User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
How Doctors Use Music to Learn Faster and Perform Better
“Because you know I’m all about that base, ‘bout that base, no acid.”
Do those words sound familiar? That’s because they’re the lyrics to Meghan Trainor’s “All About That Bass,” slightly tweaked to function as a medical study tool.
Early in med school, J.C. Sue, DO, now a family medicine physician, refashioned the song’s words to help him prepare for a test on acid extruders and loaders. Sue’s version, “All About That Base,” contained his lecture notes. During the exam, he found himself mentally singing his parody and easily recalling the information. Plus, the approach made cramming a lot more palatable.
Sound silly? It’s not. Sue’s approach is backed up by science. Recently, a 2024 study from Canada suggested that musical memory doesn’t decrease with age. And a 2023 study revealed music was a better cue than food for helping both young and older adults recall autobiographical memories.
Inspired by his success, Sue gave popular songs a medical spin throughout his medical training. “There’s no rule that says studying must be boring, tedious, or torturous,” Sue said. “If you can make it fun, why not?”
Sue isn’t alone. Many physicians say that writing songs, listening to music, or playing instruments improves their focus, energy, and work performance, along with their confidence and well-being.
Why does music work so well?
Tune Your Brain to Work With Tunes
Remember learning your ABCs to the tune of “Twinkle, Twinkle, Little Star?” (Or ask any Gen X person about Schoolhouse Rock.)
In the classroom, music is an established tool for teaching kids, said Ruth Gotian, EdD, MS, chief learning officer and associate professor of education in anesthesiology at Weill Cornell Medicine, New York City. But she said musical strategies make studying easier for adults, too, no matter how complex the material.
Christopher Emdin, PhD, Maxine Greene chair and professor of science education at Teachers College, Columbia University, New York City, shares Gotian’s view. When teaching science, engineering, technology, and mathematics (STEM) subjects to high school kids, he challenged them to write raps about the new concepts.
That’s when he saw visible results: As his students took exams, Emdin noticed them nodding and moving their mouths and heads.
“They were literally performing the songs they’d written for themselves,” Emdin said. “When you write a song to a beat, it’s almost like your heartbeat. You know it so well; you can conjure up your memories by reciting the lyrics.”
If songwriting isn’t in your repertoire, you’ll be glad to hear that just listening to music while studying can help with retention. “Music keeps both sides of the brain stimulated, which has been shown to increase focus and motivation,” explained Anita A. Paschall, MD, PhD, Medical School and Healthcare Admissions expert/director of Medical School and Healthcare Admissions at The Princeton Review.
‘Mind on a Permanent Vacation’
Paschall’s enthusiasm comes from personal experience. While preparing for her board exams, Jimmy Buffet’s catalog was her study soundtrack. “His songs stayed in my mind. I could hum along without having to think about it, so my brain was free to focus,” she recalled.
Because Paschall grew up listening to Buffet’s tunes, they also evoked relaxing moments from her earlier life, which she found comforting and uplifting. The combination helped make long, intense study sessions more pleasant. After all, when you’re “wasting away again in Margaritaville,” how can you feel stressed and despondent?
Alexander Remy Bonnel, MD, clinical assistant professor of medicine at the University of Pennsylvania and a physician at Pennsylvania Hospital, both in Philadelphia, found ways to incorporate both auditory and visual stimuli in his med school study routine. He listened to music while color-coding his notes to link both cues to the information. As with Paschall, these tactics helped reduce the monotony of learning reams of material.
That gave Bonnel an easy way to establish an important element for memory: Novelty.
“When you need to memorize so many things in a short amount of time, you’re trying to vary ways of internalizing information,” he observed. “You have a higher chance of retaining information if there’s something unique about it.”
Building Team Harmony
“Almost every single OR I rotated through in med school had music playing,” Bonnel also recalled. Furthermore, he noticed a pattern to the chosen songs: Regardless of their age, surgeons selected playlists of tunes that had been popular when they were in their 20s. Those golden oldies, from any era, could turn the OR team into a focused, cohesive unit.
Kyle McCormick, MD, a fifth-year resident in orthopedic surgery at New York–Presbyterian Hospital, Columbia University Irving Medical Center, New York City, has also noticed the ubiquity of background music in ORs. Her observation: Surgeons tend to choose universally popular, inoffensive songs, like tracks from Hall & Oates and Fleetwood Mac.
This meshes with the results of a joint survey of nearly 700 surgeons and other healthcare professionals conducted by Spotify and Figure 1 in 2021; 90% of the surgeons and surgical residents who responded said they listened to music in the OR. Rock and pop were the most popular genres, followed by classical, jazz, and then R&B.
Regardless of genre, music helped the surgical teams focus and feel less tense, the surgeons reported. But when training younger doctors, managing complications, or performing during critical points in surgery, many said they’d lower the volume.
Outside the OR, music can also help foster connection between colleagues. For Lawrence C. Loh, MD, MPH, adjunct professor at Dalla Lana School of Public Health at the University of Toronto in Ontario, Canada, playing guitar and piano has helped him connect with his staff. “I’ve played tunes at staff gatherings and recorded videos as encouragement during the emergency response for COVID-19,” he shared.
In his free time, Loh has also organized outings to his local pub’s weekly karaoke show for more than a decade. His goal: “Promote social cohesion and combat loneliness among my friend and social networks.”
Get Your Own Musical Boost
If all this sounds like music to your ears, here are some ways to try it yourself.
Find a study soundtrack. When choosing study music, follow Paschall’s lead and pick songs you know well so they’ll remain in the background. Also, compile a soundtrack you find pleasant and mood-boosting to help relieve the tedium of study and decrease stress.
Keep in mind that we all take in and process information differently, said Gotian. So background music during study sessions might not work for you. According to a 2017 study published in Frontiers in Psychology, it can be a distraction and impair learning for some. Do what works.
Get pumped with a “walkup song.” What songs make you feel like you could conquer the world? asked Emdin. Or what soundtrack would be playing if you were ascending a stage to accept an award or walking out to take the mound in the ninth inning? Those songs should be on what he calls your “superhero” or “walkup” playlist. His prescription: Tune in before you begin your workday or start a challenging procedure.
Paschall agrees and recommends her students and clients listen to music before sitting down for an exam. Forget reviewing flashcards for the nth time, she counseled. Putting on headphones (or earbuds) will put you in a “better headspace.”
Choose work and play playlists. As well as incorporating tunes in your clinic or hospital, music can help relieve stress at the end of the workday. “Medical culture can often be detrimental to doctors’ health,” said Sue, who credits music with helping him maintain equanimity.
Bonnel can relate. Practicing and performing with the Penn Medicine Symphony Orchestra offers him a sense of community and relief from the stress of modern life. “For 2 hours every Tuesday, I put my phone away and just play,” he said. “It’s nice to have those moments when I’m temporarily disconnected and can just focus on one thing: Playing.”
Scale Up Your Career
Years after med school graduation, Sue still recalls many of the tunes he wrote to help him remember information. When he sings a song in his head, he’ll get a refresher on pediatric developmental milestones, medication side effects, anatomical details, and more, which informs the treatment plans he devises for patients. To help other doctors reap these benefits, Sue created the website Tune Rx, a medical music study resource that includes many of the roughly 100 songs he’s written.
Emdin often discusses his musical strategies during talks on STEM education. Initially, people are skeptical, he said. But the idea quickly rings a bell for audience members. “They come up to me afterward to share anecdotes,” Emdin said. “If you have enough anecdotes, there’s a pattern. So let’s create a process. Let’s be intentional about using music as a learning strategy,” he urged.
A version of this article first appeared on Medscape.com.
“Because you know I’m all about that base, ‘bout that base, no acid.”
Do those words sound familiar? That’s because they’re the lyrics to Meghan Trainor’s “All About That Bass,” slightly tweaked to function as a medical study tool.
Early in med school, J.C. Sue, DO, now a family medicine physician, refashioned the song’s words to help him prepare for a test on acid extruders and loaders. Sue’s version, “All About That Base,” contained his lecture notes. During the exam, he found himself mentally singing his parody and easily recalling the information. Plus, the approach made cramming a lot more palatable.
Sound silly? It’s not. Sue’s approach is backed up by science. Recently, a 2024 study from Canada suggested that musical memory doesn’t decrease with age. And a 2023 study revealed music was a better cue than food for helping both young and older adults recall autobiographical memories.
Inspired by his success, Sue gave popular songs a medical spin throughout his medical training. “There’s no rule that says studying must be boring, tedious, or torturous,” Sue said. “If you can make it fun, why not?”
Sue isn’t alone. Many physicians say that writing songs, listening to music, or playing instruments improves their focus, energy, and work performance, along with their confidence and well-being.
Why does music work so well?
Tune Your Brain to Work With Tunes
Remember learning your ABCs to the tune of “Twinkle, Twinkle, Little Star?” (Or ask any Gen X person about Schoolhouse Rock.)
In the classroom, music is an established tool for teaching kids, said Ruth Gotian, EdD, MS, chief learning officer and associate professor of education in anesthesiology at Weill Cornell Medicine, New York City. But she said musical strategies make studying easier for adults, too, no matter how complex the material.
Christopher Emdin, PhD, Maxine Greene chair and professor of science education at Teachers College, Columbia University, New York City, shares Gotian’s view. When teaching science, engineering, technology, and mathematics (STEM) subjects to high school kids, he challenged them to write raps about the new concepts.
That’s when he saw visible results: As his students took exams, Emdin noticed them nodding and moving their mouths and heads.
“They were literally performing the songs they’d written for themselves,” Emdin said. “When you write a song to a beat, it’s almost like your heartbeat. You know it so well; you can conjure up your memories by reciting the lyrics.”
If songwriting isn’t in your repertoire, you’ll be glad to hear that just listening to music while studying can help with retention. “Music keeps both sides of the brain stimulated, which has been shown to increase focus and motivation,” explained Anita A. Paschall, MD, PhD, Medical School and Healthcare Admissions expert/director of Medical School and Healthcare Admissions at The Princeton Review.
‘Mind on a Permanent Vacation’
Paschall’s enthusiasm comes from personal experience. While preparing for her board exams, Jimmy Buffet’s catalog was her study soundtrack. “His songs stayed in my mind. I could hum along without having to think about it, so my brain was free to focus,” she recalled.
Because Paschall grew up listening to Buffet’s tunes, they also evoked relaxing moments from her earlier life, which she found comforting and uplifting. The combination helped make long, intense study sessions more pleasant. After all, when you’re “wasting away again in Margaritaville,” how can you feel stressed and despondent?
Alexander Remy Bonnel, MD, clinical assistant professor of medicine at the University of Pennsylvania and a physician at Pennsylvania Hospital, both in Philadelphia, found ways to incorporate both auditory and visual stimuli in his med school study routine. He listened to music while color-coding his notes to link both cues to the information. As with Paschall, these tactics helped reduce the monotony of learning reams of material.
That gave Bonnel an easy way to establish an important element for memory: Novelty.
“When you need to memorize so many things in a short amount of time, you’re trying to vary ways of internalizing information,” he observed. “You have a higher chance of retaining information if there’s something unique about it.”
Building Team Harmony
“Almost every single OR I rotated through in med school had music playing,” Bonnel also recalled. Furthermore, he noticed a pattern to the chosen songs: Regardless of their age, surgeons selected playlists of tunes that had been popular when they were in their 20s. Those golden oldies, from any era, could turn the OR team into a focused, cohesive unit.
Kyle McCormick, MD, a fifth-year resident in orthopedic surgery at New York–Presbyterian Hospital, Columbia University Irving Medical Center, New York City, has also noticed the ubiquity of background music in ORs. Her observation: Surgeons tend to choose universally popular, inoffensive songs, like tracks from Hall & Oates and Fleetwood Mac.
This meshes with the results of a joint survey of nearly 700 surgeons and other healthcare professionals conducted by Spotify and Figure 1 in 2021; 90% of the surgeons and surgical residents who responded said they listened to music in the OR. Rock and pop were the most popular genres, followed by classical, jazz, and then R&B.
Regardless of genre, music helped the surgical teams focus and feel less tense, the surgeons reported. But when training younger doctors, managing complications, or performing during critical points in surgery, many said they’d lower the volume.
Outside the OR, music can also help foster connection between colleagues. For Lawrence C. Loh, MD, MPH, adjunct professor at Dalla Lana School of Public Health at the University of Toronto in Ontario, Canada, playing guitar and piano has helped him connect with his staff. “I’ve played tunes at staff gatherings and recorded videos as encouragement during the emergency response for COVID-19,” he shared.
In his free time, Loh has also organized outings to his local pub’s weekly karaoke show for more than a decade. His goal: “Promote social cohesion and combat loneliness among my friend and social networks.”
Get Your Own Musical Boost
If all this sounds like music to your ears, here are some ways to try it yourself.
Find a study soundtrack. When choosing study music, follow Paschall’s lead and pick songs you know well so they’ll remain in the background. Also, compile a soundtrack you find pleasant and mood-boosting to help relieve the tedium of study and decrease stress.
Keep in mind that we all take in and process information differently, said Gotian. So background music during study sessions might not work for you. According to a 2017 study published in Frontiers in Psychology, it can be a distraction and impair learning for some. Do what works.
Get pumped with a “walkup song.” What songs make you feel like you could conquer the world? asked Emdin. Or what soundtrack would be playing if you were ascending a stage to accept an award or walking out to take the mound in the ninth inning? Those songs should be on what he calls your “superhero” or “walkup” playlist. His prescription: Tune in before you begin your workday or start a challenging procedure.
Paschall agrees and recommends her students and clients listen to music before sitting down for an exam. Forget reviewing flashcards for the nth time, she counseled. Putting on headphones (or earbuds) will put you in a “better headspace.”
Choose work and play playlists. As well as incorporating tunes in your clinic or hospital, music can help relieve stress at the end of the workday. “Medical culture can often be detrimental to doctors’ health,” said Sue, who credits music with helping him maintain equanimity.
Bonnel can relate. Practicing and performing with the Penn Medicine Symphony Orchestra offers him a sense of community and relief from the stress of modern life. “For 2 hours every Tuesday, I put my phone away and just play,” he said. “It’s nice to have those moments when I’m temporarily disconnected and can just focus on one thing: Playing.”
Scale Up Your Career
Years after med school graduation, Sue still recalls many of the tunes he wrote to help him remember information. When he sings a song in his head, he’ll get a refresher on pediatric developmental milestones, medication side effects, anatomical details, and more, which informs the treatment plans he devises for patients. To help other doctors reap these benefits, Sue created the website Tune Rx, a medical music study resource that includes many of the roughly 100 songs he’s written.
Emdin often discusses his musical strategies during talks on STEM education. Initially, people are skeptical, he said. But the idea quickly rings a bell for audience members. “They come up to me afterward to share anecdotes,” Emdin said. “If you have enough anecdotes, there’s a pattern. So let’s create a process. Let’s be intentional about using music as a learning strategy,” he urged.
A version of this article first appeared on Medscape.com.
“Because you know I’m all about that base, ‘bout that base, no acid.”
Do those words sound familiar? That’s because they’re the lyrics to Meghan Trainor’s “All About That Bass,” slightly tweaked to function as a medical study tool.
Early in med school, J.C. Sue, DO, now a family medicine physician, refashioned the song’s words to help him prepare for a test on acid extruders and loaders. Sue’s version, “All About That Base,” contained his lecture notes. During the exam, he found himself mentally singing his parody and easily recalling the information. Plus, the approach made cramming a lot more palatable.
Sound silly? It’s not. Sue’s approach is backed up by science. Recently, a 2024 study from Canada suggested that musical memory doesn’t decrease with age. And a 2023 study revealed music was a better cue than food for helping both young and older adults recall autobiographical memories.
Inspired by his success, Sue gave popular songs a medical spin throughout his medical training. “There’s no rule that says studying must be boring, tedious, or torturous,” Sue said. “If you can make it fun, why not?”
Sue isn’t alone. Many physicians say that writing songs, listening to music, or playing instruments improves their focus, energy, and work performance, along with their confidence and well-being.
Why does music work so well?
Tune Your Brain to Work With Tunes
Remember learning your ABCs to the tune of “Twinkle, Twinkle, Little Star?” (Or ask any Gen X person about Schoolhouse Rock.)
In the classroom, music is an established tool for teaching kids, said Ruth Gotian, EdD, MS, chief learning officer and associate professor of education in anesthesiology at Weill Cornell Medicine, New York City. But she said musical strategies make studying easier for adults, too, no matter how complex the material.
Christopher Emdin, PhD, Maxine Greene chair and professor of science education at Teachers College, Columbia University, New York City, shares Gotian’s view. When teaching science, engineering, technology, and mathematics (STEM) subjects to high school kids, he challenged them to write raps about the new concepts.
That’s when he saw visible results: As his students took exams, Emdin noticed them nodding and moving their mouths and heads.
“They were literally performing the songs they’d written for themselves,” Emdin said. “When you write a song to a beat, it’s almost like your heartbeat. You know it so well; you can conjure up your memories by reciting the lyrics.”
If songwriting isn’t in your repertoire, you’ll be glad to hear that just listening to music while studying can help with retention. “Music keeps both sides of the brain stimulated, which has been shown to increase focus and motivation,” explained Anita A. Paschall, MD, PhD, Medical School and Healthcare Admissions expert/director of Medical School and Healthcare Admissions at The Princeton Review.
‘Mind on a Permanent Vacation’
Paschall’s enthusiasm comes from personal experience. While preparing for her board exams, Jimmy Buffet’s catalog was her study soundtrack. “His songs stayed in my mind. I could hum along without having to think about it, so my brain was free to focus,” she recalled.
Because Paschall grew up listening to Buffet’s tunes, they also evoked relaxing moments from her earlier life, which she found comforting and uplifting. The combination helped make long, intense study sessions more pleasant. After all, when you’re “wasting away again in Margaritaville,” how can you feel stressed and despondent?
Alexander Remy Bonnel, MD, clinical assistant professor of medicine at the University of Pennsylvania and a physician at Pennsylvania Hospital, both in Philadelphia, found ways to incorporate both auditory and visual stimuli in his med school study routine. He listened to music while color-coding his notes to link both cues to the information. As with Paschall, these tactics helped reduce the monotony of learning reams of material.
That gave Bonnel an easy way to establish an important element for memory: Novelty.
“When you need to memorize so many things in a short amount of time, you’re trying to vary ways of internalizing information,” he observed. “You have a higher chance of retaining information if there’s something unique about it.”
Building Team Harmony
“Almost every single OR I rotated through in med school had music playing,” Bonnel also recalled. Furthermore, he noticed a pattern to the chosen songs: Regardless of their age, surgeons selected playlists of tunes that had been popular when they were in their 20s. Those golden oldies, from any era, could turn the OR team into a focused, cohesive unit.
Kyle McCormick, MD, a fifth-year resident in orthopedic surgery at New York–Presbyterian Hospital, Columbia University Irving Medical Center, New York City, has also noticed the ubiquity of background music in ORs. Her observation: Surgeons tend to choose universally popular, inoffensive songs, like tracks from Hall & Oates and Fleetwood Mac.
This meshes with the results of a joint survey of nearly 700 surgeons and other healthcare professionals conducted by Spotify and Figure 1 in 2021; 90% of the surgeons and surgical residents who responded said they listened to music in the OR. Rock and pop were the most popular genres, followed by classical, jazz, and then R&B.
Regardless of genre, music helped the surgical teams focus and feel less tense, the surgeons reported. But when training younger doctors, managing complications, or performing during critical points in surgery, many said they’d lower the volume.
Outside the OR, music can also help foster connection between colleagues. For Lawrence C. Loh, MD, MPH, adjunct professor at Dalla Lana School of Public Health at the University of Toronto in Ontario, Canada, playing guitar and piano has helped him connect with his staff. “I’ve played tunes at staff gatherings and recorded videos as encouragement during the emergency response for COVID-19,” he shared.
In his free time, Loh has also organized outings to his local pub’s weekly karaoke show for more than a decade. His goal: “Promote social cohesion and combat loneliness among my friend and social networks.”
Get Your Own Musical Boost
If all this sounds like music to your ears, here are some ways to try it yourself.
Find a study soundtrack. When choosing study music, follow Paschall’s lead and pick songs you know well so they’ll remain in the background. Also, compile a soundtrack you find pleasant and mood-boosting to help relieve the tedium of study and decrease stress.
Keep in mind that we all take in and process information differently, said Gotian. So background music during study sessions might not work for you. According to a 2017 study published in Frontiers in Psychology, it can be a distraction and impair learning for some. Do what works.
Get pumped with a “walkup song.” What songs make you feel like you could conquer the world? asked Emdin. Or what soundtrack would be playing if you were ascending a stage to accept an award or walking out to take the mound in the ninth inning? Those songs should be on what he calls your “superhero” or “walkup” playlist. His prescription: Tune in before you begin your workday or start a challenging procedure.
Paschall agrees and recommends her students and clients listen to music before sitting down for an exam. Forget reviewing flashcards for the nth time, she counseled. Putting on headphones (or earbuds) will put you in a “better headspace.”
Choose work and play playlists. As well as incorporating tunes in your clinic or hospital, music can help relieve stress at the end of the workday. “Medical culture can often be detrimental to doctors’ health,” said Sue, who credits music with helping him maintain equanimity.
Bonnel can relate. Practicing and performing with the Penn Medicine Symphony Orchestra offers him a sense of community and relief from the stress of modern life. “For 2 hours every Tuesday, I put my phone away and just play,” he said. “It’s nice to have those moments when I’m temporarily disconnected and can just focus on one thing: Playing.”
Scale Up Your Career
Years after med school graduation, Sue still recalls many of the tunes he wrote to help him remember information. When he sings a song in his head, he’ll get a refresher on pediatric developmental milestones, medication side effects, anatomical details, and more, which informs the treatment plans he devises for patients. To help other doctors reap these benefits, Sue created the website Tune Rx, a medical music study resource that includes many of the roughly 100 songs he’s written.
Emdin often discusses his musical strategies during talks on STEM education. Initially, people are skeptical, he said. But the idea quickly rings a bell for audience members. “They come up to me afterward to share anecdotes,” Emdin said. “If you have enough anecdotes, there’s a pattern. So let’s create a process. Let’s be intentional about using music as a learning strategy,” he urged.
A version of this article first appeared on Medscape.com.
Heard of ApoB Testing? New Guidelines
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
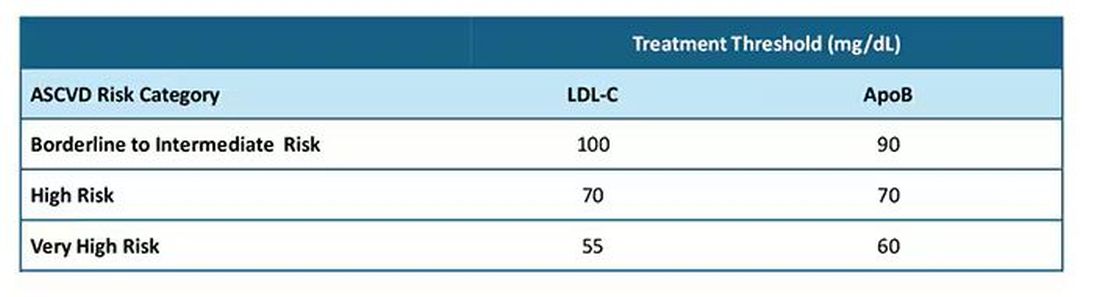
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
Fewer Recurrent Cardiovascular Events Seen With TNF Inhibitor Use in Axial Spondyloarthritis
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
70% of Doctors Would Discharge Noncompliant Patients, Medscape Survey Finds
Physicians shared their views on frequently discussed (and sometimes controversial) topics ranging from romances with patients to age-related competency tests in the latest report from Medscape Medical News.
The report captured data from over 1000 full- or part-time US physicians across more than 29 specialties who were surveyed over a 3-month period in 2024.
Responsibility toward their patients was a clear priority among the doctors surveyed.
While around 6 in 10 physicians said they would immediately discharge a patient who refused to follow their treatment recommendations, 8% said they would wait, and 31% indicated they would keep the patient.
Most doctors (91%) said they would not accept a gift of substantial monetary or sentimental value from a patient, adhering to the AMA Code of Medical Ethics.
Big gifts “may signal psychological issues, and it is not fair to patients who can’t afford big gifts, since they may encourage better care,” said Jason Doctor, PhD, a senior scholar at the USC Leonard D. Schaeffer Center for Health Policy & Economics in Los Angeles, California. “It also taints the doctor-patient relationship, which should not involve large gifts of expectations of reciprocity.”
The vast majority of doctors said a romantic relationship with a patient still in their care was unacceptable, although 1% felt it would be OK, and 9% said, “it depends.”
When asked if they might withhold information about a patient’s condition if disclosure could do more harm than good, the majority of doctors said no. But 38% said it depended on the situation.
“This is how the profession and public expectations are evolving from the old paternalistic approach,” said Peter Angood, MD, president and CEO of the American Association for Physician Leadership.
Meanwhile, most doctors (62%) said that an annual flu shot should be mandatory for physicians who see patients. And a substantial majority of doctors surveyed agreed that taking care of their physical and mental health amounts to an ethical duty.
Around three in four physicians surveyed said felt periodic bias training was necessary for doctors.
“We all need refreshers about our own bias and how to manage it,” one respondent said. But another physician said, “I think we all know what appropriate behavior is and don’t need to add yet another CME course, ugh.”
Roughly equal shares of doctors surveyed felt some obligation to take at least some Medicaid patients or felt no societal obligation. The remaining 18% were willing to treat Medicaid patients once states streamlined the rules and improved reimbursements.
And finally, nearly all the survey respondents said physicians should advise patients on the risks of marijuana, notwithstanding the number of states and localities that recently have legalized pot or cannabis products.
A version of this article first appeared on Medscape.com.
Physicians shared their views on frequently discussed (and sometimes controversial) topics ranging from romances with patients to age-related competency tests in the latest report from Medscape Medical News.
The report captured data from over 1000 full- or part-time US physicians across more than 29 specialties who were surveyed over a 3-month period in 2024.
Responsibility toward their patients was a clear priority among the doctors surveyed.
While around 6 in 10 physicians said they would immediately discharge a patient who refused to follow their treatment recommendations, 8% said they would wait, and 31% indicated they would keep the patient.
Most doctors (91%) said they would not accept a gift of substantial monetary or sentimental value from a patient, adhering to the AMA Code of Medical Ethics.
Big gifts “may signal psychological issues, and it is not fair to patients who can’t afford big gifts, since they may encourage better care,” said Jason Doctor, PhD, a senior scholar at the USC Leonard D. Schaeffer Center for Health Policy & Economics in Los Angeles, California. “It also taints the doctor-patient relationship, which should not involve large gifts of expectations of reciprocity.”
The vast majority of doctors said a romantic relationship with a patient still in their care was unacceptable, although 1% felt it would be OK, and 9% said, “it depends.”
When asked if they might withhold information about a patient’s condition if disclosure could do more harm than good, the majority of doctors said no. But 38% said it depended on the situation.
“This is how the profession and public expectations are evolving from the old paternalistic approach,” said Peter Angood, MD, president and CEO of the American Association for Physician Leadership.
Meanwhile, most doctors (62%) said that an annual flu shot should be mandatory for physicians who see patients. And a substantial majority of doctors surveyed agreed that taking care of their physical and mental health amounts to an ethical duty.
Around three in four physicians surveyed said felt periodic bias training was necessary for doctors.
“We all need refreshers about our own bias and how to manage it,” one respondent said. But another physician said, “I think we all know what appropriate behavior is and don’t need to add yet another CME course, ugh.”
Roughly equal shares of doctors surveyed felt some obligation to take at least some Medicaid patients or felt no societal obligation. The remaining 18% were willing to treat Medicaid patients once states streamlined the rules and improved reimbursements.
And finally, nearly all the survey respondents said physicians should advise patients on the risks of marijuana, notwithstanding the number of states and localities that recently have legalized pot or cannabis products.
A version of this article first appeared on Medscape.com.
Physicians shared their views on frequently discussed (and sometimes controversial) topics ranging from romances with patients to age-related competency tests in the latest report from Medscape Medical News.
The report captured data from over 1000 full- or part-time US physicians across more than 29 specialties who were surveyed over a 3-month period in 2024.
Responsibility toward their patients was a clear priority among the doctors surveyed.
While around 6 in 10 physicians said they would immediately discharge a patient who refused to follow their treatment recommendations, 8% said they would wait, and 31% indicated they would keep the patient.
Most doctors (91%) said they would not accept a gift of substantial monetary or sentimental value from a patient, adhering to the AMA Code of Medical Ethics.
Big gifts “may signal psychological issues, and it is not fair to patients who can’t afford big gifts, since they may encourage better care,” said Jason Doctor, PhD, a senior scholar at the USC Leonard D. Schaeffer Center for Health Policy & Economics in Los Angeles, California. “It also taints the doctor-patient relationship, which should not involve large gifts of expectations of reciprocity.”
The vast majority of doctors said a romantic relationship with a patient still in their care was unacceptable, although 1% felt it would be OK, and 9% said, “it depends.”
When asked if they might withhold information about a patient’s condition if disclosure could do more harm than good, the majority of doctors said no. But 38% said it depended on the situation.
“This is how the profession and public expectations are evolving from the old paternalistic approach,” said Peter Angood, MD, president and CEO of the American Association for Physician Leadership.
Meanwhile, most doctors (62%) said that an annual flu shot should be mandatory for physicians who see patients. And a substantial majority of doctors surveyed agreed that taking care of their physical and mental health amounts to an ethical duty.
Around three in four physicians surveyed said felt periodic bias training was necessary for doctors.
“We all need refreshers about our own bias and how to manage it,” one respondent said. But another physician said, “I think we all know what appropriate behavior is and don’t need to add yet another CME course, ugh.”
Roughly equal shares of doctors surveyed felt some obligation to take at least some Medicaid patients or felt no societal obligation. The remaining 18% were willing to treat Medicaid patients once states streamlined the rules and improved reimbursements.
And finally, nearly all the survey respondents said physicians should advise patients on the risks of marijuana, notwithstanding the number of states and localities that recently have legalized pot or cannabis products.
A version of this article first appeared on Medscape.com.
Heart Attack, Stroke Survivors at High Risk for Long COVID
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Genetic Risk for Gout Raises Risk for Cardiovascular Disease Independent of Urate Level
TOPLINE:
Genetic predisposition to gout, unfavorable lifestyle habits, and poor metabolic health are associated with an increased risk for cardiovascular disease (CVD); however, adherence to a healthy lifestyle can reduce this risk by up to 62%, even in individuals with high genetic risk.
METHODOLOGY:
- Researchers investigated the association between genetic predisposition to gout, combined with lifestyle habits, and the risk for CVD in two diverse prospective cohorts from different ancestral backgrounds.
- They analyzed the data of 224,689 participants of European descent from the UK Biobank (mean age, 57.0 years; 56.1% women) and 50,364 participants of East Asian descent from the Korean Genome and Epidemiology Study (KoGES; mean age, 53.7 years; 66.0% women).
- The genetic predisposition to gout was evaluated using a polygenic risk score (PRS) derived from a metagenome-wide association study, and the participants were categorized into low, intermediate, and high genetic risk groups based on their PRS for gout.
- A favorable lifestyle was defined as having ≥ 3 healthy lifestyle factors, and 0-1 metabolic syndrome factor defined the ideal metabolic health status.
- The incident CVD risk was evaluated according to genetic risk, lifestyle habits, and metabolic syndrome.
TAKEAWAY:
- Individuals in the high genetic risk group had a higher risk for CVD than those in the low genetic risk group in both the UK Biobank (adjusted hazard ratio [aHR], 1.10; P < .001) and KoGES (aHR, 1.31; P = .024) cohorts.
- In the UK Biobank cohort, individuals with a high genetic risk for gout and unfavorable lifestyle choices had a 1.99 times higher risk for incident CVD than those with low genetic risk (aHR, 1.99; P < .001); similar outcomes were observed in the KoGES cohort.
- Similarly, individuals with a high genetic risk for gout and poor metabolic health in the UK Biobank cohort had a 2.16 times higher risk for CVD than those with low genetic risk (aHR, 2.16; P < .001 for both); outcomes were no different in the KoGES cohort.
- Improving metabolic health and adhering to a healthy lifestyle reduced the risk for CVD by 62% in individuals with high genetic risk and by 46% in those with low genetic risk (P < .001 for both).
IN PRACTICE:
“PRS for gout can be used for preventing not only gout but also CVD. It is possible to identify individuals with high genetic risk for gout and strongly recommend modifying lifestyle habits. Weight reduction, smoking cessation, regular exercise, and eating healthy food are effective strategies to prevent gout and CVD,” the authors wrote.
SOURCE:
This study was led by Ki Won Moon, MD, PhD, Department of Internal Medicine, Kangwon National University School of Medicine, Chuncheon, Republic of Korea, and SangHyuk Jung, PhD, University of Pennsylvania, Philadelphia, and was published online on October 8, 2024, in RMD Open.
LIMITATIONS:
The definitions of lifestyle and metabolic syndrome were different in each cohort, which may have affected the findings. Data on lifestyle behaviors and metabolic health statuses were collected at enrollment, but these variables may have changed during the follow-up period, which potentially introduced bias into the results. This study was not able to establish causality between genetic predisposition to gout and the incident risk for CVD.
DISCLOSURES:
This study was supported by the National Institute of General Medical Sciences and the National Research Foundation of Korea. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Genetic predisposition to gout, unfavorable lifestyle habits, and poor metabolic health are associated with an increased risk for cardiovascular disease (CVD); however, adherence to a healthy lifestyle can reduce this risk by up to 62%, even in individuals with high genetic risk.
METHODOLOGY:
- Researchers investigated the association between genetic predisposition to gout, combined with lifestyle habits, and the risk for CVD in two diverse prospective cohorts from different ancestral backgrounds.
- They analyzed the data of 224,689 participants of European descent from the UK Biobank (mean age, 57.0 years; 56.1% women) and 50,364 participants of East Asian descent from the Korean Genome and Epidemiology Study (KoGES; mean age, 53.7 years; 66.0% women).
- The genetic predisposition to gout was evaluated using a polygenic risk score (PRS) derived from a metagenome-wide association study, and the participants were categorized into low, intermediate, and high genetic risk groups based on their PRS for gout.
- A favorable lifestyle was defined as having ≥ 3 healthy lifestyle factors, and 0-1 metabolic syndrome factor defined the ideal metabolic health status.
- The incident CVD risk was evaluated according to genetic risk, lifestyle habits, and metabolic syndrome.
TAKEAWAY:
- Individuals in the high genetic risk group had a higher risk for CVD than those in the low genetic risk group in both the UK Biobank (adjusted hazard ratio [aHR], 1.10; P < .001) and KoGES (aHR, 1.31; P = .024) cohorts.
- In the UK Biobank cohort, individuals with a high genetic risk for gout and unfavorable lifestyle choices had a 1.99 times higher risk for incident CVD than those with low genetic risk (aHR, 1.99; P < .001); similar outcomes were observed in the KoGES cohort.
- Similarly, individuals with a high genetic risk for gout and poor metabolic health in the UK Biobank cohort had a 2.16 times higher risk for CVD than those with low genetic risk (aHR, 2.16; P < .001 for both); outcomes were no different in the KoGES cohort.
- Improving metabolic health and adhering to a healthy lifestyle reduced the risk for CVD by 62% in individuals with high genetic risk and by 46% in those with low genetic risk (P < .001 for both).
IN PRACTICE:
“PRS for gout can be used for preventing not only gout but also CVD. It is possible to identify individuals with high genetic risk for gout and strongly recommend modifying lifestyle habits. Weight reduction, smoking cessation, regular exercise, and eating healthy food are effective strategies to prevent gout and CVD,” the authors wrote.
SOURCE:
This study was led by Ki Won Moon, MD, PhD, Department of Internal Medicine, Kangwon National University School of Medicine, Chuncheon, Republic of Korea, and SangHyuk Jung, PhD, University of Pennsylvania, Philadelphia, and was published online on October 8, 2024, in RMD Open.
LIMITATIONS:
The definitions of lifestyle and metabolic syndrome were different in each cohort, which may have affected the findings. Data on lifestyle behaviors and metabolic health statuses were collected at enrollment, but these variables may have changed during the follow-up period, which potentially introduced bias into the results. This study was not able to establish causality between genetic predisposition to gout and the incident risk for CVD.
DISCLOSURES:
This study was supported by the National Institute of General Medical Sciences and the National Research Foundation of Korea. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Genetic predisposition to gout, unfavorable lifestyle habits, and poor metabolic health are associated with an increased risk for cardiovascular disease (CVD); however, adherence to a healthy lifestyle can reduce this risk by up to 62%, even in individuals with high genetic risk.
METHODOLOGY:
- Researchers investigated the association between genetic predisposition to gout, combined with lifestyle habits, and the risk for CVD in two diverse prospective cohorts from different ancestral backgrounds.
- They analyzed the data of 224,689 participants of European descent from the UK Biobank (mean age, 57.0 years; 56.1% women) and 50,364 participants of East Asian descent from the Korean Genome and Epidemiology Study (KoGES; mean age, 53.7 years; 66.0% women).
- The genetic predisposition to gout was evaluated using a polygenic risk score (PRS) derived from a metagenome-wide association study, and the participants were categorized into low, intermediate, and high genetic risk groups based on their PRS for gout.
- A favorable lifestyle was defined as having ≥ 3 healthy lifestyle factors, and 0-1 metabolic syndrome factor defined the ideal metabolic health status.
- The incident CVD risk was evaluated according to genetic risk, lifestyle habits, and metabolic syndrome.
TAKEAWAY:
- Individuals in the high genetic risk group had a higher risk for CVD than those in the low genetic risk group in both the UK Biobank (adjusted hazard ratio [aHR], 1.10; P < .001) and KoGES (aHR, 1.31; P = .024) cohorts.
- In the UK Biobank cohort, individuals with a high genetic risk for gout and unfavorable lifestyle choices had a 1.99 times higher risk for incident CVD than those with low genetic risk (aHR, 1.99; P < .001); similar outcomes were observed in the KoGES cohort.
- Similarly, individuals with a high genetic risk for gout and poor metabolic health in the UK Biobank cohort had a 2.16 times higher risk for CVD than those with low genetic risk (aHR, 2.16; P < .001 for both); outcomes were no different in the KoGES cohort.
- Improving metabolic health and adhering to a healthy lifestyle reduced the risk for CVD by 62% in individuals with high genetic risk and by 46% in those with low genetic risk (P < .001 for both).
IN PRACTICE:
“PRS for gout can be used for preventing not only gout but also CVD. It is possible to identify individuals with high genetic risk for gout and strongly recommend modifying lifestyle habits. Weight reduction, smoking cessation, regular exercise, and eating healthy food are effective strategies to prevent gout and CVD,” the authors wrote.
SOURCE:
This study was led by Ki Won Moon, MD, PhD, Department of Internal Medicine, Kangwon National University School of Medicine, Chuncheon, Republic of Korea, and SangHyuk Jung, PhD, University of Pennsylvania, Philadelphia, and was published online on October 8, 2024, in RMD Open.
LIMITATIONS:
The definitions of lifestyle and metabolic syndrome were different in each cohort, which may have affected the findings. Data on lifestyle behaviors and metabolic health statuses were collected at enrollment, but these variables may have changed during the follow-up period, which potentially introduced bias into the results. This study was not able to establish causality between genetic predisposition to gout and the incident risk for CVD.
DISCLOSURES:
This study was supported by the National Institute of General Medical Sciences and the National Research Foundation of Korea. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Group Aims to Better Define ‘Extraordinarily Heterogeneous’ Mast Cell Activation Syndrome
Depending on one’s perspective, “mast cell activation syndrome (MCAS)” is either a relatively rare, narrowly defined severe allergic condition or a vastly underrecognized underlying cause of multiple chronic inflammatory conditions that affect roughly 17% of the entire population.
Inappropriate activation of mast cells — now termed mast cell activation disease (MCAD) — has long been known to underlie allergic symptoms and inflammation, and far less commonly, neoplasias such as mastocytosis. The concept of chronic, persistent MCAS associated with aberrant growth and dystrophism is more recent, emerging only in the last couple of decades as a separate entity under the MCAD heading.
Observational studies and clinical experience have linked signs and symptoms of MCAS with other inflammatory chronic conditions such as hypermobile Ehlers-Danlos Syndrome (EDS), postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and recently, long COVID. However, those conditions themselves are diagnostically challenging, and as yet there is no proof of causation.
The idea that MCAS is the entity — or at least, a key one — at the center of “a confoundingly, extraordinarily heterogeneous chronic multisystem polymorbidity” was the theme of a recent 4-day meeting of a professional group informally dubbed “Masterminds.” Since their first meeting in 2018, the group has grown from about 35 to nearly 650 multidisciplinary professionals.
Stephanie L. Grach, MD, assistant professor of medicine at the Mayo Clinic, Rochester, Minnesota, gave an introductory talk about the importance of changing “the medical paradigm around complex chronic illness.” Much of the rest of the meeting was devoted to sharing approaches for managing MCAS comorbidities, including dysautonomia, hypermobility, and associated craniocervical dysfunction, and various other multi-system conditions characterized by chronic pain and/or fatigue. Several talks covered the use of agents that block mast cell activity as potential treatment.
In an interview, Grach said “the meeting was an exciting example of how not only research, but also medicine, is moving forward, and it’s really cool to see that people are independently coming to very similar conclusions about shared pathologies, and because of that, the importance of overlap amongst complex medical conditions that historically have really been poorly addressed.”
She added, “mast cell activation, or mast cell hyperactivity, is one part of the greater picture. What’s important about the mast cell component is that of the multiple different targetable pathologies, it’s one that currently has potential available therapies that can be explored, some of them relatively easily.”
But Christopher Chang, MD, PhD, chief of the Pediatric Allergy and Immunology program, Joe DiMaggio Children’s Hospital, Hollywood, Florida, sees it differently. In an interview, he noted that the reason for disagreement over what constitutes MCAS is that “it doesn’t have a lot of objective findings that we can identify. ... We know that mast cells are important immune cells, just like all immune cells are important. It seems like whenever someone has unexplained symptoms, people try to blame it on mast cells. But it’s very hard to prove that.”
Two Definitions Characterize the Illness Differently
One proposed “consensus” MCAS definition was first published in 2011 by a group led by hematologist Peter Valent, MD, of the Medical University of Vienna in Austria. It has been revised since, and similar versions adopted by medical societies, including the American Academy of Allergy, Asthma & Immunology (AAAAI). The most recent versions propose three core MCAS criteria:
- Typical clinical signs of severe, recurrent (episodic) systemic (at least two organ systems) MCA are present (often in the form of anaphylaxis).
- The involvement of mast cells (MCs) is documented by biochemical studies, preferably an increase in serum tryptase levels from the individual’s baseline to plus 20% + 2 ng/mL.
- Response of symptoms to therapy with MC-stabilizing agents, drugs directed against MC mediator production, or drugs blocking mediator release or effects of MC-derived mediators.
The following year, a separate publication authored by Gerhard J. Molderings, MD, University of Bonn in Germany, and colleagues proposed a much broader MCAS definition. Also revised since, the latest “consensus-2” was published in 2020. This definition consists of one major criterion: “A constellation of clinical complaints attributable to pathologically increased MC activity, ie, MC mediator release syndrome.” This “constellation” involves conditions of nearly every organ system that, taken together, are estimated to affect up to 17% of the entire population. These are just a few examples:
- Constitutional: Chronic fatigue, flushing, or sweats
- Dermatologic: Rashes or lesions
- Ophthalmologic: dry eyes
- Oral: Burning or itching in mouth
- Pulmonary: Airway inflammation at any/all levels
- Cardiovascular: Blood pressure lability or codiagnosis of POTS is common
- Gastrointestinal: Reflux, dysphagia, or malabsorption
- Genitourinary: Endometriosis, dysmenorrhea, or dyspareunia
- Musculoskeletal/connective tissue: Fibromyalgia or diagnosis of hypermobile EDS is common
- Neurologic: Headaches or sensory neuropathies
- Psychiatric: Depression or anxiety
- Endocrinologic: Thyroid disease or dyslipidemia
- Hematologic: Polycythemia or anemia (after ruling out other causes)
The diagnosis is made by fulfilling that major criterion, plus at least one objective assessment of pathologically increased release of MC mediators, including infiltrates, abnormal MC morphology, or MC genetic changes shown to increase MC activity. Other alternatives include evidence of above-normal levels of MC mediators, including tryptase, histamine or its metabolites, heparin, or chromatin A, in whole blood, serum, plasma, or urine. Symptomatic response to MC activation inhibitors can also be used but isn’t required as it is in the other definition.
Underdiagnosis vs Overdiagnosis
Lawrence B. Afrin, MD, senior consultant in hematology/oncology at the AIM Center for Personalized Medicine, Westchester, New York, and lead author of the 2020 update of the broader “consensus-2” criteria, said in an interview, “we now know MCAS exists, and it’s prevalent, even though, for understandable and forgivable reasons, we’ve been missing it all along. ... If you see a patient who has this chronic, multisystem unwellness with general themes of inflammation plus or minus allergic issues and you can’t find some other rational explanation that better accounts for what’s going on ... then it’s reasonable to think to include MCAS in the differential diagnosis. If the patient happens not to fit the diagnostic criteria being advanced by one group, that doesn’t necessarily rule out the possibility that this is still going on.”
Afrin, along with his coauthors, faulted the narrower “consensus-1” definition for lacking data to support the “20% + 2” criteria for requiring the difficult determination of a patient’s “baseline” and for requiring evidence of response to treatment prior to making the diagnosis. Not all patients will respond to a given histamine blocker, he noted.
But Lawrence B. Schwartz, MD, PhD, an author on both the Valent and AAAAI criteria, disagreed, noting that the narrower criteria “appear to have a high degree of specificity and sensitivity when the reaction is systemic and involves hypotension. Less severe clinical events, particularly involving the gastrointestinal or central nervous systems, do not have precise clinical or biomarker criteria for identifying mast cell involvement.”
Added Schwartz, who is professor of medicine and chair of the Division of Rheumatology, Allergy, and Immunology and program director of Allergy and Immunology, Virginia Commonwealth University (VCU), Richmond, “when mast cell activation events occur only in the skin, we refer to it as chronic urticaria and in the airways or conjunctiva of allergic individuals as allergic asthma, rhinitis, and/or conjunctivitis. The absence of specific criteria for mast cell activation in the GI [gastrointestinal] tract or CNS [central nervous system] neither rules in mast cell involvement nor does it rule out mast cell involvement. Thus, more research is needed to find better diagnostic criteria.”
Schwartz also pointed to a recent paper reporting the use of artificial intelligence models to “quantify diagnostic precision and specificity” of “alternative” MCAS definitions. The conclusion was a “lack of specificity is pronounced in relation to multiple control criteria, raising the concern that alternative criteria could disproportionately contribute to MCAS overdiagnosis, to the exclusion of more appropriate diagnoses.”
During the meeting, Afrin acknowledged that the broader view risks overdiagnosis of MCAS. However, he also referenced Occam’s razor, the principle that the simplest explanation is probably the best one. “Which scenario is more likely? Multiple diagnoses and problems that are all independent of each other vs one diagnosis that’s biologically capable of causing most or all of the findings, ie, the simplest solution even if it’s not the most immediately obvious solution?”
He said in an interview: “Do we have any proof that MCAS is what’s underlying hypermobile Ehlers-Danlos or POTS or chronic fatigue? No, we don’t have any proof, not because anybody has done studies that have shown there to be no connection but simply because we’re so early in our awareness that the disease even exists that the necessary studies haven’t even been done yet.”
At the meeting, Afrin introduced proposals to turn the “Masterminds” group into a formal professional society and to launch a journal. He also gave an update on progress in developing a symptom assessment tool both for clinical use and to enable clinical trials of new drugs to target mast cells or their mediators. The plan is to field test the tool in 2025 and publish those results in 2026.
Grach, Afrin, and Chang had no disclosures. Schwartz discovered tryptase and invented the Thermo Fisher tryptase assay, for which his institution (VCU) receives royalties that are shared with him. He also invented monoclonal antibodies used for detecting mast cells or basophils, for which VCU receives royalties from several companies, including Millipore, Santa Cruz, BioLegend, and Hycult Biotech, that are also shared with him. He is a paid consultant for Blueprint Medicines, Celldex Therapeutics, Invea, Third Harmonic Bio, HYCOR Biomedical, Jasper, TerSera Therapeutics, and GLG. He also serves on an AstraZeneca data safety monitoring board for a clinical trial involving benralizumab treatment of hypereosinophilic syndrome and receives royalties from UpToDate (biomarkers for anaphylaxis) and Goldman-Cecil Medicine (anaphylaxis).
A version of this article first appeared on Medscape.com.
Depending on one’s perspective, “mast cell activation syndrome (MCAS)” is either a relatively rare, narrowly defined severe allergic condition or a vastly underrecognized underlying cause of multiple chronic inflammatory conditions that affect roughly 17% of the entire population.
Inappropriate activation of mast cells — now termed mast cell activation disease (MCAD) — has long been known to underlie allergic symptoms and inflammation, and far less commonly, neoplasias such as mastocytosis. The concept of chronic, persistent MCAS associated with aberrant growth and dystrophism is more recent, emerging only in the last couple of decades as a separate entity under the MCAD heading.
Observational studies and clinical experience have linked signs and symptoms of MCAS with other inflammatory chronic conditions such as hypermobile Ehlers-Danlos Syndrome (EDS), postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and recently, long COVID. However, those conditions themselves are diagnostically challenging, and as yet there is no proof of causation.
The idea that MCAS is the entity — or at least, a key one — at the center of “a confoundingly, extraordinarily heterogeneous chronic multisystem polymorbidity” was the theme of a recent 4-day meeting of a professional group informally dubbed “Masterminds.” Since their first meeting in 2018, the group has grown from about 35 to nearly 650 multidisciplinary professionals.
Stephanie L. Grach, MD, assistant professor of medicine at the Mayo Clinic, Rochester, Minnesota, gave an introductory talk about the importance of changing “the medical paradigm around complex chronic illness.” Much of the rest of the meeting was devoted to sharing approaches for managing MCAS comorbidities, including dysautonomia, hypermobility, and associated craniocervical dysfunction, and various other multi-system conditions characterized by chronic pain and/or fatigue. Several talks covered the use of agents that block mast cell activity as potential treatment.
In an interview, Grach said “the meeting was an exciting example of how not only research, but also medicine, is moving forward, and it’s really cool to see that people are independently coming to very similar conclusions about shared pathologies, and because of that, the importance of overlap amongst complex medical conditions that historically have really been poorly addressed.”
She added, “mast cell activation, or mast cell hyperactivity, is one part of the greater picture. What’s important about the mast cell component is that of the multiple different targetable pathologies, it’s one that currently has potential available therapies that can be explored, some of them relatively easily.”
But Christopher Chang, MD, PhD, chief of the Pediatric Allergy and Immunology program, Joe DiMaggio Children’s Hospital, Hollywood, Florida, sees it differently. In an interview, he noted that the reason for disagreement over what constitutes MCAS is that “it doesn’t have a lot of objective findings that we can identify. ... We know that mast cells are important immune cells, just like all immune cells are important. It seems like whenever someone has unexplained symptoms, people try to blame it on mast cells. But it’s very hard to prove that.”
Two Definitions Characterize the Illness Differently
One proposed “consensus” MCAS definition was first published in 2011 by a group led by hematologist Peter Valent, MD, of the Medical University of Vienna in Austria. It has been revised since, and similar versions adopted by medical societies, including the American Academy of Allergy, Asthma & Immunology (AAAAI). The most recent versions propose three core MCAS criteria:
- Typical clinical signs of severe, recurrent (episodic) systemic (at least two organ systems) MCA are present (often in the form of anaphylaxis).
- The involvement of mast cells (MCs) is documented by biochemical studies, preferably an increase in serum tryptase levels from the individual’s baseline to plus 20% + 2 ng/mL.
- Response of symptoms to therapy with MC-stabilizing agents, drugs directed against MC mediator production, or drugs blocking mediator release or effects of MC-derived mediators.
The following year, a separate publication authored by Gerhard J. Molderings, MD, University of Bonn in Germany, and colleagues proposed a much broader MCAS definition. Also revised since, the latest “consensus-2” was published in 2020. This definition consists of one major criterion: “A constellation of clinical complaints attributable to pathologically increased MC activity, ie, MC mediator release syndrome.” This “constellation” involves conditions of nearly every organ system that, taken together, are estimated to affect up to 17% of the entire population. These are just a few examples:
- Constitutional: Chronic fatigue, flushing, or sweats
- Dermatologic: Rashes or lesions
- Ophthalmologic: dry eyes
- Oral: Burning or itching in mouth
- Pulmonary: Airway inflammation at any/all levels
- Cardiovascular: Blood pressure lability or codiagnosis of POTS is common
- Gastrointestinal: Reflux, dysphagia, or malabsorption
- Genitourinary: Endometriosis, dysmenorrhea, or dyspareunia
- Musculoskeletal/connective tissue: Fibromyalgia or diagnosis of hypermobile EDS is common
- Neurologic: Headaches or sensory neuropathies
- Psychiatric: Depression or anxiety
- Endocrinologic: Thyroid disease or dyslipidemia
- Hematologic: Polycythemia or anemia (after ruling out other causes)
The diagnosis is made by fulfilling that major criterion, plus at least one objective assessment of pathologically increased release of MC mediators, including infiltrates, abnormal MC morphology, or MC genetic changes shown to increase MC activity. Other alternatives include evidence of above-normal levels of MC mediators, including tryptase, histamine or its metabolites, heparin, or chromatin A, in whole blood, serum, plasma, or urine. Symptomatic response to MC activation inhibitors can also be used but isn’t required as it is in the other definition.
Underdiagnosis vs Overdiagnosis
Lawrence B. Afrin, MD, senior consultant in hematology/oncology at the AIM Center for Personalized Medicine, Westchester, New York, and lead author of the 2020 update of the broader “consensus-2” criteria, said in an interview, “we now know MCAS exists, and it’s prevalent, even though, for understandable and forgivable reasons, we’ve been missing it all along. ... If you see a patient who has this chronic, multisystem unwellness with general themes of inflammation plus or minus allergic issues and you can’t find some other rational explanation that better accounts for what’s going on ... then it’s reasonable to think to include MCAS in the differential diagnosis. If the patient happens not to fit the diagnostic criteria being advanced by one group, that doesn’t necessarily rule out the possibility that this is still going on.”
Afrin, along with his coauthors, faulted the narrower “consensus-1” definition for lacking data to support the “20% + 2” criteria for requiring the difficult determination of a patient’s “baseline” and for requiring evidence of response to treatment prior to making the diagnosis. Not all patients will respond to a given histamine blocker, he noted.
But Lawrence B. Schwartz, MD, PhD, an author on both the Valent and AAAAI criteria, disagreed, noting that the narrower criteria “appear to have a high degree of specificity and sensitivity when the reaction is systemic and involves hypotension. Less severe clinical events, particularly involving the gastrointestinal or central nervous systems, do not have precise clinical or biomarker criteria for identifying mast cell involvement.”
Added Schwartz, who is professor of medicine and chair of the Division of Rheumatology, Allergy, and Immunology and program director of Allergy and Immunology, Virginia Commonwealth University (VCU), Richmond, “when mast cell activation events occur only in the skin, we refer to it as chronic urticaria and in the airways or conjunctiva of allergic individuals as allergic asthma, rhinitis, and/or conjunctivitis. The absence of specific criteria for mast cell activation in the GI [gastrointestinal] tract or CNS [central nervous system] neither rules in mast cell involvement nor does it rule out mast cell involvement. Thus, more research is needed to find better diagnostic criteria.”
Schwartz also pointed to a recent paper reporting the use of artificial intelligence models to “quantify diagnostic precision and specificity” of “alternative” MCAS definitions. The conclusion was a “lack of specificity is pronounced in relation to multiple control criteria, raising the concern that alternative criteria could disproportionately contribute to MCAS overdiagnosis, to the exclusion of more appropriate diagnoses.”
During the meeting, Afrin acknowledged that the broader view risks overdiagnosis of MCAS. However, he also referenced Occam’s razor, the principle that the simplest explanation is probably the best one. “Which scenario is more likely? Multiple diagnoses and problems that are all independent of each other vs one diagnosis that’s biologically capable of causing most or all of the findings, ie, the simplest solution even if it’s not the most immediately obvious solution?”
He said in an interview: “Do we have any proof that MCAS is what’s underlying hypermobile Ehlers-Danlos or POTS or chronic fatigue? No, we don’t have any proof, not because anybody has done studies that have shown there to be no connection but simply because we’re so early in our awareness that the disease even exists that the necessary studies haven’t even been done yet.”
At the meeting, Afrin introduced proposals to turn the “Masterminds” group into a formal professional society and to launch a journal. He also gave an update on progress in developing a symptom assessment tool both for clinical use and to enable clinical trials of new drugs to target mast cells or their mediators. The plan is to field test the tool in 2025 and publish those results in 2026.
Grach, Afrin, and Chang had no disclosures. Schwartz discovered tryptase and invented the Thermo Fisher tryptase assay, for which his institution (VCU) receives royalties that are shared with him. He also invented monoclonal antibodies used for detecting mast cells or basophils, for which VCU receives royalties from several companies, including Millipore, Santa Cruz, BioLegend, and Hycult Biotech, that are also shared with him. He is a paid consultant for Blueprint Medicines, Celldex Therapeutics, Invea, Third Harmonic Bio, HYCOR Biomedical, Jasper, TerSera Therapeutics, and GLG. He also serves on an AstraZeneca data safety monitoring board for a clinical trial involving benralizumab treatment of hypereosinophilic syndrome and receives royalties from UpToDate (biomarkers for anaphylaxis) and Goldman-Cecil Medicine (anaphylaxis).
A version of this article first appeared on Medscape.com.
Depending on one’s perspective, “mast cell activation syndrome (MCAS)” is either a relatively rare, narrowly defined severe allergic condition or a vastly underrecognized underlying cause of multiple chronic inflammatory conditions that affect roughly 17% of the entire population.
Inappropriate activation of mast cells — now termed mast cell activation disease (MCAD) — has long been known to underlie allergic symptoms and inflammation, and far less commonly, neoplasias such as mastocytosis. The concept of chronic, persistent MCAS associated with aberrant growth and dystrophism is more recent, emerging only in the last couple of decades as a separate entity under the MCAD heading.
Observational studies and clinical experience have linked signs and symptoms of MCAS with other inflammatory chronic conditions such as hypermobile Ehlers-Danlos Syndrome (EDS), postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and recently, long COVID. However, those conditions themselves are diagnostically challenging, and as yet there is no proof of causation.
The idea that MCAS is the entity — or at least, a key one — at the center of “a confoundingly, extraordinarily heterogeneous chronic multisystem polymorbidity” was the theme of a recent 4-day meeting of a professional group informally dubbed “Masterminds.” Since their first meeting in 2018, the group has grown from about 35 to nearly 650 multidisciplinary professionals.
Stephanie L. Grach, MD, assistant professor of medicine at the Mayo Clinic, Rochester, Minnesota, gave an introductory talk about the importance of changing “the medical paradigm around complex chronic illness.” Much of the rest of the meeting was devoted to sharing approaches for managing MCAS comorbidities, including dysautonomia, hypermobility, and associated craniocervical dysfunction, and various other multi-system conditions characterized by chronic pain and/or fatigue. Several talks covered the use of agents that block mast cell activity as potential treatment.
In an interview, Grach said “the meeting was an exciting example of how not only research, but also medicine, is moving forward, and it’s really cool to see that people are independently coming to very similar conclusions about shared pathologies, and because of that, the importance of overlap amongst complex medical conditions that historically have really been poorly addressed.”
She added, “mast cell activation, or mast cell hyperactivity, is one part of the greater picture. What’s important about the mast cell component is that of the multiple different targetable pathologies, it’s one that currently has potential available therapies that can be explored, some of them relatively easily.”
But Christopher Chang, MD, PhD, chief of the Pediatric Allergy and Immunology program, Joe DiMaggio Children’s Hospital, Hollywood, Florida, sees it differently. In an interview, he noted that the reason for disagreement over what constitutes MCAS is that “it doesn’t have a lot of objective findings that we can identify. ... We know that mast cells are important immune cells, just like all immune cells are important. It seems like whenever someone has unexplained symptoms, people try to blame it on mast cells. But it’s very hard to prove that.”
Two Definitions Characterize the Illness Differently
One proposed “consensus” MCAS definition was first published in 2011 by a group led by hematologist Peter Valent, MD, of the Medical University of Vienna in Austria. It has been revised since, and similar versions adopted by medical societies, including the American Academy of Allergy, Asthma & Immunology (AAAAI). The most recent versions propose three core MCAS criteria:
- Typical clinical signs of severe, recurrent (episodic) systemic (at least two organ systems) MCA are present (often in the form of anaphylaxis).
- The involvement of mast cells (MCs) is documented by biochemical studies, preferably an increase in serum tryptase levels from the individual’s baseline to plus 20% + 2 ng/mL.
- Response of symptoms to therapy with MC-stabilizing agents, drugs directed against MC mediator production, or drugs blocking mediator release or effects of MC-derived mediators.
The following year, a separate publication authored by Gerhard J. Molderings, MD, University of Bonn in Germany, and colleagues proposed a much broader MCAS definition. Also revised since, the latest “consensus-2” was published in 2020. This definition consists of one major criterion: “A constellation of clinical complaints attributable to pathologically increased MC activity, ie, MC mediator release syndrome.” This “constellation” involves conditions of nearly every organ system that, taken together, are estimated to affect up to 17% of the entire population. These are just a few examples:
- Constitutional: Chronic fatigue, flushing, or sweats
- Dermatologic: Rashes or lesions
- Ophthalmologic: dry eyes
- Oral: Burning or itching in mouth
- Pulmonary: Airway inflammation at any/all levels
- Cardiovascular: Blood pressure lability or codiagnosis of POTS is common
- Gastrointestinal: Reflux, dysphagia, or malabsorption
- Genitourinary: Endometriosis, dysmenorrhea, or dyspareunia
- Musculoskeletal/connective tissue: Fibromyalgia or diagnosis of hypermobile EDS is common
- Neurologic: Headaches or sensory neuropathies
- Psychiatric: Depression or anxiety
- Endocrinologic: Thyroid disease or dyslipidemia
- Hematologic: Polycythemia or anemia (after ruling out other causes)
The diagnosis is made by fulfilling that major criterion, plus at least one objective assessment of pathologically increased release of MC mediators, including infiltrates, abnormal MC morphology, or MC genetic changes shown to increase MC activity. Other alternatives include evidence of above-normal levels of MC mediators, including tryptase, histamine or its metabolites, heparin, or chromatin A, in whole blood, serum, plasma, or urine. Symptomatic response to MC activation inhibitors can also be used but isn’t required as it is in the other definition.
Underdiagnosis vs Overdiagnosis
Lawrence B. Afrin, MD, senior consultant in hematology/oncology at the AIM Center for Personalized Medicine, Westchester, New York, and lead author of the 2020 update of the broader “consensus-2” criteria, said in an interview, “we now know MCAS exists, and it’s prevalent, even though, for understandable and forgivable reasons, we’ve been missing it all along. ... If you see a patient who has this chronic, multisystem unwellness with general themes of inflammation plus or minus allergic issues and you can’t find some other rational explanation that better accounts for what’s going on ... then it’s reasonable to think to include MCAS in the differential diagnosis. If the patient happens not to fit the diagnostic criteria being advanced by one group, that doesn’t necessarily rule out the possibility that this is still going on.”
Afrin, along with his coauthors, faulted the narrower “consensus-1” definition for lacking data to support the “20% + 2” criteria for requiring the difficult determination of a patient’s “baseline” and for requiring evidence of response to treatment prior to making the diagnosis. Not all patients will respond to a given histamine blocker, he noted.
But Lawrence B. Schwartz, MD, PhD, an author on both the Valent and AAAAI criteria, disagreed, noting that the narrower criteria “appear to have a high degree of specificity and sensitivity when the reaction is systemic and involves hypotension. Less severe clinical events, particularly involving the gastrointestinal or central nervous systems, do not have precise clinical or biomarker criteria for identifying mast cell involvement.”
Added Schwartz, who is professor of medicine and chair of the Division of Rheumatology, Allergy, and Immunology and program director of Allergy and Immunology, Virginia Commonwealth University (VCU), Richmond, “when mast cell activation events occur only in the skin, we refer to it as chronic urticaria and in the airways or conjunctiva of allergic individuals as allergic asthma, rhinitis, and/or conjunctivitis. The absence of specific criteria for mast cell activation in the GI [gastrointestinal] tract or CNS [central nervous system] neither rules in mast cell involvement nor does it rule out mast cell involvement. Thus, more research is needed to find better diagnostic criteria.”
Schwartz also pointed to a recent paper reporting the use of artificial intelligence models to “quantify diagnostic precision and specificity” of “alternative” MCAS definitions. The conclusion was a “lack of specificity is pronounced in relation to multiple control criteria, raising the concern that alternative criteria could disproportionately contribute to MCAS overdiagnosis, to the exclusion of more appropriate diagnoses.”
During the meeting, Afrin acknowledged that the broader view risks overdiagnosis of MCAS. However, he also referenced Occam’s razor, the principle that the simplest explanation is probably the best one. “Which scenario is more likely? Multiple diagnoses and problems that are all independent of each other vs one diagnosis that’s biologically capable of causing most or all of the findings, ie, the simplest solution even if it’s not the most immediately obvious solution?”
He said in an interview: “Do we have any proof that MCAS is what’s underlying hypermobile Ehlers-Danlos or POTS or chronic fatigue? No, we don’t have any proof, not because anybody has done studies that have shown there to be no connection but simply because we’re so early in our awareness that the disease even exists that the necessary studies haven’t even been done yet.”
At the meeting, Afrin introduced proposals to turn the “Masterminds” group into a formal professional society and to launch a journal. He also gave an update on progress in developing a symptom assessment tool both for clinical use and to enable clinical trials of new drugs to target mast cells or their mediators. The plan is to field test the tool in 2025 and publish those results in 2026.
Grach, Afrin, and Chang had no disclosures. Schwartz discovered tryptase and invented the Thermo Fisher tryptase assay, for which his institution (VCU) receives royalties that are shared with him. He also invented monoclonal antibodies used for detecting mast cells or basophils, for which VCU receives royalties from several companies, including Millipore, Santa Cruz, BioLegend, and Hycult Biotech, that are also shared with him. He is a paid consultant for Blueprint Medicines, Celldex Therapeutics, Invea, Third Harmonic Bio, HYCOR Biomedical, Jasper, TerSera Therapeutics, and GLG. He also serves on an AstraZeneca data safety monitoring board for a clinical trial involving benralizumab treatment of hypereosinophilic syndrome and receives royalties from UpToDate (biomarkers for anaphylaxis) and Goldman-Cecil Medicine (anaphylaxis).
A version of this article first appeared on Medscape.com.
Cognitive Decline and Antihypertensive Use: New Data
TOPLINE:
a new study suggests. The association was strongest among those with dementia.
METHODOLOGY:
- The cohort study included 12,644 long-term care residents (mean age, 77.7 years; 97% men; 17.5% Black) with stays of at least 12 weeks from 2006 to 2019.
- Residents who experienced either a reduction in the total number of antihypertensive medications or a sustained 30% decrease in dosage for at least 2 weeks were classified as deprescribing users (n = 1290). Those with no medication changes were considered stable users (n = 11,354).
- The primary outcome was cognitive impairment assessed using the four-point Cognitive Function Scale (CFS), with the score proportional to the severity of impairment.
- The median follow-up duration was 23 weeks for the deprescribing users and 21 weeks for the stable users.
TAKEAWAY:
- Deprescribing antihypertensives was associated with a 12% lower likelihood of progressing to a worse CFS score per 12-week period (odds ratio [OR], 0.88; 95% CI, 0.78-0.99), compared with stable users.
- Among residents with dementia, deprescribing was associated with a 16% reduced likelihood of cognitive decline per 12-week period (OR, 0.84; 95% CI, 0.72-0.98).
- At the end of follow-up, 12% of residents had a higher CFS score and 7.7% had a lower CFS score.
- In the intention-to-treat analysis, the association between deprescribing antihypertensive medications and reduced cognitive decline remained consistent (OR, 0.94; 95% CI, 0.90-0.98).
IN PRACTICE:
“This work highlights the need for patient-centered approaches to deprescribing, ensuring that medication regimens for older adults are optimized to preserve cognitive function and minimize potential harms,” the study authors wrote.
SOURCE:
The study was led by Bocheng Jing, MS, Department of Medicine, University of California, San Francisco. It was published online in JAMA Internal Medicine.
LIMITATIONS:
The study population included predominantly men and White individuals, limiting the generalizability of the results to women and other racial and ethnic groups. The findings may not be applicable to patients with heart failure owing to their noninclusion. The specificity of dementia diagnosis was limited, as this study combined various forms of dementia, making it challenging to differentiate the impacts among subgroups.
DISCLOSURES:
This study was supported by the US National Institute on Aging. Two authors reported receiving grants, honoraria, consulting fees, or royalties from various sources. Details are provided in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
a new study suggests. The association was strongest among those with dementia.
METHODOLOGY:
- The cohort study included 12,644 long-term care residents (mean age, 77.7 years; 97% men; 17.5% Black) with stays of at least 12 weeks from 2006 to 2019.
- Residents who experienced either a reduction in the total number of antihypertensive medications or a sustained 30% decrease in dosage for at least 2 weeks were classified as deprescribing users (n = 1290). Those with no medication changes were considered stable users (n = 11,354).
- The primary outcome was cognitive impairment assessed using the four-point Cognitive Function Scale (CFS), with the score proportional to the severity of impairment.
- The median follow-up duration was 23 weeks for the deprescribing users and 21 weeks for the stable users.
TAKEAWAY:
- Deprescribing antihypertensives was associated with a 12% lower likelihood of progressing to a worse CFS score per 12-week period (odds ratio [OR], 0.88; 95% CI, 0.78-0.99), compared with stable users.
- Among residents with dementia, deprescribing was associated with a 16% reduced likelihood of cognitive decline per 12-week period (OR, 0.84; 95% CI, 0.72-0.98).
- At the end of follow-up, 12% of residents had a higher CFS score and 7.7% had a lower CFS score.
- In the intention-to-treat analysis, the association between deprescribing antihypertensive medications and reduced cognitive decline remained consistent (OR, 0.94; 95% CI, 0.90-0.98).
IN PRACTICE:
“This work highlights the need for patient-centered approaches to deprescribing, ensuring that medication regimens for older adults are optimized to preserve cognitive function and minimize potential harms,” the study authors wrote.
SOURCE:
The study was led by Bocheng Jing, MS, Department of Medicine, University of California, San Francisco. It was published online in JAMA Internal Medicine.
LIMITATIONS:
The study population included predominantly men and White individuals, limiting the generalizability of the results to women and other racial and ethnic groups. The findings may not be applicable to patients with heart failure owing to their noninclusion. The specificity of dementia diagnosis was limited, as this study combined various forms of dementia, making it challenging to differentiate the impacts among subgroups.
DISCLOSURES:
This study was supported by the US National Institute on Aging. Two authors reported receiving grants, honoraria, consulting fees, or royalties from various sources. Details are provided in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
a new study suggests. The association was strongest among those with dementia.
METHODOLOGY:
- The cohort study included 12,644 long-term care residents (mean age, 77.7 years; 97% men; 17.5% Black) with stays of at least 12 weeks from 2006 to 2019.
- Residents who experienced either a reduction in the total number of antihypertensive medications or a sustained 30% decrease in dosage for at least 2 weeks were classified as deprescribing users (n = 1290). Those with no medication changes were considered stable users (n = 11,354).
- The primary outcome was cognitive impairment assessed using the four-point Cognitive Function Scale (CFS), with the score proportional to the severity of impairment.
- The median follow-up duration was 23 weeks for the deprescribing users and 21 weeks for the stable users.
TAKEAWAY:
- Deprescribing antihypertensives was associated with a 12% lower likelihood of progressing to a worse CFS score per 12-week period (odds ratio [OR], 0.88; 95% CI, 0.78-0.99), compared with stable users.
- Among residents with dementia, deprescribing was associated with a 16% reduced likelihood of cognitive decline per 12-week period (OR, 0.84; 95% CI, 0.72-0.98).
- At the end of follow-up, 12% of residents had a higher CFS score and 7.7% had a lower CFS score.
- In the intention-to-treat analysis, the association between deprescribing antihypertensive medications and reduced cognitive decline remained consistent (OR, 0.94; 95% CI, 0.90-0.98).
IN PRACTICE:
“This work highlights the need for patient-centered approaches to deprescribing, ensuring that medication regimens for older adults are optimized to preserve cognitive function and minimize potential harms,” the study authors wrote.
SOURCE:
The study was led by Bocheng Jing, MS, Department of Medicine, University of California, San Francisco. It was published online in JAMA Internal Medicine.
LIMITATIONS:
The study population included predominantly men and White individuals, limiting the generalizability of the results to women and other racial and ethnic groups. The findings may not be applicable to patients with heart failure owing to their noninclusion. The specificity of dementia diagnosis was limited, as this study combined various forms of dementia, making it challenging to differentiate the impacts among subgroups.
DISCLOSURES:
This study was supported by the US National Institute on Aging. Two authors reported receiving grants, honoraria, consulting fees, or royalties from various sources. Details are provided in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Caffeine Brings Benefits and Risks
Coffee and tea are among the plants that are highest in caffeine. Their use as beverages makes caffeine the most consumed psychoactive agent in the world. Coffee is commonly used to increase alertness and work productivity. Synthetic caffeine is added to soft drinks, energy drinks, and products intended to reduce fatigue or promote weight loss.
The caffeine content varies with the type of drink: It is high in coffee, energy drinks, and caffeine tablets; intermediate in tea; and low in soft drinks. Coffee is the predominant source of the caffeine ingested by adults. The evidence for caffeine’s effects on people is ambiguous, and some risks and benefits deserve special attention because of the impact they may have on our health.
Characteristics of Caffeine
The half-life of caffeine varies according to age. In adults, it is 2.5-4.5 hours; in newborns, 80 hours; in children older than 6 months, it remains stable over time with respect to weight. Smoking accelerates caffeine metabolism by reducing the half-life by 50%. Oral contraceptives, however, double caffeine’s half-life. Caffeine metabolism is reduced during pregnancy (it is greater in the first trimester), with a half-life of more than 15 hours. Caffeine clearance can be slowed by several classes of drugs (eg, quinolones, cardiovascular drugs, bronchodilators, and antidepressants) that increase its half-life because they are metabolized by the same liver enzymes.
Caffeine passes the blood-brain barrier and, having an adenosine-like structure, inhibits adenosine’s effects by binding to adenosine receptors. In the brain, caffeine reduces fatigue, increases alertness, reduces reaction times, may reduce the risk for depression, and increases the effectiveness of nonsteroidal anti-inflammatory drugs in treating headaches and other types of pain.
Caffeine and Chronic Diseases
The evidence available on the relationship between caffeine and health has several methodological limitations. Observations of the acute effects of caffeine may not reflect long-term effects because tolerance to caffeine’s effects may develop over time. Smoking and unhealthy lifestyles are confounding factors in epidemiological studies of caffeine intake. In addition, the estimate of the amount and frequency of caffeine intake is often inaccurate because it is mainly based on self-assessment systems. Finally, prospective studies of caffeine consumption are mainly based on coffee and tea consumption, but it is unclear how much the observed outcomes can be translated to intake of other beverages such as energy drinks.
Considering the very high prevalence of arterial hypertension worldwide (31.1% of adults), many questions have been raised about the influence of coffee consumption on blood pressure (BP) and the risk for arterial hypertension. Administration of 200-300 mg caffeine is shown to induce a mean increase of 8.1 mm Hg systolic BP and 5.7 mm Hg diastolic BP. The increase is observed in the first hour after caffeine intake and lasts no longer than 3 hours.
Yet, the moderate and usual consumption of coffee does not increase, but may even reduce, the risk of developing high BP. In contrast, occasional coffee consumption can have hypertensive effects, and moderate and usual consumption in patients with high BP does not appear to increase the risk for uncontrolled BP and can reduce the risk for death from any cause. The inverse association between coffee consumption and hypertension risk was confirmed in a review and meta-analysis of cross-sectional and cohort studies.
With respect to lipid metabolism, cholesterol levels may increase after caffeine consumption because of cafestol. Concentrations of cafestol are high in unfiltered coffee, intermediate in espresso and moka pot coffee, and negligible in instant or filtered coffee. Studies on the impact of coffee on lipid levels have led to inconsistent results, however. Data have shown that people who drink more coffee have higher triglycerides, total cholesterol, and low-density lipoprotein cholesterol (LDL-C) levels. Other data have shown that caffeine promotes LDL receptor expression and clearance of LDL cholesterol.
Experimental and cohort studies have not shown an association between coffee consumption and atrial fibrillation (AF). In fact, evidence suggests that coffee consumption tends to reduce the risk for AF in a dose-response relationship. Similarly, coffee consumption is not associated with increased risk for cardiovascular events in the general population or among patients with a history of hypertension, diabetes, or cardiovascular disease.
The Coffee and Real-Time Atrial and Ventricular Ectopy study evaluated the acute effects of coffee consumption on cardiac ectopy using wearable sensors with continuous recording. It did not demonstrate any increase in daily premature atrial contractions with coffee consumption, compared with abstaining from caffeine.
In patients with type 2 diabetes, a study performed in Japan showed that coffee consumption was associated with reduced all-cause mortality. The results suggested a dose-response relationship, and drinking coffee and green tea appeared to reduce mortality risk further. The results were not generalizable, however, because of the study population’s ethnic homogeneity.
Dose and Toxicity
Caffeine at high doses (> 400 mg daily) and in susceptible patients can induce anxiety, but the effects of caffeine on sleep and anxiety can differ from patient to patient. This variation reflects differences in caffeine metabolism rate and adenosine receptor gene variants.
High caffeine intake can stimulate diuresis, but without causing damaging effects on hydration when taking moderate doses of caffeine (≤ 400 mg daily) for long periods. Stopping caffeine suddenly, in a regular consumer, can lead to withdrawal symptoms such as headache, asthenia, decreased attention, depressed mood, and flu-like symptoms.
The toxic effects of caffeine occur with intake > 1.2 g. A dose of 10-14 g is considered fatal. Caffeine overdose is rare when considering traditional methods of intake (coffee and tea) because 70-100 cups of coffee should be sufficient for caffeine poisoning. Severe events can occur following the use of caffeine tablets or as energy drinks for the following reasons:
- The episodic consumption of caffeine does not allow for tolerance to develop.
- Young people are more vulnerable to the effects of caffeine.
- Caffeine has a synergistic effect in combination with other components in energy drinks.
- Taking caffeine in combination with alcohol or intense exertion causes serious, even fatal, outcomes.
Products Containing Caffeine
Evidence supports the relationship between high consumption (approximately 1 L) of energy drinks with a caffeine content of 320 mg and short-term cardiovascular adverse events, such as increased BP, QT-segment prolongation corrected for heart rate, and palpitations. These tests prompt the recommendation to avoid consuming these beverages in high quantities and in association with alcohol.
Weight loss products generally contain caffeine coupled with herbal extracts that are expected to improve fat metabolism, lipolysis, and oxidation. These products, because of their easy availability, presumed benefits, and high caffeine concentration, may be more susceptible to misuse because they can be taken in larger portions than recommended. The combination of multiple ingredients, concentrated amounts of caffeine, and excessive consumption increases the likelihood of adverse effects.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Coffee and tea are among the plants that are highest in caffeine. Their use as beverages makes caffeine the most consumed psychoactive agent in the world. Coffee is commonly used to increase alertness and work productivity. Synthetic caffeine is added to soft drinks, energy drinks, and products intended to reduce fatigue or promote weight loss.
The caffeine content varies with the type of drink: It is high in coffee, energy drinks, and caffeine tablets; intermediate in tea; and low in soft drinks. Coffee is the predominant source of the caffeine ingested by adults. The evidence for caffeine’s effects on people is ambiguous, and some risks and benefits deserve special attention because of the impact they may have on our health.
Characteristics of Caffeine
The half-life of caffeine varies according to age. In adults, it is 2.5-4.5 hours; in newborns, 80 hours; in children older than 6 months, it remains stable over time with respect to weight. Smoking accelerates caffeine metabolism by reducing the half-life by 50%. Oral contraceptives, however, double caffeine’s half-life. Caffeine metabolism is reduced during pregnancy (it is greater in the first trimester), with a half-life of more than 15 hours. Caffeine clearance can be slowed by several classes of drugs (eg, quinolones, cardiovascular drugs, bronchodilators, and antidepressants) that increase its half-life because they are metabolized by the same liver enzymes.
Caffeine passes the blood-brain barrier and, having an adenosine-like structure, inhibits adenosine’s effects by binding to adenosine receptors. In the brain, caffeine reduces fatigue, increases alertness, reduces reaction times, may reduce the risk for depression, and increases the effectiveness of nonsteroidal anti-inflammatory drugs in treating headaches and other types of pain.
Caffeine and Chronic Diseases
The evidence available on the relationship between caffeine and health has several methodological limitations. Observations of the acute effects of caffeine may not reflect long-term effects because tolerance to caffeine’s effects may develop over time. Smoking and unhealthy lifestyles are confounding factors in epidemiological studies of caffeine intake. In addition, the estimate of the amount and frequency of caffeine intake is often inaccurate because it is mainly based on self-assessment systems. Finally, prospective studies of caffeine consumption are mainly based on coffee and tea consumption, but it is unclear how much the observed outcomes can be translated to intake of other beverages such as energy drinks.
Considering the very high prevalence of arterial hypertension worldwide (31.1% of adults), many questions have been raised about the influence of coffee consumption on blood pressure (BP) and the risk for arterial hypertension. Administration of 200-300 mg caffeine is shown to induce a mean increase of 8.1 mm Hg systolic BP and 5.7 mm Hg diastolic BP. The increase is observed in the first hour after caffeine intake and lasts no longer than 3 hours.
Yet, the moderate and usual consumption of coffee does not increase, but may even reduce, the risk of developing high BP. In contrast, occasional coffee consumption can have hypertensive effects, and moderate and usual consumption in patients with high BP does not appear to increase the risk for uncontrolled BP and can reduce the risk for death from any cause. The inverse association between coffee consumption and hypertension risk was confirmed in a review and meta-analysis of cross-sectional and cohort studies.
With respect to lipid metabolism, cholesterol levels may increase after caffeine consumption because of cafestol. Concentrations of cafestol are high in unfiltered coffee, intermediate in espresso and moka pot coffee, and negligible in instant or filtered coffee. Studies on the impact of coffee on lipid levels have led to inconsistent results, however. Data have shown that people who drink more coffee have higher triglycerides, total cholesterol, and low-density lipoprotein cholesterol (LDL-C) levels. Other data have shown that caffeine promotes LDL receptor expression and clearance of LDL cholesterol.
Experimental and cohort studies have not shown an association between coffee consumption and atrial fibrillation (AF). In fact, evidence suggests that coffee consumption tends to reduce the risk for AF in a dose-response relationship. Similarly, coffee consumption is not associated with increased risk for cardiovascular events in the general population or among patients with a history of hypertension, diabetes, or cardiovascular disease.
The Coffee and Real-Time Atrial and Ventricular Ectopy study evaluated the acute effects of coffee consumption on cardiac ectopy using wearable sensors with continuous recording. It did not demonstrate any increase in daily premature atrial contractions with coffee consumption, compared with abstaining from caffeine.
In patients with type 2 diabetes, a study performed in Japan showed that coffee consumption was associated with reduced all-cause mortality. The results suggested a dose-response relationship, and drinking coffee and green tea appeared to reduce mortality risk further. The results were not generalizable, however, because of the study population’s ethnic homogeneity.
Dose and Toxicity
Caffeine at high doses (> 400 mg daily) and in susceptible patients can induce anxiety, but the effects of caffeine on sleep and anxiety can differ from patient to patient. This variation reflects differences in caffeine metabolism rate and adenosine receptor gene variants.
High caffeine intake can stimulate diuresis, but without causing damaging effects on hydration when taking moderate doses of caffeine (≤ 400 mg daily) for long periods. Stopping caffeine suddenly, in a regular consumer, can lead to withdrawal symptoms such as headache, asthenia, decreased attention, depressed mood, and flu-like symptoms.
The toxic effects of caffeine occur with intake > 1.2 g. A dose of 10-14 g is considered fatal. Caffeine overdose is rare when considering traditional methods of intake (coffee and tea) because 70-100 cups of coffee should be sufficient for caffeine poisoning. Severe events can occur following the use of caffeine tablets or as energy drinks for the following reasons:
- The episodic consumption of caffeine does not allow for tolerance to develop.
- Young people are more vulnerable to the effects of caffeine.
- Caffeine has a synergistic effect in combination with other components in energy drinks.
- Taking caffeine in combination with alcohol or intense exertion causes serious, even fatal, outcomes.
Products Containing Caffeine
Evidence supports the relationship between high consumption (approximately 1 L) of energy drinks with a caffeine content of 320 mg and short-term cardiovascular adverse events, such as increased BP, QT-segment prolongation corrected for heart rate, and palpitations. These tests prompt the recommendation to avoid consuming these beverages in high quantities and in association with alcohol.
Weight loss products generally contain caffeine coupled with herbal extracts that are expected to improve fat metabolism, lipolysis, and oxidation. These products, because of their easy availability, presumed benefits, and high caffeine concentration, may be more susceptible to misuse because they can be taken in larger portions than recommended. The combination of multiple ingredients, concentrated amounts of caffeine, and excessive consumption increases the likelihood of adverse effects.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Coffee and tea are among the plants that are highest in caffeine. Their use as beverages makes caffeine the most consumed psychoactive agent in the world. Coffee is commonly used to increase alertness and work productivity. Synthetic caffeine is added to soft drinks, energy drinks, and products intended to reduce fatigue or promote weight loss.
The caffeine content varies with the type of drink: It is high in coffee, energy drinks, and caffeine tablets; intermediate in tea; and low in soft drinks. Coffee is the predominant source of the caffeine ingested by adults. The evidence for caffeine’s effects on people is ambiguous, and some risks and benefits deserve special attention because of the impact they may have on our health.
Characteristics of Caffeine
The half-life of caffeine varies according to age. In adults, it is 2.5-4.5 hours; in newborns, 80 hours; in children older than 6 months, it remains stable over time with respect to weight. Smoking accelerates caffeine metabolism by reducing the half-life by 50%. Oral contraceptives, however, double caffeine’s half-life. Caffeine metabolism is reduced during pregnancy (it is greater in the first trimester), with a half-life of more than 15 hours. Caffeine clearance can be slowed by several classes of drugs (eg, quinolones, cardiovascular drugs, bronchodilators, and antidepressants) that increase its half-life because they are metabolized by the same liver enzymes.
Caffeine passes the blood-brain barrier and, having an adenosine-like structure, inhibits adenosine’s effects by binding to adenosine receptors. In the brain, caffeine reduces fatigue, increases alertness, reduces reaction times, may reduce the risk for depression, and increases the effectiveness of nonsteroidal anti-inflammatory drugs in treating headaches and other types of pain.
Caffeine and Chronic Diseases
The evidence available on the relationship between caffeine and health has several methodological limitations. Observations of the acute effects of caffeine may not reflect long-term effects because tolerance to caffeine’s effects may develop over time. Smoking and unhealthy lifestyles are confounding factors in epidemiological studies of caffeine intake. In addition, the estimate of the amount and frequency of caffeine intake is often inaccurate because it is mainly based on self-assessment systems. Finally, prospective studies of caffeine consumption are mainly based on coffee and tea consumption, but it is unclear how much the observed outcomes can be translated to intake of other beverages such as energy drinks.
Considering the very high prevalence of arterial hypertension worldwide (31.1% of adults), many questions have been raised about the influence of coffee consumption on blood pressure (BP) and the risk for arterial hypertension. Administration of 200-300 mg caffeine is shown to induce a mean increase of 8.1 mm Hg systolic BP and 5.7 mm Hg diastolic BP. The increase is observed in the first hour after caffeine intake and lasts no longer than 3 hours.
Yet, the moderate and usual consumption of coffee does not increase, but may even reduce, the risk of developing high BP. In contrast, occasional coffee consumption can have hypertensive effects, and moderate and usual consumption in patients with high BP does not appear to increase the risk for uncontrolled BP and can reduce the risk for death from any cause. The inverse association between coffee consumption and hypertension risk was confirmed in a review and meta-analysis of cross-sectional and cohort studies.
With respect to lipid metabolism, cholesterol levels may increase after caffeine consumption because of cafestol. Concentrations of cafestol are high in unfiltered coffee, intermediate in espresso and moka pot coffee, and negligible in instant or filtered coffee. Studies on the impact of coffee on lipid levels have led to inconsistent results, however. Data have shown that people who drink more coffee have higher triglycerides, total cholesterol, and low-density lipoprotein cholesterol (LDL-C) levels. Other data have shown that caffeine promotes LDL receptor expression and clearance of LDL cholesterol.
Experimental and cohort studies have not shown an association between coffee consumption and atrial fibrillation (AF). In fact, evidence suggests that coffee consumption tends to reduce the risk for AF in a dose-response relationship. Similarly, coffee consumption is not associated with increased risk for cardiovascular events in the general population or among patients with a history of hypertension, diabetes, or cardiovascular disease.
The Coffee and Real-Time Atrial and Ventricular Ectopy study evaluated the acute effects of coffee consumption on cardiac ectopy using wearable sensors with continuous recording. It did not demonstrate any increase in daily premature atrial contractions with coffee consumption, compared with abstaining from caffeine.
In patients with type 2 diabetes, a study performed in Japan showed that coffee consumption was associated with reduced all-cause mortality. The results suggested a dose-response relationship, and drinking coffee and green tea appeared to reduce mortality risk further. The results were not generalizable, however, because of the study population’s ethnic homogeneity.
Dose and Toxicity
Caffeine at high doses (> 400 mg daily) and in susceptible patients can induce anxiety, but the effects of caffeine on sleep and anxiety can differ from patient to patient. This variation reflects differences in caffeine metabolism rate and adenosine receptor gene variants.
High caffeine intake can stimulate diuresis, but without causing damaging effects on hydration when taking moderate doses of caffeine (≤ 400 mg daily) for long periods. Stopping caffeine suddenly, in a regular consumer, can lead to withdrawal symptoms such as headache, asthenia, decreased attention, depressed mood, and flu-like symptoms.
The toxic effects of caffeine occur with intake > 1.2 g. A dose of 10-14 g is considered fatal. Caffeine overdose is rare when considering traditional methods of intake (coffee and tea) because 70-100 cups of coffee should be sufficient for caffeine poisoning. Severe events can occur following the use of caffeine tablets or as energy drinks for the following reasons:
- The episodic consumption of caffeine does not allow for tolerance to develop.
- Young people are more vulnerable to the effects of caffeine.
- Caffeine has a synergistic effect in combination with other components in energy drinks.
- Taking caffeine in combination with alcohol or intense exertion causes serious, even fatal, outcomes.
Products Containing Caffeine
Evidence supports the relationship between high consumption (approximately 1 L) of energy drinks with a caffeine content of 320 mg and short-term cardiovascular adverse events, such as increased BP, QT-segment prolongation corrected for heart rate, and palpitations. These tests prompt the recommendation to avoid consuming these beverages in high quantities and in association with alcohol.
Weight loss products generally contain caffeine coupled with herbal extracts that are expected to improve fat metabolism, lipolysis, and oxidation. These products, because of their easy availability, presumed benefits, and high caffeine concentration, may be more susceptible to misuse because they can be taken in larger portions than recommended. The combination of multiple ingredients, concentrated amounts of caffeine, and excessive consumption increases the likelihood of adverse effects.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
New Scanner Creates Highly Detailed, 3D Images of Blood Vessels in Seconds
A new scanner can provide three-dimensional (3D) photoacoustic images of millimeter-scale veins and arteries in seconds.
The scanner, developed by researchers at University College London (UCL) in England, could help clinicians better visualize and track microvascular changes for a wide range of diseases, including cancer, rheumatoid arthritis (RA), and peripheral vascular disease (PVD).
The case studies “illustrate potential areas of application that warrant future, more comprehensive clinical studies,” the authors wrote. “Moreover, they demonstrate the feasibility of using the scanner on a real-world patient cohort where imaging is more challenging due to frailty, comorbidity, or pain that may limit their ability to tolerate prolonged scan times.”
The work was published online in Nature Biomedical Engineering.
Improving Photoacoustic Imaging
PAT works using the photoacoustic effect, a phenomenon where sound waves are generated when light is absorbed by a material. When pulsed light from a laser is directed at tissue, some of that light is absorbed and causes an increase in heat in the targeted area. This localized heat also increases pressure, which generates ultrasound waves that can be detected by specialized sensors.
While previous PAT scanners translated these sound waves to electric signals directly to generate imaging, UCL engineers developed a sensor in the early 2000s that can detect these ultrasound waves using light. The result was much clearer, 3D images.
“That was great, but the problem was it was very slow, and it would take 5 minutes to get an image,” explained Paul Beard, PhD, professor of biomedical photoacoustics at UCL and senior author of the study. “That’s fine if you’re imaging a dead mouse or an anesthetized mouse, but not so useful for human imaging,” he continued, where motion would blur the image.
In this new paper, Beard and colleagues outlined how they cut scanning times to an order of seconds (or fraction of a second) rather than minutes. While previous iterations could detect only acoustic waves from one point at a time, this new scanner can detect waves from multiple points simultaneously. The scanner can visualize veins and arteries up to 15 mm deep in human tissue and can also provide dynamic, 3D images of “time-varying tissue perfusion and other hemodynamic events,” the authors wrote.
With these types of scanners, there is always a trade-off between imaging quality and imaging speed, explained Srivalleesha Mallidi, PhD, an assistant professor of biomedical engineering at Tufts University in Medford, Massachusetts. She was not involved with the work.
“With the resolution that [the authors] are providing and the depth at which they are seeing the signals, it is one of the fastest systems,” she said.
Clinical Utility
Beard and colleagues also tested the scanner to visualize blood vessels in participants with RA, suspected PVD, and skin inflammation. The scanning images “illustrated how vascular abnormalities such as increased vessel tortuosity, which has previously been linked to PVD, and the neovascularization associated with inflammation can be visualized and quantified,” the authors wrote.
The next step, Beard noted, is testing whether these characteristics can be used as a marker for the progression of disease.
Nehal Mehta, MD, a cardiologist and professor of medicine at the George Washington University, Washington, DC, agreed that more longitudinal research is needed to understand how the abnormalities captured in these images can inform detection and diagnosis of various diseases.
“You don’t know whether these images look bad because of reverse causation — the disease is doing this — or true causation — that this is actually detecting the root cause of the disease,” he explained. “Until we have a bank of normal and abnormal scans, we don’t know what any of these things mean.”
Though still some time away from entering the clinic, Mehta likened the technology to the introduction of optical coherence tomography in the 1980s. Before being adapted for clinical use, researchers first needed to visualize differences between normal coronary vasculature and myocardial infarction.
“I think this is an amazingly strong first proof of concept,” Mehta said. “This technology is showing a true promise in the field imaging.”
The work was funded by grants from Cancer Research UK, the Engineering & Physical Sciences Research Council, Wellcome Trust, the European Research Council, and the National Institute for Health and Care Research University College London Hospitals Biomedical Research Centre. Beard and two coauthors are shareholders of DeepColor Imaging to which the intellectual property associated with the new scanner has been licensed, but the company was not involved in any of this research. Mallidi and Mehta had no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new scanner can provide three-dimensional (3D) photoacoustic images of millimeter-scale veins and arteries in seconds.
The scanner, developed by researchers at University College London (UCL) in England, could help clinicians better visualize and track microvascular changes for a wide range of diseases, including cancer, rheumatoid arthritis (RA), and peripheral vascular disease (PVD).
The case studies “illustrate potential areas of application that warrant future, more comprehensive clinical studies,” the authors wrote. “Moreover, they demonstrate the feasibility of using the scanner on a real-world patient cohort where imaging is more challenging due to frailty, comorbidity, or pain that may limit their ability to tolerate prolonged scan times.”
The work was published online in Nature Biomedical Engineering.
Improving Photoacoustic Imaging
PAT works using the photoacoustic effect, a phenomenon where sound waves are generated when light is absorbed by a material. When pulsed light from a laser is directed at tissue, some of that light is absorbed and causes an increase in heat in the targeted area. This localized heat also increases pressure, which generates ultrasound waves that can be detected by specialized sensors.
While previous PAT scanners translated these sound waves to electric signals directly to generate imaging, UCL engineers developed a sensor in the early 2000s that can detect these ultrasound waves using light. The result was much clearer, 3D images.
“That was great, but the problem was it was very slow, and it would take 5 minutes to get an image,” explained Paul Beard, PhD, professor of biomedical photoacoustics at UCL and senior author of the study. “That’s fine if you’re imaging a dead mouse or an anesthetized mouse, but not so useful for human imaging,” he continued, where motion would blur the image.
In this new paper, Beard and colleagues outlined how they cut scanning times to an order of seconds (or fraction of a second) rather than minutes. While previous iterations could detect only acoustic waves from one point at a time, this new scanner can detect waves from multiple points simultaneously. The scanner can visualize veins and arteries up to 15 mm deep in human tissue and can also provide dynamic, 3D images of “time-varying tissue perfusion and other hemodynamic events,” the authors wrote.
With these types of scanners, there is always a trade-off between imaging quality and imaging speed, explained Srivalleesha Mallidi, PhD, an assistant professor of biomedical engineering at Tufts University in Medford, Massachusetts. She was not involved with the work.
“With the resolution that [the authors] are providing and the depth at which they are seeing the signals, it is one of the fastest systems,” she said.
Clinical Utility
Beard and colleagues also tested the scanner to visualize blood vessels in participants with RA, suspected PVD, and skin inflammation. The scanning images “illustrated how vascular abnormalities such as increased vessel tortuosity, which has previously been linked to PVD, and the neovascularization associated with inflammation can be visualized and quantified,” the authors wrote.
The next step, Beard noted, is testing whether these characteristics can be used as a marker for the progression of disease.
Nehal Mehta, MD, a cardiologist and professor of medicine at the George Washington University, Washington, DC, agreed that more longitudinal research is needed to understand how the abnormalities captured in these images can inform detection and diagnosis of various diseases.
“You don’t know whether these images look bad because of reverse causation — the disease is doing this — or true causation — that this is actually detecting the root cause of the disease,” he explained. “Until we have a bank of normal and abnormal scans, we don’t know what any of these things mean.”
Though still some time away from entering the clinic, Mehta likened the technology to the introduction of optical coherence tomography in the 1980s. Before being adapted for clinical use, researchers first needed to visualize differences between normal coronary vasculature and myocardial infarction.
“I think this is an amazingly strong first proof of concept,” Mehta said. “This technology is showing a true promise in the field imaging.”
The work was funded by grants from Cancer Research UK, the Engineering & Physical Sciences Research Council, Wellcome Trust, the European Research Council, and the National Institute for Health and Care Research University College London Hospitals Biomedical Research Centre. Beard and two coauthors are shareholders of DeepColor Imaging to which the intellectual property associated with the new scanner has been licensed, but the company was not involved in any of this research. Mallidi and Mehta had no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new scanner can provide three-dimensional (3D) photoacoustic images of millimeter-scale veins and arteries in seconds.
The scanner, developed by researchers at University College London (UCL) in England, could help clinicians better visualize and track microvascular changes for a wide range of diseases, including cancer, rheumatoid arthritis (RA), and peripheral vascular disease (PVD).
The case studies “illustrate potential areas of application that warrant future, more comprehensive clinical studies,” the authors wrote. “Moreover, they demonstrate the feasibility of using the scanner on a real-world patient cohort where imaging is more challenging due to frailty, comorbidity, or pain that may limit their ability to tolerate prolonged scan times.”
The work was published online in Nature Biomedical Engineering.
Improving Photoacoustic Imaging
PAT works using the photoacoustic effect, a phenomenon where sound waves are generated when light is absorbed by a material. When pulsed light from a laser is directed at tissue, some of that light is absorbed and causes an increase in heat in the targeted area. This localized heat also increases pressure, which generates ultrasound waves that can be detected by specialized sensors.
While previous PAT scanners translated these sound waves to electric signals directly to generate imaging, UCL engineers developed a sensor in the early 2000s that can detect these ultrasound waves using light. The result was much clearer, 3D images.
“That was great, but the problem was it was very slow, and it would take 5 minutes to get an image,” explained Paul Beard, PhD, professor of biomedical photoacoustics at UCL and senior author of the study. “That’s fine if you’re imaging a dead mouse or an anesthetized mouse, but not so useful for human imaging,” he continued, where motion would blur the image.
In this new paper, Beard and colleagues outlined how they cut scanning times to an order of seconds (or fraction of a second) rather than minutes. While previous iterations could detect only acoustic waves from one point at a time, this new scanner can detect waves from multiple points simultaneously. The scanner can visualize veins and arteries up to 15 mm deep in human tissue and can also provide dynamic, 3D images of “time-varying tissue perfusion and other hemodynamic events,” the authors wrote.
With these types of scanners, there is always a trade-off between imaging quality and imaging speed, explained Srivalleesha Mallidi, PhD, an assistant professor of biomedical engineering at Tufts University in Medford, Massachusetts. She was not involved with the work.
“With the resolution that [the authors] are providing and the depth at which they are seeing the signals, it is one of the fastest systems,” she said.
Clinical Utility
Beard and colleagues also tested the scanner to visualize blood vessels in participants with RA, suspected PVD, and skin inflammation. The scanning images “illustrated how vascular abnormalities such as increased vessel tortuosity, which has previously been linked to PVD, and the neovascularization associated with inflammation can be visualized and quantified,” the authors wrote.
The next step, Beard noted, is testing whether these characteristics can be used as a marker for the progression of disease.
Nehal Mehta, MD, a cardiologist and professor of medicine at the George Washington University, Washington, DC, agreed that more longitudinal research is needed to understand how the abnormalities captured in these images can inform detection and diagnosis of various diseases.
“You don’t know whether these images look bad because of reverse causation — the disease is doing this — or true causation — that this is actually detecting the root cause of the disease,” he explained. “Until we have a bank of normal and abnormal scans, we don’t know what any of these things mean.”
Though still some time away from entering the clinic, Mehta likened the technology to the introduction of optical coherence tomography in the 1980s. Before being adapted for clinical use, researchers first needed to visualize differences between normal coronary vasculature and myocardial infarction.
“I think this is an amazingly strong first proof of concept,” Mehta said. “This technology is showing a true promise in the field imaging.”
The work was funded by grants from Cancer Research UK, the Engineering & Physical Sciences Research Council, Wellcome Trust, the European Research Council, and the National Institute for Health and Care Research University College London Hospitals Biomedical Research Centre. Beard and two coauthors are shareholders of DeepColor Imaging to which the intellectual property associated with the new scanner has been licensed, but the company was not involved in any of this research. Mallidi and Mehta had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM NATURE BIOMEDICAL ENGINEERING