User login
Enterovirus D68 – An emerging threat to child health
In August 2014, we first heard of increased pediatric cases of severe respiratory tract disease, many requiring management in the ICU, and of acute flaccid myelitis/paralysis (AFM) of unknown etiology from many states across the United States. Concurrently with this outbreak in the United States, similar clinical cases were reported in Canada and Europe. Subsequently, enterovirus D68 was confirmed in some, but not all, of the paralyzed children. Although new to many of us, enterovirus D68 was already known as an atypical enterovirus sharing many of its structural and chemical properties with rhinovirus. For example, it most often was reported from respiratory samples and less common from stool samples. It also had been associated with clusters of respiratory disease since 2000 and a 2008 case of fatal AFM.
There were 120 cases of AFM, coinciding with the nationwide outbreak of enteroviral D68 disease, reported in 2014. The Centers for Disease Control and Prevention has evaluated the cerebrospinal fluid in many of these cases, and no pathogen has consistently been detected. The children were mostly school age, aged 7-11 years, presented with acute, febrile respiratory illness followed by acute onset of cranial nerve dysfunction or flaccid paralysis of one or more limbs. The CSF revealed mild pleocytosis, most often with mild elevation of protein and a normal glucose. However, the MRI was distinctly abnormal with focal lesion in the cranial nerve nuclei (in those with bulbar dysfunction) and/or in the anterior horn or spinal cord gray matter. Long-term prognosis is unknown, although most patients have persistent weakness, despite some improvement, to date.
In 2016, the CDC has reported an increase in cases after a decline in 2015 despite the absence of epidemic respiratory tract disease in the United States from enterovirus D68. In the Netherlands, an increase in respiratory disease from enterovirus D68 in children and adults also has been reported since June 2016. Respiratory disease has been observed in children as young as 3 months of age, and most of the children have underlying comorbidity, many with asthma or other pulmonary conditions. Thirteen of 17 (77%) cases in children have required ICU admission, while most of the adult cases were mild and influenzalike. One child developed bulbar dysfunction and limb weakness.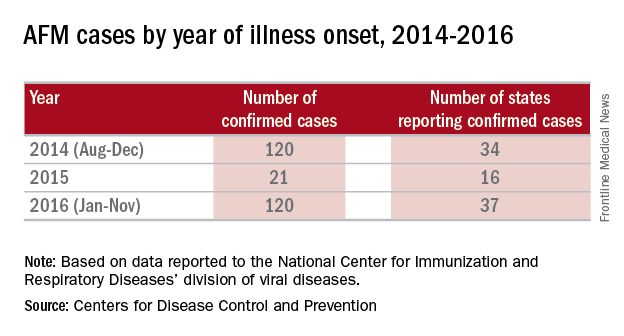
Enterovirus D68 infection should be suspected in children with moderate to severe respiratory tract infection or acute onset bulbar or flaccid paralysis of unknown etiology, especially in summer and fall. In such cases, respiratory specimens (nasopharyngeal or oral swabs or wash, tracheal secretions or bronchoalveolar lavage) should be obtained. Increasingly, hospitals and laboratories can perform multiplex polymerase chain reaction testing for enterovirus/rhinovirus. However, most do not determine the specific enterovirus. CDC and some state health departments use real-time reverse transcription polymerase chain reaction (rRT-PCR), which enables reporting of specific enterovirus species within days. CDC recommends that clinicians consider enterovirus D68 testing for children with unknown, severe respiratory illness or AFM. Details for sending specimens should be available from your state’s Department of Public Health website or the CDC.
Prevention strategies may be critical for limiting the spread of enterovirus D68 in the community. The CDC recommends:
- Wash your hands often with soap and water for 20 seconds.
- Avoid touching your eyes, nose and mouth with unwashed hands.
- Avoid close contact such as kissing, hugging, and sharing cups with people who are ill.
- Cover your coughs and sneezes with a tissue or shirt sleeve, not your hands.
- Clean and disinfect frequently touched surfaces, such as toys and doorknobs, especially if someone is sick.
- Stay home when you are ill.
In 2014, it was speculated that the epidemic might have been a one-time event. It now appears more likely that enterovirus D68 activity has been increasing since 2000, and that children and immunocompromised hosts will be at greatest risk because of a lack of neutralizing antibody. Ongoing enterovirus surveillance will be critical to understand the potential for severe respiratory disease as will the development of new and effective antivirals. A vaccine for enterovirus 71 recently demonstrated efficacy against hand, foot, and mouth disease in children and may provide insights into the development of vaccines against enterovirus D68.
References
Lancet Infect Dis. 2016 May;16(5):e64-75
Emerg Infect Dis. 2017 Jan;23(1):140-3.
J Med Virol. 2016 May;88(5):739-45
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
In August 2014, we first heard of increased pediatric cases of severe respiratory tract disease, many requiring management in the ICU, and of acute flaccid myelitis/paralysis (AFM) of unknown etiology from many states across the United States. Concurrently with this outbreak in the United States, similar clinical cases were reported in Canada and Europe. Subsequently, enterovirus D68 was confirmed in some, but not all, of the paralyzed children. Although new to many of us, enterovirus D68 was already known as an atypical enterovirus sharing many of its structural and chemical properties with rhinovirus. For example, it most often was reported from respiratory samples and less common from stool samples. It also had been associated with clusters of respiratory disease since 2000 and a 2008 case of fatal AFM.
There were 120 cases of AFM, coinciding with the nationwide outbreak of enteroviral D68 disease, reported in 2014. The Centers for Disease Control and Prevention has evaluated the cerebrospinal fluid in many of these cases, and no pathogen has consistently been detected. The children were mostly school age, aged 7-11 years, presented with acute, febrile respiratory illness followed by acute onset of cranial nerve dysfunction or flaccid paralysis of one or more limbs. The CSF revealed mild pleocytosis, most often with mild elevation of protein and a normal glucose. However, the MRI was distinctly abnormal with focal lesion in the cranial nerve nuclei (in those with bulbar dysfunction) and/or in the anterior horn or spinal cord gray matter. Long-term prognosis is unknown, although most patients have persistent weakness, despite some improvement, to date.
In 2016, the CDC has reported an increase in cases after a decline in 2015 despite the absence of epidemic respiratory tract disease in the United States from enterovirus D68. In the Netherlands, an increase in respiratory disease from enterovirus D68 in children and adults also has been reported since June 2016. Respiratory disease has been observed in children as young as 3 months of age, and most of the children have underlying comorbidity, many with asthma or other pulmonary conditions. Thirteen of 17 (77%) cases in children have required ICU admission, while most of the adult cases were mild and influenzalike. One child developed bulbar dysfunction and limb weakness.
Enterovirus D68 infection should be suspected in children with moderate to severe respiratory tract infection or acute onset bulbar or flaccid paralysis of unknown etiology, especially in summer and fall. In such cases, respiratory specimens (nasopharyngeal or oral swabs or wash, tracheal secretions or bronchoalveolar lavage) should be obtained. Increasingly, hospitals and laboratories can perform multiplex polymerase chain reaction testing for enterovirus/rhinovirus. However, most do not determine the specific enterovirus. CDC and some state health departments use real-time reverse transcription polymerase chain reaction (rRT-PCR), which enables reporting of specific enterovirus species within days. CDC recommends that clinicians consider enterovirus D68 testing for children with unknown, severe respiratory illness or AFM. Details for sending specimens should be available from your state’s Department of Public Health website or the CDC.
Prevention strategies may be critical for limiting the spread of enterovirus D68 in the community. The CDC recommends:
- Wash your hands often with soap and water for 20 seconds.
- Avoid touching your eyes, nose and mouth with unwashed hands.
- Avoid close contact such as kissing, hugging, and sharing cups with people who are ill.
- Cover your coughs and sneezes with a tissue or shirt sleeve, not your hands.
- Clean and disinfect frequently touched surfaces, such as toys and doorknobs, especially if someone is sick.
- Stay home when you are ill.
In 2014, it was speculated that the epidemic might have been a one-time event. It now appears more likely that enterovirus D68 activity has been increasing since 2000, and that children and immunocompromised hosts will be at greatest risk because of a lack of neutralizing antibody. Ongoing enterovirus surveillance will be critical to understand the potential for severe respiratory disease as will the development of new and effective antivirals. A vaccine for enterovirus 71 recently demonstrated efficacy against hand, foot, and mouth disease in children and may provide insights into the development of vaccines against enterovirus D68.
References
Lancet Infect Dis. 2016 May;16(5):e64-75
Emerg Infect Dis. 2017 Jan;23(1):140-3.
J Med Virol. 2016 May;88(5):739-45
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
In August 2014, we first heard of increased pediatric cases of severe respiratory tract disease, many requiring management in the ICU, and of acute flaccid myelitis/paralysis (AFM) of unknown etiology from many states across the United States. Concurrently with this outbreak in the United States, similar clinical cases were reported in Canada and Europe. Subsequently, enterovirus D68 was confirmed in some, but not all, of the paralyzed children. Although new to many of us, enterovirus D68 was already known as an atypical enterovirus sharing many of its structural and chemical properties with rhinovirus. For example, it most often was reported from respiratory samples and less common from stool samples. It also had been associated with clusters of respiratory disease since 2000 and a 2008 case of fatal AFM.
There were 120 cases of AFM, coinciding with the nationwide outbreak of enteroviral D68 disease, reported in 2014. The Centers for Disease Control and Prevention has evaluated the cerebrospinal fluid in many of these cases, and no pathogen has consistently been detected. The children were mostly school age, aged 7-11 years, presented with acute, febrile respiratory illness followed by acute onset of cranial nerve dysfunction or flaccid paralysis of one or more limbs. The CSF revealed mild pleocytosis, most often with mild elevation of protein and a normal glucose. However, the MRI was distinctly abnormal with focal lesion in the cranial nerve nuclei (in those with bulbar dysfunction) and/or in the anterior horn or spinal cord gray matter. Long-term prognosis is unknown, although most patients have persistent weakness, despite some improvement, to date.
In 2016, the CDC has reported an increase in cases after a decline in 2015 despite the absence of epidemic respiratory tract disease in the United States from enterovirus D68. In the Netherlands, an increase in respiratory disease from enterovirus D68 in children and adults also has been reported since June 2016. Respiratory disease has been observed in children as young as 3 months of age, and most of the children have underlying comorbidity, many with asthma or other pulmonary conditions. Thirteen of 17 (77%) cases in children have required ICU admission, while most of the adult cases were mild and influenzalike. One child developed bulbar dysfunction and limb weakness.
Enterovirus D68 infection should be suspected in children with moderate to severe respiratory tract infection or acute onset bulbar or flaccid paralysis of unknown etiology, especially in summer and fall. In such cases, respiratory specimens (nasopharyngeal or oral swabs or wash, tracheal secretions or bronchoalveolar lavage) should be obtained. Increasingly, hospitals and laboratories can perform multiplex polymerase chain reaction testing for enterovirus/rhinovirus. However, most do not determine the specific enterovirus. CDC and some state health departments use real-time reverse transcription polymerase chain reaction (rRT-PCR), which enables reporting of specific enterovirus species within days. CDC recommends that clinicians consider enterovirus D68 testing for children with unknown, severe respiratory illness or AFM. Details for sending specimens should be available from your state’s Department of Public Health website or the CDC.
Prevention strategies may be critical for limiting the spread of enterovirus D68 in the community. The CDC recommends:
- Wash your hands often with soap and water for 20 seconds.
- Avoid touching your eyes, nose and mouth with unwashed hands.
- Avoid close contact such as kissing, hugging, and sharing cups with people who are ill.
- Cover your coughs and sneezes with a tissue or shirt sleeve, not your hands.
- Clean and disinfect frequently touched surfaces, such as toys and doorknobs, especially if someone is sick.
- Stay home when you are ill.
In 2014, it was speculated that the epidemic might have been a one-time event. It now appears more likely that enterovirus D68 activity has been increasing since 2000, and that children and immunocompromised hosts will be at greatest risk because of a lack of neutralizing antibody. Ongoing enterovirus surveillance will be critical to understand the potential for severe respiratory disease as will the development of new and effective antivirals. A vaccine for enterovirus 71 recently demonstrated efficacy against hand, foot, and mouth disease in children and may provide insights into the development of vaccines against enterovirus D68.
References
Lancet Infect Dis. 2016 May;16(5):e64-75
Emerg Infect Dis. 2017 Jan;23(1):140-3.
J Med Virol. 2016 May;88(5):739-45
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Meta-analysis compares infliximab with tacrolimus in ulcerative colitis
ORLANDO – Infliximab and tacrolimus each demonstrate efficacy for treatment of moderate to severe active ulcerative colitis in published studies. However, it remains unknown if one agent offers greater efficacy than the other in this patient population, so researchers in Japan conducted a meta-analysis to find out more.
Lead investigator Shinichi Kawano, MD, at Kyushu University, Fukuoka, Japan, and his colleagues searched PubMed for relevant studies up until August 2016. They conducted a systematic review and identified 79 potential studies of tumor necrosis factor blocker infliximab (Remicade, Janssen) and the calcineurin inhibitor tacrolimus (various brands) in this patient population. They ruled out the vast majority, 75 studies, for not directly comparing therapeutic efficacy. They also excluded one additional study for insufficient data on their five outcomes of interest: rates of clinical remission, clinical response, freedom from colectomy, adverse events, and serious adverse events. They focused on three 2016 retrospective studies with a total of 244 patients, and added 13 of their own patients, 5 taking infliximab and 8 taking tacrolimus, to their dataset.
Similarly, the short-term clinical response rate favored infliximab (overall RR, 1.55), but again the difference was not statistically significant.
The investigators found the rate of colectomy was comparable between patients taking infliximab and tacrolimus (overall RR, 1.01). They reported their findings in a poster presentation at the Advances in Inflammatory Bowel Diseases meeting, sponsored by the Crohn’s & Colitis Foundation of America.
The adverse event rate favored tacrolimus over infliximab, but it was not significant (overall RR, 0.23). The serious adverse event rate slightly favored tacrolimus as well (overall RR, 0.88). The incidences of adverse events and serious adverse events were comparable between the two groups, the study authors wrote.
The trials included in the meta-analysis looked at either adults only or adults and pediatric patients with active ulcerative colitis. In one study, there were 40 patients taking infliximab and 50 taking tacrolimus (Aliment Pharmacol Ther. 2016;43:705-16); in another 48 patients took infliximab and 47 took tacrolimus (Gastroenterol Res Pract. 2016;2016:3162595); and in the third study 30 were treated with infliximab and 29 with tacrolimus (Scand J Gastroenterol. 2016;51:700-5).
“This meta-analysis demonstrates equivalent therapeutic efficacy and safety between infliximab and tacrolimus,” the authors continued. Dr. Kawano said he was not surprised by the findings. “Because there are only three retrospective studies, it is reasonable that there is no significant difference in efficacy between infliximab and tacrolimus.”
However, he added, “We think that further prospective, comparative trials are needed.”
Dr. Kawano had no relevant financial disclosures.
ORLANDO – Infliximab and tacrolimus each demonstrate efficacy for treatment of moderate to severe active ulcerative colitis in published studies. However, it remains unknown if one agent offers greater efficacy than the other in this patient population, so researchers in Japan conducted a meta-analysis to find out more.
Lead investigator Shinichi Kawano, MD, at Kyushu University, Fukuoka, Japan, and his colleagues searched PubMed for relevant studies up until August 2016. They conducted a systematic review and identified 79 potential studies of tumor necrosis factor blocker infliximab (Remicade, Janssen) and the calcineurin inhibitor tacrolimus (various brands) in this patient population. They ruled out the vast majority, 75 studies, for not directly comparing therapeutic efficacy. They also excluded one additional study for insufficient data on their five outcomes of interest: rates of clinical remission, clinical response, freedom from colectomy, adverse events, and serious adverse events. They focused on three 2016 retrospective studies with a total of 244 patients, and added 13 of their own patients, 5 taking infliximab and 8 taking tacrolimus, to their dataset.
Similarly, the short-term clinical response rate favored infliximab (overall RR, 1.55), but again the difference was not statistically significant.
The investigators found the rate of colectomy was comparable between patients taking infliximab and tacrolimus (overall RR, 1.01). They reported their findings in a poster presentation at the Advances in Inflammatory Bowel Diseases meeting, sponsored by the Crohn’s & Colitis Foundation of America.
The adverse event rate favored tacrolimus over infliximab, but it was not significant (overall RR, 0.23). The serious adverse event rate slightly favored tacrolimus as well (overall RR, 0.88). The incidences of adverse events and serious adverse events were comparable between the two groups, the study authors wrote.
The trials included in the meta-analysis looked at either adults only or adults and pediatric patients with active ulcerative colitis. In one study, there were 40 patients taking infliximab and 50 taking tacrolimus (Aliment Pharmacol Ther. 2016;43:705-16); in another 48 patients took infliximab and 47 took tacrolimus (Gastroenterol Res Pract. 2016;2016:3162595); and in the third study 30 were treated with infliximab and 29 with tacrolimus (Scand J Gastroenterol. 2016;51:700-5).
“This meta-analysis demonstrates equivalent therapeutic efficacy and safety between infliximab and tacrolimus,” the authors continued. Dr. Kawano said he was not surprised by the findings. “Because there are only three retrospective studies, it is reasonable that there is no significant difference in efficacy between infliximab and tacrolimus.”
However, he added, “We think that further prospective, comparative trials are needed.”
Dr. Kawano had no relevant financial disclosures.
ORLANDO – Infliximab and tacrolimus each demonstrate efficacy for treatment of moderate to severe active ulcerative colitis in published studies. However, it remains unknown if one agent offers greater efficacy than the other in this patient population, so researchers in Japan conducted a meta-analysis to find out more.
Lead investigator Shinichi Kawano, MD, at Kyushu University, Fukuoka, Japan, and his colleagues searched PubMed for relevant studies up until August 2016. They conducted a systematic review and identified 79 potential studies of tumor necrosis factor blocker infliximab (Remicade, Janssen) and the calcineurin inhibitor tacrolimus (various brands) in this patient population. They ruled out the vast majority, 75 studies, for not directly comparing therapeutic efficacy. They also excluded one additional study for insufficient data on their five outcomes of interest: rates of clinical remission, clinical response, freedom from colectomy, adverse events, and serious adverse events. They focused on three 2016 retrospective studies with a total of 244 patients, and added 13 of their own patients, 5 taking infliximab and 8 taking tacrolimus, to their dataset.
Similarly, the short-term clinical response rate favored infliximab (overall RR, 1.55), but again the difference was not statistically significant.
The investigators found the rate of colectomy was comparable between patients taking infliximab and tacrolimus (overall RR, 1.01). They reported their findings in a poster presentation at the Advances in Inflammatory Bowel Diseases meeting, sponsored by the Crohn’s & Colitis Foundation of America.
The adverse event rate favored tacrolimus over infliximab, but it was not significant (overall RR, 0.23). The serious adverse event rate slightly favored tacrolimus as well (overall RR, 0.88). The incidences of adverse events and serious adverse events were comparable between the two groups, the study authors wrote.
The trials included in the meta-analysis looked at either adults only or adults and pediatric patients with active ulcerative colitis. In one study, there were 40 patients taking infliximab and 50 taking tacrolimus (Aliment Pharmacol Ther. 2016;43:705-16); in another 48 patients took infliximab and 47 took tacrolimus (Gastroenterol Res Pract. 2016;2016:3162595); and in the third study 30 were treated with infliximab and 29 with tacrolimus (Scand J Gastroenterol. 2016;51:700-5).
“This meta-analysis demonstrates equivalent therapeutic efficacy and safety between infliximab and tacrolimus,” the authors continued. Dr. Kawano said he was not surprised by the findings. “Because there are only three retrospective studies, it is reasonable that there is no significant difference in efficacy between infliximab and tacrolimus.”
However, he added, “We think that further prospective, comparative trials are needed.”
Dr. Kawano had no relevant financial disclosures.
AT AIBD 2016
Key clinical point: Infliximab and tacrolimus both demonstrate efficacy for active ulcerative colitis in published studies, but few direct comparisons exist.
Major finding: The reported rate of clinical remission with infliximab was higher than with tacrolimus (risk ratio, 1.17), but the difference was not statistically significant.
Data source: Meta-analysis of relevant articles identified in a PubMed search through August 2016.
Disclosures: Dr. Kawano had no relevant financial disclosures.
FDA warns of false-positive results with Zika IgM test
, according to a safety alert issued by the Food and Drug Administration.
The ZIKV Detect IgM Capture ELISA test is the first commercially available Zika serological IgM test – it was approved by the FDA in August 2016 and is used by several commercial laboratories. The test reports only presumptive positive results and a sample has to be sent to the Centers for Disease Control and Prevention for confirmation. Final results can take up to a month to be delivered. In most instances, the preliminary test results have matched the confirmed sample results.
The FDA recommends that health care providers inform patients that presumptive positive results need to be confirmed and that they not rely on positive IgM test results as the sole basis of patient management. If a patient is pregnant, the FDA recommends contacting the laboratory to expedite the confirmation testing.
FDA officials are working with LabCorp and ZIKV Detect manufacturer InBios International to determine if the false-positive results are related to problems with the test or the commercial testing facility.
Find the full safety alert on the FDA website.
, according to a safety alert issued by the Food and Drug Administration.
The ZIKV Detect IgM Capture ELISA test is the first commercially available Zika serological IgM test – it was approved by the FDA in August 2016 and is used by several commercial laboratories. The test reports only presumptive positive results and a sample has to be sent to the Centers for Disease Control and Prevention for confirmation. Final results can take up to a month to be delivered. In most instances, the preliminary test results have matched the confirmed sample results.
The FDA recommends that health care providers inform patients that presumptive positive results need to be confirmed and that they not rely on positive IgM test results as the sole basis of patient management. If a patient is pregnant, the FDA recommends contacting the laboratory to expedite the confirmation testing.
FDA officials are working with LabCorp and ZIKV Detect manufacturer InBios International to determine if the false-positive results are related to problems with the test or the commercial testing facility.
Find the full safety alert on the FDA website.
, according to a safety alert issued by the Food and Drug Administration.
The ZIKV Detect IgM Capture ELISA test is the first commercially available Zika serological IgM test – it was approved by the FDA in August 2016 and is used by several commercial laboratories. The test reports only presumptive positive results and a sample has to be sent to the Centers for Disease Control and Prevention for confirmation. Final results can take up to a month to be delivered. In most instances, the preliminary test results have matched the confirmed sample results.
The FDA recommends that health care providers inform patients that presumptive positive results need to be confirmed and that they not rely on positive IgM test results as the sole basis of patient management. If a patient is pregnant, the FDA recommends contacting the laboratory to expedite the confirmation testing.
FDA officials are working with LabCorp and ZIKV Detect manufacturer InBios International to determine if the false-positive results are related to problems with the test or the commercial testing facility.
Find the full safety alert on the FDA website.
Conference News Roundup—Radiological Society of North America
Studies Provide More Insight Into Zika Effects
Three studies reported on the effects of the Zika virus outbreak in Brazil. The first study examined CT findings of the CNS in 16 newborn babies with congenital Zika virus infection confirmed by tests in CSF. The researchers identified a pattern of CT brain findings in the babies, including decreased brain volume, simplified gyral pattern, calcifications, ventricular dilatation, and prominent occipital bone.
"We live in Pernambuco, a state in northeastern Brazil, which had the highest number of patients with microcephaly during the Zika outbreak in our country," said Natacha Calheiros de Lima Petribu, MD, of the Department of Radiology at Barão de Lucena Hospital. "Our study proves that Zika virus infection can cause congenital brain damage in babies with and without microcephaly."
Another study analyzed the imaging results of three target groups affected by Zika: adults who developed acute neurologic syndrome, newborns with vertical infection with neurologic disorders, and pregnant women with rash outbreaks suggestive of Zika. Many of the adults had symptoms of Guillain-Barré syndrome. A few showed inflammation of the brain and spinal cord (ie, Bickerstaff's encephalitis) or brainstem and spinal cord lesions. Common MRI findings included enhancement of certain spinal and facial nerves. In the newborns, MRI showed orbital injuries and anatomical changes in brain tissue.
"It was alarming to find so many cases of neurologic syndromes in adults, some very serious, related to Zika virus infection," said study author Emerson de Melo Casagrande, MD, of the Department of Radiology at Antonio Pedro University Hospital--Federal Fluminense University. "We have also noticed a difference between these syndromes, even though the trigger was the same."
In a third study, ultrasound and fetal MRI were performed on pregnant patients with Zika virus infection at different gestational ages. Once the babies were born, they underwent ultrasound, CT, and MRI. The researchers then created 3-D virtual and physical models of the skulls. More than half of the babies had microcephaly, brain calcifications, and loss of brain tissue volume, along with other structural changes.
"The emergence of Zika virus in the Americas has coincided with increased reports of babies born with microcephaly," said study author Heron Werner Jr, MD, PhD, of the Department of Radiology at Clínica de Diagnóstico por Imagem. "An early diagnosis may help in treating these babies after birth. Moreover, the knowledge of abnormalities present in the CNS may give hints about the pathophysiology of the disease."
Head Impacts Lead to Brain Changes in High School Football Players
Brain imaging exams performed on high school football players after a single season reveal changes in the gray and white matter that correlated with exposure to head impacts, according to researchers.
"It is important to understand the potential changes occurring in the brain related to youth contact sports," said Elizabeth Moody Davenport, PhD, a postdoctoral researcher at UT Southwestern Medical Center in Dallas. "We know that some professional football players suffer from a serious condition called chronic traumatic encephalopathy or CTE. We are attempting to find out when and how that process starts, so that we can keep sports a healthy activity for millions of children and adolescents."
The study included 24 players from a high school football team in North Carolina, each of whom wore a helmet outfitted with the Head Impact Telemetry System (HITS) during all practices and games. The helmets are lined with six accelerometers that measure the magnitude, location, and direction of a hit. Data from the helmets can be uploaded to a computer for analysis.
"We saw changes in these young players' brains on both structural and functional imaging after a single season of football," said Dr. Davenport.
In the study, each player underwent pre- and post-season imaging, including a specialized MRI scan, from which diffusion tensor imaging and diffusion kurtosis imaging data were extracted to measure the brain's white matter integrity, and a magnetoencephalography (MEG) scan, which records and analyzes the magnetic fields produced by brain waves. Diffusion imaging can measure the structural white matter changes in the brain, and MEG assesses changes in function.
"MEG can be used to measure delta waves in the brain, which are a type of distress signal," said Dr. Davenport. "Delta waves represent slow wave activity that increases after brain injuries. The delta waves we saw came from the surface of the brain, while diffusion imaging is a measure of the white matter deeper in the brain."
The research team calculated the change in imaging metrics between the pre- and post-season imaging exams. They measured abnormalities observed on diffusion imaging and abnormally increased delta-wave activity on MEG. The imaging results were then combined with player-specific impact data from the HITS. None of the 24 players were diagnosed with a concussion during the study.
Players with greater head impact exposure had the greatest change in diffusion imaging and MEG metrics. "Change in diffusion imaging metrics correlated most to linear acceleration, similar to the impact of a car crash," said Dr. Davenport. "MEG changes correlated most to rotational impact, similar to a boxer's punch. These results demonstrate that you need both imaging metrics to assess impact exposure, because they correlate with different biomechanical processes."
Similar studies are being conducted this fall, and a consortium has been formed to continue the brain imaging research in youth contact sports across the country, said Dr. Davenport. "Without a larger population that is closely followed in a longitudinal study, it is difficult to know the long-term effects of these changes," she said. "We do not know if the brain's developmental trajectory is altered, or if the off-season time allows for the brain to return to normal."
Depression in Soldiers Linked to Brain Disruption From Injury
Using multiple brain imaging techniques, researchers have found that a disruption of the circuitry in the brain's cognitive-emotional pathways may provide a physical foundation for depression symptoms in some service members who have had mild traumatic brain injury (mTBI) in combat. "We can link these connectivity changes in the brain to poor top-down emotional processing and greater maladaptive rumination, or worrying, in symptomatic depressed soldiers after mTBI," said Ping-Hong Yeh, PhD, scientist and physicist at the National Intrepid Center of Excellence, Walter Reed National Military Medical Center in Bethesda, Maryland.
According to the Defense and Veterans Brain Injury Center, 352,619 service members worldwide have been diagnosed with TBI since 2000, the majority of these cases being mTBI. In addition, psychiatric disorders, such as anxiety and major depressive disorders, are becoming common in military personnel with brain injuries.
"With the increased survival of soldiers due to improvements in body armor and advanced medical care, there has been an increase in the number of soldiers surviving major trauma. Consequently, a large number of soldiers are returning from war with mTBI," said Dr. Yeh. "Mood disorders are common in military-related mTBI patients. This is an ongoing problem facing a large number of warriors in current areas of conflict, and it is likely to be a persistent problem for the foreseeable future."
For the study, researchers used diffusion-weighted imaging (DWI) and resting-state functional MRI (fMRI) to examine 130 active male service members diagnosed with mTBI and a control group of 52 men without mTBI. Depression symptoms were rated based on the Beck Depression Inventory (BDI), a 21-item, self-reporting assessment that measures characteristic attitudes and symptoms of depression. Patients with a BDI score greater than 20 are considered to have moderate to severe depression symptoms.
BDI scores showed that 75 of the patients with mTBI had moderate to severe depression symptoms. Imaging results showed that white matter tracts—the circuits that connect brain regions critical for cognitive and emotional control—were disrupted in the patients with moderate to severe depression symptoms. Researchers also saw changes in the gray matter cognitive-emotional networks in these patients.
"We found consistencies in the locations of disrupted neurocircuitry, as revealed by DWI and resting-state fMRI, that are unique to the clinical symptoms of mTBI patients," said Dr. Yeh. "We have related the brain structural and functional changes in cognitive-emotional networks to depressive symptoms in mTBI patients."
This research can possibly lead to treatment strategies in the future, he added. "Though the results of this study were not applied directly to patient care, the neuroimaging changes we found might be incorporated into treatment plans for personalized medicine in the future."
Short-Term Sleep Deprivation Affects Heart Function
Getting too little sleep takes a toll on your heart, researchers reported. People who work in fire and emergency medical services, medical residencies, and other high-stress jobs are often called upon to work 24-hour shifts with little opportunity for sleep. While it is known that extreme fatigue can affect many physical, cognitive, and emotional processes, this is the first study to examine how working a 24-hour shift specifically affects cardiac function.
"For the first time, we have shown that short-term sleep deprivation in the context of 24-hour shifts can lead to a significant increase in cardiac contractility, blood pressure, and heart rate," said study author Daniel Kuetting, MD, of the Department of Diagnostic and Interventional Radiology at the University of Bonn in Germany.
For the study, Dr. Kuetting and colleagues recruited 20 healthy radiologists (19 men) with a mean age of 31.6. Each of the study participants underwent cardiovascular magnetic resonance (CMR) imaging with strain analysis before and after a 24-hour shift with an average of three hours of sleep.
"Cardiac function in the context of sleep deprivation has not previously been investigated with CMR strain analysis, the most sensitive parameter of cardiac contractility," said Dr. Kuetting. The researchers also collected blood and urine samples from the participants and measured blood pressure and heart rate.
Following short-term sleep deprivation, the participants showed significant increases in mean peak systolic strain (-23.4 vs -21.9), systolic (118.5 mmHg vs 112.8 mmHg) and diastolic (69.2 mmHg vs 62.9 mmHg) blood pressure and heart rate (68.9 bpm vs 63.0 bpm). In addition, the participants had significant increases in levels of thyroid stimulating hormone (TSH), thyroid hormones FT3 and FT4, and cortisol.
Although the researchers were able to perform follow-up examinations of half of the participants after regular sleep, further study in a larger cohort is needed to determine possible long-term effects of sleep loss, said Dr. Kuetting.
"The study was designed to investigate real-life work-related sleep deprivation," said Dr. Kuetting. "While the participants were not permitted to consume caffeine or food and beverages containing theobromine, such as chocolate, nuts, or tea, we did not take into account factors like individual stress level or environmental stimuli."
As people continue to work longer hours or work at more than one job to make ends meet, it is critical to investigate the detrimental effects of too much work and not enough sleep. The results of this pilot study are transferable to other professions in which long periods of uninterrupted labor are common, said Dr. Kuetting. "These findings may help us better understand how workload and shift duration affect public health."
Aerobic Exercise Preserves Brain Volume and Improves Cognitive Function
Using a new MRI technique, researchers have found that adults with mild cognitive impairment (MCI) who exercised four times per week during a six-month period experienced an increase in brain volume in specific areas of the brain, but adults who participated in aerobic exercise experienced greater gains than those who just stretched.
"Even over a short period of time, we saw aerobic exercise lead to a remarkable change in the brain," said Laura D. Baker, PhD, Associate Professor of Gerontology and Geriatric Medicine at Wake Forest School of Medicine (WFSM) in Winston-Salem, North Carolina.
The study included 35 adults with MCI participating in a randomized, controlled trial of exercise intervention. The participants were separated into two groups. Sixteen adults (average age, 63) engaged in aerobic activity, including treadmill, stationary bike, or elliptical training, four times per week for six months. A control group of 19 adults (average age, 67) participated in stretching exercises with the same frequency. High-resolution brain MR images were acquired from all participants before and after the six-month activity period. The MRI results were compared using conventional and biomechanical metrics to measure the change in brain volume and shape.
"We used high-resolution MR images to measure anatomical changes within areas of the brain to obtain volumetric data and directional information," said Jeongchul Kim, PhD, a coinvestigator at WFSM.
The analysis revealed that for both the aerobic and stretching groups, brain volume increased in most gray matter regions, including the temporal lobe, which supports short-term memory.
"Compared to the stretching group, the aerobic activity group had greater preservation of total brain volume, increased local gray matter volume, and increased directional stretch of brain tissue," said Dr. Kim.
Among participants of the stretching group, the analysis revealed a local contraction, or atrophy, within the white matter connecting fibers. Such directional deformation, or shape change, is partially related to volume loss, but not always, according to Dr. Kim.
"Directional changes in the brain without local volume changes could be a novel biomarker for neurologic disease," he said. "It may be a more sensitive marker for the tiny changes that occur in a specific brain region before volumetric changes are detectable on MRI."
Both MRI measures are important to the treatment of MCI and Alzheimer's disease, which require the careful tracking of changes in the brain while patients engage in interventions, including diet and exercise, to slow the progression of the disease.
Study participants were tested to determine the effect of exercise intervention on cognitive performance. Participants in the aerobic exercise group showed statistically significant improvement in executive function after six months, whereas the stretching group did not improve.
"Any type of exercise can be beneficial," said Dr. Kim. "If possible, aerobic activity may create potential benefits for higher cognitive functioning."
Studies Provide More Insight Into Zika Effects
Three studies reported on the effects of the Zika virus outbreak in Brazil. The first study examined CT findings of the CNS in 16 newborn babies with congenital Zika virus infection confirmed by tests in CSF. The researchers identified a pattern of CT brain findings in the babies, including decreased brain volume, simplified gyral pattern, calcifications, ventricular dilatation, and prominent occipital bone.
"We live in Pernambuco, a state in northeastern Brazil, which had the highest number of patients with microcephaly during the Zika outbreak in our country," said Natacha Calheiros de Lima Petribu, MD, of the Department of Radiology at Barão de Lucena Hospital. "Our study proves that Zika virus infection can cause congenital brain damage in babies with and without microcephaly."
Another study analyzed the imaging results of three target groups affected by Zika: adults who developed acute neurologic syndrome, newborns with vertical infection with neurologic disorders, and pregnant women with rash outbreaks suggestive of Zika. Many of the adults had symptoms of Guillain-Barré syndrome. A few showed inflammation of the brain and spinal cord (ie, Bickerstaff's encephalitis) or brainstem and spinal cord lesions. Common MRI findings included enhancement of certain spinal and facial nerves. In the newborns, MRI showed orbital injuries and anatomical changes in brain tissue.
"It was alarming to find so many cases of neurologic syndromes in adults, some very serious, related to Zika virus infection," said study author Emerson de Melo Casagrande, MD, of the Department of Radiology at Antonio Pedro University Hospital--Federal Fluminense University. "We have also noticed a difference between these syndromes, even though the trigger was the same."
In a third study, ultrasound and fetal MRI were performed on pregnant patients with Zika virus infection at different gestational ages. Once the babies were born, they underwent ultrasound, CT, and MRI. The researchers then created 3-D virtual and physical models of the skulls. More than half of the babies had microcephaly, brain calcifications, and loss of brain tissue volume, along with other structural changes.
"The emergence of Zika virus in the Americas has coincided with increased reports of babies born with microcephaly," said study author Heron Werner Jr, MD, PhD, of the Department of Radiology at Clínica de Diagnóstico por Imagem. "An early diagnosis may help in treating these babies after birth. Moreover, the knowledge of abnormalities present in the CNS may give hints about the pathophysiology of the disease."
Head Impacts Lead to Brain Changes in High School Football Players
Brain imaging exams performed on high school football players after a single season reveal changes in the gray and white matter that correlated with exposure to head impacts, according to researchers.
"It is important to understand the potential changes occurring in the brain related to youth contact sports," said Elizabeth Moody Davenport, PhD, a postdoctoral researcher at UT Southwestern Medical Center in Dallas. "We know that some professional football players suffer from a serious condition called chronic traumatic encephalopathy or CTE. We are attempting to find out when and how that process starts, so that we can keep sports a healthy activity for millions of children and adolescents."
The study included 24 players from a high school football team in North Carolina, each of whom wore a helmet outfitted with the Head Impact Telemetry System (HITS) during all practices and games. The helmets are lined with six accelerometers that measure the magnitude, location, and direction of a hit. Data from the helmets can be uploaded to a computer for analysis.
"We saw changes in these young players' brains on both structural and functional imaging after a single season of football," said Dr. Davenport.
In the study, each player underwent pre- and post-season imaging, including a specialized MRI scan, from which diffusion tensor imaging and diffusion kurtosis imaging data were extracted to measure the brain's white matter integrity, and a magnetoencephalography (MEG) scan, which records and analyzes the magnetic fields produced by brain waves. Diffusion imaging can measure the structural white matter changes in the brain, and MEG assesses changes in function.
"MEG can be used to measure delta waves in the brain, which are a type of distress signal," said Dr. Davenport. "Delta waves represent slow wave activity that increases after brain injuries. The delta waves we saw came from the surface of the brain, while diffusion imaging is a measure of the white matter deeper in the brain."
The research team calculated the change in imaging metrics between the pre- and post-season imaging exams. They measured abnormalities observed on diffusion imaging and abnormally increased delta-wave activity on MEG. The imaging results were then combined with player-specific impact data from the HITS. None of the 24 players were diagnosed with a concussion during the study.
Players with greater head impact exposure had the greatest change in diffusion imaging and MEG metrics. "Change in diffusion imaging metrics correlated most to linear acceleration, similar to the impact of a car crash," said Dr. Davenport. "MEG changes correlated most to rotational impact, similar to a boxer's punch. These results demonstrate that you need both imaging metrics to assess impact exposure, because they correlate with different biomechanical processes."
Similar studies are being conducted this fall, and a consortium has been formed to continue the brain imaging research in youth contact sports across the country, said Dr. Davenport. "Without a larger population that is closely followed in a longitudinal study, it is difficult to know the long-term effects of these changes," she said. "We do not know if the brain's developmental trajectory is altered, or if the off-season time allows for the brain to return to normal."
Depression in Soldiers Linked to Brain Disruption From Injury
Using multiple brain imaging techniques, researchers have found that a disruption of the circuitry in the brain's cognitive-emotional pathways may provide a physical foundation for depression symptoms in some service members who have had mild traumatic brain injury (mTBI) in combat. "We can link these connectivity changes in the brain to poor top-down emotional processing and greater maladaptive rumination, or worrying, in symptomatic depressed soldiers after mTBI," said Ping-Hong Yeh, PhD, scientist and physicist at the National Intrepid Center of Excellence, Walter Reed National Military Medical Center in Bethesda, Maryland.
According to the Defense and Veterans Brain Injury Center, 352,619 service members worldwide have been diagnosed with TBI since 2000, the majority of these cases being mTBI. In addition, psychiatric disorders, such as anxiety and major depressive disorders, are becoming common in military personnel with brain injuries.
"With the increased survival of soldiers due to improvements in body armor and advanced medical care, there has been an increase in the number of soldiers surviving major trauma. Consequently, a large number of soldiers are returning from war with mTBI," said Dr. Yeh. "Mood disorders are common in military-related mTBI patients. This is an ongoing problem facing a large number of warriors in current areas of conflict, and it is likely to be a persistent problem for the foreseeable future."
For the study, researchers used diffusion-weighted imaging (DWI) and resting-state functional MRI (fMRI) to examine 130 active male service members diagnosed with mTBI and a control group of 52 men without mTBI. Depression symptoms were rated based on the Beck Depression Inventory (BDI), a 21-item, self-reporting assessment that measures characteristic attitudes and symptoms of depression. Patients with a BDI score greater than 20 are considered to have moderate to severe depression symptoms.
BDI scores showed that 75 of the patients with mTBI had moderate to severe depression symptoms. Imaging results showed that white matter tracts—the circuits that connect brain regions critical for cognitive and emotional control—were disrupted in the patients with moderate to severe depression symptoms. Researchers also saw changes in the gray matter cognitive-emotional networks in these patients.
"We found consistencies in the locations of disrupted neurocircuitry, as revealed by DWI and resting-state fMRI, that are unique to the clinical symptoms of mTBI patients," said Dr. Yeh. "We have related the brain structural and functional changes in cognitive-emotional networks to depressive symptoms in mTBI patients."
This research can possibly lead to treatment strategies in the future, he added. "Though the results of this study were not applied directly to patient care, the neuroimaging changes we found might be incorporated into treatment plans for personalized medicine in the future."
Short-Term Sleep Deprivation Affects Heart Function
Getting too little sleep takes a toll on your heart, researchers reported. People who work in fire and emergency medical services, medical residencies, and other high-stress jobs are often called upon to work 24-hour shifts with little opportunity for sleep. While it is known that extreme fatigue can affect many physical, cognitive, and emotional processes, this is the first study to examine how working a 24-hour shift specifically affects cardiac function.
"For the first time, we have shown that short-term sleep deprivation in the context of 24-hour shifts can lead to a significant increase in cardiac contractility, blood pressure, and heart rate," said study author Daniel Kuetting, MD, of the Department of Diagnostic and Interventional Radiology at the University of Bonn in Germany.
For the study, Dr. Kuetting and colleagues recruited 20 healthy radiologists (19 men) with a mean age of 31.6. Each of the study participants underwent cardiovascular magnetic resonance (CMR) imaging with strain analysis before and after a 24-hour shift with an average of three hours of sleep.
"Cardiac function in the context of sleep deprivation has not previously been investigated with CMR strain analysis, the most sensitive parameter of cardiac contractility," said Dr. Kuetting. The researchers also collected blood and urine samples from the participants and measured blood pressure and heart rate.
Following short-term sleep deprivation, the participants showed significant increases in mean peak systolic strain (-23.4 vs -21.9), systolic (118.5 mmHg vs 112.8 mmHg) and diastolic (69.2 mmHg vs 62.9 mmHg) blood pressure and heart rate (68.9 bpm vs 63.0 bpm). In addition, the participants had significant increases in levels of thyroid stimulating hormone (TSH), thyroid hormones FT3 and FT4, and cortisol.
Although the researchers were able to perform follow-up examinations of half of the participants after regular sleep, further study in a larger cohort is needed to determine possible long-term effects of sleep loss, said Dr. Kuetting.
"The study was designed to investigate real-life work-related sleep deprivation," said Dr. Kuetting. "While the participants were not permitted to consume caffeine or food and beverages containing theobromine, such as chocolate, nuts, or tea, we did not take into account factors like individual stress level or environmental stimuli."
As people continue to work longer hours or work at more than one job to make ends meet, it is critical to investigate the detrimental effects of too much work and not enough sleep. The results of this pilot study are transferable to other professions in which long periods of uninterrupted labor are common, said Dr. Kuetting. "These findings may help us better understand how workload and shift duration affect public health."
Aerobic Exercise Preserves Brain Volume and Improves Cognitive Function
Using a new MRI technique, researchers have found that adults with mild cognitive impairment (MCI) who exercised four times per week during a six-month period experienced an increase in brain volume in specific areas of the brain, but adults who participated in aerobic exercise experienced greater gains than those who just stretched.
"Even over a short period of time, we saw aerobic exercise lead to a remarkable change in the brain," said Laura D. Baker, PhD, Associate Professor of Gerontology and Geriatric Medicine at Wake Forest School of Medicine (WFSM) in Winston-Salem, North Carolina.
The study included 35 adults with MCI participating in a randomized, controlled trial of exercise intervention. The participants were separated into two groups. Sixteen adults (average age, 63) engaged in aerobic activity, including treadmill, stationary bike, or elliptical training, four times per week for six months. A control group of 19 adults (average age, 67) participated in stretching exercises with the same frequency. High-resolution brain MR images were acquired from all participants before and after the six-month activity period. The MRI results were compared using conventional and biomechanical metrics to measure the change in brain volume and shape.
"We used high-resolution MR images to measure anatomical changes within areas of the brain to obtain volumetric data and directional information," said Jeongchul Kim, PhD, a coinvestigator at WFSM.
The analysis revealed that for both the aerobic and stretching groups, brain volume increased in most gray matter regions, including the temporal lobe, which supports short-term memory.
"Compared to the stretching group, the aerobic activity group had greater preservation of total brain volume, increased local gray matter volume, and increased directional stretch of brain tissue," said Dr. Kim.
Among participants of the stretching group, the analysis revealed a local contraction, or atrophy, within the white matter connecting fibers. Such directional deformation, or shape change, is partially related to volume loss, but not always, according to Dr. Kim.
"Directional changes in the brain without local volume changes could be a novel biomarker for neurologic disease," he said. "It may be a more sensitive marker for the tiny changes that occur in a specific brain region before volumetric changes are detectable on MRI."
Both MRI measures are important to the treatment of MCI and Alzheimer's disease, which require the careful tracking of changes in the brain while patients engage in interventions, including diet and exercise, to slow the progression of the disease.
Study participants were tested to determine the effect of exercise intervention on cognitive performance. Participants in the aerobic exercise group showed statistically significant improvement in executive function after six months, whereas the stretching group did not improve.
"Any type of exercise can be beneficial," said Dr. Kim. "If possible, aerobic activity may create potential benefits for higher cognitive functioning."
Studies Provide More Insight Into Zika Effects
Three studies reported on the effects of the Zika virus outbreak in Brazil. The first study examined CT findings of the CNS in 16 newborn babies with congenital Zika virus infection confirmed by tests in CSF. The researchers identified a pattern of CT brain findings in the babies, including decreased brain volume, simplified gyral pattern, calcifications, ventricular dilatation, and prominent occipital bone.
"We live in Pernambuco, a state in northeastern Brazil, which had the highest number of patients with microcephaly during the Zika outbreak in our country," said Natacha Calheiros de Lima Petribu, MD, of the Department of Radiology at Barão de Lucena Hospital. "Our study proves that Zika virus infection can cause congenital brain damage in babies with and without microcephaly."
Another study analyzed the imaging results of three target groups affected by Zika: adults who developed acute neurologic syndrome, newborns with vertical infection with neurologic disorders, and pregnant women with rash outbreaks suggestive of Zika. Many of the adults had symptoms of Guillain-Barré syndrome. A few showed inflammation of the brain and spinal cord (ie, Bickerstaff's encephalitis) or brainstem and spinal cord lesions. Common MRI findings included enhancement of certain spinal and facial nerves. In the newborns, MRI showed orbital injuries and anatomical changes in brain tissue.
"It was alarming to find so many cases of neurologic syndromes in adults, some very serious, related to Zika virus infection," said study author Emerson de Melo Casagrande, MD, of the Department of Radiology at Antonio Pedro University Hospital--Federal Fluminense University. "We have also noticed a difference between these syndromes, even though the trigger was the same."
In a third study, ultrasound and fetal MRI were performed on pregnant patients with Zika virus infection at different gestational ages. Once the babies were born, they underwent ultrasound, CT, and MRI. The researchers then created 3-D virtual and physical models of the skulls. More than half of the babies had microcephaly, brain calcifications, and loss of brain tissue volume, along with other structural changes.
"The emergence of Zika virus in the Americas has coincided with increased reports of babies born with microcephaly," said study author Heron Werner Jr, MD, PhD, of the Department of Radiology at Clínica de Diagnóstico por Imagem. "An early diagnosis may help in treating these babies after birth. Moreover, the knowledge of abnormalities present in the CNS may give hints about the pathophysiology of the disease."
Head Impacts Lead to Brain Changes in High School Football Players
Brain imaging exams performed on high school football players after a single season reveal changes in the gray and white matter that correlated with exposure to head impacts, according to researchers.
"It is important to understand the potential changes occurring in the brain related to youth contact sports," said Elizabeth Moody Davenport, PhD, a postdoctoral researcher at UT Southwestern Medical Center in Dallas. "We know that some professional football players suffer from a serious condition called chronic traumatic encephalopathy or CTE. We are attempting to find out when and how that process starts, so that we can keep sports a healthy activity for millions of children and adolescents."
The study included 24 players from a high school football team in North Carolina, each of whom wore a helmet outfitted with the Head Impact Telemetry System (HITS) during all practices and games. The helmets are lined with six accelerometers that measure the magnitude, location, and direction of a hit. Data from the helmets can be uploaded to a computer for analysis.
"We saw changes in these young players' brains on both structural and functional imaging after a single season of football," said Dr. Davenport.
In the study, each player underwent pre- and post-season imaging, including a specialized MRI scan, from which diffusion tensor imaging and diffusion kurtosis imaging data were extracted to measure the brain's white matter integrity, and a magnetoencephalography (MEG) scan, which records and analyzes the magnetic fields produced by brain waves. Diffusion imaging can measure the structural white matter changes in the brain, and MEG assesses changes in function.
"MEG can be used to measure delta waves in the brain, which are a type of distress signal," said Dr. Davenport. "Delta waves represent slow wave activity that increases after brain injuries. The delta waves we saw came from the surface of the brain, while diffusion imaging is a measure of the white matter deeper in the brain."
The research team calculated the change in imaging metrics between the pre- and post-season imaging exams. They measured abnormalities observed on diffusion imaging and abnormally increased delta-wave activity on MEG. The imaging results were then combined with player-specific impact data from the HITS. None of the 24 players were diagnosed with a concussion during the study.
Players with greater head impact exposure had the greatest change in diffusion imaging and MEG metrics. "Change in diffusion imaging metrics correlated most to linear acceleration, similar to the impact of a car crash," said Dr. Davenport. "MEG changes correlated most to rotational impact, similar to a boxer's punch. These results demonstrate that you need both imaging metrics to assess impact exposure, because they correlate with different biomechanical processes."
Similar studies are being conducted this fall, and a consortium has been formed to continue the brain imaging research in youth contact sports across the country, said Dr. Davenport. "Without a larger population that is closely followed in a longitudinal study, it is difficult to know the long-term effects of these changes," she said. "We do not know if the brain's developmental trajectory is altered, or if the off-season time allows for the brain to return to normal."
Depression in Soldiers Linked to Brain Disruption From Injury
Using multiple brain imaging techniques, researchers have found that a disruption of the circuitry in the brain's cognitive-emotional pathways may provide a physical foundation for depression symptoms in some service members who have had mild traumatic brain injury (mTBI) in combat. "We can link these connectivity changes in the brain to poor top-down emotional processing and greater maladaptive rumination, or worrying, in symptomatic depressed soldiers after mTBI," said Ping-Hong Yeh, PhD, scientist and physicist at the National Intrepid Center of Excellence, Walter Reed National Military Medical Center in Bethesda, Maryland.
According to the Defense and Veterans Brain Injury Center, 352,619 service members worldwide have been diagnosed with TBI since 2000, the majority of these cases being mTBI. In addition, psychiatric disorders, such as anxiety and major depressive disorders, are becoming common in military personnel with brain injuries.
"With the increased survival of soldiers due to improvements in body armor and advanced medical care, there has been an increase in the number of soldiers surviving major trauma. Consequently, a large number of soldiers are returning from war with mTBI," said Dr. Yeh. "Mood disorders are common in military-related mTBI patients. This is an ongoing problem facing a large number of warriors in current areas of conflict, and it is likely to be a persistent problem for the foreseeable future."
For the study, researchers used diffusion-weighted imaging (DWI) and resting-state functional MRI (fMRI) to examine 130 active male service members diagnosed with mTBI and a control group of 52 men without mTBI. Depression symptoms were rated based on the Beck Depression Inventory (BDI), a 21-item, self-reporting assessment that measures characteristic attitudes and symptoms of depression. Patients with a BDI score greater than 20 are considered to have moderate to severe depression symptoms.
BDI scores showed that 75 of the patients with mTBI had moderate to severe depression symptoms. Imaging results showed that white matter tracts—the circuits that connect brain regions critical for cognitive and emotional control—were disrupted in the patients with moderate to severe depression symptoms. Researchers also saw changes in the gray matter cognitive-emotional networks in these patients.
"We found consistencies in the locations of disrupted neurocircuitry, as revealed by DWI and resting-state fMRI, that are unique to the clinical symptoms of mTBI patients," said Dr. Yeh. "We have related the brain structural and functional changes in cognitive-emotional networks to depressive symptoms in mTBI patients."
This research can possibly lead to treatment strategies in the future, he added. "Though the results of this study were not applied directly to patient care, the neuroimaging changes we found might be incorporated into treatment plans for personalized medicine in the future."
Short-Term Sleep Deprivation Affects Heart Function
Getting too little sleep takes a toll on your heart, researchers reported. People who work in fire and emergency medical services, medical residencies, and other high-stress jobs are often called upon to work 24-hour shifts with little opportunity for sleep. While it is known that extreme fatigue can affect many physical, cognitive, and emotional processes, this is the first study to examine how working a 24-hour shift specifically affects cardiac function.
"For the first time, we have shown that short-term sleep deprivation in the context of 24-hour shifts can lead to a significant increase in cardiac contractility, blood pressure, and heart rate," said study author Daniel Kuetting, MD, of the Department of Diagnostic and Interventional Radiology at the University of Bonn in Germany.
For the study, Dr. Kuetting and colleagues recruited 20 healthy radiologists (19 men) with a mean age of 31.6. Each of the study participants underwent cardiovascular magnetic resonance (CMR) imaging with strain analysis before and after a 24-hour shift with an average of three hours of sleep.
"Cardiac function in the context of sleep deprivation has not previously been investigated with CMR strain analysis, the most sensitive parameter of cardiac contractility," said Dr. Kuetting. The researchers also collected blood and urine samples from the participants and measured blood pressure and heart rate.
Following short-term sleep deprivation, the participants showed significant increases in mean peak systolic strain (-23.4 vs -21.9), systolic (118.5 mmHg vs 112.8 mmHg) and diastolic (69.2 mmHg vs 62.9 mmHg) blood pressure and heart rate (68.9 bpm vs 63.0 bpm). In addition, the participants had significant increases in levels of thyroid stimulating hormone (TSH), thyroid hormones FT3 and FT4, and cortisol.
Although the researchers were able to perform follow-up examinations of half of the participants after regular sleep, further study in a larger cohort is needed to determine possible long-term effects of sleep loss, said Dr. Kuetting.
"The study was designed to investigate real-life work-related sleep deprivation," said Dr. Kuetting. "While the participants were not permitted to consume caffeine or food and beverages containing theobromine, such as chocolate, nuts, or tea, we did not take into account factors like individual stress level or environmental stimuli."
As people continue to work longer hours or work at more than one job to make ends meet, it is critical to investigate the detrimental effects of too much work and not enough sleep. The results of this pilot study are transferable to other professions in which long periods of uninterrupted labor are common, said Dr. Kuetting. "These findings may help us better understand how workload and shift duration affect public health."
Aerobic Exercise Preserves Brain Volume and Improves Cognitive Function
Using a new MRI technique, researchers have found that adults with mild cognitive impairment (MCI) who exercised four times per week during a six-month period experienced an increase in brain volume in specific areas of the brain, but adults who participated in aerobic exercise experienced greater gains than those who just stretched.
"Even over a short period of time, we saw aerobic exercise lead to a remarkable change in the brain," said Laura D. Baker, PhD, Associate Professor of Gerontology and Geriatric Medicine at Wake Forest School of Medicine (WFSM) in Winston-Salem, North Carolina.
The study included 35 adults with MCI participating in a randomized, controlled trial of exercise intervention. The participants were separated into two groups. Sixteen adults (average age, 63) engaged in aerobic activity, including treadmill, stationary bike, or elliptical training, four times per week for six months. A control group of 19 adults (average age, 67) participated in stretching exercises with the same frequency. High-resolution brain MR images were acquired from all participants before and after the six-month activity period. The MRI results were compared using conventional and biomechanical metrics to measure the change in brain volume and shape.
"We used high-resolution MR images to measure anatomical changes within areas of the brain to obtain volumetric data and directional information," said Jeongchul Kim, PhD, a coinvestigator at WFSM.
The analysis revealed that for both the aerobic and stretching groups, brain volume increased in most gray matter regions, including the temporal lobe, which supports short-term memory.
"Compared to the stretching group, the aerobic activity group had greater preservation of total brain volume, increased local gray matter volume, and increased directional stretch of brain tissue," said Dr. Kim.
Among participants of the stretching group, the analysis revealed a local contraction, or atrophy, within the white matter connecting fibers. Such directional deformation, or shape change, is partially related to volume loss, but not always, according to Dr. Kim.
"Directional changes in the brain without local volume changes could be a novel biomarker for neurologic disease," he said. "It may be a more sensitive marker for the tiny changes that occur in a specific brain region before volumetric changes are detectable on MRI."
Both MRI measures are important to the treatment of MCI and Alzheimer's disease, which require the careful tracking of changes in the brain while patients engage in interventions, including diet and exercise, to slow the progression of the disease.
Study participants were tested to determine the effect of exercise intervention on cognitive performance. Participants in the aerobic exercise group showed statistically significant improvement in executive function after six months, whereas the stretching group did not improve.
"Any type of exercise can be beneficial," said Dr. Kim. "If possible, aerobic activity may create potential benefits for higher cognitive functioning."
Periventricular Nodular Heterotopia Poses Unique Surgical Challenges
Patients with epilepsy who also have periventricular nodular heterotopia (PVNH) are difficult to manage surgically because the relative influence of the nodular tissue and the overlying cortex on the generation of seizures is variable. A review of the relevant medical literature suggests that inter-ictal spiking from nodules often occurs in patients with PVNH, but it is rare for patients to experience seizures arising from the nodular tissue alone. It is more likely to find that the onset of seizures occurs simultaneously with overlying neocortex or mesial temporal structures.
Thompson SA, Kalamangalam GP, Tandon N. Intracranial evaluation and laser ablation for epilepsy with periventricular nodular heterotopia. Seizure. 2016;41:211-216.
Patients with epilepsy who also have periventricular nodular heterotopia (PVNH) are difficult to manage surgically because the relative influence of the nodular tissue and the overlying cortex on the generation of seizures is variable. A review of the relevant medical literature suggests that inter-ictal spiking from nodules often occurs in patients with PVNH, but it is rare for patients to experience seizures arising from the nodular tissue alone. It is more likely to find that the onset of seizures occurs simultaneously with overlying neocortex or mesial temporal structures.
Thompson SA, Kalamangalam GP, Tandon N. Intracranial evaluation and laser ablation for epilepsy with periventricular nodular heterotopia. Seizure. 2016;41:211-216.
Patients with epilepsy who also have periventricular nodular heterotopia (PVNH) are difficult to manage surgically because the relative influence of the nodular tissue and the overlying cortex on the generation of seizures is variable. A review of the relevant medical literature suggests that inter-ictal spiking from nodules often occurs in patients with PVNH, but it is rare for patients to experience seizures arising from the nodular tissue alone. It is more likely to find that the onset of seizures occurs simultaneously with overlying neocortex or mesial temporal structures.
Thompson SA, Kalamangalam GP, Tandon N. Intracranial evaluation and laser ablation for epilepsy with periventricular nodular heterotopia. Seizure. 2016;41:211-216.
Women With Epilepsy Need More Contraceptive Counseling
Despite the fact that hormonal contraceptives interact with certain antiepileptic drugs, a recent study has shown that only 35% of 397 female patients with epilepsy were given any clinician counseling about contraceptive choices during their first clinic visit. And these patients were unlikely to receive contraceptive counseling during subsequent visits. The implications of these findings are troubling: Many antiepileptic agents decrease the efficacy of hormonal contraceptives by inducing hepatic enzymes, and estrogen-containing contraceptives are known to accelerate the metabolism of lamotrigine, an antiepileptic drug commonly prescribed in women of child-bearing age. Espinera et al also found that when women with epilepsy are given advice about the advantages of IUDs, they are far more likely to switch to IUDs, which are highly effective without AED drug interactions.
Espinera AR, Gavvala J, Bellinski I, et al. Counseling by epileptologists affects contraceptive choices of women with epilepsy. Epilepsy Behav. 2016;65:1-6.
Despite the fact that hormonal contraceptives interact with certain antiepileptic drugs, a recent study has shown that only 35% of 397 female patients with epilepsy were given any clinician counseling about contraceptive choices during their first clinic visit. And these patients were unlikely to receive contraceptive counseling during subsequent visits. The implications of these findings are troubling: Many antiepileptic agents decrease the efficacy of hormonal contraceptives by inducing hepatic enzymes, and estrogen-containing contraceptives are known to accelerate the metabolism of lamotrigine, an antiepileptic drug commonly prescribed in women of child-bearing age. Espinera et al also found that when women with epilepsy are given advice about the advantages of IUDs, they are far more likely to switch to IUDs, which are highly effective without AED drug interactions.
Espinera AR, Gavvala J, Bellinski I, et al. Counseling by epileptologists affects contraceptive choices of women with epilepsy. Epilepsy Behav. 2016;65:1-6.
Despite the fact that hormonal contraceptives interact with certain antiepileptic drugs, a recent study has shown that only 35% of 397 female patients with epilepsy were given any clinician counseling about contraceptive choices during their first clinic visit. And these patients were unlikely to receive contraceptive counseling during subsequent visits. The implications of these findings are troubling: Many antiepileptic agents decrease the efficacy of hormonal contraceptives by inducing hepatic enzymes, and estrogen-containing contraceptives are known to accelerate the metabolism of lamotrigine, an antiepileptic drug commonly prescribed in women of child-bearing age. Espinera et al also found that when women with epilepsy are given advice about the advantages of IUDs, they are far more likely to switch to IUDs, which are highly effective without AED drug interactions.
Espinera AR, Gavvala J, Bellinski I, et al. Counseling by epileptologists affects contraceptive choices of women with epilepsy. Epilepsy Behav. 2016;65:1-6.
Behavioral, Neurodevelopmental Disorders More Common in Young Adults With Epilepsy
Young adults with epilepsy are at greater risk for neurodevelopmental and behavioral disorders than some other patient populations, according to a recent case-control study that looked at hospital admissions, outpatients, and ED visits for adults with epilepsy, migraine, or leg fracture. The study cohort consisted of 5666 adult epilepsy patients between 19 and 25 years of age who were seen in hospitals and EDs, 17,507 patients with migraine, and 5966 patients with leg fractures. The researchers found that 51.8% of patients with epilepsy had behavioral health issues versus 37.6% of those with migraine and 21.6% of patients with fractures. Similarly, patients with epilepsy were 297% more likely to have a neurodevelopmental disorder compared with those with migraine.
Wagner JL, Wilson DA, Kellermann T, el al. Behavioral health in young adults with epilepsy: Implications for transition of care. Epilepsy Behav. 2016;65:7-12.
Young adults with epilepsy are at greater risk for neurodevelopmental and behavioral disorders than some other patient populations, according to a recent case-control study that looked at hospital admissions, outpatients, and ED visits for adults with epilepsy, migraine, or leg fracture. The study cohort consisted of 5666 adult epilepsy patients between 19 and 25 years of age who were seen in hospitals and EDs, 17,507 patients with migraine, and 5966 patients with leg fractures. The researchers found that 51.8% of patients with epilepsy had behavioral health issues versus 37.6% of those with migraine and 21.6% of patients with fractures. Similarly, patients with epilepsy were 297% more likely to have a neurodevelopmental disorder compared with those with migraine.
Wagner JL, Wilson DA, Kellermann T, el al. Behavioral health in young adults with epilepsy: Implications for transition of care. Epilepsy Behav. 2016;65:7-12.
Young adults with epilepsy are at greater risk for neurodevelopmental and behavioral disorders than some other patient populations, according to a recent case-control study that looked at hospital admissions, outpatients, and ED visits for adults with epilepsy, migraine, or leg fracture. The study cohort consisted of 5666 adult epilepsy patients between 19 and 25 years of age who were seen in hospitals and EDs, 17,507 patients with migraine, and 5966 patients with leg fractures. The researchers found that 51.8% of patients with epilepsy had behavioral health issues versus 37.6% of those with migraine and 21.6% of patients with fractures. Similarly, patients with epilepsy were 297% more likely to have a neurodevelopmental disorder compared with those with migraine.
Wagner JL, Wilson DA, Kellermann T, el al. Behavioral health in young adults with epilepsy: Implications for transition of care. Epilepsy Behav. 2016;65:7-12.
Can Mobile Apps Improve Medication Adherence in Pregnant Patients With Epilepsy?
To determine how well pregnant women with epilepsy adhere to their medication regimen, Ernst et al studied their intake of antiepileptic medication by providing them with an iPod Touch loaded with a mobile app specifically designed to track such data. Eighty-six women with epilepsy monitored their seizures and medication use. The study found that 75% of the women had tracked their medication usage for more than 80% of the days they were enrolled in the experiment. Among this subgroup, adherence to the anti-epilepsy drug regimen was 97.7%; 44% said they had missed taking their medication for at least one day. The investigators speculate that the high adherence rate may have been the result of using the mobile app itself.
Ernst L. Harden CL, Pennell PB, et al. Medication adherence in women with epilepsy who are planning pregnancy. Epilepsia. 2016; 57(12):2039-2044.
To determine how well pregnant women with epilepsy adhere to their medication regimen, Ernst et al studied their intake of antiepileptic medication by providing them with an iPod Touch loaded with a mobile app specifically designed to track such data. Eighty-six women with epilepsy monitored their seizures and medication use. The study found that 75% of the women had tracked their medication usage for more than 80% of the days they were enrolled in the experiment. Among this subgroup, adherence to the anti-epilepsy drug regimen was 97.7%; 44% said they had missed taking their medication for at least one day. The investigators speculate that the high adherence rate may have been the result of using the mobile app itself.
Ernst L. Harden CL, Pennell PB, et al. Medication adherence in women with epilepsy who are planning pregnancy. Epilepsia. 2016; 57(12):2039-2044.
To determine how well pregnant women with epilepsy adhere to their medication regimen, Ernst et al studied their intake of antiepileptic medication by providing them with an iPod Touch loaded with a mobile app specifically designed to track such data. Eighty-six women with epilepsy monitored their seizures and medication use. The study found that 75% of the women had tracked their medication usage for more than 80% of the days they were enrolled in the experiment. Among this subgroup, adherence to the anti-epilepsy drug regimen was 97.7%; 44% said they had missed taking their medication for at least one day. The investigators speculate that the high adherence rate may have been the result of using the mobile app itself.
Ernst L. Harden CL, Pennell PB, et al. Medication adherence in women with epilepsy who are planning pregnancy. Epilepsia. 2016; 57(12):2039-2044.
Understanding the Link between Traumatic Brain Injury and Posttraumatic Seizures
Among patients who have experienced traumatic brain injury, those who have had immediate or late seizures during an acute hospital stay are at increased of developing later posttraumatic seizures. Researchers found that new onset posttraumatic seizures were mostly likely to occur between the time patients were discharged from inpatient rehabilitation and 1 year (9.2%). By year 5, the cumulative incidence of such seizures was 20.5%. A patient’s race, intracranial pathology, and neurosurgical procedures also factored into their relative risk of posttraumatic seizures.
Ritter AC, Wagner AK, Fabio A, et al. Incidence and risk factors of posttraumatic seizures following traumatic brain injury: A Traumatic Brain Injury Model Systems Study. Epilepsia. 2016;57(12):1968-1977.
Among patients who have experienced traumatic brain injury, those who have had immediate or late seizures during an acute hospital stay are at increased of developing later posttraumatic seizures. Researchers found that new onset posttraumatic seizures were mostly likely to occur between the time patients were discharged from inpatient rehabilitation and 1 year (9.2%). By year 5, the cumulative incidence of such seizures was 20.5%. A patient’s race, intracranial pathology, and neurosurgical procedures also factored into their relative risk of posttraumatic seizures.
Ritter AC, Wagner AK, Fabio A, et al. Incidence and risk factors of posttraumatic seizures following traumatic brain injury: A Traumatic Brain Injury Model Systems Study. Epilepsia. 2016;57(12):1968-1977.
Among patients who have experienced traumatic brain injury, those who have had immediate or late seizures during an acute hospital stay are at increased of developing later posttraumatic seizures. Researchers found that new onset posttraumatic seizures were mostly likely to occur between the time patients were discharged from inpatient rehabilitation and 1 year (9.2%). By year 5, the cumulative incidence of such seizures was 20.5%. A patient’s race, intracranial pathology, and neurosurgical procedures also factored into their relative risk of posttraumatic seizures.
Ritter AC, Wagner AK, Fabio A, et al. Incidence and risk factors of posttraumatic seizures following traumatic brain injury: A Traumatic Brain Injury Model Systems Study. Epilepsia. 2016;57(12):1968-1977.
Hypothermia Offers Little Benefit to Patients with Convulsive Status Epilepticus
Induced hypothermia does not improve clinical outcomes among patients with convulsive status epilepticus (CSE), according to a new multicenter study published in the New England Journal of Medicine. To reach that conclusion, investigators assigned 270 critically ill patients with CSE on mechanical ventilation to either standard care or standard care plus hypothermia, which lowered their body temperature to 32 to 34⁰C for 24 hours. To measure the impact of hypothermia, researchers used the Glasgow Outcome Scale (GOS) score and defined success as a GOS score of 5, which represents no or minimal neurologic deficit, at 90 days. Forty-nine percent of patients on hypothermia achieved a score of 5, compared to 43% of those on standard care, which was statistically insignificant (P=.43).
Legriel S, Lemiale V, Schenck, M, et al. Hypothermia for Neuroprotection in Convulsive Status Epilepticus. N Engl J Med. 2016;375(25):2457-2467.
Induced hypothermia does not improve clinical outcomes among patients with convulsive status epilepticus (CSE), according to a new multicenter study published in the New England Journal of Medicine. To reach that conclusion, investigators assigned 270 critically ill patients with CSE on mechanical ventilation to either standard care or standard care plus hypothermia, which lowered their body temperature to 32 to 34⁰C for 24 hours. To measure the impact of hypothermia, researchers used the Glasgow Outcome Scale (GOS) score and defined success as a GOS score of 5, which represents no or minimal neurologic deficit, at 90 days. Forty-nine percent of patients on hypothermia achieved a score of 5, compared to 43% of those on standard care, which was statistically insignificant (P=.43).
Legriel S, Lemiale V, Schenck, M, et al. Hypothermia for Neuroprotection in Convulsive Status Epilepticus. N Engl J Med. 2016;375(25):2457-2467.
Induced hypothermia does not improve clinical outcomes among patients with convulsive status epilepticus (CSE), according to a new multicenter study published in the New England Journal of Medicine. To reach that conclusion, investigators assigned 270 critically ill patients with CSE on mechanical ventilation to either standard care or standard care plus hypothermia, which lowered their body temperature to 32 to 34⁰C for 24 hours. To measure the impact of hypothermia, researchers used the Glasgow Outcome Scale (GOS) score and defined success as a GOS score of 5, which represents no or minimal neurologic deficit, at 90 days. Forty-nine percent of patients on hypothermia achieved a score of 5, compared to 43% of those on standard care, which was statistically insignificant (P=.43).
Legriel S, Lemiale V, Schenck, M, et al. Hypothermia for Neuroprotection in Convulsive Status Epilepticus. N Engl J Med. 2016;375(25):2457-2467.