User login
Risk factors for death from COVID-19 identified in Wuhan patients
Patients who did not survive hospitalization for COVID-19 in Wuhan were more likely to be older, have comorbidities, and elevated D-dimer, according to the first study to examine risk factors associated with death among adults hospitalized with COVID-19. “Older age, showing signs of sepsis on admission, underlying diseases like high blood pressure and diabetes, and the prolonged use of noninvasive ventilation were important factors in the deaths of these patients,” coauthor Zhibo Liu said in a news release. Abnormal blood clotting was part of the clinical picture too.
Fei Zhou, MD, from the Chinese Academy of Medical Sciences, and colleagues conducted a retrospective, observational, multicenter cohort study of 191 patients, 137 of whom were discharged and 54 of whom died in the hospital.
The study, published online today in The Lancet, included all adult inpatients with laboratory-confirmed COVID-19 from Jinyintan Hospital and Wuhan Pulmonary Hospital who had been discharged or died by January 31 of this year. Severely ill patients in the province were transferred to these hospitals until February 1.
The researchers compared demographic, clinical, treatment, and laboratory data from electronic medical records between survivors and those who succumbed to the disease. The analysis also tested serial samples for viral RNA. Overall, 91 (48%) of the 191 patients had comorbidity. Most common was hypertension (30%), followed by diabetes (19%) and coronary heart disease (8%).
The odds of dying in the hospital increased with age (odds ratio 1.10; 95% confidence interval, 1.03-1.17; per year increase in age), higher Sequential Organ Failure Assessment (SOFA) score (5.65, 2.61-12.23; P < .0001), and D-dimer level exceeding 1 mcg/L on admission. The SOFA was previously called the “sepsis-related organ failure assessment score” and assesses rate of organ failure in intensive care units. Elevated D-dimer indicates increased risk of abnormal blood clotting, such as deep vein thrombosis.
Nonsurvivors compared with survivors had higher frequencies of respiratory failure (98% vs 36%), sepsis (100%, vs 42%), and secondary infections (50% vs 1%).
The average age of survivors was 52 years compared to 69 for those who died. Liu cited weakening of the immune system and increased inflammation, which damages organs and also promotes viral replication, as explanations for the age effect.
From the time of initial symptoms, median time to discharge from the hospital was 22 days. Average time to death was 18.5 days.
Fever persisted for a median of 12 days among all patients, and cough persisted for a median 19 days; 45% of the survivors were still coughing on discharge. In survivors, shortness of breath improved after 13 days, but persisted until death in the others.
Viral shedding persisted for a median duration of 20 days in survivors, ranging from 8 to 37. The virus (SARS-CoV-2) was detectable in nonsurvivors until death. Antiviral treatment did not curtail viral shedding.
But the viral shedding data come with a caveat. “The extended viral shedding noted in our study has important implications for guiding decisions around isolation precautions and antiviral treatment in patients with confirmed COVID-19 infection. However, we need to be clear that viral shedding time should not be confused with other self-isolation guidance for people who may have been exposed to COVID-19 but do not have symptoms, as this guidance is based on the incubation time of the virus,” explained colead author Bin Cao.
“Older age, elevated D-dimer levels, and high SOFA score could help clinicians to identify at an early stage those patients with COVID-19 who have poor prognosis. Prolonged viral shedding provides the rationale for a strategy of isolation of infected patients and optimal antiviral interventions in the future,” the researchers conclude.
A limitation in interpreting the findings of the study is that hospitalized patients do not represent the entire infected population. The researchers caution that “the number of deaths does not reflect the true mortality of COVID-19.” They also note that they did not have enough genetic material to accurately assess duration of viral shedding.
This article first appeared on Medscape.com.
Patients who did not survive hospitalization for COVID-19 in Wuhan were more likely to be older, have comorbidities, and elevated D-dimer, according to the first study to examine risk factors associated with death among adults hospitalized with COVID-19. “Older age, showing signs of sepsis on admission, underlying diseases like high blood pressure and diabetes, and the prolonged use of noninvasive ventilation were important factors in the deaths of these patients,” coauthor Zhibo Liu said in a news release. Abnormal blood clotting was part of the clinical picture too.
Fei Zhou, MD, from the Chinese Academy of Medical Sciences, and colleagues conducted a retrospective, observational, multicenter cohort study of 191 patients, 137 of whom were discharged and 54 of whom died in the hospital.
The study, published online today in The Lancet, included all adult inpatients with laboratory-confirmed COVID-19 from Jinyintan Hospital and Wuhan Pulmonary Hospital who had been discharged or died by January 31 of this year. Severely ill patients in the province were transferred to these hospitals until February 1.
The researchers compared demographic, clinical, treatment, and laboratory data from electronic medical records between survivors and those who succumbed to the disease. The analysis also tested serial samples for viral RNA. Overall, 91 (48%) of the 191 patients had comorbidity. Most common was hypertension (30%), followed by diabetes (19%) and coronary heart disease (8%).
The odds of dying in the hospital increased with age (odds ratio 1.10; 95% confidence interval, 1.03-1.17; per year increase in age), higher Sequential Organ Failure Assessment (SOFA) score (5.65, 2.61-12.23; P < .0001), and D-dimer level exceeding 1 mcg/L on admission. The SOFA was previously called the “sepsis-related organ failure assessment score” and assesses rate of organ failure in intensive care units. Elevated D-dimer indicates increased risk of abnormal blood clotting, such as deep vein thrombosis.
Nonsurvivors compared with survivors had higher frequencies of respiratory failure (98% vs 36%), sepsis (100%, vs 42%), and secondary infections (50% vs 1%).
The average age of survivors was 52 years compared to 69 for those who died. Liu cited weakening of the immune system and increased inflammation, which damages organs and also promotes viral replication, as explanations for the age effect.
From the time of initial symptoms, median time to discharge from the hospital was 22 days. Average time to death was 18.5 days.
Fever persisted for a median of 12 days among all patients, and cough persisted for a median 19 days; 45% of the survivors were still coughing on discharge. In survivors, shortness of breath improved after 13 days, but persisted until death in the others.
Viral shedding persisted for a median duration of 20 days in survivors, ranging from 8 to 37. The virus (SARS-CoV-2) was detectable in nonsurvivors until death. Antiviral treatment did not curtail viral shedding.
But the viral shedding data come with a caveat. “The extended viral shedding noted in our study has important implications for guiding decisions around isolation precautions and antiviral treatment in patients with confirmed COVID-19 infection. However, we need to be clear that viral shedding time should not be confused with other self-isolation guidance for people who may have been exposed to COVID-19 but do not have symptoms, as this guidance is based on the incubation time of the virus,” explained colead author Bin Cao.
“Older age, elevated D-dimer levels, and high SOFA score could help clinicians to identify at an early stage those patients with COVID-19 who have poor prognosis. Prolonged viral shedding provides the rationale for a strategy of isolation of infected patients and optimal antiviral interventions in the future,” the researchers conclude.
A limitation in interpreting the findings of the study is that hospitalized patients do not represent the entire infected population. The researchers caution that “the number of deaths does not reflect the true mortality of COVID-19.” They also note that they did not have enough genetic material to accurately assess duration of viral shedding.
This article first appeared on Medscape.com.
Patients who did not survive hospitalization for COVID-19 in Wuhan were more likely to be older, have comorbidities, and elevated D-dimer, according to the first study to examine risk factors associated with death among adults hospitalized with COVID-19. “Older age, showing signs of sepsis on admission, underlying diseases like high blood pressure and diabetes, and the prolonged use of noninvasive ventilation were important factors in the deaths of these patients,” coauthor Zhibo Liu said in a news release. Abnormal blood clotting was part of the clinical picture too.
Fei Zhou, MD, from the Chinese Academy of Medical Sciences, and colleagues conducted a retrospective, observational, multicenter cohort study of 191 patients, 137 of whom were discharged and 54 of whom died in the hospital.
The study, published online today in The Lancet, included all adult inpatients with laboratory-confirmed COVID-19 from Jinyintan Hospital and Wuhan Pulmonary Hospital who had been discharged or died by January 31 of this year. Severely ill patients in the province were transferred to these hospitals until February 1.
The researchers compared demographic, clinical, treatment, and laboratory data from electronic medical records between survivors and those who succumbed to the disease. The analysis also tested serial samples for viral RNA. Overall, 91 (48%) of the 191 patients had comorbidity. Most common was hypertension (30%), followed by diabetes (19%) and coronary heart disease (8%).
The odds of dying in the hospital increased with age (odds ratio 1.10; 95% confidence interval, 1.03-1.17; per year increase in age), higher Sequential Organ Failure Assessment (SOFA) score (5.65, 2.61-12.23; P < .0001), and D-dimer level exceeding 1 mcg/L on admission. The SOFA was previously called the “sepsis-related organ failure assessment score” and assesses rate of organ failure in intensive care units. Elevated D-dimer indicates increased risk of abnormal blood clotting, such as deep vein thrombosis.
Nonsurvivors compared with survivors had higher frequencies of respiratory failure (98% vs 36%), sepsis (100%, vs 42%), and secondary infections (50% vs 1%).
The average age of survivors was 52 years compared to 69 for those who died. Liu cited weakening of the immune system and increased inflammation, which damages organs and also promotes viral replication, as explanations for the age effect.
From the time of initial symptoms, median time to discharge from the hospital was 22 days. Average time to death was 18.5 days.
Fever persisted for a median of 12 days among all patients, and cough persisted for a median 19 days; 45% of the survivors were still coughing on discharge. In survivors, shortness of breath improved after 13 days, but persisted until death in the others.
Viral shedding persisted for a median duration of 20 days in survivors, ranging from 8 to 37. The virus (SARS-CoV-2) was detectable in nonsurvivors until death. Antiviral treatment did not curtail viral shedding.
But the viral shedding data come with a caveat. “The extended viral shedding noted in our study has important implications for guiding decisions around isolation precautions and antiviral treatment in patients with confirmed COVID-19 infection. However, we need to be clear that viral shedding time should not be confused with other self-isolation guidance for people who may have been exposed to COVID-19 but do not have symptoms, as this guidance is based on the incubation time of the virus,” explained colead author Bin Cao.
“Older age, elevated D-dimer levels, and high SOFA score could help clinicians to identify at an early stage those patients with COVID-19 who have poor prognosis. Prolonged viral shedding provides the rationale for a strategy of isolation of infected patients and optimal antiviral interventions in the future,” the researchers conclude.
A limitation in interpreting the findings of the study is that hospitalized patients do not represent the entire infected population. The researchers caution that “the number of deaths does not reflect the true mortality of COVID-19.” They also note that they did not have enough genetic material to accurately assess duration of viral shedding.
This article first appeared on Medscape.com.
AUGUSTUS: Apixaban surpassed warfarin despite prior stroke or thromboembolism
LOS ANGELES – The edge that the direct-acting oral anticoagulant apixaban (Eliquis) has over warfarin for safely preventing ischemic events in patients with atrial fibrillation and either a recent acute coronary syndrome event or a recent percutaneous coronary intervention held up even in patients with a history of stroke, transient ischemic attack, or thromboembolic event, according to a prespecified secondary analysis of data collected in the AUGUSTUS trial.

The treatment advantages of apixaban, compared with warfarin, seen in the overall AUGUSTUS results, first reported in March 2019, “were consistent” with the benefits seen in the subgroup of enrolled patients with a prior stroke, transient ischemic attack (TIA), or thromboembolic (TE) event, M. Cecilia Bahit, MD, said at the International Stroke Conference sponsored by the American Heart Association.
All patients in AUGUSTUS received a P2Y12 inhibitor antiplatelet drug, which was clopidogrel for more than 90% of patients. The two-by-two factorial design of AUGUSTUS also assessed the safety and efficacy of either adding or withholding aspirin from the two-drug regimen that all patients in the study received with a P2Y12 inhibitor plus an anticoagulant (apixaban or warfarin). The most notable finding of the aspirin versus placebo analysis was that patients without a prior stroke, TIA, or TE event had a “more profound” increase in their rate of major or clinically relevant minor bleeds when also treated with aspirin, compared with patients who received aspirin and had a history of stroke, TIA, or TE event, reported Dr. Bahit, a chief of cardiology and director of clinical research at the INECO Foundation in Rosario, Argentina.
In general, the findings of the secondary analysis that took into account stroke, TIA, or TE history “confirmed” the main AUGUSTUS findings, Dr. Bahit said; an antithrombotic regimen of apixaban plus clopidogrel (or other P2Y12 inhibitor) without aspirin was superior for both efficacy and safety, compared with the alternative regimens that either substituted warfarin for apixaban or that added aspirin.
AUGUSTUS enrolled 4,614 atrial fibrillation (AFib) patients who either had a recent acute coronary syndrome (ACS) event or had recently undergone percutaneous coronary intervention (PCI) at any of 492 sites in 33 countries during 2015-2018. The study’s primary endpoint was the incidence of major or clinically relevant minor bleeds after 6 months, which was significantly lower in the subgroups that received apixaban instead of warfarin and in patients who received placebo instead of aspirin. The secondary endpoint of death or hospitalization after 6 months was also significantly lower in the apixaban-treated patients, compared with those on warfarin, while the aspirin and placebo subgroups showed no difference in the incidence of these events (N Engl J Med. 2019 Apr 18;380[16]:1509-24).
The results reported by Dr. Bahit also highlighted both the high risk faced by patients with AFib who also have had an ACS event or PCI, as well as a prior stroke, TIA, or TE event, noted Larry B. Goldstein, MD, professor and chairman of neurology at the University of Kentucky, Lexington. “It’s difficult, because these patients had an ACS event or PCI, and you don’t want a coronary too close up, but do these patients really need a P2Y12 inhibitor plus an anticoagulant? Could these patients do as well on apixaban only? I would have liked to see that treatment arm in the study,” Dr. Goldstein commented in an interview.
“These are challenging patients because they often require anticoagulation for the AFib as well as antiplatelet agents” for the recent PCI or ACS event, commented Mitchell S.V. Elkind, MD, professor of neurology at Columbia University, New York. “The question has always been: How many blood thinners should these patients be on? Potentially they could be on three different agents [an anticoagulant and two antiplatelet drugs], and we know that all of those drugs together pretty dramatically increase the risk of bleeding. About 15% of the patients in the overall AUGUSTUS trial had either cerebrovascular disease or systemic thromboembolism, so this was a small subgroup of the overall trial, but the overall trial was large so it’s a significant number of patients who met this criteria. The results confirmed that even in a group of patients who may be considered at high risk because they have a prior history of cerebrovascular disease use of apixaban instead of warfarin seemed safer, and that those patients did not need to be on aspirin as well as their other antiplatelet agent. Patients with a history of stroke, in fact, had a lower risk of bleeding than the other patients in this trial, so one could argue that they should be on an agent like apixaban as well as an antiplatelet agent like clopidogrel without addition of aspirin,” he said in a recorded statement.
In addition to implications for using prescription drugs like apixaban and clopidogrel, the findings also send a message about the need for very aggressive implementation of lifestyle measures that can reduce cardiovascular disease risk in these patients, added Dr. Goldstein. The AUGUSTUS outcome analyses that subdivided the study population into those with a prior stroke, TIA, or TE event – 633 patients or about 14% of the 4,581 patients eligible for this analysis – and those who did not have this history showed the extremely high, incrementally elevated risk faced by patients with these prior events.
A history of stroke, TIA, or TE event linked with a jump in the 90-day rate of major or clinically relevant minor bleeds from 13% without this history to 17%, which is a 31% relative increase; it boosted the 90-day rate of death or hospitalization from 25% to 31%, a 24% relative increase; and it jacked up the rate of death or ischemic events from 6% to 9%, a 50% relative increase, Dr. Bahit reported.
These substantial increases “suggest we need to be very aggressive” in managing these high-risk patients who combine a background of AFib, a prior stroke, TIA, or TE events, and a recent ACS event or PCI, Dr. Goldstein observed. In these patients, he suggested that clinicians make sure to address smoking cessation, obesity, exercise, diet, and statin use, and get each of these to an optimal level to further cut risk. If all five of these basic interventions were successfully administered to a patient they could collectively cut the patient’s event risk by about 80%, he added.
AUGUSTUS was funded by Bristol-Myers Squibb and Pfizer, the companies that jointly market apixaban. Dr. Bahit has received honoraria from Pfizer, and from CSL Behring and Merck. Dr. Elkind and Dr. Goldstein had no relevant disclosures.
SOURCE: Bahit MC et al. ISC 2020, Abstract LB22.
LOS ANGELES – The edge that the direct-acting oral anticoagulant apixaban (Eliquis) has over warfarin for safely preventing ischemic events in patients with atrial fibrillation and either a recent acute coronary syndrome event or a recent percutaneous coronary intervention held up even in patients with a history of stroke, transient ischemic attack, or thromboembolic event, according to a prespecified secondary analysis of data collected in the AUGUSTUS trial.
The treatment advantages of apixaban, compared with warfarin, seen in the overall AUGUSTUS results, first reported in March 2019, “were consistent” with the benefits seen in the subgroup of enrolled patients with a prior stroke, transient ischemic attack (TIA), or thromboembolic (TE) event, M. Cecilia Bahit, MD, said at the International Stroke Conference sponsored by the American Heart Association.
All patients in AUGUSTUS received a P2Y12 inhibitor antiplatelet drug, which was clopidogrel for more than 90% of patients. The two-by-two factorial design of AUGUSTUS also assessed the safety and efficacy of either adding or withholding aspirin from the two-drug regimen that all patients in the study received with a P2Y12 inhibitor plus an anticoagulant (apixaban or warfarin). The most notable finding of the aspirin versus placebo analysis was that patients without a prior stroke, TIA, or TE event had a “more profound” increase in their rate of major or clinically relevant minor bleeds when also treated with aspirin, compared with patients who received aspirin and had a history of stroke, TIA, or TE event, reported Dr. Bahit, a chief of cardiology and director of clinical research at the INECO Foundation in Rosario, Argentina.
In general, the findings of the secondary analysis that took into account stroke, TIA, or TE history “confirmed” the main AUGUSTUS findings, Dr. Bahit said; an antithrombotic regimen of apixaban plus clopidogrel (or other P2Y12 inhibitor) without aspirin was superior for both efficacy and safety, compared with the alternative regimens that either substituted warfarin for apixaban or that added aspirin.
AUGUSTUS enrolled 4,614 atrial fibrillation (AFib) patients who either had a recent acute coronary syndrome (ACS) event or had recently undergone percutaneous coronary intervention (PCI) at any of 492 sites in 33 countries during 2015-2018. The study’s primary endpoint was the incidence of major or clinically relevant minor bleeds after 6 months, which was significantly lower in the subgroups that received apixaban instead of warfarin and in patients who received placebo instead of aspirin. The secondary endpoint of death or hospitalization after 6 months was also significantly lower in the apixaban-treated patients, compared with those on warfarin, while the aspirin and placebo subgroups showed no difference in the incidence of these events (N Engl J Med. 2019 Apr 18;380[16]:1509-24).
The results reported by Dr. Bahit also highlighted both the high risk faced by patients with AFib who also have had an ACS event or PCI, as well as a prior stroke, TIA, or TE event, noted Larry B. Goldstein, MD, professor and chairman of neurology at the University of Kentucky, Lexington. “It’s difficult, because these patients had an ACS event or PCI, and you don’t want a coronary too close up, but do these patients really need a P2Y12 inhibitor plus an anticoagulant? Could these patients do as well on apixaban only? I would have liked to see that treatment arm in the study,” Dr. Goldstein commented in an interview.
“These are challenging patients because they often require anticoagulation for the AFib as well as antiplatelet agents” for the recent PCI or ACS event, commented Mitchell S.V. Elkind, MD, professor of neurology at Columbia University, New York. “The question has always been: How many blood thinners should these patients be on? Potentially they could be on three different agents [an anticoagulant and two antiplatelet drugs], and we know that all of those drugs together pretty dramatically increase the risk of bleeding. About 15% of the patients in the overall AUGUSTUS trial had either cerebrovascular disease or systemic thromboembolism, so this was a small subgroup of the overall trial, but the overall trial was large so it’s a significant number of patients who met this criteria. The results confirmed that even in a group of patients who may be considered at high risk because they have a prior history of cerebrovascular disease use of apixaban instead of warfarin seemed safer, and that those patients did not need to be on aspirin as well as their other antiplatelet agent. Patients with a history of stroke, in fact, had a lower risk of bleeding than the other patients in this trial, so one could argue that they should be on an agent like apixaban as well as an antiplatelet agent like clopidogrel without addition of aspirin,” he said in a recorded statement.
In addition to implications for using prescription drugs like apixaban and clopidogrel, the findings also send a message about the need for very aggressive implementation of lifestyle measures that can reduce cardiovascular disease risk in these patients, added Dr. Goldstein. The AUGUSTUS outcome analyses that subdivided the study population into those with a prior stroke, TIA, or TE event – 633 patients or about 14% of the 4,581 patients eligible for this analysis – and those who did not have this history showed the extremely high, incrementally elevated risk faced by patients with these prior events.
A history of stroke, TIA, or TE event linked with a jump in the 90-day rate of major or clinically relevant minor bleeds from 13% without this history to 17%, which is a 31% relative increase; it boosted the 90-day rate of death or hospitalization from 25% to 31%, a 24% relative increase; and it jacked up the rate of death or ischemic events from 6% to 9%, a 50% relative increase, Dr. Bahit reported.
These substantial increases “suggest we need to be very aggressive” in managing these high-risk patients who combine a background of AFib, a prior stroke, TIA, or TE events, and a recent ACS event or PCI, Dr. Goldstein observed. In these patients, he suggested that clinicians make sure to address smoking cessation, obesity, exercise, diet, and statin use, and get each of these to an optimal level to further cut risk. If all five of these basic interventions were successfully administered to a patient they could collectively cut the patient’s event risk by about 80%, he added.
AUGUSTUS was funded by Bristol-Myers Squibb and Pfizer, the companies that jointly market apixaban. Dr. Bahit has received honoraria from Pfizer, and from CSL Behring and Merck. Dr. Elkind and Dr. Goldstein had no relevant disclosures.
SOURCE: Bahit MC et al. ISC 2020, Abstract LB22.
LOS ANGELES – The edge that the direct-acting oral anticoagulant apixaban (Eliquis) has over warfarin for safely preventing ischemic events in patients with atrial fibrillation and either a recent acute coronary syndrome event or a recent percutaneous coronary intervention held up even in patients with a history of stroke, transient ischemic attack, or thromboembolic event, according to a prespecified secondary analysis of data collected in the AUGUSTUS trial.
The treatment advantages of apixaban, compared with warfarin, seen in the overall AUGUSTUS results, first reported in March 2019, “were consistent” with the benefits seen in the subgroup of enrolled patients with a prior stroke, transient ischemic attack (TIA), or thromboembolic (TE) event, M. Cecilia Bahit, MD, said at the International Stroke Conference sponsored by the American Heart Association.
All patients in AUGUSTUS received a P2Y12 inhibitor antiplatelet drug, which was clopidogrel for more than 90% of patients. The two-by-two factorial design of AUGUSTUS also assessed the safety and efficacy of either adding or withholding aspirin from the two-drug regimen that all patients in the study received with a P2Y12 inhibitor plus an anticoagulant (apixaban or warfarin). The most notable finding of the aspirin versus placebo analysis was that patients without a prior stroke, TIA, or TE event had a “more profound” increase in their rate of major or clinically relevant minor bleeds when also treated with aspirin, compared with patients who received aspirin and had a history of stroke, TIA, or TE event, reported Dr. Bahit, a chief of cardiology and director of clinical research at the INECO Foundation in Rosario, Argentina.
In general, the findings of the secondary analysis that took into account stroke, TIA, or TE history “confirmed” the main AUGUSTUS findings, Dr. Bahit said; an antithrombotic regimen of apixaban plus clopidogrel (or other P2Y12 inhibitor) without aspirin was superior for both efficacy and safety, compared with the alternative regimens that either substituted warfarin for apixaban or that added aspirin.
AUGUSTUS enrolled 4,614 atrial fibrillation (AFib) patients who either had a recent acute coronary syndrome (ACS) event or had recently undergone percutaneous coronary intervention (PCI) at any of 492 sites in 33 countries during 2015-2018. The study’s primary endpoint was the incidence of major or clinically relevant minor bleeds after 6 months, which was significantly lower in the subgroups that received apixaban instead of warfarin and in patients who received placebo instead of aspirin. The secondary endpoint of death or hospitalization after 6 months was also significantly lower in the apixaban-treated patients, compared with those on warfarin, while the aspirin and placebo subgroups showed no difference in the incidence of these events (N Engl J Med. 2019 Apr 18;380[16]:1509-24).
The results reported by Dr. Bahit also highlighted both the high risk faced by patients with AFib who also have had an ACS event or PCI, as well as a prior stroke, TIA, or TE event, noted Larry B. Goldstein, MD, professor and chairman of neurology at the University of Kentucky, Lexington. “It’s difficult, because these patients had an ACS event or PCI, and you don’t want a coronary too close up, but do these patients really need a P2Y12 inhibitor plus an anticoagulant? Could these patients do as well on apixaban only? I would have liked to see that treatment arm in the study,” Dr. Goldstein commented in an interview.
“These are challenging patients because they often require anticoagulation for the AFib as well as antiplatelet agents” for the recent PCI or ACS event, commented Mitchell S.V. Elkind, MD, professor of neurology at Columbia University, New York. “The question has always been: How many blood thinners should these patients be on? Potentially they could be on three different agents [an anticoagulant and two antiplatelet drugs], and we know that all of those drugs together pretty dramatically increase the risk of bleeding. About 15% of the patients in the overall AUGUSTUS trial had either cerebrovascular disease or systemic thromboembolism, so this was a small subgroup of the overall trial, but the overall trial was large so it’s a significant number of patients who met this criteria. The results confirmed that even in a group of patients who may be considered at high risk because they have a prior history of cerebrovascular disease use of apixaban instead of warfarin seemed safer, and that those patients did not need to be on aspirin as well as their other antiplatelet agent. Patients with a history of stroke, in fact, had a lower risk of bleeding than the other patients in this trial, so one could argue that they should be on an agent like apixaban as well as an antiplatelet agent like clopidogrel without addition of aspirin,” he said in a recorded statement.
In addition to implications for using prescription drugs like apixaban and clopidogrel, the findings also send a message about the need for very aggressive implementation of lifestyle measures that can reduce cardiovascular disease risk in these patients, added Dr. Goldstein. The AUGUSTUS outcome analyses that subdivided the study population into those with a prior stroke, TIA, or TE event – 633 patients or about 14% of the 4,581 patients eligible for this analysis – and those who did not have this history showed the extremely high, incrementally elevated risk faced by patients with these prior events.
A history of stroke, TIA, or TE event linked with a jump in the 90-day rate of major or clinically relevant minor bleeds from 13% without this history to 17%, which is a 31% relative increase; it boosted the 90-day rate of death or hospitalization from 25% to 31%, a 24% relative increase; and it jacked up the rate of death or ischemic events from 6% to 9%, a 50% relative increase, Dr. Bahit reported.
These substantial increases “suggest we need to be very aggressive” in managing these high-risk patients who combine a background of AFib, a prior stroke, TIA, or TE events, and a recent ACS event or PCI, Dr. Goldstein observed. In these patients, he suggested that clinicians make sure to address smoking cessation, obesity, exercise, diet, and statin use, and get each of these to an optimal level to further cut risk. If all five of these basic interventions were successfully administered to a patient they could collectively cut the patient’s event risk by about 80%, he added.
AUGUSTUS was funded by Bristol-Myers Squibb and Pfizer, the companies that jointly market apixaban. Dr. Bahit has received honoraria from Pfizer, and from CSL Behring and Merck. Dr. Elkind and Dr. Goldstein had no relevant disclosures.
SOURCE: Bahit MC et al. ISC 2020, Abstract LB22.
REPORTING FROM ISC 2020
Exercise needn’t be strenuous to reduce heart risk
PHOENIX – results from two studies presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting showed.
In one study, women who walked 2,100-4,500 steps each day reduced their risk of dying from cardiovascular disease by up to 38%, compared with those who walked fewer than 2,100 steps each day. In addition, women who walked more than 4,500 steps each day reduced their risk of cardiovascular disease (CVD) mortality risk by 48%.
The findings come from an ancillary analysis of the Women’s Health Study known as the Objective Physical Activity and Cardiovascular Health (OPACH) Study.
“Our work shows that both light-intensity and moderate-/vigorous-intensity steps are associated with reduced risk of cardiovascular disease death,” lead author Andrea Z. LaCroix, PhD, said in an interview. “And our previous studies show that all movement while standing, stepping, or just moving about at whatever intensity you choose, appears to have cardiovascular benefits, whereas long hours spent sedentary, especially prolonged sitting bouts are associated with increased risk of cardiovascular disease. These new findings on steps are best interpreted as showing that moving instead of sitting is good for your heart and blood vessels as we get older. Find the things you love to do and get moving.”
For OPACH, 6,379 women with an average age of 79 years wore ActiGraph GT3X+ triaxial accelerometers on their wrist for 7 days during 2012-2014, as a way to ascertain the number of steps they took. The researchers followed the study participants to March 1, 2019, and used Cox proportional hazard models to estimate CVD mortality across four quartiles of steps per day, adjusted for age, race/ethnicity, education, smoking, alcohol consumption, self-reported health, comorbidities, and physical function. The lowest quartile reference category was less than 2,108 steps per day. The second, third and fourth quartiles were: 2,108 to fewer than 3,136 steps, 3,136 to fewer than 4,499, and 4,500 and above.
Dr. LaCroix, distinguished professor and chief of epidemiology at the University of California, San Diego, reported that women who walked 2,100-4,500 steps daily reduced their risk of dying from CVD by up to up to 38%, compared with women who walked fewer than 2,100 daily steps. The women who walked more than 4,500 steps per day reduced their risk by 48%.
She noted that, for many years, common wisdom was that 10,000 steps per day should be used as a general fitness target, [but] that goal “was never evidence based, and so far, emerging evidence using accelerometers to measure steps shows benefit way below the level of 10,000 steps.” Dr. LaCroix added that, in this study, “we were able separate steps taken at a light intensity of energy expenditure versus a moderate or vigorous level of energy expenditure. This is like comparing slower versus faster steps. Both influenced the risk of CVD death and we found no evidence that faster steps were more beneficial for reducing risk of CVD death than slower steps. So, the main message I want my demographic [women aged over 60] to understand is that all movement appears to be good for your heart.”
Barry A. Franklin, PhD, director of preventive cardiology and cardiac rehabilitation at Beaumont Health in Royal Oak, Mich., characterized the study findings as “good news” but not entirely surprising. “It goes along with other research showing that the biggest bang from the buck is going from the least fit, least active cohort, which we call the bottom 20%, to the next lowest level,” he said in an interview. “So, by simply doing some steps, certainly less than 10,000, there were significant benefits for this older age group.”
Dr. LaCroix acknowledged certain limitations of the OPACH study, including the fact that it did not include men or women aged younger than 60 years. In addition, the accelerometer used in this and other studies may measure fewer steps than women are actually taking. “Devices vary in their accuracy,” she said. “If you are tracking steps, try to aim for 4,500 or a little more, but know that every step counts.”
In a separate study, researchers found that an increase of 30 minutes per day of low-intensity physical activity (LIPA) may lower the risk of death among older adults, regardless of the amount of moderate to vigorous physical activity (MVPA) participants are involved in or whether they have impaired physical function. In addition, an increase of 30 minutes of sedentary time per day may increase the risk of death regardless of the amount of MVPA or whether participants have impaired physical function.
Those are key findings from an analysis of 1,262 participants in the Framingham Offspring Study.
“Given that MVPA tends to decline with age, particularly during the mid- to late-life transition, promoting LIPA and reducing sedentary time may be a more practical alternative among older adults for reducing the risk of mortality,” lead author Joowon Lee, PhD, said in an interview at the meeting sponsored by the American Heart Association.
According to Dr. Lee, a postdoctoral fellow at Boston University, prior studies found that the inverse association between MVPA and cardiovascular and all-cause mortality among older adults. “However, we focused on sedentary and light-intensity physical activity, which is prevalent in older adult population,” he said. “Additionally, we looked at the association between physical activity and mortality after excluding participants with frailty as a sensitivity analysis.”
The researchers drew from accelerometry-derived physical activity data from 1,262 Framingham Offspring Study participants at their ninth examination (2011-2014). The mean age of the subjects was 69 years, 54% were women, and they had worn the accelerometers at least 10 hours per day for at least 4 days prior to the exam visit. The researchers used multivariable Cox proportional hazards regression models to relate physician activity and sedentary time with all-cause mortality adjusting for potential confounders.
During a median follow-up of 4.8 years, 67 study participants died. Dr. Lee and colleagues observed that higher total physical activity, LIPA, adherence to physical activity guidelines (at least 150 minutes of activity each week), and lower sedentary time were associated with a lower risk of all-cause mortality. Specifically, they were 67% less likely to die of any cause if they spent at least 150 minutes per week in moderate to vigorous physical activity, compared with those who did not. In addition, the researchers found that each 30-minute interval of LIPA, such as doing household chores or casual walking, was associated with a 20% lower risk of dying from any cause. On the other hand, every additional 30 minutes of being sedentary was related to a 32% higher risk of dying from any cause. The results remained statistically significant even after excluding those with frailty.
“In the present analysis, an increase of 10 minutes in MVPA was not associated with the risk of all-cause mortality although meeting physical activity guidelines [MVPA of at least 150 minutes per week] was the strongest factor associated with the risk of all-cause mortality,” Dr. Lee said.
He acknowledged certain limitations of the analysis, including the fact that the study participants were white individuals with European ancestry. “Additionally, a small number of mortality events were observed in the current investigation,” he said. “So, an additional study of larger multiethnic samples of older adults is warranted to confirm our findings.”
“We tell people: ‘You need 30 minutes of moderate intensity exercise most days of the week,’ ” Dr. Franklin said. “That’s true, but a classic study in Lancet showed that if you do 12 or 15 minutes of moderate exercise, not 30 minutes, you also get a 14% reduction in mortality. Some exercise is better than none, and for older adults, they don’t even have to do moderate intensity exercise to get benefits.”
Dr. LaCroix’s study was funded by the National Heart, Lung, and Blood Institute; Dr. LaCroix reported having no financial disclosures. Dr. Lee’s study was supported by the National Heart, Lung, and Blood Institute; Dr. Lee reported having no disclosures.
SOURCES: LaCroix A et al. Epi/Lifestyle 2020, Abstract 30; Lee J et al. Epi/Lifestyle 2020, Abstract 31.
PHOENIX – results from two studies presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting showed.
In one study, women who walked 2,100-4,500 steps each day reduced their risk of dying from cardiovascular disease by up to 38%, compared with those who walked fewer than 2,100 steps each day. In addition, women who walked more than 4,500 steps each day reduced their risk of cardiovascular disease (CVD) mortality risk by 48%.
The findings come from an ancillary analysis of the Women’s Health Study known as the Objective Physical Activity and Cardiovascular Health (OPACH) Study.
“Our work shows that both light-intensity and moderate-/vigorous-intensity steps are associated with reduced risk of cardiovascular disease death,” lead author Andrea Z. LaCroix, PhD, said in an interview. “And our previous studies show that all movement while standing, stepping, or just moving about at whatever intensity you choose, appears to have cardiovascular benefits, whereas long hours spent sedentary, especially prolonged sitting bouts are associated with increased risk of cardiovascular disease. These new findings on steps are best interpreted as showing that moving instead of sitting is good for your heart and blood vessels as we get older. Find the things you love to do and get moving.”
For OPACH, 6,379 women with an average age of 79 years wore ActiGraph GT3X+ triaxial accelerometers on their wrist for 7 days during 2012-2014, as a way to ascertain the number of steps they took. The researchers followed the study participants to March 1, 2019, and used Cox proportional hazard models to estimate CVD mortality across four quartiles of steps per day, adjusted for age, race/ethnicity, education, smoking, alcohol consumption, self-reported health, comorbidities, and physical function. The lowest quartile reference category was less than 2,108 steps per day. The second, third and fourth quartiles were: 2,108 to fewer than 3,136 steps, 3,136 to fewer than 4,499, and 4,500 and above.
Dr. LaCroix, distinguished professor and chief of epidemiology at the University of California, San Diego, reported that women who walked 2,100-4,500 steps daily reduced their risk of dying from CVD by up to up to 38%, compared with women who walked fewer than 2,100 daily steps. The women who walked more than 4,500 steps per day reduced their risk by 48%.
She noted that, for many years, common wisdom was that 10,000 steps per day should be used as a general fitness target, [but] that goal “was never evidence based, and so far, emerging evidence using accelerometers to measure steps shows benefit way below the level of 10,000 steps.” Dr. LaCroix added that, in this study, “we were able separate steps taken at a light intensity of energy expenditure versus a moderate or vigorous level of energy expenditure. This is like comparing slower versus faster steps. Both influenced the risk of CVD death and we found no evidence that faster steps were more beneficial for reducing risk of CVD death than slower steps. So, the main message I want my demographic [women aged over 60] to understand is that all movement appears to be good for your heart.”
Barry A. Franklin, PhD, director of preventive cardiology and cardiac rehabilitation at Beaumont Health in Royal Oak, Mich., characterized the study findings as “good news” but not entirely surprising. “It goes along with other research showing that the biggest bang from the buck is going from the least fit, least active cohort, which we call the bottom 20%, to the next lowest level,” he said in an interview. “So, by simply doing some steps, certainly less than 10,000, there were significant benefits for this older age group.”
Dr. LaCroix acknowledged certain limitations of the OPACH study, including the fact that it did not include men or women aged younger than 60 years. In addition, the accelerometer used in this and other studies may measure fewer steps than women are actually taking. “Devices vary in their accuracy,” she said. “If you are tracking steps, try to aim for 4,500 or a little more, but know that every step counts.”
In a separate study, researchers found that an increase of 30 minutes per day of low-intensity physical activity (LIPA) may lower the risk of death among older adults, regardless of the amount of moderate to vigorous physical activity (MVPA) participants are involved in or whether they have impaired physical function. In addition, an increase of 30 minutes of sedentary time per day may increase the risk of death regardless of the amount of MVPA or whether participants have impaired physical function.
Those are key findings from an analysis of 1,262 participants in the Framingham Offspring Study.
“Given that MVPA tends to decline with age, particularly during the mid- to late-life transition, promoting LIPA and reducing sedentary time may be a more practical alternative among older adults for reducing the risk of mortality,” lead author Joowon Lee, PhD, said in an interview at the meeting sponsored by the American Heart Association.
According to Dr. Lee, a postdoctoral fellow at Boston University, prior studies found that the inverse association between MVPA and cardiovascular and all-cause mortality among older adults. “However, we focused on sedentary and light-intensity physical activity, which is prevalent in older adult population,” he said. “Additionally, we looked at the association between physical activity and mortality after excluding participants with frailty as a sensitivity analysis.”
The researchers drew from accelerometry-derived physical activity data from 1,262 Framingham Offspring Study participants at their ninth examination (2011-2014). The mean age of the subjects was 69 years, 54% were women, and they had worn the accelerometers at least 10 hours per day for at least 4 days prior to the exam visit. The researchers used multivariable Cox proportional hazards regression models to relate physician activity and sedentary time with all-cause mortality adjusting for potential confounders.
During a median follow-up of 4.8 years, 67 study participants died. Dr. Lee and colleagues observed that higher total physical activity, LIPA, adherence to physical activity guidelines (at least 150 minutes of activity each week), and lower sedentary time were associated with a lower risk of all-cause mortality. Specifically, they were 67% less likely to die of any cause if they spent at least 150 minutes per week in moderate to vigorous physical activity, compared with those who did not. In addition, the researchers found that each 30-minute interval of LIPA, such as doing household chores or casual walking, was associated with a 20% lower risk of dying from any cause. On the other hand, every additional 30 minutes of being sedentary was related to a 32% higher risk of dying from any cause. The results remained statistically significant even after excluding those with frailty.
“In the present analysis, an increase of 10 minutes in MVPA was not associated with the risk of all-cause mortality although meeting physical activity guidelines [MVPA of at least 150 minutes per week] was the strongest factor associated with the risk of all-cause mortality,” Dr. Lee said.
He acknowledged certain limitations of the analysis, including the fact that the study participants were white individuals with European ancestry. “Additionally, a small number of mortality events were observed in the current investigation,” he said. “So, an additional study of larger multiethnic samples of older adults is warranted to confirm our findings.”
“We tell people: ‘You need 30 minutes of moderate intensity exercise most days of the week,’ ” Dr. Franklin said. “That’s true, but a classic study in Lancet showed that if you do 12 or 15 minutes of moderate exercise, not 30 minutes, you also get a 14% reduction in mortality. Some exercise is better than none, and for older adults, they don’t even have to do moderate intensity exercise to get benefits.”
Dr. LaCroix’s study was funded by the National Heart, Lung, and Blood Institute; Dr. LaCroix reported having no financial disclosures. Dr. Lee’s study was supported by the National Heart, Lung, and Blood Institute; Dr. Lee reported having no disclosures.
SOURCES: LaCroix A et al. Epi/Lifestyle 2020, Abstract 30; Lee J et al. Epi/Lifestyle 2020, Abstract 31.
PHOENIX – results from two studies presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting showed.
In one study, women who walked 2,100-4,500 steps each day reduced their risk of dying from cardiovascular disease by up to 38%, compared with those who walked fewer than 2,100 steps each day. In addition, women who walked more than 4,500 steps each day reduced their risk of cardiovascular disease (CVD) mortality risk by 48%.
The findings come from an ancillary analysis of the Women’s Health Study known as the Objective Physical Activity and Cardiovascular Health (OPACH) Study.
“Our work shows that both light-intensity and moderate-/vigorous-intensity steps are associated with reduced risk of cardiovascular disease death,” lead author Andrea Z. LaCroix, PhD, said in an interview. “And our previous studies show that all movement while standing, stepping, or just moving about at whatever intensity you choose, appears to have cardiovascular benefits, whereas long hours spent sedentary, especially prolonged sitting bouts are associated with increased risk of cardiovascular disease. These new findings on steps are best interpreted as showing that moving instead of sitting is good for your heart and blood vessels as we get older. Find the things you love to do and get moving.”
For OPACH, 6,379 women with an average age of 79 years wore ActiGraph GT3X+ triaxial accelerometers on their wrist for 7 days during 2012-2014, as a way to ascertain the number of steps they took. The researchers followed the study participants to March 1, 2019, and used Cox proportional hazard models to estimate CVD mortality across four quartiles of steps per day, adjusted for age, race/ethnicity, education, smoking, alcohol consumption, self-reported health, comorbidities, and physical function. The lowest quartile reference category was less than 2,108 steps per day. The second, third and fourth quartiles were: 2,108 to fewer than 3,136 steps, 3,136 to fewer than 4,499, and 4,500 and above.
Dr. LaCroix, distinguished professor and chief of epidemiology at the University of California, San Diego, reported that women who walked 2,100-4,500 steps daily reduced their risk of dying from CVD by up to up to 38%, compared with women who walked fewer than 2,100 daily steps. The women who walked more than 4,500 steps per day reduced their risk by 48%.
She noted that, for many years, common wisdom was that 10,000 steps per day should be used as a general fitness target, [but] that goal “was never evidence based, and so far, emerging evidence using accelerometers to measure steps shows benefit way below the level of 10,000 steps.” Dr. LaCroix added that, in this study, “we were able separate steps taken at a light intensity of energy expenditure versus a moderate or vigorous level of energy expenditure. This is like comparing slower versus faster steps. Both influenced the risk of CVD death and we found no evidence that faster steps were more beneficial for reducing risk of CVD death than slower steps. So, the main message I want my demographic [women aged over 60] to understand is that all movement appears to be good for your heart.”
Barry A. Franklin, PhD, director of preventive cardiology and cardiac rehabilitation at Beaumont Health in Royal Oak, Mich., characterized the study findings as “good news” but not entirely surprising. “It goes along with other research showing that the biggest bang from the buck is going from the least fit, least active cohort, which we call the bottom 20%, to the next lowest level,” he said in an interview. “So, by simply doing some steps, certainly less than 10,000, there were significant benefits for this older age group.”
Dr. LaCroix acknowledged certain limitations of the OPACH study, including the fact that it did not include men or women aged younger than 60 years. In addition, the accelerometer used in this and other studies may measure fewer steps than women are actually taking. “Devices vary in their accuracy,” she said. “If you are tracking steps, try to aim for 4,500 or a little more, but know that every step counts.”
In a separate study, researchers found that an increase of 30 minutes per day of low-intensity physical activity (LIPA) may lower the risk of death among older adults, regardless of the amount of moderate to vigorous physical activity (MVPA) participants are involved in or whether they have impaired physical function. In addition, an increase of 30 minutes of sedentary time per day may increase the risk of death regardless of the amount of MVPA or whether participants have impaired physical function.
Those are key findings from an analysis of 1,262 participants in the Framingham Offspring Study.
“Given that MVPA tends to decline with age, particularly during the mid- to late-life transition, promoting LIPA and reducing sedentary time may be a more practical alternative among older adults for reducing the risk of mortality,” lead author Joowon Lee, PhD, said in an interview at the meeting sponsored by the American Heart Association.
According to Dr. Lee, a postdoctoral fellow at Boston University, prior studies found that the inverse association between MVPA and cardiovascular and all-cause mortality among older adults. “However, we focused on sedentary and light-intensity physical activity, which is prevalent in older adult population,” he said. “Additionally, we looked at the association between physical activity and mortality after excluding participants with frailty as a sensitivity analysis.”
The researchers drew from accelerometry-derived physical activity data from 1,262 Framingham Offspring Study participants at their ninth examination (2011-2014). The mean age of the subjects was 69 years, 54% were women, and they had worn the accelerometers at least 10 hours per day for at least 4 days prior to the exam visit. The researchers used multivariable Cox proportional hazards regression models to relate physician activity and sedentary time with all-cause mortality adjusting for potential confounders.
During a median follow-up of 4.8 years, 67 study participants died. Dr. Lee and colleagues observed that higher total physical activity, LIPA, adherence to physical activity guidelines (at least 150 minutes of activity each week), and lower sedentary time were associated with a lower risk of all-cause mortality. Specifically, they were 67% less likely to die of any cause if they spent at least 150 minutes per week in moderate to vigorous physical activity, compared with those who did not. In addition, the researchers found that each 30-minute interval of LIPA, such as doing household chores or casual walking, was associated with a 20% lower risk of dying from any cause. On the other hand, every additional 30 minutes of being sedentary was related to a 32% higher risk of dying from any cause. The results remained statistically significant even after excluding those with frailty.
“In the present analysis, an increase of 10 minutes in MVPA was not associated with the risk of all-cause mortality although meeting physical activity guidelines [MVPA of at least 150 minutes per week] was the strongest factor associated with the risk of all-cause mortality,” Dr. Lee said.
He acknowledged certain limitations of the analysis, including the fact that the study participants were white individuals with European ancestry. “Additionally, a small number of mortality events were observed in the current investigation,” he said. “So, an additional study of larger multiethnic samples of older adults is warranted to confirm our findings.”
“We tell people: ‘You need 30 minutes of moderate intensity exercise most days of the week,’ ” Dr. Franklin said. “That’s true, but a classic study in Lancet showed that if you do 12 or 15 minutes of moderate exercise, not 30 minutes, you also get a 14% reduction in mortality. Some exercise is better than none, and for older adults, they don’t even have to do moderate intensity exercise to get benefits.”
Dr. LaCroix’s study was funded by the National Heart, Lung, and Blood Institute; Dr. LaCroix reported having no financial disclosures. Dr. Lee’s study was supported by the National Heart, Lung, and Blood Institute; Dr. Lee reported having no disclosures.
SOURCES: LaCroix A et al. Epi/Lifestyle 2020, Abstract 30; Lee J et al. Epi/Lifestyle 2020, Abstract 31.
REPORTING FROM EPI/LIFESTYLE 2020
What are the most prescribed medications for type 2 diabetes?
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
Beginning estrogen soon after menopause slows atherosclerosis progression
PHOENIX – Oral estrogen therapy taken within 6 years after the onset of menopause significantly reduced progression of lipid deposition in the carotid arterial wall, compared with placebo. However, starting oral estrogen 10 years after menopause did not confer a similar benefit.

“The clinical practice of estradiol therapy has been nothing short of a roller coaster ride,” lead study author Roksana Karim, PhD, MBBS, said in an interview at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting sponsored by the American Heart Association. “Clinicians have been sort of conservative in terms of prescribing estradiol therapy. But over the last 2 decades things have changed, and eventually the timing hypothesis evolved based on the final analysis of the Women’s Health Initiative results as well.”
The findings come from a secondary analysis of the Early Versus Late Intervention Trial With Estradiol (ELITE), which examined the effects of oral 17-beta-estradiol (estrogen) on the progression of early atherosclerosis and cognitive decline in healthy postmenopausal women.
In the original trial, 643 healthy postmenopausal women were randomized to receive 1 mg/day of estradiol or a placebo pill either within 6 years after the onset of menopause or more than a decade after menopause (N Engl J Med 2016;374[13]:1221-31). All study participants took estradiol or placebo daily for an average of 5 years. The study’s initial findings showed that the mean carotid intima-media thickness progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo, but only in women who initiated hormone therapy within 6 years of menopause onset.
For the current analysis, researchers led by Dr. Karim looked further into estradiol’s impact on heart health by using echogenicity to analyze lipids in the arterial wall among the ELITE participants. The main outcome of interest was gray-scale median (GSM, unitless), a qualitative measure of atherosclerosis based on echogenicity obtained by high-resolution ultrasonography of the common carotid arterial wall. Whereas higher GSM values result with plaques rich in calcium and fibrous tissue, lower GSM values indicate more lipid deposition.
Dr. Karim, an associate professor of clinical preventive medicine at the University of Southern California, Los Angeles, and colleagues assessed GSM and serum concentrations of estradiol every 6 months over a median 5-year trial period, and used linear mixed effects regression models to compare the rate of GSM progression between the randomized groups within time-since-menopause strata.
The researchers found that effect of estradiol on the annual rate of GSM progression significantly differed between women in the early and late postmenopause groups (P for interaction = .006). Specifically, the annual GSM progression rate among women in early postmenopause fell by 0.30 per year in women taking estradiol, compared with 1.41 per year in those in the placebo group (P less than .0001), indicating significantly more atherosclerosis in the placebo group. On the other hand, the annual GSM progression rate was not significantly different between the estradiol and placebo groups among the late postmenopausal women (P = .37).
“I think this should comfort clinicians in terms of prescribing estradiol therapy to women who don’t have any contraindications and who are within 6 years of menopause,” Dr. Karim said. “Accumulation of lipids is the key event for atherosclerosis progression.” She and her colleagues also observed that the positive association between mean on-trial serum estradiol levels and GSM progression rate was stronger and significant among early postmenopausal women (P = .008), compared with women in the late postmenopausal group (P = .003). However, this differential association between estradiol level and GSM progression rate was not statistically significant (P for interaction = .33).
“This study is important and raises a critical question: Is there a time period where getting hormone therapy would be most beneficial for the heart?” Nieca Goldberg, MD, medical director of the New York University women’s heart program and senior advisor for women’s health strategy at NYU Langone Health, said in an interview. “I think more studies and more analyses are needed, but we haven’t changed the indications for estradiol. We’re not giving estradiol to prevent progression of heart disease. We use estradiol hormone therapy as indicated for women who are having menopausal symptoms.”
Dr. Karim and colleagues plan to conduct a follow-up analysis from the same cohort of ELITE study participants to validate the findings by assessing lipid particles and markers of inflammation.
She reported having no financial disclosures. The study was funded by the National Institute on Aging.
SOURCE: Karim R et al. Epi/Lifestyle 2020, Abstract MP09.
PHOENIX – Oral estrogen therapy taken within 6 years after the onset of menopause significantly reduced progression of lipid deposition in the carotid arterial wall, compared with placebo. However, starting oral estrogen 10 years after menopause did not confer a similar benefit.
“The clinical practice of estradiol therapy has been nothing short of a roller coaster ride,” lead study author Roksana Karim, PhD, MBBS, said in an interview at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting sponsored by the American Heart Association. “Clinicians have been sort of conservative in terms of prescribing estradiol therapy. But over the last 2 decades things have changed, and eventually the timing hypothesis evolved based on the final analysis of the Women’s Health Initiative results as well.”
The findings come from a secondary analysis of the Early Versus Late Intervention Trial With Estradiol (ELITE), which examined the effects of oral 17-beta-estradiol (estrogen) on the progression of early atherosclerosis and cognitive decline in healthy postmenopausal women.
In the original trial, 643 healthy postmenopausal women were randomized to receive 1 mg/day of estradiol or a placebo pill either within 6 years after the onset of menopause or more than a decade after menopause (N Engl J Med 2016;374[13]:1221-31). All study participants took estradiol or placebo daily for an average of 5 years. The study’s initial findings showed that the mean carotid intima-media thickness progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo, but only in women who initiated hormone therapy within 6 years of menopause onset.
For the current analysis, researchers led by Dr. Karim looked further into estradiol’s impact on heart health by using echogenicity to analyze lipids in the arterial wall among the ELITE participants. The main outcome of interest was gray-scale median (GSM, unitless), a qualitative measure of atherosclerosis based on echogenicity obtained by high-resolution ultrasonography of the common carotid arterial wall. Whereas higher GSM values result with plaques rich in calcium and fibrous tissue, lower GSM values indicate more lipid deposition.
Dr. Karim, an associate professor of clinical preventive medicine at the University of Southern California, Los Angeles, and colleagues assessed GSM and serum concentrations of estradiol every 6 months over a median 5-year trial period, and used linear mixed effects regression models to compare the rate of GSM progression between the randomized groups within time-since-menopause strata.
The researchers found that effect of estradiol on the annual rate of GSM progression significantly differed between women in the early and late postmenopause groups (P for interaction = .006). Specifically, the annual GSM progression rate among women in early postmenopause fell by 0.30 per year in women taking estradiol, compared with 1.41 per year in those in the placebo group (P less than .0001), indicating significantly more atherosclerosis in the placebo group. On the other hand, the annual GSM progression rate was not significantly different between the estradiol and placebo groups among the late postmenopausal women (P = .37).
“I think this should comfort clinicians in terms of prescribing estradiol therapy to women who don’t have any contraindications and who are within 6 years of menopause,” Dr. Karim said. “Accumulation of lipids is the key event for atherosclerosis progression.” She and her colleagues also observed that the positive association between mean on-trial serum estradiol levels and GSM progression rate was stronger and significant among early postmenopausal women (P = .008), compared with women in the late postmenopausal group (P = .003). However, this differential association between estradiol level and GSM progression rate was not statistically significant (P for interaction = .33).
“This study is important and raises a critical question: Is there a time period where getting hormone therapy would be most beneficial for the heart?” Nieca Goldberg, MD, medical director of the New York University women’s heart program and senior advisor for women’s health strategy at NYU Langone Health, said in an interview. “I think more studies and more analyses are needed, but we haven’t changed the indications for estradiol. We’re not giving estradiol to prevent progression of heart disease. We use estradiol hormone therapy as indicated for women who are having menopausal symptoms.”
Dr. Karim and colleagues plan to conduct a follow-up analysis from the same cohort of ELITE study participants to validate the findings by assessing lipid particles and markers of inflammation.
She reported having no financial disclosures. The study was funded by the National Institute on Aging.
SOURCE: Karim R et al. Epi/Lifestyle 2020, Abstract MP09.
PHOENIX – Oral estrogen therapy taken within 6 years after the onset of menopause significantly reduced progression of lipid deposition in the carotid arterial wall, compared with placebo. However, starting oral estrogen 10 years after menopause did not confer a similar benefit.
“The clinical practice of estradiol therapy has been nothing short of a roller coaster ride,” lead study author Roksana Karim, PhD, MBBS, said in an interview at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting sponsored by the American Heart Association. “Clinicians have been sort of conservative in terms of prescribing estradiol therapy. But over the last 2 decades things have changed, and eventually the timing hypothesis evolved based on the final analysis of the Women’s Health Initiative results as well.”
The findings come from a secondary analysis of the Early Versus Late Intervention Trial With Estradiol (ELITE), which examined the effects of oral 17-beta-estradiol (estrogen) on the progression of early atherosclerosis and cognitive decline in healthy postmenopausal women.
In the original trial, 643 healthy postmenopausal women were randomized to receive 1 mg/day of estradiol or a placebo pill either within 6 years after the onset of menopause or more than a decade after menopause (N Engl J Med 2016;374[13]:1221-31). All study participants took estradiol or placebo daily for an average of 5 years. The study’s initial findings showed that the mean carotid intima-media thickness progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo, but only in women who initiated hormone therapy within 6 years of menopause onset.
For the current analysis, researchers led by Dr. Karim looked further into estradiol’s impact on heart health by using echogenicity to analyze lipids in the arterial wall among the ELITE participants. The main outcome of interest was gray-scale median (GSM, unitless), a qualitative measure of atherosclerosis based on echogenicity obtained by high-resolution ultrasonography of the common carotid arterial wall. Whereas higher GSM values result with plaques rich in calcium and fibrous tissue, lower GSM values indicate more lipid deposition.
Dr. Karim, an associate professor of clinical preventive medicine at the University of Southern California, Los Angeles, and colleagues assessed GSM and serum concentrations of estradiol every 6 months over a median 5-year trial period, and used linear mixed effects regression models to compare the rate of GSM progression between the randomized groups within time-since-menopause strata.
The researchers found that effect of estradiol on the annual rate of GSM progression significantly differed between women in the early and late postmenopause groups (P for interaction = .006). Specifically, the annual GSM progression rate among women in early postmenopause fell by 0.30 per year in women taking estradiol, compared with 1.41 per year in those in the placebo group (P less than .0001), indicating significantly more atherosclerosis in the placebo group. On the other hand, the annual GSM progression rate was not significantly different between the estradiol and placebo groups among the late postmenopausal women (P = .37).
“I think this should comfort clinicians in terms of prescribing estradiol therapy to women who don’t have any contraindications and who are within 6 years of menopause,” Dr. Karim said. “Accumulation of lipids is the key event for atherosclerosis progression.” She and her colleagues also observed that the positive association between mean on-trial serum estradiol levels and GSM progression rate was stronger and significant among early postmenopausal women (P = .008), compared with women in the late postmenopausal group (P = .003). However, this differential association between estradiol level and GSM progression rate was not statistically significant (P for interaction = .33).
“This study is important and raises a critical question: Is there a time period where getting hormone therapy would be most beneficial for the heart?” Nieca Goldberg, MD, medical director of the New York University women’s heart program and senior advisor for women’s health strategy at NYU Langone Health, said in an interview. “I think more studies and more analyses are needed, but we haven’t changed the indications for estradiol. We’re not giving estradiol to prevent progression of heart disease. We use estradiol hormone therapy as indicated for women who are having menopausal symptoms.”
Dr. Karim and colleagues plan to conduct a follow-up analysis from the same cohort of ELITE study participants to validate the findings by assessing lipid particles and markers of inflammation.
She reported having no financial disclosures. The study was funded by the National Institute on Aging.
SOURCE: Karim R et al. Epi/Lifestyle 2020, Abstract MP09.
REPORTING FROM EPI/LIFESTYLE 2020
AFib patients do best on a DOAC started 7-10 days post stroke
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.

The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
REPORTING FROM ISC 2020
MACE benefits with dapagliflozin improve with disease duration
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
FROM DIABETES, OBESITY AND METABOLISM
Prescription cascade more likely after CCBs than other hypertension meds
Elderly adults with hypertension who are newly prescribed a calcium-channel blocker (CCB), compared to other antihypertensive agents, are at least twice as likely to be given a loop diuretic over the following months, a large cohort study suggests.
The likelihood remained elevated for as long as a year after the start of a CCB and was more pronounced when comparing CCBs to any other kind of medication.
“Our findings suggest that many older adults who begin taking a CCB may subsequently experience a prescribing cascade” when loop diuretics are prescribed for peripheral edema, a known CCB adverse effect, that is misinterpreted as a new medical condition, Rachel D. Savage, PhD, Women’s College Hospital, Toronto, Canada, told theheart.org/Medscape Cardiology.
Edema caused by CCBs is caused by fluid redistribution, not overload, and “treating euvolemic individuals with a diuretic places them at increased risk of overdiuresis, leading to falls, urinary incontinence, acute kidney injury, electrolyte imbalances, and a cascade of other downstream consequences to which older adults are especially vulnerable,” explain Savage and coauthors of the analysis published online February 24 in JAMA Internal Medicine.
However, 1.4% of the cohort had been prescribed a loop diuretic, and 4.5% had been given any diuretic within 90 days after the start of CCBs. The corresponding rates were 0.7% and 3.4%, respectively, for patients who had started on ACE inhibitors or angiotensin receptor blocker (ARB) rather than a CCB.
Also, Savage observed, “the likelihood of being prescribed a loop diuretic following initiation of a CCB changed over time and was greatest 61 to 90 days postinitiation.” At that point, it was increased 2.4 times compared with initiation of an ACE inhibitor or an ARB in an adjusted analysis and increased almost 4 times compared with starting on any non-CCB agent.
Importantly, the actual prevalence of peripheral edema among those started on CCBs, ACE inhibitors, ARBs, or any non-CCB medication was not available in the data sets.
However, “the main message for clinicians is to consider medication side effects as a potential cause for new symptoms when patients present. We also encourage patients to ask prescribers about whether new symptoms could be caused by a medication,” senior author Lisa M. McCarthy, PharmD, told theheart.org/Medscape Cardiology.
“If a patient experiences peripheral edema while taking a CCB, we would encourage clinicians to consider whether the calcium-channel blocker is still necessary, whether it could be discontinued or the dose reduced, or whether the patient can be switched to another therapy,” she said.
Based on the current analysis, if the rate of CCB-induced peripheral edema is assumed to be 10%, which is consistent with the literature, then “potentially 7% to 14% of people who develop edema while taking a calcium channel blocker may then receive a loop diuretic,” an accompanying editorial notes.
“Patients with polypharmacy are at heightened risk of being exposed to [a] series of prescribing cascades if their current use of medications is not carefully discussed before the decision to add a new antihypertensive,” observe Timothy S. Anderson, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts, and Michael A. Steinman, MD, San Francisco Veterans Affairs Medical Center and University of California, San Francisco.
“The initial prescribing cascade can set off many other negative consequences, including adverse drug events, potentially avoidable diagnostic testing, and hospitalizations,” the editorialists caution.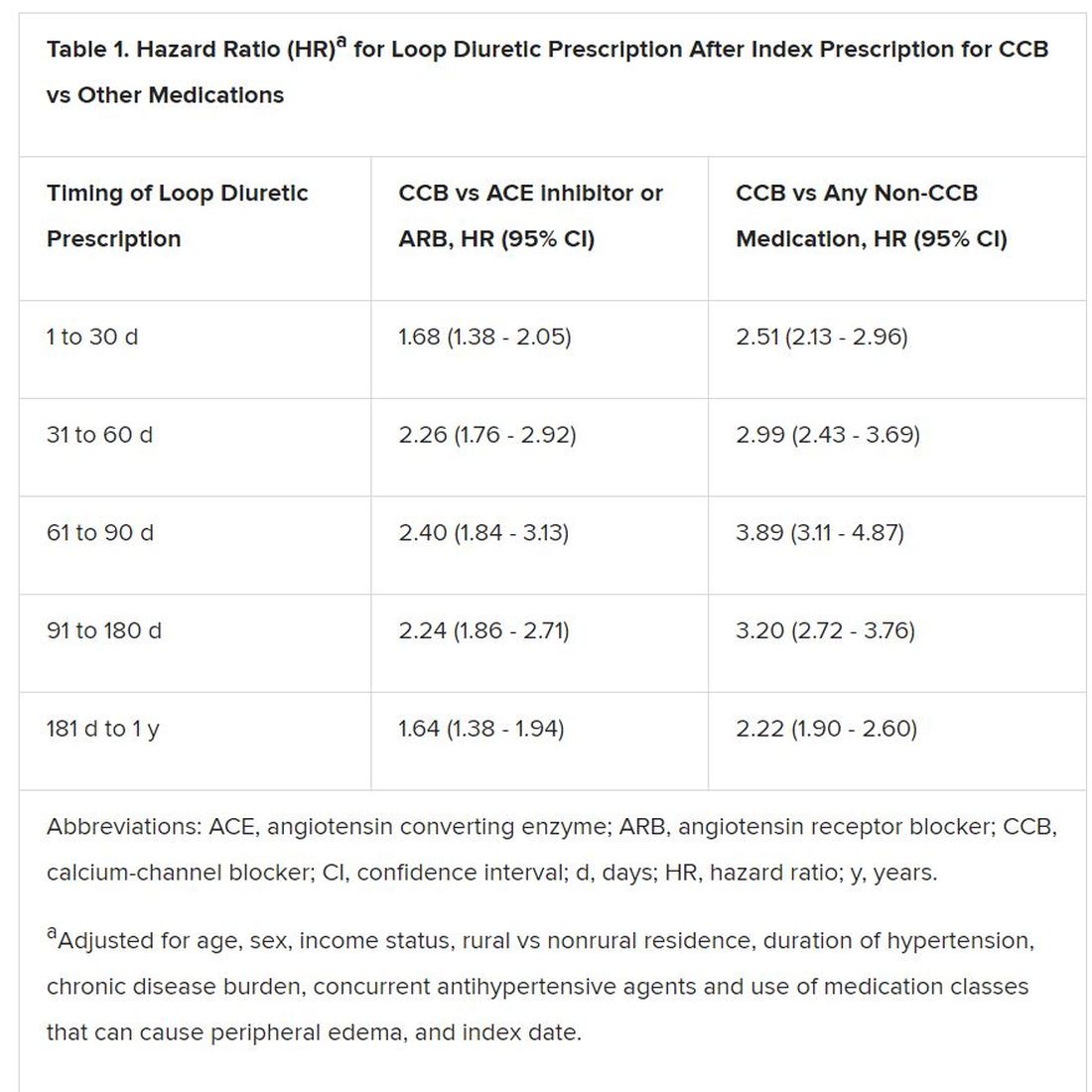
“Identifying prescribing cascades and their consequences is an important step to stem the tide of polypharmacy and inform deprescribing efforts.”
The analysis was based on administrative data from almost 340,000 adults in the community aged 66 years or older with hypertension and new drug prescriptions over 5 years ending in September 2016, the report notes. Their mean age was 74.5 years and 56.5% were women.
The data set included 41,086 patients who were newly prescribed a CCB; 66,494 who were newly prescribed an ACE inhibitor or ARB; and 231,439 newly prescribed any medication other than a CCB. The prescribed CCB was amlodipine in 79.6% of patients.
Although loop diuretics could possibly have been prescribed sometimes as a second-tier antihypertensive in the absence of peripheral edema, “we made efforts, through the design of our study, to limit this where possible,” Savage said in an interview.
For example, the focus was on loop diuretics, which aren’t generally recommended for blood-pressure lowering. Also, patients with heart failure and those with a recent history of diuretic or other antihypertensive medication use had been excluded, she said.
“As such, our cohort comprised individuals with new-onset or milder hypertension for whom diuretics would unlikely to be prescribed as part of guideline-based hypertension management.”
Although amlodipine was the most commonly prescribed CCB, the potential for a prescribing cascade seemed to be a class effect and to apply at a range of dosages.
That was unexpected, McCarthy observed, because “peripheral edema occurs more commonly in people taking dihydropyridine CCBs, like amlodipine, compared to non–dihydropyridine CCBs, such as verapamil and diltiazem.”
Savage, McCarthy, their coauthors, and the editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Elderly adults with hypertension who are newly prescribed a calcium-channel blocker (CCB), compared to other antihypertensive agents, are at least twice as likely to be given a loop diuretic over the following months, a large cohort study suggests.
The likelihood remained elevated for as long as a year after the start of a CCB and was more pronounced when comparing CCBs to any other kind of medication.
“Our findings suggest that many older adults who begin taking a CCB may subsequently experience a prescribing cascade” when loop diuretics are prescribed for peripheral edema, a known CCB adverse effect, that is misinterpreted as a new medical condition, Rachel D. Savage, PhD, Women’s College Hospital, Toronto, Canada, told theheart.org/Medscape Cardiology.
Edema caused by CCBs is caused by fluid redistribution, not overload, and “treating euvolemic individuals with a diuretic places them at increased risk of overdiuresis, leading to falls, urinary incontinence, acute kidney injury, electrolyte imbalances, and a cascade of other downstream consequences to which older adults are especially vulnerable,” explain Savage and coauthors of the analysis published online February 24 in JAMA Internal Medicine.
However, 1.4% of the cohort had been prescribed a loop diuretic, and 4.5% had been given any diuretic within 90 days after the start of CCBs. The corresponding rates were 0.7% and 3.4%, respectively, for patients who had started on ACE inhibitors or angiotensin receptor blocker (ARB) rather than a CCB.
Also, Savage observed, “the likelihood of being prescribed a loop diuretic following initiation of a CCB changed over time and was greatest 61 to 90 days postinitiation.” At that point, it was increased 2.4 times compared with initiation of an ACE inhibitor or an ARB in an adjusted analysis and increased almost 4 times compared with starting on any non-CCB agent.
Importantly, the actual prevalence of peripheral edema among those started on CCBs, ACE inhibitors, ARBs, or any non-CCB medication was not available in the data sets.
However, “the main message for clinicians is to consider medication side effects as a potential cause for new symptoms when patients present. We also encourage patients to ask prescribers about whether new symptoms could be caused by a medication,” senior author Lisa M. McCarthy, PharmD, told theheart.org/Medscape Cardiology.
“If a patient experiences peripheral edema while taking a CCB, we would encourage clinicians to consider whether the calcium-channel blocker is still necessary, whether it could be discontinued or the dose reduced, or whether the patient can be switched to another therapy,” she said.
Based on the current analysis, if the rate of CCB-induced peripheral edema is assumed to be 10%, which is consistent with the literature, then “potentially 7% to 14% of people who develop edema while taking a calcium channel blocker may then receive a loop diuretic,” an accompanying editorial notes.
“Patients with polypharmacy are at heightened risk of being exposed to [a] series of prescribing cascades if their current use of medications is not carefully discussed before the decision to add a new antihypertensive,” observe Timothy S. Anderson, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts, and Michael A. Steinman, MD, San Francisco Veterans Affairs Medical Center and University of California, San Francisco.
“The initial prescribing cascade can set off many other negative consequences, including adverse drug events, potentially avoidable diagnostic testing, and hospitalizations,” the editorialists caution.
“Identifying prescribing cascades and their consequences is an important step to stem the tide of polypharmacy and inform deprescribing efforts.”
The analysis was based on administrative data from almost 340,000 adults in the community aged 66 years or older with hypertension and new drug prescriptions over 5 years ending in September 2016, the report notes. Their mean age was 74.5 years and 56.5% were women.
The data set included 41,086 patients who were newly prescribed a CCB; 66,494 who were newly prescribed an ACE inhibitor or ARB; and 231,439 newly prescribed any medication other than a CCB. The prescribed CCB was amlodipine in 79.6% of patients.
Although loop diuretics could possibly have been prescribed sometimes as a second-tier antihypertensive in the absence of peripheral edema, “we made efforts, through the design of our study, to limit this where possible,” Savage said in an interview.
For example, the focus was on loop diuretics, which aren’t generally recommended for blood-pressure lowering. Also, patients with heart failure and those with a recent history of diuretic or other antihypertensive medication use had been excluded, she said.
“As such, our cohort comprised individuals with new-onset or milder hypertension for whom diuretics would unlikely to be prescribed as part of guideline-based hypertension management.”
Although amlodipine was the most commonly prescribed CCB, the potential for a prescribing cascade seemed to be a class effect and to apply at a range of dosages.
That was unexpected, McCarthy observed, because “peripheral edema occurs more commonly in people taking dihydropyridine CCBs, like amlodipine, compared to non–dihydropyridine CCBs, such as verapamil and diltiazem.”
Savage, McCarthy, their coauthors, and the editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Elderly adults with hypertension who are newly prescribed a calcium-channel blocker (CCB), compared to other antihypertensive agents, are at least twice as likely to be given a loop diuretic over the following months, a large cohort study suggests.
The likelihood remained elevated for as long as a year after the start of a CCB and was more pronounced when comparing CCBs to any other kind of medication.
“Our findings suggest that many older adults who begin taking a CCB may subsequently experience a prescribing cascade” when loop diuretics are prescribed for peripheral edema, a known CCB adverse effect, that is misinterpreted as a new medical condition, Rachel D. Savage, PhD, Women’s College Hospital, Toronto, Canada, told theheart.org/Medscape Cardiology.
Edema caused by CCBs is caused by fluid redistribution, not overload, and “treating euvolemic individuals with a diuretic places them at increased risk of overdiuresis, leading to falls, urinary incontinence, acute kidney injury, electrolyte imbalances, and a cascade of other downstream consequences to which older adults are especially vulnerable,” explain Savage and coauthors of the analysis published online February 24 in JAMA Internal Medicine.
However, 1.4% of the cohort had been prescribed a loop diuretic, and 4.5% had been given any diuretic within 90 days after the start of CCBs. The corresponding rates were 0.7% and 3.4%, respectively, for patients who had started on ACE inhibitors or angiotensin receptor blocker (ARB) rather than a CCB.
Also, Savage observed, “the likelihood of being prescribed a loop diuretic following initiation of a CCB changed over time and was greatest 61 to 90 days postinitiation.” At that point, it was increased 2.4 times compared with initiation of an ACE inhibitor or an ARB in an adjusted analysis and increased almost 4 times compared with starting on any non-CCB agent.
Importantly, the actual prevalence of peripheral edema among those started on CCBs, ACE inhibitors, ARBs, or any non-CCB medication was not available in the data sets.
However, “the main message for clinicians is to consider medication side effects as a potential cause for new symptoms when patients present. We also encourage patients to ask prescribers about whether new symptoms could be caused by a medication,” senior author Lisa M. McCarthy, PharmD, told theheart.org/Medscape Cardiology.
“If a patient experiences peripheral edema while taking a CCB, we would encourage clinicians to consider whether the calcium-channel blocker is still necessary, whether it could be discontinued or the dose reduced, or whether the patient can be switched to another therapy,” she said.
Based on the current analysis, if the rate of CCB-induced peripheral edema is assumed to be 10%, which is consistent with the literature, then “potentially 7% to 14% of people who develop edema while taking a calcium channel blocker may then receive a loop diuretic,” an accompanying editorial notes.
“Patients with polypharmacy are at heightened risk of being exposed to [a] series of prescribing cascades if their current use of medications is not carefully discussed before the decision to add a new antihypertensive,” observe Timothy S. Anderson, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts, and Michael A. Steinman, MD, San Francisco Veterans Affairs Medical Center and University of California, San Francisco.
“The initial prescribing cascade can set off many other negative consequences, including adverse drug events, potentially avoidable diagnostic testing, and hospitalizations,” the editorialists caution.
“Identifying prescribing cascades and their consequences is an important step to stem the tide of polypharmacy and inform deprescribing efforts.”
The analysis was based on administrative data from almost 340,000 adults in the community aged 66 years or older with hypertension and new drug prescriptions over 5 years ending in September 2016, the report notes. Their mean age was 74.5 years and 56.5% were women.
The data set included 41,086 patients who were newly prescribed a CCB; 66,494 who were newly prescribed an ACE inhibitor or ARB; and 231,439 newly prescribed any medication other than a CCB. The prescribed CCB was amlodipine in 79.6% of patients.
Although loop diuretics could possibly have been prescribed sometimes as a second-tier antihypertensive in the absence of peripheral edema, “we made efforts, through the design of our study, to limit this where possible,” Savage said in an interview.
For example, the focus was on loop diuretics, which aren’t generally recommended for blood-pressure lowering. Also, patients with heart failure and those with a recent history of diuretic or other antihypertensive medication use had been excluded, she said.
“As such, our cohort comprised individuals with new-onset or milder hypertension for whom diuretics would unlikely to be prescribed as part of guideline-based hypertension management.”
Although amlodipine was the most commonly prescribed CCB, the potential for a prescribing cascade seemed to be a class effect and to apply at a range of dosages.
That was unexpected, McCarthy observed, because “peripheral edema occurs more commonly in people taking dihydropyridine CCBs, like amlodipine, compared to non–dihydropyridine CCBs, such as verapamil and diltiazem.”
Savage, McCarthy, their coauthors, and the editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Varied nightly bedtime, sleep duration linked to CVD risk
People who frequently alter the amount of sleep and time they go to bed each night are twofold more likely to develop cardiovascular disease, independent of traditional CVD risk factors, new research suggests.
Prior studies have focused on shift workers because night shift work will influence circadian rhythm and increase CVD risk. But it is increasingly recognized that circadian disruption may occur outside of shift work and accumulate over time, particularly given modern lifestyle factors such as increased use of mobile devices and television at night, said study coauthor Tianyi Huang, ScD, MSc, of Brigham and Women’s Hospital and Harvard Medical School in Boston, Massachusetts.
“Even if they tend to go to sleep at certain times, by following that lifestyle or behavior, it can interfere with their planned sleep timing,” he said.
“One thing that surprised me in this sample is that about one third of participants have irregular sleep patterns that can put them at increased risk of cardiovascular disease. So I think the prevalence is higher than expected,” Huang added.
As reported today in the Journal of the American College of Cardiology, the investigators used data from 7-day wrist actigraphy, 1 night of at-home polysomnography, and sleep questionnaires to assess sleep duration and sleep-onset timing among 1,992 Multi-Ethnic Study of Atherosclerosis () participants, aged 45 to 84 years, who were free of CVD and prospectively followed for a me MESA dian of 4.9 years.
A total of 786 patients (39.5%) had sleep duration standard deviation (SD) > 90 minutes and 510 (25.6%) had sleep-onset timing SD > 90 minutes.
During follow-up, there were 111 incident CVD events, including myocardial infarction, coronary heart disease death, stroke, and other coronary events.
Compared with people who had less than 1 hour of variation in sleep duration, the risk for incident CVD was 9% higher for people whose sleep duration varied 61 to 90 minutes (hazard ratio [HR], 1.09; 95% confidence interval [CI], 0.62 - 1.92), even after controlling for a variety of cardiovascular and sleep-related risk factors such as body mass index, systolic blood pressure, smoking status, total cholesterol, average sleep duration, insomnia symptoms, and sleep apnea.
Moreover, the adjusted CVD risk was substantially increased with 91 to 120 minutes of variation (HR, 1.59; 95% CI, 0.91 - 2.76) and more than 120 minutes of variation in sleep duration (HR, 2.14; 95% CI, 1.24 - 3.68).
Every 1-hour increase in sleep duration SD was associated with 36% higher CVD risk (95% CI; 1.07 - 1.73).
Compared with people with no more than a half hour of variation in nightly bedtimes, the adjusted hazard ratios for CVD were 1.16 (95% CI, 0.64 - 2.13), 1.52 (95% CI, 0.81 - 2.88), and 2.11 (95% CI, 1.13 - 3.91) when bedtimes varied by 31 to 60 minutes, 61 to 90 minutes, and more than 90 minutes.
For every 1-hour increase in sleep-onset timing SD, the risk of CVD was 18% higher (95% CI; 1.06 - 1.31).
“The results are similar for the regularity of sleep timing and the regularity of sleep duration, which means that both can contribute to circadian disruption and then lead to development of cardiovascular disease,” Huang said.
This is an important article and signals how sleep is an important marker and possibly a mediator of cardiovascular risk, said Harlan Krumholz, MD, of Yale School of Medicine in New Haven, Connecticut, who was not involved with the study.
“What I like about this is it’s a nice longitudinal, epidemiologic study with not just self-report, but sensor-detected sleep, that has been correlated with well-curated and adjudicated outcomes to give us a strong sense of this association,” he told theheart.org/Medscape Cardiology. “And also, that it goes beyond just the duration — they combine the duration and timing in order to give a fuller picture of sleep.”
Nevertheless, Krumholz said researchers are only at the beginning of being able to quantify the various dimensions of sleep and the degree to which sleep is a reflection of underlying physiologic issues, or whether patients are having erratic sleep patterns that are having a toxic effect on their overall health.
Questions also remain about the mechanism behind the association, whether the increased risk is universal or more harmful for some people, and the best way to measure factors during sleep that can most comprehensively and precisely predict risk.
“As we get more information flowing in from sensors, I think we will begin to develop more sophisticated approaches toward understanding risk, and it will be accompanied by other studies that will help us understand whether, again, this is a reflection of other processes that we should be paying attention to or whether it is a cause of disease and risk,” Krumholz said.
Subgroup analyses suggested positive associations between irregular sleep and CVD in African Americans, Hispanics, and Chinese Americans but not in whites. This could be because sleep irregularity, both timing and duration, was substantially higher in minorities, especially African Americans, but may also be as a result of chance because the study sample is relatively small, Huang explained.
The authors note that the overall findings are biologically plausible because of their previous work linking sleep irregularity with metabolic risk factors that predispose to atherosclerosis, such as obesity, diabetes, and hypertension. Participants with irregular sleep tended to have worse baseline cardiometabolic profiles, but this only explained a small portion of the associations between sleep irregularity and CVD, they note.
Other possible explanations include circadian clock genes, such as clock, per2 and bmal1, which have been shown experimentally to control a broad range of cardiovascular functions, from blood pressure and endothelial functions to vascular thrombosis and cardiac remodeling.
Irregular sleep may also influence the rhythms of the autonomic nervous system, and behavioral rhythms with regard to timing and/or amount of eating or exercise.
Further research is needed to understand the mechanisms driving the associations, the impact of sleep irregularity on individual CVD outcomes, and to determine whether a 7-day SD of more than 90 minutes for either sleep duration or sleep-onset timing can be used clinically as a threshold target for promoting cardiometabolically healthy sleep, Huang said.
“When providers communicate with their patients regarding strategies for CVD prevention, usually they focus on healthy diet and physical activity; and even when they talk about sleep, they talk about whether they have good sleep quality or sufficient sleep,” he said. “But one thing they should provide is advice regarding sleep regularity and [they should] recommend their patients follow a regular sleep pattern for the purpose of cardiovascular prevention.”
In a related editorial, Olaf Oldenburg, MD, Luderus-Kliniken Münster, Clemenshospital, Münster, Germany, and Jens Spiesshoefer, MD, Institute of Life Sciences, Scuola Superiore Sant’Anna, Pisa, Italy, write that the observed independent association between sleep irregularity and CVD “is a particularly striking finding given that impaired circadian rhythm is likely to be much more prevalent than the extreme example of shift work.”
They call on researchers to utilize big data to facilitate understanding of the association and say it is essential to test whether experimental data support the hypothesis that altered circadian rhythms would translate into unfavorable changes in 24-hour sympathovagal and neurohormonal balance, and ultimately CVD.
The present study “will, and should, stimulate much needed additional research on the association between sleep and CVD that may offer novel approaches to help improve the prognosis and daily symptom burden of patients with CVD, and might make sleep itself a therapeutic target in CVD,” the editorialists conclude.
This research was supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI), and by grants from the National Center for Advancing Translational Sciences. The MESA Sleep Study was supported by an NHLBI grant. Huang was supported by a career development grant from the National Institutes of Health.
Krumholz and Oldenburg have disclosed no relevant financial relationships. Spiesshoefer is supported by grants from the Else-Kröner-Fresenius Stiftung, the Innovative Medical Research program at the University of Münster, and Deutsche Herzstiftung; and by young investigator research support from Scuola Superiore Sant’Anna Pisa. He also has received travel grants and lecture honoraria from Boehringer Ingelheim and Chiesi.
Source: J Am Coll Cardiol. 2020 Mar 2. doi: 10.1016/j.jacc.2019.12.054.
This article first appeared on Medscape.com.
People who frequently alter the amount of sleep and time they go to bed each night are twofold more likely to develop cardiovascular disease, independent of traditional CVD risk factors, new research suggests.
Prior studies have focused on shift workers because night shift work will influence circadian rhythm and increase CVD risk. But it is increasingly recognized that circadian disruption may occur outside of shift work and accumulate over time, particularly given modern lifestyle factors such as increased use of mobile devices and television at night, said study coauthor Tianyi Huang, ScD, MSc, of Brigham and Women’s Hospital and Harvard Medical School in Boston, Massachusetts.
“Even if they tend to go to sleep at certain times, by following that lifestyle or behavior, it can interfere with their planned sleep timing,” he said.
“One thing that surprised me in this sample is that about one third of participants have irregular sleep patterns that can put them at increased risk of cardiovascular disease. So I think the prevalence is higher than expected,” Huang added.
As reported today in the Journal of the American College of Cardiology, the investigators used data from 7-day wrist actigraphy, 1 night of at-home polysomnography, and sleep questionnaires to assess sleep duration and sleep-onset timing among 1,992 Multi-Ethnic Study of Atherosclerosis () participants, aged 45 to 84 years, who were free of CVD and prospectively followed for a me MESA dian of 4.9 years.
A total of 786 patients (39.5%) had sleep duration standard deviation (SD) > 90 minutes and 510 (25.6%) had sleep-onset timing SD > 90 minutes.
During follow-up, there were 111 incident CVD events, including myocardial infarction, coronary heart disease death, stroke, and other coronary events.
Compared with people who had less than 1 hour of variation in sleep duration, the risk for incident CVD was 9% higher for people whose sleep duration varied 61 to 90 minutes (hazard ratio [HR], 1.09; 95% confidence interval [CI], 0.62 - 1.92), even after controlling for a variety of cardiovascular and sleep-related risk factors such as body mass index, systolic blood pressure, smoking status, total cholesterol, average sleep duration, insomnia symptoms, and sleep apnea.
Moreover, the adjusted CVD risk was substantially increased with 91 to 120 minutes of variation (HR, 1.59; 95% CI, 0.91 - 2.76) and more than 120 minutes of variation in sleep duration (HR, 2.14; 95% CI, 1.24 - 3.68).
Every 1-hour increase in sleep duration SD was associated with 36% higher CVD risk (95% CI; 1.07 - 1.73).
Compared with people with no more than a half hour of variation in nightly bedtimes, the adjusted hazard ratios for CVD were 1.16 (95% CI, 0.64 - 2.13), 1.52 (95% CI, 0.81 - 2.88), and 2.11 (95% CI, 1.13 - 3.91) when bedtimes varied by 31 to 60 minutes, 61 to 90 minutes, and more than 90 minutes.
For every 1-hour increase in sleep-onset timing SD, the risk of CVD was 18% higher (95% CI; 1.06 - 1.31).
“The results are similar for the regularity of sleep timing and the regularity of sleep duration, which means that both can contribute to circadian disruption and then lead to development of cardiovascular disease,” Huang said.
This is an important article and signals how sleep is an important marker and possibly a mediator of cardiovascular risk, said Harlan Krumholz, MD, of Yale School of Medicine in New Haven, Connecticut, who was not involved with the study.
“What I like about this is it’s a nice longitudinal, epidemiologic study with not just self-report, but sensor-detected sleep, that has been correlated with well-curated and adjudicated outcomes to give us a strong sense of this association,” he told theheart.org/Medscape Cardiology. “And also, that it goes beyond just the duration — they combine the duration and timing in order to give a fuller picture of sleep.”
Nevertheless, Krumholz said researchers are only at the beginning of being able to quantify the various dimensions of sleep and the degree to which sleep is a reflection of underlying physiologic issues, or whether patients are having erratic sleep patterns that are having a toxic effect on their overall health.
Questions also remain about the mechanism behind the association, whether the increased risk is universal or more harmful for some people, and the best way to measure factors during sleep that can most comprehensively and precisely predict risk.
“As we get more information flowing in from sensors, I think we will begin to develop more sophisticated approaches toward understanding risk, and it will be accompanied by other studies that will help us understand whether, again, this is a reflection of other processes that we should be paying attention to or whether it is a cause of disease and risk,” Krumholz said.
Subgroup analyses suggested positive associations between irregular sleep and CVD in African Americans, Hispanics, and Chinese Americans but not in whites. This could be because sleep irregularity, both timing and duration, was substantially higher in minorities, especially African Americans, but may also be as a result of chance because the study sample is relatively small, Huang explained.
The authors note that the overall findings are biologically plausible because of their previous work linking sleep irregularity with metabolic risk factors that predispose to atherosclerosis, such as obesity, diabetes, and hypertension. Participants with irregular sleep tended to have worse baseline cardiometabolic profiles, but this only explained a small portion of the associations between sleep irregularity and CVD, they note.
Other possible explanations include circadian clock genes, such as clock, per2 and bmal1, which have been shown experimentally to control a broad range of cardiovascular functions, from blood pressure and endothelial functions to vascular thrombosis and cardiac remodeling.
Irregular sleep may also influence the rhythms of the autonomic nervous system, and behavioral rhythms with regard to timing and/or amount of eating or exercise.
Further research is needed to understand the mechanisms driving the associations, the impact of sleep irregularity on individual CVD outcomes, and to determine whether a 7-day SD of more than 90 minutes for either sleep duration or sleep-onset timing can be used clinically as a threshold target for promoting cardiometabolically healthy sleep, Huang said.
“When providers communicate with their patients regarding strategies for CVD prevention, usually they focus on healthy diet and physical activity; and even when they talk about sleep, they talk about whether they have good sleep quality or sufficient sleep,” he said. “But one thing they should provide is advice regarding sleep regularity and [they should] recommend their patients follow a regular sleep pattern for the purpose of cardiovascular prevention.”
In a related editorial, Olaf Oldenburg, MD, Luderus-Kliniken Münster, Clemenshospital, Münster, Germany, and Jens Spiesshoefer, MD, Institute of Life Sciences, Scuola Superiore Sant’Anna, Pisa, Italy, write that the observed independent association between sleep irregularity and CVD “is a particularly striking finding given that impaired circadian rhythm is likely to be much more prevalent than the extreme example of shift work.”
They call on researchers to utilize big data to facilitate understanding of the association and say it is essential to test whether experimental data support the hypothesis that altered circadian rhythms would translate into unfavorable changes in 24-hour sympathovagal and neurohormonal balance, and ultimately CVD.
The present study “will, and should, stimulate much needed additional research on the association between sleep and CVD that may offer novel approaches to help improve the prognosis and daily symptom burden of patients with CVD, and might make sleep itself a therapeutic target in CVD,” the editorialists conclude.
This research was supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI), and by grants from the National Center for Advancing Translational Sciences. The MESA Sleep Study was supported by an NHLBI grant. Huang was supported by a career development grant from the National Institutes of Health.
Krumholz and Oldenburg have disclosed no relevant financial relationships. Spiesshoefer is supported by grants from the Else-Kröner-Fresenius Stiftung, the Innovative Medical Research program at the University of Münster, and Deutsche Herzstiftung; and by young investigator research support from Scuola Superiore Sant’Anna Pisa. He also has received travel grants and lecture honoraria from Boehringer Ingelheim and Chiesi.
Source: J Am Coll Cardiol. 2020 Mar 2. doi: 10.1016/j.jacc.2019.12.054.
This article first appeared on Medscape.com.
People who frequently alter the amount of sleep and time they go to bed each night are twofold more likely to develop cardiovascular disease, independent of traditional CVD risk factors, new research suggests.
Prior studies have focused on shift workers because night shift work will influence circadian rhythm and increase CVD risk. But it is increasingly recognized that circadian disruption may occur outside of shift work and accumulate over time, particularly given modern lifestyle factors such as increased use of mobile devices and television at night, said study coauthor Tianyi Huang, ScD, MSc, of Brigham and Women’s Hospital and Harvard Medical School in Boston, Massachusetts.
“Even if they tend to go to sleep at certain times, by following that lifestyle or behavior, it can interfere with their planned sleep timing,” he said.
“One thing that surprised me in this sample is that about one third of participants have irregular sleep patterns that can put them at increased risk of cardiovascular disease. So I think the prevalence is higher than expected,” Huang added.
As reported today in the Journal of the American College of Cardiology, the investigators used data from 7-day wrist actigraphy, 1 night of at-home polysomnography, and sleep questionnaires to assess sleep duration and sleep-onset timing among 1,992 Multi-Ethnic Study of Atherosclerosis () participants, aged 45 to 84 years, who were free of CVD and prospectively followed for a me MESA dian of 4.9 years.
A total of 786 patients (39.5%) had sleep duration standard deviation (SD) > 90 minutes and 510 (25.6%) had sleep-onset timing SD > 90 minutes.
During follow-up, there were 111 incident CVD events, including myocardial infarction, coronary heart disease death, stroke, and other coronary events.
Compared with people who had less than 1 hour of variation in sleep duration, the risk for incident CVD was 9% higher for people whose sleep duration varied 61 to 90 minutes (hazard ratio [HR], 1.09; 95% confidence interval [CI], 0.62 - 1.92), even after controlling for a variety of cardiovascular and sleep-related risk factors such as body mass index, systolic blood pressure, smoking status, total cholesterol, average sleep duration, insomnia symptoms, and sleep apnea.
Moreover, the adjusted CVD risk was substantially increased with 91 to 120 minutes of variation (HR, 1.59; 95% CI, 0.91 - 2.76) and more than 120 minutes of variation in sleep duration (HR, 2.14; 95% CI, 1.24 - 3.68).
Every 1-hour increase in sleep duration SD was associated with 36% higher CVD risk (95% CI; 1.07 - 1.73).
Compared with people with no more than a half hour of variation in nightly bedtimes, the adjusted hazard ratios for CVD were 1.16 (95% CI, 0.64 - 2.13), 1.52 (95% CI, 0.81 - 2.88), and 2.11 (95% CI, 1.13 - 3.91) when bedtimes varied by 31 to 60 minutes, 61 to 90 minutes, and more than 90 minutes.
For every 1-hour increase in sleep-onset timing SD, the risk of CVD was 18% higher (95% CI; 1.06 - 1.31).
“The results are similar for the regularity of sleep timing and the regularity of sleep duration, which means that both can contribute to circadian disruption and then lead to development of cardiovascular disease,” Huang said.
This is an important article and signals how sleep is an important marker and possibly a mediator of cardiovascular risk, said Harlan Krumholz, MD, of Yale School of Medicine in New Haven, Connecticut, who was not involved with the study.
“What I like about this is it’s a nice longitudinal, epidemiologic study with not just self-report, but sensor-detected sleep, that has been correlated with well-curated and adjudicated outcomes to give us a strong sense of this association,” he told theheart.org/Medscape Cardiology. “And also, that it goes beyond just the duration — they combine the duration and timing in order to give a fuller picture of sleep.”
Nevertheless, Krumholz said researchers are only at the beginning of being able to quantify the various dimensions of sleep and the degree to which sleep is a reflection of underlying physiologic issues, or whether patients are having erratic sleep patterns that are having a toxic effect on their overall health.
Questions also remain about the mechanism behind the association, whether the increased risk is universal or more harmful for some people, and the best way to measure factors during sleep that can most comprehensively and precisely predict risk.
“As we get more information flowing in from sensors, I think we will begin to develop more sophisticated approaches toward understanding risk, and it will be accompanied by other studies that will help us understand whether, again, this is a reflection of other processes that we should be paying attention to or whether it is a cause of disease and risk,” Krumholz said.
Subgroup analyses suggested positive associations between irregular sleep and CVD in African Americans, Hispanics, and Chinese Americans but not in whites. This could be because sleep irregularity, both timing and duration, was substantially higher in minorities, especially African Americans, but may also be as a result of chance because the study sample is relatively small, Huang explained.
The authors note that the overall findings are biologically plausible because of their previous work linking sleep irregularity with metabolic risk factors that predispose to atherosclerosis, such as obesity, diabetes, and hypertension. Participants with irregular sleep tended to have worse baseline cardiometabolic profiles, but this only explained a small portion of the associations between sleep irregularity and CVD, they note.
Other possible explanations include circadian clock genes, such as clock, per2 and bmal1, which have been shown experimentally to control a broad range of cardiovascular functions, from blood pressure and endothelial functions to vascular thrombosis and cardiac remodeling.
Irregular sleep may also influence the rhythms of the autonomic nervous system, and behavioral rhythms with regard to timing and/or amount of eating or exercise.
Further research is needed to understand the mechanisms driving the associations, the impact of sleep irregularity on individual CVD outcomes, and to determine whether a 7-day SD of more than 90 minutes for either sleep duration or sleep-onset timing can be used clinically as a threshold target for promoting cardiometabolically healthy sleep, Huang said.
“When providers communicate with their patients regarding strategies for CVD prevention, usually they focus on healthy diet and physical activity; and even when they talk about sleep, they talk about whether they have good sleep quality or sufficient sleep,” he said. “But one thing they should provide is advice regarding sleep regularity and [they should] recommend their patients follow a regular sleep pattern for the purpose of cardiovascular prevention.”
In a related editorial, Olaf Oldenburg, MD, Luderus-Kliniken Münster, Clemenshospital, Münster, Germany, and Jens Spiesshoefer, MD, Institute of Life Sciences, Scuola Superiore Sant’Anna, Pisa, Italy, write that the observed independent association between sleep irregularity and CVD “is a particularly striking finding given that impaired circadian rhythm is likely to be much more prevalent than the extreme example of shift work.”
They call on researchers to utilize big data to facilitate understanding of the association and say it is essential to test whether experimental data support the hypothesis that altered circadian rhythms would translate into unfavorable changes in 24-hour sympathovagal and neurohormonal balance, and ultimately CVD.
The present study “will, and should, stimulate much needed additional research on the association between sleep and CVD that may offer novel approaches to help improve the prognosis and daily symptom burden of patients with CVD, and might make sleep itself a therapeutic target in CVD,” the editorialists conclude.
This research was supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI), and by grants from the National Center for Advancing Translational Sciences. The MESA Sleep Study was supported by an NHLBI grant. Huang was supported by a career development grant from the National Institutes of Health.
Krumholz and Oldenburg have disclosed no relevant financial relationships. Spiesshoefer is supported by grants from the Else-Kröner-Fresenius Stiftung, the Innovative Medical Research program at the University of Münster, and Deutsche Herzstiftung; and by young investigator research support from Scuola Superiore Sant’Anna Pisa. He also has received travel grants and lecture honoraria from Boehringer Ingelheim and Chiesi.
Source: J Am Coll Cardiol. 2020 Mar 2. doi: 10.1016/j.jacc.2019.12.054.
This article first appeared on Medscape.com.
New strategies cut esophageal damage from AFib catheter ablation
NATIONAL HARBOR, MD. – Thermal injury of a patient’s esophagus during radiofrequency catheter ablation of atrial fibrillation is notorious as a relatively common and problematic complication of the procedure, but two new approaches showed promise for substantially cutting the risk of esophageal thermal injury and the potential for the most severe damage: perforation.

One of these innovations is intensive esophageal cooling with a commercially marketed, fluid-chilled catheter placed in a patient’s esophagus during radiofrequency catheter ablation that keeps the inner surface of the esophagus at 4°C. This approach cut the incidence of periprocedural episodes of endoscopically detected esophageal thermal injury from 20% among controls to 3% in patients who had esophageal cooling in a randomized study with 120 patients, Mark M. Gallagher, MD, said at the annual International AF Symposium. The same device can also maintain a temperature on the inner surface of the esophagus of 42 ° C in patients undergoing cryoablation of atrial fibrillation, noted Dr. Gallagher, a cardiac electrophysiologist at St. George’s University Hospitals in London.
A second approach to cutting esophageal damage focuses on modifying the energy delivery with a radiofrequency ablation method known as high-power short-duration (HPSD). As the name says, this strategy uses a relatively high level of radiofrequency energy, 50 watts in the reported experience, for the brief interval of about 7 seconds, ideally delivering an overall Ablation Index of at least 350 but below 360, said Thomas Deneke, MD, an electrophysiologist, professor, and cochief of cardiology at the Heart Center in Bad Neustadt, Germany.
Dr. Deneke and his associates in Bad Neustadt began using this HPSD approach in mid-2019, and by early 2020 they had data from 179 patients who underwent first-time catheter ablation of atrial fibrillation (AFib), all of whom had undergone routine esophageal endoscopy 1-3 days after their treatment. Eight patients (4%) showed evidence of endoscopically detected esophageal lesions (EDEL), including three patients (2%) with an actual esophageal ulcer, and one (0.6%) who developed a perforation that healed after 52 days, Dr. Deneke reported. An additional 55 patients underwent a redo catheter ablation procedure using the HPSD method during this period, and in that group follow-up endoscopy in all patients showed EDEL in two patients (4%). In contrast, during Jan. 2012–May 2019, the same German center treated 2,102 patients who had a first radiofrequency catheter ablation using convention energy levels and treatment times, which resulted in 291 patients having an EDEL (14%), including 94 (4%) with an ulcer, and six patients (0.3%) with an esophageal perforation, he said.
His center’s recent safety experience with HPSD radiofrequncy ablation, compared with the historical controls, suggests that this technique can produce a substantial reduction in esophageal thermal injury, but HPSD has not completely eliminated the risk and hence there is need for continued alertness for this potential complication Dr. Deneke concluded. The HPSD method is also limited by having “a very narrow window” between efficacy at an Ablation Index of 350 and safety when the index remains below 360, he added.
The randomized study that Dr. Gallagher ran at St. George’s followed an analysis he and his associates recently published that suggested efficacy using esophageal cooling in prior reports when the data combined in a meta-analysis (J Interv Card Electrophysiol. 2019 Nov 22. doi: 10.1007/s10840-019-00661-5). They also concluded that the clinical setting required a temperature control device with an enhanced capacity for rapid cooling, which prior studies had lacked. So they turned to a Food and Drug Administration–approved catheter designed for placement in the esophagus for the purpose of either whole-body cooling or warming.
The study randomized a total of 187 patients, but collected follow-up endoscopy at 5-7 days after the ablation procedure on 120 patients, of whom 60 received esophageal cooling and 60 did not. The types of ablations performed on patients in the two study arms were similar, and use of esophageal cooling had no impact on treatment duration or efficacy, either acute and longer term, Dr. Gallagher reported.
Cooling had a marked and statistically significant impact on endoscopically detected thermal injury. Although two patients in the group that underwent cooling had injuries, in one of these cases the injury involved a protocol violation: Radiofrequency ablation mistakenly occurred after the cooling device shut off, and it was during this period when the injury happened. In the second case of thermal injury, blinded scoring judged the injury as grade 2 in severity – an erosion of less than 5 mm – on a nine-item scale that ranged from zero to grade 6, the most severe level denoting a fistula. By contrast, among the 12 patients with thermal injury in the nonprotected subgroup, one patient had a grade 5a lesion denoting a deep ulcer, one had a 4b denoting a superficial ulcer with a clot, and four had a 4a lesion defined as a clean superficial ulcer.
“This is really effective. It’s the first study to show reduced damage without affecting ablation efficacy,” Dr. Gallagher said. He plans to now use this method of esophageal protection routinely for his AFib ablation patients who pay privately, and for patients insured under the national U.K. system once this coverage is approved. Dr. Deneke expressed his interest in also using this approach to esophageal protection, but noted that currently he did not have access to the cooling catheter that Dr. Gallagher used because of regulatory constraints.
The esophageal cooling study was sponsored by Attune Medical, which markets the cooling device. Dr. Gallagher has received research funding from Attune Medical, and has received honoraria as a speaker on behalf of Biosense Webster and Medtronic. Dr. Deneke has been a speaker on behalf of Abbott, Biosense Webster, Biotronik, and Boston Scientific, and his institution has received research funding from Biosense Webster and Securus/Boston Scientific.
NATIONAL HARBOR, MD. – Thermal injury of a patient’s esophagus during radiofrequency catheter ablation of atrial fibrillation is notorious as a relatively common and problematic complication of the procedure, but two new approaches showed promise for substantially cutting the risk of esophageal thermal injury and the potential for the most severe damage: perforation.
One of these innovations is intensive esophageal cooling with a commercially marketed, fluid-chilled catheter placed in a patient’s esophagus during radiofrequency catheter ablation that keeps the inner surface of the esophagus at 4°C. This approach cut the incidence of periprocedural episodes of endoscopically detected esophageal thermal injury from 20% among controls to 3% in patients who had esophageal cooling in a randomized study with 120 patients, Mark M. Gallagher, MD, said at the annual International AF Symposium. The same device can also maintain a temperature on the inner surface of the esophagus of 42 ° C in patients undergoing cryoablation of atrial fibrillation, noted Dr. Gallagher, a cardiac electrophysiologist at St. George’s University Hospitals in London.
A second approach to cutting esophageal damage focuses on modifying the energy delivery with a radiofrequency ablation method known as high-power short-duration (HPSD). As the name says, this strategy uses a relatively high level of radiofrequency energy, 50 watts in the reported experience, for the brief interval of about 7 seconds, ideally delivering an overall Ablation Index of at least 350 but below 360, said Thomas Deneke, MD, an electrophysiologist, professor, and cochief of cardiology at the Heart Center in Bad Neustadt, Germany.
Dr. Deneke and his associates in Bad Neustadt began using this HPSD approach in mid-2019, and by early 2020 they had data from 179 patients who underwent first-time catheter ablation of atrial fibrillation (AFib), all of whom had undergone routine esophageal endoscopy 1-3 days after their treatment. Eight patients (4%) showed evidence of endoscopically detected esophageal lesions (EDEL), including three patients (2%) with an actual esophageal ulcer, and one (0.6%) who developed a perforation that healed after 52 days, Dr. Deneke reported. An additional 55 patients underwent a redo catheter ablation procedure using the HPSD method during this period, and in that group follow-up endoscopy in all patients showed EDEL in two patients (4%). In contrast, during Jan. 2012–May 2019, the same German center treated 2,102 patients who had a first radiofrequency catheter ablation using convention energy levels and treatment times, which resulted in 291 patients having an EDEL (14%), including 94 (4%) with an ulcer, and six patients (0.3%) with an esophageal perforation, he said.
His center’s recent safety experience with HPSD radiofrequncy ablation, compared with the historical controls, suggests that this technique can produce a substantial reduction in esophageal thermal injury, but HPSD has not completely eliminated the risk and hence there is need for continued alertness for this potential complication Dr. Deneke concluded. The HPSD method is also limited by having “a very narrow window” between efficacy at an Ablation Index of 350 and safety when the index remains below 360, he added.
The randomized study that Dr. Gallagher ran at St. George’s followed an analysis he and his associates recently published that suggested efficacy using esophageal cooling in prior reports when the data combined in a meta-analysis (J Interv Card Electrophysiol. 2019 Nov 22. doi: 10.1007/s10840-019-00661-5). They also concluded that the clinical setting required a temperature control device with an enhanced capacity for rapid cooling, which prior studies had lacked. So they turned to a Food and Drug Administration–approved catheter designed for placement in the esophagus for the purpose of either whole-body cooling or warming.
The study randomized a total of 187 patients, but collected follow-up endoscopy at 5-7 days after the ablation procedure on 120 patients, of whom 60 received esophageal cooling and 60 did not. The types of ablations performed on patients in the two study arms were similar, and use of esophageal cooling had no impact on treatment duration or efficacy, either acute and longer term, Dr. Gallagher reported.
Cooling had a marked and statistically significant impact on endoscopically detected thermal injury. Although two patients in the group that underwent cooling had injuries, in one of these cases the injury involved a protocol violation: Radiofrequency ablation mistakenly occurred after the cooling device shut off, and it was during this period when the injury happened. In the second case of thermal injury, blinded scoring judged the injury as grade 2 in severity – an erosion of less than 5 mm – on a nine-item scale that ranged from zero to grade 6, the most severe level denoting a fistula. By contrast, among the 12 patients with thermal injury in the nonprotected subgroup, one patient had a grade 5a lesion denoting a deep ulcer, one had a 4b denoting a superficial ulcer with a clot, and four had a 4a lesion defined as a clean superficial ulcer.
“This is really effective. It’s the first study to show reduced damage without affecting ablation efficacy,” Dr. Gallagher said. He plans to now use this method of esophageal protection routinely for his AFib ablation patients who pay privately, and for patients insured under the national U.K. system once this coverage is approved. Dr. Deneke expressed his interest in also using this approach to esophageal protection, but noted that currently he did not have access to the cooling catheter that Dr. Gallagher used because of regulatory constraints.
The esophageal cooling study was sponsored by Attune Medical, which markets the cooling device. Dr. Gallagher has received research funding from Attune Medical, and has received honoraria as a speaker on behalf of Biosense Webster and Medtronic. Dr. Deneke has been a speaker on behalf of Abbott, Biosense Webster, Biotronik, and Boston Scientific, and his institution has received research funding from Biosense Webster and Securus/Boston Scientific.
NATIONAL HARBOR, MD. – Thermal injury of a patient’s esophagus during radiofrequency catheter ablation of atrial fibrillation is notorious as a relatively common and problematic complication of the procedure, but two new approaches showed promise for substantially cutting the risk of esophageal thermal injury and the potential for the most severe damage: perforation.
One of these innovations is intensive esophageal cooling with a commercially marketed, fluid-chilled catheter placed in a patient’s esophagus during radiofrequency catheter ablation that keeps the inner surface of the esophagus at 4°C. This approach cut the incidence of periprocedural episodes of endoscopically detected esophageal thermal injury from 20% among controls to 3% in patients who had esophageal cooling in a randomized study with 120 patients, Mark M. Gallagher, MD, said at the annual International AF Symposium. The same device can also maintain a temperature on the inner surface of the esophagus of 42 ° C in patients undergoing cryoablation of atrial fibrillation, noted Dr. Gallagher, a cardiac electrophysiologist at St. George’s University Hospitals in London.
A second approach to cutting esophageal damage focuses on modifying the energy delivery with a radiofrequency ablation method known as high-power short-duration (HPSD). As the name says, this strategy uses a relatively high level of radiofrequency energy, 50 watts in the reported experience, for the brief interval of about 7 seconds, ideally delivering an overall Ablation Index of at least 350 but below 360, said Thomas Deneke, MD, an electrophysiologist, professor, and cochief of cardiology at the Heart Center in Bad Neustadt, Germany.
Dr. Deneke and his associates in Bad Neustadt began using this HPSD approach in mid-2019, and by early 2020 they had data from 179 patients who underwent first-time catheter ablation of atrial fibrillation (AFib), all of whom had undergone routine esophageal endoscopy 1-3 days after their treatment. Eight patients (4%) showed evidence of endoscopically detected esophageal lesions (EDEL), including three patients (2%) with an actual esophageal ulcer, and one (0.6%) who developed a perforation that healed after 52 days, Dr. Deneke reported. An additional 55 patients underwent a redo catheter ablation procedure using the HPSD method during this period, and in that group follow-up endoscopy in all patients showed EDEL in two patients (4%). In contrast, during Jan. 2012–May 2019, the same German center treated 2,102 patients who had a first radiofrequency catheter ablation using convention energy levels and treatment times, which resulted in 291 patients having an EDEL (14%), including 94 (4%) with an ulcer, and six patients (0.3%) with an esophageal perforation, he said.
His center’s recent safety experience with HPSD radiofrequncy ablation, compared with the historical controls, suggests that this technique can produce a substantial reduction in esophageal thermal injury, but HPSD has not completely eliminated the risk and hence there is need for continued alertness for this potential complication Dr. Deneke concluded. The HPSD method is also limited by having “a very narrow window” between efficacy at an Ablation Index of 350 and safety when the index remains below 360, he added.
The randomized study that Dr. Gallagher ran at St. George’s followed an analysis he and his associates recently published that suggested efficacy using esophageal cooling in prior reports when the data combined in a meta-analysis (J Interv Card Electrophysiol. 2019 Nov 22. doi: 10.1007/s10840-019-00661-5). They also concluded that the clinical setting required a temperature control device with an enhanced capacity for rapid cooling, which prior studies had lacked. So they turned to a Food and Drug Administration–approved catheter designed for placement in the esophagus for the purpose of either whole-body cooling or warming.
The study randomized a total of 187 patients, but collected follow-up endoscopy at 5-7 days after the ablation procedure on 120 patients, of whom 60 received esophageal cooling and 60 did not. The types of ablations performed on patients in the two study arms were similar, and use of esophageal cooling had no impact on treatment duration or efficacy, either acute and longer term, Dr. Gallagher reported.
Cooling had a marked and statistically significant impact on endoscopically detected thermal injury. Although two patients in the group that underwent cooling had injuries, in one of these cases the injury involved a protocol violation: Radiofrequency ablation mistakenly occurred after the cooling device shut off, and it was during this period when the injury happened. In the second case of thermal injury, blinded scoring judged the injury as grade 2 in severity – an erosion of less than 5 mm – on a nine-item scale that ranged from zero to grade 6, the most severe level denoting a fistula. By contrast, among the 12 patients with thermal injury in the nonprotected subgroup, one patient had a grade 5a lesion denoting a deep ulcer, one had a 4b denoting a superficial ulcer with a clot, and four had a 4a lesion defined as a clean superficial ulcer.
“This is really effective. It’s the first study to show reduced damage without affecting ablation efficacy,” Dr. Gallagher said. He plans to now use this method of esophageal protection routinely for his AFib ablation patients who pay privately, and for patients insured under the national U.K. system once this coverage is approved. Dr. Deneke expressed his interest in also using this approach to esophageal protection, but noted that currently he did not have access to the cooling catheter that Dr. Gallagher used because of regulatory constraints.
The esophageal cooling study was sponsored by Attune Medical, which markets the cooling device. Dr. Gallagher has received research funding from Attune Medical, and has received honoraria as a speaker on behalf of Biosense Webster and Medtronic. Dr. Deneke has been a speaker on behalf of Abbott, Biosense Webster, Biotronik, and Boston Scientific, and his institution has received research funding from Biosense Webster and Securus/Boston Scientific.
THE AF SYMPOSIUM 2020