User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
Do patients follow up on referrals after telehealth visits?
Telehealth has been a boon for modern-day patients, allowing people who might have difficulty accessing in-person appointments to continue seeing their physicians. But how many patients actually follow through on their physician’s recommendations afterward?
A new study suggests that
Investigators retrospectively examined test and referral orders for more than 4,000 patients to see how many complied with recommendations to have a colonoscopy, consult a dermatologist for a suspicious skin lesion, or undergo a cardiac stress test.
Completion of a recommended test or specialty referral was termed “diagnostic loop closure.” In particular, the researchers wanted to compare loop closure after telehealth versus in-person visits.
Rates of loop closure were low across all visit modalities but were lower for tests and referrals ordered during telehealth visits, compared with in-person visits – especially for colonoscopies.
“The take-home message for practicing clinicians is that they should be especially aware of follow-up for tests or referrals ordered during telehealth visits,” said corresponding author Maëlys Amat, MD, MBA, a primary care physician at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston.
The study was published online on in JAMA Network Open.
‘Unintended side effects’
“Diagnostic errors present a huge safety concern, impacting many patient lives and costing the health care system billions of dollars, said Dr. Amat, who is also an instructor at Harvard Medical School.
“Telehealth utilization increased rapidly during the COVID pandemic, and although there are clear benefits to utilizing telehealth, our team sought to investigate unintended side effects of this technology and highlight opportunities for improvement,” she said.
To investigate the question, the researchers reviewed medical records of 4,113 patients, with a mean age of 59 years, at two Boston-based primary care sites: an urban hospital–based primary care practice and an affiliated community health center.
Orders for tests or referrals in both centers were placed electronically through the medical record. During an in-person visit, the patient was handed a form with a phone number to call to schedule the test or referral. Patients with limited English proficiency or complex needs may have received help with the scheduling the referral during check-out.
For telehealth visits, the clinician gave the patient the phone number to call to schedule the test or referral during the visit itself. In all scenarios, patients did not receive communication after the visit reminding them about the referral or test.
A loop was considered “closed” if the orders were completed within 365 days, 90 days, or 45 days for colonoscopy, dermatology visits, or cardiac stress testing, respectively.
Of the tests, 52.4% were ordered during an in-person visit, 27.8% were ordered during a telehealth visit, and 19.7% were ordered without a visit.
Tracking systems, virtual checkout
Fewer than half of the orders (42.6%) placed during a telehealth visit were completed within the designated time frame, compared with 58.4% of the orders placed during an in-person visit and 57.4% placed without a visit.
Patients who had telehealth visits were roughly half as likely as those who had in-person visits to close the loop on high-risk tests and referrals, even in an analysis that adjusted for test type, patient demographic characteristics, comorbidities, clinical site, clinician type, and patient engagement (odds ratio, 0.55; 95% confidence interval, 0.47-0.64).
Only 39.8% of colonoscopy referrals ordered during a telehealth visit were completed during the 365-day time period, compared with 56.9% ordered during an in-person visit and 56.7% ordered without a visit.
Follow-through with dermatology referrals within 90 days was roughly the same across all types of visits (63.1% for telehealth, 61.5% for in-person, and 62.9% for no visit). No significant differences were found between telehealth and in-person visits or orders placed without a visit.
Although patients seen via telehealth were less likely than those seen in person to follow through on cardiac stress tests within the 45-day window (59.1% vs. 63.2%), this difference didn’t reach statistical significance.
“Ideally, clinicians would implement automatic tracking systems to help ensure that an ordered test or referral is completed,” Dr. Amat commented. “However, if these systems aren’t yet in place, we strongly encourage clinicians to create their own work flows for tracking tests to completion.”
Additionally, “clinicians should consider implementing a virtual checkout system, similar to what is done during in-person visits, to help patients better understand recommended next steps,” she continued.
Other potentially helpful ways to improve loop closure include automatic tracking for outstanding tests, interventions such as telephone outreach to patients, automated text and email reminders, and the use of referral managers – especially in remote, rural areas or for “disadvantaged patients with limited health care access and literacy.”
Education is key
Kisha Davis, MD, MPH, member of the board of directors of the American Academy of Family Physicians, said in an interview that being able to see a provider virtually can make the difference between a person receiving or not receiving medical care. She regards telehealth as another tool in the toolkit her practice offers to provide comprehensive health care.
Dr. Davis, a family physician in Gaithersburg, Md., who wasn’t involved with the study, described a patient with hypertension who was an Uber driver. “During the pandemic, Uber rides were down, and he couldn›t afford to pass up any opportunities, so he pulled over to the side of the road after one of his rides, did his telehealth visit, reviewed his medications, and went on to his next ride.”
The key is to make sure that patients receive adequate follow-up from the office, which Dr. Davis arranged for this patient.
She noted that telehealth “is best done if there’s an established physician-patient relationship but harder to accomplish successfully if you’ve only met the patient on telehealth and never in person.”
The study didn’t specify whether the physicians had an established relationship with their patients.
During the checkout process after an in-person appointment, patients often receive a sheet of paper with the follow-up referrals. “I can see where patients are less likely to follow through if they don’t have someone handing them that paper,” she said.
In her practice, patients’ charts are color-coded “to keep track and make sure it’s not just the ‘squeaky wheels’ that get all the attention,” she said. “The onus is on the physician and the practice, in today’s world of value-based care, to make sure that patients who don’t come into the office are getting the care they need.”
This is facilitated by a “system of care coordination” in which the office team – such as a nurse or medical assistant – follows up with patients to see if they’ve “gotten everything done without barriers,” Dr. Davis said. “Did they have trouble filling that prescription? Did they have difficulty with the referral? Or do they not think it’s necessary – for example, a patient might not go to physical therapy because the injury has improved.”
Dr. Davis wasn’t surprised that patients were less likely to close the loop for colonoscopies compared with seeking out a stress test or treatment for skin lesions.
“People who have a skin lesion may be concerned about their appearance or about skin cancer, and people who need a stress test may have had cardiac symptoms or be worried about their heart.” But a routine screening such as a colonoscopy may not mobilize the patient’s concern to the same degree.
“Additionally, a colonoscopy has an ‘ick factor,’ so there aren’t a whole lot of people who are jumping to have the procedure done.” She suggested considering newer FDA-approved stool tests to screen for colon cancer.
Dr. Amat and Dr. Davis both emphasized that educating patients – both during and after the visit – and making sure they understand the importance of their referral for tests or specialists referrals are key to ensuring that they follow through on the recommendations.
The study was funded by the Agency for Healthcare Research and Quality. Dr. Amat was supported by the Arnold Tofias and Leo Condakes Quality Scholarship Program. Dr. Amat declared no relevant financial relationships. Dr. Davis is the chief health officer for Montgomery County in Maryland.
A version of this article first appeared on Medscape.com.
Telehealth has been a boon for modern-day patients, allowing people who might have difficulty accessing in-person appointments to continue seeing their physicians. But how many patients actually follow through on their physician’s recommendations afterward?
A new study suggests that
Investigators retrospectively examined test and referral orders for more than 4,000 patients to see how many complied with recommendations to have a colonoscopy, consult a dermatologist for a suspicious skin lesion, or undergo a cardiac stress test.
Completion of a recommended test or specialty referral was termed “diagnostic loop closure.” In particular, the researchers wanted to compare loop closure after telehealth versus in-person visits.
Rates of loop closure were low across all visit modalities but were lower for tests and referrals ordered during telehealth visits, compared with in-person visits – especially for colonoscopies.
“The take-home message for practicing clinicians is that they should be especially aware of follow-up for tests or referrals ordered during telehealth visits,” said corresponding author Maëlys Amat, MD, MBA, a primary care physician at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston.
The study was published online on in JAMA Network Open.
‘Unintended side effects’
“Diagnostic errors present a huge safety concern, impacting many patient lives and costing the health care system billions of dollars, said Dr. Amat, who is also an instructor at Harvard Medical School.
“Telehealth utilization increased rapidly during the COVID pandemic, and although there are clear benefits to utilizing telehealth, our team sought to investigate unintended side effects of this technology and highlight opportunities for improvement,” she said.
To investigate the question, the researchers reviewed medical records of 4,113 patients, with a mean age of 59 years, at two Boston-based primary care sites: an urban hospital–based primary care practice and an affiliated community health center.
Orders for tests or referrals in both centers were placed electronically through the medical record. During an in-person visit, the patient was handed a form with a phone number to call to schedule the test or referral. Patients with limited English proficiency or complex needs may have received help with the scheduling the referral during check-out.
For telehealth visits, the clinician gave the patient the phone number to call to schedule the test or referral during the visit itself. In all scenarios, patients did not receive communication after the visit reminding them about the referral or test.
A loop was considered “closed” if the orders were completed within 365 days, 90 days, or 45 days for colonoscopy, dermatology visits, or cardiac stress testing, respectively.
Of the tests, 52.4% were ordered during an in-person visit, 27.8% were ordered during a telehealth visit, and 19.7% were ordered without a visit.
Tracking systems, virtual checkout
Fewer than half of the orders (42.6%) placed during a telehealth visit were completed within the designated time frame, compared with 58.4% of the orders placed during an in-person visit and 57.4% placed without a visit.
Patients who had telehealth visits were roughly half as likely as those who had in-person visits to close the loop on high-risk tests and referrals, even in an analysis that adjusted for test type, patient demographic characteristics, comorbidities, clinical site, clinician type, and patient engagement (odds ratio, 0.55; 95% confidence interval, 0.47-0.64).
Only 39.8% of colonoscopy referrals ordered during a telehealth visit were completed during the 365-day time period, compared with 56.9% ordered during an in-person visit and 56.7% ordered without a visit.
Follow-through with dermatology referrals within 90 days was roughly the same across all types of visits (63.1% for telehealth, 61.5% for in-person, and 62.9% for no visit). No significant differences were found between telehealth and in-person visits or orders placed without a visit.
Although patients seen via telehealth were less likely than those seen in person to follow through on cardiac stress tests within the 45-day window (59.1% vs. 63.2%), this difference didn’t reach statistical significance.
“Ideally, clinicians would implement automatic tracking systems to help ensure that an ordered test or referral is completed,” Dr. Amat commented. “However, if these systems aren’t yet in place, we strongly encourage clinicians to create their own work flows for tracking tests to completion.”
Additionally, “clinicians should consider implementing a virtual checkout system, similar to what is done during in-person visits, to help patients better understand recommended next steps,” she continued.
Other potentially helpful ways to improve loop closure include automatic tracking for outstanding tests, interventions such as telephone outreach to patients, automated text and email reminders, and the use of referral managers – especially in remote, rural areas or for “disadvantaged patients with limited health care access and literacy.”
Education is key
Kisha Davis, MD, MPH, member of the board of directors of the American Academy of Family Physicians, said in an interview that being able to see a provider virtually can make the difference between a person receiving or not receiving medical care. She regards telehealth as another tool in the toolkit her practice offers to provide comprehensive health care.
Dr. Davis, a family physician in Gaithersburg, Md., who wasn’t involved with the study, described a patient with hypertension who was an Uber driver. “During the pandemic, Uber rides were down, and he couldn›t afford to pass up any opportunities, so he pulled over to the side of the road after one of his rides, did his telehealth visit, reviewed his medications, and went on to his next ride.”
The key is to make sure that patients receive adequate follow-up from the office, which Dr. Davis arranged for this patient.
She noted that telehealth “is best done if there’s an established physician-patient relationship but harder to accomplish successfully if you’ve only met the patient on telehealth and never in person.”
The study didn’t specify whether the physicians had an established relationship with their patients.
During the checkout process after an in-person appointment, patients often receive a sheet of paper with the follow-up referrals. “I can see where patients are less likely to follow through if they don’t have someone handing them that paper,” she said.
In her practice, patients’ charts are color-coded “to keep track and make sure it’s not just the ‘squeaky wheels’ that get all the attention,” she said. “The onus is on the physician and the practice, in today’s world of value-based care, to make sure that patients who don’t come into the office are getting the care they need.”
This is facilitated by a “system of care coordination” in which the office team – such as a nurse or medical assistant – follows up with patients to see if they’ve “gotten everything done without barriers,” Dr. Davis said. “Did they have trouble filling that prescription? Did they have difficulty with the referral? Or do they not think it’s necessary – for example, a patient might not go to physical therapy because the injury has improved.”
Dr. Davis wasn’t surprised that patients were less likely to close the loop for colonoscopies compared with seeking out a stress test or treatment for skin lesions.
“People who have a skin lesion may be concerned about their appearance or about skin cancer, and people who need a stress test may have had cardiac symptoms or be worried about their heart.” But a routine screening such as a colonoscopy may not mobilize the patient’s concern to the same degree.
“Additionally, a colonoscopy has an ‘ick factor,’ so there aren’t a whole lot of people who are jumping to have the procedure done.” She suggested considering newer FDA-approved stool tests to screen for colon cancer.
Dr. Amat and Dr. Davis both emphasized that educating patients – both during and after the visit – and making sure they understand the importance of their referral for tests or specialists referrals are key to ensuring that they follow through on the recommendations.
The study was funded by the Agency for Healthcare Research and Quality. Dr. Amat was supported by the Arnold Tofias and Leo Condakes Quality Scholarship Program. Dr. Amat declared no relevant financial relationships. Dr. Davis is the chief health officer for Montgomery County in Maryland.
A version of this article first appeared on Medscape.com.
Telehealth has been a boon for modern-day patients, allowing people who might have difficulty accessing in-person appointments to continue seeing their physicians. But how many patients actually follow through on their physician’s recommendations afterward?
A new study suggests that
Investigators retrospectively examined test and referral orders for more than 4,000 patients to see how many complied with recommendations to have a colonoscopy, consult a dermatologist for a suspicious skin lesion, or undergo a cardiac stress test.
Completion of a recommended test or specialty referral was termed “diagnostic loop closure.” In particular, the researchers wanted to compare loop closure after telehealth versus in-person visits.
Rates of loop closure were low across all visit modalities but were lower for tests and referrals ordered during telehealth visits, compared with in-person visits – especially for colonoscopies.
“The take-home message for practicing clinicians is that they should be especially aware of follow-up for tests or referrals ordered during telehealth visits,” said corresponding author Maëlys Amat, MD, MBA, a primary care physician at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston.
The study was published online on in JAMA Network Open.
‘Unintended side effects’
“Diagnostic errors present a huge safety concern, impacting many patient lives and costing the health care system billions of dollars, said Dr. Amat, who is also an instructor at Harvard Medical School.
“Telehealth utilization increased rapidly during the COVID pandemic, and although there are clear benefits to utilizing telehealth, our team sought to investigate unintended side effects of this technology and highlight opportunities for improvement,” she said.
To investigate the question, the researchers reviewed medical records of 4,113 patients, with a mean age of 59 years, at two Boston-based primary care sites: an urban hospital–based primary care practice and an affiliated community health center.
Orders for tests or referrals in both centers were placed electronically through the medical record. During an in-person visit, the patient was handed a form with a phone number to call to schedule the test or referral. Patients with limited English proficiency or complex needs may have received help with the scheduling the referral during check-out.
For telehealth visits, the clinician gave the patient the phone number to call to schedule the test or referral during the visit itself. In all scenarios, patients did not receive communication after the visit reminding them about the referral or test.
A loop was considered “closed” if the orders were completed within 365 days, 90 days, or 45 days for colonoscopy, dermatology visits, or cardiac stress testing, respectively.
Of the tests, 52.4% were ordered during an in-person visit, 27.8% were ordered during a telehealth visit, and 19.7% were ordered without a visit.
Tracking systems, virtual checkout
Fewer than half of the orders (42.6%) placed during a telehealth visit were completed within the designated time frame, compared with 58.4% of the orders placed during an in-person visit and 57.4% placed without a visit.
Patients who had telehealth visits were roughly half as likely as those who had in-person visits to close the loop on high-risk tests and referrals, even in an analysis that adjusted for test type, patient demographic characteristics, comorbidities, clinical site, clinician type, and patient engagement (odds ratio, 0.55; 95% confidence interval, 0.47-0.64).
Only 39.8% of colonoscopy referrals ordered during a telehealth visit were completed during the 365-day time period, compared with 56.9% ordered during an in-person visit and 56.7% ordered without a visit.
Follow-through with dermatology referrals within 90 days was roughly the same across all types of visits (63.1% for telehealth, 61.5% for in-person, and 62.9% for no visit). No significant differences were found between telehealth and in-person visits or orders placed without a visit.
Although patients seen via telehealth were less likely than those seen in person to follow through on cardiac stress tests within the 45-day window (59.1% vs. 63.2%), this difference didn’t reach statistical significance.
“Ideally, clinicians would implement automatic tracking systems to help ensure that an ordered test or referral is completed,” Dr. Amat commented. “However, if these systems aren’t yet in place, we strongly encourage clinicians to create their own work flows for tracking tests to completion.”
Additionally, “clinicians should consider implementing a virtual checkout system, similar to what is done during in-person visits, to help patients better understand recommended next steps,” she continued.
Other potentially helpful ways to improve loop closure include automatic tracking for outstanding tests, interventions such as telephone outreach to patients, automated text and email reminders, and the use of referral managers – especially in remote, rural areas or for “disadvantaged patients with limited health care access and literacy.”
Education is key
Kisha Davis, MD, MPH, member of the board of directors of the American Academy of Family Physicians, said in an interview that being able to see a provider virtually can make the difference between a person receiving or not receiving medical care. She regards telehealth as another tool in the toolkit her practice offers to provide comprehensive health care.
Dr. Davis, a family physician in Gaithersburg, Md., who wasn’t involved with the study, described a patient with hypertension who was an Uber driver. “During the pandemic, Uber rides were down, and he couldn›t afford to pass up any opportunities, so he pulled over to the side of the road after one of his rides, did his telehealth visit, reviewed his medications, and went on to his next ride.”
The key is to make sure that patients receive adequate follow-up from the office, which Dr. Davis arranged for this patient.
She noted that telehealth “is best done if there’s an established physician-patient relationship but harder to accomplish successfully if you’ve only met the patient on telehealth and never in person.”
The study didn’t specify whether the physicians had an established relationship with their patients.
During the checkout process after an in-person appointment, patients often receive a sheet of paper with the follow-up referrals. “I can see where patients are less likely to follow through if they don’t have someone handing them that paper,” she said.
In her practice, patients’ charts are color-coded “to keep track and make sure it’s not just the ‘squeaky wheels’ that get all the attention,” she said. “The onus is on the physician and the practice, in today’s world of value-based care, to make sure that patients who don’t come into the office are getting the care they need.”
This is facilitated by a “system of care coordination” in which the office team – such as a nurse or medical assistant – follows up with patients to see if they’ve “gotten everything done without barriers,” Dr. Davis said. “Did they have trouble filling that prescription? Did they have difficulty with the referral? Or do they not think it’s necessary – for example, a patient might not go to physical therapy because the injury has improved.”
Dr. Davis wasn’t surprised that patients were less likely to close the loop for colonoscopies compared with seeking out a stress test or treatment for skin lesions.
“People who have a skin lesion may be concerned about their appearance or about skin cancer, and people who need a stress test may have had cardiac symptoms or be worried about their heart.” But a routine screening such as a colonoscopy may not mobilize the patient’s concern to the same degree.
“Additionally, a colonoscopy has an ‘ick factor,’ so there aren’t a whole lot of people who are jumping to have the procedure done.” She suggested considering newer FDA-approved stool tests to screen for colon cancer.
Dr. Amat and Dr. Davis both emphasized that educating patients – both during and after the visit – and making sure they understand the importance of their referral for tests or specialists referrals are key to ensuring that they follow through on the recommendations.
The study was funded by the Agency for Healthcare Research and Quality. Dr. Amat was supported by the Arnold Tofias and Leo Condakes Quality Scholarship Program. Dr. Amat declared no relevant financial relationships. Dr. Davis is the chief health officer for Montgomery County in Maryland.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Headache after drinking red wine? This could be why
This transcript has been edited for clarity.
Robert Louis Stevenson famously said, “Wine is bottled poetry.” And I think it works quite well. I’ve had wines that are simple, elegant, and unpretentious like Emily Dickinson, and passionate and mysterious like Pablo Neruda. And I’ve had wines that are more analogous to the limerick you might read scrawled on a rest-stop bathroom wall. Those ones give me headaches.
– and apparently it’s not just the alcohol.
Headaches are common, and headaches after drinking alcohol are particularly common. An interesting epidemiologic phenomenon, not yet adequately explained, is why red wine is associated with more headache than other forms of alcohol. There have been many studies fingering many suspects, from sulfites to tannins to various phenolic compounds, but none have really provided a concrete explanation for what might be going on.
A new hypothesis came to the fore on Nov. 20 in the journal Scientific Reports:
To understand the idea, first a reminder of what happens when you drink alcohol, physiologically.
Alcohol is metabolized by the enzyme alcohol dehydrogenase in the gut and then in the liver. That turns it into acetaldehyde, a toxic metabolite. In most of us, aldehyde dehydrogenase (ALDH) quickly metabolizes acetaldehyde to the inert acetate, which can be safely excreted.
I say “most of us” because some populations, particularly those with East Asian ancestry, have a mutation in the ALDH gene which can lead to accumulation of toxic acetaldehyde with alcohol consumption – leading to facial flushing, nausea, and headache.
We can also inhibit the enzyme medically. That’s what the drug disulfiram, also known as Antabuse, does. It doesn’t prevent you from wanting to drink; it makes the consequences of drinking incredibly aversive.
The researchers focused in on the aldehyde dehydrogenase enzyme and conducted a screening study. Are there any compounds in red wine that naturally inhibit ALDH?
The results pointed squarely at quercetin, and particularly its metabolite quercetin glucuronide, which, at 20 micromolar concentrations, inhibited about 80% of ALDH activity.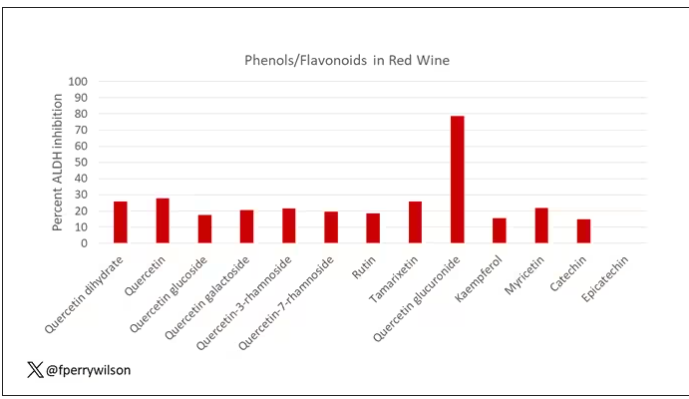
Quercetin is a flavonoid – a compound that gives color to a variety of vegetables and fruits, including grapes. In a test tube, it is an antioxidant, which is enough evidence to spawn a small quercetin-as-supplement industry, but there is no convincing evidence that it is medically useful. The authors then examined the concentration of quercetin glucuronide to achieve various inhibitions of ALDH, as you can see in this graph here.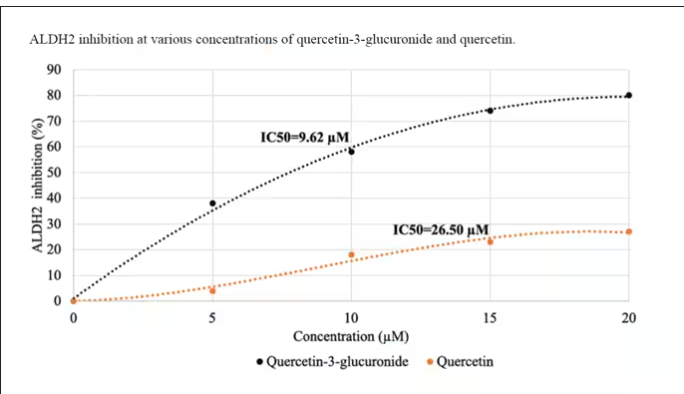
By about 10 micromolar, we see a decent amount of inhibition. Disulfiram is about 10 times more potent than that, but then again, you don’t drink three glasses of disulfiram with Thanksgiving dinner.
This is where this study stops. But it obviously tells us very little about what might be happening in the human body. For that, we need to ask the question: Can we get our quercetin levels to 10 micromolar? Is that remotely achievable?
Let’s start with how much quercetin there is in red wine. Like all things wine, it varies, but this study examining Australian wines found mean concentrations of 11 mg/L. The highest value I saw was close to 50 mg/L.
So let’s do some math. To make the numbers easy, let’s say you drank a liter of Australian wine, taking in 50 mg of quercetin glucuronide.
How much of that gets into your bloodstream? Some studies suggest a bioavailability of less than 1%, which basically means none and should probably put the quercetin hypothesis to bed. But there is some variation here too; it seems to depend on the form of quercetin you ingest.
Let’s say all 50 mg gets into your bloodstream. What blood concentration would that lead to? Well, I’ll keep the stoichiometry in the graphics and just say that if we assume that the volume of distribution of the compound is restricted to plasma alone, then you could achieve similar concentrations to what was done in petri dishes during this study.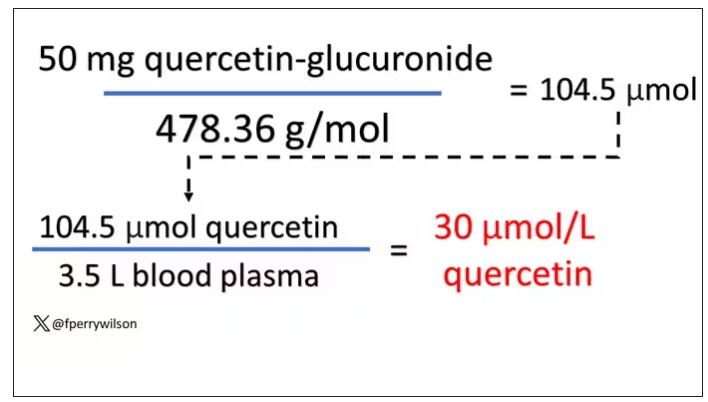
Of course, if quercetin is really the culprit behind red wine headache, I have some questions: Why aren’t the Amazon reviews of quercetin supplements chock full of warnings not to take them with alcohol? And other foods have way higher quercetin concentration than wine, but you don’t hear people warning not to take your red onions with alcohol, or your capers, or lingonberries.
There’s some more work to be done here – most importantly, some human studies. Let’s give people wine with different amounts of quercetin and see what happens. Sign me up. Seriously.
As for Thanksgiving, it’s worth noting that cranberries have a lot of quercetin in them. So between the cranberry sauce, the Beaujolais, and your uncle ranting about the contrails again, the probability of headache is pretty darn high. Stay safe out there, and Happy Thanksgiving.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Robert Louis Stevenson famously said, “Wine is bottled poetry.” And I think it works quite well. I’ve had wines that are simple, elegant, and unpretentious like Emily Dickinson, and passionate and mysterious like Pablo Neruda. And I’ve had wines that are more analogous to the limerick you might read scrawled on a rest-stop bathroom wall. Those ones give me headaches.
– and apparently it’s not just the alcohol.
Headaches are common, and headaches after drinking alcohol are particularly common. An interesting epidemiologic phenomenon, not yet adequately explained, is why red wine is associated with more headache than other forms of alcohol. There have been many studies fingering many suspects, from sulfites to tannins to various phenolic compounds, but none have really provided a concrete explanation for what might be going on.
A new hypothesis came to the fore on Nov. 20 in the journal Scientific Reports:
To understand the idea, first a reminder of what happens when you drink alcohol, physiologically.
Alcohol is metabolized by the enzyme alcohol dehydrogenase in the gut and then in the liver. That turns it into acetaldehyde, a toxic metabolite. In most of us, aldehyde dehydrogenase (ALDH) quickly metabolizes acetaldehyde to the inert acetate, which can be safely excreted.
I say “most of us” because some populations, particularly those with East Asian ancestry, have a mutation in the ALDH gene which can lead to accumulation of toxic acetaldehyde with alcohol consumption – leading to facial flushing, nausea, and headache.
We can also inhibit the enzyme medically. That’s what the drug disulfiram, also known as Antabuse, does. It doesn’t prevent you from wanting to drink; it makes the consequences of drinking incredibly aversive.
The researchers focused in on the aldehyde dehydrogenase enzyme and conducted a screening study. Are there any compounds in red wine that naturally inhibit ALDH?
The results pointed squarely at quercetin, and particularly its metabolite quercetin glucuronide, which, at 20 micromolar concentrations, inhibited about 80% of ALDH activity.
Quercetin is a flavonoid – a compound that gives color to a variety of vegetables and fruits, including grapes. In a test tube, it is an antioxidant, which is enough evidence to spawn a small quercetin-as-supplement industry, but there is no convincing evidence that it is medically useful. The authors then examined the concentration of quercetin glucuronide to achieve various inhibitions of ALDH, as you can see in this graph here.
By about 10 micromolar, we see a decent amount of inhibition. Disulfiram is about 10 times more potent than that, but then again, you don’t drink three glasses of disulfiram with Thanksgiving dinner.
This is where this study stops. But it obviously tells us very little about what might be happening in the human body. For that, we need to ask the question: Can we get our quercetin levels to 10 micromolar? Is that remotely achievable?
Let’s start with how much quercetin there is in red wine. Like all things wine, it varies, but this study examining Australian wines found mean concentrations of 11 mg/L. The highest value I saw was close to 50 mg/L.
So let’s do some math. To make the numbers easy, let’s say you drank a liter of Australian wine, taking in 50 mg of quercetin glucuronide.
How much of that gets into your bloodstream? Some studies suggest a bioavailability of less than 1%, which basically means none and should probably put the quercetin hypothesis to bed. But there is some variation here too; it seems to depend on the form of quercetin you ingest.
Let’s say all 50 mg gets into your bloodstream. What blood concentration would that lead to? Well, I’ll keep the stoichiometry in the graphics and just say that if we assume that the volume of distribution of the compound is restricted to plasma alone, then you could achieve similar concentrations to what was done in petri dishes during this study.
Of course, if quercetin is really the culprit behind red wine headache, I have some questions: Why aren’t the Amazon reviews of quercetin supplements chock full of warnings not to take them with alcohol? And other foods have way higher quercetin concentration than wine, but you don’t hear people warning not to take your red onions with alcohol, or your capers, or lingonberries.
There’s some more work to be done here – most importantly, some human studies. Let’s give people wine with different amounts of quercetin and see what happens. Sign me up. Seriously.
As for Thanksgiving, it’s worth noting that cranberries have a lot of quercetin in them. So between the cranberry sauce, the Beaujolais, and your uncle ranting about the contrails again, the probability of headache is pretty darn high. Stay safe out there, and Happy Thanksgiving.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Robert Louis Stevenson famously said, “Wine is bottled poetry.” And I think it works quite well. I’ve had wines that are simple, elegant, and unpretentious like Emily Dickinson, and passionate and mysterious like Pablo Neruda. And I’ve had wines that are more analogous to the limerick you might read scrawled on a rest-stop bathroom wall. Those ones give me headaches.
– and apparently it’s not just the alcohol.
Headaches are common, and headaches after drinking alcohol are particularly common. An interesting epidemiologic phenomenon, not yet adequately explained, is why red wine is associated with more headache than other forms of alcohol. There have been many studies fingering many suspects, from sulfites to tannins to various phenolic compounds, but none have really provided a concrete explanation for what might be going on.
A new hypothesis came to the fore on Nov. 20 in the journal Scientific Reports:
To understand the idea, first a reminder of what happens when you drink alcohol, physiologically.
Alcohol is metabolized by the enzyme alcohol dehydrogenase in the gut and then in the liver. That turns it into acetaldehyde, a toxic metabolite. In most of us, aldehyde dehydrogenase (ALDH) quickly metabolizes acetaldehyde to the inert acetate, which can be safely excreted.
I say “most of us” because some populations, particularly those with East Asian ancestry, have a mutation in the ALDH gene which can lead to accumulation of toxic acetaldehyde with alcohol consumption – leading to facial flushing, nausea, and headache.
We can also inhibit the enzyme medically. That’s what the drug disulfiram, also known as Antabuse, does. It doesn’t prevent you from wanting to drink; it makes the consequences of drinking incredibly aversive.
The researchers focused in on the aldehyde dehydrogenase enzyme and conducted a screening study. Are there any compounds in red wine that naturally inhibit ALDH?
The results pointed squarely at quercetin, and particularly its metabolite quercetin glucuronide, which, at 20 micromolar concentrations, inhibited about 80% of ALDH activity.
Quercetin is a flavonoid – a compound that gives color to a variety of vegetables and fruits, including grapes. In a test tube, it is an antioxidant, which is enough evidence to spawn a small quercetin-as-supplement industry, but there is no convincing evidence that it is medically useful. The authors then examined the concentration of quercetin glucuronide to achieve various inhibitions of ALDH, as you can see in this graph here.
By about 10 micromolar, we see a decent amount of inhibition. Disulfiram is about 10 times more potent than that, but then again, you don’t drink three glasses of disulfiram with Thanksgiving dinner.
This is where this study stops. But it obviously tells us very little about what might be happening in the human body. For that, we need to ask the question: Can we get our quercetin levels to 10 micromolar? Is that remotely achievable?
Let’s start with how much quercetin there is in red wine. Like all things wine, it varies, but this study examining Australian wines found mean concentrations of 11 mg/L. The highest value I saw was close to 50 mg/L.
So let’s do some math. To make the numbers easy, let’s say you drank a liter of Australian wine, taking in 50 mg of quercetin glucuronide.
How much of that gets into your bloodstream? Some studies suggest a bioavailability of less than 1%, which basically means none and should probably put the quercetin hypothesis to bed. But there is some variation here too; it seems to depend on the form of quercetin you ingest.
Let’s say all 50 mg gets into your bloodstream. What blood concentration would that lead to? Well, I’ll keep the stoichiometry in the graphics and just say that if we assume that the volume of distribution of the compound is restricted to plasma alone, then you could achieve similar concentrations to what was done in petri dishes during this study.
Of course, if quercetin is really the culprit behind red wine headache, I have some questions: Why aren’t the Amazon reviews of quercetin supplements chock full of warnings not to take them with alcohol? And other foods have way higher quercetin concentration than wine, but you don’t hear people warning not to take your red onions with alcohol, or your capers, or lingonberries.
There’s some more work to be done here – most importantly, some human studies. Let’s give people wine with different amounts of quercetin and see what happens. Sign me up. Seriously.
As for Thanksgiving, it’s worth noting that cranberries have a lot of quercetin in them. So between the cranberry sauce, the Beaujolais, and your uncle ranting about the contrails again, the probability of headache is pretty darn high. Stay safe out there, and Happy Thanksgiving.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
UHC accused of using AI to skirt doctors’ orders, deny claims
.
In a class action suit filed in Minnesota district court, the attorneys for the families of two deceased UHC Medicare Advantage plan policyholders say that the company uses the technology to systematically deny skilled nursing facility (SNF) claims and shirk its responsibility to adhere to Medicare’s coverage determination standards.
The case raises ethical and legal questions about whether AI can replace or supplement human tasks and interactions, particularly in a field as complex as health care. California-based public advocacy firm Clarkson Law filed a similar complaint against Cigna earlier this year and has previously sued tech giants Google and ChatGPT creator OpenAI for harvesting Internet users’ data to train their AI systems.
Clarkson Law represents the plaintiffs and says that the policyholders had to pay thousands in out-of-pocket costs or forgo the recommended postacute care owing to UHC’s faulty AI model, nH Predict. The tool has a 90% error rate, says the lawsuit, as evidenced by the number of claims that are reversed following review by a medical professional. Still, just 0.2% of policyholders appeal the denials.
nH Predict was created by naviHealth and was acquired by UnitedHealth Group, UHC’s parent company, in 2020. In a statement to Bloomberg Law, a spokesperson for naviHealth said that the lawsuit has no merit and the model was not used for making coverage determinations.
According to the complaint, nH Predict determines the appropriate amount of SNF, home health, or rehabilitation services a patient requires on the basis of the diagnosis, age, and living situation. The model compares the patient with its database of 6 million patients and estimates the ideal length of stay and target discharge date, “pinpointing the precise moment when [UHC] will cut off payment for a patient’s treatment.”
The lawsuit says that employees are instructed to strictly adhere to the AI model’s predictions, and those who do not are disciplined and terminated, even when additional care for the patient is warranted. Employees are told that the generated reports contain proprietary information and that they cannot share them with physicians and patients who inquire about extending care.
“Every patient is entitled to a nuanced evaluation of their health care needs,” Zarrina Ozari, senior associate at Clarkson Law, said in a prepared statement. “By replacing licensed practitioners with unchecked AI, UHC is telling its patients that they are completely interchangeable with one another and undervaluing the expertise of the physicians devoted to key elements of care.”
According to the complaint, Gene Lokken fell in May 2022 and fractured his leg and ankle. After a 1-month SNF stay, the 91-year-old man’s doctor ordered physical therapy. However, the insurer said Mr. Lokken was safe to be discharged home two and a half weeks later, conflicting with a physical therapist’s notes that indicated he still had paralyzed and weak muscles. The insurer denied Mr. Lokken’s appeal. He remained in the facility for another year until his death, paying about $150,000 in out-of-pocket expenses, according to the lawsuit.
Another patient, Dale H. Tetzloff, initially spent just 20 days in a SNF for stroke rehabilitation before UHC denied coverage. An appeal later extended the stay to 40 days, short of the 100 days recommended by his physician. Requests for further extensions were unsuccessful, and Mr. Tetzloff ultimately paid about $70,000 in out-of-pocket expenses over the next 10 months, according to the complaint.
New federal rules prohibit Medicare Advantage plans from relying on an algorithm or software to make medically necessary determinations instead of an individual’s specific circumstances. Any medical necessity denial must be “reviewed by a physician or other appropriate health care professional with expertise in the field of medicine or health care that is appropriate for the service at issue.”
Clarkson is demanding a jury trial and has asked the court to certify the case as a federal class action, which could open the suit to any U.S. resident who purchased a UHC Medicare Advantage plan in the past 4 years.
A version of this article appeared on Medscape.com.
.
In a class action suit filed in Minnesota district court, the attorneys for the families of two deceased UHC Medicare Advantage plan policyholders say that the company uses the technology to systematically deny skilled nursing facility (SNF) claims and shirk its responsibility to adhere to Medicare’s coverage determination standards.
The case raises ethical and legal questions about whether AI can replace or supplement human tasks and interactions, particularly in a field as complex as health care. California-based public advocacy firm Clarkson Law filed a similar complaint against Cigna earlier this year and has previously sued tech giants Google and ChatGPT creator OpenAI for harvesting Internet users’ data to train their AI systems.
Clarkson Law represents the plaintiffs and says that the policyholders had to pay thousands in out-of-pocket costs or forgo the recommended postacute care owing to UHC’s faulty AI model, nH Predict. The tool has a 90% error rate, says the lawsuit, as evidenced by the number of claims that are reversed following review by a medical professional. Still, just 0.2% of policyholders appeal the denials.
nH Predict was created by naviHealth and was acquired by UnitedHealth Group, UHC’s parent company, in 2020. In a statement to Bloomberg Law, a spokesperson for naviHealth said that the lawsuit has no merit and the model was not used for making coverage determinations.
According to the complaint, nH Predict determines the appropriate amount of SNF, home health, or rehabilitation services a patient requires on the basis of the diagnosis, age, and living situation. The model compares the patient with its database of 6 million patients and estimates the ideal length of stay and target discharge date, “pinpointing the precise moment when [UHC] will cut off payment for a patient’s treatment.”
The lawsuit says that employees are instructed to strictly adhere to the AI model’s predictions, and those who do not are disciplined and terminated, even when additional care for the patient is warranted. Employees are told that the generated reports contain proprietary information and that they cannot share them with physicians and patients who inquire about extending care.
“Every patient is entitled to a nuanced evaluation of their health care needs,” Zarrina Ozari, senior associate at Clarkson Law, said in a prepared statement. “By replacing licensed practitioners with unchecked AI, UHC is telling its patients that they are completely interchangeable with one another and undervaluing the expertise of the physicians devoted to key elements of care.”
According to the complaint, Gene Lokken fell in May 2022 and fractured his leg and ankle. After a 1-month SNF stay, the 91-year-old man’s doctor ordered physical therapy. However, the insurer said Mr. Lokken was safe to be discharged home two and a half weeks later, conflicting with a physical therapist’s notes that indicated he still had paralyzed and weak muscles. The insurer denied Mr. Lokken’s appeal. He remained in the facility for another year until his death, paying about $150,000 in out-of-pocket expenses, according to the lawsuit.
Another patient, Dale H. Tetzloff, initially spent just 20 days in a SNF for stroke rehabilitation before UHC denied coverage. An appeal later extended the stay to 40 days, short of the 100 days recommended by his physician. Requests for further extensions were unsuccessful, and Mr. Tetzloff ultimately paid about $70,000 in out-of-pocket expenses over the next 10 months, according to the complaint.
New federal rules prohibit Medicare Advantage plans from relying on an algorithm or software to make medically necessary determinations instead of an individual’s specific circumstances. Any medical necessity denial must be “reviewed by a physician or other appropriate health care professional with expertise in the field of medicine or health care that is appropriate for the service at issue.”
Clarkson is demanding a jury trial and has asked the court to certify the case as a federal class action, which could open the suit to any U.S. resident who purchased a UHC Medicare Advantage plan in the past 4 years.
A version of this article appeared on Medscape.com.
.
In a class action suit filed in Minnesota district court, the attorneys for the families of two deceased UHC Medicare Advantage plan policyholders say that the company uses the technology to systematically deny skilled nursing facility (SNF) claims and shirk its responsibility to adhere to Medicare’s coverage determination standards.
The case raises ethical and legal questions about whether AI can replace or supplement human tasks and interactions, particularly in a field as complex as health care. California-based public advocacy firm Clarkson Law filed a similar complaint against Cigna earlier this year and has previously sued tech giants Google and ChatGPT creator OpenAI for harvesting Internet users’ data to train their AI systems.
Clarkson Law represents the plaintiffs and says that the policyholders had to pay thousands in out-of-pocket costs or forgo the recommended postacute care owing to UHC’s faulty AI model, nH Predict. The tool has a 90% error rate, says the lawsuit, as evidenced by the number of claims that are reversed following review by a medical professional. Still, just 0.2% of policyholders appeal the denials.
nH Predict was created by naviHealth and was acquired by UnitedHealth Group, UHC’s parent company, in 2020. In a statement to Bloomberg Law, a spokesperson for naviHealth said that the lawsuit has no merit and the model was not used for making coverage determinations.
According to the complaint, nH Predict determines the appropriate amount of SNF, home health, or rehabilitation services a patient requires on the basis of the diagnosis, age, and living situation. The model compares the patient with its database of 6 million patients and estimates the ideal length of stay and target discharge date, “pinpointing the precise moment when [UHC] will cut off payment for a patient’s treatment.”
The lawsuit says that employees are instructed to strictly adhere to the AI model’s predictions, and those who do not are disciplined and terminated, even when additional care for the patient is warranted. Employees are told that the generated reports contain proprietary information and that they cannot share them with physicians and patients who inquire about extending care.
“Every patient is entitled to a nuanced evaluation of their health care needs,” Zarrina Ozari, senior associate at Clarkson Law, said in a prepared statement. “By replacing licensed practitioners with unchecked AI, UHC is telling its patients that they are completely interchangeable with one another and undervaluing the expertise of the physicians devoted to key elements of care.”
According to the complaint, Gene Lokken fell in May 2022 and fractured his leg and ankle. After a 1-month SNF stay, the 91-year-old man’s doctor ordered physical therapy. However, the insurer said Mr. Lokken was safe to be discharged home two and a half weeks later, conflicting with a physical therapist’s notes that indicated he still had paralyzed and weak muscles. The insurer denied Mr. Lokken’s appeal. He remained in the facility for another year until his death, paying about $150,000 in out-of-pocket expenses, according to the lawsuit.
Another patient, Dale H. Tetzloff, initially spent just 20 days in a SNF for stroke rehabilitation before UHC denied coverage. An appeal later extended the stay to 40 days, short of the 100 days recommended by his physician. Requests for further extensions were unsuccessful, and Mr. Tetzloff ultimately paid about $70,000 in out-of-pocket expenses over the next 10 months, according to the complaint.
New federal rules prohibit Medicare Advantage plans from relying on an algorithm or software to make medically necessary determinations instead of an individual’s specific circumstances. Any medical necessity denial must be “reviewed by a physician or other appropriate health care professional with expertise in the field of medicine or health care that is appropriate for the service at issue.”
Clarkson is demanding a jury trial and has asked the court to certify the case as a federal class action, which could open the suit to any U.S. resident who purchased a UHC Medicare Advantage plan in the past 4 years.
A version of this article appeared on Medscape.com.
Before signing an offer letter: Read this
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
FDA OKs symplicity renal denervation system for hypertension
the company has announced.
The Symplicity Spyral system, also known as the Symplicity blood pressure procedure, provides a catheter-based approach to denervate the renal arteries using radiofrequency energy.
Back in August, the FDA’s Circulatory System Devices Panel unanimously agreed that the Symplicity Spyral system is safe, but the panel was split on its efficacy and whether the benefits outweighed the risks associated with its use.
As part of the Medtronic SPYRAL HTN Global Clinical Program, more than 25,000 patients have been treated worldwide, both in the presence and absence of medication, and in patients with high baseline cardiovascular risk.
The SPYRAL HTN-OFF study enrolled patients with hypertension whose medications could be stopped at the start of the trial.
The primary effectiveness endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure (ASBP) from baseline to 3 months after renal denervation or sham procedure. The study showed a statistically significant reduction of 3.9 mm Hg ASBP in patients who received the device, compared with sham-control patients.
The SPYRAL HTN-ON study evaluated patients with uncontrolled hypertension who continued taking their BP medications during treatment with either the Spyral renal denervation device or a sham device.
The primary endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure at 6 months. The study showed a nonsignificant 24-hour 0.03 mm Hg reduction in ASBP in active-treatment patients, compared with sham-control patients.
“The Symplicity blood pressure procedure is safe and effective, providing significant ‘always-on’ blood pressure reductions for patients,” David Kandzari, MD, chief, Piedmont Heart Institute, Atlanta, and co–principal investigator of the SPYRAL clinical program, said in the news release.
“This approval paves the way for a transformation in hypertension treatment, offering a solution that complements medication and lifestyle changes,” added co–principal investigator Raymond Townsend, MD, with University of Pennsylvania, Philadelphia.
Medtronic notes that patient preference and shared decision-making are key components when considering the Symplicity blood pressure procedure.
In a patient preference study led by Medtronic, when presented with an interventional treatment with BP reduction and potential risks in line with those of the Symplicity blood pressure procedure, approximately one-third of patients were likely to choose the interventional treatment.
Earlier in November, the FDA also approved the Paradise Ultrasound Renal Denervation system (Recor Medical, Otsuka Medical Devices) for the treatment of hypertension.
A version of this article first appeared on Medscape.com.
the company has announced.
The Symplicity Spyral system, also known as the Symplicity blood pressure procedure, provides a catheter-based approach to denervate the renal arteries using radiofrequency energy.
Back in August, the FDA’s Circulatory System Devices Panel unanimously agreed that the Symplicity Spyral system is safe, but the panel was split on its efficacy and whether the benefits outweighed the risks associated with its use.
As part of the Medtronic SPYRAL HTN Global Clinical Program, more than 25,000 patients have been treated worldwide, both in the presence and absence of medication, and in patients with high baseline cardiovascular risk.
The SPYRAL HTN-OFF study enrolled patients with hypertension whose medications could be stopped at the start of the trial.
The primary effectiveness endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure (ASBP) from baseline to 3 months after renal denervation or sham procedure. The study showed a statistically significant reduction of 3.9 mm Hg ASBP in patients who received the device, compared with sham-control patients.
The SPYRAL HTN-ON study evaluated patients with uncontrolled hypertension who continued taking their BP medications during treatment with either the Spyral renal denervation device or a sham device.
The primary endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure at 6 months. The study showed a nonsignificant 24-hour 0.03 mm Hg reduction in ASBP in active-treatment patients, compared with sham-control patients.
“The Symplicity blood pressure procedure is safe and effective, providing significant ‘always-on’ blood pressure reductions for patients,” David Kandzari, MD, chief, Piedmont Heart Institute, Atlanta, and co–principal investigator of the SPYRAL clinical program, said in the news release.
“This approval paves the way for a transformation in hypertension treatment, offering a solution that complements medication and lifestyle changes,” added co–principal investigator Raymond Townsend, MD, with University of Pennsylvania, Philadelphia.
Medtronic notes that patient preference and shared decision-making are key components when considering the Symplicity blood pressure procedure.
In a patient preference study led by Medtronic, when presented with an interventional treatment with BP reduction and potential risks in line with those of the Symplicity blood pressure procedure, approximately one-third of patients were likely to choose the interventional treatment.
Earlier in November, the FDA also approved the Paradise Ultrasound Renal Denervation system (Recor Medical, Otsuka Medical Devices) for the treatment of hypertension.
A version of this article first appeared on Medscape.com.
the company has announced.
The Symplicity Spyral system, also known as the Symplicity blood pressure procedure, provides a catheter-based approach to denervate the renal arteries using radiofrequency energy.
Back in August, the FDA’s Circulatory System Devices Panel unanimously agreed that the Symplicity Spyral system is safe, but the panel was split on its efficacy and whether the benefits outweighed the risks associated with its use.
As part of the Medtronic SPYRAL HTN Global Clinical Program, more than 25,000 patients have been treated worldwide, both in the presence and absence of medication, and in patients with high baseline cardiovascular risk.
The SPYRAL HTN-OFF study enrolled patients with hypertension whose medications could be stopped at the start of the trial.
The primary effectiveness endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure (ASBP) from baseline to 3 months after renal denervation or sham procedure. The study showed a statistically significant reduction of 3.9 mm Hg ASBP in patients who received the device, compared with sham-control patients.
The SPYRAL HTN-ON study evaluated patients with uncontrolled hypertension who continued taking their BP medications during treatment with either the Spyral renal denervation device or a sham device.
The primary endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure at 6 months. The study showed a nonsignificant 24-hour 0.03 mm Hg reduction in ASBP in active-treatment patients, compared with sham-control patients.
“The Symplicity blood pressure procedure is safe and effective, providing significant ‘always-on’ blood pressure reductions for patients,” David Kandzari, MD, chief, Piedmont Heart Institute, Atlanta, and co–principal investigator of the SPYRAL clinical program, said in the news release.
“This approval paves the way for a transformation in hypertension treatment, offering a solution that complements medication and lifestyle changes,” added co–principal investigator Raymond Townsend, MD, with University of Pennsylvania, Philadelphia.
Medtronic notes that patient preference and shared decision-making are key components when considering the Symplicity blood pressure procedure.
In a patient preference study led by Medtronic, when presented with an interventional treatment with BP reduction and potential risks in line with those of the Symplicity blood pressure procedure, approximately one-third of patients were likely to choose the interventional treatment.
Earlier in November, the FDA also approved the Paradise Ultrasound Renal Denervation system (Recor Medical, Otsuka Medical Devices) for the treatment of hypertension.
A version of this article first appeared on Medscape.com.
Single injection reduces blood pressure for 6 months: KARDIA-1
with what appeared to be an encouraging side-effect profile, in the phase 2 dose-ranging KARDIA-1 study.
“Our study demonstrates that either quarterly or biannual doses of zilebesiran can effectively and safely lower blood pressure in patients with uncontrolled hypertension,” said senior study investigator George Bakris, MD.
“Based on these results, zilebesiran has the potential to improve medication adherence, which will, in turn, reduce cardiovascular risk in people with hypertension,” added Dr. Bakris, who is professor of medicine and director of the Comprehensive Hypertension Center at the University of Chicago Medicine.
The KARDIA-1 study was presented at the American Heart Association scientific sessions.
Dr. Bakris noted that uncontrolled hypertension is a leading cause of morbidity and mortality, and despite availability of effective antihypertensives, many adults with hypertension are untreated, and up to 80% have uncontrolled disease, both globally and in the United States.
Zilebesiran is a subcutaneous RNA interference therapeutic that binds with high affinity to the hepatic asialoglycoprotein receptor, bringing about a reduction in the synthesis of angiotensinogen, the sole precursor of all angiotensin peptides. It is hoped that its hepatocyte-targeted delivery may allow extrahepatic angiotensinogen expression to be preserved, which could limit off-target effects in the kidney and other tissues.
The KARDIA-1 trial investigated the safety and efficacy of different doses of zilebesiran in patients with mild to moderate hypertension (systolic BP of 135-160 mm Hg), who are untreated or on stable therapy with up to two antihypertensive medications.
The study included 394 such patients (average baseline systolic BP was 142 mm Hg) who were randomly assigned to receive one of four different zilebesiran doses (150 mg, 300 mg, or 600 mg once every 6 months or 300 mg once every 2 months) or a placebo. The final analysis included 377 patients (56% men, 25% Black).
Results showed sustained reductions in serum angiotensinogen (between 88% and 98%) over the 6-month follow-up period.
Ambulatory systolic BP measured over 24 hours was significantly decreased with all zilebesiran regimens, with a mean reduction from baseline to month 6 of around 10 mm Hg in the three top doses studied and by around 14 mm Hg compared with placebo.
Patients receiving zilebesiran were more likely to achieve 24-hour average systolic BP measurements of 130 mm Hg or less at 6 months.
In addition, participants in all four zilebesiran groups consistently experienced significantly greater reductions in both daytime and nighttime systolic BP.
There were four nonserious adverse reactions leading to discontinuation in the zilebesiran groups: two instances of orthostatic hypotension, one of BP elevation, and one of injection site reaction.
Most hyperkalemia adverse events, which occurred in 6% of patients, were mild, did not require intervention, and generally resolved with repeat measurement; none were associated with acute kidney injury or led to study drug discontinuation. The incidence of hypotension events was low, and no clinically relevant changes in renal or hepatic function were observed, Dr. Bakris reported.
There was one death caused by cardiopulmonary arrest in a patient receiving zilebesiran 300 mg every 3 months, but this was not classified as drug related.
Zilebesiran is being further evaluated as an add-on therapy for treatment of hypertension in the ongoing KARDIA-2 phase 2 study.
Moderator of an AHA press conference at which the study was discussed, Sandra Taler, MD, professor of medicine at the Mayo Clinic, Rochester, Minn., said that “to have an injectable medicine that gives long-term blood pressure lowering is extremely exciting.”
Dr. Taler raised the point that some patients may not return for subsequent doses, but added that with subcutaneous dosing, administration at home may be a possibility.
Also commenting at the press conference, Keith Ferdinand, MD, professor of clinical medicine at Tulane University, New Orleans, said that this study “suggests we can now target the first step in the renin-angiotensin system – angiotensinogen – which then appears to lead to robust and continued blood pressure lowering for up to 6 months, which should improve adherence.”
Noting that only 50% of patients continue to take antihypertensive drugs after 1 year, Dr. Ferdinand added: “If we can increase adherence, we will increase efficacy and perhaps protect against some of the target organ damage.”
Designated discussant of the KARDIA-1 study at the AHA late-breaking clinical trial session, Anna Dominiczak, MD, University of Glasgow, noted that hypertension affects one in three adults worldwide, but only around 20% of people have it under control.
“An increase in the number of patients effectively treated for hypertension to levels observed in high-performing countries could prevent 76 million deaths, 120 million strokes, 79 million heart attacks, and 17 million cases of heart failure between now and 2050,” she said.
Dr. Bakris has received consulting fees from Alnylam Pharmaceuticals.
A version of this article first appeared on Medscape.com.
with what appeared to be an encouraging side-effect profile, in the phase 2 dose-ranging KARDIA-1 study.
“Our study demonstrates that either quarterly or biannual doses of zilebesiran can effectively and safely lower blood pressure in patients with uncontrolled hypertension,” said senior study investigator George Bakris, MD.
“Based on these results, zilebesiran has the potential to improve medication adherence, which will, in turn, reduce cardiovascular risk in people with hypertension,” added Dr. Bakris, who is professor of medicine and director of the Comprehensive Hypertension Center at the University of Chicago Medicine.
The KARDIA-1 study was presented at the American Heart Association scientific sessions.
Dr. Bakris noted that uncontrolled hypertension is a leading cause of morbidity and mortality, and despite availability of effective antihypertensives, many adults with hypertension are untreated, and up to 80% have uncontrolled disease, both globally and in the United States.
Zilebesiran is a subcutaneous RNA interference therapeutic that binds with high affinity to the hepatic asialoglycoprotein receptor, bringing about a reduction in the synthesis of angiotensinogen, the sole precursor of all angiotensin peptides. It is hoped that its hepatocyte-targeted delivery may allow extrahepatic angiotensinogen expression to be preserved, which could limit off-target effects in the kidney and other tissues.
The KARDIA-1 trial investigated the safety and efficacy of different doses of zilebesiran in patients with mild to moderate hypertension (systolic BP of 135-160 mm Hg), who are untreated or on stable therapy with up to two antihypertensive medications.
The study included 394 such patients (average baseline systolic BP was 142 mm Hg) who were randomly assigned to receive one of four different zilebesiran doses (150 mg, 300 mg, or 600 mg once every 6 months or 300 mg once every 2 months) or a placebo. The final analysis included 377 patients (56% men, 25% Black).
Results showed sustained reductions in serum angiotensinogen (between 88% and 98%) over the 6-month follow-up period.
Ambulatory systolic BP measured over 24 hours was significantly decreased with all zilebesiran regimens, with a mean reduction from baseline to month 6 of around 10 mm Hg in the three top doses studied and by around 14 mm Hg compared with placebo.
Patients receiving zilebesiran were more likely to achieve 24-hour average systolic BP measurements of 130 mm Hg or less at 6 months.
In addition, participants in all four zilebesiran groups consistently experienced significantly greater reductions in both daytime and nighttime systolic BP.
There were four nonserious adverse reactions leading to discontinuation in the zilebesiran groups: two instances of orthostatic hypotension, one of BP elevation, and one of injection site reaction.
Most hyperkalemia adverse events, which occurred in 6% of patients, were mild, did not require intervention, and generally resolved with repeat measurement; none were associated with acute kidney injury or led to study drug discontinuation. The incidence of hypotension events was low, and no clinically relevant changes in renal or hepatic function were observed, Dr. Bakris reported.
There was one death caused by cardiopulmonary arrest in a patient receiving zilebesiran 300 mg every 3 months, but this was not classified as drug related.
Zilebesiran is being further evaluated as an add-on therapy for treatment of hypertension in the ongoing KARDIA-2 phase 2 study.
Moderator of an AHA press conference at which the study was discussed, Sandra Taler, MD, professor of medicine at the Mayo Clinic, Rochester, Minn., said that “to have an injectable medicine that gives long-term blood pressure lowering is extremely exciting.”
Dr. Taler raised the point that some patients may not return for subsequent doses, but added that with subcutaneous dosing, administration at home may be a possibility.
Also commenting at the press conference, Keith Ferdinand, MD, professor of clinical medicine at Tulane University, New Orleans, said that this study “suggests we can now target the first step in the renin-angiotensin system – angiotensinogen – which then appears to lead to robust and continued blood pressure lowering for up to 6 months, which should improve adherence.”
Noting that only 50% of patients continue to take antihypertensive drugs after 1 year, Dr. Ferdinand added: “If we can increase adherence, we will increase efficacy and perhaps protect against some of the target organ damage.”
Designated discussant of the KARDIA-1 study at the AHA late-breaking clinical trial session, Anna Dominiczak, MD, University of Glasgow, noted that hypertension affects one in three adults worldwide, but only around 20% of people have it under control.
“An increase in the number of patients effectively treated for hypertension to levels observed in high-performing countries could prevent 76 million deaths, 120 million strokes, 79 million heart attacks, and 17 million cases of heart failure between now and 2050,” she said.
Dr. Bakris has received consulting fees from Alnylam Pharmaceuticals.
A version of this article first appeared on Medscape.com.
with what appeared to be an encouraging side-effect profile, in the phase 2 dose-ranging KARDIA-1 study.
“Our study demonstrates that either quarterly or biannual doses of zilebesiran can effectively and safely lower blood pressure in patients with uncontrolled hypertension,” said senior study investigator George Bakris, MD.
“Based on these results, zilebesiran has the potential to improve medication adherence, which will, in turn, reduce cardiovascular risk in people with hypertension,” added Dr. Bakris, who is professor of medicine and director of the Comprehensive Hypertension Center at the University of Chicago Medicine.
The KARDIA-1 study was presented at the American Heart Association scientific sessions.
Dr. Bakris noted that uncontrolled hypertension is a leading cause of morbidity and mortality, and despite availability of effective antihypertensives, many adults with hypertension are untreated, and up to 80% have uncontrolled disease, both globally and in the United States.
Zilebesiran is a subcutaneous RNA interference therapeutic that binds with high affinity to the hepatic asialoglycoprotein receptor, bringing about a reduction in the synthesis of angiotensinogen, the sole precursor of all angiotensin peptides. It is hoped that its hepatocyte-targeted delivery may allow extrahepatic angiotensinogen expression to be preserved, which could limit off-target effects in the kidney and other tissues.
The KARDIA-1 trial investigated the safety and efficacy of different doses of zilebesiran in patients with mild to moderate hypertension (systolic BP of 135-160 mm Hg), who are untreated or on stable therapy with up to two antihypertensive medications.
The study included 394 such patients (average baseline systolic BP was 142 mm Hg) who were randomly assigned to receive one of four different zilebesiran doses (150 mg, 300 mg, or 600 mg once every 6 months or 300 mg once every 2 months) or a placebo. The final analysis included 377 patients (56% men, 25% Black).
Results showed sustained reductions in serum angiotensinogen (between 88% and 98%) over the 6-month follow-up period.
Ambulatory systolic BP measured over 24 hours was significantly decreased with all zilebesiran regimens, with a mean reduction from baseline to month 6 of around 10 mm Hg in the three top doses studied and by around 14 mm Hg compared with placebo.
Patients receiving zilebesiran were more likely to achieve 24-hour average systolic BP measurements of 130 mm Hg or less at 6 months.
In addition, participants in all four zilebesiran groups consistently experienced significantly greater reductions in both daytime and nighttime systolic BP.
There were four nonserious adverse reactions leading to discontinuation in the zilebesiran groups: two instances of orthostatic hypotension, one of BP elevation, and one of injection site reaction.
Most hyperkalemia adverse events, which occurred in 6% of patients, were mild, did not require intervention, and generally resolved with repeat measurement; none were associated with acute kidney injury or led to study drug discontinuation. The incidence of hypotension events was low, and no clinically relevant changes in renal or hepatic function were observed, Dr. Bakris reported.
There was one death caused by cardiopulmonary arrest in a patient receiving zilebesiran 300 mg every 3 months, but this was not classified as drug related.
Zilebesiran is being further evaluated as an add-on therapy for treatment of hypertension in the ongoing KARDIA-2 phase 2 study.
Moderator of an AHA press conference at which the study was discussed, Sandra Taler, MD, professor of medicine at the Mayo Clinic, Rochester, Minn., said that “to have an injectable medicine that gives long-term blood pressure lowering is extremely exciting.”
Dr. Taler raised the point that some patients may not return for subsequent doses, but added that with subcutaneous dosing, administration at home may be a possibility.
Also commenting at the press conference, Keith Ferdinand, MD, professor of clinical medicine at Tulane University, New Orleans, said that this study “suggests we can now target the first step in the renin-angiotensin system – angiotensinogen – which then appears to lead to robust and continued blood pressure lowering for up to 6 months, which should improve adherence.”
Noting that only 50% of patients continue to take antihypertensive drugs after 1 year, Dr. Ferdinand added: “If we can increase adherence, we will increase efficacy and perhaps protect against some of the target organ damage.”
Designated discussant of the KARDIA-1 study at the AHA late-breaking clinical trial session, Anna Dominiczak, MD, University of Glasgow, noted that hypertension affects one in three adults worldwide, but only around 20% of people have it under control.
“An increase in the number of patients effectively treated for hypertension to levels observed in high-performing countries could prevent 76 million deaths, 120 million strokes, 79 million heart attacks, and 17 million cases of heart failure between now and 2050,” she said.
Dr. Bakris has received consulting fees from Alnylam Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM AHA 2023
PREVENT: AHA’s new risk calculator incorporates CKM health
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
Alternative antirejection regimen is efficacious in pediatric heart transplant
Study challenges everolimus boxed warning
according to the first phase 3 trial to compare antirejection strategies in the pediatric setting.
Even though MMF and tacrolimus have never been evaluated for pediatric cardiac transplant in a controlled trial, this combination is widely considered a standard based on adult data, said Christopher Almond, MD, a professor of pediatric cardiology at Stanford (Calif.) Medicine.
Everolimus has not been widely used in an antirejection regimen in children following heart transplant in part because of a boxed warning. The warning was added to labeling when this agent was associated with increased infection and increased mortality in adults if given within 3 months of transplant.
In this non-inferiority trial, called TEAMMATE, patients were randomized to the MMF-based or everolimus-based regimen 6 months after transplant.
Everolimus- vs. MMF-based antirejection
The study enrolled 210 children and adolescents 21 years of age or younger. The control arm treatment consisted of MMF (660 mg/m2 every 12 hours) plus standard dose of tacrolimus (initially 7-10 ng/mL followed at 6 months by 5-8 ng/mL).
In the experimental arm, patients received everolimus (3-8 ng/mL) plus a low dose of tacrolimus (initially 3-5 ng/mL followed at 6 months by 2.5-4.5 ng/mL).
The primary endpoint was score on the major adverse transplant event (MATE-6) tool. Based on gradations of severity, this assigns values for cardiac allograft vasculopathy (CAV), chronic kidney disease (CKD), acute cellular rejection (ACR), antibody-mediated rejection, infection, and posttransplant lymphoproliferative disorder (PTLD).
Thirty months after randomization, the MATE-6 scores were 1.96 in the everolimus group and 2.18 in the MMF group, which conferred the everolimus-based regimen with a numerical but not a significant advantage over the MMF-based regimen. For the goal of noninferiority, the everolimus regimen “met the prespecified safety criterion for success,” Dr. Almond said.
Numerical advantage for everolimus on efficacy
The primary efficacy endpoint was the MATE-3 score, which is limited to CAV, CKD, and ACR. Again, the mean score on this metric (0.93 vs. 1.25) was lower on the everolimus-based regimen but not significantly different.
Looking at specific events in the MATE-6 score, the everolimus-based regimen was associated with lower numerical rates of CAV and CKD, but a higher rate of PTLD, Dr. Almond reported.
On the MATE-3 efficacy analysis, the everolimus-based regimen was again associated with lower numerical rates of CAV and CKD but higher rates of ACR.
In terms of adverse events, including those involving the gastrointestinal tract, blood cells, proteinuria, and interstitial lung disease, most did not differ markedly even if many were numerically more common in the MMF-based arm. The exception was aphthous stomatitis, which was more common on everolimus (32% vs. 7%; P < .001). There were more discontinuations for an adverse event in the MMF arm (21% vs. 12%; P < .001).
Other differences included a lower proportion of patients in the everolimus arm with anti-HLA antibodies (17% vs. 30%; P < .05). Total cholesterol levels at the end of the study were lower but not significantly different in the MMF group, while the higher median glomerular filtration rate was higher on everolimus, and this did reach statistical significance (P < .05).
Infection rates overall were similar, but cytomegalovirus (CMV) infection was more common on the MMF-based regimen. The 30% lower rate of CMV infection in the everolimus proved to be potentially clinically meaningful when it was considered in the context of MATE-3. When these two endpoints were combined (MATE-3 and CMV infection as a prespecified secondary endpoint, the difference was statistically significant (P = .03) in favor of the everolimus-based regimen,
Study supports safety of everolimus regimen
The take-home message is that the everolimus-based regimen, which “is safe in children and young adults when initiated at 6 months after transplant,” can be considered as an alternative to MFF, Dr. Almond concluded.
However, one of the coauthors of the study, Joseph Rossano, MD, chief of the division of cardiology, Children’s Hospital of Philadelphia, suggested a stronger message.
“These data provide compelling reasons to consider initiation of the combination of everolimus and tacrolimus at 6 months post transplant in pediatric heart transplant recipients,” Dr. Rossano said.
Even though the everolimus-based regimen met the terms of noninferiority overall, patients who received this combination rather than the MMF-based regimen “were less likely to have the combined endpoints of vasculopathy, CKD, rejection and CMV infection. Additionally, they were less likely to make donor specific antibodies,” he said.
He also said that this study challenges the current boxed warning for everolimus. He pointed out that the warning, based on early use of everolimus in adults, does not appear to be an issue for children treated at 6 months.
Early mortality based on infection “was not observed in our study,” he said.
The AHA-invited discussant, Antonio G. Cabrera, MD, division chief of pediatric cardiology, University of Utah, Salt Lake City, drew the same conclusions. Based on the study, the everolimus-based regimen can only be described as noninferior to the MMF-based regimen, but Dr. Cabrera listed the same relative advantages as Dr. Rossano, including better kidney function.
Overall, either regimen might be more appealing based on several variables, but Dr. Cabrera said these data suggest everolimus-based treatment “should be considered” as one of two evidence-based options,
Dr. Almond reported no potential financial conflicts of interest. Dr. Rossano reports financial relationships with Abiomed, Bayer, Cytokinetics, Merck, and Myokardia. Dr. Cabrera reported no potential financial conflicts of interest.
Study challenges everolimus boxed warning
Study challenges everolimus boxed warning
according to the first phase 3 trial to compare antirejection strategies in the pediatric setting.
Even though MMF and tacrolimus have never been evaluated for pediatric cardiac transplant in a controlled trial, this combination is widely considered a standard based on adult data, said Christopher Almond, MD, a professor of pediatric cardiology at Stanford (Calif.) Medicine.
Everolimus has not been widely used in an antirejection regimen in children following heart transplant in part because of a boxed warning. The warning was added to labeling when this agent was associated with increased infection and increased mortality in adults if given within 3 months of transplant.
In this non-inferiority trial, called TEAMMATE, patients were randomized to the MMF-based or everolimus-based regimen 6 months after transplant.
Everolimus- vs. MMF-based antirejection
The study enrolled 210 children and adolescents 21 years of age or younger. The control arm treatment consisted of MMF (660 mg/m2 every 12 hours) plus standard dose of tacrolimus (initially 7-10 ng/mL followed at 6 months by 5-8 ng/mL).
In the experimental arm, patients received everolimus (3-8 ng/mL) plus a low dose of tacrolimus (initially 3-5 ng/mL followed at 6 months by 2.5-4.5 ng/mL).
The primary endpoint was score on the major adverse transplant event (MATE-6) tool. Based on gradations of severity, this assigns values for cardiac allograft vasculopathy (CAV), chronic kidney disease (CKD), acute cellular rejection (ACR), antibody-mediated rejection, infection, and posttransplant lymphoproliferative disorder (PTLD).
Thirty months after randomization, the MATE-6 scores were 1.96 in the everolimus group and 2.18 in the MMF group, which conferred the everolimus-based regimen with a numerical but not a significant advantage over the MMF-based regimen. For the goal of noninferiority, the everolimus regimen “met the prespecified safety criterion for success,” Dr. Almond said.
Numerical advantage for everolimus on efficacy
The primary efficacy endpoint was the MATE-3 score, which is limited to CAV, CKD, and ACR. Again, the mean score on this metric (0.93 vs. 1.25) was lower on the everolimus-based regimen but not significantly different.
Looking at specific events in the MATE-6 score, the everolimus-based regimen was associated with lower numerical rates of CAV and CKD, but a higher rate of PTLD, Dr. Almond reported.
On the MATE-3 efficacy analysis, the everolimus-based regimen was again associated with lower numerical rates of CAV and CKD but higher rates of ACR.
In terms of adverse events, including those involving the gastrointestinal tract, blood cells, proteinuria, and interstitial lung disease, most did not differ markedly even if many were numerically more common in the MMF-based arm. The exception was aphthous stomatitis, which was more common on everolimus (32% vs. 7%; P < .001). There were more discontinuations for an adverse event in the MMF arm (21% vs. 12%; P < .001).
Other differences included a lower proportion of patients in the everolimus arm with anti-HLA antibodies (17% vs. 30%; P < .05). Total cholesterol levels at the end of the study were lower but not significantly different in the MMF group, while the higher median glomerular filtration rate was higher on everolimus, and this did reach statistical significance (P < .05).
Infection rates overall were similar, but cytomegalovirus (CMV) infection was more common on the MMF-based regimen. The 30% lower rate of CMV infection in the everolimus proved to be potentially clinically meaningful when it was considered in the context of MATE-3. When these two endpoints were combined (MATE-3 and CMV infection as a prespecified secondary endpoint, the difference was statistically significant (P = .03) in favor of the everolimus-based regimen,
Study supports safety of everolimus regimen
The take-home message is that the everolimus-based regimen, which “is safe in children and young adults when initiated at 6 months after transplant,” can be considered as an alternative to MFF, Dr. Almond concluded.
However, one of the coauthors of the study, Joseph Rossano, MD, chief of the division of cardiology, Children’s Hospital of Philadelphia, suggested a stronger message.
“These data provide compelling reasons to consider initiation of the combination of everolimus and tacrolimus at 6 months post transplant in pediatric heart transplant recipients,” Dr. Rossano said.
Even though the everolimus-based regimen met the terms of noninferiority overall, patients who received this combination rather than the MMF-based regimen “were less likely to have the combined endpoints of vasculopathy, CKD, rejection and CMV infection. Additionally, they were less likely to make donor specific antibodies,” he said.
He also said that this study challenges the current boxed warning for everolimus. He pointed out that the warning, based on early use of everolimus in adults, does not appear to be an issue for children treated at 6 months.
Early mortality based on infection “was not observed in our study,” he said.
The AHA-invited discussant, Antonio G. Cabrera, MD, division chief of pediatric cardiology, University of Utah, Salt Lake City, drew the same conclusions. Based on the study, the everolimus-based regimen can only be described as noninferior to the MMF-based regimen, but Dr. Cabrera listed the same relative advantages as Dr. Rossano, including better kidney function.
Overall, either regimen might be more appealing based on several variables, but Dr. Cabrera said these data suggest everolimus-based treatment “should be considered” as one of two evidence-based options,
Dr. Almond reported no potential financial conflicts of interest. Dr. Rossano reports financial relationships with Abiomed, Bayer, Cytokinetics, Merck, and Myokardia. Dr. Cabrera reported no potential financial conflicts of interest.
according to the first phase 3 trial to compare antirejection strategies in the pediatric setting.
Even though MMF and tacrolimus have never been evaluated for pediatric cardiac transplant in a controlled trial, this combination is widely considered a standard based on adult data, said Christopher Almond, MD, a professor of pediatric cardiology at Stanford (Calif.) Medicine.
Everolimus has not been widely used in an antirejection regimen in children following heart transplant in part because of a boxed warning. The warning was added to labeling when this agent was associated with increased infection and increased mortality in adults if given within 3 months of transplant.
In this non-inferiority trial, called TEAMMATE, patients were randomized to the MMF-based or everolimus-based regimen 6 months after transplant.
Everolimus- vs. MMF-based antirejection
The study enrolled 210 children and adolescents 21 years of age or younger. The control arm treatment consisted of MMF (660 mg/m2 every 12 hours) plus standard dose of tacrolimus (initially 7-10 ng/mL followed at 6 months by 5-8 ng/mL).
In the experimental arm, patients received everolimus (3-8 ng/mL) plus a low dose of tacrolimus (initially 3-5 ng/mL followed at 6 months by 2.5-4.5 ng/mL).
The primary endpoint was score on the major adverse transplant event (MATE-6) tool. Based on gradations of severity, this assigns values for cardiac allograft vasculopathy (CAV), chronic kidney disease (CKD), acute cellular rejection (ACR), antibody-mediated rejection, infection, and posttransplant lymphoproliferative disorder (PTLD).
Thirty months after randomization, the MATE-6 scores were 1.96 in the everolimus group and 2.18 in the MMF group, which conferred the everolimus-based regimen with a numerical but not a significant advantage over the MMF-based regimen. For the goal of noninferiority, the everolimus regimen “met the prespecified safety criterion for success,” Dr. Almond said.
Numerical advantage for everolimus on efficacy
The primary efficacy endpoint was the MATE-3 score, which is limited to CAV, CKD, and ACR. Again, the mean score on this metric (0.93 vs. 1.25) was lower on the everolimus-based regimen but not significantly different.
Looking at specific events in the MATE-6 score, the everolimus-based regimen was associated with lower numerical rates of CAV and CKD, but a higher rate of PTLD, Dr. Almond reported.
On the MATE-3 efficacy analysis, the everolimus-based regimen was again associated with lower numerical rates of CAV and CKD but higher rates of ACR.
In terms of adverse events, including those involving the gastrointestinal tract, blood cells, proteinuria, and interstitial lung disease, most did not differ markedly even if many were numerically more common in the MMF-based arm. The exception was aphthous stomatitis, which was more common on everolimus (32% vs. 7%; P < .001). There were more discontinuations for an adverse event in the MMF arm (21% vs. 12%; P < .001).
Other differences included a lower proportion of patients in the everolimus arm with anti-HLA antibodies (17% vs. 30%; P < .05). Total cholesterol levels at the end of the study were lower but not significantly different in the MMF group, while the higher median glomerular filtration rate was higher on everolimus, and this did reach statistical significance (P < .05).
Infection rates overall were similar, but cytomegalovirus (CMV) infection was more common on the MMF-based regimen. The 30% lower rate of CMV infection in the everolimus proved to be potentially clinically meaningful when it was considered in the context of MATE-3. When these two endpoints were combined (MATE-3 and CMV infection as a prespecified secondary endpoint, the difference was statistically significant (P = .03) in favor of the everolimus-based regimen,
Study supports safety of everolimus regimen
The take-home message is that the everolimus-based regimen, which “is safe in children and young adults when initiated at 6 months after transplant,” can be considered as an alternative to MFF, Dr. Almond concluded.
However, one of the coauthors of the study, Joseph Rossano, MD, chief of the division of cardiology, Children’s Hospital of Philadelphia, suggested a stronger message.
“These data provide compelling reasons to consider initiation of the combination of everolimus and tacrolimus at 6 months post transplant in pediatric heart transplant recipients,” Dr. Rossano said.
Even though the everolimus-based regimen met the terms of noninferiority overall, patients who received this combination rather than the MMF-based regimen “were less likely to have the combined endpoints of vasculopathy, CKD, rejection and CMV infection. Additionally, they were less likely to make donor specific antibodies,” he said.
He also said that this study challenges the current boxed warning for everolimus. He pointed out that the warning, based on early use of everolimus in adults, does not appear to be an issue for children treated at 6 months.
Early mortality based on infection “was not observed in our study,” he said.
The AHA-invited discussant, Antonio G. Cabrera, MD, division chief of pediatric cardiology, University of Utah, Salt Lake City, drew the same conclusions. Based on the study, the everolimus-based regimen can only be described as noninferior to the MMF-based regimen, but Dr. Cabrera listed the same relative advantages as Dr. Rossano, including better kidney function.
Overall, either regimen might be more appealing based on several variables, but Dr. Cabrera said these data suggest everolimus-based treatment “should be considered” as one of two evidence-based options,
Dr. Almond reported no potential financial conflicts of interest. Dr. Rossano reports financial relationships with Abiomed, Bayer, Cytokinetics, Merck, and Myokardia. Dr. Cabrera reported no potential financial conflicts of interest.
FROM AHA 2023
Infographic: Careers that tempt doctors to leave medicine
In a recently published Medscape report, 26% of American physicians said they were considering a career away from practicing medicine, for various reasons. Becoming a teacher was one of the nonclinical careers that most enthused them. What were the others?
For more details, check out the Medscape Physicians and Nonclinical Careers Report 2023.

A version of this article first appeared on Medscape.com.
In a recently published Medscape report, 26% of American physicians said they were considering a career away from practicing medicine, for various reasons. Becoming a teacher was one of the nonclinical careers that most enthused them. What were the others?
For more details, check out the Medscape Physicians and Nonclinical Careers Report 2023.
A version of this article first appeared on Medscape.com.
In a recently published Medscape report, 26% of American physicians said they were considering a career away from practicing medicine, for various reasons. Becoming a teacher was one of the nonclinical careers that most enthused them. What were the others?
For more details, check out the Medscape Physicians and Nonclinical Careers Report 2023.
A version of this article first appeared on Medscape.com.
WHO: Smoking cessation reduces risk of type 2 diabetes up to 40%
TOPLINE:
, and quitting even after one has developed type 2 diabetes is important in preventing a worsening of the disease’s many serious comorbidities, according to a new policy brief jointly issued by the World Health Organization, the International Diabetes Federation (IDF), and the University of Newcastle, Callaghan, Australia.
With type 2 diabetes representing one of the most prevalent chronic diseases worldwide and the ninth cause of death globally, the potential to reduce the risk and worsening of the disease by quitting smoking adds to the urgency of smoking cessation as a public health interest.
METHODOLOGY:
- The policy brief summarizes the evidence on the health impacts of type 2 diabetes, tobacco smoking, and the pathophysiology of tobacco use and its role in the development of type 2 diabetes.
- The brief also describes the latest data on newer products that target smokers or potential smokers, including smokeless tobacco, new nicotine and tobacco products, and their relationship with type 2 diabetes. For instance, evidence suggests that even with smokeless tobacco, heavy use or high consumption increases the risk of developing type 2 diabetes, as the products often contain nicotine, known to contribute to the development of type 2 diabetes and related health conditions.
- Evidence on the effectiveness of tobacco control interventions among those with type 2 diabetes is also summarized, including discussion of a systematic review of six studies suggesting that interventions focusing on education and the involvement of health care professionals and pharmacists can be beneficial for people with type 2 diabetes.
TAKEAWAY:
- Smoking exacerbates the known serious complications of diabetic neuropathy and foot ulcers with type 2 diabetes, while further impeding wound healing.
- Smoking also causes damage to retinal blood vessels already at risk with type 2 diabetes, increasing the risk of diabetic retinopathy and vision loss.
- Quitting tobacco use can help prevent those and other major health complications already linked to diabetes, including kidney failure and cardiovascular events.
- Studies show that key misconceptions among smokers with type 2 diabetes that can prevent cessation include concerns about post-cessation weight gain, the influence of peers who smoke, and the psychological aspect of addiction.
- Clinicians are urged to provide advice on how to stop smoking to all tobacco users during the course of a routine consultation or interaction, which can be accomplished in only a few minutes.
IN PRACTICE:
“Health professionals play a vital role in motivating and guiding individuals with type 2 diabetes in their journey to quit tobacco,” Ruediger Krech, MD, director of the Department of Health Promotion at the World Health Organization in Geneva, Switzerland, said in a press statement on the policy brief.
“Simultaneously, governments must take the crucial step of ensuring all indoor public places, workplaces, and public transport are completely smoke-free. These interventions are essential safeguards against the onset and progression of this and many other chronic diseases,” he emphasized.
SOURCE:
The policy brief was jointly developed by the World Health Organization, the International Diabetes Federation, and the University of Newcastle.
The detailed policy brief can be downloaded on the IDF website.
LIMITATIONS:
Research remains limited on some issues, including the effectiveness of tobacco control interventions and smoking cessation methods for people with type 2 diabetes.
Likewise, specific guidelines for smoking cessation in the type 2 diabetes population are lacking. However, the general approaches of building patient motivation, behavioral interventions, and pharmacological treatments are advised.
“These interventions should be at least as intensive as those for the general population, while considering the unique characteristics of the disease and the individual,” the authors asserted.
DISCLOSURES:
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
, and quitting even after one has developed type 2 diabetes is important in preventing a worsening of the disease’s many serious comorbidities, according to a new policy brief jointly issued by the World Health Organization, the International Diabetes Federation (IDF), and the University of Newcastle, Callaghan, Australia.
With type 2 diabetes representing one of the most prevalent chronic diseases worldwide and the ninth cause of death globally, the potential to reduce the risk and worsening of the disease by quitting smoking adds to the urgency of smoking cessation as a public health interest.
METHODOLOGY:
- The policy brief summarizes the evidence on the health impacts of type 2 diabetes, tobacco smoking, and the pathophysiology of tobacco use and its role in the development of type 2 diabetes.
- The brief also describes the latest data on newer products that target smokers or potential smokers, including smokeless tobacco, new nicotine and tobacco products, and their relationship with type 2 diabetes. For instance, evidence suggests that even with smokeless tobacco, heavy use or high consumption increases the risk of developing type 2 diabetes, as the products often contain nicotine, known to contribute to the development of type 2 diabetes and related health conditions.
- Evidence on the effectiveness of tobacco control interventions among those with type 2 diabetes is also summarized, including discussion of a systematic review of six studies suggesting that interventions focusing on education and the involvement of health care professionals and pharmacists can be beneficial for people with type 2 diabetes.
TAKEAWAY:
- Smoking exacerbates the known serious complications of diabetic neuropathy and foot ulcers with type 2 diabetes, while further impeding wound healing.
- Smoking also causes damage to retinal blood vessels already at risk with type 2 diabetes, increasing the risk of diabetic retinopathy and vision loss.
- Quitting tobacco use can help prevent those and other major health complications already linked to diabetes, including kidney failure and cardiovascular events.
- Studies show that key misconceptions among smokers with type 2 diabetes that can prevent cessation include concerns about post-cessation weight gain, the influence of peers who smoke, and the psychological aspect of addiction.
- Clinicians are urged to provide advice on how to stop smoking to all tobacco users during the course of a routine consultation or interaction, which can be accomplished in only a few minutes.
IN PRACTICE:
“Health professionals play a vital role in motivating and guiding individuals with type 2 diabetes in their journey to quit tobacco,” Ruediger Krech, MD, director of the Department of Health Promotion at the World Health Organization in Geneva, Switzerland, said in a press statement on the policy brief.
“Simultaneously, governments must take the crucial step of ensuring all indoor public places, workplaces, and public transport are completely smoke-free. These interventions are essential safeguards against the onset and progression of this and many other chronic diseases,” he emphasized.
SOURCE:
The policy brief was jointly developed by the World Health Organization, the International Diabetes Federation, and the University of Newcastle.
The detailed policy brief can be downloaded on the IDF website.
LIMITATIONS:
Research remains limited on some issues, including the effectiveness of tobacco control interventions and smoking cessation methods for people with type 2 diabetes.
Likewise, specific guidelines for smoking cessation in the type 2 diabetes population are lacking. However, the general approaches of building patient motivation, behavioral interventions, and pharmacological treatments are advised.
“These interventions should be at least as intensive as those for the general population, while considering the unique characteristics of the disease and the individual,” the authors asserted.
DISCLOSURES:
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
, and quitting even after one has developed type 2 diabetes is important in preventing a worsening of the disease’s many serious comorbidities, according to a new policy brief jointly issued by the World Health Organization, the International Diabetes Federation (IDF), and the University of Newcastle, Callaghan, Australia.
With type 2 diabetes representing one of the most prevalent chronic diseases worldwide and the ninth cause of death globally, the potential to reduce the risk and worsening of the disease by quitting smoking adds to the urgency of smoking cessation as a public health interest.
METHODOLOGY:
- The policy brief summarizes the evidence on the health impacts of type 2 diabetes, tobacco smoking, and the pathophysiology of tobacco use and its role in the development of type 2 diabetes.
- The brief also describes the latest data on newer products that target smokers or potential smokers, including smokeless tobacco, new nicotine and tobacco products, and their relationship with type 2 diabetes. For instance, evidence suggests that even with smokeless tobacco, heavy use or high consumption increases the risk of developing type 2 diabetes, as the products often contain nicotine, known to contribute to the development of type 2 diabetes and related health conditions.
- Evidence on the effectiveness of tobacco control interventions among those with type 2 diabetes is also summarized, including discussion of a systematic review of six studies suggesting that interventions focusing on education and the involvement of health care professionals and pharmacists can be beneficial for people with type 2 diabetes.
TAKEAWAY:
- Smoking exacerbates the known serious complications of diabetic neuropathy and foot ulcers with type 2 diabetes, while further impeding wound healing.
- Smoking also causes damage to retinal blood vessels already at risk with type 2 diabetes, increasing the risk of diabetic retinopathy and vision loss.
- Quitting tobacco use can help prevent those and other major health complications already linked to diabetes, including kidney failure and cardiovascular events.
- Studies show that key misconceptions among smokers with type 2 diabetes that can prevent cessation include concerns about post-cessation weight gain, the influence of peers who smoke, and the psychological aspect of addiction.
- Clinicians are urged to provide advice on how to stop smoking to all tobacco users during the course of a routine consultation or interaction, which can be accomplished in only a few minutes.
IN PRACTICE:
“Health professionals play a vital role in motivating and guiding individuals with type 2 diabetes in their journey to quit tobacco,” Ruediger Krech, MD, director of the Department of Health Promotion at the World Health Organization in Geneva, Switzerland, said in a press statement on the policy brief.
“Simultaneously, governments must take the crucial step of ensuring all indoor public places, workplaces, and public transport are completely smoke-free. These interventions are essential safeguards against the onset and progression of this and many other chronic diseases,” he emphasized.
SOURCE:
The policy brief was jointly developed by the World Health Organization, the International Diabetes Federation, and the University of Newcastle.
The detailed policy brief can be downloaded on the IDF website.
LIMITATIONS:
Research remains limited on some issues, including the effectiveness of tobacco control interventions and smoking cessation methods for people with type 2 diabetes.
Likewise, specific guidelines for smoking cessation in the type 2 diabetes population are lacking. However, the general approaches of building patient motivation, behavioral interventions, and pharmacological treatments are advised.
“These interventions should be at least as intensive as those for the general population, while considering the unique characteristics of the disease and the individual,” the authors asserted.
DISCLOSURES:
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.