects, including bedtime or evening for the insomnia drug Ambien, the HIV antiviral Atripla, and cholesterol-lowering Zocor. Others are intended to be taken with or after your last meal of the day, such as the long-acting insulin Levemir and the cardiovascular drug Xarelto. A morning recommendation comes with the proton pump inhibitor Nexium and the attention-deficit/hyperactivity disorder drug Ritalin.
Interest is expanding. About one third of the papers published about chronotherapy in the past 25 years have come out in the past 5 years. The May 2024 meeting of the Society for Research on Biological Rhythms featured a day-long session aimed at bringing clinicians up to speed. An organization called the International Association of Circadian Health Clinics is trying to bring circadian medicine findings to clinicians and their patients and to support research.
Moreover, while recent research suggests minding the clock could have benefits for a wide range of treatments, ignoring it could cause problems.
In a Massachusetts Institute of Technology study published in April in Science Advances, researchers looked at engineered livers made from human donor cells and found more than 300 genes that operate on a circadian schedule, many with roles in drug metabolism. They also found that circadian patterns affected the toxicity of acetaminophen and atorvastatin. Identifying the time of day to take these drugs could maximize effectiveness and minimize adverse effects, the researchers said.
Timing and the Immune System
Circadian rhythms are also seen in immune processes. In a 2023 study in The Journal of Clinical Investigation of vaccine data from 1.5 million people in Israel, researchers found that children and older adults who got their second dose of the Pfizer mRNA COVID vaccine earlier in the day were about 36% less likely to be hospitalized with SARS-CoV-2 infection than those who got an evening shot.
“The sweet spot in our data was somewhere around late morning to late afternoon,” said lead researcher Jeffrey Haspel, MD, PhD, associate professor of medicine in the division of pulmonary and critical care medicine at Washington University School of Medicine in St. Louis.
In a multicenter, 2024 analysis of 13 studies of immunotherapy for advanced cancers in 1663 people, researchers found treatment earlier in the day was associated with longer survival time and longer survival without cancer progression.
“Patients with selected metastatic cancers seemed to largely benefit from early [time of day] infusions, which is consistent with circadian mechanisms in immune-cell functions and trafficking,” the researchers noted. But “retrospective randomized trials are needed to establish recommendations for optimal circadian timing.”
Other research suggests or is investigating possible chronotherapy benefits for depression, glaucoma, respiratory diseases, stroke treatment, epilepsy, and sedatives used in surgery. So why aren’t healthcare providers adding time of day to more prescriptions? “What’s missing is more reliable data,” Dr. Dyar said.
Should You Use Chronotherapy Now?
Experts emphasize that more research is needed before doctors use chronotherapy and before medical organizations include it in treatment recommendations. But for some patients, circadian dosing may be worth a try:
Night owls whose blood pressure isn’t well controlled. Dr. Dyar and Dr. Pigazzani said night-time blood pressure drugs may be helpful for people with a “late chronotype.” Of course, patients shouldn’t change their medication schedule on their own, they said. And doctors may want to consider other concerns, like more overnight bathroom visits with evening diuretics.
In their study, the researchers determined participants’ chronotype with a few questions from the Munich Chronotype Questionnaire about what time they fell asleep and woke up on workdays and days off and whether they considered themselves “morning types” or “evening types.” (The questions can be found in supplementary data for the study.)
If a physician thinks matching the timing of a dose with chronotype would help, they can consider it, Dr. Pigazzani said. “However, I must add that this was an observational study, so I would advise healthcare practitioners to wait for our data to be confirmed in new RCTs of personalized chronotherapy of hypertension.”
Children and older adults getting vaccines. Timing COVID shots and possibly other vaccines from late morning to mid-afternoon could have a small benefit for individuals and a bigger public-health benefit, Dr. Haspel said. But the most important thing is getting vaccinated. “If you can only get one in the evening, it’s still worthwhile. Timing may add oomph at a public-health level for more vulnerable groups.”
A version of this article appeared on Medscape.com.
Do drugs work better if taken by the clock?
A new analysis published in The Lancet journal’s eClinicalMedicine suggests: Yes, they do — if you consider the patient’s individual body clock. The study is the first to find that timing blood pressure drugs to a person’s personal “chronotype” — that is, whether they are a night owl or an early bird — may reduce the risk for a heart attack.
The findings represent a significant advance in the field of circadian medicine or “chronotherapy” — timing drug administration to circadian rhythms. A growing stack of research suggests this approach could reduce side effects and improve the effectiveness of a wide range of therapies, including vaccines, cancer treatments, and drugs for depression, glaucoma, pain, seizures, and other conditions. Still, despite decades of research, time of day is rarely considered in writing prescriptions.
“We are really just at the beginning of an exciting new way of looking at patient care,” said Kenneth A. Dyar, PhD, whose lab at Helmholtz Zentrum München’s Institute for Diabetes and Cancer focuses on metabolic physiology. Dr. Dyar is co-lead author of the new blood pressure analysis.
“Chronotherapy is a rapidly growing field,” he said, “and I suspect we are soon going to see more and more studies focused on ‘personalized chronotherapy,’ not only in hypertension but also potentially in other clinical areas.”
The ‘Missing Piece’ in Chronotherapy Research
Blood pressure drugs have long been chronotherapy’s battleground. After all, blood pressure follows a circadian rhythm, peaking in the morning and dropping at night.
That healthy overnight dip can disappear in people with diabetes, kidney disease, and obstructive sleep apnea. Some physicians have suggested a bed-time dose to restore that dip. But studies have had mixed results, so “take at bedtime” has become a less common recommendation in recent years.
But the debate continued. After a large 2019 Spanish study found that bedtime doses had benefits so big that the results drew questions, an even larger, 2022 randomized, controlled trial from the University of Dundee in Dundee, Scotland — called the TIME study — aimed to settle the question.
Researchers assigned over 21,000 people to take morning or night hypertension drugs for several years and found no difference in cardiovascular outcomes.
“We did this study thinking nocturnal blood pressure tablets might be better,” said Thomas MacDonald, MD, professor emeritus of clinical pharmacology and pharmacoepidemiology at the University of Dundee and principal investigator for the TIME study and the recent chronotype analysis. “But there was no difference for heart attacks, strokes, or vascular death.”
So, the researchers then looked at participants’ chronotypes, sorting outcomes based on whether the participants were late-to-bed, late-to-rise “night owls” or early-to-bed, early-to-rise “morning larks.”
Their analysis of these 5358 TIME participants found the following results: Risk for hospitalization for a heart attack was at least 34% lower for “owls” who took their drugs at bedtime. By contrast, owls’ heart attack risk was at least 62% higher with morning doses. For “larks,” the opposite was true. Morning doses were associated with an 11% lower heart attack risk and night doses with an 11% higher risk, according to supplemental data.
The personalized approach could explain why some previous chronotherapy studies have failed to show a benefit. Those studies did not individualize drug timing as this one did. But personalization could be key to circadian medicine’s success.
“Our ‘internal personal time’ appears to be an important variable to consider when dosing antihypertensives,” said co-lead author Filippo Pigazzani, MD, PhD, clinical senior lecturer and honorary consultant cardiologist at the University of Dundee School of Medicine. “Chronotherapy research has been going on for decades. We knew there was something important with time of day. But researchers haven’t considered the internal time of individual people. I think that is the missing piece.”
The analysis has several important limitations, the researchers said. A total of 95% of participants were White. And it was an observational study, not a true randomized comparison. “We started it late in the original TIME study,” Dr. MacDonald said. “You could argue we were reporting on those who survived long enough to get into the analysis.” More research is needed, they concluded.
Looking Beyond Blood Pressure
What about the rest of the body? “Almost all the cells of our body contain ‘circadian clocks’ that are synchronized by daily environmental cues, including light-dark, activity-rest, and feeding-fasting cycles,” said Dr. Dyar.
An estimated 50% of prescription drugs hit targets in the body that have circadian patterns. So, experts suspect that syncing a drug with a person’s body clock might increase effectiveness of many drugs.
A handful of US Food and Drug Administration–approved drugs already have time-of-day recommendations on the label for effectiveness or to limit side effects, including bedtime or evening for the insomnia drug Ambien, the HIV antiviral Atripla, and cholesterol-lowering Zocor. Others are intended to be taken with or after your last meal of the day, such as the long-acting insulin Levemir and the cardiovascular drug Xarelto. A morning recommendation comes with the proton pump inhibitor Nexium and the attention-deficit/hyperactivity disorder drug Ritalin.
Interest is expanding. About one third of the papers published about chronotherapy in the past 25 years have come out in the past 5 years. The May 2024 meeting of the Society for Research on Biological Rhythms featured a day-long session aimed at bringing clinicians up to speed. An organization called the International Association of Circadian Health Clinics is trying to bring circadian medicine findings to clinicians and their patients and to support research.
Moreover, while recent research suggests minding the clock could have benefits for a wide range of treatments, ignoring it could cause problems.
In a Massachusetts Institute of Technology study published in April in Science Advances, researchers looked at engineered livers made from human donor cells and found more than 300 genes that operate on a circadian schedule, many with roles in drug metabolism. They also found that circadian patterns affected the toxicity of acetaminophen and atorvastatin. Identifying the time of day to take these drugs could maximize effectiveness and minimize adverse effects, the researchers said.
Timing and the Immune System
Circadian rhythms are also seen in immune processes. In a 2023 study in The Journal of Clinical Investigation of vaccine data from 1.5 million people in Israel, researchers found that children and older adults who got their second dose of the Pfizer mRNA COVID vaccine earlier in the day were about 36% less likely to be hospitalized with SARS-CoV-2 infection than those who got an evening shot.
“The sweet spot in our data was somewhere around late morning to late afternoon,” said lead researcher Jeffrey Haspel, MD, PhD, associate professor of medicine in the division of pulmonary and critical care medicine at Washington University School of Medicine in St. Louis.
In a multicenter, 2024 analysis of 13 studies of immunotherapy for advanced cancers in 1663 people, researchers found treatment earlier in the day was associated with longer survival time and longer survival without cancer progression.
“Patients with selected metastatic cancers seemed to largely benefit from early [time of day] infusions, which is consistent with circadian mechanisms in immune-cell functions and trafficking,” the researchers noted. But “retrospective randomized trials are needed to establish recommendations for optimal circadian timing.”
Other research suggests or is investigating possible chronotherapy benefits for depression, glaucoma, respiratory diseases, stroke treatment, epilepsy, and sedatives used in surgery. So why aren’t healthcare providers adding time of day to more prescriptions? “What’s missing is more reliable data,” Dr. Dyar said.
Should You Use Chronotherapy Now?
Experts emphasize that more research is needed before doctors use chronotherapy and before medical organizations include it in treatment recommendations. But for some patients, circadian dosing may be worth a try:
Night owls whose blood pressure isn’t well controlled. Dr. Dyar and Dr. Pigazzani said night-time blood pressure drugs may be helpful for people with a “late chronotype.” Of course, patients shouldn’t change their medication schedule on their own, they said. And doctors may want to consider other concerns, like more overnight bathroom visits with evening diuretics.
In their study, the researchers determined participants’ chronotype with a few questions from the Munich Chronotype Questionnaire about what time they fell asleep and woke up on workdays and days off and whether they considered themselves “morning types” or “evening types.” (The questions can be found in supplementary data for the study.)
If a physician thinks matching the timing of a dose with chronotype would help, they can consider it, Dr. Pigazzani said. “However, I must add that this was an observational study, so I would advise healthcare practitioners to wait for our data to be confirmed in new RCTs of personalized chronotherapy of hypertension.”
Children and older adults getting vaccines. Timing COVID shots and possibly other vaccines from late morning to mid-afternoon could have a small benefit for individuals and a bigger public-health benefit, Dr. Haspel said. But the most important thing is getting vaccinated. “If you can only get one in the evening, it’s still worthwhile. Timing may add oomph at a public-health level for more vulnerable groups.”
A version of this article appeared on Medscape.com.
Do drugs work better if taken by the clock?
A new analysis published in The Lancet journal’s eClinicalMedicine suggests: Yes, they do — if you consider the patient’s individual body clock. The study is the first to find that timing blood pressure drugs to a person’s personal “chronotype” — that is, whether they are a night owl or an early bird — may reduce the risk for a heart attack.
The findings represent a significant advance in the field of circadian medicine or “chronotherapy” — timing drug administration to circadian rhythms. A growing stack of research suggests this approach could reduce side effects and improve the effectiveness of a wide range of therapies, including vaccines, cancer treatments, and drugs for depression, glaucoma, pain, seizures, and other conditions. Still, despite decades of research, time of day is rarely considered in writing prescriptions.
“We are really just at the beginning of an exciting new way of looking at patient care,” said Kenneth A. Dyar, PhD, whose lab at Helmholtz Zentrum München’s Institute for Diabetes and Cancer focuses on metabolic physiology. Dr. Dyar is co-lead author of the new blood pressure analysis.
“Chronotherapy is a rapidly growing field,” he said, “and I suspect we are soon going to see more and more studies focused on ‘personalized chronotherapy,’ not only in hypertension but also potentially in other clinical areas.”
The ‘Missing Piece’ in Chronotherapy Research
Blood pressure drugs have long been chronotherapy’s battleground. After all, blood pressure follows a circadian rhythm, peaking in the morning and dropping at night.
That healthy overnight dip can disappear in people with diabetes, kidney disease, and obstructive sleep apnea. Some physicians have suggested a bed-time dose to restore that dip. But studies have had mixed results, so “take at bedtime” has become a less common recommendation in recent years.
But the debate continued. After a large 2019 Spanish study found that bedtime doses had benefits so big that the results drew questions, an even larger, 2022 randomized, controlled trial from the University of Dundee in Dundee, Scotland — called the TIME study — aimed to settle the question.
Researchers assigned over 21,000 people to take morning or night hypertension drugs for several years and found no difference in cardiovascular outcomes.
“We did this study thinking nocturnal blood pressure tablets might be better,” said Thomas MacDonald, MD, professor emeritus of clinical pharmacology and pharmacoepidemiology at the University of Dundee and principal investigator for the TIME study and the recent chronotype analysis. “But there was no difference for heart attacks, strokes, or vascular death.”
So, the researchers then looked at participants’ chronotypes, sorting outcomes based on whether the participants were late-to-bed, late-to-rise “night owls” or early-to-bed, early-to-rise “morning larks.”
Their analysis of these 5358 TIME participants found the following results: Risk for hospitalization for a heart attack was at least 34% lower for “owls” who took their drugs at bedtime. By contrast, owls’ heart attack risk was at least 62% higher with morning doses. For “larks,” the opposite was true. Morning doses were associated with an 11% lower heart attack risk and night doses with an 11% higher risk, according to supplemental data.
The personalized approach could explain why some previous chronotherapy studies have failed to show a benefit. Those studies did not individualize drug timing as this one did. But personalization could be key to circadian medicine’s success.
“Our ‘internal personal time’ appears to be an important variable to consider when dosing antihypertensives,” said co-lead author Filippo Pigazzani, MD, PhD, clinical senior lecturer and honorary consultant cardiologist at the University of Dundee School of Medicine. “Chronotherapy research has been going on for decades. We knew there was something important with time of day. But researchers haven’t considered the internal time of individual people. I think that is the missing piece.”
The analysis has several important limitations, the researchers said. A total of 95% of participants were White. And it was an observational study, not a true randomized comparison. “We started it late in the original TIME study,” Dr. MacDonald said. “You could argue we were reporting on those who survived long enough to get into the analysis.” More research is needed, they concluded.
Looking Beyond Blood Pressure
What about the rest of the body? “Almost all the cells of our body contain ‘circadian clocks’ that are synchronized by daily environmental cues, including light-dark, activity-rest, and feeding-fasting cycles,” said Dr. Dyar.
An estimated 50% of prescription drugs hit targets in the body that have circadian patterns. So, experts suspect that syncing a drug with a person’s body clock might increase effectiveness of many drugs.
A handful of US Food and Drug Administration–approved drugs already have time-of-day recommendations on the label for effectiveness or to limit side effects, including bedtime or evening for the insomnia drug Ambien, the HIV antiviral Atripla, and cholesterol-lowering Zocor. Others are intended to be taken with or after your last meal of the day, such as the long-acting insulin Levemir and the cardiovascular drug Xarelto. A morning recommendation comes with the proton pump inhibitor Nexium and the attention-deficit/hyperactivity disorder drug Ritalin.
Interest is expanding. About one third of the papers published about chronotherapy in the past 25 years have come out in the past 5 years. The May 2024 meeting of the Society for Research on Biological Rhythms featured a day-long session aimed at bringing clinicians up to speed. An organization called the International Association of Circadian Health Clinics is trying to bring circadian medicine findings to clinicians and their patients and to support research.
Moreover, while recent research suggests minding the clock could have benefits for a wide range of treatments, ignoring it could cause problems.
In a Massachusetts Institute of Technology study published in April in Science Advances, researchers looked at engineered livers made from human donor cells and found more than 300 genes that operate on a circadian schedule, many with roles in drug metabolism. They also found that circadian patterns affected the toxicity of acetaminophen and atorvastatin. Identifying the time of day to take these drugs could maximize effectiveness and minimize adverse effects, the researchers said.
Timing and the Immune System
Circadian rhythms are also seen in immune processes. In a 2023 study in The Journal of Clinical Investigation of vaccine data from 1.5 million people in Israel, researchers found that children and older adults who got their second dose of the Pfizer mRNA COVID vaccine earlier in the day were about 36% less likely to be hospitalized with SARS-CoV-2 infection than those who got an evening shot.
“The sweet spot in our data was somewhere around late morning to late afternoon,” said lead researcher Jeffrey Haspel, MD, PhD, associate professor of medicine in the division of pulmonary and critical care medicine at Washington University School of Medicine in St. Louis.
In a multicenter, 2024 analysis of 13 studies of immunotherapy for advanced cancers in 1663 people, researchers found treatment earlier in the day was associated with longer survival time and longer survival without cancer progression.
“Patients with selected metastatic cancers seemed to largely benefit from early [time of day] infusions, which is consistent with circadian mechanisms in immune-cell functions and trafficking,” the researchers noted. But “retrospective randomized trials are needed to establish recommendations for optimal circadian timing.”
Other research suggests or is investigating possible chronotherapy benefits for depression, glaucoma, respiratory diseases, stroke treatment, epilepsy, and sedatives used in surgery. So why aren’t healthcare providers adding time of day to more prescriptions? “What’s missing is more reliable data,” Dr. Dyar said.
Should You Use Chronotherapy Now?
Experts emphasize that more research is needed before doctors use chronotherapy and before medical organizations include it in treatment recommendations. But for some patients, circadian dosing may be worth a try:
Night owls whose blood pressure isn’t well controlled. Dr. Dyar and Dr. Pigazzani said night-time blood pressure drugs may be helpful for people with a “late chronotype.” Of course, patients shouldn’t change their medication schedule on their own, they said. And doctors may want to consider other concerns, like more overnight bathroom visits with evening diuretics.
In their study, the researchers determined participants’ chronotype with a few questions from the Munich Chronotype Questionnaire about what time they fell asleep and woke up on workdays and days off and whether they considered themselves “morning types” or “evening types.” (The questions can be found in supplementary data for the study.)
If a physician thinks matching the timing of a dose with chronotype would help, they can consider it, Dr. Pigazzani said. “However, I must add that this was an observational study, so I would advise healthcare practitioners to wait for our data to be confirmed in new RCTs of personalized chronotherapy of hypertension.”
Children and older adults getting vaccines. Timing COVID shots and possibly other vaccines from late morning to mid-afternoon could have a small benefit for individuals and a bigger public-health benefit, Dr. Haspel said. But the most important thing is getting vaccinated. “If you can only get one in the evening, it’s still worthwhile. Timing may add oomph at a public-health level for more vulnerable groups.”
A version of this article appeared on Medscape.com.
Losing Weight, Decreasing Alcohol, and Improving Sex Life?
Richard* was a master-of-the-universe type. He went to Wharton, ran a large hedge fund, and lived in Greenwich, Connecticut. His three children attended Ivy League schools. He played golf on the weekends and ate three healthy meals per day. There was just one issue: He had gained 90 pounds since the 1990s from consuming six to seven alcoholic beverages per day. He already had one DUI under his belt, and his marriage was on shaky ground. He had tried to address his alcohol abuse disorder on multiple occasions: He went to a yearlong class on alcoholism, saw a psychologist for cognitive-behavioral therapy, and joined Alcoholics Anonymous, all to no avail.
When I met him in December 2023, he had hit rock bottom and was willing to try anything.
At our first visit, I prescribed him weekly tirzepatide (Zepbound) off label, along with a small dose of naltrexone.
Richard shared some feedback after his first 2 weeks:
The naltrexone works great and is strong ... small dose for me effective ... I haven’t wanted to drink and when I do I can’t finish a glass over 2 hours … went from 25 drinks a week to about 4 … don’t notice other side effects … sleeping better too.
And after 6 weeks:
Some more feedback … on week 6-7 and all going well ... drinking very little alcohol and still on half tab of naltrexone ... that works well and have no side effects ... the Zepbound works well too. I do get hungry a few days after the shot but still don’t crave sugar or bad snacks … weight down 21 pounds since started … 292 to 271.
And finally, after 8 weeks:
Looking at my last text to you I see the progress … been incredible ... now down 35 pounds and at 257 … continue to feel excellent with plenty of energy … want to exercise more ... and no temptation to eat or drink unhealthy stuff ... I’m very happy this has surpassed my expectations on how fast it’s worked and I don’t feel any side effects. Marriage has never been better … all thanks to you.
Tirzepatide contains two hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), that are naturally produced by our bodies after meals. Scientists recently learned that the GLP-1 system contributes to the feedback loop of addictive behaviors. Increasing synthetic GLP-1, through medications like tirzepatide, appears to minimize addictive behaviors by limiting their ability to upregulate the brain’s production of dopamine.
Dopamine is a neurotransmitter produced in the brain’s reward center, which regulates how people experience pleasure and control impulses. Dopamine reinforces the pleasure experienced by certain behaviors like drinking, smoking, and eating sweets. These new medications reduce the amount of dopamine released after these activities and thereby lower the motivation to repeat these behaviors.
Contrary to some reports in the news, the vast majority of my male patients using these medications for alcohol abuse disorder experience concurrent increases in testosterone, for two reasons: (1) testosterone increases as body mass index decreases and (2) chronic alcohol use can damage the cells in the testicles that produce testosterone and also decrease the brain’s ability to stimulate the testicles to produce testosterone.
At his most recent checkup last month, Richard’s testosterone had risen from borderline to robust levels, his libido and sleep had improved, and he reported never having felt so healthy or confident. Fingers crossed that the US Food and Drug Administration won’t wait too long before approving this class of medications for more than just diabetes, heart disease, and obesity.
*Patient’s name has been changed.
Dr. Messer is clinical assistant professor, Icahn School of Medicine at Mount Sinai, New York, and associate professor, Zucker School of Medicine at Hofstra University, Hempstead, New York. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Richard* was a master-of-the-universe type. He went to Wharton, ran a large hedge fund, and lived in Greenwich, Connecticut. His three children attended Ivy League schools. He played golf on the weekends and ate three healthy meals per day. There was just one issue: He had gained 90 pounds since the 1990s from consuming six to seven alcoholic beverages per day. He already had one DUI under his belt, and his marriage was on shaky ground. He had tried to address his alcohol abuse disorder on multiple occasions: He went to a yearlong class on alcoholism, saw a psychologist for cognitive-behavioral therapy, and joined Alcoholics Anonymous, all to no avail.
When I met him in December 2023, he had hit rock bottom and was willing to try anything.
At our first visit, I prescribed him weekly tirzepatide (Zepbound) off label, along with a small dose of naltrexone.
Richard shared some feedback after his first 2 weeks:
The naltrexone works great and is strong ... small dose for me effective ... I haven’t wanted to drink and when I do I can’t finish a glass over 2 hours … went from 25 drinks a week to about 4 … don’t notice other side effects … sleeping better too.
And after 6 weeks:
Some more feedback … on week 6-7 and all going well ... drinking very little alcohol and still on half tab of naltrexone ... that works well and have no side effects ... the Zepbound works well too. I do get hungry a few days after the shot but still don’t crave sugar or bad snacks … weight down 21 pounds since started … 292 to 271.
And finally, after 8 weeks:
Looking at my last text to you I see the progress … been incredible ... now down 35 pounds and at 257 … continue to feel excellent with plenty of energy … want to exercise more ... and no temptation to eat or drink unhealthy stuff ... I’m very happy this has surpassed my expectations on how fast it’s worked and I don’t feel any side effects. Marriage has never been better … all thanks to you.
Tirzepatide contains two hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), that are naturally produced by our bodies after meals. Scientists recently learned that the GLP-1 system contributes to the feedback loop of addictive behaviors. Increasing synthetic GLP-1, through medications like tirzepatide, appears to minimize addictive behaviors by limiting their ability to upregulate the brain’s production of dopamine.
Dopamine is a neurotransmitter produced in the brain’s reward center, which regulates how people experience pleasure and control impulses. Dopamine reinforces the pleasure experienced by certain behaviors like drinking, smoking, and eating sweets. These new medications reduce the amount of dopamine released after these activities and thereby lower the motivation to repeat these behaviors.
Contrary to some reports in the news, the vast majority of my male patients using these medications for alcohol abuse disorder experience concurrent increases in testosterone, for two reasons: (1) testosterone increases as body mass index decreases and (2) chronic alcohol use can damage the cells in the testicles that produce testosterone and also decrease the brain’s ability to stimulate the testicles to produce testosterone.
At his most recent checkup last month, Richard’s testosterone had risen from borderline to robust levels, his libido and sleep had improved, and he reported never having felt so healthy or confident. Fingers crossed that the US Food and Drug Administration won’t wait too long before approving this class of medications for more than just diabetes, heart disease, and obesity.
*Patient’s name has been changed.
Dr. Messer is clinical assistant professor, Icahn School of Medicine at Mount Sinai, New York, and associate professor, Zucker School of Medicine at Hofstra University, Hempstead, New York. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Richard* was a master-of-the-universe type. He went to Wharton, ran a large hedge fund, and lived in Greenwich, Connecticut. His three children attended Ivy League schools. He played golf on the weekends and ate three healthy meals per day. There was just one issue: He had gained 90 pounds since the 1990s from consuming six to seven alcoholic beverages per day. He already had one DUI under his belt, and his marriage was on shaky ground. He had tried to address his alcohol abuse disorder on multiple occasions: He went to a yearlong class on alcoholism, saw a psychologist for cognitive-behavioral therapy, and joined Alcoholics Anonymous, all to no avail.
When I met him in December 2023, he had hit rock bottom and was willing to try anything.
At our first visit, I prescribed him weekly tirzepatide (Zepbound) off label, along with a small dose of naltrexone.
Richard shared some feedback after his first 2 weeks:
The naltrexone works great and is strong ... small dose for me effective ... I haven’t wanted to drink and when I do I can’t finish a glass over 2 hours … went from 25 drinks a week to about 4 … don’t notice other side effects … sleeping better too.
And after 6 weeks:
Some more feedback … on week 6-7 and all going well ... drinking very little alcohol and still on half tab of naltrexone ... that works well and have no side effects ... the Zepbound works well too. I do get hungry a few days after the shot but still don’t crave sugar or bad snacks … weight down 21 pounds since started … 292 to 271.
And finally, after 8 weeks:
Looking at my last text to you I see the progress … been incredible ... now down 35 pounds and at 257 … continue to feel excellent with plenty of energy … want to exercise more ... and no temptation to eat or drink unhealthy stuff ... I’m very happy this has surpassed my expectations on how fast it’s worked and I don’t feel any side effects. Marriage has never been better … all thanks to you.
Tirzepatide contains two hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), that are naturally produced by our bodies after meals. Scientists recently learned that the GLP-1 system contributes to the feedback loop of addictive behaviors. Increasing synthetic GLP-1, through medications like tirzepatide, appears to minimize addictive behaviors by limiting their ability to upregulate the brain’s production of dopamine.
Dopamine is a neurotransmitter produced in the brain’s reward center, which regulates how people experience pleasure and control impulses. Dopamine reinforces the pleasure experienced by certain behaviors like drinking, smoking, and eating sweets. These new medications reduce the amount of dopamine released after these activities and thereby lower the motivation to repeat these behaviors.
Contrary to some reports in the news, the vast majority of my male patients using these medications for alcohol abuse disorder experience concurrent increases in testosterone, for two reasons: (1) testosterone increases as body mass index decreases and (2) chronic alcohol use can damage the cells in the testicles that produce testosterone and also decrease the brain’s ability to stimulate the testicles to produce testosterone.
At his most recent checkup last month, Richard’s testosterone had risen from borderline to robust levels, his libido and sleep had improved, and he reported never having felt so healthy or confident. Fingers crossed that the US Food and Drug Administration won’t wait too long before approving this class of medications for more than just diabetes, heart disease, and obesity.
*Patient’s name has been changed.
Dr. Messer is clinical assistant professor, Icahn School of Medicine at Mount Sinai, New York, and associate professor, Zucker School of Medicine at Hofstra University, Hempstead, New York. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Cystic Fibrosis Patients Also Experience Poor Sleep, Fatigue, Depression
Non-respiratory symptoms including poor sleep, fatigue, pain, anxiety, and depressive symptoms were prevalent among adults with cystic fibrosis (AwCF) and persisted after 1 year of follow-up, based on data from more than 200 individuals in a study presented at the American Thoracic Society (ATS) 2024 International Conference.
“People with cystic fibrosis have qualitatively reported burden from extrapulmonary symptoms that were not being addressed by their health care providers; this is the first study to examine these symptoms concurrently in a large sample over time,” said lead author Kristin A. Riekert, PhD, of Johns Hopkins University, Baltimore, in an interview.
Previous cross-sectional studies have shown a high prevalence of poor sleep quality, fatigue, pain, depression, and anxiety among AwCF, but longitudinal data showing the persistence of symptoms are lacking, Dr. Riekert and colleagues noted in their abstract.
Sleep Quality, Anxiety, and Other Assessments
The researchers recruited a total of 236 AwCF aged 18 years and older from two cystic fibrosis (CF) centers between April 2021 and August 2022. They examined the prevalence of poor sleep quality, fatigue pain, depression, and anxiety in AwCF on the basis of five assessments: At baseline and at 3, 6, 9, and 12 months.
Participants were assessed via an online survey using the Fatigue Severity Scale (cutoff, > 4), Pittsburgh Sleep Quality Index (cutoff, > 5), Patient Health Questionnaire (cutoff, > 9), Generalized Anxiety Disorder (cutoff, > 9), and PROMIS Pain Intensity (cutoff, > 50 T score). Chronic symptoms were defined as positive scores on four or more assessments for individuals who completed four or five time-point assessments. The mean age of the participants was 37 years, 52% were women, 95% were non-Hispanic White, and 86% had been prescribed CF modulator therapy.
Overall, 49% of participants met the criteria for chronic poor sleep quality, and 29% met the criteria for chronic fatigue, with positive assessments at four or more time points over the course of a year. In addition, 40%, 30%, and 18% of participants reported taking medication in the past 7 days for pain, mental health, and sleep, respectively.
The findings suggest that patients with CF might benefit from routine assessments of non-pulmonary symptoms in clinical care and from access to health care providers, including mental health professionals, to address non-pulmonary concerns, the researchers wrote in their abstract.
“We delayed starting the study until elexacaftor/tezacaftor/ivacaftor (ETI) was FDA-approved because there was an assumption that people with CF would have less fatigue because of respiratory improvements from ETI,” Dr. Riekert told this news organization. “Instead, the prevalence of fatigue and poor sleep quality was higher and more chronic than we had anticipated,” she noted.
However, “we were pleasantly surprised that depression and anxiety, while still prevalent, were less prevalent and chronic than previously reported,” Dr. Riekert said in an interview. “We attribute this to the CF Foundation’s mental health initiative that has increased the frequency of annual screening for depression and anxiety and provided resources to help people with cystic fibrosis obtain mental health services,” she said.
The study findings suggest that clinicians should assess people with CF for chronic fatigue and poor sleep along with depression and anxiety and provide treatment or referral, Dr. Riekert said. “For example, cognitive behavioral therapy can effectively treat all the symptoms that were measured in our study,” she noted.
Limitations of the study include the lack of data on how the non-respiratory symptoms interact with respiratory symptoms or pulmonary exacerbations, said Dr. Riekert. “While we assessed these symptoms five times, it was for a year; longer-term follow-up seems merited given our findings,” she said. In addition, “we need to study approaches to make cognitive behavioral therapy and other therapy more accessible for people with cystic fibrosis,” Dr. Riekert said.
Targeting Non-Pulmonary Dimensions of CF Care
The current study highlights an aspect of quality of life that is often forgotten when managing adults with CF and may affect their well-being despite effective therapy to improve function and prolong life, said Wissam Chatila, MD, professor of thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia, in an interview.
The high incidence of poor sleep, fatigue, depression, and anxiety seen in the current study was “somewhat surprising,” Dr. Chatila said. Also somewhat surprising was the chronicity of the symptoms considering the cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapies (designed to correct the malfunctioning protein made by the CFTR gene) that have changed the face of CF, he noted.
However, recent growth in the number of adult patients with CF (more than 50% in certain countries) has led to a change in pathologies that physicians have to manage, and the current study addresses some of the emerging pathologies, said Dr. Chatila.
“Beyond demonstrating survival data from registries and other epidemiologic studies, this study sheds light on the need to address patient-reported outcomes that may or may not be directly related to the pulmonary and GI effects of the CFTR modulators,” he said. “Recognizing the extent of the dysfunction that many CF patients continue to suffer from will eventually lead to identifying factors that contribute to poor outcomes and the mechanisms involved,” he added.
Overall, the current study illustrates the potential benefits of offering personalized medicine to adults with CF that improves not only their physical function but also their mental health, Dr. Chatila said.
The study was funded by the Cystic Fibrosis Foundation. Dr. Riekert had no financial conflicts to disclose. Dr. Chatila had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Non-respiratory symptoms including poor sleep, fatigue, pain, anxiety, and depressive symptoms were prevalent among adults with cystic fibrosis (AwCF) and persisted after 1 year of follow-up, based on data from more than 200 individuals in a study presented at the American Thoracic Society (ATS) 2024 International Conference.
“People with cystic fibrosis have qualitatively reported burden from extrapulmonary symptoms that were not being addressed by their health care providers; this is the first study to examine these symptoms concurrently in a large sample over time,” said lead author Kristin A. Riekert, PhD, of Johns Hopkins University, Baltimore, in an interview.
Previous cross-sectional studies have shown a high prevalence of poor sleep quality, fatigue, pain, depression, and anxiety among AwCF, but longitudinal data showing the persistence of symptoms are lacking, Dr. Riekert and colleagues noted in their abstract.
Sleep Quality, Anxiety, and Other Assessments
The researchers recruited a total of 236 AwCF aged 18 years and older from two cystic fibrosis (CF) centers between April 2021 and August 2022. They examined the prevalence of poor sleep quality, fatigue pain, depression, and anxiety in AwCF on the basis of five assessments: At baseline and at 3, 6, 9, and 12 months.
Participants were assessed via an online survey using the Fatigue Severity Scale (cutoff, > 4), Pittsburgh Sleep Quality Index (cutoff, > 5), Patient Health Questionnaire (cutoff, > 9), Generalized Anxiety Disorder (cutoff, > 9), and PROMIS Pain Intensity (cutoff, > 50 T score). Chronic symptoms were defined as positive scores on four or more assessments for individuals who completed four or five time-point assessments. The mean age of the participants was 37 years, 52% were women, 95% were non-Hispanic White, and 86% had been prescribed CF modulator therapy.
Overall, 49% of participants met the criteria for chronic poor sleep quality, and 29% met the criteria for chronic fatigue, with positive assessments at four or more time points over the course of a year. In addition, 40%, 30%, and 18% of participants reported taking medication in the past 7 days for pain, mental health, and sleep, respectively.
The findings suggest that patients with CF might benefit from routine assessments of non-pulmonary symptoms in clinical care and from access to health care providers, including mental health professionals, to address non-pulmonary concerns, the researchers wrote in their abstract.
“We delayed starting the study until elexacaftor/tezacaftor/ivacaftor (ETI) was FDA-approved because there was an assumption that people with CF would have less fatigue because of respiratory improvements from ETI,” Dr. Riekert told this news organization. “Instead, the prevalence of fatigue and poor sleep quality was higher and more chronic than we had anticipated,” she noted.
However, “we were pleasantly surprised that depression and anxiety, while still prevalent, were less prevalent and chronic than previously reported,” Dr. Riekert said in an interview. “We attribute this to the CF Foundation’s mental health initiative that has increased the frequency of annual screening for depression and anxiety and provided resources to help people with cystic fibrosis obtain mental health services,” she said.
The study findings suggest that clinicians should assess people with CF for chronic fatigue and poor sleep along with depression and anxiety and provide treatment or referral, Dr. Riekert said. “For example, cognitive behavioral therapy can effectively treat all the symptoms that were measured in our study,” she noted.
Limitations of the study include the lack of data on how the non-respiratory symptoms interact with respiratory symptoms or pulmonary exacerbations, said Dr. Riekert. “While we assessed these symptoms five times, it was for a year; longer-term follow-up seems merited given our findings,” she said. In addition, “we need to study approaches to make cognitive behavioral therapy and other therapy more accessible for people with cystic fibrosis,” Dr. Riekert said.
Targeting Non-Pulmonary Dimensions of CF Care
The current study highlights an aspect of quality of life that is often forgotten when managing adults with CF and may affect their well-being despite effective therapy to improve function and prolong life, said Wissam Chatila, MD, professor of thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia, in an interview.
The high incidence of poor sleep, fatigue, depression, and anxiety seen in the current study was “somewhat surprising,” Dr. Chatila said. Also somewhat surprising was the chronicity of the symptoms considering the cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapies (designed to correct the malfunctioning protein made by the CFTR gene) that have changed the face of CF, he noted.
However, recent growth in the number of adult patients with CF (more than 50% in certain countries) has led to a change in pathologies that physicians have to manage, and the current study addresses some of the emerging pathologies, said Dr. Chatila.
“Beyond demonstrating survival data from registries and other epidemiologic studies, this study sheds light on the need to address patient-reported outcomes that may or may not be directly related to the pulmonary and GI effects of the CFTR modulators,” he said. “Recognizing the extent of the dysfunction that many CF patients continue to suffer from will eventually lead to identifying factors that contribute to poor outcomes and the mechanisms involved,” he added.
Overall, the current study illustrates the potential benefits of offering personalized medicine to adults with CF that improves not only their physical function but also their mental health, Dr. Chatila said.
The study was funded by the Cystic Fibrosis Foundation. Dr. Riekert had no financial conflicts to disclose. Dr. Chatila had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Non-respiratory symptoms including poor sleep, fatigue, pain, anxiety, and depressive symptoms were prevalent among adults with cystic fibrosis (AwCF) and persisted after 1 year of follow-up, based on data from more than 200 individuals in a study presented at the American Thoracic Society (ATS) 2024 International Conference.
“People with cystic fibrosis have qualitatively reported burden from extrapulmonary symptoms that were not being addressed by their health care providers; this is the first study to examine these symptoms concurrently in a large sample over time,” said lead author Kristin A. Riekert, PhD, of Johns Hopkins University, Baltimore, in an interview.
Previous cross-sectional studies have shown a high prevalence of poor sleep quality, fatigue, pain, depression, and anxiety among AwCF, but longitudinal data showing the persistence of symptoms are lacking, Dr. Riekert and colleagues noted in their abstract.
Sleep Quality, Anxiety, and Other Assessments
The researchers recruited a total of 236 AwCF aged 18 years and older from two cystic fibrosis (CF) centers between April 2021 and August 2022. They examined the prevalence of poor sleep quality, fatigue pain, depression, and anxiety in AwCF on the basis of five assessments: At baseline and at 3, 6, 9, and 12 months.
Participants were assessed via an online survey using the Fatigue Severity Scale (cutoff, > 4), Pittsburgh Sleep Quality Index (cutoff, > 5), Patient Health Questionnaire (cutoff, > 9), Generalized Anxiety Disorder (cutoff, > 9), and PROMIS Pain Intensity (cutoff, > 50 T score). Chronic symptoms were defined as positive scores on four or more assessments for individuals who completed four or five time-point assessments. The mean age of the participants was 37 years, 52% were women, 95% were non-Hispanic White, and 86% had been prescribed CF modulator therapy.
Overall, 49% of participants met the criteria for chronic poor sleep quality, and 29% met the criteria for chronic fatigue, with positive assessments at four or more time points over the course of a year. In addition, 40%, 30%, and 18% of participants reported taking medication in the past 7 days for pain, mental health, and sleep, respectively.
The findings suggest that patients with CF might benefit from routine assessments of non-pulmonary symptoms in clinical care and from access to health care providers, including mental health professionals, to address non-pulmonary concerns, the researchers wrote in their abstract.
“We delayed starting the study until elexacaftor/tezacaftor/ivacaftor (ETI) was FDA-approved because there was an assumption that people with CF would have less fatigue because of respiratory improvements from ETI,” Dr. Riekert told this news organization. “Instead, the prevalence of fatigue and poor sleep quality was higher and more chronic than we had anticipated,” she noted.
However, “we were pleasantly surprised that depression and anxiety, while still prevalent, were less prevalent and chronic than previously reported,” Dr. Riekert said in an interview. “We attribute this to the CF Foundation’s mental health initiative that has increased the frequency of annual screening for depression and anxiety and provided resources to help people with cystic fibrosis obtain mental health services,” she said.
The study findings suggest that clinicians should assess people with CF for chronic fatigue and poor sleep along with depression and anxiety and provide treatment or referral, Dr. Riekert said. “For example, cognitive behavioral therapy can effectively treat all the symptoms that were measured in our study,” she noted.
Limitations of the study include the lack of data on how the non-respiratory symptoms interact with respiratory symptoms or pulmonary exacerbations, said Dr. Riekert. “While we assessed these symptoms five times, it was for a year; longer-term follow-up seems merited given our findings,” she said. In addition, “we need to study approaches to make cognitive behavioral therapy and other therapy more accessible for people with cystic fibrosis,” Dr. Riekert said.
Targeting Non-Pulmonary Dimensions of CF Care
The current study highlights an aspect of quality of life that is often forgotten when managing adults with CF and may affect their well-being despite effective therapy to improve function and prolong life, said Wissam Chatila, MD, professor of thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia, in an interview.
The high incidence of poor sleep, fatigue, depression, and anxiety seen in the current study was “somewhat surprising,” Dr. Chatila said. Also somewhat surprising was the chronicity of the symptoms considering the cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapies (designed to correct the malfunctioning protein made by the CFTR gene) that have changed the face of CF, he noted.
However, recent growth in the number of adult patients with CF (more than 50% in certain countries) has led to a change in pathologies that physicians have to manage, and the current study addresses some of the emerging pathologies, said Dr. Chatila.
“Beyond demonstrating survival data from registries and other epidemiologic studies, this study sheds light on the need to address patient-reported outcomes that may or may not be directly related to the pulmonary and GI effects of the CFTR modulators,” he said. “Recognizing the extent of the dysfunction that many CF patients continue to suffer from will eventually lead to identifying factors that contribute to poor outcomes and the mechanisms involved,” he added.
Overall, the current study illustrates the potential benefits of offering personalized medicine to adults with CF that improves not only their physical function but also their mental health, Dr. Chatila said.
The study was funded by the Cystic Fibrosis Foundation. Dr. Riekert had no financial conflicts to disclose. Dr. Chatila had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Strategies for MS Fatigue and Sleep Issues
NASHVILLE, TENNESSEE —
Fatigue related to MS is complex, but it often follows a pattern. “Oftentimes when I meet with patients for the first time, they’re not always sure [what their own pattern is]. They know that the fatigue is present, and it’s limiting their activities. It’s important for us to break down and see that pattern for [the patient] specifically, and what are some ways that we can intervene to perhaps make that pattern something that improves quality of life and day-to-day living,” said Grace Tworek, PsyD, during a presentation at the annual meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
A cycle may start on a day that a patient has lots of energy. They are ambitious that day and get a lot done on their “to do” list while they have the energy. Unfortunately, they commonly overdo it, leading to fatigue the next day. Over ensuing days, the patient might feel unable to engage in everyday tasks and begin to feel they are falling behind. This in turn can affect mood, resulting in increased symptoms of depression and anxiety. That leads to days of inactivity and rest, which leads to recovery. Then comes a day with better mood and increased energy, where the cycle can begin again.
It’s an addressable problem. “What we really want to do is break this cycle, get out of those peaks and valleys of high energy days and very low energy days to try to create more sustainable patterns” said Dr. Tworek, who is a staff health psychologist at Cleveland Clinic’s Mellen Center for Multiple Sclerosis, Cleveland, Ohio.
Fatigue
When addressing fatigue in MS patients, Dr. Tworek and her colleagues begin with a fatigue diary that includes typical activities engaged in throughout the day. It also distinguishes between activities the patient feels are important and activities that give them satisfaction.
“If we can find ways to include these [satisfying] activities, and not focus only on those important activities. This is where that quality of life really comes into play. But I always say to folks, we are not striving for perfection at first. I want you to write down what’s actually happening so we can use this data to later inform how we are going to make changes,” said Dr. Tworek.
It’s also important to encourage patients to seek help. Activities that are neither important nor satisfying may not need doing at all, and they encourage patients to seek help in other tasks. As for tasks that are important in their day-to-day lives, “How can we break those down? We break those down by pacing activities,” said Dr. Tworek.
A simple way to pace yourself is to use “The rule of two.” It asks: How long can I do a task before I experience a two-point increase on a 1-10 fatigue scale. “At that time, is when we want to start inserting breaks. We want to find activities we can do that will reduce [fatigue] or get us back to baseline. Or if that’s not realistic, keep us where we are at rather than increasing fatigue,” said Dr. Tworek.
Another way to think about it is spoon theory, sometimes referred to as coin theory. The idea is that you wake up each morning with ten spoons. Each task on a given day will cost a certain number of spoons. “You might start your day, you go downstairs, you have breakfast, and you’re already down to seven points, the next day, you might still be at 10. So it’s really about monitoring where you’re at in terms of how many coins or spoons you’re spending so that we can then reflect on how many coins or spoons do I have left?” said Dr. Tworek.
The strategy can aid communication with partners or family members who may have difficulty understanding MS fatigue. “Sometimes putting a number to it can really open up the doors to having these difficult conversations with friends and family,” said Dr. Tworek.
Sleep
Fatigue and sleep are naturally intertwined, and sleep problems are also common in MS, with 30%-56% reporting problems, depending on the estimate.
One concept to think about is sleep drive. “From the moment we wake up, we are building sleep pressure, just like from the moment you stop eating, your body starts building pressure to eat again,” said Dr. Tworek.
Naps can interfere with that drive, much like a snack can rob you of a meal-time appetite. “A nap is going to curb that appetite for sleep, making it more difficult potentially to fall asleep,” said Dr. Tworek. If a nap is absolutely necessary, it’s better to do it earlier in the day to allow time to build sleep pressure again.
As with fatigue, Dr. Tworek has patients fill out a sleep diary that documents difficulty falling or staying asleep, timing and length of awakenings, quality of sleep, length and timing of any naps, and other factors. It sometimes reveals patterns, like difficulty falling asleep on specific days of the week. Such rhythms may be attributable to regular stressors, like anticipating some event the next morning. Then it might be possible to tie in other techniques like stress management to reduce accompanying anxiety.
Sleep hygiene is an important factor, employing strategies like staying off screens or social media while in bed. “About 1 hour before bedtime, we want to try to create some relaxation time,” said Dr. Tworek.
Her clinic also emphasizes consistent wake time. “If we are waking every day in about the same half hour period, we are able to build that sleep pressure consistently. [Then] your body is going to let you know when it is time for bed. You’re going to feel sleepiness,” said Dr. Tworek.
Dr. Tworek did not report any disclosures or conflicts of interest.
NASHVILLE, TENNESSEE —
Fatigue related to MS is complex, but it often follows a pattern. “Oftentimes when I meet with patients for the first time, they’re not always sure [what their own pattern is]. They know that the fatigue is present, and it’s limiting their activities. It’s important for us to break down and see that pattern for [the patient] specifically, and what are some ways that we can intervene to perhaps make that pattern something that improves quality of life and day-to-day living,” said Grace Tworek, PsyD, during a presentation at the annual meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
A cycle may start on a day that a patient has lots of energy. They are ambitious that day and get a lot done on their “to do” list while they have the energy. Unfortunately, they commonly overdo it, leading to fatigue the next day. Over ensuing days, the patient might feel unable to engage in everyday tasks and begin to feel they are falling behind. This in turn can affect mood, resulting in increased symptoms of depression and anxiety. That leads to days of inactivity and rest, which leads to recovery. Then comes a day with better mood and increased energy, where the cycle can begin again.
It’s an addressable problem. “What we really want to do is break this cycle, get out of those peaks and valleys of high energy days and very low energy days to try to create more sustainable patterns” said Dr. Tworek, who is a staff health psychologist at Cleveland Clinic’s Mellen Center for Multiple Sclerosis, Cleveland, Ohio.
Fatigue
When addressing fatigue in MS patients, Dr. Tworek and her colleagues begin with a fatigue diary that includes typical activities engaged in throughout the day. It also distinguishes between activities the patient feels are important and activities that give them satisfaction.
“If we can find ways to include these [satisfying] activities, and not focus only on those important activities. This is where that quality of life really comes into play. But I always say to folks, we are not striving for perfection at first. I want you to write down what’s actually happening so we can use this data to later inform how we are going to make changes,” said Dr. Tworek.
It’s also important to encourage patients to seek help. Activities that are neither important nor satisfying may not need doing at all, and they encourage patients to seek help in other tasks. As for tasks that are important in their day-to-day lives, “How can we break those down? We break those down by pacing activities,” said Dr. Tworek.
A simple way to pace yourself is to use “The rule of two.” It asks: How long can I do a task before I experience a two-point increase on a 1-10 fatigue scale. “At that time, is when we want to start inserting breaks. We want to find activities we can do that will reduce [fatigue] or get us back to baseline. Or if that’s not realistic, keep us where we are at rather than increasing fatigue,” said Dr. Tworek.
Another way to think about it is spoon theory, sometimes referred to as coin theory. The idea is that you wake up each morning with ten spoons. Each task on a given day will cost a certain number of spoons. “You might start your day, you go downstairs, you have breakfast, and you’re already down to seven points, the next day, you might still be at 10. So it’s really about monitoring where you’re at in terms of how many coins or spoons you’re spending so that we can then reflect on how many coins or spoons do I have left?” said Dr. Tworek.
The strategy can aid communication with partners or family members who may have difficulty understanding MS fatigue. “Sometimes putting a number to it can really open up the doors to having these difficult conversations with friends and family,” said Dr. Tworek.
Sleep
Fatigue and sleep are naturally intertwined, and sleep problems are also common in MS, with 30%-56% reporting problems, depending on the estimate.
One concept to think about is sleep drive. “From the moment we wake up, we are building sleep pressure, just like from the moment you stop eating, your body starts building pressure to eat again,” said Dr. Tworek.
Naps can interfere with that drive, much like a snack can rob you of a meal-time appetite. “A nap is going to curb that appetite for sleep, making it more difficult potentially to fall asleep,” said Dr. Tworek. If a nap is absolutely necessary, it’s better to do it earlier in the day to allow time to build sleep pressure again.
As with fatigue, Dr. Tworek has patients fill out a sleep diary that documents difficulty falling or staying asleep, timing and length of awakenings, quality of sleep, length and timing of any naps, and other factors. It sometimes reveals patterns, like difficulty falling asleep on specific days of the week. Such rhythms may be attributable to regular stressors, like anticipating some event the next morning. Then it might be possible to tie in other techniques like stress management to reduce accompanying anxiety.
Sleep hygiene is an important factor, employing strategies like staying off screens or social media while in bed. “About 1 hour before bedtime, we want to try to create some relaxation time,” said Dr. Tworek.
Her clinic also emphasizes consistent wake time. “If we are waking every day in about the same half hour period, we are able to build that sleep pressure consistently. [Then] your body is going to let you know when it is time for bed. You’re going to feel sleepiness,” said Dr. Tworek.
Dr. Tworek did not report any disclosures or conflicts of interest.
NASHVILLE, TENNESSEE —
Fatigue related to MS is complex, but it often follows a pattern. “Oftentimes when I meet with patients for the first time, they’re not always sure [what their own pattern is]. They know that the fatigue is present, and it’s limiting their activities. It’s important for us to break down and see that pattern for [the patient] specifically, and what are some ways that we can intervene to perhaps make that pattern something that improves quality of life and day-to-day living,” said Grace Tworek, PsyD, during a presentation at the annual meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
A cycle may start on a day that a patient has lots of energy. They are ambitious that day and get a lot done on their “to do” list while they have the energy. Unfortunately, they commonly overdo it, leading to fatigue the next day. Over ensuing days, the patient might feel unable to engage in everyday tasks and begin to feel they are falling behind. This in turn can affect mood, resulting in increased symptoms of depression and anxiety. That leads to days of inactivity and rest, which leads to recovery. Then comes a day with better mood and increased energy, where the cycle can begin again.
It’s an addressable problem. “What we really want to do is break this cycle, get out of those peaks and valleys of high energy days and very low energy days to try to create more sustainable patterns” said Dr. Tworek, who is a staff health psychologist at Cleveland Clinic’s Mellen Center for Multiple Sclerosis, Cleveland, Ohio.
Fatigue
When addressing fatigue in MS patients, Dr. Tworek and her colleagues begin with a fatigue diary that includes typical activities engaged in throughout the day. It also distinguishes between activities the patient feels are important and activities that give them satisfaction.
“If we can find ways to include these [satisfying] activities, and not focus only on those important activities. This is where that quality of life really comes into play. But I always say to folks, we are not striving for perfection at first. I want you to write down what’s actually happening so we can use this data to later inform how we are going to make changes,” said Dr. Tworek.
It’s also important to encourage patients to seek help. Activities that are neither important nor satisfying may not need doing at all, and they encourage patients to seek help in other tasks. As for tasks that are important in their day-to-day lives, “How can we break those down? We break those down by pacing activities,” said Dr. Tworek.
A simple way to pace yourself is to use “The rule of two.” It asks: How long can I do a task before I experience a two-point increase on a 1-10 fatigue scale. “At that time, is when we want to start inserting breaks. We want to find activities we can do that will reduce [fatigue] or get us back to baseline. Or if that’s not realistic, keep us where we are at rather than increasing fatigue,” said Dr. Tworek.
Another way to think about it is spoon theory, sometimes referred to as coin theory. The idea is that you wake up each morning with ten spoons. Each task on a given day will cost a certain number of spoons. “You might start your day, you go downstairs, you have breakfast, and you’re already down to seven points, the next day, you might still be at 10. So it’s really about monitoring where you’re at in terms of how many coins or spoons you’re spending so that we can then reflect on how many coins or spoons do I have left?” said Dr. Tworek.
The strategy can aid communication with partners or family members who may have difficulty understanding MS fatigue. “Sometimes putting a number to it can really open up the doors to having these difficult conversations with friends and family,” said Dr. Tworek.
Sleep
Fatigue and sleep are naturally intertwined, and sleep problems are also common in MS, with 30%-56% reporting problems, depending on the estimate.
One concept to think about is sleep drive. “From the moment we wake up, we are building sleep pressure, just like from the moment you stop eating, your body starts building pressure to eat again,” said Dr. Tworek.
Naps can interfere with that drive, much like a snack can rob you of a meal-time appetite. “A nap is going to curb that appetite for sleep, making it more difficult potentially to fall asleep,” said Dr. Tworek. If a nap is absolutely necessary, it’s better to do it earlier in the day to allow time to build sleep pressure again.
As with fatigue, Dr. Tworek has patients fill out a sleep diary that documents difficulty falling or staying asleep, timing and length of awakenings, quality of sleep, length and timing of any naps, and other factors. It sometimes reveals patterns, like difficulty falling asleep on specific days of the week. Such rhythms may be attributable to regular stressors, like anticipating some event the next morning. Then it might be possible to tie in other techniques like stress management to reduce accompanying anxiety.
Sleep hygiene is an important factor, employing strategies like staying off screens or social media while in bed. “About 1 hour before bedtime, we want to try to create some relaxation time,” said Dr. Tworek.
Her clinic also emphasizes consistent wake time. “If we are waking every day in about the same half hour period, we are able to build that sleep pressure consistently. [Then] your body is going to let you know when it is time for bed. You’re going to feel sleepiness,” said Dr. Tworek.
Dr. Tworek did not report any disclosures or conflicts of interest.
FROM CMSC 2024
Use of Hypoglossal Nerve Stimulation for Treating OSA in Military Patient Populations
Obstructive sleep apnea (OSA), the repetitive collapse of posterior oropharynx during sleep resulting in hypoxia and/or arousals from sleep, is the most common form of sleep disordered breathing and a common chronic respiratory disorders among middle-aged adults. OSA can lead to significant health problems, such as worsened cardiometabolic disease and cognitive impairment, which can increase morbidity and mortality.1
The gold standard for OSA diagnosis is polysomnography (PSG), although home sleep studies can be performed for select patients. OSA diagnoses are based on the number of times per hour of sleep a patient’s airway narrows or collapses, reducing or stopping airflow, scored as hypopnea or apnea events, respectively. An Apnea-Hypopnea Index (AHI) score of 5 to 14 events/hour is considered mild OSA, 15 to 30 events/hour moderate OSA, and ≥ 30 events/hour severe OSA.2
Treatment commonly includes positive airway pressure (PAP) but more than one-half of patients are not adherent to continuous PAP (CPAP) treatment after about 90 days.3 Efficacy of treatments vary as a function of disease severity and etiology, which—in addition to the classic presentation of obesity with large neck/narrowupper airway—includes craniofacial abnormalities, altered muscle function in the upper airway, pharyngeal neuropathy, and fluid shifts to the neck.
Background
The American Academy of Sleep Medicine (AASM) estimates that 10% to 17% of adults in the United States have OSA.4 Compared with civilians, the military population generally is younger and healthier. Service members have access to regular health care with yearly physical examinations, exercise scheduled into the workday, and mandatory height/weight and fitness standards. Because obesity is a major risk factor for OSA, and the incidence of obesity is relatively low in the military population (estimated at 18.8% in 2021 vs 39.8% among all US adults aged 20 to 39 years), it might be expected that incidence of OSA would be correspondingly low.5,6 However, there is evidence of a rapidly increasing incidence of OSA in military populations. A 2021 study revealed that OSA incidence rates increased from 11 to 333 per 10,000 between 2005 and 2019 across all military branches and demographics, with the highest rate among Army personnel.7 An earlier study revealed a 600% increase in OSA incidence among Army personnel between 2003 and 2011.8
Several factors likely contributed to this increase, including expanding obesity and greater physician awareness and availability of sleep study centers. Rogers and colleagues found that 40% to 50% of incident OSA diagnoses among military personnel occur within 12 months of separation, suggesting that the secondary gains associated with military disability benefits might motivate OSA evaluation.9 It is possible that secondary gain is a factor because an OSA diagnosis can range from a 0% to 100% disability rating, depending on the severity.10 This disability claim is based on evidence that untreated OSA can negatively affect long-term health and mission readiness.8 For example, untreated OSA can lead to hypertension, which contributes to a long list of adverse health and wellness consequences. Most importantly for the military, OSA has been shown to increase daytime sleepiness and reduce cognitive performance.10
The current first-line treatment for OSA is CPAP, which improves symptoms of daytime sleepiness, hypertension management, and daytime alertness.11 Despite its efficacy, nonadherence rates range from 29% to 83%.12-15 Nonadherence factors include lifestyle changes, adverse effects (eg, nasal congestion), and lack of education on proper use.11 Lifestyle changes needed to increase the likelihood of successful therapy, such as regular sleep schedules and proper CPAP cleaning and maintenance, are difficult for military personnel because of the nature of continuous or sustained operations that might require shift work and/or around-the-clock (ie, 24-hour, 7 days a week) task performance. Traveling with CPAP is an added burden for service members deployed to combat operations (ie, added luggage, weight, maintenance). Although alternate treatments such as oral appliances (ie, custom dental devices) are available, they generally are less effective than CPAP.2 Oral appliances could be a reasonable alternative treatment for some patients who cannot manage their OSA with behavioral modifications and are intolerant or unable to effectively use CPAP. This could include patients in the military who are deployed to austere environments.
Surgically implanted hypoglossal nerve stimulator (HGNS) treatment may provide long-term health benefits to service members. After the device is implanted near the hypoglossal nerve, electrical stimulation causes the tongue to move forward, which opens the airway in the anteroposterior dimension. The most important consideration is the mechanism of airway collapse. HGNS is not effective for patients whose OSA events are caused by circumferential collapse of other airway muscles. The cause of airway collapse is ascertained before surgery with drug-induced sleep endoscopy, a procedure that allows visualization of conformational changes in the upper airway during OSA events.
The US Food and Drug Administration (FDA) approved HGNS in 2014. However, it is not considered a first-line treatment for OSA by the AASM. Original candidate criteria for HGNS included an AHI score of 15 to 65 events/hour, age ≥ 18 years, failed CPAP use, body mass index (BMI) < 32, absence of palatal complete concentric collapse, and central apneas comprising < 25% of total events.16 In June 2023, the FDA expanded approval to increase the upper limit of AHI to 100 events/hour and the BMI to < 40.17
HGNS has been reported to be effective in appropriately selected patients with OSA at tertiary care centers with established multidisciplinary sleep surgical programs. These benefits have not been confirmed in larger, community-based settings, where most of these surgeries occur. In community practice, there is significant confusion among patients and clinicians about the optimal pathway for patient selection and clinical follow-up. Many patients view HGNS as a viable alternative to CPAP, but initially do not understand that it requires surgery. Surgical treatments for OSA, such as HGNS, are appealing because they suggest a 1-time intervention that permanently treats the condition, without need for follow-up or equipment resupply. HGNS might be an appealing treatment option because it is less obtrusive than CPAP and requires fewer resources for set-up and maintenance. Also, it does not cause skin irritation (a possible adverse effect of nightly use of a CPAP mask), allows the individual to sleep in a variety of positions, has less impact on social and sex life, and does not require an electric outlet. In the long term, HGNS might be more cost effective because there is no yearly physician follow-up or equipment resupply and/or maintenance.
The military population has specific demands that impact delivery and effectiveness of health care. Among service members with OSA, CPAP treatment can be challenging because of low adherence, required annual follow-up despite frequent moving cycles that pose a challenge for care continuity, and duty limitations for affected service members (ie, the requirement for a waiver to deploy and potential medical separation if symptoms are not adequately controlled). As the incidence of OSA continues to increase among service members, so does the need for OSA treatment options that are efficacious as CPAP but better tolerated and more suitable for use during military operations. The aim of this review is to assess the effectiveness of HGNS and its potential use by the military OSA patient population.
METHODS
To identify eligible studies, we employed PICOS: Population (patients aged ≥ 18 years with a history of OSA), Intervention (HGNS), Comparator (standard of care PAP therapy), Outcome (AHI or Epworth Sleepiness Scale [ESS], and Study (randomized control trial [RCT] or clinical trial). Studies were excluded if they were not written in English or included pediatric populations. The ESS is a subjective rating scale used to determine and quantify a patient’s level of daytime sleepiness, using a 4-point scale for the likelihood of falling asleep totaled across 8 different situations.18 Daytime sleepiness is considered lower normal(0-5 points), higher normal (6-10 points), mild or moderate excessive (11-15 points), and severe excessive (16-24 points).
Literature Search
We conducted a review of PubMed and Scopus for RCTs and controlled trials published from 2013 to 2023 that included the keywords and phrases: obstructive sleep apnea and either hypoglossal nerve stimulation or upper airway stimulation. The final literature search was performed December 8, 2023.
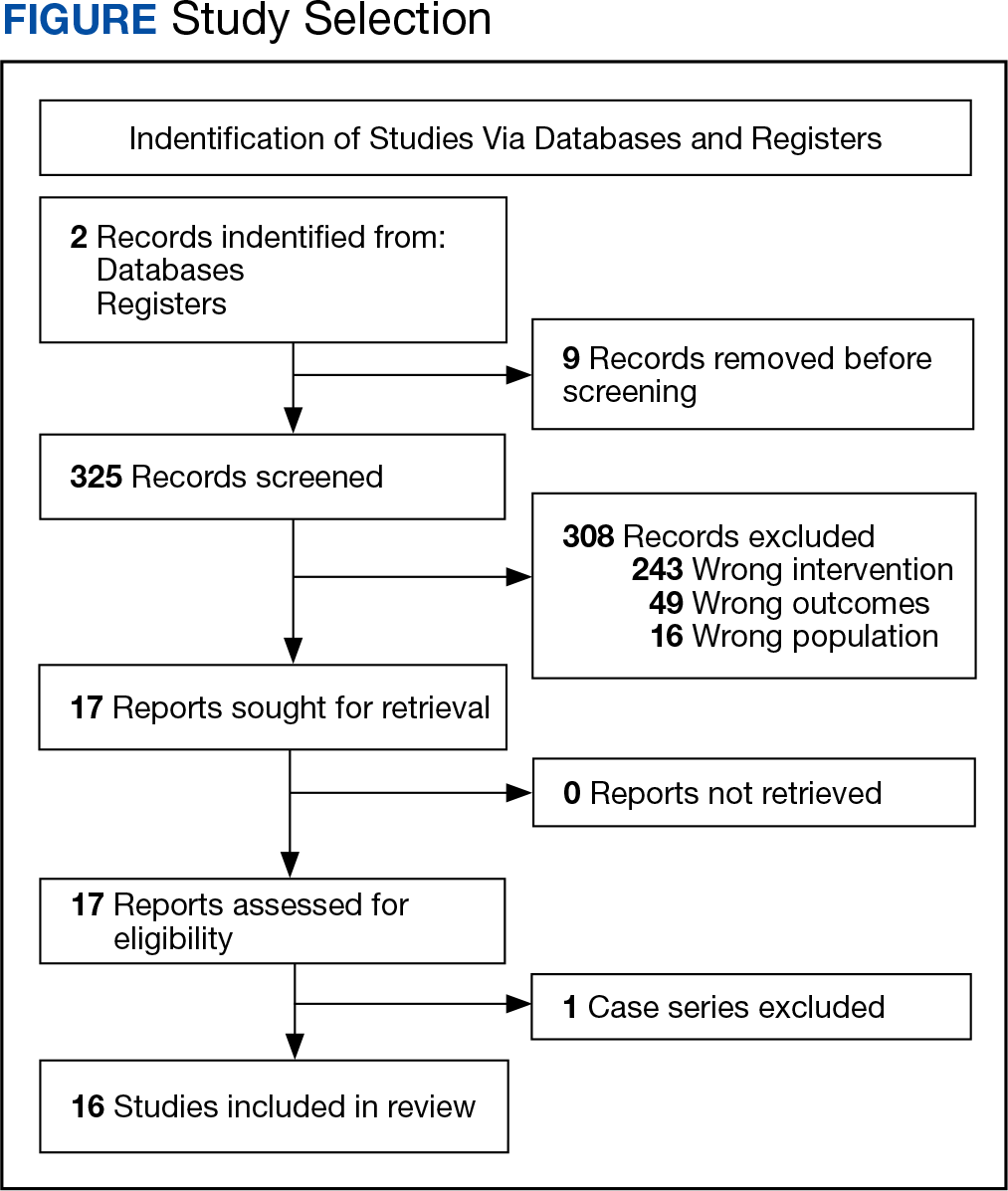
Two authors independently assessed the titles and abstracts of studies identified in the literature search based on the predefined inclusion criteria. If it was not clear whether an article met inclusion criteria based on its title and/or abstract, the 2 review authors assessed the full text of study and resolved any disagreement through consensus. If consensus was not obtained, a third author was consulted. No duplicates were identified. The PRISMA study selection process is presented in the Figure.
Data extraction was performed by 1 independent reviewer. A second author reviewed the extracted data. Any identified discrepancies were resolved through discussion and consensus. If consensus was not obtained, a third author was consulted. Study data included methods (study design and study objective), participants mean age, inclusion criteria, exclusion criteria, interventions and comparators, and primary study outcomes.
The quality of evidence was assessed using a rating of 1 to 5 based on a modified version of the Oxford Centre for Evidence-based Medicine Levels of Evidence and Grades of Recommendation.19 A rating of 1 indicated a properly powered and conducted RCT, 2 demonstrated a well-designed controlled trial without randomization or prospective comparative cohort trial, 3 designated a case-control study or retrospective cohort study, 4 signified a case series with or without intervention or a cross-sectional study, and 5 denoted an opinion of respected authorities or case reports. Two reviewers independently evaluated the quality of evidence. Any identified discrepancies were resolved through discussion and consensus. If consensus was not obtained, a third review author was consulted.
RESULTS
We identified 30 studies; 19 articles did not meet inclusion criteria. The remaining 11 articles were divided into 4 cohorts. Five articles were based on data from the STAR trial, a multicenter study that included adults with moderate-to-severe OSA and inadequate adherence to CPAP.20-24 Four articles used the same patient selection criteria as the STAR trial for a long-term German postmarket study of upper airway stimulation efficacy with OSA.25-28 The third and fourth cohorts each consist of 31 patients with moderate-to-severe OSA with CPAP nonadherence or failure.29,30 The STAR trial included follow-up at 5 years, and the German-postmarket had a follow-up at3 years. The remaining 2 cohorts have 1-year follow-ups.
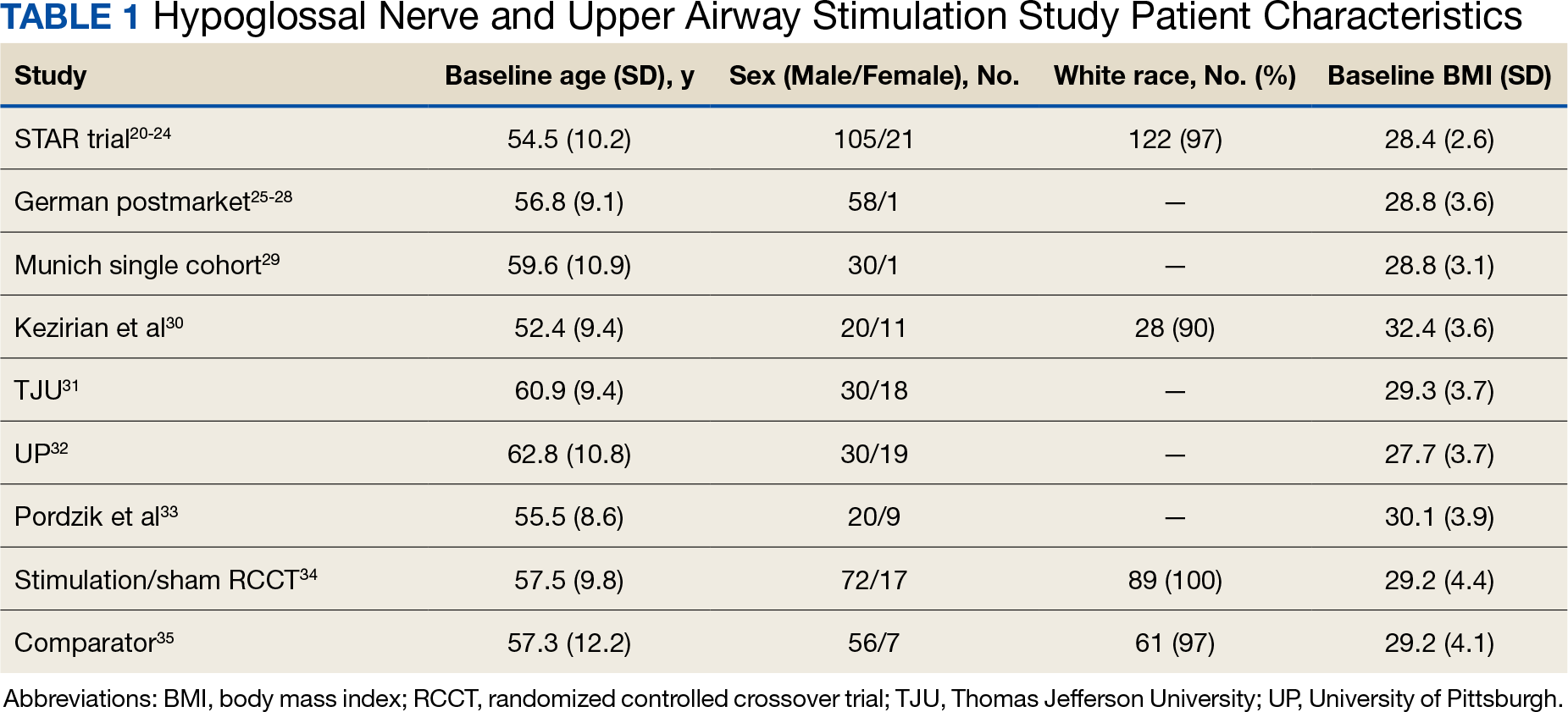
The Scopus review identified 304 studies; 299 did not meet inclusion criteria and 1 was part of the STAR trial.31 The remaining 4 articles were classified as distinct cohorts. Huntley and colleagues included patients from Thomas Jefferson University (TJU) and University of Pittsburgh (UP) academic medical centers.32 The Pordzik and colleagues cohort received implantation at a tertiary medical center, an RCCT, and a 1:1 comparator trial (Table 1).33-35
STAR Trial
This multicenter, prospective, single-group cohort study was conducted in the US, Germany, Belgium, Netherlands, and France. The STAR trial included 126 patients who were not CPAP therapy adherent. Patients were excluded if they had AHI < 20 or > 50, central sleep apnea > 25% of total AHI, anatomical abnormalities that prevent effective assessment of upper-airway stimulation, complete concentric collapse of the retropalatal airway during drug-induced sleep, neuromuscular disease, hypoglossal-nerve palsy, severe restrictive or obstructive pulmonary disease, moderate-to-severe pulmonary arterial hypertension, severe valvular heart disease, New York Heart Association class III or IV heart failure, recent myocardial infarction or severe cardiac arrhythmias (within the past 6 months), persistent uncontrolled hypertension despite medication use, active psychiatric illness, or coexisting nonrespiratory sleep disorders that would confound functional sleep assessment. Primary outcome measures included the AHI and oxygen desaturation index (ODI) with secondary outcomes using the ESS, the Functional Outcomes of Sleep Questionnaire (FOSQ), and the percentage of sleep time with oxygen saturation < 90%. Of 126 patients who received implantation, 71 underwent an overnight PSG evaluation at 5-year follow-up. Mean (SD) AHI at baseline was reduced with HGNS treatment to from 32.0 (11.8) to 12.4 (16.3). Mean (SD) ESS for 92 participants with 2 measurements declined from 11.6 (5.0) at baseline to 6.9 (4.7) at 5-year follow-up.
The STAR trial included a randomized controlled withdrawal study for 46 patients who had a positive response to therapy to evaluate efficacy and durability of upper airway stimulation. Patients were randomly assigned to therapy maintenance or therapy withdrawal groups for ≥ 1 week. The short-term withdrawal effect was assessed using the original trial outcome measures and indicated that both the withdrawal and maintenance groups showed improvements at 12 months compared with the baseline. However, after the randomized withdrawal, the withdrawal group’s outcome measures deteriorated to baseline levels while the maintenance group showed no change. At 18 months of therapy, outcome measures for both groups were similar to those observed with therapy at 12 months.24 The STAR trial included self-reported outcomes at baseline, 12 months, and 24 months that used ESS to measure daytime sleepiness. These results included subsequent STAR trial reports.20-24,31
The German Postmarket Cohort
This multicenter, prospective, single-arm study used selection criteria that were based on those used in the STAR trial and included patients with moderate-to-severe OSA and nonadherence to CPAP. Patients were excluded if they had a BMI > 35, AHI < 15 or > 65; central apnea index > 25% of total AHI; or complete concentric collapse at the velopharynx during drug-induced sleep. Measured outcomes included AHI, ODI, FOSQ, and ESS. Among the 60 participants, 38 received implantation and a 3-year follow-up. Mean (SD) AHI decreased from 31.2 (13.2) at baseline to 13.1 (14.1) at follow-up, while mean (SD) ESS decreased from 12.8 (5.3) at baseline to 6.0 (3.2) at follow-up.25-28
Munich Cohort
This single-center, prospective clinical trial included patients with AHI > 15 and < 65, central apnea index < 25% of total AHI, and nonadherence to CPAP. Patients were excluded if they had a BMI > 35, anatomical abnormalities that would prevent effective assessment of upper-airway stimulation; all other exclusion criteria matched those used in the STAR trial. Among 31 patients who received implants and completed a 1-year follow-up, mean (SD) AHI decreased from 32.9 (11.2) at baseline to 7.1 (5.9) at follow-up and mean (SD) ESS decreased from 12.6 (5.6) at baseline to 5.9 (5.2) at follow-up.29
Kezirian and Colleagues Cohort
This prospective, single-arm, open-label study was conducted at 4 Australian and 4 US sites. Selection criteria included moderate-to-severe OSA with failure of CPAP, AHI of 20 to 100 with ≥ 15 events/hour occurring in sleep that was non-REM (rapid eye movement) sleep, BMI ≤ 40 (Australia) or ≤ 37 (US), and a predominance of hypopneas (≥ 80% of disordered breathing events during sleep). Patients were excluded if they had earlier upper airway surgery, markedly enlarged tonsils, uncontrolled nasal obstruction, severe retrognathia, > 5% central or mixed apneic events, incompletely treated sleep disorders other than OSA, or a major disorder of the pulmonary, cardiac, renal, or nervous systems. Data were reported for 31 patients whose mean (SD) AHI declined from 45.4 (17.5) at baseline to 25.3 (20.6) at 1-year follow-up and mean (SD) ESS score declined from 12.1 (4.6) at baseline to 7.9 (3.8) 1 year later.30
TJU and UP Cohorts
The TJU and UP cohorts are composed of patients who underwent implantation between May 2014 and August 2016 at 2 academic centers.31,32 Selection criteria was consistent with that used in the STAR trial, and patients completed postoperative titration PSG and outpatient follow-up (48 patients at TJU and 49 at UP). Primary outcomes included AHI, ESS, and O2 nadir. Secondary outcomes consisted of surgical success and percentage of patients tolerating optimal titration setting at follow-up. Postoperative outcomes were assessed during the titration PSG. Time from initial ESS to postoperative PSG at TJU was 1.7 years and at UP was 1.9 years. Time from initial AHI to postoperative PSG at TJU was 90.4 days and 85.2 days at UP. At TJU, mean (SD) AHI and ESS dropped from 35.9 (20.8) and 11.1 (3.8), respectively at baseline to 6.3 (11.5) and 5.8 (3.4), respectively at follow-up. At UP, mean (SD) AHI and ESS fell from 35.3 (15.3) and 10.9 (4.9), respectively at baseline to 6.3 (6.1) and 6.6 (4.5), respectively at follow-up. There were no site-related differences in rates of AHI, ESS, or surgical success.31
Pordzik and Colleagues Cohort
This cohort of 29 patients underwent implantation between February 2020 and June 2022 at a tertiary university medical center with both pre- and postoperative PSG. Selection criteria was consistent with that of the German postmarket cohort. Postoperative PSG was completed a mean (SD) 96.3 (27.0) days after device activation. Mean (SD) AHI dropped from 38.6 (12.7) preoperatively to 24.4 (13.3) postoperatively. Notably, this cohort showed a much lower decrease of postoperative AHI than reported by the STAR trial and UP/TJU cohort.33
Stimulation vs Sham Trial
This multicenter, double-blinded, randomized, crossover trial assessed the effect of HGNS (stim) vs sham stimulation (sham) in 86 patients that completed both phases of the trial. Primary outcomes included AHI and ESS. Secondary outcomes included FOSQ. No carryover effect was found during the crossover phase. The difference between the phases was−15.5 (95% CI, −18.3 to −12.8) for AHI and −3.3 (95% CI, −4.4 to −2.2) for ESS.34
Comparator
The comparator study used propensity score matching to compare outcomes of HGNS and PAP therapy. Primary outcomes included sleepiness, AHI, and effectiveness with outcome measures of AHI and ESS collected at baseline and 12 months postimplantation. The article reported that 126 of 227 patients were matched 1:1. Both groups showed improvement in AHI and ESS. Mean (SD) AHI for the HGNS group at baseline started at 33.9 (15.1) and decreased to 8.1 (6.3). Mean (SD) ESS for the HGNS group at baseline was 15.4 (3.5) and decreased to 7.5 (4.7). In the PAP comparator group, mean (SD) baseline AHI was 36.8 (21.6) and at follow-up was 6.6 (8.0) and mean (SD) ESS was 14.6 (3.9) at baseline and 10.8 (5.6) at follow-up.35
DISCUSSION
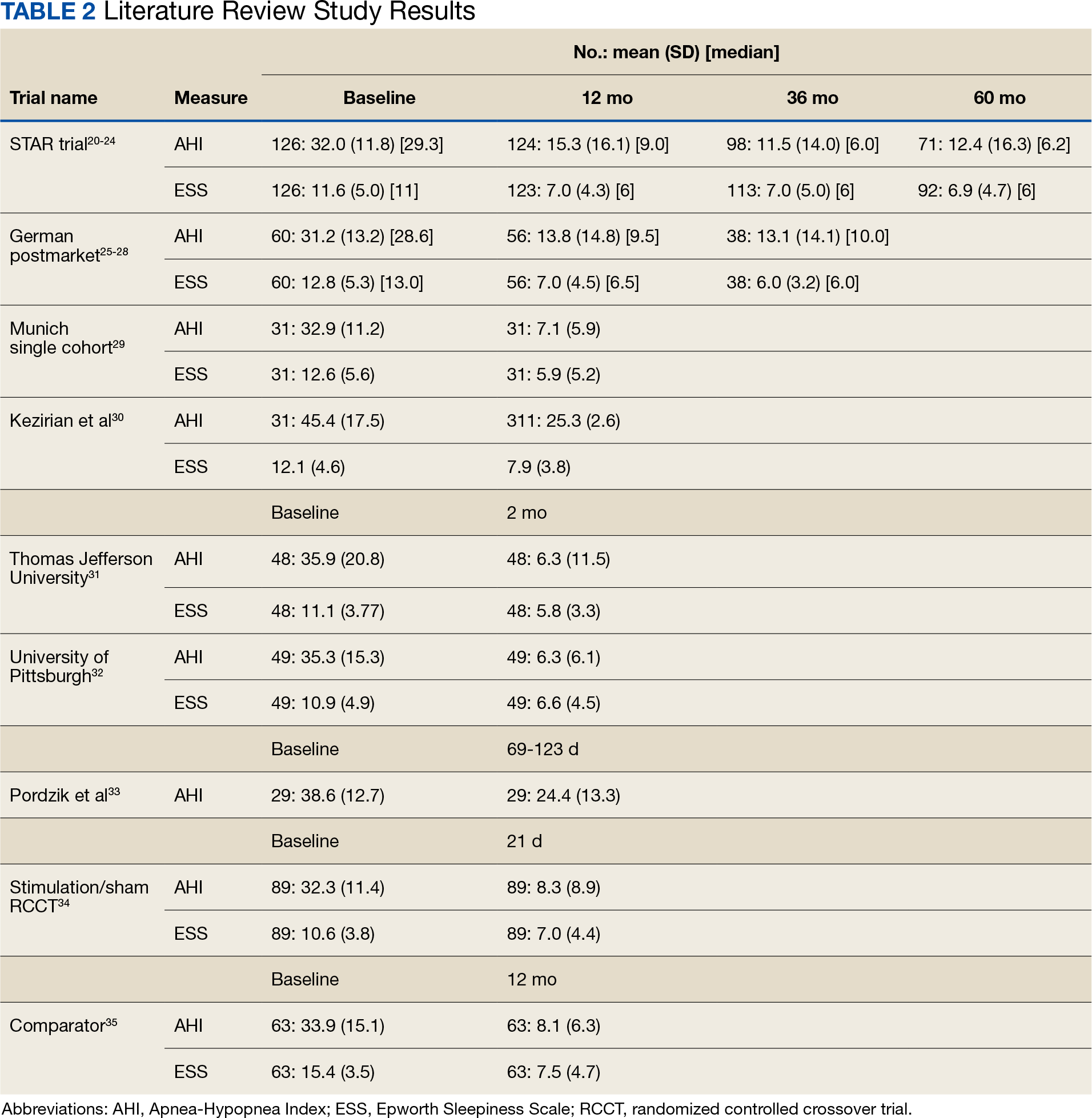
The current clinical data on HGNS suggest that this treatment is effective in adults with moderate-to-severe OSA and effects are sustained at long-term follow-up, as measured by AHI reduction and improvements in sleep related symptoms and quality of life (Table 2). These results have been consistent across several sites.
The STAR trial included a randomized control withdrawal group, for whom HGNS treatment was withdrawn after the 12-month follow-up, and then restored at 18 months.21 This revealed that withdrawal of HGNS treatment resulted in deterioration of both objective and subjective measures of OSA and sleepiness. The beneficial effects of HGNS were restored when treatment was resumed.24 Additionally, the RCCT revealed that therapeutic stimulation via HGNS significantly reduced subjective and objective measures of OSA.34 These studies provide definitive evidence of HGNS efficacy.
Currently, a diagnosis of OSA on PAP is classified as a 50% military disability rating. This rating is based primarily on epidemiologic evidence that untreated OSA is a costly disease that leads to other chronic illnesses that increases health care utilization.9 HGNS requires an initially invasive procedure and higher upfront costs, but it could result in reduced health care use and long-term costs because of improved adherence to treatment—compared with CPAP—that results in better outcomes.
Limitations to OSA Studies
The reviewed studies have several limitations that warrant caution when determining the possible benefits of HGNS treatment. The primary limitation is the lack of active control groups, therefore precluding a direct comparison of the short- and long-term effectiveness of HGNS vs other treatments (eg, CPAP). This is especially problematic because in the reviewed studies HGNS treatment efficacy is reported as a function of the mean—and SD—percent reduction in the AHI, whereas the efficacy of CPAP treatment usually is defined in terms of “adequacy of titration” as suggested by the AASM.36 It has been reported that with CPAP treatment, 50% to 60% of OSA patients achieve AASM-defined optimal improvement of respiratory disturbance index of < 5/hour during a polysomnographic sleep recording of ≥ 15 minutes duration that includes REM sleep in the supine position.37 In most of the reviewed studies, treatment success was more liberally defined as a decrease of AHI by ≥ 50%, regardless of the resulting AHI. It is notable that among the reviewed HGNS studies, the TJU and UP cohorts achieved the best outcome in short-term follow-up of 2 months with a mean (SD) AHI of 6.3 (11.5) and 6.4 (6.1), respectively. Among those cohortsassessed at a 12-month follow-up, the Munich cohort achieved the best outcome with a mean (SD) AHI of 7.1 (5.9).
Although the metrics reported in the reviewed studies are not directly comparable, the reported findings strongly suggest that HGNS generally is less effective than CPAP. How important are these differences? With findings that HGNS “reliably produces clinically meaningful (positive) effects on daytime sleepiness, daytime functioning, and sleep quality,” does it really matter if the outcome metrics for HGNS are a little less positive than those produced by CPAP?38 For individual military OSA patients the answer is yes. This is because in military operational environments—especially during deployment—sleep restriction is nearly ubiquitous, therefore any mild residual deficits in sleep quality and daytime alertness resulting from nominally adequate, but suboptimal OSA treatment, could be exacerbated by sleep restriction, therefore placing the service member and the mission at increased risk.39
Another limitation is the narrow inclusion criteria these studies employed, which limits the generalizability of the findings. Participants in the reviewed clinical trials were selected from a patient population that was mostly middle-aged, White, and obese or overweight. In a Medical Surveillance Monthly Report study, OSA was found to be highest among service members aged > 40 years, male, obese, and Black/non-Hispanic (although it should be noted that more than one-half of enlisted service members aged ≤ 25 years).40,41 Obesity has been noted as a growing concern for the military as the military population is beginning to mirror the civilian population in terms of being overweight or obese despite height and weight standards. HGNS might not be as successful in military populations with different demographics. Moreover, HGNS has been shown to have greater AHI reduction among those with higher BMI.30 Although obese service members have a 6-fold higher 12-year incidence rate of OSA than service members without obesity, this nevertheless suggests that general level of HGNS efficacy might be lower among the military patient population, because obesity is less prevalent in the military than the general population.9
Ethnicity has been found to be a relevant factor, with the highest incidence rate of OSA among non-Hispanic Black males, a demographic that was underrepresented in cohorts included in this review. Further studies will be needed to determine the extent to which findings from HGNS treatment studies are generalizable to the broader OSA patient population.
HGNS Implementation Challenges
Current impediments to widespread use of HGNS as an OSA treatment include no standardized guidance for titration and follow-on care, which varies based on the resources available. Titrating a new device for HGNS requires experienced sleep technicians who have close relationships with device representatives and can troubleshoot problems. Technical expertise, which currently is rare, is required if there are complications after placement or if adjustments to voltage settings are needed over time. In addition, patients may require multiple specialists making it easy to get lost to follow-up after implantation. This is particularly challenging in a transient community, such as the military, because there is no guarantee that a service member will have access to the same specialty care at the next duty station.
Although some evidence suggests that HGNS is a viable alternative treatment for some patients with OSA, the generalizability of these findings to the military patient population is unclear. Specialized facilities and expertise are needed for the surgical procedure and follow-up requirements, which currently constitute significant logistical constraints. As with any implantable device, there is a risk of complications including infection that could result in medical evacuation from a theater of operations. If the device malfunctions or loses effectiveness in a deployed environment, the service member might not have immediate access to medical support, potentially leading to undertreatment of OSA. In future battlefield scenarios in multidomain operations, prolonged, far-forward field care will become the new normal because the military is not expected to have air superiority or the ability to quickly evacuate service members to a higher level of medical care.42
In deployed environments, the potential limitations of HGNS become increasingly risky for the service member and the overall mission. Considering these factors, it will be important to evaluate the practicality of HGNS as a treatment option in military populations. Military-specific challenges associated with HGNS that require further study, include guidance for patient selection outside academic centers, guidance on long-term postsurgical care and device maintenance, duty limitation and military retention considerations, and limitations in training and combat environments. The military medical community needs to conduct its own studies in appropriately selected service members to guide clinical practice.
CONCLUSIONS
HGNS treatment results in improvement of both AHI and ESS scores and could be a deployable treatment option for military patients with OSA. However, HGNS has not been found to be as effective as CPAP, although the current literature is limited by small sample sizes, homogeneous populations that do not reflect the demographics of the military, and mostly short follow-up periods. Future studies should be focused on collecting data on HGNS from demographic groups that are more representative of the military OSA patient population and identifying the subpopulation of patients who derive the greatest benefit from HGNS, so that this treatment can be better individually targeted. Until data on existing military patients is published, it is not possible to fully weigh risks and benefits in this population and generalize civilian guidance to the military.
1. Cumpston E, Chen P. Sleep Apnea Syndrome. PubMed. Updated September 4, 2023. Published January 2024. https://www.ncbi.nlm.nih.gov/books/NBK564431/
2. American Academy of Sleep Medicine. Obstructive sleep apnea. Accessed November 27, 2023. https://aasm.org/resources/factsheets/sleepapnea.pdf
3. Cowen J, Harrison S, Thom L, et al. Use of historical remote monitoring data to determine predictors of CPAP non-compliance in patients with Osa. Sleep Breath. 2023;27(5):1899-1908. doi:10.1007/s11325-023-02806-3
4. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006-1014. doi:10.1093/aje/kws342
5. Stiegmann RA, Payne CB, Kiel MA, Stahlman SL. Increased Prevalence of Overweight and Obesity and Incidence of Prediabetes and Type 2 Diabetes During the COVID-19 Pandemic, Active Component Service Members, U.S. Armed Forces, 2018 to 2021. MSMR. 2023;30(1):11-18. Published 2023 Jan 20.
6. Adult obesity facts. Centers for Disease Control and Prevention. Updated May 17, 2022. Accessed November 27, 2023. https://www.cdc.gov/obesity/data/adult.html
7. Moore BA, Tison LM, Palacios JG, Peterson AL, Mysliwiec V. Incidence of insomnia and obstructive sleep apnea in active duty United States military service members. Sleep. 2021;44(7):zsab024. doi:10.1093/sleep/zsab024
8. Caldwell JA, Knapik JJ, Shing TL, Kardouni JR, Lieberman HR. The association of insomnia and sleep apnea with deployment and combat exposure in the entire population of US army soldiers from 1997 to 2011: a retrospective cohort investigation. Sleep. 2019;42(8):zsz112. doi:10.1093/sleep/zsz112
9. Rogers AE, Stahlman S, Hunt DJ, Oh GT, Clark LL. Obstructive sleep apnea and associated attrition, active component, U.S. Armed Forces, January 2004-May 2016. MSMR. 2016;23(10):2-11.
10. Veterans Affairs 38 C.F.R. § 4.97-13, Code 6847.
11. Shapiro GK, Shapiro CM. Factors that influence CPAP adherence: an overview. Sleep Breath. 2010;14(4):323-335. doi:10.1007/s11325-010-0391-y
12. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173-178. doi:10.1513/pats.200708-119mg
13. Sin DD, Mayers I, Man GCW, Pawluk L. Long-term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population-based study. Chest. 2002;121(2):430-435. doi:10.1378/chest.121.2.430
14. Nowak C, Bourgin P, Portier F, Genty E, Escourrou P, Bobin S. Obstruction nasale et compliance à la ventilation nasale à pression positive [Nasal obstruction and compliance to nasal positive airway pressure]. Ann Otolaryngol Chir Cervicofac. 2003;120(3):161-166.
15. Brin YS, Reuveni H, Greenberg S, Tal A, Tarasiuk A. Determinants affecting initiation of continuous positive airway pressure treatment. Isr Med Assoc J. 2005;7(1):13-18.
16. Suurna MV, Jacobowitz O, Chang J, et al. Improving outcomes of hypoglossal nerve stimulation therapy: current practice, future directions, and research gaps. Proceedings of the 2019 International Sleep Surgery Society Research Forum. J Clin Sleep Med. 2021;17(12):2477-2487. doi:10.5664/jcsm.9542
17. Inspire Medical Systems, Inc. Announces FDA approval for apnea hypopnea index indication expansion and increased body mass index labeling. Inspire Medical Systems, Inc. Accessed July 14, 2023. https://investors.inspiresleep.com/investors/press-releases/press-release-details/2023/Inspire-Medical-Systems-Inc.-Announces-FDA-Approval-for-Apnea-Hypopnea-Index-Indication-Expansion-and-Increased-Body-Mass-Index-Labeling/default.aspx
18. Lapin BR, Bena JF, Walia HK, Moul DE. The Epworth Sleepiness Scale: Validation of one-dimensional factor structure in a large clinical sample. J Clin Sleep Med. 2018;14(08):1293-1301. Published 2018 Aug 15. doi:10.5664/jcsm.7258
19. The Centre for Evidence-Based Medicine. November 25, 2020. http://www.cebm.net/index.aspx?o=5653
20. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149. doi:10.1056/NEJMoa1308659
21. Strollo PJ Jr, Gillespie MB, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: durability of the treatment effect at 18 months. Sleep. 2015;38(10):1593-1598. Published 2015 Oct 1. doi:10.5665/sleep.5054
22. Woodson BT, Soose RJ, Gillespie MB, et al. Three-year outcomes of cranial nerve stimulation for obstructive sleep apnea: the STAR trial. Otolaryngol Head Neck Surg. 2016;154(1):181-188. doi:10.1177/0194599815616618
23. Woodson BT, Strohl KP, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: 5-year outcomes. Otolaryngol Head Neck Surg. 2018;159(1):194-202. doi:10.1177/0194599818762383
24. Woodson BT, Gillespie MB, Soose RJ, et al. Randomized controlled withdrawal study of upper airway stimulation on OSA: short- and long-term effect. Otolaryngol Head Neck Surg. 2014;151(5):880-887. doi:10.1177/0194599814544445
25. Heiser C, Maurer JT, Hofauer B, Sommer JU, Seitz A, Steffen A. Outcomes of upper airway stimulation for obstructive sleep apnea in a multicenter German postmarket study. Otolaryngol Head Neck Surg. 2017;156(2):378-384. doi:10.1177/0194599816683378
26. Steffen A, Sommer JU, Hofauer B, Maurer JT, Hasselbacher K, Heiser C. Outcome after one year of upper airway stimulation for obstructive sleep apnea in a multicenter German post-market study. Laryngoscope. 2018;128(2):509-515. doi:10.1002/lary.26688
27. Steffen A, Sommer UJ, Maurer JT, Abrams N, Hofauer B, Heiser C. Long-term follow-up of the German post-market study for upper airway stimulation for obstructive sleep apnea. Sleep Breath. 2020;24(3):979-984. doi:10.1007/s11325-019-01933-028.
28. Hasselbacher K, Hofauer B, Maurer JT, Heiser C, Steffen A, Sommer JU. Patient-reported outcome: results of the multicenter German post-market study. Eur Arch Otorhinolaryngol. 2018;275(7):1913-1919. doi:10.1007/s00405-018-5017-129.
29. Heiser C, Knopf A, Bas M, Gahleitner C, Hofauer B. Selective upper airway stimulation for obstructive sleep apnea: a single center clinical experience. Eur Arch Otorhinolaryngol. 2017;274(3):1727-1734. doi:10.1007/s00405-016-4297-6
30. Kezirian EJ, Goding GS Jr, Malhotra A, et al. Hypoglossal nerve stimulation improves obstructive sleep apnea: 12-month outcomes. J Sleep Res. 2014;23(1):77-83. doi:10.1111/jsr.12079
31. Soose RJ, Woodson BT, Gillespie MB, et al. Upper airway stimulation for obstructive sleep apnea: self-reported outcomes at 24 months. J Clin Sleep Med. 2016;12(1):43-48. doi:10.5664/jcsm.5390
32. Huntley C, Kaffenberger T, Doghramji K, Soose R, Boon M. Upper airway stimulation for treatment of obstructive sleep apnea: an evaluation and comparison of outcomes at two academic centers. J Clin Sleep Med. 2017;13(9):1075-1079. Published 2017 Sep 15. doi:10.5664/jcsm.6726

33. Pordzik J, Seifen C, Ludwig K, et al. Short-term outcome of unilateral inspiration-coupled hypoglossal nerve stimulation in patients with obstructive sleep apnea. Int J Environ Res Public Health. 2022;19(24):16443. Published 2022 Dec 8. doi:10.3390/ijerph192416443
34. Heiser C, Steffen A, Hofauer B, et al. Effect of upper airway stimulation in patients with obstructive sleep apnea (EFFECT): a randomized controlled crossover trial. J Clin Med. 2021;10(13):2880. Published 2021 Jun 29. doi:10.3390/jcm1013288035.
35. Heiser C, Steffen A, Strollo PJ Jr, Giaie-Miniet C, Vanderveken OM, Hofauer B. Hypoglossal nerve stimulation versus positive airway pressure therapy for obstructive sleep apnea. Sleep Breath. 2023;27(2):693-701. doi:10.1007/s11325-022-02663-6
36. Kushida CA, Chediak A, Berry RB, et al. Clinical guidelines for the manual titration of positive airway pressure in patients with obstructive sleep apnea. J Clin Sleep Med. 2008;4(2):157-171.
37. Freedman N, Johnson K. Positive airway pressure treatment for obstructive sleep apnea. In: Kryger MH, Roth T, Goldstein CA, Dement WC, eds. Principles and Practice of Sleep Medicine. Elsevier; 2022:1260-1283.
38. Braun M, Stoerzel M, Wollny M, Schoebel C, Ulrich Sommer J, Heiser C. Patient-reported outcomes with hypoglossal nerve stimulation for treatment of obstructive sleep apnea: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2023;280(10):4627-4639. doi:10.1007/s00405-023-08062-1
39. Luxton DD, Greenburg D, Ryan J, Niven A, Wheeler G, Mysliwiec V. Prevalence and impact of short sleep duration in redeployed OIF soldiers. Sleep. 2011;34(9):1189-1195. doi:10.5665/SLEEP.1236
40. Rogers AE, Stahlman S, Hunt DJ, Oh GT, Clark LL. Obstructive sleep apnea and associated attrition, active component, U.S. Armed Forces, January 2004-May 2016. MSMR. 2016;23(10):2-11.
41. Office of the Deputy Assistant Secretary of Defense for Military Community and Family Policy. 2017 Demographics: Profile of the Military Community. US Dept of Defense;2017. Accessed April 4, 2024. http://download.militaryonesource.mil/12038/MOS/Reports/2017-demographics-report.pdf
42. Remondelli MH, Remick KN, Shackelford SA, et al. Casualty care implications of large-scale combat operations. J Trauma Acute Care Surg. 2023;95(2S Suppl 1): S180-S184. doi:10.1097/TA.0000000000004063
Obstructive sleep apnea (OSA), the repetitive collapse of posterior oropharynx during sleep resulting in hypoxia and/or arousals from sleep, is the most common form of sleep disordered breathing and a common chronic respiratory disorders among middle-aged adults. OSA can lead to significant health problems, such as worsened cardiometabolic disease and cognitive impairment, which can increase morbidity and mortality.1
The gold standard for OSA diagnosis is polysomnography (PSG), although home sleep studies can be performed for select patients. OSA diagnoses are based on the number of times per hour of sleep a patient’s airway narrows or collapses, reducing or stopping airflow, scored as hypopnea or apnea events, respectively. An Apnea-Hypopnea Index (AHI) score of 5 to 14 events/hour is considered mild OSA, 15 to 30 events/hour moderate OSA, and ≥ 30 events/hour severe OSA.2
Treatment commonly includes positive airway pressure (PAP) but more than one-half of patients are not adherent to continuous PAP (CPAP) treatment after about 90 days.3 Efficacy of treatments vary as a function of disease severity and etiology, which—in addition to the classic presentation of obesity with large neck/narrowupper airway—includes craniofacial abnormalities, altered muscle function in the upper airway, pharyngeal neuropathy, and fluid shifts to the neck.
Background
The American Academy of Sleep Medicine (AASM) estimates that 10% to 17% of adults in the United States have OSA.4 Compared with civilians, the military population generally is younger and healthier. Service members have access to regular health care with yearly physical examinations, exercise scheduled into the workday, and mandatory height/weight and fitness standards. Because obesity is a major risk factor for OSA, and the incidence of obesity is relatively low in the military population (estimated at 18.8% in 2021 vs 39.8% among all US adults aged 20 to 39 years), it might be expected that incidence of OSA would be correspondingly low.5,6 However, there is evidence of a rapidly increasing incidence of OSA in military populations. A 2021 study revealed that OSA incidence rates increased from 11 to 333 per 10,000 between 2005 and 2019 across all military branches and demographics, with the highest rate among Army personnel.7 An earlier study revealed a 600% increase in OSA incidence among Army personnel between 2003 and 2011.8
Several factors likely contributed to this increase, including expanding obesity and greater physician awareness and availability of sleep study centers. Rogers and colleagues found that 40% to 50% of incident OSA diagnoses among military personnel occur within 12 months of separation, suggesting that the secondary gains associated with military disability benefits might motivate OSA evaluation.9 It is possible that secondary gain is a factor because an OSA diagnosis can range from a 0% to 100% disability rating, depending on the severity.10 This disability claim is based on evidence that untreated OSA can negatively affect long-term health and mission readiness.8 For example, untreated OSA can lead to hypertension, which contributes to a long list of adverse health and wellness consequences. Most importantly for the military, OSA has been shown to increase daytime sleepiness and reduce cognitive performance.10
The current first-line treatment for OSA is CPAP, which improves symptoms of daytime sleepiness, hypertension management, and daytime alertness.11 Despite its efficacy, nonadherence rates range from 29% to 83%.12-15 Nonadherence factors include lifestyle changes, adverse effects (eg, nasal congestion), and lack of education on proper use.11 Lifestyle changes needed to increase the likelihood of successful therapy, such as regular sleep schedules and proper CPAP cleaning and maintenance, are difficult for military personnel because of the nature of continuous or sustained operations that might require shift work and/or around-the-clock (ie, 24-hour, 7 days a week) task performance. Traveling with CPAP is an added burden for service members deployed to combat operations (ie, added luggage, weight, maintenance). Although alternate treatments such as oral appliances (ie, custom dental devices) are available, they generally are less effective than CPAP.2 Oral appliances could be a reasonable alternative treatment for some patients who cannot manage their OSA with behavioral modifications and are intolerant or unable to effectively use CPAP. This could include patients in the military who are deployed to austere environments.
Surgically implanted hypoglossal nerve stimulator (HGNS) treatment may provide long-term health benefits to service members. After the device is implanted near the hypoglossal nerve, electrical stimulation causes the tongue to move forward, which opens the airway in the anteroposterior dimension. The most important consideration is the mechanism of airway collapse. HGNS is not effective for patients whose OSA events are caused by circumferential collapse of other airway muscles. The cause of airway collapse is ascertained before surgery with drug-induced sleep endoscopy, a procedure that allows visualization of conformational changes in the upper airway during OSA events.
The US Food and Drug Administration (FDA) approved HGNS in 2014. However, it is not considered a first-line treatment for OSA by the AASM. Original candidate criteria for HGNS included an AHI score of 15 to 65 events/hour, age ≥ 18 years, failed CPAP use, body mass index (BMI) < 32, absence of palatal complete concentric collapse, and central apneas comprising < 25% of total events.16 In June 2023, the FDA expanded approval to increase the upper limit of AHI to 100 events/hour and the BMI to < 40.17
HGNS has been reported to be effective in appropriately selected patients with OSA at tertiary care centers with established multidisciplinary sleep surgical programs. These benefits have not been confirmed in larger, community-based settings, where most of these surgeries occur. In community practice, there is significant confusion among patients and clinicians about the optimal pathway for patient selection and clinical follow-up. Many patients view HGNS as a viable alternative to CPAP, but initially do not understand that it requires surgery. Surgical treatments for OSA, such as HGNS, are appealing because they suggest a 1-time intervention that permanently treats the condition, without need for follow-up or equipment resupply. HGNS might be an appealing treatment option because it is less obtrusive than CPAP and requires fewer resources for set-up and maintenance. Also, it does not cause skin irritation (a possible adverse effect of nightly use of a CPAP mask), allows the individual to sleep in a variety of positions, has less impact on social and sex life, and does not require an electric outlet. In the long term, HGNS might be more cost effective because there is no yearly physician follow-up or equipment resupply and/or maintenance.
The military population has specific demands that impact delivery and effectiveness of health care. Among service members with OSA, CPAP treatment can be challenging because of low adherence, required annual follow-up despite frequent moving cycles that pose a challenge for care continuity, and duty limitations for affected service members (ie, the requirement for a waiver to deploy and potential medical separation if symptoms are not adequately controlled). As the incidence of OSA continues to increase among service members, so does the need for OSA treatment options that are efficacious as CPAP but better tolerated and more suitable for use during military operations. The aim of this review is to assess the effectiveness of HGNS and its potential use by the military OSA patient population.
METHODS
To identify eligible studies, we employed PICOS: Population (patients aged ≥ 18 years with a history of OSA), Intervention (HGNS), Comparator (standard of care PAP therapy), Outcome (AHI or Epworth Sleepiness Scale [ESS], and Study (randomized control trial [RCT] or clinical trial). Studies were excluded if they were not written in English or included pediatric populations. The ESS is a subjective rating scale used to determine and quantify a patient’s level of daytime sleepiness, using a 4-point scale for the likelihood of falling asleep totaled across 8 different situations.18 Daytime sleepiness is considered lower normal(0-5 points), higher normal (6-10 points), mild or moderate excessive (11-15 points), and severe excessive (16-24 points).
Literature Search
We conducted a review of PubMed and Scopus for RCTs and controlled trials published from 2013 to 2023 that included the keywords and phrases: obstructive sleep apnea and either hypoglossal nerve stimulation or upper airway stimulation. The final literature search was performed December 8, 2023.
Two authors independently assessed the titles and abstracts of studies identified in the literature search based on the predefined inclusion criteria. If it was not clear whether an article met inclusion criteria based on its title and/or abstract, the 2 review authors assessed the full text of study and resolved any disagreement through consensus. If consensus was not obtained, a third author was consulted. No duplicates were identified. The PRISMA study selection process is presented in the Figure.
Data extraction was performed by 1 independent reviewer. A second author reviewed the extracted data. Any identified discrepancies were resolved through discussion and consensus. If consensus was not obtained, a third author was consulted. Study data included methods (study design and study objective), participants mean age, inclusion criteria, exclusion criteria, interventions and comparators, and primary study outcomes.
The quality of evidence was assessed using a rating of 1 to 5 based on a modified version of the Oxford Centre for Evidence-based Medicine Levels of Evidence and Grades of Recommendation.19 A rating of 1 indicated a properly powered and conducted RCT, 2 demonstrated a well-designed controlled trial without randomization or prospective comparative cohort trial, 3 designated a case-control study or retrospective cohort study, 4 signified a case series with or without intervention or a cross-sectional study, and 5 denoted an opinion of respected authorities or case reports. Two reviewers independently evaluated the quality of evidence. Any identified discrepancies were resolved through discussion and consensus. If consensus was not obtained, a third review author was consulted.
RESULTS
We identified 30 studies; 19 articles did not meet inclusion criteria. The remaining 11 articles were divided into 4 cohorts. Five articles were based on data from the STAR trial, a multicenter study that included adults with moderate-to-severe OSA and inadequate adherence to CPAP.20-24 Four articles used the same patient selection criteria as the STAR trial for a long-term German postmarket study of upper airway stimulation efficacy with OSA.25-28 The third and fourth cohorts each consist of 31 patients with moderate-to-severe OSA with CPAP nonadherence or failure.29,30 The STAR trial included follow-up at 5 years, and the German-postmarket had a follow-up at3 years. The remaining 2 cohorts have 1-year follow-ups.
The Scopus review identified 304 studies; 299 did not meet inclusion criteria and 1 was part of the STAR trial.31 The remaining 4 articles were classified as distinct cohorts. Huntley and colleagues included patients from Thomas Jefferson University (TJU) and University of Pittsburgh (UP) academic medical centers.32 The Pordzik and colleagues cohort received implantation at a tertiary medical center, an RCCT, and a 1:1 comparator trial (Table 1).33-35
STAR Trial
This multicenter, prospective, single-group cohort study was conducted in the US, Germany, Belgium, Netherlands, and France. The STAR trial included 126 patients who were not CPAP therapy adherent. Patients were excluded if they had AHI < 20 or > 50, central sleep apnea > 25% of total AHI, anatomical abnormalities that prevent effective assessment of upper-airway stimulation, complete concentric collapse of the retropalatal airway during drug-induced sleep, neuromuscular disease, hypoglossal-nerve palsy, severe restrictive or obstructive pulmonary disease, moderate-to-severe pulmonary arterial hypertension, severe valvular heart disease, New York Heart Association class III or IV heart failure, recent myocardial infarction or severe cardiac arrhythmias (within the past 6 months), persistent uncontrolled hypertension despite medication use, active psychiatric illness, or coexisting nonrespiratory sleep disorders that would confound functional sleep assessment. Primary outcome measures included the AHI and oxygen desaturation index (ODI) with secondary outcomes using the ESS, the Functional Outcomes of Sleep Questionnaire (FOSQ), and the percentage of sleep time with oxygen saturation < 90%. Of 126 patients who received implantation, 71 underwent an overnight PSG evaluation at 5-year follow-up. Mean (SD) AHI at baseline was reduced with HGNS treatment to from 32.0 (11.8) to 12.4 (16.3). Mean (SD) ESS for 92 participants with 2 measurements declined from 11.6 (5.0) at baseline to 6.9 (4.7) at 5-year follow-up.
The STAR trial included a randomized controlled withdrawal study for 46 patients who had a positive response to therapy to evaluate efficacy and durability of upper airway stimulation. Patients were randomly assigned to therapy maintenance or therapy withdrawal groups for ≥ 1 week. The short-term withdrawal effect was assessed using the original trial outcome measures and indicated that both the withdrawal and maintenance groups showed improvements at 12 months compared with the baseline. However, after the randomized withdrawal, the withdrawal group’s outcome measures deteriorated to baseline levels while the maintenance group showed no change. At 18 months of therapy, outcome measures for both groups were similar to those observed with therapy at 12 months.24 The STAR trial included self-reported outcomes at baseline, 12 months, and 24 months that used ESS to measure daytime sleepiness. These results included subsequent STAR trial reports.20-24,31
The German Postmarket Cohort
This multicenter, prospective, single-arm study used selection criteria that were based on those used in the STAR trial and included patients with moderate-to-severe OSA and nonadherence to CPAP. Patients were excluded if they had a BMI > 35, AHI < 15 or > 65; central apnea index > 25% of total AHI; or complete concentric collapse at the velopharynx during drug-induced sleep. Measured outcomes included AHI, ODI, FOSQ, and ESS. Among the 60 participants, 38 received implantation and a 3-year follow-up. Mean (SD) AHI decreased from 31.2 (13.2) at baseline to 13.1 (14.1) at follow-up, while mean (SD) ESS decreased from 12.8 (5.3) at baseline to 6.0 (3.2) at follow-up.25-28
Munich Cohort
This single-center, prospective clinical trial included patients with AHI > 15 and < 65, central apnea index < 25% of total AHI, and nonadherence to CPAP. Patients were excluded if they had a BMI > 35, anatomical abnormalities that would prevent effective assessment of upper-airway stimulation; all other exclusion criteria matched those used in the STAR trial. Among 31 patients who received implants and completed a 1-year follow-up, mean (SD) AHI decreased from 32.9 (11.2) at baseline to 7.1 (5.9) at follow-up and mean (SD) ESS decreased from 12.6 (5.6) at baseline to 5.9 (5.2) at follow-up.29
Kezirian and Colleagues Cohort
This prospective, single-arm, open-label study was conducted at 4 Australian and 4 US sites. Selection criteria included moderate-to-severe OSA with failure of CPAP, AHI of 20 to 100 with ≥ 15 events/hour occurring in sleep that was non-REM (rapid eye movement) sleep, BMI ≤ 40 (Australia) or ≤ 37 (US), and a predominance of hypopneas (≥ 80% of disordered breathing events during sleep). Patients were excluded if they had earlier upper airway surgery, markedly enlarged tonsils, uncontrolled nasal obstruction, severe retrognathia, > 5% central or mixed apneic events, incompletely treated sleep disorders other than OSA, or a major disorder of the pulmonary, cardiac, renal, or nervous systems. Data were reported for 31 patients whose mean (SD) AHI declined from 45.4 (17.5) at baseline to 25.3 (20.6) at 1-year follow-up and mean (SD) ESS score declined from 12.1 (4.6) at baseline to 7.9 (3.8) 1 year later.30
TJU and UP Cohorts
The TJU and UP cohorts are composed of patients who underwent implantation between May 2014 and August 2016 at 2 academic centers.31,32 Selection criteria was consistent with that used in the STAR trial, and patients completed postoperative titration PSG and outpatient follow-up (48 patients at TJU and 49 at UP). Primary outcomes included AHI, ESS, and O2 nadir. Secondary outcomes consisted of surgical success and percentage of patients tolerating optimal titration setting at follow-up. Postoperative outcomes were assessed during the titration PSG. Time from initial ESS to postoperative PSG at TJU was 1.7 years and at UP was 1.9 years. Time from initial AHI to postoperative PSG at TJU was 90.4 days and 85.2 days at UP. At TJU, mean (SD) AHI and ESS dropped from 35.9 (20.8) and 11.1 (3.8), respectively at baseline to 6.3 (11.5) and 5.8 (3.4), respectively at follow-up. At UP, mean (SD) AHI and ESS fell from 35.3 (15.3) and 10.9 (4.9), respectively at baseline to 6.3 (6.1) and 6.6 (4.5), respectively at follow-up. There were no site-related differences in rates of AHI, ESS, or surgical success.31
Pordzik and Colleagues Cohort
This cohort of 29 patients underwent implantation between February 2020 and June 2022 at a tertiary university medical center with both pre- and postoperative PSG. Selection criteria was consistent with that of the German postmarket cohort. Postoperative PSG was completed a mean (SD) 96.3 (27.0) days after device activation. Mean (SD) AHI dropped from 38.6 (12.7) preoperatively to 24.4 (13.3) postoperatively. Notably, this cohort showed a much lower decrease of postoperative AHI than reported by the STAR trial and UP/TJU cohort.33
Stimulation vs Sham Trial
This multicenter, double-blinded, randomized, crossover trial assessed the effect of HGNS (stim) vs sham stimulation (sham) in 86 patients that completed both phases of the trial. Primary outcomes included AHI and ESS. Secondary outcomes included FOSQ. No carryover effect was found during the crossover phase. The difference between the phases was−15.5 (95% CI, −18.3 to −12.8) for AHI and −3.3 (95% CI, −4.4 to −2.2) for ESS.34
Comparator
The comparator study used propensity score matching to compare outcomes of HGNS and PAP therapy. Primary outcomes included sleepiness, AHI, and effectiveness with outcome measures of AHI and ESS collected at baseline and 12 months postimplantation. The article reported that 126 of 227 patients were matched 1:1. Both groups showed improvement in AHI and ESS. Mean (SD) AHI for the HGNS group at baseline started at 33.9 (15.1) and decreased to 8.1 (6.3). Mean (SD) ESS for the HGNS group at baseline was 15.4 (3.5) and decreased to 7.5 (4.7). In the PAP comparator group, mean (SD) baseline AHI was 36.8 (21.6) and at follow-up was 6.6 (8.0) and mean (SD) ESS was 14.6 (3.9) at baseline and 10.8 (5.6) at follow-up.35
DISCUSSION
The current clinical data on HGNS suggest that this treatment is effective in adults with moderate-to-severe OSA and effects are sustained at long-term follow-up, as measured by AHI reduction and improvements in sleep related symptoms and quality of life (Table 2). These results have been consistent across several sites.
The STAR trial included a randomized control withdrawal group, for whom HGNS treatment was withdrawn after the 12-month follow-up, and then restored at 18 months.21 This revealed that withdrawal of HGNS treatment resulted in deterioration of both objective and subjective measures of OSA and sleepiness. The beneficial effects of HGNS were restored when treatment was resumed.24 Additionally, the RCCT revealed that therapeutic stimulation via HGNS significantly reduced subjective and objective measures of OSA.34 These studies provide definitive evidence of HGNS efficacy.
Currently, a diagnosis of OSA on PAP is classified as a 50% military disability rating. This rating is based primarily on epidemiologic evidence that untreated OSA is a costly disease that leads to other chronic illnesses that increases health care utilization.9 HGNS requires an initially invasive procedure and higher upfront costs, but it could result in reduced health care use and long-term costs because of improved adherence to treatment—compared with CPAP—that results in better outcomes.
Limitations to OSA Studies
The reviewed studies have several limitations that warrant caution when determining the possible benefits of HGNS treatment. The primary limitation is the lack of active control groups, therefore precluding a direct comparison of the short- and long-term effectiveness of HGNS vs other treatments (eg, CPAP). This is especially problematic because in the reviewed studies HGNS treatment efficacy is reported as a function of the mean—and SD—percent reduction in the AHI, whereas the efficacy of CPAP treatment usually is defined in terms of “adequacy of titration” as suggested by the AASM.36 It has been reported that with CPAP treatment, 50% to 60% of OSA patients achieve AASM-defined optimal improvement of respiratory disturbance index of < 5/hour during a polysomnographic sleep recording of ≥ 15 minutes duration that includes REM sleep in the supine position.37 In most of the reviewed studies, treatment success was more liberally defined as a decrease of AHI by ≥ 50%, regardless of the resulting AHI. It is notable that among the reviewed HGNS studies, the TJU and UP cohorts achieved the best outcome in short-term follow-up of 2 months with a mean (SD) AHI of 6.3 (11.5) and 6.4 (6.1), respectively. Among those cohortsassessed at a 12-month follow-up, the Munich cohort achieved the best outcome with a mean (SD) AHI of 7.1 (5.9).
Although the metrics reported in the reviewed studies are not directly comparable, the reported findings strongly suggest that HGNS generally is less effective than CPAP. How important are these differences? With findings that HGNS “reliably produces clinically meaningful (positive) effects on daytime sleepiness, daytime functioning, and sleep quality,” does it really matter if the outcome metrics for HGNS are a little less positive than those produced by CPAP?38 For individual military OSA patients the answer is yes. This is because in military operational environments—especially during deployment—sleep restriction is nearly ubiquitous, therefore any mild residual deficits in sleep quality and daytime alertness resulting from nominally adequate, but suboptimal OSA treatment, could be exacerbated by sleep restriction, therefore placing the service member and the mission at increased risk.39
Another limitation is the narrow inclusion criteria these studies employed, which limits the generalizability of the findings. Participants in the reviewed clinical trials were selected from a patient population that was mostly middle-aged, White, and obese or overweight. In a Medical Surveillance Monthly Report study, OSA was found to be highest among service members aged > 40 years, male, obese, and Black/non-Hispanic (although it should be noted that more than one-half of enlisted service members aged ≤ 25 years).40,41 Obesity has been noted as a growing concern for the military as the military population is beginning to mirror the civilian population in terms of being overweight or obese despite height and weight standards. HGNS might not be as successful in military populations with different demographics. Moreover, HGNS has been shown to have greater AHI reduction among those with higher BMI.30 Although obese service members have a 6-fold higher 12-year incidence rate of OSA than service members without obesity, this nevertheless suggests that general level of HGNS efficacy might be lower among the military patient population, because obesity is less prevalent in the military than the general population.9
Ethnicity has been found to be a relevant factor, with the highest incidence rate of OSA among non-Hispanic Black males, a demographic that was underrepresented in cohorts included in this review. Further studies will be needed to determine the extent to which findings from HGNS treatment studies are generalizable to the broader OSA patient population.
HGNS Implementation Challenges
Current impediments to widespread use of HGNS as an OSA treatment include no standardized guidance for titration and follow-on care, which varies based on the resources available. Titrating a new device for HGNS requires experienced sleep technicians who have close relationships with device representatives and can troubleshoot problems. Technical expertise, which currently is rare, is required if there are complications after placement or if adjustments to voltage settings are needed over time. In addition, patients may require multiple specialists making it easy to get lost to follow-up after implantation. This is particularly challenging in a transient community, such as the military, because there is no guarantee that a service member will have access to the same specialty care at the next duty station.
Although some evidence suggests that HGNS is a viable alternative treatment for some patients with OSA, the generalizability of these findings to the military patient population is unclear. Specialized facilities and expertise are needed for the surgical procedure and follow-up requirements, which currently constitute significant logistical constraints. As with any implantable device, there is a risk of complications including infection that could result in medical evacuation from a theater of operations. If the device malfunctions or loses effectiveness in a deployed environment, the service member might not have immediate access to medical support, potentially leading to undertreatment of OSA. In future battlefield scenarios in multidomain operations, prolonged, far-forward field care will become the new normal because the military is not expected to have air superiority or the ability to quickly evacuate service members to a higher level of medical care.42
In deployed environments, the potential limitations of HGNS become increasingly risky for the service member and the overall mission. Considering these factors, it will be important to evaluate the practicality of HGNS as a treatment option in military populations. Military-specific challenges associated with HGNS that require further study, include guidance for patient selection outside academic centers, guidance on long-term postsurgical care and device maintenance, duty limitation and military retention considerations, and limitations in training and combat environments. The military medical community needs to conduct its own studies in appropriately selected service members to guide clinical practice.
CONCLUSIONS
HGNS treatment results in improvement of both AHI and ESS scores and could be a deployable treatment option for military patients with OSA. However, HGNS has not been found to be as effective as CPAP, although the current literature is limited by small sample sizes, homogeneous populations that do not reflect the demographics of the military, and mostly short follow-up periods. Future studies should be focused on collecting data on HGNS from demographic groups that are more representative of the military OSA patient population and identifying the subpopulation of patients who derive the greatest benefit from HGNS, so that this treatment can be better individually targeted. Until data on existing military patients is published, it is not possible to fully weigh risks and benefits in this population and generalize civilian guidance to the military.
Obstructive sleep apnea (OSA), the repetitive collapse of posterior oropharynx during sleep resulting in hypoxia and/or arousals from sleep, is the most common form of sleep disordered breathing and a common chronic respiratory disorders among middle-aged adults. OSA can lead to significant health problems, such as worsened cardiometabolic disease and cognitive impairment, which can increase morbidity and mortality.1
The gold standard for OSA diagnosis is polysomnography (PSG), although home sleep studies can be performed for select patients. OSA diagnoses are based on the number of times per hour of sleep a patient’s airway narrows or collapses, reducing or stopping airflow, scored as hypopnea or apnea events, respectively. An Apnea-Hypopnea Index (AHI) score of 5 to 14 events/hour is considered mild OSA, 15 to 30 events/hour moderate OSA, and ≥ 30 events/hour severe OSA.2
Treatment commonly includes positive airway pressure (PAP) but more than one-half of patients are not adherent to continuous PAP (CPAP) treatment after about 90 days.3 Efficacy of treatments vary as a function of disease severity and etiology, which—in addition to the classic presentation of obesity with large neck/narrowupper airway—includes craniofacial abnormalities, altered muscle function in the upper airway, pharyngeal neuropathy, and fluid shifts to the neck.
Background
The American Academy of Sleep Medicine (AASM) estimates that 10% to 17% of adults in the United States have OSA.4 Compared with civilians, the military population generally is younger and healthier. Service members have access to regular health care with yearly physical examinations, exercise scheduled into the workday, and mandatory height/weight and fitness standards. Because obesity is a major risk factor for OSA, and the incidence of obesity is relatively low in the military population (estimated at 18.8% in 2021 vs 39.8% among all US adults aged 20 to 39 years), it might be expected that incidence of OSA would be correspondingly low.5,6 However, there is evidence of a rapidly increasing incidence of OSA in military populations. A 2021 study revealed that OSA incidence rates increased from 11 to 333 per 10,000 between 2005 and 2019 across all military branches and demographics, with the highest rate among Army personnel.7 An earlier study revealed a 600% increase in OSA incidence among Army personnel between 2003 and 2011.8
Several factors likely contributed to this increase, including expanding obesity and greater physician awareness and availability of sleep study centers. Rogers and colleagues found that 40% to 50% of incident OSA diagnoses among military personnel occur within 12 months of separation, suggesting that the secondary gains associated with military disability benefits might motivate OSA evaluation.9 It is possible that secondary gain is a factor because an OSA diagnosis can range from a 0% to 100% disability rating, depending on the severity.10 This disability claim is based on evidence that untreated OSA can negatively affect long-term health and mission readiness.8 For example, untreated OSA can lead to hypertension, which contributes to a long list of adverse health and wellness consequences. Most importantly for the military, OSA has been shown to increase daytime sleepiness and reduce cognitive performance.10
The current first-line treatment for OSA is CPAP, which improves symptoms of daytime sleepiness, hypertension management, and daytime alertness.11 Despite its efficacy, nonadherence rates range from 29% to 83%.12-15 Nonadherence factors include lifestyle changes, adverse effects (eg, nasal congestion), and lack of education on proper use.11 Lifestyle changes needed to increase the likelihood of successful therapy, such as regular sleep schedules and proper CPAP cleaning and maintenance, are difficult for military personnel because of the nature of continuous or sustained operations that might require shift work and/or around-the-clock (ie, 24-hour, 7 days a week) task performance. Traveling with CPAP is an added burden for service members deployed to combat operations (ie, added luggage, weight, maintenance). Although alternate treatments such as oral appliances (ie, custom dental devices) are available, they generally are less effective than CPAP.2 Oral appliances could be a reasonable alternative treatment for some patients who cannot manage their OSA with behavioral modifications and are intolerant or unable to effectively use CPAP. This could include patients in the military who are deployed to austere environments.
Surgically implanted hypoglossal nerve stimulator (HGNS) treatment may provide long-term health benefits to service members. After the device is implanted near the hypoglossal nerve, electrical stimulation causes the tongue to move forward, which opens the airway in the anteroposterior dimension. The most important consideration is the mechanism of airway collapse. HGNS is not effective for patients whose OSA events are caused by circumferential collapse of other airway muscles. The cause of airway collapse is ascertained before surgery with drug-induced sleep endoscopy, a procedure that allows visualization of conformational changes in the upper airway during OSA events.
The US Food and Drug Administration (FDA) approved HGNS in 2014. However, it is not considered a first-line treatment for OSA by the AASM. Original candidate criteria for HGNS included an AHI score of 15 to 65 events/hour, age ≥ 18 years, failed CPAP use, body mass index (BMI) < 32, absence of palatal complete concentric collapse, and central apneas comprising < 25% of total events.16 In June 2023, the FDA expanded approval to increase the upper limit of AHI to 100 events/hour and the BMI to < 40.17
HGNS has been reported to be effective in appropriately selected patients with OSA at tertiary care centers with established multidisciplinary sleep surgical programs. These benefits have not been confirmed in larger, community-based settings, where most of these surgeries occur. In community practice, there is significant confusion among patients and clinicians about the optimal pathway for patient selection and clinical follow-up. Many patients view HGNS as a viable alternative to CPAP, but initially do not understand that it requires surgery. Surgical treatments for OSA, such as HGNS, are appealing because they suggest a 1-time intervention that permanently treats the condition, without need for follow-up or equipment resupply. HGNS might be an appealing treatment option because it is less obtrusive than CPAP and requires fewer resources for set-up and maintenance. Also, it does not cause skin irritation (a possible adverse effect of nightly use of a CPAP mask), allows the individual to sleep in a variety of positions, has less impact on social and sex life, and does not require an electric outlet. In the long term, HGNS might be more cost effective because there is no yearly physician follow-up or equipment resupply and/or maintenance.
The military population has specific demands that impact delivery and effectiveness of health care. Among service members with OSA, CPAP treatment can be challenging because of low adherence, required annual follow-up despite frequent moving cycles that pose a challenge for care continuity, and duty limitations for affected service members (ie, the requirement for a waiver to deploy and potential medical separation if symptoms are not adequately controlled). As the incidence of OSA continues to increase among service members, so does the need for OSA treatment options that are efficacious as CPAP but better tolerated and more suitable for use during military operations. The aim of this review is to assess the effectiveness of HGNS and its potential use by the military OSA patient population.
METHODS
To identify eligible studies, we employed PICOS: Population (patients aged ≥ 18 years with a history of OSA), Intervention (HGNS), Comparator (standard of care PAP therapy), Outcome (AHI or Epworth Sleepiness Scale [ESS], and Study (randomized control trial [RCT] or clinical trial). Studies were excluded if they were not written in English or included pediatric populations. The ESS is a subjective rating scale used to determine and quantify a patient’s level of daytime sleepiness, using a 4-point scale for the likelihood of falling asleep totaled across 8 different situations.18 Daytime sleepiness is considered lower normal(0-5 points), higher normal (6-10 points), mild or moderate excessive (11-15 points), and severe excessive (16-24 points).
Literature Search
We conducted a review of PubMed and Scopus for RCTs and controlled trials published from 2013 to 2023 that included the keywords and phrases: obstructive sleep apnea and either hypoglossal nerve stimulation or upper airway stimulation. The final literature search was performed December 8, 2023.
Two authors independently assessed the titles and abstracts of studies identified in the literature search based on the predefined inclusion criteria. If it was not clear whether an article met inclusion criteria based on its title and/or abstract, the 2 review authors assessed the full text of study and resolved any disagreement through consensus. If consensus was not obtained, a third author was consulted. No duplicates were identified. The PRISMA study selection process is presented in the Figure.
Data extraction was performed by 1 independent reviewer. A second author reviewed the extracted data. Any identified discrepancies were resolved through discussion and consensus. If consensus was not obtained, a third author was consulted. Study data included methods (study design and study objective), participants mean age, inclusion criteria, exclusion criteria, interventions and comparators, and primary study outcomes.
The quality of evidence was assessed using a rating of 1 to 5 based on a modified version of the Oxford Centre for Evidence-based Medicine Levels of Evidence and Grades of Recommendation.19 A rating of 1 indicated a properly powered and conducted RCT, 2 demonstrated a well-designed controlled trial without randomization or prospective comparative cohort trial, 3 designated a case-control study or retrospective cohort study, 4 signified a case series with or without intervention or a cross-sectional study, and 5 denoted an opinion of respected authorities or case reports. Two reviewers independently evaluated the quality of evidence. Any identified discrepancies were resolved through discussion and consensus. If consensus was not obtained, a third review author was consulted.
RESULTS
We identified 30 studies; 19 articles did not meet inclusion criteria. The remaining 11 articles were divided into 4 cohorts. Five articles were based on data from the STAR trial, a multicenter study that included adults with moderate-to-severe OSA and inadequate adherence to CPAP.20-24 Four articles used the same patient selection criteria as the STAR trial for a long-term German postmarket study of upper airway stimulation efficacy with OSA.25-28 The third and fourth cohorts each consist of 31 patients with moderate-to-severe OSA with CPAP nonadherence or failure.29,30 The STAR trial included follow-up at 5 years, and the German-postmarket had a follow-up at3 years. The remaining 2 cohorts have 1-year follow-ups.
The Scopus review identified 304 studies; 299 did not meet inclusion criteria and 1 was part of the STAR trial.31 The remaining 4 articles were classified as distinct cohorts. Huntley and colleagues included patients from Thomas Jefferson University (TJU) and University of Pittsburgh (UP) academic medical centers.32 The Pordzik and colleagues cohort received implantation at a tertiary medical center, an RCCT, and a 1:1 comparator trial (Table 1).33-35
STAR Trial
This multicenter, prospective, single-group cohort study was conducted in the US, Germany, Belgium, Netherlands, and France. The STAR trial included 126 patients who were not CPAP therapy adherent. Patients were excluded if they had AHI < 20 or > 50, central sleep apnea > 25% of total AHI, anatomical abnormalities that prevent effective assessment of upper-airway stimulation, complete concentric collapse of the retropalatal airway during drug-induced sleep, neuromuscular disease, hypoglossal-nerve palsy, severe restrictive or obstructive pulmonary disease, moderate-to-severe pulmonary arterial hypertension, severe valvular heart disease, New York Heart Association class III or IV heart failure, recent myocardial infarction or severe cardiac arrhythmias (within the past 6 months), persistent uncontrolled hypertension despite medication use, active psychiatric illness, or coexisting nonrespiratory sleep disorders that would confound functional sleep assessment. Primary outcome measures included the AHI and oxygen desaturation index (ODI) with secondary outcomes using the ESS, the Functional Outcomes of Sleep Questionnaire (FOSQ), and the percentage of sleep time with oxygen saturation < 90%. Of 126 patients who received implantation, 71 underwent an overnight PSG evaluation at 5-year follow-up. Mean (SD) AHI at baseline was reduced with HGNS treatment to from 32.0 (11.8) to 12.4 (16.3). Mean (SD) ESS for 92 participants with 2 measurements declined from 11.6 (5.0) at baseline to 6.9 (4.7) at 5-year follow-up.
The STAR trial included a randomized controlled withdrawal study for 46 patients who had a positive response to therapy to evaluate efficacy and durability of upper airway stimulation. Patients were randomly assigned to therapy maintenance or therapy withdrawal groups for ≥ 1 week. The short-term withdrawal effect was assessed using the original trial outcome measures and indicated that both the withdrawal and maintenance groups showed improvements at 12 months compared with the baseline. However, after the randomized withdrawal, the withdrawal group’s outcome measures deteriorated to baseline levels while the maintenance group showed no change. At 18 months of therapy, outcome measures for both groups were similar to those observed with therapy at 12 months.24 The STAR trial included self-reported outcomes at baseline, 12 months, and 24 months that used ESS to measure daytime sleepiness. These results included subsequent STAR trial reports.20-24,31
The German Postmarket Cohort
This multicenter, prospective, single-arm study used selection criteria that were based on those used in the STAR trial and included patients with moderate-to-severe OSA and nonadherence to CPAP. Patients were excluded if they had a BMI > 35, AHI < 15 or > 65; central apnea index > 25% of total AHI; or complete concentric collapse at the velopharynx during drug-induced sleep. Measured outcomes included AHI, ODI, FOSQ, and ESS. Among the 60 participants, 38 received implantation and a 3-year follow-up. Mean (SD) AHI decreased from 31.2 (13.2) at baseline to 13.1 (14.1) at follow-up, while mean (SD) ESS decreased from 12.8 (5.3) at baseline to 6.0 (3.2) at follow-up.25-28
Munich Cohort
This single-center, prospective clinical trial included patients with AHI > 15 and < 65, central apnea index < 25% of total AHI, and nonadherence to CPAP. Patients were excluded if they had a BMI > 35, anatomical abnormalities that would prevent effective assessment of upper-airway stimulation; all other exclusion criteria matched those used in the STAR trial. Among 31 patients who received implants and completed a 1-year follow-up, mean (SD) AHI decreased from 32.9 (11.2) at baseline to 7.1 (5.9) at follow-up and mean (SD) ESS decreased from 12.6 (5.6) at baseline to 5.9 (5.2) at follow-up.29
Kezirian and Colleagues Cohort
This prospective, single-arm, open-label study was conducted at 4 Australian and 4 US sites. Selection criteria included moderate-to-severe OSA with failure of CPAP, AHI of 20 to 100 with ≥ 15 events/hour occurring in sleep that was non-REM (rapid eye movement) sleep, BMI ≤ 40 (Australia) or ≤ 37 (US), and a predominance of hypopneas (≥ 80% of disordered breathing events during sleep). Patients were excluded if they had earlier upper airway surgery, markedly enlarged tonsils, uncontrolled nasal obstruction, severe retrognathia, > 5% central or mixed apneic events, incompletely treated sleep disorders other than OSA, or a major disorder of the pulmonary, cardiac, renal, or nervous systems. Data were reported for 31 patients whose mean (SD) AHI declined from 45.4 (17.5) at baseline to 25.3 (20.6) at 1-year follow-up and mean (SD) ESS score declined from 12.1 (4.6) at baseline to 7.9 (3.8) 1 year later.30
TJU and UP Cohorts
The TJU and UP cohorts are composed of patients who underwent implantation between May 2014 and August 2016 at 2 academic centers.31,32 Selection criteria was consistent with that used in the STAR trial, and patients completed postoperative titration PSG and outpatient follow-up (48 patients at TJU and 49 at UP). Primary outcomes included AHI, ESS, and O2 nadir. Secondary outcomes consisted of surgical success and percentage of patients tolerating optimal titration setting at follow-up. Postoperative outcomes were assessed during the titration PSG. Time from initial ESS to postoperative PSG at TJU was 1.7 years and at UP was 1.9 years. Time from initial AHI to postoperative PSG at TJU was 90.4 days and 85.2 days at UP. At TJU, mean (SD) AHI and ESS dropped from 35.9 (20.8) and 11.1 (3.8), respectively at baseline to 6.3 (11.5) and 5.8 (3.4), respectively at follow-up. At UP, mean (SD) AHI and ESS fell from 35.3 (15.3) and 10.9 (4.9), respectively at baseline to 6.3 (6.1) and 6.6 (4.5), respectively at follow-up. There were no site-related differences in rates of AHI, ESS, or surgical success.31
Pordzik and Colleagues Cohort
This cohort of 29 patients underwent implantation between February 2020 and June 2022 at a tertiary university medical center with both pre- and postoperative PSG. Selection criteria was consistent with that of the German postmarket cohort. Postoperative PSG was completed a mean (SD) 96.3 (27.0) days after device activation. Mean (SD) AHI dropped from 38.6 (12.7) preoperatively to 24.4 (13.3) postoperatively. Notably, this cohort showed a much lower decrease of postoperative AHI than reported by the STAR trial and UP/TJU cohort.33
Stimulation vs Sham Trial
This multicenter, double-blinded, randomized, crossover trial assessed the effect of HGNS (stim) vs sham stimulation (sham) in 86 patients that completed both phases of the trial. Primary outcomes included AHI and ESS. Secondary outcomes included FOSQ. No carryover effect was found during the crossover phase. The difference between the phases was−15.5 (95% CI, −18.3 to −12.8) for AHI and −3.3 (95% CI, −4.4 to −2.2) for ESS.34
Comparator
The comparator study used propensity score matching to compare outcomes of HGNS and PAP therapy. Primary outcomes included sleepiness, AHI, and effectiveness with outcome measures of AHI and ESS collected at baseline and 12 months postimplantation. The article reported that 126 of 227 patients were matched 1:1. Both groups showed improvement in AHI and ESS. Mean (SD) AHI for the HGNS group at baseline started at 33.9 (15.1) and decreased to 8.1 (6.3). Mean (SD) ESS for the HGNS group at baseline was 15.4 (3.5) and decreased to 7.5 (4.7). In the PAP comparator group, mean (SD) baseline AHI was 36.8 (21.6) and at follow-up was 6.6 (8.0) and mean (SD) ESS was 14.6 (3.9) at baseline and 10.8 (5.6) at follow-up.35
DISCUSSION
The current clinical data on HGNS suggest that this treatment is effective in adults with moderate-to-severe OSA and effects are sustained at long-term follow-up, as measured by AHI reduction and improvements in sleep related symptoms and quality of life (Table 2). These results have been consistent across several sites.
The STAR trial included a randomized control withdrawal group, for whom HGNS treatment was withdrawn after the 12-month follow-up, and then restored at 18 months.21 This revealed that withdrawal of HGNS treatment resulted in deterioration of both objective and subjective measures of OSA and sleepiness. The beneficial effects of HGNS were restored when treatment was resumed.24 Additionally, the RCCT revealed that therapeutic stimulation via HGNS significantly reduced subjective and objective measures of OSA.34 These studies provide definitive evidence of HGNS efficacy.
Currently, a diagnosis of OSA on PAP is classified as a 50% military disability rating. This rating is based primarily on epidemiologic evidence that untreated OSA is a costly disease that leads to other chronic illnesses that increases health care utilization.9 HGNS requires an initially invasive procedure and higher upfront costs, but it could result in reduced health care use and long-term costs because of improved adherence to treatment—compared with CPAP—that results in better outcomes.
Limitations to OSA Studies
The reviewed studies have several limitations that warrant caution when determining the possible benefits of HGNS treatment. The primary limitation is the lack of active control groups, therefore precluding a direct comparison of the short- and long-term effectiveness of HGNS vs other treatments (eg, CPAP). This is especially problematic because in the reviewed studies HGNS treatment efficacy is reported as a function of the mean—and SD—percent reduction in the AHI, whereas the efficacy of CPAP treatment usually is defined in terms of “adequacy of titration” as suggested by the AASM.36 It has been reported that with CPAP treatment, 50% to 60% of OSA patients achieve AASM-defined optimal improvement of respiratory disturbance index of < 5/hour during a polysomnographic sleep recording of ≥ 15 minutes duration that includes REM sleep in the supine position.37 In most of the reviewed studies, treatment success was more liberally defined as a decrease of AHI by ≥ 50%, regardless of the resulting AHI. It is notable that among the reviewed HGNS studies, the TJU and UP cohorts achieved the best outcome in short-term follow-up of 2 months with a mean (SD) AHI of 6.3 (11.5) and 6.4 (6.1), respectively. Among those cohortsassessed at a 12-month follow-up, the Munich cohort achieved the best outcome with a mean (SD) AHI of 7.1 (5.9).
Although the metrics reported in the reviewed studies are not directly comparable, the reported findings strongly suggest that HGNS generally is less effective than CPAP. How important are these differences? With findings that HGNS “reliably produces clinically meaningful (positive) effects on daytime sleepiness, daytime functioning, and sleep quality,” does it really matter if the outcome metrics for HGNS are a little less positive than those produced by CPAP?38 For individual military OSA patients the answer is yes. This is because in military operational environments—especially during deployment—sleep restriction is nearly ubiquitous, therefore any mild residual deficits in sleep quality and daytime alertness resulting from nominally adequate, but suboptimal OSA treatment, could be exacerbated by sleep restriction, therefore placing the service member and the mission at increased risk.39
Another limitation is the narrow inclusion criteria these studies employed, which limits the generalizability of the findings. Participants in the reviewed clinical trials were selected from a patient population that was mostly middle-aged, White, and obese or overweight. In a Medical Surveillance Monthly Report study, OSA was found to be highest among service members aged > 40 years, male, obese, and Black/non-Hispanic (although it should be noted that more than one-half of enlisted service members aged ≤ 25 years).40,41 Obesity has been noted as a growing concern for the military as the military population is beginning to mirror the civilian population in terms of being overweight or obese despite height and weight standards. HGNS might not be as successful in military populations with different demographics. Moreover, HGNS has been shown to have greater AHI reduction among those with higher BMI.30 Although obese service members have a 6-fold higher 12-year incidence rate of OSA than service members without obesity, this nevertheless suggests that general level of HGNS efficacy might be lower among the military patient population, because obesity is less prevalent in the military than the general population.9
Ethnicity has been found to be a relevant factor, with the highest incidence rate of OSA among non-Hispanic Black males, a demographic that was underrepresented in cohorts included in this review. Further studies will be needed to determine the extent to which findings from HGNS treatment studies are generalizable to the broader OSA patient population.
HGNS Implementation Challenges
Current impediments to widespread use of HGNS as an OSA treatment include no standardized guidance for titration and follow-on care, which varies based on the resources available. Titrating a new device for HGNS requires experienced sleep technicians who have close relationships with device representatives and can troubleshoot problems. Technical expertise, which currently is rare, is required if there are complications after placement or if adjustments to voltage settings are needed over time. In addition, patients may require multiple specialists making it easy to get lost to follow-up after implantation. This is particularly challenging in a transient community, such as the military, because there is no guarantee that a service member will have access to the same specialty care at the next duty station.
Although some evidence suggests that HGNS is a viable alternative treatment for some patients with OSA, the generalizability of these findings to the military patient population is unclear. Specialized facilities and expertise are needed for the surgical procedure and follow-up requirements, which currently constitute significant logistical constraints. As with any implantable device, there is a risk of complications including infection that could result in medical evacuation from a theater of operations. If the device malfunctions or loses effectiveness in a deployed environment, the service member might not have immediate access to medical support, potentially leading to undertreatment of OSA. In future battlefield scenarios in multidomain operations, prolonged, far-forward field care will become the new normal because the military is not expected to have air superiority or the ability to quickly evacuate service members to a higher level of medical care.42
In deployed environments, the potential limitations of HGNS become increasingly risky for the service member and the overall mission. Considering these factors, it will be important to evaluate the practicality of HGNS as a treatment option in military populations. Military-specific challenges associated with HGNS that require further study, include guidance for patient selection outside academic centers, guidance on long-term postsurgical care and device maintenance, duty limitation and military retention considerations, and limitations in training and combat environments. The military medical community needs to conduct its own studies in appropriately selected service members to guide clinical practice.
CONCLUSIONS
HGNS treatment results in improvement of both AHI and ESS scores and could be a deployable treatment option for military patients with OSA. However, HGNS has not been found to be as effective as CPAP, although the current literature is limited by small sample sizes, homogeneous populations that do not reflect the demographics of the military, and mostly short follow-up periods. Future studies should be focused on collecting data on HGNS from demographic groups that are more representative of the military OSA patient population and identifying the subpopulation of patients who derive the greatest benefit from HGNS, so that this treatment can be better individually targeted. Until data on existing military patients is published, it is not possible to fully weigh risks and benefits in this population and generalize civilian guidance to the military.
1. Cumpston E, Chen P. Sleep Apnea Syndrome. PubMed. Updated September 4, 2023. Published January 2024. https://www.ncbi.nlm.nih.gov/books/NBK564431/
2. American Academy of Sleep Medicine. Obstructive sleep apnea. Accessed November 27, 2023. https://aasm.org/resources/factsheets/sleepapnea.pdf
3. Cowen J, Harrison S, Thom L, et al. Use of historical remote monitoring data to determine predictors of CPAP non-compliance in patients with Osa. Sleep Breath. 2023;27(5):1899-1908. doi:10.1007/s11325-023-02806-3
4. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006-1014. doi:10.1093/aje/kws342
5. Stiegmann RA, Payne CB, Kiel MA, Stahlman SL. Increased Prevalence of Overweight and Obesity and Incidence of Prediabetes and Type 2 Diabetes During the COVID-19 Pandemic, Active Component Service Members, U.S. Armed Forces, 2018 to 2021. MSMR. 2023;30(1):11-18. Published 2023 Jan 20.
6. Adult obesity facts. Centers for Disease Control and Prevention. Updated May 17, 2022. Accessed November 27, 2023. https://www.cdc.gov/obesity/data/adult.html
7. Moore BA, Tison LM, Palacios JG, Peterson AL, Mysliwiec V. Incidence of insomnia and obstructive sleep apnea in active duty United States military service members. Sleep. 2021;44(7):zsab024. doi:10.1093/sleep/zsab024
8. Caldwell JA, Knapik JJ, Shing TL, Kardouni JR, Lieberman HR. The association of insomnia and sleep apnea with deployment and combat exposure in the entire population of US army soldiers from 1997 to 2011: a retrospective cohort investigation. Sleep. 2019;42(8):zsz112. doi:10.1093/sleep/zsz112
9. Rogers AE, Stahlman S, Hunt DJ, Oh GT, Clark LL. Obstructive sleep apnea and associated attrition, active component, U.S. Armed Forces, January 2004-May 2016. MSMR. 2016;23(10):2-11.
10. Veterans Affairs 38 C.F.R. § 4.97-13, Code 6847.
11. Shapiro GK, Shapiro CM. Factors that influence CPAP adherence: an overview. Sleep Breath. 2010;14(4):323-335. doi:10.1007/s11325-010-0391-y
12. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173-178. doi:10.1513/pats.200708-119mg
13. Sin DD, Mayers I, Man GCW, Pawluk L. Long-term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population-based study. Chest. 2002;121(2):430-435. doi:10.1378/chest.121.2.430
14. Nowak C, Bourgin P, Portier F, Genty E, Escourrou P, Bobin S. Obstruction nasale et compliance à la ventilation nasale à pression positive [Nasal obstruction and compliance to nasal positive airway pressure]. Ann Otolaryngol Chir Cervicofac. 2003;120(3):161-166.
15. Brin YS, Reuveni H, Greenberg S, Tal A, Tarasiuk A. Determinants affecting initiation of continuous positive airway pressure treatment. Isr Med Assoc J. 2005;7(1):13-18.
16. Suurna MV, Jacobowitz O, Chang J, et al. Improving outcomes of hypoglossal nerve stimulation therapy: current practice, future directions, and research gaps. Proceedings of the 2019 International Sleep Surgery Society Research Forum. J Clin Sleep Med. 2021;17(12):2477-2487. doi:10.5664/jcsm.9542
17. Inspire Medical Systems, Inc. Announces FDA approval for apnea hypopnea index indication expansion and increased body mass index labeling. Inspire Medical Systems, Inc. Accessed July 14, 2023. https://investors.inspiresleep.com/investors/press-releases/press-release-details/2023/Inspire-Medical-Systems-Inc.-Announces-FDA-Approval-for-Apnea-Hypopnea-Index-Indication-Expansion-and-Increased-Body-Mass-Index-Labeling/default.aspx
18. Lapin BR, Bena JF, Walia HK, Moul DE. The Epworth Sleepiness Scale: Validation of one-dimensional factor structure in a large clinical sample. J Clin Sleep Med. 2018;14(08):1293-1301. Published 2018 Aug 15. doi:10.5664/jcsm.7258
19. The Centre for Evidence-Based Medicine. November 25, 2020. http://www.cebm.net/index.aspx?o=5653
20. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149. doi:10.1056/NEJMoa1308659
21. Strollo PJ Jr, Gillespie MB, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: durability of the treatment effect at 18 months. Sleep. 2015;38(10):1593-1598. Published 2015 Oct 1. doi:10.5665/sleep.5054
22. Woodson BT, Soose RJ, Gillespie MB, et al. Three-year outcomes of cranial nerve stimulation for obstructive sleep apnea: the STAR trial. Otolaryngol Head Neck Surg. 2016;154(1):181-188. doi:10.1177/0194599815616618
23. Woodson BT, Strohl KP, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: 5-year outcomes. Otolaryngol Head Neck Surg. 2018;159(1):194-202. doi:10.1177/0194599818762383
24. Woodson BT, Gillespie MB, Soose RJ, et al. Randomized controlled withdrawal study of upper airway stimulation on OSA: short- and long-term effect. Otolaryngol Head Neck Surg. 2014;151(5):880-887. doi:10.1177/0194599814544445
25. Heiser C, Maurer JT, Hofauer B, Sommer JU, Seitz A, Steffen A. Outcomes of upper airway stimulation for obstructive sleep apnea in a multicenter German postmarket study. Otolaryngol Head Neck Surg. 2017;156(2):378-384. doi:10.1177/0194599816683378
26. Steffen A, Sommer JU, Hofauer B, Maurer JT, Hasselbacher K, Heiser C. Outcome after one year of upper airway stimulation for obstructive sleep apnea in a multicenter German post-market study. Laryngoscope. 2018;128(2):509-515. doi:10.1002/lary.26688
27. Steffen A, Sommer UJ, Maurer JT, Abrams N, Hofauer B, Heiser C. Long-term follow-up of the German post-market study for upper airway stimulation for obstructive sleep apnea. Sleep Breath. 2020;24(3):979-984. doi:10.1007/s11325-019-01933-028.
28. Hasselbacher K, Hofauer B, Maurer JT, Heiser C, Steffen A, Sommer JU. Patient-reported outcome: results of the multicenter German post-market study. Eur Arch Otorhinolaryngol. 2018;275(7):1913-1919. doi:10.1007/s00405-018-5017-129.
29. Heiser C, Knopf A, Bas M, Gahleitner C, Hofauer B. Selective upper airway stimulation for obstructive sleep apnea: a single center clinical experience. Eur Arch Otorhinolaryngol. 2017;274(3):1727-1734. doi:10.1007/s00405-016-4297-6
30. Kezirian EJ, Goding GS Jr, Malhotra A, et al. Hypoglossal nerve stimulation improves obstructive sleep apnea: 12-month outcomes. J Sleep Res. 2014;23(1):77-83. doi:10.1111/jsr.12079
31. Soose RJ, Woodson BT, Gillespie MB, et al. Upper airway stimulation for obstructive sleep apnea: self-reported outcomes at 24 months. J Clin Sleep Med. 2016;12(1):43-48. doi:10.5664/jcsm.5390
32. Huntley C, Kaffenberger T, Doghramji K, Soose R, Boon M. Upper airway stimulation for treatment of obstructive sleep apnea: an evaluation and comparison of outcomes at two academic centers. J Clin Sleep Med. 2017;13(9):1075-1079. Published 2017 Sep 15. doi:10.5664/jcsm.6726
33. Pordzik J, Seifen C, Ludwig K, et al. Short-term outcome of unilateral inspiration-coupled hypoglossal nerve stimulation in patients with obstructive sleep apnea. Int J Environ Res Public Health. 2022;19(24):16443. Published 2022 Dec 8. doi:10.3390/ijerph192416443
34. Heiser C, Steffen A, Hofauer B, et al. Effect of upper airway stimulation in patients with obstructive sleep apnea (EFFECT): a randomized controlled crossover trial. J Clin Med. 2021;10(13):2880. Published 2021 Jun 29. doi:10.3390/jcm1013288035.
35. Heiser C, Steffen A, Strollo PJ Jr, Giaie-Miniet C, Vanderveken OM, Hofauer B. Hypoglossal nerve stimulation versus positive airway pressure therapy for obstructive sleep apnea. Sleep Breath. 2023;27(2):693-701. doi:10.1007/s11325-022-02663-6
36. Kushida CA, Chediak A, Berry RB, et al. Clinical guidelines for the manual titration of positive airway pressure in patients with obstructive sleep apnea. J Clin Sleep Med. 2008;4(2):157-171.
37. Freedman N, Johnson K. Positive airway pressure treatment for obstructive sleep apnea. In: Kryger MH, Roth T, Goldstein CA, Dement WC, eds. Principles and Practice of Sleep Medicine. Elsevier; 2022:1260-1283.
38. Braun M, Stoerzel M, Wollny M, Schoebel C, Ulrich Sommer J, Heiser C. Patient-reported outcomes with hypoglossal nerve stimulation for treatment of obstructive sleep apnea: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2023;280(10):4627-4639. doi:10.1007/s00405-023-08062-1
39. Luxton DD, Greenburg D, Ryan J, Niven A, Wheeler G, Mysliwiec V. Prevalence and impact of short sleep duration in redeployed OIF soldiers. Sleep. 2011;34(9):1189-1195. doi:10.5665/SLEEP.1236
40. Rogers AE, Stahlman S, Hunt DJ, Oh GT, Clark LL. Obstructive sleep apnea and associated attrition, active component, U.S. Armed Forces, January 2004-May 2016. MSMR. 2016;23(10):2-11.
41. Office of the Deputy Assistant Secretary of Defense for Military Community and Family Policy. 2017 Demographics: Profile of the Military Community. US Dept of Defense;2017. Accessed April 4, 2024. http://download.militaryonesource.mil/12038/MOS/Reports/2017-demographics-report.pdf
42. Remondelli MH, Remick KN, Shackelford SA, et al. Casualty care implications of large-scale combat operations. J Trauma Acute Care Surg. 2023;95(2S Suppl 1): S180-S184. doi:10.1097/TA.0000000000004063
1. Cumpston E, Chen P. Sleep Apnea Syndrome. PubMed. Updated September 4, 2023. Published January 2024. https://www.ncbi.nlm.nih.gov/books/NBK564431/
2. American Academy of Sleep Medicine. Obstructive sleep apnea. Accessed November 27, 2023. https://aasm.org/resources/factsheets/sleepapnea.pdf
3. Cowen J, Harrison S, Thom L, et al. Use of historical remote monitoring data to determine predictors of CPAP non-compliance in patients with Osa. Sleep Breath. 2023;27(5):1899-1908. doi:10.1007/s11325-023-02806-3
4. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006-1014. doi:10.1093/aje/kws342
5. Stiegmann RA, Payne CB, Kiel MA, Stahlman SL. Increased Prevalence of Overweight and Obesity and Incidence of Prediabetes and Type 2 Diabetes During the COVID-19 Pandemic, Active Component Service Members, U.S. Armed Forces, 2018 to 2021. MSMR. 2023;30(1):11-18. Published 2023 Jan 20.
6. Adult obesity facts. Centers for Disease Control and Prevention. Updated May 17, 2022. Accessed November 27, 2023. https://www.cdc.gov/obesity/data/adult.html
7. Moore BA, Tison LM, Palacios JG, Peterson AL, Mysliwiec V. Incidence of insomnia and obstructive sleep apnea in active duty United States military service members. Sleep. 2021;44(7):zsab024. doi:10.1093/sleep/zsab024
8. Caldwell JA, Knapik JJ, Shing TL, Kardouni JR, Lieberman HR. The association of insomnia and sleep apnea with deployment and combat exposure in the entire population of US army soldiers from 1997 to 2011: a retrospective cohort investigation. Sleep. 2019;42(8):zsz112. doi:10.1093/sleep/zsz112
9. Rogers AE, Stahlman S, Hunt DJ, Oh GT, Clark LL. Obstructive sleep apnea and associated attrition, active component, U.S. Armed Forces, January 2004-May 2016. MSMR. 2016;23(10):2-11.
10. Veterans Affairs 38 C.F.R. § 4.97-13, Code 6847.
11. Shapiro GK, Shapiro CM. Factors that influence CPAP adherence: an overview. Sleep Breath. 2010;14(4):323-335. doi:10.1007/s11325-010-0391-y
12. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173-178. doi:10.1513/pats.200708-119mg
13. Sin DD, Mayers I, Man GCW, Pawluk L. Long-term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population-based study. Chest. 2002;121(2):430-435. doi:10.1378/chest.121.2.430
14. Nowak C, Bourgin P, Portier F, Genty E, Escourrou P, Bobin S. Obstruction nasale et compliance à la ventilation nasale à pression positive [Nasal obstruction and compliance to nasal positive airway pressure]. Ann Otolaryngol Chir Cervicofac. 2003;120(3):161-166.
15. Brin YS, Reuveni H, Greenberg S, Tal A, Tarasiuk A. Determinants affecting initiation of continuous positive airway pressure treatment. Isr Med Assoc J. 2005;7(1):13-18.
16. Suurna MV, Jacobowitz O, Chang J, et al. Improving outcomes of hypoglossal nerve stimulation therapy: current practice, future directions, and research gaps. Proceedings of the 2019 International Sleep Surgery Society Research Forum. J Clin Sleep Med. 2021;17(12):2477-2487. doi:10.5664/jcsm.9542
17. Inspire Medical Systems, Inc. Announces FDA approval for apnea hypopnea index indication expansion and increased body mass index labeling. Inspire Medical Systems, Inc. Accessed July 14, 2023. https://investors.inspiresleep.com/investors/press-releases/press-release-details/2023/Inspire-Medical-Systems-Inc.-Announces-FDA-Approval-for-Apnea-Hypopnea-Index-Indication-Expansion-and-Increased-Body-Mass-Index-Labeling/default.aspx
18. Lapin BR, Bena JF, Walia HK, Moul DE. The Epworth Sleepiness Scale: Validation of one-dimensional factor structure in a large clinical sample. J Clin Sleep Med. 2018;14(08):1293-1301. Published 2018 Aug 15. doi:10.5664/jcsm.7258
19. The Centre for Evidence-Based Medicine. November 25, 2020. http://www.cebm.net/index.aspx?o=5653
20. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149. doi:10.1056/NEJMoa1308659
21. Strollo PJ Jr, Gillespie MB, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: durability of the treatment effect at 18 months. Sleep. 2015;38(10):1593-1598. Published 2015 Oct 1. doi:10.5665/sleep.5054
22. Woodson BT, Soose RJ, Gillespie MB, et al. Three-year outcomes of cranial nerve stimulation for obstructive sleep apnea: the STAR trial. Otolaryngol Head Neck Surg. 2016;154(1):181-188. doi:10.1177/0194599815616618
23. Woodson BT, Strohl KP, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: 5-year outcomes. Otolaryngol Head Neck Surg. 2018;159(1):194-202. doi:10.1177/0194599818762383
24. Woodson BT, Gillespie MB, Soose RJ, et al. Randomized controlled withdrawal study of upper airway stimulation on OSA: short- and long-term effect. Otolaryngol Head Neck Surg. 2014;151(5):880-887. doi:10.1177/0194599814544445
25. Heiser C, Maurer JT, Hofauer B, Sommer JU, Seitz A, Steffen A. Outcomes of upper airway stimulation for obstructive sleep apnea in a multicenter German postmarket study. Otolaryngol Head Neck Surg. 2017;156(2):378-384. doi:10.1177/0194599816683378
26. Steffen A, Sommer JU, Hofauer B, Maurer JT, Hasselbacher K, Heiser C. Outcome after one year of upper airway stimulation for obstructive sleep apnea in a multicenter German post-market study. Laryngoscope. 2018;128(2):509-515. doi:10.1002/lary.26688
27. Steffen A, Sommer UJ, Maurer JT, Abrams N, Hofauer B, Heiser C. Long-term follow-up of the German post-market study for upper airway stimulation for obstructive sleep apnea. Sleep Breath. 2020;24(3):979-984. doi:10.1007/s11325-019-01933-028.
28. Hasselbacher K, Hofauer B, Maurer JT, Heiser C, Steffen A, Sommer JU. Patient-reported outcome: results of the multicenter German post-market study. Eur Arch Otorhinolaryngol. 2018;275(7):1913-1919. doi:10.1007/s00405-018-5017-129.
29. Heiser C, Knopf A, Bas M, Gahleitner C, Hofauer B. Selective upper airway stimulation for obstructive sleep apnea: a single center clinical experience. Eur Arch Otorhinolaryngol. 2017;274(3):1727-1734. doi:10.1007/s00405-016-4297-6
30. Kezirian EJ, Goding GS Jr, Malhotra A, et al. Hypoglossal nerve stimulation improves obstructive sleep apnea: 12-month outcomes. J Sleep Res. 2014;23(1):77-83. doi:10.1111/jsr.12079
31. Soose RJ, Woodson BT, Gillespie MB, et al. Upper airway stimulation for obstructive sleep apnea: self-reported outcomes at 24 months. J Clin Sleep Med. 2016;12(1):43-48. doi:10.5664/jcsm.5390
32. Huntley C, Kaffenberger T, Doghramji K, Soose R, Boon M. Upper airway stimulation for treatment of obstructive sleep apnea: an evaluation and comparison of outcomes at two academic centers. J Clin Sleep Med. 2017;13(9):1075-1079. Published 2017 Sep 15. doi:10.5664/jcsm.6726
33. Pordzik J, Seifen C, Ludwig K, et al. Short-term outcome of unilateral inspiration-coupled hypoglossal nerve stimulation in patients with obstructive sleep apnea. Int J Environ Res Public Health. 2022;19(24):16443. Published 2022 Dec 8. doi:10.3390/ijerph192416443
34. Heiser C, Steffen A, Hofauer B, et al. Effect of upper airway stimulation in patients with obstructive sleep apnea (EFFECT): a randomized controlled crossover trial. J Clin Med. 2021;10(13):2880. Published 2021 Jun 29. doi:10.3390/jcm1013288035.
35. Heiser C, Steffen A, Strollo PJ Jr, Giaie-Miniet C, Vanderveken OM, Hofauer B. Hypoglossal nerve stimulation versus positive airway pressure therapy for obstructive sleep apnea. Sleep Breath. 2023;27(2):693-701. doi:10.1007/s11325-022-02663-6
36. Kushida CA, Chediak A, Berry RB, et al. Clinical guidelines for the manual titration of positive airway pressure in patients with obstructive sleep apnea. J Clin Sleep Med. 2008;4(2):157-171.
37. Freedman N, Johnson K. Positive airway pressure treatment for obstructive sleep apnea. In: Kryger MH, Roth T, Goldstein CA, Dement WC, eds. Principles and Practice of Sleep Medicine. Elsevier; 2022:1260-1283.
38. Braun M, Stoerzel M, Wollny M, Schoebel C, Ulrich Sommer J, Heiser C. Patient-reported outcomes with hypoglossal nerve stimulation for treatment of obstructive sleep apnea: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2023;280(10):4627-4639. doi:10.1007/s00405-023-08062-1
39. Luxton DD, Greenburg D, Ryan J, Niven A, Wheeler G, Mysliwiec V. Prevalence and impact of short sleep duration in redeployed OIF soldiers. Sleep. 2011;34(9):1189-1195. doi:10.5665/SLEEP.1236
40. Rogers AE, Stahlman S, Hunt DJ, Oh GT, Clark LL. Obstructive sleep apnea and associated attrition, active component, U.S. Armed Forces, January 2004-May 2016. MSMR. 2016;23(10):2-11.
41. Office of the Deputy Assistant Secretary of Defense for Military Community and Family Policy. 2017 Demographics: Profile of the Military Community. US Dept of Defense;2017. Accessed April 4, 2024. http://download.militaryonesource.mil/12038/MOS/Reports/2017-demographics-report.pdf
42. Remondelli MH, Remick KN, Shackelford SA, et al. Casualty care implications of large-scale combat operations. J Trauma Acute Care Surg. 2023;95(2S Suppl 1): S180-S184. doi:10.1097/TA.0000000000004063