User login
4 Simple Hacks to Get Paid for Lifestyle Medicine
This transcript has been edited for clarity.
As primary care doctors, lifestyle medicine is supposed to be a pillar of our practice. Per the evidence, lifestyle medicine can prevent up to 80% of chronic disease. It’s a real irony, then, that it’s the thing we’re least likely to be paid to do.
Thankfully, though, there are a few hacks to help you keep your patients healthy and yourself financially healthy at the same time.
No. 1: Be as accurate in your coding as possible. We all know working on things like sleep, exercise, and diet with patients takes time, so bill for it. With time-based billing, in particular, you can account for both the time spent in face-to-face encounters and the time spent afterward on documentation and care coordination. Make sure to capture that.
No. 2: Try group visits on for size. Group visit models are great for lifestyle medicine. They give you the flexibility to include longer conversations and deeper lessons on a range of subjects while still getting paid for what you do. Want to host a cooking class? Group visit. Want to bring in a personal trainer or hold a dance class or exercise dance class? Group visit. Meditation, yoga, or even a sleep hygiene class? Group visit.
While there are a few tricks to getting paid for group visits, they’re the same things, such as documenting time and the various parts of the visit, that are key to getting paid for regular visits. They have the bonus of fighting burnout and making your own practice more meaningful as well.
No. 3: Think about joining a value-based care arrangement. While only accounting for 10% of the market right now, value-based care (VBC) is growing rapidly, and it’s easy to see why. By trading quality for the hamster wheel of billing widgets, physicians are freed up to think more about how best to take care of patients, including incorporating more lifestyle medicine. Some VBC models even have their own electronic medical records, freeing you from outdated structures when it comes to documenting patient visits.
No. 4: direct primary care. Direct primary care cuts out the middlemen of payers, letting patients pay physician practices directly for their own care. Like VBC, it opens up possibilities for practicing better medicine, including lifestyle medicine. In addition, it’s often very affordable, with a family of four often paying around $80 a month for a membership for the entire family. It’s a win-win for the doctor and the patient.
Lifestyle medicine is a great way to improve both your patients’ and your own well-being. With a few flexes, it can improve your wallet’s well-being, too.
Tamaan K. Osbourne-Roberts, President/CEO, Happiness by the Numbers, Denver, Colorado, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
As primary care doctors, lifestyle medicine is supposed to be a pillar of our practice. Per the evidence, lifestyle medicine can prevent up to 80% of chronic disease. It’s a real irony, then, that it’s the thing we’re least likely to be paid to do.
Thankfully, though, there are a few hacks to help you keep your patients healthy and yourself financially healthy at the same time.
No. 1: Be as accurate in your coding as possible. We all know working on things like sleep, exercise, and diet with patients takes time, so bill for it. With time-based billing, in particular, you can account for both the time spent in face-to-face encounters and the time spent afterward on documentation and care coordination. Make sure to capture that.
No. 2: Try group visits on for size. Group visit models are great for lifestyle medicine. They give you the flexibility to include longer conversations and deeper lessons on a range of subjects while still getting paid for what you do. Want to host a cooking class? Group visit. Want to bring in a personal trainer or hold a dance class or exercise dance class? Group visit. Meditation, yoga, or even a sleep hygiene class? Group visit.
While there are a few tricks to getting paid for group visits, they’re the same things, such as documenting time and the various parts of the visit, that are key to getting paid for regular visits. They have the bonus of fighting burnout and making your own practice more meaningful as well.
No. 3: Think about joining a value-based care arrangement. While only accounting for 10% of the market right now, value-based care (VBC) is growing rapidly, and it’s easy to see why. By trading quality for the hamster wheel of billing widgets, physicians are freed up to think more about how best to take care of patients, including incorporating more lifestyle medicine. Some VBC models even have their own electronic medical records, freeing you from outdated structures when it comes to documenting patient visits.
No. 4: direct primary care. Direct primary care cuts out the middlemen of payers, letting patients pay physician practices directly for their own care. Like VBC, it opens up possibilities for practicing better medicine, including lifestyle medicine. In addition, it’s often very affordable, with a family of four often paying around $80 a month for a membership for the entire family. It’s a win-win for the doctor and the patient.
Lifestyle medicine is a great way to improve both your patients’ and your own well-being. With a few flexes, it can improve your wallet’s well-being, too.
Tamaan K. Osbourne-Roberts, President/CEO, Happiness by the Numbers, Denver, Colorado, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
As primary care doctors, lifestyle medicine is supposed to be a pillar of our practice. Per the evidence, lifestyle medicine can prevent up to 80% of chronic disease. It’s a real irony, then, that it’s the thing we’re least likely to be paid to do.
Thankfully, though, there are a few hacks to help you keep your patients healthy and yourself financially healthy at the same time.
No. 1: Be as accurate in your coding as possible. We all know working on things like sleep, exercise, and diet with patients takes time, so bill for it. With time-based billing, in particular, you can account for both the time spent in face-to-face encounters and the time spent afterward on documentation and care coordination. Make sure to capture that.
No. 2: Try group visits on for size. Group visit models are great for lifestyle medicine. They give you the flexibility to include longer conversations and deeper lessons on a range of subjects while still getting paid for what you do. Want to host a cooking class? Group visit. Want to bring in a personal trainer or hold a dance class or exercise dance class? Group visit. Meditation, yoga, or even a sleep hygiene class? Group visit.
While there are a few tricks to getting paid for group visits, they’re the same things, such as documenting time and the various parts of the visit, that are key to getting paid for regular visits. They have the bonus of fighting burnout and making your own practice more meaningful as well.
No. 3: Think about joining a value-based care arrangement. While only accounting for 10% of the market right now, value-based care (VBC) is growing rapidly, and it’s easy to see why. By trading quality for the hamster wheel of billing widgets, physicians are freed up to think more about how best to take care of patients, including incorporating more lifestyle medicine. Some VBC models even have their own electronic medical records, freeing you from outdated structures when it comes to documenting patient visits.
No. 4: direct primary care. Direct primary care cuts out the middlemen of payers, letting patients pay physician practices directly for their own care. Like VBC, it opens up possibilities for practicing better medicine, including lifestyle medicine. In addition, it’s often very affordable, with a family of four often paying around $80 a month for a membership for the entire family. It’s a win-win for the doctor and the patient.
Lifestyle medicine is a great way to improve both your patients’ and your own well-being. With a few flexes, it can improve your wallet’s well-being, too.
Tamaan K. Osbourne-Roberts, President/CEO, Happiness by the Numbers, Denver, Colorado, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nutrition and Medical Education
How comfortable are you giving nutritional advice to your patients? When you offer it are you basing your advice on something you learned during medical school or your training? Was it included in a course devoted to nutrition? Did you learn it later as part of continuing medical education course (CME)? Or was it just something you just picked up from your experience seeing patients (osmosis)? It is very unlikely that a significant portion, or any part for that matter, of your medical training was devoted to nutrition. It certainly wasn’t during my training.
I recently read an interview with Emily M. Broad Leib, JD, faculty director of the Harvard School Center for Health Law and Policy Innovation, Cambridge, Massachusetts, who would like to correct that deficiency. She feels doctors need to know more about food and that acquiring that knowledge should be a significant component of their formal training.
In the interview, Leib said that “roughly 86% of physicians report they do not feel adequately trained to answer basic questions on diet or nutrition.” She also notes that while “72% of entering medical students report they believe food is important to health” less than 50% retained this belief after graduation.
Leib and associates feel they have recently reached a milestone in their efforts to include nutrition in the mainstream of medical education this fall by publishing a paper that demonstrates “consensus on doctor-approved nutritional standard for medical schools and residency programs.”
36 Recommended Competencies
Curious about what these nutrition experts chose to include in medical training, I decided to drill down into the list of 36 consensus-driven competencies they had agreed upon.
It was an interesting voyage into a forest of redundancies, many of which can be boiled down to having the student demonstrate that he/she understands that what we eat is important to our health and that there is a complex web of relationships connecting our society to the food consume.
Some of the recommended competencies I found make perfect sense. For example the student/trainee should be able to take a diet and food history and be able to interpret lab values and anthropometric measurements and be able to discuss the patient’s weight and diet with sensitivity while keeping in mind his/her own biases about food.
Some other recommendations are more problematic, for example, “performs a comprehensive nutrition-focused physical examination” or “demonstrates knowledge of how to create culinary nutrition SMART [Specific, Measurable, Achievable, Relevant, and Time-Bound] goals for personal use and for patient care” or “provides brief counseling interventions to help patients decrease visceral adiposity or reduce the risk of metabolic syndrome.” Including competencies like these demonstrates a lack of understanding of the time restraints and realities of a primary care physician’s life and training.
Instead of simply reinforcing the prospective physician’s preexisting assumption that food and health are entwined and discussing when and how to consult a nutrition expert, these 36 competencies seem to be an attempt to create fast-tracked part-time dietitians and nutrition advocates out of medical students and trainees who already believe that nutrition is important for health but also have a very full plate of clinical responsibilities ahead of them.
The study that Leib quotes — that 72% of medical students believed food was important in health while after graduation only 50% of agreed — doesn’t necessarily mean that professors are preaching that food was unimportant. It is more likely by the end of medical school the students have seen that food must share the spotlight with numerous other factors that influence their patients’ health.
‘A More Appropriate Focus’
In my experience, diet and lifestyle counseling done well is extremely time consuming and best done by people for whom that is their specialty. A more appropriate focus for a list of nutritional competencies for physicians in training would be for the student to achieve an understanding of when and how to consult a dietitian and then how to support and evaluate the dietitian’s recommendations to the patient.
Finally, I don’t think we can ignore a serious public relations problem that hangs like a cloud over the nutrition advocacy community. It is the same one that casts a shadow on the medical community as well. It is a common perception among the lay public that nutritionists (and physicians) are always changing their recommendations when it comes to food. What is believable? Just think about eggs, red wine, or introducing peanuts to infants, to name just a few. And what about the food pyramids that seem to have been rebuilt every several years? The problem is compounded when some “credentialed” nutritionists and physicians continue to make dietary pronouncements with only a shred of evidence or poorly documented anecdotal observations.
The first of the 36 competencies I reviewed reads: “Provide evidence-based, culturally sensitive nutrition and food recommendations for the prevention and treatment of disease.” When it comes to nutrition the “evidence” can be tough to come by. The natural experiments in which individuals and populations had extremely limited access to a certain nutrients (eg, scurvy) don’t occur very often. Animal studies don’t always extrapolate to humans. And, observational studies concerning diet often have co-factors that are difficult to control and must run over time courses that can tax even the most patient researchers.
I certainly applaud Leib and associates for promoting their primary goal of including more about of the relationship between food and health in the medical school and trainee curriculum. But I must voice a caution to be careful to keep it truly evidence-based and in a format that acknowledges the realities of the life and education of a primary care provider.
The best nutritional advice I ever received in my training was from an older pediatric professor who suggested that a healthy diet consisted of everything in moderation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
How comfortable are you giving nutritional advice to your patients? When you offer it are you basing your advice on something you learned during medical school or your training? Was it included in a course devoted to nutrition? Did you learn it later as part of continuing medical education course (CME)? Or was it just something you just picked up from your experience seeing patients (osmosis)? It is very unlikely that a significant portion, or any part for that matter, of your medical training was devoted to nutrition. It certainly wasn’t during my training.
I recently read an interview with Emily M. Broad Leib, JD, faculty director of the Harvard School Center for Health Law and Policy Innovation, Cambridge, Massachusetts, who would like to correct that deficiency. She feels doctors need to know more about food and that acquiring that knowledge should be a significant component of their formal training.
In the interview, Leib said that “roughly 86% of physicians report they do not feel adequately trained to answer basic questions on diet or nutrition.” She also notes that while “72% of entering medical students report they believe food is important to health” less than 50% retained this belief after graduation.
Leib and associates feel they have recently reached a milestone in their efforts to include nutrition in the mainstream of medical education this fall by publishing a paper that demonstrates “consensus on doctor-approved nutritional standard for medical schools and residency programs.”
36 Recommended Competencies
Curious about what these nutrition experts chose to include in medical training, I decided to drill down into the list of 36 consensus-driven competencies they had agreed upon.
It was an interesting voyage into a forest of redundancies, many of which can be boiled down to having the student demonstrate that he/she understands that what we eat is important to our health and that there is a complex web of relationships connecting our society to the food consume.
Some of the recommended competencies I found make perfect sense. For example the student/trainee should be able to take a diet and food history and be able to interpret lab values and anthropometric measurements and be able to discuss the patient’s weight and diet with sensitivity while keeping in mind his/her own biases about food.
Some other recommendations are more problematic, for example, “performs a comprehensive nutrition-focused physical examination” or “demonstrates knowledge of how to create culinary nutrition SMART [Specific, Measurable, Achievable, Relevant, and Time-Bound] goals for personal use and for patient care” or “provides brief counseling interventions to help patients decrease visceral adiposity or reduce the risk of metabolic syndrome.” Including competencies like these demonstrates a lack of understanding of the time restraints and realities of a primary care physician’s life and training.
Instead of simply reinforcing the prospective physician’s preexisting assumption that food and health are entwined and discussing when and how to consult a nutrition expert, these 36 competencies seem to be an attempt to create fast-tracked part-time dietitians and nutrition advocates out of medical students and trainees who already believe that nutrition is important for health but also have a very full plate of clinical responsibilities ahead of them.
The study that Leib quotes — that 72% of medical students believed food was important in health while after graduation only 50% of agreed — doesn’t necessarily mean that professors are preaching that food was unimportant. It is more likely by the end of medical school the students have seen that food must share the spotlight with numerous other factors that influence their patients’ health.
‘A More Appropriate Focus’
In my experience, diet and lifestyle counseling done well is extremely time consuming and best done by people for whom that is their specialty. A more appropriate focus for a list of nutritional competencies for physicians in training would be for the student to achieve an understanding of when and how to consult a dietitian and then how to support and evaluate the dietitian’s recommendations to the patient.
Finally, I don’t think we can ignore a serious public relations problem that hangs like a cloud over the nutrition advocacy community. It is the same one that casts a shadow on the medical community as well. It is a common perception among the lay public that nutritionists (and physicians) are always changing their recommendations when it comes to food. What is believable? Just think about eggs, red wine, or introducing peanuts to infants, to name just a few. And what about the food pyramids that seem to have been rebuilt every several years? The problem is compounded when some “credentialed” nutritionists and physicians continue to make dietary pronouncements with only a shred of evidence or poorly documented anecdotal observations.
The first of the 36 competencies I reviewed reads: “Provide evidence-based, culturally sensitive nutrition and food recommendations for the prevention and treatment of disease.” When it comes to nutrition the “evidence” can be tough to come by. The natural experiments in which individuals and populations had extremely limited access to a certain nutrients (eg, scurvy) don’t occur very often. Animal studies don’t always extrapolate to humans. And, observational studies concerning diet often have co-factors that are difficult to control and must run over time courses that can tax even the most patient researchers.
I certainly applaud Leib and associates for promoting their primary goal of including more about of the relationship between food and health in the medical school and trainee curriculum. But I must voice a caution to be careful to keep it truly evidence-based and in a format that acknowledges the realities of the life and education of a primary care provider.
The best nutritional advice I ever received in my training was from an older pediatric professor who suggested that a healthy diet consisted of everything in moderation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
How comfortable are you giving nutritional advice to your patients? When you offer it are you basing your advice on something you learned during medical school or your training? Was it included in a course devoted to nutrition? Did you learn it later as part of continuing medical education course (CME)? Or was it just something you just picked up from your experience seeing patients (osmosis)? It is very unlikely that a significant portion, or any part for that matter, of your medical training was devoted to nutrition. It certainly wasn’t during my training.
I recently read an interview with Emily M. Broad Leib, JD, faculty director of the Harvard School Center for Health Law and Policy Innovation, Cambridge, Massachusetts, who would like to correct that deficiency. She feels doctors need to know more about food and that acquiring that knowledge should be a significant component of their formal training.
In the interview, Leib said that “roughly 86% of physicians report they do not feel adequately trained to answer basic questions on diet or nutrition.” She also notes that while “72% of entering medical students report they believe food is important to health” less than 50% retained this belief after graduation.
Leib and associates feel they have recently reached a milestone in their efforts to include nutrition in the mainstream of medical education this fall by publishing a paper that demonstrates “consensus on doctor-approved nutritional standard for medical schools and residency programs.”
36 Recommended Competencies
Curious about what these nutrition experts chose to include in medical training, I decided to drill down into the list of 36 consensus-driven competencies they had agreed upon.
It was an interesting voyage into a forest of redundancies, many of which can be boiled down to having the student demonstrate that he/she understands that what we eat is important to our health and that there is a complex web of relationships connecting our society to the food consume.
Some of the recommended competencies I found make perfect sense. For example the student/trainee should be able to take a diet and food history and be able to interpret lab values and anthropometric measurements and be able to discuss the patient’s weight and diet with sensitivity while keeping in mind his/her own biases about food.
Some other recommendations are more problematic, for example, “performs a comprehensive nutrition-focused physical examination” or “demonstrates knowledge of how to create culinary nutrition SMART [Specific, Measurable, Achievable, Relevant, and Time-Bound] goals for personal use and for patient care” or “provides brief counseling interventions to help patients decrease visceral adiposity or reduce the risk of metabolic syndrome.” Including competencies like these demonstrates a lack of understanding of the time restraints and realities of a primary care physician’s life and training.
Instead of simply reinforcing the prospective physician’s preexisting assumption that food and health are entwined and discussing when and how to consult a nutrition expert, these 36 competencies seem to be an attempt to create fast-tracked part-time dietitians and nutrition advocates out of medical students and trainees who already believe that nutrition is important for health but also have a very full plate of clinical responsibilities ahead of them.
The study that Leib quotes — that 72% of medical students believed food was important in health while after graduation only 50% of agreed — doesn’t necessarily mean that professors are preaching that food was unimportant. It is more likely by the end of medical school the students have seen that food must share the spotlight with numerous other factors that influence their patients’ health.
‘A More Appropriate Focus’
In my experience, diet and lifestyle counseling done well is extremely time consuming and best done by people for whom that is their specialty. A more appropriate focus for a list of nutritional competencies for physicians in training would be for the student to achieve an understanding of when and how to consult a dietitian and then how to support and evaluate the dietitian’s recommendations to the patient.
Finally, I don’t think we can ignore a serious public relations problem that hangs like a cloud over the nutrition advocacy community. It is the same one that casts a shadow on the medical community as well. It is a common perception among the lay public that nutritionists (and physicians) are always changing their recommendations when it comes to food. What is believable? Just think about eggs, red wine, or introducing peanuts to infants, to name just a few. And what about the food pyramids that seem to have been rebuilt every several years? The problem is compounded when some “credentialed” nutritionists and physicians continue to make dietary pronouncements with only a shred of evidence or poorly documented anecdotal observations.
The first of the 36 competencies I reviewed reads: “Provide evidence-based, culturally sensitive nutrition and food recommendations for the prevention and treatment of disease.” When it comes to nutrition the “evidence” can be tough to come by. The natural experiments in which individuals and populations had extremely limited access to a certain nutrients (eg, scurvy) don’t occur very often. Animal studies don’t always extrapolate to humans. And, observational studies concerning diet often have co-factors that are difficult to control and must run over time courses that can tax even the most patient researchers.
I certainly applaud Leib and associates for promoting their primary goal of including more about of the relationship between food and health in the medical school and trainee curriculum. But I must voice a caution to be careful to keep it truly evidence-based and in a format that acknowledges the realities of the life and education of a primary care provider.
The best nutritional advice I ever received in my training was from an older pediatric professor who suggested that a healthy diet consisted of everything in moderation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
America’s PCPs: Take a Bow
Hi, everyone. I’m Dr. Kenny Lin. I am a family physician and associate director of the Lancaster General Hospital Family Medicine Residency, and I blog at Common Sense Family Doctor.
For the past 4 years, primary care clinicians have labored under a seemingly endless onslaught of bad news. A recent report estimated that there were over 1.3 million excess deaths in the United States from March 2020 to May 2023, including nearly half a million Americans younger than age 65. Social isolation and an ailing economy accelerated preexisting rises in drug overdoses and obesity, while teenage vaping threatened to hook a new generation on tobacco products even as adult smoking plummeted. Meanwhile, more than half of the nation’s physicians now report feelings of burnout, pay for family doctors appears to be stagnating, and our interactions with an increasing number of patients are fraught with suspicions about the value of vaccines— not just against COVID-19 but against flu and other viruses, too — and the medical system as a whole, doctors included.
Now, for the good news.
A year and a half since the end of the pandemic emergency, we are seeing gains on several fronts, and physicians deserve much of the credit. Preliminary data from the Centers for Disease Control and Prevention show that 10,000 fewer people died from drug overdoses than in the previous year. Although multiple factors contributed to this change, the elimination of the X-waiver, which had previously been required for physicians to prescribe buprenorphine for opioid use disorder, in January 2023 has improved access to medications for addiction treatment. In addition, the expansion of state requirements to check prescription drug monitoring programs when opioids or benzodiazepines are prescribed, and to prescribe naloxone to patients taking more than a certain number of morphine milligram equivalents per day, has probably reduced the harms of hazardous drug use.
On the obesity front, recent data from the National Health and Nutrition Examination Survey found that the prevalence of obesity in adults fell for the first time in more than a decade, from 41.9% to 40.3%. To be sure, obesity remains far too common, and this finding could be the result of statistical chance rather than representing a true decline. But the widespread prescribing of GLP-1 receptor agonists by primary care physicians, in particular, could have played a role in the encouraging trend.
Although more research is needed to prove causality, one analysis suggests that these drugs could easily have lowered the body mass index (BMI) of more than enough patients to account for the observed decline. What’s more, the rise in prevalence of BMIs above 40 (from 7.7% to 9.7%) could be explained by the mortality benefit of the drugs: More people remained in this severe obesity category because they didn’t die from complications of their weight. Whether future studies support keeping people on GLP-1s for life or eventually “off-ramping” them to other weight control strategies, family physicians are well positioned to help.
Finally, with little fanfare, the youth smoking rate has fallen precipitously. In 2023, 1.9% of high school students and 1.1% of middle-schoolers reported smoking cigarettes in the past 30 days. And they didn’t simply swap one form of nicotine delivery device for another. The 30-day prevalence of vaping among high school students fell from 27.5% in 2019 to 7.8% this year. Changing social norms and stricter federal regulation of tobacco products are probably more responsible for this positive trend than medical care, though the US Preventive Services Task Force recommends education or brief counseling to prevent initiation of tobacco use among school-aged children and adolescents. Should tobacco use in youth remain at these historically low levels, millions of premature deaths from lung cancer and heart disease will have been prevented.
America’s doctors have earned the right to take a bow. We have much more work to do, but our efforts are making a meaningful difference in three seemingly intractable health problems.
Dr. Lin, Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hi, everyone. I’m Dr. Kenny Lin. I am a family physician and associate director of the Lancaster General Hospital Family Medicine Residency, and I blog at Common Sense Family Doctor.
For the past 4 years, primary care clinicians have labored under a seemingly endless onslaught of bad news. A recent report estimated that there were over 1.3 million excess deaths in the United States from March 2020 to May 2023, including nearly half a million Americans younger than age 65. Social isolation and an ailing economy accelerated preexisting rises in drug overdoses and obesity, while teenage vaping threatened to hook a new generation on tobacco products even as adult smoking plummeted. Meanwhile, more than half of the nation’s physicians now report feelings of burnout, pay for family doctors appears to be stagnating, and our interactions with an increasing number of patients are fraught with suspicions about the value of vaccines— not just against COVID-19 but against flu and other viruses, too — and the medical system as a whole, doctors included.
Now, for the good news.
A year and a half since the end of the pandemic emergency, we are seeing gains on several fronts, and physicians deserve much of the credit. Preliminary data from the Centers for Disease Control and Prevention show that 10,000 fewer people died from drug overdoses than in the previous year. Although multiple factors contributed to this change, the elimination of the X-waiver, which had previously been required for physicians to prescribe buprenorphine for opioid use disorder, in January 2023 has improved access to medications for addiction treatment. In addition, the expansion of state requirements to check prescription drug monitoring programs when opioids or benzodiazepines are prescribed, and to prescribe naloxone to patients taking more than a certain number of morphine milligram equivalents per day, has probably reduced the harms of hazardous drug use.
On the obesity front, recent data from the National Health and Nutrition Examination Survey found that the prevalence of obesity in adults fell for the first time in more than a decade, from 41.9% to 40.3%. To be sure, obesity remains far too common, and this finding could be the result of statistical chance rather than representing a true decline. But the widespread prescribing of GLP-1 receptor agonists by primary care physicians, in particular, could have played a role in the encouraging trend.
Although more research is needed to prove causality, one analysis suggests that these drugs could easily have lowered the body mass index (BMI) of more than enough patients to account for the observed decline. What’s more, the rise in prevalence of BMIs above 40 (from 7.7% to 9.7%) could be explained by the mortality benefit of the drugs: More people remained in this severe obesity category because they didn’t die from complications of their weight. Whether future studies support keeping people on GLP-1s for life or eventually “off-ramping” them to other weight control strategies, family physicians are well positioned to help.
Finally, with little fanfare, the youth smoking rate has fallen precipitously. In 2023, 1.9% of high school students and 1.1% of middle-schoolers reported smoking cigarettes in the past 30 days. And they didn’t simply swap one form of nicotine delivery device for another. The 30-day prevalence of vaping among high school students fell from 27.5% in 2019 to 7.8% this year. Changing social norms and stricter federal regulation of tobacco products are probably more responsible for this positive trend than medical care, though the US Preventive Services Task Force recommends education or brief counseling to prevent initiation of tobacco use among school-aged children and adolescents. Should tobacco use in youth remain at these historically low levels, millions of premature deaths from lung cancer and heart disease will have been prevented.
America’s doctors have earned the right to take a bow. We have much more work to do, but our efforts are making a meaningful difference in three seemingly intractable health problems.
Dr. Lin, Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hi, everyone. I’m Dr. Kenny Lin. I am a family physician and associate director of the Lancaster General Hospital Family Medicine Residency, and I blog at Common Sense Family Doctor.
For the past 4 years, primary care clinicians have labored under a seemingly endless onslaught of bad news. A recent report estimated that there were over 1.3 million excess deaths in the United States from March 2020 to May 2023, including nearly half a million Americans younger than age 65. Social isolation and an ailing economy accelerated preexisting rises in drug overdoses and obesity, while teenage vaping threatened to hook a new generation on tobacco products even as adult smoking plummeted. Meanwhile, more than half of the nation’s physicians now report feelings of burnout, pay for family doctors appears to be stagnating, and our interactions with an increasing number of patients are fraught with suspicions about the value of vaccines— not just against COVID-19 but against flu and other viruses, too — and the medical system as a whole, doctors included.
Now, for the good news.
A year and a half since the end of the pandemic emergency, we are seeing gains on several fronts, and physicians deserve much of the credit. Preliminary data from the Centers for Disease Control and Prevention show that 10,000 fewer people died from drug overdoses than in the previous year. Although multiple factors contributed to this change, the elimination of the X-waiver, which had previously been required for physicians to prescribe buprenorphine for opioid use disorder, in January 2023 has improved access to medications for addiction treatment. In addition, the expansion of state requirements to check prescription drug monitoring programs when opioids or benzodiazepines are prescribed, and to prescribe naloxone to patients taking more than a certain number of morphine milligram equivalents per day, has probably reduced the harms of hazardous drug use.
On the obesity front, recent data from the National Health and Nutrition Examination Survey found that the prevalence of obesity in adults fell for the first time in more than a decade, from 41.9% to 40.3%. To be sure, obesity remains far too common, and this finding could be the result of statistical chance rather than representing a true decline. But the widespread prescribing of GLP-1 receptor agonists by primary care physicians, in particular, could have played a role in the encouraging trend.
Although more research is needed to prove causality, one analysis suggests that these drugs could easily have lowered the body mass index (BMI) of more than enough patients to account for the observed decline. What’s more, the rise in prevalence of BMIs above 40 (from 7.7% to 9.7%) could be explained by the mortality benefit of the drugs: More people remained in this severe obesity category because they didn’t die from complications of their weight. Whether future studies support keeping people on GLP-1s for life or eventually “off-ramping” them to other weight control strategies, family physicians are well positioned to help.
Finally, with little fanfare, the youth smoking rate has fallen precipitously. In 2023, 1.9% of high school students and 1.1% of middle-schoolers reported smoking cigarettes in the past 30 days. And they didn’t simply swap one form of nicotine delivery device for another. The 30-day prevalence of vaping among high school students fell from 27.5% in 2019 to 7.8% this year. Changing social norms and stricter federal regulation of tobacco products are probably more responsible for this positive trend than medical care, though the US Preventive Services Task Force recommends education or brief counseling to prevent initiation of tobacco use among school-aged children and adolescents. Should tobacco use in youth remain at these historically low levels, millions of premature deaths from lung cancer and heart disease will have been prevented.
America’s doctors have earned the right to take a bow. We have much more work to do, but our efforts are making a meaningful difference in three seemingly intractable health problems.
Dr. Lin, Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lifestyle Medicine Trends to Keep an Eye On
Our current healthcare system, which is a costly and unending cycle of merely managing chronic disease symptoms, is failing us. What we truly need is a patient-centered approach that restores health by addressing not just diagnoses but also the physical, emotional, and social needs of each individual. This is the essence of whole-person health, and transformation toward this model of care is already underway.
This shift underscores why clinicians like me support placing lifestyle medicine at the foundation of health and healthcare. Evidence-based lifestyle medicine — which applies interventions in nutrition, physical activity, restorative sleep, stress management, positive social connections, and avoidance of risky substances to prevent, treat, and when used intensively, even reverse lifestyle-related chronic disease — is a medical specialty equipped to successfully address patients’ whole-person health in an effective, high-value clinical care delivery model.
As this transformation continues, here are four key lifestyle medicine trends for 2025.
Lifestyle Medicine Becomes More Ingrained in Primary Care
The 2021 National Academies of Science, Engineering, and Medicine report, “Implementing High-Quality Primary Care” sounded the alarm about the state of primary care and outlined a comprehensive approach to transform it. Lifestyle medicine emerged as a solution as clinicians found innovative ways to integrate lifestyle behavior interventions into existing care models in a financially sustainable, scalable manner. Examples include Blue Zones Health, a new delivery model that aligns lifestyle medicine–certified clinicians with community and payers in California, and the University of Pittsburgh Medical Center lifestyle medicine program, where primary care patients are referred to virtual group coaching, a teaching kitchen, and classes on food as medicine, obesity, type 2 diabetes, and more.
Organizations dedicated to advancing primary care are paying close attention to the potential of lifestyle medicine. Currently, The Primary Care Collaborative has launched a new multi-year initiative on whole-person care and lifestyle medicine. This initiative aims to broaden the primary care community’s understanding of whole health and lifestyle medicine concepts and the evidence behind them, as well as lay the groundwork for future work to promote whole-person primary care and lifestyle medicine among an engaged and committed community of members.
Digital Tools and AI Spark Lifestyle Medicine Innovations
American College of Lifestyle Medicine partner organizations are increasingly utilizing digital tools, such as health apps tailored to lifestyle behavior interventions, to expand access to care and support behavior change. One of the biggest challenges in lifestyle interventions is the limited time during patient encounters. But artificial intelligence (AI) tools can record (with patient permission) and summarize encounters, enabling clinicians to turn away from their keyboards and be more present to learn about the unique living, environmental, and societal factors that impact every individual’s lifestyle choices. AI tools can create individualized whole-food, plant-predominant meal plans or physical activity schedules for patients in just a few seconds. The potential for AI in lifestyle medicine is vast, and its applications were further explored at the American College of Lifestyle Medicine’s annual conference in October.
Behavior Change and Sustainability of the Food-as-Medicine Movement
Significant investments have been made in food as medicine to address diet-related chronic diseases. But merely providing medically tailored meals or produce prescriptions is not enough because once the prescriptions end, so will the health benefits. Clinicians certified in lifestyle medicine are prepared to coach patients into long-term behavior change, supporting them with education and information to shop for and prepare tasty, nutritious, and affordable food. The same applies to the use of glucagon-like peptide 1 drugs. Although the initial weight loss offers motivation, lifestyle changes are necessary to sustain long-term health benefits beyond medications.
Lifestyle Medicine Emerges as a Strategy to Achieve Health Equity
Lifestyle behavior interventions have the unique ability to address health status and social drivers of health. For example, food as medicine affects an individual’s health while also addressing nutrition security. Certainly, no medication can both improve health status and feed someone. The addition of payment for the screening of social drivers of health to the 2024 Medicare Physician Fee Schedule is an important step toward connecting clinicians with community health–based organizations that can address factors that influence patients’ ability to adhere to lifestyle behavior care plans. Lifestyle medicine clinicians are poised to lead this effort because they are already having conversations with patients about their environment, living conditions, and access to nutritious food.
The changes coming to our healthcare system are exciting and long overdue. Lifestyle medicine is positioned to be at the forefront of this transformation now and in the future.
Dr. Patel, president of the American College of Lifestyle Medicine in St. Louis, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Our current healthcare system, which is a costly and unending cycle of merely managing chronic disease symptoms, is failing us. What we truly need is a patient-centered approach that restores health by addressing not just diagnoses but also the physical, emotional, and social needs of each individual. This is the essence of whole-person health, and transformation toward this model of care is already underway.
This shift underscores why clinicians like me support placing lifestyle medicine at the foundation of health and healthcare. Evidence-based lifestyle medicine — which applies interventions in nutrition, physical activity, restorative sleep, stress management, positive social connections, and avoidance of risky substances to prevent, treat, and when used intensively, even reverse lifestyle-related chronic disease — is a medical specialty equipped to successfully address patients’ whole-person health in an effective, high-value clinical care delivery model.
As this transformation continues, here are four key lifestyle medicine trends for 2025.
Lifestyle Medicine Becomes More Ingrained in Primary Care
The 2021 National Academies of Science, Engineering, and Medicine report, “Implementing High-Quality Primary Care” sounded the alarm about the state of primary care and outlined a comprehensive approach to transform it. Lifestyle medicine emerged as a solution as clinicians found innovative ways to integrate lifestyle behavior interventions into existing care models in a financially sustainable, scalable manner. Examples include Blue Zones Health, a new delivery model that aligns lifestyle medicine–certified clinicians with community and payers in California, and the University of Pittsburgh Medical Center lifestyle medicine program, where primary care patients are referred to virtual group coaching, a teaching kitchen, and classes on food as medicine, obesity, type 2 diabetes, and more.
Organizations dedicated to advancing primary care are paying close attention to the potential of lifestyle medicine. Currently, The Primary Care Collaborative has launched a new multi-year initiative on whole-person care and lifestyle medicine. This initiative aims to broaden the primary care community’s understanding of whole health and lifestyle medicine concepts and the evidence behind them, as well as lay the groundwork for future work to promote whole-person primary care and lifestyle medicine among an engaged and committed community of members.
Digital Tools and AI Spark Lifestyle Medicine Innovations
American College of Lifestyle Medicine partner organizations are increasingly utilizing digital tools, such as health apps tailored to lifestyle behavior interventions, to expand access to care and support behavior change. One of the biggest challenges in lifestyle interventions is the limited time during patient encounters. But artificial intelligence (AI) tools can record (with patient permission) and summarize encounters, enabling clinicians to turn away from their keyboards and be more present to learn about the unique living, environmental, and societal factors that impact every individual’s lifestyle choices. AI tools can create individualized whole-food, plant-predominant meal plans or physical activity schedules for patients in just a few seconds. The potential for AI in lifestyle medicine is vast, and its applications were further explored at the American College of Lifestyle Medicine’s annual conference in October.
Behavior Change and Sustainability of the Food-as-Medicine Movement
Significant investments have been made in food as medicine to address diet-related chronic diseases. But merely providing medically tailored meals or produce prescriptions is not enough because once the prescriptions end, so will the health benefits. Clinicians certified in lifestyle medicine are prepared to coach patients into long-term behavior change, supporting them with education and information to shop for and prepare tasty, nutritious, and affordable food. The same applies to the use of glucagon-like peptide 1 drugs. Although the initial weight loss offers motivation, lifestyle changes are necessary to sustain long-term health benefits beyond medications.
Lifestyle Medicine Emerges as a Strategy to Achieve Health Equity
Lifestyle behavior interventions have the unique ability to address health status and social drivers of health. For example, food as medicine affects an individual’s health while also addressing nutrition security. Certainly, no medication can both improve health status and feed someone. The addition of payment for the screening of social drivers of health to the 2024 Medicare Physician Fee Schedule is an important step toward connecting clinicians with community health–based organizations that can address factors that influence patients’ ability to adhere to lifestyle behavior care plans. Lifestyle medicine clinicians are poised to lead this effort because they are already having conversations with patients about their environment, living conditions, and access to nutritious food.
The changes coming to our healthcare system are exciting and long overdue. Lifestyle medicine is positioned to be at the forefront of this transformation now and in the future.
Dr. Patel, president of the American College of Lifestyle Medicine in St. Louis, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Our current healthcare system, which is a costly and unending cycle of merely managing chronic disease symptoms, is failing us. What we truly need is a patient-centered approach that restores health by addressing not just diagnoses but also the physical, emotional, and social needs of each individual. This is the essence of whole-person health, and transformation toward this model of care is already underway.
This shift underscores why clinicians like me support placing lifestyle medicine at the foundation of health and healthcare. Evidence-based lifestyle medicine — which applies interventions in nutrition, physical activity, restorative sleep, stress management, positive social connections, and avoidance of risky substances to prevent, treat, and when used intensively, even reverse lifestyle-related chronic disease — is a medical specialty equipped to successfully address patients’ whole-person health in an effective, high-value clinical care delivery model.
As this transformation continues, here are four key lifestyle medicine trends for 2025.
Lifestyle Medicine Becomes More Ingrained in Primary Care
The 2021 National Academies of Science, Engineering, and Medicine report, “Implementing High-Quality Primary Care” sounded the alarm about the state of primary care and outlined a comprehensive approach to transform it. Lifestyle medicine emerged as a solution as clinicians found innovative ways to integrate lifestyle behavior interventions into existing care models in a financially sustainable, scalable manner. Examples include Blue Zones Health, a new delivery model that aligns lifestyle medicine–certified clinicians with community and payers in California, and the University of Pittsburgh Medical Center lifestyle medicine program, where primary care patients are referred to virtual group coaching, a teaching kitchen, and classes on food as medicine, obesity, type 2 diabetes, and more.
Organizations dedicated to advancing primary care are paying close attention to the potential of lifestyle medicine. Currently, The Primary Care Collaborative has launched a new multi-year initiative on whole-person care and lifestyle medicine. This initiative aims to broaden the primary care community’s understanding of whole health and lifestyle medicine concepts and the evidence behind them, as well as lay the groundwork for future work to promote whole-person primary care and lifestyle medicine among an engaged and committed community of members.
Digital Tools and AI Spark Lifestyle Medicine Innovations
American College of Lifestyle Medicine partner organizations are increasingly utilizing digital tools, such as health apps tailored to lifestyle behavior interventions, to expand access to care and support behavior change. One of the biggest challenges in lifestyle interventions is the limited time during patient encounters. But artificial intelligence (AI) tools can record (with patient permission) and summarize encounters, enabling clinicians to turn away from their keyboards and be more present to learn about the unique living, environmental, and societal factors that impact every individual’s lifestyle choices. AI tools can create individualized whole-food, plant-predominant meal plans or physical activity schedules for patients in just a few seconds. The potential for AI in lifestyle medicine is vast, and its applications were further explored at the American College of Lifestyle Medicine’s annual conference in October.
Behavior Change and Sustainability of the Food-as-Medicine Movement
Significant investments have been made in food as medicine to address diet-related chronic diseases. But merely providing medically tailored meals or produce prescriptions is not enough because once the prescriptions end, so will the health benefits. Clinicians certified in lifestyle medicine are prepared to coach patients into long-term behavior change, supporting them with education and information to shop for and prepare tasty, nutritious, and affordable food. The same applies to the use of glucagon-like peptide 1 drugs. Although the initial weight loss offers motivation, lifestyle changes are necessary to sustain long-term health benefits beyond medications.
Lifestyle Medicine Emerges as a Strategy to Achieve Health Equity
Lifestyle behavior interventions have the unique ability to address health status and social drivers of health. For example, food as medicine affects an individual’s health while also addressing nutrition security. Certainly, no medication can both improve health status and feed someone. The addition of payment for the screening of social drivers of health to the 2024 Medicare Physician Fee Schedule is an important step toward connecting clinicians with community health–based organizations that can address factors that influence patients’ ability to adhere to lifestyle behavior care plans. Lifestyle medicine clinicians are poised to lead this effort because they are already having conversations with patients about their environment, living conditions, and access to nutritious food.
The changes coming to our healthcare system are exciting and long overdue. Lifestyle medicine is positioned to be at the forefront of this transformation now and in the future.
Dr. Patel, president of the American College of Lifestyle Medicine in St. Louis, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Treating Digestive Disease Across the Lifespan
Pediatric gastroenterologists are a vital, yet often overlooked segment of the GI workforce and an important part of AGA’s diverse membership. Per the American Board of Pediatrics, 2,232 pediatricians have been board certified in pediatric gastroenterology since formal certification was first offered in 1990, and AGA Institute Council’s Pediatric Gastroenterology and Developmental Biology Section has nearly 1,900 members.
According to a recently published study in the journal Pediatrics, the pediatric GI workforce is expected to double by 2040, growing at a rate faster than that of most other pediatric subspecialties. This is largely due to the increased scope and complexity of the field driven by scientific advances and the increasing prevalence of digestive and liver diseases in children, including inflammatory bowel and other diseases.
In this month’s Member Spotlight, we highlight Dr. Yoyo Zhang, a pediatric gastroenterologist at Stanford Children’s Health specializing in intestinal and liver transplantation. Her passion for her profession and for improving the lives of her patients shines brightly, and her interview provides fascinating insights into the complexities and rewards of the rapidly expanding field of pediatric gastroenterology.

Also in our November issue, we update you on the FDA’s recent approval of the “next-gen” Cologuard test and query a panel of primary care and GI experts on their thoughts regarding the role that newly FDA-approved (but not yet guideline-recommended) Guardant blood-based CRC screening test should play in CRC screening moving forward.
In our Perspectives feature, we offer expert insights on how to appropriately screen patients for certain rare malignancies. Is it worthwhile screening for pancreatic cancer, and if so, how should it be done? Likewise, diagnosing cholangiocarcinoma is challenging; how best should one evaluate for this in higher-risk populations?
We hope you enjoy all the content in our November issue – as always, thanks for reading!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Pediatric gastroenterologists are a vital, yet often overlooked segment of the GI workforce and an important part of AGA’s diverse membership. Per the American Board of Pediatrics, 2,232 pediatricians have been board certified in pediatric gastroenterology since formal certification was first offered in 1990, and AGA Institute Council’s Pediatric Gastroenterology and Developmental Biology Section has nearly 1,900 members.
According to a recently published study in the journal Pediatrics, the pediatric GI workforce is expected to double by 2040, growing at a rate faster than that of most other pediatric subspecialties. This is largely due to the increased scope and complexity of the field driven by scientific advances and the increasing prevalence of digestive and liver diseases in children, including inflammatory bowel and other diseases.
In this month’s Member Spotlight, we highlight Dr. Yoyo Zhang, a pediatric gastroenterologist at Stanford Children’s Health specializing in intestinal and liver transplantation. Her passion for her profession and for improving the lives of her patients shines brightly, and her interview provides fascinating insights into the complexities and rewards of the rapidly expanding field of pediatric gastroenterology.
Also in our November issue, we update you on the FDA’s recent approval of the “next-gen” Cologuard test and query a panel of primary care and GI experts on their thoughts regarding the role that newly FDA-approved (but not yet guideline-recommended) Guardant blood-based CRC screening test should play in CRC screening moving forward.
In our Perspectives feature, we offer expert insights on how to appropriately screen patients for certain rare malignancies. Is it worthwhile screening for pancreatic cancer, and if so, how should it be done? Likewise, diagnosing cholangiocarcinoma is challenging; how best should one evaluate for this in higher-risk populations?
We hope you enjoy all the content in our November issue – as always, thanks for reading!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Pediatric gastroenterologists are a vital, yet often overlooked segment of the GI workforce and an important part of AGA’s diverse membership. Per the American Board of Pediatrics, 2,232 pediatricians have been board certified in pediatric gastroenterology since formal certification was first offered in 1990, and AGA Institute Council’s Pediatric Gastroenterology and Developmental Biology Section has nearly 1,900 members.
According to a recently published study in the journal Pediatrics, the pediatric GI workforce is expected to double by 2040, growing at a rate faster than that of most other pediatric subspecialties. This is largely due to the increased scope and complexity of the field driven by scientific advances and the increasing prevalence of digestive and liver diseases in children, including inflammatory bowel and other diseases.
In this month’s Member Spotlight, we highlight Dr. Yoyo Zhang, a pediatric gastroenterologist at Stanford Children’s Health specializing in intestinal and liver transplantation. Her passion for her profession and for improving the lives of her patients shines brightly, and her interview provides fascinating insights into the complexities and rewards of the rapidly expanding field of pediatric gastroenterology.
Also in our November issue, we update you on the FDA’s recent approval of the “next-gen” Cologuard test and query a panel of primary care and GI experts on their thoughts regarding the role that newly FDA-approved (but not yet guideline-recommended) Guardant blood-based CRC screening test should play in CRC screening moving forward.
In our Perspectives feature, we offer expert insights on how to appropriately screen patients for certain rare malignancies. Is it worthwhile screening for pancreatic cancer, and if so, how should it be done? Likewise, diagnosing cholangiocarcinoma is challenging; how best should one evaluate for this in higher-risk populations?
We hope you enjoy all the content in our November issue – as always, thanks for reading!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Managing Age-Related Muscle Loss in Primary Care
Scene 1: Exercise Medicine Clinic, Rio de Janeiro, Brazil I just finished one evaluation on physical fitness and health and looked at my schedule. My next patient would be a 65-year-old man. How fit will he be? Will he have evident age-related muscle loss? I gave myself a short break and my mind went to the late 1970s.
Once upon a time, the practice of medicine was based primarily on the skill of your physical examination, previous experiences, and your ability to reason logically and make solid deductions. In 1979, the stethoscope was part of my dress code. After one elective semester as a research fellow at the Ambrose Cardiorespiratory Unit at McMaster University Medical Centre, in Hamilton, Canada, where I was honored to witness the dawn of evidence-based medicine, I graduated from Federal University of Rio de Janeiro. I still remember being introduced to some promising novelties in cardiology, such as M-mode echocardiograms and myocardial scintigraphy. Radiology was primarily centered on x-rays, and lab testing was basic and poorly automatized.
Over the following decades, medical practice changed dramatically with the incorporation of new technologies. Recent advances in diagnostic tools, genetics, artificial intelligence, and sophisticated statistical analyses, along with well-collected scientific data, have molded how clinicians should think and work.
At the same time, clinical profiles also changed. Internists and primary care physicians are regularly managing patients who are, on average, older and have or are on the way to having potentially life-threatening chronic diseases, accompanied by poor lifestyle habits, and, highly important, often some degree of disability, frailty, and loss of independence. Many of them exhibit age-related muscle loss.
Scene 2: Exercise Medicine Clinic, Rio de Janeiro, Brazil
Conscious of the benefits of interrupting my sitting time with activity, I left my office and walked to meet my patient in the waiting room. I called his name and introduced myself. I watched how he listened and reacted to my speech, and how easy or hard it was for him to rise from the chair — readiness, velocity, and number of supports required: none, one, or two hands. I offered my own hand to him, and when we shook, I gauged the strength of his grip.
I invited him into my office and took note of his somatotype and body composition, and whether he had any central obesity. Of course, and I should by no means miss this chance, I carefully observed how he walked in — his gait, speed, balance, posture — how he pulled up the chair, and how he managed to lower himself into his seat. Before I even sat in my own chair, I asked him if he remembered what his body weight was 5 years ago and what it was today. Before we got started in earnest, I had already managed to collect several pieces of relevant information.
Exercise Physiology: Changing Landscape
Muscle activity depends on muscle mass and function, and peaks somewhere between ages 25 and 35 before declining. The drop is slow in the early stages but accelerates rapidly after age 60 or 65.
Two of the most relevant variables in muscle function are strength and power. As a product of force and velocity, muscle power could be a more crucial factor than strength for many daily activities that demand movement against gravity or inertia, such as placing carry-on baggage in the overhead bin of an airplane or rising from the floor or chair.
The association between muscle mass and muscle strength or power is moderate, and physiologic data have indicated that the decline of muscle power with aging is faster and larger than that of muscle strength.
The term “sarcopenia” has become definitively incorporated into the medical glossary. From the Greek (“sark” and “penia”), sarcopenia was defined as reduced muscle mass, but more recently it has encompassed muscle strength in its definition. However, a recent consensus paper from the Global Leadership Initiative in Sarcopenia, using a Delphi approach, rejected the inclusion of muscle power in the concept of sarcopenia. On the other hand, a long time ago, some authors coined and advocated the use the term “dynapenia” to more precisely reflect the reduced levels of muscle strength and power that often accompany aging.
The best available intervention to counteract age-related deterioration of muscle activity is resistance exercise. The types of resistance exercises vary widely — by number of sets and repetitions, intervals between sets, speed of execution of movement, and percentage of maximal weight/load.
We recently proposed that, after an evaluation to identify the main muscle variable requiring attention, the resistance exercise program should be individually tailored and prescribed according to the objective to counteract sarcopenia or dynapenia.
What is more important for autonomy and better daily living conditions in old and very old individuals: muscle mass, muscle strength, or muscle power? More likely the response is muscle power — in practical terms, dynapenia rather than sarcopenia. This short video presents practical tips for obtaining optimal results in fighting dynapenia. The first choice should be power training or high velocity–based training, emphasizing two to three sets of six to eight repetitions performed as fast as possible (on the concentric or shortening phase of muscle contraction) with relatively high loads.
Internists and primary care physicians are most likely satisfied with the information they obtain by simple observation, and already can superficially grade the magnitude of a patient’s age-related muscle loss and its consequences to daily living.
However, those who want more objective information on nonaerobic physical fitness can add one to three simple tests to their consultation: the sitting-rising test (SRT); the 10-second one-legged test (10sOLS test); and the Flexitest. Poor performance on each of these — and particularly all three — is strongly associated with an increased risk for premature death in middle-aged and older individuals. These tests require no extra equipment and can be performed rapidly, and interpreting the results takes only a few moments using published reference values.
Age-related muscle loss profoundly affects our ability to sit and rise from the floor, so if time is limited, the SRT is the best assessment, as it measures all nonaerobic components of physical fitness. For a quick interpretation, consider that SRT scores vary from 0 to 10, do not substantially differ by sex, and that a composite score equal to or greater than 8 will reflect a minimum age-adjusted percentile of 61, most likely indicating relevant age-related muscle loss is not yet occurring.
Dr. Araújo is Professor and Dean of Research and Education, Exercise Medicine Clinic (CLINIMEX), Rio de Janeiro, Brazil. He reported conflicts of interest with INBRAMED.
A version of this article first appeared on Medscape.com.
Scene 1: Exercise Medicine Clinic, Rio de Janeiro, Brazil I just finished one evaluation on physical fitness and health and looked at my schedule. My next patient would be a 65-year-old man. How fit will he be? Will he have evident age-related muscle loss? I gave myself a short break and my mind went to the late 1970s.
Once upon a time, the practice of medicine was based primarily on the skill of your physical examination, previous experiences, and your ability to reason logically and make solid deductions. In 1979, the stethoscope was part of my dress code. After one elective semester as a research fellow at the Ambrose Cardiorespiratory Unit at McMaster University Medical Centre, in Hamilton, Canada, where I was honored to witness the dawn of evidence-based medicine, I graduated from Federal University of Rio de Janeiro. I still remember being introduced to some promising novelties in cardiology, such as M-mode echocardiograms and myocardial scintigraphy. Radiology was primarily centered on x-rays, and lab testing was basic and poorly automatized.
Over the following decades, medical practice changed dramatically with the incorporation of new technologies. Recent advances in diagnostic tools, genetics, artificial intelligence, and sophisticated statistical analyses, along with well-collected scientific data, have molded how clinicians should think and work.
At the same time, clinical profiles also changed. Internists and primary care physicians are regularly managing patients who are, on average, older and have or are on the way to having potentially life-threatening chronic diseases, accompanied by poor lifestyle habits, and, highly important, often some degree of disability, frailty, and loss of independence. Many of them exhibit age-related muscle loss.
Scene 2: Exercise Medicine Clinic, Rio de Janeiro, Brazil
Conscious of the benefits of interrupting my sitting time with activity, I left my office and walked to meet my patient in the waiting room. I called his name and introduced myself. I watched how he listened and reacted to my speech, and how easy or hard it was for him to rise from the chair — readiness, velocity, and number of supports required: none, one, or two hands. I offered my own hand to him, and when we shook, I gauged the strength of his grip.
I invited him into my office and took note of his somatotype and body composition, and whether he had any central obesity. Of course, and I should by no means miss this chance, I carefully observed how he walked in — his gait, speed, balance, posture — how he pulled up the chair, and how he managed to lower himself into his seat. Before I even sat in my own chair, I asked him if he remembered what his body weight was 5 years ago and what it was today. Before we got started in earnest, I had already managed to collect several pieces of relevant information.
Exercise Physiology: Changing Landscape
Muscle activity depends on muscle mass and function, and peaks somewhere between ages 25 and 35 before declining. The drop is slow in the early stages but accelerates rapidly after age 60 or 65.
Two of the most relevant variables in muscle function are strength and power. As a product of force and velocity, muscle power could be a more crucial factor than strength for many daily activities that demand movement against gravity or inertia, such as placing carry-on baggage in the overhead bin of an airplane or rising from the floor or chair.
The association between muscle mass and muscle strength or power is moderate, and physiologic data have indicated that the decline of muscle power with aging is faster and larger than that of muscle strength.
The term “sarcopenia” has become definitively incorporated into the medical glossary. From the Greek (“sark” and “penia”), sarcopenia was defined as reduced muscle mass, but more recently it has encompassed muscle strength in its definition. However, a recent consensus paper from the Global Leadership Initiative in Sarcopenia, using a Delphi approach, rejected the inclusion of muscle power in the concept of sarcopenia. On the other hand, a long time ago, some authors coined and advocated the use the term “dynapenia” to more precisely reflect the reduced levels of muscle strength and power that often accompany aging.
The best available intervention to counteract age-related deterioration of muscle activity is resistance exercise. The types of resistance exercises vary widely — by number of sets and repetitions, intervals between sets, speed of execution of movement, and percentage of maximal weight/load.
We recently proposed that, after an evaluation to identify the main muscle variable requiring attention, the resistance exercise program should be individually tailored and prescribed according to the objective to counteract sarcopenia or dynapenia.
What is more important for autonomy and better daily living conditions in old and very old individuals: muscle mass, muscle strength, or muscle power? More likely the response is muscle power — in practical terms, dynapenia rather than sarcopenia. This short video presents practical tips for obtaining optimal results in fighting dynapenia. The first choice should be power training or high velocity–based training, emphasizing two to three sets of six to eight repetitions performed as fast as possible (on the concentric or shortening phase of muscle contraction) with relatively high loads.
Internists and primary care physicians are most likely satisfied with the information they obtain by simple observation, and already can superficially grade the magnitude of a patient’s age-related muscle loss and its consequences to daily living.
However, those who want more objective information on nonaerobic physical fitness can add one to three simple tests to their consultation: the sitting-rising test (SRT); the 10-second one-legged test (10sOLS test); and the Flexitest. Poor performance on each of these — and particularly all three — is strongly associated with an increased risk for premature death in middle-aged and older individuals. These tests require no extra equipment and can be performed rapidly, and interpreting the results takes only a few moments using published reference values.
Age-related muscle loss profoundly affects our ability to sit and rise from the floor, so if time is limited, the SRT is the best assessment, as it measures all nonaerobic components of physical fitness. For a quick interpretation, consider that SRT scores vary from 0 to 10, do not substantially differ by sex, and that a composite score equal to or greater than 8 will reflect a minimum age-adjusted percentile of 61, most likely indicating relevant age-related muscle loss is not yet occurring.
Dr. Araújo is Professor and Dean of Research and Education, Exercise Medicine Clinic (CLINIMEX), Rio de Janeiro, Brazil. He reported conflicts of interest with INBRAMED.
A version of this article first appeared on Medscape.com.
Scene 1: Exercise Medicine Clinic, Rio de Janeiro, Brazil I just finished one evaluation on physical fitness and health and looked at my schedule. My next patient would be a 65-year-old man. How fit will he be? Will he have evident age-related muscle loss? I gave myself a short break and my mind went to the late 1970s.
Once upon a time, the practice of medicine was based primarily on the skill of your physical examination, previous experiences, and your ability to reason logically and make solid deductions. In 1979, the stethoscope was part of my dress code. After one elective semester as a research fellow at the Ambrose Cardiorespiratory Unit at McMaster University Medical Centre, in Hamilton, Canada, where I was honored to witness the dawn of evidence-based medicine, I graduated from Federal University of Rio de Janeiro. I still remember being introduced to some promising novelties in cardiology, such as M-mode echocardiograms and myocardial scintigraphy. Radiology was primarily centered on x-rays, and lab testing was basic and poorly automatized.
Over the following decades, medical practice changed dramatically with the incorporation of new technologies. Recent advances in diagnostic tools, genetics, artificial intelligence, and sophisticated statistical analyses, along with well-collected scientific data, have molded how clinicians should think and work.
At the same time, clinical profiles also changed. Internists and primary care physicians are regularly managing patients who are, on average, older and have or are on the way to having potentially life-threatening chronic diseases, accompanied by poor lifestyle habits, and, highly important, often some degree of disability, frailty, and loss of independence. Many of them exhibit age-related muscle loss.
Scene 2: Exercise Medicine Clinic, Rio de Janeiro, Brazil
Conscious of the benefits of interrupting my sitting time with activity, I left my office and walked to meet my patient in the waiting room. I called his name and introduced myself. I watched how he listened and reacted to my speech, and how easy or hard it was for him to rise from the chair — readiness, velocity, and number of supports required: none, one, or two hands. I offered my own hand to him, and when we shook, I gauged the strength of his grip.
I invited him into my office and took note of his somatotype and body composition, and whether he had any central obesity. Of course, and I should by no means miss this chance, I carefully observed how he walked in — his gait, speed, balance, posture — how he pulled up the chair, and how he managed to lower himself into his seat. Before I even sat in my own chair, I asked him if he remembered what his body weight was 5 years ago and what it was today. Before we got started in earnest, I had already managed to collect several pieces of relevant information.
Exercise Physiology: Changing Landscape
Muscle activity depends on muscle mass and function, and peaks somewhere between ages 25 and 35 before declining. The drop is slow in the early stages but accelerates rapidly after age 60 or 65.
Two of the most relevant variables in muscle function are strength and power. As a product of force and velocity, muscle power could be a more crucial factor than strength for many daily activities that demand movement against gravity or inertia, such as placing carry-on baggage in the overhead bin of an airplane or rising from the floor or chair.
The association between muscle mass and muscle strength or power is moderate, and physiologic data have indicated that the decline of muscle power with aging is faster and larger than that of muscle strength.
The term “sarcopenia” has become definitively incorporated into the medical glossary. From the Greek (“sark” and “penia”), sarcopenia was defined as reduced muscle mass, but more recently it has encompassed muscle strength in its definition. However, a recent consensus paper from the Global Leadership Initiative in Sarcopenia, using a Delphi approach, rejected the inclusion of muscle power in the concept of sarcopenia. On the other hand, a long time ago, some authors coined and advocated the use the term “dynapenia” to more precisely reflect the reduced levels of muscle strength and power that often accompany aging.
The best available intervention to counteract age-related deterioration of muscle activity is resistance exercise. The types of resistance exercises vary widely — by number of sets and repetitions, intervals between sets, speed of execution of movement, and percentage of maximal weight/load.
We recently proposed that, after an evaluation to identify the main muscle variable requiring attention, the resistance exercise program should be individually tailored and prescribed according to the objective to counteract sarcopenia or dynapenia.
What is more important for autonomy and better daily living conditions in old and very old individuals: muscle mass, muscle strength, or muscle power? More likely the response is muscle power — in practical terms, dynapenia rather than sarcopenia. This short video presents practical tips for obtaining optimal results in fighting dynapenia. The first choice should be power training or high velocity–based training, emphasizing two to three sets of six to eight repetitions performed as fast as possible (on the concentric or shortening phase of muscle contraction) with relatively high loads.
Internists and primary care physicians are most likely satisfied with the information they obtain by simple observation, and already can superficially grade the magnitude of a patient’s age-related muscle loss and its consequences to daily living.
However, those who want more objective information on nonaerobic physical fitness can add one to three simple tests to their consultation: the sitting-rising test (SRT); the 10-second one-legged test (10sOLS test); and the Flexitest. Poor performance on each of these — and particularly all three — is strongly associated with an increased risk for premature death in middle-aged and older individuals. These tests require no extra equipment and can be performed rapidly, and interpreting the results takes only a few moments using published reference values.
Age-related muscle loss profoundly affects our ability to sit and rise from the floor, so if time is limited, the SRT is the best assessment, as it measures all nonaerobic components of physical fitness. For a quick interpretation, consider that SRT scores vary from 0 to 10, do not substantially differ by sex, and that a composite score equal to or greater than 8 will reflect a minimum age-adjusted percentile of 61, most likely indicating relevant age-related muscle loss is not yet occurring.
Dr. Araújo is Professor and Dean of Research and Education, Exercise Medicine Clinic (CLINIMEX), Rio de Janeiro, Brazil. He reported conflicts of interest with INBRAMED.
A version of this article first appeared on Medscape.com.
Obesity: A Social Vulnerability
Sometime in the last year or 2 I wrote that, despite my considerable reservations, I had finally come to the conclusion that the American Medical Association’s decision to designate obesity as a disease was appropriate. My rationalization was that the disease label would open more opportunities for funding obesity treatments. However, the explosive growth and popularity of glucagon-like peptide 1 (GLP-1) agonists over the last year has had me rethinking my decision to suppress my long-held reservations about the disease designation.
So, if it’s not a disease, then what should we call it? How do we explain its surge in high-income countries that began in the 1980s? While there are still some folks who see obesity as a character flaw, I think you and I as healthcare providers have difficulty explaining the increase prevalence of obesity as either global breakdown of willpower or a widespread genetic shift as the result of burst of radiation from solar flares.
However, if we want to continue our search and finger-pointing we need to have a better definition of exactly what obesity is. If we’re going to continue calling it a disease we have done a pretty sloppy job of creating diagnostic criteria. To be honest, we aren’t doing such a hot job with “long COVID” either.
A recent article in the New York Times makes it clear that I’m not the only physician who is feeling uncomfortable with this lack of diagnostic specificity.
We know that using body mass index (BMI) as a criteria is imprecise. There are healthy individuals with elevated BMIs and there are others who are carrying an unhealthy amount of fat who have normal BMIs. And, there are individuals who have what might appear to be an excess amount of fat who are fit and healthy by other criteria.
Some investigators feel that a set of measurements that includes a waist and/or hip measurement may be a more accurate way of determining visceral adipose tissue. However, this body roundness index (BRI) currently relies on a tape measurement. Until the technique can be preformed by an inexpensive and readily available scanner, the BRI cannot be considered a practical tool for determining obesity.
Dr. Francisco Rubino, the chair of metabolic and bariatric surgery at Kings College in London, England, has been quoted as saying that, “if one defines a disease inaccurately, everything that stems from that – from diagnosis to treatment to policies – will be distorted and biased.”
Denmark has been forced to relabel obesity as a risk factor because the disease designation was stressing the financial viability of their healthcare system as more and more patients were being prescribe GLP-1 agonists, sometimes off label. A rationing strategy was resulting in suboptimal treatment of a significant portion of the obese population.
Spearheaded by Dr. Rubino, a Lancet Commission composed of physicians has tasked itself to define an “evidence-based diagnosis for obesity. Instead of relying on a single metric such as the BMI or BRI, diagnosing “clinical obesity” would involve a broad array of observations including a history, physical examination, standard laboratory and additional testing, “naming signs and symptoms, organ by organ, tissue by tissue, with plausible mechanisms for each one.” In other words, treating each patient as an individual using evidence-based criteria to make a diagnosis. While likely to be time consuming, this strategy feels like a more scientific approach. I suspect once clinical obesity is more rigorously defined it could be divided into several subtypes. For example, there would be a few conditions that were genetic; Prader-Willi syndrome being the best known.
However, I think the Lancet Commission’s strategy will find that the majority of individuals who make up this half-century global surge have become clinically obese because they have been unable to adapt to the obeseogenic forces in our society, which include diet, autocentricity, and attractive sedentary forms of entertainment, to name just three.
In some cases these unfortunate individuals are more vulnerable because there were born into an economically disadvantaged situation. In other scenarios a lack of foresight and/or political will may have left individuals with no other choice but to rely on automobiles to get around. Still others may find themselves living in a nutritional desert because all of the grocery stores have closed.
I recently encountered a descriptor in a story about the Federal Emergency Management Agency which could easily be adapted to describe this large and growing subtype of individuals with clinical obesity. “Social vulnerability” is measure of how well a community can withstand external stressors that impact human health. For example, the emergency management folks are thinking in terms of natural disaster such as hurricanes, floods, and tornadoes and are asking how well a given community can meet the challenges one would create.
But, the term social vulnerability can easily be applied to individuals living in a society in which unhealthy food is abundant, an infrastructure that discourages or outright prevents non-motorized travel, and the temptation of sedentary entertainment options is unavoidable. Fortunately, not every citizen living in an obesogenic society becomes obese. What factors have protected the non-obese individuals from these obeseogenic stressors? What are the characteristics of the unfortunate “vulnerables” living in the same society who end up being obese?
It is time to shift our focus away from a poorly defined disease model to one in which we begin looking at our society to find out why we have so many socially vulnerable individuals. The toll of obesity as it is currently defined is many order of magnitudes greater than any natural disaster. We have become communities that can no longer withstand the its obesogenic stressors many of which we have created and/or allowed to accumulate over the last century.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Sometime in the last year or 2 I wrote that, despite my considerable reservations, I had finally come to the conclusion that the American Medical Association’s decision to designate obesity as a disease was appropriate. My rationalization was that the disease label would open more opportunities for funding obesity treatments. However, the explosive growth and popularity of glucagon-like peptide 1 (GLP-1) agonists over the last year has had me rethinking my decision to suppress my long-held reservations about the disease designation.
So, if it’s not a disease, then what should we call it? How do we explain its surge in high-income countries that began in the 1980s? While there are still some folks who see obesity as a character flaw, I think you and I as healthcare providers have difficulty explaining the increase prevalence of obesity as either global breakdown of willpower or a widespread genetic shift as the result of burst of radiation from solar flares.
However, if we want to continue our search and finger-pointing we need to have a better definition of exactly what obesity is. If we’re going to continue calling it a disease we have done a pretty sloppy job of creating diagnostic criteria. To be honest, we aren’t doing such a hot job with “long COVID” either.
A recent article in the New York Times makes it clear that I’m not the only physician who is feeling uncomfortable with this lack of diagnostic specificity.
We know that using body mass index (BMI) as a criteria is imprecise. There are healthy individuals with elevated BMIs and there are others who are carrying an unhealthy amount of fat who have normal BMIs. And, there are individuals who have what might appear to be an excess amount of fat who are fit and healthy by other criteria.
Some investigators feel that a set of measurements that includes a waist and/or hip measurement may be a more accurate way of determining visceral adipose tissue. However, this body roundness index (BRI) currently relies on a tape measurement. Until the technique can be preformed by an inexpensive and readily available scanner, the BRI cannot be considered a practical tool for determining obesity.
Dr. Francisco Rubino, the chair of metabolic and bariatric surgery at Kings College in London, England, has been quoted as saying that, “if one defines a disease inaccurately, everything that stems from that – from diagnosis to treatment to policies – will be distorted and biased.”
Denmark has been forced to relabel obesity as a risk factor because the disease designation was stressing the financial viability of their healthcare system as more and more patients were being prescribe GLP-1 agonists, sometimes off label. A rationing strategy was resulting in suboptimal treatment of a significant portion of the obese population.
Spearheaded by Dr. Rubino, a Lancet Commission composed of physicians has tasked itself to define an “evidence-based diagnosis for obesity. Instead of relying on a single metric such as the BMI or BRI, diagnosing “clinical obesity” would involve a broad array of observations including a history, physical examination, standard laboratory and additional testing, “naming signs and symptoms, organ by organ, tissue by tissue, with plausible mechanisms for each one.” In other words, treating each patient as an individual using evidence-based criteria to make a diagnosis. While likely to be time consuming, this strategy feels like a more scientific approach. I suspect once clinical obesity is more rigorously defined it could be divided into several subtypes. For example, there would be a few conditions that were genetic; Prader-Willi syndrome being the best known.
However, I think the Lancet Commission’s strategy will find that the majority of individuals who make up this half-century global surge have become clinically obese because they have been unable to adapt to the obeseogenic forces in our society, which include diet, autocentricity, and attractive sedentary forms of entertainment, to name just three.
In some cases these unfortunate individuals are more vulnerable because there were born into an economically disadvantaged situation. In other scenarios a lack of foresight and/or political will may have left individuals with no other choice but to rely on automobiles to get around. Still others may find themselves living in a nutritional desert because all of the grocery stores have closed.
I recently encountered a descriptor in a story about the Federal Emergency Management Agency which could easily be adapted to describe this large and growing subtype of individuals with clinical obesity. “Social vulnerability” is measure of how well a community can withstand external stressors that impact human health. For example, the emergency management folks are thinking in terms of natural disaster such as hurricanes, floods, and tornadoes and are asking how well a given community can meet the challenges one would create.
But, the term social vulnerability can easily be applied to individuals living in a society in which unhealthy food is abundant, an infrastructure that discourages or outright prevents non-motorized travel, and the temptation of sedentary entertainment options is unavoidable. Fortunately, not every citizen living in an obesogenic society becomes obese. What factors have protected the non-obese individuals from these obeseogenic stressors? What are the characteristics of the unfortunate “vulnerables” living in the same society who end up being obese?
It is time to shift our focus away from a poorly defined disease model to one in which we begin looking at our society to find out why we have so many socially vulnerable individuals. The toll of obesity as it is currently defined is many order of magnitudes greater than any natural disaster. We have become communities that can no longer withstand the its obesogenic stressors many of which we have created and/or allowed to accumulate over the last century.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Sometime in the last year or 2 I wrote that, despite my considerable reservations, I had finally come to the conclusion that the American Medical Association’s decision to designate obesity as a disease was appropriate. My rationalization was that the disease label would open more opportunities for funding obesity treatments. However, the explosive growth and popularity of glucagon-like peptide 1 (GLP-1) agonists over the last year has had me rethinking my decision to suppress my long-held reservations about the disease designation.
So, if it’s not a disease, then what should we call it? How do we explain its surge in high-income countries that began in the 1980s? While there are still some folks who see obesity as a character flaw, I think you and I as healthcare providers have difficulty explaining the increase prevalence of obesity as either global breakdown of willpower or a widespread genetic shift as the result of burst of radiation from solar flares.
However, if we want to continue our search and finger-pointing we need to have a better definition of exactly what obesity is. If we’re going to continue calling it a disease we have done a pretty sloppy job of creating diagnostic criteria. To be honest, we aren’t doing such a hot job with “long COVID” either.
A recent article in the New York Times makes it clear that I’m not the only physician who is feeling uncomfortable with this lack of diagnostic specificity.
We know that using body mass index (BMI) as a criteria is imprecise. There are healthy individuals with elevated BMIs and there are others who are carrying an unhealthy amount of fat who have normal BMIs. And, there are individuals who have what might appear to be an excess amount of fat who are fit and healthy by other criteria.
Some investigators feel that a set of measurements that includes a waist and/or hip measurement may be a more accurate way of determining visceral adipose tissue. However, this body roundness index (BRI) currently relies on a tape measurement. Until the technique can be preformed by an inexpensive and readily available scanner, the BRI cannot be considered a practical tool for determining obesity.
Dr. Francisco Rubino, the chair of metabolic and bariatric surgery at Kings College in London, England, has been quoted as saying that, “if one defines a disease inaccurately, everything that stems from that – from diagnosis to treatment to policies – will be distorted and biased.”
Denmark has been forced to relabel obesity as a risk factor because the disease designation was stressing the financial viability of their healthcare system as more and more patients were being prescribe GLP-1 agonists, sometimes off label. A rationing strategy was resulting in suboptimal treatment of a significant portion of the obese population.
Spearheaded by Dr. Rubino, a Lancet Commission composed of physicians has tasked itself to define an “evidence-based diagnosis for obesity. Instead of relying on a single metric such as the BMI or BRI, diagnosing “clinical obesity” would involve a broad array of observations including a history, physical examination, standard laboratory and additional testing, “naming signs and symptoms, organ by organ, tissue by tissue, with plausible mechanisms for each one.” In other words, treating each patient as an individual using evidence-based criteria to make a diagnosis. While likely to be time consuming, this strategy feels like a more scientific approach. I suspect once clinical obesity is more rigorously defined it could be divided into several subtypes. For example, there would be a few conditions that were genetic; Prader-Willi syndrome being the best known.
However, I think the Lancet Commission’s strategy will find that the majority of individuals who make up this half-century global surge have become clinically obese because they have been unable to adapt to the obeseogenic forces in our society, which include diet, autocentricity, and attractive sedentary forms of entertainment, to name just three.
In some cases these unfortunate individuals are more vulnerable because there were born into an economically disadvantaged situation. In other scenarios a lack of foresight and/or political will may have left individuals with no other choice but to rely on automobiles to get around. Still others may find themselves living in a nutritional desert because all of the grocery stores have closed.
I recently encountered a descriptor in a story about the Federal Emergency Management Agency which could easily be adapted to describe this large and growing subtype of individuals with clinical obesity. “Social vulnerability” is measure of how well a community can withstand external stressors that impact human health. For example, the emergency management folks are thinking in terms of natural disaster such as hurricanes, floods, and tornadoes and are asking how well a given community can meet the challenges one would create.
But, the term social vulnerability can easily be applied to individuals living in a society in which unhealthy food is abundant, an infrastructure that discourages or outright prevents non-motorized travel, and the temptation of sedentary entertainment options is unavoidable. Fortunately, not every citizen living in an obesogenic society becomes obese. What factors have protected the non-obese individuals from these obeseogenic stressors? What are the characteristics of the unfortunate “vulnerables” living in the same society who end up being obese?
It is time to shift our focus away from a poorly defined disease model to one in which we begin looking at our society to find out why we have so many socially vulnerable individuals. The toll of obesity as it is currently defined is many order of magnitudes greater than any natural disaster. We have become communities that can no longer withstand the its obesogenic stressors many of which we have created and/or allowed to accumulate over the last century.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Preventing Pediatric Migraine
I suspect you all have some experience with childhood migraine. It can mean a painful several hours for the patient, arriving often without warning, with recurrences spaced months or sometimes even years apart. It may be accompanied by vomiting, which in some cases overshadows the severity of the headache. It can result in lost days from school and ruin family activities. It can occur so infrequently that the family can’t recall accurately when the last episode happened. In some ways it is a different animal than the adult version.
Most of the pediatric patients with migraine I have seen have experienced attacks that were occurring so infrequently that the families and I seldom discussed medication as an option. Back then imipramine was the only choice. However, currently there are more than a half dozen medications and combinations that have been tried. Recently a review of 45 clinical trials of these medications was published in JAMA Network Open.
I will let you review for yourself the details of these Iranian investigators’ network meta-analysis, but the bottom line is that some medications were associated with a reduction in migraine frequency. Others were associated with headache intensity. “However, no treatments were associated with significant improvements in quality of life or reduction of the duration of migraine attacks.”
Obviously, this paper illustrates clearly that we have not yet discovered the medicinal magic bullet for pediatric migraine prophylaxis. This doesn’t surprise me. After listening to scores of families tell their migraine stories, it became apparent to me that there was often a pattern in which the child’s headache had arrived after a period of acute sleep deprivation. For example, a trip to an amusement park in which travel or excitement may have resulted in the child going to bed later and/or getting up earlier. By afternoon the child’s reserves of something (currently unknown) were depleted to a point that the headache and/or vomiting struck.
Because these episodes were often so infrequent, separated by months, that taking a history demonstrating a recurring pattern could take considerable patience on the part of the family and the provider, even for a physician like myself who believes that better sleep is the answer for everything. However, once I could convince a family of the connection between the sleep deprivation and the headaches, they could often recall other episodes in the past that substantiated my explanation.
In some cases there was no obvious history of acute sleep deprivation, or at least it was so subtle that even a history taker with a sleep obsession couldn’t detect it. However, in these cases I could usually elicit a history of chronic sleep deprivation. For example, falling asleep instantly on automobile rides, difficulty with waking in the morning, or unhealthy bedtime routines. With this underlying vulnerability of chronic sleep deprivation, a slightly more exciting or vigorous day was all that was necessary to trigger the headache.
For those of you who don’t share my contention that childhood migraine is usually the result of sleep deprivation, consider the similarity between an epileptic seizure, which can be triggered by fatigue. Both events are usually followed by a deep sleep from which the child wakes refreshed and symptom free.
I think it is interesting that this recent meta-analysis could find no benefit in the quality of life for any of the medications. The explanation may be that the child with migraine already had a somewhat diminished quality of life as a result of the sleep deprivation, either acute or chronic.
When speaking with parents of migraine sufferers, I would tell them that once the headache had started there was little I had to offer to forestall the inevitable pain and vomiting. Certainly not in the form of an oral medication. While many adults will have an aura that warns them of the headache onset, I have found that most children don’t describe an aura. It may be they simply lack the ability to express it. Occasionally an observant parent may detect pallor or a behavior change that indicates a migraine is beginning. On rare occasions a parent may be able to abort the attack by quickly getting the child to a quiet, dark, and calm environment.
Although this recent meta-analysis review of treatment options is discouraging, it may be providing a clue to effective prophylaxis. Some of the medications that decrease the frequency of the attacks may be doing so because they improve the patient’s sleep patterns. Those that decrease the intensity of the pain are probably working on pain pathway that is not specific to migraine.
Continuing a search for a prophylactic medication is a worthy goal, particularly for those patients in which their migraines are debilitating. However, based on my experience, enhanced by my bias, the safest and most effective prophylaxis results from increasing the family’s awareness of the role that sleep deprivation plays in the illness. Even when the family buys into the message and attempts to avoid situations that will tax their vulnerable children, parents will need to accept that sometimes stuff happens even though siblings and peers may be able to tolerate the situation. Spontaneous activities can converge on a day when for whatever reason the migraine-prone child is overtired and the headache and vomiting will erupt.
A lifestyle change is always preferable to a pharmacological intervention. However, that doesn’t mean it is always easy to achieve.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
I suspect you all have some experience with childhood migraine. It can mean a painful several hours for the patient, arriving often without warning, with recurrences spaced months or sometimes even years apart. It may be accompanied by vomiting, which in some cases overshadows the severity of the headache. It can result in lost days from school and ruin family activities. It can occur so infrequently that the family can’t recall accurately when the last episode happened. In some ways it is a different animal than the adult version.
Most of the pediatric patients with migraine I have seen have experienced attacks that were occurring so infrequently that the families and I seldom discussed medication as an option. Back then imipramine was the only choice. However, currently there are more than a half dozen medications and combinations that have been tried. Recently a review of 45 clinical trials of these medications was published in JAMA Network Open.
I will let you review for yourself the details of these Iranian investigators’ network meta-analysis, but the bottom line is that some medications were associated with a reduction in migraine frequency. Others were associated with headache intensity. “However, no treatments were associated with significant improvements in quality of life or reduction of the duration of migraine attacks.”
Obviously, this paper illustrates clearly that we have not yet discovered the medicinal magic bullet for pediatric migraine prophylaxis. This doesn’t surprise me. After listening to scores of families tell their migraine stories, it became apparent to me that there was often a pattern in which the child’s headache had arrived after a period of acute sleep deprivation. For example, a trip to an amusement park in which travel or excitement may have resulted in the child going to bed later and/or getting up earlier. By afternoon the child’s reserves of something (currently unknown) were depleted to a point that the headache and/or vomiting struck.
Because these episodes were often so infrequent, separated by months, that taking a history demonstrating a recurring pattern could take considerable patience on the part of the family and the provider, even for a physician like myself who believes that better sleep is the answer for everything. However, once I could convince a family of the connection between the sleep deprivation and the headaches, they could often recall other episodes in the past that substantiated my explanation.
In some cases there was no obvious history of acute sleep deprivation, or at least it was so subtle that even a history taker with a sleep obsession couldn’t detect it. However, in these cases I could usually elicit a history of chronic sleep deprivation. For example, falling asleep instantly on automobile rides, difficulty with waking in the morning, or unhealthy bedtime routines. With this underlying vulnerability of chronic sleep deprivation, a slightly more exciting or vigorous day was all that was necessary to trigger the headache.
For those of you who don’t share my contention that childhood migraine is usually the result of sleep deprivation, consider the similarity between an epileptic seizure, which can be triggered by fatigue. Both events are usually followed by a deep sleep from which the child wakes refreshed and symptom free.
I think it is interesting that this recent meta-analysis could find no benefit in the quality of life for any of the medications. The explanation may be that the child with migraine already had a somewhat diminished quality of life as a result of the sleep deprivation, either acute or chronic.
When speaking with parents of migraine sufferers, I would tell them that once the headache had started there was little I had to offer to forestall the inevitable pain and vomiting. Certainly not in the form of an oral medication. While many adults will have an aura that warns them of the headache onset, I have found that most children don’t describe an aura. It may be they simply lack the ability to express it. Occasionally an observant parent may detect pallor or a behavior change that indicates a migraine is beginning. On rare occasions a parent may be able to abort the attack by quickly getting the child to a quiet, dark, and calm environment.
Although this recent meta-analysis review of treatment options is discouraging, it may be providing a clue to effective prophylaxis. Some of the medications that decrease the frequency of the attacks may be doing so because they improve the patient’s sleep patterns. Those that decrease the intensity of the pain are probably working on pain pathway that is not specific to migraine.
Continuing a search for a prophylactic medication is a worthy goal, particularly for those patients in which their migraines are debilitating. However, based on my experience, enhanced by my bias, the safest and most effective prophylaxis results from increasing the family’s awareness of the role that sleep deprivation plays in the illness. Even when the family buys into the message and attempts to avoid situations that will tax their vulnerable children, parents will need to accept that sometimes stuff happens even though siblings and peers may be able to tolerate the situation. Spontaneous activities can converge on a day when for whatever reason the migraine-prone child is overtired and the headache and vomiting will erupt.
A lifestyle change is always preferable to a pharmacological intervention. However, that doesn’t mean it is always easy to achieve.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
I suspect you all have some experience with childhood migraine. It can mean a painful several hours for the patient, arriving often without warning, with recurrences spaced months or sometimes even years apart. It may be accompanied by vomiting, which in some cases overshadows the severity of the headache. It can result in lost days from school and ruin family activities. It can occur so infrequently that the family can’t recall accurately when the last episode happened. In some ways it is a different animal than the adult version.
Most of the pediatric patients with migraine I have seen have experienced attacks that were occurring so infrequently that the families and I seldom discussed medication as an option. Back then imipramine was the only choice. However, currently there are more than a half dozen medications and combinations that have been tried. Recently a review of 45 clinical trials of these medications was published in JAMA Network Open.
I will let you review for yourself the details of these Iranian investigators’ network meta-analysis, but the bottom line is that some medications were associated with a reduction in migraine frequency. Others were associated with headache intensity. “However, no treatments were associated with significant improvements in quality of life or reduction of the duration of migraine attacks.”
Obviously, this paper illustrates clearly that we have not yet discovered the medicinal magic bullet for pediatric migraine prophylaxis. This doesn’t surprise me. After listening to scores of families tell their migraine stories, it became apparent to me that there was often a pattern in which the child’s headache had arrived after a period of acute sleep deprivation. For example, a trip to an amusement park in which travel or excitement may have resulted in the child going to bed later and/or getting up earlier. By afternoon the child’s reserves of something (currently unknown) were depleted to a point that the headache and/or vomiting struck.
Because these episodes were often so infrequent, separated by months, that taking a history demonstrating a recurring pattern could take considerable patience on the part of the family and the provider, even for a physician like myself who believes that better sleep is the answer for everything. However, once I could convince a family of the connection between the sleep deprivation and the headaches, they could often recall other episodes in the past that substantiated my explanation.
In some cases there was no obvious history of acute sleep deprivation, or at least it was so subtle that even a history taker with a sleep obsession couldn’t detect it. However, in these cases I could usually elicit a history of chronic sleep deprivation. For example, falling asleep instantly on automobile rides, difficulty with waking in the morning, or unhealthy bedtime routines. With this underlying vulnerability of chronic sleep deprivation, a slightly more exciting or vigorous day was all that was necessary to trigger the headache.
For those of you who don’t share my contention that childhood migraine is usually the result of sleep deprivation, consider the similarity between an epileptic seizure, which can be triggered by fatigue. Both events are usually followed by a deep sleep from which the child wakes refreshed and symptom free.
I think it is interesting that this recent meta-analysis could find no benefit in the quality of life for any of the medications. The explanation may be that the child with migraine already had a somewhat diminished quality of life as a result of the sleep deprivation, either acute or chronic.
When speaking with parents of migraine sufferers, I would tell them that once the headache had started there was little I had to offer to forestall the inevitable pain and vomiting. Certainly not in the form of an oral medication. While many adults will have an aura that warns them of the headache onset, I have found that most children don’t describe an aura. It may be they simply lack the ability to express it. Occasionally an observant parent may detect pallor or a behavior change that indicates a migraine is beginning. On rare occasions a parent may be able to abort the attack by quickly getting the child to a quiet, dark, and calm environment.
Although this recent meta-analysis review of treatment options is discouraging, it may be providing a clue to effective prophylaxis. Some of the medications that decrease the frequency of the attacks may be doing so because they improve the patient’s sleep patterns. Those that decrease the intensity of the pain are probably working on pain pathway that is not specific to migraine.
Continuing a search for a prophylactic medication is a worthy goal, particularly for those patients in which their migraines are debilitating. However, based on my experience, enhanced by my bias, the safest and most effective prophylaxis results from increasing the family’s awareness of the role that sleep deprivation plays in the illness. Even when the family buys into the message and attempts to avoid situations that will tax their vulnerable children, parents will need to accept that sometimes stuff happens even though siblings and peers may be able to tolerate the situation. Spontaneous activities can converge on a day when for whatever reason the migraine-prone child is overtired and the headache and vomiting will erupt.
A lifestyle change is always preferable to a pharmacological intervention. However, that doesn’t mean it is always easy to achieve.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Is Being ‘Manly’ a Threat to a Man’s Health?
When my normally adorable cat Biscuit bit my ankle in a playful stalking exercise gone wrong, I washed it with soap and some rubbing alcohol, slapped on a Band-Aid, and went about my day.
The next morning, when it was swollen, I told myself it was probably just a hematoma and went about my day.
The next day, when the swelling had increased and red lines started creeping up my leg, I called my doctor. Long story short, I ended up hospitalized for intravenous antibiotics.
This is all to say that, yes, I’m sort of an idiot, but also to introduce the idea that maybe I minimized my very obvious lymphangitis because I am a man.
This week, we have empirical evidence that men downplay their medical symptoms — and that manlier men downplay them even more.

I’m going to talk about a study that links manliness (or, scientifically speaking, “male gender expressivity”) to medical diagnoses that are based on hard evidence and medical diagnoses that are based on self-report. You see where this is going but I want to walk you through the methods here because they are fairly interesting.
This study used data from the US National Longitudinal Study of Adolescent to Adult Health. This study enrolled 20,000 adolescents who were in grades 7-12 in the 1994-1995 school year and has been following them ever since — about 30 years so far.
The authors wanted to link early gender roles to long-term outcomes, so they cut that 20,000 number down to the 4230 males in the group who had complete follow-up.
Now comes the first interesting question. How do you quantify the “male gender expressivity” of boys in 7th-12th grade? There was no survey item that asked them how masculine or manly they felt. What the authors did was look at the surveys that were administered and identify the questions on those surveys where boys and girls gave the most disparate answers. I have some examples here. 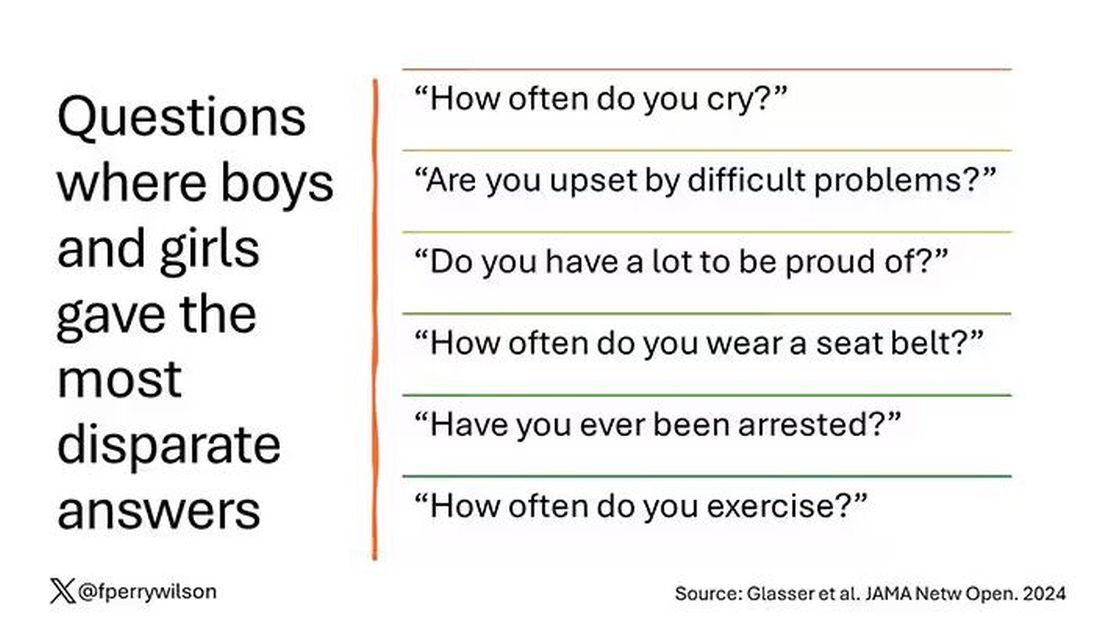
Some of these questions make sense when it comes to gender expressivity: “How often do you cry?” for example, has a lot of validity for the social construct that is gender. But some questions where boys and girls gave very different answers — like “How often do you exercise?” — don’t quite fit that mold. Regardless, this structure allowed the researchers to take individual kids’ responses to these questions and combine them into what amounts to a manliness score — how much their answers aligned with the typical male answer.
The score was established in adolescence — which is interesting because I’m sure some of this stuff may change over time — but notable because adolescence is where many gender roles develop.
Now we can fast-forward 30 years and see how these manliness scores link to various outcomes. The authors were interested in fairly common diseases: diabetes, hypertension, and hyperlipidemia.
Let’s start simply. Are males with higher gender expressivity in adolescence more or less likely to have these diseases in the future?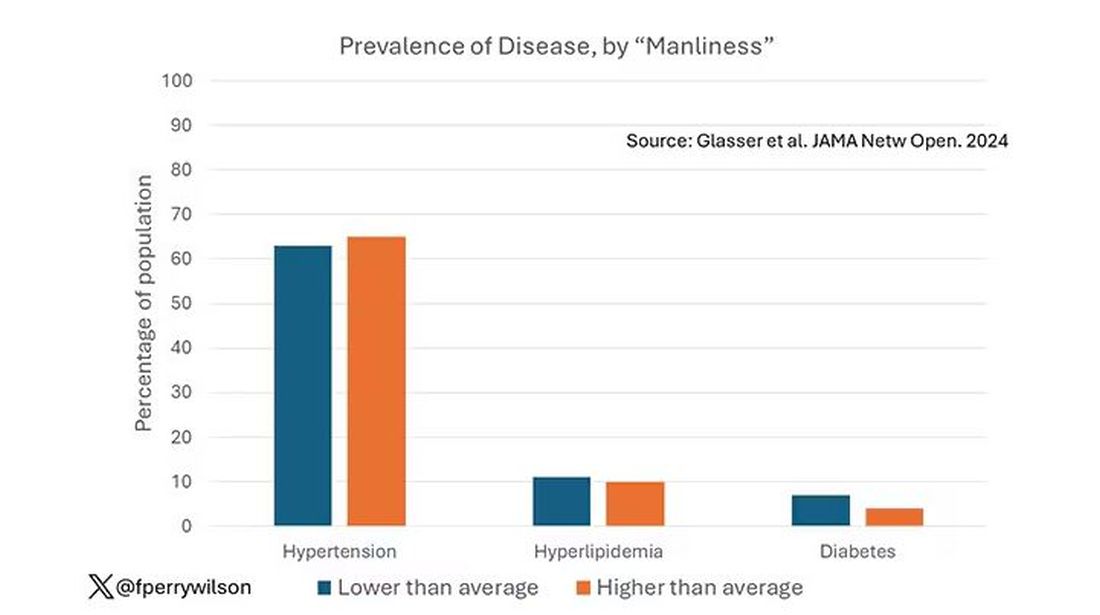
Not really. Those above the average in male gender expressivity had similar rates of hypertension and hyperlipidemia as those below the median. They were actually a bit less likely to have diabetes.
But that’s not what’s really interesting here.
I told you that there was no difference in the rate of hypertension among those with high vs low male gender expressivity. But there was a significant difference in their answer to the question “Do you have hypertension?” The same was seen for hyperlipidemia. In other words, those with higher manliness scores are less likely to admit (or perhaps know) that they have a particular disease.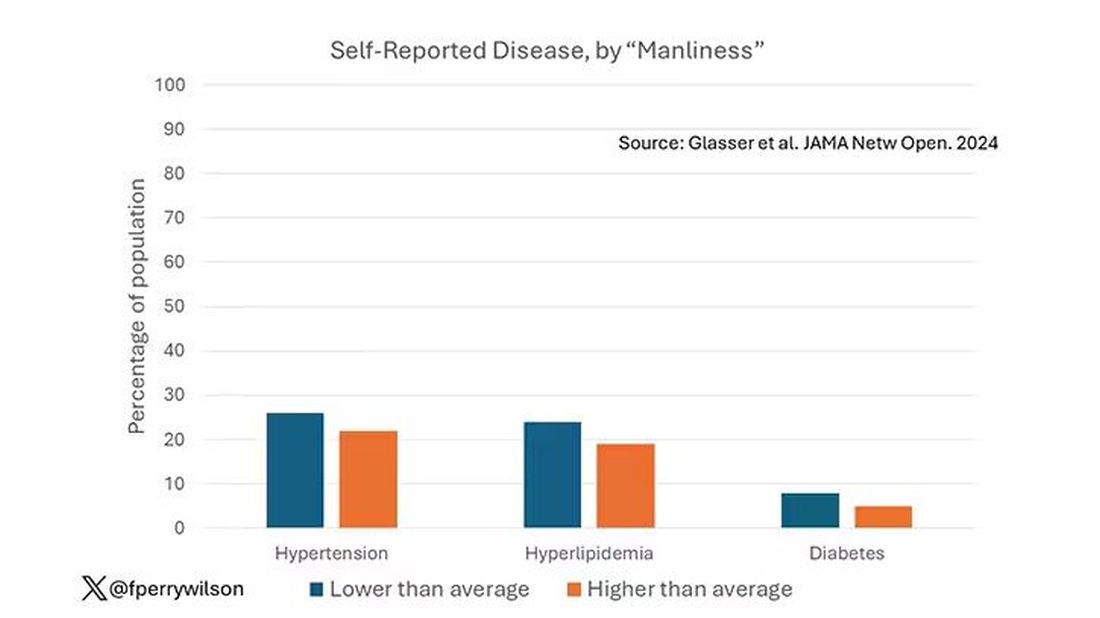
You can see the relationship across the manliness spectrum here in a series of adjusted models. The x-axis is the male gender expressivity score, and the y-axis is the percentage of people who report having the disease that we know they have based on the actual laboratory tests or vital sign measurements. As manliness increases, the self-report of a given disease decreases.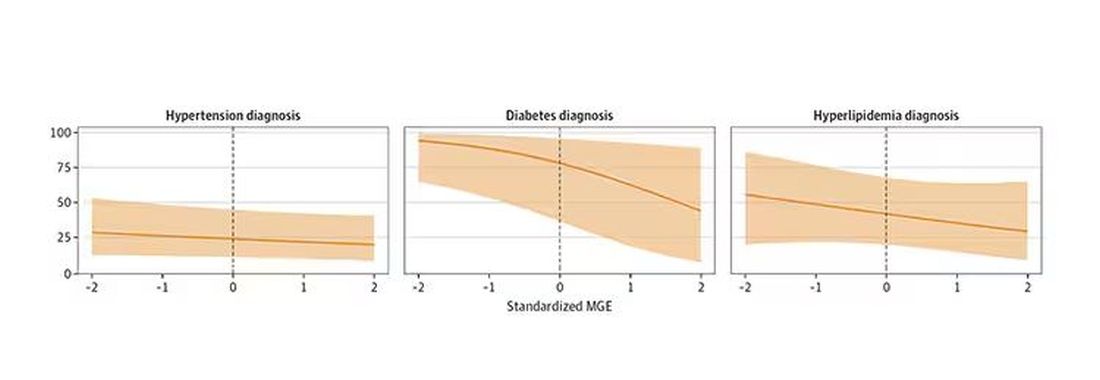
There are some important consequences of this systematic denial. Specifically, men with the diseases of interest who have higher male gender expressivity are less likely to get treatment. And, as we all know, the lack of treatment of something like hypertension puts people at risk for bad downstream outcomes.
Putting this all together, I’m not that surprised. Society trains boys from a young age to behave in certain ways: to hide emotions, to eschew vulnerability, to not complain when we are hurt. And those lessons can persist into later life. Whether the disease that strikes is hypertension or Pasteurella multocida from a slightly psychotic house cat, men are more likely to ignore it, to their detriment. 
So, gents, be brave. Get your blood tests and check your blood pressure. If there’s something wrong, admit it, and fix it. After all, fixing problems — that’s a manly thing, right?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
When my normally adorable cat Biscuit bit my ankle in a playful stalking exercise gone wrong, I washed it with soap and some rubbing alcohol, slapped on a Band-Aid, and went about my day.
The next morning, when it was swollen, I told myself it was probably just a hematoma and went about my day.
The next day, when the swelling had increased and red lines started creeping up my leg, I called my doctor. Long story short, I ended up hospitalized for intravenous antibiotics.
This is all to say that, yes, I’m sort of an idiot, but also to introduce the idea that maybe I minimized my very obvious lymphangitis because I am a man.
This week, we have empirical evidence that men downplay their medical symptoms — and that manlier men downplay them even more.
I’m going to talk about a study that links manliness (or, scientifically speaking, “male gender expressivity”) to medical diagnoses that are based on hard evidence and medical diagnoses that are based on self-report. You see where this is going but I want to walk you through the methods here because they are fairly interesting.
This study used data from the US National Longitudinal Study of Adolescent to Adult Health. This study enrolled 20,000 adolescents who were in grades 7-12 in the 1994-1995 school year and has been following them ever since — about 30 years so far.
The authors wanted to link early gender roles to long-term outcomes, so they cut that 20,000 number down to the 4230 males in the group who had complete follow-up.
Now comes the first interesting question. How do you quantify the “male gender expressivity” of boys in 7th-12th grade? There was no survey item that asked them how masculine or manly they felt. What the authors did was look at the surveys that were administered and identify the questions on those surveys where boys and girls gave the most disparate answers. I have some examples here.
Some of these questions make sense when it comes to gender expressivity: “How often do you cry?” for example, has a lot of validity for the social construct that is gender. But some questions where boys and girls gave very different answers — like “How often do you exercise?” — don’t quite fit that mold. Regardless, this structure allowed the researchers to take individual kids’ responses to these questions and combine them into what amounts to a manliness score — how much their answers aligned with the typical male answer.
The score was established in adolescence — which is interesting because I’m sure some of this stuff may change over time — but notable because adolescence is where many gender roles develop.
Now we can fast-forward 30 years and see how these manliness scores link to various outcomes. The authors were interested in fairly common diseases: diabetes, hypertension, and hyperlipidemia.
Let’s start simply. Are males with higher gender expressivity in adolescence more or less likely to have these diseases in the future?
Not really. Those above the average in male gender expressivity had similar rates of hypertension and hyperlipidemia as those below the median. They were actually a bit less likely to have diabetes.
But that’s not what’s really interesting here.
I told you that there was no difference in the rate of hypertension among those with high vs low male gender expressivity. But there was a significant difference in their answer to the question “Do you have hypertension?” The same was seen for hyperlipidemia. In other words, those with higher manliness scores are less likely to admit (or perhaps know) that they have a particular disease.
You can see the relationship across the manliness spectrum here in a series of adjusted models. The x-axis is the male gender expressivity score, and the y-axis is the percentage of people who report having the disease that we know they have based on the actual laboratory tests or vital sign measurements. As manliness increases, the self-report of a given disease decreases.
There are some important consequences of this systematic denial. Specifically, men with the diseases of interest who have higher male gender expressivity are less likely to get treatment. And, as we all know, the lack of treatment of something like hypertension puts people at risk for bad downstream outcomes.
Putting this all together, I’m not that surprised. Society trains boys from a young age to behave in certain ways: to hide emotions, to eschew vulnerability, to not complain when we are hurt. And those lessons can persist into later life. Whether the disease that strikes is hypertension or Pasteurella multocida from a slightly psychotic house cat, men are more likely to ignore it, to their detriment.
So, gents, be brave. Get your blood tests and check your blood pressure. If there’s something wrong, admit it, and fix it. After all, fixing problems — that’s a manly thing, right?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
When my normally adorable cat Biscuit bit my ankle in a playful stalking exercise gone wrong, I washed it with soap and some rubbing alcohol, slapped on a Band-Aid, and went about my day.
The next morning, when it was swollen, I told myself it was probably just a hematoma and went about my day.
The next day, when the swelling had increased and red lines started creeping up my leg, I called my doctor. Long story short, I ended up hospitalized for intravenous antibiotics.
This is all to say that, yes, I’m sort of an idiot, but also to introduce the idea that maybe I minimized my very obvious lymphangitis because I am a man.
This week, we have empirical evidence that men downplay their medical symptoms — and that manlier men downplay them even more.
I’m going to talk about a study that links manliness (or, scientifically speaking, “male gender expressivity”) to medical diagnoses that are based on hard evidence and medical diagnoses that are based on self-report. You see where this is going but I want to walk you through the methods here because they are fairly interesting.
This study used data from the US National Longitudinal Study of Adolescent to Adult Health. This study enrolled 20,000 adolescents who were in grades 7-12 in the 1994-1995 school year and has been following them ever since — about 30 years so far.
The authors wanted to link early gender roles to long-term outcomes, so they cut that 20,000 number down to the 4230 males in the group who had complete follow-up.
Now comes the first interesting question. How do you quantify the “male gender expressivity” of boys in 7th-12th grade? There was no survey item that asked them how masculine or manly they felt. What the authors did was look at the surveys that were administered and identify the questions on those surveys where boys and girls gave the most disparate answers. I have some examples here.
Some of these questions make sense when it comes to gender expressivity: “How often do you cry?” for example, has a lot of validity for the social construct that is gender. But some questions where boys and girls gave very different answers — like “How often do you exercise?” — don’t quite fit that mold. Regardless, this structure allowed the researchers to take individual kids’ responses to these questions and combine them into what amounts to a manliness score — how much their answers aligned with the typical male answer.
The score was established in adolescence — which is interesting because I’m sure some of this stuff may change over time — but notable because adolescence is where many gender roles develop.
Now we can fast-forward 30 years and see how these manliness scores link to various outcomes. The authors were interested in fairly common diseases: diabetes, hypertension, and hyperlipidemia.
Let’s start simply. Are males with higher gender expressivity in adolescence more or less likely to have these diseases in the future?
Not really. Those above the average in male gender expressivity had similar rates of hypertension and hyperlipidemia as those below the median. They were actually a bit less likely to have diabetes.
But that’s not what’s really interesting here.
I told you that there was no difference in the rate of hypertension among those with high vs low male gender expressivity. But there was a significant difference in their answer to the question “Do you have hypertension?” The same was seen for hyperlipidemia. In other words, those with higher manliness scores are less likely to admit (or perhaps know) that they have a particular disease.
You can see the relationship across the manliness spectrum here in a series of adjusted models. The x-axis is the male gender expressivity score, and the y-axis is the percentage of people who report having the disease that we know they have based on the actual laboratory tests or vital sign measurements. As manliness increases, the self-report of a given disease decreases.
There are some important consequences of this systematic denial. Specifically, men with the diseases of interest who have higher male gender expressivity are less likely to get treatment. And, as we all know, the lack of treatment of something like hypertension puts people at risk for bad downstream outcomes.
Putting this all together, I’m not that surprised. Society trains boys from a young age to behave in certain ways: to hide emotions, to eschew vulnerability, to not complain when we are hurt. And those lessons can persist into later life. Whether the disease that strikes is hypertension or Pasteurella multocida from a slightly psychotic house cat, men are more likely to ignore it, to their detriment.
So, gents, be brave. Get your blood tests and check your blood pressure. If there’s something wrong, admit it, and fix it. After all, fixing problems — that’s a manly thing, right?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Myth of the Month: Are Thickened Liquids Helpful in Dysphagia Patients?
Case: An 80-year-old man with advanced Alzheimer’s disease is admitted to the hospital after a fall. He is noted to have coughing spells after drinking liquids. He has a swallowing study done which shows severe slowing of motility in the esophagus.
What do you recommend?
A. Feeding tube
B. Thickened liquids
C. Continue current diet
The correct answer for this patient is to allow them to continue their current diet. They do not need thickened liquids. A feeding tube would not be recommended.1
So are there any data supporting the widespread use of thickened liquid diets for patients with dysphagia and aspiration?
Multiple clinical guidelines for stroke recommend the use of thickened liquids despite minimal to no evidence of efficacy.2 It is a common practice to give patients with advanced dementia thickened liquids, especially in the hospital setting. Does this help?
Makhnevich and colleagues published a cohort study of Alzheimer’s disease patients with dysphagia admitted to the hospital over a 5-year period.3 Almost half of the cohort received a thickened liquid diet; these patients were matched with patients who received a thin liquid diet. There was no significant difference in hospital mortality between the groups that received thick liquids and thin liquids (hazard ratio, 0.92; P = .46). Patients receiving thickened liquids were less likely to be intubated but were more likely to have pulmonary infections.
A 2018 Cochrane review concluded that there was no consensus on immediate and long-term effects of modifying the consistency of fluid for swallowing difficulties in dementia because too few studies have been completed.4 So why is this important information or lack of information?
What is so bad about a thickened liquid diet?
Eric Widera, MD, shared in JAMA Internal Medicine his experience along with his hospice and palliative care team of drinking thickened liquids.5 He drank only thickened liquids for a 12-hour period. “The challenge was eye-opening. It was the first time I experienced the terrible taste and texture of thickened liquids,” he wrote. He shared some of the risks of thickened liquids: dehydration, poor oral intake, and decreased quality of life.
The bottom line is that there is scant evidence for the benefit of thickened liquids, especially for patients with advanced dementia and dysphagia, and giving thickened liquids is not a benign intervention, because of poor tolerability of the diet.
References
1. American Geriatrics Society Ethics Committee and Clinical Practice and Models of Care Committee. J Am Geriatr Soc. 2014;62(8):1590-3.
2. McCurtin A et al. J Eval Clin Pract. 2020;26:1744-60.
3. Makhnevich A et al. JAMA Intern Med. 2024 Jul 1;184(7):778-85.
4. Flynn E et al. Cochrane Database Syst Rev. 2018 Sep 24;9(9):CD011077.
5. Widera E. JAMA Intern Med. 2024 Jul 1;184(7):786-7.
Case: An 80-year-old man with advanced Alzheimer’s disease is admitted to the hospital after a fall. He is noted to have coughing spells after drinking liquids. He has a swallowing study done which shows severe slowing of motility in the esophagus.
What do you recommend?
A. Feeding tube
B. Thickened liquids
C. Continue current diet
The correct answer for this patient is to allow them to continue their current diet. They do not need thickened liquids. A feeding tube would not be recommended.1
So are there any data supporting the widespread use of thickened liquid diets for patients with dysphagia and aspiration?
Multiple clinical guidelines for stroke recommend the use of thickened liquids despite minimal to no evidence of efficacy.2 It is a common practice to give patients with advanced dementia thickened liquids, especially in the hospital setting. Does this help?
Makhnevich and colleagues published a cohort study of Alzheimer’s disease patients with dysphagia admitted to the hospital over a 5-year period.3 Almost half of the cohort received a thickened liquid diet; these patients were matched with patients who received a thin liquid diet. There was no significant difference in hospital mortality between the groups that received thick liquids and thin liquids (hazard ratio, 0.92; P = .46). Patients receiving thickened liquids were less likely to be intubated but were more likely to have pulmonary infections.
A 2018 Cochrane review concluded that there was no consensus on immediate and long-term effects of modifying the consistency of fluid for swallowing difficulties in dementia because too few studies have been completed.4 So why is this important information or lack of information?
What is so bad about a thickened liquid diet?
Eric Widera, MD, shared in JAMA Internal Medicine his experience along with his hospice and palliative care team of drinking thickened liquids.5 He drank only thickened liquids for a 12-hour period. “The challenge was eye-opening. It was the first time I experienced the terrible taste and texture of thickened liquids,” he wrote. He shared some of the risks of thickened liquids: dehydration, poor oral intake, and decreased quality of life.
The bottom line is that there is scant evidence for the benefit of thickened liquids, especially for patients with advanced dementia and dysphagia, and giving thickened liquids is not a benign intervention, because of poor tolerability of the diet.
References
1. American Geriatrics Society Ethics Committee and Clinical Practice and Models of Care Committee. J Am Geriatr Soc. 2014;62(8):1590-3.
2. McCurtin A et al. J Eval Clin Pract. 2020;26:1744-60.
3. Makhnevich A et al. JAMA Intern Med. 2024 Jul 1;184(7):778-85.
4. Flynn E et al. Cochrane Database Syst Rev. 2018 Sep 24;9(9):CD011077.
5. Widera E. JAMA Intern Med. 2024 Jul 1;184(7):786-7.
Case: An 80-year-old man with advanced Alzheimer’s disease is admitted to the hospital after a fall. He is noted to have coughing spells after drinking liquids. He has a swallowing study done which shows severe slowing of motility in the esophagus.
What do you recommend?
A. Feeding tube
B. Thickened liquids
C. Continue current diet
The correct answer for this patient is to allow them to continue their current diet. They do not need thickened liquids. A feeding tube would not be recommended.1
So are there any data supporting the widespread use of thickened liquid diets for patients with dysphagia and aspiration?
Multiple clinical guidelines for stroke recommend the use of thickened liquids despite minimal to no evidence of efficacy.2 It is a common practice to give patients with advanced dementia thickened liquids, especially in the hospital setting. Does this help?
Makhnevich and colleagues published a cohort study of Alzheimer’s disease patients with dysphagia admitted to the hospital over a 5-year period.3 Almost half of the cohort received a thickened liquid diet; these patients were matched with patients who received a thin liquid diet. There was no significant difference in hospital mortality between the groups that received thick liquids and thin liquids (hazard ratio, 0.92; P = .46). Patients receiving thickened liquids were less likely to be intubated but were more likely to have pulmonary infections.
A 2018 Cochrane review concluded that there was no consensus on immediate and long-term effects of modifying the consistency of fluid for swallowing difficulties in dementia because too few studies have been completed.4 So why is this important information or lack of information?
What is so bad about a thickened liquid diet?
Eric Widera, MD, shared in JAMA Internal Medicine his experience along with his hospice and palliative care team of drinking thickened liquids.5 He drank only thickened liquids for a 12-hour period. “The challenge was eye-opening. It was the first time I experienced the terrible taste and texture of thickened liquids,” he wrote. He shared some of the risks of thickened liquids: dehydration, poor oral intake, and decreased quality of life.
The bottom line is that there is scant evidence for the benefit of thickened liquids, especially for patients with advanced dementia and dysphagia, and giving thickened liquids is not a benign intervention, because of poor tolerability of the diet.
References
1. American Geriatrics Society Ethics Committee and Clinical Practice and Models of Care Committee. J Am Geriatr Soc. 2014;62(8):1590-3.
2. McCurtin A et al. J Eval Clin Pract. 2020;26:1744-60.
3. Makhnevich A et al. JAMA Intern Med. 2024 Jul 1;184(7):778-85.
4. Flynn E et al. Cochrane Database Syst Rev. 2018 Sep 24;9(9):CD011077.
5. Widera E. JAMA Intern Med. 2024 Jul 1;184(7):786-7.