User login
New screen time guidelines address rapid changes in media environment
SAN FRANCISCO – A new set of policy statements on children’s media use from the American Academy of Pediatrics brings the recommendations into the 21st century.
The new guidance, released at the annual meeting of the AAP, synthesizes the most current evidence on mobile devices, interactivity, educational technology, sleep, obesity, cognitive development, and other aspects of the pervasive digital environment children now grow up in.
“I think our policy statement reflects the changes in the media landscape because not all media use is the same,” Megan A. Moreno, MD, lead author of the policy statement, “Media Use in School-Aged Children and Adolescents,” said during a press conference (Pediatrics. 2016, Oct. doi: 10.1542/peds.2016-2592).
The new statement both lowers the overall age at which parents can feel comfortable introducing their children to media and decreases the amount of screen time exposure per day. One key component of the new guidelines includes the unveiling of a new tool parents can use to create a Family Media Plan. The tool, available at https://www.healthychildren.org/English/media/Pages/default.aspx, enables parents to create a plan for each child in the household and reflects the individuality of each child’s use and age-appropriate guidelines.
After parents enter children’s names, the plan provides an editable template for each child that lays out screen-free zones, screen-free times, device curfews, recreational screen-time choices, alternative activities during non-screen time, media manners, digital citizenship, personal safety, sleep, and exercise.
Previous policy statements from the AAP relied primarily on research about television, a passive screen experience. In an age where many children and teens have interactive screens in their pockets and visit grandparents via video conferencing, however, the AAP Council on Communications and Media has likewise broadened its definition of media and noted the problems with applying research about television to other totally different types of screens.
“When we’re using media to connect, this is not what we’re traditionally calling screen time. These are tools,” Jenny S. Radesky, MD, lead author of the policy statement “Media and Young Minds,” said at the press conference (Pediatrics. 2016 Oct. doi: 10.1542/peds.2016-2592). She referred to the fact that many families who are spread across great distances, such as parents deployed overseas or grandparents in another state, use Skype, FaceTime, Google Hangouts, and similar programs to communicate and remain connected.
“We’re making sure our relationships are staying strong and not something to be discouraged with infants and toddlers, even though infants and toddlers will need their parent’s help to understand what they’re seeing on the screen,” said Dr. Radesky, a developmental-behavioral pediatrician at C.S. Mott Children’s Hospital at the University of Michigan in Ann Arbor.
The policy statement further notes that some emerging evidence has suggested children aged 2 and older can learn words from live video chatting with a responsive adult or by using an interactive touch screen that scaffolds learning.
An earlier introduction to screens
Among the most significant changes to the recommendations for children up to 5 years old is an allowance for introducing media before age 2, the previous policy’s age recommendation.
“If you want to introduce media, 18 months is the age when kids are cognitively ready to start, but we’re not saying parents need to introduce media then,” Dr. Radesky said, adding that more research is needed regarding devices such as tablets before it’s possible to know whether apps can be beneficial in toddlers that young. “There’s not enough evidence to know if interactivity helps or not right now,” she said.
The “Media and Young Minds” policy statement notes that children under age 2 years develop their cognitive, language, motor, and social-emotional skills through hands-on exploration and social interaction with trusted adults.
“Apps can’t do the things that parents’ minds can do or children’s minds can do on their own,” Dr. Radesky said. The policy notes that digital books, or eBooks, can be beneficial when used like a traditional physical book, but interactive elements to these eBooks could be distracting and decrease children’s comprehension.
When parents do choose to introduce media to their children, it’s “crucial that media be a shared experience” between the caregiving adult and the child, she said. “Think of media as a teaching tool, a way to connect and to create, not just to consume,” Dr. Radesky said.
What can preschoolers learn?
Although some laboratory research shows toddlers as young as 15 months can learn new words from touch screens, they have difficulty transferring that knowledge to the three-dimensional world. For children aged 3-5 years, however, both well-designed television programming and high-quality learning apps from Public Broadcasting Service (PBS) and the Sesame Workshop have shown benefits. In addition to early literacy, math, and personal and social development skills learned from shows such as Sesame Street, preschoolers have learned literacy skills from those programs’ apps.
But those apps are unfortunately in the minority.
“Most apps parents find under the ‘educational’ category in app stores have no such evidence of efficacy, target only rote academic skills, are not based on established curricula, and use little or no input from developmental specialists and educators,” the “Media and Young Minds” policy states. “The higher-order thinking skills and executive functions essential for school success, such as task persistence, impulse control, emotion regulation, and creative, flexible thinking, are best taught through unstructured and social (not digital) play, as well as responsive parent-child interactions.” 
Risks and recommendations for preschoolers
Heavy media use among preschoolers, meanwhile, carries risks of increased weight – primarily as a result of food advertising and eating while watching TV – as well as reduced sleep and cognitive, language, and social/emotional delays.
“Content is crucial,” the “Media and Young Minds” policy notes. “Experimental evidence shows that switching from violent content to educational/prosocial content results in significant improvement in behavioral symptoms, particularly for low-income boys.”
The key points of the new statement therefore include the following recommendations:
• Limit media use to 1 hour a day in children ages 2 years and older.
• Do not use screens during mealtimes and for 1 hour before bedtime.
• Start discussing family and child media use with parents early in children’s lives.
• Educate parents about early brain development and help families develop a Family Media Use Plan.
• Discourage screen use besides video-chatting in children under 18 months old.
• Encourage caregiving adults to use screen media with children aged 18-24 months, who should not use it on their own.
• Encourage parents to rely on high-quality programming products such as PBS Kids, Sesame Workshop, and Common Sense Media.
• Help parents with challenges such as setting limits, finding alternatives to screen time, and calming children without using media.
• Avoid using screens or media to calm children except during rare extenuating circumstances, such as painful medical procedures and airplane flights.
• Encourage parents to avoid fast-paced programs, apps with distracting content, any media with violent content, and any background television, which can stunt children’s early language development.
Understanding older youth’s media use
As children move into school age and adolescence, the opportunities and utilities for media use expand – and so do the risks. Children and teens can benefit from media through gaining social support, learning about healthy behaviors, and discovering new ideas and knowledge, but youth remain at risk for obesity, sleep problems, cyberbullying, compromised privacy, and exposure to inaccurate, inappropriate or unsafe content, the “Media Use in School-Aged Children and Adolescents” policy statement reports.
Despite the wide range of media types available, TV remains the most commonly used media type among school-aged children and teens and is watched an average of 2 hours a day. Still, 91% of boys have access to a video game console, and 84% report playing games online or on a mobile phone. Further, three-quarters of teens own a smartphone and 76% use at least one social media site, with more than 70% maintaining a “social media portfolio” across several platforms.
Such social media use can provide teens with helpful support networks, particularly for those with ongoing illnesses or disabilities or those needing community support as lesbian, gay, bisexual, transgender, questioning, or intersex individuals. Social media can also promote wellness and healthy behaviors such as eating well and not smoking.
Risks for school-aged children and adolescents using media
Yet social media also can open the door to cyberbullying, leading to short-term and long-term social, academic, and health problems. It carries the risk of exploitation of youth or their images, or predation from pornographers and pedophiles. Children and teens must be made aware that the “Internet is forever” and should be taught to consider privacy and confidentiality concerns in their use of social and other media.
Another concern is teens’ “sexting,” in which they share sexually explicit messages and/or partly or fully nude photos. Exposures to unhealthy behaviors, such as substance abuse, sexual behaviors, self-injury, or disordered eating are likewise among the risks of social media, as they are with television and cinema.
In fact, TV/movie content showing alcohol use, smoking, and sexual activity is linked to earlier experimentation among children and adolescents. In addition, each extra hour of television watching is associated with increase in body mass index, as is having a TV set in the bedroom. Enjoying entertainment media while doing school work is linked to poor learning and academics.
Excessive media use may lead to problematic Internet use and Internet gaming disorder as described in the DSM-5, occurring among 4%-8.5% of children and adolescents.
“Symptoms can include a preoccupation with the activity, decreased interest in offline or ‘real life’ relationships, unsuccessful attempts to decrease use and withdrawal symptoms,” the “Media Use in School-Aged Children and Adolescents” policy statement notes.
Recommendations for older children
The policy statement advises pediatricians to help families and schools promote understanding of media’s risks and benefits, including awareness of tools to screen for sexting, cyberbullying, problematic Internet use, and Internet gaming disorder. Pediatricians should advocate for training in media literacy in the community and encourage parents to follow the media, sleep, and physical activity guidelines included in the Family Media Plan.
The research was supported by the American Academy of Pediatrics. The authors reported no disclosures.
SAN FRANCISCO – A new set of policy statements on children’s media use from the American Academy of Pediatrics brings the recommendations into the 21st century.
The new guidance, released at the annual meeting of the AAP, synthesizes the most current evidence on mobile devices, interactivity, educational technology, sleep, obesity, cognitive development, and other aspects of the pervasive digital environment children now grow up in.
“I think our policy statement reflects the changes in the media landscape because not all media use is the same,” Megan A. Moreno, MD, lead author of the policy statement, “Media Use in School-Aged Children and Adolescents,” said during a press conference (Pediatrics. 2016, Oct. doi: 10.1542/peds.2016-2592).
The new statement both lowers the overall age at which parents can feel comfortable introducing their children to media and decreases the amount of screen time exposure per day. One key component of the new guidelines includes the unveiling of a new tool parents can use to create a Family Media Plan. The tool, available at https://www.healthychildren.org/English/media/Pages/default.aspx, enables parents to create a plan for each child in the household and reflects the individuality of each child’s use and age-appropriate guidelines.
After parents enter children’s names, the plan provides an editable template for each child that lays out screen-free zones, screen-free times, device curfews, recreational screen-time choices, alternative activities during non-screen time, media manners, digital citizenship, personal safety, sleep, and exercise.
Previous policy statements from the AAP relied primarily on research about television, a passive screen experience. In an age where many children and teens have interactive screens in their pockets and visit grandparents via video conferencing, however, the AAP Council on Communications and Media has likewise broadened its definition of media and noted the problems with applying research about television to other totally different types of screens.
“When we’re using media to connect, this is not what we’re traditionally calling screen time. These are tools,” Jenny S. Radesky, MD, lead author of the policy statement “Media and Young Minds,” said at the press conference (Pediatrics. 2016 Oct. doi: 10.1542/peds.2016-2592). She referred to the fact that many families who are spread across great distances, such as parents deployed overseas or grandparents in another state, use Skype, FaceTime, Google Hangouts, and similar programs to communicate and remain connected.
“We’re making sure our relationships are staying strong and not something to be discouraged with infants and toddlers, even though infants and toddlers will need their parent’s help to understand what they’re seeing on the screen,” said Dr. Radesky, a developmental-behavioral pediatrician at C.S. Mott Children’s Hospital at the University of Michigan in Ann Arbor.
The policy statement further notes that some emerging evidence has suggested children aged 2 and older can learn words from live video chatting with a responsive adult or by using an interactive touch screen that scaffolds learning.
An earlier introduction to screens
Among the most significant changes to the recommendations for children up to 5 years old is an allowance for introducing media before age 2, the previous policy’s age recommendation.
“If you want to introduce media, 18 months is the age when kids are cognitively ready to start, but we’re not saying parents need to introduce media then,” Dr. Radesky said, adding that more research is needed regarding devices such as tablets before it’s possible to know whether apps can be beneficial in toddlers that young. “There’s not enough evidence to know if interactivity helps or not right now,” she said.
The “Media and Young Minds” policy statement notes that children under age 2 years develop their cognitive, language, motor, and social-emotional skills through hands-on exploration and social interaction with trusted adults.
“Apps can’t do the things that parents’ minds can do or children’s minds can do on their own,” Dr. Radesky said. The policy notes that digital books, or eBooks, can be beneficial when used like a traditional physical book, but interactive elements to these eBooks could be distracting and decrease children’s comprehension.
When parents do choose to introduce media to their children, it’s “crucial that media be a shared experience” between the caregiving adult and the child, she said. “Think of media as a teaching tool, a way to connect and to create, not just to consume,” Dr. Radesky said.
What can preschoolers learn?
Although some laboratory research shows toddlers as young as 15 months can learn new words from touch screens, they have difficulty transferring that knowledge to the three-dimensional world. For children aged 3-5 years, however, both well-designed television programming and high-quality learning apps from Public Broadcasting Service (PBS) and the Sesame Workshop have shown benefits. In addition to early literacy, math, and personal and social development skills learned from shows such as Sesame Street, preschoolers have learned literacy skills from those programs’ apps.
But those apps are unfortunately in the minority.
“Most apps parents find under the ‘educational’ category in app stores have no such evidence of efficacy, target only rote academic skills, are not based on established curricula, and use little or no input from developmental specialists and educators,” the “Media and Young Minds” policy states. “The higher-order thinking skills and executive functions essential for school success, such as task persistence, impulse control, emotion regulation, and creative, flexible thinking, are best taught through unstructured and social (not digital) play, as well as responsive parent-child interactions.”
Risks and recommendations for preschoolers
Heavy media use among preschoolers, meanwhile, carries risks of increased weight – primarily as a result of food advertising and eating while watching TV – as well as reduced sleep and cognitive, language, and social/emotional delays.
“Content is crucial,” the “Media and Young Minds” policy notes. “Experimental evidence shows that switching from violent content to educational/prosocial content results in significant improvement in behavioral symptoms, particularly for low-income boys.”
The key points of the new statement therefore include the following recommendations:
• Limit media use to 1 hour a day in children ages 2 years and older.
• Do not use screens during mealtimes and for 1 hour before bedtime.
• Start discussing family and child media use with parents early in children’s lives.
• Educate parents about early brain development and help families develop a Family Media Use Plan.
• Discourage screen use besides video-chatting in children under 18 months old.
• Encourage caregiving adults to use screen media with children aged 18-24 months, who should not use it on their own.
• Encourage parents to rely on high-quality programming products such as PBS Kids, Sesame Workshop, and Common Sense Media.
• Help parents with challenges such as setting limits, finding alternatives to screen time, and calming children without using media.
• Avoid using screens or media to calm children except during rare extenuating circumstances, such as painful medical procedures and airplane flights.
• Encourage parents to avoid fast-paced programs, apps with distracting content, any media with violent content, and any background television, which can stunt children’s early language development.
Understanding older youth’s media use
As children move into school age and adolescence, the opportunities and utilities for media use expand – and so do the risks. Children and teens can benefit from media through gaining social support, learning about healthy behaviors, and discovering new ideas and knowledge, but youth remain at risk for obesity, sleep problems, cyberbullying, compromised privacy, and exposure to inaccurate, inappropriate or unsafe content, the “Media Use in School-Aged Children and Adolescents” policy statement reports.
Despite the wide range of media types available, TV remains the most commonly used media type among school-aged children and teens and is watched an average of 2 hours a day. Still, 91% of boys have access to a video game console, and 84% report playing games online or on a mobile phone. Further, three-quarters of teens own a smartphone and 76% use at least one social media site, with more than 70% maintaining a “social media portfolio” across several platforms.
Such social media use can provide teens with helpful support networks, particularly for those with ongoing illnesses or disabilities or those needing community support as lesbian, gay, bisexual, transgender, questioning, or intersex individuals. Social media can also promote wellness and healthy behaviors such as eating well and not smoking.
Risks for school-aged children and adolescents using media
Yet social media also can open the door to cyberbullying, leading to short-term and long-term social, academic, and health problems. It carries the risk of exploitation of youth or their images, or predation from pornographers and pedophiles. Children and teens must be made aware that the “Internet is forever” and should be taught to consider privacy and confidentiality concerns in their use of social and other media.
Another concern is teens’ “sexting,” in which they share sexually explicit messages and/or partly or fully nude photos. Exposures to unhealthy behaviors, such as substance abuse, sexual behaviors, self-injury, or disordered eating are likewise among the risks of social media, as they are with television and cinema.
In fact, TV/movie content showing alcohol use, smoking, and sexual activity is linked to earlier experimentation among children and adolescents. In addition, each extra hour of television watching is associated with increase in body mass index, as is having a TV set in the bedroom. Enjoying entertainment media while doing school work is linked to poor learning and academics.
Excessive media use may lead to problematic Internet use and Internet gaming disorder as described in the DSM-5, occurring among 4%-8.5% of children and adolescents.
“Symptoms can include a preoccupation with the activity, decreased interest in offline or ‘real life’ relationships, unsuccessful attempts to decrease use and withdrawal symptoms,” the “Media Use in School-Aged Children and Adolescents” policy statement notes.
Recommendations for older children
The policy statement advises pediatricians to help families and schools promote understanding of media’s risks and benefits, including awareness of tools to screen for sexting, cyberbullying, problematic Internet use, and Internet gaming disorder. Pediatricians should advocate for training in media literacy in the community and encourage parents to follow the media, sleep, and physical activity guidelines included in the Family Media Plan.
The research was supported by the American Academy of Pediatrics. The authors reported no disclosures.
SAN FRANCISCO – A new set of policy statements on children’s media use from the American Academy of Pediatrics brings the recommendations into the 21st century.
The new guidance, released at the annual meeting of the AAP, synthesizes the most current evidence on mobile devices, interactivity, educational technology, sleep, obesity, cognitive development, and other aspects of the pervasive digital environment children now grow up in.
“I think our policy statement reflects the changes in the media landscape because not all media use is the same,” Megan A. Moreno, MD, lead author of the policy statement, “Media Use in School-Aged Children and Adolescents,” said during a press conference (Pediatrics. 2016, Oct. doi: 10.1542/peds.2016-2592).
The new statement both lowers the overall age at which parents can feel comfortable introducing their children to media and decreases the amount of screen time exposure per day. One key component of the new guidelines includes the unveiling of a new tool parents can use to create a Family Media Plan. The tool, available at https://www.healthychildren.org/English/media/Pages/default.aspx, enables parents to create a plan for each child in the household and reflects the individuality of each child’s use and age-appropriate guidelines.
After parents enter children’s names, the plan provides an editable template for each child that lays out screen-free zones, screen-free times, device curfews, recreational screen-time choices, alternative activities during non-screen time, media manners, digital citizenship, personal safety, sleep, and exercise.
Previous policy statements from the AAP relied primarily on research about television, a passive screen experience. In an age where many children and teens have interactive screens in their pockets and visit grandparents via video conferencing, however, the AAP Council on Communications and Media has likewise broadened its definition of media and noted the problems with applying research about television to other totally different types of screens.
“When we’re using media to connect, this is not what we’re traditionally calling screen time. These are tools,” Jenny S. Radesky, MD, lead author of the policy statement “Media and Young Minds,” said at the press conference (Pediatrics. 2016 Oct. doi: 10.1542/peds.2016-2592). She referred to the fact that many families who are spread across great distances, such as parents deployed overseas or grandparents in another state, use Skype, FaceTime, Google Hangouts, and similar programs to communicate and remain connected.
“We’re making sure our relationships are staying strong and not something to be discouraged with infants and toddlers, even though infants and toddlers will need their parent’s help to understand what they’re seeing on the screen,” said Dr. Radesky, a developmental-behavioral pediatrician at C.S. Mott Children’s Hospital at the University of Michigan in Ann Arbor.
The policy statement further notes that some emerging evidence has suggested children aged 2 and older can learn words from live video chatting with a responsive adult or by using an interactive touch screen that scaffolds learning.
An earlier introduction to screens
Among the most significant changes to the recommendations for children up to 5 years old is an allowance for introducing media before age 2, the previous policy’s age recommendation.
“If you want to introduce media, 18 months is the age when kids are cognitively ready to start, but we’re not saying parents need to introduce media then,” Dr. Radesky said, adding that more research is needed regarding devices such as tablets before it’s possible to know whether apps can be beneficial in toddlers that young. “There’s not enough evidence to know if interactivity helps or not right now,” she said.
The “Media and Young Minds” policy statement notes that children under age 2 years develop their cognitive, language, motor, and social-emotional skills through hands-on exploration and social interaction with trusted adults.
“Apps can’t do the things that parents’ minds can do or children’s minds can do on their own,” Dr. Radesky said. The policy notes that digital books, or eBooks, can be beneficial when used like a traditional physical book, but interactive elements to these eBooks could be distracting and decrease children’s comprehension.
When parents do choose to introduce media to their children, it’s “crucial that media be a shared experience” between the caregiving adult and the child, she said. “Think of media as a teaching tool, a way to connect and to create, not just to consume,” Dr. Radesky said.
What can preschoolers learn?
Although some laboratory research shows toddlers as young as 15 months can learn new words from touch screens, they have difficulty transferring that knowledge to the three-dimensional world. For children aged 3-5 years, however, both well-designed television programming and high-quality learning apps from Public Broadcasting Service (PBS) and the Sesame Workshop have shown benefits. In addition to early literacy, math, and personal and social development skills learned from shows such as Sesame Street, preschoolers have learned literacy skills from those programs’ apps.
But those apps are unfortunately in the minority.
“Most apps parents find under the ‘educational’ category in app stores have no such evidence of efficacy, target only rote academic skills, are not based on established curricula, and use little or no input from developmental specialists and educators,” the “Media and Young Minds” policy states. “The higher-order thinking skills and executive functions essential for school success, such as task persistence, impulse control, emotion regulation, and creative, flexible thinking, are best taught through unstructured and social (not digital) play, as well as responsive parent-child interactions.”
Risks and recommendations for preschoolers
Heavy media use among preschoolers, meanwhile, carries risks of increased weight – primarily as a result of food advertising and eating while watching TV – as well as reduced sleep and cognitive, language, and social/emotional delays.
“Content is crucial,” the “Media and Young Minds” policy notes. “Experimental evidence shows that switching from violent content to educational/prosocial content results in significant improvement in behavioral symptoms, particularly for low-income boys.”
The key points of the new statement therefore include the following recommendations:
• Limit media use to 1 hour a day in children ages 2 years and older.
• Do not use screens during mealtimes and for 1 hour before bedtime.
• Start discussing family and child media use with parents early in children’s lives.
• Educate parents about early brain development and help families develop a Family Media Use Plan.
• Discourage screen use besides video-chatting in children under 18 months old.
• Encourage caregiving adults to use screen media with children aged 18-24 months, who should not use it on their own.
• Encourage parents to rely on high-quality programming products such as PBS Kids, Sesame Workshop, and Common Sense Media.
• Help parents with challenges such as setting limits, finding alternatives to screen time, and calming children without using media.
• Avoid using screens or media to calm children except during rare extenuating circumstances, such as painful medical procedures and airplane flights.
• Encourage parents to avoid fast-paced programs, apps with distracting content, any media with violent content, and any background television, which can stunt children’s early language development.
Understanding older youth’s media use
As children move into school age and adolescence, the opportunities and utilities for media use expand – and so do the risks. Children and teens can benefit from media through gaining social support, learning about healthy behaviors, and discovering new ideas and knowledge, but youth remain at risk for obesity, sleep problems, cyberbullying, compromised privacy, and exposure to inaccurate, inappropriate or unsafe content, the “Media Use in School-Aged Children and Adolescents” policy statement reports.
Despite the wide range of media types available, TV remains the most commonly used media type among school-aged children and teens and is watched an average of 2 hours a day. Still, 91% of boys have access to a video game console, and 84% report playing games online or on a mobile phone. Further, three-quarters of teens own a smartphone and 76% use at least one social media site, with more than 70% maintaining a “social media portfolio” across several platforms.
Such social media use can provide teens with helpful support networks, particularly for those with ongoing illnesses or disabilities or those needing community support as lesbian, gay, bisexual, transgender, questioning, or intersex individuals. Social media can also promote wellness and healthy behaviors such as eating well and not smoking.
Risks for school-aged children and adolescents using media
Yet social media also can open the door to cyberbullying, leading to short-term and long-term social, academic, and health problems. It carries the risk of exploitation of youth or their images, or predation from pornographers and pedophiles. Children and teens must be made aware that the “Internet is forever” and should be taught to consider privacy and confidentiality concerns in their use of social and other media.
Another concern is teens’ “sexting,” in which they share sexually explicit messages and/or partly or fully nude photos. Exposures to unhealthy behaviors, such as substance abuse, sexual behaviors, self-injury, or disordered eating are likewise among the risks of social media, as they are with television and cinema.
In fact, TV/movie content showing alcohol use, smoking, and sexual activity is linked to earlier experimentation among children and adolescents. In addition, each extra hour of television watching is associated with increase in body mass index, as is having a TV set in the bedroom. Enjoying entertainment media while doing school work is linked to poor learning and academics.
Excessive media use may lead to problematic Internet use and Internet gaming disorder as described in the DSM-5, occurring among 4%-8.5% of children and adolescents.
“Symptoms can include a preoccupation with the activity, decreased interest in offline or ‘real life’ relationships, unsuccessful attempts to decrease use and withdrawal symptoms,” the “Media Use in School-Aged Children and Adolescents” policy statement notes.
Recommendations for older children
The policy statement advises pediatricians to help families and schools promote understanding of media’s risks and benefits, including awareness of tools to screen for sexting, cyberbullying, problematic Internet use, and Internet gaming disorder. Pediatricians should advocate for training in media literacy in the community and encourage parents to follow the media, sleep, and physical activity guidelines included in the Family Media Plan.
The research was supported by the American Academy of Pediatrics. The authors reported no disclosures.

Deep brain stimulation for early Parkinson’s disease has long-term benefit
BALTIMORE – The use of subthalamic nucleus deep brain stimulation (DBS) along with optimal drug therapy in patients with early stage Parkinson’s disease produced clinically meaningful improvements in clinician-assessed motor control that lasted at least 5 years in a prospective pilot study.
If the findings bear out a phase III trial that has been approved, DBS may become a valuable method to achieve long-term improvement in motor skills in patients with Parkinson’s disease.
The pilot trial involved 30 patients with Parkinson’s disease, aged 50-75 years, and demonstrated the safety and benefit of DBS in conjunction with optimal drug therapy (ODT) – involving drugs such as carbidopa/levodopa, pramipexole, ropinirole, and selegiline – compared with ODT alone in improving motor scores of the patients through 2 years (Parkinsonism Relat Disord. 2014. 20[7]:731-7). The latest subanalysis of the trial data took a longer look, examining the effect of DBS through 5 years.
The subanalysis involved 28 patients; 14 in the DBS plus ODT group and 14 in the ODT-only group. Both groups were predominantly male and were similar in age at baseline (about 61 years). Motor control was assessed during the periods when DBS was applied and not applied by using the Unified Parkinson’s Disease Rating Scale (UPDRS) Part III (clinician assessed) and the Hoehn and Yahr scale.
Over the 5-year period, mean UPDRS motor scores progressively worsened for the ODT group but improved for patients receiving DBS. Patients who received DBS plus ODT had improvements relative to the ODT-only patients of 4.6 points at 1.5 years, 5.8 points at 2 years, 8.9 points at 4 years, and 10.1 points at 5 years.
“These results demonstrate that subthalamic nucleus deep brain stimulation applied in early-stage Parkinson’s disease may provide long-term, clinically meaningful improvement in motor function over standard clinical therapy,” Dr. Hacker said.
The exact mechanism of DBS is still unknown. But, there is evidence that synaptic plasticity is involved. Dr. Hacker speculated that in early Parkinson’s, the DBS intervention comes at a time of relative neuronal stability, which is then maintained.
The results of the pilot trial led to Food and Drug Administration approval of a large-scale, multicenter clinical trial. All participants will be implanted with a DBS device and will receive ODT. Some of the subjects will be randomized to receive DBS during the first 2 years, along with ODT, with the remainder receiving ODT only. In the next 2 years, all subjects will receive DBS and ODT.
Funding was provided by the National Center for Advancing Translational Science, the National Institutes of Health, Medtronic, and the Michael J. Fox Foundation for Parkinson’s Research. Dr. Hacker had no disclosures.
BALTIMORE – The use of subthalamic nucleus deep brain stimulation (DBS) along with optimal drug therapy in patients with early stage Parkinson’s disease produced clinically meaningful improvements in clinician-assessed motor control that lasted at least 5 years in a prospective pilot study.
If the findings bear out a phase III trial that has been approved, DBS may become a valuable method to achieve long-term improvement in motor skills in patients with Parkinson’s disease.
The pilot trial involved 30 patients with Parkinson’s disease, aged 50-75 years, and demonstrated the safety and benefit of DBS in conjunction with optimal drug therapy (ODT) – involving drugs such as carbidopa/levodopa, pramipexole, ropinirole, and selegiline – compared with ODT alone in improving motor scores of the patients through 2 years (Parkinsonism Relat Disord. 2014. 20[7]:731-7). The latest subanalysis of the trial data took a longer look, examining the effect of DBS through 5 years.
The subanalysis involved 28 patients; 14 in the DBS plus ODT group and 14 in the ODT-only group. Both groups were predominantly male and were similar in age at baseline (about 61 years). Motor control was assessed during the periods when DBS was applied and not applied by using the Unified Parkinson’s Disease Rating Scale (UPDRS) Part III (clinician assessed) and the Hoehn and Yahr scale.
Over the 5-year period, mean UPDRS motor scores progressively worsened for the ODT group but improved for patients receiving DBS. Patients who received DBS plus ODT had improvements relative to the ODT-only patients of 4.6 points at 1.5 years, 5.8 points at 2 years, 8.9 points at 4 years, and 10.1 points at 5 years.
“These results demonstrate that subthalamic nucleus deep brain stimulation applied in early-stage Parkinson’s disease may provide long-term, clinically meaningful improvement in motor function over standard clinical therapy,” Dr. Hacker said.
The exact mechanism of DBS is still unknown. But, there is evidence that synaptic plasticity is involved. Dr. Hacker speculated that in early Parkinson’s, the DBS intervention comes at a time of relative neuronal stability, which is then maintained.
The results of the pilot trial led to Food and Drug Administration approval of a large-scale, multicenter clinical trial. All participants will be implanted with a DBS device and will receive ODT. Some of the subjects will be randomized to receive DBS during the first 2 years, along with ODT, with the remainder receiving ODT only. In the next 2 years, all subjects will receive DBS and ODT.
Funding was provided by the National Center for Advancing Translational Science, the National Institutes of Health, Medtronic, and the Michael J. Fox Foundation for Parkinson’s Research. Dr. Hacker had no disclosures.
BALTIMORE – The use of subthalamic nucleus deep brain stimulation (DBS) along with optimal drug therapy in patients with early stage Parkinson’s disease produced clinically meaningful improvements in clinician-assessed motor control that lasted at least 5 years in a prospective pilot study.
If the findings bear out a phase III trial that has been approved, DBS may become a valuable method to achieve long-term improvement in motor skills in patients with Parkinson’s disease.
The pilot trial involved 30 patients with Parkinson’s disease, aged 50-75 years, and demonstrated the safety and benefit of DBS in conjunction with optimal drug therapy (ODT) – involving drugs such as carbidopa/levodopa, pramipexole, ropinirole, and selegiline – compared with ODT alone in improving motor scores of the patients through 2 years (Parkinsonism Relat Disord. 2014. 20[7]:731-7). The latest subanalysis of the trial data took a longer look, examining the effect of DBS through 5 years.
The subanalysis involved 28 patients; 14 in the DBS plus ODT group and 14 in the ODT-only group. Both groups were predominantly male and were similar in age at baseline (about 61 years). Motor control was assessed during the periods when DBS was applied and not applied by using the Unified Parkinson’s Disease Rating Scale (UPDRS) Part III (clinician assessed) and the Hoehn and Yahr scale.
Over the 5-year period, mean UPDRS motor scores progressively worsened for the ODT group but improved for patients receiving DBS. Patients who received DBS plus ODT had improvements relative to the ODT-only patients of 4.6 points at 1.5 years, 5.8 points at 2 years, 8.9 points at 4 years, and 10.1 points at 5 years.
“These results demonstrate that subthalamic nucleus deep brain stimulation applied in early-stage Parkinson’s disease may provide long-term, clinically meaningful improvement in motor function over standard clinical therapy,” Dr. Hacker said.
The exact mechanism of DBS is still unknown. But, there is evidence that synaptic plasticity is involved. Dr. Hacker speculated that in early Parkinson’s, the DBS intervention comes at a time of relative neuronal stability, which is then maintained.
The results of the pilot trial led to Food and Drug Administration approval of a large-scale, multicenter clinical trial. All participants will be implanted with a DBS device and will receive ODT. Some of the subjects will be randomized to receive DBS during the first 2 years, along with ODT, with the remainder receiving ODT only. In the next 2 years, all subjects will receive DBS and ODT.
Funding was provided by the National Center for Advancing Translational Science, the National Institutes of Health, Medtronic, and the Michael J. Fox Foundation for Parkinson’s Research. Dr. Hacker had no disclosures.
Key clinical point:
Major finding: Patients who received DBS plus ODT had UPDRS motor score improvements relative to the ODT-only patients of 4.6 points at 1.5 years, 5.8 points at 2 years, 8.9 points at 4 years, and 10.1 points at 5 years.
Data source: Secondary analysis of a pilot, prospective, randomized, controlled, single-blind clinical trial involving 30 patients with early Parkinson’s disease.
Disclosures: Dr. Hacker had no disclosures. Funding was provided by the National Center for Advancing Translational Science, the National Institutes of Health, Medtronic, and the Michael J. Fox Foundation for Parkinson’s Research.
Reframing views of patients who malinger advised
WASHINGTON – Imagine desperately wanting addiction treatment while living in a homeless shelter with many people who were using drugs. Could you remain sober for 6 weeks until treatment was available at an outpatient clinic – or would you bluff your way into treatment in an emergency department, where you would receive follow-up care within a week?
This is the kind of challenge that Margaret Balfour, MD, PhD, said she puts to her staff – and to anyone who treats patients they suspect are lying about this medical conditions. “Could [you], as a well-adjusted professional with reasonably good coping skills tolerate the things we ask our patients to do in order to help ‘appropriately’ ” asked Dr. Balfour, chief clinical officer at the Crisis Response Center in Tucson, Ariz., and a vice president for clinical innovation and quality at ConnectionsAZ in Tucson and Phoenix.
Signs of malingering
On average, 13% of the people presenting in the ED malinger, according to panelist Scott A. Simpson, MD, MPH, of the department of psychiatry at the University of Colorado at Denver, Aurora, and the medical director of psychiatric emergency services at Denver Health. So, how can a clinician differentiate whether a patient’s story is fact or fiction, and what can be done to get the real story?
Classic signs of malingering include a notable discrepancy between observed and reported symptoms, reports of atypical psychosis, and inexplicable cognitive symptoms. “Watch for things that seem odd, such as late-in-life onset of psychosis, Dr. Simpson said.
Patients who grow increasingly irritated during the patient interview, even to the point of threatening suicide if their treatment demands aren’t met, also can be patients who malinger However, some data do not necessarily support this as cause for alarm, according to Dr. Simpson, who cited a study showing that among 137 patients who endorsed suicidality, the 7-year suicide rate among those who did so conditionally was 0.0%, compared with 11% in those who did not have conditional suicidality (Psychiatr Serv. 2002 Jan;53[1]:92-4). The overall 7-year mortality in the first cohort was 4%, compared with 20% in the latter.
Rather than panic in such a situation, go deeper, said panelist John S. Rozel, MD, of the department of psychiatry at the University of Pittsburgh, where he also completed a master of studies in law program and serves as an adjunct professor of law. Dr. Rozel also is the medical director of the university’s re:solve Crisis Network.
“Maybe the person is worried they won’t be taken seriously,” said Dr. Rozel, explaining why some patients will escalate their claims and often are oblivious to their deceit. He shared an anecdote of having been called to treat a 14-year-old trauma patient with suicidality but who didn’t endorse any thoughts of self-harm during the patient interview. Instead, she told him that being suicidal is“what you say when you need more support, and the staff aren’t paying enough attention to you.”
Documenting the behavior
Even when clinicians are sure their patient is malingering, they often are reluctant to document it, according to Rachel Rodriguez, MD, an inpatient/emergency attending psychiatrist at Bellevue Hospital Center in New York.
“Malingering is lying, and lying is distasteful. It’s difficult to talk about,” Dr. Rodriguez said. “It’s also making a judgment about someone’s intentions, which is outside the bounds of what we are trained to do.”
Clinicians are reluctant to formally identify malingering for many reasons, Dr. Rodriguez said in an interview. Those reasons include:
• Future denial of necessary care.
• Fear of retaliation.
• Concerns about making a judgment about motives/intentions.
• Risk of misidentification.
• Fear of liability.
• Feeling sorry for the patient and helpless to address the patient’s actual needs.
Dr. Rodriguez said the underidentification and overidentification of malingering also include unique sets of risks.
At the session, Dr. Rozel agreed that an unwillingness to address malingering head-on does have its risks.
“Documentation is very important in medical malpractice. If we [record] our thinking in our notes, it’s kind of like high school math; you at least get partial credit if you show the work.” Thorough note taking includes recording the observations of all the personnel involved in the patient’s case, according to Dr. Rozel. As an example, he shared an anecdote of a patient endorsing suicidal symptoms in the interview with the clinician, but flirting with others in the waiting area, as witnessed by the admitting nurse.
Based on your observation and on a review of your patient’s prior history, Dr. Rozel suggested this partial list of notes and phrasing can be effective at establishing a “clear paper trail” should there need to be one:
• “Records show an established pattern of seeking inpatient services for ... and delaying discharge during admissions of [include dates].”
• “Review of prior records indicates no evidence of clinical improvement for brief or extended admissions similar to her current presentation.”
• “A second opinion obtained from ... concurs with ...”
• “This case has been reviewed in detail with ...”
• “Formulation and plan have been discussed with patient and other [relevant] providers, including ...”
Dr. Rozel offered this caveat: “I am not a lawyer. The only thing I promise that your lawyer and I will agree on is that they would rather you get your legal advice from them and not from me.”
Reframing the situation
Understanding yourself first will help you understand the patient better, according to Dr. Balfour: “What underlies all this is how you are feeling. Being aware of this is important.”
The range of emotional experiences when dealing with a patient who malingers can run from anger at being lied to, frustration with wasted time and resources, helplessness that nothing seems to make a difference, fear of making the wrong decision, and even hatred borne of constantly experiencing all the other emotions, she said.
Being honest about your own emotions helps keep them out of the way of delivering better care, as does being mindful of the language you use to describe patients. Describing a patient to other staff in words that connote negativity, such as “manipulative,” “attention seeking,” or “high maintenance,” might influence others to see the patient as problematic rather than someone to be helped, said Dr. Balfour, who is with the department of psychiatry at the University of Arizona, Tucson.
Instead of labeling patients, “I find using the techniques of dialectical behavioral training very effective in dealing with [this population],” Dr. Balfour said. A more effective approach includes reframing your view of patients not as liars, but as people who are doing the best they can with what they have in a system that is often set up in ways that prevent, more than augment, care.
In that case, a person who lives in a homeless shelter and who wants help with a drug addiction, for example, will “understandably come to the emergency department to try and get admitted to the inpatient unit where they can get into rehab,” Dr. Balfour said. “Sometimes, our system makes people do things we find annoying in order to get the help they need.”
Instead of making the prevention of unnecessary admissions the goal, find a way to create a rapport with patients to determine their actual problem and see what can be done to solve it. This might take several engagements with the patient, often with more than one staff member. Using the statement, “I don’t feel like I’m getting the whole story” in the patient interview is an effective way to engage patients without accusing them of lying, Dr. Balfour said. “It’s like a magic phrase. Its effectiveness is predicated on the idea that all people, even those who dissemble or embellish, have a wish on some level to reveal sensitive, personal material.”
Remembering not to take malingering personally and that your role is “to be a detective not a bouncer” will help de-escalate untruths, and can lead to a partnership with the patient rather than enmity, Dr. Balfour said.
Dr. Balfour disclosed that she is a consultant for Connections Health Solutions and Otsuka. Dr. Simpson, Dr. Rozel, and Dr. Rodriguez had no relevant disclosures.
WASHINGTON – Imagine desperately wanting addiction treatment while living in a homeless shelter with many people who were using drugs. Could you remain sober for 6 weeks until treatment was available at an outpatient clinic – or would you bluff your way into treatment in an emergency department, where you would receive follow-up care within a week?
This is the kind of challenge that Margaret Balfour, MD, PhD, said she puts to her staff – and to anyone who treats patients they suspect are lying about this medical conditions. “Could [you], as a well-adjusted professional with reasonably good coping skills tolerate the things we ask our patients to do in order to help ‘appropriately’ ” asked Dr. Balfour, chief clinical officer at the Crisis Response Center in Tucson, Ariz., and a vice president for clinical innovation and quality at ConnectionsAZ in Tucson and Phoenix.
Signs of malingering
On average, 13% of the people presenting in the ED malinger, according to panelist Scott A. Simpson, MD, MPH, of the department of psychiatry at the University of Colorado at Denver, Aurora, and the medical director of psychiatric emergency services at Denver Health. So, how can a clinician differentiate whether a patient’s story is fact or fiction, and what can be done to get the real story?
Classic signs of malingering include a notable discrepancy between observed and reported symptoms, reports of atypical psychosis, and inexplicable cognitive symptoms. “Watch for things that seem odd, such as late-in-life onset of psychosis, Dr. Simpson said.
Patients who grow increasingly irritated during the patient interview, even to the point of threatening suicide if their treatment demands aren’t met, also can be patients who malinger However, some data do not necessarily support this as cause for alarm, according to Dr. Simpson, who cited a study showing that among 137 patients who endorsed suicidality, the 7-year suicide rate among those who did so conditionally was 0.0%, compared with 11% in those who did not have conditional suicidality (Psychiatr Serv. 2002 Jan;53[1]:92-4). The overall 7-year mortality in the first cohort was 4%, compared with 20% in the latter.
Rather than panic in such a situation, go deeper, said panelist John S. Rozel, MD, of the department of psychiatry at the University of Pittsburgh, where he also completed a master of studies in law program and serves as an adjunct professor of law. Dr. Rozel also is the medical director of the university’s re:solve Crisis Network.
“Maybe the person is worried they won’t be taken seriously,” said Dr. Rozel, explaining why some patients will escalate their claims and often are oblivious to their deceit. He shared an anecdote of having been called to treat a 14-year-old trauma patient with suicidality but who didn’t endorse any thoughts of self-harm during the patient interview. Instead, she told him that being suicidal is“what you say when you need more support, and the staff aren’t paying enough attention to you.”
Documenting the behavior
Even when clinicians are sure their patient is malingering, they often are reluctant to document it, according to Rachel Rodriguez, MD, an inpatient/emergency attending psychiatrist at Bellevue Hospital Center in New York.
“Malingering is lying, and lying is distasteful. It’s difficult to talk about,” Dr. Rodriguez said. “It’s also making a judgment about someone’s intentions, which is outside the bounds of what we are trained to do.”
Clinicians are reluctant to formally identify malingering for many reasons, Dr. Rodriguez said in an interview. Those reasons include:
• Future denial of necessary care.
• Fear of retaliation.
• Concerns about making a judgment about motives/intentions.
• Risk of misidentification.
• Fear of liability.
• Feeling sorry for the patient and helpless to address the patient’s actual needs.
Dr. Rodriguez said the underidentification and overidentification of malingering also include unique sets of risks.
At the session, Dr. Rozel agreed that an unwillingness to address malingering head-on does have its risks.
“Documentation is very important in medical malpractice. If we [record] our thinking in our notes, it’s kind of like high school math; you at least get partial credit if you show the work.” Thorough note taking includes recording the observations of all the personnel involved in the patient’s case, according to Dr. Rozel. As an example, he shared an anecdote of a patient endorsing suicidal symptoms in the interview with the clinician, but flirting with others in the waiting area, as witnessed by the admitting nurse.
Based on your observation and on a review of your patient’s prior history, Dr. Rozel suggested this partial list of notes and phrasing can be effective at establishing a “clear paper trail” should there need to be one:
• “Records show an established pattern of seeking inpatient services for ... and delaying discharge during admissions of [include dates].”
• “Review of prior records indicates no evidence of clinical improvement for brief or extended admissions similar to her current presentation.”
• “A second opinion obtained from ... concurs with ...”
• “This case has been reviewed in detail with ...”
• “Formulation and plan have been discussed with patient and other [relevant] providers, including ...”
Dr. Rozel offered this caveat: “I am not a lawyer. The only thing I promise that your lawyer and I will agree on is that they would rather you get your legal advice from them and not from me.”
Reframing the situation
Understanding yourself first will help you understand the patient better, according to Dr. Balfour: “What underlies all this is how you are feeling. Being aware of this is important.”
The range of emotional experiences when dealing with a patient who malingers can run from anger at being lied to, frustration with wasted time and resources, helplessness that nothing seems to make a difference, fear of making the wrong decision, and even hatred borne of constantly experiencing all the other emotions, she said.
Being honest about your own emotions helps keep them out of the way of delivering better care, as does being mindful of the language you use to describe patients. Describing a patient to other staff in words that connote negativity, such as “manipulative,” “attention seeking,” or “high maintenance,” might influence others to see the patient as problematic rather than someone to be helped, said Dr. Balfour, who is with the department of psychiatry at the University of Arizona, Tucson.
Instead of labeling patients, “I find using the techniques of dialectical behavioral training very effective in dealing with [this population],” Dr. Balfour said. A more effective approach includes reframing your view of patients not as liars, but as people who are doing the best they can with what they have in a system that is often set up in ways that prevent, more than augment, care.
In that case, a person who lives in a homeless shelter and who wants help with a drug addiction, for example, will “understandably come to the emergency department to try and get admitted to the inpatient unit where they can get into rehab,” Dr. Balfour said. “Sometimes, our system makes people do things we find annoying in order to get the help they need.”
Instead of making the prevention of unnecessary admissions the goal, find a way to create a rapport with patients to determine their actual problem and see what can be done to solve it. This might take several engagements with the patient, often with more than one staff member. Using the statement, “I don’t feel like I’m getting the whole story” in the patient interview is an effective way to engage patients without accusing them of lying, Dr. Balfour said. “It’s like a magic phrase. Its effectiveness is predicated on the idea that all people, even those who dissemble or embellish, have a wish on some level to reveal sensitive, personal material.”
Remembering not to take malingering personally and that your role is “to be a detective not a bouncer” will help de-escalate untruths, and can lead to a partnership with the patient rather than enmity, Dr. Balfour said.
Dr. Balfour disclosed that she is a consultant for Connections Health Solutions and Otsuka. Dr. Simpson, Dr. Rozel, and Dr. Rodriguez had no relevant disclosures.
WASHINGTON – Imagine desperately wanting addiction treatment while living in a homeless shelter with many people who were using drugs. Could you remain sober for 6 weeks until treatment was available at an outpatient clinic – or would you bluff your way into treatment in an emergency department, where you would receive follow-up care within a week?
This is the kind of challenge that Margaret Balfour, MD, PhD, said she puts to her staff – and to anyone who treats patients they suspect are lying about this medical conditions. “Could [you], as a well-adjusted professional with reasonably good coping skills tolerate the things we ask our patients to do in order to help ‘appropriately’ ” asked Dr. Balfour, chief clinical officer at the Crisis Response Center in Tucson, Ariz., and a vice president for clinical innovation and quality at ConnectionsAZ in Tucson and Phoenix.
Signs of malingering
On average, 13% of the people presenting in the ED malinger, according to panelist Scott A. Simpson, MD, MPH, of the department of psychiatry at the University of Colorado at Denver, Aurora, and the medical director of psychiatric emergency services at Denver Health. So, how can a clinician differentiate whether a patient’s story is fact or fiction, and what can be done to get the real story?
Classic signs of malingering include a notable discrepancy between observed and reported symptoms, reports of atypical psychosis, and inexplicable cognitive symptoms. “Watch for things that seem odd, such as late-in-life onset of psychosis, Dr. Simpson said.
Patients who grow increasingly irritated during the patient interview, even to the point of threatening suicide if their treatment demands aren’t met, also can be patients who malinger However, some data do not necessarily support this as cause for alarm, according to Dr. Simpson, who cited a study showing that among 137 patients who endorsed suicidality, the 7-year suicide rate among those who did so conditionally was 0.0%, compared with 11% in those who did not have conditional suicidality (Psychiatr Serv. 2002 Jan;53[1]:92-4). The overall 7-year mortality in the first cohort was 4%, compared with 20% in the latter.
Rather than panic in such a situation, go deeper, said panelist John S. Rozel, MD, of the department of psychiatry at the University of Pittsburgh, where he also completed a master of studies in law program and serves as an adjunct professor of law. Dr. Rozel also is the medical director of the university’s re:solve Crisis Network.
“Maybe the person is worried they won’t be taken seriously,” said Dr. Rozel, explaining why some patients will escalate their claims and often are oblivious to their deceit. He shared an anecdote of having been called to treat a 14-year-old trauma patient with suicidality but who didn’t endorse any thoughts of self-harm during the patient interview. Instead, she told him that being suicidal is“what you say when you need more support, and the staff aren’t paying enough attention to you.”
Documenting the behavior
Even when clinicians are sure their patient is malingering, they often are reluctant to document it, according to Rachel Rodriguez, MD, an inpatient/emergency attending psychiatrist at Bellevue Hospital Center in New York.
“Malingering is lying, and lying is distasteful. It’s difficult to talk about,” Dr. Rodriguez said. “It’s also making a judgment about someone’s intentions, which is outside the bounds of what we are trained to do.”
Clinicians are reluctant to formally identify malingering for many reasons, Dr. Rodriguez said in an interview. Those reasons include:
• Future denial of necessary care.
• Fear of retaliation.
• Concerns about making a judgment about motives/intentions.
• Risk of misidentification.
• Fear of liability.
• Feeling sorry for the patient and helpless to address the patient’s actual needs.
Dr. Rodriguez said the underidentification and overidentification of malingering also include unique sets of risks.
At the session, Dr. Rozel agreed that an unwillingness to address malingering head-on does have its risks.
“Documentation is very important in medical malpractice. If we [record] our thinking in our notes, it’s kind of like high school math; you at least get partial credit if you show the work.” Thorough note taking includes recording the observations of all the personnel involved in the patient’s case, according to Dr. Rozel. As an example, he shared an anecdote of a patient endorsing suicidal symptoms in the interview with the clinician, but flirting with others in the waiting area, as witnessed by the admitting nurse.
Based on your observation and on a review of your patient’s prior history, Dr. Rozel suggested this partial list of notes and phrasing can be effective at establishing a “clear paper trail” should there need to be one:
• “Records show an established pattern of seeking inpatient services for ... and delaying discharge during admissions of [include dates].”
• “Review of prior records indicates no evidence of clinical improvement for brief or extended admissions similar to her current presentation.”
• “A second opinion obtained from ... concurs with ...”
• “This case has been reviewed in detail with ...”
• “Formulation and plan have been discussed with patient and other [relevant] providers, including ...”
Dr. Rozel offered this caveat: “I am not a lawyer. The only thing I promise that your lawyer and I will agree on is that they would rather you get your legal advice from them and not from me.”
Reframing the situation
Understanding yourself first will help you understand the patient better, according to Dr. Balfour: “What underlies all this is how you are feeling. Being aware of this is important.”
The range of emotional experiences when dealing with a patient who malingers can run from anger at being lied to, frustration with wasted time and resources, helplessness that nothing seems to make a difference, fear of making the wrong decision, and even hatred borne of constantly experiencing all the other emotions, she said.
Being honest about your own emotions helps keep them out of the way of delivering better care, as does being mindful of the language you use to describe patients. Describing a patient to other staff in words that connote negativity, such as “manipulative,” “attention seeking,” or “high maintenance,” might influence others to see the patient as problematic rather than someone to be helped, said Dr. Balfour, who is with the department of psychiatry at the University of Arizona, Tucson.
Instead of labeling patients, “I find using the techniques of dialectical behavioral training very effective in dealing with [this population],” Dr. Balfour said. A more effective approach includes reframing your view of patients not as liars, but as people who are doing the best they can with what they have in a system that is often set up in ways that prevent, more than augment, care.
In that case, a person who lives in a homeless shelter and who wants help with a drug addiction, for example, will “understandably come to the emergency department to try and get admitted to the inpatient unit where they can get into rehab,” Dr. Balfour said. “Sometimes, our system makes people do things we find annoying in order to get the help they need.”
Instead of making the prevention of unnecessary admissions the goal, find a way to create a rapport with patients to determine their actual problem and see what can be done to solve it. This might take several engagements with the patient, often with more than one staff member. Using the statement, “I don’t feel like I’m getting the whole story” in the patient interview is an effective way to engage patients without accusing them of lying, Dr. Balfour said. “It’s like a magic phrase. Its effectiveness is predicated on the idea that all people, even those who dissemble or embellish, have a wish on some level to reveal sensitive, personal material.”
Remembering not to take malingering personally and that your role is “to be a detective not a bouncer” will help de-escalate untruths, and can lead to a partnership with the patient rather than enmity, Dr. Balfour said.
Dr. Balfour disclosed that she is a consultant for Connections Health Solutions and Otsuka. Dr. Simpson, Dr. Rozel, and Dr. Rodriguez had no relevant disclosures.
FDA finalizes boxed warning for Essure
The Food and Drug Administration will require the Essure permanent birth control system to carry a boxed warning about the device’s reported adverse events, including perforation of the uterus and/or fallopian tubes, identification of inserts in the abdominal or pelvic cavity, persistent pain, and suspected allergic or hypersensitivity reactions.
The boxed warning should also state that if the device needs to be removed to address an adverse event, surgery will be necessary.
FDA officials released the final guidance Oct. 28 on labeling for permanent hysteroscopically placed tubal implants intended for sterilization, following the publication of draft labeling requirements in February 2016.
The guidance includes a Patient Decision Checklist to be signed by the patient and the physician, acknowledging that the risks and benefits of the device were discussed. The checklist is divided into sections detailing other birth control options, requirements for Essure placement (including contraindications), pregnancy risks with the device, what to expect during and after the procedure based on clinical studies, and long-term risks.
The new labeling requirements follow years of controversy about the device, which is currently the only permanent contraception option for women that can be performed without surgery.
In September 2015, the FDA Obstetrics and Gynecology Devices Panel reviewed the safety of the device after receiving more than 5,000 complaints of adverse reactions. Consensus from the 19-member panel was that there was a lack of data about the risks of the device and that patients needed better counseling before choosing it as a birth control option.
The final labeling guidance document seeks to address some of those concerns, according to the FDA.
“FDA believes this will help to ensure a woman receives and understands the benefits and risks associated with her contraceptive options so that she can make an informed decision as to whether a permanent hysteroscopically placed tubal implant intended for sterilization is the right choice for her,” according to the guidance document.
In September 2016, the FDA approved a postmarket surveillance study plan from Essure’s manufacturer, Bayer. The 3-year study will compare safety and effectiveness between women who undergo hysterocopic sterilization with Essure and those who have laparoscopic tubal sterilization.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The Food and Drug Administration will require the Essure permanent birth control system to carry a boxed warning about the device’s reported adverse events, including perforation of the uterus and/or fallopian tubes, identification of inserts in the abdominal or pelvic cavity, persistent pain, and suspected allergic or hypersensitivity reactions.
The boxed warning should also state that if the device needs to be removed to address an adverse event, surgery will be necessary.
FDA officials released the final guidance Oct. 28 on labeling for permanent hysteroscopically placed tubal implants intended for sterilization, following the publication of draft labeling requirements in February 2016.
The guidance includes a Patient Decision Checklist to be signed by the patient and the physician, acknowledging that the risks and benefits of the device were discussed. The checklist is divided into sections detailing other birth control options, requirements for Essure placement (including contraindications), pregnancy risks with the device, what to expect during and after the procedure based on clinical studies, and long-term risks.
The new labeling requirements follow years of controversy about the device, which is currently the only permanent contraception option for women that can be performed without surgery.
In September 2015, the FDA Obstetrics and Gynecology Devices Panel reviewed the safety of the device after receiving more than 5,000 complaints of adverse reactions. Consensus from the 19-member panel was that there was a lack of data about the risks of the device and that patients needed better counseling before choosing it as a birth control option.
The final labeling guidance document seeks to address some of those concerns, according to the FDA.
“FDA believes this will help to ensure a woman receives and understands the benefits and risks associated with her contraceptive options so that she can make an informed decision as to whether a permanent hysteroscopically placed tubal implant intended for sterilization is the right choice for her,” according to the guidance document.
In September 2016, the FDA approved a postmarket surveillance study plan from Essure’s manufacturer, Bayer. The 3-year study will compare safety and effectiveness between women who undergo hysterocopic sterilization with Essure and those who have laparoscopic tubal sterilization.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The Food and Drug Administration will require the Essure permanent birth control system to carry a boxed warning about the device’s reported adverse events, including perforation of the uterus and/or fallopian tubes, identification of inserts in the abdominal or pelvic cavity, persistent pain, and suspected allergic or hypersensitivity reactions.
The boxed warning should also state that if the device needs to be removed to address an adverse event, surgery will be necessary.
FDA officials released the final guidance Oct. 28 on labeling for permanent hysteroscopically placed tubal implants intended for sterilization, following the publication of draft labeling requirements in February 2016.
The guidance includes a Patient Decision Checklist to be signed by the patient and the physician, acknowledging that the risks and benefits of the device were discussed. The checklist is divided into sections detailing other birth control options, requirements for Essure placement (including contraindications), pregnancy risks with the device, what to expect during and after the procedure based on clinical studies, and long-term risks.
The new labeling requirements follow years of controversy about the device, which is currently the only permanent contraception option for women that can be performed without surgery.
In September 2015, the FDA Obstetrics and Gynecology Devices Panel reviewed the safety of the device after receiving more than 5,000 complaints of adverse reactions. Consensus from the 19-member panel was that there was a lack of data about the risks of the device and that patients needed better counseling before choosing it as a birth control option.
The final labeling guidance document seeks to address some of those concerns, according to the FDA.
“FDA believes this will help to ensure a woman receives and understands the benefits and risks associated with her contraceptive options so that she can make an informed decision as to whether a permanent hysteroscopically placed tubal implant intended for sterilization is the right choice for her,” according to the guidance document.
In September 2016, the FDA approved a postmarket surveillance study plan from Essure’s manufacturer, Bayer. The 3-year study will compare safety and effectiveness between women who undergo hysterocopic sterilization with Essure and those who have laparoscopic tubal sterilization.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Advanced heart failure symptoms linked to mortality
ORLANDO – Advanced heart failure patients who are hospitalized for heart failure and have a higher symptom burden at discharge have a significantly increased rate of death or rehospitalization over the next 6 months, based on an analysis of 393 patients enrolled in a heart failure trial.
The strong link between severe symptom burden and poor near-term outcomes persisted despite adjustment for various markers of heart failure severity, suggesting that treatment aimed at reducing symptoms may be able to reduce mortality or heart failure hospitalization in advanced heart failure patients, Ellen K. Hummel, MD, said at the annual scientific meeting of the Heart Failure Society of America.
In her analysis, a severe symptom burden at the time of hospital discharge linked with an adjusted 2.9-fold increased mortality rate and a 2.5-fold increased rate of days dead or hospitalized during the next 6 months, said Dr. Hummel, a geriatric and palliative care specialist at the University of Michigan in Ann Arbor. These elevated rate ratios for patients with severe symptoms at hospital discharge were in comparison to the ratios for advanced heart failure patients in the study with no symptoms at discharge.
Three symptoms contributed to the symptom score she used in her analysis: fatigue, scored on a scale of 0-3; dyspnea, also scored 0-3; and gastrointestinal distress, scored as 0-2, creating a maximum score of 8. Her analysis categorized mild as a total score of 1-4 and severe as 5 or greater. In the study population she used for her analysis, patients enrolled in the multicenter ESCAPE (Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness) trial, 111 of the 393 evaluable patients (28%) had none of these symptoms, 239 (61%) had mild symptoms, and 43 (11%) had severe symptoms. Scoring was done by patients based on their subjective self-assessment at the time of hospital discharge.
The absolute, observed 6-month mortality rates were roughly 45% among patients with severe symptoms, about 17% in patients with mild symptoms, and about 12% in those with no symptoms.
The primary purpose of ESCAPE was to assess the impact that routine collection of data from a pulmonary artery catheter during hospitalization has on outcomes; the results showed no significant link between improved outcomes and getting these data (JAMA. 2005 Oct 5;294[13]:1625-33). The study ran during 2000-2003 at 26 centers in the United States and Canada. Of the 433 advanced heart failure patients enrolled in ESCAPE, 393 had complete records to allow the current analysis.
The adjustments that Dr. Hummel made in the proportional hazard analysis took into account New York Heart Association class, and severity of disease at the time of hospital discharge measured by the ESCAPE Discharge Risk Score. This score takes into account age, 6-minute walk distance, blood urea nitrogen, brain natriuretic peptide levels, blood pressure, selected drug treatments, sodium level, and history of cardiopulmonary resuscitation or mechanical ventilation.
Dr. Hummel had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ORLANDO – Advanced heart failure patients who are hospitalized for heart failure and have a higher symptom burden at discharge have a significantly increased rate of death or rehospitalization over the next 6 months, based on an analysis of 393 patients enrolled in a heart failure trial.
The strong link between severe symptom burden and poor near-term outcomes persisted despite adjustment for various markers of heart failure severity, suggesting that treatment aimed at reducing symptoms may be able to reduce mortality or heart failure hospitalization in advanced heart failure patients, Ellen K. Hummel, MD, said at the annual scientific meeting of the Heart Failure Society of America.
In her analysis, a severe symptom burden at the time of hospital discharge linked with an adjusted 2.9-fold increased mortality rate and a 2.5-fold increased rate of days dead or hospitalized during the next 6 months, said Dr. Hummel, a geriatric and palliative care specialist at the University of Michigan in Ann Arbor. These elevated rate ratios for patients with severe symptoms at hospital discharge were in comparison to the ratios for advanced heart failure patients in the study with no symptoms at discharge.
Three symptoms contributed to the symptom score she used in her analysis: fatigue, scored on a scale of 0-3; dyspnea, also scored 0-3; and gastrointestinal distress, scored as 0-2, creating a maximum score of 8. Her analysis categorized mild as a total score of 1-4 and severe as 5 or greater. In the study population she used for her analysis, patients enrolled in the multicenter ESCAPE (Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness) trial, 111 of the 393 evaluable patients (28%) had none of these symptoms, 239 (61%) had mild symptoms, and 43 (11%) had severe symptoms. Scoring was done by patients based on their subjective self-assessment at the time of hospital discharge.
The absolute, observed 6-month mortality rates were roughly 45% among patients with severe symptoms, about 17% in patients with mild symptoms, and about 12% in those with no symptoms.
The primary purpose of ESCAPE was to assess the impact that routine collection of data from a pulmonary artery catheter during hospitalization has on outcomes; the results showed no significant link between improved outcomes and getting these data (JAMA. 2005 Oct 5;294[13]:1625-33). The study ran during 2000-2003 at 26 centers in the United States and Canada. Of the 433 advanced heart failure patients enrolled in ESCAPE, 393 had complete records to allow the current analysis.
The adjustments that Dr. Hummel made in the proportional hazard analysis took into account New York Heart Association class, and severity of disease at the time of hospital discharge measured by the ESCAPE Discharge Risk Score. This score takes into account age, 6-minute walk distance, blood urea nitrogen, brain natriuretic peptide levels, blood pressure, selected drug treatments, sodium level, and history of cardiopulmonary resuscitation or mechanical ventilation.
Dr. Hummel had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ORLANDO – Advanced heart failure patients who are hospitalized for heart failure and have a higher symptom burden at discharge have a significantly increased rate of death or rehospitalization over the next 6 months, based on an analysis of 393 patients enrolled in a heart failure trial.
The strong link between severe symptom burden and poor near-term outcomes persisted despite adjustment for various markers of heart failure severity, suggesting that treatment aimed at reducing symptoms may be able to reduce mortality or heart failure hospitalization in advanced heart failure patients, Ellen K. Hummel, MD, said at the annual scientific meeting of the Heart Failure Society of America.
In her analysis, a severe symptom burden at the time of hospital discharge linked with an adjusted 2.9-fold increased mortality rate and a 2.5-fold increased rate of days dead or hospitalized during the next 6 months, said Dr. Hummel, a geriatric and palliative care specialist at the University of Michigan in Ann Arbor. These elevated rate ratios for patients with severe symptoms at hospital discharge were in comparison to the ratios for advanced heart failure patients in the study with no symptoms at discharge.
Three symptoms contributed to the symptom score she used in her analysis: fatigue, scored on a scale of 0-3; dyspnea, also scored 0-3; and gastrointestinal distress, scored as 0-2, creating a maximum score of 8. Her analysis categorized mild as a total score of 1-4 and severe as 5 or greater. In the study population she used for her analysis, patients enrolled in the multicenter ESCAPE (Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness) trial, 111 of the 393 evaluable patients (28%) had none of these symptoms, 239 (61%) had mild symptoms, and 43 (11%) had severe symptoms. Scoring was done by patients based on their subjective self-assessment at the time of hospital discharge.
The absolute, observed 6-month mortality rates were roughly 45% among patients with severe symptoms, about 17% in patients with mild symptoms, and about 12% in those with no symptoms.
The primary purpose of ESCAPE was to assess the impact that routine collection of data from a pulmonary artery catheter during hospitalization has on outcomes; the results showed no significant link between improved outcomes and getting these data (JAMA. 2005 Oct 5;294[13]:1625-33). The study ran during 2000-2003 at 26 centers in the United States and Canada. Of the 433 advanced heart failure patients enrolled in ESCAPE, 393 had complete records to allow the current analysis.
The adjustments that Dr. Hummel made in the proportional hazard analysis took into account New York Heart Association class, and severity of disease at the time of hospital discharge measured by the ESCAPE Discharge Risk Score. This score takes into account age, 6-minute walk distance, blood urea nitrogen, brain natriuretic peptide levels, blood pressure, selected drug treatments, sodium level, and history of cardiopulmonary resuscitation or mechanical ventilation.
Dr. Hummel had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE HFSA ANNUAL SCIENTIFIC MEETING
Key clinical point:
Major finding: Patients with severe symptoms at discharge had a 2.9-fold increased rate of death, compared with those with no symptoms.
Data source: A post hoc analysis of data collected from 393 patients enrolled in the ESCAPE trial.
Disclosures: Dr. Hummel had no relevant financial disclosures.
Sensory-related difficulties in children
A Google search of “sensory issues in children” reveals more than 20 million results and a wide range of terminology that can be confusing to parents, providers, and youth themselves. Phenomena such as sensory processing disorder, sensory integration disorder, sensory discrimination disorder, and sensory defensiveness are noted, and autism spectrum disorder (ASD) is a label not uncommonly attached to the former terms.
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) does not include a discrete diagnosis to apply to children who have sensory differences, (meaning that they have difficulties regulating sensory input and such difficulties affect their ability to successfully relate to the world around them), but these differences are now part of the diagnostic criteria for ASD. The literature indicates that a majority of youth with ASD demonstrate features of sensory overresponsiveness (JAMA Psychiatry. 2015 Aug;72[8]:778-86), and providers should rightfully be concerned about the possibility of autism in a youngster who is presenting with severe negative responses to auditory, visual, and/or tactile stimuli.
Notably, however, even though sensory problems are considered a feature of autism, they are not pathognomonic for the disorder, and most children with these problems are, in fact, not autistic. Children with deficits in their ability to modulate sensory stimuli can present with a wide range of emotional-behavioral problems, including externalizing behaviors and internalizing symptoms manifesting with anxiety, attention challenges, mood dysregulation, and overall poor adaptive functioning. The relationship between sensory issues (both underresponsiveness and overresponsiveness) and psychopathology is rather complicated as sensory dysfunction can exist independent of a psychiatric disorder, be a significant risk factor for the development of the disorder (J Abnorm Child Psychol. 2009 Nov;37[8]:1077-87), and have symptom overlap with the disorder.
All in all, in spite of this complexity, since the 1960’s (Am J Occup Ther. 1964 Jan-Feb;18:6-11), it’s been clear that sensory dysfunction in children is associated with impairments in development, learning, and self-regulation. Parents of these children experience elevated levels of stress (J Child Fam Stud. 2013 Oct 1;22[7]:912-21), and early identification of sensory differences, psychoeducation, and referral for treatment are critical to minimize these impacts and foster positive outcomes.
Case Summary

In gathering a history and administering the Autism Diagnostic Observation Schedule (ADOS), it became clear that Sarah did not present with the social-communicative impairments that characterize ASD, but she did demonstrate repetitive hand flapping, troubles tolerating large social get-togethers, hypersensitivities, and a vulnerability to getting stuck when attempting to transition between activities. It is not uncommon for Sarah to use “fight-and-flight” reactions when faced with internal or external discomfort. Child Behavior Checklist data revealed multi-informant endorsement of clinical range symptoms across broad-band and narrow-band domains. Additionally, the Sensory Profile–2 yielded elevated scores in categories measuring sensory seeking and sensory sensitivity. The Sensory Profile is a standardized tool that uses caregiver and teacher-completed questionnaires to examine a child’s sensory processing abilities and provide data regarding the effect of such sensory processing on functional performance. Integrating all the available data, our team certainly appreciated Sarah’s profound sensory overresponsiveness, and a diagnosis of an unspecified anxiety disorder was provided along with consideration for attention-deficit/hyperactivity disorder (ADHD) (with teacher input needed to further investigate this possibility). The family history revealed anxiety disorders occurring both maternally and paternally. Additionally, Sarah’s mother’s acknowledged having her own similar sensory issues as a child.
Discussion
Associations among anxiety, sensory overresponsiveness, and ADHD are recognized in the literature (Am J Occup Ther. 2009 Jul-Aug;63[4]:433-40) and have implications for treatment. Furthermore, there is evidence that there is a heritable aspect to sensory processing abnormalities, and tactile defensiveness is associated with fearful temperament and anxiety (J Abnorm Child Psychol. 2006 Jun;34[3]:393-407). In Sarah’s case, her intense behavioral response to ordinary sensory stimuli was striking, and she had not yet been referred for an occupational therapy evaluation, which was the primary recommendation to further assess and understand her complicated sensory profile. As one component of a comprehensive treatment plan, an occupational therapist (www.aota.org), by using evidence-based practices in a sensory-integration framework, could be helpful in addressing Sarah’s range of challenges and promoting positive outcomes related to socialization, behavioral regulation, and attention. Occupational therapists, with assistance from other team members, also could work with Sarah and her family on developing relaxation skills and use exposure and response prevention–oriented intervention strategies to address anxieties. Families, however, should be counseled about the limited data on the use of sensory-based therapies (Pediatrics. 2012 Jun;129[6]:1186-9); the use of parent-management training/family coaching should also be a treatment consideration to help promote overall regulatory functioning in the household.
Clinical pearl
When encountering youth with sensory-related challenges, a clinician’s diagnostic considerations should be more than just thinking about the possibility of an autism spectrum disorder. Symptoms of sensory overresponsiveness are associated with other emotional-behavioral conditions, but also can be seen without co-occurring psychopathology. With the latter, however, providers should be mindful that family-related impairments still may be quite noteworthy (J Am Acad Child Adolesc Psychiatry. 2011 Dec;50[12]:1210-9) and associated behavior problems could be attributed incorrectly to other diagnoses (which may lead to the recommendation of ineffective and inappropriate treatments). Much more research is needed to help develop a robust framework for diagnosing and labeling sensory issues in children and studying the efficacy of available intervention strategies.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic.
A Google search of “sensory issues in children” reveals more than 20 million results and a wide range of terminology that can be confusing to parents, providers, and youth themselves. Phenomena such as sensory processing disorder, sensory integration disorder, sensory discrimination disorder, and sensory defensiveness are noted, and autism spectrum disorder (ASD) is a label not uncommonly attached to the former terms.
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) does not include a discrete diagnosis to apply to children who have sensory differences, (meaning that they have difficulties regulating sensory input and such difficulties affect their ability to successfully relate to the world around them), but these differences are now part of the diagnostic criteria for ASD. The literature indicates that a majority of youth with ASD demonstrate features of sensory overresponsiveness (JAMA Psychiatry. 2015 Aug;72[8]:778-86), and providers should rightfully be concerned about the possibility of autism in a youngster who is presenting with severe negative responses to auditory, visual, and/or tactile stimuli.
Notably, however, even though sensory problems are considered a feature of autism, they are not pathognomonic for the disorder, and most children with these problems are, in fact, not autistic. Children with deficits in their ability to modulate sensory stimuli can present with a wide range of emotional-behavioral problems, including externalizing behaviors and internalizing symptoms manifesting with anxiety, attention challenges, mood dysregulation, and overall poor adaptive functioning. The relationship between sensory issues (both underresponsiveness and overresponsiveness) and psychopathology is rather complicated as sensory dysfunction can exist independent of a psychiatric disorder, be a significant risk factor for the development of the disorder (J Abnorm Child Psychol. 2009 Nov;37[8]:1077-87), and have symptom overlap with the disorder.
All in all, in spite of this complexity, since the 1960’s (Am J Occup Ther. 1964 Jan-Feb;18:6-11), it’s been clear that sensory dysfunction in children is associated with impairments in development, learning, and self-regulation. Parents of these children experience elevated levels of stress (J Child Fam Stud. 2013 Oct 1;22[7]:912-21), and early identification of sensory differences, psychoeducation, and referral for treatment are critical to minimize these impacts and foster positive outcomes.
Case Summary
In gathering a history and administering the Autism Diagnostic Observation Schedule (ADOS), it became clear that Sarah did not present with the social-communicative impairments that characterize ASD, but she did demonstrate repetitive hand flapping, troubles tolerating large social get-togethers, hypersensitivities, and a vulnerability to getting stuck when attempting to transition between activities. It is not uncommon for Sarah to use “fight-and-flight” reactions when faced with internal or external discomfort. Child Behavior Checklist data revealed multi-informant endorsement of clinical range symptoms across broad-band and narrow-band domains. Additionally, the Sensory Profile–2 yielded elevated scores in categories measuring sensory seeking and sensory sensitivity. The Sensory Profile is a standardized tool that uses caregiver and teacher-completed questionnaires to examine a child’s sensory processing abilities and provide data regarding the effect of such sensory processing on functional performance. Integrating all the available data, our team certainly appreciated Sarah’s profound sensory overresponsiveness, and a diagnosis of an unspecified anxiety disorder was provided along with consideration for attention-deficit/hyperactivity disorder (ADHD) (with teacher input needed to further investigate this possibility). The family history revealed anxiety disorders occurring both maternally and paternally. Additionally, Sarah’s mother’s acknowledged having her own similar sensory issues as a child.
Discussion
Associations among anxiety, sensory overresponsiveness, and ADHD are recognized in the literature (Am J Occup Ther. 2009 Jul-Aug;63[4]:433-40) and have implications for treatment. Furthermore, there is evidence that there is a heritable aspect to sensory processing abnormalities, and tactile defensiveness is associated with fearful temperament and anxiety (J Abnorm Child Psychol. 2006 Jun;34[3]:393-407). In Sarah’s case, her intense behavioral response to ordinary sensory stimuli was striking, and she had not yet been referred for an occupational therapy evaluation, which was the primary recommendation to further assess and understand her complicated sensory profile. As one component of a comprehensive treatment plan, an occupational therapist (www.aota.org), by using evidence-based practices in a sensory-integration framework, could be helpful in addressing Sarah’s range of challenges and promoting positive outcomes related to socialization, behavioral regulation, and attention. Occupational therapists, with assistance from other team members, also could work with Sarah and her family on developing relaxation skills and use exposure and response prevention–oriented intervention strategies to address anxieties. Families, however, should be counseled about the limited data on the use of sensory-based therapies (Pediatrics. 2012 Jun;129[6]:1186-9); the use of parent-management training/family coaching should also be a treatment consideration to help promote overall regulatory functioning in the household.
Clinical pearl
When encountering youth with sensory-related challenges, a clinician’s diagnostic considerations should be more than just thinking about the possibility of an autism spectrum disorder. Symptoms of sensory overresponsiveness are associated with other emotional-behavioral conditions, but also can be seen without co-occurring psychopathology. With the latter, however, providers should be mindful that family-related impairments still may be quite noteworthy (J Am Acad Child Adolesc Psychiatry. 2011 Dec;50[12]:1210-9) and associated behavior problems could be attributed incorrectly to other diagnoses (which may lead to the recommendation of ineffective and inappropriate treatments). Much more research is needed to help develop a robust framework for diagnosing and labeling sensory issues in children and studying the efficacy of available intervention strategies.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic.
A Google search of “sensory issues in children” reveals more than 20 million results and a wide range of terminology that can be confusing to parents, providers, and youth themselves. Phenomena such as sensory processing disorder, sensory integration disorder, sensory discrimination disorder, and sensory defensiveness are noted, and autism spectrum disorder (ASD) is a label not uncommonly attached to the former terms.
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) does not include a discrete diagnosis to apply to children who have sensory differences, (meaning that they have difficulties regulating sensory input and such difficulties affect their ability to successfully relate to the world around them), but these differences are now part of the diagnostic criteria for ASD. The literature indicates that a majority of youth with ASD demonstrate features of sensory overresponsiveness (JAMA Psychiatry. 2015 Aug;72[8]:778-86), and providers should rightfully be concerned about the possibility of autism in a youngster who is presenting with severe negative responses to auditory, visual, and/or tactile stimuli.
Notably, however, even though sensory problems are considered a feature of autism, they are not pathognomonic for the disorder, and most children with these problems are, in fact, not autistic. Children with deficits in their ability to modulate sensory stimuli can present with a wide range of emotional-behavioral problems, including externalizing behaviors and internalizing symptoms manifesting with anxiety, attention challenges, mood dysregulation, and overall poor adaptive functioning. The relationship between sensory issues (both underresponsiveness and overresponsiveness) and psychopathology is rather complicated as sensory dysfunction can exist independent of a psychiatric disorder, be a significant risk factor for the development of the disorder (J Abnorm Child Psychol. 2009 Nov;37[8]:1077-87), and have symptom overlap with the disorder.
All in all, in spite of this complexity, since the 1960’s (Am J Occup Ther. 1964 Jan-Feb;18:6-11), it’s been clear that sensory dysfunction in children is associated with impairments in development, learning, and self-regulation. Parents of these children experience elevated levels of stress (J Child Fam Stud. 2013 Oct 1;22[7]:912-21), and early identification of sensory differences, psychoeducation, and referral for treatment are critical to minimize these impacts and foster positive outcomes.
Case Summary
In gathering a history and administering the Autism Diagnostic Observation Schedule (ADOS), it became clear that Sarah did not present with the social-communicative impairments that characterize ASD, but she did demonstrate repetitive hand flapping, troubles tolerating large social get-togethers, hypersensitivities, and a vulnerability to getting stuck when attempting to transition between activities. It is not uncommon for Sarah to use “fight-and-flight” reactions when faced with internal or external discomfort. Child Behavior Checklist data revealed multi-informant endorsement of clinical range symptoms across broad-band and narrow-band domains. Additionally, the Sensory Profile–2 yielded elevated scores in categories measuring sensory seeking and sensory sensitivity. The Sensory Profile is a standardized tool that uses caregiver and teacher-completed questionnaires to examine a child’s sensory processing abilities and provide data regarding the effect of such sensory processing on functional performance. Integrating all the available data, our team certainly appreciated Sarah’s profound sensory overresponsiveness, and a diagnosis of an unspecified anxiety disorder was provided along with consideration for attention-deficit/hyperactivity disorder (ADHD) (with teacher input needed to further investigate this possibility). The family history revealed anxiety disorders occurring both maternally and paternally. Additionally, Sarah’s mother’s acknowledged having her own similar sensory issues as a child.
Discussion
Associations among anxiety, sensory overresponsiveness, and ADHD are recognized in the literature (Am J Occup Ther. 2009 Jul-Aug;63[4]:433-40) and have implications for treatment. Furthermore, there is evidence that there is a heritable aspect to sensory processing abnormalities, and tactile defensiveness is associated with fearful temperament and anxiety (J Abnorm Child Psychol. 2006 Jun;34[3]:393-407). In Sarah’s case, her intense behavioral response to ordinary sensory stimuli was striking, and she had not yet been referred for an occupational therapy evaluation, which was the primary recommendation to further assess and understand her complicated sensory profile. As one component of a comprehensive treatment plan, an occupational therapist (www.aota.org), by using evidence-based practices in a sensory-integration framework, could be helpful in addressing Sarah’s range of challenges and promoting positive outcomes related to socialization, behavioral regulation, and attention. Occupational therapists, with assistance from other team members, also could work with Sarah and her family on developing relaxation skills and use exposure and response prevention–oriented intervention strategies to address anxieties. Families, however, should be counseled about the limited data on the use of sensory-based therapies (Pediatrics. 2012 Jun;129[6]:1186-9); the use of parent-management training/family coaching should also be a treatment consideration to help promote overall regulatory functioning in the household.
Clinical pearl
When encountering youth with sensory-related challenges, a clinician’s diagnostic considerations should be more than just thinking about the possibility of an autism spectrum disorder. Symptoms of sensory overresponsiveness are associated with other emotional-behavioral conditions, but also can be seen without co-occurring psychopathology. With the latter, however, providers should be mindful that family-related impairments still may be quite noteworthy (J Am Acad Child Adolesc Psychiatry. 2011 Dec;50[12]:1210-9) and associated behavior problems could be attributed incorrectly to other diagnoses (which may lead to the recommendation of ineffective and inappropriate treatments). Much more research is needed to help develop a robust framework for diagnosing and labeling sensory issues in children and studying the efficacy of available intervention strategies.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic.
Obesity risk rises when kids aren’t active 1 hour a day
SAN FRANCISCO – The behavioral characteristic that correlated the most with obesity in school-age children was being active less than 1 hour per day, according to findings from a prospective study.
Meredith Johnston, DO, of Eau Claire Cooperative in Columbia, S.C., performed the study with Nirupma Sharma, MD, at Children’s Hospital of Georgia in Augusta. The prospective, questionnaire-based study was conducted with 103 children, aged 5-18 years, over a 6-month period. Dr. Johnston reported the results in a poster presentation at the annual meeting of the American Academy of Pediatrics.
“Giving a child one modifiable lifestyle factor to incorporate into their lifestyle instead of overwhelming them with multiple changes is more likely to produce significant change to prevent obesity,” Dr. Johnston said in an interview. “And finding an activity that the child enjoys will produce the best adherence and greatest long-term effects.”
Considering the findings of the study, “children should exercise 30 minutes to 1 hour a day to prevent childhood obesity,” she explained.
A recent review in the Annual Review of Public Health has shown a change in teen physical activity patterns due to an increase in screen time and a decrease in opportunities for physical activities at school and in the community. Giving patients tools for exercise such as dancing to YouTube videos or playing active video games might be a good idea, Dr. Johnston said.
Drinking more than five cans of soda in a day also was significantly associated with a higher BMI (P = .001). That lifestyle factor could be addressed at subsequent well-child visits.
Such efforts are critical, she noted, because an estimated 17% of 2- to 19-year-olds are obese, and 15% are overweight.
Dr. Johnston said she had no relevant financial disclosures.
SAN FRANCISCO – The behavioral characteristic that correlated the most with obesity in school-age children was being active less than 1 hour per day, according to findings from a prospective study.
Meredith Johnston, DO, of Eau Claire Cooperative in Columbia, S.C., performed the study with Nirupma Sharma, MD, at Children’s Hospital of Georgia in Augusta. The prospective, questionnaire-based study was conducted with 103 children, aged 5-18 years, over a 6-month period. Dr. Johnston reported the results in a poster presentation at the annual meeting of the American Academy of Pediatrics.
“Giving a child one modifiable lifestyle factor to incorporate into their lifestyle instead of overwhelming them with multiple changes is more likely to produce significant change to prevent obesity,” Dr. Johnston said in an interview. “And finding an activity that the child enjoys will produce the best adherence and greatest long-term effects.”
Considering the findings of the study, “children should exercise 30 minutes to 1 hour a day to prevent childhood obesity,” she explained.
A recent review in the Annual Review of Public Health has shown a change in teen physical activity patterns due to an increase in screen time and a decrease in opportunities for physical activities at school and in the community. Giving patients tools for exercise such as dancing to YouTube videos or playing active video games might be a good idea, Dr. Johnston said.
Drinking more than five cans of soda in a day also was significantly associated with a higher BMI (P = .001). That lifestyle factor could be addressed at subsequent well-child visits.
Such efforts are critical, she noted, because an estimated 17% of 2- to 19-year-olds are obese, and 15% are overweight.
Dr. Johnston said she had no relevant financial disclosures.
SAN FRANCISCO – The behavioral characteristic that correlated the most with obesity in school-age children was being active less than 1 hour per day, according to findings from a prospective study.
Meredith Johnston, DO, of Eau Claire Cooperative in Columbia, S.C., performed the study with Nirupma Sharma, MD, at Children’s Hospital of Georgia in Augusta. The prospective, questionnaire-based study was conducted with 103 children, aged 5-18 years, over a 6-month period. Dr. Johnston reported the results in a poster presentation at the annual meeting of the American Academy of Pediatrics.
“Giving a child one modifiable lifestyle factor to incorporate into their lifestyle instead of overwhelming them with multiple changes is more likely to produce significant change to prevent obesity,” Dr. Johnston said in an interview. “And finding an activity that the child enjoys will produce the best adherence and greatest long-term effects.”
Considering the findings of the study, “children should exercise 30 minutes to 1 hour a day to prevent childhood obesity,” she explained.
A recent review in the Annual Review of Public Health has shown a change in teen physical activity patterns due to an increase in screen time and a decrease in opportunities for physical activities at school and in the community. Giving patients tools for exercise such as dancing to YouTube videos or playing active video games might be a good idea, Dr. Johnston said.
Drinking more than five cans of soda in a day also was significantly associated with a higher BMI (P = .001). That lifestyle factor could be addressed at subsequent well-child visits.
Such efforts are critical, she noted, because an estimated 17% of 2- to 19-year-olds are obese, and 15% are overweight.
Dr. Johnston said she had no relevant financial disclosures.
AT AAP 2016
Key clinical point:
Major finding: Being active less than 1 hour per day was significantly associated with a higher body mass index in children (P = .006 for 30 minutes to 1 hour, and P = .017 for less than 30 minutes).
Data source: A prospective, questionnaire-based study involving 103 children, aged 5-18 years, over a 6-month period.
Disclosures: Dr. Johnston said she had no relevant financial disclosures.
New trials address unresolved issues in endovascular therapy for acute ischemic stroke
BALTIMORE – Endovascular therapy is a bedrock of acute ischemic stroke treatment, but some vexing issues remain unresolved, according to Joseph Broderick, MD, of the University of Cincinnati.
“We have learned a tremendous amount the last few years. We know that thrombectomy can work if initiated in patients within 6 hours of stroke onset with or without TPA [tissue plasminogen activator]. The question is what we don’t know,” Dr. Broderick said.
The good news is that clinical trials are underway or planned to address several of these issues, he said at the annual meeting of the American Neurological Association.
Mechanical thrombectomy beyond 6 hours
Whether the treatment window for thrombectomy can be safely extended in appropriately selected patients beyond 6 hours from onset is “one of the most important issues we face,” Dr. Broderick said.

Along with DEFUSE 3, the DWI or CTP Assessment With Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention (DAWN) trial will examine whether medical management that includes thrombectomy delivered up to 24 hours after AIS symptoms first appear will yield better clinical outcomes than medical management alone in appropriate patients.
The use of mechanical thrombectomy up to 12 hours after symptom development in AIS patients for whom intravenous TPA can’t be used or doesn’t work will be assessed in the Perfusion Imaging Selection of Ischemic Stroke Patients for Endovascular Therapy (POSITIVE) trial. The primary objective is to show less stroke-related disability and improved good functional outcomes, compared with those who receive best medical therapy.
The first Multicenter Randomized Clinical Trial of Endovascular Treatment in the Netherlands (MR CLEAN) trial, which used stent retrievers in almost all cases, demonstrated the benefit of endovascular therapy up to 6 hours after stroke onset in the proximal anterior circulation when used along with best medical therapy (N Engl J Med. 2015;372:11-20). The MR CLEAN LATE trial involving 500 patients will expand the time window up to 12 hours.
Triage of acute stroke patients
The triage of AIS patients before their arrival at the hospital also is an evolving emergency medical service issue. While the classic triage involving CT takes time, the use of scoring systems like the National Institutes of Health Stroke Scale and the Cincinnati Stroke Triage Assessment Tool, or telemedicine-based consultation, can be done faster and with less training.
Where the patient is taken first could be important. The RACECAT trial being conducted in the Catalan territory will compare transfer of acute stroke patients with suspected large-vessel occlusion to the closest local stroke center versus direct transfer to an endovascular stroke center.
Conscious sedation or general anesthesia
Some patients undergoing thrombectomy may be able to tolerate conscious sedation in place of general anesthesia. For these patients, cost-effectiveness becomes a dominant consideration. Several anesthesia trials are addressing the issue. The Sedation Versus Intubation for Endovascular Stroke Treatment (SIESTA) trial involving 150 German patients has been completed, but the findings have not been reported. The General or Local Anaesthesia in Intra-arterial Therapy (GOLIATH) trial is recruiting patients in the Netherlands, with a target enrollment of 128. Other trials are planned in China and Sweden, but recruitment has not started.
Thrombectomy alone
For patients with AIS caused by basilar artery occlusion, stroke specialists have wondered whether intra-arterial treatment, including thrombolysis and potentially thrombectomy, could be more effective than best medical therapy, including intravenous thrombolysis. The Basilar Artery International Cooperation Study (BASICS) in Europe and the BEST trial in China are two trials in the early stages of assessing this question.
A related issue is whether thrombectomy alone is better than intravenous TPA followed by thrombectomy. This issue is being addressed in another MR CLEAN trial that is designed to compare the two approaches in 500 patients randomized to one or the other treatment.
Other intravenous antithrombotic drugs
Another unresolved issue relates to the use of other antithrombotic medications delivered intravenously in combination with TPA. This could be the sole treatment strategy, or could be used in patients who also undergo endovascular thrombectomy. The Multi-Arm Optimization of Stroke Thrombolysis (MOST) trial will randomize patients to receive argatroban or eptifibatide along with TPA, or TPA alone, within 3 hours of stroke symptom onset. Endovascular therapy will be done as indicated.
Heparin use in endovascular therapy
The proper use of antithrombotics like heparin in patients treated with endovascular therapy is unclear. The MR CLEAN MED trial will assess the benefits of two doses of unfractionated heparin and aspirin alone or in combination in 1,500 patients with AIS who receive intra-arterial treatment for confirmed anterior circulation occlusion.
On the horizon
Whether neuroprotection can improve the outcome in patients who undergo embolectomy is unclear, and will be the subject of a trial in Canada that is not yet recruiting patients. Finally, the best way to manage blood pressure following embolectomy and reperfusion is also unclear.
Dr. Broderick had no relevant financial disclosures.
BALTIMORE – Endovascular therapy is a bedrock of acute ischemic stroke treatment, but some vexing issues remain unresolved, according to Joseph Broderick, MD, of the University of Cincinnati.
“We have learned a tremendous amount the last few years. We know that thrombectomy can work if initiated in patients within 6 hours of stroke onset with or without TPA [tissue plasminogen activator]. The question is what we don’t know,” Dr. Broderick said.
The good news is that clinical trials are underway or planned to address several of these issues, he said at the annual meeting of the American Neurological Association.
Mechanical thrombectomy beyond 6 hours
Whether the treatment window for thrombectomy can be safely extended in appropriately selected patients beyond 6 hours from onset is “one of the most important issues we face,” Dr. Broderick said.
Along with DEFUSE 3, the DWI or CTP Assessment With Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention (DAWN) trial will examine whether medical management that includes thrombectomy delivered up to 24 hours after AIS symptoms first appear will yield better clinical outcomes than medical management alone in appropriate patients.
The use of mechanical thrombectomy up to 12 hours after symptom development in AIS patients for whom intravenous TPA can’t be used or doesn’t work will be assessed in the Perfusion Imaging Selection of Ischemic Stroke Patients for Endovascular Therapy (POSITIVE) trial. The primary objective is to show less stroke-related disability and improved good functional outcomes, compared with those who receive best medical therapy.
The first Multicenter Randomized Clinical Trial of Endovascular Treatment in the Netherlands (MR CLEAN) trial, which used stent retrievers in almost all cases, demonstrated the benefit of endovascular therapy up to 6 hours after stroke onset in the proximal anterior circulation when used along with best medical therapy (N Engl J Med. 2015;372:11-20). The MR CLEAN LATE trial involving 500 patients will expand the time window up to 12 hours.
Triage of acute stroke patients
The triage of AIS patients before their arrival at the hospital also is an evolving emergency medical service issue. While the classic triage involving CT takes time, the use of scoring systems like the National Institutes of Health Stroke Scale and the Cincinnati Stroke Triage Assessment Tool, or telemedicine-based consultation, can be done faster and with less training.
Where the patient is taken first could be important. The RACECAT trial being conducted in the Catalan territory will compare transfer of acute stroke patients with suspected large-vessel occlusion to the closest local stroke center versus direct transfer to an endovascular stroke center.
Conscious sedation or general anesthesia
Some patients undergoing thrombectomy may be able to tolerate conscious sedation in place of general anesthesia. For these patients, cost-effectiveness becomes a dominant consideration. Several anesthesia trials are addressing the issue. The Sedation Versus Intubation for Endovascular Stroke Treatment (SIESTA) trial involving 150 German patients has been completed, but the findings have not been reported. The General or Local Anaesthesia in Intra-arterial Therapy (GOLIATH) trial is recruiting patients in the Netherlands, with a target enrollment of 128. Other trials are planned in China and Sweden, but recruitment has not started.
Thrombectomy alone
For patients with AIS caused by basilar artery occlusion, stroke specialists have wondered whether intra-arterial treatment, including thrombolysis and potentially thrombectomy, could be more effective than best medical therapy, including intravenous thrombolysis. The Basilar Artery International Cooperation Study (BASICS) in Europe and the BEST trial in China are two trials in the early stages of assessing this question.
A related issue is whether thrombectomy alone is better than intravenous TPA followed by thrombectomy. This issue is being addressed in another MR CLEAN trial that is designed to compare the two approaches in 500 patients randomized to one or the other treatment.
Other intravenous antithrombotic drugs
Another unresolved issue relates to the use of other antithrombotic medications delivered intravenously in combination with TPA. This could be the sole treatment strategy, or could be used in patients who also undergo endovascular thrombectomy. The Multi-Arm Optimization of Stroke Thrombolysis (MOST) trial will randomize patients to receive argatroban or eptifibatide along with TPA, or TPA alone, within 3 hours of stroke symptom onset. Endovascular therapy will be done as indicated.
Heparin use in endovascular therapy
The proper use of antithrombotics like heparin in patients treated with endovascular therapy is unclear. The MR CLEAN MED trial will assess the benefits of two doses of unfractionated heparin and aspirin alone or in combination in 1,500 patients with AIS who receive intra-arterial treatment for confirmed anterior circulation occlusion.
On the horizon
Whether neuroprotection can improve the outcome in patients who undergo embolectomy is unclear, and will be the subject of a trial in Canada that is not yet recruiting patients. Finally, the best way to manage blood pressure following embolectomy and reperfusion is also unclear.
Dr. Broderick had no relevant financial disclosures.
BALTIMORE – Endovascular therapy is a bedrock of acute ischemic stroke treatment, but some vexing issues remain unresolved, according to Joseph Broderick, MD, of the University of Cincinnati.
“We have learned a tremendous amount the last few years. We know that thrombectomy can work if initiated in patients within 6 hours of stroke onset with or without TPA [tissue plasminogen activator]. The question is what we don’t know,” Dr. Broderick said.
The good news is that clinical trials are underway or planned to address several of these issues, he said at the annual meeting of the American Neurological Association.
Mechanical thrombectomy beyond 6 hours
Whether the treatment window for thrombectomy can be safely extended in appropriately selected patients beyond 6 hours from onset is “one of the most important issues we face,” Dr. Broderick said.
Along with DEFUSE 3, the DWI or CTP Assessment With Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention (DAWN) trial will examine whether medical management that includes thrombectomy delivered up to 24 hours after AIS symptoms first appear will yield better clinical outcomes than medical management alone in appropriate patients.
The use of mechanical thrombectomy up to 12 hours after symptom development in AIS patients for whom intravenous TPA can’t be used or doesn’t work will be assessed in the Perfusion Imaging Selection of Ischemic Stroke Patients for Endovascular Therapy (POSITIVE) trial. The primary objective is to show less stroke-related disability and improved good functional outcomes, compared with those who receive best medical therapy.
The first Multicenter Randomized Clinical Trial of Endovascular Treatment in the Netherlands (MR CLEAN) trial, which used stent retrievers in almost all cases, demonstrated the benefit of endovascular therapy up to 6 hours after stroke onset in the proximal anterior circulation when used along with best medical therapy (N Engl J Med. 2015;372:11-20). The MR CLEAN LATE trial involving 500 patients will expand the time window up to 12 hours.
Triage of acute stroke patients
The triage of AIS patients before their arrival at the hospital also is an evolving emergency medical service issue. While the classic triage involving CT takes time, the use of scoring systems like the National Institutes of Health Stroke Scale and the Cincinnati Stroke Triage Assessment Tool, or telemedicine-based consultation, can be done faster and with less training.
Where the patient is taken first could be important. The RACECAT trial being conducted in the Catalan territory will compare transfer of acute stroke patients with suspected large-vessel occlusion to the closest local stroke center versus direct transfer to an endovascular stroke center.
Conscious sedation or general anesthesia
Some patients undergoing thrombectomy may be able to tolerate conscious sedation in place of general anesthesia. For these patients, cost-effectiveness becomes a dominant consideration. Several anesthesia trials are addressing the issue. The Sedation Versus Intubation for Endovascular Stroke Treatment (SIESTA) trial involving 150 German patients has been completed, but the findings have not been reported. The General or Local Anaesthesia in Intra-arterial Therapy (GOLIATH) trial is recruiting patients in the Netherlands, with a target enrollment of 128. Other trials are planned in China and Sweden, but recruitment has not started.
Thrombectomy alone
For patients with AIS caused by basilar artery occlusion, stroke specialists have wondered whether intra-arterial treatment, including thrombolysis and potentially thrombectomy, could be more effective than best medical therapy, including intravenous thrombolysis. The Basilar Artery International Cooperation Study (BASICS) in Europe and the BEST trial in China are two trials in the early stages of assessing this question.
A related issue is whether thrombectomy alone is better than intravenous TPA followed by thrombectomy. This issue is being addressed in another MR CLEAN trial that is designed to compare the two approaches in 500 patients randomized to one or the other treatment.
Other intravenous antithrombotic drugs
Another unresolved issue relates to the use of other antithrombotic medications delivered intravenously in combination with TPA. This could be the sole treatment strategy, or could be used in patients who also undergo endovascular thrombectomy. The Multi-Arm Optimization of Stroke Thrombolysis (MOST) trial will randomize patients to receive argatroban or eptifibatide along with TPA, or TPA alone, within 3 hours of stroke symptom onset. Endovascular therapy will be done as indicated.
Heparin use in endovascular therapy
The proper use of antithrombotics like heparin in patients treated with endovascular therapy is unclear. The MR CLEAN MED trial will assess the benefits of two doses of unfractionated heparin and aspirin alone or in combination in 1,500 patients with AIS who receive intra-arterial treatment for confirmed anterior circulation occlusion.
On the horizon
Whether neuroprotection can improve the outcome in patients who undergo embolectomy is unclear, and will be the subject of a trial in Canada that is not yet recruiting patients. Finally, the best way to manage blood pressure following embolectomy and reperfusion is also unclear.
Dr. Broderick had no relevant financial disclosures.
United States nears 3,000 Zika-infected pregnancies
There were 54 new cases of pregnant women with laboratory evidence of Zika virus in the 50 states and the District of Columbia reported during the week ending Oct. 20 – the largest weekly increase in a month, according to the Centers for Disease Control and Prevention.
The number of cases reported in the U.S. territories, 100, was lower for the second week in a row, however, so the U.S. total for the week was a fairly average 154. The total number of pregnant women with laboratory evidence of Zika virus infection is now 2,980 for the year: 953 in the states/D.C. and 2,027 in the territories, the CDC reported.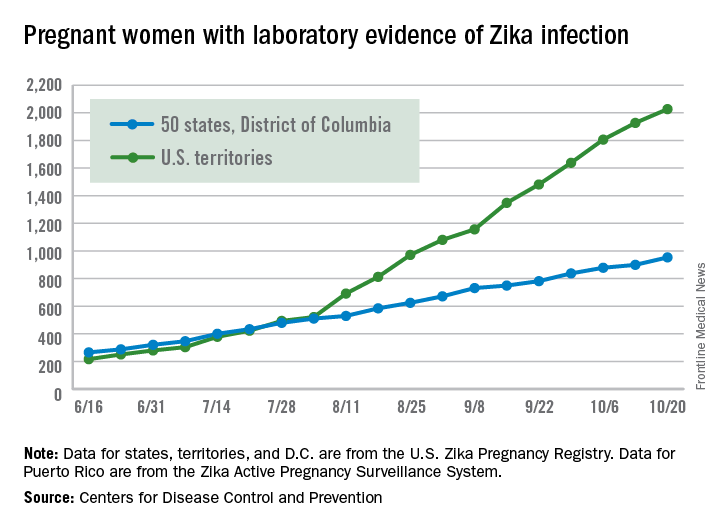
Among all Americans, the number of cases for 2015-2016 is now up to 32,814, with 1,396 new cases reported for the week ending Oct. 26: 75 in the states/D.C. and 1,321 in the territories. Almost all (98%) of the territorial cases have occurred in Puerto Rico, which continues to retroactively report cases, the CDC Arboviral Disease Branch noted.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 54 new cases of pregnant women with laboratory evidence of Zika virus in the 50 states and the District of Columbia reported during the week ending Oct. 20 – the largest weekly increase in a month, according to the Centers for Disease Control and Prevention.
The number of cases reported in the U.S. territories, 100, was lower for the second week in a row, however, so the U.S. total for the week was a fairly average 154. The total number of pregnant women with laboratory evidence of Zika virus infection is now 2,980 for the year: 953 in the states/D.C. and 2,027 in the territories, the CDC reported.
Among all Americans, the number of cases for 2015-2016 is now up to 32,814, with 1,396 new cases reported for the week ending Oct. 26: 75 in the states/D.C. and 1,321 in the territories. Almost all (98%) of the territorial cases have occurred in Puerto Rico, which continues to retroactively report cases, the CDC Arboviral Disease Branch noted.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 54 new cases of pregnant women with laboratory evidence of Zika virus in the 50 states and the District of Columbia reported during the week ending Oct. 20 – the largest weekly increase in a month, according to the Centers for Disease Control and Prevention.
The number of cases reported in the U.S. territories, 100, was lower for the second week in a row, however, so the U.S. total for the week was a fairly average 154. The total number of pregnant women with laboratory evidence of Zika virus infection is now 2,980 for the year: 953 in the states/D.C. and 2,027 in the territories, the CDC reported.
Among all Americans, the number of cases for 2015-2016 is now up to 32,814, with 1,396 new cases reported for the week ending Oct. 26: 75 in the states/D.C. and 1,321 in the territories. Almost all (98%) of the territorial cases have occurred in Puerto Rico, which continues to retroactively report cases, the CDC Arboviral Disease Branch noted.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Updated AAP safe sleep recs for infants reinforce life-saving messages
SAN FRANCISCO – At sleep time, infants should share their parents’ bedroom on a separate sleep surface without bed sharing, should be placed on their backs on a firm surface, and should have a sleep area free of blankets and soft objects, according to updated guidelines from the American Academy of Pediatrics aimed at reducing the risk of sudden infant death syndrome (SIDS) and other sleep-related infant deaths.
Drafted by a multidisciplinary task force, the set of 19 evidence-based recommendations largely reiterate messages that the academy has promoted for years such as “back to sleep for every sleep,” according to task force member Fern R. Hauck, MD, the Spencer P. Bass, MD, Twenty-First Century Professor of Family Medicine at the University of Virginia, Charlottesville. They were unveiled in a press briefing at the academy’s annual meeting and simultaneously published (Pediatrics. 2016;138[5]:e20162938).
Progress, but still a ways to go
Education campaigns that convey these and related messages to new parents and other caregivers have led to a more than halving of the rate of SIDS in recent decades. Yet, 3,500 infants are still lost each year to this syndrome and other sleep-related causes of infant death, such as unintentional suffocation, collectively called sudden unexpected infant death (SUID).

New is a recommendation for skin-to-skin care for at least the first hour of life for healthy newborns, as soon as the mother is alert enough to respond to her infant, according to Dr. Hauck. The aims here are to optimize neurodevelopment and promote temperature regulation.
There is no evidence that swaddling reduces the risk of SIDS, but parents can still use this technique if they wish as long as infants are placed on their back and it is discontinued as soon as they start to show signs of rolling over, she said. Evidence is also lacking for new technologies marketed as protective, for example, crib mattresses designed to reduce re-breathing of carbon dioxide should an infant become prone.
Sleeping in the parents’ room but on a separate surface decreases the risk of SIDS by as much as 50%, according to several studies. Bed sharing is not recommended because of the risk of suffocation, strangulation, and entrapment, the policy states.
The updated recommendations should be followed for every sleep and by every caregiver, until the child reaches 1 year of age, Dr. Hauck stressed. “This includes nap time and bedtime sleep, at home, in day care, or in any other locations where the baby is sleeping.”
“We feel that these messages need to start while the mom’s pregnant because some of the decisions that are made that are not always the best decisions, when the mother is exhausted, can occur spur of the moment,” she added. “As pediatricians, you can set up a prebirth visit to start talking about this, and obstetricians should be doing more as well to bring this up during their prenatal visits.”
Other recommendations include offering a pacifier at nap time and bedtime; avoiding smoke exposure during pregnancy and after birth; and avoiding alcohol and illicit drug use during pregnancy and after birth.
Breastfeeding issues
Although breastfeeding protects against SIDS, it can pose some problems for safe sleep practices, acknowledged Lori B. Feldman-Winter, MD, a liaison from the AAP section on breastfeeding to the task force, as well as head of the division of adolescent medicine and professor of pediatrics at Cooper University Health Care in Camden, N.J.

Bedside sleepers (also called sidecar sleepers) that attach to the parents’ bed may help facilitate the dual aims of breastfeeding and safe sleep, but they have not been formally studied to assess their impact on SIDS risk.
Raising awareness
“As a father and pediatrician, I want parents to know that their baby is safest following the AAP safe sleep recommendations, and spreading this message has become my life’s mission,” said Dr. Samuel P. Hanke, a pediatric cardiologist at the University of Cincinnati, who knows the heartbreak of SIDS firsthand.

“We know practicing safe sleep is hard. We have to be vigilant. We need to start adopting a mentality that safe sleep is not negotiable,” Dr. Hanke asserted. “We cannot emphasize enough that practicing safe sleep for every sleep is as important as buckling your child into a car seat for every drive. And just like car seats, this change won’t occur overnight.”
Federal commitment
Since the 1970s, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) in Bethesda, Md., has been supporting and performing much of the research on which the updated recommendations are based. This research continues to help identify areas where greater efforts are needed, according to acting director Catherine Y. Spong, MD.

NICHD also conducts and collaborates on related education campaigns, such as Safe to Sleep, to disseminate messages such as those in the updated AAP recommendations as widely as possible.
“I encourage all physicians, pediatricians, nurses, and other health care and child care providers to lend their authoritative voices to the Safe to Sleep effort,” Dr. Spong said. “Join us all in sharing safe infant sleep recommendations and in supporting parents and caregivers to make informed decisions that will help keep their baby safe during sleep.”
A closer look at setting
Published in conjunction with the guidelines is a study on risk factors that looked at the role of the setting in which sleep-related infant deaths occur (Pediatrics. 2016 Oct 24:e20161124).
The analysis of nearly 12,000 such deaths found that, relative to counterparts who died in their home, infants who died outside of their home were more likely to be in a stroller or car seat at the time (adjusted odds ratio, 2.6) and in other locations, such as on the floor or a futon (1.9), and to have been placed prone (1.1). They were less likely to have been sharing a bed (0.7).
The groups did not differ in terms of whether the infant was sleeping in an adult bed or on a person, on a couch or chair, or with any objects in their sleep environment.
“Caregivers should be educated on the importance of placing infants to sleep supine in cribs/bassinets to protect against sleep-related deaths, both in and out of the home,” conclude the investigators, one of whom disclosed serving as a paid expert witness in cases of sleep-related infant death.
SAN FRANCISCO – At sleep time, infants should share their parents’ bedroom on a separate sleep surface without bed sharing, should be placed on their backs on a firm surface, and should have a sleep area free of blankets and soft objects, according to updated guidelines from the American Academy of Pediatrics aimed at reducing the risk of sudden infant death syndrome (SIDS) and other sleep-related infant deaths.
Drafted by a multidisciplinary task force, the set of 19 evidence-based recommendations largely reiterate messages that the academy has promoted for years such as “back to sleep for every sleep,” according to task force member Fern R. Hauck, MD, the Spencer P. Bass, MD, Twenty-First Century Professor of Family Medicine at the University of Virginia, Charlottesville. They were unveiled in a press briefing at the academy’s annual meeting and simultaneously published (Pediatrics. 2016;138[5]:e20162938).
Progress, but still a ways to go
Education campaigns that convey these and related messages to new parents and other caregivers have led to a more than halving of the rate of SIDS in recent decades. Yet, 3,500 infants are still lost each year to this syndrome and other sleep-related causes of infant death, such as unintentional suffocation, collectively called sudden unexpected infant death (SUID).
New is a recommendation for skin-to-skin care for at least the first hour of life for healthy newborns, as soon as the mother is alert enough to respond to her infant, according to Dr. Hauck. The aims here are to optimize neurodevelopment and promote temperature regulation.
There is no evidence that swaddling reduces the risk of SIDS, but parents can still use this technique if they wish as long as infants are placed on their back and it is discontinued as soon as they start to show signs of rolling over, she said. Evidence is also lacking for new technologies marketed as protective, for example, crib mattresses designed to reduce re-breathing of carbon dioxide should an infant become prone.
Sleeping in the parents’ room but on a separate surface decreases the risk of SIDS by as much as 50%, according to several studies. Bed sharing is not recommended because of the risk of suffocation, strangulation, and entrapment, the policy states.
The updated recommendations should be followed for every sleep and by every caregiver, until the child reaches 1 year of age, Dr. Hauck stressed. “This includes nap time and bedtime sleep, at home, in day care, or in any other locations where the baby is sleeping.”
“We feel that these messages need to start while the mom’s pregnant because some of the decisions that are made that are not always the best decisions, when the mother is exhausted, can occur spur of the moment,” she added. “As pediatricians, you can set up a prebirth visit to start talking about this, and obstetricians should be doing more as well to bring this up during their prenatal visits.”
Other recommendations include offering a pacifier at nap time and bedtime; avoiding smoke exposure during pregnancy and after birth; and avoiding alcohol and illicit drug use during pregnancy and after birth.
Breastfeeding issues
Although breastfeeding protects against SIDS, it can pose some problems for safe sleep practices, acknowledged Lori B. Feldman-Winter, MD, a liaison from the AAP section on breastfeeding to the task force, as well as head of the division of adolescent medicine and professor of pediatrics at Cooper University Health Care in Camden, N.J.
Bedside sleepers (also called sidecar sleepers) that attach to the parents’ bed may help facilitate the dual aims of breastfeeding and safe sleep, but they have not been formally studied to assess their impact on SIDS risk.
Raising awareness
“As a father and pediatrician, I want parents to know that their baby is safest following the AAP safe sleep recommendations, and spreading this message has become my life’s mission,” said Dr. Samuel P. Hanke, a pediatric cardiologist at the University of Cincinnati, who knows the heartbreak of SIDS firsthand.
“We know practicing safe sleep is hard. We have to be vigilant. We need to start adopting a mentality that safe sleep is not negotiable,” Dr. Hanke asserted. “We cannot emphasize enough that practicing safe sleep for every sleep is as important as buckling your child into a car seat for every drive. And just like car seats, this change won’t occur overnight.”
Federal commitment
Since the 1970s, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) in Bethesda, Md., has been supporting and performing much of the research on which the updated recommendations are based. This research continues to help identify areas where greater efforts are needed, according to acting director Catherine Y. Spong, MD.
NICHD also conducts and collaborates on related education campaigns, such as Safe to Sleep, to disseminate messages such as those in the updated AAP recommendations as widely as possible.
“I encourage all physicians, pediatricians, nurses, and other health care and child care providers to lend their authoritative voices to the Safe to Sleep effort,” Dr. Spong said. “Join us all in sharing safe infant sleep recommendations and in supporting parents and caregivers to make informed decisions that will help keep their baby safe during sleep.”
A closer look at setting
Published in conjunction with the guidelines is a study on risk factors that looked at the role of the setting in which sleep-related infant deaths occur (Pediatrics. 2016 Oct 24:e20161124).
The analysis of nearly 12,000 such deaths found that, relative to counterparts who died in their home, infants who died outside of their home were more likely to be in a stroller or car seat at the time (adjusted odds ratio, 2.6) and in other locations, such as on the floor or a futon (1.9), and to have been placed prone (1.1). They were less likely to have been sharing a bed (0.7).
The groups did not differ in terms of whether the infant was sleeping in an adult bed or on a person, on a couch or chair, or with any objects in their sleep environment.
“Caregivers should be educated on the importance of placing infants to sleep supine in cribs/bassinets to protect against sleep-related deaths, both in and out of the home,” conclude the investigators, one of whom disclosed serving as a paid expert witness in cases of sleep-related infant death.
SAN FRANCISCO – At sleep time, infants should share their parents’ bedroom on a separate sleep surface without bed sharing, should be placed on their backs on a firm surface, and should have a sleep area free of blankets and soft objects, according to updated guidelines from the American Academy of Pediatrics aimed at reducing the risk of sudden infant death syndrome (SIDS) and other sleep-related infant deaths.
Drafted by a multidisciplinary task force, the set of 19 evidence-based recommendations largely reiterate messages that the academy has promoted for years such as “back to sleep for every sleep,” according to task force member Fern R. Hauck, MD, the Spencer P. Bass, MD, Twenty-First Century Professor of Family Medicine at the University of Virginia, Charlottesville. They were unveiled in a press briefing at the academy’s annual meeting and simultaneously published (Pediatrics. 2016;138[5]:e20162938).
Progress, but still a ways to go
Education campaigns that convey these and related messages to new parents and other caregivers have led to a more than halving of the rate of SIDS in recent decades. Yet, 3,500 infants are still lost each year to this syndrome and other sleep-related causes of infant death, such as unintentional suffocation, collectively called sudden unexpected infant death (SUID).
New is a recommendation for skin-to-skin care for at least the first hour of life for healthy newborns, as soon as the mother is alert enough to respond to her infant, according to Dr. Hauck. The aims here are to optimize neurodevelopment and promote temperature regulation.
There is no evidence that swaddling reduces the risk of SIDS, but parents can still use this technique if they wish as long as infants are placed on their back and it is discontinued as soon as they start to show signs of rolling over, she said. Evidence is also lacking for new technologies marketed as protective, for example, crib mattresses designed to reduce re-breathing of carbon dioxide should an infant become prone.
Sleeping in the parents’ room but on a separate surface decreases the risk of SIDS by as much as 50%, according to several studies. Bed sharing is not recommended because of the risk of suffocation, strangulation, and entrapment, the policy states.
The updated recommendations should be followed for every sleep and by every caregiver, until the child reaches 1 year of age, Dr. Hauck stressed. “This includes nap time and bedtime sleep, at home, in day care, or in any other locations where the baby is sleeping.”
“We feel that these messages need to start while the mom’s pregnant because some of the decisions that are made that are not always the best decisions, when the mother is exhausted, can occur spur of the moment,” she added. “As pediatricians, you can set up a prebirth visit to start talking about this, and obstetricians should be doing more as well to bring this up during their prenatal visits.”
Other recommendations include offering a pacifier at nap time and bedtime; avoiding smoke exposure during pregnancy and after birth; and avoiding alcohol and illicit drug use during pregnancy and after birth.
Breastfeeding issues
Although breastfeeding protects against SIDS, it can pose some problems for safe sleep practices, acknowledged Lori B. Feldman-Winter, MD, a liaison from the AAP section on breastfeeding to the task force, as well as head of the division of adolescent medicine and professor of pediatrics at Cooper University Health Care in Camden, N.J.
Bedside sleepers (also called sidecar sleepers) that attach to the parents’ bed may help facilitate the dual aims of breastfeeding and safe sleep, but they have not been formally studied to assess their impact on SIDS risk.
Raising awareness
“As a father and pediatrician, I want parents to know that their baby is safest following the AAP safe sleep recommendations, and spreading this message has become my life’s mission,” said Dr. Samuel P. Hanke, a pediatric cardiologist at the University of Cincinnati, who knows the heartbreak of SIDS firsthand.
“We know practicing safe sleep is hard. We have to be vigilant. We need to start adopting a mentality that safe sleep is not negotiable,” Dr. Hanke asserted. “We cannot emphasize enough that practicing safe sleep for every sleep is as important as buckling your child into a car seat for every drive. And just like car seats, this change won’t occur overnight.”
Federal commitment
Since the 1970s, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) in Bethesda, Md., has been supporting and performing much of the research on which the updated recommendations are based. This research continues to help identify areas where greater efforts are needed, according to acting director Catherine Y. Spong, MD.
NICHD also conducts and collaborates on related education campaigns, such as Safe to Sleep, to disseminate messages such as those in the updated AAP recommendations as widely as possible.
“I encourage all physicians, pediatricians, nurses, and other health care and child care providers to lend their authoritative voices to the Safe to Sleep effort,” Dr. Spong said. “Join us all in sharing safe infant sleep recommendations and in supporting parents and caregivers to make informed decisions that will help keep their baby safe during sleep.”
A closer look at setting
Published in conjunction with the guidelines is a study on risk factors that looked at the role of the setting in which sleep-related infant deaths occur (Pediatrics. 2016 Oct 24:e20161124).
The analysis of nearly 12,000 such deaths found that, relative to counterparts who died in their home, infants who died outside of their home were more likely to be in a stroller or car seat at the time (adjusted odds ratio, 2.6) and in other locations, such as on the floor or a futon (1.9), and to have been placed prone (1.1). They were less likely to have been sharing a bed (0.7).
The groups did not differ in terms of whether the infant was sleeping in an adult bed or on a person, on a couch or chair, or with any objects in their sleep environment.
“Caregivers should be educated on the importance of placing infants to sleep supine in cribs/bassinets to protect against sleep-related deaths, both in and out of the home,” conclude the investigators, one of whom disclosed serving as a paid expert witness in cases of sleep-related infant death.
EXPERT ANALYSIS FROM AAP 16