User login
New guidelines address primary cutaneous T-cell lymphoproliferative disorders
HOLLYWOOD, FLA. – The treatment of patients with lymphomatoid papulosis depends on the presentation, according to new National Comprehensive Cancer Network guidelines for managing primary cutaneous CD30+ T-cell lymphoproliferative disorders.
No treatment is needed in patients with lymphomatoid papulosis (LyP) who present without symptoms because spontaneous remission is extremely common in this disease, and these patients typically won’t have problems with progressive disease, Dr. Andrew D. Zelenetz said at the annual conference of the National Comprehensive Cancer Network.
For those who are symptomatic, topical or systemic treatments are useful in some cases.
Topical steroids "are effective, but not great," commented Dr. Zelenetz, vice chairman of medical informatics at Memorial Sloan Kettering Cancer Center, New York; professor of medicine at Cornell University, New York; and chair of the NCCN Non-Hodgkin's Lymphomas Guidelines panel.
Reported response rates are in the 50%-60% range, he said.
Bexarotene is another treatment option, although experience with this drug is quite limited. The largest series included only 11 patients. Unpublished data from that series at Memorial Sloan Kettering Cancer Center show a response rate of 45% at a maximum oral dose of 600 mg daily, Dr. Zelenetz said.
However, where this is a response, it is "dramatic and quite obvious," he noted, adding that treatment duration needs to be adequate before a patient is considered a nonresponder; the median duration of treatment in the 11-patient series was 35.5 weeks.
In a series of 57 patients from Memorial Sloan Kettering Cancer Center (including the 11 treated systemically with bexarotene), 16 received no therapy; 19 received topical treatment with steroids (13 patients), bexarotene (2 patients), UVB (2 patients), cryotherapy (1 patient), or nitrogen mustard (1 patient); and 5 received systemic treatment with methotrexate.
At follow-up, 14% of patients had no evidence of disease, and, with the exception of one who died of another cause, the remaining patients were alive with disease, Dr. Zelenetz said.
LyP is a rare CD30+ cutaneous lymphoproliferative disorder characterized by self-healing cropped or generalized eruptions of papules that come and go on the trunk or proximal extremities. In rare cases they present as solitary lesions.
"Even though many patients actually have intermittent recurrent disease ... the death rate from LyP is zero. So this is a very manageable disease; don’t overtreat these tumors," he said.
At the other end of the spectrum of CD30+ lymphoproliferative disorders addressed in the new NCCN guidelines is anaplastic large cell lymphoma (ALCL).
Primary cutaneous ALCL is characterized by skin-only presentation that is often localized but which can be disseminated in some cases. Lesions also tend to be larger and "more piled up" than those seen with LyP.
"You can get clustering in a specific area, but we don’t tend to have these big crops of lesions that we see with LyP," Dr. Zelenetz said.
The pathology is also different, with diffuse infiltration of the subcutaneous tissue. The cells are large and anaplastic, and there is intense expression of CD30.
The course of disease is usually indolent, with progression to extracutaneous sites in about 10%-15% of cases.
Nodules or tumors in cases of ALCL are less likely than LyP lesions to regress spontaneously, Dr. Zelenetz said.
This disease must be distinguished from a skin presentation of systemic ALCL, he noted.
"So what’s the big difference? In anaplastic large cell lymphoma that’s systemic, you will have multiple nodules all over and happen to have skin disease. With primary cutaneous ALCL, you have skin only or skin and some regional lymph nodes but nothing beyond that," he said, adding that these primary cutaneous tumors do extremely well nevertheless, with cumulative survival rates above 90%.
Those with systemic ALCL, however, have much lower cumulative survival, in the 25% range.
As with LyP, treatment for primary cutaneous ALCL is based on presentation.
For solitary or grouped lesions, the preferred treatment is surgical excision if needed for diagnosis or radiation if the diagnosis is already established.
Methotrexate is the preferred treatment for multifocal lesions.
The subtype that includes regional lymph nodes is typically treated with very mild chemotherapy including methotrexate or pralatrexate. Radiation can be used for locoregional disease, Dr. Zelenetz said.
An exception to the rule that patients with primary cutaneous ALCL do well is in cases of extensive limb disease. Patients with involvement of a single limb – usually lower extremity, but not always – have poor survival, and their disease is refractory to chemotherapy and radiation. It is unclear why there is a distinction in this presentation, but it is important to be aware of it, he said.
Dr. Zelenetz is a scientific adviser for Cancer Genetics Inc. and Gilead and has received consulting fees, honoraria, and/or grant or other research support from Celgene Corp., Cephalon Inc., Genentech Inc., GlaxoSmithKline, Roche Laboratories Inc., sanofi-aventis U.S., and Seattle Genetics Inc.
HOLLYWOOD, FLA. – The treatment of patients with lymphomatoid papulosis depends on the presentation, according to new National Comprehensive Cancer Network guidelines for managing primary cutaneous CD30+ T-cell lymphoproliferative disorders.
No treatment is needed in patients with lymphomatoid papulosis (LyP) who present without symptoms because spontaneous remission is extremely common in this disease, and these patients typically won’t have problems with progressive disease, Dr. Andrew D. Zelenetz said at the annual conference of the National Comprehensive Cancer Network.
For those who are symptomatic, topical or systemic treatments are useful in some cases.
Topical steroids "are effective, but not great," commented Dr. Zelenetz, vice chairman of medical informatics at Memorial Sloan Kettering Cancer Center, New York; professor of medicine at Cornell University, New York; and chair of the NCCN Non-Hodgkin's Lymphomas Guidelines panel.
Reported response rates are in the 50%-60% range, he said.
Bexarotene is another treatment option, although experience with this drug is quite limited. The largest series included only 11 patients. Unpublished data from that series at Memorial Sloan Kettering Cancer Center show a response rate of 45% at a maximum oral dose of 600 mg daily, Dr. Zelenetz said.
However, where this is a response, it is "dramatic and quite obvious," he noted, adding that treatment duration needs to be adequate before a patient is considered a nonresponder; the median duration of treatment in the 11-patient series was 35.5 weeks.
In a series of 57 patients from Memorial Sloan Kettering Cancer Center (including the 11 treated systemically with bexarotene), 16 received no therapy; 19 received topical treatment with steroids (13 patients), bexarotene (2 patients), UVB (2 patients), cryotherapy (1 patient), or nitrogen mustard (1 patient); and 5 received systemic treatment with methotrexate.
At follow-up, 14% of patients had no evidence of disease, and, with the exception of one who died of another cause, the remaining patients were alive with disease, Dr. Zelenetz said.
LyP is a rare CD30+ cutaneous lymphoproliferative disorder characterized by self-healing cropped or generalized eruptions of papules that come and go on the trunk or proximal extremities. In rare cases they present as solitary lesions.
"Even though many patients actually have intermittent recurrent disease ... the death rate from LyP is zero. So this is a very manageable disease; don’t overtreat these tumors," he said.
At the other end of the spectrum of CD30+ lymphoproliferative disorders addressed in the new NCCN guidelines is anaplastic large cell lymphoma (ALCL).
Primary cutaneous ALCL is characterized by skin-only presentation that is often localized but which can be disseminated in some cases. Lesions also tend to be larger and "more piled up" than those seen with LyP.
"You can get clustering in a specific area, but we don’t tend to have these big crops of lesions that we see with LyP," Dr. Zelenetz said.
The pathology is also different, with diffuse infiltration of the subcutaneous tissue. The cells are large and anaplastic, and there is intense expression of CD30.
The course of disease is usually indolent, with progression to extracutaneous sites in about 10%-15% of cases.
Nodules or tumors in cases of ALCL are less likely than LyP lesions to regress spontaneously, Dr. Zelenetz said.
This disease must be distinguished from a skin presentation of systemic ALCL, he noted.
"So what’s the big difference? In anaplastic large cell lymphoma that’s systemic, you will have multiple nodules all over and happen to have skin disease. With primary cutaneous ALCL, you have skin only or skin and some regional lymph nodes but nothing beyond that," he said, adding that these primary cutaneous tumors do extremely well nevertheless, with cumulative survival rates above 90%.
Those with systemic ALCL, however, have much lower cumulative survival, in the 25% range.
As with LyP, treatment for primary cutaneous ALCL is based on presentation.
For solitary or grouped lesions, the preferred treatment is surgical excision if needed for diagnosis or radiation if the diagnosis is already established.
Methotrexate is the preferred treatment for multifocal lesions.
The subtype that includes regional lymph nodes is typically treated with very mild chemotherapy including methotrexate or pralatrexate. Radiation can be used for locoregional disease, Dr. Zelenetz said.
An exception to the rule that patients with primary cutaneous ALCL do well is in cases of extensive limb disease. Patients with involvement of a single limb – usually lower extremity, but not always – have poor survival, and their disease is refractory to chemotherapy and radiation. It is unclear why there is a distinction in this presentation, but it is important to be aware of it, he said.
Dr. Zelenetz is a scientific adviser for Cancer Genetics Inc. and Gilead and has received consulting fees, honoraria, and/or grant or other research support from Celgene Corp., Cephalon Inc., Genentech Inc., GlaxoSmithKline, Roche Laboratories Inc., sanofi-aventis U.S., and Seattle Genetics Inc.
HOLLYWOOD, FLA. – The treatment of patients with lymphomatoid papulosis depends on the presentation, according to new National Comprehensive Cancer Network guidelines for managing primary cutaneous CD30+ T-cell lymphoproliferative disorders.
No treatment is needed in patients with lymphomatoid papulosis (LyP) who present without symptoms because spontaneous remission is extremely common in this disease, and these patients typically won’t have problems with progressive disease, Dr. Andrew D. Zelenetz said at the annual conference of the National Comprehensive Cancer Network.
For those who are symptomatic, topical or systemic treatments are useful in some cases.
Topical steroids "are effective, but not great," commented Dr. Zelenetz, vice chairman of medical informatics at Memorial Sloan Kettering Cancer Center, New York; professor of medicine at Cornell University, New York; and chair of the NCCN Non-Hodgkin's Lymphomas Guidelines panel.
Reported response rates are in the 50%-60% range, he said.
Bexarotene is another treatment option, although experience with this drug is quite limited. The largest series included only 11 patients. Unpublished data from that series at Memorial Sloan Kettering Cancer Center show a response rate of 45% at a maximum oral dose of 600 mg daily, Dr. Zelenetz said.
However, where this is a response, it is "dramatic and quite obvious," he noted, adding that treatment duration needs to be adequate before a patient is considered a nonresponder; the median duration of treatment in the 11-patient series was 35.5 weeks.
In a series of 57 patients from Memorial Sloan Kettering Cancer Center (including the 11 treated systemically with bexarotene), 16 received no therapy; 19 received topical treatment with steroids (13 patients), bexarotene (2 patients), UVB (2 patients), cryotherapy (1 patient), or nitrogen mustard (1 patient); and 5 received systemic treatment with methotrexate.
At follow-up, 14% of patients had no evidence of disease, and, with the exception of one who died of another cause, the remaining patients were alive with disease, Dr. Zelenetz said.
LyP is a rare CD30+ cutaneous lymphoproliferative disorder characterized by self-healing cropped or generalized eruptions of papules that come and go on the trunk or proximal extremities. In rare cases they present as solitary lesions.
"Even though many patients actually have intermittent recurrent disease ... the death rate from LyP is zero. So this is a very manageable disease; don’t overtreat these tumors," he said.
At the other end of the spectrum of CD30+ lymphoproliferative disorders addressed in the new NCCN guidelines is anaplastic large cell lymphoma (ALCL).
Primary cutaneous ALCL is characterized by skin-only presentation that is often localized but which can be disseminated in some cases. Lesions also tend to be larger and "more piled up" than those seen with LyP.
"You can get clustering in a specific area, but we don’t tend to have these big crops of lesions that we see with LyP," Dr. Zelenetz said.
The pathology is also different, with diffuse infiltration of the subcutaneous tissue. The cells are large and anaplastic, and there is intense expression of CD30.
The course of disease is usually indolent, with progression to extracutaneous sites in about 10%-15% of cases.
Nodules or tumors in cases of ALCL are less likely than LyP lesions to regress spontaneously, Dr. Zelenetz said.
This disease must be distinguished from a skin presentation of systemic ALCL, he noted.
"So what’s the big difference? In anaplastic large cell lymphoma that’s systemic, you will have multiple nodules all over and happen to have skin disease. With primary cutaneous ALCL, you have skin only or skin and some regional lymph nodes but nothing beyond that," he said, adding that these primary cutaneous tumors do extremely well nevertheless, with cumulative survival rates above 90%.
Those with systemic ALCL, however, have much lower cumulative survival, in the 25% range.
As with LyP, treatment for primary cutaneous ALCL is based on presentation.
For solitary or grouped lesions, the preferred treatment is surgical excision if needed for diagnosis or radiation if the diagnosis is already established.
Methotrexate is the preferred treatment for multifocal lesions.
The subtype that includes regional lymph nodes is typically treated with very mild chemotherapy including methotrexate or pralatrexate. Radiation can be used for locoregional disease, Dr. Zelenetz said.
An exception to the rule that patients with primary cutaneous ALCL do well is in cases of extensive limb disease. Patients with involvement of a single limb – usually lower extremity, but not always – have poor survival, and their disease is refractory to chemotherapy and radiation. It is unclear why there is a distinction in this presentation, but it is important to be aware of it, he said.
Dr. Zelenetz is a scientific adviser for Cancer Genetics Inc. and Gilead and has received consulting fees, honoraria, and/or grant or other research support from Celgene Corp., Cephalon Inc., Genentech Inc., GlaxoSmithKline, Roche Laboratories Inc., sanofi-aventis U.S., and Seattle Genetics Inc.
AT THE NCCN ANNUAL CONFERENCE
Commentary: Performing clinical research as a CT trainee
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.

So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
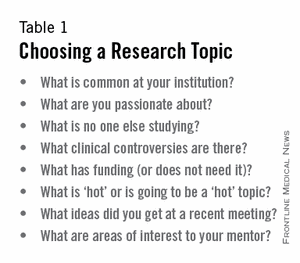
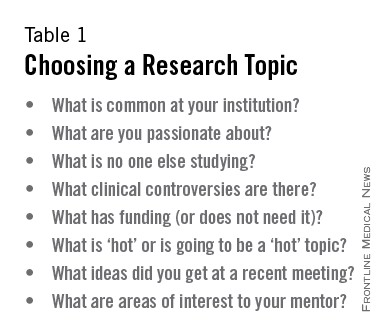
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
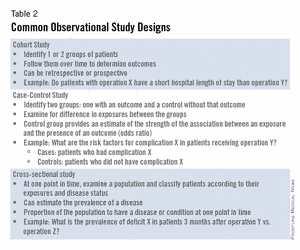
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
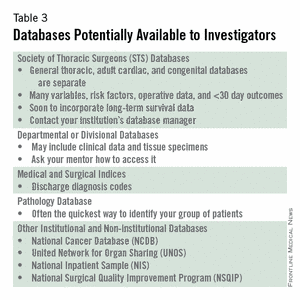
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
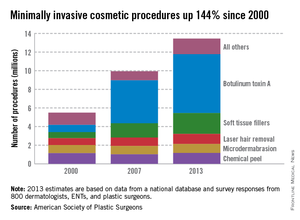
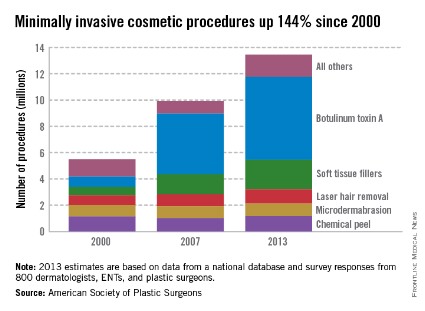
Botulinum toxin A tops list of nonsurgical cosmetic procedures in 2013
Injection of botulinum toxin type A continues to be the most popular form of minimally invasive cosmetic surgery, with a total of more than 6.3 million procedures performed in 2013, the American Society of Plastic Surgeons reported.
Overall, botulinum toxins such as Botox and Dysport accounted for 47% of the market for minimally invasive procedures, which totaled 13.4 million procedures in 2013, according to the ASPS.
The second most popular surgery was injection of soft tissue fillers, with 2.2 million procedures performed, followed by chemical peels (1.2 million procedures), laser hair removal (1.1 million), and microdermabrasion (970,000), the ASPS said.
The total number of minimally invasive procedures increased by 3% from 2012, as did the number of botulinum injections. The largest increase for a single type of procedure was seen for the soft tissue fillers, with hyaluronic acid injections up 18% from 2012 to 2013, the ASPS noted.
The estimates for 2013 are based on data from a national database and survey responses from 800 dermatologists, ENTs, and plastic surgeons.
Injection of botulinum toxin type A continues to be the most popular form of minimally invasive cosmetic surgery, with a total of more than 6.3 million procedures performed in 2013, the American Society of Plastic Surgeons reported.
Overall, botulinum toxins such as Botox and Dysport accounted for 47% of the market for minimally invasive procedures, which totaled 13.4 million procedures in 2013, according to the ASPS.
The second most popular surgery was injection of soft tissue fillers, with 2.2 million procedures performed, followed by chemical peels (1.2 million procedures), laser hair removal (1.1 million), and microdermabrasion (970,000), the ASPS said.
The total number of minimally invasive procedures increased by 3% from 2012, as did the number of botulinum injections. The largest increase for a single type of procedure was seen for the soft tissue fillers, with hyaluronic acid injections up 18% from 2012 to 2013, the ASPS noted.
The estimates for 2013 are based on data from a national database and survey responses from 800 dermatologists, ENTs, and plastic surgeons.
Injection of botulinum toxin type A continues to be the most popular form of minimally invasive cosmetic surgery, with a total of more than 6.3 million procedures performed in 2013, the American Society of Plastic Surgeons reported.
Overall, botulinum toxins such as Botox and Dysport accounted for 47% of the market for minimally invasive procedures, which totaled 13.4 million procedures in 2013, according to the ASPS.
The second most popular surgery was injection of soft tissue fillers, with 2.2 million procedures performed, followed by chemical peels (1.2 million procedures), laser hair removal (1.1 million), and microdermabrasion (970,000), the ASPS said.
The total number of minimally invasive procedures increased by 3% from 2012, as did the number of botulinum injections. The largest increase for a single type of procedure was seen for the soft tissue fillers, with hyaluronic acid injections up 18% from 2012 to 2013, the ASPS noted.
The estimates for 2013 are based on data from a national database and survey responses from 800 dermatologists, ENTs, and plastic surgeons.
They love me, they love me not ...
It was the worst of days. It was the best of days.
When I opened the mail one day last week, I found a letter from someone I’ll call Thelma. It read, in part:
"Last Monday you were kind enough to look at my rash, which you thought was just eczema. You gave me cream and asked me to e-mail you Thursday about my condition. When I did and said I was still itchy, you said I should stick with the same and that I could come back Monday, but I couldn’t wait because I itched so bad I couldn’t take it anymore. I saw another doctor Friday who said the patch was host to something called pityriasis rosea. He said the rash was so textbook it should have been picked up immediately. I had to be put on an oral steroid right away.
"I am so upset that I’m sending you back your bill [for a $15 co-pay] because I had to go to another doctor who could really help me."
I thought of a few choice words for my esteemed Friday colleague, but kept them to myself. A single scaly patch is a textbook case of pityriasis rosea? Oral steroids for pityriasis? Really?
As far as this patient is concerned, I must be a bum. Thirty-five years on the job, and I haven’t mastered the textbook yet.
Sunk in gloom, I opened an e-mail sent to my website by a patient I’ll call Louise:
"I suffer from psoriasis and have been to countless dermatologists since I was 8 years old. I recently had a terrible outbreak and was really hesitant to even go to a dermatologist because I’ve never been satisfied with any of them. Your associate is wonderful! I can’t say enough about her. She is warm, thorough, and really takes the time to sit with you and listen. You can tell she truly cares about her patients and loves her job."
I looked at the patient’s chart. What was the wonderful and satisfying treatment that my associate had prescribed to deal with this patient’s lifelong, recalcitrant psoriasis?
Betamethasone dipropionate cream 0.05%. Wow.
I e-mailed my associate at once and we shared a gratified chuckle. Guess no one ever thought of treating Louise’s psoriasis with a topical steroid before. We must be geniuses, right out there on the cutting edge.
So which are we, dear colleagues – geniuses or bums?
We’re neither, of course, which doesn’t stop our patients from forming firm opinions one way or the other. Which they can share by angry letter, fulsome e-mail, or, of course, any on-line reviews they can slip past the mysterious algorithms of the Yelps and Angie’s Lists of the world.
When I get messages like Thelma’s and Louise’s, I show them to my students and make three suggestions:
• Don’t try to look smart at someone else’s expense. Next time around a patient will be in somebody else’s office calling you a fool.
• Don’t respond to snippy patients’ complaints by contacting the complainer and trying to justify yourself. Learn something if you can, and move on.
• Be grateful for praise. Just don’t take it too seriously.
In the meantime, the insurers and assorted bureaucrats who run our lives these days are busy defining good care and claiming to measure it so they can reward quality and punish inefficiency. I’m sure they think they’re doing a fine job, although I remain deeply skeptical that what they choose to measure has much relevance to what actually goes on in offices like ours.
I could, of course, try to tell them why I think so. (I have tried, in fact.) Getting through to people with a completely different way of looking at things than yours is not very rewarding, even when large sums of money are not involved. I would have as good a chance of winning them over as I would of convincing Thelma that a scaly patch is not textbook pityriasis that needs prednisone and Louise that betamethasone cream is not the breakthrough that will change her life.
So: Not the best of times. Not the worst of times. Just another day at the office.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since 1997.
It was the worst of days. It was the best of days.
When I opened the mail one day last week, I found a letter from someone I’ll call Thelma. It read, in part:
"Last Monday you were kind enough to look at my rash, which you thought was just eczema. You gave me cream and asked me to e-mail you Thursday about my condition. When I did and said I was still itchy, you said I should stick with the same and that I could come back Monday, but I couldn’t wait because I itched so bad I couldn’t take it anymore. I saw another doctor Friday who said the patch was host to something called pityriasis rosea. He said the rash was so textbook it should have been picked up immediately. I had to be put on an oral steroid right away.
"I am so upset that I’m sending you back your bill [for a $15 co-pay] because I had to go to another doctor who could really help me."
I thought of a few choice words for my esteemed Friday colleague, but kept them to myself. A single scaly patch is a textbook case of pityriasis rosea? Oral steroids for pityriasis? Really?
As far as this patient is concerned, I must be a bum. Thirty-five years on the job, and I haven’t mastered the textbook yet.
Sunk in gloom, I opened an e-mail sent to my website by a patient I’ll call Louise:
"I suffer from psoriasis and have been to countless dermatologists since I was 8 years old. I recently had a terrible outbreak and was really hesitant to even go to a dermatologist because I’ve never been satisfied with any of them. Your associate is wonderful! I can’t say enough about her. She is warm, thorough, and really takes the time to sit with you and listen. You can tell she truly cares about her patients and loves her job."
I looked at the patient’s chart. What was the wonderful and satisfying treatment that my associate had prescribed to deal with this patient’s lifelong, recalcitrant psoriasis?
Betamethasone dipropionate cream 0.05%. Wow.
I e-mailed my associate at once and we shared a gratified chuckle. Guess no one ever thought of treating Louise’s psoriasis with a topical steroid before. We must be geniuses, right out there on the cutting edge.
So which are we, dear colleagues – geniuses or bums?
We’re neither, of course, which doesn’t stop our patients from forming firm opinions one way or the other. Which they can share by angry letter, fulsome e-mail, or, of course, any on-line reviews they can slip past the mysterious algorithms of the Yelps and Angie’s Lists of the world.
When I get messages like Thelma’s and Louise’s, I show them to my students and make three suggestions:
• Don’t try to look smart at someone else’s expense. Next time around a patient will be in somebody else’s office calling you a fool.
• Don’t respond to snippy patients’ complaints by contacting the complainer and trying to justify yourself. Learn something if you can, and move on.
• Be grateful for praise. Just don’t take it too seriously.
In the meantime, the insurers and assorted bureaucrats who run our lives these days are busy defining good care and claiming to measure it so they can reward quality and punish inefficiency. I’m sure they think they’re doing a fine job, although I remain deeply skeptical that what they choose to measure has much relevance to what actually goes on in offices like ours.
I could, of course, try to tell them why I think so. (I have tried, in fact.) Getting through to people with a completely different way of looking at things than yours is not very rewarding, even when large sums of money are not involved. I would have as good a chance of winning them over as I would of convincing Thelma that a scaly patch is not textbook pityriasis that needs prednisone and Louise that betamethasone cream is not the breakthrough that will change her life.
So: Not the best of times. Not the worst of times. Just another day at the office.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since 1997.
It was the worst of days. It was the best of days.
When I opened the mail one day last week, I found a letter from someone I’ll call Thelma. It read, in part:
"Last Monday you were kind enough to look at my rash, which you thought was just eczema. You gave me cream and asked me to e-mail you Thursday about my condition. When I did and said I was still itchy, you said I should stick with the same and that I could come back Monday, but I couldn’t wait because I itched so bad I couldn’t take it anymore. I saw another doctor Friday who said the patch was host to something called pityriasis rosea. He said the rash was so textbook it should have been picked up immediately. I had to be put on an oral steroid right away.
"I am so upset that I’m sending you back your bill [for a $15 co-pay] because I had to go to another doctor who could really help me."
I thought of a few choice words for my esteemed Friday colleague, but kept them to myself. A single scaly patch is a textbook case of pityriasis rosea? Oral steroids for pityriasis? Really?
As far as this patient is concerned, I must be a bum. Thirty-five years on the job, and I haven’t mastered the textbook yet.
Sunk in gloom, I opened an e-mail sent to my website by a patient I’ll call Louise:
"I suffer from psoriasis and have been to countless dermatologists since I was 8 years old. I recently had a terrible outbreak and was really hesitant to even go to a dermatologist because I’ve never been satisfied with any of them. Your associate is wonderful! I can’t say enough about her. She is warm, thorough, and really takes the time to sit with you and listen. You can tell she truly cares about her patients and loves her job."
I looked at the patient’s chart. What was the wonderful and satisfying treatment that my associate had prescribed to deal with this patient’s lifelong, recalcitrant psoriasis?
Betamethasone dipropionate cream 0.05%. Wow.
I e-mailed my associate at once and we shared a gratified chuckle. Guess no one ever thought of treating Louise’s psoriasis with a topical steroid before. We must be geniuses, right out there on the cutting edge.
So which are we, dear colleagues – geniuses or bums?
We’re neither, of course, which doesn’t stop our patients from forming firm opinions one way or the other. Which they can share by angry letter, fulsome e-mail, or, of course, any on-line reviews they can slip past the mysterious algorithms of the Yelps and Angie’s Lists of the world.
When I get messages like Thelma’s and Louise’s, I show them to my students and make three suggestions:
• Don’t try to look smart at someone else’s expense. Next time around a patient will be in somebody else’s office calling you a fool.
• Don’t respond to snippy patients’ complaints by contacting the complainer and trying to justify yourself. Learn something if you can, and move on.
• Be grateful for praise. Just don’t take it too seriously.
In the meantime, the insurers and assorted bureaucrats who run our lives these days are busy defining good care and claiming to measure it so they can reward quality and punish inefficiency. I’m sure they think they’re doing a fine job, although I remain deeply skeptical that what they choose to measure has much relevance to what actually goes on in offices like ours.
I could, of course, try to tell them why I think so. (I have tried, in fact.) Getting through to people with a completely different way of looking at things than yours is not very rewarding, even when large sums of money are not involved. I would have as good a chance of winning them over as I would of convincing Thelma that a scaly patch is not textbook pityriasis that needs prednisone and Louise that betamethasone cream is not the breakthrough that will change her life.
So: Not the best of times. Not the worst of times. Just another day at the office.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since 1997.

ACC/AHA cardiovascular risk equations get a thumbs-up
WASHINGTON – The controversial cardiovascular risk estimator introduced in the current American College of Cardiology/American Heart Association risk-assessment guidelines demonstrated "moderate to good" predictive performance when applied to a large U.S. cohort for whom consideration of statin therapy is clinically relevant, Paul Muntner, Ph.D., reported at the annual meeting of the American College of Cardiology.
"We believe that the current study supports the validity of the pooled cohort risk equations to inform clinical management decisions," said Dr. Muntner, professor of epidemiology and of medicine at the University of Alabama at Birmingham.
The risk estimator has come under strong criticism since the guidelines were released last November. When critics applied the risk estimator to participants in the Women's Health Study, the Physicians' Health Study, and the Women's Health Initiative, they found a big discrepancy between the observed atherosclerotic cardiovascular disease (ASCVD) event rates during follow-up and the predicted rates based on the risk calculator, with the ACC/AHA risk estimator tending to markedly overestimate risk. But those analyses involved studies lacking surveillance mechanisms to identify ASCVD events that weren’t reported by participants, according to Dr. Muntner.
"One of the challenges with those big studies is the underreporting of events. Let’s look at the Women’s Health Initiative. Roughly 25% of adjudicated events in that study were not detected because of the reliance on patient reporting. There were two reasons for this: Participants didn’t report a subsequently validated event, or hospital consent forms didn’t permit release of the chart to study investigators," he asserted.
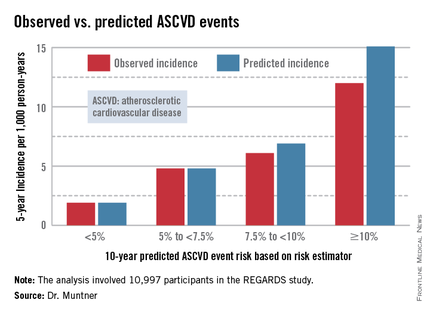
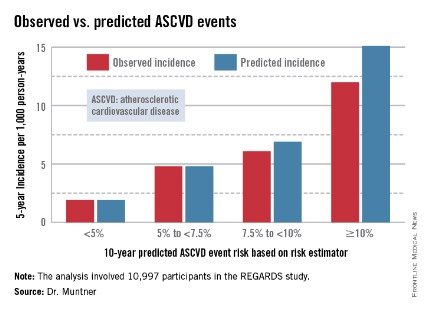
Dr. Muntner presented a new analysis in which the ASCVD risk estimator was applied to participants in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study, a prospective, observational, population-based study of more than 30,000 U.S. black and white patients. He and his coworkers compared the observed 5-year rates of the combined endpoint of death from coronary heart disease, nonfatal MI, or fatal or nonfatal stroke to rates projected by the risk equations.

The analysis was restricted to the 10,997 REGARDS participants who fell into the category of the population for whom the risk equations were designed as a guide in decision making regarding initiation of statin therapy: people aged 40-79 years without atherosclerotic cardiovascular disease or diabetes, not on a statin, and with an LDL cholesterol level of 70-189 mg/dL.
In participants in the lower 10-year ASCVD risk categories based on the equations, the predicted 5-year event rates were spot on with the observed rates. In patients at the higher end of the 10-year risk spectrum, the equations tended to overestimate the event risk (see chart). However, it should be noted that roughly 40% of the REGARDS cohort initiated statin therapy during the 5-year follow-up period, and that would have lowered their event rate, Dr. Muntner said.
The investigators also compared observed and predicted 5-year event rates in a separate REGARDS subgroup composed of 3,333 study participants with Medicare Part A insurance. In this older cohort, the risk equations tended to modestly underestimate the observed ASCVD event rate. "Overall, though, I would say this is pretty good calibration," the epidemiologist commented.
Simultaneous with Dr. Muntner’s presentation at ACC 14, the study results were published (JAMA 2014 April 9;311:1406-15).
The REGARDS study is funded by the National Institutes of Health, as was Dr. Muntner’s analysis. He reported having no relevant financial interests.
WASHINGTON – The controversial cardiovascular risk estimator introduced in the current American College of Cardiology/American Heart Association risk-assessment guidelines demonstrated "moderate to good" predictive performance when applied to a large U.S. cohort for whom consideration of statin therapy is clinically relevant, Paul Muntner, Ph.D., reported at the annual meeting of the American College of Cardiology.
"We believe that the current study supports the validity of the pooled cohort risk equations to inform clinical management decisions," said Dr. Muntner, professor of epidemiology and of medicine at the University of Alabama at Birmingham.
The risk estimator has come under strong criticism since the guidelines were released last November. When critics applied the risk estimator to participants in the Women's Health Study, the Physicians' Health Study, and the Women's Health Initiative, they found a big discrepancy between the observed atherosclerotic cardiovascular disease (ASCVD) event rates during follow-up and the predicted rates based on the risk calculator, with the ACC/AHA risk estimator tending to markedly overestimate risk. But those analyses involved studies lacking surveillance mechanisms to identify ASCVD events that weren’t reported by participants, according to Dr. Muntner.
"One of the challenges with those big studies is the underreporting of events. Let’s look at the Women’s Health Initiative. Roughly 25% of adjudicated events in that study were not detected because of the reliance on patient reporting. There were two reasons for this: Participants didn’t report a subsequently validated event, or hospital consent forms didn’t permit release of the chart to study investigators," he asserted.
Dr. Muntner presented a new analysis in which the ASCVD risk estimator was applied to participants in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study, a prospective, observational, population-based study of more than 30,000 U.S. black and white patients. He and his coworkers compared the observed 5-year rates of the combined endpoint of death from coronary heart disease, nonfatal MI, or fatal or nonfatal stroke to rates projected by the risk equations.
The analysis was restricted to the 10,997 REGARDS participants who fell into the category of the population for whom the risk equations were designed as a guide in decision making regarding initiation of statin therapy: people aged 40-79 years without atherosclerotic cardiovascular disease or diabetes, not on a statin, and with an LDL cholesterol level of 70-189 mg/dL.
In participants in the lower 10-year ASCVD risk categories based on the equations, the predicted 5-year event rates were spot on with the observed rates. In patients at the higher end of the 10-year risk spectrum, the equations tended to overestimate the event risk (see chart). However, it should be noted that roughly 40% of the REGARDS cohort initiated statin therapy during the 5-year follow-up period, and that would have lowered their event rate, Dr. Muntner said.
The investigators also compared observed and predicted 5-year event rates in a separate REGARDS subgroup composed of 3,333 study participants with Medicare Part A insurance. In this older cohort, the risk equations tended to modestly underestimate the observed ASCVD event rate. "Overall, though, I would say this is pretty good calibration," the epidemiologist commented.
Simultaneous with Dr. Muntner’s presentation at ACC 14, the study results were published (JAMA 2014 April 9;311:1406-15).
The REGARDS study is funded by the National Institutes of Health, as was Dr. Muntner’s analysis. He reported having no relevant financial interests.
WASHINGTON – The controversial cardiovascular risk estimator introduced in the current American College of Cardiology/American Heart Association risk-assessment guidelines demonstrated "moderate to good" predictive performance when applied to a large U.S. cohort for whom consideration of statin therapy is clinically relevant, Paul Muntner, Ph.D., reported at the annual meeting of the American College of Cardiology.
"We believe that the current study supports the validity of the pooled cohort risk equations to inform clinical management decisions," said Dr. Muntner, professor of epidemiology and of medicine at the University of Alabama at Birmingham.
The risk estimator has come under strong criticism since the guidelines were released last November. When critics applied the risk estimator to participants in the Women's Health Study, the Physicians' Health Study, and the Women's Health Initiative, they found a big discrepancy between the observed atherosclerotic cardiovascular disease (ASCVD) event rates during follow-up and the predicted rates based on the risk calculator, with the ACC/AHA risk estimator tending to markedly overestimate risk. But those analyses involved studies lacking surveillance mechanisms to identify ASCVD events that weren’t reported by participants, according to Dr. Muntner.
"One of the challenges with those big studies is the underreporting of events. Let’s look at the Women’s Health Initiative. Roughly 25% of adjudicated events in that study were not detected because of the reliance on patient reporting. There were two reasons for this: Participants didn’t report a subsequently validated event, or hospital consent forms didn’t permit release of the chart to study investigators," he asserted.
Dr. Muntner presented a new analysis in which the ASCVD risk estimator was applied to participants in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study, a prospective, observational, population-based study of more than 30,000 U.S. black and white patients. He and his coworkers compared the observed 5-year rates of the combined endpoint of death from coronary heart disease, nonfatal MI, or fatal or nonfatal stroke to rates projected by the risk equations.
The analysis was restricted to the 10,997 REGARDS participants who fell into the category of the population for whom the risk equations were designed as a guide in decision making regarding initiation of statin therapy: people aged 40-79 years without atherosclerotic cardiovascular disease or diabetes, not on a statin, and with an LDL cholesterol level of 70-189 mg/dL.
In participants in the lower 10-year ASCVD risk categories based on the equations, the predicted 5-year event rates were spot on with the observed rates. In patients at the higher end of the 10-year risk spectrum, the equations tended to overestimate the event risk (see chart). However, it should be noted that roughly 40% of the REGARDS cohort initiated statin therapy during the 5-year follow-up period, and that would have lowered their event rate, Dr. Muntner said.
The investigators also compared observed and predicted 5-year event rates in a separate REGARDS subgroup composed of 3,333 study participants with Medicare Part A insurance. In this older cohort, the risk equations tended to modestly underestimate the observed ASCVD event rate. "Overall, though, I would say this is pretty good calibration," the epidemiologist commented.
Simultaneous with Dr. Muntner’s presentation at ACC 14, the study results were published (JAMA 2014 April 9;311:1406-15).
The REGARDS study is funded by the National Institutes of Health, as was Dr. Muntner’s analysis. He reported having no relevant financial interests.
AT ACC 14
Major finding: The controversial cardiovascular risk equations at the heart of the latest ACC/AHA risk-assessment guidelines turned in a moderate to good performance in a validation study involving nearly 11,000 participants in a large, observational, prospective study.
Data source: The REGARDS study is a population-based study in which more than 30,000 U.S. black and white patients are being followed prospectively.
Disclosures: The analysis was funded by the National Institutes of Health. The presenter reported having no financial conflicts.
Heparanase regulates response to chemo in MM, team says
SAN DIEGO—Experiments conducted in the lab and the clinic suggest the enzyme heparanase enhances resistance to chemotherapy in multiple myeloma (MM).
Researchers first found that expression of heparanase, an endoglycosidase that cleaves heparan sulfate, is highly elevated in MM patients after chemotherapy.
The team then used MM cell lines to investigate the mechanism behind this phenomenon.
Their results indicate that, by inhibiting heparanase, we might be able to prevent or delay relapse in MM.
Vishnu Ramani, PhD, of the University of Alabama Birmingham, and his colleagues conducted this research and presented the results at the AACR Annual Meeting 2014 (abstract 1708).
Several years ago, Dr Ramani’s colleagues (in the lab of Ralph Sanderson, PhD) identified heparanase as a master regulator of aggressive MM. Since then, research has suggested that heparanase fuels aggressive MM by upregulating the expression of pro-angiogenic genes, driving osteolysis, upregulating prometastatic molecules, and controlling the tumor microenvironment.
“We have done a lot of work on the biology of how this molecule works in myeloma, but the one thing I was really interested in was its role in drug resistance,” Dr Ramani said.
So he and his colleagues decided to study heparanase levels in 9 MM patients undergoing chemotherapy. The team isolated tumor cells from patients before and after 2 rounds of chemotherapy and compared heparanase levels at the different time points.
“What we find—and this is really remarkable—is that the expression of heparanase over rounds of therapy goes up several thousand-fold, and this is in the majority of patients,” Dr Ramani said. “In 8 out of 9 patients that we studied, at the end of chemotherapy, the cells that survive have extremely high levels of heparanase.”
To gain more insight into this phenomenon, the researchers studied it in MM cell lines. The team introduced bortezomib to RPMI-8226 and CAG cells and found that heparanase levels increased “dramatically” after treatment.
“The treatment is not only increasing the heparanase expression inside the cell,” Dr Ramani explained. “What the cells do is that, if you continue the treatment, they die, but they don’t take the heparanase with them. They leave it out in the media, and this can be taken in by other cells. So this can activate other cells to promote aggressive tumor growth too.”
Additional investigation revealed that the NF-κB pathway plays a role—namely, chemotherapy activates the pathway to upregulate heparanase. But inhibiting NF-κB activity can prevent that increase in heparanase.
The researchers tested the NF-κB inhibitors BAY 11-7085 and BMS345541 in combination with bortezomib. And they found that both agents prevented bortezomib from elevating heparanase expression in CAG cells.
Dr Ramani and his colleagues also evaluated heparanase levels in chemoresistant MM cell lines. Heparanase levels were 4-fold higher in a doxorubicin-resistant MM cell line and 10-fold higher in a melphalan-resistant cell line, when compared to a wild-type MM cell line.
Next, the researchers compared MM cells with high heparanase expression to those with low heparanase expression. And they discovered that high heparanase levels protect cells from chemotherapy.
After treatment with bortezomib, cells with high heparanase expression were significantly more viable than those with low expression (P<0.05). And there was a significantly higher percentage of apoptotic cells among the low-heparanase population compared to the high-heparanase population (P<0.05).
“If you take cells that have high heparanase and another group of cells that have low heparanase and expose both of them to therapy, the cells with high heparanase always survive better because the heparanase upregulates certain pathways, like the MAP kinase pathway, which helps the cells to survive the onslaught of chemotherapy,” Dr Ramani said. “So myeloma cells are actually hijacking the heparanase pathway to survive better after therapy.”
Building upon that finding, the researchers decided to assess whether inhibiting ERK activity might help cells overcome heparanase-mediated chemoresistance. And experiments showed that the ERK inhibitor U0126 can sensitize cells with high heparanase levels to treatment with bortezomib.
To take this research to the next level, Dr Ramani and his colleagues are collaborating with a company called Sigma Tau, which is developing a heparanase inhibitor called SST-0001. A phase 1 study of the drug in MM patients has been completed, and phase 2 studies are currently recruiting patients in Europe.
Dr Ramani is now conducting experiments in mice to determine how the inhibitor might work in combination with chemotherapy and when it should be administered in order to overcome treatment resistance. He is also looking for other molecular pathways that could be involved in heparanase-related treatment resistance. ![]()
SAN DIEGO—Experiments conducted in the lab and the clinic suggest the enzyme heparanase enhances resistance to chemotherapy in multiple myeloma (MM).
Researchers first found that expression of heparanase, an endoglycosidase that cleaves heparan sulfate, is highly elevated in MM patients after chemotherapy.
The team then used MM cell lines to investigate the mechanism behind this phenomenon.
Their results indicate that, by inhibiting heparanase, we might be able to prevent or delay relapse in MM.
Vishnu Ramani, PhD, of the University of Alabama Birmingham, and his colleagues conducted this research and presented the results at the AACR Annual Meeting 2014 (abstract 1708).
Several years ago, Dr Ramani’s colleagues (in the lab of Ralph Sanderson, PhD) identified heparanase as a master regulator of aggressive MM. Since then, research has suggested that heparanase fuels aggressive MM by upregulating the expression of pro-angiogenic genes, driving osteolysis, upregulating prometastatic molecules, and controlling the tumor microenvironment.
“We have done a lot of work on the biology of how this molecule works in myeloma, but the one thing I was really interested in was its role in drug resistance,” Dr Ramani said.
So he and his colleagues decided to study heparanase levels in 9 MM patients undergoing chemotherapy. The team isolated tumor cells from patients before and after 2 rounds of chemotherapy and compared heparanase levels at the different time points.
“What we find—and this is really remarkable—is that the expression of heparanase over rounds of therapy goes up several thousand-fold, and this is in the majority of patients,” Dr Ramani said. “In 8 out of 9 patients that we studied, at the end of chemotherapy, the cells that survive have extremely high levels of heparanase.”
To gain more insight into this phenomenon, the researchers studied it in MM cell lines. The team introduced bortezomib to RPMI-8226 and CAG cells and found that heparanase levels increased “dramatically” after treatment.
“The treatment is not only increasing the heparanase expression inside the cell,” Dr Ramani explained. “What the cells do is that, if you continue the treatment, they die, but they don’t take the heparanase with them. They leave it out in the media, and this can be taken in by other cells. So this can activate other cells to promote aggressive tumor growth too.”
Additional investigation revealed that the NF-κB pathway plays a role—namely, chemotherapy activates the pathway to upregulate heparanase. But inhibiting NF-κB activity can prevent that increase in heparanase.
The researchers tested the NF-κB inhibitors BAY 11-7085 and BMS345541 in combination with bortezomib. And they found that both agents prevented bortezomib from elevating heparanase expression in CAG cells.
Dr Ramani and his colleagues also evaluated heparanase levels in chemoresistant MM cell lines. Heparanase levels were 4-fold higher in a doxorubicin-resistant MM cell line and 10-fold higher in a melphalan-resistant cell line, when compared to a wild-type MM cell line.
Next, the researchers compared MM cells with high heparanase expression to those with low heparanase expression. And they discovered that high heparanase levels protect cells from chemotherapy.
After treatment with bortezomib, cells with high heparanase expression were significantly more viable than those with low expression (P<0.05). And there was a significantly higher percentage of apoptotic cells among the low-heparanase population compared to the high-heparanase population (P<0.05).
“If you take cells that have high heparanase and another group of cells that have low heparanase and expose both of them to therapy, the cells with high heparanase always survive better because the heparanase upregulates certain pathways, like the MAP kinase pathway, which helps the cells to survive the onslaught of chemotherapy,” Dr Ramani said. “So myeloma cells are actually hijacking the heparanase pathway to survive better after therapy.”
Building upon that finding, the researchers decided to assess whether inhibiting ERK activity might help cells overcome heparanase-mediated chemoresistance. And experiments showed that the ERK inhibitor U0126 can sensitize cells with high heparanase levels to treatment with bortezomib.
To take this research to the next level, Dr Ramani and his colleagues are collaborating with a company called Sigma Tau, which is developing a heparanase inhibitor called SST-0001. A phase 1 study of the drug in MM patients has been completed, and phase 2 studies are currently recruiting patients in Europe.
Dr Ramani is now conducting experiments in mice to determine how the inhibitor might work in combination with chemotherapy and when it should be administered in order to overcome treatment resistance. He is also looking for other molecular pathways that could be involved in heparanase-related treatment resistance. ![]()
SAN DIEGO—Experiments conducted in the lab and the clinic suggest the enzyme heparanase enhances resistance to chemotherapy in multiple myeloma (MM).
Researchers first found that expression of heparanase, an endoglycosidase that cleaves heparan sulfate, is highly elevated in MM patients after chemotherapy.
The team then used MM cell lines to investigate the mechanism behind this phenomenon.
Their results indicate that, by inhibiting heparanase, we might be able to prevent or delay relapse in MM.
Vishnu Ramani, PhD, of the University of Alabama Birmingham, and his colleagues conducted this research and presented the results at the AACR Annual Meeting 2014 (abstract 1708).
Several years ago, Dr Ramani’s colleagues (in the lab of Ralph Sanderson, PhD) identified heparanase as a master regulator of aggressive MM. Since then, research has suggested that heparanase fuels aggressive MM by upregulating the expression of pro-angiogenic genes, driving osteolysis, upregulating prometastatic molecules, and controlling the tumor microenvironment.
“We have done a lot of work on the biology of how this molecule works in myeloma, but the one thing I was really interested in was its role in drug resistance,” Dr Ramani said.
So he and his colleagues decided to study heparanase levels in 9 MM patients undergoing chemotherapy. The team isolated tumor cells from patients before and after 2 rounds of chemotherapy and compared heparanase levels at the different time points.
“What we find—and this is really remarkable—is that the expression of heparanase over rounds of therapy goes up several thousand-fold, and this is in the majority of patients,” Dr Ramani said. “In 8 out of 9 patients that we studied, at the end of chemotherapy, the cells that survive have extremely high levels of heparanase.”
To gain more insight into this phenomenon, the researchers studied it in MM cell lines. The team introduced bortezomib to RPMI-8226 and CAG cells and found that heparanase levels increased “dramatically” after treatment.
“The treatment is not only increasing the heparanase expression inside the cell,” Dr Ramani explained. “What the cells do is that, if you continue the treatment, they die, but they don’t take the heparanase with them. They leave it out in the media, and this can be taken in by other cells. So this can activate other cells to promote aggressive tumor growth too.”
Additional investigation revealed that the NF-κB pathway plays a role—namely, chemotherapy activates the pathway to upregulate heparanase. But inhibiting NF-κB activity can prevent that increase in heparanase.
The researchers tested the NF-κB inhibitors BAY 11-7085 and BMS345541 in combination with bortezomib. And they found that both agents prevented bortezomib from elevating heparanase expression in CAG cells.
Dr Ramani and his colleagues also evaluated heparanase levels in chemoresistant MM cell lines. Heparanase levels were 4-fold higher in a doxorubicin-resistant MM cell line and 10-fold higher in a melphalan-resistant cell line, when compared to a wild-type MM cell line.
Next, the researchers compared MM cells with high heparanase expression to those with low heparanase expression. And they discovered that high heparanase levels protect cells from chemotherapy.
After treatment with bortezomib, cells with high heparanase expression were significantly more viable than those with low expression (P<0.05). And there was a significantly higher percentage of apoptotic cells among the low-heparanase population compared to the high-heparanase population (P<0.05).
“If you take cells that have high heparanase and another group of cells that have low heparanase and expose both of them to therapy, the cells with high heparanase always survive better because the heparanase upregulates certain pathways, like the MAP kinase pathway, which helps the cells to survive the onslaught of chemotherapy,” Dr Ramani said. “So myeloma cells are actually hijacking the heparanase pathway to survive better after therapy.”
Building upon that finding, the researchers decided to assess whether inhibiting ERK activity might help cells overcome heparanase-mediated chemoresistance. And experiments showed that the ERK inhibitor U0126 can sensitize cells with high heparanase levels to treatment with bortezomib.
To take this research to the next level, Dr Ramani and his colleagues are collaborating with a company called Sigma Tau, which is developing a heparanase inhibitor called SST-0001. A phase 1 study of the drug in MM patients has been completed, and phase 2 studies are currently recruiting patients in Europe.
Dr Ramani is now conducting experiments in mice to determine how the inhibitor might work in combination with chemotherapy and when it should be administered in order to overcome treatment resistance. He is also looking for other molecular pathways that could be involved in heparanase-related treatment resistance. ![]()
How mechanical forces affect T cells

used for T-cell force research,
with 3 glass micropipettes
shown under green light.
Georgia Tech/Rob Felt
Investigators say they’ve discovered how T-cell receptors (TCRs) use mechanical contact to decide if the cells they encounter
pose a threat to the body.
The team made their discovery using a sensor based on a red blood cell and a technique for detecting calcium ions emitted by T cells as part of the signaling process.
The researchers studied the binding of antigens to more than a hundred T cells, measuring the forces involved in the binding and the lifetimes of the bonds.
Results revealed that force prolongs TCR bonds for agonists but shortens them for antagonists. And the signaling outcome of an interaction between an antigen and a TCR depends on the magnitude, duration, frequency, and timing of the force application.
“This is the first systematic study of how T-cell recognition is affected by mechanical force, and it shows that forces play an important role in the functions of T cells,” said study author Cheng Zhu, PhD, of Georgia Tech and Emory University in Atlanta. “We think that mechanical force plays a role in almost every step of T-cell biology.”
Dr Zhu and his colleagues described this research in Cell.
The team used a biomembrane force probe to measure the strength and longevity of bonds between T cells and antigens. The probe consists, in part, of a red blood cell aspirated to a micropipette.
Attached to the red blood cell is a bead on which the investigators placed the antigen under study. Using a delicate mechanism that precisely controls motion, they moved the bead into contact with a TCR, allowing binding to take place.
To test the strength of the bond formed between an antigen and the TCR, the researchers applied piconewton forces to separate the bead holding the antigen from the TCR. The red blood cell then acted as a spring, stretching and allowing a measurement of the forces needed to separate the TCR and antigen.
To assess the impact of the binding on intracellular signaling, the investigators injected a dye into the cells that fluoresces when exposed to calcium signaling ions. Detecting the fluorescence allowed the team to determine when the mechanical force triggered T-cell signaling.
In this way, the researchers learned that interactions between the TCRs and agonist peptide-major histocompatibility complexes (MHCs) form catch bonds that become stronger with the application of additional force to initiate intracellular signaling.
And less active MHC complexes form slip bonds that weaken with force and don’t initiate signaling.
Overall, the investigators found that the signaling outcome of an interaction between an antigen and a TCR depends on the magnitude, duration, frequency, and timing of the force application.
“Force adds another dimension to interactions with T cells,” Dr Zhu explained. “Antigens that have a bond lifetime that is prolonged by force would have a higher likelihood of triggering signaling. Repeat engagements and lifetime accumulations play a role, and the decision to signal is usually made based on the accumulation of actions, not a single action.”
Researchers already have examples of how mechanical force can affect the operation of cellular systems. For instance, mechanical stress created by blood flow acting on the endothelial cells that line blood vessel walls plays a role in atherosclerosis.
So it isn’t surprising that mechanical forces play a role in the immune system, according to Dr Zhu.
“We now have a broader recognition that the physical environment and mechanical environment regulate many of the biological phenomena in the body,” he said. “When you exert a force on the TCR bonds, some of them dissociate faster, while others come off more slowly. This has an effect on the response of the T-cell receptor.”
As a next step, Dr Zhu’s team would like to explore the effects of force on T-cell development using the new experimental techniques. Evidence suggests the forces to which the cells are exposed while in a juvenile stage may affect the fates of their development. ![]()
used for T-cell force research,
with 3 glass micropipettes
shown under green light.
Georgia Tech/Rob Felt
Investigators say they’ve discovered how T-cell receptors (TCRs) use mechanical contact to decide if the cells they encounter
pose a threat to the body.
The team made their discovery using a sensor based on a red blood cell and a technique for detecting calcium ions emitted by T cells as part of the signaling process.
The researchers studied the binding of antigens to more than a hundred T cells, measuring the forces involved in the binding and the lifetimes of the bonds.
Results revealed that force prolongs TCR bonds for agonists but shortens them for antagonists. And the signaling outcome of an interaction between an antigen and a TCR depends on the magnitude, duration, frequency, and timing of the force application.
“This is the first systematic study of how T-cell recognition is affected by mechanical force, and it shows that forces play an important role in the functions of T cells,” said study author Cheng Zhu, PhD, of Georgia Tech and Emory University in Atlanta. “We think that mechanical force plays a role in almost every step of T-cell biology.”
Dr Zhu and his colleagues described this research in Cell.
The team used a biomembrane force probe to measure the strength and longevity of bonds between T cells and antigens. The probe consists, in part, of a red blood cell aspirated to a micropipette.
Attached to the red blood cell is a bead on which the investigators placed the antigen under study. Using a delicate mechanism that precisely controls motion, they moved the bead into contact with a TCR, allowing binding to take place.
To test the strength of the bond formed between an antigen and the TCR, the researchers applied piconewton forces to separate the bead holding the antigen from the TCR. The red blood cell then acted as a spring, stretching and allowing a measurement of the forces needed to separate the TCR and antigen.
To assess the impact of the binding on intracellular signaling, the investigators injected a dye into the cells that fluoresces when exposed to calcium signaling ions. Detecting the fluorescence allowed the team to determine when the mechanical force triggered T-cell signaling.
In this way, the researchers learned that interactions between the TCRs and agonist peptide-major histocompatibility complexes (MHCs) form catch bonds that become stronger with the application of additional force to initiate intracellular signaling.
And less active MHC complexes form slip bonds that weaken with force and don’t initiate signaling.
Overall, the investigators found that the signaling outcome of an interaction between an antigen and a TCR depends on the magnitude, duration, frequency, and timing of the force application.
“Force adds another dimension to interactions with T cells,” Dr Zhu explained. “Antigens that have a bond lifetime that is prolonged by force would have a higher likelihood of triggering signaling. Repeat engagements and lifetime accumulations play a role, and the decision to signal is usually made based on the accumulation of actions, not a single action.”
Researchers already have examples of how mechanical force can affect the operation of cellular systems. For instance, mechanical stress created by blood flow acting on the endothelial cells that line blood vessel walls plays a role in atherosclerosis.
So it isn’t surprising that mechanical forces play a role in the immune system, according to Dr Zhu.
“We now have a broader recognition that the physical environment and mechanical environment regulate many of the biological phenomena in the body,” he said. “When you exert a force on the TCR bonds, some of them dissociate faster, while others come off more slowly. This has an effect on the response of the T-cell receptor.”
As a next step, Dr Zhu’s team would like to explore the effects of force on T-cell development using the new experimental techniques. Evidence suggests the forces to which the cells are exposed while in a juvenile stage may affect the fates of their development. ![]()
used for T-cell force research,
with 3 glass micropipettes
shown under green light.
Georgia Tech/Rob Felt
Investigators say they’ve discovered how T-cell receptors (TCRs) use mechanical contact to decide if the cells they encounter
pose a threat to the body.
The team made their discovery using a sensor based on a red blood cell and a technique for detecting calcium ions emitted by T cells as part of the signaling process.
The researchers studied the binding of antigens to more than a hundred T cells, measuring the forces involved in the binding and the lifetimes of the bonds.
Results revealed that force prolongs TCR bonds for agonists but shortens them for antagonists. And the signaling outcome of an interaction between an antigen and a TCR depends on the magnitude, duration, frequency, and timing of the force application.
“This is the first systematic study of how T-cell recognition is affected by mechanical force, and it shows that forces play an important role in the functions of T cells,” said study author Cheng Zhu, PhD, of Georgia Tech and Emory University in Atlanta. “We think that mechanical force plays a role in almost every step of T-cell biology.”
Dr Zhu and his colleagues described this research in Cell.
The team used a biomembrane force probe to measure the strength and longevity of bonds between T cells and antigens. The probe consists, in part, of a red blood cell aspirated to a micropipette.
Attached to the red blood cell is a bead on which the investigators placed the antigen under study. Using a delicate mechanism that precisely controls motion, they moved the bead into contact with a TCR, allowing binding to take place.
To test the strength of the bond formed between an antigen and the TCR, the researchers applied piconewton forces to separate the bead holding the antigen from the TCR. The red blood cell then acted as a spring, stretching and allowing a measurement of the forces needed to separate the TCR and antigen.
To assess the impact of the binding on intracellular signaling, the investigators injected a dye into the cells that fluoresces when exposed to calcium signaling ions. Detecting the fluorescence allowed the team to determine when the mechanical force triggered T-cell signaling.
In this way, the researchers learned that interactions between the TCRs and agonist peptide-major histocompatibility complexes (MHCs) form catch bonds that become stronger with the application of additional force to initiate intracellular signaling.
And less active MHC complexes form slip bonds that weaken with force and don’t initiate signaling.
Overall, the investigators found that the signaling outcome of an interaction between an antigen and a TCR depends on the magnitude, duration, frequency, and timing of the force application.
“Force adds another dimension to interactions with T cells,” Dr Zhu explained. “Antigens that have a bond lifetime that is prolonged by force would have a higher likelihood of triggering signaling. Repeat engagements and lifetime accumulations play a role, and the decision to signal is usually made based on the accumulation of actions, not a single action.”
Researchers already have examples of how mechanical force can affect the operation of cellular systems. For instance, mechanical stress created by blood flow acting on the endothelial cells that line blood vessel walls plays a role in atherosclerosis.
So it isn’t surprising that mechanical forces play a role in the immune system, according to Dr Zhu.
“We now have a broader recognition that the physical environment and mechanical environment regulate many of the biological phenomena in the body,” he said. “When you exert a force on the TCR bonds, some of them dissociate faster, while others come off more slowly. This has an effect on the response of the T-cell receptor.”
As a next step, Dr Zhu’s team would like to explore the effects of force on T-cell development using the new experimental techniques. Evidence suggests the forces to which the cells are exposed while in a juvenile stage may affect the fates of their development. ![]()
Beware of invasive H influenzae disease among pregnant women
Experts generally have not considered H influenzae disease to be a substantial contributor to severely adverse fetal outcomes. Yet new research from England and Wales finds that even though pregnant women in their study tended to be younger and healthier than their nonpregnant counterparts, they were far more likely to develop the invasive unencapsulated form of disease and far more likely to present with bacteremia. Not to mention that almost all of their pregnancies resulted in miscarriage, stillbirth, extremely preterm birth, or, at best, the birth of infants with respiratory distress with or without sepsis.
DETAILS OF THE STUDY
Collins and colleagues queried prospectively general practitioners who cared for women of reproductive age (15 to 44 years) with invasive H influenzae disease during the 4-year period of 2009 to 2012. One hundred percent of those queried responded. The study encompassed more than 45 million woman-years of follow-up.
Of the 171 women who developed the infection (confirmed by positive culture from a normally sterile site), approximately 84% (144) had unencapsulated disease. Not quite half (44% or 75) of the 171 women were pregnant at the time of infection. The overall incidence of confirmed invasive H influenzae disease was low at 0.50 per 100,000 women of reproductive age, but the 75 pregnant women were 17.2 (95% confidence interval [CI], 12.2-24.1; P<.001) times as likely to develop the infection as the 96 nonpregnant women (2.98/100,000 woman-years versus 0.17/100,000 woman-years, respectively). And, despite being previously healthy, almost three times as many pregnant as nonpregnant women presented with bacteremia (90.3% versus 33.3%, respectively).
Of 47 women who developed unencapsulated H influenzae infection during the first 24 weeks of pregnancy, 44 lost the fetus and three had extremely preterm births. Of 28 women who developed the infection during the second half of their pregnancy, two had stillbirths. Eight of the 26 live births were preterm, and 21 of the 26 infants had respiratory distress with or without sepsis at birth. The researchers calculated that the rate of pregnancy loss following invasive H influenzae disease was almost 3 times higher than the average rate of pregnancy loss in England and Wales.
CLINICAL RECOMMENDATIONS
It is generally reported that up to one-quarter of the approximately 26,000 stillbirths occurring yearly in the United States are due to some type of maternal or fetal infection.2,3 Dr. Morven S. Edwards, in an editorial4 appearing in the same issue of JAMA as the study, comments, “Given the magnitude of the burden of perinatal deaths, clarifying the extent that bacterial infections result in stillbirth and preterm delivery could potentially inform interventions to improve child and maternal health globally.”
Experts generally have not considered H influenzae disease to be a substantial contributor to severely adverse fetal outcomes. Yet new research from England and Wales finds that even though pregnant women in their study tended to be younger and healthier than their nonpregnant counterparts, they were far more likely to develop the invasive unencapsulated form of disease and far more likely to present with bacteremia. Not to mention that almost all of their pregnancies resulted in miscarriage, stillbirth, extremely preterm birth, or, at best, the birth of infants with respiratory distress with or without sepsis.
DETAILS OF THE STUDY
Collins and colleagues queried prospectively general practitioners who cared for women of reproductive age (15 to 44 years) with invasive H influenzae disease during the 4-year period of 2009 to 2012. One hundred percent of those queried responded. The study encompassed more than 45 million woman-years of follow-up.
Of the 171 women who developed the infection (confirmed by positive culture from a normally sterile site), approximately 84% (144) had unencapsulated disease. Not quite half (44% or 75) of the 171 women were pregnant at the time of infection. The overall incidence of confirmed invasive H influenzae disease was low at 0.50 per 100,000 women of reproductive age, but the 75 pregnant women were 17.2 (95% confidence interval [CI], 12.2-24.1; P<.001) times as likely to develop the infection as the 96 nonpregnant women (2.98/100,000 woman-years versus 0.17/100,000 woman-years, respectively). And, despite being previously healthy, almost three times as many pregnant as nonpregnant women presented with bacteremia (90.3% versus 33.3%, respectively).
Of 47 women who developed unencapsulated H influenzae infection during the first 24 weeks of pregnancy, 44 lost the fetus and three had extremely preterm births. Of 28 women who developed the infection during the second half of their pregnancy, two had stillbirths. Eight of the 26 live births were preterm, and 21 of the 26 infants had respiratory distress with or without sepsis at birth. The researchers calculated that the rate of pregnancy loss following invasive H influenzae disease was almost 3 times higher than the average rate of pregnancy loss in England and Wales.
CLINICAL RECOMMENDATIONS
It is generally reported that up to one-quarter of the approximately 26,000 stillbirths occurring yearly in the United States are due to some type of maternal or fetal infection.2,3 Dr. Morven S. Edwards, in an editorial4 appearing in the same issue of JAMA as the study, comments, “Given the magnitude of the burden of perinatal deaths, clarifying the extent that bacterial infections result in stillbirth and preterm delivery could potentially inform interventions to improve child and maternal health globally.”
Experts generally have not considered H influenzae disease to be a substantial contributor to severely adverse fetal outcomes. Yet new research from England and Wales finds that even though pregnant women in their study tended to be younger and healthier than their nonpregnant counterparts, they were far more likely to develop the invasive unencapsulated form of disease and far more likely to present with bacteremia. Not to mention that almost all of their pregnancies resulted in miscarriage, stillbirth, extremely preterm birth, or, at best, the birth of infants with respiratory distress with or without sepsis.
DETAILS OF THE STUDY
Collins and colleagues queried prospectively general practitioners who cared for women of reproductive age (15 to 44 years) with invasive H influenzae disease during the 4-year period of 2009 to 2012. One hundred percent of those queried responded. The study encompassed more than 45 million woman-years of follow-up.
Of the 171 women who developed the infection (confirmed by positive culture from a normally sterile site), approximately 84% (144) had unencapsulated disease. Not quite half (44% or 75) of the 171 women were pregnant at the time of infection. The overall incidence of confirmed invasive H influenzae disease was low at 0.50 per 100,000 women of reproductive age, but the 75 pregnant women were 17.2 (95% confidence interval [CI], 12.2-24.1; P<.001) times as likely to develop the infection as the 96 nonpregnant women (2.98/100,000 woman-years versus 0.17/100,000 woman-years, respectively). And, despite being previously healthy, almost three times as many pregnant as nonpregnant women presented with bacteremia (90.3% versus 33.3%, respectively).
Of 47 women who developed unencapsulated H influenzae infection during the first 24 weeks of pregnancy, 44 lost the fetus and three had extremely preterm births. Of 28 women who developed the infection during the second half of their pregnancy, two had stillbirths. Eight of the 26 live births were preterm, and 21 of the 26 infants had respiratory distress with or without sepsis at birth. The researchers calculated that the rate of pregnancy loss following invasive H influenzae disease was almost 3 times higher than the average rate of pregnancy loss in England and Wales.
CLINICAL RECOMMENDATIONS
It is generally reported that up to one-quarter of the approximately 26,000 stillbirths occurring yearly in the United States are due to some type of maternal or fetal infection.2,3 Dr. Morven S. Edwards, in an editorial4 appearing in the same issue of JAMA as the study, comments, “Given the magnitude of the burden of perinatal deaths, clarifying the extent that bacterial infections result in stillbirth and preterm delivery could potentially inform interventions to improve child and maternal health globally.”
Predicting risk of death in childhood cancer survivors

Logan Tuttle
Factors other than cancer treatment or chronic health conditions can influence the risk of death among survivors of childhood cancers, according to a study published in the Journal of Cancer Survivorship.
The researchers found an increased risk of death among cancer survivors who rarely exercised, were underweight, visited the doctor 5 or more times a year, considered themselves in “fair” or “poor” health, and had concerns about their future health.
Cheryl Cox, PhD, of the St Jude Children’s Research Hospital in Memphis, Tennessee, and her colleagues conducted this research using data from the Childhood Cancer Survivor Study.
The team compared 7162 childhood cancer survivors to 445 subjects who survived childhood cancer but ultimately died from causes other than cancer or non-health-related events (such as accidents).
The researchers matched subjects according to their primary diagnosis, age at the time of baseline questionnaire, and the time from diagnosis to baseline questionnaire.
Among the 445 subjects who died, the median age at death was 37.6 years. Malignant neoplasms (42%), cardiac conditions (20%), and pulmonary conditions (7%) caused the most deaths.
Subjects who died were slightly older than living subjects and more often of black race (vs white, Hispanic, or “other”). They were less likely to have a post-high school education or to be married. And they were more likely to have a household income below $20,000 or have an existing grade 3 or 4 chronic health condition.
When the researchers adjusted their analyses for sociodemographic characteristics, exposure to chemotherapy and/or radiation, and the number and severity of chronic health conditions, they identified a number of factors associated with an increased risk for all-cause mortality.
One of these factors was a lack of exercise—specifically, not exercising at all (odds ratio [OR]=1.72, P<0.001) or exercising 1 to 2 days a week (OR=1.65, P=0.004), compared to exercising 3 or more days a week.
On the other hand, being overweight or obese did not significantly increase a subject’s risk of death, but being underweight did (OR=2.58, P<0.001).
As one might expect, increased use of medical care was associated with an increased risk of mortality.
Subjects who reported 5 to 6 doctor visits per year had twice the risk of death as subjects who reported 1 to 2 visits (OR=2.07, P<0.001). And subjects who reported more than 20 annual doctor visits had a nearly 4-fold greater risk of death than subjects who reported 1 to 2 visits (OR=3.87, P<0.001).
Similarly, subjects had an increased risk of mortality if they described their general health as being “poor” or “fair” (OR=1.98, P<0.001). And being “concerned” or “very concerned” about future health was associated with an increased risk of mortality as well (OR=1.54, P=0.01)
On the other hand, smoking did not have a significant impact on the risk of death, and alcohol consumption appeared to have a positive impact on life expectancy.
Subjects who reported consuming 5 or more drinks per month had a lower risk of mortality than subjects who said they did not consume alcohol at all (OR=0.75, P=0.05).
Dr Cox and her colleagues said this research has revealed novel predictors of mortality not associated with a cancer survivor’s primary disease, treatment, or late effects. And continued observation could point to interventions for reducing the risk of death in these patients. ![]()
Logan Tuttle
Factors other than cancer treatment or chronic health conditions can influence the risk of death among survivors of childhood cancers, according to a study published in the Journal of Cancer Survivorship.
The researchers found an increased risk of death among cancer survivors who rarely exercised, were underweight, visited the doctor 5 or more times a year, considered themselves in “fair” or “poor” health, and had concerns about their future health.
Cheryl Cox, PhD, of the St Jude Children’s Research Hospital in Memphis, Tennessee, and her colleagues conducted this research using data from the Childhood Cancer Survivor Study.
The team compared 7162 childhood cancer survivors to 445 subjects who survived childhood cancer but ultimately died from causes other than cancer or non-health-related events (such as accidents).
The researchers matched subjects according to their primary diagnosis, age at the time of baseline questionnaire, and the time from diagnosis to baseline questionnaire.
Among the 445 subjects who died, the median age at death was 37.6 years. Malignant neoplasms (42%), cardiac conditions (20%), and pulmonary conditions (7%) caused the most deaths.
Subjects who died were slightly older than living subjects and more often of black race (vs white, Hispanic, or “other”). They were less likely to have a post-high school education or to be married. And they were more likely to have a household income below $20,000 or have an existing grade 3 or 4 chronic health condition.
When the researchers adjusted their analyses for sociodemographic characteristics, exposure to chemotherapy and/or radiation, and the number and severity of chronic health conditions, they identified a number of factors associated with an increased risk for all-cause mortality.
One of these factors was a lack of exercise—specifically, not exercising at all (odds ratio [OR]=1.72, P<0.001) or exercising 1 to 2 days a week (OR=1.65, P=0.004), compared to exercising 3 or more days a week.
On the other hand, being overweight or obese did not significantly increase a subject’s risk of death, but being underweight did (OR=2.58, P<0.001).
As one might expect, increased use of medical care was associated with an increased risk of mortality.
Subjects who reported 5 to 6 doctor visits per year had twice the risk of death as subjects who reported 1 to 2 visits (OR=2.07, P<0.001). And subjects who reported more than 20 annual doctor visits had a nearly 4-fold greater risk of death than subjects who reported 1 to 2 visits (OR=3.87, P<0.001).
Similarly, subjects had an increased risk of mortality if they described their general health as being “poor” or “fair” (OR=1.98, P<0.001). And being “concerned” or “very concerned” about future health was associated with an increased risk of mortality as well (OR=1.54, P=0.01)
On the other hand, smoking did not have a significant impact on the risk of death, and alcohol consumption appeared to have a positive impact on life expectancy.
Subjects who reported consuming 5 or more drinks per month had a lower risk of mortality than subjects who said they did not consume alcohol at all (OR=0.75, P=0.05).
Dr Cox and her colleagues said this research has revealed novel predictors of mortality not associated with a cancer survivor’s primary disease, treatment, or late effects. And continued observation could point to interventions for reducing the risk of death in these patients. ![]()
Logan Tuttle
Factors other than cancer treatment or chronic health conditions can influence the risk of death among survivors of childhood cancers, according to a study published in the Journal of Cancer Survivorship.
The researchers found an increased risk of death among cancer survivors who rarely exercised, were underweight, visited the doctor 5 or more times a year, considered themselves in “fair” or “poor” health, and had concerns about their future health.
Cheryl Cox, PhD, of the St Jude Children’s Research Hospital in Memphis, Tennessee, and her colleagues conducted this research using data from the Childhood Cancer Survivor Study.
The team compared 7162 childhood cancer survivors to 445 subjects who survived childhood cancer but ultimately died from causes other than cancer or non-health-related events (such as accidents).
The researchers matched subjects according to their primary diagnosis, age at the time of baseline questionnaire, and the time from diagnosis to baseline questionnaire.
Among the 445 subjects who died, the median age at death was 37.6 years. Malignant neoplasms (42%), cardiac conditions (20%), and pulmonary conditions (7%) caused the most deaths.
Subjects who died were slightly older than living subjects and more often of black race (vs white, Hispanic, or “other”). They were less likely to have a post-high school education or to be married. And they were more likely to have a household income below $20,000 or have an existing grade 3 or 4 chronic health condition.
When the researchers adjusted their analyses for sociodemographic characteristics, exposure to chemotherapy and/or radiation, and the number and severity of chronic health conditions, they identified a number of factors associated with an increased risk for all-cause mortality.
One of these factors was a lack of exercise—specifically, not exercising at all (odds ratio [OR]=1.72, P<0.001) or exercising 1 to 2 days a week (OR=1.65, P=0.004), compared to exercising 3 or more days a week.
On the other hand, being overweight or obese did not significantly increase a subject’s risk of death, but being underweight did (OR=2.58, P<0.001).
As one might expect, increased use of medical care was associated with an increased risk of mortality.
Subjects who reported 5 to 6 doctor visits per year had twice the risk of death as subjects who reported 1 to 2 visits (OR=2.07, P<0.001). And subjects who reported more than 20 annual doctor visits had a nearly 4-fold greater risk of death than subjects who reported 1 to 2 visits (OR=3.87, P<0.001).
Similarly, subjects had an increased risk of mortality if they described their general health as being “poor” or “fair” (OR=1.98, P<0.001). And being “concerned” or “very concerned” about future health was associated with an increased risk of mortality as well (OR=1.54, P=0.01)
On the other hand, smoking did not have a significant impact on the risk of death, and alcohol consumption appeared to have a positive impact on life expectancy.
Subjects who reported consuming 5 or more drinks per month had a lower risk of mortality than subjects who said they did not consume alcohol at all (OR=0.75, P=0.05).
Dr Cox and her colleagues said this research has revealed novel predictors of mortality not associated with a cancer survivor’s primary disease, treatment, or late effects. And continued observation could point to interventions for reducing the risk of death in these patients. ![]()
Molecule can increase Hb in anemic cancer patients
SAN DIEGO—Results of a pilot study suggest an experimental molecule can increase hemoglobin levels in patients with hematologic malignancies who are suffering from anemia.
The molecule, lexaptepid pegol (NOX-H94), is a pegylated L-stereoisomer RNA aptamer that binds and neutralizes hepcidin.
In this phase 2 study, 5 of 12 patients who received lexaptepid pegol experienced a hemoglobin increase of 1 g/dL or greater and qualified as responders.
Researchers presented these results at the AACR Annual Meeting 2014 as abstract 3847. The study was supported by NOXXON Pharma AG, the Berlin, Germany-based company developing lexaptepid pegol.
“Our concept is to treat anemia by inhibiting the activity of hepcidin,” said study investigator Kai Riecke, MD, of NOXXON Pharma.
“Hepcidin regulates iron in the blood. The problem is that, in quite a few tumors, hepcidin reduces iron in the circulation, and, over a long period of time, that leads to iron-restricted anemia.”
So Dr Riecke and his colleagues tested their antihepcidin molecule, lexaptepid pegol, in anemic cancer patients. The team enrolled patients with hemoglobin levels less than 10 g/dL who had been diagnosed with multiple myeloma, chronic lymphocytic leukemia, Hodgkin lymphoma, or non-Hodgkin lymphoma.
The patients had a median age of 64 years (range, 35-77). At baseline, the mean hemoglobin was 9.5 ± 0.2 g/dL, the mean serum ferritin was 1067 ± 297 μg/L, the mean serum iron was 34 ± 6 μg/dL, and the mean transferrin saturation was 16.7 ± 3.4%.
The patients received twice-weekly intravenous infusions of lexaptepid pegol for 4 weeks, and the researchers observed patients for 1 month after treatment. Patients were not allowed to receive erythropoiesis-stimulating agents or iron products during the study period.
The results showed increases in hemoglobin of 1 g/dL or greater, which qualified as a response, in 5 of the 12 patients (42%). Three patients achieved a response within 2 weeks of treatment initiation. All 5 patients maintained the increase in hemoglobin throughout the follow-up period.
There was no clear difference in response among the different malignancies, Dr Reike said. But he also noted that, as the study included a small number of patients, it wasn’t really possible for the researchers to make a fair comparison.
In addition to increasing hemoglobin levels, lexaptepid pegol decreased the mean serum ferritin from 1067 μg/L to 815 μg/L in the entire cohort of patients (P=0.014) and from 772 μg/L to 462 μg/L in responders (but this was not significant).
Reticulocyte hemoglobin increased from 22.7 pg to 24.9 pg (P=0.019) in responding patients, but there was no increase in non-responders. (Data for this measurement were only available for 3 of the responders—but all 7 of the non-responders—due to differences in measurement capabilities at the different research sites).
“During the treatment, we saw a very nice increase in reticulocyte hemoglobin, which shows, in these patients, the red blood cells were able to take up iron and build up more hemoglobin,” Dr Riecke said.
The researchers also observed an increase in the mean reticulocyte index in responding patients, from 0.9 to 1.2, although the increase was not significant.
“So this shows that, not only do you have an increase in hemoglobin within each reticulocyte, but you have an increase in the number of reticulocytes—something that we didn’t really expect in the beginning,” Dr Riecke said. “And this may be a sign that the efficacy of erythropoiesis is improved.”
Additionally, responding patients experienced a decrease in soluble transferrin receptor levels, from 10.0 mg/L to 8.6 mg/L, although this was not significant. Soluble transferrin receptor levels remained unchanged in non-responders. (Data for this measurement were only available for 3 of the responders and 4 of the non-responders.)
“The decrease in soluble transferrin receptor levels is a sign that, in the beginning, the cells were very iron-hungry, and then their hunger was satisfied—at least to a certain extent—during the treatment with our drug,” Dr Reike said. “This is a sign that, by reducing hepcidin, more iron is being released into the circulation, and this iron can effectively be used for erythropoiesis.”
Dr Reike added that, although the researchers did observe some adverse effects in the patients, none of these could be clearly attributed to lexaptepid pegol.
Some of the patients did have low blood pressure shortly after treatment, but that may have been influenced by factors other than treatment, he said. Furthermore, in the phase 1 study of lexaptepid pegol in healthy subjects, the only adverse effect that occurred in the treatment arm (and not in the placebo arm) was headache.
Based on these results, NOXXON is now planning—and recruiting for—a study of lexaptepid pegol in dialysis patients. ![]()
SAN DIEGO—Results of a pilot study suggest an experimental molecule can increase hemoglobin levels in patients with hematologic malignancies who are suffering from anemia.
The molecule, lexaptepid pegol (NOX-H94), is a pegylated L-stereoisomer RNA aptamer that binds and neutralizes hepcidin.
In this phase 2 study, 5 of 12 patients who received lexaptepid pegol experienced a hemoglobin increase of 1 g/dL or greater and qualified as responders.
Researchers presented these results at the AACR Annual Meeting 2014 as abstract 3847. The study was supported by NOXXON Pharma AG, the Berlin, Germany-based company developing lexaptepid pegol.
“Our concept is to treat anemia by inhibiting the activity of hepcidin,” said study investigator Kai Riecke, MD, of NOXXON Pharma.
“Hepcidin regulates iron in the blood. The problem is that, in quite a few tumors, hepcidin reduces iron in the circulation, and, over a long period of time, that leads to iron-restricted anemia.”
So Dr Riecke and his colleagues tested their antihepcidin molecule, lexaptepid pegol, in anemic cancer patients. The team enrolled patients with hemoglobin levels less than 10 g/dL who had been diagnosed with multiple myeloma, chronic lymphocytic leukemia, Hodgkin lymphoma, or non-Hodgkin lymphoma.
The patients had a median age of 64 years (range, 35-77). At baseline, the mean hemoglobin was 9.5 ± 0.2 g/dL, the mean serum ferritin was 1067 ± 297 μg/L, the mean serum iron was 34 ± 6 μg/dL, and the mean transferrin saturation was 16.7 ± 3.4%.
The patients received twice-weekly intravenous infusions of lexaptepid pegol for 4 weeks, and the researchers observed patients for 1 month after treatment. Patients were not allowed to receive erythropoiesis-stimulating agents or iron products during the study period.
The results showed increases in hemoglobin of 1 g/dL or greater, which qualified as a response, in 5 of the 12 patients (42%). Three patients achieved a response within 2 weeks of treatment initiation. All 5 patients maintained the increase in hemoglobin throughout the follow-up period.
There was no clear difference in response among the different malignancies, Dr Reike said. But he also noted that, as the study included a small number of patients, it wasn’t really possible for the researchers to make a fair comparison.
In addition to increasing hemoglobin levels, lexaptepid pegol decreased the mean serum ferritin from 1067 μg/L to 815 μg/L in the entire cohort of patients (P=0.014) and from 772 μg/L to 462 μg/L in responders (but this was not significant).
Reticulocyte hemoglobin increased from 22.7 pg to 24.9 pg (P=0.019) in responding patients, but there was no increase in non-responders. (Data for this measurement were only available for 3 of the responders—but all 7 of the non-responders—due to differences in measurement capabilities at the different research sites).
“During the treatment, we saw a very nice increase in reticulocyte hemoglobin, which shows, in these patients, the red blood cells were able to take up iron and build up more hemoglobin,” Dr Riecke said.
The researchers also observed an increase in the mean reticulocyte index in responding patients, from 0.9 to 1.2, although the increase was not significant.
“So this shows that, not only do you have an increase in hemoglobin within each reticulocyte, but you have an increase in the number of reticulocytes—something that we didn’t really expect in the beginning,” Dr Riecke said. “And this may be a sign that the efficacy of erythropoiesis is improved.”
Additionally, responding patients experienced a decrease in soluble transferrin receptor levels, from 10.0 mg/L to 8.6 mg/L, although this was not significant. Soluble transferrin receptor levels remained unchanged in non-responders. (Data for this measurement were only available for 3 of the responders and 4 of the non-responders.)
“The decrease in soluble transferrin receptor levels is a sign that, in the beginning, the cells were very iron-hungry, and then their hunger was satisfied—at least to a certain extent—during the treatment with our drug,” Dr Reike said. “This is a sign that, by reducing hepcidin, more iron is being released into the circulation, and this iron can effectively be used for erythropoiesis.”
Dr Reike added that, although the researchers did observe some adverse effects in the patients, none of these could be clearly attributed to lexaptepid pegol.
Some of the patients did have low blood pressure shortly after treatment, but that may have been influenced by factors other than treatment, he said. Furthermore, in the phase 1 study of lexaptepid pegol in healthy subjects, the only adverse effect that occurred in the treatment arm (and not in the placebo arm) was headache.
Based on these results, NOXXON is now planning—and recruiting for—a study of lexaptepid pegol in dialysis patients. ![]()
SAN DIEGO—Results of a pilot study suggest an experimental molecule can increase hemoglobin levels in patients with hematologic malignancies who are suffering from anemia.
The molecule, lexaptepid pegol (NOX-H94), is a pegylated L-stereoisomer RNA aptamer that binds and neutralizes hepcidin.
In this phase 2 study, 5 of 12 patients who received lexaptepid pegol experienced a hemoglobin increase of 1 g/dL or greater and qualified as responders.
Researchers presented these results at the AACR Annual Meeting 2014 as abstract 3847. The study was supported by NOXXON Pharma AG, the Berlin, Germany-based company developing lexaptepid pegol.
“Our concept is to treat anemia by inhibiting the activity of hepcidin,” said study investigator Kai Riecke, MD, of NOXXON Pharma.
“Hepcidin regulates iron in the blood. The problem is that, in quite a few tumors, hepcidin reduces iron in the circulation, and, over a long period of time, that leads to iron-restricted anemia.”
So Dr Riecke and his colleagues tested their antihepcidin molecule, lexaptepid pegol, in anemic cancer patients. The team enrolled patients with hemoglobin levels less than 10 g/dL who had been diagnosed with multiple myeloma, chronic lymphocytic leukemia, Hodgkin lymphoma, or non-Hodgkin lymphoma.
The patients had a median age of 64 years (range, 35-77). At baseline, the mean hemoglobin was 9.5 ± 0.2 g/dL, the mean serum ferritin was 1067 ± 297 μg/L, the mean serum iron was 34 ± 6 μg/dL, and the mean transferrin saturation was 16.7 ± 3.4%.
The patients received twice-weekly intravenous infusions of lexaptepid pegol for 4 weeks, and the researchers observed patients for 1 month after treatment. Patients were not allowed to receive erythropoiesis-stimulating agents or iron products during the study period.
The results showed increases in hemoglobin of 1 g/dL or greater, which qualified as a response, in 5 of the 12 patients (42%). Three patients achieved a response within 2 weeks of treatment initiation. All 5 patients maintained the increase in hemoglobin throughout the follow-up period.
There was no clear difference in response among the different malignancies, Dr Reike said. But he also noted that, as the study included a small number of patients, it wasn’t really possible for the researchers to make a fair comparison.
In addition to increasing hemoglobin levels, lexaptepid pegol decreased the mean serum ferritin from 1067 μg/L to 815 μg/L in the entire cohort of patients (P=0.014) and from 772 μg/L to 462 μg/L in responders (but this was not significant).
Reticulocyte hemoglobin increased from 22.7 pg to 24.9 pg (P=0.019) in responding patients, but there was no increase in non-responders. (Data for this measurement were only available for 3 of the responders—but all 7 of the non-responders—due to differences in measurement capabilities at the different research sites).
“During the treatment, we saw a very nice increase in reticulocyte hemoglobin, which shows, in these patients, the red blood cells were able to take up iron and build up more hemoglobin,” Dr Riecke said.
The researchers also observed an increase in the mean reticulocyte index in responding patients, from 0.9 to 1.2, although the increase was not significant.
“So this shows that, not only do you have an increase in hemoglobin within each reticulocyte, but you have an increase in the number of reticulocytes—something that we didn’t really expect in the beginning,” Dr Riecke said. “And this may be a sign that the efficacy of erythropoiesis is improved.”
Additionally, responding patients experienced a decrease in soluble transferrin receptor levels, from 10.0 mg/L to 8.6 mg/L, although this was not significant. Soluble transferrin receptor levels remained unchanged in non-responders. (Data for this measurement were only available for 3 of the responders and 4 of the non-responders.)
“The decrease in soluble transferrin receptor levels is a sign that, in the beginning, the cells were very iron-hungry, and then their hunger was satisfied—at least to a certain extent—during the treatment with our drug,” Dr Reike said. “This is a sign that, by reducing hepcidin, more iron is being released into the circulation, and this iron can effectively be used for erythropoiesis.”
Dr Reike added that, although the researchers did observe some adverse effects in the patients, none of these could be clearly attributed to lexaptepid pegol.
Some of the patients did have low blood pressure shortly after treatment, but that may have been influenced by factors other than treatment, he said. Furthermore, in the phase 1 study of lexaptepid pegol in healthy subjects, the only adverse effect that occurred in the treatment arm (and not in the placebo arm) was headache.
Based on these results, NOXXON is now planning—and recruiting for—a study of lexaptepid pegol in dialysis patients. ![]()