User login
Sleep in the time of COVID-19
Mass social distancing and social isolation to prevent the spread of a deadly disease, along with technological tools that allow social communication and continued work and school, is an unprecedented situation.

The current reality of most people’s lives during the COVID-19 pandemic has the potential to induce or exacerbate sleep problems, though it may also present some with an opportunity to improve sleep, wrote Ellemarije Altena, PhD, of the University of Bordeaux (France), and her colleagues in a recent research review in the Journal of Sleep Research.
The review was conducted by a task force of the European Academy for Cognitive Behavioural Therapy for Insomnia. The European CBT-I Academy is an initiative of the European Insomnia Network to promote implementation and dissemination of treatment.
After discussing the known effects of stress, confinement, and altered schedules on sleep, the authors present recommendations on ways to manage sleep problems such as insomnia in the general public and potentially encourage people to take advantage of the opportunity to align their schedules with their natural circadian rhythms. Physicians may find the recommendations helpful in advising patients with sleep problems related to the COVID-19 emergency.
“Being forced to stay at home, work from home, do homeschooling with children, drastically minimize outings, reduce social interaction or work many more hours under stressful circumstances, and in parallel manage the attendant health risks, can have a major impact on daily functioning and nighttime sleep,” Dr. Altena and colleagues wrote.

There may also be a lag time in physicians hearing about changes in sleep or sleeping problems from patients, said Krishna M. Sundar, MD, FCCP, medical director of the Sleep-Wake Center at the University of Utah in Salt Lake City. “There may actually be some improvement in sleep durations given that most folks are working from home with more time with family and less work-related stress,” he said in an interview. “In terms of sleep or other effects on worsening of psychiatric problems, it is still not clear what the overall effects are going to be.”
Although daylight has the biggest impact on regulating circadian rhythms, artificial light, meal times, diet, and amount of physical activity can also have an influence. Negative effects on sleep can result from both excessively high activity levels, such as stress and work overload, or excessively low levels, such as from depression or confinement, the authors note.
The current situation also opens the door to interactions between stress, sleep, anxiety, and risk of PTSD. “Those sensitive to stress-related sleep disruption are more likely to develop chronic insomnia,” which, in combination with a major stressor, is a risk factor for PTSD, the authors write. They note that 7% of Wuhan residents, the city in China where the virus appears to have originated, particularly women, reported PTSD symptoms after the COVID-19 outbreak, and anxiety was highest in those under age 35 years and those who followed news about the disease for more than 3 hours a day.
Better sleep quality and fewer early morning awakenings, however, appeared to be protective against PTSD symptoms. The authors note the value of physical exercise, cognitive interventions, and relaxation techniques, including meditation, for reducing stress and milder symptoms of PTSD.
“Some patients are sleeping a bit better because of the pace of things has slowed down a bit,” said Anne C. Trainor, a nurse practitioner and instructor in the neurology department’s sleep disorders program at Oregon Health & Science University in Portland, who was not involved in the study. “Keeping a regular schedule for sleeping and eating, getting exercise daily – preferably in sunlight and not just before bedtime – and using relaxation or mindfulness practice and cognitive interventions to help manage anxiety” were the key takeaways from this review, Ms. Trainor said in an interview.
Home confinement, stressors and sleep
A wide range of stressors could affect sleep during COVID-19 social distancing interventions, including “major changes in routines, living with uncertainty,” and anxiety about health, the economic situation, and how long this situation will last, the authors write.
Parents must juggle work, homeschooling, and ordinary household errands and management. Meanwhile, entrepreneurs, small business owners ,and workers in entertainment, hospitality and food service must contend with anxiety about job uncertainty and financial security. For anyone working from home, disruptions to work and home routines can make it difficult to associate being home with relaxation – and sleep.
“The more regular our sleep schedule is the better quality our sleep tends to be, but it is a struggle when we don’t have separate spaces to work and parent in,” Ms. Trainor said.
At the same time, “confinement-related stress may be caused by an inability to engage in rewarding activities, such as visiting friends and family, shopping, attending cultural and sports events, and visiting bars or restaurants,” the authors write. “Spending more time with family in a limited space can also induce stress, particularly in situations where there are preexisting family difficulties.”
Being stuck at home may lead to less daylight exposure than usual, reduced physical activity, and increased eating, which can contribute to weight gain and other health risks. However, “the effect of stress from confinement, loss of work, and health concerns needs to be individualized and may be difficult to generalize,” Dr. Sundar said.
The authors of the review note the established associations between too little social interaction, increased stress, and poor sleep quality, though loneliness mediates this relationship. Loneliness is also a risk during this time, with or without online social interaction.
Children and teens may also have difficulty sleeping, which can affect their behavioral and emotional regulation, and primary caregivers experience more stress while juggling childcare, household duties, and work.
“While many parents share childcare and household responsibilities, in most families these tasks are still predominantly managed by mothers,” the authors added.

“Sharing responsibilities between parents and not overworking just one parent is key,” said Brandon M. Seay MD, a pediatric pulmonologist and sleep specialist at Children’s Healthcare of Atlanta. He also recommended trying to incorporate work into the day while kids are doing online learning.
Ms. Trainor agreed that trading off responsibilities between parents is ideal, though the challenge is greater for single parents. It may be possible for some to take family leave, but not all families have that option, she said.
The study authors also point out a Catch-22 for many people: The blurred boundary between home life and work life can undermine work productivity and efficiency, thereby increasing stress. “Healthy sleep may be a key protective factor to cope positively with these challenges, although adequate opportunity to sleep may be affected by increased time pressure of work, childcare, and household requirements.”
Dr. Seay advises adults to try to get at least 6-8 hours of sleep each night, even taking advantage of a later waking time – if the kids also sleep in – to help. “If anything, the ability to sleep later and wake up later is of benefit for a lot of my teenage patients,” he said in an interview.
In fact, the study authors also address possible positive effects on sleep for some people during the current situation. Since social support can improve sleep quality, social media interaction might provide some social support, though it’s not the same as meeting people in person and “screen exposure may hamper sleep quality when used close to bedtime.”
Some people may actually have an opportunity to get more daylight exposure or exercise, which can improve sleep, and some, especially night owls and teenagers, may be able to align their daily schedules more closely to their natural circadian rhythms.
“Given that we are not bound by usual work or social schedules, there may be a tendency to drift to our sleep chronotypes,” especially for teenagers, Dr. Sundar said.
For some, this may be their first opportunity to learn what their chronotype is, Dr. Seay said.
“It is always advantageous to ‘obey’ your natural sleep timing, [although] it simply isn’t always the most efficient outside of our current situation,” he said. “Use this as a time to figure out your natural sleep timing if you constantly have issues being able to wake up in the morning. Now that you don’t have to be up for work or school, you can figure out what time works for you.”
At the same time, if you have an extreme circadian rhythm disorder, especially an irregular one, it may still be best to try to keep a regular sleep schedule to avoid feeling isolated if others are socializing while you’re asleep, Ms. Trainor said.
The authors similarly note the limits of potential benefits during this time, noting that they “may not be enough to counteract the negative effects of the increased work and family requirements, as well as the overwhelming levels of stress and anxiety about the well-being of oneself and others, and the negative effects of confinement for family social reactions.”
Treating stress, anxiety, and insomnia
The first-line treatment for chronic insomnia is cognitive-behavioral therapy for insomnia, but “recent evidence shows that cognitive-behavioral therapy can also serve to treat sudden-onset (acute) insomnia due to rapid stress-causing situation changes,” the authors noted. They also reviewed the key elements of CBT-I: stimulus control, sleep hygiene, relaxation interventions, cognitive reappraisal, paradoxical intention, and sleep restriction.
CBT-I lends very naturally to telemedicine, Dr. Seay, Dr. Sundar, and Ms. Trainor all agreed.
“I actually see this current situation as an opportunity for health care practices and providers to expand the reach of telemedicine – due to necessity – which will hopefully continue after confinement has been lifted worldwide,” Dr. Seay said.
Dr. Sundar pointed to research supporting CBT-I online and several apps that can be used for it, such as SHUTi and Sleepio. Ms. Trainor noted that the Cleveland Clinic offers a basic CBT-I online class for $40.
The authors note that prescribing medication is generally discouraged because it lacks evidence for long-term effectiveness of chronic insomnia, but it might be worth considering as a second-line therapy for acute insomnia from outside stressors, such as home confinement, if CBT-I doesn’t work or isn’t possible. Pharmacologic treatment can include benzodiazepines, hypnotic benzodiazepine receptor agonists, or sedating antidepressants, particularly if used for a comorbid mood disorder.
The authors then offer general recommendations for improving sleep that doctors can pass on to their patients:
- Get up and go to bed at approximately the same times daily.
- Schedule 15-minute breaks during the day to manage stress and reflect on worries and the situation.
- Reserve the bed for sleep and sex only; not for working, watching TV, using the computer, or doing other activities.
- Try to follow your natural sleep rhythm as much as possible.
- Use social media as stress relief, an opportunity to communicate with friends and family, and distraction, especially with uplifting stories or humor.
- Leave devices out of the bedroom.
- Limit your exposure to news about the COVID-19 pandemic.
- Exercise regularly, ideally in daylight.
- Look for ways to stay busy and distracted, including making your home or bedroom more comfortable if possible.
- Get as much daylight during the day as possible, and keep lights dim or dark at night.
- Engage in familiar, comfortable, relaxing activities before bedtime.
- If your daily activity level is lower, eat less as well, ideally at least 2 hours before going to bed.
The authors also offered recommendations specifically for families:
- Divide child care, home maintenance, and chores between adults, being sure not to let the lion’s share fall on women.
- Maintain regular sleep times for children and spend the 30 minutes before their bedtime doing a calming, familiar activity that both the children and parents enjoy.
- “While using computer, smartphones, and watching TV more than usual may be inevitable in confinement, avoid technological devices after dinner or too close to bedtime.”
- Ensure your child has daily physical activity, keep a relatively consistent schedule or routine, expose them to as much daylight or bright light as possible during the day, and try to limit their bed use only to sleeping if possible. “Parents need to be involved in setting schedules for sleep and meal times so that kids do not get into sleep patterns that are difficult to change when school starts back,” Dr. Sundar said. “Limiting screen time is also important especially during nighttime.”
- Reassure children if they wake up anxious at night.
SOURCE: Altena E et al. J Sleep Res. 2020 Apr 4. doi: 10.1111/jsr.13052.
Mass social distancing and social isolation to prevent the spread of a deadly disease, along with technological tools that allow social communication and continued work and school, is an unprecedented situation.
The current reality of most people’s lives during the COVID-19 pandemic has the potential to induce or exacerbate sleep problems, though it may also present some with an opportunity to improve sleep, wrote Ellemarije Altena, PhD, of the University of Bordeaux (France), and her colleagues in a recent research review in the Journal of Sleep Research.
The review was conducted by a task force of the European Academy for Cognitive Behavioural Therapy for Insomnia. The European CBT-I Academy is an initiative of the European Insomnia Network to promote implementation and dissemination of treatment.
After discussing the known effects of stress, confinement, and altered schedules on sleep, the authors present recommendations on ways to manage sleep problems such as insomnia in the general public and potentially encourage people to take advantage of the opportunity to align their schedules with their natural circadian rhythms. Physicians may find the recommendations helpful in advising patients with sleep problems related to the COVID-19 emergency.
“Being forced to stay at home, work from home, do homeschooling with children, drastically minimize outings, reduce social interaction or work many more hours under stressful circumstances, and in parallel manage the attendant health risks, can have a major impact on daily functioning and nighttime sleep,” Dr. Altena and colleagues wrote.
There may also be a lag time in physicians hearing about changes in sleep or sleeping problems from patients, said Krishna M. Sundar, MD, FCCP, medical director of the Sleep-Wake Center at the University of Utah in Salt Lake City. “There may actually be some improvement in sleep durations given that most folks are working from home with more time with family and less work-related stress,” he said in an interview. “In terms of sleep or other effects on worsening of psychiatric problems, it is still not clear what the overall effects are going to be.”
Although daylight has the biggest impact on regulating circadian rhythms, artificial light, meal times, diet, and amount of physical activity can also have an influence. Negative effects on sleep can result from both excessively high activity levels, such as stress and work overload, or excessively low levels, such as from depression or confinement, the authors note.
The current situation also opens the door to interactions between stress, sleep, anxiety, and risk of PTSD. “Those sensitive to stress-related sleep disruption are more likely to develop chronic insomnia,” which, in combination with a major stressor, is a risk factor for PTSD, the authors write. They note that 7% of Wuhan residents, the city in China where the virus appears to have originated, particularly women, reported PTSD symptoms after the COVID-19 outbreak, and anxiety was highest in those under age 35 years and those who followed news about the disease for more than 3 hours a day.
Better sleep quality and fewer early morning awakenings, however, appeared to be protective against PTSD symptoms. The authors note the value of physical exercise, cognitive interventions, and relaxation techniques, including meditation, for reducing stress and milder symptoms of PTSD.
“Some patients are sleeping a bit better because of the pace of things has slowed down a bit,” said Anne C. Trainor, a nurse practitioner and instructor in the neurology department’s sleep disorders program at Oregon Health & Science University in Portland, who was not involved in the study. “Keeping a regular schedule for sleeping and eating, getting exercise daily – preferably in sunlight and not just before bedtime – and using relaxation or mindfulness practice and cognitive interventions to help manage anxiety” were the key takeaways from this review, Ms. Trainor said in an interview.
Home confinement, stressors and sleep
A wide range of stressors could affect sleep during COVID-19 social distancing interventions, including “major changes in routines, living with uncertainty,” and anxiety about health, the economic situation, and how long this situation will last, the authors write.
Parents must juggle work, homeschooling, and ordinary household errands and management. Meanwhile, entrepreneurs, small business owners ,and workers in entertainment, hospitality and food service must contend with anxiety about job uncertainty and financial security. For anyone working from home, disruptions to work and home routines can make it difficult to associate being home with relaxation – and sleep.
“The more regular our sleep schedule is the better quality our sleep tends to be, but it is a struggle when we don’t have separate spaces to work and parent in,” Ms. Trainor said.
At the same time, “confinement-related stress may be caused by an inability to engage in rewarding activities, such as visiting friends and family, shopping, attending cultural and sports events, and visiting bars or restaurants,” the authors write. “Spending more time with family in a limited space can also induce stress, particularly in situations where there are preexisting family difficulties.”
Being stuck at home may lead to less daylight exposure than usual, reduced physical activity, and increased eating, which can contribute to weight gain and other health risks. However, “the effect of stress from confinement, loss of work, and health concerns needs to be individualized and may be difficult to generalize,” Dr. Sundar said.
The authors of the review note the established associations between too little social interaction, increased stress, and poor sleep quality, though loneliness mediates this relationship. Loneliness is also a risk during this time, with or without online social interaction.
Children and teens may also have difficulty sleeping, which can affect their behavioral and emotional regulation, and primary caregivers experience more stress while juggling childcare, household duties, and work.
“While many parents share childcare and household responsibilities, in most families these tasks are still predominantly managed by mothers,” the authors added.
“Sharing responsibilities between parents and not overworking just one parent is key,” said Brandon M. Seay MD, a pediatric pulmonologist and sleep specialist at Children’s Healthcare of Atlanta. He also recommended trying to incorporate work into the day while kids are doing online learning.
Ms. Trainor agreed that trading off responsibilities between parents is ideal, though the challenge is greater for single parents. It may be possible for some to take family leave, but not all families have that option, she said.
The study authors also point out a Catch-22 for many people: The blurred boundary between home life and work life can undermine work productivity and efficiency, thereby increasing stress. “Healthy sleep may be a key protective factor to cope positively with these challenges, although adequate opportunity to sleep may be affected by increased time pressure of work, childcare, and household requirements.”
Dr. Seay advises adults to try to get at least 6-8 hours of sleep each night, even taking advantage of a later waking time – if the kids also sleep in – to help. “If anything, the ability to sleep later and wake up later is of benefit for a lot of my teenage patients,” he said in an interview.
In fact, the study authors also address possible positive effects on sleep for some people during the current situation. Since social support can improve sleep quality, social media interaction might provide some social support, though it’s not the same as meeting people in person and “screen exposure may hamper sleep quality when used close to bedtime.”
Some people may actually have an opportunity to get more daylight exposure or exercise, which can improve sleep, and some, especially night owls and teenagers, may be able to align their daily schedules more closely to their natural circadian rhythms.
“Given that we are not bound by usual work or social schedules, there may be a tendency to drift to our sleep chronotypes,” especially for teenagers, Dr. Sundar said.
For some, this may be their first opportunity to learn what their chronotype is, Dr. Seay said.
“It is always advantageous to ‘obey’ your natural sleep timing, [although] it simply isn’t always the most efficient outside of our current situation,” he said. “Use this as a time to figure out your natural sleep timing if you constantly have issues being able to wake up in the morning. Now that you don’t have to be up for work or school, you can figure out what time works for you.”
At the same time, if you have an extreme circadian rhythm disorder, especially an irregular one, it may still be best to try to keep a regular sleep schedule to avoid feeling isolated if others are socializing while you’re asleep, Ms. Trainor said.
The authors similarly note the limits of potential benefits during this time, noting that they “may not be enough to counteract the negative effects of the increased work and family requirements, as well as the overwhelming levels of stress and anxiety about the well-being of oneself and others, and the negative effects of confinement for family social reactions.”
Treating stress, anxiety, and insomnia
The first-line treatment for chronic insomnia is cognitive-behavioral therapy for insomnia, but “recent evidence shows that cognitive-behavioral therapy can also serve to treat sudden-onset (acute) insomnia due to rapid stress-causing situation changes,” the authors noted. They also reviewed the key elements of CBT-I: stimulus control, sleep hygiene, relaxation interventions, cognitive reappraisal, paradoxical intention, and sleep restriction.
CBT-I lends very naturally to telemedicine, Dr. Seay, Dr. Sundar, and Ms. Trainor all agreed.
“I actually see this current situation as an opportunity for health care practices and providers to expand the reach of telemedicine – due to necessity – which will hopefully continue after confinement has been lifted worldwide,” Dr. Seay said.
Dr. Sundar pointed to research supporting CBT-I online and several apps that can be used for it, such as SHUTi and Sleepio. Ms. Trainor noted that the Cleveland Clinic offers a basic CBT-I online class for $40.
The authors note that prescribing medication is generally discouraged because it lacks evidence for long-term effectiveness of chronic insomnia, but it might be worth considering as a second-line therapy for acute insomnia from outside stressors, such as home confinement, if CBT-I doesn’t work or isn’t possible. Pharmacologic treatment can include benzodiazepines, hypnotic benzodiazepine receptor agonists, or sedating antidepressants, particularly if used for a comorbid mood disorder.
The authors then offer general recommendations for improving sleep that doctors can pass on to their patients:
- Get up and go to bed at approximately the same times daily.
- Schedule 15-minute breaks during the day to manage stress and reflect on worries and the situation.
- Reserve the bed for sleep and sex only; not for working, watching TV, using the computer, or doing other activities.
- Try to follow your natural sleep rhythm as much as possible.
- Use social media as stress relief, an opportunity to communicate with friends and family, and distraction, especially with uplifting stories or humor.
- Leave devices out of the bedroom.
- Limit your exposure to news about the COVID-19 pandemic.
- Exercise regularly, ideally in daylight.
- Look for ways to stay busy and distracted, including making your home or bedroom more comfortable if possible.
- Get as much daylight during the day as possible, and keep lights dim or dark at night.
- Engage in familiar, comfortable, relaxing activities before bedtime.
- If your daily activity level is lower, eat less as well, ideally at least 2 hours before going to bed.
The authors also offered recommendations specifically for families:
- Divide child care, home maintenance, and chores between adults, being sure not to let the lion’s share fall on women.
- Maintain regular sleep times for children and spend the 30 minutes before their bedtime doing a calming, familiar activity that both the children and parents enjoy.
- “While using computer, smartphones, and watching TV more than usual may be inevitable in confinement, avoid technological devices after dinner or too close to bedtime.”
- Ensure your child has daily physical activity, keep a relatively consistent schedule or routine, expose them to as much daylight or bright light as possible during the day, and try to limit their bed use only to sleeping if possible. “Parents need to be involved in setting schedules for sleep and meal times so that kids do not get into sleep patterns that are difficult to change when school starts back,” Dr. Sundar said. “Limiting screen time is also important especially during nighttime.”
- Reassure children if they wake up anxious at night.
SOURCE: Altena E et al. J Sleep Res. 2020 Apr 4. doi: 10.1111/jsr.13052.
Mass social distancing and social isolation to prevent the spread of a deadly disease, along with technological tools that allow social communication and continued work and school, is an unprecedented situation.
The current reality of most people’s lives during the COVID-19 pandemic has the potential to induce or exacerbate sleep problems, though it may also present some with an opportunity to improve sleep, wrote Ellemarije Altena, PhD, of the University of Bordeaux (France), and her colleagues in a recent research review in the Journal of Sleep Research.
The review was conducted by a task force of the European Academy for Cognitive Behavioural Therapy for Insomnia. The European CBT-I Academy is an initiative of the European Insomnia Network to promote implementation and dissemination of treatment.
After discussing the known effects of stress, confinement, and altered schedules on sleep, the authors present recommendations on ways to manage sleep problems such as insomnia in the general public and potentially encourage people to take advantage of the opportunity to align their schedules with their natural circadian rhythms. Physicians may find the recommendations helpful in advising patients with sleep problems related to the COVID-19 emergency.
“Being forced to stay at home, work from home, do homeschooling with children, drastically minimize outings, reduce social interaction or work many more hours under stressful circumstances, and in parallel manage the attendant health risks, can have a major impact on daily functioning and nighttime sleep,” Dr. Altena and colleagues wrote.
There may also be a lag time in physicians hearing about changes in sleep or sleeping problems from patients, said Krishna M. Sundar, MD, FCCP, medical director of the Sleep-Wake Center at the University of Utah in Salt Lake City. “There may actually be some improvement in sleep durations given that most folks are working from home with more time with family and less work-related stress,” he said in an interview. “In terms of sleep or other effects on worsening of psychiatric problems, it is still not clear what the overall effects are going to be.”
Although daylight has the biggest impact on regulating circadian rhythms, artificial light, meal times, diet, and amount of physical activity can also have an influence. Negative effects on sleep can result from both excessively high activity levels, such as stress and work overload, or excessively low levels, such as from depression or confinement, the authors note.
The current situation also opens the door to interactions between stress, sleep, anxiety, and risk of PTSD. “Those sensitive to stress-related sleep disruption are more likely to develop chronic insomnia,” which, in combination with a major stressor, is a risk factor for PTSD, the authors write. They note that 7% of Wuhan residents, the city in China where the virus appears to have originated, particularly women, reported PTSD symptoms after the COVID-19 outbreak, and anxiety was highest in those under age 35 years and those who followed news about the disease for more than 3 hours a day.
Better sleep quality and fewer early morning awakenings, however, appeared to be protective against PTSD symptoms. The authors note the value of physical exercise, cognitive interventions, and relaxation techniques, including meditation, for reducing stress and milder symptoms of PTSD.
“Some patients are sleeping a bit better because of the pace of things has slowed down a bit,” said Anne C. Trainor, a nurse practitioner and instructor in the neurology department’s sleep disorders program at Oregon Health & Science University in Portland, who was not involved in the study. “Keeping a regular schedule for sleeping and eating, getting exercise daily – preferably in sunlight and not just before bedtime – and using relaxation or mindfulness practice and cognitive interventions to help manage anxiety” were the key takeaways from this review, Ms. Trainor said in an interview.
Home confinement, stressors and sleep
A wide range of stressors could affect sleep during COVID-19 social distancing interventions, including “major changes in routines, living with uncertainty,” and anxiety about health, the economic situation, and how long this situation will last, the authors write.
Parents must juggle work, homeschooling, and ordinary household errands and management. Meanwhile, entrepreneurs, small business owners ,and workers in entertainment, hospitality and food service must contend with anxiety about job uncertainty and financial security. For anyone working from home, disruptions to work and home routines can make it difficult to associate being home with relaxation – and sleep.
“The more regular our sleep schedule is the better quality our sleep tends to be, but it is a struggle when we don’t have separate spaces to work and parent in,” Ms. Trainor said.
At the same time, “confinement-related stress may be caused by an inability to engage in rewarding activities, such as visiting friends and family, shopping, attending cultural and sports events, and visiting bars or restaurants,” the authors write. “Spending more time with family in a limited space can also induce stress, particularly in situations where there are preexisting family difficulties.”
Being stuck at home may lead to less daylight exposure than usual, reduced physical activity, and increased eating, which can contribute to weight gain and other health risks. However, “the effect of stress from confinement, loss of work, and health concerns needs to be individualized and may be difficult to generalize,” Dr. Sundar said.
The authors of the review note the established associations between too little social interaction, increased stress, and poor sleep quality, though loneliness mediates this relationship. Loneliness is also a risk during this time, with or without online social interaction.
Children and teens may also have difficulty sleeping, which can affect their behavioral and emotional regulation, and primary caregivers experience more stress while juggling childcare, household duties, and work.
“While many parents share childcare and household responsibilities, in most families these tasks are still predominantly managed by mothers,” the authors added.
“Sharing responsibilities between parents and not overworking just one parent is key,” said Brandon M. Seay MD, a pediatric pulmonologist and sleep specialist at Children’s Healthcare of Atlanta. He also recommended trying to incorporate work into the day while kids are doing online learning.
Ms. Trainor agreed that trading off responsibilities between parents is ideal, though the challenge is greater for single parents. It may be possible for some to take family leave, but not all families have that option, she said.
The study authors also point out a Catch-22 for many people: The blurred boundary between home life and work life can undermine work productivity and efficiency, thereby increasing stress. “Healthy sleep may be a key protective factor to cope positively with these challenges, although adequate opportunity to sleep may be affected by increased time pressure of work, childcare, and household requirements.”
Dr. Seay advises adults to try to get at least 6-8 hours of sleep each night, even taking advantage of a later waking time – if the kids also sleep in – to help. “If anything, the ability to sleep later and wake up later is of benefit for a lot of my teenage patients,” he said in an interview.
In fact, the study authors also address possible positive effects on sleep for some people during the current situation. Since social support can improve sleep quality, social media interaction might provide some social support, though it’s not the same as meeting people in person and “screen exposure may hamper sleep quality when used close to bedtime.”
Some people may actually have an opportunity to get more daylight exposure or exercise, which can improve sleep, and some, especially night owls and teenagers, may be able to align their daily schedules more closely to their natural circadian rhythms.
“Given that we are not bound by usual work or social schedules, there may be a tendency to drift to our sleep chronotypes,” especially for teenagers, Dr. Sundar said.
For some, this may be their first opportunity to learn what their chronotype is, Dr. Seay said.
“It is always advantageous to ‘obey’ your natural sleep timing, [although] it simply isn’t always the most efficient outside of our current situation,” he said. “Use this as a time to figure out your natural sleep timing if you constantly have issues being able to wake up in the morning. Now that you don’t have to be up for work or school, you can figure out what time works for you.”
At the same time, if you have an extreme circadian rhythm disorder, especially an irregular one, it may still be best to try to keep a regular sleep schedule to avoid feeling isolated if others are socializing while you’re asleep, Ms. Trainor said.
The authors similarly note the limits of potential benefits during this time, noting that they “may not be enough to counteract the negative effects of the increased work and family requirements, as well as the overwhelming levels of stress and anxiety about the well-being of oneself and others, and the negative effects of confinement for family social reactions.”
Treating stress, anxiety, and insomnia
The first-line treatment for chronic insomnia is cognitive-behavioral therapy for insomnia, but “recent evidence shows that cognitive-behavioral therapy can also serve to treat sudden-onset (acute) insomnia due to rapid stress-causing situation changes,” the authors noted. They also reviewed the key elements of CBT-I: stimulus control, sleep hygiene, relaxation interventions, cognitive reappraisal, paradoxical intention, and sleep restriction.
CBT-I lends very naturally to telemedicine, Dr. Seay, Dr. Sundar, and Ms. Trainor all agreed.
“I actually see this current situation as an opportunity for health care practices and providers to expand the reach of telemedicine – due to necessity – which will hopefully continue after confinement has been lifted worldwide,” Dr. Seay said.
Dr. Sundar pointed to research supporting CBT-I online and several apps that can be used for it, such as SHUTi and Sleepio. Ms. Trainor noted that the Cleveland Clinic offers a basic CBT-I online class for $40.
The authors note that prescribing medication is generally discouraged because it lacks evidence for long-term effectiveness of chronic insomnia, but it might be worth considering as a second-line therapy for acute insomnia from outside stressors, such as home confinement, if CBT-I doesn’t work or isn’t possible. Pharmacologic treatment can include benzodiazepines, hypnotic benzodiazepine receptor agonists, or sedating antidepressants, particularly if used for a comorbid mood disorder.
The authors then offer general recommendations for improving sleep that doctors can pass on to their patients:
- Get up and go to bed at approximately the same times daily.
- Schedule 15-minute breaks during the day to manage stress and reflect on worries and the situation.
- Reserve the bed for sleep and sex only; not for working, watching TV, using the computer, or doing other activities.
- Try to follow your natural sleep rhythm as much as possible.
- Use social media as stress relief, an opportunity to communicate with friends and family, and distraction, especially with uplifting stories or humor.
- Leave devices out of the bedroom.
- Limit your exposure to news about the COVID-19 pandemic.
- Exercise regularly, ideally in daylight.
- Look for ways to stay busy and distracted, including making your home or bedroom more comfortable if possible.
- Get as much daylight during the day as possible, and keep lights dim or dark at night.
- Engage in familiar, comfortable, relaxing activities before bedtime.
- If your daily activity level is lower, eat less as well, ideally at least 2 hours before going to bed.
The authors also offered recommendations specifically for families:
- Divide child care, home maintenance, and chores between adults, being sure not to let the lion’s share fall on women.
- Maintain regular sleep times for children and spend the 30 minutes before their bedtime doing a calming, familiar activity that both the children and parents enjoy.
- “While using computer, smartphones, and watching TV more than usual may be inevitable in confinement, avoid technological devices after dinner or too close to bedtime.”
- Ensure your child has daily physical activity, keep a relatively consistent schedule or routine, expose them to as much daylight or bright light as possible during the day, and try to limit their bed use only to sleeping if possible. “Parents need to be involved in setting schedules for sleep and meal times so that kids do not get into sleep patterns that are difficult to change when school starts back,” Dr. Sundar said. “Limiting screen time is also important especially during nighttime.”
- Reassure children if they wake up anxious at night.
SOURCE: Altena E et al. J Sleep Res. 2020 Apr 4. doi: 10.1111/jsr.13052.
FROM JOURNAL OF SLEEP RESEARCH
'Silent Hypoxemia' and Other Curious Clinical Observations in COVID-19

This transcript has been edited for clarity.
Gary S. Ferenchick, MD, MS: I'm Gary Ferenchick with Hannah Ferenchick, who has agreed to join us to talk about what's going on in Detroit, and also about PPE and decontamination processes. Why don't you introduce yourself?
Hannah R.B. Ferenchick, MD: I am Hannah Ferenchick. I'm an ER physician and medical intensivist. I split my time between the medical ICU and the emergency department at Detroit Medical Center.
Dr Gary Ferenchick: We were talking earlier about some of the not-well-described clinical scenarios that patients with definitive COVID might present with. One of these was the idea of "silent hypoxemia." Could you describe that?
Dr Hannah Ferenchick: Silent hypoxemia is being described in many of these COVID patients. That means the patient is very hypoxemic—they may have an oxygen saturation of about 85% on room air, but clinically they look very comfortable—they are not dyspneic or tachypneic and may not even verbalize a significant sense of shortness of breath. It's not every patient, but it has been interesting to see patients sitting there looking fairly normal, with a resting oxygen saturation much lower than you would expect for someone who doesn't have underlying pulmonary disease or other symptoms.
Dr Gary Ferenchick: What abnormalities are you seeing on standard or not-so-standard lab tests?
Dr Hannah Ferenchick: Some of the characteristic lab findings we are seeing are lymphopenia and elevated inflammatory markers (eg, CRP). A couple of other atypical findings seem to be specific for COVID—elevated LDH, ferritin, CPK, and procalcitonin levels. Some of the hematologic markers that we look at—the coagulation profile studies—are also abnormal, showing thrombocytopenia and elevated D-dimer levels.
That constellation of symptoms represents more of a clinical picture. A lot of times we have only a very high clinical suspicion, because in many parts of the country it still takes days to get back a confirmatory PCR test.
Much like we do for the flu, the confirmatory test is a nasopharyngeal swab that is run for COVID/coronavirus PCR. Unfortunately the sensitivity of that test is not great. Some studies have quoted 75%-80%, so even a negative PCR does not necessarily rule out the disease, especially if you have a high clinical suspicion. A clinical suspicion is based on the typical symptoms. Many patients, although not all, will have symptoms of lower respiratory tract infection.
Dr Gary Ferenchick: So the right clinical scenario with the right hematologic/biochemical findings dramatically raises the chance that the patient has COVID?
Dr Hannah Ferenchick: Yes, and one thing that we have all been astonished by is how terrible some of these x-rays can look. There are a lot of typical findings on x-ray. Some describe them as looking like pulmonary edema, but the patient has no history of heart failure. Peripheral consolidation and ground-glass opacities are classically described. If you saw one of these x-rays from a patient with bacterial pneumonia, you would expect that patient to be very ill-appearing. Sometimes we get x-rays on patients who are sitting there, maybe mildly symptomatic on room air, and we are astonished by how terrible their x-rays look.
Unfortunately, imaging studies are something we haven't been able to rely on too much for diagnosis. Part of that is to maintain hospital safety, because to take a patient to CT scan, you have to consider the turnaround time for cleaning the CT scanner and the exposure of additional staff to a possibly infected patient. Some of those logistical considerations have limited the availability of radiography.
Gary S. Ferenchick, MD, MS, is a family physician and professor in the Department of Medicine at Michigan State University in East Lansing, Michigan. His daughter, Hannah R.B. Ferenchick, MD, is an assistant professor in the Department of Emergency Medicine, Division of Pulmonary & Critical Care and Sleep Medicine, at Wayne State University, Detroit, Michigan, and a medical intensivist and emergency medicine physician at Detroit Medical Center.
This transcript has been edited for clarity.
Gary S. Ferenchick, MD, MS: I'm Gary Ferenchick with Hannah Ferenchick, who has agreed to join us to talk about what's going on in Detroit, and also about PPE and decontamination processes. Why don't you introduce yourself?
Hannah R.B. Ferenchick, MD: I am Hannah Ferenchick. I'm an ER physician and medical intensivist. I split my time between the medical ICU and the emergency department at Detroit Medical Center.
Dr Gary Ferenchick: We were talking earlier about some of the not-well-described clinical scenarios that patients with definitive COVID might present with. One of these was the idea of "silent hypoxemia." Could you describe that?
Dr Hannah Ferenchick: Silent hypoxemia is being described in many of these COVID patients. That means the patient is very hypoxemic—they may have an oxygen saturation of about 85% on room air, but clinically they look very comfortable—they are not dyspneic or tachypneic and may not even verbalize a significant sense of shortness of breath. It's not every patient, but it has been interesting to see patients sitting there looking fairly normal, with a resting oxygen saturation much lower than you would expect for someone who doesn't have underlying pulmonary disease or other symptoms.
Dr Gary Ferenchick: What abnormalities are you seeing on standard or not-so-standard lab tests?
Dr Hannah Ferenchick: Some of the characteristic lab findings we are seeing are lymphopenia and elevated inflammatory markers (eg, CRP). A couple of other atypical findings seem to be specific for COVID—elevated LDH, ferritin, CPK, and procalcitonin levels. Some of the hematologic markers that we look at—the coagulation profile studies—are also abnormal, showing thrombocytopenia and elevated D-dimer levels.
That constellation of symptoms represents more of a clinical picture. A lot of times we have only a very high clinical suspicion, because in many parts of the country it still takes days to get back a confirmatory PCR test.
Much like we do for the flu, the confirmatory test is a nasopharyngeal swab that is run for COVID/coronavirus PCR. Unfortunately the sensitivity of that test is not great. Some studies have quoted 75%-80%, so even a negative PCR does not necessarily rule out the disease, especially if you have a high clinical suspicion. A clinical suspicion is based on the typical symptoms. Many patients, although not all, will have symptoms of lower respiratory tract infection.
Dr Gary Ferenchick: So the right clinical scenario with the right hematologic/biochemical findings dramatically raises the chance that the patient has COVID?
Dr Hannah Ferenchick: Yes, and one thing that we have all been astonished by is how terrible some of these x-rays can look. There are a lot of typical findings on x-ray. Some describe them as looking like pulmonary edema, but the patient has no history of heart failure. Peripheral consolidation and ground-glass opacities are classically described. If you saw one of these x-rays from a patient with bacterial pneumonia, you would expect that patient to be very ill-appearing. Sometimes we get x-rays on patients who are sitting there, maybe mildly symptomatic on room air, and we are astonished by how terrible their x-rays look.
Unfortunately, imaging studies are something we haven't been able to rely on too much for diagnosis. Part of that is to maintain hospital safety, because to take a patient to CT scan, you have to consider the turnaround time for cleaning the CT scanner and the exposure of additional staff to a possibly infected patient. Some of those logistical considerations have limited the availability of radiography.
Gary S. Ferenchick, MD, MS, is a family physician and professor in the Department of Medicine at Michigan State University in East Lansing, Michigan. His daughter, Hannah R.B. Ferenchick, MD, is an assistant professor in the Department of Emergency Medicine, Division of Pulmonary & Critical Care and Sleep Medicine, at Wayne State University, Detroit, Michigan, and a medical intensivist and emergency medicine physician at Detroit Medical Center.
This transcript has been edited for clarity.
Gary S. Ferenchick, MD, MS: I'm Gary Ferenchick with Hannah Ferenchick, who has agreed to join us to talk about what's going on in Detroit, and also about PPE and decontamination processes. Why don't you introduce yourself?
Hannah R.B. Ferenchick, MD: I am Hannah Ferenchick. I'm an ER physician and medical intensivist. I split my time between the medical ICU and the emergency department at Detroit Medical Center.
Dr Gary Ferenchick: We were talking earlier about some of the not-well-described clinical scenarios that patients with definitive COVID might present with. One of these was the idea of "silent hypoxemia." Could you describe that?
Dr Hannah Ferenchick: Silent hypoxemia is being described in many of these COVID patients. That means the patient is very hypoxemic—they may have an oxygen saturation of about 85% on room air, but clinically they look very comfortable—they are not dyspneic or tachypneic and may not even verbalize a significant sense of shortness of breath. It's not every patient, but it has been interesting to see patients sitting there looking fairly normal, with a resting oxygen saturation much lower than you would expect for someone who doesn't have underlying pulmonary disease or other symptoms.
Dr Gary Ferenchick: What abnormalities are you seeing on standard or not-so-standard lab tests?
Dr Hannah Ferenchick: Some of the characteristic lab findings we are seeing are lymphopenia and elevated inflammatory markers (eg, CRP). A couple of other atypical findings seem to be specific for COVID—elevated LDH, ferritin, CPK, and procalcitonin levels. Some of the hematologic markers that we look at—the coagulation profile studies—are also abnormal, showing thrombocytopenia and elevated D-dimer levels.
That constellation of symptoms represents more of a clinical picture. A lot of times we have only a very high clinical suspicion, because in many parts of the country it still takes days to get back a confirmatory PCR test.
Much like we do for the flu, the confirmatory test is a nasopharyngeal swab that is run for COVID/coronavirus PCR. Unfortunately the sensitivity of that test is not great. Some studies have quoted 75%-80%, so even a negative PCR does not necessarily rule out the disease, especially if you have a high clinical suspicion. A clinical suspicion is based on the typical symptoms. Many patients, although not all, will have symptoms of lower respiratory tract infection.
Dr Gary Ferenchick: So the right clinical scenario with the right hematologic/biochemical findings dramatically raises the chance that the patient has COVID?
Dr Hannah Ferenchick: Yes, and one thing that we have all been astonished by is how terrible some of these x-rays can look. There are a lot of typical findings on x-ray. Some describe them as looking like pulmonary edema, but the patient has no history of heart failure. Peripheral consolidation and ground-glass opacities are classically described. If you saw one of these x-rays from a patient with bacterial pneumonia, you would expect that patient to be very ill-appearing. Sometimes we get x-rays on patients who are sitting there, maybe mildly symptomatic on room air, and we are astonished by how terrible their x-rays look.
Unfortunately, imaging studies are something we haven't been able to rely on too much for diagnosis. Part of that is to maintain hospital safety, because to take a patient to CT scan, you have to consider the turnaround time for cleaning the CT scanner and the exposure of additional staff to a possibly infected patient. Some of those logistical considerations have limited the availability of radiography.
Gary S. Ferenchick, MD, MS, is a family physician and professor in the Department of Medicine at Michigan State University in East Lansing, Michigan. His daughter, Hannah R.B. Ferenchick, MD, is an assistant professor in the Department of Emergency Medicine, Division of Pulmonary & Critical Care and Sleep Medicine, at Wayne State University, Detroit, Michigan, and a medical intensivist and emergency medicine physician at Detroit Medical Center.
Senate Dems call for nationwide COVID-19 testing strategy, more funding
Senate Democrats are calling on the Trump Administration to develop a comprehensive strategy for nationwide COVID-19 testing.
Lawmakers released a “roadmap” document with the goal of including its provisions in the next legislative aid package for COVID-19. Sen. Patty Murray (D-Wash.), the ranking member of the Health, Education, Labor & Pensions committee, noted during an April 15 press conference call that testing in the United States is actually slowing because of shortages and glitches.
“At our current pace, getting 100 million tests done would already take far too long,” she said. “We absolutely cannot afford any backsliding.”
The components of the roadmap include requiring the federal government to develop and communicate a detailed strategic plan to rapidly scale and optimize COVID-19 testing, Sen. Murray said. “This is a national crisis. We need a federally coordinated, whole-of-society response, not one that leaves each state to fend for itself.”
The strategic plan called for in the roadmap would need to establish a high-functioning supply chain with a sufficient amount of available testing materials and supplies; assess potential bottlenecks in the supply chain and communicate them to all stakeholders; and develop and validate accurate and reliable tests for COVID-19, with an emphasis on tests that can deliver rapid results.
Legislation would be used to bolster the supply chain enhancements, according to the roadmap, and would include incentives for domestic manufacturing of testing supplies and compel the sharing of intellectual property and guarantees on the purchase of testing materials.
Testing would be available to patients at no cost sharing under this proposal. The plan also calls for strengthening the price gouging policy in the CARES (Coronavirus Aid, Relief, and Economic Security) Act to ensure that health care professionals are fairly reimbursed by insurers.
The roadmap calls for $30 billion in new emergency funding to enable faster scaling of testing and development of different types of test, with an emphasis on rapid response tests. The funding would also be used to address supply chain issues, according to the roadmap document.
Sen. Lamar Alexander (R.-Tenn.), who chairs the Senate Health, Education, Labor & Pensions committee, echoed the need for more testing to be done, but suggested that the funding that has already been approved by Congress should be exhausted before more is allocated.
“In the last month, Congress has given federal agencies up to $38 billion to develop tests, treatments, and vaccines. Nothing is more important than finding a new diagnostic technology that will make it possible to test tens of millions of Americans, something our country has never tried to do before,” he said in a statement issued after the roadmap’s release. “We should start by using the money Congress has already provided, put politics aside, and work together on more tests with quick results.”
Senate Democrats are calling on the Trump Administration to develop a comprehensive strategy for nationwide COVID-19 testing.
Lawmakers released a “roadmap” document with the goal of including its provisions in the next legislative aid package for COVID-19. Sen. Patty Murray (D-Wash.), the ranking member of the Health, Education, Labor & Pensions committee, noted during an April 15 press conference call that testing in the United States is actually slowing because of shortages and glitches.
“At our current pace, getting 100 million tests done would already take far too long,” she said. “We absolutely cannot afford any backsliding.”
The components of the roadmap include requiring the federal government to develop and communicate a detailed strategic plan to rapidly scale and optimize COVID-19 testing, Sen. Murray said. “This is a national crisis. We need a federally coordinated, whole-of-society response, not one that leaves each state to fend for itself.”
The strategic plan called for in the roadmap would need to establish a high-functioning supply chain with a sufficient amount of available testing materials and supplies; assess potential bottlenecks in the supply chain and communicate them to all stakeholders; and develop and validate accurate and reliable tests for COVID-19, with an emphasis on tests that can deliver rapid results.
Legislation would be used to bolster the supply chain enhancements, according to the roadmap, and would include incentives for domestic manufacturing of testing supplies and compel the sharing of intellectual property and guarantees on the purchase of testing materials.
Testing would be available to patients at no cost sharing under this proposal. The plan also calls for strengthening the price gouging policy in the CARES (Coronavirus Aid, Relief, and Economic Security) Act to ensure that health care professionals are fairly reimbursed by insurers.
The roadmap calls for $30 billion in new emergency funding to enable faster scaling of testing and development of different types of test, with an emphasis on rapid response tests. The funding would also be used to address supply chain issues, according to the roadmap document.
Sen. Lamar Alexander (R.-Tenn.), who chairs the Senate Health, Education, Labor & Pensions committee, echoed the need for more testing to be done, but suggested that the funding that has already been approved by Congress should be exhausted before more is allocated.
“In the last month, Congress has given federal agencies up to $38 billion to develop tests, treatments, and vaccines. Nothing is more important than finding a new diagnostic technology that will make it possible to test tens of millions of Americans, something our country has never tried to do before,” he said in a statement issued after the roadmap’s release. “We should start by using the money Congress has already provided, put politics aside, and work together on more tests with quick results.”
Senate Democrats are calling on the Trump Administration to develop a comprehensive strategy for nationwide COVID-19 testing.
Lawmakers released a “roadmap” document with the goal of including its provisions in the next legislative aid package for COVID-19. Sen. Patty Murray (D-Wash.), the ranking member of the Health, Education, Labor & Pensions committee, noted during an April 15 press conference call that testing in the United States is actually slowing because of shortages and glitches.
“At our current pace, getting 100 million tests done would already take far too long,” she said. “We absolutely cannot afford any backsliding.”
The components of the roadmap include requiring the federal government to develop and communicate a detailed strategic plan to rapidly scale and optimize COVID-19 testing, Sen. Murray said. “This is a national crisis. We need a federally coordinated, whole-of-society response, not one that leaves each state to fend for itself.”
The strategic plan called for in the roadmap would need to establish a high-functioning supply chain with a sufficient amount of available testing materials and supplies; assess potential bottlenecks in the supply chain and communicate them to all stakeholders; and develop and validate accurate and reliable tests for COVID-19, with an emphasis on tests that can deliver rapid results.
Legislation would be used to bolster the supply chain enhancements, according to the roadmap, and would include incentives for domestic manufacturing of testing supplies and compel the sharing of intellectual property and guarantees on the purchase of testing materials.
Testing would be available to patients at no cost sharing under this proposal. The plan also calls for strengthening the price gouging policy in the CARES (Coronavirus Aid, Relief, and Economic Security) Act to ensure that health care professionals are fairly reimbursed by insurers.
The roadmap calls for $30 billion in new emergency funding to enable faster scaling of testing and development of different types of test, with an emphasis on rapid response tests. The funding would also be used to address supply chain issues, according to the roadmap document.
Sen. Lamar Alexander (R.-Tenn.), who chairs the Senate Health, Education, Labor & Pensions committee, echoed the need for more testing to be done, but suggested that the funding that has already been approved by Congress should be exhausted before more is allocated.
“In the last month, Congress has given federal agencies up to $38 billion to develop tests, treatments, and vaccines. Nothing is more important than finding a new diagnostic technology that will make it possible to test tens of millions of Americans, something our country has never tried to do before,” he said in a statement issued after the roadmap’s release. “We should start by using the money Congress has already provided, put politics aside, and work together on more tests with quick results.”
COVID-19: When health care personnel become patients
according to the Centers for Disease Control and Prevention.
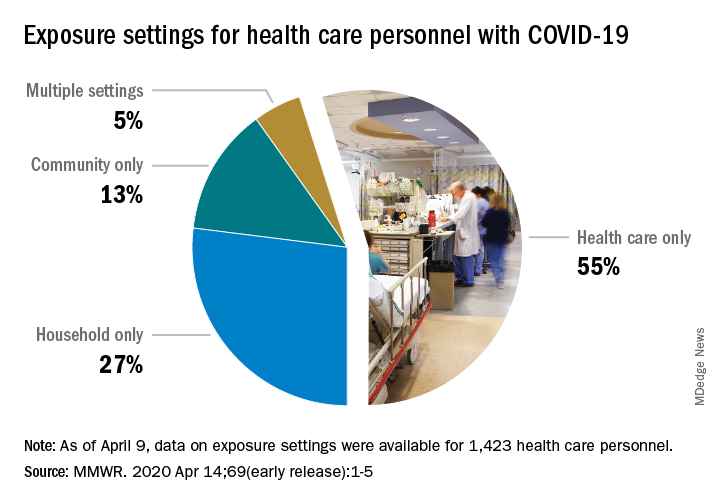
That number, however, is probably an underestimation because health care personnel (HCP) status was available for just over 49,000 of the 315,000 COVID-19 cases reported to the CDC as of April 9. Of the cases with known HCP status, 9,282 (19%) were health care personnel, Matthew J. Stuckey, PhD, and the CDC’s COVID-19 Response Team said.
“The number of cases in HCP reported here must be considered a lower bound because additional cases likely have gone unidentified or unreported,” they said.
The median age of the nearly 9,300 HCP with COVID-19 was 42 years, and the majority (55%) were aged 16-44 years; another 21% were 45-54, 18% were 55-64, and 6% were age 65 and over. The oldest group, however, represented 10 of the 27 known HCP deaths, the investigators reported in the Morbidity and Mortality Weekly Report.
The majority of infected HCP (55%) reported exposure to a COVID-19 patient in the health care setting, but “there were also known exposures in households and in the community, highlighting the potential for exposure in multiple settings, especially as community transmission increases,” the response team said.
Since “contact tracing after recognized occupational exposures likely will fail to identify many HCP at risk for developing COVID-19,” other measures will probably be needed to “reduce the risk for infected HCP transmitting the virus to colleagues and patients,” they added.
HCP with COVID-19 were less likely to be hospitalized (8%-10%) than the overall population (21%-31%), which “might reflect the younger median age … of HCP patients, compared with that of reported COVID-19 patients overall, as well as prioritization of HCP for testing, which might identify less-severe illness,” the investigators suggested.
The prevalence of underlying conditions in HCP patients, 38%, was the same as all patients with COVID-19, and 92% of the HCP patients presented with fever, cough, or shortness of breath. Two-thirds of all HCP reported muscle aches, and 65% reported headache, the CDC response team noted.
“It is critical to make every effort to ensure the health and safety of this essential national workforce of approximately 18 million HCP, both at work and in the community,” they wrote.
SOURCE: Stuckey MJ et al. MMWR. Apr 14;69(early release):1-5.
according to the Centers for Disease Control and Prevention.
That number, however, is probably an underestimation because health care personnel (HCP) status was available for just over 49,000 of the 315,000 COVID-19 cases reported to the CDC as of April 9. Of the cases with known HCP status, 9,282 (19%) were health care personnel, Matthew J. Stuckey, PhD, and the CDC’s COVID-19 Response Team said.
“The number of cases in HCP reported here must be considered a lower bound because additional cases likely have gone unidentified or unreported,” they said.
The median age of the nearly 9,300 HCP with COVID-19 was 42 years, and the majority (55%) were aged 16-44 years; another 21% were 45-54, 18% were 55-64, and 6% were age 65 and over. The oldest group, however, represented 10 of the 27 known HCP deaths, the investigators reported in the Morbidity and Mortality Weekly Report.
The majority of infected HCP (55%) reported exposure to a COVID-19 patient in the health care setting, but “there were also known exposures in households and in the community, highlighting the potential for exposure in multiple settings, especially as community transmission increases,” the response team said.
Since “contact tracing after recognized occupational exposures likely will fail to identify many HCP at risk for developing COVID-19,” other measures will probably be needed to “reduce the risk for infected HCP transmitting the virus to colleagues and patients,” they added.
HCP with COVID-19 were less likely to be hospitalized (8%-10%) than the overall population (21%-31%), which “might reflect the younger median age … of HCP patients, compared with that of reported COVID-19 patients overall, as well as prioritization of HCP for testing, which might identify less-severe illness,” the investigators suggested.
The prevalence of underlying conditions in HCP patients, 38%, was the same as all patients with COVID-19, and 92% of the HCP patients presented with fever, cough, or shortness of breath. Two-thirds of all HCP reported muscle aches, and 65% reported headache, the CDC response team noted.
“It is critical to make every effort to ensure the health and safety of this essential national workforce of approximately 18 million HCP, both at work and in the community,” they wrote.
SOURCE: Stuckey MJ et al. MMWR. Apr 14;69(early release):1-5.
according to the Centers for Disease Control and Prevention.
That number, however, is probably an underestimation because health care personnel (HCP) status was available for just over 49,000 of the 315,000 COVID-19 cases reported to the CDC as of April 9. Of the cases with known HCP status, 9,282 (19%) were health care personnel, Matthew J. Stuckey, PhD, and the CDC’s COVID-19 Response Team said.
“The number of cases in HCP reported here must be considered a lower bound because additional cases likely have gone unidentified or unreported,” they said.
The median age of the nearly 9,300 HCP with COVID-19 was 42 years, and the majority (55%) were aged 16-44 years; another 21% were 45-54, 18% were 55-64, and 6% were age 65 and over. The oldest group, however, represented 10 of the 27 known HCP deaths, the investigators reported in the Morbidity and Mortality Weekly Report.
The majority of infected HCP (55%) reported exposure to a COVID-19 patient in the health care setting, but “there were also known exposures in households and in the community, highlighting the potential for exposure in multiple settings, especially as community transmission increases,” the response team said.
Since “contact tracing after recognized occupational exposures likely will fail to identify many HCP at risk for developing COVID-19,” other measures will probably be needed to “reduce the risk for infected HCP transmitting the virus to colleagues and patients,” they added.
HCP with COVID-19 were less likely to be hospitalized (8%-10%) than the overall population (21%-31%), which “might reflect the younger median age … of HCP patients, compared with that of reported COVID-19 patients overall, as well as prioritization of HCP for testing, which might identify less-severe illness,” the investigators suggested.
The prevalence of underlying conditions in HCP patients, 38%, was the same as all patients with COVID-19, and 92% of the HCP patients presented with fever, cough, or shortness of breath. Two-thirds of all HCP reported muscle aches, and 65% reported headache, the CDC response team noted.
“It is critical to make every effort to ensure the health and safety of this essential national workforce of approximately 18 million HCP, both at work and in the community,” they wrote.
SOURCE: Stuckey MJ et al. MMWR. Apr 14;69(early release):1-5.
FROM THE MMWR
FDA approves emergency use of saliva test to detect COVID-19
As the race to develop rapid testing for COVID-19 expands, the Food and Drug Administration has granted emergency approval for an approach that uses saliva as the primary test biomaterial.

According to a document provided to the FDA, the Rutgers Clinical Genomics Laboratory TaqPath SARS-CoV-2 Assay is intended for the qualitative detection of nucleic acid from SARS-CoV-2 in oropharyngeal (throat) swab, nasopharyngeal swab, anterior nasal swab, mid-turbinate nasal swab from individuals suspected of COVID-19 by their health care clinicians. To expand on this assay, Rutgers University–based RUCDR Infinite Biologics developed a saliva collection method in partnership with Spectrum Solutions and Accurate Diagnostic Labs.
The document states that Samples are transported for RNA extraction and are tested within 48 hours of collection. In saliva samples obtained from 60 patients evaluated by the researchers, all were in agreement with the presence of COVID-19.

“If shown to be as accurate as nasopharyngeal and oropharyngeal samples, saliva as a biomatrix offers the advantage of not generating aerosols or creating as many respiratory droplets during specimen procurement, therefore decreasing the risk of transmission to the health care worker doing the testing,” said Matthew P. Cheng, MDCM, of the division of infectious diseases at McGill University Health Centre, Montreal, who was not involved in development of the test but who has written about diagnostic testing for the virus.
“Also, it may be easy enough for patients to do saliva self-collection at home. However, it is important to note that SARS-CoV-2 tests on saliva have not yet undergone the more rigorous evaluation of full FDA authorization, and saliva is not a preferred specimen type of the FDA nor the [Centers for Disease Control and Prevention] for respiratory virus testing.”
In a prepared statement, Andrew I. Brooks, PhD, chief operating officer at RUCDR Infinite Biologics, said the saliva collection method enables clinicians to preserve personal protective equipment for use in patient care instead of testing. “We can significantly increase the number of people tested each and every day as self-collection of saliva is quicker and more scalable than swab collections,” he said. “All of this combined will have a tremendous impact on testing in New Jersey and across the United States.”
The tests are currently available to the RWJBarnabas Health network, based in West Orange, N.J., which has partnered with Rutgers University.
As the race to develop rapid testing for COVID-19 expands, the Food and Drug Administration has granted emergency approval for an approach that uses saliva as the primary test biomaterial.
According to a document provided to the FDA, the Rutgers Clinical Genomics Laboratory TaqPath SARS-CoV-2 Assay is intended for the qualitative detection of nucleic acid from SARS-CoV-2 in oropharyngeal (throat) swab, nasopharyngeal swab, anterior nasal swab, mid-turbinate nasal swab from individuals suspected of COVID-19 by their health care clinicians. To expand on this assay, Rutgers University–based RUCDR Infinite Biologics developed a saliva collection method in partnership with Spectrum Solutions and Accurate Diagnostic Labs.
The document states that Samples are transported for RNA extraction and are tested within 48 hours of collection. In saliva samples obtained from 60 patients evaluated by the researchers, all were in agreement with the presence of COVID-19.
“If shown to be as accurate as nasopharyngeal and oropharyngeal samples, saliva as a biomatrix offers the advantage of not generating aerosols or creating as many respiratory droplets during specimen procurement, therefore decreasing the risk of transmission to the health care worker doing the testing,” said Matthew P. Cheng, MDCM, of the division of infectious diseases at McGill University Health Centre, Montreal, who was not involved in development of the test but who has written about diagnostic testing for the virus.
“Also, it may be easy enough for patients to do saliva self-collection at home. However, it is important to note that SARS-CoV-2 tests on saliva have not yet undergone the more rigorous evaluation of full FDA authorization, and saliva is not a preferred specimen type of the FDA nor the [Centers for Disease Control and Prevention] for respiratory virus testing.”
In a prepared statement, Andrew I. Brooks, PhD, chief operating officer at RUCDR Infinite Biologics, said the saliva collection method enables clinicians to preserve personal protective equipment for use in patient care instead of testing. “We can significantly increase the number of people tested each and every day as self-collection of saliva is quicker and more scalable than swab collections,” he said. “All of this combined will have a tremendous impact on testing in New Jersey and across the United States.”
The tests are currently available to the RWJBarnabas Health network, based in West Orange, N.J., which has partnered with Rutgers University.
As the race to develop rapid testing for COVID-19 expands, the Food and Drug Administration has granted emergency approval for an approach that uses saliva as the primary test biomaterial.
According to a document provided to the FDA, the Rutgers Clinical Genomics Laboratory TaqPath SARS-CoV-2 Assay is intended for the qualitative detection of nucleic acid from SARS-CoV-2 in oropharyngeal (throat) swab, nasopharyngeal swab, anterior nasal swab, mid-turbinate nasal swab from individuals suspected of COVID-19 by their health care clinicians. To expand on this assay, Rutgers University–based RUCDR Infinite Biologics developed a saliva collection method in partnership with Spectrum Solutions and Accurate Diagnostic Labs.
The document states that Samples are transported for RNA extraction and are tested within 48 hours of collection. In saliva samples obtained from 60 patients evaluated by the researchers, all were in agreement with the presence of COVID-19.
“If shown to be as accurate as nasopharyngeal and oropharyngeal samples, saliva as a biomatrix offers the advantage of not generating aerosols or creating as many respiratory droplets during specimen procurement, therefore decreasing the risk of transmission to the health care worker doing the testing,” said Matthew P. Cheng, MDCM, of the division of infectious diseases at McGill University Health Centre, Montreal, who was not involved in development of the test but who has written about diagnostic testing for the virus.
“Also, it may be easy enough for patients to do saliva self-collection at home. However, it is important to note that SARS-CoV-2 tests on saliva have not yet undergone the more rigorous evaluation of full FDA authorization, and saliva is not a preferred specimen type of the FDA nor the [Centers for Disease Control and Prevention] for respiratory virus testing.”
In a prepared statement, Andrew I. Brooks, PhD, chief operating officer at RUCDR Infinite Biologics, said the saliva collection method enables clinicians to preserve personal protective equipment for use in patient care instead of testing. “We can significantly increase the number of people tested each and every day as self-collection of saliva is quicker and more scalable than swab collections,” he said. “All of this combined will have a tremendous impact on testing in New Jersey and across the United States.”
The tests are currently available to the RWJBarnabas Health network, based in West Orange, N.J., which has partnered with Rutgers University.
Learning about the curve
Empty shelves that once cradled toilet paper rolls; lines of shoppers, some with masks; waiting 6 feet or at least a shopping cart length apart to get into grocery stores; hazmat-suited workers loading body bags into makeshift mortuaries ... These are the images we have come to associate with the COVID-19 pandemic. But then there also are the graphs and charts, none of them bearing good news. Some are difficult to interpret because they may be missing a key ingredient, such as a scale. Day to day fluctuations in the timeliness of the data points can make valid comparisons impossible. In most cases, it is too early to look at the graphs and hope for the big picture. Whether you are concerned about the stock market or the number of new cases of the virus in your county, you are hoping to see some graphic depiction of a favorable trend.

We have suddenly learned about the urgency of a process called “flattening the curve.” Are we doing as good a job of flattening as we could be? Are we doing better than France or Spain? Or are we heading toward an Italianesque apocalypse? Who is going to tell us when the flattening is for real and not just a 2- or 3-day statistical aberration?
The curves we are obsessed with today are those showing us new cases and new deaths. But And we won’t be seeing this curve in four-color graphics on the front page of our newspapers. It is the learning curve, and we want it to be as steep as we can make it without any hint of flattening in the foreseeable future.
We need to learn more about corona-like viruses. Why are some of us more vulnerable? We need to learn more about contagion. Does the 6-foot guideline make any sense? How long are viral particles floating in the air capable of initiating disease? What about air flow and dilution? Can we build a cruise ship or airplane that will be less of a health hazard?
More importantly, we need to learn to be better prepared. Even before the pandemic there have been shortages in intravenous solutions and drugs of critical importance to common diseases. Can we learn how to create reliable and affordable supply chains that allow researchers and developers to make a reasonable profit? Can we relearn to value science? Can we learn to invest more heavily in epidemiology and make it a specialty that attracts our best thinkers and communicators? Then can we elect officials who will share our trust in their recommendations?
Can we do a better job of resolving the tension between those who believe in a strong federal government and those who believe in local autonomy because we are seeing every day that this is an issue of survival, not just coexistence? Can we learn that the globalization that has allowed this viral spread can also be leveraged to beat it into submission?

Over the last half century there has been an unfortunate flattening of the learning curve. Ironically we have seen exponential growth among hi-tech industries that have forced us to keep abreast of new developments. But along with this has been a growing skepticism about value of scientific investigation. It is time we climbed back on that steep learning curve. The view gets better the higher we climb.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Empty shelves that once cradled toilet paper rolls; lines of shoppers, some with masks; waiting 6 feet or at least a shopping cart length apart to get into grocery stores; hazmat-suited workers loading body bags into makeshift mortuaries ... These are the images we have come to associate with the COVID-19 pandemic. But then there also are the graphs and charts, none of them bearing good news. Some are difficult to interpret because they may be missing a key ingredient, such as a scale. Day to day fluctuations in the timeliness of the data points can make valid comparisons impossible. In most cases, it is too early to look at the graphs and hope for the big picture. Whether you are concerned about the stock market or the number of new cases of the virus in your county, you are hoping to see some graphic depiction of a favorable trend.
We have suddenly learned about the urgency of a process called “flattening the curve.” Are we doing as good a job of flattening as we could be? Are we doing better than France or Spain? Or are we heading toward an Italianesque apocalypse? Who is going to tell us when the flattening is for real and not just a 2- or 3-day statistical aberration?
The curves we are obsessed with today are those showing us new cases and new deaths. But And we won’t be seeing this curve in four-color graphics on the front page of our newspapers. It is the learning curve, and we want it to be as steep as we can make it without any hint of flattening in the foreseeable future.
We need to learn more about corona-like viruses. Why are some of us more vulnerable? We need to learn more about contagion. Does the 6-foot guideline make any sense? How long are viral particles floating in the air capable of initiating disease? What about air flow and dilution? Can we build a cruise ship or airplane that will be less of a health hazard?
More importantly, we need to learn to be better prepared. Even before the pandemic there have been shortages in intravenous solutions and drugs of critical importance to common diseases. Can we learn how to create reliable and affordable supply chains that allow researchers and developers to make a reasonable profit? Can we relearn to value science? Can we learn to invest more heavily in epidemiology and make it a specialty that attracts our best thinkers and communicators? Then can we elect officials who will share our trust in their recommendations?
Can we do a better job of resolving the tension between those who believe in a strong federal government and those who believe in local autonomy because we are seeing every day that this is an issue of survival, not just coexistence? Can we learn that the globalization that has allowed this viral spread can also be leveraged to beat it into submission?
Over the last half century there has been an unfortunate flattening of the learning curve. Ironically we have seen exponential growth among hi-tech industries that have forced us to keep abreast of new developments. But along with this has been a growing skepticism about value of scientific investigation. It is time we climbed back on that steep learning curve. The view gets better the higher we climb.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Empty shelves that once cradled toilet paper rolls; lines of shoppers, some with masks; waiting 6 feet or at least a shopping cart length apart to get into grocery stores; hazmat-suited workers loading body bags into makeshift mortuaries ... These are the images we have come to associate with the COVID-19 pandemic. But then there also are the graphs and charts, none of them bearing good news. Some are difficult to interpret because they may be missing a key ingredient, such as a scale. Day to day fluctuations in the timeliness of the data points can make valid comparisons impossible. In most cases, it is too early to look at the graphs and hope for the big picture. Whether you are concerned about the stock market or the number of new cases of the virus in your county, you are hoping to see some graphic depiction of a favorable trend.
We have suddenly learned about the urgency of a process called “flattening the curve.” Are we doing as good a job of flattening as we could be? Are we doing better than France or Spain? Or are we heading toward an Italianesque apocalypse? Who is going to tell us when the flattening is for real and not just a 2- or 3-day statistical aberration?
The curves we are obsessed with today are those showing us new cases and new deaths. But And we won’t be seeing this curve in four-color graphics on the front page of our newspapers. It is the learning curve, and we want it to be as steep as we can make it without any hint of flattening in the foreseeable future.
We need to learn more about corona-like viruses. Why are some of us more vulnerable? We need to learn more about contagion. Does the 6-foot guideline make any sense? How long are viral particles floating in the air capable of initiating disease? What about air flow and dilution? Can we build a cruise ship or airplane that will be less of a health hazard?
More importantly, we need to learn to be better prepared. Even before the pandemic there have been shortages in intravenous solutions and drugs of critical importance to common diseases. Can we learn how to create reliable and affordable supply chains that allow researchers and developers to make a reasonable profit? Can we relearn to value science? Can we learn to invest more heavily in epidemiology and make it a specialty that attracts our best thinkers and communicators? Then can we elect officials who will share our trust in their recommendations?
Can we do a better job of resolving the tension between those who believe in a strong federal government and those who believe in local autonomy because we are seeing every day that this is an issue of survival, not just coexistence? Can we learn that the globalization that has allowed this viral spread can also be leveraged to beat it into submission?
Over the last half century there has been an unfortunate flattening of the learning curve. Ironically we have seen exponential growth among hi-tech industries that have forced us to keep abreast of new developments. But along with this has been a growing skepticism about value of scientific investigation. It is time we climbed back on that steep learning curve. The view gets better the higher we climb.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Social distancing comes to the medicine wards
As the coronavirus pandemic has swept across America, so have advisories for social distancing. As of April 2, stay-at-home orders had been given in 38 states and parts of 7 more, affecting about 300 million people. Most of these people have been asked to maintain 6 feet of separation to anyone outside their immediate family and to avoid all avoidable contacts.

Typical hospital medicine patients at an academic hospital, however, traditionally receive visits from their hospitalist, an intern, a resident, and sometimes several medical students, pharmacists, and case managers. At University of California, San Diego, Health, many of these visits would occur during Focused Interdisciplinary Team rounds, with providers moving together in close proximity.
Asymptomatic and presymptomatic spread of coronavirus have been documented, which means distancing is a good idea for everyone. The risks of traditional patient visits during the coronavirus pandemic include spread to both patients (at high risk of complications) and staff (taken out of the workforce during surge times). Even if coronavirus were not a risk, visits to isolation rooms consume PPE, which is in short supply.

In response to the pandemic, UCSD Hospital Medicine drafted guidelines for the reduction of patient contacts. Our slide presentations and written guidelines were then distributed to physicians, nurses, pharmacists, and other staff by our pandemic response command center. Key points include the following:
- Target one in-person MD visit per day for stable patients. This means that attending reexaminations of patients seen by residents, nurse practitioners, physician assistants, and so on would not be done for billing or teaching purposes, only when clinically necessary.
- Use phone or video conferencing for follow-up discussions unless direct patient contact is needed.
- Consider skipping daily exams on patients who do not require them, such as patients awaiting placement or stably receiving long courses of antibiotics. Interview them remotely or from the door instead.
- Conduct team rounds, patient discussions, and handoffs with all members 6 feet apart or by telephone or video. Avoid shared work rooms. Substitute video conferences for in-person meetings. Use EMR embedded messaging to reduce face-to-face discussions.
- Check if a patient is ready for a visit before donning PPE to avoid waste.
- Explain to patients that distancing is being conducted to protect them. In our experience, when patients are asked about distancing, they welcome the changes.

We have also considered that most patient visits are generated by nurses and assistants. To increase distancing and reduce PPE waste, we have encouraged nurses and pharmacists to maximize their use of remote communication with patients and to suggest changes to care plans and come up with creative solutions to reduce traffic. We specifically suggested the following changes to routine care:
- Reduce frequency of taking vital signs, such as just daily or as needed, in stable patients (for example, those awaiting placement).
- Reduce checks for alcohol withdrawal and neurologic status as soon as possible, and stop fingersticks in patients with well-controlled diabetes not receiving insulin.
- Substitute less frequently administered medications where appropriate if doing so would reduce room traffic (such as enoxaparin for heparin, ceftriaxone for cefazolin, naproxen for ibuprofen, or patient-controlled analgesia for as needed morphine).
- Place intravenous pumps in halls if needed – luckily, our situation has not required these measures in San Diego.
- Explore the possibility of increased patient self-management (self-dosed insulin or inhalers) where medically appropriate.
- Eliminate food service and janitorial trips to isolation rooms unless requested by registered nurse.

There are clear downsides to medical distancing for hospital medicine patients. Patients might have delayed diagnosis of new conditions or inadequate management of conditions requiring frequent assessment, such as alcohol withdrawal. Opportunities for miscommunication (either patient-provider or provider-provider) may be increased with distancing. Isolation also comes with emotional costs such as stress and feelings of isolation or abandonment. Given the dynamic nature of the pandemic response, we are continually reevaluating our distancing guidelines to administer the safest and most effective hospital care possible as we approach California’s expected peak coronavirus infection period.
Dr. Jenkins is professor and chair of the Patient Safety Committee in the Division of Hospital Medicine at UCSD. Dr. Seymann is clinical professor and vice chief for academic affairs, UCSD division of hospital medicine. Dr. Horman and Dr. Bell are hospitalists and associate professors of medicine at UC San Diego Health.
As the coronavirus pandemic has swept across America, so have advisories for social distancing. As of April 2, stay-at-home orders had been given in 38 states and parts of 7 more, affecting about 300 million people. Most of these people have been asked to maintain 6 feet of separation to anyone outside their immediate family and to avoid all avoidable contacts.
Typical hospital medicine patients at an academic hospital, however, traditionally receive visits from their hospitalist, an intern, a resident, and sometimes several medical students, pharmacists, and case managers. At University of California, San Diego, Health, many of these visits would occur during Focused Interdisciplinary Team rounds, with providers moving together in close proximity.
Asymptomatic and presymptomatic spread of coronavirus have been documented, which means distancing is a good idea for everyone. The risks of traditional patient visits during the coronavirus pandemic include spread to both patients (at high risk of complications) and staff (taken out of the workforce during surge times). Even if coronavirus were not a risk, visits to isolation rooms consume PPE, which is in short supply.
In response to the pandemic, UCSD Hospital Medicine drafted guidelines for the reduction of patient contacts. Our slide presentations and written guidelines were then distributed to physicians, nurses, pharmacists, and other staff by our pandemic response command center. Key points include the following:
- Target one in-person MD visit per day for stable patients. This means that attending reexaminations of patients seen by residents, nurse practitioners, physician assistants, and so on would not be done for billing or teaching purposes, only when clinically necessary.
- Use phone or video conferencing for follow-up discussions unless direct patient contact is needed.
- Consider skipping daily exams on patients who do not require them, such as patients awaiting placement or stably receiving long courses of antibiotics. Interview them remotely or from the door instead.
- Conduct team rounds, patient discussions, and handoffs with all members 6 feet apart or by telephone or video. Avoid shared work rooms. Substitute video conferences for in-person meetings. Use EMR embedded messaging to reduce face-to-face discussions.
- Check if a patient is ready for a visit before donning PPE to avoid waste.
- Explain to patients that distancing is being conducted to protect them. In our experience, when patients are asked about distancing, they welcome the changes.
We have also considered that most patient visits are generated by nurses and assistants. To increase distancing and reduce PPE waste, we have encouraged nurses and pharmacists to maximize their use of remote communication with patients and to suggest changes to care plans and come up with creative solutions to reduce traffic. We specifically suggested the following changes to routine care:
- Reduce frequency of taking vital signs, such as just daily or as needed, in stable patients (for example, those awaiting placement).
- Reduce checks for alcohol withdrawal and neurologic status as soon as possible, and stop fingersticks in patients with well-controlled diabetes not receiving insulin.
- Substitute less frequently administered medications where appropriate if doing so would reduce room traffic (such as enoxaparin for heparin, ceftriaxone for cefazolin, naproxen for ibuprofen, or patient-controlled analgesia for as needed morphine).
- Place intravenous pumps in halls if needed – luckily, our situation has not required these measures in San Diego.
- Explore the possibility of increased patient self-management (self-dosed insulin or inhalers) where medically appropriate.
- Eliminate food service and janitorial trips to isolation rooms unless requested by registered nurse.
There are clear downsides to medical distancing for hospital medicine patients. Patients might have delayed diagnosis of new conditions or inadequate management of conditions requiring frequent assessment, such as alcohol withdrawal. Opportunities for miscommunication (either patient-provider or provider-provider) may be increased with distancing. Isolation also comes with emotional costs such as stress and feelings of isolation or abandonment. Given the dynamic nature of the pandemic response, we are continually reevaluating our distancing guidelines to administer the safest and most effective hospital care possible as we approach California’s expected peak coronavirus infection period.
Dr. Jenkins is professor and chair of the Patient Safety Committee in the Division of Hospital Medicine at UCSD. Dr. Seymann is clinical professor and vice chief for academic affairs, UCSD division of hospital medicine. Dr. Horman and Dr. Bell are hospitalists and associate professors of medicine at UC San Diego Health.
As the coronavirus pandemic has swept across America, so have advisories for social distancing. As of April 2, stay-at-home orders had been given in 38 states and parts of 7 more, affecting about 300 million people. Most of these people have been asked to maintain 6 feet of separation to anyone outside their immediate family and to avoid all avoidable contacts.
Typical hospital medicine patients at an academic hospital, however, traditionally receive visits from their hospitalist, an intern, a resident, and sometimes several medical students, pharmacists, and case managers. At University of California, San Diego, Health, many of these visits would occur during Focused Interdisciplinary Team rounds, with providers moving together in close proximity.
Asymptomatic and presymptomatic spread of coronavirus have been documented, which means distancing is a good idea for everyone. The risks of traditional patient visits during the coronavirus pandemic include spread to both patients (at high risk of complications) and staff (taken out of the workforce during surge times). Even if coronavirus were not a risk, visits to isolation rooms consume PPE, which is in short supply.
In response to the pandemic, UCSD Hospital Medicine drafted guidelines for the reduction of patient contacts. Our slide presentations and written guidelines were then distributed to physicians, nurses, pharmacists, and other staff by our pandemic response command center. Key points include the following:
- Target one in-person MD visit per day for stable patients. This means that attending reexaminations of patients seen by residents, nurse practitioners, physician assistants, and so on would not be done for billing or teaching purposes, only when clinically necessary.
- Use phone or video conferencing for follow-up discussions unless direct patient contact is needed.
- Consider skipping daily exams on patients who do not require them, such as patients awaiting placement or stably receiving long courses of antibiotics. Interview them remotely or from the door instead.
- Conduct team rounds, patient discussions, and handoffs with all members 6 feet apart or by telephone or video. Avoid shared work rooms. Substitute video conferences for in-person meetings. Use EMR embedded messaging to reduce face-to-face discussions.
- Check if a patient is ready for a visit before donning PPE to avoid waste.
- Explain to patients that distancing is being conducted to protect them. In our experience, when patients are asked about distancing, they welcome the changes.
We have also considered that most patient visits are generated by nurses and assistants. To increase distancing and reduce PPE waste, we have encouraged nurses and pharmacists to maximize their use of remote communication with patients and to suggest changes to care plans and come up with creative solutions to reduce traffic. We specifically suggested the following changes to routine care:
- Reduce frequency of taking vital signs, such as just daily or as needed, in stable patients (for example, those awaiting placement).
- Reduce checks for alcohol withdrawal and neurologic status as soon as possible, and stop fingersticks in patients with well-controlled diabetes not receiving insulin.
- Substitute less frequently administered medications where appropriate if doing so would reduce room traffic (such as enoxaparin for heparin, ceftriaxone for cefazolin, naproxen for ibuprofen, or patient-controlled analgesia for as needed morphine).
- Place intravenous pumps in halls if needed – luckily, our situation has not required these measures in San Diego.
- Explore the possibility of increased patient self-management (self-dosed insulin or inhalers) where medically appropriate.
- Eliminate food service and janitorial trips to isolation rooms unless requested by registered nurse.
There are clear downsides to medical distancing for hospital medicine patients. Patients might have delayed diagnosis of new conditions or inadequate management of conditions requiring frequent assessment, such as alcohol withdrawal. Opportunities for miscommunication (either patient-provider or provider-provider) may be increased with distancing. Isolation also comes with emotional costs such as stress and feelings of isolation or abandonment. Given the dynamic nature of the pandemic response, we are continually reevaluating our distancing guidelines to administer the safest and most effective hospital care possible as we approach California’s expected peak coronavirus infection period.
Dr. Jenkins is professor and chair of the Patient Safety Committee in the Division of Hospital Medicine at UCSD. Dr. Seymann is clinical professor and vice chief for academic affairs, UCSD division of hospital medicine. Dr. Horman and Dr. Bell are hospitalists and associate professors of medicine at UC San Diego Health.
Inflammatory markers may explain COVID-19, diabetes dynamic
COVID-19 infection in patients with type 2 diabetes is associated with a greater increase in inflammatory and coagulation markers, compared with COVID-19 patients without diabetes, according to preliminary findings from a retrospective analysis of COVID-19 patients in Wuhan, China.
The results, though preliminary, could help explain why patients with diabetes and COVID-19 are at greater risk for more severe disease and death.
The results also suggest that more severe disease in patients with diabetes may be the result of a cytokine storm, in which the patient’s immune system overreacts to the virus and inflicts collateral damage on its own organs, according to Herbert I. Rettinger, MD, a clinical endocrinologist in Orange County, Calif., and member of the editorial advisory board for Clinical Endocrinology News. “Understanding the mechanism might help us understand the best way to treat,” COVID-19 in patients with diabetes, he said in an interview.
Dr. Rettinger, who was not involved in the research, noted that the study included only 24 patients with diabetes. Nevertheless, the finding of heightened inflammatory and coagulation markers was “fascinating.”
“This is the first paper I’ve seen [suggesting] that. I don’t know if we can extrapolate [the findings] to other populations, but if biomarkers are elevated in patients with COVID-19 and diabetes, then it’s something worth looking into, and to be aware of and cautious of. We need to pay attention to this,” he commented.
The study was led by Weina Guo and Desheng Hu at Huazhong University of Science and Technology in Wuhan, China, and published in Diabetes/Metabolism Research and Reviews.
The sample included 174 patients with COVID-19, who were treated consecutively during Feb. 10-29, 2020, at a single center. The researchers first assigned the patients to one of two groups – those with comorbid diabetes and those without. They further excluded all other comorbidities, focusing only on 26 patients with no comorbidities and 24 with only diabetes as a comorbidity, to remove all other comorbidities as possible confounding factors. Patients in the diabetes group were significantly older than those without diabetes (61 vs. 41 years, P < .01). The mortality rate was 16.5% in patients with diabetes and 0% in those without (P = .03).
COVID-19 patients with diabetes alone as a comorbidity had a greater risk for severe pneumonia, as evidenced by a higher mean CT score, compared with those without diabetes and no other comorbidities (P = .04). Patients with diabetes also had higher measures of release of tissue injury–related enzymes and were at higher risk of uncontrolled inflammation and hypercoagulable state. In particular, they had higher levels of interleukin-6 (13.7 vs. 4.1 pg/mL, respectively; P < .01), C-reactive protein (76.4 vs. 7.43 mg/L; P < .01), serum ferritin (764.8 vs. 128.9 ng/mL; P < .01), and D-dimer (1.16 vs. 0.25 mcg/mL; P < .01).
“It’s noteworthy that, for diseases that can induce a cytokine storm, IL-6 is a very good predictor of disease severity and prognosis, and its expression time is longer than other cytokines ([tumor necrosis factor] and IL-1). In addition, a significant rise in serum ferritin indicates the activation of the monocyte-macrophage system, which is a crucial part of inflammatory storm. These results indicate that patients with diabetes are susceptible to form an inflammatory storm, which eventually lead to rapid deterioration of COVID-19,” the authors wrote.
They also cited previous findings suggesting that coronavirus might exacerbate, or even cause, diabetes by seriously damaging islets (Acta Diabetol. 2010;47[3]:193-9). “Since viral infection may cause sharp fluctuation of the blood glucose levels of diabetes patients, which adversely affect the recovery of patients, there is reason to suspect that diabetes combined with SARS-CoV-2 pneumonia may form a vicious circle,” they wrote.
That’s one more reason to carefully monitor diabetes patients, said Dr. Rettinger. “Those patients who are able to make insulin might not be able to do so with the infection, and that may last a while, and they may require insulin. You want to keep a watch on things, and if oral agents are not working well, you want to go to insulin as quickly as you can. Probably diabetics should be way more careful and maybe visit the emergency department at earlier than a nondiabetic would.”

Raghavendra Mirmira, MD, PhD, who conducts translational research on diabetes and insulin production, said that the finding was not a complete surprise to him. “With a lot of diseases, having diabetes as a comorbidity can mean worse outcomes, and that’s certainly true of influenza. It was true for the other COVID-like illnesses, such as SARS and MERS,” Dr. Mirmira, who was not involved in the research, said in an interview.
If the findings hold up in larger numbers of patients and across multiple centers, they have the potential to inform patient management, said Dr. Mirmira, director of the Translational Research Center in the department of medicine at the University of Chicago. That will be especially true as data from long-term follow-up of become available. Elevated values in some biomarkers might dictate a patient be sent straight to the ICU or dictate admission to the hospital rather than being sent home, or it could assist patient selection for some of the new therapies that physicians hope will become available.
“The more information we get [about] total outcome, the more informed we’d be about who would benefit from some of the therapies that are in clinical trials now,” he said. Still, it will be a challenge to prove causation, because patients with diabetes have unique clinical characteristics that could also be the source of the difference.
Dr. Mirmira noted that patients with diabetes only were 20 years older on average than those with no comorbidities. “It’s really hard to know if what you’re looking at for the worse outcomes for people with diabetes is because they were older, and we know that older people tend to do much worse with COVID than younger people.” Ideally, patients would also be matched by age, but there are not enough data to do that yet.
The study was funded by
SOURCE: Guo W et al. Diabetes Metab Res Rev. 2020 Mar 31. doi: 10.1002/dmrr.3319.
COVID-19 infection in patients with type 2 diabetes is associated with a greater increase in inflammatory and coagulation markers, compared with COVID-19 patients without diabetes, according to preliminary findings from a retrospective analysis of COVID-19 patients in Wuhan, China.
The results, though preliminary, could help explain why patients with diabetes and COVID-19 are at greater risk for more severe disease and death.
The results also suggest that more severe disease in patients with diabetes may be the result of a cytokine storm, in which the patient’s immune system overreacts to the virus and inflicts collateral damage on its own organs, according to Herbert I. Rettinger, MD, a clinical endocrinologist in Orange County, Calif., and member of the editorial advisory board for Clinical Endocrinology News. “Understanding the mechanism might help us understand the best way to treat,” COVID-19 in patients with diabetes, he said in an interview.
Dr. Rettinger, who was not involved in the research, noted that the study included only 24 patients with diabetes. Nevertheless, the finding of heightened inflammatory and coagulation markers was “fascinating.”
“This is the first paper I’ve seen [suggesting] that. I don’t know if we can extrapolate [the findings] to other populations, but if biomarkers are elevated in patients with COVID-19 and diabetes, then it’s something worth looking into, and to be aware of and cautious of. We need to pay attention to this,” he commented.
The study was led by Weina Guo and Desheng Hu at Huazhong University of Science and Technology in Wuhan, China, and published in Diabetes/Metabolism Research and Reviews.
The sample included 174 patients with COVID-19, who were treated consecutively during Feb. 10-29, 2020, at a single center. The researchers first assigned the patients to one of two groups – those with comorbid diabetes and those without. They further excluded all other comorbidities, focusing only on 26 patients with no comorbidities and 24 with only diabetes as a comorbidity, to remove all other comorbidities as possible confounding factors. Patients in the diabetes group were significantly older than those without diabetes (61 vs. 41 years, P < .01). The mortality rate was 16.5% in patients with diabetes and 0% in those without (P = .03).
COVID-19 patients with diabetes alone as a comorbidity had a greater risk for severe pneumonia, as evidenced by a higher mean CT score, compared with those without diabetes and no other comorbidities (P = .04). Patients with diabetes also had higher measures of release of tissue injury–related enzymes and were at higher risk of uncontrolled inflammation and hypercoagulable state. In particular, they had higher levels of interleukin-6 (13.7 vs. 4.1 pg/mL, respectively; P < .01), C-reactive protein (76.4 vs. 7.43 mg/L; P < .01), serum ferritin (764.8 vs. 128.9 ng/mL; P < .01), and D-dimer (1.16 vs. 0.25 mcg/mL; P < .01).
“It’s noteworthy that, for diseases that can induce a cytokine storm, IL-6 is a very good predictor of disease severity and prognosis, and its expression time is longer than other cytokines ([tumor necrosis factor] and IL-1). In addition, a significant rise in serum ferritin indicates the activation of the monocyte-macrophage system, which is a crucial part of inflammatory storm. These results indicate that patients with diabetes are susceptible to form an inflammatory storm, which eventually lead to rapid deterioration of COVID-19,” the authors wrote.
They also cited previous findings suggesting that coronavirus might exacerbate, or even cause, diabetes by seriously damaging islets (Acta Diabetol. 2010;47[3]:193-9). “Since viral infection may cause sharp fluctuation of the blood glucose levels of diabetes patients, which adversely affect the recovery of patients, there is reason to suspect that diabetes combined with SARS-CoV-2 pneumonia may form a vicious circle,” they wrote.
That’s one more reason to carefully monitor diabetes patients, said Dr. Rettinger. “Those patients who are able to make insulin might not be able to do so with the infection, and that may last a while, and they may require insulin. You want to keep a watch on things, and if oral agents are not working well, you want to go to insulin as quickly as you can. Probably diabetics should be way more careful and maybe visit the emergency department at earlier than a nondiabetic would.”
Raghavendra Mirmira, MD, PhD, who conducts translational research on diabetes and insulin production, said that the finding was not a complete surprise to him. “With a lot of diseases, having diabetes as a comorbidity can mean worse outcomes, and that’s certainly true of influenza. It was true for the other COVID-like illnesses, such as SARS and MERS,” Dr. Mirmira, who was not involved in the research, said in an interview.
If the findings hold up in larger numbers of patients and across multiple centers, they have the potential to inform patient management, said Dr. Mirmira, director of the Translational Research Center in the department of medicine at the University of Chicago. That will be especially true as data from long-term follow-up of become available. Elevated values in some biomarkers might dictate a patient be sent straight to the ICU or dictate admission to the hospital rather than being sent home, or it could assist patient selection for some of the new therapies that physicians hope will become available.
“The more information we get [about] total outcome, the more informed we’d be about who would benefit from some of the therapies that are in clinical trials now,” he said. Still, it will be a challenge to prove causation, because patients with diabetes have unique clinical characteristics that could also be the source of the difference.
Dr. Mirmira noted that patients with diabetes only were 20 years older on average than those with no comorbidities. “It’s really hard to know if what you’re looking at for the worse outcomes for people with diabetes is because they were older, and we know that older people tend to do much worse with COVID than younger people.” Ideally, patients would also be matched by age, but there are not enough data to do that yet.
The study was funded by
SOURCE: Guo W et al. Diabetes Metab Res Rev. 2020 Mar 31. doi: 10.1002/dmrr.3319.
COVID-19 infection in patients with type 2 diabetes is associated with a greater increase in inflammatory and coagulation markers, compared with COVID-19 patients without diabetes, according to preliminary findings from a retrospective analysis of COVID-19 patients in Wuhan, China.
The results, though preliminary, could help explain why patients with diabetes and COVID-19 are at greater risk for more severe disease and death.
The results also suggest that more severe disease in patients with diabetes may be the result of a cytokine storm, in which the patient’s immune system overreacts to the virus and inflicts collateral damage on its own organs, according to Herbert I. Rettinger, MD, a clinical endocrinologist in Orange County, Calif., and member of the editorial advisory board for Clinical Endocrinology News. “Understanding the mechanism might help us understand the best way to treat,” COVID-19 in patients with diabetes, he said in an interview.
Dr. Rettinger, who was not involved in the research, noted that the study included only 24 patients with diabetes. Nevertheless, the finding of heightened inflammatory and coagulation markers was “fascinating.”
“This is the first paper I’ve seen [suggesting] that. I don’t know if we can extrapolate [the findings] to other populations, but if biomarkers are elevated in patients with COVID-19 and diabetes, then it’s something worth looking into, and to be aware of and cautious of. We need to pay attention to this,” he commented.
The study was led by Weina Guo and Desheng Hu at Huazhong University of Science and Technology in Wuhan, China, and published in Diabetes/Metabolism Research and Reviews.
The sample included 174 patients with COVID-19, who were treated consecutively during Feb. 10-29, 2020, at a single center. The researchers first assigned the patients to one of two groups – those with comorbid diabetes and those without. They further excluded all other comorbidities, focusing only on 26 patients with no comorbidities and 24 with only diabetes as a comorbidity, to remove all other comorbidities as possible confounding factors. Patients in the diabetes group were significantly older than those without diabetes (61 vs. 41 years, P < .01). The mortality rate was 16.5% in patients with diabetes and 0% in those without (P = .03).
COVID-19 patients with diabetes alone as a comorbidity had a greater risk for severe pneumonia, as evidenced by a higher mean CT score, compared with those without diabetes and no other comorbidities (P = .04). Patients with diabetes also had higher measures of release of tissue injury–related enzymes and were at higher risk of uncontrolled inflammation and hypercoagulable state. In particular, they had higher levels of interleukin-6 (13.7 vs. 4.1 pg/mL, respectively; P < .01), C-reactive protein (76.4 vs. 7.43 mg/L; P < .01), serum ferritin (764.8 vs. 128.9 ng/mL; P < .01), and D-dimer (1.16 vs. 0.25 mcg/mL; P < .01).
“It’s noteworthy that, for diseases that can induce a cytokine storm, IL-6 is a very good predictor of disease severity and prognosis, and its expression time is longer than other cytokines ([tumor necrosis factor] and IL-1). In addition, a significant rise in serum ferritin indicates the activation of the monocyte-macrophage system, which is a crucial part of inflammatory storm. These results indicate that patients with diabetes are susceptible to form an inflammatory storm, which eventually lead to rapid deterioration of COVID-19,” the authors wrote.
They also cited previous findings suggesting that coronavirus might exacerbate, or even cause, diabetes by seriously damaging islets (Acta Diabetol. 2010;47[3]:193-9). “Since viral infection may cause sharp fluctuation of the blood glucose levels of diabetes patients, which adversely affect the recovery of patients, there is reason to suspect that diabetes combined with SARS-CoV-2 pneumonia may form a vicious circle,” they wrote.
That’s one more reason to carefully monitor diabetes patients, said Dr. Rettinger. “Those patients who are able to make insulin might not be able to do so with the infection, and that may last a while, and they may require insulin. You want to keep a watch on things, and if oral agents are not working well, you want to go to insulin as quickly as you can. Probably diabetics should be way more careful and maybe visit the emergency department at earlier than a nondiabetic would.”
Raghavendra Mirmira, MD, PhD, who conducts translational research on diabetes and insulin production, said that the finding was not a complete surprise to him. “With a lot of diseases, having diabetes as a comorbidity can mean worse outcomes, and that’s certainly true of influenza. It was true for the other COVID-like illnesses, such as SARS and MERS,” Dr. Mirmira, who was not involved in the research, said in an interview.
If the findings hold up in larger numbers of patients and across multiple centers, they have the potential to inform patient management, said Dr. Mirmira, director of the Translational Research Center in the department of medicine at the University of Chicago. That will be especially true as data from long-term follow-up of become available. Elevated values in some biomarkers might dictate a patient be sent straight to the ICU or dictate admission to the hospital rather than being sent home, or it could assist patient selection for some of the new therapies that physicians hope will become available.
“The more information we get [about] total outcome, the more informed we’d be about who would benefit from some of the therapies that are in clinical trials now,” he said. Still, it will be a challenge to prove causation, because patients with diabetes have unique clinical characteristics that could also be the source of the difference.
Dr. Mirmira noted that patients with diabetes only were 20 years older on average than those with no comorbidities. “It’s really hard to know if what you’re looking at for the worse outcomes for people with diabetes is because they were older, and we know that older people tend to do much worse with COVID than younger people.” Ideally, patients would also be matched by age, but there are not enough data to do that yet.
The study was funded by
SOURCE: Guo W et al. Diabetes Metab Res Rev. 2020 Mar 31. doi: 10.1002/dmrr.3319.
FROM DIABETES/METABOLISM RESEARCH AND REVIEWS
AMA asks HHS for ‘immediate’ aid to ease clinicians’ COVID-19 ‘financial peril’
The American Medical Association (AMA) along with scores of specialty and state medical societies are asking the Trump administration to help the nation’s clinicians out with an immediate cash infusion that they say they need to sustain their practices, many of which have been crippled by the COVID-19 crisis.
In an April 7 letter to Secretary of US Department of Health and Human Services (HHS) Alex Azar, the AMA, backed by 137 medical groups, made the case for “immediate financial assistance” from the government for all US physicians and nurse practitioners and physician assistants enrolled in Medicare or Medicaid. These payments would be equal to roughly 1 month’s worth of prepandemic revenue from all payers.
Under the methodology laid out in the letter, HHS would use an individual clinician’s average monthly Medicare payment from October to December 2019 to determine their precrisis monthly revenue.
Because Medicare business generates an average of 35% of practice revenue in most specialties, the letter suggests that HHS triple the monthly Medicare payment to calculate the amount of emergency funding it should provide to each clinician.
The letter acknowledges that this approach wouldn’t work for certain specialties, such as psychiatry, allergy/immunology, obstetrics/gynecology, and pediatrics, which derive far less revenue from Medicare than other specialties do. These physicians’ payouts “should be adjusted upward accordingly,” the letter states.
“Physicians are continuing to put their patients’ needs first to combat this unprecedented public health emergency,” the AMA writes. “We urge you to support them against financial peril while they put their lives and businesses at risk.”
Other Emergency Funding Programs
These disbursements would be separate from the $30 billion in direct provider payments announced on April 7 by Seema Verma, the administrator of the Centers for Medicare and Medicaid Services (CMS). Because these payments are based on Medicare volume, the vast majority of this money is expected to go to hospitals.
The government is also providing financial support to hospitals, physicians, and other clinicians affected by the pandemic through CMS’s accelerated/advance payment program, as reported by Medscape Medical News. Physician practices can apply to receive upfront payments equal to 3 months’ worth of their historical Medicare payments, but they must pay back these loans, starting at 120 days after receiving them.
In addition, providers with less than 500 employees can apply for Small Business Administration (SBA) loans that were authorized by the CURES Act. If they use at least 75% of this money to cover payroll costs, the loans will be forgiven.
Medical leaders defended their request for direct physician relief in excess of what these three government programs are offering.
“From the very beginning, the AMA has been advocating for [financial] support for physician practices,” AMA President Patrice Harris, MD, told Medscape Medical News. “It’s not an either/or, it’s not a choice between hospitals or physician practices, it’s both.”
She made it clear that this applied not only to the direct payments that the CURES Act allocated to healthcare providers, but also to the SBA loans.
“We’ve been pleased to see support through the Small Business Administration, and we know that many practices have applied for loans,” Harris said. “We’ll review this, because physician practices have to be included.”
Thus far, she added, “I haven’t heard of anyone [in a medical practice] who has actually received a loan. We’ll be monitoring that, because that will be key.”
Likewise, Robert Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians (ACP), said he hadn’t heard of any practices receiving SBA loans, although many have applied.
What he has heard is that “people couldn’t even get through the SBA process and the website was freezing up. They also have to find a lender, submit documentation and get approved by the lender. And they’re competing with all the other small businesses” for a finite amount of money.
Doherty said it was unclear how many practices have received advance payments from CMS so far. CMS said it disbursed $34 billion in these payments in the first week of the program. These went to over 17,000 of the more than 25,000 applicants, CMS noted.
The ACP – which joined the AMA in its request to HHS – supports the advanced-payment program, Doherty added, but “a loan is a loan. You have to repay it. It brings in cash now, but it means you don’t have cash a few months from now. That’s different from what we’re recommending, which is an infusion of cash to practices that wouldn’t have to be repaid.”
Another advantage of the AMA-led proposal, he said, is its simplicity. It’s based on data that CMS already has, and it doesn’t require physicians to fill out forms or provide documents.
In contrast, he said, “We don’t think HHS would have the ability to process applications from thousands and thousands of physicians [for direct payments]. To create a situation where they’d have to review applications from physicians for funding out of that [CARES Act] emergency fund is probably almost impossible for HHS to administer effectively.”
Most Practices Need Help
While the medical societies’ letter makes a strong pitch for supporting physicians who are combating COVID-19, Harris and Doherty noted that physicians in all kinds of practice situations desperately need this help.
“We’ve heard from many physician practices that they have trouble making payroll,” Doherty said. “Many of them are not seeking any money out of the practices for themselves right now. They’re just trying to keep their staff employed. And some will shut their doors, unless there’s a significant and immediate infusion of money to them. From a healthcare capacity viewpoint, it’s not going to be to anyone’s benefit to see a substantial number of practices laying off staff or closing up entirely because they don’t have the money coming in to keep the doors open,” he said.
Harris agreed. “We’re hearing from practices large and small all over the country, including solo practices. Even the larger practices are losing revenue,” she pointed out. “They appropriately shut down their offices or reduced their hours. They didn’t want to contribute to the further spread of COVID-19.”
Rural practices and those launched by young physicians are facing especially difficult challenges, Harris added, and some may not make it.
It’s also important for policy makers to look ahead to what lies after the pandemic, she said. “We will come out of this, but when we come out of it there will be a lot of pent-up or unmet need where folks delayed necessary visits. Physicians and practices will have to be ready to go. If practices have to furlough some staff, it’s going to take time to ramp that up. So we’re glad to see support of physician practices so the infrastructure is strong when we start again.”
What happens if HHS turns down the medical societies’ request? “We’re hopeful that the [HHS] secretary will agree to what we’re asking,” Doherty said. While it’s always possible to ask Congress to intervene in the next stimulus bill, he said, that wouldn’t happen fast enough to get the money to physicians when they really need it.
This article first appeared on Medscape.com.
The American Medical Association (AMA) along with scores of specialty and state medical societies are asking the Trump administration to help the nation’s clinicians out with an immediate cash infusion that they say they need to sustain their practices, many of which have been crippled by the COVID-19 crisis.
In an April 7 letter to Secretary of US Department of Health and Human Services (HHS) Alex Azar, the AMA, backed by 137 medical groups, made the case for “immediate financial assistance” from the government for all US physicians and nurse practitioners and physician assistants enrolled in Medicare or Medicaid. These payments would be equal to roughly 1 month’s worth of prepandemic revenue from all payers.
Under the methodology laid out in the letter, HHS would use an individual clinician’s average monthly Medicare payment from October to December 2019 to determine their precrisis monthly revenue.
Because Medicare business generates an average of 35% of practice revenue in most specialties, the letter suggests that HHS triple the monthly Medicare payment to calculate the amount of emergency funding it should provide to each clinician.
The letter acknowledges that this approach wouldn’t work for certain specialties, such as psychiatry, allergy/immunology, obstetrics/gynecology, and pediatrics, which derive far less revenue from Medicare than other specialties do. These physicians’ payouts “should be adjusted upward accordingly,” the letter states.
“Physicians are continuing to put their patients’ needs first to combat this unprecedented public health emergency,” the AMA writes. “We urge you to support them against financial peril while they put their lives and businesses at risk.”
Other Emergency Funding Programs
These disbursements would be separate from the $30 billion in direct provider payments announced on April 7 by Seema Verma, the administrator of the Centers for Medicare and Medicaid Services (CMS). Because these payments are based on Medicare volume, the vast majority of this money is expected to go to hospitals.
The government is also providing financial support to hospitals, physicians, and other clinicians affected by the pandemic through CMS’s accelerated/advance payment program, as reported by Medscape Medical News. Physician practices can apply to receive upfront payments equal to 3 months’ worth of their historical Medicare payments, but they must pay back these loans, starting at 120 days after receiving them.
In addition, providers with less than 500 employees can apply for Small Business Administration (SBA) loans that were authorized by the CURES Act. If they use at least 75% of this money to cover payroll costs, the loans will be forgiven.
Medical leaders defended their request for direct physician relief in excess of what these three government programs are offering.
“From the very beginning, the AMA has been advocating for [financial] support for physician practices,” AMA President Patrice Harris, MD, told Medscape Medical News. “It’s not an either/or, it’s not a choice between hospitals or physician practices, it’s both.”
She made it clear that this applied not only to the direct payments that the CURES Act allocated to healthcare providers, but also to the SBA loans.
“We’ve been pleased to see support through the Small Business Administration, and we know that many practices have applied for loans,” Harris said. “We’ll review this, because physician practices have to be included.”
Thus far, she added, “I haven’t heard of anyone [in a medical practice] who has actually received a loan. We’ll be monitoring that, because that will be key.”
Likewise, Robert Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians (ACP), said he hadn’t heard of any practices receiving SBA loans, although many have applied.
What he has heard is that “people couldn’t even get through the SBA process and the website was freezing up. They also have to find a lender, submit documentation and get approved by the lender. And they’re competing with all the other small businesses” for a finite amount of money.
Doherty said it was unclear how many practices have received advance payments from CMS so far. CMS said it disbursed $34 billion in these payments in the first week of the program. These went to over 17,000 of the more than 25,000 applicants, CMS noted.
The ACP – which joined the AMA in its request to HHS – supports the advanced-payment program, Doherty added, but “a loan is a loan. You have to repay it. It brings in cash now, but it means you don’t have cash a few months from now. That’s different from what we’re recommending, which is an infusion of cash to practices that wouldn’t have to be repaid.”
Another advantage of the AMA-led proposal, he said, is its simplicity. It’s based on data that CMS already has, and it doesn’t require physicians to fill out forms or provide documents.
In contrast, he said, “We don’t think HHS would have the ability to process applications from thousands and thousands of physicians [for direct payments]. To create a situation where they’d have to review applications from physicians for funding out of that [CARES Act] emergency fund is probably almost impossible for HHS to administer effectively.”
Most Practices Need Help
While the medical societies’ letter makes a strong pitch for supporting physicians who are combating COVID-19, Harris and Doherty noted that physicians in all kinds of practice situations desperately need this help.
“We’ve heard from many physician practices that they have trouble making payroll,” Doherty said. “Many of them are not seeking any money out of the practices for themselves right now. They’re just trying to keep their staff employed. And some will shut their doors, unless there’s a significant and immediate infusion of money to them. From a healthcare capacity viewpoint, it’s not going to be to anyone’s benefit to see a substantial number of practices laying off staff or closing up entirely because they don’t have the money coming in to keep the doors open,” he said.
Harris agreed. “We’re hearing from practices large and small all over the country, including solo practices. Even the larger practices are losing revenue,” she pointed out. “They appropriately shut down their offices or reduced their hours. They didn’t want to contribute to the further spread of COVID-19.”
Rural practices and those launched by young physicians are facing especially difficult challenges, Harris added, and some may not make it.
It’s also important for policy makers to look ahead to what lies after the pandemic, she said. “We will come out of this, but when we come out of it there will be a lot of pent-up or unmet need where folks delayed necessary visits. Physicians and practices will have to be ready to go. If practices have to furlough some staff, it’s going to take time to ramp that up. So we’re glad to see support of physician practices so the infrastructure is strong when we start again.”
What happens if HHS turns down the medical societies’ request? “We’re hopeful that the [HHS] secretary will agree to what we’re asking,” Doherty said. While it’s always possible to ask Congress to intervene in the next stimulus bill, he said, that wouldn’t happen fast enough to get the money to physicians when they really need it.
This article first appeared on Medscape.com.
The American Medical Association (AMA) along with scores of specialty and state medical societies are asking the Trump administration to help the nation’s clinicians out with an immediate cash infusion that they say they need to sustain their practices, many of which have been crippled by the COVID-19 crisis.
In an April 7 letter to Secretary of US Department of Health and Human Services (HHS) Alex Azar, the AMA, backed by 137 medical groups, made the case for “immediate financial assistance” from the government for all US physicians and nurse practitioners and physician assistants enrolled in Medicare or Medicaid. These payments would be equal to roughly 1 month’s worth of prepandemic revenue from all payers.
Under the methodology laid out in the letter, HHS would use an individual clinician’s average monthly Medicare payment from October to December 2019 to determine their precrisis monthly revenue.
Because Medicare business generates an average of 35% of practice revenue in most specialties, the letter suggests that HHS triple the monthly Medicare payment to calculate the amount of emergency funding it should provide to each clinician.
The letter acknowledges that this approach wouldn’t work for certain specialties, such as psychiatry, allergy/immunology, obstetrics/gynecology, and pediatrics, which derive far less revenue from Medicare than other specialties do. These physicians’ payouts “should be adjusted upward accordingly,” the letter states.
“Physicians are continuing to put their patients’ needs first to combat this unprecedented public health emergency,” the AMA writes. “We urge you to support them against financial peril while they put their lives and businesses at risk.”
Other Emergency Funding Programs
These disbursements would be separate from the $30 billion in direct provider payments announced on April 7 by Seema Verma, the administrator of the Centers for Medicare and Medicaid Services (CMS). Because these payments are based on Medicare volume, the vast majority of this money is expected to go to hospitals.
The government is also providing financial support to hospitals, physicians, and other clinicians affected by the pandemic through CMS’s accelerated/advance payment program, as reported by Medscape Medical News. Physician practices can apply to receive upfront payments equal to 3 months’ worth of their historical Medicare payments, but they must pay back these loans, starting at 120 days after receiving them.
In addition, providers with less than 500 employees can apply for Small Business Administration (SBA) loans that were authorized by the CURES Act. If they use at least 75% of this money to cover payroll costs, the loans will be forgiven.
Medical leaders defended their request for direct physician relief in excess of what these three government programs are offering.
“From the very beginning, the AMA has been advocating for [financial] support for physician practices,” AMA President Patrice Harris, MD, told Medscape Medical News. “It’s not an either/or, it’s not a choice between hospitals or physician practices, it’s both.”
She made it clear that this applied not only to the direct payments that the CURES Act allocated to healthcare providers, but also to the SBA loans.
“We’ve been pleased to see support through the Small Business Administration, and we know that many practices have applied for loans,” Harris said. “We’ll review this, because physician practices have to be included.”
Thus far, she added, “I haven’t heard of anyone [in a medical practice] who has actually received a loan. We’ll be monitoring that, because that will be key.”
Likewise, Robert Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians (ACP), said he hadn’t heard of any practices receiving SBA loans, although many have applied.
What he has heard is that “people couldn’t even get through the SBA process and the website was freezing up. They also have to find a lender, submit documentation and get approved by the lender. And they’re competing with all the other small businesses” for a finite amount of money.
Doherty said it was unclear how many practices have received advance payments from CMS so far. CMS said it disbursed $34 billion in these payments in the first week of the program. These went to over 17,000 of the more than 25,000 applicants, CMS noted.
The ACP – which joined the AMA in its request to HHS – supports the advanced-payment program, Doherty added, but “a loan is a loan. You have to repay it. It brings in cash now, but it means you don’t have cash a few months from now. That’s different from what we’re recommending, which is an infusion of cash to practices that wouldn’t have to be repaid.”
Another advantage of the AMA-led proposal, he said, is its simplicity. It’s based on data that CMS already has, and it doesn’t require physicians to fill out forms or provide documents.
In contrast, he said, “We don’t think HHS would have the ability to process applications from thousands and thousands of physicians [for direct payments]. To create a situation where they’d have to review applications from physicians for funding out of that [CARES Act] emergency fund is probably almost impossible for HHS to administer effectively.”
Most Practices Need Help
While the medical societies’ letter makes a strong pitch for supporting physicians who are combating COVID-19, Harris and Doherty noted that physicians in all kinds of practice situations desperately need this help.
“We’ve heard from many physician practices that they have trouble making payroll,” Doherty said. “Many of them are not seeking any money out of the practices for themselves right now. They’re just trying to keep their staff employed. And some will shut their doors, unless there’s a significant and immediate infusion of money to them. From a healthcare capacity viewpoint, it’s not going to be to anyone’s benefit to see a substantial number of practices laying off staff or closing up entirely because they don’t have the money coming in to keep the doors open,” he said.
Harris agreed. “We’re hearing from practices large and small all over the country, including solo practices. Even the larger practices are losing revenue,” she pointed out. “They appropriately shut down their offices or reduced their hours. They didn’t want to contribute to the further spread of COVID-19.”
Rural practices and those launched by young physicians are facing especially difficult challenges, Harris added, and some may not make it.
It’s also important for policy makers to look ahead to what lies after the pandemic, she said. “We will come out of this, but when we come out of it there will be a lot of pent-up or unmet need where folks delayed necessary visits. Physicians and practices will have to be ready to go. If practices have to furlough some staff, it’s going to take time to ramp that up. So we’re glad to see support of physician practices so the infrastructure is strong when we start again.”
What happens if HHS turns down the medical societies’ request? “We’re hopeful that the [HHS] secretary will agree to what we’re asking,” Doherty said. While it’s always possible to ask Congress to intervene in the next stimulus bill, he said, that wouldn’t happen fast enough to get the money to physicians when they really need it.
This article first appeared on Medscape.com.
SARS-CoV-2 may confound seasons, persist in warmer months, report shows
Although conflicting, the available data indicate that SARS-CoV-2 could continue to spread in warmer spring and summer months in the US, according to a new report from the National Academies of Science, Engineering, and Medicine (NAS).
Current data suggest that the novel coronavirus may be transmitted less efficiently in higher temperatures and humidity, but the studies are not conclusive because of poor data quality, confounding factors, and the relatively short existence of the pandemic, which makes it difficult to determine its true course, writes David A. Relman, MD, a member of the NAS’ Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats, in a rapid expert consultation letter to the White House Office of Science and Technology Policy on April 7.
A number of factors could influence whether SARS-CoV-2 follows the same seasonal pattern as the influenza virus and other seasonal coronaviruses, which wane during warmer months, writes Relman, a professor of microbiology and immunology at Stanford University in California.
But he pointed out that previous coronavirus strains that have caused serious illness – SARS-CoV and MERS-CoV – “have not demonstrated any evidence of seasonality following their emergence.”
Relman cites an example from the current outbreak: “Given that countries currently in ‘summer’ climates, such as Australia and Iran, are experiencing rapid virus spread, a decrease in cases with increases in humidity and temperature elsewhere should not be assumed…Additional studies as the pandemic unfolds could shed more light on the effects of climate on transmission,” he writes.
And even if SARS-CoV-2 turns out to be less infectious in warmer months, “given the lack of host immunity globally, this reduction in transmission efficiency may not lead to a significant reduction in disease spread without the concomitant adoption of major public health interventions,” writes Relman.
Conflicting Data
Relman cites a handful of studies indicating that, on the one hand, SARS-CoV-2 has declined with increasing humidity and temperatures, but that conversely, infectivity has increased in warmer, more humid climates.
A recent study in China, published on the repository and international journal site SSRN, found that while increased temperatures and humidity decreased the infectivity, “the average R0 (R naught) was still close to 2 at maximum temperatures and humidity in their data set, suggesting that the virus will still spread exponentially at higher temperatures and humidity,” said Relman.
Several other studies found higher growth rates in temperate regions. One study, still in preprint on MedRxiv, looked at 310 geographic regions across 116 countries, and shows an inverse relationship between temperature and humidity and the incidence of COVID-19.
All the available studies so far have significant limitations, including limitation in time and location, confounding factors having to do with geography, access to and the quality of public health and health care systems, human behavior, and the availability of testing, said Relman.
However, he said, “it is useful to note that pandemic influenza strains have not exhibited the typical seasonal pattern of endemic/epidemic strains,” and, regardless of whether they started in a warmer or a cooler month, “all had a peak second wave approximately six months after the emergence in the human population.”
Worrisome Persistence on Masks
Seasonality can also be potentially gauged in the laboratory. Most of the studies on environmental persistence of SARS-CoV-2 have been conducted using virus grown in tissue culture. But that, too, is an imperfect method.
Virus disseminated into the environment from naturally infected humans likely has different survival properties than virus grown in culture, said Relman.
In addition, many labs cannot, or fail to, control and vary relative humidity, the committee letter noted. The aerosol studies so far have used humidity levels of 50% to 65%, which is more favorable to decay, while respiratory fluid is more likely to protect against infectivity, and the 20%-to-40% wintertime indoor humidity in temperate regions is more favorable for virus survival.
Even with these caveats, the committee cited worrisome studies on SARS-CoV-2 survival.
In a study published April 2 online in The Lancet, Hong Kong researchers reported significant reductions in virus in culture starting with temperatures at 37°C (98.6°F) or above.
On surfaces at a room temperature of 22°C (71.6°F) with a relative humidity of 65%, there was no infectious virus on printing paper or tissue papers after just 3 hours. It took 4 days for an infectious level to break down on glass and money, and 7 days for stainless steel and plastic. But after 7 days, investigators found 0.1% of the original inoculum on the outside of a surgical mask.
“The persistence of infectious virus on PPE is concerning,” writes Relman, noting that more studies are needed to guide healthcare workers, especially on what might be used to disinfect personal protective equipment “when they cannot be discarded after single use.”
Chad Roy, PhD, a researcher from Tulane University National Primate Research Center in New Orleans, Louisiana, told Relman by phone that in experiments where the virus was suspended as an aerosol at a temperature of 23°C (73.4° F) and about 50% humidity, SARS-CoV-2 had a longer half-life than the influenza virus, SARS-CoV-1, monkeypox virus, and Mycobacterium tuberculosis.
“This result is also concerning, but quite preliminary,” writes Relman.
This article first appeared on Medscape.com.
Although conflicting, the available data indicate that SARS-CoV-2 could continue to spread in warmer spring and summer months in the US, according to a new report from the National Academies of Science, Engineering, and Medicine (NAS).
Current data suggest that the novel coronavirus may be transmitted less efficiently in higher temperatures and humidity, but the studies are not conclusive because of poor data quality, confounding factors, and the relatively short existence of the pandemic, which makes it difficult to determine its true course, writes David A. Relman, MD, a member of the NAS’ Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats, in a rapid expert consultation letter to the White House Office of Science and Technology Policy on April 7.
A number of factors could influence whether SARS-CoV-2 follows the same seasonal pattern as the influenza virus and other seasonal coronaviruses, which wane during warmer months, writes Relman, a professor of microbiology and immunology at Stanford University in California.
But he pointed out that previous coronavirus strains that have caused serious illness – SARS-CoV and MERS-CoV – “have not demonstrated any evidence of seasonality following their emergence.”
Relman cites an example from the current outbreak: “Given that countries currently in ‘summer’ climates, such as Australia and Iran, are experiencing rapid virus spread, a decrease in cases with increases in humidity and temperature elsewhere should not be assumed…Additional studies as the pandemic unfolds could shed more light on the effects of climate on transmission,” he writes.
And even if SARS-CoV-2 turns out to be less infectious in warmer months, “given the lack of host immunity globally, this reduction in transmission efficiency may not lead to a significant reduction in disease spread without the concomitant adoption of major public health interventions,” writes Relman.
Conflicting Data
Relman cites a handful of studies indicating that, on the one hand, SARS-CoV-2 has declined with increasing humidity and temperatures, but that conversely, infectivity has increased in warmer, more humid climates.
A recent study in China, published on the repository and international journal site SSRN, found that while increased temperatures and humidity decreased the infectivity, “the average R0 (R naught) was still close to 2 at maximum temperatures and humidity in their data set, suggesting that the virus will still spread exponentially at higher temperatures and humidity,” said Relman.
Several other studies found higher growth rates in temperate regions. One study, still in preprint on MedRxiv, looked at 310 geographic regions across 116 countries, and shows an inverse relationship between temperature and humidity and the incidence of COVID-19.
All the available studies so far have significant limitations, including limitation in time and location, confounding factors having to do with geography, access to and the quality of public health and health care systems, human behavior, and the availability of testing, said Relman.
However, he said, “it is useful to note that pandemic influenza strains have not exhibited the typical seasonal pattern of endemic/epidemic strains,” and, regardless of whether they started in a warmer or a cooler month, “all had a peak second wave approximately six months after the emergence in the human population.”
Worrisome Persistence on Masks
Seasonality can also be potentially gauged in the laboratory. Most of the studies on environmental persistence of SARS-CoV-2 have been conducted using virus grown in tissue culture. But that, too, is an imperfect method.
Virus disseminated into the environment from naturally infected humans likely has different survival properties than virus grown in culture, said Relman.
In addition, many labs cannot, or fail to, control and vary relative humidity, the committee letter noted. The aerosol studies so far have used humidity levels of 50% to 65%, which is more favorable to decay, while respiratory fluid is more likely to protect against infectivity, and the 20%-to-40% wintertime indoor humidity in temperate regions is more favorable for virus survival.
Even with these caveats, the committee cited worrisome studies on SARS-CoV-2 survival.
In a study published April 2 online in The Lancet, Hong Kong researchers reported significant reductions in virus in culture starting with temperatures at 37°C (98.6°F) or above.
On surfaces at a room temperature of 22°C (71.6°F) with a relative humidity of 65%, there was no infectious virus on printing paper or tissue papers after just 3 hours. It took 4 days for an infectious level to break down on glass and money, and 7 days for stainless steel and plastic. But after 7 days, investigators found 0.1% of the original inoculum on the outside of a surgical mask.
“The persistence of infectious virus on PPE is concerning,” writes Relman, noting that more studies are needed to guide healthcare workers, especially on what might be used to disinfect personal protective equipment “when they cannot be discarded after single use.”
Chad Roy, PhD, a researcher from Tulane University National Primate Research Center in New Orleans, Louisiana, told Relman by phone that in experiments where the virus was suspended as an aerosol at a temperature of 23°C (73.4° F) and about 50% humidity, SARS-CoV-2 had a longer half-life than the influenza virus, SARS-CoV-1, monkeypox virus, and Mycobacterium tuberculosis.
“This result is also concerning, but quite preliminary,” writes Relman.
This article first appeared on Medscape.com.
Although conflicting, the available data indicate that SARS-CoV-2 could continue to spread in warmer spring and summer months in the US, according to a new report from the National Academies of Science, Engineering, and Medicine (NAS).
Current data suggest that the novel coronavirus may be transmitted less efficiently in higher temperatures and humidity, but the studies are not conclusive because of poor data quality, confounding factors, and the relatively short existence of the pandemic, which makes it difficult to determine its true course, writes David A. Relman, MD, a member of the NAS’ Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats, in a rapid expert consultation letter to the White House Office of Science and Technology Policy on April 7.
A number of factors could influence whether SARS-CoV-2 follows the same seasonal pattern as the influenza virus and other seasonal coronaviruses, which wane during warmer months, writes Relman, a professor of microbiology and immunology at Stanford University in California.
But he pointed out that previous coronavirus strains that have caused serious illness – SARS-CoV and MERS-CoV – “have not demonstrated any evidence of seasonality following their emergence.”
Relman cites an example from the current outbreak: “Given that countries currently in ‘summer’ climates, such as Australia and Iran, are experiencing rapid virus spread, a decrease in cases with increases in humidity and temperature elsewhere should not be assumed…Additional studies as the pandemic unfolds could shed more light on the effects of climate on transmission,” he writes.
And even if SARS-CoV-2 turns out to be less infectious in warmer months, “given the lack of host immunity globally, this reduction in transmission efficiency may not lead to a significant reduction in disease spread without the concomitant adoption of major public health interventions,” writes Relman.
Conflicting Data
Relman cites a handful of studies indicating that, on the one hand, SARS-CoV-2 has declined with increasing humidity and temperatures, but that conversely, infectivity has increased in warmer, more humid climates.
A recent study in China, published on the repository and international journal site SSRN, found that while increased temperatures and humidity decreased the infectivity, “the average R0 (R naught) was still close to 2 at maximum temperatures and humidity in their data set, suggesting that the virus will still spread exponentially at higher temperatures and humidity,” said Relman.
Several other studies found higher growth rates in temperate regions. One study, still in preprint on MedRxiv, looked at 310 geographic regions across 116 countries, and shows an inverse relationship between temperature and humidity and the incidence of COVID-19.
All the available studies so far have significant limitations, including limitation in time and location, confounding factors having to do with geography, access to and the quality of public health and health care systems, human behavior, and the availability of testing, said Relman.
However, he said, “it is useful to note that pandemic influenza strains have not exhibited the typical seasonal pattern of endemic/epidemic strains,” and, regardless of whether they started in a warmer or a cooler month, “all had a peak second wave approximately six months after the emergence in the human population.”
Worrisome Persistence on Masks
Seasonality can also be potentially gauged in the laboratory. Most of the studies on environmental persistence of SARS-CoV-2 have been conducted using virus grown in tissue culture. But that, too, is an imperfect method.
Virus disseminated into the environment from naturally infected humans likely has different survival properties than virus grown in culture, said Relman.
In addition, many labs cannot, or fail to, control and vary relative humidity, the committee letter noted. The aerosol studies so far have used humidity levels of 50% to 65%, which is more favorable to decay, while respiratory fluid is more likely to protect against infectivity, and the 20%-to-40% wintertime indoor humidity in temperate regions is more favorable for virus survival.
Even with these caveats, the committee cited worrisome studies on SARS-CoV-2 survival.
In a study published April 2 online in The Lancet, Hong Kong researchers reported significant reductions in virus in culture starting with temperatures at 37°C (98.6°F) or above.
On surfaces at a room temperature of 22°C (71.6°F) with a relative humidity of 65%, there was no infectious virus on printing paper or tissue papers after just 3 hours. It took 4 days for an infectious level to break down on glass and money, and 7 days for stainless steel and plastic. But after 7 days, investigators found 0.1% of the original inoculum on the outside of a surgical mask.
“The persistence of infectious virus on PPE is concerning,” writes Relman, noting that more studies are needed to guide healthcare workers, especially on what might be used to disinfect personal protective equipment “when they cannot be discarded after single use.”
Chad Roy, PhD, a researcher from Tulane University National Primate Research Center in New Orleans, Louisiana, told Relman by phone that in experiments where the virus was suspended as an aerosol at a temperature of 23°C (73.4° F) and about 50% humidity, SARS-CoV-2 had a longer half-life than the influenza virus, SARS-CoV-1, monkeypox virus, and Mycobacterium tuberculosis.
“This result is also concerning, but quite preliminary,” writes Relman.
This article first appeared on Medscape.com.