User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Next Gen Smart Pills Could Transform Personalized Care
On a November morning in 2022, James Messenger opened wide and swallowed a capsule like no other.
Messenger was no stranger to taking pills.
He’d first experimented with prescription opioids as a teenager in Morgantown, West Virginia, battled addiction on-and-off since, and known more than 70 people who had fatally overdosed. So, when asked to test a new “smart pill” that could detect an overdose in progress and call for help, he didn’t hesitate to join the study.
“I’ve lost pretty much every good friend I’ve ever had to this,” said Mr. Messenger. “This pill could save a lot of lives.”
The new Vitals Monitoring capsule he tested is just one example in a growing effort to radically rethink what the humble pill is capable of.
As far back as 1965, scientists introduced the Heidelberg capsule, an electronic pill that measured acidity from within the gut. In 1994, the University of Buffalo coined the term “smart pill” with a device promising to ferry medicine to a precise spot in the intestine, “like the tiny ship in the film Fantastic Voyage.” And in 2001, the US Food and Drug Administration (FDA) approved the first video capsule endoscope, a miniature-camera-toting pill that enabled noninvasive imaging of the small intestine.
But now, nearly 300 iterations are in various stages of development, according to a 2022 analysis. Advances in materials, imaging, and artificial intelligence (AI) are helping address everything from sleep apnea to HIV/AIDS to gut disorders via real-time tracking and real-time help.
“These technologies could enable us to shift the paradigm from ‘Let’s wait until the patient comes to us and find out what happened’ to ‘Let’s see how things are changing in real time, intervene now, and personalize that intervention,’ ” said Peter Chai, MD, associate professor of emergency medicine and health technology researcher at Brigham and Women’s Hospital in Boston.
Tracking Vitals From the Inside Out
Already, overdose-reversal agents like naloxone are saving lives. But more than 60% of overdoses occur when no one is around to administer them.
“While we need to focus on treatment, we also need to come up with more acute ways to save individuals when treatment doesn’t work or relapse occurs,” said James J. Mahoney III, PhD, director of addictions research at the Rockefeller Neuroscience Institute at West Virginia University (WVU), Morgantown.
Enter Celero Systems, a Massachusetts-based digital health company that has developed a vitamin-sized capsule packed with tiny sensors, microprocessors, and a radio antenna. It can measure breathing, heart rate, and core temperature — all from deep within the gut.
Respiratory distress is a hallmark early sign of an overdose. But it can be hard to monitor from a distance, especially in populations without access to a charged smartwatch.
Dr. Mahoney imagines a day when patients at risk could be given a weekly pill like Celero’s. If their respiratory rate drops below a dangerous level, it could alert loved ones or, better yet, release an overdose-reversal drug.
“It’s early days,” stressed Dr. Mahoney, whose team has been conducting pilot tests of the pill. “But initial data look promising.”
For one study, published in the journal Device in November 2023, the research team administered an overdose of fentanyl to anesthetized pigs with the pill in their stomachs. The capsule was able to detect respiratory depression within a minute and alert researchers via their laptop in time to step in.
When they gave the pill to 10 volunteers undergoing sleep studies at WVU, they found it could detect respiration rate with an accuracy of 93% compared with external monitoring devices — a feature that could also help diagnose sleep apnea or chronic obstructive pulmonary disease without expensive, intrusive tests.
Accuracy for heart rate was nearly 97%.
In another yet-to-be published trial, Dr. Mahoney tested the device with 10 volunteers in a residential treatment center to determine how well it could be tolerated.
Among the participants was Mr. Messenger, who said the thought of being tracked didn’t bother him.
“It was simple — just like taking a multivitamin,” said Mr. Messenger, now 34, sober, and working as a peer recovery support specialist at a hospital in his hometown. “It could be a great way to keep people alive long enough for them to get their head wrapped around the idea of treatment.”
Boosting Medication Adherence
At Brigham and Women’s Hospital, Dr. Chai is experimenting with a different smart pill — one he believes could help curb the ongoing HIV/AIDS epidemic.
Developed by Florida-based etectRx, the ID-Cap consists of a gelatin capsule embedded with a tiny radiofrequency transmitter, similar to the kind in retail antitheft devices. The capsule can be filled with a variety of medications. When swallowed, stomach acid dissolves the gel and activates the transmitter, which sends a signal to a receiver on a smartwatch, smartphone, or wall-mounted reader to confirm the medication was taken. If it isn’t, the patient’s smartphone or smart speaker might nudge them with a reminder or a family member might be notified.
In recent trials of men at a high risk for HIV, the system improved adherence to the once-daily prevention regimen pre-exposure prophylaxis (PrEP) by double digits.
“PrEP is almost 99% effective in preventing HIV, but you have to take it,” said Dr. Chai, who led the trials. “That seems like such a simple thing, but anyone who is chronically on medication can tell you just how difficult it can be.”
The pill is not the first designed to improve adherence. In 2017, the FDA approved the first digital ingestion tracking system, Abilify MyCite, for the treatment of schizophrenia and bipolar disorder. But its maker, Proteus Digital Health, filed for bankruptcy in 2020 after struggling to recruit patients willing to be tracked. (Some expressed privacy concerns. Others disliked the uncomfortable patch that received and forwarded the signal.)
More recent designs have been streamlined to ditch the patch, said etectRx senior vice president of operations Chris Carnes, PhD. And the cost of making a pill this kind of “smart” has come down to about a dollar.
So far, said Dr. Chai, in the patients he’s worked with, perceived benefits generally outweigh privacy concerns.
Studies are now underway in patients with heart disease and tuberculosis, and the company hopes to move into the aging and memory care space where medication-adherence is a serious problem.
“For us, or any company in this space, to succeed, you have to have a strong business case,” said Dr. Carnes. “If family members can keep their loved ones at home a little longer at an additional cost of $30 a month, that’s a no-brainer.”
Pillcams 2.0
Twenty-three years ago, the first video capsule endoscopy made it possible to image the small intestine via a tiny camera you swallow.
Such “pillcams” offered a more patient-friendly way to diagnose small bowel disorders, such as gastrointestinal bleeding and Crohn’s disease. Rather than undergoing sedation or anesthesia, as required during tube-based endoscopy, patients can go about their day as the pill painlessly passes through their gastrointestinal (GI) tract, capturing and recording data and images.
But the pills have their downsides.
Because they move passively, driven by movement in the intestine, they can miss trouble spots. Their ability to image the esophagus, stomach, and colon has proven limited. And unlike other procedures, like colonoscopy, they can’t intervene with therapy, like removing polyps.
The pillcam “had so much promise, to sort of revolutionize endoscopy, but it never really got the adoption that it seemed like it might,” said Andrew Meltzer, MD, professor of emergency medicine at the GW School of Medicine and Health Sciences in Washington.
That could soon change, he said, thanks to advances in locomotion and AI.
In a recent study of 40 patients, Dr. Meltzer tested a new magnetically controlled capsule endoscopy. Standing at a patient’s side, he could use a joystick to steer the pill around the stomach, capturing images in real time.
The pilot study, published in June 2023, found that the pill clearly identified six key stomach landmarks accurately 95% of the time and didn’t miss any lesions caught with traditional endoscopy. Notably, 80% of the patients preferred the pillcam over the tube.
“They are awake. They can go to work as soon as they leave. And it’s easy for them to tolerate,” Dr. Meltzer said.
More research is necessary, but Dr. Meltzer believes the technology could be particularly useful in the emergency department, allowing doctors to rule out high-risk bleeds in the stomach on the spot without admitting patients unnecessarily or making them return for a traditional scope.
“It has the potential to increase screening and provide more cost-effective care in emergencies,” he said.
It could also be useful in the telemedicine space, allowing a doctor to “drive” the pill from afar to diagnose a distant patient.
Someday, AI could enable the capsule to drive itself, so a doctor could merely press a button and wait. Or it could be adapted to treat what it finds, like administering a drug or cauterizing a bleed.
“If we can come up with a Mars rover which can explore other planets, we should be able to have something that can explore the stomach remotely,” Dr. Meltzer said.
Swallowing the Future
At the California Institute of Technology, researchers have developed a “location-aware” smart pill that uses magnetic fields to help pinpoint its location in the twists and turns of intestines. This could be useful for monitoring food in the GI tract to determine why things aren’t moving.
Other researchers are using AI models to enhance the transmission of video from inside the body and reduce the time it takes to interpret images.
One group at the Massachusetts Institute of Technology has developed a vibrating weight loss capsule designed to stimulate receptors in the gut to signal the brain that the person is full.
Not everyone is a fan of the smart-pill revolution. Some critics have raised concerns about privacy. Others fear that doctors risk yielding too much power to technology. Even those who are excited about the pills’ possibilities temper their optimism with caution.
None of these smart pills have gone mainstream yet in clinical practice, said Vivek Kaul, MD, professor of medicine at the University of Rochester Medical Center, Rochester, New York, and secretary general of the World Gastroenterology Organization.
Clinical validation, accessibility, and insurance coverage “will be critical in shaping their role,” he said. “But overall, it would be fair to state that this technology has come of age and the future is bright.”
A version of this article appeared on Medscape.com.
On a November morning in 2022, James Messenger opened wide and swallowed a capsule like no other.
Messenger was no stranger to taking pills.
He’d first experimented with prescription opioids as a teenager in Morgantown, West Virginia, battled addiction on-and-off since, and known more than 70 people who had fatally overdosed. So, when asked to test a new “smart pill” that could detect an overdose in progress and call for help, he didn’t hesitate to join the study.
“I’ve lost pretty much every good friend I’ve ever had to this,” said Mr. Messenger. “This pill could save a lot of lives.”
The new Vitals Monitoring capsule he tested is just one example in a growing effort to radically rethink what the humble pill is capable of.
As far back as 1965, scientists introduced the Heidelberg capsule, an electronic pill that measured acidity from within the gut. In 1994, the University of Buffalo coined the term “smart pill” with a device promising to ferry medicine to a precise spot in the intestine, “like the tiny ship in the film Fantastic Voyage.” And in 2001, the US Food and Drug Administration (FDA) approved the first video capsule endoscope, a miniature-camera-toting pill that enabled noninvasive imaging of the small intestine.
But now, nearly 300 iterations are in various stages of development, according to a 2022 analysis. Advances in materials, imaging, and artificial intelligence (AI) are helping address everything from sleep apnea to HIV/AIDS to gut disorders via real-time tracking and real-time help.
“These technologies could enable us to shift the paradigm from ‘Let’s wait until the patient comes to us and find out what happened’ to ‘Let’s see how things are changing in real time, intervene now, and personalize that intervention,’ ” said Peter Chai, MD, associate professor of emergency medicine and health technology researcher at Brigham and Women’s Hospital in Boston.
Tracking Vitals From the Inside Out
Already, overdose-reversal agents like naloxone are saving lives. But more than 60% of overdoses occur when no one is around to administer them.
“While we need to focus on treatment, we also need to come up with more acute ways to save individuals when treatment doesn’t work or relapse occurs,” said James J. Mahoney III, PhD, director of addictions research at the Rockefeller Neuroscience Institute at West Virginia University (WVU), Morgantown.
Enter Celero Systems, a Massachusetts-based digital health company that has developed a vitamin-sized capsule packed with tiny sensors, microprocessors, and a radio antenna. It can measure breathing, heart rate, and core temperature — all from deep within the gut.
Respiratory distress is a hallmark early sign of an overdose. But it can be hard to monitor from a distance, especially in populations without access to a charged smartwatch.
Dr. Mahoney imagines a day when patients at risk could be given a weekly pill like Celero’s. If their respiratory rate drops below a dangerous level, it could alert loved ones or, better yet, release an overdose-reversal drug.
“It’s early days,” stressed Dr. Mahoney, whose team has been conducting pilot tests of the pill. “But initial data look promising.”
For one study, published in the journal Device in November 2023, the research team administered an overdose of fentanyl to anesthetized pigs with the pill in their stomachs. The capsule was able to detect respiratory depression within a minute and alert researchers via their laptop in time to step in.
When they gave the pill to 10 volunteers undergoing sleep studies at WVU, they found it could detect respiration rate with an accuracy of 93% compared with external monitoring devices — a feature that could also help diagnose sleep apnea or chronic obstructive pulmonary disease without expensive, intrusive tests.
Accuracy for heart rate was nearly 97%.
In another yet-to-be published trial, Dr. Mahoney tested the device with 10 volunteers in a residential treatment center to determine how well it could be tolerated.
Among the participants was Mr. Messenger, who said the thought of being tracked didn’t bother him.
“It was simple — just like taking a multivitamin,” said Mr. Messenger, now 34, sober, and working as a peer recovery support specialist at a hospital in his hometown. “It could be a great way to keep people alive long enough for them to get their head wrapped around the idea of treatment.”
Boosting Medication Adherence
At Brigham and Women’s Hospital, Dr. Chai is experimenting with a different smart pill — one he believes could help curb the ongoing HIV/AIDS epidemic.
Developed by Florida-based etectRx, the ID-Cap consists of a gelatin capsule embedded with a tiny radiofrequency transmitter, similar to the kind in retail antitheft devices. The capsule can be filled with a variety of medications. When swallowed, stomach acid dissolves the gel and activates the transmitter, which sends a signal to a receiver on a smartwatch, smartphone, or wall-mounted reader to confirm the medication was taken. If it isn’t, the patient’s smartphone or smart speaker might nudge them with a reminder or a family member might be notified.
In recent trials of men at a high risk for HIV, the system improved adherence to the once-daily prevention regimen pre-exposure prophylaxis (PrEP) by double digits.
“PrEP is almost 99% effective in preventing HIV, but you have to take it,” said Dr. Chai, who led the trials. “That seems like such a simple thing, but anyone who is chronically on medication can tell you just how difficult it can be.”
The pill is not the first designed to improve adherence. In 2017, the FDA approved the first digital ingestion tracking system, Abilify MyCite, for the treatment of schizophrenia and bipolar disorder. But its maker, Proteus Digital Health, filed for bankruptcy in 2020 after struggling to recruit patients willing to be tracked. (Some expressed privacy concerns. Others disliked the uncomfortable patch that received and forwarded the signal.)
More recent designs have been streamlined to ditch the patch, said etectRx senior vice president of operations Chris Carnes, PhD. And the cost of making a pill this kind of “smart” has come down to about a dollar.
So far, said Dr. Chai, in the patients he’s worked with, perceived benefits generally outweigh privacy concerns.
Studies are now underway in patients with heart disease and tuberculosis, and the company hopes to move into the aging and memory care space where medication-adherence is a serious problem.
“For us, or any company in this space, to succeed, you have to have a strong business case,” said Dr. Carnes. “If family members can keep their loved ones at home a little longer at an additional cost of $30 a month, that’s a no-brainer.”
Pillcams 2.0
Twenty-three years ago, the first video capsule endoscopy made it possible to image the small intestine via a tiny camera you swallow.
Such “pillcams” offered a more patient-friendly way to diagnose small bowel disorders, such as gastrointestinal bleeding and Crohn’s disease. Rather than undergoing sedation or anesthesia, as required during tube-based endoscopy, patients can go about their day as the pill painlessly passes through their gastrointestinal (GI) tract, capturing and recording data and images.
But the pills have their downsides.
Because they move passively, driven by movement in the intestine, they can miss trouble spots. Their ability to image the esophagus, stomach, and colon has proven limited. And unlike other procedures, like colonoscopy, they can’t intervene with therapy, like removing polyps.
The pillcam “had so much promise, to sort of revolutionize endoscopy, but it never really got the adoption that it seemed like it might,” said Andrew Meltzer, MD, professor of emergency medicine at the GW School of Medicine and Health Sciences in Washington.
That could soon change, he said, thanks to advances in locomotion and AI.
In a recent study of 40 patients, Dr. Meltzer tested a new magnetically controlled capsule endoscopy. Standing at a patient’s side, he could use a joystick to steer the pill around the stomach, capturing images in real time.
The pilot study, published in June 2023, found that the pill clearly identified six key stomach landmarks accurately 95% of the time and didn’t miss any lesions caught with traditional endoscopy. Notably, 80% of the patients preferred the pillcam over the tube.
“They are awake. They can go to work as soon as they leave. And it’s easy for them to tolerate,” Dr. Meltzer said.
More research is necessary, but Dr. Meltzer believes the technology could be particularly useful in the emergency department, allowing doctors to rule out high-risk bleeds in the stomach on the spot without admitting patients unnecessarily or making them return for a traditional scope.
“It has the potential to increase screening and provide more cost-effective care in emergencies,” he said.
It could also be useful in the telemedicine space, allowing a doctor to “drive” the pill from afar to diagnose a distant patient.
Someday, AI could enable the capsule to drive itself, so a doctor could merely press a button and wait. Or it could be adapted to treat what it finds, like administering a drug or cauterizing a bleed.
“If we can come up with a Mars rover which can explore other planets, we should be able to have something that can explore the stomach remotely,” Dr. Meltzer said.
Swallowing the Future
At the California Institute of Technology, researchers have developed a “location-aware” smart pill that uses magnetic fields to help pinpoint its location in the twists and turns of intestines. This could be useful for monitoring food in the GI tract to determine why things aren’t moving.
Other researchers are using AI models to enhance the transmission of video from inside the body and reduce the time it takes to interpret images.
One group at the Massachusetts Institute of Technology has developed a vibrating weight loss capsule designed to stimulate receptors in the gut to signal the brain that the person is full.
Not everyone is a fan of the smart-pill revolution. Some critics have raised concerns about privacy. Others fear that doctors risk yielding too much power to technology. Even those who are excited about the pills’ possibilities temper their optimism with caution.
None of these smart pills have gone mainstream yet in clinical practice, said Vivek Kaul, MD, professor of medicine at the University of Rochester Medical Center, Rochester, New York, and secretary general of the World Gastroenterology Organization.
Clinical validation, accessibility, and insurance coverage “will be critical in shaping their role,” he said. “But overall, it would be fair to state that this technology has come of age and the future is bright.”
A version of this article appeared on Medscape.com.
On a November morning in 2022, James Messenger opened wide and swallowed a capsule like no other.
Messenger was no stranger to taking pills.
He’d first experimented with prescription opioids as a teenager in Morgantown, West Virginia, battled addiction on-and-off since, and known more than 70 people who had fatally overdosed. So, when asked to test a new “smart pill” that could detect an overdose in progress and call for help, he didn’t hesitate to join the study.
“I’ve lost pretty much every good friend I’ve ever had to this,” said Mr. Messenger. “This pill could save a lot of lives.”
The new Vitals Monitoring capsule he tested is just one example in a growing effort to radically rethink what the humble pill is capable of.
As far back as 1965, scientists introduced the Heidelberg capsule, an electronic pill that measured acidity from within the gut. In 1994, the University of Buffalo coined the term “smart pill” with a device promising to ferry medicine to a precise spot in the intestine, “like the tiny ship in the film Fantastic Voyage.” And in 2001, the US Food and Drug Administration (FDA) approved the first video capsule endoscope, a miniature-camera-toting pill that enabled noninvasive imaging of the small intestine.
But now, nearly 300 iterations are in various stages of development, according to a 2022 analysis. Advances in materials, imaging, and artificial intelligence (AI) are helping address everything from sleep apnea to HIV/AIDS to gut disorders via real-time tracking and real-time help.
“These technologies could enable us to shift the paradigm from ‘Let’s wait until the patient comes to us and find out what happened’ to ‘Let’s see how things are changing in real time, intervene now, and personalize that intervention,’ ” said Peter Chai, MD, associate professor of emergency medicine and health technology researcher at Brigham and Women’s Hospital in Boston.
Tracking Vitals From the Inside Out
Already, overdose-reversal agents like naloxone are saving lives. But more than 60% of overdoses occur when no one is around to administer them.
“While we need to focus on treatment, we also need to come up with more acute ways to save individuals when treatment doesn’t work or relapse occurs,” said James J. Mahoney III, PhD, director of addictions research at the Rockefeller Neuroscience Institute at West Virginia University (WVU), Morgantown.
Enter Celero Systems, a Massachusetts-based digital health company that has developed a vitamin-sized capsule packed with tiny sensors, microprocessors, and a radio antenna. It can measure breathing, heart rate, and core temperature — all from deep within the gut.
Respiratory distress is a hallmark early sign of an overdose. But it can be hard to monitor from a distance, especially in populations without access to a charged smartwatch.
Dr. Mahoney imagines a day when patients at risk could be given a weekly pill like Celero’s. If their respiratory rate drops below a dangerous level, it could alert loved ones or, better yet, release an overdose-reversal drug.
“It’s early days,” stressed Dr. Mahoney, whose team has been conducting pilot tests of the pill. “But initial data look promising.”
For one study, published in the journal Device in November 2023, the research team administered an overdose of fentanyl to anesthetized pigs with the pill in their stomachs. The capsule was able to detect respiratory depression within a minute and alert researchers via their laptop in time to step in.
When they gave the pill to 10 volunteers undergoing sleep studies at WVU, they found it could detect respiration rate with an accuracy of 93% compared with external monitoring devices — a feature that could also help diagnose sleep apnea or chronic obstructive pulmonary disease without expensive, intrusive tests.
Accuracy for heart rate was nearly 97%.
In another yet-to-be published trial, Dr. Mahoney tested the device with 10 volunteers in a residential treatment center to determine how well it could be tolerated.
Among the participants was Mr. Messenger, who said the thought of being tracked didn’t bother him.
“It was simple — just like taking a multivitamin,” said Mr. Messenger, now 34, sober, and working as a peer recovery support specialist at a hospital in his hometown. “It could be a great way to keep people alive long enough for them to get their head wrapped around the idea of treatment.”
Boosting Medication Adherence
At Brigham and Women’s Hospital, Dr. Chai is experimenting with a different smart pill — one he believes could help curb the ongoing HIV/AIDS epidemic.
Developed by Florida-based etectRx, the ID-Cap consists of a gelatin capsule embedded with a tiny radiofrequency transmitter, similar to the kind in retail antitheft devices. The capsule can be filled with a variety of medications. When swallowed, stomach acid dissolves the gel and activates the transmitter, which sends a signal to a receiver on a smartwatch, smartphone, or wall-mounted reader to confirm the medication was taken. If it isn’t, the patient’s smartphone or smart speaker might nudge them with a reminder or a family member might be notified.
In recent trials of men at a high risk for HIV, the system improved adherence to the once-daily prevention regimen pre-exposure prophylaxis (PrEP) by double digits.
“PrEP is almost 99% effective in preventing HIV, but you have to take it,” said Dr. Chai, who led the trials. “That seems like such a simple thing, but anyone who is chronically on medication can tell you just how difficult it can be.”
The pill is not the first designed to improve adherence. In 2017, the FDA approved the first digital ingestion tracking system, Abilify MyCite, for the treatment of schizophrenia and bipolar disorder. But its maker, Proteus Digital Health, filed for bankruptcy in 2020 after struggling to recruit patients willing to be tracked. (Some expressed privacy concerns. Others disliked the uncomfortable patch that received and forwarded the signal.)
More recent designs have been streamlined to ditch the patch, said etectRx senior vice president of operations Chris Carnes, PhD. And the cost of making a pill this kind of “smart” has come down to about a dollar.
So far, said Dr. Chai, in the patients he’s worked with, perceived benefits generally outweigh privacy concerns.
Studies are now underway in patients with heart disease and tuberculosis, and the company hopes to move into the aging and memory care space where medication-adherence is a serious problem.
“For us, or any company in this space, to succeed, you have to have a strong business case,” said Dr. Carnes. “If family members can keep their loved ones at home a little longer at an additional cost of $30 a month, that’s a no-brainer.”
Pillcams 2.0
Twenty-three years ago, the first video capsule endoscopy made it possible to image the small intestine via a tiny camera you swallow.
Such “pillcams” offered a more patient-friendly way to diagnose small bowel disorders, such as gastrointestinal bleeding and Crohn’s disease. Rather than undergoing sedation or anesthesia, as required during tube-based endoscopy, patients can go about their day as the pill painlessly passes through their gastrointestinal (GI) tract, capturing and recording data and images.
But the pills have their downsides.
Because they move passively, driven by movement in the intestine, they can miss trouble spots. Their ability to image the esophagus, stomach, and colon has proven limited. And unlike other procedures, like colonoscopy, they can’t intervene with therapy, like removing polyps.
The pillcam “had so much promise, to sort of revolutionize endoscopy, but it never really got the adoption that it seemed like it might,” said Andrew Meltzer, MD, professor of emergency medicine at the GW School of Medicine and Health Sciences in Washington.
That could soon change, he said, thanks to advances in locomotion and AI.
In a recent study of 40 patients, Dr. Meltzer tested a new magnetically controlled capsule endoscopy. Standing at a patient’s side, he could use a joystick to steer the pill around the stomach, capturing images in real time.
The pilot study, published in June 2023, found that the pill clearly identified six key stomach landmarks accurately 95% of the time and didn’t miss any lesions caught with traditional endoscopy. Notably, 80% of the patients preferred the pillcam over the tube.
“They are awake. They can go to work as soon as they leave. And it’s easy for them to tolerate,” Dr. Meltzer said.
More research is necessary, but Dr. Meltzer believes the technology could be particularly useful in the emergency department, allowing doctors to rule out high-risk bleeds in the stomach on the spot without admitting patients unnecessarily or making them return for a traditional scope.
“It has the potential to increase screening and provide more cost-effective care in emergencies,” he said.
It could also be useful in the telemedicine space, allowing a doctor to “drive” the pill from afar to diagnose a distant patient.
Someday, AI could enable the capsule to drive itself, so a doctor could merely press a button and wait. Or it could be adapted to treat what it finds, like administering a drug or cauterizing a bleed.
“If we can come up with a Mars rover which can explore other planets, we should be able to have something that can explore the stomach remotely,” Dr. Meltzer said.
Swallowing the Future
At the California Institute of Technology, researchers have developed a “location-aware” smart pill that uses magnetic fields to help pinpoint its location in the twists and turns of intestines. This could be useful for monitoring food in the GI tract to determine why things aren’t moving.
Other researchers are using AI models to enhance the transmission of video from inside the body and reduce the time it takes to interpret images.
One group at the Massachusetts Institute of Technology has developed a vibrating weight loss capsule designed to stimulate receptors in the gut to signal the brain that the person is full.
Not everyone is a fan of the smart-pill revolution. Some critics have raised concerns about privacy. Others fear that doctors risk yielding too much power to technology. Even those who are excited about the pills’ possibilities temper their optimism with caution.
None of these smart pills have gone mainstream yet in clinical practice, said Vivek Kaul, MD, professor of medicine at the University of Rochester Medical Center, Rochester, New York, and secretary general of the World Gastroenterology Organization.
Clinical validation, accessibility, and insurance coverage “will be critical in shaping their role,” he said. “But overall, it would be fair to state that this technology has come of age and the future is bright.”
A version of this article appeared on Medscape.com.
ACC Consensus Guidance on What’s New in HFrEF Treatment
The American College of Cardiology has published a new update to its consensus decision pathway for the treatment of heart failure with reduced ejection fraction (HFrEF).
Chair of the consensus document Writing Committee Thomas M. Maddox, MD, explained to this news organization that this new Decision Pathway provides a practical, streamlined update to frontline clinicians treating patients with heart failure and incorporates evidence from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“While the AHA/ACC/HFSA Guidelines are wonderful in that they collate all the latest scientific evidence, they don’t speak as much to the practicalities of delivering the care. This is what this Decision Pathway document comes in — it is designed to help frontline clinicians with the practical reality of managing these patients,” Dr. Maddox, who is director of the Healthcare Innovation Lab at BJC HealthCare and the Washington University School of Medicine in St Louis, Missouri, commented.
The document, “Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction,” was published online on March 8 in the Journal of the American College of Cardiology.
The authors provided guidance on introducing the numerous evidence-based therapies now available for HFrEF, improving adherence, overcoming treatment barriers, acknowledging contraindications and situations for which few data exist, affording expensive therapies, treating special cohorts, and making the transition to palliative care.
Rather than focusing on extensive text, the document provided practical tips, tables, and figures to make clear the steps, tools, and provisos needed to treat patients with heart failure successfully and expeditiously, they added.
Dr. Maddox reported that there are three main updated areas of advice on the treatment of heart failure in the new document.
Valsartan/Sacubitril First Line
One of the major changes involves an elevation for the status of the angiotensin receptor-neprilysin inhibitor (ARNI), Entresto (valsartan/sacubitril).
“It is now clear that this agent is superior to ACE-inhibitors or angiotensin receptor blockers in terms of reducing heart failure hospitalization and death, whereas previously it was seen as somewhat equivalent,” Dr. Maddox said. “So, barring a contraindication or another problem with getting the medication, this agent should be one of the first line medicines for all patients with heart failure and a reduced ejection fraction.”
Dual Sodium-Glucose Cotransporter 1/2 (SGLT1/2) Inhibitor
A second update involves the addition of sotagliflozin (a dual inhibitor of both SGLT1 and SGLT2) to the SGLT2 inhibitors as another first-line medication for patients with heart failure and reduced ejection fraction.
“We now have evidence that both SGLT2 and SGLT1 inhibitors are beneficial in reducing heart failure hospitalization and death. Previously we only had evidence on SGLT2 inhibitors — dapagliflozin and empagliflozin. Sotagliflozin is a newer agent, which inhibits both SGLT1 and SGLT2, and it turns out that inhibiting both are beneficial in heart failure. So, this gives us a third med in this category,” Dr. Maddox noted.
Rapid Initiation of the Four Pillars of Therapy
The document stated that more data have emerged recently to support early and rapid initiation and titration of the “four pillars” of medical therapy in heart failure to maximize the benefits of patient-reported outcomes and reduction in hospitalizations and mortality.
The four pillars of therapy are ARNI, a beta-blocker, a mineralocorticoid antagonist, and an SGLT inhibitor.
As an example, four-class medication initiation reduced the hazard of cardiovascular death or hospital admission for heart failure significantly (hazard ratio, 0.38) compared with therapy with just an angiotensin-converting enzyme inhibitor/angiotensin receptor blocker plus a beta-blocker, the document reported.
“What we realize now is that the more quickly we can get patients on all four of these drug classes and escalate to target doses or maximally tolerated doses ideally within 3 months, the better the outcome,” Dr. Maddox said.
“Unfortunately, right now there is very incomplete realization and recognition of that in clinical practice. So, we are trying to highlight the importance of this to encourage clinicians to be more aggressive in making this happen.”
“In all patients with heart failure and reduced ejection fraction, getting them on all four of these medicines as quickly as possible will give the best outcome. We’ve seen evidence in support of this from several broad population trials,” he added. “There are times when they can’t take all four but we should do our best to get there.”
Practical Considerations
Dr. Maddox pointed out that the Consensus Document is also trying to account for practical realities and barriers to heart failure treatment.
“When we think about these recommendations — and evidence that getting patients on all these medicines is valuable, we also focus on the fact that there are three major barriers that can get in the way of this and how to think about overcoming those barriers,” he said.
The barriers are comorbidities/side effects of medications, costs of the medicines, and systems of care that are needed to ensure patients can be treated with multiple medications in a timely fashion.
In terms of comorbidities/side effects, Dr. Maddox explained that patients with heart failure are generally older and are likely to have other comorbidities. “The more medicines we give, the more likely we are to run into side effects. So, we have produced some guidance on how to monitor for adverse effects and ways to mitigate these effects so the guideline recommended therapies can be continued without creating new harms.”
He gave the example of mineralocorticoid antagonists, which can sometimes elevate potassium levels, particularly if there is some underlying kidney disease, so clinicians are advised to recommend a low-potassium diet for these patients or the use of potassium binding agents that will also lower the amount of potassium in the blood stream; in this way, patients are able to continue the mineralocorticoid antagonist.
On costs, Dr. Maddox noted that the valsartan/sacubitril combination drug and SGLT inhibitors are new medicines and are expensive.
“They can be prohibitively expensive for patients who have suboptimal pharmacy benefits or who are uninsured.”
The Consensus Document therefore provided some guidance on ways to identify rebate programs, access insurance, and find different pathways to obtaining those drugs at a more reasonable price. It also advocated for policy changes to allow these medicines to be more accessible to more people.
More Use of Digital Tools
On the issue of systems of care, Dr. Maddox noted that the preexisting model of delivering care, which almost always involves the patient coming into the doctor’s office, invokes a high burden on both the system and most especially, the patient.
“Patients do not want to come back and forth to the doctor’s office multiple times in a few weeks. This is often a nonstarter, particularly for patients with busy lives,” he commented.
The Consensus Document advised more use of digital tools to provide remote care and contact with patients including sensors that can measure variables such as heart rate and blood pressure and video appointments.
“We are still working out what are the right models of care and how they can be performed safely and how they can be funded. But I think at the end of the day, this will give us more practical ways of getting people on multiple heart failure medicines and monitoring them safely without causing an undue burden for them logistically,” Dr. Maddox said.
He pointed out that there are a record number of medicines now available to treat heart failure, and while this is welcome, many of these patients are also on multiple other medications for other comorbidities as well.
“If you start giving patients seven, eight, or nine different medicines that they have to take every day, sometimes multiple times a day — that’s complicated medically, logistically, and financially. The potential for interaction and complications increases with every additional medication.”
Dr. Maddox also noted that patients have limits on how many medications they will accept. “It really helps if we have an engaged patient who has a good relationship with the care team to try to develop the right treatment plan that is going to meet their needs and give them the best possible health outcomes.”
It can take many visits to get the patient on all these medications and then up-titrate to target doses.
“We try and do a couple of things in each appointment. Often, we tend to start one or maybe two drugs at a time at a relatively low dose to avoid side effects, so we can be talking about 12-16 different encounters in total,” he said.
He recommended making a plan and the use of new technologies to manage each incremental step.
A Team Approach
Another issue that is discussed in the document is the use of a healthcare team to manage all the necessary appointments.
“It is no longer practical that one person can be the engineer for all this. It should be a team effort,” Dr. Maddox stated.
Responsibilities can be allocated across physicians, nurses, pharmacists, and even case managers, so that the team can take more of a population approach and develop a system to get patients on the multiple medications as quickly as possible.
“While this can still be quite a big burden for the patient, we need to figure out a system to make this as palatable as possible for them. Practices need to tailor this themselves according to what resources they have,” he added.
While most new patients will be routed to cardiologists to start their treatment plans, once on their initial medications and these have been up titrated to target levels, they should be able to be managed by primary care doctors, who will have the most holistic view of the patient and their other comorbidities, Dr. Maddox advised.
“Following this guidance should lead to more patients receiving evidence-based care which leads to better health outcomes, but delivered in a practical way that fits with their life reality and logistical needs,” he concluded.
A version of this article appeared on Medscape.com.
The American College of Cardiology has published a new update to its consensus decision pathway for the treatment of heart failure with reduced ejection fraction (HFrEF).
Chair of the consensus document Writing Committee Thomas M. Maddox, MD, explained to this news organization that this new Decision Pathway provides a practical, streamlined update to frontline clinicians treating patients with heart failure and incorporates evidence from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“While the AHA/ACC/HFSA Guidelines are wonderful in that they collate all the latest scientific evidence, they don’t speak as much to the practicalities of delivering the care. This is what this Decision Pathway document comes in — it is designed to help frontline clinicians with the practical reality of managing these patients,” Dr. Maddox, who is director of the Healthcare Innovation Lab at BJC HealthCare and the Washington University School of Medicine in St Louis, Missouri, commented.
The document, “Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction,” was published online on March 8 in the Journal of the American College of Cardiology.
The authors provided guidance on introducing the numerous evidence-based therapies now available for HFrEF, improving adherence, overcoming treatment barriers, acknowledging contraindications and situations for which few data exist, affording expensive therapies, treating special cohorts, and making the transition to palliative care.
Rather than focusing on extensive text, the document provided practical tips, tables, and figures to make clear the steps, tools, and provisos needed to treat patients with heart failure successfully and expeditiously, they added.
Dr. Maddox reported that there are three main updated areas of advice on the treatment of heart failure in the new document.
Valsartan/Sacubitril First Line
One of the major changes involves an elevation for the status of the angiotensin receptor-neprilysin inhibitor (ARNI), Entresto (valsartan/sacubitril).
“It is now clear that this agent is superior to ACE-inhibitors or angiotensin receptor blockers in terms of reducing heart failure hospitalization and death, whereas previously it was seen as somewhat equivalent,” Dr. Maddox said. “So, barring a contraindication or another problem with getting the medication, this agent should be one of the first line medicines for all patients with heart failure and a reduced ejection fraction.”
Dual Sodium-Glucose Cotransporter 1/2 (SGLT1/2) Inhibitor
A second update involves the addition of sotagliflozin (a dual inhibitor of both SGLT1 and SGLT2) to the SGLT2 inhibitors as another first-line medication for patients with heart failure and reduced ejection fraction.
“We now have evidence that both SGLT2 and SGLT1 inhibitors are beneficial in reducing heart failure hospitalization and death. Previously we only had evidence on SGLT2 inhibitors — dapagliflozin and empagliflozin. Sotagliflozin is a newer agent, which inhibits both SGLT1 and SGLT2, and it turns out that inhibiting both are beneficial in heart failure. So, this gives us a third med in this category,” Dr. Maddox noted.
Rapid Initiation of the Four Pillars of Therapy
The document stated that more data have emerged recently to support early and rapid initiation and titration of the “four pillars” of medical therapy in heart failure to maximize the benefits of patient-reported outcomes and reduction in hospitalizations and mortality.
The four pillars of therapy are ARNI, a beta-blocker, a mineralocorticoid antagonist, and an SGLT inhibitor.
As an example, four-class medication initiation reduced the hazard of cardiovascular death or hospital admission for heart failure significantly (hazard ratio, 0.38) compared with therapy with just an angiotensin-converting enzyme inhibitor/angiotensin receptor blocker plus a beta-blocker, the document reported.
“What we realize now is that the more quickly we can get patients on all four of these drug classes and escalate to target doses or maximally tolerated doses ideally within 3 months, the better the outcome,” Dr. Maddox said.
“Unfortunately, right now there is very incomplete realization and recognition of that in clinical practice. So, we are trying to highlight the importance of this to encourage clinicians to be more aggressive in making this happen.”
“In all patients with heart failure and reduced ejection fraction, getting them on all four of these medicines as quickly as possible will give the best outcome. We’ve seen evidence in support of this from several broad population trials,” he added. “There are times when they can’t take all four but we should do our best to get there.”
Practical Considerations
Dr. Maddox pointed out that the Consensus Document is also trying to account for practical realities and barriers to heart failure treatment.
“When we think about these recommendations — and evidence that getting patients on all these medicines is valuable, we also focus on the fact that there are three major barriers that can get in the way of this and how to think about overcoming those barriers,” he said.
The barriers are comorbidities/side effects of medications, costs of the medicines, and systems of care that are needed to ensure patients can be treated with multiple medications in a timely fashion.
In terms of comorbidities/side effects, Dr. Maddox explained that patients with heart failure are generally older and are likely to have other comorbidities. “The more medicines we give, the more likely we are to run into side effects. So, we have produced some guidance on how to monitor for adverse effects and ways to mitigate these effects so the guideline recommended therapies can be continued without creating new harms.”
He gave the example of mineralocorticoid antagonists, which can sometimes elevate potassium levels, particularly if there is some underlying kidney disease, so clinicians are advised to recommend a low-potassium diet for these patients or the use of potassium binding agents that will also lower the amount of potassium in the blood stream; in this way, patients are able to continue the mineralocorticoid antagonist.
On costs, Dr. Maddox noted that the valsartan/sacubitril combination drug and SGLT inhibitors are new medicines and are expensive.
“They can be prohibitively expensive for patients who have suboptimal pharmacy benefits or who are uninsured.”
The Consensus Document therefore provided some guidance on ways to identify rebate programs, access insurance, and find different pathways to obtaining those drugs at a more reasonable price. It also advocated for policy changes to allow these medicines to be more accessible to more people.
More Use of Digital Tools
On the issue of systems of care, Dr. Maddox noted that the preexisting model of delivering care, which almost always involves the patient coming into the doctor’s office, invokes a high burden on both the system and most especially, the patient.
“Patients do not want to come back and forth to the doctor’s office multiple times in a few weeks. This is often a nonstarter, particularly for patients with busy lives,” he commented.
The Consensus Document advised more use of digital tools to provide remote care and contact with patients including sensors that can measure variables such as heart rate and blood pressure and video appointments.
“We are still working out what are the right models of care and how they can be performed safely and how they can be funded. But I think at the end of the day, this will give us more practical ways of getting people on multiple heart failure medicines and monitoring them safely without causing an undue burden for them logistically,” Dr. Maddox said.
He pointed out that there are a record number of medicines now available to treat heart failure, and while this is welcome, many of these patients are also on multiple other medications for other comorbidities as well.
“If you start giving patients seven, eight, or nine different medicines that they have to take every day, sometimes multiple times a day — that’s complicated medically, logistically, and financially. The potential for interaction and complications increases with every additional medication.”
Dr. Maddox also noted that patients have limits on how many medications they will accept. “It really helps if we have an engaged patient who has a good relationship with the care team to try to develop the right treatment plan that is going to meet their needs and give them the best possible health outcomes.”
It can take many visits to get the patient on all these medications and then up-titrate to target doses.
“We try and do a couple of things in each appointment. Often, we tend to start one or maybe two drugs at a time at a relatively low dose to avoid side effects, so we can be talking about 12-16 different encounters in total,” he said.
He recommended making a plan and the use of new technologies to manage each incremental step.
A Team Approach
Another issue that is discussed in the document is the use of a healthcare team to manage all the necessary appointments.
“It is no longer practical that one person can be the engineer for all this. It should be a team effort,” Dr. Maddox stated.
Responsibilities can be allocated across physicians, nurses, pharmacists, and even case managers, so that the team can take more of a population approach and develop a system to get patients on the multiple medications as quickly as possible.
“While this can still be quite a big burden for the patient, we need to figure out a system to make this as palatable as possible for them. Practices need to tailor this themselves according to what resources they have,” he added.
While most new patients will be routed to cardiologists to start their treatment plans, once on their initial medications and these have been up titrated to target levels, they should be able to be managed by primary care doctors, who will have the most holistic view of the patient and their other comorbidities, Dr. Maddox advised.
“Following this guidance should lead to more patients receiving evidence-based care which leads to better health outcomes, but delivered in a practical way that fits with their life reality and logistical needs,” he concluded.
A version of this article appeared on Medscape.com.
The American College of Cardiology has published a new update to its consensus decision pathway for the treatment of heart failure with reduced ejection fraction (HFrEF).
Chair of the consensus document Writing Committee Thomas M. Maddox, MD, explained to this news organization that this new Decision Pathway provides a practical, streamlined update to frontline clinicians treating patients with heart failure and incorporates evidence from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“While the AHA/ACC/HFSA Guidelines are wonderful in that they collate all the latest scientific evidence, they don’t speak as much to the practicalities of delivering the care. This is what this Decision Pathway document comes in — it is designed to help frontline clinicians with the practical reality of managing these patients,” Dr. Maddox, who is director of the Healthcare Innovation Lab at BJC HealthCare and the Washington University School of Medicine in St Louis, Missouri, commented.
The document, “Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction,” was published online on March 8 in the Journal of the American College of Cardiology.
The authors provided guidance on introducing the numerous evidence-based therapies now available for HFrEF, improving adherence, overcoming treatment barriers, acknowledging contraindications and situations for which few data exist, affording expensive therapies, treating special cohorts, and making the transition to palliative care.
Rather than focusing on extensive text, the document provided practical tips, tables, and figures to make clear the steps, tools, and provisos needed to treat patients with heart failure successfully and expeditiously, they added.
Dr. Maddox reported that there are three main updated areas of advice on the treatment of heart failure in the new document.
Valsartan/Sacubitril First Line
One of the major changes involves an elevation for the status of the angiotensin receptor-neprilysin inhibitor (ARNI), Entresto (valsartan/sacubitril).
“It is now clear that this agent is superior to ACE-inhibitors or angiotensin receptor blockers in terms of reducing heart failure hospitalization and death, whereas previously it was seen as somewhat equivalent,” Dr. Maddox said. “So, barring a contraindication or another problem with getting the medication, this agent should be one of the first line medicines for all patients with heart failure and a reduced ejection fraction.”
Dual Sodium-Glucose Cotransporter 1/2 (SGLT1/2) Inhibitor
A second update involves the addition of sotagliflozin (a dual inhibitor of both SGLT1 and SGLT2) to the SGLT2 inhibitors as another first-line medication for patients with heart failure and reduced ejection fraction.
“We now have evidence that both SGLT2 and SGLT1 inhibitors are beneficial in reducing heart failure hospitalization and death. Previously we only had evidence on SGLT2 inhibitors — dapagliflozin and empagliflozin. Sotagliflozin is a newer agent, which inhibits both SGLT1 and SGLT2, and it turns out that inhibiting both are beneficial in heart failure. So, this gives us a third med in this category,” Dr. Maddox noted.
Rapid Initiation of the Four Pillars of Therapy
The document stated that more data have emerged recently to support early and rapid initiation and titration of the “four pillars” of medical therapy in heart failure to maximize the benefits of patient-reported outcomes and reduction in hospitalizations and mortality.
The four pillars of therapy are ARNI, a beta-blocker, a mineralocorticoid antagonist, and an SGLT inhibitor.
As an example, four-class medication initiation reduced the hazard of cardiovascular death or hospital admission for heart failure significantly (hazard ratio, 0.38) compared with therapy with just an angiotensin-converting enzyme inhibitor/angiotensin receptor blocker plus a beta-blocker, the document reported.
“What we realize now is that the more quickly we can get patients on all four of these drug classes and escalate to target doses or maximally tolerated doses ideally within 3 months, the better the outcome,” Dr. Maddox said.
“Unfortunately, right now there is very incomplete realization and recognition of that in clinical practice. So, we are trying to highlight the importance of this to encourage clinicians to be more aggressive in making this happen.”
“In all patients with heart failure and reduced ejection fraction, getting them on all four of these medicines as quickly as possible will give the best outcome. We’ve seen evidence in support of this from several broad population trials,” he added. “There are times when they can’t take all four but we should do our best to get there.”
Practical Considerations
Dr. Maddox pointed out that the Consensus Document is also trying to account for practical realities and barriers to heart failure treatment.
“When we think about these recommendations — and evidence that getting patients on all these medicines is valuable, we also focus on the fact that there are three major barriers that can get in the way of this and how to think about overcoming those barriers,” he said.
The barriers are comorbidities/side effects of medications, costs of the medicines, and systems of care that are needed to ensure patients can be treated with multiple medications in a timely fashion.
In terms of comorbidities/side effects, Dr. Maddox explained that patients with heart failure are generally older and are likely to have other comorbidities. “The more medicines we give, the more likely we are to run into side effects. So, we have produced some guidance on how to monitor for adverse effects and ways to mitigate these effects so the guideline recommended therapies can be continued without creating new harms.”
He gave the example of mineralocorticoid antagonists, which can sometimes elevate potassium levels, particularly if there is some underlying kidney disease, so clinicians are advised to recommend a low-potassium diet for these patients or the use of potassium binding agents that will also lower the amount of potassium in the blood stream; in this way, patients are able to continue the mineralocorticoid antagonist.
On costs, Dr. Maddox noted that the valsartan/sacubitril combination drug and SGLT inhibitors are new medicines and are expensive.
“They can be prohibitively expensive for patients who have suboptimal pharmacy benefits or who are uninsured.”
The Consensus Document therefore provided some guidance on ways to identify rebate programs, access insurance, and find different pathways to obtaining those drugs at a more reasonable price. It also advocated for policy changes to allow these medicines to be more accessible to more people.
More Use of Digital Tools
On the issue of systems of care, Dr. Maddox noted that the preexisting model of delivering care, which almost always involves the patient coming into the doctor’s office, invokes a high burden on both the system and most especially, the patient.
“Patients do not want to come back and forth to the doctor’s office multiple times in a few weeks. This is often a nonstarter, particularly for patients with busy lives,” he commented.
The Consensus Document advised more use of digital tools to provide remote care and contact with patients including sensors that can measure variables such as heart rate and blood pressure and video appointments.
“We are still working out what are the right models of care and how they can be performed safely and how they can be funded. But I think at the end of the day, this will give us more practical ways of getting people on multiple heart failure medicines and monitoring them safely without causing an undue burden for them logistically,” Dr. Maddox said.
He pointed out that there are a record number of medicines now available to treat heart failure, and while this is welcome, many of these patients are also on multiple other medications for other comorbidities as well.
“If you start giving patients seven, eight, or nine different medicines that they have to take every day, sometimes multiple times a day — that’s complicated medically, logistically, and financially. The potential for interaction and complications increases with every additional medication.”
Dr. Maddox also noted that patients have limits on how many medications they will accept. “It really helps if we have an engaged patient who has a good relationship with the care team to try to develop the right treatment plan that is going to meet their needs and give them the best possible health outcomes.”
It can take many visits to get the patient on all these medications and then up-titrate to target doses.
“We try and do a couple of things in each appointment. Often, we tend to start one or maybe two drugs at a time at a relatively low dose to avoid side effects, so we can be talking about 12-16 different encounters in total,” he said.
He recommended making a plan and the use of new technologies to manage each incremental step.
A Team Approach
Another issue that is discussed in the document is the use of a healthcare team to manage all the necessary appointments.
“It is no longer practical that one person can be the engineer for all this. It should be a team effort,” Dr. Maddox stated.
Responsibilities can be allocated across physicians, nurses, pharmacists, and even case managers, so that the team can take more of a population approach and develop a system to get patients on the multiple medications as quickly as possible.
“While this can still be quite a big burden for the patient, we need to figure out a system to make this as palatable as possible for them. Practices need to tailor this themselves according to what resources they have,” he added.
While most new patients will be routed to cardiologists to start their treatment plans, once on their initial medications and these have been up titrated to target levels, they should be able to be managed by primary care doctors, who will have the most holistic view of the patient and their other comorbidities, Dr. Maddox advised.
“Following this guidance should lead to more patients receiving evidence-based care which leads to better health outcomes, but delivered in a practical way that fits with their life reality and logistical needs,” he concluded.
A version of this article appeared on Medscape.com.
Allergens Present in Most ‘Hypoallergenic’ Baby Cleansers, Study Finds
TOPLINE:
METHODOLOGY:
- Many baby cleansers are marketed as “hypoallergenic,” but these claims are not validated.
- This study assessed the potential allergens and marketing claims in best-selling baby cleansers.
- The researchers collected ingredients and marketing claims of the top 50 best-selling baby body wash products sold on Amazon on April 4, 2023.
- Ingredient lists were checked for potential allergens using the 2020 American Contact Dermatitis Society (ACDS) core allergen series, which lists 90 common allergens for adults and children.
TAKEAWAY:
- In the 50 cleansers tested, 10 allergens were identified. Overall, 94% of the cleansers contained at least one allergen, averaging 2.9 allergens per product; cocamidopropyl betaine (72%), fragrance (64%), and sodium benzoate (54%) were the most common allergens.
- All cleansers had at least five marketing claims, with an average of 10.9 claims per product; the most common claims were “paraben-free” (88%), “phthalate-free” (84%), “tear-free” (74%), and “hypoallergenic” or “allergy-tested” (74%).
- There was no significant difference in the number of allergens in the cleansers marketed as “hypoallergenic” or “allergy tested” compared with cleansers that did not have these claims (P = .843).
- Fewer allergens were found in cleansers endorsed by the National Eczema Association (P = .004) or labeled “synthetic fragrance-free” (P = .003).
- There was a positive correlation between a greater number of allergens and an increased number of marketing claims (r = 0.547, P < .001) and a negative correlation between cost and number of allergens (r = −0.450, P = .001).
IN PRACTICE:
Because marketing claims like “hypoallergenic” may be misleading, “clinicians should counsel parents to carefully examine cleanser ingredients or consider selecting cleansers” endorsed by the National Eczema Association or another international eczema organization, especially for infants and children with a history of atopic dermatitis, the authors wrote.
SOURCE:
The study, led by Sasan D. Noveir, BA, from the University of California, Los Angeles, and coauthors from the division of dermatology at UCLA, was published online in Pediatric Dermatology.
LIMITATIONS:
The study only evaluated top-selling products from a single online source at a specific time, which may limit generalizability. Potential allergens not included in the ACDS core series may be present.
DISCLOSURES:
The study did not disclose any funding source. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Many baby cleansers are marketed as “hypoallergenic,” but these claims are not validated.
- This study assessed the potential allergens and marketing claims in best-selling baby cleansers.
- The researchers collected ingredients and marketing claims of the top 50 best-selling baby body wash products sold on Amazon on April 4, 2023.
- Ingredient lists were checked for potential allergens using the 2020 American Contact Dermatitis Society (ACDS) core allergen series, which lists 90 common allergens for adults and children.
TAKEAWAY:
- In the 50 cleansers tested, 10 allergens were identified. Overall, 94% of the cleansers contained at least one allergen, averaging 2.9 allergens per product; cocamidopropyl betaine (72%), fragrance (64%), and sodium benzoate (54%) were the most common allergens.
- All cleansers had at least five marketing claims, with an average of 10.9 claims per product; the most common claims were “paraben-free” (88%), “phthalate-free” (84%), “tear-free” (74%), and “hypoallergenic” or “allergy-tested” (74%).
- There was no significant difference in the number of allergens in the cleansers marketed as “hypoallergenic” or “allergy tested” compared with cleansers that did not have these claims (P = .843).
- Fewer allergens were found in cleansers endorsed by the National Eczema Association (P = .004) or labeled “synthetic fragrance-free” (P = .003).
- There was a positive correlation between a greater number of allergens and an increased number of marketing claims (r = 0.547, P < .001) and a negative correlation between cost and number of allergens (r = −0.450, P = .001).
IN PRACTICE:
Because marketing claims like “hypoallergenic” may be misleading, “clinicians should counsel parents to carefully examine cleanser ingredients or consider selecting cleansers” endorsed by the National Eczema Association or another international eczema organization, especially for infants and children with a history of atopic dermatitis, the authors wrote.
SOURCE:
The study, led by Sasan D. Noveir, BA, from the University of California, Los Angeles, and coauthors from the division of dermatology at UCLA, was published online in Pediatric Dermatology.
LIMITATIONS:
The study only evaluated top-selling products from a single online source at a specific time, which may limit generalizability. Potential allergens not included in the ACDS core series may be present.
DISCLOSURES:
The study did not disclose any funding source. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Many baby cleansers are marketed as “hypoallergenic,” but these claims are not validated.
- This study assessed the potential allergens and marketing claims in best-selling baby cleansers.
- The researchers collected ingredients and marketing claims of the top 50 best-selling baby body wash products sold on Amazon on April 4, 2023.
- Ingredient lists were checked for potential allergens using the 2020 American Contact Dermatitis Society (ACDS) core allergen series, which lists 90 common allergens for adults and children.
TAKEAWAY:
- In the 50 cleansers tested, 10 allergens were identified. Overall, 94% of the cleansers contained at least one allergen, averaging 2.9 allergens per product; cocamidopropyl betaine (72%), fragrance (64%), and sodium benzoate (54%) were the most common allergens.
- All cleansers had at least five marketing claims, with an average of 10.9 claims per product; the most common claims were “paraben-free” (88%), “phthalate-free” (84%), “tear-free” (74%), and “hypoallergenic” or “allergy-tested” (74%).
- There was no significant difference in the number of allergens in the cleansers marketed as “hypoallergenic” or “allergy tested” compared with cleansers that did not have these claims (P = .843).
- Fewer allergens were found in cleansers endorsed by the National Eczema Association (P = .004) or labeled “synthetic fragrance-free” (P = .003).
- There was a positive correlation between a greater number of allergens and an increased number of marketing claims (r = 0.547, P < .001) and a negative correlation between cost and number of allergens (r = −0.450, P = .001).
IN PRACTICE:
Because marketing claims like “hypoallergenic” may be misleading, “clinicians should counsel parents to carefully examine cleanser ingredients or consider selecting cleansers” endorsed by the National Eczema Association or another international eczema organization, especially for infants and children with a history of atopic dermatitis, the authors wrote.
SOURCE:
The study, led by Sasan D. Noveir, BA, from the University of California, Los Angeles, and coauthors from the division of dermatology at UCLA, was published online in Pediatric Dermatology.
LIMITATIONS:
The study only evaluated top-selling products from a single online source at a specific time, which may limit generalizability. Potential allergens not included in the ACDS core series may be present.
DISCLOSURES:
The study did not disclose any funding source. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Diet and Exercise in a Pill Are Real: How Mimetics Work
If couch-potato lab mice had beach-body dreams and if they could speak, they might tell you they’re thrilled by advances in the science of exercise and calorie-restriction (CR) mimetics.
In recent studies conducted at research centers across the United States, mice have chowed down, fattened up, exercised only if they felt like it, and still managed to lose body fat, improve their blood lipids, increase muscle power, avoid blood sugar problems, and boost heart function.
How did these mice get so lucky? They were given mimetics, experimental drugs that “mimic” the effects of exercise and calorie reduction in the body without the need to break a sweat or eat less.
“The mice looked like they’d done endurance training,” said Thomas Burris, PhD, chair of the Department of Pharmacodynamics at the University of Florida, Gainesville, Florida, and coauthor of a September 2023 study of the exercise mimetic SLU-PP-332, published in The Journal of Pharmacology and Experimental Therapeutics.
Meanwhile, the CR mimetic mannoheptulose (MH) “was incredibly effective at stopping the negative effects of a high-fat diet in mice,” said Donald K. Ingram, PhD, an adjunct professor at Louisiana State University’s Pennington Biomedical Research Center, Baton Rouge, Louisiana, who began studying CR mimetics at the National Institute on Aging in the 1980s. In a 2022 study published in Nutrients, MH also increased insulin sensitivity.
These “have your cake and eat it, too” drugs aren’t on the market for human use — but they’re edging closer. Several have moved into human trials with encouraging results. The National Institutes of Health and the pharmaceutical industry are taking notice, anteing up big research dollars. At the earliest, one could win US Food and Drug Administration (FDA) approval in 4-5 years, Dr. Burris said.
The medical appeal is clear: Mimetics could one day prevent and treat serious conditions such as age- and disease-related muscle loss, diabetes, heart failure, and even neurodegenerative disorders like Parkinson’s disease and Alzheimer’s disease, said the scientists studying them.
The commercial appeal is unavoidable: Mimetics have the potential to help nondieters avoid weight gain and allow dieters to build and/or preserve more calorie-burning muscle — a boon because losing weight can reduce muscle, especially with rapid loss.
How do these drugs work? What’s their downside? Like the “miracle” glucagon-like peptide 1 (GLP-1) weight-loss drugs that are now ubiquitous, are mimetics an effective pharmaceutical way to replicate two of society’s biggest lifestyle sticking points — diet and exercise?
It’s possible…
CR Mimetics: The Healthspan Drug?
From nematodes and fruit flies to yeast, Labrador Retrievers, and people, plenty of research shows that reducing calorie intake may improve health and prolong life. By how much? Cutting calories by 25% for 2 years slowed the pace of aging 2%-3% in the landmark CALERIE study of 197 adults, according to a 2023 study in Nature Aging. Sounds small, but the researchers said that equals a 10%-15% lower risk for an early death — on par with the longevity bonus you’d get from quitting smoking.
Trouble is low-cal living isn’t easy. “Diets work,” said George Roth, PhD, of GeroScience, Inc., in Pylesville, MD, who began studying CR at the National Institute on Aging in the 1980s with Ingram. “But it’s hard to sustain.”
That’s where CR mimetics come in. They activate the same health-promoting genes switched on by dieting, fasting, and extended periods of hunger, Dr. Roth said. The end result isn’t big weight loss. Instead, CR mimetics may keep us healthier and younger as we age. “Calorie restriction shifts metabolic processes in the body to protect against damage and stress,” he said.
Dr. Roth and Dr. Ingram are currently focused on the CR mimetic mannoheptulose (MH), a sugar found in unripe avocados. “It works at the first step in carbohydrate metabolism in cells throughout the body, so less energy goes through that pathway,” he said. “Glucose metabolism is reduced by 10%-15%. It’s the closest thing to actually eating less food.”
Their 2022 study found that while mice on an all-you-can-eat high-fat diet gained weight and body fat and saw blood lipids increase while insulin sensitivity decreased, mice that also got MH avoided these problems. A 2023 human study in Nutrients coauthored by Dr. Roth and Dr. Ingram found that a group consuming freeze-dried avocado had lower insulin levels than a placebo group.
Other researchers are looking at ways to stimulate the CR target nicotinamide adenine dinucleotide (NAD+). NAD+ assists sirtuins — a group of seven enzymes central to the beneficial effects of CR on aging — but levels drop with age. University of Colorado researchers are studying the effects of nicotinamide riboside (NR), an NAD+ precursor, in older adults with a $2.5 million National Institute on Aging grant. Small, preliminary human studies have found the compound reduced indicators of insulin resistance in the brain, in a January 2023 study in Aging Cell, and reduced blood pressure and arterial stiffness in a 2018 study published in Nature Communications.
Another NAD+ precursor, nicotinamide mononucleotide, reduced low-density lipoprotein cholesterol, diastolic blood pressure, and body weight in a Harvard Medical School study of 30 midlife and older adults with overweight and obesity, published in August 2023 in The Journal of Clinical Endocrinology & Metabolism. And in an April 2022 study published in Hepatology of people with nonalcoholic fatty liver disease, a proprietary supplement that included NR didn’t reduce liver fat but had a significant (vs placebo) reduction in ceramide and the liver enzyme alanine aminotransferase, a marker of inflammation.
“I think it was a pretty interesting result,” said lead researcher Leonard Guarente, PhD, professor of biology at Massachusetts Institute of Technology and founder of the supplement company Elysium. “Fatty liver progressively damages the liver. This has the potential to slow that down.”
Exercise Mimetics: Fitness in a Pill?
Physical activity builds muscle and fitness, helps keeps bones strong, sharpens thinking and memory, guards against depression, and helps discourage a slew of health concerns from weight gain and high blood pressure to diabetes and heart disease. Muscle becomes more dense, more powerful and may even burn more calories, said Dr. Burris. The problem: That pesky part about actually moving. Fewer than half of American adults get recommended amounts of aerobic exercise and fewer than a quarter fit in strength training, according to the Centers for Disease Control and Prevention.
Enter the exercise mimetics. Unlike CR mimetics, exercise mimetics affect mitochondria — the tiny power plants in muscle and every other cell in the body. They switch on genes that encourage the growth of more mitochondria and encourage them to burn fatty acids, not just glucose, for fuel.
In mice, this can keep them from gaining weight, increase insulin sensitivity, and boost exercise endurance. “We can use a drug to activate the same networks that are activated by physical activity,” said Ronald Evans, PhD, professor and director of the Gene Expression Laboratory at the Salk Institute for Biological Studies in La Jolla, California.
Among notable mimetics moving into human studies is ASP0367, a drug in a class called PPAR delta modulators first developed in Evans’ lab. ASP0367 was licensed to the pharmaceutical company Mitobridge, later acquired by Astellas. Astellas is currently running a phase 2/3 human trial of the investigational drug in people with the rare genetic disorder primary mitochondrial myopathy.
At the University of Florida, Dr. Burris and team hope to soon move the exercise mimetic SLU-PP-332 into human studies. “It targets a receptor called ERR that I’ve been working on since the 1980s,” Dr. Burris said. “We knew from genetic studies that ERR has a role in exercise’s effects on mitochondrial function in muscle.” The calorie mimetics he’s studying also activate genes for making more mitochondria and driving them to burn fatty acids. “This generates a lot of energy,” he said. In a January 2024 study in Circulation, Dr. Burris found the drug restores heart function in mice experiencing heart failure. “Very little heart function was lost,” he said. It’s had no serious side effects.
The Future of Exercise and CR Pills
The field has hit some bumps. Some feel inevitable — such as otherwise healthy people misusing the drugs. GW1516, an early experimental exercise mimetic studied by Dr. Evans and abandoned because it triggered tumor growth in lab studies, is used illegally by elite athletes as a performance-enhancing drug despite warnings from the US Anti-Doping Agency. Dr. Burris worries that future CR mimetics could be misused the same way.
But he and others see plenty of benefits in future, FDA-approved drugs. Exercise mimetics like SLU-PP-332 might one day be given to people alongside weight-loss drugs, such as Mounjaro (tirzepatide) or Ozempic (semaglutide) to prevent muscle loss. “SLU-PP-332 doesn’t affect hunger or food intake the way those drugs do,” he said. “It changes muscle.”
Mimetics may one day help older adults and people with muscle disorders rebuild muscle even when they cannot exercise and to delay a range of age-related diseases without onerous dieting. “The chance to intervene and provide a longer healthspan and lifespan — that’s been the moon shot,” Dr. Roth said.
Dr. Guarente noted that CR mimetics may work best for people who aren’t carrying extra pounds but want the health benefits of slashing calories without sacrificing meals and snacks. “Fat is still going to be a problem for joints, cholesterol, inflammation,” he said. “Calorie mimetics are not a panacea for obesity but could help preserve overall health and vitality.”
And what about the billion-dollar question: What happens when these drugs become available to a general public that has issues with actual exercise and healthy diet?
Evans sees only positives. “Our environment is designed to keep people sitting down and consuming high-calorie foods,” he said. “In the absence of people getting motivated to exercise — and there’s no evidence the country is moving in that direction on its own — a pill is an important option to have.”
A version of this article appeared on Medscape.com.
If couch-potato lab mice had beach-body dreams and if they could speak, they might tell you they’re thrilled by advances in the science of exercise and calorie-restriction (CR) mimetics.
In recent studies conducted at research centers across the United States, mice have chowed down, fattened up, exercised only if they felt like it, and still managed to lose body fat, improve their blood lipids, increase muscle power, avoid blood sugar problems, and boost heart function.
How did these mice get so lucky? They were given mimetics, experimental drugs that “mimic” the effects of exercise and calorie reduction in the body without the need to break a sweat or eat less.
“The mice looked like they’d done endurance training,” said Thomas Burris, PhD, chair of the Department of Pharmacodynamics at the University of Florida, Gainesville, Florida, and coauthor of a September 2023 study of the exercise mimetic SLU-PP-332, published in The Journal of Pharmacology and Experimental Therapeutics.
Meanwhile, the CR mimetic mannoheptulose (MH) “was incredibly effective at stopping the negative effects of a high-fat diet in mice,” said Donald K. Ingram, PhD, an adjunct professor at Louisiana State University’s Pennington Biomedical Research Center, Baton Rouge, Louisiana, who began studying CR mimetics at the National Institute on Aging in the 1980s. In a 2022 study published in Nutrients, MH also increased insulin sensitivity.
These “have your cake and eat it, too” drugs aren’t on the market for human use — but they’re edging closer. Several have moved into human trials with encouraging results. The National Institutes of Health and the pharmaceutical industry are taking notice, anteing up big research dollars. At the earliest, one could win US Food and Drug Administration (FDA) approval in 4-5 years, Dr. Burris said.
The medical appeal is clear: Mimetics could one day prevent and treat serious conditions such as age- and disease-related muscle loss, diabetes, heart failure, and even neurodegenerative disorders like Parkinson’s disease and Alzheimer’s disease, said the scientists studying them.
The commercial appeal is unavoidable: Mimetics have the potential to help nondieters avoid weight gain and allow dieters to build and/or preserve more calorie-burning muscle — a boon because losing weight can reduce muscle, especially with rapid loss.
How do these drugs work? What’s their downside? Like the “miracle” glucagon-like peptide 1 (GLP-1) weight-loss drugs that are now ubiquitous, are mimetics an effective pharmaceutical way to replicate two of society’s biggest lifestyle sticking points — diet and exercise?
It’s possible…
CR Mimetics: The Healthspan Drug?
From nematodes and fruit flies to yeast, Labrador Retrievers, and people, plenty of research shows that reducing calorie intake may improve health and prolong life. By how much? Cutting calories by 25% for 2 years slowed the pace of aging 2%-3% in the landmark CALERIE study of 197 adults, according to a 2023 study in Nature Aging. Sounds small, but the researchers said that equals a 10%-15% lower risk for an early death — on par with the longevity bonus you’d get from quitting smoking.
Trouble is low-cal living isn’t easy. “Diets work,” said George Roth, PhD, of GeroScience, Inc., in Pylesville, MD, who began studying CR at the National Institute on Aging in the 1980s with Ingram. “But it’s hard to sustain.”
That’s where CR mimetics come in. They activate the same health-promoting genes switched on by dieting, fasting, and extended periods of hunger, Dr. Roth said. The end result isn’t big weight loss. Instead, CR mimetics may keep us healthier and younger as we age. “Calorie restriction shifts metabolic processes in the body to protect against damage and stress,” he said.
Dr. Roth and Dr. Ingram are currently focused on the CR mimetic mannoheptulose (MH), a sugar found in unripe avocados. “It works at the first step in carbohydrate metabolism in cells throughout the body, so less energy goes through that pathway,” he said. “Glucose metabolism is reduced by 10%-15%. It’s the closest thing to actually eating less food.”
Their 2022 study found that while mice on an all-you-can-eat high-fat diet gained weight and body fat and saw blood lipids increase while insulin sensitivity decreased, mice that also got MH avoided these problems. A 2023 human study in Nutrients coauthored by Dr. Roth and Dr. Ingram found that a group consuming freeze-dried avocado had lower insulin levels than a placebo group.
Other researchers are looking at ways to stimulate the CR target nicotinamide adenine dinucleotide (NAD+). NAD+ assists sirtuins — a group of seven enzymes central to the beneficial effects of CR on aging — but levels drop with age. University of Colorado researchers are studying the effects of nicotinamide riboside (NR), an NAD+ precursor, in older adults with a $2.5 million National Institute on Aging grant. Small, preliminary human studies have found the compound reduced indicators of insulin resistance in the brain, in a January 2023 study in Aging Cell, and reduced blood pressure and arterial stiffness in a 2018 study published in Nature Communications.
Another NAD+ precursor, nicotinamide mononucleotide, reduced low-density lipoprotein cholesterol, diastolic blood pressure, and body weight in a Harvard Medical School study of 30 midlife and older adults with overweight and obesity, published in August 2023 in The Journal of Clinical Endocrinology & Metabolism. And in an April 2022 study published in Hepatology of people with nonalcoholic fatty liver disease, a proprietary supplement that included NR didn’t reduce liver fat but had a significant (vs placebo) reduction in ceramide and the liver enzyme alanine aminotransferase, a marker of inflammation.
“I think it was a pretty interesting result,” said lead researcher Leonard Guarente, PhD, professor of biology at Massachusetts Institute of Technology and founder of the supplement company Elysium. “Fatty liver progressively damages the liver. This has the potential to slow that down.”
Exercise Mimetics: Fitness in a Pill?
Physical activity builds muscle and fitness, helps keeps bones strong, sharpens thinking and memory, guards against depression, and helps discourage a slew of health concerns from weight gain and high blood pressure to diabetes and heart disease. Muscle becomes more dense, more powerful and may even burn more calories, said Dr. Burris. The problem: That pesky part about actually moving. Fewer than half of American adults get recommended amounts of aerobic exercise and fewer than a quarter fit in strength training, according to the Centers for Disease Control and Prevention.
Enter the exercise mimetics. Unlike CR mimetics, exercise mimetics affect mitochondria — the tiny power plants in muscle and every other cell in the body. They switch on genes that encourage the growth of more mitochondria and encourage them to burn fatty acids, not just glucose, for fuel.
In mice, this can keep them from gaining weight, increase insulin sensitivity, and boost exercise endurance. “We can use a drug to activate the same networks that are activated by physical activity,” said Ronald Evans, PhD, professor and director of the Gene Expression Laboratory at the Salk Institute for Biological Studies in La Jolla, California.
Among notable mimetics moving into human studies is ASP0367, a drug in a class called PPAR delta modulators first developed in Evans’ lab. ASP0367 was licensed to the pharmaceutical company Mitobridge, later acquired by Astellas. Astellas is currently running a phase 2/3 human trial of the investigational drug in people with the rare genetic disorder primary mitochondrial myopathy.
At the University of Florida, Dr. Burris and team hope to soon move the exercise mimetic SLU-PP-332 into human studies. “It targets a receptor called ERR that I’ve been working on since the 1980s,” Dr. Burris said. “We knew from genetic studies that ERR has a role in exercise’s effects on mitochondrial function in muscle.” The calorie mimetics he’s studying also activate genes for making more mitochondria and driving them to burn fatty acids. “This generates a lot of energy,” he said. In a January 2024 study in Circulation, Dr. Burris found the drug restores heart function in mice experiencing heart failure. “Very little heart function was lost,” he said. It’s had no serious side effects.
The Future of Exercise and CR Pills
The field has hit some bumps. Some feel inevitable — such as otherwise healthy people misusing the drugs. GW1516, an early experimental exercise mimetic studied by Dr. Evans and abandoned because it triggered tumor growth in lab studies, is used illegally by elite athletes as a performance-enhancing drug despite warnings from the US Anti-Doping Agency. Dr. Burris worries that future CR mimetics could be misused the same way.
But he and others see plenty of benefits in future, FDA-approved drugs. Exercise mimetics like SLU-PP-332 might one day be given to people alongside weight-loss drugs, such as Mounjaro (tirzepatide) or Ozempic (semaglutide) to prevent muscle loss. “SLU-PP-332 doesn’t affect hunger or food intake the way those drugs do,” he said. “It changes muscle.”
Mimetics may one day help older adults and people with muscle disorders rebuild muscle even when they cannot exercise and to delay a range of age-related diseases without onerous dieting. “The chance to intervene and provide a longer healthspan and lifespan — that’s been the moon shot,” Dr. Roth said.
Dr. Guarente noted that CR mimetics may work best for people who aren’t carrying extra pounds but want the health benefits of slashing calories without sacrificing meals and snacks. “Fat is still going to be a problem for joints, cholesterol, inflammation,” he said. “Calorie mimetics are not a panacea for obesity but could help preserve overall health and vitality.”
And what about the billion-dollar question: What happens when these drugs become available to a general public that has issues with actual exercise and healthy diet?
Evans sees only positives. “Our environment is designed to keep people sitting down and consuming high-calorie foods,” he said. “In the absence of people getting motivated to exercise — and there’s no evidence the country is moving in that direction on its own — a pill is an important option to have.”
A version of this article appeared on Medscape.com.
If couch-potato lab mice had beach-body dreams and if they could speak, they might tell you they’re thrilled by advances in the science of exercise and calorie-restriction (CR) mimetics.
In recent studies conducted at research centers across the United States, mice have chowed down, fattened up, exercised only if they felt like it, and still managed to lose body fat, improve their blood lipids, increase muscle power, avoid blood sugar problems, and boost heart function.
How did these mice get so lucky? They were given mimetics, experimental drugs that “mimic” the effects of exercise and calorie reduction in the body without the need to break a sweat or eat less.
“The mice looked like they’d done endurance training,” said Thomas Burris, PhD, chair of the Department of Pharmacodynamics at the University of Florida, Gainesville, Florida, and coauthor of a September 2023 study of the exercise mimetic SLU-PP-332, published in The Journal of Pharmacology and Experimental Therapeutics.
Meanwhile, the CR mimetic mannoheptulose (MH) “was incredibly effective at stopping the negative effects of a high-fat diet in mice,” said Donald K. Ingram, PhD, an adjunct professor at Louisiana State University’s Pennington Biomedical Research Center, Baton Rouge, Louisiana, who began studying CR mimetics at the National Institute on Aging in the 1980s. In a 2022 study published in Nutrients, MH also increased insulin sensitivity.
These “have your cake and eat it, too” drugs aren’t on the market for human use — but they’re edging closer. Several have moved into human trials with encouraging results. The National Institutes of Health and the pharmaceutical industry are taking notice, anteing up big research dollars. At the earliest, one could win US Food and Drug Administration (FDA) approval in 4-5 years, Dr. Burris said.
The medical appeal is clear: Mimetics could one day prevent and treat serious conditions such as age- and disease-related muscle loss, diabetes, heart failure, and even neurodegenerative disorders like Parkinson’s disease and Alzheimer’s disease, said the scientists studying them.
The commercial appeal is unavoidable: Mimetics have the potential to help nondieters avoid weight gain and allow dieters to build and/or preserve more calorie-burning muscle — a boon because losing weight can reduce muscle, especially with rapid loss.
How do these drugs work? What’s their downside? Like the “miracle” glucagon-like peptide 1 (GLP-1) weight-loss drugs that are now ubiquitous, are mimetics an effective pharmaceutical way to replicate two of society’s biggest lifestyle sticking points — diet and exercise?
It’s possible…
CR Mimetics: The Healthspan Drug?
From nematodes and fruit flies to yeast, Labrador Retrievers, and people, plenty of research shows that reducing calorie intake may improve health and prolong life. By how much? Cutting calories by 25% for 2 years slowed the pace of aging 2%-3% in the landmark CALERIE study of 197 adults, according to a 2023 study in Nature Aging. Sounds small, but the researchers said that equals a 10%-15% lower risk for an early death — on par with the longevity bonus you’d get from quitting smoking.
Trouble is low-cal living isn’t easy. “Diets work,” said George Roth, PhD, of GeroScience, Inc., in Pylesville, MD, who began studying CR at the National Institute on Aging in the 1980s with Ingram. “But it’s hard to sustain.”
That’s where CR mimetics come in. They activate the same health-promoting genes switched on by dieting, fasting, and extended periods of hunger, Dr. Roth said. The end result isn’t big weight loss. Instead, CR mimetics may keep us healthier and younger as we age. “Calorie restriction shifts metabolic processes in the body to protect against damage and stress,” he said.
Dr. Roth and Dr. Ingram are currently focused on the CR mimetic mannoheptulose (MH), a sugar found in unripe avocados. “It works at the first step in carbohydrate metabolism in cells throughout the body, so less energy goes through that pathway,” he said. “Glucose metabolism is reduced by 10%-15%. It’s the closest thing to actually eating less food.”
Their 2022 study found that while mice on an all-you-can-eat high-fat diet gained weight and body fat and saw blood lipids increase while insulin sensitivity decreased, mice that also got MH avoided these problems. A 2023 human study in Nutrients coauthored by Dr. Roth and Dr. Ingram found that a group consuming freeze-dried avocado had lower insulin levels than a placebo group.
Other researchers are looking at ways to stimulate the CR target nicotinamide adenine dinucleotide (NAD+). NAD+ assists sirtuins — a group of seven enzymes central to the beneficial effects of CR on aging — but levels drop with age. University of Colorado researchers are studying the effects of nicotinamide riboside (NR), an NAD+ precursor, in older adults with a $2.5 million National Institute on Aging grant. Small, preliminary human studies have found the compound reduced indicators of insulin resistance in the brain, in a January 2023 study in Aging Cell, and reduced blood pressure and arterial stiffness in a 2018 study published in Nature Communications.
Another NAD+ precursor, nicotinamide mononucleotide, reduced low-density lipoprotein cholesterol, diastolic blood pressure, and body weight in a Harvard Medical School study of 30 midlife and older adults with overweight and obesity, published in August 2023 in The Journal of Clinical Endocrinology & Metabolism. And in an April 2022 study published in Hepatology of people with nonalcoholic fatty liver disease, a proprietary supplement that included NR didn’t reduce liver fat but had a significant (vs placebo) reduction in ceramide and the liver enzyme alanine aminotransferase, a marker of inflammation.
“I think it was a pretty interesting result,” said lead researcher Leonard Guarente, PhD, professor of biology at Massachusetts Institute of Technology and founder of the supplement company Elysium. “Fatty liver progressively damages the liver. This has the potential to slow that down.”
Exercise Mimetics: Fitness in a Pill?
Physical activity builds muscle and fitness, helps keeps bones strong, sharpens thinking and memory, guards against depression, and helps discourage a slew of health concerns from weight gain and high blood pressure to diabetes and heart disease. Muscle becomes more dense, more powerful and may even burn more calories, said Dr. Burris. The problem: That pesky part about actually moving. Fewer than half of American adults get recommended amounts of aerobic exercise and fewer than a quarter fit in strength training, according to the Centers for Disease Control and Prevention.
Enter the exercise mimetics. Unlike CR mimetics, exercise mimetics affect mitochondria — the tiny power plants in muscle and every other cell in the body. They switch on genes that encourage the growth of more mitochondria and encourage them to burn fatty acids, not just glucose, for fuel.
In mice, this can keep them from gaining weight, increase insulin sensitivity, and boost exercise endurance. “We can use a drug to activate the same networks that are activated by physical activity,” said Ronald Evans, PhD, professor and director of the Gene Expression Laboratory at the Salk Institute for Biological Studies in La Jolla, California.
Among notable mimetics moving into human studies is ASP0367, a drug in a class called PPAR delta modulators first developed in Evans’ lab. ASP0367 was licensed to the pharmaceutical company Mitobridge, later acquired by Astellas. Astellas is currently running a phase 2/3 human trial of the investigational drug in people with the rare genetic disorder primary mitochondrial myopathy.
At the University of Florida, Dr. Burris and team hope to soon move the exercise mimetic SLU-PP-332 into human studies. “It targets a receptor called ERR that I’ve been working on since the 1980s,” Dr. Burris said. “We knew from genetic studies that ERR has a role in exercise’s effects on mitochondrial function in muscle.” The calorie mimetics he’s studying also activate genes for making more mitochondria and driving them to burn fatty acids. “This generates a lot of energy,” he said. In a January 2024 study in Circulation, Dr. Burris found the drug restores heart function in mice experiencing heart failure. “Very little heart function was lost,” he said. It’s had no serious side effects.
The Future of Exercise and CR Pills
The field has hit some bumps. Some feel inevitable — such as otherwise healthy people misusing the drugs. GW1516, an early experimental exercise mimetic studied by Dr. Evans and abandoned because it triggered tumor growth in lab studies, is used illegally by elite athletes as a performance-enhancing drug despite warnings from the US Anti-Doping Agency. Dr. Burris worries that future CR mimetics could be misused the same way.
But he and others see plenty of benefits in future, FDA-approved drugs. Exercise mimetics like SLU-PP-332 might one day be given to people alongside weight-loss drugs, such as Mounjaro (tirzepatide) or Ozempic (semaglutide) to prevent muscle loss. “SLU-PP-332 doesn’t affect hunger or food intake the way those drugs do,” he said. “It changes muscle.”
Mimetics may one day help older adults and people with muscle disorders rebuild muscle even when they cannot exercise and to delay a range of age-related diseases without onerous dieting. “The chance to intervene and provide a longer healthspan and lifespan — that’s been the moon shot,” Dr. Roth said.
Dr. Guarente noted that CR mimetics may work best for people who aren’t carrying extra pounds but want the health benefits of slashing calories without sacrificing meals and snacks. “Fat is still going to be a problem for joints, cholesterol, inflammation,” he said. “Calorie mimetics are not a panacea for obesity but could help preserve overall health and vitality.”
And what about the billion-dollar question: What happens when these drugs become available to a general public that has issues with actual exercise and healthy diet?
Evans sees only positives. “Our environment is designed to keep people sitting down and consuming high-calorie foods,” he said. “In the absence of people getting motivated to exercise — and there’s no evidence the country is moving in that direction on its own — a pill is an important option to have.”
A version of this article appeared on Medscape.com.
Studies Reinforce JAK Inhibitor Efficacy for Most Challenging Alopecia Types
FROM AAD 2024
SAN DIEGO — , according to late-breaking data presented at the annual meeting of the American Academy of Dermatology.
In one study of brepocitinib, the target was cicatricial alopecia (CA), a form of hair loss for which there are no approved therapies. In the other, a subanalysis from phase 3 trials of ritlecitinib for alopecia areata (AA), hair regrowth was shown in the subset of patients who entered the study with alopecia totalis or alopecia universalis (AT/AU).
Reflecting comments from several experts, including one of the late-breaking session moderators, April W. Armstrong, MD, MPH, professor and chief of dermatology, University of California, Los Angeles, said that the CA study, which matched clinical response to changes in CA biomarkers, suggested that the results are a potential breakthrough.
“This is the first placebo-controlled study with an oral JAK inhibitor that not only shows that scarring alopecia can be reversible but also gives insights to the mechanism of action and which patients might respond best,” Emma Guttman-Yassky, MD, PhD, said in an interview. Dr. Guttman-Yassky, professor of Dermatology and Immunology, and director of the Laboratory of Inflammatory Skin Diseases, Icahn School of Medicine at Mount Sinai, New York City, was the study’s senior investigator.
Scarring Alopecia and Brepocitinib
For the study of scarring alopecia, 49 patients with CA were randomized in a 3:1 ratio to brepocitinib, a first-in-class inhibitor that targets both JAK1 and TYK2, or placebo. Because of the small size of the study, the primary endpoint was the change in CA biomarkers. The secondary outcome was clinical response, but because of a correlation between the two, these were mutually reinforcing.
Of the subtypes, nine patients enrolled in the study had frontal fibrosing alopecia (FFA), 16 had lichen planopilaris (LPP) alopecia, and 24 had central centrifugal cicatricial alopecia (CCCA). All of the forms of CA are more common in women overall and women of color specifically, particularly CCCA. For this analysis, the FFA and LPP subtypes were considered similar for assessing response and were combined.
The data included a comparison of response and safety during the 24-week randomization phase, as well as an additional follow-up conducted after another 24 weeks of open-label treatment. During the second phase, all patients on placebo were switched to active treatment.
Overall, there was a reduction in all four of the key scalp inflammatory biomarkers measured among those in the combined FFA/LLP group. In the placebo group, each of these markers — interferon gamma (IFN-gamma), CCLS, CXCL10, and STAT1 — increased over the same time period. In almost all cases, the differences were statistically significant.
In the CCCA subgroup, the same pattern (an increase among those on placebo but a decrease among those on brepocitinib) was observed for CCLS and CXCL10. For IFN-gamma and STAT1, a rise was observed among those on placebo and those on active treatment, although the rise was greater for placebo.
For clinical response, improvement on brepocitinib was observed on disease activity indexes, particularly among those in the FFA/LLP group, according to Marguerite Meariman, MD, a dermatology resident at Mount Sinai, who presented the results. She called the improvement in clinical activity scores at 48 weeks “dramatic.” Moreover, improvement was apparent within 4 weeks of starting therapy.
For CCCA, a more challenging condition to treat, Dr. Meariman said that no further progression might represent an acceptable response for many patients, but there were also cases of hair regrowth in this subset. Although improvement was not generally on the order seen among those with FFA/LLP, she suggested that there is promise even in these more difficult patients.
Further studies are planned, but Dr. Meariman said that it might be important to focus on early treatment regardless of CA subtype. She noted that patients with less than 5 years disease duration typically did better than those with longer durations.
Ritlecitinib for AT/AU
The analysis of patients with AT/AU was based on a subset analysis from the ALLEGRO phase 2b/3 study of ritlecitinib, which targets JAK3 and TEC kinases. The full results of the ALLEGRO trial were published last year in The Lancet. In the new late-breaker analysis, Severity of Alopecia Tool (SALT) scores were evaluated on an observed or last-observation-carried-forward basis. Generally, responses in the subgroup of patients with AT/AU, who had a median SALT score of 80.3 (signifying 80.3% hair loss) at baseline, were only modestly lower than those in the overall trial.
At 24 months, about 50% of patients achieved a SALT score of 20, according to Melissa Piliang, MD, chair of Dermatology at the Cleveland Clinic, Cleveland, Ohio, who presented the data. In this group, as in the non-AT/AU population, responses climbed over time, and these responses have been maintained for as long as patients have remained on therapy.
At the more rigorous threshold of SALT < 10, the proportion of responders was only slightly lower, meaning a substantial proportion of patients with AT/AU “are achieving 90% or more of hair regrowth, so really an excellent response,” Dr. Piliang said.
For the subgroup with AU, specifically, regrowth of eyebrows and eyelashes was also observed in a substantial proportion, according to Dr. Piliang. Attributed to the often-devastating psychological burden of hair loss, patient-reported assessments of these responses global were generally “even better” than those reported by the investigators.
However, Dr. Piliang advised clinicians to treat AA as early as possible. Despite the benefits seen in the AT/AU subgroup, she pointed out that starting treatment before total hair loss is associated with a higher likelihood of complete or nearly complete hair regrowth.
There are no data from the ALLEGRO trial to determine how long hair regrowth persists after discontinuation of ritlecitinib, which has been approved for the treatment of AA, but Dr. Piliang said that patients should be told that lifelong therapy should be expected in the vast majority of individuals, whether or not AA has advanced to AT/AU.
“In my experience with JAK inhibitors, you lose response when you come off these drugs,” she said.
Dr. Meariman reported a financial relationship with AbbVie. Dr. Piliang reported financial relationships with Eli Lilly, Pfizer, and Proctor & Gamble. Dr. Armstrong reported financial relationships with more than 30 pharmaceutical companies, including those that manufacture JAK inhibitors. Dr. Guttman-Yassky reported financial relationships with more than 30 companies, including those that manufacture JAK inhibitors.
A version of this article appeared on Medscape.com.
FROM AAD 2024
SAN DIEGO — , according to late-breaking data presented at the annual meeting of the American Academy of Dermatology.
In one study of brepocitinib, the target was cicatricial alopecia (CA), a form of hair loss for which there are no approved therapies. In the other, a subanalysis from phase 3 trials of ritlecitinib for alopecia areata (AA), hair regrowth was shown in the subset of patients who entered the study with alopecia totalis or alopecia universalis (AT/AU).
Reflecting comments from several experts, including one of the late-breaking session moderators, April W. Armstrong, MD, MPH, professor and chief of dermatology, University of California, Los Angeles, said that the CA study, which matched clinical response to changes in CA biomarkers, suggested that the results are a potential breakthrough.
“This is the first placebo-controlled study with an oral JAK inhibitor that not only shows that scarring alopecia can be reversible but also gives insights to the mechanism of action and which patients might respond best,” Emma Guttman-Yassky, MD, PhD, said in an interview. Dr. Guttman-Yassky, professor of Dermatology and Immunology, and director of the Laboratory of Inflammatory Skin Diseases, Icahn School of Medicine at Mount Sinai, New York City, was the study’s senior investigator.
Scarring Alopecia and Brepocitinib
For the study of scarring alopecia, 49 patients with CA were randomized in a 3:1 ratio to brepocitinib, a first-in-class inhibitor that targets both JAK1 and TYK2, or placebo. Because of the small size of the study, the primary endpoint was the change in CA biomarkers. The secondary outcome was clinical response, but because of a correlation between the two, these were mutually reinforcing.
Of the subtypes, nine patients enrolled in the study had frontal fibrosing alopecia (FFA), 16 had lichen planopilaris (LPP) alopecia, and 24 had central centrifugal cicatricial alopecia (CCCA). All of the forms of CA are more common in women overall and women of color specifically, particularly CCCA. For this analysis, the FFA and LPP subtypes were considered similar for assessing response and were combined.
The data included a comparison of response and safety during the 24-week randomization phase, as well as an additional follow-up conducted after another 24 weeks of open-label treatment. During the second phase, all patients on placebo were switched to active treatment.
Overall, there was a reduction in all four of the key scalp inflammatory biomarkers measured among those in the combined FFA/LLP group. In the placebo group, each of these markers — interferon gamma (IFN-gamma), CCLS, CXCL10, and STAT1 — increased over the same time period. In almost all cases, the differences were statistically significant.
In the CCCA subgroup, the same pattern (an increase among those on placebo but a decrease among those on brepocitinib) was observed for CCLS and CXCL10. For IFN-gamma and STAT1, a rise was observed among those on placebo and those on active treatment, although the rise was greater for placebo.
For clinical response, improvement on brepocitinib was observed on disease activity indexes, particularly among those in the FFA/LLP group, according to Marguerite Meariman, MD, a dermatology resident at Mount Sinai, who presented the results. She called the improvement in clinical activity scores at 48 weeks “dramatic.” Moreover, improvement was apparent within 4 weeks of starting therapy.
For CCCA, a more challenging condition to treat, Dr. Meariman said that no further progression might represent an acceptable response for many patients, but there were also cases of hair regrowth in this subset. Although improvement was not generally on the order seen among those with FFA/LLP, she suggested that there is promise even in these more difficult patients.
Further studies are planned, but Dr. Meariman said that it might be important to focus on early treatment regardless of CA subtype. She noted that patients with less than 5 years disease duration typically did better than those with longer durations.
Ritlecitinib for AT/AU
The analysis of patients with AT/AU was based on a subset analysis from the ALLEGRO phase 2b/3 study of ritlecitinib, which targets JAK3 and TEC kinases. The full results of the ALLEGRO trial were published last year in The Lancet. In the new late-breaker analysis, Severity of Alopecia Tool (SALT) scores were evaluated on an observed or last-observation-carried-forward basis. Generally, responses in the subgroup of patients with AT/AU, who had a median SALT score of 80.3 (signifying 80.3% hair loss) at baseline, were only modestly lower than those in the overall trial.
At 24 months, about 50% of patients achieved a SALT score of 20, according to Melissa Piliang, MD, chair of Dermatology at the Cleveland Clinic, Cleveland, Ohio, who presented the data. In this group, as in the non-AT/AU population, responses climbed over time, and these responses have been maintained for as long as patients have remained on therapy.
At the more rigorous threshold of SALT < 10, the proportion of responders was only slightly lower, meaning a substantial proportion of patients with AT/AU “are achieving 90% or more of hair regrowth, so really an excellent response,” Dr. Piliang said.
For the subgroup with AU, specifically, regrowth of eyebrows and eyelashes was also observed in a substantial proportion, according to Dr. Piliang. Attributed to the often-devastating psychological burden of hair loss, patient-reported assessments of these responses global were generally “even better” than those reported by the investigators.
However, Dr. Piliang advised clinicians to treat AA as early as possible. Despite the benefits seen in the AT/AU subgroup, she pointed out that starting treatment before total hair loss is associated with a higher likelihood of complete or nearly complete hair regrowth.
There are no data from the ALLEGRO trial to determine how long hair regrowth persists after discontinuation of ritlecitinib, which has been approved for the treatment of AA, but Dr. Piliang said that patients should be told that lifelong therapy should be expected in the vast majority of individuals, whether or not AA has advanced to AT/AU.
“In my experience with JAK inhibitors, you lose response when you come off these drugs,” she said.
Dr. Meariman reported a financial relationship with AbbVie. Dr. Piliang reported financial relationships with Eli Lilly, Pfizer, and Proctor & Gamble. Dr. Armstrong reported financial relationships with more than 30 pharmaceutical companies, including those that manufacture JAK inhibitors. Dr. Guttman-Yassky reported financial relationships with more than 30 companies, including those that manufacture JAK inhibitors.
A version of this article appeared on Medscape.com.
FROM AAD 2024
SAN DIEGO — , according to late-breaking data presented at the annual meeting of the American Academy of Dermatology.
In one study of brepocitinib, the target was cicatricial alopecia (CA), a form of hair loss for which there are no approved therapies. In the other, a subanalysis from phase 3 trials of ritlecitinib for alopecia areata (AA), hair regrowth was shown in the subset of patients who entered the study with alopecia totalis or alopecia universalis (AT/AU).
Reflecting comments from several experts, including one of the late-breaking session moderators, April W. Armstrong, MD, MPH, professor and chief of dermatology, University of California, Los Angeles, said that the CA study, which matched clinical response to changes in CA biomarkers, suggested that the results are a potential breakthrough.
“This is the first placebo-controlled study with an oral JAK inhibitor that not only shows that scarring alopecia can be reversible but also gives insights to the mechanism of action and which patients might respond best,” Emma Guttman-Yassky, MD, PhD, said in an interview. Dr. Guttman-Yassky, professor of Dermatology and Immunology, and director of the Laboratory of Inflammatory Skin Diseases, Icahn School of Medicine at Mount Sinai, New York City, was the study’s senior investigator.
Scarring Alopecia and Brepocitinib
For the study of scarring alopecia, 49 patients with CA were randomized in a 3:1 ratio to brepocitinib, a first-in-class inhibitor that targets both JAK1 and TYK2, or placebo. Because of the small size of the study, the primary endpoint was the change in CA biomarkers. The secondary outcome was clinical response, but because of a correlation between the two, these were mutually reinforcing.
Of the subtypes, nine patients enrolled in the study had frontal fibrosing alopecia (FFA), 16 had lichen planopilaris (LPP) alopecia, and 24 had central centrifugal cicatricial alopecia (CCCA). All of the forms of CA are more common in women overall and women of color specifically, particularly CCCA. For this analysis, the FFA and LPP subtypes were considered similar for assessing response and were combined.
The data included a comparison of response and safety during the 24-week randomization phase, as well as an additional follow-up conducted after another 24 weeks of open-label treatment. During the second phase, all patients on placebo were switched to active treatment.
Overall, there was a reduction in all four of the key scalp inflammatory biomarkers measured among those in the combined FFA/LLP group. In the placebo group, each of these markers — interferon gamma (IFN-gamma), CCLS, CXCL10, and STAT1 — increased over the same time period. In almost all cases, the differences were statistically significant.
In the CCCA subgroup, the same pattern (an increase among those on placebo but a decrease among those on brepocitinib) was observed for CCLS and CXCL10. For IFN-gamma and STAT1, a rise was observed among those on placebo and those on active treatment, although the rise was greater for placebo.
For clinical response, improvement on brepocitinib was observed on disease activity indexes, particularly among those in the FFA/LLP group, according to Marguerite Meariman, MD, a dermatology resident at Mount Sinai, who presented the results. She called the improvement in clinical activity scores at 48 weeks “dramatic.” Moreover, improvement was apparent within 4 weeks of starting therapy.
For CCCA, a more challenging condition to treat, Dr. Meariman said that no further progression might represent an acceptable response for many patients, but there were also cases of hair regrowth in this subset. Although improvement was not generally on the order seen among those with FFA/LLP, she suggested that there is promise even in these more difficult patients.
Further studies are planned, but Dr. Meariman said that it might be important to focus on early treatment regardless of CA subtype. She noted that patients with less than 5 years disease duration typically did better than those with longer durations.
Ritlecitinib for AT/AU
The analysis of patients with AT/AU was based on a subset analysis from the ALLEGRO phase 2b/3 study of ritlecitinib, which targets JAK3 and TEC kinases. The full results of the ALLEGRO trial were published last year in The Lancet. In the new late-breaker analysis, Severity of Alopecia Tool (SALT) scores were evaluated on an observed or last-observation-carried-forward basis. Generally, responses in the subgroup of patients with AT/AU, who had a median SALT score of 80.3 (signifying 80.3% hair loss) at baseline, were only modestly lower than those in the overall trial.
At 24 months, about 50% of patients achieved a SALT score of 20, according to Melissa Piliang, MD, chair of Dermatology at the Cleveland Clinic, Cleveland, Ohio, who presented the data. In this group, as in the non-AT/AU population, responses climbed over time, and these responses have been maintained for as long as patients have remained on therapy.
At the more rigorous threshold of SALT < 10, the proportion of responders was only slightly lower, meaning a substantial proportion of patients with AT/AU “are achieving 90% or more of hair regrowth, so really an excellent response,” Dr. Piliang said.
For the subgroup with AU, specifically, regrowth of eyebrows and eyelashes was also observed in a substantial proportion, according to Dr. Piliang. Attributed to the often-devastating psychological burden of hair loss, patient-reported assessments of these responses global were generally “even better” than those reported by the investigators.
However, Dr. Piliang advised clinicians to treat AA as early as possible. Despite the benefits seen in the AT/AU subgroup, she pointed out that starting treatment before total hair loss is associated with a higher likelihood of complete or nearly complete hair regrowth.
There are no data from the ALLEGRO trial to determine how long hair regrowth persists after discontinuation of ritlecitinib, which has been approved for the treatment of AA, but Dr. Piliang said that patients should be told that lifelong therapy should be expected in the vast majority of individuals, whether or not AA has advanced to AT/AU.
“In my experience with JAK inhibitors, you lose response when you come off these drugs,” she said.
Dr. Meariman reported a financial relationship with AbbVie. Dr. Piliang reported financial relationships with Eli Lilly, Pfizer, and Proctor & Gamble. Dr. Armstrong reported financial relationships with more than 30 pharmaceutical companies, including those that manufacture JAK inhibitors. Dr. Guttman-Yassky reported financial relationships with more than 30 companies, including those that manufacture JAK inhibitors.
A version of this article appeared on Medscape.com.
Cognitive Deficits After Most Severe COVID Cases Associated With 9-Point IQ Drop
A new study from the United Kingdom provides greater clarity on how SARS-CoV-2 infection can affect cognition and memory, including novel data on how long brain fog may last after the illness resolves and which cognitive functions are most vulnerable.
In a large community sample, researchers found that on average, people who had recovered from COVID-19 showed small cognitive deficits equivalent to a 3-point loss in IQ for up to 1 year or more after recovering from the acute illness compared with peers who never had COVID-19.
However, people who had more severe cases, requiring treatment in a hospital intensive care unit, had cognitive deficits equivalent to a 9-point drop in IQ.
“People with ongoing persistent symptoms, indicative of long COVID, had larger cognitive deficits than people whose symptoms had resolved,” first author Adam Hampshire, PhD, with Imperial College London, London, England, told this news organization.
The largest deficits among cognitive tasks were in memory, reasoning, and executive function, he added.
“That is, people who had had COVID-19 were both slower and less accurate when performing tasks that measure those abilities,” Dr. Hampshire said. “The group with the largest cognitive deficits were patients who had been in intensive care for COVID-19.”
The study was published online in The New England Journal of Medicine.
Lingering Brain Fog
Cognitive symptoms after SARS-CoV-2 infection are well recognized, but whether objectively measurable cognitive deficits exist and how long they persist remains unclear.
To investigate, researchers invited 800,000 adults from the REACT study of SARS-CoV-2 transmission in England to complete an online assessment for cognitive function with eight domains.
Altogether, 141,583 participants started the cognitive battery by completing at least one task, and 112,964 completed all eight tasks.
The researchers estimated global cognitive scores among participants who had been previously infected with SARS-CoV-2 with symptoms that persisted for at least 12 weeks, whether or not resolved, and among uninfected participants.
Compared with uninfected adults, those who had COVID-19 that resolved had a small cognitive deficit, corresponding to a 3-point loss in IQ, the researchers found.
Adults with unresolved persistent COVID-19 symptoms had the equivalent of a 6-point loss in IQ, and those who had been admitted to the intensive care unit had the equivalent of a 9-point loss in IQ, in line with previous findings of cognitive deficits in patients hospitalized in a critical care unit, the researchers report.
Larger cognitive deficits were evident in adults infected early in the pandemic by the original SARS-CoV-2 virus or the B.1.1.7 variant, whereas peers infected later in the pandemic (eg., in the Omicron period), showed smaller cognitive deficits. This finding is in line with other studies suggesting that the association between COVID-19–associated cognitive deficits attenuated as the pandemic progressed, the researchers noted.
They also found that people who had COVID-19 after receiving two or more vaccinations showed better cognitive performance compared with those who had not been vaccinated.
The memory, reasoning, and executive function tasks were among the most sensitive to COVID-19–related cognitive differences and performance on these tasks differed according to illness duration and hospitalization.
Dr. Hampshire said that more research is needed to determine whether the cognitive deficits resolve with time.
“The implications of longer-term persistence of cognitive deficits and their clinical relevance remain unclear and warrant ongoing surveillance,” he said.
Larger Cognitive Deficits Likely?
These results are “a concern and the broader implications require evaluation,” wrote Ziyad Al-Aly, MD, with Washington University School of Medicine in St. Louis, Missouri, and Clifford Rosen, MD, with Tufts University School of Medicine in Boston, Massachusetts, in an accompanying editorial.
In their view, several outstanding questions remain, including what the potential functional implications of a 3-point loss in IQ may be and whether COVID-19–related cognitive deficits predispose to a higher risk for dementia later in life.
“A deeper understanding of the biology of cognitive dysfunction after SARS-CoV-2 infection and how best to prevent and treat it are critical for addressing the needs of affected persons and preserving the cognitive health of populations,” Drs. Al-Aly and Rosen concluded.
Commenting on the study for this news organization, Jacqueline Becker, PhD, clinical neuropsychologist and assistant professor of medicine, Icahn School of Medicine at Mount Sinai, New York City, noted that “one important caveat” is that the study used an online assessment tool for cognitive function and therefore the findings should be taken with “a grain of salt.”
“That said, this is a large sample, and the findings are generally consistent with what we’ve seen in terms of cognitive deficits post-COVID,” Dr. Becker said.
It’s likely that this study “underestimates” the degree of cognitive deficits that would be seen on validated neuropsychological tests, she added.
In a recent study, Dr. Becker and her colleagues investigated rates of cognitive impairment in 740 COVID-19 patients who recovered and were treated in outpatient, emergency department, or inpatient hospital settings.
Using validated neuropsychological measures, they found a relatively high frequency of cognitive impairment several months after patients contracted COVID-19. Impairments in executive functioning, processing speed, category fluency, memory encoding, and recall were predominant among hospitalized patients.
Dr. Becker noted that in her experience, cognition typically will improve in some patients 12-18 months post COVID.
Support for the study was provided by the National Institute for Health and Care Research and UK Research and Innovation and by the Department of Health and Social Care in England and the Huo Family Foundation. Disclosures for authors and editorial writers are available at NEJM.org. Dr. Becker has no relevant disclosures.
A version of this article appeared on Medscape.com.
A new study from the United Kingdom provides greater clarity on how SARS-CoV-2 infection can affect cognition and memory, including novel data on how long brain fog may last after the illness resolves and which cognitive functions are most vulnerable.
In a large community sample, researchers found that on average, people who had recovered from COVID-19 showed small cognitive deficits equivalent to a 3-point loss in IQ for up to 1 year or more after recovering from the acute illness compared with peers who never had COVID-19.
However, people who had more severe cases, requiring treatment in a hospital intensive care unit, had cognitive deficits equivalent to a 9-point drop in IQ.
“People with ongoing persistent symptoms, indicative of long COVID, had larger cognitive deficits than people whose symptoms had resolved,” first author Adam Hampshire, PhD, with Imperial College London, London, England, told this news organization.
The largest deficits among cognitive tasks were in memory, reasoning, and executive function, he added.
“That is, people who had had COVID-19 were both slower and less accurate when performing tasks that measure those abilities,” Dr. Hampshire said. “The group with the largest cognitive deficits were patients who had been in intensive care for COVID-19.”
The study was published online in The New England Journal of Medicine.
Lingering Brain Fog
Cognitive symptoms after SARS-CoV-2 infection are well recognized, but whether objectively measurable cognitive deficits exist and how long they persist remains unclear.
To investigate, researchers invited 800,000 adults from the REACT study of SARS-CoV-2 transmission in England to complete an online assessment for cognitive function with eight domains.
Altogether, 141,583 participants started the cognitive battery by completing at least one task, and 112,964 completed all eight tasks.
The researchers estimated global cognitive scores among participants who had been previously infected with SARS-CoV-2 with symptoms that persisted for at least 12 weeks, whether or not resolved, and among uninfected participants.
Compared with uninfected adults, those who had COVID-19 that resolved had a small cognitive deficit, corresponding to a 3-point loss in IQ, the researchers found.
Adults with unresolved persistent COVID-19 symptoms had the equivalent of a 6-point loss in IQ, and those who had been admitted to the intensive care unit had the equivalent of a 9-point loss in IQ, in line with previous findings of cognitive deficits in patients hospitalized in a critical care unit, the researchers report.
Larger cognitive deficits were evident in adults infected early in the pandemic by the original SARS-CoV-2 virus or the B.1.1.7 variant, whereas peers infected later in the pandemic (eg., in the Omicron period), showed smaller cognitive deficits. This finding is in line with other studies suggesting that the association between COVID-19–associated cognitive deficits attenuated as the pandemic progressed, the researchers noted.
They also found that people who had COVID-19 after receiving two or more vaccinations showed better cognitive performance compared with those who had not been vaccinated.
The memory, reasoning, and executive function tasks were among the most sensitive to COVID-19–related cognitive differences and performance on these tasks differed according to illness duration and hospitalization.
Dr. Hampshire said that more research is needed to determine whether the cognitive deficits resolve with time.
“The implications of longer-term persistence of cognitive deficits and their clinical relevance remain unclear and warrant ongoing surveillance,” he said.
Larger Cognitive Deficits Likely?
These results are “a concern and the broader implications require evaluation,” wrote Ziyad Al-Aly, MD, with Washington University School of Medicine in St. Louis, Missouri, and Clifford Rosen, MD, with Tufts University School of Medicine in Boston, Massachusetts, in an accompanying editorial.
In their view, several outstanding questions remain, including what the potential functional implications of a 3-point loss in IQ may be and whether COVID-19–related cognitive deficits predispose to a higher risk for dementia later in life.
“A deeper understanding of the biology of cognitive dysfunction after SARS-CoV-2 infection and how best to prevent and treat it are critical for addressing the needs of affected persons and preserving the cognitive health of populations,” Drs. Al-Aly and Rosen concluded.
Commenting on the study for this news organization, Jacqueline Becker, PhD, clinical neuropsychologist and assistant professor of medicine, Icahn School of Medicine at Mount Sinai, New York City, noted that “one important caveat” is that the study used an online assessment tool for cognitive function and therefore the findings should be taken with “a grain of salt.”
“That said, this is a large sample, and the findings are generally consistent with what we’ve seen in terms of cognitive deficits post-COVID,” Dr. Becker said.
It’s likely that this study “underestimates” the degree of cognitive deficits that would be seen on validated neuropsychological tests, she added.
In a recent study, Dr. Becker and her colleagues investigated rates of cognitive impairment in 740 COVID-19 patients who recovered and were treated in outpatient, emergency department, or inpatient hospital settings.
Using validated neuropsychological measures, they found a relatively high frequency of cognitive impairment several months after patients contracted COVID-19. Impairments in executive functioning, processing speed, category fluency, memory encoding, and recall were predominant among hospitalized patients.
Dr. Becker noted that in her experience, cognition typically will improve in some patients 12-18 months post COVID.
Support for the study was provided by the National Institute for Health and Care Research and UK Research and Innovation and by the Department of Health and Social Care in England and the Huo Family Foundation. Disclosures for authors and editorial writers are available at NEJM.org. Dr. Becker has no relevant disclosures.
A version of this article appeared on Medscape.com.
A new study from the United Kingdom provides greater clarity on how SARS-CoV-2 infection can affect cognition and memory, including novel data on how long brain fog may last after the illness resolves and which cognitive functions are most vulnerable.
In a large community sample, researchers found that on average, people who had recovered from COVID-19 showed small cognitive deficits equivalent to a 3-point loss in IQ for up to 1 year or more after recovering from the acute illness compared with peers who never had COVID-19.
However, people who had more severe cases, requiring treatment in a hospital intensive care unit, had cognitive deficits equivalent to a 9-point drop in IQ.
“People with ongoing persistent symptoms, indicative of long COVID, had larger cognitive deficits than people whose symptoms had resolved,” first author Adam Hampshire, PhD, with Imperial College London, London, England, told this news organization.
The largest deficits among cognitive tasks were in memory, reasoning, and executive function, he added.
“That is, people who had had COVID-19 were both slower and less accurate when performing tasks that measure those abilities,” Dr. Hampshire said. “The group with the largest cognitive deficits were patients who had been in intensive care for COVID-19.”
The study was published online in The New England Journal of Medicine.
Lingering Brain Fog
Cognitive symptoms after SARS-CoV-2 infection are well recognized, but whether objectively measurable cognitive deficits exist and how long they persist remains unclear.
To investigate, researchers invited 800,000 adults from the REACT study of SARS-CoV-2 transmission in England to complete an online assessment for cognitive function with eight domains.
Altogether, 141,583 participants started the cognitive battery by completing at least one task, and 112,964 completed all eight tasks.
The researchers estimated global cognitive scores among participants who had been previously infected with SARS-CoV-2 with symptoms that persisted for at least 12 weeks, whether or not resolved, and among uninfected participants.
Compared with uninfected adults, those who had COVID-19 that resolved had a small cognitive deficit, corresponding to a 3-point loss in IQ, the researchers found.
Adults with unresolved persistent COVID-19 symptoms had the equivalent of a 6-point loss in IQ, and those who had been admitted to the intensive care unit had the equivalent of a 9-point loss in IQ, in line with previous findings of cognitive deficits in patients hospitalized in a critical care unit, the researchers report.
Larger cognitive deficits were evident in adults infected early in the pandemic by the original SARS-CoV-2 virus or the B.1.1.7 variant, whereas peers infected later in the pandemic (eg., in the Omicron period), showed smaller cognitive deficits. This finding is in line with other studies suggesting that the association between COVID-19–associated cognitive deficits attenuated as the pandemic progressed, the researchers noted.
They also found that people who had COVID-19 after receiving two or more vaccinations showed better cognitive performance compared with those who had not been vaccinated.
The memory, reasoning, and executive function tasks were among the most sensitive to COVID-19–related cognitive differences and performance on these tasks differed according to illness duration and hospitalization.
Dr. Hampshire said that more research is needed to determine whether the cognitive deficits resolve with time.
“The implications of longer-term persistence of cognitive deficits and their clinical relevance remain unclear and warrant ongoing surveillance,” he said.
Larger Cognitive Deficits Likely?
These results are “a concern and the broader implications require evaluation,” wrote Ziyad Al-Aly, MD, with Washington University School of Medicine in St. Louis, Missouri, and Clifford Rosen, MD, with Tufts University School of Medicine in Boston, Massachusetts, in an accompanying editorial.
In their view, several outstanding questions remain, including what the potential functional implications of a 3-point loss in IQ may be and whether COVID-19–related cognitive deficits predispose to a higher risk for dementia later in life.
“A deeper understanding of the biology of cognitive dysfunction after SARS-CoV-2 infection and how best to prevent and treat it are critical for addressing the needs of affected persons and preserving the cognitive health of populations,” Drs. Al-Aly and Rosen concluded.
Commenting on the study for this news organization, Jacqueline Becker, PhD, clinical neuropsychologist and assistant professor of medicine, Icahn School of Medicine at Mount Sinai, New York City, noted that “one important caveat” is that the study used an online assessment tool for cognitive function and therefore the findings should be taken with “a grain of salt.”
“That said, this is a large sample, and the findings are generally consistent with what we’ve seen in terms of cognitive deficits post-COVID,” Dr. Becker said.
It’s likely that this study “underestimates” the degree of cognitive deficits that would be seen on validated neuropsychological tests, she added.
In a recent study, Dr. Becker and her colleagues investigated rates of cognitive impairment in 740 COVID-19 patients who recovered and were treated in outpatient, emergency department, or inpatient hospital settings.
Using validated neuropsychological measures, they found a relatively high frequency of cognitive impairment several months after patients contracted COVID-19. Impairments in executive functioning, processing speed, category fluency, memory encoding, and recall were predominant among hospitalized patients.
Dr. Becker noted that in her experience, cognition typically will improve in some patients 12-18 months post COVID.
Support for the study was provided by the National Institute for Health and Care Research and UK Research and Innovation and by the Department of Health and Social Care in England and the Huo Family Foundation. Disclosures for authors and editorial writers are available at NEJM.org. Dr. Becker has no relevant disclosures.
A version of this article appeared on Medscape.com.
Medtronic’s Duet EDMS Catheter Tubing Under Class I Recall
If this happens, potential harm to patients may include infections, cerebrospinal fluid (CSF) leakage, overdrainage of CSF, and abnormality of the ventricles. Uncontrolled overdrainage of CSF could lead to neurological injury or death if the disconnection is undetected.
The Food and Drug Administration has identified this as a Class I recall — the most serious type — due to the risk for serious injury or death. To date, there have been 26 reported injuries and no deaths related to this issue.
The recall includes 45,176 devices distributed in the United States between May 3, 2021, and January 9, 2024, with model numbers 46913, 46914, 46915, 46916, and 46917.
The Duet EDMS is used for temporary CSF drainage or sampling in patients who have surgery for open descending thoracic aortic aneurysm (TAA) or descending thoraco-abdominal aortic aneurysm (TAAA) or patients who have TAA/TAAA repair surgery and develop symptoms such as paraplegia.
Medtronic has sent an urgent medical device recall letter to all affected customers asking them to identify, quarantine, and return any unused recalled products.
Customers are also advised to check all Duet EDMS components for damage and ensure that all connections are secure and leak-free.
If a patient is currently connected to an impacted Duet EDMS and a leak or disconnection is detected, the device should be changed to a new alternative device utilizing a sterile technique.
It is not recommended that a Duet system device that is connected to a patient and working as intended be removed or replaced.
Customers in the United States with questions about this recall should contact Medtronic at 1-800-874-5797.
A version of this article appeared on Medscape.com.
If this happens, potential harm to patients may include infections, cerebrospinal fluid (CSF) leakage, overdrainage of CSF, and abnormality of the ventricles. Uncontrolled overdrainage of CSF could lead to neurological injury or death if the disconnection is undetected.
The Food and Drug Administration has identified this as a Class I recall — the most serious type — due to the risk for serious injury or death. To date, there have been 26 reported injuries and no deaths related to this issue.
The recall includes 45,176 devices distributed in the United States between May 3, 2021, and January 9, 2024, with model numbers 46913, 46914, 46915, 46916, and 46917.
The Duet EDMS is used for temporary CSF drainage or sampling in patients who have surgery for open descending thoracic aortic aneurysm (TAA) or descending thoraco-abdominal aortic aneurysm (TAAA) or patients who have TAA/TAAA repair surgery and develop symptoms such as paraplegia.
Medtronic has sent an urgent medical device recall letter to all affected customers asking them to identify, quarantine, and return any unused recalled products.
Customers are also advised to check all Duet EDMS components for damage and ensure that all connections are secure and leak-free.
If a patient is currently connected to an impacted Duet EDMS and a leak or disconnection is detected, the device should be changed to a new alternative device utilizing a sterile technique.
It is not recommended that a Duet system device that is connected to a patient and working as intended be removed or replaced.
Customers in the United States with questions about this recall should contact Medtronic at 1-800-874-5797.
A version of this article appeared on Medscape.com.
If this happens, potential harm to patients may include infections, cerebrospinal fluid (CSF) leakage, overdrainage of CSF, and abnormality of the ventricles. Uncontrolled overdrainage of CSF could lead to neurological injury or death if the disconnection is undetected.
The Food and Drug Administration has identified this as a Class I recall — the most serious type — due to the risk for serious injury or death. To date, there have been 26 reported injuries and no deaths related to this issue.
The recall includes 45,176 devices distributed in the United States between May 3, 2021, and January 9, 2024, with model numbers 46913, 46914, 46915, 46916, and 46917.
The Duet EDMS is used for temporary CSF drainage or sampling in patients who have surgery for open descending thoracic aortic aneurysm (TAA) or descending thoraco-abdominal aortic aneurysm (TAAA) or patients who have TAA/TAAA repair surgery and develop symptoms such as paraplegia.
Medtronic has sent an urgent medical device recall letter to all affected customers asking them to identify, quarantine, and return any unused recalled products.
Customers are also advised to check all Duet EDMS components for damage and ensure that all connections are secure and leak-free.
If a patient is currently connected to an impacted Duet EDMS and a leak or disconnection is detected, the device should be changed to a new alternative device utilizing a sterile technique.
It is not recommended that a Duet system device that is connected to a patient and working as intended be removed or replaced.
Customers in the United States with questions about this recall should contact Medtronic at 1-800-874-5797.
A version of this article appeared on Medscape.com.
Vitamin D Supplements May Be a Double-Edged Sword
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.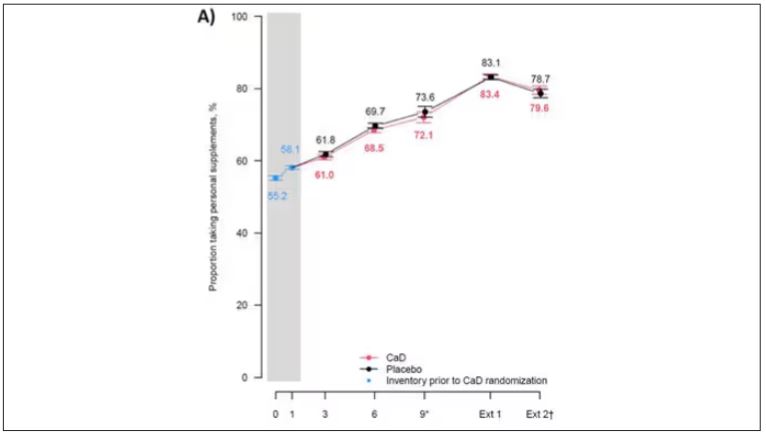
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.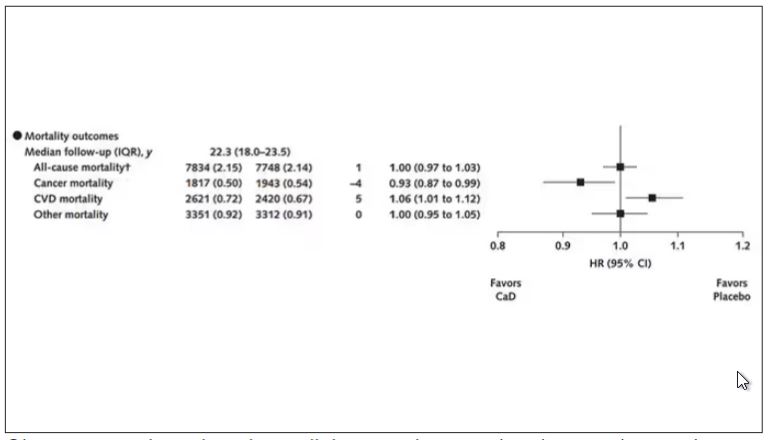
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.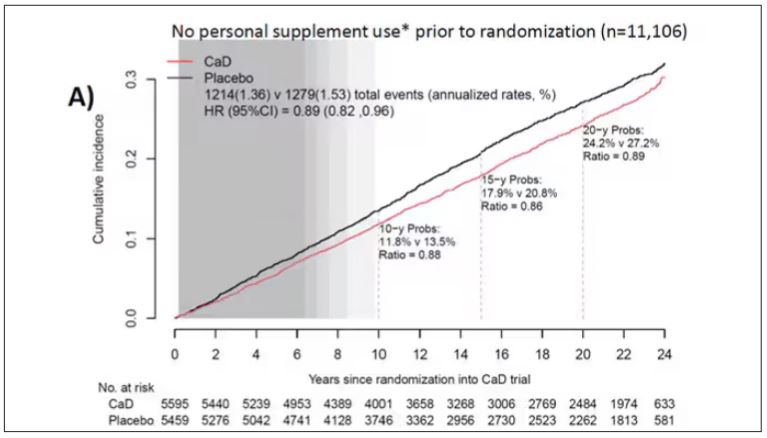
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.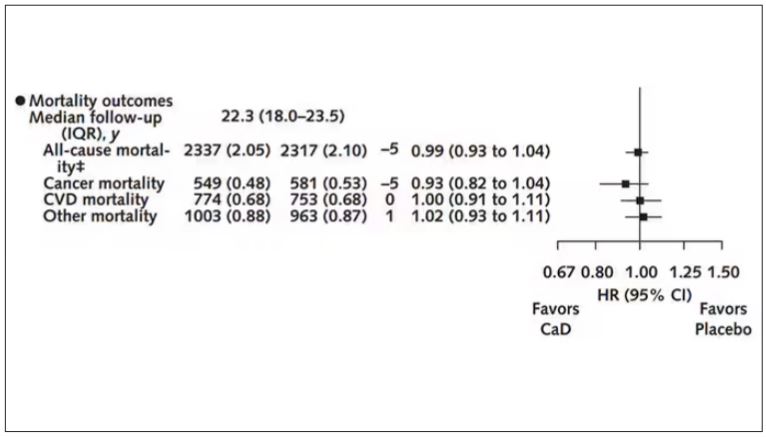
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
Long-Term Calcium and Vitamin D: Cancer Deaths Down, CVD Deaths Up in Older Women?
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.

“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.

“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”

Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.

“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.
“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.
“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”
Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.
“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.
“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.
“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”
Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.
“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
FROM ANNALS OF INTERNAL MEDICINE
Look Beyond BMI: Metabolic Factors’ Link to Cancer Explained
The new research finds that adults with persistent metabolic syndrome that worsens over time are at increased risk for any type of cancer.
The conditions that make up metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, and colleagues.
However, a single assessment of metabolic syndrome at one point in time is inadequate to show an association with cancer risk over time, they said. In the current study, the researchers used models to examine the association between trajectory patterns of metabolic syndrome over time and the risk of overall and specific cancer types. They also examined the impact of chronic inflammation concurrent with metabolic syndrome.
What We Know About Metabolic Syndrome and Cancer Risk
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2020 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
In addition, a 2022 study by some of the current study researchers of the same Chinese cohort focused on the role of inflammation in combination with metabolic syndrome on colorectal cancer specifically, and found an increased risk for cancer when both metabolic syndrome and inflammation were present.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
“There is emerging evidence that even normal weight individuals who are metabolically unhealthy may be at an elevated cancer risk, and we need better metrics to define the underlying metabolic dysfunction in obesity,” Sheetal Hardikar, MBBS, PhD, MPH, an investigator at the Huntsman Cancer Institute, University of Utah, said in an interview.
Dr. Hardikar, who serves as assistant professor in the department of population health sciences at the University of Utah, was not involved in the current study. She and her colleagues published a research paper on data from the National Health and Nutrition Examination Survey in 2023 that showed an increased risk of obesity-related cancer.
What New Study Adds to Related Research
Previous studies have consistently reported an approximately 30% increased risk of cancer with metabolic syndrome, Dr. Hardikar said. “What is unique about this study is the examination of metabolic syndrome trajectories over four years, and not just the presence of metabolic syndrome at one point in time,” she said.
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years; the mean body mass index ranged from approximately 22 kg/m2 in the low-stable group to approximately 28 kg/m2 in the elevated-increasing group.
The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
Using the International Diabetes Federation criteria was another limitation, because it prevented the assessment of cancer risk in normal weight individuals with metabolic dysfunction, Dr. Hardikar noted.
Does Metabolic Syndrome Cause Cancer?
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, noted in a statement on the study.
More research is needed to assess the impact of these interventions on cancer risk. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he continued.
“Current evidence based on this study and many other reports strongly suggests an increased risk for cancer associated with metabolic syndrome,” Dr. Hardikar said in an interview. The data serve as a reminder to clinicians to look beyond BMI as the only measure of obesity, and to consider metabolic factors together to identify individuals at increased risk for cancer, she said.
“We must continue to educate patients about obesity and all the chronic conditions it may lead to, but we cannot ignore this emerging phenotype of being of normal weight but metabolically unhealthy,” Dr. Hardikar emphasized.
What Additional Research is Needed?
Looking ahead, “we need well-designed interventions to test causality for metabolic syndrome and cancer risk, though the evidence from the observational studies is very strong,” Dr. Hardikar said.
In addition, a consensus is needed to better define metabolic dysfunction,and to explore cancer risk in normal weight but metabolically unhealthy individuals, she said.
The study was supported by the National Key Research and Development Program of China. The researchers and Dr. Hardikar had no financial conflicts to disclose.
The new research finds that adults with persistent metabolic syndrome that worsens over time are at increased risk for any type of cancer.
The conditions that make up metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, and colleagues.
However, a single assessment of metabolic syndrome at one point in time is inadequate to show an association with cancer risk over time, they said. In the current study, the researchers used models to examine the association between trajectory patterns of metabolic syndrome over time and the risk of overall and specific cancer types. They also examined the impact of chronic inflammation concurrent with metabolic syndrome.
What We Know About Metabolic Syndrome and Cancer Risk
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2020 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
In addition, a 2022 study by some of the current study researchers of the same Chinese cohort focused on the role of inflammation in combination with metabolic syndrome on colorectal cancer specifically, and found an increased risk for cancer when both metabolic syndrome and inflammation were present.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
“There is emerging evidence that even normal weight individuals who are metabolically unhealthy may be at an elevated cancer risk, and we need better metrics to define the underlying metabolic dysfunction in obesity,” Sheetal Hardikar, MBBS, PhD, MPH, an investigator at the Huntsman Cancer Institute, University of Utah, said in an interview.
Dr. Hardikar, who serves as assistant professor in the department of population health sciences at the University of Utah, was not involved in the current study. She and her colleagues published a research paper on data from the National Health and Nutrition Examination Survey in 2023 that showed an increased risk of obesity-related cancer.
What New Study Adds to Related Research
Previous studies have consistently reported an approximately 30% increased risk of cancer with metabolic syndrome, Dr. Hardikar said. “What is unique about this study is the examination of metabolic syndrome trajectories over four years, and not just the presence of metabolic syndrome at one point in time,” she said.
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years; the mean body mass index ranged from approximately 22 kg/m2 in the low-stable group to approximately 28 kg/m2 in the elevated-increasing group.
The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
Using the International Diabetes Federation criteria was another limitation, because it prevented the assessment of cancer risk in normal weight individuals with metabolic dysfunction, Dr. Hardikar noted.
Does Metabolic Syndrome Cause Cancer?
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, noted in a statement on the study.
More research is needed to assess the impact of these interventions on cancer risk. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he continued.
“Current evidence based on this study and many other reports strongly suggests an increased risk for cancer associated with metabolic syndrome,” Dr. Hardikar said in an interview. The data serve as a reminder to clinicians to look beyond BMI as the only measure of obesity, and to consider metabolic factors together to identify individuals at increased risk for cancer, she said.
“We must continue to educate patients about obesity and all the chronic conditions it may lead to, but we cannot ignore this emerging phenotype of being of normal weight but metabolically unhealthy,” Dr. Hardikar emphasized.
What Additional Research is Needed?
Looking ahead, “we need well-designed interventions to test causality for metabolic syndrome and cancer risk, though the evidence from the observational studies is very strong,” Dr. Hardikar said.
In addition, a consensus is needed to better define metabolic dysfunction,and to explore cancer risk in normal weight but metabolically unhealthy individuals, she said.
The study was supported by the National Key Research and Development Program of China. The researchers and Dr. Hardikar had no financial conflicts to disclose.
The new research finds that adults with persistent metabolic syndrome that worsens over time are at increased risk for any type of cancer.
The conditions that make up metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, and colleagues.
However, a single assessment of metabolic syndrome at one point in time is inadequate to show an association with cancer risk over time, they said. In the current study, the researchers used models to examine the association between trajectory patterns of metabolic syndrome over time and the risk of overall and specific cancer types. They also examined the impact of chronic inflammation concurrent with metabolic syndrome.
What We Know About Metabolic Syndrome and Cancer Risk
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2020 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
In addition, a 2022 study by some of the current study researchers of the same Chinese cohort focused on the role of inflammation in combination with metabolic syndrome on colorectal cancer specifically, and found an increased risk for cancer when both metabolic syndrome and inflammation were present.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
“There is emerging evidence that even normal weight individuals who are metabolically unhealthy may be at an elevated cancer risk, and we need better metrics to define the underlying metabolic dysfunction in obesity,” Sheetal Hardikar, MBBS, PhD, MPH, an investigator at the Huntsman Cancer Institute, University of Utah, said in an interview.
Dr. Hardikar, who serves as assistant professor in the department of population health sciences at the University of Utah, was not involved in the current study. She and her colleagues published a research paper on data from the National Health and Nutrition Examination Survey in 2023 that showed an increased risk of obesity-related cancer.
What New Study Adds to Related Research
Previous studies have consistently reported an approximately 30% increased risk of cancer with metabolic syndrome, Dr. Hardikar said. “What is unique about this study is the examination of metabolic syndrome trajectories over four years, and not just the presence of metabolic syndrome at one point in time,” she said.
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years; the mean body mass index ranged from approximately 22 kg/m2 in the low-stable group to approximately 28 kg/m2 in the elevated-increasing group.
The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
Using the International Diabetes Federation criteria was another limitation, because it prevented the assessment of cancer risk in normal weight individuals with metabolic dysfunction, Dr. Hardikar noted.
Does Metabolic Syndrome Cause Cancer?
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, noted in a statement on the study.
More research is needed to assess the impact of these interventions on cancer risk. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he continued.
“Current evidence based on this study and many other reports strongly suggests an increased risk for cancer associated with metabolic syndrome,” Dr. Hardikar said in an interview. The data serve as a reminder to clinicians to look beyond BMI as the only measure of obesity, and to consider metabolic factors together to identify individuals at increased risk for cancer, she said.
“We must continue to educate patients about obesity and all the chronic conditions it may lead to, but we cannot ignore this emerging phenotype of being of normal weight but metabolically unhealthy,” Dr. Hardikar emphasized.
What Additional Research is Needed?
Looking ahead, “we need well-designed interventions to test causality for metabolic syndrome and cancer risk, though the evidence from the observational studies is very strong,” Dr. Hardikar said.
In addition, a consensus is needed to better define metabolic dysfunction,and to explore cancer risk in normal weight but metabolically unhealthy individuals, she said.
The study was supported by the National Key Research and Development Program of China. The researchers and Dr. Hardikar had no financial conflicts to disclose.
FROM CANCER