User login
Vitamin D affects HSPC production, team says
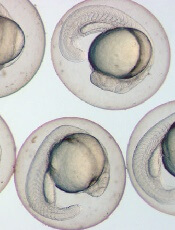
Photo by Ian Johnston
The availability of vitamin D during embryonic development can affect hematopoietic stem and progenitor cells (HSPCs), according to research published in Cell Reports.
Experiments with zebrafish embryos suggested that vitamin D acts directly on HSPCs to increase proliferation.
Similarly, in HSPCs from human umbilical cords, treatment with vitamin D enhanced hematopoietic colony numbers.
Researchers therefore theorized that vitamin D supplementation might be useful for HSPC expansion prior to transplant.
“We clearly showed that not getting enough vitamin D can alter how blood stem cells are formed,” said study author Trista North, PhD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“Vitamin D was having a direct response on the blood stem cells, and it changed what those cells did in terms of multiplying and staying alive.”
The researchers found, in both human and zebrafish tissue, that 1,25(OH)D3 (active vitamin D3) had an impact on HSPC production and function.
Investigation into the mechanism revealed that CXCL8-CXCR1/2 signaling functions downstream of 1,25(OH)D3-mediated vitamin D receptor stimulation to directly regulate HSPC production and expansion.
“What was surprising was that vitamin D is having an impact so early,” Dr North said. “We really only thought about vitamin D in terms of bone development and maintenance, but we clearly show that, whether they were zebrafish or human blood stem cells, they can respond directly to the nutrient.”
One caveat is the researchers did face difficulty testing the response in mice, as the animals don’t have the same vitamin D inflammatory targets observed in zebrafish and humans.
Additionally, the team didn’t know the vitamin D levels in the umbilical cord blood samples they tested, which may have influenced the outcome of their analysis.
As a next step, Dr North and her colleagues hope to test cord blood samples for which they know the vitamin D status to see if umbilical cords with healthy levels respond better or worse to stimulation than cords from vitamin-D-deficient donors. ![]()
Photo by Ian Johnston
The availability of vitamin D during embryonic development can affect hematopoietic stem and progenitor cells (HSPCs), according to research published in Cell Reports.
Experiments with zebrafish embryos suggested that vitamin D acts directly on HSPCs to increase proliferation.
Similarly, in HSPCs from human umbilical cords, treatment with vitamin D enhanced hematopoietic colony numbers.
Researchers therefore theorized that vitamin D supplementation might be useful for HSPC expansion prior to transplant.
“We clearly showed that not getting enough vitamin D can alter how blood stem cells are formed,” said study author Trista North, PhD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“Vitamin D was having a direct response on the blood stem cells, and it changed what those cells did in terms of multiplying and staying alive.”
The researchers found, in both human and zebrafish tissue, that 1,25(OH)D3 (active vitamin D3) had an impact on HSPC production and function.
Investigation into the mechanism revealed that CXCL8-CXCR1/2 signaling functions downstream of 1,25(OH)D3-mediated vitamin D receptor stimulation to directly regulate HSPC production and expansion.
“What was surprising was that vitamin D is having an impact so early,” Dr North said. “We really only thought about vitamin D in terms of bone development and maintenance, but we clearly show that, whether they were zebrafish or human blood stem cells, they can respond directly to the nutrient.”
One caveat is the researchers did face difficulty testing the response in mice, as the animals don’t have the same vitamin D inflammatory targets observed in zebrafish and humans.
Additionally, the team didn’t know the vitamin D levels in the umbilical cord blood samples they tested, which may have influenced the outcome of their analysis.
As a next step, Dr North and her colleagues hope to test cord blood samples for which they know the vitamin D status to see if umbilical cords with healthy levels respond better or worse to stimulation than cords from vitamin-D-deficient donors. ![]()
Photo by Ian Johnston
The availability of vitamin D during embryonic development can affect hematopoietic stem and progenitor cells (HSPCs), according to research published in Cell Reports.
Experiments with zebrafish embryos suggested that vitamin D acts directly on HSPCs to increase proliferation.
Similarly, in HSPCs from human umbilical cords, treatment with vitamin D enhanced hematopoietic colony numbers.
Researchers therefore theorized that vitamin D supplementation might be useful for HSPC expansion prior to transplant.
“We clearly showed that not getting enough vitamin D can alter how blood stem cells are formed,” said study author Trista North, PhD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“Vitamin D was having a direct response on the blood stem cells, and it changed what those cells did in terms of multiplying and staying alive.”
The researchers found, in both human and zebrafish tissue, that 1,25(OH)D3 (active vitamin D3) had an impact on HSPC production and function.
Investigation into the mechanism revealed that CXCL8-CXCR1/2 signaling functions downstream of 1,25(OH)D3-mediated vitamin D receptor stimulation to directly regulate HSPC production and expansion.
“What was surprising was that vitamin D is having an impact so early,” Dr North said. “We really only thought about vitamin D in terms of bone development and maintenance, but we clearly show that, whether they were zebrafish or human blood stem cells, they can respond directly to the nutrient.”
One caveat is the researchers did face difficulty testing the response in mice, as the animals don’t have the same vitamin D inflammatory targets observed in zebrafish and humans.
Additionally, the team didn’t know the vitamin D levels in the umbilical cord blood samples they tested, which may have influenced the outcome of their analysis.
As a next step, Dr North and her colleagues hope to test cord blood samples for which they know the vitamin D status to see if umbilical cords with healthy levels respond better or worse to stimulation than cords from vitamin-D-deficient donors. ![]()
Lifestyle may impact life expectancy in mild SCD

alongside a normal one
Image by Betty Pace
A case series published in Blood indicates that some patients with mildly symptomatic sickle cell disease (SCD) can live long lives if they
comply with treatment recommendations and lead a healthy lifestyle.
The paper includes details on 4 women with milder forms of SCD who survived beyond age 80.
“For those with mild forms of SCD, these women show that lifestyle modifications may improve disease outcomes,” said author Samir K. Ballas, MD, of Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia, Pennsylvania.
Three of the women described in this case series were treated at the Sickle Cell Center of Thomas Jefferson University, and 1 was treated in Brazil’s Instituto de Hematologia Arthur de Siqueira Cavalcanti in Rio de Janeiro.
The women had different ancestries—2 African-American, 1 Italian-American, and 1 African-Brazilian—and different diagnoses—2 with hemoglobin SC disease and 2 with sickle cell anemia. But all 4 women had what Dr Ballas called “desirable” disease states.
“These women never had a stroke, never had recurrent acute chest syndrome, had a relatively high fetal hemoglobin count, and had infrequent painful crises,” Dr Ballas said. “Patients like this usually—but not always—experience relatively mild SCD, and they live longer with better quality of life.”
In addition, all of the women took steps to maintain and improve their health and had long-term family support. Dr Ballas said these factors likely contributed to the women’s long lives and high quality of life.
“All of the women were non-smokers who consumed little to no alcohol and maintained a normal body mass index,” he said. “This was coupled with a strong compliance to their treatment regimens and excellent family support at home.”
Family support was defined as having a spouse or child who provided attentive, ongoing care. And all of the women had at least 1 such caregiver.
Treatment compliance was based on observations by healthcare providers, including study authors. According to these observations, all of the women showed “excellent” adherence when it came to medication intake, appointments, and referrals.
As the women had relatively mild disease states, none of them were qualified to receive treatment with hydroxyurea. Instead, they received hydration, vaccination (including annual flu shots), and blood transfusion and analgesics as needed.
Even with their mild disease states and healthy lifestyles, these women did not live crisis-free lives. Each experienced disease-related complications necessitating medical attention.
The women had 0 to 3 vaso-occlusive crises per year. Two women required frequent transfusions (and had iron overload), and 2 required occasional transfusions. One woman had 2 episodes of acute chest syndrome, and the second episode led to her death.
Ultimately, 3 of the women died. One died of acute chest syndrome and septicemia at age 82, and another died of cardiac complications at age 86. For a third woman, the cause of death, at age 82, was unknown. The fourth woman remains alive at age 82.
As the median life expectancy of women with SCD in the US is 47, Dr Ballas and his colleagues said these 4 women may “provide a blueprint of how to live a long life despite having a serious medical condition like SCD.”
“I would often come out to the waiting room and find these ladies talking with other SCD patients, and I could tell that they gave others hope, that just because they have SCD does not mean that they are doomed to die by their 40s . . . ,” Dr Ballas said. “[I]f they take care of themselves and live closely with those who can help keep them well, that there is hope for them to lead long, full lives.” ![]()
alongside a normal one
Image by Betty Pace
A case series published in Blood indicates that some patients with mildly symptomatic sickle cell disease (SCD) can live long lives if they
comply with treatment recommendations and lead a healthy lifestyle.
The paper includes details on 4 women with milder forms of SCD who survived beyond age 80.
“For those with mild forms of SCD, these women show that lifestyle modifications may improve disease outcomes,” said author Samir K. Ballas, MD, of Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia, Pennsylvania.
Three of the women described in this case series were treated at the Sickle Cell Center of Thomas Jefferson University, and 1 was treated in Brazil’s Instituto de Hematologia Arthur de Siqueira Cavalcanti in Rio de Janeiro.
The women had different ancestries—2 African-American, 1 Italian-American, and 1 African-Brazilian—and different diagnoses—2 with hemoglobin SC disease and 2 with sickle cell anemia. But all 4 women had what Dr Ballas called “desirable” disease states.
“These women never had a stroke, never had recurrent acute chest syndrome, had a relatively high fetal hemoglobin count, and had infrequent painful crises,” Dr Ballas said. “Patients like this usually—but not always—experience relatively mild SCD, and they live longer with better quality of life.”
In addition, all of the women took steps to maintain and improve their health and had long-term family support. Dr Ballas said these factors likely contributed to the women’s long lives and high quality of life.
“All of the women were non-smokers who consumed little to no alcohol and maintained a normal body mass index,” he said. “This was coupled with a strong compliance to their treatment regimens and excellent family support at home.”
Family support was defined as having a spouse or child who provided attentive, ongoing care. And all of the women had at least 1 such caregiver.
Treatment compliance was based on observations by healthcare providers, including study authors. According to these observations, all of the women showed “excellent” adherence when it came to medication intake, appointments, and referrals.
As the women had relatively mild disease states, none of them were qualified to receive treatment with hydroxyurea. Instead, they received hydration, vaccination (including annual flu shots), and blood transfusion and analgesics as needed.
Even with their mild disease states and healthy lifestyles, these women did not live crisis-free lives. Each experienced disease-related complications necessitating medical attention.
The women had 0 to 3 vaso-occlusive crises per year. Two women required frequent transfusions (and had iron overload), and 2 required occasional transfusions. One woman had 2 episodes of acute chest syndrome, and the second episode led to her death.
Ultimately, 3 of the women died. One died of acute chest syndrome and septicemia at age 82, and another died of cardiac complications at age 86. For a third woman, the cause of death, at age 82, was unknown. The fourth woman remains alive at age 82.
As the median life expectancy of women with SCD in the US is 47, Dr Ballas and his colleagues said these 4 women may “provide a blueprint of how to live a long life despite having a serious medical condition like SCD.”
“I would often come out to the waiting room and find these ladies talking with other SCD patients, and I could tell that they gave others hope, that just because they have SCD does not mean that they are doomed to die by their 40s . . . ,” Dr Ballas said. “[I]f they take care of themselves and live closely with those who can help keep them well, that there is hope for them to lead long, full lives.” ![]()
alongside a normal one
Image by Betty Pace
A case series published in Blood indicates that some patients with mildly symptomatic sickle cell disease (SCD) can live long lives if they
comply with treatment recommendations and lead a healthy lifestyle.
The paper includes details on 4 women with milder forms of SCD who survived beyond age 80.
“For those with mild forms of SCD, these women show that lifestyle modifications may improve disease outcomes,” said author Samir K. Ballas, MD, of Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia, Pennsylvania.
Three of the women described in this case series were treated at the Sickle Cell Center of Thomas Jefferson University, and 1 was treated in Brazil’s Instituto de Hematologia Arthur de Siqueira Cavalcanti in Rio de Janeiro.
The women had different ancestries—2 African-American, 1 Italian-American, and 1 African-Brazilian—and different diagnoses—2 with hemoglobin SC disease and 2 with sickle cell anemia. But all 4 women had what Dr Ballas called “desirable” disease states.
“These women never had a stroke, never had recurrent acute chest syndrome, had a relatively high fetal hemoglobin count, and had infrequent painful crises,” Dr Ballas said. “Patients like this usually—but not always—experience relatively mild SCD, and they live longer with better quality of life.”
In addition, all of the women took steps to maintain and improve their health and had long-term family support. Dr Ballas said these factors likely contributed to the women’s long lives and high quality of life.
“All of the women were non-smokers who consumed little to no alcohol and maintained a normal body mass index,” he said. “This was coupled with a strong compliance to their treatment regimens and excellent family support at home.”
Family support was defined as having a spouse or child who provided attentive, ongoing care. And all of the women had at least 1 such caregiver.
Treatment compliance was based on observations by healthcare providers, including study authors. According to these observations, all of the women showed “excellent” adherence when it came to medication intake, appointments, and referrals.
As the women had relatively mild disease states, none of them were qualified to receive treatment with hydroxyurea. Instead, they received hydration, vaccination (including annual flu shots), and blood transfusion and analgesics as needed.
Even with their mild disease states and healthy lifestyles, these women did not live crisis-free lives. Each experienced disease-related complications necessitating medical attention.
The women had 0 to 3 vaso-occlusive crises per year. Two women required frequent transfusions (and had iron overload), and 2 required occasional transfusions. One woman had 2 episodes of acute chest syndrome, and the second episode led to her death.
Ultimately, 3 of the women died. One died of acute chest syndrome and septicemia at age 82, and another died of cardiac complications at age 86. For a third woman, the cause of death, at age 82, was unknown. The fourth woman remains alive at age 82.
As the median life expectancy of women with SCD in the US is 47, Dr Ballas and his colleagues said these 4 women may “provide a blueprint of how to live a long life despite having a serious medical condition like SCD.”
“I would often come out to the waiting room and find these ladies talking with other SCD patients, and I could tell that they gave others hope, that just because they have SCD does not mean that they are doomed to die by their 40s . . . ,” Dr Ballas said. “[I]f they take care of themselves and live closely with those who can help keep them well, that there is hope for them to lead long, full lives.” ![]()
Factor IX therapy approved in Australia

The Australian Therapeutic Goods Administration has approved albutrepenonacog alfa (Idelvion) to treat hemophilia B patients of all ages.
Albutrepenonacog alfa is a fusion protein linking recombinant coagulation factor IX with recombinant albumin.
The product is now approved in Australia for use as routine prophylaxis to prevent and reduce the frequency of bleeding, for on-demand control of bleeding, and for perioperative management of
bleeding.
Albutrepenonacog alfa has also been approved in Canada, the European Union, Japan, Switzerland, and the US.
Albutrepenonacog alfa is being developed by CSL Behring.
The company says albutrepenonacog alfa is the first and only Australian-registered factor IX therapy that delivers high-level protection from bleeding with up to 14-day dosing for appropriate patients.
According to CSL Behring, albutrepenonacog alfa can deliver high-level protection by maintaining factor IX activity levels at an average of 20% in patients treated prophylactically every 7 days and an average of 12% in patients treated prophylactically every 14 days.
“The Australian Haemophilia Centre Directors’ Organisation (AHCDO) views the development of effective long-acting clotting factor concentrates as a major step forward in the management of our patients with hemophilia,” said Simon McRae, MMBS, consultant hematologist and chairman of AHCDO.
“The ability to maintain clotting factor levels above a level that prevent the vast majority of bleeding events with less frequent infusions has the potential to improve long-term outcomes in individuals with hemophilia.”
Phase 3 trial
The Therapeutic Goods Administration approved albutrepenonacog alfa based on results of the PROLONG-9FP clinical development program. PROLONG-9FP includes phase 1, 2, and 3 studies evaluating the safety and efficacy of albutrepenonacog alfa in adults and children (ages 1 to 61) with hemophilia B.
Data from the phase 3 study were published in Blood. The study included 63 previously treated male patients with severe hemophilia B. They had a mean age of 33 (range, 12 to 61).
The patients were divided into 2 groups. Group 1 (n=40) received routine prophylaxis with albutrepenonacog alfa once every 7 days for 26 weeks, followed by a 7-, 10-, or 14-day prophylaxis regimen for a mean of 50, 38, or 51 weeks, respectively.
Group 2 received on-demand treatment with albutrepenonacog alfa for bleeding episodes for 26 weeks (n=23) and then switched to a 7-day prophylaxis regimen for a mean of 45 weeks (n=19).
The median annualized bleeding rate (ABR) was 2.0 in the prophylaxis arm (group 1) and 23.5 in the on-demand treatment arm (group 2). The median spontaneous ABRs were 0.0 and 17.0, respectively.
For patients in group 2, there was a significant reduction in median ABRs when patients switched from on-demand treatment to prophylaxis—19.22 and 1.58, respectively (P<0.0001). And there was a significant reduction in median spontaneous ABRs—15.43 and 0.00, respectively (P<0.0001).
Overall, 98.6% of bleeding episodes were treated successfully, including 93.6% that were treated with a single injection of albutrepenonacog alfa.
None of the patients developed inhibitors or experienced thromboembolic events, anaphylaxis, or life-threatening adverse events (AEs).
There were 347 treatment-emergent AEs reported in 54 (85.7%) patients. The most common were nasopharyngitis (25.4%), headache (23.8%), arthralgia (4.3%), and influenza (11.1%).
Eleven mild/moderate AEs in 5 patients (7.9%) were considered possibly related to albutrepenonacog alfa. Two patients discontinued treatment due to AEs—1 with hypersensitivity and 1 with headache.
“I have seen first-hand the benefits Idelvion has had on children with hemophilia B,” said PROLONG-9FP investigator Julie Curtin, MBBS, PhD, of The Children’s Hospital at Westmead in New South Wales.
“Idelvion has enabled children on regular treatment with factor IX to reduce the frequency of infusions without increasing their risk of bleeding. For a child to only need an injection every 1-2 weeks is a good step forward in the management of hemophilia B, which I welcome, and I am sure my patients will welcome this improvement too.” ![]()
The Australian Therapeutic Goods Administration has approved albutrepenonacog alfa (Idelvion) to treat hemophilia B patients of all ages.
Albutrepenonacog alfa is a fusion protein linking recombinant coagulation factor IX with recombinant albumin.
The product is now approved in Australia for use as routine prophylaxis to prevent and reduce the frequency of bleeding, for on-demand control of bleeding, and for perioperative management of
bleeding.
Albutrepenonacog alfa has also been approved in Canada, the European Union, Japan, Switzerland, and the US.
Albutrepenonacog alfa is being developed by CSL Behring.
The company says albutrepenonacog alfa is the first and only Australian-registered factor IX therapy that delivers high-level protection from bleeding with up to 14-day dosing for appropriate patients.
According to CSL Behring, albutrepenonacog alfa can deliver high-level protection by maintaining factor IX activity levels at an average of 20% in patients treated prophylactically every 7 days and an average of 12% in patients treated prophylactically every 14 days.
“The Australian Haemophilia Centre Directors’ Organisation (AHCDO) views the development of effective long-acting clotting factor concentrates as a major step forward in the management of our patients with hemophilia,” said Simon McRae, MMBS, consultant hematologist and chairman of AHCDO.
“The ability to maintain clotting factor levels above a level that prevent the vast majority of bleeding events with less frequent infusions has the potential to improve long-term outcomes in individuals with hemophilia.”
Phase 3 trial
The Therapeutic Goods Administration approved albutrepenonacog alfa based on results of the PROLONG-9FP clinical development program. PROLONG-9FP includes phase 1, 2, and 3 studies evaluating the safety and efficacy of albutrepenonacog alfa in adults and children (ages 1 to 61) with hemophilia B.
Data from the phase 3 study were published in Blood. The study included 63 previously treated male patients with severe hemophilia B. They had a mean age of 33 (range, 12 to 61).
The patients were divided into 2 groups. Group 1 (n=40) received routine prophylaxis with albutrepenonacog alfa once every 7 days for 26 weeks, followed by a 7-, 10-, or 14-day prophylaxis regimen for a mean of 50, 38, or 51 weeks, respectively.
Group 2 received on-demand treatment with albutrepenonacog alfa for bleeding episodes for 26 weeks (n=23) and then switched to a 7-day prophylaxis regimen for a mean of 45 weeks (n=19).
The median annualized bleeding rate (ABR) was 2.0 in the prophylaxis arm (group 1) and 23.5 in the on-demand treatment arm (group 2). The median spontaneous ABRs were 0.0 and 17.0, respectively.
For patients in group 2, there was a significant reduction in median ABRs when patients switched from on-demand treatment to prophylaxis—19.22 and 1.58, respectively (P<0.0001). And there was a significant reduction in median spontaneous ABRs—15.43 and 0.00, respectively (P<0.0001).
Overall, 98.6% of bleeding episodes were treated successfully, including 93.6% that were treated with a single injection of albutrepenonacog alfa.
None of the patients developed inhibitors or experienced thromboembolic events, anaphylaxis, or life-threatening adverse events (AEs).
There were 347 treatment-emergent AEs reported in 54 (85.7%) patients. The most common were nasopharyngitis (25.4%), headache (23.8%), arthralgia (4.3%), and influenza (11.1%).
Eleven mild/moderate AEs in 5 patients (7.9%) were considered possibly related to albutrepenonacog alfa. Two patients discontinued treatment due to AEs—1 with hypersensitivity and 1 with headache.
“I have seen first-hand the benefits Idelvion has had on children with hemophilia B,” said PROLONG-9FP investigator Julie Curtin, MBBS, PhD, of The Children’s Hospital at Westmead in New South Wales.
“Idelvion has enabled children on regular treatment with factor IX to reduce the frequency of infusions without increasing their risk of bleeding. For a child to only need an injection every 1-2 weeks is a good step forward in the management of hemophilia B, which I welcome, and I am sure my patients will welcome this improvement too.” ![]()
The Australian Therapeutic Goods Administration has approved albutrepenonacog alfa (Idelvion) to treat hemophilia B patients of all ages.
Albutrepenonacog alfa is a fusion protein linking recombinant coagulation factor IX with recombinant albumin.
The product is now approved in Australia for use as routine prophylaxis to prevent and reduce the frequency of bleeding, for on-demand control of bleeding, and for perioperative management of
bleeding.
Albutrepenonacog alfa has also been approved in Canada, the European Union, Japan, Switzerland, and the US.
Albutrepenonacog alfa is being developed by CSL Behring.
The company says albutrepenonacog alfa is the first and only Australian-registered factor IX therapy that delivers high-level protection from bleeding with up to 14-day dosing for appropriate patients.
According to CSL Behring, albutrepenonacog alfa can deliver high-level protection by maintaining factor IX activity levels at an average of 20% in patients treated prophylactically every 7 days and an average of 12% in patients treated prophylactically every 14 days.
“The Australian Haemophilia Centre Directors’ Organisation (AHCDO) views the development of effective long-acting clotting factor concentrates as a major step forward in the management of our patients with hemophilia,” said Simon McRae, MMBS, consultant hematologist and chairman of AHCDO.
“The ability to maintain clotting factor levels above a level that prevent the vast majority of bleeding events with less frequent infusions has the potential to improve long-term outcomes in individuals with hemophilia.”
Phase 3 trial
The Therapeutic Goods Administration approved albutrepenonacog alfa based on results of the PROLONG-9FP clinical development program. PROLONG-9FP includes phase 1, 2, and 3 studies evaluating the safety and efficacy of albutrepenonacog alfa in adults and children (ages 1 to 61) with hemophilia B.
Data from the phase 3 study were published in Blood. The study included 63 previously treated male patients with severe hemophilia B. They had a mean age of 33 (range, 12 to 61).
The patients were divided into 2 groups. Group 1 (n=40) received routine prophylaxis with albutrepenonacog alfa once every 7 days for 26 weeks, followed by a 7-, 10-, or 14-day prophylaxis regimen for a mean of 50, 38, or 51 weeks, respectively.
Group 2 received on-demand treatment with albutrepenonacog alfa for bleeding episodes for 26 weeks (n=23) and then switched to a 7-day prophylaxis regimen for a mean of 45 weeks (n=19).
The median annualized bleeding rate (ABR) was 2.0 in the prophylaxis arm (group 1) and 23.5 in the on-demand treatment arm (group 2). The median spontaneous ABRs were 0.0 and 17.0, respectively.
For patients in group 2, there was a significant reduction in median ABRs when patients switched from on-demand treatment to prophylaxis—19.22 and 1.58, respectively (P<0.0001). And there was a significant reduction in median spontaneous ABRs—15.43 and 0.00, respectively (P<0.0001).
Overall, 98.6% of bleeding episodes were treated successfully, including 93.6% that were treated with a single injection of albutrepenonacog alfa.
None of the patients developed inhibitors or experienced thromboembolic events, anaphylaxis, or life-threatening adverse events (AEs).
There were 347 treatment-emergent AEs reported in 54 (85.7%) patients. The most common were nasopharyngitis (25.4%), headache (23.8%), arthralgia (4.3%), and influenza (11.1%).
Eleven mild/moderate AEs in 5 patients (7.9%) were considered possibly related to albutrepenonacog alfa. Two patients discontinued treatment due to AEs—1 with hypersensitivity and 1 with headache.
“I have seen first-hand the benefits Idelvion has had on children with hemophilia B,” said PROLONG-9FP investigator Julie Curtin, MBBS, PhD, of The Children’s Hospital at Westmead in New South Wales.
“Idelvion has enabled children on regular treatment with factor IX to reduce the frequency of infusions without increasing their risk of bleeding. For a child to only need an injection every 1-2 weeks is a good step forward in the management of hemophilia B, which I welcome, and I am sure my patients will welcome this improvement too.” ![]()
Inflammation may predict transformation to AML

Inflammatory signaling in mesenchymal niche cells can be used to predict the transformation from pre-leukemic syndrome to acute myeloid leukemia (AML), according to preclinical research published in Cell Stem Cell.
“This discovery sheds new light on the long-standing association between inflammation and cancer,” said study author Marc Raaijmakers, MD, PhD, of the Erasmus MC Cancer Institute in Rotterdam, Netherlands.
“The elucidation of the molecular mechanism underlying this concept opens the prospect of improved diagnosis of patients at increased risk for the development of leukemia and the potential of future, niche-targeted therapy to delay or prevent the development of leukemia.”
In a previous study, Dr Raaijmakers and his colleagues discovered that mutations in mesenchymal progenitor cells can induce myelodysplasia in mice and promote the development of AML.
With the current study, the researchers wanted to build upon those findings by identifying the underlying mechanisms and determining their relevance to human disease.
So the team performed massive parallel RNA sequencing of mesenchymal cells in mice with Shwachman-Diamond syndrome and bone marrow samples from patients with Shwachman-Diamond syndrome, Diamond-Blackfan anemia, and myelodysplastic syndromes (MDS).
The researchers found that mesenchymal cells in these pre-leukemic disorders are under stress. The stress leads to the release of inflammatory molecules called S100A8 and S100A9, which cause mitochondrial and DNA damage in hematopoietic stem and progenitor cells.
The team also found that activation of this inflammatory pathway in mesenchymal cells predicted the development of AML and clinical outcomes in patients with MDS.
Leukemic evolution occurred in 29.4% (5/17) of MDS patients whose mesenchymal cells overexpressed S100A8/9 and 14.2% (4/28) of MDS patients without S100A8/9 overexpression.
The time to leukemic evolution and the length of progression-free survival were both significantly shorter in niche S100A8/9+ patients than niche S100A8/9- patients.
The average time to leukemic evolution was 3.4 months and 18.5 months, respectively (P=0.03). And the median progression-free survival was 11.5 months and 53 months, respectively (P=0.03)
The researchers believe these findings, if confirmed in subsequent studies, could lead to the development of tests to identify patients with pre-leukemic syndromes who have a high risk of developing AML.
“These high-risk patients could be treated more aggressively at an earlier stage, thereby preventing or slowing down disease progression,” Dr Raaijmakers said. “Moreover, the findings suggest that new drugs targeting the inflammatory pathway should be tested in future preclinical studies.” ![]()
Inflammatory signaling in mesenchymal niche cells can be used to predict the transformation from pre-leukemic syndrome to acute myeloid leukemia (AML), according to preclinical research published in Cell Stem Cell.
“This discovery sheds new light on the long-standing association between inflammation and cancer,” said study author Marc Raaijmakers, MD, PhD, of the Erasmus MC Cancer Institute in Rotterdam, Netherlands.
“The elucidation of the molecular mechanism underlying this concept opens the prospect of improved diagnosis of patients at increased risk for the development of leukemia and the potential of future, niche-targeted therapy to delay or prevent the development of leukemia.”
In a previous study, Dr Raaijmakers and his colleagues discovered that mutations in mesenchymal progenitor cells can induce myelodysplasia in mice and promote the development of AML.
With the current study, the researchers wanted to build upon those findings by identifying the underlying mechanisms and determining their relevance to human disease.
So the team performed massive parallel RNA sequencing of mesenchymal cells in mice with Shwachman-Diamond syndrome and bone marrow samples from patients with Shwachman-Diamond syndrome, Diamond-Blackfan anemia, and myelodysplastic syndromes (MDS).
The researchers found that mesenchymal cells in these pre-leukemic disorders are under stress. The stress leads to the release of inflammatory molecules called S100A8 and S100A9, which cause mitochondrial and DNA damage in hematopoietic stem and progenitor cells.
The team also found that activation of this inflammatory pathway in mesenchymal cells predicted the development of AML and clinical outcomes in patients with MDS.
Leukemic evolution occurred in 29.4% (5/17) of MDS patients whose mesenchymal cells overexpressed S100A8/9 and 14.2% (4/28) of MDS patients without S100A8/9 overexpression.
The time to leukemic evolution and the length of progression-free survival were both significantly shorter in niche S100A8/9+ patients than niche S100A8/9- patients.
The average time to leukemic evolution was 3.4 months and 18.5 months, respectively (P=0.03). And the median progression-free survival was 11.5 months and 53 months, respectively (P=0.03)
The researchers believe these findings, if confirmed in subsequent studies, could lead to the development of tests to identify patients with pre-leukemic syndromes who have a high risk of developing AML.
“These high-risk patients could be treated more aggressively at an earlier stage, thereby preventing or slowing down disease progression,” Dr Raaijmakers said. “Moreover, the findings suggest that new drugs targeting the inflammatory pathway should be tested in future preclinical studies.” ![]()
Inflammatory signaling in mesenchymal niche cells can be used to predict the transformation from pre-leukemic syndrome to acute myeloid leukemia (AML), according to preclinical research published in Cell Stem Cell.
“This discovery sheds new light on the long-standing association between inflammation and cancer,” said study author Marc Raaijmakers, MD, PhD, of the Erasmus MC Cancer Institute in Rotterdam, Netherlands.
“The elucidation of the molecular mechanism underlying this concept opens the prospect of improved diagnosis of patients at increased risk for the development of leukemia and the potential of future, niche-targeted therapy to delay or prevent the development of leukemia.”
In a previous study, Dr Raaijmakers and his colleagues discovered that mutations in mesenchymal progenitor cells can induce myelodysplasia in mice and promote the development of AML.
With the current study, the researchers wanted to build upon those findings by identifying the underlying mechanisms and determining their relevance to human disease.
So the team performed massive parallel RNA sequencing of mesenchymal cells in mice with Shwachman-Diamond syndrome and bone marrow samples from patients with Shwachman-Diamond syndrome, Diamond-Blackfan anemia, and myelodysplastic syndromes (MDS).
The researchers found that mesenchymal cells in these pre-leukemic disorders are under stress. The stress leads to the release of inflammatory molecules called S100A8 and S100A9, which cause mitochondrial and DNA damage in hematopoietic stem and progenitor cells.
The team also found that activation of this inflammatory pathway in mesenchymal cells predicted the development of AML and clinical outcomes in patients with MDS.
Leukemic evolution occurred in 29.4% (5/17) of MDS patients whose mesenchymal cells overexpressed S100A8/9 and 14.2% (4/28) of MDS patients without S100A8/9 overexpression.
The time to leukemic evolution and the length of progression-free survival were both significantly shorter in niche S100A8/9+ patients than niche S100A8/9- patients.
The average time to leukemic evolution was 3.4 months and 18.5 months, respectively (P=0.03). And the median progression-free survival was 11.5 months and 53 months, respectively (P=0.03)
The researchers believe these findings, if confirmed in subsequent studies, could lead to the development of tests to identify patients with pre-leukemic syndromes who have a high risk of developing AML.
“These high-risk patients could be treated more aggressively at an earlier stage, thereby preventing or slowing down disease progression,” Dr Raaijmakers said. “Moreover, the findings suggest that new drugs targeting the inflammatory pathway should be tested in future preclinical studies.” ![]()
His Head Is In the Game–His Heart, Not So Much
ANSWER
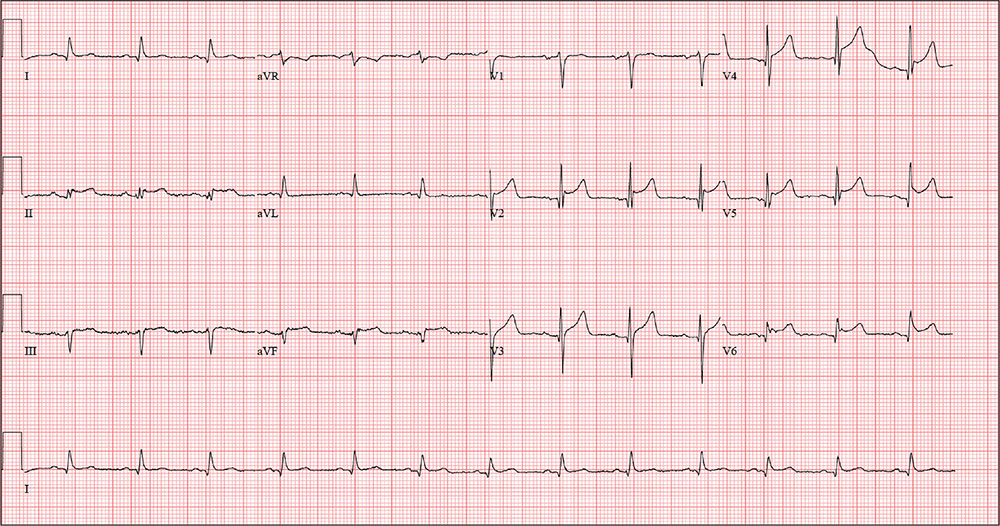
The correct interpretation includes normal sinus rhythm with a new anterior myocardial infarction (MI) and inferolateral injury.
Criteria for an anterior MI include Q waves in leads V2 to V6 and hyperacute ST-T wave changes. V1 is usually spared.
Inferolateral injury is evidenced by the presence of Q waves and absence of R waves in leads III and aVF.
The patient’s cardiac catheterization revealed left anterior descending and circumflex artery disease.
ANSWER
The correct interpretation includes normal sinus rhythm with a new anterior myocardial infarction (MI) and inferolateral injury.
Criteria for an anterior MI include Q waves in leads V2 to V6 and hyperacute ST-T wave changes. V1 is usually spared.
Inferolateral injury is evidenced by the presence of Q waves and absence of R waves in leads III and aVF.
The patient’s cardiac catheterization revealed left anterior descending and circumflex artery disease.
ANSWER
The correct interpretation includes normal sinus rhythm with a new anterior myocardial infarction (MI) and inferolateral injury.
Criteria for an anterior MI include Q waves in leads V2 to V6 and hyperacute ST-T wave changes. V1 is usually spared.
Inferolateral injury is evidenced by the presence of Q waves and absence of R waves in leads III and aVF.
The patient’s cardiac catheterization revealed left anterior descending and circumflex artery disease.
While playing in a company racquetball tournament, a 47-year-old man suddenly collapses. He is unresponsive, without a pulse, and his coworkers immediately initiate CPR. A single shock from an on-site AED successfully resuscitates him from ventricular fibrillation. Paramedics arrive within 12 minutes, by which time the patient is conscious and responsive to commands.
During transportation to the emergency department, however, he develops ventricular tachycardia and loses consciousness; a single shock cardioverts him to normal sinus rhythm. An ECG is ordered and the cardiac catheterization team mobilized.
While waiting, you contact the patient’s wife by telephone. She tells you that her husband has been complaining of chest discomfort for the past week and woke up two nights ago with what he described as “indigestion.” She says she suggested he see a clinician, and he agreed to do so—but not until after the tournament.
His medical history is remarkable only for chronic gastroesophageal reflux disease (GERD), for which he takes chewable antacids on a daily basis. He has no prior cardiac or pulmonary history. There is no surgical history apart from a tonsillectomy in childhood.
The patient is the Chief Operating Officer at a local manufacturing facility. He is married and has three children. His parents and grandparents are alive and in good health, aside from some arthritis in the older generation.
The review of systems, obtained from his wife, is noncontributory. She says he is in excellent health—he jogs, rides mountain bikes, and enjoys racquetball. Her husband attributed his recent chest discomfort to GERD; when she asked if it could be cardiac related, he adamantly denied the possibility, as he was in “excellent health” with “good genes.”
Vital signs include a blood pressure of 118/56 mm Hg; pulse, 80 beats/min; respiratory rate, 18 breaths/min-1; and O2 saturation, 100% on 2 L oxygen. He is afebrile.
Physical exam reveals a thin, otherwise healthy male who appears anxious and apprehensive. He denies ongoing chest pain but states that his chest wall is sore beneath the defibrillator pads. A focal exam reveals normal lung sounds and a regular rate and rhythm with no murmurs, gallops, or rubs. The abdomen is soft and nontender. All peripheral pulses are strong and equal bilaterally, and there are no focal neurologic signs.
The ECG taken at admission shows a ventricular rate of 80 beats/min; PR interval, 162 ms; QRS duration, 106 ms; QT/QTc interval, 370/426 ms; P axis, 51°; R axis, –20°; and T axis, 70°. What is your interpretation of the ECG?
Registry, multisite care, bundled vaccines improve HPV vaccination rate among teens
Bundling vaccines, coordinating multisite medical access, and overseeing vaccination status through an internally developed immunization registry has consistently led to Denver Health’s reporting higher-than-average HPV vaccination rates among adolescents, according to investigators.
Despite the Advisory Committee on Immunization Practice’s 2006 recommendation for routine adolescent human papillomavirus (HPV) vaccination and the Healthy People goal of 80% vaccine coverage in adolescents by 2020, HPV vaccination rates have lagged behind those of other routinely administered adolescent vaccinations, such as meningococcal conjugate vaccine (MCV4) and Tdap, reported Anna-Lisa Farmar, MD, of Denver Health, and her associates (Pediatrics. 2016 Oct 5. doi: 10.1542/peds.2015-2653).
For their study, Dr. Farmar and her associates outlined the vaccination procedures and tactics used at Denver Health’s 8 health centers and 16 school-based health centers and examined vaccine registry data for 11,463 patients to understand why the health system has been successful and to learn how it can further improve.
The multipronged vaccination procedures and tactics employed at Denver Health are designed to overcome specific HPV vaccination barriers such as concern about the vaccine’s safety, parental belief that their children are not sexually active, lack of insurance coverage, lack of knowledge about HPV, and providers missing opportunities to administer the vaccine, as well as barriers affecting low-income patients: transportation issues, low access to care, and inability to take time off work.
“For all patients presenting for acute or preventative visits, there is a standard process for the medical assistants to follow that leads to vaccines being offered to the patient,” the authors wrote. This process begins with and is organized by VaxTrax, a Denver Health internally developed immunization registry that informs medical providers of a patient’s vaccination status.
Denver Health medical providers are encouraged to bundle common vaccines together, to not present vaccines as optional or required, and to review their individual vaccine coverage rates, which are distributed monthly. In addition, school-based health centers offer vaccination drives and adolescents can receive medical care at any of the Denver Health sites, thereby increasing the opportunities for providers and patients to interact.
“Avoiding missed opportunities for vaccination and providing a strong recommendation for the HPV vaccine were key procedures that likely contributed to high coverage rates,” Dr. Farmar and her associates wrote.
The researchers found that of the 11,463 patients included in analysis, the majority completing the HPV vaccination series were female, Hispanic, and low-income. “These results are consistent with previous research examining national and state trends,” they noted.
“To our knowledge, language has not been examined as a potential factor in HPV coverage rates. The practice of continuing to approach families who have refused HPV vaccination in the past addresses the patient groups with lower vaccine completion rates, such as English-speaking and higher-income families. These families may require recurring discussion over time with a primary provider to overcome barriers to vaccination,” the researchers wrote.
This study received no external funding, and the researchers had no relevant disclosures to report.
jcraig@frontlinemedcom.com
On Twitter @jessnicolecraig
Bundling vaccines, coordinating multisite medical access, and overseeing vaccination status through an internally developed immunization registry has consistently led to Denver Health’s reporting higher-than-average HPV vaccination rates among adolescents, according to investigators.
Despite the Advisory Committee on Immunization Practice’s 2006 recommendation for routine adolescent human papillomavirus (HPV) vaccination and the Healthy People goal of 80% vaccine coverage in adolescents by 2020, HPV vaccination rates have lagged behind those of other routinely administered adolescent vaccinations, such as meningococcal conjugate vaccine (MCV4) and Tdap, reported Anna-Lisa Farmar, MD, of Denver Health, and her associates (Pediatrics. 2016 Oct 5. doi: 10.1542/peds.2015-2653).
For their study, Dr. Farmar and her associates outlined the vaccination procedures and tactics used at Denver Health’s 8 health centers and 16 school-based health centers and examined vaccine registry data for 11,463 patients to understand why the health system has been successful and to learn how it can further improve.
The multipronged vaccination procedures and tactics employed at Denver Health are designed to overcome specific HPV vaccination barriers such as concern about the vaccine’s safety, parental belief that their children are not sexually active, lack of insurance coverage, lack of knowledge about HPV, and providers missing opportunities to administer the vaccine, as well as barriers affecting low-income patients: transportation issues, low access to care, and inability to take time off work.
“For all patients presenting for acute or preventative visits, there is a standard process for the medical assistants to follow that leads to vaccines being offered to the patient,” the authors wrote. This process begins with and is organized by VaxTrax, a Denver Health internally developed immunization registry that informs medical providers of a patient’s vaccination status.
Denver Health medical providers are encouraged to bundle common vaccines together, to not present vaccines as optional or required, and to review their individual vaccine coverage rates, which are distributed monthly. In addition, school-based health centers offer vaccination drives and adolescents can receive medical care at any of the Denver Health sites, thereby increasing the opportunities for providers and patients to interact.
“Avoiding missed opportunities for vaccination and providing a strong recommendation for the HPV vaccine were key procedures that likely contributed to high coverage rates,” Dr. Farmar and her associates wrote.
The researchers found that of the 11,463 patients included in analysis, the majority completing the HPV vaccination series were female, Hispanic, and low-income. “These results are consistent with previous research examining national and state trends,” they noted.
“To our knowledge, language has not been examined as a potential factor in HPV coverage rates. The practice of continuing to approach families who have refused HPV vaccination in the past addresses the patient groups with lower vaccine completion rates, such as English-speaking and higher-income families. These families may require recurring discussion over time with a primary provider to overcome barriers to vaccination,” the researchers wrote.
This study received no external funding, and the researchers had no relevant disclosures to report.
jcraig@frontlinemedcom.com
On Twitter @jessnicolecraig
Bundling vaccines, coordinating multisite medical access, and overseeing vaccination status through an internally developed immunization registry has consistently led to Denver Health’s reporting higher-than-average HPV vaccination rates among adolescents, according to investigators.
Despite the Advisory Committee on Immunization Practice’s 2006 recommendation for routine adolescent human papillomavirus (HPV) vaccination and the Healthy People goal of 80% vaccine coverage in adolescents by 2020, HPV vaccination rates have lagged behind those of other routinely administered adolescent vaccinations, such as meningococcal conjugate vaccine (MCV4) and Tdap, reported Anna-Lisa Farmar, MD, of Denver Health, and her associates (Pediatrics. 2016 Oct 5. doi: 10.1542/peds.2015-2653).
For their study, Dr. Farmar and her associates outlined the vaccination procedures and tactics used at Denver Health’s 8 health centers and 16 school-based health centers and examined vaccine registry data for 11,463 patients to understand why the health system has been successful and to learn how it can further improve.
The multipronged vaccination procedures and tactics employed at Denver Health are designed to overcome specific HPV vaccination barriers such as concern about the vaccine’s safety, parental belief that their children are not sexually active, lack of insurance coverage, lack of knowledge about HPV, and providers missing opportunities to administer the vaccine, as well as barriers affecting low-income patients: transportation issues, low access to care, and inability to take time off work.
“For all patients presenting for acute or preventative visits, there is a standard process for the medical assistants to follow that leads to vaccines being offered to the patient,” the authors wrote. This process begins with and is organized by VaxTrax, a Denver Health internally developed immunization registry that informs medical providers of a patient’s vaccination status.
Denver Health medical providers are encouraged to bundle common vaccines together, to not present vaccines as optional or required, and to review their individual vaccine coverage rates, which are distributed monthly. In addition, school-based health centers offer vaccination drives and adolescents can receive medical care at any of the Denver Health sites, thereby increasing the opportunities for providers and patients to interact.
“Avoiding missed opportunities for vaccination and providing a strong recommendation for the HPV vaccine were key procedures that likely contributed to high coverage rates,” Dr. Farmar and her associates wrote.
The researchers found that of the 11,463 patients included in analysis, the majority completing the HPV vaccination series were female, Hispanic, and low-income. “These results are consistent with previous research examining national and state trends,” they noted.
“To our knowledge, language has not been examined as a potential factor in HPV coverage rates. The practice of continuing to approach families who have refused HPV vaccination in the past addresses the patient groups with lower vaccine completion rates, such as English-speaking and higher-income families. These families may require recurring discussion over time with a primary provider to overcome barriers to vaccination,” the researchers wrote.
This study received no external funding, and the researchers had no relevant disclosures to report.
jcraig@frontlinemedcom.com
On Twitter @jessnicolecraig
FROM PEDIATRICS
Key clinical point:
Major finding: In 2014, the national average of adolescents receiving three or more doses of the HPV vaccine was 40% for girls and 22% for boys. At Denver Health, those rates were 67% and 60%, respectively.
Data source: A retrospective study of 11,463 adolescent patients.
Disclosures: This study received no external funding, and the researchers had no relevant disclosures to report.
Laparoscopic hysterectomy best in morbidly obese uterine cancer patients
BOSTON – Total laparoscopic hysterectomy had fewer complications and a shorter length of stay among morbidly obese women with uterine cancer, compared with an abdominal approach, according to findings presented at the annual Minimally Invasive Surgery Week.
“We wanted to look at current trends and see if we’re doing more the abdominal route or adopting more minimally invasive surgery, but also find out what obesity has to do with it,” Emad Mikhail, MD, of the University of South Florida in Tampa, said in an interview. “Morbidly obese patients are a really vulnerable group of patients; they have a lot of medical comorbidities, and when they need surgery they have an increased risk of having poor perioperative outcomes because of their BMI [body mass index].”
More than half of the cases were total laparoscopic hysterectomy (1,025), a third were total abdominal hysterectomy (672), about 12% were laparoscopic assisted vaginal hysterectomy (248), and less than 3% were total vaginal hysterectomy (57).
Comparing total abdominal and total laparoscopic hysterectomy – the two most commonly performed type of hysterectomy in the study – median operative times were notably higher in total laparoscopic hysterectomy: 171 minutes versus 150 minutes (P less than .05). But the laparoscopic approach had a shorter length of stay, a lower rate of hospital readmissions, and fewer surgical complications.
Within the total laparoscopic hysterectomy cohort, length of stay averaged 1 day. Dr. Mikhail reported that this cohort also had 14 blood transfusions, 13 superficial surgical site infections, 5 deep incisional surgical site infections, and 41 readmissions within 30 days, all of which were significantly lower than in the total abdominal hysterectomy cohort (P less than .05).
Mean BMI was similar in the two groups, with 34.0 in the total abdominal hysterectomy cohort and 33.7 in the total laparoscopic hysterectomy cohort.
“As the BMI goes up, more [minimally invasive surgery] is adopted, which is a great finding,” Dr. Mikhail said. “It actually serves the purpose of vulnerable patients. Instead of having an increase in perioperative morbidity, they should benefit more from a [minimally invasive surgery] approach, which this study is showing.”
Next, Dr. Mikhail said he wants to tease out what types of procedures subspecialists are performing among morbidly obese patients with uterine cancer. This type of data collection would be easier, he added, if minimally invasive gynecologic surgeons had their own taxonomy code.
“Without a code, we cannot pull data and see if being a fellowship-trained, minimally invasive surgeon has a benefit for patients,” he said. “Are those surgeons offering more minimally invasive techniques for morbidly obese patients?”
Dr. Mikhail reported having no relevant financial disclosures. The meeting was held by the Society of Laparoendoscopic Surgeons.
BOSTON – Total laparoscopic hysterectomy had fewer complications and a shorter length of stay among morbidly obese women with uterine cancer, compared with an abdominal approach, according to findings presented at the annual Minimally Invasive Surgery Week.
“We wanted to look at current trends and see if we’re doing more the abdominal route or adopting more minimally invasive surgery, but also find out what obesity has to do with it,” Emad Mikhail, MD, of the University of South Florida in Tampa, said in an interview. “Morbidly obese patients are a really vulnerable group of patients; they have a lot of medical comorbidities, and when they need surgery they have an increased risk of having poor perioperative outcomes because of their BMI [body mass index].”
More than half of the cases were total laparoscopic hysterectomy (1,025), a third were total abdominal hysterectomy (672), about 12% were laparoscopic assisted vaginal hysterectomy (248), and less than 3% were total vaginal hysterectomy (57).
Comparing total abdominal and total laparoscopic hysterectomy – the two most commonly performed type of hysterectomy in the study – median operative times were notably higher in total laparoscopic hysterectomy: 171 minutes versus 150 minutes (P less than .05). But the laparoscopic approach had a shorter length of stay, a lower rate of hospital readmissions, and fewer surgical complications.
Within the total laparoscopic hysterectomy cohort, length of stay averaged 1 day. Dr. Mikhail reported that this cohort also had 14 blood transfusions, 13 superficial surgical site infections, 5 deep incisional surgical site infections, and 41 readmissions within 30 days, all of which were significantly lower than in the total abdominal hysterectomy cohort (P less than .05).
Mean BMI was similar in the two groups, with 34.0 in the total abdominal hysterectomy cohort and 33.7 in the total laparoscopic hysterectomy cohort.
“As the BMI goes up, more [minimally invasive surgery] is adopted, which is a great finding,” Dr. Mikhail said. “It actually serves the purpose of vulnerable patients. Instead of having an increase in perioperative morbidity, they should benefit more from a [minimally invasive surgery] approach, which this study is showing.”
Next, Dr. Mikhail said he wants to tease out what types of procedures subspecialists are performing among morbidly obese patients with uterine cancer. This type of data collection would be easier, he added, if minimally invasive gynecologic surgeons had their own taxonomy code.
“Without a code, we cannot pull data and see if being a fellowship-trained, minimally invasive surgeon has a benefit for patients,” he said. “Are those surgeons offering more minimally invasive techniques for morbidly obese patients?”
Dr. Mikhail reported having no relevant financial disclosures. The meeting was held by the Society of Laparoendoscopic Surgeons.
BOSTON – Total laparoscopic hysterectomy had fewer complications and a shorter length of stay among morbidly obese women with uterine cancer, compared with an abdominal approach, according to findings presented at the annual Minimally Invasive Surgery Week.
“We wanted to look at current trends and see if we’re doing more the abdominal route or adopting more minimally invasive surgery, but also find out what obesity has to do with it,” Emad Mikhail, MD, of the University of South Florida in Tampa, said in an interview. “Morbidly obese patients are a really vulnerable group of patients; they have a lot of medical comorbidities, and when they need surgery they have an increased risk of having poor perioperative outcomes because of their BMI [body mass index].”
More than half of the cases were total laparoscopic hysterectomy (1,025), a third were total abdominal hysterectomy (672), about 12% were laparoscopic assisted vaginal hysterectomy (248), and less than 3% were total vaginal hysterectomy (57).
Comparing total abdominal and total laparoscopic hysterectomy – the two most commonly performed type of hysterectomy in the study – median operative times were notably higher in total laparoscopic hysterectomy: 171 minutes versus 150 minutes (P less than .05). But the laparoscopic approach had a shorter length of stay, a lower rate of hospital readmissions, and fewer surgical complications.
Within the total laparoscopic hysterectomy cohort, length of stay averaged 1 day. Dr. Mikhail reported that this cohort also had 14 blood transfusions, 13 superficial surgical site infections, 5 deep incisional surgical site infections, and 41 readmissions within 30 days, all of which were significantly lower than in the total abdominal hysterectomy cohort (P less than .05).
Mean BMI was similar in the two groups, with 34.0 in the total abdominal hysterectomy cohort and 33.7 in the total laparoscopic hysterectomy cohort.
“As the BMI goes up, more [minimally invasive surgery] is adopted, which is a great finding,” Dr. Mikhail said. “It actually serves the purpose of vulnerable patients. Instead of having an increase in perioperative morbidity, they should benefit more from a [minimally invasive surgery] approach, which this study is showing.”
Next, Dr. Mikhail said he wants to tease out what types of procedures subspecialists are performing among morbidly obese patients with uterine cancer. This type of data collection would be easier, he added, if minimally invasive gynecologic surgeons had their own taxonomy code.
“Without a code, we cannot pull data and see if being a fellowship-trained, minimally invasive surgeon has a benefit for patients,” he said. “Are those surgeons offering more minimally invasive techniques for morbidly obese patients?”
Dr. Mikhail reported having no relevant financial disclosures. The meeting was held by the Society of Laparoendoscopic Surgeons.
Key clinical point:
Major finding: Total laparoscopic hysterectomy had shorter length of stay, fewer transfusions, fewer surgical site infections, and fewer readmissions, compared with total abdominal hysterectomy (P less than .05).
Data source: Retrospective review of data on 2,002 morbidly obese patients with uterine cancer in the ACS-NSQIP database.
Disclosures: Dr. Mikhail reported having no relevant financial disclosures.
Botox for overactive bladder led to low rate of catheterization
DENVER – Less than 2% of onabotulinumtoxinA injections for idiopathic detrusor overactivity resulted in clean intermittent catheterization, a substantially lower rate than previously found, Juzar Jamnagerwalla, MD, reported at Pelvic Floor Disorders Week.
These included two cases of acute urinary retention and one case in which a patient complained of problems voiding and had a postvoid residual urine volume (PVR) of 353 mL, said Dr. Jamnagerwalla of Cedars-Sinai, Los Angeles. Taken together, the findings suggest that postprocedural PVR can usually be managed safely by observation alone, which may reassure patients who are considering treatment options for overactive bladder, he added.
But these “strict” criteria contrast with real-world practice, in which patients with postprocedural PVR often are observed without CIC unless they have subjective complaints or other contraindications, Dr. Jamnagerwalla said. The discrepancy is especially relevant because patients with overactive bladder who decline onabotulinumtoxinA often cite the risk of CIC as the reason, he added.
To better understand CIC rates at Cedars-Sinai, Dr. Jamnagerwalla and his colleagues reviewed 27 months of records from patients with idiopathic detrusor overactivity who received injections of 100 U of onabotulinumtoxinA given by female pelvic medicine and reconstructive surgery physicians. The patients were followed up immediately and 2 weeks later, but underwent CIC only if they could not void or had PVRs above 350 mL and subjective voiding complaints.
In all, 99 patients received a total of 187 injections, of which only 3 (1.6%) led to urinary retention requiring CIC. The median postprocedure PVR was 117 mL. About three-quarters of patients had PVRs less than 200 mL, 29 (16%) had PVRs between 200 mL and 350 mL, and 13 (7%) had PVRs greater than 350 mL.
Age, body mass index, and preprocedure PVR did not predict urinary retention in the univariate analysis, Dr. Jamnagerwalla said at the meeting, which was sponsored by the American Urogynecologic Society.
The results support the practice of observing patients with elevated PVRs after Botox, as long as they do not develop obstructive symptoms, he advised.
“While it remains important to counsel patients on the risk of urinary retention after Botox injection for idiopathic detrusor overactivity, patients can be reassured that the true rate of retention requiring CIC is relatively low,” he said.
Dr. Jamnagerwalla reported no funding sources and reported having no financial disclosures. Two coauthors reported ties to Boston Scientific, Astora, and Allergan.
DENVER – Less than 2% of onabotulinumtoxinA injections for idiopathic detrusor overactivity resulted in clean intermittent catheterization, a substantially lower rate than previously found, Juzar Jamnagerwalla, MD, reported at Pelvic Floor Disorders Week.
These included two cases of acute urinary retention and one case in which a patient complained of problems voiding and had a postvoid residual urine volume (PVR) of 353 mL, said Dr. Jamnagerwalla of Cedars-Sinai, Los Angeles. Taken together, the findings suggest that postprocedural PVR can usually be managed safely by observation alone, which may reassure patients who are considering treatment options for overactive bladder, he added.
But these “strict” criteria contrast with real-world practice, in which patients with postprocedural PVR often are observed without CIC unless they have subjective complaints or other contraindications, Dr. Jamnagerwalla said. The discrepancy is especially relevant because patients with overactive bladder who decline onabotulinumtoxinA often cite the risk of CIC as the reason, he added.
To better understand CIC rates at Cedars-Sinai, Dr. Jamnagerwalla and his colleagues reviewed 27 months of records from patients with idiopathic detrusor overactivity who received injections of 100 U of onabotulinumtoxinA given by female pelvic medicine and reconstructive surgery physicians. The patients were followed up immediately and 2 weeks later, but underwent CIC only if they could not void or had PVRs above 350 mL and subjective voiding complaints.
In all, 99 patients received a total of 187 injections, of which only 3 (1.6%) led to urinary retention requiring CIC. The median postprocedure PVR was 117 mL. About three-quarters of patients had PVRs less than 200 mL, 29 (16%) had PVRs between 200 mL and 350 mL, and 13 (7%) had PVRs greater than 350 mL.
Age, body mass index, and preprocedure PVR did not predict urinary retention in the univariate analysis, Dr. Jamnagerwalla said at the meeting, which was sponsored by the American Urogynecologic Society.
The results support the practice of observing patients with elevated PVRs after Botox, as long as they do not develop obstructive symptoms, he advised.
“While it remains important to counsel patients on the risk of urinary retention after Botox injection for idiopathic detrusor overactivity, patients can be reassured that the true rate of retention requiring CIC is relatively low,” he said.
Dr. Jamnagerwalla reported no funding sources and reported having no financial disclosures. Two coauthors reported ties to Boston Scientific, Astora, and Allergan.
DENVER – Less than 2% of onabotulinumtoxinA injections for idiopathic detrusor overactivity resulted in clean intermittent catheterization, a substantially lower rate than previously found, Juzar Jamnagerwalla, MD, reported at Pelvic Floor Disorders Week.
These included two cases of acute urinary retention and one case in which a patient complained of problems voiding and had a postvoid residual urine volume (PVR) of 353 mL, said Dr. Jamnagerwalla of Cedars-Sinai, Los Angeles. Taken together, the findings suggest that postprocedural PVR can usually be managed safely by observation alone, which may reassure patients who are considering treatment options for overactive bladder, he added.
But these “strict” criteria contrast with real-world practice, in which patients with postprocedural PVR often are observed without CIC unless they have subjective complaints or other contraindications, Dr. Jamnagerwalla said. The discrepancy is especially relevant because patients with overactive bladder who decline onabotulinumtoxinA often cite the risk of CIC as the reason, he added.
To better understand CIC rates at Cedars-Sinai, Dr. Jamnagerwalla and his colleagues reviewed 27 months of records from patients with idiopathic detrusor overactivity who received injections of 100 U of onabotulinumtoxinA given by female pelvic medicine and reconstructive surgery physicians. The patients were followed up immediately and 2 weeks later, but underwent CIC only if they could not void or had PVRs above 350 mL and subjective voiding complaints.
In all, 99 patients received a total of 187 injections, of which only 3 (1.6%) led to urinary retention requiring CIC. The median postprocedure PVR was 117 mL. About three-quarters of patients had PVRs less than 200 mL, 29 (16%) had PVRs between 200 mL and 350 mL, and 13 (7%) had PVRs greater than 350 mL.
Age, body mass index, and preprocedure PVR did not predict urinary retention in the univariate analysis, Dr. Jamnagerwalla said at the meeting, which was sponsored by the American Urogynecologic Society.
The results support the practice of observing patients with elevated PVRs after Botox, as long as they do not develop obstructive symptoms, he advised.
“While it remains important to counsel patients on the risk of urinary retention after Botox injection for idiopathic detrusor overactivity, patients can be reassured that the true rate of retention requiring CIC is relatively low,” he said.
Dr. Jamnagerwalla reported no funding sources and reported having no financial disclosures. Two coauthors reported ties to Boston Scientific, Astora, and Allergan.
Key clinical point:
Major finding: Of 187 injections, 1.6% of led to acute urinary retention requiring clean intermittent catheterization.
Data source: A single-center, retrospective study of 99 patients receiving 187 onabotulinumtoxinA injections.
Disclosures: Dr. Jamnagerwalla and his colleagues reported no funding sources and had no disclosures.
ACS should make firearm injury prevention a priority, COT member survey says
WAIKOLOA, HAWAII – Nearly 90% of American College of Surgeons Committee on Trauma members believe that the ACS should give the highest or a high priority to reducing firearm-related injuries, according to results from a national survey.
“In the United States, we value personal liberty and personal safety highly,” Deborah A. Kuhls, MD, FACS, said at the annual meeting of the American Association for the Surgery of Trauma. “However, that sometimes leads to a polarized view on firearms. Some view it as a freedom in personal safety. Others view it as a limitation of freedom and [as promotion of] violence.”
In an effort to evaluate ACS COT member attitudes about firearm ownership, freedom, responsibility, physician/patient freedom and policy, with the objective of using survey results to inform firearm injury prevention policy development, Dr. Kuhls and the COT Injury Prevention and Control Committee developed a 32-item anonymous survey that was sent to 254 COT members between December 2015 and February 2016. Results were extracted by ACS staff.
Of 254 COT members who received the survey, 237 completed the survey, for a response rate of 93%. Their mean age was 52 years, and 88% were male, 88% were married, 85% were white, and 58% had children in the home. More than one-quarter (29%) had military experience, 88% practiced acute care, trauma, general surgery, or pediatric surgery; 43% had firearms in the home, and 33% had personal experience with a family or friend injured or killed from firearm injury. A significantly higher proportion of respondents with military experience had firearms in the home, compared with those who had no military experience (56% vs. 37%, respectively; P less than .01). By Centers for Disease Control and Prevention demographic region, the percentage of members who have firearms in their home was lowest in the Northeast (14%), followed by the West (38%), the Midwest (48%), and the South (56%).
Dr. Kuhls also reported that 88% of respondents indicated that they think the ACS should give a high or the highest level of priority to firearm injury prevention. When asked about private ownership of firearms, about 53% thought that gun ownership is generally beneficial/an important personal liberty, while 30% believed that gun ownership is generally harmful and limits personal liberty. The remaining 17% had no opinion on the issue.
The majority of respondents (95%) said that health care professionals should be allowed to counsel patients (or parents of patients) about how to prevent gun-related injuries, while 96% felt that the CDC and other federal agencies should fund research on the epidemiology and prevention of gun-related injuries.
Survey respondents were then asked to rate their opinion on the ACS initiating efforts to advocate for or support legislation on 15 possible initiatives to prevent firearm violence, ranging from “improve mental health screening and treatment to reduce suicides and gun violence” to increase penalties when guns [are] provided to others illegally including dealers” to “require safety features, including child-proof locks and ‘smart gun’ technology,” and “identify and implement evidence-based injury prevention programs.”
The greatest consensus was reached in the advocacy area titled “improve mental health screening and treatment to reduce suicides and gun violence” (ranging from 89% to 93%), while the least consensus was in the advocacy area titled “require firearms owners to be 21 years of age or older” (ranging from 41% to 71%).
The most common themes that emerged on qualitative analysis were concern that the topic is too political, as well as calls to improve existing data “to understand what role we can play in injury prevention,” and that “surgeons should be involved in solving the problem,” Dr. Kuhls said. “There were also a lot of comments on responsible ownership.” She noted that more than 90% of respondents support 7 out of 15 proposed initiatives, 80%-90% support an additional 3 initiatives, and 70%-80% support an additional 4 proposed initiatives.
The invited discussant, Ernest E. Moore, MD, FACS, a surgeon in Denver, described the effort to develop firearm injury prevention policy as laudable. However, “this process carries a risk of merely supporting the bandwagons already in motion,” Dr. Moore said. “In that light I would like to focus on the conspicuous areas of disagreement, specifically civilian access to assault rifles. The fundamental issue is the magazine capacity of rifles – housing 30 or more bullets, enabling rapid shooting. Mass shootings, defined as greater than or equal to five victims, are currently an epidemic in our country. The volatile issues are eliminating assault rifles to reduce mass shootings [and] the interpretation of the Second Amendment to keep and bear arms. I do not believe a randomized prospective trial is necessary to establish the fact that mass shootings are only feasible because irresponsible individuals have access to these weapons. The urgency in this issue is heightened by the reality that mass shootings are increasingly inspired by terrorist activity, beyond individuals traditionally considered mentally ill.”
Dr. Kuhls described the current survey as “the initial step” in an effort to develop firearm injury prevention policy. “We are just about to receive results from a survey of the Board of Governors for the ACS,” she said. “We plan to develop short- and long-term plans to address this public health challenge that leverages survey consensus findings in four ACS pillars: advocacy, quality, systems, and education. We need to continue this conversation.” She expressed gratitude to the COT Executive Committee and liaison members from the ACS Board of Regents in addition to members of the COT Injury Prevention and Control Committee. She reported having no financial disclosures.
WAIKOLOA, HAWAII – Nearly 90% of American College of Surgeons Committee on Trauma members believe that the ACS should give the highest or a high priority to reducing firearm-related injuries, according to results from a national survey.
“In the United States, we value personal liberty and personal safety highly,” Deborah A. Kuhls, MD, FACS, said at the annual meeting of the American Association for the Surgery of Trauma. “However, that sometimes leads to a polarized view on firearms. Some view it as a freedom in personal safety. Others view it as a limitation of freedom and [as promotion of] violence.”
In an effort to evaluate ACS COT member attitudes about firearm ownership, freedom, responsibility, physician/patient freedom and policy, with the objective of using survey results to inform firearm injury prevention policy development, Dr. Kuhls and the COT Injury Prevention and Control Committee developed a 32-item anonymous survey that was sent to 254 COT members between December 2015 and February 2016. Results were extracted by ACS staff.
Of 254 COT members who received the survey, 237 completed the survey, for a response rate of 93%. Their mean age was 52 years, and 88% were male, 88% were married, 85% were white, and 58% had children in the home. More than one-quarter (29%) had military experience, 88% practiced acute care, trauma, general surgery, or pediatric surgery; 43% had firearms in the home, and 33% had personal experience with a family or friend injured or killed from firearm injury. A significantly higher proportion of respondents with military experience had firearms in the home, compared with those who had no military experience (56% vs. 37%, respectively; P less than .01). By Centers for Disease Control and Prevention demographic region, the percentage of members who have firearms in their home was lowest in the Northeast (14%), followed by the West (38%), the Midwest (48%), and the South (56%).
Dr. Kuhls also reported that 88% of respondents indicated that they think the ACS should give a high or the highest level of priority to firearm injury prevention. When asked about private ownership of firearms, about 53% thought that gun ownership is generally beneficial/an important personal liberty, while 30% believed that gun ownership is generally harmful and limits personal liberty. The remaining 17% had no opinion on the issue.
The majority of respondents (95%) said that health care professionals should be allowed to counsel patients (or parents of patients) about how to prevent gun-related injuries, while 96% felt that the CDC and other federal agencies should fund research on the epidemiology and prevention of gun-related injuries.
Survey respondents were then asked to rate their opinion on the ACS initiating efforts to advocate for or support legislation on 15 possible initiatives to prevent firearm violence, ranging from “improve mental health screening and treatment to reduce suicides and gun violence” to increase penalties when guns [are] provided to others illegally including dealers” to “require safety features, including child-proof locks and ‘smart gun’ technology,” and “identify and implement evidence-based injury prevention programs.”
The greatest consensus was reached in the advocacy area titled “improve mental health screening and treatment to reduce suicides and gun violence” (ranging from 89% to 93%), while the least consensus was in the advocacy area titled “require firearms owners to be 21 years of age or older” (ranging from 41% to 71%).
The most common themes that emerged on qualitative analysis were concern that the topic is too political, as well as calls to improve existing data “to understand what role we can play in injury prevention,” and that “surgeons should be involved in solving the problem,” Dr. Kuhls said. “There were also a lot of comments on responsible ownership.” She noted that more than 90% of respondents support 7 out of 15 proposed initiatives, 80%-90% support an additional 3 initiatives, and 70%-80% support an additional 4 proposed initiatives.
The invited discussant, Ernest E. Moore, MD, FACS, a surgeon in Denver, described the effort to develop firearm injury prevention policy as laudable. However, “this process carries a risk of merely supporting the bandwagons already in motion,” Dr. Moore said. “In that light I would like to focus on the conspicuous areas of disagreement, specifically civilian access to assault rifles. The fundamental issue is the magazine capacity of rifles – housing 30 or more bullets, enabling rapid shooting. Mass shootings, defined as greater than or equal to five victims, are currently an epidemic in our country. The volatile issues are eliminating assault rifles to reduce mass shootings [and] the interpretation of the Second Amendment to keep and bear arms. I do not believe a randomized prospective trial is necessary to establish the fact that mass shootings are only feasible because irresponsible individuals have access to these weapons. The urgency in this issue is heightened by the reality that mass shootings are increasingly inspired by terrorist activity, beyond individuals traditionally considered mentally ill.”
Dr. Kuhls described the current survey as “the initial step” in an effort to develop firearm injury prevention policy. “We are just about to receive results from a survey of the Board of Governors for the ACS,” she said. “We plan to develop short- and long-term plans to address this public health challenge that leverages survey consensus findings in four ACS pillars: advocacy, quality, systems, and education. We need to continue this conversation.” She expressed gratitude to the COT Executive Committee and liaison members from the ACS Board of Regents in addition to members of the COT Injury Prevention and Control Committee. She reported having no financial disclosures.
WAIKOLOA, HAWAII – Nearly 90% of American College of Surgeons Committee on Trauma members believe that the ACS should give the highest or a high priority to reducing firearm-related injuries, according to results from a national survey.
“In the United States, we value personal liberty and personal safety highly,” Deborah A. Kuhls, MD, FACS, said at the annual meeting of the American Association for the Surgery of Trauma. “However, that sometimes leads to a polarized view on firearms. Some view it as a freedom in personal safety. Others view it as a limitation of freedom and [as promotion of] violence.”
In an effort to evaluate ACS COT member attitudes about firearm ownership, freedom, responsibility, physician/patient freedom and policy, with the objective of using survey results to inform firearm injury prevention policy development, Dr. Kuhls and the COT Injury Prevention and Control Committee developed a 32-item anonymous survey that was sent to 254 COT members between December 2015 and February 2016. Results were extracted by ACS staff.
Of 254 COT members who received the survey, 237 completed the survey, for a response rate of 93%. Their mean age was 52 years, and 88% were male, 88% were married, 85% were white, and 58% had children in the home. More than one-quarter (29%) had military experience, 88% practiced acute care, trauma, general surgery, or pediatric surgery; 43% had firearms in the home, and 33% had personal experience with a family or friend injured or killed from firearm injury. A significantly higher proportion of respondents with military experience had firearms in the home, compared with those who had no military experience (56% vs. 37%, respectively; P less than .01). By Centers for Disease Control and Prevention demographic region, the percentage of members who have firearms in their home was lowest in the Northeast (14%), followed by the West (38%), the Midwest (48%), and the South (56%).
Dr. Kuhls also reported that 88% of respondents indicated that they think the ACS should give a high or the highest level of priority to firearm injury prevention. When asked about private ownership of firearms, about 53% thought that gun ownership is generally beneficial/an important personal liberty, while 30% believed that gun ownership is generally harmful and limits personal liberty. The remaining 17% had no opinion on the issue.
The majority of respondents (95%) said that health care professionals should be allowed to counsel patients (or parents of patients) about how to prevent gun-related injuries, while 96% felt that the CDC and other federal agencies should fund research on the epidemiology and prevention of gun-related injuries.
Survey respondents were then asked to rate their opinion on the ACS initiating efforts to advocate for or support legislation on 15 possible initiatives to prevent firearm violence, ranging from “improve mental health screening and treatment to reduce suicides and gun violence” to increase penalties when guns [are] provided to others illegally including dealers” to “require safety features, including child-proof locks and ‘smart gun’ technology,” and “identify and implement evidence-based injury prevention programs.”
The greatest consensus was reached in the advocacy area titled “improve mental health screening and treatment to reduce suicides and gun violence” (ranging from 89% to 93%), while the least consensus was in the advocacy area titled “require firearms owners to be 21 years of age or older” (ranging from 41% to 71%).
The most common themes that emerged on qualitative analysis were concern that the topic is too political, as well as calls to improve existing data “to understand what role we can play in injury prevention,” and that “surgeons should be involved in solving the problem,” Dr. Kuhls said. “There were also a lot of comments on responsible ownership.” She noted that more than 90% of respondents support 7 out of 15 proposed initiatives, 80%-90% support an additional 3 initiatives, and 70%-80% support an additional 4 proposed initiatives.
The invited discussant, Ernest E. Moore, MD, FACS, a surgeon in Denver, described the effort to develop firearm injury prevention policy as laudable. However, “this process carries a risk of merely supporting the bandwagons already in motion,” Dr. Moore said. “In that light I would like to focus on the conspicuous areas of disagreement, specifically civilian access to assault rifles. The fundamental issue is the magazine capacity of rifles – housing 30 or more bullets, enabling rapid shooting. Mass shootings, defined as greater than or equal to five victims, are currently an epidemic in our country. The volatile issues are eliminating assault rifles to reduce mass shootings [and] the interpretation of the Second Amendment to keep and bear arms. I do not believe a randomized prospective trial is necessary to establish the fact that mass shootings are only feasible because irresponsible individuals have access to these weapons. The urgency in this issue is heightened by the reality that mass shootings are increasingly inspired by terrorist activity, beyond individuals traditionally considered mentally ill.”
Dr. Kuhls described the current survey as “the initial step” in an effort to develop firearm injury prevention policy. “We are just about to receive results from a survey of the Board of Governors for the ACS,” she said. “We plan to develop short- and long-term plans to address this public health challenge that leverages survey consensus findings in four ACS pillars: advocacy, quality, systems, and education. We need to continue this conversation.” She expressed gratitude to the COT Executive Committee and liaison members from the ACS Board of Regents in addition to members of the COT Injury Prevention and Control Committee. She reported having no financial disclosures.
Key clinical point:
Major finding: A majority of respondents (88%) indicated that they think the ACS should give a high or the highest level of priority to firearm injury prevention.
Data source: Responses to 32-item anonymous survey that was completed by 237 members of the ACS COT between December 2015 and February 2016.
Disclosures: Dr. Kuhls reported having no financial disclosures.
Database review supports chemoradiation for high-risk sarcomas
BOSTON – Neoadjuvant chemotherapy and radiation appear to offer long-term benefits in patients with high-risk soft tissue sarcomas of the extremities.
The key word is “appear,” however, because the idea is drawn more from inference than from evidence, and not all sarcoma specialists are convinced that neoadjuvant chemotherapy and radiation add anything more than toxicity.
In studies presented at the annual meeting of the American Society of Radiation Oncology, including a retrospective case series and a national database review, investigators found evidence supporting the use of combined modality therapy with radiation and chemotherapy in patients with soft tissue sarcomas of the extremities.
“Large high-grade extremity soft-tissue sarcomas are at high risk of failure and death compared to our typical high-risk patients who present with one [risk] factor,” said Omar Mahmoud, MD, PhD, from the Rutgers Cancer Institute of New Jersey, New Brunswick.
He and his colleagues combed through the National Cancer Database to identify 3,840 otherwise healthy patients with grade 3 or 4 soft-tissue sarcomas (STS) of the extremities of various histologies larger than 8 cm, who underwent surgical resections during 2004-2013.
They looked at overall survival in patients who received no neoadjuvant or adjuvant therapy and those who received either neoadjuvant or adjuvant chemotherapy and/or radiation therapy. They used propensity score matching to adjust for imbalances of covariates across treatment subgroups.
They found that chemotherapy was associated with significantly better 5-year overall survival, at 57%, compared with 45% with no chemotherapy (P less than .001)
In multivariate analysis, age older than 50 years, positive tumor margins, larger tumors, and tumors located in the trunk or pelvis were associated with worse prognosis, whereas receipt of chemotherapy and radiotherapy were associated independently with better prognosis.
Out to 100 months (8.3 years) of follow-up, overall survival was significantly higher for patients who received combined modality adjunctive therapies, compared with either single modality therapy (chemotherapy or radiotherapy alone) or no therapy (P less than .001).
Using propensity score matching to compare patients who received combined vs. single-modality therapy, the investigators found that combined therapies were associated with significantly better overall survival, with a hazard ratio of 0.72 (95% confidence interval, 0.62-0.84).
There was no difference in survival according to the timing of therapy, whether preoperative, postoperative, or concurrent), however.
Finally, looking at survival among all subgroups, they saw that combined therapies remained significantly better than single-modality therapies (P less than .001).
Drop the ‘D’ in MAID?
In a separate study, Neilayan Sen, MD, and colleagues from Rush University Medical Center in Chicago reported that a modified protocol involving neoadjuvant chemotherapy interdigitated with radiation followed by surgery and adjuvant chemotherapy was associated with good disease control and survival and lower toxicity in patients with large STS of the extremities or abdominal wall.
The original protocol, dubbed MAID (mesna, doxorubicin, ifosfamide, dacarbazine), was shown in the RTOG 9514 trial to be associated with higher rates of disease-free, distant disease-free, and overall survival than older regimens, but at the price of high short-term toxicities. Among 64 evaluable patients, 97% had grade 3 or higher toxicities, including three deaths, two of which were from myelodysplasia.
To see whether they could match the efficacy of MAID while reducing toxicity, the Rush team modified the MAID protocol by dropping the dacarbazine. For the radiation component, they used either 3-D conformal radiation therapy or intensity-modulated radiation therapy, set the maximum dose penetration (Dmax) at 112% or less, and used reduced volumes while maintaining the dose and fractions (44 Gy delivered in 22 fractions, 11 each between chemotherapy cycles 1-2 and 2-3). Patients then underwent surgery, followed by three additional cycles of chemotherapy.
In a retrospective analysis of 26 patients treated with the modified protocol, there were no toxicity-related amputations, and no amputations were required for tumor management. Two patients had in-field fractures.
At a median follow-up of 39 months, 25 of the 26 patients were still alive and there were no cases of treatment-related malignancies or myelodysplasia.
The 3-year actuarial results with MAI also compared favorably with those of RTOG 9514, with locoregional recurrence-free survival rates of 87.2% with the modified protocol vs. 82.4% for the original MAID protocol, distant metastasis-free survival of 67.9% vs. 64.%, respectively, disease-free survival of 67.9% vs. 56.6%, and overall survival of 93.3% vs. 75.1%.
“The omission of dacarbazine does not compromise any disease-control endpoints. With the integration of 3-D techniques as well as intensity modulation and smaller fields than were used in [RTOG] 9514, there’s a significantly reduced grade 4 and 5 toxicity rate. We think that the integration of image guidance with reduced target volume parameters further,” Dr. Sen said.
Better Agents Needed
Elizabeth H Baldini, MD, MPH, from the Dana-Farber/Brigham & Women’s Cancer Center, Boston, the invited discussant, agreed that there is a need for better systemic therapy to reduce the risk of distant recurrence in patients with high-risk localized sarcomas.
“But the bottom line is that the benefit of chemotherapy with the agents we have today is uncertain,” she said.
Assessment of systemic chemotherapy in sarcoma is hampered by the rarity of the tumors, with more than 50 different histologic subtypes, and wide tumor heterogeneity, and although the studies reported here appear to show benefit for chemotherapy, they appear to overlap with those for surgery and radiation alone, she said.
Session comoderator Yen-Lin Evelyn Chen, MD, a radiation oncologist at Massachusetts General Hospital Cancer Center, Boston, said in an interview that studies presented during the session show that, “chemotherapy in experienced hands can be delivered safely.”
Dr. Chen added, however, that the local control rates reported by Dr. Sen and colleagues were a little lower than she would have expected in the modern era, suggesting that either the radiation modification or elimination of dacarbazine may have played a role.
BOSTON – Neoadjuvant chemotherapy and radiation appear to offer long-term benefits in patients with high-risk soft tissue sarcomas of the extremities.
The key word is “appear,” however, because the idea is drawn more from inference than from evidence, and not all sarcoma specialists are convinced that neoadjuvant chemotherapy and radiation add anything more than toxicity.
In studies presented at the annual meeting of the American Society of Radiation Oncology, including a retrospective case series and a national database review, investigators found evidence supporting the use of combined modality therapy with radiation and chemotherapy in patients with soft tissue sarcomas of the extremities.
“Large high-grade extremity soft-tissue sarcomas are at high risk of failure and death compared to our typical high-risk patients who present with one [risk] factor,” said Omar Mahmoud, MD, PhD, from the Rutgers Cancer Institute of New Jersey, New Brunswick.
He and his colleagues combed through the National Cancer Database to identify 3,840 otherwise healthy patients with grade 3 or 4 soft-tissue sarcomas (STS) of the extremities of various histologies larger than 8 cm, who underwent surgical resections during 2004-2013.
They looked at overall survival in patients who received no neoadjuvant or adjuvant therapy and those who received either neoadjuvant or adjuvant chemotherapy and/or radiation therapy. They used propensity score matching to adjust for imbalances of covariates across treatment subgroups.
They found that chemotherapy was associated with significantly better 5-year overall survival, at 57%, compared with 45% with no chemotherapy (P less than .001)
In multivariate analysis, age older than 50 years, positive tumor margins, larger tumors, and tumors located in the trunk or pelvis were associated with worse prognosis, whereas receipt of chemotherapy and radiotherapy were associated independently with better prognosis.
Out to 100 months (8.3 years) of follow-up, overall survival was significantly higher for patients who received combined modality adjunctive therapies, compared with either single modality therapy (chemotherapy or radiotherapy alone) or no therapy (P less than .001).
Using propensity score matching to compare patients who received combined vs. single-modality therapy, the investigators found that combined therapies were associated with significantly better overall survival, with a hazard ratio of 0.72 (95% confidence interval, 0.62-0.84).
There was no difference in survival according to the timing of therapy, whether preoperative, postoperative, or concurrent), however.
Finally, looking at survival among all subgroups, they saw that combined therapies remained significantly better than single-modality therapies (P less than .001).
Drop the ‘D’ in MAID?
In a separate study, Neilayan Sen, MD, and colleagues from Rush University Medical Center in Chicago reported that a modified protocol involving neoadjuvant chemotherapy interdigitated with radiation followed by surgery and adjuvant chemotherapy was associated with good disease control and survival and lower toxicity in patients with large STS of the extremities or abdominal wall.
The original protocol, dubbed MAID (mesna, doxorubicin, ifosfamide, dacarbazine), was shown in the RTOG 9514 trial to be associated with higher rates of disease-free, distant disease-free, and overall survival than older regimens, but at the price of high short-term toxicities. Among 64 evaluable patients, 97% had grade 3 or higher toxicities, including three deaths, two of which were from myelodysplasia.
To see whether they could match the efficacy of MAID while reducing toxicity, the Rush team modified the MAID protocol by dropping the dacarbazine. For the radiation component, they used either 3-D conformal radiation therapy or intensity-modulated radiation therapy, set the maximum dose penetration (Dmax) at 112% or less, and used reduced volumes while maintaining the dose and fractions (44 Gy delivered in 22 fractions, 11 each between chemotherapy cycles 1-2 and 2-3). Patients then underwent surgery, followed by three additional cycles of chemotherapy.
In a retrospective analysis of 26 patients treated with the modified protocol, there were no toxicity-related amputations, and no amputations were required for tumor management. Two patients had in-field fractures.
At a median follow-up of 39 months, 25 of the 26 patients were still alive and there were no cases of treatment-related malignancies or myelodysplasia.
The 3-year actuarial results with MAI also compared favorably with those of RTOG 9514, with locoregional recurrence-free survival rates of 87.2% with the modified protocol vs. 82.4% for the original MAID protocol, distant metastasis-free survival of 67.9% vs. 64.%, respectively, disease-free survival of 67.9% vs. 56.6%, and overall survival of 93.3% vs. 75.1%.
“The omission of dacarbazine does not compromise any disease-control endpoints. With the integration of 3-D techniques as well as intensity modulation and smaller fields than were used in [RTOG] 9514, there’s a significantly reduced grade 4 and 5 toxicity rate. We think that the integration of image guidance with reduced target volume parameters further,” Dr. Sen said.
Better Agents Needed
Elizabeth H Baldini, MD, MPH, from the Dana-Farber/Brigham & Women’s Cancer Center, Boston, the invited discussant, agreed that there is a need for better systemic therapy to reduce the risk of distant recurrence in patients with high-risk localized sarcomas.
“But the bottom line is that the benefit of chemotherapy with the agents we have today is uncertain,” she said.
Assessment of systemic chemotherapy in sarcoma is hampered by the rarity of the tumors, with more than 50 different histologic subtypes, and wide tumor heterogeneity, and although the studies reported here appear to show benefit for chemotherapy, they appear to overlap with those for surgery and radiation alone, she said.
Session comoderator Yen-Lin Evelyn Chen, MD, a radiation oncologist at Massachusetts General Hospital Cancer Center, Boston, said in an interview that studies presented during the session show that, “chemotherapy in experienced hands can be delivered safely.”
Dr. Chen added, however, that the local control rates reported by Dr. Sen and colleagues were a little lower than she would have expected in the modern era, suggesting that either the radiation modification or elimination of dacarbazine may have played a role.
BOSTON – Neoadjuvant chemotherapy and radiation appear to offer long-term benefits in patients with high-risk soft tissue sarcomas of the extremities.
The key word is “appear,” however, because the idea is drawn more from inference than from evidence, and not all sarcoma specialists are convinced that neoadjuvant chemotherapy and radiation add anything more than toxicity.
In studies presented at the annual meeting of the American Society of Radiation Oncology, including a retrospective case series and a national database review, investigators found evidence supporting the use of combined modality therapy with radiation and chemotherapy in patients with soft tissue sarcomas of the extremities.
“Large high-grade extremity soft-tissue sarcomas are at high risk of failure and death compared to our typical high-risk patients who present with one [risk] factor,” said Omar Mahmoud, MD, PhD, from the Rutgers Cancer Institute of New Jersey, New Brunswick.
He and his colleagues combed through the National Cancer Database to identify 3,840 otherwise healthy patients with grade 3 or 4 soft-tissue sarcomas (STS) of the extremities of various histologies larger than 8 cm, who underwent surgical resections during 2004-2013.
They looked at overall survival in patients who received no neoadjuvant or adjuvant therapy and those who received either neoadjuvant or adjuvant chemotherapy and/or radiation therapy. They used propensity score matching to adjust for imbalances of covariates across treatment subgroups.
They found that chemotherapy was associated with significantly better 5-year overall survival, at 57%, compared with 45% with no chemotherapy (P less than .001)
In multivariate analysis, age older than 50 years, positive tumor margins, larger tumors, and tumors located in the trunk or pelvis were associated with worse prognosis, whereas receipt of chemotherapy and radiotherapy were associated independently with better prognosis.
Out to 100 months (8.3 years) of follow-up, overall survival was significantly higher for patients who received combined modality adjunctive therapies, compared with either single modality therapy (chemotherapy or radiotherapy alone) or no therapy (P less than .001).
Using propensity score matching to compare patients who received combined vs. single-modality therapy, the investigators found that combined therapies were associated with significantly better overall survival, with a hazard ratio of 0.72 (95% confidence interval, 0.62-0.84).
There was no difference in survival according to the timing of therapy, whether preoperative, postoperative, or concurrent), however.
Finally, looking at survival among all subgroups, they saw that combined therapies remained significantly better than single-modality therapies (P less than .001).
Drop the ‘D’ in MAID?
In a separate study, Neilayan Sen, MD, and colleagues from Rush University Medical Center in Chicago reported that a modified protocol involving neoadjuvant chemotherapy interdigitated with radiation followed by surgery and adjuvant chemotherapy was associated with good disease control and survival and lower toxicity in patients with large STS of the extremities or abdominal wall.
The original protocol, dubbed MAID (mesna, doxorubicin, ifosfamide, dacarbazine), was shown in the RTOG 9514 trial to be associated with higher rates of disease-free, distant disease-free, and overall survival than older regimens, but at the price of high short-term toxicities. Among 64 evaluable patients, 97% had grade 3 or higher toxicities, including three deaths, two of which were from myelodysplasia.
To see whether they could match the efficacy of MAID while reducing toxicity, the Rush team modified the MAID protocol by dropping the dacarbazine. For the radiation component, they used either 3-D conformal radiation therapy or intensity-modulated radiation therapy, set the maximum dose penetration (Dmax) at 112% or less, and used reduced volumes while maintaining the dose and fractions (44 Gy delivered in 22 fractions, 11 each between chemotherapy cycles 1-2 and 2-3). Patients then underwent surgery, followed by three additional cycles of chemotherapy.
In a retrospective analysis of 26 patients treated with the modified protocol, there were no toxicity-related amputations, and no amputations were required for tumor management. Two patients had in-field fractures.
At a median follow-up of 39 months, 25 of the 26 patients were still alive and there were no cases of treatment-related malignancies or myelodysplasia.
The 3-year actuarial results with MAI also compared favorably with those of RTOG 9514, with locoregional recurrence-free survival rates of 87.2% with the modified protocol vs. 82.4% for the original MAID protocol, distant metastasis-free survival of 67.9% vs. 64.%, respectively, disease-free survival of 67.9% vs. 56.6%, and overall survival of 93.3% vs. 75.1%.
“The omission of dacarbazine does not compromise any disease-control endpoints. With the integration of 3-D techniques as well as intensity modulation and smaller fields than were used in [RTOG] 9514, there’s a significantly reduced grade 4 and 5 toxicity rate. We think that the integration of image guidance with reduced target volume parameters further,” Dr. Sen said.
Better Agents Needed
Elizabeth H Baldini, MD, MPH, from the Dana-Farber/Brigham & Women’s Cancer Center, Boston, the invited discussant, agreed that there is a need for better systemic therapy to reduce the risk of distant recurrence in patients with high-risk localized sarcomas.
“But the bottom line is that the benefit of chemotherapy with the agents we have today is uncertain,” she said.
Assessment of systemic chemotherapy in sarcoma is hampered by the rarity of the tumors, with more than 50 different histologic subtypes, and wide tumor heterogeneity, and although the studies reported here appear to show benefit for chemotherapy, they appear to overlap with those for surgery and radiation alone, she said.
Session comoderator Yen-Lin Evelyn Chen, MD, a radiation oncologist at Massachusetts General Hospital Cancer Center, Boston, said in an interview that studies presented during the session show that, “chemotherapy in experienced hands can be delivered safely.”
Dr. Chen added, however, that the local control rates reported by Dr. Sen and colleagues were a little lower than she would have expected in the modern era, suggesting that either the radiation modification or elimination of dacarbazine may have played a role.
Key clinical point: Sarcoma specialists do not agree on whether neoadjuvant or adjuvant chemotherapy adds benefit in patients with high-risk soft-tissue sarcomas.
Major finding: In a cancer database, chemotherapy was associated with 57% 5-year overall survival, compared with 45% with no chemotherapy (P less than .001)
Data source: A National Cancer Database review of 3,840 patients with grade 3 or 4 soft-tissue sarcomas and a retrospective case series of 26 patients with large STS of the extremities or abdominal wall.
Disclosures: The studies were internally supported. The authors, Dr. Baldini and Dr. Chen, reported no relevant disclosures. Dr. Chen is the reporter’s personal radiation oncologist.