User login
Expandable cardiac valve in children found feasible
Young children and infants who require cardiac valve replacement are limited to fixed-diameter prostheses that cannot accommodate their growth, but researchers at Boston Children’s Hospital have reinforced an expandable bovine jugular vein graft using an external stent and implanted it in 42 patients with acceptable short-term results, according to a report in the Journal of Thoracic and Cardiovascular Surgery.
In 4 years, the modified Melody valve (Medtronic) has proved amenable to enlargement via catheterization as the child grows, Sitaram M. Emani, MD, and coauthors said. “The valve was competent with low gradient acutely postoperatively in all patients,” Dr. Emani and his coauthors said (J Thorac Cardiovasc Surg. 2016 Dec;152[6]:1514-23).
The Melody valve is approved for transcatheter implantation into the RVOT and can be modified for the semilunar or AV positions, Dr. Emani and his coauthors said. The valve has achieved competence within a size range of 10-22 mm.
The researchers implanted the valve in four positions: RVOT (14), mitral (24), aortic (one), or tricuspid (three). The median age at implantation was 10 months, with a range of 3 weeks to 5.8 years. The patients had an average of one previous valve replacement or repair procedure.
Six deaths occurred in the study population; three before discharge. Those three patients had replacement to salvage a moribund circulation in the setting of mechanical circulatory support and severely depressed ventricular function. The other three patients who died were able to demonstrate adequate valve function, and autopsy did not show any signs of valvular thrombosis or deterioration, the researchers said.
Using Kaplan-Meier analysis, Dr. Emani and his coauthors estimated the freedom from death or transplantation was 83% at 12 months and 77% at 24 months.
The average time between catheter-based dilations was around 10 months, they wrote, “but this might be increased by more aggressive dilation.” Early in the study, the researchers were not aggressive with dilations because of concerns about valve injury, but then they found that patients tolerated increases in valve diameter by as much as 4 mm.
“Further investigation is needed to determine whether the device retains expandability over the long term after multiple dilations,” Dr. Emani and his coauthors said.
Further refinements in valve design and implantation techniques may lead to prevention of reoperation and perivalvular complications, they suggested.
The researchers did note a couple limitations of their study: the heterogeneous cohort prohibits any generalization of the outcomes, particularly mortality, and concomitant procedures performed during the valve replacement would affect mortality.
Dr. Emani and his colleagues had no financial relationships to disclose.
In his invited commentary, Carl L. Backer, MD, of Northwestern University, Chicago, noted three advantages of the use of the stent-expandable bovine valve for infants and children: It can be used when no prosthetic is small enough to fit in the annulus, it does not require anticoagulation with warfarin after placement, and it can be dilated as the child grows (J Thorac Cardiovasc Surg. 2016 Dec:152[6];1524-5).
But, Dr. Backer added, “one note of caution that I would raise relates to the late complications noted in previous trials with tissue valves on the left side of the heart in children.” He noted such experience had been reported with the Mitroflow bovine pericardial bioprosthesis (LivaNova) (Circulation. 2014;130[1];51-60) and the Perimount Magna (Edwards Lifesciences) (Ann Thorac Surg. 2016;102[1];308-11). “The follow-up of Emani and colleagues at two years is good; however, there is always the possibility that premature calcification and stenosis of these valves, particularly those placed on the left side of the heart, could lead to the need for early explantation,” Dr. Backer said.
Nonetheless, the findings of Dr. Emani and his colleagues showed that the concept of implanting a stented jugular vein graft valve in infants and young children “is proving to be safe and efficacious,” Dr. Backer said. “In these children for whom there are limited options, this appears to be an important addition to our surgical strategies,” he concluded.
Dr. Backer had no financial relationships to disclose.
In his invited commentary, Carl L. Backer, MD, of Northwestern University, Chicago, noted three advantages of the use of the stent-expandable bovine valve for infants and children: It can be used when no prosthetic is small enough to fit in the annulus, it does not require anticoagulation with warfarin after placement, and it can be dilated as the child grows (J Thorac Cardiovasc Surg. 2016 Dec:152[6];1524-5).
But, Dr. Backer added, “one note of caution that I would raise relates to the late complications noted in previous trials with tissue valves on the left side of the heart in children.” He noted such experience had been reported with the Mitroflow bovine pericardial bioprosthesis (LivaNova) (Circulation. 2014;130[1];51-60) and the Perimount Magna (Edwards Lifesciences) (Ann Thorac Surg. 2016;102[1];308-11). “The follow-up of Emani and colleagues at two years is good; however, there is always the possibility that premature calcification and stenosis of these valves, particularly those placed on the left side of the heart, could lead to the need for early explantation,” Dr. Backer said.
Nonetheless, the findings of Dr. Emani and his colleagues showed that the concept of implanting a stented jugular vein graft valve in infants and young children “is proving to be safe and efficacious,” Dr. Backer said. “In these children for whom there are limited options, this appears to be an important addition to our surgical strategies,” he concluded.
Dr. Backer had no financial relationships to disclose.
In his invited commentary, Carl L. Backer, MD, of Northwestern University, Chicago, noted three advantages of the use of the stent-expandable bovine valve for infants and children: It can be used when no prosthetic is small enough to fit in the annulus, it does not require anticoagulation with warfarin after placement, and it can be dilated as the child grows (J Thorac Cardiovasc Surg. 2016 Dec:152[6];1524-5).
But, Dr. Backer added, “one note of caution that I would raise relates to the late complications noted in previous trials with tissue valves on the left side of the heart in children.” He noted such experience had been reported with the Mitroflow bovine pericardial bioprosthesis (LivaNova) (Circulation. 2014;130[1];51-60) and the Perimount Magna (Edwards Lifesciences) (Ann Thorac Surg. 2016;102[1];308-11). “The follow-up of Emani and colleagues at two years is good; however, there is always the possibility that premature calcification and stenosis of these valves, particularly those placed on the left side of the heart, could lead to the need for early explantation,” Dr. Backer said.
Nonetheless, the findings of Dr. Emani and his colleagues showed that the concept of implanting a stented jugular vein graft valve in infants and young children “is proving to be safe and efficacious,” Dr. Backer said. “In these children for whom there are limited options, this appears to be an important addition to our surgical strategies,” he concluded.
Dr. Backer had no financial relationships to disclose.
Young children and infants who require cardiac valve replacement are limited to fixed-diameter prostheses that cannot accommodate their growth, but researchers at Boston Children’s Hospital have reinforced an expandable bovine jugular vein graft using an external stent and implanted it in 42 patients with acceptable short-term results, according to a report in the Journal of Thoracic and Cardiovascular Surgery.
In 4 years, the modified Melody valve (Medtronic) has proved amenable to enlargement via catheterization as the child grows, Sitaram M. Emani, MD, and coauthors said. “The valve was competent with low gradient acutely postoperatively in all patients,” Dr. Emani and his coauthors said (J Thorac Cardiovasc Surg. 2016 Dec;152[6]:1514-23).
The Melody valve is approved for transcatheter implantation into the RVOT and can be modified for the semilunar or AV positions, Dr. Emani and his coauthors said. The valve has achieved competence within a size range of 10-22 mm.
The researchers implanted the valve in four positions: RVOT (14), mitral (24), aortic (one), or tricuspid (three). The median age at implantation was 10 months, with a range of 3 weeks to 5.8 years. The patients had an average of one previous valve replacement or repair procedure.
Six deaths occurred in the study population; three before discharge. Those three patients had replacement to salvage a moribund circulation in the setting of mechanical circulatory support and severely depressed ventricular function. The other three patients who died were able to demonstrate adequate valve function, and autopsy did not show any signs of valvular thrombosis or deterioration, the researchers said.
Using Kaplan-Meier analysis, Dr. Emani and his coauthors estimated the freedom from death or transplantation was 83% at 12 months and 77% at 24 months.
The average time between catheter-based dilations was around 10 months, they wrote, “but this might be increased by more aggressive dilation.” Early in the study, the researchers were not aggressive with dilations because of concerns about valve injury, but then they found that patients tolerated increases in valve diameter by as much as 4 mm.
“Further investigation is needed to determine whether the device retains expandability over the long term after multiple dilations,” Dr. Emani and his coauthors said.
Further refinements in valve design and implantation techniques may lead to prevention of reoperation and perivalvular complications, they suggested.
The researchers did note a couple limitations of their study: the heterogeneous cohort prohibits any generalization of the outcomes, particularly mortality, and concomitant procedures performed during the valve replacement would affect mortality.
Dr. Emani and his colleagues had no financial relationships to disclose.
Young children and infants who require cardiac valve replacement are limited to fixed-diameter prostheses that cannot accommodate their growth, but researchers at Boston Children’s Hospital have reinforced an expandable bovine jugular vein graft using an external stent and implanted it in 42 patients with acceptable short-term results, according to a report in the Journal of Thoracic and Cardiovascular Surgery.
In 4 years, the modified Melody valve (Medtronic) has proved amenable to enlargement via catheterization as the child grows, Sitaram M. Emani, MD, and coauthors said. “The valve was competent with low gradient acutely postoperatively in all patients,” Dr. Emani and his coauthors said (J Thorac Cardiovasc Surg. 2016 Dec;152[6]:1514-23).
The Melody valve is approved for transcatheter implantation into the RVOT and can be modified for the semilunar or AV positions, Dr. Emani and his coauthors said. The valve has achieved competence within a size range of 10-22 mm.
The researchers implanted the valve in four positions: RVOT (14), mitral (24), aortic (one), or tricuspid (three). The median age at implantation was 10 months, with a range of 3 weeks to 5.8 years. The patients had an average of one previous valve replacement or repair procedure.
Six deaths occurred in the study population; three before discharge. Those three patients had replacement to salvage a moribund circulation in the setting of mechanical circulatory support and severely depressed ventricular function. The other three patients who died were able to demonstrate adequate valve function, and autopsy did not show any signs of valvular thrombosis or deterioration, the researchers said.
Using Kaplan-Meier analysis, Dr. Emani and his coauthors estimated the freedom from death or transplantation was 83% at 12 months and 77% at 24 months.
The average time between catheter-based dilations was around 10 months, they wrote, “but this might be increased by more aggressive dilation.” Early in the study, the researchers were not aggressive with dilations because of concerns about valve injury, but then they found that patients tolerated increases in valve diameter by as much as 4 mm.
“Further investigation is needed to determine whether the device retains expandability over the long term after multiple dilations,” Dr. Emani and his coauthors said.
Further refinements in valve design and implantation techniques may lead to prevention of reoperation and perivalvular complications, they suggested.
The researchers did note a couple limitations of their study: the heterogeneous cohort prohibits any generalization of the outcomes, particularly mortality, and concomitant procedures performed during the valve replacement would affect mortality.
Dr. Emani and his colleagues had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: An expandable cardiac valve adapted for infants and children demonstrates acceptable function and can accommodate the child’s growth.
Major finding: At 12 months after implantation of a bovine jugular vein graft reinforced with an external stent modified for surgical valve replacement in pediatric patients, Kaplan-Meier analysis indicated that 83% of those surviving would be free from reoperation at 12 months.
Data source: Single-center study of 42 patients who underwent implantation between 2010 and 2014.
Disclosures: Dr. Emani and his coauthors had no financial relationships to disclose.
Four-part ‘safety bundle’ targets gynecologic surgery infections
In a new consensus safety bundle designed to reduce the frequency of infections related to gynecologic surgery, an expert panel is calling for preoperative evaluation of infection risk in every patient and surgical timeouts in every case.
The bundle, from the Council on Patient Safety in Women & Mother’s Health Care, seeks to compile existing guidelines and evidence-based recommendations in a way that can be easily implemented with whatever resources an individual institution has available.
The safety bundle covers four domains:
1. Readiness (every facility). The statement calls for standardized preoperative and postoperative care instructions and clearly defined roles for each surgical team member.
Standards should also be established regarding skin preparation, use of prophylactic antibiotics (terminate them within 24 hours after surgery completion unless medical indications are present), and temperature, such as ambient operating room temperature.
“Although the effect of temperature maintenance on surgical site infection is not definitive,” the consensus statement says, “there is no denying other benefits of normothermia; foremost among these is overall patient satisfaction and comfort.”
2. Recognition and prevention (every patient). Every patient should undergo a preoperative evaluation of infection risk based on blood glucose level, body mass index, immunodeficiency, methicillin-resistant Staphylococcus aureus (MRSA) status, nutritional status, and smoking status.
3. Response (every case). Develop “timeouts” during operations, as mandated by the Joint Commission, to address antibiotic dosage and timing, and reassess risk for infection following the procedure based on the length of surgery and blood loss.
4. Reporting and systems learning (every facility). Develop “huddles” – brief team meetings of less than 15 minutes – for high-risk patients. Surgeons and hospital officials should also create a system to report and analyze data about surgical site infections and share physician-specific infection data with all surgeons as part of ongoing professional practice evaluation.
The statement appeared in Obstetrics & Gynecology (2017;129:50-61) and was published concurrently in Anesthesia & Analgesia, the Journal of Obstetric, Gynecologic & Neonatal Nursing, and the AANA Journal.
The authors reported having no potential conflicts of interest.
In a new consensus safety bundle designed to reduce the frequency of infections related to gynecologic surgery, an expert panel is calling for preoperative evaluation of infection risk in every patient and surgical timeouts in every case.
The bundle, from the Council on Patient Safety in Women & Mother’s Health Care, seeks to compile existing guidelines and evidence-based recommendations in a way that can be easily implemented with whatever resources an individual institution has available.
The safety bundle covers four domains:
1. Readiness (every facility). The statement calls for standardized preoperative and postoperative care instructions and clearly defined roles for each surgical team member.
Standards should also be established regarding skin preparation, use of prophylactic antibiotics (terminate them within 24 hours after surgery completion unless medical indications are present), and temperature, such as ambient operating room temperature.
“Although the effect of temperature maintenance on surgical site infection is not definitive,” the consensus statement says, “there is no denying other benefits of normothermia; foremost among these is overall patient satisfaction and comfort.”
2. Recognition and prevention (every patient). Every patient should undergo a preoperative evaluation of infection risk based on blood glucose level, body mass index, immunodeficiency, methicillin-resistant Staphylococcus aureus (MRSA) status, nutritional status, and smoking status.
3. Response (every case). Develop “timeouts” during operations, as mandated by the Joint Commission, to address antibiotic dosage and timing, and reassess risk for infection following the procedure based on the length of surgery and blood loss.
4. Reporting and systems learning (every facility). Develop “huddles” – brief team meetings of less than 15 minutes – for high-risk patients. Surgeons and hospital officials should also create a system to report and analyze data about surgical site infections and share physician-specific infection data with all surgeons as part of ongoing professional practice evaluation.
The statement appeared in Obstetrics & Gynecology (2017;129:50-61) and was published concurrently in Anesthesia & Analgesia, the Journal of Obstetric, Gynecologic & Neonatal Nursing, and the AANA Journal.
The authors reported having no potential conflicts of interest.
In a new consensus safety bundle designed to reduce the frequency of infections related to gynecologic surgery, an expert panel is calling for preoperative evaluation of infection risk in every patient and surgical timeouts in every case.
The bundle, from the Council on Patient Safety in Women & Mother’s Health Care, seeks to compile existing guidelines and evidence-based recommendations in a way that can be easily implemented with whatever resources an individual institution has available.
The safety bundle covers four domains:
1. Readiness (every facility). The statement calls for standardized preoperative and postoperative care instructions and clearly defined roles for each surgical team member.
Standards should also be established regarding skin preparation, use of prophylactic antibiotics (terminate them within 24 hours after surgery completion unless medical indications are present), and temperature, such as ambient operating room temperature.
“Although the effect of temperature maintenance on surgical site infection is not definitive,” the consensus statement says, “there is no denying other benefits of normothermia; foremost among these is overall patient satisfaction and comfort.”
2. Recognition and prevention (every patient). Every patient should undergo a preoperative evaluation of infection risk based on blood glucose level, body mass index, immunodeficiency, methicillin-resistant Staphylococcus aureus (MRSA) status, nutritional status, and smoking status.
3. Response (every case). Develop “timeouts” during operations, as mandated by the Joint Commission, to address antibiotic dosage and timing, and reassess risk for infection following the procedure based on the length of surgery and blood loss.
4. Reporting and systems learning (every facility). Develop “huddles” – brief team meetings of less than 15 minutes – for high-risk patients. Surgeons and hospital officials should also create a system to report and analyze data about surgical site infections and share physician-specific infection data with all surgeons as part of ongoing professional practice evaluation.
The statement appeared in Obstetrics & Gynecology (2017;129:50-61) and was published concurrently in Anesthesia & Analgesia, the Journal of Obstetric, Gynecologic & Neonatal Nursing, and the AANA Journal.
The authors reported having no potential conflicts of interest.
FROM OBSTETRICS & GYNECOLOGY
Plasma energy ablation yields pregnancy rates similar to cystectomy
ORLANDO – The first study to directly compare plasma energy treatment of ovarian endometriomas to cystectomy demonstrates similar postintervention pregnancy rates, suggesting that plasma energy ablation may be a comparable treatment option.
Researchers evaluated 104 women seeking pregnancy after 1 year or more of infertility. Women presented with unilateral or bilateral ovarian endometriomas larger than 3 cm between January 2009 and June 2014. Clinicians treated 64 patients with plasma energy ablation and another 40 with cystectomy and followed them to compare pregnancy rates.
After at least 1 year of follow-up, pregnancy rates were 68% following plasma energy ablation, compared with 80% after cystectomy. Of the 76 pregnancies, 24 were due to spontaneous conception, including 40% of pregnancies in the plasma energy group and 18% in the cystectomy group. Even after adjustment for multiple factors, the type of intervention had no statistically significant impact on achieving a subsequent pregnancy.
“Ablation using plasma energy may be considered a valuable tool that allows a high pregnancy rate,” Basma Darwish, MD, an ob.gyn. at Rouen (France) University Hospital, said at the meeting, which was sponsored by AAGL.
These similar outcomes were observed despite a higher prevalence of risk predictors for infertility in the plasma energy group at baseline. For instance, women in this cohort were significantly older and had significantly higher revised American Fertility Society (rAFS) classification scores, as well as higher rates of pouch of Douglas obliteration, deep endometriosis, and colorectal localizations.
“Endometrial ablation using plasma energy allows good postoperative [pregnancy] rates, that is well known,” Dr. Darwish said, but the technique has not been directly compared with cystectomy outcomes.
Pregnancy rates remained similar in both groups at 24 and 36 months. The probability of pregnancy was 61% in the plasma energy group versus 69% in the cystectomy group at 24 months. At 36 months, these rates changed to 84% and 78%, respectively.
A unique property of plasma energy ablation is “very limited thermal spread, both in depth and laterally,” Dr. Darwish said.
A lack of randomization is a potential limitation of the study. “Each surgeon chose the technique he or she was best at, which may have explained our good outcomes.” Dr. Darwish said. Strengths of the study include a prospective design and follow-up to 5 years. In addition, the six centers involved in the study included both private and public hospitals, “so it’s a good reflection of what happens in real life.”
The investigators plan to conduct a randomized controlled trial to confirm these findings.
ORLANDO – The first study to directly compare plasma energy treatment of ovarian endometriomas to cystectomy demonstrates similar postintervention pregnancy rates, suggesting that plasma energy ablation may be a comparable treatment option.
Researchers evaluated 104 women seeking pregnancy after 1 year or more of infertility. Women presented with unilateral or bilateral ovarian endometriomas larger than 3 cm between January 2009 and June 2014. Clinicians treated 64 patients with plasma energy ablation and another 40 with cystectomy and followed them to compare pregnancy rates.
After at least 1 year of follow-up, pregnancy rates were 68% following plasma energy ablation, compared with 80% after cystectomy. Of the 76 pregnancies, 24 were due to spontaneous conception, including 40% of pregnancies in the plasma energy group and 18% in the cystectomy group. Even after adjustment for multiple factors, the type of intervention had no statistically significant impact on achieving a subsequent pregnancy.
“Ablation using plasma energy may be considered a valuable tool that allows a high pregnancy rate,” Basma Darwish, MD, an ob.gyn. at Rouen (France) University Hospital, said at the meeting, which was sponsored by AAGL.
These similar outcomes were observed despite a higher prevalence of risk predictors for infertility in the plasma energy group at baseline. For instance, women in this cohort were significantly older and had significantly higher revised American Fertility Society (rAFS) classification scores, as well as higher rates of pouch of Douglas obliteration, deep endometriosis, and colorectal localizations.
“Endometrial ablation using plasma energy allows good postoperative [pregnancy] rates, that is well known,” Dr. Darwish said, but the technique has not been directly compared with cystectomy outcomes.
Pregnancy rates remained similar in both groups at 24 and 36 months. The probability of pregnancy was 61% in the plasma energy group versus 69% in the cystectomy group at 24 months. At 36 months, these rates changed to 84% and 78%, respectively.
A unique property of plasma energy ablation is “very limited thermal spread, both in depth and laterally,” Dr. Darwish said.
A lack of randomization is a potential limitation of the study. “Each surgeon chose the technique he or she was best at, which may have explained our good outcomes.” Dr. Darwish said. Strengths of the study include a prospective design and follow-up to 5 years. In addition, the six centers involved in the study included both private and public hospitals, “so it’s a good reflection of what happens in real life.”
The investigators plan to conduct a randomized controlled trial to confirm these findings.
ORLANDO – The first study to directly compare plasma energy treatment of ovarian endometriomas to cystectomy demonstrates similar postintervention pregnancy rates, suggesting that plasma energy ablation may be a comparable treatment option.
Researchers evaluated 104 women seeking pregnancy after 1 year or more of infertility. Women presented with unilateral or bilateral ovarian endometriomas larger than 3 cm between January 2009 and June 2014. Clinicians treated 64 patients with plasma energy ablation and another 40 with cystectomy and followed them to compare pregnancy rates.
After at least 1 year of follow-up, pregnancy rates were 68% following plasma energy ablation, compared with 80% after cystectomy. Of the 76 pregnancies, 24 were due to spontaneous conception, including 40% of pregnancies in the plasma energy group and 18% in the cystectomy group. Even after adjustment for multiple factors, the type of intervention had no statistically significant impact on achieving a subsequent pregnancy.
“Ablation using plasma energy may be considered a valuable tool that allows a high pregnancy rate,” Basma Darwish, MD, an ob.gyn. at Rouen (France) University Hospital, said at the meeting, which was sponsored by AAGL.
These similar outcomes were observed despite a higher prevalence of risk predictors for infertility in the plasma energy group at baseline. For instance, women in this cohort were significantly older and had significantly higher revised American Fertility Society (rAFS) classification scores, as well as higher rates of pouch of Douglas obliteration, deep endometriosis, and colorectal localizations.
“Endometrial ablation using plasma energy allows good postoperative [pregnancy] rates, that is well known,” Dr. Darwish said, but the technique has not been directly compared with cystectomy outcomes.
Pregnancy rates remained similar in both groups at 24 and 36 months. The probability of pregnancy was 61% in the plasma energy group versus 69% in the cystectomy group at 24 months. At 36 months, these rates changed to 84% and 78%, respectively.
A unique property of plasma energy ablation is “very limited thermal spread, both in depth and laterally,” Dr. Darwish said.
A lack of randomization is a potential limitation of the study. “Each surgeon chose the technique he or she was best at, which may have explained our good outcomes.” Dr. Darwish said. Strengths of the study include a prospective design and follow-up to 5 years. In addition, the six centers involved in the study included both private and public hospitals, “so it’s a good reflection of what happens in real life.”
The investigators plan to conduct a randomized controlled trial to confirm these findings.
AT THE AAGL GLOBAL CONGRESS
QUIZ: What is the Rate of Postoperative Atrial Fibrillation after Non-Cardiac Surgery?
[WpProQuiz 16]
[WpProQuiz_toplist 16]
[WpProQuiz 16]
[WpProQuiz_toplist 16]
[WpProQuiz 16]
[WpProQuiz_toplist 16]
Skin cancer a concern in pediatric solid organ transplant recipients
As survival rates among pediatric organ transplant recipients increase, so do the rates of cutaneous malignancies later in life for this population, who are at a greater risk for skin cancers that include nonmelanoma skin cancers (NMSCs), melanoma, Kaposi sarcoma, and anogenital carcinoma, according to the authors of a literature review.
In studies, skin cancers account for 13%-55% of all cancers in pediatric organ transplant recipients (POTRs), according to Alexander L. Fogel of Stanford (Calif.) University and his coauthors. The review article provides an update on this topic, as well as information on the prevention and management of skin cancers in this population, and the differences between this group and adult organ transplant recipients (AOTRs).
NMSC is the most common type of skin cancer in the pediatric group – and the second most common type of malignancy (NMSCs are the most common type of cancer affecting adult organ transplant recipients). NMSCs typically appear an average of 12-18 years post transplantation in this population (at an average age of 26-34 years). Length of posttransplantation follow-up, sunlight exposure, fair skin, and Northern European ancestry are among the factors associated with increased risk. This type of cancer involves the lip nearly twice as often as in adult recipients: 23% vs. 12%. The pediatric cohort also experiences more nonmelanoma cancer spreading to the lymph nodes than do adults: 9% vs. 6%.
Among pediatric transplant recipients, squamous cell carcinomas appear 2.8 times more often than basal cell carcinomas, “a trend that is opposite that observed in the nontransplant population,” the authors wrote.
In one study, anogenital carcinomas accounted for 4% of posttransplant cancers in this cohort, at an average of 12 years after the transplant, at a mean age of 27 years.
Some data indicate that in adult transplant recipients, there is an association between the human papillomavirus, and anal and genital warts and posttransplant anogenital cancer, but there are little data looking at this association in the pediatric group, the authors noted.
Although melanoma and Kaposi sarcoma are also found in this cohort at rates greater than in the general population, and are associated with high mortality rates, the data are too few to draw conclusions, the authors wrote.
In 2014, 1,795 pediatric solid organ transplants were performed, accounting for 6% of all such transplants. The absolute number of pediatric transplants has remained fairly stable over 5 years, yet very little pediatric-specific literature exists for prevention and management of skin cancers post transplantation, the authors pointed out.
Changing immunosuppressive medications used in transplantation may be effective in reducing skin cancer risk, they said, noting that including rapamycin inhibitors in combination therapy has been shown to reduce the risk of developing skin cancers in some transplant patients by more than half.
The authors emphasized that regular sunscreen use and dermatologic checkups are also essential in this population, and that “the importance of regular dermatologic evaluation should be stressed to patients and their families.”
Mr. Fogel’s coauthors were Mari Miyar, MD, of the department of dermatology, Kaiser Permanente, San Jose, Calif., and Joyce Teng, MD, of the departments of dermatology and pediatrics, Stanford. The authors had no disclosures listed, and no funding source for the review was listed.
This article was updated 12/8/16.
As survival rates among pediatric organ transplant recipients increase, so do the rates of cutaneous malignancies later in life for this population, who are at a greater risk for skin cancers that include nonmelanoma skin cancers (NMSCs), melanoma, Kaposi sarcoma, and anogenital carcinoma, according to the authors of a literature review.
In studies, skin cancers account for 13%-55% of all cancers in pediatric organ transplant recipients (POTRs), according to Alexander L. Fogel of Stanford (Calif.) University and his coauthors. The review article provides an update on this topic, as well as information on the prevention and management of skin cancers in this population, and the differences between this group and adult organ transplant recipients (AOTRs).
NMSC is the most common type of skin cancer in the pediatric group – and the second most common type of malignancy (NMSCs are the most common type of cancer affecting adult organ transplant recipients). NMSCs typically appear an average of 12-18 years post transplantation in this population (at an average age of 26-34 years). Length of posttransplantation follow-up, sunlight exposure, fair skin, and Northern European ancestry are among the factors associated with increased risk. This type of cancer involves the lip nearly twice as often as in adult recipients: 23% vs. 12%. The pediatric cohort also experiences more nonmelanoma cancer spreading to the lymph nodes than do adults: 9% vs. 6%.
Among pediatric transplant recipients, squamous cell carcinomas appear 2.8 times more often than basal cell carcinomas, “a trend that is opposite that observed in the nontransplant population,” the authors wrote.
In one study, anogenital carcinomas accounted for 4% of posttransplant cancers in this cohort, at an average of 12 years after the transplant, at a mean age of 27 years.
Some data indicate that in adult transplant recipients, there is an association between the human papillomavirus, and anal and genital warts and posttransplant anogenital cancer, but there are little data looking at this association in the pediatric group, the authors noted.
Although melanoma and Kaposi sarcoma are also found in this cohort at rates greater than in the general population, and are associated with high mortality rates, the data are too few to draw conclusions, the authors wrote.
In 2014, 1,795 pediatric solid organ transplants were performed, accounting for 6% of all such transplants. The absolute number of pediatric transplants has remained fairly stable over 5 years, yet very little pediatric-specific literature exists for prevention and management of skin cancers post transplantation, the authors pointed out.
Changing immunosuppressive medications used in transplantation may be effective in reducing skin cancer risk, they said, noting that including rapamycin inhibitors in combination therapy has been shown to reduce the risk of developing skin cancers in some transplant patients by more than half.
The authors emphasized that regular sunscreen use and dermatologic checkups are also essential in this population, and that “the importance of regular dermatologic evaluation should be stressed to patients and their families.”
Mr. Fogel’s coauthors were Mari Miyar, MD, of the department of dermatology, Kaiser Permanente, San Jose, Calif., and Joyce Teng, MD, of the departments of dermatology and pediatrics, Stanford. The authors had no disclosures listed, and no funding source for the review was listed.
This article was updated 12/8/16.
As survival rates among pediatric organ transplant recipients increase, so do the rates of cutaneous malignancies later in life for this population, who are at a greater risk for skin cancers that include nonmelanoma skin cancers (NMSCs), melanoma, Kaposi sarcoma, and anogenital carcinoma, according to the authors of a literature review.
In studies, skin cancers account for 13%-55% of all cancers in pediatric organ transplant recipients (POTRs), according to Alexander L. Fogel of Stanford (Calif.) University and his coauthors. The review article provides an update on this topic, as well as information on the prevention and management of skin cancers in this population, and the differences between this group and adult organ transplant recipients (AOTRs).
NMSC is the most common type of skin cancer in the pediatric group – and the second most common type of malignancy (NMSCs are the most common type of cancer affecting adult organ transplant recipients). NMSCs typically appear an average of 12-18 years post transplantation in this population (at an average age of 26-34 years). Length of posttransplantation follow-up, sunlight exposure, fair skin, and Northern European ancestry are among the factors associated with increased risk. This type of cancer involves the lip nearly twice as often as in adult recipients: 23% vs. 12%. The pediatric cohort also experiences more nonmelanoma cancer spreading to the lymph nodes than do adults: 9% vs. 6%.
Among pediatric transplant recipients, squamous cell carcinomas appear 2.8 times more often than basal cell carcinomas, “a trend that is opposite that observed in the nontransplant population,” the authors wrote.
In one study, anogenital carcinomas accounted for 4% of posttransplant cancers in this cohort, at an average of 12 years after the transplant, at a mean age of 27 years.
Some data indicate that in adult transplant recipients, there is an association between the human papillomavirus, and anal and genital warts and posttransplant anogenital cancer, but there are little data looking at this association in the pediatric group, the authors noted.
Although melanoma and Kaposi sarcoma are also found in this cohort at rates greater than in the general population, and are associated with high mortality rates, the data are too few to draw conclusions, the authors wrote.
In 2014, 1,795 pediatric solid organ transplants were performed, accounting for 6% of all such transplants. The absolute number of pediatric transplants has remained fairly stable over 5 years, yet very little pediatric-specific literature exists for prevention and management of skin cancers post transplantation, the authors pointed out.
Changing immunosuppressive medications used in transplantation may be effective in reducing skin cancer risk, they said, noting that including rapamycin inhibitors in combination therapy has been shown to reduce the risk of developing skin cancers in some transplant patients by more than half.
The authors emphasized that regular sunscreen use and dermatologic checkups are also essential in this population, and that “the importance of regular dermatologic evaluation should be stressed to patients and their families.”
Mr. Fogel’s coauthors were Mari Miyar, MD, of the department of dermatology, Kaiser Permanente, San Jose, Calif., and Joyce Teng, MD, of the departments of dermatology and pediatrics, Stanford. The authors had no disclosures listed, and no funding source for the review was listed.
This article was updated 12/8/16.
FROM PEDIATRIC DERMATOLOGY
Key clinical point:
Major finding: Pediatric solid organ transplant recipients experience skin cancer rates between 13% and 55%.
Data source: A literature review of malignancies among pediatric organ transplant recipients.
Disclosures: The authors listed no disclosures, and no funding source for the review was listed.
New-onset pain rare after Essure placement
ORLANDO – While some women report new-onset pelvic pain after placement of an Essure sterilization device, results of a retrospective study suggest this pain is actually associated with placement of the device in about 1% of cases.
Among 1,430 women who had an Essure micro-insert (Bayer) placed at a tertiary care hospital in Canada from June 2002 to June 2013, 62 secondary surgeries were performed, including some for removal of fallopian tubes and removal of the device.
In total, 27 patients reported new-onset pelvic pain after Essure placement and another 11 reported worsening of previous pain. Upon further workup, 15 of the 27 women in the new-onset pain group had another possible explanation for their pain, including surgical or pathology findings of endometriosis or adenomyosis. The investigators concluded there was a link between the pain and the device in just 12 (0.8%) of the women.
Among these dozen patients, the investigators linked the pain in eight women to perforation or migration of the Essure device. Investigators found no other obvious cause for the new-onset pain in the remaining four patients and attributed it to the Essure device.
Set realistic expectations, take a comprehensive pain history, and reassure women when they report post-Essure placement pain, James Robinson, MD, a minimally invasive gynecologic surgeon at Medstar Washington Hospital in Washington, D.C., advised at the meeting, which was sponsored by AAGL.
Dr. Robinson pointed out that there is no standardized approach to managing women with complaints of pain or guidelines on how best to remove the device. Imaging to confirm proper placement and to rule out other sources of pelvic pain, followed by medical or surgical management as warranted, can be effective strategies.
“There is less science here – it’s more the art of medicine, I think,” he said.
Dr. Robinson filled in as a presenter for one of the study coauthors, John A. Thiel, MD, of the University of Saskatchewan, Saskatoon, who was unable to attend the conference.
The study by Dr. Thiel and his colleagues suggests a thorough examination will typically reveal other reasons for pelvic pain and rules out the Essure device as the cause, Dr. Robinson said. The full findings of the study are published in the Journal of Minimally Invasive Gynecology (2016 Nov-Dec;23[7]:1158-1162).
Does removal help?
In a recently published case series of 29 women who had their Essure device removed laparoscopically because of pain, 23 reported relief following excision (Contraception. 2016 Aug;94[2]:190-2).
“Again, a subset had misplaced inserts or had another condition such as endometriosis,” Dr. Robinson said.
The majority of women whose pain resolved with removal of the devices reported their pain early on, so there is an important takeaway from this,” Dr. Robinson said. “We need to listen to our patients when they report pain shortly after device placement … and respond to that.”
Dr. Robinson advised physicians to be ready to surgically remove the device if that is warranted. “I think a lot of people doing these procedures are not comfortable taking their patient back to the operating room or don’t know who to send them to,” he said. “If you are going to place the device, you should be able to take it out or know someone who can.”
The bigger picture
Even though the Essure device is not frequently the cause of pelvic pain, physicians needs to be aware that some patients are likely to assume that it is.
Dr. Robinson pointed to a case in which a woman who had the Essure micro-insert placed 7 years earlier presented with a complaint of a bilateral tingling sensation over the course of 6 months. Online research led her to suspect Essure as the cause of her symptoms. However, on further investigation, it turned out she had relatively high levels of lead in her system from leaky pipes in her home. “It wasn’t an Essure issue,” he said. “But because it’s out there, people will jump to the conclusion that the foreign body is likely the cause of their problem.”
Ob.gyns. should become familiar with websites such as essureproblems.webs.com, which chronicle problems patients have reported with the device, he said.
When talking to patients, start with informed consent and listen to their concerns, Dr. Robinson advised. As part of the counseling about Essure permanent birth control, discuss the risks and benefits of alternatives, such as laparoscopic tubal ligation, long-acting reversible contraception, and vasectomy.
“I took the time to listen to the FDA hearing in Sept 2015 and … it moved me to listen to those patients, and I’ve been a huge advocate of Essure sterilization. I felt for a while I would never do another tubal ligation,” Dr. Robinson said. “But when you listen to patients who have real complaints, what sticks out in your mind is so many of these people are upset because no one took them seriously and listened to them.”
ORLANDO – While some women report new-onset pelvic pain after placement of an Essure sterilization device, results of a retrospective study suggest this pain is actually associated with placement of the device in about 1% of cases.
Among 1,430 women who had an Essure micro-insert (Bayer) placed at a tertiary care hospital in Canada from June 2002 to June 2013, 62 secondary surgeries were performed, including some for removal of fallopian tubes and removal of the device.
In total, 27 patients reported new-onset pelvic pain after Essure placement and another 11 reported worsening of previous pain. Upon further workup, 15 of the 27 women in the new-onset pain group had another possible explanation for their pain, including surgical or pathology findings of endometriosis or adenomyosis. The investigators concluded there was a link between the pain and the device in just 12 (0.8%) of the women.
Among these dozen patients, the investigators linked the pain in eight women to perforation or migration of the Essure device. Investigators found no other obvious cause for the new-onset pain in the remaining four patients and attributed it to the Essure device.
Set realistic expectations, take a comprehensive pain history, and reassure women when they report post-Essure placement pain, James Robinson, MD, a minimally invasive gynecologic surgeon at Medstar Washington Hospital in Washington, D.C., advised at the meeting, which was sponsored by AAGL.
Dr. Robinson pointed out that there is no standardized approach to managing women with complaints of pain or guidelines on how best to remove the device. Imaging to confirm proper placement and to rule out other sources of pelvic pain, followed by medical or surgical management as warranted, can be effective strategies.
“There is less science here – it’s more the art of medicine, I think,” he said.
Dr. Robinson filled in as a presenter for one of the study coauthors, John A. Thiel, MD, of the University of Saskatchewan, Saskatoon, who was unable to attend the conference.
The study by Dr. Thiel and his colleagues suggests a thorough examination will typically reveal other reasons for pelvic pain and rules out the Essure device as the cause, Dr. Robinson said. The full findings of the study are published in the Journal of Minimally Invasive Gynecology (2016 Nov-Dec;23[7]:1158-1162).
Does removal help?
In a recently published case series of 29 women who had their Essure device removed laparoscopically because of pain, 23 reported relief following excision (Contraception. 2016 Aug;94[2]:190-2).
“Again, a subset had misplaced inserts or had another condition such as endometriosis,” Dr. Robinson said.
The majority of women whose pain resolved with removal of the devices reported their pain early on, so there is an important takeaway from this,” Dr. Robinson said. “We need to listen to our patients when they report pain shortly after device placement … and respond to that.”
Dr. Robinson advised physicians to be ready to surgically remove the device if that is warranted. “I think a lot of people doing these procedures are not comfortable taking their patient back to the operating room or don’t know who to send them to,” he said. “If you are going to place the device, you should be able to take it out or know someone who can.”
The bigger picture
Even though the Essure device is not frequently the cause of pelvic pain, physicians needs to be aware that some patients are likely to assume that it is.
Dr. Robinson pointed to a case in which a woman who had the Essure micro-insert placed 7 years earlier presented with a complaint of a bilateral tingling sensation over the course of 6 months. Online research led her to suspect Essure as the cause of her symptoms. However, on further investigation, it turned out she had relatively high levels of lead in her system from leaky pipes in her home. “It wasn’t an Essure issue,” he said. “But because it’s out there, people will jump to the conclusion that the foreign body is likely the cause of their problem.”
Ob.gyns. should become familiar with websites such as essureproblems.webs.com, which chronicle problems patients have reported with the device, he said.
When talking to patients, start with informed consent and listen to their concerns, Dr. Robinson advised. As part of the counseling about Essure permanent birth control, discuss the risks and benefits of alternatives, such as laparoscopic tubal ligation, long-acting reversible contraception, and vasectomy.
“I took the time to listen to the FDA hearing in Sept 2015 and … it moved me to listen to those patients, and I’ve been a huge advocate of Essure sterilization. I felt for a while I would never do another tubal ligation,” Dr. Robinson said. “But when you listen to patients who have real complaints, what sticks out in your mind is so many of these people are upset because no one took them seriously and listened to them.”
ORLANDO – While some women report new-onset pelvic pain after placement of an Essure sterilization device, results of a retrospective study suggest this pain is actually associated with placement of the device in about 1% of cases.
Among 1,430 women who had an Essure micro-insert (Bayer) placed at a tertiary care hospital in Canada from June 2002 to June 2013, 62 secondary surgeries were performed, including some for removal of fallopian tubes and removal of the device.
In total, 27 patients reported new-onset pelvic pain after Essure placement and another 11 reported worsening of previous pain. Upon further workup, 15 of the 27 women in the new-onset pain group had another possible explanation for their pain, including surgical or pathology findings of endometriosis or adenomyosis. The investigators concluded there was a link between the pain and the device in just 12 (0.8%) of the women.
Among these dozen patients, the investigators linked the pain in eight women to perforation or migration of the Essure device. Investigators found no other obvious cause for the new-onset pain in the remaining four patients and attributed it to the Essure device.
Set realistic expectations, take a comprehensive pain history, and reassure women when they report post-Essure placement pain, James Robinson, MD, a minimally invasive gynecologic surgeon at Medstar Washington Hospital in Washington, D.C., advised at the meeting, which was sponsored by AAGL.
Dr. Robinson pointed out that there is no standardized approach to managing women with complaints of pain or guidelines on how best to remove the device. Imaging to confirm proper placement and to rule out other sources of pelvic pain, followed by medical or surgical management as warranted, can be effective strategies.
“There is less science here – it’s more the art of medicine, I think,” he said.
Dr. Robinson filled in as a presenter for one of the study coauthors, John A. Thiel, MD, of the University of Saskatchewan, Saskatoon, who was unable to attend the conference.
The study by Dr. Thiel and his colleagues suggests a thorough examination will typically reveal other reasons for pelvic pain and rules out the Essure device as the cause, Dr. Robinson said. The full findings of the study are published in the Journal of Minimally Invasive Gynecology (2016 Nov-Dec;23[7]:1158-1162).
Does removal help?
In a recently published case series of 29 women who had their Essure device removed laparoscopically because of pain, 23 reported relief following excision (Contraception. 2016 Aug;94[2]:190-2).
“Again, a subset had misplaced inserts or had another condition such as endometriosis,” Dr. Robinson said.
The majority of women whose pain resolved with removal of the devices reported their pain early on, so there is an important takeaway from this,” Dr. Robinson said. “We need to listen to our patients when they report pain shortly after device placement … and respond to that.”
Dr. Robinson advised physicians to be ready to surgically remove the device if that is warranted. “I think a lot of people doing these procedures are not comfortable taking their patient back to the operating room or don’t know who to send them to,” he said. “If you are going to place the device, you should be able to take it out or know someone who can.”
The bigger picture
Even though the Essure device is not frequently the cause of pelvic pain, physicians needs to be aware that some patients are likely to assume that it is.
Dr. Robinson pointed to a case in which a woman who had the Essure micro-insert placed 7 years earlier presented with a complaint of a bilateral tingling sensation over the course of 6 months. Online research led her to suspect Essure as the cause of her symptoms. However, on further investigation, it turned out she had relatively high levels of lead in her system from leaky pipes in her home. “It wasn’t an Essure issue,” he said. “But because it’s out there, people will jump to the conclusion that the foreign body is likely the cause of their problem.”
Ob.gyns. should become familiar with websites such as essureproblems.webs.com, which chronicle problems patients have reported with the device, he said.
When talking to patients, start with informed consent and listen to their concerns, Dr. Robinson advised. As part of the counseling about Essure permanent birth control, discuss the risks and benefits of alternatives, such as laparoscopic tubal ligation, long-acting reversible contraception, and vasectomy.
“I took the time to listen to the FDA hearing in Sept 2015 and … it moved me to listen to those patients, and I’ve been a huge advocate of Essure sterilization. I felt for a while I would never do another tubal ligation,” Dr. Robinson said. “But when you listen to patients who have real complaints, what sticks out in your mind is so many of these people are upset because no one took them seriously and listened to them.”
Key clinical point:
Major finding: Of 1,430 women who had the Essure inserts placed, just 12 had new-onset pain that was found to be related to the device.
Data source: Retrospective cohort study of 1,430 women treated at a tertiary care hospital in Canada.
Disclosures: Dr. Robinson reported having no financial disclosures.
The war on pain
When your peer group is dominated by folks in their early 70s, conversations at dinner parties and lobster bakes invariably morph into storytelling competitions between the survivors of recent hospitalizations and medical procedures. I try to redirect this tedious and repetitive chatter with a topic from my standard collection of conversation re-starters that includes “How about those Red Sox?” and “How’s your granddaughter’s soccer season going?” But sadly I am not always successful.
Often embedded in these tales of medical misadventure are stories of unfortunate experiences with pain medications. Sometimes the story includes a description of how prescribed pain medication created symptoms that were far worse than the pain it was intended to treat. Vomiting, constipation, and “feeling goofy” are high on the list of complaints.
These caches of unused opioids, many of which were never needed in the first place, are evidence of why our health care has become so expensive, and also represent the seeds from which the addiction epidemic has grown. Ironically, they also are collateral damage from an unsuccessful and sometimes misguided war on pain.
It isn’t clear exactly when or where the war on pain began, but I’m sure those who fired the first shots were understandably concerned that many patients with incurable and terminal conditions were suffering needlessly because their pain was being under-treated. Coincidently came the realization that the sooner we could get postoperative patients on their feet and taking deep breaths, the fewer complications we would see. And the more adequately we treated their pain, the sooner we could get those patients moving and breathing optimally.
In a good faith effort to be more “scientific” about pain management, patients were asked to rate their pain and smiley face charts appeared. Unfortunately, somewhere along the line came the mantra that not only should no patient’s pain go unmeasured, but no patient’s pain should go unmedicated.
The federal government entered the war when the Centers for Medicare & Medicaid Services issued the directive that hospitals ask patients who were being discharged if their pain had been well controlled and how often did the hospital staff do what they could to ease their pain? The answers to these questions, along with others, was collected and used in assessing a hospital’s quality of care and determining its level of reimbursement.
So far, there is insufficient data to determine how frequently this directive on pain management induced hospitals to over-prescribe medication, but it certainly hasn’t been associated with a decline in opioid abuse. It is reasonable to suspect that this salvo by the government has resulted in some collateral damage as it encouraged a steady flow of unused and unnecessary prescription narcotics out of the hospital and on to the streets.
The good news is that there has been enough concern voiced about the unintended effect of these pain management questions that the CMS has decided to eliminate financial pressure clinicians might feel to over-prescribe medications by withdrawing the questions from the patient discharge questionnaire.
The bad news is that we continue to fight the war on pain with a limited arsenal. As long as clinicians simply believe that no pain should go unmedicated, they will continue to miss opportunities to use other modalities such as counseling, physical therapy, and education that can be effective without the risk of collateral damage. Instead of asking the patient (who may not know the answer), we should be asking ourselves if we have been doing everything we could to help the patient deal with his pain. The answer is often not written on prescription pads.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
When your peer group is dominated by folks in their early 70s, conversations at dinner parties and lobster bakes invariably morph into storytelling competitions between the survivors of recent hospitalizations and medical procedures. I try to redirect this tedious and repetitive chatter with a topic from my standard collection of conversation re-starters that includes “How about those Red Sox?” and “How’s your granddaughter’s soccer season going?” But sadly I am not always successful.
Often embedded in these tales of medical misadventure are stories of unfortunate experiences with pain medications. Sometimes the story includes a description of how prescribed pain medication created symptoms that were far worse than the pain it was intended to treat. Vomiting, constipation, and “feeling goofy” are high on the list of complaints.
These caches of unused opioids, many of which were never needed in the first place, are evidence of why our health care has become so expensive, and also represent the seeds from which the addiction epidemic has grown. Ironically, they also are collateral damage from an unsuccessful and sometimes misguided war on pain.
It isn’t clear exactly when or where the war on pain began, but I’m sure those who fired the first shots were understandably concerned that many patients with incurable and terminal conditions were suffering needlessly because their pain was being under-treated. Coincidently came the realization that the sooner we could get postoperative patients on their feet and taking deep breaths, the fewer complications we would see. And the more adequately we treated their pain, the sooner we could get those patients moving and breathing optimally.
In a good faith effort to be more “scientific” about pain management, patients were asked to rate their pain and smiley face charts appeared. Unfortunately, somewhere along the line came the mantra that not only should no patient’s pain go unmeasured, but no patient’s pain should go unmedicated.
The federal government entered the war when the Centers for Medicare & Medicaid Services issued the directive that hospitals ask patients who were being discharged if their pain had been well controlled and how often did the hospital staff do what they could to ease their pain? The answers to these questions, along with others, was collected and used in assessing a hospital’s quality of care and determining its level of reimbursement.
So far, there is insufficient data to determine how frequently this directive on pain management induced hospitals to over-prescribe medication, but it certainly hasn’t been associated with a decline in opioid abuse. It is reasonable to suspect that this salvo by the government has resulted in some collateral damage as it encouraged a steady flow of unused and unnecessary prescription narcotics out of the hospital and on to the streets.
The good news is that there has been enough concern voiced about the unintended effect of these pain management questions that the CMS has decided to eliminate financial pressure clinicians might feel to over-prescribe medications by withdrawing the questions from the patient discharge questionnaire.
The bad news is that we continue to fight the war on pain with a limited arsenal. As long as clinicians simply believe that no pain should go unmedicated, they will continue to miss opportunities to use other modalities such as counseling, physical therapy, and education that can be effective without the risk of collateral damage. Instead of asking the patient (who may not know the answer), we should be asking ourselves if we have been doing everything we could to help the patient deal with his pain. The answer is often not written on prescription pads.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
When your peer group is dominated by folks in their early 70s, conversations at dinner parties and lobster bakes invariably morph into storytelling competitions between the survivors of recent hospitalizations and medical procedures. I try to redirect this tedious and repetitive chatter with a topic from my standard collection of conversation re-starters that includes “How about those Red Sox?” and “How’s your granddaughter’s soccer season going?” But sadly I am not always successful.
Often embedded in these tales of medical misadventure are stories of unfortunate experiences with pain medications. Sometimes the story includes a description of how prescribed pain medication created symptoms that were far worse than the pain it was intended to treat. Vomiting, constipation, and “feeling goofy” are high on the list of complaints.
These caches of unused opioids, many of which were never needed in the first place, are evidence of why our health care has become so expensive, and also represent the seeds from which the addiction epidemic has grown. Ironically, they also are collateral damage from an unsuccessful and sometimes misguided war on pain.
It isn’t clear exactly when or where the war on pain began, but I’m sure those who fired the first shots were understandably concerned that many patients with incurable and terminal conditions were suffering needlessly because their pain was being under-treated. Coincidently came the realization that the sooner we could get postoperative patients on their feet and taking deep breaths, the fewer complications we would see. And the more adequately we treated their pain, the sooner we could get those patients moving and breathing optimally.
In a good faith effort to be more “scientific” about pain management, patients were asked to rate their pain and smiley face charts appeared. Unfortunately, somewhere along the line came the mantra that not only should no patient’s pain go unmeasured, but no patient’s pain should go unmedicated.
The federal government entered the war when the Centers for Medicare & Medicaid Services issued the directive that hospitals ask patients who were being discharged if their pain had been well controlled and how often did the hospital staff do what they could to ease their pain? The answers to these questions, along with others, was collected and used in assessing a hospital’s quality of care and determining its level of reimbursement.
So far, there is insufficient data to determine how frequently this directive on pain management induced hospitals to over-prescribe medication, but it certainly hasn’t been associated with a decline in opioid abuse. It is reasonable to suspect that this salvo by the government has resulted in some collateral damage as it encouraged a steady flow of unused and unnecessary prescription narcotics out of the hospital and on to the streets.
The good news is that there has been enough concern voiced about the unintended effect of these pain management questions that the CMS has decided to eliminate financial pressure clinicians might feel to over-prescribe medications by withdrawing the questions from the patient discharge questionnaire.
The bad news is that we continue to fight the war on pain with a limited arsenal. As long as clinicians simply believe that no pain should go unmedicated, they will continue to miss opportunities to use other modalities such as counseling, physical therapy, and education that can be effective without the risk of collateral damage. Instead of asking the patient (who may not know the answer), we should be asking ourselves if we have been doing everything we could to help the patient deal with his pain. The answer is often not written on prescription pads.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
Lower analgesic use after robotic pelvic surgery
Postoperative use of both opioid and nonopioid analgesics was lower after robotic surgery than after laparotomy for endometrial cancer, according to a report published in Gynecologic Oncology.
Researchers assessed the use of postoperative pain medication in a single-center retrospective study involving 340 consecutive robotically assisted surgeries for endometrial cancer during a 6-year period. The mean patient age was 65 years, and more than one-third of the women were aged 70 or older. Slightly more than half were obese, and 19% were morbidly obese, said Jeremie Abitbol, PhD, of the division of gynecologic oncology, Jewish General Hospital and McGill University, Montreal, and his associates.
This benefit in the use of pain medication occurred regardless of the patient’s obesity status or age, which is particularly helpful in view of the increased risk of adverse events in these two patient populations, Dr. Abitbol and his associates reported (Gynecol Oncol. 2016. doi: 10.1016/jgyno.2016.11.014).
The direct costs associated with postoperative analgesia also were commensurately lower for robotically assisted surgery ($2.52 per day) than for laparotomy ($7.89 per day).
This study was supported by grants from the Israel Cancer Research Foundation, the Gloria’s Girls Fund, the Levi Family Fund, and the Weekend to End Women’s Cancers. Dr. Abitbol reported having no relevant financial disclosures; one of his associates reported receiving a grant from Intuitive Surgical.
Postoperative use of both opioid and nonopioid analgesics was lower after robotic surgery than after laparotomy for endometrial cancer, according to a report published in Gynecologic Oncology.
Researchers assessed the use of postoperative pain medication in a single-center retrospective study involving 340 consecutive robotically assisted surgeries for endometrial cancer during a 6-year period. The mean patient age was 65 years, and more than one-third of the women were aged 70 or older. Slightly more than half were obese, and 19% were morbidly obese, said Jeremie Abitbol, PhD, of the division of gynecologic oncology, Jewish General Hospital and McGill University, Montreal, and his associates.
This benefit in the use of pain medication occurred regardless of the patient’s obesity status or age, which is particularly helpful in view of the increased risk of adverse events in these two patient populations, Dr. Abitbol and his associates reported (Gynecol Oncol. 2016. doi: 10.1016/jgyno.2016.11.014).
The direct costs associated with postoperative analgesia also were commensurately lower for robotically assisted surgery ($2.52 per day) than for laparotomy ($7.89 per day).
This study was supported by grants from the Israel Cancer Research Foundation, the Gloria’s Girls Fund, the Levi Family Fund, and the Weekend to End Women’s Cancers. Dr. Abitbol reported having no relevant financial disclosures; one of his associates reported receiving a grant from Intuitive Surgical.
Postoperative use of both opioid and nonopioid analgesics was lower after robotic surgery than after laparotomy for endometrial cancer, according to a report published in Gynecologic Oncology.
Researchers assessed the use of postoperative pain medication in a single-center retrospective study involving 340 consecutive robotically assisted surgeries for endometrial cancer during a 6-year period. The mean patient age was 65 years, and more than one-third of the women were aged 70 or older. Slightly more than half were obese, and 19% were morbidly obese, said Jeremie Abitbol, PhD, of the division of gynecologic oncology, Jewish General Hospital and McGill University, Montreal, and his associates.
This benefit in the use of pain medication occurred regardless of the patient’s obesity status or age, which is particularly helpful in view of the increased risk of adverse events in these two patient populations, Dr. Abitbol and his associates reported (Gynecol Oncol. 2016. doi: 10.1016/jgyno.2016.11.014).
The direct costs associated with postoperative analgesia also were commensurately lower for robotically assisted surgery ($2.52 per day) than for laparotomy ($7.89 per day).
This study was supported by grants from the Israel Cancer Research Foundation, the Gloria’s Girls Fund, the Levi Family Fund, and the Weekend to End Women’s Cancers. Dr. Abitbol reported having no relevant financial disclosures; one of his associates reported receiving a grant from Intuitive Surgical.
FROM GYNECOLOGIC ONCOLOGY
Key clinical point: Postoperative use of both opioid and nonopioid analgesics was lower after robotic surgery than after laparotomy for endometrial cancer.
Major finding: The robotic surgery cohort required significantly less opioids (12 mg vs. 71 mg), acetaminophen (2,151 mg vs. 4,810 mg), ibuprofen (377 mg vs. 1,892 mg), and naproxen (393 mg vs 1,470 mg), compared with an historical cohort of 59 women who underwent laparotomy.
Data source: A single-center retrospective cohort study involving 340 consecutive robotically assisted pelvic surgeries during a 6-year period.
Disclosures: This study was supported by grants from the Israel Cancer Research Foundation, the Gloria’s Girls Fund, the Levi Family Fund, and the Weekend to End Women’s Cancers. Dr. Abitbol reported having no relevant financial disclosures; one of his associates reported receiving a grant from Intuitive Surgical.

Tips for avoiding nerve injuries in gynecologic surgery
Upper- and lower-extremity injuries can occur during gynecologic surgery. The incidence of lower-extremity injury is 1.1%-1.9% and upper-extremity injuries can occur in 0.16% of cases.1-5 Fortunately, most of the injuries are transient, sensory injuries that resolve spontaneously. However, a small percentage of injuries result in long-term sequelae.
The pathophysiology of the nerve injuries can be mechanistically separated into three categories: neuropraxia, axonotmesis, and neurotmesis. Neuropraxia results from nerve demyelination at the site of injury because of compression and typically resolves within weeks to months as the nerve is remyelinated. Axonotmesis results from severe compression with axon damage. This may take up to a year to resolve as axonal regeneration proceeds at the rate of 1 mm per day. This can be separated into second and third degree and refers to the severity of damage and the resultant persistent deficit. Neurotmesis results from complete transection and is associated with a poor prognosis without reparative surgery.
Brachial plexus
Stretch injury is the most common reason for a brachial plexus injury. This can occur if the arm board is extended to greater than 90 degrees from the patient’s torso or if the patient’s arm falls off of the arm board. Careful positioning and securing the patient’s arm on the arm board before draping can avoid this injury. A brachial plexus injury can also occur if shoulder braces are placed too laterally during minimally invasive surgery. Radial nerve injuries can occur if there is too much pressure on the humerus during positioning. Ulnar injuries arise from pressure placed on the medial aspect of the elbow.
Tip #1: When tucking a patient’s arm for minimally invasive surgery, appropriate padding should be placed around the elbow and wrist, and the arm should be in the “thumbs-up” position.
Tip #2: Shoulder blocks should be placed over the acromioclavicular (AC) joint.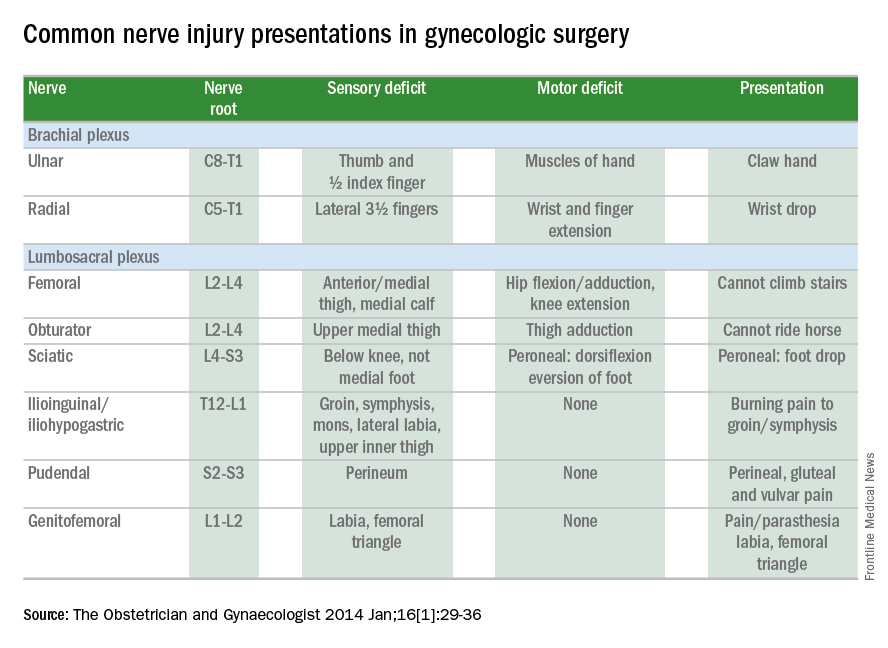
Lumbosacral plexus
The femoral nerve is the nerve most commonly injured during gynecologic surgery and this usually occurs because of compression of the nerve from the lateral blades of self-retaining retractors. One study showed an 8% incidence of injury from self-retaining retractors, compared with less than 1% when the retractors were not used.6 The femoral nerve can also be stretched when patients are placed in the lithotomy position and the hip is hyperflexed.
As with brachial injury prevention, patients should be positioned prior to draping and care must be taken to not hyperflex or externally rotate the hip during minimally invasive surgical procedures. With the introduction of robot-assisted surgery, care must be taken when docking the robot and surgeons must resist excessive movement of the stirrups.
Tip #3: During laparotomy, surgeons should use the shortest blades that allow for adequate visualization and check the blades during the procedure to ensure that excessive pressure is not placed on the psoas muscle. Consider intermittently releasing the pressure on the lateral blades during other portions of the procedure.
Tip #4: Make sure the stirrups are at the same height and that the leg is in line with the patient’s contralateral shoulder.
Obturator nerve injuries can occur during retroperitoneal dissection for pelvic lymphadenectomy (obturator nodes) and can be either a transection or a cautery injury. It can also be injured during urogynecologic procedures including paravaginal defect repairs and during the placement of transobturator tapes.
The sciatic nerve and its branch, the common peroneal, are generally injured because of excessive stretch or pressure. Both nerves can be injured from hyperflexion of the thigh and the common peroneal can suffer a pressure injury as it courses around the lateral head of the fibula. Therefore, care during lithotomy positioning with both candy cane and Allen stirrups is critical during vaginal surgery.
Tip #5: Ensure that the lateral fibula is not touching the stirrup or that padding is placed between the fibular head and the stirrup.
The ilioinguinal and iliohypogastric nerves are typically injured via suture entrapment from low transverse skin incisions, though laparoscopic injury has also been reported. The incidence after a Pfannenstiel incision is about 3.7%.7
Tip #6: Avoid extending the low transverse incision beyond the lateral margin of the rectus muscle, and do not extend the fascial closure suture more than 1.5 cm from the lateral edge of the fascial incision to avoid catching the nerve with the suture.
The pudendal nerve is most commonly injured during vaginal procedures such as sacrospinous fixation. Pain is typically worse when seated.
The genitofemoral nerve is typically injured during retroperitoneal lymph node dissection, particularly the external iliac nodes. The nerve is small and runs lateral to the external iliac artery. It can suffer cautery and transection injuries. Usually, the paresthesias over the mons pubis, labia majora, and medial inner thigh are temporary.
Tip #7: Care should be taken to identify and spare the nerve during retroperitoneal dissection or external iliac node removal.
Nerve injuries during gynecologic surgery are common and are a significant cause of potential morbidity. While occasionally unavoidable and inherent to the surgical procedure, many times the injury could be prevented with proper attention and care to patient positioning and retractor use. Gynecologists should be aware of the risks and have a through understanding of the anatomy. However, should an injury occur, the patient can be reassured that most are self-limited and full recovery is generally expected. In a prospective study, the median time to resolution of symptoms was 31.5 days (range, 1 day to 6 months).5
References
1. The Obstetrician & Gynaecologist 2014;16:29-36.
2. Gynecol Oncol. 1988 Nov;31(3):462-6.
3. Fertil Steril. 1993 Oct;60(4):729-32.
4. J Minim Invasive Gynecol. 2007 Sep-Oct;14(5):664-72.
5. Am J Obstet Gynecol. 2009 Nov;201(5):531.e1-7.
6. Eur J Obstet Gynecol Reprod Biol. 1985 Dec;20(6):385-92.
7. Obstet Gynecol. 2008 Apr;111(4):839-46.
Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. She reported having no financial disclosures relevant to this column. Email her at obnews@frontlinemedcom.com.
Upper- and lower-extremity injuries can occur during gynecologic surgery. The incidence of lower-extremity injury is 1.1%-1.9% and upper-extremity injuries can occur in 0.16% of cases.1-5 Fortunately, most of the injuries are transient, sensory injuries that resolve spontaneously. However, a small percentage of injuries result in long-term sequelae.
The pathophysiology of the nerve injuries can be mechanistically separated into three categories: neuropraxia, axonotmesis, and neurotmesis. Neuropraxia results from nerve demyelination at the site of injury because of compression and typically resolves within weeks to months as the nerve is remyelinated. Axonotmesis results from severe compression with axon damage. This may take up to a year to resolve as axonal regeneration proceeds at the rate of 1 mm per day. This can be separated into second and third degree and refers to the severity of damage and the resultant persistent deficit. Neurotmesis results from complete transection and is associated with a poor prognosis without reparative surgery.
Brachial plexus
Stretch injury is the most common reason for a brachial plexus injury. This can occur if the arm board is extended to greater than 90 degrees from the patient’s torso or if the patient’s arm falls off of the arm board. Careful positioning and securing the patient’s arm on the arm board before draping can avoid this injury. A brachial plexus injury can also occur if shoulder braces are placed too laterally during minimally invasive surgery. Radial nerve injuries can occur if there is too much pressure on the humerus during positioning. Ulnar injuries arise from pressure placed on the medial aspect of the elbow.
Tip #1: When tucking a patient’s arm for minimally invasive surgery, appropriate padding should be placed around the elbow and wrist, and the arm should be in the “thumbs-up” position.
Tip #2: Shoulder blocks should be placed over the acromioclavicular (AC) joint.
Lumbosacral plexus
The femoral nerve is the nerve most commonly injured during gynecologic surgery and this usually occurs because of compression of the nerve from the lateral blades of self-retaining retractors. One study showed an 8% incidence of injury from self-retaining retractors, compared with less than 1% when the retractors were not used.6 The femoral nerve can also be stretched when patients are placed in the lithotomy position and the hip is hyperflexed.
As with brachial injury prevention, patients should be positioned prior to draping and care must be taken to not hyperflex or externally rotate the hip during minimally invasive surgical procedures. With the introduction of robot-assisted surgery, care must be taken when docking the robot and surgeons must resist excessive movement of the stirrups.
Tip #3: During laparotomy, surgeons should use the shortest blades that allow for adequate visualization and check the blades during the procedure to ensure that excessive pressure is not placed on the psoas muscle. Consider intermittently releasing the pressure on the lateral blades during other portions of the procedure.
Tip #4: Make sure the stirrups are at the same height and that the leg is in line with the patient’s contralateral shoulder.
Obturator nerve injuries can occur during retroperitoneal dissection for pelvic lymphadenectomy (obturator nodes) and can be either a transection or a cautery injury. It can also be injured during urogynecologic procedures including paravaginal defect repairs and during the placement of transobturator tapes.
The sciatic nerve and its branch, the common peroneal, are generally injured because of excessive stretch or pressure. Both nerves can be injured from hyperflexion of the thigh and the common peroneal can suffer a pressure injury as it courses around the lateral head of the fibula. Therefore, care during lithotomy positioning with both candy cane and Allen stirrups is critical during vaginal surgery.
Tip #5: Ensure that the lateral fibula is not touching the stirrup or that padding is placed between the fibular head and the stirrup.
The ilioinguinal and iliohypogastric nerves are typically injured via suture entrapment from low transverse skin incisions, though laparoscopic injury has also been reported. The incidence after a Pfannenstiel incision is about 3.7%.7
Tip #6: Avoid extending the low transverse incision beyond the lateral margin of the rectus muscle, and do not extend the fascial closure suture more than 1.5 cm from the lateral edge of the fascial incision to avoid catching the nerve with the suture.
The pudendal nerve is most commonly injured during vaginal procedures such as sacrospinous fixation. Pain is typically worse when seated.
The genitofemoral nerve is typically injured during retroperitoneal lymph node dissection, particularly the external iliac nodes. The nerve is small and runs lateral to the external iliac artery. It can suffer cautery and transection injuries. Usually, the paresthesias over the mons pubis, labia majora, and medial inner thigh are temporary.
Tip #7: Care should be taken to identify and spare the nerve during retroperitoneal dissection or external iliac node removal.
Nerve injuries during gynecologic surgery are common and are a significant cause of potential morbidity. While occasionally unavoidable and inherent to the surgical procedure, many times the injury could be prevented with proper attention and care to patient positioning and retractor use. Gynecologists should be aware of the risks and have a through understanding of the anatomy. However, should an injury occur, the patient can be reassured that most are self-limited and full recovery is generally expected. In a prospective study, the median time to resolution of symptoms was 31.5 days (range, 1 day to 6 months).5
References
1. The Obstetrician & Gynaecologist 2014;16:29-36.
2. Gynecol Oncol. 1988 Nov;31(3):462-6.
3. Fertil Steril. 1993 Oct;60(4):729-32.
4. J Minim Invasive Gynecol. 2007 Sep-Oct;14(5):664-72.
5. Am J Obstet Gynecol. 2009 Nov;201(5):531.e1-7.
6. Eur J Obstet Gynecol Reprod Biol. 1985 Dec;20(6):385-92.
7. Obstet Gynecol. 2008 Apr;111(4):839-46.
Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. She reported having no financial disclosures relevant to this column. Email her at obnews@frontlinemedcom.com.
Upper- and lower-extremity injuries can occur during gynecologic surgery. The incidence of lower-extremity injury is 1.1%-1.9% and upper-extremity injuries can occur in 0.16% of cases.1-5 Fortunately, most of the injuries are transient, sensory injuries that resolve spontaneously. However, a small percentage of injuries result in long-term sequelae.
The pathophysiology of the nerve injuries can be mechanistically separated into three categories: neuropraxia, axonotmesis, and neurotmesis. Neuropraxia results from nerve demyelination at the site of injury because of compression and typically resolves within weeks to months as the nerve is remyelinated. Axonotmesis results from severe compression with axon damage. This may take up to a year to resolve as axonal regeneration proceeds at the rate of 1 mm per day. This can be separated into second and third degree and refers to the severity of damage and the resultant persistent deficit. Neurotmesis results from complete transection and is associated with a poor prognosis without reparative surgery.
Brachial plexus
Stretch injury is the most common reason for a brachial plexus injury. This can occur if the arm board is extended to greater than 90 degrees from the patient’s torso or if the patient’s arm falls off of the arm board. Careful positioning and securing the patient’s arm on the arm board before draping can avoid this injury. A brachial plexus injury can also occur if shoulder braces are placed too laterally during minimally invasive surgery. Radial nerve injuries can occur if there is too much pressure on the humerus during positioning. Ulnar injuries arise from pressure placed on the medial aspect of the elbow.
Tip #1: When tucking a patient’s arm for minimally invasive surgery, appropriate padding should be placed around the elbow and wrist, and the arm should be in the “thumbs-up” position.
Tip #2: Shoulder blocks should be placed over the acromioclavicular (AC) joint.
Lumbosacral plexus
The femoral nerve is the nerve most commonly injured during gynecologic surgery and this usually occurs because of compression of the nerve from the lateral blades of self-retaining retractors. One study showed an 8% incidence of injury from self-retaining retractors, compared with less than 1% when the retractors were not used.6 The femoral nerve can also be stretched when patients are placed in the lithotomy position and the hip is hyperflexed.
As with brachial injury prevention, patients should be positioned prior to draping and care must be taken to not hyperflex or externally rotate the hip during minimally invasive surgical procedures. With the introduction of robot-assisted surgery, care must be taken when docking the robot and surgeons must resist excessive movement of the stirrups.
Tip #3: During laparotomy, surgeons should use the shortest blades that allow for adequate visualization and check the blades during the procedure to ensure that excessive pressure is not placed on the psoas muscle. Consider intermittently releasing the pressure on the lateral blades during other portions of the procedure.
Tip #4: Make sure the stirrups are at the same height and that the leg is in line with the patient’s contralateral shoulder.
Obturator nerve injuries can occur during retroperitoneal dissection for pelvic lymphadenectomy (obturator nodes) and can be either a transection or a cautery injury. It can also be injured during urogynecologic procedures including paravaginal defect repairs and during the placement of transobturator tapes.
The sciatic nerve and its branch, the common peroneal, are generally injured because of excessive stretch or pressure. Both nerves can be injured from hyperflexion of the thigh and the common peroneal can suffer a pressure injury as it courses around the lateral head of the fibula. Therefore, care during lithotomy positioning with both candy cane and Allen stirrups is critical during vaginal surgery.
Tip #5: Ensure that the lateral fibula is not touching the stirrup or that padding is placed between the fibular head and the stirrup.
The ilioinguinal and iliohypogastric nerves are typically injured via suture entrapment from low transverse skin incisions, though laparoscopic injury has also been reported. The incidence after a Pfannenstiel incision is about 3.7%.7
Tip #6: Avoid extending the low transverse incision beyond the lateral margin of the rectus muscle, and do not extend the fascial closure suture more than 1.5 cm from the lateral edge of the fascial incision to avoid catching the nerve with the suture.
The pudendal nerve is most commonly injured during vaginal procedures such as sacrospinous fixation. Pain is typically worse when seated.
The genitofemoral nerve is typically injured during retroperitoneal lymph node dissection, particularly the external iliac nodes. The nerve is small and runs lateral to the external iliac artery. It can suffer cautery and transection injuries. Usually, the paresthesias over the mons pubis, labia majora, and medial inner thigh are temporary.
Tip #7: Care should be taken to identify and spare the nerve during retroperitoneal dissection or external iliac node removal.
Nerve injuries during gynecologic surgery are common and are a significant cause of potential morbidity. While occasionally unavoidable and inherent to the surgical procedure, many times the injury could be prevented with proper attention and care to patient positioning and retractor use. Gynecologists should be aware of the risks and have a through understanding of the anatomy. However, should an injury occur, the patient can be reassured that most are self-limited and full recovery is generally expected. In a prospective study, the median time to resolution of symptoms was 31.5 days (range, 1 day to 6 months).5
References
1. The Obstetrician & Gynaecologist 2014;16:29-36.
2. Gynecol Oncol. 1988 Nov;31(3):462-6.
3. Fertil Steril. 1993 Oct;60(4):729-32.
4. J Minim Invasive Gynecol. 2007 Sep-Oct;14(5):664-72.
5. Am J Obstet Gynecol. 2009 Nov;201(5):531.e1-7.
6. Eur J Obstet Gynecol Reprod Biol. 1985 Dec;20(6):385-92.
7. Obstet Gynecol. 2008 Apr;111(4):839-46.
Dr. Gehrig is professor and director of gynecologic oncology at the University of North Carolina at Chapel Hill. She reported having no financial disclosures relevant to this column. Email her at obnews@frontlinemedcom.com.
Ultrasound effective in diagnosing occult hernia in women
ORLANDO – Ultrasound appears to be an effective tool in diagnosing occult hernia in women with unexplained chronic pelvic pain, according to a retrospective cohort study of 96 women.
“As gynecologists, we are likely to see those patients with chronic pelvic pain in our clinic before other specialists due to the location of their pain,” said Joelle Aoun, MD, an ob.gyn. in the division of minimally invasive gynecologic surgery at Henry Ford Health System in Detroit. “So it’s very important to recognize women with a high clinical suspicion for occult hernia and evaluate them in order to prevent a delayed diagnosis and prolonged suffering.”
Hernias can be more difficult to diagnose in women than in men, Dr. Aoun said at the meeting sponsored by AAGL, and the literature offers conflicting findings since most hernia studies are conducted in men or with mixed gender cohorts.
Dr. Aoun and her coinvestigators conducted a retrospective cohort study from January 2005 to July 2016, identifying 96 women with chronic pelvic pain and focal inguinal tenderness. Protruding fat or visceral tissue on physical exam or observed visually led clinicians to suspect a hernia. A single sonographer performed the musculoskeletal ultrasound.
Investigators diagnosed an occult hernia in more than half of the patients (51 women) based on the physical exam and ultrasound findings. Diagnoses included inguinal, femoral, Spigelian, and umbilical hernias.
All women with an ultrasound-diagnosed hernia were referred to general surgery. A majority – 69% of women – underwent surgical exploration. The remaining 31% of women who declined tended to have lower pain scores, Dr. Aoun said. Surgeons confirmed the hernia diagnosis in 97% of the women, or 34 out of the 35 women who had consented to surgery.
The group with a hernia was older and more likely to have arthritis, but otherwise did not differ significantly from the nonhernia cohort.
“We believe musculoskeletal ultrasound is valuable as an initial imaging modality due to its high predictive value, low cost, and noninvasiveness,” Dr. Aoun said.
Chronic pelvic pain is not uncommon, affecting approximately 15% of women during their reproductive years often with significant impacts on quality of life, workplace productivity, and health care utilization, Dr. Aoun said. This presentation also accounts for about 10% outpatient gynecology consultations and approximately 40% of laparoscopies in the United States, she added.
Dr. Aoun and her colleagues are planning a subsequent study of all the women who opted not to undergo surgery to determine their follow-up pain profiles based on chart review and phone interviews.
Dr. Aoun reported having no relevant financial disclosures.
ORLANDO – Ultrasound appears to be an effective tool in diagnosing occult hernia in women with unexplained chronic pelvic pain, according to a retrospective cohort study of 96 women.
“As gynecologists, we are likely to see those patients with chronic pelvic pain in our clinic before other specialists due to the location of their pain,” said Joelle Aoun, MD, an ob.gyn. in the division of minimally invasive gynecologic surgery at Henry Ford Health System in Detroit. “So it’s very important to recognize women with a high clinical suspicion for occult hernia and evaluate them in order to prevent a delayed diagnosis and prolonged suffering.”
Hernias can be more difficult to diagnose in women than in men, Dr. Aoun said at the meeting sponsored by AAGL, and the literature offers conflicting findings since most hernia studies are conducted in men or with mixed gender cohorts.
Dr. Aoun and her coinvestigators conducted a retrospective cohort study from January 2005 to July 2016, identifying 96 women with chronic pelvic pain and focal inguinal tenderness. Protruding fat or visceral tissue on physical exam or observed visually led clinicians to suspect a hernia. A single sonographer performed the musculoskeletal ultrasound.
Investigators diagnosed an occult hernia in more than half of the patients (51 women) based on the physical exam and ultrasound findings. Diagnoses included inguinal, femoral, Spigelian, and umbilical hernias.
All women with an ultrasound-diagnosed hernia were referred to general surgery. A majority – 69% of women – underwent surgical exploration. The remaining 31% of women who declined tended to have lower pain scores, Dr. Aoun said. Surgeons confirmed the hernia diagnosis in 97% of the women, or 34 out of the 35 women who had consented to surgery.
The group with a hernia was older and more likely to have arthritis, but otherwise did not differ significantly from the nonhernia cohort.
“We believe musculoskeletal ultrasound is valuable as an initial imaging modality due to its high predictive value, low cost, and noninvasiveness,” Dr. Aoun said.
Chronic pelvic pain is not uncommon, affecting approximately 15% of women during their reproductive years often with significant impacts on quality of life, workplace productivity, and health care utilization, Dr. Aoun said. This presentation also accounts for about 10% outpatient gynecology consultations and approximately 40% of laparoscopies in the United States, she added.
Dr. Aoun and her colleagues are planning a subsequent study of all the women who opted not to undergo surgery to determine their follow-up pain profiles based on chart review and phone interviews.
Dr. Aoun reported having no relevant financial disclosures.
ORLANDO – Ultrasound appears to be an effective tool in diagnosing occult hernia in women with unexplained chronic pelvic pain, according to a retrospective cohort study of 96 women.
“As gynecologists, we are likely to see those patients with chronic pelvic pain in our clinic before other specialists due to the location of their pain,” said Joelle Aoun, MD, an ob.gyn. in the division of minimally invasive gynecologic surgery at Henry Ford Health System in Detroit. “So it’s very important to recognize women with a high clinical suspicion for occult hernia and evaluate them in order to prevent a delayed diagnosis and prolonged suffering.”
Hernias can be more difficult to diagnose in women than in men, Dr. Aoun said at the meeting sponsored by AAGL, and the literature offers conflicting findings since most hernia studies are conducted in men or with mixed gender cohorts.
Dr. Aoun and her coinvestigators conducted a retrospective cohort study from January 2005 to July 2016, identifying 96 women with chronic pelvic pain and focal inguinal tenderness. Protruding fat or visceral tissue on physical exam or observed visually led clinicians to suspect a hernia. A single sonographer performed the musculoskeletal ultrasound.
Investigators diagnosed an occult hernia in more than half of the patients (51 women) based on the physical exam and ultrasound findings. Diagnoses included inguinal, femoral, Spigelian, and umbilical hernias.
All women with an ultrasound-diagnosed hernia were referred to general surgery. A majority – 69% of women – underwent surgical exploration. The remaining 31% of women who declined tended to have lower pain scores, Dr. Aoun said. Surgeons confirmed the hernia diagnosis in 97% of the women, or 34 out of the 35 women who had consented to surgery.
The group with a hernia was older and more likely to have arthritis, but otherwise did not differ significantly from the nonhernia cohort.
“We believe musculoskeletal ultrasound is valuable as an initial imaging modality due to its high predictive value, low cost, and noninvasiveness,” Dr. Aoun said.
Chronic pelvic pain is not uncommon, affecting approximately 15% of women during their reproductive years often with significant impacts on quality of life, workplace productivity, and health care utilization, Dr. Aoun said. This presentation also accounts for about 10% outpatient gynecology consultations and approximately 40% of laparoscopies in the United States, she added.
Dr. Aoun and her colleagues are planning a subsequent study of all the women who opted not to undergo surgery to determine their follow-up pain profiles based on chart review and phone interviews.
Dr. Aoun reported having no relevant financial disclosures.
AT THE AAGL GLOBAL CONGRESS
Key clinical point:
Major finding: About 53% of women with chronic pelvic pain were diagnosed with an occult hernia following physical exam and ultrasound. Surgeons confirmed the hernia diagnosis in 34 out of 35 patients who consented to surgery.
Data source: A retrospective cohort study of 96 women with chronic pelvic pain and focal inguinal tenderness.
Disclosures: Dr. Aoun reported having no relevant financial disclosures.