User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Phototherapy for Pediatric Segmental Vitiligo
Phototherapy for Pediatric Segmental Vitiligo
To the Editor:
Segmental vitiligo (SV) accounts for a minority of vitiligo cases and most frequently occurs in children.1 It characteristically manifests unilaterally and affects a single body area with a sharp midline demarcation. In contrast to nonsegmental vitiligo (NSV), SV typically stabilizes early in the disease progression.1 The pathophysiology of this vitiligo subtype is not well established, but possible autoinflammatory mechanisms associated with somatic mosaicism, neuronal mechanisms, and/or microvascular skin-homing have been proposed.2 We present the case of a pediatric patient with segmental vitiligo of the right hemiface treated with a combination of a topical calcineurin inhibitor and narrow-band UVB (NB-UVB) phototherapy.
An otherwise healthy 7-year-old boy presented to the dermatology department for evaluation of depigmented macules and patches affecting the right hemiface (temporal, periorbital, malar, perioral, preauricular, and mandibular regions) and neck associated with homolateral leukotrichia of the scalp and facial hair as well as the eyelashes of 5 years’ duration. The findings were consistent with SV (Figure 1). The patient previously had been diagnosed based on the clinical findings and treated with continuous application of topical calcineurin inhibitors plus oral cyclosporine (3 mg/kg/d) for 1 year, but the response was poor. The condition had a severe impact on the patient’s quality of life and social relationships. Therapeutic options were discussed with the patient’s caregivers, and ultimately NB-UVB phototherapy was started twice weekly with 10% increases in the dose at each treatment. Topical tacrolimus ointment (1 mg/g) also was started, and the cyclosporine was stopped. Evaluation of treatment progress occurred every 3 months, with progressive repigmentation of the patches following a perifollicular pattern. After 6 months of phototherapy, there was notable repigmentation of the affected areas, particularly in the malar, perioral, and perinasal regions (Figure 2) and the therapeutic response improved after 1 year of treatment (Figure 3). No adverse events were noted during the treatment period.



Segmental vitiligo lacks consistently effective treatment options. This subtype of vitiligo is classically resistant to conventional therapeutic options. Surgery may be a more effective and long-lasting treatment option but is not suitable for every patient.1,3 Janus kinase (JAK) inhibitors are the newest treatment options being explored for topical and systemic treatment of vitiligo, with promising results in active and stable NSV lesions4,5; however, SV rarely is represented in case reports and clinical trials. The topical JAK inhibitor ruxolitinib has been approved for use in NSV,5 and a phase 2 trial with oral ritlecitinib only included patients with NSV.4 Furthermore, JAK inhibitors have been studied and approved for children aged 12 years or older as well as for adults,4,5 but younger age groups (4-10 years)—in whom SV most frequently manifests, as in our patient—have been excluded from these studies.1 We present a novel case of SV of the right hemiface in a child that was successfully treated with NB-UVB phototherapy in association with topical calcineurin inhibitors.
The role of phototherapy for the treatment of vitiligo has been well documented, and it frequently is combined with other therapeutic modalities, such as topical anti-inflammatory drugs or, most recently, laser and micrografting techniques.6,7 The most frequently used modality is NB-UVB. In the active phase, it performs an immunomodulatory role, while in the stable phase, it stimulates migration and activity of perilesional and hair follicle melanocytes.8 Initiating therapy early is advisable, particularly during the first 6 months of progression, as there is a higher probability of response1,3,8; nevertheless, a good response was achieved despite the 5-year evolution of vitiligo in our patient. This is a safe option for a skin condition that may begin early in life and require long-term treatment.8 A main concern would be an increased risk for skin cancer associated with repeated NB-UVB exposure, which has not been verified in a recent analysis.9
Segmental vitiligo can considerably impact the patient’s quality of life, affecting social interactions and self-perception, particularly in younger patients with facial involvement; thus, effective and safe therapeutic strategies adapted to the individual and their vitiligo lesions should be discussed. Classical treatment options remain valid and provide good results for some patients; therefore, they should not be disregarded even with the rise of innovative therapies.
- Speeckaert R, Lambert J, Bulat V, et al. Autoimmunity in segmental vitiligo. Front Immunol. 2020;11:568447. doi:10.3389/fimmu.2020.568447
- Lin X, Meng X, Lin J. Segmental vitiligo: autoimmune pathogenesis, neuronal mechanisms, and somatic mosaicism. Int J Dermatol. 2025;64:490-498. doi:10.1111/ijd.17627
- Khalili M, Amiri R, Mohammadi S, et al. Efficacy and safety of traditional and surgical treatment modalities in segmental vitiligo: a review article. J Cosmet Dermatol. 2022;21:2360-2373. doi:10.1111/jocd.14899
- Yamaguchi Y, Peeva E, Del Duca E, et al. Ritlecitinib, a JAK3/TEC family kinase inhibitor, stabilizes active lesions and repigments stable lesions in vitiligo. Arch Dermatol Res. 2024;316:478. doi:10.1007/s00403-024-03182-y
- Rosmarin D, Passeron T, Pandya AG, et al. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. N Engl J Med. 2022;387:1445-1455. doi:10.1056/NEJMoa2118828
- Chavez-Alvarez S, Herz-Ruelas M, Ocampo-Candiani J, et al. Stable segmental vitiligo treated with punch mini-grafts and narrow band UVB phototherapy. Australas J Dermatol. 2020;61:83-85. doi:10.1111/ajd.13105
- Kim WI, Kim S, Lee SH, et al. The efficacy of fractional carbon dioxide laser combined with narrow-band ultraviolet B phototherapy for non-segmental vitiligo: a systematic review and meta-analysis. Lasers Med Sci. 2021;36:165-173. doi:10.1007/s10103-020-03069-0
- Esmat S, Hegazy RA, Shalaby S, et al. Phototherapy and combination therapies for vitiligo. Dermatol Clin. 2017;35:171-192. doi:10.1016/j.det.2016.11.008
- Mimouni I, Shulman J, Unes AA, et al. Frequency of skin cancer among psoriasis, vitiligo, and mycosis fungoides patients treated with narrowband ultraviolet B phototherapy. Photodermatol Photoimmunol Photomed. 2024;40:E12936. doi:10.1111/phpp.12936
To the Editor:
Segmental vitiligo (SV) accounts for a minority of vitiligo cases and most frequently occurs in children.1 It characteristically manifests unilaterally and affects a single body area with a sharp midline demarcation. In contrast to nonsegmental vitiligo (NSV), SV typically stabilizes early in the disease progression.1 The pathophysiology of this vitiligo subtype is not well established, but possible autoinflammatory mechanisms associated with somatic mosaicism, neuronal mechanisms, and/or microvascular skin-homing have been proposed.2 We present the case of a pediatric patient with segmental vitiligo of the right hemiface treated with a combination of a topical calcineurin inhibitor and narrow-band UVB (NB-UVB) phototherapy.
An otherwise healthy 7-year-old boy presented to the dermatology department for evaluation of depigmented macules and patches affecting the right hemiface (temporal, periorbital, malar, perioral, preauricular, and mandibular regions) and neck associated with homolateral leukotrichia of the scalp and facial hair as well as the eyelashes of 5 years’ duration. The findings were consistent with SV (Figure 1). The patient previously had been diagnosed based on the clinical findings and treated with continuous application of topical calcineurin inhibitors plus oral cyclosporine (3 mg/kg/d) for 1 year, but the response was poor. The condition had a severe impact on the patient’s quality of life and social relationships. Therapeutic options were discussed with the patient’s caregivers, and ultimately NB-UVB phototherapy was started twice weekly with 10% increases in the dose at each treatment. Topical tacrolimus ointment (1 mg/g) also was started, and the cyclosporine was stopped. Evaluation of treatment progress occurred every 3 months, with progressive repigmentation of the patches following a perifollicular pattern. After 6 months of phototherapy, there was notable repigmentation of the affected areas, particularly in the malar, perioral, and perinasal regions (Figure 2) and the therapeutic response improved after 1 year of treatment (Figure 3). No adverse events were noted during the treatment period.
Segmental vitiligo lacks consistently effective treatment options. This subtype of vitiligo is classically resistant to conventional therapeutic options. Surgery may be a more effective and long-lasting treatment option but is not suitable for every patient.1,3 Janus kinase (JAK) inhibitors are the newest treatment options being explored for topical and systemic treatment of vitiligo, with promising results in active and stable NSV lesions4,5; however, SV rarely is represented in case reports and clinical trials. The topical JAK inhibitor ruxolitinib has been approved for use in NSV,5 and a phase 2 trial with oral ritlecitinib only included patients with NSV.4 Furthermore, JAK inhibitors have been studied and approved for children aged 12 years or older as well as for adults,4,5 but younger age groups (4-10 years)—in whom SV most frequently manifests, as in our patient—have been excluded from these studies.1 We present a novel case of SV of the right hemiface in a child that was successfully treated with NB-UVB phototherapy in association with topical calcineurin inhibitors.
The role of phototherapy for the treatment of vitiligo has been well documented, and it frequently is combined with other therapeutic modalities, such as topical anti-inflammatory drugs or, most recently, laser and micrografting techniques.6,7 The most frequently used modality is NB-UVB. In the active phase, it performs an immunomodulatory role, while in the stable phase, it stimulates migration and activity of perilesional and hair follicle melanocytes.8 Initiating therapy early is advisable, particularly during the first 6 months of progression, as there is a higher probability of response1,3,8; nevertheless, a good response was achieved despite the 5-year evolution of vitiligo in our patient. This is a safe option for a skin condition that may begin early in life and require long-term treatment.8 A main concern would be an increased risk for skin cancer associated with repeated NB-UVB exposure, which has not been verified in a recent analysis.9
Segmental vitiligo can considerably impact the patient’s quality of life, affecting social interactions and self-perception, particularly in younger patients with facial involvement; thus, effective and safe therapeutic strategies adapted to the individual and their vitiligo lesions should be discussed. Classical treatment options remain valid and provide good results for some patients; therefore, they should not be disregarded even with the rise of innovative therapies.
To the Editor:
Segmental vitiligo (SV) accounts for a minority of vitiligo cases and most frequently occurs in children.1 It characteristically manifests unilaterally and affects a single body area with a sharp midline demarcation. In contrast to nonsegmental vitiligo (NSV), SV typically stabilizes early in the disease progression.1 The pathophysiology of this vitiligo subtype is not well established, but possible autoinflammatory mechanisms associated with somatic mosaicism, neuronal mechanisms, and/or microvascular skin-homing have been proposed.2 We present the case of a pediatric patient with segmental vitiligo of the right hemiface treated with a combination of a topical calcineurin inhibitor and narrow-band UVB (NB-UVB) phototherapy.
An otherwise healthy 7-year-old boy presented to the dermatology department for evaluation of depigmented macules and patches affecting the right hemiface (temporal, periorbital, malar, perioral, preauricular, and mandibular regions) and neck associated with homolateral leukotrichia of the scalp and facial hair as well as the eyelashes of 5 years’ duration. The findings were consistent with SV (Figure 1). The patient previously had been diagnosed based on the clinical findings and treated with continuous application of topical calcineurin inhibitors plus oral cyclosporine (3 mg/kg/d) for 1 year, but the response was poor. The condition had a severe impact on the patient’s quality of life and social relationships. Therapeutic options were discussed with the patient’s caregivers, and ultimately NB-UVB phototherapy was started twice weekly with 10% increases in the dose at each treatment. Topical tacrolimus ointment (1 mg/g) also was started, and the cyclosporine was stopped. Evaluation of treatment progress occurred every 3 months, with progressive repigmentation of the patches following a perifollicular pattern. After 6 months of phototherapy, there was notable repigmentation of the affected areas, particularly in the malar, perioral, and perinasal regions (Figure 2) and the therapeutic response improved after 1 year of treatment (Figure 3). No adverse events were noted during the treatment period.
Segmental vitiligo lacks consistently effective treatment options. This subtype of vitiligo is classically resistant to conventional therapeutic options. Surgery may be a more effective and long-lasting treatment option but is not suitable for every patient.1,3 Janus kinase (JAK) inhibitors are the newest treatment options being explored for topical and systemic treatment of vitiligo, with promising results in active and stable NSV lesions4,5; however, SV rarely is represented in case reports and clinical trials. The topical JAK inhibitor ruxolitinib has been approved for use in NSV,5 and a phase 2 trial with oral ritlecitinib only included patients with NSV.4 Furthermore, JAK inhibitors have been studied and approved for children aged 12 years or older as well as for adults,4,5 but younger age groups (4-10 years)—in whom SV most frequently manifests, as in our patient—have been excluded from these studies.1 We present a novel case of SV of the right hemiface in a child that was successfully treated with NB-UVB phototherapy in association with topical calcineurin inhibitors.
The role of phototherapy for the treatment of vitiligo has been well documented, and it frequently is combined with other therapeutic modalities, such as topical anti-inflammatory drugs or, most recently, laser and micrografting techniques.6,7 The most frequently used modality is NB-UVB. In the active phase, it performs an immunomodulatory role, while in the stable phase, it stimulates migration and activity of perilesional and hair follicle melanocytes.8 Initiating therapy early is advisable, particularly during the first 6 months of progression, as there is a higher probability of response1,3,8; nevertheless, a good response was achieved despite the 5-year evolution of vitiligo in our patient. This is a safe option for a skin condition that may begin early in life and require long-term treatment.8 A main concern would be an increased risk for skin cancer associated with repeated NB-UVB exposure, which has not been verified in a recent analysis.9
Segmental vitiligo can considerably impact the patient’s quality of life, affecting social interactions and self-perception, particularly in younger patients with facial involvement; thus, effective and safe therapeutic strategies adapted to the individual and their vitiligo lesions should be discussed. Classical treatment options remain valid and provide good results for some patients; therefore, they should not be disregarded even with the rise of innovative therapies.
- Speeckaert R, Lambert J, Bulat V, et al. Autoimmunity in segmental vitiligo. Front Immunol. 2020;11:568447. doi:10.3389/fimmu.2020.568447
- Lin X, Meng X, Lin J. Segmental vitiligo: autoimmune pathogenesis, neuronal mechanisms, and somatic mosaicism. Int J Dermatol. 2025;64:490-498. doi:10.1111/ijd.17627
- Khalili M, Amiri R, Mohammadi S, et al. Efficacy and safety of traditional and surgical treatment modalities in segmental vitiligo: a review article. J Cosmet Dermatol. 2022;21:2360-2373. doi:10.1111/jocd.14899
- Yamaguchi Y, Peeva E, Del Duca E, et al. Ritlecitinib, a JAK3/TEC family kinase inhibitor, stabilizes active lesions and repigments stable lesions in vitiligo. Arch Dermatol Res. 2024;316:478. doi:10.1007/s00403-024-03182-y
- Rosmarin D, Passeron T, Pandya AG, et al. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. N Engl J Med. 2022;387:1445-1455. doi:10.1056/NEJMoa2118828
- Chavez-Alvarez S, Herz-Ruelas M, Ocampo-Candiani J, et al. Stable segmental vitiligo treated with punch mini-grafts and narrow band UVB phototherapy. Australas J Dermatol. 2020;61:83-85. doi:10.1111/ajd.13105
- Kim WI, Kim S, Lee SH, et al. The efficacy of fractional carbon dioxide laser combined with narrow-band ultraviolet B phototherapy for non-segmental vitiligo: a systematic review and meta-analysis. Lasers Med Sci. 2021;36:165-173. doi:10.1007/s10103-020-03069-0
- Esmat S, Hegazy RA, Shalaby S, et al. Phototherapy and combination therapies for vitiligo. Dermatol Clin. 2017;35:171-192. doi:10.1016/j.det.2016.11.008
- Mimouni I, Shulman J, Unes AA, et al. Frequency of skin cancer among psoriasis, vitiligo, and mycosis fungoides patients treated with narrowband ultraviolet B phototherapy. Photodermatol Photoimmunol Photomed. 2024;40:E12936. doi:10.1111/phpp.12936
- Speeckaert R, Lambert J, Bulat V, et al. Autoimmunity in segmental vitiligo. Front Immunol. 2020;11:568447. doi:10.3389/fimmu.2020.568447
- Lin X, Meng X, Lin J. Segmental vitiligo: autoimmune pathogenesis, neuronal mechanisms, and somatic mosaicism. Int J Dermatol. 2025;64:490-498. doi:10.1111/ijd.17627
- Khalili M, Amiri R, Mohammadi S, et al. Efficacy and safety of traditional and surgical treatment modalities in segmental vitiligo: a review article. J Cosmet Dermatol. 2022;21:2360-2373. doi:10.1111/jocd.14899
- Yamaguchi Y, Peeva E, Del Duca E, et al. Ritlecitinib, a JAK3/TEC family kinase inhibitor, stabilizes active lesions and repigments stable lesions in vitiligo. Arch Dermatol Res. 2024;316:478. doi:10.1007/s00403-024-03182-y
- Rosmarin D, Passeron T, Pandya AG, et al. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. N Engl J Med. 2022;387:1445-1455. doi:10.1056/NEJMoa2118828
- Chavez-Alvarez S, Herz-Ruelas M, Ocampo-Candiani J, et al. Stable segmental vitiligo treated with punch mini-grafts and narrow band UVB phototherapy. Australas J Dermatol. 2020;61:83-85. doi:10.1111/ajd.13105
- Kim WI, Kim S, Lee SH, et al. The efficacy of fractional carbon dioxide laser combined with narrow-band ultraviolet B phototherapy for non-segmental vitiligo: a systematic review and meta-analysis. Lasers Med Sci. 2021;36:165-173. doi:10.1007/s10103-020-03069-0
- Esmat S, Hegazy RA, Shalaby S, et al. Phototherapy and combination therapies for vitiligo. Dermatol Clin. 2017;35:171-192. doi:10.1016/j.det.2016.11.008
- Mimouni I, Shulman J, Unes AA, et al. Frequency of skin cancer among psoriasis, vitiligo, and mycosis fungoides patients treated with narrowband ultraviolet B phototherapy. Photodermatol Photoimmunol Photomed. 2024;40:E12936. doi:10.1111/phpp.12936
Phototherapy for Pediatric Segmental Vitiligo
Phototherapy for Pediatric Segmental Vitiligo
Practice Points
- Narrow-band UVB in combination with topical tacrolimus may be an effective treatment option for pediatric segmental vitiligo (SV), even in longstanding disease.
- Current evidence for Janus kinase (JAK) inhibitors largely is derived from studies in nonsegmental vitiligo and in patients aged 12 years or older.
- Segmental vitiligo is underrepresented in clinical trials, and topical and systemic JAK inhibitors are not approved for younger children, in whom SV most commonly occurs.

Black Patches on the Angles of the Mandible
Black Patches on the Angles of the Mandible
THE DIAGNOSIS: Black Dermographism
Black dermographism is characterized by asymptomatic black discoloration on the skin caused by contact with various metals, most commonly gold but also silver, nickel, zinc, lead, and aluminum.1 These metallic particles have a black appearance as they do not reflect light.2 Our patient was wearing gold hoop earrings at presentation, which were near the black patches. Certain topical products (eg, makeup, sunscreens [especially those containing zinc oxide or titanium oxide], toothpaste) can abrade metal, causing it to deposit on the skin and absorb light.3 The black discoloration is not permanent and can be prevented by avoiding contact between inciting products and metals.2 No further diagnostic testing is necessary, and the patches will self-resolve if contact with the product is avoided.
Our patient noted that she wore a physical sunscreen daily, but the black patches were present only when she wore the gold hoop earrings. Given this history and physical examination findings in the office, it was suspected she had black dermographism due to her gold earrings and topical sunscreen. The patient was advised to avoid wearing the gold earrings.
Black dermographism is a misnomer because it is not a true urticarial reaction but rather a false dermographism; therefore, patients will not experience pruritus or erythema.1 True dermographism is an inducible urticarial eruption from pressure or trauma to the skin. The clinical appearance is notable for erythematous wheals in the shape of the external force applied.4 Two other types of false dermographism include white dermographism, which occurs secondary to allergic contact dermatitis, and yellow dermographism, which is caused by bile deposits on the skin.4
Additional diagnoses were able to be ruled out for the following reasons: cutaneous mastocytosis can manifest with red-brown maculopapular lesions often accompanied by the Darier sign, which includes swelling, pruritus, and erythema but was not present in our patient.4 Allergic contact dermatitis manifests as a delayed eczematous reaction around 48 to 72 hours after exposure to an allergen. Our patient’s lesions formed while wearing gold earrings but did not manifest with a hypersensitivity reaction. Of note, symptomatic dermographism has been reported to mimic latex allergy.5 Ecchymosis may appear as erythematous, violaceous, or yellow-green patches depending on the stage but develops due to leakage from broken blood vessels secondary to trauma, which was not reported in our patient. Type I hypersensitivity reactions can occur minutes to hours after exposure to an allergen but typically manifest with a wheal-and-flare presentation.
Black dermographism from gold earrings can mimic concerning skin disorders or poor hygiene, causing unnecessary anxiety. Understanding that it is a harmless reaction between gold and certain topical products can reassure patients and prevent unnecessary testing or treatments.
- Zawar V, Kumavat S, Pawar M. Black dermographism: an uncommon cause of skin discoloration. Indian Dermatol Online J. 2018;9:216-217. doi:10.4103/idoj.IDOJ_228_17
- Lowe E, Lim S. Black dermographism. JAMA Dermatol. 2017; 153:352-353.
- Fisher AA. Black dermographism: mechanism for formation of black color. Cutis. 1993;52(1):17-19.
- Nobles T, Muse ME, Schmieder GJ. Dermatographism. In: StatPearls [Internet]. StatPearls Publishing; February 20, 2023.
- Golberg O, Johnston GA, Wilkinson M. Symptomatic dermographism mimicking latex allergy. Dermatitis. 2014;25:101-103. doi:10.1097 /DER.0000000000000016
THE DIAGNOSIS: Black Dermographism
Black dermographism is characterized by asymptomatic black discoloration on the skin caused by contact with various metals, most commonly gold but also silver, nickel, zinc, lead, and aluminum.1 These metallic particles have a black appearance as they do not reflect light.2 Our patient was wearing gold hoop earrings at presentation, which were near the black patches. Certain topical products (eg, makeup, sunscreens [especially those containing zinc oxide or titanium oxide], toothpaste) can abrade metal, causing it to deposit on the skin and absorb light.3 The black discoloration is not permanent and can be prevented by avoiding contact between inciting products and metals.2 No further diagnostic testing is necessary, and the patches will self-resolve if contact with the product is avoided.
Our patient noted that she wore a physical sunscreen daily, but the black patches were present only when she wore the gold hoop earrings. Given this history and physical examination findings in the office, it was suspected she had black dermographism due to her gold earrings and topical sunscreen. The patient was advised to avoid wearing the gold earrings.
Black dermographism is a misnomer because it is not a true urticarial reaction but rather a false dermographism; therefore, patients will not experience pruritus or erythema.1 True dermographism is an inducible urticarial eruption from pressure or trauma to the skin. The clinical appearance is notable for erythematous wheals in the shape of the external force applied.4 Two other types of false dermographism include white dermographism, which occurs secondary to allergic contact dermatitis, and yellow dermographism, which is caused by bile deposits on the skin.4
Additional diagnoses were able to be ruled out for the following reasons: cutaneous mastocytosis can manifest with red-brown maculopapular lesions often accompanied by the Darier sign, which includes swelling, pruritus, and erythema but was not present in our patient.4 Allergic contact dermatitis manifests as a delayed eczematous reaction around 48 to 72 hours after exposure to an allergen. Our patient’s lesions formed while wearing gold earrings but did not manifest with a hypersensitivity reaction. Of note, symptomatic dermographism has been reported to mimic latex allergy.5 Ecchymosis may appear as erythematous, violaceous, or yellow-green patches depending on the stage but develops due to leakage from broken blood vessels secondary to trauma, which was not reported in our patient. Type I hypersensitivity reactions can occur minutes to hours after exposure to an allergen but typically manifest with a wheal-and-flare presentation.
Black dermographism from gold earrings can mimic concerning skin disorders or poor hygiene, causing unnecessary anxiety. Understanding that it is a harmless reaction between gold and certain topical products can reassure patients and prevent unnecessary testing or treatments.
THE DIAGNOSIS: Black Dermographism
Black dermographism is characterized by asymptomatic black discoloration on the skin caused by contact with various metals, most commonly gold but also silver, nickel, zinc, lead, and aluminum.1 These metallic particles have a black appearance as they do not reflect light.2 Our patient was wearing gold hoop earrings at presentation, which were near the black patches. Certain topical products (eg, makeup, sunscreens [especially those containing zinc oxide or titanium oxide], toothpaste) can abrade metal, causing it to deposit on the skin and absorb light.3 The black discoloration is not permanent and can be prevented by avoiding contact between inciting products and metals.2 No further diagnostic testing is necessary, and the patches will self-resolve if contact with the product is avoided.
Our patient noted that she wore a physical sunscreen daily, but the black patches were present only when she wore the gold hoop earrings. Given this history and physical examination findings in the office, it was suspected she had black dermographism due to her gold earrings and topical sunscreen. The patient was advised to avoid wearing the gold earrings.
Black dermographism is a misnomer because it is not a true urticarial reaction but rather a false dermographism; therefore, patients will not experience pruritus or erythema.1 True dermographism is an inducible urticarial eruption from pressure or trauma to the skin. The clinical appearance is notable for erythematous wheals in the shape of the external force applied.4 Two other types of false dermographism include white dermographism, which occurs secondary to allergic contact dermatitis, and yellow dermographism, which is caused by bile deposits on the skin.4
Additional diagnoses were able to be ruled out for the following reasons: cutaneous mastocytosis can manifest with red-brown maculopapular lesions often accompanied by the Darier sign, which includes swelling, pruritus, and erythema but was not present in our patient.4 Allergic contact dermatitis manifests as a delayed eczematous reaction around 48 to 72 hours after exposure to an allergen. Our patient’s lesions formed while wearing gold earrings but did not manifest with a hypersensitivity reaction. Of note, symptomatic dermographism has been reported to mimic latex allergy.5 Ecchymosis may appear as erythematous, violaceous, or yellow-green patches depending on the stage but develops due to leakage from broken blood vessels secondary to trauma, which was not reported in our patient. Type I hypersensitivity reactions can occur minutes to hours after exposure to an allergen but typically manifest with a wheal-and-flare presentation.
Black dermographism from gold earrings can mimic concerning skin disorders or poor hygiene, causing unnecessary anxiety. Understanding that it is a harmless reaction between gold and certain topical products can reassure patients and prevent unnecessary testing or treatments.
- Zawar V, Kumavat S, Pawar M. Black dermographism: an uncommon cause of skin discoloration. Indian Dermatol Online J. 2018;9:216-217. doi:10.4103/idoj.IDOJ_228_17
- Lowe E, Lim S. Black dermographism. JAMA Dermatol. 2017; 153:352-353.
- Fisher AA. Black dermographism: mechanism for formation of black color. Cutis. 1993;52(1):17-19.
- Nobles T, Muse ME, Schmieder GJ. Dermatographism. In: StatPearls [Internet]. StatPearls Publishing; February 20, 2023.
- Golberg O, Johnston GA, Wilkinson M. Symptomatic dermographism mimicking latex allergy. Dermatitis. 2014;25:101-103. doi:10.1097 /DER.0000000000000016
- Zawar V, Kumavat S, Pawar M. Black dermographism: an uncommon cause of skin discoloration. Indian Dermatol Online J. 2018;9:216-217. doi:10.4103/idoj.IDOJ_228_17
- Lowe E, Lim S. Black dermographism. JAMA Dermatol. 2017; 153:352-353.
- Fisher AA. Black dermographism: mechanism for formation of black color. Cutis. 1993;52(1):17-19.
- Nobles T, Muse ME, Schmieder GJ. Dermatographism. In: StatPearls [Internet]. StatPearls Publishing; February 20, 2023.
- Golberg O, Johnston GA, Wilkinson M. Symptomatic dermographism mimicking latex allergy. Dermatitis. 2014;25:101-103. doi:10.1097 /DER.0000000000000016
Black Patches on the Angles of the Mandible
Black Patches on the Angles of the Mandible
A 30-year-old woman presented for evaluation of intermittent pigmented patches on the face of several months’ duration. The patches would form during the day and disappear when the patient woke up the next morning. She denied any associated pruritus, pain, redness, or recent trauma to the area. Her medical history was otherwise unremarkable. Physical examination revealed ill-defined black patches on both mandibular angles (top). The following day, the patient sent a photograph from home, and the patch was absent (bottom).


Diffusely Scattered Linear Folliculopapular Eruption
Diffusely Scattered Linear Folliculopapular Eruption
THE DIAGNOSIS: Disseminate and Recurrent Infundibulofolliculitis
Histopathology demonstrated a lymphocyte-predominant infundibular infiltrate with mild spongiosis and lymphocytic exocytosis; a mild, superficial perivascular infiltrate also was present. The surrounding skin was largely normal with no notable papillomatosis, acanthosis, or hyperkeratosis (Figure 1). The clinical presentation and histopathologic findings led to the diagnosis of disseminate and recurrent infundibulofolliculitis (DRIF). The patient was started on a 2-week course of once-daily ammonium lactate lotion 12% and urea cream 40% and twice-daily triamcinolone ointment 0.1%. The patient was instructed to take a 1-week break before this regimen was repeated. Isotretinoin 0.5 mg/kg/d for 2 to 4 months was considered and will be an option if there is no improvement at follow-up.
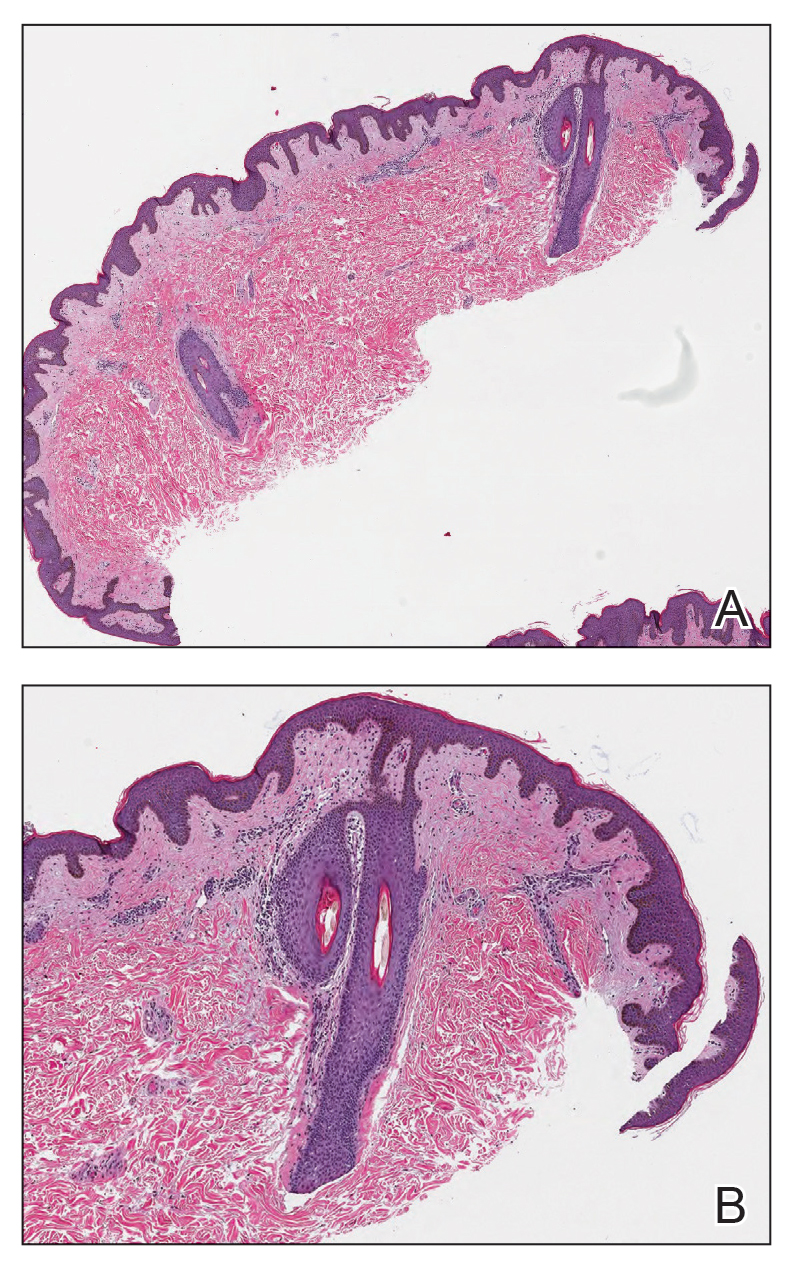
Disseminate and recurrent infundibulofolliculitis is a rare noninfectious folliculitis that initially was described by Hitch and Lund1 in 1968. Males of African descent are most commonly affected by DRIF, but the condition is not limited to this population.2,3 It manifests as asymptomatic, flesh-colored, monomorphic, follicular papules distributed on the trunk and proximal extremities. Pustules can be present, and hair may be seen protruding from them. As the name suggests, DRIF is associated with histopathologic changes that are prominent at the infundibulum of hair follicles.3,4 Disseminate and recurrent infundibulofolliculitis can persist for months to years because it often is resistant to treatment. Treatments include topical monotherapies such as corticosteroids, calcineurin inhibitors, or retinoids; combination topical treatments; antibiotics; and isotretinoin.2 Recurrent remission and exacerbation occurs in many patients.3
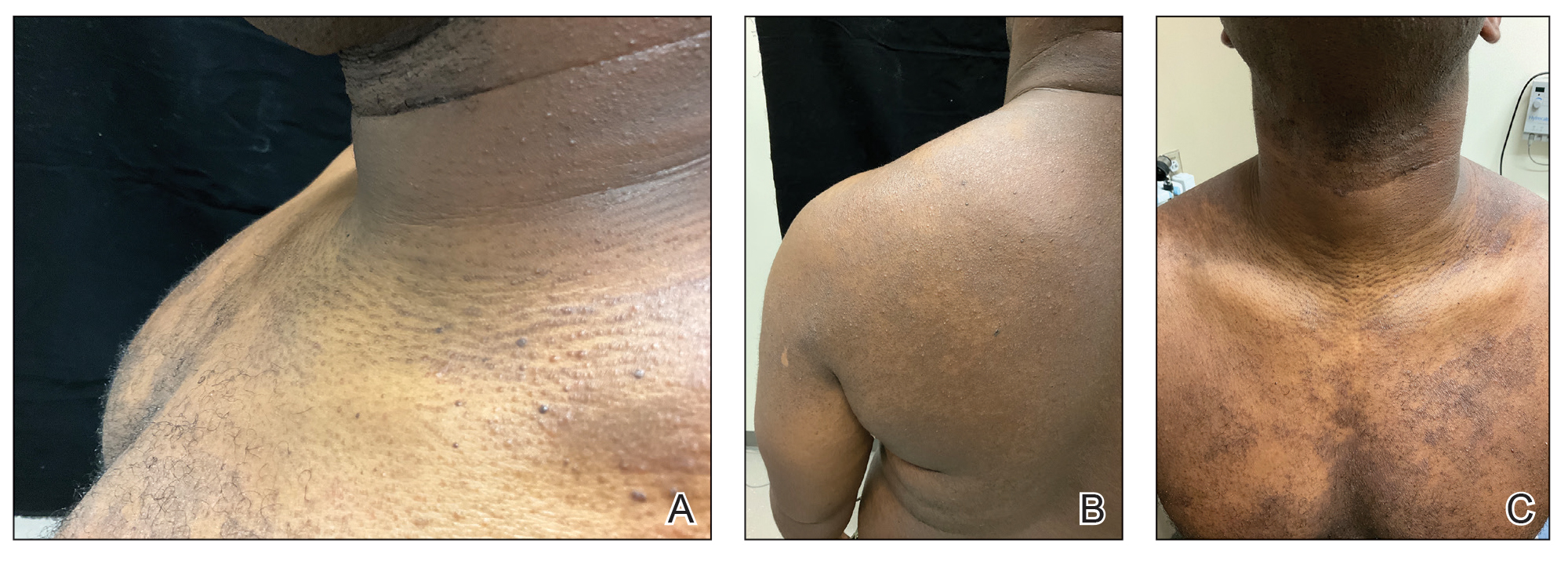
The classic manifestations of DRIF, including follicular, monomorphic, flesh-colored papules distributed on the neck, trunk, and proximal upper extremities, were seen in our patient (Figure 2). These findings along with the skin biopsy identifying a lymphocytic infundibular infiltrate led to the diagnosis of DRIF. The papules associated with DRIF can be recurrent or chronic. The lesions in this patient were chronic and persistent.
Despite limited evidence, it has been suggested that DRIF may be a manifestation of atopic dermatitis in patients with darker skin tones. In our case, the patient had a history of childhood eczema. Other hypotheses have proposed that DRIF could be a nonspecific reaction to a currently unknown antigen. A causative infectious agent has not been identified, although the search continues. There is speculation that DRIF could be an overt expression of normal follicular prominence, but the presence of occasional pustules and lymphocyte- predominant infundibular infiltrate negates that.3
Confluent and reticulated papillomatosis was included in the differential for our patient and manifests as asymptomatic hyperpigmented papules and plaques frequently occurring on the upper trunk, neck, and axilla; however, these lesions have a peripheral netlike configuration, as the name suggests. Additionally, this condition is thought to have an infectious component (Dietzia papillomatosis) and responds to antibiotic treatment.5 Follicular eczema also was high in the differential diagnosis but usually is seasonal and pruritic, and histopathology typically shows the features of spongiotic dermatitis. It also would respond well to topical steroids.6 Another condition high on the differential was juxtaclavicular beaded lines, which also manifests as flesh-colored follicular papules distributed on the upper trunk; however, histopathology usually shows features of hyperplastic pilosebaceous units along with spongiosis and exocytosis.7 Pityrosporum folliculitis initially was considered, but the patient only endorsed occasional pruritus. Additionally, no fungal elements were observed.
Currently, there are no definitive treatments for DRIF. The topical treatments available include midpotency corticosteroids, tretinoin, calcineurin inhibitors, 12% lactic acid, and 20% to 40% urea. The systemic therapies are high-dose oral vitamin A (100,000 IU/d), isotretinoin, and psoralen plus UVA.8-10
- Hitch JM, Lund HZ. Disseminate and recurrent infundibulo-folliculitis: report of a case. Arch Dermatol. 1968;97:432-435.
- Ma BC, Sahni VN, Sahni DR, et al. Disseminate and recurrent infundibulofolliculitis: an under-recognized yet treatable entity. J Drugs Dermatol. 2021;20:1353-1354. doi:10.36849/jdd.6173
- Nair SP, Gomathy M, Kumar GN. Disseminate and recurrent infundibulo- folliculitis in an Indian patient: a case report with review of literature. Indian Dermatol Online J. 2017;8:39-41. doi:10.4103/2229- 5178.198775
- Rekha S, Kumar V, Rao P, et al. Disseminate and recurrent infundibulofolliculitis. Indian J Dermatol. 2019;64:404-406. doi:10.4103/ijd.IJD_77_18
- Jones AL, Koerner RJ, Natarajan S, et al. Dietzia papillomatosis sp. nov., a novel actinomycete isolated from the skin of an immunocompetent patient with confluent and reticulated papillomatosis. Int J Syst Evol Microbiol. 2008;58(pt 1):68-72. doi:10.1099/ijs.0.65178-0
- Cohen PR. Follicular contact dermatitis revisited: a review emphasizing neomycin-associated follicular contact dermatitis. World J Clin Cases. 2014;2:815-821. doi:10.12998/wjcc.v2.i12.815
- Butterworth T, Johnson WC. Justa-clavicular beaded lines. Arch Dermatol. 1974;110:891-893.
- Calka O, Metin A, Ozen S. A case of disseminated and recurrent infundibulo-folliculitis responsive to treatment with isotretinoin. J Dermatol. 2002;29:431-434.
- Goihman-Yahr M. Disseminate and recurrent infundibulofolliculitis: response to psoralen plus UVA therapy. Int J Dermatol. 1999;38:75-76.
- Hinds GA, Heald PW. A case of disseminate and recurrent infundibulofolliculitis responsive to treatment with topical steroids. Dermatol Online J. 2008;14:11.
THE DIAGNOSIS: Disseminate and Recurrent Infundibulofolliculitis
Histopathology demonstrated a lymphocyte-predominant infundibular infiltrate with mild spongiosis and lymphocytic exocytosis; a mild, superficial perivascular infiltrate also was present. The surrounding skin was largely normal with no notable papillomatosis, acanthosis, or hyperkeratosis (Figure 1). The clinical presentation and histopathologic findings led to the diagnosis of disseminate and recurrent infundibulofolliculitis (DRIF). The patient was started on a 2-week course of once-daily ammonium lactate lotion 12% and urea cream 40% and twice-daily triamcinolone ointment 0.1%. The patient was instructed to take a 1-week break before this regimen was repeated. Isotretinoin 0.5 mg/kg/d for 2 to 4 months was considered and will be an option if there is no improvement at follow-up.
Disseminate and recurrent infundibulofolliculitis is a rare noninfectious folliculitis that initially was described by Hitch and Lund1 in 1968. Males of African descent are most commonly affected by DRIF, but the condition is not limited to this population.2,3 It manifests as asymptomatic, flesh-colored, monomorphic, follicular papules distributed on the trunk and proximal extremities. Pustules can be present, and hair may be seen protruding from them. As the name suggests, DRIF is associated with histopathologic changes that are prominent at the infundibulum of hair follicles.3,4 Disseminate and recurrent infundibulofolliculitis can persist for months to years because it often is resistant to treatment. Treatments include topical monotherapies such as corticosteroids, calcineurin inhibitors, or retinoids; combination topical treatments; antibiotics; and isotretinoin.2 Recurrent remission and exacerbation occurs in many patients.3
The classic manifestations of DRIF, including follicular, monomorphic, flesh-colored papules distributed on the neck, trunk, and proximal upper extremities, were seen in our patient (Figure 2). These findings along with the skin biopsy identifying a lymphocytic infundibular infiltrate led to the diagnosis of DRIF. The papules associated with DRIF can be recurrent or chronic. The lesions in this patient were chronic and persistent.
Despite limited evidence, it has been suggested that DRIF may be a manifestation of atopic dermatitis in patients with darker skin tones. In our case, the patient had a history of childhood eczema. Other hypotheses have proposed that DRIF could be a nonspecific reaction to a currently unknown antigen. A causative infectious agent has not been identified, although the search continues. There is speculation that DRIF could be an overt expression of normal follicular prominence, but the presence of occasional pustules and lymphocyte- predominant infundibular infiltrate negates that.3
Confluent and reticulated papillomatosis was included in the differential for our patient and manifests as asymptomatic hyperpigmented papules and plaques frequently occurring on the upper trunk, neck, and axilla; however, these lesions have a peripheral netlike configuration, as the name suggests. Additionally, this condition is thought to have an infectious component (Dietzia papillomatosis) and responds to antibiotic treatment.5 Follicular eczema also was high in the differential diagnosis but usually is seasonal and pruritic, and histopathology typically shows the features of spongiotic dermatitis. It also would respond well to topical steroids.6 Another condition high on the differential was juxtaclavicular beaded lines, which also manifests as flesh-colored follicular papules distributed on the upper trunk; however, histopathology usually shows features of hyperplastic pilosebaceous units along with spongiosis and exocytosis.7 Pityrosporum folliculitis initially was considered, but the patient only endorsed occasional pruritus. Additionally, no fungal elements were observed.
Currently, there are no definitive treatments for DRIF. The topical treatments available include midpotency corticosteroids, tretinoin, calcineurin inhibitors, 12% lactic acid, and 20% to 40% urea. The systemic therapies are high-dose oral vitamin A (100,000 IU/d), isotretinoin, and psoralen plus UVA.8-10
THE DIAGNOSIS: Disseminate and Recurrent Infundibulofolliculitis
Histopathology demonstrated a lymphocyte-predominant infundibular infiltrate with mild spongiosis and lymphocytic exocytosis; a mild, superficial perivascular infiltrate also was present. The surrounding skin was largely normal with no notable papillomatosis, acanthosis, or hyperkeratosis (Figure 1). The clinical presentation and histopathologic findings led to the diagnosis of disseminate and recurrent infundibulofolliculitis (DRIF). The patient was started on a 2-week course of once-daily ammonium lactate lotion 12% and urea cream 40% and twice-daily triamcinolone ointment 0.1%. The patient was instructed to take a 1-week break before this regimen was repeated. Isotretinoin 0.5 mg/kg/d for 2 to 4 months was considered and will be an option if there is no improvement at follow-up.
Disseminate and recurrent infundibulofolliculitis is a rare noninfectious folliculitis that initially was described by Hitch and Lund1 in 1968. Males of African descent are most commonly affected by DRIF, but the condition is not limited to this population.2,3 It manifests as asymptomatic, flesh-colored, monomorphic, follicular papules distributed on the trunk and proximal extremities. Pustules can be present, and hair may be seen protruding from them. As the name suggests, DRIF is associated with histopathologic changes that are prominent at the infundibulum of hair follicles.3,4 Disseminate and recurrent infundibulofolliculitis can persist for months to years because it often is resistant to treatment. Treatments include topical monotherapies such as corticosteroids, calcineurin inhibitors, or retinoids; combination topical treatments; antibiotics; and isotretinoin.2 Recurrent remission and exacerbation occurs in many patients.3
The classic manifestations of DRIF, including follicular, monomorphic, flesh-colored papules distributed on the neck, trunk, and proximal upper extremities, were seen in our patient (Figure 2). These findings along with the skin biopsy identifying a lymphocytic infundibular infiltrate led to the diagnosis of DRIF. The papules associated with DRIF can be recurrent or chronic. The lesions in this patient were chronic and persistent.
Despite limited evidence, it has been suggested that DRIF may be a manifestation of atopic dermatitis in patients with darker skin tones. In our case, the patient had a history of childhood eczema. Other hypotheses have proposed that DRIF could be a nonspecific reaction to a currently unknown antigen. A causative infectious agent has not been identified, although the search continues. There is speculation that DRIF could be an overt expression of normal follicular prominence, but the presence of occasional pustules and lymphocyte- predominant infundibular infiltrate negates that.3
Confluent and reticulated papillomatosis was included in the differential for our patient and manifests as asymptomatic hyperpigmented papules and plaques frequently occurring on the upper trunk, neck, and axilla; however, these lesions have a peripheral netlike configuration, as the name suggests. Additionally, this condition is thought to have an infectious component (Dietzia papillomatosis) and responds to antibiotic treatment.5 Follicular eczema also was high in the differential diagnosis but usually is seasonal and pruritic, and histopathology typically shows the features of spongiotic dermatitis. It also would respond well to topical steroids.6 Another condition high on the differential was juxtaclavicular beaded lines, which also manifests as flesh-colored follicular papules distributed on the upper trunk; however, histopathology usually shows features of hyperplastic pilosebaceous units along with spongiosis and exocytosis.7 Pityrosporum folliculitis initially was considered, but the patient only endorsed occasional pruritus. Additionally, no fungal elements were observed.
Currently, there are no definitive treatments for DRIF. The topical treatments available include midpotency corticosteroids, tretinoin, calcineurin inhibitors, 12% lactic acid, and 20% to 40% urea. The systemic therapies are high-dose oral vitamin A (100,000 IU/d), isotretinoin, and psoralen plus UVA.8-10
- Hitch JM, Lund HZ. Disseminate and recurrent infundibulo-folliculitis: report of a case. Arch Dermatol. 1968;97:432-435.
- Ma BC, Sahni VN, Sahni DR, et al. Disseminate and recurrent infundibulofolliculitis: an under-recognized yet treatable entity. J Drugs Dermatol. 2021;20:1353-1354. doi:10.36849/jdd.6173
- Nair SP, Gomathy M, Kumar GN. Disseminate and recurrent infundibulo- folliculitis in an Indian patient: a case report with review of literature. Indian Dermatol Online J. 2017;8:39-41. doi:10.4103/2229- 5178.198775
- Rekha S, Kumar V, Rao P, et al. Disseminate and recurrent infundibulofolliculitis. Indian J Dermatol. 2019;64:404-406. doi:10.4103/ijd.IJD_77_18
- Jones AL, Koerner RJ, Natarajan S, et al. Dietzia papillomatosis sp. nov., a novel actinomycete isolated from the skin of an immunocompetent patient with confluent and reticulated papillomatosis. Int J Syst Evol Microbiol. 2008;58(pt 1):68-72. doi:10.1099/ijs.0.65178-0
- Cohen PR. Follicular contact dermatitis revisited: a review emphasizing neomycin-associated follicular contact dermatitis. World J Clin Cases. 2014;2:815-821. doi:10.12998/wjcc.v2.i12.815
- Butterworth T, Johnson WC. Justa-clavicular beaded lines. Arch Dermatol. 1974;110:891-893.
- Calka O, Metin A, Ozen S. A case of disseminated and recurrent infundibulo-folliculitis responsive to treatment with isotretinoin. J Dermatol. 2002;29:431-434.
- Goihman-Yahr M. Disseminate and recurrent infundibulofolliculitis: response to psoralen plus UVA therapy. Int J Dermatol. 1999;38:75-76.
- Hinds GA, Heald PW. A case of disseminate and recurrent infundibulofolliculitis responsive to treatment with topical steroids. Dermatol Online J. 2008;14:11.
- Hitch JM, Lund HZ. Disseminate and recurrent infundibulo-folliculitis: report of a case. Arch Dermatol. 1968;97:432-435.
- Ma BC, Sahni VN, Sahni DR, et al. Disseminate and recurrent infundibulofolliculitis: an under-recognized yet treatable entity. J Drugs Dermatol. 2021;20:1353-1354. doi:10.36849/jdd.6173
- Nair SP, Gomathy M, Kumar GN. Disseminate and recurrent infundibulo- folliculitis in an Indian patient: a case report with review of literature. Indian Dermatol Online J. 2017;8:39-41. doi:10.4103/2229- 5178.198775
- Rekha S, Kumar V, Rao P, et al. Disseminate and recurrent infundibulofolliculitis. Indian J Dermatol. 2019;64:404-406. doi:10.4103/ijd.IJD_77_18
- Jones AL, Koerner RJ, Natarajan S, et al. Dietzia papillomatosis sp. nov., a novel actinomycete isolated from the skin of an immunocompetent patient with confluent and reticulated papillomatosis. Int J Syst Evol Microbiol. 2008;58(pt 1):68-72. doi:10.1099/ijs.0.65178-0
- Cohen PR. Follicular contact dermatitis revisited: a review emphasizing neomycin-associated follicular contact dermatitis. World J Clin Cases. 2014;2:815-821. doi:10.12998/wjcc.v2.i12.815
- Butterworth T, Johnson WC. Justa-clavicular beaded lines. Arch Dermatol. 1974;110:891-893.
- Calka O, Metin A, Ozen S. A case of disseminated and recurrent infundibulo-folliculitis responsive to treatment with isotretinoin. J Dermatol. 2002;29:431-434.
- Goihman-Yahr M. Disseminate and recurrent infundibulofolliculitis: response to psoralen plus UVA therapy. Int J Dermatol. 1999;38:75-76.
- Hinds GA, Heald PW. A case of disseminate and recurrent infundibulofolliculitis responsive to treatment with topical steroids. Dermatol Online J. 2008;14:11.
Diffusely Scattered Linear Folliculopapular Eruption
Diffusely Scattered Linear Folliculopapular Eruption
A 31-year-old man with a darker skin tone and a history of childhood eczema presented with papules on the trunk and upper arms of several years’ duration. The papules were persistent and were generally asymptomatic but occasionally pruritic. The patient previously had self-treated with over-the counter lotions and topical hydrocortisone with no appreciable changes. On physical examination, a hyperpigmented patch with follicular monomorphic papules was noted across the upper back along with confluent papules and plaques predominantly on the trunk and upper arms. Additionally, the patient had several monomorphic papules in a linear distribution on the neck. Review of systems and examination of the remaining skin were unremarkable. A biopsy from a representative papule on the left upper back was performed.


A Guide to Avoiding Common Procedural Coding Mistakes
A Guide to Avoiding Common Procedural Coding Mistakes
Accurate procedural coding is essential to appropriate reimbursement and regulatory compliance in dermatology. This article reviews commonly misunderstood areas of procedural coding, including new biopsy codes; coding for shave removals, destruction, excision and repair, and adjacent tissue transfer (flap closure); the National Correct Coding Initiative; Medicare payment edits; Mohs micrographic surgery (MMS) codes; and correct use of key modifiers. Practical guidance is provided to help avoid frequent errors.
NEW BIOPSY CODES
The most common questions about procedural coding relate to the new Current Procedural Terminology (CPT) biopsy codes, which are reported based on method of removal. Primary codes include the following:
- 11102: tangential biopsy of skin (eg, shave, scoop, saucerize, curette) for a single lesion
- 11104: punch biopsy of skin, including simple closure, when performed, for a single lesion
- 11106: incisional biopsy of skin (eg, wedge), including simple closure, when performed, for a single lesion
Add-on codes are used for each separate or additional lesion:
- 11103: tangential biopsy
- 11105: punch biopsy
- 11107: incisional biopsy
When multiple biopsy types are performed on the same date of service, only one primary code is reported along with add-on codes for any additional biopsies. The primary code reported should have the highest relative value unit (generally incisional > punch > tangential) plus the add-on codes for additional biopsies performed. Sampling of the stratum corneum only (eg, skin scraping or tape stripping) does not constitute a skin biopsy and is not reportable as a procedure.
SHAVE REMOVAL CODES
Shave removal codes are appropriate when the intent is removal of the entire lesion and there is only dermis remaining at the base of the wound. Tangential biopsy codes are appropriate when the intent is to sample a portion of a lesion for diagnosis. If saucerization of a lesion is appropriate and only fat remains at the base of the wound, the procedure is correctly coded as an excision. If any dermis remains at the base of the wound, the procedure is properly coded as shave removal. Shave codes do not distinguish between benign and malignant lesions and do not include the margin of normal skin, only the diameter of the lesion itself.
DESTRUCTION CODES
Destruction codes include both premalignant and benign lesions and may be reported as add-on codes or standalone codes, depending on lesion type and number. The 17000 series is used for destruction of premalignant lesions such as actinic keratosis, large cell acanthoma, actinic cheilitis, and porokeratosis:
- 17000: destruction of the first premalignant lesion
- 17003: destruction of each additional premalignant lesion (up to 13 lesions); reported in addition to 17000
- 17004: destruction of 15 or more premalignant lesions; reported as a standalone code (not in addition to 17000)
The following codes are used for destruction of benign lesions:
- 17110: destruction of benign lesions (up to 14 lesions)
- 17111: destruction of 15 or more benign lesions; reported as a standalone code (not in addition to 17110)
EXCISION AND REPAIR CODES
Individual excisions are reported separately, while repairs are reported as the sum of the lengths within grouped anatomic zones. The groupings differ for intermediate and complex closures, so be sure to refer to your coding manual. Intermediate or complex closures should be reported separately for skin excisions, whereas simple closures are already included in the excision code and are not reported separately. Excision diameter includes the margins necessary to ensure complete removal of the tumor for both benign and malignant tumors. For neoplasms of uncertain behavior, defer billing until pathology results are available to ensure accurate reporting as either a benign or malignant tumor excision. Lesion size is measured prior to excision and includes the lesion plus the narrowest intended clinical margin; this measurement reflects the width of the excised specimen rather than the length of the repair.
Malignant tumor excisions continue to be worth more because of the greater risk and preservice and postservice work involved. Only about 50% of payment relates to the procedure itself; the other 50% relates to risk and preoperative and postoperative counseling as well as bundled follow-up visits in the global period. That accounts for the difference in compensation for benign vs malignant tumors as well as the 50% multiple surgical reduction for multiple lesions, as the equipment and cognitive portion bundled into the procedure are not separate for each procedure.
Historically, Medicare has bundled complex closures with benign excisions under 0.5 cm. Medicare also applies medically unlikely edits that may limit payment when more than 5 excisions, closures, or destruction procedures (excluding add-on codes) are reported on the same date of service. Medicare may pay for the additional procedures if a copy of the record and a letter of medical necessity are included.
CODING FOR ADJACENT TISSUE TRANSFER (FLAP CLOSURE)
When reporting adjacent tissue transfers, the total size of the defect includes primary and secondary defects when calculating the area of the flap. The areas of the primary and secondary defects are added together when the flap represents a single repair. The sums are reported separately if they are distinct repairs. Adjacent tissue transfer already includes payment for the excision of malignant or benign lesions. Do not code separately for the excision.
CORRECT CODING INITIATIVE
On January 1, 1996, the Medicare program implemented the National Correct Coding Initiative (https://www.cms.gov/national-correct-coding-initiative-ncci), employing nearly 83,000 code edits, in an attempt to eliminate unbundling or other inappropriate reporting of CPT codes. When procedures are performed on separate and distinct lesions, a modifier is required to bypass the edit that would otherwise deny payment for the second procedure. Medicare publishes lists of paired codes (column 1 paired with column 2). The code in column 2 is the one that requires modifier 59 or 79.
MEDICARE PAYMENT EDITS
Mutually Exclusive Edits
Mutually exclusive edits seek to identify services that cannot reasonably be performed in the same session. The “comprehensive” code will be paid and the “component” code disallowed.
Medically Unlikely Edits
The Centers for Medicare & Medicaid Services stop paying when multiples of a procedure exceed the medically unlikely edits, but payment may be made if accompanied by a copy of the medical record and letter of medical necessity. A common example would be a transplant recipient requiring destruction of many malignant lesions in a single session, exceeding the medically unlikely edits for the procedure.
MOHS MICROGRAPHIC SURGERY CODES
Mohs micrographic surgery codes require that a single physician act as both surgeon and pathologist. Do not report 88305 separately, as the pathology interpretation is already included in the MMS reimbursement. Repairs, grafts, and adjacent tissue transfer are separately reportable with the CPT codes for MMS.
The CPT codes for MMS include skin biopsy and excision services (11102-11107, 11600-11646, and 17260-17286); however, if a suspected skin cancer is biopsied for pathologic diagnosis prior to MMS, the biopsy (11102-11107) and frozen section pathology (88331) may be reported separately utilizing modifier 59 or 58 to distinguish the diagnostic biopsy from the definitive MMS. The biopsy should not duplicate a prior biopsy unless that biopsy result cannot be located; it must be performed before MMS and must determine the subsequent procedure. Although CPT indicates that modifier 59 should be used, it also is acceptable to utilize modifier 58 to indicate that the diagnostic skin biopsy and MMS were staged or planned procedures. This may be appropriate in the following scenarios:
- The lesion for which MMS is planned has not been biopsied within the previous 60 days,
- The surgeon cannot obtain a pathology report, with reasonable effort, from the referring physician, or
- The biopsy is performed on a lesion that is not associated with the MMS.
KEY MODIFIERS AND HOW THEY ARE USED
Modifiers are essential tools in dermatology coding that are used to indicate when procedures or evaluation and management (E/M) services are distinct, staged, bilateral, or related to specific global periods. Correct application ensures accurate reimbursement, prevents claim denials, and reflects the true work performed. The following list summarizes commonly used modifiers and guidance for their proper use.
Modifier 59: Distinct Procedural Service
Modifier 59 is used to clearly designate when distinct, independent, and separate multiple procedures are provided. The procedure must not be a component of another procedure. Examples include:
- Different procedures or surgeries
- Surgery on different sites or organ systems
- Separate incision/excision
- Separate lesions
When code 17000 is paired with the new biopsy codes, modifier 59 is paired with code 17000.
Modifier 79: Distinct Procedural Service During a Postoperative Period
Modifier 79 is used to clearly designate when distinct, independent, and separate multiple procedures are provided. The procedure must not be a component of another procedure. Examples include:
- Different procedures or surgeries
- Surgery on different sites or organ systems
- Separate incision/excision
- Separate lesions
Modifier 58: Staged or Planned Procedure
Modifier 58 is most commonly used when a staged excision is planned in advance or when a positive tumor margin requires further excision during a global period.
Modifier 25: Significant, Separately Identifiable E/M Service
Modifier 25 is defined as a significant and separately identifiable E/M service performed by the same physician on the same day as a procedure or other service. It is used to describe a separate, distinctly identifiable E/M service rendered during the same visit as another procedure. The modifier must be appended to the E/M code. The decision to perform a 0- or 10-day global procedure on the same date of service is already bundled into the payment for the procedure and does not qualify as a separate billable service.
Modifier 24: Unrelated E/M Service During a Postoperative Period
Modifier 24 is defined as an unrelated E/M service performed by the same physician during a postoperative period. It is used when a separate, unrelated E/M service is provided during the global period of a surgical procedure.
Modifiers 24 and 25: Documentation and Distinction
The CPT definition of modifier 25 states that an E/M service may be prompted by the system or condition for which a separate procedure or service is needed. Neither modifier requires a separate diagnosis; however, both require clearly distinguishable cognitive services beyond those typically associated with the procedure itself. This includes evaluation beyond the examination of the lesion, discussion of risks, benefits, and alternatives, and the decision to perform a 0- or 10-day global procedure.
Modifier 50: Bilateral Procedure
Modifier 50 is defined as a bilateral procedure and is used when the same procedure is performed on both sides of the body, such as application of Unna boots. When reporting this modifier, specify the quantity applied. Because Unna boots may be required on the arms as well as the legs, the billing system cannot determine how many were applied unless the quantity is clearly indicated.
Modifier 57: Decision for Surgery
Modifier 57 is reported when an E/M service involves the decision to perform a 90-day global procedure on the same date of service. For 10-day global procedures, the decision to perform surgery on the same day does not justify a separate E/M service. The global period timing begins at midnight, with the 10-day global starting on the day of the procedure and the 90-day global starting the day before the procedure; for example, if an excision is performed today and an adjacent tissue transfer is performed tomorrow, the excision is considered within the global period.
FINAL THOUGHTS
Physicians remain responsible for accurately selecting diagnosis and procedure codes that reflect medically necessary services, and CPT codes continue to define the procedures that are reported. The Relative Value Scale Update Committee determines the value of each procedure based on physician survey data, including time and follow-up visit utilization, as well as practice expense, which represents a substantial portion of each code’s value. Our specialty relies on dedicated volunteers who devote significant time and effort to ensuring accurate representation of the work we perform for our patients. When the opportunity arises, please thank them for their service.
Accurate procedural coding is essential to appropriate reimbursement and regulatory compliance in dermatology. This article reviews commonly misunderstood areas of procedural coding, including new biopsy codes; coding for shave removals, destruction, excision and repair, and adjacent tissue transfer (flap closure); the National Correct Coding Initiative; Medicare payment edits; Mohs micrographic surgery (MMS) codes; and correct use of key modifiers. Practical guidance is provided to help avoid frequent errors.
NEW BIOPSY CODES
The most common questions about procedural coding relate to the new Current Procedural Terminology (CPT) biopsy codes, which are reported based on method of removal. Primary codes include the following:
- 11102: tangential biopsy of skin (eg, shave, scoop, saucerize, curette) for a single lesion
- 11104: punch biopsy of skin, including simple closure, when performed, for a single lesion
- 11106: incisional biopsy of skin (eg, wedge), including simple closure, when performed, for a single lesion
Add-on codes are used for each separate or additional lesion:
- 11103: tangential biopsy
- 11105: punch biopsy
- 11107: incisional biopsy
When multiple biopsy types are performed on the same date of service, only one primary code is reported along with add-on codes for any additional biopsies. The primary code reported should have the highest relative value unit (generally incisional > punch > tangential) plus the add-on codes for additional biopsies performed. Sampling of the stratum corneum only (eg, skin scraping or tape stripping) does not constitute a skin biopsy and is not reportable as a procedure.
SHAVE REMOVAL CODES
Shave removal codes are appropriate when the intent is removal of the entire lesion and there is only dermis remaining at the base of the wound. Tangential biopsy codes are appropriate when the intent is to sample a portion of a lesion for diagnosis. If saucerization of a lesion is appropriate and only fat remains at the base of the wound, the procedure is correctly coded as an excision. If any dermis remains at the base of the wound, the procedure is properly coded as shave removal. Shave codes do not distinguish between benign and malignant lesions and do not include the margin of normal skin, only the diameter of the lesion itself.
DESTRUCTION CODES
Destruction codes include both premalignant and benign lesions and may be reported as add-on codes or standalone codes, depending on lesion type and number. The 17000 series is used for destruction of premalignant lesions such as actinic keratosis, large cell acanthoma, actinic cheilitis, and porokeratosis:
- 17000: destruction of the first premalignant lesion
- 17003: destruction of each additional premalignant lesion (up to 13 lesions); reported in addition to 17000
- 17004: destruction of 15 or more premalignant lesions; reported as a standalone code (not in addition to 17000)
The following codes are used for destruction of benign lesions:
- 17110: destruction of benign lesions (up to 14 lesions)
- 17111: destruction of 15 or more benign lesions; reported as a standalone code (not in addition to 17110)
EXCISION AND REPAIR CODES
Individual excisions are reported separately, while repairs are reported as the sum of the lengths within grouped anatomic zones. The groupings differ for intermediate and complex closures, so be sure to refer to your coding manual. Intermediate or complex closures should be reported separately for skin excisions, whereas simple closures are already included in the excision code and are not reported separately. Excision diameter includes the margins necessary to ensure complete removal of the tumor for both benign and malignant tumors. For neoplasms of uncertain behavior, defer billing until pathology results are available to ensure accurate reporting as either a benign or malignant tumor excision. Lesion size is measured prior to excision and includes the lesion plus the narrowest intended clinical margin; this measurement reflects the width of the excised specimen rather than the length of the repair.
Malignant tumor excisions continue to be worth more because of the greater risk and preservice and postservice work involved. Only about 50% of payment relates to the procedure itself; the other 50% relates to risk and preoperative and postoperative counseling as well as bundled follow-up visits in the global period. That accounts for the difference in compensation for benign vs malignant tumors as well as the 50% multiple surgical reduction for multiple lesions, as the equipment and cognitive portion bundled into the procedure are not separate for each procedure.
Historically, Medicare has bundled complex closures with benign excisions under 0.5 cm. Medicare also applies medically unlikely edits that may limit payment when more than 5 excisions, closures, or destruction procedures (excluding add-on codes) are reported on the same date of service. Medicare may pay for the additional procedures if a copy of the record and a letter of medical necessity are included.
CODING FOR ADJACENT TISSUE TRANSFER (FLAP CLOSURE)
When reporting adjacent tissue transfers, the total size of the defect includes primary and secondary defects when calculating the area of the flap. The areas of the primary and secondary defects are added together when the flap represents a single repair. The sums are reported separately if they are distinct repairs. Adjacent tissue transfer already includes payment for the excision of malignant or benign lesions. Do not code separately for the excision.
CORRECT CODING INITIATIVE
On January 1, 1996, the Medicare program implemented the National Correct Coding Initiative (https://www.cms.gov/national-correct-coding-initiative-ncci), employing nearly 83,000 code edits, in an attempt to eliminate unbundling or other inappropriate reporting of CPT codes. When procedures are performed on separate and distinct lesions, a modifier is required to bypass the edit that would otherwise deny payment for the second procedure. Medicare publishes lists of paired codes (column 1 paired with column 2). The code in column 2 is the one that requires modifier 59 or 79.
MEDICARE PAYMENT EDITS
Mutually Exclusive Edits
Mutually exclusive edits seek to identify services that cannot reasonably be performed in the same session. The “comprehensive” code will be paid and the “component” code disallowed.
Medically Unlikely Edits
The Centers for Medicare & Medicaid Services stop paying when multiples of a procedure exceed the medically unlikely edits, but payment may be made if accompanied by a copy of the medical record and letter of medical necessity. A common example would be a transplant recipient requiring destruction of many malignant lesions in a single session, exceeding the medically unlikely edits for the procedure.
MOHS MICROGRAPHIC SURGERY CODES
Mohs micrographic surgery codes require that a single physician act as both surgeon and pathologist. Do not report 88305 separately, as the pathology interpretation is already included in the MMS reimbursement. Repairs, grafts, and adjacent tissue transfer are separately reportable with the CPT codes for MMS.
The CPT codes for MMS include skin biopsy and excision services (11102-11107, 11600-11646, and 17260-17286); however, if a suspected skin cancer is biopsied for pathologic diagnosis prior to MMS, the biopsy (11102-11107) and frozen section pathology (88331) may be reported separately utilizing modifier 59 or 58 to distinguish the diagnostic biopsy from the definitive MMS. The biopsy should not duplicate a prior biopsy unless that biopsy result cannot be located; it must be performed before MMS and must determine the subsequent procedure. Although CPT indicates that modifier 59 should be used, it also is acceptable to utilize modifier 58 to indicate that the diagnostic skin biopsy and MMS were staged or planned procedures. This may be appropriate in the following scenarios:
- The lesion for which MMS is planned has not been biopsied within the previous 60 days,
- The surgeon cannot obtain a pathology report, with reasonable effort, from the referring physician, or
- The biopsy is performed on a lesion that is not associated with the MMS.
KEY MODIFIERS AND HOW THEY ARE USED
Modifiers are essential tools in dermatology coding that are used to indicate when procedures or evaluation and management (E/M) services are distinct, staged, bilateral, or related to specific global periods. Correct application ensures accurate reimbursement, prevents claim denials, and reflects the true work performed. The following list summarizes commonly used modifiers and guidance for their proper use.
Modifier 59: Distinct Procedural Service
Modifier 59 is used to clearly designate when distinct, independent, and separate multiple procedures are provided. The procedure must not be a component of another procedure. Examples include:
- Different procedures or surgeries
- Surgery on different sites or organ systems
- Separate incision/excision
- Separate lesions
When code 17000 is paired with the new biopsy codes, modifier 59 is paired with code 17000.
Modifier 79: Distinct Procedural Service During a Postoperative Period
Modifier 79 is used to clearly designate when distinct, independent, and separate multiple procedures are provided. The procedure must not be a component of another procedure. Examples include:
- Different procedures or surgeries
- Surgery on different sites or organ systems
- Separate incision/excision
- Separate lesions
Modifier 58: Staged or Planned Procedure
Modifier 58 is most commonly used when a staged excision is planned in advance or when a positive tumor margin requires further excision during a global period.
Modifier 25: Significant, Separately Identifiable E/M Service
Modifier 25 is defined as a significant and separately identifiable E/M service performed by the same physician on the same day as a procedure or other service. It is used to describe a separate, distinctly identifiable E/M service rendered during the same visit as another procedure. The modifier must be appended to the E/M code. The decision to perform a 0- or 10-day global procedure on the same date of service is already bundled into the payment for the procedure and does not qualify as a separate billable service.
Modifier 24: Unrelated E/M Service During a Postoperative Period
Modifier 24 is defined as an unrelated E/M service performed by the same physician during a postoperative period. It is used when a separate, unrelated E/M service is provided during the global period of a surgical procedure.
Modifiers 24 and 25: Documentation and Distinction
The CPT definition of modifier 25 states that an E/M service may be prompted by the system or condition for which a separate procedure or service is needed. Neither modifier requires a separate diagnosis; however, both require clearly distinguishable cognitive services beyond those typically associated with the procedure itself. This includes evaluation beyond the examination of the lesion, discussion of risks, benefits, and alternatives, and the decision to perform a 0- or 10-day global procedure.
Modifier 50: Bilateral Procedure
Modifier 50 is defined as a bilateral procedure and is used when the same procedure is performed on both sides of the body, such as application of Unna boots. When reporting this modifier, specify the quantity applied. Because Unna boots may be required on the arms as well as the legs, the billing system cannot determine how many were applied unless the quantity is clearly indicated.
Modifier 57: Decision for Surgery
Modifier 57 is reported when an E/M service involves the decision to perform a 90-day global procedure on the same date of service. For 10-day global procedures, the decision to perform surgery on the same day does not justify a separate E/M service. The global period timing begins at midnight, with the 10-day global starting on the day of the procedure and the 90-day global starting the day before the procedure; for example, if an excision is performed today and an adjacent tissue transfer is performed tomorrow, the excision is considered within the global period.
FINAL THOUGHTS
Physicians remain responsible for accurately selecting diagnosis and procedure codes that reflect medically necessary services, and CPT codes continue to define the procedures that are reported. The Relative Value Scale Update Committee determines the value of each procedure based on physician survey data, including time and follow-up visit utilization, as well as practice expense, which represents a substantial portion of each code’s value. Our specialty relies on dedicated volunteers who devote significant time and effort to ensuring accurate representation of the work we perform for our patients. When the opportunity arises, please thank them for their service.
Accurate procedural coding is essential to appropriate reimbursement and regulatory compliance in dermatology. This article reviews commonly misunderstood areas of procedural coding, including new biopsy codes; coding for shave removals, destruction, excision and repair, and adjacent tissue transfer (flap closure); the National Correct Coding Initiative; Medicare payment edits; Mohs micrographic surgery (MMS) codes; and correct use of key modifiers. Practical guidance is provided to help avoid frequent errors.
NEW BIOPSY CODES
The most common questions about procedural coding relate to the new Current Procedural Terminology (CPT) biopsy codes, which are reported based on method of removal. Primary codes include the following:
- 11102: tangential biopsy of skin (eg, shave, scoop, saucerize, curette) for a single lesion
- 11104: punch biopsy of skin, including simple closure, when performed, for a single lesion
- 11106: incisional biopsy of skin (eg, wedge), including simple closure, when performed, for a single lesion
Add-on codes are used for each separate or additional lesion:
- 11103: tangential biopsy
- 11105: punch biopsy
- 11107: incisional biopsy
When multiple biopsy types are performed on the same date of service, only one primary code is reported along with add-on codes for any additional biopsies. The primary code reported should have the highest relative value unit (generally incisional > punch > tangential) plus the add-on codes for additional biopsies performed. Sampling of the stratum corneum only (eg, skin scraping or tape stripping) does not constitute a skin biopsy and is not reportable as a procedure.
SHAVE REMOVAL CODES
Shave removal codes are appropriate when the intent is removal of the entire lesion and there is only dermis remaining at the base of the wound. Tangential biopsy codes are appropriate when the intent is to sample a portion of a lesion for diagnosis. If saucerization of a lesion is appropriate and only fat remains at the base of the wound, the procedure is correctly coded as an excision. If any dermis remains at the base of the wound, the procedure is properly coded as shave removal. Shave codes do not distinguish between benign and malignant lesions and do not include the margin of normal skin, only the diameter of the lesion itself.
DESTRUCTION CODES
Destruction codes include both premalignant and benign lesions and may be reported as add-on codes or standalone codes, depending on lesion type and number. The 17000 series is used for destruction of premalignant lesions such as actinic keratosis, large cell acanthoma, actinic cheilitis, and porokeratosis:
- 17000: destruction of the first premalignant lesion
- 17003: destruction of each additional premalignant lesion (up to 13 lesions); reported in addition to 17000
- 17004: destruction of 15 or more premalignant lesions; reported as a standalone code (not in addition to 17000)
The following codes are used for destruction of benign lesions:
- 17110: destruction of benign lesions (up to 14 lesions)
- 17111: destruction of 15 or more benign lesions; reported as a standalone code (not in addition to 17110)
EXCISION AND REPAIR CODES
Individual excisions are reported separately, while repairs are reported as the sum of the lengths within grouped anatomic zones. The groupings differ for intermediate and complex closures, so be sure to refer to your coding manual. Intermediate or complex closures should be reported separately for skin excisions, whereas simple closures are already included in the excision code and are not reported separately. Excision diameter includes the margins necessary to ensure complete removal of the tumor for both benign and malignant tumors. For neoplasms of uncertain behavior, defer billing until pathology results are available to ensure accurate reporting as either a benign or malignant tumor excision. Lesion size is measured prior to excision and includes the lesion plus the narrowest intended clinical margin; this measurement reflects the width of the excised specimen rather than the length of the repair.
Malignant tumor excisions continue to be worth more because of the greater risk and preservice and postservice work involved. Only about 50% of payment relates to the procedure itself; the other 50% relates to risk and preoperative and postoperative counseling as well as bundled follow-up visits in the global period. That accounts for the difference in compensation for benign vs malignant tumors as well as the 50% multiple surgical reduction for multiple lesions, as the equipment and cognitive portion bundled into the procedure are not separate for each procedure.
Historically, Medicare has bundled complex closures with benign excisions under 0.5 cm. Medicare also applies medically unlikely edits that may limit payment when more than 5 excisions, closures, or destruction procedures (excluding add-on codes) are reported on the same date of service. Medicare may pay for the additional procedures if a copy of the record and a letter of medical necessity are included.
CODING FOR ADJACENT TISSUE TRANSFER (FLAP CLOSURE)
When reporting adjacent tissue transfers, the total size of the defect includes primary and secondary defects when calculating the area of the flap. The areas of the primary and secondary defects are added together when the flap represents a single repair. The sums are reported separately if they are distinct repairs. Adjacent tissue transfer already includes payment for the excision of malignant or benign lesions. Do not code separately for the excision.
CORRECT CODING INITIATIVE
On January 1, 1996, the Medicare program implemented the National Correct Coding Initiative (https://www.cms.gov/national-correct-coding-initiative-ncci), employing nearly 83,000 code edits, in an attempt to eliminate unbundling or other inappropriate reporting of CPT codes. When procedures are performed on separate and distinct lesions, a modifier is required to bypass the edit that would otherwise deny payment for the second procedure. Medicare publishes lists of paired codes (column 1 paired with column 2). The code in column 2 is the one that requires modifier 59 or 79.
MEDICARE PAYMENT EDITS
Mutually Exclusive Edits
Mutually exclusive edits seek to identify services that cannot reasonably be performed in the same session. The “comprehensive” code will be paid and the “component” code disallowed.
Medically Unlikely Edits
The Centers for Medicare & Medicaid Services stop paying when multiples of a procedure exceed the medically unlikely edits, but payment may be made if accompanied by a copy of the medical record and letter of medical necessity. A common example would be a transplant recipient requiring destruction of many malignant lesions in a single session, exceeding the medically unlikely edits for the procedure.
MOHS MICROGRAPHIC SURGERY CODES
Mohs micrographic surgery codes require that a single physician act as both surgeon and pathologist. Do not report 88305 separately, as the pathology interpretation is already included in the MMS reimbursement. Repairs, grafts, and adjacent tissue transfer are separately reportable with the CPT codes for MMS.
The CPT codes for MMS include skin biopsy and excision services (11102-11107, 11600-11646, and 17260-17286); however, if a suspected skin cancer is biopsied for pathologic diagnosis prior to MMS, the biopsy (11102-11107) and frozen section pathology (88331) may be reported separately utilizing modifier 59 or 58 to distinguish the diagnostic biopsy from the definitive MMS. The biopsy should not duplicate a prior biopsy unless that biopsy result cannot be located; it must be performed before MMS and must determine the subsequent procedure. Although CPT indicates that modifier 59 should be used, it also is acceptable to utilize modifier 58 to indicate that the diagnostic skin biopsy and MMS were staged or planned procedures. This may be appropriate in the following scenarios:
- The lesion for which MMS is planned has not been biopsied within the previous 60 days,
- The surgeon cannot obtain a pathology report, with reasonable effort, from the referring physician, or
- The biopsy is performed on a lesion that is not associated with the MMS.
KEY MODIFIERS AND HOW THEY ARE USED
Modifiers are essential tools in dermatology coding that are used to indicate when procedures or evaluation and management (E/M) services are distinct, staged, bilateral, or related to specific global periods. Correct application ensures accurate reimbursement, prevents claim denials, and reflects the true work performed. The following list summarizes commonly used modifiers and guidance for their proper use.
Modifier 59: Distinct Procedural Service
Modifier 59 is used to clearly designate when distinct, independent, and separate multiple procedures are provided. The procedure must not be a component of another procedure. Examples include:
- Different procedures or surgeries
- Surgery on different sites or organ systems
- Separate incision/excision
- Separate lesions
When code 17000 is paired with the new biopsy codes, modifier 59 is paired with code 17000.
Modifier 79: Distinct Procedural Service During a Postoperative Period
Modifier 79 is used to clearly designate when distinct, independent, and separate multiple procedures are provided. The procedure must not be a component of another procedure. Examples include:
- Different procedures or surgeries
- Surgery on different sites or organ systems
- Separate incision/excision
- Separate lesions
Modifier 58: Staged or Planned Procedure
Modifier 58 is most commonly used when a staged excision is planned in advance or when a positive tumor margin requires further excision during a global period.
Modifier 25: Significant, Separately Identifiable E/M Service
Modifier 25 is defined as a significant and separately identifiable E/M service performed by the same physician on the same day as a procedure or other service. It is used to describe a separate, distinctly identifiable E/M service rendered during the same visit as another procedure. The modifier must be appended to the E/M code. The decision to perform a 0- or 10-day global procedure on the same date of service is already bundled into the payment for the procedure and does not qualify as a separate billable service.
Modifier 24: Unrelated E/M Service During a Postoperative Period
Modifier 24 is defined as an unrelated E/M service performed by the same physician during a postoperative period. It is used when a separate, unrelated E/M service is provided during the global period of a surgical procedure.
Modifiers 24 and 25: Documentation and Distinction
The CPT definition of modifier 25 states that an E/M service may be prompted by the system or condition for which a separate procedure or service is needed. Neither modifier requires a separate diagnosis; however, both require clearly distinguishable cognitive services beyond those typically associated with the procedure itself. This includes evaluation beyond the examination of the lesion, discussion of risks, benefits, and alternatives, and the decision to perform a 0- or 10-day global procedure.
Modifier 50: Bilateral Procedure
Modifier 50 is defined as a bilateral procedure and is used when the same procedure is performed on both sides of the body, such as application of Unna boots. When reporting this modifier, specify the quantity applied. Because Unna boots may be required on the arms as well as the legs, the billing system cannot determine how many were applied unless the quantity is clearly indicated.
Modifier 57: Decision for Surgery
Modifier 57 is reported when an E/M service involves the decision to perform a 90-day global procedure on the same date of service. For 10-day global procedures, the decision to perform surgery on the same day does not justify a separate E/M service. The global period timing begins at midnight, with the 10-day global starting on the day of the procedure and the 90-day global starting the day before the procedure; for example, if an excision is performed today and an adjacent tissue transfer is performed tomorrow, the excision is considered within the global period.
FINAL THOUGHTS
Physicians remain responsible for accurately selecting diagnosis and procedure codes that reflect medically necessary services, and CPT codes continue to define the procedures that are reported. The Relative Value Scale Update Committee determines the value of each procedure based on physician survey data, including time and follow-up visit utilization, as well as practice expense, which represents a substantial portion of each code’s value. Our specialty relies on dedicated volunteers who devote significant time and effort to ensuring accurate representation of the work we perform for our patients. When the opportunity arises, please thank them for their service.
A Guide to Avoiding Common Procedural Coding Mistakes
A Guide to Avoiding Common Procedural Coding Mistakes
PRACTICE POINTS
- When multiple biopsy types are performed on the same date of service, only one primary code is reported, along with add-on codes for any additional biopsies.
- When multiple biopsy types are performed on the same date of service, the primary code goes to incisional biopsy if one is performed or punch biopsy if there was no incisional biopsy.

Light-Brown Macule on the Upper Arm
Light-Brown Macule on the Upper Arm
THE DIAGNOSIS: Pigmented Bowen Disease
Histopathology revealed atypical keratinocytes throughout the entire thickness of a pigmented epidermis extending from the basal layer (Figure). Diffuse epidermal hyperpigmentation and melanophages in the papillary dermis were present. There was no dermal invasion or atypical melanocytic proliferation. On dermoscopy, this lesion had small brown globules, smudging, and an asymmetric nonspecific homogeneous pattern. Based on these features as well as the clinical findings, a diagnosis of pigmented Bowen disease (PBD), a rare subtype of squamous cell carcinoma in situ, was made. Complete removal of the lesion was achieved via the biopsy, and the patient was counselled regarding the malignant but noninvasive nature of the lesion. Appropriate follow-up was recommended to monitor for recurrence.
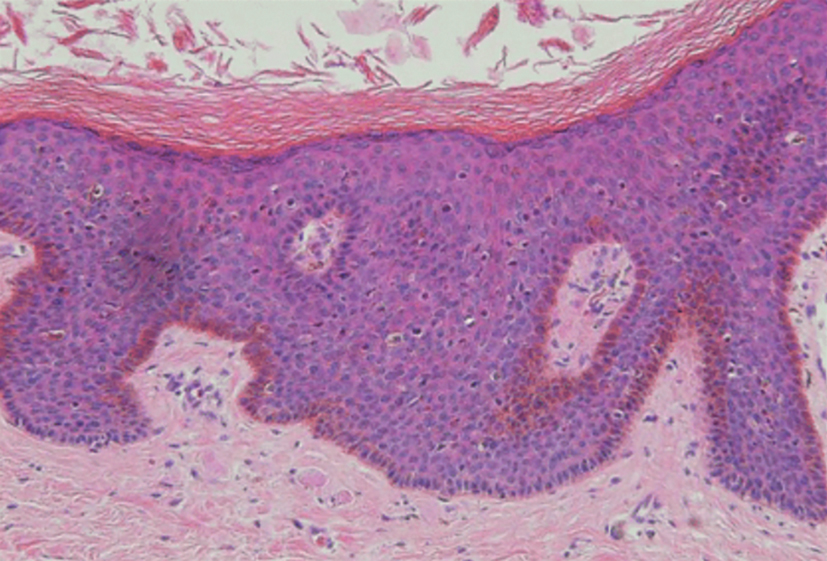
Our case presentation of PBD on the right upper arm in a female patient with a light skin tone is not classic, as PBD lesions usually manifest as well-demarcated scaly plaques on sun-protected sites in men with darker skin tones who are in the sixth to seventh decades of life.1
Dermoscopy of PBD in patients with lighter skin tones can present diagnostic challenges because characteristic clustered glomerular vessels may be faint or absent, particularly in small lesions such as this one. In such cases, PBD may instead demonstrate structureless brown pigmentation and irregular globules, patterns that overlap with pigmented actinic keratosis (PAK) and melanoma.3
Our case underscores the importance of maintaining a broad differential when evaluating small pigmented macules and reinforces biopsy as the diagnostic gold standard for PBD when dermoscopic findings are nonspecific.
- Mota AN, Piñeiro-Maceira J, Alves Mde F, et al. Pigmented Bowen’s disease. An Bras Dermatol. 2014;89:825-827. doi:10.1590 /abd1806-4841.20142725
- Lee JW, Hur J, Yeo KY, et al. A case of pigmented Bowen’s disease. Ann Dermatol. 2009;21:197-199. doi:10.5021/ad.2009.21.2.197
- Markowitz O. A Practical Guide to Dermoscopy. Philadelphia, PA: Wolters Kluwer; 2017.
- Fernández-Figueras MT, Carrato C, Sáenz X, et al. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J Eur Acad Dermatol Venereol. 2015;29:991-997. doi:10.1111/jdv.12848
THE DIAGNOSIS: Pigmented Bowen Disease
Histopathology revealed atypical keratinocytes throughout the entire thickness of a pigmented epidermis extending from the basal layer (Figure). Diffuse epidermal hyperpigmentation and melanophages in the papillary dermis were present. There was no dermal invasion or atypical melanocytic proliferation. On dermoscopy, this lesion had small brown globules, smudging, and an asymmetric nonspecific homogeneous pattern. Based on these features as well as the clinical findings, a diagnosis of pigmented Bowen disease (PBD), a rare subtype of squamous cell carcinoma in situ, was made. Complete removal of the lesion was achieved via the biopsy, and the patient was counselled regarding the malignant but noninvasive nature of the lesion. Appropriate follow-up was recommended to monitor for recurrence.
Our case presentation of PBD on the right upper arm in a female patient with a light skin tone is not classic, as PBD lesions usually manifest as well-demarcated scaly plaques on sun-protected sites in men with darker skin tones who are in the sixth to seventh decades of life.1
Dermoscopy of PBD in patients with lighter skin tones can present diagnostic challenges because characteristic clustered glomerular vessels may be faint or absent, particularly in small lesions such as this one. In such cases, PBD may instead demonstrate structureless brown pigmentation and irregular globules, patterns that overlap with pigmented actinic keratosis (PAK) and melanoma.3
Our case underscores the importance of maintaining a broad differential when evaluating small pigmented macules and reinforces biopsy as the diagnostic gold standard for PBD when dermoscopic findings are nonspecific.
THE DIAGNOSIS: Pigmented Bowen Disease
Histopathology revealed atypical keratinocytes throughout the entire thickness of a pigmented epidermis extending from the basal layer (Figure). Diffuse epidermal hyperpigmentation and melanophages in the papillary dermis were present. There was no dermal invasion or atypical melanocytic proliferation. On dermoscopy, this lesion had small brown globules, smudging, and an asymmetric nonspecific homogeneous pattern. Based on these features as well as the clinical findings, a diagnosis of pigmented Bowen disease (PBD), a rare subtype of squamous cell carcinoma in situ, was made. Complete removal of the lesion was achieved via the biopsy, and the patient was counselled regarding the malignant but noninvasive nature of the lesion. Appropriate follow-up was recommended to monitor for recurrence.
Our case presentation of PBD on the right upper arm in a female patient with a light skin tone is not classic, as PBD lesions usually manifest as well-demarcated scaly plaques on sun-protected sites in men with darker skin tones who are in the sixth to seventh decades of life.1
Dermoscopy of PBD in patients with lighter skin tones can present diagnostic challenges because characteristic clustered glomerular vessels may be faint or absent, particularly in small lesions such as this one. In such cases, PBD may instead demonstrate structureless brown pigmentation and irregular globules, patterns that overlap with pigmented actinic keratosis (PAK) and melanoma.3
Our case underscores the importance of maintaining a broad differential when evaluating small pigmented macules and reinforces biopsy as the diagnostic gold standard for PBD when dermoscopic findings are nonspecific.
- Mota AN, Piñeiro-Maceira J, Alves Mde F, et al. Pigmented Bowen’s disease. An Bras Dermatol. 2014;89:825-827. doi:10.1590 /abd1806-4841.20142725
- Lee JW, Hur J, Yeo KY, et al. A case of pigmented Bowen’s disease. Ann Dermatol. 2009;21:197-199. doi:10.5021/ad.2009.21.2.197
- Markowitz O. A Practical Guide to Dermoscopy. Philadelphia, PA: Wolters Kluwer; 2017.
- Fernández-Figueras MT, Carrato C, Sáenz X, et al. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J Eur Acad Dermatol Venereol. 2015;29:991-997. doi:10.1111/jdv.12848
- Mota AN, Piñeiro-Maceira J, Alves Mde F, et al. Pigmented Bowen’s disease. An Bras Dermatol. 2014;89:825-827. doi:10.1590 /abd1806-4841.20142725
- Lee JW, Hur J, Yeo KY, et al. A case of pigmented Bowen’s disease. Ann Dermatol. 2009;21:197-199. doi:10.5021/ad.2009.21.2.197
- Markowitz O. A Practical Guide to Dermoscopy. Philadelphia, PA: Wolters Kluwer; 2017.
- Fernández-Figueras MT, Carrato C, Sáenz X, et al. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J Eur Acad Dermatol Venereol. 2015;29:991-997. doi:10.1111/jdv.12848
Light-Brown Macule on the Upper Arm
Light-Brown Macule on the Upper Arm
An otherwise healthy 61-year-old woman with a light skin tone presented to the dermatology clinic for evaluation of a pigmented lesion on the right anterior distal upper arm of approximately 6 months’ duration. The patient reported no personal history of nonmelanoma skin cancer, atypical nevi, or melanoma but noted she had a family history of melanoma. Physical examination revealed an asymptomatic light-brown macule on the right anterior distal upper arm measuring about 3 mm with notable border irregularity and delineation. Dermoscopy findings showed a darker brown area at the lateral edge adjacent to the larger, amorphous, lighter-brown area with irregular brown globules present throughout the lesion. A biopsy of the lesion was performed.
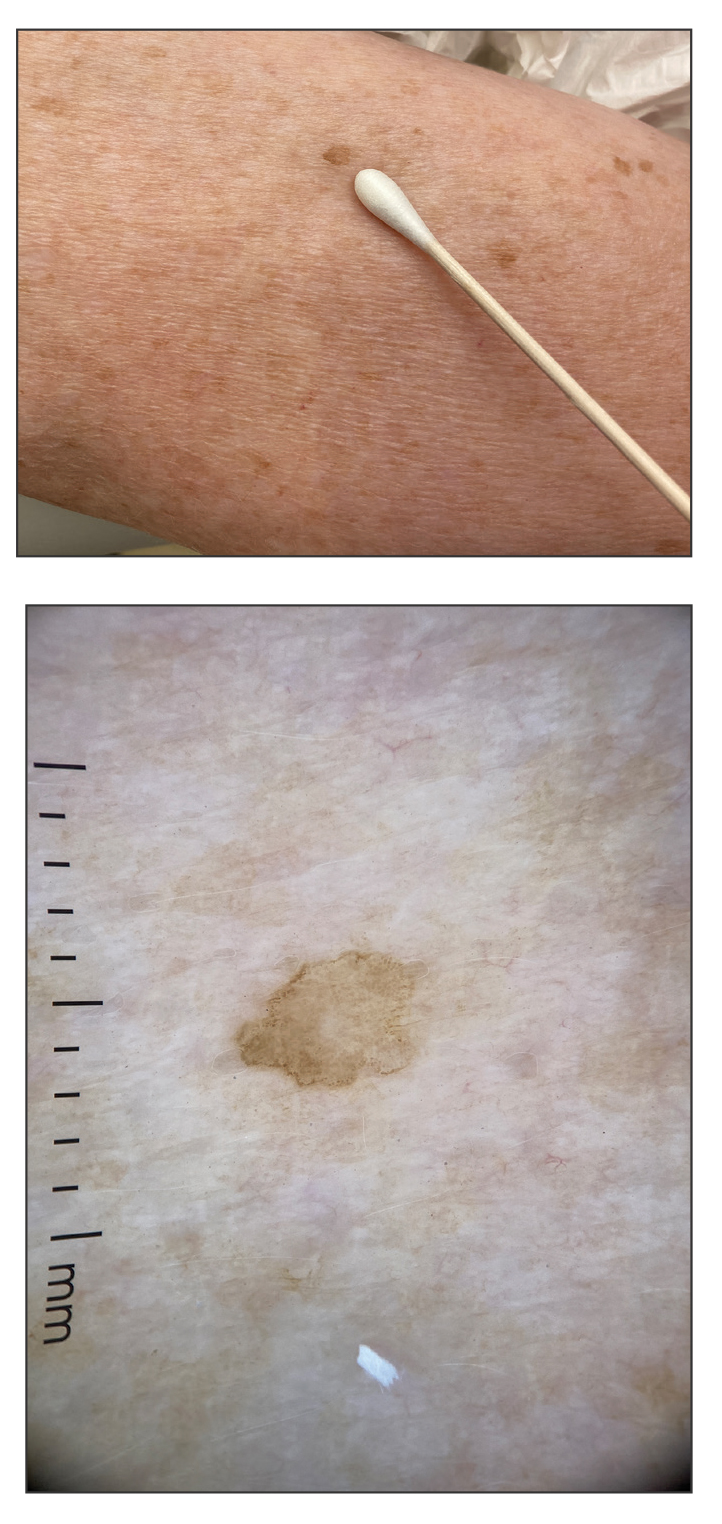

Malignancy Risk Among Psoriasis Patients Treated With Interleukin Inhibitors: A Retrospective Matched-Cohort Study
Malignancy Risk Among Psoriasis Patients Treated With Interleukin Inhibitors: A Retrospective Matched-Cohort Study
To the Editor:
Psoriasis is a chronic immune-mediated inflammatory skin disease that affects approximately 2% to 3% of the global population and an estimated 7.5 million adults in the United States.1 The condition is characterized by recurrent episodes of erythematous scaly plaques driven by dysregulated immune responses, particularly involving the interleukin (IL) 23/T-helper (Th) 17 axis.2 Although cutaneous symptoms are the most visible manifestation, psoriasis is a systemic disorder with broad multisystem involvement. Comorbidities include psoriatic arthritis, metabolic syndrome, cardiovascular disease, inflammatory bowel disease, depression, and anxiety.1 These conditions contribute to a heightened risk for premature mortality, increased health care utilization, and an estimated direct cost burden exceeding $11 billion annually in the United States alone.3 Patients with moderate to severe disease frequently require systemic therapy, and long-term disease control is essential to prevent cumulative inflammatory damage and reduce associated morbidity.4
Globally, psoriasis prevalence and disease severity vary by geography, ethnicity, and environmental factors, with higher rates in Northern Europe and North America and lower reported prevalence in East Asia and sub-Saharan Africa.5 In lower-resource settings, access to advanced therapies is limited, and patients often are treated with less effective or more toxic systemic agents, such as methotrexate or cyclosporine.5 These disparities not only affect quality of life but also may influence comorbidity and malignancy patterns, underscoring the importance of studying biologic safety in diverse real-world populations.
Over the past decade, the therapeutic landscape for psoriasis has been transformed by biologic agents targeting specific immune pathways.6 Interleukin 17 inhibitors (eg, secukinumab, ixekizumab, brodalumab, bimekizumab) act by neutralizing IL-17A, IL-17F, or the IL-17 receptor, thereby reducing keratinocyte activation, neutrophil recruitment, and downstream cytokine production.6 Interleukin 23 inhibitors (eg, guselkumab, risankizumab, tildrakizumab) block the p19 subunit of IL-23, halting the expansion and maintenance of pathogenic Th17 cells.6 Ustekinumab, an IL-12/23 inhibitor, targets the shared p40 subunit of IL-12 and IL-23, attenuating both Th1 and Th17 signaling.6 These agents achieve rapid, durable skin clearance in a large proportion of patients, improve psoriatic arthritis symptoms, and generally are well tolerated, even with long-term use.6
Although efficacy is well established, the immunomodulatory nature of IL inhibitors raises theoretical concerns about malignancy risk. Immune surveillance plays a critical role in detecting and eliminating emerging tumor cells.7 Data from other systemic immunosuppressants, such as cyclosporine, show increased risks for certain cancers8; however, the IL-17 and IL-23 pathways have dual roles in cancer biology.7 In some tumor contexts, these cytokines promote carcinogenesis through angiogenesis, epithelial proliferation, and suppression of antitumor immunity; therefore, inhibiting these pathways could theoretically reduce cancer risk.7 The uncertainty around this risk-benefit balance has made malignancy a central consideration for dermatologists, particularly when initiating therapy in patients with a history of cancer or other risk factors.
The perception of malignancy risk can influence patient willingness to start biologics as well as physician prescribing patterns.9 Some clinicians opt for alternative therapies in individuals with a personal or family history of cancer despite limited direct evidence of harm from IL inhibitors. Conversely, a reassuring malignancy safety profile may support broader adoption of these therapies, especially in patients requiring lifelong disease control.9 Shared decision-making in this context requires robust, real-world evidence that accounts for both common and rare malignancy outcomes.
Randomized controlled trials of IL inhibitors have not demonstrated a consistent malignancy signal, but these studies often are underpowered for rare outcomes and limited by short follow-up durations, typically less than 1 year. They also frequently exclude high-risk populations, limiting generalizability.10 Observational studies using real-world data can address these gaps by including more diverse patient populations, longer observation windows, and larger sample sizes capable of detecting differences in uncommon outcomes.
The TriNetX Analytics Network (http://www.trinetx.com) offers a unique platform for large-scale, real-world pharmacoepidemiologic research. This federated database aggregates deidentified electronic health record data from more than 100 million patients across the United States and internationally, including at academic medical centers, integrated delivery networks, and community hospitals.4 Data contributors refresh their datasets regularly, ensuring near-contemporary representation of prescribing trends and clinical outcomes. Standardized terminology mapping, consistent International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding, and centralized data-quality checks enhance the reliability of analyses. Governance protocols and compliance with the Health Insurance Portability and Accountability Act deidentification standards further ensure ethical use of the data. The breadth and depth of the TriNetX network make it possible to evaluate not only common malignancies but also rare cancer types that smaller studies cannot assess with sufficient statistical power.
We performed a retrospective matched-cohort study, querying data from January 1, 2014, through December 31, 2024, using TriNetX to examine whether IL inhibitor exposure is associated with differences in incident malignancy risk among adults with psoriasis. Patients aged 18 years or older with a psoriasis diagnosis (ICD-10-CM code L40.x) and documented exposure to an IL-17, IL-23, or IL-12/23 inhibitor were eligible. Patients with a prior malignancy diagnosis were excluded to reduce prevalence bias. To ensure that malignancies were incident, we included only those diagnosed at least 1 day after initiation of an IL inhibitor.
The comparison cohort consisted of psoriasis patients without IL inhibitor exposure during their observation period. We used 1:1 propensity score matching based on age, sex, race, and ethnicity, applying a caliper of 0.1 to balance baseline characteristics and minimize demographic confounding. The index date for unexposed patients was randomly assigned within their observation period to align follow-up timing with exposed patients. Outcomes were identified by ICD-10-CM codes grouped by skin, hematologic, and solid-organ malignancies. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, with statistical significance set at P<.05. Odds ratios were selected over hazard ratios due to variability in precise follow-up time capture and the primary analytic goal of comparing proportional odds within matched follow-up windows.
Propensity score matching was employed because it is a well-established technique in pharmacoepidemiology to mimic some of the balance achieved in randomized trials. By equating treatment and control groups on measured confounders, matching helps isolate the treatment effect, particularly important in nonrandomized datasets in which prescribing decisions may be influenced by baseline characteristics. Grouping cancers into clinically relevant categories allowed us to assess patterns of association, as some cancer types (eg, melanoma, lymphomas) may have pathophysiologic links to inflammatory pathways targeted by IL inhibitors.
The final cohort included 133,352 patients, with 66,676 in each group. The mean (SD) age was 49.3 (16.0) years, and demographic variables were well balanced after matching. The mean follow-up was approximately 3.8 years. Interleukin 17 inhibitors were the most frequently prescribed, followed by IL-23 inhibitors and ustekinumab. Baseline comorbidities such as cardiovascular disease, diabetes, and obesity were comparable between groups, reducing the likelihood of confounding from these factors.
Interleukin inhibitor exposure was associated with significantly reduced odds of several malignancies (eTable). Among skin cancers, melanoma risk was reduced by 36% (OR, 0.641; 95% CI, 0.534-0.77; P<.0001), basal cell carcinoma by 43% (OR, 0.565; 95% CI, 0.48-0.665; P<.0001), and squamous cell carcinoma by 18% (OR, 0.821; 95% CI, 0.676-0.996; P=.0452). Hematologic malignancies showed similar reductions, with non-Hodgkin lymphoma odds reduced by 35% (OR, 0.646; 95% CI, 0.512-0.815; P=.0002) and Hodgkin lymphoma by 50% (OR, 0.5; 95% CI, 0.292-0.855; P=.0098).
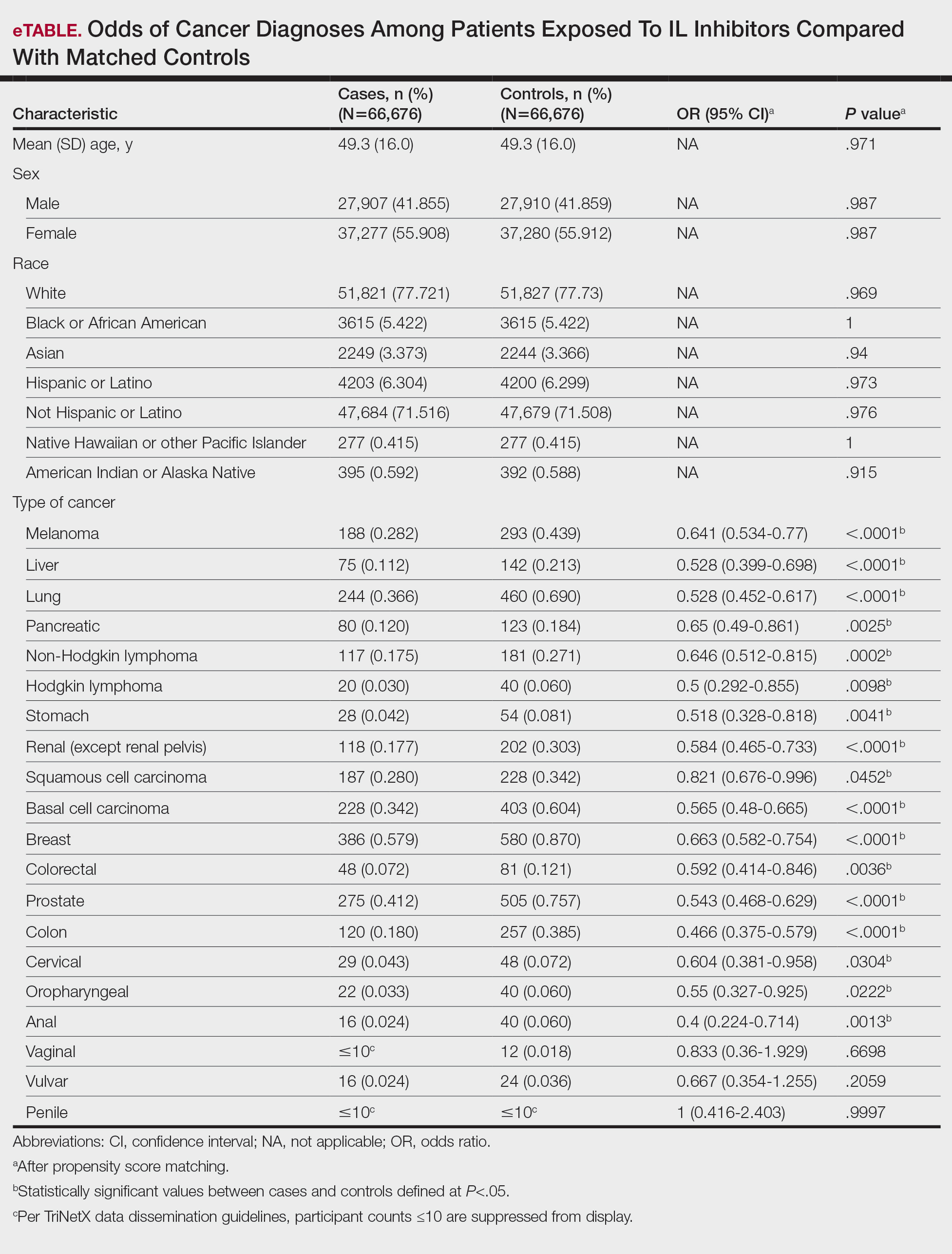
Protective associations also were observed for several solid tumors: lung (OR, 0.528; 95% CI, 0.452-0.617; P<.0001), liver (OR, 0.528; 95% CI, 0.399-0.698; P<.0001), pancreatic (OR, 0.65; 95% CI, 0.49-0.861; P=.0025), breast (OR, 0.663; 95% CI, 0.582-0.754; P<.0001), prostate (OR, 0.543; 95% CI, 0.468-0.629; P<.0001), colorectal (OR, 0.592; 95% CI, 0.414-0.846; P=.0036), colon (OR, 0.466; 95% CI, 0.375-0.579; P<.0001), and oropharyngeal (OR, 0.55; 95% CI, 0.327-0.925; P=.0222) cancers. Cervical cancer (OR, 0.604; 95% CI, 0.381-0.958; P=.0304) and anal cancer (OR, 0.4; 95% CI, 0.224-0.714; P=.0013) also showed significant reductions. Vaginal, vulvar, and penile cancers demonstrated no significant differences, likely due to their low incidence and limited statistical power.
The biological plausibility of these findings is supported by preclinical studies implicating IL-17 and IL-23 in tumor-promoting inflammation.11 These cytokines can recruit myeloid-derived suppressor cells, promote angiogenesis, and facilitate tumor-immune evasion. Inhibition may shift the immune microenvironment toward enhanced tumor surveillance, reduce protumorigenic cytokine signaling, and normalize regulatory T-cell function.11 These mechanisms could explain observed reductions in melanoma, lymphomas, and certain solid tumors.
Our results are consistent with several large registry studies showing no increased cancer incidence in IL inhibitor users and extend prior findings by demonstrating significant reductions in multiple cancer types.12 The melanoma reduction contrasts with the findings in earlier biologic safety studies, possibly due to our larger sample size, broader geographic representation, and inclusion of multiple IL inhibitor classes.13 Similar reductions have not been consistently observed with tumor necrosis factor α inhibitors, which have different immunologic targets and a more complex malignancy safety history.14
Limitations of our study include the retrospective design, potential misclassification of cancer diagnoses, and lack of data on unmeasured confounders such as sun exposure, smoking, alcohol use, and family cancer history. Surveillance bias is possible, though it would likely bias toward higher, not lower, cancer detection in biologic users. Our mean follow-up period of 3.8 years may not be sufficient for cancers with long latency periods.
If replicated, our findings could have meaningful public health implications. Reassurance regarding malignancy safety may increase patient acceptance and physician confidence in prescribing IL inhibitors, particularly for patients requiring long-term therapy. From a payer perspective, the potential for reduced cancer incidence could translate into substantial cost savings over time, offsetting the high up-front cost of biologics. Additionally, these results may be relevant to other IL inhibitor indications, including psoriatic arthritis, ankylosing spondylitis, and inflammatory bowel disease, in which similar pathophysiologic mechanisms may be at play.
In conclusion, this large matched-cohort study found that IL inhibitor therapy in psoriasis was associated with significantly reduced odds of multiple malignancies, including melanoma, lymphomas, and several solid tumors. These findings contribute to the growing body of real-world evidence supporting the long-term safety of IL inhibitors and underscore the need for continued pharmacovigilance and mechanistic research.
- Armstrong AW, Mehta MD, Schupp CW, et al. Psoriasis prevalence in adults in the United States. JAMA Dermatol. 2021;157:940-946. doi:10.1001/jamadermatol.2021.2007
- Deng Z, Wang S, Wu C, et al. IL-17 inhibitor-associated inflammatory bowel disease: a study based on literature and database analysis. Front Pharmacol. 2023;14:1124628. doi:10.3389/fphar.2023.1124628
- Al Sawah S, Foster SA, Goldblum OM, et al. Healthcare costs in psoriasis and psoriasis sub-groups over time following psoriasis diagnosis. J Med Econ. 2017;20:982-990. doi:10.1080/13696998.2017.1345749
- Korman NJ. Management of psoriasis as a systemic disease: what is the evidence? Br J Dermatol. 2020;182:840-848. doi:10.1111/bjd.18245
- Damiani G, Bragazzi NL, Karimkhani Aksut C, et al. The global, regional, and national burden of psoriasis: results and insights from the Global Burden of Disease 2019 Study. Front Med (Lausanne). 2021;8:743180. doi:10.3389/fmed.2021.743180
- Metko D, Torres T, Vender R. Viewpoint about biologic agents for psoriasis: are they immunosuppressants or immunomodulators? J Int Med Res. 2023;51:3000605231175547. doi:10.1177/03000605231175547
- Tsai YC, Tsai TF. Anti-interleukin and interleukin therapies for psoriasis: current evidence and clinical usefulness. Ther Adv Musculoskelet Dis. 2017;9:277-294. doi:10.1177/1759720X17735756
- Durnian JM, Stewart RM, Tatham R, et al. Cyclosporin-A associated malignancy. Clin Ophthalmol. 2007;1:421-430.
- DeWitt EM, Lin L, Glick HA, et al. Pattern and predictors of the initiation of biologic agents for the treatment of rheumatoid arthritis in the United States: an analysis using a large observational data bank. Clin Ther. 2009;31:1871-1858. doi:10.1016/j.clinthera.2009.08.020
- Vangilbergen M, Stockman A, Van De Velde A, et al. The role of interleukin-17 and interleukin-23 inhibitors in the development, progression, and recurrence of cancer: a systematic review. JAAD Int. 2024;17:71-79. doi:10.1016/j.jdin.2024.06.006
- Navarro-Compán V, Puig L, Vidal S, et al. The paradigm of IL-23-independent production of IL-17F and IL-17A and their role in chronic inflammatory diseases. Front Immunol. 2023;14:1191782. doi:10.3389/fimmu.2023.1191782
- Bencardino S, Bernardi F, Allocca M, et al. Advanced therapies for inflammatory bowel disease and risk of skin cancer: what’s new? Cancers (Basel). 2025;17:1710. doi:10.3390/cancers17101710
- Esse S, Mason KJ, Green AC, et al. Melanoma risk in patients treated with biologic therapy for common inflammatory diseases: a systematic review and meta-analysis. JAMA Dermatol. 2020;156:787-794. doi:10.1001/jamadermatol.2020.1300
- Solomon DH, Mercer E, Kavanaugh A. Observational studies on the risk of cancer associated with tumor necrosis factor inhibitors in rheumatoid arthritis: a review of their methodologies and results. Arthritis Rheum. 2012;64:21-32. doi:10.1002/art.30653
To the Editor:
Psoriasis is a chronic immune-mediated inflammatory skin disease that affects approximately 2% to 3% of the global population and an estimated 7.5 million adults in the United States.1 The condition is characterized by recurrent episodes of erythematous scaly plaques driven by dysregulated immune responses, particularly involving the interleukin (IL) 23/T-helper (Th) 17 axis.2 Although cutaneous symptoms are the most visible manifestation, psoriasis is a systemic disorder with broad multisystem involvement. Comorbidities include psoriatic arthritis, metabolic syndrome, cardiovascular disease, inflammatory bowel disease, depression, and anxiety.1 These conditions contribute to a heightened risk for premature mortality, increased health care utilization, and an estimated direct cost burden exceeding $11 billion annually in the United States alone.3 Patients with moderate to severe disease frequently require systemic therapy, and long-term disease control is essential to prevent cumulative inflammatory damage and reduce associated morbidity.4
Globally, psoriasis prevalence and disease severity vary by geography, ethnicity, and environmental factors, with higher rates in Northern Europe and North America and lower reported prevalence in East Asia and sub-Saharan Africa.5 In lower-resource settings, access to advanced therapies is limited, and patients often are treated with less effective or more toxic systemic agents, such as methotrexate or cyclosporine.5 These disparities not only affect quality of life but also may influence comorbidity and malignancy patterns, underscoring the importance of studying biologic safety in diverse real-world populations.
Over the past decade, the therapeutic landscape for psoriasis has been transformed by biologic agents targeting specific immune pathways.6 Interleukin 17 inhibitors (eg, secukinumab, ixekizumab, brodalumab, bimekizumab) act by neutralizing IL-17A, IL-17F, or the IL-17 receptor, thereby reducing keratinocyte activation, neutrophil recruitment, and downstream cytokine production.6 Interleukin 23 inhibitors (eg, guselkumab, risankizumab, tildrakizumab) block the p19 subunit of IL-23, halting the expansion and maintenance of pathogenic Th17 cells.6 Ustekinumab, an IL-12/23 inhibitor, targets the shared p40 subunit of IL-12 and IL-23, attenuating both Th1 and Th17 signaling.6 These agents achieve rapid, durable skin clearance in a large proportion of patients, improve psoriatic arthritis symptoms, and generally are well tolerated, even with long-term use.6
Although efficacy is well established, the immunomodulatory nature of IL inhibitors raises theoretical concerns about malignancy risk. Immune surveillance plays a critical role in detecting and eliminating emerging tumor cells.7 Data from other systemic immunosuppressants, such as cyclosporine, show increased risks for certain cancers8; however, the IL-17 and IL-23 pathways have dual roles in cancer biology.7 In some tumor contexts, these cytokines promote carcinogenesis through angiogenesis, epithelial proliferation, and suppression of antitumor immunity; therefore, inhibiting these pathways could theoretically reduce cancer risk.7 The uncertainty around this risk-benefit balance has made malignancy a central consideration for dermatologists, particularly when initiating therapy in patients with a history of cancer or other risk factors.
The perception of malignancy risk can influence patient willingness to start biologics as well as physician prescribing patterns.9 Some clinicians opt for alternative therapies in individuals with a personal or family history of cancer despite limited direct evidence of harm from IL inhibitors. Conversely, a reassuring malignancy safety profile may support broader adoption of these therapies, especially in patients requiring lifelong disease control.9 Shared decision-making in this context requires robust, real-world evidence that accounts for both common and rare malignancy outcomes.
Randomized controlled trials of IL inhibitors have not demonstrated a consistent malignancy signal, but these studies often are underpowered for rare outcomes and limited by short follow-up durations, typically less than 1 year. They also frequently exclude high-risk populations, limiting generalizability.10 Observational studies using real-world data can address these gaps by including more diverse patient populations, longer observation windows, and larger sample sizes capable of detecting differences in uncommon outcomes.
The TriNetX Analytics Network (http://www.trinetx.com) offers a unique platform for large-scale, real-world pharmacoepidemiologic research. This federated database aggregates deidentified electronic health record data from more than 100 million patients across the United States and internationally, including at academic medical centers, integrated delivery networks, and community hospitals.4 Data contributors refresh their datasets regularly, ensuring near-contemporary representation of prescribing trends and clinical outcomes. Standardized terminology mapping, consistent International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding, and centralized data-quality checks enhance the reliability of analyses. Governance protocols and compliance with the Health Insurance Portability and Accountability Act deidentification standards further ensure ethical use of the data. The breadth and depth of the TriNetX network make it possible to evaluate not only common malignancies but also rare cancer types that smaller studies cannot assess with sufficient statistical power.
We performed a retrospective matched-cohort study, querying data from January 1, 2014, through December 31, 2024, using TriNetX to examine whether IL inhibitor exposure is associated with differences in incident malignancy risk among adults with psoriasis. Patients aged 18 years or older with a psoriasis diagnosis (ICD-10-CM code L40.x) and documented exposure to an IL-17, IL-23, or IL-12/23 inhibitor were eligible. Patients with a prior malignancy diagnosis were excluded to reduce prevalence bias. To ensure that malignancies were incident, we included only those diagnosed at least 1 day after initiation of an IL inhibitor.
The comparison cohort consisted of psoriasis patients without IL inhibitor exposure during their observation period. We used 1:1 propensity score matching based on age, sex, race, and ethnicity, applying a caliper of 0.1 to balance baseline characteristics and minimize demographic confounding. The index date for unexposed patients was randomly assigned within their observation period to align follow-up timing with exposed patients. Outcomes were identified by ICD-10-CM codes grouped by skin, hematologic, and solid-organ malignancies. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, with statistical significance set at P<.05. Odds ratios were selected over hazard ratios due to variability in precise follow-up time capture and the primary analytic goal of comparing proportional odds within matched follow-up windows.
Propensity score matching was employed because it is a well-established technique in pharmacoepidemiology to mimic some of the balance achieved in randomized trials. By equating treatment and control groups on measured confounders, matching helps isolate the treatment effect, particularly important in nonrandomized datasets in which prescribing decisions may be influenced by baseline characteristics. Grouping cancers into clinically relevant categories allowed us to assess patterns of association, as some cancer types (eg, melanoma, lymphomas) may have pathophysiologic links to inflammatory pathways targeted by IL inhibitors.
The final cohort included 133,352 patients, with 66,676 in each group. The mean (SD) age was 49.3 (16.0) years, and demographic variables were well balanced after matching. The mean follow-up was approximately 3.8 years. Interleukin 17 inhibitors were the most frequently prescribed, followed by IL-23 inhibitors and ustekinumab. Baseline comorbidities such as cardiovascular disease, diabetes, and obesity were comparable between groups, reducing the likelihood of confounding from these factors.
Interleukin inhibitor exposure was associated with significantly reduced odds of several malignancies (eTable). Among skin cancers, melanoma risk was reduced by 36% (OR, 0.641; 95% CI, 0.534-0.77; P<.0001), basal cell carcinoma by 43% (OR, 0.565; 95% CI, 0.48-0.665; P<.0001), and squamous cell carcinoma by 18% (OR, 0.821; 95% CI, 0.676-0.996; P=.0452). Hematologic malignancies showed similar reductions, with non-Hodgkin lymphoma odds reduced by 35% (OR, 0.646; 95% CI, 0.512-0.815; P=.0002) and Hodgkin lymphoma by 50% (OR, 0.5; 95% CI, 0.292-0.855; P=.0098).
Protective associations also were observed for several solid tumors: lung (OR, 0.528; 95% CI, 0.452-0.617; P<.0001), liver (OR, 0.528; 95% CI, 0.399-0.698; P<.0001), pancreatic (OR, 0.65; 95% CI, 0.49-0.861; P=.0025), breast (OR, 0.663; 95% CI, 0.582-0.754; P<.0001), prostate (OR, 0.543; 95% CI, 0.468-0.629; P<.0001), colorectal (OR, 0.592; 95% CI, 0.414-0.846; P=.0036), colon (OR, 0.466; 95% CI, 0.375-0.579; P<.0001), and oropharyngeal (OR, 0.55; 95% CI, 0.327-0.925; P=.0222) cancers. Cervical cancer (OR, 0.604; 95% CI, 0.381-0.958; P=.0304) and anal cancer (OR, 0.4; 95% CI, 0.224-0.714; P=.0013) also showed significant reductions. Vaginal, vulvar, and penile cancers demonstrated no significant differences, likely due to their low incidence and limited statistical power.
The biological plausibility of these findings is supported by preclinical studies implicating IL-17 and IL-23 in tumor-promoting inflammation.11 These cytokines can recruit myeloid-derived suppressor cells, promote angiogenesis, and facilitate tumor-immune evasion. Inhibition may shift the immune microenvironment toward enhanced tumor surveillance, reduce protumorigenic cytokine signaling, and normalize regulatory T-cell function.11 These mechanisms could explain observed reductions in melanoma, lymphomas, and certain solid tumors.
Our results are consistent with several large registry studies showing no increased cancer incidence in IL inhibitor users and extend prior findings by demonstrating significant reductions in multiple cancer types.12 The melanoma reduction contrasts with the findings in earlier biologic safety studies, possibly due to our larger sample size, broader geographic representation, and inclusion of multiple IL inhibitor classes.13 Similar reductions have not been consistently observed with tumor necrosis factor α inhibitors, which have different immunologic targets and a more complex malignancy safety history.14
Limitations of our study include the retrospective design, potential misclassification of cancer diagnoses, and lack of data on unmeasured confounders such as sun exposure, smoking, alcohol use, and family cancer history. Surveillance bias is possible, though it would likely bias toward higher, not lower, cancer detection in biologic users. Our mean follow-up period of 3.8 years may not be sufficient for cancers with long latency periods.
If replicated, our findings could have meaningful public health implications. Reassurance regarding malignancy safety may increase patient acceptance and physician confidence in prescribing IL inhibitors, particularly for patients requiring long-term therapy. From a payer perspective, the potential for reduced cancer incidence could translate into substantial cost savings over time, offsetting the high up-front cost of biologics. Additionally, these results may be relevant to other IL inhibitor indications, including psoriatic arthritis, ankylosing spondylitis, and inflammatory bowel disease, in which similar pathophysiologic mechanisms may be at play.
In conclusion, this large matched-cohort study found that IL inhibitor therapy in psoriasis was associated with significantly reduced odds of multiple malignancies, including melanoma, lymphomas, and several solid tumors. These findings contribute to the growing body of real-world evidence supporting the long-term safety of IL inhibitors and underscore the need for continued pharmacovigilance and mechanistic research.
To the Editor:
Psoriasis is a chronic immune-mediated inflammatory skin disease that affects approximately 2% to 3% of the global population and an estimated 7.5 million adults in the United States.1 The condition is characterized by recurrent episodes of erythematous scaly plaques driven by dysregulated immune responses, particularly involving the interleukin (IL) 23/T-helper (Th) 17 axis.2 Although cutaneous symptoms are the most visible manifestation, psoriasis is a systemic disorder with broad multisystem involvement. Comorbidities include psoriatic arthritis, metabolic syndrome, cardiovascular disease, inflammatory bowel disease, depression, and anxiety.1 These conditions contribute to a heightened risk for premature mortality, increased health care utilization, and an estimated direct cost burden exceeding $11 billion annually in the United States alone.3 Patients with moderate to severe disease frequently require systemic therapy, and long-term disease control is essential to prevent cumulative inflammatory damage and reduce associated morbidity.4
Globally, psoriasis prevalence and disease severity vary by geography, ethnicity, and environmental factors, with higher rates in Northern Europe and North America and lower reported prevalence in East Asia and sub-Saharan Africa.5 In lower-resource settings, access to advanced therapies is limited, and patients often are treated with less effective or more toxic systemic agents, such as methotrexate or cyclosporine.5 These disparities not only affect quality of life but also may influence comorbidity and malignancy patterns, underscoring the importance of studying biologic safety in diverse real-world populations.
Over the past decade, the therapeutic landscape for psoriasis has been transformed by biologic agents targeting specific immune pathways.6 Interleukin 17 inhibitors (eg, secukinumab, ixekizumab, brodalumab, bimekizumab) act by neutralizing IL-17A, IL-17F, or the IL-17 receptor, thereby reducing keratinocyte activation, neutrophil recruitment, and downstream cytokine production.6 Interleukin 23 inhibitors (eg, guselkumab, risankizumab, tildrakizumab) block the p19 subunit of IL-23, halting the expansion and maintenance of pathogenic Th17 cells.6 Ustekinumab, an IL-12/23 inhibitor, targets the shared p40 subunit of IL-12 and IL-23, attenuating both Th1 and Th17 signaling.6 These agents achieve rapid, durable skin clearance in a large proportion of patients, improve psoriatic arthritis symptoms, and generally are well tolerated, even with long-term use.6
Although efficacy is well established, the immunomodulatory nature of IL inhibitors raises theoretical concerns about malignancy risk. Immune surveillance plays a critical role in detecting and eliminating emerging tumor cells.7 Data from other systemic immunosuppressants, such as cyclosporine, show increased risks for certain cancers8; however, the IL-17 and IL-23 pathways have dual roles in cancer biology.7 In some tumor contexts, these cytokines promote carcinogenesis through angiogenesis, epithelial proliferation, and suppression of antitumor immunity; therefore, inhibiting these pathways could theoretically reduce cancer risk.7 The uncertainty around this risk-benefit balance has made malignancy a central consideration for dermatologists, particularly when initiating therapy in patients with a history of cancer or other risk factors.
The perception of malignancy risk can influence patient willingness to start biologics as well as physician prescribing patterns.9 Some clinicians opt for alternative therapies in individuals with a personal or family history of cancer despite limited direct evidence of harm from IL inhibitors. Conversely, a reassuring malignancy safety profile may support broader adoption of these therapies, especially in patients requiring lifelong disease control.9 Shared decision-making in this context requires robust, real-world evidence that accounts for both common and rare malignancy outcomes.
Randomized controlled trials of IL inhibitors have not demonstrated a consistent malignancy signal, but these studies often are underpowered for rare outcomes and limited by short follow-up durations, typically less than 1 year. They also frequently exclude high-risk populations, limiting generalizability.10 Observational studies using real-world data can address these gaps by including more diverse patient populations, longer observation windows, and larger sample sizes capable of detecting differences in uncommon outcomes.
The TriNetX Analytics Network (http://www.trinetx.com) offers a unique platform for large-scale, real-world pharmacoepidemiologic research. This federated database aggregates deidentified electronic health record data from more than 100 million patients across the United States and internationally, including at academic medical centers, integrated delivery networks, and community hospitals.4 Data contributors refresh their datasets regularly, ensuring near-contemporary representation of prescribing trends and clinical outcomes. Standardized terminology mapping, consistent International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding, and centralized data-quality checks enhance the reliability of analyses. Governance protocols and compliance with the Health Insurance Portability and Accountability Act deidentification standards further ensure ethical use of the data. The breadth and depth of the TriNetX network make it possible to evaluate not only common malignancies but also rare cancer types that smaller studies cannot assess with sufficient statistical power.
We performed a retrospective matched-cohort study, querying data from January 1, 2014, through December 31, 2024, using TriNetX to examine whether IL inhibitor exposure is associated with differences in incident malignancy risk among adults with psoriasis. Patients aged 18 years or older with a psoriasis diagnosis (ICD-10-CM code L40.x) and documented exposure to an IL-17, IL-23, or IL-12/23 inhibitor were eligible. Patients with a prior malignancy diagnosis were excluded to reduce prevalence bias. To ensure that malignancies were incident, we included only those diagnosed at least 1 day after initiation of an IL inhibitor.
The comparison cohort consisted of psoriasis patients without IL inhibitor exposure during their observation period. We used 1:1 propensity score matching based on age, sex, race, and ethnicity, applying a caliper of 0.1 to balance baseline characteristics and minimize demographic confounding. The index date for unexposed patients was randomly assigned within their observation period to align follow-up timing with exposed patients. Outcomes were identified by ICD-10-CM codes grouped by skin, hematologic, and solid-organ malignancies. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, with statistical significance set at P<.05. Odds ratios were selected over hazard ratios due to variability in precise follow-up time capture and the primary analytic goal of comparing proportional odds within matched follow-up windows.
Propensity score matching was employed because it is a well-established technique in pharmacoepidemiology to mimic some of the balance achieved in randomized trials. By equating treatment and control groups on measured confounders, matching helps isolate the treatment effect, particularly important in nonrandomized datasets in which prescribing decisions may be influenced by baseline characteristics. Grouping cancers into clinically relevant categories allowed us to assess patterns of association, as some cancer types (eg, melanoma, lymphomas) may have pathophysiologic links to inflammatory pathways targeted by IL inhibitors.
The final cohort included 133,352 patients, with 66,676 in each group. The mean (SD) age was 49.3 (16.0) years, and demographic variables were well balanced after matching. The mean follow-up was approximately 3.8 years. Interleukin 17 inhibitors were the most frequently prescribed, followed by IL-23 inhibitors and ustekinumab. Baseline comorbidities such as cardiovascular disease, diabetes, and obesity were comparable between groups, reducing the likelihood of confounding from these factors.
Interleukin inhibitor exposure was associated with significantly reduced odds of several malignancies (eTable). Among skin cancers, melanoma risk was reduced by 36% (OR, 0.641; 95% CI, 0.534-0.77; P<.0001), basal cell carcinoma by 43% (OR, 0.565; 95% CI, 0.48-0.665; P<.0001), and squamous cell carcinoma by 18% (OR, 0.821; 95% CI, 0.676-0.996; P=.0452). Hematologic malignancies showed similar reductions, with non-Hodgkin lymphoma odds reduced by 35% (OR, 0.646; 95% CI, 0.512-0.815; P=.0002) and Hodgkin lymphoma by 50% (OR, 0.5; 95% CI, 0.292-0.855; P=.0098).
Protective associations also were observed for several solid tumors: lung (OR, 0.528; 95% CI, 0.452-0.617; P<.0001), liver (OR, 0.528; 95% CI, 0.399-0.698; P<.0001), pancreatic (OR, 0.65; 95% CI, 0.49-0.861; P=.0025), breast (OR, 0.663; 95% CI, 0.582-0.754; P<.0001), prostate (OR, 0.543; 95% CI, 0.468-0.629; P<.0001), colorectal (OR, 0.592; 95% CI, 0.414-0.846; P=.0036), colon (OR, 0.466; 95% CI, 0.375-0.579; P<.0001), and oropharyngeal (OR, 0.55; 95% CI, 0.327-0.925; P=.0222) cancers. Cervical cancer (OR, 0.604; 95% CI, 0.381-0.958; P=.0304) and anal cancer (OR, 0.4; 95% CI, 0.224-0.714; P=.0013) also showed significant reductions. Vaginal, vulvar, and penile cancers demonstrated no significant differences, likely due to their low incidence and limited statistical power.
The biological plausibility of these findings is supported by preclinical studies implicating IL-17 and IL-23 in tumor-promoting inflammation.11 These cytokines can recruit myeloid-derived suppressor cells, promote angiogenesis, and facilitate tumor-immune evasion. Inhibition may shift the immune microenvironment toward enhanced tumor surveillance, reduce protumorigenic cytokine signaling, and normalize regulatory T-cell function.11 These mechanisms could explain observed reductions in melanoma, lymphomas, and certain solid tumors.
Our results are consistent with several large registry studies showing no increased cancer incidence in IL inhibitor users and extend prior findings by demonstrating significant reductions in multiple cancer types.12 The melanoma reduction contrasts with the findings in earlier biologic safety studies, possibly due to our larger sample size, broader geographic representation, and inclusion of multiple IL inhibitor classes.13 Similar reductions have not been consistently observed with tumor necrosis factor α inhibitors, which have different immunologic targets and a more complex malignancy safety history.14
Limitations of our study include the retrospective design, potential misclassification of cancer diagnoses, and lack of data on unmeasured confounders such as sun exposure, smoking, alcohol use, and family cancer history. Surveillance bias is possible, though it would likely bias toward higher, not lower, cancer detection in biologic users. Our mean follow-up period of 3.8 years may not be sufficient for cancers with long latency periods.
If replicated, our findings could have meaningful public health implications. Reassurance regarding malignancy safety may increase patient acceptance and physician confidence in prescribing IL inhibitors, particularly for patients requiring long-term therapy. From a payer perspective, the potential for reduced cancer incidence could translate into substantial cost savings over time, offsetting the high up-front cost of biologics. Additionally, these results may be relevant to other IL inhibitor indications, including psoriatic arthritis, ankylosing spondylitis, and inflammatory bowel disease, in which similar pathophysiologic mechanisms may be at play.
In conclusion, this large matched-cohort study found that IL inhibitor therapy in psoriasis was associated with significantly reduced odds of multiple malignancies, including melanoma, lymphomas, and several solid tumors. These findings contribute to the growing body of real-world evidence supporting the long-term safety of IL inhibitors and underscore the need for continued pharmacovigilance and mechanistic research.
- Armstrong AW, Mehta MD, Schupp CW, et al. Psoriasis prevalence in adults in the United States. JAMA Dermatol. 2021;157:940-946. doi:10.1001/jamadermatol.2021.2007
- Deng Z, Wang S, Wu C, et al. IL-17 inhibitor-associated inflammatory bowel disease: a study based on literature and database analysis. Front Pharmacol. 2023;14:1124628. doi:10.3389/fphar.2023.1124628
- Al Sawah S, Foster SA, Goldblum OM, et al. Healthcare costs in psoriasis and psoriasis sub-groups over time following psoriasis diagnosis. J Med Econ. 2017;20:982-990. doi:10.1080/13696998.2017.1345749
- Korman NJ. Management of psoriasis as a systemic disease: what is the evidence? Br J Dermatol. 2020;182:840-848. doi:10.1111/bjd.18245
- Damiani G, Bragazzi NL, Karimkhani Aksut C, et al. The global, regional, and national burden of psoriasis: results and insights from the Global Burden of Disease 2019 Study. Front Med (Lausanne). 2021;8:743180. doi:10.3389/fmed.2021.743180
- Metko D, Torres T, Vender R. Viewpoint about biologic agents for psoriasis: are they immunosuppressants or immunomodulators? J Int Med Res. 2023;51:3000605231175547. doi:10.1177/03000605231175547
- Tsai YC, Tsai TF. Anti-interleukin and interleukin therapies for psoriasis: current evidence and clinical usefulness. Ther Adv Musculoskelet Dis. 2017;9:277-294. doi:10.1177/1759720X17735756
- Durnian JM, Stewart RM, Tatham R, et al. Cyclosporin-A associated malignancy. Clin Ophthalmol. 2007;1:421-430.
- DeWitt EM, Lin L, Glick HA, et al. Pattern and predictors of the initiation of biologic agents for the treatment of rheumatoid arthritis in the United States: an analysis using a large observational data bank. Clin Ther. 2009;31:1871-1858. doi:10.1016/j.clinthera.2009.08.020
- Vangilbergen M, Stockman A, Van De Velde A, et al. The role of interleukin-17 and interleukin-23 inhibitors in the development, progression, and recurrence of cancer: a systematic review. JAAD Int. 2024;17:71-79. doi:10.1016/j.jdin.2024.06.006
- Navarro-Compán V, Puig L, Vidal S, et al. The paradigm of IL-23-independent production of IL-17F and IL-17A and their role in chronic inflammatory diseases. Front Immunol. 2023;14:1191782. doi:10.3389/fimmu.2023.1191782
- Bencardino S, Bernardi F, Allocca M, et al. Advanced therapies for inflammatory bowel disease and risk of skin cancer: what’s new? Cancers (Basel). 2025;17:1710. doi:10.3390/cancers17101710
- Esse S, Mason KJ, Green AC, et al. Melanoma risk in patients treated with biologic therapy for common inflammatory diseases: a systematic review and meta-analysis. JAMA Dermatol. 2020;156:787-794. doi:10.1001/jamadermatol.2020.1300
- Solomon DH, Mercer E, Kavanaugh A. Observational studies on the risk of cancer associated with tumor necrosis factor inhibitors in rheumatoid arthritis: a review of their methodologies and results. Arthritis Rheum. 2012;64:21-32. doi:10.1002/art.30653
- Armstrong AW, Mehta MD, Schupp CW, et al. Psoriasis prevalence in adults in the United States. JAMA Dermatol. 2021;157:940-946. doi:10.1001/jamadermatol.2021.2007
- Deng Z, Wang S, Wu C, et al. IL-17 inhibitor-associated inflammatory bowel disease: a study based on literature and database analysis. Front Pharmacol. 2023;14:1124628. doi:10.3389/fphar.2023.1124628
- Al Sawah S, Foster SA, Goldblum OM, et al. Healthcare costs in psoriasis and psoriasis sub-groups over time following psoriasis diagnosis. J Med Econ. 2017;20:982-990. doi:10.1080/13696998.2017.1345749
- Korman NJ. Management of psoriasis as a systemic disease: what is the evidence? Br J Dermatol. 2020;182:840-848. doi:10.1111/bjd.18245
- Damiani G, Bragazzi NL, Karimkhani Aksut C, et al. The global, regional, and national burden of psoriasis: results and insights from the Global Burden of Disease 2019 Study. Front Med (Lausanne). 2021;8:743180. doi:10.3389/fmed.2021.743180
- Metko D, Torres T, Vender R. Viewpoint about biologic agents for psoriasis: are they immunosuppressants or immunomodulators? J Int Med Res. 2023;51:3000605231175547. doi:10.1177/03000605231175547
- Tsai YC, Tsai TF. Anti-interleukin and interleukin therapies for psoriasis: current evidence and clinical usefulness. Ther Adv Musculoskelet Dis. 2017;9:277-294. doi:10.1177/1759720X17735756
- Durnian JM, Stewart RM, Tatham R, et al. Cyclosporin-A associated malignancy. Clin Ophthalmol. 2007;1:421-430.
- DeWitt EM, Lin L, Glick HA, et al. Pattern and predictors of the initiation of biologic agents for the treatment of rheumatoid arthritis in the United States: an analysis using a large observational data bank. Clin Ther. 2009;31:1871-1858. doi:10.1016/j.clinthera.2009.08.020
- Vangilbergen M, Stockman A, Van De Velde A, et al. The role of interleukin-17 and interleukin-23 inhibitors in the development, progression, and recurrence of cancer: a systematic review. JAAD Int. 2024;17:71-79. doi:10.1016/j.jdin.2024.06.006
- Navarro-Compán V, Puig L, Vidal S, et al. The paradigm of IL-23-independent production of IL-17F and IL-17A and their role in chronic inflammatory diseases. Front Immunol. 2023;14:1191782. doi:10.3389/fimmu.2023.1191782
- Bencardino S, Bernardi F, Allocca M, et al. Advanced therapies for inflammatory bowel disease and risk of skin cancer: what’s new? Cancers (Basel). 2025;17:1710. doi:10.3390/cancers17101710
- Esse S, Mason KJ, Green AC, et al. Melanoma risk in patients treated with biologic therapy for common inflammatory diseases: a systematic review and meta-analysis. JAMA Dermatol. 2020;156:787-794. doi:10.1001/jamadermatol.2020.1300
- Solomon DH, Mercer E, Kavanaugh A. Observational studies on the risk of cancer associated with tumor necrosis factor inhibitors in rheumatoid arthritis: a review of their methodologies and results. Arthritis Rheum. 2012;64:21-32. doi:10.1002/art.30653
Malignancy Risk Among Psoriasis Patients Treated With Interleukin Inhibitors: A Retrospective Matched-Cohort Study
Malignancy Risk Among Psoriasis Patients Treated With Interleukin Inhibitors: A Retrospective Matched-Cohort Study
Practice Points
- Interleukin (IL) inhibitor therapy for psoriasis was associated with reduced odds of multiple malignancies in a large matched-cohort analysis.
- Potential mechanisms for reduced cancer risk include inhibition of tumor-promoting inflammation and restoration of antitumor immune surveillance, although further mechanistic and longitudinal studies are needed.
- These findings provide real-world evidence supporting the long-term malignancy safety of IL inhibitors, which may reassure clinicians and patients considering these agents for chronic disease management.

A Simple Alternative for Intralesional Cryosurgery of Keloids and Hypertrophic Scars Using a Disposable Infusion Set
A Simple Alternative for Intralesional Cryosurgery of Keloids and Hypertrophic Scars Using a Disposable Infusion Set
Practice Gap
Intralesional cryosurgery is a highly effective treatment for dermatologic conditions, notably keloids and hypertrophic scars.1 Conventional methods typically use specialized double-lumen intralesional probes or Luer lock adapters connected to hypodermic or lumbar puncture needles, allowing cryogen to flow internally to cool the probe or needle and treat the lesion via conduction.2 However, specialized intralesional probes are expensive and often are difficult to obtain. Furthermore, Luer lock adapters with needles directly attached to the handle unit can be ergonomically challenging, as the procedure requires simultaneous maintenance of a perpendicular handheld position, precise needle passage through the exact center of the lesion, and protection of the surrounding perilesional healthy skin from cold injury. Consequently, these limitations restrict widespread adoption, necessitating simpler, more accessible, and cost-effective alternatives. Herein, we present a novel, practical, and economical cryogen delivery method that adapts a disposable infusion set to a standard cryospray nozzle.
The Technique
This technique involves detaching the infusion set tubing and securely connecting it to the cryospray nozzle (Figure 1). Brief activation of the cryospray to constrict the nozzle or a small incision in the tubing may be required to ensure a tight fit, which can be secured with medical tape to maintain consistent cryogen flow. Local anesthesia is administered directly into and around the lesion, particularly translesionally for keloids, to avoid unnecessary trauma to the surrounding healthy skin, which could trigger further keloid formation. A needle is inserted through the lesion with the tip extending beyond its distal boundary, ensuring the tip remains outside the lesion during cryogen application to prevent cryoinsufflation. If necessary, gentle bending of the needle helps ensure optimal cryogen distribution within the lesion (Figures 2A and 2B). However, this may slightly reduce flow and extend freezing duration; therefore, bending the needle should be performed cautiously and is specifically recommended for effectively treating lesions on curved anatomic sites (eg, the auricle of the ear) to optimize freezing and protect surrounding tissues.
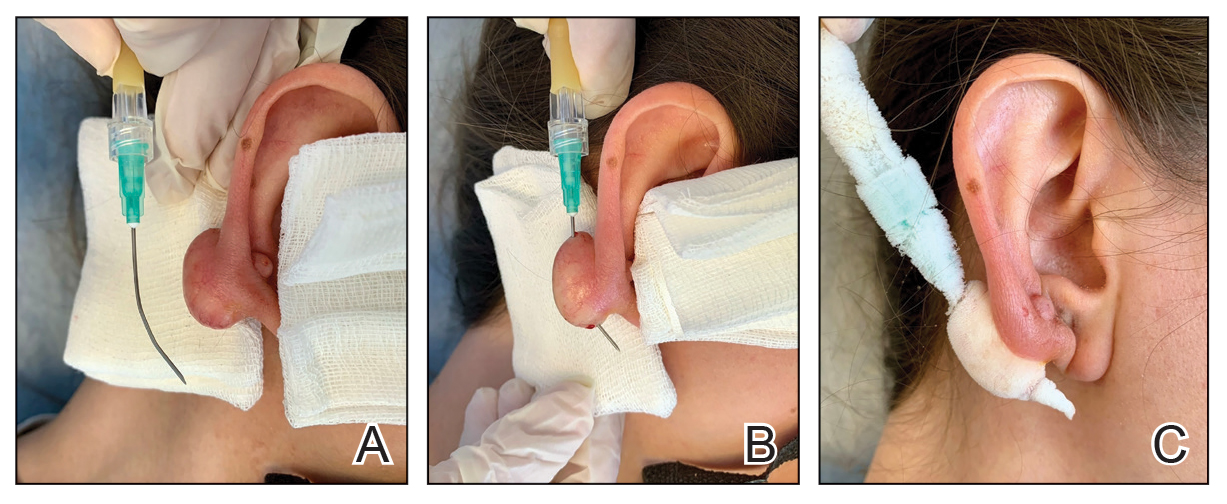
During initial cryogen release, covering the needle tip with gauze prevents aerosolization of biological debris, while placing a wooden tongue depressor between the needle tip and the patient’s skin prevents inadvertent cold injury. After cryogen flow is initiated, the lesion begins to freeze at both the needle entry and exit points, forming what is referred to as ice balls. Over time, typically within several seconds to a few minutes depending on lesion size and tissue characteristics, these ice balls merge centrally, forming a single ice ball encompassing the entire lesion (Figure 2C). Cryogen flow should be maintained during a single application until the unified ice ball appearance is achieved, confirming effective cooling.
Practice Implications
Studies have consistently shown that intralesional cryosurgery is associated with a reduction in the size and symptoms of hypertrophic scars and keloids.1,2 Multimodal treatment approaches, including intralesional methods, are especially valued for their targeted efficacy and minimal adverse effects. Our simplified method offers practical economic advantages, making it highly suitable for broad adoption across diverse clinical settings, particularly those that are resource limited. Clinicians can safely and effectively utilize this technique without specialized or costly equipment, considerably enhancing clinical efficiency and accessibility. The straightforwardness of this method also facilitates the training of medical personnel, enabling rapid integration into clinical practice and the flexibility to treat various lesion types and sizes effectively.
- McGoldrick RB, Theodorakopoulou E, Azzopardi E, et al. Lasers and ancillary treatments for scar management part 2: keloid, hypertrophic, pigmented and acne scars. Scars Burn Heal. 2017;3:1-16. doi:10.1177/2059513116689805
- Gupta S, Kumar B. Intralesional cryosurgery using lumbar puncture and/or hypodermic needles for large, bulky, recalcitrant keloids. Int J Dermatol. 2001;40:349-353. doi:10.1046/j.1365-4362.2001.01117.x
Practice Gap
Intralesional cryosurgery is a highly effective treatment for dermatologic conditions, notably keloids and hypertrophic scars.1 Conventional methods typically use specialized double-lumen intralesional probes or Luer lock adapters connected to hypodermic or lumbar puncture needles, allowing cryogen to flow internally to cool the probe or needle and treat the lesion via conduction.2 However, specialized intralesional probes are expensive and often are difficult to obtain. Furthermore, Luer lock adapters with needles directly attached to the handle unit can be ergonomically challenging, as the procedure requires simultaneous maintenance of a perpendicular handheld position, precise needle passage through the exact center of the lesion, and protection of the surrounding perilesional healthy skin from cold injury. Consequently, these limitations restrict widespread adoption, necessitating simpler, more accessible, and cost-effective alternatives. Herein, we present a novel, practical, and economical cryogen delivery method that adapts a disposable infusion set to a standard cryospray nozzle.
The Technique
This technique involves detaching the infusion set tubing and securely connecting it to the cryospray nozzle (Figure 1). Brief activation of the cryospray to constrict the nozzle or a small incision in the tubing may be required to ensure a tight fit, which can be secured with medical tape to maintain consistent cryogen flow. Local anesthesia is administered directly into and around the lesion, particularly translesionally for keloids, to avoid unnecessary trauma to the surrounding healthy skin, which could trigger further keloid formation. A needle is inserted through the lesion with the tip extending beyond its distal boundary, ensuring the tip remains outside the lesion during cryogen application to prevent cryoinsufflation. If necessary, gentle bending of the needle helps ensure optimal cryogen distribution within the lesion (Figures 2A and 2B). However, this may slightly reduce flow and extend freezing duration; therefore, bending the needle should be performed cautiously and is specifically recommended for effectively treating lesions on curved anatomic sites (eg, the auricle of the ear) to optimize freezing and protect surrounding tissues.
During initial cryogen release, covering the needle tip with gauze prevents aerosolization of biological debris, while placing a wooden tongue depressor between the needle tip and the patient’s skin prevents inadvertent cold injury. After cryogen flow is initiated, the lesion begins to freeze at both the needle entry and exit points, forming what is referred to as ice balls. Over time, typically within several seconds to a few minutes depending on lesion size and tissue characteristics, these ice balls merge centrally, forming a single ice ball encompassing the entire lesion (Figure 2C). Cryogen flow should be maintained during a single application until the unified ice ball appearance is achieved, confirming effective cooling.
Practice Implications
Studies have consistently shown that intralesional cryosurgery is associated with a reduction in the size and symptoms of hypertrophic scars and keloids.1,2 Multimodal treatment approaches, including intralesional methods, are especially valued for their targeted efficacy and minimal adverse effects. Our simplified method offers practical economic advantages, making it highly suitable for broad adoption across diverse clinical settings, particularly those that are resource limited. Clinicians can safely and effectively utilize this technique without specialized or costly equipment, considerably enhancing clinical efficiency and accessibility. The straightforwardness of this method also facilitates the training of medical personnel, enabling rapid integration into clinical practice and the flexibility to treat various lesion types and sizes effectively.
Practice Gap
Intralesional cryosurgery is a highly effective treatment for dermatologic conditions, notably keloids and hypertrophic scars.1 Conventional methods typically use specialized double-lumen intralesional probes or Luer lock adapters connected to hypodermic or lumbar puncture needles, allowing cryogen to flow internally to cool the probe or needle and treat the lesion via conduction.2 However, specialized intralesional probes are expensive and often are difficult to obtain. Furthermore, Luer lock adapters with needles directly attached to the handle unit can be ergonomically challenging, as the procedure requires simultaneous maintenance of a perpendicular handheld position, precise needle passage through the exact center of the lesion, and protection of the surrounding perilesional healthy skin from cold injury. Consequently, these limitations restrict widespread adoption, necessitating simpler, more accessible, and cost-effective alternatives. Herein, we present a novel, practical, and economical cryogen delivery method that adapts a disposable infusion set to a standard cryospray nozzle.
The Technique
This technique involves detaching the infusion set tubing and securely connecting it to the cryospray nozzle (Figure 1). Brief activation of the cryospray to constrict the nozzle or a small incision in the tubing may be required to ensure a tight fit, which can be secured with medical tape to maintain consistent cryogen flow. Local anesthesia is administered directly into and around the lesion, particularly translesionally for keloids, to avoid unnecessary trauma to the surrounding healthy skin, which could trigger further keloid formation. A needle is inserted through the lesion with the tip extending beyond its distal boundary, ensuring the tip remains outside the lesion during cryogen application to prevent cryoinsufflation. If necessary, gentle bending of the needle helps ensure optimal cryogen distribution within the lesion (Figures 2A and 2B). However, this may slightly reduce flow and extend freezing duration; therefore, bending the needle should be performed cautiously and is specifically recommended for effectively treating lesions on curved anatomic sites (eg, the auricle of the ear) to optimize freezing and protect surrounding tissues.
During initial cryogen release, covering the needle tip with gauze prevents aerosolization of biological debris, while placing a wooden tongue depressor between the needle tip and the patient’s skin prevents inadvertent cold injury. After cryogen flow is initiated, the lesion begins to freeze at both the needle entry and exit points, forming what is referred to as ice balls. Over time, typically within several seconds to a few minutes depending on lesion size and tissue characteristics, these ice balls merge centrally, forming a single ice ball encompassing the entire lesion (Figure 2C). Cryogen flow should be maintained during a single application until the unified ice ball appearance is achieved, confirming effective cooling.
Practice Implications
Studies have consistently shown that intralesional cryosurgery is associated with a reduction in the size and symptoms of hypertrophic scars and keloids.1,2 Multimodal treatment approaches, including intralesional methods, are especially valued for their targeted efficacy and minimal adverse effects. Our simplified method offers practical economic advantages, making it highly suitable for broad adoption across diverse clinical settings, particularly those that are resource limited. Clinicians can safely and effectively utilize this technique without specialized or costly equipment, considerably enhancing clinical efficiency and accessibility. The straightforwardness of this method also facilitates the training of medical personnel, enabling rapid integration into clinical practice and the flexibility to treat various lesion types and sizes effectively.
- McGoldrick RB, Theodorakopoulou E, Azzopardi E, et al. Lasers and ancillary treatments for scar management part 2: keloid, hypertrophic, pigmented and acne scars. Scars Burn Heal. 2017;3:1-16. doi:10.1177/2059513116689805
- Gupta S, Kumar B. Intralesional cryosurgery using lumbar puncture and/or hypodermic needles for large, bulky, recalcitrant keloids. Int J Dermatol. 2001;40:349-353. doi:10.1046/j.1365-4362.2001.01117.x
- McGoldrick RB, Theodorakopoulou E, Azzopardi E, et al. Lasers and ancillary treatments for scar management part 2: keloid, hypertrophic, pigmented and acne scars. Scars Burn Heal. 2017;3:1-16. doi:10.1177/2059513116689805
- Gupta S, Kumar B. Intralesional cryosurgery using lumbar puncture and/or hypodermic needles for large, bulky, recalcitrant keloids. Int J Dermatol. 2001;40:349-353. doi:10.1046/j.1365-4362.2001.01117.x
A Simple Alternative for Intralesional Cryosurgery of Keloids and Hypertrophic Scars Using a Disposable Infusion Set
A Simple Alternative for Intralesional Cryosurgery of Keloids and Hypertrophic Scars Using a Disposable Infusion Set

Thick Yellow Plaques on the Eyelids
Thick Yellow Plaques on the Eyelids
THE DIAGNOSIS: Adult-Onset Asthma With Periocular Xanthogranuloma
In the context of pre-existing sinonasal disease and features consistent with adult-onset asthma, the constellation of clinical findings including linear periorbital yellow-orange plaques, imaging demonstrating extension of xanthogranulomatous lesions into the orbital fat, histopathologic features, and serologic abnormalities including elevated IgG4 levels supported a diagnosis of adult-onset asthma with periocular xanthogranuloma (AAPOX).
Adult-onset xanthogranuloma is a non–Langerhans cell histiocytosis (historically classified as type II) within the group of adult orbital xanthogranulomatous diseases resulting from infiltration and proliferation of histiocytes in the orbital and ocular adnexal structures and eyelids. Adult orbital xanthogranulomatous diseases are classified as 4 distinct conditions: adult-onset xanthogranuloma, AAPOX, Erdheim-Chester disease, and necrobiotic xanthogranuloma (NXG). Erdheim-Chester disease is the most severe among this group and often is fatal due to infiltration of the xanthogranulomas into multiple organ systems and tissues, including the long bones, heart, lungs, and retroperitoneum. Neurologic symptoms such as incoordination can occur. Adult-onset xanthogranuloma manifests as an isolated cutaneous lesion without systemic involvement. This entity often is self-limited and does not require aggressive treatment. Adult-onset asthma with periocular xanthogranuloma affects more males than females.1 Clinically, it manifests as bilateral yellow-orange, thickened, indurated eyelid plaques that can extend to the extraocular muscles or lacrimal glands. As the name suggests, this entity is associated with adult-onset asthma or rhinosinusitis as well as lymphadenopathy and extension into the orbital fat.1
When patients present with periorbital lesions and optic symptoms such as visual disturbances, tearing, and/ or a foreign body sensation in the eyes, a work-up should be performed to rule out infiltration of orbital adnexal structures and other organ systems, as AAPOX can be associated with IgG4-related disease. Histologically, adult xanthogranulomatous diseases are characterized by sheets of foamy histiocytes accompanied by variable numbers of lymphoid aggregates, plasma cells, and Touton giant cells. These infiltrating xanthoma cells appear as a garland or wreathlike nuclei surrounded by foamy cytoplasm. Oil-red O staining of frozen sections confirms the lipid content of the xanthoma cells.2 Immunohistochemically, the foamy histiocytes are strongly positive for CD68, CD163, and factor XIIIa but usually are negative for S100, CD1a and Birbeck granules.3 More distinctively, AAPOX is associated with prominent lymphoid aggregates containing reactive germinal centers.1
Given that AAPOX is a systemic multiorgan disease, local therapies such as surgical debulking or intralesional corticosteroids generally are insufficient to address the underlying pathology and therefore necessitate systemic, often multimodal, treatment within a multidisciplinary framework.1,4 Systemic corticosteroids remain first-line therapy, with steroid-sparing agents (eg, methotrexate, azathioprine, cyclophosphamide) used in refractory cases or to reduce steroid dependence.4,5 Rituximab has demonstrated efficacy in AAPOX, further highlighting the association between AAPOX and IgG4-related disease.5 Inebilizumab, a B-cell–depleting monoclonal antibody targeting CD19 and approved for the treatment of IgG4- related disease, represents a theoretically promising therapeutic option; however, additional studies are needed to establish its efficacy and safety in AAPOX.5
Necrobiotic xanthogranuloma is another xanthogranulomatous disorder that manifests as yellow-orange papules or nodules that gradually form infiltrative plaques. Scarring and ulceration can occur in 40% to 50% of patients.6 The most common site of involvement is the periorbital area, affecting 80% of cases, often resulting in ophthalmologic complications.6 Necrobiotic xanthogranuloma lesions also can involve the trunk, arms, and legs. Extracutaneous sites include the lungs, myocardium, larynx, pharynx, skeletal muscles, kidneys, ovaries, and intestines. The prognosis of NXG is poor due to associated hematologic malignancies such as multiple myeloma and lymphoma. About 80% of patients have a serum monoclonal gammopathy.6 Histologically, NXG shows features overlapping with other xanthogranulomatous disorders, such as foamy histiocytes, multinucleated giant cells, Touton giant cells, and nodular lymphocytic aggregates6,7; however, broad zones of necrobiosis are a distinct histologic finding in NXG that helps differentiate it from other xanthogranulomatous disorders (Figure 1).6
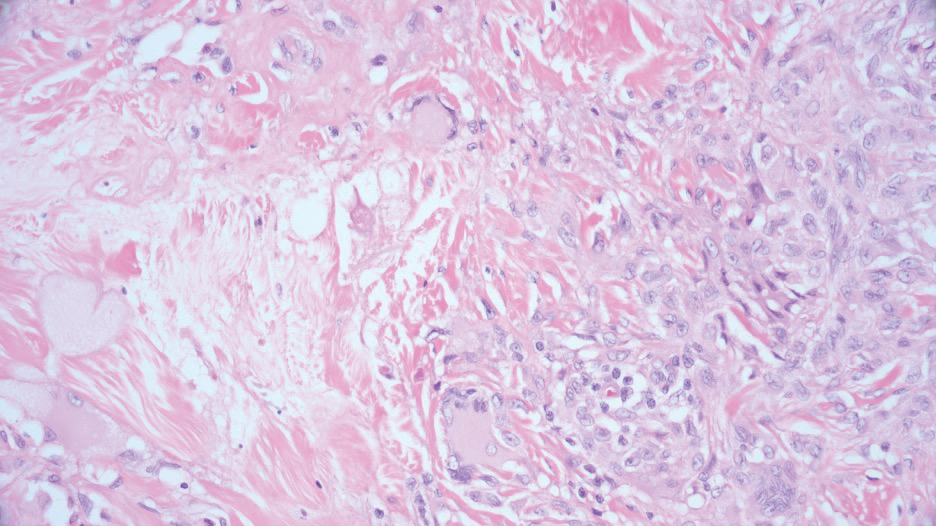
Xanthelasma manifests as yellow plaques on the medial upper and lower eyelids and lateral canthi resulting from accumulation of cholesterol-rich material in the skin, soft tissue, and sometimes the tendons. Fifty percent of patients have a primary or secondary lipid disorder such as familial dyslipidemia, thyroid disease, diabetes mellitus, or primary biliary cholangitis.8 Histologically, xanthelasmas demonstrate lipid-laden foamy histiocytes in the superficial dermis (Figure 2).8 Despite some clinical overlap in our case, the depth of orbital involvement and supportive systemic and histopathologic findings (including Touton giant cells) supported the diagnosis of AAPOX rather than xanthelasma.
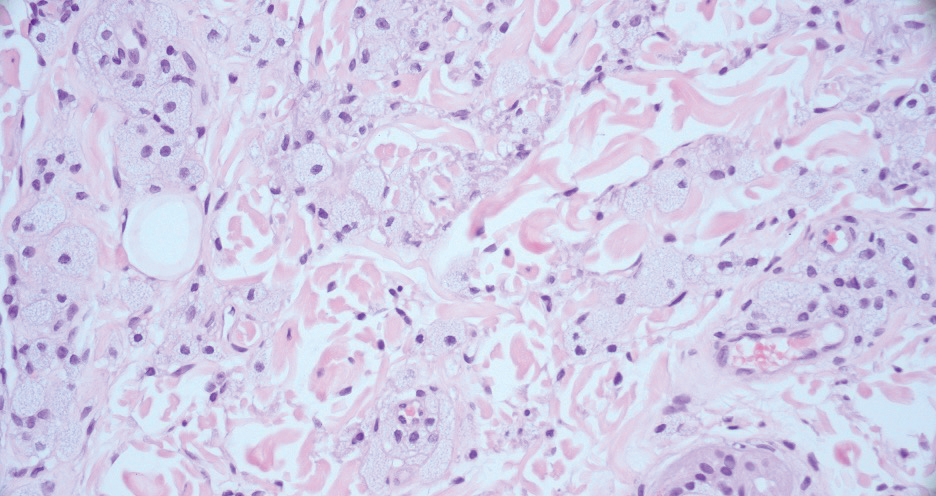
Juvenile xanthogranuloma manifests as solitary to multiple firm, yellow-orange papules or nodules on the face, neck, and upper torso. The lesions develop in early childhood, with 75% of lesions appearing in the first year of life, but rarely it may develop in adulthood.9 The most common extracutaneous manifestation involves ocular structures, most frequently the iris, followed by the lungs. Cutaneous lesions usually are asymptomatic and involute over the span of a few years. Ocular lesions can result in blindness, and juvenile xanthogranuloma also has been associated with neurofibromatosis type 1 and juvenile chronic myelogenous leukemia.9 The histopathology of juvenile xanthogranuloma often will show a dense histiocytic infiltrate in the dermis with blunting of the overlying rete ridges admixed with lymphocytes, plasma cells, and eosinophils. In the more mature phase, foam cells, foreign body giant cells, and Touton giant cells predominate. Touton giant cells have a garlandlike appearance (Figure 3).9
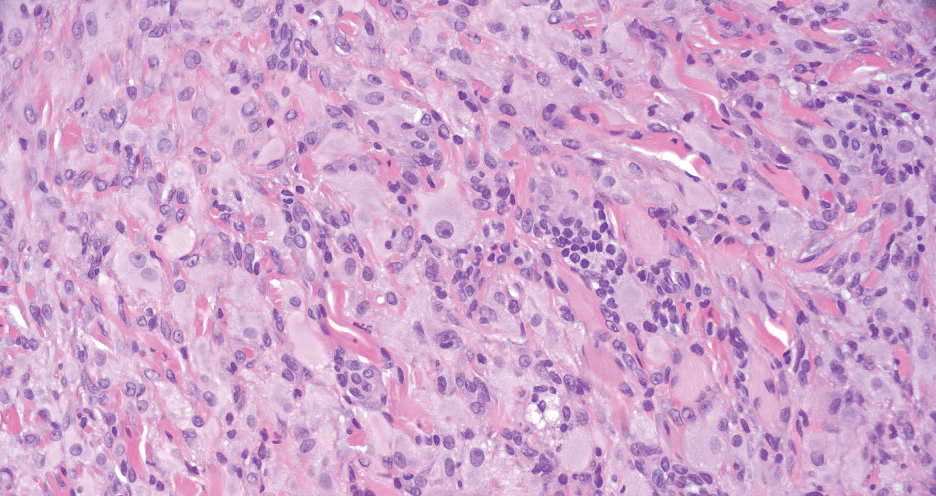
Reticulohistiocytoma (or solitary epithelioid histiocytoma) and multicentric reticulohistiocytosis are rare histiocytic proliferations. Multicentric reticulohistiocytosis refers to a systemic disease with arthropathy and multiple cutaneous histiocytic lesions located on acral sites and the face. Solitary reticulohistiocytoma manifests as papules or nodules found in many body locations, such as the trunk, arms, and legs. The lesions are uncommon on the face, which almost always is involved in multicentric reticulohistiocytosis. Solitary reticulohistiocytomas tend not to recur once excised and do not demonstrate systemic involvement. Histologically, the lesions demonstrate large eosinophilic epithelioid histiocytes with abundant glassy cytoplasm (Figure 4). Some of the epithelioid histiocytes are multinucleated, and immunophenotyping will show positivity for lysozyme, CD68, and CD163.10
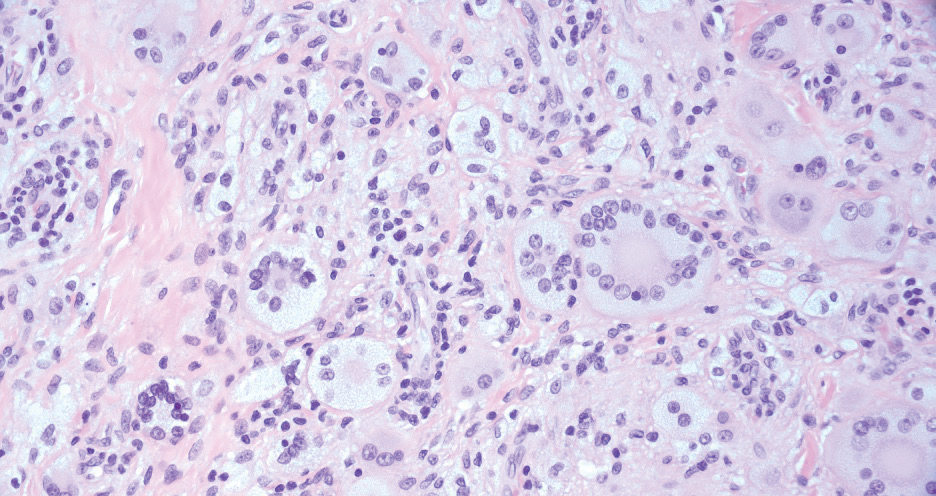
- Kerstetter J, Wang J. Adult orbital xanthogranulomatous disease: a review with emphasis on etiology, systemic associations, diagnostic tools, and treatment. Dermatol Clin. 2015;33:457-463. doi:10.1016 /j.det.2015.03.010
- Mandic` JJ, Bakula M, Šklebar LK, et al. Histiocytosis and adult-onset orbital xanthogranuloma in 2023: a review of the literature and mini case series. Int Ophthalmol. 2024;44:301. doi:10.1007/s10792-024-03181-y
- Campochiaro C, Tomelleri A, Cavalli G, et al. Erdheim-Chester disease. Eur J Intern Med. 2015;26:223-229. doi: 10.1016/j.ejim.2015.03.004
- Detiger SE, Hötte GJ, Verdijk RM, et al. Adult orbital xanthogranuloma: long-term follow-up of treated cases. Eye (Lond). 2023;37:2475-2481. doi: 10.1038/s41433-022-02357-z
- Stone JH, Khosroshahi A, Zhang W, et al. Inebilizumab for treatment of IgG4-related disease. N Engl J Med. 2025;392:1168-1177. doi:10.1056 /NEJMoa2409712
- Wood AJ, Wagner MVU, Abbott JJ, et al. Necrobiotic xanthogranuloma: a review of 17 cases with emphasis on clinical and pathologic correlation. Arch Dermatol. 2009;145:279–284. doi:10.1001 /archdermatol.2008.583
- Schadt C, Jacobsen E. Necrobiotic xanthogranuloma. In: Connor RF, ed. UpToDate. Wolters Kluwer.
- Al Aboud AM, Shah SS, Blair K, et al. Xanthelasma palpebrarum. StatPearls [Internet]. StatPearls Publishing; 2024. Updated March 1, 2024. Accessed February 10, 2026. https://www.ncbi.nlm .nih.gov/books/NBK531501/
- Collie JS, Harper CD, Fillman EP. Juvenile xanthogranuloma. StatPearls [Internet]. StatPearls Publishing; 2024. Updated August 8, 2023. Accessed February 10, 2026. https://www.ncbi.nlm.nih .gov/books/NBK526103/
- Miettinen M, Fetsch JF. Reticulohistiocytoma (solitary epithelioid histiocytoma): a clinicopathologic and immunohistochemical study of 44 cases. Am J Surg Pathol. 2006;30:521-528. doi:10.1097/00000478 -200604000-00014
THE DIAGNOSIS: Adult-Onset Asthma With Periocular Xanthogranuloma
In the context of pre-existing sinonasal disease and features consistent with adult-onset asthma, the constellation of clinical findings including linear periorbital yellow-orange plaques, imaging demonstrating extension of xanthogranulomatous lesions into the orbital fat, histopathologic features, and serologic abnormalities including elevated IgG4 levels supported a diagnosis of adult-onset asthma with periocular xanthogranuloma (AAPOX).
Adult-onset xanthogranuloma is a non–Langerhans cell histiocytosis (historically classified as type II) within the group of adult orbital xanthogranulomatous diseases resulting from infiltration and proliferation of histiocytes in the orbital and ocular adnexal structures and eyelids. Adult orbital xanthogranulomatous diseases are classified as 4 distinct conditions: adult-onset xanthogranuloma, AAPOX, Erdheim-Chester disease, and necrobiotic xanthogranuloma (NXG). Erdheim-Chester disease is the most severe among this group and often is fatal due to infiltration of the xanthogranulomas into multiple organ systems and tissues, including the long bones, heart, lungs, and retroperitoneum. Neurologic symptoms such as incoordination can occur. Adult-onset xanthogranuloma manifests as an isolated cutaneous lesion without systemic involvement. This entity often is self-limited and does not require aggressive treatment. Adult-onset asthma with periocular xanthogranuloma affects more males than females.1 Clinically, it manifests as bilateral yellow-orange, thickened, indurated eyelid plaques that can extend to the extraocular muscles or lacrimal glands. As the name suggests, this entity is associated with adult-onset asthma or rhinosinusitis as well as lymphadenopathy and extension into the orbital fat.1
When patients present with periorbital lesions and optic symptoms such as visual disturbances, tearing, and/ or a foreign body sensation in the eyes, a work-up should be performed to rule out infiltration of orbital adnexal structures and other organ systems, as AAPOX can be associated with IgG4-related disease. Histologically, adult xanthogranulomatous diseases are characterized by sheets of foamy histiocytes accompanied by variable numbers of lymphoid aggregates, plasma cells, and Touton giant cells. These infiltrating xanthoma cells appear as a garland or wreathlike nuclei surrounded by foamy cytoplasm. Oil-red O staining of frozen sections confirms the lipid content of the xanthoma cells.2 Immunohistochemically, the foamy histiocytes are strongly positive for CD68, CD163, and factor XIIIa but usually are negative for S100, CD1a and Birbeck granules.3 More distinctively, AAPOX is associated with prominent lymphoid aggregates containing reactive germinal centers.1
Given that AAPOX is a systemic multiorgan disease, local therapies such as surgical debulking or intralesional corticosteroids generally are insufficient to address the underlying pathology and therefore necessitate systemic, often multimodal, treatment within a multidisciplinary framework.1,4 Systemic corticosteroids remain first-line therapy, with steroid-sparing agents (eg, methotrexate, azathioprine, cyclophosphamide) used in refractory cases or to reduce steroid dependence.4,5 Rituximab has demonstrated efficacy in AAPOX, further highlighting the association between AAPOX and IgG4-related disease.5 Inebilizumab, a B-cell–depleting monoclonal antibody targeting CD19 and approved for the treatment of IgG4- related disease, represents a theoretically promising therapeutic option; however, additional studies are needed to establish its efficacy and safety in AAPOX.5
Necrobiotic xanthogranuloma is another xanthogranulomatous disorder that manifests as yellow-orange papules or nodules that gradually form infiltrative plaques. Scarring and ulceration can occur in 40% to 50% of patients.6 The most common site of involvement is the periorbital area, affecting 80% of cases, often resulting in ophthalmologic complications.6 Necrobiotic xanthogranuloma lesions also can involve the trunk, arms, and legs. Extracutaneous sites include the lungs, myocardium, larynx, pharynx, skeletal muscles, kidneys, ovaries, and intestines. The prognosis of NXG is poor due to associated hematologic malignancies such as multiple myeloma and lymphoma. About 80% of patients have a serum monoclonal gammopathy.6 Histologically, NXG shows features overlapping with other xanthogranulomatous disorders, such as foamy histiocytes, multinucleated giant cells, Touton giant cells, and nodular lymphocytic aggregates6,7; however, broad zones of necrobiosis are a distinct histologic finding in NXG that helps differentiate it from other xanthogranulomatous disorders (Figure 1).6
Xanthelasma manifests as yellow plaques on the medial upper and lower eyelids and lateral canthi resulting from accumulation of cholesterol-rich material in the skin, soft tissue, and sometimes the tendons. Fifty percent of patients have a primary or secondary lipid disorder such as familial dyslipidemia, thyroid disease, diabetes mellitus, or primary biliary cholangitis.8 Histologically, xanthelasmas demonstrate lipid-laden foamy histiocytes in the superficial dermis (Figure 2).8 Despite some clinical overlap in our case, the depth of orbital involvement and supportive systemic and histopathologic findings (including Touton giant cells) supported the diagnosis of AAPOX rather than xanthelasma.
Juvenile xanthogranuloma manifests as solitary to multiple firm, yellow-orange papules or nodules on the face, neck, and upper torso. The lesions develop in early childhood, with 75% of lesions appearing in the first year of life, but rarely it may develop in adulthood.9 The most common extracutaneous manifestation involves ocular structures, most frequently the iris, followed by the lungs. Cutaneous lesions usually are asymptomatic and involute over the span of a few years. Ocular lesions can result in blindness, and juvenile xanthogranuloma also has been associated with neurofibromatosis type 1 and juvenile chronic myelogenous leukemia.9 The histopathology of juvenile xanthogranuloma often will show a dense histiocytic infiltrate in the dermis with blunting of the overlying rete ridges admixed with lymphocytes, plasma cells, and eosinophils. In the more mature phase, foam cells, foreign body giant cells, and Touton giant cells predominate. Touton giant cells have a garlandlike appearance (Figure 3).9
Reticulohistiocytoma (or solitary epithelioid histiocytoma) and multicentric reticulohistiocytosis are rare histiocytic proliferations. Multicentric reticulohistiocytosis refers to a systemic disease with arthropathy and multiple cutaneous histiocytic lesions located on acral sites and the face. Solitary reticulohistiocytoma manifests as papules or nodules found in many body locations, such as the trunk, arms, and legs. The lesions are uncommon on the face, which almost always is involved in multicentric reticulohistiocytosis. Solitary reticulohistiocytomas tend not to recur once excised and do not demonstrate systemic involvement. Histologically, the lesions demonstrate large eosinophilic epithelioid histiocytes with abundant glassy cytoplasm (Figure 4). Some of the epithelioid histiocytes are multinucleated, and immunophenotyping will show positivity for lysozyme, CD68, and CD163.10
THE DIAGNOSIS: Adult-Onset Asthma With Periocular Xanthogranuloma
In the context of pre-existing sinonasal disease and features consistent with adult-onset asthma, the constellation of clinical findings including linear periorbital yellow-orange plaques, imaging demonstrating extension of xanthogranulomatous lesions into the orbital fat, histopathologic features, and serologic abnormalities including elevated IgG4 levels supported a diagnosis of adult-onset asthma with periocular xanthogranuloma (AAPOX).
Adult-onset xanthogranuloma is a non–Langerhans cell histiocytosis (historically classified as type II) within the group of adult orbital xanthogranulomatous diseases resulting from infiltration and proliferation of histiocytes in the orbital and ocular adnexal structures and eyelids. Adult orbital xanthogranulomatous diseases are classified as 4 distinct conditions: adult-onset xanthogranuloma, AAPOX, Erdheim-Chester disease, and necrobiotic xanthogranuloma (NXG). Erdheim-Chester disease is the most severe among this group and often is fatal due to infiltration of the xanthogranulomas into multiple organ systems and tissues, including the long bones, heart, lungs, and retroperitoneum. Neurologic symptoms such as incoordination can occur. Adult-onset xanthogranuloma manifests as an isolated cutaneous lesion without systemic involvement. This entity often is self-limited and does not require aggressive treatment. Adult-onset asthma with periocular xanthogranuloma affects more males than females.1 Clinically, it manifests as bilateral yellow-orange, thickened, indurated eyelid plaques that can extend to the extraocular muscles or lacrimal glands. As the name suggests, this entity is associated with adult-onset asthma or rhinosinusitis as well as lymphadenopathy and extension into the orbital fat.1
When patients present with periorbital lesions and optic symptoms such as visual disturbances, tearing, and/ or a foreign body sensation in the eyes, a work-up should be performed to rule out infiltration of orbital adnexal structures and other organ systems, as AAPOX can be associated with IgG4-related disease. Histologically, adult xanthogranulomatous diseases are characterized by sheets of foamy histiocytes accompanied by variable numbers of lymphoid aggregates, plasma cells, and Touton giant cells. These infiltrating xanthoma cells appear as a garland or wreathlike nuclei surrounded by foamy cytoplasm. Oil-red O staining of frozen sections confirms the lipid content of the xanthoma cells.2 Immunohistochemically, the foamy histiocytes are strongly positive for CD68, CD163, and factor XIIIa but usually are negative for S100, CD1a and Birbeck granules.3 More distinctively, AAPOX is associated with prominent lymphoid aggregates containing reactive germinal centers.1
Given that AAPOX is a systemic multiorgan disease, local therapies such as surgical debulking or intralesional corticosteroids generally are insufficient to address the underlying pathology and therefore necessitate systemic, often multimodal, treatment within a multidisciplinary framework.1,4 Systemic corticosteroids remain first-line therapy, with steroid-sparing agents (eg, methotrexate, azathioprine, cyclophosphamide) used in refractory cases or to reduce steroid dependence.4,5 Rituximab has demonstrated efficacy in AAPOX, further highlighting the association between AAPOX and IgG4-related disease.5 Inebilizumab, a B-cell–depleting monoclonal antibody targeting CD19 and approved for the treatment of IgG4- related disease, represents a theoretically promising therapeutic option; however, additional studies are needed to establish its efficacy and safety in AAPOX.5
Necrobiotic xanthogranuloma is another xanthogranulomatous disorder that manifests as yellow-orange papules or nodules that gradually form infiltrative plaques. Scarring and ulceration can occur in 40% to 50% of patients.6 The most common site of involvement is the periorbital area, affecting 80% of cases, often resulting in ophthalmologic complications.6 Necrobiotic xanthogranuloma lesions also can involve the trunk, arms, and legs. Extracutaneous sites include the lungs, myocardium, larynx, pharynx, skeletal muscles, kidneys, ovaries, and intestines. The prognosis of NXG is poor due to associated hematologic malignancies such as multiple myeloma and lymphoma. About 80% of patients have a serum monoclonal gammopathy.6 Histologically, NXG shows features overlapping with other xanthogranulomatous disorders, such as foamy histiocytes, multinucleated giant cells, Touton giant cells, and nodular lymphocytic aggregates6,7; however, broad zones of necrobiosis are a distinct histologic finding in NXG that helps differentiate it from other xanthogranulomatous disorders (Figure 1).6
Xanthelasma manifests as yellow plaques on the medial upper and lower eyelids and lateral canthi resulting from accumulation of cholesterol-rich material in the skin, soft tissue, and sometimes the tendons. Fifty percent of patients have a primary or secondary lipid disorder such as familial dyslipidemia, thyroid disease, diabetes mellitus, or primary biliary cholangitis.8 Histologically, xanthelasmas demonstrate lipid-laden foamy histiocytes in the superficial dermis (Figure 2).8 Despite some clinical overlap in our case, the depth of orbital involvement and supportive systemic and histopathologic findings (including Touton giant cells) supported the diagnosis of AAPOX rather than xanthelasma.
Juvenile xanthogranuloma manifests as solitary to multiple firm, yellow-orange papules or nodules on the face, neck, and upper torso. The lesions develop in early childhood, with 75% of lesions appearing in the first year of life, but rarely it may develop in adulthood.9 The most common extracutaneous manifestation involves ocular structures, most frequently the iris, followed by the lungs. Cutaneous lesions usually are asymptomatic and involute over the span of a few years. Ocular lesions can result in blindness, and juvenile xanthogranuloma also has been associated with neurofibromatosis type 1 and juvenile chronic myelogenous leukemia.9 The histopathology of juvenile xanthogranuloma often will show a dense histiocytic infiltrate in the dermis with blunting of the overlying rete ridges admixed with lymphocytes, plasma cells, and eosinophils. In the more mature phase, foam cells, foreign body giant cells, and Touton giant cells predominate. Touton giant cells have a garlandlike appearance (Figure 3).9
Reticulohistiocytoma (or solitary epithelioid histiocytoma) and multicentric reticulohistiocytosis are rare histiocytic proliferations. Multicentric reticulohistiocytosis refers to a systemic disease with arthropathy and multiple cutaneous histiocytic lesions located on acral sites and the face. Solitary reticulohistiocytoma manifests as papules or nodules found in many body locations, such as the trunk, arms, and legs. The lesions are uncommon on the face, which almost always is involved in multicentric reticulohistiocytosis. Solitary reticulohistiocytomas tend not to recur once excised and do not demonstrate systemic involvement. Histologically, the lesions demonstrate large eosinophilic epithelioid histiocytes with abundant glassy cytoplasm (Figure 4). Some of the epithelioid histiocytes are multinucleated, and immunophenotyping will show positivity for lysozyme, CD68, and CD163.10
- Kerstetter J, Wang J. Adult orbital xanthogranulomatous disease: a review with emphasis on etiology, systemic associations, diagnostic tools, and treatment. Dermatol Clin. 2015;33:457-463. doi:10.1016 /j.det.2015.03.010
- Mandic` JJ, Bakula M, Šklebar LK, et al. Histiocytosis and adult-onset orbital xanthogranuloma in 2023: a review of the literature and mini case series. Int Ophthalmol. 2024;44:301. doi:10.1007/s10792-024-03181-y
- Campochiaro C, Tomelleri A, Cavalli G, et al. Erdheim-Chester disease. Eur J Intern Med. 2015;26:223-229. doi: 10.1016/j.ejim.2015.03.004
- Detiger SE, Hötte GJ, Verdijk RM, et al. Adult orbital xanthogranuloma: long-term follow-up of treated cases. Eye (Lond). 2023;37:2475-2481. doi: 10.1038/s41433-022-02357-z
- Stone JH, Khosroshahi A, Zhang W, et al. Inebilizumab for treatment of IgG4-related disease. N Engl J Med. 2025;392:1168-1177. doi:10.1056 /NEJMoa2409712
- Wood AJ, Wagner MVU, Abbott JJ, et al. Necrobiotic xanthogranuloma: a review of 17 cases with emphasis on clinical and pathologic correlation. Arch Dermatol. 2009;145:279–284. doi:10.1001 /archdermatol.2008.583
- Schadt C, Jacobsen E. Necrobiotic xanthogranuloma. In: Connor RF, ed. UpToDate. Wolters Kluwer.
- Al Aboud AM, Shah SS, Blair K, et al. Xanthelasma palpebrarum. StatPearls [Internet]. StatPearls Publishing; 2024. Updated March 1, 2024. Accessed February 10, 2026. https://www.ncbi.nlm .nih.gov/books/NBK531501/
- Collie JS, Harper CD, Fillman EP. Juvenile xanthogranuloma. StatPearls [Internet]. StatPearls Publishing; 2024. Updated August 8, 2023. Accessed February 10, 2026. https://www.ncbi.nlm.nih .gov/books/NBK526103/
- Miettinen M, Fetsch JF. Reticulohistiocytoma (solitary epithelioid histiocytoma): a clinicopathologic and immunohistochemical study of 44 cases. Am J Surg Pathol. 2006;30:521-528. doi:10.1097/00000478 -200604000-00014
- Kerstetter J, Wang J. Adult orbital xanthogranulomatous disease: a review with emphasis on etiology, systemic associations, diagnostic tools, and treatment. Dermatol Clin. 2015;33:457-463. doi:10.1016 /j.det.2015.03.010
- Mandic` JJ, Bakula M, Šklebar LK, et al. Histiocytosis and adult-onset orbital xanthogranuloma in 2023: a review of the literature and mini case series. Int Ophthalmol. 2024;44:301. doi:10.1007/s10792-024-03181-y
- Campochiaro C, Tomelleri A, Cavalli G, et al. Erdheim-Chester disease. Eur J Intern Med. 2015;26:223-229. doi: 10.1016/j.ejim.2015.03.004
- Detiger SE, Hötte GJ, Verdijk RM, et al. Adult orbital xanthogranuloma: long-term follow-up of treated cases. Eye (Lond). 2023;37:2475-2481. doi: 10.1038/s41433-022-02357-z
- Stone JH, Khosroshahi A, Zhang W, et al. Inebilizumab for treatment of IgG4-related disease. N Engl J Med. 2025;392:1168-1177. doi:10.1056 /NEJMoa2409712
- Wood AJ, Wagner MVU, Abbott JJ, et al. Necrobiotic xanthogranuloma: a review of 17 cases with emphasis on clinical and pathologic correlation. Arch Dermatol. 2009;145:279–284. doi:10.1001 /archdermatol.2008.583
- Schadt C, Jacobsen E. Necrobiotic xanthogranuloma. In: Connor RF, ed. UpToDate. Wolters Kluwer.
- Al Aboud AM, Shah SS, Blair K, et al. Xanthelasma palpebrarum. StatPearls [Internet]. StatPearls Publishing; 2024. Updated March 1, 2024. Accessed February 10, 2026. https://www.ncbi.nlm .nih.gov/books/NBK531501/
- Collie JS, Harper CD, Fillman EP. Juvenile xanthogranuloma. StatPearls [Internet]. StatPearls Publishing; 2024. Updated August 8, 2023. Accessed February 10, 2026. https://www.ncbi.nlm.nih .gov/books/NBK526103/
- Miettinen M, Fetsch JF. Reticulohistiocytoma (solitary epithelioid histiocytoma): a clinicopathologic and immunohistochemical study of 44 cases. Am J Surg Pathol. 2006;30:521-528. doi:10.1097/00000478 -200604000-00014
Thick Yellow Plaques on the Eyelids
Thick Yellow Plaques on the Eyelids
A 54-year-old man presented to the dermatology department for evaluation of enlarging lesions on the eyelids of 18 months’ duration causing tearing, dryness, and heaviness. The patient’s medical history was positive for hyperlipidemia, chronic rhinosinusitis, and mild asthma diagnosed in adulthood. A review of systems was negative for bone pain, polyuria, polydipsia, dysuria, hematuria, decreased coordination, chest pain, palpitations, abdominal pain, easy bruising, and jaundice. Laboratory testing revealed elevated IgG4 levels and a slight increase in gamma globulins on serum protein electrophoresis, with no evidence of paraproteinemia. Liver and kidney function test results were within normal limits. Magnetic resonance imaging of the orbits revealed bilateral superolateral intraorbital masses within the extraconal fat that were displacing the superior and lateral rectus muscles. No intraconal masses were identified. Due to bilateral eyelid ptosis, the patient underwent debulking by oculoplastic surgery, and the tissue was submitted for histologic examination.
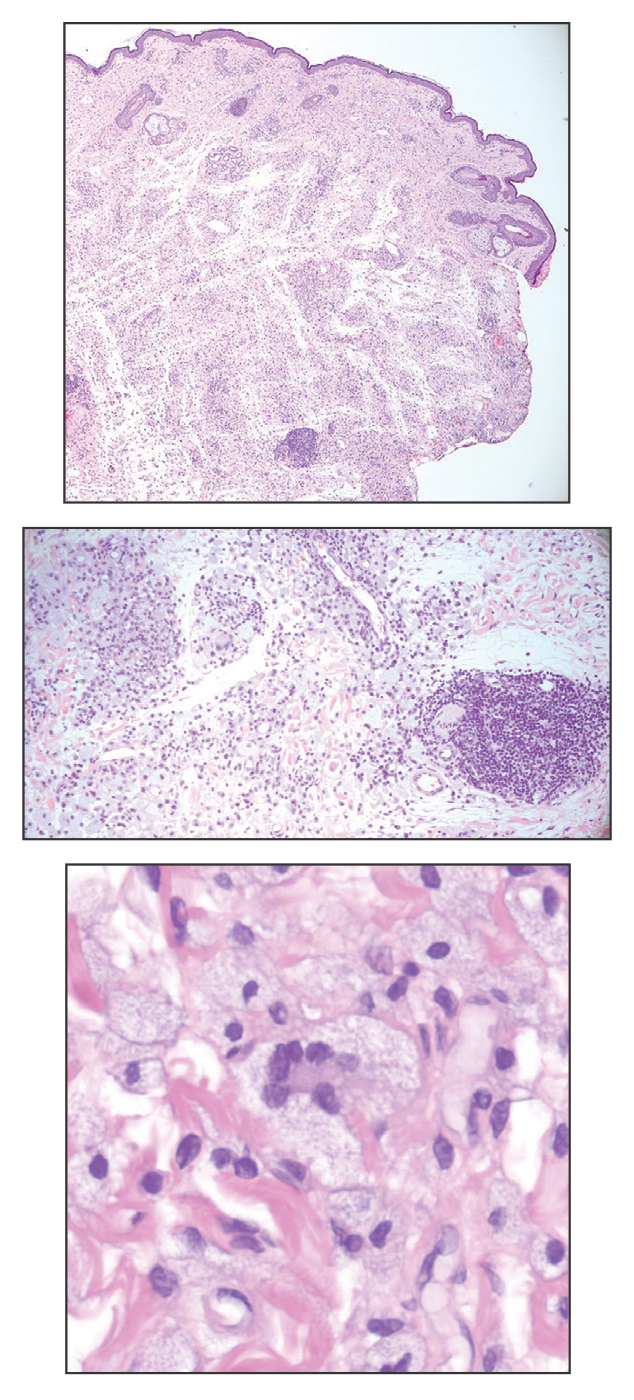

Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael
Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael
How do you distinguish active cicatricial alopecia from chronic nonprogressive hair loss in patients with skin of color, and which clinical or trichoscopic features suggest ongoing inflammation requiring treatment?
DR. McMICHAEL: Typically, I use trichoscopy to help determine if there are fine or vellus hairs in the affected area. Often, if there are vellus hairs, that means there is the potential to lengthen growth time and have thicker longer hairs in the area, even in a chronic nonprogressive hair loss state. If there is clinical or trichoscopic erythema (suggesting inflammation), that is a sure sign of active scarring. Patient-reported symptoms of itch, stinging, or pain are a sign of active scarring as well. Finally, even if none of the above are true, a biopsy can help determine if there is active inflammation, as can increasing size of the affected area on the scalp upon return visit to the clinic.
What is your initial diagnostic workup for suspected scarring alopecia in patients with skin of color, including key history, trichoscopy, and biopsy approach?
DR. McMICHAEL: In terms of historical info, I want to know how long the patient has had hair loss, what symptoms they have/had, and if there is a family history of hair loss. Also, if the patient has been treated in the past, it is helpful to know if any of the previous treatments worked. For me, the clinical exam is going to tell the most. Just the clinical location will give the first cues, followed by trichoscopy. I don’t biopsy every patient, but when there is any doubt about the form of hair loss the patient has, biopsy is important. I use the dermatoscope to guide the biopsy and perform two 4-mm punch biopsies in the appropriate area.
How do you manage active inflammatory scarring alopecias in skin of color, including first-line therapies and criteria for escalation?
DR. McMICHAEL: I like to discuss and give guidance on hair care first. Sometimes this will include increased frequency of hair washing and/or use of an antidandruff shampoo. Next, I usually start patients on a potent or ultrapotent steroid several times per week. If there is very symptomatic or clinically raging inflammation, I will begin either an oral antibiotic for 3 to 6 months or a series of intralesional steroids. Depending on the condition and patient preference, a stronger anti-inflammatory agent such as hydroxychloroquine, methotrexate, or dapsone may be used. Monitoring depends on the medication that is started. Many of the anti-inflammatory medications require laboratory monitoring every 4 or 6 months, and the drug dictates this timing. For monitoring of disease progression, questions for the patient on continued symptoms and serial clinical and trichoscopic photographs make the difference.
When and how do you use adjunctive or emerging therapies for scarring alopecias in skin of color, and what evidence and outcomes guide their use?
DR. McMICHAEL: Our research group has shown via small clinical trials and case series that both platelet-rich plasma and low-level laser light can be helpful for central centrifugal cicatricial alopecia, so I tend to begin these treatments once the inflammation is at a mild or minimal level. I often begin low-dose oral minoxidil right at the start or at any time during the course of treatment. I do not use topical minoxidil when the patient is symptomatic but often use this when patients are asymptomatic and do not wish to take oral minoxidil. There are now good case series to show minoxidil can be helpful for scarring forms of alopecia. Patients can show improvement on these treatments, but I only promise stabilization. It is difficult to predict who will have increased growth prior to treatment, and that is what I tell patients.
When are surgical options appropriate for scarring alopecia in patients with skin of color, and what precautions or criteria are required?
DR. McMICHAEL: Once everything has been done medically for scarring alopecia, surgical options can be considered. Unfortunately, these options typically are not covered by insurance, so patients have to be willing and able to pay out of pocket. Other criteria include that patients must have quiescent inflammation and enough donor hair for hair restoration via transplant. I do not personally perform hair transplantation, but I do like to refer patients with tightly coiled hair and scarring alopecia to physicians who specialize in this kind of treatment. Not all transplant surgeons have experience with skin of color or follicular unit extraction, which is sometimes needed.
What culturally tailored strategies help prevent scarring alopecia in patients with skin of color, and where are research or practice gaps?
DR. McMICHAEL: For all patients, it is important to ask about daily hair care practices, hair care at the salon, and night-time hair care before making recommendations. Any hair style that puts tension on the hair shaft needs to be discontinued as do those that are tight around the frontal or posterior hair line. Hair washing should be once per week or every 2 weeks at the least, and conditioning of the hair is important with hair trims every 2 to 3 months.
How do you distinguish active cicatricial alopecia from chronic nonprogressive hair loss in patients with skin of color, and which clinical or trichoscopic features suggest ongoing inflammation requiring treatment?
DR. McMICHAEL: Typically, I use trichoscopy to help determine if there are fine or vellus hairs in the affected area. Often, if there are vellus hairs, that means there is the potential to lengthen growth time and have thicker longer hairs in the area, even in a chronic nonprogressive hair loss state. If there is clinical or trichoscopic erythema (suggesting inflammation), that is a sure sign of active scarring. Patient-reported symptoms of itch, stinging, or pain are a sign of active scarring as well. Finally, even if none of the above are true, a biopsy can help determine if there is active inflammation, as can increasing size of the affected area on the scalp upon return visit to the clinic.
What is your initial diagnostic workup for suspected scarring alopecia in patients with skin of color, including key history, trichoscopy, and biopsy approach?
DR. McMICHAEL: In terms of historical info, I want to know how long the patient has had hair loss, what symptoms they have/had, and if there is a family history of hair loss. Also, if the patient has been treated in the past, it is helpful to know if any of the previous treatments worked. For me, the clinical exam is going to tell the most. Just the clinical location will give the first cues, followed by trichoscopy. I don’t biopsy every patient, but when there is any doubt about the form of hair loss the patient has, biopsy is important. I use the dermatoscope to guide the biopsy and perform two 4-mm punch biopsies in the appropriate area.
How do you manage active inflammatory scarring alopecias in skin of color, including first-line therapies and criteria for escalation?
DR. McMICHAEL: I like to discuss and give guidance on hair care first. Sometimes this will include increased frequency of hair washing and/or use of an antidandruff shampoo. Next, I usually start patients on a potent or ultrapotent steroid several times per week. If there is very symptomatic or clinically raging inflammation, I will begin either an oral antibiotic for 3 to 6 months or a series of intralesional steroids. Depending on the condition and patient preference, a stronger anti-inflammatory agent such as hydroxychloroquine, methotrexate, or dapsone may be used. Monitoring depends on the medication that is started. Many of the anti-inflammatory medications require laboratory monitoring every 4 or 6 months, and the drug dictates this timing. For monitoring of disease progression, questions for the patient on continued symptoms and serial clinical and trichoscopic photographs make the difference.
When and how do you use adjunctive or emerging therapies for scarring alopecias in skin of color, and what evidence and outcomes guide their use?
DR. McMICHAEL: Our research group has shown via small clinical trials and case series that both platelet-rich plasma and low-level laser light can be helpful for central centrifugal cicatricial alopecia, so I tend to begin these treatments once the inflammation is at a mild or minimal level. I often begin low-dose oral minoxidil right at the start or at any time during the course of treatment. I do not use topical minoxidil when the patient is symptomatic but often use this when patients are asymptomatic and do not wish to take oral minoxidil. There are now good case series to show minoxidil can be helpful for scarring forms of alopecia. Patients can show improvement on these treatments, but I only promise stabilization. It is difficult to predict who will have increased growth prior to treatment, and that is what I tell patients.
When are surgical options appropriate for scarring alopecia in patients with skin of color, and what precautions or criteria are required?
DR. McMICHAEL: Once everything has been done medically for scarring alopecia, surgical options can be considered. Unfortunately, these options typically are not covered by insurance, so patients have to be willing and able to pay out of pocket. Other criteria include that patients must have quiescent inflammation and enough donor hair for hair restoration via transplant. I do not personally perform hair transplantation, but I do like to refer patients with tightly coiled hair and scarring alopecia to physicians who specialize in this kind of treatment. Not all transplant surgeons have experience with skin of color or follicular unit extraction, which is sometimes needed.
What culturally tailored strategies help prevent scarring alopecia in patients with skin of color, and where are research or practice gaps?
DR. McMICHAEL: For all patients, it is important to ask about daily hair care practices, hair care at the salon, and night-time hair care before making recommendations. Any hair style that puts tension on the hair shaft needs to be discontinued as do those that are tight around the frontal or posterior hair line. Hair washing should be once per week or every 2 weeks at the least, and conditioning of the hair is important with hair trims every 2 to 3 months.
How do you distinguish active cicatricial alopecia from chronic nonprogressive hair loss in patients with skin of color, and which clinical or trichoscopic features suggest ongoing inflammation requiring treatment?
DR. McMICHAEL: Typically, I use trichoscopy to help determine if there are fine or vellus hairs in the affected area. Often, if there are vellus hairs, that means there is the potential to lengthen growth time and have thicker longer hairs in the area, even in a chronic nonprogressive hair loss state. If there is clinical or trichoscopic erythema (suggesting inflammation), that is a sure sign of active scarring. Patient-reported symptoms of itch, stinging, or pain are a sign of active scarring as well. Finally, even if none of the above are true, a biopsy can help determine if there is active inflammation, as can increasing size of the affected area on the scalp upon return visit to the clinic.
What is your initial diagnostic workup for suspected scarring alopecia in patients with skin of color, including key history, trichoscopy, and biopsy approach?
DR. McMICHAEL: In terms of historical info, I want to know how long the patient has had hair loss, what symptoms they have/had, and if there is a family history of hair loss. Also, if the patient has been treated in the past, it is helpful to know if any of the previous treatments worked. For me, the clinical exam is going to tell the most. Just the clinical location will give the first cues, followed by trichoscopy. I don’t biopsy every patient, but when there is any doubt about the form of hair loss the patient has, biopsy is important. I use the dermatoscope to guide the biopsy and perform two 4-mm punch biopsies in the appropriate area.
How do you manage active inflammatory scarring alopecias in skin of color, including first-line therapies and criteria for escalation?
DR. McMICHAEL: I like to discuss and give guidance on hair care first. Sometimes this will include increased frequency of hair washing and/or use of an antidandruff shampoo. Next, I usually start patients on a potent or ultrapotent steroid several times per week. If there is very symptomatic or clinically raging inflammation, I will begin either an oral antibiotic for 3 to 6 months or a series of intralesional steroids. Depending on the condition and patient preference, a stronger anti-inflammatory agent such as hydroxychloroquine, methotrexate, or dapsone may be used. Monitoring depends on the medication that is started. Many of the anti-inflammatory medications require laboratory monitoring every 4 or 6 months, and the drug dictates this timing. For monitoring of disease progression, questions for the patient on continued symptoms and serial clinical and trichoscopic photographs make the difference.
When and how do you use adjunctive or emerging therapies for scarring alopecias in skin of color, and what evidence and outcomes guide their use?
DR. McMICHAEL: Our research group has shown via small clinical trials and case series that both platelet-rich plasma and low-level laser light can be helpful for central centrifugal cicatricial alopecia, so I tend to begin these treatments once the inflammation is at a mild or minimal level. I often begin low-dose oral minoxidil right at the start or at any time during the course of treatment. I do not use topical minoxidil when the patient is symptomatic but often use this when patients are asymptomatic and do not wish to take oral minoxidil. There are now good case series to show minoxidil can be helpful for scarring forms of alopecia. Patients can show improvement on these treatments, but I only promise stabilization. It is difficult to predict who will have increased growth prior to treatment, and that is what I tell patients.
When are surgical options appropriate for scarring alopecia in patients with skin of color, and what precautions or criteria are required?
DR. McMICHAEL: Once everything has been done medically for scarring alopecia, surgical options can be considered. Unfortunately, these options typically are not covered by insurance, so patients have to be willing and able to pay out of pocket. Other criteria include that patients must have quiescent inflammation and enough donor hair for hair restoration via transplant. I do not personally perform hair transplantation, but I do like to refer patients with tightly coiled hair and scarring alopecia to physicians who specialize in this kind of treatment. Not all transplant surgeons have experience with skin of color or follicular unit extraction, which is sometimes needed.
What culturally tailored strategies help prevent scarring alopecia in patients with skin of color, and where are research or practice gaps?
DR. McMICHAEL: For all patients, it is important to ask about daily hair care practices, hair care at the salon, and night-time hair care before making recommendations. Any hair style that puts tension on the hair shaft needs to be discontinued as do those that are tight around the frontal or posterior hair line. Hair washing should be once per week or every 2 weeks at the least, and conditioning of the hair is important with hair trims every 2 to 3 months.
Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael
Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael

Evaluating GPT-4o for Automated Classification of Skin Lesions Using the HAM10000 Dataset
Evaluating GPT-4o for Automated Classification of Skin Lesions Using the HAM10000 Dataset
To the Editor:
The widespread availability and popularity of ChatGPT (OpenAI) have sparked interest in its potential applications within various fields, including medical diagnostics.1 In dermatology, large language models (LLMs) already are being cited as a possible way to reliably respond to common patient queries and produce concise patient education materials.2,3 That being said, there is skepticism regarding the technology’s efficacy and reliability in producing accurate treatment plans, with variability among popular LLMs; for example, a recent study by Chau et al4 demonstrated that ChatGPT was best at providing specific and accurate information regarding patient-facing responses to questions about 5 dermatologic diagnoses compared to Google Bard (now rebranded as Google Gemini) and Bing AI (now rebranded as Microsoft Copilot), which more often produced inaccurate or nonspecific responses. Google Bard also declined to answer one prompt.4 Large language models also have been evaluated in diagnosing skin lesions. In 2024, SkinGPT-4 (a pretrained multimodel LLM developed by Zhou et al5) achieved just over 80% accuracy in interpreting images of skin lesions and was considered informative by 82.5% of board-certified dermatologists, demonstrating that LLMs may have the potential to become integrated into clinical practice.5
Our study aimed to evaluate the performance of GPT-4o (OpenAI)—a widely accessible, low-cost LLM—in diagnosing dermatologic conditions using the HAM10000 dataset, a well-curated collection of dermatoscopic images developed for training and benchmarking artificial intelligence (AI) algorithms.6 HAM10000 comprises images representing 7 distinct skin conditions: actinic keratoses (ak), basal cell carcinoma (bcc), benign keratosis (bk), dermatofibroma (df), melanoma (mel), melanocytic nevi (nv), and vascular skin lesions (vsl), providing a robust platform for multiclass classification assessment. We evaluated GPT-4o using 100 dermatoscopic images per condition to assess diagnostic accuracy, potential biases, and limitations in skin lesion identification. The HAM10000 dataset was selected because it offers a large standardized reference set of dermatoscopic (rather than conventional clinical) images commonly used in dermatologic AI research. GPT-4o was chosen due to its patient-friendly interface, widespread use, and prior reports suggesting greater reliability in skin lesion assessment compared with other LLMs.
One hundred images from each of the 7 dermatologic categories were randomly selected for use in our analysis in 2024. The images were selected by our data scientist (J.C.) through random sampling from the dataset. Each image was separately presented to GPT-4o without any preprocessing or modification alongside 2 prompts designed to evaluate the diagnostic capabilities of GPT-4o. Both prompts included the same list of 7 dermatologic conditions for answer choices but differed in contextual information, where prompt 1 provided patient demographic information and localization of the dermatological condition but prompt 2 did not provide these details (Table). No follow-up questions were presented.
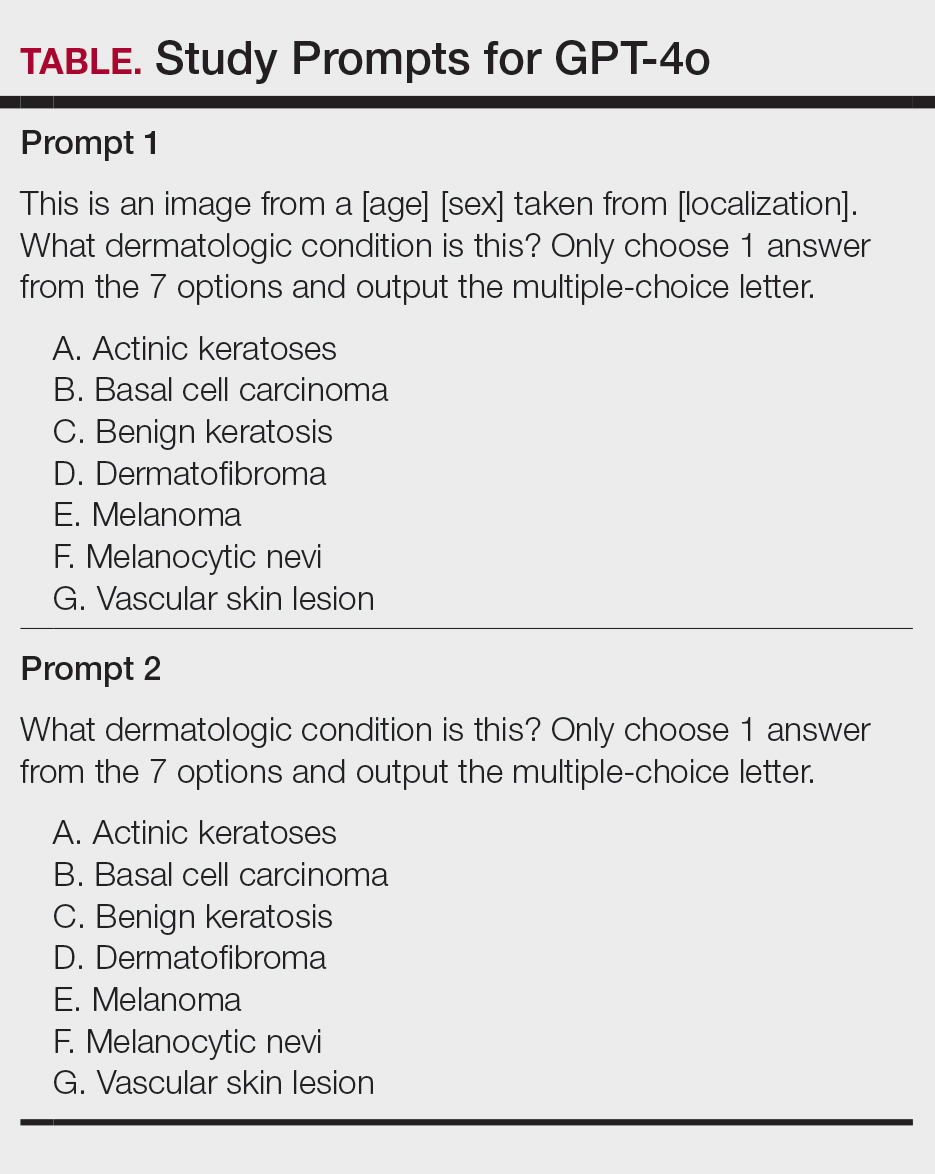
For prompt 1, the confusion matrix showed a strong bias toward detecting mel and bcc, with high true positives (mel, 83%; bcc, 37%)(eFigure 1). This pattern possibly suggests a tendency to favor malignant labels (eg, mel, BCC) when uncertainty is present. Interestingly, df and vsl also had notable true positives (46% and 37%, respectively), which is unexpected for less critical conditions because the model’s correct classifications were uneven across benign lesions. Actinic keratoses and nv showed higher misclassification rates, suggesting the model struggled to distinguish them from other lesions.
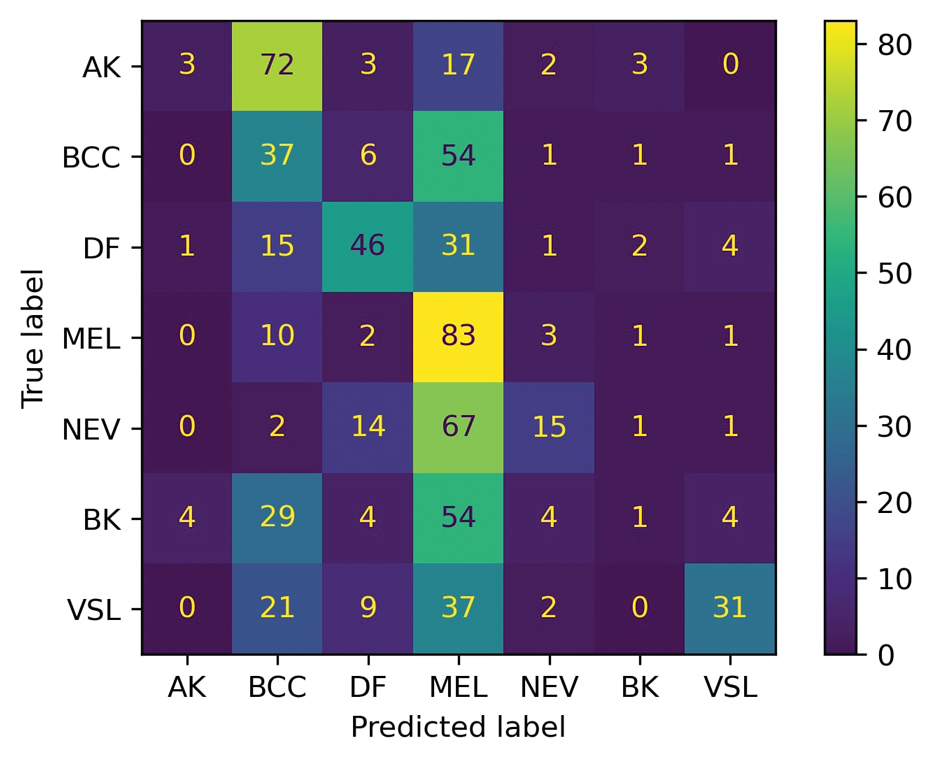
As shown in eTable 1, prompt 1 exhibited the highest recall for mel at 0.83 but performed worse in precision (0.242) and specificity (0.567) compared to ak, which had an extremely low recall (0.03) but very high specificity (0.992) and moderate precision score (0.375). The highest precision score was seen with vsl (0.738), which also achieved high scores in specificity (0.982) and accuracy (0.88) and performed moderately well in recall (0.31). All performance metrics are reported as proportions (0-1.0), wherein 1.0 indicates 100.
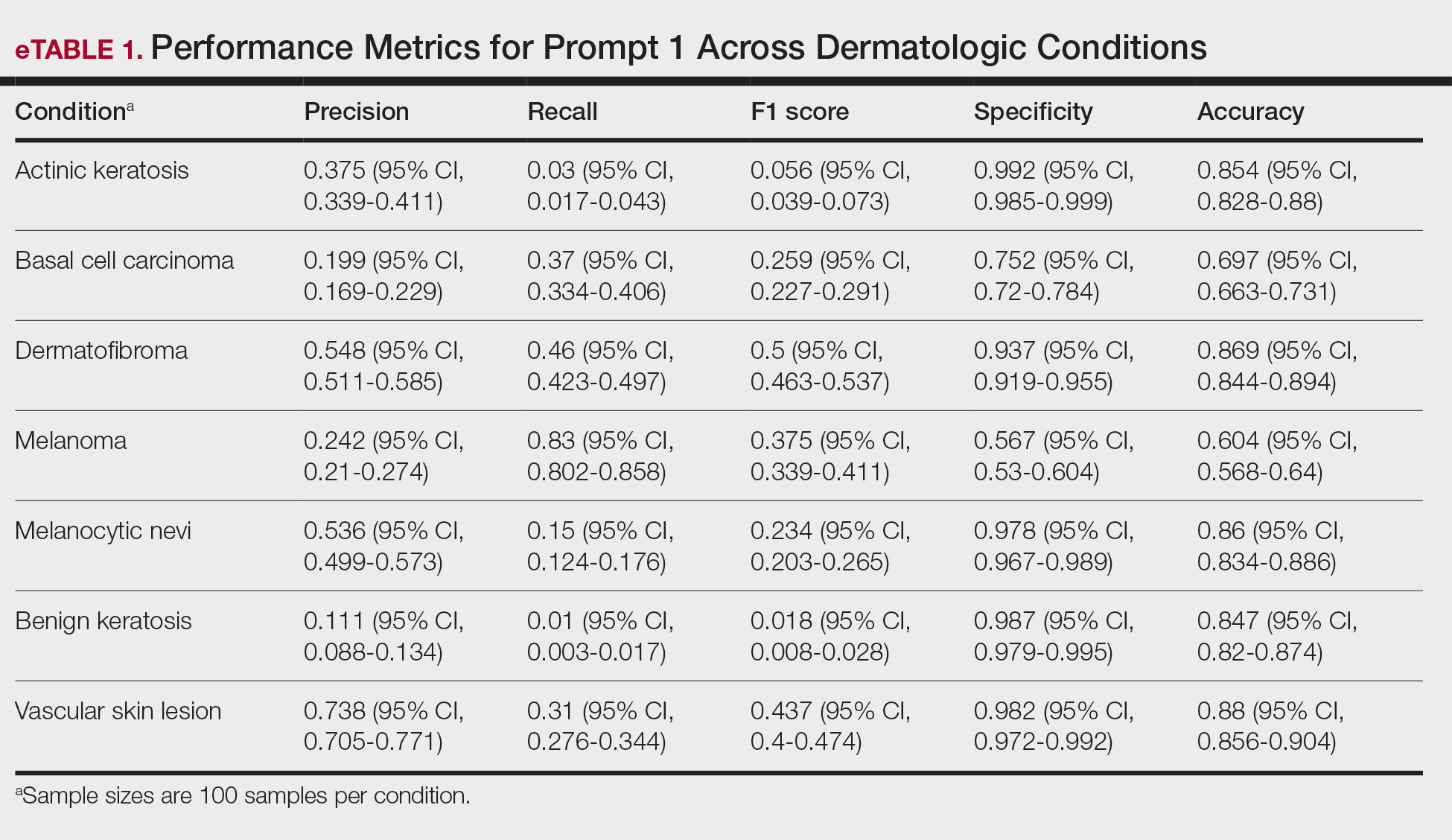
For prompt 2, the second confusion matrix followed similar trends as prompt 1 but still differed in key areas (eFigure 2). Melanoma detection remained strong (true positives, 95%), while bcc shows slightly fewer true positives (24%). Vascular skin lesions improve in true positives (40%), and df dropped slightly (33%). The model continues to struggle with ak and nv, with notable misclassifications observed across other categories
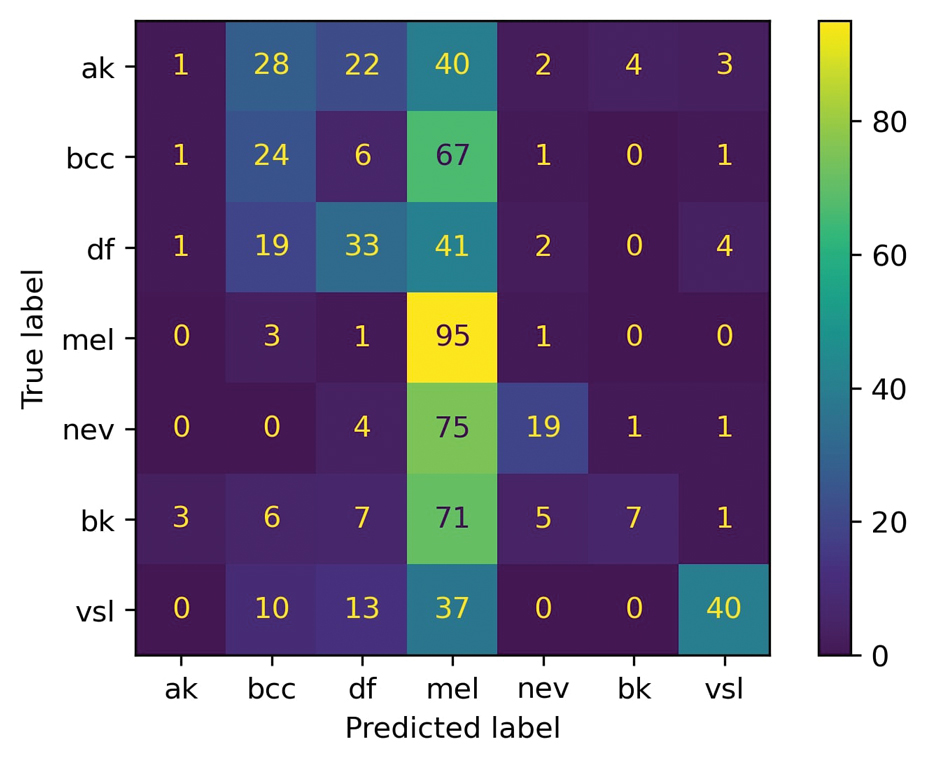
Similar to prompt 1, prompt 2 achieved its highest recall for mel (0.95%), but demonstrated lower precision (0.223%) and specificity (0.488%) for this class. Prompt 2 also produced the highest accuracy for vascular skin lesions (0.90%). The highest specificity was observed for both bk and ak (0.992% each); however, ak again demonstrated the lowest recall, with a value of 0.01%.
A previous study utilizing a model of binary classification to distinguish between mel and benign dermatologic conditions demonstrated poor performance.1 Additionally, prior studies have employed a less-strict, open-ended style question approach to examine ChatGPT’s ability to diagnose mel with limited efficacy.7 The HAM10000 dataset was specifically selected despite its limitations (including the absence of clinical images and limited diversity in skin tones) due to its comprehensive nature, robust annotation standards, and widespread acceptance in dermatologic AI research. Compared to the Diverse Dermatology Images dataset, which notably lacks skin tone diversity, HAM10000 provides a balanced representation of several dermatologic conditions crucial for multiclass classification tasks, making it suitable for benchmarking AI performance. This study aimed to eliminate these limitations by employing a multiclass classification approach; however, despite this switch, our results indicate continued and major limitations of the diagnostic capabilities of GPT-4o.
In its current form, GPT-4o appeared to demonstrate a clear accuracy bias toward correctly identifying specific and severe dermatologic conditions (eg, mel, bcc) but showed low and variable class-level performance for other categories (eg, ak, nv, df, vsl), with frequent misclassification into melanoma or basal cell carcinoma and low recall for some classes (eTables 1 and 2). This finding emphasized that GPT-4o currently lacks the reliability needed for real-life clinical applications in dermatology, as both binary and multiclass models fail to achieve consistent accurate performance across all skin conditions. Notably, GPT-4o may generate false-positive malignant classifications among patients due to its skew in predicted labels toward labeling benign lesions as malignant.
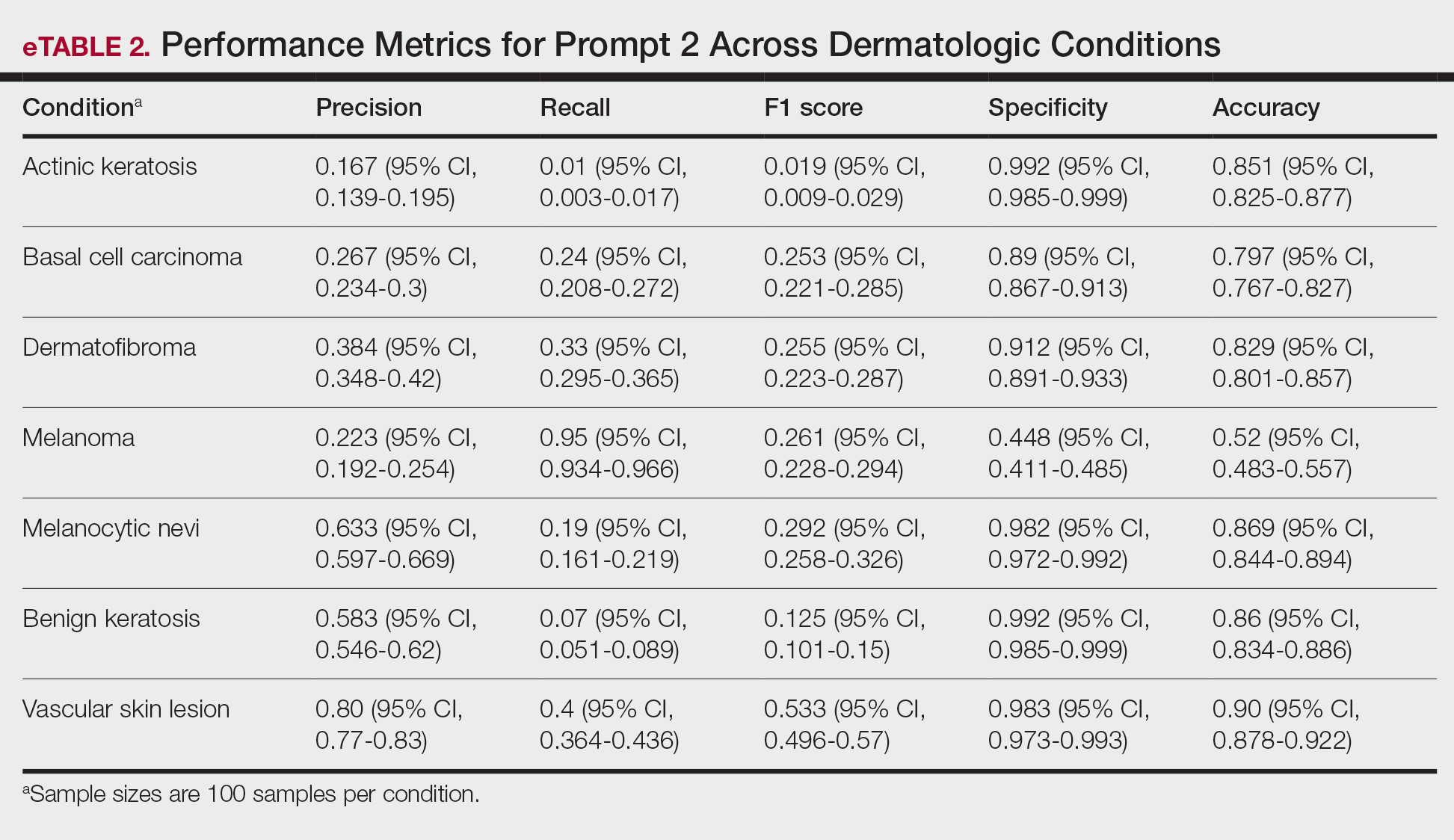
From the patient perspective, younger individuals may upload images of benign nevi only to unnecessarily fear a mel diagnosis after receiving GPT-4o results. Statistically, younger patients are less likely than older patients to have malignant lesions and more likely to instead present with common vsl or df—lesions that GPT-4o appears likely to identify correctly.8 For older users, however, the situation may differ. Beyond ak being misclassified as bcc, older patients also may encounter GPT-4o outputs that mislabel lesions as mel, raising concerns and heightening anxiety. Given the technology’s tendency to overestimate the risk of serious dermatologic conditions, this behavior poses a considerable challenge in its current state and may inadvertently intensify public anxiety around mel.
A notable limitation of our study was that, compared to publicly available datasets, the HAM10000 dataset includes only dermatoscopic images rather than a combination of clinical and dermatoscopic images. Furthermore, the HAM10000 dataset comprises images primarily from White patients, whereas other diverse databases (eg, the Diverse Dermatology Images dataset) may be more suitable for training AI algorithms to accurately diagnose skin lesions in individuals with a variety of skin tones.9
Ultimately, our results signal that major advancements in the design and training of LLMs such as GPT-4o are necessary before these systems can be integrated into dermatologic diagnostic decision-making to offer benefit rather than cause harm. Consulting a health care professional rather than relying solely on AI, which might otherwise lead to avoidable stress, unnecessary alarm, and potentially increased health care costs due to unwarranted follow-up and testing, should remain the recommended standard of care for patients suspecting a skin lesion.
- Caruccio L, Cirillo S, Polese G, et al. Can ChatGPT provide intelligent diagnoses? A comparative study between predictive models and ChatGPT to define a new medical diagnostic bot. Expert Syst Appl. 2024;235:121186. doi:10.1016/j.eswa.2023.121186
- Ferreira AL, Chu B, Grant-Kels JM, et al. Evaluation of ChatGPT dermatology responses to common patient queries. JMIR Dermatol. 2023;6:E49280. doi:10.2196/49280
- Chen R, Zhang Y, Choi S, et al. The chatbots are coming: risks and benefits of consumer-facing artificial intelligence in clinical dermatology. J Am Acad Dermatol. 2023;89:872-874. doi:10.1016/j.jaad.2023.05.088
- Chau C, Feng H, Cobos G, et al. The comparative sufficiency of ChatGPT, Google Bard, and Bing AI in answering diagnosis, treatment, and prognosis questions about common dermatological diagnoses. JMIR Dermatol. 2025;8:E60827. doi:10.2196/60827
- Zhou J, He X, Sun L, et al. Pre-trained multimodal large language model enhances dermatological diagnosis using SkinGPT-4. Nat Commun. 2024;15:5649. doi:10.1038/s41467-024-50043-3
- Tschandl P, Rosendahl C, Kittler H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci Data. 2018;5:180161. doi:10.1038/sdata.2018.161
- Shifai N, van Doorn R, Malvehy J, et al. Can ChatGPT vision diagnose melanoma? An exploratory diagnostic accuracy study. J Am Acad Dermatol. 2024;90:1057-1059. doi:10.1016/j.jaad.2023.12.062
- Cortez JL, Vasquez J, Wei ML. The impact of demographics, socioeconomics, and health care access on melanoma outcomes. J Am Acad Dermatol. 2021;84:1677-1683. doi:10.1016/j.jaad.2020.07.125
- Daneshjou R, Vodrahalli K, Novoa RA, et al. Disparities in dermatology AI performance on a diverse, curated clinical image set. Sci Adv. 2022;8:Eabq6147. doi:10.1126/sciadv.abq6147
To the Editor:
The widespread availability and popularity of ChatGPT (OpenAI) have sparked interest in its potential applications within various fields, including medical diagnostics.1 In dermatology, large language models (LLMs) already are being cited as a possible way to reliably respond to common patient queries and produce concise patient education materials.2,3 That being said, there is skepticism regarding the technology’s efficacy and reliability in producing accurate treatment plans, with variability among popular LLMs; for example, a recent study by Chau et al4 demonstrated that ChatGPT was best at providing specific and accurate information regarding patient-facing responses to questions about 5 dermatologic diagnoses compared to Google Bard (now rebranded as Google Gemini) and Bing AI (now rebranded as Microsoft Copilot), which more often produced inaccurate or nonspecific responses. Google Bard also declined to answer one prompt.4 Large language models also have been evaluated in diagnosing skin lesions. In 2024, SkinGPT-4 (a pretrained multimodel LLM developed by Zhou et al5) achieved just over 80% accuracy in interpreting images of skin lesions and was considered informative by 82.5% of board-certified dermatologists, demonstrating that LLMs may have the potential to become integrated into clinical practice.5
Our study aimed to evaluate the performance of GPT-4o (OpenAI)—a widely accessible, low-cost LLM—in diagnosing dermatologic conditions using the HAM10000 dataset, a well-curated collection of dermatoscopic images developed for training and benchmarking artificial intelligence (AI) algorithms.6 HAM10000 comprises images representing 7 distinct skin conditions: actinic keratoses (ak), basal cell carcinoma (bcc), benign keratosis (bk), dermatofibroma (df), melanoma (mel), melanocytic nevi (nv), and vascular skin lesions (vsl), providing a robust platform for multiclass classification assessment. We evaluated GPT-4o using 100 dermatoscopic images per condition to assess diagnostic accuracy, potential biases, and limitations in skin lesion identification. The HAM10000 dataset was selected because it offers a large standardized reference set of dermatoscopic (rather than conventional clinical) images commonly used in dermatologic AI research. GPT-4o was chosen due to its patient-friendly interface, widespread use, and prior reports suggesting greater reliability in skin lesion assessment compared with other LLMs.
One hundred images from each of the 7 dermatologic categories were randomly selected for use in our analysis in 2024. The images were selected by our data scientist (J.C.) through random sampling from the dataset. Each image was separately presented to GPT-4o without any preprocessing or modification alongside 2 prompts designed to evaluate the diagnostic capabilities of GPT-4o. Both prompts included the same list of 7 dermatologic conditions for answer choices but differed in contextual information, where prompt 1 provided patient demographic information and localization of the dermatological condition but prompt 2 did not provide these details (Table). No follow-up questions were presented.
For prompt 1, the confusion matrix showed a strong bias toward detecting mel and bcc, with high true positives (mel, 83%; bcc, 37%)(eFigure 1). This pattern possibly suggests a tendency to favor malignant labels (eg, mel, BCC) when uncertainty is present. Interestingly, df and vsl also had notable true positives (46% and 37%, respectively), which is unexpected for less critical conditions because the model’s correct classifications were uneven across benign lesions. Actinic keratoses and nv showed higher misclassification rates, suggesting the model struggled to distinguish them from other lesions.
As shown in eTable 1, prompt 1 exhibited the highest recall for mel at 0.83 but performed worse in precision (0.242) and specificity (0.567) compared to ak, which had an extremely low recall (0.03) but very high specificity (0.992) and moderate precision score (0.375). The highest precision score was seen with vsl (0.738), which also achieved high scores in specificity (0.982) and accuracy (0.88) and performed moderately well in recall (0.31). All performance metrics are reported as proportions (0-1.0), wherein 1.0 indicates 100.
For prompt 2, the second confusion matrix followed similar trends as prompt 1 but still differed in key areas (eFigure 2). Melanoma detection remained strong (true positives, 95%), while bcc shows slightly fewer true positives (24%). Vascular skin lesions improve in true positives (40%), and df dropped slightly (33%). The model continues to struggle with ak and nv, with notable misclassifications observed across other categories
Similar to prompt 1, prompt 2 achieved its highest recall for mel (0.95%), but demonstrated lower precision (0.223%) and specificity (0.488%) for this class. Prompt 2 also produced the highest accuracy for vascular skin lesions (0.90%). The highest specificity was observed for both bk and ak (0.992% each); however, ak again demonstrated the lowest recall, with a value of 0.01%.
A previous study utilizing a model of binary classification to distinguish between mel and benign dermatologic conditions demonstrated poor performance.1 Additionally, prior studies have employed a less-strict, open-ended style question approach to examine ChatGPT’s ability to diagnose mel with limited efficacy.7 The HAM10000 dataset was specifically selected despite its limitations (including the absence of clinical images and limited diversity in skin tones) due to its comprehensive nature, robust annotation standards, and widespread acceptance in dermatologic AI research. Compared to the Diverse Dermatology Images dataset, which notably lacks skin tone diversity, HAM10000 provides a balanced representation of several dermatologic conditions crucial for multiclass classification tasks, making it suitable for benchmarking AI performance. This study aimed to eliminate these limitations by employing a multiclass classification approach; however, despite this switch, our results indicate continued and major limitations of the diagnostic capabilities of GPT-4o.
In its current form, GPT-4o appeared to demonstrate a clear accuracy bias toward correctly identifying specific and severe dermatologic conditions (eg, mel, bcc) but showed low and variable class-level performance for other categories (eg, ak, nv, df, vsl), with frequent misclassification into melanoma or basal cell carcinoma and low recall for some classes (eTables 1 and 2). This finding emphasized that GPT-4o currently lacks the reliability needed for real-life clinical applications in dermatology, as both binary and multiclass models fail to achieve consistent accurate performance across all skin conditions. Notably, GPT-4o may generate false-positive malignant classifications among patients due to its skew in predicted labels toward labeling benign lesions as malignant.
From the patient perspective, younger individuals may upload images of benign nevi only to unnecessarily fear a mel diagnosis after receiving GPT-4o results. Statistically, younger patients are less likely than older patients to have malignant lesions and more likely to instead present with common vsl or df—lesions that GPT-4o appears likely to identify correctly.8 For older users, however, the situation may differ. Beyond ak being misclassified as bcc, older patients also may encounter GPT-4o outputs that mislabel lesions as mel, raising concerns and heightening anxiety. Given the technology’s tendency to overestimate the risk of serious dermatologic conditions, this behavior poses a considerable challenge in its current state and may inadvertently intensify public anxiety around mel.
A notable limitation of our study was that, compared to publicly available datasets, the HAM10000 dataset includes only dermatoscopic images rather than a combination of clinical and dermatoscopic images. Furthermore, the HAM10000 dataset comprises images primarily from White patients, whereas other diverse databases (eg, the Diverse Dermatology Images dataset) may be more suitable for training AI algorithms to accurately diagnose skin lesions in individuals with a variety of skin tones.9
Ultimately, our results signal that major advancements in the design and training of LLMs such as GPT-4o are necessary before these systems can be integrated into dermatologic diagnostic decision-making to offer benefit rather than cause harm. Consulting a health care professional rather than relying solely on AI, which might otherwise lead to avoidable stress, unnecessary alarm, and potentially increased health care costs due to unwarranted follow-up and testing, should remain the recommended standard of care for patients suspecting a skin lesion.
To the Editor:
The widespread availability and popularity of ChatGPT (OpenAI) have sparked interest in its potential applications within various fields, including medical diagnostics.1 In dermatology, large language models (LLMs) already are being cited as a possible way to reliably respond to common patient queries and produce concise patient education materials.2,3 That being said, there is skepticism regarding the technology’s efficacy and reliability in producing accurate treatment plans, with variability among popular LLMs; for example, a recent study by Chau et al4 demonstrated that ChatGPT was best at providing specific and accurate information regarding patient-facing responses to questions about 5 dermatologic diagnoses compared to Google Bard (now rebranded as Google Gemini) and Bing AI (now rebranded as Microsoft Copilot), which more often produced inaccurate or nonspecific responses. Google Bard also declined to answer one prompt.4 Large language models also have been evaluated in diagnosing skin lesions. In 2024, SkinGPT-4 (a pretrained multimodel LLM developed by Zhou et al5) achieved just over 80% accuracy in interpreting images of skin lesions and was considered informative by 82.5% of board-certified dermatologists, demonstrating that LLMs may have the potential to become integrated into clinical practice.5
Our study aimed to evaluate the performance of GPT-4o (OpenAI)—a widely accessible, low-cost LLM—in diagnosing dermatologic conditions using the HAM10000 dataset, a well-curated collection of dermatoscopic images developed for training and benchmarking artificial intelligence (AI) algorithms.6 HAM10000 comprises images representing 7 distinct skin conditions: actinic keratoses (ak), basal cell carcinoma (bcc), benign keratosis (bk), dermatofibroma (df), melanoma (mel), melanocytic nevi (nv), and vascular skin lesions (vsl), providing a robust platform for multiclass classification assessment. We evaluated GPT-4o using 100 dermatoscopic images per condition to assess diagnostic accuracy, potential biases, and limitations in skin lesion identification. The HAM10000 dataset was selected because it offers a large standardized reference set of dermatoscopic (rather than conventional clinical) images commonly used in dermatologic AI research. GPT-4o was chosen due to its patient-friendly interface, widespread use, and prior reports suggesting greater reliability in skin lesion assessment compared with other LLMs.
One hundred images from each of the 7 dermatologic categories were randomly selected for use in our analysis in 2024. The images were selected by our data scientist (J.C.) through random sampling from the dataset. Each image was separately presented to GPT-4o without any preprocessing or modification alongside 2 prompts designed to evaluate the diagnostic capabilities of GPT-4o. Both prompts included the same list of 7 dermatologic conditions for answer choices but differed in contextual information, where prompt 1 provided patient demographic information and localization of the dermatological condition but prompt 2 did not provide these details (Table). No follow-up questions were presented.
For prompt 1, the confusion matrix showed a strong bias toward detecting mel and bcc, with high true positives (mel, 83%; bcc, 37%)(eFigure 1). This pattern possibly suggests a tendency to favor malignant labels (eg, mel, BCC) when uncertainty is present. Interestingly, df and vsl also had notable true positives (46% and 37%, respectively), which is unexpected for less critical conditions because the model’s correct classifications were uneven across benign lesions. Actinic keratoses and nv showed higher misclassification rates, suggesting the model struggled to distinguish them from other lesions.
As shown in eTable 1, prompt 1 exhibited the highest recall for mel at 0.83 but performed worse in precision (0.242) and specificity (0.567) compared to ak, which had an extremely low recall (0.03) but very high specificity (0.992) and moderate precision score (0.375). The highest precision score was seen with vsl (0.738), which also achieved high scores in specificity (0.982) and accuracy (0.88) and performed moderately well in recall (0.31). All performance metrics are reported as proportions (0-1.0), wherein 1.0 indicates 100.
For prompt 2, the second confusion matrix followed similar trends as prompt 1 but still differed in key areas (eFigure 2). Melanoma detection remained strong (true positives, 95%), while bcc shows slightly fewer true positives (24%). Vascular skin lesions improve in true positives (40%), and df dropped slightly (33%). The model continues to struggle with ak and nv, with notable misclassifications observed across other categories
Similar to prompt 1, prompt 2 achieved its highest recall for mel (0.95%), but demonstrated lower precision (0.223%) and specificity (0.488%) for this class. Prompt 2 also produced the highest accuracy for vascular skin lesions (0.90%). The highest specificity was observed for both bk and ak (0.992% each); however, ak again demonstrated the lowest recall, with a value of 0.01%.
A previous study utilizing a model of binary classification to distinguish between mel and benign dermatologic conditions demonstrated poor performance.1 Additionally, prior studies have employed a less-strict, open-ended style question approach to examine ChatGPT’s ability to diagnose mel with limited efficacy.7 The HAM10000 dataset was specifically selected despite its limitations (including the absence of clinical images and limited diversity in skin tones) due to its comprehensive nature, robust annotation standards, and widespread acceptance in dermatologic AI research. Compared to the Diverse Dermatology Images dataset, which notably lacks skin tone diversity, HAM10000 provides a balanced representation of several dermatologic conditions crucial for multiclass classification tasks, making it suitable for benchmarking AI performance. This study aimed to eliminate these limitations by employing a multiclass classification approach; however, despite this switch, our results indicate continued and major limitations of the diagnostic capabilities of GPT-4o.
In its current form, GPT-4o appeared to demonstrate a clear accuracy bias toward correctly identifying specific and severe dermatologic conditions (eg, mel, bcc) but showed low and variable class-level performance for other categories (eg, ak, nv, df, vsl), with frequent misclassification into melanoma or basal cell carcinoma and low recall for some classes (eTables 1 and 2). This finding emphasized that GPT-4o currently lacks the reliability needed for real-life clinical applications in dermatology, as both binary and multiclass models fail to achieve consistent accurate performance across all skin conditions. Notably, GPT-4o may generate false-positive malignant classifications among patients due to its skew in predicted labels toward labeling benign lesions as malignant.
From the patient perspective, younger individuals may upload images of benign nevi only to unnecessarily fear a mel diagnosis after receiving GPT-4o results. Statistically, younger patients are less likely than older patients to have malignant lesions and more likely to instead present with common vsl or df—lesions that GPT-4o appears likely to identify correctly.8 For older users, however, the situation may differ. Beyond ak being misclassified as bcc, older patients also may encounter GPT-4o outputs that mislabel lesions as mel, raising concerns and heightening anxiety. Given the technology’s tendency to overestimate the risk of serious dermatologic conditions, this behavior poses a considerable challenge in its current state and may inadvertently intensify public anxiety around mel.
A notable limitation of our study was that, compared to publicly available datasets, the HAM10000 dataset includes only dermatoscopic images rather than a combination of clinical and dermatoscopic images. Furthermore, the HAM10000 dataset comprises images primarily from White patients, whereas other diverse databases (eg, the Diverse Dermatology Images dataset) may be more suitable for training AI algorithms to accurately diagnose skin lesions in individuals with a variety of skin tones.9
Ultimately, our results signal that major advancements in the design and training of LLMs such as GPT-4o are necessary before these systems can be integrated into dermatologic diagnostic decision-making to offer benefit rather than cause harm. Consulting a health care professional rather than relying solely on AI, which might otherwise lead to avoidable stress, unnecessary alarm, and potentially increased health care costs due to unwarranted follow-up and testing, should remain the recommended standard of care for patients suspecting a skin lesion.
- Caruccio L, Cirillo S, Polese G, et al. Can ChatGPT provide intelligent diagnoses? A comparative study between predictive models and ChatGPT to define a new medical diagnostic bot. Expert Syst Appl. 2024;235:121186. doi:10.1016/j.eswa.2023.121186
- Ferreira AL, Chu B, Grant-Kels JM, et al. Evaluation of ChatGPT dermatology responses to common patient queries. JMIR Dermatol. 2023;6:E49280. doi:10.2196/49280
- Chen R, Zhang Y, Choi S, et al. The chatbots are coming: risks and benefits of consumer-facing artificial intelligence in clinical dermatology. J Am Acad Dermatol. 2023;89:872-874. doi:10.1016/j.jaad.2023.05.088
- Chau C, Feng H, Cobos G, et al. The comparative sufficiency of ChatGPT, Google Bard, and Bing AI in answering diagnosis, treatment, and prognosis questions about common dermatological diagnoses. JMIR Dermatol. 2025;8:E60827. doi:10.2196/60827
- Zhou J, He X, Sun L, et al. Pre-trained multimodal large language model enhances dermatological diagnosis using SkinGPT-4. Nat Commun. 2024;15:5649. doi:10.1038/s41467-024-50043-3
- Tschandl P, Rosendahl C, Kittler H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci Data. 2018;5:180161. doi:10.1038/sdata.2018.161
- Shifai N, van Doorn R, Malvehy J, et al. Can ChatGPT vision diagnose melanoma? An exploratory diagnostic accuracy study. J Am Acad Dermatol. 2024;90:1057-1059. doi:10.1016/j.jaad.2023.12.062
- Cortez JL, Vasquez J, Wei ML. The impact of demographics, socioeconomics, and health care access on melanoma outcomes. J Am Acad Dermatol. 2021;84:1677-1683. doi:10.1016/j.jaad.2020.07.125
- Daneshjou R, Vodrahalli K, Novoa RA, et al. Disparities in dermatology AI performance on a diverse, curated clinical image set. Sci Adv. 2022;8:Eabq6147. doi:10.1126/sciadv.abq6147
- Caruccio L, Cirillo S, Polese G, et al. Can ChatGPT provide intelligent diagnoses? A comparative study between predictive models and ChatGPT to define a new medical diagnostic bot. Expert Syst Appl. 2024;235:121186. doi:10.1016/j.eswa.2023.121186
- Ferreira AL, Chu B, Grant-Kels JM, et al. Evaluation of ChatGPT dermatology responses to common patient queries. JMIR Dermatol. 2023;6:E49280. doi:10.2196/49280
- Chen R, Zhang Y, Choi S, et al. The chatbots are coming: risks and benefits of consumer-facing artificial intelligence in clinical dermatology. J Am Acad Dermatol. 2023;89:872-874. doi:10.1016/j.jaad.2023.05.088
- Chau C, Feng H, Cobos G, et al. The comparative sufficiency of ChatGPT, Google Bard, and Bing AI in answering diagnosis, treatment, and prognosis questions about common dermatological diagnoses. JMIR Dermatol. 2025;8:E60827. doi:10.2196/60827
- Zhou J, He X, Sun L, et al. Pre-trained multimodal large language model enhances dermatological diagnosis using SkinGPT-4. Nat Commun. 2024;15:5649. doi:10.1038/s41467-024-50043-3
- Tschandl P, Rosendahl C, Kittler H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci Data. 2018;5:180161. doi:10.1038/sdata.2018.161
- Shifai N, van Doorn R, Malvehy J, et al. Can ChatGPT vision diagnose melanoma? An exploratory diagnostic accuracy study. J Am Acad Dermatol. 2024;90:1057-1059. doi:10.1016/j.jaad.2023.12.062
- Cortez JL, Vasquez J, Wei ML. The impact of demographics, socioeconomics, and health care access on melanoma outcomes. J Am Acad Dermatol. 2021;84:1677-1683. doi:10.1016/j.jaad.2020.07.125
- Daneshjou R, Vodrahalli K, Novoa RA, et al. Disparities in dermatology AI performance on a diverse, curated clinical image set. Sci Adv. 2022;8:Eabq6147. doi:10.1126/sciadv.abq6147
Evaluating GPT-4o for Automated Classification of Skin Lesions Using the HAM10000 Dataset
Evaluating GPT-4o for Automated Classification of Skin Lesions Using the HAM10000 Dataset
Practice Points
- Even with a multiclass classification framework designed to assist GPT-4o, the model encountered notable challenges in accurately diagnosing skin lesions.
- In its current form, GPT-4o may provide inaccurate and misleading information to patients who use its interface to evaluate suspected skin lesions. Patients should continue to seek clinical consultation from health care professionals.
