User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Magic Wand Initiative Empowers Dermatologists to Innovate
NEW YORK – .
The program was founded in 2013 by two Harvard Medical School dermatologists, Lilit Garibyan, MD, PhD, the program director, and her mentor R. Rox Anderson MD, director of the Wellman Center for Photomedicine at Massachusetts General Hospital (MGH), Boston. It was based on the idea that clinicians are in a unique position to identify gaps in patient care and should be active in developing medical solutions to address those gaps.
“I truly believe that if we do a better job educating, training, and empowering our clinicians to become innovators, this will benefit patients and hospitals and physicians,” Dr. Garibyan said at the 26th annual Mount Sinai Winter Symposium — Advances in Medical and Surgical Dermatology.
One of the seeds for the project was her own experience with cryolipolysis which involves topical cooling, a noninvasive method of removing subcutaneous fat for body contouring, which relies on conducting heat from subcutaneous fat across the skin and therefore, does not reach fat far from the dermis. With Dr. Anderson’s mentorship, she developed injectable cooling technology (ICT), a procedure where “ice slurry,” composed of normal saline and glycerol, is directly injected into adipose tissue, possibly leading to more efficient and effective cryolipolysis.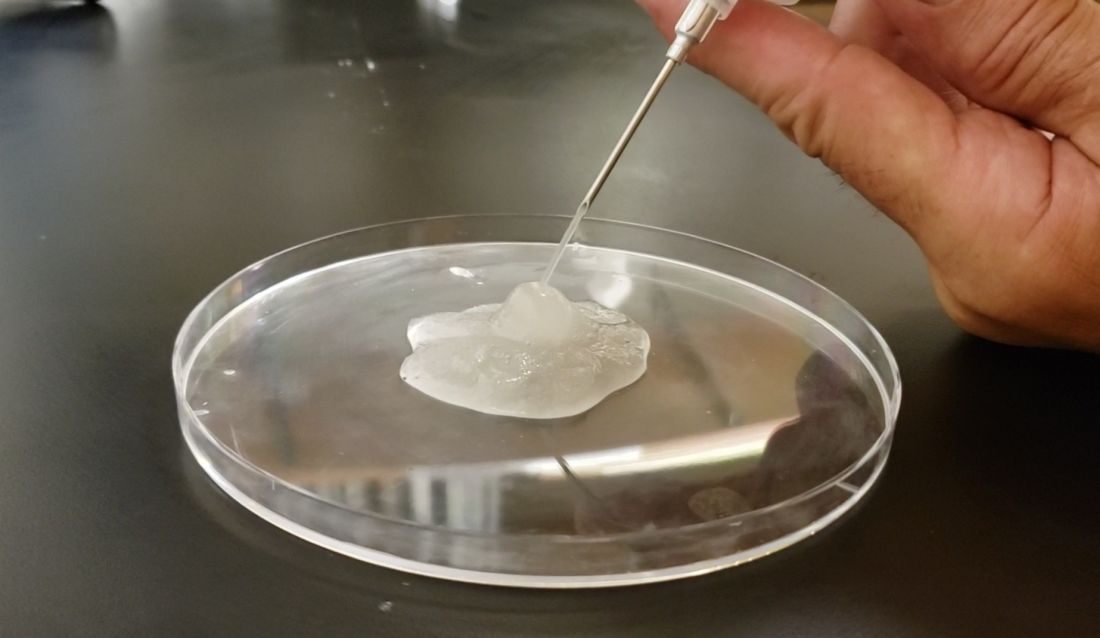
After nearly 10 years of animal studies at MGH, led by Dr. Garibyan as proof of concept trials, ice slurry (Coolio Therapy) recently received FDA breakthrough designation for long-term pain control and early-stage human trials of clinical applications are underway, she noted.
Magic Wand Program
In the Magic Wand program, participating physicians start by recording areas of unmet needs in their day-to-day practices, and in groups, engage in clinician-only brainstorming sessions to screen ideas, define problems, and generate lists of specifications and tools needed to address clinical problems. After working together to define challenges and possible solutions, they take their ideas to a development team, where scientists, engineers, regulatory experts, and industry professionals meet and help clinicians start pilot proof-of-concept projects, develop prototypes, and gain support for studies, followed by pilot feasibility studies.

Part of the project is the Virtual Magic Wand (VMW) Initiative, a 10-month online instructive and interactive course open to clinicians in the United States and Europe, designed to bring together dermatologists “interested in deeply understanding a dermatologic clinical problem worth solving,” according to Dr. Garibyan. Currently, there are more than 86 VMW scholars from 46 institutions, and military and private practice sites in the United States. The VMW was expanded to Europe in 2021 and there are plans to expand to Asia as well, she said.
The success of the program is not only attributed to its clinical methods but the fact that it provides a benefit to doctors at all stages of their careers, patients, and industry. “This is the only program that aims to engage in innovation from resident to full professor. We provide ideas that industry can then support and bring to market. Everyone including patients, doctors, and healthcare companies can benefit from active, engaged, and innovative physicians,” Dr. Garibyan said.
One of the success stories is that of Veradermics, a company founded by Kansas City dermatologist, Reid A. Waldman, MD, the company’s CEO, and Tim Durso, MD, the president, who met while participating in the VMW program in 2020, which eventually led them to start a company addressing an unmet need in dermatology, a kid-friendly treatment of warts.
In an interview with this news organization, Dr. Waldman explained how the program informed his company’s ethos. “Magic Wand Initiative is about identifying problems worth solving,” he said. At the company, “we find problems or unmet needs that are large enough to motivate prescribing changes, so we’ve really taken the philosophy I learned in the program into this company and building our portfolio.”
One of the first needs that Veradermics addressed was the fact that treatment for common warts, cryotherapy with liquid nitrogen, is painful and can frighten children, and, with a response rate of “at best, 50%,” Dr. Waldman said. Veradermics is in the process of creating a nearly painless, child-friendly wart treatment: an “immunostimulatory dissolvable microarray” patch that contains Candida antigen extract, which is currently being evaluated for treating warts in a phase 2 clinical trial started in 2023.
Although the Magic Wand Initiative was initially restricted to dermatologists at MGH, stories like that of Veradermics have made the program so popular that it has branched out to include anesthesiologists and otolaryngologists, as well as general and orthopedic surgeons at MGH, Dr. Garibyan said at the Mount Sinai meeting.
Dr. Garibyan disclosed that she is a cofounder of and has equity in Brixton Biosciences and EyeCool, and is a consultant for and/or investor in Brixton and Clarity Cosmetics. Royalties/inventorship are assigned to MGH.
NEW YORK – .
The program was founded in 2013 by two Harvard Medical School dermatologists, Lilit Garibyan, MD, PhD, the program director, and her mentor R. Rox Anderson MD, director of the Wellman Center for Photomedicine at Massachusetts General Hospital (MGH), Boston. It was based on the idea that clinicians are in a unique position to identify gaps in patient care and should be active in developing medical solutions to address those gaps.
“I truly believe that if we do a better job educating, training, and empowering our clinicians to become innovators, this will benefit patients and hospitals and physicians,” Dr. Garibyan said at the 26th annual Mount Sinai Winter Symposium — Advances in Medical and Surgical Dermatology.
One of the seeds for the project was her own experience with cryolipolysis which involves topical cooling, a noninvasive method of removing subcutaneous fat for body contouring, which relies on conducting heat from subcutaneous fat across the skin and therefore, does not reach fat far from the dermis. With Dr. Anderson’s mentorship, she developed injectable cooling technology (ICT), a procedure where “ice slurry,” composed of normal saline and glycerol, is directly injected into adipose tissue, possibly leading to more efficient and effective cryolipolysis.
After nearly 10 years of animal studies at MGH, led by Dr. Garibyan as proof of concept trials, ice slurry (Coolio Therapy) recently received FDA breakthrough designation for long-term pain control and early-stage human trials of clinical applications are underway, she noted.
Magic Wand Program
In the Magic Wand program, participating physicians start by recording areas of unmet needs in their day-to-day practices, and in groups, engage in clinician-only brainstorming sessions to screen ideas, define problems, and generate lists of specifications and tools needed to address clinical problems. After working together to define challenges and possible solutions, they take their ideas to a development team, where scientists, engineers, regulatory experts, and industry professionals meet and help clinicians start pilot proof-of-concept projects, develop prototypes, and gain support for studies, followed by pilot feasibility studies.
Part of the project is the Virtual Magic Wand (VMW) Initiative, a 10-month online instructive and interactive course open to clinicians in the United States and Europe, designed to bring together dermatologists “interested in deeply understanding a dermatologic clinical problem worth solving,” according to Dr. Garibyan. Currently, there are more than 86 VMW scholars from 46 institutions, and military and private practice sites in the United States. The VMW was expanded to Europe in 2021 and there are plans to expand to Asia as well, she said.
The success of the program is not only attributed to its clinical methods but the fact that it provides a benefit to doctors at all stages of their careers, patients, and industry. “This is the only program that aims to engage in innovation from resident to full professor. We provide ideas that industry can then support and bring to market. Everyone including patients, doctors, and healthcare companies can benefit from active, engaged, and innovative physicians,” Dr. Garibyan said.
One of the success stories is that of Veradermics, a company founded by Kansas City dermatologist, Reid A. Waldman, MD, the company’s CEO, and Tim Durso, MD, the president, who met while participating in the VMW program in 2020, which eventually led them to start a company addressing an unmet need in dermatology, a kid-friendly treatment of warts.
In an interview with this news organization, Dr. Waldman explained how the program informed his company’s ethos. “Magic Wand Initiative is about identifying problems worth solving,” he said. At the company, “we find problems or unmet needs that are large enough to motivate prescribing changes, so we’ve really taken the philosophy I learned in the program into this company and building our portfolio.”
One of the first needs that Veradermics addressed was the fact that treatment for common warts, cryotherapy with liquid nitrogen, is painful and can frighten children, and, with a response rate of “at best, 50%,” Dr. Waldman said. Veradermics is in the process of creating a nearly painless, child-friendly wart treatment: an “immunostimulatory dissolvable microarray” patch that contains Candida antigen extract, which is currently being evaluated for treating warts in a phase 2 clinical trial started in 2023.
Although the Magic Wand Initiative was initially restricted to dermatologists at MGH, stories like that of Veradermics have made the program so popular that it has branched out to include anesthesiologists and otolaryngologists, as well as general and orthopedic surgeons at MGH, Dr. Garibyan said at the Mount Sinai meeting.
Dr. Garibyan disclosed that she is a cofounder of and has equity in Brixton Biosciences and EyeCool, and is a consultant for and/or investor in Brixton and Clarity Cosmetics. Royalties/inventorship are assigned to MGH.
NEW YORK – .
The program was founded in 2013 by two Harvard Medical School dermatologists, Lilit Garibyan, MD, PhD, the program director, and her mentor R. Rox Anderson MD, director of the Wellman Center for Photomedicine at Massachusetts General Hospital (MGH), Boston. It was based on the idea that clinicians are in a unique position to identify gaps in patient care and should be active in developing medical solutions to address those gaps.
“I truly believe that if we do a better job educating, training, and empowering our clinicians to become innovators, this will benefit patients and hospitals and physicians,” Dr. Garibyan said at the 26th annual Mount Sinai Winter Symposium — Advances in Medical and Surgical Dermatology.
One of the seeds for the project was her own experience with cryolipolysis which involves topical cooling, a noninvasive method of removing subcutaneous fat for body contouring, which relies on conducting heat from subcutaneous fat across the skin and therefore, does not reach fat far from the dermis. With Dr. Anderson’s mentorship, she developed injectable cooling technology (ICT), a procedure where “ice slurry,” composed of normal saline and glycerol, is directly injected into adipose tissue, possibly leading to more efficient and effective cryolipolysis.
After nearly 10 years of animal studies at MGH, led by Dr. Garibyan as proof of concept trials, ice slurry (Coolio Therapy) recently received FDA breakthrough designation for long-term pain control and early-stage human trials of clinical applications are underway, she noted.
Magic Wand Program
In the Magic Wand program, participating physicians start by recording areas of unmet needs in their day-to-day practices, and in groups, engage in clinician-only brainstorming sessions to screen ideas, define problems, and generate lists of specifications and tools needed to address clinical problems. After working together to define challenges and possible solutions, they take their ideas to a development team, where scientists, engineers, regulatory experts, and industry professionals meet and help clinicians start pilot proof-of-concept projects, develop prototypes, and gain support for studies, followed by pilot feasibility studies.
Part of the project is the Virtual Magic Wand (VMW) Initiative, a 10-month online instructive and interactive course open to clinicians in the United States and Europe, designed to bring together dermatologists “interested in deeply understanding a dermatologic clinical problem worth solving,” according to Dr. Garibyan. Currently, there are more than 86 VMW scholars from 46 institutions, and military and private practice sites in the United States. The VMW was expanded to Europe in 2021 and there are plans to expand to Asia as well, she said.
The success of the program is not only attributed to its clinical methods but the fact that it provides a benefit to doctors at all stages of their careers, patients, and industry. “This is the only program that aims to engage in innovation from resident to full professor. We provide ideas that industry can then support and bring to market. Everyone including patients, doctors, and healthcare companies can benefit from active, engaged, and innovative physicians,” Dr. Garibyan said.
One of the success stories is that of Veradermics, a company founded by Kansas City dermatologist, Reid A. Waldman, MD, the company’s CEO, and Tim Durso, MD, the president, who met while participating in the VMW program in 2020, which eventually led them to start a company addressing an unmet need in dermatology, a kid-friendly treatment of warts.
In an interview with this news organization, Dr. Waldman explained how the program informed his company’s ethos. “Magic Wand Initiative is about identifying problems worth solving,” he said. At the company, “we find problems or unmet needs that are large enough to motivate prescribing changes, so we’ve really taken the philosophy I learned in the program into this company and building our portfolio.”
One of the first needs that Veradermics addressed was the fact that treatment for common warts, cryotherapy with liquid nitrogen, is painful and can frighten children, and, with a response rate of “at best, 50%,” Dr. Waldman said. Veradermics is in the process of creating a nearly painless, child-friendly wart treatment: an “immunostimulatory dissolvable microarray” patch that contains Candida antigen extract, which is currently being evaluated for treating warts in a phase 2 clinical trial started in 2023.
Although the Magic Wand Initiative was initially restricted to dermatologists at MGH, stories like that of Veradermics have made the program so popular that it has branched out to include anesthesiologists and otolaryngologists, as well as general and orthopedic surgeons at MGH, Dr. Garibyan said at the Mount Sinai meeting.
Dr. Garibyan disclosed that she is a cofounder of and has equity in Brixton Biosciences and EyeCool, and is a consultant for and/or investor in Brixton and Clarity Cosmetics. Royalties/inventorship are assigned to MGH.
BC axillary dissection may be unnecessary for isolated tumor cells after NAC
SAN ANTONIO — Axillary lymph node dissection is the current standard of care in breast cancer when metastases are found in sentinel lymph nodes after neoadjuvant chemotherapy.
However, what to do when isolated tumor cells instead of outright metastases are found in sentinel nodes is an open question. Some surgeons opt for a full axillary dissection while others do not, and there is no standard of care, explained Giacomo Montagna, MD, a breast cancer surgeon at Memorial Sloan Kettering Cancer Center, New York City.
The study led and presented by Dr. Montagna at the San Antonio Breast Cancer Symposium brings some much-needed clarity to the issue.
The findings argue strongly against “routine axillary lymph node dissection” — with its considerable morbidities — “in patients with residual isolated tumor cells after neoadjuvant chemotherapy,” Dr. Montagna said.
Study discussant Elizabeth Mittendorf, MD, PhD, a breast cancer surgeon at Brigham and Women’s Hospital, Boston, agreed.
“It appears that the presence of isolated tumor cells in the sentinel nodes does not negatively impact oncologic outcomes. These additional data allow us to debunk some of the surgical dogma we grew up with, specifically that lymph node dissection is required for either survival or local control,” Dr. Mittendorf said.
However, there was concern among audience members that the information gleaned from a full dissection might still be needed to guide follow-on adjuvant therapy decisions.
Dr. Mittendorf didn’t think so. Although additional positive lymph nodes were found in almost a third of women who had axillary dissections in the review, the majority of involved nodes simply had more isolated tumor cells; macrometastases were found in just 5% of cases.
So, for most patients, additional information from axillary dissections is “unlikely needed to inform adjuvant therapy, and in fact,” based on the 5% figure, “we are thinking we would have to do well over a hundred lymph node dissections in such patients to inform treatment recommendations for fewer than five. This comes at the cost of fair morbidity,” she said.
Study details
The retrospective study, dubbed OPBC05/EUBREAST-14R/ICARO, included 583 women with cT1-4 N0-3 breast cancer treated at 62 centers in 18 countries. The majority of subjects were from the United States and Europe.
Every patient was found to have isolated tumor cells (ITCs) in their sentinel lymph nodes after neoadjuvant chemotherapy (NAC), which generally included anthracycline and taxane-based regimens. The majority of patients did not have a pathologic complete response to NAC.
Overall, 182 patients (31%) had a subsequent axillary lymph node dissection; the rest did not.
Dissections were more common in the presence of lymphovascular invasion and N2/N3 disease as well as when fewer lymph nodes were removed and when ITCs were found during surgery on frozen section, which was the case in a quarter of patients.
Additional positive nodes were found in 30% of patients in the dissection group and consisted of more nodes with ITCs in 18%, micrometastases in 7%, and macrometastases in 5%. Receptor status and nodal status at presentation did not have an impact on the likelihood of finding macrometastases.
The main finding of the study was that there were no statistically significant differences in recurrence outcomes between the two groups.
The 5-year rate of isolated axillary recurrence was 1.7% with axillary lymph node dissection (ALND) versus 1.1% without it. The 5-year rate of any invasive recurrence was 16% in the ALND arm and 19% in the no-dissection group.
The median age in the study was 48 years. The majority of patients (57%) had clinical T2 tumors. Most were HR positive and either HER2 negative (41%) or HER2 positive (28%).
Regional nodal radiation was more common in the ALND group, 82% versus 75%. The dissection arm had a mean of 2.8 sentinel lymph nodes removed versus 3.5 in the no-dissection group.
“The likelihood of finding additional positive lymph nodes in patients with residual ITCs after NAC is lower than in patients with residual micro- and macrometastases. In the majority of cases, they contain ITCs. Nodal recurrence after omission of ALND is rare in this population,” the investigators concluded in their abstract.
The work was funded by EUBREAST. Dr. Montagna doesn’t have any disclosures. Dr. Mittendorf has several industry ties, including being an advisor for Roche, AstraZeneca, and Moderna and a speaker for Merck.
SAN ANTONIO — Axillary lymph node dissection is the current standard of care in breast cancer when metastases are found in sentinel lymph nodes after neoadjuvant chemotherapy.
However, what to do when isolated tumor cells instead of outright metastases are found in sentinel nodes is an open question. Some surgeons opt for a full axillary dissection while others do not, and there is no standard of care, explained Giacomo Montagna, MD, a breast cancer surgeon at Memorial Sloan Kettering Cancer Center, New York City.
The study led and presented by Dr. Montagna at the San Antonio Breast Cancer Symposium brings some much-needed clarity to the issue.
The findings argue strongly against “routine axillary lymph node dissection” — with its considerable morbidities — “in patients with residual isolated tumor cells after neoadjuvant chemotherapy,” Dr. Montagna said.
Study discussant Elizabeth Mittendorf, MD, PhD, a breast cancer surgeon at Brigham and Women’s Hospital, Boston, agreed.
“It appears that the presence of isolated tumor cells in the sentinel nodes does not negatively impact oncologic outcomes. These additional data allow us to debunk some of the surgical dogma we grew up with, specifically that lymph node dissection is required for either survival or local control,” Dr. Mittendorf said.
However, there was concern among audience members that the information gleaned from a full dissection might still be needed to guide follow-on adjuvant therapy decisions.
Dr. Mittendorf didn’t think so. Although additional positive lymph nodes were found in almost a third of women who had axillary dissections in the review, the majority of involved nodes simply had more isolated tumor cells; macrometastases were found in just 5% of cases.
So, for most patients, additional information from axillary dissections is “unlikely needed to inform adjuvant therapy, and in fact,” based on the 5% figure, “we are thinking we would have to do well over a hundred lymph node dissections in such patients to inform treatment recommendations for fewer than five. This comes at the cost of fair morbidity,” she said.
Study details
The retrospective study, dubbed OPBC05/EUBREAST-14R/ICARO, included 583 women with cT1-4 N0-3 breast cancer treated at 62 centers in 18 countries. The majority of subjects were from the United States and Europe.
Every patient was found to have isolated tumor cells (ITCs) in their sentinel lymph nodes after neoadjuvant chemotherapy (NAC), which generally included anthracycline and taxane-based regimens. The majority of patients did not have a pathologic complete response to NAC.
Overall, 182 patients (31%) had a subsequent axillary lymph node dissection; the rest did not.
Dissections were more common in the presence of lymphovascular invasion and N2/N3 disease as well as when fewer lymph nodes were removed and when ITCs were found during surgery on frozen section, which was the case in a quarter of patients.
Additional positive nodes were found in 30% of patients in the dissection group and consisted of more nodes with ITCs in 18%, micrometastases in 7%, and macrometastases in 5%. Receptor status and nodal status at presentation did not have an impact on the likelihood of finding macrometastases.
The main finding of the study was that there were no statistically significant differences in recurrence outcomes between the two groups.
The 5-year rate of isolated axillary recurrence was 1.7% with axillary lymph node dissection (ALND) versus 1.1% without it. The 5-year rate of any invasive recurrence was 16% in the ALND arm and 19% in the no-dissection group.
The median age in the study was 48 years. The majority of patients (57%) had clinical T2 tumors. Most were HR positive and either HER2 negative (41%) or HER2 positive (28%).
Regional nodal radiation was more common in the ALND group, 82% versus 75%. The dissection arm had a mean of 2.8 sentinel lymph nodes removed versus 3.5 in the no-dissection group.
“The likelihood of finding additional positive lymph nodes in patients with residual ITCs after NAC is lower than in patients with residual micro- and macrometastases. In the majority of cases, they contain ITCs. Nodal recurrence after omission of ALND is rare in this population,” the investigators concluded in their abstract.
The work was funded by EUBREAST. Dr. Montagna doesn’t have any disclosures. Dr. Mittendorf has several industry ties, including being an advisor for Roche, AstraZeneca, and Moderna and a speaker for Merck.
SAN ANTONIO — Axillary lymph node dissection is the current standard of care in breast cancer when metastases are found in sentinel lymph nodes after neoadjuvant chemotherapy.
However, what to do when isolated tumor cells instead of outright metastases are found in sentinel nodes is an open question. Some surgeons opt for a full axillary dissection while others do not, and there is no standard of care, explained Giacomo Montagna, MD, a breast cancer surgeon at Memorial Sloan Kettering Cancer Center, New York City.
The study led and presented by Dr. Montagna at the San Antonio Breast Cancer Symposium brings some much-needed clarity to the issue.
The findings argue strongly against “routine axillary lymph node dissection” — with its considerable morbidities — “in patients with residual isolated tumor cells after neoadjuvant chemotherapy,” Dr. Montagna said.
Study discussant Elizabeth Mittendorf, MD, PhD, a breast cancer surgeon at Brigham and Women’s Hospital, Boston, agreed.
“It appears that the presence of isolated tumor cells in the sentinel nodes does not negatively impact oncologic outcomes. These additional data allow us to debunk some of the surgical dogma we grew up with, specifically that lymph node dissection is required for either survival or local control,” Dr. Mittendorf said.
However, there was concern among audience members that the information gleaned from a full dissection might still be needed to guide follow-on adjuvant therapy decisions.
Dr. Mittendorf didn’t think so. Although additional positive lymph nodes were found in almost a third of women who had axillary dissections in the review, the majority of involved nodes simply had more isolated tumor cells; macrometastases were found in just 5% of cases.
So, for most patients, additional information from axillary dissections is “unlikely needed to inform adjuvant therapy, and in fact,” based on the 5% figure, “we are thinking we would have to do well over a hundred lymph node dissections in such patients to inform treatment recommendations for fewer than five. This comes at the cost of fair morbidity,” she said.
Study details
The retrospective study, dubbed OPBC05/EUBREAST-14R/ICARO, included 583 women with cT1-4 N0-3 breast cancer treated at 62 centers in 18 countries. The majority of subjects were from the United States and Europe.
Every patient was found to have isolated tumor cells (ITCs) in their sentinel lymph nodes after neoadjuvant chemotherapy (NAC), which generally included anthracycline and taxane-based regimens. The majority of patients did not have a pathologic complete response to NAC.
Overall, 182 patients (31%) had a subsequent axillary lymph node dissection; the rest did not.
Dissections were more common in the presence of lymphovascular invasion and N2/N3 disease as well as when fewer lymph nodes were removed and when ITCs were found during surgery on frozen section, which was the case in a quarter of patients.
Additional positive nodes were found in 30% of patients in the dissection group and consisted of more nodes with ITCs in 18%, micrometastases in 7%, and macrometastases in 5%. Receptor status and nodal status at presentation did not have an impact on the likelihood of finding macrometastases.
The main finding of the study was that there were no statistically significant differences in recurrence outcomes between the two groups.
The 5-year rate of isolated axillary recurrence was 1.7% with axillary lymph node dissection (ALND) versus 1.1% without it. The 5-year rate of any invasive recurrence was 16% in the ALND arm and 19% in the no-dissection group.
The median age in the study was 48 years. The majority of patients (57%) had clinical T2 tumors. Most were HR positive and either HER2 negative (41%) or HER2 positive (28%).
Regional nodal radiation was more common in the ALND group, 82% versus 75%. The dissection arm had a mean of 2.8 sentinel lymph nodes removed versus 3.5 in the no-dissection group.
“The likelihood of finding additional positive lymph nodes in patients with residual ITCs after NAC is lower than in patients with residual micro- and macrometastases. In the majority of cases, they contain ITCs. Nodal recurrence after omission of ALND is rare in this population,” the investigators concluded in their abstract.
The work was funded by EUBREAST. Dr. Montagna doesn’t have any disclosures. Dr. Mittendorf has several industry ties, including being an advisor for Roche, AstraZeneca, and Moderna and a speaker for Merck.
AT SABCS 2023
Genetic Testing Is Recommended for Adult Patients With Epilepsy
ORLANDO — The epilepsy community has yet to come to a consensus on genetic testing. During a session at the annual meeting of the American Epilepsy Society (AES), researchers and clinicians convened to share their insights on genetic testing of adult patients with epilepsy.
Colin Ellis, MD, assistant professor of neurology at the Hospital of the University of Pennsylvania in Philadelphia, shared his clinical experience to explain the importance of genetic testing in adults patients despite access challenges, limited information on certain variants, and physician reticence.
“There’s a false misconception that genetic testing should only apply to children,” Dr. Ellis told the audience. “The earlier the onset of seizures, the more likely you are to find a genetic cause.”
Guidelines Differ
The International League Against Epilepsy Task Force for Clinical Genetic Testing, Development and Epileptic Encephalopathies (DEE) recommends conducting genetic testing in patients who have focal or generalized epilepsies to whom the following circumstances apply: autism or dysmorphism, familial history, or drug-resistant epilepsy.
However, the National Society of Genetic Counselors’ guidelines recommends genetic testing for patients who have any unexplained or idiopathic epilepsies.
Guidelines identify the patients who should get tested regardless of their age.
Personal Experience
Dr. Ellis, who has spent nearly 5 years running tests on patients with epilepsy, recently tested the 300th patient at his clinic. According to him, the yield is higher in focal epilepsy than in general epilepsy — an occurrence that counters what many believe.
“Focal epilepsies are more common than monogenic epilepsies but not intuitive to many people in the industry, despite being stated in the literature,” he said. “The absence of family history shouldn’t preclude you from genetic testing because it’s still possible to have a de novo variant not inherited from either parent.”
Genetic testing can be conducted by interrogating either the exome or the genome. However, cost remains a major barrier to access.
Dr. Ellis made several arguments supporting the use of genetic testing. First, genetic testing allows for a higher diagnostic yield (i.e., 24% versus 19% in panels and 9% in microarrays). Genetic testing provides a more comprehensive overview of a patient’s genetic landscape, and it can enhance the ability to identify certain epileptic conditions, such as those caused by monogenic epilepsy — a condition associated with 926 different genes.
“You’re also less likely to find variants of uncertain significance (VUS),” Dr. Ellis said. “Regardless, you should provide the lab with phenotype information because it will help them help you.”
Variants of Uncertain Significance
The National Human Genome Research Institute defines VUS as a variant found in a patient’s genome for which it remains unclear as to whether a health condition is causing the variant. Oftentimes, such variants have very little information available due to their rarity.
In order to resolve VUS, Dr. Ellis recommended family segregation. “If the VUS appears to be de novo, you should test the parent because if they carry the gene, then it’s probably not the cause,” he said.
Dr. Ellis outlined several steps in resolving VUS.
For starters, clinicians should determine the phenotypic fit and run some ancillary tests. For example, in the case of Glu 1 abnormalities, one should consider conducting a spinal tap to determine whether the patient has cerebral spinal fluid before taking additional action.
In addition, Dr. Ellis recommends defining variant characteristics, as it becomes important in determining whether it is appropriate to take action because the majority of variances are benign.
“The take-home point is that you should not act clinically on a VUS unless you know what you’re doing,” he said. “I also disagree with the belief that VUS are rare — it’s just that they cause so much anxiety because we’re uncomfortable with this kind of testing.”
ORLANDO — The epilepsy community has yet to come to a consensus on genetic testing. During a session at the annual meeting of the American Epilepsy Society (AES), researchers and clinicians convened to share their insights on genetic testing of adult patients with epilepsy.
Colin Ellis, MD, assistant professor of neurology at the Hospital of the University of Pennsylvania in Philadelphia, shared his clinical experience to explain the importance of genetic testing in adults patients despite access challenges, limited information on certain variants, and physician reticence.
“There’s a false misconception that genetic testing should only apply to children,” Dr. Ellis told the audience. “The earlier the onset of seizures, the more likely you are to find a genetic cause.”
Guidelines Differ
The International League Against Epilepsy Task Force for Clinical Genetic Testing, Development and Epileptic Encephalopathies (DEE) recommends conducting genetic testing in patients who have focal or generalized epilepsies to whom the following circumstances apply: autism or dysmorphism, familial history, or drug-resistant epilepsy.
However, the National Society of Genetic Counselors’ guidelines recommends genetic testing for patients who have any unexplained or idiopathic epilepsies.
Guidelines identify the patients who should get tested regardless of their age.
Personal Experience
Dr. Ellis, who has spent nearly 5 years running tests on patients with epilepsy, recently tested the 300th patient at his clinic. According to him, the yield is higher in focal epilepsy than in general epilepsy — an occurrence that counters what many believe.
“Focal epilepsies are more common than monogenic epilepsies but not intuitive to many people in the industry, despite being stated in the literature,” he said. “The absence of family history shouldn’t preclude you from genetic testing because it’s still possible to have a de novo variant not inherited from either parent.”
Genetic testing can be conducted by interrogating either the exome or the genome. However, cost remains a major barrier to access.
Dr. Ellis made several arguments supporting the use of genetic testing. First, genetic testing allows for a higher diagnostic yield (i.e., 24% versus 19% in panels and 9% in microarrays). Genetic testing provides a more comprehensive overview of a patient’s genetic landscape, and it can enhance the ability to identify certain epileptic conditions, such as those caused by monogenic epilepsy — a condition associated with 926 different genes.
“You’re also less likely to find variants of uncertain significance (VUS),” Dr. Ellis said. “Regardless, you should provide the lab with phenotype information because it will help them help you.”
Variants of Uncertain Significance
The National Human Genome Research Institute defines VUS as a variant found in a patient’s genome for which it remains unclear as to whether a health condition is causing the variant. Oftentimes, such variants have very little information available due to their rarity.
In order to resolve VUS, Dr. Ellis recommended family segregation. “If the VUS appears to be de novo, you should test the parent because if they carry the gene, then it’s probably not the cause,” he said.
Dr. Ellis outlined several steps in resolving VUS.
For starters, clinicians should determine the phenotypic fit and run some ancillary tests. For example, in the case of Glu 1 abnormalities, one should consider conducting a spinal tap to determine whether the patient has cerebral spinal fluid before taking additional action.
In addition, Dr. Ellis recommends defining variant characteristics, as it becomes important in determining whether it is appropriate to take action because the majority of variances are benign.
“The take-home point is that you should not act clinically on a VUS unless you know what you’re doing,” he said. “I also disagree with the belief that VUS are rare — it’s just that they cause so much anxiety because we’re uncomfortable with this kind of testing.”
ORLANDO — The epilepsy community has yet to come to a consensus on genetic testing. During a session at the annual meeting of the American Epilepsy Society (AES), researchers and clinicians convened to share their insights on genetic testing of adult patients with epilepsy.
Colin Ellis, MD, assistant professor of neurology at the Hospital of the University of Pennsylvania in Philadelphia, shared his clinical experience to explain the importance of genetic testing in adults patients despite access challenges, limited information on certain variants, and physician reticence.
“There’s a false misconception that genetic testing should only apply to children,” Dr. Ellis told the audience. “The earlier the onset of seizures, the more likely you are to find a genetic cause.”
Guidelines Differ
The International League Against Epilepsy Task Force for Clinical Genetic Testing, Development and Epileptic Encephalopathies (DEE) recommends conducting genetic testing in patients who have focal or generalized epilepsies to whom the following circumstances apply: autism or dysmorphism, familial history, or drug-resistant epilepsy.
However, the National Society of Genetic Counselors’ guidelines recommends genetic testing for patients who have any unexplained or idiopathic epilepsies.
Guidelines identify the patients who should get tested regardless of their age.
Personal Experience
Dr. Ellis, who has spent nearly 5 years running tests on patients with epilepsy, recently tested the 300th patient at his clinic. According to him, the yield is higher in focal epilepsy than in general epilepsy — an occurrence that counters what many believe.
“Focal epilepsies are more common than monogenic epilepsies but not intuitive to many people in the industry, despite being stated in the literature,” he said. “The absence of family history shouldn’t preclude you from genetic testing because it’s still possible to have a de novo variant not inherited from either parent.”
Genetic testing can be conducted by interrogating either the exome or the genome. However, cost remains a major barrier to access.
Dr. Ellis made several arguments supporting the use of genetic testing. First, genetic testing allows for a higher diagnostic yield (i.e., 24% versus 19% in panels and 9% in microarrays). Genetic testing provides a more comprehensive overview of a patient’s genetic landscape, and it can enhance the ability to identify certain epileptic conditions, such as those caused by monogenic epilepsy — a condition associated with 926 different genes.
“You’re also less likely to find variants of uncertain significance (VUS),” Dr. Ellis said. “Regardless, you should provide the lab with phenotype information because it will help them help you.”
Variants of Uncertain Significance
The National Human Genome Research Institute defines VUS as a variant found in a patient’s genome for which it remains unclear as to whether a health condition is causing the variant. Oftentimes, such variants have very little information available due to their rarity.
In order to resolve VUS, Dr. Ellis recommended family segregation. “If the VUS appears to be de novo, you should test the parent because if they carry the gene, then it’s probably not the cause,” he said.
Dr. Ellis outlined several steps in resolving VUS.
For starters, clinicians should determine the phenotypic fit and run some ancillary tests. For example, in the case of Glu 1 abnormalities, one should consider conducting a spinal tap to determine whether the patient has cerebral spinal fluid before taking additional action.
In addition, Dr. Ellis recommends defining variant characteristics, as it becomes important in determining whether it is appropriate to take action because the majority of variances are benign.
“The take-home point is that you should not act clinically on a VUS unless you know what you’re doing,” he said. “I also disagree with the belief that VUS are rare — it’s just that they cause so much anxiety because we’re uncomfortable with this kind of testing.”
FROM AES 2023
Gestational Diabetes Treatment Moves Forward With Uncertainty And Hope
FAIRFAX, VIRGINIA — , but researchers at the biennial meeting of the Diabetes in Pregnancy Study Group of North America expressed hope for more clarity in the near future and the ability to someday individualize treatment to account for what is increasingly viewed as a heterogeneous condition.
Until studies in 2015 and 2018 cast doubt on glyburide, “we used to have 80% [of our GDM patients] on glyburide, and 20% on insulin,” Maisa Feghali, MD, of the University of Pittsburgh, said during a discussion period. “Now we have 95% on insulin and 5% on oral hypoglycemics. I rely on insulin because I don’t have a better option, and I rely on research efforts [underway to provide better options]” in the future.
The American College of Obstetricians and Gynecologists recommends insulin as the preferred first-line pharmacologic therapy for GDM when pharmacologic therapy is needed, with metformin as an option when patients decline or cannot safely use insulin. Glyburide, ACOG said in its 2018 practice bulletin on GDM (Obstet Gynecol. 2018;131[2]:e49-64), should not be recommended as a first-line pharmacologic therapy.
The Society of Maternal-Fetal Medicine, on the other hand, has accepted metformin as a “reasonable and safe” first-line alternative to insulin — while recognizing that half of women will still require insulin to achieve glycemic control — and does not rule out consideration of glyburide. In its 2018 statement on the pharmacologic treatment of GDM, the society said that the evidence of benefit of one oral agent over another remains limited.
“When you have dueling guidelines, it means the data are not that clear,” George Saade, MD, professor and chair of obstetrics and gynecology at the Eastern Virginia School of Medicine, Norfolk, said in a presentation on GDM. An upcoming $12 million multicenter study to be led by the Ohio State University College of Medicine — coined the DECIDE trial — should provide clarity, he said.
The trial, funded by the Patient-Centered Outcomes Research Institute, which funds comparative clinical effectiveness research designed to be broadly applicable to practice, will enroll and randomize over 1500 pregnant individuals with GDM to either oral metformin or insulin and will follow mothers and children until 2 years after delivery.
The study’s primary and secondary hypotheses, respectively, are that metformin is not inferior to insulin in reducing a composite adverse neonatal outcome (large for gestational age, neonatal hypoglycemia and/or hyperbilirubemia) and that metformin does not result in increased child body mass index at 2 years, compared with insulin. It will also look at patient-reported factors associated with metformin use compared to insulin use — factors that “are important ... to enable clinical implementation of study findings,” said Dr. Saade, who played a role in designing the study over the past several years.
The study will take a pragmatic, real-world approach by ensuring racial and ethnic, socioeconomic, urban and rural, and geographic diversity at both large academic and community-based sites across the United States.
The trial, to be led by Mark Landon, MD, and Kartik Venkatesh, MD, PhD, of Ohio State University, will be the first large trial in the United States to both directly compare the ability of oral hypoglycemics and insulin to prevent GDM-associated pregnancy complications, and to follow children for 2 years, Dr. Saade said. “Prior research was either outside the United States, not randomized, not adequately powered, or had no long-term child follow-up,” he added after the meeting.
The State Of Knowledge About Oral Hypoglycemics
The trial was envisioned several years ago as a three-arm comparative trial including the sulfonylurea glyburide, but data published in recent years has increasingly “not favored” glyburide, and many providers “have stopped using it,” Dr. Saade said during and after the meeting. At this point, “it would not be useful to include it” in a pragmatic trial, he said.
Glyburide became the number one agent after a seminal trial published in 2000 (N Engl J Med. 2000;343:1134-8) showed equivalent glycemic control in about 400 women with GDM who were randomized to receive insulin or glyburide. While the trial was not powered to evaluate other outcomes, there were no significant differences in neonatal complications.
In 2015, a large retrospective population-based study (JAMA Pediatr. 2015;169[5]:452-8) of more than 9,000 women with GDM showed higher risks of neonatal intensive care admission, neonatal hypoglycemia, and large-for-gestational age with glyburide compared with insulin. “It prompted a pause in thinking,” Dr. Saade recalled at the DPSG meeting. After that, several meta-analyses/systematic reviews compared the two treatments, showing varying and sometimes conflicting degrees of difference in neonatal outcomes.
In 2018, a French noninferiority randomized controlled trial (JAMA 2018;319[17]:1773-80) did not show that glyburide is not inferior to insulin in the prevention of perinatal outcomes (macrosomia, neonatal hypoglycemia, and hyperbilirubinemia). “If you add this trial to the systematic reviews, it would probably would shift more in favor of insulin,” Dr. Saade said, noting that the trial’s supplementary data included a higher rate of maternal hypoglycemia with glyburide. “I feel personally now, with all the data, that glyburide is inferior to insulin.”
A 2021 network meta-analysis (BMC Endocr Disord. 2021;21:199) that looked at glycemic control and neonatal outcomes in GDM treated with glyburide, metformin, or insulin, also offers valuable insight, Dr. Saade said. The meta-analysis used a Bayesian framework and presents results as a ranking estimated probability of a treatment being the best or worst — or in between — for different outcomes (glycemic control and neonatal outcomes), which “is one of the best ways to look at data these days,” he said.
“It tells us how likely [it is for one agent] to be better than others. Will it work most of the time? More than 60% of the time?” Dr. Saade explained. For example, the analysis “tell us that for large for gestational age, glyburide has a 94% chance of being the worst, metformin has an 80% change of being the best, and insulin a 76% chance of being in between.”
Overall, the 2021 analysis suggests that “glyburide is the most likely to be worst in most outcomes and that there is equipoise between metformin and insulin,” he said.
Meta-analyses of pharmacologic treatment of GDM have been challenged, he said, by inconsistent reporting in trials of GDM diagnostic criteria, severity of hyperglycemia, and small sample sizes (and wide confidence intervals). Criteria for supplemental insulin are also often “unclear” in trials, Dr. Saade said, as is involvement of social determinants of health and the “care package” enveloping pharmacologic interventions.
Dr. Saade, Dr. Landon, and other researchers have also lamented over the years that there is limited long-term follow-up of exposed offspring.
The Challenge of Heterogeneity
In another presentation on GDM, Maisa Feghali, MD, MS, emphasized that GDM is a heterogeneous condition, with clinical hyperglycemia not capturing individual variation in underlying physiologic processes. A 2016 study (Diabetes Care. 2016;39[6]:1052-5) assessing insulin sensitivity and secretion in 800-plus women at 24-30 weeks’ gestation found that about 50% of those with GDM had predominant insulin resistance, 30% had predominant insulin secretion deficit, and 20% were mixed.
Those with predominant insulin resistance had higher BMI, higher fasting glucose, larger infants, and greater risk of GDM-associated adverse outcomes, “suggesting that the risk is not universal or equivalent,” said Dr. Feghali, assistant professor in the department of obstetrics, gynecology and reproductive sciences at the University of Pittsburgh and the UPCM Magee-Women’s Hospital.
A 2019 multicenter European study (Diabetologia. 2019;62[11]:2118-28) found an even higher proportion of GDM involving predominant insulin resistance and, similarly, a greater risk of adverse pregnancy outcomes in these women than in insulin-sensitive women with GDM, “again suggesting that there’s probably some benefit to looking deeper at physiology to understand individual risk,” she said.
Research published decades ago showed that insulin sensitivity decreases by over 50% during pregnancy, and “what we’ve come to recognize is there [can be] insulin secretion deficiency that’s not able to surmount or overcome the insulin resistance that develops during advanced gestation,” she said. “We need to think not at the population level but at the individual level.”
Dr. Feghali is leading the MATCh-GDM (Metabolic Analysis for Treatment Choice in GDM) study, which has been randomizing women to receive either usual, unmatched treatment or treatment matched to GDM mechanism — metformin for predominant insulin resistance, glyburide, or insulin for predominant insulin secretion defects, and one of the three for combined mechanisms. Data are not available yet.
There is still more to be learned about the pharmacologic effects of oral hypoglycemics, she noted, pointing to a 2020 study (Clin Pharmacol Ther. 2020;107[6]:1362-72) that randomized women to glyburide, metformin, or glyburide/metformin combination therapy and measured insulin sensitivity, beta-cell responsivity, and disposition index. (The latter describes the overall metabolic state and is a product of insulin sensitivity and total beta-cell responsivity.)
“Somewhat surprisingly, they found metformin performed better than glyburide,” shifting the overall disposition index closer to normal, Dr. Feghali said. “But not surprisingly, they found the combination worked best.”
Total beta-cell responsivity occurred in 56% of the glyburide group and 74% of the combination group. Improvements in insulin sensitivity occurred in 84% of the metformin group and 74% of the combination group. Surprisingly, there was “a decrease in first-phase insulin secretion” with glyburide, noted Dr. Feghali — a finding that means “the glyburide story has turned out to be a little more complicated.” With metformin, there was a positive change in insulin secretion as well as insulin sensitivity.
The authors’ conclusion, she noted, “is that there’s potential in thinking about metformin first, as the primary treatment, and then adding glyburide after that.”
Future Use Of Incretin Mimetics, and Intensive Targets in Overweight/Obesity
Dr. Feghali wonders whether incretin hormone mimetics — such as glucagonlike peptide–1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP) — could play a future role in GDM treatment, helping to increase insulin secretion.
She is currently recruiting for a pilot study on the pharmacokinetics and pharmacodynamics in GDM of exenatide, a FDA-approved GLP-1 agonist that has been shown not to cross the placenta and that should, research suggests, lower the risk of maternal hypoglycemia and limit the risk of excessive fetal growth, “overcoming some of the concerns we have with glyburide,” Dr. Feghali said.
A recent study of the gut-generated incretin response during an oral glucose tolerance test in pregnant women with and without GDM showed that post-load GLP-1 and GIP were higher in women with GDM, and that the GLP-1 secretion was associated with insulin secretion only in those with GDM (J Clin Endocrinol Metab. 2022;107(6):e2425-30). “In those with normal OGTT, insulin secretion was independent of GLP-1,” she said. “This study suggests there’s a potential role for incretin mimetics in GDM.”
Also regarding the individualization of GDM treatment, patients who are overweight or obese in the prepregnancy setting and have gestational diabetes represent a different phenotype, she noted, with higher fasting and postprandial blood glucose compared to normal-weight counterparts despite higher doses of medication.
“After controlling for gestational weight gain and glycemic control, we see there’s an independent effect of prepregnancy obesity specifically for an increased risk of macrosomia, preterm birth, and hypertensive disorders of pregnancy,” said Dr. Feghali, referring to a 2015 retrospective study of GDM and obesity (Obstet Gynecol. 2015;126:316-25). “It suggests that we might think about redrawing the line, not on diagnosis and screening but on treatment.”
The randomized, controlled Intensive Glycemic Targets in Overweight and Obese Women with Gestational Diabetes Mellitus (iGDM) trial, is now recruiting at multiple centers, including at Dr. Feghali’s University of Pittsburgh, and will investigate the effect of intensive glycemic targets (fasting < 90 mg/dL, 1-hour postprandial < 120 mg/dL) versus standard glycemic targets (fasting < 95 mg/dL, 1-hour postprandial < 140 mg/dL), she said.
In another presentation on GDM, Monica Longo, MD, PhD, of the Inova Health System in Fairfax, Va., said researchers are also looking at whether nutritional supplements such as myo-inositol can reduce the risk of adverse pregnancy outcomes in GDM, and whether probiotics can improve insulin sensitivity in some patients.
Data on newer insulin analogs in pregnancy are lacking, she noted. “Preliminary data has shown no malformations in infants, but there is some increase in hypoglycemia-related admissions to the NICU,” she said. “It’s worth it [to research more].”
FAIRFAX, VIRGINIA — , but researchers at the biennial meeting of the Diabetes in Pregnancy Study Group of North America expressed hope for more clarity in the near future and the ability to someday individualize treatment to account for what is increasingly viewed as a heterogeneous condition.
Until studies in 2015 and 2018 cast doubt on glyburide, “we used to have 80% [of our GDM patients] on glyburide, and 20% on insulin,” Maisa Feghali, MD, of the University of Pittsburgh, said during a discussion period. “Now we have 95% on insulin and 5% on oral hypoglycemics. I rely on insulin because I don’t have a better option, and I rely on research efforts [underway to provide better options]” in the future.
The American College of Obstetricians and Gynecologists recommends insulin as the preferred first-line pharmacologic therapy for GDM when pharmacologic therapy is needed, with metformin as an option when patients decline or cannot safely use insulin. Glyburide, ACOG said in its 2018 practice bulletin on GDM (Obstet Gynecol. 2018;131[2]:e49-64), should not be recommended as a first-line pharmacologic therapy.
The Society of Maternal-Fetal Medicine, on the other hand, has accepted metformin as a “reasonable and safe” first-line alternative to insulin — while recognizing that half of women will still require insulin to achieve glycemic control — and does not rule out consideration of glyburide. In its 2018 statement on the pharmacologic treatment of GDM, the society said that the evidence of benefit of one oral agent over another remains limited.
“When you have dueling guidelines, it means the data are not that clear,” George Saade, MD, professor and chair of obstetrics and gynecology at the Eastern Virginia School of Medicine, Norfolk, said in a presentation on GDM. An upcoming $12 million multicenter study to be led by the Ohio State University College of Medicine — coined the DECIDE trial — should provide clarity, he said.
The trial, funded by the Patient-Centered Outcomes Research Institute, which funds comparative clinical effectiveness research designed to be broadly applicable to practice, will enroll and randomize over 1500 pregnant individuals with GDM to either oral metformin or insulin and will follow mothers and children until 2 years after delivery.
The study’s primary and secondary hypotheses, respectively, are that metformin is not inferior to insulin in reducing a composite adverse neonatal outcome (large for gestational age, neonatal hypoglycemia and/or hyperbilirubemia) and that metformin does not result in increased child body mass index at 2 years, compared with insulin. It will also look at patient-reported factors associated with metformin use compared to insulin use — factors that “are important ... to enable clinical implementation of study findings,” said Dr. Saade, who played a role in designing the study over the past several years.
The study will take a pragmatic, real-world approach by ensuring racial and ethnic, socioeconomic, urban and rural, and geographic diversity at both large academic and community-based sites across the United States.
The trial, to be led by Mark Landon, MD, and Kartik Venkatesh, MD, PhD, of Ohio State University, will be the first large trial in the United States to both directly compare the ability of oral hypoglycemics and insulin to prevent GDM-associated pregnancy complications, and to follow children for 2 years, Dr. Saade said. “Prior research was either outside the United States, not randomized, not adequately powered, or had no long-term child follow-up,” he added after the meeting.
The State Of Knowledge About Oral Hypoglycemics
The trial was envisioned several years ago as a three-arm comparative trial including the sulfonylurea glyburide, but data published in recent years has increasingly “not favored” glyburide, and many providers “have stopped using it,” Dr. Saade said during and after the meeting. At this point, “it would not be useful to include it” in a pragmatic trial, he said.
Glyburide became the number one agent after a seminal trial published in 2000 (N Engl J Med. 2000;343:1134-8) showed equivalent glycemic control in about 400 women with GDM who were randomized to receive insulin or glyburide. While the trial was not powered to evaluate other outcomes, there were no significant differences in neonatal complications.
In 2015, a large retrospective population-based study (JAMA Pediatr. 2015;169[5]:452-8) of more than 9,000 women with GDM showed higher risks of neonatal intensive care admission, neonatal hypoglycemia, and large-for-gestational age with glyburide compared with insulin. “It prompted a pause in thinking,” Dr. Saade recalled at the DPSG meeting. After that, several meta-analyses/systematic reviews compared the two treatments, showing varying and sometimes conflicting degrees of difference in neonatal outcomes.
In 2018, a French noninferiority randomized controlled trial (JAMA 2018;319[17]:1773-80) did not show that glyburide is not inferior to insulin in the prevention of perinatal outcomes (macrosomia, neonatal hypoglycemia, and hyperbilirubinemia). “If you add this trial to the systematic reviews, it would probably would shift more in favor of insulin,” Dr. Saade said, noting that the trial’s supplementary data included a higher rate of maternal hypoglycemia with glyburide. “I feel personally now, with all the data, that glyburide is inferior to insulin.”
A 2021 network meta-analysis (BMC Endocr Disord. 2021;21:199) that looked at glycemic control and neonatal outcomes in GDM treated with glyburide, metformin, or insulin, also offers valuable insight, Dr. Saade said. The meta-analysis used a Bayesian framework and presents results as a ranking estimated probability of a treatment being the best or worst — or in between — for different outcomes (glycemic control and neonatal outcomes), which “is one of the best ways to look at data these days,” he said.
“It tells us how likely [it is for one agent] to be better than others. Will it work most of the time? More than 60% of the time?” Dr. Saade explained. For example, the analysis “tell us that for large for gestational age, glyburide has a 94% chance of being the worst, metformin has an 80% change of being the best, and insulin a 76% chance of being in between.”
Overall, the 2021 analysis suggests that “glyburide is the most likely to be worst in most outcomes and that there is equipoise between metformin and insulin,” he said.
Meta-analyses of pharmacologic treatment of GDM have been challenged, he said, by inconsistent reporting in trials of GDM diagnostic criteria, severity of hyperglycemia, and small sample sizes (and wide confidence intervals). Criteria for supplemental insulin are also often “unclear” in trials, Dr. Saade said, as is involvement of social determinants of health and the “care package” enveloping pharmacologic interventions.
Dr. Saade, Dr. Landon, and other researchers have also lamented over the years that there is limited long-term follow-up of exposed offspring.
The Challenge of Heterogeneity
In another presentation on GDM, Maisa Feghali, MD, MS, emphasized that GDM is a heterogeneous condition, with clinical hyperglycemia not capturing individual variation in underlying physiologic processes. A 2016 study (Diabetes Care. 2016;39[6]:1052-5) assessing insulin sensitivity and secretion in 800-plus women at 24-30 weeks’ gestation found that about 50% of those with GDM had predominant insulin resistance, 30% had predominant insulin secretion deficit, and 20% were mixed.
Those with predominant insulin resistance had higher BMI, higher fasting glucose, larger infants, and greater risk of GDM-associated adverse outcomes, “suggesting that the risk is not universal or equivalent,” said Dr. Feghali, assistant professor in the department of obstetrics, gynecology and reproductive sciences at the University of Pittsburgh and the UPCM Magee-Women’s Hospital.
A 2019 multicenter European study (Diabetologia. 2019;62[11]:2118-28) found an even higher proportion of GDM involving predominant insulin resistance and, similarly, a greater risk of adverse pregnancy outcomes in these women than in insulin-sensitive women with GDM, “again suggesting that there’s probably some benefit to looking deeper at physiology to understand individual risk,” she said.
Research published decades ago showed that insulin sensitivity decreases by over 50% during pregnancy, and “what we’ve come to recognize is there [can be] insulin secretion deficiency that’s not able to surmount or overcome the insulin resistance that develops during advanced gestation,” she said. “We need to think not at the population level but at the individual level.”
Dr. Feghali is leading the MATCh-GDM (Metabolic Analysis for Treatment Choice in GDM) study, which has been randomizing women to receive either usual, unmatched treatment or treatment matched to GDM mechanism — metformin for predominant insulin resistance, glyburide, or insulin for predominant insulin secretion defects, and one of the three for combined mechanisms. Data are not available yet.
There is still more to be learned about the pharmacologic effects of oral hypoglycemics, she noted, pointing to a 2020 study (Clin Pharmacol Ther. 2020;107[6]:1362-72) that randomized women to glyburide, metformin, or glyburide/metformin combination therapy and measured insulin sensitivity, beta-cell responsivity, and disposition index. (The latter describes the overall metabolic state and is a product of insulin sensitivity and total beta-cell responsivity.)
“Somewhat surprisingly, they found metformin performed better than glyburide,” shifting the overall disposition index closer to normal, Dr. Feghali said. “But not surprisingly, they found the combination worked best.”
Total beta-cell responsivity occurred in 56% of the glyburide group and 74% of the combination group. Improvements in insulin sensitivity occurred in 84% of the metformin group and 74% of the combination group. Surprisingly, there was “a decrease in first-phase insulin secretion” with glyburide, noted Dr. Feghali — a finding that means “the glyburide story has turned out to be a little more complicated.” With metformin, there was a positive change in insulin secretion as well as insulin sensitivity.
The authors’ conclusion, she noted, “is that there’s potential in thinking about metformin first, as the primary treatment, and then adding glyburide after that.”
Future Use Of Incretin Mimetics, and Intensive Targets in Overweight/Obesity
Dr. Feghali wonders whether incretin hormone mimetics — such as glucagonlike peptide–1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP) — could play a future role in GDM treatment, helping to increase insulin secretion.
She is currently recruiting for a pilot study on the pharmacokinetics and pharmacodynamics in GDM of exenatide, a FDA-approved GLP-1 agonist that has been shown not to cross the placenta and that should, research suggests, lower the risk of maternal hypoglycemia and limit the risk of excessive fetal growth, “overcoming some of the concerns we have with glyburide,” Dr. Feghali said.
A recent study of the gut-generated incretin response during an oral glucose tolerance test in pregnant women with and without GDM showed that post-load GLP-1 and GIP were higher in women with GDM, and that the GLP-1 secretion was associated with insulin secretion only in those with GDM (J Clin Endocrinol Metab. 2022;107(6):e2425-30). “In those with normal OGTT, insulin secretion was independent of GLP-1,” she said. “This study suggests there’s a potential role for incretin mimetics in GDM.”
Also regarding the individualization of GDM treatment, patients who are overweight or obese in the prepregnancy setting and have gestational diabetes represent a different phenotype, she noted, with higher fasting and postprandial blood glucose compared to normal-weight counterparts despite higher doses of medication.
“After controlling for gestational weight gain and glycemic control, we see there’s an independent effect of prepregnancy obesity specifically for an increased risk of macrosomia, preterm birth, and hypertensive disorders of pregnancy,” said Dr. Feghali, referring to a 2015 retrospective study of GDM and obesity (Obstet Gynecol. 2015;126:316-25). “It suggests that we might think about redrawing the line, not on diagnosis and screening but on treatment.”
The randomized, controlled Intensive Glycemic Targets in Overweight and Obese Women with Gestational Diabetes Mellitus (iGDM) trial, is now recruiting at multiple centers, including at Dr. Feghali’s University of Pittsburgh, and will investigate the effect of intensive glycemic targets (fasting < 90 mg/dL, 1-hour postprandial < 120 mg/dL) versus standard glycemic targets (fasting < 95 mg/dL, 1-hour postprandial < 140 mg/dL), she said.
In another presentation on GDM, Monica Longo, MD, PhD, of the Inova Health System in Fairfax, Va., said researchers are also looking at whether nutritional supplements such as myo-inositol can reduce the risk of adverse pregnancy outcomes in GDM, and whether probiotics can improve insulin sensitivity in some patients.
Data on newer insulin analogs in pregnancy are lacking, she noted. “Preliminary data has shown no malformations in infants, but there is some increase in hypoglycemia-related admissions to the NICU,” she said. “It’s worth it [to research more].”
FAIRFAX, VIRGINIA — , but researchers at the biennial meeting of the Diabetes in Pregnancy Study Group of North America expressed hope for more clarity in the near future and the ability to someday individualize treatment to account for what is increasingly viewed as a heterogeneous condition.
Until studies in 2015 and 2018 cast doubt on glyburide, “we used to have 80% [of our GDM patients] on glyburide, and 20% on insulin,” Maisa Feghali, MD, of the University of Pittsburgh, said during a discussion period. “Now we have 95% on insulin and 5% on oral hypoglycemics. I rely on insulin because I don’t have a better option, and I rely on research efforts [underway to provide better options]” in the future.
The American College of Obstetricians and Gynecologists recommends insulin as the preferred first-line pharmacologic therapy for GDM when pharmacologic therapy is needed, with metformin as an option when patients decline or cannot safely use insulin. Glyburide, ACOG said in its 2018 practice bulletin on GDM (Obstet Gynecol. 2018;131[2]:e49-64), should not be recommended as a first-line pharmacologic therapy.
The Society of Maternal-Fetal Medicine, on the other hand, has accepted metformin as a “reasonable and safe” first-line alternative to insulin — while recognizing that half of women will still require insulin to achieve glycemic control — and does not rule out consideration of glyburide. In its 2018 statement on the pharmacologic treatment of GDM, the society said that the evidence of benefit of one oral agent over another remains limited.
“When you have dueling guidelines, it means the data are not that clear,” George Saade, MD, professor and chair of obstetrics and gynecology at the Eastern Virginia School of Medicine, Norfolk, said in a presentation on GDM. An upcoming $12 million multicenter study to be led by the Ohio State University College of Medicine — coined the DECIDE trial — should provide clarity, he said.
The trial, funded by the Patient-Centered Outcomes Research Institute, which funds comparative clinical effectiveness research designed to be broadly applicable to practice, will enroll and randomize over 1500 pregnant individuals with GDM to either oral metformin or insulin and will follow mothers and children until 2 years after delivery.
The study’s primary and secondary hypotheses, respectively, are that metformin is not inferior to insulin in reducing a composite adverse neonatal outcome (large for gestational age, neonatal hypoglycemia and/or hyperbilirubemia) and that metformin does not result in increased child body mass index at 2 years, compared with insulin. It will also look at patient-reported factors associated with metformin use compared to insulin use — factors that “are important ... to enable clinical implementation of study findings,” said Dr. Saade, who played a role in designing the study over the past several years.
The study will take a pragmatic, real-world approach by ensuring racial and ethnic, socioeconomic, urban and rural, and geographic diversity at both large academic and community-based sites across the United States.
The trial, to be led by Mark Landon, MD, and Kartik Venkatesh, MD, PhD, of Ohio State University, will be the first large trial in the United States to both directly compare the ability of oral hypoglycemics and insulin to prevent GDM-associated pregnancy complications, and to follow children for 2 years, Dr. Saade said. “Prior research was either outside the United States, not randomized, not adequately powered, or had no long-term child follow-up,” he added after the meeting.
The State Of Knowledge About Oral Hypoglycemics
The trial was envisioned several years ago as a three-arm comparative trial including the sulfonylurea glyburide, but data published in recent years has increasingly “not favored” glyburide, and many providers “have stopped using it,” Dr. Saade said during and after the meeting. At this point, “it would not be useful to include it” in a pragmatic trial, he said.
Glyburide became the number one agent after a seminal trial published in 2000 (N Engl J Med. 2000;343:1134-8) showed equivalent glycemic control in about 400 women with GDM who were randomized to receive insulin or glyburide. While the trial was not powered to evaluate other outcomes, there were no significant differences in neonatal complications.
In 2015, a large retrospective population-based study (JAMA Pediatr. 2015;169[5]:452-8) of more than 9,000 women with GDM showed higher risks of neonatal intensive care admission, neonatal hypoglycemia, and large-for-gestational age with glyburide compared with insulin. “It prompted a pause in thinking,” Dr. Saade recalled at the DPSG meeting. After that, several meta-analyses/systematic reviews compared the two treatments, showing varying and sometimes conflicting degrees of difference in neonatal outcomes.
In 2018, a French noninferiority randomized controlled trial (JAMA 2018;319[17]:1773-80) did not show that glyburide is not inferior to insulin in the prevention of perinatal outcomes (macrosomia, neonatal hypoglycemia, and hyperbilirubinemia). “If you add this trial to the systematic reviews, it would probably would shift more in favor of insulin,” Dr. Saade said, noting that the trial’s supplementary data included a higher rate of maternal hypoglycemia with glyburide. “I feel personally now, with all the data, that glyburide is inferior to insulin.”
A 2021 network meta-analysis (BMC Endocr Disord. 2021;21:199) that looked at glycemic control and neonatal outcomes in GDM treated with glyburide, metformin, or insulin, also offers valuable insight, Dr. Saade said. The meta-analysis used a Bayesian framework and presents results as a ranking estimated probability of a treatment being the best or worst — or in between — for different outcomes (glycemic control and neonatal outcomes), which “is one of the best ways to look at data these days,” he said.
“It tells us how likely [it is for one agent] to be better than others. Will it work most of the time? More than 60% of the time?” Dr. Saade explained. For example, the analysis “tell us that for large for gestational age, glyburide has a 94% chance of being the worst, metformin has an 80% change of being the best, and insulin a 76% chance of being in between.”
Overall, the 2021 analysis suggests that “glyburide is the most likely to be worst in most outcomes and that there is equipoise between metformin and insulin,” he said.
Meta-analyses of pharmacologic treatment of GDM have been challenged, he said, by inconsistent reporting in trials of GDM diagnostic criteria, severity of hyperglycemia, and small sample sizes (and wide confidence intervals). Criteria for supplemental insulin are also often “unclear” in trials, Dr. Saade said, as is involvement of social determinants of health and the “care package” enveloping pharmacologic interventions.
Dr. Saade, Dr. Landon, and other researchers have also lamented over the years that there is limited long-term follow-up of exposed offspring.
The Challenge of Heterogeneity
In another presentation on GDM, Maisa Feghali, MD, MS, emphasized that GDM is a heterogeneous condition, with clinical hyperglycemia not capturing individual variation in underlying physiologic processes. A 2016 study (Diabetes Care. 2016;39[6]:1052-5) assessing insulin sensitivity and secretion in 800-plus women at 24-30 weeks’ gestation found that about 50% of those with GDM had predominant insulin resistance, 30% had predominant insulin secretion deficit, and 20% were mixed.
Those with predominant insulin resistance had higher BMI, higher fasting glucose, larger infants, and greater risk of GDM-associated adverse outcomes, “suggesting that the risk is not universal or equivalent,” said Dr. Feghali, assistant professor in the department of obstetrics, gynecology and reproductive sciences at the University of Pittsburgh and the UPCM Magee-Women’s Hospital.
A 2019 multicenter European study (Diabetologia. 2019;62[11]:2118-28) found an even higher proportion of GDM involving predominant insulin resistance and, similarly, a greater risk of adverse pregnancy outcomes in these women than in insulin-sensitive women with GDM, “again suggesting that there’s probably some benefit to looking deeper at physiology to understand individual risk,” she said.
Research published decades ago showed that insulin sensitivity decreases by over 50% during pregnancy, and “what we’ve come to recognize is there [can be] insulin secretion deficiency that’s not able to surmount or overcome the insulin resistance that develops during advanced gestation,” she said. “We need to think not at the population level but at the individual level.”
Dr. Feghali is leading the MATCh-GDM (Metabolic Analysis for Treatment Choice in GDM) study, which has been randomizing women to receive either usual, unmatched treatment or treatment matched to GDM mechanism — metformin for predominant insulin resistance, glyburide, or insulin for predominant insulin secretion defects, and one of the three for combined mechanisms. Data are not available yet.
There is still more to be learned about the pharmacologic effects of oral hypoglycemics, she noted, pointing to a 2020 study (Clin Pharmacol Ther. 2020;107[6]:1362-72) that randomized women to glyburide, metformin, or glyburide/metformin combination therapy and measured insulin sensitivity, beta-cell responsivity, and disposition index. (The latter describes the overall metabolic state and is a product of insulin sensitivity and total beta-cell responsivity.)
“Somewhat surprisingly, they found metformin performed better than glyburide,” shifting the overall disposition index closer to normal, Dr. Feghali said. “But not surprisingly, they found the combination worked best.”
Total beta-cell responsivity occurred in 56% of the glyburide group and 74% of the combination group. Improvements in insulin sensitivity occurred in 84% of the metformin group and 74% of the combination group. Surprisingly, there was “a decrease in first-phase insulin secretion” with glyburide, noted Dr. Feghali — a finding that means “the glyburide story has turned out to be a little more complicated.” With metformin, there was a positive change in insulin secretion as well as insulin sensitivity.
The authors’ conclusion, she noted, “is that there’s potential in thinking about metformin first, as the primary treatment, and then adding glyburide after that.”
Future Use Of Incretin Mimetics, and Intensive Targets in Overweight/Obesity
Dr. Feghali wonders whether incretin hormone mimetics — such as glucagonlike peptide–1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP) — could play a future role in GDM treatment, helping to increase insulin secretion.
She is currently recruiting for a pilot study on the pharmacokinetics and pharmacodynamics in GDM of exenatide, a FDA-approved GLP-1 agonist that has been shown not to cross the placenta and that should, research suggests, lower the risk of maternal hypoglycemia and limit the risk of excessive fetal growth, “overcoming some of the concerns we have with glyburide,” Dr. Feghali said.
A recent study of the gut-generated incretin response during an oral glucose tolerance test in pregnant women with and without GDM showed that post-load GLP-1 and GIP were higher in women with GDM, and that the GLP-1 secretion was associated with insulin secretion only in those with GDM (J Clin Endocrinol Metab. 2022;107(6):e2425-30). “In those with normal OGTT, insulin secretion was independent of GLP-1,” she said. “This study suggests there’s a potential role for incretin mimetics in GDM.”
Also regarding the individualization of GDM treatment, patients who are overweight or obese in the prepregnancy setting and have gestational diabetes represent a different phenotype, she noted, with higher fasting and postprandial blood glucose compared to normal-weight counterparts despite higher doses of medication.
“After controlling for gestational weight gain and glycemic control, we see there’s an independent effect of prepregnancy obesity specifically for an increased risk of macrosomia, preterm birth, and hypertensive disorders of pregnancy,” said Dr. Feghali, referring to a 2015 retrospective study of GDM and obesity (Obstet Gynecol. 2015;126:316-25). “It suggests that we might think about redrawing the line, not on diagnosis and screening but on treatment.”
The randomized, controlled Intensive Glycemic Targets in Overweight and Obese Women with Gestational Diabetes Mellitus (iGDM) trial, is now recruiting at multiple centers, including at Dr. Feghali’s University of Pittsburgh, and will investigate the effect of intensive glycemic targets (fasting < 90 mg/dL, 1-hour postprandial < 120 mg/dL) versus standard glycemic targets (fasting < 95 mg/dL, 1-hour postprandial < 140 mg/dL), she said.
In another presentation on GDM, Monica Longo, MD, PhD, of the Inova Health System in Fairfax, Va., said researchers are also looking at whether nutritional supplements such as myo-inositol can reduce the risk of adverse pregnancy outcomes in GDM, and whether probiotics can improve insulin sensitivity in some patients.
Data on newer insulin analogs in pregnancy are lacking, she noted. “Preliminary data has shown no malformations in infants, but there is some increase in hypoglycemia-related admissions to the NICU,” she said. “It’s worth it [to research more].”
FROM DPSG-NA 2023
The Knowns and Unknowns About Delivery Timing in Diabetes
FAIRFAX, VIRGINIA — The lack of data on optimal timing of delivery for pregnancies complicated by diabetes remains a major challenge in obstetrics — one with considerable implications given the high and rising prevalence of pregestational and gestational diabetes, Katherine Laughon Grantz, MD, MS, of the National Institute of Child Health and Human Development, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“While 39-40 weeks might be ideal for low-risk pregnancies, the optimal timing for pregnancies with complications [like diabetes] is unknown,” said Dr. Grantz, a senior investigator in the NICHD’s epidemiology branch.
The percentage of mothers with gestational diabetes mellitus (GDM) increased from 6% in 2016 to 8% in 2021, according to the most recent data from the National Vital Statistics System of the Centers for Disease Control and Prevention (MMWR Morb Mortal Wkly Rep. 2023;72:16). Meanwhile, the prevalence of prepregnancy obesity, which raises the risk of gestational and type 2 diabetes, was 29% in 2019; this represents an 11% increase from 2015 (NCHS Data Brief. 2020;392:1-8) and has occurred across all maternal ages, races, ethnic groups, and educational levels, she said.
“The reason clinicians deliver pregnancies with diabetes earlier is because there’s a decreased risk of macrosomia, shoulder dystocia, and stillbirth. And these risks need to be balanced with the increased risk of neonatal morbidity and mortality associated with earlier delivery,” said Dr. Grantz, who noted during her talk that delivery timing also appears to influence long-term neurodevelopmental outcomes. “Yet despite [diabetes in pregnancy] being so common, there is complete uncertainty about when to deliver.”
ACOG Recommendations, Randomized Trials (New And Old)
The American College of Obstetricians and Gynecologists, in a Committee Opinion on Medically Indicated Late-Preterm and Early-Term Deliveries, published in collaboration with the Society of Maternal-Fetal Medicine, offers recommendations based on the type of diabetes and the level of control. For instance, the suggested delivery timing for well-controlled GDM is full term (39 0/7 to 40 6/7 weeks of gestation), while the recommendation for poorly controlled diabetes is individualized late preterm/early term management (Obstet Gynecol. 2021;138:e35-9).
In defining and evaluating control, she noted, “the clinical focus is on glucose, but there are likely other important parameters that are not taken into account ... which [could be] important when considering the timing of delivery.” Potentially important factors include estimated fetal weight, fetal growth velocity, lipids, and amino acids, she said.
ACOG’s recommendations are based mainly on retrospective data, Dr. Grantz said. Only two randomized controlled trials have investigated the timing of delivery in the context of diabetes, and both focused on cesarean section and were “generally underpowered to study neonatal outcomes,” she said.
The first RCT, published in 1993, enrolled 200 women with uncomplicated insulin-requiring diabetes (187 with GDM and 13 with pregestational diabetes) at 38 weeks of gestation, and compared active induction of labor within 5 days to expectant management. There was no significant difference in the cesarean delivery rate (the primary outcome), but rates of macrosomia and large for gestational age were higher in the expectant management group (27% vs. 15%, P = .05, and 23% vs. 10%, P = .02, respectively). Shoulder dystocia occurred in three deliveries, each of which was expectantly managed (Am J Obstet Gynecol. 1993;169[3]:611-5). Notably, the study included “only women with excellent glucose control,” Dr. Grantz said.
The second RCT, published in 2017 by a group in Italy, enrolled 425 patients with GDM (diagnosed by the International Association of Diabetes and Pregnancy Study Groups criteria) between week 38 and week 39 of gestation and similarly randomized them to induction of labor or expectant management. No difference in cesarean delivery was found (BJOG. 2017;124[4]:669-77). Induction of labor was associated with a higher risk of hyperbilirubinemia, and there was a trend toward a decreased risk of macrosomia, but again, the study was underpowered to detect differences in most outcomes, she said. (The study also was stopped early because of an inability to recruit, she noted.)
Dr. Grantz is currently recruiting for a randomized trial aimed at determining the optimal time between 37 and 39 weeks to initiate delivery — the time when neonatal morbidity and perinatal mortality risk is the lowest – for uncontrolled GDM-complicated pregnancies. The trial is designed to recruit up to 3,450 pregnant women with uncontrolled GDM and randomize the timing of their delivery (NCT05515744).
Those who are eligible for the study but do not consent to participate in randomization for delivery will be asked about chart review only (an estimated additional 3,000). The SPAN TIME study will also assess newborn development and behavior outcomes, as well as anthropometric measures, as secondary outcomes. An exploratory analysis will look for clinical, nonclinical or biochemical factors that could be helpful in optimizing delivery timing.
What Retrospective Studies Reveal
Factors that may influence the timing of delivery include the duration of neonatal exposure to hyperglycemia/hyperinsulinemia (pregestational vs. gestational diabetes), the level of diabetes control, and comorbidities (e.g. maternal renal disease or chronic hypertension). However, research “investigating how these factors influence morbidity and the timing of delivery is limited,” said Dr. Grantz.
Overall, it has been difficult through retrospective studies, she said, to investigate neonatal morbidity in diabetic pregnancies and tease apart the relative effects of diabetes as a precursor for early delivery and prematurity itself. Among the studies suggesting an independent risk of diabetes is a retrospective study focusing on neonatal respiratory morbidity — “one of the most common adverse outcomes associated with diabetes.”
The study, an analysis of the Consortium on Safe Labor study (an electronic medical record study of more than 220,000 singleton pregnancies), stratified morbidity by the probability of delivering at term (≥ 37 weeks). GDM and pregestational diabetes complicated 5.1% and 1.5% of the pregnancies, respectively, and were found to be associated with increased risks of neonatal respiratory morbidity compared to women without diabetes — regardless of the probability of delivering at term.
However, these associations were stronger with a higher probability of delivering at term, which suggests that the neonatal respiratory morbidity associated with diabetes is not fully explained by a greater propensity for prematurity (Am J Perinatol. 2017;34[11]:1160-8).
In addition, the rates of all neonatal respiratory morbidities and mortality were higher for pregestational diabetes compared with gestational diabetes, said Dr. Grantz, a senior author of the study. (Morbidities included neonatal intensive care unit admission, transient tachypnea of newborn, apnea, respiratory distress syndrome, mechanical ventilation, and stillbirth.)
The pathophysiology of diabetes and neonatal respiratory morbidity is “not fully known,” she said. It is believed that fetal hyperinsulinemia may cause delayed pulmonary maturation and there is evidence from animal studies that insulin decreases the incorporation of glucose and fatty acids into phospholipid phosphatidylglycerol. Indirect effects stem from the physiologic immaturity of earlier delivery and a higher cesarean delivery rate in pregnancies complicated by diabetes, Dr. Grantz said.
Among other retrospective studies was a population-based study from Canada (2004-2014), published in 2020, of large numbers of women with all types of diabetes and a comparison group of over 2.5 million without diabetes. For maternal morbidity/mortality, there were no significant differences by gestational age between iatrogenic delivery and expectant management among any form of diabetes. But for neonatal morbidity and mortality, the study found differences.
In women with gestational diabetes, iatrogenic delivery was associated with increased risk of neonatal morbidity/mortality at 36 and 37 weeks’ gestation and with decreased risk at weeks 38-40. Increased risk with iatrogenic delivery was also found for women with type 1 and type 2 diabetes at weeks 36 and 37 (Acta Obstet Gynecol Scand. 2020;99[3]:341-9).
Another retrospective study using California vital statistics (1997-2006) examined rates of stillbirth and infant death in women with GDM by gestational age at delivery (Am J Obstet Gynecol. 2012;206[4]:309.e1-e7). The 190,000-plus women with GDM had elevated risk of stillbirth at each gestational age compared to those without GDM, but “the [excess] risk for GDM was lowest at 38 weeks and again at 40 weeks,” Dr. Grantz said. The investigators concluded, she said, “that the risk of expectant management exceeded that of delivery at 38 weeks and beyond.”
Dr. Grantz reported no disclosures.
FAIRFAX, VIRGINIA — The lack of data on optimal timing of delivery for pregnancies complicated by diabetes remains a major challenge in obstetrics — one with considerable implications given the high and rising prevalence of pregestational and gestational diabetes, Katherine Laughon Grantz, MD, MS, of the National Institute of Child Health and Human Development, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“While 39-40 weeks might be ideal for low-risk pregnancies, the optimal timing for pregnancies with complications [like diabetes] is unknown,” said Dr. Grantz, a senior investigator in the NICHD’s epidemiology branch.
The percentage of mothers with gestational diabetes mellitus (GDM) increased from 6% in 2016 to 8% in 2021, according to the most recent data from the National Vital Statistics System of the Centers for Disease Control and Prevention (MMWR Morb Mortal Wkly Rep. 2023;72:16). Meanwhile, the prevalence of prepregnancy obesity, which raises the risk of gestational and type 2 diabetes, was 29% in 2019; this represents an 11% increase from 2015 (NCHS Data Brief. 2020;392:1-8) and has occurred across all maternal ages, races, ethnic groups, and educational levels, she said.
“The reason clinicians deliver pregnancies with diabetes earlier is because there’s a decreased risk of macrosomia, shoulder dystocia, and stillbirth. And these risks need to be balanced with the increased risk of neonatal morbidity and mortality associated with earlier delivery,” said Dr. Grantz, who noted during her talk that delivery timing also appears to influence long-term neurodevelopmental outcomes. “Yet despite [diabetes in pregnancy] being so common, there is complete uncertainty about when to deliver.”
ACOG Recommendations, Randomized Trials (New And Old)
The American College of Obstetricians and Gynecologists, in a Committee Opinion on Medically Indicated Late-Preterm and Early-Term Deliveries, published in collaboration with the Society of Maternal-Fetal Medicine, offers recommendations based on the type of diabetes and the level of control. For instance, the suggested delivery timing for well-controlled GDM is full term (39 0/7 to 40 6/7 weeks of gestation), while the recommendation for poorly controlled diabetes is individualized late preterm/early term management (Obstet Gynecol. 2021;138:e35-9).
In defining and evaluating control, she noted, “the clinical focus is on glucose, but there are likely other important parameters that are not taken into account ... which [could be] important when considering the timing of delivery.” Potentially important factors include estimated fetal weight, fetal growth velocity, lipids, and amino acids, she said.
ACOG’s recommendations are based mainly on retrospective data, Dr. Grantz said. Only two randomized controlled trials have investigated the timing of delivery in the context of diabetes, and both focused on cesarean section and were “generally underpowered to study neonatal outcomes,” she said.
The first RCT, published in 1993, enrolled 200 women with uncomplicated insulin-requiring diabetes (187 with GDM and 13 with pregestational diabetes) at 38 weeks of gestation, and compared active induction of labor within 5 days to expectant management. There was no significant difference in the cesarean delivery rate (the primary outcome), but rates of macrosomia and large for gestational age were higher in the expectant management group (27% vs. 15%, P = .05, and 23% vs. 10%, P = .02, respectively). Shoulder dystocia occurred in three deliveries, each of which was expectantly managed (Am J Obstet Gynecol. 1993;169[3]:611-5). Notably, the study included “only women with excellent glucose control,” Dr. Grantz said.
The second RCT, published in 2017 by a group in Italy, enrolled 425 patients with GDM (diagnosed by the International Association of Diabetes and Pregnancy Study Groups criteria) between week 38 and week 39 of gestation and similarly randomized them to induction of labor or expectant management. No difference in cesarean delivery was found (BJOG. 2017;124[4]:669-77). Induction of labor was associated with a higher risk of hyperbilirubinemia, and there was a trend toward a decreased risk of macrosomia, but again, the study was underpowered to detect differences in most outcomes, she said. (The study also was stopped early because of an inability to recruit, she noted.)
Dr. Grantz is currently recruiting for a randomized trial aimed at determining the optimal time between 37 and 39 weeks to initiate delivery — the time when neonatal morbidity and perinatal mortality risk is the lowest – for uncontrolled GDM-complicated pregnancies. The trial is designed to recruit up to 3,450 pregnant women with uncontrolled GDM and randomize the timing of their delivery (NCT05515744).
Those who are eligible for the study but do not consent to participate in randomization for delivery will be asked about chart review only (an estimated additional 3,000). The SPAN TIME study will also assess newborn development and behavior outcomes, as well as anthropometric measures, as secondary outcomes. An exploratory analysis will look for clinical, nonclinical or biochemical factors that could be helpful in optimizing delivery timing.
What Retrospective Studies Reveal
Factors that may influence the timing of delivery include the duration of neonatal exposure to hyperglycemia/hyperinsulinemia (pregestational vs. gestational diabetes), the level of diabetes control, and comorbidities (e.g. maternal renal disease or chronic hypertension). However, research “investigating how these factors influence morbidity and the timing of delivery is limited,” said Dr. Grantz.
Overall, it has been difficult through retrospective studies, she said, to investigate neonatal morbidity in diabetic pregnancies and tease apart the relative effects of diabetes as a precursor for early delivery and prematurity itself. Among the studies suggesting an independent risk of diabetes is a retrospective study focusing on neonatal respiratory morbidity — “one of the most common adverse outcomes associated with diabetes.”
The study, an analysis of the Consortium on Safe Labor study (an electronic medical record study of more than 220,000 singleton pregnancies), stratified morbidity by the probability of delivering at term (≥ 37 weeks). GDM and pregestational diabetes complicated 5.1% and 1.5% of the pregnancies, respectively, and were found to be associated with increased risks of neonatal respiratory morbidity compared to women without diabetes — regardless of the probability of delivering at term.
However, these associations were stronger with a higher probability of delivering at term, which suggests that the neonatal respiratory morbidity associated with diabetes is not fully explained by a greater propensity for prematurity (Am J Perinatol. 2017;34[11]:1160-8).
In addition, the rates of all neonatal respiratory morbidities and mortality were higher for pregestational diabetes compared with gestational diabetes, said Dr. Grantz, a senior author of the study. (Morbidities included neonatal intensive care unit admission, transient tachypnea of newborn, apnea, respiratory distress syndrome, mechanical ventilation, and stillbirth.)
The pathophysiology of diabetes and neonatal respiratory morbidity is “not fully known,” she said. It is believed that fetal hyperinsulinemia may cause delayed pulmonary maturation and there is evidence from animal studies that insulin decreases the incorporation of glucose and fatty acids into phospholipid phosphatidylglycerol. Indirect effects stem from the physiologic immaturity of earlier delivery and a higher cesarean delivery rate in pregnancies complicated by diabetes, Dr. Grantz said.
Among other retrospective studies was a population-based study from Canada (2004-2014), published in 2020, of large numbers of women with all types of diabetes and a comparison group of over 2.5 million without diabetes. For maternal morbidity/mortality, there were no significant differences by gestational age between iatrogenic delivery and expectant management among any form of diabetes. But for neonatal morbidity and mortality, the study found differences.
In women with gestational diabetes, iatrogenic delivery was associated with increased risk of neonatal morbidity/mortality at 36 and 37 weeks’ gestation and with decreased risk at weeks 38-40. Increased risk with iatrogenic delivery was also found for women with type 1 and type 2 diabetes at weeks 36 and 37 (Acta Obstet Gynecol Scand. 2020;99[3]:341-9).
Another retrospective study using California vital statistics (1997-2006) examined rates of stillbirth and infant death in women with GDM by gestational age at delivery (Am J Obstet Gynecol. 2012;206[4]:309.e1-e7). The 190,000-plus women with GDM had elevated risk of stillbirth at each gestational age compared to those without GDM, but “the [excess] risk for GDM was lowest at 38 weeks and again at 40 weeks,” Dr. Grantz said. The investigators concluded, she said, “that the risk of expectant management exceeded that of delivery at 38 weeks and beyond.”
Dr. Grantz reported no disclosures.
FAIRFAX, VIRGINIA — The lack of data on optimal timing of delivery for pregnancies complicated by diabetes remains a major challenge in obstetrics — one with considerable implications given the high and rising prevalence of pregestational and gestational diabetes, Katherine Laughon Grantz, MD, MS, of the National Institute of Child Health and Human Development, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“While 39-40 weeks might be ideal for low-risk pregnancies, the optimal timing for pregnancies with complications [like diabetes] is unknown,” said Dr. Grantz, a senior investigator in the NICHD’s epidemiology branch.
The percentage of mothers with gestational diabetes mellitus (GDM) increased from 6% in 2016 to 8% in 2021, according to the most recent data from the National Vital Statistics System of the Centers for Disease Control and Prevention (MMWR Morb Mortal Wkly Rep. 2023;72:16). Meanwhile, the prevalence of prepregnancy obesity, which raises the risk of gestational and type 2 diabetes, was 29% in 2019; this represents an 11% increase from 2015 (NCHS Data Brief. 2020;392:1-8) and has occurred across all maternal ages, races, ethnic groups, and educational levels, she said.
“The reason clinicians deliver pregnancies with diabetes earlier is because there’s a decreased risk of macrosomia, shoulder dystocia, and stillbirth. And these risks need to be balanced with the increased risk of neonatal morbidity and mortality associated with earlier delivery,” said Dr. Grantz, who noted during her talk that delivery timing also appears to influence long-term neurodevelopmental outcomes. “Yet despite [diabetes in pregnancy] being so common, there is complete uncertainty about when to deliver.”
ACOG Recommendations, Randomized Trials (New And Old)
The American College of Obstetricians and Gynecologists, in a Committee Opinion on Medically Indicated Late-Preterm and Early-Term Deliveries, published in collaboration with the Society of Maternal-Fetal Medicine, offers recommendations based on the type of diabetes and the level of control. For instance, the suggested delivery timing for well-controlled GDM is full term (39 0/7 to 40 6/7 weeks of gestation), while the recommendation for poorly controlled diabetes is individualized late preterm/early term management (Obstet Gynecol. 2021;138:e35-9).
In defining and evaluating control, she noted, “the clinical focus is on glucose, but there are likely other important parameters that are not taken into account ... which [could be] important when considering the timing of delivery.” Potentially important factors include estimated fetal weight, fetal growth velocity, lipids, and amino acids, she said.
ACOG’s recommendations are based mainly on retrospective data, Dr. Grantz said. Only two randomized controlled trials have investigated the timing of delivery in the context of diabetes, and both focused on cesarean section and were “generally underpowered to study neonatal outcomes,” she said.
The first RCT, published in 1993, enrolled 200 women with uncomplicated insulin-requiring diabetes (187 with GDM and 13 with pregestational diabetes) at 38 weeks of gestation, and compared active induction of labor within 5 days to expectant management. There was no significant difference in the cesarean delivery rate (the primary outcome), but rates of macrosomia and large for gestational age were higher in the expectant management group (27% vs. 15%, P = .05, and 23% vs. 10%, P = .02, respectively). Shoulder dystocia occurred in three deliveries, each of which was expectantly managed (Am J Obstet Gynecol. 1993;169[3]:611-5). Notably, the study included “only women with excellent glucose control,” Dr. Grantz said.
The second RCT, published in 2017 by a group in Italy, enrolled 425 patients with GDM (diagnosed by the International Association of Diabetes and Pregnancy Study Groups criteria) between week 38 and week 39 of gestation and similarly randomized them to induction of labor or expectant management. No difference in cesarean delivery was found (BJOG. 2017;124[4]:669-77). Induction of labor was associated with a higher risk of hyperbilirubinemia, and there was a trend toward a decreased risk of macrosomia, but again, the study was underpowered to detect differences in most outcomes, she said. (The study also was stopped early because of an inability to recruit, she noted.)
Dr. Grantz is currently recruiting for a randomized trial aimed at determining the optimal time between 37 and 39 weeks to initiate delivery — the time when neonatal morbidity and perinatal mortality risk is the lowest – for uncontrolled GDM-complicated pregnancies. The trial is designed to recruit up to 3,450 pregnant women with uncontrolled GDM and randomize the timing of their delivery (NCT05515744).
Those who are eligible for the study but do not consent to participate in randomization for delivery will be asked about chart review only (an estimated additional 3,000). The SPAN TIME study will also assess newborn development and behavior outcomes, as well as anthropometric measures, as secondary outcomes. An exploratory analysis will look for clinical, nonclinical or biochemical factors that could be helpful in optimizing delivery timing.
What Retrospective Studies Reveal
Factors that may influence the timing of delivery include the duration of neonatal exposure to hyperglycemia/hyperinsulinemia (pregestational vs. gestational diabetes), the level of diabetes control, and comorbidities (e.g. maternal renal disease or chronic hypertension). However, research “investigating how these factors influence morbidity and the timing of delivery is limited,” said Dr. Grantz.
Overall, it has been difficult through retrospective studies, she said, to investigate neonatal morbidity in diabetic pregnancies and tease apart the relative effects of diabetes as a precursor for early delivery and prematurity itself. Among the studies suggesting an independent risk of diabetes is a retrospective study focusing on neonatal respiratory morbidity — “one of the most common adverse outcomes associated with diabetes.”
The study, an analysis of the Consortium on Safe Labor study (an electronic medical record study of more than 220,000 singleton pregnancies), stratified morbidity by the probability of delivering at term (≥ 37 weeks). GDM and pregestational diabetes complicated 5.1% and 1.5% of the pregnancies, respectively, and were found to be associated with increased risks of neonatal respiratory morbidity compared to women without diabetes — regardless of the probability of delivering at term.
However, these associations were stronger with a higher probability of delivering at term, which suggests that the neonatal respiratory morbidity associated with diabetes is not fully explained by a greater propensity for prematurity (Am J Perinatol. 2017;34[11]:1160-8).
In addition, the rates of all neonatal respiratory morbidities and mortality were higher for pregestational diabetes compared with gestational diabetes, said Dr. Grantz, a senior author of the study. (Morbidities included neonatal intensive care unit admission, transient tachypnea of newborn, apnea, respiratory distress syndrome, mechanical ventilation, and stillbirth.)
The pathophysiology of diabetes and neonatal respiratory morbidity is “not fully known,” she said. It is believed that fetal hyperinsulinemia may cause delayed pulmonary maturation and there is evidence from animal studies that insulin decreases the incorporation of glucose and fatty acids into phospholipid phosphatidylglycerol. Indirect effects stem from the physiologic immaturity of earlier delivery and a higher cesarean delivery rate in pregnancies complicated by diabetes, Dr. Grantz said.
Among other retrospective studies was a population-based study from Canada (2004-2014), published in 2020, of large numbers of women with all types of diabetes and a comparison group of over 2.5 million without diabetes. For maternal morbidity/mortality, there were no significant differences by gestational age between iatrogenic delivery and expectant management among any form of diabetes. But for neonatal morbidity and mortality, the study found differences.
In women with gestational diabetes, iatrogenic delivery was associated with increased risk of neonatal morbidity/mortality at 36 and 37 weeks’ gestation and with decreased risk at weeks 38-40. Increased risk with iatrogenic delivery was also found for women with type 1 and type 2 diabetes at weeks 36 and 37 (Acta Obstet Gynecol Scand. 2020;99[3]:341-9).
Another retrospective study using California vital statistics (1997-2006) examined rates of stillbirth and infant death in women with GDM by gestational age at delivery (Am J Obstet Gynecol. 2012;206[4]:309.e1-e7). The 190,000-plus women with GDM had elevated risk of stillbirth at each gestational age compared to those without GDM, but “the [excess] risk for GDM was lowest at 38 weeks and again at 40 weeks,” Dr. Grantz said. The investigators concluded, she said, “that the risk of expectant management exceeded that of delivery at 38 weeks and beyond.”
Dr. Grantz reported no disclosures.
FROM DPSG-NA 2023
Myo-inositol is one of the components of an integrative approach to acne
, Jonette Elizabeth Keri, MD, PhD, professor of dermatology at the University of Miami, said during a presentation on therapies for acne at the annual Integrative Dermatology Symposium.
Probiotics and omega-3 fatty acids are among the other complementary therapies that have a role in acne treatment, she and others said during the meeting.
Myo-inositol has been well-studied in the gynecology-endocrinology community in patients with polycystic ovary syndrome (PCOS), demonstrating an ability to improve the metabolic profile and reduce acne and hirsutism, Dr. Keri said.
A study of 137 young, overweight women with PCOS and moderate acne, for example, found that compared with placebo, 6 months of myo-inositol or D-chiro-inositol, another isoform of inositol, significantly improved the acne score, endocrine and metabolic parameters, insulin resistance, and regularity of the menstrual cycle, Dr. Keri said. Both isoforms of inositol are second messengers in the signal transduction of insulin.
During a panel discussion, asked about a case of an adult female with acne, Dr. Keri said that many of her adult female patients “don’t want to do isotretinoin or antibiotics, and they don’t want to do any kind of hormonal treatment,” the options she would recommend. But for patients who do not want these treatments, she said, “I go down the route of supplements,” and myo-inositol is her “favorite” option. It’s safe to use during pregnancy, she emphasized, noting that myo-inositol is being studied for the prevention of preterm birth.
Dr. Keri, who described herself as “more of a traditionalist,” prescribes myo-inositol 2 gm twice a day in pill form. In Europe, she noted in her presentation, myo-inositol is also compounded for topical use.
Diet, probiotics, other nutraceuticals
A low-glycemic-load diet was among several complementary therapies reported in a 2015 Cochrane Database Systematic Review to have some evidence (though low-quality) of reducing total skin lesions in acne (along with tea tree oil and bee venom) and today, it is the most evidence-based dietary recommendation for acne, Dr. Keri said.

Omega-3 fatty acids and increased fruit and vegetable intake have also been reported to be acne-protective — and hyperglycemia, carbohydrates, milk and dairy products, and saturated fats and trans fats have been reported to be acne-promoting, she noted.
But, the low-glycemic-load data “is the strongest,” she said. The best advice for patients, she added, is to consume less sugar and fewer sugary drinks and “avoid white foods” such as white bread, rice, and pasta.
Probiotics can also be recommended, especially for patients on antibiotic therapy, Dr. Keri said. For “basic science evidence,” she pointed to a randomized, double-blinded, placebo-controlled study of 20 adults with acne, which evaluated the impact of a probiotic on improvement in acne and skin expression of genes involved with insulin signaling. Participants took either a liquid supplement containing Lactobacillus rhamnosus SP1 (LSP1) or placebo over a 12-week period. The investigators performed paired skin biopsies before and after 12 weeks of treatment and analyzed them for insulin-like growth factor 1 (IGF1) and forkhead box protein O1 (FOXO1) gene expression.
They found that compared with baseline, the probiotic group showed a 32% reduction in IGF1 and a 65% increase in FOXO1 gene expression (P < .0001 for both), with no such differences observed in the placebo group.
Clinically, patients in the probiotic group had an adjusted odds ratio of 28.4 (95% confidence interval, 2.2-411.1, P < .05) of acne being rated as improved or markedly improved compared with those on placebo.
Dr. Keri and others at the meeting also referenced a 2013 prospective, open-label trial that randomized 45 women with acne, ages 18-35 years, to one of three arms: Probiotic supplementation only, minocycline only, and both probiotic and minocycline. The probiotic used was a product containing Lactobacillus acidophilus, Lactobacillus bulgaricus, and Bifidobacterium bifidum. At 8 and 12 weeks, the combination group “did the best with the lowest total lesion count” compared with the probiotic group and the minocycline group, differences that were significant (P < .001 and P <.01, respectively), she said. “And they also had less candidiasis when using a probiotic than when using an antibiotic alone,” she said. Two patients in the minocycline-only group failed to complete the study because they developed vaginal candidiasis.
In addition to reducing potential adverse events secondary to chronic antibiotic use, probiotics can have synergistic anti-inflammatory effects, she said.
Dr. Keri said she recommends probiotics for patients taking antibiotics and encourages them “to get a branded probiotic,” such as Culturelle, “or if they prefer a food source, soy or almond milk–based yogurt.” As with other elements of a holistic approach to acne, she urged clinicians to consider the cost of treatment.
Probiotics (Lactobacillus plantarum) were one of four nutraceuticals determined in a 2023 systematic review to have “good-quality” evidence for potential efficacy, Dr. Keri noted, along with vitamin D, green tea extract, and cheongsangbangpoong-tang, the latter of which is an herbal therapeutic formula approved by the Korean Food and Drug Administration for use in acne.
“There were really no bad systemic effects for any of these,” she said. “The tricky part of this review is that each of the four have only one study” deemed to be a good-quality study. Omega-3 fatty acids were among several other nutraceuticals deemed to have “fair-quality” evidence for efficacy. Zinc was reported to be the most studied nutraceutical in acne, but didn’t rate as highly in the review. Dr. Keri said she likes to include zinc in her armamentarium because “it can be used in pregnant women,” noting that reviews and guidelines “are just that, a guide ... to combine with experience.”
Omega-3 fatty acids with isotretinoin
Several speakers at the meeting, including Steven Daveluy, MD, associate professor and residency program director in the department of dermatology, Wayne State University, Dearborn, Michigan, spoke about the value of omega-3 fatty acids in reducing side effects of isotretinoin. “In the FDA trials [of isotretinoin] they had patients take 50 grams of fat,” he said. “You can use the good fats to help you out.”
Research has shown that 1 gm per day of oral omega-3 reduces dryness of the lips, nose, eyes, and skin, “which are the big side effects we see with isotretinoin,” he said. An impact on triglyceride levels has also been demonstrated, Dr. Daveluy said, pointing to a longitudinal survey study of 39 patients treated with isotretinoin that showed a mean increase in triglyceride levels of 49% during treatment in patients who did not use omega-3 supplementation, compared with a mean increase of 13.9% (P =.04) in patients who used the supplements.“There is also evidence that omega-3 can decrease depression, which may or may not be a side effect of isotretinoin ... but it’s something we consider in our [acne] patients,” Dr. Daveluy said.
During a panel discussion at the meeting, Apple A. Bodemer, MD, associate professor of dermatology at the University of Wisconsin, Madison, said she usually prescribes 2 g of docosahexaenoic acid eicosapentaenoic acid combined in patients on isotretinoin because “at that dose, omega-3s have been found to be anti-inflammatory.”
Dr. Keri reported being an investigator and speaker for Galderma, and an advisory board member for Ortho Dermatologics and for Almirall. Dr. Daveluy reported no relevant disclosures.
, Jonette Elizabeth Keri, MD, PhD, professor of dermatology at the University of Miami, said during a presentation on therapies for acne at the annual Integrative Dermatology Symposium.
Probiotics and omega-3 fatty acids are among the other complementary therapies that have a role in acne treatment, she and others said during the meeting.
Myo-inositol has been well-studied in the gynecology-endocrinology community in patients with polycystic ovary syndrome (PCOS), demonstrating an ability to improve the metabolic profile and reduce acne and hirsutism, Dr. Keri said.
A study of 137 young, overweight women with PCOS and moderate acne, for example, found that compared with placebo, 6 months of myo-inositol or D-chiro-inositol, another isoform of inositol, significantly improved the acne score, endocrine and metabolic parameters, insulin resistance, and regularity of the menstrual cycle, Dr. Keri said. Both isoforms of inositol are second messengers in the signal transduction of insulin.
During a panel discussion, asked about a case of an adult female with acne, Dr. Keri said that many of her adult female patients “don’t want to do isotretinoin or antibiotics, and they don’t want to do any kind of hormonal treatment,” the options she would recommend. But for patients who do not want these treatments, she said, “I go down the route of supplements,” and myo-inositol is her “favorite” option. It’s safe to use during pregnancy, she emphasized, noting that myo-inositol is being studied for the prevention of preterm birth.
Dr. Keri, who described herself as “more of a traditionalist,” prescribes myo-inositol 2 gm twice a day in pill form. In Europe, she noted in her presentation, myo-inositol is also compounded for topical use.
Diet, probiotics, other nutraceuticals
A low-glycemic-load diet was among several complementary therapies reported in a 2015 Cochrane Database Systematic Review to have some evidence (though low-quality) of reducing total skin lesions in acne (along with tea tree oil and bee venom) and today, it is the most evidence-based dietary recommendation for acne, Dr. Keri said.
Omega-3 fatty acids and increased fruit and vegetable intake have also been reported to be acne-protective — and hyperglycemia, carbohydrates, milk and dairy products, and saturated fats and trans fats have been reported to be acne-promoting, she noted.
But, the low-glycemic-load data “is the strongest,” she said. The best advice for patients, she added, is to consume less sugar and fewer sugary drinks and “avoid white foods” such as white bread, rice, and pasta.
Probiotics can also be recommended, especially for patients on antibiotic therapy, Dr. Keri said. For “basic science evidence,” she pointed to a randomized, double-blinded, placebo-controlled study of 20 adults with acne, which evaluated the impact of a probiotic on improvement in acne and skin expression of genes involved with insulin signaling. Participants took either a liquid supplement containing Lactobacillus rhamnosus SP1 (LSP1) or placebo over a 12-week period. The investigators performed paired skin biopsies before and after 12 weeks of treatment and analyzed them for insulin-like growth factor 1 (IGF1) and forkhead box protein O1 (FOXO1) gene expression.
They found that compared with baseline, the probiotic group showed a 32% reduction in IGF1 and a 65% increase in FOXO1 gene expression (P < .0001 for both), with no such differences observed in the placebo group.
Clinically, patients in the probiotic group had an adjusted odds ratio of 28.4 (95% confidence interval, 2.2-411.1, P < .05) of acne being rated as improved or markedly improved compared with those on placebo.
Dr. Keri and others at the meeting also referenced a 2013 prospective, open-label trial that randomized 45 women with acne, ages 18-35 years, to one of three arms: Probiotic supplementation only, minocycline only, and both probiotic and minocycline. The probiotic used was a product containing Lactobacillus acidophilus, Lactobacillus bulgaricus, and Bifidobacterium bifidum. At 8 and 12 weeks, the combination group “did the best with the lowest total lesion count” compared with the probiotic group and the minocycline group, differences that were significant (P < .001 and P <.01, respectively), she said. “And they also had less candidiasis when using a probiotic than when using an antibiotic alone,” she said. Two patients in the minocycline-only group failed to complete the study because they developed vaginal candidiasis.
In addition to reducing potential adverse events secondary to chronic antibiotic use, probiotics can have synergistic anti-inflammatory effects, she said.
Dr. Keri said she recommends probiotics for patients taking antibiotics and encourages them “to get a branded probiotic,” such as Culturelle, “or if they prefer a food source, soy or almond milk–based yogurt.” As with other elements of a holistic approach to acne, she urged clinicians to consider the cost of treatment.
Probiotics (Lactobacillus plantarum) were one of four nutraceuticals determined in a 2023 systematic review to have “good-quality” evidence for potential efficacy, Dr. Keri noted, along with vitamin D, green tea extract, and cheongsangbangpoong-tang, the latter of which is an herbal therapeutic formula approved by the Korean Food and Drug Administration for use in acne.
“There were really no bad systemic effects for any of these,” she said. “The tricky part of this review is that each of the four have only one study” deemed to be a good-quality study. Omega-3 fatty acids were among several other nutraceuticals deemed to have “fair-quality” evidence for efficacy. Zinc was reported to be the most studied nutraceutical in acne, but didn’t rate as highly in the review. Dr. Keri said she likes to include zinc in her armamentarium because “it can be used in pregnant women,” noting that reviews and guidelines “are just that, a guide ... to combine with experience.”
Omega-3 fatty acids with isotretinoin
Several speakers at the meeting, including Steven Daveluy, MD, associate professor and residency program director in the department of dermatology, Wayne State University, Dearborn, Michigan, spoke about the value of omega-3 fatty acids in reducing side effects of isotretinoin. “In the FDA trials [of isotretinoin] they had patients take 50 grams of fat,” he said. “You can use the good fats to help you out.”
Research has shown that 1 gm per day of oral omega-3 reduces dryness of the lips, nose, eyes, and skin, “which are the big side effects we see with isotretinoin,” he said. An impact on triglyceride levels has also been demonstrated, Dr. Daveluy said, pointing to a longitudinal survey study of 39 patients treated with isotretinoin that showed a mean increase in triglyceride levels of 49% during treatment in patients who did not use omega-3 supplementation, compared with a mean increase of 13.9% (P =.04) in patients who used the supplements.“There is also evidence that omega-3 can decrease depression, which may or may not be a side effect of isotretinoin ... but it’s something we consider in our [acne] patients,” Dr. Daveluy said.
During a panel discussion at the meeting, Apple A. Bodemer, MD, associate professor of dermatology at the University of Wisconsin, Madison, said she usually prescribes 2 g of docosahexaenoic acid eicosapentaenoic acid combined in patients on isotretinoin because “at that dose, omega-3s have been found to be anti-inflammatory.”
Dr. Keri reported being an investigator and speaker for Galderma, and an advisory board member for Ortho Dermatologics and for Almirall. Dr. Daveluy reported no relevant disclosures.
, Jonette Elizabeth Keri, MD, PhD, professor of dermatology at the University of Miami, said during a presentation on therapies for acne at the annual Integrative Dermatology Symposium.
Probiotics and omega-3 fatty acids are among the other complementary therapies that have a role in acne treatment, she and others said during the meeting.
Myo-inositol has been well-studied in the gynecology-endocrinology community in patients with polycystic ovary syndrome (PCOS), demonstrating an ability to improve the metabolic profile and reduce acne and hirsutism, Dr. Keri said.
A study of 137 young, overweight women with PCOS and moderate acne, for example, found that compared with placebo, 6 months of myo-inositol or D-chiro-inositol, another isoform of inositol, significantly improved the acne score, endocrine and metabolic parameters, insulin resistance, and regularity of the menstrual cycle, Dr. Keri said. Both isoforms of inositol are second messengers in the signal transduction of insulin.
During a panel discussion, asked about a case of an adult female with acne, Dr. Keri said that many of her adult female patients “don’t want to do isotretinoin or antibiotics, and they don’t want to do any kind of hormonal treatment,” the options she would recommend. But for patients who do not want these treatments, she said, “I go down the route of supplements,” and myo-inositol is her “favorite” option. It’s safe to use during pregnancy, she emphasized, noting that myo-inositol is being studied for the prevention of preterm birth.
Dr. Keri, who described herself as “more of a traditionalist,” prescribes myo-inositol 2 gm twice a day in pill form. In Europe, she noted in her presentation, myo-inositol is also compounded for topical use.
Diet, probiotics, other nutraceuticals
A low-glycemic-load diet was among several complementary therapies reported in a 2015 Cochrane Database Systematic Review to have some evidence (though low-quality) of reducing total skin lesions in acne (along with tea tree oil and bee venom) and today, it is the most evidence-based dietary recommendation for acne, Dr. Keri said.
Omega-3 fatty acids and increased fruit and vegetable intake have also been reported to be acne-protective — and hyperglycemia, carbohydrates, milk and dairy products, and saturated fats and trans fats have been reported to be acne-promoting, she noted.
But, the low-glycemic-load data “is the strongest,” she said. The best advice for patients, she added, is to consume less sugar and fewer sugary drinks and “avoid white foods” such as white bread, rice, and pasta.
Probiotics can also be recommended, especially for patients on antibiotic therapy, Dr. Keri said. For “basic science evidence,” she pointed to a randomized, double-blinded, placebo-controlled study of 20 adults with acne, which evaluated the impact of a probiotic on improvement in acne and skin expression of genes involved with insulin signaling. Participants took either a liquid supplement containing Lactobacillus rhamnosus SP1 (LSP1) or placebo over a 12-week period. The investigators performed paired skin biopsies before and after 12 weeks of treatment and analyzed them for insulin-like growth factor 1 (IGF1) and forkhead box protein O1 (FOXO1) gene expression.
They found that compared with baseline, the probiotic group showed a 32% reduction in IGF1 and a 65% increase in FOXO1 gene expression (P < .0001 for both), with no such differences observed in the placebo group.
Clinically, patients in the probiotic group had an adjusted odds ratio of 28.4 (95% confidence interval, 2.2-411.1, P < .05) of acne being rated as improved or markedly improved compared with those on placebo.
Dr. Keri and others at the meeting also referenced a 2013 prospective, open-label trial that randomized 45 women with acne, ages 18-35 years, to one of three arms: Probiotic supplementation only, minocycline only, and both probiotic and minocycline. The probiotic used was a product containing Lactobacillus acidophilus, Lactobacillus bulgaricus, and Bifidobacterium bifidum. At 8 and 12 weeks, the combination group “did the best with the lowest total lesion count” compared with the probiotic group and the minocycline group, differences that were significant (P < .001 and P <.01, respectively), she said. “And they also had less candidiasis when using a probiotic than when using an antibiotic alone,” she said. Two patients in the minocycline-only group failed to complete the study because they developed vaginal candidiasis.
In addition to reducing potential adverse events secondary to chronic antibiotic use, probiotics can have synergistic anti-inflammatory effects, she said.
Dr. Keri said she recommends probiotics for patients taking antibiotics and encourages them “to get a branded probiotic,” such as Culturelle, “or if they prefer a food source, soy or almond milk–based yogurt.” As with other elements of a holistic approach to acne, she urged clinicians to consider the cost of treatment.
Probiotics (Lactobacillus plantarum) were one of four nutraceuticals determined in a 2023 systematic review to have “good-quality” evidence for potential efficacy, Dr. Keri noted, along with vitamin D, green tea extract, and cheongsangbangpoong-tang, the latter of which is an herbal therapeutic formula approved by the Korean Food and Drug Administration for use in acne.
“There were really no bad systemic effects for any of these,” she said. “The tricky part of this review is that each of the four have only one study” deemed to be a good-quality study. Omega-3 fatty acids were among several other nutraceuticals deemed to have “fair-quality” evidence for efficacy. Zinc was reported to be the most studied nutraceutical in acne, but didn’t rate as highly in the review. Dr. Keri said she likes to include zinc in her armamentarium because “it can be used in pregnant women,” noting that reviews and guidelines “are just that, a guide ... to combine with experience.”
Omega-3 fatty acids with isotretinoin
Several speakers at the meeting, including Steven Daveluy, MD, associate professor and residency program director in the department of dermatology, Wayne State University, Dearborn, Michigan, spoke about the value of omega-3 fatty acids in reducing side effects of isotretinoin. “In the FDA trials [of isotretinoin] they had patients take 50 grams of fat,” he said. “You can use the good fats to help you out.”
Research has shown that 1 gm per day of oral omega-3 reduces dryness of the lips, nose, eyes, and skin, “which are the big side effects we see with isotretinoin,” he said. An impact on triglyceride levels has also been demonstrated, Dr. Daveluy said, pointing to a longitudinal survey study of 39 patients treated with isotretinoin that showed a mean increase in triglyceride levels of 49% during treatment in patients who did not use omega-3 supplementation, compared with a mean increase of 13.9% (P =.04) in patients who used the supplements.“There is also evidence that omega-3 can decrease depression, which may or may not be a side effect of isotretinoin ... but it’s something we consider in our [acne] patients,” Dr. Daveluy said.
During a panel discussion at the meeting, Apple A. Bodemer, MD, associate professor of dermatology at the University of Wisconsin, Madison, said she usually prescribes 2 g of docosahexaenoic acid eicosapentaenoic acid combined in patients on isotretinoin because “at that dose, omega-3s have been found to be anti-inflammatory.”
Dr. Keri reported being an investigator and speaker for Galderma, and an advisory board member for Ortho Dermatologics and for Almirall. Dr. Daveluy reported no relevant disclosures.
FROM IDS 2023
ALL: What Prompts A Post-Childhood ‘Survival Cliff’?
In a session at the annual meeting of the American Society of Hematology in December, clinicians defined the extent of the problem — which one described as a “survival cliff” — and they discussed potential strategies to turn things around.
Cleveland Clinic hematologist John Molina, MD, EdM, highlighted a 2022 study that revealed “the 5-year overall survival for younger pediatric patients is quite phenomenal at 93%. But as you start shifting even to 15-19 patients, that shifts to an overall survival of 74%.”
In the rest of the young adult population, from age 20 to 39, the overall survival rate dips down to 59%. What’s going on?
As Dr. Molina noted, a 2008 study revealed that outcomes in ALL for those aged 16-20 “historically depended on which door you walked into”: the pediatric setting or the adult setting. Patients fared better on pediatric regimens.
Currently, he explained, those who begin treatment in adult oncology clinics will start with either a pediatric-inspired treatment called CALGB 10403 or HyperCVAD (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride, and dexamethasone plus methotrexate and cytarabine).
CALGB 10403 was developed based on a pediatric backbone of COG AALL0232, Dr. Molina said, and has higher doses of major myelosuppressive agents vs. HyperCVAD. A 2019 study determined that it was feasible to treat adolescents and young adults up to age 40 “with low treatment-related mortality and marked improvement in outcomes. OS [overall survival] at 3 years was 73%.”
However, Dr. Molina observed that only 39% of patients completed the treatment per protocol.
Which is better, CALGB 10403 or HyperCVAD? Dr. Molina said the risk of infertility and other long-term adverse effects is higher in HyperCVAD, but it has a lower risk of hepatic, pancreatic and thrombotic complications. And the CALGB 10403 regimen is more complicated to deliver, which is a potential obstacle in clinics without large numbers of patients.
As for outcomes, some research suggests they improve with pediatric-inspired regimens like CALGB 10403, he said, noting that “the debate continues.”
However, even with better regimens, Dr. Molina added, older ALL patients are still faring worse.
Also at the ASH presentation, Emory University/Children’s Healthcare of Atlanta pediatric cancer specialist Tamara Miller, MD, explored possible reasons that could explain the difference in outcomes based on age.
Cancer biology, response to chemotherapy, toxicities, psychosocial challenges, and low enrollment in clinical trials are all potential factors, she said. Specifically, aging into adulthood can lower tolerance of chemotherapy, and older patients are more prone to obesity, which is associated with worse outcomes, she said.
As for psychosocial challenges, it can be hard for older patients to manage their own medications, and they may lack insurance coverage, she said. Some patients may have worries about fertility, she added, and some may rebel against the requirements of treatment. Adherence is crucial to reducing risk of relapse, she added.
University of Cincinnati leukemia specialist Emily Curran, MD, told the ASH audience that researchers are exploring various avenues to improve outcomes.
Philadelphia chromosome-like (Ph-like) ALL, a subset of B-ALL, is associated with worse outcomes, she said, but it has multiple targetable pathways. An ongoing trial is exploring ruxolitinib (Jakafi) and chemotherapy in patients aged 18-39 with Ph-like ALL, Dr. Curran said.
Researchers are also wondering if up-front immunotherapy can help overcome disease biology, she said. Another potential therapy, she added, is CAR-T therapy for T-ALL.
Beyond cancer biology, “psychosocial factors are an even more challenging area in which we have fewer ongoing and less solutions,” Dr. Curran said.
Dr. Molina disclosed honoraria and consulting relationships with Autolus. Dr. Curran reported ties with Kite, Amgen, Incyte, Pfizer, Jazz, and Servier. Dr. Miller has no disclosures.
In a session at the annual meeting of the American Society of Hematology in December, clinicians defined the extent of the problem — which one described as a “survival cliff” — and they discussed potential strategies to turn things around.
Cleveland Clinic hematologist John Molina, MD, EdM, highlighted a 2022 study that revealed “the 5-year overall survival for younger pediatric patients is quite phenomenal at 93%. But as you start shifting even to 15-19 patients, that shifts to an overall survival of 74%.”
In the rest of the young adult population, from age 20 to 39, the overall survival rate dips down to 59%. What’s going on?
As Dr. Molina noted, a 2008 study revealed that outcomes in ALL for those aged 16-20 “historically depended on which door you walked into”: the pediatric setting or the adult setting. Patients fared better on pediatric regimens.
Currently, he explained, those who begin treatment in adult oncology clinics will start with either a pediatric-inspired treatment called CALGB 10403 or HyperCVAD (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride, and dexamethasone plus methotrexate and cytarabine).
CALGB 10403 was developed based on a pediatric backbone of COG AALL0232, Dr. Molina said, and has higher doses of major myelosuppressive agents vs. HyperCVAD. A 2019 study determined that it was feasible to treat adolescents and young adults up to age 40 “with low treatment-related mortality and marked improvement in outcomes. OS [overall survival] at 3 years was 73%.”
However, Dr. Molina observed that only 39% of patients completed the treatment per protocol.
Which is better, CALGB 10403 or HyperCVAD? Dr. Molina said the risk of infertility and other long-term adverse effects is higher in HyperCVAD, but it has a lower risk of hepatic, pancreatic and thrombotic complications. And the CALGB 10403 regimen is more complicated to deliver, which is a potential obstacle in clinics without large numbers of patients.
As for outcomes, some research suggests they improve with pediatric-inspired regimens like CALGB 10403, he said, noting that “the debate continues.”
However, even with better regimens, Dr. Molina added, older ALL patients are still faring worse.
Also at the ASH presentation, Emory University/Children’s Healthcare of Atlanta pediatric cancer specialist Tamara Miller, MD, explored possible reasons that could explain the difference in outcomes based on age.
Cancer biology, response to chemotherapy, toxicities, psychosocial challenges, and low enrollment in clinical trials are all potential factors, she said. Specifically, aging into adulthood can lower tolerance of chemotherapy, and older patients are more prone to obesity, which is associated with worse outcomes, she said.
As for psychosocial challenges, it can be hard for older patients to manage their own medications, and they may lack insurance coverage, she said. Some patients may have worries about fertility, she added, and some may rebel against the requirements of treatment. Adherence is crucial to reducing risk of relapse, she added.
University of Cincinnati leukemia specialist Emily Curran, MD, told the ASH audience that researchers are exploring various avenues to improve outcomes.
Philadelphia chromosome-like (Ph-like) ALL, a subset of B-ALL, is associated with worse outcomes, she said, but it has multiple targetable pathways. An ongoing trial is exploring ruxolitinib (Jakafi) and chemotherapy in patients aged 18-39 with Ph-like ALL, Dr. Curran said.
Researchers are also wondering if up-front immunotherapy can help overcome disease biology, she said. Another potential therapy, she added, is CAR-T therapy for T-ALL.
Beyond cancer biology, “psychosocial factors are an even more challenging area in which we have fewer ongoing and less solutions,” Dr. Curran said.
Dr. Molina disclosed honoraria and consulting relationships with Autolus. Dr. Curran reported ties with Kite, Amgen, Incyte, Pfizer, Jazz, and Servier. Dr. Miller has no disclosures.
In a session at the annual meeting of the American Society of Hematology in December, clinicians defined the extent of the problem — which one described as a “survival cliff” — and they discussed potential strategies to turn things around.
Cleveland Clinic hematologist John Molina, MD, EdM, highlighted a 2022 study that revealed “the 5-year overall survival for younger pediatric patients is quite phenomenal at 93%. But as you start shifting even to 15-19 patients, that shifts to an overall survival of 74%.”
In the rest of the young adult population, from age 20 to 39, the overall survival rate dips down to 59%. What’s going on?
As Dr. Molina noted, a 2008 study revealed that outcomes in ALL for those aged 16-20 “historically depended on which door you walked into”: the pediatric setting or the adult setting. Patients fared better on pediatric regimens.
Currently, he explained, those who begin treatment in adult oncology clinics will start with either a pediatric-inspired treatment called CALGB 10403 or HyperCVAD (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride, and dexamethasone plus methotrexate and cytarabine).
CALGB 10403 was developed based on a pediatric backbone of COG AALL0232, Dr. Molina said, and has higher doses of major myelosuppressive agents vs. HyperCVAD. A 2019 study determined that it was feasible to treat adolescents and young adults up to age 40 “with low treatment-related mortality and marked improvement in outcomes. OS [overall survival] at 3 years was 73%.”
However, Dr. Molina observed that only 39% of patients completed the treatment per protocol.
Which is better, CALGB 10403 or HyperCVAD? Dr. Molina said the risk of infertility and other long-term adverse effects is higher in HyperCVAD, but it has a lower risk of hepatic, pancreatic and thrombotic complications. And the CALGB 10403 regimen is more complicated to deliver, which is a potential obstacle in clinics without large numbers of patients.
As for outcomes, some research suggests they improve with pediatric-inspired regimens like CALGB 10403, he said, noting that “the debate continues.”
However, even with better regimens, Dr. Molina added, older ALL patients are still faring worse.
Also at the ASH presentation, Emory University/Children’s Healthcare of Atlanta pediatric cancer specialist Tamara Miller, MD, explored possible reasons that could explain the difference in outcomes based on age.
Cancer biology, response to chemotherapy, toxicities, psychosocial challenges, and low enrollment in clinical trials are all potential factors, she said. Specifically, aging into adulthood can lower tolerance of chemotherapy, and older patients are more prone to obesity, which is associated with worse outcomes, she said.
As for psychosocial challenges, it can be hard for older patients to manage their own medications, and they may lack insurance coverage, she said. Some patients may have worries about fertility, she added, and some may rebel against the requirements of treatment. Adherence is crucial to reducing risk of relapse, she added.
University of Cincinnati leukemia specialist Emily Curran, MD, told the ASH audience that researchers are exploring various avenues to improve outcomes.
Philadelphia chromosome-like (Ph-like) ALL, a subset of B-ALL, is associated with worse outcomes, she said, but it has multiple targetable pathways. An ongoing trial is exploring ruxolitinib (Jakafi) and chemotherapy in patients aged 18-39 with Ph-like ALL, Dr. Curran said.
Researchers are also wondering if up-front immunotherapy can help overcome disease biology, she said. Another potential therapy, she added, is CAR-T therapy for T-ALL.
Beyond cancer biology, “psychosocial factors are an even more challenging area in which we have fewer ongoing and less solutions,” Dr. Curran said.
Dr. Molina disclosed honoraria and consulting relationships with Autolus. Dr. Curran reported ties with Kite, Amgen, Incyte, Pfizer, Jazz, and Servier. Dr. Miller has no disclosures.
FROM ASH 2023
Alzheimer’s and Epilepsy: Can Shared Molecular Mechanisms Reveal New Opportunities for Epilepsy?
ORLANDO — “,” said Delia Marias Talos, MD, at a session of the annual meeting of the American Epilepsy Society (AES).
A Closer Look at the Brain
“Phosphorylated tau correlates with cognitive function and executive function recorded presurgery, but it looks like the generative changes are more associated with temporal lobe and aging.”
Alzheimer’s disease is a degenerative condition marked by progressive memory deficits and cognitive decline noted by amyloid plaques and a formation of neurofibrillary tangles resulting from tau hyperphosphorylation.
Epilepsy, on the other hand, is a multifactorial condition with causes ranging from metabolic disorders, structural defects, infections, genetic mutations, and autoimmune disorders. In addition, nearly 50% of all epileptic seizures are idiopathic in nature.
Dr. Talos, professor of neurology at the University of Pennsylvania Perlman School of Medicine in Philadelphia, and her team did not see neurofibrillary tangles in the presurgical brains of epilepsy patients they studied; however, they saw tau plaques. In the future, they seek to investigate the features that distinguish epilepsy from Alzheimer’s disease.
Toxic fragments are probably there because amyloid precursor protein is highly upregulated, she told conference attendees. “We hypothesized that amyloid plaque is cleared but not impaired in epilepsy.”
The prognosis looks comparatively worse for patients who have Alzheimer’s disease and comorbid epilepsy than for patients who have only epilepsy. In addition, Dr. Talos stated that seizures appear to have an additive effort on Alzheimer’s disease.
Fyn-disruptive Therapy
Marson Putra, MD, PhD, a neuroscientist and postdoctoral researcher at Iowa State in Ames, Iowa, presented on the potential impact of a novel fyn-tau interaction as an unexplored target for epileptogensis and epilepsy.
Dr. Putra studied whether fyn-tau interactions exist in epilepsy. In both Alzheimer’s disease and epilepsy, Fyn belongs to the Src family of nonreceptor tyrosine kinases (SFKs), which are involved in cell proliferation and migration. Fyn contains an SH3 domain, which serves as a target for tau’s proline-rich (PxxP) motif. Fyn phosphorylates tau, specifically at tyrosine residue Y18, making fyn-disruptive therapy worth exploring.
Dr. Putra shared several currently proposed mechanisms of action regarding the pathogenesis of the tau plaque. In the first theory, the tau protein assumes a closed conformation in its normal state, thereby concealing the PxxP motif. However, in the second theory, pathogenesis causes the tau protein to assume an open conformation in the disease state, exposing pAT8 sites and making them available to fyn phosphorylation. In the second scenario, which involves Alzheimer’s disease, the fyn-tau interaction still occurs in open conformation state and is thought to occur in the postsynaptic terminal of the dendritic spine.
To investigate the proposed disease-causing mechanisms, Dr. Putra and her team studied status epilepticus in a rodent model of status epilepticus (SE). They used proximity ligation assay to measure interactions between Fyn and tau. They found AT8 and Y18 Fyn and N-methyl-D-aspartate (NMDA) receptor activation in a rat model and increased Fyn interaction. In addition, neuronal nitric oxide synthase levels were elevated 24 hours post-status. When investigating the fyn activity and interactions in the human brain, they found fyn phosphorylation – something that had never been reported before.
From there, Dr. Putra’s team sought to answer whether manipulating fyn-tau interactions could modify epilepsy. To do so, they conducted an experiment using the pharmacological Fyn inhibitor sarcatinib (SAR) and found it modified dysregulated postsynaptic proteins 24 hours post-SE in rat models. Longer exposure also bore a positive effect on epileptic rats.
After treating epileptic rats with SAR for 7 weeks, Dr. Putra found that SAR therapy reduces convulsive seizures during 7 weeks post-SE in rats. Recruiting pharmacological Fyn inhibition sufficiently decreased Fyn-tau interaction, NR-PSD95 complex, and convulsive seizures in chronic epilepsy.
Ultimately, her findings showed that SE exacerbates fyn-tau interactions, with chronic epilepsy modeling showing sustained elevation. In addition, fyn-tau interactions mediate and sustain neuronal hyperexcitability in the epileptic population.
“The impact on clinical care will be bidirectional relevant therapeutic targets in epilepsy and Alzheimer’s disease,” Dr. Putra told the audience.
Trends in epilepsy comorbidity and mortality
The final presenter, University of Washington researcher Aaron del Pozo, PhD, explained the impact of early-onset Alzheimer’s disease on overall outcomes and epilepsy.
“Early-onset Alzheimer’s disease carries a high seizure risk that affects quality of life as well as mortality,” Dr. del Pozo said.
According to data published in the British Medical Journal in 2020, the number of patients with epilepsy who had degenerative disease of the central nervous system or vascular dementia and delirium increased by approximately 210% from 1999 to 2017. Cerebral palsy trailed in second place with malignant neoplasms increasing by 50%. Cerebrovascular disease–related death in the epileptic population showed nearly negligible change, and ischemic heart disease and epilepsy decreased by approximately 25% and 15%, respectively. In addition, patients who have both epilepsy and Alzheimer’s disease are less likely to survive than patients who develop epilepsy after Alzheimer’s disease.
“We found that having epilepsy alone has decreased mortality, but having it in addition to other generative diseases of the central nervous system has a 200% increase in mortality,” Dr. del Pozo said.
ORLANDO — “,” said Delia Marias Talos, MD, at a session of the annual meeting of the American Epilepsy Society (AES).
A Closer Look at the Brain
“Phosphorylated tau correlates with cognitive function and executive function recorded presurgery, but it looks like the generative changes are more associated with temporal lobe and aging.”
Alzheimer’s disease is a degenerative condition marked by progressive memory deficits and cognitive decline noted by amyloid plaques and a formation of neurofibrillary tangles resulting from tau hyperphosphorylation.
Epilepsy, on the other hand, is a multifactorial condition with causes ranging from metabolic disorders, structural defects, infections, genetic mutations, and autoimmune disorders. In addition, nearly 50% of all epileptic seizures are idiopathic in nature.
Dr. Talos, professor of neurology at the University of Pennsylvania Perlman School of Medicine in Philadelphia, and her team did not see neurofibrillary tangles in the presurgical brains of epilepsy patients they studied; however, they saw tau plaques. In the future, they seek to investigate the features that distinguish epilepsy from Alzheimer’s disease.
Toxic fragments are probably there because amyloid precursor protein is highly upregulated, she told conference attendees. “We hypothesized that amyloid plaque is cleared but not impaired in epilepsy.”
The prognosis looks comparatively worse for patients who have Alzheimer’s disease and comorbid epilepsy than for patients who have only epilepsy. In addition, Dr. Talos stated that seizures appear to have an additive effort on Alzheimer’s disease.
Fyn-disruptive Therapy
Marson Putra, MD, PhD, a neuroscientist and postdoctoral researcher at Iowa State in Ames, Iowa, presented on the potential impact of a novel fyn-tau interaction as an unexplored target for epileptogensis and epilepsy.
Dr. Putra studied whether fyn-tau interactions exist in epilepsy. In both Alzheimer’s disease and epilepsy, Fyn belongs to the Src family of nonreceptor tyrosine kinases (SFKs), which are involved in cell proliferation and migration. Fyn contains an SH3 domain, which serves as a target for tau’s proline-rich (PxxP) motif. Fyn phosphorylates tau, specifically at tyrosine residue Y18, making fyn-disruptive therapy worth exploring.
Dr. Putra shared several currently proposed mechanisms of action regarding the pathogenesis of the tau plaque. In the first theory, the tau protein assumes a closed conformation in its normal state, thereby concealing the PxxP motif. However, in the second theory, pathogenesis causes the tau protein to assume an open conformation in the disease state, exposing pAT8 sites and making them available to fyn phosphorylation. In the second scenario, which involves Alzheimer’s disease, the fyn-tau interaction still occurs in open conformation state and is thought to occur in the postsynaptic terminal of the dendritic spine.
To investigate the proposed disease-causing mechanisms, Dr. Putra and her team studied status epilepticus in a rodent model of status epilepticus (SE). They used proximity ligation assay to measure interactions between Fyn and tau. They found AT8 and Y18 Fyn and N-methyl-D-aspartate (NMDA) receptor activation in a rat model and increased Fyn interaction. In addition, neuronal nitric oxide synthase levels were elevated 24 hours post-status. When investigating the fyn activity and interactions in the human brain, they found fyn phosphorylation – something that had never been reported before.
From there, Dr. Putra’s team sought to answer whether manipulating fyn-tau interactions could modify epilepsy. To do so, they conducted an experiment using the pharmacological Fyn inhibitor sarcatinib (SAR) and found it modified dysregulated postsynaptic proteins 24 hours post-SE in rat models. Longer exposure also bore a positive effect on epileptic rats.
After treating epileptic rats with SAR for 7 weeks, Dr. Putra found that SAR therapy reduces convulsive seizures during 7 weeks post-SE in rats. Recruiting pharmacological Fyn inhibition sufficiently decreased Fyn-tau interaction, NR-PSD95 complex, and convulsive seizures in chronic epilepsy.
Ultimately, her findings showed that SE exacerbates fyn-tau interactions, with chronic epilepsy modeling showing sustained elevation. In addition, fyn-tau interactions mediate and sustain neuronal hyperexcitability in the epileptic population.
“The impact on clinical care will be bidirectional relevant therapeutic targets in epilepsy and Alzheimer’s disease,” Dr. Putra told the audience.
Trends in epilepsy comorbidity and mortality
The final presenter, University of Washington researcher Aaron del Pozo, PhD, explained the impact of early-onset Alzheimer’s disease on overall outcomes and epilepsy.
“Early-onset Alzheimer’s disease carries a high seizure risk that affects quality of life as well as mortality,” Dr. del Pozo said.
According to data published in the British Medical Journal in 2020, the number of patients with epilepsy who had degenerative disease of the central nervous system or vascular dementia and delirium increased by approximately 210% from 1999 to 2017. Cerebral palsy trailed in second place with malignant neoplasms increasing by 50%. Cerebrovascular disease–related death in the epileptic population showed nearly negligible change, and ischemic heart disease and epilepsy decreased by approximately 25% and 15%, respectively. In addition, patients who have both epilepsy and Alzheimer’s disease are less likely to survive than patients who develop epilepsy after Alzheimer’s disease.
“We found that having epilepsy alone has decreased mortality, but having it in addition to other generative diseases of the central nervous system has a 200% increase in mortality,” Dr. del Pozo said.
ORLANDO — “,” said Delia Marias Talos, MD, at a session of the annual meeting of the American Epilepsy Society (AES).
A Closer Look at the Brain
“Phosphorylated tau correlates with cognitive function and executive function recorded presurgery, but it looks like the generative changes are more associated with temporal lobe and aging.”
Alzheimer’s disease is a degenerative condition marked by progressive memory deficits and cognitive decline noted by amyloid plaques and a formation of neurofibrillary tangles resulting from tau hyperphosphorylation.
Epilepsy, on the other hand, is a multifactorial condition with causes ranging from metabolic disorders, structural defects, infections, genetic mutations, and autoimmune disorders. In addition, nearly 50% of all epileptic seizures are idiopathic in nature.
Dr. Talos, professor of neurology at the University of Pennsylvania Perlman School of Medicine in Philadelphia, and her team did not see neurofibrillary tangles in the presurgical brains of epilepsy patients they studied; however, they saw tau plaques. In the future, they seek to investigate the features that distinguish epilepsy from Alzheimer’s disease.
Toxic fragments are probably there because amyloid precursor protein is highly upregulated, she told conference attendees. “We hypothesized that amyloid plaque is cleared but not impaired in epilepsy.”
The prognosis looks comparatively worse for patients who have Alzheimer’s disease and comorbid epilepsy than for patients who have only epilepsy. In addition, Dr. Talos stated that seizures appear to have an additive effort on Alzheimer’s disease.
Fyn-disruptive Therapy
Marson Putra, MD, PhD, a neuroscientist and postdoctoral researcher at Iowa State in Ames, Iowa, presented on the potential impact of a novel fyn-tau interaction as an unexplored target for epileptogensis and epilepsy.
Dr. Putra studied whether fyn-tau interactions exist in epilepsy. In both Alzheimer’s disease and epilepsy, Fyn belongs to the Src family of nonreceptor tyrosine kinases (SFKs), which are involved in cell proliferation and migration. Fyn contains an SH3 domain, which serves as a target for tau’s proline-rich (PxxP) motif. Fyn phosphorylates tau, specifically at tyrosine residue Y18, making fyn-disruptive therapy worth exploring.
Dr. Putra shared several currently proposed mechanisms of action regarding the pathogenesis of the tau plaque. In the first theory, the tau protein assumes a closed conformation in its normal state, thereby concealing the PxxP motif. However, in the second theory, pathogenesis causes the tau protein to assume an open conformation in the disease state, exposing pAT8 sites and making them available to fyn phosphorylation. In the second scenario, which involves Alzheimer’s disease, the fyn-tau interaction still occurs in open conformation state and is thought to occur in the postsynaptic terminal of the dendritic spine.
To investigate the proposed disease-causing mechanisms, Dr. Putra and her team studied status epilepticus in a rodent model of status epilepticus (SE). They used proximity ligation assay to measure interactions between Fyn and tau. They found AT8 and Y18 Fyn and N-methyl-D-aspartate (NMDA) receptor activation in a rat model and increased Fyn interaction. In addition, neuronal nitric oxide synthase levels were elevated 24 hours post-status. When investigating the fyn activity and interactions in the human brain, they found fyn phosphorylation – something that had never been reported before.
From there, Dr. Putra’s team sought to answer whether manipulating fyn-tau interactions could modify epilepsy. To do so, they conducted an experiment using the pharmacological Fyn inhibitor sarcatinib (SAR) and found it modified dysregulated postsynaptic proteins 24 hours post-SE in rat models. Longer exposure also bore a positive effect on epileptic rats.
After treating epileptic rats with SAR for 7 weeks, Dr. Putra found that SAR therapy reduces convulsive seizures during 7 weeks post-SE in rats. Recruiting pharmacological Fyn inhibition sufficiently decreased Fyn-tau interaction, NR-PSD95 complex, and convulsive seizures in chronic epilepsy.
Ultimately, her findings showed that SE exacerbates fyn-tau interactions, with chronic epilepsy modeling showing sustained elevation. In addition, fyn-tau interactions mediate and sustain neuronal hyperexcitability in the epileptic population.
“The impact on clinical care will be bidirectional relevant therapeutic targets in epilepsy and Alzheimer’s disease,” Dr. Putra told the audience.
Trends in epilepsy comorbidity and mortality
The final presenter, University of Washington researcher Aaron del Pozo, PhD, explained the impact of early-onset Alzheimer’s disease on overall outcomes and epilepsy.
“Early-onset Alzheimer’s disease carries a high seizure risk that affects quality of life as well as mortality,” Dr. del Pozo said.
According to data published in the British Medical Journal in 2020, the number of patients with epilepsy who had degenerative disease of the central nervous system or vascular dementia and delirium increased by approximately 210% from 1999 to 2017. Cerebral palsy trailed in second place with malignant neoplasms increasing by 50%. Cerebrovascular disease–related death in the epileptic population showed nearly negligible change, and ischemic heart disease and epilepsy decreased by approximately 25% and 15%, respectively. In addition, patients who have both epilepsy and Alzheimer’s disease are less likely to survive than patients who develop epilepsy after Alzheimer’s disease.
“We found that having epilepsy alone has decreased mortality, but having it in addition to other generative diseases of the central nervous system has a 200% increase in mortality,” Dr. del Pozo said.
FROM AES 2023
ALL: ASH Draws Up Tx Guidelines For Patients 15-39
At the crux of the matter is the unusual nature of ALL, said University of Chicago leukemia specialist Wendy Stock, MD, in a presentation at the annual meeting of the American Society of Hematology in December 2023. The disease is both rare and unique since it spans the entire lifetime from infancy to old age, she said.
The guidelines will focus on adolescents and young adults, which the National Cancer Institute defines as those aged 15-39. For these patients, “treatment is administered by the whole gamut of practitioners in the world of hematology, from pediatricians to adult hematologist/oncologists, which provides unique challenges in terms of understanding and access to care,” Dr. Stock said.
As she explained, ALL “is the bread and butter of pediatric oncology, but in the world of adult hematology-oncology, many patients are treated in small-practice settings where there have been very few uniform approaches available to the treating practitioners,” she said. “There’s not going to ever be the ability to get every — or even the majority — of adults into those big academic centers.”
Meanwhile, research from around the world has highlighted major mortality gaps between pediatric and adult care in ALL. “This has been our huge challenge: Is it the treatment approach? Is it the disease biology, the patient biology, the doctors who treat these diseases? Is it the geographic location where they’re treated? Well, we now know that, of course, it’s probably all of the above, and a lot more than that.”
In light of the need for guidance in ALL treatment, it will be crucial to disseminate data and recommendations via the guidelines, she said.
In 2021, ASH members approved the development of new clinical practice guidelines for this population. The process so far has been difficult, said pediatric oncologist Sumit Gupta, MD, PhD, of the Hospital for Sick Children in Toronto, Ontario, at the ASH presentation.
“At one point,” Dr. Gupta recalled, “someone on our methodology team said this was the most challenging systematic review and guideline creation that they’d ever worked on, which is not what you want to hear as a co-chair.”
One major challenge for the guideline drafters is to balance ALL research findings that cover only certain ages, Dr. Gupta said. A study, for example, may only include patients up to age 21 or over age 35, making it difficult to decide how it fits into a larger evidence base for adolescents and young adults.
“We don’t always have perfect evidence. But we’re trying to take all of that and translate it into a formalized systematic review,” he said. “This is tricky for any guideline. But ALL poses a particular challenge because of how the evidence base is spread out.”
Another challenge is figuring out how to review psychosocial interventions in ALL. They are obviously crucial, he said. But should guidelines only take into account strategies that were tested in ALL? Or should they look at a wider perspective and encompass research into non–ALL-specific approaches?
In terms of guidance about frontline treatment, the guideline developers are focusing on several topics, said University of Rochester hematologist/oncologist Kristen O’Dwyer, MD, at the ASH presentation. These include: Should adolescents and young adults receive pediatric or adult regimens? Where do targeted therapy, immunotherapy, steroids, allogeneic stem cell transplants, and central nervous system (CNS) prophylaxis fit in?
“Finally, there are a series of questions that are addressing the toxicity prevention and management that go along with these intensive chemotherapy regimens,” she said.
On one front, there’s a “knowledge gap” about the value of stem cell transplant vs pediatric-inspired chemotherapy as postremission therapies, Dr. O’Dwyer said, because there are no direct comparisons. What to do? “There are retrospective comparisons that are emerging along with population-level analysis, single-arm observational studies that suggest that a pediatric-based chemotherapy approach is superior with similar relapse rates and less treatment-related mortality,” she said.
ASH expects to release a draft of its ALL guidelines for adolescents and young adults later this year and publish final recommendations in late 2024 or early 2025.
Dr. Stock, Dr. Gupta, and Dr. O’Dwyer have no disclosures.
At the crux of the matter is the unusual nature of ALL, said University of Chicago leukemia specialist Wendy Stock, MD, in a presentation at the annual meeting of the American Society of Hematology in December 2023. The disease is both rare and unique since it spans the entire lifetime from infancy to old age, she said.
The guidelines will focus on adolescents and young adults, which the National Cancer Institute defines as those aged 15-39. For these patients, “treatment is administered by the whole gamut of practitioners in the world of hematology, from pediatricians to adult hematologist/oncologists, which provides unique challenges in terms of understanding and access to care,” Dr. Stock said.
As she explained, ALL “is the bread and butter of pediatric oncology, but in the world of adult hematology-oncology, many patients are treated in small-practice settings where there have been very few uniform approaches available to the treating practitioners,” she said. “There’s not going to ever be the ability to get every — or even the majority — of adults into those big academic centers.”
Meanwhile, research from around the world has highlighted major mortality gaps between pediatric and adult care in ALL. “This has been our huge challenge: Is it the treatment approach? Is it the disease biology, the patient biology, the doctors who treat these diseases? Is it the geographic location where they’re treated? Well, we now know that, of course, it’s probably all of the above, and a lot more than that.”
In light of the need for guidance in ALL treatment, it will be crucial to disseminate data and recommendations via the guidelines, she said.
In 2021, ASH members approved the development of new clinical practice guidelines for this population. The process so far has been difficult, said pediatric oncologist Sumit Gupta, MD, PhD, of the Hospital for Sick Children in Toronto, Ontario, at the ASH presentation.
“At one point,” Dr. Gupta recalled, “someone on our methodology team said this was the most challenging systematic review and guideline creation that they’d ever worked on, which is not what you want to hear as a co-chair.”
One major challenge for the guideline drafters is to balance ALL research findings that cover only certain ages, Dr. Gupta said. A study, for example, may only include patients up to age 21 or over age 35, making it difficult to decide how it fits into a larger evidence base for adolescents and young adults.
“We don’t always have perfect evidence. But we’re trying to take all of that and translate it into a formalized systematic review,” he said. “This is tricky for any guideline. But ALL poses a particular challenge because of how the evidence base is spread out.”
Another challenge is figuring out how to review psychosocial interventions in ALL. They are obviously crucial, he said. But should guidelines only take into account strategies that were tested in ALL? Or should they look at a wider perspective and encompass research into non–ALL-specific approaches?
In terms of guidance about frontline treatment, the guideline developers are focusing on several topics, said University of Rochester hematologist/oncologist Kristen O’Dwyer, MD, at the ASH presentation. These include: Should adolescents and young adults receive pediatric or adult regimens? Where do targeted therapy, immunotherapy, steroids, allogeneic stem cell transplants, and central nervous system (CNS) prophylaxis fit in?
“Finally, there are a series of questions that are addressing the toxicity prevention and management that go along with these intensive chemotherapy regimens,” she said.
On one front, there’s a “knowledge gap” about the value of stem cell transplant vs pediatric-inspired chemotherapy as postremission therapies, Dr. O’Dwyer said, because there are no direct comparisons. What to do? “There are retrospective comparisons that are emerging along with population-level analysis, single-arm observational studies that suggest that a pediatric-based chemotherapy approach is superior with similar relapse rates and less treatment-related mortality,” she said.
ASH expects to release a draft of its ALL guidelines for adolescents and young adults later this year and publish final recommendations in late 2024 or early 2025.
Dr. Stock, Dr. Gupta, and Dr. O’Dwyer have no disclosures.
At the crux of the matter is the unusual nature of ALL, said University of Chicago leukemia specialist Wendy Stock, MD, in a presentation at the annual meeting of the American Society of Hematology in December 2023. The disease is both rare and unique since it spans the entire lifetime from infancy to old age, she said.
The guidelines will focus on adolescents and young adults, which the National Cancer Institute defines as those aged 15-39. For these patients, “treatment is administered by the whole gamut of practitioners in the world of hematology, from pediatricians to adult hematologist/oncologists, which provides unique challenges in terms of understanding and access to care,” Dr. Stock said.
As she explained, ALL “is the bread and butter of pediatric oncology, but in the world of adult hematology-oncology, many patients are treated in small-practice settings where there have been very few uniform approaches available to the treating practitioners,” she said. “There’s not going to ever be the ability to get every — or even the majority — of adults into those big academic centers.”
Meanwhile, research from around the world has highlighted major mortality gaps between pediatric and adult care in ALL. “This has been our huge challenge: Is it the treatment approach? Is it the disease biology, the patient biology, the doctors who treat these diseases? Is it the geographic location where they’re treated? Well, we now know that, of course, it’s probably all of the above, and a lot more than that.”
In light of the need for guidance in ALL treatment, it will be crucial to disseminate data and recommendations via the guidelines, she said.
In 2021, ASH members approved the development of new clinical practice guidelines for this population. The process so far has been difficult, said pediatric oncologist Sumit Gupta, MD, PhD, of the Hospital for Sick Children in Toronto, Ontario, at the ASH presentation.
“At one point,” Dr. Gupta recalled, “someone on our methodology team said this was the most challenging systematic review and guideline creation that they’d ever worked on, which is not what you want to hear as a co-chair.”
One major challenge for the guideline drafters is to balance ALL research findings that cover only certain ages, Dr. Gupta said. A study, for example, may only include patients up to age 21 or over age 35, making it difficult to decide how it fits into a larger evidence base for adolescents and young adults.
“We don’t always have perfect evidence. But we’re trying to take all of that and translate it into a formalized systematic review,” he said. “This is tricky for any guideline. But ALL poses a particular challenge because of how the evidence base is spread out.”
Another challenge is figuring out how to review psychosocial interventions in ALL. They are obviously crucial, he said. But should guidelines only take into account strategies that were tested in ALL? Or should they look at a wider perspective and encompass research into non–ALL-specific approaches?
In terms of guidance about frontline treatment, the guideline developers are focusing on several topics, said University of Rochester hematologist/oncologist Kristen O’Dwyer, MD, at the ASH presentation. These include: Should adolescents and young adults receive pediatric or adult regimens? Where do targeted therapy, immunotherapy, steroids, allogeneic stem cell transplants, and central nervous system (CNS) prophylaxis fit in?
“Finally, there are a series of questions that are addressing the toxicity prevention and management that go along with these intensive chemotherapy regimens,” she said.
On one front, there’s a “knowledge gap” about the value of stem cell transplant vs pediatric-inspired chemotherapy as postremission therapies, Dr. O’Dwyer said, because there are no direct comparisons. What to do? “There are retrospective comparisons that are emerging along with population-level analysis, single-arm observational studies that suggest that a pediatric-based chemotherapy approach is superior with similar relapse rates and less treatment-related mortality,” she said.
ASH expects to release a draft of its ALL guidelines for adolescents and young adults later this year and publish final recommendations in late 2024 or early 2025.
Dr. Stock, Dr. Gupta, and Dr. O’Dwyer have no disclosures.
FROM ASH 2023
Sudden Cardiac Deaths Down Among NCAA Athletes
TOPLINE:
A new study shows sudden cardiac deaths among collegiate athletes decreased over a recent 20-year period, but risks are still elevated among males, Black players, and basketball players, suggesting more intensive screening among these groups is needed.
METHODOLOGY:
- The study examined incidence and surrounding circumstances of sudden cardiac death (SCD) among student athletes who competed in at least one varsity sport at National Collegiate Athletic Association (NCAA) Division I, II, or III institutions in the 20 years from July 1, 2002, to June 30, 2022.
- Researchers determined causes of death and gathered demographic characteristics using multiple methods, including review of autopsy and other official documents, Internet searches, and contacts to next of kin, coaches, athletic trainers, coroners, medical examiners, scholarship foundations, and physicians involved in the case.
- SCD was defined as sudden unexpected death attributable to a cardiac cause, or a sudden death in a structurally normal heart with no other explanation for death and a history consistent with cardiac-related death that occurred within an hour of symptom onset, or an unwitnessed death occurring within 24 hours of the person being alive.
- Researchers calculated incidence rates over a typical 4-year collegiate career and reported these as athlete-years.
TAKEAWAY:
- The incidence of SCD, which accounted for 13% of the 1102 total deaths during the study period, decreased over time, with a 5-year incidence rate ratio (IRR) of 0.71 (95% CI, 0.61-0.82), while noncardiovascular deaths remained stable.
- IRR for males versus females was 3.79 (95% CI, 2.45-5.88) and for Black versus White athletes was 2.79 (95% CI, 1.98-3.94).
- Basketball and football players were at increased risk of SCD; for example, the incidence rate among Division I Black male basketball athletes was 1:1924 per 4-year athlete-years.
- The most common postmortem finding was autopsy-negative sudden unexplained death, at 19%, followed by idiopathic left ventricular hypertrophy/possible cardiomyopathy (17%) and hypertrophic cardiomyopathy (13%), with no cases of death attributable to COVID-19 myocarditis.
IN PRACTICE:
Although the reason for the decrease in SCD is unknown, “our data suggest that strategies to reduce SCD among competing athletes may be having a positive effect,” wrote the authors. More intensive screening strategies among groups with high SCD incidence may be warranted, they added.
SOURCE:
The study was conducted by Bradley J. Petek, MD, Sports Cardiology Program, Knight Cardiovascular Institute, Oregon Health & Science University, Portland. It was published online November 13 in Circulation and presented at the American Heart Association scientific sessions (abstract 479).
LIMITATIONS:
Some cases of SCD may have been missed as there is no mandatory reporting system in the United States. Approaches to cardiac autopsy and reporting varied significantly. The cause of death was unknown in 16 cases, and postmortem genetic testing was available for only 3% of athletes. As the study didn’t have data on resuscitated sudden cardiac arrest or preparticipation cardiovascular screening practices and findings, definitive conclusions couldn’t be drawn regarding causal factors underlying the decreased incidence of SCD.
DISCLOSURES:
There was no outside funding source. Dr. Petek has reported no relevant financial relationships. Disclosures for the other authors are listed with the article.
A version of this article appeared on Medscape.com.
TOPLINE:
A new study shows sudden cardiac deaths among collegiate athletes decreased over a recent 20-year period, but risks are still elevated among males, Black players, and basketball players, suggesting more intensive screening among these groups is needed.
METHODOLOGY:
- The study examined incidence and surrounding circumstances of sudden cardiac death (SCD) among student athletes who competed in at least one varsity sport at National Collegiate Athletic Association (NCAA) Division I, II, or III institutions in the 20 years from July 1, 2002, to June 30, 2022.
- Researchers determined causes of death and gathered demographic characteristics using multiple methods, including review of autopsy and other official documents, Internet searches, and contacts to next of kin, coaches, athletic trainers, coroners, medical examiners, scholarship foundations, and physicians involved in the case.
- SCD was defined as sudden unexpected death attributable to a cardiac cause, or a sudden death in a structurally normal heart with no other explanation for death and a history consistent with cardiac-related death that occurred within an hour of symptom onset, or an unwitnessed death occurring within 24 hours of the person being alive.
- Researchers calculated incidence rates over a typical 4-year collegiate career and reported these as athlete-years.
TAKEAWAY:
- The incidence of SCD, which accounted for 13% of the 1102 total deaths during the study period, decreased over time, with a 5-year incidence rate ratio (IRR) of 0.71 (95% CI, 0.61-0.82), while noncardiovascular deaths remained stable.
- IRR for males versus females was 3.79 (95% CI, 2.45-5.88) and for Black versus White athletes was 2.79 (95% CI, 1.98-3.94).
- Basketball and football players were at increased risk of SCD; for example, the incidence rate among Division I Black male basketball athletes was 1:1924 per 4-year athlete-years.
- The most common postmortem finding was autopsy-negative sudden unexplained death, at 19%, followed by idiopathic left ventricular hypertrophy/possible cardiomyopathy (17%) and hypertrophic cardiomyopathy (13%), with no cases of death attributable to COVID-19 myocarditis.
IN PRACTICE:
Although the reason for the decrease in SCD is unknown, “our data suggest that strategies to reduce SCD among competing athletes may be having a positive effect,” wrote the authors. More intensive screening strategies among groups with high SCD incidence may be warranted, they added.
SOURCE:
The study was conducted by Bradley J. Petek, MD, Sports Cardiology Program, Knight Cardiovascular Institute, Oregon Health & Science University, Portland. It was published online November 13 in Circulation and presented at the American Heart Association scientific sessions (abstract 479).
LIMITATIONS:
Some cases of SCD may have been missed as there is no mandatory reporting system in the United States. Approaches to cardiac autopsy and reporting varied significantly. The cause of death was unknown in 16 cases, and postmortem genetic testing was available for only 3% of athletes. As the study didn’t have data on resuscitated sudden cardiac arrest or preparticipation cardiovascular screening practices and findings, definitive conclusions couldn’t be drawn regarding causal factors underlying the decreased incidence of SCD.
DISCLOSURES:
There was no outside funding source. Dr. Petek has reported no relevant financial relationships. Disclosures for the other authors are listed with the article.
A version of this article appeared on Medscape.com.
TOPLINE:
A new study shows sudden cardiac deaths among collegiate athletes decreased over a recent 20-year period, but risks are still elevated among males, Black players, and basketball players, suggesting more intensive screening among these groups is needed.
METHODOLOGY:
- The study examined incidence and surrounding circumstances of sudden cardiac death (SCD) among student athletes who competed in at least one varsity sport at National Collegiate Athletic Association (NCAA) Division I, II, or III institutions in the 20 years from July 1, 2002, to June 30, 2022.
- Researchers determined causes of death and gathered demographic characteristics using multiple methods, including review of autopsy and other official documents, Internet searches, and contacts to next of kin, coaches, athletic trainers, coroners, medical examiners, scholarship foundations, and physicians involved in the case.
- SCD was defined as sudden unexpected death attributable to a cardiac cause, or a sudden death in a structurally normal heart with no other explanation for death and a history consistent with cardiac-related death that occurred within an hour of symptom onset, or an unwitnessed death occurring within 24 hours of the person being alive.
- Researchers calculated incidence rates over a typical 4-year collegiate career and reported these as athlete-years.
TAKEAWAY:
- The incidence of SCD, which accounted for 13% of the 1102 total deaths during the study period, decreased over time, with a 5-year incidence rate ratio (IRR) of 0.71 (95% CI, 0.61-0.82), while noncardiovascular deaths remained stable.
- IRR for males versus females was 3.79 (95% CI, 2.45-5.88) and for Black versus White athletes was 2.79 (95% CI, 1.98-3.94).
- Basketball and football players were at increased risk of SCD; for example, the incidence rate among Division I Black male basketball athletes was 1:1924 per 4-year athlete-years.
- The most common postmortem finding was autopsy-negative sudden unexplained death, at 19%, followed by idiopathic left ventricular hypertrophy/possible cardiomyopathy (17%) and hypertrophic cardiomyopathy (13%), with no cases of death attributable to COVID-19 myocarditis.
IN PRACTICE:
Although the reason for the decrease in SCD is unknown, “our data suggest that strategies to reduce SCD among competing athletes may be having a positive effect,” wrote the authors. More intensive screening strategies among groups with high SCD incidence may be warranted, they added.
SOURCE:
The study was conducted by Bradley J. Petek, MD, Sports Cardiology Program, Knight Cardiovascular Institute, Oregon Health & Science University, Portland. It was published online November 13 in Circulation and presented at the American Heart Association scientific sessions (abstract 479).
LIMITATIONS:
Some cases of SCD may have been missed as there is no mandatory reporting system in the United States. Approaches to cardiac autopsy and reporting varied significantly. The cause of death was unknown in 16 cases, and postmortem genetic testing was available for only 3% of athletes. As the study didn’t have data on resuscitated sudden cardiac arrest or preparticipation cardiovascular screening practices and findings, definitive conclusions couldn’t be drawn regarding causal factors underlying the decreased incidence of SCD.
DISCLOSURES:
There was no outside funding source. Dr. Petek has reported no relevant financial relationships. Disclosures for the other authors are listed with the article.
A version of this article appeared on Medscape.com.