Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
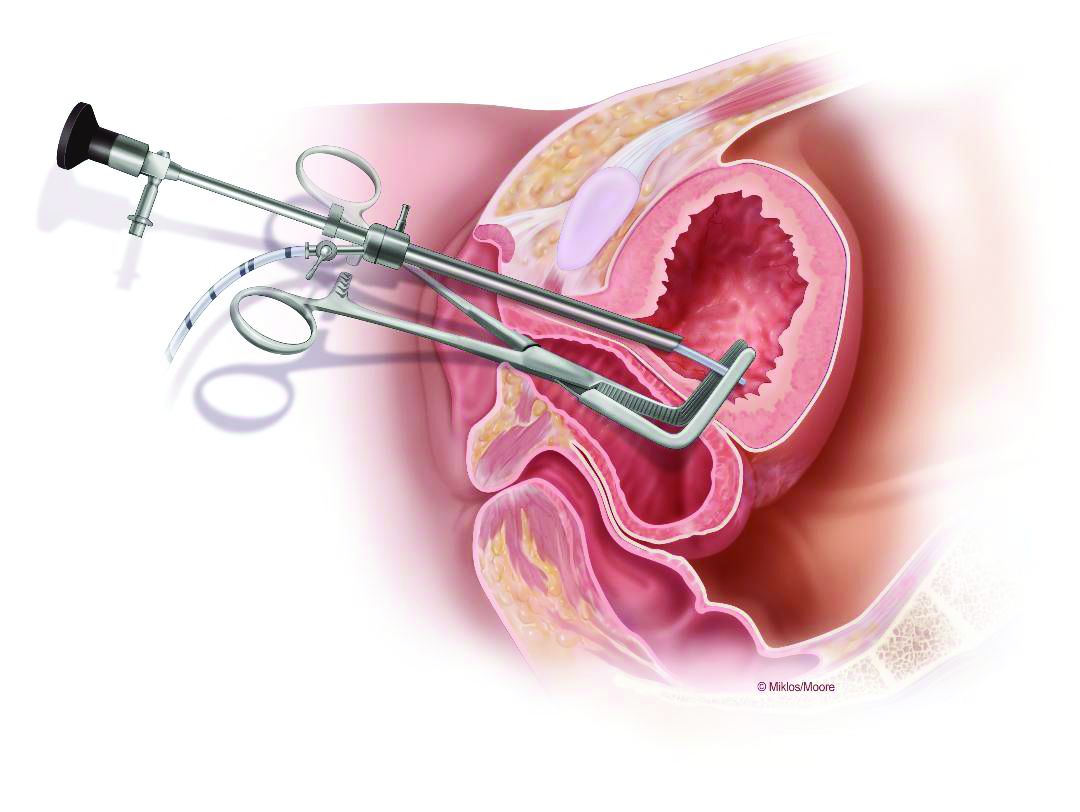
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
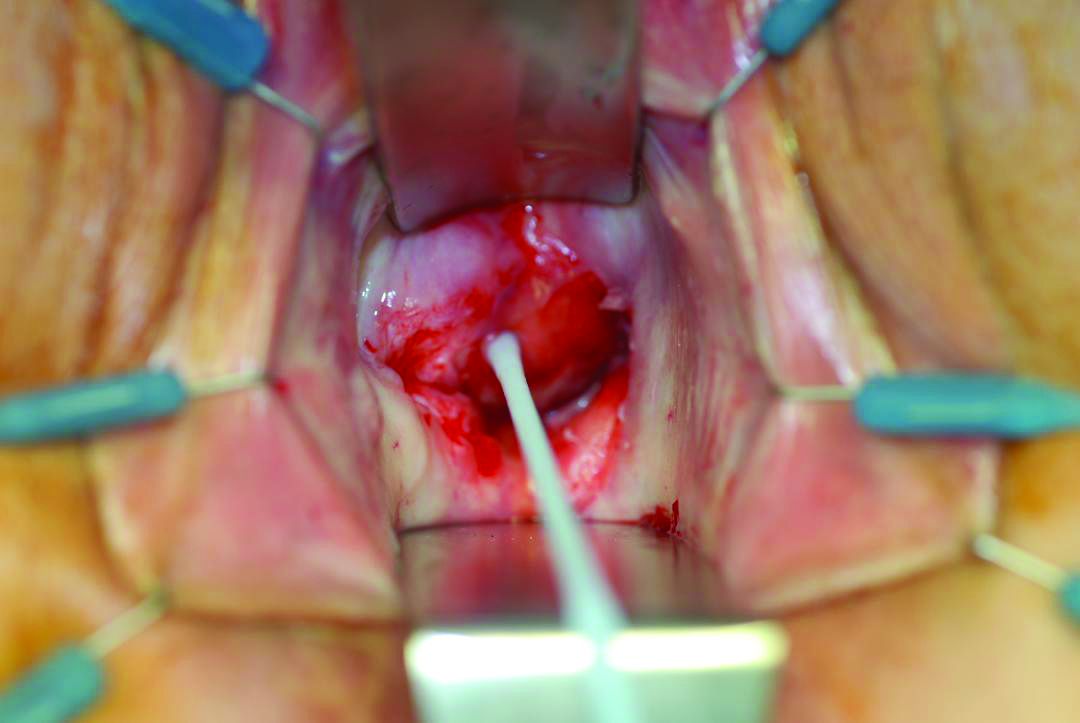
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
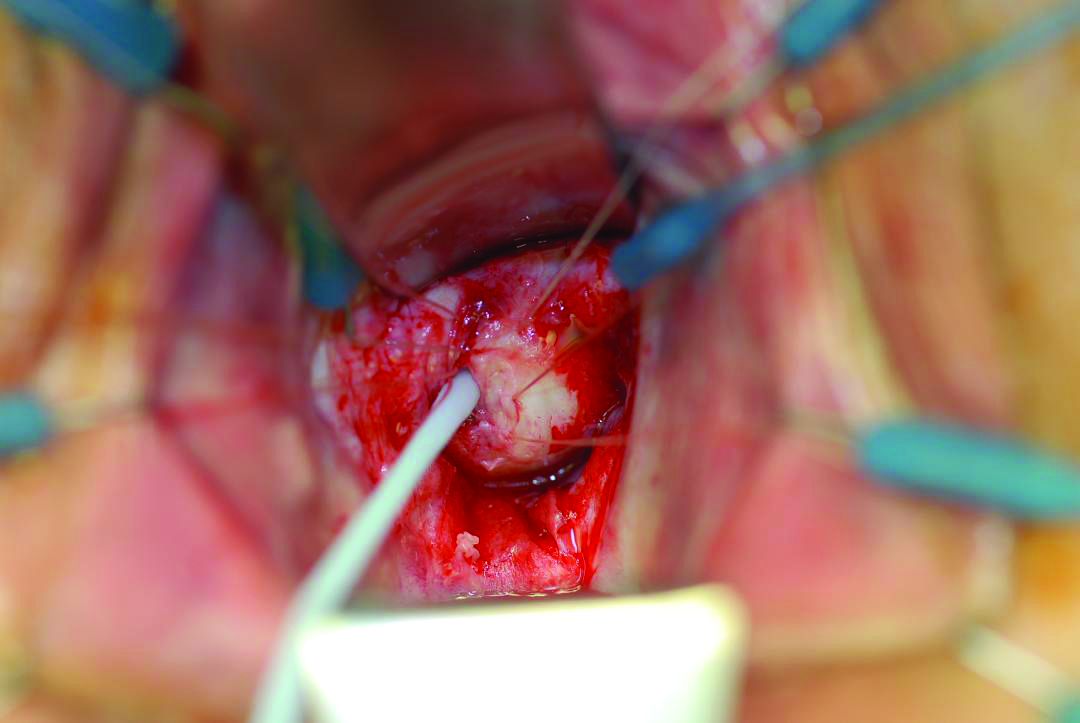
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
When a pediatric patient with acute appendicitis presents at the ED, a pediatric surgeon may not be immediately available to take the case. But a study of 220 children who had emergency appendectomies found only minor differences in outcomes between those operated on by a trauma surgeon and those by a pediatric surgeon.
“These results may be useful in optimizing the surgical workforce to care for a community,” said Derek B. Wall, MD, FACS, and Carlos Ortega, MD, FACS, of NorthShore University HealthSystem in Skokie, Ill. They noted that trauma surgeons in their group were asked to cover appendicitis in children aged 5-10 years because of the surgeons’ in-house availability and because of the difficulty pediatric surgeons often had in getting to the hospital in a timely fashion.
The study was done at Evanston (Ill.) Hospital, a Level 1 trauma center in the northern suburbs of Chicago. This trauma group were all board certified in general surgery, but none had received formal pediatric surgery fellowship training.
The study, published in the Journal of Trauma and Acute Surgery, evaluated appendectomies in children aged 5-10 years from January 2007 to December 2016. A total of 138 were performed by trauma surgeons, while 82 were done by pediatric surgeons. The patients operated on by trauma surgeons were more likely to be female (47% vs. 32%; P = .03), get to surgery more quickly (214 minutes from diagnosis vs. 318 minutes; P = .01), have a laparoscopic operation (70% vs. 55%; P = .04), have a shorter operation (40 minutes vs. 49 minutes; P less than .0001), and leave the hospital sooner (32 hours vs. 41 hours; P less than .0001). They were also more likely to be transferred from an outside hospital (60% vs. 37%; P less than .001) and less likely to be diagnosed without imaging (2% vs. 26%; P less than .0001). The study found no significant differences in complications.
Among the 31 patients who had perforated appendix, the difference in length of stay was even more pronounced: 4 days in the trauma surgery group (n = 21) versus 7.2 days in the pediatric surgery patients.
The investigators explained the rationale for focusing on the population aged 5-10 years: “We focused on a younger, narrower age range than that in previous studies, allowing comparison of outcomes in children of the same age and with equal rates of perforated appendicitis.” They noted that patients younger than age 5 are “well accepted as the domain of the pediatric surgeon,” while children over than 10 are more frequently managed by general surgeons.
At Evanston Hospital, pediatric surgeons had typically performed appendectomy in the targeted age group. But, “they cannot always quickly get to our hospital because of distance and city traffic,” the study authors noted. Therefore, the trauma surgeons were asked to cover for this population group.
They acknowledged the population size of the study was probably too small to identify any significant difference in complication rates between the two surgery groups, especially for patients who had had perforated appendicitis. Also, because of the study’s retrospective nature, most of the pediatric surgery cases were from an earlier period; therefore, later cases may have reflected advances in minimally invasive technology. “Perhaps surgical practice in a more recent time period contributes more to outcomes than specialty,” investigators wrote.
Dr. Wall and Dr. Ortega reported having no financial relationships.
When a pediatric patient with acute appendicitis presents at the ED, a pediatric surgeon may not be immediately available to take the case. But a study of 220 children who had emergency appendectomies found only minor differences in outcomes between those operated on by a trauma surgeon and those by a pediatric surgeon.
“These results may be useful in optimizing the surgical workforce to care for a community,” said Derek B. Wall, MD, FACS, and Carlos Ortega, MD, FACS, of NorthShore University HealthSystem in Skokie, Ill. They noted that trauma surgeons in their group were asked to cover appendicitis in children aged 5-10 years because of the surgeons’ in-house availability and because of the difficulty pediatric surgeons often had in getting to the hospital in a timely fashion.
The study was done at Evanston (Ill.) Hospital, a Level 1 trauma center in the northern suburbs of Chicago. This trauma group were all board certified in general surgery, but none had received formal pediatric surgery fellowship training.
The study, published in the Journal of Trauma and Acute Surgery, evaluated appendectomies in children aged 5-10 years from January 2007 to December 2016. A total of 138 were performed by trauma surgeons, while 82 were done by pediatric surgeons. The patients operated on by trauma surgeons were more likely to be female (47% vs. 32%; P = .03), get to surgery more quickly (214 minutes from diagnosis vs. 318 minutes; P = .01), have a laparoscopic operation (70% vs. 55%; P = .04), have a shorter operation (40 minutes vs. 49 minutes; P less than .0001), and leave the hospital sooner (32 hours vs. 41 hours; P less than .0001). They were also more likely to be transferred from an outside hospital (60% vs. 37%; P less than .001) and less likely to be diagnosed without imaging (2% vs. 26%; P less than .0001). The study found no significant differences in complications.
Among the 31 patients who had perforated appendix, the difference in length of stay was even more pronounced: 4 days in the trauma surgery group (n = 21) versus 7.2 days in the pediatric surgery patients.
The investigators explained the rationale for focusing on the population aged 5-10 years: “We focused on a younger, narrower age range than that in previous studies, allowing comparison of outcomes in children of the same age and with equal rates of perforated appendicitis.” They noted that patients younger than age 5 are “well accepted as the domain of the pediatric surgeon,” while children over than 10 are more frequently managed by general surgeons.
At Evanston Hospital, pediatric surgeons had typically performed appendectomy in the targeted age group. But, “they cannot always quickly get to our hospital because of distance and city traffic,” the study authors noted. Therefore, the trauma surgeons were asked to cover for this population group.
They acknowledged the population size of the study was probably too small to identify any significant difference in complication rates between the two surgery groups, especially for patients who had had perforated appendicitis. Also, because of the study’s retrospective nature, most of the pediatric surgery cases were from an earlier period; therefore, later cases may have reflected advances in minimally invasive technology. “Perhaps surgical practice in a more recent time period contributes more to outcomes than specialty,” investigators wrote.
Dr. Wall and Dr. Ortega reported having no financial relationships.
When a pediatric patient with acute appendicitis presents at the ED, a pediatric surgeon may not be immediately available to take the case. But a study of 220 children who had emergency appendectomies found only minor differences in outcomes between those operated on by a trauma surgeon and those by a pediatric surgeon.
“These results may be useful in optimizing the surgical workforce to care for a community,” said Derek B. Wall, MD, FACS, and Carlos Ortega, MD, FACS, of NorthShore University HealthSystem in Skokie, Ill. They noted that trauma surgeons in their group were asked to cover appendicitis in children aged 5-10 years because of the surgeons’ in-house availability and because of the difficulty pediatric surgeons often had in getting to the hospital in a timely fashion.
The study was done at Evanston (Ill.) Hospital, a Level 1 trauma center in the northern suburbs of Chicago. This trauma group were all board certified in general surgery, but none had received formal pediatric surgery fellowship training.
The study, published in the Journal of Trauma and Acute Surgery, evaluated appendectomies in children aged 5-10 years from January 2007 to December 2016. A total of 138 were performed by trauma surgeons, while 82 were done by pediatric surgeons. The patients operated on by trauma surgeons were more likely to be female (47% vs. 32%; P = .03), get to surgery more quickly (214 minutes from diagnosis vs. 318 minutes; P = .01), have a laparoscopic operation (70% vs. 55%; P = .04), have a shorter operation (40 minutes vs. 49 minutes; P less than .0001), and leave the hospital sooner (32 hours vs. 41 hours; P less than .0001). They were also more likely to be transferred from an outside hospital (60% vs. 37%; P less than .001) and less likely to be diagnosed without imaging (2% vs. 26%; P less than .0001). The study found no significant differences in complications.
Among the 31 patients who had perforated appendix, the difference in length of stay was even more pronounced: 4 days in the trauma surgery group (n = 21) versus 7.2 days in the pediatric surgery patients.
The investigators explained the rationale for focusing on the population aged 5-10 years: “We focused on a younger, narrower age range than that in previous studies, allowing comparison of outcomes in children of the same age and with equal rates of perforated appendicitis.” They noted that patients younger than age 5 are “well accepted as the domain of the pediatric surgeon,” while children over than 10 are more frequently managed by general surgeons.
At Evanston Hospital, pediatric surgeons had typically performed appendectomy in the targeted age group. But, “they cannot always quickly get to our hospital because of distance and city traffic,” the study authors noted. Therefore, the trauma surgeons were asked to cover for this population group.
They acknowledged the population size of the study was probably too small to identify any significant difference in complication rates between the two surgery groups, especially for patients who had had perforated appendicitis. Also, because of the study’s retrospective nature, most of the pediatric surgery cases were from an earlier period; therefore, later cases may have reflected advances in minimally invasive technology. “Perhaps surgical practice in a more recent time period contributes more to outcomes than specialty,” investigators wrote.
Dr. Wall and Dr. Ortega reported having no financial relationships.
Key clinical point: Trauma surgeons performed emergency pediatric appendectomy as well as pediatric surgeons did.
Major finding: Hospital stays averaged 32 and 41 hours for patients treated by trauma surgeons and pediatric surgeons, respectively.
Study details: Retrospective chart review of 220 children aged 5-10 years who had emergency appendectomy at a suburban Level 1 trauma center during 2007-2016.
Disclosures: The investigators reported having no financial relationships.
Source: Wall DB et al. J Trauma Acute Care Surg. 2018:85;118-21.
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
NEW ORLEANS – Comanagement of orthopedic inpatients by an internist or hospitalist can improve outcomes in myriad ways, Mary Anderson Wallace, MD, said at the annual meeting of the American College of Physicians.
She focused on patients undergoing total hip or knee arthroplasty (THA/TKA). In 2014, there were 400,000 of them under Medicare alone, accounting for $7 billion in hospitalization costs and nearly as much again in the cost of related postdischarge care.
Bruce Jancin/MDedge News
Dr. Mary Anderson Wallace So, changes in management that improve key outcomes in this population by even a small increment reap huge benefits when spread across this enormous patient population, noted Dr. Wallace, an internist and hospitalist at the University of Colorado, Denver.
Among the examples she highlighted where comanagement can have a favorable impact were optimization of perioperative pain management pathways; how to handle the use of disease-modifying antirheumatic drugs (DMARDs) in patients undergoing THA/TKA; the latest thinking on the appropriateness of low-dose aspirin for deep vein thrombosis (DVT) prophylaxis; a simple way to predict postop delirium in older individuals without known dementia; how to decide which postoperative fevers warrant a costly infectious disease workup; and the optimal wait time from arrival at the hospital with a fractured hip and THA.
These are all issues where a well-informed internist/hospitalist can be of enormous assistance to a busy orthopedic surgeon in providing high-value care, she explained.
Optimizing perioperative pain management pathways
As of 2015, orthopedists ranked as the third highest prescribers of opioids. Impressively, a retrospective cohort study of 641,941 opioid-naive, privately insured patients undergoing 1 of 11 types of surgery demonstrated that TKA was associated with a 5.1-fold increased risk for subsequent chronic opioid use in the first year after surgery, compared with 18 million opioid-naive nonsurgical controls. Indeed, TKA was the highest-risk of the 11 surgical procedures examined (JAMA Intern Med. 2016 Sep 1;176[9]:1286-93).
Another study that points to a need to develop best practices for opioid prescribing in orthopedic surgery – and other types of surgery as well – was a systematic review of six studies of patients who received prescription opioid analgesics in conjunction with seven types of surgery.
Opioid oversupply was identified as a clear problem: 67%-92% of patients in the six studies reported unused opioids. Up to 71% of opioid tablets went unused, mainly because patients felt they’d achieved adequate pain control and didn’t need them. Rates of safe disposal of unused opioids were in the single digits, suggesting that overprescribing provides a large potential reservoir of opioids that can be diverted to nonmedical use (JAMA Surg. 2017 Nov 1;152[11]:1066-71).
Moreover, a recent retrospective study of more than 1 million opioid-naive patients undergoing surgery showed that 56% of them received postoperative opioids. And each additional week of use was associated with a 44% increase in the relative risk of the composite endpoint of opioid dependence, abuse, or overdose. Duration of opioid use was a stronger predictor of this adverse outcome than was dosage (BMJ. 2018 Jan 17;360:j5790).
Other studies have shown that multimodal analgesia is utilized in only 25%-50% of surgical patients, even though it is considered the standard of care. Only 20% of patients undergoing THA/TKA receive peripheral nerve and neuraxial blocks. So, there is an opportunity for optimization of perioperative pain management pathways in orthopedic surgery patients, including avoidance of unnecessary p.r.n. prescribing, to favorably impact the national opioid epidemic, Dr. Wallace observed.
A surprise benefit of multimodal pain management that includes acetaminophen and a nonsteroidal anti-inflammatory agent is that it markedly reduces the incidence of postoperative fevers after total joint arthroplasty, compared with opioid-based pain management.
That was demonstrated in a retrospective study of 2,417 THA/TKAs in which multimodal pain management was used, and 1,484 procedures that relied on opioid-based pain relief. All of the operations were performed by the same three orthopedic surgeons. Only 5% of patients in the multimodal pain management group developed a fever greater than 38.5 degrees Celsius during the first 5 postoperative days, compared with 25% of those in the opioid-based analgesia group.
Moreover, an infectious disease workup was ordered in 2% of the multimodal analgesia group, versus 10% in the opioid-based pain management cohort, with no difference in the positive workup rates between the two groups (Clin Orthop Relat Res. 2014 May;472[5]:1489-95).
“It’s interesting that multimodal pain management has the side effect of putting you in a better position to practice high-value care, with less fever and fewer infectious disease workups,” Dr. Wallace said.
Perioperative management of DMARDs
Recent joint guidelines from the American College of Rheumatology and American Association of Hip and Knee Surgeons specifically address this issue in patients undergoing elective joint replacement (Arthritis Rheumatol. 2017 Aug;69[8]:1538-51).
“The quality of evidence isn’t high, but at least it’s a starting point,” Dr. Wallace said.
Patients with rheumatoid arthritis, systemic lupus erythematosus, spondyloarthropathies, and other rheumatic diseases who are on methotrexate or other nonbiologic DMARDs should be maintained on their current dose, according to the guidelines.
In contrast, all biologic agents should be withheld prior to surgery, which should be scheduled to coincide with the end of the dosing cycle for that specific biologic. The biologic agent should be resumed only once adequate wound healing has occurred, typically about 14 days post-THA/TKA.
Patients on daily glucocorticoids should continue on their current dose; supraphysiologic stress dosing is to be avoided.
Low-dose aspirin for VTE prophylaxis
“It seems like nothing has been such an enduring controversy in the comanagement literature as the question of whether aspirin is an effective prophylactic agent for prevention of DVT post THA/TKA,” according to Dr. Wallace.
She noted that in the space of just 4 years between the eighth and ninth editions of the American College of Chest Physician guidelines, that organization underwent a 180-degree reversal on the issue – whipsawing from a grade 1A recommendation against aspirin in 2008 to a 1B recommendation for it in 2012.
The literature is increasingly supportive of the use of aspirin for venous thromboembolism (VTE) prophylaxis in low-risk THA/TKA patients. Separate guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the Surgical Care Improvement Project, as well as the chest physicians, support the practice.
The hitch is that there is as yet no single validated risk-stratification protocol. AAOS recommends 325 mg of aspirin twice daily for 6 weeks. But a prospective crossover study of more than 4,600 total joint arthroplasty patients conducted by investigators at Thomas Jefferson University in Philadelphia showed that 81 mg BID for 4 weeks was just as effective as was 325 mg b.i.d., albeit with an incidence of GI bleeding that to their surprise wasn’t significantly lower (J Bone Joint Surg Am. 2017 Jan 18;99[2]:91-8).
Dr. Wallace anticipates definitive answers on VTE prophylaxis to come from the ongoing Patient-Centered Outcomes Research Institute-supported PEPPER (Comparative Effectiveness of Pulmonary Embolism Prevention After Hip and Knee Replacement) trial. In that study, roughly 25,000 patients undergoing THA/TKA are being randomized to prophylactic aspirin at 81 mg b.i.d., warfarin at an International Normalized Ratio of 2.0, or rivaroxaban (Xarelto). Endpoints include mortality, VTE, and bleeding. Results are expected in 2021.
Preoperative prediction of postop delirium
Unrecognized preoperative cognitive impairment in older patients without dementia who are undergoing THA/TKA is a common and powerful risk factor for postop delirium and other complications, as demonstrated recently by investigators at Harvard University and affiliated hospitals.
They had 211 patients aged 65 or older, none with known dementia, take the Mini-Cog screening test prior to their surgery. Fully 24% had probable cognitive impairment as reflected in a score of 2 or less out of a possible 5 points on this simple test, which consists of a three-word recall and clock drawing.
“I was very surprised at this high rate. These are patients who are at risk for delirium in the hospital when you’re taking care of them,” Dr. Wallace observed.
In the Harvard study, the incidence of postop delirium was 21% in patients with a Mini-Cog score of 2 or less, compared with 7% who scored 3-5, for an odds ratio of 4.5 in an age-adjusted multivariate analysis. Moreover, 67% of the low scorers were discharged somewhere other than home, in contrast to 34% of patients with a preop Mini-Cog score of 3-5, for an adjusted 3.9-fold increased risk. The group with a Mini-Cog score of 2 or less also had a significantly longer hospital length of stay (Anesthesiology. 2017 Nov;127[5]:765-74).
Perioperative gabapentin is often added to the medication regimen of older surgical patients to reduce postop delirium. The latest evidence indicates that doesn’t work, as demonstrated in a recent 697-patient randomized trial. The incidence of delirium during the first 3 days post surgery as measured by the Confusion Assessment Method was 22.4% in patients randomized to 900 mg of gabapentin per day, and 20.8% with placebo. Nearly 200 participants had THA or TKA, and in that subgroup, there was an even stronger – albeit still not statistically significant – trend for a higher delirium rate with gabapentin than with placebo (Anesthesiology. 2017 Oct.127[4]:633-44).
“Think twice about adding gabapentin to the pain regimen for THA/TKA/spine patients for the purpose of preventing postop delirium,” she advised.
When is postop fever a concern?
Up to half of patients develop fever early after THA/TKA. In most cases, this is a self-limited ancillary effect of cytokine release, with the temperature peaking on postop day 1-2.
Three strong predictors of a positive infectious disease workup are fever after postop day 3, with an associated 23.3-fold increased risk; multiple days of fever, with an odds ratio of 8.6; and a maximum temperature greater than 39.0 degrees Celsius, with a 2.4-fold increased risk. In this 7-year-old study, the cost of infectious disease workup per change in patient management was a hefty $8,209 (J Arthroplasty. 2010 Sep;25[6 Suppl]:43-8).
A retrospective study of nearly 125,000 THA/TKA patients in the American College of Surgeons National Surgical Quality Improvement Program database has important implications for clinical surveillance for postop adverse events. Stroke occurred early, on median postop day 1. The median time of acute MI and pulmonary embolism was postop day 3, and pneumonia day 4.
The key take-home message was that the median time to DVT was postop day 6, by which point most patients had been discharged. Thus, 60% of postoperative DVTs occurred after discharge. And the time to diagnosis of DVT differed markedly by surgical procedure: The median day of diagnosis was day 5 in TKA patients, compared with day 13 for THA patients. Sixty-eight percent of urinary tract infections occurred post discharge. Sepsis occurred on median day 10 post surgery, surgical site infections on day 17 (Clin Orthop Relat Res. 2017 Dec;475[12]:2952-9).
In light of ever-shortening hospital lengths of stay, Dr. Wallace noted, the findings underscore the importance of comprehensive predischarge patient counseling.
Optimal time window for hip fracture surgery
AAOS guidelines recommend that hip fracture surgery should take place within 48 hours, assuming medical comorbidities are stabilized, because complication rates go up with longer wait times.
But that is controversial. A University of Toronto retrospective cohort study of 42,430 adults with hip fracture treated at 72 Canadian hospitals during 2009-2014 found that the inflection point was 24 hours. Among 13,731 patients whose elapsed time from hospital arrival to surgery was 24 hours or less, 30-day mortality was 5.8%, significantly less than the 6.5% rate in an equal number of propensity score–matched patients with a longer wait time.
The 90- and 365-day mortality rates in the patients who received surgery within 24 hours were 10.7% and 19.3%, both significantly lower than the 12.0% and 21.6% figures in patients with longer wait times.
For the 30-day composite outcome of death, myocardial infarction, pulmonary embolism, DVT, or pneumonia, the rates were 10.1% and 12.2% – again, statistically significant and clinically meaningful. The 90- and 365-day composite outcomes followed suit (JAMA. 2017 Nov 28;318[20]:1994-2003).
But the Canadian study won’t be the final word. The ongoing international multicenter HIP ATTACK (Hip Fracture Accelerated Surgical Treatment and Care Track) trial is comparing outcomes in 3,000 patients randomized to hip fracture surgery within 6 hours versus 24 hours. Endpoints include mortality, myocardial infarction, pulmonary embolism, pneumonia, stroke, sepsis, and life-threatening and major bleeding.
Dr. Wallace reported having no financial conflicts regarding her presentation.
NEW ORLEANS – Comanagement of orthopedic inpatients by an internist or hospitalist can improve outcomes in myriad ways, Mary Anderson Wallace, MD, said at the annual meeting of the American College of Physicians.
She focused on patients undergoing total hip or knee arthroplasty (THA/TKA). In 2014, there were 400,000 of them under Medicare alone, accounting for $7 billion in hospitalization costs and nearly as much again in the cost of related postdischarge care.
Bruce Jancin/MDedge News
Dr. Mary Anderson Wallace So, changes in management that improve key outcomes in this population by even a small increment reap huge benefits when spread across this enormous patient population, noted Dr. Wallace, an internist and hospitalist at the University of Colorado, Denver.
Among the examples she highlighted where comanagement can have a favorable impact were optimization of perioperative pain management pathways; how to handle the use of disease-modifying antirheumatic drugs (DMARDs) in patients undergoing THA/TKA; the latest thinking on the appropriateness of low-dose aspirin for deep vein thrombosis (DVT) prophylaxis; a simple way to predict postop delirium in older individuals without known dementia; how to decide which postoperative fevers warrant a costly infectious disease workup; and the optimal wait time from arrival at the hospital with a fractured hip and THA.
These are all issues where a well-informed internist/hospitalist can be of enormous assistance to a busy orthopedic surgeon in providing high-value care, she explained.
Optimizing perioperative pain management pathways
As of 2015, orthopedists ranked as the third highest prescribers of opioids. Impressively, a retrospective cohort study of 641,941 opioid-naive, privately insured patients undergoing 1 of 11 types of surgery demonstrated that TKA was associated with a 5.1-fold increased risk for subsequent chronic opioid use in the first year after surgery, compared with 18 million opioid-naive nonsurgical controls. Indeed, TKA was the highest-risk of the 11 surgical procedures examined (JAMA Intern Med. 2016 Sep 1;176[9]:1286-93).
Another study that points to a need to develop best practices for opioid prescribing in orthopedic surgery – and other types of surgery as well – was a systematic review of six studies of patients who received prescription opioid analgesics in conjunction with seven types of surgery.
Opioid oversupply was identified as a clear problem: 67%-92% of patients in the six studies reported unused opioids. Up to 71% of opioid tablets went unused, mainly because patients felt they’d achieved adequate pain control and didn’t need them. Rates of safe disposal of unused opioids were in the single digits, suggesting that overprescribing provides a large potential reservoir of opioids that can be diverted to nonmedical use (JAMA Surg. 2017 Nov 1;152[11]:1066-71).
Moreover, a recent retrospective study of more than 1 million opioid-naive patients undergoing surgery showed that 56% of them received postoperative opioids. And each additional week of use was associated with a 44% increase in the relative risk of the composite endpoint of opioid dependence, abuse, or overdose. Duration of opioid use was a stronger predictor of this adverse outcome than was dosage (BMJ. 2018 Jan 17;360:j5790).
Other studies have shown that multimodal analgesia is utilized in only 25%-50% of surgical patients, even though it is considered the standard of care. Only 20% of patients undergoing THA/TKA receive peripheral nerve and neuraxial blocks. So, there is an opportunity for optimization of perioperative pain management pathways in orthopedic surgery patients, including avoidance of unnecessary p.r.n. prescribing, to favorably impact the national opioid epidemic, Dr. Wallace observed.
A surprise benefit of multimodal pain management that includes acetaminophen and a nonsteroidal anti-inflammatory agent is that it markedly reduces the incidence of postoperative fevers after total joint arthroplasty, compared with opioid-based pain management.
That was demonstrated in a retrospective study of 2,417 THA/TKAs in which multimodal pain management was used, and 1,484 procedures that relied on opioid-based pain relief. All of the operations were performed by the same three orthopedic surgeons. Only 5% of patients in the multimodal pain management group developed a fever greater than 38.5 degrees Celsius during the first 5 postoperative days, compared with 25% of those in the opioid-based analgesia group.
Moreover, an infectious disease workup was ordered in 2% of the multimodal analgesia group, versus 10% in the opioid-based pain management cohort, with no difference in the positive workup rates between the two groups (Clin Orthop Relat Res. 2014 May;472[5]:1489-95).
“It’s interesting that multimodal pain management has the side effect of putting you in a better position to practice high-value care, with less fever and fewer infectious disease workups,” Dr. Wallace said.
Perioperative management of DMARDs
Recent joint guidelines from the American College of Rheumatology and American Association of Hip and Knee Surgeons specifically address this issue in patients undergoing elective joint replacement (Arthritis Rheumatol. 2017 Aug;69[8]:1538-51).
“The quality of evidence isn’t high, but at least it’s a starting point,” Dr. Wallace said.
Patients with rheumatoid arthritis, systemic lupus erythematosus, spondyloarthropathies, and other rheumatic diseases who are on methotrexate or other nonbiologic DMARDs should be maintained on their current dose, according to the guidelines.
In contrast, all biologic agents should be withheld prior to surgery, which should be scheduled to coincide with the end of the dosing cycle for that specific biologic. The biologic agent should be resumed only once adequate wound healing has occurred, typically about 14 days post-THA/TKA.
Patients on daily glucocorticoids should continue on their current dose; supraphysiologic stress dosing is to be avoided.
Low-dose aspirin for VTE prophylaxis
“It seems like nothing has been such an enduring controversy in the comanagement literature as the question of whether aspirin is an effective prophylactic agent for prevention of DVT post THA/TKA,” according to Dr. Wallace.
She noted that in the space of just 4 years between the eighth and ninth editions of the American College of Chest Physician guidelines, that organization underwent a 180-degree reversal on the issue – whipsawing from a grade 1A recommendation against aspirin in 2008 to a 1B recommendation for it in 2012.
The literature is increasingly supportive of the use of aspirin for venous thromboembolism (VTE) prophylaxis in low-risk THA/TKA patients. Separate guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the Surgical Care Improvement Project, as well as the chest physicians, support the practice.
The hitch is that there is as yet no single validated risk-stratification protocol. AAOS recommends 325 mg of aspirin twice daily for 6 weeks. But a prospective crossover study of more than 4,600 total joint arthroplasty patients conducted by investigators at Thomas Jefferson University in Philadelphia showed that 81 mg BID for 4 weeks was just as effective as was 325 mg b.i.d., albeit with an incidence of GI bleeding that to their surprise wasn’t significantly lower (J Bone Joint Surg Am. 2017 Jan 18;99[2]:91-8).
Dr. Wallace anticipates definitive answers on VTE prophylaxis to come from the ongoing Patient-Centered Outcomes Research Institute-supported PEPPER (Comparative Effectiveness of Pulmonary Embolism Prevention After Hip and Knee Replacement) trial. In that study, roughly 25,000 patients undergoing THA/TKA are being randomized to prophylactic aspirin at 81 mg b.i.d., warfarin at an International Normalized Ratio of 2.0, or rivaroxaban (Xarelto). Endpoints include mortality, VTE, and bleeding. Results are expected in 2021.
Preoperative prediction of postop delirium
Unrecognized preoperative cognitive impairment in older patients without dementia who are undergoing THA/TKA is a common and powerful risk factor for postop delirium and other complications, as demonstrated recently by investigators at Harvard University and affiliated hospitals.
They had 211 patients aged 65 or older, none with known dementia, take the Mini-Cog screening test prior to their surgery. Fully 24% had probable cognitive impairment as reflected in a score of 2 or less out of a possible 5 points on this simple test, which consists of a three-word recall and clock drawing.
“I was very surprised at this high rate. These are patients who are at risk for delirium in the hospital when you’re taking care of them,” Dr. Wallace observed.
In the Harvard study, the incidence of postop delirium was 21% in patients with a Mini-Cog score of 2 or less, compared with 7% who scored 3-5, for an odds ratio of 4.5 in an age-adjusted multivariate analysis. Moreover, 67% of the low scorers were discharged somewhere other than home, in contrast to 34% of patients with a preop Mini-Cog score of 3-5, for an adjusted 3.9-fold increased risk. The group with a Mini-Cog score of 2 or less also had a significantly longer hospital length of stay (Anesthesiology. 2017 Nov;127[5]:765-74).
Perioperative gabapentin is often added to the medication regimen of older surgical patients to reduce postop delirium. The latest evidence indicates that doesn’t work, as demonstrated in a recent 697-patient randomized trial. The incidence of delirium during the first 3 days post surgery as measured by the Confusion Assessment Method was 22.4% in patients randomized to 900 mg of gabapentin per day, and 20.8% with placebo. Nearly 200 participants had THA or TKA, and in that subgroup, there was an even stronger – albeit still not statistically significant – trend for a higher delirium rate with gabapentin than with placebo (Anesthesiology. 2017 Oct.127[4]:633-44).
“Think twice about adding gabapentin to the pain regimen for THA/TKA/spine patients for the purpose of preventing postop delirium,” she advised.
When is postop fever a concern?
Up to half of patients develop fever early after THA/TKA. In most cases, this is a self-limited ancillary effect of cytokine release, with the temperature peaking on postop day 1-2.
Three strong predictors of a positive infectious disease workup are fever after postop day 3, with an associated 23.3-fold increased risk; multiple days of fever, with an odds ratio of 8.6; and a maximum temperature greater than 39.0 degrees Celsius, with a 2.4-fold increased risk. In this 7-year-old study, the cost of infectious disease workup per change in patient management was a hefty $8,209 (J Arthroplasty. 2010 Sep;25[6 Suppl]:43-8).
A retrospective study of nearly 125,000 THA/TKA patients in the American College of Surgeons National Surgical Quality Improvement Program database has important implications for clinical surveillance for postop adverse events. Stroke occurred early, on median postop day 1. The median time of acute MI and pulmonary embolism was postop day 3, and pneumonia day 4.
The key take-home message was that the median time to DVT was postop day 6, by which point most patients had been discharged. Thus, 60% of postoperative DVTs occurred after discharge. And the time to diagnosis of DVT differed markedly by surgical procedure: The median day of diagnosis was day 5 in TKA patients, compared with day 13 for THA patients. Sixty-eight percent of urinary tract infections occurred post discharge. Sepsis occurred on median day 10 post surgery, surgical site infections on day 17 (Clin Orthop Relat Res. 2017 Dec;475[12]:2952-9).
In light of ever-shortening hospital lengths of stay, Dr. Wallace noted, the findings underscore the importance of comprehensive predischarge patient counseling.
Optimal time window for hip fracture surgery
AAOS guidelines recommend that hip fracture surgery should take place within 48 hours, assuming medical comorbidities are stabilized, because complication rates go up with longer wait times.
But that is controversial. A University of Toronto retrospective cohort study of 42,430 adults with hip fracture treated at 72 Canadian hospitals during 2009-2014 found that the inflection point was 24 hours. Among 13,731 patients whose elapsed time from hospital arrival to surgery was 24 hours or less, 30-day mortality was 5.8%, significantly less than the 6.5% rate in an equal number of propensity score–matched patients with a longer wait time.
The 90- and 365-day mortality rates in the patients who received surgery within 24 hours were 10.7% and 19.3%, both significantly lower than the 12.0% and 21.6% figures in patients with longer wait times.
For the 30-day composite outcome of death, myocardial infarction, pulmonary embolism, DVT, or pneumonia, the rates were 10.1% and 12.2% – again, statistically significant and clinically meaningful. The 90- and 365-day composite outcomes followed suit (JAMA. 2017 Nov 28;318[20]:1994-2003).
But the Canadian study won’t be the final word. The ongoing international multicenter HIP ATTACK (Hip Fracture Accelerated Surgical Treatment and Care Track) trial is comparing outcomes in 3,000 patients randomized to hip fracture surgery within 6 hours versus 24 hours. Endpoints include mortality, myocardial infarction, pulmonary embolism, pneumonia, stroke, sepsis, and life-threatening and major bleeding.
Dr. Wallace reported having no financial conflicts regarding her presentation.
NEW ORLEANS – Comanagement of orthopedic inpatients by an internist or hospitalist can improve outcomes in myriad ways, Mary Anderson Wallace, MD, said at the annual meeting of the American College of Physicians.
She focused on patients undergoing total hip or knee arthroplasty (THA/TKA). In 2014, there were 400,000 of them under Medicare alone, accounting for $7 billion in hospitalization costs and nearly as much again in the cost of related postdischarge care.
Bruce Jancin/MDedge News
Dr. Mary Anderson Wallace So, changes in management that improve key outcomes in this population by even a small increment reap huge benefits when spread across this enormous patient population, noted Dr. Wallace, an internist and hospitalist at the University of Colorado, Denver.
Among the examples she highlighted where comanagement can have a favorable impact were optimization of perioperative pain management pathways; how to handle the use of disease-modifying antirheumatic drugs (DMARDs) in patients undergoing THA/TKA; the latest thinking on the appropriateness of low-dose aspirin for deep vein thrombosis (DVT) prophylaxis; a simple way to predict postop delirium in older individuals without known dementia; how to decide which postoperative fevers warrant a costly infectious disease workup; and the optimal wait time from arrival at the hospital with a fractured hip and THA.
These are all issues where a well-informed internist/hospitalist can be of enormous assistance to a busy orthopedic surgeon in providing high-value care, she explained.
Optimizing perioperative pain management pathways
As of 2015, orthopedists ranked as the third highest prescribers of opioids. Impressively, a retrospective cohort study of 641,941 opioid-naive, privately insured patients undergoing 1 of 11 types of surgery demonstrated that TKA was associated with a 5.1-fold increased risk for subsequent chronic opioid use in the first year after surgery, compared with 18 million opioid-naive nonsurgical controls. Indeed, TKA was the highest-risk of the 11 surgical procedures examined (JAMA Intern Med. 2016 Sep 1;176[9]:1286-93).
Another study that points to a need to develop best practices for opioid prescribing in orthopedic surgery – and other types of surgery as well – was a systematic review of six studies of patients who received prescription opioid analgesics in conjunction with seven types of surgery.
Opioid oversupply was identified as a clear problem: 67%-92% of patients in the six studies reported unused opioids. Up to 71% of opioid tablets went unused, mainly because patients felt they’d achieved adequate pain control and didn’t need them. Rates of safe disposal of unused opioids were in the single digits, suggesting that overprescribing provides a large potential reservoir of opioids that can be diverted to nonmedical use (JAMA Surg. 2017 Nov 1;152[11]:1066-71).
Moreover, a recent retrospective study of more than 1 million opioid-naive patients undergoing surgery showed that 56% of them received postoperative opioids. And each additional week of use was associated with a 44% increase in the relative risk of the composite endpoint of opioid dependence, abuse, or overdose. Duration of opioid use was a stronger predictor of this adverse outcome than was dosage (BMJ. 2018 Jan 17;360:j5790).
Other studies have shown that multimodal analgesia is utilized in only 25%-50% of surgical patients, even though it is considered the standard of care. Only 20% of patients undergoing THA/TKA receive peripheral nerve and neuraxial blocks. So, there is an opportunity for optimization of perioperative pain management pathways in orthopedic surgery patients, including avoidance of unnecessary p.r.n. prescribing, to favorably impact the national opioid epidemic, Dr. Wallace observed.
A surprise benefit of multimodal pain management that includes acetaminophen and a nonsteroidal anti-inflammatory agent is that it markedly reduces the incidence of postoperative fevers after total joint arthroplasty, compared with opioid-based pain management.
That was demonstrated in a retrospective study of 2,417 THA/TKAs in which multimodal pain management was used, and 1,484 procedures that relied on opioid-based pain relief. All of the operations were performed by the same three orthopedic surgeons. Only 5% of patients in the multimodal pain management group developed a fever greater than 38.5 degrees Celsius during the first 5 postoperative days, compared with 25% of those in the opioid-based analgesia group.
Moreover, an infectious disease workup was ordered in 2% of the multimodal analgesia group, versus 10% in the opioid-based pain management cohort, with no difference in the positive workup rates between the two groups (Clin Orthop Relat Res. 2014 May;472[5]:1489-95).
“It’s interesting that multimodal pain management has the side effect of putting you in a better position to practice high-value care, with less fever and fewer infectious disease workups,” Dr. Wallace said.
Perioperative management of DMARDs
Recent joint guidelines from the American College of Rheumatology and American Association of Hip and Knee Surgeons specifically address this issue in patients undergoing elective joint replacement (Arthritis Rheumatol. 2017 Aug;69[8]:1538-51).
“The quality of evidence isn’t high, but at least it’s a starting point,” Dr. Wallace said.
Patients with rheumatoid arthritis, systemic lupus erythematosus, spondyloarthropathies, and other rheumatic diseases who are on methotrexate or other nonbiologic DMARDs should be maintained on their current dose, according to the guidelines.
In contrast, all biologic agents should be withheld prior to surgery, which should be scheduled to coincide with the end of the dosing cycle for that specific biologic. The biologic agent should be resumed only once adequate wound healing has occurred, typically about 14 days post-THA/TKA.
Patients on daily glucocorticoids should continue on their current dose; supraphysiologic stress dosing is to be avoided.
Low-dose aspirin for VTE prophylaxis
“It seems like nothing has been such an enduring controversy in the comanagement literature as the question of whether aspirin is an effective prophylactic agent for prevention of DVT post THA/TKA,” according to Dr. Wallace.
She noted that in the space of just 4 years between the eighth and ninth editions of the American College of Chest Physician guidelines, that organization underwent a 180-degree reversal on the issue – whipsawing from a grade 1A recommendation against aspirin in 2008 to a 1B recommendation for it in 2012.
The literature is increasingly supportive of the use of aspirin for venous thromboembolism (VTE) prophylaxis in low-risk THA/TKA patients. Separate guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the Surgical Care Improvement Project, as well as the chest physicians, support the practice.
The hitch is that there is as yet no single validated risk-stratification protocol. AAOS recommends 325 mg of aspirin twice daily for 6 weeks. But a prospective crossover study of more than 4,600 total joint arthroplasty patients conducted by investigators at Thomas Jefferson University in Philadelphia showed that 81 mg BID for 4 weeks was just as effective as was 325 mg b.i.d., albeit with an incidence of GI bleeding that to their surprise wasn’t significantly lower (J Bone Joint Surg Am. 2017 Jan 18;99[2]:91-8).
Dr. Wallace anticipates definitive answers on VTE prophylaxis to come from the ongoing Patient-Centered Outcomes Research Institute-supported PEPPER (Comparative Effectiveness of Pulmonary Embolism Prevention After Hip and Knee Replacement) trial. In that study, roughly 25,000 patients undergoing THA/TKA are being randomized to prophylactic aspirin at 81 mg b.i.d., warfarin at an International Normalized Ratio of 2.0, or rivaroxaban (Xarelto). Endpoints include mortality, VTE, and bleeding. Results are expected in 2021.
Preoperative prediction of postop delirium
Unrecognized preoperative cognitive impairment in older patients without dementia who are undergoing THA/TKA is a common and powerful risk factor for postop delirium and other complications, as demonstrated recently by investigators at Harvard University and affiliated hospitals.
They had 211 patients aged 65 or older, none with known dementia, take the Mini-Cog screening test prior to their surgery. Fully 24% had probable cognitive impairment as reflected in a score of 2 or less out of a possible 5 points on this simple test, which consists of a three-word recall and clock drawing.
“I was very surprised at this high rate. These are patients who are at risk for delirium in the hospital when you’re taking care of them,” Dr. Wallace observed.
In the Harvard study, the incidence of postop delirium was 21% in patients with a Mini-Cog score of 2 or less, compared with 7% who scored 3-5, for an odds ratio of 4.5 in an age-adjusted multivariate analysis. Moreover, 67% of the low scorers were discharged somewhere other than home, in contrast to 34% of patients with a preop Mini-Cog score of 3-5, for an adjusted 3.9-fold increased risk. The group with a Mini-Cog score of 2 or less also had a significantly longer hospital length of stay (Anesthesiology. 2017 Nov;127[5]:765-74).
Perioperative gabapentin is often added to the medication regimen of older surgical patients to reduce postop delirium. The latest evidence indicates that doesn’t work, as demonstrated in a recent 697-patient randomized trial. The incidence of delirium during the first 3 days post surgery as measured by the Confusion Assessment Method was 22.4% in patients randomized to 900 mg of gabapentin per day, and 20.8% with placebo. Nearly 200 participants had THA or TKA, and in that subgroup, there was an even stronger – albeit still not statistically significant – trend for a higher delirium rate with gabapentin than with placebo (Anesthesiology. 2017 Oct.127[4]:633-44).
“Think twice about adding gabapentin to the pain regimen for THA/TKA/spine patients for the purpose of preventing postop delirium,” she advised.
When is postop fever a concern?
Up to half of patients develop fever early after THA/TKA. In most cases, this is a self-limited ancillary effect of cytokine release, with the temperature peaking on postop day 1-2.
Three strong predictors of a positive infectious disease workup are fever after postop day 3, with an associated 23.3-fold increased risk; multiple days of fever, with an odds ratio of 8.6; and a maximum temperature greater than 39.0 degrees Celsius, with a 2.4-fold increased risk. In this 7-year-old study, the cost of infectious disease workup per change in patient management was a hefty $8,209 (J Arthroplasty. 2010 Sep;25[6 Suppl]:43-8).
A retrospective study of nearly 125,000 THA/TKA patients in the American College of Surgeons National Surgical Quality Improvement Program database has important implications for clinical surveillance for postop adverse events. Stroke occurred early, on median postop day 1. The median time of acute MI and pulmonary embolism was postop day 3, and pneumonia day 4.
The key take-home message was that the median time to DVT was postop day 6, by which point most patients had been discharged. Thus, 60% of postoperative DVTs occurred after discharge. And the time to diagnosis of DVT differed markedly by surgical procedure: The median day of diagnosis was day 5 in TKA patients, compared with day 13 for THA patients. Sixty-eight percent of urinary tract infections occurred post discharge. Sepsis occurred on median day 10 post surgery, surgical site infections on day 17 (Clin Orthop Relat Res. 2017 Dec;475[12]:2952-9).
In light of ever-shortening hospital lengths of stay, Dr. Wallace noted, the findings underscore the importance of comprehensive predischarge patient counseling.
Optimal time window for hip fracture surgery
AAOS guidelines recommend that hip fracture surgery should take place within 48 hours, assuming medical comorbidities are stabilized, because complication rates go up with longer wait times.
But that is controversial. A University of Toronto retrospective cohort study of 42,430 adults with hip fracture treated at 72 Canadian hospitals during 2009-2014 found that the inflection point was 24 hours. Among 13,731 patients whose elapsed time from hospital arrival to surgery was 24 hours or less, 30-day mortality was 5.8%, significantly less than the 6.5% rate in an equal number of propensity score–matched patients with a longer wait time.
The 90- and 365-day mortality rates in the patients who received surgery within 24 hours were 10.7% and 19.3%, both significantly lower than the 12.0% and 21.6% figures in patients with longer wait times.
For the 30-day composite outcome of death, myocardial infarction, pulmonary embolism, DVT, or pneumonia, the rates were 10.1% and 12.2% – again, statistically significant and clinically meaningful. The 90- and 365-day composite outcomes followed suit (JAMA. 2017 Nov 28;318[20]:1994-2003).
But the Canadian study won’t be the final word. The ongoing international multicenter HIP ATTACK (Hip Fracture Accelerated Surgical Treatment and Care Track) trial is comparing outcomes in 3,000 patients randomized to hip fracture surgery within 6 hours versus 24 hours. Endpoints include mortality, myocardial infarction, pulmonary embolism, pneumonia, stroke, sepsis, and life-threatening and major bleeding.
Dr. Wallace reported having no financial conflicts regarding her presentation.
Preoperative opioid use was prevalent in nearly one-quarter of patients undergoing surgery at a large academic medical center, a cross-sectional observational study has determined.
Prescription or illegal opioid use can have profound implications for surgical outcomes and continued postoperative medication abuse. “Preoperative opioid use was associated with a greater burden of comorbid disease and multiple risk factors for poor recovery. ... Opioid-tolerant patients are at risk for opioid-associated adverse events and are less likely to discontinue opioid-based therapy after their surgery,” wrote Paul E. Hilliard, MD, and a team of researchers at the University of Michigan Health System. Although the question of preoperative opioid use has been examined and the Michigan findings are consistent with earlier estimates of prevalence (Ann Surg. 2017;265[4]:695-701), this study sought a more detailed profile of both the characteristics of these patients and the types of procedures correlated with opioid use.
Patient data were derived primarily from two ongoing institutional registries, the Michigan Genomics Initiative and the Analgesic Outcomes Study. Each of these projects involved recruiting nonemergency surgery patients to participate and self-report on pain and affect issues. Opioid use data were extracted from the preop anesthesia history and from physical examination. A total of 34,186 patients were recruited for this study; 54.2% were women, 89.1% were white, and the mean age was 53.1 years. Overall, 23.1% of these patients were taking opioids of various kinds, mostly by prescription along with nonprescription opioids and illegal drugs of other kinds.
The most common opioids found in this patient sample were hydrocodone bitartrate (59.4%), tramadol hydrochloride (21.2%) and oxycodone hydrochloride (18.5%), although the duration or frequency of use was not determined.
“In our experience, in surveys like this patients are pretty honest. [The data do not] track to their medical record, but was done privately for research. That having been said, I am sure there is significant underreporting,” study coauthor Michael J. Englesbe, MD, FACS, said in an interview. In addition to some nondisclosure by study participants, the exclusion of patients admitted to surgery from the ED could mean that 23.1% is a conservative estimate, he noted.
A multivariate analysis of patient characteristics found that age between 31 and 40, tobacco use, heavy alcohol use, pain score, depression, comorbidities reflected in a higher ASA score, and Charlson Comorbidity Score were all significant risk factors for presurgical opiate use.
Patients who were scheduled for surgical procedures involving lower extremities (adjusted odds ratio 3.61, 95% confidence interval, 2.81-4.64) were at the highest risk for opioid use, followed by pelvis surgery, excluding hip (aOR, 3.09, 95% CI, 1.88-5.08), upper arm or elbow (aOR, 3.07, 95% CI, 2.12-4.45), and spine surgery (aOR, 2.68, 95% CI, 2.15-3.32).
The study also broke out the data by presurgery opioid usage and surgery service. Of patients having spine neurosurgery, 55.1% were already taking opioids, and among those having orthopedic spine surgery, 65.1% were taking opioids. General surgery patients were not among those mostly likely to be using opioids (gastrointestinal surgery, 19.3% and endocrine surgery 14.3%). “Certain surgical services may be more likely to encounter patients with high comorbidities for opioid use, and more targeted opioid education strategies aimed at those services may help to mitigate risk in the postoperative period,” the authors wrote.
“All surgeons should take a preop pain history. They should ask about current pain and previous pain experiences. They should also ask about a history of substance use disorder. This should lead into a discussion of the pain expectations from the procedure. Patients should expect to be in pain, that is normal. Pain-free surgery is rare. If a patient has a complex pain history or takes chronic opioids, the surgeon should consider referring them to anesthesia for formal preop pain management planning and potentially weaning of opioid dose prior to elective surgery,” noted Dr. Englesbe, the Cyrenus G. Darling Sr., MD and Cyrenus G Darling Jr., MD Professor of Surgery, and faculty at the Center for Healthcare Outcomes & Policy, University of Michigan, Ann Arbor.
Dr. Michael J. Englesbe
Surgeons are likely to see patients with a past history of opioid dependence or who are recovering from substance abuse. “Every effort should be made to avoid opioids in these patients. We have developed a Pain Optimization Pathway which facilitates no postoperative opioids for these and other patients. These patients are at high risk to relapse and surgeons must know who these patients are so they can provide optimal care,” Dr. Englesbe added.The limitations of this study as reported by the authors include the single-center design, the nondiverse racial makeup of the sample, and the difficulty of ascertaining the dosing and duration of opioid use, both prescription and illegal.
The investigators reported no disclosures relevant to this study. This study was supported by the National Institute on Drug Abuse, National Institutes of Health, the American College of Surgeons, and other noncommercial sources.
Preoperative opioid use was prevalent in nearly one-quarter of patients undergoing surgery at a large academic medical center, a cross-sectional observational study has determined.
Prescription or illegal opioid use can have profound implications for surgical outcomes and continued postoperative medication abuse. “Preoperative opioid use was associated with a greater burden of comorbid disease and multiple risk factors for poor recovery. ... Opioid-tolerant patients are at risk for opioid-associated adverse events and are less likely to discontinue opioid-based therapy after their surgery,” wrote Paul E. Hilliard, MD, and a team of researchers at the University of Michigan Health System. Although the question of preoperative opioid use has been examined and the Michigan findings are consistent with earlier estimates of prevalence (Ann Surg. 2017;265[4]:695-701), this study sought a more detailed profile of both the characteristics of these patients and the types of procedures correlated with opioid use.
Patient data were derived primarily from two ongoing institutional registries, the Michigan Genomics Initiative and the Analgesic Outcomes Study. Each of these projects involved recruiting nonemergency surgery patients to participate and self-report on pain and affect issues. Opioid use data were extracted from the preop anesthesia history and from physical examination. A total of 34,186 patients were recruited for this study; 54.2% were women, 89.1% were white, and the mean age was 53.1 years. Overall, 23.1% of these patients were taking opioids of various kinds, mostly by prescription along with nonprescription opioids and illegal drugs of other kinds.
The most common opioids found in this patient sample were hydrocodone bitartrate (59.4%), tramadol hydrochloride (21.2%) and oxycodone hydrochloride (18.5%), although the duration or frequency of use was not determined.
“In our experience, in surveys like this patients are pretty honest. [The data do not] track to their medical record, but was done privately for research. That having been said, I am sure there is significant underreporting,” study coauthor Michael J. Englesbe, MD, FACS, said in an interview. In addition to some nondisclosure by study participants, the exclusion of patients admitted to surgery from the ED could mean that 23.1% is a conservative estimate, he noted.
A multivariate analysis of patient characteristics found that age between 31 and 40, tobacco use, heavy alcohol use, pain score, depression, comorbidities reflected in a higher ASA score, and Charlson Comorbidity Score were all significant risk factors for presurgical opiate use.
Patients who were scheduled for surgical procedures involving lower extremities (adjusted odds ratio 3.61, 95% confidence interval, 2.81-4.64) were at the highest risk for opioid use, followed by pelvis surgery, excluding hip (aOR, 3.09, 95% CI, 1.88-5.08), upper arm or elbow (aOR, 3.07, 95% CI, 2.12-4.45), and spine surgery (aOR, 2.68, 95% CI, 2.15-3.32).
The study also broke out the data by presurgery opioid usage and surgery service. Of patients having spine neurosurgery, 55.1% were already taking opioids, and among those having orthopedic spine surgery, 65.1% were taking opioids. General surgery patients were not among those mostly likely to be using opioids (gastrointestinal surgery, 19.3% and endocrine surgery 14.3%). “Certain surgical services may be more likely to encounter patients with high comorbidities for opioid use, and more targeted opioid education strategies aimed at those services may help to mitigate risk in the postoperative period,” the authors wrote.
“All surgeons should take a preop pain history. They should ask about current pain and previous pain experiences. They should also ask about a history of substance use disorder. This should lead into a discussion of the pain expectations from the procedure. Patients should expect to be in pain, that is normal. Pain-free surgery is rare. If a patient has a complex pain history or takes chronic opioids, the surgeon should consider referring them to anesthesia for formal preop pain management planning and potentially weaning of opioid dose prior to elective surgery,” noted Dr. Englesbe, the Cyrenus G. Darling Sr., MD and Cyrenus G Darling Jr., MD Professor of Surgery, and faculty at the Center for Healthcare Outcomes & Policy, University of Michigan, Ann Arbor.
Dr. Michael J. Englesbe
Surgeons are likely to see patients with a past history of opioid dependence or who are recovering from substance abuse. “Every effort should be made to avoid opioids in these patients. We have developed a Pain Optimization Pathway which facilitates no postoperative opioids for these and other patients. These patients are at high risk to relapse and surgeons must know who these patients are so they can provide optimal care,” Dr. Englesbe added.The limitations of this study as reported by the authors include the single-center design, the nondiverse racial makeup of the sample, and the difficulty of ascertaining the dosing and duration of opioid use, both prescription and illegal.
The investigators reported no disclosures relevant to this study. This study was supported by the National Institute on Drug Abuse, National Institutes of Health, the American College of Surgeons, and other noncommercial sources.
Preoperative opioid use was prevalent in nearly one-quarter of patients undergoing surgery at a large academic medical center, a cross-sectional observational study has determined.
Prescription or illegal opioid use can have profound implications for surgical outcomes and continued postoperative medication abuse. “Preoperative opioid use was associated with a greater burden of comorbid disease and multiple risk factors for poor recovery. ... Opioid-tolerant patients are at risk for opioid-associated adverse events and are less likely to discontinue opioid-based therapy after their surgery,” wrote Paul E. Hilliard, MD, and a team of researchers at the University of Michigan Health System. Although the question of preoperative opioid use has been examined and the Michigan findings are consistent with earlier estimates of prevalence (Ann Surg. 2017;265[4]:695-701), this study sought a more detailed profile of both the characteristics of these patients and the types of procedures correlated with opioid use.
Patient data were derived primarily from two ongoing institutional registries, the Michigan Genomics Initiative and the Analgesic Outcomes Study. Each of these projects involved recruiting nonemergency surgery patients to participate and self-report on pain and affect issues. Opioid use data were extracted from the preop anesthesia history and from physical examination. A total of 34,186 patients were recruited for this study; 54.2% were women, 89.1% were white, and the mean age was 53.1 years. Overall, 23.1% of these patients were taking opioids of various kinds, mostly by prescription along with nonprescription opioids and illegal drugs of other kinds.
The most common opioids found in this patient sample were hydrocodone bitartrate (59.4%), tramadol hydrochloride (21.2%) and oxycodone hydrochloride (18.5%), although the duration or frequency of use was not determined.
“In our experience, in surveys like this patients are pretty honest. [The data do not] track to their medical record, but was done privately for research. That having been said, I am sure there is significant underreporting,” study coauthor Michael J. Englesbe, MD, FACS, said in an interview. In addition to some nondisclosure by study participants, the exclusion of patients admitted to surgery from the ED could mean that 23.1% is a conservative estimate, he noted.
A multivariate analysis of patient characteristics found that age between 31 and 40, tobacco use, heavy alcohol use, pain score, depression, comorbidities reflected in a higher ASA score, and Charlson Comorbidity Score were all significant risk factors for presurgical opiate use.
Patients who were scheduled for surgical procedures involving lower extremities (adjusted odds ratio 3.61, 95% confidence interval, 2.81-4.64) were at the highest risk for opioid use, followed by pelvis surgery, excluding hip (aOR, 3.09, 95% CI, 1.88-5.08), upper arm or elbow (aOR, 3.07, 95% CI, 2.12-4.45), and spine surgery (aOR, 2.68, 95% CI, 2.15-3.32).
The study also broke out the data by presurgery opioid usage and surgery service. Of patients having spine neurosurgery, 55.1% were already taking opioids, and among those having orthopedic spine surgery, 65.1% were taking opioids. General surgery patients were not among those mostly likely to be using opioids (gastrointestinal surgery, 19.3% and endocrine surgery 14.3%). “Certain surgical services may be more likely to encounter patients with high comorbidities for opioid use, and more targeted opioid education strategies aimed at those services may help to mitigate risk in the postoperative period,” the authors wrote.
“All surgeons should take a preop pain history. They should ask about current pain and previous pain experiences. They should also ask about a history of substance use disorder. This should lead into a discussion of the pain expectations from the procedure. Patients should expect to be in pain, that is normal. Pain-free surgery is rare. If a patient has a complex pain history or takes chronic opioids, the surgeon should consider referring them to anesthesia for formal preop pain management planning and potentially weaning of opioid dose prior to elective surgery,” noted Dr. Englesbe, the Cyrenus G. Darling Sr., MD and Cyrenus G Darling Jr., MD Professor of Surgery, and faculty at the Center for Healthcare Outcomes & Policy, University of Michigan, Ann Arbor.
Dr. Michael J. Englesbe
Surgeons are likely to see patients with a past history of opioid dependence or who are recovering from substance abuse. “Every effort should be made to avoid opioids in these patients. We have developed a Pain Optimization Pathway which facilitates no postoperative opioids for these and other patients. These patients are at high risk to relapse and surgeons must know who these patients are so they can provide optimal care,” Dr. Englesbe added.The limitations of this study as reported by the authors include the single-center design, the nondiverse racial makeup of the sample, and the difficulty of ascertaining the dosing and duration of opioid use, both prescription and illegal.
The investigators reported no disclosures relevant to this study. This study was supported by the National Institute on Drug Abuse, National Institutes of Health, the American College of Surgeons, and other noncommercial sources.
Key clinical point: Preoperative opioid use is prevalent in patients who are having spinal surgery and have depression.
Major finding: Nearly one-quarter of surgical patients are taking opioids before surgery.
Study details: An observational study of 34,186 surgical patients in the University of Michigan Health system.
Disclosures: The investigators reported no disclosures relevant to this study. This study was supported by the National Institute on Drug Abuse, National Institutes of Health, the American College of Surgeons, and other noncommercial sources.
Source: Hilliard P E et al. JAMA Surg. 2018 Jul 11;. doi:10.1001/jamasurg.2018.2102.
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
Nearly three-quarters of opioid-related adverse events seen in children were related to therapeutic opioid use, based on data from more than a million prescriptions.
BackyardProduction/Thinkstock
Prescription of opioids to children for outpatient conditions may have risen along with the increased opioid prescriptions for adults, but most of the literature focuses on opioid toxicity in children, and “the incidence of adverse opioid effects for children during appropriate medical use for relatively minor conditions is unknown,” wrote Cecilia P. Chung, MD, of Vanderbilt University in Nashville, Tenn., and her colleagues.
In a retrospective study published in Pediatrics, the researchers reviewed data from 401,972 children and adolescents aged 2-17 years with no chronic or severe conditions. The patients filled a total of 1,362,503 prescriptions for opioids, with a mean 15% filling one or more opioid prescriptions a year, and 1 in every 2,611 prescriptions was followed by an emergency department visit, hospitalization, or death related to an adverse event associated with opioid use.
Approximately 20% of the prescriptions were for children aged 2-5 years, 28% for ages 6-11 years, and 52% for ages 12-17 years. The patients were enrolled in Medicaid between Jan. 1, 1999, and Dec. 31, 2014, in Tennessee, and were seen at outpatient centers. Dental procedures were the most common reasons for opioid prescriptions in the study population (31%), followed by outpatient procedures or surgeries (25%), trauma (18%), and infections (16%).
Overall, 437 cases of opioid-related adverse events were confirmed by medical record review; 89% of these were deemed related to the prescription, and 71% were related to proper therapeutic use, the researchers said. The remainder were considered to be related to unintentional overdose, abuse, self-harm, or the circumstances were not indicated.
The opioid-related symptoms most frequently were gastrointestinal, neuropsychiatric, dermatologic, and central nervous system depression.
“The incidence of opioid-related adverse events increased for children and adolescents 12-17 years of age, during current opioid use, and with higher opioid doses,” the researchers said.
The study findings were limited by several factors including the use of Medicaid patients only, the lack of clinical details such as patient weight, and the potential for incomplete medical records, Dr. Chung and her associates noted. However, the results support the need for more comprehensive guidelines in treating acute, self-limited conditions in children to reduce unnecessary opioid exposure, they said.
The researchers had no relevant financial conflicts to disclose. The study was supported by the Eunice Kennedy Shriver National Institute for Child Health and Human Development and funded by the National Institutes of Health. Dr. Chung received grant support from the National Institutes of Health and the Rheumatology Research Foundation Career Development Research K-supplement.
“We know that opioids are associated with many untoward side effects and are potentially lethal. But we believe there is a reason why opioids have been used to treat pain since the Sumerians 5,000 years ago,” Elliot J. Krane, MD, Steven J. Weisman, MD, and Gary A. Walco, PhD, wrote in an accompanying editorial.
The editorialists noted that they are not blanket advocates of opioid prescriptions for children, but they do believe in the importance of pain management for conditions including postsurgical pain, burns, physical trauma, and medical illnesses. In many cases, opioids are the most effective treatment option.
In addition, data on opioid-related deaths in the United States have been shown inaccurate for various reasons including the coding of deaths as opioid related if opioids were present among a number of other drugs, even if the cause of death was another substance or an act such as suicide, the writers noted. Even the Centers for Disease Control and Prevention has admitted overestimating the prevalence of opioid-related deaths by as much as 100%. Consequently, the opioid epidemic portrayed in the media, “pales in comparison with other public health hazards and causes of deaths in America such as tobacco-related deaths, alcoholic hepatic disease, and even hospital-acquired infections,” Dr. Krane, Dr. Weisman, and Dr. Walco said.
“The data as presented cannot be considered causal for associating opioid prescribing with severe morbidity, more hospital emergency department visits, and even death,” the editorialists concluded. They emphasized the need for good judgment on the part of clinicians when prescribing opioids to children and advocated always making good use of nonopioid alternatives, but Dr. Krane, Dr. Weisman, and Dr. Walco added that the findings of this study should not deter doctors from prescribing an opioid when they think it is the most effective and appropriate option for moderately to severely painful conditions.
“Too often, consideration of the need to prevent and treat pain can be lost in the national discussion,” they said.
Dr. Krane is affiliated with Stanford University in Palo Alto, Calif., Dr. Weisman is affiliated with the Medical College of Milwaukee, Wisc., and Dr. Walco is affiliated with the University of Washington, Seattle. Dr. Krane disclosed consulting for Collegium Pharmaceuticals and honoraria for lecturing on pain and analgesia. Dr. Weisman disclosed consulting for Grünenthal Pharmaceuticals and Pfizer Pharmaceuticals and has conducted clinical trials for Grünenthal Pharmaceuticals, Cadence Pharmaceuticals, and The Medicines Company. Their editorial accompanying the article by Chung et al. appeared in Pediatrics (2018 Jul 16. doi: 10.1542/peds.2018-1623).
“We know that opioids are associated with many untoward side effects and are potentially lethal. But we believe there is a reason why opioids have been used to treat pain since the Sumerians 5,000 years ago,” Elliot J. Krane, MD, Steven J. Weisman, MD, and Gary A. Walco, PhD, wrote in an accompanying editorial.
The editorialists noted that they are not blanket advocates of opioid prescriptions for children, but they do believe in the importance of pain management for conditions including postsurgical pain, burns, physical trauma, and medical illnesses. In many cases, opioids are the most effective treatment option.
In addition, data on opioid-related deaths in the United States have been shown inaccurate for various reasons including the coding of deaths as opioid related if opioids were present among a number of other drugs, even if the cause of death was another substance or an act such as suicide, the writers noted. Even the Centers for Disease Control and Prevention has admitted overestimating the prevalence of opioid-related deaths by as much as 100%. Consequently, the opioid epidemic portrayed in the media, “pales in comparison with other public health hazards and causes of deaths in America such as tobacco-related deaths, alcoholic hepatic disease, and even hospital-acquired infections,” Dr. Krane, Dr. Weisman, and Dr. Walco said.
“The data as presented cannot be considered causal for associating opioid prescribing with severe morbidity, more hospital emergency department visits, and even death,” the editorialists concluded. They emphasized the need for good judgment on the part of clinicians when prescribing opioids to children and advocated always making good use of nonopioid alternatives, but Dr. Krane, Dr. Weisman, and Dr. Walco added that the findings of this study should not deter doctors from prescribing an opioid when they think it is the most effective and appropriate option for moderately to severely painful conditions.
“Too often, consideration of the need to prevent and treat pain can be lost in the national discussion,” they said.
Dr. Krane is affiliated with Stanford University in Palo Alto, Calif., Dr. Weisman is affiliated with the Medical College of Milwaukee, Wisc., and Dr. Walco is affiliated with the University of Washington, Seattle. Dr. Krane disclosed consulting for Collegium Pharmaceuticals and honoraria for lecturing on pain and analgesia. Dr. Weisman disclosed consulting for Grünenthal Pharmaceuticals and Pfizer Pharmaceuticals and has conducted clinical trials for Grünenthal Pharmaceuticals, Cadence Pharmaceuticals, and The Medicines Company. Their editorial accompanying the article by Chung et al. appeared in Pediatrics (2018 Jul 16. doi: 10.1542/peds.2018-1623).
Body
“We know that opioids are associated with many untoward side effects and are potentially lethal. But we believe there is a reason why opioids have been used to treat pain since the Sumerians 5,000 years ago,” Elliot J. Krane, MD, Steven J. Weisman, MD, and Gary A. Walco, PhD, wrote in an accompanying editorial.
The editorialists noted that they are not blanket advocates of opioid prescriptions for children, but they do believe in the importance of pain management for conditions including postsurgical pain, burns, physical trauma, and medical illnesses. In many cases, opioids are the most effective treatment option.
In addition, data on opioid-related deaths in the United States have been shown inaccurate for various reasons including the coding of deaths as opioid related if opioids were present among a number of other drugs, even if the cause of death was another substance or an act such as suicide, the writers noted. Even the Centers for Disease Control and Prevention has admitted overestimating the prevalence of opioid-related deaths by as much as 100%. Consequently, the opioid epidemic portrayed in the media, “pales in comparison with other public health hazards and causes of deaths in America such as tobacco-related deaths, alcoholic hepatic disease, and even hospital-acquired infections,” Dr. Krane, Dr. Weisman, and Dr. Walco said.
“The data as presented cannot be considered causal for associating opioid prescribing with severe morbidity, more hospital emergency department visits, and even death,” the editorialists concluded. They emphasized the need for good judgment on the part of clinicians when prescribing opioids to children and advocated always making good use of nonopioid alternatives, but Dr. Krane, Dr. Weisman, and Dr. Walco added that the findings of this study should not deter doctors from prescribing an opioid when they think it is the most effective and appropriate option for moderately to severely painful conditions.
“Too often, consideration of the need to prevent and treat pain can be lost in the national discussion,” they said.
Dr. Krane is affiliated with Stanford University in Palo Alto, Calif., Dr. Weisman is affiliated with the Medical College of Milwaukee, Wisc., and Dr. Walco is affiliated with the University of Washington, Seattle. Dr. Krane disclosed consulting for Collegium Pharmaceuticals and honoraria for lecturing on pain and analgesia. Dr. Weisman disclosed consulting for Grünenthal Pharmaceuticals and Pfizer Pharmaceuticals and has conducted clinical trials for Grünenthal Pharmaceuticals, Cadence Pharmaceuticals, and The Medicines Company. Their editorial accompanying the article by Chung et al. appeared in Pediatrics (2018 Jul 16. doi: 10.1542/peds.2018-1623).
Title
Pain relief may outweigh side effects in pediatric opioid use
Pain relief may outweigh side effects in pediatric opioid use
Nearly three-quarters of opioid-related adverse events seen in children were related to therapeutic opioid use, based on data from more than a million prescriptions.
BackyardProduction/Thinkstock
Prescription of opioids to children for outpatient conditions may have risen along with the increased opioid prescriptions for adults, but most of the literature focuses on opioid toxicity in children, and “the incidence of adverse opioid effects for children during appropriate medical use for relatively minor conditions is unknown,” wrote Cecilia P. Chung, MD, of Vanderbilt University in Nashville, Tenn., and her colleagues.
In a retrospective study published in Pediatrics, the researchers reviewed data from 401,972 children and adolescents aged 2-17 years with no chronic or severe conditions. The patients filled a total of 1,362,503 prescriptions for opioids, with a mean 15% filling one or more opioid prescriptions a year, and 1 in every 2,611 prescriptions was followed by an emergency department visit, hospitalization, or death related to an adverse event associated with opioid use.
Approximately 20% of the prescriptions were for children aged 2-5 years, 28% for ages 6-11 years, and 52% for ages 12-17 years. The patients were enrolled in Medicaid between Jan. 1, 1999, and Dec. 31, 2014, in Tennessee, and were seen at outpatient centers. Dental procedures were the most common reasons for opioid prescriptions in the study population (31%), followed by outpatient procedures or surgeries (25%), trauma (18%), and infections (16%).
Overall, 437 cases of opioid-related adverse events were confirmed by medical record review; 89% of these were deemed related to the prescription, and 71% were related to proper therapeutic use, the researchers said. The remainder were considered to be related to unintentional overdose, abuse, self-harm, or the circumstances were not indicated.
The opioid-related symptoms most frequently were gastrointestinal, neuropsychiatric, dermatologic, and central nervous system depression.
“The incidence of opioid-related adverse events increased for children and adolescents 12-17 years of age, during current opioid use, and with higher opioid doses,” the researchers said.
The study findings were limited by several factors including the use of Medicaid patients only, the lack of clinical details such as patient weight, and the potential for incomplete medical records, Dr. Chung and her associates noted. However, the results support the need for more comprehensive guidelines in treating acute, self-limited conditions in children to reduce unnecessary opioid exposure, they said.
The researchers had no relevant financial conflicts to disclose. The study was supported by the Eunice Kennedy Shriver National Institute for Child Health and Human Development and funded by the National Institutes of Health. Dr. Chung received grant support from the National Institutes of Health and the Rheumatology Research Foundation Career Development Research K-supplement.
Nearly three-quarters of opioid-related adverse events seen in children were related to therapeutic opioid use, based on data from more than a million prescriptions.
BackyardProduction/Thinkstock
Prescription of opioids to children for outpatient conditions may have risen along with the increased opioid prescriptions for adults, but most of the literature focuses on opioid toxicity in children, and “the incidence of adverse opioid effects for children during appropriate medical use for relatively minor conditions is unknown,” wrote Cecilia P. Chung, MD, of Vanderbilt University in Nashville, Tenn., and her colleagues.
In a retrospective study published in Pediatrics, the researchers reviewed data from 401,972 children and adolescents aged 2-17 years with no chronic or severe conditions. The patients filled a total of 1,362,503 prescriptions for opioids, with a mean 15% filling one or more opioid prescriptions a year, and 1 in every 2,611 prescriptions was followed by an emergency department visit, hospitalization, or death related to an adverse event associated with opioid use.
Approximately 20% of the prescriptions were for children aged 2-5 years, 28% for ages 6-11 years, and 52% for ages 12-17 years. The patients were enrolled in Medicaid between Jan. 1, 1999, and Dec. 31, 2014, in Tennessee, and were seen at outpatient centers. Dental procedures were the most common reasons for opioid prescriptions in the study population (31%), followed by outpatient procedures or surgeries (25%), trauma (18%), and infections (16%).
Overall, 437 cases of opioid-related adverse events were confirmed by medical record review; 89% of these were deemed related to the prescription, and 71% were related to proper therapeutic use, the researchers said. The remainder were considered to be related to unintentional overdose, abuse, self-harm, or the circumstances were not indicated.
The opioid-related symptoms most frequently were gastrointestinal, neuropsychiatric, dermatologic, and central nervous system depression.
“The incidence of opioid-related adverse events increased for children and adolescents 12-17 years of age, during current opioid use, and with higher opioid doses,” the researchers said.
The study findings were limited by several factors including the use of Medicaid patients only, the lack of clinical details such as patient weight, and the potential for incomplete medical records, Dr. Chung and her associates noted. However, the results support the need for more comprehensive guidelines in treating acute, self-limited conditions in children to reduce unnecessary opioid exposure, they said.
The researchers had no relevant financial conflicts to disclose. The study was supported by the Eunice Kennedy Shriver National Institute for Child Health and Human Development and funded by the National Institutes of Health. Dr. Chung received grant support from the National Institutes of Health and the Rheumatology Research Foundation Career Development Research K-supplement.
Key clinical point: One in every 2,611 opioid prescriptions in children and teens was followed by an ED visit, hospitalization, or death related to an adverse event associated with opioid use.
Major finding: A total of 437 cases of opioid-related adverse events were confirmed; most were associated with therapeutic medication use.
Study details: The data come from a retrospective cohort study of 401,972 children aged 2-17 years enrolled in Medicaid between Jan. 1, 1999, and Dec. 31, 2014.
Disclosures: The researchers had no relevant financial conflicts to disclose. The study was supported by the Eunice Kennedy Shriver National Institute for Child Health and Human Development, and funded by the National Institutes of Health. Dr. Chung received grant support from the National Institutes of Health and the Rheumatology Research Foundation Career Development Research K-supplement.
Source: Chung C et al. Pediatrics. 2018 Jul 16. doi: 10.1542/peds.2017-2156
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
In this Update I highlight 5 interesting investigations on infectious diseases. The first addresses the value of applying prophylactically a negative-pressure wound dressing to prevent surgical site infection (SSI) in obese women having cesarean delivery (CD). The second report assesses the effectiveness of a preoperative vaginal wash in reducing the frequency of postcesarean endometritis. The third investigation examines the role of systemic antibiotics, combined with surgical drainage, for patients who have subcutaneous abscesses ranging in size up to 5 cm. The fourth study presents new information about the major risk factors for Clostridium difficile infections in obstetric patients. The final study presents valuable sobering new data about the risks of congenital Zika virus infection.
Negative-pressure wound therapy after CD shows some benefit in preventing SSI
Yu L, Kronen RJ, Simon LE, Stoll CR, Colditz GA, Tuuli MG. Prophylactic negative-pressure wound therapy after cesarean is associated with reduced risk of surgical site infection: a systematic review and meta-analysis. Am J Obstet Gynecol. 2018;218(2):200-210.e1.
Illustration: Used with permission. Courtesy of KCI, an Acelity Company
Yu and colleagues sought to determine if the prophylactic use of negative-pressure devices, compared with standard wound dressing, was effective in reducing the frequency of SSI after CD.
The authors searched multiple databases and initially identified 161 randomized controlled trials and cohort studies for further assessment. After applying rigorous exclusion criteria, they ultimately selected 9 studies for systematic review and meta-analysis. Six studies were randomized controlled trials (RCTs), 2 were retrospective cohort studies, and 1 was a prospective cohort study. Five studies were considered high quality; 4 were of low quality.
Details of the study
Several types of negative-pressure devices were used, but the 2 most common were the Prevena incision management system (KCI, San Antonio, Texas) and PICO negative- pressure wound therapy (Smith & Nephew, St. Petersburg, Florida). The majority of patients in all groups were at high risk for wound complications because of obesity.
The primary outcome of interest was the frequency of SSI. Secondary outcomes included dehiscence, seroma, endometritis, a composite measure for all wound complications, and hospital readmission.
The absolute risk of SSI in the intervention group was 5% (95% confidence interval [CI], 2.0%-7.0%) compared with 11% (95% CI, 7.0%-16.0%) in the standard dressing group. The pooled risk ratio was 0.45 (95% CI, 0.31-0.66). The absolute risk reduction was 6% (95% CI, -10.0% to -3.0%), and the number needed to treat was 17.
There were no significant differences in the rate of any of the secondary outcomes other than the composite of all wound complications. This difference was largely accounted for by the difference in the rate of SSI.
Illustration: Used with permission. Courtesy of KCI, an Acelity Company
Passive wound closure (left) compared with negative-pressure wound therapy with the Prevena incision management system (right).
How negative-pressure devices aid wound healing
Yu and colleagues explained that negative-pressure devices exert their beneficial effects in various ways, including:
shrinking the wound
inducing cellular stretch
removing extracellular fluids
creating a favorable environment for healing
promoting angiogenesis and neurogenesis.
Multiple studies in nonobstetric patients have shown that prophylactic use of negative-pressure devices is beneficial in reducing the rate of SSI.1 Yu and colleagues' systematic review and meta-analysis confirms those findings in a high-risk population of women having CD.
Study limitations
Before routinely adopting the use of negative-pressure devices for all women having CD, however, obstetricians should consider the following caveats:
The investigations included in the study by Yu and colleagues did not consistently distinguish between scheduled versus unscheduled CDs.
The reports did not systematically consider other major risk factors for wound complications besides obesity, and they did not control for these confounders in the statistical analyses.
The studies included in the meta-analysis did not provide full descriptions of other measures that might influence the rate of SSIs, such as timing and selection of prophylactic antibiotics, selection of suture material, preoperative skin preparation, and closure techniques for the deep subcutaneous tissue and skin.
None of the included studies systematically considered the cost-effectiveness of the negative-pressure devices. This is an important consideration given that the acquisition cost of these devices ranges from $200 to $500.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Results of the systematic review and meta-analysis by Yu and colleagues suggest that prophylactic negative-pressure wound therapy in high-risk mostly obese women after CD reduces SSI and overall wound complications. The study's limitations, however, must be kept in mind, and more data are needed. It would be most helpful if a large, well-designed RCT was conducted and included 2 groups with comparable multiple major risk factors for wound complications, and in which all women received the following important interventions2-4:
removal of hair in the surgical site with a clipper, not a razor
cleansing of the skin with a chlorhexidine rather than an iodophor solution
closure of the deep subcutaneous tissue if the total subcutaneous layer exceeds 2 cm in depth
closure of the skin with suture rather than staples
administration of antibiotic prophylaxis, ideally with a combination of cefazolin plus azithromycin, prior to the surgical incision.
Vaginal cleansing before CD lowers risk of postop endometritis
Caissutti C, Saccone G, Zullo F, et al. Vaginal cleansing before cesarean delivery: a systematic review and meta-analysis. Obstet Gynecol. 2017;130(3):527-538.
Photo: Shutterstock
Caissutti and colleagues aimed to determine if cleansing the vagina with an antiseptic solution prior to surgery reduced the frequency of postcesarean endometritis. They included 16 RCTs (4,837 patients) in their systematic review and meta-analysis. The primary outcome was the frequency of postoperative endometritis.
Details of the study
The studies were conducted in several countries and included patients of various socioeconomic classes. Six trials included only patients having a scheduled CD; 9 included both scheduled and unscheduled cesareans; and 1 included only unscheduled cesareans. In 11 studies, povidone-iodine was the antiseptic solution used. Two trials used chlorhexidine diacetate 0.2%, and 1 used chlorhexidine diacetate 0.4%. One trial used metronidazole 0.5% gel, and another used the antiseptic cetrimide, which is a mixture of different quaternary ammonium salts, including cetrimonium bromide.
In all trials, patients received prophylactic antibiotics. The antibiotics were administered prior to the surgical incision in 6 trials; they were given after the umbilical cord was clamped in 6 trials. In 2 trials, the antibiotics were given at varying times, and in the final 2 trials, the timing of antibiotic administration was not reported. Of note, no trials described the method of placenta removal, a factor of considerable significance in influencing the rate of postoperative endometritis.5,6
Endometritis frequency reduced with vaginal cleansing; benefit greater in certain groups. Overall, in the 15 trials in which vaginal cleansing was compared with placebo or with no treatment, women in the treatment group had a significantly lower rate of endometritis (4.5% compared with 8.8%; relative risk [RR], 0.52; 95% CI, 0.37-0.72). When only women in labor were considered, the frequency of endometritis was 8.1% in the intervention group compared with 13.8% in the control group (RR, 0.52; 95% CI, 0.28-0.97). In the women who were not in labor, the difference in the incidence of endometritis was not statistically significant (3.5% vs 6.6%; RR, 0.62; 95% CI, 0.34-1.15).
In the subgroup analysis of women with ruptured membranes at the time of surgery, the incidence of endometritis was 4.3% in the treatment group compared with 20.1% in the control group (RR, 0.23; 95% CI, 0.10-0.52). In women with intact membranes at the time of surgery, the incidence of endometritis was not significantly reduced in the treatment group.
Interestingly, in the subgroup analysis of the 10 trials that used povidone-iodine, the reduction in the frequency of postcesarean endometritis was statistically significant (2.8% vs 6.3%; RR, 0.42; 95% CI, 0.25-0.71). However, this same protective effect was not observed in the women treated with chlorhexidine. In the 1 trial that directly compared povidone-iodine with chlorhexidine, there was no statistically significant difference in outcome.
Simple intervention, solid benefit
Endometritis is the most common complication following CD. The infection is polymicrobial, with mixed aerobic and anaerobic organisms. The principal risk factors for postcesarean endometritis are low socioeconomic status, extended duration of labor and ruptured membranes, multiple vaginal examinations, internal fetal monitoring, and pre-existing vaginal infections (principally, bacterial vaginosis and group B streptococcal colonization).
Two interventions are clearly of value in reducing the incidence of endometritis: administration of prophylactic antibiotics prior to the surgical incision and removal of the placenta by traction on the cord as opposed to manual extraction.5,6
The assessment by Caissutti and colleagues confirms that a third measure — preoperative vaginal cleansing — also helps reduce the incidence of postcesarean endometritis. The principal benefit is seen in women who have been in labor with ruptured membranes, although certainly it is not harmful in lower-risk patients. The intervention is simple and straightforward: a 30-second vaginal wash with a povidone-iodine solution just prior to surgery.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
From my perspective, the interesting unanswered question is why a chlorhexidine solution with low alcohol content was not more effective than povidone-iodine, given that a chlorhexidine abdominal wash is superior to povidone-iodine in preventing wound infection after cesarean delivery.7 Until additional studies confirm the effectiveness of vaginal cleansing with chlorhexidine, I recommend the routine use of the povidone-iodine solution in all women having CD.
Treat smaller skin abscesses with antibiotics after surgical drainage? Yes.
Daum RS, Miller LG, Immergluck L, et al; for the DMID 07-0051 Team. A placebo-controlled trial of antibiotics for smaller skin abscesses. N Engl J Med. 2017;376(26):2545-2555.
Photo: Shutterstock
For treatment of subcutaneous abscesses that were 5 cm or smaller in diameter, investigators sought to determine if surgical drainage alone was equivalent to surgical drainage plus systemic antibiotics. After their abscess was drained, patients were randomly assigned to receive either clindamycin (300 mg 3 times daily) or trimethoprim-sulfamethoxazole (80 mg/400 mg twice daily) or placebo for 10 days. The primary outcome was clinical cure 7 to 10 days after treatment.
Details of the study
Daum and colleagues enrolled 786 participants (505 adults, 281 children) in the prospective double-blind study. Staphylococcus aureus was isolated from 527 patients (67.0%); methicillin-resistant S aureus (MRSA) was isolated from 388 (49.4%). The cure rate was similar in patients in the clindamycin group (83.1%) and the trimethoprim-sulfamethoxazole group (81.7%), and the cure rate in each antibiotic group was significantly higher than that in the placebo group (68.9%; P<.001 for both comparisons). The difference in treatment effect was specifically limited to patients who had S aureus isolated from their lesions.
Findings at follow-up. At 1 month of follow-up, new infections were less common in the clindamycin group (6.8%) than in the trimethoprim-sulfamethoxazole group (13.5%; P = .03) or the placebo group (12.4%; P = .06). However, the highest frequency of adverse effects occurred in the patients who received clindamycin (21.9% vs 11.1% vs 12.5%). No adverse effects were judged to be serious, and all resolved without sequela.
Controversy remains on antibiotic use after drainage
This study is important for 2 major reasons. First, soft tissue infections are quite commonand can evolve into serious problems, especially when the offending pathogen is MRSA. Second, controversy exists about whether systemic antibiotics are indicated if the subcutaneous abscess is relatively small and is adequately drained. For example, Talan and colleagues demonstrated that, in settings with a high prevalence of MRSA, surgical drainage combined with trimethoprim-sulfamethoxazole (1 double-strength tablet orally twice daily) was superior to drainage plus placebo.8 However, Daum and Gold recently debated the issue of drainage plus antibiotics in a case vignette and reached opposite conclusions.9
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In my opinion, this investigation by Daum and colleagues supports a role for consistent use of systemic antibiotics following surgical drainage of clinically significant subcutaneous abscesses that have a 5 cm or smaller diameter. Several oral antibiotics are effective against S aureus, including MRSA.10 These drugs include trimethoprim-sulfamethoxazole (1 double-strength tablet orally twice daily), clindamycin (300-450 mg 3 times daily), doxycycline (100 mg twice daily), and minocycline (200 mg initially, then 100 mg every 12 hours).
Of these drugs, I prefer trimethoprim-sulfamethoxazole, provided that the patient does not have an allergy to sulfonamides. Trimethoprim-sulfamethoxazole is significantly less expensive than the other 3 drugs and usually is better tolerated. In particular, compared with clindamycin, trimethoprim-sulfamethoxazole is less likely to cause antibiotic-associated diarrhea, including Clostridium difficile infection. Trimethoprim-sulfamethoxazole should not be used in the first trimester of pregnancy because of concerns about fetal teratogenicity.
Antibiotic use, common in the obstetric population, raises risk for C difficile infection
Ruiter-Ligeti J, Vincent S, Czuzoj-Shulman N, Abenhaim HA. Risk factors, incidence, and morbidity associated with obstetric Clostridium difficile infection. Obstet Gynecol. 2018;131(2):387-391.
Photo: Shutterstock
The objective of this investigation was to identify risk factors for Clostridium difficile infection (previously termed pseudomembranous enterocolitis) in obstetric patients. The authors performed a retrospective cohort study using information from a large database maintained by the Agency for Healthcare Research and Quality. This database provides information about inpatient hospital stays in the United States, and it is the largest repository of its kind. It includes data from a sample of 1,000 US hospitals.
Details of the study
Ruiter-Ligeti and colleagues reviewed 13,881,592 births during 1999-2013 and identified 2,757 (0.02%) admissions for delivery complicated by C difficile infection, a rate of 20 admissions per 100,000 deliveries per year (95% CI, 19.13-20.62). The rate of admissions with this diagnosis doubled from 1999 (15 per 100,000) to 2013 (30 per 100,000, P<.001).
Among these obstetric patients, the principal risk factors for C difficile infection were older age, multiple gestation, long-term antibiotic use (not precisely defined), and concurrent diagnosis of inflammatory bowel disease. In addition, patients with pyelonephritis, perineal or cesarean wound infections, or pneumonia also were at increased risk, presumably because those patients required longer courses of broad-spectrum antibiotics.
Of additional note, when compared with women who did not have C difficile infection, patients with infection were more likely to develop a thromboembolic event (38.4 per 1,000), paralytic ileus (58.0 per 1,000), sepsis (46.4 per 1,000), and death (8.0 per 1,000).
Be on guard for C difficile infection in antibiotic-treated obstetric patients
C difficile infection is an uncommon but potentially very serious complication of antibiotic therapy. Given that approximately half of all women admitted for delivery are exposed to antibiotics because of prophylaxis for group B streptococcus infection, prophylaxis for CD, and treatment of chorioamnionitis and puerperal endometritis, clinicians constantly need to be vigilant for this complication.11
Affected patients typically present with frequent loose, watery stools and lower abdominal cramping. In severe cases, blood may be present in the stool, and signs of intestinal distention and even acute peritonitis may be evident. The diagnosis can be established by documenting a positive culture or polymerase chain reaction (PCR) assay for C difficile and a positive cytotoxin assay for toxins A and/or B. In addition, if endoscopy is performed, the characteristic gray membranous plaques can be visualized on the rectal and colonic mucosa.11
Discontinue antibiotic therapy. The first step in managing affected patients is to stop all antibiotics, if possible, or at least the one most likely to be the causative agent of C difficile infection. Patients with relatively mild clinical findings should be treated with oral metronidazole, 500 mg every 8 hours for 10 to 14 days. Patients with severe findings should be treated with oral vancomycin, 500 mg every 6 hours, plus IV metronidazole, 500 mg every 8 hours. The more seriously ill patient must be observed carefully for signs of bowel obstruction, intestinal perforation, peritonitis, and sepsis.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Clearly, clinicians should make every effort to prevent C difficile infection in the first place. The following preventive measures are essential:
Avoid the use of extremely broad-spectrum antibiotics for prophylaxis for CD.
When using therapeutic antibiotics, keep the spectrum as narrow as possible, consistent with adequately treating the pathogens causing the infection.
Administer antibiotics for the shortest time possible, consistent with achieving a clinical cure or providing appropriate prophylaxis for surgical procedures (usually, a maximum of 3 doses).
If a patient receiving antibiotics experiences more than 3 loose stools in 24 hours, either discontinue all antibiotics or substitute another drug for the most likely offending agent, depending on the clinical situation.
If, after stopping or changing antibiotics, the clinical findings do not resolve promptly, perform a culture or PCR assay for C difficile and assays for the C difficile toxin. Treat as outlined above if these tests are positive.
Danger for birth defects with maternal Zika infection present in all trimesters, but greatest in first
Hoen B, Schaub B, Funk AL, et al. Pregnancy outcomes after ZIKV infection in French territories in the Americas. N Engl J Med. 2018;378(11):985-994.
Photo: Shutterstock
To estimate the risk of congenital neurologic defects associated with Zika virus infection, Hoen and colleagues conducted a prospective cohort study of pregnant women with symptomatic Zika virus infection who were enrolled during March through November 2016 in French Guiana, Guadeloupe, and Martinique. All women had Zika virus infection confirmed by PCR assay.
Details of the study
The investigators reviewed 546 pregnancies, which resulted in the birth of 555 fetuses and infants. Thirty-nine fetuses and neonates (7%; 95% CI, 5.0-9.5) had neurologic and ocular findings known to be associated with Zika virus infection. Of these, 10 pregnancies were terminated, 1 fetus was stillborn, and 28 were live-born.
Microcephaly (defined as head circumference more than 2 SD below the mean) was present in 32 fetuses and infants (5.8%); 9 had severe microcephaly, defined as head circumference more than 3 SD below the mean. Neurologic and ocular abnormalities were more common when maternal infection occurred during the first trimester (24 of 189 fetuses and infants, 12.7%) compared with infection during the second trimester (9 of 252, 3.6%) or third trimester (6 of 114, 5.3%) (P = .001).
Studies report similar rates of fetal injury
Zika virus infection primarily is caused by a bite from the Aedes aegypti mosquito. The infection also can be transmitted by sexual contact, laboratory accident, and blood transfusion. Eighty percent of infected persons are asymptomatic. In symptomatic patients, the most common clinical manifestations are low-grade fever, a disseminated maculopapular rash, arthralgias, swelling of the hands and feet, and nonpurulent conjunctivitis.
The most ominous manifestation of congenital Zika virus infection is microcephaly. Other important manifestations include lissencephaly, pachygyria, cortical atrophy, ventriculomegaly, subcortical calcifications, ocular abnormalities, and arthrogryposis. Although most of these abnormalities are immediately visible in the neonate, some may not appear until the child is older.
The present study is an excellent complement to 2 recent reports that defined the risk of Zika virus-related fetal injury in patients in the United States and its territories. Based on an analysis of data from the US Zika Pregnancy Registry, Honein and colleagues reported an overall rate of congenital infection of 6%.12 The rate of fetal injury was 11% when the mother was infected in the first trimester and 0% when the infection occurred in the second or third trimester. The overall rate of infection and the first trimester rate of infection were similar to those reported by Hoen and colleagues.
Conversely, Shapiro-Mendoza and colleagues evaluated rates of infection in US territories (American Samoa, Puerto Rico, and the US Virgin Islands) and observed cases of fetal injury associated with second- and third-trimester maternal infection.13 These authors reported an overall rate of infection of 5% and an 8% rate of infection with first-trimester maternal infection. When maternal infection occurred in the second and third trimesters, the rates of fetal injury were 5% and 4%, respectively, figures almost identical to those reported by Hoen and colleagues. Of note, the investigations by Honein and Shapiro-Mendoza included women with both symptomatic and asymptomatic infection.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Taken together, the studies discussed provide 2 clear take-home messages:
Both symptomatic and asymptomatic maternal infection pose a significant risk of injury to the fetus and neonate.
Although the risk of fetal injury is greatest when maternal infection occurs in the first trimester, exposure in the second and third trimesters is still dangerous. The Zika virus is quite pathogenic and can cause debilitating injury to the developing fetus at any stage of gestation.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
References
Hyldig N, Birke-Sorensen H, Kruse M, et al. Meta-analysis of negative-pressure wound therapy for closed surgical incisions. Br J Surg. 2016;103(5):477–486.
Duff P. A simple checklist for preventing major complications associated with cesarean delivery. Obstet Gynecol. 2010;116(6):1393–1396.
Patrick KE, Deatsman SL, Duff P. Preventing infection after cesarean delivery: evidence-based guidance. OBG Manag. 2016;28(11):41–47.
Patrick KE, Deatsman SL, Duff P. Preventing infection after cesarean delivery: 5 more evidence-based measures to consider. OBG Manag. 2016;28(12):18–22.
Lasley DS, Eblen A, Yancey MK, Duff P. The effect of placental removal method on the incidence of postcesarean infections. Am J Obstet Gynecol. 1997;176(6):1250–1254.
Duff P. A simple checklist for preventing major complications associated with cesarean delivery. Obstet Gynecol. 2010;116(6):1393–1396.
Tuuli MG, Liu J, Stout MJ, et al. A randomized trial comparing skin antiseptic agents at cesarean delivery. N Engl J Med. 2016;374(7):647–655.
Talan DA, Mower WR, Krishnadasan A, et al. Trimethoprim-sulfamethoxazole versus placebo for uncomplicated skin abscess. N Engl J Med. 2016;374(9):823–832.
Singer AJ, Talan DA. Management of skin abscesses in the era of methicillin-resistant Staphylococcus aureus. N Engl J Med. 2014;370(11):1039–1047.
Unger JA, Whimbey E, Gravett MG, Eschenbach DA. The emergence of Clostridium difficile infection among peripartum women: a case-control study of a C difficile outbreak on an obstetrical service. Infect Dis Obstet Gynecol. 2011;267249. doi:10.1155/2011/267249.
Honein MA, Dawson AL, Petersen EE, et al; US Zika Pregnancy Registry Collaboration. Birth defects among fetuses and infants of US women with evidence of possible Zika virus infection during pregnancy. JAMA. 2017;317(1):59–68.
Shapiro-Mendoza CK, Rice ME, Galang RR, et al; Zika Pregnancy and Infant Registries Working Group. Pregnancy outcomes after maternal Zika virus infection during pregnancy — US territories. January 1, 2016-April 25, 2017. MMWR Morb Mortal Wkly Rep. 2017;66(23):615–621.
In this Update I highlight 5 interesting investigations on infectious diseases. The first addresses the value of applying prophylactically a negative-pressure wound dressing to prevent surgical site infection (SSI) in obese women having cesarean delivery (CD). The second report assesses the effectiveness of a preoperative vaginal wash in reducing the frequency of postcesarean endometritis. The third investigation examines the role of systemic antibiotics, combined with surgical drainage, for patients who have subcutaneous abscesses ranging in size up to 5 cm. The fourth study presents new information about the major risk factors for Clostridium difficile infections in obstetric patients. The final study presents valuable sobering new data about the risks of congenital Zika virus infection.
Negative-pressure wound therapy after CD shows some benefit in preventing SSI
Yu L, Kronen RJ, Simon LE, Stoll CR, Colditz GA, Tuuli MG. Prophylactic negative-pressure wound therapy after cesarean is associated with reduced risk of surgical site infection: a systematic review and meta-analysis. Am J Obstet Gynecol. 2018;218(2):200-210.e1.
Illustration: Used with permission. Courtesy of KCI, an Acelity Company
Yu and colleagues sought to determine if the prophylactic use of negative-pressure devices, compared with standard wound dressing, was effective in reducing the frequency of SSI after CD.
The authors searched multiple databases and initially identified 161 randomized controlled trials and cohort studies for further assessment. After applying rigorous exclusion criteria, they ultimately selected 9 studies for systematic review and meta-analysis. Six studies were randomized controlled trials (RCTs), 2 were retrospective cohort studies, and 1 was a prospective cohort study. Five studies were considered high quality; 4 were of low quality.
Details of the study
Several types of negative-pressure devices were used, but the 2 most common were the Prevena incision management system (KCI, San Antonio, Texas) and PICO negative- pressure wound therapy (Smith & Nephew, St. Petersburg, Florida). The majority of patients in all groups were at high risk for wound complications because of obesity.
The primary outcome of interest was the frequency of SSI. Secondary outcomes included dehiscence, seroma, endometritis, a composite measure for all wound complications, and hospital readmission.
The absolute risk of SSI in the intervention group was 5% (95% confidence interval [CI], 2.0%-7.0%) compared with 11% (95% CI, 7.0%-16.0%) in the standard dressing group. The pooled risk ratio was 0.45 (95% CI, 0.31-0.66). The absolute risk reduction was 6% (95% CI, -10.0% to -3.0%), and the number needed to treat was 17.
There were no significant differences in the rate of any of the secondary outcomes other than the composite of all wound complications. This difference was largely accounted for by the difference in the rate of SSI.
Illustration: Used with permission. Courtesy of KCI, an Acelity Company
Passive wound closure (left) compared with negative-pressure wound therapy with the Prevena incision management system (right).
How negative-pressure devices aid wound healing
Yu and colleagues explained that negative-pressure devices exert their beneficial effects in various ways, including:
shrinking the wound
inducing cellular stretch
removing extracellular fluids
creating a favorable environment for healing
promoting angiogenesis and neurogenesis.
Multiple studies in nonobstetric patients have shown that prophylactic use of negative-pressure devices is beneficial in reducing the rate of SSI.1 Yu and colleagues' systematic review and meta-analysis confirms those findings in a high-risk population of women having CD.
Study limitations
Before routinely adopting the use of negative-pressure devices for all women having CD, however, obstetricians should consider the following caveats:
The investigations included in the study by Yu and colleagues did not consistently distinguish between scheduled versus unscheduled CDs.
The reports did not systematically consider other major risk factors for wound complications besides obesity, and they did not control for these confounders in the statistical analyses.
The studies included in the meta-analysis did not provide full descriptions of other measures that might influence the rate of SSIs, such as timing and selection of prophylactic antibiotics, selection of suture material, preoperative skin preparation, and closure techniques for the deep subcutaneous tissue and skin.
None of the included studies systematically considered the cost-effectiveness of the negative-pressure devices. This is an important consideration given that the acquisition cost of these devices ranges from $200 to $500.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Results of the systematic review and meta-analysis by Yu and colleagues suggest that prophylactic negative-pressure wound therapy in high-risk mostly obese women after CD reduces SSI and overall wound complications. The study's limitations, however, must be kept in mind, and more data are needed. It would be most helpful if a large, well-designed RCT was conducted and included 2 groups with comparable multiple major risk factors for wound complications, and in which all women received the following important interventions2-4:
removal of hair in the surgical site with a clipper, not a razor
cleansing of the skin with a chlorhexidine rather than an iodophor solution
closure of the deep subcutaneous tissue if the total subcutaneous layer exceeds 2 cm in depth
closure of the skin with suture rather than staples
administration of antibiotic prophylaxis, ideally with a combination of cefazolin plus azithromycin, prior to the surgical incision.
Vaginal cleansing before CD lowers risk of postop endometritis
Caissutti C, Saccone G, Zullo F, et al. Vaginal cleansing before cesarean delivery: a systematic review and meta-analysis. Obstet Gynecol. 2017;130(3):527-538.
Photo: Shutterstock
Caissutti and colleagues aimed to determine if cleansing the vagina with an antiseptic solution prior to surgery reduced the frequency of postcesarean endometritis. They included 16 RCTs (4,837 patients) in their systematic review and meta-analysis. The primary outcome was the frequency of postoperative endometritis.
Details of the study
The studies were conducted in several countries and included patients of various socioeconomic classes. Six trials included only patients having a scheduled CD; 9 included both scheduled and unscheduled cesareans; and 1 included only unscheduled cesareans. In 11 studies, povidone-iodine was the antiseptic solution used. Two trials used chlorhexidine diacetate 0.2%, and 1 used chlorhexidine diacetate 0.4%. One trial used metronidazole 0.5% gel, and another used the antiseptic cetrimide, which is a mixture of different quaternary ammonium salts, including cetrimonium bromide.
In all trials, patients received prophylactic antibiotics. The antibiotics were administered prior to the surgical incision in 6 trials; they were given after the umbilical cord was clamped in 6 trials. In 2 trials, the antibiotics were given at varying times, and in the final 2 trials, the timing of antibiotic administration was not reported. Of note, no trials described the method of placenta removal, a factor of considerable significance in influencing the rate of postoperative endometritis.5,6
Endometritis frequency reduced with vaginal cleansing; benefit greater in certain groups. Overall, in the 15 trials in which vaginal cleansing was compared with placebo or with no treatment, women in the treatment group had a significantly lower rate of endometritis (4.5% compared with 8.8%; relative risk [RR], 0.52; 95% CI, 0.37-0.72). When only women in labor were considered, the frequency of endometritis was 8.1% in the intervention group compared with 13.8% in the control group (RR, 0.52; 95% CI, 0.28-0.97). In the women who were not in labor, the difference in the incidence of endometritis was not statistically significant (3.5% vs 6.6%; RR, 0.62; 95% CI, 0.34-1.15).
In the subgroup analysis of women with ruptured membranes at the time of surgery, the incidence of endometritis was 4.3% in the treatment group compared with 20.1% in the control group (RR, 0.23; 95% CI, 0.10-0.52). In women with intact membranes at the time of surgery, the incidence of endometritis was not significantly reduced in the treatment group.
Interestingly, in the subgroup analysis of the 10 trials that used povidone-iodine, the reduction in the frequency of postcesarean endometritis was statistically significant (2.8% vs 6.3%; RR, 0.42; 95% CI, 0.25-0.71). However, this same protective effect was not observed in the women treated with chlorhexidine. In the 1 trial that directly compared povidone-iodine with chlorhexidine, there was no statistically significant difference in outcome.
Simple intervention, solid benefit
Endometritis is the most common complication following CD. The infection is polymicrobial, with mixed aerobic and anaerobic organisms. The principal risk factors for postcesarean endometritis are low socioeconomic status, extended duration of labor and ruptured membranes, multiple vaginal examinations, internal fetal monitoring, and pre-existing vaginal infections (principally, bacterial vaginosis and group B streptococcal colonization).
Two interventions are clearly of value in reducing the incidence of endometritis: administration of prophylactic antibiotics prior to the surgical incision and removal of the placenta by traction on the cord as opposed to manual extraction.5,6
The assessment by Caissutti and colleagues confirms that a third measure — preoperative vaginal cleansing — also helps reduce the incidence of postcesarean endometritis. The principal benefit is seen in women who have been in labor with ruptured membranes, although certainly it is not harmful in lower-risk patients. The intervention is simple and straightforward: a 30-second vaginal wash with a povidone-iodine solution just prior to surgery.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
From my perspective, the interesting unanswered question is why a chlorhexidine solution with low alcohol content was not more effective than povidone-iodine, given that a chlorhexidine abdominal wash is superior to povidone-iodine in preventing wound infection after cesarean delivery.7 Until additional studies confirm the effectiveness of vaginal cleansing with chlorhexidine, I recommend the routine use of the povidone-iodine solution in all women having CD.
Treat smaller skin abscesses with antibiotics after surgical drainage? Yes.
Daum RS, Miller LG, Immergluck L, et al; for the DMID 07-0051 Team. A placebo-controlled trial of antibiotics for smaller skin abscesses. N Engl J Med. 2017;376(26):2545-2555.
Photo: Shutterstock
For treatment of subcutaneous abscesses that were 5 cm or smaller in diameter, investigators sought to determine if surgical drainage alone was equivalent to surgical drainage plus systemic antibiotics. After their abscess was drained, patients were randomly assigned to receive either clindamycin (300 mg 3 times daily) or trimethoprim-sulfamethoxazole (80 mg/400 mg twice daily) or placebo for 10 days. The primary outcome was clinical cure 7 to 10 days after treatment.
Details of the study
Daum and colleagues enrolled 786 participants (505 adults, 281 children) in the prospective double-blind study. Staphylococcus aureus was isolated from 527 patients (67.0%); methicillin-resistant S aureus (MRSA) was isolated from 388 (49.4%). The cure rate was similar in patients in the clindamycin group (83.1%) and the trimethoprim-sulfamethoxazole group (81.7%), and the cure rate in each antibiotic group was significantly higher than that in the placebo group (68.9%; P<.001 for both comparisons). The difference in treatment effect was specifically limited to patients who had S aureus isolated from their lesions.
Findings at follow-up. At 1 month of follow-up, new infections were less common in the clindamycin group (6.8%) than in the trimethoprim-sulfamethoxazole group (13.5%; P = .03) or the placebo group (12.4%; P = .06). However, the highest frequency of adverse effects occurred in the patients who received clindamycin (21.9% vs 11.1% vs 12.5%). No adverse effects were judged to be serious, and all resolved without sequela.
Controversy remains on antibiotic use after drainage
This study is important for 2 major reasons. First, soft tissue infections are quite commonand can evolve into serious problems, especially when the offending pathogen is MRSA. Second, controversy exists about whether systemic antibiotics are indicated if the subcutaneous abscess is relatively small and is adequately drained. For example, Talan and colleagues demonstrated that, in settings with a high prevalence of MRSA, surgical drainage combined with trimethoprim-sulfamethoxazole (1 double-strength tablet orally twice daily) was superior to drainage plus placebo.8 However, Daum and Gold recently debated the issue of drainage plus antibiotics in a case vignette and reached opposite conclusions.9
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In my opinion, this investigation by Daum and colleagues supports a role for consistent use of systemic antibiotics following surgical drainage of clinically significant subcutaneous abscesses that have a 5 cm or smaller diameter. Several oral antibiotics are effective against S aureus, including MRSA.10 These drugs include trimethoprim-sulfamethoxazole (1 double-strength tablet orally twice daily), clindamycin (300-450 mg 3 times daily), doxycycline (100 mg twice daily), and minocycline (200 mg initially, then 100 mg every 12 hours).
Of these drugs, I prefer trimethoprim-sulfamethoxazole, provided that the patient does not have an allergy to sulfonamides. Trimethoprim-sulfamethoxazole is significantly less expensive than the other 3 drugs and usually is better tolerated. In particular, compared with clindamycin, trimethoprim-sulfamethoxazole is less likely to cause antibiotic-associated diarrhea, including Clostridium difficile infection. Trimethoprim-sulfamethoxazole should not be used in the first trimester of pregnancy because of concerns about fetal teratogenicity.
Antibiotic use, common in the obstetric population, raises risk for C difficile infection
Ruiter-Ligeti J, Vincent S, Czuzoj-Shulman N, Abenhaim HA. Risk factors, incidence, and morbidity associated with obstetric Clostridium difficile infection. Obstet Gynecol. 2018;131(2):387-391.
Photo: Shutterstock
The objective of this investigation was to identify risk factors for Clostridium difficile infection (previously termed pseudomembranous enterocolitis) in obstetric patients. The authors performed a retrospective cohort study using information from a large database maintained by the Agency for Healthcare Research and Quality. This database provides information about inpatient hospital stays in the United States, and it is the largest repository of its kind. It includes data from a sample of 1,000 US hospitals.
Details of the study
Ruiter-Ligeti and colleagues reviewed 13,881,592 births during 1999-2013 and identified 2,757 (0.02%) admissions for delivery complicated by C difficile infection, a rate of 20 admissions per 100,000 deliveries per year (95% CI, 19.13-20.62). The rate of admissions with this diagnosis doubled from 1999 (15 per 100,000) to 2013 (30 per 100,000, P<.001).
Among these obstetric patients, the principal risk factors for C difficile infection were older age, multiple gestation, long-term antibiotic use (not precisely defined), and concurrent diagnosis of inflammatory bowel disease. In addition, patients with pyelonephritis, perineal or cesarean wound infections, or pneumonia also were at increased risk, presumably because those patients required longer courses of broad-spectrum antibiotics.
Of additional note, when compared with women who did not have C difficile infection, patients with infection were more likely to develop a thromboembolic event (38.4 per 1,000), paralytic ileus (58.0 per 1,000), sepsis (46.4 per 1,000), and death (8.0 per 1,000).
Be on guard for C difficile infection in antibiotic-treated obstetric patients
C difficile infection is an uncommon but potentially very serious complication of antibiotic therapy. Given that approximately half of all women admitted for delivery are exposed to antibiotics because of prophylaxis for group B streptococcus infection, prophylaxis for CD, and treatment of chorioamnionitis and puerperal endometritis, clinicians constantly need to be vigilant for this complication.11
Affected patients typically present with frequent loose, watery stools and lower abdominal cramping. In severe cases, blood may be present in the stool, and signs of intestinal distention and even acute peritonitis may be evident. The diagnosis can be established by documenting a positive culture or polymerase chain reaction (PCR) assay for C difficile and a positive cytotoxin assay for toxins A and/or B. In addition, if endoscopy is performed, the characteristic gray membranous plaques can be visualized on the rectal and colonic mucosa.11
Discontinue antibiotic therapy. The first step in managing affected patients is to stop all antibiotics, if possible, or at least the one most likely to be the causative agent of C difficile infection. Patients with relatively mild clinical findings should be treated with oral metronidazole, 500 mg every 8 hours for 10 to 14 days. Patients with severe findings should be treated with oral vancomycin, 500 mg every 6 hours, plus IV metronidazole, 500 mg every 8 hours. The more seriously ill patient must be observed carefully for signs of bowel obstruction, intestinal perforation, peritonitis, and sepsis.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Clearly, clinicians should make every effort to prevent C difficile infection in the first place. The following preventive measures are essential:
Avoid the use of extremely broad-spectrum antibiotics for prophylaxis for CD.
When using therapeutic antibiotics, keep the spectrum as narrow as possible, consistent with adequately treating the pathogens causing the infection.
Administer antibiotics for the shortest time possible, consistent with achieving a clinical cure or providing appropriate prophylaxis for surgical procedures (usually, a maximum of 3 doses).
If a patient receiving antibiotics experiences more than 3 loose stools in 24 hours, either discontinue all antibiotics or substitute another drug for the most likely offending agent, depending on the clinical situation.
If, after stopping or changing antibiotics, the clinical findings do not resolve promptly, perform a culture or PCR assay for C difficile and assays for the C difficile toxin. Treat as outlined above if these tests are positive.
Danger for birth defects with maternal Zika infection present in all trimesters, but greatest in first
Hoen B, Schaub B, Funk AL, et al. Pregnancy outcomes after ZIKV infection in French territories in the Americas. N Engl J Med. 2018;378(11):985-994.
Photo: Shutterstock
To estimate the risk of congenital neurologic defects associated with Zika virus infection, Hoen and colleagues conducted a prospective cohort study of pregnant women with symptomatic Zika virus infection who were enrolled during March through November 2016 in French Guiana, Guadeloupe, and Martinique. All women had Zika virus infection confirmed by PCR assay.
Details of the study
The investigators reviewed 546 pregnancies, which resulted in the birth of 555 fetuses and infants. Thirty-nine fetuses and neonates (7%; 95% CI, 5.0-9.5) had neurologic and ocular findings known to be associated with Zika virus infection. Of these, 10 pregnancies were terminated, 1 fetus was stillborn, and 28 were live-born.
Microcephaly (defined as head circumference more than 2 SD below the mean) was present in 32 fetuses and infants (5.8%); 9 had severe microcephaly, defined as head circumference more than 3 SD below the mean. Neurologic and ocular abnormalities were more common when maternal infection occurred during the first trimester (24 of 189 fetuses and infants, 12.7%) compared with infection during the second trimester (9 of 252, 3.6%) or third trimester (6 of 114, 5.3%) (P = .001).
Studies report similar rates of fetal injury
Zika virus infection primarily is caused by a bite from the Aedes aegypti mosquito. The infection also can be transmitted by sexual contact, laboratory accident, and blood transfusion. Eighty percent of infected persons are asymptomatic. In symptomatic patients, the most common clinical manifestations are low-grade fever, a disseminated maculopapular rash, arthralgias, swelling of the hands and feet, and nonpurulent conjunctivitis.
The most ominous manifestation of congenital Zika virus infection is microcephaly. Other important manifestations include lissencephaly, pachygyria, cortical atrophy, ventriculomegaly, subcortical calcifications, ocular abnormalities, and arthrogryposis. Although most of these abnormalities are immediately visible in the neonate, some may not appear until the child is older.
The present study is an excellent complement to 2 recent reports that defined the risk of Zika virus-related fetal injury in patients in the United States and its territories. Based on an analysis of data from the US Zika Pregnancy Registry, Honein and colleagues reported an overall rate of congenital infection of 6%.12 The rate of fetal injury was 11% when the mother was infected in the first trimester and 0% when the infection occurred in the second or third trimester. The overall rate of infection and the first trimester rate of infection were similar to those reported by Hoen and colleagues.
Conversely, Shapiro-Mendoza and colleagues evaluated rates of infection in US territories (American Samoa, Puerto Rico, and the US Virgin Islands) and observed cases of fetal injury associated with second- and third-trimester maternal infection.13 These authors reported an overall rate of infection of 5% and an 8% rate of infection with first-trimester maternal infection. When maternal infection occurred in the second and third trimesters, the rates of fetal injury were 5% and 4%, respectively, figures almost identical to those reported by Hoen and colleagues. Of note, the investigations by Honein and Shapiro-Mendoza included women with both symptomatic and asymptomatic infection.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Taken together, the studies discussed provide 2 clear take-home messages:
Both symptomatic and asymptomatic maternal infection pose a significant risk of injury to the fetus and neonate.
Although the risk of fetal injury is greatest when maternal infection occurs in the first trimester, exposure in the second and third trimesters is still dangerous. The Zika virus is quite pathogenic and can cause debilitating injury to the developing fetus at any stage of gestation.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
In this Update I highlight 5 interesting investigations on infectious diseases. The first addresses the value of applying prophylactically a negative-pressure wound dressing to prevent surgical site infection (SSI) in obese women having cesarean delivery (CD). The second report assesses the effectiveness of a preoperative vaginal wash in reducing the frequency of postcesarean endometritis. The third investigation examines the role of systemic antibiotics, combined with surgical drainage, for patients who have subcutaneous abscesses ranging in size up to 5 cm. The fourth study presents new information about the major risk factors for Clostridium difficile infections in obstetric patients. The final study presents valuable sobering new data about the risks of congenital Zika virus infection.
Negative-pressure wound therapy after CD shows some benefit in preventing SSI
Yu L, Kronen RJ, Simon LE, Stoll CR, Colditz GA, Tuuli MG. Prophylactic negative-pressure wound therapy after cesarean is associated with reduced risk of surgical site infection: a systematic review and meta-analysis. Am J Obstet Gynecol. 2018;218(2):200-210.e1.
Illustration: Used with permission. Courtesy of KCI, an Acelity Company
Yu and colleagues sought to determine if the prophylactic use of negative-pressure devices, compared with standard wound dressing, was effective in reducing the frequency of SSI after CD.
The authors searched multiple databases and initially identified 161 randomized controlled trials and cohort studies for further assessment. After applying rigorous exclusion criteria, they ultimately selected 9 studies for systematic review and meta-analysis. Six studies were randomized controlled trials (RCTs), 2 were retrospective cohort studies, and 1 was a prospective cohort study. Five studies were considered high quality; 4 were of low quality.
Details of the study
Several types of negative-pressure devices were used, but the 2 most common were the Prevena incision management system (KCI, San Antonio, Texas) and PICO negative- pressure wound therapy (Smith & Nephew, St. Petersburg, Florida). The majority of patients in all groups were at high risk for wound complications because of obesity.
The primary outcome of interest was the frequency of SSI. Secondary outcomes included dehiscence, seroma, endometritis, a composite measure for all wound complications, and hospital readmission.
The absolute risk of SSI in the intervention group was 5% (95% confidence interval [CI], 2.0%-7.0%) compared with 11% (95% CI, 7.0%-16.0%) in the standard dressing group. The pooled risk ratio was 0.45 (95% CI, 0.31-0.66). The absolute risk reduction was 6% (95% CI, -10.0% to -3.0%), and the number needed to treat was 17.
There were no significant differences in the rate of any of the secondary outcomes other than the composite of all wound complications. This difference was largely accounted for by the difference in the rate of SSI.
Illustration: Used with permission. Courtesy of KCI, an Acelity Company
Passive wound closure (left) compared with negative-pressure wound therapy with the Prevena incision management system (right).
How negative-pressure devices aid wound healing
Yu and colleagues explained that negative-pressure devices exert their beneficial effects in various ways, including:
shrinking the wound
inducing cellular stretch
removing extracellular fluids
creating a favorable environment for healing
promoting angiogenesis and neurogenesis.
Multiple studies in nonobstetric patients have shown that prophylactic use of negative-pressure devices is beneficial in reducing the rate of SSI.1 Yu and colleagues' systematic review and meta-analysis confirms those findings in a high-risk population of women having CD.
Study limitations
Before routinely adopting the use of negative-pressure devices for all women having CD, however, obstetricians should consider the following caveats:
The investigations included in the study by Yu and colleagues did not consistently distinguish between scheduled versus unscheduled CDs.
The reports did not systematically consider other major risk factors for wound complications besides obesity, and they did not control for these confounders in the statistical analyses.
The studies included in the meta-analysis did not provide full descriptions of other measures that might influence the rate of SSIs, such as timing and selection of prophylactic antibiotics, selection of suture material, preoperative skin preparation, and closure techniques for the deep subcutaneous tissue and skin.
None of the included studies systematically considered the cost-effectiveness of the negative-pressure devices. This is an important consideration given that the acquisition cost of these devices ranges from $200 to $500.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Results of the systematic review and meta-analysis by Yu and colleagues suggest that prophylactic negative-pressure wound therapy in high-risk mostly obese women after CD reduces SSI and overall wound complications. The study's limitations, however, must be kept in mind, and more data are needed. It would be most helpful if a large, well-designed RCT was conducted and included 2 groups with comparable multiple major risk factors for wound complications, and in which all women received the following important interventions2-4:
removal of hair in the surgical site with a clipper, not a razor
cleansing of the skin with a chlorhexidine rather than an iodophor solution
closure of the deep subcutaneous tissue if the total subcutaneous layer exceeds 2 cm in depth
closure of the skin with suture rather than staples
administration of antibiotic prophylaxis, ideally with a combination of cefazolin plus azithromycin, prior to the surgical incision.
Vaginal cleansing before CD lowers risk of postop endometritis
Caissutti C, Saccone G, Zullo F, et al. Vaginal cleansing before cesarean delivery: a systematic review and meta-analysis. Obstet Gynecol. 2017;130(3):527-538.
Photo: Shutterstock
Caissutti and colleagues aimed to determine if cleansing the vagina with an antiseptic solution prior to surgery reduced the frequency of postcesarean endometritis. They included 16 RCTs (4,837 patients) in their systematic review and meta-analysis. The primary outcome was the frequency of postoperative endometritis.
Details of the study
The studies were conducted in several countries and included patients of various socioeconomic classes. Six trials included only patients having a scheduled CD; 9 included both scheduled and unscheduled cesareans; and 1 included only unscheduled cesareans. In 11 studies, povidone-iodine was the antiseptic solution used. Two trials used chlorhexidine diacetate 0.2%, and 1 used chlorhexidine diacetate 0.4%. One trial used metronidazole 0.5% gel, and another used the antiseptic cetrimide, which is a mixture of different quaternary ammonium salts, including cetrimonium bromide.
In all trials, patients received prophylactic antibiotics. The antibiotics were administered prior to the surgical incision in 6 trials; they were given after the umbilical cord was clamped in 6 trials. In 2 trials, the antibiotics were given at varying times, and in the final 2 trials, the timing of antibiotic administration was not reported. Of note, no trials described the method of placenta removal, a factor of considerable significance in influencing the rate of postoperative endometritis.5,6
Endometritis frequency reduced with vaginal cleansing; benefit greater in certain groups. Overall, in the 15 trials in which vaginal cleansing was compared with placebo or with no treatment, women in the treatment group had a significantly lower rate of endometritis (4.5% compared with 8.8%; relative risk [RR], 0.52; 95% CI, 0.37-0.72). When only women in labor were considered, the frequency of endometritis was 8.1% in the intervention group compared with 13.8% in the control group (RR, 0.52; 95% CI, 0.28-0.97). In the women who were not in labor, the difference in the incidence of endometritis was not statistically significant (3.5% vs 6.6%; RR, 0.62; 95% CI, 0.34-1.15).
In the subgroup analysis of women with ruptured membranes at the time of surgery, the incidence of endometritis was 4.3% in the treatment group compared with 20.1% in the control group (RR, 0.23; 95% CI, 0.10-0.52). In women with intact membranes at the time of surgery, the incidence of endometritis was not significantly reduced in the treatment group.
Interestingly, in the subgroup analysis of the 10 trials that used povidone-iodine, the reduction in the frequency of postcesarean endometritis was statistically significant (2.8% vs 6.3%; RR, 0.42; 95% CI, 0.25-0.71). However, this same protective effect was not observed in the women treated with chlorhexidine. In the 1 trial that directly compared povidone-iodine with chlorhexidine, there was no statistically significant difference in outcome.
Simple intervention, solid benefit
Endometritis is the most common complication following CD. The infection is polymicrobial, with mixed aerobic and anaerobic organisms. The principal risk factors for postcesarean endometritis are low socioeconomic status, extended duration of labor and ruptured membranes, multiple vaginal examinations, internal fetal monitoring, and pre-existing vaginal infections (principally, bacterial vaginosis and group B streptococcal colonization).
Two interventions are clearly of value in reducing the incidence of endometritis: administration of prophylactic antibiotics prior to the surgical incision and removal of the placenta by traction on the cord as opposed to manual extraction.5,6
The assessment by Caissutti and colleagues confirms that a third measure — preoperative vaginal cleansing — also helps reduce the incidence of postcesarean endometritis. The principal benefit is seen in women who have been in labor with ruptured membranes, although certainly it is not harmful in lower-risk patients. The intervention is simple and straightforward: a 30-second vaginal wash with a povidone-iodine solution just prior to surgery.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
From my perspective, the interesting unanswered question is why a chlorhexidine solution with low alcohol content was not more effective than povidone-iodine, given that a chlorhexidine abdominal wash is superior to povidone-iodine in preventing wound infection after cesarean delivery.7 Until additional studies confirm the effectiveness of vaginal cleansing with chlorhexidine, I recommend the routine use of the povidone-iodine solution in all women having CD.
Treat smaller skin abscesses with antibiotics after surgical drainage? Yes.
Daum RS, Miller LG, Immergluck L, et al; for the DMID 07-0051 Team. A placebo-controlled trial of antibiotics for smaller skin abscesses. N Engl J Med. 2017;376(26):2545-2555.
Photo: Shutterstock
For treatment of subcutaneous abscesses that were 5 cm or smaller in diameter, investigators sought to determine if surgical drainage alone was equivalent to surgical drainage plus systemic antibiotics. After their abscess was drained, patients were randomly assigned to receive either clindamycin (300 mg 3 times daily) or trimethoprim-sulfamethoxazole (80 mg/400 mg twice daily) or placebo for 10 days. The primary outcome was clinical cure 7 to 10 days after treatment.
Details of the study
Daum and colleagues enrolled 786 participants (505 adults, 281 children) in the prospective double-blind study. Staphylococcus aureus was isolated from 527 patients (67.0%); methicillin-resistant S aureus (MRSA) was isolated from 388 (49.4%). The cure rate was similar in patients in the clindamycin group (83.1%) and the trimethoprim-sulfamethoxazole group (81.7%), and the cure rate in each antibiotic group was significantly higher than that in the placebo group (68.9%; P<.001 for both comparisons). The difference in treatment effect was specifically limited to patients who had S aureus isolated from their lesions.
Findings at follow-up. At 1 month of follow-up, new infections were less common in the clindamycin group (6.8%) than in the trimethoprim-sulfamethoxazole group (13.5%; P = .03) or the placebo group (12.4%; P = .06). However, the highest frequency of adverse effects occurred in the patients who received clindamycin (21.9% vs 11.1% vs 12.5%). No adverse effects were judged to be serious, and all resolved without sequela.
Controversy remains on antibiotic use after drainage
This study is important for 2 major reasons. First, soft tissue infections are quite commonand can evolve into serious problems, especially when the offending pathogen is MRSA. Second, controversy exists about whether systemic antibiotics are indicated if the subcutaneous abscess is relatively small and is adequately drained. For example, Talan and colleagues demonstrated that, in settings with a high prevalence of MRSA, surgical drainage combined with trimethoprim-sulfamethoxazole (1 double-strength tablet orally twice daily) was superior to drainage plus placebo.8 However, Daum and Gold recently debated the issue of drainage plus antibiotics in a case vignette and reached opposite conclusions.9
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In my opinion, this investigation by Daum and colleagues supports a role for consistent use of systemic antibiotics following surgical drainage of clinically significant subcutaneous abscesses that have a 5 cm or smaller diameter. Several oral antibiotics are effective against S aureus, including MRSA.10 These drugs include trimethoprim-sulfamethoxazole (1 double-strength tablet orally twice daily), clindamycin (300-450 mg 3 times daily), doxycycline (100 mg twice daily), and minocycline (200 mg initially, then 100 mg every 12 hours).
Of these drugs, I prefer trimethoprim-sulfamethoxazole, provided that the patient does not have an allergy to sulfonamides. Trimethoprim-sulfamethoxazole is significantly less expensive than the other 3 drugs and usually is better tolerated. In particular, compared with clindamycin, trimethoprim-sulfamethoxazole is less likely to cause antibiotic-associated diarrhea, including Clostridium difficile infection. Trimethoprim-sulfamethoxazole should not be used in the first trimester of pregnancy because of concerns about fetal teratogenicity.
Antibiotic use, common in the obstetric population, raises risk for C difficile infection
Ruiter-Ligeti J, Vincent S, Czuzoj-Shulman N, Abenhaim HA. Risk factors, incidence, and morbidity associated with obstetric Clostridium difficile infection. Obstet Gynecol. 2018;131(2):387-391.
Photo: Shutterstock
The objective of this investigation was to identify risk factors for Clostridium difficile infection (previously termed pseudomembranous enterocolitis) in obstetric patients. The authors performed a retrospective cohort study using information from a large database maintained by the Agency for Healthcare Research and Quality. This database provides information about inpatient hospital stays in the United States, and it is the largest repository of its kind. It includes data from a sample of 1,000 US hospitals.
Details of the study
Ruiter-Ligeti and colleagues reviewed 13,881,592 births during 1999-2013 and identified 2,757 (0.02%) admissions for delivery complicated by C difficile infection, a rate of 20 admissions per 100,000 deliveries per year (95% CI, 19.13-20.62). The rate of admissions with this diagnosis doubled from 1999 (15 per 100,000) to 2013 (30 per 100,000, P<.001).
Among these obstetric patients, the principal risk factors for C difficile infection were older age, multiple gestation, long-term antibiotic use (not precisely defined), and concurrent diagnosis of inflammatory bowel disease. In addition, patients with pyelonephritis, perineal or cesarean wound infections, or pneumonia also were at increased risk, presumably because those patients required longer courses of broad-spectrum antibiotics.
Of additional note, when compared with women who did not have C difficile infection, patients with infection were more likely to develop a thromboembolic event (38.4 per 1,000), paralytic ileus (58.0 per 1,000), sepsis (46.4 per 1,000), and death (8.0 per 1,000).
Be on guard for C difficile infection in antibiotic-treated obstetric patients
C difficile infection is an uncommon but potentially very serious complication of antibiotic therapy. Given that approximately half of all women admitted for delivery are exposed to antibiotics because of prophylaxis for group B streptococcus infection, prophylaxis for CD, and treatment of chorioamnionitis and puerperal endometritis, clinicians constantly need to be vigilant for this complication.11
Affected patients typically present with frequent loose, watery stools and lower abdominal cramping. In severe cases, blood may be present in the stool, and signs of intestinal distention and even acute peritonitis may be evident. The diagnosis can be established by documenting a positive culture or polymerase chain reaction (PCR) assay for C difficile and a positive cytotoxin assay for toxins A and/or B. In addition, if endoscopy is performed, the characteristic gray membranous plaques can be visualized on the rectal and colonic mucosa.11
Discontinue antibiotic therapy. The first step in managing affected patients is to stop all antibiotics, if possible, or at least the one most likely to be the causative agent of C difficile infection. Patients with relatively mild clinical findings should be treated with oral metronidazole, 500 mg every 8 hours for 10 to 14 days. Patients with severe findings should be treated with oral vancomycin, 500 mg every 6 hours, plus IV metronidazole, 500 mg every 8 hours. The more seriously ill patient must be observed carefully for signs of bowel obstruction, intestinal perforation, peritonitis, and sepsis.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Clearly, clinicians should make every effort to prevent C difficile infection in the first place. The following preventive measures are essential:
Avoid the use of extremely broad-spectrum antibiotics for prophylaxis for CD.
When using therapeutic antibiotics, keep the spectrum as narrow as possible, consistent with adequately treating the pathogens causing the infection.
Administer antibiotics for the shortest time possible, consistent with achieving a clinical cure or providing appropriate prophylaxis for surgical procedures (usually, a maximum of 3 doses).
If a patient receiving antibiotics experiences more than 3 loose stools in 24 hours, either discontinue all antibiotics or substitute another drug for the most likely offending agent, depending on the clinical situation.
If, after stopping or changing antibiotics, the clinical findings do not resolve promptly, perform a culture or PCR assay for C difficile and assays for the C difficile toxin. Treat as outlined above if these tests are positive.
Danger for birth defects with maternal Zika infection present in all trimesters, but greatest in first
Hoen B, Schaub B, Funk AL, et al. Pregnancy outcomes after ZIKV infection in French territories in the Americas. N Engl J Med. 2018;378(11):985-994.
Photo: Shutterstock
To estimate the risk of congenital neurologic defects associated with Zika virus infection, Hoen and colleagues conducted a prospective cohort study of pregnant women with symptomatic Zika virus infection who were enrolled during March through November 2016 in French Guiana, Guadeloupe, and Martinique. All women had Zika virus infection confirmed by PCR assay.
Details of the study
The investigators reviewed 546 pregnancies, which resulted in the birth of 555 fetuses and infants. Thirty-nine fetuses and neonates (7%; 95% CI, 5.0-9.5) had neurologic and ocular findings known to be associated with Zika virus infection. Of these, 10 pregnancies were terminated, 1 fetus was stillborn, and 28 were live-born.
Microcephaly (defined as head circumference more than 2 SD below the mean) was present in 32 fetuses and infants (5.8%); 9 had severe microcephaly, defined as head circumference more than 3 SD below the mean. Neurologic and ocular abnormalities were more common when maternal infection occurred during the first trimester (24 of 189 fetuses and infants, 12.7%) compared with infection during the second trimester (9 of 252, 3.6%) or third trimester (6 of 114, 5.3%) (P = .001).
Studies report similar rates of fetal injury
Zika virus infection primarily is caused by a bite from the Aedes aegypti mosquito. The infection also can be transmitted by sexual contact, laboratory accident, and blood transfusion. Eighty percent of infected persons are asymptomatic. In symptomatic patients, the most common clinical manifestations are low-grade fever, a disseminated maculopapular rash, arthralgias, swelling of the hands and feet, and nonpurulent conjunctivitis.
The most ominous manifestation of congenital Zika virus infection is microcephaly. Other important manifestations include lissencephaly, pachygyria, cortical atrophy, ventriculomegaly, subcortical calcifications, ocular abnormalities, and arthrogryposis. Although most of these abnormalities are immediately visible in the neonate, some may not appear until the child is older.
The present study is an excellent complement to 2 recent reports that defined the risk of Zika virus-related fetal injury in patients in the United States and its territories. Based on an analysis of data from the US Zika Pregnancy Registry, Honein and colleagues reported an overall rate of congenital infection of 6%.12 The rate of fetal injury was 11% when the mother was infected in the first trimester and 0% when the infection occurred in the second or third trimester. The overall rate of infection and the first trimester rate of infection were similar to those reported by Hoen and colleagues.
Conversely, Shapiro-Mendoza and colleagues evaluated rates of infection in US territories (American Samoa, Puerto Rico, and the US Virgin Islands) and observed cases of fetal injury associated with second- and third-trimester maternal infection.13 These authors reported an overall rate of infection of 5% and an 8% rate of infection with first-trimester maternal infection. When maternal infection occurred in the second and third trimesters, the rates of fetal injury were 5% and 4%, respectively, figures almost identical to those reported by Hoen and colleagues. Of note, the investigations by Honein and Shapiro-Mendoza included women with both symptomatic and asymptomatic infection.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Taken together, the studies discussed provide 2 clear take-home messages:
Both symptomatic and asymptomatic maternal infection pose a significant risk of injury to the fetus and neonate.
Although the risk of fetal injury is greatest when maternal infection occurs in the first trimester, exposure in the second and third trimesters is still dangerous. The Zika virus is quite pathogenic and can cause debilitating injury to the developing fetus at any stage of gestation.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
References
Hyldig N, Birke-Sorensen H, Kruse M, et al. Meta-analysis of negative-pressure wound therapy for closed surgical incisions. Br J Surg. 2016;103(5):477–486.
Duff P. A simple checklist for preventing major complications associated with cesarean delivery. Obstet Gynecol. 2010;116(6):1393–1396.
Patrick KE, Deatsman SL, Duff P. Preventing infection after cesarean delivery: evidence-based guidance. OBG Manag. 2016;28(11):41–47.
Patrick KE, Deatsman SL, Duff P. Preventing infection after cesarean delivery: 5 more evidence-based measures to consider. OBG Manag. 2016;28(12):18–22.
Lasley DS, Eblen A, Yancey MK, Duff P. The effect of placental removal method on the incidence of postcesarean infections. Am J Obstet Gynecol. 1997;176(6):1250–1254.
Duff P. A simple checklist for preventing major complications associated with cesarean delivery. Obstet Gynecol. 2010;116(6):1393–1396.
Tuuli MG, Liu J, Stout MJ, et al. A randomized trial comparing skin antiseptic agents at cesarean delivery. N Engl J Med. 2016;374(7):647–655.
Talan DA, Mower WR, Krishnadasan A, et al. Trimethoprim-sulfamethoxazole versus placebo for uncomplicated skin abscess. N Engl J Med. 2016;374(9):823–832.
Singer AJ, Talan DA. Management of skin abscesses in the era of methicillin-resistant Staphylococcus aureus. N Engl J Med. 2014;370(11):1039–1047.
Unger JA, Whimbey E, Gravett MG, Eschenbach DA. The emergence of Clostridium difficile infection among peripartum women: a case-control study of a C difficile outbreak on an obstetrical service. Infect Dis Obstet Gynecol. 2011;267249. doi:10.1155/2011/267249.
Honein MA, Dawson AL, Petersen EE, et al; US Zika Pregnancy Registry Collaboration. Birth defects among fetuses and infants of US women with evidence of possible Zika virus infection during pregnancy. JAMA. 2017;317(1):59–68.
Shapiro-Mendoza CK, Rice ME, Galang RR, et al; Zika Pregnancy and Infant Registries Working Group. Pregnancy outcomes after maternal Zika virus infection during pregnancy — US territories. January 1, 2016-April 25, 2017. MMWR Morb Mortal Wkly Rep. 2017;66(23):615–621.
References
Hyldig N, Birke-Sorensen H, Kruse M, et al. Meta-analysis of negative-pressure wound therapy for closed surgical incisions. Br J Surg. 2016;103(5):477–486.
Duff P. A simple checklist for preventing major complications associated with cesarean delivery. Obstet Gynecol. 2010;116(6):1393–1396.
Patrick KE, Deatsman SL, Duff P. Preventing infection after cesarean delivery: evidence-based guidance. OBG Manag. 2016;28(11):41–47.
Patrick KE, Deatsman SL, Duff P. Preventing infection after cesarean delivery: 5 more evidence-based measures to consider. OBG Manag. 2016;28(12):18–22.
Lasley DS, Eblen A, Yancey MK, Duff P. The effect of placental removal method on the incidence of postcesarean infections. Am J Obstet Gynecol. 1997;176(6):1250–1254.
Duff P. A simple checklist for preventing major complications associated with cesarean delivery. Obstet Gynecol. 2010;116(6):1393–1396.
Tuuli MG, Liu J, Stout MJ, et al. A randomized trial comparing skin antiseptic agents at cesarean delivery. N Engl J Med. 2016;374(7):647–655.
Talan DA, Mower WR, Krishnadasan A, et al. Trimethoprim-sulfamethoxazole versus placebo for uncomplicated skin abscess. N Engl J Med. 2016;374(9):823–832.
Singer AJ, Talan DA. Management of skin abscesses in the era of methicillin-resistant Staphylococcus aureus. N Engl J Med. 2014;370(11):1039–1047.
Unger JA, Whimbey E, Gravett MG, Eschenbach DA. The emergence of Clostridium difficile infection among peripartum women: a case-control study of a C difficile outbreak on an obstetrical service. Infect Dis Obstet Gynecol. 2011;267249. doi:10.1155/2011/267249.
Honein MA, Dawson AL, Petersen EE, et al; US Zika Pregnancy Registry Collaboration. Birth defects among fetuses and infants of US women with evidence of possible Zika virus infection during pregnancy. JAMA. 2017;317(1):59–68.
Shapiro-Mendoza CK, Rice ME, Galang RR, et al; Zika Pregnancy and Infant Registries Working Group. Pregnancy outcomes after maternal Zika virus infection during pregnancy — US territories. January 1, 2016-April 25, 2017. MMWR Morb Mortal Wkly Rep. 2017;66(23):615–621.
ORLANDO – The risk of perioperative MI or death associated with noncardiac surgery is vanishingly low in patients free of diabetes, hypertension, and smoking, Tanya Wilcox, MD, reported at the annual meeting of the American College of Cardiology.
How small is the risk? A mere 1 in 1,000, according to her analysis of more than 3.8 million major noncardiac surgeries in the American College of Surgeons National Surgical Quality Improvement Program database for 2009-2015, according to Dr. Wilcox of New York University.
Physicians are frequently asked by surgeons to clear patients for noncardiac surgery in terms of cardiovascular risk. Because current risk scores are complex, aren’t amenable to rapid bedside calculations, and may entail cardiac stress testing, Dr. Wilcox decided it was worth assessing the impact of three straightforward cardiovascular risk factors – current smoking and treatment for hypertension or diabetes – on 30-day postoperative MI-free survival. For this purpose she turned to the National Surgical Quality Improvement Program database, a validated, risk-adjusted, outcomes-based program to measure and improve the quality of surgical care utilizing data from 250 U.S. surgical centers.
Of the 3,817,113 patients who underwent major noncardiac surgery, 1,586,020 (42%) of them had none of the three cardiovascular risk factors of interest, 1,541,846 (40%) had one, 643,424 (17%) had two, and 45,823, or 1.2%, had all three. The patients’ mean age was 57, 75% were white, and 57% were women. About half of all patients underwent various operations within the realm of general surgery; next most frequent were orthopedic procedures, accounting for 18% of total noncardiac surgery. Of note, only 23% of patients with zero risk factors were American Society of Anesthesiologists Class 3-5, compared with 51% of those with one cardiovascular risk factor, 76% with two, and 71% with all three.
The incidence of acute MI or death within 30 days of noncardiac surgery climbed in stepwise fashion according to a patient’s risk factor burden. In a multivariate analysis adjusted for age, race, and gender, patients with any one of the cardiovascular risk factors had a 30-day risk of acute MI or death that was 1.52 times greater than those with no risk factors, patients with two risk factors were at 2.4-fold increased risk, and those with all three were at 3.63-fold greater risk than those with none. The degree of increased risk associated with any single risk factor ranged from 1.47-fold for hypertension to 1.94-fold for smoking.
“Further study is needed to determine whether aggressive risk factor modifications in the form of blood pressure control, glycemic control, and smoking cessation could reduce the incidence of postoperative MI,” Dr. Wilcox observed.
She reported having no financial conflicts regarding her study.
ORLANDO – The risk of perioperative MI or death associated with noncardiac surgery is vanishingly low in patients free of diabetes, hypertension, and smoking, Tanya Wilcox, MD, reported at the annual meeting of the American College of Cardiology.
How small is the risk? A mere 1 in 1,000, according to her analysis of more than 3.8 million major noncardiac surgeries in the American College of Surgeons National Surgical Quality Improvement Program database for 2009-2015, according to Dr. Wilcox of New York University.
Physicians are frequently asked by surgeons to clear patients for noncardiac surgery in terms of cardiovascular risk. Because current risk scores are complex, aren’t amenable to rapid bedside calculations, and may entail cardiac stress testing, Dr. Wilcox decided it was worth assessing the impact of three straightforward cardiovascular risk factors – current smoking and treatment for hypertension or diabetes – on 30-day postoperative MI-free survival. For this purpose she turned to the National Surgical Quality Improvement Program database, a validated, risk-adjusted, outcomes-based program to measure and improve the quality of surgical care utilizing data from 250 U.S. surgical centers.
Of the 3,817,113 patients who underwent major noncardiac surgery, 1,586,020 (42%) of them had none of the three cardiovascular risk factors of interest, 1,541,846 (40%) had one, 643,424 (17%) had two, and 45,823, or 1.2%, had all three. The patients’ mean age was 57, 75% were white, and 57% were women. About half of all patients underwent various operations within the realm of general surgery; next most frequent were orthopedic procedures, accounting for 18% of total noncardiac surgery. Of note, only 23% of patients with zero risk factors were American Society of Anesthesiologists Class 3-5, compared with 51% of those with one cardiovascular risk factor, 76% with two, and 71% with all three.
The incidence of acute MI or death within 30 days of noncardiac surgery climbed in stepwise fashion according to a patient’s risk factor burden. In a multivariate analysis adjusted for age, race, and gender, patients with any one of the cardiovascular risk factors had a 30-day risk of acute MI or death that was 1.52 times greater than those with no risk factors, patients with two risk factors were at 2.4-fold increased risk, and those with all three were at 3.63-fold greater risk than those with none. The degree of increased risk associated with any single risk factor ranged from 1.47-fold for hypertension to 1.94-fold for smoking.
“Further study is needed to determine whether aggressive risk factor modifications in the form of blood pressure control, glycemic control, and smoking cessation could reduce the incidence of postoperative MI,” Dr. Wilcox observed.
She reported having no financial conflicts regarding her study.
ORLANDO – The risk of perioperative MI or death associated with noncardiac surgery is vanishingly low in patients free of diabetes, hypertension, and smoking, Tanya Wilcox, MD, reported at the annual meeting of the American College of Cardiology.
How small is the risk? A mere 1 in 1,000, according to her analysis of more than 3.8 million major noncardiac surgeries in the American College of Surgeons National Surgical Quality Improvement Program database for 2009-2015, according to Dr. Wilcox of New York University.
Physicians are frequently asked by surgeons to clear patients for noncardiac surgery in terms of cardiovascular risk. Because current risk scores are complex, aren’t amenable to rapid bedside calculations, and may entail cardiac stress testing, Dr. Wilcox decided it was worth assessing the impact of three straightforward cardiovascular risk factors – current smoking and treatment for hypertension or diabetes – on 30-day postoperative MI-free survival. For this purpose she turned to the National Surgical Quality Improvement Program database, a validated, risk-adjusted, outcomes-based program to measure and improve the quality of surgical care utilizing data from 250 U.S. surgical centers.
Of the 3,817,113 patients who underwent major noncardiac surgery, 1,586,020 (42%) of them had none of the three cardiovascular risk factors of interest, 1,541,846 (40%) had one, 643,424 (17%) had two, and 45,823, or 1.2%, had all three. The patients’ mean age was 57, 75% were white, and 57% were women. About half of all patients underwent various operations within the realm of general surgery; next most frequent were orthopedic procedures, accounting for 18% of total noncardiac surgery. Of note, only 23% of patients with zero risk factors were American Society of Anesthesiologists Class 3-5, compared with 51% of those with one cardiovascular risk factor, 76% with two, and 71% with all three.
The incidence of acute MI or death within 30 days of noncardiac surgery climbed in stepwise fashion according to a patient’s risk factor burden. In a multivariate analysis adjusted for age, race, and gender, patients with any one of the cardiovascular risk factors had a 30-day risk of acute MI or death that was 1.52 times greater than those with no risk factors, patients with two risk factors were at 2.4-fold increased risk, and those with all three were at 3.63-fold greater risk than those with none. The degree of increased risk associated with any single risk factor ranged from 1.47-fold for hypertension to 1.94-fold for smoking.
“Further study is needed to determine whether aggressive risk factor modifications in the form of blood pressure control, glycemic control, and smoking cessation could reduce the incidence of postoperative MI,” Dr. Wilcox observed.
She reported having no financial conflicts regarding her study.
Key clinical point: Noncardiac surgery patients can breathe easier regarding perioperative cardiovascular risk provided they don’t smoke and aren’t hypertensive or diabetic.
Major finding: The risk of perioperative MI or death associated with noncardiac surgery in nonsmokers free of diabetes or hypertension was just 1 in 1,000.
Study details: This was a retrospective analysis of more than 3.8 million noncardiac surgeries contained in the American College of Surgeons National Surgical Quality Improvement Program database for 2009-2015.
Disclosures: The study presenter reported having no financial conflicts.
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
Dr. Lum is Clinical Assistant Professor, Department of Obstetrics and Gynecology, and Director, Minimally Invasive Gynecologic Surgery, Stanford University, Stanford, California.
The author reports no financial relationships relevant to this video.
Dr. Lum is Clinical Assistant Professor, Department of Obstetrics and Gynecology, and Director, Minimally Invasive Gynecologic Surgery, Stanford University, Stanford, California.
The author reports no financial relationships relevant to this video.
Author and Disclosure Information
Dr. Lum is Clinical Assistant Professor, Department of Obstetrics and Gynecology, and Director, Minimally Invasive Gynecologic Surgery, Stanford University, Stanford, California.
The author reports no financial relationships relevant to this video.
Vidyard Video
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings: