User login
JIA arthritis and uveitis flares ‘often run parallel’
Children with juvenile idiopathic arthritis–associated uveitis (JIA-U) are significantly more likely to experience a flare in their eye disease if their arthritis is also worsening, a team of U.S.-based researchers has found.
In a longitudinal cohort study, children with active arthritis at the time of a routine rheumatology assessment had an almost 2.5-fold increased risk of also having active uveitis 45 days before or after the assessment than did children whose arthritis was not flaring at the rheumatology assessment.
“We demonstrate that the two diseases often run parallel courses,” corresponding author Emily J. Liebling, MD, of the Children’s Hospital of Philadelphia and associates state in Arthritis Care & Research, noting that the magnitude of the association is striking.
“Although there are known risk factors associated with uveitis development in children with JIA, less data are available about factors associated with uveitis flare or activity,” said Sheila T. Angeles-Han, MD, MSc, of the departments of pediatrics and ophthalmology at Cincinnati Children’s Hospital Medical Center who commented on the study in an interview.
“If proven, this knowledge has the potential to impact practice patterns and current guidelines wherein a pediatric rheumatologist who evaluates a child with JIA-associated uveitis and finds active arthritis would request an expedited ophthalmic examination,” Dr. Angeles-Han suggested.
Dr. Angeles-Han led the development of the first American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring, and Treatment of JIA-Associated Uveitis, which recommends regular screening for uveitis in all children with JIA. Children found to have uveitis should then be screened at least every 3 months, and more frequently if they are taking glucocorticoids and treatment is being tapered.

JIA-associated uveitis accounts for around 20%-40% of all cases of noninfectious childhood eye inflammation, and it can run an insidious and chronic course.
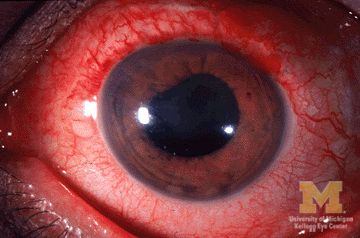
“Children with acute anterior uveitis are symptomatic and tend to have a painful red eye, thus prompting an ophthalmic evaluation,” Dr. Angeles-Han explained. “This is different from children with chronic anterior uveitis who tend not to have any symptoms, thus a screening examination is critical to detect ocular inflammation.”
While the ACR/AF guideline distinguishes between acute and chronic uveitis, Dr. Liebling and colleagues explain that they did not because their experience shows that “even patients with chronic anterior uveitis, typically thought to have silent disease, may exhibit symptoms of eye pain, redness, vision changes, and photophobia.”
Conversely, they say “the JIA subtypes usually associated with acute anterior uveitis may instead manifest as asymptomatic eye disease.”
For their study, Dr. Liebling and coinvestigators examined the records of children seen at the Children’s Hospital of Philadelphia over a 6.5-year period. For inclusion, children had to have a physician diagnosis of JIA of any subtype and a history of uveitis.
A total of 98 children were included in the retrospective evaluation; the median age at diagnosis of JIA was 3.3 years, and the median age at first uveitis diagnosis was 5.1 years. The majority (82%) were female, 69% were antinuclear antibody (ANA) positive, and 60% had oligoarthritis – all of which have been associated with having a higher risk for developing uveitis.
However, independent of these and several other factors, the probability of having active uveitis within 45 days of a rheumatology assessment was 65% in those with active arthritis versus 42% for those with no active joints.
Their data are based on 1,229 rheumatology visits that occurred between 2013 and 2019, with a median of 13 visits per patient. Overall, arthritis was defined as being active in 17% of visits, and active uveitis was observed in 18% of rheumatology visits.
Concordance between arthritis and uveitis activity was observed 73% of the time, the researchers reported. A sensitivity analysis that excluded children with the enthesitis-related arthritis subtype of JIA, who may not undergo frequent eye exams, did not change their findings.
Decreased odds of active uveitis at any time point were seen with the use of combination biologic and nonbiologic disease-modifying antirheumatic drugs. Years from uveitis diagnosis was also associated with lower odds of active uveitis over time.
Other factors associated with lower odds of uveitis were female sex, HLA-B27 positivity, and having any subtype of JIA other than the oligoarticular subtype.
Dr. Liebling and coinvestigators concluded that, contrary to the historical dogma, arthritis and uveitis do not run distinct and unrelated courses: “In patients with JIA-U, there is a significant temporal association between arthritis and uveitis disease activity.”
The study was sponsored by the Children’s Hospital of Philadelphia Rheumatology Research Fund. The investigators for the study had no financial support from commercial sources or any other potential conflicts of interest. Dr. Angeles-Han had no conflicts of interest to disclose.
SOURCE: Liebling EJ et al. Arthritis Care Res. 2020 Oct 12. doi: 10.1002/acr.24483.
Children with juvenile idiopathic arthritis–associated uveitis (JIA-U) are significantly more likely to experience a flare in their eye disease if their arthritis is also worsening, a team of U.S.-based researchers has found.
In a longitudinal cohort study, children with active arthritis at the time of a routine rheumatology assessment had an almost 2.5-fold increased risk of also having active uveitis 45 days before or after the assessment than did children whose arthritis was not flaring at the rheumatology assessment.
“We demonstrate that the two diseases often run parallel courses,” corresponding author Emily J. Liebling, MD, of the Children’s Hospital of Philadelphia and associates state in Arthritis Care & Research, noting that the magnitude of the association is striking.
“Although there are known risk factors associated with uveitis development in children with JIA, less data are available about factors associated with uveitis flare or activity,” said Sheila T. Angeles-Han, MD, MSc, of the departments of pediatrics and ophthalmology at Cincinnati Children’s Hospital Medical Center who commented on the study in an interview.
“If proven, this knowledge has the potential to impact practice patterns and current guidelines wherein a pediatric rheumatologist who evaluates a child with JIA-associated uveitis and finds active arthritis would request an expedited ophthalmic examination,” Dr. Angeles-Han suggested.
Dr. Angeles-Han led the development of the first American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring, and Treatment of JIA-Associated Uveitis, which recommends regular screening for uveitis in all children with JIA. Children found to have uveitis should then be screened at least every 3 months, and more frequently if they are taking glucocorticoids and treatment is being tapered.
JIA-associated uveitis accounts for around 20%-40% of all cases of noninfectious childhood eye inflammation, and it can run an insidious and chronic course.
“Children with acute anterior uveitis are symptomatic and tend to have a painful red eye, thus prompting an ophthalmic evaluation,” Dr. Angeles-Han explained. “This is different from children with chronic anterior uveitis who tend not to have any symptoms, thus a screening examination is critical to detect ocular inflammation.”
While the ACR/AF guideline distinguishes between acute and chronic uveitis, Dr. Liebling and colleagues explain that they did not because their experience shows that “even patients with chronic anterior uveitis, typically thought to have silent disease, may exhibit symptoms of eye pain, redness, vision changes, and photophobia.”
Conversely, they say “the JIA subtypes usually associated with acute anterior uveitis may instead manifest as asymptomatic eye disease.”
For their study, Dr. Liebling and coinvestigators examined the records of children seen at the Children’s Hospital of Philadelphia over a 6.5-year period. For inclusion, children had to have a physician diagnosis of JIA of any subtype and a history of uveitis.
A total of 98 children were included in the retrospective evaluation; the median age at diagnosis of JIA was 3.3 years, and the median age at first uveitis diagnosis was 5.1 years. The majority (82%) were female, 69% were antinuclear antibody (ANA) positive, and 60% had oligoarthritis – all of which have been associated with having a higher risk for developing uveitis.
However, independent of these and several other factors, the probability of having active uveitis within 45 days of a rheumatology assessment was 65% in those with active arthritis versus 42% for those with no active joints.
Their data are based on 1,229 rheumatology visits that occurred between 2013 and 2019, with a median of 13 visits per patient. Overall, arthritis was defined as being active in 17% of visits, and active uveitis was observed in 18% of rheumatology visits.
Concordance between arthritis and uveitis activity was observed 73% of the time, the researchers reported. A sensitivity analysis that excluded children with the enthesitis-related arthritis subtype of JIA, who may not undergo frequent eye exams, did not change their findings.
Decreased odds of active uveitis at any time point were seen with the use of combination biologic and nonbiologic disease-modifying antirheumatic drugs. Years from uveitis diagnosis was also associated with lower odds of active uveitis over time.
Other factors associated with lower odds of uveitis were female sex, HLA-B27 positivity, and having any subtype of JIA other than the oligoarticular subtype.
Dr. Liebling and coinvestigators concluded that, contrary to the historical dogma, arthritis and uveitis do not run distinct and unrelated courses: “In patients with JIA-U, there is a significant temporal association between arthritis and uveitis disease activity.”
The study was sponsored by the Children’s Hospital of Philadelphia Rheumatology Research Fund. The investigators for the study had no financial support from commercial sources or any other potential conflicts of interest. Dr. Angeles-Han had no conflicts of interest to disclose.
SOURCE: Liebling EJ et al. Arthritis Care Res. 2020 Oct 12. doi: 10.1002/acr.24483.
Children with juvenile idiopathic arthritis–associated uveitis (JIA-U) are significantly more likely to experience a flare in their eye disease if their arthritis is also worsening, a team of U.S.-based researchers has found.
In a longitudinal cohort study, children with active arthritis at the time of a routine rheumatology assessment had an almost 2.5-fold increased risk of also having active uveitis 45 days before or after the assessment than did children whose arthritis was not flaring at the rheumatology assessment.
“We demonstrate that the two diseases often run parallel courses,” corresponding author Emily J. Liebling, MD, of the Children’s Hospital of Philadelphia and associates state in Arthritis Care & Research, noting that the magnitude of the association is striking.
“Although there are known risk factors associated with uveitis development in children with JIA, less data are available about factors associated with uveitis flare or activity,” said Sheila T. Angeles-Han, MD, MSc, of the departments of pediatrics and ophthalmology at Cincinnati Children’s Hospital Medical Center who commented on the study in an interview.
“If proven, this knowledge has the potential to impact practice patterns and current guidelines wherein a pediatric rheumatologist who evaluates a child with JIA-associated uveitis and finds active arthritis would request an expedited ophthalmic examination,” Dr. Angeles-Han suggested.
Dr. Angeles-Han led the development of the first American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring, and Treatment of JIA-Associated Uveitis, which recommends regular screening for uveitis in all children with JIA. Children found to have uveitis should then be screened at least every 3 months, and more frequently if they are taking glucocorticoids and treatment is being tapered.
JIA-associated uveitis accounts for around 20%-40% of all cases of noninfectious childhood eye inflammation, and it can run an insidious and chronic course.
“Children with acute anterior uveitis are symptomatic and tend to have a painful red eye, thus prompting an ophthalmic evaluation,” Dr. Angeles-Han explained. “This is different from children with chronic anterior uveitis who tend not to have any symptoms, thus a screening examination is critical to detect ocular inflammation.”
While the ACR/AF guideline distinguishes between acute and chronic uveitis, Dr. Liebling and colleagues explain that they did not because their experience shows that “even patients with chronic anterior uveitis, typically thought to have silent disease, may exhibit symptoms of eye pain, redness, vision changes, and photophobia.”
Conversely, they say “the JIA subtypes usually associated with acute anterior uveitis may instead manifest as asymptomatic eye disease.”
For their study, Dr. Liebling and coinvestigators examined the records of children seen at the Children’s Hospital of Philadelphia over a 6.5-year period. For inclusion, children had to have a physician diagnosis of JIA of any subtype and a history of uveitis.
A total of 98 children were included in the retrospective evaluation; the median age at diagnosis of JIA was 3.3 years, and the median age at first uveitis diagnosis was 5.1 years. The majority (82%) were female, 69% were antinuclear antibody (ANA) positive, and 60% had oligoarthritis – all of which have been associated with having a higher risk for developing uveitis.
However, independent of these and several other factors, the probability of having active uveitis within 45 days of a rheumatology assessment was 65% in those with active arthritis versus 42% for those with no active joints.
Their data are based on 1,229 rheumatology visits that occurred between 2013 and 2019, with a median of 13 visits per patient. Overall, arthritis was defined as being active in 17% of visits, and active uveitis was observed in 18% of rheumatology visits.
Concordance between arthritis and uveitis activity was observed 73% of the time, the researchers reported. A sensitivity analysis that excluded children with the enthesitis-related arthritis subtype of JIA, who may not undergo frequent eye exams, did not change their findings.
Decreased odds of active uveitis at any time point were seen with the use of combination biologic and nonbiologic disease-modifying antirheumatic drugs. Years from uveitis diagnosis was also associated with lower odds of active uveitis over time.
Other factors associated with lower odds of uveitis were female sex, HLA-B27 positivity, and having any subtype of JIA other than the oligoarticular subtype.
Dr. Liebling and coinvestigators concluded that, contrary to the historical dogma, arthritis and uveitis do not run distinct and unrelated courses: “In patients with JIA-U, there is a significant temporal association between arthritis and uveitis disease activity.”
The study was sponsored by the Children’s Hospital of Philadelphia Rheumatology Research Fund. The investigators for the study had no financial support from commercial sources or any other potential conflicts of interest. Dr. Angeles-Han had no conflicts of interest to disclose.
SOURCE: Liebling EJ et al. Arthritis Care Res. 2020 Oct 12. doi: 10.1002/acr.24483.
FROM ARTHRITIS CARE & RESEARCH
‘Modest’ benefit for post-MI T2D glucose monitoring
Following a heart attack, there appears to be a “modest” benefit of using flash glucose monitoring over fingerstick testing to monitor blood glucose levels in patients with type 2 diabetes being treated with insulin or a sulfonylurea, according to investigators of the LIBERATES trial.
The results showed a nonsignificant increase in the time that subjects’ blood glucose was spent in the target range of 3.9-10.00 mmol/L (70-180 mg/dL) 3 months after experiencing an acute coronary syndrome (ACS).
At best, flash monitoring using Abbott’s Freestyle Libre system was associated with an increase in time spent in range (TIR) of 17-28 or 48 minutes per day over self-monitoring of blood glucose (SMBG), depending on the type of statistical analysis used. There was no difference in glycated hemoglobin A1c levels between the two groups, but there was a trend for less time spent in hypoglycemia in the flash monitoring arm.
Viewers underwhelmed
“My overall impression is that the effects were less pronounced than anticipated,” Kare Birkeland, MD, PhD, a specialist in internal medicine and endocrinology at Oslo University Hospital, Rikshospitalet, Norway, observed after the findings were presented at the virtual annual meeting of the European Association for the Study of Diabetes.
Others who had watched the live session seemed similarly underwhelmed by the findings, with one viewer questioning the value of devoting an hour-and-a-half session to the phase 2 trial.
However, the session chair Simon Heller, BA, MB, BChir, DM, professor of clinical diabetes at the University of Sheffield, and trial coinvestigator, defended the detailed look at the trial’s findings, noting that it was worthwhile to present the data from the trial as it “really helps explain why we do phase 2 and phase 3 trials.”

Strong rationale for monitoring post-MI
There is a strong rationale for ensuring that blood glucose is well controlled in type 2 diabetes patients who have experienced a myocardial infarction, observed Robert Storey, BSc, BM, DM, professor of cardiology at the University of Sheffield. One way to do that potentially is through improved glucose monitoring.
“There’s clearly a close link between diabetes and the risk of MI: Both high and low HbA1c are associated with adverse outcome, and high and low glucose levels following MI are also associated with adverse outcome,” he observed, noting also that hypoglycemia was not given enough attention in post-ACS patients.

“The hypothesis of the LIBERATES study was that a modern glycemic monitoring strategy can optimize blood glucose levels in type 2 diabetes patients following MI with the potential to reduce mortality and morbidity and improve quality of life,” Dr. Storey said. “The main research question of LIBERATES says, ‘Do new approaches in glucose monitoring increase the time in range and reduce hypoglycemia?’ ”
Pragmatic trial design
LIBERATES was a prospective, multicenter, parallel group, randomized controlled trial, explained the study’s statistician Deborah Stocken, PhD, professor of clinical trials research at the University of Leeds. There was “limited ability to blind the interventions,” so it was an open-label design.
“The patient population in LIBERATES was kept as inclusive and as pragmatic as possible to ensure that the results at the end of the trial are generalizable,” said Dr. Stocken. Patients with type 2 diabetes were recruited within 5 days of hospital admission for ACS, which could include both ST- and non-ST elevation MI. In all, 141 of a calculated 150 patients that would be needed were recruited and randomized to the flash monitoring (69) or SMBG (72) arm.
Dr. Stocken noted that early in the recruitment phase, the trials oversight committee recommended that Bayesian methodology should be used as the most robust analytical approach.
“Essentially, a Bayesian approach would avoid a hypothesis test, and instead would provide a probability of there being a treatment benefit for continuous monitoring. And if this probability was high enough, this would warrant further research in the phase 3 setting,” Dr. Stocken said.
What else was shown?
“We had a number of prespecified secondary endpoints, which to me are equally important,” said Ramzi Ajjan, MD, MMed.Sci, PhD, associate professor and consultant in diabetes and endocrinology at Leeds University and Leeds Teaching Hospitals Trust.
Among these was the TIR at days 16-30, which showed a 90-minute increase per day in favor of flash monitoring over SMBG. This “seems to be driven by those who are an insulin,” Dr. Ajjan said, adding that “you get almost a 3-hour increase in time in range in people who are on insulin at baseline, and you don’t see that in people who are on sulfonylurea.”
Conversely, sulfonylurea treatment seemed to drive the reduction in the time spent in hypoglycemia defined as 3.9 mmol/L (70 g/dL) at 3 months. For the whole group, there was a 1.3-hour reduction in hypoglycemia per day with flash monitoring versus SMBG, which increased to 2 hours for those on sulfonylureas.
There also was a “pattern of reduction” in time spent in hypoglycemia defined as less than 3.0 mmol/L (54 g/dL) both early on and becoming more pronounced with time.
“Flash glucose monitoring is associated with higher treatment satisfaction score, compared with SMBG,” Dr. Ajjan said.
Although A1c dropped in both groups to a similar extent, he noted that the reduction seen in the flash monitoring group was associated with a decrease in hypoglycemia.
There was a huge amount of data collected during the trial and there are many more analyses that could be done, Dr. Ajjan said. The outcome of those may determine whether a phase 3 trial is likely, assuming sponsorship can be secured.
The LIBERATES Trial was funded by grants from the UK National Institute for Health Research and Abbott Diabetes Care. None of the investigators were additionally compensated for their work within the trial. Dr. Stocken had no disclosures in relation to this trial. Dr. Ajjan has received research funding and other financial support from Abbott, Bayer, Eli Lilly, Johnson & Johnson, and Novo Nordisk.
SOURCE: Ajjan R et al. EASD 2020. S11 – The LIBERATES Trial.
Following a heart attack, there appears to be a “modest” benefit of using flash glucose monitoring over fingerstick testing to monitor blood glucose levels in patients with type 2 diabetes being treated with insulin or a sulfonylurea, according to investigators of the LIBERATES trial.
The results showed a nonsignificant increase in the time that subjects’ blood glucose was spent in the target range of 3.9-10.00 mmol/L (70-180 mg/dL) 3 months after experiencing an acute coronary syndrome (ACS).
At best, flash monitoring using Abbott’s Freestyle Libre system was associated with an increase in time spent in range (TIR) of 17-28 or 48 minutes per day over self-monitoring of blood glucose (SMBG), depending on the type of statistical analysis used. There was no difference in glycated hemoglobin A1c levels between the two groups, but there was a trend for less time spent in hypoglycemia in the flash monitoring arm.
Viewers underwhelmed
“My overall impression is that the effects were less pronounced than anticipated,” Kare Birkeland, MD, PhD, a specialist in internal medicine and endocrinology at Oslo University Hospital, Rikshospitalet, Norway, observed after the findings were presented at the virtual annual meeting of the European Association for the Study of Diabetes.
Others who had watched the live session seemed similarly underwhelmed by the findings, with one viewer questioning the value of devoting an hour-and-a-half session to the phase 2 trial.
However, the session chair Simon Heller, BA, MB, BChir, DM, professor of clinical diabetes at the University of Sheffield, and trial coinvestigator, defended the detailed look at the trial’s findings, noting that it was worthwhile to present the data from the trial as it “really helps explain why we do phase 2 and phase 3 trials.”
Strong rationale for monitoring post-MI
There is a strong rationale for ensuring that blood glucose is well controlled in type 2 diabetes patients who have experienced a myocardial infarction, observed Robert Storey, BSc, BM, DM, professor of cardiology at the University of Sheffield. One way to do that potentially is through improved glucose monitoring.
“There’s clearly a close link between diabetes and the risk of MI: Both high and low HbA1c are associated with adverse outcome, and high and low glucose levels following MI are also associated with adverse outcome,” he observed, noting also that hypoglycemia was not given enough attention in post-ACS patients.
“The hypothesis of the LIBERATES study was that a modern glycemic monitoring strategy can optimize blood glucose levels in type 2 diabetes patients following MI with the potential to reduce mortality and morbidity and improve quality of life,” Dr. Storey said. “The main research question of LIBERATES says, ‘Do new approaches in glucose monitoring increase the time in range and reduce hypoglycemia?’ ”
Pragmatic trial design
LIBERATES was a prospective, multicenter, parallel group, randomized controlled trial, explained the study’s statistician Deborah Stocken, PhD, professor of clinical trials research at the University of Leeds. There was “limited ability to blind the interventions,” so it was an open-label design.
“The patient population in LIBERATES was kept as inclusive and as pragmatic as possible to ensure that the results at the end of the trial are generalizable,” said Dr. Stocken. Patients with type 2 diabetes were recruited within 5 days of hospital admission for ACS, which could include both ST- and non-ST elevation MI. In all, 141 of a calculated 150 patients that would be needed were recruited and randomized to the flash monitoring (69) or SMBG (72) arm.
Dr. Stocken noted that early in the recruitment phase, the trials oversight committee recommended that Bayesian methodology should be used as the most robust analytical approach.
“Essentially, a Bayesian approach would avoid a hypothesis test, and instead would provide a probability of there being a treatment benefit for continuous monitoring. And if this probability was high enough, this would warrant further research in the phase 3 setting,” Dr. Stocken said.
What else was shown?
“We had a number of prespecified secondary endpoints, which to me are equally important,” said Ramzi Ajjan, MD, MMed.Sci, PhD, associate professor and consultant in diabetes and endocrinology at Leeds University and Leeds Teaching Hospitals Trust.
Among these was the TIR at days 16-30, which showed a 90-minute increase per day in favor of flash monitoring over SMBG. This “seems to be driven by those who are an insulin,” Dr. Ajjan said, adding that “you get almost a 3-hour increase in time in range in people who are on insulin at baseline, and you don’t see that in people who are on sulfonylurea.”
Conversely, sulfonylurea treatment seemed to drive the reduction in the time spent in hypoglycemia defined as 3.9 mmol/L (70 g/dL) at 3 months. For the whole group, there was a 1.3-hour reduction in hypoglycemia per day with flash monitoring versus SMBG, which increased to 2 hours for those on sulfonylureas.
There also was a “pattern of reduction” in time spent in hypoglycemia defined as less than 3.0 mmol/L (54 g/dL) both early on and becoming more pronounced with time.
“Flash glucose monitoring is associated with higher treatment satisfaction score, compared with SMBG,” Dr. Ajjan said.
Although A1c dropped in both groups to a similar extent, he noted that the reduction seen in the flash monitoring group was associated with a decrease in hypoglycemia.
There was a huge amount of data collected during the trial and there are many more analyses that could be done, Dr. Ajjan said. The outcome of those may determine whether a phase 3 trial is likely, assuming sponsorship can be secured.
The LIBERATES Trial was funded by grants from the UK National Institute for Health Research and Abbott Diabetes Care. None of the investigators were additionally compensated for their work within the trial. Dr. Stocken had no disclosures in relation to this trial. Dr. Ajjan has received research funding and other financial support from Abbott, Bayer, Eli Lilly, Johnson & Johnson, and Novo Nordisk.
SOURCE: Ajjan R et al. EASD 2020. S11 – The LIBERATES Trial.
Following a heart attack, there appears to be a “modest” benefit of using flash glucose monitoring over fingerstick testing to monitor blood glucose levels in patients with type 2 diabetes being treated with insulin or a sulfonylurea, according to investigators of the LIBERATES trial.
The results showed a nonsignificant increase in the time that subjects’ blood glucose was spent in the target range of 3.9-10.00 mmol/L (70-180 mg/dL) 3 months after experiencing an acute coronary syndrome (ACS).
At best, flash monitoring using Abbott’s Freestyle Libre system was associated with an increase in time spent in range (TIR) of 17-28 or 48 minutes per day over self-monitoring of blood glucose (SMBG), depending on the type of statistical analysis used. There was no difference in glycated hemoglobin A1c levels between the two groups, but there was a trend for less time spent in hypoglycemia in the flash monitoring arm.
Viewers underwhelmed
“My overall impression is that the effects were less pronounced than anticipated,” Kare Birkeland, MD, PhD, a specialist in internal medicine and endocrinology at Oslo University Hospital, Rikshospitalet, Norway, observed after the findings were presented at the virtual annual meeting of the European Association for the Study of Diabetes.
Others who had watched the live session seemed similarly underwhelmed by the findings, with one viewer questioning the value of devoting an hour-and-a-half session to the phase 2 trial.
However, the session chair Simon Heller, BA, MB, BChir, DM, professor of clinical diabetes at the University of Sheffield, and trial coinvestigator, defended the detailed look at the trial’s findings, noting that it was worthwhile to present the data from the trial as it “really helps explain why we do phase 2 and phase 3 trials.”
Strong rationale for monitoring post-MI
There is a strong rationale for ensuring that blood glucose is well controlled in type 2 diabetes patients who have experienced a myocardial infarction, observed Robert Storey, BSc, BM, DM, professor of cardiology at the University of Sheffield. One way to do that potentially is through improved glucose monitoring.
“There’s clearly a close link between diabetes and the risk of MI: Both high and low HbA1c are associated with adverse outcome, and high and low glucose levels following MI are also associated with adverse outcome,” he observed, noting also that hypoglycemia was not given enough attention in post-ACS patients.
“The hypothesis of the LIBERATES study was that a modern glycemic monitoring strategy can optimize blood glucose levels in type 2 diabetes patients following MI with the potential to reduce mortality and morbidity and improve quality of life,” Dr. Storey said. “The main research question of LIBERATES says, ‘Do new approaches in glucose monitoring increase the time in range and reduce hypoglycemia?’ ”
Pragmatic trial design
LIBERATES was a prospective, multicenter, parallel group, randomized controlled trial, explained the study’s statistician Deborah Stocken, PhD, professor of clinical trials research at the University of Leeds. There was “limited ability to blind the interventions,” so it was an open-label design.
“The patient population in LIBERATES was kept as inclusive and as pragmatic as possible to ensure that the results at the end of the trial are generalizable,” said Dr. Stocken. Patients with type 2 diabetes were recruited within 5 days of hospital admission for ACS, which could include both ST- and non-ST elevation MI. In all, 141 of a calculated 150 patients that would be needed were recruited and randomized to the flash monitoring (69) or SMBG (72) arm.
Dr. Stocken noted that early in the recruitment phase, the trials oversight committee recommended that Bayesian methodology should be used as the most robust analytical approach.
“Essentially, a Bayesian approach would avoid a hypothesis test, and instead would provide a probability of there being a treatment benefit for continuous monitoring. And if this probability was high enough, this would warrant further research in the phase 3 setting,” Dr. Stocken said.
What else was shown?
“We had a number of prespecified secondary endpoints, which to me are equally important,” said Ramzi Ajjan, MD, MMed.Sci, PhD, associate professor and consultant in diabetes and endocrinology at Leeds University and Leeds Teaching Hospitals Trust.
Among these was the TIR at days 16-30, which showed a 90-minute increase per day in favor of flash monitoring over SMBG. This “seems to be driven by those who are an insulin,” Dr. Ajjan said, adding that “you get almost a 3-hour increase in time in range in people who are on insulin at baseline, and you don’t see that in people who are on sulfonylurea.”
Conversely, sulfonylurea treatment seemed to drive the reduction in the time spent in hypoglycemia defined as 3.9 mmol/L (70 g/dL) at 3 months. For the whole group, there was a 1.3-hour reduction in hypoglycemia per day with flash monitoring versus SMBG, which increased to 2 hours for those on sulfonylureas.
There also was a “pattern of reduction” in time spent in hypoglycemia defined as less than 3.0 mmol/L (54 g/dL) both early on and becoming more pronounced with time.
“Flash glucose monitoring is associated with higher treatment satisfaction score, compared with SMBG,” Dr. Ajjan said.
Although A1c dropped in both groups to a similar extent, he noted that the reduction seen in the flash monitoring group was associated with a decrease in hypoglycemia.
There was a huge amount of data collected during the trial and there are many more analyses that could be done, Dr. Ajjan said. The outcome of those may determine whether a phase 3 trial is likely, assuming sponsorship can be secured.
The LIBERATES Trial was funded by grants from the UK National Institute for Health Research and Abbott Diabetes Care. None of the investigators were additionally compensated for their work within the trial. Dr. Stocken had no disclosures in relation to this trial. Dr. Ajjan has received research funding and other financial support from Abbott, Bayer, Eli Lilly, Johnson & Johnson, and Novo Nordisk.
SOURCE: Ajjan R et al. EASD 2020. S11 – The LIBERATES Trial.
FROM EASD 2020
Diabetic neuropathic pain linked to brain bioenergic anomalies
Abnormal mitochondrial activity in pain-processing areas of the brain may explain why some persons with type 2 diabetes experience painful peripheral neuropathy while others do not, new U.K. study findings have suggested.
A greater ratio of adenosine triphosphate (ATP) – “the cellular energy currency of all life” – to phosphocreatine (PCr) was observed in the somatosensory cortex and right thalamus in those with painful diabetic peripheral neuropathy (DPN). Importantly, this correlated with neuropathic pain symptom intensity as measured by the Neuropathic Pain Symptom Inventory (NPSI) and the Doleur Neuroathique en 4 (DN4).
The findings suggest that altered cerebral phosphorus metabolite ratios may serve as a biomarker of DPN, said the study’s investigators.
“Normally the ATP:Cr ratio will be unaltered, but there’s stress to the brain that might change,” Gordon Sloan, a clinical research fellow within the Diabetes Research Unit at the Royal Hallamshire Hospital in Sheffield (England) said at the virtual annual meeting of the European Association for the Study of Diabetes.
DPN affects around a quarter of patients with type 2 diabetes but treatments are “inadequate”, and “unfortunately fewer than a third of individuals receive 50% or greater pain relief from current neuropathic pain treatments,” Mr. Sloan said. “Ultimately, this lack of understanding of the pathophysiology of the condition is therefore clear rationale to investigate the disease mechanisms further and to find novel targets for treatments,” he added.
Brain metabolites offer clues to neuropathic pain levels
The thalamus and primary somatosensory cortex are two key areas of the brain that are involved in the perception of painful stimuli, Mr. Sloan explained. “The thalamus receives most of the slowest sensory impulses from the peripheral nervous system modulating and processing them for relaying the signals to the rest of the pain matrix, including the somatosensory cortex where these sensations are interpreted and localized.”
Prior imaging work by Mr. Sloan’s group and others have shown that there are alterations in the functioning of both these brain areas in those with painful DPN versus healthy volunteers and those with type 2 diabetes but no DPN. So for their current study, Mr. Sloan and associates from Sheffield University and Sheffield Teaching Hospitals National Health Service Trust, used an advanced imaging method – phosphorus magnetic resonance spectroscopy (MRS) – to scan the thalamus and somatosensory cortex of 43 persons with type 2 diabetes and 12 healthy volunteers. Of those with diabetes, 11 had no DPN, 12 had DPN but were not currently in pain, and 20 had painful DPN.
From the scans, three phosphorus metabolite ratios were calculated, which gave an indication of mitochondrial activity: first, the ATP to PCr ratio, which gives a measure of cellular energy status; second, the ATP to inorganic phosphate (Pi) ratio, which measures oxidative phosphorylation; and third, the ratio of phosphomonoesters (PME) to phosphodiesters (PDE), which gives a measure of cell membrane turnover.
“We have measured the ratio of high-energy phosphate levels which are an indirect representation of the balance between energy generation, reserve and usage in the brain,” Mr. Sloan said.
The subjects studied were of a similar age, around 63 years on average, and well matched in terms of their sex and body mass index. Those with diabetes of course had higher blood glucose and glycated hemoglobin than did the healthy volunteers during the scans. Among those with diabetes, those with DPN were significantly more likely to have a longer duration of diabetes (12.5 years for painful DPN and 15.8 years for nonpainful DPN) than were those with no DPN (8.7 years).
Furthermore, those with DPN had higher scores on the Neuropathic Pain Symptom Inventory (NPSI) than did those without, although there was not much difference between those with painful or nonpainful DPN. On the other had, those with painful DPN were more likely to have higher scores when using the Doleur Neuroathique en 4 (DN4) to assess their pain level.
Results showed significant changes in cerebral cellular bioenergetics in the pain processing regions of the brain in those with painful DPN. The ATP:PCr at the thalamus and at the somatosensory cortex was significantly higher in those with painful DPN, compared with healthy volunteers. The other measures of phosphorus metabolite levels (ATP:Pi and PME:PDE) were unaltered.
“We hypothesize that the findings of the study are suggestive of increased energy demands in regions of pain perception due to increased neuronal activity” said Dr. Sloan.
The study’s results add further evidence for cerebral alterations playing a key role in the generation and maintenance of pain in painful DPN.
SOURCE: Sloan S et al. EASD 2020, oral presentation 181.
Abnormal mitochondrial activity in pain-processing areas of the brain may explain why some persons with type 2 diabetes experience painful peripheral neuropathy while others do not, new U.K. study findings have suggested.
A greater ratio of adenosine triphosphate (ATP) – “the cellular energy currency of all life” – to phosphocreatine (PCr) was observed in the somatosensory cortex and right thalamus in those with painful diabetic peripheral neuropathy (DPN). Importantly, this correlated with neuropathic pain symptom intensity as measured by the Neuropathic Pain Symptom Inventory (NPSI) and the Doleur Neuroathique en 4 (DN4).
The findings suggest that altered cerebral phosphorus metabolite ratios may serve as a biomarker of DPN, said the study’s investigators.
“Normally the ATP:Cr ratio will be unaltered, but there’s stress to the brain that might change,” Gordon Sloan, a clinical research fellow within the Diabetes Research Unit at the Royal Hallamshire Hospital in Sheffield (England) said at the virtual annual meeting of the European Association for the Study of Diabetes.
DPN affects around a quarter of patients with type 2 diabetes but treatments are “inadequate”, and “unfortunately fewer than a third of individuals receive 50% or greater pain relief from current neuropathic pain treatments,” Mr. Sloan said. “Ultimately, this lack of understanding of the pathophysiology of the condition is therefore clear rationale to investigate the disease mechanisms further and to find novel targets for treatments,” he added.
Brain metabolites offer clues to neuropathic pain levels
The thalamus and primary somatosensory cortex are two key areas of the brain that are involved in the perception of painful stimuli, Mr. Sloan explained. “The thalamus receives most of the slowest sensory impulses from the peripheral nervous system modulating and processing them for relaying the signals to the rest of the pain matrix, including the somatosensory cortex where these sensations are interpreted and localized.”
Prior imaging work by Mr. Sloan’s group and others have shown that there are alterations in the functioning of both these brain areas in those with painful DPN versus healthy volunteers and those with type 2 diabetes but no DPN. So for their current study, Mr. Sloan and associates from Sheffield University and Sheffield Teaching Hospitals National Health Service Trust, used an advanced imaging method – phosphorus magnetic resonance spectroscopy (MRS) – to scan the thalamus and somatosensory cortex of 43 persons with type 2 diabetes and 12 healthy volunteers. Of those with diabetes, 11 had no DPN, 12 had DPN but were not currently in pain, and 20 had painful DPN.
From the scans, three phosphorus metabolite ratios were calculated, which gave an indication of mitochondrial activity: first, the ATP to PCr ratio, which gives a measure of cellular energy status; second, the ATP to inorganic phosphate (Pi) ratio, which measures oxidative phosphorylation; and third, the ratio of phosphomonoesters (PME) to phosphodiesters (PDE), which gives a measure of cell membrane turnover.
“We have measured the ratio of high-energy phosphate levels which are an indirect representation of the balance between energy generation, reserve and usage in the brain,” Mr. Sloan said.
The subjects studied were of a similar age, around 63 years on average, and well matched in terms of their sex and body mass index. Those with diabetes of course had higher blood glucose and glycated hemoglobin than did the healthy volunteers during the scans. Among those with diabetes, those with DPN were significantly more likely to have a longer duration of diabetes (12.5 years for painful DPN and 15.8 years for nonpainful DPN) than were those with no DPN (8.7 years).
Furthermore, those with DPN had higher scores on the Neuropathic Pain Symptom Inventory (NPSI) than did those without, although there was not much difference between those with painful or nonpainful DPN. On the other had, those with painful DPN were more likely to have higher scores when using the Doleur Neuroathique en 4 (DN4) to assess their pain level.
Results showed significant changes in cerebral cellular bioenergetics in the pain processing regions of the brain in those with painful DPN. The ATP:PCr at the thalamus and at the somatosensory cortex was significantly higher in those with painful DPN, compared with healthy volunteers. The other measures of phosphorus metabolite levels (ATP:Pi and PME:PDE) were unaltered.
“We hypothesize that the findings of the study are suggestive of increased energy demands in regions of pain perception due to increased neuronal activity” said Dr. Sloan.
The study’s results add further evidence for cerebral alterations playing a key role in the generation and maintenance of pain in painful DPN.
SOURCE: Sloan S et al. EASD 2020, oral presentation 181.
Abnormal mitochondrial activity in pain-processing areas of the brain may explain why some persons with type 2 diabetes experience painful peripheral neuropathy while others do not, new U.K. study findings have suggested.
A greater ratio of adenosine triphosphate (ATP) – “the cellular energy currency of all life” – to phosphocreatine (PCr) was observed in the somatosensory cortex and right thalamus in those with painful diabetic peripheral neuropathy (DPN). Importantly, this correlated with neuropathic pain symptom intensity as measured by the Neuropathic Pain Symptom Inventory (NPSI) and the Doleur Neuroathique en 4 (DN4).
The findings suggest that altered cerebral phosphorus metabolite ratios may serve as a biomarker of DPN, said the study’s investigators.
“Normally the ATP:Cr ratio will be unaltered, but there’s stress to the brain that might change,” Gordon Sloan, a clinical research fellow within the Diabetes Research Unit at the Royal Hallamshire Hospital in Sheffield (England) said at the virtual annual meeting of the European Association for the Study of Diabetes.
DPN affects around a quarter of patients with type 2 diabetes but treatments are “inadequate”, and “unfortunately fewer than a third of individuals receive 50% or greater pain relief from current neuropathic pain treatments,” Mr. Sloan said. “Ultimately, this lack of understanding of the pathophysiology of the condition is therefore clear rationale to investigate the disease mechanisms further and to find novel targets for treatments,” he added.
Brain metabolites offer clues to neuropathic pain levels
The thalamus and primary somatosensory cortex are two key areas of the brain that are involved in the perception of painful stimuli, Mr. Sloan explained. “The thalamus receives most of the slowest sensory impulses from the peripheral nervous system modulating and processing them for relaying the signals to the rest of the pain matrix, including the somatosensory cortex where these sensations are interpreted and localized.”
Prior imaging work by Mr. Sloan’s group and others have shown that there are alterations in the functioning of both these brain areas in those with painful DPN versus healthy volunteers and those with type 2 diabetes but no DPN. So for their current study, Mr. Sloan and associates from Sheffield University and Sheffield Teaching Hospitals National Health Service Trust, used an advanced imaging method – phosphorus magnetic resonance spectroscopy (MRS) – to scan the thalamus and somatosensory cortex of 43 persons with type 2 diabetes and 12 healthy volunteers. Of those with diabetes, 11 had no DPN, 12 had DPN but were not currently in pain, and 20 had painful DPN.
From the scans, three phosphorus metabolite ratios were calculated, which gave an indication of mitochondrial activity: first, the ATP to PCr ratio, which gives a measure of cellular energy status; second, the ATP to inorganic phosphate (Pi) ratio, which measures oxidative phosphorylation; and third, the ratio of phosphomonoesters (PME) to phosphodiesters (PDE), which gives a measure of cell membrane turnover.
“We have measured the ratio of high-energy phosphate levels which are an indirect representation of the balance between energy generation, reserve and usage in the brain,” Mr. Sloan said.
The subjects studied were of a similar age, around 63 years on average, and well matched in terms of their sex and body mass index. Those with diabetes of course had higher blood glucose and glycated hemoglobin than did the healthy volunteers during the scans. Among those with diabetes, those with DPN were significantly more likely to have a longer duration of diabetes (12.5 years for painful DPN and 15.8 years for nonpainful DPN) than were those with no DPN (8.7 years).
Furthermore, those with DPN had higher scores on the Neuropathic Pain Symptom Inventory (NPSI) than did those without, although there was not much difference between those with painful or nonpainful DPN. On the other had, those with painful DPN were more likely to have higher scores when using the Doleur Neuroathique en 4 (DN4) to assess their pain level.
Results showed significant changes in cerebral cellular bioenergetics in the pain processing regions of the brain in those with painful DPN. The ATP:PCr at the thalamus and at the somatosensory cortex was significantly higher in those with painful DPN, compared with healthy volunteers. The other measures of phosphorus metabolite levels (ATP:Pi and PME:PDE) were unaltered.
“We hypothesize that the findings of the study are suggestive of increased energy demands in regions of pain perception due to increased neuronal activity” said Dr. Sloan.
The study’s results add further evidence for cerebral alterations playing a key role in the generation and maintenance of pain in painful DPN.
SOURCE: Sloan S et al. EASD 2020, oral presentation 181.
FROM EASD 2020
Substance in tears could be used for diabetes monitoring
Measuring glycated albumin (glycoalbumin, GA) in tears could be a future way for those with diabetes to monitor their blood sugar levels noninvasively.

In a 100-patient trial, levels of GA in tears were found to be strongly correlated (r = .722; P < .001) with those in the blood.
“GA levels in blood are widely measured in clinical practice in Japan,” said study investigator Masakazu Aihara, MD, PhD, in an interview.
“It’s a biomarker that reflects the 2-week average blood glucose level like fructosamine,” explained the researcher from the department of diabetes and metabolic diseases in the Graduate School of Medicine at the University of Tokyo.
This could make it a better biomarker for detecting earlier changes in blood glucose than glycated hemoglobin (HbA1c), which reflects changes in blood glucose over the preceding 2-3 months.
Prior studies had shown that glucose levels can be measured in tear samples and that tear glucose levels correlated with blood glucose levels, Dr. Aihara and fellow researchers observed in a poster presentation at the virtual annual meeting of the European Association for the Study of Diabetes.
“While looking for noninvasive diabetes-related markers, we found that tears contained albumin. Based on this fact, we thought that GA could be measured in tears,” Dr. Aihara explained.
Using tears to test for biomarkers is not a new idea – tears not only protect the eye, they contain a variety of large proteins, and their composition can change with disease. Indeed, researchers have been looking at their usefulness in helping find biomarkers for Parkinson’s disease and diabetic peripheral neuropathy.
During their study, Dr. Aihara and associates collected tear and blood samples at the same time. Tear samples were assessed using liquid chromatography (LC) and mass spectrometry (MS). An enzymic method was used to measure GA levels in blood. Several diagnosis assay kits for GA are sold in Japan, Dr. Aihara said, and at least one of these has U.S. Food and Drug Administration approval.
Multiple regression analysis revealed that the correlation between GA levels in tears and in blood was maintained even after adjustment for age, gender, nephropathy stage, and obesity (P < .001). The results obtained from the tests were thought unlikely to be affected by any changes in the concentration or dilution of tear samples.
“Since GA levels in blood are clinically used in all types of diabetes, GA levels in tears is also expected to be useful in all types of diabetes,” Dr. Aihara said, noting that the effects of receiving treatment on GA levels in tears is something that he would like to look at.
The team would also like to optimize how tear samples are collected and reduce the volume of tears that are required for analysis. At the moment tears are collected via a dropper and about 100 mcL of tear fluid is required for measurement.
“At present, it is difficult to measure for dry eye patients because sufficient tears cannot be collected, but if the required amount of tears decreases in the future, it may be indicated for dry eye patients,” Dr. Aihara noted.
Discussing further research plans, he added: “We would like to examine the conditions of LC-MS/MS so that the correlation coefficient with GA in blood can be improved.
“Since LC-MS/MS is a large equipment in the laboratory, I would like to develop a device that can measure at the clinic or at home in the future.”
The study was funded by a grant from the Japan Agency for Medical Research and Development. Dr. Aihara had no conflicts of interest.
SOURCE: Aihara M et al. EASD 2020, poster presentation 624.
Measuring glycated albumin (glycoalbumin, GA) in tears could be a future way for those with diabetes to monitor their blood sugar levels noninvasively.
In a 100-patient trial, levels of GA in tears were found to be strongly correlated (r = .722; P < .001) with those in the blood.
“GA levels in blood are widely measured in clinical practice in Japan,” said study investigator Masakazu Aihara, MD, PhD, in an interview.
“It’s a biomarker that reflects the 2-week average blood glucose level like fructosamine,” explained the researcher from the department of diabetes and metabolic diseases in the Graduate School of Medicine at the University of Tokyo.
This could make it a better biomarker for detecting earlier changes in blood glucose than glycated hemoglobin (HbA1c), which reflects changes in blood glucose over the preceding 2-3 months.
Prior studies had shown that glucose levels can be measured in tear samples and that tear glucose levels correlated with blood glucose levels, Dr. Aihara and fellow researchers observed in a poster presentation at the virtual annual meeting of the European Association for the Study of Diabetes.
“While looking for noninvasive diabetes-related markers, we found that tears contained albumin. Based on this fact, we thought that GA could be measured in tears,” Dr. Aihara explained.
Using tears to test for biomarkers is not a new idea – tears not only protect the eye, they contain a variety of large proteins, and their composition can change with disease. Indeed, researchers have been looking at their usefulness in helping find biomarkers for Parkinson’s disease and diabetic peripheral neuropathy.
During their study, Dr. Aihara and associates collected tear and blood samples at the same time. Tear samples were assessed using liquid chromatography (LC) and mass spectrometry (MS). An enzymic method was used to measure GA levels in blood. Several diagnosis assay kits for GA are sold in Japan, Dr. Aihara said, and at least one of these has U.S. Food and Drug Administration approval.
Multiple regression analysis revealed that the correlation between GA levels in tears and in blood was maintained even after adjustment for age, gender, nephropathy stage, and obesity (P < .001). The results obtained from the tests were thought unlikely to be affected by any changes in the concentration or dilution of tear samples.
“Since GA levels in blood are clinically used in all types of diabetes, GA levels in tears is also expected to be useful in all types of diabetes,” Dr. Aihara said, noting that the effects of receiving treatment on GA levels in tears is something that he would like to look at.
The team would also like to optimize how tear samples are collected and reduce the volume of tears that are required for analysis. At the moment tears are collected via a dropper and about 100 mcL of tear fluid is required for measurement.
“At present, it is difficult to measure for dry eye patients because sufficient tears cannot be collected, but if the required amount of tears decreases in the future, it may be indicated for dry eye patients,” Dr. Aihara noted.
Discussing further research plans, he added: “We would like to examine the conditions of LC-MS/MS so that the correlation coefficient with GA in blood can be improved.
“Since LC-MS/MS is a large equipment in the laboratory, I would like to develop a device that can measure at the clinic or at home in the future.”
The study was funded by a grant from the Japan Agency for Medical Research and Development. Dr. Aihara had no conflicts of interest.
SOURCE: Aihara M et al. EASD 2020, poster presentation 624.
Measuring glycated albumin (glycoalbumin, GA) in tears could be a future way for those with diabetes to monitor their blood sugar levels noninvasively.
In a 100-patient trial, levels of GA in tears were found to be strongly correlated (r = .722; P < .001) with those in the blood.
“GA levels in blood are widely measured in clinical practice in Japan,” said study investigator Masakazu Aihara, MD, PhD, in an interview.
“It’s a biomarker that reflects the 2-week average blood glucose level like fructosamine,” explained the researcher from the department of diabetes and metabolic diseases in the Graduate School of Medicine at the University of Tokyo.
This could make it a better biomarker for detecting earlier changes in blood glucose than glycated hemoglobin (HbA1c), which reflects changes in blood glucose over the preceding 2-3 months.
Prior studies had shown that glucose levels can be measured in tear samples and that tear glucose levels correlated with blood glucose levels, Dr. Aihara and fellow researchers observed in a poster presentation at the virtual annual meeting of the European Association for the Study of Diabetes.
“While looking for noninvasive diabetes-related markers, we found that tears contained albumin. Based on this fact, we thought that GA could be measured in tears,” Dr. Aihara explained.
Using tears to test for biomarkers is not a new idea – tears not only protect the eye, they contain a variety of large proteins, and their composition can change with disease. Indeed, researchers have been looking at their usefulness in helping find biomarkers for Parkinson’s disease and diabetic peripheral neuropathy.
During their study, Dr. Aihara and associates collected tear and blood samples at the same time. Tear samples were assessed using liquid chromatography (LC) and mass spectrometry (MS). An enzymic method was used to measure GA levels in blood. Several diagnosis assay kits for GA are sold in Japan, Dr. Aihara said, and at least one of these has U.S. Food and Drug Administration approval.
Multiple regression analysis revealed that the correlation between GA levels in tears and in blood was maintained even after adjustment for age, gender, nephropathy stage, and obesity (P < .001). The results obtained from the tests were thought unlikely to be affected by any changes in the concentration or dilution of tear samples.
“Since GA levels in blood are clinically used in all types of diabetes, GA levels in tears is also expected to be useful in all types of diabetes,” Dr. Aihara said, noting that the effects of receiving treatment on GA levels in tears is something that he would like to look at.
The team would also like to optimize how tear samples are collected and reduce the volume of tears that are required for analysis. At the moment tears are collected via a dropper and about 100 mcL of tear fluid is required for measurement.
“At present, it is difficult to measure for dry eye patients because sufficient tears cannot be collected, but if the required amount of tears decreases in the future, it may be indicated for dry eye patients,” Dr. Aihara noted.
Discussing further research plans, he added: “We would like to examine the conditions of LC-MS/MS so that the correlation coefficient with GA in blood can be improved.
“Since LC-MS/MS is a large equipment in the laboratory, I would like to develop a device that can measure at the clinic or at home in the future.”
The study was funded by a grant from the Japan Agency for Medical Research and Development. Dr. Aihara had no conflicts of interest.
SOURCE: Aihara M et al. EASD 2020, poster presentation 624.
FROM EASD 2020
Time to screen for liver disease in type 2 diabetes?
With high rates of fatty liver disease known to occur among people with type 2 diabetes, is it time to introduce routine liver screening into daily diabetes practice? The answer depends on whom you ask, and then there are still some important caveats.

From the hepatologist’s perspective, there is no excuse not to consider liver surveillance now that noninvasive screening methods are available, suggested Michael Trauner, MD, of the Medical University of Vienna.
“From a practical standpoint, I think every type 2 diabetic over 50 years of age is at high risk,” and consequently should be screened at diagnosis, Dr. Trauner said during a debate at the virtual annual meeting of the European Association for the Study of Diabetes. “I would screen at diagnosis and then decide on recall depending on noninvasive fibrosis markers.”
“It’s a rising problem that we are facing these days,” observed Michael Roden, MD, chair and professor of internal medicine, endocrinology and metabolic diseases at Heinrich-Heine University in Düsseldorf, Germany, and who cochaired the session. Not only do people with type 2 diabetes have an increased risk for developing liver diseases, but also there’s a higher risk for those with fatty liver diseases developing type 2 diabetes.
A meta-analysis published in Gut in just last week illustrates just how big a problem this is – nonalcoholic fatty liver disease (NAFLD) “doubled the risk of type 2 diabetes,” said Dr Rosen, who is also the director of the division of endocrinology and diabetology at University Clinics Düsseldorf. That analysis was based on more than 500,000 people, almost 28,000 of whom had incident diabetes over a 5-year period.
Screening tools scarce
This makes liver screening in type 2 diabetes patients “a formidable challenge,” cautioned Gianluca Perseghin, MD, professor of endocrinology at the Monza (Italy) Polyclinic and the University of Milano-Bicocca in Milan.
“Hepatologists generally see only the most severe cases,” Dr. Perseghin said. Diabetologists and endocrinologists would be likely to see huge numbers of patients that could potentially be at risk for liver disease and following the recommendations set out in the joint European Association for the Study of the Liver/EASD/European Association for the Study of Obesity guidelines would result in a huge number of patients being identified and potentially needing referral, he argued.
“At this stage, we need to build friendly, reliable and cost-effective screening process to be applied in the health systems,” Dr. Perseghin suggested. He proposed that liver surveillance would need to be not only personalized on a patient level, but also at the infrastructure level. Measuring liver enzymes, for example, was going to be less accurate in picking up liver disease but blood tests were widely available, whereas imaging methods were not going to be something all diabetes clinics would have immediate access to.
“There are clearly a lot of provocative decisions still to be made,” acknowledged Philip Newsome, PhD, FRCPE, an honorary consultant hepatologist at the University of Birmingham (England) and who cochaired the debate.
“We need to demonstrate that looking for the presence of liver disease in this cohort changes their outcomes in a way that is cost effective,” Dr. Newsome, who is also the secretary general of EASL.
“Tests are evolving, but more importantly, treatments are evolving. So, the decision around cost effectiveness will clearly change,” he added.
NAFLD therapies unclar
“There are still a lot of questions,” Dr. Newsome said during a Novo-Nordisk–sponsored “Meet the Expert” session discussing EASL-EASD-EASO guidelines. “We don’t have any licensed therapies at the moment. But there’s been a huge amount of investment, looking at all sorts of different approaches.”
Dr. Newsome added: “We also don’t know how to monitor these patients. Most of the noninvasive are very useful for staging patients, but we don’t really understand how useful they are for monitoring changes in fibrosis.”
Diabetologist Hannele Yki-Järvinen, MD, PhD, of the University of Helsinki, gave her thoughts on the topic during the same session.
“We should add FIB-4 [Fibrosis-4 index] to the annual exam and ask the lab to calculate FIB-4 automatically,” Dr. Yki-Järvinen said. FIB-4is calculated using the patients age and the results of readily available blood tests that measure the AST/ALT ratio and the platelet count.
Dr. Trauner has received advisory fees and grant support from various companies with an interest in developing liver-directed therapies, and is also a coinventor of 24-norursodeoxycholic acid under development for cholestatic liver disease and potentially NAFLD. Dr. Perseghin has received honoraria and grant support from various pharmaceutical companies with an interest in diabetes care. Dr. Roden did not provide any disclosures. Dr. Newsome has received research grants from Boehringer Ingelheim and Novo Nordisk and acted as a consultant to many pharmaceutical companies. Dr. Yki-Järvinen disclosed receiving consultancy fees from Eli Lilly, MSD, and Novo Nordisk.
SOURCE: Trauner M; Persghin G. EASD 2020, Session S27.
With high rates of fatty liver disease known to occur among people with type 2 diabetes, is it time to introduce routine liver screening into daily diabetes practice? The answer depends on whom you ask, and then there are still some important caveats.
From the hepatologist’s perspective, there is no excuse not to consider liver surveillance now that noninvasive screening methods are available, suggested Michael Trauner, MD, of the Medical University of Vienna.
“From a practical standpoint, I think every type 2 diabetic over 50 years of age is at high risk,” and consequently should be screened at diagnosis, Dr. Trauner said during a debate at the virtual annual meeting of the European Association for the Study of Diabetes. “I would screen at diagnosis and then decide on recall depending on noninvasive fibrosis markers.”
“It’s a rising problem that we are facing these days,” observed Michael Roden, MD, chair and professor of internal medicine, endocrinology and metabolic diseases at Heinrich-Heine University in Düsseldorf, Germany, and who cochaired the session. Not only do people with type 2 diabetes have an increased risk for developing liver diseases, but also there’s a higher risk for those with fatty liver diseases developing type 2 diabetes.
A meta-analysis published in Gut in just last week illustrates just how big a problem this is – nonalcoholic fatty liver disease (NAFLD) “doubled the risk of type 2 diabetes,” said Dr Rosen, who is also the director of the division of endocrinology and diabetology at University Clinics Düsseldorf. That analysis was based on more than 500,000 people, almost 28,000 of whom had incident diabetes over a 5-year period.
Screening tools scarce
This makes liver screening in type 2 diabetes patients “a formidable challenge,” cautioned Gianluca Perseghin, MD, professor of endocrinology at the Monza (Italy) Polyclinic and the University of Milano-Bicocca in Milan.
“Hepatologists generally see only the most severe cases,” Dr. Perseghin said. Diabetologists and endocrinologists would be likely to see huge numbers of patients that could potentially be at risk for liver disease and following the recommendations set out in the joint European Association for the Study of the Liver/EASD/European Association for the Study of Obesity guidelines would result in a huge number of patients being identified and potentially needing referral, he argued.
“At this stage, we need to build friendly, reliable and cost-effective screening process to be applied in the health systems,” Dr. Perseghin suggested. He proposed that liver surveillance would need to be not only personalized on a patient level, but also at the infrastructure level. Measuring liver enzymes, for example, was going to be less accurate in picking up liver disease but blood tests were widely available, whereas imaging methods were not going to be something all diabetes clinics would have immediate access to.
“There are clearly a lot of provocative decisions still to be made,” acknowledged Philip Newsome, PhD, FRCPE, an honorary consultant hepatologist at the University of Birmingham (England) and who cochaired the debate.
“We need to demonstrate that looking for the presence of liver disease in this cohort changes their outcomes in a way that is cost effective,” Dr. Newsome, who is also the secretary general of EASL.
“Tests are evolving, but more importantly, treatments are evolving. So, the decision around cost effectiveness will clearly change,” he added.
NAFLD therapies unclar
“There are still a lot of questions,” Dr. Newsome said during a Novo-Nordisk–sponsored “Meet the Expert” session discussing EASL-EASD-EASO guidelines. “We don’t have any licensed therapies at the moment. But there’s been a huge amount of investment, looking at all sorts of different approaches.”
Dr. Newsome added: “We also don’t know how to monitor these patients. Most of the noninvasive are very useful for staging patients, but we don’t really understand how useful they are for monitoring changes in fibrosis.”
Diabetologist Hannele Yki-Järvinen, MD, PhD, of the University of Helsinki, gave her thoughts on the topic during the same session.
“We should add FIB-4 [Fibrosis-4 index] to the annual exam and ask the lab to calculate FIB-4 automatically,” Dr. Yki-Järvinen said. FIB-4is calculated using the patients age and the results of readily available blood tests that measure the AST/ALT ratio and the platelet count.
Dr. Trauner has received advisory fees and grant support from various companies with an interest in developing liver-directed therapies, and is also a coinventor of 24-norursodeoxycholic acid under development for cholestatic liver disease and potentially NAFLD. Dr. Perseghin has received honoraria and grant support from various pharmaceutical companies with an interest in diabetes care. Dr. Roden did not provide any disclosures. Dr. Newsome has received research grants from Boehringer Ingelheim and Novo Nordisk and acted as a consultant to many pharmaceutical companies. Dr. Yki-Järvinen disclosed receiving consultancy fees from Eli Lilly, MSD, and Novo Nordisk.
SOURCE: Trauner M; Persghin G. EASD 2020, Session S27.
With high rates of fatty liver disease known to occur among people with type 2 diabetes, is it time to introduce routine liver screening into daily diabetes practice? The answer depends on whom you ask, and then there are still some important caveats.
From the hepatologist’s perspective, there is no excuse not to consider liver surveillance now that noninvasive screening methods are available, suggested Michael Trauner, MD, of the Medical University of Vienna.
“From a practical standpoint, I think every type 2 diabetic over 50 years of age is at high risk,” and consequently should be screened at diagnosis, Dr. Trauner said during a debate at the virtual annual meeting of the European Association for the Study of Diabetes. “I would screen at diagnosis and then decide on recall depending on noninvasive fibrosis markers.”
“It’s a rising problem that we are facing these days,” observed Michael Roden, MD, chair and professor of internal medicine, endocrinology and metabolic diseases at Heinrich-Heine University in Düsseldorf, Germany, and who cochaired the session. Not only do people with type 2 diabetes have an increased risk for developing liver diseases, but also there’s a higher risk for those with fatty liver diseases developing type 2 diabetes.
A meta-analysis published in Gut in just last week illustrates just how big a problem this is – nonalcoholic fatty liver disease (NAFLD) “doubled the risk of type 2 diabetes,” said Dr Rosen, who is also the director of the division of endocrinology and diabetology at University Clinics Düsseldorf. That analysis was based on more than 500,000 people, almost 28,000 of whom had incident diabetes over a 5-year period.
Screening tools scarce
This makes liver screening in type 2 diabetes patients “a formidable challenge,” cautioned Gianluca Perseghin, MD, professor of endocrinology at the Monza (Italy) Polyclinic and the University of Milano-Bicocca in Milan.
“Hepatologists generally see only the most severe cases,” Dr. Perseghin said. Diabetologists and endocrinologists would be likely to see huge numbers of patients that could potentially be at risk for liver disease and following the recommendations set out in the joint European Association for the Study of the Liver/EASD/European Association for the Study of Obesity guidelines would result in a huge number of patients being identified and potentially needing referral, he argued.
“At this stage, we need to build friendly, reliable and cost-effective screening process to be applied in the health systems,” Dr. Perseghin suggested. He proposed that liver surveillance would need to be not only personalized on a patient level, but also at the infrastructure level. Measuring liver enzymes, for example, was going to be less accurate in picking up liver disease but blood tests were widely available, whereas imaging methods were not going to be something all diabetes clinics would have immediate access to.
“There are clearly a lot of provocative decisions still to be made,” acknowledged Philip Newsome, PhD, FRCPE, an honorary consultant hepatologist at the University of Birmingham (England) and who cochaired the debate.
“We need to demonstrate that looking for the presence of liver disease in this cohort changes their outcomes in a way that is cost effective,” Dr. Newsome, who is also the secretary general of EASL.
“Tests are evolving, but more importantly, treatments are evolving. So, the decision around cost effectiveness will clearly change,” he added.
NAFLD therapies unclar
“There are still a lot of questions,” Dr. Newsome said during a Novo-Nordisk–sponsored “Meet the Expert” session discussing EASL-EASD-EASO guidelines. “We don’t have any licensed therapies at the moment. But there’s been a huge amount of investment, looking at all sorts of different approaches.”
Dr. Newsome added: “We also don’t know how to monitor these patients. Most of the noninvasive are very useful for staging patients, but we don’t really understand how useful they are for monitoring changes in fibrosis.”
Diabetologist Hannele Yki-Järvinen, MD, PhD, of the University of Helsinki, gave her thoughts on the topic during the same session.
“We should add FIB-4 [Fibrosis-4 index] to the annual exam and ask the lab to calculate FIB-4 automatically,” Dr. Yki-Järvinen said. FIB-4is calculated using the patients age and the results of readily available blood tests that measure the AST/ALT ratio and the platelet count.
Dr. Trauner has received advisory fees and grant support from various companies with an interest in developing liver-directed therapies, and is also a coinventor of 24-norursodeoxycholic acid under development for cholestatic liver disease and potentially NAFLD. Dr. Perseghin has received honoraria and grant support from various pharmaceutical companies with an interest in diabetes care. Dr. Roden did not provide any disclosures. Dr. Newsome has received research grants from Boehringer Ingelheim and Novo Nordisk and acted as a consultant to many pharmaceutical companies. Dr. Yki-Järvinen disclosed receiving consultancy fees from Eli Lilly, MSD, and Novo Nordisk.
SOURCE: Trauner M; Persghin G. EASD 2020, Session S27.
REPORTING FROM EASD 2020
Exercise cuts diabetes death risk by a third in two studies
Type 2 diabetes patients could lower their risk for death from any cause by up to a third by exercising at a moderate to high level or by cycling, according to data from two studies reported at the virtual annual meeting of the European Association for the Study of Diabetes.

Yun-Ju Lai, MD, and colleagues from the Puli branch of Taichung Veterans General Hospital in Nantou, Taiwan, found that persons with type 2 diabetes who exercised at moderate to high intensity had a 25%-32% decreased risk for death, compared with those who did not exercise.
In a separate study, Mathias Ried-Larsen, MSc, PhD, group leader at the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and associates found that cycling was associated with a 25%-31% decreased risk for all-cause death compared to no cycling, and that cycling also reduced cardiovascular mortality.
Results fit with ADA recommendations
“There is really nothing surprising about these results as others have shown that regular participation in physical activity lowers both overall mortality rates and morbidity,” commented Sheri Colberg-Ochs, PhD, professor emerita in exercise science at Old Dominion University in Norfolk, Va., in an interview.

“Regular exercise participation lowers the risk of mortality in almost all populations with many different health conditions. It is not specific to people with type 2 diabetes,” Dr. Colberg-Ochs said. “These data add further support to the ADA [American Diabetes Association] recommendations by again suggesting that being more active leads to many health benefits for people with type 2 diabetes.”
Dr. Colberg-Ochs, who was not involved in either study, is recognized by the ADA as an Outstanding Educator in Diabetes. She was also involved in writing the ADA’s position statement on physical activity/exercise in diabetes, which advocate that adults with type 2 diabetes should reduce sedentary time and undertake both aerobic and resistance exercise training to help optimize their glycemic and general health outcomes.
Asian population understudied
In an interview Dr. Lai acknowledged that epidemiologic studies had shown that exercise reduced the risk of cardiovascular events and mortality in subjects with type 2 diabetes. “However, the dose of exercise capacity for reducing mortality risk in people with type 2 diabetes was not yet well investigated, especially in the Asian population.”
Dr. Lai and colleagues analyzed data on 4,859 subjects drawn from two Taiwanese databases – the National Health Interview Survey and the National Health Insurance research database – to study what effect exercise “capacity” had on the risk for death in those with type 2 diabetes.
“Information about physical activity during leisure time was collected by asking the questions: ‘How often do you exercise every week? What kind of exercise do you do? How long do you do the exercise?’, Dr. Lai said. “We included nearly all kinds of exercise in the analysis, such as jogging, swimming, walking, dancing, riding, and so on.”
Each exercise had an activity intensity code expressed as kilocalories per minute. This was used to determine the exercise “capacity” by multiplying it by how frequently the exercise was performed per week and for how long each time.
“I don’t think ‘capacity’ is the right word to use here. The equation they used describes their exercise ‘volume,’ not their capacity. Self-reported exercise is notoriously inaccurate,” Dr. Colberg-Ochs observed. Furthermore, “just asking people how much they exercise and at what intensity [without using a validated exercise questionnaire] gives questionable results.”
The study’s findings, however, were clear: Those who exercised at a higher level had a significantly decreased risk for all-cause mortality than did those with no exercise habits. The hazard ratio for death by any cause was 0.75 for those who undertook a moderate level of exercise, burning 0-800 kcal per week. Exercising at a higher level burned more than 800 kcal had a HR of 0.68. A significant (P < .01) trend in favor of more exercise was noted.
Cycling reduces all-cause and cardiovascular mortality
In their prospective cohort study, Dr. Ried-Larsen and associates took a more specific look at the effects of exercise on mortality in diabetes by studying a single exercise: cycling. They sampled data on more than 5,000 people collected as part of the European Prospective Investigation into Cancer and Nutrition study. First, they identified participants with diabetes – although they couldn’t distinguish type 1 from type 2 forms because this was self-reported or obtained from registries. They then identified those who reported cycling at their baseline assessment and those who reported a change in cycling habits at their second examination around 5 years later.
At baseline, 38% of participants reported that they cycled every week. The mean age was 56 years, diabetes duration was 8 years, one-fifth were smokers, and the average body mass index was 29 kg/m2.
Participants who reported cycling up to 1 hour every week at baseline had a 25% reduction in all-cause mortality, compared with those who did not cycle. The biggest reduction (31%) in all-cause mortality was seen for cycling 2.5-5 hours a week; cycling for 1-2.5 hours, and for more than 5 hours, yielded 23% and 24% risk reductions, respectively.
A reverse J–shaped relationship between cycling duration and reduction in all-cause mortality was seen, Dr. Ried-Larsen noted during a live oral session at the virtual meeting. “The maximum benefit [was at] around 5 hours per week, and the benefits persisted until around 9 hours per week.” Adjustment for the prevalence of stroke, MI, cancer, hyperlipidemia, hypertension, and central obesity did not alter the findings.
“The direction of the association was the same for cardiovascular mortality as all-cause mortality, although a bit weaker, with the maximum benefit being around 4 hours per week, and that persisted up until around 8 hours per week,” Dr. Ried-Larsen said.
The benefits of cycling on all-cause and cardiovascular mortality were lost, however, if those who cycled at baseline stopped by the second examination. Those who did not cycle at the first but did at the second examination got a benefit on both, as did those who continued cycling.
“Cycling is among one of the preferred activities for diabetes patients, so it actually may help them to achieve the recommend level of physical activity,” Dr. Ried-Larsen said.
Tailored exercise program important
Advice for exercise “should be tailored to the individual and based on starting fitness levels and activity levels,” Dr. Colberg-Ochs recommended.
“Those who are the most sedentary and the least fit have the most to gain from doing any activity. They should be advised to start out slowly and progress slowly with both aerobic activities and some resistance training,” Dr. Colberg-Ochs said.
She added: “In addition, individuals over 40 should engage in regular balance training, and all individuals should do some flexibility exercises.”
The studies received no commercial funding and all those mentioned in this article had no conflicts of interest to disclose.
SOURCE: Lai Y-J et al. EASD 2020, Poster presentation 267; Ried-Larsen M et al. EASD 2020, Oral presentation 194.
Type 2 diabetes patients could lower their risk for death from any cause by up to a third by exercising at a moderate to high level or by cycling, according to data from two studies reported at the virtual annual meeting of the European Association for the Study of Diabetes.
Yun-Ju Lai, MD, and colleagues from the Puli branch of Taichung Veterans General Hospital in Nantou, Taiwan, found that persons with type 2 diabetes who exercised at moderate to high intensity had a 25%-32% decreased risk for death, compared with those who did not exercise.
In a separate study, Mathias Ried-Larsen, MSc, PhD, group leader at the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and associates found that cycling was associated with a 25%-31% decreased risk for all-cause death compared to no cycling, and that cycling also reduced cardiovascular mortality.
Results fit with ADA recommendations
“There is really nothing surprising about these results as others have shown that regular participation in physical activity lowers both overall mortality rates and morbidity,” commented Sheri Colberg-Ochs, PhD, professor emerita in exercise science at Old Dominion University in Norfolk, Va., in an interview.
“Regular exercise participation lowers the risk of mortality in almost all populations with many different health conditions. It is not specific to people with type 2 diabetes,” Dr. Colberg-Ochs said. “These data add further support to the ADA [American Diabetes Association] recommendations by again suggesting that being more active leads to many health benefits for people with type 2 diabetes.”
Dr. Colberg-Ochs, who was not involved in either study, is recognized by the ADA as an Outstanding Educator in Diabetes. She was also involved in writing the ADA’s position statement on physical activity/exercise in diabetes, which advocate that adults with type 2 diabetes should reduce sedentary time and undertake both aerobic and resistance exercise training to help optimize their glycemic and general health outcomes.
Asian population understudied
In an interview Dr. Lai acknowledged that epidemiologic studies had shown that exercise reduced the risk of cardiovascular events and mortality in subjects with type 2 diabetes. “However, the dose of exercise capacity for reducing mortality risk in people with type 2 diabetes was not yet well investigated, especially in the Asian population.”
Dr. Lai and colleagues analyzed data on 4,859 subjects drawn from two Taiwanese databases – the National Health Interview Survey and the National Health Insurance research database – to study what effect exercise “capacity” had on the risk for death in those with type 2 diabetes.
“Information about physical activity during leisure time was collected by asking the questions: ‘How often do you exercise every week? What kind of exercise do you do? How long do you do the exercise?’, Dr. Lai said. “We included nearly all kinds of exercise in the analysis, such as jogging, swimming, walking, dancing, riding, and so on.”
Each exercise had an activity intensity code expressed as kilocalories per minute. This was used to determine the exercise “capacity” by multiplying it by how frequently the exercise was performed per week and for how long each time.
“I don’t think ‘capacity’ is the right word to use here. The equation they used describes their exercise ‘volume,’ not their capacity. Self-reported exercise is notoriously inaccurate,” Dr. Colberg-Ochs observed. Furthermore, “just asking people how much they exercise and at what intensity [without using a validated exercise questionnaire] gives questionable results.”
The study’s findings, however, were clear: Those who exercised at a higher level had a significantly decreased risk for all-cause mortality than did those with no exercise habits. The hazard ratio for death by any cause was 0.75 for those who undertook a moderate level of exercise, burning 0-800 kcal per week. Exercising at a higher level burned more than 800 kcal had a HR of 0.68. A significant (P < .01) trend in favor of more exercise was noted.
Cycling reduces all-cause and cardiovascular mortality
In their prospective cohort study, Dr. Ried-Larsen and associates took a more specific look at the effects of exercise on mortality in diabetes by studying a single exercise: cycling. They sampled data on more than 5,000 people collected as part of the European Prospective Investigation into Cancer and Nutrition study. First, they identified participants with diabetes – although they couldn’t distinguish type 1 from type 2 forms because this was self-reported or obtained from registries. They then identified those who reported cycling at their baseline assessment and those who reported a change in cycling habits at their second examination around 5 years later.
At baseline, 38% of participants reported that they cycled every week. The mean age was 56 years, diabetes duration was 8 years, one-fifth were smokers, and the average body mass index was 29 kg/m2.
Participants who reported cycling up to 1 hour every week at baseline had a 25% reduction in all-cause mortality, compared with those who did not cycle. The biggest reduction (31%) in all-cause mortality was seen for cycling 2.5-5 hours a week; cycling for 1-2.5 hours, and for more than 5 hours, yielded 23% and 24% risk reductions, respectively.
A reverse J–shaped relationship between cycling duration and reduction in all-cause mortality was seen, Dr. Ried-Larsen noted during a live oral session at the virtual meeting. “The maximum benefit [was at] around 5 hours per week, and the benefits persisted until around 9 hours per week.” Adjustment for the prevalence of stroke, MI, cancer, hyperlipidemia, hypertension, and central obesity did not alter the findings.
“The direction of the association was the same for cardiovascular mortality as all-cause mortality, although a bit weaker, with the maximum benefit being around 4 hours per week, and that persisted up until around 8 hours per week,” Dr. Ried-Larsen said.
The benefits of cycling on all-cause and cardiovascular mortality were lost, however, if those who cycled at baseline stopped by the second examination. Those who did not cycle at the first but did at the second examination got a benefit on both, as did those who continued cycling.
“Cycling is among one of the preferred activities for diabetes patients, so it actually may help them to achieve the recommend level of physical activity,” Dr. Ried-Larsen said.
Tailored exercise program important
Advice for exercise “should be tailored to the individual and based on starting fitness levels and activity levels,” Dr. Colberg-Ochs recommended.
“Those who are the most sedentary and the least fit have the most to gain from doing any activity. They should be advised to start out slowly and progress slowly with both aerobic activities and some resistance training,” Dr. Colberg-Ochs said.
She added: “In addition, individuals over 40 should engage in regular balance training, and all individuals should do some flexibility exercises.”
The studies received no commercial funding and all those mentioned in this article had no conflicts of interest to disclose.
SOURCE: Lai Y-J et al. EASD 2020, Poster presentation 267; Ried-Larsen M et al. EASD 2020, Oral presentation 194.
Type 2 diabetes patients could lower their risk for death from any cause by up to a third by exercising at a moderate to high level or by cycling, according to data from two studies reported at the virtual annual meeting of the European Association for the Study of Diabetes.
Yun-Ju Lai, MD, and colleagues from the Puli branch of Taichung Veterans General Hospital in Nantou, Taiwan, found that persons with type 2 diabetes who exercised at moderate to high intensity had a 25%-32% decreased risk for death, compared with those who did not exercise.
In a separate study, Mathias Ried-Larsen, MSc, PhD, group leader at the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and associates found that cycling was associated with a 25%-31% decreased risk for all-cause death compared to no cycling, and that cycling also reduced cardiovascular mortality.
Results fit with ADA recommendations
“There is really nothing surprising about these results as others have shown that regular participation in physical activity lowers both overall mortality rates and morbidity,” commented Sheri Colberg-Ochs, PhD, professor emerita in exercise science at Old Dominion University in Norfolk, Va., in an interview.
“Regular exercise participation lowers the risk of mortality in almost all populations with many different health conditions. It is not specific to people with type 2 diabetes,” Dr. Colberg-Ochs said. “These data add further support to the ADA [American Diabetes Association] recommendations by again suggesting that being more active leads to many health benefits for people with type 2 diabetes.”
Dr. Colberg-Ochs, who was not involved in either study, is recognized by the ADA as an Outstanding Educator in Diabetes. She was also involved in writing the ADA’s position statement on physical activity/exercise in diabetes, which advocate that adults with type 2 diabetes should reduce sedentary time and undertake both aerobic and resistance exercise training to help optimize their glycemic and general health outcomes.
Asian population understudied
In an interview Dr. Lai acknowledged that epidemiologic studies had shown that exercise reduced the risk of cardiovascular events and mortality in subjects with type 2 diabetes. “However, the dose of exercise capacity for reducing mortality risk in people with type 2 diabetes was not yet well investigated, especially in the Asian population.”
Dr. Lai and colleagues analyzed data on 4,859 subjects drawn from two Taiwanese databases – the National Health Interview Survey and the National Health Insurance research database – to study what effect exercise “capacity” had on the risk for death in those with type 2 diabetes.
“Information about physical activity during leisure time was collected by asking the questions: ‘How often do you exercise every week? What kind of exercise do you do? How long do you do the exercise?’, Dr. Lai said. “We included nearly all kinds of exercise in the analysis, such as jogging, swimming, walking, dancing, riding, and so on.”
Each exercise had an activity intensity code expressed as kilocalories per minute. This was used to determine the exercise “capacity” by multiplying it by how frequently the exercise was performed per week and for how long each time.
“I don’t think ‘capacity’ is the right word to use here. The equation they used describes their exercise ‘volume,’ not their capacity. Self-reported exercise is notoriously inaccurate,” Dr. Colberg-Ochs observed. Furthermore, “just asking people how much they exercise and at what intensity [without using a validated exercise questionnaire] gives questionable results.”
The study’s findings, however, were clear: Those who exercised at a higher level had a significantly decreased risk for all-cause mortality than did those with no exercise habits. The hazard ratio for death by any cause was 0.75 for those who undertook a moderate level of exercise, burning 0-800 kcal per week. Exercising at a higher level burned more than 800 kcal had a HR of 0.68. A significant (P < .01) trend in favor of more exercise was noted.
Cycling reduces all-cause and cardiovascular mortality
In their prospective cohort study, Dr. Ried-Larsen and associates took a more specific look at the effects of exercise on mortality in diabetes by studying a single exercise: cycling. They sampled data on more than 5,000 people collected as part of the European Prospective Investigation into Cancer and Nutrition study. First, they identified participants with diabetes – although they couldn’t distinguish type 1 from type 2 forms because this was self-reported or obtained from registries. They then identified those who reported cycling at their baseline assessment and those who reported a change in cycling habits at their second examination around 5 years later.
At baseline, 38% of participants reported that they cycled every week. The mean age was 56 years, diabetes duration was 8 years, one-fifth were smokers, and the average body mass index was 29 kg/m2.
Participants who reported cycling up to 1 hour every week at baseline had a 25% reduction in all-cause mortality, compared with those who did not cycle. The biggest reduction (31%) in all-cause mortality was seen for cycling 2.5-5 hours a week; cycling for 1-2.5 hours, and for more than 5 hours, yielded 23% and 24% risk reductions, respectively.
A reverse J–shaped relationship between cycling duration and reduction in all-cause mortality was seen, Dr. Ried-Larsen noted during a live oral session at the virtual meeting. “The maximum benefit [was at] around 5 hours per week, and the benefits persisted until around 9 hours per week.” Adjustment for the prevalence of stroke, MI, cancer, hyperlipidemia, hypertension, and central obesity did not alter the findings.
“The direction of the association was the same for cardiovascular mortality as all-cause mortality, although a bit weaker, with the maximum benefit being around 4 hours per week, and that persisted up until around 8 hours per week,” Dr. Ried-Larsen said.
The benefits of cycling on all-cause and cardiovascular mortality were lost, however, if those who cycled at baseline stopped by the second examination. Those who did not cycle at the first but did at the second examination got a benefit on both, as did those who continued cycling.
“Cycling is among one of the preferred activities for diabetes patients, so it actually may help them to achieve the recommend level of physical activity,” Dr. Ried-Larsen said.
Tailored exercise program important
Advice for exercise “should be tailored to the individual and based on starting fitness levels and activity levels,” Dr. Colberg-Ochs recommended.
“Those who are the most sedentary and the least fit have the most to gain from doing any activity. They should be advised to start out slowly and progress slowly with both aerobic activities and some resistance training,” Dr. Colberg-Ochs said.
She added: “In addition, individuals over 40 should engage in regular balance training, and all individuals should do some flexibility exercises.”
The studies received no commercial funding and all those mentioned in this article had no conflicts of interest to disclose.
SOURCE: Lai Y-J et al. EASD 2020, Poster presentation 267; Ried-Larsen M et al. EASD 2020, Oral presentation 194.
FROM EASD 2020
No prior use of insulin predicts postsurgical diabetes remission
Type 2 diabetes patients who had never used insulin showed sustained remission 10 years after bariatric surgery in a prospective study of 85 patients.
Having diabetes for less than 5 years was also predictive of achieving long-term diabetes remission, Diego Moriconi, MD, of the University of Pisa (Italy) and presenting study investigator, reported at the virtual annual meeting of the European Association for the Study of Diabetes.
“Weight loss was associated with type 2 diabetes remission 1 year after surgery, but it had no impact on the long-term relapse of diabetes,” Dr. Moriconi said.
The findings are important, commented Tina Vilsbøll, MD, DMSc, chief consultant at the Steno Diabetes Centre Copenhagen, who chaired the session. They’re important because they would help “to set the expectations for patients before they have surgery, what to expect in respect to resolution or remission of diabetes.”
If patients were taking insulin, for instance, the take home would seem to be not to expect too much in terms of remission of their diabetes, Dr. Vilsbøll said. She added: “Usually I am not a big fan of [relying on] diabetes duration, because often we know that patients with type 2 diabetes have had diabetes for a long time before they’re actually diagnosed.” However, “it seems to be very important here.”
Dr. Moriconi reported the findings of an observational study that had started in 2006 and recruited individuals about to undergo bariatric surgery for type 2 diabetes. Participants were evaluated before surgery and every 6-12 months after, undergoing various clinical and laboratory investigations, for a period of 10 years.
The majority of the recruited patients (76%) were women. Most (also 76%) had undergone gastric bypass (Roux-en-Y) surgery, and the remainder had undergone sleeve gastrectomy. Both types of surgery were equally as good at getting people into remission, as defined by the American Diabetes Association Standards of Medical Care in Diabetes, Dr. Moriconi said. As such, remission was achieved if the fasting blood glucose fell below 100 mg/dL and the hemoglobin A1c below 5.7%.
In the first year following surgery, 75% of patients had met diabetes remission criteria. This fell to 61% of patients after 5 years, and to 55% at 10 years. At each of these time points, 25% of patients had type 2 diabetes, with 14% relapsing back at 5 years and 20% at 10 years.
Dr. Moriconi pointed out some of the different characteristics of the 47 patients who had achieved diabetes remission at 10 years, compared with the 17 who had “relapsed” back to having type 2 diabetes and the 21 who had remained with type 2 diabetes.
The decrease in body mass index achieved at 10 years was no different between the three groups. However, 1 year after surgery, there had been a significantly greater drop in body in those who achieved remission, compared with those who did not (P = .04).
“Glycemic control improved with time in all the three groups after bariatric surgery, although more markedly so in the remission group,” Dr. Moriconi said.
He highlighted how none of the patients who had achieved remission had used insulin, whereas 12% of those who had relapsed and half (52%) of those who remained with type 2 diabetes had used insulin (P < .0001).
Patients who achieved remission at 1, 5, and 10 years were more likely to have had diabetes for less than 5 years than those who remained with type 2 diabetes. The average duration of diabetes was 2 years in those achieving remission versus 8 years in those who had relapsed and 13 years in those who had remained diabetic (P < .0001).
Logistic regression analysis, which adjusted for all major confounding factors such as age, sex, and type of surgery, showed that only the duration of diabetes and insulin therapy before surgery were the only predictors of long-term diabetes remission.
The study had no commercial funding. Dr. Moriconi and Dr. Vilsbøll had no conflicts of interest to disclose.
SOURCE: Moriconi D. EASD 2020, Oral presentation 120.
Type 2 diabetes patients who had never used insulin showed sustained remission 10 years after bariatric surgery in a prospective study of 85 patients.
Having diabetes for less than 5 years was also predictive of achieving long-term diabetes remission, Diego Moriconi, MD, of the University of Pisa (Italy) and presenting study investigator, reported at the virtual annual meeting of the European Association for the Study of Diabetes.
“Weight loss was associated with type 2 diabetes remission 1 year after surgery, but it had no impact on the long-term relapse of diabetes,” Dr. Moriconi said.
The findings are important, commented Tina Vilsbøll, MD, DMSc, chief consultant at the Steno Diabetes Centre Copenhagen, who chaired the session. They’re important because they would help “to set the expectations for patients before they have surgery, what to expect in respect to resolution or remission of diabetes.”
If patients were taking insulin, for instance, the take home would seem to be not to expect too much in terms of remission of their diabetes, Dr. Vilsbøll said. She added: “Usually I am not a big fan of [relying on] diabetes duration, because often we know that patients with type 2 diabetes have had diabetes for a long time before they’re actually diagnosed.” However, “it seems to be very important here.”
Dr. Moriconi reported the findings of an observational study that had started in 2006 and recruited individuals about to undergo bariatric surgery for type 2 diabetes. Participants were evaluated before surgery and every 6-12 months after, undergoing various clinical and laboratory investigations, for a period of 10 years.
The majority of the recruited patients (76%) were women. Most (also 76%) had undergone gastric bypass (Roux-en-Y) surgery, and the remainder had undergone sleeve gastrectomy. Both types of surgery were equally as good at getting people into remission, as defined by the American Diabetes Association Standards of Medical Care in Diabetes, Dr. Moriconi said. As such, remission was achieved if the fasting blood glucose fell below 100 mg/dL and the hemoglobin A1c below 5.7%.
In the first year following surgery, 75% of patients had met diabetes remission criteria. This fell to 61% of patients after 5 years, and to 55% at 10 years. At each of these time points, 25% of patients had type 2 diabetes, with 14% relapsing back at 5 years and 20% at 10 years.
Dr. Moriconi pointed out some of the different characteristics of the 47 patients who had achieved diabetes remission at 10 years, compared with the 17 who had “relapsed” back to having type 2 diabetes and the 21 who had remained with type 2 diabetes.
The decrease in body mass index achieved at 10 years was no different between the three groups. However, 1 year after surgery, there had been a significantly greater drop in body in those who achieved remission, compared with those who did not (P = .04).
“Glycemic control improved with time in all the three groups after bariatric surgery, although more markedly so in the remission group,” Dr. Moriconi said.
He highlighted how none of the patients who had achieved remission had used insulin, whereas 12% of those who had relapsed and half (52%) of those who remained with type 2 diabetes had used insulin (P < .0001).
Patients who achieved remission at 1, 5, and 10 years were more likely to have had diabetes for less than 5 years than those who remained with type 2 diabetes. The average duration of diabetes was 2 years in those achieving remission versus 8 years in those who had relapsed and 13 years in those who had remained diabetic (P < .0001).
Logistic regression analysis, which adjusted for all major confounding factors such as age, sex, and type of surgery, showed that only the duration of diabetes and insulin therapy before surgery were the only predictors of long-term diabetes remission.
The study had no commercial funding. Dr. Moriconi and Dr. Vilsbøll had no conflicts of interest to disclose.
SOURCE: Moriconi D. EASD 2020, Oral presentation 120.
Type 2 diabetes patients who had never used insulin showed sustained remission 10 years after bariatric surgery in a prospective study of 85 patients.
Having diabetes for less than 5 years was also predictive of achieving long-term diabetes remission, Diego Moriconi, MD, of the University of Pisa (Italy) and presenting study investigator, reported at the virtual annual meeting of the European Association for the Study of Diabetes.
“Weight loss was associated with type 2 diabetes remission 1 year after surgery, but it had no impact on the long-term relapse of diabetes,” Dr. Moriconi said.
The findings are important, commented Tina Vilsbøll, MD, DMSc, chief consultant at the Steno Diabetes Centre Copenhagen, who chaired the session. They’re important because they would help “to set the expectations for patients before they have surgery, what to expect in respect to resolution or remission of diabetes.”
If patients were taking insulin, for instance, the take home would seem to be not to expect too much in terms of remission of their diabetes, Dr. Vilsbøll said. She added: “Usually I am not a big fan of [relying on] diabetes duration, because often we know that patients with type 2 diabetes have had diabetes for a long time before they’re actually diagnosed.” However, “it seems to be very important here.”
Dr. Moriconi reported the findings of an observational study that had started in 2006 and recruited individuals about to undergo bariatric surgery for type 2 diabetes. Participants were evaluated before surgery and every 6-12 months after, undergoing various clinical and laboratory investigations, for a period of 10 years.
The majority of the recruited patients (76%) were women. Most (also 76%) had undergone gastric bypass (Roux-en-Y) surgery, and the remainder had undergone sleeve gastrectomy. Both types of surgery were equally as good at getting people into remission, as defined by the American Diabetes Association Standards of Medical Care in Diabetes, Dr. Moriconi said. As such, remission was achieved if the fasting blood glucose fell below 100 mg/dL and the hemoglobin A1c below 5.7%.
In the first year following surgery, 75% of patients had met diabetes remission criteria. This fell to 61% of patients after 5 years, and to 55% at 10 years. At each of these time points, 25% of patients had type 2 diabetes, with 14% relapsing back at 5 years and 20% at 10 years.
Dr. Moriconi pointed out some of the different characteristics of the 47 patients who had achieved diabetes remission at 10 years, compared with the 17 who had “relapsed” back to having type 2 diabetes and the 21 who had remained with type 2 diabetes.
The decrease in body mass index achieved at 10 years was no different between the three groups. However, 1 year after surgery, there had been a significantly greater drop in body in those who achieved remission, compared with those who did not (P = .04).
“Glycemic control improved with time in all the three groups after bariatric surgery, although more markedly so in the remission group,” Dr. Moriconi said.
He highlighted how none of the patients who had achieved remission had used insulin, whereas 12% of those who had relapsed and half (52%) of those who remained with type 2 diabetes had used insulin (P < .0001).
Patients who achieved remission at 1, 5, and 10 years were more likely to have had diabetes for less than 5 years than those who remained with type 2 diabetes. The average duration of diabetes was 2 years in those achieving remission versus 8 years in those who had relapsed and 13 years in those who had remained diabetic (P < .0001).
Logistic regression analysis, which adjusted for all major confounding factors such as age, sex, and type of surgery, showed that only the duration of diabetes and insulin therapy before surgery were the only predictors of long-term diabetes remission.
The study had no commercial funding. Dr. Moriconi and Dr. Vilsbøll had no conflicts of interest to disclose.
SOURCE: Moriconi D. EASD 2020, Oral presentation 120.
FROM EASD 2020
Vascular dementia risk particularly high in type 2 diabetes
Persons with type 2 diabetes may be at heightened risk for developing vascular dementia than other types of dementia, a team of international researchers has found.

Compared with a nondiabetic control population, those with type 2 diabetes had a statistically significant 35% increased chance of having vascular dementia in a large observational study.
By comparison, the risk for nonvascular dementia was increased by a “more modest” 8%, said the researchers from the University of Glasgow and the University of Gothenburg (Sweden), while the risk for Alzheimer’s dementia appeared to be reduced by 8%.
The link between type 2 diabetes and dementia is not new, observed Carlos Celis-Morales, PhD, who presented the study’s findings at the virtual annual meeting of the European Association for the Study of Diabetes. With people living longer thanks to improved preventative strategies and treatments, there is a risk for developing other chronic conditions, such as dementia.
“A third of all dementia cases may be attributable to modifiable risk factors, among them type 2 diabetes, which accounts for 3.2% of all dementia cases,” said Dr. Celis-Morales, a research fellow at the University of Glasgow’s Institute of Cardiovascular and Medical Sciences.
“Although we know that diabetes is linked to dementia, what we don’t know really well is how much of this association between diabetes and dementia outcomes are explained by modifiable and nonmodifiable risk factors,” Dr. Celis-Morales added.
“Diabetes and dementia share certain risk factors,” commented coinvestigator Naveed Sattar, MD, in a press release issued by the EASD. These include obesity, smoking, and lack of physical activity and might explain part of the association between the two conditions.
Dr. Sattar said that the heightened vascular dementia risk found in the study was “in itself an argument for preventive measures such as healthier lifestyle,” adding that “the importance of prevention is underscored by the fact that, for the majority of dementia diseases, there is no good treatment.”
Using data from the Swedish National Diabetes Register, the research team set out to determine the extent to which type 2 diabetes was associated with dementia and the incidence of different subtypes of dementia. They also looked to see if there were any associations with blood glucose control and what risk factors may be involved.
In total, data on 378,299 individuals with type 2 diabetes were compared with data on 1,886,022 similarly aged (average, 64 years) and gender-matched controls from the general population.
After a mean 7 years of follow-up, 10,143 people with and 46,479 people without type 2 diabetes developed dementia. Nonvascular dementia was the most common type of dementia recorded, followed by Alzheimer’s disease and then vascular dementia.
“Within type 2 diabetes individuals, poor glycemic [control] increased the risk of dementia especially for vascular dementia and nonvascular dementia. However, these associations were not as evident for Alzheimer’s disease,” Dr. Celis-Morales reported.
Comparing those with hemoglobin bA1c of less than 52 mmol/mol (7%) with those whose A1c was above 87 mmol/mol (10.1%), there was 93% increase in the risk for vascular dementia, a 67% increase in the risk for nonvascular dementia, and a 34% higher risk for Alzheimer’s disease–associated dementia.
“We have focused on high levels of HbA1c, but what happens if you have really low limits? It’s something we’re working on right now,” Dr. Celis-Morales said.
Importantly, cardiovascular-related risk factors – some of which, like systolic blood pressure and body weight, were potentially modifiable – accounted for more than 40% of the risk for dementia in type 2 diabetes. This suggests that a large percentage of the dementia risk could perhaps be addressed by identifying high-risk individuals and tailoring interventions accordingly.
“These are observational findings, so we need to be careful before we translate to any sort of recommendation,” Dr. Celis-Morales said.
The study was financed by the Swedish state under the agreement between the government and the county councils, the ALF agreement, as well as grant from the Novo Nordisk Foundation and the Swedish Association of Local Authorities and Regions. Dr. Celis-Morales and Dr. Sattar had no conflicts of interest.
SOURCE: Celis-Morales C et al. EASD 2020, Oral presentation 06.
Persons with type 2 diabetes may be at heightened risk for developing vascular dementia than other types of dementia, a team of international researchers has found.
Compared with a nondiabetic control population, those with type 2 diabetes had a statistically significant 35% increased chance of having vascular dementia in a large observational study.
By comparison, the risk for nonvascular dementia was increased by a “more modest” 8%, said the researchers from the University of Glasgow and the University of Gothenburg (Sweden), while the risk for Alzheimer’s dementia appeared to be reduced by 8%.
The link between type 2 diabetes and dementia is not new, observed Carlos Celis-Morales, PhD, who presented the study’s findings at the virtual annual meeting of the European Association for the Study of Diabetes. With people living longer thanks to improved preventative strategies and treatments, there is a risk for developing other chronic conditions, such as dementia.
“A third of all dementia cases may be attributable to modifiable risk factors, among them type 2 diabetes, which accounts for 3.2% of all dementia cases,” said Dr. Celis-Morales, a research fellow at the University of Glasgow’s Institute of Cardiovascular and Medical Sciences.
“Although we know that diabetes is linked to dementia, what we don’t know really well is how much of this association between diabetes and dementia outcomes are explained by modifiable and nonmodifiable risk factors,” Dr. Celis-Morales added.
“Diabetes and dementia share certain risk factors,” commented coinvestigator Naveed Sattar, MD, in a press release issued by the EASD. These include obesity, smoking, and lack of physical activity and might explain part of the association between the two conditions.
Dr. Sattar said that the heightened vascular dementia risk found in the study was “in itself an argument for preventive measures such as healthier lifestyle,” adding that “the importance of prevention is underscored by the fact that, for the majority of dementia diseases, there is no good treatment.”
Using data from the Swedish National Diabetes Register, the research team set out to determine the extent to which type 2 diabetes was associated with dementia and the incidence of different subtypes of dementia. They also looked to see if there were any associations with blood glucose control and what risk factors may be involved.
In total, data on 378,299 individuals with type 2 diabetes were compared with data on 1,886,022 similarly aged (average, 64 years) and gender-matched controls from the general population.
After a mean 7 years of follow-up, 10,143 people with and 46,479 people without type 2 diabetes developed dementia. Nonvascular dementia was the most common type of dementia recorded, followed by Alzheimer’s disease and then vascular dementia.
“Within type 2 diabetes individuals, poor glycemic [control] increased the risk of dementia especially for vascular dementia and nonvascular dementia. However, these associations were not as evident for Alzheimer’s disease,” Dr. Celis-Morales reported.
Comparing those with hemoglobin bA1c of less than 52 mmol/mol (7%) with those whose A1c was above 87 mmol/mol (10.1%), there was 93% increase in the risk for vascular dementia, a 67% increase in the risk for nonvascular dementia, and a 34% higher risk for Alzheimer’s disease–associated dementia.
“We have focused on high levels of HbA1c, but what happens if you have really low limits? It’s something we’re working on right now,” Dr. Celis-Morales said.
Importantly, cardiovascular-related risk factors – some of which, like systolic blood pressure and body weight, were potentially modifiable – accounted for more than 40% of the risk for dementia in type 2 diabetes. This suggests that a large percentage of the dementia risk could perhaps be addressed by identifying high-risk individuals and tailoring interventions accordingly.
“These are observational findings, so we need to be careful before we translate to any sort of recommendation,” Dr. Celis-Morales said.
The study was financed by the Swedish state under the agreement between the government and the county councils, the ALF agreement, as well as grant from the Novo Nordisk Foundation and the Swedish Association of Local Authorities and Regions. Dr. Celis-Morales and Dr. Sattar had no conflicts of interest.
SOURCE: Celis-Morales C et al. EASD 2020, Oral presentation 06.
Persons with type 2 diabetes may be at heightened risk for developing vascular dementia than other types of dementia, a team of international researchers has found.
Compared with a nondiabetic control population, those with type 2 diabetes had a statistically significant 35% increased chance of having vascular dementia in a large observational study.
By comparison, the risk for nonvascular dementia was increased by a “more modest” 8%, said the researchers from the University of Glasgow and the University of Gothenburg (Sweden), while the risk for Alzheimer’s dementia appeared to be reduced by 8%.
The link between type 2 diabetes and dementia is not new, observed Carlos Celis-Morales, PhD, who presented the study’s findings at the virtual annual meeting of the European Association for the Study of Diabetes. With people living longer thanks to improved preventative strategies and treatments, there is a risk for developing other chronic conditions, such as dementia.
“A third of all dementia cases may be attributable to modifiable risk factors, among them type 2 diabetes, which accounts for 3.2% of all dementia cases,” said Dr. Celis-Morales, a research fellow at the University of Glasgow’s Institute of Cardiovascular and Medical Sciences.
“Although we know that diabetes is linked to dementia, what we don’t know really well is how much of this association between diabetes and dementia outcomes are explained by modifiable and nonmodifiable risk factors,” Dr. Celis-Morales added.
“Diabetes and dementia share certain risk factors,” commented coinvestigator Naveed Sattar, MD, in a press release issued by the EASD. These include obesity, smoking, and lack of physical activity and might explain part of the association between the two conditions.
Dr. Sattar said that the heightened vascular dementia risk found in the study was “in itself an argument for preventive measures such as healthier lifestyle,” adding that “the importance of prevention is underscored by the fact that, for the majority of dementia diseases, there is no good treatment.”
Using data from the Swedish National Diabetes Register, the research team set out to determine the extent to which type 2 diabetes was associated with dementia and the incidence of different subtypes of dementia. They also looked to see if there were any associations with blood glucose control and what risk factors may be involved.
In total, data on 378,299 individuals with type 2 diabetes were compared with data on 1,886,022 similarly aged (average, 64 years) and gender-matched controls from the general population.
After a mean 7 years of follow-up, 10,143 people with and 46,479 people without type 2 diabetes developed dementia. Nonvascular dementia was the most common type of dementia recorded, followed by Alzheimer’s disease and then vascular dementia.
“Within type 2 diabetes individuals, poor glycemic [control] increased the risk of dementia especially for vascular dementia and nonvascular dementia. However, these associations were not as evident for Alzheimer’s disease,” Dr. Celis-Morales reported.
Comparing those with hemoglobin bA1c of less than 52 mmol/mol (7%) with those whose A1c was above 87 mmol/mol (10.1%), there was 93% increase in the risk for vascular dementia, a 67% increase in the risk for nonvascular dementia, and a 34% higher risk for Alzheimer’s disease–associated dementia.
“We have focused on high levels of HbA1c, but what happens if you have really low limits? It’s something we’re working on right now,” Dr. Celis-Morales said.
Importantly, cardiovascular-related risk factors – some of which, like systolic blood pressure and body weight, were potentially modifiable – accounted for more than 40% of the risk for dementia in type 2 diabetes. This suggests that a large percentage of the dementia risk could perhaps be addressed by identifying high-risk individuals and tailoring interventions accordingly.
“These are observational findings, so we need to be careful before we translate to any sort of recommendation,” Dr. Celis-Morales said.
The study was financed by the Swedish state under the agreement between the government and the county councils, the ALF agreement, as well as grant from the Novo Nordisk Foundation and the Swedish Association of Local Authorities and Regions. Dr. Celis-Morales and Dr. Sattar had no conflicts of interest.
SOURCE: Celis-Morales C et al. EASD 2020, Oral presentation 06.
FROM EASD 2020
Large waistline linked to higher risk of prostate cancer death
Men with prostate cancer may be wise to watch their waistlines, according to the findings of a large observational study in which patients with the highest waist measurements had a higher chance of dying from prostate cancer.

Researchers found that, over a 10.8-year period, men with the largest waist circumferences appeared 35% more likely to die from prostate cancer, when compared to men with the smallest waist circumferences (hazard ratio = 1.35, 95% confidence interval [CI], 1.05–1.73).
Men in the highest quartile for waist-to-hip ratio measurements also had a 34% higher risk of dying from prostate cancer, when compared to men in the lowest quartile (HR = 1.34, 95% CI, 1.04–1.72).
There was no association between the total body fat percentage (HR = 1.00, 95% CI, 0.79–1.28) or body mass index (HR = 1.00, 95% CI, 0.78–1.28) and the risk for prostate cancer death.
The findings – reported in a late-breaking poster at the European and International Conference on Obesity (ECOICO) – provide further insight into how fat and its distribution may be associated with prostate cancer death.
A ‘complex’ relationship
“Obesity is a known risk factor for many cancer sites, but its association with prostate cancer is less clear. It’s very complex,” said study investigator Aurora Pérez-Cornago, PhD, a nutritional epidemiologist in the Nuffield Department of Population Health at University of Oxford, England.
Three years ago, Dr. Pérez-Cornago and collaborators looked for risk factors for prostate cancer among men who had volunteered to participate in the prospective UK Biobank cohort study.
One of the group’s findings was that excess adiposity and body fat were not associated with an increase in the development of prostate cancer (Br J Cancer. 2017 Nov 7;117[10]:1562-71). In fact, these factors were associated with a lower risk. This inverse association likely had more to do with prostate-specific antigen screening than a true effect of body weight, as men with obesity were potentially less likely to be screened or have lower prostate-specific antigen levels, Dr. Pérez-Cornago said.
For the present study, attention was turned to men with aggressive prostate tumors as “these are the kind of tumors we are more interested in because they are the ones that can kill these men,” Dr. Pérez-Cornago said.
There was also previous evidence suggesting that adiposity may be associated with a higher risk of aggressive disease.
Data on 218,225 men with no previous cancer when they enrolled in the UK Biobank cohort study were linked to health care administrative databases that provided information on prostate cancer deaths. This showed that 571 men died from prostate cancer over a 10.8-year follow-up period.
“When we looked at the association of adiposity measurements – we looked at [body mass index] and body fat percentage as markers of total adiposity, and waist circumference and waist-to-hip ratio as markers of central adiposity – we found that the association seems to be more specific for fat located around the waist,” Dr. Pérez-Cornago said.
“Excessive fat accumulation around your belly is likely to be visceral fat, which may induce metabolic and hormonal dysfunction that, in turn, may help prostate cancer cells to develop and to progress,” she added.
Study strengths and next steps
As this was an observational study, the researchers could not confirm a causal association between central adiposity and prostate cancer death. That is why Dr. Perez-Cornago and collaborators plan to do further work that will include biomarker studies. The team also will look at stage and grade data when available in the UK Biobank.
“There is strong evidence that men with greater body fat are at a higher risk of advanced and fatal prostate cancer. It is time to build on this,” said Barbra Dickerman, PhD, who has looked at the relationship between obesity and prostate cancer progression (Cancer. 2019 Aug 15;125[16]:2877-85).
“First, predictive analyses of directly measured body fat distribution may sharpen our view of who is at the highest risk,” observed Dr. Dickerman, a research fellow in the department of epidemiology at Harvard T.H. Chan School of Public Health in Boston.
“Second, causal analyses of precisely defined energy balance strategies may help to identify targeted prevention strategies that minimize that risk,” she added.
One of the strengths of Dr. Pérez-Cornago’s work was that it used data from a large, prospective study to examine the link between adiposity and the risk of fatal prostate cancer, observed Ying Wang, PhD, a senior principal scientist of epidemiology research at The American Cancer Society.
“In addition to the large sample size, anthropometric measurements were obtained by trained research clinic staff rather than self-reported by participants, which is a strength compared with many other studies,” Dr. Wang noted.
Furthermore, Dr. Wang said, “The study was also able to control for multiple confounders, including lifestyle factors such as smoking and physical activity. Future studies need to confirm their findings.”
The study was supported by a fellowship from Cancer Research UK. The investigators, Dr. Dickerman, and Dr. Wang had no conflicts of interest to disclose.
SOURCE: Pérez-Cornago A et al. ECOICO 2020. LBP-075.
Men with prostate cancer may be wise to watch their waistlines, according to the findings of a large observational study in which patients with the highest waist measurements had a higher chance of dying from prostate cancer.
Researchers found that, over a 10.8-year period, men with the largest waist circumferences appeared 35% more likely to die from prostate cancer, when compared to men with the smallest waist circumferences (hazard ratio = 1.35, 95% confidence interval [CI], 1.05–1.73).
Men in the highest quartile for waist-to-hip ratio measurements also had a 34% higher risk of dying from prostate cancer, when compared to men in the lowest quartile (HR = 1.34, 95% CI, 1.04–1.72).
There was no association between the total body fat percentage (HR = 1.00, 95% CI, 0.79–1.28) or body mass index (HR = 1.00, 95% CI, 0.78–1.28) and the risk for prostate cancer death.
The findings – reported in a late-breaking poster at the European and International Conference on Obesity (ECOICO) – provide further insight into how fat and its distribution may be associated with prostate cancer death.
A ‘complex’ relationship
“Obesity is a known risk factor for many cancer sites, but its association with prostate cancer is less clear. It’s very complex,” said study investigator Aurora Pérez-Cornago, PhD, a nutritional epidemiologist in the Nuffield Department of Population Health at University of Oxford, England.
Three years ago, Dr. Pérez-Cornago and collaborators looked for risk factors for prostate cancer among men who had volunteered to participate in the prospective UK Biobank cohort study.
One of the group’s findings was that excess adiposity and body fat were not associated with an increase in the development of prostate cancer (Br J Cancer. 2017 Nov 7;117[10]:1562-71). In fact, these factors were associated with a lower risk. This inverse association likely had more to do with prostate-specific antigen screening than a true effect of body weight, as men with obesity were potentially less likely to be screened or have lower prostate-specific antigen levels, Dr. Pérez-Cornago said.
For the present study, attention was turned to men with aggressive prostate tumors as “these are the kind of tumors we are more interested in because they are the ones that can kill these men,” Dr. Pérez-Cornago said.
There was also previous evidence suggesting that adiposity may be associated with a higher risk of aggressive disease.
Data on 218,225 men with no previous cancer when they enrolled in the UK Biobank cohort study were linked to health care administrative databases that provided information on prostate cancer deaths. This showed that 571 men died from prostate cancer over a 10.8-year follow-up period.
“When we looked at the association of adiposity measurements – we looked at [body mass index] and body fat percentage as markers of total adiposity, and waist circumference and waist-to-hip ratio as markers of central adiposity – we found that the association seems to be more specific for fat located around the waist,” Dr. Pérez-Cornago said.
“Excessive fat accumulation around your belly is likely to be visceral fat, which may induce metabolic and hormonal dysfunction that, in turn, may help prostate cancer cells to develop and to progress,” she added.
Study strengths and next steps
As this was an observational study, the researchers could not confirm a causal association between central adiposity and prostate cancer death. That is why Dr. Perez-Cornago and collaborators plan to do further work that will include biomarker studies. The team also will look at stage and grade data when available in the UK Biobank.
“There is strong evidence that men with greater body fat are at a higher risk of advanced and fatal prostate cancer. It is time to build on this,” said Barbra Dickerman, PhD, who has looked at the relationship between obesity and prostate cancer progression (Cancer. 2019 Aug 15;125[16]:2877-85).
“First, predictive analyses of directly measured body fat distribution may sharpen our view of who is at the highest risk,” observed Dr. Dickerman, a research fellow in the department of epidemiology at Harvard T.H. Chan School of Public Health in Boston.
“Second, causal analyses of precisely defined energy balance strategies may help to identify targeted prevention strategies that minimize that risk,” she added.
One of the strengths of Dr. Pérez-Cornago’s work was that it used data from a large, prospective study to examine the link between adiposity and the risk of fatal prostate cancer, observed Ying Wang, PhD, a senior principal scientist of epidemiology research at The American Cancer Society.
“In addition to the large sample size, anthropometric measurements were obtained by trained research clinic staff rather than self-reported by participants, which is a strength compared with many other studies,” Dr. Wang noted.
Furthermore, Dr. Wang said, “The study was also able to control for multiple confounders, including lifestyle factors such as smoking and physical activity. Future studies need to confirm their findings.”
The study was supported by a fellowship from Cancer Research UK. The investigators, Dr. Dickerman, and Dr. Wang had no conflicts of interest to disclose.
SOURCE: Pérez-Cornago A et al. ECOICO 2020. LBP-075.
Men with prostate cancer may be wise to watch their waistlines, according to the findings of a large observational study in which patients with the highest waist measurements had a higher chance of dying from prostate cancer.
Researchers found that, over a 10.8-year period, men with the largest waist circumferences appeared 35% more likely to die from prostate cancer, when compared to men with the smallest waist circumferences (hazard ratio = 1.35, 95% confidence interval [CI], 1.05–1.73).
Men in the highest quartile for waist-to-hip ratio measurements also had a 34% higher risk of dying from prostate cancer, when compared to men in the lowest quartile (HR = 1.34, 95% CI, 1.04–1.72).
There was no association between the total body fat percentage (HR = 1.00, 95% CI, 0.79–1.28) or body mass index (HR = 1.00, 95% CI, 0.78–1.28) and the risk for prostate cancer death.
The findings – reported in a late-breaking poster at the European and International Conference on Obesity (ECOICO) – provide further insight into how fat and its distribution may be associated with prostate cancer death.
A ‘complex’ relationship
“Obesity is a known risk factor for many cancer sites, but its association with prostate cancer is less clear. It’s very complex,” said study investigator Aurora Pérez-Cornago, PhD, a nutritional epidemiologist in the Nuffield Department of Population Health at University of Oxford, England.
Three years ago, Dr. Pérez-Cornago and collaborators looked for risk factors for prostate cancer among men who had volunteered to participate in the prospective UK Biobank cohort study.
One of the group’s findings was that excess adiposity and body fat were not associated with an increase in the development of prostate cancer (Br J Cancer. 2017 Nov 7;117[10]:1562-71). In fact, these factors were associated with a lower risk. This inverse association likely had more to do with prostate-specific antigen screening than a true effect of body weight, as men with obesity were potentially less likely to be screened or have lower prostate-specific antigen levels, Dr. Pérez-Cornago said.
For the present study, attention was turned to men with aggressive prostate tumors as “these are the kind of tumors we are more interested in because they are the ones that can kill these men,” Dr. Pérez-Cornago said.
There was also previous evidence suggesting that adiposity may be associated with a higher risk of aggressive disease.
Data on 218,225 men with no previous cancer when they enrolled in the UK Biobank cohort study were linked to health care administrative databases that provided information on prostate cancer deaths. This showed that 571 men died from prostate cancer over a 10.8-year follow-up period.
“When we looked at the association of adiposity measurements – we looked at [body mass index] and body fat percentage as markers of total adiposity, and waist circumference and waist-to-hip ratio as markers of central adiposity – we found that the association seems to be more specific for fat located around the waist,” Dr. Pérez-Cornago said.
“Excessive fat accumulation around your belly is likely to be visceral fat, which may induce metabolic and hormonal dysfunction that, in turn, may help prostate cancer cells to develop and to progress,” she added.
Study strengths and next steps
As this was an observational study, the researchers could not confirm a causal association between central adiposity and prostate cancer death. That is why Dr. Perez-Cornago and collaborators plan to do further work that will include biomarker studies. The team also will look at stage and grade data when available in the UK Biobank.
“There is strong evidence that men with greater body fat are at a higher risk of advanced and fatal prostate cancer. It is time to build on this,” said Barbra Dickerman, PhD, who has looked at the relationship between obesity and prostate cancer progression (Cancer. 2019 Aug 15;125[16]:2877-85).
“First, predictive analyses of directly measured body fat distribution may sharpen our view of who is at the highest risk,” observed Dr. Dickerman, a research fellow in the department of epidemiology at Harvard T.H. Chan School of Public Health in Boston.
“Second, causal analyses of precisely defined energy balance strategies may help to identify targeted prevention strategies that minimize that risk,” she added.
One of the strengths of Dr. Pérez-Cornago’s work was that it used data from a large, prospective study to examine the link between adiposity and the risk of fatal prostate cancer, observed Ying Wang, PhD, a senior principal scientist of epidemiology research at The American Cancer Society.
“In addition to the large sample size, anthropometric measurements were obtained by trained research clinic staff rather than self-reported by participants, which is a strength compared with many other studies,” Dr. Wang noted.
Furthermore, Dr. Wang said, “The study was also able to control for multiple confounders, including lifestyle factors such as smoking and physical activity. Future studies need to confirm their findings.”
The study was supported by a fellowship from Cancer Research UK. The investigators, Dr. Dickerman, and Dr. Wang had no conflicts of interest to disclose.
SOURCE: Pérez-Cornago A et al. ECOICO 2020. LBP-075.
FROM ECOICO 2020
Diffuse idiopathic skeletal hyperostosis heart risk higher than expected
More people with diffuse idiopathic skeletal hyperostosis (DISH) develop cardiovascular disease (CVD) than is predicted by the Framingham Risk Score, results of an observational study have shown.
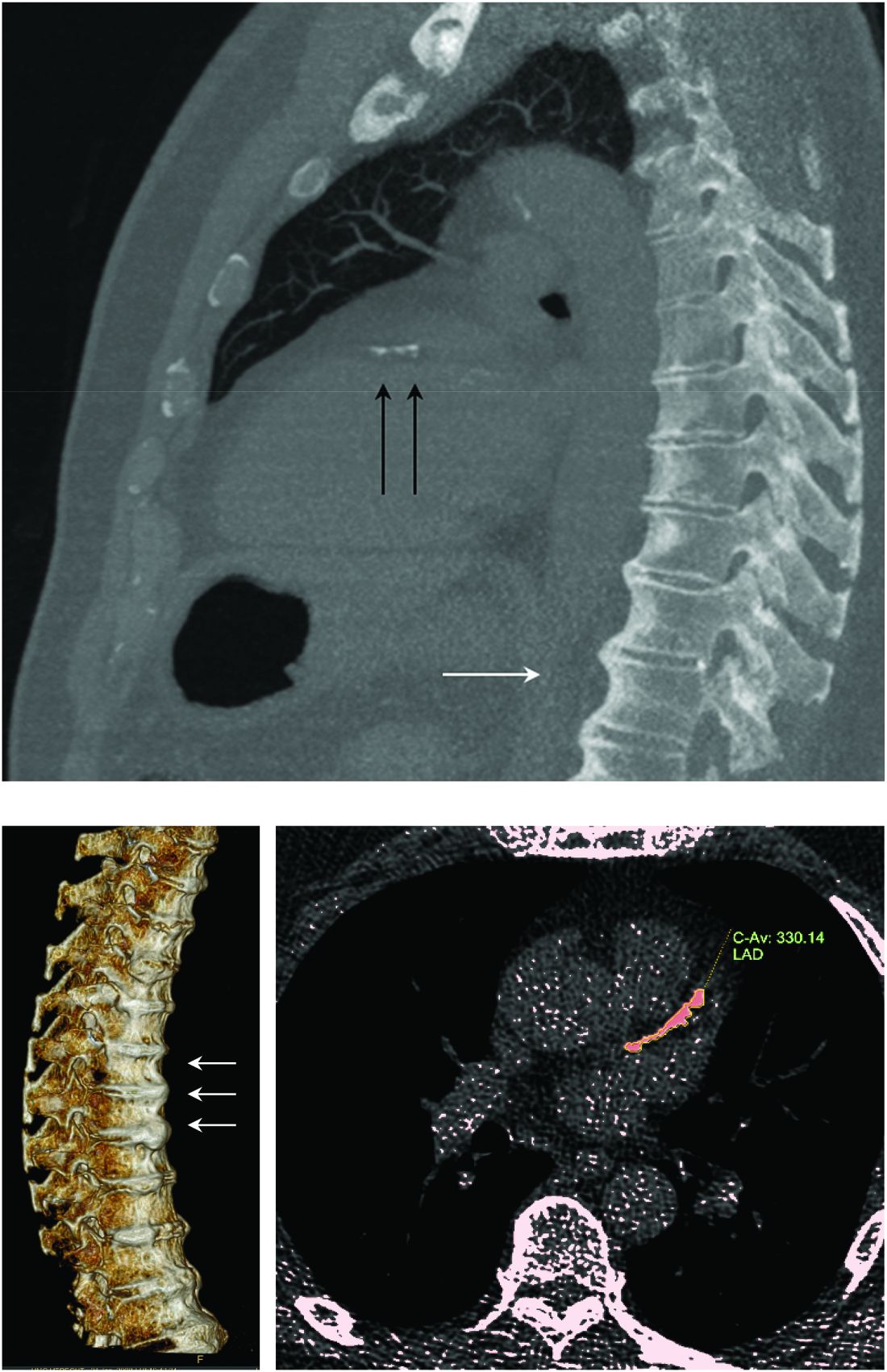
Notably, a higher rate of myocardial infarction (MI) was seen in those with DISH than in those without DISH over the 10-year follow-up period (24.4% vs. 4.3%; P = .0055).
“We propose more scrutiny is warranted in evaluating CV risk in these patients, more demanding treatment target goals should be established, and as a result, earlier and more aggressive preventive medical interventions instituted,” corresponding author Reuven Mader, MD, and associates wrote in Arthritis Research & Therapy.
“What Mader’s study is pointing out is that it’s worth the radiologist reporting [DISH],” Elizabeth A. Regan, MD, PhD, from the National Jewish Health Center in Denver, said in an interview.
DISH on a chest x-ray or CT scan should be another “red flag to be even more attentive to cardiovascular risk,” she added, particularly because studies have shown that people with DISH tend to be obese, have metabolic syndrome, or diabetes – all of which independently increase their risk for cardiovascular disease.
An old condition often found by accident
Physicians have known about DISH for many years, Dr. Mader of Ha’Emek Medical Center in Afula, Israel, observed in an interview. Historical evidence suggests it was present more than a thousand years ago, but it wasn’t until the 1950s that it gained scientific interest. Originally coined Forestier’s disease, it was renamed DISH in the late 1960s following the realization that it was not limited to the spine.
“It is a condition which is characterized by new bone formation,” Dr. Mader explained. This new bone formation has some predilection for the entheses – the tendons, ligaments, or joint capsules, that attach to the bone.
“Diagnosis of the disease is based mainly on radiographs, especially of the thoracic spine, and it requires the formation of bridges that connect at least four contiguous vertebra,” he continued.
“The bridges are usually right-sided and usually the intervertebral spaces are spared. Classically there is no involvement of the sacroiliac joints, although there are some changes that might involve the sacroiliac joints but in a different manner than in inflammatory sacroiliitis.”
DISH was originally thought to be a pain syndrome, which has “not played out,” Dr. Regan noted in her interview. While there may be people who experience pain as a result of DISH, most cases are asymptomatic and usually picked up incidentally on a chest x-ray or CT scan.
“It’s something that’s not obvious,” she said. One of the main problems it can cause is stiffness and lack of mobility in the spine and this can lead to quite severe fractures in some cases, such as during a car accident. Hence spinal surgeons and other orthopedic specialists, such as Dr. Regan, have also taken an interest in the condition.
“Apart from the thoracic spine, DISH may also involve the cervical spine; there have been many reports about difficulty in swallowing, breathing, and in the lumbar spine, spinal stenosis and so forth,” Dr. Mader said. The differential diagnosis includes ankylosing spondylitis, although there is some evidence that the two can coexist.
“The diagnosis depends on the alertness of the examining physician,” he added, noting that rheumatologists and other specialists would be “very aware of this condition” and “sensitive to changes that we see when we examine these patients.”
DISH and heightened cardiovascular risk
Previous work by Dr. Mader and associates has shown that people with DISH are more often affected by the metabolic syndrome than are those without DISH. The cross-sectional study had excluded those with preexisting CVD and found that people with DISH had a significantly higher Framingham Risk Score, compared with a control group of people with osteoarthritis and no DISH (P = .004), which in turn meant they had a significantly (P = .007) higher 10-year risk for developing CVD.
The aim of their most recent study was to compare the actual rate of CV events in 2016 versus those predicted by the Framingham Risk Score in 2006. To do this, they compared the available electronic medical records of 45 individuals with DISH and 47 without it.
The results showed that almost 39% of people with DISH had developed CVD, whereas the Framingham Risk Score had estimated that just under 27% would develop CVD.
For every 1% increase in the CVD risk calculated by the Framingham Risk Score, the odds of CVD increased by 4% in the DISH group versus the control group (P = .02).
While there was a significant (P < .003) difference in the Framingham Risk Score between the DISH and control groups in 2006 (28.6% vs. 17.8%), there was no overall statistical difference (P = .2) in the composite CVD outcome (38.8% vs. 25.5%) 10 years later, as calculated by the revised Framingham Risk Score, which included MI, cerebrovascular accident, transient ischemic attack, peripheral artery disease, and heart failure with preserved ejection fraction.
“We are dealing with patients who are in their 70s. So, it is expected that this group of patients will be more often affected by cardiovascular disease” than younger individuals, Dr. Mader observed. That said, the study’s findings “confirm the theory that patients with DISH have a high likelihood of developing cardiovascular disease,” he added, acknowledging that it was only the risk for MI that was statistically significantly higher in people with DISH than in the controls.
DISH and coronary artery calcification
“It might be even more interesting to have a different control population that had no osteoarthritis,” Dr. Regan observed.
As the associate director of the COPDGene study, Dr. Regan has access to data collected from a large cohort of people with chronic obstructive pulmonary disease (COPD; n = 2,728), around 13% of whom were identified as having DISH in one recent study.
In that study, the presence of DISH versus no DISH was associated with a 37% higher risk for having coronary artery calcification (CAC) – a marker for atherosclerosis and cardiovascular disease. Two-thirds of people with DISH had CAC, compared with 46.9% of those without DISH (P < .001). The prevalence of DISH was 8.8% in those without CAC, 12.8% in those with a CAC score of 1-100, 20% in those with a CAC score of 100-400, and 24.7% in those with a CAC score of more than 400, which is associated with a very high risk for coronary artery disease.
Dr. Regan observed that information on heart attacks and strokes were collected within the COPDGene study, so it would be possible to look at cardiovascular risk in their patients with DISH and confirm the findings of Mader and colleagues.
“I think the most important thing is recognizing that there are things going on in the spine that are important to people’s general health,” Dr. Regan said.
Dr. Mader noted: “It makes sense that patients with DISH should be more meticulously followed for at least the traditional risk factors and better treated because they are at a higher risk for these events.”
The study received no financial support. Neither Dr. Mader nor Dr. Regan had any conflicts of interest to disclose.
SOURCE: Glick K et al. Arthritis Res Ther. 2020. doi: 10.1186/s13075-020-02278-w.
More people with diffuse idiopathic skeletal hyperostosis (DISH) develop cardiovascular disease (CVD) than is predicted by the Framingham Risk Score, results of an observational study have shown.
Notably, a higher rate of myocardial infarction (MI) was seen in those with DISH than in those without DISH over the 10-year follow-up period (24.4% vs. 4.3%; P = .0055).
“We propose more scrutiny is warranted in evaluating CV risk in these patients, more demanding treatment target goals should be established, and as a result, earlier and more aggressive preventive medical interventions instituted,” corresponding author Reuven Mader, MD, and associates wrote in Arthritis Research & Therapy.
“What Mader’s study is pointing out is that it’s worth the radiologist reporting [DISH],” Elizabeth A. Regan, MD, PhD, from the National Jewish Health Center in Denver, said in an interview.
DISH on a chest x-ray or CT scan should be another “red flag to be even more attentive to cardiovascular risk,” she added, particularly because studies have shown that people with DISH tend to be obese, have metabolic syndrome, or diabetes – all of which independently increase their risk for cardiovascular disease.
An old condition often found by accident
Physicians have known about DISH for many years, Dr. Mader of Ha’Emek Medical Center in Afula, Israel, observed in an interview. Historical evidence suggests it was present more than a thousand years ago, but it wasn’t until the 1950s that it gained scientific interest. Originally coined Forestier’s disease, it was renamed DISH in the late 1960s following the realization that it was not limited to the spine.
“It is a condition which is characterized by new bone formation,” Dr. Mader explained. This new bone formation has some predilection for the entheses – the tendons, ligaments, or joint capsules, that attach to the bone.
“Diagnosis of the disease is based mainly on radiographs, especially of the thoracic spine, and it requires the formation of bridges that connect at least four contiguous vertebra,” he continued.
“The bridges are usually right-sided and usually the intervertebral spaces are spared. Classically there is no involvement of the sacroiliac joints, although there are some changes that might involve the sacroiliac joints but in a different manner than in inflammatory sacroiliitis.”
DISH was originally thought to be a pain syndrome, which has “not played out,” Dr. Regan noted in her interview. While there may be people who experience pain as a result of DISH, most cases are asymptomatic and usually picked up incidentally on a chest x-ray or CT scan.
“It’s something that’s not obvious,” she said. One of the main problems it can cause is stiffness and lack of mobility in the spine and this can lead to quite severe fractures in some cases, such as during a car accident. Hence spinal surgeons and other orthopedic specialists, such as Dr. Regan, have also taken an interest in the condition.
“Apart from the thoracic spine, DISH may also involve the cervical spine; there have been many reports about difficulty in swallowing, breathing, and in the lumbar spine, spinal stenosis and so forth,” Dr. Mader said. The differential diagnosis includes ankylosing spondylitis, although there is some evidence that the two can coexist.
“The diagnosis depends on the alertness of the examining physician,” he added, noting that rheumatologists and other specialists would be “very aware of this condition” and “sensitive to changes that we see when we examine these patients.”
DISH and heightened cardiovascular risk
Previous work by Dr. Mader and associates has shown that people with DISH are more often affected by the metabolic syndrome than are those without DISH. The cross-sectional study had excluded those with preexisting CVD and found that people with DISH had a significantly higher Framingham Risk Score, compared with a control group of people with osteoarthritis and no DISH (P = .004), which in turn meant they had a significantly (P = .007) higher 10-year risk for developing CVD.
The aim of their most recent study was to compare the actual rate of CV events in 2016 versus those predicted by the Framingham Risk Score in 2006. To do this, they compared the available electronic medical records of 45 individuals with DISH and 47 without it.
The results showed that almost 39% of people with DISH had developed CVD, whereas the Framingham Risk Score had estimated that just under 27% would develop CVD.
For every 1% increase in the CVD risk calculated by the Framingham Risk Score, the odds of CVD increased by 4% in the DISH group versus the control group (P = .02).
While there was a significant (P < .003) difference in the Framingham Risk Score between the DISH and control groups in 2006 (28.6% vs. 17.8%), there was no overall statistical difference (P = .2) in the composite CVD outcome (38.8% vs. 25.5%) 10 years later, as calculated by the revised Framingham Risk Score, which included MI, cerebrovascular accident, transient ischemic attack, peripheral artery disease, and heart failure with preserved ejection fraction.
“We are dealing with patients who are in their 70s. So, it is expected that this group of patients will be more often affected by cardiovascular disease” than younger individuals, Dr. Mader observed. That said, the study’s findings “confirm the theory that patients with DISH have a high likelihood of developing cardiovascular disease,” he added, acknowledging that it was only the risk for MI that was statistically significantly higher in people with DISH than in the controls.
DISH and coronary artery calcification
“It might be even more interesting to have a different control population that had no osteoarthritis,” Dr. Regan observed.
As the associate director of the COPDGene study, Dr. Regan has access to data collected from a large cohort of people with chronic obstructive pulmonary disease (COPD; n = 2,728), around 13% of whom were identified as having DISH in one recent study.
In that study, the presence of DISH versus no DISH was associated with a 37% higher risk for having coronary artery calcification (CAC) – a marker for atherosclerosis and cardiovascular disease. Two-thirds of people with DISH had CAC, compared with 46.9% of those without DISH (P < .001). The prevalence of DISH was 8.8% in those without CAC, 12.8% in those with a CAC score of 1-100, 20% in those with a CAC score of 100-400, and 24.7% in those with a CAC score of more than 400, which is associated with a very high risk for coronary artery disease.
Dr. Regan observed that information on heart attacks and strokes were collected within the COPDGene study, so it would be possible to look at cardiovascular risk in their patients with DISH and confirm the findings of Mader and colleagues.
“I think the most important thing is recognizing that there are things going on in the spine that are important to people’s general health,” Dr. Regan said.
Dr. Mader noted: “It makes sense that patients with DISH should be more meticulously followed for at least the traditional risk factors and better treated because they are at a higher risk for these events.”
The study received no financial support. Neither Dr. Mader nor Dr. Regan had any conflicts of interest to disclose.
SOURCE: Glick K et al. Arthritis Res Ther. 2020. doi: 10.1186/s13075-020-02278-w.
More people with diffuse idiopathic skeletal hyperostosis (DISH) develop cardiovascular disease (CVD) than is predicted by the Framingham Risk Score, results of an observational study have shown.
Notably, a higher rate of myocardial infarction (MI) was seen in those with DISH than in those without DISH over the 10-year follow-up period (24.4% vs. 4.3%; P = .0055).
“We propose more scrutiny is warranted in evaluating CV risk in these patients, more demanding treatment target goals should be established, and as a result, earlier and more aggressive preventive medical interventions instituted,” corresponding author Reuven Mader, MD, and associates wrote in Arthritis Research & Therapy.
“What Mader’s study is pointing out is that it’s worth the radiologist reporting [DISH],” Elizabeth A. Regan, MD, PhD, from the National Jewish Health Center in Denver, said in an interview.
DISH on a chest x-ray or CT scan should be another “red flag to be even more attentive to cardiovascular risk,” she added, particularly because studies have shown that people with DISH tend to be obese, have metabolic syndrome, or diabetes – all of which independently increase their risk for cardiovascular disease.
An old condition often found by accident
Physicians have known about DISH for many years, Dr. Mader of Ha’Emek Medical Center in Afula, Israel, observed in an interview. Historical evidence suggests it was present more than a thousand years ago, but it wasn’t until the 1950s that it gained scientific interest. Originally coined Forestier’s disease, it was renamed DISH in the late 1960s following the realization that it was not limited to the spine.
“It is a condition which is characterized by new bone formation,” Dr. Mader explained. This new bone formation has some predilection for the entheses – the tendons, ligaments, or joint capsules, that attach to the bone.
“Diagnosis of the disease is based mainly on radiographs, especially of the thoracic spine, and it requires the formation of bridges that connect at least four contiguous vertebra,” he continued.
“The bridges are usually right-sided and usually the intervertebral spaces are spared. Classically there is no involvement of the sacroiliac joints, although there are some changes that might involve the sacroiliac joints but in a different manner than in inflammatory sacroiliitis.”
DISH was originally thought to be a pain syndrome, which has “not played out,” Dr. Regan noted in her interview. While there may be people who experience pain as a result of DISH, most cases are asymptomatic and usually picked up incidentally on a chest x-ray or CT scan.
“It’s something that’s not obvious,” she said. One of the main problems it can cause is stiffness and lack of mobility in the spine and this can lead to quite severe fractures in some cases, such as during a car accident. Hence spinal surgeons and other orthopedic specialists, such as Dr. Regan, have also taken an interest in the condition.
“Apart from the thoracic spine, DISH may also involve the cervical spine; there have been many reports about difficulty in swallowing, breathing, and in the lumbar spine, spinal stenosis and so forth,” Dr. Mader said. The differential diagnosis includes ankylosing spondylitis, although there is some evidence that the two can coexist.
“The diagnosis depends on the alertness of the examining physician,” he added, noting that rheumatologists and other specialists would be “very aware of this condition” and “sensitive to changes that we see when we examine these patients.”
DISH and heightened cardiovascular risk
Previous work by Dr. Mader and associates has shown that people with DISH are more often affected by the metabolic syndrome than are those without DISH. The cross-sectional study had excluded those with preexisting CVD and found that people with DISH had a significantly higher Framingham Risk Score, compared with a control group of people with osteoarthritis and no DISH (P = .004), which in turn meant they had a significantly (P = .007) higher 10-year risk for developing CVD.
The aim of their most recent study was to compare the actual rate of CV events in 2016 versus those predicted by the Framingham Risk Score in 2006. To do this, they compared the available electronic medical records of 45 individuals with DISH and 47 without it.
The results showed that almost 39% of people with DISH had developed CVD, whereas the Framingham Risk Score had estimated that just under 27% would develop CVD.
For every 1% increase in the CVD risk calculated by the Framingham Risk Score, the odds of CVD increased by 4% in the DISH group versus the control group (P = .02).
While there was a significant (P < .003) difference in the Framingham Risk Score between the DISH and control groups in 2006 (28.6% vs. 17.8%), there was no overall statistical difference (P = .2) in the composite CVD outcome (38.8% vs. 25.5%) 10 years later, as calculated by the revised Framingham Risk Score, which included MI, cerebrovascular accident, transient ischemic attack, peripheral artery disease, and heart failure with preserved ejection fraction.
“We are dealing with patients who are in their 70s. So, it is expected that this group of patients will be more often affected by cardiovascular disease” than younger individuals, Dr. Mader observed. That said, the study’s findings “confirm the theory that patients with DISH have a high likelihood of developing cardiovascular disease,” he added, acknowledging that it was only the risk for MI that was statistically significantly higher in people with DISH than in the controls.
DISH and coronary artery calcification
“It might be even more interesting to have a different control population that had no osteoarthritis,” Dr. Regan observed.
As the associate director of the COPDGene study, Dr. Regan has access to data collected from a large cohort of people with chronic obstructive pulmonary disease (COPD; n = 2,728), around 13% of whom were identified as having DISH in one recent study.
In that study, the presence of DISH versus no DISH was associated with a 37% higher risk for having coronary artery calcification (CAC) – a marker for atherosclerosis and cardiovascular disease. Two-thirds of people with DISH had CAC, compared with 46.9% of those without DISH (P < .001). The prevalence of DISH was 8.8% in those without CAC, 12.8% in those with a CAC score of 1-100, 20% in those with a CAC score of 100-400, and 24.7% in those with a CAC score of more than 400, which is associated with a very high risk for coronary artery disease.
Dr. Regan observed that information on heart attacks and strokes were collected within the COPDGene study, so it would be possible to look at cardiovascular risk in their patients with DISH and confirm the findings of Mader and colleagues.
“I think the most important thing is recognizing that there are things going on in the spine that are important to people’s general health,” Dr. Regan said.
Dr. Mader noted: “It makes sense that patients with DISH should be more meticulously followed for at least the traditional risk factors and better treated because they are at a higher risk for these events.”
The study received no financial support. Neither Dr. Mader nor Dr. Regan had any conflicts of interest to disclose.
SOURCE: Glick K et al. Arthritis Res Ther. 2020. doi: 10.1186/s13075-020-02278-w.
FROM ARTHRITIS RESEARCH & THERAPY