User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
US Hospitals Prone to Cyberattacks Like One That Impacted Patient Care at Ascension, Experts Say
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Should You Offer Medical Credit Cards?
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.

Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
Latest Izokibep Trial for PsA Shows Promise But Misses on Enthesitis
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.
At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.

“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.

More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.
At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.
“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.
More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.
At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.
“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.
More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
Selective JAK 1 Inhibitor for RA Proves Promising in Phase 3 Trial
VIENNA — The highly selective oral Janus kinase (JAK) inhibitor SHR0302 (ivarmacitinib) enables more patients with active rheumatoid arthritis to meet American College of Rheumatology (ACR) response criteria than placebo, the results of a phase 3 trial showed.
After 24 weeks of daily treatment, the primary endpoint of an ACR20 response was met by 40.4% of those who had been given placebo, 70.4% who had received a 4-mg dose, and 75.1% given an 8-mg dose. At the same time point, ACR50 responses were a respective 15.4%, 46.0%, and 57.1%, and ACR70 responses were 6.9%, 22.2%, and 31.7%. All analyses comparing SHR0302 vs placebo were highly significant (P < .0001).
First Phase 3 Trial in China
“This is the first highly selective JAK inhibitor originally developed, and a phase 3 clinical trial conducted, [exclusively] in China,” Jinjing Liu, from the department of rheumatology at Peking Union Medical College Hospital in Beijing, China, said in an interview.

Ms. Liu presented the results at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting, during the Abstract Plenary, which highlights the best-scored abstracts of the meeting.
“We are working our best to provide more choices for Chinese patients,” Ms. Liu said, which includes lowering the financial cost of treatments. A locally developed JAK inhibitor could potentially be a much cheaper option than other alternatives that are currently available, she said.
But it is more than that, Ms. Liu said. “The selectivity of SHR0302 for JAK 1 is nine times greater than for JAK 2, so it surpasses either tofacitinib or baricitinib.” The theory is that this higher selectivity for JAK 1 over JAK 2 could lead to fewer adverse events (AEs).
“Maybe it will result in lower JAK 2–associated hematologic side effects,” Ms. Liu said.
“We have noticed that, throughout the clinical trial, the most commonly reported AEs in the drug groups were upper extremity infection [21.7%-22.8% vs 13.8% for placebo] and hyperlipidemia [12.2%-15.3% vs 5.3%].” And for the control group, she said that anemia was the second highest reported AE, at 11.7% vs 6.3% and 7.4% for SHR0302 4 and 8 mg, respectively.
Standard Design
The trial design was typical for a phase 3 study: Multicenter, randomized, placebo controlled, and double blind for the first 24 weeks, followed by an extension period out to 52 weeks. For inclusion in the study, patients had to be aged 18-75 years and have active rheumatoid arthritis and an inadequate response to previous treatment with conventional synthetic disease-modifying antirheumatic drugs.
Of 1085 patients who were initially screened, 566 were randomly allocated to receive placebo (n = 188), SHR0302 4 mg (n = 189), or SHR0302 8 mg (n = 189). The average age of patients was 51 years, and 13.3% of patients were older than 65 years.
Additional Results
Alongside improvements in ACR responses, Ms Liu reported that a significantly higher proportion of patients treated with SHR0302 vs placebo achieved a Disease Activity Score in 28 joints based on C-reactive protein less than 2.6 (29.6% with 4 mg and 39.2% with 8 mg vs 4.2% with placebo; both P < .0001) and at least 3.2 (57.1% and 46.0% vs 15.4%; both P < .0001) at 24 weeks.
There were also greater improvements seen in Health Assessment Questionnaire-Disability Index, 36-item Short-Form (SF36) physical component summary, and SF36 mental component summary scores for active vs placebo treatment.
As for AEs, there were no surprises. During the main 24-week trial period, 81.5%, 90.5%, and 79.3% of patients treated with SHR0302 4 and 8 mg and placebo, respectively, experienced any AE.
Infection-related treatment-emergent adverse effects occurred slightly more often in the SHR0302-treated groups (40.2% for 4 mg and 40.7% for 8 mg) than in the placebo group (34.0%). There was a single case of serious infection that required treatment in the SHR0302 8 mg–treated group but no cases of systemic opportunistic infection.
There was one thromboembolic event and one major cardiovascular event in the 24-week period, both occurring in patients treated with SHR0302 8 mg. There were also single cases of each reported during the extension phase of the trial, but both were in the placebo arm.
Two cases of liver function abnormality — one each in the SHR0302 4- and 8-mg groups — were recorded during the main part of the trial and two cases — both in the SHR0302 4-mg group — during the extension phase.
As for malignancy, there was a single, newly diagnosed case in the SHR0302 4 mg group in the first part of the trial and two cases, both in the SHR0302 4-mg group, during the extension phase.
“We hope this [JAK inhibitor] will be for everybody. But, you know, if it’s for patients, globally, more clinical trials would be required,” Ms. Liu said in an interview. The future, she added, was to start accumulating some real-world data and perhaps do a trial comparing SHR0302 with another JAK inhibitor or a tumor necrosis factor inhibitor.
Another JAK in the Box?
Following her presentation, Ms. Liu at EULAR 2024 was quizzed as to why there were so many screening failures. She responded that she did not have the full data to answer the question but noted that some patients in her center had been worried about being randomized to a placebo. This trial has also been conducted during the COVID-19 pandemic, so that may have been a contributing factor with patients unable to get to their follow-up appointments.

Iain B. McInnes, MD, PhD, vice principal, professor of rheumatology, and head of the College of Medical, Veterinary & Life Sciences at the University of Glasgow, Glasgow, Scotland, commented on the study, saying: “The JAK field is in evolution. We need to understand the broader toxicities. There is an unexplained mechanism driving potential cardiovascular and malignant risk in a small proportion of patients receiving the drugs.”
Dr. McInnes added, “It’s really unclear whether the solution is going to be greater selectivity and potency, or whether we need to think really about selecting the right patients for a JAK inhibitor.”
The study was funded by Jiangsu Hengrui Pharmaceuticals. Two of the 18 authors of the abstract were employees of the sponsoring company, but Ms. Liu reported having no conflicts of interest. Dr. McInnes reported serving on speaker’s bureaus for AbbVie and UCB; receiving consulting fees received from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Causeway Therapeutics, Cabaletta Bio, Compugen, Eli Lilly, Evelo, Gilead, Janssen, Novartis, MoonLake Immunotherapeutics, Pfizer, Sanofi Regeneron, and UCB; and receiving grant/research support from GlaxoSmithKline, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
VIENNA — The highly selective oral Janus kinase (JAK) inhibitor SHR0302 (ivarmacitinib) enables more patients with active rheumatoid arthritis to meet American College of Rheumatology (ACR) response criteria than placebo, the results of a phase 3 trial showed.
After 24 weeks of daily treatment, the primary endpoint of an ACR20 response was met by 40.4% of those who had been given placebo, 70.4% who had received a 4-mg dose, and 75.1% given an 8-mg dose. At the same time point, ACR50 responses were a respective 15.4%, 46.0%, and 57.1%, and ACR70 responses were 6.9%, 22.2%, and 31.7%. All analyses comparing SHR0302 vs placebo were highly significant (P < .0001).
First Phase 3 Trial in China
“This is the first highly selective JAK inhibitor originally developed, and a phase 3 clinical trial conducted, [exclusively] in China,” Jinjing Liu, from the department of rheumatology at Peking Union Medical College Hospital in Beijing, China, said in an interview.
Ms. Liu presented the results at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting, during the Abstract Plenary, which highlights the best-scored abstracts of the meeting.
“We are working our best to provide more choices for Chinese patients,” Ms. Liu said, which includes lowering the financial cost of treatments. A locally developed JAK inhibitor could potentially be a much cheaper option than other alternatives that are currently available, she said.
But it is more than that, Ms. Liu said. “The selectivity of SHR0302 for JAK 1 is nine times greater than for JAK 2, so it surpasses either tofacitinib or baricitinib.” The theory is that this higher selectivity for JAK 1 over JAK 2 could lead to fewer adverse events (AEs).
“Maybe it will result in lower JAK 2–associated hematologic side effects,” Ms. Liu said.
“We have noticed that, throughout the clinical trial, the most commonly reported AEs in the drug groups were upper extremity infection [21.7%-22.8% vs 13.8% for placebo] and hyperlipidemia [12.2%-15.3% vs 5.3%].” And for the control group, she said that anemia was the second highest reported AE, at 11.7% vs 6.3% and 7.4% for SHR0302 4 and 8 mg, respectively.
Standard Design
The trial design was typical for a phase 3 study: Multicenter, randomized, placebo controlled, and double blind for the first 24 weeks, followed by an extension period out to 52 weeks. For inclusion in the study, patients had to be aged 18-75 years and have active rheumatoid arthritis and an inadequate response to previous treatment with conventional synthetic disease-modifying antirheumatic drugs.
Of 1085 patients who were initially screened, 566 were randomly allocated to receive placebo (n = 188), SHR0302 4 mg (n = 189), or SHR0302 8 mg (n = 189). The average age of patients was 51 years, and 13.3% of patients were older than 65 years.
Additional Results
Alongside improvements in ACR responses, Ms Liu reported that a significantly higher proportion of patients treated with SHR0302 vs placebo achieved a Disease Activity Score in 28 joints based on C-reactive protein less than 2.6 (29.6% with 4 mg and 39.2% with 8 mg vs 4.2% with placebo; both P < .0001) and at least 3.2 (57.1% and 46.0% vs 15.4%; both P < .0001) at 24 weeks.
There were also greater improvements seen in Health Assessment Questionnaire-Disability Index, 36-item Short-Form (SF36) physical component summary, and SF36 mental component summary scores for active vs placebo treatment.
As for AEs, there were no surprises. During the main 24-week trial period, 81.5%, 90.5%, and 79.3% of patients treated with SHR0302 4 and 8 mg and placebo, respectively, experienced any AE.
Infection-related treatment-emergent adverse effects occurred slightly more often in the SHR0302-treated groups (40.2% for 4 mg and 40.7% for 8 mg) than in the placebo group (34.0%). There was a single case of serious infection that required treatment in the SHR0302 8 mg–treated group but no cases of systemic opportunistic infection.
There was one thromboembolic event and one major cardiovascular event in the 24-week period, both occurring in patients treated with SHR0302 8 mg. There were also single cases of each reported during the extension phase of the trial, but both were in the placebo arm.
Two cases of liver function abnormality — one each in the SHR0302 4- and 8-mg groups — were recorded during the main part of the trial and two cases — both in the SHR0302 4-mg group — during the extension phase.
As for malignancy, there was a single, newly diagnosed case in the SHR0302 4 mg group in the first part of the trial and two cases, both in the SHR0302 4-mg group, during the extension phase.
“We hope this [JAK inhibitor] will be for everybody. But, you know, if it’s for patients, globally, more clinical trials would be required,” Ms. Liu said in an interview. The future, she added, was to start accumulating some real-world data and perhaps do a trial comparing SHR0302 with another JAK inhibitor or a tumor necrosis factor inhibitor.
Another JAK in the Box?
Following her presentation, Ms. Liu at EULAR 2024 was quizzed as to why there were so many screening failures. She responded that she did not have the full data to answer the question but noted that some patients in her center had been worried about being randomized to a placebo. This trial has also been conducted during the COVID-19 pandemic, so that may have been a contributing factor with patients unable to get to their follow-up appointments.
Iain B. McInnes, MD, PhD, vice principal, professor of rheumatology, and head of the College of Medical, Veterinary & Life Sciences at the University of Glasgow, Glasgow, Scotland, commented on the study, saying: “The JAK field is in evolution. We need to understand the broader toxicities. There is an unexplained mechanism driving potential cardiovascular and malignant risk in a small proportion of patients receiving the drugs.”
Dr. McInnes added, “It’s really unclear whether the solution is going to be greater selectivity and potency, or whether we need to think really about selecting the right patients for a JAK inhibitor.”
The study was funded by Jiangsu Hengrui Pharmaceuticals. Two of the 18 authors of the abstract were employees of the sponsoring company, but Ms. Liu reported having no conflicts of interest. Dr. McInnes reported serving on speaker’s bureaus for AbbVie and UCB; receiving consulting fees received from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Causeway Therapeutics, Cabaletta Bio, Compugen, Eli Lilly, Evelo, Gilead, Janssen, Novartis, MoonLake Immunotherapeutics, Pfizer, Sanofi Regeneron, and UCB; and receiving grant/research support from GlaxoSmithKline, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
VIENNA — The highly selective oral Janus kinase (JAK) inhibitor SHR0302 (ivarmacitinib) enables more patients with active rheumatoid arthritis to meet American College of Rheumatology (ACR) response criteria than placebo, the results of a phase 3 trial showed.
After 24 weeks of daily treatment, the primary endpoint of an ACR20 response was met by 40.4% of those who had been given placebo, 70.4% who had received a 4-mg dose, and 75.1% given an 8-mg dose. At the same time point, ACR50 responses were a respective 15.4%, 46.0%, and 57.1%, and ACR70 responses were 6.9%, 22.2%, and 31.7%. All analyses comparing SHR0302 vs placebo were highly significant (P < .0001).
First Phase 3 Trial in China
“This is the first highly selective JAK inhibitor originally developed, and a phase 3 clinical trial conducted, [exclusively] in China,” Jinjing Liu, from the department of rheumatology at Peking Union Medical College Hospital in Beijing, China, said in an interview.
Ms. Liu presented the results at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting, during the Abstract Plenary, which highlights the best-scored abstracts of the meeting.
“We are working our best to provide more choices for Chinese patients,” Ms. Liu said, which includes lowering the financial cost of treatments. A locally developed JAK inhibitor could potentially be a much cheaper option than other alternatives that are currently available, she said.
But it is more than that, Ms. Liu said. “The selectivity of SHR0302 for JAK 1 is nine times greater than for JAK 2, so it surpasses either tofacitinib or baricitinib.” The theory is that this higher selectivity for JAK 1 over JAK 2 could lead to fewer adverse events (AEs).
“Maybe it will result in lower JAK 2–associated hematologic side effects,” Ms. Liu said.
“We have noticed that, throughout the clinical trial, the most commonly reported AEs in the drug groups were upper extremity infection [21.7%-22.8% vs 13.8% for placebo] and hyperlipidemia [12.2%-15.3% vs 5.3%].” And for the control group, she said that anemia was the second highest reported AE, at 11.7% vs 6.3% and 7.4% for SHR0302 4 and 8 mg, respectively.
Standard Design
The trial design was typical for a phase 3 study: Multicenter, randomized, placebo controlled, and double blind for the first 24 weeks, followed by an extension period out to 52 weeks. For inclusion in the study, patients had to be aged 18-75 years and have active rheumatoid arthritis and an inadequate response to previous treatment with conventional synthetic disease-modifying antirheumatic drugs.
Of 1085 patients who were initially screened, 566 were randomly allocated to receive placebo (n = 188), SHR0302 4 mg (n = 189), or SHR0302 8 mg (n = 189). The average age of patients was 51 years, and 13.3% of patients were older than 65 years.
Additional Results
Alongside improvements in ACR responses, Ms Liu reported that a significantly higher proportion of patients treated with SHR0302 vs placebo achieved a Disease Activity Score in 28 joints based on C-reactive protein less than 2.6 (29.6% with 4 mg and 39.2% with 8 mg vs 4.2% with placebo; both P < .0001) and at least 3.2 (57.1% and 46.0% vs 15.4%; both P < .0001) at 24 weeks.
There were also greater improvements seen in Health Assessment Questionnaire-Disability Index, 36-item Short-Form (SF36) physical component summary, and SF36 mental component summary scores for active vs placebo treatment.
As for AEs, there were no surprises. During the main 24-week trial period, 81.5%, 90.5%, and 79.3% of patients treated with SHR0302 4 and 8 mg and placebo, respectively, experienced any AE.
Infection-related treatment-emergent adverse effects occurred slightly more often in the SHR0302-treated groups (40.2% for 4 mg and 40.7% for 8 mg) than in the placebo group (34.0%). There was a single case of serious infection that required treatment in the SHR0302 8 mg–treated group but no cases of systemic opportunistic infection.
There was one thromboembolic event and one major cardiovascular event in the 24-week period, both occurring in patients treated with SHR0302 8 mg. There were also single cases of each reported during the extension phase of the trial, but both were in the placebo arm.
Two cases of liver function abnormality — one each in the SHR0302 4- and 8-mg groups — were recorded during the main part of the trial and two cases — both in the SHR0302 4-mg group — during the extension phase.
As for malignancy, there was a single, newly diagnosed case in the SHR0302 4 mg group in the first part of the trial and two cases, both in the SHR0302 4-mg group, during the extension phase.
“We hope this [JAK inhibitor] will be for everybody. But, you know, if it’s for patients, globally, more clinical trials would be required,” Ms. Liu said in an interview. The future, she added, was to start accumulating some real-world data and perhaps do a trial comparing SHR0302 with another JAK inhibitor or a tumor necrosis factor inhibitor.
Another JAK in the Box?
Following her presentation, Ms. Liu at EULAR 2024 was quizzed as to why there were so many screening failures. She responded that she did not have the full data to answer the question but noted that some patients in her center had been worried about being randomized to a placebo. This trial has also been conducted during the COVID-19 pandemic, so that may have been a contributing factor with patients unable to get to their follow-up appointments.
Iain B. McInnes, MD, PhD, vice principal, professor of rheumatology, and head of the College of Medical, Veterinary & Life Sciences at the University of Glasgow, Glasgow, Scotland, commented on the study, saying: “The JAK field is in evolution. We need to understand the broader toxicities. There is an unexplained mechanism driving potential cardiovascular and malignant risk in a small proportion of patients receiving the drugs.”
Dr. McInnes added, “It’s really unclear whether the solution is going to be greater selectivity and potency, or whether we need to think really about selecting the right patients for a JAK inhibitor.”
The study was funded by Jiangsu Hengrui Pharmaceuticals. Two of the 18 authors of the abstract were employees of the sponsoring company, but Ms. Liu reported having no conflicts of interest. Dr. McInnes reported serving on speaker’s bureaus for AbbVie and UCB; receiving consulting fees received from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Causeway Therapeutics, Cabaletta Bio, Compugen, Eli Lilly, Evelo, Gilead, Janssen, Novartis, MoonLake Immunotherapeutics, Pfizer, Sanofi Regeneron, and UCB; and receiving grant/research support from GlaxoSmithKline, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
VEXAS Syndrome: Study Highlights Cutaneous Symptoms
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.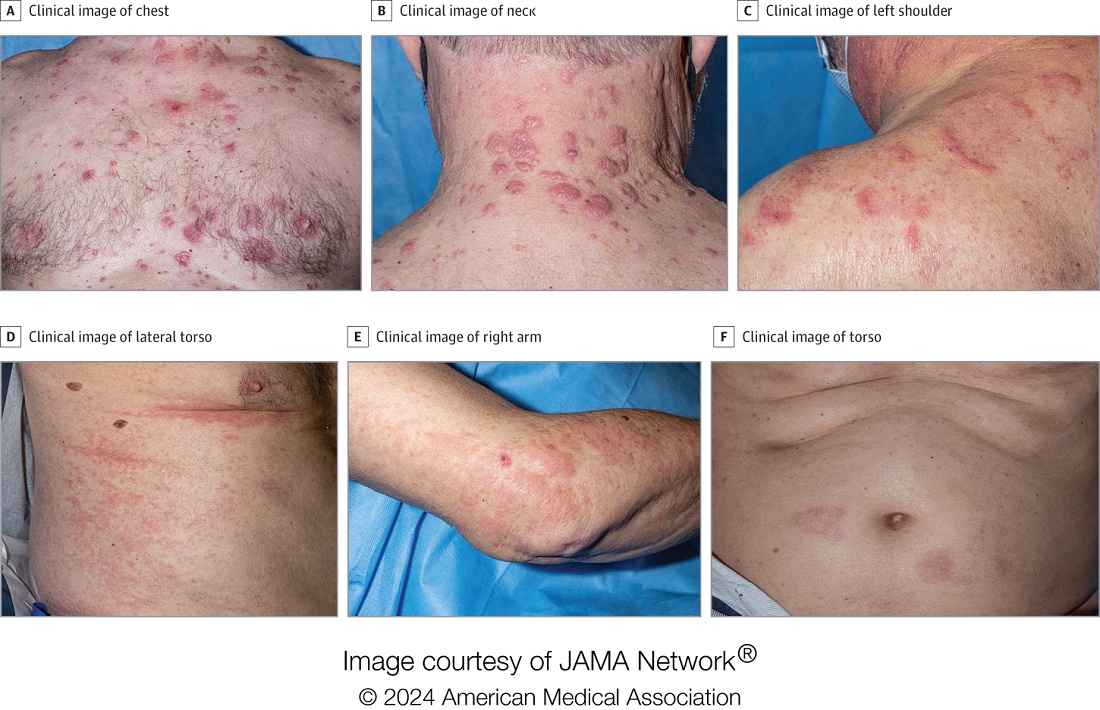
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
FROM JAMA DERMATOLOGY
A New Psychotherapeutic ‘Gold Standard’ for Chronic Pain?
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
Doctors Endorsing Products on X May Not Disclose Company Ties
Lead author Aaron Mitchell, MD, MPH, a medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, told this news organization that he and his colleagues undertook the study in part to see whether physicians were adhering to professional and industry guidelines regarding marketing communications.
The team reviewed posts by physicians on X during 2022, looking for key words that might indicate that the posts were intended as endorsements of a product. The researchers then delved into the Centers for Medicare and Medicaid Services Open Payments database to see how many of those identified as having endorsed a product were paid by the manufacturers.
What Dr. Mitchell found concerned him, he said.
Overall, the researchers identified 28 physician endorsers who received a total of $1.4 million from sponsors in 2022. Among these, 26 physicians (93%) received payments from the product’s manufacturer, totaling $713,976, and 24 physicians (86%) accepted payments related to the endorsed drug or device, totaling $492,098.
While most did disclose that the posts were sponsored — by adding the word “sponsored” or using #sponsored — nine physicians did not.
Although 28 physician endorsers represent a “small fraction” of the overall number of physicians who use X, each endorsement was ultimately posted dozens, if not hundreds of times, said Dr. Mitchell. In fact, he said he saw the same particular endorsement post every time he opened his X app for months.
Overall, Dr. Mitchell noted that it’s less about the fact that the endorsements are occurring on social media and more that there are these paid endorsements taking place at all.
Among the physician specialties promoting a product, urologists and oncologists dominated. Almost one third were urologists, and 57% were oncologists — six medical oncologists, six radiation oncologists, and four gynecologic oncologists. Of the remaining three physicians, two were internists and one was a pulmonary and critical care medicine specialist.
The authors tracked posts from physicians and industry accounts. Many of the posts on industry accounts were physician testimonials, usually videos. Almost half — 8 of 17 — of those testimonials did not disclose that the doctor was being paid by the manufacturer. In another case, a physician did not disclose that they were paid to endorse a white paper.
Fifteen promotional posts were for a Boston Scientific product, followed by six for GlaxoSmithKline, two for Eisai, two for Exelixis, and one each for AstraZeneca, Novartis, and Pfizer.
In general, Dr. Mitchell said, industry guidelines suggest that manufacturer-paid speakers or consultants should have well-regarded expertise in the area they are being asked to weigh in on, but most physician endorsers in the study were not key opinion leaders or experts.
The authors examined the paid endorsers’ H-index — a measure of academic productivity provided by Scopus. Overall, 19 of the 28 physicians had an H-index below 20, which is considered less accomplished, and 14 had no published research related to the endorsed product.
Ten received payments from manufacturers for research purposes, and only one received research payments related to the endorsed product ($224,577).
“Physicians’ participation in industry marketing raises questions regarding professionalism and their responsibilities as patient advocates,” the JAMA authors wrote.
The study was supported by grants from the National Cancer Institute. Dr. Mitchell reported no relevant financial relationships. Coauthors Samer Al Hadidi, MD, reported receiving personal fees from Pfizer, Sanofi, and Janssen during the conduct of the study, and Timothy S. Anderson, MD, reported receiving grants from the National Institute on Aging, the American Heart Association, and the American College of Cardiology, and receiving consulting fees from the American Medical Student Association. Dr. Anderson is also an associate editor of JAMA Internal Medicine.
A version of this article appeared on Medscape.com.
Lead author Aaron Mitchell, MD, MPH, a medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, told this news organization that he and his colleagues undertook the study in part to see whether physicians were adhering to professional and industry guidelines regarding marketing communications.
The team reviewed posts by physicians on X during 2022, looking for key words that might indicate that the posts were intended as endorsements of a product. The researchers then delved into the Centers for Medicare and Medicaid Services Open Payments database to see how many of those identified as having endorsed a product were paid by the manufacturers.
What Dr. Mitchell found concerned him, he said.
Overall, the researchers identified 28 physician endorsers who received a total of $1.4 million from sponsors in 2022. Among these, 26 physicians (93%) received payments from the product’s manufacturer, totaling $713,976, and 24 physicians (86%) accepted payments related to the endorsed drug or device, totaling $492,098.
While most did disclose that the posts were sponsored — by adding the word “sponsored” or using #sponsored — nine physicians did not.
Although 28 physician endorsers represent a “small fraction” of the overall number of physicians who use X, each endorsement was ultimately posted dozens, if not hundreds of times, said Dr. Mitchell. In fact, he said he saw the same particular endorsement post every time he opened his X app for months.
Overall, Dr. Mitchell noted that it’s less about the fact that the endorsements are occurring on social media and more that there are these paid endorsements taking place at all.
Among the physician specialties promoting a product, urologists and oncologists dominated. Almost one third were urologists, and 57% were oncologists — six medical oncologists, six radiation oncologists, and four gynecologic oncologists. Of the remaining three physicians, two were internists and one was a pulmonary and critical care medicine specialist.
The authors tracked posts from physicians and industry accounts. Many of the posts on industry accounts were physician testimonials, usually videos. Almost half — 8 of 17 — of those testimonials did not disclose that the doctor was being paid by the manufacturer. In another case, a physician did not disclose that they were paid to endorse a white paper.
Fifteen promotional posts were for a Boston Scientific product, followed by six for GlaxoSmithKline, two for Eisai, two for Exelixis, and one each for AstraZeneca, Novartis, and Pfizer.
In general, Dr. Mitchell said, industry guidelines suggest that manufacturer-paid speakers or consultants should have well-regarded expertise in the area they are being asked to weigh in on, but most physician endorsers in the study were not key opinion leaders or experts.
The authors examined the paid endorsers’ H-index — a measure of academic productivity provided by Scopus. Overall, 19 of the 28 physicians had an H-index below 20, which is considered less accomplished, and 14 had no published research related to the endorsed product.
Ten received payments from manufacturers for research purposes, and only one received research payments related to the endorsed product ($224,577).
“Physicians’ participation in industry marketing raises questions regarding professionalism and their responsibilities as patient advocates,” the JAMA authors wrote.
The study was supported by grants from the National Cancer Institute. Dr. Mitchell reported no relevant financial relationships. Coauthors Samer Al Hadidi, MD, reported receiving personal fees from Pfizer, Sanofi, and Janssen during the conduct of the study, and Timothy S. Anderson, MD, reported receiving grants from the National Institute on Aging, the American Heart Association, and the American College of Cardiology, and receiving consulting fees from the American Medical Student Association. Dr. Anderson is also an associate editor of JAMA Internal Medicine.
A version of this article appeared on Medscape.com.
Lead author Aaron Mitchell, MD, MPH, a medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, told this news organization that he and his colleagues undertook the study in part to see whether physicians were adhering to professional and industry guidelines regarding marketing communications.
The team reviewed posts by physicians on X during 2022, looking for key words that might indicate that the posts were intended as endorsements of a product. The researchers then delved into the Centers for Medicare and Medicaid Services Open Payments database to see how many of those identified as having endorsed a product were paid by the manufacturers.
What Dr. Mitchell found concerned him, he said.
Overall, the researchers identified 28 physician endorsers who received a total of $1.4 million from sponsors in 2022. Among these, 26 physicians (93%) received payments from the product’s manufacturer, totaling $713,976, and 24 physicians (86%) accepted payments related to the endorsed drug or device, totaling $492,098.
While most did disclose that the posts were sponsored — by adding the word “sponsored” or using #sponsored — nine physicians did not.
Although 28 physician endorsers represent a “small fraction” of the overall number of physicians who use X, each endorsement was ultimately posted dozens, if not hundreds of times, said Dr. Mitchell. In fact, he said he saw the same particular endorsement post every time he opened his X app for months.
Overall, Dr. Mitchell noted that it’s less about the fact that the endorsements are occurring on social media and more that there are these paid endorsements taking place at all.
Among the physician specialties promoting a product, urologists and oncologists dominated. Almost one third were urologists, and 57% were oncologists — six medical oncologists, six radiation oncologists, and four gynecologic oncologists. Of the remaining three physicians, two were internists and one was a pulmonary and critical care medicine specialist.
The authors tracked posts from physicians and industry accounts. Many of the posts on industry accounts were physician testimonials, usually videos. Almost half — 8 of 17 — of those testimonials did not disclose that the doctor was being paid by the manufacturer. In another case, a physician did not disclose that they were paid to endorse a white paper.
Fifteen promotional posts were for a Boston Scientific product, followed by six for GlaxoSmithKline, two for Eisai, two for Exelixis, and one each for AstraZeneca, Novartis, and Pfizer.
In general, Dr. Mitchell said, industry guidelines suggest that manufacturer-paid speakers or consultants should have well-regarded expertise in the area they are being asked to weigh in on, but most physician endorsers in the study were not key opinion leaders or experts.
The authors examined the paid endorsers’ H-index — a measure of academic productivity provided by Scopus. Overall, 19 of the 28 physicians had an H-index below 20, which is considered less accomplished, and 14 had no published research related to the endorsed product.
Ten received payments from manufacturers for research purposes, and only one received research payments related to the endorsed product ($224,577).
“Physicians’ participation in industry marketing raises questions regarding professionalism and their responsibilities as patient advocates,” the JAMA authors wrote.
The study was supported by grants from the National Cancer Institute. Dr. Mitchell reported no relevant financial relationships. Coauthors Samer Al Hadidi, MD, reported receiving personal fees from Pfizer, Sanofi, and Janssen during the conduct of the study, and Timothy S. Anderson, MD, reported receiving grants from the National Institute on Aging, the American Heart Association, and the American College of Cardiology, and receiving consulting fees from the American Medical Student Association. Dr. Anderson is also an associate editor of JAMA Internal Medicine.
A version of this article appeared on Medscape.com.
Long-Term OA, RA Symptom Improvement Seen with Plant-Based Diet, Lifestyle Changes
VIENNA — An intervention consisting of a plant-based diet, exercise, and sleep and stress advice improved pain, stiffness, and physical function in people with knee and/or hip osteoarthritis (OA) and metabolic syndrome, while in patients with rheumatoid arthritis (RA), disease activity improved significantly, and medication use was reduced.
At the annual European Congress of Rheumatology, Carlijn Wagenaar, MD, a PhD candidate in Clinical Immunology and Rheumatology at Amsterdam University Medical Center, presented 2-year extension study results for OA and RA and an overview of the possible biological mechanisms underpinning the plant-based intervention in RA.
“At 2 years, RA patients on the PFJ [Plants for Joints] intervention resulted in a significant improvement in disease activity of RA, and these outcomes were maintained 2 years after program end,” Dr. Wagenaar reported.
“Some initial improvements in body composition and metabolic outcomes were also maintained at the end of the 2-year extension phase, and there was a net decrease in antirheumatic medication use,” she continued.
In the patients with OA, Dr. Wagenaar said the PFJ intervention improved pain, stiffness, and physical function in people with knee and/or hip OA and metabolic syndrome. “In the 2-year extension study, these effects were maintained, and we saw lasting body composition changes and a decrease in cholesterol-lowering medications. There was also high acceptability of the program; the study shows long-term maintenance of clinically relevant effects.”
Significant Improvement in OA Pain, Stiffness, Physical Function
In the OA randomized controlled trial, 64 people with hip and/or knee OA and metabolic syndrome were randomized to the PFJ intervention or usual care (waitlist control group). A total of 62 participants (including those in the control group previously) entered the long-term effectiveness study, and 44 had 2 years of follow-up data for analysis. Twenty participants dropped out, with most being unreachable or too busy.
“The PFJ program is a theoretical and practical program where people learn about and follow a whole food, plant-based diet, and receive advice on sleep and stress management and exercise,” said Dr. Wagenaar.
The program lasted 16 weeks with group sessions of 6-12 participants. The diet was a plant-based version of the Dutch dietary guidelines with a focus on unprocessed food. It was rich in whole grains, legumes, nuts, seeds, fruit, and vegetables, but without calorie restrictions and participants had one-to-one contact with a dietitian. The exercise advice followed the Dutch exercise guidelines, which advise 150 minutes of moderate to intense exercise per week, as well as twice-weekly muscle strength exercises, noted Dr. Wagenaar.
The 2-year follow-up study involved twice-yearly visits and six adherence-promoting webinars per year, as well as monthly newsletters. Researchers also monitored changes in medication intensity (classified as “increased,” “stable,” or “decreased/stopped”) between the start of the PFJ intervention and end of the 2-year extension study, and they were grouped into medications for pain, blood pressure, glucose, and cholesterol.
Participants were encouraged to try to avoid making changes to medication during the intervention phase, but they could do so during the 2-year extension study, said Dr. Wagenaar. In fact, the researchers actively monitored and quantified medication changes between the start of the PFJ intervention and end of the 2-year follow-up period.
Patients in the 16-week trial had an average age of 64 years, 84% were women, and their mean body mass index (BMI) was 33 kg/m2. A total of 73% had knee OA and 78% hip OA, and their mean WOMAC score was 38.2, indicative of moderate to severe OA.
In participants who completed the 2-year extension study, the primary outcome (WOMAC score for mean stiffness and physical function) showed a significant improvement of −9.1 (95% CI, −12.8 to −5.3; P < .0001) compared with the start of the PFJ intervention.
“Looking at individual components of the WOMAC score — pain, stiffness, and physical function — we found these also all significantly improved at the end of the 2-year extension phase,” reported Dr. Wagenaar.
She added that after 2 years, there were significant improvements in weight loss (from 94.9 to 92.1 kg), BMI (from 33.3 to 32 kg/m2), and waist circumference (from 110 to 106.7 cm).
By the end of the trial and at 1 year of the extension study, there were significant improvements in A1c, fasting blood glucose, and low-density lipoprotein cholesterol, but at 2 years, these were no longer significant.
Regarding medications use, Dr. Wagenaar reported that, overall, there was no net change in use of pain, glucose-lowering, or hypertension medications, but 44% of patients using cholesterol-lowering medications were able to lower their dose or stop them.
Disease Activity Improvement and Medication Reduction in RA
Turning to the study of the intervention in patients with RA, 77 people (DAS28 ≥ 2.6 and ≤ 5.1, mild to moderate disease) were randomized to receive either the PFJ intervention in addition to usual care or only usual care (control group). Of these, 48 (62%) from both the intervention and control groups also completed the 2-year follow-up. The details of the PFJ intervention and the extension study for RA were the same as for the OA patient group.
Dr. Wagenaar commented on how they tried to individualize the exercise part of the program. “We noticed many of the RA patients asked too much of their body, while in contrast, those with OA were too hesitant,” she said. “We decided to focus on people’s own physical barriers, and we wanted to protect these. Sometimes, people needed to move more, and at other times, we had to tell people to slow down. Often, we advised people to move more by integrating exercise into their daily life.”
Similar to the OA study, patients were asked to try to avoid changing their medications in the 16-week study. “In the extension study, they were encouraged to reduce their medication in collaboration with their rheumatologist,” explained Wagenaar, who monitored any changes.
Differences were quantified according to medication groups comprising rheumatic medications, as well as pain, blood pressure, glucose-lowering, and cholesterol medications, and changes were categorized as increased, stable, or decreased/stopped.
Again, participants were mostly women (92%) with an average age of 55 years, BMI of 26 kg/m2, and DAS28 of 3.85 at baseline. Dropout reasons were similar to those for OA, and over 85% of participants were on medications.
During the 16-week trial period, the DAS28 changed more in the intervention participants than in the controls, and after 2 years of follow-up, DAS28 was significantly lower than baseline with a mean difference of −0.9 (95% CI, −1.2 to −0.6; P < .0001).
“Comparing with the literature, the drop in DAS28 was similar to that seen with medication, so it’s a very significant reduction,” remarked Dr. Wagenaar.
Mean tender joint count dropped from 3 to 0, and general health components of the DAS28 improved significantly over the intervention and over the 2-year follow-up, whereas there was no significant difference in the already low erythrocyte sedimentation rate and swollen joint count compared with baseline. C-reactive protein (CRP) changed from 3.2 to 1.3 mg/L over the 2-year follow-up. High-density lipoprotein increased from 1.6 to 1.8 mmol/L.
A total of 44% of people using antirheumatic medication decreased or stopped them after the 2-year extension.
Dr. Wagenaar went on to say that focus group findings suggested that “participants were very enthusiastic about the program despite it largely involving lifestyle change, and this is reflected in our low dropout rates after the trial and 1-year extension [20% for OA and RA].” There were more dropouts in year 2 of the extension.
In an interview, Dr. Wagenaar explained why she felt the program had been so well received. “People in the program felt like they had more control over their disease, and they felt listened to.”
Mechanisms Underpinning PFJ
Dr. Wagenaar and colleagues also sought to determine the possible mechanisms underlying the clinical effects of the plant-based diet on RA. “With RA, we have the mucosal origins hypothesis, which suggests RA is triggered at the mucosal site [of the gut] in genetically predisposed individuals, and this consequently transfers to the synovial [fluid in] joints,” she said.
“On top of this, we know that fiber protects our gut barrier and therefore reduces inflammation. The PFJ intervention is a very high-fiber program, so our hypothesis is that it might help [strengthen] the barrier,” she explained.
Dr. Wagenaar and colleagues collected fecal samples from patients and measured the albumin and calprotectin in them, which are both indicators of the gut barrier function. The researchers analyzed metabolomic data and found that fecal albumin — considered a gut barrier integrity marker — decreased significantly in the intervention group. In patients with RA, this improvement corresponded with an improvement in DAS28, the researchers reported in a poster at the meeting.
“Patients who had the greatest improvement in their gut barrier function also showed the greatest improvement in the DAS28 score, suggestive of a possible link between gut barrier improvement and clinical effects.”
They did not identify any change in calprotectin, an inflammation marker, but Dr. Wagenaar said this might change later. “We found that in those on the intervention, at 4 months, the CRP wasn’t reduced, but 1 year later it was.”
The metabolite lenticin, a lentil intake biomarker considered protective against inflammation and osteoclastic differentiation, also increased. Tryptophan was also reduced in people on the PFJ intervention.
Fernando Estevez-Lopez, PhD, a sports scientist at Harvard T.H. Chan School of Public Health, Boston, who specializes in physical activity and behavioral change in rheumatology patients, co-moderated the session and remarked that, “In this study, they did a brilliant job with encouraging participants to follow the program. The design and methods were really good — the sample size was good, and they followed people up. Also, these researchers come from Reade [a medical research center in Amsterdam University Medical Center] where they are well known for applying their research findings to the clinic,” he said.
“In terms of physical activity, we really mean increasing the time spent moving, for example, gentle activity such as walking, or changing behaviors in people with OA and RA. We don’t want them to have more pain the next day.”
Dr. Wagenaar reported receiving a grant from ZonMw (The Netherlands Organization for Health Research and Development). She and colleagues hold shares in Plants for Health, a limited liability company. Dr. Estevez-Lopez reported having no relevant disclosures.
A version of this article appeared on Medscape.com.
VIENNA — An intervention consisting of a plant-based diet, exercise, and sleep and stress advice improved pain, stiffness, and physical function in people with knee and/or hip osteoarthritis (OA) and metabolic syndrome, while in patients with rheumatoid arthritis (RA), disease activity improved significantly, and medication use was reduced.
At the annual European Congress of Rheumatology, Carlijn Wagenaar, MD, a PhD candidate in Clinical Immunology and Rheumatology at Amsterdam University Medical Center, presented 2-year extension study results for OA and RA and an overview of the possible biological mechanisms underpinning the plant-based intervention in RA.
“At 2 years, RA patients on the PFJ [Plants for Joints] intervention resulted in a significant improvement in disease activity of RA, and these outcomes were maintained 2 years after program end,” Dr. Wagenaar reported.
“Some initial improvements in body composition and metabolic outcomes were also maintained at the end of the 2-year extension phase, and there was a net decrease in antirheumatic medication use,” she continued.
In the patients with OA, Dr. Wagenaar said the PFJ intervention improved pain, stiffness, and physical function in people with knee and/or hip OA and metabolic syndrome. “In the 2-year extension study, these effects were maintained, and we saw lasting body composition changes and a decrease in cholesterol-lowering medications. There was also high acceptability of the program; the study shows long-term maintenance of clinically relevant effects.”
Significant Improvement in OA Pain, Stiffness, Physical Function
In the OA randomized controlled trial, 64 people with hip and/or knee OA and metabolic syndrome were randomized to the PFJ intervention or usual care (waitlist control group). A total of 62 participants (including those in the control group previously) entered the long-term effectiveness study, and 44 had 2 years of follow-up data for analysis. Twenty participants dropped out, with most being unreachable or too busy.
“The PFJ program is a theoretical and practical program where people learn about and follow a whole food, plant-based diet, and receive advice on sleep and stress management and exercise,” said Dr. Wagenaar.
The program lasted 16 weeks with group sessions of 6-12 participants. The diet was a plant-based version of the Dutch dietary guidelines with a focus on unprocessed food. It was rich in whole grains, legumes, nuts, seeds, fruit, and vegetables, but without calorie restrictions and participants had one-to-one contact with a dietitian. The exercise advice followed the Dutch exercise guidelines, which advise 150 minutes of moderate to intense exercise per week, as well as twice-weekly muscle strength exercises, noted Dr. Wagenaar.
The 2-year follow-up study involved twice-yearly visits and six adherence-promoting webinars per year, as well as monthly newsletters. Researchers also monitored changes in medication intensity (classified as “increased,” “stable,” or “decreased/stopped”) between the start of the PFJ intervention and end of the 2-year extension study, and they were grouped into medications for pain, blood pressure, glucose, and cholesterol.
Participants were encouraged to try to avoid making changes to medication during the intervention phase, but they could do so during the 2-year extension study, said Dr. Wagenaar. In fact, the researchers actively monitored and quantified medication changes between the start of the PFJ intervention and end of the 2-year follow-up period.
Patients in the 16-week trial had an average age of 64 years, 84% were women, and their mean body mass index (BMI) was 33 kg/m2. A total of 73% had knee OA and 78% hip OA, and their mean WOMAC score was 38.2, indicative of moderate to severe OA.
In participants who completed the 2-year extension study, the primary outcome (WOMAC score for mean stiffness and physical function) showed a significant improvement of −9.1 (95% CI, −12.8 to −5.3; P < .0001) compared with the start of the PFJ intervention.
“Looking at individual components of the WOMAC score — pain, stiffness, and physical function — we found these also all significantly improved at the end of the 2-year extension phase,” reported Dr. Wagenaar.
She added that after 2 years, there were significant improvements in weight loss (from 94.9 to 92.1 kg), BMI (from 33.3 to 32 kg/m2), and waist circumference (from 110 to 106.7 cm).
By the end of the trial and at 1 year of the extension study, there were significant improvements in A1c, fasting blood glucose, and low-density lipoprotein cholesterol, but at 2 years, these were no longer significant.
Regarding medications use, Dr. Wagenaar reported that, overall, there was no net change in use of pain, glucose-lowering, or hypertension medications, but 44% of patients using cholesterol-lowering medications were able to lower their dose or stop them.
Disease Activity Improvement and Medication Reduction in RA
Turning to the study of the intervention in patients with RA, 77 people (DAS28 ≥ 2.6 and ≤ 5.1, mild to moderate disease) were randomized to receive either the PFJ intervention in addition to usual care or only usual care (control group). Of these, 48 (62%) from both the intervention and control groups also completed the 2-year follow-up. The details of the PFJ intervention and the extension study for RA were the same as for the OA patient group.
Dr. Wagenaar commented on how they tried to individualize the exercise part of the program. “We noticed many of the RA patients asked too much of their body, while in contrast, those with OA were too hesitant,” she said. “We decided to focus on people’s own physical barriers, and we wanted to protect these. Sometimes, people needed to move more, and at other times, we had to tell people to slow down. Often, we advised people to move more by integrating exercise into their daily life.”
Similar to the OA study, patients were asked to try to avoid changing their medications in the 16-week study. “In the extension study, they were encouraged to reduce their medication in collaboration with their rheumatologist,” explained Wagenaar, who monitored any changes.
Differences were quantified according to medication groups comprising rheumatic medications, as well as pain, blood pressure, glucose-lowering, and cholesterol medications, and changes were categorized as increased, stable, or decreased/stopped.
Again, participants were mostly women (92%) with an average age of 55 years, BMI of 26 kg/m2, and DAS28 of 3.85 at baseline. Dropout reasons were similar to those for OA, and over 85% of participants were on medications.
During the 16-week trial period, the DAS28 changed more in the intervention participants than in the controls, and after 2 years of follow-up, DAS28 was significantly lower than baseline with a mean difference of −0.9 (95% CI, −1.2 to −0.6; P < .0001).
“Comparing with the literature, the drop in DAS28 was similar to that seen with medication, so it’s a very significant reduction,” remarked Dr. Wagenaar.
Mean tender joint count dropped from 3 to 0, and general health components of the DAS28 improved significantly over the intervention and over the 2-year follow-up, whereas there was no significant difference in the already low erythrocyte sedimentation rate and swollen joint count compared with baseline. C-reactive protein (CRP) changed from 3.2 to 1.3 mg/L over the 2-year follow-up. High-density lipoprotein increased from 1.6 to 1.8 mmol/L.
A total of 44% of people using antirheumatic medication decreased or stopped them after the 2-year extension.
Dr. Wagenaar went on to say that focus group findings suggested that “participants were very enthusiastic about the program despite it largely involving lifestyle change, and this is reflected in our low dropout rates after the trial and 1-year extension [20% for OA and RA].” There were more dropouts in year 2 of the extension.
In an interview, Dr. Wagenaar explained why she felt the program had been so well received. “People in the program felt like they had more control over their disease, and they felt listened to.”
Mechanisms Underpinning PFJ
Dr. Wagenaar and colleagues also sought to determine the possible mechanisms underlying the clinical effects of the plant-based diet on RA. “With RA, we have the mucosal origins hypothesis, which suggests RA is triggered at the mucosal site [of the gut] in genetically predisposed individuals, and this consequently transfers to the synovial [fluid in] joints,” she said.
“On top of this, we know that fiber protects our gut barrier and therefore reduces inflammation. The PFJ intervention is a very high-fiber program, so our hypothesis is that it might help [strengthen] the barrier,” she explained.
Dr. Wagenaar and colleagues collected fecal samples from patients and measured the albumin and calprotectin in them, which are both indicators of the gut barrier function. The researchers analyzed metabolomic data and found that fecal albumin — considered a gut barrier integrity marker — decreased significantly in the intervention group. In patients with RA, this improvement corresponded with an improvement in DAS28, the researchers reported in a poster at the meeting.
“Patients who had the greatest improvement in their gut barrier function also showed the greatest improvement in the DAS28 score, suggestive of a possible link between gut barrier improvement and clinical effects.”
They did not identify any change in calprotectin, an inflammation marker, but Dr. Wagenaar said this might change later. “We found that in those on the intervention, at 4 months, the CRP wasn’t reduced, but 1 year later it was.”
The metabolite lenticin, a lentil intake biomarker considered protective against inflammation and osteoclastic differentiation, also increased. Tryptophan was also reduced in people on the PFJ intervention.
Fernando Estevez-Lopez, PhD, a sports scientist at Harvard T.H. Chan School of Public Health, Boston, who specializes in physical activity and behavioral change in rheumatology patients, co-moderated the session and remarked that, “In this study, they did a brilliant job with encouraging participants to follow the program. The design and methods were really good — the sample size was good, and they followed people up. Also, these researchers come from Reade [a medical research center in Amsterdam University Medical Center] where they are well known for applying their research findings to the clinic,” he said.
“In terms of physical activity, we really mean increasing the time spent moving, for example, gentle activity such as walking, or changing behaviors in people with OA and RA. We don’t want them to have more pain the next day.”
Dr. Wagenaar reported receiving a grant from ZonMw (The Netherlands Organization for Health Research and Development). She and colleagues hold shares in Plants for Health, a limited liability company. Dr. Estevez-Lopez reported having no relevant disclosures.
A version of this article appeared on Medscape.com.
VIENNA — An intervention consisting of a plant-based diet, exercise, and sleep and stress advice improved pain, stiffness, and physical function in people with knee and/or hip osteoarthritis (OA) and metabolic syndrome, while in patients with rheumatoid arthritis (RA), disease activity improved significantly, and medication use was reduced.
At the annual European Congress of Rheumatology, Carlijn Wagenaar, MD, a PhD candidate in Clinical Immunology and Rheumatology at Amsterdam University Medical Center, presented 2-year extension study results for OA and RA and an overview of the possible biological mechanisms underpinning the plant-based intervention in RA.
“At 2 years, RA patients on the PFJ [Plants for Joints] intervention resulted in a significant improvement in disease activity of RA, and these outcomes were maintained 2 years after program end,” Dr. Wagenaar reported.
“Some initial improvements in body composition and metabolic outcomes were also maintained at the end of the 2-year extension phase, and there was a net decrease in antirheumatic medication use,” she continued.
In the patients with OA, Dr. Wagenaar said the PFJ intervention improved pain, stiffness, and physical function in people with knee and/or hip OA and metabolic syndrome. “In the 2-year extension study, these effects were maintained, and we saw lasting body composition changes and a decrease in cholesterol-lowering medications. There was also high acceptability of the program; the study shows long-term maintenance of clinically relevant effects.”
Significant Improvement in OA Pain, Stiffness, Physical Function
In the OA randomized controlled trial, 64 people with hip and/or knee OA and metabolic syndrome were randomized to the PFJ intervention or usual care (waitlist control group). A total of 62 participants (including those in the control group previously) entered the long-term effectiveness study, and 44 had 2 years of follow-up data for analysis. Twenty participants dropped out, with most being unreachable or too busy.
“The PFJ program is a theoretical and practical program where people learn about and follow a whole food, plant-based diet, and receive advice on sleep and stress management and exercise,” said Dr. Wagenaar.
The program lasted 16 weeks with group sessions of 6-12 participants. The diet was a plant-based version of the Dutch dietary guidelines with a focus on unprocessed food. It was rich in whole grains, legumes, nuts, seeds, fruit, and vegetables, but without calorie restrictions and participants had one-to-one contact with a dietitian. The exercise advice followed the Dutch exercise guidelines, which advise 150 minutes of moderate to intense exercise per week, as well as twice-weekly muscle strength exercises, noted Dr. Wagenaar.
The 2-year follow-up study involved twice-yearly visits and six adherence-promoting webinars per year, as well as monthly newsletters. Researchers also monitored changes in medication intensity (classified as “increased,” “stable,” or “decreased/stopped”) between the start of the PFJ intervention and end of the 2-year extension study, and they were grouped into medications for pain, blood pressure, glucose, and cholesterol.
Participants were encouraged to try to avoid making changes to medication during the intervention phase, but they could do so during the 2-year extension study, said Dr. Wagenaar. In fact, the researchers actively monitored and quantified medication changes between the start of the PFJ intervention and end of the 2-year follow-up period.
Patients in the 16-week trial had an average age of 64 years, 84% were women, and their mean body mass index (BMI) was 33 kg/m2. A total of 73% had knee OA and 78% hip OA, and their mean WOMAC score was 38.2, indicative of moderate to severe OA.
In participants who completed the 2-year extension study, the primary outcome (WOMAC score for mean stiffness and physical function) showed a significant improvement of −9.1 (95% CI, −12.8 to −5.3; P < .0001) compared with the start of the PFJ intervention.
“Looking at individual components of the WOMAC score — pain, stiffness, and physical function — we found these also all significantly improved at the end of the 2-year extension phase,” reported Dr. Wagenaar.
She added that after 2 years, there were significant improvements in weight loss (from 94.9 to 92.1 kg), BMI (from 33.3 to 32 kg/m2), and waist circumference (from 110 to 106.7 cm).
By the end of the trial and at 1 year of the extension study, there were significant improvements in A1c, fasting blood glucose, and low-density lipoprotein cholesterol, but at 2 years, these were no longer significant.
Regarding medications use, Dr. Wagenaar reported that, overall, there was no net change in use of pain, glucose-lowering, or hypertension medications, but 44% of patients using cholesterol-lowering medications were able to lower their dose or stop them.
Disease Activity Improvement and Medication Reduction in RA
Turning to the study of the intervention in patients with RA, 77 people (DAS28 ≥ 2.6 and ≤ 5.1, mild to moderate disease) were randomized to receive either the PFJ intervention in addition to usual care or only usual care (control group). Of these, 48 (62%) from both the intervention and control groups also completed the 2-year follow-up. The details of the PFJ intervention and the extension study for RA were the same as for the OA patient group.
Dr. Wagenaar commented on how they tried to individualize the exercise part of the program. “We noticed many of the RA patients asked too much of their body, while in contrast, those with OA were too hesitant,” she said. “We decided to focus on people’s own physical barriers, and we wanted to protect these. Sometimes, people needed to move more, and at other times, we had to tell people to slow down. Often, we advised people to move more by integrating exercise into their daily life.”
Similar to the OA study, patients were asked to try to avoid changing their medications in the 16-week study. “In the extension study, they were encouraged to reduce their medication in collaboration with their rheumatologist,” explained Wagenaar, who monitored any changes.
Differences were quantified according to medication groups comprising rheumatic medications, as well as pain, blood pressure, glucose-lowering, and cholesterol medications, and changes were categorized as increased, stable, or decreased/stopped.
Again, participants were mostly women (92%) with an average age of 55 years, BMI of 26 kg/m2, and DAS28 of 3.85 at baseline. Dropout reasons were similar to those for OA, and over 85% of participants were on medications.
During the 16-week trial period, the DAS28 changed more in the intervention participants than in the controls, and after 2 years of follow-up, DAS28 was significantly lower than baseline with a mean difference of −0.9 (95% CI, −1.2 to −0.6; P < .0001).
“Comparing with the literature, the drop in DAS28 was similar to that seen with medication, so it’s a very significant reduction,” remarked Dr. Wagenaar.
Mean tender joint count dropped from 3 to 0, and general health components of the DAS28 improved significantly over the intervention and over the 2-year follow-up, whereas there was no significant difference in the already low erythrocyte sedimentation rate and swollen joint count compared with baseline. C-reactive protein (CRP) changed from 3.2 to 1.3 mg/L over the 2-year follow-up. High-density lipoprotein increased from 1.6 to 1.8 mmol/L.
A total of 44% of people using antirheumatic medication decreased or stopped them after the 2-year extension.
Dr. Wagenaar went on to say that focus group findings suggested that “participants were very enthusiastic about the program despite it largely involving lifestyle change, and this is reflected in our low dropout rates after the trial and 1-year extension [20% for OA and RA].” There were more dropouts in year 2 of the extension.
In an interview, Dr. Wagenaar explained why she felt the program had been so well received. “People in the program felt like they had more control over their disease, and they felt listened to.”
Mechanisms Underpinning PFJ
Dr. Wagenaar and colleagues also sought to determine the possible mechanisms underlying the clinical effects of the plant-based diet on RA. “With RA, we have the mucosal origins hypothesis, which suggests RA is triggered at the mucosal site [of the gut] in genetically predisposed individuals, and this consequently transfers to the synovial [fluid in] joints,” she said.
“On top of this, we know that fiber protects our gut barrier and therefore reduces inflammation. The PFJ intervention is a very high-fiber program, so our hypothesis is that it might help [strengthen] the barrier,” she explained.
Dr. Wagenaar and colleagues collected fecal samples from patients and measured the albumin and calprotectin in them, which are both indicators of the gut barrier function. The researchers analyzed metabolomic data and found that fecal albumin — considered a gut barrier integrity marker — decreased significantly in the intervention group. In patients with RA, this improvement corresponded with an improvement in DAS28, the researchers reported in a poster at the meeting.
“Patients who had the greatest improvement in their gut barrier function also showed the greatest improvement in the DAS28 score, suggestive of a possible link between gut barrier improvement and clinical effects.”
They did not identify any change in calprotectin, an inflammation marker, but Dr. Wagenaar said this might change later. “We found that in those on the intervention, at 4 months, the CRP wasn’t reduced, but 1 year later it was.”
The metabolite lenticin, a lentil intake biomarker considered protective against inflammation and osteoclastic differentiation, also increased. Tryptophan was also reduced in people on the PFJ intervention.
Fernando Estevez-Lopez, PhD, a sports scientist at Harvard T.H. Chan School of Public Health, Boston, who specializes in physical activity and behavioral change in rheumatology patients, co-moderated the session and remarked that, “In this study, they did a brilliant job with encouraging participants to follow the program. The design and methods were really good — the sample size was good, and they followed people up. Also, these researchers come from Reade [a medical research center in Amsterdam University Medical Center] where they are well known for applying their research findings to the clinic,” he said.
“In terms of physical activity, we really mean increasing the time spent moving, for example, gentle activity such as walking, or changing behaviors in people with OA and RA. We don’t want them to have more pain the next day.”
Dr. Wagenaar reported receiving a grant from ZonMw (The Netherlands Organization for Health Research and Development). She and colleagues hold shares in Plants for Health, a limited liability company. Dr. Estevez-Lopez reported having no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
Trial Confirms Treating Gout Based on Uric Acid Level, Not Symptoms
UPDATED July 8, 2024 // Editor's note: This article has been revised to give a more nuanced view from Yael Klionsky, MD, about the need for more accurate and consistent gout management guidelines for busy primary care clinicians who often rely on them in clinical practice.
VIENNA — The first multicenter randomized trial in gout to compare treat-to-target (T2T) and treat for symptom avoidance (T2S) strategies has finally generated data to make the guideline-recommended practice of T2T evidence-based.
The T2T strategy may be guideline-endorsed, but it has never been validated, contended Anusha Moses, MSc, a researcher and PhD candidate at the University of Twente, Enschede, the Netherlands. She argued that this controlled trial fills an evidence gap.
T2T is defined as maintaining a serum uric acid (sUA) level below the physiologic threshold level of 36 mmol/L (< 6 mg/dL). T2S, in contrast, is a strategy of symptom control, typically basing therapy on suppression of symptoms independent of sUA, Dr. Moses explained. 
Both the American College of Rheumatology and European Alliance of Associations for Rheumatology (EULAR) have already endorsed T2T, but other organizations, such as the American College of Physicians (ACP), still accept symptom-based treatment in its gout clinical practice guideline, according to Dr. Moses.
The results of the trial were not surprising based on the pathophysiology of gout. Elevated sUA is considered the driver of both flares and the complications of gout. This well-established association led to endorsement of T2T in guidelines from organizations such as EULAR, but Dr. Moses said a controlled trial allows this to be declared as evidence based.
To provide proof that T2T is superior, 308 gout patients at eight centers were randomized to one of the two strategies in a trial called GO TEST OVERTURE. In the T2T arm, commonly used therapies, such as allopurinol, benzbromarone, and febuxostat were employed to achieve and maintain a target sUA of < 0.36 mmol/L. In the T2S comparator arm, the same drugs were offered to control symptoms and prevent recurrences, but sUA levels were not used to guide treatment.
The 1-year results of a planned 2-year study were presented in an oral abstract session at the annual European Congress of Rheumatology. For this analysis, outcomes were compared in the last 6 months prior to the 1-year data analysis. When assessed at 2 years, the comparison will again be made in the prior 6 months of the study.
For the primary endpoint of flares defined by the validated Gallo criteria, the mean rates were 1.3 for T2T and 1.85 for T2S (P < .001), Dr. Moses reported.
The reduced risk for flares correlated with the greater proportion of patients with sUA < 0.36 mmol/L. These proportions were 72% and 26% (P < .001) for the T2T and T2S groups, respectively. The mean sUA levels were 0.31 mmol/L and 0.42 mmol/L (P < .001), respectively.
At the 1-year mark, none of the secondary endpoints reached statistical significance. These included mean numeric rating pain scale (2.46 vs 2.41), the proportion of patients in remission (8% vs 5.7%), and the mean Health Assessment Questionnaire-Disability Index score (0.65 vs 0.62), according to Dr. Moses, who said all of these endpoints will continue to be followed in the planned second year of the study.
At baseline, there were no differences in any of the variables evaluated, including age (about 62.5 years in both groups), proportion of patients with a body mass index > 30 kg/m2 (about 62%), sUA (about 0.5 mmol/L), or estimated glomerular filtration rate (about 70 mL/min/1.73 m2).
Nonspecialists Should Heed the Results
According to Yael Klionsky, MD, a clinical assistant professor of rheumatology and immunology at Wake Forest University School of Medicine, Winston-Salem, North Carolina, these data are not a surprise.
Even before this trial was completed, the message for clinicians is that they “should be focused on maintaining serum uric acid levels below physiological levels to improve outcomes” in patients with recurrent flares, said Klionsky, citing the validated EULAR and ACR guidelines.
While the ACP does still consider T2S acceptable as a strategy for chronic gout management, Klionsky pointed out that those guidelines have not been updated recently. Specialists in the treatment of gout do not need any more evidence that the T2T approach leads to better outcomes.
However, she agreed with the principle that non-rheumatologists need to be reached with better guidance in regard to gout management. While she expects the ACP to endorse T2T the next time their guidelines are updated, she hopes that primary care physicians recognize that T2T should now be a standard.
“In a 10- to 20-minute visit, managing multiple chronic conditions can be a challenge in primary care,” Klionsky said. “Many clinicians rely on guidelines so it is important to have consistent and accurate information.”
There is currently some distance between specialists and primary care physicians regarding the goals of gout management, according to a study that Klionsky presented at EULAR 2024. In a survey, nonspecialists and specialists did not perceive treatment priorities in the same way.
In this survey, which elicited responses from 151 rheumatologists, 150 nephrologists, and 102 primary care physicians, there was general agreement that preventing flares is a priority, but only 30% of primary care physicians and 35% of nephrologists vs 64% of rheumatologists identified the T2T target of < 0.36 mmol/L as a key step in reaching this goal.
Conversely, 58% of primary care physicians and 42% of nephrologists vs only 34% of rheumatologists considered absence of gout pain to be in the top three criteria.
In addition to the fact that primary care physicians differ from specialists in their goals for gout treatment, these data “highlight the need for the importance of a standardized definition of gout remission that includes serum uric acid control,” Dr. Klionsky said. She further thinks that this type of guidance should be disseminated to nonspecialists.
Dr. Moses reported no potential conflicts of interest. Dr. Klionsky reported financial relationships with Amgen, AstraZeneca, Eli Lilly, and MedIQ.
A version of this article appeared on Medscape.com.
UPDATED July 8, 2024 // Editor's note: This article has been revised to give a more nuanced view from Yael Klionsky, MD, about the need for more accurate and consistent gout management guidelines for busy primary care clinicians who often rely on them in clinical practice.
VIENNA — The first multicenter randomized trial in gout to compare treat-to-target (T2T) and treat for symptom avoidance (T2S) strategies has finally generated data to make the guideline-recommended practice of T2T evidence-based.
The T2T strategy may be guideline-endorsed, but it has never been validated, contended Anusha Moses, MSc, a researcher and PhD candidate at the University of Twente, Enschede, the Netherlands. She argued that this controlled trial fills an evidence gap.
T2T is defined as maintaining a serum uric acid (sUA) level below the physiologic threshold level of 36 mmol/L (< 6 mg/dL). T2S, in contrast, is a strategy of symptom control, typically basing therapy on suppression of symptoms independent of sUA, Dr. Moses explained.
Both the American College of Rheumatology and European Alliance of Associations for Rheumatology (EULAR) have already endorsed T2T, but other organizations, such as the American College of Physicians (ACP), still accept symptom-based treatment in its gout clinical practice guideline, according to Dr. Moses.
The results of the trial were not surprising based on the pathophysiology of gout. Elevated sUA is considered the driver of both flares and the complications of gout. This well-established association led to endorsement of T2T in guidelines from organizations such as EULAR, but Dr. Moses said a controlled trial allows this to be declared as evidence based.
To provide proof that T2T is superior, 308 gout patients at eight centers were randomized to one of the two strategies in a trial called GO TEST OVERTURE. In the T2T arm, commonly used therapies, such as allopurinol, benzbromarone, and febuxostat were employed to achieve and maintain a target sUA of < 0.36 mmol/L. In the T2S comparator arm, the same drugs were offered to control symptoms and prevent recurrences, but sUA levels were not used to guide treatment.
The 1-year results of a planned 2-year study were presented in an oral abstract session at the annual European Congress of Rheumatology. For this analysis, outcomes were compared in the last 6 months prior to the 1-year data analysis. When assessed at 2 years, the comparison will again be made in the prior 6 months of the study.
For the primary endpoint of flares defined by the validated Gallo criteria, the mean rates were 1.3 for T2T and 1.85 for T2S (P < .001), Dr. Moses reported.
The reduced risk for flares correlated with the greater proportion of patients with sUA < 0.36 mmol/L. These proportions were 72% and 26% (P < .001) for the T2T and T2S groups, respectively. The mean sUA levels were 0.31 mmol/L and 0.42 mmol/L (P < .001), respectively.
At the 1-year mark, none of the secondary endpoints reached statistical significance. These included mean numeric rating pain scale (2.46 vs 2.41), the proportion of patients in remission (8% vs 5.7%), and the mean Health Assessment Questionnaire-Disability Index score (0.65 vs 0.62), according to Dr. Moses, who said all of these endpoints will continue to be followed in the planned second year of the study.
At baseline, there were no differences in any of the variables evaluated, including age (about 62.5 years in both groups), proportion of patients with a body mass index > 30 kg/m2 (about 62%), sUA (about 0.5 mmol/L), or estimated glomerular filtration rate (about 70 mL/min/1.73 m2).
Nonspecialists Should Heed the Results
According to Yael Klionsky, MD, a clinical assistant professor of rheumatology and immunology at Wake Forest University School of Medicine, Winston-Salem, North Carolina, these data are not a surprise.
Even before this trial was completed, the message for clinicians is that they “should be focused on maintaining serum uric acid levels below physiological levels to improve outcomes” in patients with recurrent flares, said Klionsky, citing the validated EULAR and ACR guidelines.
While the ACP does still consider T2S acceptable as a strategy for chronic gout management, Klionsky pointed out that those guidelines have not been updated recently. Specialists in the treatment of gout do not need any more evidence that the T2T approach leads to better outcomes.
However, she agreed with the principle that non-rheumatologists need to be reached with better guidance in regard to gout management. While she expects the ACP to endorse T2T the next time their guidelines are updated, she hopes that primary care physicians recognize that T2T should now be a standard.
“In a 10- to 20-minute visit, managing multiple chronic conditions can be a challenge in primary care,” Klionsky said. “Many clinicians rely on guidelines so it is important to have consistent and accurate information.”
There is currently some distance between specialists and primary care physicians regarding the goals of gout management, according to a study that Klionsky presented at EULAR 2024. In a survey, nonspecialists and specialists did not perceive treatment priorities in the same way.
In this survey, which elicited responses from 151 rheumatologists, 150 nephrologists, and 102 primary care physicians, there was general agreement that preventing flares is a priority, but only 30% of primary care physicians and 35% of nephrologists vs 64% of rheumatologists identified the T2T target of < 0.36 mmol/L as a key step in reaching this goal.
Conversely, 58% of primary care physicians and 42% of nephrologists vs only 34% of rheumatologists considered absence of gout pain to be in the top three criteria.
In addition to the fact that primary care physicians differ from specialists in their goals for gout treatment, these data “highlight the need for the importance of a standardized definition of gout remission that includes serum uric acid control,” Dr. Klionsky said. She further thinks that this type of guidance should be disseminated to nonspecialists.
Dr. Moses reported no potential conflicts of interest. Dr. Klionsky reported financial relationships with Amgen, AstraZeneca, Eli Lilly, and MedIQ.
A version of this article appeared on Medscape.com.
UPDATED July 8, 2024 // Editor's note: This article has been revised to give a more nuanced view from Yael Klionsky, MD, about the need for more accurate and consistent gout management guidelines for busy primary care clinicians who often rely on them in clinical practice.
VIENNA — The first multicenter randomized trial in gout to compare treat-to-target (T2T) and treat for symptom avoidance (T2S) strategies has finally generated data to make the guideline-recommended practice of T2T evidence-based.
The T2T strategy may be guideline-endorsed, but it has never been validated, contended Anusha Moses, MSc, a researcher and PhD candidate at the University of Twente, Enschede, the Netherlands. She argued that this controlled trial fills an evidence gap.
T2T is defined as maintaining a serum uric acid (sUA) level below the physiologic threshold level of 36 mmol/L (< 6 mg/dL). T2S, in contrast, is a strategy of symptom control, typically basing therapy on suppression of symptoms independent of sUA, Dr. Moses explained.
Both the American College of Rheumatology and European Alliance of Associations for Rheumatology (EULAR) have already endorsed T2T, but other organizations, such as the American College of Physicians (ACP), still accept symptom-based treatment in its gout clinical practice guideline, according to Dr. Moses.
The results of the trial were not surprising based on the pathophysiology of gout. Elevated sUA is considered the driver of both flares and the complications of gout. This well-established association led to endorsement of T2T in guidelines from organizations such as EULAR, but Dr. Moses said a controlled trial allows this to be declared as evidence based.
To provide proof that T2T is superior, 308 gout patients at eight centers were randomized to one of the two strategies in a trial called GO TEST OVERTURE. In the T2T arm, commonly used therapies, such as allopurinol, benzbromarone, and febuxostat were employed to achieve and maintain a target sUA of < 0.36 mmol/L. In the T2S comparator arm, the same drugs were offered to control symptoms and prevent recurrences, but sUA levels were not used to guide treatment.
The 1-year results of a planned 2-year study were presented in an oral abstract session at the annual European Congress of Rheumatology. For this analysis, outcomes were compared in the last 6 months prior to the 1-year data analysis. When assessed at 2 years, the comparison will again be made in the prior 6 months of the study.
For the primary endpoint of flares defined by the validated Gallo criteria, the mean rates were 1.3 for T2T and 1.85 for T2S (P < .001), Dr. Moses reported.
The reduced risk for flares correlated with the greater proportion of patients with sUA < 0.36 mmol/L. These proportions were 72% and 26% (P < .001) for the T2T and T2S groups, respectively. The mean sUA levels were 0.31 mmol/L and 0.42 mmol/L (P < .001), respectively.
At the 1-year mark, none of the secondary endpoints reached statistical significance. These included mean numeric rating pain scale (2.46 vs 2.41), the proportion of patients in remission (8% vs 5.7%), and the mean Health Assessment Questionnaire-Disability Index score (0.65 vs 0.62), according to Dr. Moses, who said all of these endpoints will continue to be followed in the planned second year of the study.
At baseline, there were no differences in any of the variables evaluated, including age (about 62.5 years in both groups), proportion of patients with a body mass index > 30 kg/m2 (about 62%), sUA (about 0.5 mmol/L), or estimated glomerular filtration rate (about 70 mL/min/1.73 m2).
Nonspecialists Should Heed the Results
According to Yael Klionsky, MD, a clinical assistant professor of rheumatology and immunology at Wake Forest University School of Medicine, Winston-Salem, North Carolina, these data are not a surprise.
Even before this trial was completed, the message for clinicians is that they “should be focused on maintaining serum uric acid levels below physiological levels to improve outcomes” in patients with recurrent flares, said Klionsky, citing the validated EULAR and ACR guidelines.
While the ACP does still consider T2S acceptable as a strategy for chronic gout management, Klionsky pointed out that those guidelines have not been updated recently. Specialists in the treatment of gout do not need any more evidence that the T2T approach leads to better outcomes.
However, she agreed with the principle that non-rheumatologists need to be reached with better guidance in regard to gout management. While she expects the ACP to endorse T2T the next time their guidelines are updated, she hopes that primary care physicians recognize that T2T should now be a standard.
“In a 10- to 20-minute visit, managing multiple chronic conditions can be a challenge in primary care,” Klionsky said. “Many clinicians rely on guidelines so it is important to have consistent and accurate information.”
There is currently some distance between specialists and primary care physicians regarding the goals of gout management, according to a study that Klionsky presented at EULAR 2024. In a survey, nonspecialists and specialists did not perceive treatment priorities in the same way.
In this survey, which elicited responses from 151 rheumatologists, 150 nephrologists, and 102 primary care physicians, there was general agreement that preventing flares is a priority, but only 30% of primary care physicians and 35% of nephrologists vs 64% of rheumatologists identified the T2T target of < 0.36 mmol/L as a key step in reaching this goal.
Conversely, 58% of primary care physicians and 42% of nephrologists vs only 34% of rheumatologists considered absence of gout pain to be in the top three criteria.
In addition to the fact that primary care physicians differ from specialists in their goals for gout treatment, these data “highlight the need for the importance of a standardized definition of gout remission that includes serum uric acid control,” Dr. Klionsky said. She further thinks that this type of guidance should be disseminated to nonspecialists.
Dr. Moses reported no potential conflicts of interest. Dr. Klionsky reported financial relationships with Amgen, AstraZeneca, Eli Lilly, and MedIQ.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
Timing Pneumococcal Vaccination in Patients with RA Starting Methotrexate: When’s Best?
VIENNA — Pneumococcal vaccination administered 1 month prior to starting methotrexate (MTX) in patients with rheumatoid arthritis (RA) allows a significantly higher immunological response at 1 month and does not affect disease control at 1 year, compared with starting MTX simultaneously with the vaccination, according to data from a randomized trial presented at the annual European Congress of Rheumatology.
“Our patients are more susceptible to infection due to immunosuppressive therapy, and it’s recommended they receive vaccination against pneumococcal infection,” the lead author Jacques Morel, MD, PhD, said in his presentation of results from the VACIMRA study.
Timing the vaccination against pneumococcal disease when initiating MTX in clinical practice has been a point of uncertainty, noted Dr. Morel, a rheumatologist from Centre Hospitalier Universitaire, Montpellier, France.
“How can we deal with this in clinical practice where one recommendation is to vaccine before initiation of methotrexate, but it is also recommended to start methotrexate as soon as the diagnosis of RA is made?” he asked.
Comparing Humoral Response of MTX Started Immediately or 1 Month Post-Vaccination
The prospective, randomized, multicenter trial aimed to compare the rate of humoral immunological response against pneumococcal 13-valent conjugate vaccine (PCV13) in patients with RA who had a Disease Activity Score in 28 joints (DAS28) > 3.2, never taken MTX, and never been vaccinated against pneumococcus. Patients were vaccinated either 1 month before MTX initiation (n = 126) or simultaneously with MTX (n = 123). Oral glucocorticoids were allowed but only at < 10 mg/d. Following PCV13 vaccination, all patients also received the 23-valent pneumococcal polysaccharide vaccine (PPV23) 2 months later.
Concentrations of immunoglobulin (Ig) G antibodies against the 13 serotypes contained within PCV13 were measured using enzyme-linked immunosorbent assay (ELISA) and opsonophagocytic killing assay (OPA) at baseline and during follow-up at 1, 3, 6, and 12 months.
Positive antibody response was defined as a twofold or more increase in the IgG concentration using ELISA. The main outcome was the responder rates at 1 month after PCV13, defined by at least three positive antibody responses out of five of the target PVC13 serotypes (1, 3, 5, 7F, and 19A) using ELISA or OPA. Secondary outcomes included comparisons of the percentage of patients responding to each of the 13 vaccine serotypes at 1 month and after the boost with PPV23 and at 3, 6, and 12 months after vaccination with PCV13. The researchers also measured disease activity, infections, and side effects throughout the study.
Dr. Morel highlighted that all the patients had very early RA of less than 6 months, and that their characteristics at baseline were similar in both groups with 70% women, mean age 55.6 years, RA duration 2 months, 69% positive for anticitrullinated protein antibodies, 21% with erosive disease, and a DAS28 based on C-reactive protein of 4.6.
Response rates in those receiving MTX 1 month after vaccination were significantly higher at 88% with ELISA than those at 75% for immediate vaccination (P < .01) and 96% vs 88% with OPA (P = .02). These responder proportions persisted at the 12-month follow-up measurements, remaining higher in the delayed MTX group for both assays and across the 13 serotypes.
Showing a graph of the antibody responses, Dr. Morel explained that “at 12 months, the curves start to converge, but the difference in antibody titers were still significant for eight of the 13 serotypes.”
Disease Activity Not Adversely Affected by Starting MTX 1 Month Later
Regarding medication doses at 12 months, the cumulative glucocorticoid doses were similar between groups during the follow-up. As expected, the 1-year cumulative dose of MTX was higher in those given the drug immediately after vaccination vs delayed (826 vs 734 mg), but the weekly mean doses of MTX were similar at 3, 6, and 12 months between the two groups, and likewise, the use of targeted disease-modifying antirheumatic drugs (DMARDs) at 1 year was comparable. The cumulative glucocorticoid dose at 12 months was similar at 1716 mg with delayed MTX and 1613 mg with immediate MTX.
Not unexpectedly, at 1 month, DAS28 scores were higher with delayed vs immediate MTX at 3.95 vs 3.38 for DAS28-ESR and 3.54 vs 3.01 for DAS28-CRP (P < .01), but after the first month, DAS28 scores were similar between the two groups.
No significant differences were found between the groups for adverse event rates within 7 days of receiving PCV13, with local and systemic reactions occurring at 60%-61% and 50%-58%, respectively; fever at 0%-4%; and severe infections at 12%.
Finally, no difference was found in terms of serious adverse events between groups, with one pneumococcal infection with delayed MTX during follow-up, and there were no unexpected side effects observed with the PCV13 and PPV23 vaccinations.
Rheumatologists’ Reactions
Ernest Choy, MD, head of rheumatology and translational research at the Institute of Infection and Immunity, Cardiff University School of Medicine, Cardiff, Wales, asked if any individual showed no humoral response at all rather than a reduced response. “I ask because if there is no humoral response, then they are at very high risk, and there will be clinical relevance to that.”
Dr. Morel replied that “one serotype showed no response, at least according to the assays used, but we don’t know why. We analyzed at the population [level], not at the individual level, so it is difficult to answer the question.”
Another delegate asked what the participants thought about delaying MTX by 1 month. “When we tell the patient we need to vaccinate before we can use methotrexate [because] otherwise, we will reduce the response to the vaccination, then patient accepts it,” said Dr. Morel, adding that, “we allowed a minimal dose of steroids, and we saw from the results that the DAS28 at 1 month had changed.”
Co-moderator Katerina Chatzidionysiou, MD, PhD, a consultant rheumatologist and head of the Clinical Trial Department Rheumatology Unit, Karolinska University Hospital, Stockholm, Sweden, said that “As a physician, I’d feel uncomfortable delaying MTX if they had very active disease even for a short period of time.”
Dr. Morel replied that, “Today, we have so many drugs that can control the disease, for example, the targeted DMARDs. Progression does not show much variation, and we know x-ray progression with today’s drugs is a lot less than previously.”
Dr. Morel reported financial relationships with AbbVie, Amgen, Biogen, Bristol Myers Squibb, Fresenius Kabi, Galapagos, GlaxoSmithKline, Lilly, Medac, Nordic Pharma, Novartis, Pfizer, Sandoz, Sanofi, Boehringer Ingelheim, and Servier. Dr. Choy had no relevant financial relationships of relevance to this study.
A version of this article appeared on Medscape.com.
VIENNA — Pneumococcal vaccination administered 1 month prior to starting methotrexate (MTX) in patients with rheumatoid arthritis (RA) allows a significantly higher immunological response at 1 month and does not affect disease control at 1 year, compared with starting MTX simultaneously with the vaccination, according to data from a randomized trial presented at the annual European Congress of Rheumatology.
“Our patients are more susceptible to infection due to immunosuppressive therapy, and it’s recommended they receive vaccination against pneumococcal infection,” the lead author Jacques Morel, MD, PhD, said in his presentation of results from the VACIMRA study.
Timing the vaccination against pneumococcal disease when initiating MTX in clinical practice has been a point of uncertainty, noted Dr. Morel, a rheumatologist from Centre Hospitalier Universitaire, Montpellier, France.
“How can we deal with this in clinical practice where one recommendation is to vaccine before initiation of methotrexate, but it is also recommended to start methotrexate as soon as the diagnosis of RA is made?” he asked.
Comparing Humoral Response of MTX Started Immediately or 1 Month Post-Vaccination
The prospective, randomized, multicenter trial aimed to compare the rate of humoral immunological response against pneumococcal 13-valent conjugate vaccine (PCV13) in patients with RA who had a Disease Activity Score in 28 joints (DAS28) > 3.2, never taken MTX, and never been vaccinated against pneumococcus. Patients were vaccinated either 1 month before MTX initiation (n = 126) or simultaneously with MTX (n = 123). Oral glucocorticoids were allowed but only at < 10 mg/d. Following PCV13 vaccination, all patients also received the 23-valent pneumococcal polysaccharide vaccine (PPV23) 2 months later.
Concentrations of immunoglobulin (Ig) G antibodies against the 13 serotypes contained within PCV13 were measured using enzyme-linked immunosorbent assay (ELISA) and opsonophagocytic killing assay (OPA) at baseline and during follow-up at 1, 3, 6, and 12 months.
Positive antibody response was defined as a twofold or more increase in the IgG concentration using ELISA. The main outcome was the responder rates at 1 month after PCV13, defined by at least three positive antibody responses out of five of the target PVC13 serotypes (1, 3, 5, 7F, and 19A) using ELISA or OPA. Secondary outcomes included comparisons of the percentage of patients responding to each of the 13 vaccine serotypes at 1 month and after the boost with PPV23 and at 3, 6, and 12 months after vaccination with PCV13. The researchers also measured disease activity, infections, and side effects throughout the study.
Dr. Morel highlighted that all the patients had very early RA of less than 6 months, and that their characteristics at baseline were similar in both groups with 70% women, mean age 55.6 years, RA duration 2 months, 69% positive for anticitrullinated protein antibodies, 21% with erosive disease, and a DAS28 based on C-reactive protein of 4.6.
Response rates in those receiving MTX 1 month after vaccination were significantly higher at 88% with ELISA than those at 75% for immediate vaccination (P < .01) and 96% vs 88% with OPA (P = .02). These responder proportions persisted at the 12-month follow-up measurements, remaining higher in the delayed MTX group for both assays and across the 13 serotypes.
Showing a graph of the antibody responses, Dr. Morel explained that “at 12 months, the curves start to converge, but the difference in antibody titers were still significant for eight of the 13 serotypes.”
Disease Activity Not Adversely Affected by Starting MTX 1 Month Later
Regarding medication doses at 12 months, the cumulative glucocorticoid doses were similar between groups during the follow-up. As expected, the 1-year cumulative dose of MTX was higher in those given the drug immediately after vaccination vs delayed (826 vs 734 mg), but the weekly mean doses of MTX were similar at 3, 6, and 12 months between the two groups, and likewise, the use of targeted disease-modifying antirheumatic drugs (DMARDs) at 1 year was comparable. The cumulative glucocorticoid dose at 12 months was similar at 1716 mg with delayed MTX and 1613 mg with immediate MTX.
Not unexpectedly, at 1 month, DAS28 scores were higher with delayed vs immediate MTX at 3.95 vs 3.38 for DAS28-ESR and 3.54 vs 3.01 for DAS28-CRP (P < .01), but after the first month, DAS28 scores were similar between the two groups.
No significant differences were found between the groups for adverse event rates within 7 days of receiving PCV13, with local and systemic reactions occurring at 60%-61% and 50%-58%, respectively; fever at 0%-4%; and severe infections at 12%.
Finally, no difference was found in terms of serious adverse events between groups, with one pneumococcal infection with delayed MTX during follow-up, and there were no unexpected side effects observed with the PCV13 and PPV23 vaccinations.
Rheumatologists’ Reactions
Ernest Choy, MD, head of rheumatology and translational research at the Institute of Infection and Immunity, Cardiff University School of Medicine, Cardiff, Wales, asked if any individual showed no humoral response at all rather than a reduced response. “I ask because if there is no humoral response, then they are at very high risk, and there will be clinical relevance to that.”
Dr. Morel replied that “one serotype showed no response, at least according to the assays used, but we don’t know why. We analyzed at the population [level], not at the individual level, so it is difficult to answer the question.”
Another delegate asked what the participants thought about delaying MTX by 1 month. “When we tell the patient we need to vaccinate before we can use methotrexate [because] otherwise, we will reduce the response to the vaccination, then patient accepts it,” said Dr. Morel, adding that, “we allowed a minimal dose of steroids, and we saw from the results that the DAS28 at 1 month had changed.”
Co-moderator Katerina Chatzidionysiou, MD, PhD, a consultant rheumatologist and head of the Clinical Trial Department Rheumatology Unit, Karolinska University Hospital, Stockholm, Sweden, said that “As a physician, I’d feel uncomfortable delaying MTX if they had very active disease even for a short period of time.”
Dr. Morel replied that, “Today, we have so many drugs that can control the disease, for example, the targeted DMARDs. Progression does not show much variation, and we know x-ray progression with today’s drugs is a lot less than previously.”
Dr. Morel reported financial relationships with AbbVie, Amgen, Biogen, Bristol Myers Squibb, Fresenius Kabi, Galapagos, GlaxoSmithKline, Lilly, Medac, Nordic Pharma, Novartis, Pfizer, Sandoz, Sanofi, Boehringer Ingelheim, and Servier. Dr. Choy had no relevant financial relationships of relevance to this study.
A version of this article appeared on Medscape.com.
VIENNA — Pneumococcal vaccination administered 1 month prior to starting methotrexate (MTX) in patients with rheumatoid arthritis (RA) allows a significantly higher immunological response at 1 month and does not affect disease control at 1 year, compared with starting MTX simultaneously with the vaccination, according to data from a randomized trial presented at the annual European Congress of Rheumatology.
“Our patients are more susceptible to infection due to immunosuppressive therapy, and it’s recommended they receive vaccination against pneumococcal infection,” the lead author Jacques Morel, MD, PhD, said in his presentation of results from the VACIMRA study.
Timing the vaccination against pneumococcal disease when initiating MTX in clinical practice has been a point of uncertainty, noted Dr. Morel, a rheumatologist from Centre Hospitalier Universitaire, Montpellier, France.
“How can we deal with this in clinical practice where one recommendation is to vaccine before initiation of methotrexate, but it is also recommended to start methotrexate as soon as the diagnosis of RA is made?” he asked.
Comparing Humoral Response of MTX Started Immediately or 1 Month Post-Vaccination
The prospective, randomized, multicenter trial aimed to compare the rate of humoral immunological response against pneumococcal 13-valent conjugate vaccine (PCV13) in patients with RA who had a Disease Activity Score in 28 joints (DAS28) > 3.2, never taken MTX, and never been vaccinated against pneumococcus. Patients were vaccinated either 1 month before MTX initiation (n = 126) or simultaneously with MTX (n = 123). Oral glucocorticoids were allowed but only at < 10 mg/d. Following PCV13 vaccination, all patients also received the 23-valent pneumococcal polysaccharide vaccine (PPV23) 2 months later.
Concentrations of immunoglobulin (Ig) G antibodies against the 13 serotypes contained within PCV13 were measured using enzyme-linked immunosorbent assay (ELISA) and opsonophagocytic killing assay (OPA) at baseline and during follow-up at 1, 3, 6, and 12 months.
Positive antibody response was defined as a twofold or more increase in the IgG concentration using ELISA. The main outcome was the responder rates at 1 month after PCV13, defined by at least three positive antibody responses out of five of the target PVC13 serotypes (1, 3, 5, 7F, and 19A) using ELISA or OPA. Secondary outcomes included comparisons of the percentage of patients responding to each of the 13 vaccine serotypes at 1 month and after the boost with PPV23 and at 3, 6, and 12 months after vaccination with PCV13. The researchers also measured disease activity, infections, and side effects throughout the study.
Dr. Morel highlighted that all the patients had very early RA of less than 6 months, and that their characteristics at baseline were similar in both groups with 70% women, mean age 55.6 years, RA duration 2 months, 69% positive for anticitrullinated protein antibodies, 21% with erosive disease, and a DAS28 based on C-reactive protein of 4.6.
Response rates in those receiving MTX 1 month after vaccination were significantly higher at 88% with ELISA than those at 75% for immediate vaccination (P < .01) and 96% vs 88% with OPA (P = .02). These responder proportions persisted at the 12-month follow-up measurements, remaining higher in the delayed MTX group for both assays and across the 13 serotypes.
Showing a graph of the antibody responses, Dr. Morel explained that “at 12 months, the curves start to converge, but the difference in antibody titers were still significant for eight of the 13 serotypes.”
Disease Activity Not Adversely Affected by Starting MTX 1 Month Later
Regarding medication doses at 12 months, the cumulative glucocorticoid doses were similar between groups during the follow-up. As expected, the 1-year cumulative dose of MTX was higher in those given the drug immediately after vaccination vs delayed (826 vs 734 mg), but the weekly mean doses of MTX were similar at 3, 6, and 12 months between the two groups, and likewise, the use of targeted disease-modifying antirheumatic drugs (DMARDs) at 1 year was comparable. The cumulative glucocorticoid dose at 12 months was similar at 1716 mg with delayed MTX and 1613 mg with immediate MTX.
Not unexpectedly, at 1 month, DAS28 scores were higher with delayed vs immediate MTX at 3.95 vs 3.38 for DAS28-ESR and 3.54 vs 3.01 for DAS28-CRP (P < .01), but after the first month, DAS28 scores were similar between the two groups.
No significant differences were found between the groups for adverse event rates within 7 days of receiving PCV13, with local and systemic reactions occurring at 60%-61% and 50%-58%, respectively; fever at 0%-4%; and severe infections at 12%.
Finally, no difference was found in terms of serious adverse events between groups, with one pneumococcal infection with delayed MTX during follow-up, and there were no unexpected side effects observed with the PCV13 and PPV23 vaccinations.
Rheumatologists’ Reactions
Ernest Choy, MD, head of rheumatology and translational research at the Institute of Infection and Immunity, Cardiff University School of Medicine, Cardiff, Wales, asked if any individual showed no humoral response at all rather than a reduced response. “I ask because if there is no humoral response, then they are at very high risk, and there will be clinical relevance to that.”
Dr. Morel replied that “one serotype showed no response, at least according to the assays used, but we don’t know why. We analyzed at the population [level], not at the individual level, so it is difficult to answer the question.”
Another delegate asked what the participants thought about delaying MTX by 1 month. “When we tell the patient we need to vaccinate before we can use methotrexate [because] otherwise, we will reduce the response to the vaccination, then patient accepts it,” said Dr. Morel, adding that, “we allowed a minimal dose of steroids, and we saw from the results that the DAS28 at 1 month had changed.”
Co-moderator Katerina Chatzidionysiou, MD, PhD, a consultant rheumatologist and head of the Clinical Trial Department Rheumatology Unit, Karolinska University Hospital, Stockholm, Sweden, said that “As a physician, I’d feel uncomfortable delaying MTX if they had very active disease even for a short period of time.”
Dr. Morel replied that, “Today, we have so many drugs that can control the disease, for example, the targeted DMARDs. Progression does not show much variation, and we know x-ray progression with today’s drugs is a lot less than previously.”
Dr. Morel reported financial relationships with AbbVie, Amgen, Biogen, Bristol Myers Squibb, Fresenius Kabi, Galapagos, GlaxoSmithKline, Lilly, Medac, Nordic Pharma, Novartis, Pfizer, Sandoz, Sanofi, Boehringer Ingelheim, and Servier. Dr. Choy had no relevant financial relationships of relevance to this study.
A version of this article appeared on Medscape.com.
FROM EULAR 2024