User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Shingles infection rates higher in patients with MS
DENVER – , according to research presented at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Herpes zoster and its complications are associated with increased health care cost and decreased quality of life,” lead author Nikita Stempniewicz, MSc, director of U.S. Health Outcomes & Epidemiology at GSK Vaccines, Alexandria, Va., reported.
“The take-home finding is that herpes zoster incidence is high among people with MS overall,” Mr. Stempniewicz said in an interview. “We also found that herpes zoster incidence is numerically higher among MS patients with higher levels of baseline immunosuppression, so another conclusion is that herpes zoster prevention may be warranted among this population given the high level of immunosuppression and the high risk of developing herpes zoster infection.” GSK manufactures Shingrix, the only currently approved and recommended herpes zoster vaccine available in the United States
Lawrence Steinman, MD, a professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) Medicine, was not involved in the research but said in an interview that the findings “raise the issue of whether not enough individuals with MS are getting Shingrix, and also whether there is a need for rapid intervention with an antiviral, for those individuals who develop shingles.”
Real-world data
For the study, researchers analyzed U.S. administrative claims data from the Optum Research Database between October 2015 and March 2022 to compare shingles infections between adults with MS (and no other immunocompromising conditions) and a random sample of one million people without any immunocompromising conditions. The study excluded anyone who had been vaccinated against herpes zoster or diagnosed with it in the year before October 2015.
Among the 42,185 adults with MS included in the cohort, just over half (53%) were commercially insured, and 47% had Medicare Advantage. Their average age was 53, and 75% were female. Just over half the cohort (55%) had no immunosuppression because of medications while 35% had low immunosuppression from MS therapy and 10% had high immunosuppression from therapy. High suppression meant patients were taking fingolimod, siponimod, ozanimod, ponesimod, cladribine, or a monoclonal antibody except natalizumab. Those with low suppression were taking natalizumab, fumarates, IVIG, glatiramer acetate, interferon beta or a related drug, teriflunomide, azathioprine, methotrexate, or mycophenolate mofetil.
The rate of shingles infections in the MS patient population was 13.8 per 1,000 people per year, compared with 5.6 infections per 1,000 immunocompetent people per year (adjusted incident rate ratio, 1.69; 95% confidenceinterval, 1.58-1.81. When broken down by age, younger adults aged 18-49 with MS were more than three times more likely to develop shingles (incidence rate, 11.6 per 1,000 people per year) than immunocompetent younger adults (IR, 3.5). The gap was narrower for those age 50 and older, where adults with MS had a rate of 15.2 infections per 1,000 people per year versus 8.6 per 1,000 immunocompetent people per year.
Although MS patients with a higher baseline level of immunosuppression from therapy had higher herpes zoster infection rates (18 cases per 1,000 people per year) than those with low immunosuppression (14 cases per 1,000 people per year) or no immunosuppression from medication (13 cases per 1,000 people per year), rates for all three remained higher than for the immunocompetent population.
Herpes and MS: Some questions still unanswered
“We’ve known that herpes zoster is more common in people with MS, and we’ve known that it is seen in people on MS therapies,” Robert Fox, MD, a staff neurologist at the Mellen Center for MS and vice-chair for research at the Neurological Institute at the Cleveland Clinic, said in an interview. “What we haven’t known is just how much more common it is in people with MS than the rest of the adult population and whether it truly is more common in people taking MS therapies than people not taking MS therapies. This study puts real, population-based numbers on the incidence rates.”
Dr. Fox, who was not involved in the research, noted that a limitation of the study was the inability to know the risk of shingles according to specific MS therapies since all the therapies were grouped together.
”So I can’t say to a patient that their particular therapy increases their risk,” Dr. Fox said. “Similarly with the MS therapies listed in the ‘high’ immunosuppression category: We don’t know that each of the therapies listed do in fact increase the rate of herpes zoster. We just know that the group of MS therapies bunched into the ‘high’ category, on the whole, increase the rate of herpes zoster.”
The study does not provide any information about the impact of Shingrix vaccination, he added, since vaccinated individuals were excluded from the analysis.
Timing the vaccination with MS therapy
Dr. Steinman said in an interview that he recommends herpes zoster vaccination to his patients with MS.
“The mistake that people make with MS is that they don’t want to take the [herpes zoster] vaccine, and they should be taking it,”
Dr. Steinman said. “In a perfect world, they would get it before they went on their [immunosuppressive] drug. But now we’ll have a lot of people who didn’t take the vaccine; they can get it while they’re on their drug.” Although it depends on the particular therapy they’re taking, Dr. Steinman said that most people can get the shingles vaccine while continuing their medication.
The Centers for Disease Control and Prevention recommends that adults who are or will be immunodeficient or immunosuppressed because of a disease or therapy get two doses of the Shingrix vaccine against herpes zoster, regardless of whether they have previously been vaccinated with Zostavax or have ever had shingles. The agency has also issued detailed clinical guidance regarding how to administer the vaccine to individuals taking immunosuppressive therapy, including the option to administer the second dose 1-2 months after the first instead of 2-6 months to “facilitate avoiding vaccination during periods of more intense immunosuppression,” the agency wrote.
The research was sponsored, funded, and analyzed by GSK, which manufactures the shingles vaccine Shingrix, and Mr. Stempniewicz is a GSK employee. Two other authors are GSK employees, and three authors are employees of Optum who received fees from GSK for this study. Dr. Steinman and Dr. Fox reported no relevant disclosures.
DENVER – , according to research presented at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Herpes zoster and its complications are associated with increased health care cost and decreased quality of life,” lead author Nikita Stempniewicz, MSc, director of U.S. Health Outcomes & Epidemiology at GSK Vaccines, Alexandria, Va., reported.
“The take-home finding is that herpes zoster incidence is high among people with MS overall,” Mr. Stempniewicz said in an interview. “We also found that herpes zoster incidence is numerically higher among MS patients with higher levels of baseline immunosuppression, so another conclusion is that herpes zoster prevention may be warranted among this population given the high level of immunosuppression and the high risk of developing herpes zoster infection.” GSK manufactures Shingrix, the only currently approved and recommended herpes zoster vaccine available in the United States
Lawrence Steinman, MD, a professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) Medicine, was not involved in the research but said in an interview that the findings “raise the issue of whether not enough individuals with MS are getting Shingrix, and also whether there is a need for rapid intervention with an antiviral, for those individuals who develop shingles.”
Real-world data
For the study, researchers analyzed U.S. administrative claims data from the Optum Research Database between October 2015 and March 2022 to compare shingles infections between adults with MS (and no other immunocompromising conditions) and a random sample of one million people without any immunocompromising conditions. The study excluded anyone who had been vaccinated against herpes zoster or diagnosed with it in the year before October 2015.
Among the 42,185 adults with MS included in the cohort, just over half (53%) were commercially insured, and 47% had Medicare Advantage. Their average age was 53, and 75% were female. Just over half the cohort (55%) had no immunosuppression because of medications while 35% had low immunosuppression from MS therapy and 10% had high immunosuppression from therapy. High suppression meant patients were taking fingolimod, siponimod, ozanimod, ponesimod, cladribine, or a monoclonal antibody except natalizumab. Those with low suppression were taking natalizumab, fumarates, IVIG, glatiramer acetate, interferon beta or a related drug, teriflunomide, azathioprine, methotrexate, or mycophenolate mofetil.
The rate of shingles infections in the MS patient population was 13.8 per 1,000 people per year, compared with 5.6 infections per 1,000 immunocompetent people per year (adjusted incident rate ratio, 1.69; 95% confidenceinterval, 1.58-1.81. When broken down by age, younger adults aged 18-49 with MS were more than three times more likely to develop shingles (incidence rate, 11.6 per 1,000 people per year) than immunocompetent younger adults (IR, 3.5). The gap was narrower for those age 50 and older, where adults with MS had a rate of 15.2 infections per 1,000 people per year versus 8.6 per 1,000 immunocompetent people per year.
Although MS patients with a higher baseline level of immunosuppression from therapy had higher herpes zoster infection rates (18 cases per 1,000 people per year) than those with low immunosuppression (14 cases per 1,000 people per year) or no immunosuppression from medication (13 cases per 1,000 people per year), rates for all three remained higher than for the immunocompetent population.
Herpes and MS: Some questions still unanswered
“We’ve known that herpes zoster is more common in people with MS, and we’ve known that it is seen in people on MS therapies,” Robert Fox, MD, a staff neurologist at the Mellen Center for MS and vice-chair for research at the Neurological Institute at the Cleveland Clinic, said in an interview. “What we haven’t known is just how much more common it is in people with MS than the rest of the adult population and whether it truly is more common in people taking MS therapies than people not taking MS therapies. This study puts real, population-based numbers on the incidence rates.”
Dr. Fox, who was not involved in the research, noted that a limitation of the study was the inability to know the risk of shingles according to specific MS therapies since all the therapies were grouped together.
”So I can’t say to a patient that their particular therapy increases their risk,” Dr. Fox said. “Similarly with the MS therapies listed in the ‘high’ immunosuppression category: We don’t know that each of the therapies listed do in fact increase the rate of herpes zoster. We just know that the group of MS therapies bunched into the ‘high’ category, on the whole, increase the rate of herpes zoster.”
The study does not provide any information about the impact of Shingrix vaccination, he added, since vaccinated individuals were excluded from the analysis.
Timing the vaccination with MS therapy
Dr. Steinman said in an interview that he recommends herpes zoster vaccination to his patients with MS.
“The mistake that people make with MS is that they don’t want to take the [herpes zoster] vaccine, and they should be taking it,”
Dr. Steinman said. “In a perfect world, they would get it before they went on their [immunosuppressive] drug. But now we’ll have a lot of people who didn’t take the vaccine; they can get it while they’re on their drug.” Although it depends on the particular therapy they’re taking, Dr. Steinman said that most people can get the shingles vaccine while continuing their medication.
The Centers for Disease Control and Prevention recommends that adults who are or will be immunodeficient or immunosuppressed because of a disease or therapy get two doses of the Shingrix vaccine against herpes zoster, regardless of whether they have previously been vaccinated with Zostavax or have ever had shingles. The agency has also issued detailed clinical guidance regarding how to administer the vaccine to individuals taking immunosuppressive therapy, including the option to administer the second dose 1-2 months after the first instead of 2-6 months to “facilitate avoiding vaccination during periods of more intense immunosuppression,” the agency wrote.
The research was sponsored, funded, and analyzed by GSK, which manufactures the shingles vaccine Shingrix, and Mr. Stempniewicz is a GSK employee. Two other authors are GSK employees, and three authors are employees of Optum who received fees from GSK for this study. Dr. Steinman and Dr. Fox reported no relevant disclosures.
DENVER – , according to research presented at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Herpes zoster and its complications are associated with increased health care cost and decreased quality of life,” lead author Nikita Stempniewicz, MSc, director of U.S. Health Outcomes & Epidemiology at GSK Vaccines, Alexandria, Va., reported.
“The take-home finding is that herpes zoster incidence is high among people with MS overall,” Mr. Stempniewicz said in an interview. “We also found that herpes zoster incidence is numerically higher among MS patients with higher levels of baseline immunosuppression, so another conclusion is that herpes zoster prevention may be warranted among this population given the high level of immunosuppression and the high risk of developing herpes zoster infection.” GSK manufactures Shingrix, the only currently approved and recommended herpes zoster vaccine available in the United States
Lawrence Steinman, MD, a professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) Medicine, was not involved in the research but said in an interview that the findings “raise the issue of whether not enough individuals with MS are getting Shingrix, and also whether there is a need for rapid intervention with an antiviral, for those individuals who develop shingles.”
Real-world data
For the study, researchers analyzed U.S. administrative claims data from the Optum Research Database between October 2015 and March 2022 to compare shingles infections between adults with MS (and no other immunocompromising conditions) and a random sample of one million people without any immunocompromising conditions. The study excluded anyone who had been vaccinated against herpes zoster or diagnosed with it in the year before October 2015.
Among the 42,185 adults with MS included in the cohort, just over half (53%) were commercially insured, and 47% had Medicare Advantage. Their average age was 53, and 75% were female. Just over half the cohort (55%) had no immunosuppression because of medications while 35% had low immunosuppression from MS therapy and 10% had high immunosuppression from therapy. High suppression meant patients were taking fingolimod, siponimod, ozanimod, ponesimod, cladribine, or a monoclonal antibody except natalizumab. Those with low suppression were taking natalizumab, fumarates, IVIG, glatiramer acetate, interferon beta or a related drug, teriflunomide, azathioprine, methotrexate, or mycophenolate mofetil.
The rate of shingles infections in the MS patient population was 13.8 per 1,000 people per year, compared with 5.6 infections per 1,000 immunocompetent people per year (adjusted incident rate ratio, 1.69; 95% confidenceinterval, 1.58-1.81. When broken down by age, younger adults aged 18-49 with MS were more than three times more likely to develop shingles (incidence rate, 11.6 per 1,000 people per year) than immunocompetent younger adults (IR, 3.5). The gap was narrower for those age 50 and older, where adults with MS had a rate of 15.2 infections per 1,000 people per year versus 8.6 per 1,000 immunocompetent people per year.
Although MS patients with a higher baseline level of immunosuppression from therapy had higher herpes zoster infection rates (18 cases per 1,000 people per year) than those with low immunosuppression (14 cases per 1,000 people per year) or no immunosuppression from medication (13 cases per 1,000 people per year), rates for all three remained higher than for the immunocompetent population.
Herpes and MS: Some questions still unanswered
“We’ve known that herpes zoster is more common in people with MS, and we’ve known that it is seen in people on MS therapies,” Robert Fox, MD, a staff neurologist at the Mellen Center for MS and vice-chair for research at the Neurological Institute at the Cleveland Clinic, said in an interview. “What we haven’t known is just how much more common it is in people with MS than the rest of the adult population and whether it truly is more common in people taking MS therapies than people not taking MS therapies. This study puts real, population-based numbers on the incidence rates.”
Dr. Fox, who was not involved in the research, noted that a limitation of the study was the inability to know the risk of shingles according to specific MS therapies since all the therapies were grouped together.
”So I can’t say to a patient that their particular therapy increases their risk,” Dr. Fox said. “Similarly with the MS therapies listed in the ‘high’ immunosuppression category: We don’t know that each of the therapies listed do in fact increase the rate of herpes zoster. We just know that the group of MS therapies bunched into the ‘high’ category, on the whole, increase the rate of herpes zoster.”
The study does not provide any information about the impact of Shingrix vaccination, he added, since vaccinated individuals were excluded from the analysis.
Timing the vaccination with MS therapy
Dr. Steinman said in an interview that he recommends herpes zoster vaccination to his patients with MS.
“The mistake that people make with MS is that they don’t want to take the [herpes zoster] vaccine, and they should be taking it,”
Dr. Steinman said. “In a perfect world, they would get it before they went on their [immunosuppressive] drug. But now we’ll have a lot of people who didn’t take the vaccine; they can get it while they’re on their drug.” Although it depends on the particular therapy they’re taking, Dr. Steinman said that most people can get the shingles vaccine while continuing their medication.
The Centers for Disease Control and Prevention recommends that adults who are or will be immunodeficient or immunosuppressed because of a disease or therapy get two doses of the Shingrix vaccine against herpes zoster, regardless of whether they have previously been vaccinated with Zostavax or have ever had shingles. The agency has also issued detailed clinical guidance regarding how to administer the vaccine to individuals taking immunosuppressive therapy, including the option to administer the second dose 1-2 months after the first instead of 2-6 months to “facilitate avoiding vaccination during periods of more intense immunosuppression,” the agency wrote.
The research was sponsored, funded, and analyzed by GSK, which manufactures the shingles vaccine Shingrix, and Mr. Stempniewicz is a GSK employee. Two other authors are GSK employees, and three authors are employees of Optum who received fees from GSK for this study. Dr. Steinman and Dr. Fox reported no relevant disclosures.
AT CMSC 2023
More support for thrombectomy in large-core strokes: TESLA, MAGNA
Although not quite meeting its primary endpoint,
And a new meta-analysis (MAGNA) of previous studies in a similar population has provided more detailed estimates of the treatment benefit of thrombectomy in these patients.
The TESLA trial, which included patients with large-core infarcts (ASPECTS score 2-5) within 24 hours of symptom onset, showed encouraging trends towards a benefit with thrombectomy for the primary outcome of 90-day utility-weighted scores on the modified Rankin scale (mRS), but this did not reach the prespecified Bayesian superiority threshold.
Several secondary efficacy endpoints also showed suggestions of benefits with thrombectomy.
“The interventional group had higher mean or average utility-weighted mRS scores than the control group which means that their functional recovery at 90 days was trending for better outcome and less disability,” lead TESLA investigator, Osama Zaidat, MD, neuroscience & stroke director at Mercy St. Vincent Medical Center, Toledo, Ohio, said in an interview. “They also showed better neurological improvement and a higher chance of achieving a good outcome (mRS 0-3).”
These patients with large-core infarct strokes were not included in the initial trials of endovascular therapy in patients presenting in the late time window, up to 24 hours, as it was thought they would not benefit. However, three recent trials (RESCUE-Japan LIMIT; ANGEL ASPECT; and SELECT 2) have shown that patients with large core infarcts can still benefit from endovascular thrombectomy.
While these three previous trials used sophisticated imaging techniques (MRI or CT perfusion) to select patients, and restricted patients included to those with an ASPECTS score of 3-5, the TESLA study had a more pragmatic design, using just noncontrast CT scan evaluation without advanced imaging to select patients, and extending the inclusion criteria to patients with an ASPECTS score of 2.
“Noncontrast CT scans are available at all stroke centers so this study is more practical, highly generalizable, and more applicable globally,” Dr. Zaidat commented.
“However, our results suggest that when using noncontrast CT only to select patients, the gain or treatment effect of thrombectomy seems to be smaller than when using sophisticated advanced imaging to make the decision to go for thrombectomy or not as in the other trials,” he added.
The TESLA trial results were presented at the recent European Stroke Organisation Conference, held in Munich.
The study included 300 stroke patients with anterior circulation large‐vessel occlusion (NIHSS of 6 or more) with a large‐core infarction (investigator read ASPECTS Score 2-5), selected on the basis of noncontrast CT scan, who were randomized to undergo intra-arterial thrombectomy or best medical management (control) up to 24 hours from last known well.
The trial had a Bayesian probabilities design, with a primary endpoint of the 90-day utility-weighted mRS (uw-mRS), a relatively new patient-centered outcome used in stroke trials, which includes a quality-of-life measurement. Utilities represent preferences for mRS health states and range from 0 (death) to 1 (perfect health), so in contrast to the traditional mRS scores, a higher uw-mRS score is better.
The 90-day uw-MRS scores were 2.93 in the thrombectomy group vs. 2.27 in the control group.
The Bayesian probability of thrombectomy superiority was 0.957, which Dr. Zaidat said was “similar” to a P value of .043, but this was less than the prespecified superiority probability of > .975 to declare efficacy.
A separate analysis in a population of patients selected by core-lab read noncontrast CT scan, showed a Bayesian probability of benefit with thrombectomy of 0.98, “similar” to one-sided P value of .02.
In terms of secondary endpoints, there were also some encouraging trends, including a suggestion of benefit in the 90-day mRS ordinal shift (odds ratio 1.40; P = .06).
The number of patients achieving functional independence (mRS 0-2) was 14% in the thrombectomy groups vs. 9% in the control group (P = .09); and a good functional outcome (mRS 0-3) was achieved in 30% of thrombectomy patients vs. 20% of those in the control group (P = .03).
Major neurological improvement (NIHSS scale of 0-2 or improvement of 8 points or more) occurred in 26% of thrombectomy patients vs. 13% of controls (P = .0008).
Quality of life, measured by the EuroQol 5-Dimension 5-Level survey, also showed a trend towards improvement in the thrombectomy group with mean scores of 53 vs. 46 (P = .058).
In terms of safety, all-cause mortality was similar in the two groups (35% thrombectomy and 33% control) and symptomatic intracerebral hemmorhage (ICH) occurred in 3.97% of thrombectomy vs. 1.34% of control patients (relative risk, 2.96).
“Cost-effective analysis and additional subgroup studies will provide more insight about the training needs to read the CT scan and if there is any value to treat patients with an ASPECTS score of 2,” Dr. Zaidat concluded.
“Larger pooled analysis will also be very useful in understanding the threshold of brain volume with irreversible damage beyond which thrombectomy wouldn’t be helpful,” he added.
Meta-analysis of previous studies: MAGNA
Another presentation at the ESOC meeting reported an individual patient data meta-analysis (MAGNA) of the three previous trials suggesting benefit of thrombectomy in patients with large-core ischemic strokes of the anterior circulation up to 24 hours of last known well.
The RESCUE Japan Limit trial was conducted in Japan; the SELECT-2 trial in North America, Europe, Australia, and New Zealand; and the ANGEL ASPECT trial in China.
In total, the meta-analysis included 1,009 patients, half of whom received thrombectomy and half received medical management only.
Results showed that in the whole population in the three trials, the use of thrombectomy improved functional outcomes, with an adjusted odds ratio of 1.78 (P < .001).
Functional independence (mRS 0-2) was also increased (23% vs. 9%; adjusted risk ratio, 2.62; P < .001); as was independent ambulation (mRS, 0-3; 41% vs. 24%; aRR, 1.76; P < .001).
But early neurological worsening was more frequent with thrombectomy (aRR 1.42, 1.09-1.84, P = .010).
No difference in mortality was identified between thrombectomy (27%) and medical management (28%) or in rates of symptomatic ICH (1.8% thrombectomy vs. 1.6% medical management).
“The results from the previously published large-core trials and from this pooled dataset provide unequivocal evidence on the efficacy and safety of endovascular thrombectomy in patients with large-core infarcts,” lead author of the MAGNA meta-analysis, Amrou Sarraj, MD, professor of neurology at University Hospitals Cleveland Medical Center, affiliate of Case Western Reserve University in Cleveland, concluded.
“The benefit persists across the spectrum of age, clinical severity, and time, with clear benefit up to an estimated ischemic core volume of 150 mL,” he added. “We have great hopes that these results will lead to more patients being treated and achieving improved functional outcomes.”
On how the TESLA results fit in with the previous three trials, Dr. Sarraj pointed out to this news organization that the TESLA trial was conducted in the United States and enrolled patients based on ASPECTS 2-5 on noncontrast CT.
“The primary outcome for intention-to-treat analysis did not reach the prespecified threshold for efficacy, but the results were largely in the same direction as shown in SELECT2, ANGEL ASPECT, and RESCUE Japan Limit,” he said. “These findings further emphasize the efficacy and safety of thrombectomy in patients with large ischemic core, at the same time reinforcing the need to provide results from pooled data from all large-core trials.”
He noted that results from two further trials of thrombectomy in large core strokes, TENSION and LASTE – both of which have now been stopped early because of the positive findings from the previous studies – are expected soon, and the MAGNA meta-analysis will be updated to include data from all six trials.
“This will increase the accuracy of the estimation of the treatment effect and will give even more power to look further into the details related to subgroups and selection imaging modalities,” Dr. Sarraj added.
The research team hopes that this joint effort will eventually set the pathway for selection algorithms and treatment boundaries in patients with large-vessel occlusion.
TESLA was an investigator-initiated study funded by unrestricted grants from Cerenovus, Penumbra, Medtronic, Stryker, and Genentech. Dr. Zaidat is a consultant for Stryker, Cerenovus, Penumbra, and Medtronic.
A version of this article first appeared on Medscape.com.
Although not quite meeting its primary endpoint,
And a new meta-analysis (MAGNA) of previous studies in a similar population has provided more detailed estimates of the treatment benefit of thrombectomy in these patients.
The TESLA trial, which included patients with large-core infarcts (ASPECTS score 2-5) within 24 hours of symptom onset, showed encouraging trends towards a benefit with thrombectomy for the primary outcome of 90-day utility-weighted scores on the modified Rankin scale (mRS), but this did not reach the prespecified Bayesian superiority threshold.
Several secondary efficacy endpoints also showed suggestions of benefits with thrombectomy.
“The interventional group had higher mean or average utility-weighted mRS scores than the control group which means that their functional recovery at 90 days was trending for better outcome and less disability,” lead TESLA investigator, Osama Zaidat, MD, neuroscience & stroke director at Mercy St. Vincent Medical Center, Toledo, Ohio, said in an interview. “They also showed better neurological improvement and a higher chance of achieving a good outcome (mRS 0-3).”
These patients with large-core infarct strokes were not included in the initial trials of endovascular therapy in patients presenting in the late time window, up to 24 hours, as it was thought they would not benefit. However, three recent trials (RESCUE-Japan LIMIT; ANGEL ASPECT; and SELECT 2) have shown that patients with large core infarcts can still benefit from endovascular thrombectomy.
While these three previous trials used sophisticated imaging techniques (MRI or CT perfusion) to select patients, and restricted patients included to those with an ASPECTS score of 3-5, the TESLA study had a more pragmatic design, using just noncontrast CT scan evaluation without advanced imaging to select patients, and extending the inclusion criteria to patients with an ASPECTS score of 2.
“Noncontrast CT scans are available at all stroke centers so this study is more practical, highly generalizable, and more applicable globally,” Dr. Zaidat commented.
“However, our results suggest that when using noncontrast CT only to select patients, the gain or treatment effect of thrombectomy seems to be smaller than when using sophisticated advanced imaging to make the decision to go for thrombectomy or not as in the other trials,” he added.
The TESLA trial results were presented at the recent European Stroke Organisation Conference, held in Munich.
The study included 300 stroke patients with anterior circulation large‐vessel occlusion (NIHSS of 6 or more) with a large‐core infarction (investigator read ASPECTS Score 2-5), selected on the basis of noncontrast CT scan, who were randomized to undergo intra-arterial thrombectomy or best medical management (control) up to 24 hours from last known well.
The trial had a Bayesian probabilities design, with a primary endpoint of the 90-day utility-weighted mRS (uw-mRS), a relatively new patient-centered outcome used in stroke trials, which includes a quality-of-life measurement. Utilities represent preferences for mRS health states and range from 0 (death) to 1 (perfect health), so in contrast to the traditional mRS scores, a higher uw-mRS score is better.
The 90-day uw-MRS scores were 2.93 in the thrombectomy group vs. 2.27 in the control group.
The Bayesian probability of thrombectomy superiority was 0.957, which Dr. Zaidat said was “similar” to a P value of .043, but this was less than the prespecified superiority probability of > .975 to declare efficacy.
A separate analysis in a population of patients selected by core-lab read noncontrast CT scan, showed a Bayesian probability of benefit with thrombectomy of 0.98, “similar” to one-sided P value of .02.
In terms of secondary endpoints, there were also some encouraging trends, including a suggestion of benefit in the 90-day mRS ordinal shift (odds ratio 1.40; P = .06).
The number of patients achieving functional independence (mRS 0-2) was 14% in the thrombectomy groups vs. 9% in the control group (P = .09); and a good functional outcome (mRS 0-3) was achieved in 30% of thrombectomy patients vs. 20% of those in the control group (P = .03).
Major neurological improvement (NIHSS scale of 0-2 or improvement of 8 points or more) occurred in 26% of thrombectomy patients vs. 13% of controls (P = .0008).
Quality of life, measured by the EuroQol 5-Dimension 5-Level survey, also showed a trend towards improvement in the thrombectomy group with mean scores of 53 vs. 46 (P = .058).
In terms of safety, all-cause mortality was similar in the two groups (35% thrombectomy and 33% control) and symptomatic intracerebral hemmorhage (ICH) occurred in 3.97% of thrombectomy vs. 1.34% of control patients (relative risk, 2.96).
“Cost-effective analysis and additional subgroup studies will provide more insight about the training needs to read the CT scan and if there is any value to treat patients with an ASPECTS score of 2,” Dr. Zaidat concluded.
“Larger pooled analysis will also be very useful in understanding the threshold of brain volume with irreversible damage beyond which thrombectomy wouldn’t be helpful,” he added.
Meta-analysis of previous studies: MAGNA
Another presentation at the ESOC meeting reported an individual patient data meta-analysis (MAGNA) of the three previous trials suggesting benefit of thrombectomy in patients with large-core ischemic strokes of the anterior circulation up to 24 hours of last known well.
The RESCUE Japan Limit trial was conducted in Japan; the SELECT-2 trial in North America, Europe, Australia, and New Zealand; and the ANGEL ASPECT trial in China.
In total, the meta-analysis included 1,009 patients, half of whom received thrombectomy and half received medical management only.
Results showed that in the whole population in the three trials, the use of thrombectomy improved functional outcomes, with an adjusted odds ratio of 1.78 (P < .001).
Functional independence (mRS 0-2) was also increased (23% vs. 9%; adjusted risk ratio, 2.62; P < .001); as was independent ambulation (mRS, 0-3; 41% vs. 24%; aRR, 1.76; P < .001).
But early neurological worsening was more frequent with thrombectomy (aRR 1.42, 1.09-1.84, P = .010).
No difference in mortality was identified between thrombectomy (27%) and medical management (28%) or in rates of symptomatic ICH (1.8% thrombectomy vs. 1.6% medical management).
“The results from the previously published large-core trials and from this pooled dataset provide unequivocal evidence on the efficacy and safety of endovascular thrombectomy in patients with large-core infarcts,” lead author of the MAGNA meta-analysis, Amrou Sarraj, MD, professor of neurology at University Hospitals Cleveland Medical Center, affiliate of Case Western Reserve University in Cleveland, concluded.
“The benefit persists across the spectrum of age, clinical severity, and time, with clear benefit up to an estimated ischemic core volume of 150 mL,” he added. “We have great hopes that these results will lead to more patients being treated and achieving improved functional outcomes.”
On how the TESLA results fit in with the previous three trials, Dr. Sarraj pointed out to this news organization that the TESLA trial was conducted in the United States and enrolled patients based on ASPECTS 2-5 on noncontrast CT.
“The primary outcome for intention-to-treat analysis did not reach the prespecified threshold for efficacy, but the results were largely in the same direction as shown in SELECT2, ANGEL ASPECT, and RESCUE Japan Limit,” he said. “These findings further emphasize the efficacy and safety of thrombectomy in patients with large ischemic core, at the same time reinforcing the need to provide results from pooled data from all large-core trials.”
He noted that results from two further trials of thrombectomy in large core strokes, TENSION and LASTE – both of which have now been stopped early because of the positive findings from the previous studies – are expected soon, and the MAGNA meta-analysis will be updated to include data from all six trials.
“This will increase the accuracy of the estimation of the treatment effect and will give even more power to look further into the details related to subgroups and selection imaging modalities,” Dr. Sarraj added.
The research team hopes that this joint effort will eventually set the pathway for selection algorithms and treatment boundaries in patients with large-vessel occlusion.
TESLA was an investigator-initiated study funded by unrestricted grants from Cerenovus, Penumbra, Medtronic, Stryker, and Genentech. Dr. Zaidat is a consultant for Stryker, Cerenovus, Penumbra, and Medtronic.
A version of this article first appeared on Medscape.com.
Although not quite meeting its primary endpoint,
And a new meta-analysis (MAGNA) of previous studies in a similar population has provided more detailed estimates of the treatment benefit of thrombectomy in these patients.
The TESLA trial, which included patients with large-core infarcts (ASPECTS score 2-5) within 24 hours of symptom onset, showed encouraging trends towards a benefit with thrombectomy for the primary outcome of 90-day utility-weighted scores on the modified Rankin scale (mRS), but this did not reach the prespecified Bayesian superiority threshold.
Several secondary efficacy endpoints also showed suggestions of benefits with thrombectomy.
“The interventional group had higher mean or average utility-weighted mRS scores than the control group which means that their functional recovery at 90 days was trending for better outcome and less disability,” lead TESLA investigator, Osama Zaidat, MD, neuroscience & stroke director at Mercy St. Vincent Medical Center, Toledo, Ohio, said in an interview. “They also showed better neurological improvement and a higher chance of achieving a good outcome (mRS 0-3).”
These patients with large-core infarct strokes were not included in the initial trials of endovascular therapy in patients presenting in the late time window, up to 24 hours, as it was thought they would not benefit. However, three recent trials (RESCUE-Japan LIMIT; ANGEL ASPECT; and SELECT 2) have shown that patients with large core infarcts can still benefit from endovascular thrombectomy.
While these three previous trials used sophisticated imaging techniques (MRI or CT perfusion) to select patients, and restricted patients included to those with an ASPECTS score of 3-5, the TESLA study had a more pragmatic design, using just noncontrast CT scan evaluation without advanced imaging to select patients, and extending the inclusion criteria to patients with an ASPECTS score of 2.
“Noncontrast CT scans are available at all stroke centers so this study is more practical, highly generalizable, and more applicable globally,” Dr. Zaidat commented.
“However, our results suggest that when using noncontrast CT only to select patients, the gain or treatment effect of thrombectomy seems to be smaller than when using sophisticated advanced imaging to make the decision to go for thrombectomy or not as in the other trials,” he added.
The TESLA trial results were presented at the recent European Stroke Organisation Conference, held in Munich.
The study included 300 stroke patients with anterior circulation large‐vessel occlusion (NIHSS of 6 or more) with a large‐core infarction (investigator read ASPECTS Score 2-5), selected on the basis of noncontrast CT scan, who were randomized to undergo intra-arterial thrombectomy or best medical management (control) up to 24 hours from last known well.
The trial had a Bayesian probabilities design, with a primary endpoint of the 90-day utility-weighted mRS (uw-mRS), a relatively new patient-centered outcome used in stroke trials, which includes a quality-of-life measurement. Utilities represent preferences for mRS health states and range from 0 (death) to 1 (perfect health), so in contrast to the traditional mRS scores, a higher uw-mRS score is better.
The 90-day uw-MRS scores were 2.93 in the thrombectomy group vs. 2.27 in the control group.
The Bayesian probability of thrombectomy superiority was 0.957, which Dr. Zaidat said was “similar” to a P value of .043, but this was less than the prespecified superiority probability of > .975 to declare efficacy.
A separate analysis in a population of patients selected by core-lab read noncontrast CT scan, showed a Bayesian probability of benefit with thrombectomy of 0.98, “similar” to one-sided P value of .02.
In terms of secondary endpoints, there were also some encouraging trends, including a suggestion of benefit in the 90-day mRS ordinal shift (odds ratio 1.40; P = .06).
The number of patients achieving functional independence (mRS 0-2) was 14% in the thrombectomy groups vs. 9% in the control group (P = .09); and a good functional outcome (mRS 0-3) was achieved in 30% of thrombectomy patients vs. 20% of those in the control group (P = .03).
Major neurological improvement (NIHSS scale of 0-2 or improvement of 8 points or more) occurred in 26% of thrombectomy patients vs. 13% of controls (P = .0008).
Quality of life, measured by the EuroQol 5-Dimension 5-Level survey, also showed a trend towards improvement in the thrombectomy group with mean scores of 53 vs. 46 (P = .058).
In terms of safety, all-cause mortality was similar in the two groups (35% thrombectomy and 33% control) and symptomatic intracerebral hemmorhage (ICH) occurred in 3.97% of thrombectomy vs. 1.34% of control patients (relative risk, 2.96).
“Cost-effective analysis and additional subgroup studies will provide more insight about the training needs to read the CT scan and if there is any value to treat patients with an ASPECTS score of 2,” Dr. Zaidat concluded.
“Larger pooled analysis will also be very useful in understanding the threshold of brain volume with irreversible damage beyond which thrombectomy wouldn’t be helpful,” he added.
Meta-analysis of previous studies: MAGNA
Another presentation at the ESOC meeting reported an individual patient data meta-analysis (MAGNA) of the three previous trials suggesting benefit of thrombectomy in patients with large-core ischemic strokes of the anterior circulation up to 24 hours of last known well.
The RESCUE Japan Limit trial was conducted in Japan; the SELECT-2 trial in North America, Europe, Australia, and New Zealand; and the ANGEL ASPECT trial in China.
In total, the meta-analysis included 1,009 patients, half of whom received thrombectomy and half received medical management only.
Results showed that in the whole population in the three trials, the use of thrombectomy improved functional outcomes, with an adjusted odds ratio of 1.78 (P < .001).
Functional independence (mRS 0-2) was also increased (23% vs. 9%; adjusted risk ratio, 2.62; P < .001); as was independent ambulation (mRS, 0-3; 41% vs. 24%; aRR, 1.76; P < .001).
But early neurological worsening was more frequent with thrombectomy (aRR 1.42, 1.09-1.84, P = .010).
No difference in mortality was identified between thrombectomy (27%) and medical management (28%) or in rates of symptomatic ICH (1.8% thrombectomy vs. 1.6% medical management).
“The results from the previously published large-core trials and from this pooled dataset provide unequivocal evidence on the efficacy and safety of endovascular thrombectomy in patients with large-core infarcts,” lead author of the MAGNA meta-analysis, Amrou Sarraj, MD, professor of neurology at University Hospitals Cleveland Medical Center, affiliate of Case Western Reserve University in Cleveland, concluded.
“The benefit persists across the spectrum of age, clinical severity, and time, with clear benefit up to an estimated ischemic core volume of 150 mL,” he added. “We have great hopes that these results will lead to more patients being treated and achieving improved functional outcomes.”
On how the TESLA results fit in with the previous three trials, Dr. Sarraj pointed out to this news organization that the TESLA trial was conducted in the United States and enrolled patients based on ASPECTS 2-5 on noncontrast CT.
“The primary outcome for intention-to-treat analysis did not reach the prespecified threshold for efficacy, but the results were largely in the same direction as shown in SELECT2, ANGEL ASPECT, and RESCUE Japan Limit,” he said. “These findings further emphasize the efficacy and safety of thrombectomy in patients with large ischemic core, at the same time reinforcing the need to provide results from pooled data from all large-core trials.”
He noted that results from two further trials of thrombectomy in large core strokes, TENSION and LASTE – both of which have now been stopped early because of the positive findings from the previous studies – are expected soon, and the MAGNA meta-analysis will be updated to include data from all six trials.
“This will increase the accuracy of the estimation of the treatment effect and will give even more power to look further into the details related to subgroups and selection imaging modalities,” Dr. Sarraj added.
The research team hopes that this joint effort will eventually set the pathway for selection algorithms and treatment boundaries in patients with large-vessel occlusion.
TESLA was an investigator-initiated study funded by unrestricted grants from Cerenovus, Penumbra, Medtronic, Stryker, and Genentech. Dr. Zaidat is a consultant for Stryker, Cerenovus, Penumbra, and Medtronic.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023
Ozanimod for relapsing MS shows long-term safety, efficacy with age differences
AURORA, COLO. – , according to research presented at the annual meeting of the Consortium of Multiple Sclerosis Centers.
Research from the phase 3 DAYBREAK trial had already shown the safety of ozanimod, and the Food and Drug Administration approved the drug as an oral disease-modifying therapy for relapsing forms of MS in 2020.
“In the DAYBREAK study, we already have shown that the clinical and radiological disease was quite low in these patients who received the higher dose of ozanimod, and those who switched from the lower dose of the interferon to this active treatment also had decreases in their annualized relapse rate and their MRI lesion counts,” Sarah Morrow, MD, associate professor of neurology at Western University in London, Ontario, told attendees. She presented the data on behalf of senior author Bruce Cree, MD, PhD, professor of neurology and clinical research director at the University of California, San Francisco, Multiple Sclerosis Center, and the other authors. “But what was not known was whether there’s a difference in efficacy based on age, and we know that disease activity can differ based on age in person with relapsing multiple sclerosis.”
Examining efficacy by age
Analysis of data from DAYBREAK and an open-label extension study revealed that respiratory infections were more common in patients younger than 35, and urinary tract infections, dizziness, and treatment-emergent depressive symptoms became were common in patients age 50 and older. “Serious infections did not vary by age, and there were too few serious events to identify any age-related trends by specific TEAE,” the authors reported. During the open-label extension of the study, no new adverse events emerged, “confirming the ozanimod safety profile reported in the parent trials,” SUNBEAM and RADIANCE, the authors reported.
The phase 3 parent trials compared 30 mcg once weekly of intramuscular interferon beta-1a to 0.92 mg of once-daily oral ozanimod and 0.46 mg of once-daily oral ozanimod. In the DAYBREAK open-label extension, 2,256 participants underwent a dose escalation over 1 week until all reached 0.92 mg of ozanimod, where they remained for approximately 5 years of follow-up. The researchers then analyzed TEAEs, serious adverse events, and TEAEs leading to discontinuation in four age categories: 18-25, 26-35, 36-49, and 50 and older.
Respiratory infections occurred more often in those aged 18-25 (10.9%) and 26-35 (6.1%) than in those 36-49 (5.8%) and 50 and older (3.4%). However, UTIs occurred most in those age 50 and older (9.2%), versus occurring in 6.6% of those 36-49, 4.3% of those aged 26-35, and 4.6% of those 18-25.
High cholesterol occurred significantly less often in those 18-25 (1.4%) and 26-35 (2%) than in those 36-49 (5%) and 50 and older (8%), and hypertension showed a similar pattern: 2% in the youngest group, 4.7% in those aged 26-35, 12.8% in those aged 36-49, and 16.7% in those aged 50 and older.
Other TEAEs that occurred more often in older patients included depression/depressive symptoms, dizziness, back pain, joint pain, osteoarthritis, and high gamma-glutamyl transferase (GGT) levels. Overall cardiac and vascular disorders and malignancies were also more common as participants’ age increased.
Bigger concerns?
The increase in malignancy risk by age surprised Shailee Shah, MD, assistant professor of neuroimmunology and neurology at Vanderbilt University Medical Center, Nashville, Tenn., who was not involved in the research. This increase in risk was “not expanded upon much in this abstract or compared to population estimates, as this may ultimately be one of the bigger concerns with long-term use of this drug,” Dr. Shah said.
She further noted that “older patients may be at higher risk of infections and multiple cardiovascular risk factors, and so if patients already have comorbid disease, I may be less inclined to use this agent and likely less so in older individuals.”
Dr. Shah said these drugs are often recommended to individuals in their 20s and 30s at time of diagnosis. “If a patient is given this drug and tolerates it and finds it efficacious, we might continue this indefinitely, so looking at how the risk profile of young patients on this drug changes over time will be important,” Dr. Shah said. “I am also concerned about the malignancy risk and would want this elaborated upon.”
Overall efficacy across age groups
Serious infections occurred at relatively similar rates across all age groups. Incidence of any serious adverse event was 27 per 1,000 people per year in the youngest group compared with 24 events in the 26-35 group, 35 events in the 36-49 group, and 62 events per 1,000 people per year in those 50 and older.
“Patients in the 50 and older age group had a numerically lower adjusted annualized relapse rate and less gadolinium-enhancing lesions and new or enlarging T2 lesions per scan and were generally more likely to be free of gadolinium-enhancing lesions or new or enlarging T2 lesions than the 25 and younger age group,” Dr. Morrow told attendees, “but we feel that that’s more in keeping with the natural history of disease. And, overall, ozanimod, regardless of the age group, showed decreasing disease activity in the inflammatory part of disease, showing with annualized relapse rate, gad-enhancing lesions, and T2 lesions.”
Older participants were substantially more likely to withdraw from the trial because of adverse events. While 8% of the youngest group and 7.6% of participants aged 26-35 withdrew because of adverse events, 24.5% of those aged 36-49 and 18.5% of those aged 50 and older withdrew because of adverse events.
Dr. Shah said it was reassuring that no new safety signals emerged, “but based on this data, you would be concerned that long-term risk of cardiovascular disease may result in more serious adverse events over a longer period of time and will need to be considered as we see people increasingly on this drug.”
The research was funded by Bristol-Myers Squibb. The authors reported a wide range of financial disclosures, including personal fees, research funding, advisory board, and speakers fees, for multiple pharmaceutical companies, including Bristol-Myers Squibb, and five authors are employees and/or shareholders of the company. Dr. Shah has served on advisory boards for Alexion, Genentech, and Horizon.
AURORA, COLO. – , according to research presented at the annual meeting of the Consortium of Multiple Sclerosis Centers.
Research from the phase 3 DAYBREAK trial had already shown the safety of ozanimod, and the Food and Drug Administration approved the drug as an oral disease-modifying therapy for relapsing forms of MS in 2020.
“In the DAYBREAK study, we already have shown that the clinical and radiological disease was quite low in these patients who received the higher dose of ozanimod, and those who switched from the lower dose of the interferon to this active treatment also had decreases in their annualized relapse rate and their MRI lesion counts,” Sarah Morrow, MD, associate professor of neurology at Western University in London, Ontario, told attendees. She presented the data on behalf of senior author Bruce Cree, MD, PhD, professor of neurology and clinical research director at the University of California, San Francisco, Multiple Sclerosis Center, and the other authors. “But what was not known was whether there’s a difference in efficacy based on age, and we know that disease activity can differ based on age in person with relapsing multiple sclerosis.”
Examining efficacy by age
Analysis of data from DAYBREAK and an open-label extension study revealed that respiratory infections were more common in patients younger than 35, and urinary tract infections, dizziness, and treatment-emergent depressive symptoms became were common in patients age 50 and older. “Serious infections did not vary by age, and there were too few serious events to identify any age-related trends by specific TEAE,” the authors reported. During the open-label extension of the study, no new adverse events emerged, “confirming the ozanimod safety profile reported in the parent trials,” SUNBEAM and RADIANCE, the authors reported.
The phase 3 parent trials compared 30 mcg once weekly of intramuscular interferon beta-1a to 0.92 mg of once-daily oral ozanimod and 0.46 mg of once-daily oral ozanimod. In the DAYBREAK open-label extension, 2,256 participants underwent a dose escalation over 1 week until all reached 0.92 mg of ozanimod, where they remained for approximately 5 years of follow-up. The researchers then analyzed TEAEs, serious adverse events, and TEAEs leading to discontinuation in four age categories: 18-25, 26-35, 36-49, and 50 and older.
Respiratory infections occurred more often in those aged 18-25 (10.9%) and 26-35 (6.1%) than in those 36-49 (5.8%) and 50 and older (3.4%). However, UTIs occurred most in those age 50 and older (9.2%), versus occurring in 6.6% of those 36-49, 4.3% of those aged 26-35, and 4.6% of those 18-25.
High cholesterol occurred significantly less often in those 18-25 (1.4%) and 26-35 (2%) than in those 36-49 (5%) and 50 and older (8%), and hypertension showed a similar pattern: 2% in the youngest group, 4.7% in those aged 26-35, 12.8% in those aged 36-49, and 16.7% in those aged 50 and older.
Other TEAEs that occurred more often in older patients included depression/depressive symptoms, dizziness, back pain, joint pain, osteoarthritis, and high gamma-glutamyl transferase (GGT) levels. Overall cardiac and vascular disorders and malignancies were also more common as participants’ age increased.
Bigger concerns?
The increase in malignancy risk by age surprised Shailee Shah, MD, assistant professor of neuroimmunology and neurology at Vanderbilt University Medical Center, Nashville, Tenn., who was not involved in the research. This increase in risk was “not expanded upon much in this abstract or compared to population estimates, as this may ultimately be one of the bigger concerns with long-term use of this drug,” Dr. Shah said.
She further noted that “older patients may be at higher risk of infections and multiple cardiovascular risk factors, and so if patients already have comorbid disease, I may be less inclined to use this agent and likely less so in older individuals.”
Dr. Shah said these drugs are often recommended to individuals in their 20s and 30s at time of diagnosis. “If a patient is given this drug and tolerates it and finds it efficacious, we might continue this indefinitely, so looking at how the risk profile of young patients on this drug changes over time will be important,” Dr. Shah said. “I am also concerned about the malignancy risk and would want this elaborated upon.”
Overall efficacy across age groups
Serious infections occurred at relatively similar rates across all age groups. Incidence of any serious adverse event was 27 per 1,000 people per year in the youngest group compared with 24 events in the 26-35 group, 35 events in the 36-49 group, and 62 events per 1,000 people per year in those 50 and older.
“Patients in the 50 and older age group had a numerically lower adjusted annualized relapse rate and less gadolinium-enhancing lesions and new or enlarging T2 lesions per scan and were generally more likely to be free of gadolinium-enhancing lesions or new or enlarging T2 lesions than the 25 and younger age group,” Dr. Morrow told attendees, “but we feel that that’s more in keeping with the natural history of disease. And, overall, ozanimod, regardless of the age group, showed decreasing disease activity in the inflammatory part of disease, showing with annualized relapse rate, gad-enhancing lesions, and T2 lesions.”
Older participants were substantially more likely to withdraw from the trial because of adverse events. While 8% of the youngest group and 7.6% of participants aged 26-35 withdrew because of adverse events, 24.5% of those aged 36-49 and 18.5% of those aged 50 and older withdrew because of adverse events.
Dr. Shah said it was reassuring that no new safety signals emerged, “but based on this data, you would be concerned that long-term risk of cardiovascular disease may result in more serious adverse events over a longer period of time and will need to be considered as we see people increasingly on this drug.”
The research was funded by Bristol-Myers Squibb. The authors reported a wide range of financial disclosures, including personal fees, research funding, advisory board, and speakers fees, for multiple pharmaceutical companies, including Bristol-Myers Squibb, and five authors are employees and/or shareholders of the company. Dr. Shah has served on advisory boards for Alexion, Genentech, and Horizon.
AURORA, COLO. – , according to research presented at the annual meeting of the Consortium of Multiple Sclerosis Centers.
Research from the phase 3 DAYBREAK trial had already shown the safety of ozanimod, and the Food and Drug Administration approved the drug as an oral disease-modifying therapy for relapsing forms of MS in 2020.
“In the DAYBREAK study, we already have shown that the clinical and radiological disease was quite low in these patients who received the higher dose of ozanimod, and those who switched from the lower dose of the interferon to this active treatment also had decreases in their annualized relapse rate and their MRI lesion counts,” Sarah Morrow, MD, associate professor of neurology at Western University in London, Ontario, told attendees. She presented the data on behalf of senior author Bruce Cree, MD, PhD, professor of neurology and clinical research director at the University of California, San Francisco, Multiple Sclerosis Center, and the other authors. “But what was not known was whether there’s a difference in efficacy based on age, and we know that disease activity can differ based on age in person with relapsing multiple sclerosis.”
Examining efficacy by age
Analysis of data from DAYBREAK and an open-label extension study revealed that respiratory infections were more common in patients younger than 35, and urinary tract infections, dizziness, and treatment-emergent depressive symptoms became were common in patients age 50 and older. “Serious infections did not vary by age, and there were too few serious events to identify any age-related trends by specific TEAE,” the authors reported. During the open-label extension of the study, no new adverse events emerged, “confirming the ozanimod safety profile reported in the parent trials,” SUNBEAM and RADIANCE, the authors reported.
The phase 3 parent trials compared 30 mcg once weekly of intramuscular interferon beta-1a to 0.92 mg of once-daily oral ozanimod and 0.46 mg of once-daily oral ozanimod. In the DAYBREAK open-label extension, 2,256 participants underwent a dose escalation over 1 week until all reached 0.92 mg of ozanimod, where they remained for approximately 5 years of follow-up. The researchers then analyzed TEAEs, serious adverse events, and TEAEs leading to discontinuation in four age categories: 18-25, 26-35, 36-49, and 50 and older.
Respiratory infections occurred more often in those aged 18-25 (10.9%) and 26-35 (6.1%) than in those 36-49 (5.8%) and 50 and older (3.4%). However, UTIs occurred most in those age 50 and older (9.2%), versus occurring in 6.6% of those 36-49, 4.3% of those aged 26-35, and 4.6% of those 18-25.
High cholesterol occurred significantly less often in those 18-25 (1.4%) and 26-35 (2%) than in those 36-49 (5%) and 50 and older (8%), and hypertension showed a similar pattern: 2% in the youngest group, 4.7% in those aged 26-35, 12.8% in those aged 36-49, and 16.7% in those aged 50 and older.
Other TEAEs that occurred more often in older patients included depression/depressive symptoms, dizziness, back pain, joint pain, osteoarthritis, and high gamma-glutamyl transferase (GGT) levels. Overall cardiac and vascular disorders and malignancies were also more common as participants’ age increased.
Bigger concerns?
The increase in malignancy risk by age surprised Shailee Shah, MD, assistant professor of neuroimmunology and neurology at Vanderbilt University Medical Center, Nashville, Tenn., who was not involved in the research. This increase in risk was “not expanded upon much in this abstract or compared to population estimates, as this may ultimately be one of the bigger concerns with long-term use of this drug,” Dr. Shah said.
She further noted that “older patients may be at higher risk of infections and multiple cardiovascular risk factors, and so if patients already have comorbid disease, I may be less inclined to use this agent and likely less so in older individuals.”
Dr. Shah said these drugs are often recommended to individuals in their 20s and 30s at time of diagnosis. “If a patient is given this drug and tolerates it and finds it efficacious, we might continue this indefinitely, so looking at how the risk profile of young patients on this drug changes over time will be important,” Dr. Shah said. “I am also concerned about the malignancy risk and would want this elaborated upon.”
Overall efficacy across age groups
Serious infections occurred at relatively similar rates across all age groups. Incidence of any serious adverse event was 27 per 1,000 people per year in the youngest group compared with 24 events in the 26-35 group, 35 events in the 36-49 group, and 62 events per 1,000 people per year in those 50 and older.
“Patients in the 50 and older age group had a numerically lower adjusted annualized relapse rate and less gadolinium-enhancing lesions and new or enlarging T2 lesions per scan and were generally more likely to be free of gadolinium-enhancing lesions or new or enlarging T2 lesions than the 25 and younger age group,” Dr. Morrow told attendees, “but we feel that that’s more in keeping with the natural history of disease. And, overall, ozanimod, regardless of the age group, showed decreasing disease activity in the inflammatory part of disease, showing with annualized relapse rate, gad-enhancing lesions, and T2 lesions.”
Older participants were substantially more likely to withdraw from the trial because of adverse events. While 8% of the youngest group and 7.6% of participants aged 26-35 withdrew because of adverse events, 24.5% of those aged 36-49 and 18.5% of those aged 50 and older withdrew because of adverse events.
Dr. Shah said it was reassuring that no new safety signals emerged, “but based on this data, you would be concerned that long-term risk of cardiovascular disease may result in more serious adverse events over a longer period of time and will need to be considered as we see people increasingly on this drug.”
The research was funded by Bristol-Myers Squibb. The authors reported a wide range of financial disclosures, including personal fees, research funding, advisory board, and speakers fees, for multiple pharmaceutical companies, including Bristol-Myers Squibb, and five authors are employees and/or shareholders of the company. Dr. Shah has served on advisory boards for Alexion, Genentech, and Horizon.
AT CMSC 2023
When could you be sued for AI malpractice? You’re likely using it now
The ways in which artificial intelligence (AI) may transform the future of medicine is making headlines across the globe. But chances are, you’re already using AI in your practice every day – you may just not realize it.
And whether you recognize the presence of AI or not, the technology could be putting you in danger of a lawsuit, legal experts say.
“For physicians, AI has also not yet drastically changed or improved the way care is provided or consumed,” said Michael LeTang, chief nursing informatics officer and vice president of risk management and patient safety at Healthcare Risk Advisors, part of TDC Group. “Consequently, it may seem like AI is not present in their work streams, but in reality, it has been utilized in health care for several years. As AI technologies continue to develop and become more sophisticated, we can expect them to play an increasingly significant role in health care.”
Today, most AI applications in health care use narrow AI, which is designed to complete a single task without human assistance, as opposed to artificial general intelligence (AGI), which pertains to human-level reasoning and problem solving across a broad spectrum. Here are some ways doctors are using AI throughout the day – sometimes being aware of its assistance, and sometimes being unaware:
- Many doctors use electronic health records (EHRs) with integrated AI that include computerized clinical decision support tools designed to reduce the risk of diagnostic error and to integrate decision-making in the medication ordering function.
- Cardiologists, pathologists, and dermatologists use AI in the interpretation of vast amounts of images, tracings, and complex patterns.
- Surgeons are using AI-enhanced surgical robotics for orthopedic surgeries, such as joint replacement and spine surgery.
- A growing number of doctors are using ChatGPT to assist in drafting prior authorization letters for insurers. Experts say more doctors are also experimenting with ChatGPT to support medical decision-making.
- Within oncology, physicians use machine learning techniques in the form of computer-aided detection systems for early breast cancer detection.
- AI algorithms are often used by health systems for workflow, staffing optimization, population management, and care coordination.
- Some systems within EHRs use AI to indicate high-risk patients.
- Physicians are using AI applications for the early recognition of sepsis, including EHR-integrated decision tools, such as the Hospital Corporation of America Healthcare’s Sepsis Prediction and Optimization Therapy and the Sepsis Early Risk Assessment algorithm.
- About 30% of radiologists use AI in their practice to analyze x-rays and CT scans.
- Epic Systems recently announced a partnership with Microsoft to integrate ChatGPT into MyChart, Epic’s patient portal system. Pilot hospitals will utilize ChatGPT to automatically generate responses to patient-generated questions sent via the portal.
The growth of AI in health care has been enormous, and it’s only going to continue, said Ravi B. Parikh, MD, an assistant professor in the department of medical ethics and health policy and medicine at the University of Pennsylvania, Philadelphia.
“What’s really critical is that physicians, clinicians, and nurses using AI are provided with the tools to understand how artificial intelligence works and, most importantly, understand that they are still accountable for making the ultimate decision,” Mr. LeTang said, “The information is not always going to be the right thing to do or the most accurate thing to do. They’re still liable for making a bad decision, even if AI is driving that.”
What are the top AI legal dangers of today?
A pressing legal risk is becoming too reliant on the suggestions that AI-based systems provide, which can lead to poor care decisions, said Kenneth Rashbaum, a New York–based cybersecurity attorney with more than 25 years of experience in medical malpractice defense.
This can occur, for example, when using clinical support systems that leverage AI, machine learning, or statistical pattern recognition. Today, clinical support systems are commonly administered through EHRs and other computerized clinical workflows. In general, such systems match a patient’s characteristics to a computerized clinical knowledge base. An assessment or recommendation is then presented to the physician for a decision.
“If the clinician blindly accepts it without considering whether it’s appropriate for this patient at this time with this presentation, the clinician may bear some responsibility if there is an untoward result,” Mr. Rashbaum said.
“A common claim even in the days before the EMR [electronic medical record] and AI, was that the clinician did not take all available information into account in rendering treatment, including history of past and present condition, as reflected in the records, communication with past and other present treating clinicians, lab and radiology results, discussions with the patient, and physical examination findings,” he said. “So, if the clinician relied upon the support prompt to the exclusion of these other sources of information, that could be a very strong argument for the plaintiff.”
Chatbots, such OpenAI’s ChatGPT, are another form of AI raising legal red flags. ChatGPT, trained on a massive set of text data, can carry out conversations, write code, draft emails, and answer any question posed. The chatbot has gained considerable credibility for accurately diagnosing rare conditions in seconds, and it recently passed the U.S. Medical Licensing Examination.
It’s unclear how many doctors are signing onto the ChatGPT website daily, but physicians are actively using the chatbot, particularly for assistance with prior authorization letters and to support decision-making processes in their practices, said Mr. LeTang.
When physicians ask ChatGPT a question, however, they should be mindful that ChatGPT could “hallucinate,” a term that refers to a generated response that sounds plausible but is factually incorrect or is unrelated to the context, explains Harvey Castro, MD, an emergency physician, ChatGPT health care expert, and author of the 2023 book “ChatGPT and Healthcare: Unlocking the Potential of Patient Empowerment.”
Acting on ChatGPT’s response without vetting the information places doctors at serious risk of a lawsuit, he said.
“Sometimes, the response is half true and half false,” he said. “Say, I go outside my specialty of emergency medicine and ask it about a pediatric surgical procedure. It could give me a response that sounds medically correct, but then I ask a pediatric cardiologist, and he says, ‘We don’t even do this. This doesn’t even exist!’ Physicians really have to make sure they are vetting the information provided.”
In response to ChatGPT’s growing usage by health care professionals, hospitals and practices are quickly implementing guidelines, policies, and restrictions that caution physicians about the accuracy of ChatGPT-generated information, adds Mr. LeTang.
Emerging best practices include avoiding the input of patient health information, personally identifiable information, or any data that could be commercially valuable or considered the intellectual property of a hospital or health system, he said.
“Another crucial guideline is not to rely solely on ChatGPT as a definitive source for clinical decision-making; physicians must exercise their professional judgment,” he said. “If best practices are not adhered to, the associated risks are present today. However, these risks may become more significant as AI technologies continue to evolve and become increasingly integrated into health care.”
The potential for misdiagnosis by AI systems and the risk of unnecessary procedures if physicians do not thoroughly evaluate and validate AI predictions are other dangers.
As an example, Mr. LeTang described a case in which a physician documents in the EHR that a patient has presented to the emergency department with chest pains and other signs of a heart attack, and an AI algorithm predicts that the patient is experiencing an active myocardial infarction. If the physician then sends the patient for stenting or an angioplasty without other concrete evidence or tests to confirm the diagnosis, the doctor could later face a misdiagnosis complaint if the costly procedures were unnecessary.
“That’s one of the risks of using artificial intelligence,” he said. “A large percentage of malpractice claims is failure to diagnose, delayed diagnosis, or inaccurate diagnosis. What falls in the category of failure to diagnose is sending a patient for an unnecessary procedure or having an adverse event or bad outcome because of the failure to diagnose.”
So far, no AI lawsuits have been filed, but they may make an appearance soon, said Sue Boisvert, senior patient safety risk manager at The Doctors Company, a national medical liability insurer.
“There are hundreds of AI programs currently in use in health care,” she said. “At some point, a provider will make a decision that is contrary to what the AI recommended. The AI may be wrong, or the provider may be wrong. Either way, the provider will neglect to document their clinical reasoning, a patient will be harmed, and we will have the first AI claim.”
Upcoming AI legal risks to watch for
Lawsuits that allege biased patient care by physicians on the basis of algorithmic bias may also be forthcoming, analysts warn.
Much has been written about algorithmic bias that compounds and worsens inequities in socioeconomic status, ethnicity, sexual orientation, and gender in health systems. In 2019, a groundbreaking article in Science shed light on commonly used algorithms that are considered racially biased and how health care professionals often use such information to make medical decisions.
No claims involving AI bias have come down the pipeline yet, but it’s an area to watch, said Ms. Boisvert. She noted a website that highlights complaints and accusations of AI bias, including in health care.
“We need to be sure the training of the AI is appropriate, current, and broad enough so that there is no bias in the AI when it’s participating in the decision-making,” said Ms. Boisvert. “Imagine if the AI is diagnosing based on a dataset that is not local. It doesn’t represent the population at that particular hospital, and it’s providing inaccurate information to the physicians who are then making decisions about treatment.”
In pain management, for example, there are known differences in how patients experience pain, Ms. Boisvert said. If AI was being used to develop an algorithm for how a particular patient’s postoperative pain should be managed, and the algorithm did not include the differences, the pain control for a certain patient could be inappropriate. A poor outcome resulting from the treatment could lead to a claim against the physician or hospital that used the biased AI system, she said.
In the future, as AI becomes more integrated and accepted in medicine, there may be a risk of legal complaints against doctors for not using AI, said Saurabh Jha, MD, an associate professor of radiology at the University of Pennsylvania, Philadelphia, and a scholar of AI in radiology.
“Ultimately, we might get to a place where AI starts helping physicians detect more or reduce the miss of certain conditions, and it becomes the standard of care,” Dr. Jha said. “For example, if it became part of the standard of care for pulmonary embolism [PE] detection, and you didn’t use it for PE detection, and there was a miss. That could put you at legal risk. We’re not at that stage yet, but that is one future possibility.”
Dr. Parikh envisions an even cloudier liability landscape as the potential grows for AI to control patient care decisions. In such a scenario, rather than just issuing an alert or prediction to a physician, the AI system could trigger an action.
For instance, if an algorithm is trained to predict sepsis and, once triggered, the AI could initiate a nurse-led rapid response or a change in patient care outside the clinician’s control, said Dr. Parikh, who coauthored a recent article on AI and medical liability in The Milbank Quarterly.
“That’s still very much the minority of how AI is being used, but as evidence is growing that AI-based diagnostic tools perform equivalent or even superior to physicians, these autonomous workflows are being considered,” Dr. Parikh said. “When the ultimate action upon the patient is more determined by the AI than what the clinician does, then I think the liability picture gets murkier, and we should be thinking about how we can respond to that from a liability framework.”
How you can prevent AI-related lawsuits
The first step to preventing an AI-related claim is being aware of when and how you are using AI.
Ensure you’re informed about how the AI was trained, Ms. Boisvert stresses.
“Ask questions!” she said. “Is the AI safe? Are the recommendations accurate? Does the AI perform better than current systems? In what way? What databases were used, and did the programmers consider bias? Do I understand how to use the results?”
Never blindly trust the AI but rather view it as a data point in a medical decision, said Dr. Parikh. Ensure that other sources of medical information are properly accessed and that best practices for your specialty are still being followed.
When using any form of AI, document your usage, adds Mr. Rashbaum. A record that clearly outlines how the physician incorporated the AI is critical if a claim later arises in which the doctor is accused of AI-related malpractice, he said.
“Indicating how the AI tool was used, why it was used, and that it was used in conjunction with available clinical information and the clinician’s best judgment could reduce the risk of being found responsible as a result of AI use in a particular case,” he said.
Use chatbots, such as ChatGPT, the way they were intended, as support tools, rather than definitive diagnostic instruments, adds Dr. Castro.
“Doctors should also be well-trained in interpreting and understanding the suggestions provided by ChatGPT and should use their clinical judgment and experience alongside the AI tool for more accurate decision-making,” he said.
In addition, because no AI insurance product exists on the market, physicians and organizations using AI – particularly for direct health care – should evaluate their current insurance or insurance-like products to determine where a claim involving AI might fall and whether the policy would respond, said Ms. Boisvert. The AI vendor/manufacturer will likely have indemnified themselves in the purchase and sale agreement or contract, she said.
It will also become increasingly important for medical practices, hospitals, and health systems to put in place strong data governance strategies, Mr. LeTang said.
“AI relies on good data,” he said. “A data governance strategy is a key component to making sure we understand where the data is coming from, what is represents, how accurate it is, if it’s reproducible, what controls are in place to ensure the right people have the right access, and that if we’re starting to use it to build algorithms, that it’s deidentified.”
While no malpractice claims associated with the use of AI have yet surfaced, this may change as legal courts catch up on the backlog of malpractice claims that were delayed because of COVID-19, and even more so as AI becomes more prevalent in health care, Mr. LeTang said.
“Similar to the attention that autonomous driving systems, like Tesla, receive when the system fails and accidents occur, we can be assured that media outlets will widely publicize AI-related medical adverse events,” he said. “It is crucial for health care professionals, AI developers, and regulatory authorities to work together to ensure the responsible use of AI in health care, with patient safety as the top priority. By doing so, they can mitigate the risks associated with AI implementation and minimize the potential for legal disputes arising from AI-related medical errors.”
A version of this article first appeared on Medscape.com.
The ways in which artificial intelligence (AI) may transform the future of medicine is making headlines across the globe. But chances are, you’re already using AI in your practice every day – you may just not realize it.
And whether you recognize the presence of AI or not, the technology could be putting you in danger of a lawsuit, legal experts say.
“For physicians, AI has also not yet drastically changed or improved the way care is provided or consumed,” said Michael LeTang, chief nursing informatics officer and vice president of risk management and patient safety at Healthcare Risk Advisors, part of TDC Group. “Consequently, it may seem like AI is not present in their work streams, but in reality, it has been utilized in health care for several years. As AI technologies continue to develop and become more sophisticated, we can expect them to play an increasingly significant role in health care.”
Today, most AI applications in health care use narrow AI, which is designed to complete a single task without human assistance, as opposed to artificial general intelligence (AGI), which pertains to human-level reasoning and problem solving across a broad spectrum. Here are some ways doctors are using AI throughout the day – sometimes being aware of its assistance, and sometimes being unaware:
- Many doctors use electronic health records (EHRs) with integrated AI that include computerized clinical decision support tools designed to reduce the risk of diagnostic error and to integrate decision-making in the medication ordering function.
- Cardiologists, pathologists, and dermatologists use AI in the interpretation of vast amounts of images, tracings, and complex patterns.
- Surgeons are using AI-enhanced surgical robotics for orthopedic surgeries, such as joint replacement and spine surgery.
- A growing number of doctors are using ChatGPT to assist in drafting prior authorization letters for insurers. Experts say more doctors are also experimenting with ChatGPT to support medical decision-making.
- Within oncology, physicians use machine learning techniques in the form of computer-aided detection systems for early breast cancer detection.
- AI algorithms are often used by health systems for workflow, staffing optimization, population management, and care coordination.
- Some systems within EHRs use AI to indicate high-risk patients.
- Physicians are using AI applications for the early recognition of sepsis, including EHR-integrated decision tools, such as the Hospital Corporation of America Healthcare’s Sepsis Prediction and Optimization Therapy and the Sepsis Early Risk Assessment algorithm.
- About 30% of radiologists use AI in their practice to analyze x-rays and CT scans.
- Epic Systems recently announced a partnership with Microsoft to integrate ChatGPT into MyChart, Epic’s patient portal system. Pilot hospitals will utilize ChatGPT to automatically generate responses to patient-generated questions sent via the portal.
The growth of AI in health care has been enormous, and it’s only going to continue, said Ravi B. Parikh, MD, an assistant professor in the department of medical ethics and health policy and medicine at the University of Pennsylvania, Philadelphia.
“What’s really critical is that physicians, clinicians, and nurses using AI are provided with the tools to understand how artificial intelligence works and, most importantly, understand that they are still accountable for making the ultimate decision,” Mr. LeTang said, “The information is not always going to be the right thing to do or the most accurate thing to do. They’re still liable for making a bad decision, even if AI is driving that.”
What are the top AI legal dangers of today?
A pressing legal risk is becoming too reliant on the suggestions that AI-based systems provide, which can lead to poor care decisions, said Kenneth Rashbaum, a New York–based cybersecurity attorney with more than 25 years of experience in medical malpractice defense.
This can occur, for example, when using clinical support systems that leverage AI, machine learning, or statistical pattern recognition. Today, clinical support systems are commonly administered through EHRs and other computerized clinical workflows. In general, such systems match a patient’s characteristics to a computerized clinical knowledge base. An assessment or recommendation is then presented to the physician for a decision.
“If the clinician blindly accepts it without considering whether it’s appropriate for this patient at this time with this presentation, the clinician may bear some responsibility if there is an untoward result,” Mr. Rashbaum said.
“A common claim even in the days before the EMR [electronic medical record] and AI, was that the clinician did not take all available information into account in rendering treatment, including history of past and present condition, as reflected in the records, communication with past and other present treating clinicians, lab and radiology results, discussions with the patient, and physical examination findings,” he said. “So, if the clinician relied upon the support prompt to the exclusion of these other sources of information, that could be a very strong argument for the plaintiff.”
Chatbots, such OpenAI’s ChatGPT, are another form of AI raising legal red flags. ChatGPT, trained on a massive set of text data, can carry out conversations, write code, draft emails, and answer any question posed. The chatbot has gained considerable credibility for accurately diagnosing rare conditions in seconds, and it recently passed the U.S. Medical Licensing Examination.
It’s unclear how many doctors are signing onto the ChatGPT website daily, but physicians are actively using the chatbot, particularly for assistance with prior authorization letters and to support decision-making processes in their practices, said Mr. LeTang.
When physicians ask ChatGPT a question, however, they should be mindful that ChatGPT could “hallucinate,” a term that refers to a generated response that sounds plausible but is factually incorrect or is unrelated to the context, explains Harvey Castro, MD, an emergency physician, ChatGPT health care expert, and author of the 2023 book “ChatGPT and Healthcare: Unlocking the Potential of Patient Empowerment.”
Acting on ChatGPT’s response without vetting the information places doctors at serious risk of a lawsuit, he said.
“Sometimes, the response is half true and half false,” he said. “Say, I go outside my specialty of emergency medicine and ask it about a pediatric surgical procedure. It could give me a response that sounds medically correct, but then I ask a pediatric cardiologist, and he says, ‘We don’t even do this. This doesn’t even exist!’ Physicians really have to make sure they are vetting the information provided.”
In response to ChatGPT’s growing usage by health care professionals, hospitals and practices are quickly implementing guidelines, policies, and restrictions that caution physicians about the accuracy of ChatGPT-generated information, adds Mr. LeTang.
Emerging best practices include avoiding the input of patient health information, personally identifiable information, or any data that could be commercially valuable or considered the intellectual property of a hospital or health system, he said.
“Another crucial guideline is not to rely solely on ChatGPT as a definitive source for clinical decision-making; physicians must exercise their professional judgment,” he said. “If best practices are not adhered to, the associated risks are present today. However, these risks may become more significant as AI technologies continue to evolve and become increasingly integrated into health care.”
The potential for misdiagnosis by AI systems and the risk of unnecessary procedures if physicians do not thoroughly evaluate and validate AI predictions are other dangers.
As an example, Mr. LeTang described a case in which a physician documents in the EHR that a patient has presented to the emergency department with chest pains and other signs of a heart attack, and an AI algorithm predicts that the patient is experiencing an active myocardial infarction. If the physician then sends the patient for stenting or an angioplasty without other concrete evidence or tests to confirm the diagnosis, the doctor could later face a misdiagnosis complaint if the costly procedures were unnecessary.
“That’s one of the risks of using artificial intelligence,” he said. “A large percentage of malpractice claims is failure to diagnose, delayed diagnosis, or inaccurate diagnosis. What falls in the category of failure to diagnose is sending a patient for an unnecessary procedure or having an adverse event or bad outcome because of the failure to diagnose.”
So far, no AI lawsuits have been filed, but they may make an appearance soon, said Sue Boisvert, senior patient safety risk manager at The Doctors Company, a national medical liability insurer.
“There are hundreds of AI programs currently in use in health care,” she said. “At some point, a provider will make a decision that is contrary to what the AI recommended. The AI may be wrong, or the provider may be wrong. Either way, the provider will neglect to document their clinical reasoning, a patient will be harmed, and we will have the first AI claim.”
Upcoming AI legal risks to watch for
Lawsuits that allege biased patient care by physicians on the basis of algorithmic bias may also be forthcoming, analysts warn.
Much has been written about algorithmic bias that compounds and worsens inequities in socioeconomic status, ethnicity, sexual orientation, and gender in health systems. In 2019, a groundbreaking article in Science shed light on commonly used algorithms that are considered racially biased and how health care professionals often use such information to make medical decisions.
No claims involving AI bias have come down the pipeline yet, but it’s an area to watch, said Ms. Boisvert. She noted a website that highlights complaints and accusations of AI bias, including in health care.
“We need to be sure the training of the AI is appropriate, current, and broad enough so that there is no bias in the AI when it’s participating in the decision-making,” said Ms. Boisvert. “Imagine if the AI is diagnosing based on a dataset that is not local. It doesn’t represent the population at that particular hospital, and it’s providing inaccurate information to the physicians who are then making decisions about treatment.”
In pain management, for example, there are known differences in how patients experience pain, Ms. Boisvert said. If AI was being used to develop an algorithm for how a particular patient’s postoperative pain should be managed, and the algorithm did not include the differences, the pain control for a certain patient could be inappropriate. A poor outcome resulting from the treatment could lead to a claim against the physician or hospital that used the biased AI system, she said.
In the future, as AI becomes more integrated and accepted in medicine, there may be a risk of legal complaints against doctors for not using AI, said Saurabh Jha, MD, an associate professor of radiology at the University of Pennsylvania, Philadelphia, and a scholar of AI in radiology.
“Ultimately, we might get to a place where AI starts helping physicians detect more or reduce the miss of certain conditions, and it becomes the standard of care,” Dr. Jha said. “For example, if it became part of the standard of care for pulmonary embolism [PE] detection, and you didn’t use it for PE detection, and there was a miss. That could put you at legal risk. We’re not at that stage yet, but that is one future possibility.”
Dr. Parikh envisions an even cloudier liability landscape as the potential grows for AI to control patient care decisions. In such a scenario, rather than just issuing an alert or prediction to a physician, the AI system could trigger an action.
For instance, if an algorithm is trained to predict sepsis and, once triggered, the AI could initiate a nurse-led rapid response or a change in patient care outside the clinician’s control, said Dr. Parikh, who coauthored a recent article on AI and medical liability in The Milbank Quarterly.
“That’s still very much the minority of how AI is being used, but as evidence is growing that AI-based diagnostic tools perform equivalent or even superior to physicians, these autonomous workflows are being considered,” Dr. Parikh said. “When the ultimate action upon the patient is more determined by the AI than what the clinician does, then I think the liability picture gets murkier, and we should be thinking about how we can respond to that from a liability framework.”
How you can prevent AI-related lawsuits
The first step to preventing an AI-related claim is being aware of when and how you are using AI.
Ensure you’re informed about how the AI was trained, Ms. Boisvert stresses.
“Ask questions!” she said. “Is the AI safe? Are the recommendations accurate? Does the AI perform better than current systems? In what way? What databases were used, and did the programmers consider bias? Do I understand how to use the results?”
Never blindly trust the AI but rather view it as a data point in a medical decision, said Dr. Parikh. Ensure that other sources of medical information are properly accessed and that best practices for your specialty are still being followed.
When using any form of AI, document your usage, adds Mr. Rashbaum. A record that clearly outlines how the physician incorporated the AI is critical if a claim later arises in which the doctor is accused of AI-related malpractice, he said.
“Indicating how the AI tool was used, why it was used, and that it was used in conjunction with available clinical information and the clinician’s best judgment could reduce the risk of being found responsible as a result of AI use in a particular case,” he said.
Use chatbots, such as ChatGPT, the way they were intended, as support tools, rather than definitive diagnostic instruments, adds Dr. Castro.
“Doctors should also be well-trained in interpreting and understanding the suggestions provided by ChatGPT and should use their clinical judgment and experience alongside the AI tool for more accurate decision-making,” he said.
In addition, because no AI insurance product exists on the market, physicians and organizations using AI – particularly for direct health care – should evaluate their current insurance or insurance-like products to determine where a claim involving AI might fall and whether the policy would respond, said Ms. Boisvert. The AI vendor/manufacturer will likely have indemnified themselves in the purchase and sale agreement or contract, she said.
It will also become increasingly important for medical practices, hospitals, and health systems to put in place strong data governance strategies, Mr. LeTang said.
“AI relies on good data,” he said. “A data governance strategy is a key component to making sure we understand where the data is coming from, what is represents, how accurate it is, if it’s reproducible, what controls are in place to ensure the right people have the right access, and that if we’re starting to use it to build algorithms, that it’s deidentified.”
While no malpractice claims associated with the use of AI have yet surfaced, this may change as legal courts catch up on the backlog of malpractice claims that were delayed because of COVID-19, and even more so as AI becomes more prevalent in health care, Mr. LeTang said.
“Similar to the attention that autonomous driving systems, like Tesla, receive when the system fails and accidents occur, we can be assured that media outlets will widely publicize AI-related medical adverse events,” he said. “It is crucial for health care professionals, AI developers, and regulatory authorities to work together to ensure the responsible use of AI in health care, with patient safety as the top priority. By doing so, they can mitigate the risks associated with AI implementation and minimize the potential for legal disputes arising from AI-related medical errors.”
A version of this article first appeared on Medscape.com.
The ways in which artificial intelligence (AI) may transform the future of medicine is making headlines across the globe. But chances are, you’re already using AI in your practice every day – you may just not realize it.
And whether you recognize the presence of AI or not, the technology could be putting you in danger of a lawsuit, legal experts say.
“For physicians, AI has also not yet drastically changed or improved the way care is provided or consumed,” said Michael LeTang, chief nursing informatics officer and vice president of risk management and patient safety at Healthcare Risk Advisors, part of TDC Group. “Consequently, it may seem like AI is not present in their work streams, but in reality, it has been utilized in health care for several years. As AI technologies continue to develop and become more sophisticated, we can expect them to play an increasingly significant role in health care.”
Today, most AI applications in health care use narrow AI, which is designed to complete a single task without human assistance, as opposed to artificial general intelligence (AGI), which pertains to human-level reasoning and problem solving across a broad spectrum. Here are some ways doctors are using AI throughout the day – sometimes being aware of its assistance, and sometimes being unaware:
- Many doctors use electronic health records (EHRs) with integrated AI that include computerized clinical decision support tools designed to reduce the risk of diagnostic error and to integrate decision-making in the medication ordering function.
- Cardiologists, pathologists, and dermatologists use AI in the interpretation of vast amounts of images, tracings, and complex patterns.
- Surgeons are using AI-enhanced surgical robotics for orthopedic surgeries, such as joint replacement and spine surgery.
- A growing number of doctors are using ChatGPT to assist in drafting prior authorization letters for insurers. Experts say more doctors are also experimenting with ChatGPT to support medical decision-making.
- Within oncology, physicians use machine learning techniques in the form of computer-aided detection systems for early breast cancer detection.
- AI algorithms are often used by health systems for workflow, staffing optimization, population management, and care coordination.
- Some systems within EHRs use AI to indicate high-risk patients.
- Physicians are using AI applications for the early recognition of sepsis, including EHR-integrated decision tools, such as the Hospital Corporation of America Healthcare’s Sepsis Prediction and Optimization Therapy and the Sepsis Early Risk Assessment algorithm.
- About 30% of radiologists use AI in their practice to analyze x-rays and CT scans.
- Epic Systems recently announced a partnership with Microsoft to integrate ChatGPT into MyChart, Epic’s patient portal system. Pilot hospitals will utilize ChatGPT to automatically generate responses to patient-generated questions sent via the portal.
The growth of AI in health care has been enormous, and it’s only going to continue, said Ravi B. Parikh, MD, an assistant professor in the department of medical ethics and health policy and medicine at the University of Pennsylvania, Philadelphia.
“What’s really critical is that physicians, clinicians, and nurses using AI are provided with the tools to understand how artificial intelligence works and, most importantly, understand that they are still accountable for making the ultimate decision,” Mr. LeTang said, “The information is not always going to be the right thing to do or the most accurate thing to do. They’re still liable for making a bad decision, even if AI is driving that.”
What are the top AI legal dangers of today?
A pressing legal risk is becoming too reliant on the suggestions that AI-based systems provide, which can lead to poor care decisions, said Kenneth Rashbaum, a New York–based cybersecurity attorney with more than 25 years of experience in medical malpractice defense.
This can occur, for example, when using clinical support systems that leverage AI, machine learning, or statistical pattern recognition. Today, clinical support systems are commonly administered through EHRs and other computerized clinical workflows. In general, such systems match a patient’s characteristics to a computerized clinical knowledge base. An assessment or recommendation is then presented to the physician for a decision.
“If the clinician blindly accepts it without considering whether it’s appropriate for this patient at this time with this presentation, the clinician may bear some responsibility if there is an untoward result,” Mr. Rashbaum said.
“A common claim even in the days before the EMR [electronic medical record] and AI, was that the clinician did not take all available information into account in rendering treatment, including history of past and present condition, as reflected in the records, communication with past and other present treating clinicians, lab and radiology results, discussions with the patient, and physical examination findings,” he said. “So, if the clinician relied upon the support prompt to the exclusion of these other sources of information, that could be a very strong argument for the plaintiff.”
Chatbots, such OpenAI’s ChatGPT, are another form of AI raising legal red flags. ChatGPT, trained on a massive set of text data, can carry out conversations, write code, draft emails, and answer any question posed. The chatbot has gained considerable credibility for accurately diagnosing rare conditions in seconds, and it recently passed the U.S. Medical Licensing Examination.
It’s unclear how many doctors are signing onto the ChatGPT website daily, but physicians are actively using the chatbot, particularly for assistance with prior authorization letters and to support decision-making processes in their practices, said Mr. LeTang.
When physicians ask ChatGPT a question, however, they should be mindful that ChatGPT could “hallucinate,” a term that refers to a generated response that sounds plausible but is factually incorrect or is unrelated to the context, explains Harvey Castro, MD, an emergency physician, ChatGPT health care expert, and author of the 2023 book “ChatGPT and Healthcare: Unlocking the Potential of Patient Empowerment.”
Acting on ChatGPT’s response without vetting the information places doctors at serious risk of a lawsuit, he said.
“Sometimes, the response is half true and half false,” he said. “Say, I go outside my specialty of emergency medicine and ask it about a pediatric surgical procedure. It could give me a response that sounds medically correct, but then I ask a pediatric cardiologist, and he says, ‘We don’t even do this. This doesn’t even exist!’ Physicians really have to make sure they are vetting the information provided.”
In response to ChatGPT’s growing usage by health care professionals, hospitals and practices are quickly implementing guidelines, policies, and restrictions that caution physicians about the accuracy of ChatGPT-generated information, adds Mr. LeTang.
Emerging best practices include avoiding the input of patient health information, personally identifiable information, or any data that could be commercially valuable or considered the intellectual property of a hospital or health system, he said.
“Another crucial guideline is not to rely solely on ChatGPT as a definitive source for clinical decision-making; physicians must exercise their professional judgment,” he said. “If best practices are not adhered to, the associated risks are present today. However, these risks may become more significant as AI technologies continue to evolve and become increasingly integrated into health care.”
The potential for misdiagnosis by AI systems and the risk of unnecessary procedures if physicians do not thoroughly evaluate and validate AI predictions are other dangers.
As an example, Mr. LeTang described a case in which a physician documents in the EHR that a patient has presented to the emergency department with chest pains and other signs of a heart attack, and an AI algorithm predicts that the patient is experiencing an active myocardial infarction. If the physician then sends the patient for stenting or an angioplasty without other concrete evidence or tests to confirm the diagnosis, the doctor could later face a misdiagnosis complaint if the costly procedures were unnecessary.
“That’s one of the risks of using artificial intelligence,” he said. “A large percentage of malpractice claims is failure to diagnose, delayed diagnosis, or inaccurate diagnosis. What falls in the category of failure to diagnose is sending a patient for an unnecessary procedure or having an adverse event or bad outcome because of the failure to diagnose.”
So far, no AI lawsuits have been filed, but they may make an appearance soon, said Sue Boisvert, senior patient safety risk manager at The Doctors Company, a national medical liability insurer.
“There are hundreds of AI programs currently in use in health care,” she said. “At some point, a provider will make a decision that is contrary to what the AI recommended. The AI may be wrong, or the provider may be wrong. Either way, the provider will neglect to document their clinical reasoning, a patient will be harmed, and we will have the first AI claim.”
Upcoming AI legal risks to watch for
Lawsuits that allege biased patient care by physicians on the basis of algorithmic bias may also be forthcoming, analysts warn.
Much has been written about algorithmic bias that compounds and worsens inequities in socioeconomic status, ethnicity, sexual orientation, and gender in health systems. In 2019, a groundbreaking article in Science shed light on commonly used algorithms that are considered racially biased and how health care professionals often use such information to make medical decisions.
No claims involving AI bias have come down the pipeline yet, but it’s an area to watch, said Ms. Boisvert. She noted a website that highlights complaints and accusations of AI bias, including in health care.
“We need to be sure the training of the AI is appropriate, current, and broad enough so that there is no bias in the AI when it’s participating in the decision-making,” said Ms. Boisvert. “Imagine if the AI is diagnosing based on a dataset that is not local. It doesn’t represent the population at that particular hospital, and it’s providing inaccurate information to the physicians who are then making decisions about treatment.”
In pain management, for example, there are known differences in how patients experience pain, Ms. Boisvert said. If AI was being used to develop an algorithm for how a particular patient’s postoperative pain should be managed, and the algorithm did not include the differences, the pain control for a certain patient could be inappropriate. A poor outcome resulting from the treatment could lead to a claim against the physician or hospital that used the biased AI system, she said.
In the future, as AI becomes more integrated and accepted in medicine, there may be a risk of legal complaints against doctors for not using AI, said Saurabh Jha, MD, an associate professor of radiology at the University of Pennsylvania, Philadelphia, and a scholar of AI in radiology.
“Ultimately, we might get to a place where AI starts helping physicians detect more or reduce the miss of certain conditions, and it becomes the standard of care,” Dr. Jha said. “For example, if it became part of the standard of care for pulmonary embolism [PE] detection, and you didn’t use it for PE detection, and there was a miss. That could put you at legal risk. We’re not at that stage yet, but that is one future possibility.”
Dr. Parikh envisions an even cloudier liability landscape as the potential grows for AI to control patient care decisions. In such a scenario, rather than just issuing an alert or prediction to a physician, the AI system could trigger an action.
For instance, if an algorithm is trained to predict sepsis and, once triggered, the AI could initiate a nurse-led rapid response or a change in patient care outside the clinician’s control, said Dr. Parikh, who coauthored a recent article on AI and medical liability in The Milbank Quarterly.
“That’s still very much the minority of how AI is being used, but as evidence is growing that AI-based diagnostic tools perform equivalent or even superior to physicians, these autonomous workflows are being considered,” Dr. Parikh said. “When the ultimate action upon the patient is more determined by the AI than what the clinician does, then I think the liability picture gets murkier, and we should be thinking about how we can respond to that from a liability framework.”
How you can prevent AI-related lawsuits
The first step to preventing an AI-related claim is being aware of when and how you are using AI.
Ensure you’re informed about how the AI was trained, Ms. Boisvert stresses.
“Ask questions!” she said. “Is the AI safe? Are the recommendations accurate? Does the AI perform better than current systems? In what way? What databases were used, and did the programmers consider bias? Do I understand how to use the results?”
Never blindly trust the AI but rather view it as a data point in a medical decision, said Dr. Parikh. Ensure that other sources of medical information are properly accessed and that best practices for your specialty are still being followed.
When using any form of AI, document your usage, adds Mr. Rashbaum. A record that clearly outlines how the physician incorporated the AI is critical if a claim later arises in which the doctor is accused of AI-related malpractice, he said.
“Indicating how the AI tool was used, why it was used, and that it was used in conjunction with available clinical information and the clinician’s best judgment could reduce the risk of being found responsible as a result of AI use in a particular case,” he said.
Use chatbots, such as ChatGPT, the way they were intended, as support tools, rather than definitive diagnostic instruments, adds Dr. Castro.
“Doctors should also be well-trained in interpreting and understanding the suggestions provided by ChatGPT and should use their clinical judgment and experience alongside the AI tool for more accurate decision-making,” he said.
In addition, because no AI insurance product exists on the market, physicians and organizations using AI – particularly for direct health care – should evaluate their current insurance or insurance-like products to determine where a claim involving AI might fall and whether the policy would respond, said Ms. Boisvert. The AI vendor/manufacturer will likely have indemnified themselves in the purchase and sale agreement or contract, she said.
It will also become increasingly important for medical practices, hospitals, and health systems to put in place strong data governance strategies, Mr. LeTang said.
“AI relies on good data,” he said. “A data governance strategy is a key component to making sure we understand where the data is coming from, what is represents, how accurate it is, if it’s reproducible, what controls are in place to ensure the right people have the right access, and that if we’re starting to use it to build algorithms, that it’s deidentified.”
While no malpractice claims associated with the use of AI have yet surfaced, this may change as legal courts catch up on the backlog of malpractice claims that were delayed because of COVID-19, and even more so as AI becomes more prevalent in health care, Mr. LeTang said.
“Similar to the attention that autonomous driving systems, like Tesla, receive when the system fails and accidents occur, we can be assured that media outlets will widely publicize AI-related medical adverse events,” he said. “It is crucial for health care professionals, AI developers, and regulatory authorities to work together to ensure the responsible use of AI in health care, with patient safety as the top priority. By doing so, they can mitigate the risks associated with AI implementation and minimize the potential for legal disputes arising from AI-related medical errors.”
A version of this article first appeared on Medscape.com.
Blood biomarker may help predict who will develop Alzheimer’s
A blood biomarker that measures astrocyte reactivity may help determine who, among cognitively unimpaired older adults with amyloid-beta, will go on to develop Alzheimer’s disease (AD), new research suggests.
Investigators tested the blood of 1,000 cognitively healthy individuals with and without amyloid-beta pathology and found that only those with a combination of amyloid-beta burden and abnormal astrocyte activation subsequently progressed to AD.
“Our study argues that testing for the presence of brain amyloid along with blood biomarkers of astrocyte reactivity is the optimal screening to identify patients who are most at risk for progressing to Alzheimer’s disease,” senior investigator Tharick A. Pascoal, MD, PhD, associate professor of psychiatry and neurology, University of Pittsburgh, said in a release.
At this point, the biomarker is a research tool, but its application in clinical practice “is not very far away,” Dr. Pascoal told this news organization.
The study was published online in Nature Medicine.
Multicenter study
In AD, accumulation of amyloid-beta in the brain precedes tau pathology, but not everyone with amyloid-beta develops tau, and, consequently, clinical symptoms. Approximately 30% of older adults have brain amyloid but many never progress to AD, said Dr. Pascoal.
This suggests other biological processes may trigger the deleterious effects of amyloid-beta in the early stages of AD.
Finding predictive markers of early amyloid-beta–related tau pathology would help identify cognitively normal individuals who are more likely to develop AD.
Post-mortem studies show astrocyte reactivity – changes in glial cells in the brain and spinal cord because of an insult in the brain – is an early AD abnormality. Other research suggests a close link between amyloid-beta, astrocyte reactivity, and tau.
In addition, evidence suggests plasma measures of glial fibrillary acidic protein (GFAP) could be a strong proxy of astrocyte reactivity in the brain. Dr. Pascoal explained that when astrocytes are changed or become bigger, more GFAP is released.
The study included 1,016 cognitively normal individuals from three centers; some had amyloid pathology, some did not. Participants’ mean age was 69.6 years, and all were deemed negative or positive for astrocyte reactivity based on plasma GFAP levels.
Results showed amyloid-beta is associated with increased plasma phosphorylated tau only in individuals positive for astrocyte reactivity. In addition, analyses using PET scans showed an AD-like pattern of tau tangle accumulation as a function of amyloid-beta exclusively in those same individuals.
Early upstream event
The findings suggest abnormalities in astrocyte reactivity is an early upstream event that likely occurs prior to tau pathology, which is closely related to the development of neurodegeneration and cognitive decline.
It’s likely many types of insults or processes can lead to astrocyte reactivity, possibly including COVID, but more research in this area is needed, said Dr. Pascoal.
“Our study only looked at the consequence of having both amyloid and astrocyte reactivity; it did not elucidate what is causing either of them,” he said.
Although “we were able to have very good results” in the current study, additional studies are needed to better establish the cut-off for GFAP levels that signal progression, said Dr. Pascoal.
The effect of astrocyte reactivity on the association between amyloid-beta and tau phosphorylation was greater in men than women. Dr. Pascoal noted anti-amyloid therapies, which might be modifying the amyloid-beta-astrocyte-tau pathway, tend to have a much larger effect in men than women.
Further studies that measure amyloid-beta, tau, and GFAP biomarkers at multiple timepoints, and with long follow-up, are needed, the investigators note.
The results may have implications for clinical trials, which have increasingly focused on individuals in the earliest preclinical phases of AD. Future studies should include cognitively normal patients who are positive for both amyloid pathology and astrocyte reactivity but have no overt p-tau abnormality, said Dr. Pascoal.
This may provide a time window for interventions very early in the disease process in those at increased risk for AD-related progression.
The study did not determine whether participants with both amyloid and astrocyte reactivity will inevitably develop AD, and to do so would require a longer follow up. “Our outcome was correlation to tau in the brain, which is something we know will lead to AD.”
Although the cohort represents significant socioeconomic diversity, a main limitation of the study was that subjects were mainly White, which limits the generalizability of the findings to a more diverse population.
The study received support from the National Institute of Aging; National Heart Lung and Blood Institute; Alzheimer’s Association; Fonds de Recherche du Québec-Santé; Canadian Consortium of Neurodegeneration in Aging; Weston Brain Institute; Colin Adair Charitable Foundation; Swedish Research Council; Wallenberg Scholar; BrightFocus Foundation; Swedish Alzheimer Foundation; Swedish Brain Foundation; Agneta Prytz-Folkes & Gösta Folkes Foundation; European Union; Swedish State Support for Clinical Research; Alzheimer Drug Discovery Foundation; Bluefield Project, the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden; the UK Dementia Research Institute at UCL; National Academy of Neuropsychology; Fundação de Amparo a pesquisa do Rio Grande do Sul; Instituto Serrapilheira; and Hjärnfonden.
Dr. Pascoal reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A blood biomarker that measures astrocyte reactivity may help determine who, among cognitively unimpaired older adults with amyloid-beta, will go on to develop Alzheimer’s disease (AD), new research suggests.
Investigators tested the blood of 1,000 cognitively healthy individuals with and without amyloid-beta pathology and found that only those with a combination of amyloid-beta burden and abnormal astrocyte activation subsequently progressed to AD.
“Our study argues that testing for the presence of brain amyloid along with blood biomarkers of astrocyte reactivity is the optimal screening to identify patients who are most at risk for progressing to Alzheimer’s disease,” senior investigator Tharick A. Pascoal, MD, PhD, associate professor of psychiatry and neurology, University of Pittsburgh, said in a release.
At this point, the biomarker is a research tool, but its application in clinical practice “is not very far away,” Dr. Pascoal told this news organization.
The study was published online in Nature Medicine.
Multicenter study
In AD, accumulation of amyloid-beta in the brain precedes tau pathology, but not everyone with amyloid-beta develops tau, and, consequently, clinical symptoms. Approximately 30% of older adults have brain amyloid but many never progress to AD, said Dr. Pascoal.
This suggests other biological processes may trigger the deleterious effects of amyloid-beta in the early stages of AD.
Finding predictive markers of early amyloid-beta–related tau pathology would help identify cognitively normal individuals who are more likely to develop AD.
Post-mortem studies show astrocyte reactivity – changes in glial cells in the brain and spinal cord because of an insult in the brain – is an early AD abnormality. Other research suggests a close link between amyloid-beta, astrocyte reactivity, and tau.
In addition, evidence suggests plasma measures of glial fibrillary acidic protein (GFAP) could be a strong proxy of astrocyte reactivity in the brain. Dr. Pascoal explained that when astrocytes are changed or become bigger, more GFAP is released.
The study included 1,016 cognitively normal individuals from three centers; some had amyloid pathology, some did not. Participants’ mean age was 69.6 years, and all were deemed negative or positive for astrocyte reactivity based on plasma GFAP levels.
Results showed amyloid-beta is associated with increased plasma phosphorylated tau only in individuals positive for astrocyte reactivity. In addition, analyses using PET scans showed an AD-like pattern of tau tangle accumulation as a function of amyloid-beta exclusively in those same individuals.
Early upstream event
The findings suggest abnormalities in astrocyte reactivity is an early upstream event that likely occurs prior to tau pathology, which is closely related to the development of neurodegeneration and cognitive decline.
It’s likely many types of insults or processes can lead to astrocyte reactivity, possibly including COVID, but more research in this area is needed, said Dr. Pascoal.
“Our study only looked at the consequence of having both amyloid and astrocyte reactivity; it did not elucidate what is causing either of them,” he said.
Although “we were able to have very good results” in the current study, additional studies are needed to better establish the cut-off for GFAP levels that signal progression, said Dr. Pascoal.
The effect of astrocyte reactivity on the association between amyloid-beta and tau phosphorylation was greater in men than women. Dr. Pascoal noted anti-amyloid therapies, which might be modifying the amyloid-beta-astrocyte-tau pathway, tend to have a much larger effect in men than women.
Further studies that measure amyloid-beta, tau, and GFAP biomarkers at multiple timepoints, and with long follow-up, are needed, the investigators note.
The results may have implications for clinical trials, which have increasingly focused on individuals in the earliest preclinical phases of AD. Future studies should include cognitively normal patients who are positive for both amyloid pathology and astrocyte reactivity but have no overt p-tau abnormality, said Dr. Pascoal.
This may provide a time window for interventions very early in the disease process in those at increased risk for AD-related progression.
The study did not determine whether participants with both amyloid and astrocyte reactivity will inevitably develop AD, and to do so would require a longer follow up. “Our outcome was correlation to tau in the brain, which is something we know will lead to AD.”
Although the cohort represents significant socioeconomic diversity, a main limitation of the study was that subjects were mainly White, which limits the generalizability of the findings to a more diverse population.
The study received support from the National Institute of Aging; National Heart Lung and Blood Institute; Alzheimer’s Association; Fonds de Recherche du Québec-Santé; Canadian Consortium of Neurodegeneration in Aging; Weston Brain Institute; Colin Adair Charitable Foundation; Swedish Research Council; Wallenberg Scholar; BrightFocus Foundation; Swedish Alzheimer Foundation; Swedish Brain Foundation; Agneta Prytz-Folkes & Gösta Folkes Foundation; European Union; Swedish State Support for Clinical Research; Alzheimer Drug Discovery Foundation; Bluefield Project, the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden; the UK Dementia Research Institute at UCL; National Academy of Neuropsychology; Fundação de Amparo a pesquisa do Rio Grande do Sul; Instituto Serrapilheira; and Hjärnfonden.
Dr. Pascoal reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A blood biomarker that measures astrocyte reactivity may help determine who, among cognitively unimpaired older adults with amyloid-beta, will go on to develop Alzheimer’s disease (AD), new research suggests.
Investigators tested the blood of 1,000 cognitively healthy individuals with and without amyloid-beta pathology and found that only those with a combination of amyloid-beta burden and abnormal astrocyte activation subsequently progressed to AD.
“Our study argues that testing for the presence of brain amyloid along with blood biomarkers of astrocyte reactivity is the optimal screening to identify patients who are most at risk for progressing to Alzheimer’s disease,” senior investigator Tharick A. Pascoal, MD, PhD, associate professor of psychiatry and neurology, University of Pittsburgh, said in a release.
At this point, the biomarker is a research tool, but its application in clinical practice “is not very far away,” Dr. Pascoal told this news organization.
The study was published online in Nature Medicine.
Multicenter study
In AD, accumulation of amyloid-beta in the brain precedes tau pathology, but not everyone with amyloid-beta develops tau, and, consequently, clinical symptoms. Approximately 30% of older adults have brain amyloid but many never progress to AD, said Dr. Pascoal.
This suggests other biological processes may trigger the deleterious effects of amyloid-beta in the early stages of AD.
Finding predictive markers of early amyloid-beta–related tau pathology would help identify cognitively normal individuals who are more likely to develop AD.
Post-mortem studies show astrocyte reactivity – changes in glial cells in the brain and spinal cord because of an insult in the brain – is an early AD abnormality. Other research suggests a close link between amyloid-beta, astrocyte reactivity, and tau.
In addition, evidence suggests plasma measures of glial fibrillary acidic protein (GFAP) could be a strong proxy of astrocyte reactivity in the brain. Dr. Pascoal explained that when astrocytes are changed or become bigger, more GFAP is released.
The study included 1,016 cognitively normal individuals from three centers; some had amyloid pathology, some did not. Participants’ mean age was 69.6 years, and all were deemed negative or positive for astrocyte reactivity based on plasma GFAP levels.
Results showed amyloid-beta is associated with increased plasma phosphorylated tau only in individuals positive for astrocyte reactivity. In addition, analyses using PET scans showed an AD-like pattern of tau tangle accumulation as a function of amyloid-beta exclusively in those same individuals.
Early upstream event
The findings suggest abnormalities in astrocyte reactivity is an early upstream event that likely occurs prior to tau pathology, which is closely related to the development of neurodegeneration and cognitive decline.
It’s likely many types of insults or processes can lead to astrocyte reactivity, possibly including COVID, but more research in this area is needed, said Dr. Pascoal.
“Our study only looked at the consequence of having both amyloid and astrocyte reactivity; it did not elucidate what is causing either of them,” he said.
Although “we were able to have very good results” in the current study, additional studies are needed to better establish the cut-off for GFAP levels that signal progression, said Dr. Pascoal.
The effect of astrocyte reactivity on the association between amyloid-beta and tau phosphorylation was greater in men than women. Dr. Pascoal noted anti-amyloid therapies, which might be modifying the amyloid-beta-astrocyte-tau pathway, tend to have a much larger effect in men than women.
Further studies that measure amyloid-beta, tau, and GFAP biomarkers at multiple timepoints, and with long follow-up, are needed, the investigators note.
The results may have implications for clinical trials, which have increasingly focused on individuals in the earliest preclinical phases of AD. Future studies should include cognitively normal patients who are positive for both amyloid pathology and astrocyte reactivity but have no overt p-tau abnormality, said Dr. Pascoal.
This may provide a time window for interventions very early in the disease process in those at increased risk for AD-related progression.
The study did not determine whether participants with both amyloid and astrocyte reactivity will inevitably develop AD, and to do so would require a longer follow up. “Our outcome was correlation to tau in the brain, which is something we know will lead to AD.”
Although the cohort represents significant socioeconomic diversity, a main limitation of the study was that subjects were mainly White, which limits the generalizability of the findings to a more diverse population.
The study received support from the National Institute of Aging; National Heart Lung and Blood Institute; Alzheimer’s Association; Fonds de Recherche du Québec-Santé; Canadian Consortium of Neurodegeneration in Aging; Weston Brain Institute; Colin Adair Charitable Foundation; Swedish Research Council; Wallenberg Scholar; BrightFocus Foundation; Swedish Alzheimer Foundation; Swedish Brain Foundation; Agneta Prytz-Folkes & Gösta Folkes Foundation; European Union; Swedish State Support for Clinical Research; Alzheimer Drug Discovery Foundation; Bluefield Project, the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden; the UK Dementia Research Institute at UCL; National Academy of Neuropsychology; Fundação de Amparo a pesquisa do Rio Grande do Sul; Instituto Serrapilheira; and Hjärnfonden.
Dr. Pascoal reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The enemy of carcinogenic fumes is my friendly begonia
Sowing the seeds of cancer prevention
Are you looking to add to your quality of life, even though pets are not your speed? Might we suggest something with lower maintenance? Something a little greener?
Indoor plants can purify the air that comes from outside. Researchers at the University of Technology Sydney, in partnership with the plantscaping company Ambius, showed that a “green wall” made up of mixed indoor plants was able to suck up 97% of “the most toxic compounds” from the air in just 8 hours. We’re talking about lung-irritating, headache-inducing, cancer risk–boosting compounds from gasoline fumes, including benzene.
Public health initiatives often strive to reduce cardiovascular and obesity risks, but breathing seems pretty important too. According to the World Health Organization, household air pollution is responsible for about 2.5 million global premature deaths each year. And since 2020 we’ve become accustomed to spending more time inside and at home.
“This new research proves that plants should not just be seen as ‘nice to have,’ but rather a crucial part of every workplace wellness plan,” Ambius General Manager Johan Hodgson said in statement released by the university.
So don’t spend hundreds of dollars on a fancy air filtration system when a wall of plants can do that for next to nothing. Find what works for you and your space and become a plant parent today! Your lungs will thank you.
But officer, I had to swerve to miss the duodenal ampulla
Tiny video capsule endoscopes have been around for many years, but they have one big weakness: The ingestible cameras’ journey through the GI tract is passively driven by gravity and the natural movement of the body, so they often miss potential problem areas.
Not anymore. That flaw has been addressed by medical technology company AnX Robotica, which has taken endoscopy to the next level by adding that wondrous directional control device of the modern electronic age, a joystick.
The new system “uses an external magnet and hand-held video game style joysticks to move the capsule in three dimensions,” which allows physicians to “remotely drive a miniature video capsule to all regions of the stomach to visualize and photograph potential problem areas,” according to Andrew C. Meltzer, MD, of George Washington University and associates, who conducted a pilot study funded by AnX Robotica.
The video capsule provided a 95% rate of visualization in the stomachs of 40 patients who were examined at a medical office building by an emergency medicine physician who had no previous specialty training in endoscopy. “Capsules were driven by the ER physician and then the study reports were reviewed by an attending gastroenterologist who was physically off site,” the investigators said in a written statement.
The capsule operator did receive some additional training, and development of artificial intelligence to self-drive the capsule is in the works, but for now, we’re talking about a device controlled by a human using a joystick. And we all know that 50-year-olds are not especially known for their joystick skills. For that we need real experts. Yup, we need to put those joystick-controlled capsule endoscopes in the hands of teenage gamers. Who wants to go first?
Maybe AI isn’t ready for the big time after all
“How long before some intrepid stockholder says: ‘Hey, instead of paying doctors, why don’t we just use the free robot instead?’ ” Those words appeared on LOTME but a month ago. After all, the AI is supposed to be smarter and more empathetic than a doctor. And did we mention it’s free? Or at least extremely cheap. Cheaper than, say, a group of recently unionized health care workers.

In early May, the paid employees manning the National Eating Disorders Association emergency hotline voted to unionize, as they felt overwhelmed and underpaid. Apparently, paying six people an extra few thousand a year was too much for NEDA’s leadership, as they decided a few weeks later to fire those workers, fully closing down the hotline. Instead of talking to a real person, people “calling in” for support would be met with Tessa, a wellness chatbot that would hopefully guide them through their crisis. Key word, hopefully.
In perhaps the least surprising twist of the year, NEDA was forced to walk back its decision about a week after its initial announcement. It all started with a viral Instagram post from a woman who called in and received the following advice from Tessa: Lose 1-2 pounds a week, count calories and work for a 500- to 1,000-calorie deficit, weigh herself weekly, and restrict her diet. Unfortunately, all of these suggestions were things that led to the development of the woman’s eating disorder.
Naturally, NEDA responded in good grace, accusing the woman of lying. A NEDA vice president even left some nasty comments on the post, but hastily deleted them a day later when NEDA announced it was shutting down Tessa “until further notice for a complete investigation.” NEDA’s CEO insisted they hadn’t seen that behavior from Tessa before, calling it a “bug” and insisting the bot would only be down temporarily until the triggers causing the bug were fixed.
In the aftermath, several doctors and psychologists chimed in, terming the rush to automate human roles dangerous and risky. After all, much of what makes these hotlines effective is the volunteers speaking from their own experience. An unsupervised bot doesn’t seem to have what it takes to deal with a mental health crisis, but we’re betting that Tessa will be back. As a wise cephalopod once said: Nobody gives a care about the fate of labor as long as they can get their instant gratification.
You can’t spell existential without s-t-e-n-t
This week, we’re including a special “bonus” item that, to be honest, has nothing to do with stents. That’s why our editor is making us call this a “bonus” (and making us use quote marks, too): It doesn’t really have anything to do with stents or health care or those who practice health care. Actually, his exact words were, “You can’t just give the readers someone else’s ****ing list and expect to get paid for it.” Did we mention that he looks like Jack Nicklaus but acts like BoJack Horseman?
Anywaaay, we’re pretty sure that the list in question – “America’s Top 10 Most Googled Existential Questions” – says something about the human condition, just not about stents:
1. Why is the sky blue?
2. What do dreams mean?
3. What is the meaning of life?
4. Why am I so tired?
5. Who am I?
6. What is love?
7. Is a hot dog a sandwich?
8. What came first, the chicken or the egg?
9. What should I do?
10. Do animals have souls?
Sowing the seeds of cancer prevention
Are you looking to add to your quality of life, even though pets are not your speed? Might we suggest something with lower maintenance? Something a little greener?
Indoor plants can purify the air that comes from outside. Researchers at the University of Technology Sydney, in partnership with the plantscaping company Ambius, showed that a “green wall” made up of mixed indoor plants was able to suck up 97% of “the most toxic compounds” from the air in just 8 hours. We’re talking about lung-irritating, headache-inducing, cancer risk–boosting compounds from gasoline fumes, including benzene.
Public health initiatives often strive to reduce cardiovascular and obesity risks, but breathing seems pretty important too. According to the World Health Organization, household air pollution is responsible for about 2.5 million global premature deaths each year. And since 2020 we’ve become accustomed to spending more time inside and at home.
“This new research proves that plants should not just be seen as ‘nice to have,’ but rather a crucial part of every workplace wellness plan,” Ambius General Manager Johan Hodgson said in statement released by the university.
So don’t spend hundreds of dollars on a fancy air filtration system when a wall of plants can do that for next to nothing. Find what works for you and your space and become a plant parent today! Your lungs will thank you.
But officer, I had to swerve to miss the duodenal ampulla
Tiny video capsule endoscopes have been around for many years, but they have one big weakness: The ingestible cameras’ journey through the GI tract is passively driven by gravity and the natural movement of the body, so they often miss potential problem areas.
Not anymore. That flaw has been addressed by medical technology company AnX Robotica, which has taken endoscopy to the next level by adding that wondrous directional control device of the modern electronic age, a joystick.
The new system “uses an external magnet and hand-held video game style joysticks to move the capsule in three dimensions,” which allows physicians to “remotely drive a miniature video capsule to all regions of the stomach to visualize and photograph potential problem areas,” according to Andrew C. Meltzer, MD, of George Washington University and associates, who conducted a pilot study funded by AnX Robotica.
The video capsule provided a 95% rate of visualization in the stomachs of 40 patients who were examined at a medical office building by an emergency medicine physician who had no previous specialty training in endoscopy. “Capsules were driven by the ER physician and then the study reports were reviewed by an attending gastroenterologist who was physically off site,” the investigators said in a written statement.
The capsule operator did receive some additional training, and development of artificial intelligence to self-drive the capsule is in the works, but for now, we’re talking about a device controlled by a human using a joystick. And we all know that 50-year-olds are not especially known for their joystick skills. For that we need real experts. Yup, we need to put those joystick-controlled capsule endoscopes in the hands of teenage gamers. Who wants to go first?
Maybe AI isn’t ready for the big time after all
“How long before some intrepid stockholder says: ‘Hey, instead of paying doctors, why don’t we just use the free robot instead?’ ” Those words appeared on LOTME but a month ago. After all, the AI is supposed to be smarter and more empathetic than a doctor. And did we mention it’s free? Or at least extremely cheap. Cheaper than, say, a group of recently unionized health care workers.
In early May, the paid employees manning the National Eating Disorders Association emergency hotline voted to unionize, as they felt overwhelmed and underpaid. Apparently, paying six people an extra few thousand a year was too much for NEDA’s leadership, as they decided a few weeks later to fire those workers, fully closing down the hotline. Instead of talking to a real person, people “calling in” for support would be met with Tessa, a wellness chatbot that would hopefully guide them through their crisis. Key word, hopefully.
In perhaps the least surprising twist of the year, NEDA was forced to walk back its decision about a week after its initial announcement. It all started with a viral Instagram post from a woman who called in and received the following advice from Tessa: Lose 1-2 pounds a week, count calories and work for a 500- to 1,000-calorie deficit, weigh herself weekly, and restrict her diet. Unfortunately, all of these suggestions were things that led to the development of the woman’s eating disorder.
Naturally, NEDA responded in good grace, accusing the woman of lying. A NEDA vice president even left some nasty comments on the post, but hastily deleted them a day later when NEDA announced it was shutting down Tessa “until further notice for a complete investigation.” NEDA’s CEO insisted they hadn’t seen that behavior from Tessa before, calling it a “bug” and insisting the bot would only be down temporarily until the triggers causing the bug were fixed.
In the aftermath, several doctors and psychologists chimed in, terming the rush to automate human roles dangerous and risky. After all, much of what makes these hotlines effective is the volunteers speaking from their own experience. An unsupervised bot doesn’t seem to have what it takes to deal with a mental health crisis, but we’re betting that Tessa will be back. As a wise cephalopod once said: Nobody gives a care about the fate of labor as long as they can get their instant gratification.
You can’t spell existential without s-t-e-n-t
This week, we’re including a special “bonus” item that, to be honest, has nothing to do with stents. That’s why our editor is making us call this a “bonus” (and making us use quote marks, too): It doesn’t really have anything to do with stents or health care or those who practice health care. Actually, his exact words were, “You can’t just give the readers someone else’s ****ing list and expect to get paid for it.” Did we mention that he looks like Jack Nicklaus but acts like BoJack Horseman?
Anywaaay, we’re pretty sure that the list in question – “America’s Top 10 Most Googled Existential Questions” – says something about the human condition, just not about stents:
1. Why is the sky blue?
2. What do dreams mean?
3. What is the meaning of life?
4. Why am I so tired?
5. Who am I?
6. What is love?
7. Is a hot dog a sandwich?
8. What came first, the chicken or the egg?
9. What should I do?
10. Do animals have souls?
Sowing the seeds of cancer prevention
Are you looking to add to your quality of life, even though pets are not your speed? Might we suggest something with lower maintenance? Something a little greener?
Indoor plants can purify the air that comes from outside. Researchers at the University of Technology Sydney, in partnership with the plantscaping company Ambius, showed that a “green wall” made up of mixed indoor plants was able to suck up 97% of “the most toxic compounds” from the air in just 8 hours. We’re talking about lung-irritating, headache-inducing, cancer risk–boosting compounds from gasoline fumes, including benzene.
Public health initiatives often strive to reduce cardiovascular and obesity risks, but breathing seems pretty important too. According to the World Health Organization, household air pollution is responsible for about 2.5 million global premature deaths each year. And since 2020 we’ve become accustomed to spending more time inside and at home.
“This new research proves that plants should not just be seen as ‘nice to have,’ but rather a crucial part of every workplace wellness plan,” Ambius General Manager Johan Hodgson said in statement released by the university.
So don’t spend hundreds of dollars on a fancy air filtration system when a wall of plants can do that for next to nothing. Find what works for you and your space and become a plant parent today! Your lungs will thank you.
But officer, I had to swerve to miss the duodenal ampulla
Tiny video capsule endoscopes have been around for many years, but they have one big weakness: The ingestible cameras’ journey through the GI tract is passively driven by gravity and the natural movement of the body, so they often miss potential problem areas.
Not anymore. That flaw has been addressed by medical technology company AnX Robotica, which has taken endoscopy to the next level by adding that wondrous directional control device of the modern electronic age, a joystick.
The new system “uses an external magnet and hand-held video game style joysticks to move the capsule in three dimensions,” which allows physicians to “remotely drive a miniature video capsule to all regions of the stomach to visualize and photograph potential problem areas,” according to Andrew C. Meltzer, MD, of George Washington University and associates, who conducted a pilot study funded by AnX Robotica.
The video capsule provided a 95% rate of visualization in the stomachs of 40 patients who were examined at a medical office building by an emergency medicine physician who had no previous specialty training in endoscopy. “Capsules were driven by the ER physician and then the study reports were reviewed by an attending gastroenterologist who was physically off site,” the investigators said in a written statement.
The capsule operator did receive some additional training, and development of artificial intelligence to self-drive the capsule is in the works, but for now, we’re talking about a device controlled by a human using a joystick. And we all know that 50-year-olds are not especially known for their joystick skills. For that we need real experts. Yup, we need to put those joystick-controlled capsule endoscopes in the hands of teenage gamers. Who wants to go first?
Maybe AI isn’t ready for the big time after all
“How long before some intrepid stockholder says: ‘Hey, instead of paying doctors, why don’t we just use the free robot instead?’ ” Those words appeared on LOTME but a month ago. After all, the AI is supposed to be smarter and more empathetic than a doctor. And did we mention it’s free? Or at least extremely cheap. Cheaper than, say, a group of recently unionized health care workers.
In early May, the paid employees manning the National Eating Disorders Association emergency hotline voted to unionize, as they felt overwhelmed and underpaid. Apparently, paying six people an extra few thousand a year was too much for NEDA’s leadership, as they decided a few weeks later to fire those workers, fully closing down the hotline. Instead of talking to a real person, people “calling in” for support would be met with Tessa, a wellness chatbot that would hopefully guide them through their crisis. Key word, hopefully.
In perhaps the least surprising twist of the year, NEDA was forced to walk back its decision about a week after its initial announcement. It all started with a viral Instagram post from a woman who called in and received the following advice from Tessa: Lose 1-2 pounds a week, count calories and work for a 500- to 1,000-calorie deficit, weigh herself weekly, and restrict her diet. Unfortunately, all of these suggestions were things that led to the development of the woman’s eating disorder.
Naturally, NEDA responded in good grace, accusing the woman of lying. A NEDA vice president even left some nasty comments on the post, but hastily deleted them a day later when NEDA announced it was shutting down Tessa “until further notice for a complete investigation.” NEDA’s CEO insisted they hadn’t seen that behavior from Tessa before, calling it a “bug” and insisting the bot would only be down temporarily until the triggers causing the bug were fixed.
In the aftermath, several doctors and psychologists chimed in, terming the rush to automate human roles dangerous and risky. After all, much of what makes these hotlines effective is the volunteers speaking from their own experience. An unsupervised bot doesn’t seem to have what it takes to deal with a mental health crisis, but we’re betting that Tessa will be back. As a wise cephalopod once said: Nobody gives a care about the fate of labor as long as they can get their instant gratification.
You can’t spell existential without s-t-e-n-t
This week, we’re including a special “bonus” item that, to be honest, has nothing to do with stents. That’s why our editor is making us call this a “bonus” (and making us use quote marks, too): It doesn’t really have anything to do with stents or health care or those who practice health care. Actually, his exact words were, “You can’t just give the readers someone else’s ****ing list and expect to get paid for it.” Did we mention that he looks like Jack Nicklaus but acts like BoJack Horseman?
Anywaaay, we’re pretty sure that the list in question – “America’s Top 10 Most Googled Existential Questions” – says something about the human condition, just not about stents:
1. Why is the sky blue?
2. What do dreams mean?
3. What is the meaning of life?
4. Why am I so tired?
5. Who am I?
6. What is love?
7. Is a hot dog a sandwich?
8. What came first, the chicken or the egg?
9. What should I do?
10. Do animals have souls?
Gout linked to smaller brain volume, higher likelihood of neurodegenerative diseases
Patients with gout may have smaller brain volumes and higher brain iron markers than people without gout, and also be more likely to develop Parkinson’s disease, probable essential tremor, and dementia, researchers in the United Kingdom report.
“We were surprised about the regions of the brain affected by gout, several of which are important for motor function. The other intriguing finding was that the risk of dementia amongst gout patients was strongly time-dependent: highest in the first 3 years after their gout diagnosis,” lead study author Anya Topiwala, BMBCh, DPhil, said in an interview.
“Our combination of traditional and genetic approaches increases the confidence that gout is causing the brain findings,” said Dr. Topiwala, a clinical research fellow and consultant psychiatrist in the Nuffield Department of Population Health at the University of Oxford, England.
“We suggest that clinicians be vigilant for cognitive and motor problems after gout diagnosis, particularly in the early stages,” she added.
Links between gout and neurodegenerative diseases debated in earlier studies
Gout, the most common inflammatory arthritis, affects around 1%-4% of people, the authors wrote, with monosodium urate crystal deposits causing acute flares of pain and swelling in joints and periarticular tissues.
Whether and how gout may affect the brain has been debated in the literature. Gout and hyperuricemia have been linked with elevated stroke risk; and although observational studies have linked hyperuricemia with lower dementia risk, especially Alzheimer’s disease, Mendelian randomization studies have had conflicting results in Alzheimer’s disease.
A novel approach that analyzes brain structure and genetics
In a study published in Nature Communications, Dr. Topiwala and her colleagues combined observational and Mendelian randomization techniques to explore relationships between gout and neurodegenerative diseases. They analyzed data from over 303,000 volunteer participants between 40 and 69 years of age recruited between 2006 and 2010 to contribute their detailed genetic and health information to the U.K. Biobank, a large-scale biomedical database and research resource.
Patients with gout tended to be older and male. At baseline, all participants’ serum urate levels were measured, and 30.8% of patients with gout reported that they currently used urate-lowering therapy.
MRI shows brain changes in patients with gout
In what the authors said is the first investigation of neuroimaging markers in patients with gout, they compared differences in gray matter volumes found in the 1,165 participants with gout and the 32,202 controls without gout who had MRI data.
They found no marked sex differences in associations. Urate was inversely linked with global brain volume and with gray and white matter volumes, and gout appeared to age global gray matter by 2 years.
Patients with gout and higher urate showed significant differences in regional gray matter volumes, especially in the cerebellum, pons, and midbrain, as well as subcortical differences in the nucleus accumbens, putamen, and caudate. They also showed significant differences in white matter tract microstructure in the fornix.
Patients with gout were more likely to develop dementia (average hazard ratio [HR] over study = 1.60), especially in the first 3 years after gout diagnosis (HR = 7.40). They were also at higher risk for vascular dementia (average HR = 2.41), compared with all-cause dementia, but not for Alzheimer’s disease (average HR = 1.62).
In asymptomatic participants though, urate and dementia were inversely linked (HR = 0.85), with no time dependence.
Gout was linked with higher incidence of Parkinson’s disease (HR = 1.43) and probable essential tremor (HR = 6.75). In asymptomatic participants, urate and Parkinson’s disease (HR = 0.89), but not probable essential tremor, were inversely linked.
Genetic analyses reinforce MRI results
Using Mendelian randomization estimates, the authors found that genetic links generally reflected their observational findings. Both genetically predicted gout and serum urate were significantly linked with regional gray matter volumes, including cerebellar, midbrain, pons, and brainstem.
They also found significant links with higher magnetic susceptibility in the putamen and caudate, markers of higher iron. But while genetically predicted gout was significantly linked with global gray matter volume, urate was not.
In males, but not in females, urate was positively linked with alcohol intake and lower socioeconomic status.
Dr. Topiwala acknowledged several limitations to the study, writing that “the results from the volunteer participants may not apply to other populations; the cross-sectional serum urate measurements may not reflect chronic exposure; and Parkinson’s disease and essential tremor may have been diagnostically confounded.”
A novel approach that suggests further related research
Asked to comment on the study, Puja Khanna, MD, MPH, a rheumatologist and clinical associate professor of medicine at the University of Michigan, Ann Arbor, called its novel use of neuroimaging interesting.

Dr. Khanna, who was not involved in the study, said she would like to know more about the role that horizontal pleiotropy – one genetic variant having independent effects on multiple traits – plays in this disease process, and about the impact of the antioxidative properties of urate in maintaining neuroprotection.
“[The] U.K. Biobank is an excellent database to look at questions of association,” John D. FitzGerald, MD, PhD, MPH, MBA, professor and clinical chief of rheumatology at the University of California, Los Angeles, said in an interview.

“This is a fairly rigorous study,” added Dr. FitzGerald, also not involved in the study. “While it has lots of strengths,” including its large sample size and Mendelian randomization, it also has “abundant weaknesses,” he added. “It is largely cross-sectional, with single urate measurement and single brain MRI.”
“Causation is the big question,” Dr. FitzGerald noted. “Does treating gout (or urate) help prevent dementia or neurodegenerative decline?”
Early diagnosis benefits patients
Dr. Khanna and Dr. FitzGerald joined the authors in advising doctors to monitor their gout patients for cognitive and motor symptoms of neurodegenerative disease.
“It is clearly important to pay close attention to the neurologic exam and history in gout, especially because it is a disease of the aging population,” Dr. Khanna advised. “Addressing dementia when gout is diagnosed can lead to prompt mitigation strategies that can hugely impact patients.”
Dr. Topiwala and her colleagues would like to investigate why the dementia risk was time-dependent. “Is this because of the acute inflammatory response in gout, or could it just be that patients with gout visit their doctors more frequently, so any cognitive problems are picked up sooner?” she asked.
The authors, and Dr. Khanna and Dr. FitzGerald, report no relevant financial relationships. The Wellcome Trust; the U.K. Medical Research Council; the European Commission Horizon 2020 research and innovation program; the British Heart Foundation; the U.S. National Institutes of Health; the Engineering and Physical Sciences Research Council; and the National Institute for Health and Care Research funded the study.
Patients with gout may have smaller brain volumes and higher brain iron markers than people without gout, and also be more likely to develop Parkinson’s disease, probable essential tremor, and dementia, researchers in the United Kingdom report.
“We were surprised about the regions of the brain affected by gout, several of which are important for motor function. The other intriguing finding was that the risk of dementia amongst gout patients was strongly time-dependent: highest in the first 3 years after their gout diagnosis,” lead study author Anya Topiwala, BMBCh, DPhil, said in an interview.
“Our combination of traditional and genetic approaches increases the confidence that gout is causing the brain findings,” said Dr. Topiwala, a clinical research fellow and consultant psychiatrist in the Nuffield Department of Population Health at the University of Oxford, England.
“We suggest that clinicians be vigilant for cognitive and motor problems after gout diagnosis, particularly in the early stages,” she added.
Links between gout and neurodegenerative diseases debated in earlier studies
Gout, the most common inflammatory arthritis, affects around 1%-4% of people, the authors wrote, with monosodium urate crystal deposits causing acute flares of pain and swelling in joints and periarticular tissues.
Whether and how gout may affect the brain has been debated in the literature. Gout and hyperuricemia have been linked with elevated stroke risk; and although observational studies have linked hyperuricemia with lower dementia risk, especially Alzheimer’s disease, Mendelian randomization studies have had conflicting results in Alzheimer’s disease.
A novel approach that analyzes brain structure and genetics
In a study published in Nature Communications, Dr. Topiwala and her colleagues combined observational and Mendelian randomization techniques to explore relationships between gout and neurodegenerative diseases. They analyzed data from over 303,000 volunteer participants between 40 and 69 years of age recruited between 2006 and 2010 to contribute their detailed genetic and health information to the U.K. Biobank, a large-scale biomedical database and research resource.
Patients with gout tended to be older and male. At baseline, all participants’ serum urate levels were measured, and 30.8% of patients with gout reported that they currently used urate-lowering therapy.
MRI shows brain changes in patients with gout
In what the authors said is the first investigation of neuroimaging markers in patients with gout, they compared differences in gray matter volumes found in the 1,165 participants with gout and the 32,202 controls without gout who had MRI data.
They found no marked sex differences in associations. Urate was inversely linked with global brain volume and with gray and white matter volumes, and gout appeared to age global gray matter by 2 years.
Patients with gout and higher urate showed significant differences in regional gray matter volumes, especially in the cerebellum, pons, and midbrain, as well as subcortical differences in the nucleus accumbens, putamen, and caudate. They also showed significant differences in white matter tract microstructure in the fornix.
Patients with gout were more likely to develop dementia (average hazard ratio [HR] over study = 1.60), especially in the first 3 years after gout diagnosis (HR = 7.40). They were also at higher risk for vascular dementia (average HR = 2.41), compared with all-cause dementia, but not for Alzheimer’s disease (average HR = 1.62).
In asymptomatic participants though, urate and dementia were inversely linked (HR = 0.85), with no time dependence.
Gout was linked with higher incidence of Parkinson’s disease (HR = 1.43) and probable essential tremor (HR = 6.75). In asymptomatic participants, urate and Parkinson’s disease (HR = 0.89), but not probable essential tremor, were inversely linked.
Genetic analyses reinforce MRI results
Using Mendelian randomization estimates, the authors found that genetic links generally reflected their observational findings. Both genetically predicted gout and serum urate were significantly linked with regional gray matter volumes, including cerebellar, midbrain, pons, and brainstem.
They also found significant links with higher magnetic susceptibility in the putamen and caudate, markers of higher iron. But while genetically predicted gout was significantly linked with global gray matter volume, urate was not.
In males, but not in females, urate was positively linked with alcohol intake and lower socioeconomic status.
Dr. Topiwala acknowledged several limitations to the study, writing that “the results from the volunteer participants may not apply to other populations; the cross-sectional serum urate measurements may not reflect chronic exposure; and Parkinson’s disease and essential tremor may have been diagnostically confounded.”
A novel approach that suggests further related research
Asked to comment on the study, Puja Khanna, MD, MPH, a rheumatologist and clinical associate professor of medicine at the University of Michigan, Ann Arbor, called its novel use of neuroimaging interesting.
Dr. Khanna, who was not involved in the study, said she would like to know more about the role that horizontal pleiotropy – one genetic variant having independent effects on multiple traits – plays in this disease process, and about the impact of the antioxidative properties of urate in maintaining neuroprotection.
“[The] U.K. Biobank is an excellent database to look at questions of association,” John D. FitzGerald, MD, PhD, MPH, MBA, professor and clinical chief of rheumatology at the University of California, Los Angeles, said in an interview.
“This is a fairly rigorous study,” added Dr. FitzGerald, also not involved in the study. “While it has lots of strengths,” including its large sample size and Mendelian randomization, it also has “abundant weaknesses,” he added. “It is largely cross-sectional, with single urate measurement and single brain MRI.”
“Causation is the big question,” Dr. FitzGerald noted. “Does treating gout (or urate) help prevent dementia or neurodegenerative decline?”
Early diagnosis benefits patients
Dr. Khanna and Dr. FitzGerald joined the authors in advising doctors to monitor their gout patients for cognitive and motor symptoms of neurodegenerative disease.
“It is clearly important to pay close attention to the neurologic exam and history in gout, especially because it is a disease of the aging population,” Dr. Khanna advised. “Addressing dementia when gout is diagnosed can lead to prompt mitigation strategies that can hugely impact patients.”
Dr. Topiwala and her colleagues would like to investigate why the dementia risk was time-dependent. “Is this because of the acute inflammatory response in gout, or could it just be that patients with gout visit their doctors more frequently, so any cognitive problems are picked up sooner?” she asked.
The authors, and Dr. Khanna and Dr. FitzGerald, report no relevant financial relationships. The Wellcome Trust; the U.K. Medical Research Council; the European Commission Horizon 2020 research and innovation program; the British Heart Foundation; the U.S. National Institutes of Health; the Engineering and Physical Sciences Research Council; and the National Institute for Health and Care Research funded the study.
Patients with gout may have smaller brain volumes and higher brain iron markers than people without gout, and also be more likely to develop Parkinson’s disease, probable essential tremor, and dementia, researchers in the United Kingdom report.
“We were surprised about the regions of the brain affected by gout, several of which are important for motor function. The other intriguing finding was that the risk of dementia amongst gout patients was strongly time-dependent: highest in the first 3 years after their gout diagnosis,” lead study author Anya Topiwala, BMBCh, DPhil, said in an interview.
“Our combination of traditional and genetic approaches increases the confidence that gout is causing the brain findings,” said Dr. Topiwala, a clinical research fellow and consultant psychiatrist in the Nuffield Department of Population Health at the University of Oxford, England.
“We suggest that clinicians be vigilant for cognitive and motor problems after gout diagnosis, particularly in the early stages,” she added.
Links between gout and neurodegenerative diseases debated in earlier studies
Gout, the most common inflammatory arthritis, affects around 1%-4% of people, the authors wrote, with monosodium urate crystal deposits causing acute flares of pain and swelling in joints and periarticular tissues.
Whether and how gout may affect the brain has been debated in the literature. Gout and hyperuricemia have been linked with elevated stroke risk; and although observational studies have linked hyperuricemia with lower dementia risk, especially Alzheimer’s disease, Mendelian randomization studies have had conflicting results in Alzheimer’s disease.
A novel approach that analyzes brain structure and genetics
In a study published in Nature Communications, Dr. Topiwala and her colleagues combined observational and Mendelian randomization techniques to explore relationships between gout and neurodegenerative diseases. They analyzed data from over 303,000 volunteer participants between 40 and 69 years of age recruited between 2006 and 2010 to contribute their detailed genetic and health information to the U.K. Biobank, a large-scale biomedical database and research resource.
Patients with gout tended to be older and male. At baseline, all participants’ serum urate levels were measured, and 30.8% of patients with gout reported that they currently used urate-lowering therapy.
MRI shows brain changes in patients with gout
In what the authors said is the first investigation of neuroimaging markers in patients with gout, they compared differences in gray matter volumes found in the 1,165 participants with gout and the 32,202 controls without gout who had MRI data.
They found no marked sex differences in associations. Urate was inversely linked with global brain volume and with gray and white matter volumes, and gout appeared to age global gray matter by 2 years.
Patients with gout and higher urate showed significant differences in regional gray matter volumes, especially in the cerebellum, pons, and midbrain, as well as subcortical differences in the nucleus accumbens, putamen, and caudate. They also showed significant differences in white matter tract microstructure in the fornix.
Patients with gout were more likely to develop dementia (average hazard ratio [HR] over study = 1.60), especially in the first 3 years after gout diagnosis (HR = 7.40). They were also at higher risk for vascular dementia (average HR = 2.41), compared with all-cause dementia, but not for Alzheimer’s disease (average HR = 1.62).
In asymptomatic participants though, urate and dementia were inversely linked (HR = 0.85), with no time dependence.
Gout was linked with higher incidence of Parkinson’s disease (HR = 1.43) and probable essential tremor (HR = 6.75). In asymptomatic participants, urate and Parkinson’s disease (HR = 0.89), but not probable essential tremor, were inversely linked.
Genetic analyses reinforce MRI results
Using Mendelian randomization estimates, the authors found that genetic links generally reflected their observational findings. Both genetically predicted gout and serum urate were significantly linked with regional gray matter volumes, including cerebellar, midbrain, pons, and brainstem.
They also found significant links with higher magnetic susceptibility in the putamen and caudate, markers of higher iron. But while genetically predicted gout was significantly linked with global gray matter volume, urate was not.
In males, but not in females, urate was positively linked with alcohol intake and lower socioeconomic status.
Dr. Topiwala acknowledged several limitations to the study, writing that “the results from the volunteer participants may not apply to other populations; the cross-sectional serum urate measurements may not reflect chronic exposure; and Parkinson’s disease and essential tremor may have been diagnostically confounded.”
A novel approach that suggests further related research
Asked to comment on the study, Puja Khanna, MD, MPH, a rheumatologist and clinical associate professor of medicine at the University of Michigan, Ann Arbor, called its novel use of neuroimaging interesting.
Dr. Khanna, who was not involved in the study, said she would like to know more about the role that horizontal pleiotropy – one genetic variant having independent effects on multiple traits – plays in this disease process, and about the impact of the antioxidative properties of urate in maintaining neuroprotection.
“[The] U.K. Biobank is an excellent database to look at questions of association,” John D. FitzGerald, MD, PhD, MPH, MBA, professor and clinical chief of rheumatology at the University of California, Los Angeles, said in an interview.
“This is a fairly rigorous study,” added Dr. FitzGerald, also not involved in the study. “While it has lots of strengths,” including its large sample size and Mendelian randomization, it also has “abundant weaknesses,” he added. “It is largely cross-sectional, with single urate measurement and single brain MRI.”
“Causation is the big question,” Dr. FitzGerald noted. “Does treating gout (or urate) help prevent dementia or neurodegenerative decline?”
Early diagnosis benefits patients
Dr. Khanna and Dr. FitzGerald joined the authors in advising doctors to monitor their gout patients for cognitive and motor symptoms of neurodegenerative disease.
“It is clearly important to pay close attention to the neurologic exam and history in gout, especially because it is a disease of the aging population,” Dr. Khanna advised. “Addressing dementia when gout is diagnosed can lead to prompt mitigation strategies that can hugely impact patients.”
Dr. Topiwala and her colleagues would like to investigate why the dementia risk was time-dependent. “Is this because of the acute inflammatory response in gout, or could it just be that patients with gout visit their doctors more frequently, so any cognitive problems are picked up sooner?” she asked.
The authors, and Dr. Khanna and Dr. FitzGerald, report no relevant financial relationships. The Wellcome Trust; the U.K. Medical Research Council; the European Commission Horizon 2020 research and innovation program; the British Heart Foundation; the U.S. National Institutes of Health; the Engineering and Physical Sciences Research Council; and the National Institute for Health and Care Research funded the study.
FROM NATURE COMMUNICATIONS
How can we make medical training less ‘toxic’?
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
Game-changing Alzheimer’s research: The latest on biomarkers
The field of neurodegenerative dementias, particularly Alzheimer’s disease (AD), has been revolutionized by the development of imaging and cerebrospinal fluid biomarkers and is on the brink of a new development: emerging plasma biomarkers. Research now recognizes the relationship between the cognitive-behavioral syndromic diagnosis (that is, the illness) and the etiologic diagnosis (the disease) – and the need to consider each separately when developing a diagnostic formulation. The National Institute on Aging and Alzheimer’s Association Research Framework uses the amyloid, tau, and neurodegeneration system to define AD biologically in living patients. Here is an overview of the framework, which requires biomarker evidence of amyloid plaques (amyloid positivity) and neurofibrillary tangles (tau positivity), with evidence of neurodegeneration (neurodegeneration positivity) to support the diagnosis.
The diagnostic approach for symptomatic patients
The differential diagnosis in symptomatic patients with mild cognitive impairment (MCI), mild behavioral impairment, or dementia is broad and includes multiple neurodegenerative diseases (for example, AD, frontotemporal lobar degeneration, dementia with Lewy bodies, argyrophilic grain disease, hippocampal sclerosis); vascular ischemic brain injury (for example, stroke); tumors; infectious, inflammatory, paraneoplastic, or demyelinating diseases; trauma; hydrocephalus; toxic/metabolic insults; and other rare diseases. The patient’s clinical syndrome narrows the differential diagnosis.
Once the clinician has a prioritized differential diagnosis of the brain disease or condition that is probably causing or contributing to the patient’s signs and symptoms, they can then select appropriate assessments and tests, typically starting with a laboratory panel and brain MRI. Strong evidence backed by practice recommendations also supports the use of fluorodeoxyglucose PET as a marker of functional brain abnormalities associated with dementia. Although molecular biomarkers are typically considered at the later stage of the clinical workup, the anticipated future availability of plasma biomarkers will probably change the timing of molecular biomarker assessment in patients with suspected cognitive impairment owing to AD.
Molecular PET biomarkers
Three PET tracers approved by the U.S. Food and Drug Administration for the detection of cerebral amyloid plaques have high sensitivity (89%-98%) and specificity (88%-100%), compared with autopsy, the gold standard diagnostic tool. However, these scans are costly and are not reimbursed by Medicare and Medicaid. Because all amyloid PET scans are covered by the Veterans Administration, this test is more readily accessible for patients receiving VA benefits.
The appropriate-use criteria developed by the Amyloid Imaging Task Force recommends amyloid PET for patients with persistent or progressive MCI or dementia. In such patients, a negative amyloid PET scan would strongly weigh against AD, supporting a differential diagnosis of other etiologies. Although a positive amyloid PET scan in patients with MCI or dementia indicates the presence of amyloid plaques, it does not necessarily confirm AD as the cause. Cerebral amyloid plaques may coexist with other pathologies and increase with age, even in cognitively normal individuals.
The IDEAS study looked at the clinical utility of amyloid PET in a real-world dementia specialist setting. In the study, dementia subspecialists documented their presumed etiologic diagnosis (and level of confidence) before and after amyloid PET. Of the 11,409 patients who completed the study, the etiologic diagnosis changed from AD to non-AD in just over 25% of cases and from non-AD to AD in 10.5%. Clinical management changed in about 60% of patients with MCI and 63.5% of patients with dementia.
In May 2020, the FDA approved flortaucipir F-18, the first diagnostic tau radiotracer for use with PET to estimate the density and distribution of aggregated tau neurofibrillary tangles in adults with cognitive impairment undergoing evaluation for AD. Regulatory approval of flortaucipir F-18 was based on findings from two clinical trials of terminally ill patients who were followed to autopsy. The studies included patients with a spectrum of clinically diagnosed dementias and those with normal cognition. The primary outcome of the studies was accurate visual interpretation of the images in detecting advanced AD tau neurofibrillary tangle pathology (Braak stage V or VI tau pathology). Sensitivity of five trained readers ranged from 68% to 86%, and specificity ranged from 63% to 100%; interrater agreement was 0.87. Tau PET is not yet reimbursed and is therefore not yet readily available in the clinical setting. Moreover, appropriate use criteria have not yet been published.
Molecular fluid biomarkers
Cerebrospinal fluid (CSF) analysis is currently the most readily available and reimbursed test to aid in diagnosing AD, with appropriate-use criteria for patients with suspected AD. CSF biomarkers for AD are useful in cognitively impaired patients when the etiologic diagnosis is equivocal, there is only an intermediate level of diagnostic confidence, or there is very high confidence in the etiologic diagnosis. Testing for CSF biomarkers is also recommended for patients at very early clinical stages (for example, early MCI) or with atypical clinical presentations.
A decreased concentration of amyloid-beta 42 in CSF is a marker of amyloid neuritic plaques in the brain. An increased concentration of total tau in CSF reflects injury to neurons, and an increased concentration of specific isoforms of hyperphosphorylated tau reflects neurofibrillary tangles. Presently, the ratios of t-tau to amyloid-beta 42, amyloid-beta 42 to amyloid-beta 40, and phosphorylated-tau 181 to amyloid-beta 42 are the best-performing markers of AD neuropathologic changes and are more accurate than assessing individual biomarkers. These CSF biomarkers of AD have been validated against autopsy, and ratio values of CSF amyloid-beta 42 have been further validated against amyloid PET, with overall sensitivity and specificity of approximately 90% and 84%, respectively.
Some of the most exciting recent advances in AD center around the measurement of these proteins and others in plasma. Appropriate-use criteria for plasma biomarkers in the evaluation of patients with cognitive impairment were published in 2022. In addition to their use in clinical trials, these criteria cautiously recommend using these biomarkers in specialized memory clinics in the diagnostic workup of patients with cognitive symptoms, along with confirmatory CSF markers or PET. Additional data are needed before plasma biomarkers of AD are used as standalone diagnostic markers or considered in the primary care setting.
We have made remarkable progress toward more precise molecular diagnosis of brain diseases underlying cognitive impairment and dementia. Ongoing efforts to evaluate the utility of these measures in clinical practice include the need to increase diversity of patients and providers. Ultimately, the tremendous progress in molecular biomarkers for the diseases causing dementia will help the field work toward our common goal of early and accurate diagnosis, better management, and hope for people living with these diseases.
Bradford C. Dickerson, MD, MMSc, is a professor, department of neurology, Harvard Medical School, and director, Frontotemporal Disorders Unit, department of neurology, at Massachusetts General Hospital, both in Boston.
A version of this article first appeared on Medscape.com.
The field of neurodegenerative dementias, particularly Alzheimer’s disease (AD), has been revolutionized by the development of imaging and cerebrospinal fluid biomarkers and is on the brink of a new development: emerging plasma biomarkers. Research now recognizes the relationship between the cognitive-behavioral syndromic diagnosis (that is, the illness) and the etiologic diagnosis (the disease) – and the need to consider each separately when developing a diagnostic formulation. The National Institute on Aging and Alzheimer’s Association Research Framework uses the amyloid, tau, and neurodegeneration system to define AD biologically in living patients. Here is an overview of the framework, which requires biomarker evidence of amyloid plaques (amyloid positivity) and neurofibrillary tangles (tau positivity), with evidence of neurodegeneration (neurodegeneration positivity) to support the diagnosis.
The diagnostic approach for symptomatic patients
The differential diagnosis in symptomatic patients with mild cognitive impairment (MCI), mild behavioral impairment, or dementia is broad and includes multiple neurodegenerative diseases (for example, AD, frontotemporal lobar degeneration, dementia with Lewy bodies, argyrophilic grain disease, hippocampal sclerosis); vascular ischemic brain injury (for example, stroke); tumors; infectious, inflammatory, paraneoplastic, or demyelinating diseases; trauma; hydrocephalus; toxic/metabolic insults; and other rare diseases. The patient’s clinical syndrome narrows the differential diagnosis.
Once the clinician has a prioritized differential diagnosis of the brain disease or condition that is probably causing or contributing to the patient’s signs and symptoms, they can then select appropriate assessments and tests, typically starting with a laboratory panel and brain MRI. Strong evidence backed by practice recommendations also supports the use of fluorodeoxyglucose PET as a marker of functional brain abnormalities associated with dementia. Although molecular biomarkers are typically considered at the later stage of the clinical workup, the anticipated future availability of plasma biomarkers will probably change the timing of molecular biomarker assessment in patients with suspected cognitive impairment owing to AD.
Molecular PET biomarkers
Three PET tracers approved by the U.S. Food and Drug Administration for the detection of cerebral amyloid plaques have high sensitivity (89%-98%) and specificity (88%-100%), compared with autopsy, the gold standard diagnostic tool. However, these scans are costly and are not reimbursed by Medicare and Medicaid. Because all amyloid PET scans are covered by the Veterans Administration, this test is more readily accessible for patients receiving VA benefits.
The appropriate-use criteria developed by the Amyloid Imaging Task Force recommends amyloid PET for patients with persistent or progressive MCI or dementia. In such patients, a negative amyloid PET scan would strongly weigh against AD, supporting a differential diagnosis of other etiologies. Although a positive amyloid PET scan in patients with MCI or dementia indicates the presence of amyloid plaques, it does not necessarily confirm AD as the cause. Cerebral amyloid plaques may coexist with other pathologies and increase with age, even in cognitively normal individuals.
The IDEAS study looked at the clinical utility of amyloid PET in a real-world dementia specialist setting. In the study, dementia subspecialists documented their presumed etiologic diagnosis (and level of confidence) before and after amyloid PET. Of the 11,409 patients who completed the study, the etiologic diagnosis changed from AD to non-AD in just over 25% of cases and from non-AD to AD in 10.5%. Clinical management changed in about 60% of patients with MCI and 63.5% of patients with dementia.
In May 2020, the FDA approved flortaucipir F-18, the first diagnostic tau radiotracer for use with PET to estimate the density and distribution of aggregated tau neurofibrillary tangles in adults with cognitive impairment undergoing evaluation for AD. Regulatory approval of flortaucipir F-18 was based on findings from two clinical trials of terminally ill patients who were followed to autopsy. The studies included patients with a spectrum of clinically diagnosed dementias and those with normal cognition. The primary outcome of the studies was accurate visual interpretation of the images in detecting advanced AD tau neurofibrillary tangle pathology (Braak stage V or VI tau pathology). Sensitivity of five trained readers ranged from 68% to 86%, and specificity ranged from 63% to 100%; interrater agreement was 0.87. Tau PET is not yet reimbursed and is therefore not yet readily available in the clinical setting. Moreover, appropriate use criteria have not yet been published.
Molecular fluid biomarkers
Cerebrospinal fluid (CSF) analysis is currently the most readily available and reimbursed test to aid in diagnosing AD, with appropriate-use criteria for patients with suspected AD. CSF biomarkers for AD are useful in cognitively impaired patients when the etiologic diagnosis is equivocal, there is only an intermediate level of diagnostic confidence, or there is very high confidence in the etiologic diagnosis. Testing for CSF biomarkers is also recommended for patients at very early clinical stages (for example, early MCI) or with atypical clinical presentations.
A decreased concentration of amyloid-beta 42 in CSF is a marker of amyloid neuritic plaques in the brain. An increased concentration of total tau in CSF reflects injury to neurons, and an increased concentration of specific isoforms of hyperphosphorylated tau reflects neurofibrillary tangles. Presently, the ratios of t-tau to amyloid-beta 42, amyloid-beta 42 to amyloid-beta 40, and phosphorylated-tau 181 to amyloid-beta 42 are the best-performing markers of AD neuropathologic changes and are more accurate than assessing individual biomarkers. These CSF biomarkers of AD have been validated against autopsy, and ratio values of CSF amyloid-beta 42 have been further validated against amyloid PET, with overall sensitivity and specificity of approximately 90% and 84%, respectively.
Some of the most exciting recent advances in AD center around the measurement of these proteins and others in plasma. Appropriate-use criteria for plasma biomarkers in the evaluation of patients with cognitive impairment were published in 2022. In addition to their use in clinical trials, these criteria cautiously recommend using these biomarkers in specialized memory clinics in the diagnostic workup of patients with cognitive symptoms, along with confirmatory CSF markers or PET. Additional data are needed before plasma biomarkers of AD are used as standalone diagnostic markers or considered in the primary care setting.
We have made remarkable progress toward more precise molecular diagnosis of brain diseases underlying cognitive impairment and dementia. Ongoing efforts to evaluate the utility of these measures in clinical practice include the need to increase diversity of patients and providers. Ultimately, the tremendous progress in molecular biomarkers for the diseases causing dementia will help the field work toward our common goal of early and accurate diagnosis, better management, and hope for people living with these diseases.
Bradford C. Dickerson, MD, MMSc, is a professor, department of neurology, Harvard Medical School, and director, Frontotemporal Disorders Unit, department of neurology, at Massachusetts General Hospital, both in Boston.
A version of this article first appeared on Medscape.com.
The field of neurodegenerative dementias, particularly Alzheimer’s disease (AD), has been revolutionized by the development of imaging and cerebrospinal fluid biomarkers and is on the brink of a new development: emerging plasma biomarkers. Research now recognizes the relationship between the cognitive-behavioral syndromic diagnosis (that is, the illness) and the etiologic diagnosis (the disease) – and the need to consider each separately when developing a diagnostic formulation. The National Institute on Aging and Alzheimer’s Association Research Framework uses the amyloid, tau, and neurodegeneration system to define AD biologically in living patients. Here is an overview of the framework, which requires biomarker evidence of amyloid plaques (amyloid positivity) and neurofibrillary tangles (tau positivity), with evidence of neurodegeneration (neurodegeneration positivity) to support the diagnosis.
The diagnostic approach for symptomatic patients
The differential diagnosis in symptomatic patients with mild cognitive impairment (MCI), mild behavioral impairment, or dementia is broad and includes multiple neurodegenerative diseases (for example, AD, frontotemporal lobar degeneration, dementia with Lewy bodies, argyrophilic grain disease, hippocampal sclerosis); vascular ischemic brain injury (for example, stroke); tumors; infectious, inflammatory, paraneoplastic, or demyelinating diseases; trauma; hydrocephalus; toxic/metabolic insults; and other rare diseases. The patient’s clinical syndrome narrows the differential diagnosis.
Once the clinician has a prioritized differential diagnosis of the brain disease or condition that is probably causing or contributing to the patient’s signs and symptoms, they can then select appropriate assessments and tests, typically starting with a laboratory panel and brain MRI. Strong evidence backed by practice recommendations also supports the use of fluorodeoxyglucose PET as a marker of functional brain abnormalities associated with dementia. Although molecular biomarkers are typically considered at the later stage of the clinical workup, the anticipated future availability of plasma biomarkers will probably change the timing of molecular biomarker assessment in patients with suspected cognitive impairment owing to AD.
Molecular PET biomarkers
Three PET tracers approved by the U.S. Food and Drug Administration for the detection of cerebral amyloid plaques have high sensitivity (89%-98%) and specificity (88%-100%), compared with autopsy, the gold standard diagnostic tool. However, these scans are costly and are not reimbursed by Medicare and Medicaid. Because all amyloid PET scans are covered by the Veterans Administration, this test is more readily accessible for patients receiving VA benefits.
The appropriate-use criteria developed by the Amyloid Imaging Task Force recommends amyloid PET for patients with persistent or progressive MCI or dementia. In such patients, a negative amyloid PET scan would strongly weigh against AD, supporting a differential diagnosis of other etiologies. Although a positive amyloid PET scan in patients with MCI or dementia indicates the presence of amyloid plaques, it does not necessarily confirm AD as the cause. Cerebral amyloid plaques may coexist with other pathologies and increase with age, even in cognitively normal individuals.
The IDEAS study looked at the clinical utility of amyloid PET in a real-world dementia specialist setting. In the study, dementia subspecialists documented their presumed etiologic diagnosis (and level of confidence) before and after amyloid PET. Of the 11,409 patients who completed the study, the etiologic diagnosis changed from AD to non-AD in just over 25% of cases and from non-AD to AD in 10.5%. Clinical management changed in about 60% of patients with MCI and 63.5% of patients with dementia.
In May 2020, the FDA approved flortaucipir F-18, the first diagnostic tau radiotracer for use with PET to estimate the density and distribution of aggregated tau neurofibrillary tangles in adults with cognitive impairment undergoing evaluation for AD. Regulatory approval of flortaucipir F-18 was based on findings from two clinical trials of terminally ill patients who were followed to autopsy. The studies included patients with a spectrum of clinically diagnosed dementias and those with normal cognition. The primary outcome of the studies was accurate visual interpretation of the images in detecting advanced AD tau neurofibrillary tangle pathology (Braak stage V or VI tau pathology). Sensitivity of five trained readers ranged from 68% to 86%, and specificity ranged from 63% to 100%; interrater agreement was 0.87. Tau PET is not yet reimbursed and is therefore not yet readily available in the clinical setting. Moreover, appropriate use criteria have not yet been published.
Molecular fluid biomarkers
Cerebrospinal fluid (CSF) analysis is currently the most readily available and reimbursed test to aid in diagnosing AD, with appropriate-use criteria for patients with suspected AD. CSF biomarkers for AD are useful in cognitively impaired patients when the etiologic diagnosis is equivocal, there is only an intermediate level of diagnostic confidence, or there is very high confidence in the etiologic diagnosis. Testing for CSF biomarkers is also recommended for patients at very early clinical stages (for example, early MCI) or with atypical clinical presentations.
A decreased concentration of amyloid-beta 42 in CSF is a marker of amyloid neuritic plaques in the brain. An increased concentration of total tau in CSF reflects injury to neurons, and an increased concentration of specific isoforms of hyperphosphorylated tau reflects neurofibrillary tangles. Presently, the ratios of t-tau to amyloid-beta 42, amyloid-beta 42 to amyloid-beta 40, and phosphorylated-tau 181 to amyloid-beta 42 are the best-performing markers of AD neuropathologic changes and are more accurate than assessing individual biomarkers. These CSF biomarkers of AD have been validated against autopsy, and ratio values of CSF amyloid-beta 42 have been further validated against amyloid PET, with overall sensitivity and specificity of approximately 90% and 84%, respectively.
Some of the most exciting recent advances in AD center around the measurement of these proteins and others in plasma. Appropriate-use criteria for plasma biomarkers in the evaluation of patients with cognitive impairment were published in 2022. In addition to their use in clinical trials, these criteria cautiously recommend using these biomarkers in specialized memory clinics in the diagnostic workup of patients with cognitive symptoms, along with confirmatory CSF markers or PET. Additional data are needed before plasma biomarkers of AD are used as standalone diagnostic markers or considered in the primary care setting.
We have made remarkable progress toward more precise molecular diagnosis of brain diseases underlying cognitive impairment and dementia. Ongoing efforts to evaluate the utility of these measures in clinical practice include the need to increase diversity of patients and providers. Ultimately, the tremendous progress in molecular biomarkers for the diseases causing dementia will help the field work toward our common goal of early and accurate diagnosis, better management, and hope for people living with these diseases.
Bradford C. Dickerson, MD, MMSc, is a professor, department of neurology, Harvard Medical School, and director, Frontotemporal Disorders Unit, department of neurology, at Massachusetts General Hospital, both in Boston.
A version of this article first appeared on Medscape.com.
Unlocking the riddle of REM sleep
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.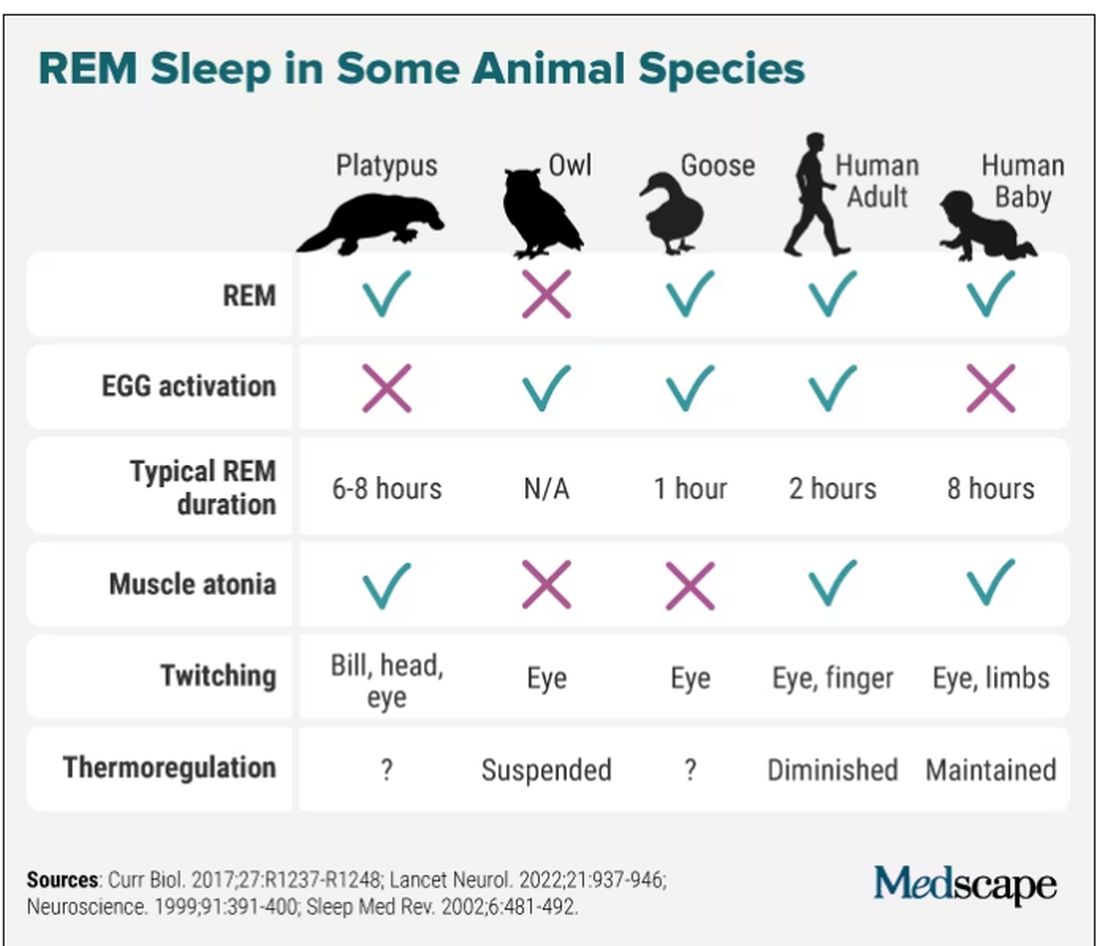
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.