User login
First-line nivolumab plus platinum/etoposide effective in extensive-stage SCLC
While nivolumab plus doublet chemotherapy was effective in extensive-stage small-cell lung cancer (ES-SCLC) in a recent randomized trial, the results might not be sufficient to change current clinical practice, in which two first-line chemo-immunotherapies are already approved and recommended, sources said.
Nivolumab added to platinum/etoposide doublet chemotherapy was well tolerated and significantly improved progression-free survival (PFS) and overall survival (OS) compared to chemotherapy alone, according to results of ECOG-ACRIN EA5161, a randomized, phase 2 trial including 160 patients with ES-SCLC.
Risks of progression and death were reduced by 32% and 27%, respectively, when the immune checkpoint inhibitor was given along with chemotherapy, according to data presented by investigator Ticiana A. Leal, MD, of the University of Wisconsin Carbone Cancer Center in Madison.
“Our study, EA5161, confirms the efficacy of nivolumab in extensive-stage small cell lung cancer,” Dr. Leal said in a presentation she gave as part of the American Society of Clinical Oncology virtual scientific program.
Nivolumab did demonstrate a clear PFS advantage in EA5161, but “more surprisingly for a small trial” it also showed a clear OS advantage, said Taofeek K. Owonikoko, MD, PhD, in a commentary on the study.
“While the study as currently reported is insufficient to change practice, it does however provide very strong data to make the combination of nivolumab and platinum doublet acceptable as a platform for future clinical trials,” he said in the commentary, which was also included in the virtual ASCO proceedings.
Going forward, it would be difficult to justify another nondefinitive randomized phase 2 chemo-immunotherapy trial, especially if there are no “immediate plans” for a confirmatory phase 3 trial, added Dr. Owonikoko, who is director of thoracic oncology at Winship Cancer Institute of Emory University in Atlanta.
Nivolumab wasn’t the only immune checkpoint with new first-line data in ES-SCLC at ASCO. In the randomized, double-blind, phase 3 KEYNOTE-604 trial, pembrolizumab added to etoposide and platinum significantly prolonged PFS and showed a trend toward improved OS. However, the significance threshold for OS was missed, according to the report.
While these pembrolizumab data are also insufficient to change today’s practice standards, results for both the pembrolizumab- and nivolumab-containing regimens are nevertheless compelling to support their use as a platform for new treatment strategies, according to Dr. Owonikoko.
With these new ASCO data, there are now randomized data confirming a benefit of immune checkpoint inhibitor–based regimens in ES-SCLC, according to Lauren A. Byers, MD, from the department of thoracic/head and neck medical oncology at The University of Texas MD Anderson Cancer Center in Houston.
Immune checkpoint inhibitors that are approved by the Food and Drug Administration for first-line treatment of ES-SCLC include atezolizumab (in combination with carboplatin and etoposide) and durvalumab (in combination with either carboplatin or cisplatin plus etoposide). In current National Comprehensive Cancer Network (NCCN) guidelines, both are described as “preferred” regimens for primary or adjuvant therapy.
“A lot of times in oncology we have trials with similar drugs, and you get somewhat different answers in terms of the outcome of the trials, so we’re kind of trying to tease them apart,” Dr. Byers said in an interview.
“I think in this situation, we’ve got four studies, and they essentially are extremely similar in terms of the result, which just gives us even more confidence that there is benefit, at least for a subset of patients.”
The EA5161 study was developed to evaluate the role of nivolumab in ES-SCLC, Dr. Leal said in her virtual ASCO presentation.
Of the 160 patients enrolled and randomized, 145 were eligible and treated, including 75 in the nivolumab plus chemotherapy arm and 70 in the chemotherapy arm. Participants were evenly split between performance status 0 and 1, and little more than half of patients were women, and a median of five treatment cycles were delivered in each arm.
Median PFS, the primary end point of the trial, was 5.5 months for nivolumab plus chemotherapy versus 4.7 months for chemotherapy alone for all eligible and treated patients (hazard ratio, 0.68; 95% confidence interval, 0.48-1.00; P = .047). In the intent-to-treat population, median PFS was 5.5 and 4.6 months in the respective arms (HR, 0.65; 95% CI, 0.46-0.91; P = .012).
Median overall survival was 11.3 months and 9.3 months for the nivolumab plus chemotherapy and chemotherapy-only arms, respectively, for all eligible and treated patients (HR, 0.73; 95% CI, 0.49-1.1), and in the intent-to-treat population, median OS was 11.3 and 8.5 months for the respective arms (HR, 0.67; 95% CI, 0.46-0.98; P = .038).
The overall response rate was 52% for nivolumab plus chemotherapy and 47% for chemotherapy alone, with a median duration of response of 5.6 and 3.3 months, respectively, Dr. Leal reported.
Treatment was generally well tolerated in both arms, according to the investigator, with no safety signals observed. Toxicities resulting in death occurred in nine patients in the nivolumab plus chemotherapy arm and seven in the chemotherapy-only arm. “Most of the events were related to progression of disease,” Dr. Leal said.
While nivolumab and pembrolizumab’s use in the first-line setting may be uncertain, it is currently approved for metastatic SCLC that has progressed following platinum-based chemotherapy and at least one more line of therapy, according to the drug’s package insert.
The EA5161 study was sponsored by the National Cancer Institute. Dr. Leal provided disclosures related to AbbVie, AstraZeneca, Bayer, BeyondSpring, Bristol-Myers Squibb, Genentech, InvisionFirst Lung, Merck, Mirati, Novocure, and Takeda.
Dr. Owonikoko provided disclosures related to Bristol-Myers Squibb, Novartis, Celgene, Lilly, Sandoz, AbbVie, Eisai, and Takeda, among others. Dr. Byers reported disclosures related to Bristol-Myers Squibb, AstraZeneca, AbbVie, GenMab, PharmaMar, and Sierra Oncology, Tolero, Alethia, Merck, Jazz Pharmaceuticals, and Pfizer.
SOURCE: Leal TA et al. ASCO 2020, Abstract 9000.
While nivolumab plus doublet chemotherapy was effective in extensive-stage small-cell lung cancer (ES-SCLC) in a recent randomized trial, the results might not be sufficient to change current clinical practice, in which two first-line chemo-immunotherapies are already approved and recommended, sources said.
Nivolumab added to platinum/etoposide doublet chemotherapy was well tolerated and significantly improved progression-free survival (PFS) and overall survival (OS) compared to chemotherapy alone, according to results of ECOG-ACRIN EA5161, a randomized, phase 2 trial including 160 patients with ES-SCLC.
Risks of progression and death were reduced by 32% and 27%, respectively, when the immune checkpoint inhibitor was given along with chemotherapy, according to data presented by investigator Ticiana A. Leal, MD, of the University of Wisconsin Carbone Cancer Center in Madison.
“Our study, EA5161, confirms the efficacy of nivolumab in extensive-stage small cell lung cancer,” Dr. Leal said in a presentation she gave as part of the American Society of Clinical Oncology virtual scientific program.
Nivolumab did demonstrate a clear PFS advantage in EA5161, but “more surprisingly for a small trial” it also showed a clear OS advantage, said Taofeek K. Owonikoko, MD, PhD, in a commentary on the study.
“While the study as currently reported is insufficient to change practice, it does however provide very strong data to make the combination of nivolumab and platinum doublet acceptable as a platform for future clinical trials,” he said in the commentary, which was also included in the virtual ASCO proceedings.
Going forward, it would be difficult to justify another nondefinitive randomized phase 2 chemo-immunotherapy trial, especially if there are no “immediate plans” for a confirmatory phase 3 trial, added Dr. Owonikoko, who is director of thoracic oncology at Winship Cancer Institute of Emory University in Atlanta.
Nivolumab wasn’t the only immune checkpoint with new first-line data in ES-SCLC at ASCO. In the randomized, double-blind, phase 3 KEYNOTE-604 trial, pembrolizumab added to etoposide and platinum significantly prolonged PFS and showed a trend toward improved OS. However, the significance threshold for OS was missed, according to the report.
While these pembrolizumab data are also insufficient to change today’s practice standards, results for both the pembrolizumab- and nivolumab-containing regimens are nevertheless compelling to support their use as a platform for new treatment strategies, according to Dr. Owonikoko.
With these new ASCO data, there are now randomized data confirming a benefit of immune checkpoint inhibitor–based regimens in ES-SCLC, according to Lauren A. Byers, MD, from the department of thoracic/head and neck medical oncology at The University of Texas MD Anderson Cancer Center in Houston.
Immune checkpoint inhibitors that are approved by the Food and Drug Administration for first-line treatment of ES-SCLC include atezolizumab (in combination with carboplatin and etoposide) and durvalumab (in combination with either carboplatin or cisplatin plus etoposide). In current National Comprehensive Cancer Network (NCCN) guidelines, both are described as “preferred” regimens for primary or adjuvant therapy.
“A lot of times in oncology we have trials with similar drugs, and you get somewhat different answers in terms of the outcome of the trials, so we’re kind of trying to tease them apart,” Dr. Byers said in an interview.
“I think in this situation, we’ve got four studies, and they essentially are extremely similar in terms of the result, which just gives us even more confidence that there is benefit, at least for a subset of patients.”
The EA5161 study was developed to evaluate the role of nivolumab in ES-SCLC, Dr. Leal said in her virtual ASCO presentation.
Of the 160 patients enrolled and randomized, 145 were eligible and treated, including 75 in the nivolumab plus chemotherapy arm and 70 in the chemotherapy arm. Participants were evenly split between performance status 0 and 1, and little more than half of patients were women, and a median of five treatment cycles were delivered in each arm.
Median PFS, the primary end point of the trial, was 5.5 months for nivolumab plus chemotherapy versus 4.7 months for chemotherapy alone for all eligible and treated patients (hazard ratio, 0.68; 95% confidence interval, 0.48-1.00; P = .047). In the intent-to-treat population, median PFS was 5.5 and 4.6 months in the respective arms (HR, 0.65; 95% CI, 0.46-0.91; P = .012).
Median overall survival was 11.3 months and 9.3 months for the nivolumab plus chemotherapy and chemotherapy-only arms, respectively, for all eligible and treated patients (HR, 0.73; 95% CI, 0.49-1.1), and in the intent-to-treat population, median OS was 11.3 and 8.5 months for the respective arms (HR, 0.67; 95% CI, 0.46-0.98; P = .038).
The overall response rate was 52% for nivolumab plus chemotherapy and 47% for chemotherapy alone, with a median duration of response of 5.6 and 3.3 months, respectively, Dr. Leal reported.
Treatment was generally well tolerated in both arms, according to the investigator, with no safety signals observed. Toxicities resulting in death occurred in nine patients in the nivolumab plus chemotherapy arm and seven in the chemotherapy-only arm. “Most of the events were related to progression of disease,” Dr. Leal said.
While nivolumab and pembrolizumab’s use in the first-line setting may be uncertain, it is currently approved for metastatic SCLC that has progressed following platinum-based chemotherapy and at least one more line of therapy, according to the drug’s package insert.
The EA5161 study was sponsored by the National Cancer Institute. Dr. Leal provided disclosures related to AbbVie, AstraZeneca, Bayer, BeyondSpring, Bristol-Myers Squibb, Genentech, InvisionFirst Lung, Merck, Mirati, Novocure, and Takeda.
Dr. Owonikoko provided disclosures related to Bristol-Myers Squibb, Novartis, Celgene, Lilly, Sandoz, AbbVie, Eisai, and Takeda, among others. Dr. Byers reported disclosures related to Bristol-Myers Squibb, AstraZeneca, AbbVie, GenMab, PharmaMar, and Sierra Oncology, Tolero, Alethia, Merck, Jazz Pharmaceuticals, and Pfizer.
SOURCE: Leal TA et al. ASCO 2020, Abstract 9000.
While nivolumab plus doublet chemotherapy was effective in extensive-stage small-cell lung cancer (ES-SCLC) in a recent randomized trial, the results might not be sufficient to change current clinical practice, in which two first-line chemo-immunotherapies are already approved and recommended, sources said.
Nivolumab added to platinum/etoposide doublet chemotherapy was well tolerated and significantly improved progression-free survival (PFS) and overall survival (OS) compared to chemotherapy alone, according to results of ECOG-ACRIN EA5161, a randomized, phase 2 trial including 160 patients with ES-SCLC.
Risks of progression and death were reduced by 32% and 27%, respectively, when the immune checkpoint inhibitor was given along with chemotherapy, according to data presented by investigator Ticiana A. Leal, MD, of the University of Wisconsin Carbone Cancer Center in Madison.
“Our study, EA5161, confirms the efficacy of nivolumab in extensive-stage small cell lung cancer,” Dr. Leal said in a presentation she gave as part of the American Society of Clinical Oncology virtual scientific program.
Nivolumab did demonstrate a clear PFS advantage in EA5161, but “more surprisingly for a small trial” it also showed a clear OS advantage, said Taofeek K. Owonikoko, MD, PhD, in a commentary on the study.
“While the study as currently reported is insufficient to change practice, it does however provide very strong data to make the combination of nivolumab and platinum doublet acceptable as a platform for future clinical trials,” he said in the commentary, which was also included in the virtual ASCO proceedings.
Going forward, it would be difficult to justify another nondefinitive randomized phase 2 chemo-immunotherapy trial, especially if there are no “immediate plans” for a confirmatory phase 3 trial, added Dr. Owonikoko, who is director of thoracic oncology at Winship Cancer Institute of Emory University in Atlanta.
Nivolumab wasn’t the only immune checkpoint with new first-line data in ES-SCLC at ASCO. In the randomized, double-blind, phase 3 KEYNOTE-604 trial, pembrolizumab added to etoposide and platinum significantly prolonged PFS and showed a trend toward improved OS. However, the significance threshold for OS was missed, according to the report.
While these pembrolizumab data are also insufficient to change today’s practice standards, results for both the pembrolizumab- and nivolumab-containing regimens are nevertheless compelling to support their use as a platform for new treatment strategies, according to Dr. Owonikoko.
With these new ASCO data, there are now randomized data confirming a benefit of immune checkpoint inhibitor–based regimens in ES-SCLC, according to Lauren A. Byers, MD, from the department of thoracic/head and neck medical oncology at The University of Texas MD Anderson Cancer Center in Houston.
Immune checkpoint inhibitors that are approved by the Food and Drug Administration for first-line treatment of ES-SCLC include atezolizumab (in combination with carboplatin and etoposide) and durvalumab (in combination with either carboplatin or cisplatin plus etoposide). In current National Comprehensive Cancer Network (NCCN) guidelines, both are described as “preferred” regimens for primary or adjuvant therapy.
“A lot of times in oncology we have trials with similar drugs, and you get somewhat different answers in terms of the outcome of the trials, so we’re kind of trying to tease them apart,” Dr. Byers said in an interview.
“I think in this situation, we’ve got four studies, and they essentially are extremely similar in terms of the result, which just gives us even more confidence that there is benefit, at least for a subset of patients.”
The EA5161 study was developed to evaluate the role of nivolumab in ES-SCLC, Dr. Leal said in her virtual ASCO presentation.
Of the 160 patients enrolled and randomized, 145 were eligible and treated, including 75 in the nivolumab plus chemotherapy arm and 70 in the chemotherapy arm. Participants were evenly split between performance status 0 and 1, and little more than half of patients were women, and a median of five treatment cycles were delivered in each arm.
Median PFS, the primary end point of the trial, was 5.5 months for nivolumab plus chemotherapy versus 4.7 months for chemotherapy alone for all eligible and treated patients (hazard ratio, 0.68; 95% confidence interval, 0.48-1.00; P = .047). In the intent-to-treat population, median PFS was 5.5 and 4.6 months in the respective arms (HR, 0.65; 95% CI, 0.46-0.91; P = .012).
Median overall survival was 11.3 months and 9.3 months for the nivolumab plus chemotherapy and chemotherapy-only arms, respectively, for all eligible and treated patients (HR, 0.73; 95% CI, 0.49-1.1), and in the intent-to-treat population, median OS was 11.3 and 8.5 months for the respective arms (HR, 0.67; 95% CI, 0.46-0.98; P = .038).
The overall response rate was 52% for nivolumab plus chemotherapy and 47% for chemotherapy alone, with a median duration of response of 5.6 and 3.3 months, respectively, Dr. Leal reported.
Treatment was generally well tolerated in both arms, according to the investigator, with no safety signals observed. Toxicities resulting in death occurred in nine patients in the nivolumab plus chemotherapy arm and seven in the chemotherapy-only arm. “Most of the events were related to progression of disease,” Dr. Leal said.
While nivolumab and pembrolizumab’s use in the first-line setting may be uncertain, it is currently approved for metastatic SCLC that has progressed following platinum-based chemotherapy and at least one more line of therapy, according to the drug’s package insert.
The EA5161 study was sponsored by the National Cancer Institute. Dr. Leal provided disclosures related to AbbVie, AstraZeneca, Bayer, BeyondSpring, Bristol-Myers Squibb, Genentech, InvisionFirst Lung, Merck, Mirati, Novocure, and Takeda.
Dr. Owonikoko provided disclosures related to Bristol-Myers Squibb, Novartis, Celgene, Lilly, Sandoz, AbbVie, Eisai, and Takeda, among others. Dr. Byers reported disclosures related to Bristol-Myers Squibb, AstraZeneca, AbbVie, GenMab, PharmaMar, and Sierra Oncology, Tolero, Alethia, Merck, Jazz Pharmaceuticals, and Pfizer.
SOURCE: Leal TA et al. ASCO 2020, Abstract 9000.
FROM ASCO 2020
Clinicians still unaware of need for genetic testing in NSCLC
Moreover, the majority of these clinicians believe that fewer than 50% of patients in their country undergo molecular testing, the same survey showed.
The survey was conducted by the International Association for the Study of Lung Cancer (IASLC); 2537 questionnaires from 102 countries were returned and analyzed.
It was published online May 20 in the Journal of Thoracic Oncology.
The results are concerning because “the risk of death for patients with NSCLC is substantially reduced when a gene alteration is identified and the available targeted therapy is administered,” the authors emphasize.
“Specific protocols to initiate reflex testing for guideline-recommended molecular markers would help providers consider molecular testing earlier and optimize tissue,” they suggest.
Surprised that clinicians were unaware of guidelines
“I was not surprised that we found suboptimal testing rates based on other research that has demonstrated the need to improve the quality of lung cancer in some areas,” corresponding author Matthew Smeltzer, PhD, University of Memphis, Tennessee, told Medscape Medical News in an email.
“However, I was surprised that so many respondents were unaware of guidelines,” he said.
The College of American Pathologists, IASLC, and Association for Molecular Pathology established evidence-based standards for the selection of NSCLC patients for molecular testing in 2013, and these guidelines were subsequently endorsed by the American Society of Clinical Oncology.
“We suspect that the level of access a provider has to targeted therapies does affect molecular testing rates,” Smeltzer acknowledged.
Molecular testing survey
“The survey included a seven-question introduction for all respondents and then divided respondents into one of three tracks,” the authors explain.
These tracks included respondents who requested tests and who treated patients (medical oncologists), those who analyzed and interpreted assays (pathologists), and those who acquired tissue samples (surgeons, pulmonologists, radiologists).
Countries were also grouped into five geographic regions — Asia, Europe, Latin America, United States, and Canada — and the rest of the world (ROW).
“Overall, respondents reported that molecular testing rates were lower than we would like but they were not satisfied with the current state of testing, and they reported higher testing rates in their own clinics,” Smeltzer noted.
However, when tests were ordered, “we found 99% of respondents in the requesting/treating track ordered tests for EGFR, 95% for ALK, 79% for ROS1, and < 50% ordered other tests,” the authors observe.
Indeed, EGFR, ALK, and ROS1 were the top three tests ordered across all regions, though less frequently so in the ROW, they add.
More than half of requesting/treating track respondents also order multiplex assays, although Latin America and the ROW did this less frequently than other regions.
Over 90% of respondents who perform or interpret assays indicated that they perform EGFR testing, while 83% of the same group do ALK testing; 69% tested for KRAS; 68% for BRAF, 64% for ROS1, and 56% for HER2. Fewer than half of them performed other tests.
Survey results also showed that EGFR, ALK, and KRAS are the top three tests performed across all regions, with no regional differences.
“Respondents also reported on the acquisition and testing of liquid biopsies,” survey authors point out.
Here, 87% of requesting/treating track respondents indicated that they “sometimes” request molecular testing on liquid biopsies, but the proportions of those who sometimes use liquid biopsy varied by region and were lowest in Latin America and the ROW.
A lower proportion of those who perform and interpret assays, at 69%, also offer tests on liquid biopsies, but this percentage, too, varied significantly by region, being the least frequently done in the United States and Canada, as well as in the ROW.
All the above tests are for genetic mutations or alterations that guide clinicians on use of targeted therapy directed at particular mutations, for example, drugs like erlotinib for EGFR and crizotinib for ALK.
However, immunotherapy with checkpoint inhibitors has also made a big impact on the treatment of NSCLC, and the use of these agents is sometimes guided by testing for programmed cell-death ligand (PD-L1).
PD-L1 is not a molecular marker per se, the authors note.
Nevertheless, “we found that 84% of respondents in the requesting/treating track ordered PD-L1 and 68% of respondents who perform or interpret assays report PD-L1 is offered in their own lab,” the authors observe.
Smeltzer commented that both approaches — targeted therapies and immunotherapy — have made inroads into the treatment of NSCLC, in some cases replacing chemotherapy.
He emphasized that “it is important to know if a specific oncogene driver is present before initiating immunotherapy treatment,” and noted that when tissue is sent out for both types of testing, the results for PD-L1 are usually available before the results for the full molecular testing panel are back.
Barriers to testing
“The most frequent barrier to molecular testing in every region was cost,” the survey authors note.
Insufficient amount of tumor cells was the main reason for molecular testing failures along with inadequate tissue quality.
The majority of respondents who order tests and treat patients were sure that the laboratories they use perform appropriate validation of molecular tests, while almost all of those who perform or interpret assays said they perform validation tests in their labs.
Only 30% of respondents who request tests and treat patients have access to molecular testing labs within their own institutions; the remaining respondents have to outsource testing completely or partially.
Most respondents who test and treat patients also have multidisciplinary tumor boards to discuss patients with NSCLC, but almost one quarter of the same group indicated their board met less than once a month.
“Turnaround time is a barrier to molecular testing across the world,” the authors continue, with 29% of those who request tests and treat patients reporting that it typically takes 10 days or more to receive molecular testing results.
Interestingly, the highest percentage of respondents who reported this long turnaround time were in North America.
Perhaps encouragingly, 41% of respondents who perform or interpret assays indicated they were dissatisfied with the condition of molecular testing in their country, although in this regard, the United States and Canada had the lowest rates of dissatisfaction.
In fact, 39% of those who request tests and treat patients ranked the conditions of molecular testing in their country as “average or below,” while 42% of respondents in the tissue acquisition track ranked the conditions of molecular testing as average or below, the worst rankings coming from Latin America and the ROW.
Low quality of tissue samples was another reason respondents expressed dissatisfaction with the current state of molecular testing in their country.
Smeltzer is a research consultant for the Association of Community Cancer Centers.
This article first appeared on Medscape.com.
Moreover, the majority of these clinicians believe that fewer than 50% of patients in their country undergo molecular testing, the same survey showed.
The survey was conducted by the International Association for the Study of Lung Cancer (IASLC); 2537 questionnaires from 102 countries were returned and analyzed.
It was published online May 20 in the Journal of Thoracic Oncology.
The results are concerning because “the risk of death for patients with NSCLC is substantially reduced when a gene alteration is identified and the available targeted therapy is administered,” the authors emphasize.
“Specific protocols to initiate reflex testing for guideline-recommended molecular markers would help providers consider molecular testing earlier and optimize tissue,” they suggest.
Surprised that clinicians were unaware of guidelines
“I was not surprised that we found suboptimal testing rates based on other research that has demonstrated the need to improve the quality of lung cancer in some areas,” corresponding author Matthew Smeltzer, PhD, University of Memphis, Tennessee, told Medscape Medical News in an email.
“However, I was surprised that so many respondents were unaware of guidelines,” he said.
The College of American Pathologists, IASLC, and Association for Molecular Pathology established evidence-based standards for the selection of NSCLC patients for molecular testing in 2013, and these guidelines were subsequently endorsed by the American Society of Clinical Oncology.
“We suspect that the level of access a provider has to targeted therapies does affect molecular testing rates,” Smeltzer acknowledged.
Molecular testing survey
“The survey included a seven-question introduction for all respondents and then divided respondents into one of three tracks,” the authors explain.
These tracks included respondents who requested tests and who treated patients (medical oncologists), those who analyzed and interpreted assays (pathologists), and those who acquired tissue samples (surgeons, pulmonologists, radiologists).
Countries were also grouped into five geographic regions — Asia, Europe, Latin America, United States, and Canada — and the rest of the world (ROW).
“Overall, respondents reported that molecular testing rates were lower than we would like but they were not satisfied with the current state of testing, and they reported higher testing rates in their own clinics,” Smeltzer noted.
However, when tests were ordered, “we found 99% of respondents in the requesting/treating track ordered tests for EGFR, 95% for ALK, 79% for ROS1, and < 50% ordered other tests,” the authors observe.
Indeed, EGFR, ALK, and ROS1 were the top three tests ordered across all regions, though less frequently so in the ROW, they add.
More than half of requesting/treating track respondents also order multiplex assays, although Latin America and the ROW did this less frequently than other regions.
Over 90% of respondents who perform or interpret assays indicated that they perform EGFR testing, while 83% of the same group do ALK testing; 69% tested for KRAS; 68% for BRAF, 64% for ROS1, and 56% for HER2. Fewer than half of them performed other tests.
Survey results also showed that EGFR, ALK, and KRAS are the top three tests performed across all regions, with no regional differences.
“Respondents also reported on the acquisition and testing of liquid biopsies,” survey authors point out.
Here, 87% of requesting/treating track respondents indicated that they “sometimes” request molecular testing on liquid biopsies, but the proportions of those who sometimes use liquid biopsy varied by region and were lowest in Latin America and the ROW.
A lower proportion of those who perform and interpret assays, at 69%, also offer tests on liquid biopsies, but this percentage, too, varied significantly by region, being the least frequently done in the United States and Canada, as well as in the ROW.
All the above tests are for genetic mutations or alterations that guide clinicians on use of targeted therapy directed at particular mutations, for example, drugs like erlotinib for EGFR and crizotinib for ALK.
However, immunotherapy with checkpoint inhibitors has also made a big impact on the treatment of NSCLC, and the use of these agents is sometimes guided by testing for programmed cell-death ligand (PD-L1).
PD-L1 is not a molecular marker per se, the authors note.
Nevertheless, “we found that 84% of respondents in the requesting/treating track ordered PD-L1 and 68% of respondents who perform or interpret assays report PD-L1 is offered in their own lab,” the authors observe.
Smeltzer commented that both approaches — targeted therapies and immunotherapy — have made inroads into the treatment of NSCLC, in some cases replacing chemotherapy.
He emphasized that “it is important to know if a specific oncogene driver is present before initiating immunotherapy treatment,” and noted that when tissue is sent out for both types of testing, the results for PD-L1 are usually available before the results for the full molecular testing panel are back.
Barriers to testing
“The most frequent barrier to molecular testing in every region was cost,” the survey authors note.
Insufficient amount of tumor cells was the main reason for molecular testing failures along with inadequate tissue quality.
The majority of respondents who order tests and treat patients were sure that the laboratories they use perform appropriate validation of molecular tests, while almost all of those who perform or interpret assays said they perform validation tests in their labs.
Only 30% of respondents who request tests and treat patients have access to molecular testing labs within their own institutions; the remaining respondents have to outsource testing completely or partially.
Most respondents who test and treat patients also have multidisciplinary tumor boards to discuss patients with NSCLC, but almost one quarter of the same group indicated their board met less than once a month.
“Turnaround time is a barrier to molecular testing across the world,” the authors continue, with 29% of those who request tests and treat patients reporting that it typically takes 10 days or more to receive molecular testing results.
Interestingly, the highest percentage of respondents who reported this long turnaround time were in North America.
Perhaps encouragingly, 41% of respondents who perform or interpret assays indicated they were dissatisfied with the condition of molecular testing in their country, although in this regard, the United States and Canada had the lowest rates of dissatisfaction.
In fact, 39% of those who request tests and treat patients ranked the conditions of molecular testing in their country as “average or below,” while 42% of respondents in the tissue acquisition track ranked the conditions of molecular testing as average or below, the worst rankings coming from Latin America and the ROW.
Low quality of tissue samples was another reason respondents expressed dissatisfaction with the current state of molecular testing in their country.
Smeltzer is a research consultant for the Association of Community Cancer Centers.
This article first appeared on Medscape.com.
Moreover, the majority of these clinicians believe that fewer than 50% of patients in their country undergo molecular testing, the same survey showed.
The survey was conducted by the International Association for the Study of Lung Cancer (IASLC); 2537 questionnaires from 102 countries were returned and analyzed.
It was published online May 20 in the Journal of Thoracic Oncology.
The results are concerning because “the risk of death for patients with NSCLC is substantially reduced when a gene alteration is identified and the available targeted therapy is administered,” the authors emphasize.
“Specific protocols to initiate reflex testing for guideline-recommended molecular markers would help providers consider molecular testing earlier and optimize tissue,” they suggest.
Surprised that clinicians were unaware of guidelines
“I was not surprised that we found suboptimal testing rates based on other research that has demonstrated the need to improve the quality of lung cancer in some areas,” corresponding author Matthew Smeltzer, PhD, University of Memphis, Tennessee, told Medscape Medical News in an email.
“However, I was surprised that so many respondents were unaware of guidelines,” he said.
The College of American Pathologists, IASLC, and Association for Molecular Pathology established evidence-based standards for the selection of NSCLC patients for molecular testing in 2013, and these guidelines were subsequently endorsed by the American Society of Clinical Oncology.
“We suspect that the level of access a provider has to targeted therapies does affect molecular testing rates,” Smeltzer acknowledged.
Molecular testing survey
“The survey included a seven-question introduction for all respondents and then divided respondents into one of three tracks,” the authors explain.
These tracks included respondents who requested tests and who treated patients (medical oncologists), those who analyzed and interpreted assays (pathologists), and those who acquired tissue samples (surgeons, pulmonologists, radiologists).
Countries were also grouped into five geographic regions — Asia, Europe, Latin America, United States, and Canada — and the rest of the world (ROW).
“Overall, respondents reported that molecular testing rates were lower than we would like but they were not satisfied with the current state of testing, and they reported higher testing rates in their own clinics,” Smeltzer noted.
However, when tests were ordered, “we found 99% of respondents in the requesting/treating track ordered tests for EGFR, 95% for ALK, 79% for ROS1, and < 50% ordered other tests,” the authors observe.
Indeed, EGFR, ALK, and ROS1 were the top three tests ordered across all regions, though less frequently so in the ROW, they add.
More than half of requesting/treating track respondents also order multiplex assays, although Latin America and the ROW did this less frequently than other regions.
Over 90% of respondents who perform or interpret assays indicated that they perform EGFR testing, while 83% of the same group do ALK testing; 69% tested for KRAS; 68% for BRAF, 64% for ROS1, and 56% for HER2. Fewer than half of them performed other tests.
Survey results also showed that EGFR, ALK, and KRAS are the top three tests performed across all regions, with no regional differences.
“Respondents also reported on the acquisition and testing of liquid biopsies,” survey authors point out.
Here, 87% of requesting/treating track respondents indicated that they “sometimes” request molecular testing on liquid biopsies, but the proportions of those who sometimes use liquid biopsy varied by region and were lowest in Latin America and the ROW.
A lower proportion of those who perform and interpret assays, at 69%, also offer tests on liquid biopsies, but this percentage, too, varied significantly by region, being the least frequently done in the United States and Canada, as well as in the ROW.
All the above tests are for genetic mutations or alterations that guide clinicians on use of targeted therapy directed at particular mutations, for example, drugs like erlotinib for EGFR and crizotinib for ALK.
However, immunotherapy with checkpoint inhibitors has also made a big impact on the treatment of NSCLC, and the use of these agents is sometimes guided by testing for programmed cell-death ligand (PD-L1).
PD-L1 is not a molecular marker per se, the authors note.
Nevertheless, “we found that 84% of respondents in the requesting/treating track ordered PD-L1 and 68% of respondents who perform or interpret assays report PD-L1 is offered in their own lab,” the authors observe.
Smeltzer commented that both approaches — targeted therapies and immunotherapy — have made inroads into the treatment of NSCLC, in some cases replacing chemotherapy.
He emphasized that “it is important to know if a specific oncogene driver is present before initiating immunotherapy treatment,” and noted that when tissue is sent out for both types of testing, the results for PD-L1 are usually available before the results for the full molecular testing panel are back.
Barriers to testing
“The most frequent barrier to molecular testing in every region was cost,” the survey authors note.
Insufficient amount of tumor cells was the main reason for molecular testing failures along with inadequate tissue quality.
The majority of respondents who order tests and treat patients were sure that the laboratories they use perform appropriate validation of molecular tests, while almost all of those who perform or interpret assays said they perform validation tests in their labs.
Only 30% of respondents who request tests and treat patients have access to molecular testing labs within their own institutions; the remaining respondents have to outsource testing completely or partially.
Most respondents who test and treat patients also have multidisciplinary tumor boards to discuss patients with NSCLC, but almost one quarter of the same group indicated their board met less than once a month.
“Turnaround time is a barrier to molecular testing across the world,” the authors continue, with 29% of those who request tests and treat patients reporting that it typically takes 10 days or more to receive molecular testing results.
Interestingly, the highest percentage of respondents who reported this long turnaround time were in North America.
Perhaps encouragingly, 41% of respondents who perform or interpret assays indicated they were dissatisfied with the condition of molecular testing in their country, although in this regard, the United States and Canada had the lowest rates of dissatisfaction.
In fact, 39% of those who request tests and treat patients ranked the conditions of molecular testing in their country as “average or below,” while 42% of respondents in the tissue acquisition track ranked the conditions of molecular testing as average or below, the worst rankings coming from Latin America and the ROW.
Low quality of tissue samples was another reason respondents expressed dissatisfaction with the current state of molecular testing in their country.
Smeltzer is a research consultant for the Association of Community Cancer Centers.
This article first appeared on Medscape.com.
Active cancer increases death risk in patients with COVID-19
Patients with COVID-19 and progressing cancer had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer, according to data from the COVID-19 and Cancer Consortium (CCC19) registry.

Other independent risk factors for death in patients with COVID-19 and cancer were older age, male sex, former smoking, number of comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater, and treatment with hydroxychloroquine plus azithromycin.
In fact, patients who received hydroxychloroquine and azithromycin had a nearly threefold higher risk of death than did patients who had not received the combination. However, this finding was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville, Tennessee.
Dr. Warner presented these findings in an online press briefing. Additional findings from the CCC19 registry are set to be presented as part of the American Society of Clinical Oncology (ASCO) virtual scientific program. The findings were also published in The Lancet.
‘Severe impact’ in cancer patients
“For people with cancer, the impact of COVID-19 is especially severe, whether they have been exposed to the virus or not. Patients with cancer are typically older adults, often with other underlying conditions, and their immune systems may be suppressed by the cancer, or due to chemotherapy, radiation, or other treatment,” commented ASCO President Howard A. Burris III, MD, who moderated the press briefing but was not involved in the study of CCC19 registry data.
“ASCO members tell us that they have had to delay or modify treatment plans to reduce patients’ risk of infection, and we’re unclear what the impact of these changes will be. Delays in cancer screening and diagnosis are also a major concern,” Dr. Burris continued.
“This does confirm reports that have come out from other centers, including other parts of the world, where they have found that people who have cancer and COVID-19 have a worse outcome,” said Andrew T. Chan, MD, MPH, of Massachusetts General Hospital in Boston, who was not involved in the research.
Dr. Chan’s group has developed a COVID-19 symptom study app with the aim of defining whether people living with cancer are at increased risk for infections, in addition to whether cancer is an independent risk factor for COVID-19 severity or mortality.
“Using data from our app, we were able to show that people who reported living with cancer did have a higher risk of developing COVID and were more likely to be hospitalized related to COVID,” Dr. Chan said in an interview.
Study details
The CCC19 registry collects information from 104 participating institutions in the United States and Canada, as well as anonymous data from individuals in the United States, Argentina, Canada, the European Union, and the United Kingdom.
The sample of 928 patients Dr. Warner presented was evenly balanced by sex. The median age was 66 years, and 30% of patients were aged 75 years or older.
In all, 39% of patients were on active anticancer therapy, and 43% had measurable disease. Breast cancer was the most common diagnosis, followed by prostate cancer, gastrointestinal cancers, lymphomas, and thoracic cancers.
Two-thirds of the patients (68%) had an ECOG performance status of 0 or 1, 8% had a performance status of 2, and 5% a status of 3 or 4. The remaining patients had unknown performance status.
Slightly more than half of patients (52%) were never smokers, 37% were former smokers, and 5% were current smokers. The remaining 6% of patients had unknown smoking status.
At a median follow-up of 21 days, 121 patients (13%) had died. All deaths occurred within 30 days of COVID-19 diagnosis. Among patients who died, 78 were male, 64 were former smokers, 70 were aged 75 years or older, 41 had active stable or responding cancer, 25 had progressing cancer, and 42 had an ECOG performance status of 2 or higher.
In all, 466 patients were hospitalized, and 106 in this group (23%) died. Among the 132 patients admitted to an ICU, 50 (38%) died, including 27 patients aged 75 years or older, and 15 with an ECOG performance status of 2 or greater. Of the 116 patients who required intubation, 50 (43%) died, including 26 who were 75 years or older, and 11 who had a performance status of 2 or greater.
It’s early days yet, and a larger sample size with longer follow-up will be needed to get a more complete picture of how COVID-19 affects specific patient subsets over time, Dr. Warner said.
ASCO has established its own COVID-19 registry to collect both near-term and longitudinal data during the pandemic.
“We’ll be able to learn about both how the pandemic has impacted delivery of cancer care, as well as the longer-term effects of COVID-19 on cancer patients and understand what care approaches are working best,” said Richard L. Schilsky, MD, chief medical officer and executive vice president of ASCO, during the briefing.
The study of CCC19 registry data was supported in part by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed stock/ownership in HemOnc.org, consulting for IBM and Westat, and travel expenses from IBM. Dr. Burris, Dr. Schilsky, and Dr. Chan reported no disclosures relevant to the study.
SOURCE: Warner J L et al. ASCO 2020, Abstract LBA110.
Patients with COVID-19 and progressing cancer had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer, according to data from the COVID-19 and Cancer Consortium (CCC19) registry.
Other independent risk factors for death in patients with COVID-19 and cancer were older age, male sex, former smoking, number of comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater, and treatment with hydroxychloroquine plus azithromycin.
In fact, patients who received hydroxychloroquine and azithromycin had a nearly threefold higher risk of death than did patients who had not received the combination. However, this finding was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville, Tennessee.
Dr. Warner presented these findings in an online press briefing. Additional findings from the CCC19 registry are set to be presented as part of the American Society of Clinical Oncology (ASCO) virtual scientific program. The findings were also published in The Lancet.
‘Severe impact’ in cancer patients
“For people with cancer, the impact of COVID-19 is especially severe, whether they have been exposed to the virus or not. Patients with cancer are typically older adults, often with other underlying conditions, and their immune systems may be suppressed by the cancer, or due to chemotherapy, radiation, or other treatment,” commented ASCO President Howard A. Burris III, MD, who moderated the press briefing but was not involved in the study of CCC19 registry data.
“ASCO members tell us that they have had to delay or modify treatment plans to reduce patients’ risk of infection, and we’re unclear what the impact of these changes will be. Delays in cancer screening and diagnosis are also a major concern,” Dr. Burris continued.
“This does confirm reports that have come out from other centers, including other parts of the world, where they have found that people who have cancer and COVID-19 have a worse outcome,” said Andrew T. Chan, MD, MPH, of Massachusetts General Hospital in Boston, who was not involved in the research.
Dr. Chan’s group has developed a COVID-19 symptom study app with the aim of defining whether people living with cancer are at increased risk for infections, in addition to whether cancer is an independent risk factor for COVID-19 severity or mortality.
“Using data from our app, we were able to show that people who reported living with cancer did have a higher risk of developing COVID and were more likely to be hospitalized related to COVID,” Dr. Chan said in an interview.
Study details
The CCC19 registry collects information from 104 participating institutions in the United States and Canada, as well as anonymous data from individuals in the United States, Argentina, Canada, the European Union, and the United Kingdom.
The sample of 928 patients Dr. Warner presented was evenly balanced by sex. The median age was 66 years, and 30% of patients were aged 75 years or older.
In all, 39% of patients were on active anticancer therapy, and 43% had measurable disease. Breast cancer was the most common diagnosis, followed by prostate cancer, gastrointestinal cancers, lymphomas, and thoracic cancers.
Two-thirds of the patients (68%) had an ECOG performance status of 0 or 1, 8% had a performance status of 2, and 5% a status of 3 or 4. The remaining patients had unknown performance status.
Slightly more than half of patients (52%) were never smokers, 37% were former smokers, and 5% were current smokers. The remaining 6% of patients had unknown smoking status.
At a median follow-up of 21 days, 121 patients (13%) had died. All deaths occurred within 30 days of COVID-19 diagnosis. Among patients who died, 78 were male, 64 were former smokers, 70 were aged 75 years or older, 41 had active stable or responding cancer, 25 had progressing cancer, and 42 had an ECOG performance status of 2 or higher.
In all, 466 patients were hospitalized, and 106 in this group (23%) died. Among the 132 patients admitted to an ICU, 50 (38%) died, including 27 patients aged 75 years or older, and 15 with an ECOG performance status of 2 or greater. Of the 116 patients who required intubation, 50 (43%) died, including 26 who were 75 years or older, and 11 who had a performance status of 2 or greater.
It’s early days yet, and a larger sample size with longer follow-up will be needed to get a more complete picture of how COVID-19 affects specific patient subsets over time, Dr. Warner said.
ASCO has established its own COVID-19 registry to collect both near-term and longitudinal data during the pandemic.
“We’ll be able to learn about both how the pandemic has impacted delivery of cancer care, as well as the longer-term effects of COVID-19 on cancer patients and understand what care approaches are working best,” said Richard L. Schilsky, MD, chief medical officer and executive vice president of ASCO, during the briefing.
The study of CCC19 registry data was supported in part by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed stock/ownership in HemOnc.org, consulting for IBM and Westat, and travel expenses from IBM. Dr. Burris, Dr. Schilsky, and Dr. Chan reported no disclosures relevant to the study.
SOURCE: Warner J L et al. ASCO 2020, Abstract LBA110.
Patients with COVID-19 and progressing cancer had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer, according to data from the COVID-19 and Cancer Consortium (CCC19) registry.
Other independent risk factors for death in patients with COVID-19 and cancer were older age, male sex, former smoking, number of comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater, and treatment with hydroxychloroquine plus azithromycin.
In fact, patients who received hydroxychloroquine and azithromycin had a nearly threefold higher risk of death than did patients who had not received the combination. However, this finding was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville, Tennessee.
Dr. Warner presented these findings in an online press briefing. Additional findings from the CCC19 registry are set to be presented as part of the American Society of Clinical Oncology (ASCO) virtual scientific program. The findings were also published in The Lancet.
‘Severe impact’ in cancer patients
“For people with cancer, the impact of COVID-19 is especially severe, whether they have been exposed to the virus or not. Patients with cancer are typically older adults, often with other underlying conditions, and their immune systems may be suppressed by the cancer, or due to chemotherapy, radiation, or other treatment,” commented ASCO President Howard A. Burris III, MD, who moderated the press briefing but was not involved in the study of CCC19 registry data.
“ASCO members tell us that they have had to delay or modify treatment plans to reduce patients’ risk of infection, and we’re unclear what the impact of these changes will be. Delays in cancer screening and diagnosis are also a major concern,” Dr. Burris continued.
“This does confirm reports that have come out from other centers, including other parts of the world, where they have found that people who have cancer and COVID-19 have a worse outcome,” said Andrew T. Chan, MD, MPH, of Massachusetts General Hospital in Boston, who was not involved in the research.
Dr. Chan’s group has developed a COVID-19 symptom study app with the aim of defining whether people living with cancer are at increased risk for infections, in addition to whether cancer is an independent risk factor for COVID-19 severity or mortality.
“Using data from our app, we were able to show that people who reported living with cancer did have a higher risk of developing COVID and were more likely to be hospitalized related to COVID,” Dr. Chan said in an interview.
Study details
The CCC19 registry collects information from 104 participating institutions in the United States and Canada, as well as anonymous data from individuals in the United States, Argentina, Canada, the European Union, and the United Kingdom.
The sample of 928 patients Dr. Warner presented was evenly balanced by sex. The median age was 66 years, and 30% of patients were aged 75 years or older.
In all, 39% of patients were on active anticancer therapy, and 43% had measurable disease. Breast cancer was the most common diagnosis, followed by prostate cancer, gastrointestinal cancers, lymphomas, and thoracic cancers.
Two-thirds of the patients (68%) had an ECOG performance status of 0 or 1, 8% had a performance status of 2, and 5% a status of 3 or 4. The remaining patients had unknown performance status.
Slightly more than half of patients (52%) were never smokers, 37% were former smokers, and 5% were current smokers. The remaining 6% of patients had unknown smoking status.
At a median follow-up of 21 days, 121 patients (13%) had died. All deaths occurred within 30 days of COVID-19 diagnosis. Among patients who died, 78 were male, 64 were former smokers, 70 were aged 75 years or older, 41 had active stable or responding cancer, 25 had progressing cancer, and 42 had an ECOG performance status of 2 or higher.
In all, 466 patients were hospitalized, and 106 in this group (23%) died. Among the 132 patients admitted to an ICU, 50 (38%) died, including 27 patients aged 75 years or older, and 15 with an ECOG performance status of 2 or greater. Of the 116 patients who required intubation, 50 (43%) died, including 26 who were 75 years or older, and 11 who had a performance status of 2 or greater.
It’s early days yet, and a larger sample size with longer follow-up will be needed to get a more complete picture of how COVID-19 affects specific patient subsets over time, Dr. Warner said.
ASCO has established its own COVID-19 registry to collect both near-term and longitudinal data during the pandemic.
“We’ll be able to learn about both how the pandemic has impacted delivery of cancer care, as well as the longer-term effects of COVID-19 on cancer patients and understand what care approaches are working best,” said Richard L. Schilsky, MD, chief medical officer and executive vice president of ASCO, during the briefing.
The study of CCC19 registry data was supported in part by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed stock/ownership in HemOnc.org, consulting for IBM and Westat, and travel expenses from IBM. Dr. Burris, Dr. Schilsky, and Dr. Chan reported no disclosures relevant to the study.
SOURCE: Warner J L et al. ASCO 2020, Abstract LBA110.
FROM ASCO 2020
Key clinical point: Patients with progressing cancer and COVID-19 are at an especially high risk of 30-day mortality.
Major finding: Patients with COVID-19 whose cancers were progressing had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients in remission or with no evidence of cancer.
Study details: Analysis of data on 928 patients enrolled in the COVID-19 and Cancer Consortium (CCC19) registry.
Disclosures: The research was supported, in part, by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed relationships with HemOnc.org, IBM, and Westat.
Source: Warner J L et al. ASCO 2020, Abstract LBA110.

Adjuvant osimertinib extends DFS in localized NSCLC
, results of the ADAURA trial showed.
The randomized, phase 3 trial was a comparison of osimertinib treatment with placebo following complete resection of localized or locally advanced NSCLC with negative margins. The trial was unblinded early and halted on the recommendation of the independent data-monitoring committee, due to the efficacy of osimertinib.
“If I were on the committee, I would have done the same thing. These are extraordinary results,” said study investigator Roy S. Herbst, MD, PhD, chief of medical oncology at the Yale Cancer Center and Smilow Cancer Center at Yale University in New Haven, Conn.
Dr. Herbst is scheduled to present results from ADAURA as part of the American Society of Clinical Oncology virtual scientific program.
In an online briefing prior to the meeting, Dr. Herbst said the impressive results reminded him of a lesson imparted by his mentor, the late Isaiah Fidler, DVM, PhD.
“He taught me, he taught all of us, that metastasis is a spread of tumor that kills patients,” Dr. Herbst said. “Drugs such as this, based on biology, given to patients at the earliest possible time, prevent those metastases and allow patients to live longer and with a better quality of life.”
Results from the ADAURA trial provide compelling evidence of the benefit of adjuvant osimertinib for a select group of patients, according to Tina Cascone, MD, PhD, assistant professor in the department of thoracic head and neck medical oncology at The University of Texas MD Anderson Cancer Center in Houston. She was not involved in the study.
“These are unprecedented results for a potentially curable, resected population of patients,” Dr. Cascone said in an interview. “This definitely has the potential to shift the paradigm in the treatments that we have available for patients with resected disease. It’s very important to emphasize how much we’ve learned from the metastatic setting and how we’re bringing what we’ve learned into early stage disease.”
High recurrence rates
An estimated 30% of patients with NSCLC present with resectable disease at diagnosis, but 5-year recurrence rates following surgery and cisplatin-based adjuvant chemotherapy remain high, ranging from 45% among patients with stage IB disease to 62% for patients with stage II NSCLC and 76% for patients with stage III disease, Dr. Herbst noted.
Osimertinib is a third-generation tyrosine kinase inhibitor (TKI) targeted to EGFR. It has been shown to offer improvements in both progression-free survival and overall survival compared with the EGFR-TKIs erlotinib and gefitinib for patients with advanced EGFR-mutated NSCLC, as well as in patients with central nervous system metastases.
Osimertinib’s efficacy and safety profile against advanced disease suggests it may also be effective against early stage disease, a hypothesis the ADAURA trial was designed to test.
Study details
The phase 3, randomized, double-blind trial was conducted at centers in the United States, Europe, Asia, and Australia. A total of 682 patients with completely resected stage IB, II, or IIIA NSCLC, with or without planned adjuvant chemotherapy, were enrolled.
After stratification by stage, EGFR mutation, and race (Asian vs. non-Asian), patients were randomized on a 1:1 basis to receive either osimertinib at 80 mg once daily or placebo. The planned treatment duration was a maximum of 3 years.
Members of the independent data-monitoring committee held a meeting in April 2020. Although they had not planned an efficacy analysis at that time, they decided the results were clearly in favor of osimertinib. So they recommended unblinding and halting of the trial.
At the time of unblinding, the study had completed enrollment, and all patients had been followed for at least 1 year.
Efficacy and safety
For the primary endpoint of disease-free survival (DFS) in patients with stage II to IIIA disease, the median DFS was not reached for patients assigned to osimertinib, but it was 20.4 months for patients assigned to placebo (hazard ratio, 0.17; P < .0001).
The numbers were similar for the secondary endpoint of DFS in the overall population, including patients with stage IB disease. The median DFS was not reached for patients on osimertinib but was 28.1 months for patients on placebo (HR, 0.21; P < .0001).
DFS was significantly superior with osimertinib across all subgroups in the overall population, including sex, age, smoking status, race, stage, EGFR mutation, and adjuvant chemotherapy (yes or no).
Dr. Herbst said patients tolerated osimertinib well, and the drug’s safety profile was consistent with that already known. There were no adverse events leading to death in the osimertinib arm, and the incidence of grade 3 or 4 adverse events of any kind was low.
In all, 10 patients (3%) in the osimertinib arm were reported to have interstitial lung disease. Prolongation of the QT interval was reported in 22 patients (7%) on osimertinib and 4 patients (1%) in the placebo arm.
The results show that “adjuvant osimertinib provides a highly effective, practice-changing treatment for patients with stage IB, II, IIIA, EGFR mutation-positive non–small cell lung cancer after complete tumor resection,” Dr. Herbst said.
Dr. Herbst disclosed relationships with AstraZeneca, which funded the study, as well as Jun Shi Pharmaceuticals and other companies. Dr. Cascone is the international principal investigator of the NeoCOAST trial evaluating durvalumab, an AstraZeneca product.
SOURCE: Herbst RS et al. ASCO 2020, Abstract LBA5.
, results of the ADAURA trial showed.
The randomized, phase 3 trial was a comparison of osimertinib treatment with placebo following complete resection of localized or locally advanced NSCLC with negative margins. The trial was unblinded early and halted on the recommendation of the independent data-monitoring committee, due to the efficacy of osimertinib.
“If I were on the committee, I would have done the same thing. These are extraordinary results,” said study investigator Roy S. Herbst, MD, PhD, chief of medical oncology at the Yale Cancer Center and Smilow Cancer Center at Yale University in New Haven, Conn.
Dr. Herbst is scheduled to present results from ADAURA as part of the American Society of Clinical Oncology virtual scientific program.
In an online briefing prior to the meeting, Dr. Herbst said the impressive results reminded him of a lesson imparted by his mentor, the late Isaiah Fidler, DVM, PhD.
“He taught me, he taught all of us, that metastasis is a spread of tumor that kills patients,” Dr. Herbst said. “Drugs such as this, based on biology, given to patients at the earliest possible time, prevent those metastases and allow patients to live longer and with a better quality of life.”
Results from the ADAURA trial provide compelling evidence of the benefit of adjuvant osimertinib for a select group of patients, according to Tina Cascone, MD, PhD, assistant professor in the department of thoracic head and neck medical oncology at The University of Texas MD Anderson Cancer Center in Houston. She was not involved in the study.
“These are unprecedented results for a potentially curable, resected population of patients,” Dr. Cascone said in an interview. “This definitely has the potential to shift the paradigm in the treatments that we have available for patients with resected disease. It’s very important to emphasize how much we’ve learned from the metastatic setting and how we’re bringing what we’ve learned into early stage disease.”
High recurrence rates
An estimated 30% of patients with NSCLC present with resectable disease at diagnosis, but 5-year recurrence rates following surgery and cisplatin-based adjuvant chemotherapy remain high, ranging from 45% among patients with stage IB disease to 62% for patients with stage II NSCLC and 76% for patients with stage III disease, Dr. Herbst noted.
Osimertinib is a third-generation tyrosine kinase inhibitor (TKI) targeted to EGFR. It has been shown to offer improvements in both progression-free survival and overall survival compared with the EGFR-TKIs erlotinib and gefitinib for patients with advanced EGFR-mutated NSCLC, as well as in patients with central nervous system metastases.
Osimertinib’s efficacy and safety profile against advanced disease suggests it may also be effective against early stage disease, a hypothesis the ADAURA trial was designed to test.
Study details
The phase 3, randomized, double-blind trial was conducted at centers in the United States, Europe, Asia, and Australia. A total of 682 patients with completely resected stage IB, II, or IIIA NSCLC, with or without planned adjuvant chemotherapy, were enrolled.
After stratification by stage, EGFR mutation, and race (Asian vs. non-Asian), patients were randomized on a 1:1 basis to receive either osimertinib at 80 mg once daily or placebo. The planned treatment duration was a maximum of 3 years.
Members of the independent data-monitoring committee held a meeting in April 2020. Although they had not planned an efficacy analysis at that time, they decided the results were clearly in favor of osimertinib. So they recommended unblinding and halting of the trial.
At the time of unblinding, the study had completed enrollment, and all patients had been followed for at least 1 year.
Efficacy and safety
For the primary endpoint of disease-free survival (DFS) in patients with stage II to IIIA disease, the median DFS was not reached for patients assigned to osimertinib, but it was 20.4 months for patients assigned to placebo (hazard ratio, 0.17; P < .0001).
The numbers were similar for the secondary endpoint of DFS in the overall population, including patients with stage IB disease. The median DFS was not reached for patients on osimertinib but was 28.1 months for patients on placebo (HR, 0.21; P < .0001).
DFS was significantly superior with osimertinib across all subgroups in the overall population, including sex, age, smoking status, race, stage, EGFR mutation, and adjuvant chemotherapy (yes or no).
Dr. Herbst said patients tolerated osimertinib well, and the drug’s safety profile was consistent with that already known. There were no adverse events leading to death in the osimertinib arm, and the incidence of grade 3 or 4 adverse events of any kind was low.
In all, 10 patients (3%) in the osimertinib arm were reported to have interstitial lung disease. Prolongation of the QT interval was reported in 22 patients (7%) on osimertinib and 4 patients (1%) in the placebo arm.
The results show that “adjuvant osimertinib provides a highly effective, practice-changing treatment for patients with stage IB, II, IIIA, EGFR mutation-positive non–small cell lung cancer after complete tumor resection,” Dr. Herbst said.
Dr. Herbst disclosed relationships with AstraZeneca, which funded the study, as well as Jun Shi Pharmaceuticals and other companies. Dr. Cascone is the international principal investigator of the NeoCOAST trial evaluating durvalumab, an AstraZeneca product.
SOURCE: Herbst RS et al. ASCO 2020, Abstract LBA5.
, results of the ADAURA trial showed.
The randomized, phase 3 trial was a comparison of osimertinib treatment with placebo following complete resection of localized or locally advanced NSCLC with negative margins. The trial was unblinded early and halted on the recommendation of the independent data-monitoring committee, due to the efficacy of osimertinib.
“If I were on the committee, I would have done the same thing. These are extraordinary results,” said study investigator Roy S. Herbst, MD, PhD, chief of medical oncology at the Yale Cancer Center and Smilow Cancer Center at Yale University in New Haven, Conn.
Dr. Herbst is scheduled to present results from ADAURA as part of the American Society of Clinical Oncology virtual scientific program.
In an online briefing prior to the meeting, Dr. Herbst said the impressive results reminded him of a lesson imparted by his mentor, the late Isaiah Fidler, DVM, PhD.
“He taught me, he taught all of us, that metastasis is a spread of tumor that kills patients,” Dr. Herbst said. “Drugs such as this, based on biology, given to patients at the earliest possible time, prevent those metastases and allow patients to live longer and with a better quality of life.”
Results from the ADAURA trial provide compelling evidence of the benefit of adjuvant osimertinib for a select group of patients, according to Tina Cascone, MD, PhD, assistant professor in the department of thoracic head and neck medical oncology at The University of Texas MD Anderson Cancer Center in Houston. She was not involved in the study.
“These are unprecedented results for a potentially curable, resected population of patients,” Dr. Cascone said in an interview. “This definitely has the potential to shift the paradigm in the treatments that we have available for patients with resected disease. It’s very important to emphasize how much we’ve learned from the metastatic setting and how we’re bringing what we’ve learned into early stage disease.”
High recurrence rates
An estimated 30% of patients with NSCLC present with resectable disease at diagnosis, but 5-year recurrence rates following surgery and cisplatin-based adjuvant chemotherapy remain high, ranging from 45% among patients with stage IB disease to 62% for patients with stage II NSCLC and 76% for patients with stage III disease, Dr. Herbst noted.
Osimertinib is a third-generation tyrosine kinase inhibitor (TKI) targeted to EGFR. It has been shown to offer improvements in both progression-free survival and overall survival compared with the EGFR-TKIs erlotinib and gefitinib for patients with advanced EGFR-mutated NSCLC, as well as in patients with central nervous system metastases.
Osimertinib’s efficacy and safety profile against advanced disease suggests it may also be effective against early stage disease, a hypothesis the ADAURA trial was designed to test.
Study details
The phase 3, randomized, double-blind trial was conducted at centers in the United States, Europe, Asia, and Australia. A total of 682 patients with completely resected stage IB, II, or IIIA NSCLC, with or without planned adjuvant chemotherapy, were enrolled.
After stratification by stage, EGFR mutation, and race (Asian vs. non-Asian), patients were randomized on a 1:1 basis to receive either osimertinib at 80 mg once daily or placebo. The planned treatment duration was a maximum of 3 years.
Members of the independent data-monitoring committee held a meeting in April 2020. Although they had not planned an efficacy analysis at that time, they decided the results were clearly in favor of osimertinib. So they recommended unblinding and halting of the trial.
At the time of unblinding, the study had completed enrollment, and all patients had been followed for at least 1 year.
Efficacy and safety
For the primary endpoint of disease-free survival (DFS) in patients with stage II to IIIA disease, the median DFS was not reached for patients assigned to osimertinib, but it was 20.4 months for patients assigned to placebo (hazard ratio, 0.17; P < .0001).
The numbers were similar for the secondary endpoint of DFS in the overall population, including patients with stage IB disease. The median DFS was not reached for patients on osimertinib but was 28.1 months for patients on placebo (HR, 0.21; P < .0001).
DFS was significantly superior with osimertinib across all subgroups in the overall population, including sex, age, smoking status, race, stage, EGFR mutation, and adjuvant chemotherapy (yes or no).
Dr. Herbst said patients tolerated osimertinib well, and the drug’s safety profile was consistent with that already known. There were no adverse events leading to death in the osimertinib arm, and the incidence of grade 3 or 4 adverse events of any kind was low.
In all, 10 patients (3%) in the osimertinib arm were reported to have interstitial lung disease. Prolongation of the QT interval was reported in 22 patients (7%) on osimertinib and 4 patients (1%) in the placebo arm.
The results show that “adjuvant osimertinib provides a highly effective, practice-changing treatment for patients with stage IB, II, IIIA, EGFR mutation-positive non–small cell lung cancer after complete tumor resection,” Dr. Herbst said.
Dr. Herbst disclosed relationships with AstraZeneca, which funded the study, as well as Jun Shi Pharmaceuticals and other companies. Dr. Cascone is the international principal investigator of the NeoCOAST trial evaluating durvalumab, an AstraZeneca product.
SOURCE: Herbst RS et al. ASCO 2020, Abstract LBA5.
FROM ASCO 2020
Key clinical point: Adjuvant osimertinib extended disease-free survival, compared with placebo, in patients with EGFR-mutated non–small cell lung cancer.
Major finding: In the overall population, the median disease-free survival was not reached for patients on osimertinib and was 28.1 months for patients on placebo (hazard ratio, 0.21, P < .0001).
Study details: Randomized, double-blind, phase 3 trial of 682 patients with stage IB-IIIA non–small cell lung cancer bearing EGFR mutations.
Disclosures: Dr. Herbst disclosed relationships with AstraZeneca, which funded the study, as well as Jun Shi Pharmaceuticals and other companies.
Source: Herbst RS et al. ASCO 2020, Abstract LBA5.
Frontline nivo-ipi plus chemo approved for metastatic NSCLC
The Food and Drug Administration has approved the combination of nivolumab (Opdivo), ipilimumab (Yervoy), and two cycles of platinum-doublet chemotherapy as frontline treatment for patients with metastatic or recurrent non–small cell lung cancer (NSCLC) who have no EGFR or ALK genomic tumor aberrations.
The FDA collaborated with the Australian Therapeutic Goods Administration, Health Canada, and Singapore’s Health Sciences Authority on the review that led to this approval, as part of Project Orbis. The FDA approved the application 2 months ahead of schedule.
The combination chemotherapy was investigated in the CHECKMATE-9LA trial (NCT03215706), which enrolled patients with metastatic or recurrent NSCLC.
Patients were randomized to receive nivolumab plus ipilimumab and two cycles of platinum-doublet chemotherapy (n = 361) or platinum-doublet chemotherapy for four cycles (n = 358).
There was a significant overall survival benefit in the nivolumab-ipilimumab arm, compared with the chemotherapy-only arm. The median overall survival was 14.1 months and 10.7 months, respectively (hazard ratio, 0.69; P = .0006).
The median progression-free survival was 6.8 months in the nivolumab-ipilimumab arm and 5 months in the chemotherapy-only arm (HR, 0.70; P = .0001). The overall response rate was 38% and 25%, respectively (P = .0003).
The most common adverse events in the nivolumab-ipilimumab arm, which occurred in at least 20% of patients, were fatigue, musculoskeletal pain, nausea, diarrhea, rash, decreased appetite, constipation, and pruritus.
Serious adverse events occurred in 57% of patients in the nivolumab-ipilimumab arm. Fatal adverse events occurred in seven patients (2%) in that arm. Fatal events were hepatic toxicity, acute renal failure, sepsis, pneumonitis, diarrhea with hypokalemia, and massive hemoptysis in the setting of thrombocytopenia.
For more details, see the full prescribing information for nivolumab or ipilimumab. Nivolumab and ipilimumab are both products of Bristol-Myers Squibb.
The Food and Drug Administration has approved the combination of nivolumab (Opdivo), ipilimumab (Yervoy), and two cycles of platinum-doublet chemotherapy as frontline treatment for patients with metastatic or recurrent non–small cell lung cancer (NSCLC) who have no EGFR or ALK genomic tumor aberrations.
The FDA collaborated with the Australian Therapeutic Goods Administration, Health Canada, and Singapore’s Health Sciences Authority on the review that led to this approval, as part of Project Orbis. The FDA approved the application 2 months ahead of schedule.
The combination chemotherapy was investigated in the CHECKMATE-9LA trial (NCT03215706), which enrolled patients with metastatic or recurrent NSCLC.
Patients were randomized to receive nivolumab plus ipilimumab and two cycles of platinum-doublet chemotherapy (n = 361) or platinum-doublet chemotherapy for four cycles (n = 358).
There was a significant overall survival benefit in the nivolumab-ipilimumab arm, compared with the chemotherapy-only arm. The median overall survival was 14.1 months and 10.7 months, respectively (hazard ratio, 0.69; P = .0006).
The median progression-free survival was 6.8 months in the nivolumab-ipilimumab arm and 5 months in the chemotherapy-only arm (HR, 0.70; P = .0001). The overall response rate was 38% and 25%, respectively (P = .0003).
The most common adverse events in the nivolumab-ipilimumab arm, which occurred in at least 20% of patients, were fatigue, musculoskeletal pain, nausea, diarrhea, rash, decreased appetite, constipation, and pruritus.
Serious adverse events occurred in 57% of patients in the nivolumab-ipilimumab arm. Fatal adverse events occurred in seven patients (2%) in that arm. Fatal events were hepatic toxicity, acute renal failure, sepsis, pneumonitis, diarrhea with hypokalemia, and massive hemoptysis in the setting of thrombocytopenia.
For more details, see the full prescribing information for nivolumab or ipilimumab. Nivolumab and ipilimumab are both products of Bristol-Myers Squibb.
The Food and Drug Administration has approved the combination of nivolumab (Opdivo), ipilimumab (Yervoy), and two cycles of platinum-doublet chemotherapy as frontline treatment for patients with metastatic or recurrent non–small cell lung cancer (NSCLC) who have no EGFR or ALK genomic tumor aberrations.
The FDA collaborated with the Australian Therapeutic Goods Administration, Health Canada, and Singapore’s Health Sciences Authority on the review that led to this approval, as part of Project Orbis. The FDA approved the application 2 months ahead of schedule.
The combination chemotherapy was investigated in the CHECKMATE-9LA trial (NCT03215706), which enrolled patients with metastatic or recurrent NSCLC.
Patients were randomized to receive nivolumab plus ipilimumab and two cycles of platinum-doublet chemotherapy (n = 361) or platinum-doublet chemotherapy for four cycles (n = 358).
There was a significant overall survival benefit in the nivolumab-ipilimumab arm, compared with the chemotherapy-only arm. The median overall survival was 14.1 months and 10.7 months, respectively (hazard ratio, 0.69; P = .0006).
The median progression-free survival was 6.8 months in the nivolumab-ipilimumab arm and 5 months in the chemotherapy-only arm (HR, 0.70; P = .0001). The overall response rate was 38% and 25%, respectively (P = .0003).
The most common adverse events in the nivolumab-ipilimumab arm, which occurred in at least 20% of patients, were fatigue, musculoskeletal pain, nausea, diarrhea, rash, decreased appetite, constipation, and pruritus.
Serious adverse events occurred in 57% of patients in the nivolumab-ipilimumab arm. Fatal adverse events occurred in seven patients (2%) in that arm. Fatal events were hepatic toxicity, acute renal failure, sepsis, pneumonitis, diarrhea with hypokalemia, and massive hemoptysis in the setting of thrombocytopenia.
For more details, see the full prescribing information for nivolumab or ipilimumab. Nivolumab and ipilimumab are both products of Bristol-Myers Squibb.
FDA approves brigatinib and companion diagnostic for NSCLC
The Food and Drug Administration has approved brigatinib (Alunbrig) to treat adults with ALK-positive metastatic non–small cell lung cancer (NSCLC) as detected by an FDA-approved test.
The FDA also approved the Vysis ALK Break Apart FISH Probe Kit as a companion diagnostic for brigatinib.
Brigatinib and the companion diagnostic were both evaluated in the ALTA 1L trial (NCT02737501). The trial enrolled adults with advanced ALK-positive NSCLC who had not previously received an ALK-targeted therapy. Patients had to have an ALK rearrangement based on a local standard of care test.
Clinical samples from trial participants were retrospectively tested with the Vysis ALK Break Apart FISH Probe Kit. Of the 275 patients enrolled in the trial, 239 were ALK positive according to the test. Results were negative for 20 patients and unavailable for 16 patients.
Patients were randomized to receive brigatinib at 180 mg once daily with a 7-day lead-in at 90 mg once daily (n = 137) or crizotinib at 250 mg twice daily (n = 138).
The estimated median progression-free survival was 24 months in the brigatinib arm and 11 months in the crizotinib arm (hazard ratio, 0.49; P < .0001). The overall response rate was 74% in the brigatinib arm and 62% in the crizotinib arm.
The most common adverse events in the brigatinib arm, occurring in at least 20% of patients, were diarrhea, fatigue, nausea, rash, cough, myalgia, headache, hypertension, vomiting, abdominal pain, pruritus, back pain, and dyspnea.
Serious adverse events occurred in 33% of patients in the brigatinib arm, and fatal adverse events included in 2.9%. The fatal events were pneumonia (1.5%), cerebrovascular accident (0.7%), and multiple organ dysfunction syndrome (0.7%).
For more details on the ALTA 1L trial, see the full prescribing information for brigatinib.
The approval of brigatinib was granted to ARIAD Pharmaceuticals. The approval of the Vysis ALK Break Apart FISH Probe Kit was granted to Abbott Molecular.
The Food and Drug Administration has approved brigatinib (Alunbrig) to treat adults with ALK-positive metastatic non–small cell lung cancer (NSCLC) as detected by an FDA-approved test.
The FDA also approved the Vysis ALK Break Apart FISH Probe Kit as a companion diagnostic for brigatinib.
Brigatinib and the companion diagnostic were both evaluated in the ALTA 1L trial (NCT02737501). The trial enrolled adults with advanced ALK-positive NSCLC who had not previously received an ALK-targeted therapy. Patients had to have an ALK rearrangement based on a local standard of care test.
Clinical samples from trial participants were retrospectively tested with the Vysis ALK Break Apart FISH Probe Kit. Of the 275 patients enrolled in the trial, 239 were ALK positive according to the test. Results were negative for 20 patients and unavailable for 16 patients.
Patients were randomized to receive brigatinib at 180 mg once daily with a 7-day lead-in at 90 mg once daily (n = 137) or crizotinib at 250 mg twice daily (n = 138).
The estimated median progression-free survival was 24 months in the brigatinib arm and 11 months in the crizotinib arm (hazard ratio, 0.49; P < .0001). The overall response rate was 74% in the brigatinib arm and 62% in the crizotinib arm.
The most common adverse events in the brigatinib arm, occurring in at least 20% of patients, were diarrhea, fatigue, nausea, rash, cough, myalgia, headache, hypertension, vomiting, abdominal pain, pruritus, back pain, and dyspnea.
Serious adverse events occurred in 33% of patients in the brigatinib arm, and fatal adverse events included in 2.9%. The fatal events were pneumonia (1.5%), cerebrovascular accident (0.7%), and multiple organ dysfunction syndrome (0.7%).
For more details on the ALTA 1L trial, see the full prescribing information for brigatinib.
The approval of brigatinib was granted to ARIAD Pharmaceuticals. The approval of the Vysis ALK Break Apart FISH Probe Kit was granted to Abbott Molecular.
The Food and Drug Administration has approved brigatinib (Alunbrig) to treat adults with ALK-positive metastatic non–small cell lung cancer (NSCLC) as detected by an FDA-approved test.
The FDA also approved the Vysis ALK Break Apart FISH Probe Kit as a companion diagnostic for brigatinib.
Brigatinib and the companion diagnostic were both evaluated in the ALTA 1L trial (NCT02737501). The trial enrolled adults with advanced ALK-positive NSCLC who had not previously received an ALK-targeted therapy. Patients had to have an ALK rearrangement based on a local standard of care test.
Clinical samples from trial participants were retrospectively tested with the Vysis ALK Break Apart FISH Probe Kit. Of the 275 patients enrolled in the trial, 239 were ALK positive according to the test. Results were negative for 20 patients and unavailable for 16 patients.
Patients were randomized to receive brigatinib at 180 mg once daily with a 7-day lead-in at 90 mg once daily (n = 137) or crizotinib at 250 mg twice daily (n = 138).
The estimated median progression-free survival was 24 months in the brigatinib arm and 11 months in the crizotinib arm (hazard ratio, 0.49; P < .0001). The overall response rate was 74% in the brigatinib arm and 62% in the crizotinib arm.
The most common adverse events in the brigatinib arm, occurring in at least 20% of patients, were diarrhea, fatigue, nausea, rash, cough, myalgia, headache, hypertension, vomiting, abdominal pain, pruritus, back pain, and dyspnea.
Serious adverse events occurred in 33% of patients in the brigatinib arm, and fatal adverse events included in 2.9%. The fatal events were pneumonia (1.5%), cerebrovascular accident (0.7%), and multiple organ dysfunction syndrome (0.7%).
For more details on the ALTA 1L trial, see the full prescribing information for brigatinib.
The approval of brigatinib was granted to ARIAD Pharmaceuticals. The approval of the Vysis ALK Break Apart FISH Probe Kit was granted to Abbott Molecular.
Patient-focused precautions, testing help blunt pandemic effects on heme-onc unit
Keeping hematologic oncology patients on their treatment regimens and caring for inpatients with hematologic malignancies remained “manageable” during the first 2 months of the COVID-19 pandemic at Levine Cancer Institute in Charlotte, N.C.

That level of manageability has partly been because a surge in cases so far hasn’t arrived at Levine or in most of the surrounding North Carolina and South Carolina communities it serves. As of May 15, 2020, the total number of confirmed and reported COVID-19 cases had reached about 19,000 in North Carolina, and just under 9,000 in South Carolina, out of a total population in the two states of close to 16 million. What’s happened instead at Levine Cancer Institute (LCI) has been a steady but low drumbeat of cases that, by mid-May 2020, totaled fewer than 10 patients with hematologic malignancies diagnosed with COVID-19.
“For a large system with multiple sites throughout North and South Carolina that saw 17,200 new patients in 2019 – including solid tumor, benign hematology, and malignant hematology patients – with 198,000 total patient visits, it is safe to say that we are off to a good start. However, we remain in the early throes of the pandemic and we will need to remain vigilant going forward,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in LCI’s Department of Hematologic Oncology and Blood Disorders.
The limited effects to date of COVID-19 at LCI has been thanks to a regimen of great caution for preventing infections that’s been consistently conveyed to LCI patients from before the pandemic’s onset, liberal testing that started early, a proactive plan to defer and temporarily replace infusion care when medically appropriate, a novel staffing approach designed to minimize and contain potential staff outbreaks, and an early pivot to virtual patient contact when feasible.
COVID-19 has had limited penetration into the LCI case load because patients have, in general, “been very careful,” said Dr. Voorhees.
“My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious even before the coronavirus using distancing, masking, and meticulous hand hygiene,” he said in an interview that reviewed the steps LCI took starting in March to confront and manage the effects of the then-nascent pandemic. “Since we started screening asymptomatic patients in the inpatient and outpatient settings we have identified only one patient with COVID-19 infection, which supports the low rate of infection in our patient population thus far.”
Another key step was the launch of “robust” testing for the COVID-19 virus starting on March 9, using an in-house assay from LCI’s parent health system, Atrium Health, that delivered results within 24 hours. Testing became available at LCI “earlier than at many other health systems.” At first, testing was limited to patients or staff presenting with symptoms, but in the following weeks, it expanded to more patients, including those without symptoms who were scheduled for treatment at the apheresis center, cell donors and cell recipients, patients arriving for inpatient chemotherapy or cellular therapy, patients arriving from a skilled nursing facility or similar environments, and more recently, outpatient chemotherapy patients. “We’re now doing a lot of screening,” Dr. Voorhees said. “In general, screening has been well received because patients recognize that it’s for their own safety.”
Another piece of COVID-19 preparedness was a move toward technology as an alternative to face-to-face encounters between patients and staff. “We adopted virtual technology early.” When medically appropriate, they provided either video consultations with more tech-savvy patients or telephone-based virtual visits for patients who preferred a more familiar interface. As LCI starts the process of reentry for patients whose face-to-face encounters were deferred, virtual visits will remain an important facet of maintaining care while limiting exposure for appropriate patients and facilitating adequate space for social distancing in the clinics and infusion centers.
Atrium Health also launched a “virtual hospital” geared to intensified remote management of COVID-19 patients who aren’t sick enough for hospitalization. “People who test positive automatically enter the virtual hospital and have regular interactions with their team of providers,” with LCI providing additional support for their patients who get infected. Patients receive an equipment kit that lets them monitor and transmit their vital signs. The virtual hospital program also helps expedite personal needs like delivery of prescriptions and food. “It helps patients manage at home, and has been incredibly useful,” said Dr. Voorhees.
Perhaps the most challenging step LCI clinicians took to preclude a potential COVID-19 case surge was to review all patients receiving infusional therapy or planned cellular therapy and triage those who could potentially tolerate a temporary change to either an oral, at-home regimen or to a brief hold on their treatment. Some patients on maintenance, outpatient infusion-therapy regimens “expressed concern about coming to the clinic. We looked at the patients scheduled to come for infusions and decided which visits were essential and which were deferrable without disrupting care by briefly using a noninfusional approach,” said Dr. Voorhees. The number of patients who had their regimens modified or held was “relatively small,” and with the recent recognition that a surge of infections has not occurred, “we’re now rolling out cautious reentry of those patients back to their originally prescribed chemotherapy.”
In addition to concerns of exposure at infusion clinics, there are concerns about the heightened susceptibility of immunosuppressed hematologic oncology patients to COVID-19 and their risk for more severe infection. “Our view is that, if patients tested positive, continuing immunosuppressive treatment would likely be detrimental,” so when possible treatment is temporarily suspended and then resumed when the infection has cleared. “When patients test positive for a prolonged period, a decision to resume treatment must be in the best interests of the patient and weigh the benefits of resuming therapy against the risks of incurring a more severe infection by restarting potentially immunosuppressive therapy,” Dr. Voorhees said.
The enhanced risk that cancer patients face if they develop COVID-19 was documented in a recent review of 218 cancer patients hospitalized for COVID-19 during parts of March and April in a large New York health system. The results showed an overall mortality rate of 28%, including a 37% rate among 54 patients with hematologic malignancies and a 25% rate among 164 patients with solid tumors. The mortality rate “may not be quite as high as they reported because that depends on how many patients you test, but there is no question that patients with more comorbidities are at higher risk. Patients with active cancer on chemotherapy are a particularly vulnerable population, and many have expressed concerns about their vulnerability,” he observed.
For the few LCI patients who developed COVID-19 infection, the medical staff has had several therapeutic options they could match to each patient’s needs, with help from the Atrium Health infectious disease team. LCI and Atrium Health are participating in several COVID-19 clinical treatment trials, including an investigational convalescent plasma protocol spearheaded by the Mayo Clinic. They have also opened a randomized, phase 2 trial evaluating the safety and efficacy of selinexor (Xpovio), an oral drug that’s Food and Drug Administration approved for patients with multiple myeloma, for treatment of moderate or severe COVID-19 infection. Additional studies evaluating blockade of granulocyte-macrophage colony-stimulating factor, as well as inhaled antiviral therapy, have recently launched, and several additional studies are poised to open in the coming weeks.
The LCI and Atrium Health team also has a supply of the antiviral agent remdesivir as part of the FDA’s expanded access protocol and emergency use authorization. They also have a supply of and experience administering the interleukin-6 receptor inhibitor tocilizumab (Actemra), which showed some suggestion of efficacy in limited experience treating patients with severe or critical COVID-19 infections. Clinicians at LCI have not used the investigational and unproven agents hydroxychloroquine, chloroquine, and azithromycin to either prevent or treat COVID-19.
LCI also instituted measures to try to minimize the risk that staff members could become infected and transmit the virus while asymptomatic. Following conversations held early on with COVID-19–experienced health authorities in China and Italy, the patient-facing LCI staff split into two teams starting on March 23 that alternated responsibility for direct patient interactions every 2 weeks. When one of these teams was off from direct patient contact they continued to care for patients remotely through virtual technologies. The concept was that, if a staffer became infected while remaining asymptomatic during their contact with patients, their status would either become diagnosable or resolve during their 2 weeks away from seeing any patients. Perhaps in part because of this approach infections among staff members “have not been a big issue. We’ve had an incredibly low infection rate among the LCI staff,” Dr. Voorhees noted.
By mid-May, with the imminent threat of a sudden CODIV-19 surge moderated, heme-onc operations at LCI began to cautiously revert to more normal operations. “We’re continuing patient screening for signs and symptoms of COVID-19 infection, testing for asymptomatic infections, and requiring masking and social distancing in the clinics and hospitals, but we’re starting to slowly restore the number of patients at our clinics [virtual and face to face[ and infusion centers,” and the staff’s division into two teams ended. “The idea was to get past a surge and make sure our system was not overwhelmed. We anticipated a local surge in late April, but then it kept getting pushed back. Current projections are for the infection rate among LCI patients to remain low provided that community spread remains stable or, ideally, decreases.” The LCI infectious disease staff is closely monitoring infection rates for early recognition of an outbreak, with plans to follow any new cases with contact tracing. So far, the COVID-19 pandemic at LCI “has been very manageable,” Dr. Voorhees concluded.
“We’re now better positioned to deal with a case surge if it were to happen. We could resume the two-team approach, hospital-wide plans are now in place for a future surge, and we are now up and running with robust testing and inpatient and outpatient virtual technology. The first time, we were all learning on the fly.”
The LCI biostatistics team has been prospectively collecting the Institutes’s COVID-19 patient data, with plans to report their findings.
Dr. Voorhees has had financial relationships with Bristol-Myers Squibb/Celgene, Janssen, Novartis, and Oncopeptides, none of which are relevant to this article.
Keeping hematologic oncology patients on their treatment regimens and caring for inpatients with hematologic malignancies remained “manageable” during the first 2 months of the COVID-19 pandemic at Levine Cancer Institute in Charlotte, N.C.
That level of manageability has partly been because a surge in cases so far hasn’t arrived at Levine or in most of the surrounding North Carolina and South Carolina communities it serves. As of May 15, 2020, the total number of confirmed and reported COVID-19 cases had reached about 19,000 in North Carolina, and just under 9,000 in South Carolina, out of a total population in the two states of close to 16 million. What’s happened instead at Levine Cancer Institute (LCI) has been a steady but low drumbeat of cases that, by mid-May 2020, totaled fewer than 10 patients with hematologic malignancies diagnosed with COVID-19.
“For a large system with multiple sites throughout North and South Carolina that saw 17,200 new patients in 2019 – including solid tumor, benign hematology, and malignant hematology patients – with 198,000 total patient visits, it is safe to say that we are off to a good start. However, we remain in the early throes of the pandemic and we will need to remain vigilant going forward,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in LCI’s Department of Hematologic Oncology and Blood Disorders.
The limited effects to date of COVID-19 at LCI has been thanks to a regimen of great caution for preventing infections that’s been consistently conveyed to LCI patients from before the pandemic’s onset, liberal testing that started early, a proactive plan to defer and temporarily replace infusion care when medically appropriate, a novel staffing approach designed to minimize and contain potential staff outbreaks, and an early pivot to virtual patient contact when feasible.
COVID-19 has had limited penetration into the LCI case load because patients have, in general, “been very careful,” said Dr. Voorhees.
“My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious even before the coronavirus using distancing, masking, and meticulous hand hygiene,” he said in an interview that reviewed the steps LCI took starting in March to confront and manage the effects of the then-nascent pandemic. “Since we started screening asymptomatic patients in the inpatient and outpatient settings we have identified only one patient with COVID-19 infection, which supports the low rate of infection in our patient population thus far.”
Another key step was the launch of “robust” testing for the COVID-19 virus starting on March 9, using an in-house assay from LCI’s parent health system, Atrium Health, that delivered results within 24 hours. Testing became available at LCI “earlier than at many other health systems.” At first, testing was limited to patients or staff presenting with symptoms, but in the following weeks, it expanded to more patients, including those without symptoms who were scheduled for treatment at the apheresis center, cell donors and cell recipients, patients arriving for inpatient chemotherapy or cellular therapy, patients arriving from a skilled nursing facility or similar environments, and more recently, outpatient chemotherapy patients. “We’re now doing a lot of screening,” Dr. Voorhees said. “In general, screening has been well received because patients recognize that it’s for their own safety.”
Another piece of COVID-19 preparedness was a move toward technology as an alternative to face-to-face encounters between patients and staff. “We adopted virtual technology early.” When medically appropriate, they provided either video consultations with more tech-savvy patients or telephone-based virtual visits for patients who preferred a more familiar interface. As LCI starts the process of reentry for patients whose face-to-face encounters were deferred, virtual visits will remain an important facet of maintaining care while limiting exposure for appropriate patients and facilitating adequate space for social distancing in the clinics and infusion centers.
Atrium Health also launched a “virtual hospital” geared to intensified remote management of COVID-19 patients who aren’t sick enough for hospitalization. “People who test positive automatically enter the virtual hospital and have regular interactions with their team of providers,” with LCI providing additional support for their patients who get infected. Patients receive an equipment kit that lets them monitor and transmit their vital signs. The virtual hospital program also helps expedite personal needs like delivery of prescriptions and food. “It helps patients manage at home, and has been incredibly useful,” said Dr. Voorhees.
Perhaps the most challenging step LCI clinicians took to preclude a potential COVID-19 case surge was to review all patients receiving infusional therapy or planned cellular therapy and triage those who could potentially tolerate a temporary change to either an oral, at-home regimen or to a brief hold on their treatment. Some patients on maintenance, outpatient infusion-therapy regimens “expressed concern about coming to the clinic. We looked at the patients scheduled to come for infusions and decided which visits were essential and which were deferrable without disrupting care by briefly using a noninfusional approach,” said Dr. Voorhees. The number of patients who had their regimens modified or held was “relatively small,” and with the recent recognition that a surge of infections has not occurred, “we’re now rolling out cautious reentry of those patients back to their originally prescribed chemotherapy.”
In addition to concerns of exposure at infusion clinics, there are concerns about the heightened susceptibility of immunosuppressed hematologic oncology patients to COVID-19 and their risk for more severe infection. “Our view is that, if patients tested positive, continuing immunosuppressive treatment would likely be detrimental,” so when possible treatment is temporarily suspended and then resumed when the infection has cleared. “When patients test positive for a prolonged period, a decision to resume treatment must be in the best interests of the patient and weigh the benefits of resuming therapy against the risks of incurring a more severe infection by restarting potentially immunosuppressive therapy,” Dr. Voorhees said.
The enhanced risk that cancer patients face if they develop COVID-19 was documented in a recent review of 218 cancer patients hospitalized for COVID-19 during parts of March and April in a large New York health system. The results showed an overall mortality rate of 28%, including a 37% rate among 54 patients with hematologic malignancies and a 25% rate among 164 patients with solid tumors. The mortality rate “may not be quite as high as they reported because that depends on how many patients you test, but there is no question that patients with more comorbidities are at higher risk. Patients with active cancer on chemotherapy are a particularly vulnerable population, and many have expressed concerns about their vulnerability,” he observed.
For the few LCI patients who developed COVID-19 infection, the medical staff has had several therapeutic options they could match to each patient’s needs, with help from the Atrium Health infectious disease team. LCI and Atrium Health are participating in several COVID-19 clinical treatment trials, including an investigational convalescent plasma protocol spearheaded by the Mayo Clinic. They have also opened a randomized, phase 2 trial evaluating the safety and efficacy of selinexor (Xpovio), an oral drug that’s Food and Drug Administration approved for patients with multiple myeloma, for treatment of moderate or severe COVID-19 infection. Additional studies evaluating blockade of granulocyte-macrophage colony-stimulating factor, as well as inhaled antiviral therapy, have recently launched, and several additional studies are poised to open in the coming weeks.
The LCI and Atrium Health team also has a supply of the antiviral agent remdesivir as part of the FDA’s expanded access protocol and emergency use authorization. They also have a supply of and experience administering the interleukin-6 receptor inhibitor tocilizumab (Actemra), which showed some suggestion of efficacy in limited experience treating patients with severe or critical COVID-19 infections. Clinicians at LCI have not used the investigational and unproven agents hydroxychloroquine, chloroquine, and azithromycin to either prevent or treat COVID-19.
LCI also instituted measures to try to minimize the risk that staff members could become infected and transmit the virus while asymptomatic. Following conversations held early on with COVID-19–experienced health authorities in China and Italy, the patient-facing LCI staff split into two teams starting on March 23 that alternated responsibility for direct patient interactions every 2 weeks. When one of these teams was off from direct patient contact they continued to care for patients remotely through virtual technologies. The concept was that, if a staffer became infected while remaining asymptomatic during their contact with patients, their status would either become diagnosable or resolve during their 2 weeks away from seeing any patients. Perhaps in part because of this approach infections among staff members “have not been a big issue. We’ve had an incredibly low infection rate among the LCI staff,” Dr. Voorhees noted.
By mid-May, with the imminent threat of a sudden CODIV-19 surge moderated, heme-onc operations at LCI began to cautiously revert to more normal operations. “We’re continuing patient screening for signs and symptoms of COVID-19 infection, testing for asymptomatic infections, and requiring masking and social distancing in the clinics and hospitals, but we’re starting to slowly restore the number of patients at our clinics [virtual and face to face[ and infusion centers,” and the staff’s division into two teams ended. “The idea was to get past a surge and make sure our system was not overwhelmed. We anticipated a local surge in late April, but then it kept getting pushed back. Current projections are for the infection rate among LCI patients to remain low provided that community spread remains stable or, ideally, decreases.” The LCI infectious disease staff is closely monitoring infection rates for early recognition of an outbreak, with plans to follow any new cases with contact tracing. So far, the COVID-19 pandemic at LCI “has been very manageable,” Dr. Voorhees concluded.
“We’re now better positioned to deal with a case surge if it were to happen. We could resume the two-team approach, hospital-wide plans are now in place for a future surge, and we are now up and running with robust testing and inpatient and outpatient virtual technology. The first time, we were all learning on the fly.”
The LCI biostatistics team has been prospectively collecting the Institutes’s COVID-19 patient data, with plans to report their findings.
Dr. Voorhees has had financial relationships with Bristol-Myers Squibb/Celgene, Janssen, Novartis, and Oncopeptides, none of which are relevant to this article.
Keeping hematologic oncology patients on their treatment regimens and caring for inpatients with hematologic malignancies remained “manageable” during the first 2 months of the COVID-19 pandemic at Levine Cancer Institute in Charlotte, N.C.
That level of manageability has partly been because a surge in cases so far hasn’t arrived at Levine or in most of the surrounding North Carolina and South Carolina communities it serves. As of May 15, 2020, the total number of confirmed and reported COVID-19 cases had reached about 19,000 in North Carolina, and just under 9,000 in South Carolina, out of a total population in the two states of close to 16 million. What’s happened instead at Levine Cancer Institute (LCI) has been a steady but low drumbeat of cases that, by mid-May 2020, totaled fewer than 10 patients with hematologic malignancies diagnosed with COVID-19.
“For a large system with multiple sites throughout North and South Carolina that saw 17,200 new patients in 2019 – including solid tumor, benign hematology, and malignant hematology patients – with 198,000 total patient visits, it is safe to say that we are off to a good start. However, we remain in the early throes of the pandemic and we will need to remain vigilant going forward,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in LCI’s Department of Hematologic Oncology and Blood Disorders.
The limited effects to date of COVID-19 at LCI has been thanks to a regimen of great caution for preventing infections that’s been consistently conveyed to LCI patients from before the pandemic’s onset, liberal testing that started early, a proactive plan to defer and temporarily replace infusion care when medically appropriate, a novel staffing approach designed to minimize and contain potential staff outbreaks, and an early pivot to virtual patient contact when feasible.
COVID-19 has had limited penetration into the LCI case load because patients have, in general, “been very careful,” said Dr. Voorhees.
“My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious even before the coronavirus using distancing, masking, and meticulous hand hygiene,” he said in an interview that reviewed the steps LCI took starting in March to confront and manage the effects of the then-nascent pandemic. “Since we started screening asymptomatic patients in the inpatient and outpatient settings we have identified only one patient with COVID-19 infection, which supports the low rate of infection in our patient population thus far.”
Another key step was the launch of “robust” testing for the COVID-19 virus starting on March 9, using an in-house assay from LCI’s parent health system, Atrium Health, that delivered results within 24 hours. Testing became available at LCI “earlier than at many other health systems.” At first, testing was limited to patients or staff presenting with symptoms, but in the following weeks, it expanded to more patients, including those without symptoms who were scheduled for treatment at the apheresis center, cell donors and cell recipients, patients arriving for inpatient chemotherapy or cellular therapy, patients arriving from a skilled nursing facility or similar environments, and more recently, outpatient chemotherapy patients. “We’re now doing a lot of screening,” Dr. Voorhees said. “In general, screening has been well received because patients recognize that it’s for their own safety.”
Another piece of COVID-19 preparedness was a move toward technology as an alternative to face-to-face encounters between patients and staff. “We adopted virtual technology early.” When medically appropriate, they provided either video consultations with more tech-savvy patients or telephone-based virtual visits for patients who preferred a more familiar interface. As LCI starts the process of reentry for patients whose face-to-face encounters were deferred, virtual visits will remain an important facet of maintaining care while limiting exposure for appropriate patients and facilitating adequate space for social distancing in the clinics and infusion centers.
Atrium Health also launched a “virtual hospital” geared to intensified remote management of COVID-19 patients who aren’t sick enough for hospitalization. “People who test positive automatically enter the virtual hospital and have regular interactions with their team of providers,” with LCI providing additional support for their patients who get infected. Patients receive an equipment kit that lets them monitor and transmit their vital signs. The virtual hospital program also helps expedite personal needs like delivery of prescriptions and food. “It helps patients manage at home, and has been incredibly useful,” said Dr. Voorhees.
Perhaps the most challenging step LCI clinicians took to preclude a potential COVID-19 case surge was to review all patients receiving infusional therapy or planned cellular therapy and triage those who could potentially tolerate a temporary change to either an oral, at-home regimen or to a brief hold on their treatment. Some patients on maintenance, outpatient infusion-therapy regimens “expressed concern about coming to the clinic. We looked at the patients scheduled to come for infusions and decided which visits were essential and which were deferrable without disrupting care by briefly using a noninfusional approach,” said Dr. Voorhees. The number of patients who had their regimens modified or held was “relatively small,” and with the recent recognition that a surge of infections has not occurred, “we’re now rolling out cautious reentry of those patients back to their originally prescribed chemotherapy.”
In addition to concerns of exposure at infusion clinics, there are concerns about the heightened susceptibility of immunosuppressed hematologic oncology patients to COVID-19 and their risk for more severe infection. “Our view is that, if patients tested positive, continuing immunosuppressive treatment would likely be detrimental,” so when possible treatment is temporarily suspended and then resumed when the infection has cleared. “When patients test positive for a prolonged period, a decision to resume treatment must be in the best interests of the patient and weigh the benefits of resuming therapy against the risks of incurring a more severe infection by restarting potentially immunosuppressive therapy,” Dr. Voorhees said.
The enhanced risk that cancer patients face if they develop COVID-19 was documented in a recent review of 218 cancer patients hospitalized for COVID-19 during parts of March and April in a large New York health system. The results showed an overall mortality rate of 28%, including a 37% rate among 54 patients with hematologic malignancies and a 25% rate among 164 patients with solid tumors. The mortality rate “may not be quite as high as they reported because that depends on how many patients you test, but there is no question that patients with more comorbidities are at higher risk. Patients with active cancer on chemotherapy are a particularly vulnerable population, and many have expressed concerns about their vulnerability,” he observed.
For the few LCI patients who developed COVID-19 infection, the medical staff has had several therapeutic options they could match to each patient’s needs, with help from the Atrium Health infectious disease team. LCI and Atrium Health are participating in several COVID-19 clinical treatment trials, including an investigational convalescent plasma protocol spearheaded by the Mayo Clinic. They have also opened a randomized, phase 2 trial evaluating the safety and efficacy of selinexor (Xpovio), an oral drug that’s Food and Drug Administration approved for patients with multiple myeloma, for treatment of moderate or severe COVID-19 infection. Additional studies evaluating blockade of granulocyte-macrophage colony-stimulating factor, as well as inhaled antiviral therapy, have recently launched, and several additional studies are poised to open in the coming weeks.
The LCI and Atrium Health team also has a supply of the antiviral agent remdesivir as part of the FDA’s expanded access protocol and emergency use authorization. They also have a supply of and experience administering the interleukin-6 receptor inhibitor tocilizumab (Actemra), which showed some suggestion of efficacy in limited experience treating patients with severe or critical COVID-19 infections. Clinicians at LCI have not used the investigational and unproven agents hydroxychloroquine, chloroquine, and azithromycin to either prevent or treat COVID-19.
LCI also instituted measures to try to minimize the risk that staff members could become infected and transmit the virus while asymptomatic. Following conversations held early on with COVID-19–experienced health authorities in China and Italy, the patient-facing LCI staff split into two teams starting on March 23 that alternated responsibility for direct patient interactions every 2 weeks. When one of these teams was off from direct patient contact they continued to care for patients remotely through virtual technologies. The concept was that, if a staffer became infected while remaining asymptomatic during their contact with patients, their status would either become diagnosable or resolve during their 2 weeks away from seeing any patients. Perhaps in part because of this approach infections among staff members “have not been a big issue. We’ve had an incredibly low infection rate among the LCI staff,” Dr. Voorhees noted.
By mid-May, with the imminent threat of a sudden CODIV-19 surge moderated, heme-onc operations at LCI began to cautiously revert to more normal operations. “We’re continuing patient screening for signs and symptoms of COVID-19 infection, testing for asymptomatic infections, and requiring masking and social distancing in the clinics and hospitals, but we’re starting to slowly restore the number of patients at our clinics [virtual and face to face[ and infusion centers,” and the staff’s division into two teams ended. “The idea was to get past a surge and make sure our system was not overwhelmed. We anticipated a local surge in late April, but then it kept getting pushed back. Current projections are for the infection rate among LCI patients to remain low provided that community spread remains stable or, ideally, decreases.” The LCI infectious disease staff is closely monitoring infection rates for early recognition of an outbreak, with plans to follow any new cases with contact tracing. So far, the COVID-19 pandemic at LCI “has been very manageable,” Dr. Voorhees concluded.
“We’re now better positioned to deal with a case surge if it were to happen. We could resume the two-team approach, hospital-wide plans are now in place for a future surge, and we are now up and running with robust testing and inpatient and outpatient virtual technology. The first time, we were all learning on the fly.”
The LCI biostatistics team has been prospectively collecting the Institutes’s COVID-19 patient data, with plans to report their findings.
Dr. Voorhees has had financial relationships with Bristol-Myers Squibb/Celgene, Janssen, Novartis, and Oncopeptides, none of which are relevant to this article.
Low-dose erlotinib seems feasible for frail, elderly patients with NSCLC
, according to researchers.
They conducted a phase 2 trial to investigate whether one-third of the maximum tolerated dose of erlotinib could maintain sufficient plasma concentration of the drug while avoiding the adverse effects of higher doses. The results were published in JAMA Oncology.
Erlotinib and other epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) have demonstrated efficacy in elderly patients with EGFR-positive NSCLC, according to study author Shingo Miyamoto, MD, of Japanese Red Cross Medical Center in Tokyo, and colleagues.
“With the increasing number of elderly patients with cancer, many of whom also have significant comorbidities, there is a considerable value in investigating whether EGFR-TKIs are effective for the frail population,” the authors wrote. They also noted that it is “difficult to identify the appropriate dose of molecular-targeted drugs.”
With this in mind, Dr. Miyamoto and colleagues conducted a single-arm, phase 2 trial of low-dose erlotinib in 80 chemotherapy-naive frail or elderly patients with EGFR-positive NSCLC. Frailty was defined by age and the Charlson Comorbidity Index. The patients’ median age was 80 years (range, 49-90 years).
Patients received erlotinib at 50 mg per day, which is one-third of the established maximum tolerated dose, for 4 weeks. Then, they were evaluated with radiologic imaging. Treatment continued until disease progression or unacceptable adverse events. Dosing was modified by treatment response or by adverse events.
Results
At last follow-up, 7 of the 80 patients were still receiving low-dose erlotinib. Reasons for discontinuation were disease progression (n = 60), patient request (n = 6), adverse events (n = 4), and death (n = 3).
The overall response rate was 60%, and the disease control rate was 90%. The researchers measured plasma erlotinib concentration in 48 patients and found it did not correlate with response.
The median progression-free survival was 9.3 months, and the median overall survival was 26.2 months.
Ten patients had erlotinib temporarily suspended because of adverse events. Five patients had their dose reduced to 25 mg because of adverse events, including oral mucositis, paronychia, erythema multiforme, diarrhea, and anorexia.
Two patients discontinued treatment because of adverse events. One patient had a cutaneous ulcer and bone infection. The other had oral mucositis.
Dr. Miyamoto and colleagues concluded that, “low-dose erlotinib was associated with efficacy and safety in frail patients with EGFR mutation–positive lung cancer. More research on the dosing strategy of target-based drugs is warranted, especially in frail patients in the real-world setting.”
Less is more
Sometimes, less can be more, said Mellar P. Davis, MD, an oncologist and section head of the palliative care department at Geisinger Medical System in Danville, Penn., who was not involved in this study.
“Why do patients benefit from small doses? It may be that there are fewer drug interruptions over time and patients are able to stay on schedule,” Dr. Davis said. “It may also be that erlotinib clearance is reduced in the elderly and comorbid patient. The reduced dose may, in fact, be the ‘therapeutic’ dose in this special population.”
Plasma levels were frequently in therapeutic ranges in this study, but patients who had subtherapeutic plasma levels also responded to therapy, Dr. Davis pointed out. The lower dose was shown to maintain sufficient concentrations of the treatment while reducing adverse effects.
However, Dr. Davis noted, this was not a randomized trial. “It is always a risk hedging bets on single-arm trials,” he said. “Randomized trials often prove phase 2 single-arm trials wrong.”
He added that quality-of-life measures are absent from the study. Erlotinib is a palliative drug with side effects, Dr. Davis noted.
“Control of cancer and cancer regression should improve symptoms and quality of life when balanced against treatment toxicity,” he said. “In this study, I would have thought that symptom improvement, performance score, and quality of life would have been the primary outcome or the co-primary outcome with disease control.”
Should a randomized, controlled trial of low-dose erlotinib be conducted in the frail/elderly population? “If one believes trials should be quantitatively based, the answer would be no,” Dr. Davis said. “Responses may be the same, and it would be expensive to prove that low-dose erlotinib is the same as standard doses when comparing survival.”
However, if one is interested in quality of life, particularly in this growing population, a trial that incorporated quality-of-life measures would make more sense, according to Dr. Davis. “For if one can achieve less toxicity and treat more patients and get the same duration of clinical benefit, then less will be more,” he concluded.
Dr. Davis reported having no conflicts of interest. Study authors disclosed relationships with Astellas Pharma, AstraZeneca, Bristol-Myers Squibb, and many other companies. Erlotinib is manufactured for OSI Pharmaceuticals, an affiliate of Astellas Pharma, and distributed by Genentech, a member of the Roche Group.
The study was supported by the Japan Agency for Medical Research and Development.
SOURCE: Miyamoto S et al. JAMA Oncol. 2020 May 14; e201250. doi: 10.1001/jamaoncol.2020.1250.
, according to researchers.
They conducted a phase 2 trial to investigate whether one-third of the maximum tolerated dose of erlotinib could maintain sufficient plasma concentration of the drug while avoiding the adverse effects of higher doses. The results were published in JAMA Oncology.
Erlotinib and other epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) have demonstrated efficacy in elderly patients with EGFR-positive NSCLC, according to study author Shingo Miyamoto, MD, of Japanese Red Cross Medical Center in Tokyo, and colleagues.
“With the increasing number of elderly patients with cancer, many of whom also have significant comorbidities, there is a considerable value in investigating whether EGFR-TKIs are effective for the frail population,” the authors wrote. They also noted that it is “difficult to identify the appropriate dose of molecular-targeted drugs.”
With this in mind, Dr. Miyamoto and colleagues conducted a single-arm, phase 2 trial of low-dose erlotinib in 80 chemotherapy-naive frail or elderly patients with EGFR-positive NSCLC. Frailty was defined by age and the Charlson Comorbidity Index. The patients’ median age was 80 years (range, 49-90 years).
Patients received erlotinib at 50 mg per day, which is one-third of the established maximum tolerated dose, for 4 weeks. Then, they were evaluated with radiologic imaging. Treatment continued until disease progression or unacceptable adverse events. Dosing was modified by treatment response or by adverse events.
Results
At last follow-up, 7 of the 80 patients were still receiving low-dose erlotinib. Reasons for discontinuation were disease progression (n = 60), patient request (n = 6), adverse events (n = 4), and death (n = 3).
The overall response rate was 60%, and the disease control rate was 90%. The researchers measured plasma erlotinib concentration in 48 patients and found it did not correlate with response.
The median progression-free survival was 9.3 months, and the median overall survival was 26.2 months.
Ten patients had erlotinib temporarily suspended because of adverse events. Five patients had their dose reduced to 25 mg because of adverse events, including oral mucositis, paronychia, erythema multiforme, diarrhea, and anorexia.
Two patients discontinued treatment because of adverse events. One patient had a cutaneous ulcer and bone infection. The other had oral mucositis.
Dr. Miyamoto and colleagues concluded that, “low-dose erlotinib was associated with efficacy and safety in frail patients with EGFR mutation–positive lung cancer. More research on the dosing strategy of target-based drugs is warranted, especially in frail patients in the real-world setting.”
Less is more
Sometimes, less can be more, said Mellar P. Davis, MD, an oncologist and section head of the palliative care department at Geisinger Medical System in Danville, Penn., who was not involved in this study.
“Why do patients benefit from small doses? It may be that there are fewer drug interruptions over time and patients are able to stay on schedule,” Dr. Davis said. “It may also be that erlotinib clearance is reduced in the elderly and comorbid patient. The reduced dose may, in fact, be the ‘therapeutic’ dose in this special population.”
Plasma levels were frequently in therapeutic ranges in this study, but patients who had subtherapeutic plasma levels also responded to therapy, Dr. Davis pointed out. The lower dose was shown to maintain sufficient concentrations of the treatment while reducing adverse effects.
However, Dr. Davis noted, this was not a randomized trial. “It is always a risk hedging bets on single-arm trials,” he said. “Randomized trials often prove phase 2 single-arm trials wrong.”
He added that quality-of-life measures are absent from the study. Erlotinib is a palliative drug with side effects, Dr. Davis noted.
“Control of cancer and cancer regression should improve symptoms and quality of life when balanced against treatment toxicity,” he said. “In this study, I would have thought that symptom improvement, performance score, and quality of life would have been the primary outcome or the co-primary outcome with disease control.”
Should a randomized, controlled trial of low-dose erlotinib be conducted in the frail/elderly population? “If one believes trials should be quantitatively based, the answer would be no,” Dr. Davis said. “Responses may be the same, and it would be expensive to prove that low-dose erlotinib is the same as standard doses when comparing survival.”
However, if one is interested in quality of life, particularly in this growing population, a trial that incorporated quality-of-life measures would make more sense, according to Dr. Davis. “For if one can achieve less toxicity and treat more patients and get the same duration of clinical benefit, then less will be more,” he concluded.
Dr. Davis reported having no conflicts of interest. Study authors disclosed relationships with Astellas Pharma, AstraZeneca, Bristol-Myers Squibb, and many other companies. Erlotinib is manufactured for OSI Pharmaceuticals, an affiliate of Astellas Pharma, and distributed by Genentech, a member of the Roche Group.
The study was supported by the Japan Agency for Medical Research and Development.
SOURCE: Miyamoto S et al. JAMA Oncol. 2020 May 14; e201250. doi: 10.1001/jamaoncol.2020.1250.
, according to researchers.
They conducted a phase 2 trial to investigate whether one-third of the maximum tolerated dose of erlotinib could maintain sufficient plasma concentration of the drug while avoiding the adverse effects of higher doses. The results were published in JAMA Oncology.
Erlotinib and other epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) have demonstrated efficacy in elderly patients with EGFR-positive NSCLC, according to study author Shingo Miyamoto, MD, of Japanese Red Cross Medical Center in Tokyo, and colleagues.
“With the increasing number of elderly patients with cancer, many of whom also have significant comorbidities, there is a considerable value in investigating whether EGFR-TKIs are effective for the frail population,” the authors wrote. They also noted that it is “difficult to identify the appropriate dose of molecular-targeted drugs.”
With this in mind, Dr. Miyamoto and colleagues conducted a single-arm, phase 2 trial of low-dose erlotinib in 80 chemotherapy-naive frail or elderly patients with EGFR-positive NSCLC. Frailty was defined by age and the Charlson Comorbidity Index. The patients’ median age was 80 years (range, 49-90 years).
Patients received erlotinib at 50 mg per day, which is one-third of the established maximum tolerated dose, for 4 weeks. Then, they were evaluated with radiologic imaging. Treatment continued until disease progression or unacceptable adverse events. Dosing was modified by treatment response or by adverse events.
Results
At last follow-up, 7 of the 80 patients were still receiving low-dose erlotinib. Reasons for discontinuation were disease progression (n = 60), patient request (n = 6), adverse events (n = 4), and death (n = 3).
The overall response rate was 60%, and the disease control rate was 90%. The researchers measured plasma erlotinib concentration in 48 patients and found it did not correlate with response.
The median progression-free survival was 9.3 months, and the median overall survival was 26.2 months.
Ten patients had erlotinib temporarily suspended because of adverse events. Five patients had their dose reduced to 25 mg because of adverse events, including oral mucositis, paronychia, erythema multiforme, diarrhea, and anorexia.
Two patients discontinued treatment because of adverse events. One patient had a cutaneous ulcer and bone infection. The other had oral mucositis.
Dr. Miyamoto and colleagues concluded that, “low-dose erlotinib was associated with efficacy and safety in frail patients with EGFR mutation–positive lung cancer. More research on the dosing strategy of target-based drugs is warranted, especially in frail patients in the real-world setting.”
Less is more
Sometimes, less can be more, said Mellar P. Davis, MD, an oncologist and section head of the palliative care department at Geisinger Medical System in Danville, Penn., who was not involved in this study.
“Why do patients benefit from small doses? It may be that there are fewer drug interruptions over time and patients are able to stay on schedule,” Dr. Davis said. “It may also be that erlotinib clearance is reduced in the elderly and comorbid patient. The reduced dose may, in fact, be the ‘therapeutic’ dose in this special population.”
Plasma levels were frequently in therapeutic ranges in this study, but patients who had subtherapeutic plasma levels also responded to therapy, Dr. Davis pointed out. The lower dose was shown to maintain sufficient concentrations of the treatment while reducing adverse effects.
However, Dr. Davis noted, this was not a randomized trial. “It is always a risk hedging bets on single-arm trials,” he said. “Randomized trials often prove phase 2 single-arm trials wrong.”
He added that quality-of-life measures are absent from the study. Erlotinib is a palliative drug with side effects, Dr. Davis noted.
“Control of cancer and cancer regression should improve symptoms and quality of life when balanced against treatment toxicity,” he said. “In this study, I would have thought that symptom improvement, performance score, and quality of life would have been the primary outcome or the co-primary outcome with disease control.”
Should a randomized, controlled trial of low-dose erlotinib be conducted in the frail/elderly population? “If one believes trials should be quantitatively based, the answer would be no,” Dr. Davis said. “Responses may be the same, and it would be expensive to prove that low-dose erlotinib is the same as standard doses when comparing survival.”
However, if one is interested in quality of life, particularly in this growing population, a trial that incorporated quality-of-life measures would make more sense, according to Dr. Davis. “For if one can achieve less toxicity and treat more patients and get the same duration of clinical benefit, then less will be more,” he concluded.
Dr. Davis reported having no conflicts of interest. Study authors disclosed relationships with Astellas Pharma, AstraZeneca, Bristol-Myers Squibb, and many other companies. Erlotinib is manufactured for OSI Pharmaceuticals, an affiliate of Astellas Pharma, and distributed by Genentech, a member of the Roche Group.
The study was supported by the Japan Agency for Medical Research and Development.
SOURCE: Miyamoto S et al. JAMA Oncol. 2020 May 14; e201250. doi: 10.1001/jamaoncol.2020.1250.
Oncologists’ income and satisfaction are up
Oncologists continue to rank above the middle range for all specialties in annual compensation for physicians, according to findings from the newly released Medscape Oncologist Compensation Report 2020.
The average earnings for oncologists who participated in the survey was $377,000, which was a 5% increase from the $359,000 reported for 2018.
Just over two-thirds (67%) of oncologists reported that they felt that they were fairly compensated, which is quite a jump from 53% last year.
In addition, oncologists appear to be very satisfied with their profession. Similar to last year’s findings, 84% said they would choose medicine again, and 96% said they would choose the specialty of oncology again.
Earning in top third of all specialties
The average annual earnings reported by oncologists put this specialty in eleventh place among 29 specialties. Orthopedic specialists remain at the head of the list, with estimated earnings of $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according to Medscape’s compensation report, which included responses from 17,461 physicians in over 30 specialties.
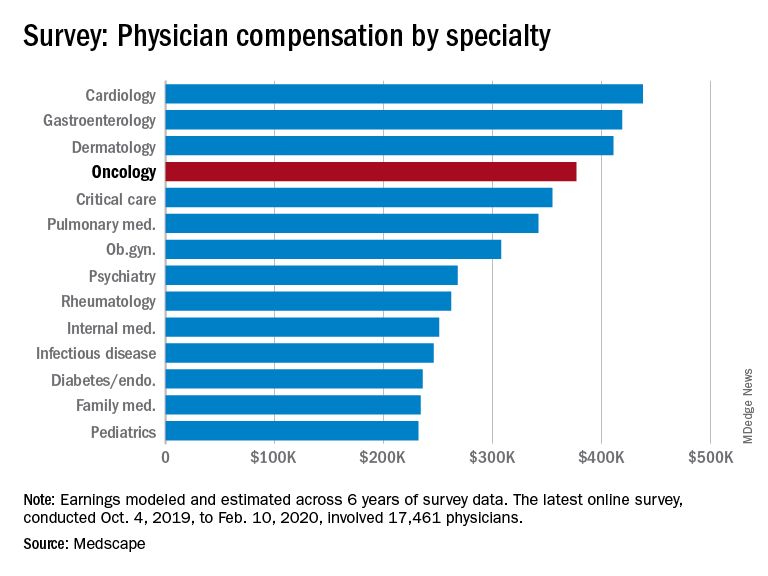
At the bottom of the estimated earnings list were public health and preventive medicine doctors and pediatricians. For both specialties, the reported annual earnings was $232,000. Family medicine specialists were only marginally higher at $234,000.
Radiologists ($427,000), gastroenterologists ($419,000), and urologists ($417,000) all reported higher earnings than oncologists, whereas neurologists, at $280,000, rheumatologists, at $262,000, and internal medicine physicians, at $251,000, earned less.
The report also found that gender disparities in income persist, with male oncologists earning 17% more than their female colleagues. The gender gap in oncology is somewhat less than that seen for all specialties combined, in which men earned 31% more than women, similar to last year’s figure of 33%.
Male oncologists reported spending 38.8 hours per week seeing patients, compared with 34.9 hours reported by female oncologists. This could be a factor contributing to the gender pay disparity. Overall, the average amount of time seeing patients was 37.9 hours per week.
Frustrations with paperwork and denied claims
Surveyed oncologists cited some of the frustrations they are facing, such as spending nearly 17 hours a week on paperwork and administrative tasks. They reported that 16% of claims are denied or have to be resubmitted. As for the most challenging part of the job, oncologists (22%), similar to physicians overall (26%), found that having so many rules and regulations takes first place, followed by working with electronic health record systems (20%), difficulties getting fair reimbursement (19%), having to work long hours (12%), and dealing with difficult patients (8%). Few oncologists were concerned about lawsuits (4%), and 4% reported that there were no challenges.
Oncologists reported that the most rewarding part of their job was gratitude/relationships with patients (31%), followed by knowing that they are making the world a better place (27%). After that, oncologists agreed with statements about being very good at what they do/finding answers/diagnoses (22%), having pride in being a doctor (9%), and making good money at a job they like (8%).
Other key findings
Other key findings from the Medscape Oncologist Compensation Report 2020 included the following:
- Regarding payment models, 80% take insurance, 41% are in fee-for-service arrangements, and 18% are in accountable care organizations (21%). Only 3% are in direct primary care, and 1% are cash-only practices or have a concierge practice.
- 65% of oncologists state that they will continue taking new and current Medicare/Medicaid patients. None said that they would not take on new Medicare/Medicaid patients, and 35% remain undecided. These numbers differed from physicians overall; 73% of all physicians surveyed said they would continue taking new/current Medicare/Medicaid patients, 6% said that will not take on new Medicare patients, and 4% said they will not take new Medicaid patients. In addition, 3% and 2% said that they would stop treating some or all of their Medicare and Medicaid patients, respectively.
- About half (51%) of oncologists use nurse practitioners, about a third (34%) use physician assistants, and 37% use neither. This was about the same as physicians overall.
- A larger percentage of oncologists (38%) expect to participate in MIPS (merit-based incentive payment system), and only 8% expect to participate in APMs (alternative payment models). This was similar to the findings for physicians overall, with more than one-third (37%) expecting to participate in MIPS and 9% planning to take part in APMs.
Impact of COVID-19 pandemic
The Medscape compensation reports also gives a glimpse of the impact the COVID-19 pandemic is having on physician compensation.
Since the beginning of the pandemic, practices have reported a 55% decrease in revenue and a 60% drop in patient volume. Physician practices and hospitals have laid off or furloughed personnel and have cut pay, and 9% of practices have closed their doors, at least for the time being.
A total of 43,000 health care workers were laid off in March, the report notes.
The findings tie in with those reported elsewhere. For example, a survey conducted by the Medical Group Management Association, which was reported by Medscape Medical News, found that 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
Specialties were hard hit, especially those that rely on elective procedures, such as dermatology and cardiology. Oncology care has also been disrupted. For example, a survey conducted by the American Cancer Society Cancer Action Network found that half of the cancer patients and survivors who responded reported changes, delays, or disruptions to the care they were receiving.
This article first appeared on Medscape.com.
Oncologists continue to rank above the middle range for all specialties in annual compensation for physicians, according to findings from the newly released Medscape Oncologist Compensation Report 2020.
The average earnings for oncologists who participated in the survey was $377,000, which was a 5% increase from the $359,000 reported for 2018.
Just over two-thirds (67%) of oncologists reported that they felt that they were fairly compensated, which is quite a jump from 53% last year.
In addition, oncologists appear to be very satisfied with their profession. Similar to last year’s findings, 84% said they would choose medicine again, and 96% said they would choose the specialty of oncology again.
Earning in top third of all specialties
The average annual earnings reported by oncologists put this specialty in eleventh place among 29 specialties. Orthopedic specialists remain at the head of the list, with estimated earnings of $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according to Medscape’s compensation report, which included responses from 17,461 physicians in over 30 specialties.
At the bottom of the estimated earnings list were public health and preventive medicine doctors and pediatricians. For both specialties, the reported annual earnings was $232,000. Family medicine specialists were only marginally higher at $234,000.
Radiologists ($427,000), gastroenterologists ($419,000), and urologists ($417,000) all reported higher earnings than oncologists, whereas neurologists, at $280,000, rheumatologists, at $262,000, and internal medicine physicians, at $251,000, earned less.
The report also found that gender disparities in income persist, with male oncologists earning 17% more than their female colleagues. The gender gap in oncology is somewhat less than that seen for all specialties combined, in which men earned 31% more than women, similar to last year’s figure of 33%.
Male oncologists reported spending 38.8 hours per week seeing patients, compared with 34.9 hours reported by female oncologists. This could be a factor contributing to the gender pay disparity. Overall, the average amount of time seeing patients was 37.9 hours per week.
Frustrations with paperwork and denied claims
Surveyed oncologists cited some of the frustrations they are facing, such as spending nearly 17 hours a week on paperwork and administrative tasks. They reported that 16% of claims are denied or have to be resubmitted. As for the most challenging part of the job, oncologists (22%), similar to physicians overall (26%), found that having so many rules and regulations takes first place, followed by working with electronic health record systems (20%), difficulties getting fair reimbursement (19%), having to work long hours (12%), and dealing with difficult patients (8%). Few oncologists were concerned about lawsuits (4%), and 4% reported that there were no challenges.
Oncologists reported that the most rewarding part of their job was gratitude/relationships with patients (31%), followed by knowing that they are making the world a better place (27%). After that, oncologists agreed with statements about being very good at what they do/finding answers/diagnoses (22%), having pride in being a doctor (9%), and making good money at a job they like (8%).
Other key findings
Other key findings from the Medscape Oncologist Compensation Report 2020 included the following:
- Regarding payment models, 80% take insurance, 41% are in fee-for-service arrangements, and 18% are in accountable care organizations (21%). Only 3% are in direct primary care, and 1% are cash-only practices or have a concierge practice.
- 65% of oncologists state that they will continue taking new and current Medicare/Medicaid patients. None said that they would not take on new Medicare/Medicaid patients, and 35% remain undecided. These numbers differed from physicians overall; 73% of all physicians surveyed said they would continue taking new/current Medicare/Medicaid patients, 6% said that will not take on new Medicare patients, and 4% said they will not take new Medicaid patients. In addition, 3% and 2% said that they would stop treating some or all of their Medicare and Medicaid patients, respectively.
- About half (51%) of oncologists use nurse practitioners, about a third (34%) use physician assistants, and 37% use neither. This was about the same as physicians overall.
- A larger percentage of oncologists (38%) expect to participate in MIPS (merit-based incentive payment system), and only 8% expect to participate in APMs (alternative payment models). This was similar to the findings for physicians overall, with more than one-third (37%) expecting to participate in MIPS and 9% planning to take part in APMs.
Impact of COVID-19 pandemic
The Medscape compensation reports also gives a glimpse of the impact the COVID-19 pandemic is having on physician compensation.
Since the beginning of the pandemic, practices have reported a 55% decrease in revenue and a 60% drop in patient volume. Physician practices and hospitals have laid off or furloughed personnel and have cut pay, and 9% of practices have closed their doors, at least for the time being.
A total of 43,000 health care workers were laid off in March, the report notes.
The findings tie in with those reported elsewhere. For example, a survey conducted by the Medical Group Management Association, which was reported by Medscape Medical News, found that 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
Specialties were hard hit, especially those that rely on elective procedures, such as dermatology and cardiology. Oncology care has also been disrupted. For example, a survey conducted by the American Cancer Society Cancer Action Network found that half of the cancer patients and survivors who responded reported changes, delays, or disruptions to the care they were receiving.
This article first appeared on Medscape.com.
Oncologists continue to rank above the middle range for all specialties in annual compensation for physicians, according to findings from the newly released Medscape Oncologist Compensation Report 2020.
The average earnings for oncologists who participated in the survey was $377,000, which was a 5% increase from the $359,000 reported for 2018.
Just over two-thirds (67%) of oncologists reported that they felt that they were fairly compensated, which is quite a jump from 53% last year.
In addition, oncologists appear to be very satisfied with their profession. Similar to last year’s findings, 84% said they would choose medicine again, and 96% said they would choose the specialty of oncology again.
Earning in top third of all specialties
The average annual earnings reported by oncologists put this specialty in eleventh place among 29 specialties. Orthopedic specialists remain at the head of the list, with estimated earnings of $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according to Medscape’s compensation report, which included responses from 17,461 physicians in over 30 specialties.
At the bottom of the estimated earnings list were public health and preventive medicine doctors and pediatricians. For both specialties, the reported annual earnings was $232,000. Family medicine specialists were only marginally higher at $234,000.
Radiologists ($427,000), gastroenterologists ($419,000), and urologists ($417,000) all reported higher earnings than oncologists, whereas neurologists, at $280,000, rheumatologists, at $262,000, and internal medicine physicians, at $251,000, earned less.
The report also found that gender disparities in income persist, with male oncologists earning 17% more than their female colleagues. The gender gap in oncology is somewhat less than that seen for all specialties combined, in which men earned 31% more than women, similar to last year’s figure of 33%.
Male oncologists reported spending 38.8 hours per week seeing patients, compared with 34.9 hours reported by female oncologists. This could be a factor contributing to the gender pay disparity. Overall, the average amount of time seeing patients was 37.9 hours per week.
Frustrations with paperwork and denied claims
Surveyed oncologists cited some of the frustrations they are facing, such as spending nearly 17 hours a week on paperwork and administrative tasks. They reported that 16% of claims are denied or have to be resubmitted. As for the most challenging part of the job, oncologists (22%), similar to physicians overall (26%), found that having so many rules and regulations takes first place, followed by working with electronic health record systems (20%), difficulties getting fair reimbursement (19%), having to work long hours (12%), and dealing with difficult patients (8%). Few oncologists were concerned about lawsuits (4%), and 4% reported that there were no challenges.
Oncologists reported that the most rewarding part of their job was gratitude/relationships with patients (31%), followed by knowing that they are making the world a better place (27%). After that, oncologists agreed with statements about being very good at what they do/finding answers/diagnoses (22%), having pride in being a doctor (9%), and making good money at a job they like (8%).
Other key findings
Other key findings from the Medscape Oncologist Compensation Report 2020 included the following:
- Regarding payment models, 80% take insurance, 41% are in fee-for-service arrangements, and 18% are in accountable care organizations (21%). Only 3% are in direct primary care, and 1% are cash-only practices or have a concierge practice.
- 65% of oncologists state that they will continue taking new and current Medicare/Medicaid patients. None said that they would not take on new Medicare/Medicaid patients, and 35% remain undecided. These numbers differed from physicians overall; 73% of all physicians surveyed said they would continue taking new/current Medicare/Medicaid patients, 6% said that will not take on new Medicare patients, and 4% said they will not take new Medicaid patients. In addition, 3% and 2% said that they would stop treating some or all of their Medicare and Medicaid patients, respectively.
- About half (51%) of oncologists use nurse practitioners, about a third (34%) use physician assistants, and 37% use neither. This was about the same as physicians overall.
- A larger percentage of oncologists (38%) expect to participate in MIPS (merit-based incentive payment system), and only 8% expect to participate in APMs (alternative payment models). This was similar to the findings for physicians overall, with more than one-third (37%) expecting to participate in MIPS and 9% planning to take part in APMs.
Impact of COVID-19 pandemic
The Medscape compensation reports also gives a glimpse of the impact the COVID-19 pandemic is having on physician compensation.
Since the beginning of the pandemic, practices have reported a 55% decrease in revenue and a 60% drop in patient volume. Physician practices and hospitals have laid off or furloughed personnel and have cut pay, and 9% of practices have closed their doors, at least for the time being.
A total of 43,000 health care workers were laid off in March, the report notes.
The findings tie in with those reported elsewhere. For example, a survey conducted by the Medical Group Management Association, which was reported by Medscape Medical News, found that 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
Specialties were hard hit, especially those that rely on elective procedures, such as dermatology and cardiology. Oncology care has also been disrupted. For example, a survey conducted by the American Cancer Society Cancer Action Network found that half of the cancer patients and survivors who responded reported changes, delays, or disruptions to the care they were receiving.
This article first appeared on Medscape.com.
FDA expands approval of atezolizumab in NSCLC
The Food and Drug Administration has expanded the approved indication for atezolizumab (Tecentriq) in patients with non–small cell lung cancer (NSCLC).

Atezolizumab is now approved as first-line monotherapy for adults with metastatic NSCLC whose tumors are EGFR and ALK wild-type but have high PD-L1 expression (PD-L1 stained ≥50% of tumor cells or PD-L1 stained tumor-infiltrating immune cells covering ≥10% of the tumor area).
The FDA also approved the VENTANA PD-L1 (SP142) Assay as a companion diagnostic to identify patients with NSCLC who are eligible for treatment with atezolizumab.
The drug was evaluated in the IMpower110 trial (NCT02409342), which enrolled patients with stage IV, PD-L1–positive (tumor cells [TC] ≥1% or immune cells [IC] ≥1%) NSCLC who had received no prior chemotherapy for metastatic disease.
The patients were randomized to receive atezolizumab at 1,200 mg every 3 weeks (n = 286) or platinum-based chemotherapy (n = 263), which consisted of carboplatin or cisplatin with either pemetrexed or gemcitabine, until disease progression or unacceptable toxicity.
Overall survival was superior in the atezolizumab arm, but only among patients with high PD-L1 expression (TC ≥50% or IC ≥10%). The median overall survival was 20.2 months among PD-L1–high patients in the atezolizumab arm and 13.1 months among PD-L1–high patients in the chemotherapy arm (hazard ratio, 0.59; P = .0106). There was no significant difference in overall survival between the treatment arms for patients in the other two PD-L1 subgroups – TC ≥5% or IC ≥5% and TC ≥1% or IC ≥1%.
Serious adverse events occurred in 28% of patients receiving atezolizumab. The most frequent of these were pneumonia (2.8%), chronic obstructive pulmonary disease (2.1%), and pneumonitis (2.1%). Fatal adverse events in the atezolizumab arm included unexplained death, aspiration, chronic obstructive pulmonary disease, pulmonary embolism, acute myocardial infarction, cardiac arrest, mechanical ileus, sepsis, cerebral infraction, and device occlusion (one patient each).
For more details on atezolizumab, see the full prescribing information.
The FDA has granted the approval of atezolizumab to Genentech and the approval of the VENTANA PD-L1 (SP142) Assay to Ventana Medical Systems.
The Food and Drug Administration has expanded the approved indication for atezolizumab (Tecentriq) in patients with non–small cell lung cancer (NSCLC).
Atezolizumab is now approved as first-line monotherapy for adults with metastatic NSCLC whose tumors are EGFR and ALK wild-type but have high PD-L1 expression (PD-L1 stained ≥50% of tumor cells or PD-L1 stained tumor-infiltrating immune cells covering ≥10% of the tumor area).
The FDA also approved the VENTANA PD-L1 (SP142) Assay as a companion diagnostic to identify patients with NSCLC who are eligible for treatment with atezolizumab.
The drug was evaluated in the IMpower110 trial (NCT02409342), which enrolled patients with stage IV, PD-L1–positive (tumor cells [TC] ≥1% or immune cells [IC] ≥1%) NSCLC who had received no prior chemotherapy for metastatic disease.
The patients were randomized to receive atezolizumab at 1,200 mg every 3 weeks (n = 286) or platinum-based chemotherapy (n = 263), which consisted of carboplatin or cisplatin with either pemetrexed or gemcitabine, until disease progression or unacceptable toxicity.
Overall survival was superior in the atezolizumab arm, but only among patients with high PD-L1 expression (TC ≥50% or IC ≥10%). The median overall survival was 20.2 months among PD-L1–high patients in the atezolizumab arm and 13.1 months among PD-L1–high patients in the chemotherapy arm (hazard ratio, 0.59; P = .0106). There was no significant difference in overall survival between the treatment arms for patients in the other two PD-L1 subgroups – TC ≥5% or IC ≥5% and TC ≥1% or IC ≥1%.
Serious adverse events occurred in 28% of patients receiving atezolizumab. The most frequent of these were pneumonia (2.8%), chronic obstructive pulmonary disease (2.1%), and pneumonitis (2.1%). Fatal adverse events in the atezolizumab arm included unexplained death, aspiration, chronic obstructive pulmonary disease, pulmonary embolism, acute myocardial infarction, cardiac arrest, mechanical ileus, sepsis, cerebral infraction, and device occlusion (one patient each).
For more details on atezolizumab, see the full prescribing information.
The FDA has granted the approval of atezolizumab to Genentech and the approval of the VENTANA PD-L1 (SP142) Assay to Ventana Medical Systems.
The Food and Drug Administration has expanded the approved indication for atezolizumab (Tecentriq) in patients with non–small cell lung cancer (NSCLC).
Atezolizumab is now approved as first-line monotherapy for adults with metastatic NSCLC whose tumors are EGFR and ALK wild-type but have high PD-L1 expression (PD-L1 stained ≥50% of tumor cells or PD-L1 stained tumor-infiltrating immune cells covering ≥10% of the tumor area).
The FDA also approved the VENTANA PD-L1 (SP142) Assay as a companion diagnostic to identify patients with NSCLC who are eligible for treatment with atezolizumab.
The drug was evaluated in the IMpower110 trial (NCT02409342), which enrolled patients with stage IV, PD-L1–positive (tumor cells [TC] ≥1% or immune cells [IC] ≥1%) NSCLC who had received no prior chemotherapy for metastatic disease.
The patients were randomized to receive atezolizumab at 1,200 mg every 3 weeks (n = 286) or platinum-based chemotherapy (n = 263), which consisted of carboplatin or cisplatin with either pemetrexed or gemcitabine, until disease progression or unacceptable toxicity.
Overall survival was superior in the atezolizumab arm, but only among patients with high PD-L1 expression (TC ≥50% or IC ≥10%). The median overall survival was 20.2 months among PD-L1–high patients in the atezolizumab arm and 13.1 months among PD-L1–high patients in the chemotherapy arm (hazard ratio, 0.59; P = .0106). There was no significant difference in overall survival between the treatment arms for patients in the other two PD-L1 subgroups – TC ≥5% or IC ≥5% and TC ≥1% or IC ≥1%.
Serious adverse events occurred in 28% of patients receiving atezolizumab. The most frequent of these were pneumonia (2.8%), chronic obstructive pulmonary disease (2.1%), and pneumonitis (2.1%). Fatal adverse events in the atezolizumab arm included unexplained death, aspiration, chronic obstructive pulmonary disease, pulmonary embolism, acute myocardial infarction, cardiac arrest, mechanical ileus, sepsis, cerebral infraction, and device occlusion (one patient each).
For more details on atezolizumab, see the full prescribing information.
The FDA has granted the approval of atezolizumab to Genentech and the approval of the VENTANA PD-L1 (SP142) Assay to Ventana Medical Systems.