User login
Too Many Chest CTs for Incidental Lung Nodules?
Too Many Chest CTs for Incidental Lung Nodules?
Chest CT is being ordered too often for incidental pulmonary nodules found on neck imaging, according to a study at one US health system.
It’s not uncommon for neck CT or MRI to show nodules in the lung apices, but there’s been no data on how often those incidental findings turn out to be lung cancer.
For the new study, researchers analyzed data of 22,173 patients who underwent neck, brachial plexus, or parathyroid imaging at the Massachusetts General Brigham in Boston.
Of those patients, 273 (1.2%) had requests for supplemental chest CTs due to incidental lung findings. Ultimately, only one new lung cancer was detected — an indolent adenocarcinoma — yielding a 2-year incidence rate of 0.40%.
The results suggest that recommendations for chest CT “should likely be substantially decreased,” the researchers conclude in the Journal of the American College of Radiology — though they also acknowledge a need for studies of larger datasets.
As for what drives such CT requests, study co-author Mark Hammer, MD, a thoracic radiologist at Brigham and Women’s Hospital, Harvard Medical School in Boston, offered one possibility: Neuroradiologists, who typically interpret neck imaging, might be less familiar with lung nodule follow-up guidelines.
At his institution, Hammer told Medscape Medical News, thoracic radiologists generally follow the Fleischner Society guidelines on management of incidentally detected pulmonary nodules.
“The reality is that neuroradiologists are often unfamiliar with those guidelines and may recommend follow-up for nodules that do not require it,” he said.
The Fleischner guidelines don’t recommend imaging nodules smaller than 6 mm given the very low cancer risk. For nodules of 6-8 mm, they recommend follow-up chest CTs at 3-12 months to see if the nodule has grown or changed. For larger or otherwise suspicious lesions, they advise prompt evaluation.
But while guidelines exist, follow-up decisions after neck imaging are largely at the discretion of the provider, said Dave Yousem, MD, MBA, a neuroradiologist at Johns Hopkins University in Baltimore.
According to Yousem, some physicians might be comfortable with the possibility of missing a low-risk indolent cancer to spare many patients from unnecessary CTs. But there’s also concern that overlooking even one tumor could trigger litigation, he said.
Hammer’s team found that of all patients with chest CT recommendations, only 171 (62.6%) underwent scanning — a rate consistent with previous reports of incidentaloma follow-up.
Hammer said, thoracic radiologists might have been applying the Fleischner guidelines, but some patients might simply have been lost to follow-up, among other possibilities.
He and his colleagues said recommendations for additional imaging should be evidence-based and judicious to ensure “appropriate follow-up and early detection of lung cancer.”
Potential solutions, they added, include incidentaloma tracking systems, improved communication between providers, and AI-assisted image interpretation.
The study was funded by the Association of University Radiologists and the Agency for Healthcare Research and Quality. Hammer and Yousem had no relevant disclosures.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. He is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net.
A version of this article first appeared on Medscape.com.
Chest CT is being ordered too often for incidental pulmonary nodules found on neck imaging, according to a study at one US health system.
It’s not uncommon for neck CT or MRI to show nodules in the lung apices, but there’s been no data on how often those incidental findings turn out to be lung cancer.
For the new study, researchers analyzed data of 22,173 patients who underwent neck, brachial plexus, or parathyroid imaging at the Massachusetts General Brigham in Boston.
Of those patients, 273 (1.2%) had requests for supplemental chest CTs due to incidental lung findings. Ultimately, only one new lung cancer was detected — an indolent adenocarcinoma — yielding a 2-year incidence rate of 0.40%.
The results suggest that recommendations for chest CT “should likely be substantially decreased,” the researchers conclude in the Journal of the American College of Radiology — though they also acknowledge a need for studies of larger datasets.
As for what drives such CT requests, study co-author Mark Hammer, MD, a thoracic radiologist at Brigham and Women’s Hospital, Harvard Medical School in Boston, offered one possibility: Neuroradiologists, who typically interpret neck imaging, might be less familiar with lung nodule follow-up guidelines.
At his institution, Hammer told Medscape Medical News, thoracic radiologists generally follow the Fleischner Society guidelines on management of incidentally detected pulmonary nodules.
“The reality is that neuroradiologists are often unfamiliar with those guidelines and may recommend follow-up for nodules that do not require it,” he said.
The Fleischner guidelines don’t recommend imaging nodules smaller than 6 mm given the very low cancer risk. For nodules of 6-8 mm, they recommend follow-up chest CTs at 3-12 months to see if the nodule has grown or changed. For larger or otherwise suspicious lesions, they advise prompt evaluation.
But while guidelines exist, follow-up decisions after neck imaging are largely at the discretion of the provider, said Dave Yousem, MD, MBA, a neuroradiologist at Johns Hopkins University in Baltimore.
According to Yousem, some physicians might be comfortable with the possibility of missing a low-risk indolent cancer to spare many patients from unnecessary CTs. But there’s also concern that overlooking even one tumor could trigger litigation, he said.
Hammer’s team found that of all patients with chest CT recommendations, only 171 (62.6%) underwent scanning — a rate consistent with previous reports of incidentaloma follow-up.
Hammer said, thoracic radiologists might have been applying the Fleischner guidelines, but some patients might simply have been lost to follow-up, among other possibilities.
He and his colleagues said recommendations for additional imaging should be evidence-based and judicious to ensure “appropriate follow-up and early detection of lung cancer.”
Potential solutions, they added, include incidentaloma tracking systems, improved communication between providers, and AI-assisted image interpretation.
The study was funded by the Association of University Radiologists and the Agency for Healthcare Research and Quality. Hammer and Yousem had no relevant disclosures.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. He is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net.
A version of this article first appeared on Medscape.com.
Chest CT is being ordered too often for incidental pulmonary nodules found on neck imaging, according to a study at one US health system.
It’s not uncommon for neck CT or MRI to show nodules in the lung apices, but there’s been no data on how often those incidental findings turn out to be lung cancer.
For the new study, researchers analyzed data of 22,173 patients who underwent neck, brachial plexus, or parathyroid imaging at the Massachusetts General Brigham in Boston.
Of those patients, 273 (1.2%) had requests for supplemental chest CTs due to incidental lung findings. Ultimately, only one new lung cancer was detected — an indolent adenocarcinoma — yielding a 2-year incidence rate of 0.40%.
The results suggest that recommendations for chest CT “should likely be substantially decreased,” the researchers conclude in the Journal of the American College of Radiology — though they also acknowledge a need for studies of larger datasets.
As for what drives such CT requests, study co-author Mark Hammer, MD, a thoracic radiologist at Brigham and Women’s Hospital, Harvard Medical School in Boston, offered one possibility: Neuroradiologists, who typically interpret neck imaging, might be less familiar with lung nodule follow-up guidelines.
At his institution, Hammer told Medscape Medical News, thoracic radiologists generally follow the Fleischner Society guidelines on management of incidentally detected pulmonary nodules.
“The reality is that neuroradiologists are often unfamiliar with those guidelines and may recommend follow-up for nodules that do not require it,” he said.
The Fleischner guidelines don’t recommend imaging nodules smaller than 6 mm given the very low cancer risk. For nodules of 6-8 mm, they recommend follow-up chest CTs at 3-12 months to see if the nodule has grown or changed. For larger or otherwise suspicious lesions, they advise prompt evaluation.
But while guidelines exist, follow-up decisions after neck imaging are largely at the discretion of the provider, said Dave Yousem, MD, MBA, a neuroradiologist at Johns Hopkins University in Baltimore.
According to Yousem, some physicians might be comfortable with the possibility of missing a low-risk indolent cancer to spare many patients from unnecessary CTs. But there’s also concern that overlooking even one tumor could trigger litigation, he said.
Hammer’s team found that of all patients with chest CT recommendations, only 171 (62.6%) underwent scanning — a rate consistent with previous reports of incidentaloma follow-up.
Hammer said, thoracic radiologists might have been applying the Fleischner guidelines, but some patients might simply have been lost to follow-up, among other possibilities.
He and his colleagues said recommendations for additional imaging should be evidence-based and judicious to ensure “appropriate follow-up and early detection of lung cancer.”
Potential solutions, they added, include incidentaloma tracking systems, improved communication between providers, and AI-assisted image interpretation.
The study was funded by the Association of University Radiologists and the Agency for Healthcare Research and Quality. Hammer and Yousem had no relevant disclosures.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. He is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net.
A version of this article first appeared on Medscape.com.
Too Many Chest CTs for Incidental Lung Nodules?
Too Many Chest CTs for Incidental Lung Nodules?
Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Several newly identified biomarkers can help distinguish invasive aspergillosis from aspergillus colonization in lung transplant recipients, according to data from a new study presented at the annual meeting of the International Society for Heart and Lung Transplantation.
Aspergillus, a common environmental mold, can cause potentially serious infection or asymptomatic colonization in patients who have significant lung disease or are immunosuppressed, said Aaron Mishkin, MD, associate professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, who was not involved in the study.
“Determining if the aspergillus that is present is a colonizing organism vs disease is challenging clinically,” Mishkin said. Clinicians currently rely on criteria including a compatible patient, imaging findings, and a laboratory-based diagnostic such as tissue from a biopsy, cultures, polymerase chain reaction (PCR), or fungal antigen detection, said Mishkin. “Fungal antigen detection has variable specificity and sensitivity,” he noted. New biomarkers that look for an immune response could help differentiate between colonization and infection by assessing an immune-mediated inflammatory response, the hallmark of infection, he said.
To tease out potential biomarkers associated with invasive aspergillosis, Christine Ng, MS, a researcher at the University Health Network, Toronto, Ontario, Canada, and colleagues performed RNA sequencing on samples from 14 control lung transplant patients, 34 with aspergillus colonization, and seven with invasive aspergillosis. They identified potential candidate genes in 15 control samples, 17 aspergillus colonization samples, and 15 invasive aspergillosis samples.
Overall, signaling pathway analysis showed robust immune response, T-cell immunity, and leukocyte immunity in patients with invasive aspergillosis. By contrast, patients with aspergillus colonization showed enriched cellular responses (response to stimuli, epithelium development).
In a real-time quantitative PCR analysis, the researchers validated three biomarkers specific to invasive aspergillosis (IRF7, ZBP1, CYP27B1). Biomarkers AKR1C2, FGF10, and VGLL3 demonstrated specificity for aspergillus colonization. Additionally, biomarkers PTGER3, LPAR3, and COL14A1 were significant when aspergillus colonization was compared to controls but not in comparisons between invasive aspergillosis and aspergillus colonization.
The study findings were limited by the small sample size, and larger studies are needed before they can be implemented in clinical practice, the researchers wrote. However, the results suggest that the new biomarkers reveal distinct host immune patterns and may improve differentiation of aspergillosis from colonization in lung transplant recipients, they concluded.
Clinical Implications and Next Steps
RNA testing can help differentiate colonization vs infection, Mishkin said. “Colonization is not typically treated, whereas infection would be treated with an anti-fungal and, in the case of a transplant recipient, a reduction in immunosuppression,” he said. “In lung transplantation, a delicate equilibrium must be maintained between achieving optimal immunosuppression and minimizing or treating infection. Any tools that can aid in this decision-making have the potential to enhance patient outcomes,” he added.
The current study was limited by the use of data only from a single center, and the broader applicability to additional populations, broader geographic areas, and a larger number of organisms remains unknown, Mishkin said. “This type of assay does have the possibility of applicability to a larger number of fungal and even bacterial species,” he noted.
A version of this article first appeared on Medscape.com.
Several newly identified biomarkers can help distinguish invasive aspergillosis from aspergillus colonization in lung transplant recipients, according to data from a new study presented at the annual meeting of the International Society for Heart and Lung Transplantation.
Aspergillus, a common environmental mold, can cause potentially serious infection or asymptomatic colonization in patients who have significant lung disease or are immunosuppressed, said Aaron Mishkin, MD, associate professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, who was not involved in the study.
“Determining if the aspergillus that is present is a colonizing organism vs disease is challenging clinically,” Mishkin said. Clinicians currently rely on criteria including a compatible patient, imaging findings, and a laboratory-based diagnostic such as tissue from a biopsy, cultures, polymerase chain reaction (PCR), or fungal antigen detection, said Mishkin. “Fungal antigen detection has variable specificity and sensitivity,” he noted. New biomarkers that look for an immune response could help differentiate between colonization and infection by assessing an immune-mediated inflammatory response, the hallmark of infection, he said.
To tease out potential biomarkers associated with invasive aspergillosis, Christine Ng, MS, a researcher at the University Health Network, Toronto, Ontario, Canada, and colleagues performed RNA sequencing on samples from 14 control lung transplant patients, 34 with aspergillus colonization, and seven with invasive aspergillosis. They identified potential candidate genes in 15 control samples, 17 aspergillus colonization samples, and 15 invasive aspergillosis samples.
Overall, signaling pathway analysis showed robust immune response, T-cell immunity, and leukocyte immunity in patients with invasive aspergillosis. By contrast, patients with aspergillus colonization showed enriched cellular responses (response to stimuli, epithelium development).
In a real-time quantitative PCR analysis, the researchers validated three biomarkers specific to invasive aspergillosis (IRF7, ZBP1, CYP27B1). Biomarkers AKR1C2, FGF10, and VGLL3 demonstrated specificity for aspergillus colonization. Additionally, biomarkers PTGER3, LPAR3, and COL14A1 were significant when aspergillus colonization was compared to controls but not in comparisons between invasive aspergillosis and aspergillus colonization.
The study findings were limited by the small sample size, and larger studies are needed before they can be implemented in clinical practice, the researchers wrote. However, the results suggest that the new biomarkers reveal distinct host immune patterns and may improve differentiation of aspergillosis from colonization in lung transplant recipients, they concluded.
Clinical Implications and Next Steps
RNA testing can help differentiate colonization vs infection, Mishkin said. “Colonization is not typically treated, whereas infection would be treated with an anti-fungal and, in the case of a transplant recipient, a reduction in immunosuppression,” he said. “In lung transplantation, a delicate equilibrium must be maintained between achieving optimal immunosuppression and minimizing or treating infection. Any tools that can aid in this decision-making have the potential to enhance patient outcomes,” he added.
The current study was limited by the use of data only from a single center, and the broader applicability to additional populations, broader geographic areas, and a larger number of organisms remains unknown, Mishkin said. “This type of assay does have the possibility of applicability to a larger number of fungal and even bacterial species,” he noted.
A version of this article first appeared on Medscape.com.
Several newly identified biomarkers can help distinguish invasive aspergillosis from aspergillus colonization in lung transplant recipients, according to data from a new study presented at the annual meeting of the International Society for Heart and Lung Transplantation.
Aspergillus, a common environmental mold, can cause potentially serious infection or asymptomatic colonization in patients who have significant lung disease or are immunosuppressed, said Aaron Mishkin, MD, associate professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, who was not involved in the study.
“Determining if the aspergillus that is present is a colonizing organism vs disease is challenging clinically,” Mishkin said. Clinicians currently rely on criteria including a compatible patient, imaging findings, and a laboratory-based diagnostic such as tissue from a biopsy, cultures, polymerase chain reaction (PCR), or fungal antigen detection, said Mishkin. “Fungal antigen detection has variable specificity and sensitivity,” he noted. New biomarkers that look for an immune response could help differentiate between colonization and infection by assessing an immune-mediated inflammatory response, the hallmark of infection, he said.
To tease out potential biomarkers associated with invasive aspergillosis, Christine Ng, MS, a researcher at the University Health Network, Toronto, Ontario, Canada, and colleagues performed RNA sequencing on samples from 14 control lung transplant patients, 34 with aspergillus colonization, and seven with invasive aspergillosis. They identified potential candidate genes in 15 control samples, 17 aspergillus colonization samples, and 15 invasive aspergillosis samples.
Overall, signaling pathway analysis showed robust immune response, T-cell immunity, and leukocyte immunity in patients with invasive aspergillosis. By contrast, patients with aspergillus colonization showed enriched cellular responses (response to stimuli, epithelium development).
In a real-time quantitative PCR analysis, the researchers validated three biomarkers specific to invasive aspergillosis (IRF7, ZBP1, CYP27B1). Biomarkers AKR1C2, FGF10, and VGLL3 demonstrated specificity for aspergillus colonization. Additionally, biomarkers PTGER3, LPAR3, and COL14A1 were significant when aspergillus colonization was compared to controls but not in comparisons between invasive aspergillosis and aspergillus colonization.
The study findings were limited by the small sample size, and larger studies are needed before they can be implemented in clinical practice, the researchers wrote. However, the results suggest that the new biomarkers reveal distinct host immune patterns and may improve differentiation of aspergillosis from colonization in lung transplant recipients, they concluded.
Clinical Implications and Next Steps
RNA testing can help differentiate colonization vs infection, Mishkin said. “Colonization is not typically treated, whereas infection would be treated with an anti-fungal and, in the case of a transplant recipient, a reduction in immunosuppression,” he said. “In lung transplantation, a delicate equilibrium must be maintained between achieving optimal immunosuppression and minimizing or treating infection. Any tools that can aid in this decision-making have the potential to enhance patient outcomes,” he added.
The current study was limited by the use of data only from a single center, and the broader applicability to additional populations, broader geographic areas, and a larger number of organisms remains unknown, Mishkin said. “This type of assay does have the possibility of applicability to a larger number of fungal and even bacterial species,” he noted.
A version of this article first appeared on Medscape.com.
Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Cervical Cancer Screening Gaps Persist After 65 Years of Age
Cervical Cancer Screening Gaps Persist After 65 Years of Age
TOPLINE:
Among women aged > 65 years who were at a high risk for cervical cancer and required screening, only 5.2% received appropriate screening. Women with a history of high-grade cervical dysplasia had a greater likelihood of appropriate screening.
METHODOLOGY:
- Researchers conducted a retrospective study to assess the rates of appropriate cervical cancer screening among 1787 women aged 66 years or older (median, 76 years; 96.3% White) who had a Medicare wellness visit or an annual gynecologic visit in a healthcare system in 2022.
- Data on age at the last cervical cancer screening, history of hysterectomy, human papillomavirus (HPV) status, and history of a diagnosis of cervical cancer or cervical dysplasia, high-grade dysplasia, and immune deficiency status were assessed.
- Participants were categorized into 2 groups: those at high risk for cervical cancer (prior high-grade cervical dysplasia or cancer, an immunocompromised status, or lack of two normal cytology results in the past 10 years; n = 250) and those at average risk (having no high-risk features and adequate prior screening or having a prior hysterectomy with no history of high-grade cervical dysplasia; n = 1537).
- The screening cessation criteria were based on adequate prior screening, defined as two prior negative cervical cancer screenings in the past 10 years, the absence of high-grade cervical dysplasia or cervical cancer, and no immune deficiency.
TAKEAWAY:
- Overall, 4.9% of patients had a history of inadequate prior screening; among women at high risk, 5.2% were appropriately screened.
- The odds of continued screening were greater for women with a history of a positive HPV test results (adjusted odds ratio [aOR], 3.4; P = .016), a history of high-grade cervical dysplasia (aOR, 3.8; P = .009), and those without prior hysterectomy (aOR, 2.2; P = .005).
- Among women at high risk for cervical cancer, those with a history of high-grade cervical dysplasia had increased odds of appropriate screening (aOR, 6.7; P = .002), whereas the odds decreased with every 5-year increase in age (aOR, 0.5; P = .031). Women with prior hysterectomy were less likely to be over-screened (aOR, 0.3; P < .001) than those without.
- Among the 79 women who underwent screening, 97.5% had normal cytology results; the remaining women had abnormal cytology results (atypical squamous cells of undetermined significance or atypical squamous cells); all patients with abnormal cytology results met high-risk criteria and were screened appropriately.
IN PRACTICE:
“[The study] findings suggest that most clinicians and patients are aware of recommendations to stop cervical cancer screening after age 65 years. However, there may be a lack of awareness regarding continued screening in high-risk patients or those with inadequate prior screening. The lack of prior screening history and results in the medical record suggests that providers may not understand the importance of these factors to inform cervical cancer screening in older patients,” the authors of the study wrote.
SOURCE:
The study was led by Daniel Rodriguez, BS, Kolschowsky Research and Education Institute, Sarasota Memorial Health Care System, Sarasota, Florida. It was published online on April 23, 2026, in the Journal of Lower Genital Tract Disease.
LIMITATIONS:
Screening history in electronic medical records may be incomplete.
DISCLOSURES:
The Sarasota Memorial Healthcare Foundation provided financial support for this research. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among women aged > 65 years who were at a high risk for cervical cancer and required screening, only 5.2% received appropriate screening. Women with a history of high-grade cervical dysplasia had a greater likelihood of appropriate screening.
METHODOLOGY:
- Researchers conducted a retrospective study to assess the rates of appropriate cervical cancer screening among 1787 women aged 66 years or older (median, 76 years; 96.3% White) who had a Medicare wellness visit or an annual gynecologic visit in a healthcare system in 2022.
- Data on age at the last cervical cancer screening, history of hysterectomy, human papillomavirus (HPV) status, and history of a diagnosis of cervical cancer or cervical dysplasia, high-grade dysplasia, and immune deficiency status were assessed.
- Participants were categorized into 2 groups: those at high risk for cervical cancer (prior high-grade cervical dysplasia or cancer, an immunocompromised status, or lack of two normal cytology results in the past 10 years; n = 250) and those at average risk (having no high-risk features and adequate prior screening or having a prior hysterectomy with no history of high-grade cervical dysplasia; n = 1537).
- The screening cessation criteria were based on adequate prior screening, defined as two prior negative cervical cancer screenings in the past 10 years, the absence of high-grade cervical dysplasia or cervical cancer, and no immune deficiency.
TAKEAWAY:
- Overall, 4.9% of patients had a history of inadequate prior screening; among women at high risk, 5.2% were appropriately screened.
- The odds of continued screening were greater for women with a history of a positive HPV test results (adjusted odds ratio [aOR], 3.4; P = .016), a history of high-grade cervical dysplasia (aOR, 3.8; P = .009), and those without prior hysterectomy (aOR, 2.2; P = .005).
- Among women at high risk for cervical cancer, those with a history of high-grade cervical dysplasia had increased odds of appropriate screening (aOR, 6.7; P = .002), whereas the odds decreased with every 5-year increase in age (aOR, 0.5; P = .031). Women with prior hysterectomy were less likely to be over-screened (aOR, 0.3; P < .001) than those without.
- Among the 79 women who underwent screening, 97.5% had normal cytology results; the remaining women had abnormal cytology results (atypical squamous cells of undetermined significance or atypical squamous cells); all patients with abnormal cytology results met high-risk criteria and were screened appropriately.
IN PRACTICE:
“[The study] findings suggest that most clinicians and patients are aware of recommendations to stop cervical cancer screening after age 65 years. However, there may be a lack of awareness regarding continued screening in high-risk patients or those with inadequate prior screening. The lack of prior screening history and results in the medical record suggests that providers may not understand the importance of these factors to inform cervical cancer screening in older patients,” the authors of the study wrote.
SOURCE:
The study was led by Daniel Rodriguez, BS, Kolschowsky Research and Education Institute, Sarasota Memorial Health Care System, Sarasota, Florida. It was published online on April 23, 2026, in the Journal of Lower Genital Tract Disease.
LIMITATIONS:
Screening history in electronic medical records may be incomplete.
DISCLOSURES:
The Sarasota Memorial Healthcare Foundation provided financial support for this research. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among women aged > 65 years who were at a high risk for cervical cancer and required screening, only 5.2% received appropriate screening. Women with a history of high-grade cervical dysplasia had a greater likelihood of appropriate screening.
METHODOLOGY:
- Researchers conducted a retrospective study to assess the rates of appropriate cervical cancer screening among 1787 women aged 66 years or older (median, 76 years; 96.3% White) who had a Medicare wellness visit or an annual gynecologic visit in a healthcare system in 2022.
- Data on age at the last cervical cancer screening, history of hysterectomy, human papillomavirus (HPV) status, and history of a diagnosis of cervical cancer or cervical dysplasia, high-grade dysplasia, and immune deficiency status were assessed.
- Participants were categorized into 2 groups: those at high risk for cervical cancer (prior high-grade cervical dysplasia or cancer, an immunocompromised status, or lack of two normal cytology results in the past 10 years; n = 250) and those at average risk (having no high-risk features and adequate prior screening or having a prior hysterectomy with no history of high-grade cervical dysplasia; n = 1537).
- The screening cessation criteria were based on adequate prior screening, defined as two prior negative cervical cancer screenings in the past 10 years, the absence of high-grade cervical dysplasia or cervical cancer, and no immune deficiency.
TAKEAWAY:
- Overall, 4.9% of patients had a history of inadequate prior screening; among women at high risk, 5.2% were appropriately screened.
- The odds of continued screening were greater for women with a history of a positive HPV test results (adjusted odds ratio [aOR], 3.4; P = .016), a history of high-grade cervical dysplasia (aOR, 3.8; P = .009), and those without prior hysterectomy (aOR, 2.2; P = .005).
- Among women at high risk for cervical cancer, those with a history of high-grade cervical dysplasia had increased odds of appropriate screening (aOR, 6.7; P = .002), whereas the odds decreased with every 5-year increase in age (aOR, 0.5; P = .031). Women with prior hysterectomy were less likely to be over-screened (aOR, 0.3; P < .001) than those without.
- Among the 79 women who underwent screening, 97.5% had normal cytology results; the remaining women had abnormal cytology results (atypical squamous cells of undetermined significance or atypical squamous cells); all patients with abnormal cytology results met high-risk criteria and were screened appropriately.
IN PRACTICE:
“[The study] findings suggest that most clinicians and patients are aware of recommendations to stop cervical cancer screening after age 65 years. However, there may be a lack of awareness regarding continued screening in high-risk patients or those with inadequate prior screening. The lack of prior screening history and results in the medical record suggests that providers may not understand the importance of these factors to inform cervical cancer screening in older patients,” the authors of the study wrote.
SOURCE:
The study was led by Daniel Rodriguez, BS, Kolschowsky Research and Education Institute, Sarasota Memorial Health Care System, Sarasota, Florida. It was published online on April 23, 2026, in the Journal of Lower Genital Tract Disease.
LIMITATIONS:
Screening history in electronic medical records may be incomplete.
DISCLOSURES:
The Sarasota Memorial Healthcare Foundation provided financial support for this research. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Cervical Cancer Screening Gaps Persist After 65 Years of Age
Cervical Cancer Screening Gaps Persist After 65 Years of Age
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Dual checkpoint blockade allowed 70.6% of patients with microsatellite instability-high (MSI-H) resectable gastric or gastroesophageal junction adenocarcinoma (G/GEJAC) to avoid surgery in a small cohort of the INFINITY study.
MSI-H tumors account for roughly 10% of early G/GEJACs. They respond well to immunotherapy, with high rates of pathologic complete responses. The Italian INFINITY trial set out to test whether some patients with these tumors might not need gastrectomy.
The trial treated MSI-H patients with durvalumab 1500 mg once a month for 3 months along with 1 300-mg dose of the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blocker tremelimumab on day 1. The 18 patients in cohort 1 proceeded to surgery, with a 60% pathologic complete response rate. An additional 18 patients in cohort 2 were the subject of a presentation at the American Association for Cancer Research (AACR) Annual Meeting 2026. These patients were assessed for clinical complete response; if present, they went on to surveillance; if not, they had surgery.
To qualify for a clinical complete response and surveillance, patients were required to have negative findings on CT and PET scans; tumor-informed circulating tumor DNA (ctDNA); and upper endoscopy with ultrasound, including bite-on-bite biopsies and nodal sampling. Surveillance afterward included CT, endoscopy with biopsies, and ctDNA every 12 weeks for up to 2 years.
Among 17 evaluable patients, 1 withdrew consent during immunotherapy, 13 (76%) had a clinical complete response and started surveillance, and the other 4 went to surgery. One patient in the surveillance group had a local regrowth after 4 months, underwent salvage surgery, and remained disease-free. At a median follow-up of 27.1 months, there were no additional progression events.
Overall, 12 of the 17 patients (70.6%) were gastrectomy-free at 2 years without additional treatment. Progression-free survival was 94.1%, and all patients were alive.
“The results are very encouraging,” lead investigator Alberto Leone, MD, said while presenting the results at the AACR annual meeting.
“Nonoperative management could be a safe and effective strategy for patients achieving a clinical complete response after only 3 months of dual immunotherapy,” said Leone, who is a gastrointestinal medical oncologist at the Istituto Nazionale dei Tumori, Milan, Italy. “However, the optimal strategy needs to be established in larger randomized trials.”
Study discussant Yelena Janjagian, MD, gastrointestinal medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, said the findings were important, particularly given that 70.6% of patients avoided a potentially life-altering gastrectomy.
In addition to surgery, the study also calls into question the need for chemotherapy, long the backbone of management alongside surgery, she said. To replace it, however, “it appears that dual checkpoint blockade will be required for a chemotherapy-free approach to achieve organ preservation.”
“Anti-PD-1 alone is not sufficient; we need CTLA-4 to expand and reactivate tumor-specific immunity,” Janjagian continued.
Ultimately, she expects immunotherapy to shift management of MSI-H cancers away from surgery, although some patients will still likely need an operation.
In addition to being MSI-H, patients in the study were mismatch repair deficient and Epstein-Barr virus-negative with T2/T3 tumors; T4 tumors were excluded.
Tumor-agnostic plasma ctDNA was positive at baseline in 13 patients and cleared in 11 after treatment. Higher baseline plasma ctDNA trended toward a lower likelihood of reaching a clinical complete response. Specificity was 100%, so when positive, the test was “very highly informative,” Leone said.
Three patients had grade 3 adverse events (hyperthyroidism, increased gamma-glutamyl transferase, and colitis) that resolved with steroids. There were no grade 4 events, treatment discontinuation, or deaths.
The work was funded by the GONO Foundation and AstraZeneca, the maker of durvalumab and tremelimumab. Leone reported having no disclosures. Janjagian reported having extensive industry ties, including travel funding, consulting fees, and research support from AstraZeneca.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net
A version of this article first appeared on Medscape.com.
Dual checkpoint blockade allowed 70.6% of patients with microsatellite instability-high (MSI-H) resectable gastric or gastroesophageal junction adenocarcinoma (G/GEJAC) to avoid surgery in a small cohort of the INFINITY study.
MSI-H tumors account for roughly 10% of early G/GEJACs. They respond well to immunotherapy, with high rates of pathologic complete responses. The Italian INFINITY trial set out to test whether some patients with these tumors might not need gastrectomy.
The trial treated MSI-H patients with durvalumab 1500 mg once a month for 3 months along with 1 300-mg dose of the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blocker tremelimumab on day 1. The 18 patients in cohort 1 proceeded to surgery, with a 60% pathologic complete response rate. An additional 18 patients in cohort 2 were the subject of a presentation at the American Association for Cancer Research (AACR) Annual Meeting 2026. These patients were assessed for clinical complete response; if present, they went on to surveillance; if not, they had surgery.
To qualify for a clinical complete response and surveillance, patients were required to have negative findings on CT and PET scans; tumor-informed circulating tumor DNA (ctDNA); and upper endoscopy with ultrasound, including bite-on-bite biopsies and nodal sampling. Surveillance afterward included CT, endoscopy with biopsies, and ctDNA every 12 weeks for up to 2 years.
Among 17 evaluable patients, 1 withdrew consent during immunotherapy, 13 (76%) had a clinical complete response and started surveillance, and the other 4 went to surgery. One patient in the surveillance group had a local regrowth after 4 months, underwent salvage surgery, and remained disease-free. At a median follow-up of 27.1 months, there were no additional progression events.
Overall, 12 of the 17 patients (70.6%) were gastrectomy-free at 2 years without additional treatment. Progression-free survival was 94.1%, and all patients were alive.
“The results are very encouraging,” lead investigator Alberto Leone, MD, said while presenting the results at the AACR annual meeting.
“Nonoperative management could be a safe and effective strategy for patients achieving a clinical complete response after only 3 months of dual immunotherapy,” said Leone, who is a gastrointestinal medical oncologist at the Istituto Nazionale dei Tumori, Milan, Italy. “However, the optimal strategy needs to be established in larger randomized trials.”
Study discussant Yelena Janjagian, MD, gastrointestinal medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, said the findings were important, particularly given that 70.6% of patients avoided a potentially life-altering gastrectomy.
In addition to surgery, the study also calls into question the need for chemotherapy, long the backbone of management alongside surgery, she said. To replace it, however, “it appears that dual checkpoint blockade will be required for a chemotherapy-free approach to achieve organ preservation.”
“Anti-PD-1 alone is not sufficient; we need CTLA-4 to expand and reactivate tumor-specific immunity,” Janjagian continued.
Ultimately, she expects immunotherapy to shift management of MSI-H cancers away from surgery, although some patients will still likely need an operation.
In addition to being MSI-H, patients in the study were mismatch repair deficient and Epstein-Barr virus-negative with T2/T3 tumors; T4 tumors were excluded.
Tumor-agnostic plasma ctDNA was positive at baseline in 13 patients and cleared in 11 after treatment. Higher baseline plasma ctDNA trended toward a lower likelihood of reaching a clinical complete response. Specificity was 100%, so when positive, the test was “very highly informative,” Leone said.
Three patients had grade 3 adverse events (hyperthyroidism, increased gamma-glutamyl transferase, and colitis) that resolved with steroids. There were no grade 4 events, treatment discontinuation, or deaths.
The work was funded by the GONO Foundation and AstraZeneca, the maker of durvalumab and tremelimumab. Leone reported having no disclosures. Janjagian reported having extensive industry ties, including travel funding, consulting fees, and research support from AstraZeneca.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net
A version of this article first appeared on Medscape.com.
Dual checkpoint blockade allowed 70.6% of patients with microsatellite instability-high (MSI-H) resectable gastric or gastroesophageal junction adenocarcinoma (G/GEJAC) to avoid surgery in a small cohort of the INFINITY study.
MSI-H tumors account for roughly 10% of early G/GEJACs. They respond well to immunotherapy, with high rates of pathologic complete responses. The Italian INFINITY trial set out to test whether some patients with these tumors might not need gastrectomy.
The trial treated MSI-H patients with durvalumab 1500 mg once a month for 3 months along with 1 300-mg dose of the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blocker tremelimumab on day 1. The 18 patients in cohort 1 proceeded to surgery, with a 60% pathologic complete response rate. An additional 18 patients in cohort 2 were the subject of a presentation at the American Association for Cancer Research (AACR) Annual Meeting 2026. These patients were assessed for clinical complete response; if present, they went on to surveillance; if not, they had surgery.
To qualify for a clinical complete response and surveillance, patients were required to have negative findings on CT and PET scans; tumor-informed circulating tumor DNA (ctDNA); and upper endoscopy with ultrasound, including bite-on-bite biopsies and nodal sampling. Surveillance afterward included CT, endoscopy with biopsies, and ctDNA every 12 weeks for up to 2 years.
Among 17 evaluable patients, 1 withdrew consent during immunotherapy, 13 (76%) had a clinical complete response and started surveillance, and the other 4 went to surgery. One patient in the surveillance group had a local regrowth after 4 months, underwent salvage surgery, and remained disease-free. At a median follow-up of 27.1 months, there were no additional progression events.
Overall, 12 of the 17 patients (70.6%) were gastrectomy-free at 2 years without additional treatment. Progression-free survival was 94.1%, and all patients were alive.
“The results are very encouraging,” lead investigator Alberto Leone, MD, said while presenting the results at the AACR annual meeting.
“Nonoperative management could be a safe and effective strategy for patients achieving a clinical complete response after only 3 months of dual immunotherapy,” said Leone, who is a gastrointestinal medical oncologist at the Istituto Nazionale dei Tumori, Milan, Italy. “However, the optimal strategy needs to be established in larger randomized trials.”
Study discussant Yelena Janjagian, MD, gastrointestinal medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, said the findings were important, particularly given that 70.6% of patients avoided a potentially life-altering gastrectomy.
In addition to surgery, the study also calls into question the need for chemotherapy, long the backbone of management alongside surgery, she said. To replace it, however, “it appears that dual checkpoint blockade will be required for a chemotherapy-free approach to achieve organ preservation.”
“Anti-PD-1 alone is not sufficient; we need CTLA-4 to expand and reactivate tumor-specific immunity,” Janjagian continued.
Ultimately, she expects immunotherapy to shift management of MSI-H cancers away from surgery, although some patients will still likely need an operation.
In addition to being MSI-H, patients in the study were mismatch repair deficient and Epstein-Barr virus-negative with T2/T3 tumors; T4 tumors were excluded.
Tumor-agnostic plasma ctDNA was positive at baseline in 13 patients and cleared in 11 after treatment. Higher baseline plasma ctDNA trended toward a lower likelihood of reaching a clinical complete response. Specificity was 100%, so when positive, the test was “very highly informative,” Leone said.
Three patients had grade 3 adverse events (hyperthyroidism, increased gamma-glutamyl transferase, and colitis) that resolved with steroids. There were no grade 4 events, treatment discontinuation, or deaths.
The work was funded by the GONO Foundation and AstraZeneca, the maker of durvalumab and tremelimumab. Leone reported having no disclosures. Janjagian reported having extensive industry ties, including travel funding, consulting fees, and research support from AstraZeneca.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net
A version of this article first appeared on Medscape.com.
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
A personalized messenger RNA (mRNA) vaccine for pancreatic cancer continues to show promise for improving patient survival, according to 6-year follow-up results of a phase 1 clinical study.
Among the 8 out of 16 patients in the study who initially experienced an immune response to the vaccine, seven (87.5%) were still alive at follow-up, lead investigator Vinod P. Balachandran, MD, reported at the American Association for Cancer Research (AACR) Annual Meeting 2026.
Of the eight patients who did not respond, two (25%) were still alive, with a median survival time of 3.4 years. “This suggests that personalized vaccines can stimulate the immune system in some pancreatic cancer patients, and that these patients continue to do well for several years after vaccination,” said Balachandran, director of the Olayan Center for Cancer Vaccines at Memorial Sloan Kettering Cancer Center in New York City.
The findings suggest that this vaccine has the potential to improve outcomes in patients with pancreatic cancer, which is one of the deadliest cancers, he said.
The 5-year survival rate for pancreatic cancer is currently 13%, according to the American Cancer Society’s Cancer Statistics 2026 report.
Initial results of the trial evaluating the individualized neoantigen vaccine — autogene cevumeran, which is being developed by BioNTech and Genentech — were published in Nature in February 2025.
After pancreatic cancer surgery and chemo-immunotherapy, patients with pancreatic ductal adenocarcinoma (PDAC) received a vaccine personalized to each patient based on unique changes in their tumor DNA.
The eight patients with vaccine-induced T cells had prolonged recurrence-free survival (RFS; median not reached), whereas nonresponders had a median RFS of 13.4 months, the authors had reported in the Nature paper.
This correlation was not confounded by other factors, including those associated with the patient, tumor, treatment, and host immune fitness, Balachandran noted.
In the responders, the T-cell clones had “high magnitude and exceptional longevity,” with an average estimated lifespan of 7.7 years, he said.
A fundamental challenge in developing cancer vaccines has been generating durable functional T cells specific for tumor antigens, and these findings suggest that mRNA-lipoplex vaccines against somatic mutation-derived neoantigens like autogene cevumeran may help overcome this challenge in pancreatic cancer, he and his colleagues concluded in the Nature paper.
The latest findings presented at the AACR annual meeting further underscore the potential of this approach.
At the 6-year follow-up, median RFS was “still not reached” in the vaccine responders vs 1.1 year in the nonresponders, he noted.
“This translates to a difference in overall survival,” he said. “Seven of eight [responders to the vaccine] are still alive 4.5-6 years after surgery.”
And of the 2 of 8 nonresponders still alive, one appears to be mounting a subclinical vaccine-induced T-cell response, he added, noting that this “suggests that inducible vaccine immunity may also impact survival in PDAC.”
“The implication here, we believe, is that even if a cancer has very mutational by-products [like PDAC], these mutational by-products can empower potent and composite immunity,” he said. “This is important because it could potentially expand vaccine eligibility to many cancers.”
Currently, there are about 50 neoantigen vaccine trials in solid tumors ongoing worldwide, he noted.
Memorial Sloan Kettering reports that Genentech and BioNTech are now testing autogene cevumeran in a larger patient population at numerous sites worldwide.
Balachandran reported receiving research support from Genentech, Merck Sharp & Dohme, and AbbVie.
Sharon Worcester, MA, is an award-winning medical journalist based in Birmingham, Alabama, writing for Medscape, MDedge, and other affiliate sites. She currently covers oncology, but she has also written on a variety of other medical specialties and healthcare topics. She can be reached at sworcester@mdedge.com or on X: @SW_MedReporter.
A version of this article first appeared on Medscape.com.
A personalized messenger RNA (mRNA) vaccine for pancreatic cancer continues to show promise for improving patient survival, according to 6-year follow-up results of a phase 1 clinical study.
Among the 8 out of 16 patients in the study who initially experienced an immune response to the vaccine, seven (87.5%) were still alive at follow-up, lead investigator Vinod P. Balachandran, MD, reported at the American Association for Cancer Research (AACR) Annual Meeting 2026.
Of the eight patients who did not respond, two (25%) were still alive, with a median survival time of 3.4 years. “This suggests that personalized vaccines can stimulate the immune system in some pancreatic cancer patients, and that these patients continue to do well for several years after vaccination,” said Balachandran, director of the Olayan Center for Cancer Vaccines at Memorial Sloan Kettering Cancer Center in New York City.
The findings suggest that this vaccine has the potential to improve outcomes in patients with pancreatic cancer, which is one of the deadliest cancers, he said.
The 5-year survival rate for pancreatic cancer is currently 13%, according to the American Cancer Society’s Cancer Statistics 2026 report.
Initial results of the trial evaluating the individualized neoantigen vaccine — autogene cevumeran, which is being developed by BioNTech and Genentech — were published in Nature in February 2025.
After pancreatic cancer surgery and chemo-immunotherapy, patients with pancreatic ductal adenocarcinoma (PDAC) received a vaccine personalized to each patient based on unique changes in their tumor DNA.
The eight patients with vaccine-induced T cells had prolonged recurrence-free survival (RFS; median not reached), whereas nonresponders had a median RFS of 13.4 months, the authors had reported in the Nature paper.
This correlation was not confounded by other factors, including those associated with the patient, tumor, treatment, and host immune fitness, Balachandran noted.
In the responders, the T-cell clones had “high magnitude and exceptional longevity,” with an average estimated lifespan of 7.7 years, he said.
A fundamental challenge in developing cancer vaccines has been generating durable functional T cells specific for tumor antigens, and these findings suggest that mRNA-lipoplex vaccines against somatic mutation-derived neoantigens like autogene cevumeran may help overcome this challenge in pancreatic cancer, he and his colleagues concluded in the Nature paper.
The latest findings presented at the AACR annual meeting further underscore the potential of this approach.
At the 6-year follow-up, median RFS was “still not reached” in the vaccine responders vs 1.1 year in the nonresponders, he noted.
“This translates to a difference in overall survival,” he said. “Seven of eight [responders to the vaccine] are still alive 4.5-6 years after surgery.”
And of the 2 of 8 nonresponders still alive, one appears to be mounting a subclinical vaccine-induced T-cell response, he added, noting that this “suggests that inducible vaccine immunity may also impact survival in PDAC.”
“The implication here, we believe, is that even if a cancer has very mutational by-products [like PDAC], these mutational by-products can empower potent and composite immunity,” he said. “This is important because it could potentially expand vaccine eligibility to many cancers.”
Currently, there are about 50 neoantigen vaccine trials in solid tumors ongoing worldwide, he noted.
Memorial Sloan Kettering reports that Genentech and BioNTech are now testing autogene cevumeran in a larger patient population at numerous sites worldwide.
Balachandran reported receiving research support from Genentech, Merck Sharp & Dohme, and AbbVie.
Sharon Worcester, MA, is an award-winning medical journalist based in Birmingham, Alabama, writing for Medscape, MDedge, and other affiliate sites. She currently covers oncology, but she has also written on a variety of other medical specialties and healthcare topics. She can be reached at sworcester@mdedge.com or on X: @SW_MedReporter.
A version of this article first appeared on Medscape.com.
A personalized messenger RNA (mRNA) vaccine for pancreatic cancer continues to show promise for improving patient survival, according to 6-year follow-up results of a phase 1 clinical study.
Among the 8 out of 16 patients in the study who initially experienced an immune response to the vaccine, seven (87.5%) were still alive at follow-up, lead investigator Vinod P. Balachandran, MD, reported at the American Association for Cancer Research (AACR) Annual Meeting 2026.
Of the eight patients who did not respond, two (25%) were still alive, with a median survival time of 3.4 years. “This suggests that personalized vaccines can stimulate the immune system in some pancreatic cancer patients, and that these patients continue to do well for several years after vaccination,” said Balachandran, director of the Olayan Center for Cancer Vaccines at Memorial Sloan Kettering Cancer Center in New York City.
The findings suggest that this vaccine has the potential to improve outcomes in patients with pancreatic cancer, which is one of the deadliest cancers, he said.
The 5-year survival rate for pancreatic cancer is currently 13%, according to the American Cancer Society’s Cancer Statistics 2026 report.
Initial results of the trial evaluating the individualized neoantigen vaccine — autogene cevumeran, which is being developed by BioNTech and Genentech — were published in Nature in February 2025.
After pancreatic cancer surgery and chemo-immunotherapy, patients with pancreatic ductal adenocarcinoma (PDAC) received a vaccine personalized to each patient based on unique changes in their tumor DNA.
The eight patients with vaccine-induced T cells had prolonged recurrence-free survival (RFS; median not reached), whereas nonresponders had a median RFS of 13.4 months, the authors had reported in the Nature paper.
This correlation was not confounded by other factors, including those associated with the patient, tumor, treatment, and host immune fitness, Balachandran noted.
In the responders, the T-cell clones had “high magnitude and exceptional longevity,” with an average estimated lifespan of 7.7 years, he said.
A fundamental challenge in developing cancer vaccines has been generating durable functional T cells specific for tumor antigens, and these findings suggest that mRNA-lipoplex vaccines against somatic mutation-derived neoantigens like autogene cevumeran may help overcome this challenge in pancreatic cancer, he and his colleagues concluded in the Nature paper.
The latest findings presented at the AACR annual meeting further underscore the potential of this approach.
At the 6-year follow-up, median RFS was “still not reached” in the vaccine responders vs 1.1 year in the nonresponders, he noted.
“This translates to a difference in overall survival,” he said. “Seven of eight [responders to the vaccine] are still alive 4.5-6 years after surgery.”
And of the 2 of 8 nonresponders still alive, one appears to be mounting a subclinical vaccine-induced T-cell response, he added, noting that this “suggests that inducible vaccine immunity may also impact survival in PDAC.”
“The implication here, we believe, is that even if a cancer has very mutational by-products [like PDAC], these mutational by-products can empower potent and composite immunity,” he said. “This is important because it could potentially expand vaccine eligibility to many cancers.”
Currently, there are about 50 neoantigen vaccine trials in solid tumors ongoing worldwide, he noted.
Memorial Sloan Kettering reports that Genentech and BioNTech are now testing autogene cevumeran in a larger patient population at numerous sites worldwide.
Balachandran reported receiving research support from Genentech, Merck Sharp & Dohme, and AbbVie.
Sharon Worcester, MA, is an award-winning medical journalist based in Birmingham, Alabama, writing for Medscape, MDedge, and other affiliate sites. She currently covers oncology, but she has also written on a variety of other medical specialties and healthcare topics. She can be reached at sworcester@mdedge.com or on X: @SW_MedReporter.
A version of this article first appeared on Medscape.com.
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
GLP-1 Drugs May Modestly Raise Optic Neuropathy Risk in T2D
GLP-1 Drugs May Modestly Raise Optic Neuropathy Risk in T2D
TOPLINE:
A large cohort study found that the use of GLP-1 receptor agonists (GLP-1 RAs) over 3 years was associated with a modestly increased risk for nonarteritic anterior ischemic optic neuropathy (NAION) compared with the use of SGLT2 inhibitors in veterans with type 2 diabetes (T2D).
METHODOLOGY:
- Pharmacovigilance reports and emerging, but inconsistent, population-based studies suggest that the use of GLP-1 RAs may be linked to ocular adverse events, including a possible increased risk for NAION; however, it remains unclear whether the association is specific to NAION as compared with other optic disorders.
- Researchers conducted a target trial emulation study using nationwide electronic health records from the US Department of Veterans Affairs to compare the 3-year risk for NAION among veterans with T2D who initiated GLP-1 RAs vs SGLT2 inhibitors.
- The study included 588,168 veterans with T2D, of whom 139,546 initiated GLP-1 RA therapy (mean age, 65.33 years; 90.2% male) and 448,622 initiated SGLT2 inhibitor therapy (mean age, 67.94 years; 95.3% male) between 2017 and 2024; groups were subsequently matched using propensity score-based inverse probability weighting.
- Cases of NAION were identified from medical records using standard diagnostic codes; cases diagnosed by an eye care specialist and repeat diagnoses were also evaluated.
- The 3-year cumulative incidence, cumulative incidence difference (CID), and cumulative incidence ratio of NAION were estimated.
TAKEAWAY:
- Over 3 years, individuals who started GLP-1 RAs had a small but statistically significant increase in the risk for NAION compared with those who started SGLT2 inhibitors — 39.07 vs 29.33 cases per 10,000 people (CID, 9.98 per 10,000 people; 95% CI, 3.48-14.03) — and a relative increase of about 35% (cumulative incidence ratio, 1.35; 95% CI, 1.11-1.51).
- The increased risk for NAION with the use of GLP-1 RAs was consistent across definitions: diagnosis by an eye care specialist (CID, 8.73; 95% CI, 2.46-12.89), repeat diagnoses (CID, 6.35; 95% CI, 2.40-9.65), and repeat diagnoses with a specialist (CID, 5.91; 95% CI, 2.00-8.88).
- Compared with the use of SGLT2 inhibitors, the use of GLP-1 RAs was not associated with an increased risk for other optic disorders such as diabetic retinopathy, macular degeneration, retinal vascular occlusion, or optic neuritis.
- The frequency of ophthalmology or optometry clinic visits during follow-up was found to be similar between the two groups, suggesting that the association with NAION was not due to differential surveillance.
IN PRACTICE
“GLP-1 RA use was associated with a modestly increased risk of NAION compared with [SGLT2 inhibitor] use. While the absolute risk remains low, the specificity of this finding may warrant heightened vigilance,” the authors of the study wrote.
SOURCE:
The study was led by Taeyoung Choi, MS, Clinical Epidemiology Center, Research and Development Service, VA St Louis Health Care System, St. Louis. It was published online on April 30, 2026, in JAMA Network Open.
LIMITATIONS:
The study cohort was older and predominantly male, limiting generalizability to other populations. Residual confounding, selection bias, and outcome misclassification could not be fully excluded.
DISCLOSURES:
The study was funded by the US Department of Veterans Affairs. Two authors reported being uncompensated consultants for Pfizer.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A large cohort study found that the use of GLP-1 receptor agonists (GLP-1 RAs) over 3 years was associated with a modestly increased risk for nonarteritic anterior ischemic optic neuropathy (NAION) compared with the use of SGLT2 inhibitors in veterans with type 2 diabetes (T2D).
METHODOLOGY:
- Pharmacovigilance reports and emerging, but inconsistent, population-based studies suggest that the use of GLP-1 RAs may be linked to ocular adverse events, including a possible increased risk for NAION; however, it remains unclear whether the association is specific to NAION as compared with other optic disorders.
- Researchers conducted a target trial emulation study using nationwide electronic health records from the US Department of Veterans Affairs to compare the 3-year risk for NAION among veterans with T2D who initiated GLP-1 RAs vs SGLT2 inhibitors.
- The study included 588,168 veterans with T2D, of whom 139,546 initiated GLP-1 RA therapy (mean age, 65.33 years; 90.2% male) and 448,622 initiated SGLT2 inhibitor therapy (mean age, 67.94 years; 95.3% male) between 2017 and 2024; groups were subsequently matched using propensity score-based inverse probability weighting.
- Cases of NAION were identified from medical records using standard diagnostic codes; cases diagnosed by an eye care specialist and repeat diagnoses were also evaluated.
- The 3-year cumulative incidence, cumulative incidence difference (CID), and cumulative incidence ratio of NAION were estimated.
TAKEAWAY:
- Over 3 years, individuals who started GLP-1 RAs had a small but statistically significant increase in the risk for NAION compared with those who started SGLT2 inhibitors — 39.07 vs 29.33 cases per 10,000 people (CID, 9.98 per 10,000 people; 95% CI, 3.48-14.03) — and a relative increase of about 35% (cumulative incidence ratio, 1.35; 95% CI, 1.11-1.51).
- The increased risk for NAION with the use of GLP-1 RAs was consistent across definitions: diagnosis by an eye care specialist (CID, 8.73; 95% CI, 2.46-12.89), repeat diagnoses (CID, 6.35; 95% CI, 2.40-9.65), and repeat diagnoses with a specialist (CID, 5.91; 95% CI, 2.00-8.88).
- Compared with the use of SGLT2 inhibitors, the use of GLP-1 RAs was not associated with an increased risk for other optic disorders such as diabetic retinopathy, macular degeneration, retinal vascular occlusion, or optic neuritis.
- The frequency of ophthalmology or optometry clinic visits during follow-up was found to be similar between the two groups, suggesting that the association with NAION was not due to differential surveillance.
IN PRACTICE
“GLP-1 RA use was associated with a modestly increased risk of NAION compared with [SGLT2 inhibitor] use. While the absolute risk remains low, the specificity of this finding may warrant heightened vigilance,” the authors of the study wrote.
SOURCE:
The study was led by Taeyoung Choi, MS, Clinical Epidemiology Center, Research and Development Service, VA St Louis Health Care System, St. Louis. It was published online on April 30, 2026, in JAMA Network Open.
LIMITATIONS:
The study cohort was older and predominantly male, limiting generalizability to other populations. Residual confounding, selection bias, and outcome misclassification could not be fully excluded.
DISCLOSURES:
The study was funded by the US Department of Veterans Affairs. Two authors reported being uncompensated consultants for Pfizer.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A large cohort study found that the use of GLP-1 receptor agonists (GLP-1 RAs) over 3 years was associated with a modestly increased risk for nonarteritic anterior ischemic optic neuropathy (NAION) compared with the use of SGLT2 inhibitors in veterans with type 2 diabetes (T2D).
METHODOLOGY:
- Pharmacovigilance reports and emerging, but inconsistent, population-based studies suggest that the use of GLP-1 RAs may be linked to ocular adverse events, including a possible increased risk for NAION; however, it remains unclear whether the association is specific to NAION as compared with other optic disorders.
- Researchers conducted a target trial emulation study using nationwide electronic health records from the US Department of Veterans Affairs to compare the 3-year risk for NAION among veterans with T2D who initiated GLP-1 RAs vs SGLT2 inhibitors.
- The study included 588,168 veterans with T2D, of whom 139,546 initiated GLP-1 RA therapy (mean age, 65.33 years; 90.2% male) and 448,622 initiated SGLT2 inhibitor therapy (mean age, 67.94 years; 95.3% male) between 2017 and 2024; groups were subsequently matched using propensity score-based inverse probability weighting.
- Cases of NAION were identified from medical records using standard diagnostic codes; cases diagnosed by an eye care specialist and repeat diagnoses were also evaluated.
- The 3-year cumulative incidence, cumulative incidence difference (CID), and cumulative incidence ratio of NAION were estimated.
TAKEAWAY:
- Over 3 years, individuals who started GLP-1 RAs had a small but statistically significant increase in the risk for NAION compared with those who started SGLT2 inhibitors — 39.07 vs 29.33 cases per 10,000 people (CID, 9.98 per 10,000 people; 95% CI, 3.48-14.03) — and a relative increase of about 35% (cumulative incidence ratio, 1.35; 95% CI, 1.11-1.51).
- The increased risk for NAION with the use of GLP-1 RAs was consistent across definitions: diagnosis by an eye care specialist (CID, 8.73; 95% CI, 2.46-12.89), repeat diagnoses (CID, 6.35; 95% CI, 2.40-9.65), and repeat diagnoses with a specialist (CID, 5.91; 95% CI, 2.00-8.88).
- Compared with the use of SGLT2 inhibitors, the use of GLP-1 RAs was not associated with an increased risk for other optic disorders such as diabetic retinopathy, macular degeneration, retinal vascular occlusion, or optic neuritis.
- The frequency of ophthalmology or optometry clinic visits during follow-up was found to be similar between the two groups, suggesting that the association with NAION was not due to differential surveillance.
IN PRACTICE
“GLP-1 RA use was associated with a modestly increased risk of NAION compared with [SGLT2 inhibitor] use. While the absolute risk remains low, the specificity of this finding may warrant heightened vigilance,” the authors of the study wrote.
SOURCE:
The study was led by Taeyoung Choi, MS, Clinical Epidemiology Center, Research and Development Service, VA St Louis Health Care System, St. Louis. It was published online on April 30, 2026, in JAMA Network Open.
LIMITATIONS:
The study cohort was older and predominantly male, limiting generalizability to other populations. Residual confounding, selection bias, and outcome misclassification could not be fully excluded.
DISCLOSURES:
The study was funded by the US Department of Veterans Affairs. Two authors reported being uncompensated consultants for Pfizer.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
GLP-1 Drugs May Modestly Raise Optic Neuropathy Risk in T2D
GLP-1 Drugs May Modestly Raise Optic Neuropathy Risk in T2D
End-of-Life Palliative Care Rare for VA Patients With COPD
End-of-Life Palliative Care Rare for VA Patients With COPD
Though end-of-life care for veterans with chronic obstructive pulmonary disease (COPD) in the US Department of Veterans Affairs (VA) has become more prevalent in recent years, a recent retrospective cohort study found that most patients do not receive palliative care or inpatient VA hospice over the past year of life, with rates lower than for other terminal illnesses.
Among 332,770 decedents traced from 2010 through 2020, only 16.8% received either palliative or inpatient hospice care in the year before their death. The median time between their first palliative care appointment and death was 46 days, reported pulmonologist Natalia Smirnova, MD, assistant professor of medicine, Emory School of Medicine, Atlanta, et al in CHEST Pulmonary.
A total of 15.9% of the decedents received inpatient hospice care from the VA.
“These findings point to an opportunity to improve access to palliative care and hospice services for veterans with COPD, including earlier identification of need and stronger access pathways across care settings,” Smirnova told Federal Practitioner.
COPD Common Among Vets
An estimated 8%-19% of US veterans have COPD, higher than the estimated rate of 6% in adults from the general population. The condition is believed to be underdiagnosed in veterans.
“Palliative care should be integrated early into routine care, when symptoms start,” Kathleen Lindell, PhD, RN, associate professor and chair, Palliative Care Health, School of Nursing, Medical University of South Carolina, Charleston, explained in a Federal Practitioner interview. “COPD is a serious respiratory illness, and patients experience progressively debilitating dyspnea or shortness of breath, frequent hospitalizations. And they frequently experience high rates of anxiety and depression,”
Lindell is familiar with the study findings but didn’t take part in the research.
“Early palliative care,” she said, “addresses symptom management and advance care planning to reduce suffering and ensure what matters most to the patient as the disease progresses.”
Smirnova noted that “hospice is a related but distinct service for veterans with a terminal condition, generally when life expectancy is < 6 months and the veteran is no longer seeking treatment other than palliative care.”
The study analyzed electronic health records and patterns of palliative and hospice care in the year before death. The 332,770 patients were mostly male (98.1%) and White (81.0%). Many had comorbidities such as congestive heart failure (30.0%), depression (26.0%), coronary artery disease (25.5%), anxiety (13.4%), and lung cancer (12.1%).
Researchers found that palliative care was mostly (61.6% of encounters) delivered in the inpatient setting, where it occurred a median 30 days before death. In the outpatient setting, it began a median of 71 days before death.
From 2010 through 2020, the prevalence of palliative care increased from 10.4% to 16.0%, and the prevalence of VA inpatient hospice care increased from 15.0% to 18.0%. Some veterans may have received hospice services in other settings; in-home hospice is common.
Who is More Likely to Receive Palliative Care?
Black patients (adjusted odds ratio [AOR], 1.21), Latino/Hispanic ethnicity (AOR, 1.22), patients with housing instability (AOR, 1.38) and who were underweight (AOR, 1.75) were linked to more palliative care use. Black patients were especially likely to get inpatient palliative care, a fact that “may, in part, be driven by increased care intensity at the end of life, as has been demonstrated in prior studies,” the authors noted.
Marriage (AOR, 0.88) was linked to less palliative care use, while patients with lung cancer were especially likely to receive it (AOR, 2.48). There were similar differences in use of hospice care apart from higher use for Black patients.
Smirnova said the study was not designed to determine the causes of patterns in palliative care use. However, important factors appear to include hospitalization, comorbidities, and access to care at health care sites. (Usage rates were lower at rural centers and higher at more complex centers.)
COPD vs Other Terminal Diseases
“The modest increases in utilization of palliative care and VA inpatient hospice from 2010 to 2020 align with previous work [research] in inpatients with COPD and heart failure,” the researchers wrote, “possibly reflecting the effect of international professional society guidelines, increased acceptance of palliative care, improvements related to VA end-of-life care and life-sustaining treatment decisions initiatives, and increases in the specialist palliative care workforce.”
Still, there appears to be a major discrepancy regarding the use of palliative care for COPD within the VA compared with other diseases. A study of data from 2014 through 2017 found that for patients with several comorbidities—including COPD, heart failure, cancer, and dementia—inpatient palliative care was introduced a median of 58 days before death and outpatient care 160 days before death.
“This suggests that veterans with COPD receive palliative care later than those with other serious illnesses,” the authors argued.
Don’t Wait for the ‘Right Time’
Sarah Miller, PhD, RN, associate professor, and assistant dean, PhD Nursing Science Program, School of Nursing, Medical University of South Carolina, Charleston, praised the study in an interview and noted that uncertainty about the “right time” to refer patients to palliative care could play a role in the findings. Miller is familiar with the study but did not participate in the research.
Lindell, the chair of Palliative Care Health, agreed.
“With COPD—a chronic, progressive disease—decline can be gradual, which makes it difficult to identify a clear transition point,” Lindell told Federal Practitioner. “This has contributed to many palliative referrals happening only when patients are clearly deteriorating or nearing the end of life. But palliative care should not be introduced reactively; it should be integrated early, alongside disease-directed treatment.”
For her part, Miller noted that “many veterans with COPD are navigating complex comorbidities and fragmented care across settings. Diseases like COPD don’t follow a predictable path, so referrals don’t always happen like they should.”
Moving forward, “if symptoms are present, early palliative care is appropriate,” Lindell said. These conversations should happen early and over time.
“The VA should prioritize early referral and access to palliative care for patients with COPD to provide the best care for these individuals.”
No study funding was reported. Smirnova discloses relationships with the CHEST Foundation and National Heart, Lung, and Blood Institute. Other authors disclose relationships with various grantors.
Miller discloses a relationship with AstraZeneca. Lindell discloses relationships with Boehringer Ingelheim and Heart & Lung: The Journal of Acute and Critical Care.
Though end-of-life care for veterans with chronic obstructive pulmonary disease (COPD) in the US Department of Veterans Affairs (VA) has become more prevalent in recent years, a recent retrospective cohort study found that most patients do not receive palliative care or inpatient VA hospice over the past year of life, with rates lower than for other terminal illnesses.
Among 332,770 decedents traced from 2010 through 2020, only 16.8% received either palliative or inpatient hospice care in the year before their death. The median time between their first palliative care appointment and death was 46 days, reported pulmonologist Natalia Smirnova, MD, assistant professor of medicine, Emory School of Medicine, Atlanta, et al in CHEST Pulmonary.
A total of 15.9% of the decedents received inpatient hospice care from the VA.
“These findings point to an opportunity to improve access to palliative care and hospice services for veterans with COPD, including earlier identification of need and stronger access pathways across care settings,” Smirnova told Federal Practitioner.
COPD Common Among Vets
An estimated 8%-19% of US veterans have COPD, higher than the estimated rate of 6% in adults from the general population. The condition is believed to be underdiagnosed in veterans.
“Palliative care should be integrated early into routine care, when symptoms start,” Kathleen Lindell, PhD, RN, associate professor and chair, Palliative Care Health, School of Nursing, Medical University of South Carolina, Charleston, explained in a Federal Practitioner interview. “COPD is a serious respiratory illness, and patients experience progressively debilitating dyspnea or shortness of breath, frequent hospitalizations. And they frequently experience high rates of anxiety and depression,”
Lindell is familiar with the study findings but didn’t take part in the research.
“Early palliative care,” she said, “addresses symptom management and advance care planning to reduce suffering and ensure what matters most to the patient as the disease progresses.”
Smirnova noted that “hospice is a related but distinct service for veterans with a terminal condition, generally when life expectancy is < 6 months and the veteran is no longer seeking treatment other than palliative care.”
The study analyzed electronic health records and patterns of palliative and hospice care in the year before death. The 332,770 patients were mostly male (98.1%) and White (81.0%). Many had comorbidities such as congestive heart failure (30.0%), depression (26.0%), coronary artery disease (25.5%), anxiety (13.4%), and lung cancer (12.1%).
Researchers found that palliative care was mostly (61.6% of encounters) delivered in the inpatient setting, where it occurred a median 30 days before death. In the outpatient setting, it began a median of 71 days before death.
From 2010 through 2020, the prevalence of palliative care increased from 10.4% to 16.0%, and the prevalence of VA inpatient hospice care increased from 15.0% to 18.0%. Some veterans may have received hospice services in other settings; in-home hospice is common.
Who is More Likely to Receive Palliative Care?
Black patients (adjusted odds ratio [AOR], 1.21), Latino/Hispanic ethnicity (AOR, 1.22), patients with housing instability (AOR, 1.38) and who were underweight (AOR, 1.75) were linked to more palliative care use. Black patients were especially likely to get inpatient palliative care, a fact that “may, in part, be driven by increased care intensity at the end of life, as has been demonstrated in prior studies,” the authors noted.
Marriage (AOR, 0.88) was linked to less palliative care use, while patients with lung cancer were especially likely to receive it (AOR, 2.48). There were similar differences in use of hospice care apart from higher use for Black patients.
Smirnova said the study was not designed to determine the causes of patterns in palliative care use. However, important factors appear to include hospitalization, comorbidities, and access to care at health care sites. (Usage rates were lower at rural centers and higher at more complex centers.)
COPD vs Other Terminal Diseases
“The modest increases in utilization of palliative care and VA inpatient hospice from 2010 to 2020 align with previous work [research] in inpatients with COPD and heart failure,” the researchers wrote, “possibly reflecting the effect of international professional society guidelines, increased acceptance of palliative care, improvements related to VA end-of-life care and life-sustaining treatment decisions initiatives, and increases in the specialist palliative care workforce.”
Still, there appears to be a major discrepancy regarding the use of palliative care for COPD within the VA compared with other diseases. A study of data from 2014 through 2017 found that for patients with several comorbidities—including COPD, heart failure, cancer, and dementia—inpatient palliative care was introduced a median of 58 days before death and outpatient care 160 days before death.
“This suggests that veterans with COPD receive palliative care later than those with other serious illnesses,” the authors argued.
Don’t Wait for the ‘Right Time’
Sarah Miller, PhD, RN, associate professor, and assistant dean, PhD Nursing Science Program, School of Nursing, Medical University of South Carolina, Charleston, praised the study in an interview and noted that uncertainty about the “right time” to refer patients to palliative care could play a role in the findings. Miller is familiar with the study but did not participate in the research.
Lindell, the chair of Palliative Care Health, agreed.
“With COPD—a chronic, progressive disease—decline can be gradual, which makes it difficult to identify a clear transition point,” Lindell told Federal Practitioner. “This has contributed to many palliative referrals happening only when patients are clearly deteriorating or nearing the end of life. But palliative care should not be introduced reactively; it should be integrated early, alongside disease-directed treatment.”
For her part, Miller noted that “many veterans with COPD are navigating complex comorbidities and fragmented care across settings. Diseases like COPD don’t follow a predictable path, so referrals don’t always happen like they should.”
Moving forward, “if symptoms are present, early palliative care is appropriate,” Lindell said. These conversations should happen early and over time.
“The VA should prioritize early referral and access to palliative care for patients with COPD to provide the best care for these individuals.”
No study funding was reported. Smirnova discloses relationships with the CHEST Foundation and National Heart, Lung, and Blood Institute. Other authors disclose relationships with various grantors.
Miller discloses a relationship with AstraZeneca. Lindell discloses relationships with Boehringer Ingelheim and Heart & Lung: The Journal of Acute and Critical Care.
Though end-of-life care for veterans with chronic obstructive pulmonary disease (COPD) in the US Department of Veterans Affairs (VA) has become more prevalent in recent years, a recent retrospective cohort study found that most patients do not receive palliative care or inpatient VA hospice over the past year of life, with rates lower than for other terminal illnesses.
Among 332,770 decedents traced from 2010 through 2020, only 16.8% received either palliative or inpatient hospice care in the year before their death. The median time between their first palliative care appointment and death was 46 days, reported pulmonologist Natalia Smirnova, MD, assistant professor of medicine, Emory School of Medicine, Atlanta, et al in CHEST Pulmonary.
A total of 15.9% of the decedents received inpatient hospice care from the VA.
“These findings point to an opportunity to improve access to palliative care and hospice services for veterans with COPD, including earlier identification of need and stronger access pathways across care settings,” Smirnova told Federal Practitioner.
COPD Common Among Vets
An estimated 8%-19% of US veterans have COPD, higher than the estimated rate of 6% in adults from the general population. The condition is believed to be underdiagnosed in veterans.
“Palliative care should be integrated early into routine care, when symptoms start,” Kathleen Lindell, PhD, RN, associate professor and chair, Palliative Care Health, School of Nursing, Medical University of South Carolina, Charleston, explained in a Federal Practitioner interview. “COPD is a serious respiratory illness, and patients experience progressively debilitating dyspnea or shortness of breath, frequent hospitalizations. And they frequently experience high rates of anxiety and depression,”
Lindell is familiar with the study findings but didn’t take part in the research.
“Early palliative care,” she said, “addresses symptom management and advance care planning to reduce suffering and ensure what matters most to the patient as the disease progresses.”
Smirnova noted that “hospice is a related but distinct service for veterans with a terminal condition, generally when life expectancy is < 6 months and the veteran is no longer seeking treatment other than palliative care.”
The study analyzed electronic health records and patterns of palliative and hospice care in the year before death. The 332,770 patients were mostly male (98.1%) and White (81.0%). Many had comorbidities such as congestive heart failure (30.0%), depression (26.0%), coronary artery disease (25.5%), anxiety (13.4%), and lung cancer (12.1%).
Researchers found that palliative care was mostly (61.6% of encounters) delivered in the inpatient setting, where it occurred a median 30 days before death. In the outpatient setting, it began a median of 71 days before death.
From 2010 through 2020, the prevalence of palliative care increased from 10.4% to 16.0%, and the prevalence of VA inpatient hospice care increased from 15.0% to 18.0%. Some veterans may have received hospice services in other settings; in-home hospice is common.
Who is More Likely to Receive Palliative Care?
Black patients (adjusted odds ratio [AOR], 1.21), Latino/Hispanic ethnicity (AOR, 1.22), patients with housing instability (AOR, 1.38) and who were underweight (AOR, 1.75) were linked to more palliative care use. Black patients were especially likely to get inpatient palliative care, a fact that “may, in part, be driven by increased care intensity at the end of life, as has been demonstrated in prior studies,” the authors noted.
Marriage (AOR, 0.88) was linked to less palliative care use, while patients with lung cancer were especially likely to receive it (AOR, 2.48). There were similar differences in use of hospice care apart from higher use for Black patients.
Smirnova said the study was not designed to determine the causes of patterns in palliative care use. However, important factors appear to include hospitalization, comorbidities, and access to care at health care sites. (Usage rates were lower at rural centers and higher at more complex centers.)
COPD vs Other Terminal Diseases
“The modest increases in utilization of palliative care and VA inpatient hospice from 2010 to 2020 align with previous work [research] in inpatients with COPD and heart failure,” the researchers wrote, “possibly reflecting the effect of international professional society guidelines, increased acceptance of palliative care, improvements related to VA end-of-life care and life-sustaining treatment decisions initiatives, and increases in the specialist palliative care workforce.”
Still, there appears to be a major discrepancy regarding the use of palliative care for COPD within the VA compared with other diseases. A study of data from 2014 through 2017 found that for patients with several comorbidities—including COPD, heart failure, cancer, and dementia—inpatient palliative care was introduced a median of 58 days before death and outpatient care 160 days before death.
“This suggests that veterans with COPD receive palliative care later than those with other serious illnesses,” the authors argued.
Don’t Wait for the ‘Right Time’
Sarah Miller, PhD, RN, associate professor, and assistant dean, PhD Nursing Science Program, School of Nursing, Medical University of South Carolina, Charleston, praised the study in an interview and noted that uncertainty about the “right time” to refer patients to palliative care could play a role in the findings. Miller is familiar with the study but did not participate in the research.
Lindell, the chair of Palliative Care Health, agreed.
“With COPD—a chronic, progressive disease—decline can be gradual, which makes it difficult to identify a clear transition point,” Lindell told Federal Practitioner. “This has contributed to many palliative referrals happening only when patients are clearly deteriorating or nearing the end of life. But palliative care should not be introduced reactively; it should be integrated early, alongside disease-directed treatment.”
For her part, Miller noted that “many veterans with COPD are navigating complex comorbidities and fragmented care across settings. Diseases like COPD don’t follow a predictable path, so referrals don’t always happen like they should.”
Moving forward, “if symptoms are present, early palliative care is appropriate,” Lindell said. These conversations should happen early and over time.
“The VA should prioritize early referral and access to palliative care for patients with COPD to provide the best care for these individuals.”
No study funding was reported. Smirnova discloses relationships with the CHEST Foundation and National Heart, Lung, and Blood Institute. Other authors disclose relationships with various grantors.
Miller discloses a relationship with AstraZeneca. Lindell discloses relationships with Boehringer Ingelheim and Heart & Lung: The Journal of Acute and Critical Care.
End-of-Life Palliative Care Rare for VA Patients With COPD
End-of-Life Palliative Care Rare for VA Patients With COPD
Rising Lung Cancer Burden Among Women
Rising Lung Cancer Burden Among Women
While the incidence of lung cancer is decreasing in men, it continues to rise in women. With more than 19,000 new cases in France each year, lung cancer is now the third most commonly diagnosed cancer among women. This trend is also seen in other European countries but appears to be region-specific because other continents report a decline in incidence among women. Moreover, although overall prognosis remains better in the female population, the trend is worrying: Mortality associated with the disease is increasing in women, unlike in men with lung cancer. A session at the French-Language Pneumology Congress held from January 30 to February 1, 2026, in Lille, France, provided an opportunity to review the situation.
Efficacy and Toxicity
Lung tumors in women have a distinct tumor profile: Women have a higher proportion of adenocarcinomas than men and a higher frequency of somatic mutations (EGFR, BRAF, or HER2), including in nonsmokers. In addition, 65% of lung cancers in women are associated with smoking compared with 87% of those in men.
The role of estrogens is central because they interact directly with tumor growth signaling pathways. Moreover, “sex is the second leading factor of variability in drug pharmacokinetics after weight and accounts for 28% of anticancer drug kinetics,” emphasized Julien Mazières, pulmonologist, Toulouse University Hospital, Toulouse, France. Also involved in this equation are a higher body fat percentage, lower gastric acidity, and, above all, reduced renal and hepatic clearance.
As a result, exposure to drugs — represented by the area under the curve — is often greater in women and translates into not only improved progression-free survival with targeted therapies and chemotherapy but also increased toxicity. Carboplatin and paclitaxel are among the drugs whose kinetics are most affected by clearance. There are differences in clearance of more than 20% for these drugs in women vs men, though dosages are not systematically adjusted except for weight-based dosing. This vulnerability to adverse effects is particularly pronounced with targeted therapies, with more neuropsychiatric and gastrointestinal disorders. Data on the efficacy of immunotherapy in lung cancer by sex are contradictory. However, endocrine-related adverse effects and pneumonitis are more frequent in women, especially before menopause.
Women remain underrepresented in clinical trials, and sex-specific analyses of results are too rarely performed, which limits understanding of mechanisms and prevents tailoring management recommendations according to sex.
Impaired Quality of Life
Lung cancer most severely impairs physical functioning in women. “In the absence of sex-stratified studies, psycho-oncologists’ experience suggests that women have more cognitive disorders, anxiety, and depression associated with this disease. Its impact on quality of life is major, with deterioration of social relationships and reduced treatment adherence,” summarized Céline Mascaux, MD, PhD, pulmonologist, Strasbourg University Hospital, Strasbourg, France. Women also face social and family pressure — a mental burden that pushes them to “hold on” for their loved ones. Regarding sexual health, women with lung cancer who are sexually active often report dissatisfaction with the quality of their sexual relations because of fatigue, lack of energy, sadness, and shortness of breath, not to mention treatment-related sexual dysfunction. These problems are often not given sufficient attention by physicians.
Finally, fertility requires greater attention from the medical community: According to the VICAN study conducted by France’s National Health Insurance Fund, a discussion about fertility preservation did not take place at the time of cancer diagnosis for 60% of men and 67% of women of childbearing age. “In lung cancer specifically, the desire for children nevertheless exists in nearly 40% of patients of childbearing age,” regretted Jacques Cadranel, pulmonologist, Tenon Hospital, Paris, France. This desire does not appear to have influenced therapeutic strategy, and fertility preservation was ultimately proposed in only a third of cases and was carried out in only 3% of women compared with21% of men.
This story has been translated from Univadis France, part of the Medscape Professional Network.
A version of this story first appeared on Medscape.com
While the incidence of lung cancer is decreasing in men, it continues to rise in women. With more than 19,000 new cases in France each year, lung cancer is now the third most commonly diagnosed cancer among women. This trend is also seen in other European countries but appears to be region-specific because other continents report a decline in incidence among women. Moreover, although overall prognosis remains better in the female population, the trend is worrying: Mortality associated with the disease is increasing in women, unlike in men with lung cancer. A session at the French-Language Pneumology Congress held from January 30 to February 1, 2026, in Lille, France, provided an opportunity to review the situation.
Efficacy and Toxicity
Lung tumors in women have a distinct tumor profile: Women have a higher proportion of adenocarcinomas than men and a higher frequency of somatic mutations (EGFR, BRAF, or HER2), including in nonsmokers. In addition, 65% of lung cancers in women are associated with smoking compared with 87% of those in men.
The role of estrogens is central because they interact directly with tumor growth signaling pathways. Moreover, “sex is the second leading factor of variability in drug pharmacokinetics after weight and accounts for 28% of anticancer drug kinetics,” emphasized Julien Mazières, pulmonologist, Toulouse University Hospital, Toulouse, France. Also involved in this equation are a higher body fat percentage, lower gastric acidity, and, above all, reduced renal and hepatic clearance.
As a result, exposure to drugs — represented by the area under the curve — is often greater in women and translates into not only improved progression-free survival with targeted therapies and chemotherapy but also increased toxicity. Carboplatin and paclitaxel are among the drugs whose kinetics are most affected by clearance. There are differences in clearance of more than 20% for these drugs in women vs men, though dosages are not systematically adjusted except for weight-based dosing. This vulnerability to adverse effects is particularly pronounced with targeted therapies, with more neuropsychiatric and gastrointestinal disorders. Data on the efficacy of immunotherapy in lung cancer by sex are contradictory. However, endocrine-related adverse effects and pneumonitis are more frequent in women, especially before menopause.
Women remain underrepresented in clinical trials, and sex-specific analyses of results are too rarely performed, which limits understanding of mechanisms and prevents tailoring management recommendations according to sex.
Impaired Quality of Life
Lung cancer most severely impairs physical functioning in women. “In the absence of sex-stratified studies, psycho-oncologists’ experience suggests that women have more cognitive disorders, anxiety, and depression associated with this disease. Its impact on quality of life is major, with deterioration of social relationships and reduced treatment adherence,” summarized Céline Mascaux, MD, PhD, pulmonologist, Strasbourg University Hospital, Strasbourg, France. Women also face social and family pressure — a mental burden that pushes them to “hold on” for their loved ones. Regarding sexual health, women with lung cancer who are sexually active often report dissatisfaction with the quality of their sexual relations because of fatigue, lack of energy, sadness, and shortness of breath, not to mention treatment-related sexual dysfunction. These problems are often not given sufficient attention by physicians.
Finally, fertility requires greater attention from the medical community: According to the VICAN study conducted by France’s National Health Insurance Fund, a discussion about fertility preservation did not take place at the time of cancer diagnosis for 60% of men and 67% of women of childbearing age. “In lung cancer specifically, the desire for children nevertheless exists in nearly 40% of patients of childbearing age,” regretted Jacques Cadranel, pulmonologist, Tenon Hospital, Paris, France. This desire does not appear to have influenced therapeutic strategy, and fertility preservation was ultimately proposed in only a third of cases and was carried out in only 3% of women compared with21% of men.
This story has been translated from Univadis France, part of the Medscape Professional Network.
A version of this story first appeared on Medscape.com
While the incidence of lung cancer is decreasing in men, it continues to rise in women. With more than 19,000 new cases in France each year, lung cancer is now the third most commonly diagnosed cancer among women. This trend is also seen in other European countries but appears to be region-specific because other continents report a decline in incidence among women. Moreover, although overall prognosis remains better in the female population, the trend is worrying: Mortality associated with the disease is increasing in women, unlike in men with lung cancer. A session at the French-Language Pneumology Congress held from January 30 to February 1, 2026, in Lille, France, provided an opportunity to review the situation.
Efficacy and Toxicity
Lung tumors in women have a distinct tumor profile: Women have a higher proportion of adenocarcinomas than men and a higher frequency of somatic mutations (EGFR, BRAF, or HER2), including in nonsmokers. In addition, 65% of lung cancers in women are associated with smoking compared with 87% of those in men.
The role of estrogens is central because they interact directly with tumor growth signaling pathways. Moreover, “sex is the second leading factor of variability in drug pharmacokinetics after weight and accounts for 28% of anticancer drug kinetics,” emphasized Julien Mazières, pulmonologist, Toulouse University Hospital, Toulouse, France. Also involved in this equation are a higher body fat percentage, lower gastric acidity, and, above all, reduced renal and hepatic clearance.
As a result, exposure to drugs — represented by the area under the curve — is often greater in women and translates into not only improved progression-free survival with targeted therapies and chemotherapy but also increased toxicity. Carboplatin and paclitaxel are among the drugs whose kinetics are most affected by clearance. There are differences in clearance of more than 20% for these drugs in women vs men, though dosages are not systematically adjusted except for weight-based dosing. This vulnerability to adverse effects is particularly pronounced with targeted therapies, with more neuropsychiatric and gastrointestinal disorders. Data on the efficacy of immunotherapy in lung cancer by sex are contradictory. However, endocrine-related adverse effects and pneumonitis are more frequent in women, especially before menopause.
Women remain underrepresented in clinical trials, and sex-specific analyses of results are too rarely performed, which limits understanding of mechanisms and prevents tailoring management recommendations according to sex.
Impaired Quality of Life
Lung cancer most severely impairs physical functioning in women. “In the absence of sex-stratified studies, psycho-oncologists’ experience suggests that women have more cognitive disorders, anxiety, and depression associated with this disease. Its impact on quality of life is major, with deterioration of social relationships and reduced treatment adherence,” summarized Céline Mascaux, MD, PhD, pulmonologist, Strasbourg University Hospital, Strasbourg, France. Women also face social and family pressure — a mental burden that pushes them to “hold on” for their loved ones. Regarding sexual health, women with lung cancer who are sexually active often report dissatisfaction with the quality of their sexual relations because of fatigue, lack of energy, sadness, and shortness of breath, not to mention treatment-related sexual dysfunction. These problems are often not given sufficient attention by physicians.
Finally, fertility requires greater attention from the medical community: According to the VICAN study conducted by France’s National Health Insurance Fund, a discussion about fertility preservation did not take place at the time of cancer diagnosis for 60% of men and 67% of women of childbearing age. “In lung cancer specifically, the desire for children nevertheless exists in nearly 40% of patients of childbearing age,” regretted Jacques Cadranel, pulmonologist, Tenon Hospital, Paris, France. This desire does not appear to have influenced therapeutic strategy, and fertility preservation was ultimately proposed in only a third of cases and was carried out in only 3% of women compared with21% of men.
This story has been translated from Univadis France, part of the Medscape Professional Network.
A version of this story first appeared on Medscape.com
Rising Lung Cancer Burden Among Women
Rising Lung Cancer Burden Among Women
Evaluation of Pharmacist-Driven Inhaled Corticosteroid De-escalation in Veterans
Evaluation of Pharmacist-Driven Inhaled Corticosteroid De-escalation in Veterans
Systemic glucocorticoids play an important role in the treatment of chronic obstructive pulmonary disease (COPD) exacerbations. They are recommended to shorten recovery time and increase forced expiratory volume in 1 second (FEV1) during exacerbations.1 However, the role of the chronic use of inhaled corticosteroids (ICSs) in the treatment of COPD is less clear.
When added to inhaled β-2 agonists and muscarinic antagonists, ICSs can decrease the risk of exacerbations.1 However, not all patients with COPD benefit from ICS therapy. The degree of benefit an ICS can provide has been shown to correlate with eosinophil count—a marker of inflammation. The expected benefit of using an ICS increases as the eosinophil count increases.1 Maximum benefit can be observed with eosinophil counts ≥ 300 cells/µL, and minimal benefit is observed with eosinophil counts < 100 cells/µL. Adverse effects (AEs) of ICSs include a hoarse voice, oral candidiasis, and an increased risk of pneumonia.1 Given the risk of AEs, it is important to limit ICS use in patients who are unlikely to reap any benefits.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines suggest the use of ICSs in patients who experience exacerbations while using long-acting β agonist (LABA) plus long-acting muscarinic antagonist (LAMA) therapy and have an eosinophil count ≥ 100 cells/µL. Switching from LABA or LAMA monotherapy to triple therapy with LAMA/LABA/ICS may be considered if patients have continued exacerbations and an eosinophil count ≥ 300 cells/µL. De-escalation of ICS therapy should be considered if patients do not meet these criteria or if patients experience ICS AEs, such as pneumonia. The patients most likely to have increased exacerbations or decreased FEV1 with ICS withdrawal are those with eosinophil counts ≥ 300 cells/µL.1,2
Several studies have explored the effects of ICS de-escalation in real-world clinical settings. A systematic review of 11 studies indicated that de-escalation of ICS in COPD does not result in increased exacerbations.3 A prospective study by Rossi et al found that in a 6-month period, 141 of 482 patients on ICS therapy (29%) had an exacerbation. In the opposing arm of the study, 88 of 334 patients (26%) with deprescribed ICS experienced an exacerbation. The difference between these 2 groups was not statistically significant.4 The researchers concluded that in real-world practice, ICS withdrawal can be safe in patients at low risk of exacerbation.
About 25% of veterans (1.25 million) have been diagnosed with COPD.5 To address this, the US Department of Veterans Affairs (VA) and US Department of Defense published updated COPD guidelines in 2021 that specify criteria for de-escalation of ICS.6 Guidelines, however, may not be reflected in common clinical practice for several years following publication. The VA Academic Detailing Service (ADS) provides tools to help clinicians identify patients who may benefit from changes in treatment plans. A recent ADS focus was the implementation of a COPD dashboard, which identifies patients with COPD who are candidates for ICS de-escalation based on comorbid diagnoses, exacerbation history, and eosinophil count. VA pharmacists have an expanded role in the management of primary care disease states and are therefore well-positioned to increase adherence to guideline-directed therapy. The objective of this quality improvement project was to determine the impact of pharmacist-driven de-escalation on ICS usage in veterans with COPD.
Methods
This project was conducted in an outpatient clinic at the Robley Rex VA Medical Center beginning September 21, 2023, with a progress note in the Computerized Patient Record System (CPRS). Eligible patients were selected using the COPD Dashboard provided by ADS. The COPD Dashboard defined patients with COPD as those with ≥ 2 outpatient COPD diagnoses in the past 2 years, 1 inpatient discharge COPD diagnosis in the past year, or COPD listed as an active problem. COPD diagnoses were identified using International Statistical Classification of Disease, Tenth Revision (ICD-10) codes
Candidates identified for ICS de-escalation by the dashboard were excluded if they had a history of COPD exacerbation in the previous 2 years. The dashboard identified COPD exacerbations via ICD-10 codes for COPD or acute respiratory failure for inpatient discharges, emergency department (ED) visits, urgent care visits, and community care consults with 1 of the following terms: emergency, inpatient, hospital, urgent, ED (self). The COPD dashboard excluded patients with a diagnosis of asthma.
After patients were selected, they were screened for additional exclusion criteria. Patients were excluded if a pulmonary care practitioner managed their COPD; if identified via an active pulmonary consult in CPRS; if a non-VA clinician prescribed their ICS; or if they were being treated with roflumilast, theophylline, or chronic azithromycin. Individuals taking these 3 drugs were excluded due to potential severe and/or refractory COPD. Patients also were excluded if they: (1) had prior ICS de-escalation failure (defined as a COPD exacerbation following ICS de-escalation that resulted in ICS resumption); (2) had a COPD exacerbation requiring systemic corticosteroids or antibiotics in the previous year; (3) had active lung cancer; (4) did not have any eosinophil levels in CPRS within the previous 2 years; or (5) had any eosinophil levels ≥ 300 cells/µL in the previous year.
Each patient who met the inclusion criteria and was not excluded received a focused medication review by a pharmacist who created a templated progress note, with patient-specific recommendations, that was entered in the CPRS (eAppendix). The recommendations were also attached as an addendum to the patient’s last primary care visit note, and the primary care practitioner (PCP) was alerted via CPRS to consider ICS de-escalation and non-ICS alternatives. Tapering of ICS therapy was offered as an option to de-escalate if abrupt discontinuation was deemed inappropriate. PCPs were also prompted to consider referral to a primary care clinical pharmacy specialist for management and follow-up of ICS de-escalation.
The primary outcome was the number of patients with de-escalated ICS at 3 and 6 months following the recommendation. Secondary outcomes included the number of: patients who were no longer prescribed an ICS or who had a non-ICS alternative initiated at a pharmacist’s recommendation; patients who were referred to a primary care clinical pharmacy specialist for ICS de-escalation; COPD exacerbations requiring systemic steroids or antibiotics, or requiring an ED visit, inpatient admission, or urgent-care clinic visit; and cases of pneumonia or oral candidiasis. Primary and secondary outcomes were evaluated via chart review in CPRS. For secondary outcomes of pneumonia and COPD exacerbation, identification was made by documented diagnosis in CPRS. For continuous data such as age, the mean was calculated.
Results
Pharmacist ICS de-escalation recommendations were made between September 21, 2023, and November 19, 2023, for 106 patients. The mean age was 72 years and 99 (93%) patients were male (Table 1). Forty-one (39%) of the patients used tobacco at the time of the study. FEV1 was available for 69 patients with a mean of 63% (GOLD grade 2).1 Based on FEV1 values, 16 patients had mild COPD (GOLD grade 1), 37 patients had moderate COPD (GOLD grade 2), 14 patients had severe COPD (GOLD grade 3), and 2 patients had very severe COPD (GOLD grade 4).1 Thirty-four patients received LABA + LAMA + ICS, 65 received LABA + ICS, 2 received LAMA + ICS, and 5 received ICS monotherapy. The most common dose of ICS was a moderate dose (Table 2). Only 2 patients had an ICS AE in the previous year.
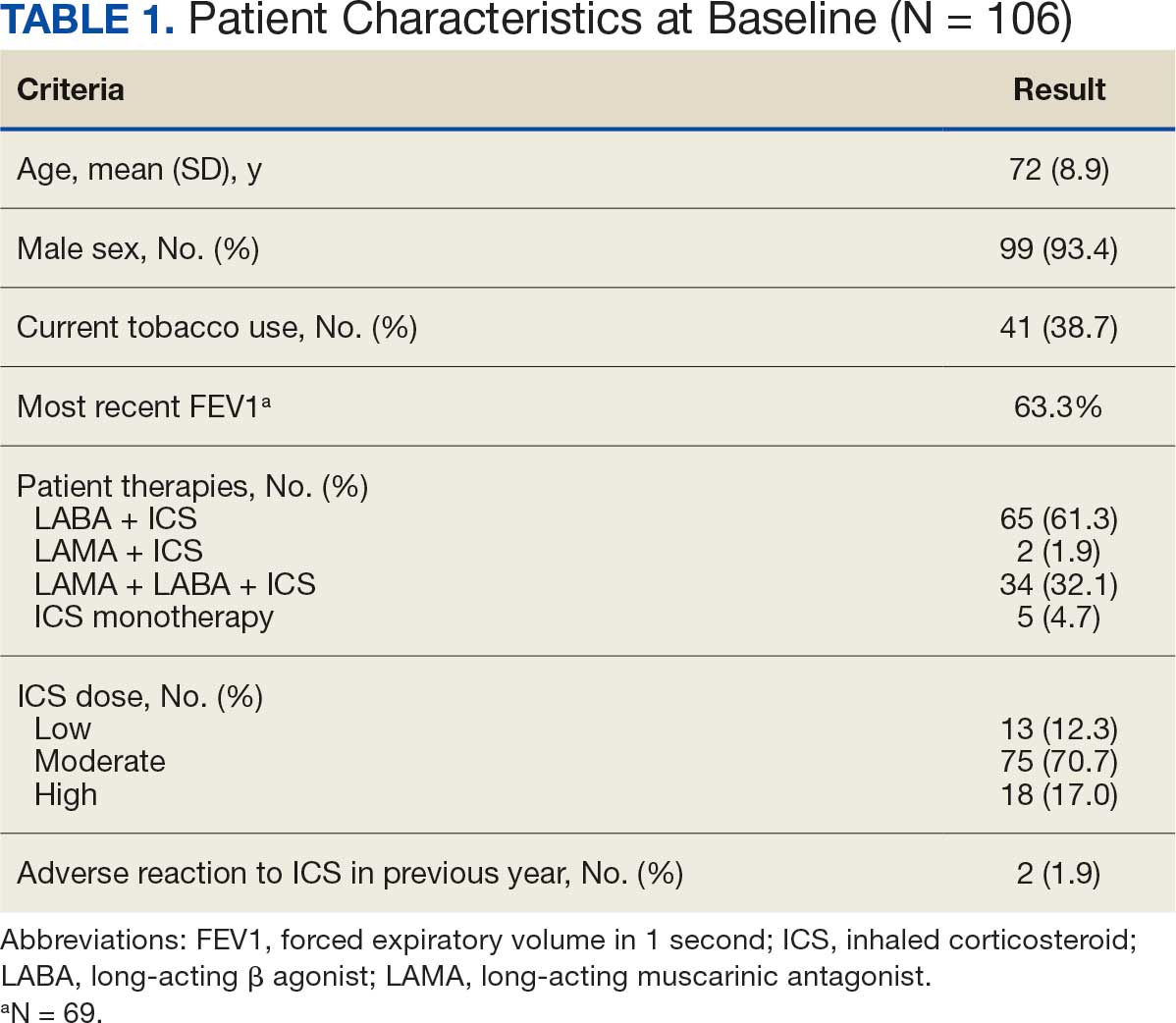
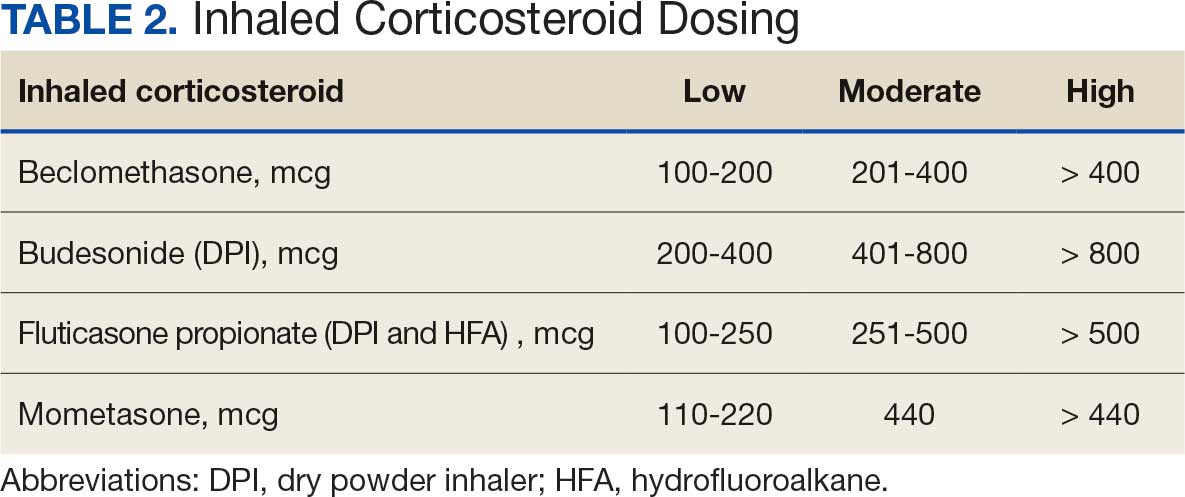
ICS de-escalation recommendations resulted in ICS de-escalation in 50 (47.2%) and 62 (58.5%) patients at 3 and 6 months, respectively. The 6-month ICS de-escalation rate by ICS dose at baseline was 72.2% (high dose), 60.0% (moderate), and 30.8% (low). De-escalation at 6 months by GOLD grade at baseline was 56.3% (9 of 16 patients, GOLD 1), 64.9% (24 of 37 patients, GOLD 2), 50% (7 of 14 patients, GOLD 3), and 50% (1 of 2 patients, GOLD 4). Six months after the ICS de-escalation recommendation appeared in the CPRS, the percentage of patients on LABA + ICS therapy dropped from 65 patients (61.3%) at baseline to 25 patients (23.6%).
Secondary outcomes were assessed at 3 and 6 months following the recommendation. Most patients with de-escalated ICS had their ICS discontinued and a non-ICS alternative initiated per pharmacist recommendations. At 6 months, 39 patients (36.8%) patients were referred to a patient aligned care team (PACT) pharmacist for de-escalation. Of the 39 patients referred to pharmacists, 69.2% (27 patients) were de-escalated; this compared to 52.2% (35 patients) who were not referred to pharmacists (Table 3).
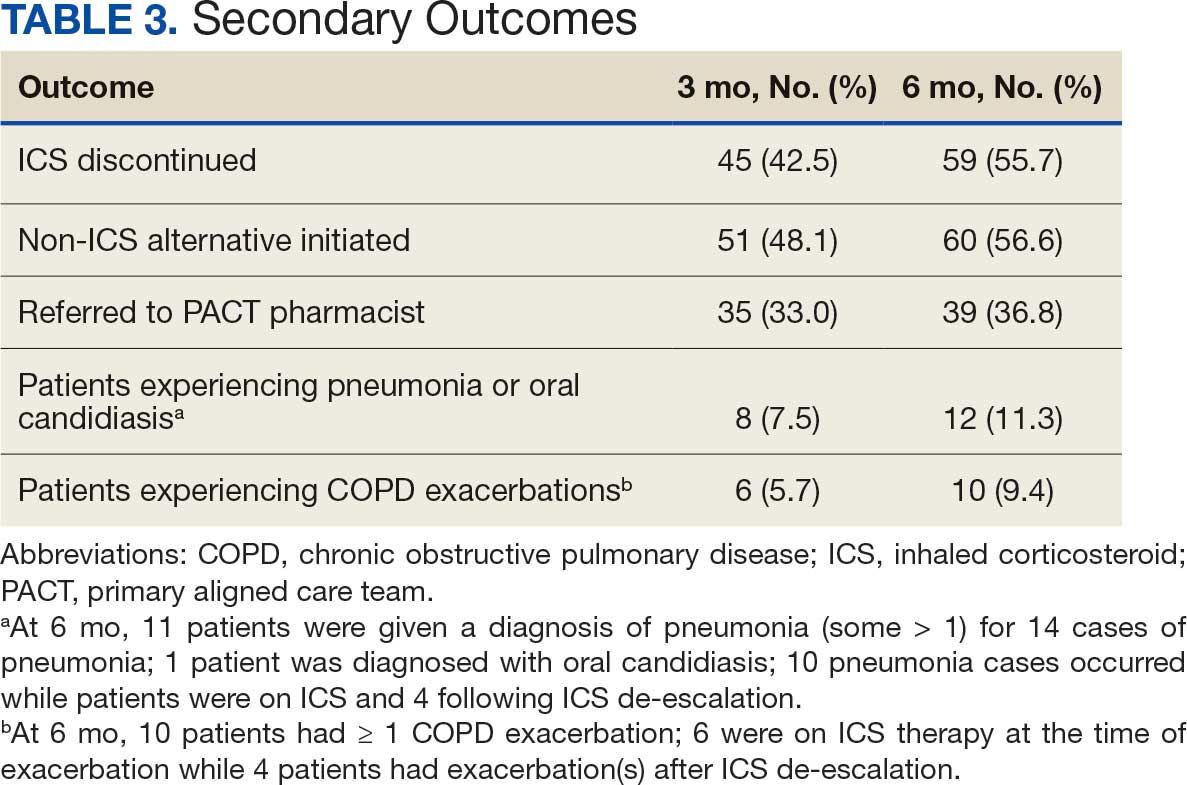
ICS use increases the risk of pneumonia.1 At 6 months, 11 patients were diagnosed with pneumonia; 3 patients were diagnosed with pneumonia twice, resulting in a total of 14 cases. Ten cases occurred while patients were on ICS and 4 cases occurred following ICS de-escalation. One patient had a documented case of oral candidiasis that occurred while on ICS therapy; no patients with discontinued ICS were diagnosed with oral candidiasis. In addition, 10 patients had COPD exacerbations; however no patients had exacerbations both before and after de-escalation. Six patients were on ICS therapy when they experienced an exacerbation, and 4 patients had an exacerbation after ICS de-escalation.
Discussion
More than half of patients receiving the pharmacist intervention achieved the primary outcome of ICS de-escalation at 6 months. Furthermore, a larger percentage of patients referred to pharmacists for the management of ICS de-escalation successfully achieved de-escalation compared to those who were not referred. These outcomes reflect the important role pharmacists can play in identifying appropriate candidates for ICS de-escalation and assisting in the management of ICS de-escalation. Patients referred to pharmacists also received other services such as smoking cessation pharmacotherapy and counseling on inhaler technique and adherence. These interventions can support improved COPD clinical outcomes.
The purpose of de-escalating ICS therapy is to reduce the risk of AEs such as pneumonia and oral candidiasis.1 The secondary outcomes of this study support previous evidence that patients who have de-escalated ICS therapy may have reduced risk of AEs compared to those who remain on ICS therapy.3 Specifically, of the 14 cases of pneumonia that occurred during the study, 10 cases occurred while patients were on ICS and 4 cases occurred following ICS de-escalation.
ICS de-escalation may increase risk of increased COPD exacerbations.1 However, the secondary outcomes of this study do not indicate that those with de-escalated ICS had more COPD exacerbations compared to those who continued on ICS. Pharmacists’ recommendations were more effective for patients with less severe COPD based on baseline FEV1.
The previous GOLD Guidelines for COPD suggested LABA + ICS therapy as an option for patients with a high symptom and exacerbation burden (previously known as GOLD Group D). Guidelines no longer recommend LABA + ICS therapy due to the superiority of triple inhaled therapy for exacerbations and the superiority of LAMA + LABA therapy for dyspnea.7 A majority of identified patients in this project were on LABA + ICS therapy alone at baseline. The ICS de-escalation recommendation resulted in a 61.5% reduction in patients on LABA + ICS therapy at 6 months. By decreasing the number of patients on LABA + ICS without LAMA, recommendations increased the number of patients on guideline-directed therapy.
Limitations
This study lacked a control group, and the rate of ICS de-escalation in patients who did not receive a pharmacist recommendation was not assessed. Therefore, it could not be determined whether the pharmacist recommendation is more effective than no recommendation. Another limitation was our inability to access records from non-VA health care facilities. This may have resulted in missed COPD exacerbations, pneumonia, and oral candidiasis prior to or following the pharmacist recommendation.
In addition, the method used to notify PCPs of the pharmacist recommendation was a CPRS alert. Clinicians often receive multiple daily alerts and may not always pay close attention to them due to alert fatigue. Early in the study, some PCPs were unknowingly omitted from the alert of the pharmacist recommendation for 10 patients due to human error. For 8 of these 10 patients, the PCP was notified of the recommendations during the 3-month follow-up period. However, 2 patients had COPD exacerbations during the 3-month follow-up period. In these cases, the PCP was not alerted to de-escalate ICS. The data for these patients were collected at 3 and 6 months in the same manner as all other patients. Also, 7 of 35 patients who were referred to a pharmacist for ICS de-escalation did not have a scheduled appointment. These patients were considered to be lost to follow-up and this may have resulted in an underestimation of the ability of pharmacists to successfully de-escalate ICS in patients with COPD.
Other studies have evaluated the efficacy of a pharmacy-driven ICS de-escalation.8,9 Hegland et al reported ICS de-escalation for 22% of 141 eligible ambulatory patients with COPD on triple inhaled therapy following pharmacist appointments.8 A study by Hahn et al resulted in 63.8% of 58 patients with COPD being maintained off ICS following a pharmacist de-escalation initiative.9 However, these studies relied upon more time-consuming de-escalation interventions, including at least 1 phone, video, or in-person patient visit.8,9
This project used a single chart review and templated progress note to recommend ICS de-escalation and achieved similar or improved de-escalation rates compared to previous studies.8,9 Previous studies were conducted prior to the updated 2023 GOLD guidelines for COPD which no longer recommend LABA + ICS therapy. This project addressed ICS de-escalation in patients on LABA + ICS therapy in addition to those on triple inhaled therapy. Additionally, previous studies did not address rates of moderate to severe COPD exacerbation and adverse events to ICS following the pharmacist intervention.8,9
This study included COPD exacerbations and cases of pneumonia or oral candidiasis as secondary outcomes to assess the safety and efficacy of the ICS de-escalation. It appeared there were similar or lower rates of COPD exacerbations, pneumonia, and oral candidiasis in those with de-escalated ICS therapy in this study. However, these secondary outcomes are exploratory and would need to be confirmed by larger studies powered to address these outcomes.
CONCLUSIONS
Pharmacist-driven ICS de-escalation may be an effective method for reducing ICS usage in veterans as seen in this study. Additional controlled studies are required to evaluate the efficacy and safety of pharmacist-driven ICS de-escalation.
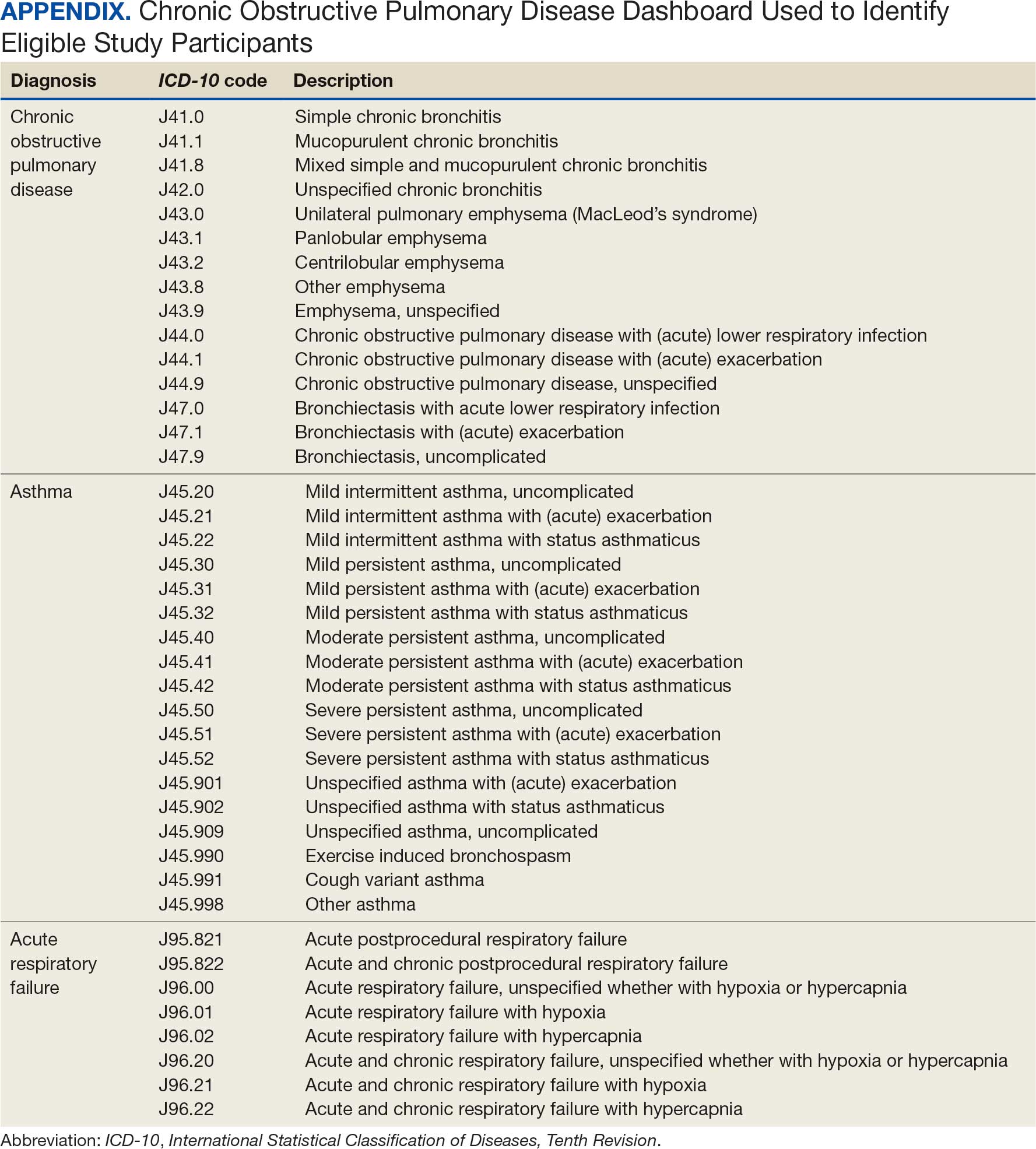
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2024 Report). Accessed October 14, 2025. https://goldcopd.org/2024-gold-report/
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2025 Report). Accessed November 14, 2025. https://goldcopd.org/2025-gold-report/
- Rogliani P, Ritondo BL, Gabriele M, et al. Optimizing de-escalation of inhaled corticosteroids in COPD: a systematic review of real-world findings. Expert Rev Clin Pharmacol. 2020;13(9):977-990. doi:10.1080/17512433.2020.1817739
- Rossi A, Guerriero M, Corrado A; OPTIMO/AIPO Study Group. Withdrawal of inhaled corticosteroids can be safe in COPD patients at low risk of exacerbation: a real-life study on the appropriateness of treatment in moderate COPD patients (OPTIMO). Respir Res. 2014;15(1):77. doi:10.1186/1465-9921-15-77
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26(2):63-68. doi:10.37765/ajmc.2020.42394
- US Department of Veterans Affairs, US Department of Defense. VA/DoD Clinical Practice Guideline for the Management of Chronic Obstructive Pulmonary Disease. 2021. Accessed October 14, 2025. https://www.healthquality.va.gov/guidelines/CD/copd/
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Accessed October 14, 2025. https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf
- Hegland AJ, Bolduc J, Jones L, Kunisaki KM, Melzer AC. Pharmacist-driven deprescribing of inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2021;18(4):730-733. doi:10.1513/AnnalsATS.202007-871RL
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13(1):10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
Systemic glucocorticoids play an important role in the treatment of chronic obstructive pulmonary disease (COPD) exacerbations. They are recommended to shorten recovery time and increase forced expiratory volume in 1 second (FEV1) during exacerbations.1 However, the role of the chronic use of inhaled corticosteroids (ICSs) in the treatment of COPD is less clear.
When added to inhaled β-2 agonists and muscarinic antagonists, ICSs can decrease the risk of exacerbations.1 However, not all patients with COPD benefit from ICS therapy. The degree of benefit an ICS can provide has been shown to correlate with eosinophil count—a marker of inflammation. The expected benefit of using an ICS increases as the eosinophil count increases.1 Maximum benefit can be observed with eosinophil counts ≥ 300 cells/µL, and minimal benefit is observed with eosinophil counts < 100 cells/µL. Adverse effects (AEs) of ICSs include a hoarse voice, oral candidiasis, and an increased risk of pneumonia.1 Given the risk of AEs, it is important to limit ICS use in patients who are unlikely to reap any benefits.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines suggest the use of ICSs in patients who experience exacerbations while using long-acting β agonist (LABA) plus long-acting muscarinic antagonist (LAMA) therapy and have an eosinophil count ≥ 100 cells/µL. Switching from LABA or LAMA monotherapy to triple therapy with LAMA/LABA/ICS may be considered if patients have continued exacerbations and an eosinophil count ≥ 300 cells/µL. De-escalation of ICS therapy should be considered if patients do not meet these criteria or if patients experience ICS AEs, such as pneumonia. The patients most likely to have increased exacerbations or decreased FEV1 with ICS withdrawal are those with eosinophil counts ≥ 300 cells/µL.1,2
Several studies have explored the effects of ICS de-escalation in real-world clinical settings. A systematic review of 11 studies indicated that de-escalation of ICS in COPD does not result in increased exacerbations.3 A prospective study by Rossi et al found that in a 6-month period, 141 of 482 patients on ICS therapy (29%) had an exacerbation. In the opposing arm of the study, 88 of 334 patients (26%) with deprescribed ICS experienced an exacerbation. The difference between these 2 groups was not statistically significant.4 The researchers concluded that in real-world practice, ICS withdrawal can be safe in patients at low risk of exacerbation.
About 25% of veterans (1.25 million) have been diagnosed with COPD.5 To address this, the US Department of Veterans Affairs (VA) and US Department of Defense published updated COPD guidelines in 2021 that specify criteria for de-escalation of ICS.6 Guidelines, however, may not be reflected in common clinical practice for several years following publication. The VA Academic Detailing Service (ADS) provides tools to help clinicians identify patients who may benefit from changes in treatment plans. A recent ADS focus was the implementation of a COPD dashboard, which identifies patients with COPD who are candidates for ICS de-escalation based on comorbid diagnoses, exacerbation history, and eosinophil count. VA pharmacists have an expanded role in the management of primary care disease states and are therefore well-positioned to increase adherence to guideline-directed therapy. The objective of this quality improvement project was to determine the impact of pharmacist-driven de-escalation on ICS usage in veterans with COPD.
Methods
This project was conducted in an outpatient clinic at the Robley Rex VA Medical Center beginning September 21, 2023, with a progress note in the Computerized Patient Record System (CPRS). Eligible patients were selected using the COPD Dashboard provided by ADS. The COPD Dashboard defined patients with COPD as those with ≥ 2 outpatient COPD diagnoses in the past 2 years, 1 inpatient discharge COPD diagnosis in the past year, or COPD listed as an active problem. COPD diagnoses were identified using International Statistical Classification of Disease, Tenth Revision (ICD-10) codes
Candidates identified for ICS de-escalation by the dashboard were excluded if they had a history of COPD exacerbation in the previous 2 years. The dashboard identified COPD exacerbations via ICD-10 codes for COPD or acute respiratory failure for inpatient discharges, emergency department (ED) visits, urgent care visits, and community care consults with 1 of the following terms: emergency, inpatient, hospital, urgent, ED (self). The COPD dashboard excluded patients with a diagnosis of asthma.
After patients were selected, they were screened for additional exclusion criteria. Patients were excluded if a pulmonary care practitioner managed their COPD; if identified via an active pulmonary consult in CPRS; if a non-VA clinician prescribed their ICS; or if they were being treated with roflumilast, theophylline, or chronic azithromycin. Individuals taking these 3 drugs were excluded due to potential severe and/or refractory COPD. Patients also were excluded if they: (1) had prior ICS de-escalation failure (defined as a COPD exacerbation following ICS de-escalation that resulted in ICS resumption); (2) had a COPD exacerbation requiring systemic corticosteroids or antibiotics in the previous year; (3) had active lung cancer; (4) did not have any eosinophil levels in CPRS within the previous 2 years; or (5) had any eosinophil levels ≥ 300 cells/µL in the previous year.
Each patient who met the inclusion criteria and was not excluded received a focused medication review by a pharmacist who created a templated progress note, with patient-specific recommendations, that was entered in the CPRS (eAppendix). The recommendations were also attached as an addendum to the patient’s last primary care visit note, and the primary care practitioner (PCP) was alerted via CPRS to consider ICS de-escalation and non-ICS alternatives. Tapering of ICS therapy was offered as an option to de-escalate if abrupt discontinuation was deemed inappropriate. PCPs were also prompted to consider referral to a primary care clinical pharmacy specialist for management and follow-up of ICS de-escalation.
The primary outcome was the number of patients with de-escalated ICS at 3 and 6 months following the recommendation. Secondary outcomes included the number of: patients who were no longer prescribed an ICS or who had a non-ICS alternative initiated at a pharmacist’s recommendation; patients who were referred to a primary care clinical pharmacy specialist for ICS de-escalation; COPD exacerbations requiring systemic steroids or antibiotics, or requiring an ED visit, inpatient admission, or urgent-care clinic visit; and cases of pneumonia or oral candidiasis. Primary and secondary outcomes were evaluated via chart review in CPRS. For secondary outcomes of pneumonia and COPD exacerbation, identification was made by documented diagnosis in CPRS. For continuous data such as age, the mean was calculated.
Results
Pharmacist ICS de-escalation recommendations were made between September 21, 2023, and November 19, 2023, for 106 patients. The mean age was 72 years and 99 (93%) patients were male (Table 1). Forty-one (39%) of the patients used tobacco at the time of the study. FEV1 was available for 69 patients with a mean of 63% (GOLD grade 2).1 Based on FEV1 values, 16 patients had mild COPD (GOLD grade 1), 37 patients had moderate COPD (GOLD grade 2), 14 patients had severe COPD (GOLD grade 3), and 2 patients had very severe COPD (GOLD grade 4).1 Thirty-four patients received LABA + LAMA + ICS, 65 received LABA + ICS, 2 received LAMA + ICS, and 5 received ICS monotherapy. The most common dose of ICS was a moderate dose (Table 2). Only 2 patients had an ICS AE in the previous year.
ICS de-escalation recommendations resulted in ICS de-escalation in 50 (47.2%) and 62 (58.5%) patients at 3 and 6 months, respectively. The 6-month ICS de-escalation rate by ICS dose at baseline was 72.2% (high dose), 60.0% (moderate), and 30.8% (low). De-escalation at 6 months by GOLD grade at baseline was 56.3% (9 of 16 patients, GOLD 1), 64.9% (24 of 37 patients, GOLD 2), 50% (7 of 14 patients, GOLD 3), and 50% (1 of 2 patients, GOLD 4). Six months after the ICS de-escalation recommendation appeared in the CPRS, the percentage of patients on LABA + ICS therapy dropped from 65 patients (61.3%) at baseline to 25 patients (23.6%).
Secondary outcomes were assessed at 3 and 6 months following the recommendation. Most patients with de-escalated ICS had their ICS discontinued and a non-ICS alternative initiated per pharmacist recommendations. At 6 months, 39 patients (36.8%) patients were referred to a patient aligned care team (PACT) pharmacist for de-escalation. Of the 39 patients referred to pharmacists, 69.2% (27 patients) were de-escalated; this compared to 52.2% (35 patients) who were not referred to pharmacists (Table 3).
ICS use increases the risk of pneumonia.1 At 6 months, 11 patients were diagnosed with pneumonia; 3 patients were diagnosed with pneumonia twice, resulting in a total of 14 cases. Ten cases occurred while patients were on ICS and 4 cases occurred following ICS de-escalation. One patient had a documented case of oral candidiasis that occurred while on ICS therapy; no patients with discontinued ICS were diagnosed with oral candidiasis. In addition, 10 patients had COPD exacerbations; however no patients had exacerbations both before and after de-escalation. Six patients were on ICS therapy when they experienced an exacerbation, and 4 patients had an exacerbation after ICS de-escalation.
Discussion
More than half of patients receiving the pharmacist intervention achieved the primary outcome of ICS de-escalation at 6 months. Furthermore, a larger percentage of patients referred to pharmacists for the management of ICS de-escalation successfully achieved de-escalation compared to those who were not referred. These outcomes reflect the important role pharmacists can play in identifying appropriate candidates for ICS de-escalation and assisting in the management of ICS de-escalation. Patients referred to pharmacists also received other services such as smoking cessation pharmacotherapy and counseling on inhaler technique and adherence. These interventions can support improved COPD clinical outcomes.
The purpose of de-escalating ICS therapy is to reduce the risk of AEs such as pneumonia and oral candidiasis.1 The secondary outcomes of this study support previous evidence that patients who have de-escalated ICS therapy may have reduced risk of AEs compared to those who remain on ICS therapy.3 Specifically, of the 14 cases of pneumonia that occurred during the study, 10 cases occurred while patients were on ICS and 4 cases occurred following ICS de-escalation.
ICS de-escalation may increase risk of increased COPD exacerbations.1 However, the secondary outcomes of this study do not indicate that those with de-escalated ICS had more COPD exacerbations compared to those who continued on ICS. Pharmacists’ recommendations were more effective for patients with less severe COPD based on baseline FEV1.
The previous GOLD Guidelines for COPD suggested LABA + ICS therapy as an option for patients with a high symptom and exacerbation burden (previously known as GOLD Group D). Guidelines no longer recommend LABA + ICS therapy due to the superiority of triple inhaled therapy for exacerbations and the superiority of LAMA + LABA therapy for dyspnea.7 A majority of identified patients in this project were on LABA + ICS therapy alone at baseline. The ICS de-escalation recommendation resulted in a 61.5% reduction in patients on LABA + ICS therapy at 6 months. By decreasing the number of patients on LABA + ICS without LAMA, recommendations increased the number of patients on guideline-directed therapy.
Limitations
This study lacked a control group, and the rate of ICS de-escalation in patients who did not receive a pharmacist recommendation was not assessed. Therefore, it could not be determined whether the pharmacist recommendation is more effective than no recommendation. Another limitation was our inability to access records from non-VA health care facilities. This may have resulted in missed COPD exacerbations, pneumonia, and oral candidiasis prior to or following the pharmacist recommendation.
In addition, the method used to notify PCPs of the pharmacist recommendation was a CPRS alert. Clinicians often receive multiple daily alerts and may not always pay close attention to them due to alert fatigue. Early in the study, some PCPs were unknowingly omitted from the alert of the pharmacist recommendation for 10 patients due to human error. For 8 of these 10 patients, the PCP was notified of the recommendations during the 3-month follow-up period. However, 2 patients had COPD exacerbations during the 3-month follow-up period. In these cases, the PCP was not alerted to de-escalate ICS. The data for these patients were collected at 3 and 6 months in the same manner as all other patients. Also, 7 of 35 patients who were referred to a pharmacist for ICS de-escalation did not have a scheduled appointment. These patients were considered to be lost to follow-up and this may have resulted in an underestimation of the ability of pharmacists to successfully de-escalate ICS in patients with COPD.
Other studies have evaluated the efficacy of a pharmacy-driven ICS de-escalation.8,9 Hegland et al reported ICS de-escalation for 22% of 141 eligible ambulatory patients with COPD on triple inhaled therapy following pharmacist appointments.8 A study by Hahn et al resulted in 63.8% of 58 patients with COPD being maintained off ICS following a pharmacist de-escalation initiative.9 However, these studies relied upon more time-consuming de-escalation interventions, including at least 1 phone, video, or in-person patient visit.8,9
This project used a single chart review and templated progress note to recommend ICS de-escalation and achieved similar or improved de-escalation rates compared to previous studies.8,9 Previous studies were conducted prior to the updated 2023 GOLD guidelines for COPD which no longer recommend LABA + ICS therapy. This project addressed ICS de-escalation in patients on LABA + ICS therapy in addition to those on triple inhaled therapy. Additionally, previous studies did not address rates of moderate to severe COPD exacerbation and adverse events to ICS following the pharmacist intervention.8,9
This study included COPD exacerbations and cases of pneumonia or oral candidiasis as secondary outcomes to assess the safety and efficacy of the ICS de-escalation. It appeared there were similar or lower rates of COPD exacerbations, pneumonia, and oral candidiasis in those with de-escalated ICS therapy in this study. However, these secondary outcomes are exploratory and would need to be confirmed by larger studies powered to address these outcomes.
CONCLUSIONS
Pharmacist-driven ICS de-escalation may be an effective method for reducing ICS usage in veterans as seen in this study. Additional controlled studies are required to evaluate the efficacy and safety of pharmacist-driven ICS de-escalation.
Systemic glucocorticoids play an important role in the treatment of chronic obstructive pulmonary disease (COPD) exacerbations. They are recommended to shorten recovery time and increase forced expiratory volume in 1 second (FEV1) during exacerbations.1 However, the role of the chronic use of inhaled corticosteroids (ICSs) in the treatment of COPD is less clear.
When added to inhaled β-2 agonists and muscarinic antagonists, ICSs can decrease the risk of exacerbations.1 However, not all patients with COPD benefit from ICS therapy. The degree of benefit an ICS can provide has been shown to correlate with eosinophil count—a marker of inflammation. The expected benefit of using an ICS increases as the eosinophil count increases.1 Maximum benefit can be observed with eosinophil counts ≥ 300 cells/µL, and minimal benefit is observed with eosinophil counts < 100 cells/µL. Adverse effects (AEs) of ICSs include a hoarse voice, oral candidiasis, and an increased risk of pneumonia.1 Given the risk of AEs, it is important to limit ICS use in patients who are unlikely to reap any benefits.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines suggest the use of ICSs in patients who experience exacerbations while using long-acting β agonist (LABA) plus long-acting muscarinic antagonist (LAMA) therapy and have an eosinophil count ≥ 100 cells/µL. Switching from LABA or LAMA monotherapy to triple therapy with LAMA/LABA/ICS may be considered if patients have continued exacerbations and an eosinophil count ≥ 300 cells/µL. De-escalation of ICS therapy should be considered if patients do not meet these criteria or if patients experience ICS AEs, such as pneumonia. The patients most likely to have increased exacerbations or decreased FEV1 with ICS withdrawal are those with eosinophil counts ≥ 300 cells/µL.1,2
Several studies have explored the effects of ICS de-escalation in real-world clinical settings. A systematic review of 11 studies indicated that de-escalation of ICS in COPD does not result in increased exacerbations.3 A prospective study by Rossi et al found that in a 6-month period, 141 of 482 patients on ICS therapy (29%) had an exacerbation. In the opposing arm of the study, 88 of 334 patients (26%) with deprescribed ICS experienced an exacerbation. The difference between these 2 groups was not statistically significant.4 The researchers concluded that in real-world practice, ICS withdrawal can be safe in patients at low risk of exacerbation.
About 25% of veterans (1.25 million) have been diagnosed with COPD.5 To address this, the US Department of Veterans Affairs (VA) and US Department of Defense published updated COPD guidelines in 2021 that specify criteria for de-escalation of ICS.6 Guidelines, however, may not be reflected in common clinical practice for several years following publication. The VA Academic Detailing Service (ADS) provides tools to help clinicians identify patients who may benefit from changes in treatment plans. A recent ADS focus was the implementation of a COPD dashboard, which identifies patients with COPD who are candidates for ICS de-escalation based on comorbid diagnoses, exacerbation history, and eosinophil count. VA pharmacists have an expanded role in the management of primary care disease states and are therefore well-positioned to increase adherence to guideline-directed therapy. The objective of this quality improvement project was to determine the impact of pharmacist-driven de-escalation on ICS usage in veterans with COPD.
Methods
This project was conducted in an outpatient clinic at the Robley Rex VA Medical Center beginning September 21, 2023, with a progress note in the Computerized Patient Record System (CPRS). Eligible patients were selected using the COPD Dashboard provided by ADS. The COPD Dashboard defined patients with COPD as those with ≥ 2 outpatient COPD diagnoses in the past 2 years, 1 inpatient discharge COPD diagnosis in the past year, or COPD listed as an active problem. COPD diagnoses were identified using International Statistical Classification of Disease, Tenth Revision (ICD-10) codes
Candidates identified for ICS de-escalation by the dashboard were excluded if they had a history of COPD exacerbation in the previous 2 years. The dashboard identified COPD exacerbations via ICD-10 codes for COPD or acute respiratory failure for inpatient discharges, emergency department (ED) visits, urgent care visits, and community care consults with 1 of the following terms: emergency, inpatient, hospital, urgent, ED (self). The COPD dashboard excluded patients with a diagnosis of asthma.
After patients were selected, they were screened for additional exclusion criteria. Patients were excluded if a pulmonary care practitioner managed their COPD; if identified via an active pulmonary consult in CPRS; if a non-VA clinician prescribed their ICS; or if they were being treated with roflumilast, theophylline, or chronic azithromycin. Individuals taking these 3 drugs were excluded due to potential severe and/or refractory COPD. Patients also were excluded if they: (1) had prior ICS de-escalation failure (defined as a COPD exacerbation following ICS de-escalation that resulted in ICS resumption); (2) had a COPD exacerbation requiring systemic corticosteroids or antibiotics in the previous year; (3) had active lung cancer; (4) did not have any eosinophil levels in CPRS within the previous 2 years; or (5) had any eosinophil levels ≥ 300 cells/µL in the previous year.
Each patient who met the inclusion criteria and was not excluded received a focused medication review by a pharmacist who created a templated progress note, with patient-specific recommendations, that was entered in the CPRS (eAppendix). The recommendations were also attached as an addendum to the patient’s last primary care visit note, and the primary care practitioner (PCP) was alerted via CPRS to consider ICS de-escalation and non-ICS alternatives. Tapering of ICS therapy was offered as an option to de-escalate if abrupt discontinuation was deemed inappropriate. PCPs were also prompted to consider referral to a primary care clinical pharmacy specialist for management and follow-up of ICS de-escalation.
The primary outcome was the number of patients with de-escalated ICS at 3 and 6 months following the recommendation. Secondary outcomes included the number of: patients who were no longer prescribed an ICS or who had a non-ICS alternative initiated at a pharmacist’s recommendation; patients who were referred to a primary care clinical pharmacy specialist for ICS de-escalation; COPD exacerbations requiring systemic steroids or antibiotics, or requiring an ED visit, inpatient admission, or urgent-care clinic visit; and cases of pneumonia or oral candidiasis. Primary and secondary outcomes were evaluated via chart review in CPRS. For secondary outcomes of pneumonia and COPD exacerbation, identification was made by documented diagnosis in CPRS. For continuous data such as age, the mean was calculated.
Results
Pharmacist ICS de-escalation recommendations were made between September 21, 2023, and November 19, 2023, for 106 patients. The mean age was 72 years and 99 (93%) patients were male (Table 1). Forty-one (39%) of the patients used tobacco at the time of the study. FEV1 was available for 69 patients with a mean of 63% (GOLD grade 2).1 Based on FEV1 values, 16 patients had mild COPD (GOLD grade 1), 37 patients had moderate COPD (GOLD grade 2), 14 patients had severe COPD (GOLD grade 3), and 2 patients had very severe COPD (GOLD grade 4).1 Thirty-four patients received LABA + LAMA + ICS, 65 received LABA + ICS, 2 received LAMA + ICS, and 5 received ICS monotherapy. The most common dose of ICS was a moderate dose (Table 2). Only 2 patients had an ICS AE in the previous year.
ICS de-escalation recommendations resulted in ICS de-escalation in 50 (47.2%) and 62 (58.5%) patients at 3 and 6 months, respectively. The 6-month ICS de-escalation rate by ICS dose at baseline was 72.2% (high dose), 60.0% (moderate), and 30.8% (low). De-escalation at 6 months by GOLD grade at baseline was 56.3% (9 of 16 patients, GOLD 1), 64.9% (24 of 37 patients, GOLD 2), 50% (7 of 14 patients, GOLD 3), and 50% (1 of 2 patients, GOLD 4). Six months after the ICS de-escalation recommendation appeared in the CPRS, the percentage of patients on LABA + ICS therapy dropped from 65 patients (61.3%) at baseline to 25 patients (23.6%).
Secondary outcomes were assessed at 3 and 6 months following the recommendation. Most patients with de-escalated ICS had their ICS discontinued and a non-ICS alternative initiated per pharmacist recommendations. At 6 months, 39 patients (36.8%) patients were referred to a patient aligned care team (PACT) pharmacist for de-escalation. Of the 39 patients referred to pharmacists, 69.2% (27 patients) were de-escalated; this compared to 52.2% (35 patients) who were not referred to pharmacists (Table 3).
ICS use increases the risk of pneumonia.1 At 6 months, 11 patients were diagnosed with pneumonia; 3 patients were diagnosed with pneumonia twice, resulting in a total of 14 cases. Ten cases occurred while patients were on ICS and 4 cases occurred following ICS de-escalation. One patient had a documented case of oral candidiasis that occurred while on ICS therapy; no patients with discontinued ICS were diagnosed with oral candidiasis. In addition, 10 patients had COPD exacerbations; however no patients had exacerbations both before and after de-escalation. Six patients were on ICS therapy when they experienced an exacerbation, and 4 patients had an exacerbation after ICS de-escalation.
Discussion
More than half of patients receiving the pharmacist intervention achieved the primary outcome of ICS de-escalation at 6 months. Furthermore, a larger percentage of patients referred to pharmacists for the management of ICS de-escalation successfully achieved de-escalation compared to those who were not referred. These outcomes reflect the important role pharmacists can play in identifying appropriate candidates for ICS de-escalation and assisting in the management of ICS de-escalation. Patients referred to pharmacists also received other services such as smoking cessation pharmacotherapy and counseling on inhaler technique and adherence. These interventions can support improved COPD clinical outcomes.
The purpose of de-escalating ICS therapy is to reduce the risk of AEs such as pneumonia and oral candidiasis.1 The secondary outcomes of this study support previous evidence that patients who have de-escalated ICS therapy may have reduced risk of AEs compared to those who remain on ICS therapy.3 Specifically, of the 14 cases of pneumonia that occurred during the study, 10 cases occurred while patients were on ICS and 4 cases occurred following ICS de-escalation.
ICS de-escalation may increase risk of increased COPD exacerbations.1 However, the secondary outcomes of this study do not indicate that those with de-escalated ICS had more COPD exacerbations compared to those who continued on ICS. Pharmacists’ recommendations were more effective for patients with less severe COPD based on baseline FEV1.
The previous GOLD Guidelines for COPD suggested LABA + ICS therapy as an option for patients with a high symptom and exacerbation burden (previously known as GOLD Group D). Guidelines no longer recommend LABA + ICS therapy due to the superiority of triple inhaled therapy for exacerbations and the superiority of LAMA + LABA therapy for dyspnea.7 A majority of identified patients in this project were on LABA + ICS therapy alone at baseline. The ICS de-escalation recommendation resulted in a 61.5% reduction in patients on LABA + ICS therapy at 6 months. By decreasing the number of patients on LABA + ICS without LAMA, recommendations increased the number of patients on guideline-directed therapy.
Limitations
This study lacked a control group, and the rate of ICS de-escalation in patients who did not receive a pharmacist recommendation was not assessed. Therefore, it could not be determined whether the pharmacist recommendation is more effective than no recommendation. Another limitation was our inability to access records from non-VA health care facilities. This may have resulted in missed COPD exacerbations, pneumonia, and oral candidiasis prior to or following the pharmacist recommendation.
In addition, the method used to notify PCPs of the pharmacist recommendation was a CPRS alert. Clinicians often receive multiple daily alerts and may not always pay close attention to them due to alert fatigue. Early in the study, some PCPs were unknowingly omitted from the alert of the pharmacist recommendation for 10 patients due to human error. For 8 of these 10 patients, the PCP was notified of the recommendations during the 3-month follow-up period. However, 2 patients had COPD exacerbations during the 3-month follow-up period. In these cases, the PCP was not alerted to de-escalate ICS. The data for these patients were collected at 3 and 6 months in the same manner as all other patients. Also, 7 of 35 patients who were referred to a pharmacist for ICS de-escalation did not have a scheduled appointment. These patients were considered to be lost to follow-up and this may have resulted in an underestimation of the ability of pharmacists to successfully de-escalate ICS in patients with COPD.
Other studies have evaluated the efficacy of a pharmacy-driven ICS de-escalation.8,9 Hegland et al reported ICS de-escalation for 22% of 141 eligible ambulatory patients with COPD on triple inhaled therapy following pharmacist appointments.8 A study by Hahn et al resulted in 63.8% of 58 patients with COPD being maintained off ICS following a pharmacist de-escalation initiative.9 However, these studies relied upon more time-consuming de-escalation interventions, including at least 1 phone, video, or in-person patient visit.8,9
This project used a single chart review and templated progress note to recommend ICS de-escalation and achieved similar or improved de-escalation rates compared to previous studies.8,9 Previous studies were conducted prior to the updated 2023 GOLD guidelines for COPD which no longer recommend LABA + ICS therapy. This project addressed ICS de-escalation in patients on LABA + ICS therapy in addition to those on triple inhaled therapy. Additionally, previous studies did not address rates of moderate to severe COPD exacerbation and adverse events to ICS following the pharmacist intervention.8,9
This study included COPD exacerbations and cases of pneumonia or oral candidiasis as secondary outcomes to assess the safety and efficacy of the ICS de-escalation. It appeared there were similar or lower rates of COPD exacerbations, pneumonia, and oral candidiasis in those with de-escalated ICS therapy in this study. However, these secondary outcomes are exploratory and would need to be confirmed by larger studies powered to address these outcomes.
CONCLUSIONS
Pharmacist-driven ICS de-escalation may be an effective method for reducing ICS usage in veterans as seen in this study. Additional controlled studies are required to evaluate the efficacy and safety of pharmacist-driven ICS de-escalation.
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2024 Report). Accessed October 14, 2025. https://goldcopd.org/2024-gold-report/
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2025 Report). Accessed November 14, 2025. https://goldcopd.org/2025-gold-report/
- Rogliani P, Ritondo BL, Gabriele M, et al. Optimizing de-escalation of inhaled corticosteroids in COPD: a systematic review of real-world findings. Expert Rev Clin Pharmacol. 2020;13(9):977-990. doi:10.1080/17512433.2020.1817739
- Rossi A, Guerriero M, Corrado A; OPTIMO/AIPO Study Group. Withdrawal of inhaled corticosteroids can be safe in COPD patients at low risk of exacerbation: a real-life study on the appropriateness of treatment in moderate COPD patients (OPTIMO). Respir Res. 2014;15(1):77. doi:10.1186/1465-9921-15-77
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26(2):63-68. doi:10.37765/ajmc.2020.42394
- US Department of Veterans Affairs, US Department of Defense. VA/DoD Clinical Practice Guideline for the Management of Chronic Obstructive Pulmonary Disease. 2021. Accessed October 14, 2025. https://www.healthquality.va.gov/guidelines/CD/copd/
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Accessed October 14, 2025. https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf
- Hegland AJ, Bolduc J, Jones L, Kunisaki KM, Melzer AC. Pharmacist-driven deprescribing of inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2021;18(4):730-733. doi:10.1513/AnnalsATS.202007-871RL
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13(1):10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2024 Report). Accessed October 14, 2025. https://goldcopd.org/2024-gold-report/
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2025 Report). Accessed November 14, 2025. https://goldcopd.org/2025-gold-report/
- Rogliani P, Ritondo BL, Gabriele M, et al. Optimizing de-escalation of inhaled corticosteroids in COPD: a systematic review of real-world findings. Expert Rev Clin Pharmacol. 2020;13(9):977-990. doi:10.1080/17512433.2020.1817739
- Rossi A, Guerriero M, Corrado A; OPTIMO/AIPO Study Group. Withdrawal of inhaled corticosteroids can be safe in COPD patients at low risk of exacerbation: a real-life study on the appropriateness of treatment in moderate COPD patients (OPTIMO). Respir Res. 2014;15(1):77. doi:10.1186/1465-9921-15-77
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26(2):63-68. doi:10.37765/ajmc.2020.42394
- US Department of Veterans Affairs, US Department of Defense. VA/DoD Clinical Practice Guideline for the Management of Chronic Obstructive Pulmonary Disease. 2021. Accessed October 14, 2025. https://www.healthquality.va.gov/guidelines/CD/copd/
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Accessed October 14, 2025. https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf
- Hegland AJ, Bolduc J, Jones L, Kunisaki KM, Melzer AC. Pharmacist-driven deprescribing of inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2021;18(4):730-733. doi:10.1513/AnnalsATS.202007-871RL
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13(1):10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
Evaluation of Pharmacist-Driven Inhaled Corticosteroid De-escalation in Veterans
Evaluation of Pharmacist-Driven Inhaled Corticosteroid De-escalation in Veterans

Military Deployment Raises Respiratory Disease Risk
Individuals who served in Iraq or Afghanistan had significantly higher rates of new-onset respiratory diseases after deployment compared to non-deployed control peers, based on data from more than 48,000 veterans. The findings were presented at the American College of Allergy, Asthma, and Immunology (ACAAI) 2025 Annual Meeting.
“Veterans deployed to Iraq and Afghanistan were often exposed to airborne hazards such as burn pits and dust storms,” said Patrick Gleeson, MD, an allergist at the University of Pennsylvania Perelman School of Medicine, Philadelphia, in a press release.
“We found that these exposures may have long-term health impacts, particularly for respiratory diseases that can affect quality of life for years after service,” said Gleeson, who presented the results at the meeting.
Gleeson and colleagues used data from the Veterans Affairs Corporate Data Warehouse and Observational Medical Outcomes Partnership to identify veterans with a single deployment as part of Operation Iraqi Freedom or Operation Enduring Freedom. Participants had at least one outpatient visit prior to deployment with no baseline history of asthma, chronic rhinitis, chronic rhinosinusitis, or nasal polyposis. The mean age of the participants at deployment was 26.7 years, 84% were male, 75% were White, and 11% were Hispanic or Latino. Each was matched with a similar non-deployed veteran control.
The primary outcome was outpatient diagnoses or problem list entries for asthma, chronic rhinitis, chronic rhinosinusitis, or nasal polyposis.
Compared to non-deployed peers, deployed veterans had a 55% increased risk of asthma, a 48% increased risk of nasal polyposis, a 41% increased risk of chronic rhinitis, and a 27% increased risk of chronic rhinosinusitis, based on Cox proportional hazards models (P < .0005 for all).
The findings were limited by the retrospective design. However, “Recognizing the link between deployment and respiratory disease can help guide medical support, policy, and preventive strategies for those affected,” Gleeson said in the press release.
The study received no outside funding. The researchers disclosed no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Individuals who served in Iraq or Afghanistan had significantly higher rates of new-onset respiratory diseases after deployment compared to non-deployed control peers, based on data from more than 48,000 veterans. The findings were presented at the American College of Allergy, Asthma, and Immunology (ACAAI) 2025 Annual Meeting.
“Veterans deployed to Iraq and Afghanistan were often exposed to airborne hazards such as burn pits and dust storms,” said Patrick Gleeson, MD, an allergist at the University of Pennsylvania Perelman School of Medicine, Philadelphia, in a press release.
“We found that these exposures may have long-term health impacts, particularly for respiratory diseases that can affect quality of life for years after service,” said Gleeson, who presented the results at the meeting.
Gleeson and colleagues used data from the Veterans Affairs Corporate Data Warehouse and Observational Medical Outcomes Partnership to identify veterans with a single deployment as part of Operation Iraqi Freedom or Operation Enduring Freedom. Participants had at least one outpatient visit prior to deployment with no baseline history of asthma, chronic rhinitis, chronic rhinosinusitis, or nasal polyposis. The mean age of the participants at deployment was 26.7 years, 84% were male, 75% were White, and 11% were Hispanic or Latino. Each was matched with a similar non-deployed veteran control.
The primary outcome was outpatient diagnoses or problem list entries for asthma, chronic rhinitis, chronic rhinosinusitis, or nasal polyposis.
Compared to non-deployed peers, deployed veterans had a 55% increased risk of asthma, a 48% increased risk of nasal polyposis, a 41% increased risk of chronic rhinitis, and a 27% increased risk of chronic rhinosinusitis, based on Cox proportional hazards models (P < .0005 for all).
The findings were limited by the retrospective design. However, “Recognizing the link between deployment and respiratory disease can help guide medical support, policy, and preventive strategies for those affected,” Gleeson said in the press release.
The study received no outside funding. The researchers disclosed no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Individuals who served in Iraq or Afghanistan had significantly higher rates of new-onset respiratory diseases after deployment compared to non-deployed control peers, based on data from more than 48,000 veterans. The findings were presented at the American College of Allergy, Asthma, and Immunology (ACAAI) 2025 Annual Meeting.
“Veterans deployed to Iraq and Afghanistan were often exposed to airborne hazards such as burn pits and dust storms,” said Patrick Gleeson, MD, an allergist at the University of Pennsylvania Perelman School of Medicine, Philadelphia, in a press release.
“We found that these exposures may have long-term health impacts, particularly for respiratory diseases that can affect quality of life for years after service,” said Gleeson, who presented the results at the meeting.
Gleeson and colleagues used data from the Veterans Affairs Corporate Data Warehouse and Observational Medical Outcomes Partnership to identify veterans with a single deployment as part of Operation Iraqi Freedom or Operation Enduring Freedom. Participants had at least one outpatient visit prior to deployment with no baseline history of asthma, chronic rhinitis, chronic rhinosinusitis, or nasal polyposis. The mean age of the participants at deployment was 26.7 years, 84% were male, 75% were White, and 11% were Hispanic or Latino. Each was matched with a similar non-deployed veteran control.
The primary outcome was outpatient diagnoses or problem list entries for asthma, chronic rhinitis, chronic rhinosinusitis, or nasal polyposis.
Compared to non-deployed peers, deployed veterans had a 55% increased risk of asthma, a 48% increased risk of nasal polyposis, a 41% increased risk of chronic rhinitis, and a 27% increased risk of chronic rhinosinusitis, based on Cox proportional hazards models (P < .0005 for all).
The findings were limited by the retrospective design. However, “Recognizing the link between deployment and respiratory disease can help guide medical support, policy, and preventive strategies for those affected,” Gleeson said in the press release.
The study received no outside funding. The researchers disclosed no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM ACAAI 2025