User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Patient aggression against receptionists demands protocols
“I’ve been hit in the head by a walking stick,” a primary care receptionist reported.
“A mother came in and was screaming and swearing at me because she couldn’t get an appointment for her daughters,” another receptionist reported.
“I’ve had people throw a bag of syringes at me because we don’t accept syringes,” said another.
Reports such as these are part of the literature supporting a review that finds patient aggression against receptionists is a serious safety concern for primary care offices and affects delivery of health care.
The review was published online in the BMJ’s Family Medicine and Community Health journal.
“Receptionists in general practice deserve evidence-based measures to improve their working conditions and well-being,” say the authors, led by Fiona Willer, PhD, of the Centre for Community Health and Wellbeing at the University of Queensland, Brisbane, Australia.
Though the study looked primarily at European and Australian practices, physicians in the United States say the incidences are familiar.
Cause often lack of access
Dr. Willer and colleagues point out that the root cause of patient regression is typically related to operational factors, such as inefficient scheduling or lack of access to the medical providers.
“However, reception staff are placed in the unenviable position of having to deal with the aftermath of the poor function of these systems without having the status or autonomy to overhaul them,” the authors note.
Authors analyzed 20 studies on aggression against receptionists.
Among the findings:
- All studies reported that patient hostility and verbal abuse of receptionists “was a frequent, routine, and relatively unavoidable occurrence in general practice.”
- Nine studies reported acts of physical violence toward receptionists, with all reporting that physical abuse occurred much less frequently than verbal abuse.
- Some acts were very severe, including being hit, shaken, held at gunpoint, stalked, and threatened with a razorblade.
The studies also discussed ways to prevent potential aggression or react to it, including:
- Regular staff training for managing patient aggression.
- Designing clinics with “safe rooms” and “cool down” spaces.
- Providing clear acrylic shields between receptionists and patients.
- Developing formal policy/procedure/protocol/action guides relating to management of patients.
Behavior can interrupt health care delivery
Carrie Janiski, DO, regional medical director at Golden Valley Health Centers in California, who was not part of the review, said she has seen the aggressive behavior the authors document in her practice’s lobby, “including yelling, name-calling, and threatening language or physical behavior.”
The instances disrupt health care delivery to the patient, who is often in crisis, and all patients and staff in the clinic, she said.
“The patient needs help and the aggressive way they are seeking it could cause harm to others or prevent them from receiving all the help they need,” she said.
She says in practices she has worked in, some effective mitigation strategies have included open-access scheduling, increased walk-in availability for appointments, de-escalation training for front-line staff, and office and exam room layout designed for safety.
She added that incident review is important and should include a process for patient dismissal from the practice.
Dustin Arnold, DO, an internal medicine specialist and chief medical officer at UnityPoint Health-St. Luke’s Hospital, Cedar Rapids, IA, said he agrees with the authors on the urgency for action.
“This is an urgent concern for practices across the country. Your receptionist is the face of your practice, and you should invest in them,” said Dr. Arnold, who was not part of the review.
He said he has seen “verbal abuse and generalized incivility” from patients against receptionists in practices where he has worked.
He said the measure the authors list that he thinks is most effective is staff de-escalation training.
“However, the best preventative measure is for the physician to be on time and minimize cancellation of appointments,” he said. “These are the two primary triggers of a patient becoming disruptive.”
He said his practice has installed a panic button at the front desk and built an alert into the electronic health record indicating that a patient has shown disruptive behavior in the past.
The authors conclude: “Staff training and protocols to manage patient aggression and ongoing structured staff support should be considered essential in general practice. Evidence-based strategies to prevent, manage, and mitigate the harms of patient aggression towards general practice reception staff are urgently needed.”
The authors and Dr. Janiski and Dr. Arnold declared no relevant financial relationships.
“I’ve been hit in the head by a walking stick,” a primary care receptionist reported.
“A mother came in and was screaming and swearing at me because she couldn’t get an appointment for her daughters,” another receptionist reported.
“I’ve had people throw a bag of syringes at me because we don’t accept syringes,” said another.
Reports such as these are part of the literature supporting a review that finds patient aggression against receptionists is a serious safety concern for primary care offices and affects delivery of health care.
The review was published online in the BMJ’s Family Medicine and Community Health journal.
“Receptionists in general practice deserve evidence-based measures to improve their working conditions and well-being,” say the authors, led by Fiona Willer, PhD, of the Centre for Community Health and Wellbeing at the University of Queensland, Brisbane, Australia.
Though the study looked primarily at European and Australian practices, physicians in the United States say the incidences are familiar.
Cause often lack of access
Dr. Willer and colleagues point out that the root cause of patient regression is typically related to operational factors, such as inefficient scheduling or lack of access to the medical providers.
“However, reception staff are placed in the unenviable position of having to deal with the aftermath of the poor function of these systems without having the status or autonomy to overhaul them,” the authors note.
Authors analyzed 20 studies on aggression against receptionists.
Among the findings:
- All studies reported that patient hostility and verbal abuse of receptionists “was a frequent, routine, and relatively unavoidable occurrence in general practice.”
- Nine studies reported acts of physical violence toward receptionists, with all reporting that physical abuse occurred much less frequently than verbal abuse.
- Some acts were very severe, including being hit, shaken, held at gunpoint, stalked, and threatened with a razorblade.
The studies also discussed ways to prevent potential aggression or react to it, including:
- Regular staff training for managing patient aggression.
- Designing clinics with “safe rooms” and “cool down” spaces.
- Providing clear acrylic shields between receptionists and patients.
- Developing formal policy/procedure/protocol/action guides relating to management of patients.
Behavior can interrupt health care delivery
Carrie Janiski, DO, regional medical director at Golden Valley Health Centers in California, who was not part of the review, said she has seen the aggressive behavior the authors document in her practice’s lobby, “including yelling, name-calling, and threatening language or physical behavior.”
The instances disrupt health care delivery to the patient, who is often in crisis, and all patients and staff in the clinic, she said.
“The patient needs help and the aggressive way they are seeking it could cause harm to others or prevent them from receiving all the help they need,” she said.
She says in practices she has worked in, some effective mitigation strategies have included open-access scheduling, increased walk-in availability for appointments, de-escalation training for front-line staff, and office and exam room layout designed for safety.
She added that incident review is important and should include a process for patient dismissal from the practice.
Dustin Arnold, DO, an internal medicine specialist and chief medical officer at UnityPoint Health-St. Luke’s Hospital, Cedar Rapids, IA, said he agrees with the authors on the urgency for action.
“This is an urgent concern for practices across the country. Your receptionist is the face of your practice, and you should invest in them,” said Dr. Arnold, who was not part of the review.
He said he has seen “verbal abuse and generalized incivility” from patients against receptionists in practices where he has worked.
He said the measure the authors list that he thinks is most effective is staff de-escalation training.
“However, the best preventative measure is for the physician to be on time and minimize cancellation of appointments,” he said. “These are the two primary triggers of a patient becoming disruptive.”
He said his practice has installed a panic button at the front desk and built an alert into the electronic health record indicating that a patient has shown disruptive behavior in the past.
The authors conclude: “Staff training and protocols to manage patient aggression and ongoing structured staff support should be considered essential in general practice. Evidence-based strategies to prevent, manage, and mitigate the harms of patient aggression towards general practice reception staff are urgently needed.”
The authors and Dr. Janiski and Dr. Arnold declared no relevant financial relationships.
“I’ve been hit in the head by a walking stick,” a primary care receptionist reported.
“A mother came in and was screaming and swearing at me because she couldn’t get an appointment for her daughters,” another receptionist reported.
“I’ve had people throw a bag of syringes at me because we don’t accept syringes,” said another.
Reports such as these are part of the literature supporting a review that finds patient aggression against receptionists is a serious safety concern for primary care offices and affects delivery of health care.
The review was published online in the BMJ’s Family Medicine and Community Health journal.
“Receptionists in general practice deserve evidence-based measures to improve their working conditions and well-being,” say the authors, led by Fiona Willer, PhD, of the Centre for Community Health and Wellbeing at the University of Queensland, Brisbane, Australia.
Though the study looked primarily at European and Australian practices, physicians in the United States say the incidences are familiar.
Cause often lack of access
Dr. Willer and colleagues point out that the root cause of patient regression is typically related to operational factors, such as inefficient scheduling or lack of access to the medical providers.
“However, reception staff are placed in the unenviable position of having to deal with the aftermath of the poor function of these systems without having the status or autonomy to overhaul them,” the authors note.
Authors analyzed 20 studies on aggression against receptionists.
Among the findings:
- All studies reported that patient hostility and verbal abuse of receptionists “was a frequent, routine, and relatively unavoidable occurrence in general practice.”
- Nine studies reported acts of physical violence toward receptionists, with all reporting that physical abuse occurred much less frequently than verbal abuse.
- Some acts were very severe, including being hit, shaken, held at gunpoint, stalked, and threatened with a razorblade.
The studies also discussed ways to prevent potential aggression or react to it, including:
- Regular staff training for managing patient aggression.
- Designing clinics with “safe rooms” and “cool down” spaces.
- Providing clear acrylic shields between receptionists and patients.
- Developing formal policy/procedure/protocol/action guides relating to management of patients.
Behavior can interrupt health care delivery
Carrie Janiski, DO, regional medical director at Golden Valley Health Centers in California, who was not part of the review, said she has seen the aggressive behavior the authors document in her practice’s lobby, “including yelling, name-calling, and threatening language or physical behavior.”
The instances disrupt health care delivery to the patient, who is often in crisis, and all patients and staff in the clinic, she said.
“The patient needs help and the aggressive way they are seeking it could cause harm to others or prevent them from receiving all the help they need,” she said.
She says in practices she has worked in, some effective mitigation strategies have included open-access scheduling, increased walk-in availability for appointments, de-escalation training for front-line staff, and office and exam room layout designed for safety.
She added that incident review is important and should include a process for patient dismissal from the practice.
Dustin Arnold, DO, an internal medicine specialist and chief medical officer at UnityPoint Health-St. Luke’s Hospital, Cedar Rapids, IA, said he agrees with the authors on the urgency for action.
“This is an urgent concern for practices across the country. Your receptionist is the face of your practice, and you should invest in them,” said Dr. Arnold, who was not part of the review.
He said he has seen “verbal abuse and generalized incivility” from patients against receptionists in practices where he has worked.
He said the measure the authors list that he thinks is most effective is staff de-escalation training.
“However, the best preventative measure is for the physician to be on time and minimize cancellation of appointments,” he said. “These are the two primary triggers of a patient becoming disruptive.”
He said his practice has installed a panic button at the front desk and built an alert into the electronic health record indicating that a patient has shown disruptive behavior in the past.
The authors conclude: “Staff training and protocols to manage patient aggression and ongoing structured staff support should be considered essential in general practice. Evidence-based strategies to prevent, manage, and mitigate the harms of patient aggression towards general practice reception staff are urgently needed.”
The authors and Dr. Janiski and Dr. Arnold declared no relevant financial relationships.
FROM FAMILY MEDICINE AND COMMUNITY HEALTH
High-dose vitamin D may cut risk for new atrial fibrillation
TOPLINE:
a post hoc analysis from a randomized trial conducted in Finland suggests.

METHODOLOGY:
- Observational studies have suggested that vitamin D deficiency is associated with increased risk for AFib, but few randomized trials have looked at the effect of vitamin D supplementation on AFib incidence in healthy people.
- The study, a post hoc analysis from a trial that explored the effects of vitamin D3 supplementation on incidence of cardiovascular diseases and cancer, included 2,495 vitamin D–sufficient healthy older adults, mean age 68.2 years, of whom 43% were women.
- Participants had been randomized to one of three groups in which they received vitamin D3 at either 1,600 IU/day or 3,200 IU/day, or placebo.
- Serum 25(OH)D3 concentrations were measured and data on incident AFib were gathered from national health records.
TAKEAWAY:
- Atrial fibrillation was diagnosed in 190 participants.
- Over a follow-up averaging 4.1 years, risk for incident AFib was reduced by 27% for participants who received the 1,600 IU/day dose, compared with placebo; hazard ratio, 0.73 (95% confidence interval, 0.52-1.02; P = .07), and by 32% for those in the 3,200 IU/day arm; HR, 0.68 (95% CI, 0.48-0.96; P = .03).
- The incident-AFib risk was reduced by 30% in a comparison of the two vitamin D groups combined versus the placebo group; HR, 0.70 (95% CI, 0.53-0.94; P = .02).
- After exclusion of 122 participants who reported being on antiarrhythmic medications at baseline, the 1,600 IU/day group showed a significant 27% reduction in risk for AF (95% CI, 4%-58%; P = .03) and the 3,200 IU/day group a nonsignificant 30% (95% CI, 5%-53%; P = .08) reduction in risk.
IN PRACTICE:
High-dose vitamin D3 supplementation may reduce incidence of AFib in a generally healthy, largely vitamin D–sufficient elderly population, the authors proposed. Additional controlled trials are needed, especially in diverse populations.
STUDY DETAILS:
The study was conducted by Jyrki K. Virtanen, PhD, University of Eastern Finland, Institute of Public Health and Clinical Nutrition, Kuopio, and colleagues. It was published in the American Heart Journal.
LIMITATIONS:
Atrial fibrillation was not prespecified as a primary outcome, and the results differ from those of other randomized controlled trials. Information on type of AFib (whether paroxysmal or nonparoxysmal, for example) wasn’t available nor were participants’ history of AFib. All participants were White and from Finland, limiting generalizability of the results.
DISCLOSURES:
The study was supported by the Academy of Finland, University of Eastern Finland, the Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and the Finnish Cultural Foundation. One coauthor disclosed receiving grants from the National Institutes of Health and Mars Edge. Another coauthor disclosed receipt of a grant from Orion. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
a post hoc analysis from a randomized trial conducted in Finland suggests.
METHODOLOGY:
- Observational studies have suggested that vitamin D deficiency is associated with increased risk for AFib, but few randomized trials have looked at the effect of vitamin D supplementation on AFib incidence in healthy people.
- The study, a post hoc analysis from a trial that explored the effects of vitamin D3 supplementation on incidence of cardiovascular diseases and cancer, included 2,495 vitamin D–sufficient healthy older adults, mean age 68.2 years, of whom 43% were women.
- Participants had been randomized to one of three groups in which they received vitamin D3 at either 1,600 IU/day or 3,200 IU/day, or placebo.
- Serum 25(OH)D3 concentrations were measured and data on incident AFib were gathered from national health records.
TAKEAWAY:
- Atrial fibrillation was diagnosed in 190 participants.
- Over a follow-up averaging 4.1 years, risk for incident AFib was reduced by 27% for participants who received the 1,600 IU/day dose, compared with placebo; hazard ratio, 0.73 (95% confidence interval, 0.52-1.02; P = .07), and by 32% for those in the 3,200 IU/day arm; HR, 0.68 (95% CI, 0.48-0.96; P = .03).
- The incident-AFib risk was reduced by 30% in a comparison of the two vitamin D groups combined versus the placebo group; HR, 0.70 (95% CI, 0.53-0.94; P = .02).
- After exclusion of 122 participants who reported being on antiarrhythmic medications at baseline, the 1,600 IU/day group showed a significant 27% reduction in risk for AF (95% CI, 4%-58%; P = .03) and the 3,200 IU/day group a nonsignificant 30% (95% CI, 5%-53%; P = .08) reduction in risk.
IN PRACTICE:
High-dose vitamin D3 supplementation may reduce incidence of AFib in a generally healthy, largely vitamin D–sufficient elderly population, the authors proposed. Additional controlled trials are needed, especially in diverse populations.
STUDY DETAILS:
The study was conducted by Jyrki K. Virtanen, PhD, University of Eastern Finland, Institute of Public Health and Clinical Nutrition, Kuopio, and colleagues. It was published in the American Heart Journal.
LIMITATIONS:
Atrial fibrillation was not prespecified as a primary outcome, and the results differ from those of other randomized controlled trials. Information on type of AFib (whether paroxysmal or nonparoxysmal, for example) wasn’t available nor were participants’ history of AFib. All participants were White and from Finland, limiting generalizability of the results.
DISCLOSURES:
The study was supported by the Academy of Finland, University of Eastern Finland, the Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and the Finnish Cultural Foundation. One coauthor disclosed receiving grants from the National Institutes of Health and Mars Edge. Another coauthor disclosed receipt of a grant from Orion. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
a post hoc analysis from a randomized trial conducted in Finland suggests.
METHODOLOGY:
- Observational studies have suggested that vitamin D deficiency is associated with increased risk for AFib, but few randomized trials have looked at the effect of vitamin D supplementation on AFib incidence in healthy people.
- The study, a post hoc analysis from a trial that explored the effects of vitamin D3 supplementation on incidence of cardiovascular diseases and cancer, included 2,495 vitamin D–sufficient healthy older adults, mean age 68.2 years, of whom 43% were women.
- Participants had been randomized to one of three groups in which they received vitamin D3 at either 1,600 IU/day or 3,200 IU/day, or placebo.
- Serum 25(OH)D3 concentrations were measured and data on incident AFib were gathered from national health records.
TAKEAWAY:
- Atrial fibrillation was diagnosed in 190 participants.
- Over a follow-up averaging 4.1 years, risk for incident AFib was reduced by 27% for participants who received the 1,600 IU/day dose, compared with placebo; hazard ratio, 0.73 (95% confidence interval, 0.52-1.02; P = .07), and by 32% for those in the 3,200 IU/day arm; HR, 0.68 (95% CI, 0.48-0.96; P = .03).
- The incident-AFib risk was reduced by 30% in a comparison of the two vitamin D groups combined versus the placebo group; HR, 0.70 (95% CI, 0.53-0.94; P = .02).
- After exclusion of 122 participants who reported being on antiarrhythmic medications at baseline, the 1,600 IU/day group showed a significant 27% reduction in risk for AF (95% CI, 4%-58%; P = .03) and the 3,200 IU/day group a nonsignificant 30% (95% CI, 5%-53%; P = .08) reduction in risk.
IN PRACTICE:
High-dose vitamin D3 supplementation may reduce incidence of AFib in a generally healthy, largely vitamin D–sufficient elderly population, the authors proposed. Additional controlled trials are needed, especially in diverse populations.
STUDY DETAILS:
The study was conducted by Jyrki K. Virtanen, PhD, University of Eastern Finland, Institute of Public Health and Clinical Nutrition, Kuopio, and colleagues. It was published in the American Heart Journal.
LIMITATIONS:
Atrial fibrillation was not prespecified as a primary outcome, and the results differ from those of other randomized controlled trials. Information on type of AFib (whether paroxysmal or nonparoxysmal, for example) wasn’t available nor were participants’ history of AFib. All participants were White and from Finland, limiting generalizability of the results.
DISCLOSURES:
The study was supported by the Academy of Finland, University of Eastern Finland, the Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and the Finnish Cultural Foundation. One coauthor disclosed receiving grants from the National Institutes of Health and Mars Edge. Another coauthor disclosed receipt of a grant from Orion. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.

Cardiorespiratory fitness linked to cancer risk, mortality?
TOPLINE:
a large Swedish cohort study suggests.
METHODOLOGY:
- A prospective cohort study included 177,709 Swedish men (mean age, 42; mean body mass index, 26 kg/m2) who completed an occupational health profile assessment and were followed for a mean of 9.6 years.
- CRF was assessed by determining maximal oxygen consumption during an aerobic fitness test, known as a submaximal Åstrand cycle ergometer test.
- Participants reported physical activity habits, lifestyle, and perceived health.
- Data on prostate, colon, and lung cancer incidence and mortality were derived from national registers.
- Outcomes from three higher CRF groups (low, > 25-35; moderate, > 35-45; high, > 45 mL/min per kg) were compared with those from the very low CRF group (25 mL/min per kg or less). Models were adjusted for various factors, including age, BMI, education, dietary habits, comorbidity, and smoking.
TAKEAWAY:
- During follow-up, investigators identified 1,918 prostate, 499 colon, and 283 lung cancer cases as well as 141 prostate, 207 lung, and 152 colon cancer deaths.
- In the fully adjusted model, higher CRF levels were associated with a significantly lower risk for colon cancer (hazard ratio, 0.72 for moderate; HR, 0.63 for high).
- In this model, higher CRF was also associated with a lower risk of death from prostate cancer (HR, 0.67 for low; HR, 0.57 for moderate; HR, 0.29 for high).
- For lung cancer mortality, only high CRF was associated with a significantly lower risk of death (HR, 0.41).
- An association between CRF and lung cancer incidence (HR, 0.99) and death (HR, 0.99) was only evident among adults aged 60 and older.
IN PRACTICE:
“The clinical implications of these findings further emphasize the importance of CRF for possibly reducing cancer incidence and mortality,” the authors concluded. “It is important for the general public to understand that higher-intensity [physical activity] has greater effects on CRF and is likely to be more protective against the risk of developing and dying from certain cancers.”
SOURCE:
The study was led by Elin Ekblom-Bak, PhD, from the Swedish School of Sport and Health Sciences, Stockholm. It was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by voluntary participation, inclusion of only employed individuals, and estimations of CRF via submaximal tests. Data on smoking status were not optimal and there was a small number of cancer cases and deaths.
DISCLOSURES:
Funding was provided by the Swedish Cancer Society. The authors have reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
a large Swedish cohort study suggests.
METHODOLOGY:
- A prospective cohort study included 177,709 Swedish men (mean age, 42; mean body mass index, 26 kg/m2) who completed an occupational health profile assessment and were followed for a mean of 9.6 years.
- CRF was assessed by determining maximal oxygen consumption during an aerobic fitness test, known as a submaximal Åstrand cycle ergometer test.
- Participants reported physical activity habits, lifestyle, and perceived health.
- Data on prostate, colon, and lung cancer incidence and mortality were derived from national registers.
- Outcomes from three higher CRF groups (low, > 25-35; moderate, > 35-45; high, > 45 mL/min per kg) were compared with those from the very low CRF group (25 mL/min per kg or less). Models were adjusted for various factors, including age, BMI, education, dietary habits, comorbidity, and smoking.
TAKEAWAY:
- During follow-up, investigators identified 1,918 prostate, 499 colon, and 283 lung cancer cases as well as 141 prostate, 207 lung, and 152 colon cancer deaths.
- In the fully adjusted model, higher CRF levels were associated with a significantly lower risk for colon cancer (hazard ratio, 0.72 for moderate; HR, 0.63 for high).
- In this model, higher CRF was also associated with a lower risk of death from prostate cancer (HR, 0.67 for low; HR, 0.57 for moderate; HR, 0.29 for high).
- For lung cancer mortality, only high CRF was associated with a significantly lower risk of death (HR, 0.41).
- An association between CRF and lung cancer incidence (HR, 0.99) and death (HR, 0.99) was only evident among adults aged 60 and older.
IN PRACTICE:
“The clinical implications of these findings further emphasize the importance of CRF for possibly reducing cancer incidence and mortality,” the authors concluded. “It is important for the general public to understand that higher-intensity [physical activity] has greater effects on CRF and is likely to be more protective against the risk of developing and dying from certain cancers.”
SOURCE:
The study was led by Elin Ekblom-Bak, PhD, from the Swedish School of Sport and Health Sciences, Stockholm. It was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by voluntary participation, inclusion of only employed individuals, and estimations of CRF via submaximal tests. Data on smoking status were not optimal and there was a small number of cancer cases and deaths.
DISCLOSURES:
Funding was provided by the Swedish Cancer Society. The authors have reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
a large Swedish cohort study suggests.
METHODOLOGY:
- A prospective cohort study included 177,709 Swedish men (mean age, 42; mean body mass index, 26 kg/m2) who completed an occupational health profile assessment and were followed for a mean of 9.6 years.
- CRF was assessed by determining maximal oxygen consumption during an aerobic fitness test, known as a submaximal Åstrand cycle ergometer test.
- Participants reported physical activity habits, lifestyle, and perceived health.
- Data on prostate, colon, and lung cancer incidence and mortality were derived from national registers.
- Outcomes from three higher CRF groups (low, > 25-35; moderate, > 35-45; high, > 45 mL/min per kg) were compared with those from the very low CRF group (25 mL/min per kg or less). Models were adjusted for various factors, including age, BMI, education, dietary habits, comorbidity, and smoking.
TAKEAWAY:
- During follow-up, investigators identified 1,918 prostate, 499 colon, and 283 lung cancer cases as well as 141 prostate, 207 lung, and 152 colon cancer deaths.
- In the fully adjusted model, higher CRF levels were associated with a significantly lower risk for colon cancer (hazard ratio, 0.72 for moderate; HR, 0.63 for high).
- In this model, higher CRF was also associated with a lower risk of death from prostate cancer (HR, 0.67 for low; HR, 0.57 for moderate; HR, 0.29 for high).
- For lung cancer mortality, only high CRF was associated with a significantly lower risk of death (HR, 0.41).
- An association between CRF and lung cancer incidence (HR, 0.99) and death (HR, 0.99) was only evident among adults aged 60 and older.
IN PRACTICE:
“The clinical implications of these findings further emphasize the importance of CRF for possibly reducing cancer incidence and mortality,” the authors concluded. “It is important for the general public to understand that higher-intensity [physical activity] has greater effects on CRF and is likely to be more protective against the risk of developing and dying from certain cancers.”
SOURCE:
The study was led by Elin Ekblom-Bak, PhD, from the Swedish School of Sport and Health Sciences, Stockholm. It was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by voluntary participation, inclusion of only employed individuals, and estimations of CRF via submaximal tests. Data on smoking status were not optimal and there was a small number of cancer cases and deaths.
DISCLOSURES:
Funding was provided by the Swedish Cancer Society. The authors have reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
PCPs key to heart failure care after discharge
Madeline Sterling, MD, knew something was wrong when she heard her patient’s voice on the phone. The patient was breathing too fast and sounded fatigued. Like many people with heart failure, this patient had several comorbidities: diabetes, high blood pressure, and cancer, which was in remission.
The patient had been in and out of the hospital several times and was afraid of going back, but Dr. Sterling, a primary care physician, advised her that it was the safe thing to do.
During the woman’s stay, the inpatient cardiology team called Dr. Sterling to provide status updates and ask for input. When the patient was discharged, Dr. Sterling received information on what medicines had been changed and scheduled follow-up care within 10 days. Dr. Sterling, who’d cared for the woman for many years, called her family, her home health aide, and another caregiver to discuss the plan.
“When you know these patients really well, it’s helpful,” Dr. Sterling, a professor of medicine at Weill Cornell Medicine, New York, said. Primary care clinicians have “an appreciation for how all these conditions fit together, how the medicines fit together, and how to put that patient’s priorities at the front of the equation.”
Research has shown that follow-up care within 7-10 days after discharge, especially for patients with heart failure, can prevent hospital readmissions. Patients’ health can change rapidly following discharge: They may start retaining fluid or may not know how to maintain a low-sodium diet, or they might have trouble obtaining medication. Primary care clinicians spot these early warning signs in follow-up visits.
Heart failure affects more than 6 million adults in the United States, according to the Centers for Disease Control and Prevention. The condition is a common cause of hospital readmissions within 30 days of discharge, according to research published by the American Heart Association.
Patients with heart failure are particularly challenging to care for because of comorbidities.
“They’re a very, very sick group of patients that are very difficult to manage,” said Noah Moss, MD, an advanced heart failure and transplant cardiologist at Mount Sinai Hospital, New York.
But patients do not always receive the follow-up care they need, some studies have found.
Right drugs at the right time
Kelly Axsom, MD, a cardiologist at the Columbia University Medical Center, New York, and director of the centralized heart failure management program at the New York–Presbyterian Hospital System, called the primary care clinician the “captain of the ship,” ensuring that medications are reconciled and providing education about what to eat after discharge.
“It’s actually pretty complicated to go from being in the hospital to being at home,” Dr. Axsom said. “There are often many medication changes, there are lots of instructions that are told to you as a patient that are hard to remember.”
A patient’s weight might fluctuate in the days following discharge because the dose of diuretics might be too low or too high and need to be adjusted, according to Ishani Ganguli, MD, MPH, an assistant professor of medicine and a general internist in the Division of General Internal Medicine and Primary Care at Harvard Medical School and Brigham and Women’s Hospital, Boston.
K. Melissa Hayes, DNP, ANP-BC, CHFN, an assistant professor in the adult gerontology primary care program at the Vanderbilt University School of Nursing, Nashville, Tenn., recalled one patient who was given a months’ worth of medications following his discharge from the hospital.
“He was given expensive medications he couldn’t afford and not any refills or how to get those medications,” Dr. Hayes said.
Sometimes patients have no way to get to the pharmacy, or their pharmacy doesn’t have the medication they need, or their insurance doesn’t cover the drugs.
“The average patient is on at least six medications for heart failure, maybe even seven, and then that’s not including all their other medications,” Dr. Hayes said. “That can be a lot for people to keep up with.”
Dr. Hayes talks to her patients with heart failure about what drugs they have been prescribed and what medications they require more of, and she deprescribes any that are duplicative.
Helping patients understand why they are taking each drug encourages them to stick to the regimen. Diuretics, for example, can lead to frequent urination. If patients are unable to take regular bathroom breaks, they may be tempted to stop using the medication – a potentially catastrophic mistake.
“Often I have patients say, ‘Nobody ever explained it to me that way,’ ” Dr. Hayes said. “Someone can have a PhD but not understand their medications.”
Clinicians also can alert patients to commonly used medications that can worsen heart failure, such as diabetes drugs and over-the-counter medications such as ibuprofen.
Patients should be prescribed a combination of four recommended medications. But several studies have found that clinicians often fail to achieve the target doses for those medications. The use of guideline-directed medications reduces mortality and hospitalization rates, according to multiple clinical trials.
Eyes and ears on the patient
Once home, patients must stick to the right diet, weigh themselves every day, and monitor their blood pressure. But changing behaviors can be a struggle.
“Being seen quickly within a couple of days of discharge, you can catch things,” said Dr. Hayes, who has edited a book on managing patients with heart failure in primary care.
“It’s an opportunity to see how they’re doing at home, make sure they have their medications, make sure there’s been no misunderstanding or miscommunication about what they’re supposed to be doing at home,” says Marc Itskowitz, MD, a primary care physician affiliated with Allegheny General Hospital, Pittsburgh.
Ideally, a record that readily integrates information from wearables – such as blood pressure and weight – would make it easier to spot abnormalities, Dr. Itskowtiz said. “I think we’re still in the infancy of the electronic health record,” he said.
Ensuring that follow-up visits are as accessible as possible for patients is also important. Telehealth makes it easier for patients after they return home from the hospital, Dr. Itskowitz said.
More infrastructure
Another challenge of providing follow-up care for patients with heart failure is completing all the tasks a clinician must do within a 20-minute visit: an examination; education on the condition and medications; counseling on diet and exercise; coordination of medical equipment, such as a blood pressure cuff for home use; and making appointments with specialists.
“In the current system, additional support for primary care is needed so we can do all this,” Dr. Sterling said.
Staff at primary care clinics should be trained to answer calls from patients when they experience changes in their weight or are worried about other potential problems. “A lot of primary care practices are bare bones,” Dr. Hayes said, meaning they might not have the staff to field those calls. Educating patients as to when they should call their physician, especially after experiencing worsening symptoms, is also important.
Dr. Hayes suggests setting aside time in the schedule each week to see patients who have been recently discharged from the hospital. In the Cardiology and Vascular Clinic at Nashville General Hospital, Tenn., where she spends half a day each week, Dr. Hayes requests 30 minutes to see patients who have recently been discharged from hospital.
Even when the process goes smoothly, some patients will return to the hospital because of the progressive nature of heart failure, according to Dr. Hayes. Improving care following their hospitalization can keep these people from rapidly declining.
“Most patients with heart failure want to be taking care of the grandchildren or be able to enjoy family dinners together,” Dr. Axsom said. “I think anything we can do to help improve their quality of life is really important.”
Take-home
- See heart failure patients early after their discharge from hospital, ideally within 7-10 days.
- Make sure patients have access to the right medications at the right dosages and that they know why they’re taking them.
- Educate patients about the diet they should be following.
- Have a system to monitor patients’ symptoms and let them know when they should call.
A version of this article first appeared on Medscape.com.
Madeline Sterling, MD, knew something was wrong when she heard her patient’s voice on the phone. The patient was breathing too fast and sounded fatigued. Like many people with heart failure, this patient had several comorbidities: diabetes, high blood pressure, and cancer, which was in remission.
The patient had been in and out of the hospital several times and was afraid of going back, but Dr. Sterling, a primary care physician, advised her that it was the safe thing to do.
During the woman’s stay, the inpatient cardiology team called Dr. Sterling to provide status updates and ask for input. When the patient was discharged, Dr. Sterling received information on what medicines had been changed and scheduled follow-up care within 10 days. Dr. Sterling, who’d cared for the woman for many years, called her family, her home health aide, and another caregiver to discuss the plan.
“When you know these patients really well, it’s helpful,” Dr. Sterling, a professor of medicine at Weill Cornell Medicine, New York, said. Primary care clinicians have “an appreciation for how all these conditions fit together, how the medicines fit together, and how to put that patient’s priorities at the front of the equation.”
Research has shown that follow-up care within 7-10 days after discharge, especially for patients with heart failure, can prevent hospital readmissions. Patients’ health can change rapidly following discharge: They may start retaining fluid or may not know how to maintain a low-sodium diet, or they might have trouble obtaining medication. Primary care clinicians spot these early warning signs in follow-up visits.
Heart failure affects more than 6 million adults in the United States, according to the Centers for Disease Control and Prevention. The condition is a common cause of hospital readmissions within 30 days of discharge, according to research published by the American Heart Association.
Patients with heart failure are particularly challenging to care for because of comorbidities.
“They’re a very, very sick group of patients that are very difficult to manage,” said Noah Moss, MD, an advanced heart failure and transplant cardiologist at Mount Sinai Hospital, New York.
But patients do not always receive the follow-up care they need, some studies have found.
Right drugs at the right time
Kelly Axsom, MD, a cardiologist at the Columbia University Medical Center, New York, and director of the centralized heart failure management program at the New York–Presbyterian Hospital System, called the primary care clinician the “captain of the ship,” ensuring that medications are reconciled and providing education about what to eat after discharge.
“It’s actually pretty complicated to go from being in the hospital to being at home,” Dr. Axsom said. “There are often many medication changes, there are lots of instructions that are told to you as a patient that are hard to remember.”
A patient’s weight might fluctuate in the days following discharge because the dose of diuretics might be too low or too high and need to be adjusted, according to Ishani Ganguli, MD, MPH, an assistant professor of medicine and a general internist in the Division of General Internal Medicine and Primary Care at Harvard Medical School and Brigham and Women’s Hospital, Boston.
K. Melissa Hayes, DNP, ANP-BC, CHFN, an assistant professor in the adult gerontology primary care program at the Vanderbilt University School of Nursing, Nashville, Tenn., recalled one patient who was given a months’ worth of medications following his discharge from the hospital.
“He was given expensive medications he couldn’t afford and not any refills or how to get those medications,” Dr. Hayes said.
Sometimes patients have no way to get to the pharmacy, or their pharmacy doesn’t have the medication they need, or their insurance doesn’t cover the drugs.
“The average patient is on at least six medications for heart failure, maybe even seven, and then that’s not including all their other medications,” Dr. Hayes said. “That can be a lot for people to keep up with.”
Dr. Hayes talks to her patients with heart failure about what drugs they have been prescribed and what medications they require more of, and she deprescribes any that are duplicative.
Helping patients understand why they are taking each drug encourages them to stick to the regimen. Diuretics, for example, can lead to frequent urination. If patients are unable to take regular bathroom breaks, they may be tempted to stop using the medication – a potentially catastrophic mistake.
“Often I have patients say, ‘Nobody ever explained it to me that way,’ ” Dr. Hayes said. “Someone can have a PhD but not understand their medications.”
Clinicians also can alert patients to commonly used medications that can worsen heart failure, such as diabetes drugs and over-the-counter medications such as ibuprofen.
Patients should be prescribed a combination of four recommended medications. But several studies have found that clinicians often fail to achieve the target doses for those medications. The use of guideline-directed medications reduces mortality and hospitalization rates, according to multiple clinical trials.
Eyes and ears on the patient
Once home, patients must stick to the right diet, weigh themselves every day, and monitor their blood pressure. But changing behaviors can be a struggle.
“Being seen quickly within a couple of days of discharge, you can catch things,” said Dr. Hayes, who has edited a book on managing patients with heart failure in primary care.
“It’s an opportunity to see how they’re doing at home, make sure they have their medications, make sure there’s been no misunderstanding or miscommunication about what they’re supposed to be doing at home,” says Marc Itskowitz, MD, a primary care physician affiliated with Allegheny General Hospital, Pittsburgh.
Ideally, a record that readily integrates information from wearables – such as blood pressure and weight – would make it easier to spot abnormalities, Dr. Itskowtiz said. “I think we’re still in the infancy of the electronic health record,” he said.
Ensuring that follow-up visits are as accessible as possible for patients is also important. Telehealth makes it easier for patients after they return home from the hospital, Dr. Itskowitz said.
More infrastructure
Another challenge of providing follow-up care for patients with heart failure is completing all the tasks a clinician must do within a 20-minute visit: an examination; education on the condition and medications; counseling on diet and exercise; coordination of medical equipment, such as a blood pressure cuff for home use; and making appointments with specialists.
“In the current system, additional support for primary care is needed so we can do all this,” Dr. Sterling said.
Staff at primary care clinics should be trained to answer calls from patients when they experience changes in their weight or are worried about other potential problems. “A lot of primary care practices are bare bones,” Dr. Hayes said, meaning they might not have the staff to field those calls. Educating patients as to when they should call their physician, especially after experiencing worsening symptoms, is also important.
Dr. Hayes suggests setting aside time in the schedule each week to see patients who have been recently discharged from the hospital. In the Cardiology and Vascular Clinic at Nashville General Hospital, Tenn., where she spends half a day each week, Dr. Hayes requests 30 minutes to see patients who have recently been discharged from hospital.
Even when the process goes smoothly, some patients will return to the hospital because of the progressive nature of heart failure, according to Dr. Hayes. Improving care following their hospitalization can keep these people from rapidly declining.
“Most patients with heart failure want to be taking care of the grandchildren or be able to enjoy family dinners together,” Dr. Axsom said. “I think anything we can do to help improve their quality of life is really important.”
Take-home
- See heart failure patients early after their discharge from hospital, ideally within 7-10 days.
- Make sure patients have access to the right medications at the right dosages and that they know why they’re taking them.
- Educate patients about the diet they should be following.
- Have a system to monitor patients’ symptoms and let them know when they should call.
A version of this article first appeared on Medscape.com.
Madeline Sterling, MD, knew something was wrong when she heard her patient’s voice on the phone. The patient was breathing too fast and sounded fatigued. Like many people with heart failure, this patient had several comorbidities: diabetes, high blood pressure, and cancer, which was in remission.
The patient had been in and out of the hospital several times and was afraid of going back, but Dr. Sterling, a primary care physician, advised her that it was the safe thing to do.
During the woman’s stay, the inpatient cardiology team called Dr. Sterling to provide status updates and ask for input. When the patient was discharged, Dr. Sterling received information on what medicines had been changed and scheduled follow-up care within 10 days. Dr. Sterling, who’d cared for the woman for many years, called her family, her home health aide, and another caregiver to discuss the plan.
“When you know these patients really well, it’s helpful,” Dr. Sterling, a professor of medicine at Weill Cornell Medicine, New York, said. Primary care clinicians have “an appreciation for how all these conditions fit together, how the medicines fit together, and how to put that patient’s priorities at the front of the equation.”
Research has shown that follow-up care within 7-10 days after discharge, especially for patients with heart failure, can prevent hospital readmissions. Patients’ health can change rapidly following discharge: They may start retaining fluid or may not know how to maintain a low-sodium diet, or they might have trouble obtaining medication. Primary care clinicians spot these early warning signs in follow-up visits.
Heart failure affects more than 6 million adults in the United States, according to the Centers for Disease Control and Prevention. The condition is a common cause of hospital readmissions within 30 days of discharge, according to research published by the American Heart Association.
Patients with heart failure are particularly challenging to care for because of comorbidities.
“They’re a very, very sick group of patients that are very difficult to manage,” said Noah Moss, MD, an advanced heart failure and transplant cardiologist at Mount Sinai Hospital, New York.
But patients do not always receive the follow-up care they need, some studies have found.
Right drugs at the right time
Kelly Axsom, MD, a cardiologist at the Columbia University Medical Center, New York, and director of the centralized heart failure management program at the New York–Presbyterian Hospital System, called the primary care clinician the “captain of the ship,” ensuring that medications are reconciled and providing education about what to eat after discharge.
“It’s actually pretty complicated to go from being in the hospital to being at home,” Dr. Axsom said. “There are often many medication changes, there are lots of instructions that are told to you as a patient that are hard to remember.”
A patient’s weight might fluctuate in the days following discharge because the dose of diuretics might be too low or too high and need to be adjusted, according to Ishani Ganguli, MD, MPH, an assistant professor of medicine and a general internist in the Division of General Internal Medicine and Primary Care at Harvard Medical School and Brigham and Women’s Hospital, Boston.
K. Melissa Hayes, DNP, ANP-BC, CHFN, an assistant professor in the adult gerontology primary care program at the Vanderbilt University School of Nursing, Nashville, Tenn., recalled one patient who was given a months’ worth of medications following his discharge from the hospital.
“He was given expensive medications he couldn’t afford and not any refills or how to get those medications,” Dr. Hayes said.
Sometimes patients have no way to get to the pharmacy, or their pharmacy doesn’t have the medication they need, or their insurance doesn’t cover the drugs.
“The average patient is on at least six medications for heart failure, maybe even seven, and then that’s not including all their other medications,” Dr. Hayes said. “That can be a lot for people to keep up with.”
Dr. Hayes talks to her patients with heart failure about what drugs they have been prescribed and what medications they require more of, and she deprescribes any that are duplicative.
Helping patients understand why they are taking each drug encourages them to stick to the regimen. Diuretics, for example, can lead to frequent urination. If patients are unable to take regular bathroom breaks, they may be tempted to stop using the medication – a potentially catastrophic mistake.
“Often I have patients say, ‘Nobody ever explained it to me that way,’ ” Dr. Hayes said. “Someone can have a PhD but not understand their medications.”
Clinicians also can alert patients to commonly used medications that can worsen heart failure, such as diabetes drugs and over-the-counter medications such as ibuprofen.
Patients should be prescribed a combination of four recommended medications. But several studies have found that clinicians often fail to achieve the target doses for those medications. The use of guideline-directed medications reduces mortality and hospitalization rates, according to multiple clinical trials.
Eyes and ears on the patient
Once home, patients must stick to the right diet, weigh themselves every day, and monitor their blood pressure. But changing behaviors can be a struggle.
“Being seen quickly within a couple of days of discharge, you can catch things,” said Dr. Hayes, who has edited a book on managing patients with heart failure in primary care.
“It’s an opportunity to see how they’re doing at home, make sure they have their medications, make sure there’s been no misunderstanding or miscommunication about what they’re supposed to be doing at home,” says Marc Itskowitz, MD, a primary care physician affiliated with Allegheny General Hospital, Pittsburgh.
Ideally, a record that readily integrates information from wearables – such as blood pressure and weight – would make it easier to spot abnormalities, Dr. Itskowtiz said. “I think we’re still in the infancy of the electronic health record,” he said.
Ensuring that follow-up visits are as accessible as possible for patients is also important. Telehealth makes it easier for patients after they return home from the hospital, Dr. Itskowitz said.
More infrastructure
Another challenge of providing follow-up care for patients with heart failure is completing all the tasks a clinician must do within a 20-minute visit: an examination; education on the condition and medications; counseling on diet and exercise; coordination of medical equipment, such as a blood pressure cuff for home use; and making appointments with specialists.
“In the current system, additional support for primary care is needed so we can do all this,” Dr. Sterling said.
Staff at primary care clinics should be trained to answer calls from patients when they experience changes in their weight or are worried about other potential problems. “A lot of primary care practices are bare bones,” Dr. Hayes said, meaning they might not have the staff to field those calls. Educating patients as to when they should call their physician, especially after experiencing worsening symptoms, is also important.
Dr. Hayes suggests setting aside time in the schedule each week to see patients who have been recently discharged from the hospital. In the Cardiology and Vascular Clinic at Nashville General Hospital, Tenn., where she spends half a day each week, Dr. Hayes requests 30 minutes to see patients who have recently been discharged from hospital.
Even when the process goes smoothly, some patients will return to the hospital because of the progressive nature of heart failure, according to Dr. Hayes. Improving care following their hospitalization can keep these people from rapidly declining.
“Most patients with heart failure want to be taking care of the grandchildren or be able to enjoy family dinners together,” Dr. Axsom said. “I think anything we can do to help improve their quality of life is really important.”
Take-home
- See heart failure patients early after their discharge from hospital, ideally within 7-10 days.
- Make sure patients have access to the right medications at the right dosages and that they know why they’re taking them.
- Educate patients about the diet they should be following.
- Have a system to monitor patients’ symptoms and let them know when they should call.
A version of this article first appeared on Medscape.com.
FDA approves first leadless dual-chamber pacing system
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.

The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.
The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.
The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
Peripartum cardiomyopathy raises risks at future pregnancy despite LV recovery
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
New ESH hypertension guidelines aim for simplified message
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
New definition for iron deficiency in CV disease proposed
with implications that may extend to cardiovascular disease in general.
In the study involving more than 900 patients with PH, investigators at seven U.S. centers determined the prevalence of iron deficiency by two separate definitions and assessed its associations with functional measures and quality of life (QoL) scores.
An iron deficiency definition used conventionally in heart failure (HF) – ferritin less than 100 g/mL or 100-299 ng/mL with transferrin saturation (TSAT) less than 20% – failed to discriminate patients with reduced peak oxygen consumption (peakVO2), 6-minute walk test (6MWT) results, and QoL scores on the 36-item Short Form Survey (SF-36).
But an alternative definition for iron deficiency, simply a TSAT less than 21%, did predict such patients with reduced peakVO2, 6MWT, and QoL. It was also associated with an increased mortality risk. The study was published in the European Heart Journal.
“A low TSAT, less than 21%, is key in the pathophysiology of iron deficiency in pulmonary hypertension” and is associated with those important clinical and functional characteristics, lead author Pieter Martens MD, PhD, said in an interview. The study “underscores the importance of these criteria in future intervention studies in the field of pulmonary hypertension testing iron therapies.”
A broader implication is that “we should revise how we define iron deficiency in heart failure and cardiovascular disease in general and how we select patients for iron therapies,” said Dr. Martens, of the Heart, Vascular & Thoracic Institute of the Cleveland Clinic.
Iron’s role in pulmonary vascular disease
“Iron deficiency is associated with an energetic deficit, especially in high energy–demanding tissue, leading to early skeletal muscle acidification and diminished left and right ventricular (RV) contractile reserve during exercise,” the published report states. It can lead to “maladaptive RV remodeling,” which is a “hallmark feature” predictive of morbidity and mortality in patients with pulmonary vascular disease (PVD).
Some studies have suggested that iron deficiency is a common comorbidity in patients with PVD, their estimates of its prevalence ranging widely due in part to the “absence of a uniform definition,” write the authors.
Dr. Martens said the current study was conducted partly in response to the increasingly common observation that the HF-associated definition of iron deficiency “has limitations.” Yet, “without validation in the field of pulmonary hypertension, the 2022 pulmonary hypertension guidelines endorse this definition.”
As iron deficiency is a causal risk factor for HF progression, Dr. Martens added, the HF field has “taught us the importance of using validated definitions for iron deficiency when selecting patients for iron treatment in randomized controlled trials.”
Moreover, some evidence suggests that iron deficiency by some definitions may be associated with diminished exercise capacity and QoL in patients with PVD, which are associations that have not been confirmed in large studies, the report notes.
Therefore, it continues, the study sought to “determine and validate” the optimal definition of iron deficiency in patients with PVD; document its prevalence; and explore associations between iron deficiency and exercise capacity, QoL, and cardiac and pulmonary vascular remodeling.
Evaluating definitions of iron deficiency
The prospective study, called PVDOMICS, entered 1,195 subjects with available iron levels. After exclusion of 38 patients with sarcoidosis, myeloproliferative disease, or hemoglobinopathy, there remained 693 patients with “overt” PH, 225 with a milder form of PH who served as PVD comparators, and 90 age-, sex-, race/ethnicity- matched “healthy” adults who served as controls.
According to the conventional HF definition of iron deficiency – that is, ferritin 100-299 ng/mL and TSAT less than 20% – the prevalences were 74% in patients with overt PH and 72% of those “across the PVD spectrum.”
But by that definition, iron deficient and non-iron deficient patients didn’t differ significantly in peakVO2, 6MWT distance, or SF-36 physical component scores.
In contrast, patients meeting the alternative definition of iron deficiency of TSAT less than 21% showed significantly reduced functional and QoL measures, compared with those with TSAT greater than or equal to 21%.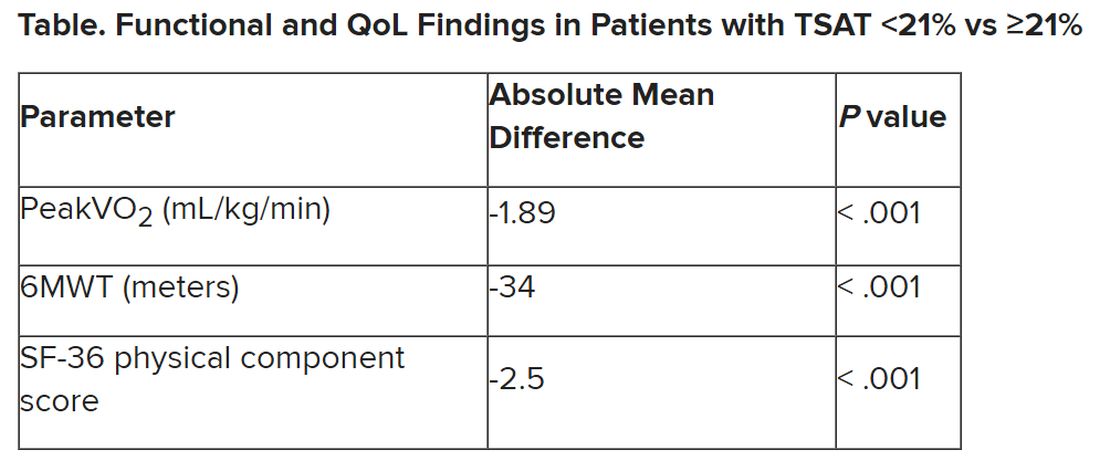
The group with TSAT less than 21% also showed significantly more RV remodeling at cardiac MRI, compared with those who had TSAT greater than or equal to 21%, but their invasively measured pulmonary vascular resistance was comparable.
Of note, those with TSAT less than 21% also showed significantly increased all-cause mortality (hazard ratio, 1.63; 95% confidence interval, 1.13-2.34; P = .009) after adjustment for age, sex, hemoglobin, and natriuretic peptide levels.
“Proper validation of the definition of iron deficiency is important for prognostication,” the published report states, “but also for providing a working definition that can be used to identify suitable patients for inclusion in randomized controlled trials” of drugs for iron deficiency.
Additionally, the finding that TSAT less than 21% points to patients with diminished functional and exercise capacity is “consistent with more recent studies in the field of heart failure” that suggest “functional abnormalities and adverse cardiac remodeling are worse in patients with a low TSAT.” Indeed, the report states, such treatment effects have been “the most convincing” in HF trials.
Broader implications
An accompanying editorial agrees that the study’s implications apply well beyond PH. It highlights that iron deficiency is common in PH, while such PH is “not substantially different from the problem in patients with heart failure, chronic kidney disease, and cardiovascular disease in general,” lead editorialist John G.F. Cleland, MD, PhD, University of Glasgow, said in an interview. “It’s also common as people get older, even in those without these diseases.”
Dr. Cleland said the anemia definition currently used in cardiovascular research and practice is based on a hemoglobin concentration below the 5th percentile of age and sex in primarily young, healthy people, and not on its association with clinical outcomes.
“We recently analyzed data on a large population in the United Kingdom with a broad range of cardiovascular diseases and found that unless anemia is severe, [other] markers of iron deficiency are usually not measured,” he said. A low hemoglobin and TSAT, but not low ferritin levels, are associated with worse prognosis.
Dr. Cleland agreed that the HF-oriented definition is “poor,” with profound implications for the conduct of clinical trials. “If the definition of iron deficiency lacks specificity, then clinical trials will include many patients without iron deficiency who are unlikely to benefit from and might be harmed by IV iron.” Inclusion of such patients may also “dilute” any benefit that might emerge and render the outcome inaccurate.
But if the definition of iron deficiency lacks sensitivity, “then in clinical practice, many patients with iron deficiency may be denied a simple and effective treatment.”
Measuring serum iron could potentially be useful, but it’s usually not done in randomized trials “especially since taking an iron tablet can give a temporary ‘blip’ in serum iron,” Dr. Cleland said. “So TSAT is a reasonable compromise.” He said he “looks forward” to any further data on serum iron as a way of assessing iron deficiency and anemia.
Half full vs. half empty
Dr. Cleland likened the question of whom to treat with iron supplementation as a “glass half full versus half empty” clinical dilemma. “One approach is to give iron to everyone unless there’s evidence that they’re overloaded,” he said, “while the other is to withhold iron from everyone unless there’s evidence that they’re iron depleted.”
Recent evidence from the IRONMAN trial suggested that its patients with HF who received intravenous iron were less likely to be hospitalized for infections, particularly COVID-19, than a usual-care group. The treatment may also help reduce frailty.
“So should we be offering IV iron specifically to people considered iron deficient, or should we be ensuring that everyone over age 70 get iron supplements?” Dr. Cleland mused rhetorically. On a cautionary note, he added, perhaps iron supplementation will be harmful if it’s not necessary.
Dr. Cleland proposed “focusing for the moment on people who are iron deficient but investigating the possibility that we are being overly restrictive and should be giving iron to a much broader population.” That course, however, would require large population-based studies.
“We need more experience,” Dr. Cleland said, “to make sure that the benefits outweigh any risks before we can just give iron to everyone.”
Dr. Martens has received consultancy fees from AstraZeneca, Abbott, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Novo Nordisk, and Vifor Pharma. Dr. Cleland declares grant support, support for travel, and personal honoraria from Pharmacosmos and Vifor. Disclosures for other authors are in the published report and editorial.
A version of this article first appeared on Medscape.com.
with implications that may extend to cardiovascular disease in general.
In the study involving more than 900 patients with PH, investigators at seven U.S. centers determined the prevalence of iron deficiency by two separate definitions and assessed its associations with functional measures and quality of life (QoL) scores.
An iron deficiency definition used conventionally in heart failure (HF) – ferritin less than 100 g/mL or 100-299 ng/mL with transferrin saturation (TSAT) less than 20% – failed to discriminate patients with reduced peak oxygen consumption (peakVO2), 6-minute walk test (6MWT) results, and QoL scores on the 36-item Short Form Survey (SF-36).
But an alternative definition for iron deficiency, simply a TSAT less than 21%, did predict such patients with reduced peakVO2, 6MWT, and QoL. It was also associated with an increased mortality risk. The study was published in the European Heart Journal.
“A low TSAT, less than 21%, is key in the pathophysiology of iron deficiency in pulmonary hypertension” and is associated with those important clinical and functional characteristics, lead author Pieter Martens MD, PhD, said in an interview. The study “underscores the importance of these criteria in future intervention studies in the field of pulmonary hypertension testing iron therapies.”
A broader implication is that “we should revise how we define iron deficiency in heart failure and cardiovascular disease in general and how we select patients for iron therapies,” said Dr. Martens, of the Heart, Vascular & Thoracic Institute of the Cleveland Clinic.
Iron’s role in pulmonary vascular disease
“Iron deficiency is associated with an energetic deficit, especially in high energy–demanding tissue, leading to early skeletal muscle acidification and diminished left and right ventricular (RV) contractile reserve during exercise,” the published report states. It can lead to “maladaptive RV remodeling,” which is a “hallmark feature” predictive of morbidity and mortality in patients with pulmonary vascular disease (PVD).
Some studies have suggested that iron deficiency is a common comorbidity in patients with PVD, their estimates of its prevalence ranging widely due in part to the “absence of a uniform definition,” write the authors.
Dr. Martens said the current study was conducted partly in response to the increasingly common observation that the HF-associated definition of iron deficiency “has limitations.” Yet, “without validation in the field of pulmonary hypertension, the 2022 pulmonary hypertension guidelines endorse this definition.”
As iron deficiency is a causal risk factor for HF progression, Dr. Martens added, the HF field has “taught us the importance of using validated definitions for iron deficiency when selecting patients for iron treatment in randomized controlled trials.”
Moreover, some evidence suggests that iron deficiency by some definitions may be associated with diminished exercise capacity and QoL in patients with PVD, which are associations that have not been confirmed in large studies, the report notes.
Therefore, it continues, the study sought to “determine and validate” the optimal definition of iron deficiency in patients with PVD; document its prevalence; and explore associations between iron deficiency and exercise capacity, QoL, and cardiac and pulmonary vascular remodeling.
Evaluating definitions of iron deficiency
The prospective study, called PVDOMICS, entered 1,195 subjects with available iron levels. After exclusion of 38 patients with sarcoidosis, myeloproliferative disease, or hemoglobinopathy, there remained 693 patients with “overt” PH, 225 with a milder form of PH who served as PVD comparators, and 90 age-, sex-, race/ethnicity- matched “healthy” adults who served as controls.
According to the conventional HF definition of iron deficiency – that is, ferritin 100-299 ng/mL and TSAT less than 20% – the prevalences were 74% in patients with overt PH and 72% of those “across the PVD spectrum.”
But by that definition, iron deficient and non-iron deficient patients didn’t differ significantly in peakVO2, 6MWT distance, or SF-36 physical component scores.
In contrast, patients meeting the alternative definition of iron deficiency of TSAT less than 21% showed significantly reduced functional and QoL measures, compared with those with TSAT greater than or equal to 21%.
The group with TSAT less than 21% also showed significantly more RV remodeling at cardiac MRI, compared with those who had TSAT greater than or equal to 21%, but their invasively measured pulmonary vascular resistance was comparable.
Of note, those with TSAT less than 21% also showed significantly increased all-cause mortality (hazard ratio, 1.63; 95% confidence interval, 1.13-2.34; P = .009) after adjustment for age, sex, hemoglobin, and natriuretic peptide levels.
“Proper validation of the definition of iron deficiency is important for prognostication,” the published report states, “but also for providing a working definition that can be used to identify suitable patients for inclusion in randomized controlled trials” of drugs for iron deficiency.
Additionally, the finding that TSAT less than 21% points to patients with diminished functional and exercise capacity is “consistent with more recent studies in the field of heart failure” that suggest “functional abnormalities and adverse cardiac remodeling are worse in patients with a low TSAT.” Indeed, the report states, such treatment effects have been “the most convincing” in HF trials.
Broader implications
An accompanying editorial agrees that the study’s implications apply well beyond PH. It highlights that iron deficiency is common in PH, while such PH is “not substantially different from the problem in patients with heart failure, chronic kidney disease, and cardiovascular disease in general,” lead editorialist John G.F. Cleland, MD, PhD, University of Glasgow, said in an interview. “It’s also common as people get older, even in those without these diseases.”
Dr. Cleland said the anemia definition currently used in cardiovascular research and practice is based on a hemoglobin concentration below the 5th percentile of age and sex in primarily young, healthy people, and not on its association with clinical outcomes.
“We recently analyzed data on a large population in the United Kingdom with a broad range of cardiovascular diseases and found that unless anemia is severe, [other] markers of iron deficiency are usually not measured,” he said. A low hemoglobin and TSAT, but not low ferritin levels, are associated with worse prognosis.
Dr. Cleland agreed that the HF-oriented definition is “poor,” with profound implications for the conduct of clinical trials. “If the definition of iron deficiency lacks specificity, then clinical trials will include many patients without iron deficiency who are unlikely to benefit from and might be harmed by IV iron.” Inclusion of such patients may also “dilute” any benefit that might emerge and render the outcome inaccurate.
But if the definition of iron deficiency lacks sensitivity, “then in clinical practice, many patients with iron deficiency may be denied a simple and effective treatment.”
Measuring serum iron could potentially be useful, but it’s usually not done in randomized trials “especially since taking an iron tablet can give a temporary ‘blip’ in serum iron,” Dr. Cleland said. “So TSAT is a reasonable compromise.” He said he “looks forward” to any further data on serum iron as a way of assessing iron deficiency and anemia.
Half full vs. half empty
Dr. Cleland likened the question of whom to treat with iron supplementation as a “glass half full versus half empty” clinical dilemma. “One approach is to give iron to everyone unless there’s evidence that they’re overloaded,” he said, “while the other is to withhold iron from everyone unless there’s evidence that they’re iron depleted.”
Recent evidence from the IRONMAN trial suggested that its patients with HF who received intravenous iron were less likely to be hospitalized for infections, particularly COVID-19, than a usual-care group. The treatment may also help reduce frailty.
“So should we be offering IV iron specifically to people considered iron deficient, or should we be ensuring that everyone over age 70 get iron supplements?” Dr. Cleland mused rhetorically. On a cautionary note, he added, perhaps iron supplementation will be harmful if it’s not necessary.
Dr. Cleland proposed “focusing for the moment on people who are iron deficient but investigating the possibility that we are being overly restrictive and should be giving iron to a much broader population.” That course, however, would require large population-based studies.
“We need more experience,” Dr. Cleland said, “to make sure that the benefits outweigh any risks before we can just give iron to everyone.”
Dr. Martens has received consultancy fees from AstraZeneca, Abbott, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Novo Nordisk, and Vifor Pharma. Dr. Cleland declares grant support, support for travel, and personal honoraria from Pharmacosmos and Vifor. Disclosures for other authors are in the published report and editorial.
A version of this article first appeared on Medscape.com.
with implications that may extend to cardiovascular disease in general.
In the study involving more than 900 patients with PH, investigators at seven U.S. centers determined the prevalence of iron deficiency by two separate definitions and assessed its associations with functional measures and quality of life (QoL) scores.
An iron deficiency definition used conventionally in heart failure (HF) – ferritin less than 100 g/mL or 100-299 ng/mL with transferrin saturation (TSAT) less than 20% – failed to discriminate patients with reduced peak oxygen consumption (peakVO2), 6-minute walk test (6MWT) results, and QoL scores on the 36-item Short Form Survey (SF-36).
But an alternative definition for iron deficiency, simply a TSAT less than 21%, did predict such patients with reduced peakVO2, 6MWT, and QoL. It was also associated with an increased mortality risk. The study was published in the European Heart Journal.
“A low TSAT, less than 21%, is key in the pathophysiology of iron deficiency in pulmonary hypertension” and is associated with those important clinical and functional characteristics, lead author Pieter Martens MD, PhD, said in an interview. The study “underscores the importance of these criteria in future intervention studies in the field of pulmonary hypertension testing iron therapies.”
A broader implication is that “we should revise how we define iron deficiency in heart failure and cardiovascular disease in general and how we select patients for iron therapies,” said Dr. Martens, of the Heart, Vascular & Thoracic Institute of the Cleveland Clinic.
Iron’s role in pulmonary vascular disease
“Iron deficiency is associated with an energetic deficit, especially in high energy–demanding tissue, leading to early skeletal muscle acidification and diminished left and right ventricular (RV) contractile reserve during exercise,” the published report states. It can lead to “maladaptive RV remodeling,” which is a “hallmark feature” predictive of morbidity and mortality in patients with pulmonary vascular disease (PVD).
Some studies have suggested that iron deficiency is a common comorbidity in patients with PVD, their estimates of its prevalence ranging widely due in part to the “absence of a uniform definition,” write the authors.
Dr. Martens said the current study was conducted partly in response to the increasingly common observation that the HF-associated definition of iron deficiency “has limitations.” Yet, “without validation in the field of pulmonary hypertension, the 2022 pulmonary hypertension guidelines endorse this definition.”
As iron deficiency is a causal risk factor for HF progression, Dr. Martens added, the HF field has “taught us the importance of using validated definitions for iron deficiency when selecting patients for iron treatment in randomized controlled trials.”
Moreover, some evidence suggests that iron deficiency by some definitions may be associated with diminished exercise capacity and QoL in patients with PVD, which are associations that have not been confirmed in large studies, the report notes.
Therefore, it continues, the study sought to “determine and validate” the optimal definition of iron deficiency in patients with PVD; document its prevalence; and explore associations between iron deficiency and exercise capacity, QoL, and cardiac and pulmonary vascular remodeling.
Evaluating definitions of iron deficiency
The prospective study, called PVDOMICS, entered 1,195 subjects with available iron levels. After exclusion of 38 patients with sarcoidosis, myeloproliferative disease, or hemoglobinopathy, there remained 693 patients with “overt” PH, 225 with a milder form of PH who served as PVD comparators, and 90 age-, sex-, race/ethnicity- matched “healthy” adults who served as controls.
According to the conventional HF definition of iron deficiency – that is, ferritin 100-299 ng/mL and TSAT less than 20% – the prevalences were 74% in patients with overt PH and 72% of those “across the PVD spectrum.”
But by that definition, iron deficient and non-iron deficient patients didn’t differ significantly in peakVO2, 6MWT distance, or SF-36 physical component scores.
In contrast, patients meeting the alternative definition of iron deficiency of TSAT less than 21% showed significantly reduced functional and QoL measures, compared with those with TSAT greater than or equal to 21%.
The group with TSAT less than 21% also showed significantly more RV remodeling at cardiac MRI, compared with those who had TSAT greater than or equal to 21%, but their invasively measured pulmonary vascular resistance was comparable.
Of note, those with TSAT less than 21% also showed significantly increased all-cause mortality (hazard ratio, 1.63; 95% confidence interval, 1.13-2.34; P = .009) after adjustment for age, sex, hemoglobin, and natriuretic peptide levels.
“Proper validation of the definition of iron deficiency is important for prognostication,” the published report states, “but also for providing a working definition that can be used to identify suitable patients for inclusion in randomized controlled trials” of drugs for iron deficiency.
Additionally, the finding that TSAT less than 21% points to patients with diminished functional and exercise capacity is “consistent with more recent studies in the field of heart failure” that suggest “functional abnormalities and adverse cardiac remodeling are worse in patients with a low TSAT.” Indeed, the report states, such treatment effects have been “the most convincing” in HF trials.
Broader implications
An accompanying editorial agrees that the study’s implications apply well beyond PH. It highlights that iron deficiency is common in PH, while such PH is “not substantially different from the problem in patients with heart failure, chronic kidney disease, and cardiovascular disease in general,” lead editorialist John G.F. Cleland, MD, PhD, University of Glasgow, said in an interview. “It’s also common as people get older, even in those without these diseases.”
Dr. Cleland said the anemia definition currently used in cardiovascular research and practice is based on a hemoglobin concentration below the 5th percentile of age and sex in primarily young, healthy people, and not on its association with clinical outcomes.
“We recently analyzed data on a large population in the United Kingdom with a broad range of cardiovascular diseases and found that unless anemia is severe, [other] markers of iron deficiency are usually not measured,” he said. A low hemoglobin and TSAT, but not low ferritin levels, are associated with worse prognosis.
Dr. Cleland agreed that the HF-oriented definition is “poor,” with profound implications for the conduct of clinical trials. “If the definition of iron deficiency lacks specificity, then clinical trials will include many patients without iron deficiency who are unlikely to benefit from and might be harmed by IV iron.” Inclusion of such patients may also “dilute” any benefit that might emerge and render the outcome inaccurate.
But if the definition of iron deficiency lacks sensitivity, “then in clinical practice, many patients with iron deficiency may be denied a simple and effective treatment.”
Measuring serum iron could potentially be useful, but it’s usually not done in randomized trials “especially since taking an iron tablet can give a temporary ‘blip’ in serum iron,” Dr. Cleland said. “So TSAT is a reasonable compromise.” He said he “looks forward” to any further data on serum iron as a way of assessing iron deficiency and anemia.
Half full vs. half empty
Dr. Cleland likened the question of whom to treat with iron supplementation as a “glass half full versus half empty” clinical dilemma. “One approach is to give iron to everyone unless there’s evidence that they’re overloaded,” he said, “while the other is to withhold iron from everyone unless there’s evidence that they’re iron depleted.”
Recent evidence from the IRONMAN trial suggested that its patients with HF who received intravenous iron were less likely to be hospitalized for infections, particularly COVID-19, than a usual-care group. The treatment may also help reduce frailty.
“So should we be offering IV iron specifically to people considered iron deficient, or should we be ensuring that everyone over age 70 get iron supplements?” Dr. Cleland mused rhetorically. On a cautionary note, he added, perhaps iron supplementation will be harmful if it’s not necessary.
Dr. Cleland proposed “focusing for the moment on people who are iron deficient but investigating the possibility that we are being overly restrictive and should be giving iron to a much broader population.” That course, however, would require large population-based studies.
“We need more experience,” Dr. Cleland said, “to make sure that the benefits outweigh any risks before we can just give iron to everyone.”
Dr. Martens has received consultancy fees from AstraZeneca, Abbott, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Novo Nordisk, and Vifor Pharma. Dr. Cleland declares grant support, support for travel, and personal honoraria from Pharmacosmos and Vifor. Disclosures for other authors are in the published report and editorial.
A version of this article first appeared on Medscape.com.
FROM EUROPEAN HEART JOURNAL
Pulmonary embolism confers higher mortality long term
Topline
Long-term mortality rates among individuals who have had a pulmonary embolism are significantly higher than rates in the general population.
Methodology
Researchers investigated long-term outcomes of patients with pulmonary embolism in a single-center registry.
They followed 896 patients for up to 14 years.
Data were from consecutive cases treated between May 2005 and December 2017.
Takeaway
The total follow-up time was 3,908 patient-years (median, 3.1 years).
One-year and five-year mortality rates were 19.7% (95% confidence interval, 17.2%-22.4%) and 37.1% (95% CI, 33.6%-40.5%), respectively, for patients with pulmonary embolism.
The most frequent causes of death were cancer (28.5%), pulmonary embolism (19.4%), infections (13.9%), and cardiovascular events (11.6%).
Late mortality (>30 days) was more frequent than in the general population for patients with cancer (5-year standardized mortality ratio, 2.77; 95% CI, 2.41-3.16) and for patients without cancer (1.80; 95% CI, 1.50-2.14), compared with expected rates.
In practice
stated Johannes Eckelt, Clinic of Cardiology and Pneumology, University Medical Center Göttingen (Germany).
Source
“Long-term Mortality in Pulmonary Embolism: Results in a Single-Center Registry,” by Mr. Eckelt and colleagues was published in Research and Practice in Thrombosis and Haemostasis.
Limitations
Owing to the single-center study design, selection bias cannot be excluded, limiting the generalizability of the study findings, the authors stated.
Disclosures
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Topline
Long-term mortality rates among individuals who have had a pulmonary embolism are significantly higher than rates in the general population.
Methodology
Researchers investigated long-term outcomes of patients with pulmonary embolism in a single-center registry.
They followed 896 patients for up to 14 years.
Data were from consecutive cases treated between May 2005 and December 2017.
Takeaway
The total follow-up time was 3,908 patient-years (median, 3.1 years).
One-year and five-year mortality rates were 19.7% (95% confidence interval, 17.2%-22.4%) and 37.1% (95% CI, 33.6%-40.5%), respectively, for patients with pulmonary embolism.
The most frequent causes of death were cancer (28.5%), pulmonary embolism (19.4%), infections (13.9%), and cardiovascular events (11.6%).
Late mortality (>30 days) was more frequent than in the general population for patients with cancer (5-year standardized mortality ratio, 2.77; 95% CI, 2.41-3.16) and for patients without cancer (1.80; 95% CI, 1.50-2.14), compared with expected rates.
In practice
stated Johannes Eckelt, Clinic of Cardiology and Pneumology, University Medical Center Göttingen (Germany).
Source
“Long-term Mortality in Pulmonary Embolism: Results in a Single-Center Registry,” by Mr. Eckelt and colleagues was published in Research and Practice in Thrombosis and Haemostasis.
Limitations
Owing to the single-center study design, selection bias cannot be excluded, limiting the generalizability of the study findings, the authors stated.
Disclosures
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Topline
Long-term mortality rates among individuals who have had a pulmonary embolism are significantly higher than rates in the general population.
Methodology
Researchers investigated long-term outcomes of patients with pulmonary embolism in a single-center registry.
They followed 896 patients for up to 14 years.
Data were from consecutive cases treated between May 2005 and December 2017.
Takeaway
The total follow-up time was 3,908 patient-years (median, 3.1 years).
One-year and five-year mortality rates were 19.7% (95% confidence interval, 17.2%-22.4%) and 37.1% (95% CI, 33.6%-40.5%), respectively, for patients with pulmonary embolism.
The most frequent causes of death were cancer (28.5%), pulmonary embolism (19.4%), infections (13.9%), and cardiovascular events (11.6%).
Late mortality (>30 days) was more frequent than in the general population for patients with cancer (5-year standardized mortality ratio, 2.77; 95% CI, 2.41-3.16) and for patients without cancer (1.80; 95% CI, 1.50-2.14), compared with expected rates.
In practice
stated Johannes Eckelt, Clinic of Cardiology and Pneumology, University Medical Center Göttingen (Germany).
Source
“Long-term Mortality in Pulmonary Embolism: Results in a Single-Center Registry,” by Mr. Eckelt and colleagues was published in Research and Practice in Thrombosis and Haemostasis.
Limitations
Owing to the single-center study design, selection bias cannot be excluded, limiting the generalizability of the study findings, the authors stated.
Disclosures
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
CV benefit from vitamin D caps hinted in huge D-Health trial
in an analysis from a large prospective randomized trial.
Risk reductions on vitamin D in the mixed primary- and secondary-prevention population were slight in absolute terms but reached a significant 19% in the case of myocardial infarction (MI).
Over 5 years, 6.6% of those in placebo group experienced major CV events, the primary endpoint, compared with 6% in the vitamin D group. The difference, which corresponded to 5.8 fewer events per 1,000 participants, was short of significance in adjusted analysis.
Still, vitamin-D supplementation was associated with the potential MI benefit and an 11% drop in risk for coronary revascularization.
Also, a subgroup analysis hinted at a potentially reduced CV-event risk from vitamin-D supplementation among individuals who entered the trial on statins or other CV medications generally.
“Most other studies have not found benefit for vitamin D for major CV events,” senior investigator Rachel E. Neale, PhD, said in an interview. Although there was a significant effect for MI, the difference in the composite primary endpoint fell short of significance “in keeping with the other studies.”
“However, the effects for myocardial infarction in people taking statins or cardiovascular disease drugs at baseline are suggestive of benefit,” said Dr. Neale, of QIMR Berghofer Medical Research Institute, Queensland, Australia. Still, “it is important to keep in mind that these may be chance findings.”
The analysis based on the D-Health study was published online in The BMJ.
Benefits minimal
The 21,302 patients in the D-Health trial, conducted in Australia from 2014 to 2020, were randomly assigned double-blind to receive either placebo or vitamin D3 supplements for a planned 5 years. They were instructed to take one placebo or vitamin D capsule per month, each active capsule containing 60,000 IU of the vitamin.
People with self-reported hypercalcemia, hyperparathyroidism, kidney stones, osteomalacia, or sarcoidosis, and those taking greater than 500 IU/day vitamin D supplements were excluded from enrollment. Participants ranged in age from 60 to 84 at randomization and 46% were women.
With 80% of the 10,658 participants assigned to vitamin D and 78% of the 10,644 control subjects completing the 5-year intervention, 6% and 6.6%, respectively, met the primary endpoint of a major CV event, defined as MI, stroke, or coronary revascularization.
The hazard ratio for a vitamin-D effect on the primary endpoint was 0.91 (95% confidence interval, 0.81-1.01). The number needed to treat to avoid one major CV event was 172.
The HR for MI was 0.81 (95% CI, 0.67-0.98), for coronary intervention was 0.89 (0.78-1.01), and for stroke was 0.99 (0.80-1.23).
Adverse event rates were similar at about 16% in both groups and included hypercalcemia, kidney stones, gastrointestinal issues, and skin rash.
Vitamin D at moderate dosages has low toxicity, Dr. Neale said, “so I think it would be reasonable for clinicians to consider supplementing elderly people who do not have contraindications, particularly those who have underlying risk factors for CV disease,” Dr. Neale said. But patients should be told that the evidence for such a recommendation is not strong, so they can make an informed decision, she added.
Also, in general “we would be cautious about extrapolating to formulations other than those used in the study,” Dr. Neale said. “However, in this case, I think it would be reasonable to extrapolate to the use of 2,000 IU per day taken orally, provided that the same adherence can be maintained for a lengthy period.”
Chance findings?
Based on the current study and in light of prior research, “it is premature to recommend vitamin D supplementation for cardiovascular disease prevention specifically,” Nour Makarem, PhD, of the Mailman School of Public Health, Columbia University, New York, said in an interview.
“Prior clinical trials did not show an association between vitamin D supplementation and cardiovascular events,” observed Dr. Makarem, who is not affiliated with the current study. Also, she agreed, it looked at “multiple outcomes, which increases the likelihood that findings may be due to chance.”
She added that the study’s authors observed a possible vitamin-D protective effect “among people who were vitamin D sufficient at baseline but not among those who were insufficient. It is important to interpret this finding with caution because they used predicted, not measured, vitamin D status for these analyses.”
There’s a need for studies in other populations, including younger persons and “particularly populations with higher rates of vitamin D deficiency,” Dr. Makarem observed. Also, further research should aim to “understand the interactions between vitamin D supplementation and cardiovascular medications, including statins.”
The D-Health Trial is funded by National Health and Medical Research Council project grants. Dr. Neale was supported by fellowships from the NHMRC. Neither she nor Dr. Makarem reported any relevant financial relationships.
A version of this article first appeared on Medscape.com.
in an analysis from a large prospective randomized trial.
Risk reductions on vitamin D in the mixed primary- and secondary-prevention population were slight in absolute terms but reached a significant 19% in the case of myocardial infarction (MI).
Over 5 years, 6.6% of those in placebo group experienced major CV events, the primary endpoint, compared with 6% in the vitamin D group. The difference, which corresponded to 5.8 fewer events per 1,000 participants, was short of significance in adjusted analysis.
Still, vitamin-D supplementation was associated with the potential MI benefit and an 11% drop in risk for coronary revascularization.
Also, a subgroup analysis hinted at a potentially reduced CV-event risk from vitamin-D supplementation among individuals who entered the trial on statins or other CV medications generally.
“Most other studies have not found benefit for vitamin D for major CV events,” senior investigator Rachel E. Neale, PhD, said in an interview. Although there was a significant effect for MI, the difference in the composite primary endpoint fell short of significance “in keeping with the other studies.”
“However, the effects for myocardial infarction in people taking statins or cardiovascular disease drugs at baseline are suggestive of benefit,” said Dr. Neale, of QIMR Berghofer Medical Research Institute, Queensland, Australia. Still, “it is important to keep in mind that these may be chance findings.”
The analysis based on the D-Health study was published online in The BMJ.
Benefits minimal
The 21,302 patients in the D-Health trial, conducted in Australia from 2014 to 2020, were randomly assigned double-blind to receive either placebo or vitamin D3 supplements for a planned 5 years. They were instructed to take one placebo or vitamin D capsule per month, each active capsule containing 60,000 IU of the vitamin.
People with self-reported hypercalcemia, hyperparathyroidism, kidney stones, osteomalacia, or sarcoidosis, and those taking greater than 500 IU/day vitamin D supplements were excluded from enrollment. Participants ranged in age from 60 to 84 at randomization and 46% were women.
With 80% of the 10,658 participants assigned to vitamin D and 78% of the 10,644 control subjects completing the 5-year intervention, 6% and 6.6%, respectively, met the primary endpoint of a major CV event, defined as MI, stroke, or coronary revascularization.
The hazard ratio for a vitamin-D effect on the primary endpoint was 0.91 (95% confidence interval, 0.81-1.01). The number needed to treat to avoid one major CV event was 172.
The HR for MI was 0.81 (95% CI, 0.67-0.98), for coronary intervention was 0.89 (0.78-1.01), and for stroke was 0.99 (0.80-1.23).
Adverse event rates were similar at about 16% in both groups and included hypercalcemia, kidney stones, gastrointestinal issues, and skin rash.
Vitamin D at moderate dosages has low toxicity, Dr. Neale said, “so I think it would be reasonable for clinicians to consider supplementing elderly people who do not have contraindications, particularly those who have underlying risk factors for CV disease,” Dr. Neale said. But patients should be told that the evidence for such a recommendation is not strong, so they can make an informed decision, she added.
Also, in general “we would be cautious about extrapolating to formulations other than those used in the study,” Dr. Neale said. “However, in this case, I think it would be reasonable to extrapolate to the use of 2,000 IU per day taken orally, provided that the same adherence can be maintained for a lengthy period.”
Chance findings?
Based on the current study and in light of prior research, “it is premature to recommend vitamin D supplementation for cardiovascular disease prevention specifically,” Nour Makarem, PhD, of the Mailman School of Public Health, Columbia University, New York, said in an interview.
“Prior clinical trials did not show an association between vitamin D supplementation and cardiovascular events,” observed Dr. Makarem, who is not affiliated with the current study. Also, she agreed, it looked at “multiple outcomes, which increases the likelihood that findings may be due to chance.”
She added that the study’s authors observed a possible vitamin-D protective effect “among people who were vitamin D sufficient at baseline but not among those who were insufficient. It is important to interpret this finding with caution because they used predicted, not measured, vitamin D status for these analyses.”
There’s a need for studies in other populations, including younger persons and “particularly populations with higher rates of vitamin D deficiency,” Dr. Makarem observed. Also, further research should aim to “understand the interactions between vitamin D supplementation and cardiovascular medications, including statins.”
The D-Health Trial is funded by National Health and Medical Research Council project grants. Dr. Neale was supported by fellowships from the NHMRC. Neither she nor Dr. Makarem reported any relevant financial relationships.
A version of this article first appeared on Medscape.com.
in an analysis from a large prospective randomized trial.
Risk reductions on vitamin D in the mixed primary- and secondary-prevention population were slight in absolute terms but reached a significant 19% in the case of myocardial infarction (MI).
Over 5 years, 6.6% of those in placebo group experienced major CV events, the primary endpoint, compared with 6% in the vitamin D group. The difference, which corresponded to 5.8 fewer events per 1,000 participants, was short of significance in adjusted analysis.
Still, vitamin-D supplementation was associated with the potential MI benefit and an 11% drop in risk for coronary revascularization.
Also, a subgroup analysis hinted at a potentially reduced CV-event risk from vitamin-D supplementation among individuals who entered the trial on statins or other CV medications generally.
“Most other studies have not found benefit for vitamin D for major CV events,” senior investigator Rachel E. Neale, PhD, said in an interview. Although there was a significant effect for MI, the difference in the composite primary endpoint fell short of significance “in keeping with the other studies.”
“However, the effects for myocardial infarction in people taking statins or cardiovascular disease drugs at baseline are suggestive of benefit,” said Dr. Neale, of QIMR Berghofer Medical Research Institute, Queensland, Australia. Still, “it is important to keep in mind that these may be chance findings.”
The analysis based on the D-Health study was published online in The BMJ.
Benefits minimal
The 21,302 patients in the D-Health trial, conducted in Australia from 2014 to 2020, were randomly assigned double-blind to receive either placebo or vitamin D3 supplements for a planned 5 years. They were instructed to take one placebo or vitamin D capsule per month, each active capsule containing 60,000 IU of the vitamin.
People with self-reported hypercalcemia, hyperparathyroidism, kidney stones, osteomalacia, or sarcoidosis, and those taking greater than 500 IU/day vitamin D supplements were excluded from enrollment. Participants ranged in age from 60 to 84 at randomization and 46% were women.
With 80% of the 10,658 participants assigned to vitamin D and 78% of the 10,644 control subjects completing the 5-year intervention, 6% and 6.6%, respectively, met the primary endpoint of a major CV event, defined as MI, stroke, or coronary revascularization.
The hazard ratio for a vitamin-D effect on the primary endpoint was 0.91 (95% confidence interval, 0.81-1.01). The number needed to treat to avoid one major CV event was 172.
The HR for MI was 0.81 (95% CI, 0.67-0.98), for coronary intervention was 0.89 (0.78-1.01), and for stroke was 0.99 (0.80-1.23).
Adverse event rates were similar at about 16% in both groups and included hypercalcemia, kidney stones, gastrointestinal issues, and skin rash.
Vitamin D at moderate dosages has low toxicity, Dr. Neale said, “so I think it would be reasonable for clinicians to consider supplementing elderly people who do not have contraindications, particularly those who have underlying risk factors for CV disease,” Dr. Neale said. But patients should be told that the evidence for such a recommendation is not strong, so they can make an informed decision, she added.
Also, in general “we would be cautious about extrapolating to formulations other than those used in the study,” Dr. Neale said. “However, in this case, I think it would be reasonable to extrapolate to the use of 2,000 IU per day taken orally, provided that the same adherence can be maintained for a lengthy period.”
Chance findings?
Based on the current study and in light of prior research, “it is premature to recommend vitamin D supplementation for cardiovascular disease prevention specifically,” Nour Makarem, PhD, of the Mailman School of Public Health, Columbia University, New York, said in an interview.
“Prior clinical trials did not show an association between vitamin D supplementation and cardiovascular events,” observed Dr. Makarem, who is not affiliated with the current study. Also, she agreed, it looked at “multiple outcomes, which increases the likelihood that findings may be due to chance.”
She added that the study’s authors observed a possible vitamin-D protective effect “among people who were vitamin D sufficient at baseline but not among those who were insufficient. It is important to interpret this finding with caution because they used predicted, not measured, vitamin D status for these analyses.”
There’s a need for studies in other populations, including younger persons and “particularly populations with higher rates of vitamin D deficiency,” Dr. Makarem observed. Also, further research should aim to “understand the interactions between vitamin D supplementation and cardiovascular medications, including statins.”
The D-Health Trial is funded by National Health and Medical Research Council project grants. Dr. Neale was supported by fellowships from the NHMRC. Neither she nor Dr. Makarem reported any relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE BMJ