User login
Children with BCP-ALL show inflammatory marker differences at birth
Patients who develop B-cell precursor acute lymphoblastic leukemia (BCP-ALL) in childhood may have dysregulated immune function at birth, according to a study published in Cancer Research.
Investigators evaluated neonatal concentrations of inflammatory markers and found significant differences between children who were later diagnosed with BCP-ALL and leukemia-free control subjects.
“Our findings suggest that children who develop ALL are immunologically disparate already at birth,” said study author Signe Holst Søegaard, PhD, of Statens Serum Institut in Copenhagen. “This may link to other observations suggesting that children who develop ALL respond differently to infections in early childhood, potentially promoting subsequent genetic events required for transformation to ALL, or speculations that they are unable to eliminate preleukemic cells.”
She noted that the study could not determine if the associations shown are causal or consequential so further studies will be needed both to confirm the findings and identify the underlying mechanisms.
For this study, Dr. Søegaard and her colleagues measured concentrations of 10 inflammatory markers on neonatal dried blood spots from 178 patients with BCP-ALL and 178 matched controls. The patients were diagnosed with BCP-ALL at ages 1-9 years.
Compared with controls, children who later developed BCP-ALL had significantly different neonatal concentrations of eight inflammatory markers.
Concentrations of interleukin (IL)–8, soluble receptor sIL-6R alpha, transforming growth factor (TGF)–beta 1, monocyte chemotactic protein (MCP)–1, and C-reactive protein (CRP) were significantly lower among the BCP-ALL patients.
On the other hand, concentrations of IL-6, IL-17, and IL-18 were significantly higher among BCP-ALL patients than controls.
The investigators noted that IL-10 concentrations were too low for accurate measurement in all patients and controls. Additionally, a “large proportion” of patients and controls had IL-6 and IL-17 concentrations that were below the limit of detection.
“We also demonstrated that several previously shown ALL risk factors – namely, birth order, gestational age, and sex – were associated with the neonatal concentrations of inflammatory markers,” Dr. Søegaard said. “These findings raise the interesting possibility that the effects of some known ALL risk factors partly act through prenatal programming of immune function.”
The investigators found that increasing birth order was associated with significantly higher IL-18 and lower CRP concentrations.
Increasing gestational age was associated with significantly lower sIL-6R alpha and TGF-beta 1 concentrations and higher CRP concentrations. And boys had significantly lower sIL-6R alpha and IL-8 concentrations and higher CRP concentrations than girls.
However, none of the following factors were significantly associated with concentrations of inflammatory biomarkers: maternal age at delivery, maternal hospital contact attributable to infection during pregnancy, maternal prescription for antimicrobials during pregnancy, birth weight, and mode of delivery.
“Our findings underline the role the child’s baseline immune characteristics may play in the development of ALL,” Dr. Søegaard said. “However, we cannot yet use our research results to predict who will develop childhood ALL.”
The study was sponsored by the Dagmar Marshall Foundation, the A.P. Møller Foundation, the Danish Childhood Cancer Foundation, the Arvid Nilsson Foundation, and the Danish Cancer Research Foundation. The investigators reported having no conflicts of interest.
SOURCE: Søegaard SH et al. Cancer Res. 2018;78(18);5458-63.
Patients who develop B-cell precursor acute lymphoblastic leukemia (BCP-ALL) in childhood may have dysregulated immune function at birth, according to a study published in Cancer Research.
Investigators evaluated neonatal concentrations of inflammatory markers and found significant differences between children who were later diagnosed with BCP-ALL and leukemia-free control subjects.
“Our findings suggest that children who develop ALL are immunologically disparate already at birth,” said study author Signe Holst Søegaard, PhD, of Statens Serum Institut in Copenhagen. “This may link to other observations suggesting that children who develop ALL respond differently to infections in early childhood, potentially promoting subsequent genetic events required for transformation to ALL, or speculations that they are unable to eliminate preleukemic cells.”
She noted that the study could not determine if the associations shown are causal or consequential so further studies will be needed both to confirm the findings and identify the underlying mechanisms.
For this study, Dr. Søegaard and her colleagues measured concentrations of 10 inflammatory markers on neonatal dried blood spots from 178 patients with BCP-ALL and 178 matched controls. The patients were diagnosed with BCP-ALL at ages 1-9 years.
Compared with controls, children who later developed BCP-ALL had significantly different neonatal concentrations of eight inflammatory markers.
Concentrations of interleukin (IL)–8, soluble receptor sIL-6R alpha, transforming growth factor (TGF)–beta 1, monocyte chemotactic protein (MCP)–1, and C-reactive protein (CRP) were significantly lower among the BCP-ALL patients.
On the other hand, concentrations of IL-6, IL-17, and IL-18 were significantly higher among BCP-ALL patients than controls.
The investigators noted that IL-10 concentrations were too low for accurate measurement in all patients and controls. Additionally, a “large proportion” of patients and controls had IL-6 and IL-17 concentrations that were below the limit of detection.
“We also demonstrated that several previously shown ALL risk factors – namely, birth order, gestational age, and sex – were associated with the neonatal concentrations of inflammatory markers,” Dr. Søegaard said. “These findings raise the interesting possibility that the effects of some known ALL risk factors partly act through prenatal programming of immune function.”
The investigators found that increasing birth order was associated with significantly higher IL-18 and lower CRP concentrations.
Increasing gestational age was associated with significantly lower sIL-6R alpha and TGF-beta 1 concentrations and higher CRP concentrations. And boys had significantly lower sIL-6R alpha and IL-8 concentrations and higher CRP concentrations than girls.
However, none of the following factors were significantly associated with concentrations of inflammatory biomarkers: maternal age at delivery, maternal hospital contact attributable to infection during pregnancy, maternal prescription for antimicrobials during pregnancy, birth weight, and mode of delivery.
“Our findings underline the role the child’s baseline immune characteristics may play in the development of ALL,” Dr. Søegaard said. “However, we cannot yet use our research results to predict who will develop childhood ALL.”
The study was sponsored by the Dagmar Marshall Foundation, the A.P. Møller Foundation, the Danish Childhood Cancer Foundation, the Arvid Nilsson Foundation, and the Danish Cancer Research Foundation. The investigators reported having no conflicts of interest.
SOURCE: Søegaard SH et al. Cancer Res. 2018;78(18);5458-63.
Patients who develop B-cell precursor acute lymphoblastic leukemia (BCP-ALL) in childhood may have dysregulated immune function at birth, according to a study published in Cancer Research.
Investigators evaluated neonatal concentrations of inflammatory markers and found significant differences between children who were later diagnosed with BCP-ALL and leukemia-free control subjects.
“Our findings suggest that children who develop ALL are immunologically disparate already at birth,” said study author Signe Holst Søegaard, PhD, of Statens Serum Institut in Copenhagen. “This may link to other observations suggesting that children who develop ALL respond differently to infections in early childhood, potentially promoting subsequent genetic events required for transformation to ALL, or speculations that they are unable to eliminate preleukemic cells.”
She noted that the study could not determine if the associations shown are causal or consequential so further studies will be needed both to confirm the findings and identify the underlying mechanisms.
For this study, Dr. Søegaard and her colleagues measured concentrations of 10 inflammatory markers on neonatal dried blood spots from 178 patients with BCP-ALL and 178 matched controls. The patients were diagnosed with BCP-ALL at ages 1-9 years.
Compared with controls, children who later developed BCP-ALL had significantly different neonatal concentrations of eight inflammatory markers.
Concentrations of interleukin (IL)–8, soluble receptor sIL-6R alpha, transforming growth factor (TGF)–beta 1, monocyte chemotactic protein (MCP)–1, and C-reactive protein (CRP) were significantly lower among the BCP-ALL patients.
On the other hand, concentrations of IL-6, IL-17, and IL-18 were significantly higher among BCP-ALL patients than controls.
The investigators noted that IL-10 concentrations were too low for accurate measurement in all patients and controls. Additionally, a “large proportion” of patients and controls had IL-6 and IL-17 concentrations that were below the limit of detection.
“We also demonstrated that several previously shown ALL risk factors – namely, birth order, gestational age, and sex – were associated with the neonatal concentrations of inflammatory markers,” Dr. Søegaard said. “These findings raise the interesting possibility that the effects of some known ALL risk factors partly act through prenatal programming of immune function.”
The investigators found that increasing birth order was associated with significantly higher IL-18 and lower CRP concentrations.
Increasing gestational age was associated with significantly lower sIL-6R alpha and TGF-beta 1 concentrations and higher CRP concentrations. And boys had significantly lower sIL-6R alpha and IL-8 concentrations and higher CRP concentrations than girls.
However, none of the following factors were significantly associated with concentrations of inflammatory biomarkers: maternal age at delivery, maternal hospital contact attributable to infection during pregnancy, maternal prescription for antimicrobials during pregnancy, birth weight, and mode of delivery.
“Our findings underline the role the child’s baseline immune characteristics may play in the development of ALL,” Dr. Søegaard said. “However, we cannot yet use our research results to predict who will develop childhood ALL.”
The study was sponsored by the Dagmar Marshall Foundation, the A.P. Møller Foundation, the Danish Childhood Cancer Foundation, the Arvid Nilsson Foundation, and the Danish Cancer Research Foundation. The investigators reported having no conflicts of interest.
SOURCE: Søegaard SH et al. Cancer Res. 2018;78(18);5458-63.
FROM CANCER RESEARCH
Key clinical point:
Major finding: Neonatal concentrations of some inflammatory markers were significantly different between BCP-ALL patients and controls.
Study details: Ten markers were measured in 178 patients with BCP-ALL and 178 matched controls.
Disclosures: The study was sponsored by the Dagmar Marshall Foundation, the A.P. Møller Foundation, the Danish Childhood Cancer Foundation, the Arvid Nilsson Foundation, and the Danish Cancer Research Foundation. The investigators reported having no conflicts of interest.
Source: Søegaard SH et al. Cancer Res. 2018;78(18);5458-63.
Azithromycin for COPD exacerbations may reduce treatment failure
PARIS – In patients with a chronic obstructive pulmonary disease (provided improvement in a variety of outcomes at 90 days, including risk of death, according to a placebo-controlled trial presented as a late-breaker at the annual congress of the European Respiratory Society.

In patients with COPD, “azithromycin initiated in the acute setting and continued for 3 months appears to be safe and potentially effective,” reported Wim Janssens, MD, PhD, division of respiratory medicine, University Hospital, Leuven, Belgium.
The phrase “potentially effective” was used because the primary endpoint, which was time to treatment failure, fell just short of statistical significance (P = .053), but the rate of treatment failures, which was a coprimary endpoint (P = .04), and all of the secondary endpoints, including mortality at 90 days (P = .027), need for treatment intensification (P = .02) and need for an intensive care unit (ICU) admission (P = .003), were significantly lower in the group receiving azithromycin rather than placebo.
In a previous trial, chronic azithromycin therapy on top of usual care in patients frequently hospitalized for COPD was associated with a reduction in the risk of exacerbations and an improvement in quality of life (N Engl J Med. 2011;365:689-98). However, Dr. Janssens explained that this strategy is not commonly used because it was associated with a variety of adverse events, not least of which was QTc prolongation.
The study at the meeting, called the BACE trial, was designed to test whether azithromycin could be employed in a more targeted approach to control exacerbations. In the study, 301 COPD patients hospitalized with an acute exacerbation were randomized within 48 hours of admission to azithromycin or placebo. For the first 3 days, azithromycin was administered in a 500-mg dose. Thereafter, the dose was 250 mg every second day. Treatment was stopped at 90 days.
The primary outcome was time to treatment failure, a novel composite endpoint of any of three events: the need for treatment intensification, the need for step-up hospital care (either ICU admission or hospital readmission), or death by any cause. The two treatment arms were also compared for safety, including QTc prolongation.
The treatment failure rates were 49% in the azithromycin arm and 60% in the placebo arm, producing a hazard ratio (HR) of 0.73. Although this outcome fell short of significance, Dr. Janssens suggested that benefits over the 90 days of treatment are supported by the secondary outcomes. However, he also cautioned that most relative advantages for azithromycin over placebo were found to dissipate over time.
“The maximum separation between the azithromycin and placebo arms [for the primary outcome] occurred at 120 days or 30 days after the medication was stopped,” Dr. Janssens reported. After this point, the two arms converged and eventually overlapped.
However, the acute benefits appeared to be substantial. For example, average hospital stay over the 90-day treatment period was reduced from 40 to 10 days (P = .0061), and the ICU days fell from 11 days to 3 days in the azithromycin relative to the placebo group. According to Dr. Janssens, the difference in hospital stay carries “important health economic potential that deserves further attention.”
Of the three QTc events that occurred during the course of the study, one was observed in the placebo group. There was no significant difference in this or other adverse events, according to Dr. Janssens.
It is notable that the design for the BACE trial called for 500 patients. When enrollment was slow, the design was changed on the basis of power calculations indicating that 300 patients would be sufficient to demonstrate a difference. It is unclear whether a larger study would have permitted the difference in the primary endpoint to advance from a trend.
Dr. Janssens reports no conflicts of interest relevant to this study.
PARIS – In patients with a chronic obstructive pulmonary disease (provided improvement in a variety of outcomes at 90 days, including risk of death, according to a placebo-controlled trial presented as a late-breaker at the annual congress of the European Respiratory Society.
In patients with COPD, “azithromycin initiated in the acute setting and continued for 3 months appears to be safe and potentially effective,” reported Wim Janssens, MD, PhD, division of respiratory medicine, University Hospital, Leuven, Belgium.
The phrase “potentially effective” was used because the primary endpoint, which was time to treatment failure, fell just short of statistical significance (P = .053), but the rate of treatment failures, which was a coprimary endpoint (P = .04), and all of the secondary endpoints, including mortality at 90 days (P = .027), need for treatment intensification (P = .02) and need for an intensive care unit (ICU) admission (P = .003), were significantly lower in the group receiving azithromycin rather than placebo.
In a previous trial, chronic azithromycin therapy on top of usual care in patients frequently hospitalized for COPD was associated with a reduction in the risk of exacerbations and an improvement in quality of life (N Engl J Med. 2011;365:689-98). However, Dr. Janssens explained that this strategy is not commonly used because it was associated with a variety of adverse events, not least of which was QTc prolongation.
The study at the meeting, called the BACE trial, was designed to test whether azithromycin could be employed in a more targeted approach to control exacerbations. In the study, 301 COPD patients hospitalized with an acute exacerbation were randomized within 48 hours of admission to azithromycin or placebo. For the first 3 days, azithromycin was administered in a 500-mg dose. Thereafter, the dose was 250 mg every second day. Treatment was stopped at 90 days.
The primary outcome was time to treatment failure, a novel composite endpoint of any of three events: the need for treatment intensification, the need for step-up hospital care (either ICU admission or hospital readmission), or death by any cause. The two treatment arms were also compared for safety, including QTc prolongation.
The treatment failure rates were 49% in the azithromycin arm and 60% in the placebo arm, producing a hazard ratio (HR) of 0.73. Although this outcome fell short of significance, Dr. Janssens suggested that benefits over the 90 days of treatment are supported by the secondary outcomes. However, he also cautioned that most relative advantages for azithromycin over placebo were found to dissipate over time.
“The maximum separation between the azithromycin and placebo arms [for the primary outcome] occurred at 120 days or 30 days after the medication was stopped,” Dr. Janssens reported. After this point, the two arms converged and eventually overlapped.
However, the acute benefits appeared to be substantial. For example, average hospital stay over the 90-day treatment period was reduced from 40 to 10 days (P = .0061), and the ICU days fell from 11 days to 3 days in the azithromycin relative to the placebo group. According to Dr. Janssens, the difference in hospital stay carries “important health economic potential that deserves further attention.”
Of the three QTc events that occurred during the course of the study, one was observed in the placebo group. There was no significant difference in this or other adverse events, according to Dr. Janssens.
It is notable that the design for the BACE trial called for 500 patients. When enrollment was slow, the design was changed on the basis of power calculations indicating that 300 patients would be sufficient to demonstrate a difference. It is unclear whether a larger study would have permitted the difference in the primary endpoint to advance from a trend.
Dr. Janssens reports no conflicts of interest relevant to this study.
PARIS – In patients with a chronic obstructive pulmonary disease (provided improvement in a variety of outcomes at 90 days, including risk of death, according to a placebo-controlled trial presented as a late-breaker at the annual congress of the European Respiratory Society.
In patients with COPD, “azithromycin initiated in the acute setting and continued for 3 months appears to be safe and potentially effective,” reported Wim Janssens, MD, PhD, division of respiratory medicine, University Hospital, Leuven, Belgium.
The phrase “potentially effective” was used because the primary endpoint, which was time to treatment failure, fell just short of statistical significance (P = .053), but the rate of treatment failures, which was a coprimary endpoint (P = .04), and all of the secondary endpoints, including mortality at 90 days (P = .027), need for treatment intensification (P = .02) and need for an intensive care unit (ICU) admission (P = .003), were significantly lower in the group receiving azithromycin rather than placebo.
In a previous trial, chronic azithromycin therapy on top of usual care in patients frequently hospitalized for COPD was associated with a reduction in the risk of exacerbations and an improvement in quality of life (N Engl J Med. 2011;365:689-98). However, Dr. Janssens explained that this strategy is not commonly used because it was associated with a variety of adverse events, not least of which was QTc prolongation.
The study at the meeting, called the BACE trial, was designed to test whether azithromycin could be employed in a more targeted approach to control exacerbations. In the study, 301 COPD patients hospitalized with an acute exacerbation were randomized within 48 hours of admission to azithromycin or placebo. For the first 3 days, azithromycin was administered in a 500-mg dose. Thereafter, the dose was 250 mg every second day. Treatment was stopped at 90 days.
The primary outcome was time to treatment failure, a novel composite endpoint of any of three events: the need for treatment intensification, the need for step-up hospital care (either ICU admission or hospital readmission), or death by any cause. The two treatment arms were also compared for safety, including QTc prolongation.
The treatment failure rates were 49% in the azithromycin arm and 60% in the placebo arm, producing a hazard ratio (HR) of 0.73. Although this outcome fell short of significance, Dr. Janssens suggested that benefits over the 90 days of treatment are supported by the secondary outcomes. However, he also cautioned that most relative advantages for azithromycin over placebo were found to dissipate over time.
“The maximum separation between the azithromycin and placebo arms [for the primary outcome] occurred at 120 days or 30 days after the medication was stopped,” Dr. Janssens reported. After this point, the two arms converged and eventually overlapped.
However, the acute benefits appeared to be substantial. For example, average hospital stay over the 90-day treatment period was reduced from 40 to 10 days (P = .0061), and the ICU days fell from 11 days to 3 days in the azithromycin relative to the placebo group. According to Dr. Janssens, the difference in hospital stay carries “important health economic potential that deserves further attention.”
Of the three QTc events that occurred during the course of the study, one was observed in the placebo group. There was no significant difference in this or other adverse events, according to Dr. Janssens.
It is notable that the design for the BACE trial called for 500 patients. When enrollment was slow, the design was changed on the basis of power calculations indicating that 300 patients would be sufficient to demonstrate a difference. It is unclear whether a larger study would have permitted the difference in the primary endpoint to advance from a trend.
Dr. Janssens reports no conflicts of interest relevant to this study.
REPORTING FROM THE ERS CONGRESS 2018
Key clinical point: Initiating azithromycin in patients with COPD exacerbation at the time of hospitalization improves short-term outcomes.
Major finding: Relative to placebo, azithromycin provided a borderline reduction in treatment failure (P = .053) while reducing mortality (P = .027).
Study details: Multicenter, placebo-controlled trial.
Disclosures: Dr. Janssens reports no conflicts of interest relevant to this study.
Ob.Gyn. News welcomes Dr. Badell to the Board

Dr. Badell is an assistant professor of gynecology and obstetrics in the division of maternal-fetal medicine at Emory University in Atlanta. She also is director of the Perinatal Center at Emory University Hospital Midtown.
Dr. Badell has been a primary author or coauthor of 35 articles published and accepted in refereed medical publications on topics including Zika infection during pregnancy, HIV infection during pregnancy, use of complementary and alternative medication in obstetrics and gynecology, botulism during pregnancy, maternal and fetal risk associated with assisted reproductive technology, and perinatal outcomes among women with congenital heart disease. She also has written several book chapters, and she currently is involved in research involving pediatric and maternal HIV/AIDS, as well as chronic hypertension during pregnancy.
Dr. Badell serves on a number of committees at Emory for the department of obstetrics and gynecology, including the clinical competency committee and program evaluation committee, as well as similar committees for the maternal-fetal medicine fellowship program. She also is a member of the Emory University Hospital Midtown’s quality enhancement committee.
Dr. Badell graduated with distinction from the University of Rochester (N.Y.), did a clinical research fellowship in obstetrics and gynecology at Baylor College of Medicine in Houston, and a fellowship in maternal-fetal medicine at Emory University. Dr. Badell has won too many honors and awards to mention, but a few of them are membership in Phi Beta Kappa; an outstanding clinician award in maternal-fetal medicine; an excellence in teaching, maternal-fetal medicine award; and a faculty recognition “Hidden Gem” award.
Dr. Badell is an assistant professor of gynecology and obstetrics in the division of maternal-fetal medicine at Emory University in Atlanta. She also is director of the Perinatal Center at Emory University Hospital Midtown.
Dr. Badell has been a primary author or coauthor of 35 articles published and accepted in refereed medical publications on topics including Zika infection during pregnancy, HIV infection during pregnancy, use of complementary and alternative medication in obstetrics and gynecology, botulism during pregnancy, maternal and fetal risk associated with assisted reproductive technology, and perinatal outcomes among women with congenital heart disease. She also has written several book chapters, and she currently is involved in research involving pediatric and maternal HIV/AIDS, as well as chronic hypertension during pregnancy.
Dr. Badell serves on a number of committees at Emory for the department of obstetrics and gynecology, including the clinical competency committee and program evaluation committee, as well as similar committees for the maternal-fetal medicine fellowship program. She also is a member of the Emory University Hospital Midtown’s quality enhancement committee.
Dr. Badell graduated with distinction from the University of Rochester (N.Y.), did a clinical research fellowship in obstetrics and gynecology at Baylor College of Medicine in Houston, and a fellowship in maternal-fetal medicine at Emory University. Dr. Badell has won too many honors and awards to mention, but a few of them are membership in Phi Beta Kappa; an outstanding clinician award in maternal-fetal medicine; an excellence in teaching, maternal-fetal medicine award; and a faculty recognition “Hidden Gem” award.
Dr. Badell is an assistant professor of gynecology and obstetrics in the division of maternal-fetal medicine at Emory University in Atlanta. She also is director of the Perinatal Center at Emory University Hospital Midtown.
Dr. Badell has been a primary author or coauthor of 35 articles published and accepted in refereed medical publications on topics including Zika infection during pregnancy, HIV infection during pregnancy, use of complementary and alternative medication in obstetrics and gynecology, botulism during pregnancy, maternal and fetal risk associated with assisted reproductive technology, and perinatal outcomes among women with congenital heart disease. She also has written several book chapters, and she currently is involved in research involving pediatric and maternal HIV/AIDS, as well as chronic hypertension during pregnancy.
Dr. Badell serves on a number of committees at Emory for the department of obstetrics and gynecology, including the clinical competency committee and program evaluation committee, as well as similar committees for the maternal-fetal medicine fellowship program. She also is a member of the Emory University Hospital Midtown’s quality enhancement committee.
Dr. Badell graduated with distinction from the University of Rochester (N.Y.), did a clinical research fellowship in obstetrics and gynecology at Baylor College of Medicine in Houston, and a fellowship in maternal-fetal medicine at Emory University. Dr. Badell has won too many honors and awards to mention, but a few of them are membership in Phi Beta Kappa; an outstanding clinician award in maternal-fetal medicine; an excellence in teaching, maternal-fetal medicine award; and a faculty recognition “Hidden Gem” award.
SBRT controls oligometastatic RCC in majority of patients
Stereotactic body radiation therapy (SBRT) is a safe and effective treatment option for patients with oligometastatic renal cell carcinoma (RCC), according to investigators.
Patients with clear cell RCC who had previously received systemic therapy were more likely to achieve local control, reported Ciro Franzese, MD of Humanitas Clinical and Research Center in Milan, and his coauthors.
These findings contribute to a shifting landscape in RCC; modern techniques are opening doors once closed by disappointing historical results. Several recent SBRT studies have demonstrated local control rates of approximately 90%, compared with conventional RT rates of 20%.
“While the outcomes from conventional RT were quite poor, with SBRT, different biological mechanisms occur due to the use of higher doses per fraction,” the authors wrote in The Journal of Urology.
The present retrospective study involved 58 patients with oligometastatic RCC who were treated with SBRT between 2004 and 2006. Patients previously underwent primary tumor excision, had no greater than three distant extracranial metastases, and were not surgical candidates. Study endpoints included median overall survival (OS), progression-free survival (PFS), and in-field local control (LC). Stratified analysis was also performed in patients with clear cell RCC.
Just over 90% of patients achieved LC at 18 months. Slightly less than half (46.2%) were progression-free at 1 year, and this number dropped to one-third (35%) by 18 months. Median OS was just over 2 years (28 months). Although all patients (100%) were alive at 2 years, this rate dropped to 83% by the 5-year mark.
In patients with clear cell RCC, those treated with systemic therapy prior to SBRT were more likely to achieve LC compared with patients who did not receive systemic therapy (HR 0.15; P = .032).
Overall, SBRT was well tolerated. No grade 3 or higher adverse events occurred. The most common adverse events were pain, fatigue, nausea, and vomiting.
The authors concluded that SBRT is a safe and effective option for patients with oligometastatic RCC. They called for future research to address “the radiobiology of RCC” in order to “understand the role of SBRT and, particularly, its possible interaction with medical therapies.”
The authors reported no conflicts of interest.
SOURCE: Franzese et al. J Urol. 2018 Sep 1. doi: 10.1016/j.juro.2018.08.049.
Stereotactic body radiation therapy (SBRT) is a safe and effective treatment option for patients with oligometastatic renal cell carcinoma (RCC), according to investigators.
Patients with clear cell RCC who had previously received systemic therapy were more likely to achieve local control, reported Ciro Franzese, MD of Humanitas Clinical and Research Center in Milan, and his coauthors.
These findings contribute to a shifting landscape in RCC; modern techniques are opening doors once closed by disappointing historical results. Several recent SBRT studies have demonstrated local control rates of approximately 90%, compared with conventional RT rates of 20%.
“While the outcomes from conventional RT were quite poor, with SBRT, different biological mechanisms occur due to the use of higher doses per fraction,” the authors wrote in The Journal of Urology.
The present retrospective study involved 58 patients with oligometastatic RCC who were treated with SBRT between 2004 and 2006. Patients previously underwent primary tumor excision, had no greater than three distant extracranial metastases, and were not surgical candidates. Study endpoints included median overall survival (OS), progression-free survival (PFS), and in-field local control (LC). Stratified analysis was also performed in patients with clear cell RCC.
Just over 90% of patients achieved LC at 18 months. Slightly less than half (46.2%) were progression-free at 1 year, and this number dropped to one-third (35%) by 18 months. Median OS was just over 2 years (28 months). Although all patients (100%) were alive at 2 years, this rate dropped to 83% by the 5-year mark.
In patients with clear cell RCC, those treated with systemic therapy prior to SBRT were more likely to achieve LC compared with patients who did not receive systemic therapy (HR 0.15; P = .032).
Overall, SBRT was well tolerated. No grade 3 or higher adverse events occurred. The most common adverse events were pain, fatigue, nausea, and vomiting.
The authors concluded that SBRT is a safe and effective option for patients with oligometastatic RCC. They called for future research to address “the radiobiology of RCC” in order to “understand the role of SBRT and, particularly, its possible interaction with medical therapies.”
The authors reported no conflicts of interest.
SOURCE: Franzese et al. J Urol. 2018 Sep 1. doi: 10.1016/j.juro.2018.08.049.
Stereotactic body radiation therapy (SBRT) is a safe and effective treatment option for patients with oligometastatic renal cell carcinoma (RCC), according to investigators.
Patients with clear cell RCC who had previously received systemic therapy were more likely to achieve local control, reported Ciro Franzese, MD of Humanitas Clinical and Research Center in Milan, and his coauthors.
These findings contribute to a shifting landscape in RCC; modern techniques are opening doors once closed by disappointing historical results. Several recent SBRT studies have demonstrated local control rates of approximately 90%, compared with conventional RT rates of 20%.
“While the outcomes from conventional RT were quite poor, with SBRT, different biological mechanisms occur due to the use of higher doses per fraction,” the authors wrote in The Journal of Urology.
The present retrospective study involved 58 patients with oligometastatic RCC who were treated with SBRT between 2004 and 2006. Patients previously underwent primary tumor excision, had no greater than three distant extracranial metastases, and were not surgical candidates. Study endpoints included median overall survival (OS), progression-free survival (PFS), and in-field local control (LC). Stratified analysis was also performed in patients with clear cell RCC.
Just over 90% of patients achieved LC at 18 months. Slightly less than half (46.2%) were progression-free at 1 year, and this number dropped to one-third (35%) by 18 months. Median OS was just over 2 years (28 months). Although all patients (100%) were alive at 2 years, this rate dropped to 83% by the 5-year mark.
In patients with clear cell RCC, those treated with systemic therapy prior to SBRT were more likely to achieve LC compared with patients who did not receive systemic therapy (HR 0.15; P = .032).
Overall, SBRT was well tolerated. No grade 3 or higher adverse events occurred. The most common adverse events were pain, fatigue, nausea, and vomiting.
The authors concluded that SBRT is a safe and effective option for patients with oligometastatic RCC. They called for future research to address “the radiobiology of RCC” in order to “understand the role of SBRT and, particularly, its possible interaction with medical therapies.”
The authors reported no conflicts of interest.
SOURCE: Franzese et al. J Urol. 2018 Sep 1. doi: 10.1016/j.juro.2018.08.049.
FROM THE JOURNAL OF UROLOGY
Key clinical point: For patients with oligometastatic renal cell carcinoma (RCC), stereotactic body radiation therapy (SBRT) is a safe and effective treatment option.
Major finding: The local control rate 18 months after SBRT was 90.2%.
Study details: A retrospective study involving 58 patients with oligometastatic RCC who were treated with SBRT between 2004 and 2006.
Disclosures: None.
Source: Franzese et al. J Urol. 2018 Sep 1. doi: 10.1016/j.juro.2018.08.049.
Female Gender, High Stress Levels, and Migraine
A recent study found a 10.7% prevalence of migraines and synergism between female gender and stress on risk of migraine, suggesting health interventions targeting women under stress may be beneficial. Researchers used data from 42,282 persons aged ≥12 years who participated in a 2013–2014 community health survey. A multivariate log-binomial model was used to calculate adjusted prevalence ratios for migraines associated with individual and joint exposures of female gender and stress. They used relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (S index) to measure additive interaction. They found:
- The prevalence of migraines was 10.7%.
- The adjusted prevalence ratios were 2.37 for female vs male, 1.63 for persons with high vs low levels of stress, and 3.38 for women with high stress vs men with low stress.
- The RERI estimate was 0.38, the AP estimate was 0.11, and the S index was 1.19.
Slatculescu AM, Chen Y. Synergism between female gender and high levels of daily stress associated with migraine headaches in Ontario, Canada. [Published online ahead of print August 28, 2018]. Neuroepidemiol. doi:10.1159/000492503.
A recent study found a 10.7% prevalence of migraines and synergism between female gender and stress on risk of migraine, suggesting health interventions targeting women under stress may be beneficial. Researchers used data from 42,282 persons aged ≥12 years who participated in a 2013–2014 community health survey. A multivariate log-binomial model was used to calculate adjusted prevalence ratios for migraines associated with individual and joint exposures of female gender and stress. They used relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (S index) to measure additive interaction. They found:
- The prevalence of migraines was 10.7%.
- The adjusted prevalence ratios were 2.37 for female vs male, 1.63 for persons with high vs low levels of stress, and 3.38 for women with high stress vs men with low stress.
- The RERI estimate was 0.38, the AP estimate was 0.11, and the S index was 1.19.
Slatculescu AM, Chen Y. Synergism between female gender and high levels of daily stress associated with migraine headaches in Ontario, Canada. [Published online ahead of print August 28, 2018]. Neuroepidemiol. doi:10.1159/000492503.
A recent study found a 10.7% prevalence of migraines and synergism between female gender and stress on risk of migraine, suggesting health interventions targeting women under stress may be beneficial. Researchers used data from 42,282 persons aged ≥12 years who participated in a 2013–2014 community health survey. A multivariate log-binomial model was used to calculate adjusted prevalence ratios for migraines associated with individual and joint exposures of female gender and stress. They used relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (S index) to measure additive interaction. They found:
- The prevalence of migraines was 10.7%.
- The adjusted prevalence ratios were 2.37 for female vs male, 1.63 for persons with high vs low levels of stress, and 3.38 for women with high stress vs men with low stress.
- The RERI estimate was 0.38, the AP estimate was 0.11, and the S index was 1.19.
Slatculescu AM, Chen Y. Synergism between female gender and high levels of daily stress associated with migraine headaches in Ontario, Canada. [Published online ahead of print August 28, 2018]. Neuroepidemiol. doi:10.1159/000492503.
Decrease Found in ED Return Rates for Migraine
For patients with migraine in the emergency department (ED), the use of IV fluids, dopamine receptor antagonists (DRA), nonsteroidal anti-Inflammatory drugs, and corticosteroids increased whereas the use of narcotics and discharge prescriptions for narcotics decreased, according to a recent study. Researchers also found that the return rates for migraines decreased and they speculate that the increased use of non-narcotic medications contributed to this decrease. In this study, they examined a multi-hospital retrospective cohort consisting of consecutive ED patients from January 1, 1999, to September 31, 2014. They examined charts at the beginning and end of the time period and found:
- Of the 2,824,710 total visits, 8046 (0.28%) were for migraine.
- 290 charts (147 in 1999–2000 and 143 in 2014) were reviewed to determine migraine treatments.
- Of the 8046 migraine patients, 624 (8%) returned within 72 hours.
- The return rate decreased from 1999–2000 to 2014 from 12% to 4% (difference = 8%).
Ruzek M, Richman P, Eskin B, Allegra JR. ED treatment of migraine patients has changed. [Published online ahead of print August 20, 2018]. Am J Emerg Med. doi:10.1016/j.ajem.2018.08.051.
For patients with migraine in the emergency department (ED), the use of IV fluids, dopamine receptor antagonists (DRA), nonsteroidal anti-Inflammatory drugs, and corticosteroids increased whereas the use of narcotics and discharge prescriptions for narcotics decreased, according to a recent study. Researchers also found that the return rates for migraines decreased and they speculate that the increased use of non-narcotic medications contributed to this decrease. In this study, they examined a multi-hospital retrospective cohort consisting of consecutive ED patients from January 1, 1999, to September 31, 2014. They examined charts at the beginning and end of the time period and found:
- Of the 2,824,710 total visits, 8046 (0.28%) were for migraine.
- 290 charts (147 in 1999–2000 and 143 in 2014) were reviewed to determine migraine treatments.
- Of the 8046 migraine patients, 624 (8%) returned within 72 hours.
- The return rate decreased from 1999–2000 to 2014 from 12% to 4% (difference = 8%).
Ruzek M, Richman P, Eskin B, Allegra JR. ED treatment of migraine patients has changed. [Published online ahead of print August 20, 2018]. Am J Emerg Med. doi:10.1016/j.ajem.2018.08.051.
For patients with migraine in the emergency department (ED), the use of IV fluids, dopamine receptor antagonists (DRA), nonsteroidal anti-Inflammatory drugs, and corticosteroids increased whereas the use of narcotics and discharge prescriptions for narcotics decreased, according to a recent study. Researchers also found that the return rates for migraines decreased and they speculate that the increased use of non-narcotic medications contributed to this decrease. In this study, they examined a multi-hospital retrospective cohort consisting of consecutive ED patients from January 1, 1999, to September 31, 2014. They examined charts at the beginning and end of the time period and found:
- Of the 2,824,710 total visits, 8046 (0.28%) were for migraine.
- 290 charts (147 in 1999–2000 and 143 in 2014) were reviewed to determine migraine treatments.
- Of the 8046 migraine patients, 624 (8%) returned within 72 hours.
- The return rate decreased from 1999–2000 to 2014 from 12% to 4% (difference = 8%).
Ruzek M, Richman P, Eskin B, Allegra JR. ED treatment of migraine patients has changed. [Published online ahead of print August 20, 2018]. Am J Emerg Med. doi:10.1016/j.ajem.2018.08.051.
Sunscreens: Survey of the Cutis Editorial Board
To improve patient care and outcomes, leading dermatologists from the Cutis Editorial Board answered 5 questions on sunscreens. Here’s what we found.
What sun protection factor (SPF) do you recommend for the majority of your patients?

Fifty percent of dermatologists we surveyed recommend SPF 30. SPF 50 was recommended by 26%, SPF 50+ by 21%, and SPF 15 by only 2%.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Half of our Editorial Board recommends sunscreen with SPF 30, with many recommending SPF 50 or higher. This trend toward sunscreens with higher SPF is consistent with a survey-based study with 97% of dermatologists stating they were comfortable recommending sunscreens with an SPF of 50 or higher and 83.3% stating that they believe that high SPF sunscreens provide an additional margin of safety (Farberg et al). These trends are supported by a randomized, double-blind, split-face clinical trial in which participants applied either SPF 50+ or SPF 100+ sunscreen after exposure to natural sunlight. The results showed that SPF 100+ sunscreen was remarkably more effective in protecting against sunburn than SPF 50+ sunscreen in actual use conditions (Williams et al).
Next page: Spray sunscreens
Which patient populations do you feel may benefit from spray sunscreens?
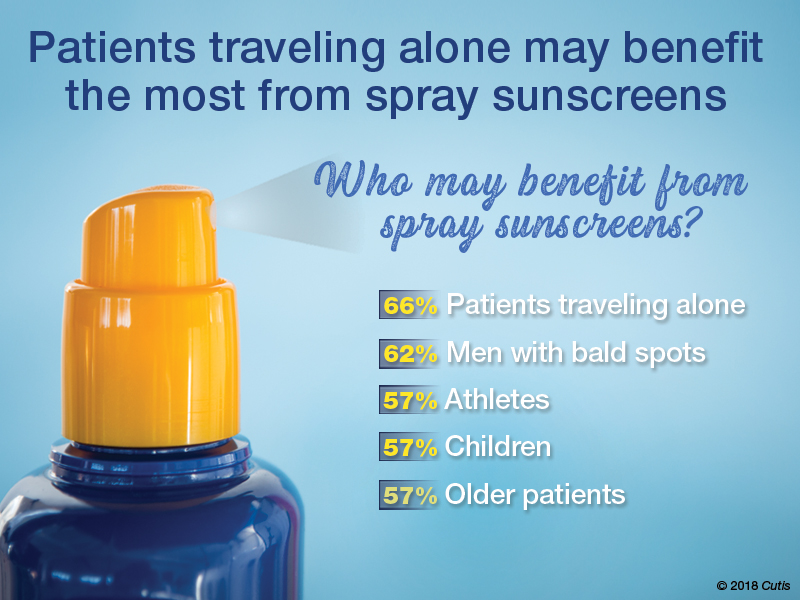
Two-thirds of dermatologists indicated that spray sunscreens may benefit patients traveling alone. Men with bald spots also may benefit (62%), as well as athletes, children, and older patients (57% each).
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
As dermatologists, we tell our patients that the best sunscreens are ones that are used consistently. Spray sunscreens are likely as effective as lotions (Ou-Yang et al). There has been a clear trend in consumer purchasing of spray sunscreens from 2011 to 2016 (Teplitz et al). Spray sunscreens may benefit those traveling alone, particularly for hard-to-reach areas.
Next page: Supplemental vitamin D
In patients who apply sunscreen regularly, do you recommend supplemental vitamin D3?

More than half (53%) of dermatologists recommend supplemental vitamin D3.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Because use of photoprotection results in decreased vitamin D levels in most individuals, it is good practice to recommend vitamin D supplementation in patients who are applying sunscreen regularly (Bogaczewicz et al).
Next page: Sunscreen compliance
What is the most often heard reason(s) for not using sunscreen in your patients?
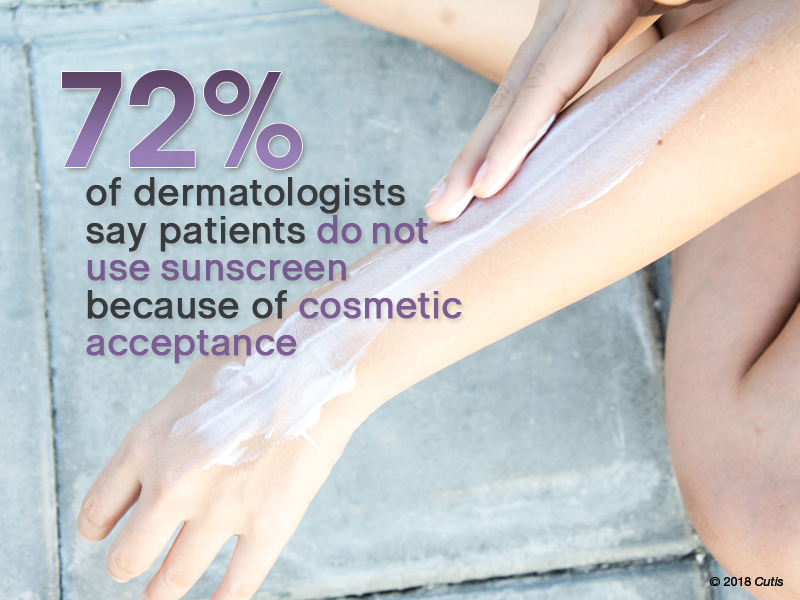
Nearly three-quarters (72%) of dermatologists reported that patients do not use sunscreen because of cosmetic acceptance. Almost one-third (31%) said their patients prefer “natural” products. Price was a factor for 26%. Fewer dermatologists indicated risk of environmental damage (14%), allergy (12%), cancer induction (5%), and hormonal alteration (5%) were reasons patients are not compliant.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Cosmetic acceptance is paramount for patient compliance for sunscreen application. These results from our Editorial Board echo a study on sunscreen product performance and other determinants of consumer preferences, which cited “cosmetic elegance” as an important factor in choosing sunscreens (Xu et al). Dermatologists must stress to patients to find a sunscreen that they find acceptable in terms of vehicle and price to increase compliance.
Next page: Sunscreens in pregnant women
What sunscreens do you recommend to pregnant women and children?

Most dermatologists (86%) recommend physical blockers “chemical-free” only sunscreens to pregnant women and children.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
While absorption of sunscreen by human embryos is likely negligible, because there is limited data on sunscreen effects in embryos and children, it is reasonable to recommend physical blockers for pregnant women and children.
Next page: More tips from derms
More Tips From Dermatologists
The dermatologists we polled had the following advice for their peers:
As a dermatologist married to a pediatrician, I try to get my kids to embrace sun-protection strategies. For the little ones it’s hard, but as they have gotten older and been exposed to more derm journals sitting around with pretty graphic pictures, they seem to get on board, even when away at summer camp on their own. If only our patients knew what our kids do.—Joel L. Cohen, MD (Denver, Colorado)
The most important factor in getting patient compliance with sunscreen usage is “cosmetic acceptance.” If they or their children or their spouse don’t like the feel, they won’t use it.—Vincent A. DeLeo, MD (Los Angeles, California)
Not using photoprotection with sunscreen is like crossing a busy road without looking both ways first.—James Q. Del Rosso, DO (Las Vegas, Nevada)
I do not recommend spray sunscreens. At least half of the spray seems to go in the air rather than on the skin. And people often do not rub the spray into their skin well enough. Lotions are better!—Lawrence J. Green, MD (Washington, DC)
The most important factor in sunscreen is not SPF; educate patients on the important role vehicle and sweating play in the length of sun protection.—Orit Markowitz, MD (New York, New York)
Reapplying sunscreen in the appropriate amount is key to blocking the danger rays of the sun.—Vineet Mishra, MD (San Antonio, Texas)
A good sunscreen is the one you put on properly. Regardless of the formulation, make sure you apply the sunscreen evenly to all exposed skin and reapply according to directions on the container. Remember, a regular white T-shirt has minimal SPF 4-5. Either wear sun-protective clothing or wear sunscreen underneath!—Larisa Ravitskiy, MD (Gahanna, Ohio)
Sun protection and sunscreen application go hand-in-hand. We can still enjoy the outdoors without getting excessive UV exposure.—Anthony M. Rossi, MD (New York, New York)
Sunscreens are only part of sun protection. Make sure to reapply them regularly, try to avoid direct sun between about 10 AM and 2 PM if possible, and wear a hat with a wide brim (not a baseball cap, which, after all, is designed for catching baseballs, not sun protection).—Robert I. Rudolph, MD (Wyomissing, Pennsylvania)
Sunscreens keep you younger looking longer!—Richard K. Scher, MD (New York, New York)
The dentist says only floss the teeth you want to keep. I tell patients to only sun block the skin they want to keep.—Daniel M. Siegel, MD, MS (Brooklyn, New York)
The best sunscreen is the one that is used! If it's too greasy or drying, smells bad or stings, it won't be used. Stick to the one YOU like, but at least SPF 30 or better.—Stephen P. Stone, MD, (Springfield, Illinois)
Sunscreen can be a meaningful part of your sun-protection regimen used in conjunction with sun-protective clothing, sun safe behaviors, and a diet rich in natural antioxidants.—Michelle Tarbox, MD (Lubbock, Texas)
About This Survey
The survey was fielded electronically to Cutis Editorial Board Members within the United States from August 2, 2018, to September 2, 2018. A total of 42 usable responses were received.
Bogaczewicz J, Karczmarewicz E, Pludowski P, et al. Requirement for vitamin D supplementation in patients using photoprotection: variations in vitamin D levels and bone formation markers. Int J Dermatol. 2016;55:e176-e183.
Farberg AS, Glazer AM, Rigel AC, et al. Dermatologists’ perceptions, recommendations, and use of sunscreen. JAMA Dermatol. 2017;153:99-101.
Ou-Yang H, Stanfield J, Cole C, et al. High-SPF sunscreens (SPF ≥ 70) may provide ultraviolet protection above minimal recommended levels by adequately compensating for lower sunscreen user application amounts. J Am Acad Dermatol. 2012;67:1220-1227.
Teplitz RW, Glazer AM, Svoboda RM, et al. Trends in US sunscreen formulations: impact of increasing spray usage. J Am Acad Dermatol. 2018;78:187-189.
Williams JD, Maitra P, Atillasoy E, et al. SPF 100+ sunscreen is more protective against sunburn than SPF 50+ in actual use: Results of a randomized, double-blind, split-face, natural sunlight exposure clinical trial. J Am Acad Dermatol. 2018;78:902.e2-910.e2.
Xu S, Kwa M, Agarwal A, et al. Sunscreen product performance and other determinants of consumer preferences. JAMA Dermatol. 2016;152:920-927.
To improve patient care and outcomes, leading dermatologists from the Cutis Editorial Board answered 5 questions on sunscreens. Here’s what we found.
What sun protection factor (SPF) do you recommend for the majority of your patients?
Fifty percent of dermatologists we surveyed recommend SPF 30. SPF 50 was recommended by 26%, SPF 50+ by 21%, and SPF 15 by only 2%.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Half of our Editorial Board recommends sunscreen with SPF 30, with many recommending SPF 50 or higher. This trend toward sunscreens with higher SPF is consistent with a survey-based study with 97% of dermatologists stating they were comfortable recommending sunscreens with an SPF of 50 or higher and 83.3% stating that they believe that high SPF sunscreens provide an additional margin of safety (Farberg et al). These trends are supported by a randomized, double-blind, split-face clinical trial in which participants applied either SPF 50+ or SPF 100+ sunscreen after exposure to natural sunlight. The results showed that SPF 100+ sunscreen was remarkably more effective in protecting against sunburn than SPF 50+ sunscreen in actual use conditions (Williams et al).
Next page: Spray sunscreens
Which patient populations do you feel may benefit from spray sunscreens?
Two-thirds of dermatologists indicated that spray sunscreens may benefit patients traveling alone. Men with bald spots also may benefit (62%), as well as athletes, children, and older patients (57% each).
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
As dermatologists, we tell our patients that the best sunscreens are ones that are used consistently. Spray sunscreens are likely as effective as lotions (Ou-Yang et al). There has been a clear trend in consumer purchasing of spray sunscreens from 2011 to 2016 (Teplitz et al). Spray sunscreens may benefit those traveling alone, particularly for hard-to-reach areas.
Next page: Supplemental vitamin D
In patients who apply sunscreen regularly, do you recommend supplemental vitamin D3?
More than half (53%) of dermatologists recommend supplemental vitamin D3.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Because use of photoprotection results in decreased vitamin D levels in most individuals, it is good practice to recommend vitamin D supplementation in patients who are applying sunscreen regularly (Bogaczewicz et al).
Next page: Sunscreen compliance
What is the most often heard reason(s) for not using sunscreen in your patients?
Nearly three-quarters (72%) of dermatologists reported that patients do not use sunscreen because of cosmetic acceptance. Almost one-third (31%) said their patients prefer “natural” products. Price was a factor for 26%. Fewer dermatologists indicated risk of environmental damage (14%), allergy (12%), cancer induction (5%), and hormonal alteration (5%) were reasons patients are not compliant.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Cosmetic acceptance is paramount for patient compliance for sunscreen application. These results from our Editorial Board echo a study on sunscreen product performance and other determinants of consumer preferences, which cited “cosmetic elegance” as an important factor in choosing sunscreens (Xu et al). Dermatologists must stress to patients to find a sunscreen that they find acceptable in terms of vehicle and price to increase compliance.
Next page: Sunscreens in pregnant women
What sunscreens do you recommend to pregnant women and children?
Most dermatologists (86%) recommend physical blockers “chemical-free” only sunscreens to pregnant women and children.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
While absorption of sunscreen by human embryos is likely negligible, because there is limited data on sunscreen effects in embryos and children, it is reasonable to recommend physical blockers for pregnant women and children.
Next page: More tips from derms
More Tips From Dermatologists
The dermatologists we polled had the following advice for their peers:
As a dermatologist married to a pediatrician, I try to get my kids to embrace sun-protection strategies. For the little ones it’s hard, but as they have gotten older and been exposed to more derm journals sitting around with pretty graphic pictures, they seem to get on board, even when away at summer camp on their own. If only our patients knew what our kids do.—Joel L. Cohen, MD (Denver, Colorado)
The most important factor in getting patient compliance with sunscreen usage is “cosmetic acceptance.” If they or their children or their spouse don’t like the feel, they won’t use it.—Vincent A. DeLeo, MD (Los Angeles, California)
Not using photoprotection with sunscreen is like crossing a busy road without looking both ways first.—James Q. Del Rosso, DO (Las Vegas, Nevada)
I do not recommend spray sunscreens. At least half of the spray seems to go in the air rather than on the skin. And people often do not rub the spray into their skin well enough. Lotions are better!—Lawrence J. Green, MD (Washington, DC)
The most important factor in sunscreen is not SPF; educate patients on the important role vehicle and sweating play in the length of sun protection.—Orit Markowitz, MD (New York, New York)
Reapplying sunscreen in the appropriate amount is key to blocking the danger rays of the sun.—Vineet Mishra, MD (San Antonio, Texas)
A good sunscreen is the one you put on properly. Regardless of the formulation, make sure you apply the sunscreen evenly to all exposed skin and reapply according to directions on the container. Remember, a regular white T-shirt has minimal SPF 4-5. Either wear sun-protective clothing or wear sunscreen underneath!—Larisa Ravitskiy, MD (Gahanna, Ohio)
Sun protection and sunscreen application go hand-in-hand. We can still enjoy the outdoors without getting excessive UV exposure.—Anthony M. Rossi, MD (New York, New York)
Sunscreens are only part of sun protection. Make sure to reapply them regularly, try to avoid direct sun between about 10 AM and 2 PM if possible, and wear a hat with a wide brim (not a baseball cap, which, after all, is designed for catching baseballs, not sun protection).—Robert I. Rudolph, MD (Wyomissing, Pennsylvania)
Sunscreens keep you younger looking longer!—Richard K. Scher, MD (New York, New York)
The dentist says only floss the teeth you want to keep. I tell patients to only sun block the skin they want to keep.—Daniel M. Siegel, MD, MS (Brooklyn, New York)
The best sunscreen is the one that is used! If it's too greasy or drying, smells bad or stings, it won't be used. Stick to the one YOU like, but at least SPF 30 or better.—Stephen P. Stone, MD, (Springfield, Illinois)
Sunscreen can be a meaningful part of your sun-protection regimen used in conjunction with sun-protective clothing, sun safe behaviors, and a diet rich in natural antioxidants.—Michelle Tarbox, MD (Lubbock, Texas)
About This Survey
The survey was fielded electronically to Cutis Editorial Board Members within the United States from August 2, 2018, to September 2, 2018. A total of 42 usable responses were received.
To improve patient care and outcomes, leading dermatologists from the Cutis Editorial Board answered 5 questions on sunscreens. Here’s what we found.
What sun protection factor (SPF) do you recommend for the majority of your patients?
Fifty percent of dermatologists we surveyed recommend SPF 30. SPF 50 was recommended by 26%, SPF 50+ by 21%, and SPF 15 by only 2%.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Half of our Editorial Board recommends sunscreen with SPF 30, with many recommending SPF 50 or higher. This trend toward sunscreens with higher SPF is consistent with a survey-based study with 97% of dermatologists stating they were comfortable recommending sunscreens with an SPF of 50 or higher and 83.3% stating that they believe that high SPF sunscreens provide an additional margin of safety (Farberg et al). These trends are supported by a randomized, double-blind, split-face clinical trial in which participants applied either SPF 50+ or SPF 100+ sunscreen after exposure to natural sunlight. The results showed that SPF 100+ sunscreen was remarkably more effective in protecting against sunburn than SPF 50+ sunscreen in actual use conditions (Williams et al).
Next page: Spray sunscreens
Which patient populations do you feel may benefit from spray sunscreens?
Two-thirds of dermatologists indicated that spray sunscreens may benefit patients traveling alone. Men with bald spots also may benefit (62%), as well as athletes, children, and older patients (57% each).
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
As dermatologists, we tell our patients that the best sunscreens are ones that are used consistently. Spray sunscreens are likely as effective as lotions (Ou-Yang et al). There has been a clear trend in consumer purchasing of spray sunscreens from 2011 to 2016 (Teplitz et al). Spray sunscreens may benefit those traveling alone, particularly for hard-to-reach areas.
Next page: Supplemental vitamin D
In patients who apply sunscreen regularly, do you recommend supplemental vitamin D3?
More than half (53%) of dermatologists recommend supplemental vitamin D3.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Because use of photoprotection results in decreased vitamin D levels in most individuals, it is good practice to recommend vitamin D supplementation in patients who are applying sunscreen regularly (Bogaczewicz et al).
Next page: Sunscreen compliance
What is the most often heard reason(s) for not using sunscreen in your patients?
Nearly three-quarters (72%) of dermatologists reported that patients do not use sunscreen because of cosmetic acceptance. Almost one-third (31%) said their patients prefer “natural” products. Price was a factor for 26%. Fewer dermatologists indicated risk of environmental damage (14%), allergy (12%), cancer induction (5%), and hormonal alteration (5%) were reasons patients are not compliant.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
Cosmetic acceptance is paramount for patient compliance for sunscreen application. These results from our Editorial Board echo a study on sunscreen product performance and other determinants of consumer preferences, which cited “cosmetic elegance” as an important factor in choosing sunscreens (Xu et al). Dermatologists must stress to patients to find a sunscreen that they find acceptable in terms of vehicle and price to increase compliance.
Next page: Sunscreens in pregnant women
What sunscreens do you recommend to pregnant women and children?
Most dermatologists (86%) recommend physical blockers “chemical-free” only sunscreens to pregnant women and children.
Expert Commentary
Provided by Shari R. Lipner, MD, PhD (New York, New York)
While absorption of sunscreen by human embryos is likely negligible, because there is limited data on sunscreen effects in embryos and children, it is reasonable to recommend physical blockers for pregnant women and children.
Next page: More tips from derms
More Tips From Dermatologists
The dermatologists we polled had the following advice for their peers:
As a dermatologist married to a pediatrician, I try to get my kids to embrace sun-protection strategies. For the little ones it’s hard, but as they have gotten older and been exposed to more derm journals sitting around with pretty graphic pictures, they seem to get on board, even when away at summer camp on their own. If only our patients knew what our kids do.—Joel L. Cohen, MD (Denver, Colorado)
The most important factor in getting patient compliance with sunscreen usage is “cosmetic acceptance.” If they or their children or their spouse don’t like the feel, they won’t use it.—Vincent A. DeLeo, MD (Los Angeles, California)
Not using photoprotection with sunscreen is like crossing a busy road without looking both ways first.—James Q. Del Rosso, DO (Las Vegas, Nevada)
I do not recommend spray sunscreens. At least half of the spray seems to go in the air rather than on the skin. And people often do not rub the spray into their skin well enough. Lotions are better!—Lawrence J. Green, MD (Washington, DC)
The most important factor in sunscreen is not SPF; educate patients on the important role vehicle and sweating play in the length of sun protection.—Orit Markowitz, MD (New York, New York)
Reapplying sunscreen in the appropriate amount is key to blocking the danger rays of the sun.—Vineet Mishra, MD (San Antonio, Texas)
A good sunscreen is the one you put on properly. Regardless of the formulation, make sure you apply the sunscreen evenly to all exposed skin and reapply according to directions on the container. Remember, a regular white T-shirt has minimal SPF 4-5. Either wear sun-protective clothing or wear sunscreen underneath!—Larisa Ravitskiy, MD (Gahanna, Ohio)
Sun protection and sunscreen application go hand-in-hand. We can still enjoy the outdoors without getting excessive UV exposure.—Anthony M. Rossi, MD (New York, New York)
Sunscreens are only part of sun protection. Make sure to reapply them regularly, try to avoid direct sun between about 10 AM and 2 PM if possible, and wear a hat with a wide brim (not a baseball cap, which, after all, is designed for catching baseballs, not sun protection).—Robert I. Rudolph, MD (Wyomissing, Pennsylvania)
Sunscreens keep you younger looking longer!—Richard K. Scher, MD (New York, New York)
The dentist says only floss the teeth you want to keep. I tell patients to only sun block the skin they want to keep.—Daniel M. Siegel, MD, MS (Brooklyn, New York)
The best sunscreen is the one that is used! If it's too greasy or drying, smells bad or stings, it won't be used. Stick to the one YOU like, but at least SPF 30 or better.—Stephen P. Stone, MD, (Springfield, Illinois)
Sunscreen can be a meaningful part of your sun-protection regimen used in conjunction with sun-protective clothing, sun safe behaviors, and a diet rich in natural antioxidants.—Michelle Tarbox, MD (Lubbock, Texas)
About This Survey
The survey was fielded electronically to Cutis Editorial Board Members within the United States from August 2, 2018, to September 2, 2018. A total of 42 usable responses were received.
Bogaczewicz J, Karczmarewicz E, Pludowski P, et al. Requirement for vitamin D supplementation in patients using photoprotection: variations in vitamin D levels and bone formation markers. Int J Dermatol. 2016;55:e176-e183.
Farberg AS, Glazer AM, Rigel AC, et al. Dermatologists’ perceptions, recommendations, and use of sunscreen. JAMA Dermatol. 2017;153:99-101.
Ou-Yang H, Stanfield J, Cole C, et al. High-SPF sunscreens (SPF ≥ 70) may provide ultraviolet protection above minimal recommended levels by adequately compensating for lower sunscreen user application amounts. J Am Acad Dermatol. 2012;67:1220-1227.
Teplitz RW, Glazer AM, Svoboda RM, et al. Trends in US sunscreen formulations: impact of increasing spray usage. J Am Acad Dermatol. 2018;78:187-189.
Williams JD, Maitra P, Atillasoy E, et al. SPF 100+ sunscreen is more protective against sunburn than SPF 50+ in actual use: Results of a randomized, double-blind, split-face, natural sunlight exposure clinical trial. J Am Acad Dermatol. 2018;78:902.e2-910.e2.
Xu S, Kwa M, Agarwal A, et al. Sunscreen product performance and other determinants of consumer preferences. JAMA Dermatol. 2016;152:920-927.
Bogaczewicz J, Karczmarewicz E, Pludowski P, et al. Requirement for vitamin D supplementation in patients using photoprotection: variations in vitamin D levels and bone formation markers. Int J Dermatol. 2016;55:e176-e183.
Farberg AS, Glazer AM, Rigel AC, et al. Dermatologists’ perceptions, recommendations, and use of sunscreen. JAMA Dermatol. 2017;153:99-101.
Ou-Yang H, Stanfield J, Cole C, et al. High-SPF sunscreens (SPF ≥ 70) may provide ultraviolet protection above minimal recommended levels by adequately compensating for lower sunscreen user application amounts. J Am Acad Dermatol. 2012;67:1220-1227.
Teplitz RW, Glazer AM, Svoboda RM, et al. Trends in US sunscreen formulations: impact of increasing spray usage. J Am Acad Dermatol. 2018;78:187-189.
Williams JD, Maitra P, Atillasoy E, et al. SPF 100+ sunscreen is more protective against sunburn than SPF 50+ in actual use: Results of a randomized, double-blind, split-face, natural sunlight exposure clinical trial. J Am Acad Dermatol. 2018;78:902.e2-910.e2.
Xu S, Kwa M, Agarwal A, et al. Sunscreen product performance and other determinants of consumer preferences. JAMA Dermatol. 2016;152:920-927.
Autonomic Dysfunction Greater in PPTH than Migraine
Symptoms of autonomic dysfunction were greatest among those with persistent posttraumatic headaches (PPTH) compared to migraine and healthy controls (HCs), a recent study found. In addition, among individuals with PPTH, number of lifetime traumatic brain injuries (TBIs) was associated with greater symptoms of autonomic dysfunction, while greater headache burden was associated with higher vasomotor domain autonomic dysfunction subscores, potentially indicating that PPTH patients with higher disease burden have an increased risk for having autonomic dysfunction. Individuals with PPTH (n=56) (87.5% of whom had a migraine/probable migraine phenotype), migraine (n=30), and HCs (n=36) were prospectively assessed in this cross‐sectional cohort study using the COMPASS‐31 questionnaire. Total COMPASS‐31 scores and individual domain scores were compared between subject groups. Researchers found:
- COMPASS‐31 mean total weighted score was 37.22 ± 15.44 in the PPTH group, 27.15 ± 14.37 in the migraine group, and 11.67 ± 8.98 for HCs.
- COMPASS‐31 mean weighted total scores were significantly higher in those with PPTH vs migraine, for PPTH vs HCs, and for migraine vs HCs.
Howard L, Dumkrieger G, Chong CD, Ross K, Berisha V, Schwedt TJ. Symptoms of autonomic dysfunction among those with persistent posttraumatic headache attributed to mild traumatic brain injury: A comparison to migraine and healthy controls. [Published online ahead of print August 29, 2018]. Headache. doi:10.1111/head.13396.
Symptoms of autonomic dysfunction were greatest among those with persistent posttraumatic headaches (PPTH) compared to migraine and healthy controls (HCs), a recent study found. In addition, among individuals with PPTH, number of lifetime traumatic brain injuries (TBIs) was associated with greater symptoms of autonomic dysfunction, while greater headache burden was associated with higher vasomotor domain autonomic dysfunction subscores, potentially indicating that PPTH patients with higher disease burden have an increased risk for having autonomic dysfunction. Individuals with PPTH (n=56) (87.5% of whom had a migraine/probable migraine phenotype), migraine (n=30), and HCs (n=36) were prospectively assessed in this cross‐sectional cohort study using the COMPASS‐31 questionnaire. Total COMPASS‐31 scores and individual domain scores were compared between subject groups. Researchers found:
- COMPASS‐31 mean total weighted score was 37.22 ± 15.44 in the PPTH group, 27.15 ± 14.37 in the migraine group, and 11.67 ± 8.98 for HCs.
- COMPASS‐31 mean weighted total scores were significantly higher in those with PPTH vs migraine, for PPTH vs HCs, and for migraine vs HCs.
Howard L, Dumkrieger G, Chong CD, Ross K, Berisha V, Schwedt TJ. Symptoms of autonomic dysfunction among those with persistent posttraumatic headache attributed to mild traumatic brain injury: A comparison to migraine and healthy controls. [Published online ahead of print August 29, 2018]. Headache. doi:10.1111/head.13396.
Symptoms of autonomic dysfunction were greatest among those with persistent posttraumatic headaches (PPTH) compared to migraine and healthy controls (HCs), a recent study found. In addition, among individuals with PPTH, number of lifetime traumatic brain injuries (TBIs) was associated with greater symptoms of autonomic dysfunction, while greater headache burden was associated with higher vasomotor domain autonomic dysfunction subscores, potentially indicating that PPTH patients with higher disease burden have an increased risk for having autonomic dysfunction. Individuals with PPTH (n=56) (87.5% of whom had a migraine/probable migraine phenotype), migraine (n=30), and HCs (n=36) were prospectively assessed in this cross‐sectional cohort study using the COMPASS‐31 questionnaire. Total COMPASS‐31 scores and individual domain scores were compared between subject groups. Researchers found:
- COMPASS‐31 mean total weighted score was 37.22 ± 15.44 in the PPTH group, 27.15 ± 14.37 in the migraine group, and 11.67 ± 8.98 for HCs.
- COMPASS‐31 mean weighted total scores were significantly higher in those with PPTH vs migraine, for PPTH vs HCs, and for migraine vs HCs.
Howard L, Dumkrieger G, Chong CD, Ross K, Berisha V, Schwedt TJ. Symptoms of autonomic dysfunction among those with persistent posttraumatic headache attributed to mild traumatic brain injury: A comparison to migraine and healthy controls. [Published online ahead of print August 29, 2018]. Headache. doi:10.1111/head.13396.
What’s in that e-cigarette? It may be cannabis
Nearly 1 in 11 U.S. middle and high school students have used a cannabis product in an e-cigarette, according to a school-based survey of 20,675 students.

The survey found that 8.9% of students in grades 6-12 said they had used an e-cigarette with marijuana, tetrahydrocannabinol or hash oil, or tetrahydrocannabinol wax. Among the students who reported ever using e-cigarettes, 30.6% had used a cannabis product in the device. The findings were published in JAMA Pediatrics.
This translated to around 1.7 million high school students and 425,000 middle school students who had ever used cannabis in e-cigarettes; figures the authors said were consistent with or higher than previous reports among U.S. and Canadian students.
Katrina F. Trivers, PhD, and her colleagues from the Centers for Disease Control and Prevention, noted that the U.S. Surgeon General has found e-cigarette aerosol can contain potentially harmful ingredients. Additionally, the National Academies of Sciences has said youth cannabis use can harm learning and memory.
“Strategies to reduce cannabis use in e-cigarettes are critical for protecting young people from these potential health risks,” the researchers wrote.
Male students and high school students were significantly more likely to report using cannabis products in an e-cigarette (10.6% and 12.4%, respectively), compared with female or middle school students.
Among current users of e-cigarettes, 39.5% reported using cannabis in the e-cigarette, while among those who used other tobacco products, 38.5% used cannabis in e-cigarettes. Higher e-cigarette use was also associated with use of cannabis products in e-cigarettes.
Living with someone who used tobacco products was associated with a higher incidence of cannabis in e-cigarette use (13%). Researchers also saw a higher use of cannabis in e-cigarettes among students of Hispanic ethnicity, compared with other ethnicities.
In 2015, around one-third of U.S. middle and high school students said they had used nonnicotine substances in e-cigarettes, but the use of cannabis in e-cigarettes could increase as several states consider legalizing cannabis sales for adults. “Given the high concurrent use of tobacco and other substances, it is important to monitor the substances youth use in e-cigarettes,” they wrote.
The researchers reported having no financial disclosures.
SOURCE: Trivers KF et al. JAMA Pediatr. 2018 Sep 17. doi: 10.1001/jamapediatrics.2018.1920.
Nearly 1 in 11 U.S. middle and high school students have used a cannabis product in an e-cigarette, according to a school-based survey of 20,675 students.
The survey found that 8.9% of students in grades 6-12 said they had used an e-cigarette with marijuana, tetrahydrocannabinol or hash oil, or tetrahydrocannabinol wax. Among the students who reported ever using e-cigarettes, 30.6% had used a cannabis product in the device. The findings were published in JAMA Pediatrics.
This translated to around 1.7 million high school students and 425,000 middle school students who had ever used cannabis in e-cigarettes; figures the authors said were consistent with or higher than previous reports among U.S. and Canadian students.
Katrina F. Trivers, PhD, and her colleagues from the Centers for Disease Control and Prevention, noted that the U.S. Surgeon General has found e-cigarette aerosol can contain potentially harmful ingredients. Additionally, the National Academies of Sciences has said youth cannabis use can harm learning and memory.
“Strategies to reduce cannabis use in e-cigarettes are critical for protecting young people from these potential health risks,” the researchers wrote.
Male students and high school students were significantly more likely to report using cannabis products in an e-cigarette (10.6% and 12.4%, respectively), compared with female or middle school students.
Among current users of e-cigarettes, 39.5% reported using cannabis in the e-cigarette, while among those who used other tobacco products, 38.5% used cannabis in e-cigarettes. Higher e-cigarette use was also associated with use of cannabis products in e-cigarettes.
Living with someone who used tobacco products was associated with a higher incidence of cannabis in e-cigarette use (13%). Researchers also saw a higher use of cannabis in e-cigarettes among students of Hispanic ethnicity, compared with other ethnicities.
In 2015, around one-third of U.S. middle and high school students said they had used nonnicotine substances in e-cigarettes, but the use of cannabis in e-cigarettes could increase as several states consider legalizing cannabis sales for adults. “Given the high concurrent use of tobacco and other substances, it is important to monitor the substances youth use in e-cigarettes,” they wrote.
The researchers reported having no financial disclosures.
SOURCE: Trivers KF et al. JAMA Pediatr. 2018 Sep 17. doi: 10.1001/jamapediatrics.2018.1920.
Nearly 1 in 11 U.S. middle and high school students have used a cannabis product in an e-cigarette, according to a school-based survey of 20,675 students.
The survey found that 8.9% of students in grades 6-12 said they had used an e-cigarette with marijuana, tetrahydrocannabinol or hash oil, or tetrahydrocannabinol wax. Among the students who reported ever using e-cigarettes, 30.6% had used a cannabis product in the device. The findings were published in JAMA Pediatrics.
This translated to around 1.7 million high school students and 425,000 middle school students who had ever used cannabis in e-cigarettes; figures the authors said were consistent with or higher than previous reports among U.S. and Canadian students.
Katrina F. Trivers, PhD, and her colleagues from the Centers for Disease Control and Prevention, noted that the U.S. Surgeon General has found e-cigarette aerosol can contain potentially harmful ingredients. Additionally, the National Academies of Sciences has said youth cannabis use can harm learning and memory.
“Strategies to reduce cannabis use in e-cigarettes are critical for protecting young people from these potential health risks,” the researchers wrote.
Male students and high school students were significantly more likely to report using cannabis products in an e-cigarette (10.6% and 12.4%, respectively), compared with female or middle school students.
Among current users of e-cigarettes, 39.5% reported using cannabis in the e-cigarette, while among those who used other tobacco products, 38.5% used cannabis in e-cigarettes. Higher e-cigarette use was also associated with use of cannabis products in e-cigarettes.
Living with someone who used tobacco products was associated with a higher incidence of cannabis in e-cigarette use (13%). Researchers also saw a higher use of cannabis in e-cigarettes among students of Hispanic ethnicity, compared with other ethnicities.
In 2015, around one-third of U.S. middle and high school students said they had used nonnicotine substances in e-cigarettes, but the use of cannabis in e-cigarettes could increase as several states consider legalizing cannabis sales for adults. “Given the high concurrent use of tobacco and other substances, it is important to monitor the substances youth use in e-cigarettes,” they wrote.
The researchers reported having no financial disclosures.
SOURCE: Trivers KF et al. JAMA Pediatr. 2018 Sep 17. doi: 10.1001/jamapediatrics.2018.1920.
FROM JAMA PEDIATRICS
Key clinical point:
Major finding: A survey of U.S. students showed that 8.9% have used cannabis in an e-cigarette. Among e-cigarette users, cannabis use in e-cigarettes was reported by 30.6% of students.
Study details: A school-based survey of 20,675 students.
Disclosures: The researchers reported having no financial disclosures.
Source: Trivers KF et al. JAMA Pediatr. 2018 Sep 17. doi: 10.1001/jamapediatrics.2018.1920.
Metastatic breast cancer lesions immunologically depleted compared with primary
The immune microenvironment of metastatic breast cancer lesions is relatively inert and depleted versus primary tumors, results of a recent study suggest.
“These results predict that immune therapy may be more successful in early stage breast cancers rather than in metastatic disease,” Lajos Pusztai, MD, and study coinvestigators reported in Annals of Oncology.
However, metastatic breast cancers showed high expression levels of some targetable molecules that may provide a “foundation for rational immunotherapy combination strategies,” wrote Dr. Pusztai, director of breast cancer translational research at Yale Cancer Center, New Haven, Conn., and his coinvestigators.
The investigators looked at tumor PD-L1 protein expression, tumor infiltrating lymphocyte (TIL) count, and mRNA expression for 730 immune-related genes in both primary and metastatic cancer samples obtained from pathologists at Yale.
The study included one cohort with full sections of paired metastatic and primary tumors from 45 patients, and a second cohort of tissue microarrays from 55 other patients.
Compared with primary lesions, metastatic lesions had substantially lower levels of PD-L1 expression and TIL counts, the investigators found.
Staining of PD-L1 was primarily seen in stromal immune cells, rather than tumor cells, according to investigators. The median stromal PD-L1 positivity was 14% for metastases and 52% for primary tumors in the first cohort (P = .0004), and 7% for metastases and 22% for primary tumors in the second cohort (P = .03).
They also reported significant decreased TIL counts in metastatic lesions for both the first (P = .026) and second (P = .089) cohorts, the report shows.
Immune gene expression profiling results, similarly, showed that most immune cell types and functions were “depleted” in the metastatic lesions, including a decreased mRNA expression of CTLA4, Dr. Pusztai and his colleagues reported.
The “lesser immunogenicity” of metastatic breast cancer cells was shown by decreased expression of immune proteasome and MHC class I genes, along with increased expression of HLA-E, which has been shown to suppress immunity, and reduced presence of dendritic cells, they said.
However, they also found high expression of targetable molecules in metastatic lesions. Those included macrophage markers such as CD68 and CD163, cytokine ligand/receptor pairs that mediate pro-tumorigenic effects, such as CCL2/CCR2 and CXCR4/CXCL12, and signaling molecules such as STAT-3 and JAK2, among others.
“We suggest that targeting these molecules may lead to synergy with PD1/PD-L1 blockade in metastatic breast cancer,” they wrote.
The work by Dr. Pusztai and his colleagues was supported by the Breast Cancer Research Foundation, Susan G Komen for the Cure, Department of Defense Breast Cancer Research Program Awards, and the Rosztoczy Foundation. The authors declared no conflicts of interest.
SOURCE: Szekely B, et al. Ann Oncol. 2018 Sep 10. doi: 10.1093/annonc/mdy399.
The immune microenvironment of metastatic breast cancer lesions is relatively inert and depleted versus primary tumors, results of a recent study suggest.
“These results predict that immune therapy may be more successful in early stage breast cancers rather than in metastatic disease,” Lajos Pusztai, MD, and study coinvestigators reported in Annals of Oncology.
However, metastatic breast cancers showed high expression levels of some targetable molecules that may provide a “foundation for rational immunotherapy combination strategies,” wrote Dr. Pusztai, director of breast cancer translational research at Yale Cancer Center, New Haven, Conn., and his coinvestigators.
The investigators looked at tumor PD-L1 protein expression, tumor infiltrating lymphocyte (TIL) count, and mRNA expression for 730 immune-related genes in both primary and metastatic cancer samples obtained from pathologists at Yale.
The study included one cohort with full sections of paired metastatic and primary tumors from 45 patients, and a second cohort of tissue microarrays from 55 other patients.
Compared with primary lesions, metastatic lesions had substantially lower levels of PD-L1 expression and TIL counts, the investigators found.
Staining of PD-L1 was primarily seen in stromal immune cells, rather than tumor cells, according to investigators. The median stromal PD-L1 positivity was 14% for metastases and 52% for primary tumors in the first cohort (P = .0004), and 7% for metastases and 22% for primary tumors in the second cohort (P = .03).
They also reported significant decreased TIL counts in metastatic lesions for both the first (P = .026) and second (P = .089) cohorts, the report shows.
Immune gene expression profiling results, similarly, showed that most immune cell types and functions were “depleted” in the metastatic lesions, including a decreased mRNA expression of CTLA4, Dr. Pusztai and his colleagues reported.
The “lesser immunogenicity” of metastatic breast cancer cells was shown by decreased expression of immune proteasome and MHC class I genes, along with increased expression of HLA-E, which has been shown to suppress immunity, and reduced presence of dendritic cells, they said.
However, they also found high expression of targetable molecules in metastatic lesions. Those included macrophage markers such as CD68 and CD163, cytokine ligand/receptor pairs that mediate pro-tumorigenic effects, such as CCL2/CCR2 and CXCR4/CXCL12, and signaling molecules such as STAT-3 and JAK2, among others.
“We suggest that targeting these molecules may lead to synergy with PD1/PD-L1 blockade in metastatic breast cancer,” they wrote.
The work by Dr. Pusztai and his colleagues was supported by the Breast Cancer Research Foundation, Susan G Komen for the Cure, Department of Defense Breast Cancer Research Program Awards, and the Rosztoczy Foundation. The authors declared no conflicts of interest.
SOURCE: Szekely B, et al. Ann Oncol. 2018 Sep 10. doi: 10.1093/annonc/mdy399.
The immune microenvironment of metastatic breast cancer lesions is relatively inert and depleted versus primary tumors, results of a recent study suggest.
“These results predict that immune therapy may be more successful in early stage breast cancers rather than in metastatic disease,” Lajos Pusztai, MD, and study coinvestigators reported in Annals of Oncology.
However, metastatic breast cancers showed high expression levels of some targetable molecules that may provide a “foundation for rational immunotherapy combination strategies,” wrote Dr. Pusztai, director of breast cancer translational research at Yale Cancer Center, New Haven, Conn., and his coinvestigators.
The investigators looked at tumor PD-L1 protein expression, tumor infiltrating lymphocyte (TIL) count, and mRNA expression for 730 immune-related genes in both primary and metastatic cancer samples obtained from pathologists at Yale.
The study included one cohort with full sections of paired metastatic and primary tumors from 45 patients, and a second cohort of tissue microarrays from 55 other patients.
Compared with primary lesions, metastatic lesions had substantially lower levels of PD-L1 expression and TIL counts, the investigators found.
Staining of PD-L1 was primarily seen in stromal immune cells, rather than tumor cells, according to investigators. The median stromal PD-L1 positivity was 14% for metastases and 52% for primary tumors in the first cohort (P = .0004), and 7% for metastases and 22% for primary tumors in the second cohort (P = .03).
They also reported significant decreased TIL counts in metastatic lesions for both the first (P = .026) and second (P = .089) cohorts, the report shows.
Immune gene expression profiling results, similarly, showed that most immune cell types and functions were “depleted” in the metastatic lesions, including a decreased mRNA expression of CTLA4, Dr. Pusztai and his colleagues reported.
The “lesser immunogenicity” of metastatic breast cancer cells was shown by decreased expression of immune proteasome and MHC class I genes, along with increased expression of HLA-E, which has been shown to suppress immunity, and reduced presence of dendritic cells, they said.
However, they also found high expression of targetable molecules in metastatic lesions. Those included macrophage markers such as CD68 and CD163, cytokine ligand/receptor pairs that mediate pro-tumorigenic effects, such as CCL2/CCR2 and CXCR4/CXCL12, and signaling molecules such as STAT-3 and JAK2, among others.
“We suggest that targeting these molecules may lead to synergy with PD1/PD-L1 blockade in metastatic breast cancer,” they wrote.
The work by Dr. Pusztai and his colleagues was supported by the Breast Cancer Research Foundation, Susan G Komen for the Cure, Department of Defense Breast Cancer Research Program Awards, and the Rosztoczy Foundation. The authors declared no conflicts of interest.
SOURCE: Szekely B, et al. Ann Oncol. 2018 Sep 10. doi: 10.1093/annonc/mdy399.
FROM ANNALS OF ONCOLOGY
Key clinical point: The immune microenvironment of metastatic breast cancer lesions is relatively inert and depleted versus primary tumors.
Major finding: Median stromal PD-L1 positivity was 14% for metastases and 52% for primary tumors in one cohort (P = .0004), and 7% versus 22% in a second (P = .03).
Study details: Analysis of breast cancer tissue samples (primary tumor and metastatic lesions) from 90 patients
Disclosures: The work was supported by the Breast Cancer Research Foundation, the Susan Komen for the Cure, Department of Defense Breast Cancer Research Program Awards, and the Rosztoczy Foundation. The study authors declared no conflicts of interest.
Source: Szekely B et al. Ann Oncol. 2018 Sep 10. doi: 10.1093/annonc/mdy399.