User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Frequent cannabis use tied to coronary artery disease
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
FROM ACC 2023
New data strengthen case for oral immunotherapy in tots
The buzz surrounding OIT – which involves ingesting daily doses of the culprit food to raise the threshold that would trigger a reaction – grew with the approval, by the U.S. Food and Drug Administration of Palforzia, of the peanut OIT pill in January 2020. Yet many allergists remained wary about the treatment, a monthslong regimen that can itself trigger allergic reactions.
Now, accumulating research points to “a possible window of opportunity early in life, less than 3 years of age, for more successful disease remission,” Justin Schwartz, MD, PhD, an allergist at Cincinnati Children’s Hospital, told a crowd at the annual meeting of the American Academy of Allergy, Asthma, & Immunology.
His presentation about OIT in toddlers kicked off a 3-hour clinical practice course, one of several dozen conference offerings highlighting this emerging approach.
Several AAAAI posters add to prior studies (for example, DEVIL and IMPACT) suggesting that OIT proceeds more smoothly and faster during a child’s earliest years – a season fraught with accidental exposures and reactions.
One poster described a retrospective study of 73 children younger than 4 years who underwent OIT at the Cleveland Clinic Food Allergy Center. Sixty-four were treated for peanut allergies, and seven patients received OIT for multiple foods, including tree nuts, milk, wheat, and sesame.
Of the 80 total OIT courses, 76 (95%) reached maintenance – meaning the child tolerated a small amount (for example, 1-2 peanuts) without reacting – in a median of 104 days (~3.4 months).
That is “quite impressive,” said allergist Hugh Windom, MD, whose clinic in Sarasota, Fla., has offered OIT since 2012.
Older children typically have 80%-90% success and take longer (6-8 months) to reach maintenance because of busier schedules and reactions that slow them down, he said. In his clinic’s larger retrospective analysis of preschool-aged OIT patients, presented at the 2022 AAAAI meeting, 89% of patients with peanut allergies and 72% of children with multiple food allergies achieved maintenance.
In the Cleveland Clinic study, children with favorable lab test results after receiving the maintenance dose for 6 months were offered an oral food challenge. Of 24 patients who completed the challenge, 75% “passed with a normal serving size of the treated food (for example, two tablespoons of peanut butter),” Sarah Johnson, MD, lead author and Cleveland Clinic allergy/immunology fellow, said in an interview.
Plus, OIT seemed safer for toddlers. Although 41% of the children had reactions during clinic updosing and 48% had reactions at home, only ~3% of toddler OIT courses required epinephrine. By comparison, ~11% of treatments required epinephrine in a large OIT study of older children.
When a child reacts, “you might keep them on the dose or go a little slower,” said Johnson, who worked with allergist Jaclyn Bjelac, MD, on the study. These setbacks occurred less frequently in toddlers, allowing their OIT to “go a lot faster” than in older children. And so far, Dr. Johnson said, none of the toddlers have shown signs of eosinophilic esophagitis, a rare complication that can develop during OIT.
A smaller analysis of real-world outcomes in an academic clinical setting also found that OIT was well tolerated at very young ages. Since 2020, this ongoing study at UVA Children’s Hospital in Charlottesville has enrolled 22 peanut-allergic children (aged 6 months to 3 years) for OIT. Three patients have dropped out, four are in the buildup phrase, and 15 have reached maintenance dosing. None have reported having to use epinephrine.
Three patients have completed 1 year of maintenance therapy, and another patient accidentally consumed ~3,000 mg of peanut protein (equivalent to ~10 peanuts) after 5 months of maintenance. All four “now incorporate peanut into their diets ad lib,” according to lead author and allergist Jonathan Hemler, MD, who directs the UVA pediatric food allergy program.
These findings are “really reassuring – because even if you may not offer OIT, you’re still going to get questions about it,” said Ama Alexis, MD, an allergist/immunologist in private practice in New York and a clinical assistant professor at NYU Grossmann School of Medicine, commenting on the Cleveland Clinic study.
“It’s great that we’re hearing and seeing so much about OIT,” she added. While training as an allergy/immunology fellow 15 years ago, many saw the treatment as dangerous – “an absolute no-no,” she said.
The AAAAI still considers OIT “investigational,” yet this year’s annual meeting featured 22 posters – plus a course, workshop, seminar, and oral abstract session – on the approach.
The “thought process has shifted,” Dr. Alexis said. “It’s good to see all these numbers, these results. I think once you’re comfortable, you should embrace new therapies.”
Dr. Schwartz has consulted for Shire/Takeda and has received research funding from Knopp Biosciences. Dr. Alexis consults for AbbVie, serves on advisory boards for Jansen and Eli Lilli, and is a member of Pfizer’s advisory board and speaker’s bureau. Dr. Johnson, Dr. Windom, and Dr. Hemler report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The buzz surrounding OIT – which involves ingesting daily doses of the culprit food to raise the threshold that would trigger a reaction – grew with the approval, by the U.S. Food and Drug Administration of Palforzia, of the peanut OIT pill in January 2020. Yet many allergists remained wary about the treatment, a monthslong regimen that can itself trigger allergic reactions.
Now, accumulating research points to “a possible window of opportunity early in life, less than 3 years of age, for more successful disease remission,” Justin Schwartz, MD, PhD, an allergist at Cincinnati Children’s Hospital, told a crowd at the annual meeting of the American Academy of Allergy, Asthma, & Immunology.
His presentation about OIT in toddlers kicked off a 3-hour clinical practice course, one of several dozen conference offerings highlighting this emerging approach.
Several AAAAI posters add to prior studies (for example, DEVIL and IMPACT) suggesting that OIT proceeds more smoothly and faster during a child’s earliest years – a season fraught with accidental exposures and reactions.
One poster described a retrospective study of 73 children younger than 4 years who underwent OIT at the Cleveland Clinic Food Allergy Center. Sixty-four were treated for peanut allergies, and seven patients received OIT for multiple foods, including tree nuts, milk, wheat, and sesame.
Of the 80 total OIT courses, 76 (95%) reached maintenance – meaning the child tolerated a small amount (for example, 1-2 peanuts) without reacting – in a median of 104 days (~3.4 months).
That is “quite impressive,” said allergist Hugh Windom, MD, whose clinic in Sarasota, Fla., has offered OIT since 2012.
Older children typically have 80%-90% success and take longer (6-8 months) to reach maintenance because of busier schedules and reactions that slow them down, he said. In his clinic’s larger retrospective analysis of preschool-aged OIT patients, presented at the 2022 AAAAI meeting, 89% of patients with peanut allergies and 72% of children with multiple food allergies achieved maintenance.
In the Cleveland Clinic study, children with favorable lab test results after receiving the maintenance dose for 6 months were offered an oral food challenge. Of 24 patients who completed the challenge, 75% “passed with a normal serving size of the treated food (for example, two tablespoons of peanut butter),” Sarah Johnson, MD, lead author and Cleveland Clinic allergy/immunology fellow, said in an interview.
Plus, OIT seemed safer for toddlers. Although 41% of the children had reactions during clinic updosing and 48% had reactions at home, only ~3% of toddler OIT courses required epinephrine. By comparison, ~11% of treatments required epinephrine in a large OIT study of older children.
When a child reacts, “you might keep them on the dose or go a little slower,” said Johnson, who worked with allergist Jaclyn Bjelac, MD, on the study. These setbacks occurred less frequently in toddlers, allowing their OIT to “go a lot faster” than in older children. And so far, Dr. Johnson said, none of the toddlers have shown signs of eosinophilic esophagitis, a rare complication that can develop during OIT.
A smaller analysis of real-world outcomes in an academic clinical setting also found that OIT was well tolerated at very young ages. Since 2020, this ongoing study at UVA Children’s Hospital in Charlottesville has enrolled 22 peanut-allergic children (aged 6 months to 3 years) for OIT. Three patients have dropped out, four are in the buildup phrase, and 15 have reached maintenance dosing. None have reported having to use epinephrine.
Three patients have completed 1 year of maintenance therapy, and another patient accidentally consumed ~3,000 mg of peanut protein (equivalent to ~10 peanuts) after 5 months of maintenance. All four “now incorporate peanut into their diets ad lib,” according to lead author and allergist Jonathan Hemler, MD, who directs the UVA pediatric food allergy program.
These findings are “really reassuring – because even if you may not offer OIT, you’re still going to get questions about it,” said Ama Alexis, MD, an allergist/immunologist in private practice in New York and a clinical assistant professor at NYU Grossmann School of Medicine, commenting on the Cleveland Clinic study.
“It’s great that we’re hearing and seeing so much about OIT,” she added. While training as an allergy/immunology fellow 15 years ago, many saw the treatment as dangerous – “an absolute no-no,” she said.
The AAAAI still considers OIT “investigational,” yet this year’s annual meeting featured 22 posters – plus a course, workshop, seminar, and oral abstract session – on the approach.
The “thought process has shifted,” Dr. Alexis said. “It’s good to see all these numbers, these results. I think once you’re comfortable, you should embrace new therapies.”
Dr. Schwartz has consulted for Shire/Takeda and has received research funding from Knopp Biosciences. Dr. Alexis consults for AbbVie, serves on advisory boards for Jansen and Eli Lilli, and is a member of Pfizer’s advisory board and speaker’s bureau. Dr. Johnson, Dr. Windom, and Dr. Hemler report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The buzz surrounding OIT – which involves ingesting daily doses of the culprit food to raise the threshold that would trigger a reaction – grew with the approval, by the U.S. Food and Drug Administration of Palforzia, of the peanut OIT pill in January 2020. Yet many allergists remained wary about the treatment, a monthslong regimen that can itself trigger allergic reactions.
Now, accumulating research points to “a possible window of opportunity early in life, less than 3 years of age, for more successful disease remission,” Justin Schwartz, MD, PhD, an allergist at Cincinnati Children’s Hospital, told a crowd at the annual meeting of the American Academy of Allergy, Asthma, & Immunology.
His presentation about OIT in toddlers kicked off a 3-hour clinical practice course, one of several dozen conference offerings highlighting this emerging approach.
Several AAAAI posters add to prior studies (for example, DEVIL and IMPACT) suggesting that OIT proceeds more smoothly and faster during a child’s earliest years – a season fraught with accidental exposures and reactions.
One poster described a retrospective study of 73 children younger than 4 years who underwent OIT at the Cleveland Clinic Food Allergy Center. Sixty-four were treated for peanut allergies, and seven patients received OIT for multiple foods, including tree nuts, milk, wheat, and sesame.
Of the 80 total OIT courses, 76 (95%) reached maintenance – meaning the child tolerated a small amount (for example, 1-2 peanuts) without reacting – in a median of 104 days (~3.4 months).
That is “quite impressive,” said allergist Hugh Windom, MD, whose clinic in Sarasota, Fla., has offered OIT since 2012.
Older children typically have 80%-90% success and take longer (6-8 months) to reach maintenance because of busier schedules and reactions that slow them down, he said. In his clinic’s larger retrospective analysis of preschool-aged OIT patients, presented at the 2022 AAAAI meeting, 89% of patients with peanut allergies and 72% of children with multiple food allergies achieved maintenance.
In the Cleveland Clinic study, children with favorable lab test results after receiving the maintenance dose for 6 months were offered an oral food challenge. Of 24 patients who completed the challenge, 75% “passed with a normal serving size of the treated food (for example, two tablespoons of peanut butter),” Sarah Johnson, MD, lead author and Cleveland Clinic allergy/immunology fellow, said in an interview.
Plus, OIT seemed safer for toddlers. Although 41% of the children had reactions during clinic updosing and 48% had reactions at home, only ~3% of toddler OIT courses required epinephrine. By comparison, ~11% of treatments required epinephrine in a large OIT study of older children.
When a child reacts, “you might keep them on the dose or go a little slower,” said Johnson, who worked with allergist Jaclyn Bjelac, MD, on the study. These setbacks occurred less frequently in toddlers, allowing their OIT to “go a lot faster” than in older children. And so far, Dr. Johnson said, none of the toddlers have shown signs of eosinophilic esophagitis, a rare complication that can develop during OIT.
A smaller analysis of real-world outcomes in an academic clinical setting also found that OIT was well tolerated at very young ages. Since 2020, this ongoing study at UVA Children’s Hospital in Charlottesville has enrolled 22 peanut-allergic children (aged 6 months to 3 years) for OIT. Three patients have dropped out, four are in the buildup phrase, and 15 have reached maintenance dosing. None have reported having to use epinephrine.
Three patients have completed 1 year of maintenance therapy, and another patient accidentally consumed ~3,000 mg of peanut protein (equivalent to ~10 peanuts) after 5 months of maintenance. All four “now incorporate peanut into their diets ad lib,” according to lead author and allergist Jonathan Hemler, MD, who directs the UVA pediatric food allergy program.
These findings are “really reassuring – because even if you may not offer OIT, you’re still going to get questions about it,” said Ama Alexis, MD, an allergist/immunologist in private practice in New York and a clinical assistant professor at NYU Grossmann School of Medicine, commenting on the Cleveland Clinic study.
“It’s great that we’re hearing and seeing so much about OIT,” she added. While training as an allergy/immunology fellow 15 years ago, many saw the treatment as dangerous – “an absolute no-no,” she said.
The AAAAI still considers OIT “investigational,” yet this year’s annual meeting featured 22 posters – plus a course, workshop, seminar, and oral abstract session – on the approach.
The “thought process has shifted,” Dr. Alexis said. “It’s good to see all these numbers, these results. I think once you’re comfortable, you should embrace new therapies.”
Dr. Schwartz has consulted for Shire/Takeda and has received research funding from Knopp Biosciences. Dr. Alexis consults for AbbVie, serves on advisory boards for Jansen and Eli Lilli, and is a member of Pfizer’s advisory board and speaker’s bureau. Dr. Johnson, Dr. Windom, and Dr. Hemler report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAAAI 2023
Prostate cancer subgroup may benefit from intensified therapy
SAN FRANCISCO – For patients with prostate cancer who have unfavorable features and a detectable PSA following a radical prostatectomy, the standard of care is treatment with 6 months of a gonadotropin-releasing hormone (GnRH) agonist with salvage radiation therapy (SRT), as established by the GETUG-AFU 16 trial.
A new trial, dubbed FORMULA-509, explored whether outcomes could be improved by intensifying the drug treatment by adding 6 months of abiraterone acetate plus prednisone as well as apalutamide on top of the GnRH agonist alongside the salvage radiotherapy.
However, the combination did significantly improve PFS and MFS in a subset of men with PSA levels greater than 0.5 ng/mL.
“Although this primary analysis did not meet the prespecified threshold for statistical significance, it does strongly suggest that the addition of abiraterone acetate/prednisone/apalutamide to salvage radiotherapy plus 6 months of ADT [androgen deprivation therapy] may improve progression-free survival and metastasis-free survival,” said lead author Paul L. Nguyen, MD, of the Dana-Farber Cancer Institute in Boston, and professor of radiation oncology at Harvard Medical School.
“This may be particularly evident in the subgroup of patients with PSA greater that 0.5 ng/mL where a preplanned subgroup analysis by stratification factors observed a statistically significant benefit for both progression-free survival and metastasis-free survival,” he said. “Six months of intensified ADT with next generation anti-androgens may provide an attractive alternative to lengthening ADT for patients with rising PSA and unfavorable features after radical prostatectomy.”
The study results were presented at the ASCO Genitourinary Cancers Symposium.
Benefit in subset
The FORMULA-509 trial included 305 patients with PSA ≥ 0.1 ng/mL who had undergone a radical prostatectomy, and who had one or more unfavorable risk features (Gleason 8-10 disease, PSA > 0.5 ng/mL, pT3/T4, pN1 or radiographic N1, PSA doubling time < 10 months, negative margins, persistent PSA, gross local/regional disease).
“This was a pretty high-risk population,” Dr. Nguyen emphasized, as 35% had Gleason score of 9, about a third (31%) a PSA >0.5, and 29% were pathologic node positive.
All patients received salvage radiotherapy plus 6 months of GnRH agonist (bicalutamide 50 mg), and half were randomly assigned to also receive abiraterone acetate/prednisone 1,000 mg/5 mg + apalutamide 240 mg daily.
At a median follow-up of 34 months, the 3-year PFS rate was 74.9% in the AAP-apalutamide arm vs. 68.5% for the control group (hazard ratio [HR], 0.71; P = .06), and the 3-year MFS rate was 90.6% vs. 87.2%, respectively (HR, 0.57; P = .05).
In the subset of patients with a PSA greater than 0.5 ng/mL, the 3-year PFS and MFS rates were significantly higher with in the AAP-apalutamide group: the 3-year PFS rate was 67.2% vs. 46.8% (HR, 0.50; P = .03), and the 3-year MFS rate was 84.3% vs. 66.1% (HR, 0.32; P = .02).
Adverse events were consistent with the known safety profiles of the agents being studied, Dr. Nguyen noted. The most common toxicities for AAP-apalutamide vs. controls were hypertension (21.8% vs. 13.3%), maculopapular rash (11.5% vs. 0.6%), diarrhea (8.5% vs. 4.8%), and fatigue (7.9% vs. 6.1%).
Dr. Nguyen noted that even though “we’re not supposed to compare clinical trials,” the results of this study appeared to compare favorably with those of another trial, RADICALS-HD, which was presented at the 2022 European Society of Medical Oncology Congress. That study showed that in patients undergoing postoperative radiation therapy, 24 months of ADT was superior to 6 months of ADT in improving both time to salvage ADT and MFS.
However, Dr. Nguyen emphasized that it would have to be formally tested, to see if “FORMULA-509 is performing in the ballpark of what 24 months of ADT would do.
“And I think that compared to 6 months of ADT, we can say it is certainly performing in the ballpark,” he said. “So, for patients with higher risk features, intensifying 6 months of ADT, I think, may be an appealing alternative to lengthening the ADT duration to 24 months.”
He added that this concept would be formally tested in the upcoming PROSTATE IQ study.
Strong evidence, standardization needed
In a discussion of the paper, Tyler Seibert, MD, PhD, of the University of California San Diego, said that “escalation by 24 months has the strongest evidence today, specifically from the RADICALS-HD trial, with more than 1,500 men with 10 years of follow-up and a clear statistically significant result.
“Intensification for 6 months is a very compelling concept, as most patients are not getting 2 years of androgen deprivation therapy at this point post prostatectomy,” he continued. “While we await the long term follow-up of this study and the pending PROSTATE IQ trial, and if only 6 months of therapy is acceptable or feasible, the FORMULA-509 [trial] provides convincing evidence that select patients would benefit from intensification with AAP and apalutamide.”
Another expert weighed in on the data. Approached by this news organization for an independent comment, Jeff M. Michalski, MD, MBA, professor of radiation oncology at Washington University, St Louis, and president of the American Society of Radiation Oncology, noted a few issues in the study.
He said that standards had changed since this study was first approved and had begun accrual several years ago. “In context of today’s era, the current standard is to do a PET scan if patients have a chemical failure after surgery,” he said. “The PSA levels of patients who were treated [in this trial] were very high, and many patients do not want to wait until they reach that level.”
Dr. Michalski also pointed out the number of patients getting radiation was less than the number who had node-positive disease. “This shows that patients had received suboptimal therapy late in the disease,” he said.
Overall, most patients in the study did not receive lymph node radiation, even though they had high-risk features. “A recent study of almost 1,800 patients that was published in The Lancet found that there is a benefit to pelvic lymph node radiation,” he said. “Because it wasn’t mandated, most of the patients did not receive pelvic lymph node radiation, which we now understand offers some benefit.”
The reasons for not giving pelvic radiation to these men is unclear. “Treatment was left at the discretion of the physician and this could create bias,” Dr. Michalski said. “It could drive one arm more than another.”
The study also wasn’t controlled for pelvic radiation. “Most of the nodal positive patients received it, but the other patients were undertreated,” he noted.
Dr. Michalski added that he hopes that in the forthcoming PROSTATE IQ study, lymph node radiation and imaging are standardized.
The trial was supported by Janssen Oncology. Dr. Nguyen disclosed relationships with, and/or support from, Volatilyx, Bayer, Blue Earth Diagnostics, Boston Scientific, Janssen Oncology, Myovant Sciences, Astellas Pharma, and Janssen. Dr. Seibert disclosed relationships with, and/or support from, CorTechs Labs, Varian Medical Systems, and GE Healthcare.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – For patients with prostate cancer who have unfavorable features and a detectable PSA following a radical prostatectomy, the standard of care is treatment with 6 months of a gonadotropin-releasing hormone (GnRH) agonist with salvage radiation therapy (SRT), as established by the GETUG-AFU 16 trial.
A new trial, dubbed FORMULA-509, explored whether outcomes could be improved by intensifying the drug treatment by adding 6 months of abiraterone acetate plus prednisone as well as apalutamide on top of the GnRH agonist alongside the salvage radiotherapy.
However, the combination did significantly improve PFS and MFS in a subset of men with PSA levels greater than 0.5 ng/mL.
“Although this primary analysis did not meet the prespecified threshold for statistical significance, it does strongly suggest that the addition of abiraterone acetate/prednisone/apalutamide to salvage radiotherapy plus 6 months of ADT [androgen deprivation therapy] may improve progression-free survival and metastasis-free survival,” said lead author Paul L. Nguyen, MD, of the Dana-Farber Cancer Institute in Boston, and professor of radiation oncology at Harvard Medical School.
“This may be particularly evident in the subgroup of patients with PSA greater that 0.5 ng/mL where a preplanned subgroup analysis by stratification factors observed a statistically significant benefit for both progression-free survival and metastasis-free survival,” he said. “Six months of intensified ADT with next generation anti-androgens may provide an attractive alternative to lengthening ADT for patients with rising PSA and unfavorable features after radical prostatectomy.”
The study results were presented at the ASCO Genitourinary Cancers Symposium.
Benefit in subset
The FORMULA-509 trial included 305 patients with PSA ≥ 0.1 ng/mL who had undergone a radical prostatectomy, and who had one or more unfavorable risk features (Gleason 8-10 disease, PSA > 0.5 ng/mL, pT3/T4, pN1 or radiographic N1, PSA doubling time < 10 months, negative margins, persistent PSA, gross local/regional disease).
“This was a pretty high-risk population,” Dr. Nguyen emphasized, as 35% had Gleason score of 9, about a third (31%) a PSA >0.5, and 29% were pathologic node positive.
All patients received salvage radiotherapy plus 6 months of GnRH agonist (bicalutamide 50 mg), and half were randomly assigned to also receive abiraterone acetate/prednisone 1,000 mg/5 mg + apalutamide 240 mg daily.
At a median follow-up of 34 months, the 3-year PFS rate was 74.9% in the AAP-apalutamide arm vs. 68.5% for the control group (hazard ratio [HR], 0.71; P = .06), and the 3-year MFS rate was 90.6% vs. 87.2%, respectively (HR, 0.57; P = .05).
In the subset of patients with a PSA greater than 0.5 ng/mL, the 3-year PFS and MFS rates were significantly higher with in the AAP-apalutamide group: the 3-year PFS rate was 67.2% vs. 46.8% (HR, 0.50; P = .03), and the 3-year MFS rate was 84.3% vs. 66.1% (HR, 0.32; P = .02).
Adverse events were consistent with the known safety profiles of the agents being studied, Dr. Nguyen noted. The most common toxicities for AAP-apalutamide vs. controls were hypertension (21.8% vs. 13.3%), maculopapular rash (11.5% vs. 0.6%), diarrhea (8.5% vs. 4.8%), and fatigue (7.9% vs. 6.1%).
Dr. Nguyen noted that even though “we’re not supposed to compare clinical trials,” the results of this study appeared to compare favorably with those of another trial, RADICALS-HD, which was presented at the 2022 European Society of Medical Oncology Congress. That study showed that in patients undergoing postoperative radiation therapy, 24 months of ADT was superior to 6 months of ADT in improving both time to salvage ADT and MFS.
However, Dr. Nguyen emphasized that it would have to be formally tested, to see if “FORMULA-509 is performing in the ballpark of what 24 months of ADT would do.
“And I think that compared to 6 months of ADT, we can say it is certainly performing in the ballpark,” he said. “So, for patients with higher risk features, intensifying 6 months of ADT, I think, may be an appealing alternative to lengthening the ADT duration to 24 months.”
He added that this concept would be formally tested in the upcoming PROSTATE IQ study.
Strong evidence, standardization needed
In a discussion of the paper, Tyler Seibert, MD, PhD, of the University of California San Diego, said that “escalation by 24 months has the strongest evidence today, specifically from the RADICALS-HD trial, with more than 1,500 men with 10 years of follow-up and a clear statistically significant result.
“Intensification for 6 months is a very compelling concept, as most patients are not getting 2 years of androgen deprivation therapy at this point post prostatectomy,” he continued. “While we await the long term follow-up of this study and the pending PROSTATE IQ trial, and if only 6 months of therapy is acceptable or feasible, the FORMULA-509 [trial] provides convincing evidence that select patients would benefit from intensification with AAP and apalutamide.”
Another expert weighed in on the data. Approached by this news organization for an independent comment, Jeff M. Michalski, MD, MBA, professor of radiation oncology at Washington University, St Louis, and president of the American Society of Radiation Oncology, noted a few issues in the study.
He said that standards had changed since this study was first approved and had begun accrual several years ago. “In context of today’s era, the current standard is to do a PET scan if patients have a chemical failure after surgery,” he said. “The PSA levels of patients who were treated [in this trial] were very high, and many patients do not want to wait until they reach that level.”
Dr. Michalski also pointed out the number of patients getting radiation was less than the number who had node-positive disease. “This shows that patients had received suboptimal therapy late in the disease,” he said.
Overall, most patients in the study did not receive lymph node radiation, even though they had high-risk features. “A recent study of almost 1,800 patients that was published in The Lancet found that there is a benefit to pelvic lymph node radiation,” he said. “Because it wasn’t mandated, most of the patients did not receive pelvic lymph node radiation, which we now understand offers some benefit.”
The reasons for not giving pelvic radiation to these men is unclear. “Treatment was left at the discretion of the physician and this could create bias,” Dr. Michalski said. “It could drive one arm more than another.”
The study also wasn’t controlled for pelvic radiation. “Most of the nodal positive patients received it, but the other patients were undertreated,” he noted.
Dr. Michalski added that he hopes that in the forthcoming PROSTATE IQ study, lymph node radiation and imaging are standardized.
The trial was supported by Janssen Oncology. Dr. Nguyen disclosed relationships with, and/or support from, Volatilyx, Bayer, Blue Earth Diagnostics, Boston Scientific, Janssen Oncology, Myovant Sciences, Astellas Pharma, and Janssen. Dr. Seibert disclosed relationships with, and/or support from, CorTechs Labs, Varian Medical Systems, and GE Healthcare.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – For patients with prostate cancer who have unfavorable features and a detectable PSA following a radical prostatectomy, the standard of care is treatment with 6 months of a gonadotropin-releasing hormone (GnRH) agonist with salvage radiation therapy (SRT), as established by the GETUG-AFU 16 trial.
A new trial, dubbed FORMULA-509, explored whether outcomes could be improved by intensifying the drug treatment by adding 6 months of abiraterone acetate plus prednisone as well as apalutamide on top of the GnRH agonist alongside the salvage radiotherapy.
However, the combination did significantly improve PFS and MFS in a subset of men with PSA levels greater than 0.5 ng/mL.
“Although this primary analysis did not meet the prespecified threshold for statistical significance, it does strongly suggest that the addition of abiraterone acetate/prednisone/apalutamide to salvage radiotherapy plus 6 months of ADT [androgen deprivation therapy] may improve progression-free survival and metastasis-free survival,” said lead author Paul L. Nguyen, MD, of the Dana-Farber Cancer Institute in Boston, and professor of radiation oncology at Harvard Medical School.
“This may be particularly evident in the subgroup of patients with PSA greater that 0.5 ng/mL where a preplanned subgroup analysis by stratification factors observed a statistically significant benefit for both progression-free survival and metastasis-free survival,” he said. “Six months of intensified ADT with next generation anti-androgens may provide an attractive alternative to lengthening ADT for patients with rising PSA and unfavorable features after radical prostatectomy.”
The study results were presented at the ASCO Genitourinary Cancers Symposium.
Benefit in subset
The FORMULA-509 trial included 305 patients with PSA ≥ 0.1 ng/mL who had undergone a radical prostatectomy, and who had one or more unfavorable risk features (Gleason 8-10 disease, PSA > 0.5 ng/mL, pT3/T4, pN1 or radiographic N1, PSA doubling time < 10 months, negative margins, persistent PSA, gross local/regional disease).
“This was a pretty high-risk population,” Dr. Nguyen emphasized, as 35% had Gleason score of 9, about a third (31%) a PSA >0.5, and 29% were pathologic node positive.
All patients received salvage radiotherapy plus 6 months of GnRH agonist (bicalutamide 50 mg), and half were randomly assigned to also receive abiraterone acetate/prednisone 1,000 mg/5 mg + apalutamide 240 mg daily.
At a median follow-up of 34 months, the 3-year PFS rate was 74.9% in the AAP-apalutamide arm vs. 68.5% for the control group (hazard ratio [HR], 0.71; P = .06), and the 3-year MFS rate was 90.6% vs. 87.2%, respectively (HR, 0.57; P = .05).
In the subset of patients with a PSA greater than 0.5 ng/mL, the 3-year PFS and MFS rates were significantly higher with in the AAP-apalutamide group: the 3-year PFS rate was 67.2% vs. 46.8% (HR, 0.50; P = .03), and the 3-year MFS rate was 84.3% vs. 66.1% (HR, 0.32; P = .02).
Adverse events were consistent with the known safety profiles of the agents being studied, Dr. Nguyen noted. The most common toxicities for AAP-apalutamide vs. controls were hypertension (21.8% vs. 13.3%), maculopapular rash (11.5% vs. 0.6%), diarrhea (8.5% vs. 4.8%), and fatigue (7.9% vs. 6.1%).
Dr. Nguyen noted that even though “we’re not supposed to compare clinical trials,” the results of this study appeared to compare favorably with those of another trial, RADICALS-HD, which was presented at the 2022 European Society of Medical Oncology Congress. That study showed that in patients undergoing postoperative radiation therapy, 24 months of ADT was superior to 6 months of ADT in improving both time to salvage ADT and MFS.
However, Dr. Nguyen emphasized that it would have to be formally tested, to see if “FORMULA-509 is performing in the ballpark of what 24 months of ADT would do.
“And I think that compared to 6 months of ADT, we can say it is certainly performing in the ballpark,” he said. “So, for patients with higher risk features, intensifying 6 months of ADT, I think, may be an appealing alternative to lengthening the ADT duration to 24 months.”
He added that this concept would be formally tested in the upcoming PROSTATE IQ study.
Strong evidence, standardization needed
In a discussion of the paper, Tyler Seibert, MD, PhD, of the University of California San Diego, said that “escalation by 24 months has the strongest evidence today, specifically from the RADICALS-HD trial, with more than 1,500 men with 10 years of follow-up and a clear statistically significant result.
“Intensification for 6 months is a very compelling concept, as most patients are not getting 2 years of androgen deprivation therapy at this point post prostatectomy,” he continued. “While we await the long term follow-up of this study and the pending PROSTATE IQ trial, and if only 6 months of therapy is acceptable or feasible, the FORMULA-509 [trial] provides convincing evidence that select patients would benefit from intensification with AAP and apalutamide.”
Another expert weighed in on the data. Approached by this news organization for an independent comment, Jeff M. Michalski, MD, MBA, professor of radiation oncology at Washington University, St Louis, and president of the American Society of Radiation Oncology, noted a few issues in the study.
He said that standards had changed since this study was first approved and had begun accrual several years ago. “In context of today’s era, the current standard is to do a PET scan if patients have a chemical failure after surgery,” he said. “The PSA levels of patients who were treated [in this trial] were very high, and many patients do not want to wait until they reach that level.”
Dr. Michalski also pointed out the number of patients getting radiation was less than the number who had node-positive disease. “This shows that patients had received suboptimal therapy late in the disease,” he said.
Overall, most patients in the study did not receive lymph node radiation, even though they had high-risk features. “A recent study of almost 1,800 patients that was published in The Lancet found that there is a benefit to pelvic lymph node radiation,” he said. “Because it wasn’t mandated, most of the patients did not receive pelvic lymph node radiation, which we now understand offers some benefit.”
The reasons for not giving pelvic radiation to these men is unclear. “Treatment was left at the discretion of the physician and this could create bias,” Dr. Michalski said. “It could drive one arm more than another.”
The study also wasn’t controlled for pelvic radiation. “Most of the nodal positive patients received it, but the other patients were undertreated,” he noted.
Dr. Michalski added that he hopes that in the forthcoming PROSTATE IQ study, lymph node radiation and imaging are standardized.
The trial was supported by Janssen Oncology. Dr. Nguyen disclosed relationships with, and/or support from, Volatilyx, Bayer, Blue Earth Diagnostics, Boston Scientific, Janssen Oncology, Myovant Sciences, Astellas Pharma, and Janssen. Dr. Seibert disclosed relationships with, and/or support from, CorTechs Labs, Varian Medical Systems, and GE Healthcare.
A version of this article first appeared on Medscape.com.
AT ASCO GU 2023
Expert dispels myths about hair care in patients with skin of color
HONOLULU –
“This is false,” Dr. Heath, director of pediatric dermatology at Temple University, Philadelphia, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! With little manipulation, length may be retained, since tightly coiled hair has a higher likelihood of breakage, she said. “But washing the scalp and hair is recommended for tightly coiled hair weekly or every other week. Exclusively co-washing – a technique where hair conditioner is used instead of shampooing – is also not advised due to scalp build-up.”
Other myths she addressed include the following:
“I have a weak spot (or stress spot) on the top of my scalp.” These terms may be used to describe hair on a spot that goes through cycles of breaking off and re-growing. This is false. “If someone were to say that, and we see short hairs on the top of a patient’s scalp, with or without tenderness, pruritus, or pain, we want to recognize that as possibly an early sign of central centrifugal cicatricial alopecia [CCCA],” she said. “We want to pick up cases of CCCA forme fruste [central hair breakage] early.”
Medicated shampoos are helpful for all patients with seborrheic dermatitis. This notion is more complicated. “In theory, medicated shampoos like ketoconazole should be helpful, but if the shampoos are too drying for the hair and they cause further hair breakage, that’s going to be a problem as well,” explained Dr. Heath, who was the senior author of an article on how to address common conditions affecting pediatric and adolescent patients with skin of color. For patients with tightly coiled hair, she recommends applying antifungal shampoos to the scalp only, waiting 5-10 minutes, rinsing, and shampooing the scalp and hair with a moisturizing shampoo and rinsing. They can then condition with a moisturizing conditioner and style their hair as desired.

Don’t touch a Black woman’s hair. That unwritten rule may apply to a woman you pass on the street, she said, but not during clinical exams in cases where clinicians and patients seeking hair loss treatment have different hair types. “Touch the hair; don’t do a lean-in exam,” emphasized Dr. Heath, who is the inaugural faculty scholar at Temple University Lewis Katz School of Medicine’s Office of Health Equity Diversity, and Inclusion. “You want to perform the scalp and hair exam with cultural humility.” Understanding the patient’s hair care goals and perspective allows dermatologists to take a more individualized approach to their concerns, especially in race-discordant patient-physician interactions.
Going natural (chemical-free) will solve scarring hair loss problems. This is false. “Genetic defects in the hair shaft have been described as the cause of some CCCA cases, so we need to stop solely blaming the patient for that condition,” she said. Dr. Heath noted that the transition point between natural hair and relaxed hair is highly prone to breakage. She suggests low or lower tension options such as knotless braids, and crochet hairstyles, and when patients have locs, they should be shoulder length or higher to reduce tension.
Dr. Heath disclosed that she has served as a consultant or adviser for Arcutis, CeraVe, Janssen Pharmaceuticals, Johnson & Johnson Pharmaceutical Research & Development, Leo, Lilly, Pfizer, and Regeneron Pharmaceuticals.
Medscape and this news organization are owned by the same parent company.
HONOLULU –
“This is false,” Dr. Heath, director of pediatric dermatology at Temple University, Philadelphia, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! With little manipulation, length may be retained, since tightly coiled hair has a higher likelihood of breakage, she said. “But washing the scalp and hair is recommended for tightly coiled hair weekly or every other week. Exclusively co-washing – a technique where hair conditioner is used instead of shampooing – is also not advised due to scalp build-up.”
Other myths she addressed include the following:
“I have a weak spot (or stress spot) on the top of my scalp.” These terms may be used to describe hair on a spot that goes through cycles of breaking off and re-growing. This is false. “If someone were to say that, and we see short hairs on the top of a patient’s scalp, with or without tenderness, pruritus, or pain, we want to recognize that as possibly an early sign of central centrifugal cicatricial alopecia [CCCA],” she said. “We want to pick up cases of CCCA forme fruste [central hair breakage] early.”
Medicated shampoos are helpful for all patients with seborrheic dermatitis. This notion is more complicated. “In theory, medicated shampoos like ketoconazole should be helpful, but if the shampoos are too drying for the hair and they cause further hair breakage, that’s going to be a problem as well,” explained Dr. Heath, who was the senior author of an article on how to address common conditions affecting pediatric and adolescent patients with skin of color. For patients with tightly coiled hair, she recommends applying antifungal shampoos to the scalp only, waiting 5-10 minutes, rinsing, and shampooing the scalp and hair with a moisturizing shampoo and rinsing. They can then condition with a moisturizing conditioner and style their hair as desired.
Don’t touch a Black woman’s hair. That unwritten rule may apply to a woman you pass on the street, she said, but not during clinical exams in cases where clinicians and patients seeking hair loss treatment have different hair types. “Touch the hair; don’t do a lean-in exam,” emphasized Dr. Heath, who is the inaugural faculty scholar at Temple University Lewis Katz School of Medicine’s Office of Health Equity Diversity, and Inclusion. “You want to perform the scalp and hair exam with cultural humility.” Understanding the patient’s hair care goals and perspective allows dermatologists to take a more individualized approach to their concerns, especially in race-discordant patient-physician interactions.
Going natural (chemical-free) will solve scarring hair loss problems. This is false. “Genetic defects in the hair shaft have been described as the cause of some CCCA cases, so we need to stop solely blaming the patient for that condition,” she said. Dr. Heath noted that the transition point between natural hair and relaxed hair is highly prone to breakage. She suggests low or lower tension options such as knotless braids, and crochet hairstyles, and when patients have locs, they should be shoulder length or higher to reduce tension.
Dr. Heath disclosed that she has served as a consultant or adviser for Arcutis, CeraVe, Janssen Pharmaceuticals, Johnson & Johnson Pharmaceutical Research & Development, Leo, Lilly, Pfizer, and Regeneron Pharmaceuticals.
Medscape and this news organization are owned by the same parent company.
HONOLULU –
“This is false,” Dr. Heath, director of pediatric dermatology at Temple University, Philadelphia, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! With little manipulation, length may be retained, since tightly coiled hair has a higher likelihood of breakage, she said. “But washing the scalp and hair is recommended for tightly coiled hair weekly or every other week. Exclusively co-washing – a technique where hair conditioner is used instead of shampooing – is also not advised due to scalp build-up.”
Other myths she addressed include the following:
“I have a weak spot (or stress spot) on the top of my scalp.” These terms may be used to describe hair on a spot that goes through cycles of breaking off and re-growing. This is false. “If someone were to say that, and we see short hairs on the top of a patient’s scalp, with or without tenderness, pruritus, or pain, we want to recognize that as possibly an early sign of central centrifugal cicatricial alopecia [CCCA],” she said. “We want to pick up cases of CCCA forme fruste [central hair breakage] early.”
Medicated shampoos are helpful for all patients with seborrheic dermatitis. This notion is more complicated. “In theory, medicated shampoos like ketoconazole should be helpful, but if the shampoos are too drying for the hair and they cause further hair breakage, that’s going to be a problem as well,” explained Dr. Heath, who was the senior author of an article on how to address common conditions affecting pediatric and adolescent patients with skin of color. For patients with tightly coiled hair, she recommends applying antifungal shampoos to the scalp only, waiting 5-10 minutes, rinsing, and shampooing the scalp and hair with a moisturizing shampoo and rinsing. They can then condition with a moisturizing conditioner and style their hair as desired.
Don’t touch a Black woman’s hair. That unwritten rule may apply to a woman you pass on the street, she said, but not during clinical exams in cases where clinicians and patients seeking hair loss treatment have different hair types. “Touch the hair; don’t do a lean-in exam,” emphasized Dr. Heath, who is the inaugural faculty scholar at Temple University Lewis Katz School of Medicine’s Office of Health Equity Diversity, and Inclusion. “You want to perform the scalp and hair exam with cultural humility.” Understanding the patient’s hair care goals and perspective allows dermatologists to take a more individualized approach to their concerns, especially in race-discordant patient-physician interactions.
Going natural (chemical-free) will solve scarring hair loss problems. This is false. “Genetic defects in the hair shaft have been described as the cause of some CCCA cases, so we need to stop solely blaming the patient for that condition,” she said. Dr. Heath noted that the transition point between natural hair and relaxed hair is highly prone to breakage. She suggests low or lower tension options such as knotless braids, and crochet hairstyles, and when patients have locs, they should be shoulder length or higher to reduce tension.
Dr. Heath disclosed that she has served as a consultant or adviser for Arcutis, CeraVe, Janssen Pharmaceuticals, Johnson & Johnson Pharmaceutical Research & Development, Leo, Lilly, Pfizer, and Regeneron Pharmaceuticals.
Medscape and this news organization are owned by the same parent company.
AT THE MEDSCAPE LIVE! HAWAII DERMATOLOGY SEMINAR
Old drug verapamil may have new use in type 1 diabetes
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
Insomnia, short sleep linked to greater risk for MI
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.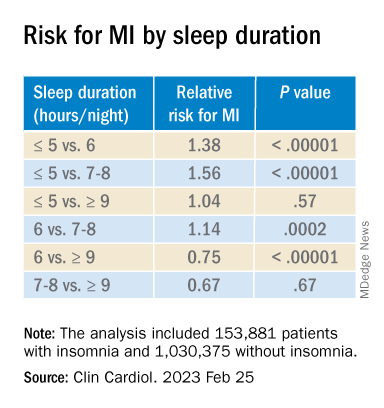
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
To prevent MS, should we target EBV?
SAN DIEGO – Although most adults have been exposed, it is very rare to find MS in an individual with no prior EBV exposure.
That apparent relationship has driven interest in a vaccine against EBV in an effort to reduce MS incidence on a population level.
At a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS), two researchers debated the potential benefits and pitfalls of such a program. The issues included the possible benefit in MS and other EBV-related conditions such as mononucleosis and various cancers, and whether EBV infection is a sufficient cause for MS, as well as concerns about vaccinating a healthy at-risk population.
Reducing the risk of MS by targeting EBV
Jeffrey I. Cohen, MD, spoke first, and cited several lines of evidence supporting the importance of EBV in MS. One study showed a 32-fold increased risk of MS following primary infection with EBV, and another showed that higher EBV nuclear antigen (EBNA) antibody titers were associated with a 36-fold higher risk of MS. “So we have two completely independent studies suggesting that EBV is really very important as a cofactor for development of MS,” said Dr. Cohen, chief of the laboratory of infectious diseases and chief of the medical virology section at the National Institutes of Health, Bethesda, Md.

EBV is also latent in B cells, and anti-B cell therapy is an effective therapeutic strategy for MS. However, the mechanism remains unknown.
Targeting EBV could involve attacking infected cells, or a therapeutic vaccine could be employed to treat EVB-infected individuals, similar to the shingles vaccine. “In all of these methods, one would end up with fewer EBV infected B cells and as a result, presumably you’d have reduced antigenic stimulation of EBV-infected B cells to stimulate either antibodies or T cells that could damage the nervous system. By reducing this, one might be able to [treat] multiple sclerosis,” said Dr. Cohen.
He did acknowledge concerns. It isn’t yet understood whether destroying EBV-infected cells would actually improve outcomes. It also may be more difficult to reduce a latent infection than to prevent infection, since almost all B cells become latently infected. “Thus we think perhaps a role for preventing infection or modifying the initial infection could be important,” said Dr. Cohen.
The most advanced vaccine candidate is a soluble form of EBV glycoprotein gp 350, which is the dominant glycoprotein on the surface of the virus and infected cells. It reduced the risk of mononucleosis by 78%, but it did not prevent EBV infection. There were no safety concerns. Two more vaccines are currently in clinical trials – an mRNA vaccine against a gp 350 sponsored by Moderna, and a gp 350 nanoparticle vaccine by the NIH.
Dr. Cohen acknowledged that safety is the most important factor, since it would be given to healthy individuals, and probably children. There are worries that a vaccine using EBV proteins could worsen MS. In particular, higher titers of antibodies against EBNA have been linked to developing MS and the anti-EBNA antibody has been implicated in molecular mimicry related to MS. However, the current vaccines avoid EBNA. Another worry is that a vaccine could delay onset of disease to an older age, when infection might be more dangerous. However, no delay in onset has been noted with the varicella vaccine or polio vaccines, which prompted similar concerns.
Vaccinating against EBV could also reduce other conditions such as mononucleosis and several cancers.
Does EBV infection even matter?
In his talk, Peter Calabresi, MD, made the case that EBV is not the sole cause of MS, and thus targeting it may prove ineffective. Dr. Calabresi is director of the division of neuroimmunology at Johns Hopkins Medicine, Baltimore.
Why was he asked to provide a rebuttal? “About this time last year, I commented at a meeting that we should be thoughtful as we think about what to do about EBV and MS. I do believe that constructive dialogue is the foundation of science,” he said. He also stated that he is not opposed to vaccines. “I congratulate Dr. Cohen on all of his vaccine successes,” he said.

Still, he is unconvinced that EBV is solely responsible for MS. “I think it’s hard to draw a straight line between EBV and MS as one might with HPV [human papillomavirus] and cervical cancer. For example, we know that EBV accounts for more than 1% of all cancers, and EBV can also cause other autoimmune diseases such as lupus and Sjogren’s, so it’s complicated. And MS of course has genetic susceptibility that’s not limited to the major histocompatibility complex (MHC) genes that are associated with presenting viral peptides,” said Dr. Calabresi.
Evidence relating MS vulnerability to other genetic and environmental factors, including diet, sunlight, smoking, and even pollution, calls into question a direct causal relationship between EBV and MS, he said.
The age prevalence of EBV would complicate efforts to eradicate it. Seroprevalence is 55% by age 5-11 and 75% among university students. “This is important because the duration of the vaccine response–induced protection in young seronegative children is not lengthy. Vaccinated individuals may become susceptible to natural infection at an age where the consequences of infection are more severe, especially leading to infectious mononucleosis, and hopefully not MS. This then raises the issue of the need for boosters, which we’re all well aware of during the COVID pandemic. This may be a problem, especially in young adults due to noncompliance,” said Dr. Calabresi.
He pointed out that not all vaccine attempts went well. In the 1960s, early respiratory syncytial virus (RSV) vaccines caused enhanced respiratory disease and 2 deaths. “We need to be careful when we think about targeting healthy at-risk young people,” said Dr. Calabresi.
Rather than pursue vaccination, Dr. Calabresi favors research into EBV latency in B cells as well as how EBV-infected B cells may cause or exacerbate MS, with the hopes of developing interventions. “It’s tempting to speculate that the success of the anti-CD 20 monoclonal antibody therapies is related to depletion of EBV infected B cells. In fact, I think that may be the case,” he said.
Dr. Cohen has no relevant financial disclosures. Dr. Calabresi has served on a scientific advisory board or data monitoring board for Biogen and Disarm Therapeutics.
SAN DIEGO – Although most adults have been exposed, it is very rare to find MS in an individual with no prior EBV exposure.
That apparent relationship has driven interest in a vaccine against EBV in an effort to reduce MS incidence on a population level.
At a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS), two researchers debated the potential benefits and pitfalls of such a program. The issues included the possible benefit in MS and other EBV-related conditions such as mononucleosis and various cancers, and whether EBV infection is a sufficient cause for MS, as well as concerns about vaccinating a healthy at-risk population.
Reducing the risk of MS by targeting EBV
Jeffrey I. Cohen, MD, spoke first, and cited several lines of evidence supporting the importance of EBV in MS. One study showed a 32-fold increased risk of MS following primary infection with EBV, and another showed that higher EBV nuclear antigen (EBNA) antibody titers were associated with a 36-fold higher risk of MS. “So we have two completely independent studies suggesting that EBV is really very important as a cofactor for development of MS,” said Dr. Cohen, chief of the laboratory of infectious diseases and chief of the medical virology section at the National Institutes of Health, Bethesda, Md.
EBV is also latent in B cells, and anti-B cell therapy is an effective therapeutic strategy for MS. However, the mechanism remains unknown.
Targeting EBV could involve attacking infected cells, or a therapeutic vaccine could be employed to treat EVB-infected individuals, similar to the shingles vaccine. “In all of these methods, one would end up with fewer EBV infected B cells and as a result, presumably you’d have reduced antigenic stimulation of EBV-infected B cells to stimulate either antibodies or T cells that could damage the nervous system. By reducing this, one might be able to [treat] multiple sclerosis,” said Dr. Cohen.
He did acknowledge concerns. It isn’t yet understood whether destroying EBV-infected cells would actually improve outcomes. It also may be more difficult to reduce a latent infection than to prevent infection, since almost all B cells become latently infected. “Thus we think perhaps a role for preventing infection or modifying the initial infection could be important,” said Dr. Cohen.
The most advanced vaccine candidate is a soluble form of EBV glycoprotein gp 350, which is the dominant glycoprotein on the surface of the virus and infected cells. It reduced the risk of mononucleosis by 78%, but it did not prevent EBV infection. There were no safety concerns. Two more vaccines are currently in clinical trials – an mRNA vaccine against a gp 350 sponsored by Moderna, and a gp 350 nanoparticle vaccine by the NIH.
Dr. Cohen acknowledged that safety is the most important factor, since it would be given to healthy individuals, and probably children. There are worries that a vaccine using EBV proteins could worsen MS. In particular, higher titers of antibodies against EBNA have been linked to developing MS and the anti-EBNA antibody has been implicated in molecular mimicry related to MS. However, the current vaccines avoid EBNA. Another worry is that a vaccine could delay onset of disease to an older age, when infection might be more dangerous. However, no delay in onset has been noted with the varicella vaccine or polio vaccines, which prompted similar concerns.
Vaccinating against EBV could also reduce other conditions such as mononucleosis and several cancers.
Does EBV infection even matter?
In his talk, Peter Calabresi, MD, made the case that EBV is not the sole cause of MS, and thus targeting it may prove ineffective. Dr. Calabresi is director of the division of neuroimmunology at Johns Hopkins Medicine, Baltimore.
Why was he asked to provide a rebuttal? “About this time last year, I commented at a meeting that we should be thoughtful as we think about what to do about EBV and MS. I do believe that constructive dialogue is the foundation of science,” he said. He also stated that he is not opposed to vaccines. “I congratulate Dr. Cohen on all of his vaccine successes,” he said.
Still, he is unconvinced that EBV is solely responsible for MS. “I think it’s hard to draw a straight line between EBV and MS as one might with HPV [human papillomavirus] and cervical cancer. For example, we know that EBV accounts for more than 1% of all cancers, and EBV can also cause other autoimmune diseases such as lupus and Sjogren’s, so it’s complicated. And MS of course has genetic susceptibility that’s not limited to the major histocompatibility complex (MHC) genes that are associated with presenting viral peptides,” said Dr. Calabresi.
Evidence relating MS vulnerability to other genetic and environmental factors, including diet, sunlight, smoking, and even pollution, calls into question a direct causal relationship between EBV and MS, he said.
The age prevalence of EBV would complicate efforts to eradicate it. Seroprevalence is 55% by age 5-11 and 75% among university students. “This is important because the duration of the vaccine response–induced protection in young seronegative children is not lengthy. Vaccinated individuals may become susceptible to natural infection at an age where the consequences of infection are more severe, especially leading to infectious mononucleosis, and hopefully not MS. This then raises the issue of the need for boosters, which we’re all well aware of during the COVID pandemic. This may be a problem, especially in young adults due to noncompliance,” said Dr. Calabresi.
He pointed out that not all vaccine attempts went well. In the 1960s, early respiratory syncytial virus (RSV) vaccines caused enhanced respiratory disease and 2 deaths. “We need to be careful when we think about targeting healthy at-risk young people,” said Dr. Calabresi.
Rather than pursue vaccination, Dr. Calabresi favors research into EBV latency in B cells as well as how EBV-infected B cells may cause or exacerbate MS, with the hopes of developing interventions. “It’s tempting to speculate that the success of the anti-CD 20 monoclonal antibody therapies is related to depletion of EBV infected B cells. In fact, I think that may be the case,” he said.
Dr. Cohen has no relevant financial disclosures. Dr. Calabresi has served on a scientific advisory board or data monitoring board for Biogen and Disarm Therapeutics.
SAN DIEGO – Although most adults have been exposed, it is very rare to find MS in an individual with no prior EBV exposure.
That apparent relationship has driven interest in a vaccine against EBV in an effort to reduce MS incidence on a population level.
At a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS), two researchers debated the potential benefits and pitfalls of such a program. The issues included the possible benefit in MS and other EBV-related conditions such as mononucleosis and various cancers, and whether EBV infection is a sufficient cause for MS, as well as concerns about vaccinating a healthy at-risk population.
Reducing the risk of MS by targeting EBV
Jeffrey I. Cohen, MD, spoke first, and cited several lines of evidence supporting the importance of EBV in MS. One study showed a 32-fold increased risk of MS following primary infection with EBV, and another showed that higher EBV nuclear antigen (EBNA) antibody titers were associated with a 36-fold higher risk of MS. “So we have two completely independent studies suggesting that EBV is really very important as a cofactor for development of MS,” said Dr. Cohen, chief of the laboratory of infectious diseases and chief of the medical virology section at the National Institutes of Health, Bethesda, Md.
EBV is also latent in B cells, and anti-B cell therapy is an effective therapeutic strategy for MS. However, the mechanism remains unknown.
Targeting EBV could involve attacking infected cells, or a therapeutic vaccine could be employed to treat EVB-infected individuals, similar to the shingles vaccine. “In all of these methods, one would end up with fewer EBV infected B cells and as a result, presumably you’d have reduced antigenic stimulation of EBV-infected B cells to stimulate either antibodies or T cells that could damage the nervous system. By reducing this, one might be able to [treat] multiple sclerosis,” said Dr. Cohen.
He did acknowledge concerns. It isn’t yet understood whether destroying EBV-infected cells would actually improve outcomes. It also may be more difficult to reduce a latent infection than to prevent infection, since almost all B cells become latently infected. “Thus we think perhaps a role for preventing infection or modifying the initial infection could be important,” said Dr. Cohen.
The most advanced vaccine candidate is a soluble form of EBV glycoprotein gp 350, which is the dominant glycoprotein on the surface of the virus and infected cells. It reduced the risk of mononucleosis by 78%, but it did not prevent EBV infection. There were no safety concerns. Two more vaccines are currently in clinical trials – an mRNA vaccine against a gp 350 sponsored by Moderna, and a gp 350 nanoparticle vaccine by the NIH.
Dr. Cohen acknowledged that safety is the most important factor, since it would be given to healthy individuals, and probably children. There are worries that a vaccine using EBV proteins could worsen MS. In particular, higher titers of antibodies against EBNA have been linked to developing MS and the anti-EBNA antibody has been implicated in molecular mimicry related to MS. However, the current vaccines avoid EBNA. Another worry is that a vaccine could delay onset of disease to an older age, when infection might be more dangerous. However, no delay in onset has been noted with the varicella vaccine or polio vaccines, which prompted similar concerns.
Vaccinating against EBV could also reduce other conditions such as mononucleosis and several cancers.
Does EBV infection even matter?
In his talk, Peter Calabresi, MD, made the case that EBV is not the sole cause of MS, and thus targeting it may prove ineffective. Dr. Calabresi is director of the division of neuroimmunology at Johns Hopkins Medicine, Baltimore.
Why was he asked to provide a rebuttal? “About this time last year, I commented at a meeting that we should be thoughtful as we think about what to do about EBV and MS. I do believe that constructive dialogue is the foundation of science,” he said. He also stated that he is not opposed to vaccines. “I congratulate Dr. Cohen on all of his vaccine successes,” he said.
Still, he is unconvinced that EBV is solely responsible for MS. “I think it’s hard to draw a straight line between EBV and MS as one might with HPV [human papillomavirus] and cervical cancer. For example, we know that EBV accounts for more than 1% of all cancers, and EBV can also cause other autoimmune diseases such as lupus and Sjogren’s, so it’s complicated. And MS of course has genetic susceptibility that’s not limited to the major histocompatibility complex (MHC) genes that are associated with presenting viral peptides,” said Dr. Calabresi.
Evidence relating MS vulnerability to other genetic and environmental factors, including diet, sunlight, smoking, and even pollution, calls into question a direct causal relationship between EBV and MS, he said.
The age prevalence of EBV would complicate efforts to eradicate it. Seroprevalence is 55% by age 5-11 and 75% among university students. “This is important because the duration of the vaccine response–induced protection in young seronegative children is not lengthy. Vaccinated individuals may become susceptible to natural infection at an age where the consequences of infection are more severe, especially leading to infectious mononucleosis, and hopefully not MS. This then raises the issue of the need for boosters, which we’re all well aware of during the COVID pandemic. This may be a problem, especially in young adults due to noncompliance,” said Dr. Calabresi.
He pointed out that not all vaccine attempts went well. In the 1960s, early respiratory syncytial virus (RSV) vaccines caused enhanced respiratory disease and 2 deaths. “We need to be careful when we think about targeting healthy at-risk young people,” said Dr. Calabresi.
Rather than pursue vaccination, Dr. Calabresi favors research into EBV latency in B cells as well as how EBV-infected B cells may cause or exacerbate MS, with the hopes of developing interventions. “It’s tempting to speculate that the success of the anti-CD 20 monoclonal antibody therapies is related to depletion of EBV infected B cells. In fact, I think that may be the case,” he said.
Dr. Cohen has no relevant financial disclosures. Dr. Calabresi has served on a scientific advisory board or data monitoring board for Biogen and Disarm Therapeutics.
FROM ACTRIMS FORUM 2023
Differential diagnosis in MS: What to watch for
SAN DIEGO –
The problem is that MS can vary greatly in its presentation, and many symptoms can mimic other conditions, according to Eoin Flanagan, MBBCh, who discussed the issue during a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Mimics and red flags
Dr. Flanagan noted a study that found common themes among MS misdiagnoses. “Many of these conditions are common conditions that we see in our neurology clinic – for example, migraine, fibromyalgia, nonspecific symptoms with an abnormal MRI, or functional neurologic disorder. If you’re teaching medical students or trainees about MS misdiagnosis, it’s important to give this example to show that these are not the zebras that are misdiagnosed, but actually common conditions that we see in our clinics,” said Dr. Flanagan, a neurologist at Mayo Clinic in Rochester, Minn.
Evaluation of MS mimics isn’t always necessary. Much of the time, typical clinical, neurologic, and imaging features provide a clear diagnosis. But some features can be red flags that MS may not be the cause. These can include a cerebrospinal fluid white blood cell count higher than 50, elevated CSF protein with normal white cell counts, low glucose, and negative oligoclonal bands, all of which could signify a range of other conditions.
These and other red flags should prompt a careful look to get the right diagnosis.
Earlier diagnosis = better outcomes
“[Evidence has] shown recently that as the diagnostic criteria have become more sensitive and we diagnose MS earlier, patients have had better outcomes because they’ve been able to initiate treatment earlier,” said Andrew Solomon, MD, who is an associate professor of neurologic sciences and division chief of multiple sclerosis at University of Vermont, Burlington. Dr. Solomon, Dr. Flanagan, and others are currently writing a review article on differential diagnosis of MS that will update the last review, published in 2008.
“Differential diagnosis has become more complex as we’ve had a broader understanding of disorders that can mimic MS. In the meantime, we still don’t have a highly sensitive and specific biomarker for MS that can help guide us when we first see somebody,” said Dr. Solomon.
Look for patterns and imaging clues
Dr. Flanagan’s talk had several points of emphasis. A key feature is the length of time between when the patient develops the first symptom and maximal symptoms. “If that’s very quick, then that suggests it’s a spinal cord stroke. If it comes down over days to a few weeks, then that suggests inflammation like MS, or like neuromyelitis optica [NMO] or myelin oligodendrocyte glycoprotein antibody-associated disease [MOGAD]. As it progresses beyond 21 days, then we’re going to be thinking about a different diagnosis,” said Dr. Flanagan.
Dr. Flanagan also noted the usefulness of specific features of the spinal cord MRI. Variables like lesion length, location in the center or periphery of the spinal cord, and characteristics of the enhancement pattern may be useful. “The pattern of gadolinium enhancement can be useful in narrowing your differential diagnosis and suggesting the correct diagnosis. For example, the flat pancake-like enhancement on sagittal images can suggest cervical spondylosis, while trident sign on axial images can suggest spinal cord sarcoidosis. Prior studies have shown that education on these patterns can enhance diagnosis.”
Dr. Flanagan suggested that both radiologists and neurologists should be trained to recognize such patterns. “If you educate radiologists or neurologists on these patterns, it can help them with diagnosis.”
Common mistakes
MOGAD and aquaporin 4–positive NMO spectrum disorder (AQP4+NMOSD) can be easily mistaken for MS, but there are some key differences. MOGAD and AQP4+NMOSD attacks are more severe than MS attacks, leaving patients more likely to be blind following an optic neuritis attack or wheelchair bound because of myelitis. More than 85% of CSF from patients with MS have oligoclonal bands versus about 15% of CSF from patients with MOGAD or AQP4+NMOSD. There is also a difference in lesion dynamics over time: MOGAD T2 lesions frequently resolve over follow-up while AQP4+NMOSD and MS lesions typically continue and leave a scar and persist. Silent lesions are more likely during surveillance MRI among MS patients, but are rare in MOGAD and AQP4+NMOSD, according to Dr. Flanagan. “One caveat to this is that with stronger MS medications we are seeing less silent lesions accumulating as we use those treatments more often.”
Dr. Solomon has been done nonpromotional speaking for EMD Serono. He has received research funding from Bristol-Myers Squibb. He has been on an advisory board or consulted for Greenwich Biosciences, TG Therapeutics, Octave Bioscience, and Horizon Therapeutics. Dr. Flanagan has no relevant financial disclosures. Dr. Flanagan has served on advisory boards for Alexion, Genentech, Horizon Therapeutics, and UCB.
SAN DIEGO –
The problem is that MS can vary greatly in its presentation, and many symptoms can mimic other conditions, according to Eoin Flanagan, MBBCh, who discussed the issue during a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Mimics and red flags
Dr. Flanagan noted a study that found common themes among MS misdiagnoses. “Many of these conditions are common conditions that we see in our neurology clinic – for example, migraine, fibromyalgia, nonspecific symptoms with an abnormal MRI, or functional neurologic disorder. If you’re teaching medical students or trainees about MS misdiagnosis, it’s important to give this example to show that these are not the zebras that are misdiagnosed, but actually common conditions that we see in our clinics,” said Dr. Flanagan, a neurologist at Mayo Clinic in Rochester, Minn.
Evaluation of MS mimics isn’t always necessary. Much of the time, typical clinical, neurologic, and imaging features provide a clear diagnosis. But some features can be red flags that MS may not be the cause. These can include a cerebrospinal fluid white blood cell count higher than 50, elevated CSF protein with normal white cell counts, low glucose, and negative oligoclonal bands, all of which could signify a range of other conditions.
These and other red flags should prompt a careful look to get the right diagnosis.
Earlier diagnosis = better outcomes
“[Evidence has] shown recently that as the diagnostic criteria have become more sensitive and we diagnose MS earlier, patients have had better outcomes because they’ve been able to initiate treatment earlier,” said Andrew Solomon, MD, who is an associate professor of neurologic sciences and division chief of multiple sclerosis at University of Vermont, Burlington. Dr. Solomon, Dr. Flanagan, and others are currently writing a review article on differential diagnosis of MS that will update the last review, published in 2008.
“Differential diagnosis has become more complex as we’ve had a broader understanding of disorders that can mimic MS. In the meantime, we still don’t have a highly sensitive and specific biomarker for MS that can help guide us when we first see somebody,” said Dr. Solomon.
Look for patterns and imaging clues
Dr. Flanagan’s talk had several points of emphasis. A key feature is the length of time between when the patient develops the first symptom and maximal symptoms. “If that’s very quick, then that suggests it’s a spinal cord stroke. If it comes down over days to a few weeks, then that suggests inflammation like MS, or like neuromyelitis optica [NMO] or myelin oligodendrocyte glycoprotein antibody-associated disease [MOGAD]. As it progresses beyond 21 days, then we’re going to be thinking about a different diagnosis,” said Dr. Flanagan.
Dr. Flanagan also noted the usefulness of specific features of the spinal cord MRI. Variables like lesion length, location in the center or periphery of the spinal cord, and characteristics of the enhancement pattern may be useful. “The pattern of gadolinium enhancement can be useful in narrowing your differential diagnosis and suggesting the correct diagnosis. For example, the flat pancake-like enhancement on sagittal images can suggest cervical spondylosis, while trident sign on axial images can suggest spinal cord sarcoidosis. Prior studies have shown that education on these patterns can enhance diagnosis.”
Dr. Flanagan suggested that both radiologists and neurologists should be trained to recognize such patterns. “If you educate radiologists or neurologists on these patterns, it can help them with diagnosis.”
Common mistakes
MOGAD and aquaporin 4–positive NMO spectrum disorder (AQP4+NMOSD) can be easily mistaken for MS, but there are some key differences. MOGAD and AQP4+NMOSD attacks are more severe than MS attacks, leaving patients more likely to be blind following an optic neuritis attack or wheelchair bound because of myelitis. More than 85% of CSF from patients with MS have oligoclonal bands versus about 15% of CSF from patients with MOGAD or AQP4+NMOSD. There is also a difference in lesion dynamics over time: MOGAD T2 lesions frequently resolve over follow-up while AQP4+NMOSD and MS lesions typically continue and leave a scar and persist. Silent lesions are more likely during surveillance MRI among MS patients, but are rare in MOGAD and AQP4+NMOSD, according to Dr. Flanagan. “One caveat to this is that with stronger MS medications we are seeing less silent lesions accumulating as we use those treatments more often.”
Dr. Solomon has been done nonpromotional speaking for EMD Serono. He has received research funding from Bristol-Myers Squibb. He has been on an advisory board or consulted for Greenwich Biosciences, TG Therapeutics, Octave Bioscience, and Horizon Therapeutics. Dr. Flanagan has no relevant financial disclosures. Dr. Flanagan has served on advisory boards for Alexion, Genentech, Horizon Therapeutics, and UCB.
SAN DIEGO –
The problem is that MS can vary greatly in its presentation, and many symptoms can mimic other conditions, according to Eoin Flanagan, MBBCh, who discussed the issue during a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Mimics and red flags
Dr. Flanagan noted a study that found common themes among MS misdiagnoses. “Many of these conditions are common conditions that we see in our neurology clinic – for example, migraine, fibromyalgia, nonspecific symptoms with an abnormal MRI, or functional neurologic disorder. If you’re teaching medical students or trainees about MS misdiagnosis, it’s important to give this example to show that these are not the zebras that are misdiagnosed, but actually common conditions that we see in our clinics,” said Dr. Flanagan, a neurologist at Mayo Clinic in Rochester, Minn.
Evaluation of MS mimics isn’t always necessary. Much of the time, typical clinical, neurologic, and imaging features provide a clear diagnosis. But some features can be red flags that MS may not be the cause. These can include a cerebrospinal fluid white blood cell count higher than 50, elevated CSF protein with normal white cell counts, low glucose, and negative oligoclonal bands, all of which could signify a range of other conditions.
These and other red flags should prompt a careful look to get the right diagnosis.
Earlier diagnosis = better outcomes
“[Evidence has] shown recently that as the diagnostic criteria have become more sensitive and we diagnose MS earlier, patients have had better outcomes because they’ve been able to initiate treatment earlier,” said Andrew Solomon, MD, who is an associate professor of neurologic sciences and division chief of multiple sclerosis at University of Vermont, Burlington. Dr. Solomon, Dr. Flanagan, and others are currently writing a review article on differential diagnosis of MS that will update the last review, published in 2008.
“Differential diagnosis has become more complex as we’ve had a broader understanding of disorders that can mimic MS. In the meantime, we still don’t have a highly sensitive and specific biomarker for MS that can help guide us when we first see somebody,” said Dr. Solomon.
Look for patterns and imaging clues
Dr. Flanagan’s talk had several points of emphasis. A key feature is the length of time between when the patient develops the first symptom and maximal symptoms. “If that’s very quick, then that suggests it’s a spinal cord stroke. If it comes down over days to a few weeks, then that suggests inflammation like MS, or like neuromyelitis optica [NMO] or myelin oligodendrocyte glycoprotein antibody-associated disease [MOGAD]. As it progresses beyond 21 days, then we’re going to be thinking about a different diagnosis,” said Dr. Flanagan.
Dr. Flanagan also noted the usefulness of specific features of the spinal cord MRI. Variables like lesion length, location in the center or periphery of the spinal cord, and characteristics of the enhancement pattern may be useful. “The pattern of gadolinium enhancement can be useful in narrowing your differential diagnosis and suggesting the correct diagnosis. For example, the flat pancake-like enhancement on sagittal images can suggest cervical spondylosis, while trident sign on axial images can suggest spinal cord sarcoidosis. Prior studies have shown that education on these patterns can enhance diagnosis.”
Dr. Flanagan suggested that both radiologists and neurologists should be trained to recognize such patterns. “If you educate radiologists or neurologists on these patterns, it can help them with diagnosis.”
Common mistakes
MOGAD and aquaporin 4–positive NMO spectrum disorder (AQP4+NMOSD) can be easily mistaken for MS, but there are some key differences. MOGAD and AQP4+NMOSD attacks are more severe than MS attacks, leaving patients more likely to be blind following an optic neuritis attack or wheelchair bound because of myelitis. More than 85% of CSF from patients with MS have oligoclonal bands versus about 15% of CSF from patients with MOGAD or AQP4+NMOSD. There is also a difference in lesion dynamics over time: MOGAD T2 lesions frequently resolve over follow-up while AQP4+NMOSD and MS lesions typically continue and leave a scar and persist. Silent lesions are more likely during surveillance MRI among MS patients, but are rare in MOGAD and AQP4+NMOSD, according to Dr. Flanagan. “One caveat to this is that with stronger MS medications we are seeing less silent lesions accumulating as we use those treatments more often.”
Dr. Solomon has been done nonpromotional speaking for EMD Serono. He has received research funding from Bristol-Myers Squibb. He has been on an advisory board or consulted for Greenwich Biosciences, TG Therapeutics, Octave Bioscience, and Horizon Therapeutics. Dr. Flanagan has no relevant financial disclosures. Dr. Flanagan has served on advisory boards for Alexion, Genentech, Horizon Therapeutics, and UCB.
FROM ACTRIMS FORUM 2023
Topical or intralesional cidofovir an option for recalcitrant warts
HONOLULU – Combining or those located in areas that are challenging to treat, according to John S. Barbieri, MD, MBA.
“There are 5 million office visits per year in the United States for warts and molluscum, and they’re most common in pediatrics,” Dr. Barbieri, of the department of dermatology at Brigham and Women’s Hospital, Boston, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! “In fact, some studies have suggested that one in three children in primary school suffers from warts.”
According to a 2012 Cochrane review of topical therapies for warts, first-line treatments such as salicylic acid, cryotherapy, 5-FU, or Candida antigen injection often have modest efficacy when used alone. For example, the authors found that salicylic acid and cryotherapy cleared warts in about 60%-70% of cases, respectively, but clearance rates were improved by combining the two therapies.
In an earlier literature review and meta-analysis, investigators evaluated the effect of 5-FU plus salicylic acid or salicylic acid alone. The therapeutic effect for common warts across all studies was a 63.4% response rate (complete healing) for 5-FU/SA vversus 23.1% for the 5-FU–free controls, respectively. For plantar warts, the response rate was 63% versus 11%, respectively.
“But what about the person with multiple warts or those in challenging locations where you might worry about destructive treatments hurting the nail fold or causing nail dystrophy?” Dr. Barbieri asked. “Maybe they’ve used salicylic acid or intralesional Candida and they’re still not getting better. What can we do for these patients?”
Emerging research suggests that topical cidofovir can be a valuable option for recalcitrant warts or those in sensitive locations. In a case report of a 10-year-old boy with more than 50 severe verrucous papules on his hands and face that were recalcitrant to multiple conventional therapies, topical 1% cidofovir applied daily for 8 weeks was effective, with no adverse side effects. A young female patient who presented to Dr. Barbieri with multiple warts around the nail matrix of several fingers experienced complete clearance after treatment with topical cidofovir, he said. Other researchers found this approach to be effective for plantar warts as well, in a report of two brothers with severe combined immunodeficiency after hematopoietic stem cell transplantation with persistent warts that did not respond to traditional topical treatments.
“Topical cidofovir is typically a painless treatment, which is nice, especially for our pediatric patients who might be afraid of other therapies like or cryotherapy or intralesional injections,” One limitation is that it is “a bit expensive,” Dr. Barbieri said. “To have topical cidofovir compounded is typically $100-$300, depending on the quantity and strength that you ask for.”
Intralesional cidofovir is another treatment option. In a retrospective study of 58 patients, Dr. Barbieri and colleagues evaluated the outcome of intralesional cidofovir treatment of warts in immunocompromised and nonimmunocompromised patients. Rates of improvement ranged from 98.3% to 100%, while resolution rates ranged from 75.9% to 97.6%.
“Most of the patients had warts for more than 5 years and almost half of them had recalcitrant warts,” Dr. Barbieri said. “These were mostly adult patients, but I think this is a treatment that can work in younger populations as well. About 10%-15% had HIV or cancer or diabetes or were transplant recipients, but despite these challenges and despite these recalcitrant warts, about 100% had improvement.”
He pointed out that cidofovir is available as a 75 mg/mL vial that comes with a 5 mL single-use vial. He dilutes this with normal saline to create a 15 mg/mL solution.
“If you want to be efficient you can try to schedule multiple patients together on the same day as a single vial is sufficient to treat about 25 patients,” assuming about 1 mL is injected per patient, he said. “The challenge with intralesional cidofovir is that it’s painful beyond just the needle part of the injection. Sometimes a nerve block can be helpful. But this can be an effective treatment for patients with recalcitrant warts or those with comorbidities.”
Other intralesional therapies to try for recalcitrant warts, he said, include bleomycin (1 U/mL solution, 1-2 mL per treatment, spaced every 2-4 weeks), and 5-FU (a 4:1 mixture of 5-FU [50 mg/mL] and 2% lidocaine).
Dr. Barbieri disclosed that he receives consulting fees from Dexcel for work unrelated to his presentation. Medscape and this news organization are owned by the same parent company.
HONOLULU – Combining or those located in areas that are challenging to treat, according to John S. Barbieri, MD, MBA.
“There are 5 million office visits per year in the United States for warts and molluscum, and they’re most common in pediatrics,” Dr. Barbieri, of the department of dermatology at Brigham and Women’s Hospital, Boston, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! “In fact, some studies have suggested that one in three children in primary school suffers from warts.”
According to a 2012 Cochrane review of topical therapies for warts, first-line treatments such as salicylic acid, cryotherapy, 5-FU, or Candida antigen injection often have modest efficacy when used alone. For example, the authors found that salicylic acid and cryotherapy cleared warts in about 60%-70% of cases, respectively, but clearance rates were improved by combining the two therapies.
In an earlier literature review and meta-analysis, investigators evaluated the effect of 5-FU plus salicylic acid or salicylic acid alone. The therapeutic effect for common warts across all studies was a 63.4% response rate (complete healing) for 5-FU/SA vversus 23.1% for the 5-FU–free controls, respectively. For plantar warts, the response rate was 63% versus 11%, respectively.
“But what about the person with multiple warts or those in challenging locations where you might worry about destructive treatments hurting the nail fold or causing nail dystrophy?” Dr. Barbieri asked. “Maybe they’ve used salicylic acid or intralesional Candida and they’re still not getting better. What can we do for these patients?”
Emerging research suggests that topical cidofovir can be a valuable option for recalcitrant warts or those in sensitive locations. In a case report of a 10-year-old boy with more than 50 severe verrucous papules on his hands and face that were recalcitrant to multiple conventional therapies, topical 1% cidofovir applied daily for 8 weeks was effective, with no adverse side effects. A young female patient who presented to Dr. Barbieri with multiple warts around the nail matrix of several fingers experienced complete clearance after treatment with topical cidofovir, he said. Other researchers found this approach to be effective for plantar warts as well, in a report of two brothers with severe combined immunodeficiency after hematopoietic stem cell transplantation with persistent warts that did not respond to traditional topical treatments.
“Topical cidofovir is typically a painless treatment, which is nice, especially for our pediatric patients who might be afraid of other therapies like or cryotherapy or intralesional injections,” One limitation is that it is “a bit expensive,” Dr. Barbieri said. “To have topical cidofovir compounded is typically $100-$300, depending on the quantity and strength that you ask for.”
Intralesional cidofovir is another treatment option. In a retrospective study of 58 patients, Dr. Barbieri and colleagues evaluated the outcome of intralesional cidofovir treatment of warts in immunocompromised and nonimmunocompromised patients. Rates of improvement ranged from 98.3% to 100%, while resolution rates ranged from 75.9% to 97.6%.
“Most of the patients had warts for more than 5 years and almost half of them had recalcitrant warts,” Dr. Barbieri said. “These were mostly adult patients, but I think this is a treatment that can work in younger populations as well. About 10%-15% had HIV or cancer or diabetes or were transplant recipients, but despite these challenges and despite these recalcitrant warts, about 100% had improvement.”
He pointed out that cidofovir is available as a 75 mg/mL vial that comes with a 5 mL single-use vial. He dilutes this with normal saline to create a 15 mg/mL solution.
“If you want to be efficient you can try to schedule multiple patients together on the same day as a single vial is sufficient to treat about 25 patients,” assuming about 1 mL is injected per patient, he said. “The challenge with intralesional cidofovir is that it’s painful beyond just the needle part of the injection. Sometimes a nerve block can be helpful. But this can be an effective treatment for patients with recalcitrant warts or those with comorbidities.”
Other intralesional therapies to try for recalcitrant warts, he said, include bleomycin (1 U/mL solution, 1-2 mL per treatment, spaced every 2-4 weeks), and 5-FU (a 4:1 mixture of 5-FU [50 mg/mL] and 2% lidocaine).
Dr. Barbieri disclosed that he receives consulting fees from Dexcel for work unrelated to his presentation. Medscape and this news organization are owned by the same parent company.
HONOLULU – Combining or those located in areas that are challenging to treat, according to John S. Barbieri, MD, MBA.
“There are 5 million office visits per year in the United States for warts and molluscum, and they’re most common in pediatrics,” Dr. Barbieri, of the department of dermatology at Brigham and Women’s Hospital, Boston, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! “In fact, some studies have suggested that one in three children in primary school suffers from warts.”
According to a 2012 Cochrane review of topical therapies for warts, first-line treatments such as salicylic acid, cryotherapy, 5-FU, or Candida antigen injection often have modest efficacy when used alone. For example, the authors found that salicylic acid and cryotherapy cleared warts in about 60%-70% of cases, respectively, but clearance rates were improved by combining the two therapies.
In an earlier literature review and meta-analysis, investigators evaluated the effect of 5-FU plus salicylic acid or salicylic acid alone. The therapeutic effect for common warts across all studies was a 63.4% response rate (complete healing) for 5-FU/SA vversus 23.1% for the 5-FU–free controls, respectively. For plantar warts, the response rate was 63% versus 11%, respectively.
“But what about the person with multiple warts or those in challenging locations where you might worry about destructive treatments hurting the nail fold or causing nail dystrophy?” Dr. Barbieri asked. “Maybe they’ve used salicylic acid or intralesional Candida and they’re still not getting better. What can we do for these patients?”
Emerging research suggests that topical cidofovir can be a valuable option for recalcitrant warts or those in sensitive locations. In a case report of a 10-year-old boy with more than 50 severe verrucous papules on his hands and face that were recalcitrant to multiple conventional therapies, topical 1% cidofovir applied daily for 8 weeks was effective, with no adverse side effects. A young female patient who presented to Dr. Barbieri with multiple warts around the nail matrix of several fingers experienced complete clearance after treatment with topical cidofovir, he said. Other researchers found this approach to be effective for plantar warts as well, in a report of two brothers with severe combined immunodeficiency after hematopoietic stem cell transplantation with persistent warts that did not respond to traditional topical treatments.
“Topical cidofovir is typically a painless treatment, which is nice, especially for our pediatric patients who might be afraid of other therapies like or cryotherapy or intralesional injections,” One limitation is that it is “a bit expensive,” Dr. Barbieri said. “To have topical cidofovir compounded is typically $100-$300, depending on the quantity and strength that you ask for.”
Intralesional cidofovir is another treatment option. In a retrospective study of 58 patients, Dr. Barbieri and colleagues evaluated the outcome of intralesional cidofovir treatment of warts in immunocompromised and nonimmunocompromised patients. Rates of improvement ranged from 98.3% to 100%, while resolution rates ranged from 75.9% to 97.6%.
“Most of the patients had warts for more than 5 years and almost half of them had recalcitrant warts,” Dr. Barbieri said. “These were mostly adult patients, but I think this is a treatment that can work in younger populations as well. About 10%-15% had HIV or cancer or diabetes or were transplant recipients, but despite these challenges and despite these recalcitrant warts, about 100% had improvement.”
He pointed out that cidofovir is available as a 75 mg/mL vial that comes with a 5 mL single-use vial. He dilutes this with normal saline to create a 15 mg/mL solution.
“If you want to be efficient you can try to schedule multiple patients together on the same day as a single vial is sufficient to treat about 25 patients,” assuming about 1 mL is injected per patient, he said. “The challenge with intralesional cidofovir is that it’s painful beyond just the needle part of the injection. Sometimes a nerve block can be helpful. But this can be an effective treatment for patients with recalcitrant warts or those with comorbidities.”
Other intralesional therapies to try for recalcitrant warts, he said, include bleomycin (1 U/mL solution, 1-2 mL per treatment, spaced every 2-4 weeks), and 5-FU (a 4:1 mixture of 5-FU [50 mg/mL] and 2% lidocaine).
Dr. Barbieri disclosed that he receives consulting fees from Dexcel for work unrelated to his presentation. Medscape and this news organization are owned by the same parent company.
AT THE MEDSCAPELIVE! HAWAII DERMATOLOGY SEMINAR
In weighing PCI vs. CABG for left main disease, diabetes matters
WASHINGTON – For patients with diabetes, there are trade-offs for selecting a percutaneous intervention (PCI) over coronary artery bypass grafting (CABG) for left main artery disease when either can be considered, according to a hypothesis-generating pooled analysis.
The pooled data from four trials indicate that either method of revascularization is “reasonable,” but risk of myocardial infarction and revascularization is higher and risk of stroke is lower in patients with diabetes following PCI relative to CABG, Prakriti Gaba, MD, said in presenting the analysis at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
Despite decades of advances in both PCI and CABG, the findings are remarkably similar to those of Emory Angioplasty Versus Surgery Trial (EAST), the first major study to compare PCI to CABG, which were published almost 30 years ago. In the new analysis, like in EAST, PCI and CABG were comparable for a primary composite endpoint overall, but patients with diabetes were the exception. In those, outcomes were modestly better after CABG, said Dr. Gaba, a cardiology fellow at Brigham and Women’s Hospital, Harvard Medical School, both in Boston.
“More and more I am hearing from practitioners that diabetes does not matter, but what I get from your data is that diabetes still matters,” said Spencer B. King, MD, a pioneer of PCI affiliated with Emory University, Atlanta.
Dr. King, the first author of the 1994 paper and a panelist in the late-breaking trial session where the new data were presented, pointed out that a relatively limited proportion of patients with diabetes are equally suitable for PCI and CABG because of other considerations. However, he said an updated look once again suggesting that PCI and CABG are not equivalent for left main lesions in patients with diabetes “is helpful to see.”
CABG traditionally preferred for left main revascularization
The issue was revisited because CABG has been preferred traditionally for left main disease, but there was increasing evidence that PCI is associated with similar survival, according to Dr. Gaba. These new data support that contention, even if it shows that outcomes are not the same in those with diabetes relative to those without.
In this pooled analysis, data were drawn from four trials. Each compared PCI with drug-eluting stents with CABG in patients that were considered suitable for either. From the four trials, the numbers in this analysis included 705 patients from SYNTAX, 600 patients from PRECOMBAT, 1,184 patients from NOBLE, and 1,905 patients from EXCEL.
The focus was on the 1,104 patients with diabetes relative to the 3,289 without. The primary endpoint was all-cause death at 5 years. The multiple secondary endpoints included cardiovascular (CV) death, MI, stroke, and revascularization.
Overall, the 5-year mortality, independent of revascularization procedure, was 14.8% for those with diabetes and 9.3% for those without (P < .001). For this endpoint, the rates were numerically lower but not statistically different for CABG whether patients had diabetes (14.1% vs. 15.3%) or no diabetes (8.9% vs. 9.7%).
However, the rate of spontaneous MI was twice as great with PCI than with CABG for those with diabetes (8.9% vs. 4.4%), which doubled the hazard ratio within significant confidence intervals (HR, 2.01; 95% CI, 1.21-3.35). The rates of revascularization were also about twice as great with PCI than with CABG (24.5% vs. 12.4%), again producing a twofold increase in risk (HR, 2.12; 95% CI, 1.56-2.87).
For stroke in patients with diabetes, there was no difference in events at 5 years for PCI relative to CABG (2.1% in both groups). However, in those without diabetes, a trend approaching significance favored CABG over PCI (1.2% vs. 2.1%; HR, 0.177; 95% CI, 0.99-1.77). This difference was concentrated in the first year, when stroke rates among those treated with CABG were more than double the rates among those treated with PCI. Over time, this difference dissipated so that the difference was reduced to a trend at the end of follow-up.
Data considered hypothesis generating
Although patients with diabetes were prespecified as a subgroup of interest in these studies, Dr. Gaba said that the data can only be considered hypothesis generating and pointed out several limitations, including the fact that these studies preceded some therapies, such as sodium-glucose cotransporter 2 inhibitors, that are known to affect CV outcomes.
However, Dr. King was not alone in suggesting that these data once again show that diabetes matters. Several panelists agreed, including the moderator of the session, Robert A Byrne, MBBcH, PhD, director of cardiology, Mater Private Hospital, Dublin.
“Of course, there has been a lot of discussion over the last 4 or 5 years about this issue since the long-term EXCEL data were presented,” Dr. Byrne said. He added that the team of investigators who put this together “have done a great service to the community” by providing a detailed combined analysis to explore the interaction between diabetes and outcomes relative to method of revascularization. Although PCI and CABG are not always equivalent choices for reasons other than diabetes, he echoed the sentiment that diabetes likely remains a variable to consider when considering revascularization of left main artery disease.
Dr. Gabi, Dr. Spencer, and Dr. Byrne report no potential conflicts of interest.
WASHINGTON – For patients with diabetes, there are trade-offs for selecting a percutaneous intervention (PCI) over coronary artery bypass grafting (CABG) for left main artery disease when either can be considered, according to a hypothesis-generating pooled analysis.
The pooled data from four trials indicate that either method of revascularization is “reasonable,” but risk of myocardial infarction and revascularization is higher and risk of stroke is lower in patients with diabetes following PCI relative to CABG, Prakriti Gaba, MD, said in presenting the analysis at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
Despite decades of advances in both PCI and CABG, the findings are remarkably similar to those of Emory Angioplasty Versus Surgery Trial (EAST), the first major study to compare PCI to CABG, which were published almost 30 years ago. In the new analysis, like in EAST, PCI and CABG were comparable for a primary composite endpoint overall, but patients with diabetes were the exception. In those, outcomes were modestly better after CABG, said Dr. Gaba, a cardiology fellow at Brigham and Women’s Hospital, Harvard Medical School, both in Boston.
“More and more I am hearing from practitioners that diabetes does not matter, but what I get from your data is that diabetes still matters,” said Spencer B. King, MD, a pioneer of PCI affiliated with Emory University, Atlanta.
Dr. King, the first author of the 1994 paper and a panelist in the late-breaking trial session where the new data were presented, pointed out that a relatively limited proportion of patients with diabetes are equally suitable for PCI and CABG because of other considerations. However, he said an updated look once again suggesting that PCI and CABG are not equivalent for left main lesions in patients with diabetes “is helpful to see.”
CABG traditionally preferred for left main revascularization
The issue was revisited because CABG has been preferred traditionally for left main disease, but there was increasing evidence that PCI is associated with similar survival, according to Dr. Gaba. These new data support that contention, even if it shows that outcomes are not the same in those with diabetes relative to those without.
In this pooled analysis, data were drawn from four trials. Each compared PCI with drug-eluting stents with CABG in patients that were considered suitable for either. From the four trials, the numbers in this analysis included 705 patients from SYNTAX, 600 patients from PRECOMBAT, 1,184 patients from NOBLE, and 1,905 patients from EXCEL.
The focus was on the 1,104 patients with diabetes relative to the 3,289 without. The primary endpoint was all-cause death at 5 years. The multiple secondary endpoints included cardiovascular (CV) death, MI, stroke, and revascularization.
Overall, the 5-year mortality, independent of revascularization procedure, was 14.8% for those with diabetes and 9.3% for those without (P < .001). For this endpoint, the rates were numerically lower but not statistically different for CABG whether patients had diabetes (14.1% vs. 15.3%) or no diabetes (8.9% vs. 9.7%).
However, the rate of spontaneous MI was twice as great with PCI than with CABG for those with diabetes (8.9% vs. 4.4%), which doubled the hazard ratio within significant confidence intervals (HR, 2.01; 95% CI, 1.21-3.35). The rates of revascularization were also about twice as great with PCI than with CABG (24.5% vs. 12.4%), again producing a twofold increase in risk (HR, 2.12; 95% CI, 1.56-2.87).
For stroke in patients with diabetes, there was no difference in events at 5 years for PCI relative to CABG (2.1% in both groups). However, in those without diabetes, a trend approaching significance favored CABG over PCI (1.2% vs. 2.1%; HR, 0.177; 95% CI, 0.99-1.77). This difference was concentrated in the first year, when stroke rates among those treated with CABG were more than double the rates among those treated with PCI. Over time, this difference dissipated so that the difference was reduced to a trend at the end of follow-up.
Data considered hypothesis generating
Although patients with diabetes were prespecified as a subgroup of interest in these studies, Dr. Gaba said that the data can only be considered hypothesis generating and pointed out several limitations, including the fact that these studies preceded some therapies, such as sodium-glucose cotransporter 2 inhibitors, that are known to affect CV outcomes.
However, Dr. King was not alone in suggesting that these data once again show that diabetes matters. Several panelists agreed, including the moderator of the session, Robert A Byrne, MBBcH, PhD, director of cardiology, Mater Private Hospital, Dublin.
“Of course, there has been a lot of discussion over the last 4 or 5 years about this issue since the long-term EXCEL data were presented,” Dr. Byrne said. He added that the team of investigators who put this together “have done a great service to the community” by providing a detailed combined analysis to explore the interaction between diabetes and outcomes relative to method of revascularization. Although PCI and CABG are not always equivalent choices for reasons other than diabetes, he echoed the sentiment that diabetes likely remains a variable to consider when considering revascularization of left main artery disease.
Dr. Gabi, Dr. Spencer, and Dr. Byrne report no potential conflicts of interest.
WASHINGTON – For patients with diabetes, there are trade-offs for selecting a percutaneous intervention (PCI) over coronary artery bypass grafting (CABG) for left main artery disease when either can be considered, according to a hypothesis-generating pooled analysis.
The pooled data from four trials indicate that either method of revascularization is “reasonable,” but risk of myocardial infarction and revascularization is higher and risk of stroke is lower in patients with diabetes following PCI relative to CABG, Prakriti Gaba, MD, said in presenting the analysis at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
Despite decades of advances in both PCI and CABG, the findings are remarkably similar to those of Emory Angioplasty Versus Surgery Trial (EAST), the first major study to compare PCI to CABG, which were published almost 30 years ago. In the new analysis, like in EAST, PCI and CABG were comparable for a primary composite endpoint overall, but patients with diabetes were the exception. In those, outcomes were modestly better after CABG, said Dr. Gaba, a cardiology fellow at Brigham and Women’s Hospital, Harvard Medical School, both in Boston.
“More and more I am hearing from practitioners that diabetes does not matter, but what I get from your data is that diabetes still matters,” said Spencer B. King, MD, a pioneer of PCI affiliated with Emory University, Atlanta.
Dr. King, the first author of the 1994 paper and a panelist in the late-breaking trial session where the new data were presented, pointed out that a relatively limited proportion of patients with diabetes are equally suitable for PCI and CABG because of other considerations. However, he said an updated look once again suggesting that PCI and CABG are not equivalent for left main lesions in patients with diabetes “is helpful to see.”
CABG traditionally preferred for left main revascularization
The issue was revisited because CABG has been preferred traditionally for left main disease, but there was increasing evidence that PCI is associated with similar survival, according to Dr. Gaba. These new data support that contention, even if it shows that outcomes are not the same in those with diabetes relative to those without.
In this pooled analysis, data were drawn from four trials. Each compared PCI with drug-eluting stents with CABG in patients that were considered suitable for either. From the four trials, the numbers in this analysis included 705 patients from SYNTAX, 600 patients from PRECOMBAT, 1,184 patients from NOBLE, and 1,905 patients from EXCEL.
The focus was on the 1,104 patients with diabetes relative to the 3,289 without. The primary endpoint was all-cause death at 5 years. The multiple secondary endpoints included cardiovascular (CV) death, MI, stroke, and revascularization.
Overall, the 5-year mortality, independent of revascularization procedure, was 14.8% for those with diabetes and 9.3% for those without (P < .001). For this endpoint, the rates were numerically lower but not statistically different for CABG whether patients had diabetes (14.1% vs. 15.3%) or no diabetes (8.9% vs. 9.7%).
However, the rate of spontaneous MI was twice as great with PCI than with CABG for those with diabetes (8.9% vs. 4.4%), which doubled the hazard ratio within significant confidence intervals (HR, 2.01; 95% CI, 1.21-3.35). The rates of revascularization were also about twice as great with PCI than with CABG (24.5% vs. 12.4%), again producing a twofold increase in risk (HR, 2.12; 95% CI, 1.56-2.87).
For stroke in patients with diabetes, there was no difference in events at 5 years for PCI relative to CABG (2.1% in both groups). However, in those without diabetes, a trend approaching significance favored CABG over PCI (1.2% vs. 2.1%; HR, 0.177; 95% CI, 0.99-1.77). This difference was concentrated in the first year, when stroke rates among those treated with CABG were more than double the rates among those treated with PCI. Over time, this difference dissipated so that the difference was reduced to a trend at the end of follow-up.
Data considered hypothesis generating
Although patients with diabetes were prespecified as a subgroup of interest in these studies, Dr. Gaba said that the data can only be considered hypothesis generating and pointed out several limitations, including the fact that these studies preceded some therapies, such as sodium-glucose cotransporter 2 inhibitors, that are known to affect CV outcomes.
However, Dr. King was not alone in suggesting that these data once again show that diabetes matters. Several panelists agreed, including the moderator of the session, Robert A Byrne, MBBcH, PhD, director of cardiology, Mater Private Hospital, Dublin.
“Of course, there has been a lot of discussion over the last 4 or 5 years about this issue since the long-term EXCEL data were presented,” Dr. Byrne said. He added that the team of investigators who put this together “have done a great service to the community” by providing a detailed combined analysis to explore the interaction between diabetes and outcomes relative to method of revascularization. Although PCI and CABG are not always equivalent choices for reasons other than diabetes, he echoed the sentiment that diabetes likely remains a variable to consider when considering revascularization of left main artery disease.
Dr. Gabi, Dr. Spencer, and Dr. Byrne report no potential conflicts of interest.
AT CRT 2023