User login
In praise of parents and children
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.

Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”

This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at pdnews@mdedge.com.
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.
Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”
This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at pdnews@mdedge.com.
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.
Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”
This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at pdnews@mdedge.com.
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
2019-2020 flu season ends with ‘very high’ activity in New Jersey
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
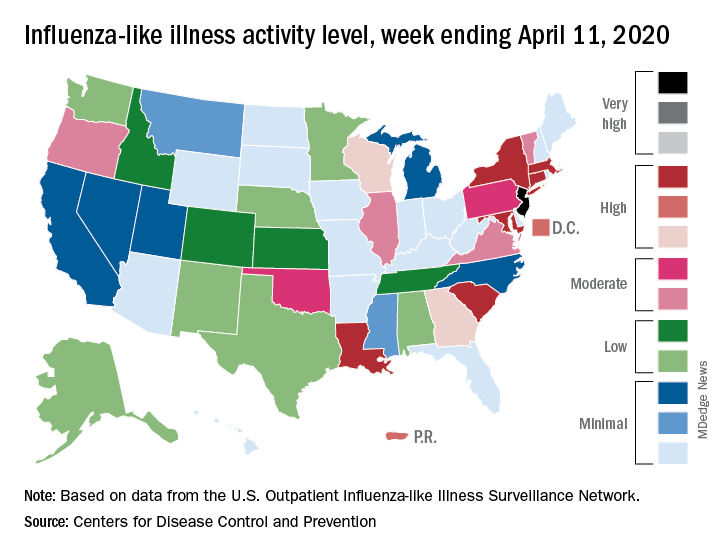
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
N.Y. universal testing: Many COVID-19+ pregnant women are asymptomatic
based on data from 215 pregnant women in New York City.

“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.

However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.

“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
based on data from 215 pregnant women in New York City.
“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.
However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.
“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
based on data from 215 pregnant women in New York City.
“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.
However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.
“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Universal COVID-19 testing for pregnant women entering hospitals for delivery could better protect patients and staff.
Major finding: Approximately 88% of 33 pregnant women who tested positive for COVID-19 infection at hospital admission were asymptomatic; about 14% of the 215 women overall tested positive for the novel coronavirus.
Study details: The data come from a review of 215 pregnant women who delivered infants between March 22 and April 4, 2020, in New York City.
Disclosures: The authors had no financial conflicts to disclose.
Source: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
Infectious disease experts say testing is key to reopening
The key to opening up the American economy rests on the ability to conduct mass testing, according to the Infectious Diseases Society of America (IDSA).
As policymakers weigh how to safely reopen parts of the United States, the IDSA, along with its HIV Medicine Association, issued a set of recommendations outlining the steps that would be necessary in order to begin easing physical distancing measures.
“A stepwise approach to reopening should reflect early diagnosis and enhanced surveillance for COVID-19 cases, linkage of cases to appropriate levels of care, isolation and/or quarantine, contact tracing, and data processing capabilities for state and local public health departments,” according to the recommendation document.
Some of the recommended steps include the following:
- Widespread testing and surveillance, including use of validated nucleic acid amplification assays and anti–SARS-CoV-2 antibody detection.
- The ability to diagnose, treat, and isolate individuals with COVID-19.
- Scaling up of health care capacity and supplies to manage recurrent episodic outbreaks.
- Maintaining a degree of physical distancing to prevent recurrent outbreaks, including use of masks, limiting gatherings, and continued distancing for susceptible adults.
“The recommendations stress that physical distancing policy changes must be based on relevant data and adequate public health resources and capacities and calls for a rolling and incremental approach to lifting these restrictions, ” Thomas File Jr., MD, IDSA president and a professor at Northeastern Ohio Universities, Rootstown, said during an April 17 press briefing.
The rolling approach “must reflect state and regional capacities for diagnosing, isolating, and treating people with the virus, tracing their contacts, protecting health care workers, and addressing the needs of populations disproportionately affected by COVID-19,” he continued.
In order to fully lift physical distancing restrictions, there would need to be effective treatments for COVID-19 and a protective vaccine that can be deployed to key at-risk populations, according to the recommendations.
During the call, Tina Q. Tan, MD, professor of pediatrics at Northwestern University, Chicago, and a member of the IDSA board of directors, said that easing social distancing requirements requires comprehensive data and that “one of the major missing data points” is the number of people who are currently infected or have been infected. She warned that easing restrictions too soon could have “disastrous consequences,” including an increase in spread of infection, hospitalization, and death rates, as well as overwhelming health care facilities.
“In order to reopen, we have to have the ability to safely, successfully, and rapidly diagnose and treat, as well as isolate, individuals with COVID-19, as well as track their contacts,” she said.
The implementation of more widespread, comprehensive testing would better enable targeting of resources, such as personal protective equipment, ICU beds, and ventilators, Dr. Tan said. “This is needed in order to ensure that, if there is an outbreak and it does occur again, the health care system and the first responders are ready for this,” she said.
The key to opening up the American economy rests on the ability to conduct mass testing, according to the Infectious Diseases Society of America (IDSA).
As policymakers weigh how to safely reopen parts of the United States, the IDSA, along with its HIV Medicine Association, issued a set of recommendations outlining the steps that would be necessary in order to begin easing physical distancing measures.
“A stepwise approach to reopening should reflect early diagnosis and enhanced surveillance for COVID-19 cases, linkage of cases to appropriate levels of care, isolation and/or quarantine, contact tracing, and data processing capabilities for state and local public health departments,” according to the recommendation document.
Some of the recommended steps include the following:
- Widespread testing and surveillance, including use of validated nucleic acid amplification assays and anti–SARS-CoV-2 antibody detection.
- The ability to diagnose, treat, and isolate individuals with COVID-19.
- Scaling up of health care capacity and supplies to manage recurrent episodic outbreaks.
- Maintaining a degree of physical distancing to prevent recurrent outbreaks, including use of masks, limiting gatherings, and continued distancing for susceptible adults.
“The recommendations stress that physical distancing policy changes must be based on relevant data and adequate public health resources and capacities and calls for a rolling and incremental approach to lifting these restrictions, ” Thomas File Jr., MD, IDSA president and a professor at Northeastern Ohio Universities, Rootstown, said during an April 17 press briefing.
The rolling approach “must reflect state and regional capacities for diagnosing, isolating, and treating people with the virus, tracing their contacts, protecting health care workers, and addressing the needs of populations disproportionately affected by COVID-19,” he continued.
In order to fully lift physical distancing restrictions, there would need to be effective treatments for COVID-19 and a protective vaccine that can be deployed to key at-risk populations, according to the recommendations.
During the call, Tina Q. Tan, MD, professor of pediatrics at Northwestern University, Chicago, and a member of the IDSA board of directors, said that easing social distancing requirements requires comprehensive data and that “one of the major missing data points” is the number of people who are currently infected or have been infected. She warned that easing restrictions too soon could have “disastrous consequences,” including an increase in spread of infection, hospitalization, and death rates, as well as overwhelming health care facilities.
“In order to reopen, we have to have the ability to safely, successfully, and rapidly diagnose and treat, as well as isolate, individuals with COVID-19, as well as track their contacts,” she said.
The implementation of more widespread, comprehensive testing would better enable targeting of resources, such as personal protective equipment, ICU beds, and ventilators, Dr. Tan said. “This is needed in order to ensure that, if there is an outbreak and it does occur again, the health care system and the first responders are ready for this,” she said.
The key to opening up the American economy rests on the ability to conduct mass testing, according to the Infectious Diseases Society of America (IDSA).
As policymakers weigh how to safely reopen parts of the United States, the IDSA, along with its HIV Medicine Association, issued a set of recommendations outlining the steps that would be necessary in order to begin easing physical distancing measures.
“A stepwise approach to reopening should reflect early diagnosis and enhanced surveillance for COVID-19 cases, linkage of cases to appropriate levels of care, isolation and/or quarantine, contact tracing, and data processing capabilities for state and local public health departments,” according to the recommendation document.
Some of the recommended steps include the following:
- Widespread testing and surveillance, including use of validated nucleic acid amplification assays and anti–SARS-CoV-2 antibody detection.
- The ability to diagnose, treat, and isolate individuals with COVID-19.
- Scaling up of health care capacity and supplies to manage recurrent episodic outbreaks.
- Maintaining a degree of physical distancing to prevent recurrent outbreaks, including use of masks, limiting gatherings, and continued distancing for susceptible adults.
“The recommendations stress that physical distancing policy changes must be based on relevant data and adequate public health resources and capacities and calls for a rolling and incremental approach to lifting these restrictions, ” Thomas File Jr., MD, IDSA president and a professor at Northeastern Ohio Universities, Rootstown, said during an April 17 press briefing.
The rolling approach “must reflect state and regional capacities for diagnosing, isolating, and treating people with the virus, tracing their contacts, protecting health care workers, and addressing the needs of populations disproportionately affected by COVID-19,” he continued.
In order to fully lift physical distancing restrictions, there would need to be effective treatments for COVID-19 and a protective vaccine that can be deployed to key at-risk populations, according to the recommendations.
During the call, Tina Q. Tan, MD, professor of pediatrics at Northwestern University, Chicago, and a member of the IDSA board of directors, said that easing social distancing requirements requires comprehensive data and that “one of the major missing data points” is the number of people who are currently infected or have been infected. She warned that easing restrictions too soon could have “disastrous consequences,” including an increase in spread of infection, hospitalization, and death rates, as well as overwhelming health care facilities.
“In order to reopen, we have to have the ability to safely, successfully, and rapidly diagnose and treat, as well as isolate, individuals with COVID-19, as well as track their contacts,” she said.
The implementation of more widespread, comprehensive testing would better enable targeting of resources, such as personal protective equipment, ICU beds, and ventilators, Dr. Tan said. “This is needed in order to ensure that, if there is an outbreak and it does occur again, the health care system and the first responders are ready for this,” she said.
How to sanitize N95 masks for reuse: NIH study
Exposing contaminated N95 respirators to vaporized hydrogen peroxide (VHP) or ultraviolet (UV) light appears to eliminate the SARS-CoV-2 virus from the material and preserve the integrity of the masks fit for up to three uses, a National Institutes of Health (NIH) study shows.
Dry heat (70° C) was also found to eliminate the virus on masks but was effective for two uses instead of three.
Robert Fischer, PhD, with the National Institute of Allergy and Infectious Diseases in Hamilton, Montana, and colleagues posted the findings on a preprint server on April 15. The paper has not yet been peer reviewed.
Four methods tested
Fischer and colleagues compared four methods for decontaminating the masks, which are designed for one-time use: UV radiation (260-285 nm); 70° C dry heat; 70% ethanol spray; and VHP.
For each method, the researchers compared the rate at which SARS-CoV-2 is inactivated on N95 filter fabric to that on stainless steel.
All four methods eliminated detectable SARS-CoV-2 virus from the fabric test samples, though the time needed for decontamination varied. VHP was the quickest, requiring 10 minutes. Dry heat and UV light each required approximately 60 minutes. Ethanol required an intermediate amount of time.
To test durability over three uses, the researchers treated intact, clean masks with the same decontamination method and assessed function via quantitative fit testing.
Volunteers from the Rocky Mountain laboratory wore the masks for 2 hours to test fit and seal.
The researchers found that masks that had been decontaminated with ethanol spray did not function effectively after decontamination, and they did not recommend use of that method.
By contrast, masks decontaminated with UV and VHP could be used up to three times and function properly. Masks decontaminated with dry heat could be used two times before function declined.
“Our results indicate that N95 respirators can be decontaminated and reused in times of shortage for up to three times for UV and HPV, and up to two times for dry heat,” the authors write. “However, utmost care should be given to ensure the proper functioning of the N95 respirator after each decontamination using readily available qualitative fit testing tools and to ensure that treatments are carried out for sufficient time to achieve desired risk-reduction.”
Reassurance for clinicians
The results will reassure clinicians, many of whom are already using these decontamination methods, Ravina Kullar, PharmD, MPH, an infectious disease expert with the Infectious Diseases Society of America, told Medscape Medical News.
Kullar, who is also an adjunct faculty member at the David Geffen School of Medicine of the University of California, Los Angeles, said the most widely used methods have been UV light and VPH.
UV light has been used for years to decontaminate rooms, she said. She also said that so far, supplies of hydrogen peroxide are adequate.
A shortcoming of the study, Kullar said, is that it tested the masks for only 2 hours, whereas in clinical practice, they are being worn for much longer periods.
After the study is peer reviewed, the Centers for Disease Control and Prevention (CDC) may update its recommendations, she said.
So far, she noted, the CDC has not approved any method for decontaminating masks, “but it has said that it does not object to using these sterilizers, disinfectants, devices, and air purifiers for effectively killing this virus.”
Safe, multiple use of the masks is critical in the COVID-19 crisis, she said.
“We have to look at other mechanisms to keep these N95 respirators in use when there’s such a shortage,” she said.
Integrity of the fit was an important factor in the study.
“All health care workers have to go through a fitting to have that mask fitted appropriately. That’s why these N95s are only approved for health care professionals, not the lay public,” she said.
The study was supported by the National Institutes of Health; the Defense Advanced Research Projects Agency; the University of California, Los Angeles; the US National Science Foundation; and the US Department of Defense.
This article first appeared on Medscape.com.
Exposing contaminated N95 respirators to vaporized hydrogen peroxide (VHP) or ultraviolet (UV) light appears to eliminate the SARS-CoV-2 virus from the material and preserve the integrity of the masks fit for up to three uses, a National Institutes of Health (NIH) study shows.
Dry heat (70° C) was also found to eliminate the virus on masks but was effective for two uses instead of three.
Robert Fischer, PhD, with the National Institute of Allergy and Infectious Diseases in Hamilton, Montana, and colleagues posted the findings on a preprint server on April 15. The paper has not yet been peer reviewed.
Four methods tested
Fischer and colleagues compared four methods for decontaminating the masks, which are designed for one-time use: UV radiation (260-285 nm); 70° C dry heat; 70% ethanol spray; and VHP.
For each method, the researchers compared the rate at which SARS-CoV-2 is inactivated on N95 filter fabric to that on stainless steel.
All four methods eliminated detectable SARS-CoV-2 virus from the fabric test samples, though the time needed for decontamination varied. VHP was the quickest, requiring 10 minutes. Dry heat and UV light each required approximately 60 minutes. Ethanol required an intermediate amount of time.
To test durability over three uses, the researchers treated intact, clean masks with the same decontamination method and assessed function via quantitative fit testing.
Volunteers from the Rocky Mountain laboratory wore the masks for 2 hours to test fit and seal.
The researchers found that masks that had been decontaminated with ethanol spray did not function effectively after decontamination, and they did not recommend use of that method.
By contrast, masks decontaminated with UV and VHP could be used up to three times and function properly. Masks decontaminated with dry heat could be used two times before function declined.
“Our results indicate that N95 respirators can be decontaminated and reused in times of shortage for up to three times for UV and HPV, and up to two times for dry heat,” the authors write. “However, utmost care should be given to ensure the proper functioning of the N95 respirator after each decontamination using readily available qualitative fit testing tools and to ensure that treatments are carried out for sufficient time to achieve desired risk-reduction.”
Reassurance for clinicians
The results will reassure clinicians, many of whom are already using these decontamination methods, Ravina Kullar, PharmD, MPH, an infectious disease expert with the Infectious Diseases Society of America, told Medscape Medical News.
Kullar, who is also an adjunct faculty member at the David Geffen School of Medicine of the University of California, Los Angeles, said the most widely used methods have been UV light and VPH.
UV light has been used for years to decontaminate rooms, she said. She also said that so far, supplies of hydrogen peroxide are adequate.
A shortcoming of the study, Kullar said, is that it tested the masks for only 2 hours, whereas in clinical practice, they are being worn for much longer periods.
After the study is peer reviewed, the Centers for Disease Control and Prevention (CDC) may update its recommendations, she said.
So far, she noted, the CDC has not approved any method for decontaminating masks, “but it has said that it does not object to using these sterilizers, disinfectants, devices, and air purifiers for effectively killing this virus.”
Safe, multiple use of the masks is critical in the COVID-19 crisis, she said.
“We have to look at other mechanisms to keep these N95 respirators in use when there’s such a shortage,” she said.
Integrity of the fit was an important factor in the study.
“All health care workers have to go through a fitting to have that mask fitted appropriately. That’s why these N95s are only approved for health care professionals, not the lay public,” she said.
The study was supported by the National Institutes of Health; the Defense Advanced Research Projects Agency; the University of California, Los Angeles; the US National Science Foundation; and the US Department of Defense.
This article first appeared on Medscape.com.
Exposing contaminated N95 respirators to vaporized hydrogen peroxide (VHP) or ultraviolet (UV) light appears to eliminate the SARS-CoV-2 virus from the material and preserve the integrity of the masks fit for up to three uses, a National Institutes of Health (NIH) study shows.
Dry heat (70° C) was also found to eliminate the virus on masks but was effective for two uses instead of three.
Robert Fischer, PhD, with the National Institute of Allergy and Infectious Diseases in Hamilton, Montana, and colleagues posted the findings on a preprint server on April 15. The paper has not yet been peer reviewed.
Four methods tested
Fischer and colleagues compared four methods for decontaminating the masks, which are designed for one-time use: UV radiation (260-285 nm); 70° C dry heat; 70% ethanol spray; and VHP.
For each method, the researchers compared the rate at which SARS-CoV-2 is inactivated on N95 filter fabric to that on stainless steel.
All four methods eliminated detectable SARS-CoV-2 virus from the fabric test samples, though the time needed for decontamination varied. VHP was the quickest, requiring 10 minutes. Dry heat and UV light each required approximately 60 minutes. Ethanol required an intermediate amount of time.
To test durability over three uses, the researchers treated intact, clean masks with the same decontamination method and assessed function via quantitative fit testing.
Volunteers from the Rocky Mountain laboratory wore the masks for 2 hours to test fit and seal.
The researchers found that masks that had been decontaminated with ethanol spray did not function effectively after decontamination, and they did not recommend use of that method.
By contrast, masks decontaminated with UV and VHP could be used up to three times and function properly. Masks decontaminated with dry heat could be used two times before function declined.
“Our results indicate that N95 respirators can be decontaminated and reused in times of shortage for up to three times for UV and HPV, and up to two times for dry heat,” the authors write. “However, utmost care should be given to ensure the proper functioning of the N95 respirator after each decontamination using readily available qualitative fit testing tools and to ensure that treatments are carried out for sufficient time to achieve desired risk-reduction.”
Reassurance for clinicians
The results will reassure clinicians, many of whom are already using these decontamination methods, Ravina Kullar, PharmD, MPH, an infectious disease expert with the Infectious Diseases Society of America, told Medscape Medical News.
Kullar, who is also an adjunct faculty member at the David Geffen School of Medicine of the University of California, Los Angeles, said the most widely used methods have been UV light and VPH.
UV light has been used for years to decontaminate rooms, she said. She also said that so far, supplies of hydrogen peroxide are adequate.
A shortcoming of the study, Kullar said, is that it tested the masks for only 2 hours, whereas in clinical practice, they are being worn for much longer periods.
After the study is peer reviewed, the Centers for Disease Control and Prevention (CDC) may update its recommendations, she said.
So far, she noted, the CDC has not approved any method for decontaminating masks, “but it has said that it does not object to using these sterilizers, disinfectants, devices, and air purifiers for effectively killing this virus.”
Safe, multiple use of the masks is critical in the COVID-19 crisis, she said.
“We have to look at other mechanisms to keep these N95 respirators in use when there’s such a shortage,” she said.
Integrity of the fit was an important factor in the study.
“All health care workers have to go through a fitting to have that mask fitted appropriately. That’s why these N95s are only approved for health care professionals, not the lay public,” she said.
The study was supported by the National Institutes of Health; the Defense Advanced Research Projects Agency; the University of California, Los Angeles; the US National Science Foundation; and the US Department of Defense.
This article first appeared on Medscape.com.
Protean manifestations of COVID-19: “Our ignorance is profound”

Although a cause-and-effect relationship is unknown, people with the virus have presented with or developed heart disease, acute liver injury, ongoing GI issues, skin manifestations, neurologic damage, and other problems, especially among sicker people.
For example, French physicians described an association with encephalopathy, agitation, confusion, and corticospinal tract signs among 58 people hospitalized with acute respiratory distress (N Engl J Med. 2020 Apr 15. doi: 10.1056/NEJMc2008597).
In particular, Yale New Haven (Conn.) Hospital is dealing with unexpected complications up close. Almost half of the beds there are occupied by COVID-19 patients. Over 100 people are in the ICU, and almost 70 intubated. Of the more than 750 COVID admissions so far, only about 350 have been discharged. “Even in a bad flu season, you never see something like this; it’s just unheard of,” said Harlan Krumholz, MD, a Yale cardiologist and professor of medicine helping lead the efforts there.
Kidney injuries prominent
“When they get to the ICU, we are seeing lots of people with acute kidney injuries; lots of people developing endocrine problems; people having blood sugar control issues, coagulation issues, blood clots. We are just waking up to the wide range of ways this virus can affect people. Our ignorance is profound,” Dr. Krumholz said, but physicians “recognize that this thing has the capability of attacking almost every single organ system, and it may or may not present with respiratory symptoms.”

It’s a similar story at Mt. Sinai South Nassau, a hospital in Oceanside, N.Y. “We’ve seen a lot of renal injury in people having complications, a lot of acute dialysis,” but it’s unclear how much is caused by the virus and how much is simply because people are so sick, said Aaron Glatt, MD, infectious disease professor and chair of medicine at the hospital. However, he said things are looking brighter than at Yale.
“We are not seeing the same level of increase in cases that we had previously, and we are starting to see extubations and discharges. We’ve treated a number of patients with plasma therapy, and hopefully that will be of benefit. We’ve seen some response to” the immunosuppressive “tocilizumab [Actemra], and a lot of response to very good respiratory therapy. I think we are starting to flatten the curve,” Dr. Glatt said.
“Look for tricky symptoms”
The growing awareness of COVID’s protean manifestations is evident in Medscape’s Consult forum, an online community where physicians and medical students share information and seek advice; there’s been over 200 COVID-19 cases and questions since January.
Early on, traffic was mostly about typical pulmonary presentations, but lately it’s shifted to nonrespiratory involvement. Physicians want to know if what they are seeing is related to the virus, and if other people are seeing the same things.
There’s a case on Consult of a 37-year-old man with stomach pain, vomiting, and diarrhea, but no respiratory symptoms and a positive COVID test. A chest CT incidental to his abdominal scan revealed significant bilateral lung involvement.
A 69-year-old woman with a history of laparotomy and new onset intestinal subocclusion had only adhesions on a subsequent exploratory laparotomy, and was doing okay otherwise. She suddenly went into respiratory failure with progressive bradycardia and died 3 days later. Aspiration pneumonia, pulmonary embolism, and MI had been ruled out. “The pattern of cardiovascular failure was in favor of myocarditis, but we don’t have any other clue,” the physician said after describing a second similar case.
Another doctor on the forum reported elevated cardiac enzymes without coronary artery obstruction in a positive patient who went into shock, with an ejection fraction of 40% and markedly increased heart wall thickness, but no lung involvement. There are also two cases of idiopathic thrombocytopenia without fever of hypoxia.
An Italian gastroenterologist said: “Look for tricky symptoms.” Expand “patient history, asking about the sudden occurrence of dysgeusia and/or anosmia. These symptoms have become my guiding diagnostic light” in Verona. “Most patients become nauseated, [and] the taste of any food is unbearable. When I find these symptoms by history, the patient is COVID positive 100%.”
‘Make sure that they didn’t die in vain’
There was interest in those and other reports on Consult, and comments from physicians who have theories, but no certain answers about what is, and is not, caused by the virus.
Direct viral attack is likely a part of it, said Stanley Perlman, MD, PhD, a professor of microbiology and immunology at the University of Iowa, Iowa City.
The ACE2 receptor the virus uses to enter cells is common in many organs, plus there were extrapulmonary manifestations with severe acute respiratory syndrome (SARS), another pandemic caused by a zoonotic coronavirus almost 20 years ago. At least with SARS, “many organs were infected when examined at autopsy,” he said.

The body’s inflammatory response is almost certainly also in play. Progressive derangements in inflammatory markers – C-reactive protein, D-dimer, ferritin – correlate with worse prognosis, and “the cytokine storm that occurs in these patients can lead to a degree of encephalopathy, myocarditis, liver impairment, and kidney impairment; multiorgan dysfunction, in other words,” said William Shaffner, MD, a professor of preventive medicine and infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn.
But in some cases, the virus might simply be a bystander to an unrelated disease process; in others, the experimental treatments being used might cause problems. Indeed, cardiology groups recently warned of torsade de pointes – a dangerously abnormal heart rhythm – with hydroxychloroquine and azithromycin.
“We think it’s some combination,” but don’t really know, Dr. Krumholz said. In the meantime, “we are forced to treat patients by instinct and first principles,” and long-term sequelae are unknown. “We don’t want to be in this position for long.”
To that end, he said, “this is the time for us all to hold hands and be together because we need to learn rapidly from each other. Our job is both to care for the people in front of us and make sure that they didn’t die in vain, that the experience they had is funneled into a larger set of data to make sure the next person is better off.”
Although a cause-and-effect relationship is unknown, people with the virus have presented with or developed heart disease, acute liver injury, ongoing GI issues, skin manifestations, neurologic damage, and other problems, especially among sicker people.
For example, French physicians described an association with encephalopathy, agitation, confusion, and corticospinal tract signs among 58 people hospitalized with acute respiratory distress (N Engl J Med. 2020 Apr 15. doi: 10.1056/NEJMc2008597).
In particular, Yale New Haven (Conn.) Hospital is dealing with unexpected complications up close. Almost half of the beds there are occupied by COVID-19 patients. Over 100 people are in the ICU, and almost 70 intubated. Of the more than 750 COVID admissions so far, only about 350 have been discharged. “Even in a bad flu season, you never see something like this; it’s just unheard of,” said Harlan Krumholz, MD, a Yale cardiologist and professor of medicine helping lead the efforts there.
Kidney injuries prominent
“When they get to the ICU, we are seeing lots of people with acute kidney injuries; lots of people developing endocrine problems; people having blood sugar control issues, coagulation issues, blood clots. We are just waking up to the wide range of ways this virus can affect people. Our ignorance is profound,” Dr. Krumholz said, but physicians “recognize that this thing has the capability of attacking almost every single organ system, and it may or may not present with respiratory symptoms.”
It’s a similar story at Mt. Sinai South Nassau, a hospital in Oceanside, N.Y. “We’ve seen a lot of renal injury in people having complications, a lot of acute dialysis,” but it’s unclear how much is caused by the virus and how much is simply because people are so sick, said Aaron Glatt, MD, infectious disease professor and chair of medicine at the hospital. However, he said things are looking brighter than at Yale.
“We are not seeing the same level of increase in cases that we had previously, and we are starting to see extubations and discharges. We’ve treated a number of patients with plasma therapy, and hopefully that will be of benefit. We’ve seen some response to” the immunosuppressive “tocilizumab [Actemra], and a lot of response to very good respiratory therapy. I think we are starting to flatten the curve,” Dr. Glatt said.
“Look for tricky symptoms”
The growing awareness of COVID’s protean manifestations is evident in Medscape’s Consult forum, an online community where physicians and medical students share information and seek advice; there’s been over 200 COVID-19 cases and questions since January.
Early on, traffic was mostly about typical pulmonary presentations, but lately it’s shifted to nonrespiratory involvement. Physicians want to know if what they are seeing is related to the virus, and if other people are seeing the same things.
There’s a case on Consult of a 37-year-old man with stomach pain, vomiting, and diarrhea, but no respiratory symptoms and a positive COVID test. A chest CT incidental to his abdominal scan revealed significant bilateral lung involvement.
A 69-year-old woman with a history of laparotomy and new onset intestinal subocclusion had only adhesions on a subsequent exploratory laparotomy, and was doing okay otherwise. She suddenly went into respiratory failure with progressive bradycardia and died 3 days later. Aspiration pneumonia, pulmonary embolism, and MI had been ruled out. “The pattern of cardiovascular failure was in favor of myocarditis, but we don’t have any other clue,” the physician said after describing a second similar case.
Another doctor on the forum reported elevated cardiac enzymes without coronary artery obstruction in a positive patient who went into shock, with an ejection fraction of 40% and markedly increased heart wall thickness, but no lung involvement. There are also two cases of idiopathic thrombocytopenia without fever of hypoxia.
An Italian gastroenterologist said: “Look for tricky symptoms.” Expand “patient history, asking about the sudden occurrence of dysgeusia and/or anosmia. These symptoms have become my guiding diagnostic light” in Verona. “Most patients become nauseated, [and] the taste of any food is unbearable. When I find these symptoms by history, the patient is COVID positive 100%.”
‘Make sure that they didn’t die in vain’
There was interest in those and other reports on Consult, and comments from physicians who have theories, but no certain answers about what is, and is not, caused by the virus.
Direct viral attack is likely a part of it, said Stanley Perlman, MD, PhD, a professor of microbiology and immunology at the University of Iowa, Iowa City.
The ACE2 receptor the virus uses to enter cells is common in many organs, plus there were extrapulmonary manifestations with severe acute respiratory syndrome (SARS), another pandemic caused by a zoonotic coronavirus almost 20 years ago. At least with SARS, “many organs were infected when examined at autopsy,” he said.
The body’s inflammatory response is almost certainly also in play. Progressive derangements in inflammatory markers – C-reactive protein, D-dimer, ferritin – correlate with worse prognosis, and “the cytokine storm that occurs in these patients can lead to a degree of encephalopathy, myocarditis, liver impairment, and kidney impairment; multiorgan dysfunction, in other words,” said William Shaffner, MD, a professor of preventive medicine and infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn.
But in some cases, the virus might simply be a bystander to an unrelated disease process; in others, the experimental treatments being used might cause problems. Indeed, cardiology groups recently warned of torsade de pointes – a dangerously abnormal heart rhythm – with hydroxychloroquine and azithromycin.
“We think it’s some combination,” but don’t really know, Dr. Krumholz said. In the meantime, “we are forced to treat patients by instinct and first principles,” and long-term sequelae are unknown. “We don’t want to be in this position for long.”
To that end, he said, “this is the time for us all to hold hands and be together because we need to learn rapidly from each other. Our job is both to care for the people in front of us and make sure that they didn’t die in vain, that the experience they had is funneled into a larger set of data to make sure the next person is better off.”
Although a cause-and-effect relationship is unknown, people with the virus have presented with or developed heart disease, acute liver injury, ongoing GI issues, skin manifestations, neurologic damage, and other problems, especially among sicker people.
For example, French physicians described an association with encephalopathy, agitation, confusion, and corticospinal tract signs among 58 people hospitalized with acute respiratory distress (N Engl J Med. 2020 Apr 15. doi: 10.1056/NEJMc2008597).
In particular, Yale New Haven (Conn.) Hospital is dealing with unexpected complications up close. Almost half of the beds there are occupied by COVID-19 patients. Over 100 people are in the ICU, and almost 70 intubated. Of the more than 750 COVID admissions so far, only about 350 have been discharged. “Even in a bad flu season, you never see something like this; it’s just unheard of,” said Harlan Krumholz, MD, a Yale cardiologist and professor of medicine helping lead the efforts there.
Kidney injuries prominent
“When they get to the ICU, we are seeing lots of people with acute kidney injuries; lots of people developing endocrine problems; people having blood sugar control issues, coagulation issues, blood clots. We are just waking up to the wide range of ways this virus can affect people. Our ignorance is profound,” Dr. Krumholz said, but physicians “recognize that this thing has the capability of attacking almost every single organ system, and it may or may not present with respiratory symptoms.”
It’s a similar story at Mt. Sinai South Nassau, a hospital in Oceanside, N.Y. “We’ve seen a lot of renal injury in people having complications, a lot of acute dialysis,” but it’s unclear how much is caused by the virus and how much is simply because people are so sick, said Aaron Glatt, MD, infectious disease professor and chair of medicine at the hospital. However, he said things are looking brighter than at Yale.
“We are not seeing the same level of increase in cases that we had previously, and we are starting to see extubations and discharges. We’ve treated a number of patients with plasma therapy, and hopefully that will be of benefit. We’ve seen some response to” the immunosuppressive “tocilizumab [Actemra], and a lot of response to very good respiratory therapy. I think we are starting to flatten the curve,” Dr. Glatt said.
“Look for tricky symptoms”
The growing awareness of COVID’s protean manifestations is evident in Medscape’s Consult forum, an online community where physicians and medical students share information and seek advice; there’s been over 200 COVID-19 cases and questions since January.
Early on, traffic was mostly about typical pulmonary presentations, but lately it’s shifted to nonrespiratory involvement. Physicians want to know if what they are seeing is related to the virus, and if other people are seeing the same things.
There’s a case on Consult of a 37-year-old man with stomach pain, vomiting, and diarrhea, but no respiratory symptoms and a positive COVID test. A chest CT incidental to his abdominal scan revealed significant bilateral lung involvement.
A 69-year-old woman with a history of laparotomy and new onset intestinal subocclusion had only adhesions on a subsequent exploratory laparotomy, and was doing okay otherwise. She suddenly went into respiratory failure with progressive bradycardia and died 3 days later. Aspiration pneumonia, pulmonary embolism, and MI had been ruled out. “The pattern of cardiovascular failure was in favor of myocarditis, but we don’t have any other clue,” the physician said after describing a second similar case.
Another doctor on the forum reported elevated cardiac enzymes without coronary artery obstruction in a positive patient who went into shock, with an ejection fraction of 40% and markedly increased heart wall thickness, but no lung involvement. There are also two cases of idiopathic thrombocytopenia without fever of hypoxia.
An Italian gastroenterologist said: “Look for tricky symptoms.” Expand “patient history, asking about the sudden occurrence of dysgeusia and/or anosmia. These symptoms have become my guiding diagnostic light” in Verona. “Most patients become nauseated, [and] the taste of any food is unbearable. When I find these symptoms by history, the patient is COVID positive 100%.”
‘Make sure that they didn’t die in vain’
There was interest in those and other reports on Consult, and comments from physicians who have theories, but no certain answers about what is, and is not, caused by the virus.
Direct viral attack is likely a part of it, said Stanley Perlman, MD, PhD, a professor of microbiology and immunology at the University of Iowa, Iowa City.
The ACE2 receptor the virus uses to enter cells is common in many organs, plus there were extrapulmonary manifestations with severe acute respiratory syndrome (SARS), another pandemic caused by a zoonotic coronavirus almost 20 years ago. At least with SARS, “many organs were infected when examined at autopsy,” he said.
The body’s inflammatory response is almost certainly also in play. Progressive derangements in inflammatory markers – C-reactive protein, D-dimer, ferritin – correlate with worse prognosis, and “the cytokine storm that occurs in these patients can lead to a degree of encephalopathy, myocarditis, liver impairment, and kidney impairment; multiorgan dysfunction, in other words,” said William Shaffner, MD, a professor of preventive medicine and infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn.
But in some cases, the virus might simply be a bystander to an unrelated disease process; in others, the experimental treatments being used might cause problems. Indeed, cardiology groups recently warned of torsade de pointes – a dangerously abnormal heart rhythm – with hydroxychloroquine and azithromycin.
“We think it’s some combination,” but don’t really know, Dr. Krumholz said. In the meantime, “we are forced to treat patients by instinct and first principles,” and long-term sequelae are unknown. “We don’t want to be in this position for long.”
To that end, he said, “this is the time for us all to hold hands and be together because we need to learn rapidly from each other. Our job is both to care for the people in front of us and make sure that they didn’t die in vain, that the experience they had is funneled into a larger set of data to make sure the next person is better off.”
COVID-19: Press pause on assisted reproduction?
The SARS-CoV-2 novel coronavirus has dramatically altered specialty practice across the board, including the practice of infertility treatment. Reproductive medicine societies recommend suspending new infertility treatment cycles during this time. Women and couples who have already invested time and money in their treatment may be understandably frustrated and worried about the impact of this enforced – and indefinite – delay on their chances of conceiving. This puts the physician, who can’t even guarantee when treatment can resume, in the difficult position of trying to balance the patient’s needs with expert recommendations and government mandates.
Infertility Care During COVID-19
European and American reproductive medicine societies have both offered guidelines regarding infertility care during the pandemic. Both recommend shifting to the use of telehealth rather than in-person visits when possible for initial consultations and follow-up discussions.
With respect to infertility treatments during the COVID-19 pandemic, the American Society for Reproductive Medicine (ASRM) advises the following:
- Suspend initiation of new treatment cycles, including ovulation induction; intrauterine insemination; and in vitro fertilization, including retrievals and frozen embryo transfers, and suspend nonurgent gamete cryopreservation.
- Strongly consider cancellation of all embryo transfers, whether fresh or frozen.
- Continue to care for patients who are currently “in cycle” or who require urgent stimulation and cryopreservation.
- Suspend elective surgeries and nonurgent diagnostic procedures.
In most countries, including the United States, all healthcare providers have been asked to put elective and nonurgent medical interventions on hold to ensure that personal protective equipment and other resources are available for the management of patients with COVID-19.
Infertility is a disease and, as such, not all infertility care should be considered elective. Still, for most patients, the overall chances of conceiving will not be compromised by a short delay (1-3 months) in treatment. A longer wait could have more impact on older patients or those who already have reduced ovarian reserve, but these are not indications for urgent fertility treatment.
There are clearly some cases in which infertility treatment cannot be delayed: for example, fertility preservation (oocyte or embryo vitrification) for patients who need to undergo immediate gonadotoxic oncology treatment. These patients need to be able to freeze oocytes/embryos so that later on, they have the option of having a family.
Another situation that could require new infertility treatment is a woman who needs urgent surgery for a condition such as severe symptomatic endometriosis causing ureteral or bowel stenosis/obstruction. Because the surgery itself can compromise fertility, the patient may elect to undergo oocyte embryo cryopreservation or ovarian tissue cryopreservation before the surgical procedure.
Pregnancy and COVID-19
As a precautionary measure during the COVID-19 pandemic, it is recommended that planned pregnancy be avoided. The available data on the risks presented by planning a pregnancy during the COVID pandemic are reassuring but limited.
Pregnancy itself has not been shown to alter the course of COVID-19, and most affected pregnant women will experience only mild or moderate flulike symptoms. Patients with cardiovascular or metabolic comorbidities or those requiring immunosuppressants are expected to be at increased risk for more severe forms of the infection. Currently, no strong evidence suggests a higher risk for miscarriage, stillbirth, or adverse neonatal outcomes with maternal COVID-19 infection.
A report based on 38 cases found no evidence for vertical transmission from mother to fetus, and all neonatal specimens (placental tissue) tested negative for the virus. Moreover, no maternal deaths were reported among these 38 infected women. Another study of 11 infected pregnant women likewise found no increased risk for perinatal morbidity or mortality.
On the other hand, a recent article on the perinatal outcomes of 33 neonates born to mothers with confirmed COVID-19 reported three cases of neonatal COVID-19 as a result of possible vertical transmission. In two cases, symptoms were mild and initial positive coronavirus test results turned negative within a few days. The third case – a pregnancy delivered by emergency cesarean section at 31 weeks for fetal distress – was complicated by bacterial sepsis, thrombocytopenia, and coagulopathy, but once again, the initially positive coronavirus test was negative by day 7.
No neonatal deaths were reported in these 33 cases. The authors could not rule out the possibility of vertical transmission in the three COVID-positive newborns because strict infection control measures were implemented during the care of the patients.
Counseling Patients About Suspending Infertility Treatments
Counseling women is the key to acceptance of the need to suspend or postpone infertility treatments during the pandemic. In addition to the economic hardships that some patients may face as a consequence of the pandemic, an obvious source of frustration stems from not knowing how long delays in treatment might be necessary. A discussion with patients or couples may reassure them that delaying conception is the safest route. For some women, other treatment options might be offered, such as the use of a donor gamete.
Some patients, even when counseled appropriately, may elect to accept the unknown risks. These patients should be counseled about the benefits of cryopreservation with delayed transfer. This could be a compromise, because their overall chances of pregnancy will not be affected but they will have to wait to become pregnant.
Counseling patients about the true impact of delaying treatment in their individual circumstances, providing them with emotional and (if needed) psychological support is important while they wait for their treatment to start. For now, the vast majority of the patients understand the need for delay, appreciate the opportunity to consult the physician over the phone, and are demonstrating patience as they wait for their treatment to start or resume.
Resuming Infertility Care
Recommendations could change as the pandemic continues and more information becomes available about the impact of coronavirus infection during pregnancy and the overall capacity of the healthcare system improves. ASRM acknowledges that “reproductive care professionals, in consultation with their patients, will have to consider reassessing the criteria of what represents urgent and non-urgent care.” If the data remain reassuring and social distancing measures are able to slow down the spread of the disease, the infertility care of those couples who would be most affected by a delay in their treatment could gradually be resumed. On April 14, ASRM updated its recommendations about resuming infertility treatment: “ While it is not yet prudent to resume nonemergency infertility procedures, the Task Force recognizes it is also time to begin to consider strategies and best practices for resuming time-sensitive fertility treatments in the face of COVID-19.”
It is likely that the return to “normal” daily practice will be done in a stepwise fashion. I expect the practices first to open for diagnostic infertility testing, then for the less invasive procedures (frozen embryo transfer, intrauterine insemination) and finally for the more invasive lengthy procedures (stimulation with retrieval and embryo transfer). During the reopening of practice, strict infection control measures will need to be observed.
Dr. Kovacs is the medical director of Kaali Institute IVF Center in Budapest, Hungary. He has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The SARS-CoV-2 novel coronavirus has dramatically altered specialty practice across the board, including the practice of infertility treatment. Reproductive medicine societies recommend suspending new infertility treatment cycles during this time. Women and couples who have already invested time and money in their treatment may be understandably frustrated and worried about the impact of this enforced – and indefinite – delay on their chances of conceiving. This puts the physician, who can’t even guarantee when treatment can resume, in the difficult position of trying to balance the patient’s needs with expert recommendations and government mandates.
Infertility Care During COVID-19
European and American reproductive medicine societies have both offered guidelines regarding infertility care during the pandemic. Both recommend shifting to the use of telehealth rather than in-person visits when possible for initial consultations and follow-up discussions.
With respect to infertility treatments during the COVID-19 pandemic, the American Society for Reproductive Medicine (ASRM) advises the following:
- Suspend initiation of new treatment cycles, including ovulation induction; intrauterine insemination; and in vitro fertilization, including retrievals and frozen embryo transfers, and suspend nonurgent gamete cryopreservation.
- Strongly consider cancellation of all embryo transfers, whether fresh or frozen.
- Continue to care for patients who are currently “in cycle” or who require urgent stimulation and cryopreservation.
- Suspend elective surgeries and nonurgent diagnostic procedures.
In most countries, including the United States, all healthcare providers have been asked to put elective and nonurgent medical interventions on hold to ensure that personal protective equipment and other resources are available for the management of patients with COVID-19.
Infertility is a disease and, as such, not all infertility care should be considered elective. Still, for most patients, the overall chances of conceiving will not be compromised by a short delay (1-3 months) in treatment. A longer wait could have more impact on older patients or those who already have reduced ovarian reserve, but these are not indications for urgent fertility treatment.
There are clearly some cases in which infertility treatment cannot be delayed: for example, fertility preservation (oocyte or embryo vitrification) for patients who need to undergo immediate gonadotoxic oncology treatment. These patients need to be able to freeze oocytes/embryos so that later on, they have the option of having a family.
Another situation that could require new infertility treatment is a woman who needs urgent surgery for a condition such as severe symptomatic endometriosis causing ureteral or bowel stenosis/obstruction. Because the surgery itself can compromise fertility, the patient may elect to undergo oocyte embryo cryopreservation or ovarian tissue cryopreservation before the surgical procedure.
Pregnancy and COVID-19
As a precautionary measure during the COVID-19 pandemic, it is recommended that planned pregnancy be avoided. The available data on the risks presented by planning a pregnancy during the COVID pandemic are reassuring but limited.
Pregnancy itself has not been shown to alter the course of COVID-19, and most affected pregnant women will experience only mild or moderate flulike symptoms. Patients with cardiovascular or metabolic comorbidities or those requiring immunosuppressants are expected to be at increased risk for more severe forms of the infection. Currently, no strong evidence suggests a higher risk for miscarriage, stillbirth, or adverse neonatal outcomes with maternal COVID-19 infection.
A report based on 38 cases found no evidence for vertical transmission from mother to fetus, and all neonatal specimens (placental tissue) tested negative for the virus. Moreover, no maternal deaths were reported among these 38 infected women. Another study of 11 infected pregnant women likewise found no increased risk for perinatal morbidity or mortality.
On the other hand, a recent article on the perinatal outcomes of 33 neonates born to mothers with confirmed COVID-19 reported three cases of neonatal COVID-19 as a result of possible vertical transmission. In two cases, symptoms were mild and initial positive coronavirus test results turned negative within a few days. The third case – a pregnancy delivered by emergency cesarean section at 31 weeks for fetal distress – was complicated by bacterial sepsis, thrombocytopenia, and coagulopathy, but once again, the initially positive coronavirus test was negative by day 7.
No neonatal deaths were reported in these 33 cases. The authors could not rule out the possibility of vertical transmission in the three COVID-positive newborns because strict infection control measures were implemented during the care of the patients.
Counseling Patients About Suspending Infertility Treatments
Counseling women is the key to acceptance of the need to suspend or postpone infertility treatments during the pandemic. In addition to the economic hardships that some patients may face as a consequence of the pandemic, an obvious source of frustration stems from not knowing how long delays in treatment might be necessary. A discussion with patients or couples may reassure them that delaying conception is the safest route. For some women, other treatment options might be offered, such as the use of a donor gamete.
Some patients, even when counseled appropriately, may elect to accept the unknown risks. These patients should be counseled about the benefits of cryopreservation with delayed transfer. This could be a compromise, because their overall chances of pregnancy will not be affected but they will have to wait to become pregnant.
Counseling patients about the true impact of delaying treatment in their individual circumstances, providing them with emotional and (if needed) psychological support is important while they wait for their treatment to start. For now, the vast majority of the patients understand the need for delay, appreciate the opportunity to consult the physician over the phone, and are demonstrating patience as they wait for their treatment to start or resume.
Resuming Infertility Care
Recommendations could change as the pandemic continues and more information becomes available about the impact of coronavirus infection during pregnancy and the overall capacity of the healthcare system improves. ASRM acknowledges that “reproductive care professionals, in consultation with their patients, will have to consider reassessing the criteria of what represents urgent and non-urgent care.” If the data remain reassuring and social distancing measures are able to slow down the spread of the disease, the infertility care of those couples who would be most affected by a delay in their treatment could gradually be resumed. On April 14, ASRM updated its recommendations about resuming infertility treatment: “ While it is not yet prudent to resume nonemergency infertility procedures, the Task Force recognizes it is also time to begin to consider strategies and best practices for resuming time-sensitive fertility treatments in the face of COVID-19.”
It is likely that the return to “normal” daily practice will be done in a stepwise fashion. I expect the practices first to open for diagnostic infertility testing, then for the less invasive procedures (frozen embryo transfer, intrauterine insemination) and finally for the more invasive lengthy procedures (stimulation with retrieval and embryo transfer). During the reopening of practice, strict infection control measures will need to be observed.
Dr. Kovacs is the medical director of Kaali Institute IVF Center in Budapest, Hungary. He has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The SARS-CoV-2 novel coronavirus has dramatically altered specialty practice across the board, including the practice of infertility treatment. Reproductive medicine societies recommend suspending new infertility treatment cycles during this time. Women and couples who have already invested time and money in their treatment may be understandably frustrated and worried about the impact of this enforced – and indefinite – delay on their chances of conceiving. This puts the physician, who can’t even guarantee when treatment can resume, in the difficult position of trying to balance the patient’s needs with expert recommendations and government mandates.
Infertility Care During COVID-19
European and American reproductive medicine societies have both offered guidelines regarding infertility care during the pandemic. Both recommend shifting to the use of telehealth rather than in-person visits when possible for initial consultations and follow-up discussions.
With respect to infertility treatments during the COVID-19 pandemic, the American Society for Reproductive Medicine (ASRM) advises the following:
- Suspend initiation of new treatment cycles, including ovulation induction; intrauterine insemination; and in vitro fertilization, including retrievals and frozen embryo transfers, and suspend nonurgent gamete cryopreservation.
- Strongly consider cancellation of all embryo transfers, whether fresh or frozen.
- Continue to care for patients who are currently “in cycle” or who require urgent stimulation and cryopreservation.
- Suspend elective surgeries and nonurgent diagnostic procedures.
In most countries, including the United States, all healthcare providers have been asked to put elective and nonurgent medical interventions on hold to ensure that personal protective equipment and other resources are available for the management of patients with COVID-19.
Infertility is a disease and, as such, not all infertility care should be considered elective. Still, for most patients, the overall chances of conceiving will not be compromised by a short delay (1-3 months) in treatment. A longer wait could have more impact on older patients or those who already have reduced ovarian reserve, but these are not indications for urgent fertility treatment.
There are clearly some cases in which infertility treatment cannot be delayed: for example, fertility preservation (oocyte or embryo vitrification) for patients who need to undergo immediate gonadotoxic oncology treatment. These patients need to be able to freeze oocytes/embryos so that later on, they have the option of having a family.
Another situation that could require new infertility treatment is a woman who needs urgent surgery for a condition such as severe symptomatic endometriosis causing ureteral or bowel stenosis/obstruction. Because the surgery itself can compromise fertility, the patient may elect to undergo oocyte embryo cryopreservation or ovarian tissue cryopreservation before the surgical procedure.
Pregnancy and COVID-19
As a precautionary measure during the COVID-19 pandemic, it is recommended that planned pregnancy be avoided. The available data on the risks presented by planning a pregnancy during the COVID pandemic are reassuring but limited.
Pregnancy itself has not been shown to alter the course of COVID-19, and most affected pregnant women will experience only mild or moderate flulike symptoms. Patients with cardiovascular or metabolic comorbidities or those requiring immunosuppressants are expected to be at increased risk for more severe forms of the infection. Currently, no strong evidence suggests a higher risk for miscarriage, stillbirth, or adverse neonatal outcomes with maternal COVID-19 infection.
A report based on 38 cases found no evidence for vertical transmission from mother to fetus, and all neonatal specimens (placental tissue) tested negative for the virus. Moreover, no maternal deaths were reported among these 38 infected women. Another study of 11 infected pregnant women likewise found no increased risk for perinatal morbidity or mortality.
On the other hand, a recent article on the perinatal outcomes of 33 neonates born to mothers with confirmed COVID-19 reported three cases of neonatal COVID-19 as a result of possible vertical transmission. In two cases, symptoms were mild and initial positive coronavirus test results turned negative within a few days. The third case – a pregnancy delivered by emergency cesarean section at 31 weeks for fetal distress – was complicated by bacterial sepsis, thrombocytopenia, and coagulopathy, but once again, the initially positive coronavirus test was negative by day 7.
No neonatal deaths were reported in these 33 cases. The authors could not rule out the possibility of vertical transmission in the three COVID-positive newborns because strict infection control measures were implemented during the care of the patients.
Counseling Patients About Suspending Infertility Treatments
Counseling women is the key to acceptance of the need to suspend or postpone infertility treatments during the pandemic. In addition to the economic hardships that some patients may face as a consequence of the pandemic, an obvious source of frustration stems from not knowing how long delays in treatment might be necessary. A discussion with patients or couples may reassure them that delaying conception is the safest route. For some women, other treatment options might be offered, such as the use of a donor gamete.
Some patients, even when counseled appropriately, may elect to accept the unknown risks. These patients should be counseled about the benefits of cryopreservation with delayed transfer. This could be a compromise, because their overall chances of pregnancy will not be affected but they will have to wait to become pregnant.
Counseling patients about the true impact of delaying treatment in their individual circumstances, providing them with emotional and (if needed) psychological support is important while they wait for their treatment to start. For now, the vast majority of the patients understand the need for delay, appreciate the opportunity to consult the physician over the phone, and are demonstrating patience as they wait for their treatment to start or resume.
Resuming Infertility Care
Recommendations could change as the pandemic continues and more information becomes available about the impact of coronavirus infection during pregnancy and the overall capacity of the healthcare system improves. ASRM acknowledges that “reproductive care professionals, in consultation with their patients, will have to consider reassessing the criteria of what represents urgent and non-urgent care.” If the data remain reassuring and social distancing measures are able to slow down the spread of the disease, the infertility care of those couples who would be most affected by a delay in their treatment could gradually be resumed. On April 14, ASRM updated its recommendations about resuming infertility treatment: “ While it is not yet prudent to resume nonemergency infertility procedures, the Task Force recognizes it is also time to begin to consider strategies and best practices for resuming time-sensitive fertility treatments in the face of COVID-19.”
It is likely that the return to “normal” daily practice will be done in a stepwise fashion. I expect the practices first to open for diagnostic infertility testing, then for the less invasive procedures (frozen embryo transfer, intrauterine insemination) and finally for the more invasive lengthy procedures (stimulation with retrieval and embryo transfer). During the reopening of practice, strict infection control measures will need to be observed.
Dr. Kovacs is the medical director of Kaali Institute IVF Center in Budapest, Hungary. He has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
COVID-19 pandemic spells trouble for children’s health
Although priority number one lies in controlling the spread of COVID-19, public health researchers are calling attention to the long-term repercussions of the pandemic on children’s health.
School closures could noticeably worsen the epidemic of childhood obesity that already threatens many children in the United States, say Paul Rundle, DrPH, and colleagues from Columbia University Mailman School of Public Health, New York City, in a perspective published online March 30 in Obesity.
“In part, we wrote the perspective to remind people that summer unhealthy weight gain seems to accumulate year to year,” he told Medscape Medical News in an email.
Rundle and colleagues estimate that time spent out of school will double this year because of school closures due to COVID-19. That, along with shelter-in-place orders, will pose challenges both for physical activity and healthy eating among children.
In addition, playgrounds have closed in many areas, and even where parks remain open, social distancing decreases opportunities for exercise. Team sports are on hold, and without physical education taught in schools, many children will not be getting as much active outdoor play as needed.
That’s especially true for children in urban areas, who may find it even more difficult to exercise inside cramped apartments, they add.
As a result, more and more children may turn to sedentary activities, and increased screen time goes hand in hand with childhood overweight and obesity, not just because of the lack of exercise but also because of snacking on unhealthy, empty-calorie foods while glued to the screen.
“We were hoping to get the word out on this issue, do some education or reminding, and at least let people know that this should be something to keep an eye on, among so many other things,” Rundle added.
Excess Eating Because of Stress and Boredom
Jessica Sparks Lilley, MD, director of the Pediatric Diabetes and Lipid Program at the Mississippi Center for Advanced Medicine in Madison, agrees that it is crucial to address these issues.
“Just like adults, children eat in response to emotions, including stress and boredom, and stress levels are high during these uncertain times,” she told Medscape Medical News.
Although both Rundle and Sparks Lilley acknowledged the challenges of finding good solutions at this time, they do offer some tips.
Schools should make physical education and at-home exercise a priority alongside other remote teaching. Physical education teachers could even stream exercise classes to children at home.
Even just walking in the park while maintaining social distancing could be better than nothing, and a brisk walk is probably even better.
Depending on the age of the child, online yoga may also be useful. Even though yoga burns relatively few calories, it incorporates mindfulness training that may be helpful.
“I think focusing on promoting mindful eating as compared to mindless or distracted eating is important. Even in the best of circumstances, it is hard to exercise enough to burn off high energy snacks,” Rundle said.
Additional Stressors From Poverty: Schools Can Help With Meals
Children living in poverty, already the most vulnerable to obesity and related health problems, have additional stressors, add the two experts.
“As more Americans are losing jobs, poverty is a real threat to many of the children I care for. Families living in poverty often rely on processed, high-calorie, low-nutrient foods for survival, because they are inexpensive and shelf-stable,” Sparks Lilley said.
Rundle and colleagues agree: “Our own experiences in supermarkets show...shelves that held...crackers, chips, ramen noodles, soda, sugary cereals, and processed ready-to-eat meals are quite empty. We anticipate that many children will experience higher calorie diets during the pandemic response.”
Similar to how they address food insecurity during summer holidays, school districts have responded by offering grab-and-go meals, Rundle and colleagues note.
To maintain social distancing for people with vulnerable family members, some school districts have also started delivering food using school buses that run along regularly scheduled routes.
Rundle also stresses that farmers’ markets, which often provide foods that appeal to immigrant and ethnic communities, should be considered part of essential food services.
As such, social distancing protocols should be established for them and they should be allowed to stay open, he argues.
“The safety of American children is at stake in many ways. The threat to themselves or their caregivers being infected with COVID-19 is rightly foremost in our concerns,” Sparks Lilley stressed.
“However, there is other fallout to consider. We’ve seen very clearly the need for public health and preventive medicine and can’t let vulnerable children fall through the cracks.”
Rundle agrees. Although it is a “priority” to mitigate the immediate impact of COVID-19, “it is important to consider ways to prevent its long-term effects, including new risks for childhood obesity.”
Rundle and coauthors, as well as Sparks Lilley, have reported no relevant financial relationships.
This article first appeared on Medscape.com.
Although priority number one lies in controlling the spread of COVID-19, public health researchers are calling attention to the long-term repercussions of the pandemic on children’s health.
School closures could noticeably worsen the epidemic of childhood obesity that already threatens many children in the United States, say Paul Rundle, DrPH, and colleagues from Columbia University Mailman School of Public Health, New York City, in a perspective published online March 30 in Obesity.
“In part, we wrote the perspective to remind people that summer unhealthy weight gain seems to accumulate year to year,” he told Medscape Medical News in an email.
Rundle and colleagues estimate that time spent out of school will double this year because of school closures due to COVID-19. That, along with shelter-in-place orders, will pose challenges both for physical activity and healthy eating among children.
In addition, playgrounds have closed in many areas, and even where parks remain open, social distancing decreases opportunities for exercise. Team sports are on hold, and without physical education taught in schools, many children will not be getting as much active outdoor play as needed.
That’s especially true for children in urban areas, who may find it even more difficult to exercise inside cramped apartments, they add.
As a result, more and more children may turn to sedentary activities, and increased screen time goes hand in hand with childhood overweight and obesity, not just because of the lack of exercise but also because of snacking on unhealthy, empty-calorie foods while glued to the screen.
“We were hoping to get the word out on this issue, do some education or reminding, and at least let people know that this should be something to keep an eye on, among so many other things,” Rundle added.
Excess Eating Because of Stress and Boredom
Jessica Sparks Lilley, MD, director of the Pediatric Diabetes and Lipid Program at the Mississippi Center for Advanced Medicine in Madison, agrees that it is crucial to address these issues.
“Just like adults, children eat in response to emotions, including stress and boredom, and stress levels are high during these uncertain times,” she told Medscape Medical News.
Although both Rundle and Sparks Lilley acknowledged the challenges of finding good solutions at this time, they do offer some tips.
Schools should make physical education and at-home exercise a priority alongside other remote teaching. Physical education teachers could even stream exercise classes to children at home.
Even just walking in the park while maintaining social distancing could be better than nothing, and a brisk walk is probably even better.
Depending on the age of the child, online yoga may also be useful. Even though yoga burns relatively few calories, it incorporates mindfulness training that may be helpful.
“I think focusing on promoting mindful eating as compared to mindless or distracted eating is important. Even in the best of circumstances, it is hard to exercise enough to burn off high energy snacks,” Rundle said.
Additional Stressors From Poverty: Schools Can Help With Meals
Children living in poverty, already the most vulnerable to obesity and related health problems, have additional stressors, add the two experts.
“As more Americans are losing jobs, poverty is a real threat to many of the children I care for. Families living in poverty often rely on processed, high-calorie, low-nutrient foods for survival, because they are inexpensive and shelf-stable,” Sparks Lilley said.
Rundle and colleagues agree: “Our own experiences in supermarkets show...shelves that held...crackers, chips, ramen noodles, soda, sugary cereals, and processed ready-to-eat meals are quite empty. We anticipate that many children will experience higher calorie diets during the pandemic response.”
Similar to how they address food insecurity during summer holidays, school districts have responded by offering grab-and-go meals, Rundle and colleagues note.
To maintain social distancing for people with vulnerable family members, some school districts have also started delivering food using school buses that run along regularly scheduled routes.
Rundle also stresses that farmers’ markets, which often provide foods that appeal to immigrant and ethnic communities, should be considered part of essential food services.
As such, social distancing protocols should be established for them and they should be allowed to stay open, he argues.
“The safety of American children is at stake in many ways. The threat to themselves or their caregivers being infected with COVID-19 is rightly foremost in our concerns,” Sparks Lilley stressed.
“However, there is other fallout to consider. We’ve seen very clearly the need for public health and preventive medicine and can’t let vulnerable children fall through the cracks.”
Rundle agrees. Although it is a “priority” to mitigate the immediate impact of COVID-19, “it is important to consider ways to prevent its long-term effects, including new risks for childhood obesity.”
Rundle and coauthors, as well as Sparks Lilley, have reported no relevant financial relationships.
This article first appeared on Medscape.com.
Although priority number one lies in controlling the spread of COVID-19, public health researchers are calling attention to the long-term repercussions of the pandemic on children’s health.
School closures could noticeably worsen the epidemic of childhood obesity that already threatens many children in the United States, say Paul Rundle, DrPH, and colleagues from Columbia University Mailman School of Public Health, New York City, in a perspective published online March 30 in Obesity.
“In part, we wrote the perspective to remind people that summer unhealthy weight gain seems to accumulate year to year,” he told Medscape Medical News in an email.
Rundle and colleagues estimate that time spent out of school will double this year because of school closures due to COVID-19. That, along with shelter-in-place orders, will pose challenges both for physical activity and healthy eating among children.
In addition, playgrounds have closed in many areas, and even where parks remain open, social distancing decreases opportunities for exercise. Team sports are on hold, and without physical education taught in schools, many children will not be getting as much active outdoor play as needed.
That’s especially true for children in urban areas, who may find it even more difficult to exercise inside cramped apartments, they add.
As a result, more and more children may turn to sedentary activities, and increased screen time goes hand in hand with childhood overweight and obesity, not just because of the lack of exercise but also because of snacking on unhealthy, empty-calorie foods while glued to the screen.
“We were hoping to get the word out on this issue, do some education or reminding, and at least let people know that this should be something to keep an eye on, among so many other things,” Rundle added.
Excess Eating Because of Stress and Boredom
Jessica Sparks Lilley, MD, director of the Pediatric Diabetes and Lipid Program at the Mississippi Center for Advanced Medicine in Madison, agrees that it is crucial to address these issues.
“Just like adults, children eat in response to emotions, including stress and boredom, and stress levels are high during these uncertain times,” she told Medscape Medical News.
Although both Rundle and Sparks Lilley acknowledged the challenges of finding good solutions at this time, they do offer some tips.
Schools should make physical education and at-home exercise a priority alongside other remote teaching. Physical education teachers could even stream exercise classes to children at home.
Even just walking in the park while maintaining social distancing could be better than nothing, and a brisk walk is probably even better.
Depending on the age of the child, online yoga may also be useful. Even though yoga burns relatively few calories, it incorporates mindfulness training that may be helpful.
“I think focusing on promoting mindful eating as compared to mindless or distracted eating is important. Even in the best of circumstances, it is hard to exercise enough to burn off high energy snacks,” Rundle said.
Additional Stressors From Poverty: Schools Can Help With Meals
Children living in poverty, already the most vulnerable to obesity and related health problems, have additional stressors, add the two experts.
“As more Americans are losing jobs, poverty is a real threat to many of the children I care for. Families living in poverty often rely on processed, high-calorie, low-nutrient foods for survival, because they are inexpensive and shelf-stable,” Sparks Lilley said.
Rundle and colleagues agree: “Our own experiences in supermarkets show...shelves that held...crackers, chips, ramen noodles, soda, sugary cereals, and processed ready-to-eat meals are quite empty. We anticipate that many children will experience higher calorie diets during the pandemic response.”
Similar to how they address food insecurity during summer holidays, school districts have responded by offering grab-and-go meals, Rundle and colleagues note.
To maintain social distancing for people with vulnerable family members, some school districts have also started delivering food using school buses that run along regularly scheduled routes.
Rundle also stresses that farmers’ markets, which often provide foods that appeal to immigrant and ethnic communities, should be considered part of essential food services.
As such, social distancing protocols should be established for them and they should be allowed to stay open, he argues.
“The safety of American children is at stake in many ways. The threat to themselves or their caregivers being infected with COVID-19 is rightly foremost in our concerns,” Sparks Lilley stressed.
“However, there is other fallout to consider. We’ve seen very clearly the need for public health and preventive medicine and can’t let vulnerable children fall through the cracks.”
Rundle agrees. Although it is a “priority” to mitigate the immediate impact of COVID-19, “it is important to consider ways to prevent its long-term effects, including new risks for childhood obesity.”
Rundle and coauthors, as well as Sparks Lilley, have reported no relevant financial relationships.
This article first appeared on Medscape.com.
Imaging recommendations issued for COVID-19 patients
A consensus statement on the role of imaging during the acute work-up of COVID-19 patients called for liberal use in patients with moderate to severe clinical features indicative of infection, regardless of their COVID-19 test results, but limited use in patients who present with mild symptoms or are asymptomatic.

The consensus statement on The Role of Imaging in Patient Management during the COVID-19 Pandemic released by the Fleischner Society on April 7 was designed to highlight the “key decision points around imaging” in COVID-19 patients.
“We developed the statement to be applicable across settings” so that each clinic or hospital managing COVID-19 patients could decide the situations where chest radiography (CXR) or CT would work best, said Geoffrey D. Rubin, MD, professor of cardiovascular research, radiology, and bioengineering at Duke University in Durham, N.C., and lead author of the statement.
Written by 15 thoracic radiologists and 10 pulmonologists/intensivists including an anesthesiologist, a pathologist, and additional experts in emergency medicine, infection control, and laboratory medicine, and with members from any of 10 countries on three continents, the panel arrived at agreement by more than 70% for each of the 14 questions.
“I was impressed and a little surprised that consensus was achieved for every question” posed to the panel by the Fleischner Society for Thoracic Imaging and Diagnosis, Dr. Rubin said in an interview. The panel also placed their 14 decisions about imaging within the context of three distinct clinical scenarios chosen to mirror common real-world situations: mild COVID-19 features, moderate to severe features with no critical-resource constraints, and moderate to severe features with constrained resources. The statement also summarized its conclusions as five main recommendations and three additional recommendations.
Main recommendations
- Imaging is not routinely indicated for COVID-19 screening in asymptomatic people.
- Imaging is not indicated for patients with mild features of COVID-19 unless they are at risk for disease progression.
- Imaging is indicated for patients with features of moderate to severe COVID-19 regardless of COVID-19 test results.
- Imaging is indicated for patients with COVID-19 and evidence of worsening respiratory status.
- When access to CT is limited, chest radiography may be preferred for COVID-19 patients unless features of respiratory worsening warrant using CT.
Additional recommendations
- Daily chest radiographs are not indicated in stable, intubated patients with COVID-19.
- CT is indicated in patients with functional impairment, hypoxemia, or both, after COVID-19 recovery.
- COVID-19 testing is warranted in patients incidentally found to have findings suggestive of COVID-19 on a CT scan.
The statement particularly called out one of its recommendations – that a COVID-19 diagnosis “may be presumed when imaging findings are strongly suggestive of COVID-19 despite negative COVID-19 testing” in a patient who has moderate to severe clinical features of COVID-19 and whose pretest probability is high. The panel voted unanimously in favor of this concept, that imaging is “indicated” in hospitalized patients with moderate to severe symptoms consistent with COVID-19 despite a negative COVID-19 test result. “This guidance represents variance from other published recommendations which advise against the use of imaging for the initial diagnosis of COVID-19,” the statement acknowledged and specifically cited the recommendations issued in March 2020 by the American College of Radiology. Despite that, the ACR and Fleischner recommendations “are not at odds with one another,” maintained Dr. Rubin. The panel based its take on this question on the “direct experience” of its members caring for COVID-19 patients, according to the statement.

“I wholeheartedly agree with the suggested uses of imaging outlined by the panel,” commented Sachin Gupta, MD, FCCP, a pulmonologist and critical care physician in San Francisco. “The consensus statement brings a practical way to consider obtaining imaging. It leaves the door open to local standards and best judgment for using CXR or CT. Many physicians are unclear whether to image low-risk and mildly symptomatic patients. This statement gives support to a watchful waiting approach.” Another recommendation advises against daily CXR in stable, intubated COVID-19 patients. This “now gives backing from an important society and thought leaders while giving an explanation” for why daily imaging is problematic, he noted in an interview. The daily CXR in these patients adds no value, and skipping unneeded imaging minimizes SARS-CoV-2 exposure to radiology personnel, and conserves personal protection equipment, said the statement.
“The Fleischner Society is known worldwide for its recommendations. Having the society lend its weight on triage with imaging for COVID-19 patients is important. I suspect it will help standardize practice.”
Dr. Gupta also highlighted that lung imaging with a portable ultrasound unit has quickly become recognized as a very useful imaging tool with increasing use as the pandemic has unfolded, an option not covered by the Fleischner statement. Study results have “confirmed excellent sensitivity, specificity, and reproducibility” with lung ultrasound, and it’s also “easy to use,” Dr. Gupta said.
Ultrasound chest imaging of COVID-19 patients did not get included in the statement despite the reliance some U.S. sites have already placed on it largely because few on the panel had direct experience using it. “We didn’t feel we could contribute” to a discussion of ultrasound, Dr. Rubin said.
The statement’s recommendations appear to have already begun influencing practice. “The feedback I’ve gotten is that people are relying on them,” said Dr. Rubin, and some programs have sent him screen shots of the recommendations embedded in their local electronic health record.
The Radiological Society of North America is hosting a webinar on the statement on April 17.
A consensus statement on the role of imaging during the acute work-up of COVID-19 patients called for liberal use in patients with moderate to severe clinical features indicative of infection, regardless of their COVID-19 test results, but limited use in patients who present with mild symptoms or are asymptomatic.
The consensus statement on The Role of Imaging in Patient Management during the COVID-19 Pandemic released by the Fleischner Society on April 7 was designed to highlight the “key decision points around imaging” in COVID-19 patients.
“We developed the statement to be applicable across settings” so that each clinic or hospital managing COVID-19 patients could decide the situations where chest radiography (CXR) or CT would work best, said Geoffrey D. Rubin, MD, professor of cardiovascular research, radiology, and bioengineering at Duke University in Durham, N.C., and lead author of the statement.
Written by 15 thoracic radiologists and 10 pulmonologists/intensivists including an anesthesiologist, a pathologist, and additional experts in emergency medicine, infection control, and laboratory medicine, and with members from any of 10 countries on three continents, the panel arrived at agreement by more than 70% for each of the 14 questions.
“I was impressed and a little surprised that consensus was achieved for every question” posed to the panel by the Fleischner Society for Thoracic Imaging and Diagnosis, Dr. Rubin said in an interview. The panel also placed their 14 decisions about imaging within the context of three distinct clinical scenarios chosen to mirror common real-world situations: mild COVID-19 features, moderate to severe features with no critical-resource constraints, and moderate to severe features with constrained resources. The statement also summarized its conclusions as five main recommendations and three additional recommendations.
Main recommendations
- Imaging is not routinely indicated for COVID-19 screening in asymptomatic people.
- Imaging is not indicated for patients with mild features of COVID-19 unless they are at risk for disease progression.
- Imaging is indicated for patients with features of moderate to severe COVID-19 regardless of COVID-19 test results.
- Imaging is indicated for patients with COVID-19 and evidence of worsening respiratory status.
- When access to CT is limited, chest radiography may be preferred for COVID-19 patients unless features of respiratory worsening warrant using CT.
Additional recommendations
- Daily chest radiographs are not indicated in stable, intubated patients with COVID-19.
- CT is indicated in patients with functional impairment, hypoxemia, or both, after COVID-19 recovery.
- COVID-19 testing is warranted in patients incidentally found to have findings suggestive of COVID-19 on a CT scan.
The statement particularly called out one of its recommendations – that a COVID-19 diagnosis “may be presumed when imaging findings are strongly suggestive of COVID-19 despite negative COVID-19 testing” in a patient who has moderate to severe clinical features of COVID-19 and whose pretest probability is high. The panel voted unanimously in favor of this concept, that imaging is “indicated” in hospitalized patients with moderate to severe symptoms consistent with COVID-19 despite a negative COVID-19 test result. “This guidance represents variance from other published recommendations which advise against the use of imaging for the initial diagnosis of COVID-19,” the statement acknowledged and specifically cited the recommendations issued in March 2020 by the American College of Radiology. Despite that, the ACR and Fleischner recommendations “are not at odds with one another,” maintained Dr. Rubin. The panel based its take on this question on the “direct experience” of its members caring for COVID-19 patients, according to the statement.
“I wholeheartedly agree with the suggested uses of imaging outlined by the panel,” commented Sachin Gupta, MD, FCCP, a pulmonologist and critical care physician in San Francisco. “The consensus statement brings a practical way to consider obtaining imaging. It leaves the door open to local standards and best judgment for using CXR or CT. Many physicians are unclear whether to image low-risk and mildly symptomatic patients. This statement gives support to a watchful waiting approach.” Another recommendation advises against daily CXR in stable, intubated COVID-19 patients. This “now gives backing from an important society and thought leaders while giving an explanation” for why daily imaging is problematic, he noted in an interview. The daily CXR in these patients adds no value, and skipping unneeded imaging minimizes SARS-CoV-2 exposure to radiology personnel, and conserves personal protection equipment, said the statement.
“The Fleischner Society is known worldwide for its recommendations. Having the society lend its weight on triage with imaging for COVID-19 patients is important. I suspect it will help standardize practice.”
Dr. Gupta also highlighted that lung imaging with a portable ultrasound unit has quickly become recognized as a very useful imaging tool with increasing use as the pandemic has unfolded, an option not covered by the Fleischner statement. Study results have “confirmed excellent sensitivity, specificity, and reproducibility” with lung ultrasound, and it’s also “easy to use,” Dr. Gupta said.
Ultrasound chest imaging of COVID-19 patients did not get included in the statement despite the reliance some U.S. sites have already placed on it largely because few on the panel had direct experience using it. “We didn’t feel we could contribute” to a discussion of ultrasound, Dr. Rubin said.
The statement’s recommendations appear to have already begun influencing practice. “The feedback I’ve gotten is that people are relying on them,” said Dr. Rubin, and some programs have sent him screen shots of the recommendations embedded in their local electronic health record.
The Radiological Society of North America is hosting a webinar on the statement on April 17.
A consensus statement on the role of imaging during the acute work-up of COVID-19 patients called for liberal use in patients with moderate to severe clinical features indicative of infection, regardless of their COVID-19 test results, but limited use in patients who present with mild symptoms or are asymptomatic.
The consensus statement on The Role of Imaging in Patient Management during the COVID-19 Pandemic released by the Fleischner Society on April 7 was designed to highlight the “key decision points around imaging” in COVID-19 patients.
“We developed the statement to be applicable across settings” so that each clinic or hospital managing COVID-19 patients could decide the situations where chest radiography (CXR) or CT would work best, said Geoffrey D. Rubin, MD, professor of cardiovascular research, radiology, and bioengineering at Duke University in Durham, N.C., and lead author of the statement.
Written by 15 thoracic radiologists and 10 pulmonologists/intensivists including an anesthesiologist, a pathologist, and additional experts in emergency medicine, infection control, and laboratory medicine, and with members from any of 10 countries on three continents, the panel arrived at agreement by more than 70% for each of the 14 questions.
“I was impressed and a little surprised that consensus was achieved for every question” posed to the panel by the Fleischner Society for Thoracic Imaging and Diagnosis, Dr. Rubin said in an interview. The panel also placed their 14 decisions about imaging within the context of three distinct clinical scenarios chosen to mirror common real-world situations: mild COVID-19 features, moderate to severe features with no critical-resource constraints, and moderate to severe features with constrained resources. The statement also summarized its conclusions as five main recommendations and three additional recommendations.
Main recommendations
- Imaging is not routinely indicated for COVID-19 screening in asymptomatic people.
- Imaging is not indicated for patients with mild features of COVID-19 unless they are at risk for disease progression.
- Imaging is indicated for patients with features of moderate to severe COVID-19 regardless of COVID-19 test results.
- Imaging is indicated for patients with COVID-19 and evidence of worsening respiratory status.
- When access to CT is limited, chest radiography may be preferred for COVID-19 patients unless features of respiratory worsening warrant using CT.
Additional recommendations
- Daily chest radiographs are not indicated in stable, intubated patients with COVID-19.
- CT is indicated in patients with functional impairment, hypoxemia, or both, after COVID-19 recovery.
- COVID-19 testing is warranted in patients incidentally found to have findings suggestive of COVID-19 on a CT scan.
The statement particularly called out one of its recommendations – that a COVID-19 diagnosis “may be presumed when imaging findings are strongly suggestive of COVID-19 despite negative COVID-19 testing” in a patient who has moderate to severe clinical features of COVID-19 and whose pretest probability is high. The panel voted unanimously in favor of this concept, that imaging is “indicated” in hospitalized patients with moderate to severe symptoms consistent with COVID-19 despite a negative COVID-19 test result. “This guidance represents variance from other published recommendations which advise against the use of imaging for the initial diagnosis of COVID-19,” the statement acknowledged and specifically cited the recommendations issued in March 2020 by the American College of Radiology. Despite that, the ACR and Fleischner recommendations “are not at odds with one another,” maintained Dr. Rubin. The panel based its take on this question on the “direct experience” of its members caring for COVID-19 patients, according to the statement.
“I wholeheartedly agree with the suggested uses of imaging outlined by the panel,” commented Sachin Gupta, MD, FCCP, a pulmonologist and critical care physician in San Francisco. “The consensus statement brings a practical way to consider obtaining imaging. It leaves the door open to local standards and best judgment for using CXR or CT. Many physicians are unclear whether to image low-risk and mildly symptomatic patients. This statement gives support to a watchful waiting approach.” Another recommendation advises against daily CXR in stable, intubated COVID-19 patients. This “now gives backing from an important society and thought leaders while giving an explanation” for why daily imaging is problematic, he noted in an interview. The daily CXR in these patients adds no value, and skipping unneeded imaging minimizes SARS-CoV-2 exposure to radiology personnel, and conserves personal protection equipment, said the statement.
“The Fleischner Society is known worldwide for its recommendations. Having the society lend its weight on triage with imaging for COVID-19 patients is important. I suspect it will help standardize practice.”
Dr. Gupta also highlighted that lung imaging with a portable ultrasound unit has quickly become recognized as a very useful imaging tool with increasing use as the pandemic has unfolded, an option not covered by the Fleischner statement. Study results have “confirmed excellent sensitivity, specificity, and reproducibility” with lung ultrasound, and it’s also “easy to use,” Dr. Gupta said.
Ultrasound chest imaging of COVID-19 patients did not get included in the statement despite the reliance some U.S. sites have already placed on it largely because few on the panel had direct experience using it. “We didn’t feel we could contribute” to a discussion of ultrasound, Dr. Rubin said.
The statement’s recommendations appear to have already begun influencing practice. “The feedback I’ve gotten is that people are relying on them,” said Dr. Rubin, and some programs have sent him screen shots of the recommendations embedded in their local electronic health record.
The Radiological Society of North America is hosting a webinar on the statement on April 17.
FROM CHEST
Evidence suggests possible RAS-blocker benefit in COVID-19 patients
Patients infected by the COVID-19 virus may benefit from treatments that dampen the renin-angiotensin system, according to a review of several animal studies. These preclinical findings generally support the positions taken in recent week by several cardiology societies that recommended patients taking drugs that moderate the renin-angiotensin system stay on these treatments.
“In patients with cardiovascular disease and SARS-CoV2, the use of ACE inhibitors, ARBs [angiotensin receptor blockers], or MRAs [mineralocorticoid-receptor antagonists] may be favorable as a method to endogenously upregulate ACE2 as a compensatory mechanism that provides anti-inflammatory, antifibrotic, and antithrombotic support as well as reduction in progression of vascular/cardiac remodeling and heart failure,” wrote Jeffrey Bander, MD, and his associates in a report published online (J Am Coll Cardiol. 2020 Apr 15. doi: 10.1016/j.jacc.2020.04.028).
“Based on our review, we hypothesize cardiovascular patients with COVID-19 should remain on RAS [renin-angiotensin system] inhibitors given the protective effects of the ACE2 pathway until RAS blockade is proven to increase the risk to COVID-19,” said the researchers, who are affiliated with the Icahn School of Medicine at Mount Sinai in New York.
The ACE2 protein, found both in human blood as well as in cell membranes, especially cells of the lungs, heart, kidneys, and gastrointestinal tissues, functions as both a key enzyme in RAS regulation as well as the primary cell receptor for entry of SARS-CoV2.
Their conclusion jibed with both a joint statement in March from the American College of Cardiology, American Heart Association, and the Heart Failure Society of America; and with the conclusions of a review organized by the European Society of Hypertension’s COVID-19 Task Force (Cardiovasc Res. 2020 Apr 15. doi: 10.1093/cvr/cvaa097).
In their review, the Mount Sinai authors described results from several animal studies suggesting that ACE2 and its associated signaling proteins could potentially be a “valuable therapeutic target.” They also highlighted several clinical intervention studies recently launched to target ACE2, related proteins, and regulation of this arm of the RAS.
Currently, “no data support any conclusive effects of the use of RAS inhibitors in patients with COVID-19,” they concluded. They acknowledged that “the question remains whether the use of ACE inhibitors, ARBs, and MRAs should be avoided in the setting of SARS-CoV infection,” but emphasized that “adequate data on the effects of RAS inhibition in COVID-19 patients is not available,” with more data becoming available soon from ongoing clinical studies.
None of the authors had any disclosures.
Patients infected by the COVID-19 virus may benefit from treatments that dampen the renin-angiotensin system, according to a review of several animal studies. These preclinical findings generally support the positions taken in recent week by several cardiology societies that recommended patients taking drugs that moderate the renin-angiotensin system stay on these treatments.
“In patients with cardiovascular disease and SARS-CoV2, the use of ACE inhibitors, ARBs [angiotensin receptor blockers], or MRAs [mineralocorticoid-receptor antagonists] may be favorable as a method to endogenously upregulate ACE2 as a compensatory mechanism that provides anti-inflammatory, antifibrotic, and antithrombotic support as well as reduction in progression of vascular/cardiac remodeling and heart failure,” wrote Jeffrey Bander, MD, and his associates in a report published online (J Am Coll Cardiol. 2020 Apr 15. doi: 10.1016/j.jacc.2020.04.028).
“Based on our review, we hypothesize cardiovascular patients with COVID-19 should remain on RAS [renin-angiotensin system] inhibitors given the protective effects of the ACE2 pathway until RAS blockade is proven to increase the risk to COVID-19,” said the researchers, who are affiliated with the Icahn School of Medicine at Mount Sinai in New York.
The ACE2 protein, found both in human blood as well as in cell membranes, especially cells of the lungs, heart, kidneys, and gastrointestinal tissues, functions as both a key enzyme in RAS regulation as well as the primary cell receptor for entry of SARS-CoV2.
Their conclusion jibed with both a joint statement in March from the American College of Cardiology, American Heart Association, and the Heart Failure Society of America; and with the conclusions of a review organized by the European Society of Hypertension’s COVID-19 Task Force (Cardiovasc Res. 2020 Apr 15. doi: 10.1093/cvr/cvaa097).
In their review, the Mount Sinai authors described results from several animal studies suggesting that ACE2 and its associated signaling proteins could potentially be a “valuable therapeutic target.” They also highlighted several clinical intervention studies recently launched to target ACE2, related proteins, and regulation of this arm of the RAS.
Currently, “no data support any conclusive effects of the use of RAS inhibitors in patients with COVID-19,” they concluded. They acknowledged that “the question remains whether the use of ACE inhibitors, ARBs, and MRAs should be avoided in the setting of SARS-CoV infection,” but emphasized that “adequate data on the effects of RAS inhibition in COVID-19 patients is not available,” with more data becoming available soon from ongoing clinical studies.
None of the authors had any disclosures.
Patients infected by the COVID-19 virus may benefit from treatments that dampen the renin-angiotensin system, according to a review of several animal studies. These preclinical findings generally support the positions taken in recent week by several cardiology societies that recommended patients taking drugs that moderate the renin-angiotensin system stay on these treatments.
“In patients with cardiovascular disease and SARS-CoV2, the use of ACE inhibitors, ARBs [angiotensin receptor blockers], or MRAs [mineralocorticoid-receptor antagonists] may be favorable as a method to endogenously upregulate ACE2 as a compensatory mechanism that provides anti-inflammatory, antifibrotic, and antithrombotic support as well as reduction in progression of vascular/cardiac remodeling and heart failure,” wrote Jeffrey Bander, MD, and his associates in a report published online (J Am Coll Cardiol. 2020 Apr 15. doi: 10.1016/j.jacc.2020.04.028).
“Based on our review, we hypothesize cardiovascular patients with COVID-19 should remain on RAS [renin-angiotensin system] inhibitors given the protective effects of the ACE2 pathway until RAS blockade is proven to increase the risk to COVID-19,” said the researchers, who are affiliated with the Icahn School of Medicine at Mount Sinai in New York.
The ACE2 protein, found both in human blood as well as in cell membranes, especially cells of the lungs, heart, kidneys, and gastrointestinal tissues, functions as both a key enzyme in RAS regulation as well as the primary cell receptor for entry of SARS-CoV2.
Their conclusion jibed with both a joint statement in March from the American College of Cardiology, American Heart Association, and the Heart Failure Society of America; and with the conclusions of a review organized by the European Society of Hypertension’s COVID-19 Task Force (Cardiovasc Res. 2020 Apr 15. doi: 10.1093/cvr/cvaa097).
In their review, the Mount Sinai authors described results from several animal studies suggesting that ACE2 and its associated signaling proteins could potentially be a “valuable therapeutic target.” They also highlighted several clinical intervention studies recently launched to target ACE2, related proteins, and regulation of this arm of the RAS.
Currently, “no data support any conclusive effects of the use of RAS inhibitors in patients with COVID-19,” they concluded. They acknowledged that “the question remains whether the use of ACE inhibitors, ARBs, and MRAs should be avoided in the setting of SARS-CoV infection,” but emphasized that “adequate data on the effects of RAS inhibition in COVID-19 patients is not available,” with more data becoming available soon from ongoing clinical studies.
None of the authors had any disclosures.
REPORTING FROM JACC