User login
Higher buprenorphine doses help OUD patients stay in treatment
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
AT APA 2023
Peak seasons, times for suicidal thoughts, attempts identified
In addition, the results from Harvard University’s Project Implicit Health also show that people are most likely to make an attempt at suicide between 4 and 6 a.m.
“No research has demonstrated a peak in suicidal ideation in winter until our paper,” study investigator Brian O’Shea, PhD, assistant professor of social psychology at the University of Nottingham, England, told this news organization.
“Most people incorrectly assume that suicide behaviours peak in winter and are surprised, as I was, when learning about this phenomenon, that suicide actually peaks in spring/early summer,” he added.
However, at least one expert cautioned that the database, which comprises mostly responses from younger women, doesn’t capture responses from those who are most likely to attempt suicide: older men with substance abuse.
The findings were published online in Translational Psychiatry.
New insight into suicide risk
Previous studies examining the seasonality of suicides and suicide attempts have reported a peak in spring and early summer, but there has been very little information about why this may be, the investigators noted.
Dr. O’Shea and his colleague from the University of Amsterdam, René Freichel, mined one of the databases from Project Implicit Health, which contains self-report measures on suicidal ideation, self-harm, and past suicide attempts, as well as respondents’ implicit biases on these topics.
The analysis included data from 10,000 respondents living in the United States, United Kingdom, and Canada provided between April 2012 and November 2018.
The sample was predominantly young and female, with 38% (3,247) of the sample reporting that they had made at least one suicide attempt.
The researchers found a peak in negative mood and desire to die occurring in December, especially among those who reported attempting suicide (P ≤ .001)
Suicidal ideation peaked approximately 3-4 months before the annual seasonal crest of suicide attempts in early spring and summer.
“Affected individuals may become severely depressed and experience a lack of energy throughout the winter months. Essentially, this period may put them below a threshold of severe suicide risk as the high level of suicidal ideation coincides with a low level of energy,” said Dr. O’Shea.
When the days get longer, brighter, and warmer, these changes likely improve an individuals’ mood, he explained. “Hence, the most at-risk individuals become slightly less depressed and may gain more energy to contemplate and plan their method to attempt suicide,” Dr. O’Shea noted.
A major limitation of the study is that all responses included in analysis were based on self-report.
To confirm the findings, future research should include ecological momentary assessment, which involves using a large community sample to question participants about suicidal intent at various time points, along with real-time monitoring of vital signs, said Dr. O’Shea.
Ideally, the investigators noted, the study’s findings will inform clinician assessments of patients who are at risk for suicide.
A research gap?
Commenting on the findings, Justin Shuster, MD, MPH, assistant professor of psychiatry at the University of Pittsburgh and medical director of two psychiatric units at Western Psychiatric Hospital, noted that the database used in the study did not include responses from those who were most likely to attempt or commit suicide: older men with a history of substance abuse, who require social supports, and who have a family history of suicide.
Though Dr. Shuster agreed with Dr. O’Shea about the possibility that spring brought energy to a desire to take one’s life, he had another theory.
“When people are depressed in the winter, they expect to feel better with the advent of the warmer weather in spring. When they don’t feel better, they may think to themselves, ‘If I’m going to feel like this forever, I may as well follow through with these plans,’ ” he said.
As for the early morning attempts, he noted that 4-6 a.m. is often when people are alone, and there are fewer distractions.
“The other thing I see a great deal of clinically is intoxication,” said Dr. Shuster. “Either intoxication with substances or alcohol, or the fact that intoxication is waning at those early morning hours, and people are becoming desperate as they face a new day,” he said.
The study was funded by a German Academic Exchange Service Scholarship and an EU Horizon 2020 Fellowship. Dr. O’Shea reports being an unpaid member of Project Implicit’s scientific advisory board and is on the executive committee of Project Implicit Health.
A version of this article first appeared on Medscape.com.
In addition, the results from Harvard University’s Project Implicit Health also show that people are most likely to make an attempt at suicide between 4 and 6 a.m.
“No research has demonstrated a peak in suicidal ideation in winter until our paper,” study investigator Brian O’Shea, PhD, assistant professor of social psychology at the University of Nottingham, England, told this news organization.
“Most people incorrectly assume that suicide behaviours peak in winter and are surprised, as I was, when learning about this phenomenon, that suicide actually peaks in spring/early summer,” he added.
However, at least one expert cautioned that the database, which comprises mostly responses from younger women, doesn’t capture responses from those who are most likely to attempt suicide: older men with substance abuse.
The findings were published online in Translational Psychiatry.
New insight into suicide risk
Previous studies examining the seasonality of suicides and suicide attempts have reported a peak in spring and early summer, but there has been very little information about why this may be, the investigators noted.
Dr. O’Shea and his colleague from the University of Amsterdam, René Freichel, mined one of the databases from Project Implicit Health, which contains self-report measures on suicidal ideation, self-harm, and past suicide attempts, as well as respondents’ implicit biases on these topics.
The analysis included data from 10,000 respondents living in the United States, United Kingdom, and Canada provided between April 2012 and November 2018.
The sample was predominantly young and female, with 38% (3,247) of the sample reporting that they had made at least one suicide attempt.
The researchers found a peak in negative mood and desire to die occurring in December, especially among those who reported attempting suicide (P ≤ .001)
Suicidal ideation peaked approximately 3-4 months before the annual seasonal crest of suicide attempts in early spring and summer.
“Affected individuals may become severely depressed and experience a lack of energy throughout the winter months. Essentially, this period may put them below a threshold of severe suicide risk as the high level of suicidal ideation coincides with a low level of energy,” said Dr. O’Shea.
When the days get longer, brighter, and warmer, these changes likely improve an individuals’ mood, he explained. “Hence, the most at-risk individuals become slightly less depressed and may gain more energy to contemplate and plan their method to attempt suicide,” Dr. O’Shea noted.
A major limitation of the study is that all responses included in analysis were based on self-report.
To confirm the findings, future research should include ecological momentary assessment, which involves using a large community sample to question participants about suicidal intent at various time points, along with real-time monitoring of vital signs, said Dr. O’Shea.
Ideally, the investigators noted, the study’s findings will inform clinician assessments of patients who are at risk for suicide.
A research gap?
Commenting on the findings, Justin Shuster, MD, MPH, assistant professor of psychiatry at the University of Pittsburgh and medical director of two psychiatric units at Western Psychiatric Hospital, noted that the database used in the study did not include responses from those who were most likely to attempt or commit suicide: older men with a history of substance abuse, who require social supports, and who have a family history of suicide.
Though Dr. Shuster agreed with Dr. O’Shea about the possibility that spring brought energy to a desire to take one’s life, he had another theory.
“When people are depressed in the winter, they expect to feel better with the advent of the warmer weather in spring. When they don’t feel better, they may think to themselves, ‘If I’m going to feel like this forever, I may as well follow through with these plans,’ ” he said.
As for the early morning attempts, he noted that 4-6 a.m. is often when people are alone, and there are fewer distractions.
“The other thing I see a great deal of clinically is intoxication,” said Dr. Shuster. “Either intoxication with substances or alcohol, or the fact that intoxication is waning at those early morning hours, and people are becoming desperate as they face a new day,” he said.
The study was funded by a German Academic Exchange Service Scholarship and an EU Horizon 2020 Fellowship. Dr. O’Shea reports being an unpaid member of Project Implicit’s scientific advisory board and is on the executive committee of Project Implicit Health.
A version of this article first appeared on Medscape.com.
In addition, the results from Harvard University’s Project Implicit Health also show that people are most likely to make an attempt at suicide between 4 and 6 a.m.
“No research has demonstrated a peak in suicidal ideation in winter until our paper,” study investigator Brian O’Shea, PhD, assistant professor of social psychology at the University of Nottingham, England, told this news organization.
“Most people incorrectly assume that suicide behaviours peak in winter and are surprised, as I was, when learning about this phenomenon, that suicide actually peaks in spring/early summer,” he added.
However, at least one expert cautioned that the database, which comprises mostly responses from younger women, doesn’t capture responses from those who are most likely to attempt suicide: older men with substance abuse.
The findings were published online in Translational Psychiatry.
New insight into suicide risk
Previous studies examining the seasonality of suicides and suicide attempts have reported a peak in spring and early summer, but there has been very little information about why this may be, the investigators noted.
Dr. O’Shea and his colleague from the University of Amsterdam, René Freichel, mined one of the databases from Project Implicit Health, which contains self-report measures on suicidal ideation, self-harm, and past suicide attempts, as well as respondents’ implicit biases on these topics.
The analysis included data from 10,000 respondents living in the United States, United Kingdom, and Canada provided between April 2012 and November 2018.
The sample was predominantly young and female, with 38% (3,247) of the sample reporting that they had made at least one suicide attempt.
The researchers found a peak in negative mood and desire to die occurring in December, especially among those who reported attempting suicide (P ≤ .001)
Suicidal ideation peaked approximately 3-4 months before the annual seasonal crest of suicide attempts in early spring and summer.
“Affected individuals may become severely depressed and experience a lack of energy throughout the winter months. Essentially, this period may put them below a threshold of severe suicide risk as the high level of suicidal ideation coincides with a low level of energy,” said Dr. O’Shea.
When the days get longer, brighter, and warmer, these changes likely improve an individuals’ mood, he explained. “Hence, the most at-risk individuals become slightly less depressed and may gain more energy to contemplate and plan their method to attempt suicide,” Dr. O’Shea noted.
A major limitation of the study is that all responses included in analysis were based on self-report.
To confirm the findings, future research should include ecological momentary assessment, which involves using a large community sample to question participants about suicidal intent at various time points, along with real-time monitoring of vital signs, said Dr. O’Shea.
Ideally, the investigators noted, the study’s findings will inform clinician assessments of patients who are at risk for suicide.
A research gap?
Commenting on the findings, Justin Shuster, MD, MPH, assistant professor of psychiatry at the University of Pittsburgh and medical director of two psychiatric units at Western Psychiatric Hospital, noted that the database used in the study did not include responses from those who were most likely to attempt or commit suicide: older men with a history of substance abuse, who require social supports, and who have a family history of suicide.
Though Dr. Shuster agreed with Dr. O’Shea about the possibility that spring brought energy to a desire to take one’s life, he had another theory.
“When people are depressed in the winter, they expect to feel better with the advent of the warmer weather in spring. When they don’t feel better, they may think to themselves, ‘If I’m going to feel like this forever, I may as well follow through with these plans,’ ” he said.
As for the early morning attempts, he noted that 4-6 a.m. is often when people are alone, and there are fewer distractions.
“The other thing I see a great deal of clinically is intoxication,” said Dr. Shuster. “Either intoxication with substances or alcohol, or the fact that intoxication is waning at those early morning hours, and people are becoming desperate as they face a new day,” he said.
The study was funded by a German Academic Exchange Service Scholarship and an EU Horizon 2020 Fellowship. Dr. O’Shea reports being an unpaid member of Project Implicit’s scientific advisory board and is on the executive committee of Project Implicit Health.
A version of this article first appeared on Medscape.com.
FROM TRANSLATIONAL PSYCHIATRY
Prenatal sleep problems, depression linked to poorer outcomes
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
AT ACOG 2023
APA launches online eating disorder assessment tool
The American Psychiatric Association has released an online screening and assessment tool for eating disorders.
“People with eating disorders have a high rate of mortality and [the disorder is] growing in prevalence among young adults and adolescents,” APA CEO and medical director Saul Levin, MD, MPA, said in a news release.
“It is vital that we equip our clinicians, especially primary care clinicians, with the latest evidence from the APA to empower their decision-making and improve care for their patients,” Dr. Levin added.
The clinical decision support tool was developed by the APA’s guideline writing group in collaboration with AvoMD, a software company that translates clinical evidence into the workflow.
The tool guides clinicians through the screening, assessing, diagnosing, and treatment planning of patients with anorexia nervosa, bulimia nervosa, binge-eating disorder, and other eating disorders.
It’s available free in the electronic health record, on the APA website, and on the AvoMD mobile app.
The tool is based on the APA’s updated practice guidelines for the management of eating disorders, which were released in March.
The tool incorporates guidance on screening tools, levels of care, nutrition, exercise, psychotherapy, and more. Additionally, the tool provides a summary of responses that can be leveraged for easy documentation.
It is intended for use by pediatricians, family physicians, and other primary care and mental health clinicians, including psychiatrists and therapists.
Data published earlier this year show that more than 1 in 5 children worldwide are at risk of developing an eating disorder. Girls are significantly more likely than boys to have disordered eating.
Early diagnosis and treatment are associated with a higher rate of recovery, and extended illness is associated with potentially devastating consequences, the APA notes.
“As an internal medicine physician myself, I see a wide variety of patients and clinical issues,” Joongheum Park, MD, head of product and engineering at AvoMD, said in the release.
“Easy access to the expertise in me and my peers’ workflow is essential to ensuring high-quality care, and partnering with the leading authority on eating disorders to provide this tool will improve clinician efficiency and most importantly, patient outcomes,” Dr. Park added.
A version of this article first appeared on Medscape.com.
The American Psychiatric Association has released an online screening and assessment tool for eating disorders.
“People with eating disorders have a high rate of mortality and [the disorder is] growing in prevalence among young adults and adolescents,” APA CEO and medical director Saul Levin, MD, MPA, said in a news release.
“It is vital that we equip our clinicians, especially primary care clinicians, with the latest evidence from the APA to empower their decision-making and improve care for their patients,” Dr. Levin added.
The clinical decision support tool was developed by the APA’s guideline writing group in collaboration with AvoMD, a software company that translates clinical evidence into the workflow.
The tool guides clinicians through the screening, assessing, diagnosing, and treatment planning of patients with anorexia nervosa, bulimia nervosa, binge-eating disorder, and other eating disorders.
It’s available free in the electronic health record, on the APA website, and on the AvoMD mobile app.
The tool is based on the APA’s updated practice guidelines for the management of eating disorders, which were released in March.
The tool incorporates guidance on screening tools, levels of care, nutrition, exercise, psychotherapy, and more. Additionally, the tool provides a summary of responses that can be leveraged for easy documentation.
It is intended for use by pediatricians, family physicians, and other primary care and mental health clinicians, including psychiatrists and therapists.
Data published earlier this year show that more than 1 in 5 children worldwide are at risk of developing an eating disorder. Girls are significantly more likely than boys to have disordered eating.
Early diagnosis and treatment are associated with a higher rate of recovery, and extended illness is associated with potentially devastating consequences, the APA notes.
“As an internal medicine physician myself, I see a wide variety of patients and clinical issues,” Joongheum Park, MD, head of product and engineering at AvoMD, said in the release.
“Easy access to the expertise in me and my peers’ workflow is essential to ensuring high-quality care, and partnering with the leading authority on eating disorders to provide this tool will improve clinician efficiency and most importantly, patient outcomes,” Dr. Park added.
A version of this article first appeared on Medscape.com.
The American Psychiatric Association has released an online screening and assessment tool for eating disorders.
“People with eating disorders have a high rate of mortality and [the disorder is] growing in prevalence among young adults and adolescents,” APA CEO and medical director Saul Levin, MD, MPA, said in a news release.
“It is vital that we equip our clinicians, especially primary care clinicians, with the latest evidence from the APA to empower their decision-making and improve care for their patients,” Dr. Levin added.
The clinical decision support tool was developed by the APA’s guideline writing group in collaboration with AvoMD, a software company that translates clinical evidence into the workflow.
The tool guides clinicians through the screening, assessing, diagnosing, and treatment planning of patients with anorexia nervosa, bulimia nervosa, binge-eating disorder, and other eating disorders.
It’s available free in the electronic health record, on the APA website, and on the AvoMD mobile app.
The tool is based on the APA’s updated practice guidelines for the management of eating disorders, which were released in March.
The tool incorporates guidance on screening tools, levels of care, nutrition, exercise, psychotherapy, and more. Additionally, the tool provides a summary of responses that can be leveraged for easy documentation.
It is intended for use by pediatricians, family physicians, and other primary care and mental health clinicians, including psychiatrists and therapists.
Data published earlier this year show that more than 1 in 5 children worldwide are at risk of developing an eating disorder. Girls are significantly more likely than boys to have disordered eating.
Early diagnosis and treatment are associated with a higher rate of recovery, and extended illness is associated with potentially devastating consequences, the APA notes.
“As an internal medicine physician myself, I see a wide variety of patients and clinical issues,” Joongheum Park, MD, head of product and engineering at AvoMD, said in the release.
“Easy access to the expertise in me and my peers’ workflow is essential to ensuring high-quality care, and partnering with the leading authority on eating disorders to provide this tool will improve clinician efficiency and most importantly, patient outcomes,” Dr. Park added.
A version of this article first appeared on Medscape.com.
Buprenorphine update: Looser rules and a helpful injectable
SAN FRANCISCO – As the opioid epidemic continues to grow and evolve, the federal government is trying to make it easier for clinicians to treat abusers with the drug buprenorphine, psychiatrists told colleagues at the annual meeting of the American Psychiatric Association. And an injectable version of the drug is making a big difference.
John A. Renner Jr., MD, of Boston University, said in a presentation at the APA meeting.
As Dr. Renner explained, the United States is now in the fourth wave of nearly a quarter-century of opioid overdose-related deaths. The outbreak began in 1999 as prescription opioids spurred deaths, and heroin overdoses began to rise in 2010. The third wave brought rises in deaths from synthetic opioids such as fentanyl in 2013. In 2015, the fourth wave – driven by deaths from combinations of synthetic opioids and psychostimulants like methamphetamines – started in 2015.
COVID-19 seems to have played a role too: In 2020, opioid overdose deaths spiked during the early months of the pandemic. In 2021, drug-related overdose deaths overall hit a high of 106,889, including 80,411 linked to opioids. In contrast, fewer than 20,000 drug-related overdose deaths were reported in 1999.
On the other hand, deaths from prescription drug overdoses are falling, Dr. Renner said, suggesting “improvement in terms of how clinicians are handling medications and our prescribing practices. But that’s being masked by what’s happened with fentanyl and methamphetamine.”
Buprenorphine (Subutex), used to treat opioid use withdrawal, is itself an opioid and can cause addiction and death in some cases. However, Dr. Renner highlighted a 2023 study that determined that efforts to increase its use from 2019 to 2021 didn’t appear to boost buprenorphine-related overdose deaths in the United States.
New federal regulations aim to make it easier to prescribe buprenorphine. Thanks to Congressional legislation, the Drug Enforcement Administration in January 2023 eliminated regulations requiring clinicians to undergo special training to get an “X-waiver” to be able to prescribe buprenorphine. But they’re not off the hook entirely: As of June 27, 2023, providers must have undergone training in order to apply for – or renew – a DEA license to prescribe certain controlled substances like buprenorphine.
“I’m afraid that people will be able to meet that requirement easily, and they’re not going to get good coordinated teaching,” Dr. Renner said. “I’m not sure that’s really going to improve the quality of care that we’re delivering.”
In regard to treatment, psychiatrist Dong Chan Park, MD, of Boston University, touted a long-acting injectable form of buprenorphine known by the brand name Sublocade. The FDA approved Sublocade in 2017 for patients who’ve been taking sublingual buprenorphine for at least 7 days, although Dr. Park said research suggests the 7-day period may not be necessary.
“We’ve utilized this about 2.5-plus years in my hospital, and it’s really been a game changer for some of our sickest, most challenging patients,” he said at the APA presentation. As he explained, one benefit is that patients can’t repeatedly avoid doses depending on how they feel, as they may do with the sublingual version. “On the first day of injection, you can actually stop the sublingual buprenorphine.”
Dr. Renner emphasized the importance of getting users on buprenorphine as fast as possible. If the treatment begins in the ED, he said, “they need to have a system that is going to be able to pick them up and continue the care.”
Otherwise, the risk is high. “We’re in a very dangerous era,” he said, “where the patient walks out the door, and then they die.”
Dr. Park had no disclosures, and Dr. Renner disclosed royalties from the APA.
SAN FRANCISCO – As the opioid epidemic continues to grow and evolve, the federal government is trying to make it easier for clinicians to treat abusers with the drug buprenorphine, psychiatrists told colleagues at the annual meeting of the American Psychiatric Association. And an injectable version of the drug is making a big difference.
John A. Renner Jr., MD, of Boston University, said in a presentation at the APA meeting.
As Dr. Renner explained, the United States is now in the fourth wave of nearly a quarter-century of opioid overdose-related deaths. The outbreak began in 1999 as prescription opioids spurred deaths, and heroin overdoses began to rise in 2010. The third wave brought rises in deaths from synthetic opioids such as fentanyl in 2013. In 2015, the fourth wave – driven by deaths from combinations of synthetic opioids and psychostimulants like methamphetamines – started in 2015.
COVID-19 seems to have played a role too: In 2020, opioid overdose deaths spiked during the early months of the pandemic. In 2021, drug-related overdose deaths overall hit a high of 106,889, including 80,411 linked to opioids. In contrast, fewer than 20,000 drug-related overdose deaths were reported in 1999.
On the other hand, deaths from prescription drug overdoses are falling, Dr. Renner said, suggesting “improvement in terms of how clinicians are handling medications and our prescribing practices. But that’s being masked by what’s happened with fentanyl and methamphetamine.”
Buprenorphine (Subutex), used to treat opioid use withdrawal, is itself an opioid and can cause addiction and death in some cases. However, Dr. Renner highlighted a 2023 study that determined that efforts to increase its use from 2019 to 2021 didn’t appear to boost buprenorphine-related overdose deaths in the United States.
New federal regulations aim to make it easier to prescribe buprenorphine. Thanks to Congressional legislation, the Drug Enforcement Administration in January 2023 eliminated regulations requiring clinicians to undergo special training to get an “X-waiver” to be able to prescribe buprenorphine. But they’re not off the hook entirely: As of June 27, 2023, providers must have undergone training in order to apply for – or renew – a DEA license to prescribe certain controlled substances like buprenorphine.
“I’m afraid that people will be able to meet that requirement easily, and they’re not going to get good coordinated teaching,” Dr. Renner said. “I’m not sure that’s really going to improve the quality of care that we’re delivering.”
In regard to treatment, psychiatrist Dong Chan Park, MD, of Boston University, touted a long-acting injectable form of buprenorphine known by the brand name Sublocade. The FDA approved Sublocade in 2017 for patients who’ve been taking sublingual buprenorphine for at least 7 days, although Dr. Park said research suggests the 7-day period may not be necessary.
“We’ve utilized this about 2.5-plus years in my hospital, and it’s really been a game changer for some of our sickest, most challenging patients,” he said at the APA presentation. As he explained, one benefit is that patients can’t repeatedly avoid doses depending on how they feel, as they may do with the sublingual version. “On the first day of injection, you can actually stop the sublingual buprenorphine.”
Dr. Renner emphasized the importance of getting users on buprenorphine as fast as possible. If the treatment begins in the ED, he said, “they need to have a system that is going to be able to pick them up and continue the care.”
Otherwise, the risk is high. “We’re in a very dangerous era,” he said, “where the patient walks out the door, and then they die.”
Dr. Park had no disclosures, and Dr. Renner disclosed royalties from the APA.
SAN FRANCISCO – As the opioid epidemic continues to grow and evolve, the federal government is trying to make it easier for clinicians to treat abusers with the drug buprenorphine, psychiatrists told colleagues at the annual meeting of the American Psychiatric Association. And an injectable version of the drug is making a big difference.
John A. Renner Jr., MD, of Boston University, said in a presentation at the APA meeting.
As Dr. Renner explained, the United States is now in the fourth wave of nearly a quarter-century of opioid overdose-related deaths. The outbreak began in 1999 as prescription opioids spurred deaths, and heroin overdoses began to rise in 2010. The third wave brought rises in deaths from synthetic opioids such as fentanyl in 2013. In 2015, the fourth wave – driven by deaths from combinations of synthetic opioids and psychostimulants like methamphetamines – started in 2015.
COVID-19 seems to have played a role too: In 2020, opioid overdose deaths spiked during the early months of the pandemic. In 2021, drug-related overdose deaths overall hit a high of 106,889, including 80,411 linked to opioids. In contrast, fewer than 20,000 drug-related overdose deaths were reported in 1999.
On the other hand, deaths from prescription drug overdoses are falling, Dr. Renner said, suggesting “improvement in terms of how clinicians are handling medications and our prescribing practices. But that’s being masked by what’s happened with fentanyl and methamphetamine.”
Buprenorphine (Subutex), used to treat opioid use withdrawal, is itself an opioid and can cause addiction and death in some cases. However, Dr. Renner highlighted a 2023 study that determined that efforts to increase its use from 2019 to 2021 didn’t appear to boost buprenorphine-related overdose deaths in the United States.
New federal regulations aim to make it easier to prescribe buprenorphine. Thanks to Congressional legislation, the Drug Enforcement Administration in January 2023 eliminated regulations requiring clinicians to undergo special training to get an “X-waiver” to be able to prescribe buprenorphine. But they’re not off the hook entirely: As of June 27, 2023, providers must have undergone training in order to apply for – or renew – a DEA license to prescribe certain controlled substances like buprenorphine.
“I’m afraid that people will be able to meet that requirement easily, and they’re not going to get good coordinated teaching,” Dr. Renner said. “I’m not sure that’s really going to improve the quality of care that we’re delivering.”
In regard to treatment, psychiatrist Dong Chan Park, MD, of Boston University, touted a long-acting injectable form of buprenorphine known by the brand name Sublocade. The FDA approved Sublocade in 2017 for patients who’ve been taking sublingual buprenorphine for at least 7 days, although Dr. Park said research suggests the 7-day period may not be necessary.
“We’ve utilized this about 2.5-plus years in my hospital, and it’s really been a game changer for some of our sickest, most challenging patients,” he said at the APA presentation. As he explained, one benefit is that patients can’t repeatedly avoid doses depending on how they feel, as they may do with the sublingual version. “On the first day of injection, you can actually stop the sublingual buprenorphine.”
Dr. Renner emphasized the importance of getting users on buprenorphine as fast as possible. If the treatment begins in the ED, he said, “they need to have a system that is going to be able to pick them up and continue the care.”
Otherwise, the risk is high. “We’re in a very dangerous era,” he said, “where the patient walks out the door, and then they die.”
Dr. Park had no disclosures, and Dr. Renner disclosed royalties from the APA.
AT APA 2023
Family placement better for deprived kids than institutions
SAN FRANCISCO – results of a new study suggest.
The study shows that sustained recovery is possible after severe, early-life adversity, study author Kathryn L. Humphreys, PhD, assistant professor, department of psychology and human development, Vanderbilt University, Nashville, Tenn., said in an interview.

“Given the strong evidence from the present study, I hope physicians will play a role in promoting family placements as an alternative to institutional care for children who have been orphaned,” she said.
The findings were presented at the annual meeting of the American Psychiatric Association and were published online in the American Journal of Psychiatry.
Millions of children around the world experience psychosocial deprivation while living in institutions, and many more are neglected in their families of origin. In addition, about 6.7 million children lost a parent or caregiver during the COVID-19 pandemic.
In particular, Romania has a history of institutionalizing children. Through decades of repressive policies from the Romanian dictator Nicolae Ceausescu, child abandonment became a national disaster. Families couldn’t afford to keep their children and were encouraged to turn them over to the state.
The current study was part of the Bucharest Early Intervention Project, initiated in 2001 to examine the impact of high-quality, family-based care on development. It included 136 Romanian children (mean age, about 22 months) who were abandoned at or shortly after birth and were placed in an institution.
Researchers randomly assigned each toddler to 1 of 56 foster families or to continue living in an institution (care as usual). The researchers had to create a foster care network, because such care was extremely limited at the start of the study.
Providing stimulating care
Foster parents in the study received regular support from social workers and U.S.-based psychologists. They were encouraged to “make a commitment to treat the child as if it was their own, providing sensitive, stimulating, and nurturing care, not just in the short term but for their whole life,” said Dr. Humphreys.
Foster care programs in the United States have been criticized for focusing on short-term care, she said. “It’s really just a bed to sleep on, clothes to wear, and food to eat rather than the psychological component we think is really important for child development.”
For the study, the researchers assessed the children across multiple developmental domains at baseline and at ages 30, 42, and 54 months. They conducted additional assessments when the kids were aged 8, 12, and 16-18 years.
The primary outcomes were cognitive functioning (IQ), physical growth (height, weight, head circumference), brain electrical activity (relative electroencephalography power in the alpha frequency band), and symptoms of five types of psychopathology (disinhibited social engagement disorder, reactive attachment disorder, ADHD symptoms, externalizing symptoms, and internalizing symptoms).
From over 7,000 observations analyzed across follow-ups, the investigators found that the intervention had an overall significant effect on cognitive, physical, and neural outcomes when considered collectively across waves (beta, 0.26; 95% confidence interval, 0.07-0.46; P = .012). Compared to children who received care as usual, those in foster homes had significantly higher average IQ scores (P < .001) and physical size (P = .008).
The intervention had an overall beneficial effect in regard to psychopathology. The greatest impact involved a reduction in symptoms of reactive attachment disorder (P < .001).
“There are a few forms of psychopathology that seem to almost entirely occur after severe neglect, including reactive attachment disorder; we think of these as disorders of social relatedness that derive from aberrant or insufficient early caregiving experiences,” said Dr. Humphreys. “Being placed in a family reduced the symptoms of reactive attachment disorder to pretty much nonexistent.”
To a lesser extent, the intervention reduced symptoms of disinhibited social engagement disorder. The foster care group also had significantly fewer internalizing symptoms than did children in the care-as-usual group.
But there was no significant overall effect of the intervention on symptoms of ADHD or externalizing problems.
Positive effects persisted
For the most part, the positive effects of the intervention on children’s functioning persisted during nearly 2 decades of follow-up. The impact of the intervention “can be described as rapidly apparent by age 30 months and sustained through late adolescence,” wrote the authors.
Regarding the impact of age at the time of placement, the study found that, compared with children placed into foster care later, those who entered foster care earlier (younger than 33 months) had significantly higher IQ scores and relative alpha power, but there was no difference in physical growth.
For some outcomes, the benefits of earlier placement were apparent in early childhood but faded by adolescence. But Dr. Humphreys noted all placements were early by most definitions.
The researchers also assessed stability of foster care placements. Children were considered “stable” if they remained with their original foster family; they were considered “disrupted” if they no longer resided with the family.
Here, the study found some “striking results,” said Dr. Humphreys. The effect of placement stability was largest in adolescence, when, overall, those who had remained with their original foster family had better cognitive and physical outcomes and less severe symptoms of psychopathology compared to those who experienced placement disruptions.
As for sex differences, “it’s a mixed bag,” said Dr. Humphreys, although overall, “we didn’t see strong evidence of sex differences” in terms of outcomes.
The investigators were unable to examine trajectories of children’s functioning, which would have provided important information on aspects such as rate of growth and the shape of growth curves. Specific features of the institutional or foster care environment in Bucharest during the study may limit the generalizability of the findings to other settings.
Absolutely unique project
The study examined an “absolutely unique project” and had “very exciting” results that should have “important clinical implications,” commented the American Journal of Psychiatry editor-in-chief Ned Kalin, MD, Hedberg Professor and chair, department of psychiatry, University of Wisconsin–Madison.
The findings are “pretty dramatic,” added Dr. Kalin. “This is probably the study to be thinking about when considering the future of treatment and interventions in children who have suffered from this type of neglect, which is unfortunately extremely common worldwide, including in the U.S.”
In particular, the findings regarding improved psychopathology “bode well for the future,” said Dr. Kalin. “We know these types of problems are risk factors for the later development of depression and anxiety disorders. It will be really interesting to find out, but my guess is these kids will be protected as they mature further.”
The study was supported by the NIH, the John D. and Catherine T. MacArthur Foundation, the Palix Foundation, and the Jacobs Foundation. Dr. Humphreys has received research funding from the Brain and Behavior Research Foundation, the Caplan Foundation, the Jacobs Foundation, the National Science Foundation, the NIH, the Vanderbilt Institute for Clinical and Translational Research, the Vanderbilt Kennedy Center, and Vanderbilt University; she has received honoraria from the Journal of Clinical Child and Adolescent Psychology Future Directions Forum, Learning Grove, the University of Iowa, the University of Texas at Austin, and ZERO TO THREE.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – results of a new study suggest.
The study shows that sustained recovery is possible after severe, early-life adversity, study author Kathryn L. Humphreys, PhD, assistant professor, department of psychology and human development, Vanderbilt University, Nashville, Tenn., said in an interview.
“Given the strong evidence from the present study, I hope physicians will play a role in promoting family placements as an alternative to institutional care for children who have been orphaned,” she said.
The findings were presented at the annual meeting of the American Psychiatric Association and were published online in the American Journal of Psychiatry.
Millions of children around the world experience psychosocial deprivation while living in institutions, and many more are neglected in their families of origin. In addition, about 6.7 million children lost a parent or caregiver during the COVID-19 pandemic.
In particular, Romania has a history of institutionalizing children. Through decades of repressive policies from the Romanian dictator Nicolae Ceausescu, child abandonment became a national disaster. Families couldn’t afford to keep their children and were encouraged to turn them over to the state.
The current study was part of the Bucharest Early Intervention Project, initiated in 2001 to examine the impact of high-quality, family-based care on development. It included 136 Romanian children (mean age, about 22 months) who were abandoned at or shortly after birth and were placed in an institution.
Researchers randomly assigned each toddler to 1 of 56 foster families or to continue living in an institution (care as usual). The researchers had to create a foster care network, because such care was extremely limited at the start of the study.
Providing stimulating care
Foster parents in the study received regular support from social workers and U.S.-based psychologists. They were encouraged to “make a commitment to treat the child as if it was their own, providing sensitive, stimulating, and nurturing care, not just in the short term but for their whole life,” said Dr. Humphreys.
Foster care programs in the United States have been criticized for focusing on short-term care, she said. “It’s really just a bed to sleep on, clothes to wear, and food to eat rather than the psychological component we think is really important for child development.”
For the study, the researchers assessed the children across multiple developmental domains at baseline and at ages 30, 42, and 54 months. They conducted additional assessments when the kids were aged 8, 12, and 16-18 years.
The primary outcomes were cognitive functioning (IQ), physical growth (height, weight, head circumference), brain electrical activity (relative electroencephalography power in the alpha frequency band), and symptoms of five types of psychopathology (disinhibited social engagement disorder, reactive attachment disorder, ADHD symptoms, externalizing symptoms, and internalizing symptoms).
From over 7,000 observations analyzed across follow-ups, the investigators found that the intervention had an overall significant effect on cognitive, physical, and neural outcomes when considered collectively across waves (beta, 0.26; 95% confidence interval, 0.07-0.46; P = .012). Compared to children who received care as usual, those in foster homes had significantly higher average IQ scores (P < .001) and physical size (P = .008).
The intervention had an overall beneficial effect in regard to psychopathology. The greatest impact involved a reduction in symptoms of reactive attachment disorder (P < .001).
“There are a few forms of psychopathology that seem to almost entirely occur after severe neglect, including reactive attachment disorder; we think of these as disorders of social relatedness that derive from aberrant or insufficient early caregiving experiences,” said Dr. Humphreys. “Being placed in a family reduced the symptoms of reactive attachment disorder to pretty much nonexistent.”
To a lesser extent, the intervention reduced symptoms of disinhibited social engagement disorder. The foster care group also had significantly fewer internalizing symptoms than did children in the care-as-usual group.
But there was no significant overall effect of the intervention on symptoms of ADHD or externalizing problems.
Positive effects persisted
For the most part, the positive effects of the intervention on children’s functioning persisted during nearly 2 decades of follow-up. The impact of the intervention “can be described as rapidly apparent by age 30 months and sustained through late adolescence,” wrote the authors.
Regarding the impact of age at the time of placement, the study found that, compared with children placed into foster care later, those who entered foster care earlier (younger than 33 months) had significantly higher IQ scores and relative alpha power, but there was no difference in physical growth.
For some outcomes, the benefits of earlier placement were apparent in early childhood but faded by adolescence. But Dr. Humphreys noted all placements were early by most definitions.
The researchers also assessed stability of foster care placements. Children were considered “stable” if they remained with their original foster family; they were considered “disrupted” if they no longer resided with the family.
Here, the study found some “striking results,” said Dr. Humphreys. The effect of placement stability was largest in adolescence, when, overall, those who had remained with their original foster family had better cognitive and physical outcomes and less severe symptoms of psychopathology compared to those who experienced placement disruptions.
As for sex differences, “it’s a mixed bag,” said Dr. Humphreys, although overall, “we didn’t see strong evidence of sex differences” in terms of outcomes.
The investigators were unable to examine trajectories of children’s functioning, which would have provided important information on aspects such as rate of growth and the shape of growth curves. Specific features of the institutional or foster care environment in Bucharest during the study may limit the generalizability of the findings to other settings.
Absolutely unique project
The study examined an “absolutely unique project” and had “very exciting” results that should have “important clinical implications,” commented the American Journal of Psychiatry editor-in-chief Ned Kalin, MD, Hedberg Professor and chair, department of psychiatry, University of Wisconsin–Madison.
The findings are “pretty dramatic,” added Dr. Kalin. “This is probably the study to be thinking about when considering the future of treatment and interventions in children who have suffered from this type of neglect, which is unfortunately extremely common worldwide, including in the U.S.”
In particular, the findings regarding improved psychopathology “bode well for the future,” said Dr. Kalin. “We know these types of problems are risk factors for the later development of depression and anxiety disorders. It will be really interesting to find out, but my guess is these kids will be protected as they mature further.”
The study was supported by the NIH, the John D. and Catherine T. MacArthur Foundation, the Palix Foundation, and the Jacobs Foundation. Dr. Humphreys has received research funding from the Brain and Behavior Research Foundation, the Caplan Foundation, the Jacobs Foundation, the National Science Foundation, the NIH, the Vanderbilt Institute for Clinical and Translational Research, the Vanderbilt Kennedy Center, and Vanderbilt University; she has received honoraria from the Journal of Clinical Child and Adolescent Psychology Future Directions Forum, Learning Grove, the University of Iowa, the University of Texas at Austin, and ZERO TO THREE.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – results of a new study suggest.
The study shows that sustained recovery is possible after severe, early-life adversity, study author Kathryn L. Humphreys, PhD, assistant professor, department of psychology and human development, Vanderbilt University, Nashville, Tenn., said in an interview.
“Given the strong evidence from the present study, I hope physicians will play a role in promoting family placements as an alternative to institutional care for children who have been orphaned,” she said.
The findings were presented at the annual meeting of the American Psychiatric Association and were published online in the American Journal of Psychiatry.
Millions of children around the world experience psychosocial deprivation while living in institutions, and many more are neglected in their families of origin. In addition, about 6.7 million children lost a parent or caregiver during the COVID-19 pandemic.
In particular, Romania has a history of institutionalizing children. Through decades of repressive policies from the Romanian dictator Nicolae Ceausescu, child abandonment became a national disaster. Families couldn’t afford to keep their children and were encouraged to turn them over to the state.
The current study was part of the Bucharest Early Intervention Project, initiated in 2001 to examine the impact of high-quality, family-based care on development. It included 136 Romanian children (mean age, about 22 months) who were abandoned at or shortly after birth and were placed in an institution.
Researchers randomly assigned each toddler to 1 of 56 foster families or to continue living in an institution (care as usual). The researchers had to create a foster care network, because such care was extremely limited at the start of the study.
Providing stimulating care
Foster parents in the study received regular support from social workers and U.S.-based psychologists. They were encouraged to “make a commitment to treat the child as if it was their own, providing sensitive, stimulating, and nurturing care, not just in the short term but for their whole life,” said Dr. Humphreys.
Foster care programs in the United States have been criticized for focusing on short-term care, she said. “It’s really just a bed to sleep on, clothes to wear, and food to eat rather than the psychological component we think is really important for child development.”
For the study, the researchers assessed the children across multiple developmental domains at baseline and at ages 30, 42, and 54 months. They conducted additional assessments when the kids were aged 8, 12, and 16-18 years.
The primary outcomes were cognitive functioning (IQ), physical growth (height, weight, head circumference), brain electrical activity (relative electroencephalography power in the alpha frequency band), and symptoms of five types of psychopathology (disinhibited social engagement disorder, reactive attachment disorder, ADHD symptoms, externalizing symptoms, and internalizing symptoms).
From over 7,000 observations analyzed across follow-ups, the investigators found that the intervention had an overall significant effect on cognitive, physical, and neural outcomes when considered collectively across waves (beta, 0.26; 95% confidence interval, 0.07-0.46; P = .012). Compared to children who received care as usual, those in foster homes had significantly higher average IQ scores (P < .001) and physical size (P = .008).
The intervention had an overall beneficial effect in regard to psychopathology. The greatest impact involved a reduction in symptoms of reactive attachment disorder (P < .001).
“There are a few forms of psychopathology that seem to almost entirely occur after severe neglect, including reactive attachment disorder; we think of these as disorders of social relatedness that derive from aberrant or insufficient early caregiving experiences,” said Dr. Humphreys. “Being placed in a family reduced the symptoms of reactive attachment disorder to pretty much nonexistent.”
To a lesser extent, the intervention reduced symptoms of disinhibited social engagement disorder. The foster care group also had significantly fewer internalizing symptoms than did children in the care-as-usual group.
But there was no significant overall effect of the intervention on symptoms of ADHD or externalizing problems.
Positive effects persisted
For the most part, the positive effects of the intervention on children’s functioning persisted during nearly 2 decades of follow-up. The impact of the intervention “can be described as rapidly apparent by age 30 months and sustained through late adolescence,” wrote the authors.
Regarding the impact of age at the time of placement, the study found that, compared with children placed into foster care later, those who entered foster care earlier (younger than 33 months) had significantly higher IQ scores and relative alpha power, but there was no difference in physical growth.
For some outcomes, the benefits of earlier placement were apparent in early childhood but faded by adolescence. But Dr. Humphreys noted all placements were early by most definitions.
The researchers also assessed stability of foster care placements. Children were considered “stable” if they remained with their original foster family; they were considered “disrupted” if they no longer resided with the family.
Here, the study found some “striking results,” said Dr. Humphreys. The effect of placement stability was largest in adolescence, when, overall, those who had remained with their original foster family had better cognitive and physical outcomes and less severe symptoms of psychopathology compared to those who experienced placement disruptions.
As for sex differences, “it’s a mixed bag,” said Dr. Humphreys, although overall, “we didn’t see strong evidence of sex differences” in terms of outcomes.
The investigators were unable to examine trajectories of children’s functioning, which would have provided important information on aspects such as rate of growth and the shape of growth curves. Specific features of the institutional or foster care environment in Bucharest during the study may limit the generalizability of the findings to other settings.
Absolutely unique project
The study examined an “absolutely unique project” and had “very exciting” results that should have “important clinical implications,” commented the American Journal of Psychiatry editor-in-chief Ned Kalin, MD, Hedberg Professor and chair, department of psychiatry, University of Wisconsin–Madison.
The findings are “pretty dramatic,” added Dr. Kalin. “This is probably the study to be thinking about when considering the future of treatment and interventions in children who have suffered from this type of neglect, which is unfortunately extremely common worldwide, including in the U.S.”
In particular, the findings regarding improved psychopathology “bode well for the future,” said Dr. Kalin. “We know these types of problems are risk factors for the later development of depression and anxiety disorders. It will be really interesting to find out, but my guess is these kids will be protected as they mature further.”
The study was supported by the NIH, the John D. and Catherine T. MacArthur Foundation, the Palix Foundation, and the Jacobs Foundation. Dr. Humphreys has received research funding from the Brain and Behavior Research Foundation, the Caplan Foundation, the Jacobs Foundation, the National Science Foundation, the NIH, the Vanderbilt Institute for Clinical and Translational Research, the Vanderbilt Kennedy Center, and Vanderbilt University; she has received honoraria from the Journal of Clinical Child and Adolescent Psychology Future Directions Forum, Learning Grove, the University of Iowa, the University of Texas at Austin, and ZERO TO THREE.
A version of this article first appeared on Medscape.com.
AT APA 2023
Significant increase in vitamin D deficiency in kids with major depressive disorder
SAN FRANCISCO – , according to new findings that suggest spending more time indoors may have fueled this uptick.
“We suspect that this may be due to the COVID lockdowns and kids schooling from home and having less time outside,” study investigator Oluwatomiwa Babade, MD, MPH, with Virginia Tech Carilion School of Medicine, Roanoke, Va., said in an interview.
The study was presented at the annual meeting of the American Psychiatric Association.
Anecdotal observation confirmed
During the pandemic, investigators noticed an uptick in the number of children and adolescents attending their clinic for psychiatric hospitalization who had low vitamin D levels.
To investigate, they analyzed the records of all patients aged 6-17 years with psychiatric diagnoses and vitamin D level assessment who were admitted into the inpatient psychiatry unit from March 18, 2020, to June 30, 2021.
Among 599 unique patients, 275 (83% female) had a diagnosis of MDD and 226 of these patients were vitamin D deficient (< 30 ng/mL) – a prevalence rate of roughly 82%. Among 246 patients with psychiatric disorders other than MDD, the prevalence of vitamin D deficiency was 76%.
“This was very surprising and much higher than prior to the pandemic. Prior to COVID, the prevalence of vitamin D deficiency was around 14% in similar patients,” Dr. Babade said.
“Now that we are post-lockdown, it would be good to repeat the study. I think the prevalence should drop. That’s my guess,” he added.
Important research, no surprises
In a comment, Cemre Robinson, MD, director of the Mount Sinai Pediatric Bone Health and Calcium Metabolism Clinic, New York, said that although the study’s findings aren’t surprising, “it’s important to present such data in adolescents with major depression.”
“These findings reiterate the importance of screening for vitamin D deficiency in children and adolescents, with or without depression, particularly during winter, which is associated with less sun exposure,” Dr. Robinson, assistant professor of pediatrics, endocrinology, and diabetes at Icahn School of Medicine at Mount Sinai, said.
She noted that vitamin D deficiency is prevalent in the general population, and it can be easily corrected with supplementation.
“Vitamin D is important for bone growth, mineralization, and accretion as well as calcium absorption. Adolescence, in particular, is a period of rapid physical, cognitive, and psychosocial growth,” Dr. Robinson said.
“The requirement of all minerals and vitamins changes in this phase of life. Therefore, it is important to have sufficient vitamin D levels during adolescence for several health benefits,” she noted.
Dr. Robinson said that “more research is needed to validate the present findings in adolescents with major depression, and larger studies, including randomized control trials, are required to establish a causal association between MDD and vitamin D deficiency.”
The study had no specific funding. Dr. Babade and Dr. Robinson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , according to new findings that suggest spending more time indoors may have fueled this uptick.
“We suspect that this may be due to the COVID lockdowns and kids schooling from home and having less time outside,” study investigator Oluwatomiwa Babade, MD, MPH, with Virginia Tech Carilion School of Medicine, Roanoke, Va., said in an interview.
The study was presented at the annual meeting of the American Psychiatric Association.
Anecdotal observation confirmed
During the pandemic, investigators noticed an uptick in the number of children and adolescents attending their clinic for psychiatric hospitalization who had low vitamin D levels.
To investigate, they analyzed the records of all patients aged 6-17 years with psychiatric diagnoses and vitamin D level assessment who were admitted into the inpatient psychiatry unit from March 18, 2020, to June 30, 2021.
Among 599 unique patients, 275 (83% female) had a diagnosis of MDD and 226 of these patients were vitamin D deficient (< 30 ng/mL) – a prevalence rate of roughly 82%. Among 246 patients with psychiatric disorders other than MDD, the prevalence of vitamin D deficiency was 76%.
“This was very surprising and much higher than prior to the pandemic. Prior to COVID, the prevalence of vitamin D deficiency was around 14% in similar patients,” Dr. Babade said.
“Now that we are post-lockdown, it would be good to repeat the study. I think the prevalence should drop. That’s my guess,” he added.
Important research, no surprises
In a comment, Cemre Robinson, MD, director of the Mount Sinai Pediatric Bone Health and Calcium Metabolism Clinic, New York, said that although the study’s findings aren’t surprising, “it’s important to present such data in adolescents with major depression.”
“These findings reiterate the importance of screening for vitamin D deficiency in children and adolescents, with or without depression, particularly during winter, which is associated with less sun exposure,” Dr. Robinson, assistant professor of pediatrics, endocrinology, and diabetes at Icahn School of Medicine at Mount Sinai, said.
She noted that vitamin D deficiency is prevalent in the general population, and it can be easily corrected with supplementation.
“Vitamin D is important for bone growth, mineralization, and accretion as well as calcium absorption. Adolescence, in particular, is a period of rapid physical, cognitive, and psychosocial growth,” Dr. Robinson said.
“The requirement of all minerals and vitamins changes in this phase of life. Therefore, it is important to have sufficient vitamin D levels during adolescence for several health benefits,” she noted.
Dr. Robinson said that “more research is needed to validate the present findings in adolescents with major depression, and larger studies, including randomized control trials, are required to establish a causal association between MDD and vitamin D deficiency.”
The study had no specific funding. Dr. Babade and Dr. Robinson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , according to new findings that suggest spending more time indoors may have fueled this uptick.
“We suspect that this may be due to the COVID lockdowns and kids schooling from home and having less time outside,” study investigator Oluwatomiwa Babade, MD, MPH, with Virginia Tech Carilion School of Medicine, Roanoke, Va., said in an interview.
The study was presented at the annual meeting of the American Psychiatric Association.
Anecdotal observation confirmed
During the pandemic, investigators noticed an uptick in the number of children and adolescents attending their clinic for psychiatric hospitalization who had low vitamin D levels.
To investigate, they analyzed the records of all patients aged 6-17 years with psychiatric diagnoses and vitamin D level assessment who were admitted into the inpatient psychiatry unit from March 18, 2020, to June 30, 2021.
Among 599 unique patients, 275 (83% female) had a diagnosis of MDD and 226 of these patients were vitamin D deficient (< 30 ng/mL) – a prevalence rate of roughly 82%. Among 246 patients with psychiatric disorders other than MDD, the prevalence of vitamin D deficiency was 76%.
“This was very surprising and much higher than prior to the pandemic. Prior to COVID, the prevalence of vitamin D deficiency was around 14% in similar patients,” Dr. Babade said.
“Now that we are post-lockdown, it would be good to repeat the study. I think the prevalence should drop. That’s my guess,” he added.
Important research, no surprises
In a comment, Cemre Robinson, MD, director of the Mount Sinai Pediatric Bone Health and Calcium Metabolism Clinic, New York, said that although the study’s findings aren’t surprising, “it’s important to present such data in adolescents with major depression.”
“These findings reiterate the importance of screening for vitamin D deficiency in children and adolescents, with or without depression, particularly during winter, which is associated with less sun exposure,” Dr. Robinson, assistant professor of pediatrics, endocrinology, and diabetes at Icahn School of Medicine at Mount Sinai, said.
She noted that vitamin D deficiency is prevalent in the general population, and it can be easily corrected with supplementation.
“Vitamin D is important for bone growth, mineralization, and accretion as well as calcium absorption. Adolescence, in particular, is a period of rapid physical, cognitive, and psychosocial growth,” Dr. Robinson said.
“The requirement of all minerals and vitamins changes in this phase of life. Therefore, it is important to have sufficient vitamin D levels during adolescence for several health benefits,” she noted.
Dr. Robinson said that “more research is needed to validate the present findings in adolescents with major depression, and larger studies, including randomized control trials, are required to establish a causal association between MDD and vitamin D deficiency.”
The study had no specific funding. Dr. Babade and Dr. Robinson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT APA 2023
Quick medication, better communication linked to less violence at inpatient psych unit
SAN FRANCISCO – Physically violent events at an inpatient psychiatric unit in Pennsylvania dropped by 59.8% in the months after it implemented a plan to administer antipsychotic medications to patients more quickly – both in the emergency department and in the unit – and improve handoffs between providers and nurses, researchers reported.
“We were able to significantly reduce violence,” said Michael Chen, MD, Lehigh Valley Health Network psychiatry resident and lead author of an abstract presented at the annual meeting of the American Psychiatric Association. “Furthermore, the interventions were effective in reducing episodes of violence rather than redirecting it. And the overall feeling of safety on the inpatient psychiatric unit improved.”
Violence is common in psychiatric units, although it’s not clear how often it occurs. “The data has shown that patients with a psychotic disorder such as schizophrenia or a mood disorder with psychotic features such as bipolar disorder tend to account for most of the episodes of violence on the unit,” Dr. Chen said in an interview. “This inevitably results in a higher risk for violence on inpatient psychiatric units as a large portion of patients admitted to inpatient psychiatric units have these diagnoses.”
Enlisting the pharmacy department
For the new study, investigators tracked episodes of violence – including verbal attacks – at an Allentown, Penn.–area inpatient psychiatric unit from December 2021 to September 2022. According to Dr. Chen, unit leaders implemented the new plan in May 2022 in the wake of higher levels of violence during the COVID-19 pandemic and the concurrent staff shortages.
Clinic leaders sought to identify potentially aggressive patients in the emergency department and treat them with antipsychotics prior to admission to the psychiatric unit, ensure that the pharmacy provides access to as-needed or standing medications, and develop “standardized huddles to ensure proper handoffs between providers and nurses.”
Medical staff relied on the Dynamic Appraisal of Situational Aggression scale, risk factors, and clinical judgment to determine which patients had the potential to be violent, Dr. Chen said.
As for treatment, first-line antipsychotics are typically given orally, but they can be injected if patients must be treated over their objections, he said. “We would only consider starting standing medications against objections in patients who are involuntarily committed.”
During the 5 months before the intervention was implemented versus the following 5 months, the average monthly number of physically violent events in the psychiatric unit fell from 12.4 to 4.8 (–61.1%, P = .04), and verbal threats dipped from 7.2 to 4 (–44.4%, P = .15). The total average number of violent events per month, including violence against property, fell from an average of 25.4 to 10.2 (–59.8%, P = .03).
The total patient population didn’t vary significantly over time, Dr. Chen said. “Thus, the decrease in violence was not correlated with a decrease in patient load.”
While “there were concerns that there would just be higher episodes of violence in the ED while psychiatry patients awaited placement,” Dr. Chen said, the numbers actually showed reductions in violence in that setting. The average number of physically violent events per month in the ED fell from 49.6 to 39.4 (–20.6%, P = .03). Verbal threats dropped from 38 to 34.6 (–8.9%, P = .5) and overall violent events dipped from 87.6 to 74 (–15.6%, P = .08).
Why did the interventions seem to work? “Standing doses as well as as-needed medications started for psychiatric patients in the emergency department have been crucial to prevent delay of care,” Dr. Chen said. Enlisting the pharmacy department “helped ensure all patients had appropriate as-needed medications to prevent them from decompensating on the units,” he added, and “involvement of nursing and ancillary staff in high-risk rounds allowed the treatment team to rapidly anticipate and address concerns.”
The study authors also reported that nursing staff felt safer. Scores on a perception-of-safety scale – with 1 most unsafe and 7 most safe – improved from 3.3 to 4.2 (+27%, P < .01).
Dr. Chen said there was a “minimal” increase in cost to implement the intervention, although coordination is necessary. “The emergency department and psychiatry department have to work together to initiate treatment in the ED while awaiting beds,” he said. “The treatment team needs to communicate concerns during rounds. The pharmacist and psychiatrist need to work together to ensure that proper as-needed medications are available.”
‘Good clinical practice’
In an interview, psychiatrist Mark J. Russ, MD, of NewYork-Presbyterian/Westchester Behavioral Health and Weill Cornell Medical College, said violent incidents in inpatient psychiatric units are influenced by many factors, such as history of violence, substance use, history of trauma, psychosis/paranoia, and medical problems.
The units themselves can contribute to the risk of violence through power struggles and lack of attention paid to respect and dignity, he said. “Attention to these issues is important in reducing violence,” he noted. “Generalized training for staff in de-escalation techniques and trauma-informed care is imperative. There may be value in developing specialized psychiatric ICUs where staff are meticulously trained in these and other approaches.”
The new study, Dr. Russ said, suggests that “early identification of patients at risk of engaging in violent behavior on the inpatient unit, pharmacologic treatment, and good communication helps reduce violence.” The findings, he added, suggest that “interventions known to constitute good clinical practice are indeed helpful.”
However, he cautioned that “treating all at-risk patients with antipsychotics, regardless of their psychiatric diagnosis, might well be considered chemical restraint, depending on [the] circumstances.”
There was no study funding. The study authors and Dr. Russ have no disclosures.
SAN FRANCISCO – Physically violent events at an inpatient psychiatric unit in Pennsylvania dropped by 59.8% in the months after it implemented a plan to administer antipsychotic medications to patients more quickly – both in the emergency department and in the unit – and improve handoffs between providers and nurses, researchers reported.
“We were able to significantly reduce violence,” said Michael Chen, MD, Lehigh Valley Health Network psychiatry resident and lead author of an abstract presented at the annual meeting of the American Psychiatric Association. “Furthermore, the interventions were effective in reducing episodes of violence rather than redirecting it. And the overall feeling of safety on the inpatient psychiatric unit improved.”
Violence is common in psychiatric units, although it’s not clear how often it occurs. “The data has shown that patients with a psychotic disorder such as schizophrenia or a mood disorder with psychotic features such as bipolar disorder tend to account for most of the episodes of violence on the unit,” Dr. Chen said in an interview. “This inevitably results in a higher risk for violence on inpatient psychiatric units as a large portion of patients admitted to inpatient psychiatric units have these diagnoses.”
Enlisting the pharmacy department
For the new study, investigators tracked episodes of violence – including verbal attacks – at an Allentown, Penn.–area inpatient psychiatric unit from December 2021 to September 2022. According to Dr. Chen, unit leaders implemented the new plan in May 2022 in the wake of higher levels of violence during the COVID-19 pandemic and the concurrent staff shortages.
Clinic leaders sought to identify potentially aggressive patients in the emergency department and treat them with antipsychotics prior to admission to the psychiatric unit, ensure that the pharmacy provides access to as-needed or standing medications, and develop “standardized huddles to ensure proper handoffs between providers and nurses.”
Medical staff relied on the Dynamic Appraisal of Situational Aggression scale, risk factors, and clinical judgment to determine which patients had the potential to be violent, Dr. Chen said.
As for treatment, first-line antipsychotics are typically given orally, but they can be injected if patients must be treated over their objections, he said. “We would only consider starting standing medications against objections in patients who are involuntarily committed.”
During the 5 months before the intervention was implemented versus the following 5 months, the average monthly number of physically violent events in the psychiatric unit fell from 12.4 to 4.8 (–61.1%, P = .04), and verbal threats dipped from 7.2 to 4 (–44.4%, P = .15). The total average number of violent events per month, including violence against property, fell from an average of 25.4 to 10.2 (–59.8%, P = .03).
The total patient population didn’t vary significantly over time, Dr. Chen said. “Thus, the decrease in violence was not correlated with a decrease in patient load.”
While “there were concerns that there would just be higher episodes of violence in the ED while psychiatry patients awaited placement,” Dr. Chen said, the numbers actually showed reductions in violence in that setting. The average number of physically violent events per month in the ED fell from 49.6 to 39.4 (–20.6%, P = .03). Verbal threats dropped from 38 to 34.6 (–8.9%, P = .5) and overall violent events dipped from 87.6 to 74 (–15.6%, P = .08).
Why did the interventions seem to work? “Standing doses as well as as-needed medications started for psychiatric patients in the emergency department have been crucial to prevent delay of care,” Dr. Chen said. Enlisting the pharmacy department “helped ensure all patients had appropriate as-needed medications to prevent them from decompensating on the units,” he added, and “involvement of nursing and ancillary staff in high-risk rounds allowed the treatment team to rapidly anticipate and address concerns.”
The study authors also reported that nursing staff felt safer. Scores on a perception-of-safety scale – with 1 most unsafe and 7 most safe – improved from 3.3 to 4.2 (+27%, P < .01).
Dr. Chen said there was a “minimal” increase in cost to implement the intervention, although coordination is necessary. “The emergency department and psychiatry department have to work together to initiate treatment in the ED while awaiting beds,” he said. “The treatment team needs to communicate concerns during rounds. The pharmacist and psychiatrist need to work together to ensure that proper as-needed medications are available.”
‘Good clinical practice’
In an interview, psychiatrist Mark J. Russ, MD, of NewYork-Presbyterian/Westchester Behavioral Health and Weill Cornell Medical College, said violent incidents in inpatient psychiatric units are influenced by many factors, such as history of violence, substance use, history of trauma, psychosis/paranoia, and medical problems.
The units themselves can contribute to the risk of violence through power struggles and lack of attention paid to respect and dignity, he said. “Attention to these issues is important in reducing violence,” he noted. “Generalized training for staff in de-escalation techniques and trauma-informed care is imperative. There may be value in developing specialized psychiatric ICUs where staff are meticulously trained in these and other approaches.”
The new study, Dr. Russ said, suggests that “early identification of patients at risk of engaging in violent behavior on the inpatient unit, pharmacologic treatment, and good communication helps reduce violence.” The findings, he added, suggest that “interventions known to constitute good clinical practice are indeed helpful.”
However, he cautioned that “treating all at-risk patients with antipsychotics, regardless of their psychiatric diagnosis, might well be considered chemical restraint, depending on [the] circumstances.”
There was no study funding. The study authors and Dr. Russ have no disclosures.
SAN FRANCISCO – Physically violent events at an inpatient psychiatric unit in Pennsylvania dropped by 59.8% in the months after it implemented a plan to administer antipsychotic medications to patients more quickly – both in the emergency department and in the unit – and improve handoffs between providers and nurses, researchers reported.
“We were able to significantly reduce violence,” said Michael Chen, MD, Lehigh Valley Health Network psychiatry resident and lead author of an abstract presented at the annual meeting of the American Psychiatric Association. “Furthermore, the interventions were effective in reducing episodes of violence rather than redirecting it. And the overall feeling of safety on the inpatient psychiatric unit improved.”
Violence is common in psychiatric units, although it’s not clear how often it occurs. “The data has shown that patients with a psychotic disorder such as schizophrenia or a mood disorder with psychotic features such as bipolar disorder tend to account for most of the episodes of violence on the unit,” Dr. Chen said in an interview. “This inevitably results in a higher risk for violence on inpatient psychiatric units as a large portion of patients admitted to inpatient psychiatric units have these diagnoses.”
Enlisting the pharmacy department
For the new study, investigators tracked episodes of violence – including verbal attacks – at an Allentown, Penn.–area inpatient psychiatric unit from December 2021 to September 2022. According to Dr. Chen, unit leaders implemented the new plan in May 2022 in the wake of higher levels of violence during the COVID-19 pandemic and the concurrent staff shortages.
Clinic leaders sought to identify potentially aggressive patients in the emergency department and treat them with antipsychotics prior to admission to the psychiatric unit, ensure that the pharmacy provides access to as-needed or standing medications, and develop “standardized huddles to ensure proper handoffs between providers and nurses.”
Medical staff relied on the Dynamic Appraisal of Situational Aggression scale, risk factors, and clinical judgment to determine which patients had the potential to be violent, Dr. Chen said.
As for treatment, first-line antipsychotics are typically given orally, but they can be injected if patients must be treated over their objections, he said. “We would only consider starting standing medications against objections in patients who are involuntarily committed.”
During the 5 months before the intervention was implemented versus the following 5 months, the average monthly number of physically violent events in the psychiatric unit fell from 12.4 to 4.8 (–61.1%, P = .04), and verbal threats dipped from 7.2 to 4 (–44.4%, P = .15). The total average number of violent events per month, including violence against property, fell from an average of 25.4 to 10.2 (–59.8%, P = .03).
The total patient population didn’t vary significantly over time, Dr. Chen said. “Thus, the decrease in violence was not correlated with a decrease in patient load.”
While “there were concerns that there would just be higher episodes of violence in the ED while psychiatry patients awaited placement,” Dr. Chen said, the numbers actually showed reductions in violence in that setting. The average number of physically violent events per month in the ED fell from 49.6 to 39.4 (–20.6%, P = .03). Verbal threats dropped from 38 to 34.6 (–8.9%, P = .5) and overall violent events dipped from 87.6 to 74 (–15.6%, P = .08).
Why did the interventions seem to work? “Standing doses as well as as-needed medications started for psychiatric patients in the emergency department have been crucial to prevent delay of care,” Dr. Chen said. Enlisting the pharmacy department “helped ensure all patients had appropriate as-needed medications to prevent them from decompensating on the units,” he added, and “involvement of nursing and ancillary staff in high-risk rounds allowed the treatment team to rapidly anticipate and address concerns.”
The study authors also reported that nursing staff felt safer. Scores on a perception-of-safety scale – with 1 most unsafe and 7 most safe – improved from 3.3 to 4.2 (+27%, P < .01).
Dr. Chen said there was a “minimal” increase in cost to implement the intervention, although coordination is necessary. “The emergency department and psychiatry department have to work together to initiate treatment in the ED while awaiting beds,” he said. “The treatment team needs to communicate concerns during rounds. The pharmacist and psychiatrist need to work together to ensure that proper as-needed medications are available.”
‘Good clinical practice’
In an interview, psychiatrist Mark J. Russ, MD, of NewYork-Presbyterian/Westchester Behavioral Health and Weill Cornell Medical College, said violent incidents in inpatient psychiatric units are influenced by many factors, such as history of violence, substance use, history of trauma, psychosis/paranoia, and medical problems.
The units themselves can contribute to the risk of violence through power struggles and lack of attention paid to respect and dignity, he said. “Attention to these issues is important in reducing violence,” he noted. “Generalized training for staff in de-escalation techniques and trauma-informed care is imperative. There may be value in developing specialized psychiatric ICUs where staff are meticulously trained in these and other approaches.”
The new study, Dr. Russ said, suggests that “early identification of patients at risk of engaging in violent behavior on the inpatient unit, pharmacologic treatment, and good communication helps reduce violence.” The findings, he added, suggest that “interventions known to constitute good clinical practice are indeed helpful.”
However, he cautioned that “treating all at-risk patients with antipsychotics, regardless of their psychiatric diagnosis, might well be considered chemical restraint, depending on [the] circumstances.”
There was no study funding. The study authors and Dr. Russ have no disclosures.
AT APA 2023
PTSD, anxiety linked to out-of-hospital cardiac arrest
Investigators compared more than 35,000 OHCA case patients with a similar number of matched control persons and found an almost 1.5 times higher hazard of long-term stress conditions among OHCA case patients, compared with control persons, with a similar hazard for anxiety. Posttraumatic stress disorder was associated with an almost twofold higher risk of OHCA.
The findings applied equally to men and women and were independent of the presence of cardiovascular disease (CVD).
“This study raises awareness of the higher risks of OHCA and early risk monitoring to prevent OHCA in patients with stress-related disorders and anxiety,” write Talip Eroglu, of the department of cardiology, Copenhagen University Hospital, and colleagues.
The study was published online in BMJ Open Heart.
Stress disorders and anxiety overrepresented
OHCA “predominantly arises from lethal cardiac arrhythmias ... that occur most frequently in the setting of coronary heart disease,” the authors write. However, increasing evidence suggests that rates of OHCA may also be increased in association with noncardiac diseases.
Individuals with stress-related disorders and anxiety are “overrepresented” among victims of cardiac arrest as well as those with multiple CVDs. But previous studies of OHCA have been limited by small numbers of cardiac arrests. In addition, those studies involved only data from selected populations or used in-hospital diagnosis to identify cardiac arrest, thereby potentially omitting OHCA patients who died prior to hospital admission.
The researchers therefore turned to data from Danish health registries that include a large, unselected cohort of patients with OHCA to investigate whether long-term stress conditions (that is, PTSD and adjustment disorder) or anxiety disorder were associated with OHCA.
They stratified the cohort according to sex, age, and CVD to identify which risk factor confers the highest risk of OHCA in patients with long-term stress conditions or anxiety, and they conducted sensitivity analyses of potential confounders, such as depression.
The design was a nested-case control model in which records at an individual patient level across registries were cross-linked to data from other national registries and were compared to matched control persons from the general population (35,195 OHCAs and 351,950 matched control persons; median IQR age, 72 [62-81] years; 66.82% men).
The prevalence of comorbidities and use of cardiovascular drugs were higher among OHCA case patients than among non-OHCA control persons.
Keep aware of stress and anxiety as risk factors
Among OHCA and non-OHCA participants, long-term stress conditions were diagnosed in 0.92% and 0.45%, respectively. Anxiety was diagnosed in 0.85% of OHCA case patients and in 0.37% of non-OHCA control persons.
These conditions were associated with a higher rate of OHCA after adjustment for common OHCA risk factors.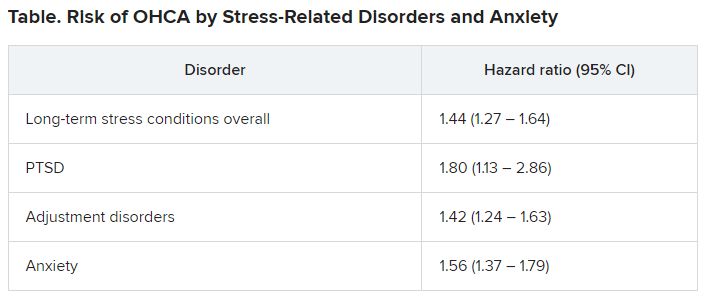
There were no significant differences in results when the researchers adjusted for the use of anxiolytics and antidepressants.
When they examined the prevalence of concomitant medication use or comorbidities, they found that depression was more frequent among patients with long-term stress and anxiety, compared with individuals with neither of those diagnoses. Additionally, patients with long-term stress and anxiety more often used anxiolytics, antidepressants, and QT-prolonging drugs.
Stratification of the analyses according to sex revealed that the OHCA rate was increased in both women and men with long-term stress and anxiety. There were no significant differences between the sexes. There were also no significant differences between the association among different age groups, nor between patients with and those without CVD, ischemic heart disease, or heart failure.
Previous research has shown associations of stress-related disorders or anxiety with cardiovascular outcomes, including myocardial infarction, heart failure, and cerebrovascular disease. These disorders might be “biological mediators in the causal pathway of OHCA” and contribute to the increased OHCA rate associated with stress-related disorders and anxiety, the authors suggest.
Nevertheless, they note, stress-related disorders and anxiety remained significantly associated with OHCA after controlling for these variables, “suggesting that it is unlikely that traditional risk factors of OHCA alone explain this relationship.”
They suggest several potential mechanisms. One is that the relationship is likely mediated by the activity of the sympathetic autonomic nervous system, which “leads to an increase in heart rate, release of neurotransmitters into the circulation, and local release of neurotransmitters in the heart.”
Each of these factors “may potentially influence cardiac electrophysiology and facilitate ventricular arrhythmias and OHCA.”
In addition to a biological mechanism, behavioral and psychosocial factors may also contribute to OHCA risk, since stress-related disorders and anxiety “often lead to unhealthy lifestyle, such as smoking and lower physical activity, which in turn may increase the risk of OHCA.” Given the absence of data on these features in the registries the investigators used, they were unable to account for them.
However, “it is unlikely that knowledge of these factors would have altered our conclusions considering that we have adjusted for all the relevant cardiovascular comorbidities.”
Similarly, other psychiatric disorders, such as depression, can contribute to OHCA risk, but they adjusted for depression in their multivariable analyses.
“Awareness of the higher risks of OHCA in patients with stress-related disorders and anxiety is important when treating these patients,” they conclude.
Detrimental to the heart, not just the psyche
Glenn Levine, MD, master clinician and professor of medicine, Baylor College of Medicine, Houston, called it an “important study in that it is a large, nationwide cohort study and thus provides important information to complement much smaller, focused studies.”
Like those other studies, “it finds that negative psychological health, specifically, long-term stress (as well as anxiety), is associated with a significantly increased risk of out-of-hospital cardiac arrest,” continued Dr. Levine, who is the chief of the cardiology section at Michael E. DeBakey VA Medical Center, Houston, and was not involved with the study.
Dr. Levine thinks the study “does a good job, as best one can for such a study, in trying to control for other factors, and zeroing in specifically on stress (and anxiety), trying to assess their independent contributions to the risk of developing cardiac arrest.”
The take-home message for clinicians and patients “is that negative psychological stress factors, such as stress and anxiety, are not only detrimental to one’s psychological health but likely increase one’s risk for adverse cardiac events, such as cardiac arrest,” he stated.
No specific funding for the study was disclosed. Mr. Eroglu has disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original article. Dr. Levine reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators compared more than 35,000 OHCA case patients with a similar number of matched control persons and found an almost 1.5 times higher hazard of long-term stress conditions among OHCA case patients, compared with control persons, with a similar hazard for anxiety. Posttraumatic stress disorder was associated with an almost twofold higher risk of OHCA.
The findings applied equally to men and women and were independent of the presence of cardiovascular disease (CVD).
“This study raises awareness of the higher risks of OHCA and early risk monitoring to prevent OHCA in patients with stress-related disorders and anxiety,” write Talip Eroglu, of the department of cardiology, Copenhagen University Hospital, and colleagues.
The study was published online in BMJ Open Heart.
Stress disorders and anxiety overrepresented
OHCA “predominantly arises from lethal cardiac arrhythmias ... that occur most frequently in the setting of coronary heart disease,” the authors write. However, increasing evidence suggests that rates of OHCA may also be increased in association with noncardiac diseases.
Individuals with stress-related disorders and anxiety are “overrepresented” among victims of cardiac arrest as well as those with multiple CVDs. But previous studies of OHCA have been limited by small numbers of cardiac arrests. In addition, those studies involved only data from selected populations or used in-hospital diagnosis to identify cardiac arrest, thereby potentially omitting OHCA patients who died prior to hospital admission.
The researchers therefore turned to data from Danish health registries that include a large, unselected cohort of patients with OHCA to investigate whether long-term stress conditions (that is, PTSD and adjustment disorder) or anxiety disorder were associated with OHCA.
They stratified the cohort according to sex, age, and CVD to identify which risk factor confers the highest risk of OHCA in patients with long-term stress conditions or anxiety, and they conducted sensitivity analyses of potential confounders, such as depression.
The design was a nested-case control model in which records at an individual patient level across registries were cross-linked to data from other national registries and were compared to matched control persons from the general population (35,195 OHCAs and 351,950 matched control persons; median IQR age, 72 [62-81] years; 66.82% men).
The prevalence of comorbidities and use of cardiovascular drugs were higher among OHCA case patients than among non-OHCA control persons.
Keep aware of stress and anxiety as risk factors
Among OHCA and non-OHCA participants, long-term stress conditions were diagnosed in 0.92% and 0.45%, respectively. Anxiety was diagnosed in 0.85% of OHCA case patients and in 0.37% of non-OHCA control persons.
These conditions were associated with a higher rate of OHCA after adjustment for common OHCA risk factors.
There were no significant differences in results when the researchers adjusted for the use of anxiolytics and antidepressants.
When they examined the prevalence of concomitant medication use or comorbidities, they found that depression was more frequent among patients with long-term stress and anxiety, compared with individuals with neither of those diagnoses. Additionally, patients with long-term stress and anxiety more often used anxiolytics, antidepressants, and QT-prolonging drugs.
Stratification of the analyses according to sex revealed that the OHCA rate was increased in both women and men with long-term stress and anxiety. There were no significant differences between the sexes. There were also no significant differences between the association among different age groups, nor between patients with and those without CVD, ischemic heart disease, or heart failure.
Previous research has shown associations of stress-related disorders or anxiety with cardiovascular outcomes, including myocardial infarction, heart failure, and cerebrovascular disease. These disorders might be “biological mediators in the causal pathway of OHCA” and contribute to the increased OHCA rate associated with stress-related disorders and anxiety, the authors suggest.
Nevertheless, they note, stress-related disorders and anxiety remained significantly associated with OHCA after controlling for these variables, “suggesting that it is unlikely that traditional risk factors of OHCA alone explain this relationship.”
They suggest several potential mechanisms. One is that the relationship is likely mediated by the activity of the sympathetic autonomic nervous system, which “leads to an increase in heart rate, release of neurotransmitters into the circulation, and local release of neurotransmitters in the heart.”
Each of these factors “may potentially influence cardiac electrophysiology and facilitate ventricular arrhythmias and OHCA.”
In addition to a biological mechanism, behavioral and psychosocial factors may also contribute to OHCA risk, since stress-related disorders and anxiety “often lead to unhealthy lifestyle, such as smoking and lower physical activity, which in turn may increase the risk of OHCA.” Given the absence of data on these features in the registries the investigators used, they were unable to account for them.
However, “it is unlikely that knowledge of these factors would have altered our conclusions considering that we have adjusted for all the relevant cardiovascular comorbidities.”
Similarly, other psychiatric disorders, such as depression, can contribute to OHCA risk, but they adjusted for depression in their multivariable analyses.
“Awareness of the higher risks of OHCA in patients with stress-related disorders and anxiety is important when treating these patients,” they conclude.
Detrimental to the heart, not just the psyche
Glenn Levine, MD, master clinician and professor of medicine, Baylor College of Medicine, Houston, called it an “important study in that it is a large, nationwide cohort study and thus provides important information to complement much smaller, focused studies.”
Like those other studies, “it finds that negative psychological health, specifically, long-term stress (as well as anxiety), is associated with a significantly increased risk of out-of-hospital cardiac arrest,” continued Dr. Levine, who is the chief of the cardiology section at Michael E. DeBakey VA Medical Center, Houston, and was not involved with the study.
Dr. Levine thinks the study “does a good job, as best one can for such a study, in trying to control for other factors, and zeroing in specifically on stress (and anxiety), trying to assess their independent contributions to the risk of developing cardiac arrest.”
The take-home message for clinicians and patients “is that negative psychological stress factors, such as stress and anxiety, are not only detrimental to one’s psychological health but likely increase one’s risk for adverse cardiac events, such as cardiac arrest,” he stated.
No specific funding for the study was disclosed. Mr. Eroglu has disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original article. Dr. Levine reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators compared more than 35,000 OHCA case patients with a similar number of matched control persons and found an almost 1.5 times higher hazard of long-term stress conditions among OHCA case patients, compared with control persons, with a similar hazard for anxiety. Posttraumatic stress disorder was associated with an almost twofold higher risk of OHCA.
The findings applied equally to men and women and were independent of the presence of cardiovascular disease (CVD).
“This study raises awareness of the higher risks of OHCA and early risk monitoring to prevent OHCA in patients with stress-related disorders and anxiety,” write Talip Eroglu, of the department of cardiology, Copenhagen University Hospital, and colleagues.
The study was published online in BMJ Open Heart.
Stress disorders and anxiety overrepresented
OHCA “predominantly arises from lethal cardiac arrhythmias ... that occur most frequently in the setting of coronary heart disease,” the authors write. However, increasing evidence suggests that rates of OHCA may also be increased in association with noncardiac diseases.
Individuals with stress-related disorders and anxiety are “overrepresented” among victims of cardiac arrest as well as those with multiple CVDs. But previous studies of OHCA have been limited by small numbers of cardiac arrests. In addition, those studies involved only data from selected populations or used in-hospital diagnosis to identify cardiac arrest, thereby potentially omitting OHCA patients who died prior to hospital admission.
The researchers therefore turned to data from Danish health registries that include a large, unselected cohort of patients with OHCA to investigate whether long-term stress conditions (that is, PTSD and adjustment disorder) or anxiety disorder were associated with OHCA.
They stratified the cohort according to sex, age, and CVD to identify which risk factor confers the highest risk of OHCA in patients with long-term stress conditions or anxiety, and they conducted sensitivity analyses of potential confounders, such as depression.
The design was a nested-case control model in which records at an individual patient level across registries were cross-linked to data from other national registries and were compared to matched control persons from the general population (35,195 OHCAs and 351,950 matched control persons; median IQR age, 72 [62-81] years; 66.82% men).
The prevalence of comorbidities and use of cardiovascular drugs were higher among OHCA case patients than among non-OHCA control persons.
Keep aware of stress and anxiety as risk factors
Among OHCA and non-OHCA participants, long-term stress conditions were diagnosed in 0.92% and 0.45%, respectively. Anxiety was diagnosed in 0.85% of OHCA case patients and in 0.37% of non-OHCA control persons.
These conditions were associated with a higher rate of OHCA after adjustment for common OHCA risk factors.
There were no significant differences in results when the researchers adjusted for the use of anxiolytics and antidepressants.
When they examined the prevalence of concomitant medication use or comorbidities, they found that depression was more frequent among patients with long-term stress and anxiety, compared with individuals with neither of those diagnoses. Additionally, patients with long-term stress and anxiety more often used anxiolytics, antidepressants, and QT-prolonging drugs.
Stratification of the analyses according to sex revealed that the OHCA rate was increased in both women and men with long-term stress and anxiety. There were no significant differences between the sexes. There were also no significant differences between the association among different age groups, nor between patients with and those without CVD, ischemic heart disease, or heart failure.
Previous research has shown associations of stress-related disorders or anxiety with cardiovascular outcomes, including myocardial infarction, heart failure, and cerebrovascular disease. These disorders might be “biological mediators in the causal pathway of OHCA” and contribute to the increased OHCA rate associated with stress-related disorders and anxiety, the authors suggest.
Nevertheless, they note, stress-related disorders and anxiety remained significantly associated with OHCA after controlling for these variables, “suggesting that it is unlikely that traditional risk factors of OHCA alone explain this relationship.”
They suggest several potential mechanisms. One is that the relationship is likely mediated by the activity of the sympathetic autonomic nervous system, which “leads to an increase in heart rate, release of neurotransmitters into the circulation, and local release of neurotransmitters in the heart.”
Each of these factors “may potentially influence cardiac electrophysiology and facilitate ventricular arrhythmias and OHCA.”
In addition to a biological mechanism, behavioral and psychosocial factors may also contribute to OHCA risk, since stress-related disorders and anxiety “often lead to unhealthy lifestyle, such as smoking and lower physical activity, which in turn may increase the risk of OHCA.” Given the absence of data on these features in the registries the investigators used, they were unable to account for them.
However, “it is unlikely that knowledge of these factors would have altered our conclusions considering that we have adjusted for all the relevant cardiovascular comorbidities.”
Similarly, other psychiatric disorders, such as depression, can contribute to OHCA risk, but they adjusted for depression in their multivariable analyses.
“Awareness of the higher risks of OHCA in patients with stress-related disorders and anxiety is important when treating these patients,” they conclude.
Detrimental to the heart, not just the psyche
Glenn Levine, MD, master clinician and professor of medicine, Baylor College of Medicine, Houston, called it an “important study in that it is a large, nationwide cohort study and thus provides important information to complement much smaller, focused studies.”
Like those other studies, “it finds that negative psychological health, specifically, long-term stress (as well as anxiety), is associated with a significantly increased risk of out-of-hospital cardiac arrest,” continued Dr. Levine, who is the chief of the cardiology section at Michael E. DeBakey VA Medical Center, Houston, and was not involved with the study.
Dr. Levine thinks the study “does a good job, as best one can for such a study, in trying to control for other factors, and zeroing in specifically on stress (and anxiety), trying to assess their independent contributions to the risk of developing cardiac arrest.”
The take-home message for clinicians and patients “is that negative psychological stress factors, such as stress and anxiety, are not only detrimental to one’s psychological health but likely increase one’s risk for adverse cardiac events, such as cardiac arrest,” he stated.
No specific funding for the study was disclosed. Mr. Eroglu has disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original article. Dr. Levine reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM BMJ OPEN HEART
Serious mental illness not a factor in most mass school shootings
Mass shootings, often on school campuses, have become a regular and sad reality in the United States.
The statistics are grim. Every day 12 children die from gun violence in America and another 32 are shot and injured. Since the Columbine High School shooting in 1999, more than 338,000 students in the United States have experienced school gun violence, according to the nonprofit organization Sandy Hook Promise.
A new analysis from the Columbia Mass Murder Database (CMMD) sheds fresh light on the debate over whether mental illness or easy access to guns is the key driver of mass shootings.
The findings, which are published in the Journal of Forensic Sciences, show that most perpetrators of mass school shootings are young, White men without serious mental illness.
A ‘straw man’
Mental health is often used as a “straw man” in debates about mass shootings, lead investigator Ragy Girgis, MD, told this news organization.
“There are many factors that contribute to the mass shooting epidemic, including gun access, criminality, substance use and misuse, and many others. Mental illness is incidental in the vast majority of cases,” said Dr. Girgis, with Columbia University Irving Medical Center, New York, and the New York State Psychiatric Institute.
“People with serious mental illness constitute only a small portion of the perpetrators of gun violence in this country,” coinvestigator Paul Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, told this news organization.
Using the CMMD, the researchers examined 82 incidents of mass murder perpetrated in academic settings including schools, colleges, and universities. The average number of victims of these incidents was eight. More than half (60%) of mass school shootings involved at least one semi- or fully automatic firearm.
All 82 incidents were initiated by men (mean age, 28), and 67% were White. About two-thirds (63%) involved guns.
More than three-quarters (77%) of all perpetrators of mass murders in academic settings had no recorded history of psychotic symptoms.
Despite the absence of serious mental illness, almost half (46%) of the mass school shooters took their own lives at the scene, suggesting that they viewed themselves as engaging in some form of “final act,” the researchers note.
“The major difference between mass shooters in school settings and elsewhere is the higher rate of suicide by the perpetrators in school settings. That suggests that the shootings are often part of a preexisting intent to die on the part of the shooter,” said Dr. Appelbaum.
Epidemic of emptiness
He noted that the typical profile of a mass school shooter is that of “a young male with anger problems, often as a result of bullying or abuse, frequently described as a loner, who has signaled a desire to kill other people.”
“If we only focus on mental illness, we will miss the warning signs in the majority of cases associated with victimization (such as bullying) and consequent anger,” Dr. Appelbaum said.
Dr. Girgis said there is a need to deal with the “epidemic of emptiness, narcissism, anger, and societal rejection felt by many young men/boys who, when combined with a desire to take their own lives and a great need for notoriety, feel that perpetrating a mass school shooting is their only option.”
“We also need to understand why it is so easy for so many mass school shooters to obtain firearms that are not theirs – either illegally or from someone else who themselves may have obtained the firearm legally,” Dr. Girgis said.
“All countries have people with mental illness,” Dr. Appelbaum said, “but among developed countries the U.S. is unique in the easy availability of weapons and in our disproportionate rate of murders.”
He also noted that school shootings are not a problem that clinicians are going to solve.
“Although they can be alert to signals from their patients of an intent to harm people in a school (or other) setting, the vast majority of shooters are not receiving treatment for a mental disorder,” Dr. Appelbaum said.
“This is a problem that can only be substantially diminished by reducing access to firearms, which includes requirements for safe storage, universal background checks, waiting periods to purchase firearms, and similar means-oriented interventions,” he added.
Need for regular mental health checks
Thea Gallagher, PsyD, who was not involved in the study, noted that mass school shooters may not have a psychotic illness, but with mental health there is a “spectrum, and obviously, that individual is struggling to some extent, most likely, mentally, if they are at a place where they are willing to take the lives of others and themselves.”
“We need to understand more about how people get to this place and the issues people are struggling with. We need to push for yearly mental health checks just like the yearly physical,” Dr. Gallagher, with the department of psychiatry at NYU Langone Health, New York, told this news organization.
“The more that we create conversation and moments to talk about how people are feeling internally, the better chance we have to give people who are struggling healthy coping strategies and the opportunity to process their emotions and not bury them,” Dr. Gallagher said.
Support for the study was provided in part by the New York State Office of Mental Hygiene, and the Elizabeth K. Dollard Charitable Trust. Dr. Girgis has received royalties and/or advances from books on mental health published by Wipf and Stock, and Routledge/Taylor and Francis. He has consulted for Noble Insights, IMS Expert Services, and Fowler White Burnett. Dr. Appelbaum and Dr. Gallagher report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Mass shootings, often on school campuses, have become a regular and sad reality in the United States.
The statistics are grim. Every day 12 children die from gun violence in America and another 32 are shot and injured. Since the Columbine High School shooting in 1999, more than 338,000 students in the United States have experienced school gun violence, according to the nonprofit organization Sandy Hook Promise.
A new analysis from the Columbia Mass Murder Database (CMMD) sheds fresh light on the debate over whether mental illness or easy access to guns is the key driver of mass shootings.
The findings, which are published in the Journal of Forensic Sciences, show that most perpetrators of mass school shootings are young, White men without serious mental illness.
A ‘straw man’
Mental health is often used as a “straw man” in debates about mass shootings, lead investigator Ragy Girgis, MD, told this news organization.
“There are many factors that contribute to the mass shooting epidemic, including gun access, criminality, substance use and misuse, and many others. Mental illness is incidental in the vast majority of cases,” said Dr. Girgis, with Columbia University Irving Medical Center, New York, and the New York State Psychiatric Institute.
“People with serious mental illness constitute only a small portion of the perpetrators of gun violence in this country,” coinvestigator Paul Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, told this news organization.
Using the CMMD, the researchers examined 82 incidents of mass murder perpetrated in academic settings including schools, colleges, and universities. The average number of victims of these incidents was eight. More than half (60%) of mass school shootings involved at least one semi- or fully automatic firearm.
All 82 incidents were initiated by men (mean age, 28), and 67% were White. About two-thirds (63%) involved guns.
More than three-quarters (77%) of all perpetrators of mass murders in academic settings had no recorded history of psychotic symptoms.
Despite the absence of serious mental illness, almost half (46%) of the mass school shooters took their own lives at the scene, suggesting that they viewed themselves as engaging in some form of “final act,” the researchers note.
“The major difference between mass shooters in school settings and elsewhere is the higher rate of suicide by the perpetrators in school settings. That suggests that the shootings are often part of a preexisting intent to die on the part of the shooter,” said Dr. Appelbaum.
Epidemic of emptiness
He noted that the typical profile of a mass school shooter is that of “a young male with anger problems, often as a result of bullying or abuse, frequently described as a loner, who has signaled a desire to kill other people.”
“If we only focus on mental illness, we will miss the warning signs in the majority of cases associated with victimization (such as bullying) and consequent anger,” Dr. Appelbaum said.
Dr. Girgis said there is a need to deal with the “epidemic of emptiness, narcissism, anger, and societal rejection felt by many young men/boys who, when combined with a desire to take their own lives and a great need for notoriety, feel that perpetrating a mass school shooting is their only option.”
“We also need to understand why it is so easy for so many mass school shooters to obtain firearms that are not theirs – either illegally or from someone else who themselves may have obtained the firearm legally,” Dr. Girgis said.
“All countries have people with mental illness,” Dr. Appelbaum said, “but among developed countries the U.S. is unique in the easy availability of weapons and in our disproportionate rate of murders.”
He also noted that school shootings are not a problem that clinicians are going to solve.
“Although they can be alert to signals from their patients of an intent to harm people in a school (or other) setting, the vast majority of shooters are not receiving treatment for a mental disorder,” Dr. Appelbaum said.
“This is a problem that can only be substantially diminished by reducing access to firearms, which includes requirements for safe storage, universal background checks, waiting periods to purchase firearms, and similar means-oriented interventions,” he added.
Need for regular mental health checks
Thea Gallagher, PsyD, who was not involved in the study, noted that mass school shooters may not have a psychotic illness, but with mental health there is a “spectrum, and obviously, that individual is struggling to some extent, most likely, mentally, if they are at a place where they are willing to take the lives of others and themselves.”
“We need to understand more about how people get to this place and the issues people are struggling with. We need to push for yearly mental health checks just like the yearly physical,” Dr. Gallagher, with the department of psychiatry at NYU Langone Health, New York, told this news organization.
“The more that we create conversation and moments to talk about how people are feeling internally, the better chance we have to give people who are struggling healthy coping strategies and the opportunity to process their emotions and not bury them,” Dr. Gallagher said.
Support for the study was provided in part by the New York State Office of Mental Hygiene, and the Elizabeth K. Dollard Charitable Trust. Dr. Girgis has received royalties and/or advances from books on mental health published by Wipf and Stock, and Routledge/Taylor and Francis. He has consulted for Noble Insights, IMS Expert Services, and Fowler White Burnett. Dr. Appelbaum and Dr. Gallagher report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Mass shootings, often on school campuses, have become a regular and sad reality in the United States.
The statistics are grim. Every day 12 children die from gun violence in America and another 32 are shot and injured. Since the Columbine High School shooting in 1999, more than 338,000 students in the United States have experienced school gun violence, according to the nonprofit organization Sandy Hook Promise.
A new analysis from the Columbia Mass Murder Database (CMMD) sheds fresh light on the debate over whether mental illness or easy access to guns is the key driver of mass shootings.
The findings, which are published in the Journal of Forensic Sciences, show that most perpetrators of mass school shootings are young, White men without serious mental illness.
A ‘straw man’
Mental health is often used as a “straw man” in debates about mass shootings, lead investigator Ragy Girgis, MD, told this news organization.
“There are many factors that contribute to the mass shooting epidemic, including gun access, criminality, substance use and misuse, and many others. Mental illness is incidental in the vast majority of cases,” said Dr. Girgis, with Columbia University Irving Medical Center, New York, and the New York State Psychiatric Institute.
“People with serious mental illness constitute only a small portion of the perpetrators of gun violence in this country,” coinvestigator Paul Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, told this news organization.
Using the CMMD, the researchers examined 82 incidents of mass murder perpetrated in academic settings including schools, colleges, and universities. The average number of victims of these incidents was eight. More than half (60%) of mass school shootings involved at least one semi- or fully automatic firearm.
All 82 incidents were initiated by men (mean age, 28), and 67% were White. About two-thirds (63%) involved guns.
More than three-quarters (77%) of all perpetrators of mass murders in academic settings had no recorded history of psychotic symptoms.
Despite the absence of serious mental illness, almost half (46%) of the mass school shooters took their own lives at the scene, suggesting that they viewed themselves as engaging in some form of “final act,” the researchers note.
“The major difference between mass shooters in school settings and elsewhere is the higher rate of suicide by the perpetrators in school settings. That suggests that the shootings are often part of a preexisting intent to die on the part of the shooter,” said Dr. Appelbaum.
Epidemic of emptiness
He noted that the typical profile of a mass school shooter is that of “a young male with anger problems, often as a result of bullying or abuse, frequently described as a loner, who has signaled a desire to kill other people.”
“If we only focus on mental illness, we will miss the warning signs in the majority of cases associated with victimization (such as bullying) and consequent anger,” Dr. Appelbaum said.
Dr. Girgis said there is a need to deal with the “epidemic of emptiness, narcissism, anger, and societal rejection felt by many young men/boys who, when combined with a desire to take their own lives and a great need for notoriety, feel that perpetrating a mass school shooting is their only option.”
“We also need to understand why it is so easy for so many mass school shooters to obtain firearms that are not theirs – either illegally or from someone else who themselves may have obtained the firearm legally,” Dr. Girgis said.
“All countries have people with mental illness,” Dr. Appelbaum said, “but among developed countries the U.S. is unique in the easy availability of weapons and in our disproportionate rate of murders.”
He also noted that school shootings are not a problem that clinicians are going to solve.
“Although they can be alert to signals from their patients of an intent to harm people in a school (or other) setting, the vast majority of shooters are not receiving treatment for a mental disorder,” Dr. Appelbaum said.
“This is a problem that can only be substantially diminished by reducing access to firearms, which includes requirements for safe storage, universal background checks, waiting periods to purchase firearms, and similar means-oriented interventions,” he added.
Need for regular mental health checks
Thea Gallagher, PsyD, who was not involved in the study, noted that mass school shooters may not have a psychotic illness, but with mental health there is a “spectrum, and obviously, that individual is struggling to some extent, most likely, mentally, if they are at a place where they are willing to take the lives of others and themselves.”
“We need to understand more about how people get to this place and the issues people are struggling with. We need to push for yearly mental health checks just like the yearly physical,” Dr. Gallagher, with the department of psychiatry at NYU Langone Health, New York, told this news organization.
“The more that we create conversation and moments to talk about how people are feeling internally, the better chance we have to give people who are struggling healthy coping strategies and the opportunity to process their emotions and not bury them,” Dr. Gallagher said.
Support for the study was provided in part by the New York State Office of Mental Hygiene, and the Elizabeth K. Dollard Charitable Trust. Dr. Girgis has received royalties and/or advances from books on mental health published by Wipf and Stock, and Routledge/Taylor and Francis. He has consulted for Noble Insights, IMS Expert Services, and Fowler White Burnett. Dr. Appelbaum and Dr. Gallagher report no relevant financial relationships.
A version of this article first appeared on Medscape.com.