User login
In Case You Missed It: COVID
Advanced Primary Care program boosts COVID-19 results
The better outcomes were seen in higher vaccination rates and fewer infections, hospitalizations, and deaths from the disease, according to study authors, led by Emily Gruber, MBA, MPH, with the Maryland Primary Care Program, Maryland Department of Health in Baltimore.
The results were published online in JAMA Network Open.
The study population was divided into MDPCP participants (n = 208,146) and a matched cohort (n = 37,203) of beneficiaries not attributed to MDPCP practices but who met eligibility criteria for study participation from Jan. 1, 2020, through Dec. 31, 2021.
More vaccinations, more antibody treatments
Researchers broke down the comparisons of better outcomes: 84.47% of MDPCP beneficiaries were fully vaccinated vs. 77.93% of nonparticipating beneficiaries (P less than .001). COVID-19–positive program beneficiaries also received monoclonal antibody treatment more often (8.45% vs. 6.11%; P less than .001).
Plus, program participants received more care via telehealth (62.95% vs. 54.53%; P less than .001) compared with those not participating.
Regarding secondary outcomes, MDPCP beneficiaries had lower rates of COVID cases (6.55% vs. 7.09%; P less than .001), lower rates of COVID-19 hospitalizations (1.81% vs. 2.06%; P = .001), and lower rates of death due to COVID-19 (0.56% vs. 0.77%; P less than .001).
Program components
Enrollment in the MDPCP is voluntary, and primary care practices can apply each year to be part of the program.
The model integrates primary care and public health in the pandemic response. It was created by the Maryland Department of Health (MDH) and the Centers for Medicare & Medicaid Services (CMS).
It expands the role of primary care to include services such as expanded care management, integrated behavioral health, data-driven care, and screenings and referrals to address social needs.
Coauthor Howard Haft, MD, MMM, with the Maryland Department of Public Health, said in an interview that among the most important factors in the program’s success were giving providers vaccines to distribute and then giving providers data on how many patients are vaccinated, and who’s not vaccinated but at high risk, and how those rates compare to other practices.
As to whether this could be a widespread model, Dr. Haft said, “It’s highly replicable.”
“Every state in the nation overall has all of these resources. It’s a matter of having the operational and political will to put those resources together. Almost every state has the technological ability to use their health information exchange to help tie pieces together.”
Vaccines and testing made available to providers
Making ample vaccines and testing available to providers in their offices helped patients get those services in a place they trust, Dr. Haft said.
The model also included a payment system for providers that included a significant amount of non–visit-based payments when many locations were closed in the height of the pandemic.
“That helped financially,” as did providing free telehealth platforms to practices with training on how to use them, Dr. Haft said.
‘Innovative and important’
Renu Tipirneni, MD, an assistant professor of internal medicine at the University of Michigan and at the Institute for Healthcare Policy and Innovation in Ann Arbor, said Maryland is out front putting into practice what practices nationwide aspire to do – coordinating physical and mental health and social needs and integrating primary and public health. Dr. Tipirneni, who was not involved with the study, said she was impressed the researchers were able to show statistically significant improvement with COVID-19 outcomes in the first 2 years.
“In terms of health outcomes, we often have to wait longer to see good outcomes,” she said. “It’s a really innovative and important model.”
She said states can learn from each other and this model is an example.
Integrating primary care and public health and addressing social needs may be the biggest challenges for states, she said, as those realms typically have been siloed.
“But they may be the key components to achieving these outcomes,” she said.
Take-home message
The most important benefit of the program is that data suggest it saves lives, according to Dr. Haft. While the actual difference between COVID deaths in the program and nonprogram groups was small, multiplying that savings across the nation shows substantial potential benefit, he explained.
“At a time when we were losing lives at an unconscionable rate, we were able to make a difference in saving lives,” Dr. Haft said.
Authors report no relevant financial disclosures.
The study received financial support from the Maryland Department of Health.
Dr. Tiperneni is helping evaluate Michigan’s Medicaid contract.
The better outcomes were seen in higher vaccination rates and fewer infections, hospitalizations, and deaths from the disease, according to study authors, led by Emily Gruber, MBA, MPH, with the Maryland Primary Care Program, Maryland Department of Health in Baltimore.
The results were published online in JAMA Network Open.
The study population was divided into MDPCP participants (n = 208,146) and a matched cohort (n = 37,203) of beneficiaries not attributed to MDPCP practices but who met eligibility criteria for study participation from Jan. 1, 2020, through Dec. 31, 2021.
More vaccinations, more antibody treatments
Researchers broke down the comparisons of better outcomes: 84.47% of MDPCP beneficiaries were fully vaccinated vs. 77.93% of nonparticipating beneficiaries (P less than .001). COVID-19–positive program beneficiaries also received monoclonal antibody treatment more often (8.45% vs. 6.11%; P less than .001).
Plus, program participants received more care via telehealth (62.95% vs. 54.53%; P less than .001) compared with those not participating.
Regarding secondary outcomes, MDPCP beneficiaries had lower rates of COVID cases (6.55% vs. 7.09%; P less than .001), lower rates of COVID-19 hospitalizations (1.81% vs. 2.06%; P = .001), and lower rates of death due to COVID-19 (0.56% vs. 0.77%; P less than .001).
Program components
Enrollment in the MDPCP is voluntary, and primary care practices can apply each year to be part of the program.
The model integrates primary care and public health in the pandemic response. It was created by the Maryland Department of Health (MDH) and the Centers for Medicare & Medicaid Services (CMS).
It expands the role of primary care to include services such as expanded care management, integrated behavioral health, data-driven care, and screenings and referrals to address social needs.
Coauthor Howard Haft, MD, MMM, with the Maryland Department of Public Health, said in an interview that among the most important factors in the program’s success were giving providers vaccines to distribute and then giving providers data on how many patients are vaccinated, and who’s not vaccinated but at high risk, and how those rates compare to other practices.
As to whether this could be a widespread model, Dr. Haft said, “It’s highly replicable.”
“Every state in the nation overall has all of these resources. It’s a matter of having the operational and political will to put those resources together. Almost every state has the technological ability to use their health information exchange to help tie pieces together.”
Vaccines and testing made available to providers
Making ample vaccines and testing available to providers in their offices helped patients get those services in a place they trust, Dr. Haft said.
The model also included a payment system for providers that included a significant amount of non–visit-based payments when many locations were closed in the height of the pandemic.
“That helped financially,” as did providing free telehealth platforms to practices with training on how to use them, Dr. Haft said.
‘Innovative and important’
Renu Tipirneni, MD, an assistant professor of internal medicine at the University of Michigan and at the Institute for Healthcare Policy and Innovation in Ann Arbor, said Maryland is out front putting into practice what practices nationwide aspire to do – coordinating physical and mental health and social needs and integrating primary and public health. Dr. Tipirneni, who was not involved with the study, said she was impressed the researchers were able to show statistically significant improvement with COVID-19 outcomes in the first 2 years.
“In terms of health outcomes, we often have to wait longer to see good outcomes,” she said. “It’s a really innovative and important model.”
She said states can learn from each other and this model is an example.
Integrating primary care and public health and addressing social needs may be the biggest challenges for states, she said, as those realms typically have been siloed.
“But they may be the key components to achieving these outcomes,” she said.
Take-home message
The most important benefit of the program is that data suggest it saves lives, according to Dr. Haft. While the actual difference between COVID deaths in the program and nonprogram groups was small, multiplying that savings across the nation shows substantial potential benefit, he explained.
“At a time when we were losing lives at an unconscionable rate, we were able to make a difference in saving lives,” Dr. Haft said.
Authors report no relevant financial disclosures.
The study received financial support from the Maryland Department of Health.
Dr. Tiperneni is helping evaluate Michigan’s Medicaid contract.
The better outcomes were seen in higher vaccination rates and fewer infections, hospitalizations, and deaths from the disease, according to study authors, led by Emily Gruber, MBA, MPH, with the Maryland Primary Care Program, Maryland Department of Health in Baltimore.
The results were published online in JAMA Network Open.
The study population was divided into MDPCP participants (n = 208,146) and a matched cohort (n = 37,203) of beneficiaries not attributed to MDPCP practices but who met eligibility criteria for study participation from Jan. 1, 2020, through Dec. 31, 2021.
More vaccinations, more antibody treatments
Researchers broke down the comparisons of better outcomes: 84.47% of MDPCP beneficiaries were fully vaccinated vs. 77.93% of nonparticipating beneficiaries (P less than .001). COVID-19–positive program beneficiaries also received monoclonal antibody treatment more often (8.45% vs. 6.11%; P less than .001).
Plus, program participants received more care via telehealth (62.95% vs. 54.53%; P less than .001) compared with those not participating.
Regarding secondary outcomes, MDPCP beneficiaries had lower rates of COVID cases (6.55% vs. 7.09%; P less than .001), lower rates of COVID-19 hospitalizations (1.81% vs. 2.06%; P = .001), and lower rates of death due to COVID-19 (0.56% vs. 0.77%; P less than .001).
Program components
Enrollment in the MDPCP is voluntary, and primary care practices can apply each year to be part of the program.
The model integrates primary care and public health in the pandemic response. It was created by the Maryland Department of Health (MDH) and the Centers for Medicare & Medicaid Services (CMS).
It expands the role of primary care to include services such as expanded care management, integrated behavioral health, data-driven care, and screenings and referrals to address social needs.
Coauthor Howard Haft, MD, MMM, with the Maryland Department of Public Health, said in an interview that among the most important factors in the program’s success were giving providers vaccines to distribute and then giving providers data on how many patients are vaccinated, and who’s not vaccinated but at high risk, and how those rates compare to other practices.
As to whether this could be a widespread model, Dr. Haft said, “It’s highly replicable.”
“Every state in the nation overall has all of these resources. It’s a matter of having the operational and political will to put those resources together. Almost every state has the technological ability to use their health information exchange to help tie pieces together.”
Vaccines and testing made available to providers
Making ample vaccines and testing available to providers in their offices helped patients get those services in a place they trust, Dr. Haft said.
The model also included a payment system for providers that included a significant amount of non–visit-based payments when many locations were closed in the height of the pandemic.
“That helped financially,” as did providing free telehealth platforms to practices with training on how to use them, Dr. Haft said.
‘Innovative and important’
Renu Tipirneni, MD, an assistant professor of internal medicine at the University of Michigan and at the Institute for Healthcare Policy and Innovation in Ann Arbor, said Maryland is out front putting into practice what practices nationwide aspire to do – coordinating physical and mental health and social needs and integrating primary and public health. Dr. Tipirneni, who was not involved with the study, said she was impressed the researchers were able to show statistically significant improvement with COVID-19 outcomes in the first 2 years.
“In terms of health outcomes, we often have to wait longer to see good outcomes,” she said. “It’s a really innovative and important model.”
She said states can learn from each other and this model is an example.
Integrating primary care and public health and addressing social needs may be the biggest challenges for states, she said, as those realms typically have been siloed.
“But they may be the key components to achieving these outcomes,” she said.
Take-home message
The most important benefit of the program is that data suggest it saves lives, according to Dr. Haft. While the actual difference between COVID deaths in the program and nonprogram groups was small, multiplying that savings across the nation shows substantial potential benefit, he explained.
“At a time when we were losing lives at an unconscionable rate, we were able to make a difference in saving lives,” Dr. Haft said.
Authors report no relevant financial disclosures.
The study received financial support from the Maryland Department of Health.
Dr. Tiperneni is helping evaluate Michigan’s Medicaid contract.
FROM JAMA NETWORK OPEN
Gene associated with vision loss also linked to COVID: Study
age-related macular degeneration.
The findings show that COVID and AMD were associated with variations in what is called the PDGFB gene, which has a role in new blood vessel formation and is linked to abnormal blood vessel changes that occur in AMD. The study was published in the Journal of Clinical Medicine. The analysis included genetic data from more than 16,000 people with AMD, more than 50,000 people with COVID, plus control groups.
Age-related macular degeneration is a vision problem that occurs when a part of the retina – the macula – is damaged, according to the American Academy of Ophthalmology. The result is that central vision is lost, but peripheral vision remains normal, so it is difficult to see fine details. For example, a person with AMD can see a clock’s numbers but not its hands.
“Our analysis lends credence to previously reported clinical studies that found those with AMD have a higher risk for COVID-19 infection and severe disease, and that this increased risk may have a genetic basis,” Boston University researcher Lindsay Farrer, PhD, chief of biomedical genetics, explained in a news release.
Previous research has shown that people with AMD have a 25% increased risk of respiratory failure or death due to COVID, which is higher than other well-known risk factors such as type 2 diabetes (21%) or obesity (13%), according to the news release.
A version of this article first appeared on WebMD.com.
age-related macular degeneration.
The findings show that COVID and AMD were associated with variations in what is called the PDGFB gene, which has a role in new blood vessel formation and is linked to abnormal blood vessel changes that occur in AMD. The study was published in the Journal of Clinical Medicine. The analysis included genetic data from more than 16,000 people with AMD, more than 50,000 people with COVID, plus control groups.
Age-related macular degeneration is a vision problem that occurs when a part of the retina – the macula – is damaged, according to the American Academy of Ophthalmology. The result is that central vision is lost, but peripheral vision remains normal, so it is difficult to see fine details. For example, a person with AMD can see a clock’s numbers but not its hands.
“Our analysis lends credence to previously reported clinical studies that found those with AMD have a higher risk for COVID-19 infection and severe disease, and that this increased risk may have a genetic basis,” Boston University researcher Lindsay Farrer, PhD, chief of biomedical genetics, explained in a news release.
Previous research has shown that people with AMD have a 25% increased risk of respiratory failure or death due to COVID, which is higher than other well-known risk factors such as type 2 diabetes (21%) or obesity (13%), according to the news release.
A version of this article first appeared on WebMD.com.
age-related macular degeneration.
The findings show that COVID and AMD were associated with variations in what is called the PDGFB gene, which has a role in new blood vessel formation and is linked to abnormal blood vessel changes that occur in AMD. The study was published in the Journal of Clinical Medicine. The analysis included genetic data from more than 16,000 people with AMD, more than 50,000 people with COVID, plus control groups.
Age-related macular degeneration is a vision problem that occurs when a part of the retina – the macula – is damaged, according to the American Academy of Ophthalmology. The result is that central vision is lost, but peripheral vision remains normal, so it is difficult to see fine details. For example, a person with AMD can see a clock’s numbers but not its hands.
“Our analysis lends credence to previously reported clinical studies that found those with AMD have a higher risk for COVID-19 infection and severe disease, and that this increased risk may have a genetic basis,” Boston University researcher Lindsay Farrer, PhD, chief of biomedical genetics, explained in a news release.
Previous research has shown that people with AMD have a 25% increased risk of respiratory failure or death due to COVID, which is higher than other well-known risk factors such as type 2 diabetes (21%) or obesity (13%), according to the news release.
A version of this article first appeared on WebMD.com.
FROM THE JOURNAL OF CLINICAL MEDICINE
Long COVID clinical trials may offer shortcut to new treatments
With no proven treatments for long COVID, millions of Americans struggling with debilitating symptoms may be wondering whether it’s worth it to try something they’ve never considered before: a clinical trial.
But it may take years for these trials to prove which drugs, devices, and behavioral therapies are safe and effective.
“We’re not in warp speed,” said Kanecia Zimmerman, MD, a principal investigator at the Duke Clinical Research Institute in Durham, N.C., who is overseeing long COVID trials for the NIH. Operation Warp Speed – the 2020-2021 federal effort to get COVID vaccines designed, tested, authorized and distributed – benefited from existing scientific knowledge about other coronaviruses and about vaccines in general. But there’s no similar foundation of scientific knowledge about long COVID.
“We are in a place of not really knowing anything,” Dr. Zimmerman said.
But some glimmers of hope are emerging. A Veterans Affairs study recently found the antiviral Paxlovid might help prevent long COVID. A small case study at Yale found the ADHD drug guanfacine may ease brain fog from long COVID. And preliminary results from an NIH-funded study suggest COVID vaccines might help children with a rare but serious inflammatory condition known as multisystem inflammatory syndrome (MIS-C).
More results are expected very soon from the trial for kids with MIS-C, which can strike suddenly long after a COVID infection clears up. While the exact causes aren’t yet clear, MIS-C can cause dangerous inflammation in the heart, lungs, kidneys, brain, skin, eyes, or gastrointestinal system.
Because the virus often triggered a delayed response of MIS-C in kids who had few if any symptoms of acute COVID-19, scientists wondered whether children infected with the virus might respond to a vaccine dose to prevent MIS-C from developing, Gary Gibbons, MD, director of the National Heart, Lung, and Blood Institute, said during a Dec. 9 presentation at the NIH. It’s not yet clear if vaccination helps, but it doesn’t harm the children, Dr. Gibbons said.
“Indeed, the studies suggest with some relief that yes, these children could be vaccinated safely,” he said.
Several new trials are also testing Paxlovid against long COVID, including one late-stage study that may have results in about a year.
“We already know that Paxlovid reduces the risk of developing long COVID, but it would be a game changer if it can improve long COVID symptoms as well,” said Surendra Barshikar, MD, an associate professor and medical director of the COVID Recover program at the University of Texas Southwestern Medical Center, Dallas.
In other studies, researchers are looking at a wide variety of previously approved and experimental drugs and devices. For example, scientists in New York are testing the mood stabilizer lithium to treat brain fog and fatigue. And researchers in Illinois are investigating efgartigimod, a drug approved for the rare muscle-weakening autoimmune disorder myasthenia gravis, to see if it helps ease a long COVID complication known as POTS that can cause a sudden rapid heart rate and chronic fatigue.
“The good news is that enrollment will proceed quickly, given the vast number of patients,” said Kristin Englund, MD, director of the reCOVer Center of Excellence at the Cleveland Clinic.
This is all encouraging because roughly one in five American adults who have acute COVID infections develop persistent symptoms of long COVID, also known as post–acute sequelae of SARS-CoV-2 (PASC). And many of these long COVID patients have complex, overlapping clusters of symptoms that make traditional treatment approaches largely ineffective against this new, formidable disease.
But not every patient living with long COVID will qualify for trials or find it easy to take part even if they do. Patients should consider how severe their symptoms are, the potential risks of any experimental treatments, and the many challenges they may have with getting to and from clinical trial sites that are largely concentrated around major cities and might be far from home.
While this holds true for any type of trial, it’s essential for long COVID patients, who may have fatigue, muscle weakness, and other symptoms that make distance an impossible factor to ignore, said Aaron Friedberg, MD, clinical colead of the post–COVID-19 recovery program at the Ohio State University Wexner Medical Center, Columbus.
“I think it is a personal decision, since the fatigue and pain that patients with PASC can experience can make it very challenging to travel long distances,” Dr. Friedberg said. “I would recommend calling or messaging ahead to find out exactly what type of travel might be required because there may be steps that can be completed by email or video, which could make it easier to participate, and some trials may be entirely remote.”
Even when patients feel up to the travel, they still might not be a good fit for a clinical trial. Scientists often look for people who didn’t have pre-existing health problems before they got long COVID, Dr. Barshikar noted. Patients taking medications may also be unable to participate in drug trials, particularly for experimental treatments because of concerns about unknown side effects from drug interactions.
When clinical trials do seem like a good option, patients may want to consider seeking treatment at an academic medical center that is already doing long COVID research, particularly if their symptoms are too complex or severe to manage only through their primary care provider, said Jonathan Whiteson, MD, who helped draft long COVID treatment guidelines for the American Academy of Physical Medicine and Rehabilitation. He also serves as codirector of the New York University Langone Health post–COVID care program.
Many health care professionals on the front lines treating long COVID patients are optimistic that the sheer number of trials and the vast number of patients taking part should ultimately produce some better treatment options than people have right now. It’s just not going to happen overnight.
“I suspect that while we will see some new treatments coming in the next 1-2 years, it may be several years before targets can be identified and full trials conducted to see results,” Dr. Friedberg said. “Getting good data takes time.”
A version of this article first appeared on WebMD.com.
With no proven treatments for long COVID, millions of Americans struggling with debilitating symptoms may be wondering whether it’s worth it to try something they’ve never considered before: a clinical trial.
But it may take years for these trials to prove which drugs, devices, and behavioral therapies are safe and effective.
“We’re not in warp speed,” said Kanecia Zimmerman, MD, a principal investigator at the Duke Clinical Research Institute in Durham, N.C., who is overseeing long COVID trials for the NIH. Operation Warp Speed – the 2020-2021 federal effort to get COVID vaccines designed, tested, authorized and distributed – benefited from existing scientific knowledge about other coronaviruses and about vaccines in general. But there’s no similar foundation of scientific knowledge about long COVID.
“We are in a place of not really knowing anything,” Dr. Zimmerman said.
But some glimmers of hope are emerging. A Veterans Affairs study recently found the antiviral Paxlovid might help prevent long COVID. A small case study at Yale found the ADHD drug guanfacine may ease brain fog from long COVID. And preliminary results from an NIH-funded study suggest COVID vaccines might help children with a rare but serious inflammatory condition known as multisystem inflammatory syndrome (MIS-C).
More results are expected very soon from the trial for kids with MIS-C, which can strike suddenly long after a COVID infection clears up. While the exact causes aren’t yet clear, MIS-C can cause dangerous inflammation in the heart, lungs, kidneys, brain, skin, eyes, or gastrointestinal system.
Because the virus often triggered a delayed response of MIS-C in kids who had few if any symptoms of acute COVID-19, scientists wondered whether children infected with the virus might respond to a vaccine dose to prevent MIS-C from developing, Gary Gibbons, MD, director of the National Heart, Lung, and Blood Institute, said during a Dec. 9 presentation at the NIH. It’s not yet clear if vaccination helps, but it doesn’t harm the children, Dr. Gibbons said.
“Indeed, the studies suggest with some relief that yes, these children could be vaccinated safely,” he said.
Several new trials are also testing Paxlovid against long COVID, including one late-stage study that may have results in about a year.
“We already know that Paxlovid reduces the risk of developing long COVID, but it would be a game changer if it can improve long COVID symptoms as well,” said Surendra Barshikar, MD, an associate professor and medical director of the COVID Recover program at the University of Texas Southwestern Medical Center, Dallas.
In other studies, researchers are looking at a wide variety of previously approved and experimental drugs and devices. For example, scientists in New York are testing the mood stabilizer lithium to treat brain fog and fatigue. And researchers in Illinois are investigating efgartigimod, a drug approved for the rare muscle-weakening autoimmune disorder myasthenia gravis, to see if it helps ease a long COVID complication known as POTS that can cause a sudden rapid heart rate and chronic fatigue.
“The good news is that enrollment will proceed quickly, given the vast number of patients,” said Kristin Englund, MD, director of the reCOVer Center of Excellence at the Cleveland Clinic.
This is all encouraging because roughly one in five American adults who have acute COVID infections develop persistent symptoms of long COVID, also known as post–acute sequelae of SARS-CoV-2 (PASC). And many of these long COVID patients have complex, overlapping clusters of symptoms that make traditional treatment approaches largely ineffective against this new, formidable disease.
But not every patient living with long COVID will qualify for trials or find it easy to take part even if they do. Patients should consider how severe their symptoms are, the potential risks of any experimental treatments, and the many challenges they may have with getting to and from clinical trial sites that are largely concentrated around major cities and might be far from home.
While this holds true for any type of trial, it’s essential for long COVID patients, who may have fatigue, muscle weakness, and other symptoms that make distance an impossible factor to ignore, said Aaron Friedberg, MD, clinical colead of the post–COVID-19 recovery program at the Ohio State University Wexner Medical Center, Columbus.
“I think it is a personal decision, since the fatigue and pain that patients with PASC can experience can make it very challenging to travel long distances,” Dr. Friedberg said. “I would recommend calling or messaging ahead to find out exactly what type of travel might be required because there may be steps that can be completed by email or video, which could make it easier to participate, and some trials may be entirely remote.”
Even when patients feel up to the travel, they still might not be a good fit for a clinical trial. Scientists often look for people who didn’t have pre-existing health problems before they got long COVID, Dr. Barshikar noted. Patients taking medications may also be unable to participate in drug trials, particularly for experimental treatments because of concerns about unknown side effects from drug interactions.
When clinical trials do seem like a good option, patients may want to consider seeking treatment at an academic medical center that is already doing long COVID research, particularly if their symptoms are too complex or severe to manage only through their primary care provider, said Jonathan Whiteson, MD, who helped draft long COVID treatment guidelines for the American Academy of Physical Medicine and Rehabilitation. He also serves as codirector of the New York University Langone Health post–COVID care program.
Many health care professionals on the front lines treating long COVID patients are optimistic that the sheer number of trials and the vast number of patients taking part should ultimately produce some better treatment options than people have right now. It’s just not going to happen overnight.
“I suspect that while we will see some new treatments coming in the next 1-2 years, it may be several years before targets can be identified and full trials conducted to see results,” Dr. Friedberg said. “Getting good data takes time.”
A version of this article first appeared on WebMD.com.
With no proven treatments for long COVID, millions of Americans struggling with debilitating symptoms may be wondering whether it’s worth it to try something they’ve never considered before: a clinical trial.
But it may take years for these trials to prove which drugs, devices, and behavioral therapies are safe and effective.
“We’re not in warp speed,” said Kanecia Zimmerman, MD, a principal investigator at the Duke Clinical Research Institute in Durham, N.C., who is overseeing long COVID trials for the NIH. Operation Warp Speed – the 2020-2021 federal effort to get COVID vaccines designed, tested, authorized and distributed – benefited from existing scientific knowledge about other coronaviruses and about vaccines in general. But there’s no similar foundation of scientific knowledge about long COVID.
“We are in a place of not really knowing anything,” Dr. Zimmerman said.
But some glimmers of hope are emerging. A Veterans Affairs study recently found the antiviral Paxlovid might help prevent long COVID. A small case study at Yale found the ADHD drug guanfacine may ease brain fog from long COVID. And preliminary results from an NIH-funded study suggest COVID vaccines might help children with a rare but serious inflammatory condition known as multisystem inflammatory syndrome (MIS-C).
More results are expected very soon from the trial for kids with MIS-C, which can strike suddenly long after a COVID infection clears up. While the exact causes aren’t yet clear, MIS-C can cause dangerous inflammation in the heart, lungs, kidneys, brain, skin, eyes, or gastrointestinal system.
Because the virus often triggered a delayed response of MIS-C in kids who had few if any symptoms of acute COVID-19, scientists wondered whether children infected with the virus might respond to a vaccine dose to prevent MIS-C from developing, Gary Gibbons, MD, director of the National Heart, Lung, and Blood Institute, said during a Dec. 9 presentation at the NIH. It’s not yet clear if vaccination helps, but it doesn’t harm the children, Dr. Gibbons said.
“Indeed, the studies suggest with some relief that yes, these children could be vaccinated safely,” he said.
Several new trials are also testing Paxlovid against long COVID, including one late-stage study that may have results in about a year.
“We already know that Paxlovid reduces the risk of developing long COVID, but it would be a game changer if it can improve long COVID symptoms as well,” said Surendra Barshikar, MD, an associate professor and medical director of the COVID Recover program at the University of Texas Southwestern Medical Center, Dallas.
In other studies, researchers are looking at a wide variety of previously approved and experimental drugs and devices. For example, scientists in New York are testing the mood stabilizer lithium to treat brain fog and fatigue. And researchers in Illinois are investigating efgartigimod, a drug approved for the rare muscle-weakening autoimmune disorder myasthenia gravis, to see if it helps ease a long COVID complication known as POTS that can cause a sudden rapid heart rate and chronic fatigue.
“The good news is that enrollment will proceed quickly, given the vast number of patients,” said Kristin Englund, MD, director of the reCOVer Center of Excellence at the Cleveland Clinic.
This is all encouraging because roughly one in five American adults who have acute COVID infections develop persistent symptoms of long COVID, also known as post–acute sequelae of SARS-CoV-2 (PASC). And many of these long COVID patients have complex, overlapping clusters of symptoms that make traditional treatment approaches largely ineffective against this new, formidable disease.
But not every patient living with long COVID will qualify for trials or find it easy to take part even if they do. Patients should consider how severe their symptoms are, the potential risks of any experimental treatments, and the many challenges they may have with getting to and from clinical trial sites that are largely concentrated around major cities and might be far from home.
While this holds true for any type of trial, it’s essential for long COVID patients, who may have fatigue, muscle weakness, and other symptoms that make distance an impossible factor to ignore, said Aaron Friedberg, MD, clinical colead of the post–COVID-19 recovery program at the Ohio State University Wexner Medical Center, Columbus.
“I think it is a personal decision, since the fatigue and pain that patients with PASC can experience can make it very challenging to travel long distances,” Dr. Friedberg said. “I would recommend calling or messaging ahead to find out exactly what type of travel might be required because there may be steps that can be completed by email or video, which could make it easier to participate, and some trials may be entirely remote.”
Even when patients feel up to the travel, they still might not be a good fit for a clinical trial. Scientists often look for people who didn’t have pre-existing health problems before they got long COVID, Dr. Barshikar noted. Patients taking medications may also be unable to participate in drug trials, particularly for experimental treatments because of concerns about unknown side effects from drug interactions.
When clinical trials do seem like a good option, patients may want to consider seeking treatment at an academic medical center that is already doing long COVID research, particularly if their symptoms are too complex or severe to manage only through their primary care provider, said Jonathan Whiteson, MD, who helped draft long COVID treatment guidelines for the American Academy of Physical Medicine and Rehabilitation. He also serves as codirector of the New York University Langone Health post–COVID care program.
Many health care professionals on the front lines treating long COVID patients are optimistic that the sheer number of trials and the vast number of patients taking part should ultimately produce some better treatment options than people have right now. It’s just not going to happen overnight.
“I suspect that while we will see some new treatments coming in the next 1-2 years, it may be several years before targets can be identified and full trials conducted to see results,” Dr. Friedberg said. “Getting good data takes time.”
A version of this article first appeared on WebMD.com.
What’s next for COVID? Here’s what to know
As holiday celebrations wind down in the United States, COVID is on the rise.
Will there be another winter surge? If so, can we minimize it? How big a role might the boosters play in that? Are more mandates coming, along with a return to closed offices and businesses? Read on for a look at the latest info.
Cases, hospitalizations, deaths
As of Dec. 27, the latest statistics, the Centers for Disease Control and Prevention reports more than 487,000 weekly cases, compared to about 265,000 for the week ending Oct. 12. On average, 4,938 people were admitted to the hospital daily from Dec. 19 to 25, down about 6% from the 5,257 admitted daily the week before.
Deaths totaled 2,952 weekly as of Dec. 21, up from 2,699 on Dec. 14.
“What’s sobering overall is still seeing about 400 deaths a day in the U.S.,” said Peter Chin-Hong, MD, professor of medicine and infectious disease specialist at the University of California, San Francisco. “It’s still very high.”
As of Dec. 17, the variants predominating are BQ.1, BQ.1.1, and XBB. Experts said they are paying close attention to XBB, which is increasing quickly in the Northeast.
Predicting a winter surge
Experts tracking the pandemic agree there will be a surge.
“We are in the midst of it now,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape (MDedge’s sister site). “It’s not nearly like what we’ve had in Omicron or other waves; it’s not as severe. But it’s being particularly felt by seniors.”
One bit of good news: “Outside of that group it doesn’t look like – so far – it is going to be as bad a wave [as in the past],” Dr. Topol said.
Predicting the extent of the post-holiday surge “is the billion-dollar question right now,” said Katelyn Jetelina, PhD, a San Diego epidemiologist and author of the newsletter Your Local Epidemiologist.
“Much of these waves are not being driven by subvariants of concern but rather behavior,” she said.
People are opening up their social networks to gather for celebrations and family time. That’s unique to this winter, she said.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
Others point out that the surge doesn’t involve just COVID.
“We are expecting a Christmas surge and we are concerned it might be a triple surge,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University, Nashville, Tenn., referring to the rising cases of flu and RSV (respiratory syncytial virus).
Dr. Jetelina shares that concern, worrying that those illnesses may be what overwhelms hospital capacity.
Another wild card is the situation in China. With the easing of China’s “zero COVID” policies, cases there are rising dramatically. Some models are predicting up to 1 million COVID deaths could occur in China in 2023. (The United States is now requiring travelers from China to show a negative COVID test before entering. Italy and Japan have taken similar measures.)
“The suffering that is going to occur in China is not good news at all,” Dr. Topol said. “We are going to be seeing that for many weeks if not months ahead.”
Theoretically, uncontained spread such as what is expected there could generate a whole new family of variants, he said. But “the main hit is going to be in China,” he predicted. “But it’s hard to project with accuracy.”
“China is 20% of the global population, so we can’t ignore it,” Dr. Jetelina said. “The question is, what’s the probability of a subvariant of concern coming from China? I think the probability is pretty low, but the possibility is there.”
What happens with cases in China may “throw a wrench” in the transition from pandemic to endemic, Dr. Chin-Hong said. But even if the rising cases in China do result in a new variant, “there’s so much T cell and B cell immunity [here], your average person is still not going to get seriously ill, even if the variant looks really scary.”
Minimizing the damage
Experts echo the same advice on stemming the surge, especially for adults who are 65 or older: Get the bivalent booster, and get it now.
“The same with the influenza vaccine,” Dr. Schaffner said.
Both the booster vaccine and the flu vaccine have been underused this year, he said. “It’s part of the general vaccine fatigue.”
The low uptake of the booster vaccine is concerning, Dr. Topol said, especially among adults aged 65 and older, the age group most vulnerable to severe disease. Just 35.7% of U.S. adults 65 and older have gotten the booster, according to the CDC. Dr. Topol calls that a tragedy.
Younger people have not taken to the booster, either. Overall, only 14.1% of people aged 5 and up have gotten an updated booster dose, according to the CDC.
Recent studies find value in the boosters. One study looked only at adults age 65 or older, finding that the bivalent booster reduced the risk of hospitalization by 84% compared to someone not vaccinated, and 73% compared to someone who had received only the monovalent vaccine. Another study of adults found those who had gotten the bivalent were less likely to need COVID-related emergency room care or urgent care.
In a Dec. 21 report in the New England Journal of Medicine, researchers took plasma samples from people who had gotten either one or two monovalent boosters or the bivalent to determine how well they worked against the circulating Omicron subvariants BA.1, BA.5, BA.2.75.2, BQ.1.1, and XBB. The bivalent worked better than the monovalent against all the Omicron subvariants, but especially against BA.2.75.2, BQ.1.1, and XBB.
Rapid testing can help minimize transmission. On Dec. 15, the Biden administration announced its Winter Preparedness Plan, urging Americans to test before and after travel as well as indoor visiting with vulnerable individuals, providing another round of free at-home tests, continuing to make community testing available and continuing to provide vaccines.
Besides the general precautions, Dr. Schaffner suggested: “Look at yourself. Who are you? If you are older than 65, or have underlying illness or are immunocompromised, or are pregnant, please put your mask back on. And think about social distancing. It might be time to worship at home and stream a movie,” instead of going to the theaters, he said.
Back to mandates?
On Dec. 9, the New York City Commissioner of Health and Mental Hygiene urged a return to masking indoors, saying people “should” mask up, including in schools, stores, offices, and when in crowded outdoor settings.
On the same date, the County of Los Angeles Public Health urged a return to masking for everyone aged 2 and older when indoors, including at schools, in transit, or in work sites when around others.
While the CDC order requiring masks on public transportation is no longer in effect, the agency continues to recommend that those using public transportation do so.
But some are taking that further. In Philadelphia, for example, School Superintendent Tony B. Watlington Sr., EdD, announced before the winter break that indoor masking would be required for all students and staff for the first 2 weeks of school return, through Jan. 13, citing guidance from the Philadelphia Department of Public Health.
Universal masking in schools does reduce COVID transmission, as a study published in late November suggests. After Massachusetts dropped the statewide universal masking policy in public schools in February 2022, researchers compared the incidence of COVID in 70 school districts there that dropped the mandate with two school districts that kept it. In the 15 weeks after the policy was rescinded, the lifting of the mandate was linked with an additional 44.9 cases of COVID per 1,000 students and staff. That corresponded to an estimated 11,901 cases and to nearly 30% of the cases in all districts during that time.
That said, experts see mandates as the exception rather than the rule, at least for now, citing public backlash against mandates to mask or follow other restrictions.
“Mandating, we know, it shuts people off,” Dr. Topol said. “It’s unenforceable. If you have a very strong recommendation, that’s probably as good as you’re going to be able to do right now.”
There may be communities where mandates go over better than others, Dr. Schaffner said, such as communities where people have confidence in their public health authorities.
Glimmers of hope
Despite uncertainties, experts offered some not-so-dismal perspectives as well.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
A version of this article first appeared on WebMD.com.
As holiday celebrations wind down in the United States, COVID is on the rise.
Will there be another winter surge? If so, can we minimize it? How big a role might the boosters play in that? Are more mandates coming, along with a return to closed offices and businesses? Read on for a look at the latest info.
Cases, hospitalizations, deaths
As of Dec. 27, the latest statistics, the Centers for Disease Control and Prevention reports more than 487,000 weekly cases, compared to about 265,000 for the week ending Oct. 12. On average, 4,938 people were admitted to the hospital daily from Dec. 19 to 25, down about 6% from the 5,257 admitted daily the week before.
Deaths totaled 2,952 weekly as of Dec. 21, up from 2,699 on Dec. 14.
“What’s sobering overall is still seeing about 400 deaths a day in the U.S.,” said Peter Chin-Hong, MD, professor of medicine and infectious disease specialist at the University of California, San Francisco. “It’s still very high.”
As of Dec. 17, the variants predominating are BQ.1, BQ.1.1, and XBB. Experts said they are paying close attention to XBB, which is increasing quickly in the Northeast.
Predicting a winter surge
Experts tracking the pandemic agree there will be a surge.
“We are in the midst of it now,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape (MDedge’s sister site). “It’s not nearly like what we’ve had in Omicron or other waves; it’s not as severe. But it’s being particularly felt by seniors.”
One bit of good news: “Outside of that group it doesn’t look like – so far – it is going to be as bad a wave [as in the past],” Dr. Topol said.
Predicting the extent of the post-holiday surge “is the billion-dollar question right now,” said Katelyn Jetelina, PhD, a San Diego epidemiologist and author of the newsletter Your Local Epidemiologist.
“Much of these waves are not being driven by subvariants of concern but rather behavior,” she said.
People are opening up their social networks to gather for celebrations and family time. That’s unique to this winter, she said.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
Others point out that the surge doesn’t involve just COVID.
“We are expecting a Christmas surge and we are concerned it might be a triple surge,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University, Nashville, Tenn., referring to the rising cases of flu and RSV (respiratory syncytial virus).
Dr. Jetelina shares that concern, worrying that those illnesses may be what overwhelms hospital capacity.
Another wild card is the situation in China. With the easing of China’s “zero COVID” policies, cases there are rising dramatically. Some models are predicting up to 1 million COVID deaths could occur in China in 2023. (The United States is now requiring travelers from China to show a negative COVID test before entering. Italy and Japan have taken similar measures.)
“The suffering that is going to occur in China is not good news at all,” Dr. Topol said. “We are going to be seeing that for many weeks if not months ahead.”
Theoretically, uncontained spread such as what is expected there could generate a whole new family of variants, he said. But “the main hit is going to be in China,” he predicted. “But it’s hard to project with accuracy.”
“China is 20% of the global population, so we can’t ignore it,” Dr. Jetelina said. “The question is, what’s the probability of a subvariant of concern coming from China? I think the probability is pretty low, but the possibility is there.”
What happens with cases in China may “throw a wrench” in the transition from pandemic to endemic, Dr. Chin-Hong said. But even if the rising cases in China do result in a new variant, “there’s so much T cell and B cell immunity [here], your average person is still not going to get seriously ill, even if the variant looks really scary.”
Minimizing the damage
Experts echo the same advice on stemming the surge, especially for adults who are 65 or older: Get the bivalent booster, and get it now.
“The same with the influenza vaccine,” Dr. Schaffner said.
Both the booster vaccine and the flu vaccine have been underused this year, he said. “It’s part of the general vaccine fatigue.”
The low uptake of the booster vaccine is concerning, Dr. Topol said, especially among adults aged 65 and older, the age group most vulnerable to severe disease. Just 35.7% of U.S. adults 65 and older have gotten the booster, according to the CDC. Dr. Topol calls that a tragedy.
Younger people have not taken to the booster, either. Overall, only 14.1% of people aged 5 and up have gotten an updated booster dose, according to the CDC.
Recent studies find value in the boosters. One study looked only at adults age 65 or older, finding that the bivalent booster reduced the risk of hospitalization by 84% compared to someone not vaccinated, and 73% compared to someone who had received only the monovalent vaccine. Another study of adults found those who had gotten the bivalent were less likely to need COVID-related emergency room care or urgent care.
In a Dec. 21 report in the New England Journal of Medicine, researchers took plasma samples from people who had gotten either one or two monovalent boosters or the bivalent to determine how well they worked against the circulating Omicron subvariants BA.1, BA.5, BA.2.75.2, BQ.1.1, and XBB. The bivalent worked better than the monovalent against all the Omicron subvariants, but especially against BA.2.75.2, BQ.1.1, and XBB.
Rapid testing can help minimize transmission. On Dec. 15, the Biden administration announced its Winter Preparedness Plan, urging Americans to test before and after travel as well as indoor visiting with vulnerable individuals, providing another round of free at-home tests, continuing to make community testing available and continuing to provide vaccines.
Besides the general precautions, Dr. Schaffner suggested: “Look at yourself. Who are you? If you are older than 65, or have underlying illness or are immunocompromised, or are pregnant, please put your mask back on. And think about social distancing. It might be time to worship at home and stream a movie,” instead of going to the theaters, he said.
Back to mandates?
On Dec. 9, the New York City Commissioner of Health and Mental Hygiene urged a return to masking indoors, saying people “should” mask up, including in schools, stores, offices, and when in crowded outdoor settings.
On the same date, the County of Los Angeles Public Health urged a return to masking for everyone aged 2 and older when indoors, including at schools, in transit, or in work sites when around others.
While the CDC order requiring masks on public transportation is no longer in effect, the agency continues to recommend that those using public transportation do so.
But some are taking that further. In Philadelphia, for example, School Superintendent Tony B. Watlington Sr., EdD, announced before the winter break that indoor masking would be required for all students and staff for the first 2 weeks of school return, through Jan. 13, citing guidance from the Philadelphia Department of Public Health.
Universal masking in schools does reduce COVID transmission, as a study published in late November suggests. After Massachusetts dropped the statewide universal masking policy in public schools in February 2022, researchers compared the incidence of COVID in 70 school districts there that dropped the mandate with two school districts that kept it. In the 15 weeks after the policy was rescinded, the lifting of the mandate was linked with an additional 44.9 cases of COVID per 1,000 students and staff. That corresponded to an estimated 11,901 cases and to nearly 30% of the cases in all districts during that time.
That said, experts see mandates as the exception rather than the rule, at least for now, citing public backlash against mandates to mask or follow other restrictions.
“Mandating, we know, it shuts people off,” Dr. Topol said. “It’s unenforceable. If you have a very strong recommendation, that’s probably as good as you’re going to be able to do right now.”
There may be communities where mandates go over better than others, Dr. Schaffner said, such as communities where people have confidence in their public health authorities.
Glimmers of hope
Despite uncertainties, experts offered some not-so-dismal perspectives as well.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
A version of this article first appeared on WebMD.com.
As holiday celebrations wind down in the United States, COVID is on the rise.
Will there be another winter surge? If so, can we minimize it? How big a role might the boosters play in that? Are more mandates coming, along with a return to closed offices and businesses? Read on for a look at the latest info.
Cases, hospitalizations, deaths
As of Dec. 27, the latest statistics, the Centers for Disease Control and Prevention reports more than 487,000 weekly cases, compared to about 265,000 for the week ending Oct. 12. On average, 4,938 people were admitted to the hospital daily from Dec. 19 to 25, down about 6% from the 5,257 admitted daily the week before.
Deaths totaled 2,952 weekly as of Dec. 21, up from 2,699 on Dec. 14.
“What’s sobering overall is still seeing about 400 deaths a day in the U.S.,” said Peter Chin-Hong, MD, professor of medicine and infectious disease specialist at the University of California, San Francisco. “It’s still very high.”
As of Dec. 17, the variants predominating are BQ.1, BQ.1.1, and XBB. Experts said they are paying close attention to XBB, which is increasing quickly in the Northeast.
Predicting a winter surge
Experts tracking the pandemic agree there will be a surge.
“We are in the midst of it now,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape (MDedge’s sister site). “It’s not nearly like what we’ve had in Omicron or other waves; it’s not as severe. But it’s being particularly felt by seniors.”
One bit of good news: “Outside of that group it doesn’t look like – so far – it is going to be as bad a wave [as in the past],” Dr. Topol said.
Predicting the extent of the post-holiday surge “is the billion-dollar question right now,” said Katelyn Jetelina, PhD, a San Diego epidemiologist and author of the newsletter Your Local Epidemiologist.
“Much of these waves are not being driven by subvariants of concern but rather behavior,” she said.
People are opening up their social networks to gather for celebrations and family time. That’s unique to this winter, she said.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
Others point out that the surge doesn’t involve just COVID.
“We are expecting a Christmas surge and we are concerned it might be a triple surge,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University, Nashville, Tenn., referring to the rising cases of flu and RSV (respiratory syncytial virus).
Dr. Jetelina shares that concern, worrying that those illnesses may be what overwhelms hospital capacity.
Another wild card is the situation in China. With the easing of China’s “zero COVID” policies, cases there are rising dramatically. Some models are predicting up to 1 million COVID deaths could occur in China in 2023. (The United States is now requiring travelers from China to show a negative COVID test before entering. Italy and Japan have taken similar measures.)
“The suffering that is going to occur in China is not good news at all,” Dr. Topol said. “We are going to be seeing that for many weeks if not months ahead.”
Theoretically, uncontained spread such as what is expected there could generate a whole new family of variants, he said. But “the main hit is going to be in China,” he predicted. “But it’s hard to project with accuracy.”
“China is 20% of the global population, so we can’t ignore it,” Dr. Jetelina said. “The question is, what’s the probability of a subvariant of concern coming from China? I think the probability is pretty low, but the possibility is there.”
What happens with cases in China may “throw a wrench” in the transition from pandemic to endemic, Dr. Chin-Hong said. But even if the rising cases in China do result in a new variant, “there’s so much T cell and B cell immunity [here], your average person is still not going to get seriously ill, even if the variant looks really scary.”
Minimizing the damage
Experts echo the same advice on stemming the surge, especially for adults who are 65 or older: Get the bivalent booster, and get it now.
“The same with the influenza vaccine,” Dr. Schaffner said.
Both the booster vaccine and the flu vaccine have been underused this year, he said. “It’s part of the general vaccine fatigue.”
The low uptake of the booster vaccine is concerning, Dr. Topol said, especially among adults aged 65 and older, the age group most vulnerable to severe disease. Just 35.7% of U.S. adults 65 and older have gotten the booster, according to the CDC. Dr. Topol calls that a tragedy.
Younger people have not taken to the booster, either. Overall, only 14.1% of people aged 5 and up have gotten an updated booster dose, according to the CDC.
Recent studies find value in the boosters. One study looked only at adults age 65 or older, finding that the bivalent booster reduced the risk of hospitalization by 84% compared to someone not vaccinated, and 73% compared to someone who had received only the monovalent vaccine. Another study of adults found those who had gotten the bivalent were less likely to need COVID-related emergency room care or urgent care.
In a Dec. 21 report in the New England Journal of Medicine, researchers took plasma samples from people who had gotten either one or two monovalent boosters or the bivalent to determine how well they worked against the circulating Omicron subvariants BA.1, BA.5, BA.2.75.2, BQ.1.1, and XBB. The bivalent worked better than the monovalent against all the Omicron subvariants, but especially against BA.2.75.2, BQ.1.1, and XBB.
Rapid testing can help minimize transmission. On Dec. 15, the Biden administration announced its Winter Preparedness Plan, urging Americans to test before and after travel as well as indoor visiting with vulnerable individuals, providing another round of free at-home tests, continuing to make community testing available and continuing to provide vaccines.
Besides the general precautions, Dr. Schaffner suggested: “Look at yourself. Who are you? If you are older than 65, or have underlying illness or are immunocompromised, or are pregnant, please put your mask back on. And think about social distancing. It might be time to worship at home and stream a movie,” instead of going to the theaters, he said.
Back to mandates?
On Dec. 9, the New York City Commissioner of Health and Mental Hygiene urged a return to masking indoors, saying people “should” mask up, including in schools, stores, offices, and when in crowded outdoor settings.
On the same date, the County of Los Angeles Public Health urged a return to masking for everyone aged 2 and older when indoors, including at schools, in transit, or in work sites when around others.
While the CDC order requiring masks on public transportation is no longer in effect, the agency continues to recommend that those using public transportation do so.
But some are taking that further. In Philadelphia, for example, School Superintendent Tony B. Watlington Sr., EdD, announced before the winter break that indoor masking would be required for all students and staff for the first 2 weeks of school return, through Jan. 13, citing guidance from the Philadelphia Department of Public Health.
Universal masking in schools does reduce COVID transmission, as a study published in late November suggests. After Massachusetts dropped the statewide universal masking policy in public schools in February 2022, researchers compared the incidence of COVID in 70 school districts there that dropped the mandate with two school districts that kept it. In the 15 weeks after the policy was rescinded, the lifting of the mandate was linked with an additional 44.9 cases of COVID per 1,000 students and staff. That corresponded to an estimated 11,901 cases and to nearly 30% of the cases in all districts during that time.
That said, experts see mandates as the exception rather than the rule, at least for now, citing public backlash against mandates to mask or follow other restrictions.
“Mandating, we know, it shuts people off,” Dr. Topol said. “It’s unenforceable. If you have a very strong recommendation, that’s probably as good as you’re going to be able to do right now.”
There may be communities where mandates go over better than others, Dr. Schaffner said, such as communities where people have confidence in their public health authorities.
Glimmers of hope
Despite uncertainties, experts offered some not-so-dismal perspectives as well.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
A version of this article first appeared on WebMD.com.
IBD patients have limited protection against Omicron with third vaccine dose
For people with inflammatory bowel disease (IBD) taking immunosuppressive medication, a third dose of a COVID-19 mRNA vaccine significantly increases neutralizing antibodies against the original SARS-CoV-2 strain, but the picture is more complicated for protection against the Omicron variant, according to a research letter published in Gastroenterology.
“As further mutations in the viral genome accumulate over time, with the attendant risk of immune evasion, it remains important to continue to reappraise vaccination strategy, including the implementation of personalized approaches for some patients, such as those treated with anti-TNF drugs and JAK inhibitors,” wrote Zhigang Liu, PhD, a research associate in the department of metabolism, digestion, and reproduction at Imperial College London, and his colleagues. “Preferential use of bivalent vaccines may be especially valuable in IBD patients taking anti-TNF agents or JAK inhibitors,” they wrote. Their study did not assess neutralizing antibodies resulting from use of the bivalent vaccine, however.
The researchers tracked 268 participants, including 49 healthy participants serving as controls, from May 2021 through March 2022. The other participants had IBD and included 51 patients taking thiopurines, 36 patients taking infliximab, 39 taking both infliximab and thiopurines, 39 taking ustekinumab, 38 taking vedolizumab, and 16 taking tofacitinib. The IBD patients were all enrolled in the SARS-CoV-2 Vaccination Immunogenicity in Immunosuppressed Inflammatory Bowel Disease Patients (VIP) cohort.
None of the participants had evidence of a SARS-CoV-2 infection at baseline. All had received two doses of an mRNA COVID-19 vaccine (all received Pfizer, except two controls who received Moderna) or two doses of the AstraZeneca vaccine as their primary vaccination. All received an mRNA vaccine for their third dose. Among the IBD patients, 137 received the AstraZeneca in their primary two-dose series, and 82 received Pfizer.
First the researchers assessed the participants’ humoral response to the vaccine against the original SARS-CoV-2 strain and against the Omicron BA.1 variant. Neutralizing antibody titers rose significantly against both strains after the third vaccine dose for all participants.
“However, 50% neutralization titer (NT50) values were significantly lower against Omicron than against the ancestral strain in all study groups, irrespective of the immunosuppressive treatment regimen,” the authors reported. NT50 values are a measure that reflect a vaccine-induced humoral immunity against SARS-CoV-2 after vaccination.
Compared to the healthy controls, individuals receiving infliximab, tofacitinib, or infliximab/thiopurine combination therapy showed significantly lower responses after the second and third vaccine doses. Thirteen patients did not generate NT50 against Omicron after the second vaccine dose, and 7 of them were on infliximab monotherapy. They represented nearly 20% of all infliximab monotherapy participants.
Next the researchers assessed the risk of a breakthrough infection according to neutralizing titer thresholds. Individuals with an NT50 less than 500 had 1.6 times greater odds of a breakthrough infection than those with an NT50 above 500, they noted. After two vaccine doses, 46% of participants with IBD had an NT50 above 500 for the ancestral strain, which rose to 85% of those with IBD after a third dose.
In the healthy control group, 35% had an NT50 under 500 after two doses, and 14% of them had a breakthrough infection, all of which were mild and none of which required hospitalization. The NT50 in healthy controls, however, was not significantly associated with risk of breakthrough infection.
“In this study, neutralizing titers elicited against the omicron variant were generally poor for all individuals and were substantially lower in recipients of infliximab, infliximab/thiopurine combination, or tofacitinib therapy,” the authors concluded. “This raises concerns about whether currently available vaccines will be sufficient to protect against continually evolving SARS-CoV-2 variants, especially in patients established on certain immunosuppressive drugs.”
The small population sizes for each subgroup based on medication was one of the study’s limitations. Another was the fact that it was underpowered to conclusively determine whether an increased risk of breakthrough infection exists in IBD patients who have lower titers of neutralizing antibodies. A limitation for generalization to U.S. patients is that just 64% of the IBD patients received the AstraZeneca vaccine, which is not offered in the United States, for their first two doses before receiving the third mRNA (Pfizer) dose.
The study was funded by Pfizer in an independent research grant and by the NIHR Biomedical Research Centres in Imperial College London and Imperial College Healthcare NHS Trust and Cambridge, and the NIHR Clinical Research Facility Cambridge.
Dr. Liu and one other author had no disclosures. The other 18 authors have a range of disclosures related to various pharmaceutical companies, including Pfizer.
Understanding how inflammatory bowel disease (IBD) impacts COVID-19 infection risk and how IBD medications influence this risk remains an ever-evolving discussion, particularly with the emergence of new SARS-CoV-2 variants and booster vaccines. In this study, Liu et al. further shape this conversation: They show that a third mRNA COVID-19 vaccine dose increases neutralizing antibody levels against the Omicron variant in IBD patients compared to the level following a second vaccine dose, but that infliximab and tofacitinib significantly attenuate this response. They additionally suggest that IBD patients achieve lower neutralizing antibody levels after a third COVID-19 vaccine and may have a higher breakthrough infection risk compared to healthy controls without IBD.

Whether to change booster vaccination recommendations specifically for IBD patients on tofacitinib or infliximab, however, remains an unanswered question. The small sample of patients on tofacitinib precludes definitive conclusions regarding tofacitinib’s impact on vaccine response. Moreover, this humoral antibody-based study tells only half the story: We need analyses of the cell-mediated booster vaccine response to truly understand vaccine efficacy during immunosuppressant use. Lastly, future studies including the bivalent booster will provide the most up-to-date information on protecting our IBD patients from the Omicron variant.
Dr. Erica J. Brenner MD, MSCR is an Assistant Professor, Department of Pediatrics, Division of Pediatric Gastroenterology, University of North Carolina School of Medicine; and a cofounder of the Surveillance Epidemiology of Coronavirus Under Research Exclusion for Inflammatory Bowel Disease (SECURE-IBD) Registry. She has no relevant financial conflicts of interest.
Understanding how inflammatory bowel disease (IBD) impacts COVID-19 infection risk and how IBD medications influence this risk remains an ever-evolving discussion, particularly with the emergence of new SARS-CoV-2 variants and booster vaccines. In this study, Liu et al. further shape this conversation: They show that a third mRNA COVID-19 vaccine dose increases neutralizing antibody levels against the Omicron variant in IBD patients compared to the level following a second vaccine dose, but that infliximab and tofacitinib significantly attenuate this response. They additionally suggest that IBD patients achieve lower neutralizing antibody levels after a third COVID-19 vaccine and may have a higher breakthrough infection risk compared to healthy controls without IBD.
Whether to change booster vaccination recommendations specifically for IBD patients on tofacitinib or infliximab, however, remains an unanswered question. The small sample of patients on tofacitinib precludes definitive conclusions regarding tofacitinib’s impact on vaccine response. Moreover, this humoral antibody-based study tells only half the story: We need analyses of the cell-mediated booster vaccine response to truly understand vaccine efficacy during immunosuppressant use. Lastly, future studies including the bivalent booster will provide the most up-to-date information on protecting our IBD patients from the Omicron variant.
Dr. Erica J. Brenner MD, MSCR is an Assistant Professor, Department of Pediatrics, Division of Pediatric Gastroenterology, University of North Carolina School of Medicine; and a cofounder of the Surveillance Epidemiology of Coronavirus Under Research Exclusion for Inflammatory Bowel Disease (SECURE-IBD) Registry. She has no relevant financial conflicts of interest.
Understanding how inflammatory bowel disease (IBD) impacts COVID-19 infection risk and how IBD medications influence this risk remains an ever-evolving discussion, particularly with the emergence of new SARS-CoV-2 variants and booster vaccines. In this study, Liu et al. further shape this conversation: They show that a third mRNA COVID-19 vaccine dose increases neutralizing antibody levels against the Omicron variant in IBD patients compared to the level following a second vaccine dose, but that infliximab and tofacitinib significantly attenuate this response. They additionally suggest that IBD patients achieve lower neutralizing antibody levels after a third COVID-19 vaccine and may have a higher breakthrough infection risk compared to healthy controls without IBD.
Whether to change booster vaccination recommendations specifically for IBD patients on tofacitinib or infliximab, however, remains an unanswered question. The small sample of patients on tofacitinib precludes definitive conclusions regarding tofacitinib’s impact on vaccine response. Moreover, this humoral antibody-based study tells only half the story: We need analyses of the cell-mediated booster vaccine response to truly understand vaccine efficacy during immunosuppressant use. Lastly, future studies including the bivalent booster will provide the most up-to-date information on protecting our IBD patients from the Omicron variant.
Dr. Erica J. Brenner MD, MSCR is an Assistant Professor, Department of Pediatrics, Division of Pediatric Gastroenterology, University of North Carolina School of Medicine; and a cofounder of the Surveillance Epidemiology of Coronavirus Under Research Exclusion for Inflammatory Bowel Disease (SECURE-IBD) Registry. She has no relevant financial conflicts of interest.
For people with inflammatory bowel disease (IBD) taking immunosuppressive medication, a third dose of a COVID-19 mRNA vaccine significantly increases neutralizing antibodies against the original SARS-CoV-2 strain, but the picture is more complicated for protection against the Omicron variant, according to a research letter published in Gastroenterology.
“As further mutations in the viral genome accumulate over time, with the attendant risk of immune evasion, it remains important to continue to reappraise vaccination strategy, including the implementation of personalized approaches for some patients, such as those treated with anti-TNF drugs and JAK inhibitors,” wrote Zhigang Liu, PhD, a research associate in the department of metabolism, digestion, and reproduction at Imperial College London, and his colleagues. “Preferential use of bivalent vaccines may be especially valuable in IBD patients taking anti-TNF agents or JAK inhibitors,” they wrote. Their study did not assess neutralizing antibodies resulting from use of the bivalent vaccine, however.
The researchers tracked 268 participants, including 49 healthy participants serving as controls, from May 2021 through March 2022. The other participants had IBD and included 51 patients taking thiopurines, 36 patients taking infliximab, 39 taking both infliximab and thiopurines, 39 taking ustekinumab, 38 taking vedolizumab, and 16 taking tofacitinib. The IBD patients were all enrolled in the SARS-CoV-2 Vaccination Immunogenicity in Immunosuppressed Inflammatory Bowel Disease Patients (VIP) cohort.
None of the participants had evidence of a SARS-CoV-2 infection at baseline. All had received two doses of an mRNA COVID-19 vaccine (all received Pfizer, except two controls who received Moderna) or two doses of the AstraZeneca vaccine as their primary vaccination. All received an mRNA vaccine for their third dose. Among the IBD patients, 137 received the AstraZeneca in their primary two-dose series, and 82 received Pfizer.
First the researchers assessed the participants’ humoral response to the vaccine against the original SARS-CoV-2 strain and against the Omicron BA.1 variant. Neutralizing antibody titers rose significantly against both strains after the third vaccine dose for all participants.
“However, 50% neutralization titer (NT50) values were significantly lower against Omicron than against the ancestral strain in all study groups, irrespective of the immunosuppressive treatment regimen,” the authors reported. NT50 values are a measure that reflect a vaccine-induced humoral immunity against SARS-CoV-2 after vaccination.
Compared to the healthy controls, individuals receiving infliximab, tofacitinib, or infliximab/thiopurine combination therapy showed significantly lower responses after the second and third vaccine doses. Thirteen patients did not generate NT50 against Omicron after the second vaccine dose, and 7 of them were on infliximab monotherapy. They represented nearly 20% of all infliximab monotherapy participants.
Next the researchers assessed the risk of a breakthrough infection according to neutralizing titer thresholds. Individuals with an NT50 less than 500 had 1.6 times greater odds of a breakthrough infection than those with an NT50 above 500, they noted. After two vaccine doses, 46% of participants with IBD had an NT50 above 500 for the ancestral strain, which rose to 85% of those with IBD after a third dose.
In the healthy control group, 35% had an NT50 under 500 after two doses, and 14% of them had a breakthrough infection, all of which were mild and none of which required hospitalization. The NT50 in healthy controls, however, was not significantly associated with risk of breakthrough infection.
“In this study, neutralizing titers elicited against the omicron variant were generally poor for all individuals and were substantially lower in recipients of infliximab, infliximab/thiopurine combination, or tofacitinib therapy,” the authors concluded. “This raises concerns about whether currently available vaccines will be sufficient to protect against continually evolving SARS-CoV-2 variants, especially in patients established on certain immunosuppressive drugs.”
The small population sizes for each subgroup based on medication was one of the study’s limitations. Another was the fact that it was underpowered to conclusively determine whether an increased risk of breakthrough infection exists in IBD patients who have lower titers of neutralizing antibodies. A limitation for generalization to U.S. patients is that just 64% of the IBD patients received the AstraZeneca vaccine, which is not offered in the United States, for their first two doses before receiving the third mRNA (Pfizer) dose.
The study was funded by Pfizer in an independent research grant and by the NIHR Biomedical Research Centres in Imperial College London and Imperial College Healthcare NHS Trust and Cambridge, and the NIHR Clinical Research Facility Cambridge.
Dr. Liu and one other author had no disclosures. The other 18 authors have a range of disclosures related to various pharmaceutical companies, including Pfizer.
For people with inflammatory bowel disease (IBD) taking immunosuppressive medication, a third dose of a COVID-19 mRNA vaccine significantly increases neutralizing antibodies against the original SARS-CoV-2 strain, but the picture is more complicated for protection against the Omicron variant, according to a research letter published in Gastroenterology.
“As further mutations in the viral genome accumulate over time, with the attendant risk of immune evasion, it remains important to continue to reappraise vaccination strategy, including the implementation of personalized approaches for some patients, such as those treated with anti-TNF drugs and JAK inhibitors,” wrote Zhigang Liu, PhD, a research associate in the department of metabolism, digestion, and reproduction at Imperial College London, and his colleagues. “Preferential use of bivalent vaccines may be especially valuable in IBD patients taking anti-TNF agents or JAK inhibitors,” they wrote. Their study did not assess neutralizing antibodies resulting from use of the bivalent vaccine, however.
The researchers tracked 268 participants, including 49 healthy participants serving as controls, from May 2021 through March 2022. The other participants had IBD and included 51 patients taking thiopurines, 36 patients taking infliximab, 39 taking both infliximab and thiopurines, 39 taking ustekinumab, 38 taking vedolizumab, and 16 taking tofacitinib. The IBD patients were all enrolled in the SARS-CoV-2 Vaccination Immunogenicity in Immunosuppressed Inflammatory Bowel Disease Patients (VIP) cohort.
None of the participants had evidence of a SARS-CoV-2 infection at baseline. All had received two doses of an mRNA COVID-19 vaccine (all received Pfizer, except two controls who received Moderna) or two doses of the AstraZeneca vaccine as their primary vaccination. All received an mRNA vaccine for their third dose. Among the IBD patients, 137 received the AstraZeneca in their primary two-dose series, and 82 received Pfizer.
First the researchers assessed the participants’ humoral response to the vaccine against the original SARS-CoV-2 strain and against the Omicron BA.1 variant. Neutralizing antibody titers rose significantly against both strains after the third vaccine dose for all participants.
“However, 50% neutralization titer (NT50) values were significantly lower against Omicron than against the ancestral strain in all study groups, irrespective of the immunosuppressive treatment regimen,” the authors reported. NT50 values are a measure that reflect a vaccine-induced humoral immunity against SARS-CoV-2 after vaccination.
Compared to the healthy controls, individuals receiving infliximab, tofacitinib, or infliximab/thiopurine combination therapy showed significantly lower responses after the second and third vaccine doses. Thirteen patients did not generate NT50 against Omicron after the second vaccine dose, and 7 of them were on infliximab monotherapy. They represented nearly 20% of all infliximab monotherapy participants.
Next the researchers assessed the risk of a breakthrough infection according to neutralizing titer thresholds. Individuals with an NT50 less than 500 had 1.6 times greater odds of a breakthrough infection than those with an NT50 above 500, they noted. After two vaccine doses, 46% of participants with IBD had an NT50 above 500 for the ancestral strain, which rose to 85% of those with IBD after a third dose.
In the healthy control group, 35% had an NT50 under 500 after two doses, and 14% of them had a breakthrough infection, all of which were mild and none of which required hospitalization. The NT50 in healthy controls, however, was not significantly associated with risk of breakthrough infection.
“In this study, neutralizing titers elicited against the omicron variant were generally poor for all individuals and were substantially lower in recipients of infliximab, infliximab/thiopurine combination, or tofacitinib therapy,” the authors concluded. “This raises concerns about whether currently available vaccines will be sufficient to protect against continually evolving SARS-CoV-2 variants, especially in patients established on certain immunosuppressive drugs.”
The small population sizes for each subgroup based on medication was one of the study’s limitations. Another was the fact that it was underpowered to conclusively determine whether an increased risk of breakthrough infection exists in IBD patients who have lower titers of neutralizing antibodies. A limitation for generalization to U.S. patients is that just 64% of the IBD patients received the AstraZeneca vaccine, which is not offered in the United States, for their first two doses before receiving the third mRNA (Pfizer) dose.
The study was funded by Pfizer in an independent research grant and by the NIHR Biomedical Research Centres in Imperial College London and Imperial College Healthcare NHS Trust and Cambridge, and the NIHR Clinical Research Facility Cambridge.
Dr. Liu and one other author had no disclosures. The other 18 authors have a range of disclosures related to various pharmaceutical companies, including Pfizer.
FROM GASTROENTEROLOGY
Children and COVID: New cases fell as the old year ended
The end of 2022 saw a drop in new COVID-19 cases in children, even as rates of emergency department visits continued upward trends that began in late October.
New cases for the week of Dec. 23-29 fell for the first time since late November, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The AAP/CHA analysis of publicly available state data differs somewhat from figures reported by the Centers for Disease Control and Prevention, which has new cases for the latest available week, Dec.18-24, at just over 27,000 after 3 straight weeks of declines from a count of almost 63,000 for the week ending Nov. 26. The CDC, however, updates previously reported data on a regular basis, so that 27,000 is likely to increase in the coming weeks.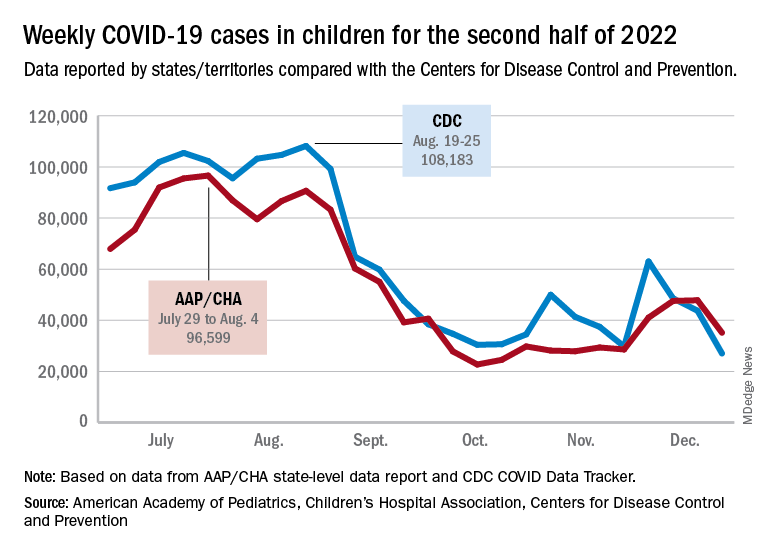
The CDC line on the graph also shows a peak for the week of Oct. 30 to Nov. 5 when new cases reached almost 50,000, compared with almost 30,000 reported for the week of Oct. 28 to Nov. 3 by the AAP and CHA in their report of state-level data. The AAP and CHA put the total number of child COVID cases since the start of the pandemic at 15.2 million as of Dec. 29, while the CDC reports 16.2 million cases as of Dec. 28.
There have been 1,975 deaths from COVID-19 in children aged 0-17 years, according to the CDC, which amounts to just over 0.2% of all COVID deaths for which age group data were available.
CDC data on emergency department visits involving diagnosed COVID-19 have been rising since late October. In children aged 0-11 years, for example, COVID was involved in 1.0% of ED visits (7-day average) as late as Nov. 4, but by Dec. 27 that rate was 2.6%. Children aged 12-15 years went from 0.6% on Oct. 28 to 1.5% on Dec. 27, while 16- to 17-year-olds had ED visit rates of 0.6% on Oct. 19 and 1.7% on Dec. 27, the CDC said on its COVID Data Tracker.
New hospital admissions with diagnosed COVID, which had been following the same upward trend as ED visits since late October, halted that rise in children aged 0-17 years and have gone no higher than 0.29 per 100,000 population since Dec. 9, the CDC data show.
The end of 2022 saw a drop in new COVID-19 cases in children, even as rates of emergency department visits continued upward trends that began in late October.
New cases for the week of Dec. 23-29 fell for the first time since late November, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The AAP/CHA analysis of publicly available state data differs somewhat from figures reported by the Centers for Disease Control and Prevention, which has new cases for the latest available week, Dec.18-24, at just over 27,000 after 3 straight weeks of declines from a count of almost 63,000 for the week ending Nov. 26. The CDC, however, updates previously reported data on a regular basis, so that 27,000 is likely to increase in the coming weeks.
The CDC line on the graph also shows a peak for the week of Oct. 30 to Nov. 5 when new cases reached almost 50,000, compared with almost 30,000 reported for the week of Oct. 28 to Nov. 3 by the AAP and CHA in their report of state-level data. The AAP and CHA put the total number of child COVID cases since the start of the pandemic at 15.2 million as of Dec. 29, while the CDC reports 16.2 million cases as of Dec. 28.
There have been 1,975 deaths from COVID-19 in children aged 0-17 years, according to the CDC, which amounts to just over 0.2% of all COVID deaths for which age group data were available.
CDC data on emergency department visits involving diagnosed COVID-19 have been rising since late October. In children aged 0-11 years, for example, COVID was involved in 1.0% of ED visits (7-day average) as late as Nov. 4, but by Dec. 27 that rate was 2.6%. Children aged 12-15 years went from 0.6% on Oct. 28 to 1.5% on Dec. 27, while 16- to 17-year-olds had ED visit rates of 0.6% on Oct. 19 and 1.7% on Dec. 27, the CDC said on its COVID Data Tracker.
New hospital admissions with diagnosed COVID, which had been following the same upward trend as ED visits since late October, halted that rise in children aged 0-17 years and have gone no higher than 0.29 per 100,000 population since Dec. 9, the CDC data show.
The end of 2022 saw a drop in new COVID-19 cases in children, even as rates of emergency department visits continued upward trends that began in late October.
New cases for the week of Dec. 23-29 fell for the first time since late November, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The AAP/CHA analysis of publicly available state data differs somewhat from figures reported by the Centers for Disease Control and Prevention, which has new cases for the latest available week, Dec.18-24, at just over 27,000 after 3 straight weeks of declines from a count of almost 63,000 for the week ending Nov. 26. The CDC, however, updates previously reported data on a regular basis, so that 27,000 is likely to increase in the coming weeks.
The CDC line on the graph also shows a peak for the week of Oct. 30 to Nov. 5 when new cases reached almost 50,000, compared with almost 30,000 reported for the week of Oct. 28 to Nov. 3 by the AAP and CHA in their report of state-level data. The AAP and CHA put the total number of child COVID cases since the start of the pandemic at 15.2 million as of Dec. 29, while the CDC reports 16.2 million cases as of Dec. 28.
There have been 1,975 deaths from COVID-19 in children aged 0-17 years, according to the CDC, which amounts to just over 0.2% of all COVID deaths for which age group data were available.
CDC data on emergency department visits involving diagnosed COVID-19 have been rising since late October. In children aged 0-11 years, for example, COVID was involved in 1.0% of ED visits (7-day average) as late as Nov. 4, but by Dec. 27 that rate was 2.6%. Children aged 12-15 years went from 0.6% on Oct. 28 to 1.5% on Dec. 27, while 16- to 17-year-olds had ED visit rates of 0.6% on Oct. 19 and 1.7% on Dec. 27, the CDC said on its COVID Data Tracker.
New hospital admissions with diagnosed COVID, which had been following the same upward trend as ED visits since late October, halted that rise in children aged 0-17 years and have gone no higher than 0.29 per 100,000 population since Dec. 9, the CDC data show.
SARS-CoV-2 seroprevalence grew rapidly in pandemic’s early waves
By August 2022, two-and-a-half years into the COVID-19 pandemic, most children as well as most adults under age 60 years had evidence of SARS-CoV-2 vaccination and/or infection, a Canadian seroprevalence study of almost 14,000 people over the first seven waves of the pandemic reports.
However, fewer than 50% people older than age 60, the age group most vulnerable to severe outcomes, showed evidence of immunity from infection or vaccination. The authors noted that older adults – who have the lowest infection rates but highest risk of severe outcomes – continue to warrant prioritized vaccination, writing online in the Canadian Medical Association Journal.

Previous evidence suggests that a combination of both infection and vaccination exposure may induce more robust and durable hybrid immunity than either exposure alone, according to lead author Danuta M. Skowronski, MD, MHSc, an epidemiologist at the British Columbia Centre for Disease Control in Vancouver.
“Our main objective was to chronicle the changing proportion of the population considered immunologically naive and therefore susceptible to SARS-CoV-2,” Dr. Skowronski said in an interview. “It’s relevant for risk assessment to know what proportion have acquired some priming for more efficient immune memory response to the virus because that reduces the likelihood of severe outcomes.” Standardized seroprevalence studies are essential to inform COVID-19 response, particularly in resource-limited regions.
The study
Conducted in British Columbia’s Greater Vancouver and Fraser Valley, the analysis found that in the first year of the pandemic, when extraordinary measures were in place to curtail transmission, virtually everyone remained immunologically naive. Thereafter, however, age-based vaccine rollouts dramatically changed the immuno-epidemiological landscape so that by September 2021, more than 80% of the study population had antibody evidence of immunological priming, while more than 85% remained uninfected.
By August 2022, after the Omicron-variant waves, overall vaccine- and infection-induced seroprevalence exceeded 95%, with 60% having been actually infected, including at least three-quarters of children. Fewer than 50% of older adults, however, showed immunological evidence of exposure.
The study results were based on anonymized residual sera from children and adults in an outpatient laboratory network. At least three immunoassays per serosurvey were used to detect antibodies to SARS-CoV-2 spike (from vaccine) and to nucleocapsid antibodies (from infection).
The researchers assessed any seroprevalence – vaccine-, infection-induced, or both – as defined by positivity on any two assays. Infection-induced seroprevalence was also defined by dual-assay positivity but required both antinucleocapsid and antispike detection. Their estimates of infection-induced seroprevalence indicated considerable under-ascertainment of infections by standard surveillance case reports.
Results
During the first year of the pandemic, fewer than 1% manifested seroprevalence during the first three snapshots and fewer than 5% by January 2021. With vaccine rollout, however, seroprevalence increased dramatically during the first half of 2021 to 56% by May/June 2021 and to 83% by September/October 2021.
In addition, infection-induced seroprevalence was low at less than 15% in September/October 2021 until the arrival of the Omicron waves, after which it rose to 42% by March 2022 and 61% by July/August 2022. Combined seroprevalence for vaccination or infection was more than 95% by the summer, with most children but less than half of adults older than 60 years showing evidence of having been infected.
“We found the highest infection rates among children, closely followed by young adults, which may reflect their greater interconnectedness, including between siblings and parents in the household, as well as with peers in schools and the community,” the authors wrote, adding that the low cumulative infection rates among older adults may reflect their higher vaccination rates and greater social isolation.
U.S. data show similar age-related infection rates, but data among children from other Canadian provinces are limited, the authors said.
Commenting on the survey but not involved in it, infectious diseases expert Marc Germain, MD, PhD, a vice president at Héma-Québec in Quebec City, believes the pattern observed in British Columbia is fairly representative of what happened across Canada and the United States, including the sweeping effect of the Omicron variant and the differential impact according to age.

“But regional differences might very well exist – for example, due to differential vaccine uptake – and are also probably related in part to the different testing platforms being used,” Dr. Germain told this news organization.
Caroline Quach-Tanh, MD, PhD, a pediatrician and epidemiologist/infectologist at the University of Montreal, pointed out that Quebec seroprevalence surveys using residual blood samples from children and adults visiting emergency departments for any reason showed higher rates of prior infection than did the BC surveys. “But Dr. Skowronski’s findings are likely applicable to settings where some nonpharmacological interventions were put in place, but without strict confinement – and thus are likely applicable to most settings in the U.S. and Canada.”
Dr. Quach-Tanh added that there is always a risk of bias with the use of residual blood samples, “but the fact that the study method was stable should have captured a similar population from time to time. It would be unlikely to result in a major overestimation in the proportion of individuals positive for SARS-CoV-2 antibodies.”
A recent global meta-analysis found that while global seroprevalence has risen considerably, albeit variably by region, more than a third of the world’s population is still seronegative to the SARS-CoV-2 virus.
Dr. Skowronski reported institutional grants from the Canadian Institutes of Health Research and the British Columbia Centre for Disease Control Foundation for Public Health for other SARSCoV-2 work. Coauthor Romina C. Reyes, MD, chairs the BC Diagnostic Accreditation Program committee. Coauthor Mel Krajden, MD, reported institutional grants from Roche, Hologic, and Siemens. Dr. Germain and Dr. Quach-Tanh disclosed no competing interests relevant to their comments.
By August 2022, two-and-a-half years into the COVID-19 pandemic, most children as well as most adults under age 60 years had evidence of SARS-CoV-2 vaccination and/or infection, a Canadian seroprevalence study of almost 14,000 people over the first seven waves of the pandemic reports.
However, fewer than 50% people older than age 60, the age group most vulnerable to severe outcomes, showed evidence of immunity from infection or vaccination. The authors noted that older adults – who have the lowest infection rates but highest risk of severe outcomes – continue to warrant prioritized vaccination, writing online in the Canadian Medical Association Journal.
Previous evidence suggests that a combination of both infection and vaccination exposure may induce more robust and durable hybrid immunity than either exposure alone, according to lead author Danuta M. Skowronski, MD, MHSc, an epidemiologist at the British Columbia Centre for Disease Control in Vancouver.
“Our main objective was to chronicle the changing proportion of the population considered immunologically naive and therefore susceptible to SARS-CoV-2,” Dr. Skowronski said in an interview. “It’s relevant for risk assessment to know what proportion have acquired some priming for more efficient immune memory response to the virus because that reduces the likelihood of severe outcomes.” Standardized seroprevalence studies are essential to inform COVID-19 response, particularly in resource-limited regions.
The study
Conducted in British Columbia’s Greater Vancouver and Fraser Valley, the analysis found that in the first year of the pandemic, when extraordinary measures were in place to curtail transmission, virtually everyone remained immunologically naive. Thereafter, however, age-based vaccine rollouts dramatically changed the immuno-epidemiological landscape so that by September 2021, more than 80% of the study population had antibody evidence of immunological priming, while more than 85% remained uninfected.
By August 2022, after the Omicron-variant waves, overall vaccine- and infection-induced seroprevalence exceeded 95%, with 60% having been actually infected, including at least three-quarters of children. Fewer than 50% of older adults, however, showed immunological evidence of exposure.
The study results were based on anonymized residual sera from children and adults in an outpatient laboratory network. At least three immunoassays per serosurvey were used to detect antibodies to SARS-CoV-2 spike (from vaccine) and to nucleocapsid antibodies (from infection).
The researchers assessed any seroprevalence – vaccine-, infection-induced, or both – as defined by positivity on any two assays. Infection-induced seroprevalence was also defined by dual-assay positivity but required both antinucleocapsid and antispike detection. Their estimates of infection-induced seroprevalence indicated considerable under-ascertainment of infections by standard surveillance case reports.
Results
During the first year of the pandemic, fewer than 1% manifested seroprevalence during the first three snapshots and fewer than 5% by January 2021. With vaccine rollout, however, seroprevalence increased dramatically during the first half of 2021 to 56% by May/June 2021 and to 83% by September/October 2021.
In addition, infection-induced seroprevalence was low at less than 15% in September/October 2021 until the arrival of the Omicron waves, after which it rose to 42% by March 2022 and 61% by July/August 2022. Combined seroprevalence for vaccination or infection was more than 95% by the summer, with most children but less than half of adults older than 60 years showing evidence of having been infected.
“We found the highest infection rates among children, closely followed by young adults, which may reflect their greater interconnectedness, including between siblings and parents in the household, as well as with peers in schools and the community,” the authors wrote, adding that the low cumulative infection rates among older adults may reflect their higher vaccination rates and greater social isolation.
U.S. data show similar age-related infection rates, but data among children from other Canadian provinces are limited, the authors said.
Commenting on the survey but not involved in it, infectious diseases expert Marc Germain, MD, PhD, a vice president at Héma-Québec in Quebec City, believes the pattern observed in British Columbia is fairly representative of what happened across Canada and the United States, including the sweeping effect of the Omicron variant and the differential impact according to age.
“But regional differences might very well exist – for example, due to differential vaccine uptake – and are also probably related in part to the different testing platforms being used,” Dr. Germain told this news organization.
Caroline Quach-Tanh, MD, PhD, a pediatrician and epidemiologist/infectologist at the University of Montreal, pointed out that Quebec seroprevalence surveys using residual blood samples from children and adults visiting emergency departments for any reason showed higher rates of prior infection than did the BC surveys. “But Dr. Skowronski’s findings are likely applicable to settings where some nonpharmacological interventions were put in place, but without strict confinement – and thus are likely applicable to most settings in the U.S. and Canada.”
Dr. Quach-Tanh added that there is always a risk of bias with the use of residual blood samples, “but the fact that the study method was stable should have captured a similar population from time to time. It would be unlikely to result in a major overestimation in the proportion of individuals positive for SARS-CoV-2 antibodies.”
A recent global meta-analysis found that while global seroprevalence has risen considerably, albeit variably by region, more than a third of the world’s population is still seronegative to the SARS-CoV-2 virus.
Dr. Skowronski reported institutional grants from the Canadian Institutes of Health Research and the British Columbia Centre for Disease Control Foundation for Public Health for other SARSCoV-2 work. Coauthor Romina C. Reyes, MD, chairs the BC Diagnostic Accreditation Program committee. Coauthor Mel Krajden, MD, reported institutional grants from Roche, Hologic, and Siemens. Dr. Germain and Dr. Quach-Tanh disclosed no competing interests relevant to their comments.
By August 2022, two-and-a-half years into the COVID-19 pandemic, most children as well as most adults under age 60 years had evidence of SARS-CoV-2 vaccination and/or infection, a Canadian seroprevalence study of almost 14,000 people over the first seven waves of the pandemic reports.
However, fewer than 50% people older than age 60, the age group most vulnerable to severe outcomes, showed evidence of immunity from infection or vaccination. The authors noted that older adults – who have the lowest infection rates but highest risk of severe outcomes – continue to warrant prioritized vaccination, writing online in the Canadian Medical Association Journal.
Previous evidence suggests that a combination of both infection and vaccination exposure may induce more robust and durable hybrid immunity than either exposure alone, according to lead author Danuta M. Skowronski, MD, MHSc, an epidemiologist at the British Columbia Centre for Disease Control in Vancouver.
“Our main objective was to chronicle the changing proportion of the population considered immunologically naive and therefore susceptible to SARS-CoV-2,” Dr. Skowronski said in an interview. “It’s relevant for risk assessment to know what proportion have acquired some priming for more efficient immune memory response to the virus because that reduces the likelihood of severe outcomes.” Standardized seroprevalence studies are essential to inform COVID-19 response, particularly in resource-limited regions.
The study
Conducted in British Columbia’s Greater Vancouver and Fraser Valley, the analysis found that in the first year of the pandemic, when extraordinary measures were in place to curtail transmission, virtually everyone remained immunologically naive. Thereafter, however, age-based vaccine rollouts dramatically changed the immuno-epidemiological landscape so that by September 2021, more than 80% of the study population had antibody evidence of immunological priming, while more than 85% remained uninfected.
By August 2022, after the Omicron-variant waves, overall vaccine- and infection-induced seroprevalence exceeded 95%, with 60% having been actually infected, including at least three-quarters of children. Fewer than 50% of older adults, however, showed immunological evidence of exposure.
The study results were based on anonymized residual sera from children and adults in an outpatient laboratory network. At least three immunoassays per serosurvey were used to detect antibodies to SARS-CoV-2 spike (from vaccine) and to nucleocapsid antibodies (from infection).
The researchers assessed any seroprevalence – vaccine-, infection-induced, or both – as defined by positivity on any two assays. Infection-induced seroprevalence was also defined by dual-assay positivity but required both antinucleocapsid and antispike detection. Their estimates of infection-induced seroprevalence indicated considerable under-ascertainment of infections by standard surveillance case reports.
Results
During the first year of the pandemic, fewer than 1% manifested seroprevalence during the first three snapshots and fewer than 5% by January 2021. With vaccine rollout, however, seroprevalence increased dramatically during the first half of 2021 to 56% by May/June 2021 and to 83% by September/October 2021.
In addition, infection-induced seroprevalence was low at less than 15% in September/October 2021 until the arrival of the Omicron waves, after which it rose to 42% by March 2022 and 61% by July/August 2022. Combined seroprevalence for vaccination or infection was more than 95% by the summer, with most children but less than half of adults older than 60 years showing evidence of having been infected.
“We found the highest infection rates among children, closely followed by young adults, which may reflect their greater interconnectedness, including between siblings and parents in the household, as well as with peers in schools and the community,” the authors wrote, adding that the low cumulative infection rates among older adults may reflect their higher vaccination rates and greater social isolation.
U.S. data show similar age-related infection rates, but data among children from other Canadian provinces are limited, the authors said.
Commenting on the survey but not involved in it, infectious diseases expert Marc Germain, MD, PhD, a vice president at Héma-Québec in Quebec City, believes the pattern observed in British Columbia is fairly representative of what happened across Canada and the United States, including the sweeping effect of the Omicron variant and the differential impact according to age.
“But regional differences might very well exist – for example, due to differential vaccine uptake – and are also probably related in part to the different testing platforms being used,” Dr. Germain told this news organization.
Caroline Quach-Tanh, MD, PhD, a pediatrician and epidemiologist/infectologist at the University of Montreal, pointed out that Quebec seroprevalence surveys using residual blood samples from children and adults visiting emergency departments for any reason showed higher rates of prior infection than did the BC surveys. “But Dr. Skowronski’s findings are likely applicable to settings where some nonpharmacological interventions were put in place, but without strict confinement – and thus are likely applicable to most settings in the U.S. and Canada.”
Dr. Quach-Tanh added that there is always a risk of bias with the use of residual blood samples, “but the fact that the study method was stable should have captured a similar population from time to time. It would be unlikely to result in a major overestimation in the proportion of individuals positive for SARS-CoV-2 antibodies.”
A recent global meta-analysis found that while global seroprevalence has risen considerably, albeit variably by region, more than a third of the world’s population is still seronegative to the SARS-CoV-2 virus.
Dr. Skowronski reported institutional grants from the Canadian Institutes of Health Research and the British Columbia Centre for Disease Control Foundation for Public Health for other SARSCoV-2 work. Coauthor Romina C. Reyes, MD, chairs the BC Diagnostic Accreditation Program committee. Coauthor Mel Krajden, MD, reported institutional grants from Roche, Hologic, and Siemens. Dr. Germain and Dr. Quach-Tanh disclosed no competing interests relevant to their comments.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
Study of beliefs about what causes cancer sparks debate
The study, entitled, “Everything Causes Cancer? Beliefs and Attitudes Towards Cancer Prevention Among Anti-Vaxxers, Flat Earthers, and Reptilian Conspiracists: Online Cross Sectional Survey,” was published in the Christmas 2022 issue of The British Medical Journal (BMJ).
The authors explain that they set out to evaluate “the patterns of beliefs about cancer among people who believed in conspiracies, rejected the COVID-19 vaccine, or preferred alternative medicine.”
They sought such people on social media and online chat platforms and asked them questions about real and mythical causes of cancer.
Almost half of survey participants agreed with the statement, “It seems like everything causes cancer.”
Overall, among all participants, awareness of the actual causes of cancer was greater than awareness of the mythical causes of cancer, the authors report. However, awareness of the actual causes of cancer was lower among the unvaccinated and members of conspiracy groups than among their counterparts.
The authors are concerned that their findings suggest “a direct connection between digital misinformation and consequent potential erroneous health decisions, which may represent a further preventable fraction of cancer.”
Backlash and criticism
The study “highlights the difficulty society encounters in distinguishing the actual causes of cancer from mythical causes,” The BMJ commented on Twitter.
However, both the study and the journal received some backlash.
This is a “horrible article seeking to smear people with concerns about COVID vaccines,” commented Clare Craig, a British consultant pathologist who specializes in cancer diagnostics.
The study and its methodology were also harshly criticized on Twitter by Normal Fenton, professor of risk information management at the Queen Mary University of London.
The senior author of the study, Laura Costas, a medical epidemiologist with the Catalan Institute of Oncology, Barcelona, told this news organization that the naysayers on social media, many of whom focused their comments on the COVID-19 vaccine, prove the purpose of the study – that misinformation spreads widely on the internet.
“Most comments focused on spreading COVID-19 myths, which were not the direct subject of the study, and questioned the motivations of BMJ authors and the scientific community, assuming they had a common malevolent hidden agenda,” Ms. Costas said.
“They stated the need of having critical thinking, a trait in common with the scientific method, but dogmatically dismissed any information that comes from official sources,” she added.
Ms. Costas commented that “society encounters difficulty in differentiating actual from mythical causes of cancer owing to mass information. We therefore planned this study with a certain satire, which is in line with the essence of The BMJ Christmas issue.”
The BMJ has a long history of publishing a lighthearted Christmas edition full of original, satirical, and nontraditional studies. Previous years have seen studies that explored potential harms from holly and ivy, survival time of chocolates on hospital wards, and the question, “Were James Bond’s drinks shaken because of alcohol induced tremor?”
Study details
Ms. Costas and colleagues sought participants for their survey from online forums that included 4chan and Reddit, which are known for their controversial content posted by anonymous users. Data were also collected from ForoCoches and HispaChan, well-known Spanish online forums. These online sites were intentionally chosen because researchers thought “conspiracy beliefs would be more prevalent,” according to Ms. Costas.
Across the multiple forums, there were 1,494 participants. Of these, 209 participants were unvaccinated against COVID-19, 112 preferred alternatives rather than conventional medicine, and 62 reported that they believed the earth was flat or believed that humanoids take reptilian forms to manipulate human societies.
The team then sought to assess beliefs about actual and mythical (nonestablished) causes of cancer by presenting the participants with the closed risk factor questions on two validated scales – the Cancer Awareness Measure (CAM) and CAM–Mythical Causes Scale (CAM-MYCS).
Responses to both were recorded on a five-point scale; answers ranged from “strongly disagree” to “strongly agree.”
The CAM assesses cancer risk perceptions of 11 established risk factors for cancer: smoking actively or passively, consuming alcohol, low levels of physical activity, consuming red or processed meat, getting sunburnt as a child, family history of cancer, human papillomavirus infection, being overweight, age greater than or equal to 70 years, and low vegetable and fruit consumption.
The CAM-MYCS measure includes 12 questions on risk perceptions of mythical causes of cancer – nonestablished causes that are commonly believed to cause cancer but for which there is no supporting scientific evidence, the authors explain. These items include drinking from plastic bottles; eating food containing artificial sweeteners or additives and genetically modified food; using microwave ovens, aerosol containers, mobile phones, and cleaning products; living near power lines; feeling stressed; experiencing physical trauma; and being exposed to electromagnetic frequencies/non-ionizing radiation, such as wi-fi networks, radio, and television.
The most endorsed mythical causes of cancer were eating food containing additives (63.9%) or sweeteners (50.7%), feeling stressed (59.7%), and eating genetically modified foods (38.4%).
A version of this article first appeared on Medscape.com.
The study, entitled, “Everything Causes Cancer? Beliefs and Attitudes Towards Cancer Prevention Among Anti-Vaxxers, Flat Earthers, and Reptilian Conspiracists: Online Cross Sectional Survey,” was published in the Christmas 2022 issue of The British Medical Journal (BMJ).
The authors explain that they set out to evaluate “the patterns of beliefs about cancer among people who believed in conspiracies, rejected the COVID-19 vaccine, or preferred alternative medicine.”
They sought such people on social media and online chat platforms and asked them questions about real and mythical causes of cancer.
Almost half of survey participants agreed with the statement, “It seems like everything causes cancer.”
Overall, among all participants, awareness of the actual causes of cancer was greater than awareness of the mythical causes of cancer, the authors report. However, awareness of the actual causes of cancer was lower among the unvaccinated and members of conspiracy groups than among their counterparts.
The authors are concerned that their findings suggest “a direct connection between digital misinformation and consequent potential erroneous health decisions, which may represent a further preventable fraction of cancer.”
Backlash and criticism
The study “highlights the difficulty society encounters in distinguishing the actual causes of cancer from mythical causes,” The BMJ commented on Twitter.
However, both the study and the journal received some backlash.
This is a “horrible article seeking to smear people with concerns about COVID vaccines,” commented Clare Craig, a British consultant pathologist who specializes in cancer diagnostics.
The study and its methodology were also harshly criticized on Twitter by Normal Fenton, professor of risk information management at the Queen Mary University of London.
The senior author of the study, Laura Costas, a medical epidemiologist with the Catalan Institute of Oncology, Barcelona, told this news organization that the naysayers on social media, many of whom focused their comments on the COVID-19 vaccine, prove the purpose of the study – that misinformation spreads widely on the internet.
“Most comments focused on spreading COVID-19 myths, which were not the direct subject of the study, and questioned the motivations of BMJ authors and the scientific community, assuming they had a common malevolent hidden agenda,” Ms. Costas said.
“They stated the need of having critical thinking, a trait in common with the scientific method, but dogmatically dismissed any information that comes from official sources,” she added.
Ms. Costas commented that “society encounters difficulty in differentiating actual from mythical causes of cancer owing to mass information. We therefore planned this study with a certain satire, which is in line with the essence of The BMJ Christmas issue.”
The BMJ has a long history of publishing a lighthearted Christmas edition full of original, satirical, and nontraditional studies. Previous years have seen studies that explored potential harms from holly and ivy, survival time of chocolates on hospital wards, and the question, “Were James Bond’s drinks shaken because of alcohol induced tremor?”
Study details
Ms. Costas and colleagues sought participants for their survey from online forums that included 4chan and Reddit, which are known for their controversial content posted by anonymous users. Data were also collected from ForoCoches and HispaChan, well-known Spanish online forums. These online sites were intentionally chosen because researchers thought “conspiracy beliefs would be more prevalent,” according to Ms. Costas.
Across the multiple forums, there were 1,494 participants. Of these, 209 participants were unvaccinated against COVID-19, 112 preferred alternatives rather than conventional medicine, and 62 reported that they believed the earth was flat or believed that humanoids take reptilian forms to manipulate human societies.
The team then sought to assess beliefs about actual and mythical (nonestablished) causes of cancer by presenting the participants with the closed risk factor questions on two validated scales – the Cancer Awareness Measure (CAM) and CAM–Mythical Causes Scale (CAM-MYCS).
Responses to both were recorded on a five-point scale; answers ranged from “strongly disagree” to “strongly agree.”
The CAM assesses cancer risk perceptions of 11 established risk factors for cancer: smoking actively or passively, consuming alcohol, low levels of physical activity, consuming red or processed meat, getting sunburnt as a child, family history of cancer, human papillomavirus infection, being overweight, age greater than or equal to 70 years, and low vegetable and fruit consumption.
The CAM-MYCS measure includes 12 questions on risk perceptions of mythical causes of cancer – nonestablished causes that are commonly believed to cause cancer but for which there is no supporting scientific evidence, the authors explain. These items include drinking from plastic bottles; eating food containing artificial sweeteners or additives and genetically modified food; using microwave ovens, aerosol containers, mobile phones, and cleaning products; living near power lines; feeling stressed; experiencing physical trauma; and being exposed to electromagnetic frequencies/non-ionizing radiation, such as wi-fi networks, radio, and television.
The most endorsed mythical causes of cancer were eating food containing additives (63.9%) or sweeteners (50.7%), feeling stressed (59.7%), and eating genetically modified foods (38.4%).
A version of this article first appeared on Medscape.com.
The study, entitled, “Everything Causes Cancer? Beliefs and Attitudes Towards Cancer Prevention Among Anti-Vaxxers, Flat Earthers, and Reptilian Conspiracists: Online Cross Sectional Survey,” was published in the Christmas 2022 issue of The British Medical Journal (BMJ).
The authors explain that they set out to evaluate “the patterns of beliefs about cancer among people who believed in conspiracies, rejected the COVID-19 vaccine, or preferred alternative medicine.”
They sought such people on social media and online chat platforms and asked them questions about real and mythical causes of cancer.
Almost half of survey participants agreed with the statement, “It seems like everything causes cancer.”
Overall, among all participants, awareness of the actual causes of cancer was greater than awareness of the mythical causes of cancer, the authors report. However, awareness of the actual causes of cancer was lower among the unvaccinated and members of conspiracy groups than among their counterparts.
The authors are concerned that their findings suggest “a direct connection between digital misinformation and consequent potential erroneous health decisions, which may represent a further preventable fraction of cancer.”
Backlash and criticism
The study “highlights the difficulty society encounters in distinguishing the actual causes of cancer from mythical causes,” The BMJ commented on Twitter.
However, both the study and the journal received some backlash.
This is a “horrible article seeking to smear people with concerns about COVID vaccines,” commented Clare Craig, a British consultant pathologist who specializes in cancer diagnostics.
The study and its methodology were also harshly criticized on Twitter by Normal Fenton, professor of risk information management at the Queen Mary University of London.
The senior author of the study, Laura Costas, a medical epidemiologist with the Catalan Institute of Oncology, Barcelona, told this news organization that the naysayers on social media, many of whom focused their comments on the COVID-19 vaccine, prove the purpose of the study – that misinformation spreads widely on the internet.
“Most comments focused on spreading COVID-19 myths, which were not the direct subject of the study, and questioned the motivations of BMJ authors and the scientific community, assuming they had a common malevolent hidden agenda,” Ms. Costas said.
“They stated the need of having critical thinking, a trait in common with the scientific method, but dogmatically dismissed any information that comes from official sources,” she added.
Ms. Costas commented that “society encounters difficulty in differentiating actual from mythical causes of cancer owing to mass information. We therefore planned this study with a certain satire, which is in line with the essence of The BMJ Christmas issue.”
The BMJ has a long history of publishing a lighthearted Christmas edition full of original, satirical, and nontraditional studies. Previous years have seen studies that explored potential harms from holly and ivy, survival time of chocolates on hospital wards, and the question, “Were James Bond’s drinks shaken because of alcohol induced tremor?”
Study details
Ms. Costas and colleagues sought participants for their survey from online forums that included 4chan and Reddit, which are known for their controversial content posted by anonymous users. Data were also collected from ForoCoches and HispaChan, well-known Spanish online forums. These online sites were intentionally chosen because researchers thought “conspiracy beliefs would be more prevalent,” according to Ms. Costas.
Across the multiple forums, there were 1,494 participants. Of these, 209 participants were unvaccinated against COVID-19, 112 preferred alternatives rather than conventional medicine, and 62 reported that they believed the earth was flat or believed that humanoids take reptilian forms to manipulate human societies.
The team then sought to assess beliefs about actual and mythical (nonestablished) causes of cancer by presenting the participants with the closed risk factor questions on two validated scales – the Cancer Awareness Measure (CAM) and CAM–Mythical Causes Scale (CAM-MYCS).
Responses to both were recorded on a five-point scale; answers ranged from “strongly disagree” to “strongly agree.”
The CAM assesses cancer risk perceptions of 11 established risk factors for cancer: smoking actively or passively, consuming alcohol, low levels of physical activity, consuming red or processed meat, getting sunburnt as a child, family history of cancer, human papillomavirus infection, being overweight, age greater than or equal to 70 years, and low vegetable and fruit consumption.
The CAM-MYCS measure includes 12 questions on risk perceptions of mythical causes of cancer – nonestablished causes that are commonly believed to cause cancer but for which there is no supporting scientific evidence, the authors explain. These items include drinking from plastic bottles; eating food containing artificial sweeteners or additives and genetically modified food; using microwave ovens, aerosol containers, mobile phones, and cleaning products; living near power lines; feeling stressed; experiencing physical trauma; and being exposed to electromagnetic frequencies/non-ionizing radiation, such as wi-fi networks, radio, and television.
The most endorsed mythical causes of cancer were eating food containing additives (63.9%) or sweeteners (50.7%), feeling stressed (59.7%), and eating genetically modified foods (38.4%).
A version of this article first appeared on Medscape.com.
COVID isolated people. Long COVID makes it worse
A year ago in December, mapping specialist Whitney Tyshynski, 35, was working out 5 days a week with a personal trainer near her home in Alberta, Canada, doing 5k trail runs, lifting heavy weights, and feeling good. Then, in January she got COVID-19. The symptoms never went away.
Nowadays, Ms. Tyshynski needs a walker to retrieve her mail, a half-block trip she can’t make without fear of fainting. Because she gets dizzy when she drives, she rarely goes anywhere in her car. Going for a dog walk with a friend means sitting in a car and watching the friend and the dogs in an open field. And since fainting at Costco during the summer, she’s afraid to shop by herself.
Because she lives alone and her closest relatives are an hour and a half away, Ms. Tyshynski is dependent on friends. But she’s reluctant to lean on them because they already have trouble understanding how debilitating her lingering symptoms can be.
“I’ve had people pretty much insinuate that I’m lazy,” she says.
There’s no question that COVID-19 cut people off from one another. But for those like Ms. Tyshynski who have long COVID, that disconnect has never ended. that the condition is real.
At worst, as Ms. Tyshynski has discovered, people don’t take it seriously and accuse those who have it of exaggerating their health woes. In that way, long COVID can be as isolating as the original illness.
“Isolation in long COVID comes in various forms and it’s not primarily just that physical isolation,” says Yochai Re’em, MD, a psychiatrist in private practice in New York who has experienced long COVID and blogs about the condition for Psychology Today. “A different yet equally challenging type of isolation is the emotional isolation, where you need more emotional support, connection with other people who can appreciate what it is you are going through without putting their own needs and desires onto you – and that can be hard to find.”
It’s hard to find in part because of what Dr. Re’em sees as a collective belief that anyone who feels bad should be able to get better by exercising, researching, or going to a doctor.
“Society thinks you need to take some kind of action and usually that’s a physical action,” he says. “And that attitude is tremendously problematic in this illness because of the postexertional malaise that people experience: When people exert themselves, their symptoms get worse. And so the action that people take can’t be that traditional action that we’re used to taking in our society.”
Long COVID patients often have their feelings invalidated not just by friends, loved ones, and extended family, but by health care providers. That can heighten feelings of isolation, particularly for people who live alone, says Jordan Anderson, DO, a neuropsychiatrist and assistant professor of psychiatry at Oregon Health & Science University in Portland.
The first patients Dr. Anderson saw as part of OHSU’s long COVID program contracted the virus in February 2020. Because the program addresses both the physical and mental health components of the condition, Dr. Anderson has seen a lot of people whose emotional challenges are similar to those Ms. Tyshynski faces.
“I think there’s a lack of understanding that leads to people just not necessarily taking it seriously,” he says. “Plus, the symptoms of long COVID do wax and wane. They’re not static. So people can be feeling pretty good one day and be feeling terrible the next. There’s some predictability to it, but it’s not absolutely predictable. It can be difficult for people to understand.”
Both Dr. Anderson and Dr. Re’em stress that long COVID patients need to prioritize their own energy regardless of what they’re being told by those who don’t understand the illness. Dr. Anderson offers to speak to his patients’ spouses to educate them about the realities of the condition because, he says, “any kind of lack of awareness or understanding in a family member or close support could potentially isolate the person struggling with long COVID.”
Depending on how open-minded and motivated a friend or relative is, they might develop more empathy with time and education, Dr. Re’em says. But for others, dealing with a confusing, unfamiliar chronic illness can be overwhelming and provoke anxiety.
“The hopelessness is too much for them to sit with, so instead they say things like ‘just push through it,’ or ‘just do X, Y, and Z,’ because psychologically it’s too much for them to take on that burden,” he says.
The good news is that there are plenty of web-based support groups for people with long COVID, including Body Politic (which Dr. Re’em is affiliated with), Survivor Corps, and on Facebook. “The patient community with this illness is tremendous, absolutely tremendous,” Dr. Re’em says. “Those people can be found and they can support each other.”
Some long COVID clinics run groups, as do individual practitioners such as Dr. Re’em, although those can be challenging to join. For instance, Dr. Re’em’s are only for New York state residents.
The key to finding a group is to be patient, because finding the right one takes time and energy.
“There are support groups that exist, but they are not as prevalent as I would like them to be,” Dr. Anderson says.
OHSU had an educational support group run by a social worker affiliated with the long COVID hub, but when the social worker left the program, the program was put on hold.
There’s a psychotherapy group operating out of the psychiatry department, but the patients are recruited exclusively from Dr. Anderson’s clinic and access is limited.
“The services exist, but I think that generally they’re sparse and pretty geographically dependent,” Dr. Anderson says. “I think you’d probably more likely be able to find something like this in a city or an area that has an academic institution or a place with a lot of resources rather than out in a rural community.”
Ms. Tyshynski opted not to join a group for fear it would increase the depression and anxiety that she had even before developing long COVID. When she and her family joined a cancer support group when her father was ill, she found it more depressing than helpful. Where she has found support is from the cofounder of the animal rescue society where she volunteers, a woman who has had long COVID for more than 2 years and has been a source of comfort and advice.
It’s one of the rare reminders Ms. Tyshynski has that even though she may live alone, she’s not completely alone. “Other people are going through this, too,” she says. “It helps to remember that.”
A version of this article first appeared on WebMD.com.
A year ago in December, mapping specialist Whitney Tyshynski, 35, was working out 5 days a week with a personal trainer near her home in Alberta, Canada, doing 5k trail runs, lifting heavy weights, and feeling good. Then, in January she got COVID-19. The symptoms never went away.
Nowadays, Ms. Tyshynski needs a walker to retrieve her mail, a half-block trip she can’t make without fear of fainting. Because she gets dizzy when she drives, she rarely goes anywhere in her car. Going for a dog walk with a friend means sitting in a car and watching the friend and the dogs in an open field. And since fainting at Costco during the summer, she’s afraid to shop by herself.
Because she lives alone and her closest relatives are an hour and a half away, Ms. Tyshynski is dependent on friends. But she’s reluctant to lean on them because they already have trouble understanding how debilitating her lingering symptoms can be.
“I’ve had people pretty much insinuate that I’m lazy,” she says.
There’s no question that COVID-19 cut people off from one another. But for those like Ms. Tyshynski who have long COVID, that disconnect has never ended. that the condition is real.
At worst, as Ms. Tyshynski has discovered, people don’t take it seriously and accuse those who have it of exaggerating their health woes. In that way, long COVID can be as isolating as the original illness.
“Isolation in long COVID comes in various forms and it’s not primarily just that physical isolation,” says Yochai Re’em, MD, a psychiatrist in private practice in New York who has experienced long COVID and blogs about the condition for Psychology Today. “A different yet equally challenging type of isolation is the emotional isolation, where you need more emotional support, connection with other people who can appreciate what it is you are going through without putting their own needs and desires onto you – and that can be hard to find.”
It’s hard to find in part because of what Dr. Re’em sees as a collective belief that anyone who feels bad should be able to get better by exercising, researching, or going to a doctor.
“Society thinks you need to take some kind of action and usually that’s a physical action,” he says. “And that attitude is tremendously problematic in this illness because of the postexertional malaise that people experience: When people exert themselves, their symptoms get worse. And so the action that people take can’t be that traditional action that we’re used to taking in our society.”
Long COVID patients often have their feelings invalidated not just by friends, loved ones, and extended family, but by health care providers. That can heighten feelings of isolation, particularly for people who live alone, says Jordan Anderson, DO, a neuropsychiatrist and assistant professor of psychiatry at Oregon Health & Science University in Portland.
The first patients Dr. Anderson saw as part of OHSU’s long COVID program contracted the virus in February 2020. Because the program addresses both the physical and mental health components of the condition, Dr. Anderson has seen a lot of people whose emotional challenges are similar to those Ms. Tyshynski faces.
“I think there’s a lack of understanding that leads to people just not necessarily taking it seriously,” he says. “Plus, the symptoms of long COVID do wax and wane. They’re not static. So people can be feeling pretty good one day and be feeling terrible the next. There’s some predictability to it, but it’s not absolutely predictable. It can be difficult for people to understand.”
Both Dr. Anderson and Dr. Re’em stress that long COVID patients need to prioritize their own energy regardless of what they’re being told by those who don’t understand the illness. Dr. Anderson offers to speak to his patients’ spouses to educate them about the realities of the condition because, he says, “any kind of lack of awareness or understanding in a family member or close support could potentially isolate the person struggling with long COVID.”
Depending on how open-minded and motivated a friend or relative is, they might develop more empathy with time and education, Dr. Re’em says. But for others, dealing with a confusing, unfamiliar chronic illness can be overwhelming and provoke anxiety.
“The hopelessness is too much for them to sit with, so instead they say things like ‘just push through it,’ or ‘just do X, Y, and Z,’ because psychologically it’s too much for them to take on that burden,” he says.
The good news is that there are plenty of web-based support groups for people with long COVID, including Body Politic (which Dr. Re’em is affiliated with), Survivor Corps, and on Facebook. “The patient community with this illness is tremendous, absolutely tremendous,” Dr. Re’em says. “Those people can be found and they can support each other.”
Some long COVID clinics run groups, as do individual practitioners such as Dr. Re’em, although those can be challenging to join. For instance, Dr. Re’em’s are only for New York state residents.
The key to finding a group is to be patient, because finding the right one takes time and energy.
“There are support groups that exist, but they are not as prevalent as I would like them to be,” Dr. Anderson says.
OHSU had an educational support group run by a social worker affiliated with the long COVID hub, but when the social worker left the program, the program was put on hold.
There’s a psychotherapy group operating out of the psychiatry department, but the patients are recruited exclusively from Dr. Anderson’s clinic and access is limited.
“The services exist, but I think that generally they’re sparse and pretty geographically dependent,” Dr. Anderson says. “I think you’d probably more likely be able to find something like this in a city or an area that has an academic institution or a place with a lot of resources rather than out in a rural community.”
Ms. Tyshynski opted not to join a group for fear it would increase the depression and anxiety that she had even before developing long COVID. When she and her family joined a cancer support group when her father was ill, she found it more depressing than helpful. Where she has found support is from the cofounder of the animal rescue society where she volunteers, a woman who has had long COVID for more than 2 years and has been a source of comfort and advice.
It’s one of the rare reminders Ms. Tyshynski has that even though she may live alone, she’s not completely alone. “Other people are going through this, too,” she says. “It helps to remember that.”
A version of this article first appeared on WebMD.com.
A year ago in December, mapping specialist Whitney Tyshynski, 35, was working out 5 days a week with a personal trainer near her home in Alberta, Canada, doing 5k trail runs, lifting heavy weights, and feeling good. Then, in January she got COVID-19. The symptoms never went away.
Nowadays, Ms. Tyshynski needs a walker to retrieve her mail, a half-block trip she can’t make without fear of fainting. Because she gets dizzy when she drives, she rarely goes anywhere in her car. Going for a dog walk with a friend means sitting in a car and watching the friend and the dogs in an open field. And since fainting at Costco during the summer, she’s afraid to shop by herself.
Because she lives alone and her closest relatives are an hour and a half away, Ms. Tyshynski is dependent on friends. But she’s reluctant to lean on them because they already have trouble understanding how debilitating her lingering symptoms can be.
“I’ve had people pretty much insinuate that I’m lazy,” she says.
There’s no question that COVID-19 cut people off from one another. But for those like Ms. Tyshynski who have long COVID, that disconnect has never ended. that the condition is real.
At worst, as Ms. Tyshynski has discovered, people don’t take it seriously and accuse those who have it of exaggerating their health woes. In that way, long COVID can be as isolating as the original illness.
“Isolation in long COVID comes in various forms and it’s not primarily just that physical isolation,” says Yochai Re’em, MD, a psychiatrist in private practice in New York who has experienced long COVID and blogs about the condition for Psychology Today. “A different yet equally challenging type of isolation is the emotional isolation, where you need more emotional support, connection with other people who can appreciate what it is you are going through without putting their own needs and desires onto you – and that can be hard to find.”
It’s hard to find in part because of what Dr. Re’em sees as a collective belief that anyone who feels bad should be able to get better by exercising, researching, or going to a doctor.
“Society thinks you need to take some kind of action and usually that’s a physical action,” he says. “And that attitude is tremendously problematic in this illness because of the postexertional malaise that people experience: When people exert themselves, their symptoms get worse. And so the action that people take can’t be that traditional action that we’re used to taking in our society.”
Long COVID patients often have their feelings invalidated not just by friends, loved ones, and extended family, but by health care providers. That can heighten feelings of isolation, particularly for people who live alone, says Jordan Anderson, DO, a neuropsychiatrist and assistant professor of psychiatry at Oregon Health & Science University in Portland.
The first patients Dr. Anderson saw as part of OHSU’s long COVID program contracted the virus in February 2020. Because the program addresses both the physical and mental health components of the condition, Dr. Anderson has seen a lot of people whose emotional challenges are similar to those Ms. Tyshynski faces.
“I think there’s a lack of understanding that leads to people just not necessarily taking it seriously,” he says. “Plus, the symptoms of long COVID do wax and wane. They’re not static. So people can be feeling pretty good one day and be feeling terrible the next. There’s some predictability to it, but it’s not absolutely predictable. It can be difficult for people to understand.”
Both Dr. Anderson and Dr. Re’em stress that long COVID patients need to prioritize their own energy regardless of what they’re being told by those who don’t understand the illness. Dr. Anderson offers to speak to his patients’ spouses to educate them about the realities of the condition because, he says, “any kind of lack of awareness or understanding in a family member or close support could potentially isolate the person struggling with long COVID.”
Depending on how open-minded and motivated a friend or relative is, they might develop more empathy with time and education, Dr. Re’em says. But for others, dealing with a confusing, unfamiliar chronic illness can be overwhelming and provoke anxiety.
“The hopelessness is too much for them to sit with, so instead they say things like ‘just push through it,’ or ‘just do X, Y, and Z,’ because psychologically it’s too much for them to take on that burden,” he says.
The good news is that there are plenty of web-based support groups for people with long COVID, including Body Politic (which Dr. Re’em is affiliated with), Survivor Corps, and on Facebook. “The patient community with this illness is tremendous, absolutely tremendous,” Dr. Re’em says. “Those people can be found and they can support each other.”
Some long COVID clinics run groups, as do individual practitioners such as Dr. Re’em, although those can be challenging to join. For instance, Dr. Re’em’s are only for New York state residents.
The key to finding a group is to be patient, because finding the right one takes time and energy.
“There are support groups that exist, but they are not as prevalent as I would like them to be,” Dr. Anderson says.
OHSU had an educational support group run by a social worker affiliated with the long COVID hub, but when the social worker left the program, the program was put on hold.
There’s a psychotherapy group operating out of the psychiatry department, but the patients are recruited exclusively from Dr. Anderson’s clinic and access is limited.
“The services exist, but I think that generally they’re sparse and pretty geographically dependent,” Dr. Anderson says. “I think you’d probably more likely be able to find something like this in a city or an area that has an academic institution or a place with a lot of resources rather than out in a rural community.”
Ms. Tyshynski opted not to join a group for fear it would increase the depression and anxiety that she had even before developing long COVID. When she and her family joined a cancer support group when her father was ill, she found it more depressing than helpful. Where she has found support is from the cofounder of the animal rescue society where she volunteers, a woman who has had long COVID for more than 2 years and has been a source of comfort and advice.
It’s one of the rare reminders Ms. Tyshynski has that even though she may live alone, she’s not completely alone. “Other people are going through this, too,” she says. “It helps to remember that.”
A version of this article first appeared on WebMD.com.
COVID update: ASH experts discuss thrombosis, immunity
NEW ORLEANS –

In a presidential symposium at the annual meeting of the American Society of Hematology, La Jolla Institute of Immunology scientist Shane Crotty, PhD, explained that COVID-19 has a “superpower” that allows it to be “extraordinarily stealthy.”
The virus, he said, can sneak past the body’s innate immune system, which normally responds to viral invaders within minutes to hours. “This is why you have people with high viral loads who are presymptomatic. Their innate immune system hasn’t even recognized that these people are infected.”
The adaptive immune system kicks in later. As Dr. Crotty noted, adaptive immunity is composed of three branches: B cells (the source of antibodies), CD4 “helper” T cells, and CD8 “killer” T cells. In the first year of COVID-19, his team tracked 188 subjects post infection in what he said was the largest study of its kind ever for any viral infection.
“In 8 months, 95% of people who had been infected still had measurable immune memory. In fact, most of them had multiple different compartments of immune memory still detectable, and it was likely that these individuals would still have that memory years into the future. Based on that, we made the prediction that most people who have had COVID-19 would likely be protected from reinfection – at least by severe infections – for 3 years into the future. That prediction has widely held up even in the presence of variants which weren’t around at the time.”
How do vaccines fit into the immunity picture? Dr. Crotty’s lab has tracked subjects who received 4 vaccines – Moderna, Pfizer/BioNTech, Janssen/Johnson & Johnson, and Novavax. Researchers found that the mRNA vaccines, Moderna and Pfizer/BioNTech, “are fantastic at eliciting neutralizing antibodies quickly, but then they drop off rapidly at two doses and actually continue to drop for 10 months.”
Still, he said, “when we take a look at 6 months, actually the vaccines are doing pretty incredibly well. If we compare them to an average infected individual, the mRNA vaccines all have higher neutralizing antibody titers.”
What’s happening? According to Dr. Crotty, B cells are “making guesses about what other variants might look like.” But he said research suggests that an important component of this process – germinal centers – aren’t made in some vaccinated people who are immunocompromised. (Germinal centers have been described as “microbial boot camps” for B cells.)
The good news, Dr. Crotty noted, is that a greater understanding of how COVID-19 penetrates various layers of adaptive immune defenses will lead to better ways to protect the immunocompromised. “If you think about immunity in this layered defense way, there are various ways that it could be enhanced for individuals in different categories,” he said.
Hematologist Beverley J. Hunt, MD, OBE, of St. Thomas’ Hospital/King’s Healthcare Partners in London, spoke at the ASH presidential symposium about blood clots and COVID-19. As she noted, concern arose about vaccine-related blood clots. A British team “managed quickly to come up with a diagnostic criteria,” she said. “We looked at nearly 300 patients and essentially came up with a scoring system.”
The diagnostic criteria was based on an analysis of definite or probable cases of vaccine-induced immune thrombocytopenia and thrombosis (VITT) – all related to the AstraZeneca vaccine. The criteria appeared in a 2021 study in the New England Journal of Medicine.
The report’s data didn’t allow it to compare the efficacy of anticoagulants. However, Dr. Hunt noted that clinicians turned to plasma exchange in patients with low platelet counts and extensive thrombosis. The report stated “survival after plasma exchange was 90%, considerably better than would be predicted given the baseline characteristics.”
“Now we’re following up,” Dr. Hunt said. One question to answer: Is long-term anticoagulation helpful? “We have many patients,” she said, “who are taking an anti-platelet factor out of habit.”
Dr. Crotty and Dr. Hunt report no disclosures. This reporter is a paid participant in a COVID vaccine study run by Dr. Crotty’s lab.
NEW ORLEANS –
In a presidential symposium at the annual meeting of the American Society of Hematology, La Jolla Institute of Immunology scientist Shane Crotty, PhD, explained that COVID-19 has a “superpower” that allows it to be “extraordinarily stealthy.”
The virus, he said, can sneak past the body’s innate immune system, which normally responds to viral invaders within minutes to hours. “This is why you have people with high viral loads who are presymptomatic. Their innate immune system hasn’t even recognized that these people are infected.”
The adaptive immune system kicks in later. As Dr. Crotty noted, adaptive immunity is composed of three branches: B cells (the source of antibodies), CD4 “helper” T cells, and CD8 “killer” T cells. In the first year of COVID-19, his team tracked 188 subjects post infection in what he said was the largest study of its kind ever for any viral infection.
“In 8 months, 95% of people who had been infected still had measurable immune memory. In fact, most of them had multiple different compartments of immune memory still detectable, and it was likely that these individuals would still have that memory years into the future. Based on that, we made the prediction that most people who have had COVID-19 would likely be protected from reinfection – at least by severe infections – for 3 years into the future. That prediction has widely held up even in the presence of variants which weren’t around at the time.”
How do vaccines fit into the immunity picture? Dr. Crotty’s lab has tracked subjects who received 4 vaccines – Moderna, Pfizer/BioNTech, Janssen/Johnson & Johnson, and Novavax. Researchers found that the mRNA vaccines, Moderna and Pfizer/BioNTech, “are fantastic at eliciting neutralizing antibodies quickly, but then they drop off rapidly at two doses and actually continue to drop for 10 months.”
Still, he said, “when we take a look at 6 months, actually the vaccines are doing pretty incredibly well. If we compare them to an average infected individual, the mRNA vaccines all have higher neutralizing antibody titers.”
What’s happening? According to Dr. Crotty, B cells are “making guesses about what other variants might look like.” But he said research suggests that an important component of this process – germinal centers – aren’t made in some vaccinated people who are immunocompromised. (Germinal centers have been described as “microbial boot camps” for B cells.)
The good news, Dr. Crotty noted, is that a greater understanding of how COVID-19 penetrates various layers of adaptive immune defenses will lead to better ways to protect the immunocompromised. “If you think about immunity in this layered defense way, there are various ways that it could be enhanced for individuals in different categories,” he said.
Hematologist Beverley J. Hunt, MD, OBE, of St. Thomas’ Hospital/King’s Healthcare Partners in London, spoke at the ASH presidential symposium about blood clots and COVID-19. As she noted, concern arose about vaccine-related blood clots. A British team “managed quickly to come up with a diagnostic criteria,” she said. “We looked at nearly 300 patients and essentially came up with a scoring system.”
The diagnostic criteria was based on an analysis of definite or probable cases of vaccine-induced immune thrombocytopenia and thrombosis (VITT) – all related to the AstraZeneca vaccine. The criteria appeared in a 2021 study in the New England Journal of Medicine.
The report’s data didn’t allow it to compare the efficacy of anticoagulants. However, Dr. Hunt noted that clinicians turned to plasma exchange in patients with low platelet counts and extensive thrombosis. The report stated “survival after plasma exchange was 90%, considerably better than would be predicted given the baseline characteristics.”
“Now we’re following up,” Dr. Hunt said. One question to answer: Is long-term anticoagulation helpful? “We have many patients,” she said, “who are taking an anti-platelet factor out of habit.”
Dr. Crotty and Dr. Hunt report no disclosures. This reporter is a paid participant in a COVID vaccine study run by Dr. Crotty’s lab.
NEW ORLEANS –
In a presidential symposium at the annual meeting of the American Society of Hematology, La Jolla Institute of Immunology scientist Shane Crotty, PhD, explained that COVID-19 has a “superpower” that allows it to be “extraordinarily stealthy.”
The virus, he said, can sneak past the body’s innate immune system, which normally responds to viral invaders within minutes to hours. “This is why you have people with high viral loads who are presymptomatic. Their innate immune system hasn’t even recognized that these people are infected.”
The adaptive immune system kicks in later. As Dr. Crotty noted, adaptive immunity is composed of three branches: B cells (the source of antibodies), CD4 “helper” T cells, and CD8 “killer” T cells. In the first year of COVID-19, his team tracked 188 subjects post infection in what he said was the largest study of its kind ever for any viral infection.
“In 8 months, 95% of people who had been infected still had measurable immune memory. In fact, most of them had multiple different compartments of immune memory still detectable, and it was likely that these individuals would still have that memory years into the future. Based on that, we made the prediction that most people who have had COVID-19 would likely be protected from reinfection – at least by severe infections – for 3 years into the future. That prediction has widely held up even in the presence of variants which weren’t around at the time.”
How do vaccines fit into the immunity picture? Dr. Crotty’s lab has tracked subjects who received 4 vaccines – Moderna, Pfizer/BioNTech, Janssen/Johnson & Johnson, and Novavax. Researchers found that the mRNA vaccines, Moderna and Pfizer/BioNTech, “are fantastic at eliciting neutralizing antibodies quickly, but then they drop off rapidly at two doses and actually continue to drop for 10 months.”
Still, he said, “when we take a look at 6 months, actually the vaccines are doing pretty incredibly well. If we compare them to an average infected individual, the mRNA vaccines all have higher neutralizing antibody titers.”
What’s happening? According to Dr. Crotty, B cells are “making guesses about what other variants might look like.” But he said research suggests that an important component of this process – germinal centers – aren’t made in some vaccinated people who are immunocompromised. (Germinal centers have been described as “microbial boot camps” for B cells.)
The good news, Dr. Crotty noted, is that a greater understanding of how COVID-19 penetrates various layers of adaptive immune defenses will lead to better ways to protect the immunocompromised. “If you think about immunity in this layered defense way, there are various ways that it could be enhanced for individuals in different categories,” he said.
Hematologist Beverley J. Hunt, MD, OBE, of St. Thomas’ Hospital/King’s Healthcare Partners in London, spoke at the ASH presidential symposium about blood clots and COVID-19. As she noted, concern arose about vaccine-related blood clots. A British team “managed quickly to come up with a diagnostic criteria,” she said. “We looked at nearly 300 patients and essentially came up with a scoring system.”
The diagnostic criteria was based on an analysis of definite or probable cases of vaccine-induced immune thrombocytopenia and thrombosis (VITT) – all related to the AstraZeneca vaccine. The criteria appeared in a 2021 study in the New England Journal of Medicine.
The report’s data didn’t allow it to compare the efficacy of anticoagulants. However, Dr. Hunt noted that clinicians turned to plasma exchange in patients with low platelet counts and extensive thrombosis. The report stated “survival after plasma exchange was 90%, considerably better than would be predicted given the baseline characteristics.”
“Now we’re following up,” Dr. Hunt said. One question to answer: Is long-term anticoagulation helpful? “We have many patients,” she said, “who are taking an anti-platelet factor out of habit.”
Dr. Crotty and Dr. Hunt report no disclosures. This reporter is a paid participant in a COVID vaccine study run by Dr. Crotty’s lab.
AT ASH 2022