User login
Antibiotic-resistant bacteria emerging in community settings
A new study from the Centers for Disease Control and Prevention found that
Traditionally, CRE has been thought of as a nosocomial infection, acquired in a hospital or other health care facility (nursing home, long-term acute care hospital, dialysis center, etc.). This is the first population-level study to show otherwise, with fully 10% of the CRE isolates found to be community acquired.
CREs are a group of multidrug-resistant bacteria considered an urgent health threat by the CDC because they can rapidly spread between patients, especially those who are most seriously ill and vulnerable, and because they are so difficult to treat. These patients often require treatment with toxic antibiotics, such as colistin, and carry a high mortality rate – up to 50% in some studies.
Overall, 30% of CREs carry a carbapenemase – an enzyme that can make them resistant to carbapenem antibiotics. The genes for this are readily transferable between bacteria and help account for their spread in hospitals.
But in this study, published in the American Journal of Infection Control, of the 12 isolates that underwent whole-genome sequencing, 42% of the CA-CRE isolates carried the carbapenemase gene. Lead author Sandra Bulens, MPH, a health scientist in the CDC’s division of health care quality promotion, said in an interview, “The findings highlight the potential for CP-CRE to move from health care settings into the community. The fact that 5 of the 12 isolates harbored a carbapenemase gene introduces new challenges for controlling spread of CP-CRE.”
CDC researchers analyzed data from eight U.S. metropolitan areas between 2012 and 2015 as part of the CDC’s Emerging Infections Program (EIP) health care–associated infections – community interface activity, which conducts surveillance for CRE and other drug-resistant gram-negative bacteria. Cases of CA-CRE were compared with HCA-CRE, with 1499 cases in 1,194 case-patients being analyzed. Though Klebsiella pneumoniae was the most common isolate, there were some differences between metropolitan areas.
The incidence of CRE cases per 100,000 population was 2.96 (95% confidence interval, 2.81-3.11) overall and 0.29 (95% CI, 0.25-0.25) for CA-CRE. Most CA-CRE cases were in White persons (73%) and women (84%). Urine cultures were the source of 98% of all CA-CRE cases, compared with 86% of HCA-CRE cases (P < .001). Though small numbers, the numbers of patients with CA-CRE without apparent underlying medical condition (n = 51; 37%) was greater when compared with patients with HCA-CRE (n = 36; 3%; P < .001).
Asked for independent comment, Lance Price, PhD, of George Washington University and the founding director of GW’s Antibiotic Resistance Action Center, Washington, said, “what’s striking about these data is that: ‘Who is the front line, at least in the United States for CRE?’ It’s women, older women. ... At some point, we have to frame drug resistance as a women’s health issue.”
Dr. Price noted that the 10% of patients with CA-CRE acquired it in the community. “I would argue that probably none of them had any idea, because there’s this silent community epidemic,” he said. “It’s asymptomatic carriage and transmission in the community. Somebody can be this walking reservoir of these really dangerous bacteria and have no idea.”
This is an increasingly serious problem for women, Dr. Price said, because, “with a community-acquired bladder infection, you’re going to call your doctor or go to an urgent care, and they’re not going to test you. They’re going to guess what you have, and they’re going to prescribe an antibiotic, and that antibiotic is going to fail. So then your bladder infection continues, and then you wait a few more days, and you start to get flank pain and kidney infection. ... If you start getting a fever, they might admit you. They are going to start treating you immediately, and they might miss it because you’ve got this organism that’s resistant to all the best antibiotics. ... The gateway to the blood is the UTI.”
Because of such empiric treatment and increasing resistance, the risk for treatment failure is quite high, especially for older women. Ms. Bulens, however, said that, “[although] 10% of CRE were in persons without health care risk factors, the proportion of all UTIs in this population that are CRE is going to be very, very small.”
This study involved cultures from 2012 to 2015. Before the pandemic, from 2012 to 2017, U.S. deaths from antibiotic resistance fell by 18% overall and by 30% in hospitals.
But in the first year of the COVID-19 pandemic, there was a 15% increase in infections and deaths from antibiotic-resistant (AMR), hospital-acquired bacteria. In 2020, 29,400 patients died from AMR infections. There was a 78% increase in carbapenem-resistant Acinetobacter baumannii health care–associated infections, a 35% increase in carbapenem-resistant Enterobacterales, and 32% increases in both multidrug-resistant Pseudomonas aeruginosa and extended-spectrum beta-lactamase–producing Enterobacterales. Aside from gram-negative bacteria, methicillin-resistant Staphylococcus aureus rose 13%, and Candida auris rose 60%. But owing to limited surveillance, recent sound figures are lacking.
Ms. Bulens and Dr. Price reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study from the Centers for Disease Control and Prevention found that
Traditionally, CRE has been thought of as a nosocomial infection, acquired in a hospital or other health care facility (nursing home, long-term acute care hospital, dialysis center, etc.). This is the first population-level study to show otherwise, with fully 10% of the CRE isolates found to be community acquired.
CREs are a group of multidrug-resistant bacteria considered an urgent health threat by the CDC because they can rapidly spread between patients, especially those who are most seriously ill and vulnerable, and because they are so difficult to treat. These patients often require treatment with toxic antibiotics, such as colistin, and carry a high mortality rate – up to 50% in some studies.
Overall, 30% of CREs carry a carbapenemase – an enzyme that can make them resistant to carbapenem antibiotics. The genes for this are readily transferable between bacteria and help account for their spread in hospitals.
But in this study, published in the American Journal of Infection Control, of the 12 isolates that underwent whole-genome sequencing, 42% of the CA-CRE isolates carried the carbapenemase gene. Lead author Sandra Bulens, MPH, a health scientist in the CDC’s division of health care quality promotion, said in an interview, “The findings highlight the potential for CP-CRE to move from health care settings into the community. The fact that 5 of the 12 isolates harbored a carbapenemase gene introduces new challenges for controlling spread of CP-CRE.”
CDC researchers analyzed data from eight U.S. metropolitan areas between 2012 and 2015 as part of the CDC’s Emerging Infections Program (EIP) health care–associated infections – community interface activity, which conducts surveillance for CRE and other drug-resistant gram-negative bacteria. Cases of CA-CRE were compared with HCA-CRE, with 1499 cases in 1,194 case-patients being analyzed. Though Klebsiella pneumoniae was the most common isolate, there were some differences between metropolitan areas.
The incidence of CRE cases per 100,000 population was 2.96 (95% confidence interval, 2.81-3.11) overall and 0.29 (95% CI, 0.25-0.25) for CA-CRE. Most CA-CRE cases were in White persons (73%) and women (84%). Urine cultures were the source of 98% of all CA-CRE cases, compared with 86% of HCA-CRE cases (P < .001). Though small numbers, the numbers of patients with CA-CRE without apparent underlying medical condition (n = 51; 37%) was greater when compared with patients with HCA-CRE (n = 36; 3%; P < .001).
Asked for independent comment, Lance Price, PhD, of George Washington University and the founding director of GW’s Antibiotic Resistance Action Center, Washington, said, “what’s striking about these data is that: ‘Who is the front line, at least in the United States for CRE?’ It’s women, older women. ... At some point, we have to frame drug resistance as a women’s health issue.”
Dr. Price noted that the 10% of patients with CA-CRE acquired it in the community. “I would argue that probably none of them had any idea, because there’s this silent community epidemic,” he said. “It’s asymptomatic carriage and transmission in the community. Somebody can be this walking reservoir of these really dangerous bacteria and have no idea.”
This is an increasingly serious problem for women, Dr. Price said, because, “with a community-acquired bladder infection, you’re going to call your doctor or go to an urgent care, and they’re not going to test you. They’re going to guess what you have, and they’re going to prescribe an antibiotic, and that antibiotic is going to fail. So then your bladder infection continues, and then you wait a few more days, and you start to get flank pain and kidney infection. ... If you start getting a fever, they might admit you. They are going to start treating you immediately, and they might miss it because you’ve got this organism that’s resistant to all the best antibiotics. ... The gateway to the blood is the UTI.”
Because of such empiric treatment and increasing resistance, the risk for treatment failure is quite high, especially for older women. Ms. Bulens, however, said that, “[although] 10% of CRE were in persons without health care risk factors, the proportion of all UTIs in this population that are CRE is going to be very, very small.”
This study involved cultures from 2012 to 2015. Before the pandemic, from 2012 to 2017, U.S. deaths from antibiotic resistance fell by 18% overall and by 30% in hospitals.
But in the first year of the COVID-19 pandemic, there was a 15% increase in infections and deaths from antibiotic-resistant (AMR), hospital-acquired bacteria. In 2020, 29,400 patients died from AMR infections. There was a 78% increase in carbapenem-resistant Acinetobacter baumannii health care–associated infections, a 35% increase in carbapenem-resistant Enterobacterales, and 32% increases in both multidrug-resistant Pseudomonas aeruginosa and extended-spectrum beta-lactamase–producing Enterobacterales. Aside from gram-negative bacteria, methicillin-resistant Staphylococcus aureus rose 13%, and Candida auris rose 60%. But owing to limited surveillance, recent sound figures are lacking.
Ms. Bulens and Dr. Price reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study from the Centers for Disease Control and Prevention found that
Traditionally, CRE has been thought of as a nosocomial infection, acquired in a hospital or other health care facility (nursing home, long-term acute care hospital, dialysis center, etc.). This is the first population-level study to show otherwise, with fully 10% of the CRE isolates found to be community acquired.
CREs are a group of multidrug-resistant bacteria considered an urgent health threat by the CDC because they can rapidly spread between patients, especially those who are most seriously ill and vulnerable, and because they are so difficult to treat. These patients often require treatment with toxic antibiotics, such as colistin, and carry a high mortality rate – up to 50% in some studies.
Overall, 30% of CREs carry a carbapenemase – an enzyme that can make them resistant to carbapenem antibiotics. The genes for this are readily transferable between bacteria and help account for their spread in hospitals.
But in this study, published in the American Journal of Infection Control, of the 12 isolates that underwent whole-genome sequencing, 42% of the CA-CRE isolates carried the carbapenemase gene. Lead author Sandra Bulens, MPH, a health scientist in the CDC’s division of health care quality promotion, said in an interview, “The findings highlight the potential for CP-CRE to move from health care settings into the community. The fact that 5 of the 12 isolates harbored a carbapenemase gene introduces new challenges for controlling spread of CP-CRE.”
CDC researchers analyzed data from eight U.S. metropolitan areas between 2012 and 2015 as part of the CDC’s Emerging Infections Program (EIP) health care–associated infections – community interface activity, which conducts surveillance for CRE and other drug-resistant gram-negative bacteria. Cases of CA-CRE were compared with HCA-CRE, with 1499 cases in 1,194 case-patients being analyzed. Though Klebsiella pneumoniae was the most common isolate, there were some differences between metropolitan areas.
The incidence of CRE cases per 100,000 population was 2.96 (95% confidence interval, 2.81-3.11) overall and 0.29 (95% CI, 0.25-0.25) for CA-CRE. Most CA-CRE cases were in White persons (73%) and women (84%). Urine cultures were the source of 98% of all CA-CRE cases, compared with 86% of HCA-CRE cases (P < .001). Though small numbers, the numbers of patients with CA-CRE without apparent underlying medical condition (n = 51; 37%) was greater when compared with patients with HCA-CRE (n = 36; 3%; P < .001).
Asked for independent comment, Lance Price, PhD, of George Washington University and the founding director of GW’s Antibiotic Resistance Action Center, Washington, said, “what’s striking about these data is that: ‘Who is the front line, at least in the United States for CRE?’ It’s women, older women. ... At some point, we have to frame drug resistance as a women’s health issue.”
Dr. Price noted that the 10% of patients with CA-CRE acquired it in the community. “I would argue that probably none of them had any idea, because there’s this silent community epidemic,” he said. “It’s asymptomatic carriage and transmission in the community. Somebody can be this walking reservoir of these really dangerous bacteria and have no idea.”
This is an increasingly serious problem for women, Dr. Price said, because, “with a community-acquired bladder infection, you’re going to call your doctor or go to an urgent care, and they’re not going to test you. They’re going to guess what you have, and they’re going to prescribe an antibiotic, and that antibiotic is going to fail. So then your bladder infection continues, and then you wait a few more days, and you start to get flank pain and kidney infection. ... If you start getting a fever, they might admit you. They are going to start treating you immediately, and they might miss it because you’ve got this organism that’s resistant to all the best antibiotics. ... The gateway to the blood is the UTI.”
Because of such empiric treatment and increasing resistance, the risk for treatment failure is quite high, especially for older women. Ms. Bulens, however, said that, “[although] 10% of CRE were in persons without health care risk factors, the proportion of all UTIs in this population that are CRE is going to be very, very small.”
This study involved cultures from 2012 to 2015. Before the pandemic, from 2012 to 2017, U.S. deaths from antibiotic resistance fell by 18% overall and by 30% in hospitals.
But in the first year of the COVID-19 pandemic, there was a 15% increase in infections and deaths from antibiotic-resistant (AMR), hospital-acquired bacteria. In 2020, 29,400 patients died from AMR infections. There was a 78% increase in carbapenem-resistant Acinetobacter baumannii health care–associated infections, a 35% increase in carbapenem-resistant Enterobacterales, and 32% increases in both multidrug-resistant Pseudomonas aeruginosa and extended-spectrum beta-lactamase–producing Enterobacterales. Aside from gram-negative bacteria, methicillin-resistant Staphylococcus aureus rose 13%, and Candida auris rose 60%. But owing to limited surveillance, recent sound figures are lacking.
Ms. Bulens and Dr. Price reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF INFECTION CONTROL
White House declares monkeypox a public health emergency
There have been more than 6,600 reported cases of the disease in the United States, up from less than 5,000 cases reported last week.
“This public health emergency will allow us to explore additional strategies to get vaccines and treatments more quickly out in the affected communities. And it will allow us to get more data from jurisdictions so we can effectively track and attack this outbreak,” Robert Fenton, who was named as the national monkeypox response coordinator this week, said at a news briefing Aug. 4.
Those who catch the virus usually have fever-like symptoms, followed by red lesions on the body that can raise and develop pus. Those at highest risk of monkeypox are gay and bisexual men, as well as men who have sex with other men. There are between 1.6 million and 1.7 million Americans in this high-risk group, Health and Human Services Secretary Xavier Becerra said at the briefing.
The Jynneos vaccine is being distributed to protect against monkeypox and can prevent severe symptoms. It’s mostly going to those with the greatest risk of catching the virus.
Last week, the Biden administration made over 1.1 million doses of the Jynneos vaccine available – of which over 600,000 doses have already been distributed across the country – and have secured over 6.9 million Jynneos doses altogether.
Around 786,000 vaccines have already been allocated, and the first doses were shipped this week. States will be able to order more doses beginning Aug. 15. If a state has used 90% or more of its vaccine supply, it will be eligible to order more doses before Aug. 15, according to Dawn O’Connell, JD, assistant secretary for preparedness and response at the U.S. Department of Health and Human Services.
An additional 150,000 doses will be added to the national stockpile in September, with more doses to come later this year, Ms. O’Connell says.
The administration is also stressing the importance of monkeypox testing and says it can now distribute 80,000 monkeypox tests per week.
An antiviral drug – known as TPOXX – is also available to treat severe cases of monkeypox. Around 1,700,000 doses are available in the Strategic National Stockpile, public health officials say.
“We are prepared to take our response to the next level, and we urge every American to take this seriously and to take responsibility to help us tackle this virus,” Secretary Becerra told reporters.
The White House says it will continue reaching out to doctors, public health partners, LGBTQ advocates, and other impacted communities.
“The public health emergency further raises awareness about monkeypox, which will encourage clinicians to test for it,” Rochelle Walensky, MD, director of the Centers for Disease Control and Prevention, said at the briefing.
This week, President Joe Biden appointed a new White House monkeypox response team. Besides Mr. Fenton as the response coordinator, Demetre Daskalakis, MD, will serve as the White House national monkeypox response deputy coordinator. He is the director of the CDC’s Division of HIV Prevention.
“This virus is moving fast. This is a unique outbreak that is spreading faster than previous outbreaks,” Mr. Fenton told reporters Aug. 4. “That’s why the president asked me to explore everything we can do to combat monkeypox and protect communities at risk.”
This article was updated 8/4/22.
There have been more than 6,600 reported cases of the disease in the United States, up from less than 5,000 cases reported last week.
“This public health emergency will allow us to explore additional strategies to get vaccines and treatments more quickly out in the affected communities. And it will allow us to get more data from jurisdictions so we can effectively track and attack this outbreak,” Robert Fenton, who was named as the national monkeypox response coordinator this week, said at a news briefing Aug. 4.
Those who catch the virus usually have fever-like symptoms, followed by red lesions on the body that can raise and develop pus. Those at highest risk of monkeypox are gay and bisexual men, as well as men who have sex with other men. There are between 1.6 million and 1.7 million Americans in this high-risk group, Health and Human Services Secretary Xavier Becerra said at the briefing.
The Jynneos vaccine is being distributed to protect against monkeypox and can prevent severe symptoms. It’s mostly going to those with the greatest risk of catching the virus.
Last week, the Biden administration made over 1.1 million doses of the Jynneos vaccine available – of which over 600,000 doses have already been distributed across the country – and have secured over 6.9 million Jynneos doses altogether.
Around 786,000 vaccines have already been allocated, and the first doses were shipped this week. States will be able to order more doses beginning Aug. 15. If a state has used 90% or more of its vaccine supply, it will be eligible to order more doses before Aug. 15, according to Dawn O’Connell, JD, assistant secretary for preparedness and response at the U.S. Department of Health and Human Services.
An additional 150,000 doses will be added to the national stockpile in September, with more doses to come later this year, Ms. O’Connell says.
The administration is also stressing the importance of monkeypox testing and says it can now distribute 80,000 monkeypox tests per week.
An antiviral drug – known as TPOXX – is also available to treat severe cases of monkeypox. Around 1,700,000 doses are available in the Strategic National Stockpile, public health officials say.
“We are prepared to take our response to the next level, and we urge every American to take this seriously and to take responsibility to help us tackle this virus,” Secretary Becerra told reporters.
The White House says it will continue reaching out to doctors, public health partners, LGBTQ advocates, and other impacted communities.
“The public health emergency further raises awareness about monkeypox, which will encourage clinicians to test for it,” Rochelle Walensky, MD, director of the Centers for Disease Control and Prevention, said at the briefing.
This week, President Joe Biden appointed a new White House monkeypox response team. Besides Mr. Fenton as the response coordinator, Demetre Daskalakis, MD, will serve as the White House national monkeypox response deputy coordinator. He is the director of the CDC’s Division of HIV Prevention.
“This virus is moving fast. This is a unique outbreak that is spreading faster than previous outbreaks,” Mr. Fenton told reporters Aug. 4. “That’s why the president asked me to explore everything we can do to combat monkeypox and protect communities at risk.”
This article was updated 8/4/22.
There have been more than 6,600 reported cases of the disease in the United States, up from less than 5,000 cases reported last week.
“This public health emergency will allow us to explore additional strategies to get vaccines and treatments more quickly out in the affected communities. And it will allow us to get more data from jurisdictions so we can effectively track and attack this outbreak,” Robert Fenton, who was named as the national monkeypox response coordinator this week, said at a news briefing Aug. 4.
Those who catch the virus usually have fever-like symptoms, followed by red lesions on the body that can raise and develop pus. Those at highest risk of monkeypox are gay and bisexual men, as well as men who have sex with other men. There are between 1.6 million and 1.7 million Americans in this high-risk group, Health and Human Services Secretary Xavier Becerra said at the briefing.
The Jynneos vaccine is being distributed to protect against monkeypox and can prevent severe symptoms. It’s mostly going to those with the greatest risk of catching the virus.
Last week, the Biden administration made over 1.1 million doses of the Jynneos vaccine available – of which over 600,000 doses have already been distributed across the country – and have secured over 6.9 million Jynneos doses altogether.
Around 786,000 vaccines have already been allocated, and the first doses were shipped this week. States will be able to order more doses beginning Aug. 15. If a state has used 90% or more of its vaccine supply, it will be eligible to order more doses before Aug. 15, according to Dawn O’Connell, JD, assistant secretary for preparedness and response at the U.S. Department of Health and Human Services.
An additional 150,000 doses will be added to the national stockpile in September, with more doses to come later this year, Ms. O’Connell says.
The administration is also stressing the importance of monkeypox testing and says it can now distribute 80,000 monkeypox tests per week.
An antiviral drug – known as TPOXX – is also available to treat severe cases of monkeypox. Around 1,700,000 doses are available in the Strategic National Stockpile, public health officials say.
“We are prepared to take our response to the next level, and we urge every American to take this seriously and to take responsibility to help us tackle this virus,” Secretary Becerra told reporters.
The White House says it will continue reaching out to doctors, public health partners, LGBTQ advocates, and other impacted communities.
“The public health emergency further raises awareness about monkeypox, which will encourage clinicians to test for it,” Rochelle Walensky, MD, director of the Centers for Disease Control and Prevention, said at the briefing.
This week, President Joe Biden appointed a new White House monkeypox response team. Besides Mr. Fenton as the response coordinator, Demetre Daskalakis, MD, will serve as the White House national monkeypox response deputy coordinator. He is the director of the CDC’s Division of HIV Prevention.
“This virus is moving fast. This is a unique outbreak that is spreading faster than previous outbreaks,” Mr. Fenton told reporters Aug. 4. “That’s why the president asked me to explore everything we can do to combat monkeypox and protect communities at risk.”
This article was updated 8/4/22.
New Omicron COVID boosters coming soon: What to know now
– a month ahead of schedule, the Biden administration announced this week.
Moderna has signed a $1.74 billion federal contract to supply 66 million initial doses of the “bivalent” booster, which includes the original “ancestral” virus strain and elements of the Omicron BA.4 and BA.5 variants. Pfizer also announced a $3.2 billion U.S. agreement for another 105 million shots. Both vaccine suppliers have signed options to provide millions more boosters in the months ahead.
About 83.5% of Americans have received at least one COVID-19 shot, with 71.5% fully vaccinated with the initial series, 48% receiving one booster shot, and 31% two boosters, according to the CDC. With about 130,000 new COVID cases per day, and about 440 deaths, officials say the updated boosters may help rein in those figures by targeting the highly transmissible and widely circulating Omicron strains.
Federal health officials are still hammering out details of guidelines and recommendations of who should get the boosters, which are expected to come from the CDC and FDA. For now, authorities have decided not to expand eligibility for second boosters of the existing vaccines – now recommended only for adults over 50 and those 12 and older with immune deficiencies. Children 5 through 11 are advised to receive a single booster, 5 months after their initial vaccine series.
For a preview of what to expect from the CDC and FDA, this news organization spoke with Keri Althoff, PhD, an epidemiologist at Johns Hopkins University, Baltimore.
Q: Based on what we know now, who should be getting one of these new bivalent boosters?A: Of course, there is a process here regarding the specific recommendations, but it appears there will likely be a recommendation for all individuals to get this bivalent booster, similar to the first booster. And there will likely be a recommended time frame as to time since the last booster.
Right now, we have a recommendation for adults over the age of 50 or adults who are at higher risk for severe COVID-related illness [to get] a second booster. For them, there will probably be a timeline that says you should get the booster if you’re X amount of months or more from your second booster; or X amount of months or more from your first booster, if you’ve only had one.
Q: What about pregnant women or those being treated for chronic health conditions?A: I would imagine that once this bivalent booster becomes available, it will be recommended for all adults.
Q: And for children?A: That’s a good question. It’s something I have been digging into, [and] I think parents are really interested in this. Most kids, 5 and above, are supposed to be boosted with one shot right now, if they’re X amount of days from their primary vaccine series. Of course those 6 months to 4.99 years are not yet eligible [for boosters].
As a parent, I would love to see my children become eligible for the bivalent booster. It would be great if these boosters are conveying some additional protection that the kids could get access to before we send them off to school this fall. But there are questions as to whether or not that is going to happen.
Q: If you never received a booster, but only the preliminary vaccine series, do you need to get those earlier boosters before having the new bivalent booster shot?A: I don’t think they will likely make that a requirement – to restrict the bivalent booster only to those who are already boosted or up to date on their vaccines at the time the bivalent booster becomes available. But that will be up to the [CDC] vaccine recommendation committee to decide.
Q: Are there any new risks associated with these boosters, since they were developed so rapidly?A: No. We continue to monitor this technology, and with all the mRNA vaccines that have been delivered, you have seen all that monitoring play out with the detection, for example, of different forms of inflammation of the heart tissue and who that may impact. So, those monitoring systems work, and they work really, really well, so we can detect those things. And we know these vaccines are definitely safe.
Q: Some health experts are concerned “vaccine fatigue” will have an impact on the booster campaign. What’s your take?A: We have seen this fatigue in the proportion of individuals who are boosted with a first booster and even boosted with a second. But having those earlier boosters along with this new bivalent booster is important, because essentially, what we’re doing is really priming the immune system.
We’re trying to expedite the process of getting people’s immune system up to speed so that when the virus comes our way – as we know it will, because [of] these Omicron strains that are highly infectious and really whipping through our communities – we’re able to get the highest level of population immunity, you don’t end up in the hospital.
Q: What other challenges do you see in persuading Americans to get another round of boosters?A: One of the things that I’ve been hearing a lot, which I get very nervous about, is people saying: “Oh, I got fully vaccinated, I did or did not get the booster, and I had COVID anyway and it was really nothing, it didn’t feel like much to me, and so I’m not going to be boosted anymore.” We are not in a place quite yet where those guidelines are being rolled back in any way, shape, or form. We still have highly vulnerable people to severe disease and death in our communities, and we’re seeing hundreds of deaths every day.
There are consequences, even if it isn’t in severity of disease, meaning hospitalization and death. And let’s not let the actual quality of the vaccine being so successful that it can keep you out of the hospital. Don’t mistake that for “I don’t need another one.”
Q: Unlike the flu shot, which is reformulated each year to match circulating strains, the new COVID boosters offer protection against older strains as well as the newer ones. Why?A: It’s all about creating a broader immune response in individuals so that as more strains emerge, which they likely will, we can create a broader population immune response [to all strains]. Our individual bodies are seeing differences in these strains through vaccination that helps everyone stay healthy.
Q: There haven’t been clinical trials of these new mRNA boosters. How strong is the evidence that they will be effective against the emerging Omicron variants?A: There have been some studies – some great studies – looking at things like neutralizing antibodies, which we use as a surrogate for clinical trials. But that is not the same as studying the outcome of interest, which would be hospitalizations. So, part of the challenge is to be able to say: “Okay, this is what we know about the safety and effectiveness of the prior vaccines ... and how can we relate that to outcomes with these new boosters at an earlier stage [before] clinical data is available?”
Q: How long will the new boosters’ protections last – do we know yet?A: That timing is still a question, but of course what plays a big role in that is what COVID strains are circulating. If we prep these boosters that are Omicron specific, and then we have something totally new emerge ... we have to be more nimble because the variants are outpacing what we’re able to do.
This turns out to be a bit of a game of probability – the more infection we have, the more replication of the virus; the more replication, the more opportunity for mutations and subsequent variants.
Q: What about a combined flu-COVID vaccine; is that on the horizon?A: My children, who like most children do not like vaccines, always tell me: “Mom, why can’t they just put the influenza vaccine and the COVID vaccine into the same shot?” And I’m like: “Oh, from your lips to some scientist’s ears.”
At a time like this, where mRNA technology has totally disrupted what we can do with vaccines, in such a good way, I think we should push for the limits, because that would be incredible.
Q: If you’ve received a non-mRNA COVID vaccine, like those produced by Johnson & Johnson and Novavax, should you also get an mRNA booster?A: Right now, the CDC guidelines do state that if your primary vaccine series was not with an mRNA vaccine then being boosted with an mRNA is a fine thing to do, and it’s actually encouraged. So that’s not going to change with the bivalent booster.
Q: Is it okay to get a flu shot and a COVID booster at the same time, as the Centers for Disease Control and Prevention has recommended with past vaccines?A: I don’t anticipate there being recommendations against that. But I would also say watch for the recommendations that come out this fall on the bivalent boosters.
I do hope in the recommendations the CDC makes about the COVID boosters, they will say think about also getting your influenza vaccine, too. You could also get your COVID booster first, then by October get your influenza vaccine.
Q: Once you’re fully boosted, is it safe to stop wearing a mask, social distancing, avoiding crowded indoor spaces, and taking other precautions to avoid COVID-19?A: The virus is going to do what it does, which is infect whomever it can, and make them sick. So, if you see a lot of community transmission – you know who is ill with COVID in your kids’ schools, you know in your workplace and when people go out – that still signals there’s some increases in the circulation of virus. So, look at that to understand what your risk is.
If you know someone or have a colleague who is currently pregnant or immune suppressed, think about how you can protect them with mask-wearing, even if it’s just when you’re in one-on-one closed-door meetings with that individual.
So, your masking question is an important one, and it’s important for people to continue to hang onto those masks and wear them the week before you go see Grandma, for instance, to further reduce your risk so you don’t bring anything to here.
The high-level community risk nationwide is high right now. COVID is here.
A version of this article first appeared on WebMd.com.
– a month ahead of schedule, the Biden administration announced this week.
Moderna has signed a $1.74 billion federal contract to supply 66 million initial doses of the “bivalent” booster, which includes the original “ancestral” virus strain and elements of the Omicron BA.4 and BA.5 variants. Pfizer also announced a $3.2 billion U.S. agreement for another 105 million shots. Both vaccine suppliers have signed options to provide millions more boosters in the months ahead.
About 83.5% of Americans have received at least one COVID-19 shot, with 71.5% fully vaccinated with the initial series, 48% receiving one booster shot, and 31% two boosters, according to the CDC. With about 130,000 new COVID cases per day, and about 440 deaths, officials say the updated boosters may help rein in those figures by targeting the highly transmissible and widely circulating Omicron strains.
Federal health officials are still hammering out details of guidelines and recommendations of who should get the boosters, which are expected to come from the CDC and FDA. For now, authorities have decided not to expand eligibility for second boosters of the existing vaccines – now recommended only for adults over 50 and those 12 and older with immune deficiencies. Children 5 through 11 are advised to receive a single booster, 5 months after their initial vaccine series.
For a preview of what to expect from the CDC and FDA, this news organization spoke with Keri Althoff, PhD, an epidemiologist at Johns Hopkins University, Baltimore.
Q: Based on what we know now, who should be getting one of these new bivalent boosters?A: Of course, there is a process here regarding the specific recommendations, but it appears there will likely be a recommendation for all individuals to get this bivalent booster, similar to the first booster. And there will likely be a recommended time frame as to time since the last booster.
Right now, we have a recommendation for adults over the age of 50 or adults who are at higher risk for severe COVID-related illness [to get] a second booster. For them, there will probably be a timeline that says you should get the booster if you’re X amount of months or more from your second booster; or X amount of months or more from your first booster, if you’ve only had one.
Q: What about pregnant women or those being treated for chronic health conditions?A: I would imagine that once this bivalent booster becomes available, it will be recommended for all adults.
Q: And for children?A: That’s a good question. It’s something I have been digging into, [and] I think parents are really interested in this. Most kids, 5 and above, are supposed to be boosted with one shot right now, if they’re X amount of days from their primary vaccine series. Of course those 6 months to 4.99 years are not yet eligible [for boosters].
As a parent, I would love to see my children become eligible for the bivalent booster. It would be great if these boosters are conveying some additional protection that the kids could get access to before we send them off to school this fall. But there are questions as to whether or not that is going to happen.
Q: If you never received a booster, but only the preliminary vaccine series, do you need to get those earlier boosters before having the new bivalent booster shot?A: I don’t think they will likely make that a requirement – to restrict the bivalent booster only to those who are already boosted or up to date on their vaccines at the time the bivalent booster becomes available. But that will be up to the [CDC] vaccine recommendation committee to decide.
Q: Are there any new risks associated with these boosters, since they were developed so rapidly?A: No. We continue to monitor this technology, and with all the mRNA vaccines that have been delivered, you have seen all that monitoring play out with the detection, for example, of different forms of inflammation of the heart tissue and who that may impact. So, those monitoring systems work, and they work really, really well, so we can detect those things. And we know these vaccines are definitely safe.
Q: Some health experts are concerned “vaccine fatigue” will have an impact on the booster campaign. What’s your take?A: We have seen this fatigue in the proportion of individuals who are boosted with a first booster and even boosted with a second. But having those earlier boosters along with this new bivalent booster is important, because essentially, what we’re doing is really priming the immune system.
We’re trying to expedite the process of getting people’s immune system up to speed so that when the virus comes our way – as we know it will, because [of] these Omicron strains that are highly infectious and really whipping through our communities – we’re able to get the highest level of population immunity, you don’t end up in the hospital.
Q: What other challenges do you see in persuading Americans to get another round of boosters?A: One of the things that I’ve been hearing a lot, which I get very nervous about, is people saying: “Oh, I got fully vaccinated, I did or did not get the booster, and I had COVID anyway and it was really nothing, it didn’t feel like much to me, and so I’m not going to be boosted anymore.” We are not in a place quite yet where those guidelines are being rolled back in any way, shape, or form. We still have highly vulnerable people to severe disease and death in our communities, and we’re seeing hundreds of deaths every day.
There are consequences, even if it isn’t in severity of disease, meaning hospitalization and death. And let’s not let the actual quality of the vaccine being so successful that it can keep you out of the hospital. Don’t mistake that for “I don’t need another one.”
Q: Unlike the flu shot, which is reformulated each year to match circulating strains, the new COVID boosters offer protection against older strains as well as the newer ones. Why?A: It’s all about creating a broader immune response in individuals so that as more strains emerge, which they likely will, we can create a broader population immune response [to all strains]. Our individual bodies are seeing differences in these strains through vaccination that helps everyone stay healthy.
Q: There haven’t been clinical trials of these new mRNA boosters. How strong is the evidence that they will be effective against the emerging Omicron variants?A: There have been some studies – some great studies – looking at things like neutralizing antibodies, which we use as a surrogate for clinical trials. But that is not the same as studying the outcome of interest, which would be hospitalizations. So, part of the challenge is to be able to say: “Okay, this is what we know about the safety and effectiveness of the prior vaccines ... and how can we relate that to outcomes with these new boosters at an earlier stage [before] clinical data is available?”
Q: How long will the new boosters’ protections last – do we know yet?A: That timing is still a question, but of course what plays a big role in that is what COVID strains are circulating. If we prep these boosters that are Omicron specific, and then we have something totally new emerge ... we have to be more nimble because the variants are outpacing what we’re able to do.
This turns out to be a bit of a game of probability – the more infection we have, the more replication of the virus; the more replication, the more opportunity for mutations and subsequent variants.
Q: What about a combined flu-COVID vaccine; is that on the horizon?A: My children, who like most children do not like vaccines, always tell me: “Mom, why can’t they just put the influenza vaccine and the COVID vaccine into the same shot?” And I’m like: “Oh, from your lips to some scientist’s ears.”
At a time like this, where mRNA technology has totally disrupted what we can do with vaccines, in such a good way, I think we should push for the limits, because that would be incredible.
Q: If you’ve received a non-mRNA COVID vaccine, like those produced by Johnson & Johnson and Novavax, should you also get an mRNA booster?A: Right now, the CDC guidelines do state that if your primary vaccine series was not with an mRNA vaccine then being boosted with an mRNA is a fine thing to do, and it’s actually encouraged. So that’s not going to change with the bivalent booster.
Q: Is it okay to get a flu shot and a COVID booster at the same time, as the Centers for Disease Control and Prevention has recommended with past vaccines?A: I don’t anticipate there being recommendations against that. But I would also say watch for the recommendations that come out this fall on the bivalent boosters.
I do hope in the recommendations the CDC makes about the COVID boosters, they will say think about also getting your influenza vaccine, too. You could also get your COVID booster first, then by October get your influenza vaccine.
Q: Once you’re fully boosted, is it safe to stop wearing a mask, social distancing, avoiding crowded indoor spaces, and taking other precautions to avoid COVID-19?A: The virus is going to do what it does, which is infect whomever it can, and make them sick. So, if you see a lot of community transmission – you know who is ill with COVID in your kids’ schools, you know in your workplace and when people go out – that still signals there’s some increases in the circulation of virus. So, look at that to understand what your risk is.
If you know someone or have a colleague who is currently pregnant or immune suppressed, think about how you can protect them with mask-wearing, even if it’s just when you’re in one-on-one closed-door meetings with that individual.
So, your masking question is an important one, and it’s important for people to continue to hang onto those masks and wear them the week before you go see Grandma, for instance, to further reduce your risk so you don’t bring anything to here.
The high-level community risk nationwide is high right now. COVID is here.
A version of this article first appeared on WebMd.com.
– a month ahead of schedule, the Biden administration announced this week.
Moderna has signed a $1.74 billion federal contract to supply 66 million initial doses of the “bivalent” booster, which includes the original “ancestral” virus strain and elements of the Omicron BA.4 and BA.5 variants. Pfizer also announced a $3.2 billion U.S. agreement for another 105 million shots. Both vaccine suppliers have signed options to provide millions more boosters in the months ahead.
About 83.5% of Americans have received at least one COVID-19 shot, with 71.5% fully vaccinated with the initial series, 48% receiving one booster shot, and 31% two boosters, according to the CDC. With about 130,000 new COVID cases per day, and about 440 deaths, officials say the updated boosters may help rein in those figures by targeting the highly transmissible and widely circulating Omicron strains.
Federal health officials are still hammering out details of guidelines and recommendations of who should get the boosters, which are expected to come from the CDC and FDA. For now, authorities have decided not to expand eligibility for second boosters of the existing vaccines – now recommended only for adults over 50 and those 12 and older with immune deficiencies. Children 5 through 11 are advised to receive a single booster, 5 months after their initial vaccine series.
For a preview of what to expect from the CDC and FDA, this news organization spoke with Keri Althoff, PhD, an epidemiologist at Johns Hopkins University, Baltimore.
Q: Based on what we know now, who should be getting one of these new bivalent boosters?A: Of course, there is a process here regarding the specific recommendations, but it appears there will likely be a recommendation for all individuals to get this bivalent booster, similar to the first booster. And there will likely be a recommended time frame as to time since the last booster.
Right now, we have a recommendation for adults over the age of 50 or adults who are at higher risk for severe COVID-related illness [to get] a second booster. For them, there will probably be a timeline that says you should get the booster if you’re X amount of months or more from your second booster; or X amount of months or more from your first booster, if you’ve only had one.
Q: What about pregnant women or those being treated for chronic health conditions?A: I would imagine that once this bivalent booster becomes available, it will be recommended for all adults.
Q: And for children?A: That’s a good question. It’s something I have been digging into, [and] I think parents are really interested in this. Most kids, 5 and above, are supposed to be boosted with one shot right now, if they’re X amount of days from their primary vaccine series. Of course those 6 months to 4.99 years are not yet eligible [for boosters].
As a parent, I would love to see my children become eligible for the bivalent booster. It would be great if these boosters are conveying some additional protection that the kids could get access to before we send them off to school this fall. But there are questions as to whether or not that is going to happen.
Q: If you never received a booster, but only the preliminary vaccine series, do you need to get those earlier boosters before having the new bivalent booster shot?A: I don’t think they will likely make that a requirement – to restrict the bivalent booster only to those who are already boosted or up to date on their vaccines at the time the bivalent booster becomes available. But that will be up to the [CDC] vaccine recommendation committee to decide.
Q: Are there any new risks associated with these boosters, since they were developed so rapidly?A: No. We continue to monitor this technology, and with all the mRNA vaccines that have been delivered, you have seen all that monitoring play out with the detection, for example, of different forms of inflammation of the heart tissue and who that may impact. So, those monitoring systems work, and they work really, really well, so we can detect those things. And we know these vaccines are definitely safe.
Q: Some health experts are concerned “vaccine fatigue” will have an impact on the booster campaign. What’s your take?A: We have seen this fatigue in the proportion of individuals who are boosted with a first booster and even boosted with a second. But having those earlier boosters along with this new bivalent booster is important, because essentially, what we’re doing is really priming the immune system.
We’re trying to expedite the process of getting people’s immune system up to speed so that when the virus comes our way – as we know it will, because [of] these Omicron strains that are highly infectious and really whipping through our communities – we’re able to get the highest level of population immunity, you don’t end up in the hospital.
Q: What other challenges do you see in persuading Americans to get another round of boosters?A: One of the things that I’ve been hearing a lot, which I get very nervous about, is people saying: “Oh, I got fully vaccinated, I did or did not get the booster, and I had COVID anyway and it was really nothing, it didn’t feel like much to me, and so I’m not going to be boosted anymore.” We are not in a place quite yet where those guidelines are being rolled back in any way, shape, or form. We still have highly vulnerable people to severe disease and death in our communities, and we’re seeing hundreds of deaths every day.
There are consequences, even if it isn’t in severity of disease, meaning hospitalization and death. And let’s not let the actual quality of the vaccine being so successful that it can keep you out of the hospital. Don’t mistake that for “I don’t need another one.”
Q: Unlike the flu shot, which is reformulated each year to match circulating strains, the new COVID boosters offer protection against older strains as well as the newer ones. Why?A: It’s all about creating a broader immune response in individuals so that as more strains emerge, which they likely will, we can create a broader population immune response [to all strains]. Our individual bodies are seeing differences in these strains through vaccination that helps everyone stay healthy.
Q: There haven’t been clinical trials of these new mRNA boosters. How strong is the evidence that they will be effective against the emerging Omicron variants?A: There have been some studies – some great studies – looking at things like neutralizing antibodies, which we use as a surrogate for clinical trials. But that is not the same as studying the outcome of interest, which would be hospitalizations. So, part of the challenge is to be able to say: “Okay, this is what we know about the safety and effectiveness of the prior vaccines ... and how can we relate that to outcomes with these new boosters at an earlier stage [before] clinical data is available?”
Q: How long will the new boosters’ protections last – do we know yet?A: That timing is still a question, but of course what plays a big role in that is what COVID strains are circulating. If we prep these boosters that are Omicron specific, and then we have something totally new emerge ... we have to be more nimble because the variants are outpacing what we’re able to do.
This turns out to be a bit of a game of probability – the more infection we have, the more replication of the virus; the more replication, the more opportunity for mutations and subsequent variants.
Q: What about a combined flu-COVID vaccine; is that on the horizon?A: My children, who like most children do not like vaccines, always tell me: “Mom, why can’t they just put the influenza vaccine and the COVID vaccine into the same shot?” And I’m like: “Oh, from your lips to some scientist’s ears.”
At a time like this, where mRNA technology has totally disrupted what we can do with vaccines, in such a good way, I think we should push for the limits, because that would be incredible.
Q: If you’ve received a non-mRNA COVID vaccine, like those produced by Johnson & Johnson and Novavax, should you also get an mRNA booster?A: Right now, the CDC guidelines do state that if your primary vaccine series was not with an mRNA vaccine then being boosted with an mRNA is a fine thing to do, and it’s actually encouraged. So that’s not going to change with the bivalent booster.
Q: Is it okay to get a flu shot and a COVID booster at the same time, as the Centers for Disease Control and Prevention has recommended with past vaccines?A: I don’t anticipate there being recommendations against that. But I would also say watch for the recommendations that come out this fall on the bivalent boosters.
I do hope in the recommendations the CDC makes about the COVID boosters, they will say think about also getting your influenza vaccine, too. You could also get your COVID booster first, then by October get your influenza vaccine.
Q: Once you’re fully boosted, is it safe to stop wearing a mask, social distancing, avoiding crowded indoor spaces, and taking other precautions to avoid COVID-19?A: The virus is going to do what it does, which is infect whomever it can, and make them sick. So, if you see a lot of community transmission – you know who is ill with COVID in your kids’ schools, you know in your workplace and when people go out – that still signals there’s some increases in the circulation of virus. So, look at that to understand what your risk is.
If you know someone or have a colleague who is currently pregnant or immune suppressed, think about how you can protect them with mask-wearing, even if it’s just when you’re in one-on-one closed-door meetings with that individual.
So, your masking question is an important one, and it’s important for people to continue to hang onto those masks and wear them the week before you go see Grandma, for instance, to further reduce your risk so you don’t bring anything to here.
The high-level community risk nationwide is high right now. COVID is here.
A version of this article first appeared on WebMd.com.
Should patients undergoing surgical treatment for cervical lesions also receive an HPV vaccination?
Human papillomavirus (HPV) vaccine given around the time women have surgery for precancerous cervical lesions might lead to a reduction in the risk of lesions returning, as well as other HPV-related diseases, but the effects of this remain unclear.
The authors of the new study, published in The BMJ, explained that women who have been treated for high-grade cervical intra-epithelial neoplasia (CIN) have a “lifelong residual high risk of cervical cancer and other malignancies related to HPV infection,” and some research suggests that giving a preventive HPV vaccine alongside treatment for CIN might help to “reduce the risk in these women.”
HPV vaccination is highly effective at preventing the development of precancerous cervical lesions, CIN, and in the U.K., HPV vaccination is offered to girls and boys around the age of 12 or 13.
Eluned Hughes, head of information and engagement at Jo’s Cervical Cancer Trust, said: “Recent evidence has found that cases of cervical cancer have fallen 87% since the introduction of the HPV vaccine program in U.K. schools in 2008.”
“However, women over the age of 27, for whom the vaccine was not available, remain at increased risk of cervical cancer,” she highlighted.
Significant risk of bias and scarcity of data
In the study, researchers set out to explore the efficacy of HPV vaccination on the risk of HPV infection and recurrent diseases related to HPV infection in individuals undergoing local surgical treatment of preinvasive genital disease.
The systematic review and meta-analysis, led by researchers at Imperial College London, screened data from PubMed (Medline), Scopus, Cochrane, Web of Science, and ClinicalTrials.gov from inception to March 31, 2021.
The researchers analyzed the results of 18 studies – two randomized controlled trials (RCTs), 12 observational studies, and four post-hoc analyses of RCTs.
The authors said that the two RCTs were classified as low risk of bias, while in the observational studies and post-hoc analyses, risk of bias was moderate for seven, serious for seven, and critical for two. Average length of follow-up was 36 months.
There was a reduction of 57% in the risk of recurrence of high-grade pre-invasive disease (CIN2+) in individuals who were vaccinated, compared with those who were not vaccinated. “The effect estimate was “even more pronounced” – a relative 74% reduction – when the risk of recurrence of CIN2+ was assessed for disease related to the two high-risk HPV types – HPV16 and HPV18,” explained the authors.
However, the researchers noted that these effects are unclear because of the “scarcity of data” and the “moderate to high overall risk of bias” of the available studies.
Quality of evidence inconclusive – more trials needed
With regards to CIN3, the risk of recurrence of was also reduced in patients who were vaccinated, but there was a high level of uncertainty about the quality of this evidence, cautioned the authors.
Evidence was also lacking on the benefit of HPV vaccination for recurrence of vulvar, vaginal, and anal lesions, as well as genital warts.
Analysis of the post-hoc studies from randomized controlled trial data with historic vaccination at randomization before the development of the disease reported inconsistent results, the authors said.
Several study limitations were acknowledged by the authors, including that most of the studies were observational, of low to moderate quality, and with relatively short follow-up times, which they pointed out prevented assessment of long-term effects. In addition, the average age of participants was not provided in most studies, and factors such as smoking – associated with a higher risk of recurrence – were not controlled for in many studies.
“HPV vaccination might reduce the risk of recurrence of CIN, in particular when related to HPV16 or HPV18, in women treated with local excision,” they concluded. However, they cautioned that “quality of evidence indicated that the data were inconclusive.”
“Large, appropriately powered, randomized controlled trials are required to establish the effectiveness of adjuvant HPV vaccination at the time of local surgical treatment of CIN,” they recommended.
“Given that the incidence of recurrence of high-grade disease is low in quality assured national screening programs, such as in the United Kingdom, absolute risks and a cost effectiveness analysis would be important in determining the implementation strategy of HPV vaccination after treatment,” the authors said.
Ms. Hughes said that the charity was pleased to see emerging research into the value of using the HPV vaccine to prevent the recurrence of cervical cell changes. She said that the charity looks forward to seeing “further large-scale studies into the effectiveness of this method.”
In the meantime, the charity encourages all women and other people with a cervix to attend their cervical screening and for young people to have the HPV vaccination when invited, as “these are the best tools we currently have to prevent cervical cancer,” she said.
A version of this article first appeared on Medscape UK.
Human papillomavirus (HPV) vaccine given around the time women have surgery for precancerous cervical lesions might lead to a reduction in the risk of lesions returning, as well as other HPV-related diseases, but the effects of this remain unclear.
The authors of the new study, published in The BMJ, explained that women who have been treated for high-grade cervical intra-epithelial neoplasia (CIN) have a “lifelong residual high risk of cervical cancer and other malignancies related to HPV infection,” and some research suggests that giving a preventive HPV vaccine alongside treatment for CIN might help to “reduce the risk in these women.”
HPV vaccination is highly effective at preventing the development of precancerous cervical lesions, CIN, and in the U.K., HPV vaccination is offered to girls and boys around the age of 12 or 13.
Eluned Hughes, head of information and engagement at Jo’s Cervical Cancer Trust, said: “Recent evidence has found that cases of cervical cancer have fallen 87% since the introduction of the HPV vaccine program in U.K. schools in 2008.”
“However, women over the age of 27, for whom the vaccine was not available, remain at increased risk of cervical cancer,” she highlighted.
Significant risk of bias and scarcity of data
In the study, researchers set out to explore the efficacy of HPV vaccination on the risk of HPV infection and recurrent diseases related to HPV infection in individuals undergoing local surgical treatment of preinvasive genital disease.
The systematic review and meta-analysis, led by researchers at Imperial College London, screened data from PubMed (Medline), Scopus, Cochrane, Web of Science, and ClinicalTrials.gov from inception to March 31, 2021.
The researchers analyzed the results of 18 studies – two randomized controlled trials (RCTs), 12 observational studies, and four post-hoc analyses of RCTs.
The authors said that the two RCTs were classified as low risk of bias, while in the observational studies and post-hoc analyses, risk of bias was moderate for seven, serious for seven, and critical for two. Average length of follow-up was 36 months.
There was a reduction of 57% in the risk of recurrence of high-grade pre-invasive disease (CIN2+) in individuals who were vaccinated, compared with those who were not vaccinated. “The effect estimate was “even more pronounced” – a relative 74% reduction – when the risk of recurrence of CIN2+ was assessed for disease related to the two high-risk HPV types – HPV16 and HPV18,” explained the authors.
However, the researchers noted that these effects are unclear because of the “scarcity of data” and the “moderate to high overall risk of bias” of the available studies.
Quality of evidence inconclusive – more trials needed
With regards to CIN3, the risk of recurrence of was also reduced in patients who were vaccinated, but there was a high level of uncertainty about the quality of this evidence, cautioned the authors.
Evidence was also lacking on the benefit of HPV vaccination for recurrence of vulvar, vaginal, and anal lesions, as well as genital warts.
Analysis of the post-hoc studies from randomized controlled trial data with historic vaccination at randomization before the development of the disease reported inconsistent results, the authors said.
Several study limitations were acknowledged by the authors, including that most of the studies were observational, of low to moderate quality, and with relatively short follow-up times, which they pointed out prevented assessment of long-term effects. In addition, the average age of participants was not provided in most studies, and factors such as smoking – associated with a higher risk of recurrence – were not controlled for in many studies.
“HPV vaccination might reduce the risk of recurrence of CIN, in particular when related to HPV16 or HPV18, in women treated with local excision,” they concluded. However, they cautioned that “quality of evidence indicated that the data were inconclusive.”
“Large, appropriately powered, randomized controlled trials are required to establish the effectiveness of adjuvant HPV vaccination at the time of local surgical treatment of CIN,” they recommended.
“Given that the incidence of recurrence of high-grade disease is low in quality assured national screening programs, such as in the United Kingdom, absolute risks and a cost effectiveness analysis would be important in determining the implementation strategy of HPV vaccination after treatment,” the authors said.
Ms. Hughes said that the charity was pleased to see emerging research into the value of using the HPV vaccine to prevent the recurrence of cervical cell changes. She said that the charity looks forward to seeing “further large-scale studies into the effectiveness of this method.”
In the meantime, the charity encourages all women and other people with a cervix to attend their cervical screening and for young people to have the HPV vaccination when invited, as “these are the best tools we currently have to prevent cervical cancer,” she said.
A version of this article first appeared on Medscape UK.
Human papillomavirus (HPV) vaccine given around the time women have surgery for precancerous cervical lesions might lead to a reduction in the risk of lesions returning, as well as other HPV-related diseases, but the effects of this remain unclear.
The authors of the new study, published in The BMJ, explained that women who have been treated for high-grade cervical intra-epithelial neoplasia (CIN) have a “lifelong residual high risk of cervical cancer and other malignancies related to HPV infection,” and some research suggests that giving a preventive HPV vaccine alongside treatment for CIN might help to “reduce the risk in these women.”
HPV vaccination is highly effective at preventing the development of precancerous cervical lesions, CIN, and in the U.K., HPV vaccination is offered to girls and boys around the age of 12 or 13.
Eluned Hughes, head of information and engagement at Jo’s Cervical Cancer Trust, said: “Recent evidence has found that cases of cervical cancer have fallen 87% since the introduction of the HPV vaccine program in U.K. schools in 2008.”
“However, women over the age of 27, for whom the vaccine was not available, remain at increased risk of cervical cancer,” she highlighted.
Significant risk of bias and scarcity of data
In the study, researchers set out to explore the efficacy of HPV vaccination on the risk of HPV infection and recurrent diseases related to HPV infection in individuals undergoing local surgical treatment of preinvasive genital disease.
The systematic review and meta-analysis, led by researchers at Imperial College London, screened data from PubMed (Medline), Scopus, Cochrane, Web of Science, and ClinicalTrials.gov from inception to March 31, 2021.
The researchers analyzed the results of 18 studies – two randomized controlled trials (RCTs), 12 observational studies, and four post-hoc analyses of RCTs.
The authors said that the two RCTs were classified as low risk of bias, while in the observational studies and post-hoc analyses, risk of bias was moderate for seven, serious for seven, and critical for two. Average length of follow-up was 36 months.
There was a reduction of 57% in the risk of recurrence of high-grade pre-invasive disease (CIN2+) in individuals who were vaccinated, compared with those who were not vaccinated. “The effect estimate was “even more pronounced” – a relative 74% reduction – when the risk of recurrence of CIN2+ was assessed for disease related to the two high-risk HPV types – HPV16 and HPV18,” explained the authors.
However, the researchers noted that these effects are unclear because of the “scarcity of data” and the “moderate to high overall risk of bias” of the available studies.
Quality of evidence inconclusive – more trials needed
With regards to CIN3, the risk of recurrence of was also reduced in patients who were vaccinated, but there was a high level of uncertainty about the quality of this evidence, cautioned the authors.
Evidence was also lacking on the benefit of HPV vaccination for recurrence of vulvar, vaginal, and anal lesions, as well as genital warts.
Analysis of the post-hoc studies from randomized controlled trial data with historic vaccination at randomization before the development of the disease reported inconsistent results, the authors said.
Several study limitations were acknowledged by the authors, including that most of the studies were observational, of low to moderate quality, and with relatively short follow-up times, which they pointed out prevented assessment of long-term effects. In addition, the average age of participants was not provided in most studies, and factors such as smoking – associated with a higher risk of recurrence – were not controlled for in many studies.
“HPV vaccination might reduce the risk of recurrence of CIN, in particular when related to HPV16 or HPV18, in women treated with local excision,” they concluded. However, they cautioned that “quality of evidence indicated that the data were inconclusive.”
“Large, appropriately powered, randomized controlled trials are required to establish the effectiveness of adjuvant HPV vaccination at the time of local surgical treatment of CIN,” they recommended.
“Given that the incidence of recurrence of high-grade disease is low in quality assured national screening programs, such as in the United Kingdom, absolute risks and a cost effectiveness analysis would be important in determining the implementation strategy of HPV vaccination after treatment,” the authors said.
Ms. Hughes said that the charity was pleased to see emerging research into the value of using the HPV vaccine to prevent the recurrence of cervical cell changes. She said that the charity looks forward to seeing “further large-scale studies into the effectiveness of this method.”
In the meantime, the charity encourages all women and other people with a cervix to attend their cervical screening and for young people to have the HPV vaccination when invited, as “these are the best tools we currently have to prevent cervical cancer,” she said.
A version of this article first appeared on Medscape UK.
COVID-19 and IPF: Fundamental similarities found
An AI-guided analysis of more than 1,000 human lung transcriptomic datasets found that COVID-19 resembles idiopathic pulmonary fibrosis (IPF) at a fundamental level, according to a study published in eBiomedicine, part of The Lancet Discovery Science.
In the aftermath of COVID-19, a significant number of patients develop a fibrotic lung disease, for which insights into pathogenesis, disease models, or treatment options are lacking, according to researchers Dr. Sinha and colleagues. This long-haul form of the disease culminates in a fibrotic type of interstitial lung disease (ILD). While the actual prevalence of post–COVID-19 ILD (PCLD) is still emerging, early analysis indicates that more than a third of COVID-19 survivors develop fibrotic abnormalities, according to the authors.
Previous research has shown that one of the important determinants for PCLD is the duration of disease. Among patients who developed fibrosis, approximately 4% of patients had a disease duration of less than 1 week; approximately 24% had a disease duration between 1 and 3 weeks; and around 61% had a disease duration longer than 3 weeks, the authors stated.
The lung transcriptomic datasets compared in their study were associated with various lung conditions. The researchers used two viral pandemic signatures (ViP and sViP) and one COVID lung-derived signature. They found that the resemblances included that COVID-19 recapitulates the gene expression patterns (ViP and IPF signatures), cytokine storm (IL15-centric), and the AT2 cytopathic changes, for example, injury, DNA damage, arrest in a transient, damage-induced progenitor state, and senescence-associated secretory phenotype (SASP).
In laboratory experiments, Dr. Sinha and colleagues were able to induce these same immunocytopathic features in preclinical COVID-19 models (human adult lung organoid and hamster) and to reverse them in the hamster model with effective anti–CoV-2 therapeutics.
PPI-network analyses pinpointed endoplasmic reticulum (ER) stress as one of the shared early triggers of both IPF and COVID-19, and immunohistochemistry studies validated the same in the lungs of deceased subjects with COVID-19 and the SARS-CoV-2–challenged hamster lungs. Additionally, lungs from transgenic mice, in which ER stress was induced specifically in the AT2 cells, faithfully recapitulated the host immune response and alveolar cytopathic changes that are induced by SARS-CoV-2.
stated corresponding author Pradipta Ghosh, MD, professor in the departments of medicine and cellular and molecular medicine, University of California, San Diego. “If proven in prospective studies, this biomarker could indicate who is at greatest risk for progressive fibrosis and may require lung transplantation,” she said in an interview.
Dr. Ghosh stated further, “When it comes to therapeutics in COVID lung or IPF, we also found that shared fundamental pathogenic mechanisms present excellent opportunities for developing therapeutics that can arrest the fibrogenic drivers in both diseases. One clue that emerged is a specific cytokine that is at the heart of the smoldering inflammation which is invariably associated with fibrosis. That is interleukin 15 [IL-15] and its receptor.” Dr. Ghosh observed that there are two Food and Drug Administration–approved drugs for IPF. “None are very effective in arresting this invariably fatal disease. Hence, finding better options to treat IPF is an urgent and an unmet need.”
Preclinical testing of hypotheses, Dr. Ghosh said, is next on the path to clinical trials. “We have the advantage of using human lung organoids (mini-lungs grown using stem cells) in a dish, adding additional cells to the system (like fibroblasts and immune cells), infecting them with the virus, or subjecting them to the IL-15 cytokine and monitoring lung fibrosis progression in a dish. Anti–IL-15 therapy can then be initiated to observe reversal of the fibrogenic cascade.” Hamsters have also been shown to provide appropriate models for mimicking lung fibrosis, Dr. Ghosh said.
“The report by Sinha and colleagues describes the fascinating similarities between drivers of post-COVID lung disease and idiopathic pulmonary fibrosis,” stated David Bowton, MD, professor emeritus, section on critical care, department of anesthesiology, Wake Forest University, Winston-Salem, N.C., in an interview. He added that, “Central to the mechanisms of induction of fibrosis in both disorders appears to be endoplasmic reticulum stress in alveolar type II cells (AT2). ER stress induces the unfolded protein response (UPR) that halts protein translation and promotes the degradation of misfolded proteins. Prolonged UPR can reprogram the cell or trigger apoptosis pathways. ER stress in the lung has been reported in a variety of cell lines including AT2 in IPF, bronchial and alveolar epithelial cells in asthma and [chronic obstructive pulmonary disease], and endothelial cells in pulmonary hypertension.”
Dr. Bowton commented further, including a caution, “Sinha and colleagues suggest that the identification of these gene signatures and mechanisms will be a fruitful avenue for developing effective therapeutics for IPF and other fibrotic lung diseases. I am hopeful that these data may offer clues that expedite this process. However, the redundancy of triggers for effector pathways in biologic systems argues that, even if successful, this will be [a] long and fraught process.”
The research study was supported by National Institutes of Health grants and funding from the Tobacco-Related Disease Research Program.
Dr. Sinha, Dr. Ghosh, and Dr. Bowton reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
An AI-guided analysis of more than 1,000 human lung transcriptomic datasets found that COVID-19 resembles idiopathic pulmonary fibrosis (IPF) at a fundamental level, according to a study published in eBiomedicine, part of The Lancet Discovery Science.
In the aftermath of COVID-19, a significant number of patients develop a fibrotic lung disease, for which insights into pathogenesis, disease models, or treatment options are lacking, according to researchers Dr. Sinha and colleagues. This long-haul form of the disease culminates in a fibrotic type of interstitial lung disease (ILD). While the actual prevalence of post–COVID-19 ILD (PCLD) is still emerging, early analysis indicates that more than a third of COVID-19 survivors develop fibrotic abnormalities, according to the authors.
Previous research has shown that one of the important determinants for PCLD is the duration of disease. Among patients who developed fibrosis, approximately 4% of patients had a disease duration of less than 1 week; approximately 24% had a disease duration between 1 and 3 weeks; and around 61% had a disease duration longer than 3 weeks, the authors stated.
The lung transcriptomic datasets compared in their study were associated with various lung conditions. The researchers used two viral pandemic signatures (ViP and sViP) and one COVID lung-derived signature. They found that the resemblances included that COVID-19 recapitulates the gene expression patterns (ViP and IPF signatures), cytokine storm (IL15-centric), and the AT2 cytopathic changes, for example, injury, DNA damage, arrest in a transient, damage-induced progenitor state, and senescence-associated secretory phenotype (SASP).
In laboratory experiments, Dr. Sinha and colleagues were able to induce these same immunocytopathic features in preclinical COVID-19 models (human adult lung organoid and hamster) and to reverse them in the hamster model with effective anti–CoV-2 therapeutics.
PPI-network analyses pinpointed endoplasmic reticulum (ER) stress as one of the shared early triggers of both IPF and COVID-19, and immunohistochemistry studies validated the same in the lungs of deceased subjects with COVID-19 and the SARS-CoV-2–challenged hamster lungs. Additionally, lungs from transgenic mice, in which ER stress was induced specifically in the AT2 cells, faithfully recapitulated the host immune response and alveolar cytopathic changes that are induced by SARS-CoV-2.
stated corresponding author Pradipta Ghosh, MD, professor in the departments of medicine and cellular and molecular medicine, University of California, San Diego. “If proven in prospective studies, this biomarker could indicate who is at greatest risk for progressive fibrosis and may require lung transplantation,” she said in an interview.
Dr. Ghosh stated further, “When it comes to therapeutics in COVID lung or IPF, we also found that shared fundamental pathogenic mechanisms present excellent opportunities for developing therapeutics that can arrest the fibrogenic drivers in both diseases. One clue that emerged is a specific cytokine that is at the heart of the smoldering inflammation which is invariably associated with fibrosis. That is interleukin 15 [IL-15] and its receptor.” Dr. Ghosh observed that there are two Food and Drug Administration–approved drugs for IPF. “None are very effective in arresting this invariably fatal disease. Hence, finding better options to treat IPF is an urgent and an unmet need.”
Preclinical testing of hypotheses, Dr. Ghosh said, is next on the path to clinical trials. “We have the advantage of using human lung organoids (mini-lungs grown using stem cells) in a dish, adding additional cells to the system (like fibroblasts and immune cells), infecting them with the virus, or subjecting them to the IL-15 cytokine and monitoring lung fibrosis progression in a dish. Anti–IL-15 therapy can then be initiated to observe reversal of the fibrogenic cascade.” Hamsters have also been shown to provide appropriate models for mimicking lung fibrosis, Dr. Ghosh said.
“The report by Sinha and colleagues describes the fascinating similarities between drivers of post-COVID lung disease and idiopathic pulmonary fibrosis,” stated David Bowton, MD, professor emeritus, section on critical care, department of anesthesiology, Wake Forest University, Winston-Salem, N.C., in an interview. He added that, “Central to the mechanisms of induction of fibrosis in both disorders appears to be endoplasmic reticulum stress in alveolar type II cells (AT2). ER stress induces the unfolded protein response (UPR) that halts protein translation and promotes the degradation of misfolded proteins. Prolonged UPR can reprogram the cell or trigger apoptosis pathways. ER stress in the lung has been reported in a variety of cell lines including AT2 in IPF, bronchial and alveolar epithelial cells in asthma and [chronic obstructive pulmonary disease], and endothelial cells in pulmonary hypertension.”
Dr. Bowton commented further, including a caution, “Sinha and colleagues suggest that the identification of these gene signatures and mechanisms will be a fruitful avenue for developing effective therapeutics for IPF and other fibrotic lung diseases. I am hopeful that these data may offer clues that expedite this process. However, the redundancy of triggers for effector pathways in biologic systems argues that, even if successful, this will be [a] long and fraught process.”
The research study was supported by National Institutes of Health grants and funding from the Tobacco-Related Disease Research Program.
Dr. Sinha, Dr. Ghosh, and Dr. Bowton reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
An AI-guided analysis of more than 1,000 human lung transcriptomic datasets found that COVID-19 resembles idiopathic pulmonary fibrosis (IPF) at a fundamental level, according to a study published in eBiomedicine, part of The Lancet Discovery Science.
In the aftermath of COVID-19, a significant number of patients develop a fibrotic lung disease, for which insights into pathogenesis, disease models, or treatment options are lacking, according to researchers Dr. Sinha and colleagues. This long-haul form of the disease culminates in a fibrotic type of interstitial lung disease (ILD). While the actual prevalence of post–COVID-19 ILD (PCLD) is still emerging, early analysis indicates that more than a third of COVID-19 survivors develop fibrotic abnormalities, according to the authors.
Previous research has shown that one of the important determinants for PCLD is the duration of disease. Among patients who developed fibrosis, approximately 4% of patients had a disease duration of less than 1 week; approximately 24% had a disease duration between 1 and 3 weeks; and around 61% had a disease duration longer than 3 weeks, the authors stated.
The lung transcriptomic datasets compared in their study were associated with various lung conditions. The researchers used two viral pandemic signatures (ViP and sViP) and one COVID lung-derived signature. They found that the resemblances included that COVID-19 recapitulates the gene expression patterns (ViP and IPF signatures), cytokine storm (IL15-centric), and the AT2 cytopathic changes, for example, injury, DNA damage, arrest in a transient, damage-induced progenitor state, and senescence-associated secretory phenotype (SASP).
In laboratory experiments, Dr. Sinha and colleagues were able to induce these same immunocytopathic features in preclinical COVID-19 models (human adult lung organoid and hamster) and to reverse them in the hamster model with effective anti–CoV-2 therapeutics.
PPI-network analyses pinpointed endoplasmic reticulum (ER) stress as one of the shared early triggers of both IPF and COVID-19, and immunohistochemistry studies validated the same in the lungs of deceased subjects with COVID-19 and the SARS-CoV-2–challenged hamster lungs. Additionally, lungs from transgenic mice, in which ER stress was induced specifically in the AT2 cells, faithfully recapitulated the host immune response and alveolar cytopathic changes that are induced by SARS-CoV-2.
stated corresponding author Pradipta Ghosh, MD, professor in the departments of medicine and cellular and molecular medicine, University of California, San Diego. “If proven in prospective studies, this biomarker could indicate who is at greatest risk for progressive fibrosis and may require lung transplantation,” she said in an interview.
Dr. Ghosh stated further, “When it comes to therapeutics in COVID lung or IPF, we also found that shared fundamental pathogenic mechanisms present excellent opportunities for developing therapeutics that can arrest the fibrogenic drivers in both diseases. One clue that emerged is a specific cytokine that is at the heart of the smoldering inflammation which is invariably associated with fibrosis. That is interleukin 15 [IL-15] and its receptor.” Dr. Ghosh observed that there are two Food and Drug Administration–approved drugs for IPF. “None are very effective in arresting this invariably fatal disease. Hence, finding better options to treat IPF is an urgent and an unmet need.”
Preclinical testing of hypotheses, Dr. Ghosh said, is next on the path to clinical trials. “We have the advantage of using human lung organoids (mini-lungs grown using stem cells) in a dish, adding additional cells to the system (like fibroblasts and immune cells), infecting them with the virus, or subjecting them to the IL-15 cytokine and monitoring lung fibrosis progression in a dish. Anti–IL-15 therapy can then be initiated to observe reversal of the fibrogenic cascade.” Hamsters have also been shown to provide appropriate models for mimicking lung fibrosis, Dr. Ghosh said.
“The report by Sinha and colleagues describes the fascinating similarities between drivers of post-COVID lung disease and idiopathic pulmonary fibrosis,” stated David Bowton, MD, professor emeritus, section on critical care, department of anesthesiology, Wake Forest University, Winston-Salem, N.C., in an interview. He added that, “Central to the mechanisms of induction of fibrosis in both disorders appears to be endoplasmic reticulum stress in alveolar type II cells (AT2). ER stress induces the unfolded protein response (UPR) that halts protein translation and promotes the degradation of misfolded proteins. Prolonged UPR can reprogram the cell or trigger apoptosis pathways. ER stress in the lung has been reported in a variety of cell lines including AT2 in IPF, bronchial and alveolar epithelial cells in asthma and [chronic obstructive pulmonary disease], and endothelial cells in pulmonary hypertension.”
Dr. Bowton commented further, including a caution, “Sinha and colleagues suggest that the identification of these gene signatures and mechanisms will be a fruitful avenue for developing effective therapeutics for IPF and other fibrotic lung diseases. I am hopeful that these data may offer clues that expedite this process. However, the redundancy of triggers for effector pathways in biologic systems argues that, even if successful, this will be [a] long and fraught process.”
The research study was supported by National Institutes of Health grants and funding from the Tobacco-Related Disease Research Program.
Dr. Sinha, Dr. Ghosh, and Dr. Bowton reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM eBIOMEDICINE
Researcher revisits ‘03 guidance on monkeypox in pregnant women
In creating a guide about monkeypox for ob.gyns., Denise J. Jamieson, MD, MPH, turned to research she relied on during another outbreak of the disease nearly 20 years ago.
Dr. Jamieson, the James Robert McCord Professor and chair of the department of gynecology and obstetrics at Emory Healthcare, Atlanta, had been working for the Centers for Disease Control and Prevention in 2003 when doctors diagnosed monkeypox in several states.
That year, the virus was mainly transmitted by contact with pet prairie dogs, including in childcare and school settings. Of the approximately 70 suspected and confirmed cases, 55% occurred in female patients, according to one study .
Dr. Jamieson, an obstetrician with a focus on emerging infectious diseases, and colleagues at the agency published a commentary in Obstetrics & Gynecology highlighting the need for physicians to stay up to date with relevant information about the virus.
Fast forward to 2022: Dr. Jamieson – again with coauthors from the CDC – is delivering a similar message in the same journal about the need for clinicians to be prepared for this virus.
“Most ob.gyns. have never seen a case of monkeypox virus infection and may not be aware of testing, treatment, or pre-exposure or postexposure vaccine options,” she and her coauthors wrote in a primer published online.
But if a woman were to contract the virus, her ob.gyn. might well be the first clinician she called. “We are often the first people, the first physicians to see and evaluate women with various symptoms,” Dr. Jamieson said.
To promptly diagnose, treat, and prevent further spread of monkeypox, ob.gyns. need up-to-date information, Dr. Jamieson and colleagues said.
Based on data from related viruses like smallpox, monkeypox may be more severe in pregnant women and entail risk for adverse pregnancy outcomes, Dr. Jamieson said.
Outliers
So far this year, monkeypox has predominantly spread among men who have sex with men. Cases have occurred in women, however, some of whom have required hospitalization.
According to the CDC, as of July 25, 1,373 cases of monkeypox in the United States were in men and 13 in women. The total confirmed case count exceeded 5,800 as of Aug. 1. The agency recently announced that it planned to make the disease a reportable condition.
In the United Kingdom, which has been hit hard by the outbreak, researchers are keeping a close eye on the number of cases in women to assess how the disease is spreading.
At least one case of monkeypox in the United States has occurred in a pregnant woman who delivered. The mother and baby, who received immune globulin as a preventive measure, are doing well, according to health officials.
“We know that infection can occur through placental transfer. In the case that we are aware of presently, it does not appear that the virus was transmitted,” said John T. Brooks, MD, the CDC’s chief medical officer in the division of HIV prevention, on a July 23 call with clinicians.
While monkeypox can be transmitted in utero and during sexual activity, it also can spread through any close contact with skin lesions or body fluids and possibly through touching contaminated items like clothing or linens, according to the CDC.
A preferred vaccine and antiviral in pregnancy
One monkeypox vaccine, Jynneos, is preferred for use during pregnancy, while another, ACAM2000, is contraindicated, the CDC advises.
Jynneos can be offered to people who are pregnant or breastfeeding who are eligible for vaccination based on confirmed or likely contact with cases, ideally within 4 days of exposure. People at high risk for exposure, such as laboratory workers, may receive the vaccine in advance.
Developmental toxicity studies in animals showed no evidence of harm with the Jynneos vaccine, Dr. Jamieson said.
ACAM2000, however, can cause fetal vaccinia and should not be used in people who are pregnant or breastfeeding, according to the CDC.
The Society for Maternal-Fetal Medicine notes that, if treatment for monkeypox is warranted, tecovirimat should be considered the first-line antiviral for pregnant, recently pregnant, and breastfeeding people, in line with CDC guidance.
Current outbreak ‘very different,’ but lessons apply
In 2003, some women exposed to monkeypox through contact with infected prairie dogs were pregnant – which is how Dr. Jamieson came to be involved in responding to the outbreak and studying the effects of the virus in pregnancy.
“When this resurfaced this year, of course it caught my attention,” Dr. Jamieson said. The extensive person-to-person transmission and far greater number of cases today make the current outbreak “very different” from the prior one, she said.
But key principles in managing the disease and understanding its potential risks in pregnancy – despite relatively limited information – remain the same.
“Whenever you are looking at an infectious disease, you want to think about, are pregnant persons more susceptible or more likely to have severe disease,” Dr. Jamieson said. Smallpox, a similar orthopoxvirus, “is more severe during pregnancy with a higher case fatality rate,” which is one reason for concern with monkeypox in this population.
In terms of pregnancy outcomes, researchers have data from only a handful of confirmed cases of monkeypox, which makes it difficult to draw conclusions, Dr. Jamieson said. A review of five cases from outside the United States in prior years found that three resulted in loss of the pregnancy. One resulted in preterm delivery of an infant who subsequently died. One child was apparently healthy and born at term.
Addition to the differential diagnosis
A separate team of researchers has proposed a clinical management algorithm for pregnant women with suspected exposure to monkeypox.
“Clinicians must maintain a high index of suspicion for monkeypox virus in any pregnant woman presenting with lymphadenopathy and vesiculopustular rash – including rash localized to the genital or perianal region – even if there are no apparent epidemiological links,” Pradip Dashraath, MBBS, National University Hospital, Singapore, and coauthors wrote in The Lancet.
Jamieson echoed the call for increased vigilance.
“As ob.gyns., people may present to us with genital lesions concerning for sexually transmitted infection. And it is important to include monkeypox in our differential,” Dr. Jamieson said. “We are trying to get the word out that it needs to be part of what you think about when you see a patient with genital ulcers.”
Health care professionals have acquired monkeypox through contact with patients or fomites, so clinicians should be sure to use appropriate precautions when evaluating patients who might have monkeypox, Dr. Jamieson added. Appropriate protective measures include wearing a gown, gloves, eye protection, and an N95.
A version of this article first appeared on Medscape.com.
In creating a guide about monkeypox for ob.gyns., Denise J. Jamieson, MD, MPH, turned to research she relied on during another outbreak of the disease nearly 20 years ago.
Dr. Jamieson, the James Robert McCord Professor and chair of the department of gynecology and obstetrics at Emory Healthcare, Atlanta, had been working for the Centers for Disease Control and Prevention in 2003 when doctors diagnosed monkeypox in several states.
That year, the virus was mainly transmitted by contact with pet prairie dogs, including in childcare and school settings. Of the approximately 70 suspected and confirmed cases, 55% occurred in female patients, according to one study .
Dr. Jamieson, an obstetrician with a focus on emerging infectious diseases, and colleagues at the agency published a commentary in Obstetrics & Gynecology highlighting the need for physicians to stay up to date with relevant information about the virus.
Fast forward to 2022: Dr. Jamieson – again with coauthors from the CDC – is delivering a similar message in the same journal about the need for clinicians to be prepared for this virus.
“Most ob.gyns. have never seen a case of monkeypox virus infection and may not be aware of testing, treatment, or pre-exposure or postexposure vaccine options,” she and her coauthors wrote in a primer published online.
But if a woman were to contract the virus, her ob.gyn. might well be the first clinician she called. “We are often the first people, the first physicians to see and evaluate women with various symptoms,” Dr. Jamieson said.
To promptly diagnose, treat, and prevent further spread of monkeypox, ob.gyns. need up-to-date information, Dr. Jamieson and colleagues said.
Based on data from related viruses like smallpox, monkeypox may be more severe in pregnant women and entail risk for adverse pregnancy outcomes, Dr. Jamieson said.
Outliers
So far this year, monkeypox has predominantly spread among men who have sex with men. Cases have occurred in women, however, some of whom have required hospitalization.
According to the CDC, as of July 25, 1,373 cases of monkeypox in the United States were in men and 13 in women. The total confirmed case count exceeded 5,800 as of Aug. 1. The agency recently announced that it planned to make the disease a reportable condition.
In the United Kingdom, which has been hit hard by the outbreak, researchers are keeping a close eye on the number of cases in women to assess how the disease is spreading.
At least one case of monkeypox in the United States has occurred in a pregnant woman who delivered. The mother and baby, who received immune globulin as a preventive measure, are doing well, according to health officials.
“We know that infection can occur through placental transfer. In the case that we are aware of presently, it does not appear that the virus was transmitted,” said John T. Brooks, MD, the CDC’s chief medical officer in the division of HIV prevention, on a July 23 call with clinicians.
While monkeypox can be transmitted in utero and during sexual activity, it also can spread through any close contact with skin lesions or body fluids and possibly through touching contaminated items like clothing or linens, according to the CDC.
A preferred vaccine and antiviral in pregnancy
One monkeypox vaccine, Jynneos, is preferred for use during pregnancy, while another, ACAM2000, is contraindicated, the CDC advises.
Jynneos can be offered to people who are pregnant or breastfeeding who are eligible for vaccination based on confirmed or likely contact with cases, ideally within 4 days of exposure. People at high risk for exposure, such as laboratory workers, may receive the vaccine in advance.
Developmental toxicity studies in animals showed no evidence of harm with the Jynneos vaccine, Dr. Jamieson said.
ACAM2000, however, can cause fetal vaccinia and should not be used in people who are pregnant or breastfeeding, according to the CDC.
The Society for Maternal-Fetal Medicine notes that, if treatment for monkeypox is warranted, tecovirimat should be considered the first-line antiviral for pregnant, recently pregnant, and breastfeeding people, in line with CDC guidance.
Current outbreak ‘very different,’ but lessons apply
In 2003, some women exposed to monkeypox through contact with infected prairie dogs were pregnant – which is how Dr. Jamieson came to be involved in responding to the outbreak and studying the effects of the virus in pregnancy.
“When this resurfaced this year, of course it caught my attention,” Dr. Jamieson said. The extensive person-to-person transmission and far greater number of cases today make the current outbreak “very different” from the prior one, she said.
But key principles in managing the disease and understanding its potential risks in pregnancy – despite relatively limited information – remain the same.
“Whenever you are looking at an infectious disease, you want to think about, are pregnant persons more susceptible or more likely to have severe disease,” Dr. Jamieson said. Smallpox, a similar orthopoxvirus, “is more severe during pregnancy with a higher case fatality rate,” which is one reason for concern with monkeypox in this population.
In terms of pregnancy outcomes, researchers have data from only a handful of confirmed cases of monkeypox, which makes it difficult to draw conclusions, Dr. Jamieson said. A review of five cases from outside the United States in prior years found that three resulted in loss of the pregnancy. One resulted in preterm delivery of an infant who subsequently died. One child was apparently healthy and born at term.
Addition to the differential diagnosis
A separate team of researchers has proposed a clinical management algorithm for pregnant women with suspected exposure to monkeypox.
“Clinicians must maintain a high index of suspicion for monkeypox virus in any pregnant woman presenting with lymphadenopathy and vesiculopustular rash – including rash localized to the genital or perianal region – even if there are no apparent epidemiological links,” Pradip Dashraath, MBBS, National University Hospital, Singapore, and coauthors wrote in The Lancet.
Jamieson echoed the call for increased vigilance.
“As ob.gyns., people may present to us with genital lesions concerning for sexually transmitted infection. And it is important to include monkeypox in our differential,” Dr. Jamieson said. “We are trying to get the word out that it needs to be part of what you think about when you see a patient with genital ulcers.”
Health care professionals have acquired monkeypox through contact with patients or fomites, so clinicians should be sure to use appropriate precautions when evaluating patients who might have monkeypox, Dr. Jamieson added. Appropriate protective measures include wearing a gown, gloves, eye protection, and an N95.
A version of this article first appeared on Medscape.com.
In creating a guide about monkeypox for ob.gyns., Denise J. Jamieson, MD, MPH, turned to research she relied on during another outbreak of the disease nearly 20 years ago.
Dr. Jamieson, the James Robert McCord Professor and chair of the department of gynecology and obstetrics at Emory Healthcare, Atlanta, had been working for the Centers for Disease Control and Prevention in 2003 when doctors diagnosed monkeypox in several states.
That year, the virus was mainly transmitted by contact with pet prairie dogs, including in childcare and school settings. Of the approximately 70 suspected and confirmed cases, 55% occurred in female patients, according to one study .
Dr. Jamieson, an obstetrician with a focus on emerging infectious diseases, and colleagues at the agency published a commentary in Obstetrics & Gynecology highlighting the need for physicians to stay up to date with relevant information about the virus.
Fast forward to 2022: Dr. Jamieson – again with coauthors from the CDC – is delivering a similar message in the same journal about the need for clinicians to be prepared for this virus.
“Most ob.gyns. have never seen a case of monkeypox virus infection and may not be aware of testing, treatment, or pre-exposure or postexposure vaccine options,” she and her coauthors wrote in a primer published online.
But if a woman were to contract the virus, her ob.gyn. might well be the first clinician she called. “We are often the first people, the first physicians to see and evaluate women with various symptoms,” Dr. Jamieson said.
To promptly diagnose, treat, and prevent further spread of monkeypox, ob.gyns. need up-to-date information, Dr. Jamieson and colleagues said.
Based on data from related viruses like smallpox, monkeypox may be more severe in pregnant women and entail risk for adverse pregnancy outcomes, Dr. Jamieson said.
Outliers
So far this year, monkeypox has predominantly spread among men who have sex with men. Cases have occurred in women, however, some of whom have required hospitalization.
According to the CDC, as of July 25, 1,373 cases of monkeypox in the United States were in men and 13 in women. The total confirmed case count exceeded 5,800 as of Aug. 1. The agency recently announced that it planned to make the disease a reportable condition.
In the United Kingdom, which has been hit hard by the outbreak, researchers are keeping a close eye on the number of cases in women to assess how the disease is spreading.
At least one case of monkeypox in the United States has occurred in a pregnant woman who delivered. The mother and baby, who received immune globulin as a preventive measure, are doing well, according to health officials.
“We know that infection can occur through placental transfer. In the case that we are aware of presently, it does not appear that the virus was transmitted,” said John T. Brooks, MD, the CDC’s chief medical officer in the division of HIV prevention, on a July 23 call with clinicians.
While monkeypox can be transmitted in utero and during sexual activity, it also can spread through any close contact with skin lesions or body fluids and possibly through touching contaminated items like clothing or linens, according to the CDC.
A preferred vaccine and antiviral in pregnancy
One monkeypox vaccine, Jynneos, is preferred for use during pregnancy, while another, ACAM2000, is contraindicated, the CDC advises.
Jynneos can be offered to people who are pregnant or breastfeeding who are eligible for vaccination based on confirmed or likely contact with cases, ideally within 4 days of exposure. People at high risk for exposure, such as laboratory workers, may receive the vaccine in advance.
Developmental toxicity studies in animals showed no evidence of harm with the Jynneos vaccine, Dr. Jamieson said.
ACAM2000, however, can cause fetal vaccinia and should not be used in people who are pregnant or breastfeeding, according to the CDC.
The Society for Maternal-Fetal Medicine notes that, if treatment for monkeypox is warranted, tecovirimat should be considered the first-line antiviral for pregnant, recently pregnant, and breastfeeding people, in line with CDC guidance.
Current outbreak ‘very different,’ but lessons apply
In 2003, some women exposed to monkeypox through contact with infected prairie dogs were pregnant – which is how Dr. Jamieson came to be involved in responding to the outbreak and studying the effects of the virus in pregnancy.
“When this resurfaced this year, of course it caught my attention,” Dr. Jamieson said. The extensive person-to-person transmission and far greater number of cases today make the current outbreak “very different” from the prior one, she said.
But key principles in managing the disease and understanding its potential risks in pregnancy – despite relatively limited information – remain the same.
“Whenever you are looking at an infectious disease, you want to think about, are pregnant persons more susceptible or more likely to have severe disease,” Dr. Jamieson said. Smallpox, a similar orthopoxvirus, “is more severe during pregnancy with a higher case fatality rate,” which is one reason for concern with monkeypox in this population.
In terms of pregnancy outcomes, researchers have data from only a handful of confirmed cases of monkeypox, which makes it difficult to draw conclusions, Dr. Jamieson said. A review of five cases from outside the United States in prior years found that three resulted in loss of the pregnancy. One resulted in preterm delivery of an infant who subsequently died. One child was apparently healthy and born at term.
Addition to the differential diagnosis
A separate team of researchers has proposed a clinical management algorithm for pregnant women with suspected exposure to monkeypox.
“Clinicians must maintain a high index of suspicion for monkeypox virus in any pregnant woman presenting with lymphadenopathy and vesiculopustular rash – including rash localized to the genital or perianal region – even if there are no apparent epidemiological links,” Pradip Dashraath, MBBS, National University Hospital, Singapore, and coauthors wrote in The Lancet.
Jamieson echoed the call for increased vigilance.
“As ob.gyns., people may present to us with genital lesions concerning for sexually transmitted infection. And it is important to include monkeypox in our differential,” Dr. Jamieson said. “We are trying to get the word out that it needs to be part of what you think about when you see a patient with genital ulcers.”
Health care professionals have acquired monkeypox through contact with patients or fomites, so clinicians should be sure to use appropriate precautions when evaluating patients who might have monkeypox, Dr. Jamieson added. Appropriate protective measures include wearing a gown, gloves, eye protection, and an N95.
A version of this article first appeared on Medscape.com.
FROM OBSTETRICS AND GYNECOLOGY
Summer flu, RSV in July, ‘super colds?’
Richard Martinello, MD, a professor of medicine and pediatric infectious diseases at Yale University, New haven, Conn., doesn’t expect to see a child hospitalized with respiratory syncytial virus (RSV) in the middle of summer. The illness, which can strike infants and older adults especially hard, is known as a “winter virus.”
But not this year. Over the last several weeks, he says, admissions for children with RSV have increased at the Yale New Haven Children’s Hospital. While the numbers aren’t large, they are out of the ordinary, he says, “because usually, at this time of year, we see zero. For lack of a better term, it’s weird.”
Likewise, William Schaffner, MD, a professor of infectious diseases at Vanderbilt University in Nashville, says RSV is on the rise there. Tennessee is one of 10 states taking part in a Centers for Disease Control and Prevention surveillance system that tracks influenza, RSV, and COVID-19.
He says RSV cases have risen by at least a third during the past week, including all age ranges. At this time of year, he says, “We aren’t supposed to have any RSV.”
RSV isn’t the only virus thriving out of season or otherwise acting strangely. Since the pandemic began, flu seasons have been out of whack – sometimes nearly nonexistent and other times extending well beyond “normal” seasons. Some experts say one influenza “B” strain may now be extinct, while others say it will be back.
Severe colds – what some call “super colds” – also seem to be on the rise in recent warm-weather months, although that evidence is mostly based on personal experience, not science.
Trying to explain these out-of-season variations has sparked much discussion among epidemiologists and virologists, Dr. Schaffner says, with debates ongoing about whether human behavior and habits or the seasons play a bigger role in the transmission of viral illness.
On top of that, scientists are also looking at the interactions between the SARS-CoV-2 virus that causes COVID-19 and other viruses. When people get hit with COVID-19 and other viruses at the same time, does that make COVID-19 more severe, or less?
Research is conflicting.
Summer of 2022: A repeat of 2021?
RSV. Most children contract the virus by age 2, and while it’s generally mild, about 58,000 children under age 5 years are hospitalized each year. During the pandemic, RSV cases decreased from January to April 2020, the CDC reported, and then remained at “historically low levels”: less than 1% positive RSV results a week, for the next year.
But cases began rising in April 2021.
“Last year, we did have an unusual summer,” Dr. Schaffner says. After lockdown ended, to everyone’s surprise, RSV infections rose.
That increase triggered a CDC health advisory in June 2021, telling doctors and caregivers about the increase in “interseasonal” RSV cases across parts of the Southern United States, recommending broader testing for RSV in patients who had a respiratory illness but tested negative for COVID.
Because of the reduced circulation of RSV during the winter of 2020 to 2021, the CDC warned, older infants and toddlers might have a higher risk of RSV since they weren’t exposed to typical levels of RSV for the previous 15 months.
What about 2022? “At the moment,” Dr. Schaffner says, “it looks like we are having a repeat [of 2021].”
On Twitter, other pediatricians, including those from Maine and Texas, have reported an increase in RSV cases this summer.
Influenza. From October 2020 until May 2021, flu activity was lower than during any previous flu season since at least 1997, according to the CDC.
In late 2021, researchers suggested that one line of influenza known as B/Yamagata may have become extinct.
The 2021-2022 flu season has been mild, the CDC says, but it has come in two waves, with the second wave lingering longer than previous ones. While flu activity is decreasing, last week the CDC said doctors should be alert to flu infections throughout the summer.
Colds. In reports on colds that aren’t based on science, several doctors say they are seeing more colds than usual in the summer, and they’re more severe than usual. According to the CDC, common coronaviruses and respiratory adenoviruses have been increasing since early 2021, and rhinoviruses since June 2020.
Behavior vs. seasons
In explaining the spread of viral respiratory diseases, infectious disease doctors consider two things. “One is that temperature and humidity in the winter favors longer survival of some viruses, leading to longer periods of possible transmission,” says Dean Blumberg, MD, a professor of pediatrics and chief of pediatric infectious disease at University of California Davis Health.
“The other is differences in human behavior, with people spending more time outside in the summer, which results in more distancing and [less] virus concentration due to very large air volume,” he says, and vice versa in winter.
What about the “super colds?” COVID-19 lockdowns and social distancing greatly reduced people’s exposure to common viruses like those that cause colds, says Neil A. Mabbott, PhD, a professor of immunopathology at the University of Edinburgh (Scotland).
“Immunity to these common cold viruses gained through natural infection is considered to last around 8 or 9 months or so,” he says. “Each winter, when we are exposed to the new circulating variants of these viruses, our immunity receives a natural boost.”
That explains why most people get a cold that’s relatively mild. But with all the pandemic lockdowns and the use of hand sanitizers, most people had limited exposure to other viruses, including the common cold. When people emerged from lockdown, the common cold viruses were beginning to circulate again.
“Our immune systems were less able to clear the infection than previously,” Dr. Mabbott says. “As a consequence, some may have experienced increased symptoms, giving the impression of being infected with a ‘super cold.’ ”
“The colds themselves are probably not different to those we got prepandemic,” says Ian Mackay, PhD, a virologist at the University of Queensland, Brisbane, Australia. “But there might be more of them. So I doubt they are ‘super colds’ as much as they are ‘super-perfect circumstances.’ ”
The colds themselves are probably not different to those we got prepandemic. But there might be more of them.
Those super-perfect circumstances, he says, include people gathering after lockdown; a lack of immunity in new babies; viruses that have remained, even if at low levels, but continue to mutate; and our waning immunity to the range of viruses we’d normally encounter.
While lack of exposure may partly explain why some viruses become rampant out of season, it’s likely not the only reason. For example, the reduced circulation of RSV in the population as a whole also may have reduced the transfer of immunity from mothers to infants, some researchers say, making those infants more vulnerable than usual.
Interactions of viruses
Another thing that may be driving the different behavior of viruses is that the SARS-CoV-2 virus could somehow be interacting with other respiratory viruses, Dr. Schaffner says. “And if so, what sort of interactions?”
Many researchers are looking into that, and how coinfections with other respiratory diseases, including the common cold and flu, may affect the course of COVID-19. Some studies have found that the T cells – a source of deeper, cellular immunity in people – generated after a common cold “may also provide cross-protection in some people against COVID-19.”
But another study found immunity against common cold–causing coronaviruses might make COVID-19 more severe.
When researchers in the United Kingdom studied nearly 7,000 patients infected with COVID-19, including 583 also infected with RSV, flu, or adenoviruses (causing flulike or coldlike illness), those with flu or adenovirus, compared with the others, were at higher risk of death.
To be continued …
Exactly how COVID-19 will be changing what we know of other viruses is yet to be determined, too.
Even before the pandemic, Dr. Martinello says, there were already some shifts in RSV. Florida, for instance, has an RSV season longer than the rest of the country, mimicking the pattern in the tropics.
Will the atypical patterns continue? “My guess is that this will settle out,” he says, with some sort of pattern developing. At this point, there are many unknowns. “We still can’t answer whether there will be some seasonality to COVID.”
A version of this article first appeared on WebMD.com.
Richard Martinello, MD, a professor of medicine and pediatric infectious diseases at Yale University, New haven, Conn., doesn’t expect to see a child hospitalized with respiratory syncytial virus (RSV) in the middle of summer. The illness, which can strike infants and older adults especially hard, is known as a “winter virus.”
But not this year. Over the last several weeks, he says, admissions for children with RSV have increased at the Yale New Haven Children’s Hospital. While the numbers aren’t large, they are out of the ordinary, he says, “because usually, at this time of year, we see zero. For lack of a better term, it’s weird.”
Likewise, William Schaffner, MD, a professor of infectious diseases at Vanderbilt University in Nashville, says RSV is on the rise there. Tennessee is one of 10 states taking part in a Centers for Disease Control and Prevention surveillance system that tracks influenza, RSV, and COVID-19.
He says RSV cases have risen by at least a third during the past week, including all age ranges. At this time of year, he says, “We aren’t supposed to have any RSV.”
RSV isn’t the only virus thriving out of season or otherwise acting strangely. Since the pandemic began, flu seasons have been out of whack – sometimes nearly nonexistent and other times extending well beyond “normal” seasons. Some experts say one influenza “B” strain may now be extinct, while others say it will be back.
Severe colds – what some call “super colds” – also seem to be on the rise in recent warm-weather months, although that evidence is mostly based on personal experience, not science.
Trying to explain these out-of-season variations has sparked much discussion among epidemiologists and virologists, Dr. Schaffner says, with debates ongoing about whether human behavior and habits or the seasons play a bigger role in the transmission of viral illness.
On top of that, scientists are also looking at the interactions between the SARS-CoV-2 virus that causes COVID-19 and other viruses. When people get hit with COVID-19 and other viruses at the same time, does that make COVID-19 more severe, or less?
Research is conflicting.
Summer of 2022: A repeat of 2021?
RSV. Most children contract the virus by age 2, and while it’s generally mild, about 58,000 children under age 5 years are hospitalized each year. During the pandemic, RSV cases decreased from January to April 2020, the CDC reported, and then remained at “historically low levels”: less than 1% positive RSV results a week, for the next year.
But cases began rising in April 2021.
“Last year, we did have an unusual summer,” Dr. Schaffner says. After lockdown ended, to everyone’s surprise, RSV infections rose.
That increase triggered a CDC health advisory in June 2021, telling doctors and caregivers about the increase in “interseasonal” RSV cases across parts of the Southern United States, recommending broader testing for RSV in patients who had a respiratory illness but tested negative for COVID.
Because of the reduced circulation of RSV during the winter of 2020 to 2021, the CDC warned, older infants and toddlers might have a higher risk of RSV since they weren’t exposed to typical levels of RSV for the previous 15 months.
What about 2022? “At the moment,” Dr. Schaffner says, “it looks like we are having a repeat [of 2021].”
On Twitter, other pediatricians, including those from Maine and Texas, have reported an increase in RSV cases this summer.
Influenza. From October 2020 until May 2021, flu activity was lower than during any previous flu season since at least 1997, according to the CDC.
In late 2021, researchers suggested that one line of influenza known as B/Yamagata may have become extinct.
The 2021-2022 flu season has been mild, the CDC says, but it has come in two waves, with the second wave lingering longer than previous ones. While flu activity is decreasing, last week the CDC said doctors should be alert to flu infections throughout the summer.
Colds. In reports on colds that aren’t based on science, several doctors say they are seeing more colds than usual in the summer, and they’re more severe than usual. According to the CDC, common coronaviruses and respiratory adenoviruses have been increasing since early 2021, and rhinoviruses since June 2020.
Behavior vs. seasons
In explaining the spread of viral respiratory diseases, infectious disease doctors consider two things. “One is that temperature and humidity in the winter favors longer survival of some viruses, leading to longer periods of possible transmission,” says Dean Blumberg, MD, a professor of pediatrics and chief of pediatric infectious disease at University of California Davis Health.
“The other is differences in human behavior, with people spending more time outside in the summer, which results in more distancing and [less] virus concentration due to very large air volume,” he says, and vice versa in winter.
What about the “super colds?” COVID-19 lockdowns and social distancing greatly reduced people’s exposure to common viruses like those that cause colds, says Neil A. Mabbott, PhD, a professor of immunopathology at the University of Edinburgh (Scotland).
“Immunity to these common cold viruses gained through natural infection is considered to last around 8 or 9 months or so,” he says. “Each winter, when we are exposed to the new circulating variants of these viruses, our immunity receives a natural boost.”
That explains why most people get a cold that’s relatively mild. But with all the pandemic lockdowns and the use of hand sanitizers, most people had limited exposure to other viruses, including the common cold. When people emerged from lockdown, the common cold viruses were beginning to circulate again.
“Our immune systems were less able to clear the infection than previously,” Dr. Mabbott says. “As a consequence, some may have experienced increased symptoms, giving the impression of being infected with a ‘super cold.’ ”
“The colds themselves are probably not different to those we got prepandemic,” says Ian Mackay, PhD, a virologist at the University of Queensland, Brisbane, Australia. “But there might be more of them. So I doubt they are ‘super colds’ as much as they are ‘super-perfect circumstances.’ ”
The colds themselves are probably not different to those we got prepandemic. But there might be more of them.
Those super-perfect circumstances, he says, include people gathering after lockdown; a lack of immunity in new babies; viruses that have remained, even if at low levels, but continue to mutate; and our waning immunity to the range of viruses we’d normally encounter.
While lack of exposure may partly explain why some viruses become rampant out of season, it’s likely not the only reason. For example, the reduced circulation of RSV in the population as a whole also may have reduced the transfer of immunity from mothers to infants, some researchers say, making those infants more vulnerable than usual.
Interactions of viruses
Another thing that may be driving the different behavior of viruses is that the SARS-CoV-2 virus could somehow be interacting with other respiratory viruses, Dr. Schaffner says. “And if so, what sort of interactions?”
Many researchers are looking into that, and how coinfections with other respiratory diseases, including the common cold and flu, may affect the course of COVID-19. Some studies have found that the T cells – a source of deeper, cellular immunity in people – generated after a common cold “may also provide cross-protection in some people against COVID-19.”
But another study found immunity against common cold–causing coronaviruses might make COVID-19 more severe.
When researchers in the United Kingdom studied nearly 7,000 patients infected with COVID-19, including 583 also infected with RSV, flu, or adenoviruses (causing flulike or coldlike illness), those with flu or adenovirus, compared with the others, were at higher risk of death.
To be continued …
Exactly how COVID-19 will be changing what we know of other viruses is yet to be determined, too.
Even before the pandemic, Dr. Martinello says, there were already some shifts in RSV. Florida, for instance, has an RSV season longer than the rest of the country, mimicking the pattern in the tropics.
Will the atypical patterns continue? “My guess is that this will settle out,” he says, with some sort of pattern developing. At this point, there are many unknowns. “We still can’t answer whether there will be some seasonality to COVID.”
A version of this article first appeared on WebMD.com.
Richard Martinello, MD, a professor of medicine and pediatric infectious diseases at Yale University, New haven, Conn., doesn’t expect to see a child hospitalized with respiratory syncytial virus (RSV) in the middle of summer. The illness, which can strike infants and older adults especially hard, is known as a “winter virus.”
But not this year. Over the last several weeks, he says, admissions for children with RSV have increased at the Yale New Haven Children’s Hospital. While the numbers aren’t large, they are out of the ordinary, he says, “because usually, at this time of year, we see zero. For lack of a better term, it’s weird.”
Likewise, William Schaffner, MD, a professor of infectious diseases at Vanderbilt University in Nashville, says RSV is on the rise there. Tennessee is one of 10 states taking part in a Centers for Disease Control and Prevention surveillance system that tracks influenza, RSV, and COVID-19.
He says RSV cases have risen by at least a third during the past week, including all age ranges. At this time of year, he says, “We aren’t supposed to have any RSV.”
RSV isn’t the only virus thriving out of season or otherwise acting strangely. Since the pandemic began, flu seasons have been out of whack – sometimes nearly nonexistent and other times extending well beyond “normal” seasons. Some experts say one influenza “B” strain may now be extinct, while others say it will be back.
Severe colds – what some call “super colds” – also seem to be on the rise in recent warm-weather months, although that evidence is mostly based on personal experience, not science.
Trying to explain these out-of-season variations has sparked much discussion among epidemiologists and virologists, Dr. Schaffner says, with debates ongoing about whether human behavior and habits or the seasons play a bigger role in the transmission of viral illness.
On top of that, scientists are also looking at the interactions between the SARS-CoV-2 virus that causes COVID-19 and other viruses. When people get hit with COVID-19 and other viruses at the same time, does that make COVID-19 more severe, or less?
Research is conflicting.
Summer of 2022: A repeat of 2021?
RSV. Most children contract the virus by age 2, and while it’s generally mild, about 58,000 children under age 5 years are hospitalized each year. During the pandemic, RSV cases decreased from January to April 2020, the CDC reported, and then remained at “historically low levels”: less than 1% positive RSV results a week, for the next year.
But cases began rising in April 2021.
“Last year, we did have an unusual summer,” Dr. Schaffner says. After lockdown ended, to everyone’s surprise, RSV infections rose.
That increase triggered a CDC health advisory in June 2021, telling doctors and caregivers about the increase in “interseasonal” RSV cases across parts of the Southern United States, recommending broader testing for RSV in patients who had a respiratory illness but tested negative for COVID.
Because of the reduced circulation of RSV during the winter of 2020 to 2021, the CDC warned, older infants and toddlers might have a higher risk of RSV since they weren’t exposed to typical levels of RSV for the previous 15 months.
What about 2022? “At the moment,” Dr. Schaffner says, “it looks like we are having a repeat [of 2021].”
On Twitter, other pediatricians, including those from Maine and Texas, have reported an increase in RSV cases this summer.
Influenza. From October 2020 until May 2021, flu activity was lower than during any previous flu season since at least 1997, according to the CDC.
In late 2021, researchers suggested that one line of influenza known as B/Yamagata may have become extinct.
The 2021-2022 flu season has been mild, the CDC says, but it has come in two waves, with the second wave lingering longer than previous ones. While flu activity is decreasing, last week the CDC said doctors should be alert to flu infections throughout the summer.
Colds. In reports on colds that aren’t based on science, several doctors say they are seeing more colds than usual in the summer, and they’re more severe than usual. According to the CDC, common coronaviruses and respiratory adenoviruses have been increasing since early 2021, and rhinoviruses since June 2020.
Behavior vs. seasons
In explaining the spread of viral respiratory diseases, infectious disease doctors consider two things. “One is that temperature and humidity in the winter favors longer survival of some viruses, leading to longer periods of possible transmission,” says Dean Blumberg, MD, a professor of pediatrics and chief of pediatric infectious disease at University of California Davis Health.
“The other is differences in human behavior, with people spending more time outside in the summer, which results in more distancing and [less] virus concentration due to very large air volume,” he says, and vice versa in winter.
What about the “super colds?” COVID-19 lockdowns and social distancing greatly reduced people’s exposure to common viruses like those that cause colds, says Neil A. Mabbott, PhD, a professor of immunopathology at the University of Edinburgh (Scotland).
“Immunity to these common cold viruses gained through natural infection is considered to last around 8 or 9 months or so,” he says. “Each winter, when we are exposed to the new circulating variants of these viruses, our immunity receives a natural boost.”
That explains why most people get a cold that’s relatively mild. But with all the pandemic lockdowns and the use of hand sanitizers, most people had limited exposure to other viruses, including the common cold. When people emerged from lockdown, the common cold viruses were beginning to circulate again.
“Our immune systems were less able to clear the infection than previously,” Dr. Mabbott says. “As a consequence, some may have experienced increased symptoms, giving the impression of being infected with a ‘super cold.’ ”
“The colds themselves are probably not different to those we got prepandemic,” says Ian Mackay, PhD, a virologist at the University of Queensland, Brisbane, Australia. “But there might be more of them. So I doubt they are ‘super colds’ as much as they are ‘super-perfect circumstances.’ ”
The colds themselves are probably not different to those we got prepandemic. But there might be more of them.
Those super-perfect circumstances, he says, include people gathering after lockdown; a lack of immunity in new babies; viruses that have remained, even if at low levels, but continue to mutate; and our waning immunity to the range of viruses we’d normally encounter.
While lack of exposure may partly explain why some viruses become rampant out of season, it’s likely not the only reason. For example, the reduced circulation of RSV in the population as a whole also may have reduced the transfer of immunity from mothers to infants, some researchers say, making those infants more vulnerable than usual.
Interactions of viruses
Another thing that may be driving the different behavior of viruses is that the SARS-CoV-2 virus could somehow be interacting with other respiratory viruses, Dr. Schaffner says. “And if so, what sort of interactions?”
Many researchers are looking into that, and how coinfections with other respiratory diseases, including the common cold and flu, may affect the course of COVID-19. Some studies have found that the T cells – a source of deeper, cellular immunity in people – generated after a common cold “may also provide cross-protection in some people against COVID-19.”
But another study found immunity against common cold–causing coronaviruses might make COVID-19 more severe.
When researchers in the United Kingdom studied nearly 7,000 patients infected with COVID-19, including 583 also infected with RSV, flu, or adenoviruses (causing flulike or coldlike illness), those with flu or adenovirus, compared with the others, were at higher risk of death.
To be continued …
Exactly how COVID-19 will be changing what we know of other viruses is yet to be determined, too.
Even before the pandemic, Dr. Martinello says, there were already some shifts in RSV. Florida, for instance, has an RSV season longer than the rest of the country, mimicking the pattern in the tropics.
Will the atypical patterns continue? “My guess is that this will settle out,” he says, with some sort of pattern developing. At this point, there are many unknowns. “We still can’t answer whether there will be some seasonality to COVID.”
A version of this article first appeared on WebMD.com.
Injectable HIV prevention better than pills in two trials
MONTREAL – , according to new data from two HIV Prevention Trials Network (HPTN) studies reported at the International AIDS Society Conference.
Follow-up data from the HPTN 084 trial, which compared the two regimens in 3,224 sub-Saharan persons who were assigned female sex at birth, show that three new HIV infections occurred in the CAB LA group in the 12 months since the study was unblinded, versus 20 new infections among the TDF-FTC group. That translates to an 89% lower risk of infection in the CAB LA arm across both the blinded and unblinded phases of the trial, said lead investigator Sinead Delany-Moretlwe, MD, PhD, director of research, Wits Reproductive Health and HIV Institute, the University of the Witwatersrand, Johannesburg, South Africa, during a press conference.
“The trial was designed with the assumption that both drugs were highly effective in preventing HIV infection but that, given the challenges with taking a pill a day, that injectable cabotegravir may offer an adherence advantage,” she said in an interview. “Our data appear to confirm this, as most of the participants in the TDF-FTC arm who became infected with HIV had evidence of poor or inconsistent use of PrEP.”
The study also found that pregnancy incidence increased “two- to threefold” between the blinded and the unblinded period, “and this emphasizes to us the desire of women to conceive safely, without the threat of HIV, and the importance of us continuing to evaluate the safety and pharmacology of cabotegravir in pregnant and breastfeeding women during open-label extension phase of HPTN 084, so that [they] are not excluded from access to this highly effective PrEP agent,” she said. To date, no congenital anomalies have been reported in babies born during the study.
In an update report from HPTN 083, which also showed superiority of CAB LA over TDF-FTC in cisgender men and transgender women (TGW), researchers reported the safety and efficacy of CAB LA use in TGW using gender-affirming hormone therapy (GAHT).
Among the 4,566 participants in HPTN 083, 570 were TGW, and of those, 58% used GAHT at baseline, reported Beatriz Grinsztejn, MD, PhD, head of the STD/AIDS Clinical Research Laboratory at the Instituto Nacional de Infectologicia/Fundação Oswaldo Cruz.
CAB LA drug concentrations measured in a subset of 53 TGW who received on-time CAB injections were comparable between those taking (n = 30) and those not taking GAHT (n = 23), “suggesting the lack of a gender-affirming hormone effect on CAB pharmacokinetics,” she said. “These are very promising results, as we all know that the use of gender-affirming hormone therapy is a major priority for our transgender women community, ... so the lack of drug-drug interaction is really a very important result.”
“Cabotegravir long-acting PrEP is now approved for all at-risk populations, including men who have sex with men, transgender women, and cisgender women, after the results of HPTN 083 and 084,” commented Monica Gandhi, MD, MPH, an infectious disease physician, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco (UCSF).
Dr. Gandhi, who was not involved in either study, is also director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “The incredible efficacy of long-acting PrEP for cisgender women shown by HPTN 084 is game-changing for our practice, and we have already instituted CAB LA across a range of populations at Ward 86,” she said in an interview. “The durability of the 89% additional efficacy of CAB LA over oral TDF/FTC is thrilling and will lead to a greater use of long-acting options.”
She acknowledged that information on potential interactions of GAHT was needed from the HPTN 083 trial. “That cabotegravir levels did not change with the use of estradiol or spironolactone for gender-affirming therapy is important news for our practice and to reassure our TGW that they can safely and effectively use CAB LA for HIV prevention.”
The HPTN 084 and 083 trials were funded by the National Institutes for Allergy and Infectious Diseases. Dr. Delany-Moretlwe, Dr. Grinsztejn, and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – , according to new data from two HIV Prevention Trials Network (HPTN) studies reported at the International AIDS Society Conference.
Follow-up data from the HPTN 084 trial, which compared the two regimens in 3,224 sub-Saharan persons who were assigned female sex at birth, show that three new HIV infections occurred in the CAB LA group in the 12 months since the study was unblinded, versus 20 new infections among the TDF-FTC group. That translates to an 89% lower risk of infection in the CAB LA arm across both the blinded and unblinded phases of the trial, said lead investigator Sinead Delany-Moretlwe, MD, PhD, director of research, Wits Reproductive Health and HIV Institute, the University of the Witwatersrand, Johannesburg, South Africa, during a press conference.
“The trial was designed with the assumption that both drugs were highly effective in preventing HIV infection but that, given the challenges with taking a pill a day, that injectable cabotegravir may offer an adherence advantage,” she said in an interview. “Our data appear to confirm this, as most of the participants in the TDF-FTC arm who became infected with HIV had evidence of poor or inconsistent use of PrEP.”
The study also found that pregnancy incidence increased “two- to threefold” between the blinded and the unblinded period, “and this emphasizes to us the desire of women to conceive safely, without the threat of HIV, and the importance of us continuing to evaluate the safety and pharmacology of cabotegravir in pregnant and breastfeeding women during open-label extension phase of HPTN 084, so that [they] are not excluded from access to this highly effective PrEP agent,” she said. To date, no congenital anomalies have been reported in babies born during the study.
In an update report from HPTN 083, which also showed superiority of CAB LA over TDF-FTC in cisgender men and transgender women (TGW), researchers reported the safety and efficacy of CAB LA use in TGW using gender-affirming hormone therapy (GAHT).
Among the 4,566 participants in HPTN 083, 570 were TGW, and of those, 58% used GAHT at baseline, reported Beatriz Grinsztejn, MD, PhD, head of the STD/AIDS Clinical Research Laboratory at the Instituto Nacional de Infectologicia/Fundação Oswaldo Cruz.
CAB LA drug concentrations measured in a subset of 53 TGW who received on-time CAB injections were comparable between those taking (n = 30) and those not taking GAHT (n = 23), “suggesting the lack of a gender-affirming hormone effect on CAB pharmacokinetics,” she said. “These are very promising results, as we all know that the use of gender-affirming hormone therapy is a major priority for our transgender women community, ... so the lack of drug-drug interaction is really a very important result.”
“Cabotegravir long-acting PrEP is now approved for all at-risk populations, including men who have sex with men, transgender women, and cisgender women, after the results of HPTN 083 and 084,” commented Monica Gandhi, MD, MPH, an infectious disease physician, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco (UCSF).
Dr. Gandhi, who was not involved in either study, is also director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “The incredible efficacy of long-acting PrEP for cisgender women shown by HPTN 084 is game-changing for our practice, and we have already instituted CAB LA across a range of populations at Ward 86,” she said in an interview. “The durability of the 89% additional efficacy of CAB LA over oral TDF/FTC is thrilling and will lead to a greater use of long-acting options.”
She acknowledged that information on potential interactions of GAHT was needed from the HPTN 083 trial. “That cabotegravir levels did not change with the use of estradiol or spironolactone for gender-affirming therapy is important news for our practice and to reassure our TGW that they can safely and effectively use CAB LA for HIV prevention.”
The HPTN 084 and 083 trials were funded by the National Institutes for Allergy and Infectious Diseases. Dr. Delany-Moretlwe, Dr. Grinsztejn, and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – , according to new data from two HIV Prevention Trials Network (HPTN) studies reported at the International AIDS Society Conference.
Follow-up data from the HPTN 084 trial, which compared the two regimens in 3,224 sub-Saharan persons who were assigned female sex at birth, show that three new HIV infections occurred in the CAB LA group in the 12 months since the study was unblinded, versus 20 new infections among the TDF-FTC group. That translates to an 89% lower risk of infection in the CAB LA arm across both the blinded and unblinded phases of the trial, said lead investigator Sinead Delany-Moretlwe, MD, PhD, director of research, Wits Reproductive Health and HIV Institute, the University of the Witwatersrand, Johannesburg, South Africa, during a press conference.
“The trial was designed with the assumption that both drugs were highly effective in preventing HIV infection but that, given the challenges with taking a pill a day, that injectable cabotegravir may offer an adherence advantage,” she said in an interview. “Our data appear to confirm this, as most of the participants in the TDF-FTC arm who became infected with HIV had evidence of poor or inconsistent use of PrEP.”
The study also found that pregnancy incidence increased “two- to threefold” between the blinded and the unblinded period, “and this emphasizes to us the desire of women to conceive safely, without the threat of HIV, and the importance of us continuing to evaluate the safety and pharmacology of cabotegravir in pregnant and breastfeeding women during open-label extension phase of HPTN 084, so that [they] are not excluded from access to this highly effective PrEP agent,” she said. To date, no congenital anomalies have been reported in babies born during the study.
In an update report from HPTN 083, which also showed superiority of CAB LA over TDF-FTC in cisgender men and transgender women (TGW), researchers reported the safety and efficacy of CAB LA use in TGW using gender-affirming hormone therapy (GAHT).
Among the 4,566 participants in HPTN 083, 570 were TGW, and of those, 58% used GAHT at baseline, reported Beatriz Grinsztejn, MD, PhD, head of the STD/AIDS Clinical Research Laboratory at the Instituto Nacional de Infectologicia/Fundação Oswaldo Cruz.
CAB LA drug concentrations measured in a subset of 53 TGW who received on-time CAB injections were comparable between those taking (n = 30) and those not taking GAHT (n = 23), “suggesting the lack of a gender-affirming hormone effect on CAB pharmacokinetics,” she said. “These are very promising results, as we all know that the use of gender-affirming hormone therapy is a major priority for our transgender women community, ... so the lack of drug-drug interaction is really a very important result.”
“Cabotegravir long-acting PrEP is now approved for all at-risk populations, including men who have sex with men, transgender women, and cisgender women, after the results of HPTN 083 and 084,” commented Monica Gandhi, MD, MPH, an infectious disease physician, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco (UCSF).
Dr. Gandhi, who was not involved in either study, is also director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “The incredible efficacy of long-acting PrEP for cisgender women shown by HPTN 084 is game-changing for our practice, and we have already instituted CAB LA across a range of populations at Ward 86,” she said in an interview. “The durability of the 89% additional efficacy of CAB LA over oral TDF/FTC is thrilling and will lead to a greater use of long-acting options.”
She acknowledged that information on potential interactions of GAHT was needed from the HPTN 083 trial. “That cabotegravir levels did not change with the use of estradiol or spironolactone for gender-affirming therapy is important news for our practice and to reassure our TGW that they can safely and effectively use CAB LA for HIV prevention.”
The HPTN 084 and 083 trials were funded by the National Institutes for Allergy and Infectious Diseases. Dr. Delany-Moretlwe, Dr. Grinsztejn, and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AIDS 2022
Children and COVID: Weekly cases top 95,000, admissions continue to rise
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.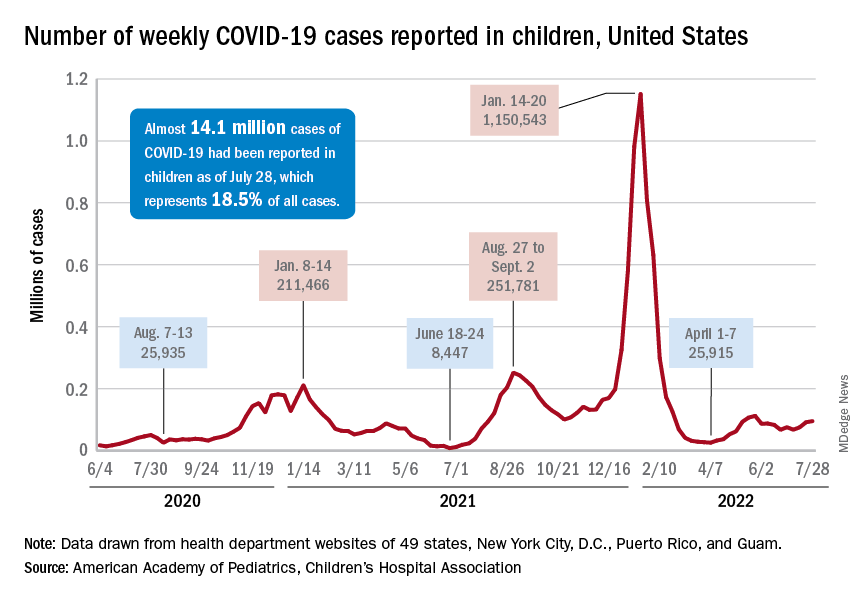
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.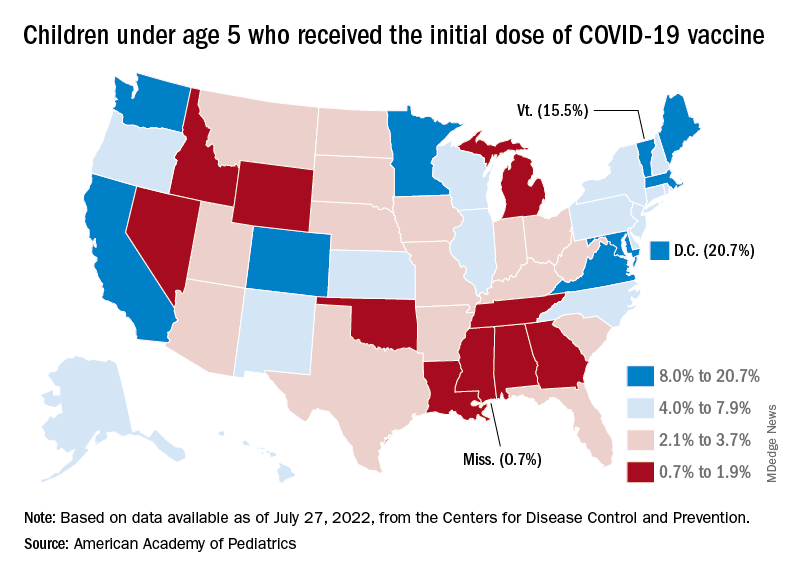
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
COVID skin manifestations vary by type of variant, U.K. study finds
during the Omicron and Delta waves.
Among the key findings, the study shows that skin involvement during the Omicron wave was less frequent than during the Delta wave (11.4% vs. 17.6%), skin symptoms generally resolved more quickly, and that the risk for skin symptoms was similar whether patients had or had not been vaccinated, according to a team led by Alessia Visconti, PhD, a research fellow in the department of twin research and genetic epidemiology, King’s College, London.
These data are consistent with the experience of those dermatologists who have been following this area closely, according to Esther Freeman, MD, PhD, associate professor of dermatology at Harvard Medical School and director of MGH Global Health Dermatology at Massachusetts General Hospital, both in Boston.
“Anecdotally, we thought we were seeing fewer skin symptoms with Omicron versus Delta and the ancestral strains, and now this study shows it is true,” said Dr. Freeman, who is also principal investigator of the American Academy of Dermatology’s International Dermatology COVID-19 Registry.
The data also confirm that the skin is less likely to be involved than in past waves of COVID-19 infections.
“Up to this point, it was hard to know if we were seeing fewer referrals for COVID-related skin rashes or if clinicians had just become more comfortable with these rashes and were not referring them as often,” added Dr. Freeman, who was among the study coauthors.
Data captured from 348,691 patients
The data from the study was generated by 348,691 users in the United Kingdom of the ZOE COVID study app, a smartphone-based tool introduced relatively early in the pandemic. It asked users to provide demographic data, information on COVID-19 symptoms, including those involving the skin, and treatments. Of 33 COVID-related symptoms included in the app, five related to the skin (acral rash, burning rash, erythematopapular rash, urticarial rash, and unusual hair loss).
While the focus of this study was to compare skin manifestations during the Omicron wave with the Delta wave of COVID-19, the investigators also had data on the experience in 2020 with wild-type COVID-19 that preceded both variants. Overall, this showed a stepwise decline in skin symptoms overall, as well in as skin symptoms that occurred in the absence of systemic symptoms.
“The shift in the skin manifestations makes sense when you think about the change that is also being seen in the systemic symptoms,” said Dr. Freeman, referring to lower rates of cough and loss of smell but higher rates of sore throat and fatigue. “Omicron is achieving immune escape, which is why there is a shift in involved tissues,” she said in an interview.
Previous data collected during the wild-type COVID-19 stage of the pandemic by the same group of investigators showed that 17% of patients reported skin rash as the first symptom of COVID-19 infection, and 21% reported skin rash as the only clinical sign of infection.
In the Delta and Omicron waves, skin rash was an isolated initial symptom in only 0.8% and 0.5% of patients, respectively. (The authors noted that, in the United Kingdom, the first documented samples of the Delta variant were detected in October 2020, and the first documented samples of the Omicron variant were detected in November 2021.)
During the early stages of wild-type COVID, an acral rash was characteristic, occurring in 3.1% of patients, according to the U.K. data. In the Delta wave, acral rashes, at an incidence of 1.1% remained positively correlated with a diagnosis of COVID-19 infection. In the Omicron wave, acral rashes were observed in only 0.7% of patients and were no longer statistically correlated with a positive COVID diagnosis.
Characteristic cutaneous symptoms are evolving
Early in the course of the COVID-19 epidemic, more than 30 types of rashes were observed in patients with COVID-19 infection. Cutaneous symptoms continue to be diverse, but some, such as acral rash, are being seen less frequently. For example, the odds ratio of a positive COVID-19 diagnosis among those with an erythematopapular rash fell from 1.76 to 1.08 between the Delta and Omicron waves.
While specific cutaneous symptoms are less predictive of a diagnosis of COVID-19, clinicians should not discount cutaneous symptoms as a sign of disease, according to Veronique Bataille, MD, PhD, a consultant dermatologist at King’s College.
“You need to keep an open mind” regarding cutaneous signs and a diagnosis of COVID-19, Dr. Bataille, one of the coauthors of the U.K. report, said in an interview. In general, she considers a low threshold of suspicion appropriate. “If the patient has no past history of skin disease and no other triggers for a rash, then, in a high prevalence area, COVID must be suspected.”
In most cases, the rash resolves on its own, but Dr. Bataille emphasized the need for individualized care. Even as the risk of life-threatening COVID-19 infections appears to be diminishing with current variants, cutaneous manifestations can be severe.
“There are cases of long COVID affecting the skin, such as urticaria or a lichenoid erythematopapular rash, both of which can be very pruritic and difficult to control,” she said.
Dr. Freeman echoed the importance of an individualized approach. She agreed that most cutaneous symptoms are self-limited, but there are exceptions and treatments vary for the different types of skin involvement. “I think another point to consider when examining skin lesions is monkey pox. The fact that these are overlapping outbreaks should not be ignored. You need to be alert for both.”
Dr. Visconti, Dr. Freeman, and Dr. Bataille reported no potential conflicts of interest.
during the Omicron and Delta waves.
Among the key findings, the study shows that skin involvement during the Omicron wave was less frequent than during the Delta wave (11.4% vs. 17.6%), skin symptoms generally resolved more quickly, and that the risk for skin symptoms was similar whether patients had or had not been vaccinated, according to a team led by Alessia Visconti, PhD, a research fellow in the department of twin research and genetic epidemiology, King’s College, London.
These data are consistent with the experience of those dermatologists who have been following this area closely, according to Esther Freeman, MD, PhD, associate professor of dermatology at Harvard Medical School and director of MGH Global Health Dermatology at Massachusetts General Hospital, both in Boston.
“Anecdotally, we thought we were seeing fewer skin symptoms with Omicron versus Delta and the ancestral strains, and now this study shows it is true,” said Dr. Freeman, who is also principal investigator of the American Academy of Dermatology’s International Dermatology COVID-19 Registry.
The data also confirm that the skin is less likely to be involved than in past waves of COVID-19 infections.
“Up to this point, it was hard to know if we were seeing fewer referrals for COVID-related skin rashes or if clinicians had just become more comfortable with these rashes and were not referring them as often,” added Dr. Freeman, who was among the study coauthors.
Data captured from 348,691 patients
The data from the study was generated by 348,691 users in the United Kingdom of the ZOE COVID study app, a smartphone-based tool introduced relatively early in the pandemic. It asked users to provide demographic data, information on COVID-19 symptoms, including those involving the skin, and treatments. Of 33 COVID-related symptoms included in the app, five related to the skin (acral rash, burning rash, erythematopapular rash, urticarial rash, and unusual hair loss).
While the focus of this study was to compare skin manifestations during the Omicron wave with the Delta wave of COVID-19, the investigators also had data on the experience in 2020 with wild-type COVID-19 that preceded both variants. Overall, this showed a stepwise decline in skin symptoms overall, as well in as skin symptoms that occurred in the absence of systemic symptoms.
“The shift in the skin manifestations makes sense when you think about the change that is also being seen in the systemic symptoms,” said Dr. Freeman, referring to lower rates of cough and loss of smell but higher rates of sore throat and fatigue. “Omicron is achieving immune escape, which is why there is a shift in involved tissues,” she said in an interview.
Previous data collected during the wild-type COVID-19 stage of the pandemic by the same group of investigators showed that 17% of patients reported skin rash as the first symptom of COVID-19 infection, and 21% reported skin rash as the only clinical sign of infection.
In the Delta and Omicron waves, skin rash was an isolated initial symptom in only 0.8% and 0.5% of patients, respectively. (The authors noted that, in the United Kingdom, the first documented samples of the Delta variant were detected in October 2020, and the first documented samples of the Omicron variant were detected in November 2021.)
During the early stages of wild-type COVID, an acral rash was characteristic, occurring in 3.1% of patients, according to the U.K. data. In the Delta wave, acral rashes, at an incidence of 1.1% remained positively correlated with a diagnosis of COVID-19 infection. In the Omicron wave, acral rashes were observed in only 0.7% of patients and were no longer statistically correlated with a positive COVID diagnosis.
Characteristic cutaneous symptoms are evolving
Early in the course of the COVID-19 epidemic, more than 30 types of rashes were observed in patients with COVID-19 infection. Cutaneous symptoms continue to be diverse, but some, such as acral rash, are being seen less frequently. For example, the odds ratio of a positive COVID-19 diagnosis among those with an erythematopapular rash fell from 1.76 to 1.08 between the Delta and Omicron waves.
While specific cutaneous symptoms are less predictive of a diagnosis of COVID-19, clinicians should not discount cutaneous symptoms as a sign of disease, according to Veronique Bataille, MD, PhD, a consultant dermatologist at King’s College.
“You need to keep an open mind” regarding cutaneous signs and a diagnosis of COVID-19, Dr. Bataille, one of the coauthors of the U.K. report, said in an interview. In general, she considers a low threshold of suspicion appropriate. “If the patient has no past history of skin disease and no other triggers for a rash, then, in a high prevalence area, COVID must be suspected.”
In most cases, the rash resolves on its own, but Dr. Bataille emphasized the need for individualized care. Even as the risk of life-threatening COVID-19 infections appears to be diminishing with current variants, cutaneous manifestations can be severe.
“There are cases of long COVID affecting the skin, such as urticaria or a lichenoid erythematopapular rash, both of which can be very pruritic and difficult to control,” she said.
Dr. Freeman echoed the importance of an individualized approach. She agreed that most cutaneous symptoms are self-limited, but there are exceptions and treatments vary for the different types of skin involvement. “I think another point to consider when examining skin lesions is monkey pox. The fact that these are overlapping outbreaks should not be ignored. You need to be alert for both.”
Dr. Visconti, Dr. Freeman, and Dr. Bataille reported no potential conflicts of interest.
during the Omicron and Delta waves.
Among the key findings, the study shows that skin involvement during the Omicron wave was less frequent than during the Delta wave (11.4% vs. 17.6%), skin symptoms generally resolved more quickly, and that the risk for skin symptoms was similar whether patients had or had not been vaccinated, according to a team led by Alessia Visconti, PhD, a research fellow in the department of twin research and genetic epidemiology, King’s College, London.
These data are consistent with the experience of those dermatologists who have been following this area closely, according to Esther Freeman, MD, PhD, associate professor of dermatology at Harvard Medical School and director of MGH Global Health Dermatology at Massachusetts General Hospital, both in Boston.
“Anecdotally, we thought we were seeing fewer skin symptoms with Omicron versus Delta and the ancestral strains, and now this study shows it is true,” said Dr. Freeman, who is also principal investigator of the American Academy of Dermatology’s International Dermatology COVID-19 Registry.
The data also confirm that the skin is less likely to be involved than in past waves of COVID-19 infections.
“Up to this point, it was hard to know if we were seeing fewer referrals for COVID-related skin rashes or if clinicians had just become more comfortable with these rashes and were not referring them as often,” added Dr. Freeman, who was among the study coauthors.
Data captured from 348,691 patients
The data from the study was generated by 348,691 users in the United Kingdom of the ZOE COVID study app, a smartphone-based tool introduced relatively early in the pandemic. It asked users to provide demographic data, information on COVID-19 symptoms, including those involving the skin, and treatments. Of 33 COVID-related symptoms included in the app, five related to the skin (acral rash, burning rash, erythematopapular rash, urticarial rash, and unusual hair loss).
While the focus of this study was to compare skin manifestations during the Omicron wave with the Delta wave of COVID-19, the investigators also had data on the experience in 2020 with wild-type COVID-19 that preceded both variants. Overall, this showed a stepwise decline in skin symptoms overall, as well in as skin symptoms that occurred in the absence of systemic symptoms.
“The shift in the skin manifestations makes sense when you think about the change that is also being seen in the systemic symptoms,” said Dr. Freeman, referring to lower rates of cough and loss of smell but higher rates of sore throat and fatigue. “Omicron is achieving immune escape, which is why there is a shift in involved tissues,” she said in an interview.
Previous data collected during the wild-type COVID-19 stage of the pandemic by the same group of investigators showed that 17% of patients reported skin rash as the first symptom of COVID-19 infection, and 21% reported skin rash as the only clinical sign of infection.
In the Delta and Omicron waves, skin rash was an isolated initial symptom in only 0.8% and 0.5% of patients, respectively. (The authors noted that, in the United Kingdom, the first documented samples of the Delta variant were detected in October 2020, and the first documented samples of the Omicron variant were detected in November 2021.)
During the early stages of wild-type COVID, an acral rash was characteristic, occurring in 3.1% of patients, according to the U.K. data. In the Delta wave, acral rashes, at an incidence of 1.1% remained positively correlated with a diagnosis of COVID-19 infection. In the Omicron wave, acral rashes were observed in only 0.7% of patients and were no longer statistically correlated with a positive COVID diagnosis.
Characteristic cutaneous symptoms are evolving
Early in the course of the COVID-19 epidemic, more than 30 types of rashes were observed in patients with COVID-19 infection. Cutaneous symptoms continue to be diverse, but some, such as acral rash, are being seen less frequently. For example, the odds ratio of a positive COVID-19 diagnosis among those with an erythematopapular rash fell from 1.76 to 1.08 between the Delta and Omicron waves.
While specific cutaneous symptoms are less predictive of a diagnosis of COVID-19, clinicians should not discount cutaneous symptoms as a sign of disease, according to Veronique Bataille, MD, PhD, a consultant dermatologist at King’s College.
“You need to keep an open mind” regarding cutaneous signs and a diagnosis of COVID-19, Dr. Bataille, one of the coauthors of the U.K. report, said in an interview. In general, she considers a low threshold of suspicion appropriate. “If the patient has no past history of skin disease and no other triggers for a rash, then, in a high prevalence area, COVID must be suspected.”
In most cases, the rash resolves on its own, but Dr. Bataille emphasized the need for individualized care. Even as the risk of life-threatening COVID-19 infections appears to be diminishing with current variants, cutaneous manifestations can be severe.
“There are cases of long COVID affecting the skin, such as urticaria or a lichenoid erythematopapular rash, both of which can be very pruritic and difficult to control,” she said.
Dr. Freeman echoed the importance of an individualized approach. She agreed that most cutaneous symptoms are self-limited, but there are exceptions and treatments vary for the different types of skin involvement. “I think another point to consider when examining skin lesions is monkey pox. The fact that these are overlapping outbreaks should not be ignored. You need to be alert for both.”
Dr. Visconti, Dr. Freeman, and Dr. Bataille reported no potential conflicts of interest.
FROM THE BRITISH JOURNAL OF DERMATOLOGY