User login
Pneumonia Prevalence Highest of Health Care-Associated Infections
SAN DIEGO – The overall prevalence of health care–associated infections among inpatients in the United States stands at 4%, with the most common types of infections being a combination of pneumonia and lower respiratory infections.
Those are key preliminary findings from the Centers for Disease Control and Prevention’s first large-scale health care–associated infection (HAI) prevalence survey in more than 30 years, Dr. Shelley S. Magill reported during IDWeek 2012, the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The data "can help us better understand the factors that influence HAI prevalence," said Dr. Magill of the division of health care quality promotion at the Centers for Disease Control and Prevention, Atlanta. "We can also clarify the burden of different HAI types and pathogens across the hospital, which can suggest areas to target for prevention."
The phase 3 survey was conducted in 2011 in 183 hospitals in 10 states: California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee. Dr. Magill reported results from 11,282 patients who were surveyed in the 183 hospitals. Of these, 452 patients had HAIs, for a prevalence of 4%.
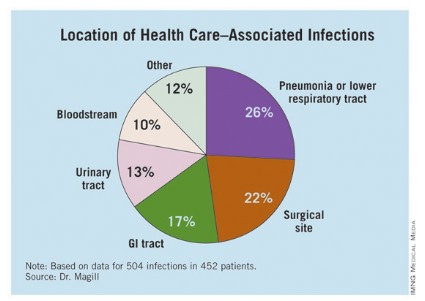
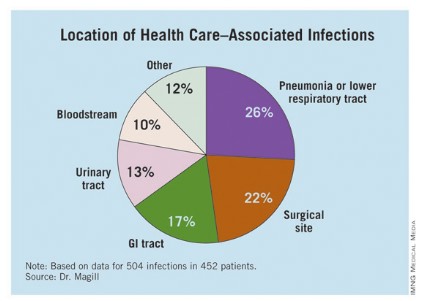
The researchers identified 504 HAIs in the 452 patients. Of these, the highest proportion (26%) were pneumonia or lower respiratory infections. "Of the pneumonia events, 39% were ventilator-associated infections," Dr. Magill said.
Surgical-site infections were the second most common infection type, representing 22% of all HAIs, followed by GI infections (17%), urinary tract infections (13%), and bloodstream infections (10%). "About two-third of UTIs were catheter associated and about 84% of the bloodstream infections were central-line associated," Dr. Magill noted.
Other infections made up the remaining 12% of HAIs.
Dr. Magill also reported that 56% of HAIs were attributed to non-ICU locations in the hospital while 53% were not directly associated with a device or with a procedure.
After multivariable regression analysis, patients with the following factors were at higher risk of having HAIs:
• Older age (risk ratio, 4.60 for patients older than age 77 compared with patients younger than 3 months old).
• Inpatient in a large hospital – defined as having 400 or more beds (RR, 1.24).
• Inpatient in a critical care unit (RR ,1.96 compared with all other units),
• Inpatient for more than 2 weeks at the time of the survey (RR, 26.09 compared with patients in the hospital for 3 days or fewer).
Pathogens were reported for 372 of the 504 HAIs. Clostridium difficile was the most common pathogen, accounting for 12% of all HAIs that were identified. Staphylococcus aureus was the second most common pathogen (11%; about half of these cases were methicillin-resistant S. aureus), followed by Klebsiella pneumoniae and Klebsiella oxytoca (10%).
Dr. Magill acknowledged certain limitations of the survey, including the fact that a small number of patients surveyed in each hospital "make results of limited use to individual facilities," she said. "We also had a relatively small number of hospitals in 10 states participate. This survey method provides a single snapshot of HAIs based on a retrospective review of medical record data, which is sometimes not complete. Finally, we were not able to collect a lot of detailed patient information, such as underlying illnesses and severity of illness."
She and her associates are currently planning a phase 4 survey, anticipated to occur in 2014.
Dr. Magill said she had no relevant financial conflicts to disclose.
SAN DIEGO – The overall prevalence of health care–associated infections among inpatients in the United States stands at 4%, with the most common types of infections being a combination of pneumonia and lower respiratory infections.
Those are key preliminary findings from the Centers for Disease Control and Prevention’s first large-scale health care–associated infection (HAI) prevalence survey in more than 30 years, Dr. Shelley S. Magill reported during IDWeek 2012, the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The data "can help us better understand the factors that influence HAI prevalence," said Dr. Magill of the division of health care quality promotion at the Centers for Disease Control and Prevention, Atlanta. "We can also clarify the burden of different HAI types and pathogens across the hospital, which can suggest areas to target for prevention."
The phase 3 survey was conducted in 2011 in 183 hospitals in 10 states: California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee. Dr. Magill reported results from 11,282 patients who were surveyed in the 183 hospitals. Of these, 452 patients had HAIs, for a prevalence of 4%.
The researchers identified 504 HAIs in the 452 patients. Of these, the highest proportion (26%) were pneumonia or lower respiratory infections. "Of the pneumonia events, 39% were ventilator-associated infections," Dr. Magill said.
Surgical-site infections were the second most common infection type, representing 22% of all HAIs, followed by GI infections (17%), urinary tract infections (13%), and bloodstream infections (10%). "About two-third of UTIs were catheter associated and about 84% of the bloodstream infections were central-line associated," Dr. Magill noted.
Other infections made up the remaining 12% of HAIs.
Dr. Magill also reported that 56% of HAIs were attributed to non-ICU locations in the hospital while 53% were not directly associated with a device or with a procedure.
After multivariable regression analysis, patients with the following factors were at higher risk of having HAIs:
• Older age (risk ratio, 4.60 for patients older than age 77 compared with patients younger than 3 months old).
• Inpatient in a large hospital – defined as having 400 or more beds (RR, 1.24).
• Inpatient in a critical care unit (RR ,1.96 compared with all other units),
• Inpatient for more than 2 weeks at the time of the survey (RR, 26.09 compared with patients in the hospital for 3 days or fewer).
Pathogens were reported for 372 of the 504 HAIs. Clostridium difficile was the most common pathogen, accounting for 12% of all HAIs that were identified. Staphylococcus aureus was the second most common pathogen (11%; about half of these cases were methicillin-resistant S. aureus), followed by Klebsiella pneumoniae and Klebsiella oxytoca (10%).
Dr. Magill acknowledged certain limitations of the survey, including the fact that a small number of patients surveyed in each hospital "make results of limited use to individual facilities," she said. "We also had a relatively small number of hospitals in 10 states participate. This survey method provides a single snapshot of HAIs based on a retrospective review of medical record data, which is sometimes not complete. Finally, we were not able to collect a lot of detailed patient information, such as underlying illnesses and severity of illness."
She and her associates are currently planning a phase 4 survey, anticipated to occur in 2014.
Dr. Magill said she had no relevant financial conflicts to disclose.
SAN DIEGO – The overall prevalence of health care–associated infections among inpatients in the United States stands at 4%, with the most common types of infections being a combination of pneumonia and lower respiratory infections.
Those are key preliminary findings from the Centers for Disease Control and Prevention’s first large-scale health care–associated infection (HAI) prevalence survey in more than 30 years, Dr. Shelley S. Magill reported during IDWeek 2012, the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The data "can help us better understand the factors that influence HAI prevalence," said Dr. Magill of the division of health care quality promotion at the Centers for Disease Control and Prevention, Atlanta. "We can also clarify the burden of different HAI types and pathogens across the hospital, which can suggest areas to target for prevention."
The phase 3 survey was conducted in 2011 in 183 hospitals in 10 states: California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee. Dr. Magill reported results from 11,282 patients who were surveyed in the 183 hospitals. Of these, 452 patients had HAIs, for a prevalence of 4%.
The researchers identified 504 HAIs in the 452 patients. Of these, the highest proportion (26%) were pneumonia or lower respiratory infections. "Of the pneumonia events, 39% were ventilator-associated infections," Dr. Magill said.
Surgical-site infections were the second most common infection type, representing 22% of all HAIs, followed by GI infections (17%), urinary tract infections (13%), and bloodstream infections (10%). "About two-third of UTIs were catheter associated and about 84% of the bloodstream infections were central-line associated," Dr. Magill noted.
Other infections made up the remaining 12% of HAIs.
Dr. Magill also reported that 56% of HAIs were attributed to non-ICU locations in the hospital while 53% were not directly associated with a device or with a procedure.
After multivariable regression analysis, patients with the following factors were at higher risk of having HAIs:
• Older age (risk ratio, 4.60 for patients older than age 77 compared with patients younger than 3 months old).
• Inpatient in a large hospital – defined as having 400 or more beds (RR, 1.24).
• Inpatient in a critical care unit (RR ,1.96 compared with all other units),
• Inpatient for more than 2 weeks at the time of the survey (RR, 26.09 compared with patients in the hospital for 3 days or fewer).
Pathogens were reported for 372 of the 504 HAIs. Clostridium difficile was the most common pathogen, accounting for 12% of all HAIs that were identified. Staphylococcus aureus was the second most common pathogen (11%; about half of these cases were methicillin-resistant S. aureus), followed by Klebsiella pneumoniae and Klebsiella oxytoca (10%).
Dr. Magill acknowledged certain limitations of the survey, including the fact that a small number of patients surveyed in each hospital "make results of limited use to individual facilities," she said. "We also had a relatively small number of hospitals in 10 states participate. This survey method provides a single snapshot of HAIs based on a retrospective review of medical record data, which is sometimes not complete. Finally, we were not able to collect a lot of detailed patient information, such as underlying illnesses and severity of illness."
She and her associates are currently planning a phase 4 survey, anticipated to occur in 2014.
Dr. Magill said she had no relevant financial conflicts to disclose.
AT IDWEEK 2012
Major Finding: The overall prevalence of health care–associated infections among hospitalized patients nationwide was 4%.
Data Source: Preliminary results were obtained from a 2011 survey of 11,282 inpatients at 183 hospitals located in 10 states.
Disclosures: The study was conducted by the Centers for Disease Control and Prevention. Dr. Magill said she had no relevant financial conflicts to disclose.
Quality Initiative Generates Widespread Improvements for Hospitals
Aligning Forces for Quality, an 18-month virtual quality collaborative launched in 16 targeted communities, generated measurable improvements for 90% of the 100 participating hospitals. The project, sponsored by the Robert Wood Johnson Foundation (www.forces4quality.org), is focused on reducing avoidable hospital readmissions; improving ED timeliness, efficiency, and patient flow; and eliminating patient-language barriers via standardized collection of data on race, ethnicity, and language preferences.
The collaborative showed 60% of participating hospitals improved 30-day readmission rates for heart failure patients, and 75% improved adherence to heart failure care standards.
“Hospitals are willing to really take stock of what they are doing well and where they could improve,” Susan Mende, BSN, MPH, of the foundation’s senior program office noted in a prepared statement.
Hospitalist William C. Cook, DO, chief of hospital medicine for the Ohio Permanente Medical Group, served as co-chair of the steering committee for transitional care for Better Care Greater Cleveland, one of the 16 community coalitions, and led two other work groups targeting care transitions. “I also had the opportunity to meet and work with Eric Coleman, MD,” of the University of Colorado Denver and creator of the widely implemented Care Transitions Program that coaches patients discharged from the hospital.
The foundation’s program promoted a vision for addressing readmissions across Dr. Cook’s region. “From the hospitalist perspective, our role is to try to make transitions as safe and predictable as possible,” Dr. Cook says.
Aligning Forces for Quality, an 18-month virtual quality collaborative launched in 16 targeted communities, generated measurable improvements for 90% of the 100 participating hospitals. The project, sponsored by the Robert Wood Johnson Foundation (www.forces4quality.org), is focused on reducing avoidable hospital readmissions; improving ED timeliness, efficiency, and patient flow; and eliminating patient-language barriers via standardized collection of data on race, ethnicity, and language preferences.
The collaborative showed 60% of participating hospitals improved 30-day readmission rates for heart failure patients, and 75% improved adherence to heart failure care standards.
“Hospitals are willing to really take stock of what they are doing well and where they could improve,” Susan Mende, BSN, MPH, of the foundation’s senior program office noted in a prepared statement.
Hospitalist William C. Cook, DO, chief of hospital medicine for the Ohio Permanente Medical Group, served as co-chair of the steering committee for transitional care for Better Care Greater Cleveland, one of the 16 community coalitions, and led two other work groups targeting care transitions. “I also had the opportunity to meet and work with Eric Coleman, MD,” of the University of Colorado Denver and creator of the widely implemented Care Transitions Program that coaches patients discharged from the hospital.
The foundation’s program promoted a vision for addressing readmissions across Dr. Cook’s region. “From the hospitalist perspective, our role is to try to make transitions as safe and predictable as possible,” Dr. Cook says.
Aligning Forces for Quality, an 18-month virtual quality collaborative launched in 16 targeted communities, generated measurable improvements for 90% of the 100 participating hospitals. The project, sponsored by the Robert Wood Johnson Foundation (www.forces4quality.org), is focused on reducing avoidable hospital readmissions; improving ED timeliness, efficiency, and patient flow; and eliminating patient-language barriers via standardized collection of data on race, ethnicity, and language preferences.
The collaborative showed 60% of participating hospitals improved 30-day readmission rates for heart failure patients, and 75% improved adherence to heart failure care standards.
“Hospitals are willing to really take stock of what they are doing well and where they could improve,” Susan Mende, BSN, MPH, of the foundation’s senior program office noted in a prepared statement.
Hospitalist William C. Cook, DO, chief of hospital medicine for the Ohio Permanente Medical Group, served as co-chair of the steering committee for transitional care for Better Care Greater Cleveland, one of the 16 community coalitions, and led two other work groups targeting care transitions. “I also had the opportunity to meet and work with Eric Coleman, MD,” of the University of Colorado Denver and creator of the widely implemented Care Transitions Program that coaches patients discharged from the hospital.
The foundation’s program promoted a vision for addressing readmissions across Dr. Cook’s region. “From the hospitalist perspective, our role is to try to make transitions as safe and predictable as possible,” Dr. Cook says.
Palliative Care Teams in 65% of Hospitals
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Professional Medical Coders Increase Hospitalist Group Reimbursement
What is the hospitalist’s optimal role in professional services billing? According to Leonard Noronha, MD, who was until recently a hospitalist practicing at the University of New Mexico (UNM), “physicians often find E/M (evaluation and management) coding rules confusing and frustrating,” leading to delinquent or tardy bills. Yet some feel apprehensive about turning billing and coding decisions over to professional coders because the physician retains legal responsibility for the accuracy of coding.
In a poster presented at HM12 in San Diego, Dr. Noronha described a 2010 decision by the academic group at UNM to have coders assign service levels to physician visits, retrieving the data from typed progress notes in the medical center’s newly implemented electronic health record (EHR). There were concerns that this new approach might lead to decreased revenue, but in practice, it led to both increased charges and collections (18%) and faster bill submissions (to 14 days from 16 days). The UNM hospitalists are incentivized to submit daily patient lists and to respond promptly to documentation completion requests.
“Working in a community hospital setting for five years and then in an academic practice for four years exposed me to a variety of approaches,” Dr. Noronha says. “My opinion is that coders have degrees and professional certifications and, thus, are capable of taking on this responsibility.”
Physicians still need to review submissions within specified time frames, and the system is yet to incorporate regular audits to ensure the quality of the coding.
What is the hospitalist’s optimal role in professional services billing? According to Leonard Noronha, MD, who was until recently a hospitalist practicing at the University of New Mexico (UNM), “physicians often find E/M (evaluation and management) coding rules confusing and frustrating,” leading to delinquent or tardy bills. Yet some feel apprehensive about turning billing and coding decisions over to professional coders because the physician retains legal responsibility for the accuracy of coding.
In a poster presented at HM12 in San Diego, Dr. Noronha described a 2010 decision by the academic group at UNM to have coders assign service levels to physician visits, retrieving the data from typed progress notes in the medical center’s newly implemented electronic health record (EHR). There were concerns that this new approach might lead to decreased revenue, but in practice, it led to both increased charges and collections (18%) and faster bill submissions (to 14 days from 16 days). The UNM hospitalists are incentivized to submit daily patient lists and to respond promptly to documentation completion requests.
“Working in a community hospital setting for five years and then in an academic practice for four years exposed me to a variety of approaches,” Dr. Noronha says. “My opinion is that coders have degrees and professional certifications and, thus, are capable of taking on this responsibility.”
Physicians still need to review submissions within specified time frames, and the system is yet to incorporate regular audits to ensure the quality of the coding.
What is the hospitalist’s optimal role in professional services billing? According to Leonard Noronha, MD, who was until recently a hospitalist practicing at the University of New Mexico (UNM), “physicians often find E/M (evaluation and management) coding rules confusing and frustrating,” leading to delinquent or tardy bills. Yet some feel apprehensive about turning billing and coding decisions over to professional coders because the physician retains legal responsibility for the accuracy of coding.
In a poster presented at HM12 in San Diego, Dr. Noronha described a 2010 decision by the academic group at UNM to have coders assign service levels to physician visits, retrieving the data from typed progress notes in the medical center’s newly implemented electronic health record (EHR). There were concerns that this new approach might lead to decreased revenue, but in practice, it led to both increased charges and collections (18%) and faster bill submissions (to 14 days from 16 days). The UNM hospitalists are incentivized to submit daily patient lists and to respond promptly to documentation completion requests.
“Working in a community hospital setting for five years and then in an academic practice for four years exposed me to a variety of approaches,” Dr. Noronha says. “My opinion is that coders have degrees and professional certifications and, thus, are capable of taking on this responsibility.”
Physicians still need to review submissions within specified time frames, and the system is yet to incorporate regular audits to ensure the quality of the coding.
U.S. Army Supports Rapid Deployment of Hospital Practice



A U.S. military combat-support hospital team based at Fort Polk near Leesville, La., works hard year-round to remain ready to erect a temporary, fully functioning tent hospital within 72 hours whenever and wherever it’s needed. That could mean an overseas war zone or closer to home for Americans hit by a tornado or hurricane.
The 115th Forward Support Battalion, led by Col. Kevin J. Stevens, has practiced assembling the temporary hospital three times this year, with another exercise planned for October. In its last run-through, a 24-hour acute-care hospital of 84 beds was erected in 66 hours. It included two operating rooms, two 24-bed ICUs with ventilators, patient wards, a six-bay ED, specialty clinics, and lab, pathology, biomedical, pharmacy, and blood services.
All of the needed equipment can be moved by truck, airplane, or boat in 32 20-foot-long vehicles, Stevens says. The staging team lays out the perimeter, perhaps in a parking lot or an existing structure, such as a school. Heating and cooling systems, water, oxygen, and power generators are brought in, and the team establishes a landing pad for helicopters.
“We bring all that wherever we go. But setting it up is the easy part,” Stevens says, adding that staffing and managing an acute-care hospital is the hard part.
When fully operational, the temporary hospital employs a professional staff of 75 to 80, including medical specialists. Some are based year-round at Fort Polk, keeping the equipment maintained. Others practice at hospitals across the country but are on the “call list” when a deployment is ordered. A new set of up-to-date, interlocking equipment for the temporary hospital was issued in March.
“Getting better at this is my mission,” says Stevens, a soldier since 1974 who has deployed with Forward Support Hospitals in both Iraq and Afghanistan. “We work to keep medical and deployment skills sharp at all times. Everything we do is meant to save soldier and civilian lives.”
Larry Beresford is a freelance writer in Oakland, Calif.
A U.S. military combat-support hospital team based at Fort Polk near Leesville, La., works hard year-round to remain ready to erect a temporary, fully functioning tent hospital within 72 hours whenever and wherever it’s needed. That could mean an overseas war zone or closer to home for Americans hit by a tornado or hurricane.
The 115th Forward Support Battalion, led by Col. Kevin J. Stevens, has practiced assembling the temporary hospital three times this year, with another exercise planned for October. In its last run-through, a 24-hour acute-care hospital of 84 beds was erected in 66 hours. It included two operating rooms, two 24-bed ICUs with ventilators, patient wards, a six-bay ED, specialty clinics, and lab, pathology, biomedical, pharmacy, and blood services.
All of the needed equipment can be moved by truck, airplane, or boat in 32 20-foot-long vehicles, Stevens says. The staging team lays out the perimeter, perhaps in a parking lot or an existing structure, such as a school. Heating and cooling systems, water, oxygen, and power generators are brought in, and the team establishes a landing pad for helicopters.
“We bring all that wherever we go. But setting it up is the easy part,” Stevens says, adding that staffing and managing an acute-care hospital is the hard part.
When fully operational, the temporary hospital employs a professional staff of 75 to 80, including medical specialists. Some are based year-round at Fort Polk, keeping the equipment maintained. Others practice at hospitals across the country but are on the “call list” when a deployment is ordered. A new set of up-to-date, interlocking equipment for the temporary hospital was issued in March.
“Getting better at this is my mission,” says Stevens, a soldier since 1974 who has deployed with Forward Support Hospitals in both Iraq and Afghanistan. “We work to keep medical and deployment skills sharp at all times. Everything we do is meant to save soldier and civilian lives.”
Larry Beresford is a freelance writer in Oakland, Calif.
A U.S. military combat-support hospital team based at Fort Polk near Leesville, La., works hard year-round to remain ready to erect a temporary, fully functioning tent hospital within 72 hours whenever and wherever it’s needed. That could mean an overseas war zone or closer to home for Americans hit by a tornado or hurricane.
The 115th Forward Support Battalion, led by Col. Kevin J. Stevens, has practiced assembling the temporary hospital three times this year, with another exercise planned for October. In its last run-through, a 24-hour acute-care hospital of 84 beds was erected in 66 hours. It included two operating rooms, two 24-bed ICUs with ventilators, patient wards, a six-bay ED, specialty clinics, and lab, pathology, biomedical, pharmacy, and blood services.
All of the needed equipment can be moved by truck, airplane, or boat in 32 20-foot-long vehicles, Stevens says. The staging team lays out the perimeter, perhaps in a parking lot or an existing structure, such as a school. Heating and cooling systems, water, oxygen, and power generators are brought in, and the team establishes a landing pad for helicopters.
“We bring all that wherever we go. But setting it up is the easy part,” Stevens says, adding that staffing and managing an acute-care hospital is the hard part.
When fully operational, the temporary hospital employs a professional staff of 75 to 80, including medical specialists. Some are based year-round at Fort Polk, keeping the equipment maintained. Others practice at hospitals across the country but are on the “call list” when a deployment is ordered. A new set of up-to-date, interlocking equipment for the temporary hospital was issued in March.
“Getting better at this is my mission,” says Stevens, a soldier since 1974 who has deployed with Forward Support Hospitals in both Iraq and Afghanistan. “We work to keep medical and deployment skills sharp at all times. Everything we do is meant to save soldier and civilian lives.”
Larry Beresford is a freelance writer in Oakland, Calif.
Win Whitcomb: Hospitalists Must Grin and Bear the Hospital-Acquired Conditions Program

The Inpatient Prospective Payment System FY2013 Final Rule charts a different future: By fiscal-year 2015 (October 2014), it will morph into a set of measures that are vetted by the National Quality Forum. Hopefully, this will be an improvement.
In recent years, hospitalists have been deluged with rules about documentation, being asked to use medical vocabulary in ways that were foreign to many of us during our training years. Much of the focus on documentation has been propelled by hospitals’ quest to optimize (“maximize” is a forbidden term) reimbursement, which is purely a function of what is written by “licensed providers” (doctors, physician assistants, and nurse practitioners) in the medical chart.
But another powerful driver of documentation practices of late is the hospital-acquired conditions (HAC) program developed by the Centers for Medicare & Medicaid Services (CMS) and enacted in 2009.
Origins of the HAC List
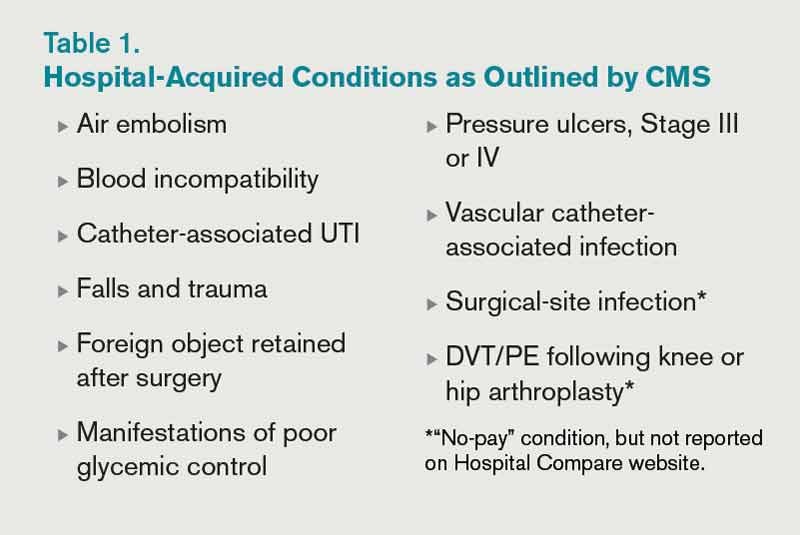
CMS disliked the fact that they were paying for conditions acquired in the hospital that were “reasonably preventable” if evidence-based—or at least “best”—practice was applied. After all, who likes to pay for a punctured gas tank when you brought the minivan in for an oil change? CMS worked with stakeholder groups, including SHM, to create a list of conditions known as hospital-acquired conditions (see Table 1, right).
(As an aside, SHM was supportive of CMS. In fact, we provided direct input into the final rule, recognizing some of the drawbacks of the CMS approach but understanding the larger objective of reengineering a flawed incentive system.)
The idea was that if a hospital submitted a bill to CMS that contained one of these conditions, the hospital would not be paid the amount by which that condition increased total reimbursement for that hospitalization. Note that if you’ve been told your hospital isn’t getting paid at all for patients with one of these conditions, that is not quite correct. Instead, your hospital may not get paid the added amount that is derived from having one of the diagnoses on the list submitted in your hospital’s bill to CMS for a given patient. At the end of the day, this might be a few hundred dollars each time one of these is documented—or $0, if your hospital biller can add another diagnosis in its place to capture the higher payment.
How big a hit to a hospital’s bottom line is this? Meddings and colleagues recently reported that a measly 0.003% of all hospitalizations in Michigan in 2009 saw payments lowered as a result of hospital-acquired catheter-associated UTI, one of the list’s HACs (Ann Int Med. 2012;157:305-312). When all the HACs are added together, one can extrapolate that they haven’t exactly had a big impact on hospital payments.
If the specter of nonpayment for one of these is not enough of a motivator (and it shouldn’t be, given the paltry financial stakes), the rate of HACs are now reported for all hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov). If a small poke to the pocketbook doesn’t work, maybe public humiliation will.
The Problem with HACs
Although CMS’ intent in creating the HAC program—to eliminate payment for “reasonably preventable” hospital-acquired conditions, thereby improving patient safety—was good, in practice, the program has turned out to be as much about documentation as it is about providing good care. For example, if I forget to write that a Stage III pressure ulcer was present on admission, it gets coded as hospital-acquired and my hospital gets dinged.
It’s important to note that HACs as quality measures were never endorsed by the National Quality Forum (NQF), and without such an endorsement, a quality measure suffers from Rodney Dangerfield syndrome: It don’t get no respect.
Finally, it is disquieting that Meddings et al showed that hospital-acquired catheter-associated UTI rates derived from chart documentation for HACs were but a small fraction of rates determined from rigorous epidemiologic studies, demonstrating that using claims data for determining rates for that specific HAC is flawed. We can only wonder how divergent reported vs. actual rates for the other HACs are.
The Future of the HAC Program
The Affordable Care Act specifies that the lowest-performing quartile of U.S. hospitals for HAC rates will see a 1% Medicare reimbursement reduction beginning in fiscal-year 2015. That’s right: Hospitals facing possible readmissions penalties and losses under value-based purchasing also will face a HAC penalty.
Thankfully, the recently released Inpatient Prospective Payment System FY2013 Final Rule, CMS’ annual update of how hospitals are paid, specifies that the HAC measures are to be removed from public reporting on the Hospital Compare website effective Oct. 1, 2014. They will be replaced by a new set of measures that will (hopefully) be more methodologically sound, because they will require the scrutiny required for endorsement by the NQF. Exactly how these measures will look is not certain, as the rule-making has not yet occurred.
We do know that the three infection measures—catheter-associated UTI, surgical-site infection, and vascular catheter infection—will be generated from clinical data and, therefore, more methodologically sound under the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network. The derivation of the other measures will have to wait until the rule is written next year.
So, until further notice, pay attention to the queries of your hospital’s documentation experts when they approach you about a potential HAC!
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is involved in influencing HAC definitions and the methods in which those definitions are used, in an attempt to “keep it real.” It is important for hospitalists to understand how the HACs can influence care, reimbursement, and their medical center’s strategic priorities. SHM has provided input to CMS, the CDC, and the NQF on the critical role hospitalists have in reducing or preventing HACs. SHM also has played a national role by leading an effort to reduce catheter-associated UTIs through the Partnership for Patients program, a national campaign with a goal of reducing hospital-acquired infections by 40% by the end of 2013.
SHM offers a variety of resources and programs related to reducing HACs, allowing hospitalists to improve patient safety and provide value to their hospital’s leadership. These include:
- Step-by-step implementation guides for reducing hospital-acquired VTE and hyper- and hypoglycemia;
- VTE and glycemic control mentored implementation programs that offer physician experts for tailored coaching on implementing best practices; and
- A fully functioning data repository and reporting engine for glycemic control parameters and hypoglycemia rates and management (eQUIPS).
The Inpatient Prospective Payment System FY2013 Final Rule charts a different future: By fiscal-year 2015 (October 2014), it will morph into a set of measures that are vetted by the National Quality Forum. Hopefully, this will be an improvement.
In recent years, hospitalists have been deluged with rules about documentation, being asked to use medical vocabulary in ways that were foreign to many of us during our training years. Much of the focus on documentation has been propelled by hospitals’ quest to optimize (“maximize” is a forbidden term) reimbursement, which is purely a function of what is written by “licensed providers” (doctors, physician assistants, and nurse practitioners) in the medical chart.
But another powerful driver of documentation practices of late is the hospital-acquired conditions (HAC) program developed by the Centers for Medicare & Medicaid Services (CMS) and enacted in 2009.
Origins of the HAC List
CMS disliked the fact that they were paying for conditions acquired in the hospital that were “reasonably preventable” if evidence-based—or at least “best”—practice was applied. After all, who likes to pay for a punctured gas tank when you brought the minivan in for an oil change? CMS worked with stakeholder groups, including SHM, to create a list of conditions known as hospital-acquired conditions (see Table 1, right).
(As an aside, SHM was supportive of CMS. In fact, we provided direct input into the final rule, recognizing some of the drawbacks of the CMS approach but understanding the larger objective of reengineering a flawed incentive system.)
The idea was that if a hospital submitted a bill to CMS that contained one of these conditions, the hospital would not be paid the amount by which that condition increased total reimbursement for that hospitalization. Note that if you’ve been told your hospital isn’t getting paid at all for patients with one of these conditions, that is not quite correct. Instead, your hospital may not get paid the added amount that is derived from having one of the diagnoses on the list submitted in your hospital’s bill to CMS for a given patient. At the end of the day, this might be a few hundred dollars each time one of these is documented—or $0, if your hospital biller can add another diagnosis in its place to capture the higher payment.
How big a hit to a hospital’s bottom line is this? Meddings and colleagues recently reported that a measly 0.003% of all hospitalizations in Michigan in 2009 saw payments lowered as a result of hospital-acquired catheter-associated UTI, one of the list’s HACs (Ann Int Med. 2012;157:305-312). When all the HACs are added together, one can extrapolate that they haven’t exactly had a big impact on hospital payments.
If the specter of nonpayment for one of these is not enough of a motivator (and it shouldn’t be, given the paltry financial stakes), the rate of HACs are now reported for all hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov). If a small poke to the pocketbook doesn’t work, maybe public humiliation will.
The Problem with HACs
Although CMS’ intent in creating the HAC program—to eliminate payment for “reasonably preventable” hospital-acquired conditions, thereby improving patient safety—was good, in practice, the program has turned out to be as much about documentation as it is about providing good care. For example, if I forget to write that a Stage III pressure ulcer was present on admission, it gets coded as hospital-acquired and my hospital gets dinged.
It’s important to note that HACs as quality measures were never endorsed by the National Quality Forum (NQF), and without such an endorsement, a quality measure suffers from Rodney Dangerfield syndrome: It don’t get no respect.
Finally, it is disquieting that Meddings et al showed that hospital-acquired catheter-associated UTI rates derived from chart documentation for HACs were but a small fraction of rates determined from rigorous epidemiologic studies, demonstrating that using claims data for determining rates for that specific HAC is flawed. We can only wonder how divergent reported vs. actual rates for the other HACs are.
The Future of the HAC Program
The Affordable Care Act specifies that the lowest-performing quartile of U.S. hospitals for HAC rates will see a 1% Medicare reimbursement reduction beginning in fiscal-year 2015. That’s right: Hospitals facing possible readmissions penalties and losses under value-based purchasing also will face a HAC penalty.
Thankfully, the recently released Inpatient Prospective Payment System FY2013 Final Rule, CMS’ annual update of how hospitals are paid, specifies that the HAC measures are to be removed from public reporting on the Hospital Compare website effective Oct. 1, 2014. They will be replaced by a new set of measures that will (hopefully) be more methodologically sound, because they will require the scrutiny required for endorsement by the NQF. Exactly how these measures will look is not certain, as the rule-making has not yet occurred.
We do know that the three infection measures—catheter-associated UTI, surgical-site infection, and vascular catheter infection—will be generated from clinical data and, therefore, more methodologically sound under the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network. The derivation of the other measures will have to wait until the rule is written next year.
So, until further notice, pay attention to the queries of your hospital’s documentation experts when they approach you about a potential HAC!
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is involved in influencing HAC definitions and the methods in which those definitions are used, in an attempt to “keep it real.” It is important for hospitalists to understand how the HACs can influence care, reimbursement, and their medical center’s strategic priorities. SHM has provided input to CMS, the CDC, and the NQF on the critical role hospitalists have in reducing or preventing HACs. SHM also has played a national role by leading an effort to reduce catheter-associated UTIs through the Partnership for Patients program, a national campaign with a goal of reducing hospital-acquired infections by 40% by the end of 2013.
SHM offers a variety of resources and programs related to reducing HACs, allowing hospitalists to improve patient safety and provide value to their hospital’s leadership. These include:
- Step-by-step implementation guides for reducing hospital-acquired VTE and hyper- and hypoglycemia;
- VTE and glycemic control mentored implementation programs that offer physician experts for tailored coaching on implementing best practices; and
- A fully functioning data repository and reporting engine for glycemic control parameters and hypoglycemia rates and management (eQUIPS).
The Inpatient Prospective Payment System FY2013 Final Rule charts a different future: By fiscal-year 2015 (October 2014), it will morph into a set of measures that are vetted by the National Quality Forum. Hopefully, this will be an improvement.
In recent years, hospitalists have been deluged with rules about documentation, being asked to use medical vocabulary in ways that were foreign to many of us during our training years. Much of the focus on documentation has been propelled by hospitals’ quest to optimize (“maximize” is a forbidden term) reimbursement, which is purely a function of what is written by “licensed providers” (doctors, physician assistants, and nurse practitioners) in the medical chart.
But another powerful driver of documentation practices of late is the hospital-acquired conditions (HAC) program developed by the Centers for Medicare & Medicaid Services (CMS) and enacted in 2009.
Origins of the HAC List
CMS disliked the fact that they were paying for conditions acquired in the hospital that were “reasonably preventable” if evidence-based—or at least “best”—practice was applied. After all, who likes to pay for a punctured gas tank when you brought the minivan in for an oil change? CMS worked with stakeholder groups, including SHM, to create a list of conditions known as hospital-acquired conditions (see Table 1, right).
(As an aside, SHM was supportive of CMS. In fact, we provided direct input into the final rule, recognizing some of the drawbacks of the CMS approach but understanding the larger objective of reengineering a flawed incentive system.)
The idea was that if a hospital submitted a bill to CMS that contained one of these conditions, the hospital would not be paid the amount by which that condition increased total reimbursement for that hospitalization. Note that if you’ve been told your hospital isn’t getting paid at all for patients with one of these conditions, that is not quite correct. Instead, your hospital may not get paid the added amount that is derived from having one of the diagnoses on the list submitted in your hospital’s bill to CMS for a given patient. At the end of the day, this might be a few hundred dollars each time one of these is documented—or $0, if your hospital biller can add another diagnosis in its place to capture the higher payment.
How big a hit to a hospital’s bottom line is this? Meddings and colleagues recently reported that a measly 0.003% of all hospitalizations in Michigan in 2009 saw payments lowered as a result of hospital-acquired catheter-associated UTI, one of the list’s HACs (Ann Int Med. 2012;157:305-312). When all the HACs are added together, one can extrapolate that they haven’t exactly had a big impact on hospital payments.
If the specter of nonpayment for one of these is not enough of a motivator (and it shouldn’t be, given the paltry financial stakes), the rate of HACs are now reported for all hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov). If a small poke to the pocketbook doesn’t work, maybe public humiliation will.
The Problem with HACs
Although CMS’ intent in creating the HAC program—to eliminate payment for “reasonably preventable” hospital-acquired conditions, thereby improving patient safety—was good, in practice, the program has turned out to be as much about documentation as it is about providing good care. For example, if I forget to write that a Stage III pressure ulcer was present on admission, it gets coded as hospital-acquired and my hospital gets dinged.
It’s important to note that HACs as quality measures were never endorsed by the National Quality Forum (NQF), and without such an endorsement, a quality measure suffers from Rodney Dangerfield syndrome: It don’t get no respect.
Finally, it is disquieting that Meddings et al showed that hospital-acquired catheter-associated UTI rates derived from chart documentation for HACs were but a small fraction of rates determined from rigorous epidemiologic studies, demonstrating that using claims data for determining rates for that specific HAC is flawed. We can only wonder how divergent reported vs. actual rates for the other HACs are.
The Future of the HAC Program
The Affordable Care Act specifies that the lowest-performing quartile of U.S. hospitals for HAC rates will see a 1% Medicare reimbursement reduction beginning in fiscal-year 2015. That’s right: Hospitals facing possible readmissions penalties and losses under value-based purchasing also will face a HAC penalty.
Thankfully, the recently released Inpatient Prospective Payment System FY2013 Final Rule, CMS’ annual update of how hospitals are paid, specifies that the HAC measures are to be removed from public reporting on the Hospital Compare website effective Oct. 1, 2014. They will be replaced by a new set of measures that will (hopefully) be more methodologically sound, because they will require the scrutiny required for endorsement by the NQF. Exactly how these measures will look is not certain, as the rule-making has not yet occurred.
We do know that the three infection measures—catheter-associated UTI, surgical-site infection, and vascular catheter infection—will be generated from clinical data and, therefore, more methodologically sound under the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network. The derivation of the other measures will have to wait until the rule is written next year.
So, until further notice, pay attention to the queries of your hospital’s documentation experts when they approach you about a potential HAC!
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is involved in influencing HAC definitions and the methods in which those definitions are used, in an attempt to “keep it real.” It is important for hospitalists to understand how the HACs can influence care, reimbursement, and their medical center’s strategic priorities. SHM has provided input to CMS, the CDC, and the NQF on the critical role hospitalists have in reducing or preventing HACs. SHM also has played a national role by leading an effort to reduce catheter-associated UTIs through the Partnership for Patients program, a national campaign with a goal of reducing hospital-acquired infections by 40% by the end of 2013.
SHM offers a variety of resources and programs related to reducing HACs, allowing hospitalists to improve patient safety and provide value to their hospital’s leadership. These include:
- Step-by-step implementation guides for reducing hospital-acquired VTE and hyper- and hypoglycemia;
- VTE and glycemic control mentored implementation programs that offer physician experts for tailored coaching on implementing best practices; and
- A fully functioning data repository and reporting engine for glycemic control parameters and hypoglycemia rates and management (eQUIPS).
The Quality Journey of Hospitalist David J. Yu
Hospitalist David J. Yu, MD, FACP, MBA, SFHM, medical director of the adult inpatient service at Presbyterian Healthcare Services in Albuquerque, N.M., began his quality journey by earning an MBA, then spending a week at University of Toyota in Gardena, Calif., to learn its Lean process-management techniques. He presented a Research, Innovations, and Clinical Vignettes poster at HM12 that outlined the multidisciplinary quality initiative at 453-bed Presbyterian Hospital in Albuquerque.
The project identified problems of throughput, ED diversion, disjointed team rounding, inadequate communication, multiple patient handoffs, low staff morale, and greater-than-expected length of stay (LOS).
“We really dug into the issues on a granular level,” with the participation of finance, nursing, care coordinators, physical therapy, and other staffers alongside the hospitalists, Dr. Yu says. The project ended up changing the practice from a model in which 11 hospitalist teams and five admitting hospitalists cared for patients throughout the hospital’s various floors while carrying caseloads too high to manage optimally. They replaced it with a unit-based rounding model, with hospitalists and care coordinators geographically segregated on units and multidisciplinary rounds to improve the efficiency of team communication (see “A Holy Grail,” July 2012, p. 30).
The group also used data to persuade the hospital’s administration to add hospitalist FTEs. As a result, LOS on two pilot units decreased by nearly half a day, with increased inpatient volume, higher patient satisfaction scores on Press-Ganey surveys, and an estimated net financial benefit of nearly $3.5 million between April 2010 and December 2011—even counting the additional hospitalist FTEs. This model has since spread to all medical units in the hospital.
“We need to be in the business of producing ‘defect-free’ discharges,” Dr. Yu quips. “Every group needs a local solution. But the mantra for this work is standardization....That’s where the leadership of the hospitalist comes in. It’s not, ‘Follow me,’ but ‘Hey, join us in collaborating together to come up with a solution.’
“It has been a two-year journey, and we’re still learning.”
Hospitalist David J. Yu, MD, FACP, MBA, SFHM, medical director of the adult inpatient service at Presbyterian Healthcare Services in Albuquerque, N.M., began his quality journey by earning an MBA, then spending a week at University of Toyota in Gardena, Calif., to learn its Lean process-management techniques. He presented a Research, Innovations, and Clinical Vignettes poster at HM12 that outlined the multidisciplinary quality initiative at 453-bed Presbyterian Hospital in Albuquerque.
The project identified problems of throughput, ED diversion, disjointed team rounding, inadequate communication, multiple patient handoffs, low staff morale, and greater-than-expected length of stay (LOS).
“We really dug into the issues on a granular level,” with the participation of finance, nursing, care coordinators, physical therapy, and other staffers alongside the hospitalists, Dr. Yu says. The project ended up changing the practice from a model in which 11 hospitalist teams and five admitting hospitalists cared for patients throughout the hospital’s various floors while carrying caseloads too high to manage optimally. They replaced it with a unit-based rounding model, with hospitalists and care coordinators geographically segregated on units and multidisciplinary rounds to improve the efficiency of team communication (see “A Holy Grail,” July 2012, p. 30).
The group also used data to persuade the hospital’s administration to add hospitalist FTEs. As a result, LOS on two pilot units decreased by nearly half a day, with increased inpatient volume, higher patient satisfaction scores on Press-Ganey surveys, and an estimated net financial benefit of nearly $3.5 million between April 2010 and December 2011—even counting the additional hospitalist FTEs. This model has since spread to all medical units in the hospital.
“We need to be in the business of producing ‘defect-free’ discharges,” Dr. Yu quips. “Every group needs a local solution. But the mantra for this work is standardization....That’s where the leadership of the hospitalist comes in. It’s not, ‘Follow me,’ but ‘Hey, join us in collaborating together to come up with a solution.’
“It has been a two-year journey, and we’re still learning.”
Hospitalist David J. Yu, MD, FACP, MBA, SFHM, medical director of the adult inpatient service at Presbyterian Healthcare Services in Albuquerque, N.M., began his quality journey by earning an MBA, then spending a week at University of Toyota in Gardena, Calif., to learn its Lean process-management techniques. He presented a Research, Innovations, and Clinical Vignettes poster at HM12 that outlined the multidisciplinary quality initiative at 453-bed Presbyterian Hospital in Albuquerque.
The project identified problems of throughput, ED diversion, disjointed team rounding, inadequate communication, multiple patient handoffs, low staff morale, and greater-than-expected length of stay (LOS).
“We really dug into the issues on a granular level,” with the participation of finance, nursing, care coordinators, physical therapy, and other staffers alongside the hospitalists, Dr. Yu says. The project ended up changing the practice from a model in which 11 hospitalist teams and five admitting hospitalists cared for patients throughout the hospital’s various floors while carrying caseloads too high to manage optimally. They replaced it with a unit-based rounding model, with hospitalists and care coordinators geographically segregated on units and multidisciplinary rounds to improve the efficiency of team communication (see “A Holy Grail,” July 2012, p. 30).
The group also used data to persuade the hospital’s administration to add hospitalist FTEs. As a result, LOS on two pilot units decreased by nearly half a day, with increased inpatient volume, higher patient satisfaction scores on Press-Ganey surveys, and an estimated net financial benefit of nearly $3.5 million between April 2010 and December 2011—even counting the additional hospitalist FTEs. This model has since spread to all medical units in the hospital.
“We need to be in the business of producing ‘defect-free’ discharges,” Dr. Yu quips. “Every group needs a local solution. But the mantra for this work is standardization....That’s where the leadership of the hospitalist comes in. It’s not, ‘Follow me,’ but ‘Hey, join us in collaborating together to come up with a solution.’
“It has been a two-year journey, and we’re still learning.”
Defining and Protecting Scope of Practice Critical for Hospitalists
Scope creep can lead to suboptimal clinical outcomes if hospitalist practices fail to plan appropriately, Dr. Simone says. The plan must include “development of a staffing and schedule model to accommodate service expansion (when applicable), creation of policies and procedures addressing the new services, and hospitalist training (when appropriate) to ensure competently trained providers,” he adds.
Before any HM group agrees to comanagement, it should first understand the reasons for the request, Dr. Siegal says. According to a presentation he gave at HM07 on the topic, group leaders should:
- Determine if comanagement is a reasonable solution to the problem.
- Identify stakeholders and understand their goals, concerns, and expectations.
- Ask what might be jeopardized if hospitalists participate: Will it overload an already busy service, compromise care elsewhere, or set unrealistic service expectations?
- Set measurable outcomes to quantify the success (or failure) of the new arrangement.
It’s also important to define responsibilities, establish clear lines of communication, and determine how disagreements will be adjudicated. Establish your scope of practice and stick to it, Dr. Siegal says. A big red flag is when your group does things on nights, weekends, or holidays that it doesn’t do during the week.
Scope creep can lead to suboptimal clinical outcomes if hospitalist practices fail to plan appropriately, Dr. Simone says. The plan must include “development of a staffing and schedule model to accommodate service expansion (when applicable), creation of policies and procedures addressing the new services, and hospitalist training (when appropriate) to ensure competently trained providers,” he adds.
Before any HM group agrees to comanagement, it should first understand the reasons for the request, Dr. Siegal says. According to a presentation he gave at HM07 on the topic, group leaders should:
- Determine if comanagement is a reasonable solution to the problem.
- Identify stakeholders and understand their goals, concerns, and expectations.
- Ask what might be jeopardized if hospitalists participate: Will it overload an already busy service, compromise care elsewhere, or set unrealistic service expectations?
- Set measurable outcomes to quantify the success (or failure) of the new arrangement.
It’s also important to define responsibilities, establish clear lines of communication, and determine how disagreements will be adjudicated. Establish your scope of practice and stick to it, Dr. Siegal says. A big red flag is when your group does things on nights, weekends, or holidays that it doesn’t do during the week.
Scope creep can lead to suboptimal clinical outcomes if hospitalist practices fail to plan appropriately, Dr. Simone says. The plan must include “development of a staffing and schedule model to accommodate service expansion (when applicable), creation of policies and procedures addressing the new services, and hospitalist training (when appropriate) to ensure competently trained providers,” he adds.
Before any HM group agrees to comanagement, it should first understand the reasons for the request, Dr. Siegal says. According to a presentation he gave at HM07 on the topic, group leaders should:
- Determine if comanagement is a reasonable solution to the problem.
- Identify stakeholders and understand their goals, concerns, and expectations.
- Ask what might be jeopardized if hospitalists participate: Will it overload an already busy service, compromise care elsewhere, or set unrealistic service expectations?
- Set measurable outcomes to quantify the success (or failure) of the new arrangement.
It’s also important to define responsibilities, establish clear lines of communication, and determine how disagreements will be adjudicated. Establish your scope of practice and stick to it, Dr. Siegal says. A big red flag is when your group does things on nights, weekends, or holidays that it doesn’t do during the week.
Five Ways Hospitalists Can Prevent Overextending Their Services
1. Do not feel sorry for yourself; it can become a self-fulfilling prophecy.
“Most of what is happening in medicine is outside of our control,” Dr. Nelson says. “We need to realize that our role is going to change, and we should not perceive ourselves as the low person on the totem pole.”
2. Increase “face time” with your specialist colleagues.
Join them for lunch in the physician’s lounge, call your colleagues by their first names, engage in meaningful discussions about cases, and show empathy for them and their patients. Look for opportunities to do mutual education with other services.
3. Know when to draw the line.
“HM leaders should have the skills to analyze an opportunity and assess whether their program has the staffing capacity and clinical skills to successfully deliver a requested service,” Dr. Simone says. “‘No’ is an acceptable answer, if there are clear and reasonable reasons that support that decision.”
4. Make it about the patient.
Whenever your HM service is approached about comanagement, phrase your decision within the context of ensuring patient safety and delivering quality care. In that way, Dr. Siy says, you will be on solid footing.
5. Openly promote strategic “yes” answers.
Instead of digging in their heels, HM groups can periodically examine all requests, pick one or two to begin with, then promote successful outcomes to boost the group’s value.
1. Do not feel sorry for yourself; it can become a self-fulfilling prophecy.
“Most of what is happening in medicine is outside of our control,” Dr. Nelson says. “We need to realize that our role is going to change, and we should not perceive ourselves as the low person on the totem pole.”
2. Increase “face time” with your specialist colleagues.
Join them for lunch in the physician’s lounge, call your colleagues by their first names, engage in meaningful discussions about cases, and show empathy for them and their patients. Look for opportunities to do mutual education with other services.
3. Know when to draw the line.
“HM leaders should have the skills to analyze an opportunity and assess whether their program has the staffing capacity and clinical skills to successfully deliver a requested service,” Dr. Simone says. “‘No’ is an acceptable answer, if there are clear and reasonable reasons that support that decision.”
4. Make it about the patient.
Whenever your HM service is approached about comanagement, phrase your decision within the context of ensuring patient safety and delivering quality care. In that way, Dr. Siy says, you will be on solid footing.
5. Openly promote strategic “yes” answers.
Instead of digging in their heels, HM groups can periodically examine all requests, pick one or two to begin with, then promote successful outcomes to boost the group’s value.
1. Do not feel sorry for yourself; it can become a self-fulfilling prophecy.
“Most of what is happening in medicine is outside of our control,” Dr. Nelson says. “We need to realize that our role is going to change, and we should not perceive ourselves as the low person on the totem pole.”
2. Increase “face time” with your specialist colleagues.
Join them for lunch in the physician’s lounge, call your colleagues by their first names, engage in meaningful discussions about cases, and show empathy for them and their patients. Look for opportunities to do mutual education with other services.
3. Know when to draw the line.
“HM leaders should have the skills to analyze an opportunity and assess whether their program has the staffing capacity and clinical skills to successfully deliver a requested service,” Dr. Simone says. “‘No’ is an acceptable answer, if there are clear and reasonable reasons that support that decision.”
4. Make it about the patient.
Whenever your HM service is approached about comanagement, phrase your decision within the context of ensuring patient safety and delivering quality care. In that way, Dr. Siy says, you will be on solid footing.
5. Openly promote strategic “yes” answers.
Instead of digging in their heels, HM groups can periodically examine all requests, pick one or two to begin with, then promote successful outcomes to boost the group’s value.
Shaun Frost: Society of Hospital Medicine Supports the Choosing Wisely Campaign (CWC)

SHM is participating in the ABIM Foundation's Choosing Wisely Campaign (CWC).1 Launched earlier this year, the CWC aims to increase awareness about medical practices that may be of little or no benefit to patients. Presently, 26 physician organizations have teamed with the ABIM Foundation to each create a list of “five things physicians and patients should question.” In addition, Consumer Reports (the product ratings organization well known for grading the quality of such items as automobiles and vacuum cleaners) is coordinating the efforts of 11 consumer groups to advance the CWC agenda.
The CWC aims to highlight two pillars of healthcare reform that will receive enhanced attention in the near future: 1. Cost of care, and 2. Patient experience of care. Heretofore healthcare reform efforts have largely been focused on the quality and patient-safety movements. Equally important, however, to policymakers is affordability and care experience. By focusing on tests and procedures of questionable benefit, the CWC aims to directly address costly unnecessary treatment by encouraging care planning that incorporates patient preferences. This is necessary work because research suggests that physician decisions account for 80% of healthcare expenditures, while the tradition of patients entrusting their doctors with complete decision-making authority leads to care that they do not want.2
Choosing Wisely Begins with Medical Professionalism
In 2002, the ABIM Foundation collaborated with the American College of Physicians Foundation and the European Federation of Internal Medicine to jointly author “Medical Professionalism in the New Millennium: A Physician Charter.”3 The charter has since been endorsed by more than 130 organizations and triggered countless improvement initiatives to advance its fundamental principles of patient welfare, patient autonomy, and social justice.
Through project grant support, the ABIM Foundation is emphasizing two key Physician Charter commitments (see Table 1) to advance appropriate healthcare decision-making and encourage stewardship of healthcare resources. The CWC naturally augments this work by focusing on care affordability and decision-making through shared discussions between patients and providers.
SHM’s Involvement
SHM convened a workgroup of hospital medicine quality improvement experts led by John Bulger, DO, the chief quality officer at Geisinger Health System in Pennsylvania. This group solicited from SHM committee members 150 suggested tests and treatments that HM clinicians and their patients should question. After critical analysis, the list was narrowed to exclude suggestions already being advanced by the CWC while focusing on those that represent the largest opportunity for hospitalists to impact on affordability and patient experience.
The list was then submitted to SHM members for comment via survey, resulting in 11 recommended medical interventions that were subjected to comprehensive literature review. Workgroup members then rated these 11 interventions according to the following criteria: validity of supporting evidence, feasibility and degree of hospitalist impact, frequency of occurrence, and cost of occurrence.
Finally, the workgroup collaborated with the SHM board of directors to submit to the ABIM Foundation the ultimate list of “five things hospitalists and their patients should question.” Ricardo Quinonez, MD, at Baylor College of Medicine in Houston, Texas, led a similar process that generated a list of questionable practices in pediatric HM. It, too, was submitted to the ABIM Foundation.
The CWC anticipates publishing SHM’s list in February 2013. In the meantime, please consult the CWC website to find practices commonly performed by hospitalists that have been deemed to be of unclear benefit by other professional medical societies (see “2012 CWC Recommendations for Hospitalists,” left).
SHM plans to build upon this work in the future. Expect to see Choosing Wisely sessions and discussions at the HM13 SHM Annual Meeting in May (www.hospitalmedicine2013.org) focused on creating and teaching QI strategies to implement CWC recommendations. Furthermore, the Center for Hospital Innovation and Improvement will be identifying opportunities to develop mentored implementation QI programs related to Choosing Wisely and its principles.
What You Can Do
Hospitalists can make a huge impact on affordability and patient experience given that most of the country’s healthcare dollar is spent in the hospital, and patients are at their most vulnerable to receiving treatment that they may not want when they are acutely ill. Hospitalists, thus, are uniquely positioned to make a positive impact by embracing the Choosing Wisely Campaign’s principles.
Please commit to assisting SHM by visiting the CWC website and learning about other medical society’s thoughts on “things physicians and patients should question.” Pledge thereafter to engage your patients and their families in healthcare decision-making, especially in situations where the benefits of tests and therapies are unclear.
Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same.
Dr. Frost is president of SHM.
References
- The ABIM Foundation. Choosing Wisely: An initiative of the ABIM Foundation. Choosing Wisely website. Available at: http://www.choosingwisely.org. Accessed Sept. 25, 2012.
- The ABIM Foundation. Principles Guiding Wise Choices. ABIM Foundation website. Available at: www.abimfoundation.org/Initiatives/~/media/Files/2011-Forum/110411_ABIM%20Stewardship.ashx. Accessed Sept. 25, 2012.
- ABIM Foundation, ACP–ASIM Foundation, European Federation of Internal Medicine. Medical Professionalism in the New Millennium: A Physician Charter. Ann Intern Med. 2002;136(3):243.
SHM is participating in the ABIM Foundation's Choosing Wisely Campaign (CWC).1 Launched earlier this year, the CWC aims to increase awareness about medical practices that may be of little or no benefit to patients. Presently, 26 physician organizations have teamed with the ABIM Foundation to each create a list of “five things physicians and patients should question.” In addition, Consumer Reports (the product ratings organization well known for grading the quality of such items as automobiles and vacuum cleaners) is coordinating the efforts of 11 consumer groups to advance the CWC agenda.
The CWC aims to highlight two pillars of healthcare reform that will receive enhanced attention in the near future: 1. Cost of care, and 2. Patient experience of care. Heretofore healthcare reform efforts have largely been focused on the quality and patient-safety movements. Equally important, however, to policymakers is affordability and care experience. By focusing on tests and procedures of questionable benefit, the CWC aims to directly address costly unnecessary treatment by encouraging care planning that incorporates patient preferences. This is necessary work because research suggests that physician decisions account for 80% of healthcare expenditures, while the tradition of patients entrusting their doctors with complete decision-making authority leads to care that they do not want.2
Choosing Wisely Begins with Medical Professionalism
In 2002, the ABIM Foundation collaborated with the American College of Physicians Foundation and the European Federation of Internal Medicine to jointly author “Medical Professionalism in the New Millennium: A Physician Charter.”3 The charter has since been endorsed by more than 130 organizations and triggered countless improvement initiatives to advance its fundamental principles of patient welfare, patient autonomy, and social justice.
Through project grant support, the ABIM Foundation is emphasizing two key Physician Charter commitments (see Table 1) to advance appropriate healthcare decision-making and encourage stewardship of healthcare resources. The CWC naturally augments this work by focusing on care affordability and decision-making through shared discussions between patients and providers.
SHM’s Involvement
SHM convened a workgroup of hospital medicine quality improvement experts led by John Bulger, DO, the chief quality officer at Geisinger Health System in Pennsylvania. This group solicited from SHM committee members 150 suggested tests and treatments that HM clinicians and their patients should question. After critical analysis, the list was narrowed to exclude suggestions already being advanced by the CWC while focusing on those that represent the largest opportunity for hospitalists to impact on affordability and patient experience.
The list was then submitted to SHM members for comment via survey, resulting in 11 recommended medical interventions that were subjected to comprehensive literature review. Workgroup members then rated these 11 interventions according to the following criteria: validity of supporting evidence, feasibility and degree of hospitalist impact, frequency of occurrence, and cost of occurrence.
Finally, the workgroup collaborated with the SHM board of directors to submit to the ABIM Foundation the ultimate list of “five things hospitalists and their patients should question.” Ricardo Quinonez, MD, at Baylor College of Medicine in Houston, Texas, led a similar process that generated a list of questionable practices in pediatric HM. It, too, was submitted to the ABIM Foundation.
The CWC anticipates publishing SHM’s list in February 2013. In the meantime, please consult the CWC website to find practices commonly performed by hospitalists that have been deemed to be of unclear benefit by other professional medical societies (see “2012 CWC Recommendations for Hospitalists,” left).
SHM plans to build upon this work in the future. Expect to see Choosing Wisely sessions and discussions at the HM13 SHM Annual Meeting in May (www.hospitalmedicine2013.org) focused on creating and teaching QI strategies to implement CWC recommendations. Furthermore, the Center for Hospital Innovation and Improvement will be identifying opportunities to develop mentored implementation QI programs related to Choosing Wisely and its principles.
What You Can Do
Hospitalists can make a huge impact on affordability and patient experience given that most of the country’s healthcare dollar is spent in the hospital, and patients are at their most vulnerable to receiving treatment that they may not want when they are acutely ill. Hospitalists, thus, are uniquely positioned to make a positive impact by embracing the Choosing Wisely Campaign’s principles.
Please commit to assisting SHM by visiting the CWC website and learning about other medical society’s thoughts on “things physicians and patients should question.” Pledge thereafter to engage your patients and their families in healthcare decision-making, especially in situations where the benefits of tests and therapies are unclear.
Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same.
Dr. Frost is president of SHM.
References
- The ABIM Foundation. Choosing Wisely: An initiative of the ABIM Foundation. Choosing Wisely website. Available at: http://www.choosingwisely.org. Accessed Sept. 25, 2012.
- The ABIM Foundation. Principles Guiding Wise Choices. ABIM Foundation website. Available at: www.abimfoundation.org/Initiatives/~/media/Files/2011-Forum/110411_ABIM%20Stewardship.ashx. Accessed Sept. 25, 2012.
- ABIM Foundation, ACP–ASIM Foundation, European Federation of Internal Medicine. Medical Professionalism in the New Millennium: A Physician Charter. Ann Intern Med. 2002;136(3):243.
SHM is participating in the ABIM Foundation's Choosing Wisely Campaign (CWC).1 Launched earlier this year, the CWC aims to increase awareness about medical practices that may be of little or no benefit to patients. Presently, 26 physician organizations have teamed with the ABIM Foundation to each create a list of “five things physicians and patients should question.” In addition, Consumer Reports (the product ratings organization well known for grading the quality of such items as automobiles and vacuum cleaners) is coordinating the efforts of 11 consumer groups to advance the CWC agenda.
The CWC aims to highlight two pillars of healthcare reform that will receive enhanced attention in the near future: 1. Cost of care, and 2. Patient experience of care. Heretofore healthcare reform efforts have largely been focused on the quality and patient-safety movements. Equally important, however, to policymakers is affordability and care experience. By focusing on tests and procedures of questionable benefit, the CWC aims to directly address costly unnecessary treatment by encouraging care planning that incorporates patient preferences. This is necessary work because research suggests that physician decisions account for 80% of healthcare expenditures, while the tradition of patients entrusting their doctors with complete decision-making authority leads to care that they do not want.2
Choosing Wisely Begins with Medical Professionalism
In 2002, the ABIM Foundation collaborated with the American College of Physicians Foundation and the European Federation of Internal Medicine to jointly author “Medical Professionalism in the New Millennium: A Physician Charter.”3 The charter has since been endorsed by more than 130 organizations and triggered countless improvement initiatives to advance its fundamental principles of patient welfare, patient autonomy, and social justice.
Through project grant support, the ABIM Foundation is emphasizing two key Physician Charter commitments (see Table 1) to advance appropriate healthcare decision-making and encourage stewardship of healthcare resources. The CWC naturally augments this work by focusing on care affordability and decision-making through shared discussions between patients and providers.
SHM’s Involvement
SHM convened a workgroup of hospital medicine quality improvement experts led by John Bulger, DO, the chief quality officer at Geisinger Health System in Pennsylvania. This group solicited from SHM committee members 150 suggested tests and treatments that HM clinicians and their patients should question. After critical analysis, the list was narrowed to exclude suggestions already being advanced by the CWC while focusing on those that represent the largest opportunity for hospitalists to impact on affordability and patient experience.
The list was then submitted to SHM members for comment via survey, resulting in 11 recommended medical interventions that were subjected to comprehensive literature review. Workgroup members then rated these 11 interventions according to the following criteria: validity of supporting evidence, feasibility and degree of hospitalist impact, frequency of occurrence, and cost of occurrence.
Finally, the workgroup collaborated with the SHM board of directors to submit to the ABIM Foundation the ultimate list of “five things hospitalists and their patients should question.” Ricardo Quinonez, MD, at Baylor College of Medicine in Houston, Texas, led a similar process that generated a list of questionable practices in pediatric HM. It, too, was submitted to the ABIM Foundation.
The CWC anticipates publishing SHM’s list in February 2013. In the meantime, please consult the CWC website to find practices commonly performed by hospitalists that have been deemed to be of unclear benefit by other professional medical societies (see “2012 CWC Recommendations for Hospitalists,” left).
SHM plans to build upon this work in the future. Expect to see Choosing Wisely sessions and discussions at the HM13 SHM Annual Meeting in May (www.hospitalmedicine2013.org) focused on creating and teaching QI strategies to implement CWC recommendations. Furthermore, the Center for Hospital Innovation and Improvement will be identifying opportunities to develop mentored implementation QI programs related to Choosing Wisely and its principles.
What You Can Do
Hospitalists can make a huge impact on affordability and patient experience given that most of the country’s healthcare dollar is spent in the hospital, and patients are at their most vulnerable to receiving treatment that they may not want when they are acutely ill. Hospitalists, thus, are uniquely positioned to make a positive impact by embracing the Choosing Wisely Campaign’s principles.
Please commit to assisting SHM by visiting the CWC website and learning about other medical society’s thoughts on “things physicians and patients should question.” Pledge thereafter to engage your patients and their families in healthcare decision-making, especially in situations where the benefits of tests and therapies are unclear.
Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same.
Dr. Frost is president of SHM.
References
- The ABIM Foundation. Choosing Wisely: An initiative of the ABIM Foundation. Choosing Wisely website. Available at: http://www.choosingwisely.org. Accessed Sept. 25, 2012.
- The ABIM Foundation. Principles Guiding Wise Choices. ABIM Foundation website. Available at: www.abimfoundation.org/Initiatives/~/media/Files/2011-Forum/110411_ABIM%20Stewardship.ashx. Accessed Sept. 25, 2012.
- ABIM Foundation, ACP–ASIM Foundation, European Federation of Internal Medicine. Medical Professionalism in the New Millennium: A Physician Charter. Ann Intern Med. 2002;136(3):243.