User login
How not to establish rapport with your patient
1. Stride confidently into the room to greet your 84-year-old female patient.
2. Introduce yourself saying, “Hi, I’m Dr. Jeff Benabio.”
3. Extend your clenched fist toward her chest and wait for her to reciprocate.
4. Smile awkwardly behind your mask while you wait.
5. Advise that you are doing a fist bump instead of a handshake to prevent the spread of viruses.
6. Wait.
7. Explain that she can bump, also known as “dap,” you back by extending her clenched fist and bumping into yours.
8. Wait a bit more.
9. Lower your fist and pat her on the shoulder with your left hand. Do so gently so it doesn’t seem like you just did a quick right jab followed by a left hook.
10. Sit down diffidently and pray that you can help her so this office visit is not an utter disaster.
It seemed a good idea for 2020: Let’s stop shaking hands while we wait out this viral apocalypse. Sensible, but entering a patient room and just sitting down didn’t work. It felt cold, impolite – this isn’t the DMV. In medicine, a complete stranger has to trust us to get naked, tell intimate secrets, even be stuck by needles all within minutes of meeting. We needed a trust-building substitute greeting.
There was the Muslim hand-on-my-heart greeting. Or the Hindu “namaste” or Buddhist “amituofo” folded hands. Or perhaps the paternalistic shoulder pat? I went with the fist bump. With some of my partner docs, my old MBA squad, my neighbor, the fist bump felt natural, reciprocated without hesitation. But it fails with many patients. To understand why, it’s helpful to know the history of the fist bump, also known as the dap.
Dap is an acronym for Dignity And Pride. It’s a variation of a handshake that originated among Black soldiers in the Vietnam war as a means of showing fraternity and establishing connectedness. In Vietnam, 30% of the combat battalions were Black. Marginalized in the military and at home, they created a greeting that was meaningful and unique. The dap was a series of shakes, bumps, slaps, and hugs that was symbolic. It was a means of showing respect and humility, that no one is above others, that I’ve got your back and you’ve got mine. It was a powerful recognition of humanity and effective means of personal connection. It spread from the Black community to the general population and it exists still today. The choreographed pregame handshake you see so many NBA players engage in is a descendant of the dap. Like many rituals, it reinforces bonds with those who are your people, your team, those you trust.
The more generalized version is the simple fist bump. It is widely used, notably by President Obama, and in the appropriate circumstance, will almost always be reciprocated. But it doesn’t work well to create trust with a stranger. With a patient for example, you are not showing them respect for some accomplishment. Nor are we connecting with them as a member of your team. Unless this is a patient whom you’ve seen many times before, a fist bump attempt might be met with “are you serious?” In fact, a survey done in 2016 asking infectious disease professionals what they thought of fist bumps as a greeting, very few replied it was a good idea. Most felt it was unprofessional. Not to mention that a fist bump does not symbolize an agreement in the way that a handshake does (and has done since at least the 9th century BC).
With COVID waning and masks doffed, I’ve found myself back to handshaking. Yes, I sanitize before and after, another ritual that has symbolic as well as practical significance. I get fewer sideways glances from my geriatric patients for sure. But I do still offer a little dap for my liquid nitrogen–survivor kids and for the occasional fellow Gen Xer. “Wonder Twin powers, activate!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com
1. Stride confidently into the room to greet your 84-year-old female patient.
2. Introduce yourself saying, “Hi, I’m Dr. Jeff Benabio.”
3. Extend your clenched fist toward her chest and wait for her to reciprocate.
4. Smile awkwardly behind your mask while you wait.
5. Advise that you are doing a fist bump instead of a handshake to prevent the spread of viruses.
6. Wait.
7. Explain that she can bump, also known as “dap,” you back by extending her clenched fist and bumping into yours.
8. Wait a bit more.
9. Lower your fist and pat her on the shoulder with your left hand. Do so gently so it doesn’t seem like you just did a quick right jab followed by a left hook.
10. Sit down diffidently and pray that you can help her so this office visit is not an utter disaster.
It seemed a good idea for 2020: Let’s stop shaking hands while we wait out this viral apocalypse. Sensible, but entering a patient room and just sitting down didn’t work. It felt cold, impolite – this isn’t the DMV. In medicine, a complete stranger has to trust us to get naked, tell intimate secrets, even be stuck by needles all within minutes of meeting. We needed a trust-building substitute greeting.
There was the Muslim hand-on-my-heart greeting. Or the Hindu “namaste” or Buddhist “amituofo” folded hands. Or perhaps the paternalistic shoulder pat? I went with the fist bump. With some of my partner docs, my old MBA squad, my neighbor, the fist bump felt natural, reciprocated without hesitation. But it fails with many patients. To understand why, it’s helpful to know the history of the fist bump, also known as the dap.
Dap is an acronym for Dignity And Pride. It’s a variation of a handshake that originated among Black soldiers in the Vietnam war as a means of showing fraternity and establishing connectedness. In Vietnam, 30% of the combat battalions were Black. Marginalized in the military and at home, they created a greeting that was meaningful and unique. The dap was a series of shakes, bumps, slaps, and hugs that was symbolic. It was a means of showing respect and humility, that no one is above others, that I’ve got your back and you’ve got mine. It was a powerful recognition of humanity and effective means of personal connection. It spread from the Black community to the general population and it exists still today. The choreographed pregame handshake you see so many NBA players engage in is a descendant of the dap. Like many rituals, it reinforces bonds with those who are your people, your team, those you trust.
The more generalized version is the simple fist bump. It is widely used, notably by President Obama, and in the appropriate circumstance, will almost always be reciprocated. But it doesn’t work well to create trust with a stranger. With a patient for example, you are not showing them respect for some accomplishment. Nor are we connecting with them as a member of your team. Unless this is a patient whom you’ve seen many times before, a fist bump attempt might be met with “are you serious?” In fact, a survey done in 2016 asking infectious disease professionals what they thought of fist bumps as a greeting, very few replied it was a good idea. Most felt it was unprofessional. Not to mention that a fist bump does not symbolize an agreement in the way that a handshake does (and has done since at least the 9th century BC).
With COVID waning and masks doffed, I’ve found myself back to handshaking. Yes, I sanitize before and after, another ritual that has symbolic as well as practical significance. I get fewer sideways glances from my geriatric patients for sure. But I do still offer a little dap for my liquid nitrogen–survivor kids and for the occasional fellow Gen Xer. “Wonder Twin powers, activate!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com
1. Stride confidently into the room to greet your 84-year-old female patient.
2. Introduce yourself saying, “Hi, I’m Dr. Jeff Benabio.”
3. Extend your clenched fist toward her chest and wait for her to reciprocate.
4. Smile awkwardly behind your mask while you wait.
5. Advise that you are doing a fist bump instead of a handshake to prevent the spread of viruses.
6. Wait.
7. Explain that she can bump, also known as “dap,” you back by extending her clenched fist and bumping into yours.
8. Wait a bit more.
9. Lower your fist and pat her on the shoulder with your left hand. Do so gently so it doesn’t seem like you just did a quick right jab followed by a left hook.
10. Sit down diffidently and pray that you can help her so this office visit is not an utter disaster.
It seemed a good idea for 2020: Let’s stop shaking hands while we wait out this viral apocalypse. Sensible, but entering a patient room and just sitting down didn’t work. It felt cold, impolite – this isn’t the DMV. In medicine, a complete stranger has to trust us to get naked, tell intimate secrets, even be stuck by needles all within minutes of meeting. We needed a trust-building substitute greeting.
There was the Muslim hand-on-my-heart greeting. Or the Hindu “namaste” or Buddhist “amituofo” folded hands. Or perhaps the paternalistic shoulder pat? I went with the fist bump. With some of my partner docs, my old MBA squad, my neighbor, the fist bump felt natural, reciprocated without hesitation. But it fails with many patients. To understand why, it’s helpful to know the history of the fist bump, also known as the dap.
Dap is an acronym for Dignity And Pride. It’s a variation of a handshake that originated among Black soldiers in the Vietnam war as a means of showing fraternity and establishing connectedness. In Vietnam, 30% of the combat battalions were Black. Marginalized in the military and at home, they created a greeting that was meaningful and unique. The dap was a series of shakes, bumps, slaps, and hugs that was symbolic. It was a means of showing respect and humility, that no one is above others, that I’ve got your back and you’ve got mine. It was a powerful recognition of humanity and effective means of personal connection. It spread from the Black community to the general population and it exists still today. The choreographed pregame handshake you see so many NBA players engage in is a descendant of the dap. Like many rituals, it reinforces bonds with those who are your people, your team, those you trust.
The more generalized version is the simple fist bump. It is widely used, notably by President Obama, and in the appropriate circumstance, will almost always be reciprocated. But it doesn’t work well to create trust with a stranger. With a patient for example, you are not showing them respect for some accomplishment. Nor are we connecting with them as a member of your team. Unless this is a patient whom you’ve seen many times before, a fist bump attempt might be met with “are you serious?” In fact, a survey done in 2016 asking infectious disease professionals what they thought of fist bumps as a greeting, very few replied it was a good idea. Most felt it was unprofessional. Not to mention that a fist bump does not symbolize an agreement in the way that a handshake does (and has done since at least the 9th century BC).
With COVID waning and masks doffed, I’ve found myself back to handshaking. Yes, I sanitize before and after, another ritual that has symbolic as well as practical significance. I get fewer sideways glances from my geriatric patients for sure. But I do still offer a little dap for my liquid nitrogen–survivor kids and for the occasional fellow Gen Xer. “Wonder Twin powers, activate!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com
Book review: “Sexual Citizens”
The Sexual Health Initiative to Foster Transformation (SHIFT)1 is a landmark study about sexual assault at college, which has generated 20 scientific articles and several chapters in books, but unfortunately, has not made its way into the psychiatric literature.
“Sexual Citizens: Sex, Power and Assault on Campus,” by Jennifer Hirsch and Shamus Khan, (available in audio book and paperback) was written as a follow up to the SHIFT study, so the rest of us can absorb the findings.2 This mixed-methods study included a survey of over 1,600 students aged 18-29 from Columbia University and Barnard College regarding their relationships and sexual histories, including assault. Data were collected using daily diaries, focus groups, and hundreds of hours of field work observation by young researchers. One- to 3-hour in-depth interviews exploring sexual experiences on campus were conducted with 151 students. These interviews are the focus of the book. It is a well-written, provocative story brimming with insights for those of us who lack the time to scour social science literature.
“Sexual Citizens” and the SHIFT study confirmed much of what we know. Sexual assault is common and has enduring effects. The study found that 36% of women and 15% of men had experienced unwanted, nonconsensual sexual contact by senior year. Twenty percent of women and 6% of men were rape survivors. Freshman, LGBTQ, and minority students were found at highest risk of assault. SHIFT reaffirmed that abstinence-only education is not a protective factor against college sexual assault, but neither was knowledge of affirmative consent (the practice of “ongoing and explicit” checking-in with partners) which few students ever employed. Encouragingly, students taught refusal skills were less likely to experience sexual assault.
Many of the book’s valuable lessons fall under the umbrella of failures of language and communication. For example, after drinking, they went to his room. She was expecting a social interaction, but with no other place to sit, they sat on his bed where she was coaxed or pressured into a sexual encounter. Afterward, she leaves, and it is never discussed again. One partner desires emotional intimacy, and the other, bragging rights in the fraternity or at the girls’ weekly brunch. Numerous personal stories like these, though at times heart wrenching, provide perspective on the barriers to addressing assault.
Subjects relayed experiences of assault by strangers or friends, and some provided details of their own actions as perpetrators. Stumbling around words and emotions, an avoidance of explicit language stemmed from shame, a fear of personal responsibility, the desire to maintain social cohesion, and concern for potential consequences for the perpetrator. Many subjects were resistant to calling nonconsensual sexual activity rape or even assault. Some who had perpetrated were unaware their behavior may have been experienced as assault, with recognition of this fact dawning during interviews.
This apparent limitation in self-reflective capacity may be in part due to the conceptualization of what assault is. Focus groups identified a discernible difference in how men and women understood assaults, with men believing rapes looked like a woman fighting back and screaming for help ... which is rarely what happens.
Notably absent among the interviewed are any flagrant perpetrators. The methodology section theorizes that individuals who intentionally harmed their peers were unlikely to choose to participate in this study. In addition, the characterization of assailants as “sociopathic predators” is based in a history of racialized imagery that leads us astray from the truth about campus sexual assault. Most assaults do not involve force, and SHIFT data showed 75% of victims knew their assailants. Ultimately, a major aim of the research was to study assault alongside healthy sex to “understand those pivotal moments when encounters change from being sex, to being assault.” Doing this requires understanding the where, how, and why students have sex, a more complicated undertaking than we may think.
In discussing their sexual lives, subjects frequently noted they did not have space to talk about their assaults. Though 81% of students discussed their experiences with someone, friend groups were often overburdened with stories, which minimized the victim’s experience. Furthermore, most had not sought help from the student counseling centers. Students navigating this complex field were frequently doing so in isolation. SHIFT found subjects to be eager to participate; they would often express thankfulness, and a sense of freedom in sharing with researchers. Commonly, students expressly did not want retribution for perpetrators, but simply a place to be heard without challenge. The current legal system precludes that possibility, leaving individuals without the option to confront perpetrators, and perpetrators often not knowing the extent of the damage they caused.
Where can psychiatrists have an impact right now? “Sexual Citizens” identifies four key areas for intervention to work toward a world with less sexual assault. These are:
- Improving diversity, inequality, and power distortions.
- Education about sex and sexual assault.
- Substance use.
- Mental health.
Substance use and mental health are especially relevant for psychiatrists (That substance use contributes to sexual assault is known by approximately ... everybody!). Unwanted sexual contact prior to college (20% of students) increased the odds of experiencing assault during college. Harm reduction strategies should be introduced before college, according to the SHIFT research, particularly in skills-based training on how to say “No” to unwanted sex. Psychiatrists are likely used to asking brief history questions related to sexual assault and rape. “Sexual Citizens” highlights the inadequacy of this blunt language and guides the reader toward a refined knowledge of the language needed to address sexual assault.
Dr. Whisler is a child and adolescent psychiatry fellow at the Stanford (Calif.) University. Dr. Higgins is affiliate associate professor of psychiatry and family medicine at the Medical University of South Carolina, Charleston.
References
1. Hirsch JS et al. Social dimensions of sexual consent among cisgender heterosexual college students: Insights from ethnographic research. J Adolesc Health. 2019 Jan;64(1):26-35. doi: 10.1016/j.jadohealth.2018.06.011.
2. Hirsch JS and Khan S. Sexual citizens: Sex, power, and assault on campus. New York: W.W. Norton & Company, 2020.
The Sexual Health Initiative to Foster Transformation (SHIFT)1 is a landmark study about sexual assault at college, which has generated 20 scientific articles and several chapters in books, but unfortunately, has not made its way into the psychiatric literature.
“Sexual Citizens: Sex, Power and Assault on Campus,” by Jennifer Hirsch and Shamus Khan, (available in audio book and paperback) was written as a follow up to the SHIFT study, so the rest of us can absorb the findings.2 This mixed-methods study included a survey of over 1,600 students aged 18-29 from Columbia University and Barnard College regarding their relationships and sexual histories, including assault. Data were collected using daily diaries, focus groups, and hundreds of hours of field work observation by young researchers. One- to 3-hour in-depth interviews exploring sexual experiences on campus were conducted with 151 students. These interviews are the focus of the book. It is a well-written, provocative story brimming with insights for those of us who lack the time to scour social science literature.
“Sexual Citizens” and the SHIFT study confirmed much of what we know. Sexual assault is common and has enduring effects. The study found that 36% of women and 15% of men had experienced unwanted, nonconsensual sexual contact by senior year. Twenty percent of women and 6% of men were rape survivors. Freshman, LGBTQ, and minority students were found at highest risk of assault. SHIFT reaffirmed that abstinence-only education is not a protective factor against college sexual assault, but neither was knowledge of affirmative consent (the practice of “ongoing and explicit” checking-in with partners) which few students ever employed. Encouragingly, students taught refusal skills were less likely to experience sexual assault.
Many of the book’s valuable lessons fall under the umbrella of failures of language and communication. For example, after drinking, they went to his room. She was expecting a social interaction, but with no other place to sit, they sat on his bed where she was coaxed or pressured into a sexual encounter. Afterward, she leaves, and it is never discussed again. One partner desires emotional intimacy, and the other, bragging rights in the fraternity or at the girls’ weekly brunch. Numerous personal stories like these, though at times heart wrenching, provide perspective on the barriers to addressing assault.
Subjects relayed experiences of assault by strangers or friends, and some provided details of their own actions as perpetrators. Stumbling around words and emotions, an avoidance of explicit language stemmed from shame, a fear of personal responsibility, the desire to maintain social cohesion, and concern for potential consequences for the perpetrator. Many subjects were resistant to calling nonconsensual sexual activity rape or even assault. Some who had perpetrated were unaware their behavior may have been experienced as assault, with recognition of this fact dawning during interviews.
This apparent limitation in self-reflective capacity may be in part due to the conceptualization of what assault is. Focus groups identified a discernible difference in how men and women understood assaults, with men believing rapes looked like a woman fighting back and screaming for help ... which is rarely what happens.
Notably absent among the interviewed are any flagrant perpetrators. The methodology section theorizes that individuals who intentionally harmed their peers were unlikely to choose to participate in this study. In addition, the characterization of assailants as “sociopathic predators” is based in a history of racialized imagery that leads us astray from the truth about campus sexual assault. Most assaults do not involve force, and SHIFT data showed 75% of victims knew their assailants. Ultimately, a major aim of the research was to study assault alongside healthy sex to “understand those pivotal moments when encounters change from being sex, to being assault.” Doing this requires understanding the where, how, and why students have sex, a more complicated undertaking than we may think.
In discussing their sexual lives, subjects frequently noted they did not have space to talk about their assaults. Though 81% of students discussed their experiences with someone, friend groups were often overburdened with stories, which minimized the victim’s experience. Furthermore, most had not sought help from the student counseling centers. Students navigating this complex field were frequently doing so in isolation. SHIFT found subjects to be eager to participate; they would often express thankfulness, and a sense of freedom in sharing with researchers. Commonly, students expressly did not want retribution for perpetrators, but simply a place to be heard without challenge. The current legal system precludes that possibility, leaving individuals without the option to confront perpetrators, and perpetrators often not knowing the extent of the damage they caused.
Where can psychiatrists have an impact right now? “Sexual Citizens” identifies four key areas for intervention to work toward a world with less sexual assault. These are:
- Improving diversity, inequality, and power distortions.
- Education about sex and sexual assault.
- Substance use.
- Mental health.
Substance use and mental health are especially relevant for psychiatrists (That substance use contributes to sexual assault is known by approximately ... everybody!). Unwanted sexual contact prior to college (20% of students) increased the odds of experiencing assault during college. Harm reduction strategies should be introduced before college, according to the SHIFT research, particularly in skills-based training on how to say “No” to unwanted sex. Psychiatrists are likely used to asking brief history questions related to sexual assault and rape. “Sexual Citizens” highlights the inadequacy of this blunt language and guides the reader toward a refined knowledge of the language needed to address sexual assault.
Dr. Whisler is a child and adolescent psychiatry fellow at the Stanford (Calif.) University. Dr. Higgins is affiliate associate professor of psychiatry and family medicine at the Medical University of South Carolina, Charleston.
References
1. Hirsch JS et al. Social dimensions of sexual consent among cisgender heterosexual college students: Insights from ethnographic research. J Adolesc Health. 2019 Jan;64(1):26-35. doi: 10.1016/j.jadohealth.2018.06.011.
2. Hirsch JS and Khan S. Sexual citizens: Sex, power, and assault on campus. New York: W.W. Norton & Company, 2020.
The Sexual Health Initiative to Foster Transformation (SHIFT)1 is a landmark study about sexual assault at college, which has generated 20 scientific articles and several chapters in books, but unfortunately, has not made its way into the psychiatric literature.
“Sexual Citizens: Sex, Power and Assault on Campus,” by Jennifer Hirsch and Shamus Khan, (available in audio book and paperback) was written as a follow up to the SHIFT study, so the rest of us can absorb the findings.2 This mixed-methods study included a survey of over 1,600 students aged 18-29 from Columbia University and Barnard College regarding their relationships and sexual histories, including assault. Data were collected using daily diaries, focus groups, and hundreds of hours of field work observation by young researchers. One- to 3-hour in-depth interviews exploring sexual experiences on campus were conducted with 151 students. These interviews are the focus of the book. It is a well-written, provocative story brimming with insights for those of us who lack the time to scour social science literature.
“Sexual Citizens” and the SHIFT study confirmed much of what we know. Sexual assault is common and has enduring effects. The study found that 36% of women and 15% of men had experienced unwanted, nonconsensual sexual contact by senior year. Twenty percent of women and 6% of men were rape survivors. Freshman, LGBTQ, and minority students were found at highest risk of assault. SHIFT reaffirmed that abstinence-only education is not a protective factor against college sexual assault, but neither was knowledge of affirmative consent (the practice of “ongoing and explicit” checking-in with partners) which few students ever employed. Encouragingly, students taught refusal skills were less likely to experience sexual assault.
Many of the book’s valuable lessons fall under the umbrella of failures of language and communication. For example, after drinking, they went to his room. She was expecting a social interaction, but with no other place to sit, they sat on his bed where she was coaxed or pressured into a sexual encounter. Afterward, she leaves, and it is never discussed again. One partner desires emotional intimacy, and the other, bragging rights in the fraternity or at the girls’ weekly brunch. Numerous personal stories like these, though at times heart wrenching, provide perspective on the barriers to addressing assault.
Subjects relayed experiences of assault by strangers or friends, and some provided details of their own actions as perpetrators. Stumbling around words and emotions, an avoidance of explicit language stemmed from shame, a fear of personal responsibility, the desire to maintain social cohesion, and concern for potential consequences for the perpetrator. Many subjects were resistant to calling nonconsensual sexual activity rape or even assault. Some who had perpetrated were unaware their behavior may have been experienced as assault, with recognition of this fact dawning during interviews.
This apparent limitation in self-reflective capacity may be in part due to the conceptualization of what assault is. Focus groups identified a discernible difference in how men and women understood assaults, with men believing rapes looked like a woman fighting back and screaming for help ... which is rarely what happens.
Notably absent among the interviewed are any flagrant perpetrators. The methodology section theorizes that individuals who intentionally harmed their peers were unlikely to choose to participate in this study. In addition, the characterization of assailants as “sociopathic predators” is based in a history of racialized imagery that leads us astray from the truth about campus sexual assault. Most assaults do not involve force, and SHIFT data showed 75% of victims knew their assailants. Ultimately, a major aim of the research was to study assault alongside healthy sex to “understand those pivotal moments when encounters change from being sex, to being assault.” Doing this requires understanding the where, how, and why students have sex, a more complicated undertaking than we may think.
In discussing their sexual lives, subjects frequently noted they did not have space to talk about their assaults. Though 81% of students discussed their experiences with someone, friend groups were often overburdened with stories, which minimized the victim’s experience. Furthermore, most had not sought help from the student counseling centers. Students navigating this complex field were frequently doing so in isolation. SHIFT found subjects to be eager to participate; they would often express thankfulness, and a sense of freedom in sharing with researchers. Commonly, students expressly did not want retribution for perpetrators, but simply a place to be heard without challenge. The current legal system precludes that possibility, leaving individuals without the option to confront perpetrators, and perpetrators often not knowing the extent of the damage they caused.
Where can psychiatrists have an impact right now? “Sexual Citizens” identifies four key areas for intervention to work toward a world with less sexual assault. These are:
- Improving diversity, inequality, and power distortions.
- Education about sex and sexual assault.
- Substance use.
- Mental health.
Substance use and mental health are especially relevant for psychiatrists (That substance use contributes to sexual assault is known by approximately ... everybody!). Unwanted sexual contact prior to college (20% of students) increased the odds of experiencing assault during college. Harm reduction strategies should be introduced before college, according to the SHIFT research, particularly in skills-based training on how to say “No” to unwanted sex. Psychiatrists are likely used to asking brief history questions related to sexual assault and rape. “Sexual Citizens” highlights the inadequacy of this blunt language and guides the reader toward a refined knowledge of the language needed to address sexual assault.
Dr. Whisler is a child and adolescent psychiatry fellow at the Stanford (Calif.) University. Dr. Higgins is affiliate associate professor of psychiatry and family medicine at the Medical University of South Carolina, Charleston.
References
1. Hirsch JS et al. Social dimensions of sexual consent among cisgender heterosexual college students: Insights from ethnographic research. J Adolesc Health. 2019 Jan;64(1):26-35. doi: 10.1016/j.jadohealth.2018.06.011.
2. Hirsch JS and Khan S. Sexual citizens: Sex, power, and assault on campus. New York: W.W. Norton & Company, 2020.
A 63-year-old male presented for evaluation of worsening genital lesions and associated swelling
.1 Clinically, ENV presents as verrucous, hyperkeratotic, cobblestone-like patches, plaques, and nodules with associated nonpitting edema of the affected body area.1 Secondary bacterial infections are common and often worsen the clinical course. The etiology of ENV involves chronic lymphatic obstruction and venous insufficiency, with additional risk factors including obesity, chronic lymphedema, bacterial infection, surgery or trauma, neoplasia, radiation, congestive heart failure, or scleroderma.2,3 While most commonly presenting on the lower extremities, cases have been reported involving the abdomen, sacrum, ears, buttocks, and penoscrotal area.1,2

Regardless of location, the pathogenesis of ENV remains the same. Chronic lymphatic obstruction results in accumulation and lymphostasis of protein-rich dermal fluid, which subsequently precipitates fibroblast proliferation and activation, suppression of the local immune response and development of recurrent lymphangitis, chronic inflammation, and potential secondary bacterial infection.2,4
There is no standard of care for the treatment and management of ENV and recurrence is common. Interventions often involve those used for chronic lymphedema – including leg elevation, compression stockings or devices, skin hygiene, and lymphatic pumping.2,3 Medical management with topical and oral retinoids has been reported, as well as emphasis on weight loss and infection control.1,4 Surgical intervention is often reserved for refractory cases that fail to respond to more conservative management, or severe presentations resulting in extensive functional and aesthetic impairment. Less commonly reported treatment modalities include lymphaticovenular anastomosis and ablative carbon dioxide laser use, although this latter intervention demonstrated minimal improvement in this patient.5,6
Penoscrotal ENV is a rare form of ENV affecting the genital region of males, often resulting in significant disfigurement, functional impairment, and psychosocial distress. Penoscrotal elephantiasis can be idiopathic, due to filarial infections, scleroinflammatory stricture of the urethra, Chlamydia trachomatis infection, and lymphostasis secondary to chronic inflammatory conditions such as streptococcal infections, radiotherapy, surgery, chronic venous stasis, or Kaposi sarcoma.7
In addition, hidradenitis suppurativa (HS) has been documented multiple times in the literature in association with the development of ENV, detailing lymphatic scarring secondary to chronic inguinal HS as the main pathogenic factor.8,9
Surgery is the mainstay of treatment for penoscrotal ENV, which not only improves functionality and cosmesis, but also aids in prevention of rare malignant sequelae, such as lymphangiosarcoma.10 Such interventions can involve lymphangioplasty to aid in lymphatic drainage or excision of the mass and subcutaneous tissue with full-thickness skin grafting for reconstruction.7 Collaboration between urology, plastic surgery, and dermatology is often essential to obtain adequate care with satisfactory outcomes and minimal recurrence for patients with this uncommon condition.
This case and photo were submitted by Marlee Hill, a medical student at the University of Oklahoma, Oklahoma City; and Michael Franzetti, MD, and Jeffrey McBride, MD, department of dermatology, University of Oklahoma Health Sciences Center. The column was edited by Donna Bilu Martin, MD.
Dr. Donna Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Hadian Y et al. Dermatol Online J. 2019 Dec 15;25(12):13030/qt6rn1s8ff.
2. Judge N and Kilic A. J Dermatol Case Rep. 2016 Nov 13;10(2):32-4.
3. Dean SM et al. J Am Acad Dermatol. 2011 Jun;64(6):1104-10.
4. Sisto K and Khachemoune A. Am J Clin Dermatol. 2008;9(3):141-6.
5. Motegi S et al. Dermatology. 2007;215(2):147-51.
6. Robinson CG et al. J Cutan Med Surg. 2018;22(6):611-3.
7. Koualla S et al. Ann Chir Plast Esthet. 2023 Apr 10;S0294-1260(23)00035-3.
8. Lelonek E et al. Acta Derm Venereol. 2021 Feb 11;101(2):adv00389.
9. Good LM et al. J Am Acad Dermatol. 2011 May;64(5):993-4.
10. Cerri A et al. Eur J Dermatol. 1998 Oct-Nov;8(7):511-4.
.1 Clinically, ENV presents as verrucous, hyperkeratotic, cobblestone-like patches, plaques, and nodules with associated nonpitting edema of the affected body area.1 Secondary bacterial infections are common and often worsen the clinical course. The etiology of ENV involves chronic lymphatic obstruction and venous insufficiency, with additional risk factors including obesity, chronic lymphedema, bacterial infection, surgery or trauma, neoplasia, radiation, congestive heart failure, or scleroderma.2,3 While most commonly presenting on the lower extremities, cases have been reported involving the abdomen, sacrum, ears, buttocks, and penoscrotal area.1,2
Regardless of location, the pathogenesis of ENV remains the same. Chronic lymphatic obstruction results in accumulation and lymphostasis of protein-rich dermal fluid, which subsequently precipitates fibroblast proliferation and activation, suppression of the local immune response and development of recurrent lymphangitis, chronic inflammation, and potential secondary bacterial infection.2,4
There is no standard of care for the treatment and management of ENV and recurrence is common. Interventions often involve those used for chronic lymphedema – including leg elevation, compression stockings or devices, skin hygiene, and lymphatic pumping.2,3 Medical management with topical and oral retinoids has been reported, as well as emphasis on weight loss and infection control.1,4 Surgical intervention is often reserved for refractory cases that fail to respond to more conservative management, or severe presentations resulting in extensive functional and aesthetic impairment. Less commonly reported treatment modalities include lymphaticovenular anastomosis and ablative carbon dioxide laser use, although this latter intervention demonstrated minimal improvement in this patient.5,6
Penoscrotal ENV is a rare form of ENV affecting the genital region of males, often resulting in significant disfigurement, functional impairment, and psychosocial distress. Penoscrotal elephantiasis can be idiopathic, due to filarial infections, scleroinflammatory stricture of the urethra, Chlamydia trachomatis infection, and lymphostasis secondary to chronic inflammatory conditions such as streptococcal infections, radiotherapy, surgery, chronic venous stasis, or Kaposi sarcoma.7
In addition, hidradenitis suppurativa (HS) has been documented multiple times in the literature in association with the development of ENV, detailing lymphatic scarring secondary to chronic inguinal HS as the main pathogenic factor.8,9
Surgery is the mainstay of treatment for penoscrotal ENV, which not only improves functionality and cosmesis, but also aids in prevention of rare malignant sequelae, such as lymphangiosarcoma.10 Such interventions can involve lymphangioplasty to aid in lymphatic drainage or excision of the mass and subcutaneous tissue with full-thickness skin grafting for reconstruction.7 Collaboration between urology, plastic surgery, and dermatology is often essential to obtain adequate care with satisfactory outcomes and minimal recurrence for patients with this uncommon condition.
This case and photo were submitted by Marlee Hill, a medical student at the University of Oklahoma, Oklahoma City; and Michael Franzetti, MD, and Jeffrey McBride, MD, department of dermatology, University of Oklahoma Health Sciences Center. The column was edited by Donna Bilu Martin, MD.
Dr. Donna Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Hadian Y et al. Dermatol Online J. 2019 Dec 15;25(12):13030/qt6rn1s8ff.
2. Judge N and Kilic A. J Dermatol Case Rep. 2016 Nov 13;10(2):32-4.
3. Dean SM et al. J Am Acad Dermatol. 2011 Jun;64(6):1104-10.
4. Sisto K and Khachemoune A. Am J Clin Dermatol. 2008;9(3):141-6.
5. Motegi S et al. Dermatology. 2007;215(2):147-51.
6. Robinson CG et al. J Cutan Med Surg. 2018;22(6):611-3.
7. Koualla S et al. Ann Chir Plast Esthet. 2023 Apr 10;S0294-1260(23)00035-3.
8. Lelonek E et al. Acta Derm Venereol. 2021 Feb 11;101(2):adv00389.
9. Good LM et al. J Am Acad Dermatol. 2011 May;64(5):993-4.
10. Cerri A et al. Eur J Dermatol. 1998 Oct-Nov;8(7):511-4.
.1 Clinically, ENV presents as verrucous, hyperkeratotic, cobblestone-like patches, plaques, and nodules with associated nonpitting edema of the affected body area.1 Secondary bacterial infections are common and often worsen the clinical course. The etiology of ENV involves chronic lymphatic obstruction and venous insufficiency, with additional risk factors including obesity, chronic lymphedema, bacterial infection, surgery or trauma, neoplasia, radiation, congestive heart failure, or scleroderma.2,3 While most commonly presenting on the lower extremities, cases have been reported involving the abdomen, sacrum, ears, buttocks, and penoscrotal area.1,2
Regardless of location, the pathogenesis of ENV remains the same. Chronic lymphatic obstruction results in accumulation and lymphostasis of protein-rich dermal fluid, which subsequently precipitates fibroblast proliferation and activation, suppression of the local immune response and development of recurrent lymphangitis, chronic inflammation, and potential secondary bacterial infection.2,4
There is no standard of care for the treatment and management of ENV and recurrence is common. Interventions often involve those used for chronic lymphedema – including leg elevation, compression stockings or devices, skin hygiene, and lymphatic pumping.2,3 Medical management with topical and oral retinoids has been reported, as well as emphasis on weight loss and infection control.1,4 Surgical intervention is often reserved for refractory cases that fail to respond to more conservative management, or severe presentations resulting in extensive functional and aesthetic impairment. Less commonly reported treatment modalities include lymphaticovenular anastomosis and ablative carbon dioxide laser use, although this latter intervention demonstrated minimal improvement in this patient.5,6
Penoscrotal ENV is a rare form of ENV affecting the genital region of males, often resulting in significant disfigurement, functional impairment, and psychosocial distress. Penoscrotal elephantiasis can be idiopathic, due to filarial infections, scleroinflammatory stricture of the urethra, Chlamydia trachomatis infection, and lymphostasis secondary to chronic inflammatory conditions such as streptococcal infections, radiotherapy, surgery, chronic venous stasis, or Kaposi sarcoma.7
In addition, hidradenitis suppurativa (HS) has been documented multiple times in the literature in association with the development of ENV, detailing lymphatic scarring secondary to chronic inguinal HS as the main pathogenic factor.8,9
Surgery is the mainstay of treatment for penoscrotal ENV, which not only improves functionality and cosmesis, but also aids in prevention of rare malignant sequelae, such as lymphangiosarcoma.10 Such interventions can involve lymphangioplasty to aid in lymphatic drainage or excision of the mass and subcutaneous tissue with full-thickness skin grafting for reconstruction.7 Collaboration between urology, plastic surgery, and dermatology is often essential to obtain adequate care with satisfactory outcomes and minimal recurrence for patients with this uncommon condition.
This case and photo were submitted by Marlee Hill, a medical student at the University of Oklahoma, Oklahoma City; and Michael Franzetti, MD, and Jeffrey McBride, MD, department of dermatology, University of Oklahoma Health Sciences Center. The column was edited by Donna Bilu Martin, MD.
Dr. Donna Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
References
1. Hadian Y et al. Dermatol Online J. 2019 Dec 15;25(12):13030/qt6rn1s8ff.
2. Judge N and Kilic A. J Dermatol Case Rep. 2016 Nov 13;10(2):32-4.
3. Dean SM et al. J Am Acad Dermatol. 2011 Jun;64(6):1104-10.
4. Sisto K and Khachemoune A. Am J Clin Dermatol. 2008;9(3):141-6.
5. Motegi S et al. Dermatology. 2007;215(2):147-51.
6. Robinson CG et al. J Cutan Med Surg. 2018;22(6):611-3.
7. Koualla S et al. Ann Chir Plast Esthet. 2023 Apr 10;S0294-1260(23)00035-3.
8. Lelonek E et al. Acta Derm Venereol. 2021 Feb 11;101(2):adv00389.
9. Good LM et al. J Am Acad Dermatol. 2011 May;64(5):993-4.
10. Cerri A et al. Eur J Dermatol. 1998 Oct-Nov;8(7):511-4.

You’ve been warned
Recently, Canada announced new regulations on tobacco, with warnings printed on individual cigarettes, such as “poison in every puff.” This is on top of the packaging already required to have 75% of its space devoted to similar warnings, often with graphic pictures, of the potential consequences.
Make no mistake, I don’t like cigarettes and try to get smokers to quit.
But I have to wonder how successful this is going to be. I mean, you’d have to have lived under a rock for the last 70 years (or more) to not know that cigarettes (and tobacco in general) aren’t good for you, and can cause stroke, heart disease, and a multitude of cancers.
I suppose you could ban cigarettes, but that only opens up a black market. From 1920 to 1933 the United States set an example for the world with prohibition, showing how such an idea can backfire horribly.
Realistically, there are always going to be people making bad health decisions of one kind or another, including myself. Whether it’s tobacco, alcohol, or a cheeseburger and fries.
Tobacco, of course, has a much worse track record than that of the cheeseburger. We all have to eat, even though some choices are better than others. Tobacco has absolutely no biological necessity, as do food, air, and water.
But it’s remarkably addictive, not to mention profitable. Those factors will always guarantee it a place in society.
At this point,
There’s a legitimate argument to be made in trying to keep people from starting. The teenage years, where we all tend to believe we’re immortal, are when a lot of habits (good and bad) form. If gruesome pictures and repeated warnings cut down on those numbers, then in the long run it’s a very good thing. Given that Canada’s goal is to cut tobacco use from 13% down to less than 5% by 2035, this could happen. Only time will tell how it plays out.
On a side note, here in the United States tobacco use is 19% of the population. This is actually somewhat surprising to me, as a brief, not particularly scientific, review of my charts for the past few weeks found that less than 5% of my patients do it. So either some are lying or (more likely), it’s just the demographics of my practice area.
But at some point it doesn’t matter how many warnings or gory pictures people see, or where they encounter them. Some will keep smoking out of habit. Some because they actually like it. Some to be defiant. Some just because they can. And no amount of warnings is going to change their minds.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, Canada announced new regulations on tobacco, with warnings printed on individual cigarettes, such as “poison in every puff.” This is on top of the packaging already required to have 75% of its space devoted to similar warnings, often with graphic pictures, of the potential consequences.
Make no mistake, I don’t like cigarettes and try to get smokers to quit.
But I have to wonder how successful this is going to be. I mean, you’d have to have lived under a rock for the last 70 years (or more) to not know that cigarettes (and tobacco in general) aren’t good for you, and can cause stroke, heart disease, and a multitude of cancers.
I suppose you could ban cigarettes, but that only opens up a black market. From 1920 to 1933 the United States set an example for the world with prohibition, showing how such an idea can backfire horribly.
Realistically, there are always going to be people making bad health decisions of one kind or another, including myself. Whether it’s tobacco, alcohol, or a cheeseburger and fries.
Tobacco, of course, has a much worse track record than that of the cheeseburger. We all have to eat, even though some choices are better than others. Tobacco has absolutely no biological necessity, as do food, air, and water.
But it’s remarkably addictive, not to mention profitable. Those factors will always guarantee it a place in society.
At this point,
There’s a legitimate argument to be made in trying to keep people from starting. The teenage years, where we all tend to believe we’re immortal, are when a lot of habits (good and bad) form. If gruesome pictures and repeated warnings cut down on those numbers, then in the long run it’s a very good thing. Given that Canada’s goal is to cut tobacco use from 13% down to less than 5% by 2035, this could happen. Only time will tell how it plays out.
On a side note, here in the United States tobacco use is 19% of the population. This is actually somewhat surprising to me, as a brief, not particularly scientific, review of my charts for the past few weeks found that less than 5% of my patients do it. So either some are lying or (more likely), it’s just the demographics of my practice area.
But at some point it doesn’t matter how many warnings or gory pictures people see, or where they encounter them. Some will keep smoking out of habit. Some because they actually like it. Some to be defiant. Some just because they can. And no amount of warnings is going to change their minds.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, Canada announced new regulations on tobacco, with warnings printed on individual cigarettes, such as “poison in every puff.” This is on top of the packaging already required to have 75% of its space devoted to similar warnings, often with graphic pictures, of the potential consequences.
Make no mistake, I don’t like cigarettes and try to get smokers to quit.
But I have to wonder how successful this is going to be. I mean, you’d have to have lived under a rock for the last 70 years (or more) to not know that cigarettes (and tobacco in general) aren’t good for you, and can cause stroke, heart disease, and a multitude of cancers.
I suppose you could ban cigarettes, but that only opens up a black market. From 1920 to 1933 the United States set an example for the world with prohibition, showing how such an idea can backfire horribly.
Realistically, there are always going to be people making bad health decisions of one kind or another, including myself. Whether it’s tobacco, alcohol, or a cheeseburger and fries.
Tobacco, of course, has a much worse track record than that of the cheeseburger. We all have to eat, even though some choices are better than others. Tobacco has absolutely no biological necessity, as do food, air, and water.
But it’s remarkably addictive, not to mention profitable. Those factors will always guarantee it a place in society.
At this point,
There’s a legitimate argument to be made in trying to keep people from starting. The teenage years, where we all tend to believe we’re immortal, are when a lot of habits (good and bad) form. If gruesome pictures and repeated warnings cut down on those numbers, then in the long run it’s a very good thing. Given that Canada’s goal is to cut tobacco use from 13% down to less than 5% by 2035, this could happen. Only time will tell how it plays out.
On a side note, here in the United States tobacco use is 19% of the population. This is actually somewhat surprising to me, as a brief, not particularly scientific, review of my charts for the past few weeks found that less than 5% of my patients do it. So either some are lying or (more likely), it’s just the demographics of my practice area.
But at some point it doesn’t matter how many warnings or gory pictures people see, or where they encounter them. Some will keep smoking out of habit. Some because they actually like it. Some to be defiant. Some just because they can. And no amount of warnings is going to change their minds.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A new nonhormonal option for menopausal hot flashes: What prescribers should know
This transcript has been edited for clarity.
Hello. I am Dr. JoAnn Pinkerton, professor of obstetrics and gynecology at the University of Virginia and a North American Menopause Society–credentialed menopause specialist.
I am excited to tell you about a brand-new, just-approved non-estrogen therapy for treatment of menopausal symptoms. . The manufacturer, Astellas, is expected to make fezolinetant available at pharmacies before the end of this year. This medication binds to and blocks the neurokinin 3 (NK3) receptor, which plays a role in regulating body temperature, leading to a reduction in hot flashes.
For women suffering from frequent moderate to severe hot flashes, fezolinetant is an exciting breakthrough in women’s health as it is a highly effective nonhormonal treatment that reduces hot flashes and improves quality of life.
In two phase 3 clinical trials (Johnson et al. and Lederman et al.), fezolinetant 45 mg reduced the frequency of vasomotor symptoms by about 65%, significantly more than placebo, and similar to the 75% reduction seen with hormone therapy. Fezolinetant’s efficacy becomes evident within 1 week, reducing both frequency and severity of hot flashes.
With respect to side effects, 1%-2% of the menopausal women participating in clinical trials reported adverse events, including headaches, abdominal pain, diarrhea, insomnia, back pain, hot flushes, and reversible elevated hepatic transaminases. Serious adverse events were infrequent.
Subgroup analysis of data presented at ACOG’s 2023 annual meeting noted fezolinetant’s effectiveness among diverse populations, including White or Black race, body mass index of 30 or higher, those younger or older than age 55, smokers, former smokers, and never smokers, in U.S. as well as in European trial participants.
With respect to safety, a 52-week placebo-controlled safety trial confirmed safety for this time period. Adverse effects on the endometrium were neither seen nor expected, as fezolinetant is a centrally acting non–estrogen-containing medication. In addition, no loss of bone density was seen.
Prior trials of neurokinin receptor antagonists suggested the potential for hepatotoxicity. Increases in ALT or AST noted in one of the phase 3 trials of fezolinetant were described as asymptomatic, isolated, intermittent, or transient and returned to baseline during treatment or after discontinuation. However, the FDA placed a warning about liver injury potential. Package labeling recommends baseline liver function tests before starting fezolinetant and at 3, 6, and 9 months. In addition, concomitant use of moderate CYP1A2 inhibitors, including many antidepressants and cimetidine, should be avoided.
As with other recently approved medications, I am concerned that high cost could prevent appropriate candidates from having access.
Until now, the FDA had approved only one nonhormone therapy for vasomotor symptoms, 7.5 mg paroxetine salt. However, neither this formulation nor off-label use of other SSRIs, SNRIs, gabapentinoids, oxybutynin, or clonidine are as effective as hormone therapy or fezolinetant for moderate to severe vasomotor symptoms.
For women with bothersome menopausal hot flashes who can’t or choose not to use hormone therapy, including those with estrogen-sensitive breast or uterine cancers, fezolinetant offers a much-needed, highly effective, safe, nonhormone/non-estrogen option to treat their hot flashes.
The FDA approved it for treating vasomotor symptoms of menopause (hot flashes and night sweats) but it also appears to improve sleep disruption, mood, and quality of life.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. I am Dr. JoAnn Pinkerton, professor of obstetrics and gynecology at the University of Virginia and a North American Menopause Society–credentialed menopause specialist.
I am excited to tell you about a brand-new, just-approved non-estrogen therapy for treatment of menopausal symptoms. . The manufacturer, Astellas, is expected to make fezolinetant available at pharmacies before the end of this year. This medication binds to and blocks the neurokinin 3 (NK3) receptor, which plays a role in regulating body temperature, leading to a reduction in hot flashes.
For women suffering from frequent moderate to severe hot flashes, fezolinetant is an exciting breakthrough in women’s health as it is a highly effective nonhormonal treatment that reduces hot flashes and improves quality of life.
In two phase 3 clinical trials (Johnson et al. and Lederman et al.), fezolinetant 45 mg reduced the frequency of vasomotor symptoms by about 65%, significantly more than placebo, and similar to the 75% reduction seen with hormone therapy. Fezolinetant’s efficacy becomes evident within 1 week, reducing both frequency and severity of hot flashes.
With respect to side effects, 1%-2% of the menopausal women participating in clinical trials reported adverse events, including headaches, abdominal pain, diarrhea, insomnia, back pain, hot flushes, and reversible elevated hepatic transaminases. Serious adverse events were infrequent.
Subgroup analysis of data presented at ACOG’s 2023 annual meeting noted fezolinetant’s effectiveness among diverse populations, including White or Black race, body mass index of 30 or higher, those younger or older than age 55, smokers, former smokers, and never smokers, in U.S. as well as in European trial participants.
With respect to safety, a 52-week placebo-controlled safety trial confirmed safety for this time period. Adverse effects on the endometrium were neither seen nor expected, as fezolinetant is a centrally acting non–estrogen-containing medication. In addition, no loss of bone density was seen.
Prior trials of neurokinin receptor antagonists suggested the potential for hepatotoxicity. Increases in ALT or AST noted in one of the phase 3 trials of fezolinetant were described as asymptomatic, isolated, intermittent, or transient and returned to baseline during treatment or after discontinuation. However, the FDA placed a warning about liver injury potential. Package labeling recommends baseline liver function tests before starting fezolinetant and at 3, 6, and 9 months. In addition, concomitant use of moderate CYP1A2 inhibitors, including many antidepressants and cimetidine, should be avoided.
As with other recently approved medications, I am concerned that high cost could prevent appropriate candidates from having access.
Until now, the FDA had approved only one nonhormone therapy for vasomotor symptoms, 7.5 mg paroxetine salt. However, neither this formulation nor off-label use of other SSRIs, SNRIs, gabapentinoids, oxybutynin, or clonidine are as effective as hormone therapy or fezolinetant for moderate to severe vasomotor symptoms.
For women with bothersome menopausal hot flashes who can’t or choose not to use hormone therapy, including those with estrogen-sensitive breast or uterine cancers, fezolinetant offers a much-needed, highly effective, safe, nonhormone/non-estrogen option to treat their hot flashes.
The FDA approved it for treating vasomotor symptoms of menopause (hot flashes and night sweats) but it also appears to improve sleep disruption, mood, and quality of life.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. I am Dr. JoAnn Pinkerton, professor of obstetrics and gynecology at the University of Virginia and a North American Menopause Society–credentialed menopause specialist.
I am excited to tell you about a brand-new, just-approved non-estrogen therapy for treatment of menopausal symptoms. . The manufacturer, Astellas, is expected to make fezolinetant available at pharmacies before the end of this year. This medication binds to and blocks the neurokinin 3 (NK3) receptor, which plays a role in regulating body temperature, leading to a reduction in hot flashes.
For women suffering from frequent moderate to severe hot flashes, fezolinetant is an exciting breakthrough in women’s health as it is a highly effective nonhormonal treatment that reduces hot flashes and improves quality of life.
In two phase 3 clinical trials (Johnson et al. and Lederman et al.), fezolinetant 45 mg reduced the frequency of vasomotor symptoms by about 65%, significantly more than placebo, and similar to the 75% reduction seen with hormone therapy. Fezolinetant’s efficacy becomes evident within 1 week, reducing both frequency and severity of hot flashes.
With respect to side effects, 1%-2% of the menopausal women participating in clinical trials reported adverse events, including headaches, abdominal pain, diarrhea, insomnia, back pain, hot flushes, and reversible elevated hepatic transaminases. Serious adverse events were infrequent.
Subgroup analysis of data presented at ACOG’s 2023 annual meeting noted fezolinetant’s effectiveness among diverse populations, including White or Black race, body mass index of 30 or higher, those younger or older than age 55, smokers, former smokers, and never smokers, in U.S. as well as in European trial participants.
With respect to safety, a 52-week placebo-controlled safety trial confirmed safety for this time period. Adverse effects on the endometrium were neither seen nor expected, as fezolinetant is a centrally acting non–estrogen-containing medication. In addition, no loss of bone density was seen.
Prior trials of neurokinin receptor antagonists suggested the potential for hepatotoxicity. Increases in ALT or AST noted in one of the phase 3 trials of fezolinetant were described as asymptomatic, isolated, intermittent, or transient and returned to baseline during treatment or after discontinuation. However, the FDA placed a warning about liver injury potential. Package labeling recommends baseline liver function tests before starting fezolinetant and at 3, 6, and 9 months. In addition, concomitant use of moderate CYP1A2 inhibitors, including many antidepressants and cimetidine, should be avoided.
As with other recently approved medications, I am concerned that high cost could prevent appropriate candidates from having access.
Until now, the FDA had approved only one nonhormone therapy for vasomotor symptoms, 7.5 mg paroxetine salt. However, neither this formulation nor off-label use of other SSRIs, SNRIs, gabapentinoids, oxybutynin, or clonidine are as effective as hormone therapy or fezolinetant for moderate to severe vasomotor symptoms.
For women with bothersome menopausal hot flashes who can’t or choose not to use hormone therapy, including those with estrogen-sensitive breast or uterine cancers, fezolinetant offers a much-needed, highly effective, safe, nonhormone/non-estrogen option to treat their hot flashes.
The FDA approved it for treating vasomotor symptoms of menopause (hot flashes and night sweats) but it also appears to improve sleep disruption, mood, and quality of life.
A version of this article first appeared on Medscape.com.
Are you a physician ... or a vending machine?
When we address this problem with patients, some become immediately defensive, making it difficult to modify treatment regimens. It’s almost as if people believe that they have a “right” to their medications and nobody should dare take them away. Even when I think the interaction goes relatively smoothly, the outcome usually shows otherwise.
I will decrease gabapentin from 3,200 mg per day and they will come back with cyclobenzaprine from the urgent care center down the block.
I try to stop an abused amphetamine and dextroamphetamine, and not only do the drugs show up in the urine toxicology test a month later (from the brother’s girlfriend’s sister) but the screening will be positive for cocaine (from the sister’s boyfriend’s brother) and probably alprazolam, too.
People want what they want, and I believe what they want is the overwhelming need not to feel, and especially to not feel our natural and uncomfortable states of pain, sadness, anxiety, fatigue, and discomfort (sometimes all at once). They will use anything orally or intravenously or nasally to make those feelings go away.
I am an addiction specialist so I write this commentary out of care and concern and recognition of how much, pain both physical and psychic, people suffer.
Perhaps we as physicians are conditioned to believe that we must prescribe “something” to the patient who is uncomfortable and sitting in front of us. In general we are sympathetic to the needs of those who come to us in distress, and we try our best to help reduce their symptoms.
I know that we cannot simply “fire” people, because these patients are ours to take care of; they are our responsibility, though this is our overused response to “difficult” patients.
And I know that we have insufficient replacements for these medications. We stopped prescribing oxycodone and now people are on gabapentin in the highest doses, diversion is up, and so is its abuse.
Many of us regularly teach about breathing and mindfulness. I discuss trauma and talk therapy. I order physical therapy and walking regimens and podcasts. But our relationship is transactional, and in prescribing a medication, I have shown them that I am hearing them. I hate this feeling of being trapped.
I spend much of my day negotiating and drive home at night feeling like nothing more than a vending machine.
Dr. Hambright is with the department of addiction medicine at Samaritan Daytop Village, Ellenville, N.Y., and Samadhi Recovery Community Outreach Center, Kingston, N.Y. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
When we address this problem with patients, some become immediately defensive, making it difficult to modify treatment regimens. It’s almost as if people believe that they have a “right” to their medications and nobody should dare take them away. Even when I think the interaction goes relatively smoothly, the outcome usually shows otherwise.
I will decrease gabapentin from 3,200 mg per day and they will come back with cyclobenzaprine from the urgent care center down the block.
I try to stop an abused amphetamine and dextroamphetamine, and not only do the drugs show up in the urine toxicology test a month later (from the brother’s girlfriend’s sister) but the screening will be positive for cocaine (from the sister’s boyfriend’s brother) and probably alprazolam, too.
People want what they want, and I believe what they want is the overwhelming need not to feel, and especially to not feel our natural and uncomfortable states of pain, sadness, anxiety, fatigue, and discomfort (sometimes all at once). They will use anything orally or intravenously or nasally to make those feelings go away.
I am an addiction specialist so I write this commentary out of care and concern and recognition of how much, pain both physical and psychic, people suffer.
Perhaps we as physicians are conditioned to believe that we must prescribe “something” to the patient who is uncomfortable and sitting in front of us. In general we are sympathetic to the needs of those who come to us in distress, and we try our best to help reduce their symptoms.
I know that we cannot simply “fire” people, because these patients are ours to take care of; they are our responsibility, though this is our overused response to “difficult” patients.
And I know that we have insufficient replacements for these medications. We stopped prescribing oxycodone and now people are on gabapentin in the highest doses, diversion is up, and so is its abuse.
Many of us regularly teach about breathing and mindfulness. I discuss trauma and talk therapy. I order physical therapy and walking regimens and podcasts. But our relationship is transactional, and in prescribing a medication, I have shown them that I am hearing them. I hate this feeling of being trapped.
I spend much of my day negotiating and drive home at night feeling like nothing more than a vending machine.
Dr. Hambright is with the department of addiction medicine at Samaritan Daytop Village, Ellenville, N.Y., and Samadhi Recovery Community Outreach Center, Kingston, N.Y. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
When we address this problem with patients, some become immediately defensive, making it difficult to modify treatment regimens. It’s almost as if people believe that they have a “right” to their medications and nobody should dare take them away. Even when I think the interaction goes relatively smoothly, the outcome usually shows otherwise.
I will decrease gabapentin from 3,200 mg per day and they will come back with cyclobenzaprine from the urgent care center down the block.
I try to stop an abused amphetamine and dextroamphetamine, and not only do the drugs show up in the urine toxicology test a month later (from the brother’s girlfriend’s sister) but the screening will be positive for cocaine (from the sister’s boyfriend’s brother) and probably alprazolam, too.
People want what they want, and I believe what they want is the overwhelming need not to feel, and especially to not feel our natural and uncomfortable states of pain, sadness, anxiety, fatigue, and discomfort (sometimes all at once). They will use anything orally or intravenously or nasally to make those feelings go away.
I am an addiction specialist so I write this commentary out of care and concern and recognition of how much, pain both physical and psychic, people suffer.
Perhaps we as physicians are conditioned to believe that we must prescribe “something” to the patient who is uncomfortable and sitting in front of us. In general we are sympathetic to the needs of those who come to us in distress, and we try our best to help reduce their symptoms.
I know that we cannot simply “fire” people, because these patients are ours to take care of; they are our responsibility, though this is our overused response to “difficult” patients.
And I know that we have insufficient replacements for these medications. We stopped prescribing oxycodone and now people are on gabapentin in the highest doses, diversion is up, and so is its abuse.
Many of us regularly teach about breathing and mindfulness. I discuss trauma and talk therapy. I order physical therapy and walking regimens and podcasts. But our relationship is transactional, and in prescribing a medication, I have shown them that I am hearing them. I hate this feeling of being trapped.
I spend much of my day negotiating and drive home at night feeling like nothing more than a vending machine.
Dr. Hambright is with the department of addiction medicine at Samaritan Daytop Village, Ellenville, N.Y., and Samadhi Recovery Community Outreach Center, Kingston, N.Y. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
ASCO 2023: Promising results in breast cancer from NATALEE and PHERGain
This transcript has been edited for clarity.
Hi. It’s Dr. Kathy Miller from Indiana University, coming to you today from the 2023 ASCO annual meeting in Chicago.
It’s been an exciting year for breast cancer news. I want to make sure that you hear about the two studies that I find the most impactful. One is the NATALEE study looking at ribociclib in adjuvant ER-positive patients at high risk for recurrence. You saw the press release a few weeks ago, and we now have the data. There is no doubt that this is a positive trial.
The details here are important. These were pre- or postmenopausal women, and men as well. Premenopausal women and men also had an LHRH agonist in addition to an aromatase inhibitor – that could have been either letrozole or anastrozole – then randomized to ribociclib or placebo.
The dose of ribociclib that you’re used to thinking about is 600 mg daily for 3 weeks and 7 days off. That’s the approved dose in the metastatic setting. In the adjuvant trial, they used 400 mg, and that was intentional to try to reduce some of the toxicity because the plan was for 3 years of therapy. Managing toxicity and really making this tolerable for patients was crucial.
We’ve now seen the efficacy results, with a roughly 3% reduction in the risk for recurrence; 90% disease-free survival in the ribociclib arm, 87% in the control arm, some patients still having prolongation of QTc but no serious arrhythmias; some patients still with myelosuppression, but risk for serious infections was really very low.
We have no head-to-head trials in any setting, and I doubt that our industry colleagues are going to be interested in a head-to-head setting.
We’re going to need to pay particular attention to long-term follow-up and to quality of life and toxicity data as to which our patients prefer. We may need to think about other ways of doing those direct comparisons with public funding, where we can get the answers our patients deserve.
I also want to think about the other end of the spectrum, those patients with HER2-positive disease. We saw fantastic results from the PHERGain study from our colleagues in Spain. This was a trial that took patients with predominantly stage II and III HER2-positive breast cancer. These are patients that we would treat with neoadjuvant chemotherapy, with dual HER2-targeted therapy.
Years ago, we saw results of some small, single-arm, phase 2 studies, suggesting that some of those patients may be so sensitive to biologic therapy that they have a pathologic complete response with HER2-targeted therapy – HER2-targeted therapy with endocrine therapy if they are positive – with no chemotherapy at all. Our question has always been how to identify those patients. Can we identify them well enough that we would be comfortable not treating them with chemotherapy? Importantly, If they didn’t get chemotherapy, what’s their long-term outcome?
The PHERGain trial lets us look at all those things. The PHERGain trial gave patients two cycles of dual HER2-targeted therapy, pertuzumab and trastuzumab, hormone therapy if also ER positive, and they got an FDG-PET scan after two cycles of therapy.
If they had a significant PET response, those patients were then randomized to switch to chemotherapy, standard TCHP, or continue biologic therapy alone for a total of six cycles. They then went to surgery. If they had a pathologic complete response, whether they had gotten chemotherapy or no chemotherapy, they completed the HER2-targeted therapy. If they still had residual disease, they got chemotherapy if chemotherapy had not been administered before, and they may have gotten other HER2-targeted therapies if they had already received chemotherapy.
There were over 300 patients in this trial, and my memory is that roughly two thirds of them had a PET response. About 86 patients randomized to continue biologic therapy had a pathologic complete response, so about one-third of those for whom the PET imaging said they were responding with biologic therapy only had a pathologic complete response.
They have now been followed for 3 years. The 3-year disease-free survival results look very reassuring. Of those 86 patients, one patient had a local recurrence and no patient had a distant recurrence.
This is what we’ve been waiting for. Can we identify those patients who have an excellent prognosis with biologic therapy alone so that we can avoid the toxicities? This is really where you’ll see the research over the coming years in breast cancer, looking at additional therapies in high-risk patients who don’t do so well with our standard therapies, and better stratification of patients who do so well with our standard therapies that we may be able to do less.
This is one of the ways that we’ll be able to do that. I look forward to sharing those results with you over coming years.
Kathy D. Miller, MD, is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. It’s Dr. Kathy Miller from Indiana University, coming to you today from the 2023 ASCO annual meeting in Chicago.
It’s been an exciting year for breast cancer news. I want to make sure that you hear about the two studies that I find the most impactful. One is the NATALEE study looking at ribociclib in adjuvant ER-positive patients at high risk for recurrence. You saw the press release a few weeks ago, and we now have the data. There is no doubt that this is a positive trial.
The details here are important. These were pre- or postmenopausal women, and men as well. Premenopausal women and men also had an LHRH agonist in addition to an aromatase inhibitor – that could have been either letrozole or anastrozole – then randomized to ribociclib or placebo.
The dose of ribociclib that you’re used to thinking about is 600 mg daily for 3 weeks and 7 days off. That’s the approved dose in the metastatic setting. In the adjuvant trial, they used 400 mg, and that was intentional to try to reduce some of the toxicity because the plan was for 3 years of therapy. Managing toxicity and really making this tolerable for patients was crucial.
We’ve now seen the efficacy results, with a roughly 3% reduction in the risk for recurrence; 90% disease-free survival in the ribociclib arm, 87% in the control arm, some patients still having prolongation of QTc but no serious arrhythmias; some patients still with myelosuppression, but risk for serious infections was really very low.
We have no head-to-head trials in any setting, and I doubt that our industry colleagues are going to be interested in a head-to-head setting.
We’re going to need to pay particular attention to long-term follow-up and to quality of life and toxicity data as to which our patients prefer. We may need to think about other ways of doing those direct comparisons with public funding, where we can get the answers our patients deserve.
I also want to think about the other end of the spectrum, those patients with HER2-positive disease. We saw fantastic results from the PHERGain study from our colleagues in Spain. This was a trial that took patients with predominantly stage II and III HER2-positive breast cancer. These are patients that we would treat with neoadjuvant chemotherapy, with dual HER2-targeted therapy.
Years ago, we saw results of some small, single-arm, phase 2 studies, suggesting that some of those patients may be so sensitive to biologic therapy that they have a pathologic complete response with HER2-targeted therapy – HER2-targeted therapy with endocrine therapy if they are positive – with no chemotherapy at all. Our question has always been how to identify those patients. Can we identify them well enough that we would be comfortable not treating them with chemotherapy? Importantly, If they didn’t get chemotherapy, what’s their long-term outcome?
The PHERGain trial lets us look at all those things. The PHERGain trial gave patients two cycles of dual HER2-targeted therapy, pertuzumab and trastuzumab, hormone therapy if also ER positive, and they got an FDG-PET scan after two cycles of therapy.
If they had a significant PET response, those patients were then randomized to switch to chemotherapy, standard TCHP, or continue biologic therapy alone for a total of six cycles. They then went to surgery. If they had a pathologic complete response, whether they had gotten chemotherapy or no chemotherapy, they completed the HER2-targeted therapy. If they still had residual disease, they got chemotherapy if chemotherapy had not been administered before, and they may have gotten other HER2-targeted therapies if they had already received chemotherapy.
There were over 300 patients in this trial, and my memory is that roughly two thirds of them had a PET response. About 86 patients randomized to continue biologic therapy had a pathologic complete response, so about one-third of those for whom the PET imaging said they were responding with biologic therapy only had a pathologic complete response.
They have now been followed for 3 years. The 3-year disease-free survival results look very reassuring. Of those 86 patients, one patient had a local recurrence and no patient had a distant recurrence.
This is what we’ve been waiting for. Can we identify those patients who have an excellent prognosis with biologic therapy alone so that we can avoid the toxicities? This is really where you’ll see the research over the coming years in breast cancer, looking at additional therapies in high-risk patients who don’t do so well with our standard therapies, and better stratification of patients who do so well with our standard therapies that we may be able to do less.
This is one of the ways that we’ll be able to do that. I look forward to sharing those results with you over coming years.
Kathy D. Miller, MD, is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. It’s Dr. Kathy Miller from Indiana University, coming to you today from the 2023 ASCO annual meeting in Chicago.
It’s been an exciting year for breast cancer news. I want to make sure that you hear about the two studies that I find the most impactful. One is the NATALEE study looking at ribociclib in adjuvant ER-positive patients at high risk for recurrence. You saw the press release a few weeks ago, and we now have the data. There is no doubt that this is a positive trial.
The details here are important. These were pre- or postmenopausal women, and men as well. Premenopausal women and men also had an LHRH agonist in addition to an aromatase inhibitor – that could have been either letrozole or anastrozole – then randomized to ribociclib or placebo.
The dose of ribociclib that you’re used to thinking about is 600 mg daily for 3 weeks and 7 days off. That’s the approved dose in the metastatic setting. In the adjuvant trial, they used 400 mg, and that was intentional to try to reduce some of the toxicity because the plan was for 3 years of therapy. Managing toxicity and really making this tolerable for patients was crucial.
We’ve now seen the efficacy results, with a roughly 3% reduction in the risk for recurrence; 90% disease-free survival in the ribociclib arm, 87% in the control arm, some patients still having prolongation of QTc but no serious arrhythmias; some patients still with myelosuppression, but risk for serious infections was really very low.
We have no head-to-head trials in any setting, and I doubt that our industry colleagues are going to be interested in a head-to-head setting.
We’re going to need to pay particular attention to long-term follow-up and to quality of life and toxicity data as to which our patients prefer. We may need to think about other ways of doing those direct comparisons with public funding, where we can get the answers our patients deserve.
I also want to think about the other end of the spectrum, those patients with HER2-positive disease. We saw fantastic results from the PHERGain study from our colleagues in Spain. This was a trial that took patients with predominantly stage II and III HER2-positive breast cancer. These are patients that we would treat with neoadjuvant chemotherapy, with dual HER2-targeted therapy.
Years ago, we saw results of some small, single-arm, phase 2 studies, suggesting that some of those patients may be so sensitive to biologic therapy that they have a pathologic complete response with HER2-targeted therapy – HER2-targeted therapy with endocrine therapy if they are positive – with no chemotherapy at all. Our question has always been how to identify those patients. Can we identify them well enough that we would be comfortable not treating them with chemotherapy? Importantly, If they didn’t get chemotherapy, what’s their long-term outcome?
The PHERGain trial lets us look at all those things. The PHERGain trial gave patients two cycles of dual HER2-targeted therapy, pertuzumab and trastuzumab, hormone therapy if also ER positive, and they got an FDG-PET scan after two cycles of therapy.
If they had a significant PET response, those patients were then randomized to switch to chemotherapy, standard TCHP, or continue biologic therapy alone for a total of six cycles. They then went to surgery. If they had a pathologic complete response, whether they had gotten chemotherapy or no chemotherapy, they completed the HER2-targeted therapy. If they still had residual disease, they got chemotherapy if chemotherapy had not been administered before, and they may have gotten other HER2-targeted therapies if they had already received chemotherapy.
There were over 300 patients in this trial, and my memory is that roughly two thirds of them had a PET response. About 86 patients randomized to continue biologic therapy had a pathologic complete response, so about one-third of those for whom the PET imaging said they were responding with biologic therapy only had a pathologic complete response.
They have now been followed for 3 years. The 3-year disease-free survival results look very reassuring. Of those 86 patients, one patient had a local recurrence and no patient had a distant recurrence.
This is what we’ve been waiting for. Can we identify those patients who have an excellent prognosis with biologic therapy alone so that we can avoid the toxicities? This is really where you’ll see the research over the coming years in breast cancer, looking at additional therapies in high-risk patients who don’t do so well with our standard therapies, and better stratification of patients who do so well with our standard therapies that we may be able to do less.
This is one of the ways that we’ll be able to do that. I look forward to sharing those results with you over coming years.
Kathy D. Miller, MD, is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Self-talk overhaul may help patients achieve weight loss
It’s common knowledge that the recommended first-line treatment for obesity is behavioral or “lifestyle” intervention, with the goal of losing a modest amount of weight to gain significant health benefits. Unfortunately, when pursuing weight loss, patients often think they need to beat themselves up to stay motivated. I’ve heard patients call themselves “weak,” saying they need to “stop being lazy” and gain some self-control in order to be less of a “failure.” They label their bodies as “disgusting” and themselves as “worthless,” all because of their weight.
Some patients may worry that if they are kind to themselves or “too accepting” of their bodies, they’ll lose motivation to stick with their health behavior goals. That’s a question that my colleagues and I have explored in recent research that attempts to reduce weight stigma as part of standard weight-related care.
Misguided societal view drives blame game
This tendency for people to blame and disparage themselves for their weight is largely driven by the misguided societal view of body weight as an issue of personal responsibility. We’re constantly exposed to messages telling us that there’s a narrow range of acceptable body weights and sizes, and that if we have enough willpower and discipline to eat healthily and exercise, then we should be able to control our weight. These messages are prevalent in the news and in social media, but often they are communicated in health care settings too. Narratives of this kind usually ignore the complex environmental and biological factors that contribute to body size and shape, instead attributing high body weight to laziness and moral failings.
Such messages exemplify weight bias and stigma, or the negative attitudes toward and mistreatment of individuals with a high body weight. Given society’s harsh judgment of people with larger bodies, it’s no surprise that many individuals internalize these beliefs and stigmatize themselves for their weight. This internalized or self-directed stigma is known to be harmful to mental and physical health.
Contrary to beliefs that negative self-talk and self-blame can be motivators to improve health, we know that high levels of weight self-stigma are linked to unhealthy eating behaviors and less engagement in physical activity, among other poor health outcomes. Thus, ironically, internalizing weight stigma actually undermines efforts to lose weight and maintain weight loss, rather than motivating healthy behavior change.
Combating internalized weight stigma
How do we combat these negative weight messages in our culture and reduce, or ideally prevent, internalization of judgment and blame? Fundamental changes in policies, health care practices, and public attitudes are needed to eradicate weight stigma. While such initiatives are underway, there are many individuals who have already experienced and internalized weight stigma and need support now. Interventions such as peer support and psychological counseling may be helpful for challenging negative, internalized beliefs about weight; learning to cope with exposure to weight stigma without internalizing it; increasing self-acceptance and self-compassion; and feeling empowered to fight back against weight bias and stigma.
In our latest study, my colleagues and I tested the long-term effects of including a group intervention to address weight stigma in a standard behavioral weight management program. More than 100 adults with obesity who had experienced and internalized weight stigma were recruited for this clinical trial, which randomly assigned participants to receive either the Weight Bias Internalization and Stigma (Weight BIAS) program combined with standard behavioral weight loss treatment, or standard weight loss treatment alone.
The Weight BIAS program adapted evidence-based psychotherapy techniques to target weight self-stigma, while also providing peer support in a group treatment format. Specific topics included challenging myths and stereotypes about weight; identifying and changing negative thought patterns related to weight and how they affect emotions and behaviors; and responding to experiences of weight stigma.
For example, to challenge negative thoughts (for example, that they were a “failure” because of their weight), patients worked together to examine all of the evidence that proved these beliefs were not true, and came up with ideas for how to revise these thoughts to be less judgmental and more fair and accurate.
Other topics focused on building confidence, increasing body- and self-acceptance, and advocating for themselves and others who are mistreated because of their weight. Many patients shared examples of stigmatizing experiences in health care settings and discussed what they could say or do when facing judgment or discrimination from health care providers, as well as the importance of finding health care providers who treated them with respect. Group discussions also tied in information relevant to health behavior goals, such as overcoming self-consciousness about weight to enjoy physical activity.
Participants were offered weekly group meetings for 20 weeks, followed by a year of less frequent meetings. At the study’s end, participants in the group that received weight loss treatment with the Weight BIAS program on average lost about 7% of their starting weight, compared with an average weight loss of about 5% in the group that received weight loss treatment alone. Weight losses of these magnitudes are known to have meaningful health benefits. Results from our study showed comparable improvements in most outcomes across groups, with some added benefit of the Weight BIAS program for certain psychological and behavioral outcomes. These findings challenge the notion that reducing weight stigma and promoting body acceptance will undermine motivation to engage in healthy behaviors and lose weight. We found no such effect.
What did participants say?
When asked questions such as how much they liked the program, what they learned, and how they used the new skills and changed their self-perceptions, participants who received the Weight BIAS program gave higher ratings than those who received only the weight loss treatment. Positive feedback from free-response questions indicated that many participants identified social support as their favorite aspect of the program. Others highlighted how the program helped them to gain “the ability to think differently about myself and other people” and “an understanding that weight really is separate from the person.” They also described how they brought together the goals of weight loss and body and self-acceptance, saying, “I am more accepting of me and at the same time more dedicated to obtaining a healthier weight,” and “It’s okay to be happy the way I am and still want to change.”
Participants who didn’t receive the Weight BIAS program also shared positive feedback, writing that their favorite part of the program was “being part of such a supportive group of people who can relate to the things that I think and feel” and that they learned “how not to be so hard on myself.” This might suggest that even without an intervention specifically for weight stigma, providing respectful, compassionate care and peer support may help patients to feel less alone and to be kinder to themselves.
Our study results suggest that reducing negative self-talk and internalized beliefs about weight certainly won’t undermine treatment outcomes and may have some benefits beyond standard weight loss treatment. At the same time, we also all need to do our part to change how society views and treats people with larger bodies and prevent the harms of experiencing and internalizing weight stigma.
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL140176. The content is solely the responsibility of the author and does not necessarily reflect the official views of the National Institutes of Health.
Dr. Pearl is assistant professor, clinical and health psychology, University of Florida, Gainesville. She has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
It’s common knowledge that the recommended first-line treatment for obesity is behavioral or “lifestyle” intervention, with the goal of losing a modest amount of weight to gain significant health benefits. Unfortunately, when pursuing weight loss, patients often think they need to beat themselves up to stay motivated. I’ve heard patients call themselves “weak,” saying they need to “stop being lazy” and gain some self-control in order to be less of a “failure.” They label their bodies as “disgusting” and themselves as “worthless,” all because of their weight.
Some patients may worry that if they are kind to themselves or “too accepting” of their bodies, they’ll lose motivation to stick with their health behavior goals. That’s a question that my colleagues and I have explored in recent research that attempts to reduce weight stigma as part of standard weight-related care.
Misguided societal view drives blame game
This tendency for people to blame and disparage themselves for their weight is largely driven by the misguided societal view of body weight as an issue of personal responsibility. We’re constantly exposed to messages telling us that there’s a narrow range of acceptable body weights and sizes, and that if we have enough willpower and discipline to eat healthily and exercise, then we should be able to control our weight. These messages are prevalent in the news and in social media, but often they are communicated in health care settings too. Narratives of this kind usually ignore the complex environmental and biological factors that contribute to body size and shape, instead attributing high body weight to laziness and moral failings.
Such messages exemplify weight bias and stigma, or the negative attitudes toward and mistreatment of individuals with a high body weight. Given society’s harsh judgment of people with larger bodies, it’s no surprise that many individuals internalize these beliefs and stigmatize themselves for their weight. This internalized or self-directed stigma is known to be harmful to mental and physical health.
Contrary to beliefs that negative self-talk and self-blame can be motivators to improve health, we know that high levels of weight self-stigma are linked to unhealthy eating behaviors and less engagement in physical activity, among other poor health outcomes. Thus, ironically, internalizing weight stigma actually undermines efforts to lose weight and maintain weight loss, rather than motivating healthy behavior change.
Combating internalized weight stigma
How do we combat these negative weight messages in our culture and reduce, or ideally prevent, internalization of judgment and blame? Fundamental changes in policies, health care practices, and public attitudes are needed to eradicate weight stigma. While such initiatives are underway, there are many individuals who have already experienced and internalized weight stigma and need support now. Interventions such as peer support and psychological counseling may be helpful for challenging negative, internalized beliefs about weight; learning to cope with exposure to weight stigma without internalizing it; increasing self-acceptance and self-compassion; and feeling empowered to fight back against weight bias and stigma.
In our latest study, my colleagues and I tested the long-term effects of including a group intervention to address weight stigma in a standard behavioral weight management program. More than 100 adults with obesity who had experienced and internalized weight stigma were recruited for this clinical trial, which randomly assigned participants to receive either the Weight Bias Internalization and Stigma (Weight BIAS) program combined with standard behavioral weight loss treatment, or standard weight loss treatment alone.
The Weight BIAS program adapted evidence-based psychotherapy techniques to target weight self-stigma, while also providing peer support in a group treatment format. Specific topics included challenging myths and stereotypes about weight; identifying and changing negative thought patterns related to weight and how they affect emotions and behaviors; and responding to experiences of weight stigma.
For example, to challenge negative thoughts (for example, that they were a “failure” because of their weight), patients worked together to examine all of the evidence that proved these beliefs were not true, and came up with ideas for how to revise these thoughts to be less judgmental and more fair and accurate.
Other topics focused on building confidence, increasing body- and self-acceptance, and advocating for themselves and others who are mistreated because of their weight. Many patients shared examples of stigmatizing experiences in health care settings and discussed what they could say or do when facing judgment or discrimination from health care providers, as well as the importance of finding health care providers who treated them with respect. Group discussions also tied in information relevant to health behavior goals, such as overcoming self-consciousness about weight to enjoy physical activity.
Participants were offered weekly group meetings for 20 weeks, followed by a year of less frequent meetings. At the study’s end, participants in the group that received weight loss treatment with the Weight BIAS program on average lost about 7% of their starting weight, compared with an average weight loss of about 5% in the group that received weight loss treatment alone. Weight losses of these magnitudes are known to have meaningful health benefits. Results from our study showed comparable improvements in most outcomes across groups, with some added benefit of the Weight BIAS program for certain psychological and behavioral outcomes. These findings challenge the notion that reducing weight stigma and promoting body acceptance will undermine motivation to engage in healthy behaviors and lose weight. We found no such effect.
What did participants say?
When asked questions such as how much they liked the program, what they learned, and how they used the new skills and changed their self-perceptions, participants who received the Weight BIAS program gave higher ratings than those who received only the weight loss treatment. Positive feedback from free-response questions indicated that many participants identified social support as their favorite aspect of the program. Others highlighted how the program helped them to gain “the ability to think differently about myself and other people” and “an understanding that weight really is separate from the person.” They also described how they brought together the goals of weight loss and body and self-acceptance, saying, “I am more accepting of me and at the same time more dedicated to obtaining a healthier weight,” and “It’s okay to be happy the way I am and still want to change.”
Participants who didn’t receive the Weight BIAS program also shared positive feedback, writing that their favorite part of the program was “being part of such a supportive group of people who can relate to the things that I think and feel” and that they learned “how not to be so hard on myself.” This might suggest that even without an intervention specifically for weight stigma, providing respectful, compassionate care and peer support may help patients to feel less alone and to be kinder to themselves.
Our study results suggest that reducing negative self-talk and internalized beliefs about weight certainly won’t undermine treatment outcomes and may have some benefits beyond standard weight loss treatment. At the same time, we also all need to do our part to change how society views and treats people with larger bodies and prevent the harms of experiencing and internalizing weight stigma.
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL140176. The content is solely the responsibility of the author and does not necessarily reflect the official views of the National Institutes of Health.
Dr. Pearl is assistant professor, clinical and health psychology, University of Florida, Gainesville. She has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
It’s common knowledge that the recommended first-line treatment for obesity is behavioral or “lifestyle” intervention, with the goal of losing a modest amount of weight to gain significant health benefits. Unfortunately, when pursuing weight loss, patients often think they need to beat themselves up to stay motivated. I’ve heard patients call themselves “weak,” saying they need to “stop being lazy” and gain some self-control in order to be less of a “failure.” They label their bodies as “disgusting” and themselves as “worthless,” all because of their weight.
Some patients may worry that if they are kind to themselves or “too accepting” of their bodies, they’ll lose motivation to stick with their health behavior goals. That’s a question that my colleagues and I have explored in recent research that attempts to reduce weight stigma as part of standard weight-related care.
Misguided societal view drives blame game
This tendency for people to blame and disparage themselves for their weight is largely driven by the misguided societal view of body weight as an issue of personal responsibility. We’re constantly exposed to messages telling us that there’s a narrow range of acceptable body weights and sizes, and that if we have enough willpower and discipline to eat healthily and exercise, then we should be able to control our weight. These messages are prevalent in the news and in social media, but often they are communicated in health care settings too. Narratives of this kind usually ignore the complex environmental and biological factors that contribute to body size and shape, instead attributing high body weight to laziness and moral failings.
Such messages exemplify weight bias and stigma, or the negative attitudes toward and mistreatment of individuals with a high body weight. Given society’s harsh judgment of people with larger bodies, it’s no surprise that many individuals internalize these beliefs and stigmatize themselves for their weight. This internalized or self-directed stigma is known to be harmful to mental and physical health.
Contrary to beliefs that negative self-talk and self-blame can be motivators to improve health, we know that high levels of weight self-stigma are linked to unhealthy eating behaviors and less engagement in physical activity, among other poor health outcomes. Thus, ironically, internalizing weight stigma actually undermines efforts to lose weight and maintain weight loss, rather than motivating healthy behavior change.
Combating internalized weight stigma
How do we combat these negative weight messages in our culture and reduce, or ideally prevent, internalization of judgment and blame? Fundamental changes in policies, health care practices, and public attitudes are needed to eradicate weight stigma. While such initiatives are underway, there are many individuals who have already experienced and internalized weight stigma and need support now. Interventions such as peer support and psychological counseling may be helpful for challenging negative, internalized beliefs about weight; learning to cope with exposure to weight stigma without internalizing it; increasing self-acceptance and self-compassion; and feeling empowered to fight back against weight bias and stigma.
In our latest study, my colleagues and I tested the long-term effects of including a group intervention to address weight stigma in a standard behavioral weight management program. More than 100 adults with obesity who had experienced and internalized weight stigma were recruited for this clinical trial, which randomly assigned participants to receive either the Weight Bias Internalization and Stigma (Weight BIAS) program combined with standard behavioral weight loss treatment, or standard weight loss treatment alone.
The Weight BIAS program adapted evidence-based psychotherapy techniques to target weight self-stigma, while also providing peer support in a group treatment format. Specific topics included challenging myths and stereotypes about weight; identifying and changing negative thought patterns related to weight and how they affect emotions and behaviors; and responding to experiences of weight stigma.
For example, to challenge negative thoughts (for example, that they were a “failure” because of their weight), patients worked together to examine all of the evidence that proved these beliefs were not true, and came up with ideas for how to revise these thoughts to be less judgmental and more fair and accurate.
Other topics focused on building confidence, increasing body- and self-acceptance, and advocating for themselves and others who are mistreated because of their weight. Many patients shared examples of stigmatizing experiences in health care settings and discussed what they could say or do when facing judgment or discrimination from health care providers, as well as the importance of finding health care providers who treated them with respect. Group discussions also tied in information relevant to health behavior goals, such as overcoming self-consciousness about weight to enjoy physical activity.
Participants were offered weekly group meetings for 20 weeks, followed by a year of less frequent meetings. At the study’s end, participants in the group that received weight loss treatment with the Weight BIAS program on average lost about 7% of their starting weight, compared with an average weight loss of about 5% in the group that received weight loss treatment alone. Weight losses of these magnitudes are known to have meaningful health benefits. Results from our study showed comparable improvements in most outcomes across groups, with some added benefit of the Weight BIAS program for certain psychological and behavioral outcomes. These findings challenge the notion that reducing weight stigma and promoting body acceptance will undermine motivation to engage in healthy behaviors and lose weight. We found no such effect.
What did participants say?
When asked questions such as how much they liked the program, what they learned, and how they used the new skills and changed their self-perceptions, participants who received the Weight BIAS program gave higher ratings than those who received only the weight loss treatment. Positive feedback from free-response questions indicated that many participants identified social support as their favorite aspect of the program. Others highlighted how the program helped them to gain “the ability to think differently about myself and other people” and “an understanding that weight really is separate from the person.” They also described how they brought together the goals of weight loss and body and self-acceptance, saying, “I am more accepting of me and at the same time more dedicated to obtaining a healthier weight,” and “It’s okay to be happy the way I am and still want to change.”
Participants who didn’t receive the Weight BIAS program also shared positive feedback, writing that their favorite part of the program was “being part of such a supportive group of people who can relate to the things that I think and feel” and that they learned “how not to be so hard on myself.” This might suggest that even without an intervention specifically for weight stigma, providing respectful, compassionate care and peer support may help patients to feel less alone and to be kinder to themselves.
Our study results suggest that reducing negative self-talk and internalized beliefs about weight certainly won’t undermine treatment outcomes and may have some benefits beyond standard weight loss treatment. At the same time, we also all need to do our part to change how society views and treats people with larger bodies and prevent the harms of experiencing and internalizing weight stigma.
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL140176. The content is solely the responsibility of the author and does not necessarily reflect the official views of the National Institutes of Health.
Dr. Pearl is assistant professor, clinical and health psychology, University of Florida, Gainesville. She has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Protecting your practice data
While data protection is important in any industry, it is particularly critical in health care because in addition to the usual financial records, trade secrets, and other valuable data, confidential patient information is also at risk.
You may think that your computer vendor is responsible for safeguarding your data, but third parties can only do so much. And if your data is compromised, the ultimate responsibility is yours – not to mention the financial loss, and the damage to your practice’s reputation.
In addition to the security vulnerabilities inherent in any system, there are external vulnerabilities, such as weak passwords, viruses, and hacking (either externally or internally). And as hardware becomes more and more portable, there is the increasing risk of theft of platforms and storage media containing confidential data.
A close and ongoing relationship with your hardware and software vendors is essential to good data protection. Your office should have a permanent contact at each company, and you should talk to them regularly. Ask them what sort of firewalls, antivirus software, and other safeguards are in place to protect your system. Whenever they identify a bug or other vulnerability, you should know about it. They should tell you about each software update, what improvements it makes, and what defects it fixes. You should also know about any changes to your data encryption.
Encryption has become an essential component of data protection. It is especially important if you use portable devices such as laptops, pads, or smart phones to store and transport patient information. If you lose one of these devices, or a thumb drive or other storage media, HIPAA will probably not consider it a breach if the data it contains is encrypted.
Encryption isn’t perfect, of course. Log-in credentials can be stolen; and data that is stored in house is can be hacked with malware and phishing techniques, especially if the key to decryption is located on that server. And make sure that employees are not putting any medical data on their own private (unencrypted) devices.
Each employee should have his or her own password, and sharing should be strictly prohibited. Multifactor authentication is becoming increasingly popular for an extra level of security.
Your vendor should require you to change your passwords every few months. If it doesn’t, you need to establish a timetable to do it yourself. All passwords should be strong (no birthdays, pet names, etc.), and they shouldn’t be the same or similar to old passwords.
In some offices, I’ve been surprised to see that every employee has unrestricted access to all practice data. The vulnerabilities of such an arrangement are obvious. There is no reason why receptionists, for example, should have access to medical histories, and insurance people don’t need to know what medications a patient is on. Your vendor can help you design partitions that restrict each employee to only the information they need access to.
Ask if your vendor provides security training for employees. If not, look into hiring a security firm to do it. Regular security training can help employees to recognize data security attacks like phishing, and instills a heightened sense of security awareness and vigilance among staff. They will also gain a better understanding of the role they play in maintaining the overall security of your office.
It goes without saying that third parties, such as business vendors, payers, and managed care providers, should never have access to patient records or other personal health information.
Backing up data
I have written many times about the importance of regularly backing up your data. Industry statistics show that fully 10% of hard drives fail in any given year, and 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, email, documents, and other important information. Recovery of lost data, when it’s possible at all, can be very expensive.
Even if your EHR vendor backs up your data, you should consider making a separate backup of your own. Backup drives have been known to fail too; and if you decide to switch computer vendors, you don’t want to be at the mercy of the old company that might be reluctant to transfer your data without a hefty payment.
The first rule of backing up is to store your backup drives in a different location from your computers. Unfortunately, that’s a pain; and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup. Several companies offer that service, and the cost is very reasonable for individual computers. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it’s still very reasonable and includes other services, such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and how fast your Internet connection runs. After that the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service’s data center, making them HIPAA compliant and, theoretically, only accessible by you.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
While data protection is important in any industry, it is particularly critical in health care because in addition to the usual financial records, trade secrets, and other valuable data, confidential patient information is also at risk.
You may think that your computer vendor is responsible for safeguarding your data, but third parties can only do so much. And if your data is compromised, the ultimate responsibility is yours – not to mention the financial loss, and the damage to your practice’s reputation.
In addition to the security vulnerabilities inherent in any system, there are external vulnerabilities, such as weak passwords, viruses, and hacking (either externally or internally). And as hardware becomes more and more portable, there is the increasing risk of theft of platforms and storage media containing confidential data.
A close and ongoing relationship with your hardware and software vendors is essential to good data protection. Your office should have a permanent contact at each company, and you should talk to them regularly. Ask them what sort of firewalls, antivirus software, and other safeguards are in place to protect your system. Whenever they identify a bug or other vulnerability, you should know about it. They should tell you about each software update, what improvements it makes, and what defects it fixes. You should also know about any changes to your data encryption.
Encryption has become an essential component of data protection. It is especially important if you use portable devices such as laptops, pads, or smart phones to store and transport patient information. If you lose one of these devices, or a thumb drive or other storage media, HIPAA will probably not consider it a breach if the data it contains is encrypted.
Encryption isn’t perfect, of course. Log-in credentials can be stolen; and data that is stored in house is can be hacked with malware and phishing techniques, especially if the key to decryption is located on that server. And make sure that employees are not putting any medical data on their own private (unencrypted) devices.
Each employee should have his or her own password, and sharing should be strictly prohibited. Multifactor authentication is becoming increasingly popular for an extra level of security.
Your vendor should require you to change your passwords every few months. If it doesn’t, you need to establish a timetable to do it yourself. All passwords should be strong (no birthdays, pet names, etc.), and they shouldn’t be the same or similar to old passwords.
In some offices, I’ve been surprised to see that every employee has unrestricted access to all practice data. The vulnerabilities of such an arrangement are obvious. There is no reason why receptionists, for example, should have access to medical histories, and insurance people don’t need to know what medications a patient is on. Your vendor can help you design partitions that restrict each employee to only the information they need access to.
Ask if your vendor provides security training for employees. If not, look into hiring a security firm to do it. Regular security training can help employees to recognize data security attacks like phishing, and instills a heightened sense of security awareness and vigilance among staff. They will also gain a better understanding of the role they play in maintaining the overall security of your office.
It goes without saying that third parties, such as business vendors, payers, and managed care providers, should never have access to patient records or other personal health information.
Backing up data
I have written many times about the importance of regularly backing up your data. Industry statistics show that fully 10% of hard drives fail in any given year, and 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, email, documents, and other important information. Recovery of lost data, when it’s possible at all, can be very expensive.
Even if your EHR vendor backs up your data, you should consider making a separate backup of your own. Backup drives have been known to fail too; and if you decide to switch computer vendors, you don’t want to be at the mercy of the old company that might be reluctant to transfer your data without a hefty payment.
The first rule of backing up is to store your backup drives in a different location from your computers. Unfortunately, that’s a pain; and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup. Several companies offer that service, and the cost is very reasonable for individual computers. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it’s still very reasonable and includes other services, such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and how fast your Internet connection runs. After that the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service’s data center, making them HIPAA compliant and, theoretically, only accessible by you.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
While data protection is important in any industry, it is particularly critical in health care because in addition to the usual financial records, trade secrets, and other valuable data, confidential patient information is also at risk.
You may think that your computer vendor is responsible for safeguarding your data, but third parties can only do so much. And if your data is compromised, the ultimate responsibility is yours – not to mention the financial loss, and the damage to your practice’s reputation.
In addition to the security vulnerabilities inherent in any system, there are external vulnerabilities, such as weak passwords, viruses, and hacking (either externally or internally). And as hardware becomes more and more portable, there is the increasing risk of theft of platforms and storage media containing confidential data.
A close and ongoing relationship with your hardware and software vendors is essential to good data protection. Your office should have a permanent contact at each company, and you should talk to them regularly. Ask them what sort of firewalls, antivirus software, and other safeguards are in place to protect your system. Whenever they identify a bug or other vulnerability, you should know about it. They should tell you about each software update, what improvements it makes, and what defects it fixes. You should also know about any changes to your data encryption.
Encryption has become an essential component of data protection. It is especially important if you use portable devices such as laptops, pads, or smart phones to store and transport patient information. If you lose one of these devices, or a thumb drive or other storage media, HIPAA will probably not consider it a breach if the data it contains is encrypted.
Encryption isn’t perfect, of course. Log-in credentials can be stolen; and data that is stored in house is can be hacked with malware and phishing techniques, especially if the key to decryption is located on that server. And make sure that employees are not putting any medical data on their own private (unencrypted) devices.
Each employee should have his or her own password, and sharing should be strictly prohibited. Multifactor authentication is becoming increasingly popular for an extra level of security.
Your vendor should require you to change your passwords every few months. If it doesn’t, you need to establish a timetable to do it yourself. All passwords should be strong (no birthdays, pet names, etc.), and they shouldn’t be the same or similar to old passwords.
In some offices, I’ve been surprised to see that every employee has unrestricted access to all practice data. The vulnerabilities of such an arrangement are obvious. There is no reason why receptionists, for example, should have access to medical histories, and insurance people don’t need to know what medications a patient is on. Your vendor can help you design partitions that restrict each employee to only the information they need access to.
Ask if your vendor provides security training for employees. If not, look into hiring a security firm to do it. Regular security training can help employees to recognize data security attacks like phishing, and instills a heightened sense of security awareness and vigilance among staff. They will also gain a better understanding of the role they play in maintaining the overall security of your office.
It goes without saying that third parties, such as business vendors, payers, and managed care providers, should never have access to patient records or other personal health information.
Backing up data
I have written many times about the importance of regularly backing up your data. Industry statistics show that fully 10% of hard drives fail in any given year, and 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, email, documents, and other important information. Recovery of lost data, when it’s possible at all, can be very expensive.
Even if your EHR vendor backs up your data, you should consider making a separate backup of your own. Backup drives have been known to fail too; and if you decide to switch computer vendors, you don’t want to be at the mercy of the old company that might be reluctant to transfer your data without a hefty payment.
The first rule of backing up is to store your backup drives in a different location from your computers. Unfortunately, that’s a pain; and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup. Several companies offer that service, and the cost is very reasonable for individual computers. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it’s still very reasonable and includes other services, such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and how fast your Internet connection runs. After that the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service’s data center, making them HIPAA compliant and, theoretically, only accessible by you.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

The cardiopulmonary effects of mask wearing
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.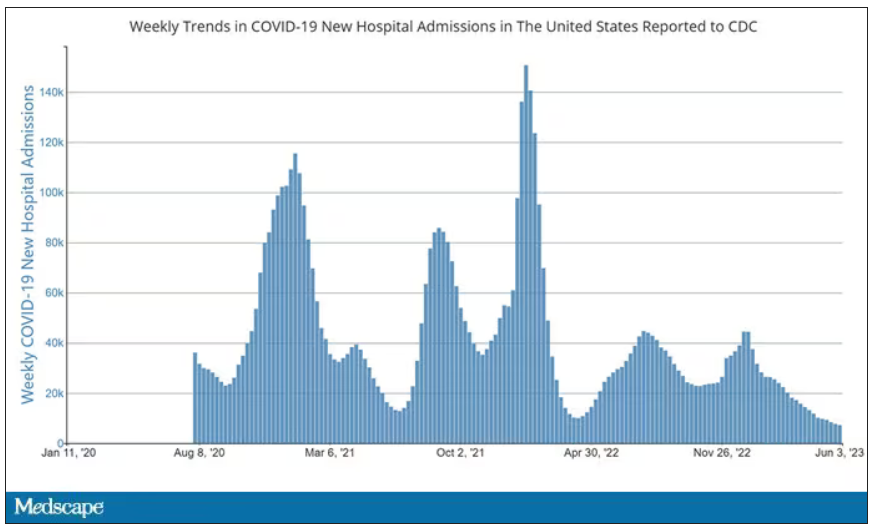
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.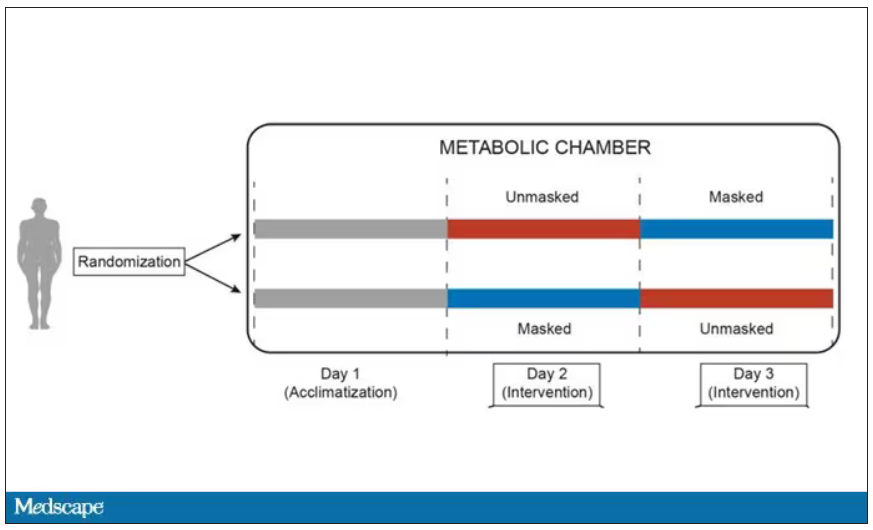
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.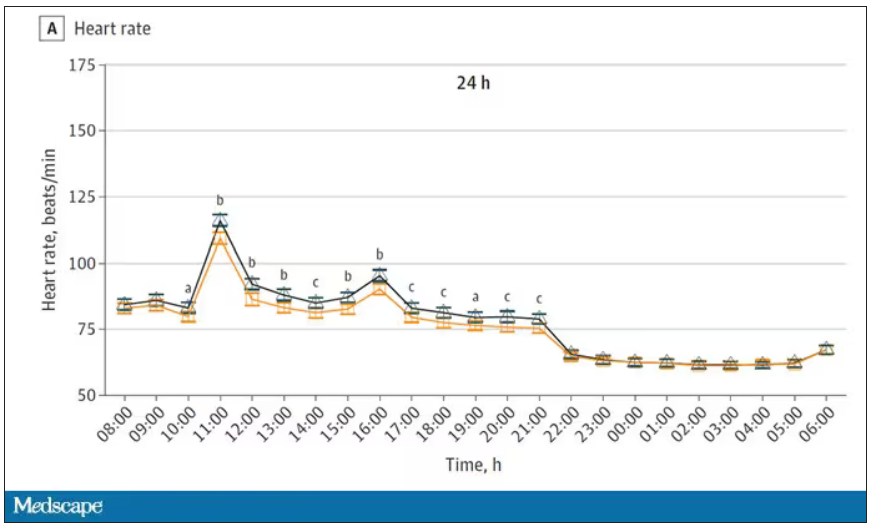
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.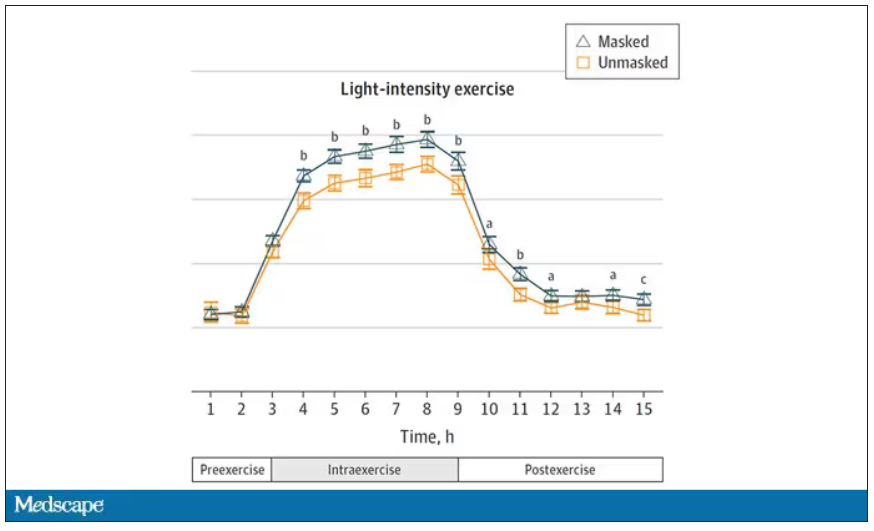
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.