User login
Lung Cancer Screening Unveils Hidden Health Risks
The reason is because the low-dose CT scans used for screening cover the lower neck down to the upper abdomen, revealing far more anatomy than simply the lungs.
In fact, lung cancer screening can provide information on three of the top 10 causes of death worldwide: ischemic heart disease, chronic obstructive pulmonary disease, and, of course, lung cancer.
With lung cancer screening, “we are basically targeting many birds with one low-dose stone,” explained Jelena Spasic MD, PhD, at the European Lung Cancer Congress (ELCC) 2024.
Dr. Spasic, a medical oncologist at the Institute for Oncology and Radiology of Serbia in Belgrade, was the discussant on a study that gave an indication on just how useful screening can be for other diseases.
The study, dubbed 4-IN-THE-LUNG-RUN trial (4ITLR), is an ongoing prospective trial in six European countries that is using lung cancer screening scans to also look for coronary artery calcifications, a marker of atherosclerosis.
Usually, coronary calcifications are considered incidental findings on lung cancer screenings and reported to subjects’ physicians for heart disease risk assessment.
The difference in 4ITLR is that investigators are actively looking for the lesions and quantifying the extent of calcifications.
It’s made possible by the artificial intelligence-based software being used to read the scans. In addition to generating reports on lung nodules, it also automatically calculates an Agatston score, a quantification of the degree of coronary artery calcification for each subject.
At the meeting, which was organized by the European Society for Clinical Oncology, 4ITLR investigator Daiwei Han, MD, PhD, a research associate at the Institute for Diagnostic Accuracy in Groningen, the Netherlands, reported outcomes in the first 2487 of the 24,000 planned subjects.
To be eligible for screening, participants had to be 60-79 years old and either current smokers, past smokers who had quit within 10 years, or people with a 35 or more pack-year history. The median age in the study was 68.1 years.
Overall, 53% of subjects had Agatston scores of 100 or more, indicating the need for treatment to prevent active coronary artery disease, Dr. Han said.
Fifteen percent were at high risk for heart disease with scores of 400-999, indicating extensive coronary artery calcification, and 16.2% were at very high risk, with scores of 1000 or higher. The information is being shared with participants’ physicians.
The risk of heart disease was far higher in men, who made up 56% of the study population. While women had a median Agatston score of 61, the median score for men was 211.1.
The findings illustrate the potential of dedicated cardiovascular screening within lung cancer screening programs, Dr. Han said, noting that 4ITLR will also incorporate COPD risk assessment.
The study also shows the increased impact lung cancer screening programs could have if greater use were made of the CT images to look for other diseases, Dr. Spasic said.
4ITLR is funded by the European Union’s Horizon 2020 Program. Dr. Spasic and Dr. Han didn’t have any relevant disclosures.
The reason is because the low-dose CT scans used for screening cover the lower neck down to the upper abdomen, revealing far more anatomy than simply the lungs.
In fact, lung cancer screening can provide information on three of the top 10 causes of death worldwide: ischemic heart disease, chronic obstructive pulmonary disease, and, of course, lung cancer.
With lung cancer screening, “we are basically targeting many birds with one low-dose stone,” explained Jelena Spasic MD, PhD, at the European Lung Cancer Congress (ELCC) 2024.
Dr. Spasic, a medical oncologist at the Institute for Oncology and Radiology of Serbia in Belgrade, was the discussant on a study that gave an indication on just how useful screening can be for other diseases.
The study, dubbed 4-IN-THE-LUNG-RUN trial (4ITLR), is an ongoing prospective trial in six European countries that is using lung cancer screening scans to also look for coronary artery calcifications, a marker of atherosclerosis.
Usually, coronary calcifications are considered incidental findings on lung cancer screenings and reported to subjects’ physicians for heart disease risk assessment.
The difference in 4ITLR is that investigators are actively looking for the lesions and quantifying the extent of calcifications.
It’s made possible by the artificial intelligence-based software being used to read the scans. In addition to generating reports on lung nodules, it also automatically calculates an Agatston score, a quantification of the degree of coronary artery calcification for each subject.
At the meeting, which was organized by the European Society for Clinical Oncology, 4ITLR investigator Daiwei Han, MD, PhD, a research associate at the Institute for Diagnostic Accuracy in Groningen, the Netherlands, reported outcomes in the first 2487 of the 24,000 planned subjects.
To be eligible for screening, participants had to be 60-79 years old and either current smokers, past smokers who had quit within 10 years, or people with a 35 or more pack-year history. The median age in the study was 68.1 years.
Overall, 53% of subjects had Agatston scores of 100 or more, indicating the need for treatment to prevent active coronary artery disease, Dr. Han said.
Fifteen percent were at high risk for heart disease with scores of 400-999, indicating extensive coronary artery calcification, and 16.2% were at very high risk, with scores of 1000 or higher. The information is being shared with participants’ physicians.
The risk of heart disease was far higher in men, who made up 56% of the study population. While women had a median Agatston score of 61, the median score for men was 211.1.
The findings illustrate the potential of dedicated cardiovascular screening within lung cancer screening programs, Dr. Han said, noting that 4ITLR will also incorporate COPD risk assessment.
The study also shows the increased impact lung cancer screening programs could have if greater use were made of the CT images to look for other diseases, Dr. Spasic said.
4ITLR is funded by the European Union’s Horizon 2020 Program. Dr. Spasic and Dr. Han didn’t have any relevant disclosures.
The reason is because the low-dose CT scans used for screening cover the lower neck down to the upper abdomen, revealing far more anatomy than simply the lungs.
In fact, lung cancer screening can provide information on three of the top 10 causes of death worldwide: ischemic heart disease, chronic obstructive pulmonary disease, and, of course, lung cancer.
With lung cancer screening, “we are basically targeting many birds with one low-dose stone,” explained Jelena Spasic MD, PhD, at the European Lung Cancer Congress (ELCC) 2024.
Dr. Spasic, a medical oncologist at the Institute for Oncology and Radiology of Serbia in Belgrade, was the discussant on a study that gave an indication on just how useful screening can be for other diseases.
The study, dubbed 4-IN-THE-LUNG-RUN trial (4ITLR), is an ongoing prospective trial in six European countries that is using lung cancer screening scans to also look for coronary artery calcifications, a marker of atherosclerosis.
Usually, coronary calcifications are considered incidental findings on lung cancer screenings and reported to subjects’ physicians for heart disease risk assessment.
The difference in 4ITLR is that investigators are actively looking for the lesions and quantifying the extent of calcifications.
It’s made possible by the artificial intelligence-based software being used to read the scans. In addition to generating reports on lung nodules, it also automatically calculates an Agatston score, a quantification of the degree of coronary artery calcification for each subject.
At the meeting, which was organized by the European Society for Clinical Oncology, 4ITLR investigator Daiwei Han, MD, PhD, a research associate at the Institute for Diagnostic Accuracy in Groningen, the Netherlands, reported outcomes in the first 2487 of the 24,000 planned subjects.
To be eligible for screening, participants had to be 60-79 years old and either current smokers, past smokers who had quit within 10 years, or people with a 35 or more pack-year history. The median age in the study was 68.1 years.
Overall, 53% of subjects had Agatston scores of 100 or more, indicating the need for treatment to prevent active coronary artery disease, Dr. Han said.
Fifteen percent were at high risk for heart disease with scores of 400-999, indicating extensive coronary artery calcification, and 16.2% were at very high risk, with scores of 1000 or higher. The information is being shared with participants’ physicians.
The risk of heart disease was far higher in men, who made up 56% of the study population. While women had a median Agatston score of 61, the median score for men was 211.1.
The findings illustrate the potential of dedicated cardiovascular screening within lung cancer screening programs, Dr. Han said, noting that 4ITLR will also incorporate COPD risk assessment.
The study also shows the increased impact lung cancer screening programs could have if greater use were made of the CT images to look for other diseases, Dr. Spasic said.
4ITLR is funded by the European Union’s Horizon 2020 Program. Dr. Spasic and Dr. Han didn’t have any relevant disclosures.
FROM ELCC 2024
Is Melatonin a Valuable Resource or Children’s Health Risk?
For Courtney Stinson, ensuring her daughter’s comfort is a constant battle against the challenges of congenital myopathy. At 9 years old, she relies on a ventilator to breathe, has multiple respiratory treatments daily, and is under the constant care of rotating skilled caregivers. Last year alone, she endured 36 doctor appointments.
To ease her daughter’s struggles with sleep, and after consulting a pediatrician, Ms. Stinson turned to melatonin, a hormone naturally produced by the body to manage sleep. She gave her daughter a low dose of melatonin and saw significant improvement in her ability to settle down, especially when her mind raced.
“She would have such a hard time sleeping when everything is swirling in her head,” said Ms. Stinson, a mother of two who lives in Milan, Michigan. “It’s really been helpful when her brain is moving 100 miles an hour.”
Melatonin is sold without a prescription as a sleep aid in the form of a supplement.
Recent data from the CDC illustrates one of these drawbacks: a significant surge in accidental melatonin ingestion among young children over the past 2 decades.
Between 2012 and 2021, poison center calls related to pediatric melatonin exposures skyrocketed by 530%, while emergency department visits for unsupervised melatonin ingestion by infants and young children surged by 420% from 2009 to 2020, according to the CDC report.
Between 2019 and 2022, an estimated 10,930 emergency room visits were linked to 295 cases of children under the age of 6 ingesting melatonin. These incidents accounted for 7.1% of all emergency department visits for medication exposures in this age group, according to the report.
The share of U.S. adults using melatonin increased from 0.4% during 1999 to 2000 to 2.1% during 2017 to 2018.
Doctors say the escalating number of melatonin-related incidents underscores the need for increased awareness and safety measures to protect young children from unintentional overdose, which can cause nausea, vomiting, diarrhea, dizziness, and confusion.
“I do think there is a safe way to use it in certain children, but it should only be used under the guidance of a physician,” said Laura Sterni, MD, director of the Johns Hopkins Pediatric Sleep Center. “There are dangers to using it without that guidance.”
Almost 1 in 5 Children Use Melatonin
Nearly 1 in 5 school-age children and preteens take melatonin for sleep, according to research published last year in JAMA Pediatrics, which also found that 18% of children between 5 and 9 take the supplement.
The American Academy of Sleep Medicine issued a warning in 2022 advising parents to approach the sleep aid with caution.
“While melatonin can be useful in treating certain sleep-wake disorders, like jet lag, there is much less evidence it can help healthy children or adults fall asleep faster,” M. Adeel Rishi, MD, vice chair of the Academy of Sleep Medicine’s Public Safety Committee, warned on the academy’s site. “Instead of turning to melatonin, parents should work on encouraging their children to develop good sleep habits, like setting a regular bedtime and wake time, having a bedtime routine, and limiting screen time as bedtime approaches.”
What’s the Best Way to Give Kids Melatonin?
Melatonin has been found to work well for children with attention deficit hyperactive disorder (ADHD), autism spectrum disorder, or other conditions like blindness that can hinder the development of a normal circadian rhythm.
But beyond consulting a pediatrician, caregivers whose children are otherwise healthy should consider trying other approaches to sleep disruption first, Dr. Sterni said, and things like proper sleep hygiene and anxiety should be addressed first.
“Most sleep problems in children really should be managed with behavioral therapy alone,” she said. “To first pull out a medication to treat that I think is the wrong approach.”
Sterni also recommends starting with the lowest dose possible, which is 0.5 milligrams, with the help of pediatrician. It should be taken 1 to 2 hours before bedtime and 2 hours after their last meal, she said.
But she notes that because melatonin is sold as a supplement and is not regulated by the FDA, it is impossible to know the exact amount in each dose.
According to JAMA, out of 25 supplements of melatonin, most of the products contained up to 50% more melatonin than what was listed.
Dangers of Keeping It Within Reach
One of the biggest dangers for children is that melatonin is often sold in the form of gummies or chewable tablets — things that appeal to children, said Jenna Wheeler, MD, a pediatric critical care doctor at Orlando Health Arnold Palmer Hospital for Children.
Because it is sold as a supplement, there are no child-safe packaging requirements.
“From a critical care standpoint, just remember to keep it up high, not on the nightstand or in a drawer,” Dr. Wheeler said. “A child may eat the whole bottle, thinking, ‘This is just like fruits snacks.’ ”
She noted that the amount people need is often lower than what they buy at the store, and that regardless of whether it is used in proper amounts, it is not meant to be a long-term supplement — for adults or for children.
“Like with anything that’s out there, it’s all about how it’s used,” Dr. Wheeler said. “The problem is when kids get into it accidentally or when it’s not used appropriately.”
A version of this article appeared on WebMD.com.
For Courtney Stinson, ensuring her daughter’s comfort is a constant battle against the challenges of congenital myopathy. At 9 years old, she relies on a ventilator to breathe, has multiple respiratory treatments daily, and is under the constant care of rotating skilled caregivers. Last year alone, she endured 36 doctor appointments.
To ease her daughter’s struggles with sleep, and after consulting a pediatrician, Ms. Stinson turned to melatonin, a hormone naturally produced by the body to manage sleep. She gave her daughter a low dose of melatonin and saw significant improvement in her ability to settle down, especially when her mind raced.
“She would have such a hard time sleeping when everything is swirling in her head,” said Ms. Stinson, a mother of two who lives in Milan, Michigan. “It’s really been helpful when her brain is moving 100 miles an hour.”
Melatonin is sold without a prescription as a sleep aid in the form of a supplement.
Recent data from the CDC illustrates one of these drawbacks: a significant surge in accidental melatonin ingestion among young children over the past 2 decades.
Between 2012 and 2021, poison center calls related to pediatric melatonin exposures skyrocketed by 530%, while emergency department visits for unsupervised melatonin ingestion by infants and young children surged by 420% from 2009 to 2020, according to the CDC report.
Between 2019 and 2022, an estimated 10,930 emergency room visits were linked to 295 cases of children under the age of 6 ingesting melatonin. These incidents accounted for 7.1% of all emergency department visits for medication exposures in this age group, according to the report.
The share of U.S. adults using melatonin increased from 0.4% during 1999 to 2000 to 2.1% during 2017 to 2018.
Doctors say the escalating number of melatonin-related incidents underscores the need for increased awareness and safety measures to protect young children from unintentional overdose, which can cause nausea, vomiting, diarrhea, dizziness, and confusion.
“I do think there is a safe way to use it in certain children, but it should only be used under the guidance of a physician,” said Laura Sterni, MD, director of the Johns Hopkins Pediatric Sleep Center. “There are dangers to using it without that guidance.”
Almost 1 in 5 Children Use Melatonin
Nearly 1 in 5 school-age children and preteens take melatonin for sleep, according to research published last year in JAMA Pediatrics, which also found that 18% of children between 5 and 9 take the supplement.
The American Academy of Sleep Medicine issued a warning in 2022 advising parents to approach the sleep aid with caution.
“While melatonin can be useful in treating certain sleep-wake disorders, like jet lag, there is much less evidence it can help healthy children or adults fall asleep faster,” M. Adeel Rishi, MD, vice chair of the Academy of Sleep Medicine’s Public Safety Committee, warned on the academy’s site. “Instead of turning to melatonin, parents should work on encouraging their children to develop good sleep habits, like setting a regular bedtime and wake time, having a bedtime routine, and limiting screen time as bedtime approaches.”
What’s the Best Way to Give Kids Melatonin?
Melatonin has been found to work well for children with attention deficit hyperactive disorder (ADHD), autism spectrum disorder, or other conditions like blindness that can hinder the development of a normal circadian rhythm.
But beyond consulting a pediatrician, caregivers whose children are otherwise healthy should consider trying other approaches to sleep disruption first, Dr. Sterni said, and things like proper sleep hygiene and anxiety should be addressed first.
“Most sleep problems in children really should be managed with behavioral therapy alone,” she said. “To first pull out a medication to treat that I think is the wrong approach.”
Sterni also recommends starting with the lowest dose possible, which is 0.5 milligrams, with the help of pediatrician. It should be taken 1 to 2 hours before bedtime and 2 hours after their last meal, she said.
But she notes that because melatonin is sold as a supplement and is not regulated by the FDA, it is impossible to know the exact amount in each dose.
According to JAMA, out of 25 supplements of melatonin, most of the products contained up to 50% more melatonin than what was listed.
Dangers of Keeping It Within Reach
One of the biggest dangers for children is that melatonin is often sold in the form of gummies or chewable tablets — things that appeal to children, said Jenna Wheeler, MD, a pediatric critical care doctor at Orlando Health Arnold Palmer Hospital for Children.
Because it is sold as a supplement, there are no child-safe packaging requirements.
“From a critical care standpoint, just remember to keep it up high, not on the nightstand or in a drawer,” Dr. Wheeler said. “A child may eat the whole bottle, thinking, ‘This is just like fruits snacks.’ ”
She noted that the amount people need is often lower than what they buy at the store, and that regardless of whether it is used in proper amounts, it is not meant to be a long-term supplement — for adults or for children.
“Like with anything that’s out there, it’s all about how it’s used,” Dr. Wheeler said. “The problem is when kids get into it accidentally or when it’s not used appropriately.”
A version of this article appeared on WebMD.com.
For Courtney Stinson, ensuring her daughter’s comfort is a constant battle against the challenges of congenital myopathy. At 9 years old, she relies on a ventilator to breathe, has multiple respiratory treatments daily, and is under the constant care of rotating skilled caregivers. Last year alone, she endured 36 doctor appointments.
To ease her daughter’s struggles with sleep, and after consulting a pediatrician, Ms. Stinson turned to melatonin, a hormone naturally produced by the body to manage sleep. She gave her daughter a low dose of melatonin and saw significant improvement in her ability to settle down, especially when her mind raced.
“She would have such a hard time sleeping when everything is swirling in her head,” said Ms. Stinson, a mother of two who lives in Milan, Michigan. “It’s really been helpful when her brain is moving 100 miles an hour.”
Melatonin is sold without a prescription as a sleep aid in the form of a supplement.
Recent data from the CDC illustrates one of these drawbacks: a significant surge in accidental melatonin ingestion among young children over the past 2 decades.
Between 2012 and 2021, poison center calls related to pediatric melatonin exposures skyrocketed by 530%, while emergency department visits for unsupervised melatonin ingestion by infants and young children surged by 420% from 2009 to 2020, according to the CDC report.
Between 2019 and 2022, an estimated 10,930 emergency room visits were linked to 295 cases of children under the age of 6 ingesting melatonin. These incidents accounted for 7.1% of all emergency department visits for medication exposures in this age group, according to the report.
The share of U.S. adults using melatonin increased from 0.4% during 1999 to 2000 to 2.1% during 2017 to 2018.
Doctors say the escalating number of melatonin-related incidents underscores the need for increased awareness and safety measures to protect young children from unintentional overdose, which can cause nausea, vomiting, diarrhea, dizziness, and confusion.
“I do think there is a safe way to use it in certain children, but it should only be used under the guidance of a physician,” said Laura Sterni, MD, director of the Johns Hopkins Pediatric Sleep Center. “There are dangers to using it without that guidance.”
Almost 1 in 5 Children Use Melatonin
Nearly 1 in 5 school-age children and preteens take melatonin for sleep, according to research published last year in JAMA Pediatrics, which also found that 18% of children between 5 and 9 take the supplement.
The American Academy of Sleep Medicine issued a warning in 2022 advising parents to approach the sleep aid with caution.
“While melatonin can be useful in treating certain sleep-wake disorders, like jet lag, there is much less evidence it can help healthy children or adults fall asleep faster,” M. Adeel Rishi, MD, vice chair of the Academy of Sleep Medicine’s Public Safety Committee, warned on the academy’s site. “Instead of turning to melatonin, parents should work on encouraging their children to develop good sleep habits, like setting a regular bedtime and wake time, having a bedtime routine, and limiting screen time as bedtime approaches.”
What’s the Best Way to Give Kids Melatonin?
Melatonin has been found to work well for children with attention deficit hyperactive disorder (ADHD), autism spectrum disorder, or other conditions like blindness that can hinder the development of a normal circadian rhythm.
But beyond consulting a pediatrician, caregivers whose children are otherwise healthy should consider trying other approaches to sleep disruption first, Dr. Sterni said, and things like proper sleep hygiene and anxiety should be addressed first.
“Most sleep problems in children really should be managed with behavioral therapy alone,” she said. “To first pull out a medication to treat that I think is the wrong approach.”
Sterni also recommends starting with the lowest dose possible, which is 0.5 milligrams, with the help of pediatrician. It should be taken 1 to 2 hours before bedtime and 2 hours after their last meal, she said.
But she notes that because melatonin is sold as a supplement and is not regulated by the FDA, it is impossible to know the exact amount in each dose.
According to JAMA, out of 25 supplements of melatonin, most of the products contained up to 50% more melatonin than what was listed.
Dangers of Keeping It Within Reach
One of the biggest dangers for children is that melatonin is often sold in the form of gummies or chewable tablets — things that appeal to children, said Jenna Wheeler, MD, a pediatric critical care doctor at Orlando Health Arnold Palmer Hospital for Children.
Because it is sold as a supplement, there are no child-safe packaging requirements.
“From a critical care standpoint, just remember to keep it up high, not on the nightstand or in a drawer,” Dr. Wheeler said. “A child may eat the whole bottle, thinking, ‘This is just like fruits snacks.’ ”
She noted that the amount people need is often lower than what they buy at the store, and that regardless of whether it is used in proper amounts, it is not meant to be a long-term supplement — for adults or for children.
“Like with anything that’s out there, it’s all about how it’s used,” Dr. Wheeler said. “The problem is when kids get into it accidentally or when it’s not used appropriately.”
A version of this article appeared on WebMD.com.
Systematic Viral Testing in Emergency Departments Has Limited Benefit for General Population
Routine use of rapid respiratory virus testing in the emergency department (ED) appears to show limited benefit among patients with signs and symptoms of acute respiratory infection (ARI), according to a new study.
Rapid viral testing wasn’t associated with reduced antibiotic use, ED length of stay, or rates of ED return visits or hospitalization. However, testing was associated with a small increase in antiviral prescriptions and a small reduction in blood tests and chest x-rays.
“Our interest in studying the benefits of rapid viral testing in emergency departments comes from a commitment to diagnostic stewardship — ensuring that the right tests are administered to the right patients at the right time while also curbing overuse,” said lead author Tilmann Schober, MD, a resident in pediatric infectious disease at McGill University and Montreal Children’s Hospital.
“Following the SARS-CoV-2 pandemic, we have seen a surge in the availability of rapid viral testing, including molecular multiplex panels,” he said. “However, the actual impact of these advancements on patient care in the ED remains uncertain.”
The study was published online on March 4, 2024, in JAMA Internal Medicine).
Rapid Viral Testing
Dr. Schober and colleagues conducted a systematic review and meta-analysis of 11 randomized clinical trials to understand whether rapid testing for respiratory viruses was associated with patient treatment in the ED.
In particular, the research team looked at whether testing in patients with suspected ARI was associated with decreased antibiotic use, ancillary tests, ED length of stay, ED return visits, hospitalization, and increased influenza antiviral treatment.
Among the trials, seven studies included molecular testing, and eight used multiplex panels, including influenza and respiratory syncytial virus (RSV), influenza/RSV/adenovirus/parainfluenza, or a panel of 15 or more respiratory viruses. No study evaluated testing for SARS-CoV-2. The research team reported risk ratios (RRs) and risk difference estimates.
In general, routine rapid viral testing was associated with higher use of influenza antivirals (RR, 1.33) and lower use of chest radiography (RR, 0.88) and blood tests (RR, 0.81). However, the magnitude of these effects was small. For instance, to achieve one additional viral prescription, 70 patients would need to be tested, and to save one x-ray, 30 patients would need to be tested.
“This suggests that, while statistically significant, the practical impact of these secondary outcomes may not justify the extensive effort and resources involved in widespread testing,” Dr. Schober said.
In addition, there was no association between rapid testing and antibiotic use (RR, 0.99), urine testing (RR, 0.95), ED length of stay (0 h), return visits (RR, 0.93), or hospitalization (RR, 1.01).
Notably, there was no association between rapid viral testing and antibiotic use in any prespecified subgroup based on age, test method, publication date, number of viral targets, risk of bias, or industry funding, the authors said. They concluded that rapid virus testing should be reserved for patients for whom the testing will change treatment, such as high-risk patients or those with severe disease.
“It’s crucial to note that our study specifically evaluated the impact of systematic testing of patients with signs and symptoms of acute respiratory infection. Our findings do not advocate against rapid respiratory virus testing in general,” Dr. Schober said. “There is well-established evidence supporting the benefits of viral testing in certain contexts, such as hospitalized patients, to guide infection control practices or in specific high-risk populations.”
Future Research
Additional studies should look at testing among subgroups, particularly those with high-risk conditions, the study authors wrote. In addition, the research team would like to study the implementation of novel diagnostic stewardship programs as compared with well-established antibiotic stewardship programs.
“Acute respiratory tract illnesses represent one of the most common reasons for being evaluated in an acute care setting, especially in pediatrics, and these visits have traditionally resulted in excessive antibiotic prescribing, despite the etiology of the infection mostly being viral,” said Suchitra Rao, MBBS, associate professor of pediatrics at the University of Colorado School of Medicine and associate medical director of infection prevention and control at Children’s Hospital Colorado, Aurora.
Dr. Rao, who wasn’t involved with this study, has surveyed ED providers about respiratory viral testing and changes in clinical decision-making. She and colleagues found that providers most commonly changed clinical decision-making while prescribing an antiviral if influenza was detected or withholding antivirals if influenza wasn’t detected.
“Multiplex testing for respiratory viruses and atypical bacteria is becoming more widespread, with newer-generation platforms having shorter turnaround times, and offers the potential to impact point-of-care decision-making,” she said. “However, these tests are expensive, and more studies are needed to explore whether respiratory pathogen panel testing in the acute care setting has an impact in terms of reduced antibiotic use as well as other outcomes, including ED visits, health-seeking behaviors, and hospitalization.”
For instance, more recent studies around SARS-CoV-2 with newer-generation panels may make a difference, as well as multiplex panels that include numerous viral targets, she said.
“Further RCTs are required to evaluate the impact of influenza/RSV/SARS-CoV-2 panels, as well as respiratory pathogen panel testing in conjunction with antimicrobial and diagnostic stewardship efforts, which have been associated with improved outcomes for other rapid molecular platforms, such as blood culture identification panels,” Rao said.
The study was funded by the Research Institute of the McGill University Health Center. Dr. Schober reported no disclosures, and several study authors reported grants or personal fees from companies outside of this research. Dr. Rao disclosed no relevant relationships.
A version of this article appeared on Medscape.com .
Routine use of rapid respiratory virus testing in the emergency department (ED) appears to show limited benefit among patients with signs and symptoms of acute respiratory infection (ARI), according to a new study.
Rapid viral testing wasn’t associated with reduced antibiotic use, ED length of stay, or rates of ED return visits or hospitalization. However, testing was associated with a small increase in antiviral prescriptions and a small reduction in blood tests and chest x-rays.
“Our interest in studying the benefits of rapid viral testing in emergency departments comes from a commitment to diagnostic stewardship — ensuring that the right tests are administered to the right patients at the right time while also curbing overuse,” said lead author Tilmann Schober, MD, a resident in pediatric infectious disease at McGill University and Montreal Children’s Hospital.
“Following the SARS-CoV-2 pandemic, we have seen a surge in the availability of rapid viral testing, including molecular multiplex panels,” he said. “However, the actual impact of these advancements on patient care in the ED remains uncertain.”
The study was published online on March 4, 2024, in JAMA Internal Medicine).
Rapid Viral Testing
Dr. Schober and colleagues conducted a systematic review and meta-analysis of 11 randomized clinical trials to understand whether rapid testing for respiratory viruses was associated with patient treatment in the ED.
In particular, the research team looked at whether testing in patients with suspected ARI was associated with decreased antibiotic use, ancillary tests, ED length of stay, ED return visits, hospitalization, and increased influenza antiviral treatment.
Among the trials, seven studies included molecular testing, and eight used multiplex panels, including influenza and respiratory syncytial virus (RSV), influenza/RSV/adenovirus/parainfluenza, or a panel of 15 or more respiratory viruses. No study evaluated testing for SARS-CoV-2. The research team reported risk ratios (RRs) and risk difference estimates.
In general, routine rapid viral testing was associated with higher use of influenza antivirals (RR, 1.33) and lower use of chest radiography (RR, 0.88) and blood tests (RR, 0.81). However, the magnitude of these effects was small. For instance, to achieve one additional viral prescription, 70 patients would need to be tested, and to save one x-ray, 30 patients would need to be tested.
“This suggests that, while statistically significant, the practical impact of these secondary outcomes may not justify the extensive effort and resources involved in widespread testing,” Dr. Schober said.
In addition, there was no association between rapid testing and antibiotic use (RR, 0.99), urine testing (RR, 0.95), ED length of stay (0 h), return visits (RR, 0.93), or hospitalization (RR, 1.01).
Notably, there was no association between rapid viral testing and antibiotic use in any prespecified subgroup based on age, test method, publication date, number of viral targets, risk of bias, or industry funding, the authors said. They concluded that rapid virus testing should be reserved for patients for whom the testing will change treatment, such as high-risk patients or those with severe disease.
“It’s crucial to note that our study specifically evaluated the impact of systematic testing of patients with signs and symptoms of acute respiratory infection. Our findings do not advocate against rapid respiratory virus testing in general,” Dr. Schober said. “There is well-established evidence supporting the benefits of viral testing in certain contexts, such as hospitalized patients, to guide infection control practices or in specific high-risk populations.”
Future Research
Additional studies should look at testing among subgroups, particularly those with high-risk conditions, the study authors wrote. In addition, the research team would like to study the implementation of novel diagnostic stewardship programs as compared with well-established antibiotic stewardship programs.
“Acute respiratory tract illnesses represent one of the most common reasons for being evaluated in an acute care setting, especially in pediatrics, and these visits have traditionally resulted in excessive antibiotic prescribing, despite the etiology of the infection mostly being viral,” said Suchitra Rao, MBBS, associate professor of pediatrics at the University of Colorado School of Medicine and associate medical director of infection prevention and control at Children’s Hospital Colorado, Aurora.
Dr. Rao, who wasn’t involved with this study, has surveyed ED providers about respiratory viral testing and changes in clinical decision-making. She and colleagues found that providers most commonly changed clinical decision-making while prescribing an antiviral if influenza was detected or withholding antivirals if influenza wasn’t detected.
“Multiplex testing for respiratory viruses and atypical bacteria is becoming more widespread, with newer-generation platforms having shorter turnaround times, and offers the potential to impact point-of-care decision-making,” she said. “However, these tests are expensive, and more studies are needed to explore whether respiratory pathogen panel testing in the acute care setting has an impact in terms of reduced antibiotic use as well as other outcomes, including ED visits, health-seeking behaviors, and hospitalization.”
For instance, more recent studies around SARS-CoV-2 with newer-generation panels may make a difference, as well as multiplex panels that include numerous viral targets, she said.
“Further RCTs are required to evaluate the impact of influenza/RSV/SARS-CoV-2 panels, as well as respiratory pathogen panel testing in conjunction with antimicrobial and diagnostic stewardship efforts, which have been associated with improved outcomes for other rapid molecular platforms, such as blood culture identification panels,” Rao said.
The study was funded by the Research Institute of the McGill University Health Center. Dr. Schober reported no disclosures, and several study authors reported grants or personal fees from companies outside of this research. Dr. Rao disclosed no relevant relationships.
A version of this article appeared on Medscape.com .
Routine use of rapid respiratory virus testing in the emergency department (ED) appears to show limited benefit among patients with signs and symptoms of acute respiratory infection (ARI), according to a new study.
Rapid viral testing wasn’t associated with reduced antibiotic use, ED length of stay, or rates of ED return visits or hospitalization. However, testing was associated with a small increase in antiviral prescriptions and a small reduction in blood tests and chest x-rays.
“Our interest in studying the benefits of rapid viral testing in emergency departments comes from a commitment to diagnostic stewardship — ensuring that the right tests are administered to the right patients at the right time while also curbing overuse,” said lead author Tilmann Schober, MD, a resident in pediatric infectious disease at McGill University and Montreal Children’s Hospital.
“Following the SARS-CoV-2 pandemic, we have seen a surge in the availability of rapid viral testing, including molecular multiplex panels,” he said. “However, the actual impact of these advancements on patient care in the ED remains uncertain.”
The study was published online on March 4, 2024, in JAMA Internal Medicine).
Rapid Viral Testing
Dr. Schober and colleagues conducted a systematic review and meta-analysis of 11 randomized clinical trials to understand whether rapid testing for respiratory viruses was associated with patient treatment in the ED.
In particular, the research team looked at whether testing in patients with suspected ARI was associated with decreased antibiotic use, ancillary tests, ED length of stay, ED return visits, hospitalization, and increased influenza antiviral treatment.
Among the trials, seven studies included molecular testing, and eight used multiplex panels, including influenza and respiratory syncytial virus (RSV), influenza/RSV/adenovirus/parainfluenza, or a panel of 15 or more respiratory viruses. No study evaluated testing for SARS-CoV-2. The research team reported risk ratios (RRs) and risk difference estimates.
In general, routine rapid viral testing was associated with higher use of influenza antivirals (RR, 1.33) and lower use of chest radiography (RR, 0.88) and blood tests (RR, 0.81). However, the magnitude of these effects was small. For instance, to achieve one additional viral prescription, 70 patients would need to be tested, and to save one x-ray, 30 patients would need to be tested.
“This suggests that, while statistically significant, the practical impact of these secondary outcomes may not justify the extensive effort and resources involved in widespread testing,” Dr. Schober said.
In addition, there was no association between rapid testing and antibiotic use (RR, 0.99), urine testing (RR, 0.95), ED length of stay (0 h), return visits (RR, 0.93), or hospitalization (RR, 1.01).
Notably, there was no association between rapid viral testing and antibiotic use in any prespecified subgroup based on age, test method, publication date, number of viral targets, risk of bias, or industry funding, the authors said. They concluded that rapid virus testing should be reserved for patients for whom the testing will change treatment, such as high-risk patients or those with severe disease.
“It’s crucial to note that our study specifically evaluated the impact of systematic testing of patients with signs and symptoms of acute respiratory infection. Our findings do not advocate against rapid respiratory virus testing in general,” Dr. Schober said. “There is well-established evidence supporting the benefits of viral testing in certain contexts, such as hospitalized patients, to guide infection control practices or in specific high-risk populations.”
Future Research
Additional studies should look at testing among subgroups, particularly those with high-risk conditions, the study authors wrote. In addition, the research team would like to study the implementation of novel diagnostic stewardship programs as compared with well-established antibiotic stewardship programs.
“Acute respiratory tract illnesses represent one of the most common reasons for being evaluated in an acute care setting, especially in pediatrics, and these visits have traditionally resulted in excessive antibiotic prescribing, despite the etiology of the infection mostly being viral,” said Suchitra Rao, MBBS, associate professor of pediatrics at the University of Colorado School of Medicine and associate medical director of infection prevention and control at Children’s Hospital Colorado, Aurora.
Dr. Rao, who wasn’t involved with this study, has surveyed ED providers about respiratory viral testing and changes in clinical decision-making. She and colleagues found that providers most commonly changed clinical decision-making while prescribing an antiviral if influenza was detected or withholding antivirals if influenza wasn’t detected.
“Multiplex testing for respiratory viruses and atypical bacteria is becoming more widespread, with newer-generation platforms having shorter turnaround times, and offers the potential to impact point-of-care decision-making,” she said. “However, these tests are expensive, and more studies are needed to explore whether respiratory pathogen panel testing in the acute care setting has an impact in terms of reduced antibiotic use as well as other outcomes, including ED visits, health-seeking behaviors, and hospitalization.”
For instance, more recent studies around SARS-CoV-2 with newer-generation panels may make a difference, as well as multiplex panels that include numerous viral targets, she said.
“Further RCTs are required to evaluate the impact of influenza/RSV/SARS-CoV-2 panels, as well as respiratory pathogen panel testing in conjunction with antimicrobial and diagnostic stewardship efforts, which have been associated with improved outcomes for other rapid molecular platforms, such as blood culture identification panels,” Rao said.
The study was funded by the Research Institute of the McGill University Health Center. Dr. Schober reported no disclosures, and several study authors reported grants or personal fees from companies outside of this research. Dr. Rao disclosed no relevant relationships.
A version of this article appeared on Medscape.com .
New Infant RSV Antibody Treatment Shows Strong Results
The new RSV antibody treatment for babies has been highly effective in its first season, according to a first look at data from four children’s hospitals.
Babies who received the new preventive treatment for RSV shortly after birth were 90% less likely to be severely sickened with the potentially deadly respiratory illness, according to the new estimate published by the Centers for Disease Control and Prevention. It is the first real-world evaluation of Beyfortus (the generic name is nirsevimab), which was approved by the Food and Drug Administration last July.
RSV is a seasonal illness that affects more people — particularly infants and the elderly — in the fall and winter. Symptoms are usually mild in healthy adults, but infants are particularly at risk of getting bronchiolitis, which results in exhausting wheezing and coughing in babies due to swelling in their airways and lungs. Babies who are hospitalized may need fluids and medical devices to help them breathe.
RSV peaked this season from November to January, with more than 10,000 monthly diagnoses reported to the CDC.
The new CDC analysis was conducted among about 700 babies hospitalized for severe respiratory problems from October to the end of February. Among the babies in the study, 407 were diagnosed with RSV and 292 tested negative. The researchers found that 1% of babies in the study who were diagnosed with RSV had received Beyfortus, while the remaining babies who were positive for the virus had not.
Among the babies hospitalized for other severe respiratory problems, 18% had received Beyfortus. Overall, just 59 babies among the nearly 700 in the study received Beyfortus, perhaps reflecting the short supply of the medicine the first season it was available. The report authors noted that babies in the study who did receive Beyfortus also tended to have high-risk medical conditions.
The number of babies nationwide who received Beyfortus during this first season of availability is unclear, but a January CDC survey showed that 4 in 10 parents said their babies under 8 months old had received the treatment. The Wall Street Journal reported recently that a shortage last fall resulted from underestimated demand and from production plans that were set before the CDC decided to recommend that all infants under 8 months old receive Beyfortus if their mothers did not get a maternal vaccine that can protect infants from RSV.
Both the antibody treatment for infants and the maternal vaccine were shown in clinical trials to be about 80% effective at preventing severe illness stemming from RSV.
The authors of the latest CDC report concluded that “this early estimate supports the current nirsevimab recommendation for the prevention of severe RSV disease in infants. Infants should be protected by maternal RSV vaccination or infant receipt of nirsevimab.”
A version of this article appeared on WebMD.com.
The new RSV antibody treatment for babies has been highly effective in its first season, according to a first look at data from four children’s hospitals.
Babies who received the new preventive treatment for RSV shortly after birth were 90% less likely to be severely sickened with the potentially deadly respiratory illness, according to the new estimate published by the Centers for Disease Control and Prevention. It is the first real-world evaluation of Beyfortus (the generic name is nirsevimab), which was approved by the Food and Drug Administration last July.
RSV is a seasonal illness that affects more people — particularly infants and the elderly — in the fall and winter. Symptoms are usually mild in healthy adults, but infants are particularly at risk of getting bronchiolitis, which results in exhausting wheezing and coughing in babies due to swelling in their airways and lungs. Babies who are hospitalized may need fluids and medical devices to help them breathe.
RSV peaked this season from November to January, with more than 10,000 monthly diagnoses reported to the CDC.
The new CDC analysis was conducted among about 700 babies hospitalized for severe respiratory problems from October to the end of February. Among the babies in the study, 407 were diagnosed with RSV and 292 tested negative. The researchers found that 1% of babies in the study who were diagnosed with RSV had received Beyfortus, while the remaining babies who were positive for the virus had not.
Among the babies hospitalized for other severe respiratory problems, 18% had received Beyfortus. Overall, just 59 babies among the nearly 700 in the study received Beyfortus, perhaps reflecting the short supply of the medicine the first season it was available. The report authors noted that babies in the study who did receive Beyfortus also tended to have high-risk medical conditions.
The number of babies nationwide who received Beyfortus during this first season of availability is unclear, but a January CDC survey showed that 4 in 10 parents said their babies under 8 months old had received the treatment. The Wall Street Journal reported recently that a shortage last fall resulted from underestimated demand and from production plans that were set before the CDC decided to recommend that all infants under 8 months old receive Beyfortus if their mothers did not get a maternal vaccine that can protect infants from RSV.
Both the antibody treatment for infants and the maternal vaccine were shown in clinical trials to be about 80% effective at preventing severe illness stemming from RSV.
The authors of the latest CDC report concluded that “this early estimate supports the current nirsevimab recommendation for the prevention of severe RSV disease in infants. Infants should be protected by maternal RSV vaccination or infant receipt of nirsevimab.”
A version of this article appeared on WebMD.com.
The new RSV antibody treatment for babies has been highly effective in its first season, according to a first look at data from four children’s hospitals.
Babies who received the new preventive treatment for RSV shortly after birth were 90% less likely to be severely sickened with the potentially deadly respiratory illness, according to the new estimate published by the Centers for Disease Control and Prevention. It is the first real-world evaluation of Beyfortus (the generic name is nirsevimab), which was approved by the Food and Drug Administration last July.
RSV is a seasonal illness that affects more people — particularly infants and the elderly — in the fall and winter. Symptoms are usually mild in healthy adults, but infants are particularly at risk of getting bronchiolitis, which results in exhausting wheezing and coughing in babies due to swelling in their airways and lungs. Babies who are hospitalized may need fluids and medical devices to help them breathe.
RSV peaked this season from November to January, with more than 10,000 monthly diagnoses reported to the CDC.
The new CDC analysis was conducted among about 700 babies hospitalized for severe respiratory problems from October to the end of February. Among the babies in the study, 407 were diagnosed with RSV and 292 tested negative. The researchers found that 1% of babies in the study who were diagnosed with RSV had received Beyfortus, while the remaining babies who were positive for the virus had not.
Among the babies hospitalized for other severe respiratory problems, 18% had received Beyfortus. Overall, just 59 babies among the nearly 700 in the study received Beyfortus, perhaps reflecting the short supply of the medicine the first season it was available. The report authors noted that babies in the study who did receive Beyfortus also tended to have high-risk medical conditions.
The number of babies nationwide who received Beyfortus during this first season of availability is unclear, but a January CDC survey showed that 4 in 10 parents said their babies under 8 months old had received the treatment. The Wall Street Journal reported recently that a shortage last fall resulted from underestimated demand and from production plans that were set before the CDC decided to recommend that all infants under 8 months old receive Beyfortus if their mothers did not get a maternal vaccine that can protect infants from RSV.
Both the antibody treatment for infants and the maternal vaccine were shown in clinical trials to be about 80% effective at preventing severe illness stemming from RSV.
The authors of the latest CDC report concluded that “this early estimate supports the current nirsevimab recommendation for the prevention of severe RSV disease in infants. Infants should be protected by maternal RSV vaccination or infant receipt of nirsevimab.”
A version of this article appeared on WebMD.com.
Smoking Cessation Before Age 40 Years Brings Great Benefits
Chronic smoking remains a major cause of premature mortality on a global scale. Despite intensified efforts to combat this scourge, a quarter of deaths among middle-aged adults in Europe and North America are attributed to it. However, over the past decades, antismoking campaigns have borne fruit, and many smokers have quit before the age of 40 years, enabling some case-control studies.
Among those abstainers who made the right choice, the excess mortality attributable to smoking over a lifetime would be reduced by 90% compared with controls who continued smoking. The estimated benefit is clear, but the analysis lacks nuance. Is smoking cessation beneficial even at older ages? If so, is the effect measurable in terms of magnitude and speed of the effect? An article published online in The New England Journal of Medicine Evidence provided some answers to these questions.
Four-Cohort Meta-Analysis
The study was a meta-analysis of individual data collected within four national cohort studies that were linked to each country’s death registry. Two of these studies were nationally representative. The National Health Interview Survey involved a sample of US citizens living in the community, aged 20-79 years, who were included annually in the cohort between 1997 and 2018. The second, the Canadian Community Health Survey, included subjects in the same age group, with samples analyzed between 2000 and 2014.
In Norway, three cohort studies conducted between 1974 and 2003, in which participants aged 25-79 years were included, were combined to form the Norwegian Health Screening Survey. These were the Counties Study (1974-1988), the 40 Years Study (1985-1999), and the Cohort of Norway (1994-2003), respectively. The fourth cohort was established through recruitment via the UK Biobank, with adults aged 40-73 years invited to participate in the survey. The data analysis ultimately covered a relatively heterogeneous total population of 1.48 million adults, all from high-income countries and followed for 15 years. It relied on the Cox proportional hazards model applied to each study, considering smoker vs nonsmoker status, as well as the time elapsed since smoking cessation (less than 3 years, between 3 and 9 years, or at least 10 years). Statistical adjustments made in the context of multivariate Cox analysis considered age, education, alcohol consumption, and obesity.
Excess Mortality Confirmed
At the end of follow-up, 122,697 deaths were recorded. The comparison of smokers and nonsmokers confirmed smoking-related excess mortality, with adjusted hazard ratios (HRs) estimated at 2.80 for women and 2.70 for men. Smoking shortened life expectancy in the 40- to 79-year-age group by 12 years for women and 13 years for men, in terms of overall mortality. In terms of smoking-attributable specific mortality, the corresponding figures reached 24 and 26 years, respectively. Respiratory diseases ranked highest in both sexes (HR, 7.6 for women and 6.3 for men), followed by cardiovascular diseases (HR, 3.1 for women and 2.9 for men) and cancers (HR, 2.8 for women and 3.1 for men).
The Earlier, the Better
Smoking cessation halves overall excess mortality. Above all, quitting before age 40 years brings overall mortality back to the level of nonsmokers as early as the third year after quitting. The excess mortality decreases even more as the cessation period is prolonged, even after age 40 years. Thus, cessation ≥ 10 years in smokers aged 40-49 years almost cancels out overall excess mortality (-99% in women, -96% in men). The trend is almost as favorable in the older age group (50-59 years), with corresponding figures of -95% and -92%, respectively.
Long-term survival increases in the early years after cessation, especially if it occurs at a younger age, but the benefit remains tangible even in older smokers. Thus, cessation of less than 3 years, effective in patients aged 50-59 years, reduces overall excess mortality by 63% in women and 54% in men. In patients aged 60-79 years, the figures are -40% and -33%, respectively.
Naturally, the earlier the cessation, the greater the number of years gained. It is 12 years for cessation before age 40 years, reduced to 6 years for cessation between 40 and 49 years, and 2.5 years when it is even later (50-59 years). These quantitative results are approximate, given the methodology (a meta-analysis) and some heterogeneity in the studies, as well as the multitude of potential confounding factors that have not all been considered. Nevertheless, the results probably contain a kernel of truth, and their optimistic implications should be highlighted to encourage smokers to abstain, even older ones. Better late than never, even if the benefit of cessation is maximal when it occurs as early as possible, knowing that a minimum of 3 years of cessation would be sufficient to gain years of life.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Chronic smoking remains a major cause of premature mortality on a global scale. Despite intensified efforts to combat this scourge, a quarter of deaths among middle-aged adults in Europe and North America are attributed to it. However, over the past decades, antismoking campaigns have borne fruit, and many smokers have quit before the age of 40 years, enabling some case-control studies.
Among those abstainers who made the right choice, the excess mortality attributable to smoking over a lifetime would be reduced by 90% compared with controls who continued smoking. The estimated benefit is clear, but the analysis lacks nuance. Is smoking cessation beneficial even at older ages? If so, is the effect measurable in terms of magnitude and speed of the effect? An article published online in The New England Journal of Medicine Evidence provided some answers to these questions.
Four-Cohort Meta-Analysis
The study was a meta-analysis of individual data collected within four national cohort studies that were linked to each country’s death registry. Two of these studies were nationally representative. The National Health Interview Survey involved a sample of US citizens living in the community, aged 20-79 years, who were included annually in the cohort between 1997 and 2018. The second, the Canadian Community Health Survey, included subjects in the same age group, with samples analyzed between 2000 and 2014.
In Norway, three cohort studies conducted between 1974 and 2003, in which participants aged 25-79 years were included, were combined to form the Norwegian Health Screening Survey. These were the Counties Study (1974-1988), the 40 Years Study (1985-1999), and the Cohort of Norway (1994-2003), respectively. The fourth cohort was established through recruitment via the UK Biobank, with adults aged 40-73 years invited to participate in the survey. The data analysis ultimately covered a relatively heterogeneous total population of 1.48 million adults, all from high-income countries and followed for 15 years. It relied on the Cox proportional hazards model applied to each study, considering smoker vs nonsmoker status, as well as the time elapsed since smoking cessation (less than 3 years, between 3 and 9 years, or at least 10 years). Statistical adjustments made in the context of multivariate Cox analysis considered age, education, alcohol consumption, and obesity.
Excess Mortality Confirmed
At the end of follow-up, 122,697 deaths were recorded. The comparison of smokers and nonsmokers confirmed smoking-related excess mortality, with adjusted hazard ratios (HRs) estimated at 2.80 for women and 2.70 for men. Smoking shortened life expectancy in the 40- to 79-year-age group by 12 years for women and 13 years for men, in terms of overall mortality. In terms of smoking-attributable specific mortality, the corresponding figures reached 24 and 26 years, respectively. Respiratory diseases ranked highest in both sexes (HR, 7.6 for women and 6.3 for men), followed by cardiovascular diseases (HR, 3.1 for women and 2.9 for men) and cancers (HR, 2.8 for women and 3.1 for men).
The Earlier, the Better
Smoking cessation halves overall excess mortality. Above all, quitting before age 40 years brings overall mortality back to the level of nonsmokers as early as the third year after quitting. The excess mortality decreases even more as the cessation period is prolonged, even after age 40 years. Thus, cessation ≥ 10 years in smokers aged 40-49 years almost cancels out overall excess mortality (-99% in women, -96% in men). The trend is almost as favorable in the older age group (50-59 years), with corresponding figures of -95% and -92%, respectively.
Long-term survival increases in the early years after cessation, especially if it occurs at a younger age, but the benefit remains tangible even in older smokers. Thus, cessation of less than 3 years, effective in patients aged 50-59 years, reduces overall excess mortality by 63% in women and 54% in men. In patients aged 60-79 years, the figures are -40% and -33%, respectively.
Naturally, the earlier the cessation, the greater the number of years gained. It is 12 years for cessation before age 40 years, reduced to 6 years for cessation between 40 and 49 years, and 2.5 years when it is even later (50-59 years). These quantitative results are approximate, given the methodology (a meta-analysis) and some heterogeneity in the studies, as well as the multitude of potential confounding factors that have not all been considered. Nevertheless, the results probably contain a kernel of truth, and their optimistic implications should be highlighted to encourage smokers to abstain, even older ones. Better late than never, even if the benefit of cessation is maximal when it occurs as early as possible, knowing that a minimum of 3 years of cessation would be sufficient to gain years of life.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Chronic smoking remains a major cause of premature mortality on a global scale. Despite intensified efforts to combat this scourge, a quarter of deaths among middle-aged adults in Europe and North America are attributed to it. However, over the past decades, antismoking campaigns have borne fruit, and many smokers have quit before the age of 40 years, enabling some case-control studies.
Among those abstainers who made the right choice, the excess mortality attributable to smoking over a lifetime would be reduced by 90% compared with controls who continued smoking. The estimated benefit is clear, but the analysis lacks nuance. Is smoking cessation beneficial even at older ages? If so, is the effect measurable in terms of magnitude and speed of the effect? An article published online in The New England Journal of Medicine Evidence provided some answers to these questions.
Four-Cohort Meta-Analysis
The study was a meta-analysis of individual data collected within four national cohort studies that were linked to each country’s death registry. Two of these studies were nationally representative. The National Health Interview Survey involved a sample of US citizens living in the community, aged 20-79 years, who were included annually in the cohort between 1997 and 2018. The second, the Canadian Community Health Survey, included subjects in the same age group, with samples analyzed between 2000 and 2014.
In Norway, three cohort studies conducted between 1974 and 2003, in which participants aged 25-79 years were included, were combined to form the Norwegian Health Screening Survey. These were the Counties Study (1974-1988), the 40 Years Study (1985-1999), and the Cohort of Norway (1994-2003), respectively. The fourth cohort was established through recruitment via the UK Biobank, with adults aged 40-73 years invited to participate in the survey. The data analysis ultimately covered a relatively heterogeneous total population of 1.48 million adults, all from high-income countries and followed for 15 years. It relied on the Cox proportional hazards model applied to each study, considering smoker vs nonsmoker status, as well as the time elapsed since smoking cessation (less than 3 years, between 3 and 9 years, or at least 10 years). Statistical adjustments made in the context of multivariate Cox analysis considered age, education, alcohol consumption, and obesity.
Excess Mortality Confirmed
At the end of follow-up, 122,697 deaths were recorded. The comparison of smokers and nonsmokers confirmed smoking-related excess mortality, with adjusted hazard ratios (HRs) estimated at 2.80 for women and 2.70 for men. Smoking shortened life expectancy in the 40- to 79-year-age group by 12 years for women and 13 years for men, in terms of overall mortality. In terms of smoking-attributable specific mortality, the corresponding figures reached 24 and 26 years, respectively. Respiratory diseases ranked highest in both sexes (HR, 7.6 for women and 6.3 for men), followed by cardiovascular diseases (HR, 3.1 for women and 2.9 for men) and cancers (HR, 2.8 for women and 3.1 for men).
The Earlier, the Better
Smoking cessation halves overall excess mortality. Above all, quitting before age 40 years brings overall mortality back to the level of nonsmokers as early as the third year after quitting. The excess mortality decreases even more as the cessation period is prolonged, even after age 40 years. Thus, cessation ≥ 10 years in smokers aged 40-49 years almost cancels out overall excess mortality (-99% in women, -96% in men). The trend is almost as favorable in the older age group (50-59 years), with corresponding figures of -95% and -92%, respectively.
Long-term survival increases in the early years after cessation, especially if it occurs at a younger age, but the benefit remains tangible even in older smokers. Thus, cessation of less than 3 years, effective in patients aged 50-59 years, reduces overall excess mortality by 63% in women and 54% in men. In patients aged 60-79 years, the figures are -40% and -33%, respectively.
Naturally, the earlier the cessation, the greater the number of years gained. It is 12 years for cessation before age 40 years, reduced to 6 years for cessation between 40 and 49 years, and 2.5 years when it is even later (50-59 years). These quantitative results are approximate, given the methodology (a meta-analysis) and some heterogeneity in the studies, as well as the multitude of potential confounding factors that have not all been considered. Nevertheless, the results probably contain a kernel of truth, and their optimistic implications should be highlighted to encourage smokers to abstain, even older ones. Better late than never, even if the benefit of cessation is maximal when it occurs as early as possible, knowing that a minimum of 3 years of cessation would be sufficient to gain years of life.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Study Sounds Alert About GLP-1 RA Use and Aspiration Risk
TOPLINE:
Patients on weekly glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have high residual gastric content, a major risk factor for aspiration under anesthesia, despite following fasting guidelines before undergoing elective procedures.
METHODOLOGY:
- The increasing use of GLP-1 RAs to manage weight and hyperglycemia has sparked safety concerns because of the drugs’ association with slow gastric emptying, a major risk factor for aspiration under anesthesia.
- This cross-sectional study used gastric ultrasonography to examine the link between GLP-1 RA use and the prevalence of increased residual gastric content.
- All 124 participants (median age, 56 years; 60% women) — half of whom received once-weekly GLP-1 RAs such as semaglutide, dulaglutide, or tirzepatide — adhered to the guideline-recommended fasting duration before undergoing elective procedures under anesthesia.
- The primary outcome focused on identifying increased residual gastric content, defined by the presence of solids, thick liquids, or > 1.5 mL/kg of clear liquids on ultrasound.
- An exploratory analysis examined the association between the duration of GLP-1 RA discontinuation and increased residual gastric content.
TAKEAWAY:
- The adjusted prevalence of increased residual gastric content was 30.5% (95% CI, 9.9%-51.2%) higher in participants who received GLP-1 RA than those who did not.
- Most patients took their last dose of GLP-1 RA within 5 days before their procedure, but elevated residual gastric content persisted even after 7 days of GLP-1 RA discontinuation.
- There was also no significant association between the type of GLP-1 RA used and the prevalence of increased residual gastric content.
IN PRACTICE:
“We expect healthcare professionals will encounter these classes of drugs with increasing frequency in the perioperative period. Perioperative physicians, including anesthesiologists, surgeons, and primary care physicians, should be well-informed about the safety implications of GLP-1 RA drugs,” the authors wrote.
SOURCE:
The study was led by Sudipta Sen, MD, from the Department of Anesthesiology, Critical Care and Pain Medicine, McGovern Medical School, University of Texas Health Center at Houston, Houston, Texas, and published online in JAMA Surgery.
LIMITATIONS:
Residual gastric content, the primary outcome, served as a proxy for aspiration risk and does not have an exact threshold of volume associated with increased risk. The study did not directly evaluate aspiration events. The authors also acknowledged potential bias from unmeasured confounders owing to the observational nature of this study. A small sample size limited the ability to detect a risk difference for each additional day of drug discontinuation before surgery.
DISCLOSURES:
One of the authors reported receiving a grant from the National Institutes of Health. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients on weekly glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have high residual gastric content, a major risk factor for aspiration under anesthesia, despite following fasting guidelines before undergoing elective procedures.
METHODOLOGY:
- The increasing use of GLP-1 RAs to manage weight and hyperglycemia has sparked safety concerns because of the drugs’ association with slow gastric emptying, a major risk factor for aspiration under anesthesia.
- This cross-sectional study used gastric ultrasonography to examine the link between GLP-1 RA use and the prevalence of increased residual gastric content.
- All 124 participants (median age, 56 years; 60% women) — half of whom received once-weekly GLP-1 RAs such as semaglutide, dulaglutide, or tirzepatide — adhered to the guideline-recommended fasting duration before undergoing elective procedures under anesthesia.
- The primary outcome focused on identifying increased residual gastric content, defined by the presence of solids, thick liquids, or > 1.5 mL/kg of clear liquids on ultrasound.
- An exploratory analysis examined the association between the duration of GLP-1 RA discontinuation and increased residual gastric content.
TAKEAWAY:
- The adjusted prevalence of increased residual gastric content was 30.5% (95% CI, 9.9%-51.2%) higher in participants who received GLP-1 RA than those who did not.
- Most patients took their last dose of GLP-1 RA within 5 days before their procedure, but elevated residual gastric content persisted even after 7 days of GLP-1 RA discontinuation.
- There was also no significant association between the type of GLP-1 RA used and the prevalence of increased residual gastric content.
IN PRACTICE:
“We expect healthcare professionals will encounter these classes of drugs with increasing frequency in the perioperative period. Perioperative physicians, including anesthesiologists, surgeons, and primary care physicians, should be well-informed about the safety implications of GLP-1 RA drugs,” the authors wrote.
SOURCE:
The study was led by Sudipta Sen, MD, from the Department of Anesthesiology, Critical Care and Pain Medicine, McGovern Medical School, University of Texas Health Center at Houston, Houston, Texas, and published online in JAMA Surgery.
LIMITATIONS:
Residual gastric content, the primary outcome, served as a proxy for aspiration risk and does not have an exact threshold of volume associated with increased risk. The study did not directly evaluate aspiration events. The authors also acknowledged potential bias from unmeasured confounders owing to the observational nature of this study. A small sample size limited the ability to detect a risk difference for each additional day of drug discontinuation before surgery.
DISCLOSURES:
One of the authors reported receiving a grant from the National Institutes of Health. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients on weekly glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have high residual gastric content, a major risk factor for aspiration under anesthesia, despite following fasting guidelines before undergoing elective procedures.
METHODOLOGY:
- The increasing use of GLP-1 RAs to manage weight and hyperglycemia has sparked safety concerns because of the drugs’ association with slow gastric emptying, a major risk factor for aspiration under anesthesia.
- This cross-sectional study used gastric ultrasonography to examine the link between GLP-1 RA use and the prevalence of increased residual gastric content.
- All 124 participants (median age, 56 years; 60% women) — half of whom received once-weekly GLP-1 RAs such as semaglutide, dulaglutide, or tirzepatide — adhered to the guideline-recommended fasting duration before undergoing elective procedures under anesthesia.
- The primary outcome focused on identifying increased residual gastric content, defined by the presence of solids, thick liquids, or > 1.5 mL/kg of clear liquids on ultrasound.
- An exploratory analysis examined the association between the duration of GLP-1 RA discontinuation and increased residual gastric content.
TAKEAWAY:
- The adjusted prevalence of increased residual gastric content was 30.5% (95% CI, 9.9%-51.2%) higher in participants who received GLP-1 RA than those who did not.
- Most patients took their last dose of GLP-1 RA within 5 days before their procedure, but elevated residual gastric content persisted even after 7 days of GLP-1 RA discontinuation.
- There was also no significant association between the type of GLP-1 RA used and the prevalence of increased residual gastric content.
IN PRACTICE:
“We expect healthcare professionals will encounter these classes of drugs with increasing frequency in the perioperative period. Perioperative physicians, including anesthesiologists, surgeons, and primary care physicians, should be well-informed about the safety implications of GLP-1 RA drugs,” the authors wrote.
SOURCE:
The study was led by Sudipta Sen, MD, from the Department of Anesthesiology, Critical Care and Pain Medicine, McGovern Medical School, University of Texas Health Center at Houston, Houston, Texas, and published online in JAMA Surgery.
LIMITATIONS:
Residual gastric content, the primary outcome, served as a proxy for aspiration risk and does not have an exact threshold of volume associated with increased risk. The study did not directly evaluate aspiration events. The authors also acknowledged potential bias from unmeasured confounders owing to the observational nature of this study. A small sample size limited the ability to detect a risk difference for each additional day of drug discontinuation before surgery.
DISCLOSURES:
One of the authors reported receiving a grant from the National Institutes of Health. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Does Exercise Reduce Cancer Risk? It’s Just Not That Simple
“Exercise is medicine” has become something of a mantra, with good reason. There’s no doubt that regular physical activity has a broad range of health benefits. Exercise can improve circulation, help control weight, reduce stress, and boost mood — take your pick.
Lower cancer risk is also on the list — with exercise promoted as a risk-cutting strategy in government guidelines and in recommendations from professional groups such as the American Cancer Society.
The bulk of the data hangs on less rigorous, observational studies that have linked physical activity to lower risks for certain cancers, but plenty of questions remain.
What are the cancer types where exercise makes a difference? How significant is that impact? And what, exactly, defines a physical activity pattern powerful enough to move the needle on cancer risk?
Here’s an overview of the state of the evidence.
Exercise and Cancer Types: A Mixed Bag
When it comes to cancer prevention strategies, guidelines uniformly endorse less couch time and more movement. But a deeper look at the science reveals a complex and often poorly understood connection between exercise and cancer risk.
For certain cancer types, the benefits of exercise on cancer risk seem fairly well established.
The latest edition of the Physical Activity Guidelines for Americans, published in 2018, cites “strong evidence” that regular exercise might curb the risks for breast and colon cancers as well as bladder, endometrial, esophageal, kidney, and gastric cancers. These guidelines also point to “moderate”-strength evidence of a protective association with lung cancer.
The evidence of a protective effect, however, is strongest for breast and colon cancers, said Jennifer Ligibel, MD, senior physician in the Breast Oncology Center at Dana-Farber Cancer Institute, Boston, . “But,” she pointed out, “that may be because they’re some of the most common cancers, and it’s been easier to detect an association.”
Guidelines from the American Cancer Society, published in 2020, align with the 2018 recommendations.
“We believe there’s strong evidence to suggest at least eight different types of cancer are associated with physical activity,” said Erika Rees-Punia, PhD, MPH, senior principal scientist, epidemiology and behavioral research at the American Cancer Society.
That view is not universal, however. Current recommendations from the World Cancer Research Fund and American Institute for Cancer Research, for example, are more circumspect, citing only three cancers with good evidence of a protective effect from exercise: Breast (postmenopausal), colon, and endometrial.
“We definitely can’t say exercise reduces the risk of all cancers,” said Lee Jones, PhD, head of the Exercise Oncology Program at Memorial Sloan Kettering Cancer Center in New York City. “The data suggest it’s just not that simple.”
And it’s challenging to put all the evidence together, Dr. Jones added.
The physical activity guidelines are based on published systematic reviews, meta-analyses, and pooled analyses of data from observational studies that examined the relationship between physical activity — aerobic exercise, specifically — and cancer incidence. That means the evidence comes with all the limitations observational studies entail, such as how they collect information on participants’ exercise habits — which, Dr. Jones noted, is typically done via “monster questionnaires” that gauge physical activity in broad strokes.
Pooling all those findings into a meta-analysis is tricky, Dr. Jones added, because individual studies vary in important ways — from follow-up periods to how they quantify exercise and track cancer incidence.
In a study published in February in Cancer Cell, Dr. Jones and his colleagues attempted to address some of those issues by leveraging data from the PLCO screening trial.
The PLCO was a prospective study of over 60,000 US adults that compared the effects of annual screening vs usual care on cancer mortality. At enrollment, participants completed questionnaires that included an assessment of “vigorous” exercise. Based on that, Dr. Jones and his colleagues classified 55% as “exercisers” — meaning they reported 2 or more hours of vigorous exercise per week. The remaining 45%, who were in the 0 to 1 hour per week range, were deemed non-exercisers.
Over a median of 18 years, nearly 16,000 first-time invasive cancers were diagnosed, and some interesting differences between exercisers and non-exercisers emerged. The active group had lower risks for three cancers: Head and neck, with a 26% lower risk (hazard ratio [HR], 0.74), lung (a 20% lower risk), and breast (an 11% lower risk).
What was striking, however, was the lack of connection between exercise and many cancers cited in the guidelines, including colon, gastric, bladder, endometrial, and renal cancers.
Perhaps even more surprising — exercisers had higher risks for prostate cancer (12%) and melanoma (20%). This finding, Dr. Jones said, is in line with a previous pooled analysis of data from 12 US and European prospective cohorts. In this study, the most physically active participants (90th percentile) had higher risks for melanoma and prostate cancer, compared with the least active group (10th percentile).
The melanoma findings do make sense, Dr. Jones said, given that highly active people may spend a lot of time in the sun. “My advice,” Dr. Jones said, “is, if you’re exercising outside, wear sunscreen.” The prostate cancer findings, however, are more puzzling and warrant further research, he noted.
But the bottom line is that the relationship between exercise and cancer types is mixed and far from nailed down.
How Big Is the Effect?
Even if exercise reduces the risk for only certain cancers, that’s still important, particularly when those links appear strongest for common cancer types, such as breast and colon.
But how much of a difference can exercise make?
Based on the evidence, it may only be a modest one. A 2019 systematic review by the Physical Activity Guidelines Advisory Committee provided a rough estimate: Across hundreds of epidemiological studies, people with the highest physical activity levels had a 10%-20% lower risk for the cancers cited in the 2018 exercise guidelines compared with people who were least active.
These figures, however, are probably an underestimate, said Anne McTiernan, MD, PhD, a member of the advisory committee and professor of epidemiology, at Fred Hutchinson Cancer Center, Seattle.
“This is what we usually see when a factor is not measured very well,” said Dr. McTiernan, explaining that the individual studies differed in their categories of “highest” and “lowest” physical activity, such that one study’s “highest” could be another’s mid-range.
“In other words, the effects of physical activity are likely larger” than the review found, Dr. McTiernan said.
The next logical question is whether a bigger exercise “dose” — more time or higher intensity — would have a greater impact on cancer risk. A 2019 study published in the Journal of Clinical Oncology tried to clarify that by pooling data on over 750,000 participants from nine prospective cohorts.
Overall, people meeting government recommendations for exercise — equivalent to about 2.5-5 hours of weekly moderate activity, such as a brisk walk, or about 1.25-2.5 hours of more vigorous activities, like running — had lower risks for seven of 15 cancer types studied compared with less active people.
For cancers with positive findings, being on the higher end of the recommended 2.5- to 5-hour weekly range was better. Risk reductions for breast cancer, for instance, were 6% at 2.5 hours of physical activity per week and 10% at 5 hours per week. Similar trends emerged for other cancer types, including colon (8%-14%), endometrial (10%-18%), liver cancer (18%-27%), and non-Hodgkin lymphoma in women (11%-18%).
But there may be an exercise sweet spot that maximizes the cancer risk benefit.
Among people who surpassed the recommendations — exercising for more time or more intensely — the risk reduction benefit did not necessarily improve in a linear fashion. For certain cancer types, such as colon and endometrial, the benefits of more vigorous exercise “eroded at higher levels of activity,” the authors said.
The issue here is that most studies have not dug deeply into aerobic exercise habits. Often, studies present participants with a list of activities — walking, biking, and running — and ask them to estimate how often and for what duration they do each.
Plus, “we’ve usually lumped moderate and vigorous activities together,” Dr. Rees-Punia said, which means there’s a lack of “granular data” to say whether certain intensities or frequencies of exercise are optimal and for whom.
Why Exercise May Lower Cancer Risk
Exercise habits do not, of course, exist in a vacuum. Highly active people, Dr. Ligibel said, tend to be of higher socioeconomic status, leaner, and have generally healthier lifestyles than sedentary people.
Body weight is a big confounder as well. However, Dr. Rees-Punia noted, it’s also probably a reason that exercise is linked to lower cancer risks, particularly by preventing weight gain. Still, studies have found that the association between exercise and many cancers remains significant after adjusting for body mass index.
The why remains unclear, though some studies offer clues.
“There’s been some really interesting mechanistic research, suggesting that exercise may help inhibit tumor growth or upregulate the immune system,” Dr. Ligibel said.
That includes not only lab research but small intervention studies. While these studies have largely involved people who already have cancer, some have also focused on healthy individuals.
A 2019 study from Dr. Ligibel and her colleagues, which randomly assigned 49 women newly diagnosed with breast cancer to start either an exercise program or mind-body practices ahead of surgery, found exercisers, who had been active for about a month at the time of surgery, showed signs of immune system upregulation in their tumors, while the control group did not.
Among healthy postmenopausal women, a meta-analysis of six clinical trials from Dr. McTiernan and her colleagues found that exercise plus calorie reduction can reduce levels of breast cancer-related endogenous hormones, more so than calorie-cutting alone. And a 2023 study found that high-intensity exercise boosted the ranks of certain immune cells and reduced inflammation in the colon among people at high risk for colon and endometrial cancers due to Lynch syndrome.
Defining an Exercise ‘Prescription’
Despite the gaps and uncertainties in the research, government guidelines as well as those from the American Cancer Society and other medical groups are in lockstep in their exercise recommendations: Adults should strive for 150-300 minutes of moderate-intensity aerobic exercise (like brisk walking), 75-150 minutes of vigorous activity (like running), or some combination each week.
The guidelines also encourage strength training twice a week — advice that’s based on research tying those activity levels to lower risks for heart disease, diabetes, and other chronic conditions.
But there’s no “best” exercise prescription for lowering cancer risk specifically. Most epidemiological studies have examined only aerobic activity, Dr. Rees-Punia said, and there’s very little known about whether strength conditioning or other moderate heart rate-elevating activities, such as daily household chores, may reduce the risk for cancer.
Given the lack of nuance in the literature, it’s hard to say what intensities, types, or amounts of exercise are best for each individual.
Going forward, device-based measurements of physical activity could “help us sort out the effects of different intensities of exercise and possibly types,” Dr. Rees-Punia said.
But overall, Dr. McTiernan said, the data do show that the risks for several cancers are lower at the widely recommended activity levels.
“The bottom-line advice is still to exercise at least 150 minutes per week at a moderate-intensity level or greater,” Dr. McTiernan said.
Or put another way, moving beats being sedentary. It’s probably wise for everyone to sit less, noted Dr. Rees-Punia, for overall health and based on evidence tying sedentary time to the risks for certain cancers, including colon, endometrial, and lung.
There’s a practical element to consider in all of this: What physical activities will people actually do on the regular? In the big epidemiological studies, Dr. McTiernan noted, middle-aged and older adults most often report walking, suggesting that’s the preferred, or most accessible activity, for many.
“You can only benefit from the physical activity you’ll actually do,” Dr. Rees-Punia said.
Dr. Ligibel echoed that sentiment, saying she encourages patients to think about physical activity as a process: “You need to find things you like to do and work them into your daily life, in a sustainable way.
“People often talk about exercise being medicine,” Dr. Ligibel said. “But I think you could take that too far. If we get too prescriptive about it, that could take the joy away.”
A version of this article appeared on Medscape.com.
“Exercise is medicine” has become something of a mantra, with good reason. There’s no doubt that regular physical activity has a broad range of health benefits. Exercise can improve circulation, help control weight, reduce stress, and boost mood — take your pick.
Lower cancer risk is also on the list — with exercise promoted as a risk-cutting strategy in government guidelines and in recommendations from professional groups such as the American Cancer Society.
The bulk of the data hangs on less rigorous, observational studies that have linked physical activity to lower risks for certain cancers, but plenty of questions remain.
What are the cancer types where exercise makes a difference? How significant is that impact? And what, exactly, defines a physical activity pattern powerful enough to move the needle on cancer risk?
Here’s an overview of the state of the evidence.
Exercise and Cancer Types: A Mixed Bag
When it comes to cancer prevention strategies, guidelines uniformly endorse less couch time and more movement. But a deeper look at the science reveals a complex and often poorly understood connection between exercise and cancer risk.
For certain cancer types, the benefits of exercise on cancer risk seem fairly well established.
The latest edition of the Physical Activity Guidelines for Americans, published in 2018, cites “strong evidence” that regular exercise might curb the risks for breast and colon cancers as well as bladder, endometrial, esophageal, kidney, and gastric cancers. These guidelines also point to “moderate”-strength evidence of a protective association with lung cancer.
The evidence of a protective effect, however, is strongest for breast and colon cancers, said Jennifer Ligibel, MD, senior physician in the Breast Oncology Center at Dana-Farber Cancer Institute, Boston, . “But,” she pointed out, “that may be because they’re some of the most common cancers, and it’s been easier to detect an association.”
Guidelines from the American Cancer Society, published in 2020, align with the 2018 recommendations.
“We believe there’s strong evidence to suggest at least eight different types of cancer are associated with physical activity,” said Erika Rees-Punia, PhD, MPH, senior principal scientist, epidemiology and behavioral research at the American Cancer Society.
That view is not universal, however. Current recommendations from the World Cancer Research Fund and American Institute for Cancer Research, for example, are more circumspect, citing only three cancers with good evidence of a protective effect from exercise: Breast (postmenopausal), colon, and endometrial.
“We definitely can’t say exercise reduces the risk of all cancers,” said Lee Jones, PhD, head of the Exercise Oncology Program at Memorial Sloan Kettering Cancer Center in New York City. “The data suggest it’s just not that simple.”
And it’s challenging to put all the evidence together, Dr. Jones added.
The physical activity guidelines are based on published systematic reviews, meta-analyses, and pooled analyses of data from observational studies that examined the relationship between physical activity — aerobic exercise, specifically — and cancer incidence. That means the evidence comes with all the limitations observational studies entail, such as how they collect information on participants’ exercise habits — which, Dr. Jones noted, is typically done via “monster questionnaires” that gauge physical activity in broad strokes.
Pooling all those findings into a meta-analysis is tricky, Dr. Jones added, because individual studies vary in important ways — from follow-up periods to how they quantify exercise and track cancer incidence.
In a study published in February in Cancer Cell, Dr. Jones and his colleagues attempted to address some of those issues by leveraging data from the PLCO screening trial.
The PLCO was a prospective study of over 60,000 US adults that compared the effects of annual screening vs usual care on cancer mortality. At enrollment, participants completed questionnaires that included an assessment of “vigorous” exercise. Based on that, Dr. Jones and his colleagues classified 55% as “exercisers” — meaning they reported 2 or more hours of vigorous exercise per week. The remaining 45%, who were in the 0 to 1 hour per week range, were deemed non-exercisers.
Over a median of 18 years, nearly 16,000 first-time invasive cancers were diagnosed, and some interesting differences between exercisers and non-exercisers emerged. The active group had lower risks for three cancers: Head and neck, with a 26% lower risk (hazard ratio [HR], 0.74), lung (a 20% lower risk), and breast (an 11% lower risk).
What was striking, however, was the lack of connection between exercise and many cancers cited in the guidelines, including colon, gastric, bladder, endometrial, and renal cancers.
Perhaps even more surprising — exercisers had higher risks for prostate cancer (12%) and melanoma (20%). This finding, Dr. Jones said, is in line with a previous pooled analysis of data from 12 US and European prospective cohorts. In this study, the most physically active participants (90th percentile) had higher risks for melanoma and prostate cancer, compared with the least active group (10th percentile).
The melanoma findings do make sense, Dr. Jones said, given that highly active people may spend a lot of time in the sun. “My advice,” Dr. Jones said, “is, if you’re exercising outside, wear sunscreen.” The prostate cancer findings, however, are more puzzling and warrant further research, he noted.
But the bottom line is that the relationship between exercise and cancer types is mixed and far from nailed down.
How Big Is the Effect?
Even if exercise reduces the risk for only certain cancers, that’s still important, particularly when those links appear strongest for common cancer types, such as breast and colon.
But how much of a difference can exercise make?
Based on the evidence, it may only be a modest one. A 2019 systematic review by the Physical Activity Guidelines Advisory Committee provided a rough estimate: Across hundreds of epidemiological studies, people with the highest physical activity levels had a 10%-20% lower risk for the cancers cited in the 2018 exercise guidelines compared with people who were least active.
These figures, however, are probably an underestimate, said Anne McTiernan, MD, PhD, a member of the advisory committee and professor of epidemiology, at Fred Hutchinson Cancer Center, Seattle.
“This is what we usually see when a factor is not measured very well,” said Dr. McTiernan, explaining that the individual studies differed in their categories of “highest” and “lowest” physical activity, such that one study’s “highest” could be another’s mid-range.
“In other words, the effects of physical activity are likely larger” than the review found, Dr. McTiernan said.
The next logical question is whether a bigger exercise “dose” — more time or higher intensity — would have a greater impact on cancer risk. A 2019 study published in the Journal of Clinical Oncology tried to clarify that by pooling data on over 750,000 participants from nine prospective cohorts.
Overall, people meeting government recommendations for exercise — equivalent to about 2.5-5 hours of weekly moderate activity, such as a brisk walk, or about 1.25-2.5 hours of more vigorous activities, like running — had lower risks for seven of 15 cancer types studied compared with less active people.
For cancers with positive findings, being on the higher end of the recommended 2.5- to 5-hour weekly range was better. Risk reductions for breast cancer, for instance, were 6% at 2.5 hours of physical activity per week and 10% at 5 hours per week. Similar trends emerged for other cancer types, including colon (8%-14%), endometrial (10%-18%), liver cancer (18%-27%), and non-Hodgkin lymphoma in women (11%-18%).
But there may be an exercise sweet spot that maximizes the cancer risk benefit.
Among people who surpassed the recommendations — exercising for more time or more intensely — the risk reduction benefit did not necessarily improve in a linear fashion. For certain cancer types, such as colon and endometrial, the benefits of more vigorous exercise “eroded at higher levels of activity,” the authors said.
The issue here is that most studies have not dug deeply into aerobic exercise habits. Often, studies present participants with a list of activities — walking, biking, and running — and ask them to estimate how often and for what duration they do each.
Plus, “we’ve usually lumped moderate and vigorous activities together,” Dr. Rees-Punia said, which means there’s a lack of “granular data” to say whether certain intensities or frequencies of exercise are optimal and for whom.
Why Exercise May Lower Cancer Risk
Exercise habits do not, of course, exist in a vacuum. Highly active people, Dr. Ligibel said, tend to be of higher socioeconomic status, leaner, and have generally healthier lifestyles than sedentary people.
Body weight is a big confounder as well. However, Dr. Rees-Punia noted, it’s also probably a reason that exercise is linked to lower cancer risks, particularly by preventing weight gain. Still, studies have found that the association between exercise and many cancers remains significant after adjusting for body mass index.
The why remains unclear, though some studies offer clues.
“There’s been some really interesting mechanistic research, suggesting that exercise may help inhibit tumor growth or upregulate the immune system,” Dr. Ligibel said.
That includes not only lab research but small intervention studies. While these studies have largely involved people who already have cancer, some have also focused on healthy individuals.
A 2019 study from Dr. Ligibel and her colleagues, which randomly assigned 49 women newly diagnosed with breast cancer to start either an exercise program or mind-body practices ahead of surgery, found exercisers, who had been active for about a month at the time of surgery, showed signs of immune system upregulation in their tumors, while the control group did not.
Among healthy postmenopausal women, a meta-analysis of six clinical trials from Dr. McTiernan and her colleagues found that exercise plus calorie reduction can reduce levels of breast cancer-related endogenous hormones, more so than calorie-cutting alone. And a 2023 study found that high-intensity exercise boosted the ranks of certain immune cells and reduced inflammation in the colon among people at high risk for colon and endometrial cancers due to Lynch syndrome.
Defining an Exercise ‘Prescription’
Despite the gaps and uncertainties in the research, government guidelines as well as those from the American Cancer Society and other medical groups are in lockstep in their exercise recommendations: Adults should strive for 150-300 minutes of moderate-intensity aerobic exercise (like brisk walking), 75-150 minutes of vigorous activity (like running), or some combination each week.
The guidelines also encourage strength training twice a week — advice that’s based on research tying those activity levels to lower risks for heart disease, diabetes, and other chronic conditions.
But there’s no “best” exercise prescription for lowering cancer risk specifically. Most epidemiological studies have examined only aerobic activity, Dr. Rees-Punia said, and there’s very little known about whether strength conditioning or other moderate heart rate-elevating activities, such as daily household chores, may reduce the risk for cancer.
Given the lack of nuance in the literature, it’s hard to say what intensities, types, or amounts of exercise are best for each individual.
Going forward, device-based measurements of physical activity could “help us sort out the effects of different intensities of exercise and possibly types,” Dr. Rees-Punia said.
But overall, Dr. McTiernan said, the data do show that the risks for several cancers are lower at the widely recommended activity levels.
“The bottom-line advice is still to exercise at least 150 minutes per week at a moderate-intensity level or greater,” Dr. McTiernan said.
Or put another way, moving beats being sedentary. It’s probably wise for everyone to sit less, noted Dr. Rees-Punia, for overall health and based on evidence tying sedentary time to the risks for certain cancers, including colon, endometrial, and lung.
There’s a practical element to consider in all of this: What physical activities will people actually do on the regular? In the big epidemiological studies, Dr. McTiernan noted, middle-aged and older adults most often report walking, suggesting that’s the preferred, or most accessible activity, for many.
“You can only benefit from the physical activity you’ll actually do,” Dr. Rees-Punia said.
Dr. Ligibel echoed that sentiment, saying she encourages patients to think about physical activity as a process: “You need to find things you like to do and work them into your daily life, in a sustainable way.
“People often talk about exercise being medicine,” Dr. Ligibel said. “But I think you could take that too far. If we get too prescriptive about it, that could take the joy away.”
A version of this article appeared on Medscape.com.
“Exercise is medicine” has become something of a mantra, with good reason. There’s no doubt that regular physical activity has a broad range of health benefits. Exercise can improve circulation, help control weight, reduce stress, and boost mood — take your pick.
Lower cancer risk is also on the list — with exercise promoted as a risk-cutting strategy in government guidelines and in recommendations from professional groups such as the American Cancer Society.
The bulk of the data hangs on less rigorous, observational studies that have linked physical activity to lower risks for certain cancers, but plenty of questions remain.
What are the cancer types where exercise makes a difference? How significant is that impact? And what, exactly, defines a physical activity pattern powerful enough to move the needle on cancer risk?
Here’s an overview of the state of the evidence.
Exercise and Cancer Types: A Mixed Bag
When it comes to cancer prevention strategies, guidelines uniformly endorse less couch time and more movement. But a deeper look at the science reveals a complex and often poorly understood connection between exercise and cancer risk.
For certain cancer types, the benefits of exercise on cancer risk seem fairly well established.
The latest edition of the Physical Activity Guidelines for Americans, published in 2018, cites “strong evidence” that regular exercise might curb the risks for breast and colon cancers as well as bladder, endometrial, esophageal, kidney, and gastric cancers. These guidelines also point to “moderate”-strength evidence of a protective association with lung cancer.
The evidence of a protective effect, however, is strongest for breast and colon cancers, said Jennifer Ligibel, MD, senior physician in the Breast Oncology Center at Dana-Farber Cancer Institute, Boston, . “But,” she pointed out, “that may be because they’re some of the most common cancers, and it’s been easier to detect an association.”
Guidelines from the American Cancer Society, published in 2020, align with the 2018 recommendations.
“We believe there’s strong evidence to suggest at least eight different types of cancer are associated with physical activity,” said Erika Rees-Punia, PhD, MPH, senior principal scientist, epidemiology and behavioral research at the American Cancer Society.
That view is not universal, however. Current recommendations from the World Cancer Research Fund and American Institute for Cancer Research, for example, are more circumspect, citing only three cancers with good evidence of a protective effect from exercise: Breast (postmenopausal), colon, and endometrial.
“We definitely can’t say exercise reduces the risk of all cancers,” said Lee Jones, PhD, head of the Exercise Oncology Program at Memorial Sloan Kettering Cancer Center in New York City. “The data suggest it’s just not that simple.”
And it’s challenging to put all the evidence together, Dr. Jones added.
The physical activity guidelines are based on published systematic reviews, meta-analyses, and pooled analyses of data from observational studies that examined the relationship between physical activity — aerobic exercise, specifically — and cancer incidence. That means the evidence comes with all the limitations observational studies entail, such as how they collect information on participants’ exercise habits — which, Dr. Jones noted, is typically done via “monster questionnaires” that gauge physical activity in broad strokes.
Pooling all those findings into a meta-analysis is tricky, Dr. Jones added, because individual studies vary in important ways — from follow-up periods to how they quantify exercise and track cancer incidence.
In a study published in February in Cancer Cell, Dr. Jones and his colleagues attempted to address some of those issues by leveraging data from the PLCO screening trial.
The PLCO was a prospective study of over 60,000 US adults that compared the effects of annual screening vs usual care on cancer mortality. At enrollment, participants completed questionnaires that included an assessment of “vigorous” exercise. Based on that, Dr. Jones and his colleagues classified 55% as “exercisers” — meaning they reported 2 or more hours of vigorous exercise per week. The remaining 45%, who were in the 0 to 1 hour per week range, were deemed non-exercisers.
Over a median of 18 years, nearly 16,000 first-time invasive cancers were diagnosed, and some interesting differences between exercisers and non-exercisers emerged. The active group had lower risks for three cancers: Head and neck, with a 26% lower risk (hazard ratio [HR], 0.74), lung (a 20% lower risk), and breast (an 11% lower risk).
What was striking, however, was the lack of connection between exercise and many cancers cited in the guidelines, including colon, gastric, bladder, endometrial, and renal cancers.
Perhaps even more surprising — exercisers had higher risks for prostate cancer (12%) and melanoma (20%). This finding, Dr. Jones said, is in line with a previous pooled analysis of data from 12 US and European prospective cohorts. In this study, the most physically active participants (90th percentile) had higher risks for melanoma and prostate cancer, compared with the least active group (10th percentile).
The melanoma findings do make sense, Dr. Jones said, given that highly active people may spend a lot of time in the sun. “My advice,” Dr. Jones said, “is, if you’re exercising outside, wear sunscreen.” The prostate cancer findings, however, are more puzzling and warrant further research, he noted.
But the bottom line is that the relationship between exercise and cancer types is mixed and far from nailed down.
How Big Is the Effect?
Even if exercise reduces the risk for only certain cancers, that’s still important, particularly when those links appear strongest for common cancer types, such as breast and colon.
But how much of a difference can exercise make?
Based on the evidence, it may only be a modest one. A 2019 systematic review by the Physical Activity Guidelines Advisory Committee provided a rough estimate: Across hundreds of epidemiological studies, people with the highest physical activity levels had a 10%-20% lower risk for the cancers cited in the 2018 exercise guidelines compared with people who were least active.
These figures, however, are probably an underestimate, said Anne McTiernan, MD, PhD, a member of the advisory committee and professor of epidemiology, at Fred Hutchinson Cancer Center, Seattle.
“This is what we usually see when a factor is not measured very well,” said Dr. McTiernan, explaining that the individual studies differed in their categories of “highest” and “lowest” physical activity, such that one study’s “highest” could be another’s mid-range.
“In other words, the effects of physical activity are likely larger” than the review found, Dr. McTiernan said.
The next logical question is whether a bigger exercise “dose” — more time or higher intensity — would have a greater impact on cancer risk. A 2019 study published in the Journal of Clinical Oncology tried to clarify that by pooling data on over 750,000 participants from nine prospective cohorts.
Overall, people meeting government recommendations for exercise — equivalent to about 2.5-5 hours of weekly moderate activity, such as a brisk walk, or about 1.25-2.5 hours of more vigorous activities, like running — had lower risks for seven of 15 cancer types studied compared with less active people.
For cancers with positive findings, being on the higher end of the recommended 2.5- to 5-hour weekly range was better. Risk reductions for breast cancer, for instance, were 6% at 2.5 hours of physical activity per week and 10% at 5 hours per week. Similar trends emerged for other cancer types, including colon (8%-14%), endometrial (10%-18%), liver cancer (18%-27%), and non-Hodgkin lymphoma in women (11%-18%).
But there may be an exercise sweet spot that maximizes the cancer risk benefit.
Among people who surpassed the recommendations — exercising for more time or more intensely — the risk reduction benefit did not necessarily improve in a linear fashion. For certain cancer types, such as colon and endometrial, the benefits of more vigorous exercise “eroded at higher levels of activity,” the authors said.
The issue here is that most studies have not dug deeply into aerobic exercise habits. Often, studies present participants with a list of activities — walking, biking, and running — and ask them to estimate how often and for what duration they do each.
Plus, “we’ve usually lumped moderate and vigorous activities together,” Dr. Rees-Punia said, which means there’s a lack of “granular data” to say whether certain intensities or frequencies of exercise are optimal and for whom.
Why Exercise May Lower Cancer Risk
Exercise habits do not, of course, exist in a vacuum. Highly active people, Dr. Ligibel said, tend to be of higher socioeconomic status, leaner, and have generally healthier lifestyles than sedentary people.
Body weight is a big confounder as well. However, Dr. Rees-Punia noted, it’s also probably a reason that exercise is linked to lower cancer risks, particularly by preventing weight gain. Still, studies have found that the association between exercise and many cancers remains significant after adjusting for body mass index.
The why remains unclear, though some studies offer clues.
“There’s been some really interesting mechanistic research, suggesting that exercise may help inhibit tumor growth or upregulate the immune system,” Dr. Ligibel said.
That includes not only lab research but small intervention studies. While these studies have largely involved people who already have cancer, some have also focused on healthy individuals.
A 2019 study from Dr. Ligibel and her colleagues, which randomly assigned 49 women newly diagnosed with breast cancer to start either an exercise program or mind-body practices ahead of surgery, found exercisers, who had been active for about a month at the time of surgery, showed signs of immune system upregulation in their tumors, while the control group did not.
Among healthy postmenopausal women, a meta-analysis of six clinical trials from Dr. McTiernan and her colleagues found that exercise plus calorie reduction can reduce levels of breast cancer-related endogenous hormones, more so than calorie-cutting alone. And a 2023 study found that high-intensity exercise boosted the ranks of certain immune cells and reduced inflammation in the colon among people at high risk for colon and endometrial cancers due to Lynch syndrome.
Defining an Exercise ‘Prescription’
Despite the gaps and uncertainties in the research, government guidelines as well as those from the American Cancer Society and other medical groups are in lockstep in their exercise recommendations: Adults should strive for 150-300 minutes of moderate-intensity aerobic exercise (like brisk walking), 75-150 minutes of vigorous activity (like running), or some combination each week.
The guidelines also encourage strength training twice a week — advice that’s based on research tying those activity levels to lower risks for heart disease, diabetes, and other chronic conditions.
But there’s no “best” exercise prescription for lowering cancer risk specifically. Most epidemiological studies have examined only aerobic activity, Dr. Rees-Punia said, and there’s very little known about whether strength conditioning or other moderate heart rate-elevating activities, such as daily household chores, may reduce the risk for cancer.
Given the lack of nuance in the literature, it’s hard to say what intensities, types, or amounts of exercise are best for each individual.
Going forward, device-based measurements of physical activity could “help us sort out the effects of different intensities of exercise and possibly types,” Dr. Rees-Punia said.
But overall, Dr. McTiernan said, the data do show that the risks for several cancers are lower at the widely recommended activity levels.
“The bottom-line advice is still to exercise at least 150 minutes per week at a moderate-intensity level or greater,” Dr. McTiernan said.
Or put another way, moving beats being sedentary. It’s probably wise for everyone to sit less, noted Dr. Rees-Punia, for overall health and based on evidence tying sedentary time to the risks for certain cancers, including colon, endometrial, and lung.
There’s a practical element to consider in all of this: What physical activities will people actually do on the regular? In the big epidemiological studies, Dr. McTiernan noted, middle-aged and older adults most often report walking, suggesting that’s the preferred, or most accessible activity, for many.
“You can only benefit from the physical activity you’ll actually do,” Dr. Rees-Punia said.
Dr. Ligibel echoed that sentiment, saying she encourages patients to think about physical activity as a process: “You need to find things you like to do and work them into your daily life, in a sustainable way.
“People often talk about exercise being medicine,” Dr. Ligibel said. “But I think you could take that too far. If we get too prescriptive about it, that could take the joy away.”
A version of this article appeared on Medscape.com.
Air Pollution Tied to Greater Amyloid Burden in the Brain
TOPLINE:
, a new postmortem study showed.
METHODOLOGY:
- Investigators examined the brain tissue of 224 people living in the Atlanta area who agreed to donate their brains after death (average age of death, 76 years) for the presence of amyloid plaques and tau tangles.
- They also studied the amount of fine particulate matter < 2.5 microns (PM2.5) from traffic-related air pollution at participants’ home addresses at 1, 3, and 5 years before death.
- The presence of the APOE e4 gene was examined for evidence of any effect on the relationship between air pollution and evidence of Alzheimer’s disease (AD).
TAKEAWAY:
The average level of exposure in the year before death was 1.32 µg/m3 and 1.35 µg/m3 in the 3 years before death.
People with 1 µg/m3 higher PM2.5 exposure in the year before death were nearly twice as likely to have higher levels of plaques (odds ratio [OR], 1.92; 95% CI, 1.12-3.30), while those with higher exposure in the 3 years before death were 87% more likely to have higher levels of plaques (OR, 1.87; 95% CI, 1.01-3.17).
A little more than half (56%) of the sample were positive for the APOE e4 genotype, but the strongest association between pollution and neuropathology markers was for noncarriers of the genotype, although this relationship did not reach statistical significance.
IN PRACTICE:
“More research is needed to establish causality for the association between PM2.5 and AD, including epidemiologic and mechanistic studies. Future studies should also investigate the association between PM2.5 and other dementia-related pathologies, including cerebrovascular pathology,” the study authors wrote.
SOURCE:
Anke Hüls, PhD, of Emory University in Atlanta, led the study, which was published online on February 21, 2024, in Neurology.
LIMITATIONS:
The sample was not population-based but a convenience sample composed mostly of highly educated White participants.
DISCLOSURES:
The study was funded by the National Institute of Environmental Health Sciences, the Goizueta Alzheimer’s Disease Research Center, the National Institute on Aging, and the National Institutes of Health. There were no relevant disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
, a new postmortem study showed.
METHODOLOGY:
- Investigators examined the brain tissue of 224 people living in the Atlanta area who agreed to donate their brains after death (average age of death, 76 years) for the presence of amyloid plaques and tau tangles.
- They also studied the amount of fine particulate matter < 2.5 microns (PM2.5) from traffic-related air pollution at participants’ home addresses at 1, 3, and 5 years before death.
- The presence of the APOE e4 gene was examined for evidence of any effect on the relationship between air pollution and evidence of Alzheimer’s disease (AD).
TAKEAWAY:
The average level of exposure in the year before death was 1.32 µg/m3 and 1.35 µg/m3 in the 3 years before death.
People with 1 µg/m3 higher PM2.5 exposure in the year before death were nearly twice as likely to have higher levels of plaques (odds ratio [OR], 1.92; 95% CI, 1.12-3.30), while those with higher exposure in the 3 years before death were 87% more likely to have higher levels of plaques (OR, 1.87; 95% CI, 1.01-3.17).
A little more than half (56%) of the sample were positive for the APOE e4 genotype, but the strongest association between pollution and neuropathology markers was for noncarriers of the genotype, although this relationship did not reach statistical significance.
IN PRACTICE:
“More research is needed to establish causality for the association between PM2.5 and AD, including epidemiologic and mechanistic studies. Future studies should also investigate the association between PM2.5 and other dementia-related pathologies, including cerebrovascular pathology,” the study authors wrote.
SOURCE:
Anke Hüls, PhD, of Emory University in Atlanta, led the study, which was published online on February 21, 2024, in Neurology.
LIMITATIONS:
The sample was not population-based but a convenience sample composed mostly of highly educated White participants.
DISCLOSURES:
The study was funded by the National Institute of Environmental Health Sciences, the Goizueta Alzheimer’s Disease Research Center, the National Institute on Aging, and the National Institutes of Health. There were no relevant disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
, a new postmortem study showed.
METHODOLOGY:
- Investigators examined the brain tissue of 224 people living in the Atlanta area who agreed to donate their brains after death (average age of death, 76 years) for the presence of amyloid plaques and tau tangles.
- They also studied the amount of fine particulate matter < 2.5 microns (PM2.5) from traffic-related air pollution at participants’ home addresses at 1, 3, and 5 years before death.
- The presence of the APOE e4 gene was examined for evidence of any effect on the relationship between air pollution and evidence of Alzheimer’s disease (AD).
TAKEAWAY:
The average level of exposure in the year before death was 1.32 µg/m3 and 1.35 µg/m3 in the 3 years before death.
People with 1 µg/m3 higher PM2.5 exposure in the year before death were nearly twice as likely to have higher levels of plaques (odds ratio [OR], 1.92; 95% CI, 1.12-3.30), while those with higher exposure in the 3 years before death were 87% more likely to have higher levels of plaques (OR, 1.87; 95% CI, 1.01-3.17).
A little more than half (56%) of the sample were positive for the APOE e4 genotype, but the strongest association between pollution and neuropathology markers was for noncarriers of the genotype, although this relationship did not reach statistical significance.
IN PRACTICE:
“More research is needed to establish causality for the association between PM2.5 and AD, including epidemiologic and mechanistic studies. Future studies should also investigate the association between PM2.5 and other dementia-related pathologies, including cerebrovascular pathology,” the study authors wrote.
SOURCE:
Anke Hüls, PhD, of Emory University in Atlanta, led the study, which was published online on February 21, 2024, in Neurology.
LIMITATIONS:
The sample was not population-based but a convenience sample composed mostly of highly educated White participants.
DISCLOSURES:
The study was funded by the National Institute of Environmental Health Sciences, the Goizueta Alzheimer’s Disease Research Center, the National Institute on Aging, and the National Institutes of Health. There were no relevant disclosures.
A version of this article appeared on Medscape.com.
‘Thunderstorm Asthma’ Could Strike More Often With Climate Change
Thunderstorm asthma can strike with little warning, leaving people with the symptoms of an asthma attack during or after the dark clouds pass.
If you’re unfamiliar, the risk for a thunderstorm asthma attack grows when heavy storms arrive on a day with very high pollen or spores. The storm uplifts these particles, adds water, and causes them to explode into smaller grains. The electrical activity in a storm can do the same. Next, strong winds sweep these particles down and across the ground. People in the path of the storm can experience shortness of breath, coughing, and wheezing.
“Yes, if only because the amount of pollen appears to be increasing in many areas due to climate change,” said Frank S. Virant, MD, chief of the Allergy Division at Seattle Children’s Hospital in Washington.
Most cases of thunderstorm asthma occur in the spring and early summer, but that also could change. Pollen seasons “have been getting longer and more intense,” said Shaan M. Waqar, MD, an allergist at ENT and Allergy Associates in Plainview, NY.
“Thunderstorm asthma events are rare, but our changing environment and the increase in the number of people with allergies may make such events more common and more severe into the future,” agreed Paul J. Beggs, PhD, associate professor in the School of Natural Sciences at Macquarie University in Sydney, Australia.
How to Minimize Your Risk
If your patients are sensitive to pollen, advise them to continue to monitor outdoor levels, particularly during tree, grass, and weed pollen season, Dr. Virant recommended. Also patients should pay attention to weather reports. Watch for thunderstorms that could “amplify exposure to the pollen with 40-plus mile per hour winds and often colder air downdrafts.” Cold is an additional asthma trigger, he noted.
People with asthma should try to stay indoors with windows and doors closed during strong thunderstorms and for several hours afterward. Using air filters can also help reduce risk, said Deepti V. Manian, MD, an allergist and immunologist at Stormont Vail Health in Topeka, Kansas.
Patients should continue controller therapies -- such as longer-acting inhalers and allergy medications -- and use a rescue inhaler or nebulizer for prompt treatment of symptoms, recommended Donald J. Dvorin, MD, of The Allergy and Asthma Doctors in Mount Laurel, NJ. Ideally, people seeking shelter indoors during storms should be “accompanied by friends or family who can help them transport quickly to a hospital if needed.”
Asthma Diagnosis Not Required
Even peoples who would not consider themselves to have asthma can be seriously affected. For example, people with hay fever, or allergic rhinitis as it’s also known, are also at risk, said Ajay Kevat, MBBS, MPH, of the respiratory department at Queensland Children’s Hospital in Brisbane, Australia.
People with hay fever can also experience stronger symptoms during and after thunderstorms. Optimally treating allergic rhinitis during the pollen season with non-sedation antihistamines and nasal steroids can help, Dr. Virant said, instead of “chasing symptoms with medication after they are already severe.”
Part of the challenge is connecting severe weather to worse asthma symptoms. “In my experience, there is a lack of awareness surrounding thunderstorm asthma,” Dr. Manian said. For example, people with non-allergic rhinitis, also known as vasomotor rhinitis, can also experience the effects. “It often surprises many of my patients when I introduce the concept of vasomotor rhinitis, which can be triggered by environmental fluctuations.”
Gathering Clouds, Gathering Evidence
Climate change could also change which Americans experience the most storms. Researchers in a June 2022 study predicted fewer storms in the Southern plains and more storms in the Midwest and the Southeastern United States in the future.
Dr. Dvorin practices in Southern New Jersey, and in this area, “we fortunate in this area not to experience thunderstorm-induced asthma exacerbations,” he said.
But climate change means that in the future, thunderstorm asthma could strike in places it has never been seen before, said Dr. Kevat, who wrote a thunderstorm asthma review article published online June 2020 in the Journal of Asthma and Allergy.
And this is not just a concern in the United States. Major thunderstorm asthma events have been reported in Italy, the United Kingdom, the Middle East, Asia, and Australia. In November 2016, for instance, a strong set of storms swept across Melbourne, Australia. Temperatures dropped 10C (about 18F), humidity rose above 70%, and particulate matter like pollen became more concentrated in the air.
This event spurred a “thunderstorm asthma epidemic of unprecedented magnitude, tempo, and geographical range and severity,” Dr. Beggs and colleagues wrote in their June 2018 report in The Lancet Planetary Health.
Large-scale events like this can affect entire communities and quickly overwhelm local health care resources. Within 30 hours of the Melbourne storms, 3,365 people more than usual came to local emergency departments with respiratory issues — and 476 with asthma were admitted to the hospital. Ten people died: five in the hospital and five who could not be resuscitated or died while waiting for emergency services.
More research is needed “so as to best prepare for this unpredictable, significant public health threat,” Dr. Kevat wrote.
People whose asthma is triggered by pollen or mold spores are particularly at risk for thunderstorm asthma, Dr. Waqar said. If you’re unsure, an allergist can help diagnose and treat your allergic risks.
More severe thunderstorms are just one asthma trigger associated with climate change. Last summer, Canadian wildfires sent smoke across the northern U.S. and triggered widespread asthma exacerbations.
A version of this article appeared on WebMD.com.
Thunderstorm asthma can strike with little warning, leaving people with the symptoms of an asthma attack during or after the dark clouds pass.
If you’re unfamiliar, the risk for a thunderstorm asthma attack grows when heavy storms arrive on a day with very high pollen or spores. The storm uplifts these particles, adds water, and causes them to explode into smaller grains. The electrical activity in a storm can do the same. Next, strong winds sweep these particles down and across the ground. People in the path of the storm can experience shortness of breath, coughing, and wheezing.
“Yes, if only because the amount of pollen appears to be increasing in many areas due to climate change,” said Frank S. Virant, MD, chief of the Allergy Division at Seattle Children’s Hospital in Washington.
Most cases of thunderstorm asthma occur in the spring and early summer, but that also could change. Pollen seasons “have been getting longer and more intense,” said Shaan M. Waqar, MD, an allergist at ENT and Allergy Associates in Plainview, NY.
“Thunderstorm asthma events are rare, but our changing environment and the increase in the number of people with allergies may make such events more common and more severe into the future,” agreed Paul J. Beggs, PhD, associate professor in the School of Natural Sciences at Macquarie University in Sydney, Australia.
How to Minimize Your Risk
If your patients are sensitive to pollen, advise them to continue to monitor outdoor levels, particularly during tree, grass, and weed pollen season, Dr. Virant recommended. Also patients should pay attention to weather reports. Watch for thunderstorms that could “amplify exposure to the pollen with 40-plus mile per hour winds and often colder air downdrafts.” Cold is an additional asthma trigger, he noted.
People with asthma should try to stay indoors with windows and doors closed during strong thunderstorms and for several hours afterward. Using air filters can also help reduce risk, said Deepti V. Manian, MD, an allergist and immunologist at Stormont Vail Health in Topeka, Kansas.
Patients should continue controller therapies -- such as longer-acting inhalers and allergy medications -- and use a rescue inhaler or nebulizer for prompt treatment of symptoms, recommended Donald J. Dvorin, MD, of The Allergy and Asthma Doctors in Mount Laurel, NJ. Ideally, people seeking shelter indoors during storms should be “accompanied by friends or family who can help them transport quickly to a hospital if needed.”
Asthma Diagnosis Not Required
Even peoples who would not consider themselves to have asthma can be seriously affected. For example, people with hay fever, or allergic rhinitis as it’s also known, are also at risk, said Ajay Kevat, MBBS, MPH, of the respiratory department at Queensland Children’s Hospital in Brisbane, Australia.
People with hay fever can also experience stronger symptoms during and after thunderstorms. Optimally treating allergic rhinitis during the pollen season with non-sedation antihistamines and nasal steroids can help, Dr. Virant said, instead of “chasing symptoms with medication after they are already severe.”
Part of the challenge is connecting severe weather to worse asthma symptoms. “In my experience, there is a lack of awareness surrounding thunderstorm asthma,” Dr. Manian said. For example, people with non-allergic rhinitis, also known as vasomotor rhinitis, can also experience the effects. “It often surprises many of my patients when I introduce the concept of vasomotor rhinitis, which can be triggered by environmental fluctuations.”
Gathering Clouds, Gathering Evidence
Climate change could also change which Americans experience the most storms. Researchers in a June 2022 study predicted fewer storms in the Southern plains and more storms in the Midwest and the Southeastern United States in the future.
Dr. Dvorin practices in Southern New Jersey, and in this area, “we fortunate in this area not to experience thunderstorm-induced asthma exacerbations,” he said.
But climate change means that in the future, thunderstorm asthma could strike in places it has never been seen before, said Dr. Kevat, who wrote a thunderstorm asthma review article published online June 2020 in the Journal of Asthma and Allergy.
And this is not just a concern in the United States. Major thunderstorm asthma events have been reported in Italy, the United Kingdom, the Middle East, Asia, and Australia. In November 2016, for instance, a strong set of storms swept across Melbourne, Australia. Temperatures dropped 10C (about 18F), humidity rose above 70%, and particulate matter like pollen became more concentrated in the air.
This event spurred a “thunderstorm asthma epidemic of unprecedented magnitude, tempo, and geographical range and severity,” Dr. Beggs and colleagues wrote in their June 2018 report in The Lancet Planetary Health.
Large-scale events like this can affect entire communities and quickly overwhelm local health care resources. Within 30 hours of the Melbourne storms, 3,365 people more than usual came to local emergency departments with respiratory issues — and 476 with asthma were admitted to the hospital. Ten people died: five in the hospital and five who could not be resuscitated or died while waiting for emergency services.
More research is needed “so as to best prepare for this unpredictable, significant public health threat,” Dr. Kevat wrote.
People whose asthma is triggered by pollen or mold spores are particularly at risk for thunderstorm asthma, Dr. Waqar said. If you’re unsure, an allergist can help diagnose and treat your allergic risks.
More severe thunderstorms are just one asthma trigger associated with climate change. Last summer, Canadian wildfires sent smoke across the northern U.S. and triggered widespread asthma exacerbations.
A version of this article appeared on WebMD.com.
Thunderstorm asthma can strike with little warning, leaving people with the symptoms of an asthma attack during or after the dark clouds pass.
If you’re unfamiliar, the risk for a thunderstorm asthma attack grows when heavy storms arrive on a day with very high pollen or spores. The storm uplifts these particles, adds water, and causes them to explode into smaller grains. The electrical activity in a storm can do the same. Next, strong winds sweep these particles down and across the ground. People in the path of the storm can experience shortness of breath, coughing, and wheezing.
“Yes, if only because the amount of pollen appears to be increasing in many areas due to climate change,” said Frank S. Virant, MD, chief of the Allergy Division at Seattle Children’s Hospital in Washington.
Most cases of thunderstorm asthma occur in the spring and early summer, but that also could change. Pollen seasons “have been getting longer and more intense,” said Shaan M. Waqar, MD, an allergist at ENT and Allergy Associates in Plainview, NY.
“Thunderstorm asthma events are rare, but our changing environment and the increase in the number of people with allergies may make such events more common and more severe into the future,” agreed Paul J. Beggs, PhD, associate professor in the School of Natural Sciences at Macquarie University in Sydney, Australia.
How to Minimize Your Risk
If your patients are sensitive to pollen, advise them to continue to monitor outdoor levels, particularly during tree, grass, and weed pollen season, Dr. Virant recommended. Also patients should pay attention to weather reports. Watch for thunderstorms that could “amplify exposure to the pollen with 40-plus mile per hour winds and often colder air downdrafts.” Cold is an additional asthma trigger, he noted.
People with asthma should try to stay indoors with windows and doors closed during strong thunderstorms and for several hours afterward. Using air filters can also help reduce risk, said Deepti V. Manian, MD, an allergist and immunologist at Stormont Vail Health in Topeka, Kansas.
Patients should continue controller therapies -- such as longer-acting inhalers and allergy medications -- and use a rescue inhaler or nebulizer for prompt treatment of symptoms, recommended Donald J. Dvorin, MD, of The Allergy and Asthma Doctors in Mount Laurel, NJ. Ideally, people seeking shelter indoors during storms should be “accompanied by friends or family who can help them transport quickly to a hospital if needed.”
Asthma Diagnosis Not Required
Even peoples who would not consider themselves to have asthma can be seriously affected. For example, people with hay fever, or allergic rhinitis as it’s also known, are also at risk, said Ajay Kevat, MBBS, MPH, of the respiratory department at Queensland Children’s Hospital in Brisbane, Australia.
People with hay fever can also experience stronger symptoms during and after thunderstorms. Optimally treating allergic rhinitis during the pollen season with non-sedation antihistamines and nasal steroids can help, Dr. Virant said, instead of “chasing symptoms with medication after they are already severe.”
Part of the challenge is connecting severe weather to worse asthma symptoms. “In my experience, there is a lack of awareness surrounding thunderstorm asthma,” Dr. Manian said. For example, people with non-allergic rhinitis, also known as vasomotor rhinitis, can also experience the effects. “It often surprises many of my patients when I introduce the concept of vasomotor rhinitis, which can be triggered by environmental fluctuations.”
Gathering Clouds, Gathering Evidence
Climate change could also change which Americans experience the most storms. Researchers in a June 2022 study predicted fewer storms in the Southern plains and more storms in the Midwest and the Southeastern United States in the future.
Dr. Dvorin practices in Southern New Jersey, and in this area, “we fortunate in this area not to experience thunderstorm-induced asthma exacerbations,” he said.
But climate change means that in the future, thunderstorm asthma could strike in places it has never been seen before, said Dr. Kevat, who wrote a thunderstorm asthma review article published online June 2020 in the Journal of Asthma and Allergy.
And this is not just a concern in the United States. Major thunderstorm asthma events have been reported in Italy, the United Kingdom, the Middle East, Asia, and Australia. In November 2016, for instance, a strong set of storms swept across Melbourne, Australia. Temperatures dropped 10C (about 18F), humidity rose above 70%, and particulate matter like pollen became more concentrated in the air.
This event spurred a “thunderstorm asthma epidemic of unprecedented magnitude, tempo, and geographical range and severity,” Dr. Beggs and colleagues wrote in their June 2018 report in The Lancet Planetary Health.
Large-scale events like this can affect entire communities and quickly overwhelm local health care resources. Within 30 hours of the Melbourne storms, 3,365 people more than usual came to local emergency departments with respiratory issues — and 476 with asthma were admitted to the hospital. Ten people died: five in the hospital and five who could not be resuscitated or died while waiting for emergency services.
More research is needed “so as to best prepare for this unpredictable, significant public health threat,” Dr. Kevat wrote.
People whose asthma is triggered by pollen or mold spores are particularly at risk for thunderstorm asthma, Dr. Waqar said. If you’re unsure, an allergist can help diagnose and treat your allergic risks.
More severe thunderstorms are just one asthma trigger associated with climate change. Last summer, Canadian wildfires sent smoke across the northern U.S. and triggered widespread asthma exacerbations.
A version of this article appeared on WebMD.com.
COVID-19 Is a Very Weird Virus
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.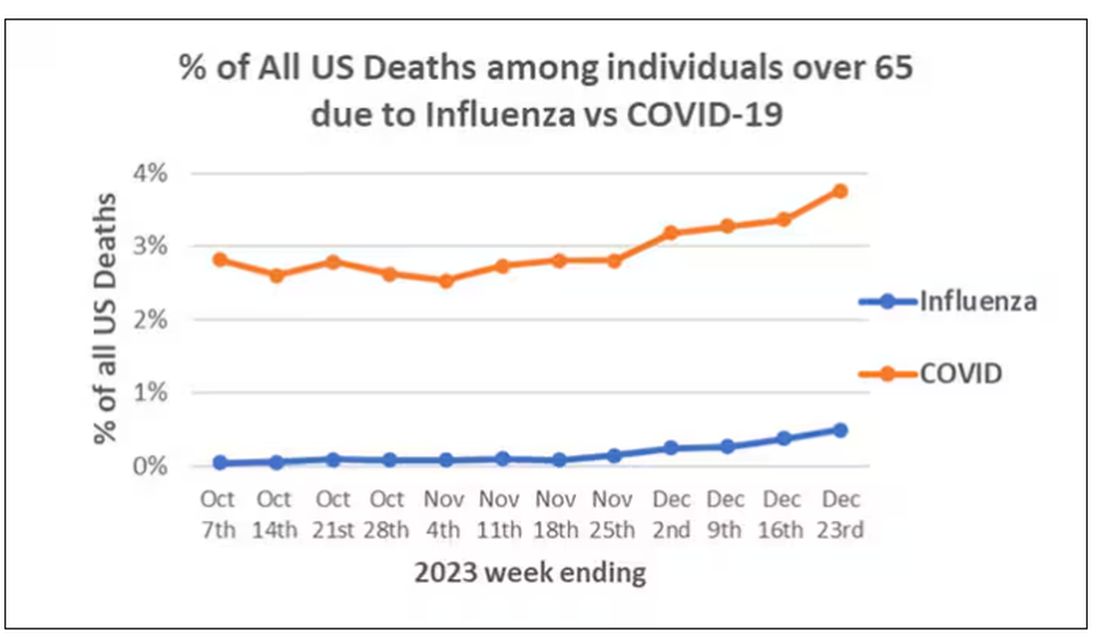
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)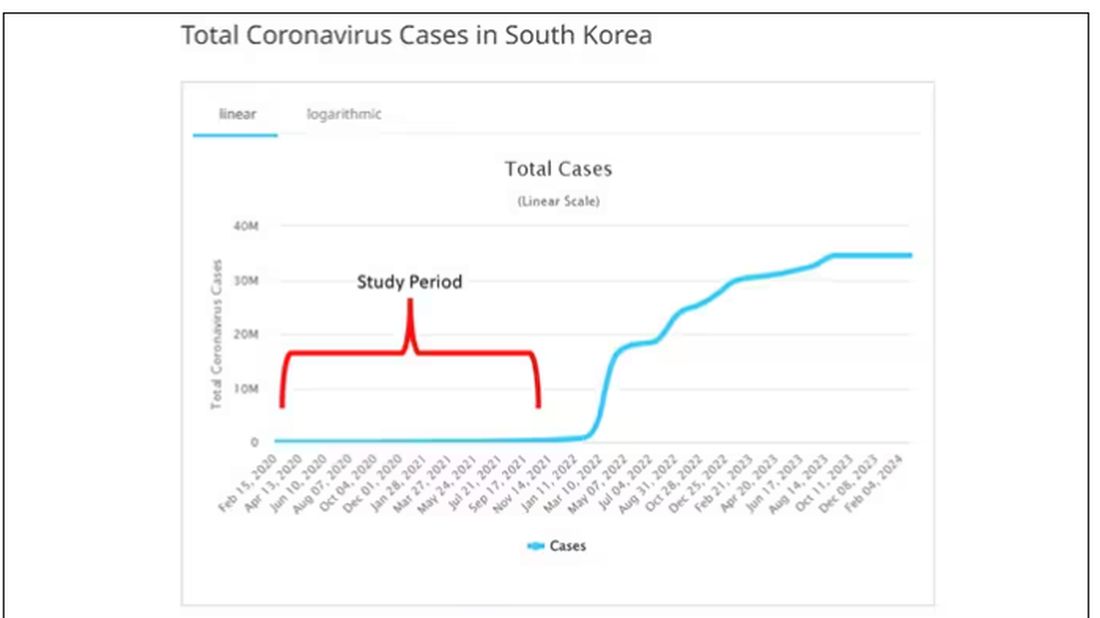
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.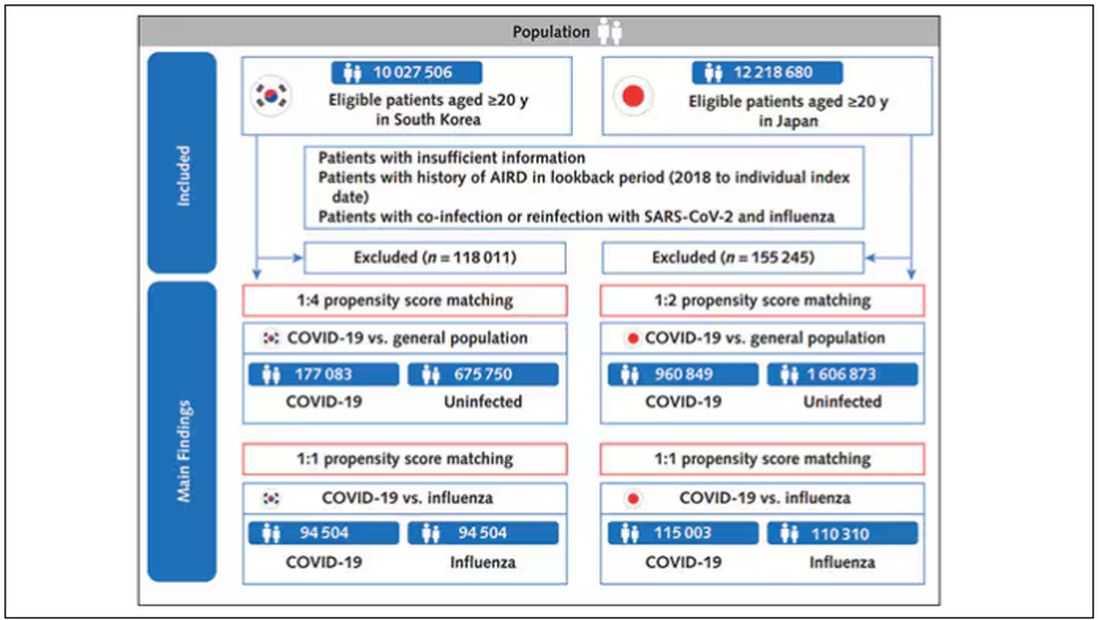
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).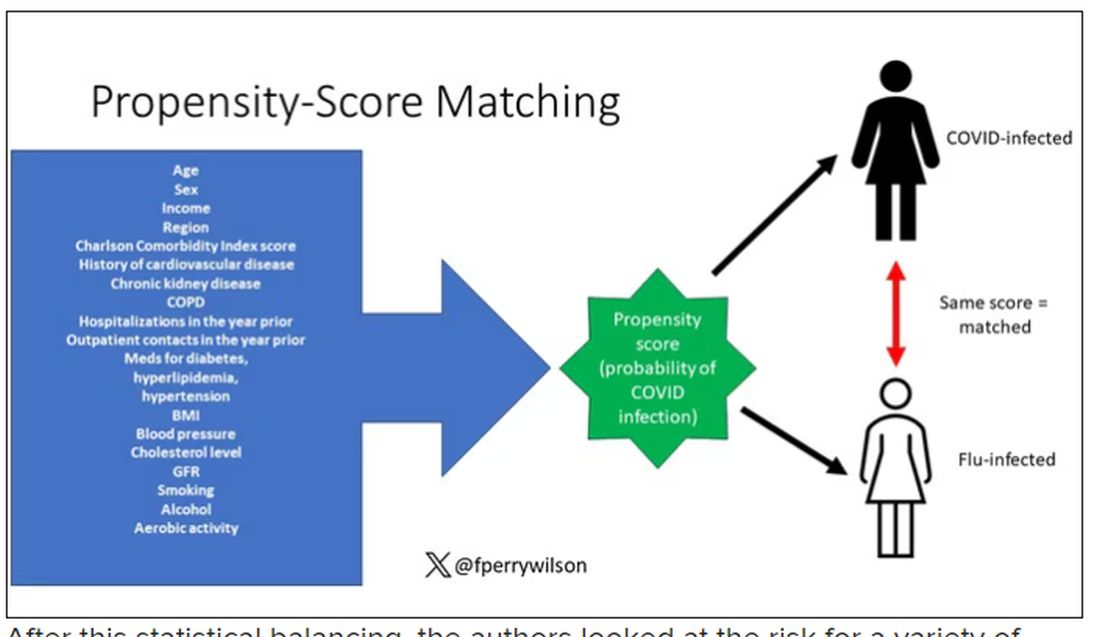
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.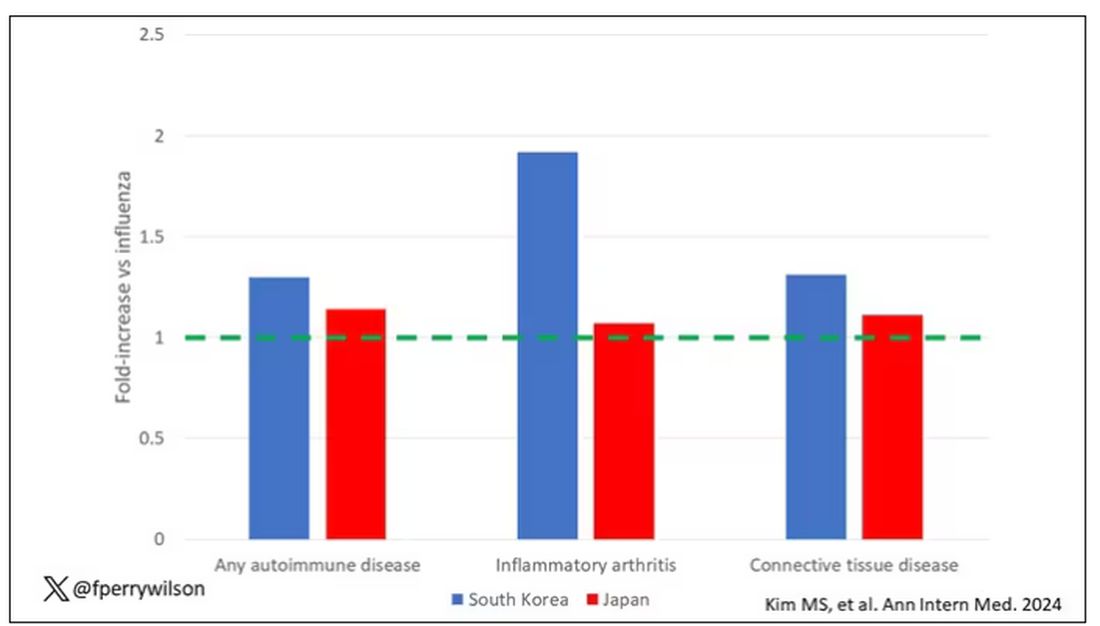
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.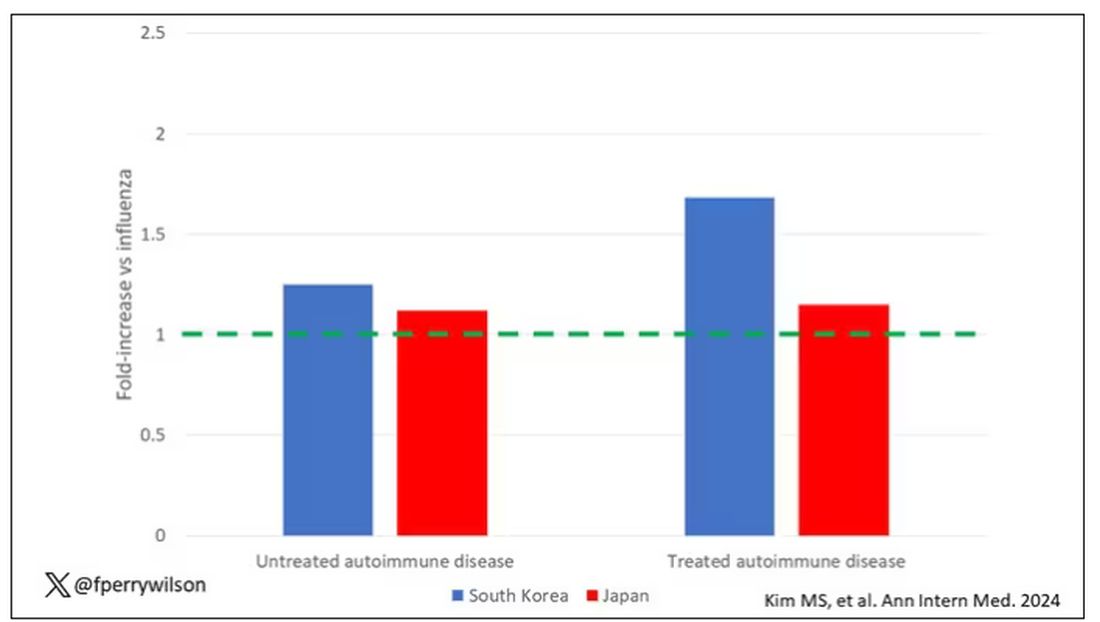
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.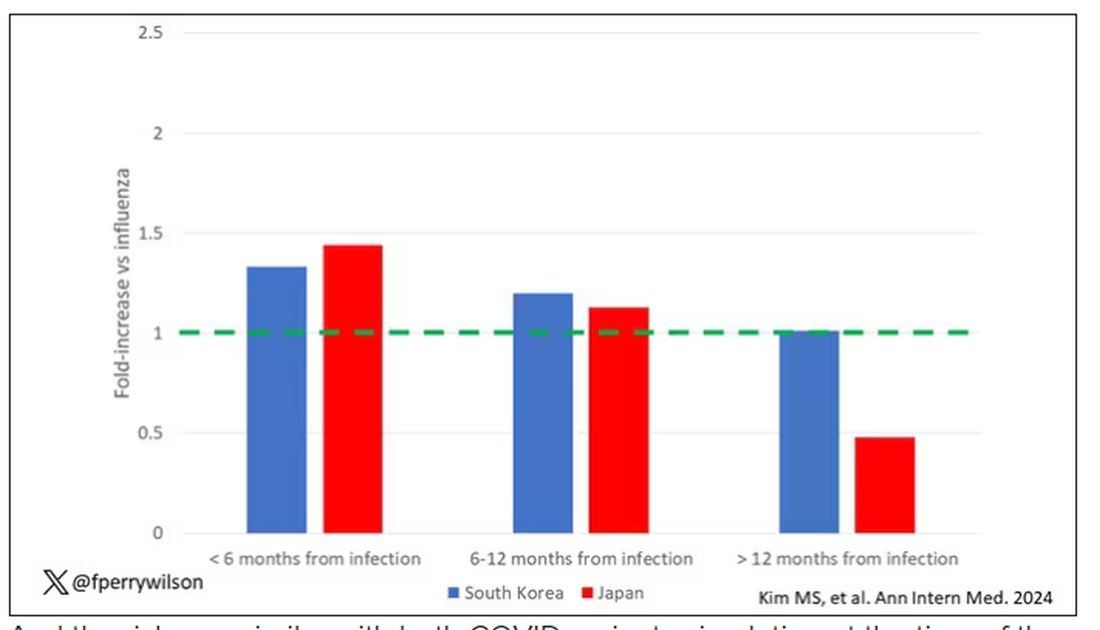
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?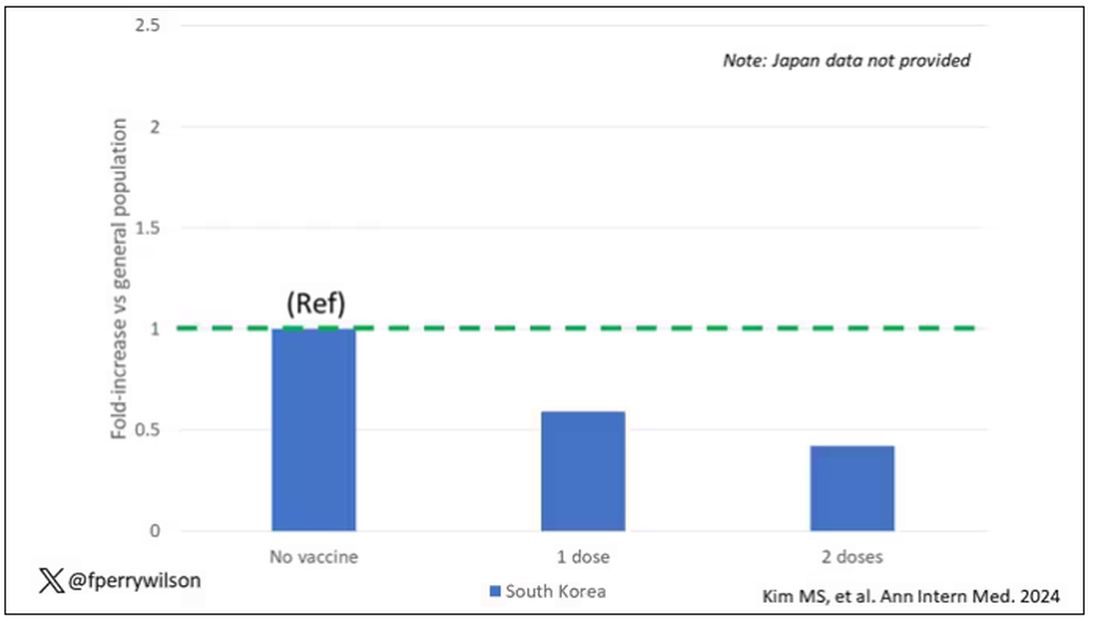
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.