User login
Maternal pertussis vax effective for infants in most vulnerable months
Maternal pertussis vaccinations, given during pregnancy, prevent an estimated 65% of pertussis infections in infants, new research indicates.
The study, led by Annette K. Regan, PhD, MPH, a perinatal and pediatric infectious disease epidemiologist at Curtin University, Perth, Australia, was published online in Pediatrics.
Dr. Regan – who is also with the University of San Francisco and the University of California, Los Angeles – and colleagues reviewed data on 279,418 infants born to 252,444 mothers in Australia.
There, about 52% of the women in this study received the Tdap vaccine through a maternal pertussis vaccination program.
Duration of effectiveness in infants was one of the main questions the study sought to answer.
The authors wrote that they assessed vaccine effectiveness through 18 months of age. “We observed significant protection against disease until at least 8 months of age, 2 months longer than reported in previous studies.” From 70% to 90% of all pertussis-attributable hospitalizations and death occur in infancy.
Answering the ‘blunting’ question
This study also set out to clarify an important clinical question regarding a potential “blunting” effect in infants. Previous work had suggested that maternal antibodies from the vaccination could interfere with the effectiveness of infants’ DtaP (the version of Tdap for infants) and other vaccines.
Dr. Regan and colleagues found that, “although we observed slightly lower VE [vaccine effectiveness] point estimates for the third dose of infant pertussis vaccine among maternally vaccinated compared with unvaccinated infants (76.5% vs. 92.9%, P = .002), we did not observe higher rates of pertussis infection (hazard ratio, 0.70; 95% confidence interval, 0.61-3.39).
Best time to give mothers the vaccine
Another clinical debate has centered on when to give the mother the vaccine during pregnancy. The authors concluded: “Our findings support the infant health benefits of recommendations to administer a booster dose of pertussis vaccine near 28 weeks of gestational age.”
That 28-week mark was associated with lower risk of infection in infants through 8 months of age, they wrote.
Positive results in the United States
In an invited commentary, Kathryn M. Edwards, MD, with the division of infectious diseases, department of pediatrics, at Vanderbilt University Medical Center, Nashville, Tenn., highlighted similar positive findings for maternal pertussis vaccination in the United States.
The Centers for Disease Control and Prevention did an ecologic study of infant pertussis cases reported between Jan. 1, 2000, and Dec. 31, 2019. Rates were compared for the years before maternal Tdap vaccinations were recommended against the 7-year period after they were implemented.
That study found that in the period before maternal Tdap vaccination, annual pertussis incidence did not change among infants younger than 2 months and increased slightly in infants 6-12 months.
However, during the period after maternal Tdap vaccination had started (2012-2019), pertussis incidence significantly decreased in infants younger than 2 months and was unchanged in infants 6-12 months.
“As with the Australian data, the U.S. data support the overall benefit of the maternal Tdap program and, as with the Australian data, do not suggest that blunting has led to an increase in cases within the first year of life,” Dr. Edwards wrote.
The CDC notes that pertussis cases are rising and outbreaks are happening across the United States.
“On average, about 1,000 infants are hospitalized and typically between 5 and 15 infants die each year in the United States due to pertussis,” the CDC states.
Uptake low despite positive data
Dr. Edwards noted that, despite positive data supporting maternal vaccination to reduce pertussis, uptake rates are low – between 50% and 60% in Australia, the United Kingdom, and the United States. “Active engagement to increase these rates should be implemented.”
Maternal vaccination might also be implemented soon to protect against other diseases including respiratory syncytial virus and group B streptococcal disease after promising study data, she said.
As with pertussis, the potential “blunting” effect will need to be carefully monitored, she said, “as was done in the carefully conducted study of pertussis reported in this issue of Pediatrics.”
One coauthor has received institutional honoraria for participation in advisory groups for Merck Sharpe & Dohme and Pfizer unrelated to this work. Another coauthor was supported by scholarships provided by the Wesfarmers Centre of Vaccines and Infectious Disease at the Telethon Kids Institute. Dr. Edwards reported receiving grants from the CDC and consulting for Bionet, Dynavax, and IBM. She is a member of the data safety and monitoring board for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, Merck, Roche, Novavax, and Brighton Collaboration.
Maternal pertussis vaccinations, given during pregnancy, prevent an estimated 65% of pertussis infections in infants, new research indicates.
The study, led by Annette K. Regan, PhD, MPH, a perinatal and pediatric infectious disease epidemiologist at Curtin University, Perth, Australia, was published online in Pediatrics.
Dr. Regan – who is also with the University of San Francisco and the University of California, Los Angeles – and colleagues reviewed data on 279,418 infants born to 252,444 mothers in Australia.
There, about 52% of the women in this study received the Tdap vaccine through a maternal pertussis vaccination program.
Duration of effectiveness in infants was one of the main questions the study sought to answer.
The authors wrote that they assessed vaccine effectiveness through 18 months of age. “We observed significant protection against disease until at least 8 months of age, 2 months longer than reported in previous studies.” From 70% to 90% of all pertussis-attributable hospitalizations and death occur in infancy.
Answering the ‘blunting’ question
This study also set out to clarify an important clinical question regarding a potential “blunting” effect in infants. Previous work had suggested that maternal antibodies from the vaccination could interfere with the effectiveness of infants’ DtaP (the version of Tdap for infants) and other vaccines.
Dr. Regan and colleagues found that, “although we observed slightly lower VE [vaccine effectiveness] point estimates for the third dose of infant pertussis vaccine among maternally vaccinated compared with unvaccinated infants (76.5% vs. 92.9%, P = .002), we did not observe higher rates of pertussis infection (hazard ratio, 0.70; 95% confidence interval, 0.61-3.39).
Best time to give mothers the vaccine
Another clinical debate has centered on when to give the mother the vaccine during pregnancy. The authors concluded: “Our findings support the infant health benefits of recommendations to administer a booster dose of pertussis vaccine near 28 weeks of gestational age.”
That 28-week mark was associated with lower risk of infection in infants through 8 months of age, they wrote.
Positive results in the United States
In an invited commentary, Kathryn M. Edwards, MD, with the division of infectious diseases, department of pediatrics, at Vanderbilt University Medical Center, Nashville, Tenn., highlighted similar positive findings for maternal pertussis vaccination in the United States.
The Centers for Disease Control and Prevention did an ecologic study of infant pertussis cases reported between Jan. 1, 2000, and Dec. 31, 2019. Rates were compared for the years before maternal Tdap vaccinations were recommended against the 7-year period after they were implemented.
That study found that in the period before maternal Tdap vaccination, annual pertussis incidence did not change among infants younger than 2 months and increased slightly in infants 6-12 months.
However, during the period after maternal Tdap vaccination had started (2012-2019), pertussis incidence significantly decreased in infants younger than 2 months and was unchanged in infants 6-12 months.
“As with the Australian data, the U.S. data support the overall benefit of the maternal Tdap program and, as with the Australian data, do not suggest that blunting has led to an increase in cases within the first year of life,” Dr. Edwards wrote.
The CDC notes that pertussis cases are rising and outbreaks are happening across the United States.
“On average, about 1,000 infants are hospitalized and typically between 5 and 15 infants die each year in the United States due to pertussis,” the CDC states.
Uptake low despite positive data
Dr. Edwards noted that, despite positive data supporting maternal vaccination to reduce pertussis, uptake rates are low – between 50% and 60% in Australia, the United Kingdom, and the United States. “Active engagement to increase these rates should be implemented.”
Maternal vaccination might also be implemented soon to protect against other diseases including respiratory syncytial virus and group B streptococcal disease after promising study data, she said.
As with pertussis, the potential “blunting” effect will need to be carefully monitored, she said, “as was done in the carefully conducted study of pertussis reported in this issue of Pediatrics.”
One coauthor has received institutional honoraria for participation in advisory groups for Merck Sharpe & Dohme and Pfizer unrelated to this work. Another coauthor was supported by scholarships provided by the Wesfarmers Centre of Vaccines and Infectious Disease at the Telethon Kids Institute. Dr. Edwards reported receiving grants from the CDC and consulting for Bionet, Dynavax, and IBM. She is a member of the data safety and monitoring board for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, Merck, Roche, Novavax, and Brighton Collaboration.
Maternal pertussis vaccinations, given during pregnancy, prevent an estimated 65% of pertussis infections in infants, new research indicates.
The study, led by Annette K. Regan, PhD, MPH, a perinatal and pediatric infectious disease epidemiologist at Curtin University, Perth, Australia, was published online in Pediatrics.
Dr. Regan – who is also with the University of San Francisco and the University of California, Los Angeles – and colleagues reviewed data on 279,418 infants born to 252,444 mothers in Australia.
There, about 52% of the women in this study received the Tdap vaccine through a maternal pertussis vaccination program.
Duration of effectiveness in infants was one of the main questions the study sought to answer.
The authors wrote that they assessed vaccine effectiveness through 18 months of age. “We observed significant protection against disease until at least 8 months of age, 2 months longer than reported in previous studies.” From 70% to 90% of all pertussis-attributable hospitalizations and death occur in infancy.
Answering the ‘blunting’ question
This study also set out to clarify an important clinical question regarding a potential “blunting” effect in infants. Previous work had suggested that maternal antibodies from the vaccination could interfere with the effectiveness of infants’ DtaP (the version of Tdap for infants) and other vaccines.
Dr. Regan and colleagues found that, “although we observed slightly lower VE [vaccine effectiveness] point estimates for the third dose of infant pertussis vaccine among maternally vaccinated compared with unvaccinated infants (76.5% vs. 92.9%, P = .002), we did not observe higher rates of pertussis infection (hazard ratio, 0.70; 95% confidence interval, 0.61-3.39).
Best time to give mothers the vaccine
Another clinical debate has centered on when to give the mother the vaccine during pregnancy. The authors concluded: “Our findings support the infant health benefits of recommendations to administer a booster dose of pertussis vaccine near 28 weeks of gestational age.”
That 28-week mark was associated with lower risk of infection in infants through 8 months of age, they wrote.
Positive results in the United States
In an invited commentary, Kathryn M. Edwards, MD, with the division of infectious diseases, department of pediatrics, at Vanderbilt University Medical Center, Nashville, Tenn., highlighted similar positive findings for maternal pertussis vaccination in the United States.
The Centers for Disease Control and Prevention did an ecologic study of infant pertussis cases reported between Jan. 1, 2000, and Dec. 31, 2019. Rates were compared for the years before maternal Tdap vaccinations were recommended against the 7-year period after they were implemented.
That study found that in the period before maternal Tdap vaccination, annual pertussis incidence did not change among infants younger than 2 months and increased slightly in infants 6-12 months.
However, during the period after maternal Tdap vaccination had started (2012-2019), pertussis incidence significantly decreased in infants younger than 2 months and was unchanged in infants 6-12 months.
“As with the Australian data, the U.S. data support the overall benefit of the maternal Tdap program and, as with the Australian data, do not suggest that blunting has led to an increase in cases within the first year of life,” Dr. Edwards wrote.
The CDC notes that pertussis cases are rising and outbreaks are happening across the United States.
“On average, about 1,000 infants are hospitalized and typically between 5 and 15 infants die each year in the United States due to pertussis,” the CDC states.
Uptake low despite positive data
Dr. Edwards noted that, despite positive data supporting maternal vaccination to reduce pertussis, uptake rates are low – between 50% and 60% in Australia, the United Kingdom, and the United States. “Active engagement to increase these rates should be implemented.”
Maternal vaccination might also be implemented soon to protect against other diseases including respiratory syncytial virus and group B streptococcal disease after promising study data, she said.
As with pertussis, the potential “blunting” effect will need to be carefully monitored, she said, “as was done in the carefully conducted study of pertussis reported in this issue of Pediatrics.”
One coauthor has received institutional honoraria for participation in advisory groups for Merck Sharpe & Dohme and Pfizer unrelated to this work. Another coauthor was supported by scholarships provided by the Wesfarmers Centre of Vaccines and Infectious Disease at the Telethon Kids Institute. Dr. Edwards reported receiving grants from the CDC and consulting for Bionet, Dynavax, and IBM. She is a member of the data safety and monitoring board for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, Merck, Roche, Novavax, and Brighton Collaboration.
FROM PEDIATRICS
Long-Awaited RSV Vaccines Now Available for Older Adults and Pediatric Patients
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
Preparing for the viral trifecta: RSV, influenza, and COVID-19
New armamentaria available to fight an old disease.
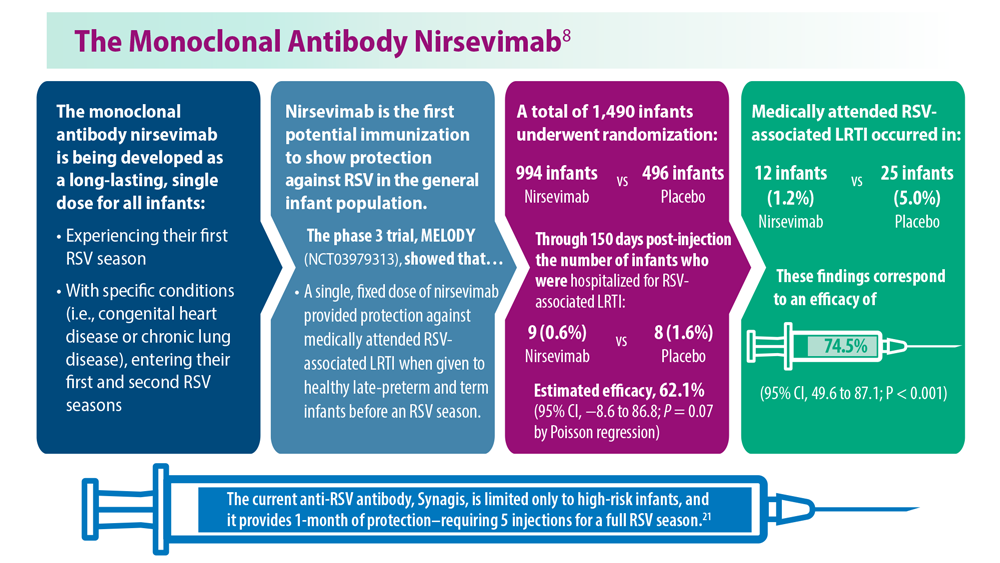
In July 2023, nirsevimab (Beyfortus), a monoclonal antibody, was approved by the Food and Drug Administration for the prevention of respiratory syncytial virus (RSV) disease in infants and children younger than 2 years of age. On Aug. 3, 2023, the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention recommended routine use of it for all infants younger than 8 months of age born during or entering their first RSV season. Its use is also recommended for certain children 8-19 months of age who are at increased risk for severe RSV disease at the start of their second RSV season. Hearing the approval, I immediately had a flashback to residency, recalling the multiple infants admitted each fall and winter exhibiting classic symptoms including cough, rhinorrhea, nasal flaring, retractions, and wheezing with many having oxygen requirements and others needing intubation. Only supportive care was available.
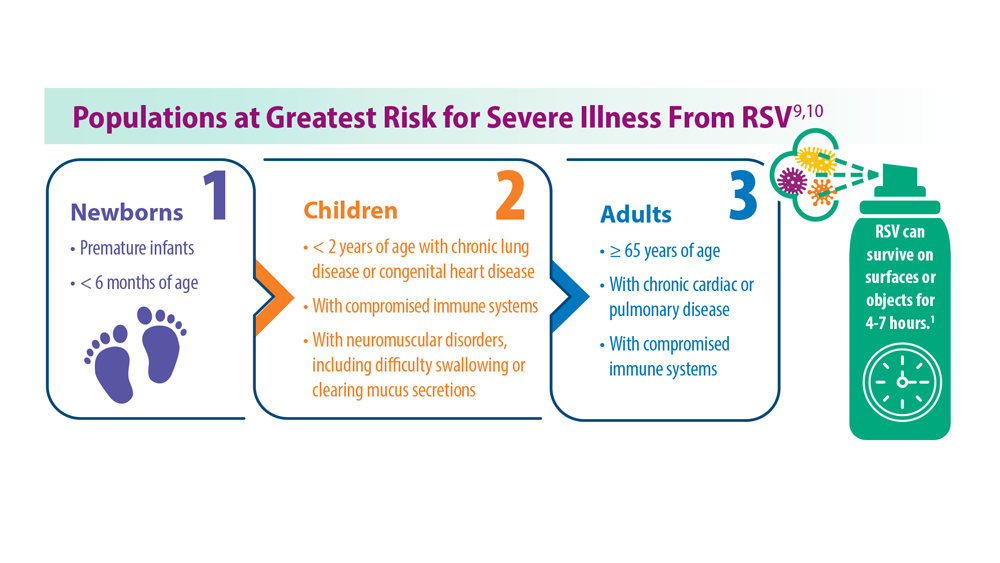
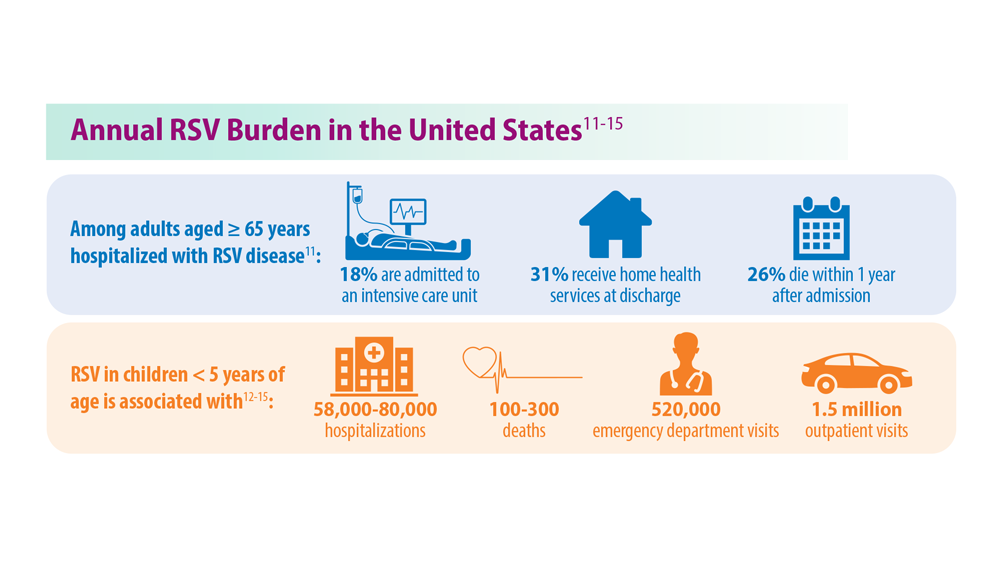
RSV is the leading cause of infant hospitalizations. Annually, the CDC estimates there are 50,000-80,000 RSV hospitalizations and 100-300 RSV-related deaths in the United States in persons younger than 5 years of age. While premature infants have the highest rates of hospitalization (three times a term infant) about 79% of hospitalized children younger than 2 years have no underlying medical risks.1 The majority of children will experience RSV as an upper respiratory infection within the first 2 years of life. However, severe disease requiring hospitalization is more likely to occur in premature infants and children younger than 6 months; children younger than 2 with congenital heart disease and/or chronic lung disease; children with severe cystic fibrosis; as well as the immunocompromised child and individuals with neuromuscular disorders that preclude clearing mucous secretions or have difficulty swallowing.

Palivizumab (Synagis), the first monoclonal antibody to prevent RSV in infants was licensed in 1998. Its use was limited to infants meeting specific criteria developed by the American Academy of Pediatrics. Only 5% of infants had access to it. It was a short-acting agent requiring monthly injections, which were very costly ($1,661-$2,584 per dose). Eligible infants could receive up to five injections per season. Several studies proved its use was not cost beneficial.
What are the advantages of nirsevimab? It’s a long-acting monoclonal antibody. Only one dose is required per season. Costs will significantly diminish. It is recommended for all infants younger than 8 months of age born during RSV season. Those children 8-19 months at risk for severe RSV disease can receive it prior to the start of their second RSV season. During RSV season (October 1 to March 31), the initial dose should be administered to newborns just prior to hospital discharge. Older infants and newborns who did not receive it prior to hospital discharge can receive it at their medical home. Newborns should receive it within the first week of life. It is covered by the Vaccine for Children Program. Simultaneous administration with routine childhood immunizations is recommended. Finally, RSV season may vary in tropical areas (Southern Florida, Puerto Rico. etc.) and Alaska. The timing of nirsevimab administration should be based on local RSV activity provided by state and local authorities.
In addition, the FDA approved an RSV vaccine (Abrysvo) for use in adults at least 60 years of age and in pregnant women at 32-36 weeks’ gestation. The latter is administered to prevent lower respiratory tract infection in infants from birth to 6 months. Recommendations have been published for administration in nonpregnant adults. Specific information is forthcoming in terms timing of administration of nirsevimab in infants whose mothers receive Abrysvo.
RSV season is quickly approaching. Detailed recommendations for administration and FAQ questions related to nirsevimab and palivizumab can be found at https://www.aap.org or https://www.cdc.gov/vaccines/hcp/acip-recs/index.html.
Influenza
So, what about influenza? Vaccine composition has been tweaked to match the circulating viruses but the recommended age for annual routine administration remains unchanged. All persons at least 6 months of age should be vaccinated. Children between 6 months and 8 years need two doses at least 4 weeks apart when receiving vaccine for the first time. Immunizing everyone in the household is encouraged especially if there are household contacts at risk for developing severe disease, including infants too young to be vaccinated. Keep in mind children may be coinfected with multiple viruses. Adams and colleagues reviewed the prevalence of coinfection of influenza and Sars-CoV-2 in persons younger than 18 years reported to three CDC surveillance platforms during the 2021-2022 season.2 Thirty-two of 575 hospitalized (6%) coinfections were analyzed and 7 of 44 (16%) deaths. Compared with patients without coinfections, the coinfected patients were more likely to require mechanical ventilation (13% vs. 4%) or CPAP (16% vs. 6%). Only 4 of 23 who were influenza vaccine eligible were vaccinated. Of seven coinfected children who died, none had received influenza vaccine and only one received an antiviral. Only 5 of 31 (16%) infected only with influenza were vaccinated.3
Influenza activity was lower than usual during the 2021-2022 season. However, this report revealed underuse of both influenza vaccine and antiviral therapy, both of which are routinely recommended.
COVID-19
What’s new with COVID-19? On Sept. 12, 2023, ACIP recommended that everyone at least 6 months of age receive the 2023-2024 (monovalent, XBB containing) COVID-19 vaccines. Children at least 5 years of age need one dose and those younger need one or two doses depending on the number of doses previously received. Why the change? Circulating variants continue to change. There is a current uptick in cases including hospitalizations (7.7%) and deaths (4.5%) and it’s just the beginning of the season.4 Symptoms, risk groups and complications have not changed. The primary goal is to prevent infection, hospitalization, long term complications, and death.
We are now armed with the most up-to-date interventions to help prevent the acquisition of these three viruses. Our next step is recommending and delivering them to our patients.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She reported no relevant financial disclosures.
References
1.Suh M et al. J Infect Dis. 2022;226(Suppl 2):S154-36. doi: 10.1093/infdis/jiac120.
2. Adams K et al. MMWR Morb Mortal Wkly Rep. 2022;71:1589-96. doi: http://dx.doi.org/10.15585/mmwr.mm7150a4.
3. Pingali C et al. MMWR Morb Mortal Wkly Rep. 2023 Aug 25;72:912-9. doi: http://dx.doi.org/10.15585/mmwr.mm7234a3.
4. CDC Covid Data Tracker.
New armamentaria available to fight an old disease.
New armamentaria available to fight an old disease.
In July 2023, nirsevimab (Beyfortus), a monoclonal antibody, was approved by the Food and Drug Administration for the prevention of respiratory syncytial virus (RSV) disease in infants and children younger than 2 years of age. On Aug. 3, 2023, the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention recommended routine use of it for all infants younger than 8 months of age born during or entering their first RSV season. Its use is also recommended for certain children 8-19 months of age who are at increased risk for severe RSV disease at the start of their second RSV season. Hearing the approval, I immediately had a flashback to residency, recalling the multiple infants admitted each fall and winter exhibiting classic symptoms including cough, rhinorrhea, nasal flaring, retractions, and wheezing with many having oxygen requirements and others needing intubation. Only supportive care was available.
RSV is the leading cause of infant hospitalizations. Annually, the CDC estimates there are 50,000-80,000 RSV hospitalizations and 100-300 RSV-related deaths in the United States in persons younger than 5 years of age. While premature infants have the highest rates of hospitalization (three times a term infant) about 79% of hospitalized children younger than 2 years have no underlying medical risks.1 The majority of children will experience RSV as an upper respiratory infection within the first 2 years of life. However, severe disease requiring hospitalization is more likely to occur in premature infants and children younger than 6 months; children younger than 2 with congenital heart disease and/or chronic lung disease; children with severe cystic fibrosis; as well as the immunocompromised child and individuals with neuromuscular disorders that preclude clearing mucous secretions or have difficulty swallowing.
Palivizumab (Synagis), the first monoclonal antibody to prevent RSV in infants was licensed in 1998. Its use was limited to infants meeting specific criteria developed by the American Academy of Pediatrics. Only 5% of infants had access to it. It was a short-acting agent requiring monthly injections, which were very costly ($1,661-$2,584 per dose). Eligible infants could receive up to five injections per season. Several studies proved its use was not cost beneficial.
What are the advantages of nirsevimab? It’s a long-acting monoclonal antibody. Only one dose is required per season. Costs will significantly diminish. It is recommended for all infants younger than 8 months of age born during RSV season. Those children 8-19 months at risk for severe RSV disease can receive it prior to the start of their second RSV season. During RSV season (October 1 to March 31), the initial dose should be administered to newborns just prior to hospital discharge. Older infants and newborns who did not receive it prior to hospital discharge can receive it at their medical home. Newborns should receive it within the first week of life. It is covered by the Vaccine for Children Program. Simultaneous administration with routine childhood immunizations is recommended. Finally, RSV season may vary in tropical areas (Southern Florida, Puerto Rico. etc.) and Alaska. The timing of nirsevimab administration should be based on local RSV activity provided by state and local authorities.
In addition, the FDA approved an RSV vaccine (Abrysvo) for use in adults at least 60 years of age and in pregnant women at 32-36 weeks’ gestation. The latter is administered to prevent lower respiratory tract infection in infants from birth to 6 months. Recommendations have been published for administration in nonpregnant adults. Specific information is forthcoming in terms timing of administration of nirsevimab in infants whose mothers receive Abrysvo.
RSV season is quickly approaching. Detailed recommendations for administration and FAQ questions related to nirsevimab and palivizumab can be found at https://www.aap.org or https://www.cdc.gov/vaccines/hcp/acip-recs/index.html.
Influenza
So, what about influenza? Vaccine composition has been tweaked to match the circulating viruses but the recommended age for annual routine administration remains unchanged. All persons at least 6 months of age should be vaccinated. Children between 6 months and 8 years need two doses at least 4 weeks apart when receiving vaccine for the first time. Immunizing everyone in the household is encouraged especially if there are household contacts at risk for developing severe disease, including infants too young to be vaccinated. Keep in mind children may be coinfected with multiple viruses. Adams and colleagues reviewed the prevalence of coinfection of influenza and Sars-CoV-2 in persons younger than 18 years reported to three CDC surveillance platforms during the 2021-2022 season.2 Thirty-two of 575 hospitalized (6%) coinfections were analyzed and 7 of 44 (16%) deaths. Compared with patients without coinfections, the coinfected patients were more likely to require mechanical ventilation (13% vs. 4%) or CPAP (16% vs. 6%). Only 4 of 23 who were influenza vaccine eligible were vaccinated. Of seven coinfected children who died, none had received influenza vaccine and only one received an antiviral. Only 5 of 31 (16%) infected only with influenza were vaccinated.3
Influenza activity was lower than usual during the 2021-2022 season. However, this report revealed underuse of both influenza vaccine and antiviral therapy, both of which are routinely recommended.
COVID-19
What’s new with COVID-19? On Sept. 12, 2023, ACIP recommended that everyone at least 6 months of age receive the 2023-2024 (monovalent, XBB containing) COVID-19 vaccines. Children at least 5 years of age need one dose and those younger need one or two doses depending on the number of doses previously received. Why the change? Circulating variants continue to change. There is a current uptick in cases including hospitalizations (7.7%) and deaths (4.5%) and it’s just the beginning of the season.4 Symptoms, risk groups and complications have not changed. The primary goal is to prevent infection, hospitalization, long term complications, and death.
We are now armed with the most up-to-date interventions to help prevent the acquisition of these three viruses. Our next step is recommending and delivering them to our patients.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She reported no relevant financial disclosures.
References
1.Suh M et al. J Infect Dis. 2022;226(Suppl 2):S154-36. doi: 10.1093/infdis/jiac120.
2. Adams K et al. MMWR Morb Mortal Wkly Rep. 2022;71:1589-96. doi: http://dx.doi.org/10.15585/mmwr.mm7150a4.
3. Pingali C et al. MMWR Morb Mortal Wkly Rep. 2023 Aug 25;72:912-9. doi: http://dx.doi.org/10.15585/mmwr.mm7234a3.
4. CDC Covid Data Tracker.
In July 2023, nirsevimab (Beyfortus), a monoclonal antibody, was approved by the Food and Drug Administration for the prevention of respiratory syncytial virus (RSV) disease in infants and children younger than 2 years of age. On Aug. 3, 2023, the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention recommended routine use of it for all infants younger than 8 months of age born during or entering their first RSV season. Its use is also recommended for certain children 8-19 months of age who are at increased risk for severe RSV disease at the start of their second RSV season. Hearing the approval, I immediately had a flashback to residency, recalling the multiple infants admitted each fall and winter exhibiting classic symptoms including cough, rhinorrhea, nasal flaring, retractions, and wheezing with many having oxygen requirements and others needing intubation. Only supportive care was available.
RSV is the leading cause of infant hospitalizations. Annually, the CDC estimates there are 50,000-80,000 RSV hospitalizations and 100-300 RSV-related deaths in the United States in persons younger than 5 years of age. While premature infants have the highest rates of hospitalization (three times a term infant) about 79% of hospitalized children younger than 2 years have no underlying medical risks.1 The majority of children will experience RSV as an upper respiratory infection within the first 2 years of life. However, severe disease requiring hospitalization is more likely to occur in premature infants and children younger than 6 months; children younger than 2 with congenital heart disease and/or chronic lung disease; children with severe cystic fibrosis; as well as the immunocompromised child and individuals with neuromuscular disorders that preclude clearing mucous secretions or have difficulty swallowing.
Palivizumab (Synagis), the first monoclonal antibody to prevent RSV in infants was licensed in 1998. Its use was limited to infants meeting specific criteria developed by the American Academy of Pediatrics. Only 5% of infants had access to it. It was a short-acting agent requiring monthly injections, which were very costly ($1,661-$2,584 per dose). Eligible infants could receive up to five injections per season. Several studies proved its use was not cost beneficial.
What are the advantages of nirsevimab? It’s a long-acting monoclonal antibody. Only one dose is required per season. Costs will significantly diminish. It is recommended for all infants younger than 8 months of age born during RSV season. Those children 8-19 months at risk for severe RSV disease can receive it prior to the start of their second RSV season. During RSV season (October 1 to March 31), the initial dose should be administered to newborns just prior to hospital discharge. Older infants and newborns who did not receive it prior to hospital discharge can receive it at their medical home. Newborns should receive it within the first week of life. It is covered by the Vaccine for Children Program. Simultaneous administration with routine childhood immunizations is recommended. Finally, RSV season may vary in tropical areas (Southern Florida, Puerto Rico. etc.) and Alaska. The timing of nirsevimab administration should be based on local RSV activity provided by state and local authorities.
In addition, the FDA approved an RSV vaccine (Abrysvo) for use in adults at least 60 years of age and in pregnant women at 32-36 weeks’ gestation. The latter is administered to prevent lower respiratory tract infection in infants from birth to 6 months. Recommendations have been published for administration in nonpregnant adults. Specific information is forthcoming in terms timing of administration of nirsevimab in infants whose mothers receive Abrysvo.
RSV season is quickly approaching. Detailed recommendations for administration and FAQ questions related to nirsevimab and palivizumab can be found at https://www.aap.org or https://www.cdc.gov/vaccines/hcp/acip-recs/index.html.
Influenza
So, what about influenza? Vaccine composition has been tweaked to match the circulating viruses but the recommended age for annual routine administration remains unchanged. All persons at least 6 months of age should be vaccinated. Children between 6 months and 8 years need two doses at least 4 weeks apart when receiving vaccine for the first time. Immunizing everyone in the household is encouraged especially if there are household contacts at risk for developing severe disease, including infants too young to be vaccinated. Keep in mind children may be coinfected with multiple viruses. Adams and colleagues reviewed the prevalence of coinfection of influenza and Sars-CoV-2 in persons younger than 18 years reported to three CDC surveillance platforms during the 2021-2022 season.2 Thirty-two of 575 hospitalized (6%) coinfections were analyzed and 7 of 44 (16%) deaths. Compared with patients without coinfections, the coinfected patients were more likely to require mechanical ventilation (13% vs. 4%) or CPAP (16% vs. 6%). Only 4 of 23 who were influenza vaccine eligible were vaccinated. Of seven coinfected children who died, none had received influenza vaccine and only one received an antiviral. Only 5 of 31 (16%) infected only with influenza were vaccinated.3
Influenza activity was lower than usual during the 2021-2022 season. However, this report revealed underuse of both influenza vaccine and antiviral therapy, both of which are routinely recommended.
COVID-19
What’s new with COVID-19? On Sept. 12, 2023, ACIP recommended that everyone at least 6 months of age receive the 2023-2024 (monovalent, XBB containing) COVID-19 vaccines. Children at least 5 years of age need one dose and those younger need one or two doses depending on the number of doses previously received. Why the change? Circulating variants continue to change. There is a current uptick in cases including hospitalizations (7.7%) and deaths (4.5%) and it’s just the beginning of the season.4 Symptoms, risk groups and complications have not changed. The primary goal is to prevent infection, hospitalization, long term complications, and death.
We are now armed with the most up-to-date interventions to help prevent the acquisition of these three viruses. Our next step is recommending and delivering them to our patients.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She reported no relevant financial disclosures.
References
1.Suh M et al. J Infect Dis. 2022;226(Suppl 2):S154-36. doi: 10.1093/infdis/jiac120.
2. Adams K et al. MMWR Morb Mortal Wkly Rep. 2022;71:1589-96. doi: http://dx.doi.org/10.15585/mmwr.mm7150a4.
3. Pingali C et al. MMWR Morb Mortal Wkly Rep. 2023 Aug 25;72:912-9. doi: http://dx.doi.org/10.15585/mmwr.mm7234a3.
4. CDC Covid Data Tracker.
Study: Unexpected vaginal bleeding rises after COVID vaccination
The researchers suggested it could have been connected to the SARS-CoV-2 spike protein in the vaccines. The study was published in Science Advances.
After vaccinations became widely available, many women reported heavier menstrual bleeding than normal. Researchers at the Norwegian Institute of Public Health in Oslo examined the data, particularly among women who do not have periods, such as those who have been through menopause or are taking contraceptives.
The researchers used an ongoing population health survey called the Norwegian Mother, Father, and Child Cohort Study, Nature reported. They examined more than 21,000 responses from postmenopausal, perimenopausal, and nonmenstruating premenopausal women. Some were on long-term hormonal contraceptives.
They learned that 252 postmenopausal women, 1,008 perimenopausal women, and 924 premenopausal women reported having unexpected vaginal bleeding.
About half said the bleeding occurred within 4 weeks of the first or second shot or both. The risk of bleeding was up three to five times for premenopausal and perimenopausal women, and two to three times for postmenopausal women, the researchers found.
Postmenopausal bleeding is usually serious and can be a sign of cancer. “Knowing a patient’s vaccination status could put their bleeding incidence into context,” said Kate Clancy, a biological anthropologist at the University of Illinois at Urbana-Champaign.
The study received funding through the Norwegian Institute of Public Health and Research Council of Norway. The researchers reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
The researchers suggested it could have been connected to the SARS-CoV-2 spike protein in the vaccines. The study was published in Science Advances.
After vaccinations became widely available, many women reported heavier menstrual bleeding than normal. Researchers at the Norwegian Institute of Public Health in Oslo examined the data, particularly among women who do not have periods, such as those who have been through menopause or are taking contraceptives.
The researchers used an ongoing population health survey called the Norwegian Mother, Father, and Child Cohort Study, Nature reported. They examined more than 21,000 responses from postmenopausal, perimenopausal, and nonmenstruating premenopausal women. Some were on long-term hormonal contraceptives.
They learned that 252 postmenopausal women, 1,008 perimenopausal women, and 924 premenopausal women reported having unexpected vaginal bleeding.
About half said the bleeding occurred within 4 weeks of the first or second shot or both. The risk of bleeding was up three to five times for premenopausal and perimenopausal women, and two to three times for postmenopausal women, the researchers found.
Postmenopausal bleeding is usually serious and can be a sign of cancer. “Knowing a patient’s vaccination status could put their bleeding incidence into context,” said Kate Clancy, a biological anthropologist at the University of Illinois at Urbana-Champaign.
The study received funding through the Norwegian Institute of Public Health and Research Council of Norway. The researchers reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
The researchers suggested it could have been connected to the SARS-CoV-2 spike protein in the vaccines. The study was published in Science Advances.
After vaccinations became widely available, many women reported heavier menstrual bleeding than normal. Researchers at the Norwegian Institute of Public Health in Oslo examined the data, particularly among women who do not have periods, such as those who have been through menopause or are taking contraceptives.
The researchers used an ongoing population health survey called the Norwegian Mother, Father, and Child Cohort Study, Nature reported. They examined more than 21,000 responses from postmenopausal, perimenopausal, and nonmenstruating premenopausal women. Some were on long-term hormonal contraceptives.
They learned that 252 postmenopausal women, 1,008 perimenopausal women, and 924 premenopausal women reported having unexpected vaginal bleeding.
About half said the bleeding occurred within 4 weeks of the first or second shot or both. The risk of bleeding was up three to five times for premenopausal and perimenopausal women, and two to three times for postmenopausal women, the researchers found.
Postmenopausal bleeding is usually serious and can be a sign of cancer. “Knowing a patient’s vaccination status could put their bleeding incidence into context,” said Kate Clancy, a biological anthropologist at the University of Illinois at Urbana-Champaign.
The study received funding through the Norwegian Institute of Public Health and Research Council of Norway. The researchers reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
FROM SCIENCE ADVANCES
Effect of COVID-19 infection or vaccination on migraine frequency
Key clinical point: In patients with migraine, COVID-19 vaccination worsened the overall migraine symptoms in the first month post-vaccination; however, COVID-19 infection solely increased the number of acute medication intake days in the first month following infection.
Major finding: COVID-19 vaccination led to a significant increase in the number of monthly migraine days (MMD), monthly headache days (MHD), and monthly acute medication days (MAMD) by 1.06, 1.52, and 0.72, respectively (all P < .001) in the first month post-vaccination. COVID-19 infection solely increased MAMD by 1.11 (P = .027) in the first month following infection, with no significant effects on MMD and MHD.
Study details: This longitudinal cohort study identified 547 patients with migraine, of whom 147 were included in the vaccine analysis and 59 in the infection analysis.
Disclosures: This study did not receive any funding. BWH van der Arend and GM Terwindt declared receiving independent support and consultancy or industry support from various sources. The other authors declared no conflicts of interest.
Source: van der Arend BWH et al. Effect of COVID vaccination on monthly migraine days: A longitudinal cohort study. Cephalalgia. 2023;43(9) (Sep 8). doi: 10.1177/03331024231198792
Key clinical point: In patients with migraine, COVID-19 vaccination worsened the overall migraine symptoms in the first month post-vaccination; however, COVID-19 infection solely increased the number of acute medication intake days in the first month following infection.
Major finding: COVID-19 vaccination led to a significant increase in the number of monthly migraine days (MMD), monthly headache days (MHD), and monthly acute medication days (MAMD) by 1.06, 1.52, and 0.72, respectively (all P < .001) in the first month post-vaccination. COVID-19 infection solely increased MAMD by 1.11 (P = .027) in the first month following infection, with no significant effects on MMD and MHD.
Study details: This longitudinal cohort study identified 547 patients with migraine, of whom 147 were included in the vaccine analysis and 59 in the infection analysis.
Disclosures: This study did not receive any funding. BWH van der Arend and GM Terwindt declared receiving independent support and consultancy or industry support from various sources. The other authors declared no conflicts of interest.
Source: van der Arend BWH et al. Effect of COVID vaccination on monthly migraine days: A longitudinal cohort study. Cephalalgia. 2023;43(9) (Sep 8). doi: 10.1177/03331024231198792
Key clinical point: In patients with migraine, COVID-19 vaccination worsened the overall migraine symptoms in the first month post-vaccination; however, COVID-19 infection solely increased the number of acute medication intake days in the first month following infection.
Major finding: COVID-19 vaccination led to a significant increase in the number of monthly migraine days (MMD), monthly headache days (MHD), and monthly acute medication days (MAMD) by 1.06, 1.52, and 0.72, respectively (all P < .001) in the first month post-vaccination. COVID-19 infection solely increased MAMD by 1.11 (P = .027) in the first month following infection, with no significant effects on MMD and MHD.
Study details: This longitudinal cohort study identified 547 patients with migraine, of whom 147 were included in the vaccine analysis and 59 in the infection analysis.
Disclosures: This study did not receive any funding. BWH van der Arend and GM Terwindt declared receiving independent support and consultancy or industry support from various sources. The other authors declared no conflicts of interest.
Source: van der Arend BWH et al. Effect of COVID vaccination on monthly migraine days: A longitudinal cohort study. Cephalalgia. 2023;43(9) (Sep 8). doi: 10.1177/03331024231198792
CPT updates for 2024 include new RSV vaccines, Spanish translation
The American Medical Association recently released the Current Procedural Terminology (CPT) 2024 Code Set. The update included 349 editorial changes, including 230 additions, 49 deletions, and 70 revisions. With more than 11,100 codes in use, the CPT system continues “to grow and evolve with the rapid pace of innovation in medical science and health technology,” AMA said.
The AMA said the CPT update includes five new codes created to report product-specific RSV products (90380, 90381, 90683, 90679, and 90678) for better tracking, reporting and analysis that supports data-driven planning and allocation, AMA said.
There’s been a flurry of new U.S. vaccines and drugs to address RSV. The Food and Drug Administration in May granted the first U.S. approval of an RSV vaccine to Arexy, manufactured by GSK. The FDA cleared it for prevention of lower respiratory tract disease caused by RSV in adults age 60 years and older.
In June, Pfizer won FDA approval of Abrysvo, another vaccine meant to protect adults older than 60 years from RSV. The following month, the FDA approved nirsevimab (Beyfortus, AstraZeneca/Sanofi), for the prevention of RSV in neonates and infants entering their first RSV season, and in children up to 24 months of age who remain vulnerable to severe RSV disease through their second RSV season. (This is not a vaccine, but a monoclonal antibody used for prevention. There has been confusion on this issue in part because monoclonal antibodies are often used for treatment rather than prevention.)
The FDA also has approved Abrysvo for use in pregnant individuals.
In addition, new CPT codes aim to streamline COVID-19 immunizations reporting. A new code (90480) was approved for reporting the administration of any COVID-19 vaccine for any patient. New provisional codes (91318-91322) will identify monovalent vaccine products from Moderna and Pfizer for immunization against COVID-19.
These provisional codes will be effective for use when the monovalent vaccine products from Moderna and Pfizer receive FDA approval, AMA said.
More codes explained in Spanish
The 2024 update includes more code descriptions in Spanish. Many hospitals, health plans, and medical offices already incorporate CPT descriptors in English-language medical documents, insurance forms, price sheets, and patient portals. This expansion is intended to help patients who may not read English well or at all.
“Providing approximately 41 million Spanish-speaking individuals in the United States with an easy-to-understand description of medical procedures and services can help build a more inclusive health care environment, where language is no longer a barrier and patients can actively engage in their own care,” Lori Prestesater, AMA’s senior vice president of health solutions, said in a statement.
In addition, the 2024 update includes clarifications sought by the Centers for Medicare & Medicaid Services about the reporting of evaluation and management (E/M) services. The revisions include:
- Removal of time ranges from office or other outpatient visit codes (99202-99205, 99212-99215) and format alignment with other E/M codes.
- Definition of the “substantive portion” of a split/shared E/M visit in which a physician and a nonphysician practitioner work jointly to furnish all the work related to the visit.
- Instructions for reporting hospital inpatient or observation care services and admission and discharge services for the use of codes. 99234-99236 when the patient stay crosses over two calendar dates.
A version of this article appeared on Medscape.com.
The American Medical Association recently released the Current Procedural Terminology (CPT) 2024 Code Set. The update included 349 editorial changes, including 230 additions, 49 deletions, and 70 revisions. With more than 11,100 codes in use, the CPT system continues “to grow and evolve with the rapid pace of innovation in medical science and health technology,” AMA said.
The AMA said the CPT update includes five new codes created to report product-specific RSV products (90380, 90381, 90683, 90679, and 90678) for better tracking, reporting and analysis that supports data-driven planning and allocation, AMA said.
There’s been a flurry of new U.S. vaccines and drugs to address RSV. The Food and Drug Administration in May granted the first U.S. approval of an RSV vaccine to Arexy, manufactured by GSK. The FDA cleared it for prevention of lower respiratory tract disease caused by RSV in adults age 60 years and older.
In June, Pfizer won FDA approval of Abrysvo, another vaccine meant to protect adults older than 60 years from RSV. The following month, the FDA approved nirsevimab (Beyfortus, AstraZeneca/Sanofi), for the prevention of RSV in neonates and infants entering their first RSV season, and in children up to 24 months of age who remain vulnerable to severe RSV disease through their second RSV season. (This is not a vaccine, but a monoclonal antibody used for prevention. There has been confusion on this issue in part because monoclonal antibodies are often used for treatment rather than prevention.)
The FDA also has approved Abrysvo for use in pregnant individuals.
In addition, new CPT codes aim to streamline COVID-19 immunizations reporting. A new code (90480) was approved for reporting the administration of any COVID-19 vaccine for any patient. New provisional codes (91318-91322) will identify monovalent vaccine products from Moderna and Pfizer for immunization against COVID-19.
These provisional codes will be effective for use when the monovalent vaccine products from Moderna and Pfizer receive FDA approval, AMA said.
More codes explained in Spanish
The 2024 update includes more code descriptions in Spanish. Many hospitals, health plans, and medical offices already incorporate CPT descriptors in English-language medical documents, insurance forms, price sheets, and patient portals. This expansion is intended to help patients who may not read English well or at all.
“Providing approximately 41 million Spanish-speaking individuals in the United States with an easy-to-understand description of medical procedures and services can help build a more inclusive health care environment, where language is no longer a barrier and patients can actively engage in their own care,” Lori Prestesater, AMA’s senior vice president of health solutions, said in a statement.
In addition, the 2024 update includes clarifications sought by the Centers for Medicare & Medicaid Services about the reporting of evaluation and management (E/M) services. The revisions include:
- Removal of time ranges from office or other outpatient visit codes (99202-99205, 99212-99215) and format alignment with other E/M codes.
- Definition of the “substantive portion” of a split/shared E/M visit in which a physician and a nonphysician practitioner work jointly to furnish all the work related to the visit.
- Instructions for reporting hospital inpatient or observation care services and admission and discharge services for the use of codes. 99234-99236 when the patient stay crosses over two calendar dates.
A version of this article appeared on Medscape.com.
The American Medical Association recently released the Current Procedural Terminology (CPT) 2024 Code Set. The update included 349 editorial changes, including 230 additions, 49 deletions, and 70 revisions. With more than 11,100 codes in use, the CPT system continues “to grow and evolve with the rapid pace of innovation in medical science and health technology,” AMA said.
The AMA said the CPT update includes five new codes created to report product-specific RSV products (90380, 90381, 90683, 90679, and 90678) for better tracking, reporting and analysis that supports data-driven planning and allocation, AMA said.
There’s been a flurry of new U.S. vaccines and drugs to address RSV. The Food and Drug Administration in May granted the first U.S. approval of an RSV vaccine to Arexy, manufactured by GSK. The FDA cleared it for prevention of lower respiratory tract disease caused by RSV in adults age 60 years and older.
In June, Pfizer won FDA approval of Abrysvo, another vaccine meant to protect adults older than 60 years from RSV. The following month, the FDA approved nirsevimab (Beyfortus, AstraZeneca/Sanofi), for the prevention of RSV in neonates and infants entering their first RSV season, and in children up to 24 months of age who remain vulnerable to severe RSV disease through their second RSV season. (This is not a vaccine, but a monoclonal antibody used for prevention. There has been confusion on this issue in part because monoclonal antibodies are often used for treatment rather than prevention.)
The FDA also has approved Abrysvo for use in pregnant individuals.
In addition, new CPT codes aim to streamline COVID-19 immunizations reporting. A new code (90480) was approved for reporting the administration of any COVID-19 vaccine for any patient. New provisional codes (91318-91322) will identify monovalent vaccine products from Moderna and Pfizer for immunization against COVID-19.
These provisional codes will be effective for use when the monovalent vaccine products from Moderna and Pfizer receive FDA approval, AMA said.
More codes explained in Spanish
The 2024 update includes more code descriptions in Spanish. Many hospitals, health plans, and medical offices already incorporate CPT descriptors in English-language medical documents, insurance forms, price sheets, and patient portals. This expansion is intended to help patients who may not read English well or at all.
“Providing approximately 41 million Spanish-speaking individuals in the United States with an easy-to-understand description of medical procedures and services can help build a more inclusive health care environment, where language is no longer a barrier and patients can actively engage in their own care,” Lori Prestesater, AMA’s senior vice president of health solutions, said in a statement.
In addition, the 2024 update includes clarifications sought by the Centers for Medicare & Medicaid Services about the reporting of evaluation and management (E/M) services. The revisions include:
- Removal of time ranges from office or other outpatient visit codes (99202-99205, 99212-99215) and format alignment with other E/M codes.
- Definition of the “substantive portion” of a split/shared E/M visit in which a physician and a nonphysician practitioner work jointly to furnish all the work related to the visit.
- Instructions for reporting hospital inpatient or observation care services and admission and discharge services for the use of codes. 99234-99236 when the patient stay crosses over two calendar dates.
A version of this article appeared on Medscape.com.
PCPs prep for ‘less predictable’ respiratory virus season
Hospitalizations for COVID-19 in the United States have increased for 8 weeks in a row.
Data from Florida and Georgia signal that respiratory syncytial virus (RSV) season has begun.
As for flu shots, experts say patients with long COVID should get them in 2023, although federal health agencies have not addressed that specific question.
Paul G. Auwaerter, MD, MBA, an infectious disease consultant, said many patients in his primary care practice worry about “the big three” – COVID, influenza, and RSV.
They discussed how to handle COVID boosters, the use of Paxlovid, vaccine hesitancy, and the correct order of operations for patients getting vaccinated against all three diseases.
Paul G. Auwaerter, MD, MBA, clinical director of the division of infectious diseases and the Sherrilyn and Ken Fisher Professor of Medicine at Johns Hopkins University, BaltimoreQuestion: How should primary care physicians be preparing to handle what everyone is predicting will be a major surge in cases of respiratory infections?
Auwaerter: Although I’m an infectious disease consultant, I still have a small primary care practice. So, I field questions for my patients all the time, and many patients, especially those with health problems, are worried about the big three: RSV, COVID, and influenza – at least, my more motivated patients are.
People frequently ask if they need the COVID booster. I think that’s been something many people think maybe they can avoid. The good news is that the early in vitro data suggest that the XBB1.5x-based vaccine seems to offer sufficient neutralizing activity against the circulating newer variants since the vaccine was approved earlier this year. I am suggesting that everyone get a booster, especially those at high risk, because we know that the risk for hospitalization decreases based on earlier studies for 4-6 months after a COVID booster. We can simultaneously administer the revised COVID booster vaccine and the annual influenza vaccine. The timing is good, as influenza immunization should be accomplished by October or early November at the latest. Like many parts of the country, we in Maryland are in the middle of a COVID boomlet. I have issued more Paxlovid prescriptions since mid-August than I did all spring and early summer.
Q: Are you seeing a lot of rebound COVID in your patients taking Paxlovid [nirmatrelvir/ritonavir]?
Dr. Auwaerter: I think the frequency is probably around 10%. It has been quoted much higher – at 20% – but careful studies have put it down at just single digits. I think it just depends on symptomatology and how you ask the question. But I think it’s important that I try to persuade people to take a direct-acting antiviral if they’re in a high-risk category rather than tough it out. Increasing data suggest taking an antiviral also reduces the risk for long COVID. Also, we know that rebound symptoms are not always infectious virus. Sometimes, they’re just inflammatory. Unless a person is immune suppressed, they rarely have a culturable virus 7-8 days after onset of symptoms. So, for most people, I don’t administer second courses of Paxlovid, although I know some physicians do. One has to realize the risk for hospitalization from a rebound is tiny, and many people don’t even have infectious virus when they take the second course of a drug such as Paxlovid.
Q: You mentioned motivated patients, which seems to be an important factor to consider, particularly for new vaccines.
Dr. Auwaerter: There are always early adopters who are less afraid. And then some people say: This is a brand-new vaccine; I’m going to wait for a year to let this shake out, and make sure it seems safe. People more engaged in their health have asked me about the RSV vaccine. For anyone who has cardiopulmonary problems and other major health problems, I’ve advised it. But if someone’s in good health and 65 or 70, the RSV illness is probably pretty mild if they get it. For them, I would say the vaccine is optional.
For people over 75, I have been advising the RSV vaccine because that is a group we tend to see hospitalized with RSV; they’re the highest-risk group, similar to COVID. The older you are, the more likely this infection will land you in the hospital. You can acquire RSV even if you don’t have young grandchildren around.
Q: You have called respiratory virus seasons unstable? What does it mean, and what is the significance for clinicians?
Dr. Auwaerter: It’s less predictable than in the past. If you had a cough and fever, you could think it was influenza if you knew you had influenza circulating in your community. Maybe you thought about RSV for your immunocompromised or older patients, but we didn’t have any therapy for it anyway. I sometimes refer to the respiratory virus season as a cage match between the major infections. Last year, RSV came out first, and we got some influenza and COVID. What does the situation look like this year? I don’t know at this point, but we are seeing more COVID earlier. What’s different is we continue to have the emergence of viral variants of SARS-CoV-2. Also, with both influenza and COVID, it’s harder to make a clinical judgment about what people have.
I think we have to rely more on tests to treat these patients. Options include having point of care testing in the office for rapid results (molecular assays preferred) for both influenza and SARS-CoV-2 or home antigen testing. There are home kits that do test for both if influenza is known to be circulating significantly in the community. But there are still barriers. For one, COVID and COVID/influenza antigen kits are no longer free, although some health insurance companies do provide COVID kits free of charge. In offices, you don’t want to have ill people with respiratory infections in your waiting room unless you can isolate or have negative pressure rooms. Do you ask for masking in your offices? Telemedicine has been a big help since the pandemic in managing nonsevere respiratory infections at home; however, you must be licensed in the state to practice, which limits helping your out-of-state patients.
Q: How has the advent of in-home antigen tests changed practice?
Dr. Auwaerter: Home antigen tests have been groundbreaking in facilitating care. When I see patients via telemedicine, I don’t want to prescribe medications for influenza and COVID to people simultaneously. I want to pick one or the other – and now I’m able to ask for a COVID test or a COVID/influenza test if the patient or family is able to get a kit. Some offices do have real-time molecular testing, which is the ideal and the CDC-recommended approach, but they’re expensive, and not everyone has access to them.
Q: People talk about the “tripledemic,” but does doing so ignore the fourth horseman of the respiratory apocalypse: pneumococcal pneumonia?
Dr. Auwaerter: Pneumonia remains a leading cause of hospitalization, except we’ve seen much more viral than bacterial pneumonia in recent years of the pandemic. We’ve lost sight, and pneumococcal pneumonia is important, especially in older patients. What we have seen pretty clearly is a rise in group A streptococcal infections. This is another consequence of the pandemic, where people did not socialize for a year or 2. There was much less group A strep infection in younger children, and even in adults, the amount of invasive group A streptococcal infections has clearly taken a jump, according to the NHS in Great Britain. Our pediatric practices here at Johns Hopkins are seeing far more cases of acute rheumatic fever than they’ve seen in decades. And I think, again, this is a consequence of the frequency of group A strep infections definitely taking an uptick. And that was no doubt probably from social mitigation measures and just an interruption in normal circumstances that bacterial and respiratory pathogens tend to circulate and colonize.
Q: Do you have any concerns about immunogenicity or side effects associated with receiving several vaccines at once?
Dr. Auwaerter: I think three injections at once is only for the heroic, and there is actually no guidance for getting all three at the moment. COVID, RSV, and influenza are not live vaccines. I’ve been recommending the new COVID booster and flu together, and then wait 2 weeks and then get RSV or vice-versa. A part of the reason is RSV is new. People have gotten COVID and flu vaccines before; they’re no different than in the past in terms of anticipating adverse effects. But RSV is new, so I’ve usually been recommending that as a standalone to gauge if there are issues as an RSV booster may be recommended at some point down the road.
Q: Unfortunately, some people are going to see or hear misinformation that the COVID boosters have not been properly tested or proven safe. What’s your response to the patient who says something to that effect?
Dr. Auwaerter: My response is, the basic components of the vaccine are the same, right? If you have the mRNA vaccine, you’re getting the vaccine components, the lipids, and the mRNA coding for spike proteins, which has just been modified slightly to adjust to the Omicron subvariant composition. We do the same thing with the influenza vaccine every year, and we don’t see much change in the side effect profile. I think it’s important for my staff in the office and myself to be very comfortable to field questions such as these.
We try to inform all of our staff about a vaccine, especially a new one like RSV, just so they have some comfort level with it, whether they’re getting it or not. Vaccine-hesitant patients need very little to dissuade and to take a pass – to the probable detriment of their health and their family’s health. We know the influenza vaccine helps reduce absenteeism and transmission in addition to reducing serious illness in high-risk patients. Even COVID vaccine efficacy is not as robust as initially reported, falling from 95% to under 70% depending on the study – you are provided with protection against serious illness and hospitalization. The same goes for influenza, and that’s how we try to pitch it to people. Are they going to get the flu? Maybe, but you didn’t land in the hospital. That’s why it’s these vaccines are so important.
Spencer H. Durham, PharmD, associate clinical professor in the department of pharmacy practice at Auburn (Ala.) University, and clinical pharmacist, Internal Medicine & Infectious Diseases, at the UAB Heersink School of Medicine in Huntsville.Q: What is known, if anything, about the risks/desirability of giving three vaccinations at once to patients (particularly older patients) – flu, COVID-19 and RSV? Any potential vaccine interactions physicians should know about?
Dr. Durham: There are currently no data about giving all three of these vaccines together at the same time. However, there is both data and practical experience of giving both the flu and COVID vaccines at the same time. The best approach right now for these three vaccines would be to get the flu and COVID vaccines at the same time, then give the RSV vaccine at a different date. In general, they should be separated by about 2 weeks, although it does not matter in what order they are given (that is, patients could get RSV first, then flu/COVID, or they could get flu/COVID first, followed by RSV).
Having said this, there is no theoretical reason why patients couldn’t get all three at once, so if there is only one opportunity to vaccinate a patient, then it would be okay to give all three. But, if the patient can come for two separate visits, the recommendation would currently be to separate these. In the future, there likely will be data on giving all three vaccines at once, so it may not be an issue to administer all three at the same time.
Lastly, I would point out that the RSV vaccine is not necessarily recommended for everyone age 60 and above. The Advisory Committee on Immunization Practices recommends using shared clinical decision-making to determine if that vaccine is right for the patient. In general, the flu and COVID vaccines are recommended for everyone, although the specific COVID recommendations for fall 2023 have not yet been released. There are no particular vaccine interactions that are concerning with these vaccines.
Q: What if any special considerations are there regarding the storage, handling, and ordering of these vaccines? Should primary care practices take any special steps they might not already be taking?
Dr. Durham: I don’t think there are any special considerations that providers might not already be doing. All of the vaccines do require refrigeration, but each individual product may vary some on beyond-use dates or how long they are good after being reconstituted. All providers administering these vaccines should carefully examine the labeling of each individual product to ensure correct storage and handling. In addition, the Centers for Disease Control and Prevention has an online toolkit for vaccine storage and handling and can be found at https://www.cdc.gov/vaccines/hcp/admin/storage/toolkit/index.html.
Santina J. G. Wheat, MD, MPH, vice chair of diversity, equity, and inclusion, department of family and community medicine, and associate professor of family and community medicine, Northwestern University, ChicagoQ: What can primary care doctors/family physicians and their staff do to increase patient access to the vaccines? Any lessons learned from the earlier phases of the pandemic that might pertain not only to COVID-19 but also to RSV and/or influenza?
Dr. Wheat: I think the most important thing family physicians can do is speak with their patients about the importance of vaccines and specific recommendations they have for the situations of individuals and families. When vaccines started becoming available, I had many patients who wanted to hear from me – as their primary physician – what I truly thought and what I was planning to do for my own family.
I also think if our teams can know where vaccines are easily accessible, that makes it much easier for our patients. I have heard great stories and seen my own clinical support staff look at websites with patients to help them find the best location to get vaccines. In particular, about the RSV vaccine, I have had a handful of patients already come to ask me about my recommendations. When vaccines are available at my location, I find it much easier for my patients to be willing to get vaccinated. Similarly, if I am sending patients to pick up a prescription and they can get it at the same time, I have found success in them being willing to be vaccinated while picking up their prescription. In both instances, they do not need to make an additional stop; they are just able to be vaccinated while already at the clinic or pharmacy.
Q: Do you see any extra difficulties involved in trying to get groups of patients – in this case, older people – to be receptive to three vaccines, especially in this climate where it appears a growing number of people are hostile to immunization?
Dr. Wheat: Recently, I have found myself negotiating vaccines with patients not just with these, but as recommendations have changed for vaccines such as the pneumococcal vaccines and the hepatitis B vaccines. I think primary care providers can recommend all of them, but still help patients prioritize what is most important for that patient and family. For example, if welcoming a new baby soon, they might prioritize the vaccines for pertussis or influenza over the hepatitis vaccine with a plan to revisit the conversations later.
I have had some patients tell me they have gotten enough vaccines – and we know that even before the pandemic there was resistance to the influenza vaccine for some. I think we need to be prepared to address the concerns and, at times, the apathy. We also need to ask every time, because we never know which visit will be the one when a patient agrees.
Dr. Auwaerter reported financial relationships with Pfizer, Shionogi, Gilead, and Wellstat. Dr. Durham and Dr. Wheat disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Hospitalizations for COVID-19 in the United States have increased for 8 weeks in a row.
Data from Florida and Georgia signal that respiratory syncytial virus (RSV) season has begun.
As for flu shots, experts say patients with long COVID should get them in 2023, although federal health agencies have not addressed that specific question.
Paul G. Auwaerter, MD, MBA, an infectious disease consultant, said many patients in his primary care practice worry about “the big three” – COVID, influenza, and RSV.
They discussed how to handle COVID boosters, the use of Paxlovid, vaccine hesitancy, and the correct order of operations for patients getting vaccinated against all three diseases.
Paul G. Auwaerter, MD, MBA, clinical director of the division of infectious diseases and the Sherrilyn and Ken Fisher Professor of Medicine at Johns Hopkins University, BaltimoreQuestion: How should primary care physicians be preparing to handle what everyone is predicting will be a major surge in cases of respiratory infections?
Auwaerter: Although I’m an infectious disease consultant, I still have a small primary care practice. So, I field questions for my patients all the time, and many patients, especially those with health problems, are worried about the big three: RSV, COVID, and influenza – at least, my more motivated patients are.
People frequently ask if they need the COVID booster. I think that’s been something many people think maybe they can avoid. The good news is that the early in vitro data suggest that the XBB1.5x-based vaccine seems to offer sufficient neutralizing activity against the circulating newer variants since the vaccine was approved earlier this year. I am suggesting that everyone get a booster, especially those at high risk, because we know that the risk for hospitalization decreases based on earlier studies for 4-6 months after a COVID booster. We can simultaneously administer the revised COVID booster vaccine and the annual influenza vaccine. The timing is good, as influenza immunization should be accomplished by October or early November at the latest. Like many parts of the country, we in Maryland are in the middle of a COVID boomlet. I have issued more Paxlovid prescriptions since mid-August than I did all spring and early summer.
Q: Are you seeing a lot of rebound COVID in your patients taking Paxlovid [nirmatrelvir/ritonavir]?
Dr. Auwaerter: I think the frequency is probably around 10%. It has been quoted much higher – at 20% – but careful studies have put it down at just single digits. I think it just depends on symptomatology and how you ask the question. But I think it’s important that I try to persuade people to take a direct-acting antiviral if they’re in a high-risk category rather than tough it out. Increasing data suggest taking an antiviral also reduces the risk for long COVID. Also, we know that rebound symptoms are not always infectious virus. Sometimes, they’re just inflammatory. Unless a person is immune suppressed, they rarely have a culturable virus 7-8 days after onset of symptoms. So, for most people, I don’t administer second courses of Paxlovid, although I know some physicians do. One has to realize the risk for hospitalization from a rebound is tiny, and many people don’t even have infectious virus when they take the second course of a drug such as Paxlovid.
Q: You mentioned motivated patients, which seems to be an important factor to consider, particularly for new vaccines.
Dr. Auwaerter: There are always early adopters who are less afraid. And then some people say: This is a brand-new vaccine; I’m going to wait for a year to let this shake out, and make sure it seems safe. People more engaged in their health have asked me about the RSV vaccine. For anyone who has cardiopulmonary problems and other major health problems, I’ve advised it. But if someone’s in good health and 65 or 70, the RSV illness is probably pretty mild if they get it. For them, I would say the vaccine is optional.
For people over 75, I have been advising the RSV vaccine because that is a group we tend to see hospitalized with RSV; they’re the highest-risk group, similar to COVID. The older you are, the more likely this infection will land you in the hospital. You can acquire RSV even if you don’t have young grandchildren around.
Q: You have called respiratory virus seasons unstable? What does it mean, and what is the significance for clinicians?
Dr. Auwaerter: It’s less predictable than in the past. If you had a cough and fever, you could think it was influenza if you knew you had influenza circulating in your community. Maybe you thought about RSV for your immunocompromised or older patients, but we didn’t have any therapy for it anyway. I sometimes refer to the respiratory virus season as a cage match between the major infections. Last year, RSV came out first, and we got some influenza and COVID. What does the situation look like this year? I don’t know at this point, but we are seeing more COVID earlier. What’s different is we continue to have the emergence of viral variants of SARS-CoV-2. Also, with both influenza and COVID, it’s harder to make a clinical judgment about what people have.
I think we have to rely more on tests to treat these patients. Options include having point of care testing in the office for rapid results (molecular assays preferred) for both influenza and SARS-CoV-2 or home antigen testing. There are home kits that do test for both if influenza is known to be circulating significantly in the community. But there are still barriers. For one, COVID and COVID/influenza antigen kits are no longer free, although some health insurance companies do provide COVID kits free of charge. In offices, you don’t want to have ill people with respiratory infections in your waiting room unless you can isolate or have negative pressure rooms. Do you ask for masking in your offices? Telemedicine has been a big help since the pandemic in managing nonsevere respiratory infections at home; however, you must be licensed in the state to practice, which limits helping your out-of-state patients.
Q: How has the advent of in-home antigen tests changed practice?
Dr. Auwaerter: Home antigen tests have been groundbreaking in facilitating care. When I see patients via telemedicine, I don’t want to prescribe medications for influenza and COVID to people simultaneously. I want to pick one or the other – and now I’m able to ask for a COVID test or a COVID/influenza test if the patient or family is able to get a kit. Some offices do have real-time molecular testing, which is the ideal and the CDC-recommended approach, but they’re expensive, and not everyone has access to them.
Q: People talk about the “tripledemic,” but does doing so ignore the fourth horseman of the respiratory apocalypse: pneumococcal pneumonia?
Dr. Auwaerter: Pneumonia remains a leading cause of hospitalization, except we’ve seen much more viral than bacterial pneumonia in recent years of the pandemic. We’ve lost sight, and pneumococcal pneumonia is important, especially in older patients. What we have seen pretty clearly is a rise in group A streptococcal infections. This is another consequence of the pandemic, where people did not socialize for a year or 2. There was much less group A strep infection in younger children, and even in adults, the amount of invasive group A streptococcal infections has clearly taken a jump, according to the NHS in Great Britain. Our pediatric practices here at Johns Hopkins are seeing far more cases of acute rheumatic fever than they’ve seen in decades. And I think, again, this is a consequence of the frequency of group A strep infections definitely taking an uptick. And that was no doubt probably from social mitigation measures and just an interruption in normal circumstances that bacterial and respiratory pathogens tend to circulate and colonize.
Q: Do you have any concerns about immunogenicity or side effects associated with receiving several vaccines at once?
Dr. Auwaerter: I think three injections at once is only for the heroic, and there is actually no guidance for getting all three at the moment. COVID, RSV, and influenza are not live vaccines. I’ve been recommending the new COVID booster and flu together, and then wait 2 weeks and then get RSV or vice-versa. A part of the reason is RSV is new. People have gotten COVID and flu vaccines before; they’re no different than in the past in terms of anticipating adverse effects. But RSV is new, so I’ve usually been recommending that as a standalone to gauge if there are issues as an RSV booster may be recommended at some point down the road.
Q: Unfortunately, some people are going to see or hear misinformation that the COVID boosters have not been properly tested or proven safe. What’s your response to the patient who says something to that effect?
Dr. Auwaerter: My response is, the basic components of the vaccine are the same, right? If you have the mRNA vaccine, you’re getting the vaccine components, the lipids, and the mRNA coding for spike proteins, which has just been modified slightly to adjust to the Omicron subvariant composition. We do the same thing with the influenza vaccine every year, and we don’t see much change in the side effect profile. I think it’s important for my staff in the office and myself to be very comfortable to field questions such as these.
We try to inform all of our staff about a vaccine, especially a new one like RSV, just so they have some comfort level with it, whether they’re getting it or not. Vaccine-hesitant patients need very little to dissuade and to take a pass – to the probable detriment of their health and their family’s health. We know the influenza vaccine helps reduce absenteeism and transmission in addition to reducing serious illness in high-risk patients. Even COVID vaccine efficacy is not as robust as initially reported, falling from 95% to under 70% depending on the study – you are provided with protection against serious illness and hospitalization. The same goes for influenza, and that’s how we try to pitch it to people. Are they going to get the flu? Maybe, but you didn’t land in the hospital. That’s why it’s these vaccines are so important.
Spencer H. Durham, PharmD, associate clinical professor in the department of pharmacy practice at Auburn (Ala.) University, and clinical pharmacist, Internal Medicine & Infectious Diseases, at the UAB Heersink School of Medicine in Huntsville.Q: What is known, if anything, about the risks/desirability of giving three vaccinations at once to patients (particularly older patients) – flu, COVID-19 and RSV? Any potential vaccine interactions physicians should know about?
Dr. Durham: There are currently no data about giving all three of these vaccines together at the same time. However, there is both data and practical experience of giving both the flu and COVID vaccines at the same time. The best approach right now for these three vaccines would be to get the flu and COVID vaccines at the same time, then give the RSV vaccine at a different date. In general, they should be separated by about 2 weeks, although it does not matter in what order they are given (that is, patients could get RSV first, then flu/COVID, or they could get flu/COVID first, followed by RSV).
Having said this, there is no theoretical reason why patients couldn’t get all three at once, so if there is only one opportunity to vaccinate a patient, then it would be okay to give all three. But, if the patient can come for two separate visits, the recommendation would currently be to separate these. In the future, there likely will be data on giving all three vaccines at once, so it may not be an issue to administer all three at the same time.
Lastly, I would point out that the RSV vaccine is not necessarily recommended for everyone age 60 and above. The Advisory Committee on Immunization Practices recommends using shared clinical decision-making to determine if that vaccine is right for the patient. In general, the flu and COVID vaccines are recommended for everyone, although the specific COVID recommendations for fall 2023 have not yet been released. There are no particular vaccine interactions that are concerning with these vaccines.
Q: What if any special considerations are there regarding the storage, handling, and ordering of these vaccines? Should primary care practices take any special steps they might not already be taking?
Dr. Durham: I don’t think there are any special considerations that providers might not already be doing. All of the vaccines do require refrigeration, but each individual product may vary some on beyond-use dates or how long they are good after being reconstituted. All providers administering these vaccines should carefully examine the labeling of each individual product to ensure correct storage and handling. In addition, the Centers for Disease Control and Prevention has an online toolkit for vaccine storage and handling and can be found at https://www.cdc.gov/vaccines/hcp/admin/storage/toolkit/index.html.
Santina J. G. Wheat, MD, MPH, vice chair of diversity, equity, and inclusion, department of family and community medicine, and associate professor of family and community medicine, Northwestern University, ChicagoQ: What can primary care doctors/family physicians and their staff do to increase patient access to the vaccines? Any lessons learned from the earlier phases of the pandemic that might pertain not only to COVID-19 but also to RSV and/or influenza?
Dr. Wheat: I think the most important thing family physicians can do is speak with their patients about the importance of vaccines and specific recommendations they have for the situations of individuals and families. When vaccines started becoming available, I had many patients who wanted to hear from me – as their primary physician – what I truly thought and what I was planning to do for my own family.
I also think if our teams can know where vaccines are easily accessible, that makes it much easier for our patients. I have heard great stories and seen my own clinical support staff look at websites with patients to help them find the best location to get vaccines. In particular, about the RSV vaccine, I have had a handful of patients already come to ask me about my recommendations. When vaccines are available at my location, I find it much easier for my patients to be willing to get vaccinated. Similarly, if I am sending patients to pick up a prescription and they can get it at the same time, I have found success in them being willing to be vaccinated while picking up their prescription. In both instances, they do not need to make an additional stop; they are just able to be vaccinated while already at the clinic or pharmacy.
Q: Do you see any extra difficulties involved in trying to get groups of patients – in this case, older people – to be receptive to three vaccines, especially in this climate where it appears a growing number of people are hostile to immunization?
Dr. Wheat: Recently, I have found myself negotiating vaccines with patients not just with these, but as recommendations have changed for vaccines such as the pneumococcal vaccines and the hepatitis B vaccines. I think primary care providers can recommend all of them, but still help patients prioritize what is most important for that patient and family. For example, if welcoming a new baby soon, they might prioritize the vaccines for pertussis or influenza over the hepatitis vaccine with a plan to revisit the conversations later.
I have had some patients tell me they have gotten enough vaccines – and we know that even before the pandemic there was resistance to the influenza vaccine for some. I think we need to be prepared to address the concerns and, at times, the apathy. We also need to ask every time, because we never know which visit will be the one when a patient agrees.
Dr. Auwaerter reported financial relationships with Pfizer, Shionogi, Gilead, and Wellstat. Dr. Durham and Dr. Wheat disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Hospitalizations for COVID-19 in the United States have increased for 8 weeks in a row.
Data from Florida and Georgia signal that respiratory syncytial virus (RSV) season has begun.
As for flu shots, experts say patients with long COVID should get them in 2023, although federal health agencies have not addressed that specific question.
Paul G. Auwaerter, MD, MBA, an infectious disease consultant, said many patients in his primary care practice worry about “the big three” – COVID, influenza, and RSV.
They discussed how to handle COVID boosters, the use of Paxlovid, vaccine hesitancy, and the correct order of operations for patients getting vaccinated against all three diseases.
Paul G. Auwaerter, MD, MBA, clinical director of the division of infectious diseases and the Sherrilyn and Ken Fisher Professor of Medicine at Johns Hopkins University, BaltimoreQuestion: How should primary care physicians be preparing to handle what everyone is predicting will be a major surge in cases of respiratory infections?
Auwaerter: Although I’m an infectious disease consultant, I still have a small primary care practice. So, I field questions for my patients all the time, and many patients, especially those with health problems, are worried about the big three: RSV, COVID, and influenza – at least, my more motivated patients are.
People frequently ask if they need the COVID booster. I think that’s been something many people think maybe they can avoid. The good news is that the early in vitro data suggest that the XBB1.5x-based vaccine seems to offer sufficient neutralizing activity against the circulating newer variants since the vaccine was approved earlier this year. I am suggesting that everyone get a booster, especially those at high risk, because we know that the risk for hospitalization decreases based on earlier studies for 4-6 months after a COVID booster. We can simultaneously administer the revised COVID booster vaccine and the annual influenza vaccine. The timing is good, as influenza immunization should be accomplished by October or early November at the latest. Like many parts of the country, we in Maryland are in the middle of a COVID boomlet. I have issued more Paxlovid prescriptions since mid-August than I did all spring and early summer.
Q: Are you seeing a lot of rebound COVID in your patients taking Paxlovid [nirmatrelvir/ritonavir]?
Dr. Auwaerter: I think the frequency is probably around 10%. It has been quoted much higher – at 20% – but careful studies have put it down at just single digits. I think it just depends on symptomatology and how you ask the question. But I think it’s important that I try to persuade people to take a direct-acting antiviral if they’re in a high-risk category rather than tough it out. Increasing data suggest taking an antiviral also reduces the risk for long COVID. Also, we know that rebound symptoms are not always infectious virus. Sometimes, they’re just inflammatory. Unless a person is immune suppressed, they rarely have a culturable virus 7-8 days after onset of symptoms. So, for most people, I don’t administer second courses of Paxlovid, although I know some physicians do. One has to realize the risk for hospitalization from a rebound is tiny, and many people don’t even have infectious virus when they take the second course of a drug such as Paxlovid.
Q: You mentioned motivated patients, which seems to be an important factor to consider, particularly for new vaccines.
Dr. Auwaerter: There are always early adopters who are less afraid. And then some people say: This is a brand-new vaccine; I’m going to wait for a year to let this shake out, and make sure it seems safe. People more engaged in their health have asked me about the RSV vaccine. For anyone who has cardiopulmonary problems and other major health problems, I’ve advised it. But if someone’s in good health and 65 or 70, the RSV illness is probably pretty mild if they get it. For them, I would say the vaccine is optional.
For people over 75, I have been advising the RSV vaccine because that is a group we tend to see hospitalized with RSV; they’re the highest-risk group, similar to COVID. The older you are, the more likely this infection will land you in the hospital. You can acquire RSV even if you don’t have young grandchildren around.
Q: You have called respiratory virus seasons unstable? What does it mean, and what is the significance for clinicians?
Dr. Auwaerter: It’s less predictable than in the past. If you had a cough and fever, you could think it was influenza if you knew you had influenza circulating in your community. Maybe you thought about RSV for your immunocompromised or older patients, but we didn’t have any therapy for it anyway. I sometimes refer to the respiratory virus season as a cage match between the major infections. Last year, RSV came out first, and we got some influenza and COVID. What does the situation look like this year? I don’t know at this point, but we are seeing more COVID earlier. What’s different is we continue to have the emergence of viral variants of SARS-CoV-2. Also, with both influenza and COVID, it’s harder to make a clinical judgment about what people have.
I think we have to rely more on tests to treat these patients. Options include having point of care testing in the office for rapid results (molecular assays preferred) for both influenza and SARS-CoV-2 or home antigen testing. There are home kits that do test for both if influenza is known to be circulating significantly in the community. But there are still barriers. For one, COVID and COVID/influenza antigen kits are no longer free, although some health insurance companies do provide COVID kits free of charge. In offices, you don’t want to have ill people with respiratory infections in your waiting room unless you can isolate or have negative pressure rooms. Do you ask for masking in your offices? Telemedicine has been a big help since the pandemic in managing nonsevere respiratory infections at home; however, you must be licensed in the state to practice, which limits helping your out-of-state patients.
Q: How has the advent of in-home antigen tests changed practice?
Dr. Auwaerter: Home antigen tests have been groundbreaking in facilitating care. When I see patients via telemedicine, I don’t want to prescribe medications for influenza and COVID to people simultaneously. I want to pick one or the other – and now I’m able to ask for a COVID test or a COVID/influenza test if the patient or family is able to get a kit. Some offices do have real-time molecular testing, which is the ideal and the CDC-recommended approach, but they’re expensive, and not everyone has access to them.
Q: People talk about the “tripledemic,” but does doing so ignore the fourth horseman of the respiratory apocalypse: pneumococcal pneumonia?
Dr. Auwaerter: Pneumonia remains a leading cause of hospitalization, except we’ve seen much more viral than bacterial pneumonia in recent years of the pandemic. We’ve lost sight, and pneumococcal pneumonia is important, especially in older patients. What we have seen pretty clearly is a rise in group A streptococcal infections. This is another consequence of the pandemic, where people did not socialize for a year or 2. There was much less group A strep infection in younger children, and even in adults, the amount of invasive group A streptococcal infections has clearly taken a jump, according to the NHS in Great Britain. Our pediatric practices here at Johns Hopkins are seeing far more cases of acute rheumatic fever than they’ve seen in decades. And I think, again, this is a consequence of the frequency of group A strep infections definitely taking an uptick. And that was no doubt probably from social mitigation measures and just an interruption in normal circumstances that bacterial and respiratory pathogens tend to circulate and colonize.
Q: Do you have any concerns about immunogenicity or side effects associated with receiving several vaccines at once?
Dr. Auwaerter: I think three injections at once is only for the heroic, and there is actually no guidance for getting all three at the moment. COVID, RSV, and influenza are not live vaccines. I’ve been recommending the new COVID booster and flu together, and then wait 2 weeks and then get RSV or vice-versa. A part of the reason is RSV is new. People have gotten COVID and flu vaccines before; they’re no different than in the past in terms of anticipating adverse effects. But RSV is new, so I’ve usually been recommending that as a standalone to gauge if there are issues as an RSV booster may be recommended at some point down the road.
Q: Unfortunately, some people are going to see or hear misinformation that the COVID boosters have not been properly tested or proven safe. What’s your response to the patient who says something to that effect?
Dr. Auwaerter: My response is, the basic components of the vaccine are the same, right? If you have the mRNA vaccine, you’re getting the vaccine components, the lipids, and the mRNA coding for spike proteins, which has just been modified slightly to adjust to the Omicron subvariant composition. We do the same thing with the influenza vaccine every year, and we don’t see much change in the side effect profile. I think it’s important for my staff in the office and myself to be very comfortable to field questions such as these.
We try to inform all of our staff about a vaccine, especially a new one like RSV, just so they have some comfort level with it, whether they’re getting it or not. Vaccine-hesitant patients need very little to dissuade and to take a pass – to the probable detriment of their health and their family’s health. We know the influenza vaccine helps reduce absenteeism and transmission in addition to reducing serious illness in high-risk patients. Even COVID vaccine efficacy is not as robust as initially reported, falling from 95% to under 70% depending on the study – you are provided with protection against serious illness and hospitalization. The same goes for influenza, and that’s how we try to pitch it to people. Are they going to get the flu? Maybe, but you didn’t land in the hospital. That’s why it’s these vaccines are so important.
Spencer H. Durham, PharmD, associate clinical professor in the department of pharmacy practice at Auburn (Ala.) University, and clinical pharmacist, Internal Medicine & Infectious Diseases, at the UAB Heersink School of Medicine in Huntsville.Q: What is known, if anything, about the risks/desirability of giving three vaccinations at once to patients (particularly older patients) – flu, COVID-19 and RSV? Any potential vaccine interactions physicians should know about?
Dr. Durham: There are currently no data about giving all three of these vaccines together at the same time. However, there is both data and practical experience of giving both the flu and COVID vaccines at the same time. The best approach right now for these three vaccines would be to get the flu and COVID vaccines at the same time, then give the RSV vaccine at a different date. In general, they should be separated by about 2 weeks, although it does not matter in what order they are given (that is, patients could get RSV first, then flu/COVID, or they could get flu/COVID first, followed by RSV).
Having said this, there is no theoretical reason why patients couldn’t get all three at once, so if there is only one opportunity to vaccinate a patient, then it would be okay to give all three. But, if the patient can come for two separate visits, the recommendation would currently be to separate these. In the future, there likely will be data on giving all three vaccines at once, so it may not be an issue to administer all three at the same time.
Lastly, I would point out that the RSV vaccine is not necessarily recommended for everyone age 60 and above. The Advisory Committee on Immunization Practices recommends using shared clinical decision-making to determine if that vaccine is right for the patient. In general, the flu and COVID vaccines are recommended for everyone, although the specific COVID recommendations for fall 2023 have not yet been released. There are no particular vaccine interactions that are concerning with these vaccines.
Q: What if any special considerations are there regarding the storage, handling, and ordering of these vaccines? Should primary care practices take any special steps they might not already be taking?
Dr. Durham: I don’t think there are any special considerations that providers might not already be doing. All of the vaccines do require refrigeration, but each individual product may vary some on beyond-use dates or how long they are good after being reconstituted. All providers administering these vaccines should carefully examine the labeling of each individual product to ensure correct storage and handling. In addition, the Centers for Disease Control and Prevention has an online toolkit for vaccine storage and handling and can be found at https://www.cdc.gov/vaccines/hcp/admin/storage/toolkit/index.html.
Santina J. G. Wheat, MD, MPH, vice chair of diversity, equity, and inclusion, department of family and community medicine, and associate professor of family and community medicine, Northwestern University, ChicagoQ: What can primary care doctors/family physicians and their staff do to increase patient access to the vaccines? Any lessons learned from the earlier phases of the pandemic that might pertain not only to COVID-19 but also to RSV and/or influenza?
Dr. Wheat: I think the most important thing family physicians can do is speak with their patients about the importance of vaccines and specific recommendations they have for the situations of individuals and families. When vaccines started becoming available, I had many patients who wanted to hear from me – as their primary physician – what I truly thought and what I was planning to do for my own family.
I also think if our teams can know where vaccines are easily accessible, that makes it much easier for our patients. I have heard great stories and seen my own clinical support staff look at websites with patients to help them find the best location to get vaccines. In particular, about the RSV vaccine, I have had a handful of patients already come to ask me about my recommendations. When vaccines are available at my location, I find it much easier for my patients to be willing to get vaccinated. Similarly, if I am sending patients to pick up a prescription and they can get it at the same time, I have found success in them being willing to be vaccinated while picking up their prescription. In both instances, they do not need to make an additional stop; they are just able to be vaccinated while already at the clinic or pharmacy.
Q: Do you see any extra difficulties involved in trying to get groups of patients – in this case, older people – to be receptive to three vaccines, especially in this climate where it appears a growing number of people are hostile to immunization?
Dr. Wheat: Recently, I have found myself negotiating vaccines with patients not just with these, but as recommendations have changed for vaccines such as the pneumococcal vaccines and the hepatitis B vaccines. I think primary care providers can recommend all of them, but still help patients prioritize what is most important for that patient and family. For example, if welcoming a new baby soon, they might prioritize the vaccines for pertussis or influenza over the hepatitis vaccine with a plan to revisit the conversations later.
I have had some patients tell me they have gotten enough vaccines – and we know that even before the pandemic there was resistance to the influenza vaccine for some. I think we need to be prepared to address the concerns and, at times, the apathy. We also need to ask every time, because we never know which visit will be the one when a patient agrees.
Dr. Auwaerter reported financial relationships with Pfizer, Shionogi, Gilead, and Wellstat. Dr. Durham and Dr. Wheat disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Olfactory Hallucinations Following COVID-19 Vaccination
The rapid development of multiple vaccines for COVID-19 significantly contributed to reducing the morbidity and mortality associated with COVID-19 infection.1 The vaccination campaign against COVID-19 started in December 2020 within the US Department of Veterans Affairs (VA) health care system with the Pfizer-BioNTech and Moderna COVID-19 mRNA vaccines followed by the Johnson & Johnson (J&J) vaccine in March 2021.2,3
Because of the importance of maintaining a safe vaccination campaign, surveillance reports documenting cases of malignant or benign adverse effects (AEs) are fundamental to generate awareness and accurate knowledge on these newly developed vaccines. Here we report the case of a veteran who developed olfactory hallucinations following the administration of the J&J COVID-19 vaccine.
Case Presentation
A 39-year-old veteran with a history of tension-type headaches presented to the neurology clinic with concern of a burning smell sensation in the absence of an identifiable source. He first noticed this symptom approximately 3 weeks after he received the J&J COVID-19 vaccine about 4 months prior. At the symptom’s first occurrence, he underwent a nasal swab antigen COVID-19 test, which was negative. Initially, symptoms would occur daily lasting about 1 hour. Thereafter, they started to decrease in duration, frequency, and intensity, and about 11 months postvaccination, milder episodes were occurring 1 to 2 times weekly. These episodes lasted nearly 2 years (21 months postvaccination). They happened randomly during the day and were not associated with any other symptoms. Specifically, there were no headaches, loss of consciousness, abnormal movements, nausea, vomiting, photophobia or phonophobia, or alteration of consciousness, such as confusion or drowsiness during or after the events. Additionally, there were no clear triggers the veteran could identify. The veteran did not sustain any head injuries or exposure to toxic odors before the onset of symptoms.
At the time of his presentation to the clinic, both his general and neurological examinations were unremarkable.

Discussion
It has been previously observed that infection with COVID-19 can lead to the loss of taste and smell, but only less commonly olfactory hallucination.4 The pathophysiology of olfactory hallucinations following COVID-19 infection is unknown, but several mechanisms have been proposed. These include obstruction of the olfactory cleft; infection of the sustentacular supporting cells, which express angiotensin‐converting enzyme 2 (ACE‐2); injury to olfactory sensory cells via neuropilin‐1 receptors (NRP1); and injury to the olfactory bulb.5
The case we present represents the only report of phantosmia following a J&J COVID-19 vaccination. Phantosmia, featured by a burning or smoke odor, has been reported prior in a case of a 57-year-old woman following the administration of the Pfizer-BioNTech mRNA vaccine.6 Similar to our case, symptoms were not associated with a concurrent COVID-19 infection ruled out via a COVID-19 polymerase chain reaction test. For the Pfizer-BioNTech phantosmia case, a 3 Tesla (T) brain MRI showed left greater than right olfactory bulb and tract gadolinium enhancement on T1-weighted postcontrast images. On axial T2-weighted fluid-attenuated inversion recovery images, hyperintensity along the left olfactory bulb and bilateral olfactory tracts was noted and interpreted as edema. On sagittal thin sections of T2-weighted images, the olfactory nerve filia were thickened and clumped.6 On the contrary, in the case we present, a brain MRI obtained with a 1.5 T magnet showed no abnormalities. It is possible that a high-resolution scan targeting the olfactory bulb could have disclosed pathological changes. At the time when the veteran presented to the neurology clinic, symptoms were already improving, and repeat MRI was deferred as it would not have changed the clinical management.
Konstantinidis and colleagues reported hyposmia in 2 patients following Pfizer-BioNTech COVID-19 vaccination.5 Both patients, 42- and 39-year-old women, experienced hyposmia following their second dose of the vaccine with symptom onset 3 and 5 days after vaccination, respectively. The first patient reported improvement of symptoms after 1 week, while the second patient participated in olfactory training and experienced only partial recovery after 1 month. Multiple studies have reported cranial nerve involvement secondary to other COVID-19 vaccines, including olfactory dysfunction, optic neuritis, acute abducens nerve palsy, Bell palsy, tinnitus, and cochleopathy.7
There are no previous reports of phantosmia following the J&J COVID-19 vaccine. In our case, reported symptoms were mild, although they persisted for nearly 2 years following vaccination.
In the evaluation of this veteran, although the timing between symptom onset and vaccination was indicative of a possible link between the 2, other etiologies of phantosmia were ruled out. Isolated olfactory hallucination is most associated with temporal lobe epilepsy, which is the most common form of epilepsy to present in adulthood. However, given the absence of other symptoms suggestive of epilepsy and the duration of the episodes (approximately 1 hour), the clinical suspicion was low. This was reinforced by the EEG that showed no abnormalities in the temporal region. Notwithstanding these considerations, one must keep in mind that no episodes of phantosmia occurred during the EEG recording, the correlates of which are the gold standard to rule out a diagnosis of epilepsy.
A normal brain MRI argued against possible structural abnormalities leading to these symptoms. Thus, the origin of these symptoms remains unknown.
Conclusions
The emergency approval and use of vaccines against COVID-19 was a major victory for public health in 2021. However, given the rapid rollout of these vaccines, the medical community is responsible for reporting adverse effects as they are observed. The authors believe that the clinical events featuring the J&J COVID-19 vaccine in this veteran should not discourage the use of the COVID-19 vaccine. However, sharing the clinical outcome of this veteran is relevant to inform the community regarding this rare and benign possible adverse effect of the J&J COVID-19 vaccine.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Tennessee Valley Veteran Healthcare System (Nashville). The authors thank Dr. Martin Gallagher (Tennessee Valley Veteran Healthcare System) for providing clinical expertise with electroencephalogram interpretation.
1. Xu S, Huang R, Sy LS, et al. COVID-19 vaccination and non-COVID-19 mortality risk - seven integrated health care organizations, United States, December 14, 2020-July 31, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(43):1520-1524. Published 2021 Oct 29. doi:10.15585/mmwr.mm7043e2
2. Der-Martirosian C, Steers WN, Northcraft H, Chu K, Dobalian A. Vaccinating veterans for COVID-19 at the U.S. Department of Veterans Affairs. Am J Prev Med. 2022;62(6):e317-e324. doi:10.1016/j.amepre.2021.12.016
3. Bagnato F, Wallin M. COVID-19 vaccine in veterans with multiple sclerosis: protect the vulnerable. Fed Pract. 2021;38(suppl 1):S28-S32. doi:10.12788/fp.0113
4. Işlek A, Balcı MK. Phantosmia with COVID-19 related olfactory dysfunction: report of nine cases. Indian J Otolaryngol Head Neck Surg. 2022;74(suppl 2):2891-2893. doi:10.1007/s12070-021-02505-z
5. Konstantinidis I, Tsakiropoulou E, Hähner A, de With K, Poulas K, Hummel T. Olfactory dysfunction after coronavirus disease 2019 (COVID-19) vaccination. Int Forum Allergy Rhinol. 2021;11(9):1399-1401. doi:10.1002/alr.22809
6. Keir G, Maria NI, Kirsch CFE. Unique imaging findings of neurologic phantosmia following Pfizer-BioNtech COVID-19 vaccination: a case report. Top Magn Reson Imaging. 2021;30(3):133-137. doi:10.1097/RMR.0000000000000287
7. Garg RK, Paliwal VK. Spectrum of neurological complications following COVID-19 vaccination. Neurol Sci. 2022;43(1):3-40. doi:10.1007/s10072-021-05662-9
The rapid development of multiple vaccines for COVID-19 significantly contributed to reducing the morbidity and mortality associated with COVID-19 infection.1 The vaccination campaign against COVID-19 started in December 2020 within the US Department of Veterans Affairs (VA) health care system with the Pfizer-BioNTech and Moderna COVID-19 mRNA vaccines followed by the Johnson & Johnson (J&J) vaccine in March 2021.2,3
Because of the importance of maintaining a safe vaccination campaign, surveillance reports documenting cases of malignant or benign adverse effects (AEs) are fundamental to generate awareness and accurate knowledge on these newly developed vaccines. Here we report the case of a veteran who developed olfactory hallucinations following the administration of the J&J COVID-19 vaccine.
Case Presentation
A 39-year-old veteran with a history of tension-type headaches presented to the neurology clinic with concern of a burning smell sensation in the absence of an identifiable source. He first noticed this symptom approximately 3 weeks after he received the J&J COVID-19 vaccine about 4 months prior. At the symptom’s first occurrence, he underwent a nasal swab antigen COVID-19 test, which was negative. Initially, symptoms would occur daily lasting about 1 hour. Thereafter, they started to decrease in duration, frequency, and intensity, and about 11 months postvaccination, milder episodes were occurring 1 to 2 times weekly. These episodes lasted nearly 2 years (21 months postvaccination). They happened randomly during the day and were not associated with any other symptoms. Specifically, there were no headaches, loss of consciousness, abnormal movements, nausea, vomiting, photophobia or phonophobia, or alteration of consciousness, such as confusion or drowsiness during or after the events. Additionally, there were no clear triggers the veteran could identify. The veteran did not sustain any head injuries or exposure to toxic odors before the onset of symptoms.
At the time of his presentation to the clinic, both his general and neurological examinations were unremarkable.
Discussion
It has been previously observed that infection with COVID-19 can lead to the loss of taste and smell, but only less commonly olfactory hallucination.4 The pathophysiology of olfactory hallucinations following COVID-19 infection is unknown, but several mechanisms have been proposed. These include obstruction of the olfactory cleft; infection of the sustentacular supporting cells, which express angiotensin‐converting enzyme 2 (ACE‐2); injury to olfactory sensory cells via neuropilin‐1 receptors (NRP1); and injury to the olfactory bulb.5
The case we present represents the only report of phantosmia following a J&J COVID-19 vaccination. Phantosmia, featured by a burning or smoke odor, has been reported prior in a case of a 57-year-old woman following the administration of the Pfizer-BioNTech mRNA vaccine.6 Similar to our case, symptoms were not associated with a concurrent COVID-19 infection ruled out via a COVID-19 polymerase chain reaction test. For the Pfizer-BioNTech phantosmia case, a 3 Tesla (T) brain MRI showed left greater than right olfactory bulb and tract gadolinium enhancement on T1-weighted postcontrast images. On axial T2-weighted fluid-attenuated inversion recovery images, hyperintensity along the left olfactory bulb and bilateral olfactory tracts was noted and interpreted as edema. On sagittal thin sections of T2-weighted images, the olfactory nerve filia were thickened and clumped.6 On the contrary, in the case we present, a brain MRI obtained with a 1.5 T magnet showed no abnormalities. It is possible that a high-resolution scan targeting the olfactory bulb could have disclosed pathological changes. At the time when the veteran presented to the neurology clinic, symptoms were already improving, and repeat MRI was deferred as it would not have changed the clinical management.
Konstantinidis and colleagues reported hyposmia in 2 patients following Pfizer-BioNTech COVID-19 vaccination.5 Both patients, 42- and 39-year-old women, experienced hyposmia following their second dose of the vaccine with symptom onset 3 and 5 days after vaccination, respectively. The first patient reported improvement of symptoms after 1 week, while the second patient participated in olfactory training and experienced only partial recovery after 1 month. Multiple studies have reported cranial nerve involvement secondary to other COVID-19 vaccines, including olfactory dysfunction, optic neuritis, acute abducens nerve palsy, Bell palsy, tinnitus, and cochleopathy.7
There are no previous reports of phantosmia following the J&J COVID-19 vaccine. In our case, reported symptoms were mild, although they persisted for nearly 2 years following vaccination.
In the evaluation of this veteran, although the timing between symptom onset and vaccination was indicative of a possible link between the 2, other etiologies of phantosmia were ruled out. Isolated olfactory hallucination is most associated with temporal lobe epilepsy, which is the most common form of epilepsy to present in adulthood. However, given the absence of other symptoms suggestive of epilepsy and the duration of the episodes (approximately 1 hour), the clinical suspicion was low. This was reinforced by the EEG that showed no abnormalities in the temporal region. Notwithstanding these considerations, one must keep in mind that no episodes of phantosmia occurred during the EEG recording, the correlates of which are the gold standard to rule out a diagnosis of epilepsy.
A normal brain MRI argued against possible structural abnormalities leading to these symptoms. Thus, the origin of these symptoms remains unknown.
Conclusions
The emergency approval and use of vaccines against COVID-19 was a major victory for public health in 2021. However, given the rapid rollout of these vaccines, the medical community is responsible for reporting adverse effects as they are observed. The authors believe that the clinical events featuring the J&J COVID-19 vaccine in this veteran should not discourage the use of the COVID-19 vaccine. However, sharing the clinical outcome of this veteran is relevant to inform the community regarding this rare and benign possible adverse effect of the J&J COVID-19 vaccine.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Tennessee Valley Veteran Healthcare System (Nashville). The authors thank Dr. Martin Gallagher (Tennessee Valley Veteran Healthcare System) for providing clinical expertise with electroencephalogram interpretation.
The rapid development of multiple vaccines for COVID-19 significantly contributed to reducing the morbidity and mortality associated with COVID-19 infection.1 The vaccination campaign against COVID-19 started in December 2020 within the US Department of Veterans Affairs (VA) health care system with the Pfizer-BioNTech and Moderna COVID-19 mRNA vaccines followed by the Johnson & Johnson (J&J) vaccine in March 2021.2,3
Because of the importance of maintaining a safe vaccination campaign, surveillance reports documenting cases of malignant or benign adverse effects (AEs) are fundamental to generate awareness and accurate knowledge on these newly developed vaccines. Here we report the case of a veteran who developed olfactory hallucinations following the administration of the J&J COVID-19 vaccine.
Case Presentation
A 39-year-old veteran with a history of tension-type headaches presented to the neurology clinic with concern of a burning smell sensation in the absence of an identifiable source. He first noticed this symptom approximately 3 weeks after he received the J&J COVID-19 vaccine about 4 months prior. At the symptom’s first occurrence, he underwent a nasal swab antigen COVID-19 test, which was negative. Initially, symptoms would occur daily lasting about 1 hour. Thereafter, they started to decrease in duration, frequency, and intensity, and about 11 months postvaccination, milder episodes were occurring 1 to 2 times weekly. These episodes lasted nearly 2 years (21 months postvaccination). They happened randomly during the day and were not associated with any other symptoms. Specifically, there were no headaches, loss of consciousness, abnormal movements, nausea, vomiting, photophobia or phonophobia, or alteration of consciousness, such as confusion or drowsiness during or after the events. Additionally, there were no clear triggers the veteran could identify. The veteran did not sustain any head injuries or exposure to toxic odors before the onset of symptoms.
At the time of his presentation to the clinic, both his general and neurological examinations were unremarkable.
Discussion
It has been previously observed that infection with COVID-19 can lead to the loss of taste and smell, but only less commonly olfactory hallucination.4 The pathophysiology of olfactory hallucinations following COVID-19 infection is unknown, but several mechanisms have been proposed. These include obstruction of the olfactory cleft; infection of the sustentacular supporting cells, which express angiotensin‐converting enzyme 2 (ACE‐2); injury to olfactory sensory cells via neuropilin‐1 receptors (NRP1); and injury to the olfactory bulb.5
The case we present represents the only report of phantosmia following a J&J COVID-19 vaccination. Phantosmia, featured by a burning or smoke odor, has been reported prior in a case of a 57-year-old woman following the administration of the Pfizer-BioNTech mRNA vaccine.6 Similar to our case, symptoms were not associated with a concurrent COVID-19 infection ruled out via a COVID-19 polymerase chain reaction test. For the Pfizer-BioNTech phantosmia case, a 3 Tesla (T) brain MRI showed left greater than right olfactory bulb and tract gadolinium enhancement on T1-weighted postcontrast images. On axial T2-weighted fluid-attenuated inversion recovery images, hyperintensity along the left olfactory bulb and bilateral olfactory tracts was noted and interpreted as edema. On sagittal thin sections of T2-weighted images, the olfactory nerve filia were thickened and clumped.6 On the contrary, in the case we present, a brain MRI obtained with a 1.5 T magnet showed no abnormalities. It is possible that a high-resolution scan targeting the olfactory bulb could have disclosed pathological changes. At the time when the veteran presented to the neurology clinic, symptoms were already improving, and repeat MRI was deferred as it would not have changed the clinical management.
Konstantinidis and colleagues reported hyposmia in 2 patients following Pfizer-BioNTech COVID-19 vaccination.5 Both patients, 42- and 39-year-old women, experienced hyposmia following their second dose of the vaccine with symptom onset 3 and 5 days after vaccination, respectively. The first patient reported improvement of symptoms after 1 week, while the second patient participated in olfactory training and experienced only partial recovery after 1 month. Multiple studies have reported cranial nerve involvement secondary to other COVID-19 vaccines, including olfactory dysfunction, optic neuritis, acute abducens nerve palsy, Bell palsy, tinnitus, and cochleopathy.7
There are no previous reports of phantosmia following the J&J COVID-19 vaccine. In our case, reported symptoms were mild, although they persisted for nearly 2 years following vaccination.
In the evaluation of this veteran, although the timing between symptom onset and vaccination was indicative of a possible link between the 2, other etiologies of phantosmia were ruled out. Isolated olfactory hallucination is most associated with temporal lobe epilepsy, which is the most common form of epilepsy to present in adulthood. However, given the absence of other symptoms suggestive of epilepsy and the duration of the episodes (approximately 1 hour), the clinical suspicion was low. This was reinforced by the EEG that showed no abnormalities in the temporal region. Notwithstanding these considerations, one must keep in mind that no episodes of phantosmia occurred during the EEG recording, the correlates of which are the gold standard to rule out a diagnosis of epilepsy.
A normal brain MRI argued against possible structural abnormalities leading to these symptoms. Thus, the origin of these symptoms remains unknown.
Conclusions
The emergency approval and use of vaccines against COVID-19 was a major victory for public health in 2021. However, given the rapid rollout of these vaccines, the medical community is responsible for reporting adverse effects as they are observed. The authors believe that the clinical events featuring the J&J COVID-19 vaccine in this veteran should not discourage the use of the COVID-19 vaccine. However, sharing the clinical outcome of this veteran is relevant to inform the community regarding this rare and benign possible adverse effect of the J&J COVID-19 vaccine.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Tennessee Valley Veteran Healthcare System (Nashville). The authors thank Dr. Martin Gallagher (Tennessee Valley Veteran Healthcare System) for providing clinical expertise with electroencephalogram interpretation.
1. Xu S, Huang R, Sy LS, et al. COVID-19 vaccination and non-COVID-19 mortality risk - seven integrated health care organizations, United States, December 14, 2020-July 31, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(43):1520-1524. Published 2021 Oct 29. doi:10.15585/mmwr.mm7043e2
2. Der-Martirosian C, Steers WN, Northcraft H, Chu K, Dobalian A. Vaccinating veterans for COVID-19 at the U.S. Department of Veterans Affairs. Am J Prev Med. 2022;62(6):e317-e324. doi:10.1016/j.amepre.2021.12.016
3. Bagnato F, Wallin M. COVID-19 vaccine in veterans with multiple sclerosis: protect the vulnerable. Fed Pract. 2021;38(suppl 1):S28-S32. doi:10.12788/fp.0113
4. Işlek A, Balcı MK. Phantosmia with COVID-19 related olfactory dysfunction: report of nine cases. Indian J Otolaryngol Head Neck Surg. 2022;74(suppl 2):2891-2893. doi:10.1007/s12070-021-02505-z
5. Konstantinidis I, Tsakiropoulou E, Hähner A, de With K, Poulas K, Hummel T. Olfactory dysfunction after coronavirus disease 2019 (COVID-19) vaccination. Int Forum Allergy Rhinol. 2021;11(9):1399-1401. doi:10.1002/alr.22809
6. Keir G, Maria NI, Kirsch CFE. Unique imaging findings of neurologic phantosmia following Pfizer-BioNtech COVID-19 vaccination: a case report. Top Magn Reson Imaging. 2021;30(3):133-137. doi:10.1097/RMR.0000000000000287
7. Garg RK, Paliwal VK. Spectrum of neurological complications following COVID-19 vaccination. Neurol Sci. 2022;43(1):3-40. doi:10.1007/s10072-021-05662-9
1. Xu S, Huang R, Sy LS, et al. COVID-19 vaccination and non-COVID-19 mortality risk - seven integrated health care organizations, United States, December 14, 2020-July 31, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(43):1520-1524. Published 2021 Oct 29. doi:10.15585/mmwr.mm7043e2
2. Der-Martirosian C, Steers WN, Northcraft H, Chu K, Dobalian A. Vaccinating veterans for COVID-19 at the U.S. Department of Veterans Affairs. Am J Prev Med. 2022;62(6):e317-e324. doi:10.1016/j.amepre.2021.12.016
3. Bagnato F, Wallin M. COVID-19 vaccine in veterans with multiple sclerosis: protect the vulnerable. Fed Pract. 2021;38(suppl 1):S28-S32. doi:10.12788/fp.0113
4. Işlek A, Balcı MK. Phantosmia with COVID-19 related olfactory dysfunction: report of nine cases. Indian J Otolaryngol Head Neck Surg. 2022;74(suppl 2):2891-2893. doi:10.1007/s12070-021-02505-z
5. Konstantinidis I, Tsakiropoulou E, Hähner A, de With K, Poulas K, Hummel T. Olfactory dysfunction after coronavirus disease 2019 (COVID-19) vaccination. Int Forum Allergy Rhinol. 2021;11(9):1399-1401. doi:10.1002/alr.22809
6. Keir G, Maria NI, Kirsch CFE. Unique imaging findings of neurologic phantosmia following Pfizer-BioNtech COVID-19 vaccination: a case report. Top Magn Reson Imaging. 2021;30(3):133-137. doi:10.1097/RMR.0000000000000287
7. Garg RK, Paliwal VK. Spectrum of neurological complications following COVID-19 vaccination. Neurol Sci. 2022;43(1):3-40. doi:10.1007/s10072-021-05662-9
New COVID vaccines force bivalents out
COVID vaccines will have a new formulation in 2023, according to a decision announced by the U.S. Food and Drug Administration, that will focus efforts on circulating variants. The move pushes last year’s bivalent vaccines out of circulation because they will no longer be authorized for use in the United States.
The updated mRNA vaccines for 2023-2024 are being revised to include a single component that corresponds to the Omicron variant XBB.1.5. Like the bivalents offered before, the new monovalents are being manufactured by Moderna and Pfizer.
The new vaccines are authorized for use in individuals age 6 months and older. And the new options are being developed using a similar process as previous formulations, according to the FDA.
Targeting circulating variants
In recent studies, regulators point out the extent of neutralization observed by the updated vaccines against currently circulating viral variants causing COVID-19, including EG.5, BA.2.86, appears to be of a similar magnitude to the extent of neutralization observed with previous versions of the vaccines against corresponding prior variants.
“This suggests that the vaccines are a good match for protecting against the currently circulating COVID-19 variants,” according to the report.
Hundreds of millions of people in the United States have already received previously approved mRNA COVID vaccines, according to regulators who say the benefit-to-risk profile is well understood as they move forward with new formulations.
“Vaccination remains critical to public health and continued protection against serious consequences of COVID-19, including hospitalization and death,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in a statement. “The public can be assured that these updated vaccines have met the agency’s rigorous scientific standards for safety, effectiveness, and manufacturing quality. We very much encourage those who are eligible to consider getting vaccinated.”
Timing the effort
On Sept. 12 the U.S. Centers for Disease Control and Prevention recommended that everyone 6 months and older get an updated COVID-19 vaccine. Updated vaccines from Pfizer-BioNTech and Moderna will be available later this week, according to the agency.
This article was updated 9/14/23.
A version of this article appeared on Medscape.com.
COVID vaccines will have a new formulation in 2023, according to a decision announced by the U.S. Food and Drug Administration, that will focus efforts on circulating variants. The move pushes last year’s bivalent vaccines out of circulation because they will no longer be authorized for use in the United States.
The updated mRNA vaccines for 2023-2024 are being revised to include a single component that corresponds to the Omicron variant XBB.1.5. Like the bivalents offered before, the new monovalents are being manufactured by Moderna and Pfizer.
The new vaccines are authorized for use in individuals age 6 months and older. And the new options are being developed using a similar process as previous formulations, according to the FDA.
Targeting circulating variants
In recent studies, regulators point out the extent of neutralization observed by the updated vaccines against currently circulating viral variants causing COVID-19, including EG.5, BA.2.86, appears to be of a similar magnitude to the extent of neutralization observed with previous versions of the vaccines against corresponding prior variants.
“This suggests that the vaccines are a good match for protecting against the currently circulating COVID-19 variants,” according to the report.
Hundreds of millions of people in the United States have already received previously approved mRNA COVID vaccines, according to regulators who say the benefit-to-risk profile is well understood as they move forward with new formulations.
“Vaccination remains critical to public health and continued protection against serious consequences of COVID-19, including hospitalization and death,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in a statement. “The public can be assured that these updated vaccines have met the agency’s rigorous scientific standards for safety, effectiveness, and manufacturing quality. We very much encourage those who are eligible to consider getting vaccinated.”
Timing the effort
On Sept. 12 the U.S. Centers for Disease Control and Prevention recommended that everyone 6 months and older get an updated COVID-19 vaccine. Updated vaccines from Pfizer-BioNTech and Moderna will be available later this week, according to the agency.
This article was updated 9/14/23.
A version of this article appeared on Medscape.com.
COVID vaccines will have a new formulation in 2023, according to a decision announced by the U.S. Food and Drug Administration, that will focus efforts on circulating variants. The move pushes last year’s bivalent vaccines out of circulation because they will no longer be authorized for use in the United States.
The updated mRNA vaccines for 2023-2024 are being revised to include a single component that corresponds to the Omicron variant XBB.1.5. Like the bivalents offered before, the new monovalents are being manufactured by Moderna and Pfizer.
The new vaccines are authorized for use in individuals age 6 months and older. And the new options are being developed using a similar process as previous formulations, according to the FDA.
Targeting circulating variants
In recent studies, regulators point out the extent of neutralization observed by the updated vaccines against currently circulating viral variants causing COVID-19, including EG.5, BA.2.86, appears to be of a similar magnitude to the extent of neutralization observed with previous versions of the vaccines against corresponding prior variants.
“This suggests that the vaccines are a good match for protecting against the currently circulating COVID-19 variants,” according to the report.
Hundreds of millions of people in the United States have already received previously approved mRNA COVID vaccines, according to regulators who say the benefit-to-risk profile is well understood as they move forward with new formulations.
“Vaccination remains critical to public health and continued protection against serious consequences of COVID-19, including hospitalization and death,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in a statement. “The public can be assured that these updated vaccines have met the agency’s rigorous scientific standards for safety, effectiveness, and manufacturing quality. We very much encourage those who are eligible to consider getting vaccinated.”
Timing the effort
On Sept. 12 the U.S. Centers for Disease Control and Prevention recommended that everyone 6 months and older get an updated COVID-19 vaccine. Updated vaccines from Pfizer-BioNTech and Moderna will be available later this week, according to the agency.
This article was updated 9/14/23.
A version of this article appeared on Medscape.com.
Effect of COVID-19 Vaccination on Disease Severity in Patients With Stable Plaque Psoriasis: A Cross-sectional Study
To the Editor:
COVID-19 infection has resulted in 6.9 million deaths worldwide. India has the third highest mortality from COVID-19 infection after the United States and Brazil.1 Vaccination plays a crucial role in containing COVID-19 infection and reducing its severity. At present, 11 vaccines have been approved by the World Health Organization. India started its vaccination program on January 16, 2021, with approval for use of Covaxin (Bharat Biotech) and Covishield (Oxford/AstraZeneca formulation)(Serum Institute of India). More than 2 billion doses have been administered since then.2,3
Patients with psoriasis are prone to develop a severe form of COVID-19 due to comorbidities and the intake of immunosuppressive drugs.4 These patients often are hesitant to receive the vaccine without an expert opinion. COVID-19 vaccines are considered to increase tumor necrosis factor α (TNF-α) and IFN-γ production by CD4+ T cells. Tumor necrosis factor α is a key proinflammatory cytokine implicated in the pathogenesis of psoriasis. COVID-19 messenger RNA vaccines induce elevation of IL-6 and helper T cells (TH17), which can induce a flare of psoriasis in a subset of patients.5The International Psoriasis Council recommends that patients with psoriasis receive one of the vaccines approved to prevent COVID-19 infection as soon as possible.6 Reports of new-onset psoriasis and flare of psoriasis after the use of COVID-19 vaccines, such as those manufactured by Pfizer-BioNTech, Moderna, and AstraZeneca, have been published from different parts of the world.7 India used locally developed whole virion inactivated BBV152 (Covaxin) and nonreplicating viral vaccine ChAdOx1 nCoV-19 (Covishield) in its vaccination program and exported them to other developing countries. There is a dearth of data on the safety of these vaccines in patients with psoriasis, which needs to be assessed. Later, Covaxin, ZyCoV-D (DNA plasmid vaccine; Cadila Healthcare), and CorbeVax (protein subunit vaccine; Biological E) were approved for usage in children.8 We conducted a cross-sectional study using the direct interview method.
Patients with psoriasis who attended the outpatient department of the Postgraduate Institute of Medical Education and Research (Chandigarh, India) from April 2022 to June 2022 were invited to participate in the study after written informed consent was received. Patients 18 years and older with chronic plaque psoriasis who had received a COVID-19 vaccine dose in the last 90 days were enrolled. Data on demographics, comorbidities, treatment received for psoriasis, vaccination concerns, history of COVID-19 infection, type of vaccine received with doses, adverse effects, and psoriasis flare after receiving the vaccine (considered up to 2 weeks from the date of vaccination) were collected. Ordinal logistic regression was used to identify factors associated with a psoriasis flare following vaccination. P<.05 was considered statistically significant.
A total of 202 patients with chronic plaque psoriasis who received either Covaxin or Covishield were enrolled during the study period. The mean age (SD) was 40.3 (13.1) years, and 149 (73.8%) patients were male. One hundred thirty-five (66.8%) patients completed 2 doses of the vaccine. eTable 1 provides the clinicodemographic details of the patients. Eighty-three (41.1%) patients had a fear of psoriasis flare after vaccination. Seventy-two (35.6%) patients received the vaccine after clearance from their treating physician/dermatologist. One hundred sixty-four (81.2%) patients received the Covishield vaccine, and 38 (18.8%) patients received Covaxin. Eighty-three (41.1%) patients reported flulike symptoms, such as fever, myalgia, or body pain, within the first week of vaccination. Sixty-one (30.2%) patients reported a psoriasis flare after vaccination in the form of new lesions or worsening of pre-existing lesions. Of these patients, 51 reported a flare after receiving the first dose of vaccine, 8 patients reported a flare after receiving the second dose of vaccine, and 2 patients reported a flare after receiving both doses of vaccine. The mean (SD) flare onset was 8.1 (3.4) days after the vaccination. Eighteen patients considered the flare to be severe. Seventeen (8.4%) patients reported a positive history of COVID-19 infection before vaccination. None of the patients reported breakthrough COVID-19 infection or pustular aggravation of psoriasis following the vaccination.

The self-reported psoriasis flare after receiving the COVID-19 vaccine was significantly higher in patients who experienced immediate adverse effects (P=.005), which included fever, myalgia, joint pain, and injection-site reaction. The reported postvaccination psoriasis flare was not significantly associated with patient sex, history of COVID-19 infection, type of vaccine received, comorbidities, or therapy for psoriasis (eTable 2).

Nearly 30% of our patients reported a postvaccination psoriasis flare, which was more common after the first vaccine dose. Sotiriou et al7 reported 14 cases of psoriasis flare in patients after receiving Pfizer-BioNTech, Moderna, and AstraZeneca COVID-19 vaccines. These patients experienced an exacerbation of disease soon after the second dose of vaccine (mean [SD], 10.36 [7.71] days), and 21% of the 713 enrolled patients wanted to forego the immunization due to concern of a postvaccination psoriasis flare.7 In another report, 14 (27%) patients developed a psoriasis flare after COVID-19 vaccination; the mean (SD) flare onset was 9.3 (4.3) days after vaccination.9
Data on the safety of the COVID-19 vaccine in patients using immunosuppressive drugs are limited. We did not find a significant association between the psoriasis flare and use of immunosuppressive drugs or type of vaccine received. Huang and Tsai9 observed similar results, with no association between psoriasis flare and use of immunosuppressive drugs or biologics, while Damiani et al10 demonstrated a protective role of biologics in preventing vaccine-induced psoriasis flare.
Similar to another study from India,11 the immediate adverse effects due to immunization with Covaxin and Covishield were mild in our study and resolved within a week. The incidence of psoriasis flare was significantly higher in patients who reported adverse effects (P=.005). Activation of immune response after vaccination leads to the release of proinflammatory and pyrogenic cytokines (ie, IL-1, IL-6, TNF-α), which may explain the higher incidence of psoriasis flare in patients experiencing adverse effects to vaccination.12
Our study showed approximately 30% of patients developed a psoriasis flare after COVID-19 vaccination, with no patients experiencing any vaccine-related serious adverse events, which suggests that Covaxin and Covishield are safe for patients with psoriasis in India. Limitations of our study include potential inaccuracy of the patient’s self-assessment of symptoms and disease flare, recall bias that may lead to errors in estimating patient-reported outcomes, the flare of psoriasis potentially being a part of disease fluctuation, and flare being enhanced by the psychological stress of vaccination.
Considering a high risk for severe COVID-19 infection in patients with psoriasis with comorbidities and those using immunosuppressive drugs, Covaxin and Covishield can be safely recommended in India. However, caution needs to be exercised when vaccinating patients with an unstable disease or severe psoriasis.
- COVID-19 coronavirus pandemic: weekly trends. Worldometer. Accessed August 21, 2023. https://www.worldometers.info/coronavirus/
- National COVID-19 vaccination programme meets its goals by overcoming R&D and logistical challenges, says economic survey 2022-23. Government of India Press Information Bureau website. Published January 31, 2023. Accessed August 24, 2023. https://pib.gov.in/PressReleasePage.aspx?PRID=1894907
- Ministry of Health and Family Welfare. CoWIN. Accessed August 21, 2023. https://www.cowin.gov.in/
- Griffiths CEM, Armstrong AW, Gudjonsson JE, et al. Psoriasis. Lancet. 2021;397:1301-1315.
- Wu D, Yang XO. TH17 responses in cytokine storm of COVID-19: anemerging target of JAK2 inhibitor fedratinib. J Microbiol Immunol Infect. 2020;53:368-370.
- International Psoriasis Council. Revised IPC statement on COVID-19. Published December 19, 2022. Accessed August 24, 2023. https://psoriasiscouncil.org/covid-19/revised-statement-covid-19/
- Sotiriou E, Tsentemeidou A, Bakirtzi K, et al. Psoriasis exacerbation after COVID-19 vaccination: a report of 14 cases from a single centre. J Eur Acad Dermatol Venereol. 2021;35:E857-E859.
- Kaul R. India clears 2 vaccines for kids under 12 years. Hindustan Times. Published April 27, 2022. Accessed August 24, 2023. https://www.hindustantimes.com/india-news/india-clears-2-vaccines-for-kids-under-12-years-101650998027336.html
- Huang YW, Tsai TF. Exacerbation of psoriasis following COVID-19 vaccination: report from a single center. Front Med (Lausanne). 2021;8:812010.
- Damiani G, Allocco F, Young Dermatologists Italian Network, et al. COVID-19 vaccination and patients with psoriasis under biologics: real-life evidence on safety and effectiveness from Italian vaccinated healthcare workers. Clin Exp Dermatol. 2021;460:1106-1108.
- Joshi RK, Muralidharan CG, Gulati DS, et al. Higher incidence of reported adverse events following immunisation (AEFI) after first dose of COVID-19 vaccine among previously infected health care workers. Med J Armed Forces India. 2021;77(suppl 2):S505-S507.
- Hervé C, Laupèze B, Del Giudice G, et al. The how’s and what’s of vaccine reactogenicity. NPJ Vaccines. 2019;4:39.
To the Editor:
COVID-19 infection has resulted in 6.9 million deaths worldwide. India has the third highest mortality from COVID-19 infection after the United States and Brazil.1 Vaccination plays a crucial role in containing COVID-19 infection and reducing its severity. At present, 11 vaccines have been approved by the World Health Organization. India started its vaccination program on January 16, 2021, with approval for use of Covaxin (Bharat Biotech) and Covishield (Oxford/AstraZeneca formulation)(Serum Institute of India). More than 2 billion doses have been administered since then.2,3
Patients with psoriasis are prone to develop a severe form of COVID-19 due to comorbidities and the intake of immunosuppressive drugs.4 These patients often are hesitant to receive the vaccine without an expert opinion. COVID-19 vaccines are considered to increase tumor necrosis factor α (TNF-α) and IFN-γ production by CD4+ T cells. Tumor necrosis factor α is a key proinflammatory cytokine implicated in the pathogenesis of psoriasis. COVID-19 messenger RNA vaccines induce elevation of IL-6 and helper T cells (TH17), which can induce a flare of psoriasis in a subset of patients.5The International Psoriasis Council recommends that patients with psoriasis receive one of the vaccines approved to prevent COVID-19 infection as soon as possible.6 Reports of new-onset psoriasis and flare of psoriasis after the use of COVID-19 vaccines, such as those manufactured by Pfizer-BioNTech, Moderna, and AstraZeneca, have been published from different parts of the world.7 India used locally developed whole virion inactivated BBV152 (Covaxin) and nonreplicating viral vaccine ChAdOx1 nCoV-19 (Covishield) in its vaccination program and exported them to other developing countries. There is a dearth of data on the safety of these vaccines in patients with psoriasis, which needs to be assessed. Later, Covaxin, ZyCoV-D (DNA plasmid vaccine; Cadila Healthcare), and CorbeVax (protein subunit vaccine; Biological E) were approved for usage in children.8 We conducted a cross-sectional study using the direct interview method.
Patients with psoriasis who attended the outpatient department of the Postgraduate Institute of Medical Education and Research (Chandigarh, India) from April 2022 to June 2022 were invited to participate in the study after written informed consent was received. Patients 18 years and older with chronic plaque psoriasis who had received a COVID-19 vaccine dose in the last 90 days were enrolled. Data on demographics, comorbidities, treatment received for psoriasis, vaccination concerns, history of COVID-19 infection, type of vaccine received with doses, adverse effects, and psoriasis flare after receiving the vaccine (considered up to 2 weeks from the date of vaccination) were collected. Ordinal logistic regression was used to identify factors associated with a psoriasis flare following vaccination. P<.05 was considered statistically significant.
A total of 202 patients with chronic plaque psoriasis who received either Covaxin or Covishield were enrolled during the study period. The mean age (SD) was 40.3 (13.1) years, and 149 (73.8%) patients were male. One hundred thirty-five (66.8%) patients completed 2 doses of the vaccine. eTable 1 provides the clinicodemographic details of the patients. Eighty-three (41.1%) patients had a fear of psoriasis flare after vaccination. Seventy-two (35.6%) patients received the vaccine after clearance from their treating physician/dermatologist. One hundred sixty-four (81.2%) patients received the Covishield vaccine, and 38 (18.8%) patients received Covaxin. Eighty-three (41.1%) patients reported flulike symptoms, such as fever, myalgia, or body pain, within the first week of vaccination. Sixty-one (30.2%) patients reported a psoriasis flare after vaccination in the form of new lesions or worsening of pre-existing lesions. Of these patients, 51 reported a flare after receiving the first dose of vaccine, 8 patients reported a flare after receiving the second dose of vaccine, and 2 patients reported a flare after receiving both doses of vaccine. The mean (SD) flare onset was 8.1 (3.4) days after the vaccination. Eighteen patients considered the flare to be severe. Seventeen (8.4%) patients reported a positive history of COVID-19 infection before vaccination. None of the patients reported breakthrough COVID-19 infection or pustular aggravation of psoriasis following the vaccination.
The self-reported psoriasis flare after receiving the COVID-19 vaccine was significantly higher in patients who experienced immediate adverse effects (P=.005), which included fever, myalgia, joint pain, and injection-site reaction. The reported postvaccination psoriasis flare was not significantly associated with patient sex, history of COVID-19 infection, type of vaccine received, comorbidities, or therapy for psoriasis (eTable 2).
Nearly 30% of our patients reported a postvaccination psoriasis flare, which was more common after the first vaccine dose. Sotiriou et al7 reported 14 cases of psoriasis flare in patients after receiving Pfizer-BioNTech, Moderna, and AstraZeneca COVID-19 vaccines. These patients experienced an exacerbation of disease soon after the second dose of vaccine (mean [SD], 10.36 [7.71] days), and 21% of the 713 enrolled patients wanted to forego the immunization due to concern of a postvaccination psoriasis flare.7 In another report, 14 (27%) patients developed a psoriasis flare after COVID-19 vaccination; the mean (SD) flare onset was 9.3 (4.3) days after vaccination.9
Data on the safety of the COVID-19 vaccine in patients using immunosuppressive drugs are limited. We did not find a significant association between the psoriasis flare and use of immunosuppressive drugs or type of vaccine received. Huang and Tsai9 observed similar results, with no association between psoriasis flare and use of immunosuppressive drugs or biologics, while Damiani et al10 demonstrated a protective role of biologics in preventing vaccine-induced psoriasis flare.
Similar to another study from India,11 the immediate adverse effects due to immunization with Covaxin and Covishield were mild in our study and resolved within a week. The incidence of psoriasis flare was significantly higher in patients who reported adverse effects (P=.005). Activation of immune response after vaccination leads to the release of proinflammatory and pyrogenic cytokines (ie, IL-1, IL-6, TNF-α), which may explain the higher incidence of psoriasis flare in patients experiencing adverse effects to vaccination.12
Our study showed approximately 30% of patients developed a psoriasis flare after COVID-19 vaccination, with no patients experiencing any vaccine-related serious adverse events, which suggests that Covaxin and Covishield are safe for patients with psoriasis in India. Limitations of our study include potential inaccuracy of the patient’s self-assessment of symptoms and disease flare, recall bias that may lead to errors in estimating patient-reported outcomes, the flare of psoriasis potentially being a part of disease fluctuation, and flare being enhanced by the psychological stress of vaccination.
Considering a high risk for severe COVID-19 infection in patients with psoriasis with comorbidities and those using immunosuppressive drugs, Covaxin and Covishield can be safely recommended in India. However, caution needs to be exercised when vaccinating patients with an unstable disease or severe psoriasis.
To the Editor:
COVID-19 infection has resulted in 6.9 million deaths worldwide. India has the third highest mortality from COVID-19 infection after the United States and Brazil.1 Vaccination plays a crucial role in containing COVID-19 infection and reducing its severity. At present, 11 vaccines have been approved by the World Health Organization. India started its vaccination program on January 16, 2021, with approval for use of Covaxin (Bharat Biotech) and Covishield (Oxford/AstraZeneca formulation)(Serum Institute of India). More than 2 billion doses have been administered since then.2,3
Patients with psoriasis are prone to develop a severe form of COVID-19 due to comorbidities and the intake of immunosuppressive drugs.4 These patients often are hesitant to receive the vaccine without an expert opinion. COVID-19 vaccines are considered to increase tumor necrosis factor α (TNF-α) and IFN-γ production by CD4+ T cells. Tumor necrosis factor α is a key proinflammatory cytokine implicated in the pathogenesis of psoriasis. COVID-19 messenger RNA vaccines induce elevation of IL-6 and helper T cells (TH17), which can induce a flare of psoriasis in a subset of patients.5The International Psoriasis Council recommends that patients with psoriasis receive one of the vaccines approved to prevent COVID-19 infection as soon as possible.6 Reports of new-onset psoriasis and flare of psoriasis after the use of COVID-19 vaccines, such as those manufactured by Pfizer-BioNTech, Moderna, and AstraZeneca, have been published from different parts of the world.7 India used locally developed whole virion inactivated BBV152 (Covaxin) and nonreplicating viral vaccine ChAdOx1 nCoV-19 (Covishield) in its vaccination program and exported them to other developing countries. There is a dearth of data on the safety of these vaccines in patients with psoriasis, which needs to be assessed. Later, Covaxin, ZyCoV-D (DNA plasmid vaccine; Cadila Healthcare), and CorbeVax (protein subunit vaccine; Biological E) were approved for usage in children.8 We conducted a cross-sectional study using the direct interview method.
Patients with psoriasis who attended the outpatient department of the Postgraduate Institute of Medical Education and Research (Chandigarh, India) from April 2022 to June 2022 were invited to participate in the study after written informed consent was received. Patients 18 years and older with chronic plaque psoriasis who had received a COVID-19 vaccine dose in the last 90 days were enrolled. Data on demographics, comorbidities, treatment received for psoriasis, vaccination concerns, history of COVID-19 infection, type of vaccine received with doses, adverse effects, and psoriasis flare after receiving the vaccine (considered up to 2 weeks from the date of vaccination) were collected. Ordinal logistic regression was used to identify factors associated with a psoriasis flare following vaccination. P<.05 was considered statistically significant.
A total of 202 patients with chronic plaque psoriasis who received either Covaxin or Covishield were enrolled during the study period. The mean age (SD) was 40.3 (13.1) years, and 149 (73.8%) patients were male. One hundred thirty-five (66.8%) patients completed 2 doses of the vaccine. eTable 1 provides the clinicodemographic details of the patients. Eighty-three (41.1%) patients had a fear of psoriasis flare after vaccination. Seventy-two (35.6%) patients received the vaccine after clearance from their treating physician/dermatologist. One hundred sixty-four (81.2%) patients received the Covishield vaccine, and 38 (18.8%) patients received Covaxin. Eighty-three (41.1%) patients reported flulike symptoms, such as fever, myalgia, or body pain, within the first week of vaccination. Sixty-one (30.2%) patients reported a psoriasis flare after vaccination in the form of new lesions or worsening of pre-existing lesions. Of these patients, 51 reported a flare after receiving the first dose of vaccine, 8 patients reported a flare after receiving the second dose of vaccine, and 2 patients reported a flare after receiving both doses of vaccine. The mean (SD) flare onset was 8.1 (3.4) days after the vaccination. Eighteen patients considered the flare to be severe. Seventeen (8.4%) patients reported a positive history of COVID-19 infection before vaccination. None of the patients reported breakthrough COVID-19 infection or pustular aggravation of psoriasis following the vaccination.
The self-reported psoriasis flare after receiving the COVID-19 vaccine was significantly higher in patients who experienced immediate adverse effects (P=.005), which included fever, myalgia, joint pain, and injection-site reaction. The reported postvaccination psoriasis flare was not significantly associated with patient sex, history of COVID-19 infection, type of vaccine received, comorbidities, or therapy for psoriasis (eTable 2).
Nearly 30% of our patients reported a postvaccination psoriasis flare, which was more common after the first vaccine dose. Sotiriou et al7 reported 14 cases of psoriasis flare in patients after receiving Pfizer-BioNTech, Moderna, and AstraZeneca COVID-19 vaccines. These patients experienced an exacerbation of disease soon after the second dose of vaccine (mean [SD], 10.36 [7.71] days), and 21% of the 713 enrolled patients wanted to forego the immunization due to concern of a postvaccination psoriasis flare.7 In another report, 14 (27%) patients developed a psoriasis flare after COVID-19 vaccination; the mean (SD) flare onset was 9.3 (4.3) days after vaccination.9
Data on the safety of the COVID-19 vaccine in patients using immunosuppressive drugs are limited. We did not find a significant association between the psoriasis flare and use of immunosuppressive drugs or type of vaccine received. Huang and Tsai9 observed similar results, with no association between psoriasis flare and use of immunosuppressive drugs or biologics, while Damiani et al10 demonstrated a protective role of biologics in preventing vaccine-induced psoriasis flare.
Similar to another study from India,11 the immediate adverse effects due to immunization with Covaxin and Covishield were mild in our study and resolved within a week. The incidence of psoriasis flare was significantly higher in patients who reported adverse effects (P=.005). Activation of immune response after vaccination leads to the release of proinflammatory and pyrogenic cytokines (ie, IL-1, IL-6, TNF-α), which may explain the higher incidence of psoriasis flare in patients experiencing adverse effects to vaccination.12
Our study showed approximately 30% of patients developed a psoriasis flare after COVID-19 vaccination, with no patients experiencing any vaccine-related serious adverse events, which suggests that Covaxin and Covishield are safe for patients with psoriasis in India. Limitations of our study include potential inaccuracy of the patient’s self-assessment of symptoms and disease flare, recall bias that may lead to errors in estimating patient-reported outcomes, the flare of psoriasis potentially being a part of disease fluctuation, and flare being enhanced by the psychological stress of vaccination.
Considering a high risk for severe COVID-19 infection in patients with psoriasis with comorbidities and those using immunosuppressive drugs, Covaxin and Covishield can be safely recommended in India. However, caution needs to be exercised when vaccinating patients with an unstable disease or severe psoriasis.
- COVID-19 coronavirus pandemic: weekly trends. Worldometer. Accessed August 21, 2023. https://www.worldometers.info/coronavirus/
- National COVID-19 vaccination programme meets its goals by overcoming R&D and logistical challenges, says economic survey 2022-23. Government of India Press Information Bureau website. Published January 31, 2023. Accessed August 24, 2023. https://pib.gov.in/PressReleasePage.aspx?PRID=1894907
- Ministry of Health and Family Welfare. CoWIN. Accessed August 21, 2023. https://www.cowin.gov.in/
- Griffiths CEM, Armstrong AW, Gudjonsson JE, et al. Psoriasis. Lancet. 2021;397:1301-1315.
- Wu D, Yang XO. TH17 responses in cytokine storm of COVID-19: anemerging target of JAK2 inhibitor fedratinib. J Microbiol Immunol Infect. 2020;53:368-370.
- International Psoriasis Council. Revised IPC statement on COVID-19. Published December 19, 2022. Accessed August 24, 2023. https://psoriasiscouncil.org/covid-19/revised-statement-covid-19/
- Sotiriou E, Tsentemeidou A, Bakirtzi K, et al. Psoriasis exacerbation after COVID-19 vaccination: a report of 14 cases from a single centre. J Eur Acad Dermatol Venereol. 2021;35:E857-E859.
- Kaul R. India clears 2 vaccines for kids under 12 years. Hindustan Times. Published April 27, 2022. Accessed August 24, 2023. https://www.hindustantimes.com/india-news/india-clears-2-vaccines-for-kids-under-12-years-101650998027336.html
- Huang YW, Tsai TF. Exacerbation of psoriasis following COVID-19 vaccination: report from a single center. Front Med (Lausanne). 2021;8:812010.
- Damiani G, Allocco F, Young Dermatologists Italian Network, et al. COVID-19 vaccination and patients with psoriasis under biologics: real-life evidence on safety and effectiveness from Italian vaccinated healthcare workers. Clin Exp Dermatol. 2021;460:1106-1108.
- Joshi RK, Muralidharan CG, Gulati DS, et al. Higher incidence of reported adverse events following immunisation (AEFI) after first dose of COVID-19 vaccine among previously infected health care workers. Med J Armed Forces India. 2021;77(suppl 2):S505-S507.
- Hervé C, Laupèze B, Del Giudice G, et al. The how’s and what’s of vaccine reactogenicity. NPJ Vaccines. 2019;4:39.
- COVID-19 coronavirus pandemic: weekly trends. Worldometer. Accessed August 21, 2023. https://www.worldometers.info/coronavirus/
- National COVID-19 vaccination programme meets its goals by overcoming R&D and logistical challenges, says economic survey 2022-23. Government of India Press Information Bureau website. Published January 31, 2023. Accessed August 24, 2023. https://pib.gov.in/PressReleasePage.aspx?PRID=1894907
- Ministry of Health and Family Welfare. CoWIN. Accessed August 21, 2023. https://www.cowin.gov.in/
- Griffiths CEM, Armstrong AW, Gudjonsson JE, et al. Psoriasis. Lancet. 2021;397:1301-1315.
- Wu D, Yang XO. TH17 responses in cytokine storm of COVID-19: anemerging target of JAK2 inhibitor fedratinib. J Microbiol Immunol Infect. 2020;53:368-370.
- International Psoriasis Council. Revised IPC statement on COVID-19. Published December 19, 2022. Accessed August 24, 2023. https://psoriasiscouncil.org/covid-19/revised-statement-covid-19/
- Sotiriou E, Tsentemeidou A, Bakirtzi K, et al. Psoriasis exacerbation after COVID-19 vaccination: a report of 14 cases from a single centre. J Eur Acad Dermatol Venereol. 2021;35:E857-E859.
- Kaul R. India clears 2 vaccines for kids under 12 years. Hindustan Times. Published April 27, 2022. Accessed August 24, 2023. https://www.hindustantimes.com/india-news/india-clears-2-vaccines-for-kids-under-12-years-101650998027336.html
- Huang YW, Tsai TF. Exacerbation of psoriasis following COVID-19 vaccination: report from a single center. Front Med (Lausanne). 2021;8:812010.
- Damiani G, Allocco F, Young Dermatologists Italian Network, et al. COVID-19 vaccination and patients with psoriasis under biologics: real-life evidence on safety and effectiveness from Italian vaccinated healthcare workers. Clin Exp Dermatol. 2021;460:1106-1108.
- Joshi RK, Muralidharan CG, Gulati DS, et al. Higher incidence of reported adverse events following immunisation (AEFI) after first dose of COVID-19 vaccine among previously infected health care workers. Med J Armed Forces India. 2021;77(suppl 2):S505-S507.
- Hervé C, Laupèze B, Del Giudice G, et al. The how’s and what’s of vaccine reactogenicity. NPJ Vaccines. 2019;4:39.
Practice Points
- Vaccines are known to induce a psoriasis flare.
- Given the high risk for severe COVID infection in individuals with psoriasis who have comorbidities, vaccination with Covaxin and Covishield can be safely recommended in India for this population.