User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
In utero COVID exposure tied to developmental differences in infants
suggests a small-scale analysis that points to the need for further study and monitoring during pregnancy.
The study included 24 pregnant women, half of whom had COVID-19 during pregnancy, and their offspring. It showed impairments at 6 weeks of age on the social interactive dimension of a neonatal assessment.
“Not all babies born to mothers infected with COVID show neurodevelopmental differences, but our data show that their risk is increased in comparison to those not exposed to COVID in the womb. We need a bigger study to confirm the exact extent of the difference,” said lead researcher Rosa Ayesa Arriola, PhD, Valdecilla Research Institute (IDIVAL), Hospital Universitario Marqués de Valdecilla, Santander, Spain, in a release.
The findings were presented at the virtual European Psychiatric Association 2022 Congress.
Differing responses to cuddling
Coauthor Águeda Castro Quintas, PhD student, Network Centre for Biomedical Research in Mental Health, University of Barcelona, explained that the tests showed the children born to mothers who had COVID-19 during pregnancy reacted “slightly differently to being held, or cuddled.”
“We need to note that these are preliminary results, but this is part of a project following a larger sample of 100 mothers and their babies,” she added. The authors plan to compare their results with those from a similar study.
The group will also monitor infant language and motor development aged between 18 and 42 months.
“This is an ongoing project, and we are at an early stage,” Ms. Castro Quintas said. “We don’t know if these effects will result in any longer-term issues,” but longer-term observation “may help us understand this.”
“Of course, in babies who are so young, there are several things we just can’t measure, such as language skills or cognition,” added coinvestigator Nerea San Martín González, department of evolutionary biology, ecology and environmental sciences, University of Barcelona.
While emphasizing the need for larger sample sizes, she said that “in the meantime, we need to stress the importance of medical monitoring to facilitate a healthy pregnancy.”
The researchers note that the consequences of the COVID-19 pandemic for the newborns of affected mothers remain “unknown.”
However, previous studies of other infections during pregnancy suggest that offspring could be “especially vulnerable,”as the pathophysiological mechanisms of the infection, such as cytokine storms and microcoagulation, “could clearly compromise fetal neurodevelopment.”
To investigate further, they examined the neurodevelopment of infants born both immediately before and during the COVID-19 pandemic, from 2017 to 2021.
Twenty-one women who had COVID-19 during pregnancy were matched with 21 healthy controls. They were studied both during pregnancy and in the postpartum period, completing hormonal and other biochemical tests, salivary tests, movement assessments, and psychological questionnaires, adjusted for various factors.
The team also administered the Brazelton Neonatal Behavioural Assessment Scale (NBAS) to the offspring at 6 weeks of age to evaluate neurologic, social, and behavioral aspects of function.
“We have been especially sensitive in how we have conducted these tests,” said Ms. Castro Quintas. “Each mother and baby were closely examined by clinicians with expert training in the field and in the tests.”
Among those offspring exposed to COVID-19 during pregnancy, there was a significant decrease in scores on the social interactive dimension of the NBAS, particularly if infection occurred before week 20 of gestation.
Other NBAS subscales were not associated with maternal COVID-19 during pregnancy.
More research needed
Commenting on the findings, Livio Provenzi, PhD, a psychologist and researcher in developmental psychobiology at the University of Pavia (Italy), noted there is a “great need” to study the direct and indirect effect of the COVID-19 pandemic on parents and their children. “Pregnancy is a period of life which shapes much of our subsequent development, and exposure to adversity in pregnancy can leave long-lasting biological footprints.”
Dr. Provenzi, who was not involved in the study, added in the release that the findings reinforce “evidence of epigenetic alterations in infants born from mothers exposed to pandemic-related stress during pregnancy.
“It shows we need more large-scale, international research to allow us to understand the developmental effects of this health emergency and to deliver better quality of care to parents and infants.”
The study was funded by the Spanish Ministry of Economy and Competitiveness, Instituto de Salud Carlos III through the University of Barcelona multicenter project and the Government of Cantabria. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
suggests a small-scale analysis that points to the need for further study and monitoring during pregnancy.
The study included 24 pregnant women, half of whom had COVID-19 during pregnancy, and their offspring. It showed impairments at 6 weeks of age on the social interactive dimension of a neonatal assessment.
“Not all babies born to mothers infected with COVID show neurodevelopmental differences, but our data show that their risk is increased in comparison to those not exposed to COVID in the womb. We need a bigger study to confirm the exact extent of the difference,” said lead researcher Rosa Ayesa Arriola, PhD, Valdecilla Research Institute (IDIVAL), Hospital Universitario Marqués de Valdecilla, Santander, Spain, in a release.
The findings were presented at the virtual European Psychiatric Association 2022 Congress.
Differing responses to cuddling
Coauthor Águeda Castro Quintas, PhD student, Network Centre for Biomedical Research in Mental Health, University of Barcelona, explained that the tests showed the children born to mothers who had COVID-19 during pregnancy reacted “slightly differently to being held, or cuddled.”
“We need to note that these are preliminary results, but this is part of a project following a larger sample of 100 mothers and their babies,” she added. The authors plan to compare their results with those from a similar study.
The group will also monitor infant language and motor development aged between 18 and 42 months.
“This is an ongoing project, and we are at an early stage,” Ms. Castro Quintas said. “We don’t know if these effects will result in any longer-term issues,” but longer-term observation “may help us understand this.”
“Of course, in babies who are so young, there are several things we just can’t measure, such as language skills or cognition,” added coinvestigator Nerea San Martín González, department of evolutionary biology, ecology and environmental sciences, University of Barcelona.
While emphasizing the need for larger sample sizes, she said that “in the meantime, we need to stress the importance of medical monitoring to facilitate a healthy pregnancy.”
The researchers note that the consequences of the COVID-19 pandemic for the newborns of affected mothers remain “unknown.”
However, previous studies of other infections during pregnancy suggest that offspring could be “especially vulnerable,”as the pathophysiological mechanisms of the infection, such as cytokine storms and microcoagulation, “could clearly compromise fetal neurodevelopment.”
To investigate further, they examined the neurodevelopment of infants born both immediately before and during the COVID-19 pandemic, from 2017 to 2021.
Twenty-one women who had COVID-19 during pregnancy were matched with 21 healthy controls. They were studied both during pregnancy and in the postpartum period, completing hormonal and other biochemical tests, salivary tests, movement assessments, and psychological questionnaires, adjusted for various factors.
The team also administered the Brazelton Neonatal Behavioural Assessment Scale (NBAS) to the offspring at 6 weeks of age to evaluate neurologic, social, and behavioral aspects of function.
“We have been especially sensitive in how we have conducted these tests,” said Ms. Castro Quintas. “Each mother and baby were closely examined by clinicians with expert training in the field and in the tests.”
Among those offspring exposed to COVID-19 during pregnancy, there was a significant decrease in scores on the social interactive dimension of the NBAS, particularly if infection occurred before week 20 of gestation.
Other NBAS subscales were not associated with maternal COVID-19 during pregnancy.
More research needed
Commenting on the findings, Livio Provenzi, PhD, a psychologist and researcher in developmental psychobiology at the University of Pavia (Italy), noted there is a “great need” to study the direct and indirect effect of the COVID-19 pandemic on parents and their children. “Pregnancy is a period of life which shapes much of our subsequent development, and exposure to adversity in pregnancy can leave long-lasting biological footprints.”
Dr. Provenzi, who was not involved in the study, added in the release that the findings reinforce “evidence of epigenetic alterations in infants born from mothers exposed to pandemic-related stress during pregnancy.
“It shows we need more large-scale, international research to allow us to understand the developmental effects of this health emergency and to deliver better quality of care to parents and infants.”
The study was funded by the Spanish Ministry of Economy and Competitiveness, Instituto de Salud Carlos III through the University of Barcelona multicenter project and the Government of Cantabria. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
suggests a small-scale analysis that points to the need for further study and monitoring during pregnancy.
The study included 24 pregnant women, half of whom had COVID-19 during pregnancy, and their offspring. It showed impairments at 6 weeks of age on the social interactive dimension of a neonatal assessment.
“Not all babies born to mothers infected with COVID show neurodevelopmental differences, but our data show that their risk is increased in comparison to those not exposed to COVID in the womb. We need a bigger study to confirm the exact extent of the difference,” said lead researcher Rosa Ayesa Arriola, PhD, Valdecilla Research Institute (IDIVAL), Hospital Universitario Marqués de Valdecilla, Santander, Spain, in a release.
The findings were presented at the virtual European Psychiatric Association 2022 Congress.
Differing responses to cuddling
Coauthor Águeda Castro Quintas, PhD student, Network Centre for Biomedical Research in Mental Health, University of Barcelona, explained that the tests showed the children born to mothers who had COVID-19 during pregnancy reacted “slightly differently to being held, or cuddled.”
“We need to note that these are preliminary results, but this is part of a project following a larger sample of 100 mothers and their babies,” she added. The authors plan to compare their results with those from a similar study.
The group will also monitor infant language and motor development aged between 18 and 42 months.
“This is an ongoing project, and we are at an early stage,” Ms. Castro Quintas said. “We don’t know if these effects will result in any longer-term issues,” but longer-term observation “may help us understand this.”
“Of course, in babies who are so young, there are several things we just can’t measure, such as language skills or cognition,” added coinvestigator Nerea San Martín González, department of evolutionary biology, ecology and environmental sciences, University of Barcelona.
While emphasizing the need for larger sample sizes, she said that “in the meantime, we need to stress the importance of medical monitoring to facilitate a healthy pregnancy.”
The researchers note that the consequences of the COVID-19 pandemic for the newborns of affected mothers remain “unknown.”
However, previous studies of other infections during pregnancy suggest that offspring could be “especially vulnerable,”as the pathophysiological mechanisms of the infection, such as cytokine storms and microcoagulation, “could clearly compromise fetal neurodevelopment.”
To investigate further, they examined the neurodevelopment of infants born both immediately before and during the COVID-19 pandemic, from 2017 to 2021.
Twenty-one women who had COVID-19 during pregnancy were matched with 21 healthy controls. They were studied both during pregnancy and in the postpartum period, completing hormonal and other biochemical tests, salivary tests, movement assessments, and psychological questionnaires, adjusted for various factors.
The team also administered the Brazelton Neonatal Behavioural Assessment Scale (NBAS) to the offspring at 6 weeks of age to evaluate neurologic, social, and behavioral aspects of function.
“We have been especially sensitive in how we have conducted these tests,” said Ms. Castro Quintas. “Each mother and baby were closely examined by clinicians with expert training in the field and in the tests.”
Among those offspring exposed to COVID-19 during pregnancy, there was a significant decrease in scores on the social interactive dimension of the NBAS, particularly if infection occurred before week 20 of gestation.
Other NBAS subscales were not associated with maternal COVID-19 during pregnancy.
More research needed
Commenting on the findings, Livio Provenzi, PhD, a psychologist and researcher in developmental psychobiology at the University of Pavia (Italy), noted there is a “great need” to study the direct and indirect effect of the COVID-19 pandemic on parents and their children. “Pregnancy is a period of life which shapes much of our subsequent development, and exposure to adversity in pregnancy can leave long-lasting biological footprints.”
Dr. Provenzi, who was not involved in the study, added in the release that the findings reinforce “evidence of epigenetic alterations in infants born from mothers exposed to pandemic-related stress during pregnancy.
“It shows we need more large-scale, international research to allow us to understand the developmental effects of this health emergency and to deliver better quality of care to parents and infants.”
The study was funded by the Spanish Ministry of Economy and Competitiveness, Instituto de Salud Carlos III through the University of Barcelona multicenter project and the Government of Cantabria. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
FROM EPA 2022
Motor abnormalities drive decreased function in schizophrenia
Approximately half of adults with schizophrenia suffer from motor abnormalities that may impair their ability to work and decrease their quality of life, wrote Niluja Nadesalingam, MD, of the University of Bern, Switzerland, and colleagues. “Although previous reports show strong associations between single movement abnormalities and global as well as social functioning, we still struggle to understand the contribution of various motor domains,” they said.
The impact of these abnormalities on social and global functioning and on functional capacity remains unclear, but the researchers proposed that motor abnormalities would be associated with worse functional outcomes in schizophrenia patients.
In a study published in Comprehensive Psychiatry, the researchers identified patients with diagnosed schizophrenia spectrum disorders who were treated on an inpatient or outpatient basis at a single center. They collected data on five motor abnormalities: parkinsonism, catatonia, dyskinesia, neurological soft signs (NSS), and psychomotor slowing (PS). They assessed functional outcomes using the Global Assessment of Functioning (GAF), the Social and Occupational Functioning Assessment Scale (SOFAS), and the UCSD Performance-Based Skills Assessment (UPSA-B). The average age of the participants was 37.9 years and 88 of the 156 were male. The average duration of illness was 12.5 years.
Overall, patients with catatonia and parkinsonism scored significantly lower on GAF and SOFAS scale compared to those without catatonia and parkinsonism (P < .035 and P < .027, respectively).
No significant differences in functional outcomes appeared between patients with and without dyskinesia.
However, significant negative correlations were identified for parkinsonism and PS with GAF, SOFAS, and UPSA-B (P < .036 for all). “Our study further found that parkinsonism and psychomotor slowing also impair the functional capacity of patients,” which may be influenced by factors including deficits in social interaction and cognitive impairment, the researchers said.
Overall, the study findings demonstrate that motor abnormalities in patients with schizophrenia are strongly associated with poor functional outcomes, and the stronger the motor impairment, the worse the global and social functioning, the researchers said.
As for potential pathways, “motor abnormalities are readily observable signs, allowing laypersons to perceive subjects with schizophrenia as somebody with severe mental illness. Thus, motor abnormalities might lead to stigmatization of patients suffering from schizophrenia,” they wrote in their discussion.
The researchers emphasized the need to explore alternative treatment options that might improve motor abnormalities, such as transcranial magnetic stimulation, given the potential of antipsychotic medications to introduce additional motor abnormalities.
The study findings were limited by several factors including the potential for missed confounding variables, the small number of patients with dyskinesia, and the inability to deduce the course of illness because most of the patients were in psychotic episodes, the researchers noted.
However, the results suggest that specific motor abnormalities are associated with poor global and social functioning, and with reduced functional capacity, in adults with schizophrenia, the researchers said. “Future studies need to test whether amelioration of motor abnormalities may improve community functioning,” they concluded.
The study was supported by the Swiss National Science Foundation, the Bangerter Rhyner Foundation, and the Adrian and Simone Frutiger Foundation. Lead author Dr. Nadesalingam had no financial conflicts to disclose.
Approximately half of adults with schizophrenia suffer from motor abnormalities that may impair their ability to work and decrease their quality of life, wrote Niluja Nadesalingam, MD, of the University of Bern, Switzerland, and colleagues. “Although previous reports show strong associations between single movement abnormalities and global as well as social functioning, we still struggle to understand the contribution of various motor domains,” they said.
The impact of these abnormalities on social and global functioning and on functional capacity remains unclear, but the researchers proposed that motor abnormalities would be associated with worse functional outcomes in schizophrenia patients.
In a study published in Comprehensive Psychiatry, the researchers identified patients with diagnosed schizophrenia spectrum disorders who were treated on an inpatient or outpatient basis at a single center. They collected data on five motor abnormalities: parkinsonism, catatonia, dyskinesia, neurological soft signs (NSS), and psychomotor slowing (PS). They assessed functional outcomes using the Global Assessment of Functioning (GAF), the Social and Occupational Functioning Assessment Scale (SOFAS), and the UCSD Performance-Based Skills Assessment (UPSA-B). The average age of the participants was 37.9 years and 88 of the 156 were male. The average duration of illness was 12.5 years.
Overall, patients with catatonia and parkinsonism scored significantly lower on GAF and SOFAS scale compared to those without catatonia and parkinsonism (P < .035 and P < .027, respectively).
No significant differences in functional outcomes appeared between patients with and without dyskinesia.
However, significant negative correlations were identified for parkinsonism and PS with GAF, SOFAS, and UPSA-B (P < .036 for all). “Our study further found that parkinsonism and psychomotor slowing also impair the functional capacity of patients,” which may be influenced by factors including deficits in social interaction and cognitive impairment, the researchers said.
Overall, the study findings demonstrate that motor abnormalities in patients with schizophrenia are strongly associated with poor functional outcomes, and the stronger the motor impairment, the worse the global and social functioning, the researchers said.
As for potential pathways, “motor abnormalities are readily observable signs, allowing laypersons to perceive subjects with schizophrenia as somebody with severe mental illness. Thus, motor abnormalities might lead to stigmatization of patients suffering from schizophrenia,” they wrote in their discussion.
The researchers emphasized the need to explore alternative treatment options that might improve motor abnormalities, such as transcranial magnetic stimulation, given the potential of antipsychotic medications to introduce additional motor abnormalities.
The study findings were limited by several factors including the potential for missed confounding variables, the small number of patients with dyskinesia, and the inability to deduce the course of illness because most of the patients were in psychotic episodes, the researchers noted.
However, the results suggest that specific motor abnormalities are associated with poor global and social functioning, and with reduced functional capacity, in adults with schizophrenia, the researchers said. “Future studies need to test whether amelioration of motor abnormalities may improve community functioning,” they concluded.
The study was supported by the Swiss National Science Foundation, the Bangerter Rhyner Foundation, and the Adrian and Simone Frutiger Foundation. Lead author Dr. Nadesalingam had no financial conflicts to disclose.
Approximately half of adults with schizophrenia suffer from motor abnormalities that may impair their ability to work and decrease their quality of life, wrote Niluja Nadesalingam, MD, of the University of Bern, Switzerland, and colleagues. “Although previous reports show strong associations between single movement abnormalities and global as well as social functioning, we still struggle to understand the contribution of various motor domains,” they said.
The impact of these abnormalities on social and global functioning and on functional capacity remains unclear, but the researchers proposed that motor abnormalities would be associated with worse functional outcomes in schizophrenia patients.
In a study published in Comprehensive Psychiatry, the researchers identified patients with diagnosed schizophrenia spectrum disorders who were treated on an inpatient or outpatient basis at a single center. They collected data on five motor abnormalities: parkinsonism, catatonia, dyskinesia, neurological soft signs (NSS), and psychomotor slowing (PS). They assessed functional outcomes using the Global Assessment of Functioning (GAF), the Social and Occupational Functioning Assessment Scale (SOFAS), and the UCSD Performance-Based Skills Assessment (UPSA-B). The average age of the participants was 37.9 years and 88 of the 156 were male. The average duration of illness was 12.5 years.
Overall, patients with catatonia and parkinsonism scored significantly lower on GAF and SOFAS scale compared to those without catatonia and parkinsonism (P < .035 and P < .027, respectively).
No significant differences in functional outcomes appeared between patients with and without dyskinesia.
However, significant negative correlations were identified for parkinsonism and PS with GAF, SOFAS, and UPSA-B (P < .036 for all). “Our study further found that parkinsonism and psychomotor slowing also impair the functional capacity of patients,” which may be influenced by factors including deficits in social interaction and cognitive impairment, the researchers said.
Overall, the study findings demonstrate that motor abnormalities in patients with schizophrenia are strongly associated with poor functional outcomes, and the stronger the motor impairment, the worse the global and social functioning, the researchers said.
As for potential pathways, “motor abnormalities are readily observable signs, allowing laypersons to perceive subjects with schizophrenia as somebody with severe mental illness. Thus, motor abnormalities might lead to stigmatization of patients suffering from schizophrenia,” they wrote in their discussion.
The researchers emphasized the need to explore alternative treatment options that might improve motor abnormalities, such as transcranial magnetic stimulation, given the potential of antipsychotic medications to introduce additional motor abnormalities.
The study findings were limited by several factors including the potential for missed confounding variables, the small number of patients with dyskinesia, and the inability to deduce the course of illness because most of the patients were in psychotic episodes, the researchers noted.
However, the results suggest that specific motor abnormalities are associated with poor global and social functioning, and with reduced functional capacity, in adults with schizophrenia, the researchers said. “Future studies need to test whether amelioration of motor abnormalities may improve community functioning,” they concluded.
The study was supported by the Swiss National Science Foundation, the Bangerter Rhyner Foundation, and the Adrian and Simone Frutiger Foundation. Lead author Dr. Nadesalingam had no financial conflicts to disclose.
FROM COMPREHENSIVE PSYCHIATRY
Novel drug ‘promising’ for concomitant depression, insomnia
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.

“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”

“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.
“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”
“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.
“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”
“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
‘Alarming’ new data on disordered sleep after COVID-19
Such disturbances are especially common among Black people, new research shows.
The “high” prevalence of moderate to severe sleep disturbances is “alarming,” study investigator Cinthya Pena Orbea, MD, sleep specialist at the Cleveland Clinic, said in an interview.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Dr. Pena and colleagues analyzed data on 962 patients with PASC seen at the Cleveland Clinic ReCOVer Clinic between February 2021 and April 2022.
More than two-thirds of patients (67.2%) reported at least moderate fatigue, while 21.8% reported severe fatigue, Dr. Pena reported.
In addition, 41.3% reported at least moderate sleep disturbances, while 8% of patients reported severe sleep disturbances, including insomnia, “which may impair quality of life,” Dr. Pena said.
Obesity, mood disorders, and Black race emerged as contributors to problems with sleep and fatigue after COVID.
Notably, after adjusting for demographics, Black race conferred threefold higher odds of moderate to severe sleep disturbances.
“We don’t know why this is, and one of our next steps is to better understand race-specific determinants of sleep disturbances after COVID and create targeted interventions,” Dr. Pena said.
How long after COVID the fatigue and sleep problems last “remains uncertain,” Dr. Pena acknowledged. However, in her clinical experience with therapy, patients’ sleep and fatigue may improve after 6 or 8 months.
Ruth Benca, MD, PhD, cochair of the Alliance for Sleep, is not surprised by the Cleveland Clinic findings.
“Sleep disturbances and fatigue are part of the sequelae of COVID,” Dr. Benca, who was not involved in the study, said in an interview.
“We know that people who have had COVID have more trouble sleeping afterwards. There is the COVID insomnia created in all of us just out of our worries, fears, isolation, and stress. And then there’s an actual impact of having the infection itself on worsening sleep,” said Dr. Benca, with Wake Forest University and Atrium Health Wake Forest Baptist, both in Winston-Salem, N.C.
The study had no specific funding. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Such disturbances are especially common among Black people, new research shows.
The “high” prevalence of moderate to severe sleep disturbances is “alarming,” study investigator Cinthya Pena Orbea, MD, sleep specialist at the Cleveland Clinic, said in an interview.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Dr. Pena and colleagues analyzed data on 962 patients with PASC seen at the Cleveland Clinic ReCOVer Clinic between February 2021 and April 2022.
More than two-thirds of patients (67.2%) reported at least moderate fatigue, while 21.8% reported severe fatigue, Dr. Pena reported.
In addition, 41.3% reported at least moderate sleep disturbances, while 8% of patients reported severe sleep disturbances, including insomnia, “which may impair quality of life,” Dr. Pena said.
Obesity, mood disorders, and Black race emerged as contributors to problems with sleep and fatigue after COVID.
Notably, after adjusting for demographics, Black race conferred threefold higher odds of moderate to severe sleep disturbances.
“We don’t know why this is, and one of our next steps is to better understand race-specific determinants of sleep disturbances after COVID and create targeted interventions,” Dr. Pena said.
How long after COVID the fatigue and sleep problems last “remains uncertain,” Dr. Pena acknowledged. However, in her clinical experience with therapy, patients’ sleep and fatigue may improve after 6 or 8 months.
Ruth Benca, MD, PhD, cochair of the Alliance for Sleep, is not surprised by the Cleveland Clinic findings.
“Sleep disturbances and fatigue are part of the sequelae of COVID,” Dr. Benca, who was not involved in the study, said in an interview.
“We know that people who have had COVID have more trouble sleeping afterwards. There is the COVID insomnia created in all of us just out of our worries, fears, isolation, and stress. And then there’s an actual impact of having the infection itself on worsening sleep,” said Dr. Benca, with Wake Forest University and Atrium Health Wake Forest Baptist, both in Winston-Salem, N.C.
The study had no specific funding. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Such disturbances are especially common among Black people, new research shows.
The “high” prevalence of moderate to severe sleep disturbances is “alarming,” study investigator Cinthya Pena Orbea, MD, sleep specialist at the Cleveland Clinic, said in an interview.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Dr. Pena and colleagues analyzed data on 962 patients with PASC seen at the Cleveland Clinic ReCOVer Clinic between February 2021 and April 2022.
More than two-thirds of patients (67.2%) reported at least moderate fatigue, while 21.8% reported severe fatigue, Dr. Pena reported.
In addition, 41.3% reported at least moderate sleep disturbances, while 8% of patients reported severe sleep disturbances, including insomnia, “which may impair quality of life,” Dr. Pena said.
Obesity, mood disorders, and Black race emerged as contributors to problems with sleep and fatigue after COVID.
Notably, after adjusting for demographics, Black race conferred threefold higher odds of moderate to severe sleep disturbances.
“We don’t know why this is, and one of our next steps is to better understand race-specific determinants of sleep disturbances after COVID and create targeted interventions,” Dr. Pena said.
How long after COVID the fatigue and sleep problems last “remains uncertain,” Dr. Pena acknowledged. However, in her clinical experience with therapy, patients’ sleep and fatigue may improve after 6 or 8 months.
Ruth Benca, MD, PhD, cochair of the Alliance for Sleep, is not surprised by the Cleveland Clinic findings.
“Sleep disturbances and fatigue are part of the sequelae of COVID,” Dr. Benca, who was not involved in the study, said in an interview.
“We know that people who have had COVID have more trouble sleeping afterwards. There is the COVID insomnia created in all of us just out of our worries, fears, isolation, and stress. And then there’s an actual impact of having the infection itself on worsening sleep,” said Dr. Benca, with Wake Forest University and Atrium Health Wake Forest Baptist, both in Winston-Salem, N.C.
The study had no specific funding. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2022
Substance use the main cause of physician license actions
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
FROM JAMA
FDA panel strongly backs protein-based Novavax COVID-19 vaccine
than the cutting-edge technology used in mRNA-based shots.
The Vaccines and Related Biological Products Advisory Committee of the Food and Drug Administration voted almost unanimously June 7 in favor of Novavax’s two-dose COVID-19 vaccine for those 18 or older – despite some concerns over rare events of myocarditis and pericarditis.
The tally was 21 “yes” votes, without any “no” votes, but one abstention from a panelist who then offered a largely positive take on this vaccine.
Panelist Bruce Gellin, MD, explained at the end of the meeting that he would have cast a conditional vote in favor of the Novavax vaccine, called NVX-CoV2373, had that been an option. Dr. Gellin, chief of global public health strategy for the Rockefeller Foundation and a vaccine expert, said he didn’t want his abstention to be considered as signaling opposition to the Novavax shot.
Instead, he said, he expects FDA officials will gather more data and evidence about the Novavax vaccine, especially in relation to certain manufacturing issues, before making its decision on the company’s application.
Earlier in the day, a top FDA vaccine reviewer, Doran Fink, MD, PhD, noted that there were important manufacturing differences between the Novavax vaccine supply used in different projects, complicating efforts to assess the company’s application for emergency use authorization (EUA).
But Dr. Fink noted that the FDA staff already had made a convincing case in its briefing document, with enough evidence for an initial conditional clearance to be found in available data.
The FDA is not bound to follow the suggestions of its advisory committees but it often does.
Using the ‘bully pulpit’
At the beginning of the meeting, Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said he was seizing the “bully pulpit” in addressing the need to persuade more people in the United States to take shots against COVID-19.
About 67% of people in the United States aged 18 and older are fully vaccinated, but only about 50% of those in this group have had a first booster, according to the Centers for Disease Control and Prevention.
The two-dose mRNA vaccines from Pfizer and Moderna have been the subject of intense misinformation campaigns on social media, despite efforts by the FDA and other public health officials to convey the message about their strong benefit-risk profile. The FDA in May limited the authorized use of Johnson & Johnson’s single-dose COVID-19 shot, which is based on a different technology, because of concerns about rare and potentially life-threatening blood clots.
Novavax has been described as a more traditional vaccine – a protein subunit shot similar to one people have long received for protection against influenza, pertussis (whooping cough), diphtheria, and tetanus.
“Having a protein-based alternative may be more comfortable for some in terms of their acceptance of vaccines,” Dr. Marks said. “We do have a problem with vaccine uptake that is very serious in the United States. And anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do.”
Dr. Marks offered these remarks in answer to an FDA panelist’s question about the need to consider an EUA for yet another vaccine.
EUAs are special clearances the FDA can grant in connection with public health emergencies such as the pandemic. The FDA used EUAs for the initial December 2020 clearances of the Pfizer-BioNTech and Moderna vaccines. It has since granted normal approvals for both of these mRNA-based vaccines, based on larger bodies of evidence gathered and submitted by their developers.
During the meeting, the FDA panelists in general appeared comfortable with the idea of granting another EUA for a vaccine. There was agreement that the shot appeared to work in key tests, although these were done before the rise of the Omicron variant.
In a key test, known as study 301, the Novavax vaccine was judged to be 90.4% effective. In the study, 17 of the 17,272 people who got the Novavax vaccine developed COVID-19, compared with 79 of the 8,385 in the placebo group.
Panelists expressed disappointment with the lack of information about how the shot would work now.
“We’re looking at the efficacy against strains that don’t exist any longer,” said panelist Eric J. Rubin, MD, PhD, a Harvard professor and editor of the New England Journal of Medicine.
Still, Dr. Rubin added that he agreed with the argument the FDA’s Dr. Marks had made earlier for an EUA for the Novavax vaccine.
“If there really is a population of patients who are willing to take this and not willing to take the existing vaccines, I think it’s pretty compelling,” Dr. Rubin said.
Other FDA panelists were skeptical of this argument. Jay Portnoy, MD, who was listed on the FDA roster as the panel’s consumer representative, said he has close friends who are vaccine skeptics.
“Their hesitancy is more ideological than technological,” said Dr. Portnoy of Children’s Mercy Hospital, Kansas City, Mo. “So I really doubt that this vaccine is going to crack that nut, but perhaps some individuals would get this when they wouldn’t get the other ones.”
Myocarditis, pericarditis
The Novavax vaccine is already authorized in other countries, including Canada. Novavax in February announced that it had begun shipping its first doses of the vaccine to European Union member states. The vaccine can be moved through existing vaccine supply and cold chain channels instead of requiring complex new delivery procedures.
That could prove an advantage in time, said FDA panelist Michael Nelson, MD, PhD, of the University of Virginia, Charlottesville.
“Who knows even with supply chain challenges down the road, it will be nice to have options going forward,” Dr. Nelson said.
As with other COVID-19 vaccines, clinicians and researchers are still working to understand the potential risk for inflammation of heart muscle and nearby tissue with vaccination. Most patients with myocarditis or pericarditis who sought medical care for these conditions responded well to medicine and rest and felt better quickly, the CDC says on its website. They usually return to their normal daily activities after their symptoms improve.
At the June 7 meeting, Dr. Nelson said there may be cases of myocarditis that go undetected.
“Our signals are those who get admitted to the emergency room and the hospital,” he said. “I’m quite convinced that there are others who are experiencing cardiac events of lesser severity that are worthy of being studied, both from mechanistic and outcomes standpoints. So we have a lot of work to do.”
In looking at results for an initial pool of 40,000 people who received the Novavax vaccine, there were five reported cases of myocarditis or pericarditis developing within 20 days of people getting the shot, the FDA staff said in its presentation on safety.
In a briefing document released ahead of the advisory committee meeting, the FDA staff flagged this number of cases in a relatively small database as a concern, noting it “could be higher than reported during postauthorization use of mRNA COVID-19 vaccines (for which no cases were identified in preauthorization evaluation).”
Novavax officials took a somewhat unusual step of responding in public. The Gaithersburg, Md.–based company on June 3 issued a statement saying researchers had come to “expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.”
The data from the company’s placebo-controlled studies show that, overall, in its clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%), Novavax said.
At the June 7 meeting, FDA panelists including Dr. Nelson, and Paul A. Offit, MD, of Children’s Hospital of Philadelphia, urged continued study to try to determine whether and how the vaccines could trigger myocarditis. Investments made now in pursuing these questions related to COVID-19 shots may pay off later, Dr. Offit said.
“We can use that knowledge to make safer vaccines for a disease that is going to be with us for decades, if not longer,” he said.
A version of this article first appeared on Medscape.com.
than the cutting-edge technology used in mRNA-based shots.
The Vaccines and Related Biological Products Advisory Committee of the Food and Drug Administration voted almost unanimously June 7 in favor of Novavax’s two-dose COVID-19 vaccine for those 18 or older – despite some concerns over rare events of myocarditis and pericarditis.
The tally was 21 “yes” votes, without any “no” votes, but one abstention from a panelist who then offered a largely positive take on this vaccine.
Panelist Bruce Gellin, MD, explained at the end of the meeting that he would have cast a conditional vote in favor of the Novavax vaccine, called NVX-CoV2373, had that been an option. Dr. Gellin, chief of global public health strategy for the Rockefeller Foundation and a vaccine expert, said he didn’t want his abstention to be considered as signaling opposition to the Novavax shot.
Instead, he said, he expects FDA officials will gather more data and evidence about the Novavax vaccine, especially in relation to certain manufacturing issues, before making its decision on the company’s application.
Earlier in the day, a top FDA vaccine reviewer, Doran Fink, MD, PhD, noted that there were important manufacturing differences between the Novavax vaccine supply used in different projects, complicating efforts to assess the company’s application for emergency use authorization (EUA).
But Dr. Fink noted that the FDA staff already had made a convincing case in its briefing document, with enough evidence for an initial conditional clearance to be found in available data.
The FDA is not bound to follow the suggestions of its advisory committees but it often does.
Using the ‘bully pulpit’
At the beginning of the meeting, Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said he was seizing the “bully pulpit” in addressing the need to persuade more people in the United States to take shots against COVID-19.
About 67% of people in the United States aged 18 and older are fully vaccinated, but only about 50% of those in this group have had a first booster, according to the Centers for Disease Control and Prevention.
The two-dose mRNA vaccines from Pfizer and Moderna have been the subject of intense misinformation campaigns on social media, despite efforts by the FDA and other public health officials to convey the message about their strong benefit-risk profile. The FDA in May limited the authorized use of Johnson & Johnson’s single-dose COVID-19 shot, which is based on a different technology, because of concerns about rare and potentially life-threatening blood clots.
Novavax has been described as a more traditional vaccine – a protein subunit shot similar to one people have long received for protection against influenza, pertussis (whooping cough), diphtheria, and tetanus.
“Having a protein-based alternative may be more comfortable for some in terms of their acceptance of vaccines,” Dr. Marks said. “We do have a problem with vaccine uptake that is very serious in the United States. And anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do.”
Dr. Marks offered these remarks in answer to an FDA panelist’s question about the need to consider an EUA for yet another vaccine.
EUAs are special clearances the FDA can grant in connection with public health emergencies such as the pandemic. The FDA used EUAs for the initial December 2020 clearances of the Pfizer-BioNTech and Moderna vaccines. It has since granted normal approvals for both of these mRNA-based vaccines, based on larger bodies of evidence gathered and submitted by their developers.
During the meeting, the FDA panelists in general appeared comfortable with the idea of granting another EUA for a vaccine. There was agreement that the shot appeared to work in key tests, although these were done before the rise of the Omicron variant.
In a key test, known as study 301, the Novavax vaccine was judged to be 90.4% effective. In the study, 17 of the 17,272 people who got the Novavax vaccine developed COVID-19, compared with 79 of the 8,385 in the placebo group.
Panelists expressed disappointment with the lack of information about how the shot would work now.
“We’re looking at the efficacy against strains that don’t exist any longer,” said panelist Eric J. Rubin, MD, PhD, a Harvard professor and editor of the New England Journal of Medicine.
Still, Dr. Rubin added that he agreed with the argument the FDA’s Dr. Marks had made earlier for an EUA for the Novavax vaccine.
“If there really is a population of patients who are willing to take this and not willing to take the existing vaccines, I think it’s pretty compelling,” Dr. Rubin said.
Other FDA panelists were skeptical of this argument. Jay Portnoy, MD, who was listed on the FDA roster as the panel’s consumer representative, said he has close friends who are vaccine skeptics.
“Their hesitancy is more ideological than technological,” said Dr. Portnoy of Children’s Mercy Hospital, Kansas City, Mo. “So I really doubt that this vaccine is going to crack that nut, but perhaps some individuals would get this when they wouldn’t get the other ones.”
Myocarditis, pericarditis
The Novavax vaccine is already authorized in other countries, including Canada. Novavax in February announced that it had begun shipping its first doses of the vaccine to European Union member states. The vaccine can be moved through existing vaccine supply and cold chain channels instead of requiring complex new delivery procedures.
That could prove an advantage in time, said FDA panelist Michael Nelson, MD, PhD, of the University of Virginia, Charlottesville.
“Who knows even with supply chain challenges down the road, it will be nice to have options going forward,” Dr. Nelson said.
As with other COVID-19 vaccines, clinicians and researchers are still working to understand the potential risk for inflammation of heart muscle and nearby tissue with vaccination. Most patients with myocarditis or pericarditis who sought medical care for these conditions responded well to medicine and rest and felt better quickly, the CDC says on its website. They usually return to their normal daily activities after their symptoms improve.
At the June 7 meeting, Dr. Nelson said there may be cases of myocarditis that go undetected.
“Our signals are those who get admitted to the emergency room and the hospital,” he said. “I’m quite convinced that there are others who are experiencing cardiac events of lesser severity that are worthy of being studied, both from mechanistic and outcomes standpoints. So we have a lot of work to do.”
In looking at results for an initial pool of 40,000 people who received the Novavax vaccine, there were five reported cases of myocarditis or pericarditis developing within 20 days of people getting the shot, the FDA staff said in its presentation on safety.
In a briefing document released ahead of the advisory committee meeting, the FDA staff flagged this number of cases in a relatively small database as a concern, noting it “could be higher than reported during postauthorization use of mRNA COVID-19 vaccines (for which no cases were identified in preauthorization evaluation).”
Novavax officials took a somewhat unusual step of responding in public. The Gaithersburg, Md.–based company on June 3 issued a statement saying researchers had come to “expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.”
The data from the company’s placebo-controlled studies show that, overall, in its clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%), Novavax said.
At the June 7 meeting, FDA panelists including Dr. Nelson, and Paul A. Offit, MD, of Children’s Hospital of Philadelphia, urged continued study to try to determine whether and how the vaccines could trigger myocarditis. Investments made now in pursuing these questions related to COVID-19 shots may pay off later, Dr. Offit said.
“We can use that knowledge to make safer vaccines for a disease that is going to be with us for decades, if not longer,” he said.
A version of this article first appeared on Medscape.com.
than the cutting-edge technology used in mRNA-based shots.
The Vaccines and Related Biological Products Advisory Committee of the Food and Drug Administration voted almost unanimously June 7 in favor of Novavax’s two-dose COVID-19 vaccine for those 18 or older – despite some concerns over rare events of myocarditis and pericarditis.
The tally was 21 “yes” votes, without any “no” votes, but one abstention from a panelist who then offered a largely positive take on this vaccine.
Panelist Bruce Gellin, MD, explained at the end of the meeting that he would have cast a conditional vote in favor of the Novavax vaccine, called NVX-CoV2373, had that been an option. Dr. Gellin, chief of global public health strategy for the Rockefeller Foundation and a vaccine expert, said he didn’t want his abstention to be considered as signaling opposition to the Novavax shot.
Instead, he said, he expects FDA officials will gather more data and evidence about the Novavax vaccine, especially in relation to certain manufacturing issues, before making its decision on the company’s application.
Earlier in the day, a top FDA vaccine reviewer, Doran Fink, MD, PhD, noted that there were important manufacturing differences between the Novavax vaccine supply used in different projects, complicating efforts to assess the company’s application for emergency use authorization (EUA).
But Dr. Fink noted that the FDA staff already had made a convincing case in its briefing document, with enough evidence for an initial conditional clearance to be found in available data.
The FDA is not bound to follow the suggestions of its advisory committees but it often does.
Using the ‘bully pulpit’
At the beginning of the meeting, Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said he was seizing the “bully pulpit” in addressing the need to persuade more people in the United States to take shots against COVID-19.
About 67% of people in the United States aged 18 and older are fully vaccinated, but only about 50% of those in this group have had a first booster, according to the Centers for Disease Control and Prevention.
The two-dose mRNA vaccines from Pfizer and Moderna have been the subject of intense misinformation campaigns on social media, despite efforts by the FDA and other public health officials to convey the message about their strong benefit-risk profile. The FDA in May limited the authorized use of Johnson & Johnson’s single-dose COVID-19 shot, which is based on a different technology, because of concerns about rare and potentially life-threatening blood clots.
Novavax has been described as a more traditional vaccine – a protein subunit shot similar to one people have long received for protection against influenza, pertussis (whooping cough), diphtheria, and tetanus.
“Having a protein-based alternative may be more comfortable for some in terms of their acceptance of vaccines,” Dr. Marks said. “We do have a problem with vaccine uptake that is very serious in the United States. And anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do.”
Dr. Marks offered these remarks in answer to an FDA panelist’s question about the need to consider an EUA for yet another vaccine.
EUAs are special clearances the FDA can grant in connection with public health emergencies such as the pandemic. The FDA used EUAs for the initial December 2020 clearances of the Pfizer-BioNTech and Moderna vaccines. It has since granted normal approvals for both of these mRNA-based vaccines, based on larger bodies of evidence gathered and submitted by their developers.
During the meeting, the FDA panelists in general appeared comfortable with the idea of granting another EUA for a vaccine. There was agreement that the shot appeared to work in key tests, although these were done before the rise of the Omicron variant.
In a key test, known as study 301, the Novavax vaccine was judged to be 90.4% effective. In the study, 17 of the 17,272 people who got the Novavax vaccine developed COVID-19, compared with 79 of the 8,385 in the placebo group.
Panelists expressed disappointment with the lack of information about how the shot would work now.
“We’re looking at the efficacy against strains that don’t exist any longer,” said panelist Eric J. Rubin, MD, PhD, a Harvard professor and editor of the New England Journal of Medicine.
Still, Dr. Rubin added that he agreed with the argument the FDA’s Dr. Marks had made earlier for an EUA for the Novavax vaccine.
“If there really is a population of patients who are willing to take this and not willing to take the existing vaccines, I think it’s pretty compelling,” Dr. Rubin said.
Other FDA panelists were skeptical of this argument. Jay Portnoy, MD, who was listed on the FDA roster as the panel’s consumer representative, said he has close friends who are vaccine skeptics.
“Their hesitancy is more ideological than technological,” said Dr. Portnoy of Children’s Mercy Hospital, Kansas City, Mo. “So I really doubt that this vaccine is going to crack that nut, but perhaps some individuals would get this when they wouldn’t get the other ones.”
Myocarditis, pericarditis
The Novavax vaccine is already authorized in other countries, including Canada. Novavax in February announced that it had begun shipping its first doses of the vaccine to European Union member states. The vaccine can be moved through existing vaccine supply and cold chain channels instead of requiring complex new delivery procedures.
That could prove an advantage in time, said FDA panelist Michael Nelson, MD, PhD, of the University of Virginia, Charlottesville.
“Who knows even with supply chain challenges down the road, it will be nice to have options going forward,” Dr. Nelson said.
As with other COVID-19 vaccines, clinicians and researchers are still working to understand the potential risk for inflammation of heart muscle and nearby tissue with vaccination. Most patients with myocarditis or pericarditis who sought medical care for these conditions responded well to medicine and rest and felt better quickly, the CDC says on its website. They usually return to their normal daily activities after their symptoms improve.
At the June 7 meeting, Dr. Nelson said there may be cases of myocarditis that go undetected.
“Our signals are those who get admitted to the emergency room and the hospital,” he said. “I’m quite convinced that there are others who are experiencing cardiac events of lesser severity that are worthy of being studied, both from mechanistic and outcomes standpoints. So we have a lot of work to do.”
In looking at results for an initial pool of 40,000 people who received the Novavax vaccine, there were five reported cases of myocarditis or pericarditis developing within 20 days of people getting the shot, the FDA staff said in its presentation on safety.
In a briefing document released ahead of the advisory committee meeting, the FDA staff flagged this number of cases in a relatively small database as a concern, noting it “could be higher than reported during postauthorization use of mRNA COVID-19 vaccines (for which no cases were identified in preauthorization evaluation).”
Novavax officials took a somewhat unusual step of responding in public. The Gaithersburg, Md.–based company on June 3 issued a statement saying researchers had come to “expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.”
The data from the company’s placebo-controlled studies show that, overall, in its clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%), Novavax said.
At the June 7 meeting, FDA panelists including Dr. Nelson, and Paul A. Offit, MD, of Children’s Hospital of Philadelphia, urged continued study to try to determine whether and how the vaccines could trigger myocarditis. Investments made now in pursuing these questions related to COVID-19 shots may pay off later, Dr. Offit said.
“We can use that knowledge to make safer vaccines for a disease that is going to be with us for decades, if not longer,” he said.
A version of this article first appeared on Medscape.com.
Social activities may offset psychosis risk in poor communities
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.

The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
Antipsychotic tied to dose-related weight gain, higher cholesterol
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.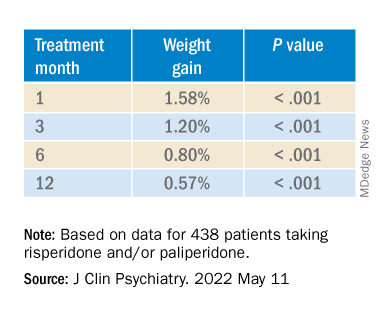
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.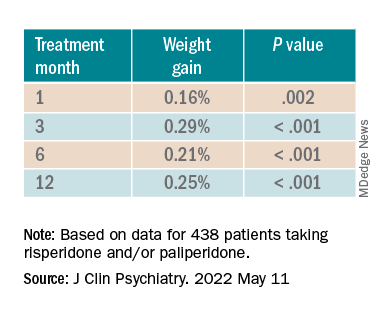
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.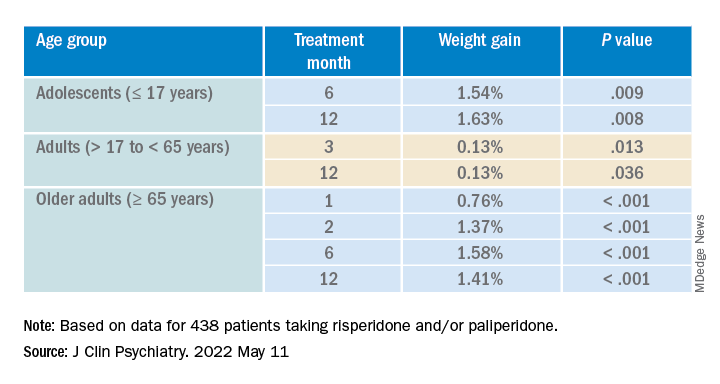
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”

It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Cannabis may relieve pain as effectively as opioids, but more research is needed
Several other systematic reviews have recently evaluated cannabinoids for treating chronic pain, but the new study’s methodology was “distinct” in “important ways,” leading to “conclusions that differ from other reviews,” according to the authors of the paper published in the Annals of Internal Medicine.
In the new systematic review, synthetic products with high THC:CBD ratios were associated with moderate improvements in pain, whereas plant-based products with comparable THC:CBD ratios offered less relief, said study author Marian S. McDonagh, PharmD, professor of medical informatics and clinical epidemiology, and codirector of the Evidence-based Practice Center at Oregon Health & Science University, Portland, and colleagues.
Specifically, the investigators stratified cannabis-based interventions according to relative content of two key cannabinoids: THC and CBD. Products were sorted into five categories: high THC:CBD ratio (at least 2:1), comparable THC:CBD ratio (less than 2:1 but more than 1:2), low THC:CBD ratio (no more than 1:2), whole-plant cannabis products, and other cannabinoids.
“In preclinical studies, THC and related compounds have demonstrated analgesic properties, although its psychoactive effects and addiction potential may limit its suitability as an analgesic,” the investigators wrote. “CBD and other cannabinoids may also have some analgesic or anti-inflammatory properties and are not believed to be psychoactive or addictive. Given the variation in analgesic effect with THC and CBD, response may differ according to the ratio of THC to CBD in products used to treat pain.”
The final analysis included 18 randomized placebo-controlled trials involving 1,740 individuals and 7 cohort studies involving 13,095 individuals. Most of the studies were short-term, lasting 1-6 months.
Pain was scored on a ten-point scale, with improvements reported as the mean difference from baseline to post treatment. A mean difference in pain score of 0.5-1.0 was considered a “small effect,” an improvement of 1-2 points was considered a “moderate effect,” and an improvement greater than 2 points was considered a “large effect.”
Cannabis-based products with relatively high THC:CBD ratios showed efficacy
Synthetic products with high THC:CBD ratios offered moderate pain relief, based on a mean difference in pain score of –1.15 (95% confidence interval, –1.99 to –0.54), whereas products with comparable THC:CBD ratios were associated with a small effect on pain, with a mean difference of –0.52 (95% CI, –0.95 to –0.19).
According to Dr. McDonagh, treatment response rates were on par with response rates for more conventional treatments, “such as opioids or specific antidepressant drugs,” but data for the cannabis-based products are weaker.
“The amount of evidence available for cannabis-related products is very limited for [response rates], and therefore less certain,” Dr. McDonagh said in an interview. “The average reduction in pain severity is also similar to some other treatments, but we do not have studies directly comparing these treatments to draw conclusions.”
Although the cannabis-based products with relatively high and comparable THC:CBD ratios showed efficacy, they were also associated with “moderate to large increased risk for dizziness, sedation, and nausea,” the investigators wrote, noting that evidence was insufficient to characterize other “key adverse event outcomes” that may occur with long-term use, such as “psychosis, cannabis use disorder, and cognitive deficits.”
For products with low THC:CBD ratios, or without reported THC:CBD ratios, data were too scarce to reach any conclusions at all about safety or efficacy, highlighting the sizable knowledge gaps that remain in the area, the authors said.
“The current evidence on cannabis-related products for chronic pain is quite limited,” Dr. McDonagh said in an interview. “Patients with chronic pain should consult with their doctor to discuss which of the many options for treating chronic pain is best for them to start with.”
Patients may face resistance when asking about cannabis
According to Kevin F. Boehnke, PhD, and Daniel J. Clauw, MD, of the anesthesiology department and Chronic Pain and Fatigue Research Center at the University of Michigan, Ann Arbor, patients with chronic pain may face resistance, or even risk of being reported, when asking about cannabis-based products.
“Some physicians cite lack of data as rationale for not engaging with patients who wish to use or currently use cannabis,” Dr. Boehnke and Dr. Clauw wrote in an accompanying editorial. “Such practices may reflect consideration of cannabis solely as a drug of misuse (even in the 37 states where medical cannabis is legal) and requirements to refer patients who disclose or test positive for cannabis use to addiction services or decline to refill opioid prescriptions.”
Instead of shutting patients out, Dr. Boehnke and Dr. Clauw suggested clinicians engage in an “open information exchange” with their patients that focuses on “pragmatism, patient experience, known cannabinoid effects, and harm reduction.” In these conversations, the editorialists recommend noting that, “as with other analgesics, some persons will benefit, and others will not.”
They also offered some practical guidance: “Clinicians could suggest using tinctures (effect onset, 15-45 minutes) for breakthrough pain and edibles or capsules (which last about 6-8 hours) for extended relief. ... The scientific literature suggests that CBD doses could start at 5-10 mg twice daily and increase to 40-50 mg daily, whereas THC doses could start at 0.5-3 mg (initially at night) and increase to 30-40 mg/day.”
David Copenhaver, MD, MPH, clinical professor and chief of the division of pain medicine at UC Davis Health, Sacramento, shared a similar clinical mindset for patients choosing between opioids and cannabis-based products, specifically, CBD.
Compared with opioids, “the side-effect profile for CBD is less and the risk of mortality is less,” Dr. Copenhaver said in an interview, pointing out that nobody, to his knowledge, has ever died from an overdose of cannabis alone, and that CBD doses up to 1,000 mg/kg have been safely tolerated in people. “You present that, and most patients will say, ‘You know, I’d like to give this a try.’”
If so, Dr. Copenhaver makes sure patients know about a nonmedical risk: “The risk to the pocketbook.” Unlike opioids, which are covered under most insurance policies, most cannabis-based therapies are self-pay.
Buyers may get what they pay for, Dr. Copenhaver said, since products vary in quality, as do the dispensaries, from “very modest,” to highly sophisticated, with some even using chromatographic datasets to support the purity of their products.
Dr. Copenhaver steers his patients toward these more sophisticated retailers. Their expertise appears to be paying off, he said, not only in relief for patients, but also in market share. “Survival of the most fit will occur in the marketplace based on the results,” he said. “Unfortunately, some of that information doesn’t get percolated out into the literature.”
For investigators to fully uncover what cannabis-based products can do for chronic pain, Dr. Copenhaver said they need to get as “granular” as the leading dispensaries, which may first require recognition of the “very expansive opportunity” that less-studied cannabinoids may provide.
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators, Dr. Boehnke, Dr. Clauw, and Dr. Copenhaver, disclosed no conflicts of interest.
Several other systematic reviews have recently evaluated cannabinoids for treating chronic pain, but the new study’s methodology was “distinct” in “important ways,” leading to “conclusions that differ from other reviews,” according to the authors of the paper published in the Annals of Internal Medicine.
In the new systematic review, synthetic products with high THC:CBD ratios were associated with moderate improvements in pain, whereas plant-based products with comparable THC:CBD ratios offered less relief, said study author Marian S. McDonagh, PharmD, professor of medical informatics and clinical epidemiology, and codirector of the Evidence-based Practice Center at Oregon Health & Science University, Portland, and colleagues.
Specifically, the investigators stratified cannabis-based interventions according to relative content of two key cannabinoids: THC and CBD. Products were sorted into five categories: high THC:CBD ratio (at least 2:1), comparable THC:CBD ratio (less than 2:1 but more than 1:2), low THC:CBD ratio (no more than 1:2), whole-plant cannabis products, and other cannabinoids.
“In preclinical studies, THC and related compounds have demonstrated analgesic properties, although its psychoactive effects and addiction potential may limit its suitability as an analgesic,” the investigators wrote. “CBD and other cannabinoids may also have some analgesic or anti-inflammatory properties and are not believed to be psychoactive or addictive. Given the variation in analgesic effect with THC and CBD, response may differ according to the ratio of THC to CBD in products used to treat pain.”
The final analysis included 18 randomized placebo-controlled trials involving 1,740 individuals and 7 cohort studies involving 13,095 individuals. Most of the studies were short-term, lasting 1-6 months.
Pain was scored on a ten-point scale, with improvements reported as the mean difference from baseline to post treatment. A mean difference in pain score of 0.5-1.0 was considered a “small effect,” an improvement of 1-2 points was considered a “moderate effect,” and an improvement greater than 2 points was considered a “large effect.”
Cannabis-based products with relatively high THC:CBD ratios showed efficacy
Synthetic products with high THC:CBD ratios offered moderate pain relief, based on a mean difference in pain score of –1.15 (95% confidence interval, –1.99 to –0.54), whereas products with comparable THC:CBD ratios were associated with a small effect on pain, with a mean difference of –0.52 (95% CI, –0.95 to –0.19).
According to Dr. McDonagh, treatment response rates were on par with response rates for more conventional treatments, “such as opioids or specific antidepressant drugs,” but data for the cannabis-based products are weaker.
“The amount of evidence available for cannabis-related products is very limited for [response rates], and therefore less certain,” Dr. McDonagh said in an interview. “The average reduction in pain severity is also similar to some other treatments, but we do not have studies directly comparing these treatments to draw conclusions.”
Although the cannabis-based products with relatively high and comparable THC:CBD ratios showed efficacy, they were also associated with “moderate to large increased risk for dizziness, sedation, and nausea,” the investigators wrote, noting that evidence was insufficient to characterize other “key adverse event outcomes” that may occur with long-term use, such as “psychosis, cannabis use disorder, and cognitive deficits.”
For products with low THC:CBD ratios, or without reported THC:CBD ratios, data were too scarce to reach any conclusions at all about safety or efficacy, highlighting the sizable knowledge gaps that remain in the area, the authors said.
“The current evidence on cannabis-related products for chronic pain is quite limited,” Dr. McDonagh said in an interview. “Patients with chronic pain should consult with their doctor to discuss which of the many options for treating chronic pain is best for them to start with.”
Patients may face resistance when asking about cannabis
According to Kevin F. Boehnke, PhD, and Daniel J. Clauw, MD, of the anesthesiology department and Chronic Pain and Fatigue Research Center at the University of Michigan, Ann Arbor, patients with chronic pain may face resistance, or even risk of being reported, when asking about cannabis-based products.
“Some physicians cite lack of data as rationale for not engaging with patients who wish to use or currently use cannabis,” Dr. Boehnke and Dr. Clauw wrote in an accompanying editorial. “Such practices may reflect consideration of cannabis solely as a drug of misuse (even in the 37 states where medical cannabis is legal) and requirements to refer patients who disclose or test positive for cannabis use to addiction services or decline to refill opioid prescriptions.”
Instead of shutting patients out, Dr. Boehnke and Dr. Clauw suggested clinicians engage in an “open information exchange” with their patients that focuses on “pragmatism, patient experience, known cannabinoid effects, and harm reduction.” In these conversations, the editorialists recommend noting that, “as with other analgesics, some persons will benefit, and others will not.”
They also offered some practical guidance: “Clinicians could suggest using tinctures (effect onset, 15-45 minutes) for breakthrough pain and edibles or capsules (which last about 6-8 hours) for extended relief. ... The scientific literature suggests that CBD doses could start at 5-10 mg twice daily and increase to 40-50 mg daily, whereas THC doses could start at 0.5-3 mg (initially at night) and increase to 30-40 mg/day.”
David Copenhaver, MD, MPH, clinical professor and chief of the division of pain medicine at UC Davis Health, Sacramento, shared a similar clinical mindset for patients choosing between opioids and cannabis-based products, specifically, CBD.
Compared with opioids, “the side-effect profile for CBD is less and the risk of mortality is less,” Dr. Copenhaver said in an interview, pointing out that nobody, to his knowledge, has ever died from an overdose of cannabis alone, and that CBD doses up to 1,000 mg/kg have been safely tolerated in people. “You present that, and most patients will say, ‘You know, I’d like to give this a try.’”
If so, Dr. Copenhaver makes sure patients know about a nonmedical risk: “The risk to the pocketbook.” Unlike opioids, which are covered under most insurance policies, most cannabis-based therapies are self-pay.
Buyers may get what they pay for, Dr. Copenhaver said, since products vary in quality, as do the dispensaries, from “very modest,” to highly sophisticated, with some even using chromatographic datasets to support the purity of their products.
Dr. Copenhaver steers his patients toward these more sophisticated retailers. Their expertise appears to be paying off, he said, not only in relief for patients, but also in market share. “Survival of the most fit will occur in the marketplace based on the results,” he said. “Unfortunately, some of that information doesn’t get percolated out into the literature.”
For investigators to fully uncover what cannabis-based products can do for chronic pain, Dr. Copenhaver said they need to get as “granular” as the leading dispensaries, which may first require recognition of the “very expansive opportunity” that less-studied cannabinoids may provide.
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators, Dr. Boehnke, Dr. Clauw, and Dr. Copenhaver, disclosed no conflicts of interest.
Several other systematic reviews have recently evaluated cannabinoids for treating chronic pain, but the new study’s methodology was “distinct” in “important ways,” leading to “conclusions that differ from other reviews,” according to the authors of the paper published in the Annals of Internal Medicine.
In the new systematic review, synthetic products with high THC:CBD ratios were associated with moderate improvements in pain, whereas plant-based products with comparable THC:CBD ratios offered less relief, said study author Marian S. McDonagh, PharmD, professor of medical informatics and clinical epidemiology, and codirector of the Evidence-based Practice Center at Oregon Health & Science University, Portland, and colleagues.
Specifically, the investigators stratified cannabis-based interventions according to relative content of two key cannabinoids: THC and CBD. Products were sorted into five categories: high THC:CBD ratio (at least 2:1), comparable THC:CBD ratio (less than 2:1 but more than 1:2), low THC:CBD ratio (no more than 1:2), whole-plant cannabis products, and other cannabinoids.
“In preclinical studies, THC and related compounds have demonstrated analgesic properties, although its psychoactive effects and addiction potential may limit its suitability as an analgesic,” the investigators wrote. “CBD and other cannabinoids may also have some analgesic or anti-inflammatory properties and are not believed to be psychoactive or addictive. Given the variation in analgesic effect with THC and CBD, response may differ according to the ratio of THC to CBD in products used to treat pain.”
The final analysis included 18 randomized placebo-controlled trials involving 1,740 individuals and 7 cohort studies involving 13,095 individuals. Most of the studies were short-term, lasting 1-6 months.
Pain was scored on a ten-point scale, with improvements reported as the mean difference from baseline to post treatment. A mean difference in pain score of 0.5-1.0 was considered a “small effect,” an improvement of 1-2 points was considered a “moderate effect,” and an improvement greater than 2 points was considered a “large effect.”
Cannabis-based products with relatively high THC:CBD ratios showed efficacy
Synthetic products with high THC:CBD ratios offered moderate pain relief, based on a mean difference in pain score of –1.15 (95% confidence interval, –1.99 to –0.54), whereas products with comparable THC:CBD ratios were associated with a small effect on pain, with a mean difference of –0.52 (95% CI, –0.95 to –0.19).
According to Dr. McDonagh, treatment response rates were on par with response rates for more conventional treatments, “such as opioids or specific antidepressant drugs,” but data for the cannabis-based products are weaker.
“The amount of evidence available for cannabis-related products is very limited for [response rates], and therefore less certain,” Dr. McDonagh said in an interview. “The average reduction in pain severity is also similar to some other treatments, but we do not have studies directly comparing these treatments to draw conclusions.”
Although the cannabis-based products with relatively high and comparable THC:CBD ratios showed efficacy, they were also associated with “moderate to large increased risk for dizziness, sedation, and nausea,” the investigators wrote, noting that evidence was insufficient to characterize other “key adverse event outcomes” that may occur with long-term use, such as “psychosis, cannabis use disorder, and cognitive deficits.”
For products with low THC:CBD ratios, or without reported THC:CBD ratios, data were too scarce to reach any conclusions at all about safety or efficacy, highlighting the sizable knowledge gaps that remain in the area, the authors said.
“The current evidence on cannabis-related products for chronic pain is quite limited,” Dr. McDonagh said in an interview. “Patients with chronic pain should consult with their doctor to discuss which of the many options for treating chronic pain is best for them to start with.”
Patients may face resistance when asking about cannabis
According to Kevin F. Boehnke, PhD, and Daniel J. Clauw, MD, of the anesthesiology department and Chronic Pain and Fatigue Research Center at the University of Michigan, Ann Arbor, patients with chronic pain may face resistance, or even risk of being reported, when asking about cannabis-based products.
“Some physicians cite lack of data as rationale for not engaging with patients who wish to use or currently use cannabis,” Dr. Boehnke and Dr. Clauw wrote in an accompanying editorial. “Such practices may reflect consideration of cannabis solely as a drug of misuse (even in the 37 states where medical cannabis is legal) and requirements to refer patients who disclose or test positive for cannabis use to addiction services or decline to refill opioid prescriptions.”
Instead of shutting patients out, Dr. Boehnke and Dr. Clauw suggested clinicians engage in an “open information exchange” with their patients that focuses on “pragmatism, patient experience, known cannabinoid effects, and harm reduction.” In these conversations, the editorialists recommend noting that, “as with other analgesics, some persons will benefit, and others will not.”
They also offered some practical guidance: “Clinicians could suggest using tinctures (effect onset, 15-45 minutes) for breakthrough pain and edibles or capsules (which last about 6-8 hours) for extended relief. ... The scientific literature suggests that CBD doses could start at 5-10 mg twice daily and increase to 40-50 mg daily, whereas THC doses could start at 0.5-3 mg (initially at night) and increase to 30-40 mg/day.”
David Copenhaver, MD, MPH, clinical professor and chief of the division of pain medicine at UC Davis Health, Sacramento, shared a similar clinical mindset for patients choosing between opioids and cannabis-based products, specifically, CBD.
Compared with opioids, “the side-effect profile for CBD is less and the risk of mortality is less,” Dr. Copenhaver said in an interview, pointing out that nobody, to his knowledge, has ever died from an overdose of cannabis alone, and that CBD doses up to 1,000 mg/kg have been safely tolerated in people. “You present that, and most patients will say, ‘You know, I’d like to give this a try.’”
If so, Dr. Copenhaver makes sure patients know about a nonmedical risk: “The risk to the pocketbook.” Unlike opioids, which are covered under most insurance policies, most cannabis-based therapies are self-pay.
Buyers may get what they pay for, Dr. Copenhaver said, since products vary in quality, as do the dispensaries, from “very modest,” to highly sophisticated, with some even using chromatographic datasets to support the purity of their products.
Dr. Copenhaver steers his patients toward these more sophisticated retailers. Their expertise appears to be paying off, he said, not only in relief for patients, but also in market share. “Survival of the most fit will occur in the marketplace based on the results,” he said. “Unfortunately, some of that information doesn’t get percolated out into the literature.”
For investigators to fully uncover what cannabis-based products can do for chronic pain, Dr. Copenhaver said they need to get as “granular” as the leading dispensaries, which may first require recognition of the “very expansive opportunity” that less-studied cannabinoids may provide.
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators, Dr. Boehnke, Dr. Clauw, and Dr. Copenhaver, disclosed no conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE

The mental health of health care professionals takes center stage
Mental illness has been waiting in the wings for years; ignored, ridiculed, minimized, and stigmatized. Those who succumbed to it tried to lend testimonials, but to no avail. Those who were spared its effects remained in disbelief. So, it stayed on the sidelines, growing in intensity and breadth, yet stifled by the masses, until 2 years ago.
In March 2020, when COVID-19 became a pandemic, the importance of mental health finally became undeniable. As the pandemic’s effects progressed and wreaked havoc on our nation, our mental illness rates simultaneously surged. This surge paralleled that of the COVID-19 pandemic’s and in fact, contributed to a secondary crisis, allowing mental health to finally be addressed and gain center stage status.
But “mental health” is not easily defined, as it takes on many forms and is expressed in a variety of ways and via a myriad of symptoms. It does not discriminate by gender, race, age, socioeconomic status, educational level, profession, religion, or geography. At times, mental health status is consistent but at other times it can fluctuate in intensity, duration, and expression. It can be difficult to manage, yet there are various treatment modalities that can be implemented to lessen the impact of mental illness. Stressful events seem to potentiate its manifestation and yet, there are times it seems to appear spontaneously, much as an uninvited guest.
Mental health has a strong synergistic relationship with physical health, as they are very interdependent and allow us to function at our best only when they are both operating optimally. It should come as no surprise then, that the COVID-19 pandemic contributed to the exponential surge of mental illnesses. Capitalizing on its nondiscriminatory nature, mental illness impacted a large segment of the population – both those suffering from COVID-19 as well as those treating them.
As the nation starts to heal from the immediate and lingering physical and emotional consequences of the COVID-19 pandemic, President Biden has chosen to address and try to meet the needs of the health care heroes, the healers. The signing of H.R. 1667, the Dr. Lorna Breen Health Care Provider Protection Act into law on March 18, 2022, showed dedication to the health care community that has given tirelessly to our nation during the COVID-19 pandemic, and is itself recuperating from that effort.
Taking a top-down approach is essential to assuring the health of the nation. If our healers are not healthy, physically and mentally, they will not be able treat those whom they are dedicated to helping. Openly discussing and acknowledging the mental health problems of health care workers as a community makes it okay to not be okay. It normalizes the need for health care workers to prioritize their own mental health. It can also start to ease the fear of professional backlash or repercussions for practicing self-care.
I, for one, am very grateful for the prioritizing and promoting of the importance of mental health and wellness amongst health care workers. This helps to reduce the stigma of mental illness, helps us understand its impact, and allows us to formulate strategies and solutions to address its effects. The time has come.
Dr. Jarkon is a psychiatrist and director of the Center for Behavioral Health at the New York Institute of Technology College of Osteopathic Medicine in Old Westbury, N.Y.
Mental illness has been waiting in the wings for years; ignored, ridiculed, minimized, and stigmatized. Those who succumbed to it tried to lend testimonials, but to no avail. Those who were spared its effects remained in disbelief. So, it stayed on the sidelines, growing in intensity and breadth, yet stifled by the masses, until 2 years ago.
In March 2020, when COVID-19 became a pandemic, the importance of mental health finally became undeniable. As the pandemic’s effects progressed and wreaked havoc on our nation, our mental illness rates simultaneously surged. This surge paralleled that of the COVID-19 pandemic’s and in fact, contributed to a secondary crisis, allowing mental health to finally be addressed and gain center stage status.
But “mental health” is not easily defined, as it takes on many forms and is expressed in a variety of ways and via a myriad of symptoms. It does not discriminate by gender, race, age, socioeconomic status, educational level, profession, religion, or geography. At times, mental health status is consistent but at other times it can fluctuate in intensity, duration, and expression. It can be difficult to manage, yet there are various treatment modalities that can be implemented to lessen the impact of mental illness. Stressful events seem to potentiate its manifestation and yet, there are times it seems to appear spontaneously, much as an uninvited guest.
Mental health has a strong synergistic relationship with physical health, as they are very interdependent and allow us to function at our best only when they are both operating optimally. It should come as no surprise then, that the COVID-19 pandemic contributed to the exponential surge of mental illnesses. Capitalizing on its nondiscriminatory nature, mental illness impacted a large segment of the population – both those suffering from COVID-19 as well as those treating them.
As the nation starts to heal from the immediate and lingering physical and emotional consequences of the COVID-19 pandemic, President Biden has chosen to address and try to meet the needs of the health care heroes, the healers. The signing of H.R. 1667, the Dr. Lorna Breen Health Care Provider Protection Act into law on March 18, 2022, showed dedication to the health care community that has given tirelessly to our nation during the COVID-19 pandemic, and is itself recuperating from that effort.
Taking a top-down approach is essential to assuring the health of the nation. If our healers are not healthy, physically and mentally, they will not be able treat those whom they are dedicated to helping. Openly discussing and acknowledging the mental health problems of health care workers as a community makes it okay to not be okay. It normalizes the need for health care workers to prioritize their own mental health. It can also start to ease the fear of professional backlash or repercussions for practicing self-care.
I, for one, am very grateful for the prioritizing and promoting of the importance of mental health and wellness amongst health care workers. This helps to reduce the stigma of mental illness, helps us understand its impact, and allows us to formulate strategies and solutions to address its effects. The time has come.
Dr. Jarkon is a psychiatrist and director of the Center for Behavioral Health at the New York Institute of Technology College of Osteopathic Medicine in Old Westbury, N.Y.
Mental illness has been waiting in the wings for years; ignored, ridiculed, minimized, and stigmatized. Those who succumbed to it tried to lend testimonials, but to no avail. Those who were spared its effects remained in disbelief. So, it stayed on the sidelines, growing in intensity and breadth, yet stifled by the masses, until 2 years ago.
In March 2020, when COVID-19 became a pandemic, the importance of mental health finally became undeniable. As the pandemic’s effects progressed and wreaked havoc on our nation, our mental illness rates simultaneously surged. This surge paralleled that of the COVID-19 pandemic’s and in fact, contributed to a secondary crisis, allowing mental health to finally be addressed and gain center stage status.
But “mental health” is not easily defined, as it takes on many forms and is expressed in a variety of ways and via a myriad of symptoms. It does not discriminate by gender, race, age, socioeconomic status, educational level, profession, religion, or geography. At times, mental health status is consistent but at other times it can fluctuate in intensity, duration, and expression. It can be difficult to manage, yet there are various treatment modalities that can be implemented to lessen the impact of mental illness. Stressful events seem to potentiate its manifestation and yet, there are times it seems to appear spontaneously, much as an uninvited guest.
Mental health has a strong synergistic relationship with physical health, as they are very interdependent and allow us to function at our best only when they are both operating optimally. It should come as no surprise then, that the COVID-19 pandemic contributed to the exponential surge of mental illnesses. Capitalizing on its nondiscriminatory nature, mental illness impacted a large segment of the population – both those suffering from COVID-19 as well as those treating them.
As the nation starts to heal from the immediate and lingering physical and emotional consequences of the COVID-19 pandemic, President Biden has chosen to address and try to meet the needs of the health care heroes, the healers. The signing of H.R. 1667, the Dr. Lorna Breen Health Care Provider Protection Act into law on March 18, 2022, showed dedication to the health care community that has given tirelessly to our nation during the COVID-19 pandemic, and is itself recuperating from that effort.
Taking a top-down approach is essential to assuring the health of the nation. If our healers are not healthy, physically and mentally, they will not be able treat those whom they are dedicated to helping. Openly discussing and acknowledging the mental health problems of health care workers as a community makes it okay to not be okay. It normalizes the need for health care workers to prioritize their own mental health. It can also start to ease the fear of professional backlash or repercussions for practicing self-care.
I, for one, am very grateful for the prioritizing and promoting of the importance of mental health and wellness amongst health care workers. This helps to reduce the stigma of mental illness, helps us understand its impact, and allows us to formulate strategies and solutions to address its effects. The time has come.
Dr. Jarkon is a psychiatrist and director of the Center for Behavioral Health at the New York Institute of Technology College of Osteopathic Medicine in Old Westbury, N.Y.