User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
500 more steps a day tied to 14% lower CVD risk in older adults
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.
The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.
The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.
The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
FROM EPI/LIFESTYLE 2023
Lilly cuts insulin price by 70%, caps out-of-pocket cost
Eli Lilly will cut prices for most of its insulins in the United States by 70% and cap out-of-pocket costs for insulin at $35 per month, the company announced on March 1.
“Lilly is taking these actions to make it easier to access Lilly insulin and help Americans who may have difficulty navigating a complex healthcare system that may keep them from getting affordable insulin,” the company said in a statement.
The $35 price cap is effective immediately at participating retail pharmacies for people with commercial insurance. Those without insurance can go to InsulinAffordability.com and download the Lilly Insulin Value Program savings card to receive Lilly insulins for $35 per month.
The company says it will cut the list price of its nonbranded Insulin Lispro Injection 100 units/mL to $25 a vial, effective May 1, 2023. The list price of the branded Humalog (insulin lispro injection) 100 units/mL will be cut by 70%, effective in the fourth quarter of 2023.
Lilly is among the three main companies that manufacture insulin, along with Novo Nordisk and Sanofi, that have come under fire over the cost of insulin in the US. Studies have shown that up to 25% of people with type 1 diabetes ration insulin because of costs, putting their health and often their lives in jeopardy.
Prices in the United States are around 10 times higher than in other countries. California is the latest state to say it plans to sue these big three companies over the high price of insulin and has announced plans to make its own cheaper versions.
Asked at a telephone press briefing if the lawsuit prompted the company’s move, Lilly chair and CEO David A. Ricks said: “Of course there are complaints against the industry and the company. We see those as completely unfounded. However, we can probably all agree that patients should have a consistent and lower-cost experience at the pharmacy counter, and that’s what today’s announcement is about. We’re doing this completely voluntarily because it’s time and it’s the right thing to do.”
On hearing the company announcement, Laura Nally, MD, a pediatric endocrinologist living with type 1 diabetes, @drnallypants, tweeted: “YES. After years of advocacy, the list price of Lispro/Humalog is now similar to what it was in the late 1990s. Cheers to all the #pwd [people with diabetes] who have advocated through #insulin4all! But we still have work to do to improve access to other diabetes medications & supplies.”
#insulin4all is a worldwide campaign to ensure that people with type 1 diabetes have access to affordable insulin and other supplies needed to manage the condition, such as glucose strips. It is supported, among others, by the advocacy group T1International.
Also giving his reaction to the Lilly announcement, Chuck Henderson, CEO of the American Diabetes Association, said: “We applaud Eli Lilly for taking the important step to limit cost-sharing for its insulin, and we encourage other insulin manufacturers to do the same.
“While we have been able to help achieve significant progress on the issue of insulin affordability, including Medicare’s new out-of-pocket cost cap on insulin, state copay caps, and patient assistance developments from insulin manufacturers, we know that our work is not done,” he added.
“ADA will work to ensure that Eli Lilly’s patient assistance program is benefiting patients as intended and continue the fight so that everyone who needs insulin has access.”
And Endocrine Society chief medical officer Robert Lash, MD, said: “Lilly’s move to apply a $35/month cap for people with private insurance will be a significant improvement for adults and children with diabetes who use Lilly’s products.
“We encourage all insulin manufacturers to join in the effort to reduce out-of-pocket costs for people who need insulin.”
Lilly will also launch a new insulin biosimilar, Rezvoglar (insulin glargine-aglr) injection, which is similar to and interchangeable with insulin glargine (Lantus). The cost will by $92 for a five pack of KwikPens, a 78% discount, compared with the cost of Lantus, beginning April 1, 2023.
A version of this article first appeared on Medscape.com.
Eli Lilly will cut prices for most of its insulins in the United States by 70% and cap out-of-pocket costs for insulin at $35 per month, the company announced on March 1.
“Lilly is taking these actions to make it easier to access Lilly insulin and help Americans who may have difficulty navigating a complex healthcare system that may keep them from getting affordable insulin,” the company said in a statement.
The $35 price cap is effective immediately at participating retail pharmacies for people with commercial insurance. Those without insurance can go to InsulinAffordability.com and download the Lilly Insulin Value Program savings card to receive Lilly insulins for $35 per month.
The company says it will cut the list price of its nonbranded Insulin Lispro Injection 100 units/mL to $25 a vial, effective May 1, 2023. The list price of the branded Humalog (insulin lispro injection) 100 units/mL will be cut by 70%, effective in the fourth quarter of 2023.
Lilly is among the three main companies that manufacture insulin, along with Novo Nordisk and Sanofi, that have come under fire over the cost of insulin in the US. Studies have shown that up to 25% of people with type 1 diabetes ration insulin because of costs, putting their health and often their lives in jeopardy.
Prices in the United States are around 10 times higher than in other countries. California is the latest state to say it plans to sue these big three companies over the high price of insulin and has announced plans to make its own cheaper versions.
Asked at a telephone press briefing if the lawsuit prompted the company’s move, Lilly chair and CEO David A. Ricks said: “Of course there are complaints against the industry and the company. We see those as completely unfounded. However, we can probably all agree that patients should have a consistent and lower-cost experience at the pharmacy counter, and that’s what today’s announcement is about. We’re doing this completely voluntarily because it’s time and it’s the right thing to do.”
On hearing the company announcement, Laura Nally, MD, a pediatric endocrinologist living with type 1 diabetes, @drnallypants, tweeted: “YES. After years of advocacy, the list price of Lispro/Humalog is now similar to what it was in the late 1990s. Cheers to all the #pwd [people with diabetes] who have advocated through #insulin4all! But we still have work to do to improve access to other diabetes medications & supplies.”
#insulin4all is a worldwide campaign to ensure that people with type 1 diabetes have access to affordable insulin and other supplies needed to manage the condition, such as glucose strips. It is supported, among others, by the advocacy group T1International.
Also giving his reaction to the Lilly announcement, Chuck Henderson, CEO of the American Diabetes Association, said: “We applaud Eli Lilly for taking the important step to limit cost-sharing for its insulin, and we encourage other insulin manufacturers to do the same.
“While we have been able to help achieve significant progress on the issue of insulin affordability, including Medicare’s new out-of-pocket cost cap on insulin, state copay caps, and patient assistance developments from insulin manufacturers, we know that our work is not done,” he added.
“ADA will work to ensure that Eli Lilly’s patient assistance program is benefiting patients as intended and continue the fight so that everyone who needs insulin has access.”
And Endocrine Society chief medical officer Robert Lash, MD, said: “Lilly’s move to apply a $35/month cap for people with private insurance will be a significant improvement for adults and children with diabetes who use Lilly’s products.
“We encourage all insulin manufacturers to join in the effort to reduce out-of-pocket costs for people who need insulin.”
Lilly will also launch a new insulin biosimilar, Rezvoglar (insulin glargine-aglr) injection, which is similar to and interchangeable with insulin glargine (Lantus). The cost will by $92 for a five pack of KwikPens, a 78% discount, compared with the cost of Lantus, beginning April 1, 2023.
A version of this article first appeared on Medscape.com.
Eli Lilly will cut prices for most of its insulins in the United States by 70% and cap out-of-pocket costs for insulin at $35 per month, the company announced on March 1.
“Lilly is taking these actions to make it easier to access Lilly insulin and help Americans who may have difficulty navigating a complex healthcare system that may keep them from getting affordable insulin,” the company said in a statement.
The $35 price cap is effective immediately at participating retail pharmacies for people with commercial insurance. Those without insurance can go to InsulinAffordability.com and download the Lilly Insulin Value Program savings card to receive Lilly insulins for $35 per month.
The company says it will cut the list price of its nonbranded Insulin Lispro Injection 100 units/mL to $25 a vial, effective May 1, 2023. The list price of the branded Humalog (insulin lispro injection) 100 units/mL will be cut by 70%, effective in the fourth quarter of 2023.
Lilly is among the three main companies that manufacture insulin, along with Novo Nordisk and Sanofi, that have come under fire over the cost of insulin in the US. Studies have shown that up to 25% of people with type 1 diabetes ration insulin because of costs, putting their health and often their lives in jeopardy.
Prices in the United States are around 10 times higher than in other countries. California is the latest state to say it plans to sue these big three companies over the high price of insulin and has announced plans to make its own cheaper versions.
Asked at a telephone press briefing if the lawsuit prompted the company’s move, Lilly chair and CEO David A. Ricks said: “Of course there are complaints against the industry and the company. We see those as completely unfounded. However, we can probably all agree that patients should have a consistent and lower-cost experience at the pharmacy counter, and that’s what today’s announcement is about. We’re doing this completely voluntarily because it’s time and it’s the right thing to do.”
On hearing the company announcement, Laura Nally, MD, a pediatric endocrinologist living with type 1 diabetes, @drnallypants, tweeted: “YES. After years of advocacy, the list price of Lispro/Humalog is now similar to what it was in the late 1990s. Cheers to all the #pwd [people with diabetes] who have advocated through #insulin4all! But we still have work to do to improve access to other diabetes medications & supplies.”
#insulin4all is a worldwide campaign to ensure that people with type 1 diabetes have access to affordable insulin and other supplies needed to manage the condition, such as glucose strips. It is supported, among others, by the advocacy group T1International.
Also giving his reaction to the Lilly announcement, Chuck Henderson, CEO of the American Diabetes Association, said: “We applaud Eli Lilly for taking the important step to limit cost-sharing for its insulin, and we encourage other insulin manufacturers to do the same.
“While we have been able to help achieve significant progress on the issue of insulin affordability, including Medicare’s new out-of-pocket cost cap on insulin, state copay caps, and patient assistance developments from insulin manufacturers, we know that our work is not done,” he added.
“ADA will work to ensure that Eli Lilly’s patient assistance program is benefiting patients as intended and continue the fight so that everyone who needs insulin has access.”
And Endocrine Society chief medical officer Robert Lash, MD, said: “Lilly’s move to apply a $35/month cap for people with private insurance will be a significant improvement for adults and children with diabetes who use Lilly’s products.
“We encourage all insulin manufacturers to join in the effort to reduce out-of-pocket costs for people who need insulin.”
Lilly will also launch a new insulin biosimilar, Rezvoglar (insulin glargine-aglr) injection, which is similar to and interchangeable with insulin glargine (Lantus). The cost will by $92 for a five pack of KwikPens, a 78% discount, compared with the cost of Lantus, beginning April 1, 2023.
A version of this article first appeared on Medscape.com.
FDA declines approval for omecamtiv mecarbil in HFrEF
The Food and Drug Administration has declined to approve omecamtiv mecarbil (Cytokinetics) for treatment of adults with chronic heart failure with reduced ejection fraction (HFrEF), citing a lack of evidence on efficacy.

Omecamtiv mecarbil is a first-in-class, selective cardiac myosin activator designed to improve cardiac performance.
Last December, a panel of FDA advisers recommended against approval of omecamtiv mecarbil for chronic HFrEF, as reported by this news organization.
The FDA Cardiovascular and Renal Drugs Advisory Committee voted 8 to 3 (with no abstentions) that the benefits of omecamtiv mecarbil do not outweigh the risks for HFrEF. The drug had a PDUFA date of February 28.
The committee’s decision was based on results from the phase 3 GALACTIC-HF trial, which enrolled 8,256 patients with HFrEF who were at risk of hospitalization and death, despite standard-of-care therapy.
As previously reported by this news organization, omecamtiv mecarbil produced a positive result for the study’s primary endpoint, with a 2.1% absolute reduction in the combined rate of cardiovascular (CV) death, first HF hospitalization, or first urgent visit for HF, compared with placebo during a median follow-up of about 22 months.
This represented an 8% relative risk reduction and broke down as a 0.6% absolute drop in CV death, compared with placebo, a 0.7% cut in HF hospitalization, and a 0.8% drop in urgent outpatient HF visits.
In a complete response letter, the FDA said GALACTIC-HF is “not sufficiently persuasive to establish substantial evidence of effectiveness for reducing the risk of heart failure events and cardiovascular death” in adults with HFrEF, Cytokinetics shared in a news release.
Further, the FDA said results from an additional clinical trial of omecamtiv mecarbil are required to establish substantial evidence of effectiveness for the treatment of HFrEF, with benefits that outweigh the risks, Cytokinetics said.
The company said it will request a meeting with the FDA to gain a better understanding of what may be required to support potential approval of omecamtiv mecarbil. However, the company also said it has “no plans” to conduct an additional clinical trial of omecamtiv mecarbil.
Instead, the company said its focus remains on the development of aficamten, the next-in-class cardiac myosin inhibitor, currently the subject of SEQUOIA-HCM, a phase 3 clinical trial in patients with obstructive hypertrophic cardiomyopathy.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has declined to approve omecamtiv mecarbil (Cytokinetics) for treatment of adults with chronic heart failure with reduced ejection fraction (HFrEF), citing a lack of evidence on efficacy.
Omecamtiv mecarbil is a first-in-class, selective cardiac myosin activator designed to improve cardiac performance.
Last December, a panel of FDA advisers recommended against approval of omecamtiv mecarbil for chronic HFrEF, as reported by this news organization.
The FDA Cardiovascular and Renal Drugs Advisory Committee voted 8 to 3 (with no abstentions) that the benefits of omecamtiv mecarbil do not outweigh the risks for HFrEF. The drug had a PDUFA date of February 28.
The committee’s decision was based on results from the phase 3 GALACTIC-HF trial, which enrolled 8,256 patients with HFrEF who were at risk of hospitalization and death, despite standard-of-care therapy.
As previously reported by this news organization, omecamtiv mecarbil produced a positive result for the study’s primary endpoint, with a 2.1% absolute reduction in the combined rate of cardiovascular (CV) death, first HF hospitalization, or first urgent visit for HF, compared with placebo during a median follow-up of about 22 months.
This represented an 8% relative risk reduction and broke down as a 0.6% absolute drop in CV death, compared with placebo, a 0.7% cut in HF hospitalization, and a 0.8% drop in urgent outpatient HF visits.
In a complete response letter, the FDA said GALACTIC-HF is “not sufficiently persuasive to establish substantial evidence of effectiveness for reducing the risk of heart failure events and cardiovascular death” in adults with HFrEF, Cytokinetics shared in a news release.
Further, the FDA said results from an additional clinical trial of omecamtiv mecarbil are required to establish substantial evidence of effectiveness for the treatment of HFrEF, with benefits that outweigh the risks, Cytokinetics said.
The company said it will request a meeting with the FDA to gain a better understanding of what may be required to support potential approval of omecamtiv mecarbil. However, the company also said it has “no plans” to conduct an additional clinical trial of omecamtiv mecarbil.
Instead, the company said its focus remains on the development of aficamten, the next-in-class cardiac myosin inhibitor, currently the subject of SEQUOIA-HCM, a phase 3 clinical trial in patients with obstructive hypertrophic cardiomyopathy.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has declined to approve omecamtiv mecarbil (Cytokinetics) for treatment of adults with chronic heart failure with reduced ejection fraction (HFrEF), citing a lack of evidence on efficacy.
Omecamtiv mecarbil is a first-in-class, selective cardiac myosin activator designed to improve cardiac performance.
Last December, a panel of FDA advisers recommended against approval of omecamtiv mecarbil for chronic HFrEF, as reported by this news organization.
The FDA Cardiovascular and Renal Drugs Advisory Committee voted 8 to 3 (with no abstentions) that the benefits of omecamtiv mecarbil do not outweigh the risks for HFrEF. The drug had a PDUFA date of February 28.
The committee’s decision was based on results from the phase 3 GALACTIC-HF trial, which enrolled 8,256 patients with HFrEF who were at risk of hospitalization and death, despite standard-of-care therapy.
As previously reported by this news organization, omecamtiv mecarbil produced a positive result for the study’s primary endpoint, with a 2.1% absolute reduction in the combined rate of cardiovascular (CV) death, first HF hospitalization, or first urgent visit for HF, compared with placebo during a median follow-up of about 22 months.
This represented an 8% relative risk reduction and broke down as a 0.6% absolute drop in CV death, compared with placebo, a 0.7% cut in HF hospitalization, and a 0.8% drop in urgent outpatient HF visits.
In a complete response letter, the FDA said GALACTIC-HF is “not sufficiently persuasive to establish substantial evidence of effectiveness for reducing the risk of heart failure events and cardiovascular death” in adults with HFrEF, Cytokinetics shared in a news release.
Further, the FDA said results from an additional clinical trial of omecamtiv mecarbil are required to establish substantial evidence of effectiveness for the treatment of HFrEF, with benefits that outweigh the risks, Cytokinetics said.
The company said it will request a meeting with the FDA to gain a better understanding of what may be required to support potential approval of omecamtiv mecarbil. However, the company also said it has “no plans” to conduct an additional clinical trial of omecamtiv mecarbil.
Instead, the company said its focus remains on the development of aficamten, the next-in-class cardiac myosin inhibitor, currently the subject of SEQUOIA-HCM, a phase 3 clinical trial in patients with obstructive hypertrophic cardiomyopathy.
A version of this article first appeared on Medscape.com.

Transplant surgeon to 30,000 marathoners: Give me that liver
Surgeon goes the extra half mile for his patient
Sorry medical profession, but it’s Adam Bodzin’s world now. When a donor liver got stuck in the middle of the Philadelphia Half Marathon’s 30,000 participants, Dr. Bodzin, the transplant team’s lead surgeon, took matters into his own hands. And by hands, of course, we mean feet.

Still wearing his hospital scrubs, Dr. Bodzin ran more than half a mile to where the van carrying the liver was stranded, according to the Philadelphia Inquirer. Fortunately, he was able to hitch a ride in a police car for the return trip and didn’t have to run back through the crowd carrying his somewhat unusual package. By package, of course, we mean human liver.
It’s been 3 months since the surgery/marathon and it’s still not clear why the driver had such trouble getting through – he had been trying for more than an hour and half by the time Dr. Bodzin reached him – but the surgery half of the big event was deemed a success and the patient has recovered.
Rick Hasz, president and chief executive officer of the Gift of Life Donor Program, which coordinates organ donation for transplants in the Philadelphia region, told the newspaper that “Dr. Bodzin’s quick action demonstrated his commitment to honoring the selfless generosity of all donors and their families and gives hope to everyone waiting for a second chance at life.”
Should Dr. Bodzin consider a step up from the transplant team to another group that’s fighting for the common good? The recipient of the liver in question seems to think so. “I guess he has a cape on under that white jacket,” 66-year-old Charles Rowe told Fox29. You already know where we’re going with this, right?
Avengers … Assemble.
Your spleen’s due for its 5,000-mile oil change
The human body is an incredible biological machine, capable of performing a countless array of tasks automatically and essentially without flaw, but there’s always room for improvement. After all, there are animals that can regrow entire missing limbs or live for up to 500 years. It would be nice if we could get some of that going.

Rather than any of that cool stuff, a recent survey of 2,000 average Americans revealed that our ambitions for improving the human body are a bit more mundane. The big thing that would make our lives better and easier, according to three-fourths of Americans, would be a built-in “check engine” light in our bodies. Come on guys, starfish can literally be cut in half and not only survive, but become two starfish. Mantis shrimp can punch with a force thousands of times their own weight. If we could punch like they could, we could literally break steel with our fists. Wouldn’t we rather have that?
Apparently not. Fine, we’ll stick with the check engine light.
Maybe it isn’t a huge surprise that we’d like the extra help in figuring out what our body needs. According to the survey, more than 60% of Americans struggle to identify when their body is trying to tell them something important, and only one-third actively checked in with their health every day. Considering about 40% said they feel tired for much of the day and nearly half reported not having a meal with fruits or vegetables in the past 3 days, perhaps a gentle reminder wouldn’t be the worst thing in the world.
So, if we did have a built-in check engine light, what would we use it for? A majority said they’d like to be reminded to drink a glass of water, with 45% saying they wanted to know when to take a nap. Feeling thirsty or tired isn’t quite enough, it seems.
Of course, the technology certainly exists to make the human check engine light a reality. An implanted microchip could absolutely tell us to drink a glass of water, but that would put our health in the hands of tech companies, and you just know Meta and Elon Muskrat wouldn’t pass up the chance for monetization. “Oh, sorry, we could have notified the hospital that you were about to have a heart attack, but you didn’t pay your life subscription this month.”
Sext offenders show more than their, well, you know
As we have become more and more attached to our phones, especially post pandemic, it’s no surprise that sexting – sending sexually explicit images and messages with those phones – has become a fairly common way for people to sexually communicate. And with dating apps just another venture in the dating landscape, regardless of age, sexting is an easy avenue to incite a mood without being physically present.

A recent study, though, has linked sexting with anxiety, sleep issues, depression, and compulsive sexual behaviors. Yikes.
Although the researchers noted that sexting was primarily reciprocal (sending and receiving), “over 50% of adults report sending a sext, while women are up to four times more likely than men to report having received nonconsensual sexts,” said Brenda K. Wiederhold, PhD, editor-in-chief of Cyberpsychology, Behavior, and Social Networking, which published the study, in which Dr. Wiederhold was not involved.
Among the 2,160 U.S. college students who were involved, participants who had only sent sexts reported more anxiety, depression, and sleep problems than other groups (no sexting, received only, reciprocal). There was also a possible connection between sexting, marijuana use, and compulsive sexual behavior, the investigators said in a written statement.
Considering the study population, these data are perhaps not that surprising. For young adults, to receive or send an elusive nude is as common as it once was to give someone flowers. Not that the two things elicit the same reactions. “Many individuals reveal they enjoy consensual sexting and feel it empowers them and builds self-confidence,” Dr. Wiederhold added.
Receiving a nonconsensual sext, though, is definitely going to result in feeling violated and super awkward. Senders beware: Don’t be surprised if you’re ghosted after that.
Surgeon goes the extra half mile for his patient
Sorry medical profession, but it’s Adam Bodzin’s world now. When a donor liver got stuck in the middle of the Philadelphia Half Marathon’s 30,000 participants, Dr. Bodzin, the transplant team’s lead surgeon, took matters into his own hands. And by hands, of course, we mean feet.
Still wearing his hospital scrubs, Dr. Bodzin ran more than half a mile to where the van carrying the liver was stranded, according to the Philadelphia Inquirer. Fortunately, he was able to hitch a ride in a police car for the return trip and didn’t have to run back through the crowd carrying his somewhat unusual package. By package, of course, we mean human liver.
It’s been 3 months since the surgery/marathon and it’s still not clear why the driver had such trouble getting through – he had been trying for more than an hour and half by the time Dr. Bodzin reached him – but the surgery half of the big event was deemed a success and the patient has recovered.
Rick Hasz, president and chief executive officer of the Gift of Life Donor Program, which coordinates organ donation for transplants in the Philadelphia region, told the newspaper that “Dr. Bodzin’s quick action demonstrated his commitment to honoring the selfless generosity of all donors and their families and gives hope to everyone waiting for a second chance at life.”
Should Dr. Bodzin consider a step up from the transplant team to another group that’s fighting for the common good? The recipient of the liver in question seems to think so. “I guess he has a cape on under that white jacket,” 66-year-old Charles Rowe told Fox29. You already know where we’re going with this, right?
Avengers … Assemble.
Your spleen’s due for its 5,000-mile oil change
The human body is an incredible biological machine, capable of performing a countless array of tasks automatically and essentially without flaw, but there’s always room for improvement. After all, there are animals that can regrow entire missing limbs or live for up to 500 years. It would be nice if we could get some of that going.
Rather than any of that cool stuff, a recent survey of 2,000 average Americans revealed that our ambitions for improving the human body are a bit more mundane. The big thing that would make our lives better and easier, according to three-fourths of Americans, would be a built-in “check engine” light in our bodies. Come on guys, starfish can literally be cut in half and not only survive, but become two starfish. Mantis shrimp can punch with a force thousands of times their own weight. If we could punch like they could, we could literally break steel with our fists. Wouldn’t we rather have that?
Apparently not. Fine, we’ll stick with the check engine light.
Maybe it isn’t a huge surprise that we’d like the extra help in figuring out what our body needs. According to the survey, more than 60% of Americans struggle to identify when their body is trying to tell them something important, and only one-third actively checked in with their health every day. Considering about 40% said they feel tired for much of the day and nearly half reported not having a meal with fruits or vegetables in the past 3 days, perhaps a gentle reminder wouldn’t be the worst thing in the world.
So, if we did have a built-in check engine light, what would we use it for? A majority said they’d like to be reminded to drink a glass of water, with 45% saying they wanted to know when to take a nap. Feeling thirsty or tired isn’t quite enough, it seems.
Of course, the technology certainly exists to make the human check engine light a reality. An implanted microchip could absolutely tell us to drink a glass of water, but that would put our health in the hands of tech companies, and you just know Meta and Elon Muskrat wouldn’t pass up the chance for monetization. “Oh, sorry, we could have notified the hospital that you were about to have a heart attack, but you didn’t pay your life subscription this month.”
Sext offenders show more than their, well, you know
As we have become more and more attached to our phones, especially post pandemic, it’s no surprise that sexting – sending sexually explicit images and messages with those phones – has become a fairly common way for people to sexually communicate. And with dating apps just another venture in the dating landscape, regardless of age, sexting is an easy avenue to incite a mood without being physically present.
A recent study, though, has linked sexting with anxiety, sleep issues, depression, and compulsive sexual behaviors. Yikes.
Although the researchers noted that sexting was primarily reciprocal (sending and receiving), “over 50% of adults report sending a sext, while women are up to four times more likely than men to report having received nonconsensual sexts,” said Brenda K. Wiederhold, PhD, editor-in-chief of Cyberpsychology, Behavior, and Social Networking, which published the study, in which Dr. Wiederhold was not involved.
Among the 2,160 U.S. college students who were involved, participants who had only sent sexts reported more anxiety, depression, and sleep problems than other groups (no sexting, received only, reciprocal). There was also a possible connection between sexting, marijuana use, and compulsive sexual behavior, the investigators said in a written statement.
Considering the study population, these data are perhaps not that surprising. For young adults, to receive or send an elusive nude is as common as it once was to give someone flowers. Not that the two things elicit the same reactions. “Many individuals reveal they enjoy consensual sexting and feel it empowers them and builds self-confidence,” Dr. Wiederhold added.
Receiving a nonconsensual sext, though, is definitely going to result in feeling violated and super awkward. Senders beware: Don’t be surprised if you’re ghosted after that.
Surgeon goes the extra half mile for his patient
Sorry medical profession, but it’s Adam Bodzin’s world now. When a donor liver got stuck in the middle of the Philadelphia Half Marathon’s 30,000 participants, Dr. Bodzin, the transplant team’s lead surgeon, took matters into his own hands. And by hands, of course, we mean feet.
Still wearing his hospital scrubs, Dr. Bodzin ran more than half a mile to where the van carrying the liver was stranded, according to the Philadelphia Inquirer. Fortunately, he was able to hitch a ride in a police car for the return trip and didn’t have to run back through the crowd carrying his somewhat unusual package. By package, of course, we mean human liver.
It’s been 3 months since the surgery/marathon and it’s still not clear why the driver had such trouble getting through – he had been trying for more than an hour and half by the time Dr. Bodzin reached him – but the surgery half of the big event was deemed a success and the patient has recovered.
Rick Hasz, president and chief executive officer of the Gift of Life Donor Program, which coordinates organ donation for transplants in the Philadelphia region, told the newspaper that “Dr. Bodzin’s quick action demonstrated his commitment to honoring the selfless generosity of all donors and their families and gives hope to everyone waiting for a second chance at life.”
Should Dr. Bodzin consider a step up from the transplant team to another group that’s fighting for the common good? The recipient of the liver in question seems to think so. “I guess he has a cape on under that white jacket,” 66-year-old Charles Rowe told Fox29. You already know where we’re going with this, right?
Avengers … Assemble.
Your spleen’s due for its 5,000-mile oil change
The human body is an incredible biological machine, capable of performing a countless array of tasks automatically and essentially without flaw, but there’s always room for improvement. After all, there are animals that can regrow entire missing limbs or live for up to 500 years. It would be nice if we could get some of that going.
Rather than any of that cool stuff, a recent survey of 2,000 average Americans revealed that our ambitions for improving the human body are a bit more mundane. The big thing that would make our lives better and easier, according to three-fourths of Americans, would be a built-in “check engine” light in our bodies. Come on guys, starfish can literally be cut in half and not only survive, but become two starfish. Mantis shrimp can punch with a force thousands of times their own weight. If we could punch like they could, we could literally break steel with our fists. Wouldn’t we rather have that?
Apparently not. Fine, we’ll stick with the check engine light.
Maybe it isn’t a huge surprise that we’d like the extra help in figuring out what our body needs. According to the survey, more than 60% of Americans struggle to identify when their body is trying to tell them something important, and only one-third actively checked in with their health every day. Considering about 40% said they feel tired for much of the day and nearly half reported not having a meal with fruits or vegetables in the past 3 days, perhaps a gentle reminder wouldn’t be the worst thing in the world.
So, if we did have a built-in check engine light, what would we use it for? A majority said they’d like to be reminded to drink a glass of water, with 45% saying they wanted to know when to take a nap. Feeling thirsty or tired isn’t quite enough, it seems.
Of course, the technology certainly exists to make the human check engine light a reality. An implanted microchip could absolutely tell us to drink a glass of water, but that would put our health in the hands of tech companies, and you just know Meta and Elon Muskrat wouldn’t pass up the chance for monetization. “Oh, sorry, we could have notified the hospital that you were about to have a heart attack, but you didn’t pay your life subscription this month.”
Sext offenders show more than their, well, you know
As we have become more and more attached to our phones, especially post pandemic, it’s no surprise that sexting – sending sexually explicit images and messages with those phones – has become a fairly common way for people to sexually communicate. And with dating apps just another venture in the dating landscape, regardless of age, sexting is an easy avenue to incite a mood without being physically present.
A recent study, though, has linked sexting with anxiety, sleep issues, depression, and compulsive sexual behaviors. Yikes.
Although the researchers noted that sexting was primarily reciprocal (sending and receiving), “over 50% of adults report sending a sext, while women are up to four times more likely than men to report having received nonconsensual sexts,” said Brenda K. Wiederhold, PhD, editor-in-chief of Cyberpsychology, Behavior, and Social Networking, which published the study, in which Dr. Wiederhold was not involved.
Among the 2,160 U.S. college students who were involved, participants who had only sent sexts reported more anxiety, depression, and sleep problems than other groups (no sexting, received only, reciprocal). There was also a possible connection between sexting, marijuana use, and compulsive sexual behavior, the investigators said in a written statement.
Considering the study population, these data are perhaps not that surprising. For young adults, to receive or send an elusive nude is as common as it once was to give someone flowers. Not that the two things elicit the same reactions. “Many individuals reveal they enjoy consensual sexting and feel it empowers them and builds self-confidence,” Dr. Wiederhold added.
Receiving a nonconsensual sext, though, is definitely going to result in feeling violated and super awkward. Senders beware: Don’t be surprised if you’re ghosted after that.
Is cellular senescence related to post–COVID-19 syndrome?
Proinflammatory elements mediated through metabolic pathways related to obesity and increased cellular senescence in CD57 expression in CD8+ T cells are associated with postacute sequelae of COVID-19 (PASC), according to a Mexican study. The researchers followed a Mexican cohort of 102 patients 3 months and 6 months after acute SARS-CoV-2 infection.
The study’s principal investigator was Diana Gómez-Martín, MD, PhD, of the department of immunology and rheumatology at the Salvador Zubirán National Institute of Medical Sciences and Nutrition, Mexico City. She told this news organization that follow-up of the patients began with the objective of understanding the determinative clinical, genetic, metabolic, and immunological factors in the progression of the acute disease. However, clinical aspects associated with PASC developed in the selected cohort. As a result, the study was extended, and the clinical, metabolic, and immunologic conditions in this single-center Mexican cohort were evaluated 3 months 6 months after the onset of infection.
Dr. Gómez-Martín explained that the immune senescence in CD57 of CD8+ T cells is one of the best-known findings of the present study. If it is confirmed in future studies, it could have important implications. “Its main implication is the possibility of better understanding the physiopathology of the clinical aspects associated with postacute sequelae of COVID-19, potentially being used for early detection and to provide follow-up aimed at patients, in addition to eventually developing targeted therapeutic strategies, such as immunometabolism regulation, in certain populations.”
Patients with PASC
The study was conducted from August 2020 to August 2021. Investigators recruited 102 patients (median age, 50.5 years; 55% were women) at the Mexico City Temporary Unit with a confirmed diagnosis of SARS-CoV-2. Of the patients, 44% had mild or moderate COVID-19, 30% had severe cases, and 26% of patients had critical cases. The most frequent comorbidities were obesity (44%), hypertension (24%), and type 2 diabetes (24%). The authors used a questionnaire to assess the presence of symptoms during follow-up. They analyzed immunologic variables at the time of recruitment, as well as levels of cytokines, immunoglobulin G against SARS-CoV-2, and neutrophil extracellular traps (NETs) at 1, 3, and 6 months. At 6 months’ follow-up, 12.7% of the cohort had symptoms compatible with PASC, which was defined for the study as the presence and report of three or more symptoms at 6 months’ follow-up.
As in similar studies, the authors found that female gender, remaining in intensive care, and having had more symptoms and greater titers of anti-SARS-CoV-2 antibodies during the acute infection were associated with the development of clinical aspects associated with PASC. Patients who had the disease at 6 months had increased serum levels of interleukin-1 alpha (6.21 pg/mL vs. 2.21 pg/mL), granulocyte colony-stimulating factor (55.08 pg/mL vs. 14.68 pg/mL), and interferon gamma-induced protein 10 (2,309.40 pg/mL vs. 780 pg/mL). Also, there was a trend toward an increase in serum concentration of interleukin-1 beta, interleukin-6, and interferon-gamma.
Patients whose condition met the definition of persistent PASC had increased expression of CD57 in CD8+ T cells (42,714 arbitrary units vs. 28,506) 6 months after the acute infection. The authors reported that there was no association between the persistence of PASC and the baseline amount of NETs, TRIM63, and anticellular antibodies. Nor was there an association between PASC and the titers of anti-SARS-CoV-2 antibodies at baseline and 1 month after COVID-19 diagnosis. Nonetheless, patients with persistent PASC had higher titers of anti-SARS-CoV-2 IgGs 3 months after the onset of COVID-19.
On the basis of previous data, the researchers aimed to construct a preliminary explanatory model to address the clinical and immunologic features associated with persistent PASC 6 months after SARS-CoV-2 infection. In the univariate analysis, the variables associated with the diagnosis of persistent PASC were the serum levels of granulocyte colony-stimulating factor (odds ratio, 1.01), macrophage inflammatory protein-1 alpha (OR, 1.13), interferon gamma-induced protein 10 (OR, 1.00), interleukin-6 (OR, 1.03), the expression of CD57 in CD8+ T cells (OR, 1.00), and the titers of anti-SARS-CoV-2 IgG at 1 month (OR, 1.45).
, such as obesity, greater levels of macrophage inflammatory protein-1 alpha and interferon gamma-induced protein 10 in peripheral blood, greater expression of the senescence CD57 marker in CD8+ T lymphocytes, and persistent symptoms at 3 months.
Using these parameters to construct a predictive model after 3 months, the authors found a sensitivity of 97.7%, specificity of 53.8%, positive predictive value of 93.5%, and a negative predictive value of 77.7% for the diagnosis of clinical aspects associated with PASC at 6 months.
Interpreting CD57
One of the researchers who participated in the study was Luis Martínez-Juárez, MD, MPH, DrPH. He is on the operative solutions team at the Carlos Slim Foundation. Dr. Martínez-Juárez pointed out that one of the contributions of this study was that it specifically examined the Mexican population. He noted that “according to the findings, obesity is not only a comorbidity associated with more severe progressions during acute COVID-19 disease, but also, through inflammation parameters, such as interleukin-6, interferon gamma-induced protein 10, and macrophage inflammatory protein-1 alpha, it’s involved in the development of clinical aspects related to postacute sequelae of COVID-19.”
Dr. Gómez-Martín added that finding proinflammatory and obesity parameters in the patients could potentially support the hypothesis of the persistence of virus fragments in adipose tissue as possibly involved in clinical aspects associated with PASC, as some groups have reported in the medical literature.
Angélica Cuapio, MD, DrMed, an immunologist and senior investigator at the Karolinska Institute, Stockholm, who did not participate in the study, said in an interview that the authors’ findings on the sustained increase of the CD57 marker in CD8+ lymphocytes are of notable interest. They may be associated with senescence states or cellular aging or with a stage of chronic viral infections. Therefore, Dr. Cuapio argued, it would have been valuable to include cellular markers of the innate system, such as natural killer cells, since in various infections, an increase in CD57 in lymphocytes is accompanied by an almost proportional increase of this marker in natural killer cells.
“This information would help to determine more accurately if we are talking about a cellular senescence or more about a chronic infection in persistent COVID-19.” The finding is important, but future research is needed in this developing field.
Dr. Cuapio pointed out that the authors found an interesting elevation in interleukin-1 alpha in patients with clinical aspects associated with PASC in a clinically well-characterized population in Mexico. “It is possible that this is a specific marker either of a specific population or location, or this could be an association with a humoral response. Despite the fact that this finding is new and unclear, it is worth investigating. This study is of great value for the scientific community because it’s one more piece in the complex puzzle of clinical aspects associated with postacute sequelae of COVID-19.”
Dr. Gómez-Martín noted that the main limitations of the study consist of its single-center design and the small patient sample. Dr. Martínez-Juárez added that the study did not consider reinfections. In future studies, it would be ideal to integrate other molecular assessments associated with various hypotheses of the physiopathology of clinical aspects associated with PASC, such as microbiota alteration, coagulation anomalies, endothelial damage, and dysfunctional neurologic signaling.
The study was supported and funded by the Carlos Slim Foundation. Dr. Gómez-Martín, Dr. Martínez-Juárez, and Dr. Cuapio have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Proinflammatory elements mediated through metabolic pathways related to obesity and increased cellular senescence in CD57 expression in CD8+ T cells are associated with postacute sequelae of COVID-19 (PASC), according to a Mexican study. The researchers followed a Mexican cohort of 102 patients 3 months and 6 months after acute SARS-CoV-2 infection.
The study’s principal investigator was Diana Gómez-Martín, MD, PhD, of the department of immunology and rheumatology at the Salvador Zubirán National Institute of Medical Sciences and Nutrition, Mexico City. She told this news organization that follow-up of the patients began with the objective of understanding the determinative clinical, genetic, metabolic, and immunological factors in the progression of the acute disease. However, clinical aspects associated with PASC developed in the selected cohort. As a result, the study was extended, and the clinical, metabolic, and immunologic conditions in this single-center Mexican cohort were evaluated 3 months 6 months after the onset of infection.
Dr. Gómez-Martín explained that the immune senescence in CD57 of CD8+ T cells is one of the best-known findings of the present study. If it is confirmed in future studies, it could have important implications. “Its main implication is the possibility of better understanding the physiopathology of the clinical aspects associated with postacute sequelae of COVID-19, potentially being used for early detection and to provide follow-up aimed at patients, in addition to eventually developing targeted therapeutic strategies, such as immunometabolism regulation, in certain populations.”
Patients with PASC
The study was conducted from August 2020 to August 2021. Investigators recruited 102 patients (median age, 50.5 years; 55% were women) at the Mexico City Temporary Unit with a confirmed diagnosis of SARS-CoV-2. Of the patients, 44% had mild or moderate COVID-19, 30% had severe cases, and 26% of patients had critical cases. The most frequent comorbidities were obesity (44%), hypertension (24%), and type 2 diabetes (24%). The authors used a questionnaire to assess the presence of symptoms during follow-up. They analyzed immunologic variables at the time of recruitment, as well as levels of cytokines, immunoglobulin G against SARS-CoV-2, and neutrophil extracellular traps (NETs) at 1, 3, and 6 months. At 6 months’ follow-up, 12.7% of the cohort had symptoms compatible with PASC, which was defined for the study as the presence and report of three or more symptoms at 6 months’ follow-up.
As in similar studies, the authors found that female gender, remaining in intensive care, and having had more symptoms and greater titers of anti-SARS-CoV-2 antibodies during the acute infection were associated with the development of clinical aspects associated with PASC. Patients who had the disease at 6 months had increased serum levels of interleukin-1 alpha (6.21 pg/mL vs. 2.21 pg/mL), granulocyte colony-stimulating factor (55.08 pg/mL vs. 14.68 pg/mL), and interferon gamma-induced protein 10 (2,309.40 pg/mL vs. 780 pg/mL). Also, there was a trend toward an increase in serum concentration of interleukin-1 beta, interleukin-6, and interferon-gamma.
Patients whose condition met the definition of persistent PASC had increased expression of CD57 in CD8+ T cells (42,714 arbitrary units vs. 28,506) 6 months after the acute infection. The authors reported that there was no association between the persistence of PASC and the baseline amount of NETs, TRIM63, and anticellular antibodies. Nor was there an association between PASC and the titers of anti-SARS-CoV-2 antibodies at baseline and 1 month after COVID-19 diagnosis. Nonetheless, patients with persistent PASC had higher titers of anti-SARS-CoV-2 IgGs 3 months after the onset of COVID-19.
On the basis of previous data, the researchers aimed to construct a preliminary explanatory model to address the clinical and immunologic features associated with persistent PASC 6 months after SARS-CoV-2 infection. In the univariate analysis, the variables associated with the diagnosis of persistent PASC were the serum levels of granulocyte colony-stimulating factor (odds ratio, 1.01), macrophage inflammatory protein-1 alpha (OR, 1.13), interferon gamma-induced protein 10 (OR, 1.00), interleukin-6 (OR, 1.03), the expression of CD57 in CD8+ T cells (OR, 1.00), and the titers of anti-SARS-CoV-2 IgG at 1 month (OR, 1.45).
, such as obesity, greater levels of macrophage inflammatory protein-1 alpha and interferon gamma-induced protein 10 in peripheral blood, greater expression of the senescence CD57 marker in CD8+ T lymphocytes, and persistent symptoms at 3 months.
Using these parameters to construct a predictive model after 3 months, the authors found a sensitivity of 97.7%, specificity of 53.8%, positive predictive value of 93.5%, and a negative predictive value of 77.7% for the diagnosis of clinical aspects associated with PASC at 6 months.
Interpreting CD57
One of the researchers who participated in the study was Luis Martínez-Juárez, MD, MPH, DrPH. He is on the operative solutions team at the Carlos Slim Foundation. Dr. Martínez-Juárez pointed out that one of the contributions of this study was that it specifically examined the Mexican population. He noted that “according to the findings, obesity is not only a comorbidity associated with more severe progressions during acute COVID-19 disease, but also, through inflammation parameters, such as interleukin-6, interferon gamma-induced protein 10, and macrophage inflammatory protein-1 alpha, it’s involved in the development of clinical aspects related to postacute sequelae of COVID-19.”
Dr. Gómez-Martín added that finding proinflammatory and obesity parameters in the patients could potentially support the hypothesis of the persistence of virus fragments in adipose tissue as possibly involved in clinical aspects associated with PASC, as some groups have reported in the medical literature.
Angélica Cuapio, MD, DrMed, an immunologist and senior investigator at the Karolinska Institute, Stockholm, who did not participate in the study, said in an interview that the authors’ findings on the sustained increase of the CD57 marker in CD8+ lymphocytes are of notable interest. They may be associated with senescence states or cellular aging or with a stage of chronic viral infections. Therefore, Dr. Cuapio argued, it would have been valuable to include cellular markers of the innate system, such as natural killer cells, since in various infections, an increase in CD57 in lymphocytes is accompanied by an almost proportional increase of this marker in natural killer cells.
“This information would help to determine more accurately if we are talking about a cellular senescence or more about a chronic infection in persistent COVID-19.” The finding is important, but future research is needed in this developing field.
Dr. Cuapio pointed out that the authors found an interesting elevation in interleukin-1 alpha in patients with clinical aspects associated with PASC in a clinically well-characterized population in Mexico. “It is possible that this is a specific marker either of a specific population or location, or this could be an association with a humoral response. Despite the fact that this finding is new and unclear, it is worth investigating. This study is of great value for the scientific community because it’s one more piece in the complex puzzle of clinical aspects associated with postacute sequelae of COVID-19.”
Dr. Gómez-Martín noted that the main limitations of the study consist of its single-center design and the small patient sample. Dr. Martínez-Juárez added that the study did not consider reinfections. In future studies, it would be ideal to integrate other molecular assessments associated with various hypotheses of the physiopathology of clinical aspects associated with PASC, such as microbiota alteration, coagulation anomalies, endothelial damage, and dysfunctional neurologic signaling.
The study was supported and funded by the Carlos Slim Foundation. Dr. Gómez-Martín, Dr. Martínez-Juárez, and Dr. Cuapio have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Proinflammatory elements mediated through metabolic pathways related to obesity and increased cellular senescence in CD57 expression in CD8+ T cells are associated with postacute sequelae of COVID-19 (PASC), according to a Mexican study. The researchers followed a Mexican cohort of 102 patients 3 months and 6 months after acute SARS-CoV-2 infection.
The study’s principal investigator was Diana Gómez-Martín, MD, PhD, of the department of immunology and rheumatology at the Salvador Zubirán National Institute of Medical Sciences and Nutrition, Mexico City. She told this news organization that follow-up of the patients began with the objective of understanding the determinative clinical, genetic, metabolic, and immunological factors in the progression of the acute disease. However, clinical aspects associated with PASC developed in the selected cohort. As a result, the study was extended, and the clinical, metabolic, and immunologic conditions in this single-center Mexican cohort were evaluated 3 months 6 months after the onset of infection.
Dr. Gómez-Martín explained that the immune senescence in CD57 of CD8+ T cells is one of the best-known findings of the present study. If it is confirmed in future studies, it could have important implications. “Its main implication is the possibility of better understanding the physiopathology of the clinical aspects associated with postacute sequelae of COVID-19, potentially being used for early detection and to provide follow-up aimed at patients, in addition to eventually developing targeted therapeutic strategies, such as immunometabolism regulation, in certain populations.”
Patients with PASC
The study was conducted from August 2020 to August 2021. Investigators recruited 102 patients (median age, 50.5 years; 55% were women) at the Mexico City Temporary Unit with a confirmed diagnosis of SARS-CoV-2. Of the patients, 44% had mild or moderate COVID-19, 30% had severe cases, and 26% of patients had critical cases. The most frequent comorbidities were obesity (44%), hypertension (24%), and type 2 diabetes (24%). The authors used a questionnaire to assess the presence of symptoms during follow-up. They analyzed immunologic variables at the time of recruitment, as well as levels of cytokines, immunoglobulin G against SARS-CoV-2, and neutrophil extracellular traps (NETs) at 1, 3, and 6 months. At 6 months’ follow-up, 12.7% of the cohort had symptoms compatible with PASC, which was defined for the study as the presence and report of three or more symptoms at 6 months’ follow-up.
As in similar studies, the authors found that female gender, remaining in intensive care, and having had more symptoms and greater titers of anti-SARS-CoV-2 antibodies during the acute infection were associated with the development of clinical aspects associated with PASC. Patients who had the disease at 6 months had increased serum levels of interleukin-1 alpha (6.21 pg/mL vs. 2.21 pg/mL), granulocyte colony-stimulating factor (55.08 pg/mL vs. 14.68 pg/mL), and interferon gamma-induced protein 10 (2,309.40 pg/mL vs. 780 pg/mL). Also, there was a trend toward an increase in serum concentration of interleukin-1 beta, interleukin-6, and interferon-gamma.
Patients whose condition met the definition of persistent PASC had increased expression of CD57 in CD8+ T cells (42,714 arbitrary units vs. 28,506) 6 months after the acute infection. The authors reported that there was no association between the persistence of PASC and the baseline amount of NETs, TRIM63, and anticellular antibodies. Nor was there an association between PASC and the titers of anti-SARS-CoV-2 antibodies at baseline and 1 month after COVID-19 diagnosis. Nonetheless, patients with persistent PASC had higher titers of anti-SARS-CoV-2 IgGs 3 months after the onset of COVID-19.
On the basis of previous data, the researchers aimed to construct a preliminary explanatory model to address the clinical and immunologic features associated with persistent PASC 6 months after SARS-CoV-2 infection. In the univariate analysis, the variables associated with the diagnosis of persistent PASC were the serum levels of granulocyte colony-stimulating factor (odds ratio, 1.01), macrophage inflammatory protein-1 alpha (OR, 1.13), interferon gamma-induced protein 10 (OR, 1.00), interleukin-6 (OR, 1.03), the expression of CD57 in CD8+ T cells (OR, 1.00), and the titers of anti-SARS-CoV-2 IgG at 1 month (OR, 1.45).
, such as obesity, greater levels of macrophage inflammatory protein-1 alpha and interferon gamma-induced protein 10 in peripheral blood, greater expression of the senescence CD57 marker in CD8+ T lymphocytes, and persistent symptoms at 3 months.
Using these parameters to construct a predictive model after 3 months, the authors found a sensitivity of 97.7%, specificity of 53.8%, positive predictive value of 93.5%, and a negative predictive value of 77.7% for the diagnosis of clinical aspects associated with PASC at 6 months.
Interpreting CD57
One of the researchers who participated in the study was Luis Martínez-Juárez, MD, MPH, DrPH. He is on the operative solutions team at the Carlos Slim Foundation. Dr. Martínez-Juárez pointed out that one of the contributions of this study was that it specifically examined the Mexican population. He noted that “according to the findings, obesity is not only a comorbidity associated with more severe progressions during acute COVID-19 disease, but also, through inflammation parameters, such as interleukin-6, interferon gamma-induced protein 10, and macrophage inflammatory protein-1 alpha, it’s involved in the development of clinical aspects related to postacute sequelae of COVID-19.”
Dr. Gómez-Martín added that finding proinflammatory and obesity parameters in the patients could potentially support the hypothesis of the persistence of virus fragments in adipose tissue as possibly involved in clinical aspects associated with PASC, as some groups have reported in the medical literature.
Angélica Cuapio, MD, DrMed, an immunologist and senior investigator at the Karolinska Institute, Stockholm, who did not participate in the study, said in an interview that the authors’ findings on the sustained increase of the CD57 marker in CD8+ lymphocytes are of notable interest. They may be associated with senescence states or cellular aging or with a stage of chronic viral infections. Therefore, Dr. Cuapio argued, it would have been valuable to include cellular markers of the innate system, such as natural killer cells, since in various infections, an increase in CD57 in lymphocytes is accompanied by an almost proportional increase of this marker in natural killer cells.
“This information would help to determine more accurately if we are talking about a cellular senescence or more about a chronic infection in persistent COVID-19.” The finding is important, but future research is needed in this developing field.
Dr. Cuapio pointed out that the authors found an interesting elevation in interleukin-1 alpha in patients with clinical aspects associated with PASC in a clinically well-characterized population in Mexico. “It is possible that this is a specific marker either of a specific population or location, or this could be an association with a humoral response. Despite the fact that this finding is new and unclear, it is worth investigating. This study is of great value for the scientific community because it’s one more piece in the complex puzzle of clinical aspects associated with postacute sequelae of COVID-19.”
Dr. Gómez-Martín noted that the main limitations of the study consist of its single-center design and the small patient sample. Dr. Martínez-Juárez added that the study did not consider reinfections. In future studies, it would be ideal to integrate other molecular assessments associated with various hypotheses of the physiopathology of clinical aspects associated with PASC, such as microbiota alteration, coagulation anomalies, endothelial damage, and dysfunctional neurologic signaling.
The study was supported and funded by the Carlos Slim Foundation. Dr. Gómez-Martín, Dr. Martínez-Juárez, and Dr. Cuapio have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Frequent cannabis use tied to coronary artery disease
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
FROM ACC 2023
Old drug verapamil may have new use in type 1 diabetes
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
Insomnia, short sleep linked to greater risk for MI
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.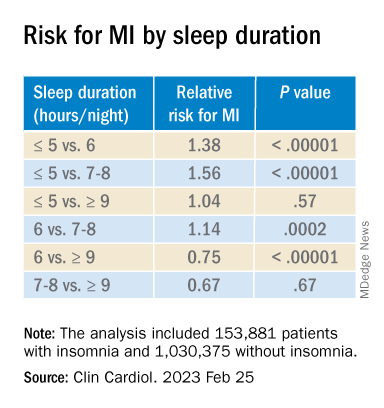
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
FDA warns of potential problems with Abbott Trifecta valves
There is a potential risk of early structural valve deterioration with the Abbott Trifecta valve and Trifecta valve with glide technology (Trifecta GT), the U.S. Food and Drug Administration says in a letter to health care professionals posted on its website.
Evidence in the literature suggests a higher cumulative incidence of early structural valve deterioration (SVD) and a lower freedom from reintervention due to SVD with the Trifecta valves, compared with other commercially available bovine pericardial valves, the FDA says.
The Trifecta and Trifecta GT valves are heart valve replacement devices intended to treat diseased, damaged, or malfunctioning native or prosthetic aortic heart valves, the letter notes. The first-generation Trifecta valve was approved in 2011 but is no longer marketed in the United States. The Trifecta GT valve was approved in 2016.
Medical device reports (MDRs) received by the FDA describe early SVD with Trifecta valves, with a peak time to SVD of 3 to 4 years post-implant. “Reported outcomes include surgical valve explant/replacement, transcatheter valve-in-valve intervention, and in some cases death,” the FDA notes.
In a letter to customers, Abbott says a “complaint analysis has shown that most cases of early SVD which occur within 5 years post-implant are characterized as a non-calcific leaflet tear, while most cases of late SVD which occur beyond 5 years post-implant are characterized as a fibrous-calcific SVD.”
The FDA recommends that health care providers take the following actions:
- Be aware of the potential risk of early SVD with Trifecta valves, and current patient management considerations, as communicated by Abbott.
- Discuss the risks and benefits of all available aortic valve treatment options with patients and caregivers as part of shared clinical decision-making prior to surgery.
- Read and carefully follow the Instructions for Use when implanting a Trifecta GT valve.
- Monitor patients who have undergone implantation with Trifecta valves for signs and symptoms of potential SVD.
- Instruct patients to seek medical attention with new onset of symptoms such as shortness of breath or fatigue.
- Ensure lifelong follow-up visits, conducted at least yearly, including transthoracic echocardiogram assessment of the valve beginning 1-year post-implant.
The FDA is working with Abbott to further evaluate the issue and develop additional patient management strategies, if needed. The FDA says it will continue to monitor the literature and reports of adverse events related to the issue.
Clinicians are encouraged to report any adverse events or quality problems with the Trifecta valves to their local Abbott representative or the customer service department at 1-800-544-1664.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
There is a potential risk of early structural valve deterioration with the Abbott Trifecta valve and Trifecta valve with glide technology (Trifecta GT), the U.S. Food and Drug Administration says in a letter to health care professionals posted on its website.
Evidence in the literature suggests a higher cumulative incidence of early structural valve deterioration (SVD) and a lower freedom from reintervention due to SVD with the Trifecta valves, compared with other commercially available bovine pericardial valves, the FDA says.
The Trifecta and Trifecta GT valves are heart valve replacement devices intended to treat diseased, damaged, or malfunctioning native or prosthetic aortic heart valves, the letter notes. The first-generation Trifecta valve was approved in 2011 but is no longer marketed in the United States. The Trifecta GT valve was approved in 2016.
Medical device reports (MDRs) received by the FDA describe early SVD with Trifecta valves, with a peak time to SVD of 3 to 4 years post-implant. “Reported outcomes include surgical valve explant/replacement, transcatheter valve-in-valve intervention, and in some cases death,” the FDA notes.
In a letter to customers, Abbott says a “complaint analysis has shown that most cases of early SVD which occur within 5 years post-implant are characterized as a non-calcific leaflet tear, while most cases of late SVD which occur beyond 5 years post-implant are characterized as a fibrous-calcific SVD.”
The FDA recommends that health care providers take the following actions:
- Be aware of the potential risk of early SVD with Trifecta valves, and current patient management considerations, as communicated by Abbott.
- Discuss the risks and benefits of all available aortic valve treatment options with patients and caregivers as part of shared clinical decision-making prior to surgery.
- Read and carefully follow the Instructions for Use when implanting a Trifecta GT valve.
- Monitor patients who have undergone implantation with Trifecta valves for signs and symptoms of potential SVD.
- Instruct patients to seek medical attention with new onset of symptoms such as shortness of breath or fatigue.
- Ensure lifelong follow-up visits, conducted at least yearly, including transthoracic echocardiogram assessment of the valve beginning 1-year post-implant.
The FDA is working with Abbott to further evaluate the issue and develop additional patient management strategies, if needed. The FDA says it will continue to monitor the literature and reports of adverse events related to the issue.
Clinicians are encouraged to report any adverse events or quality problems with the Trifecta valves to their local Abbott representative or the customer service department at 1-800-544-1664.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
There is a potential risk of early structural valve deterioration with the Abbott Trifecta valve and Trifecta valve with glide technology (Trifecta GT), the U.S. Food and Drug Administration says in a letter to health care professionals posted on its website.
Evidence in the literature suggests a higher cumulative incidence of early structural valve deterioration (SVD) and a lower freedom from reintervention due to SVD with the Trifecta valves, compared with other commercially available bovine pericardial valves, the FDA says.
The Trifecta and Trifecta GT valves are heart valve replacement devices intended to treat diseased, damaged, or malfunctioning native or prosthetic aortic heart valves, the letter notes. The first-generation Trifecta valve was approved in 2011 but is no longer marketed in the United States. The Trifecta GT valve was approved in 2016.
Medical device reports (MDRs) received by the FDA describe early SVD with Trifecta valves, with a peak time to SVD of 3 to 4 years post-implant. “Reported outcomes include surgical valve explant/replacement, transcatheter valve-in-valve intervention, and in some cases death,” the FDA notes.
In a letter to customers, Abbott says a “complaint analysis has shown that most cases of early SVD which occur within 5 years post-implant are characterized as a non-calcific leaflet tear, while most cases of late SVD which occur beyond 5 years post-implant are characterized as a fibrous-calcific SVD.”
The FDA recommends that health care providers take the following actions:
- Be aware of the potential risk of early SVD with Trifecta valves, and current patient management considerations, as communicated by Abbott.
- Discuss the risks and benefits of all available aortic valve treatment options with patients and caregivers as part of shared clinical decision-making prior to surgery.
- Read and carefully follow the Instructions for Use when implanting a Trifecta GT valve.
- Monitor patients who have undergone implantation with Trifecta valves for signs and symptoms of potential SVD.
- Instruct patients to seek medical attention with new onset of symptoms such as shortness of breath or fatigue.
- Ensure lifelong follow-up visits, conducted at least yearly, including transthoracic echocardiogram assessment of the valve beginning 1-year post-implant.
The FDA is working with Abbott to further evaluate the issue and develop additional patient management strategies, if needed. The FDA says it will continue to monitor the literature and reports of adverse events related to the issue.
Clinicians are encouraged to report any adverse events or quality problems with the Trifecta valves to their local Abbott representative or the customer service department at 1-800-544-1664.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Fewer than 10% of eligible type 2 diabetes patients get new, pricey drugs
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE