User login
Formerly Skin & Allergy News
ass lick
assault rifle
balls
ballsac
black jack
bleach
Boko Haram
bondage
causas
cheap
child abuse
cocaine
compulsive behaviors
cost of miracles
cunt
Daech
display network stats
drug paraphernalia
explosion
fart
fda and death
fda AND warn
fda AND warning
fda AND warns
feom
fuck
gambling
gfc
gun
human trafficking
humira AND expensive
illegal
ISIL
ISIS
Islamic caliphate
Islamic state
madvocate
masturbation
mixed martial arts
MMA
molestation
national rifle association
NRA
nsfw
nuccitelli
pedophile
pedophilia
poker
porn
porn
pornography
psychedelic drug
recreational drug
sex slave rings
shit
slot machine
snort
substance abuse
terrorism
terrorist
texarkana
Texas hold 'em
UFC
section[contains(@class, 'nav-hidden')]
section[contains(@class, 'nav-hidden active')]
The leading independent newspaper covering dermatology news and commentary.
Pityriasis rosea carries few risks for pregnant women
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Circadian rhythms, part 2: Can treating cutaneous conditions at different times of the day improve outcomes?
We continue with a focus on when possible, as well as clinical studies that may shed light on how to time skin care treatments.

It is important to remember that several studies in the last 20 years have revealed cutaneous tendencies based on the time of day. For instance, sebum production is known to be highest around noon, and pH also peaks during the day and is at its lowest at night.1-5
Skin aging
In 2019, Dong and associates showed that blue light at 410 nm reduces PER1 transcription in keratinocytes, indicating that epidermal cells have the capacity to directly sense light and regulate their own clock gene expression. With the introduction of blue light at night, circadian rhythm is disrupted as epidermal skin cells act as if it is daytime. The investigators also considered blue light–induced damage to skin cells at various doses and exposure times in comparison with cells that remained unexposed to light. The production of reactive oxygen species increased in the exposed cells, as did DNA impairment and the emergence of inflammatory mediators, all of which have the potential to hasten aging.6
Early this year, Dong and associates demonstrated that melatonin can dose-dependently stimulate PER1 clock gene expression in normal human dermal fibroblasts and normal human epidermal keratinocytes, and verified that the MT-1 melatonin receptor in such fibroblasts manifests a marked decline with age. The researchers concluded that the melatonin pathway contributes significantly in cutaneous aging and impairment, and that its relationship with skin circadian rhythm points to a possible role in slowing the rate of skin aging through the modulation of cutaneous melatonin receptors.7
Wound healing
In 2019, Walker and associates investigated the effects of dim artificial light at night on wound healing in female C57BL/6 mice, and found that those conditions prior to wounding reduced healing. They concluded that such information might warrant consideration in prescribing treatment.8
Atopic dermatitis
Vaughn and associates contended that alterations in circadian rhythm may contribute to the development of atopic dermatitis.9 A good example of the impact of circadian rhythms on cutaneous health is the nocturnal exacerbation of atopic dermatitis, particularly in children.10
Psoriasis
According to Plikus and associates, recent evidence has emerged showing that the circadian clock regulates UVB-induced DNA damage and cutaneous cancers, and it is also associated with the immune-mediated disorder psoriasis.11
Clinical studies
In 2018, Deshayes and associates conducted a clinical study to evaluate the precursors and stem cell attributes of hHF (human hair follicle keratinocytes), hEpi (human interfollicular epidermal keratinocytes), and hHFDP (hair follicle dermal papilla stem cells) in response to clock pathway changes caused by long-term deregulation of circadian rhythms. A total of 20 women participated in the study, 10 in each group (day workers were the control group and compared with shift workers). Two 3-mm fresh punch biopsies were collected from the occipital region of each participant. The investigators reported that chronic circadian rhythm deregulation influenced clock pathway protein expression and correlated with changes in hHF, hEpi, and hHFDP. They concluded that their findings represented the first data in humans suggesting that deregulation of the clock pathway modulates regenerative activity in human cutaneous and hair precursor cells.12

Later that year, Wu and associates reported on the role of the circadian clock in the transcriptional regulation of human epidermis. Investigators sampled 20 human participants through a 24-hour period and a population of 219 people once, finding a potent circadian oscillator in human epidermis at the population level, hundreds of rhythmically expressed genes, as well as a biomarker set for human epidermis that can, with one sample, highlight circadian phase within a 3-hour time frame. The team concluded that rhythms in human epidermis persist at the population level, and that they were able to present an effective single-sample circadian biomarker.13 This is important, as Morris pointed out, because the standard practice for measuring an individual’s internal clock is to use a dim-light melatonin onset assay over the course of a day.14 In 2019, Jia and associates studied the skin surface lipid profiles of young women to evaluate and characterize circadian human facial surface lipid composition. The investigators identified significant markers of circadian rhythm, with glycerolipids most affected. They ascribed changes in skin barrier function, such as variable pH and transepidermal water loss, to alterations in triacylglycerol levels as well as free fatty acid chain lengths and content that were affected by variations in circadian rhythm.15
Sleep and the timing of topicals
Based on their recent review of the literature on circadian rhythm and skin, Lyons and associates argued that an understanding of circadian rhythm helps dermatologists in recommending the optimal times for patients to apply topical medications. They added that urging patients to get sufficient sleep is important because DNA repair of the skin occurs best at that time.16
Conclusions
Doctors have known for half a century that timing drug delivery to a patient’s circadian clock can enhance outcomes. Chronobiological research into how circadian rhythms work at the cellular level, and in cutaneous cells in particular, is a fascinating and expanding area of inquiry that could help dermatologists more accurately recommend timing for skin care regimens. Much more research, especially in clinical trials, is necessary to further elucidate how to best work with the skin’s natural rhythms.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions, a company that independently tests skin care products and makes recommendations to physicians on skin care technologies. Write to her at dermnews@mdedge.com.
References
1. Mehling A et al. Skin Pharmacol Physiol. 2006;19(4):182-9.
2. Latreille J et al. Skin Pharmacol Physiol. 2004 May-Jun;17(3):133-40.
3. Le Fur I et al. J Invest Dermatol. 2001 Sep;117(3):718-24.
4. Verschoore M et al. Chronobiol Int. 1993 Oct;10(5):349-59.
5. Yosipovitch G et al. J Invest Dermatol. 1998 Jan;110(1):20-3.
6. Dong K et al. Int J Cosmet Sci. 2019 Dec;41(6):558-62.
7. Dong K et al. Int J Mol Sci. 2020 Jan 3;21(1):326.
8. Walker WH II et al. Arch Dermatol Res. 2019 Sep;311(7):573-6.
9. Vaughn AR et al. Pediatr Dermatol. 2018 Jan;35(1):152-7.
10. Fishbein AB et al. J Allergy Clin Immunol. 2015 Nov;136(5):1170-7.
11. Plikus MV et al. J Biol Rhythms. 2015 Jun;30(3):163-82.
12. Deshayes N et al. Eur J Dermatol. 2018 Aug 1;28(4):467-75.
13. Wu G et al. Proc Natl Acad Sci U S A. 2018 Nov 27;115(48):12313-8.
14. Morris A. Nat Rev Endocrinol. 2018 Dec;15(1):3.
15. Jia Y et al. Exp Dermatol. 2019 Jul;28(7):858-62.
16. Lyons AB et al. J Clin Aesthet Dermatol. 2019 Sep;12(9):42-5.
We continue with a focus on when possible, as well as clinical studies that may shed light on how to time skin care treatments.
It is important to remember that several studies in the last 20 years have revealed cutaneous tendencies based on the time of day. For instance, sebum production is known to be highest around noon, and pH also peaks during the day and is at its lowest at night.1-5
Skin aging
In 2019, Dong and associates showed that blue light at 410 nm reduces PER1 transcription in keratinocytes, indicating that epidermal cells have the capacity to directly sense light and regulate their own clock gene expression. With the introduction of blue light at night, circadian rhythm is disrupted as epidermal skin cells act as if it is daytime. The investigators also considered blue light–induced damage to skin cells at various doses and exposure times in comparison with cells that remained unexposed to light. The production of reactive oxygen species increased in the exposed cells, as did DNA impairment and the emergence of inflammatory mediators, all of which have the potential to hasten aging.6
Early this year, Dong and associates demonstrated that melatonin can dose-dependently stimulate PER1 clock gene expression in normal human dermal fibroblasts and normal human epidermal keratinocytes, and verified that the MT-1 melatonin receptor in such fibroblasts manifests a marked decline with age. The researchers concluded that the melatonin pathway contributes significantly in cutaneous aging and impairment, and that its relationship with skin circadian rhythm points to a possible role in slowing the rate of skin aging through the modulation of cutaneous melatonin receptors.7
Wound healing
In 2019, Walker and associates investigated the effects of dim artificial light at night on wound healing in female C57BL/6 mice, and found that those conditions prior to wounding reduced healing. They concluded that such information might warrant consideration in prescribing treatment.8
Atopic dermatitis
Vaughn and associates contended that alterations in circadian rhythm may contribute to the development of atopic dermatitis.9 A good example of the impact of circadian rhythms on cutaneous health is the nocturnal exacerbation of atopic dermatitis, particularly in children.10
Psoriasis
According to Plikus and associates, recent evidence has emerged showing that the circadian clock regulates UVB-induced DNA damage and cutaneous cancers, and it is also associated with the immune-mediated disorder psoriasis.11
Clinical studies
In 2018, Deshayes and associates conducted a clinical study to evaluate the precursors and stem cell attributes of hHF (human hair follicle keratinocytes), hEpi (human interfollicular epidermal keratinocytes), and hHFDP (hair follicle dermal papilla stem cells) in response to clock pathway changes caused by long-term deregulation of circadian rhythms. A total of 20 women participated in the study, 10 in each group (day workers were the control group and compared with shift workers). Two 3-mm fresh punch biopsies were collected from the occipital region of each participant. The investigators reported that chronic circadian rhythm deregulation influenced clock pathway protein expression and correlated with changes in hHF, hEpi, and hHFDP. They concluded that their findings represented the first data in humans suggesting that deregulation of the clock pathway modulates regenerative activity in human cutaneous and hair precursor cells.12
Later that year, Wu and associates reported on the role of the circadian clock in the transcriptional regulation of human epidermis. Investigators sampled 20 human participants through a 24-hour period and a population of 219 people once, finding a potent circadian oscillator in human epidermis at the population level, hundreds of rhythmically expressed genes, as well as a biomarker set for human epidermis that can, with one sample, highlight circadian phase within a 3-hour time frame. The team concluded that rhythms in human epidermis persist at the population level, and that they were able to present an effective single-sample circadian biomarker.13 This is important, as Morris pointed out, because the standard practice for measuring an individual’s internal clock is to use a dim-light melatonin onset assay over the course of a day.14 In 2019, Jia and associates studied the skin surface lipid profiles of young women to evaluate and characterize circadian human facial surface lipid composition. The investigators identified significant markers of circadian rhythm, with glycerolipids most affected. They ascribed changes in skin barrier function, such as variable pH and transepidermal water loss, to alterations in triacylglycerol levels as well as free fatty acid chain lengths and content that were affected by variations in circadian rhythm.15
Sleep and the timing of topicals
Based on their recent review of the literature on circadian rhythm and skin, Lyons and associates argued that an understanding of circadian rhythm helps dermatologists in recommending the optimal times for patients to apply topical medications. They added that urging patients to get sufficient sleep is important because DNA repair of the skin occurs best at that time.16
Conclusions
Doctors have known for half a century that timing drug delivery to a patient’s circadian clock can enhance outcomes. Chronobiological research into how circadian rhythms work at the cellular level, and in cutaneous cells in particular, is a fascinating and expanding area of inquiry that could help dermatologists more accurately recommend timing for skin care regimens. Much more research, especially in clinical trials, is necessary to further elucidate how to best work with the skin’s natural rhythms.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions, a company that independently tests skin care products and makes recommendations to physicians on skin care technologies. Write to her at dermnews@mdedge.com.
References
1. Mehling A et al. Skin Pharmacol Physiol. 2006;19(4):182-9.
2. Latreille J et al. Skin Pharmacol Physiol. 2004 May-Jun;17(3):133-40.
3. Le Fur I et al. J Invest Dermatol. 2001 Sep;117(3):718-24.
4. Verschoore M et al. Chronobiol Int. 1993 Oct;10(5):349-59.
5. Yosipovitch G et al. J Invest Dermatol. 1998 Jan;110(1):20-3.
6. Dong K et al. Int J Cosmet Sci. 2019 Dec;41(6):558-62.
7. Dong K et al. Int J Mol Sci. 2020 Jan 3;21(1):326.
8. Walker WH II et al. Arch Dermatol Res. 2019 Sep;311(7):573-6.
9. Vaughn AR et al. Pediatr Dermatol. 2018 Jan;35(1):152-7.
10. Fishbein AB et al. J Allergy Clin Immunol. 2015 Nov;136(5):1170-7.
11. Plikus MV et al. J Biol Rhythms. 2015 Jun;30(3):163-82.
12. Deshayes N et al. Eur J Dermatol. 2018 Aug 1;28(4):467-75.
13. Wu G et al. Proc Natl Acad Sci U S A. 2018 Nov 27;115(48):12313-8.
14. Morris A. Nat Rev Endocrinol. 2018 Dec;15(1):3.
15. Jia Y et al. Exp Dermatol. 2019 Jul;28(7):858-62.
16. Lyons AB et al. J Clin Aesthet Dermatol. 2019 Sep;12(9):42-5.
We continue with a focus on when possible, as well as clinical studies that may shed light on how to time skin care treatments.
It is important to remember that several studies in the last 20 years have revealed cutaneous tendencies based on the time of day. For instance, sebum production is known to be highest around noon, and pH also peaks during the day and is at its lowest at night.1-5
Skin aging
In 2019, Dong and associates showed that blue light at 410 nm reduces PER1 transcription in keratinocytes, indicating that epidermal cells have the capacity to directly sense light and regulate their own clock gene expression. With the introduction of blue light at night, circadian rhythm is disrupted as epidermal skin cells act as if it is daytime. The investigators also considered blue light–induced damage to skin cells at various doses and exposure times in comparison with cells that remained unexposed to light. The production of reactive oxygen species increased in the exposed cells, as did DNA impairment and the emergence of inflammatory mediators, all of which have the potential to hasten aging.6
Early this year, Dong and associates demonstrated that melatonin can dose-dependently stimulate PER1 clock gene expression in normal human dermal fibroblasts and normal human epidermal keratinocytes, and verified that the MT-1 melatonin receptor in such fibroblasts manifests a marked decline with age. The researchers concluded that the melatonin pathway contributes significantly in cutaneous aging and impairment, and that its relationship with skin circadian rhythm points to a possible role in slowing the rate of skin aging through the modulation of cutaneous melatonin receptors.7
Wound healing
In 2019, Walker and associates investigated the effects of dim artificial light at night on wound healing in female C57BL/6 mice, and found that those conditions prior to wounding reduced healing. They concluded that such information might warrant consideration in prescribing treatment.8
Atopic dermatitis
Vaughn and associates contended that alterations in circadian rhythm may contribute to the development of atopic dermatitis.9 A good example of the impact of circadian rhythms on cutaneous health is the nocturnal exacerbation of atopic dermatitis, particularly in children.10
Psoriasis
According to Plikus and associates, recent evidence has emerged showing that the circadian clock regulates UVB-induced DNA damage and cutaneous cancers, and it is also associated with the immune-mediated disorder psoriasis.11
Clinical studies
In 2018, Deshayes and associates conducted a clinical study to evaluate the precursors and stem cell attributes of hHF (human hair follicle keratinocytes), hEpi (human interfollicular epidermal keratinocytes), and hHFDP (hair follicle dermal papilla stem cells) in response to clock pathway changes caused by long-term deregulation of circadian rhythms. A total of 20 women participated in the study, 10 in each group (day workers were the control group and compared with shift workers). Two 3-mm fresh punch biopsies were collected from the occipital region of each participant. The investigators reported that chronic circadian rhythm deregulation influenced clock pathway protein expression and correlated with changes in hHF, hEpi, and hHFDP. They concluded that their findings represented the first data in humans suggesting that deregulation of the clock pathway modulates regenerative activity in human cutaneous and hair precursor cells.12
Later that year, Wu and associates reported on the role of the circadian clock in the transcriptional regulation of human epidermis. Investigators sampled 20 human participants through a 24-hour period and a population of 219 people once, finding a potent circadian oscillator in human epidermis at the population level, hundreds of rhythmically expressed genes, as well as a biomarker set for human epidermis that can, with one sample, highlight circadian phase within a 3-hour time frame. The team concluded that rhythms in human epidermis persist at the population level, and that they were able to present an effective single-sample circadian biomarker.13 This is important, as Morris pointed out, because the standard practice for measuring an individual’s internal clock is to use a dim-light melatonin onset assay over the course of a day.14 In 2019, Jia and associates studied the skin surface lipid profiles of young women to evaluate and characterize circadian human facial surface lipid composition. The investigators identified significant markers of circadian rhythm, with glycerolipids most affected. They ascribed changes in skin barrier function, such as variable pH and transepidermal water loss, to alterations in triacylglycerol levels as well as free fatty acid chain lengths and content that were affected by variations in circadian rhythm.15
Sleep and the timing of topicals
Based on their recent review of the literature on circadian rhythm and skin, Lyons and associates argued that an understanding of circadian rhythm helps dermatologists in recommending the optimal times for patients to apply topical medications. They added that urging patients to get sufficient sleep is important because DNA repair of the skin occurs best at that time.16
Conclusions
Doctors have known for half a century that timing drug delivery to a patient’s circadian clock can enhance outcomes. Chronobiological research into how circadian rhythms work at the cellular level, and in cutaneous cells in particular, is a fascinating and expanding area of inquiry that could help dermatologists more accurately recommend timing for skin care regimens. Much more research, especially in clinical trials, is necessary to further elucidate how to best work with the skin’s natural rhythms.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions, a company that independently tests skin care products and makes recommendations to physicians on skin care technologies. Write to her at dermnews@mdedge.com.
References
1. Mehling A et al. Skin Pharmacol Physiol. 2006;19(4):182-9.
2. Latreille J et al. Skin Pharmacol Physiol. 2004 May-Jun;17(3):133-40.
3. Le Fur I et al. J Invest Dermatol. 2001 Sep;117(3):718-24.
4. Verschoore M et al. Chronobiol Int. 1993 Oct;10(5):349-59.
5. Yosipovitch G et al. J Invest Dermatol. 1998 Jan;110(1):20-3.
6. Dong K et al. Int J Cosmet Sci. 2019 Dec;41(6):558-62.
7. Dong K et al. Int J Mol Sci. 2020 Jan 3;21(1):326.
8. Walker WH II et al. Arch Dermatol Res. 2019 Sep;311(7):573-6.
9. Vaughn AR et al. Pediatr Dermatol. 2018 Jan;35(1):152-7.
10. Fishbein AB et al. J Allergy Clin Immunol. 2015 Nov;136(5):1170-7.
11. Plikus MV et al. J Biol Rhythms. 2015 Jun;30(3):163-82.
12. Deshayes N et al. Eur J Dermatol. 2018 Aug 1;28(4):467-75.
13. Wu G et al. Proc Natl Acad Sci U S A. 2018 Nov 27;115(48):12313-8.
14. Morris A. Nat Rev Endocrinol. 2018 Dec;15(1):3.
15. Jia Y et al. Exp Dermatol. 2019 Jul;28(7):858-62.
16. Lyons AB et al. J Clin Aesthet Dermatol. 2019 Sep;12(9):42-5.
Adjuvant nivolumab plus ipilimumab shows strong results in resected stage IV melanoma
Results of the

IMMUNED was a multicenter German double-blind, placebo-controlled, phase 2 trial conducted by the Dermatologic Cooperative Oncology Group. It included 167 patients with resected stage IV melanoma and no evidence of disease who were randomized to adjuvant nivolumab (Opdivo) plus placebo, nivolumab plus ipilimumab (Yervoy), or double placebo, with relapse-free survival as the primary outcome, Merrick I. Ross, MD, explained at a forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
“The patients who received adjuvant ipilimumab and nivolumab had amazing 24-month outcomes: a relapse-free survival of 70% versus 42% with nivolumab and 14% with placebo,” observed Dr. Ross, professor of surgical oncology and chief of the melanoma section at the University of Texas M.D. Anderson Cancer Center, Houston.
“It’s not a long-term survival outcome, but we’ll see what happens long term. This could be a very interesting approach to move forward with,” he commented.
By way of background, the cancer surgeon noted that nivolumab has achieved standard-of-care status as adjuvant immunotherapy in patients with resected stage IIIB-C and stage IV melanoma, largely on the strength of the CheckMate-238 trial, which randomized 906 such patients at 130 academic centers in 25 countries to 1 year of adjuvant therapy with either intravenous nivolumab or ipilimumab. In the study, nivolumab emerged as the clear winner, with a 4-year recurrence-free survival of 51.7%, compared with 41.2% for ipilimumab, for a 29% relative risk reduction. Ipilimumab was associated with greater toxicity.
The between-group difference in relapse-free survival in the overall study population also held true in the subgroup comprised of 169 CheckMate 238 participants with resected stage IV melanoma and no evidence of disease at enrollment, Dr. Ross noted.
In the IMMUNED trial, the superior outcome achieved with adjuvant nivolumab plus ipilimumab came at the cost of significantly greater toxicity than with nivolumab alone. Treatment-related adverse events led to medication discontinuation in 62% of the dual-adjuvant therapy group, compared with 13% of those on adjuvant nivolumab.
IMMUNED was funded by Bristol-Myers Squibb.
Dr. Ross reported having no financial conflicts regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
Results of the
IMMUNED was a multicenter German double-blind, placebo-controlled, phase 2 trial conducted by the Dermatologic Cooperative Oncology Group. It included 167 patients with resected stage IV melanoma and no evidence of disease who were randomized to adjuvant nivolumab (Opdivo) plus placebo, nivolumab plus ipilimumab (Yervoy), or double placebo, with relapse-free survival as the primary outcome, Merrick I. Ross, MD, explained at a forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
“The patients who received adjuvant ipilimumab and nivolumab had amazing 24-month outcomes: a relapse-free survival of 70% versus 42% with nivolumab and 14% with placebo,” observed Dr. Ross, professor of surgical oncology and chief of the melanoma section at the University of Texas M.D. Anderson Cancer Center, Houston.
“It’s not a long-term survival outcome, but we’ll see what happens long term. This could be a very interesting approach to move forward with,” he commented.
By way of background, the cancer surgeon noted that nivolumab has achieved standard-of-care status as adjuvant immunotherapy in patients with resected stage IIIB-C and stage IV melanoma, largely on the strength of the CheckMate-238 trial, which randomized 906 such patients at 130 academic centers in 25 countries to 1 year of adjuvant therapy with either intravenous nivolumab or ipilimumab. In the study, nivolumab emerged as the clear winner, with a 4-year recurrence-free survival of 51.7%, compared with 41.2% for ipilimumab, for a 29% relative risk reduction. Ipilimumab was associated with greater toxicity.
The between-group difference in relapse-free survival in the overall study population also held true in the subgroup comprised of 169 CheckMate 238 participants with resected stage IV melanoma and no evidence of disease at enrollment, Dr. Ross noted.
In the IMMUNED trial, the superior outcome achieved with adjuvant nivolumab plus ipilimumab came at the cost of significantly greater toxicity than with nivolumab alone. Treatment-related adverse events led to medication discontinuation in 62% of the dual-adjuvant therapy group, compared with 13% of those on adjuvant nivolumab.
IMMUNED was funded by Bristol-Myers Squibb.
Dr. Ross reported having no financial conflicts regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
Results of the
IMMUNED was a multicenter German double-blind, placebo-controlled, phase 2 trial conducted by the Dermatologic Cooperative Oncology Group. It included 167 patients with resected stage IV melanoma and no evidence of disease who were randomized to adjuvant nivolumab (Opdivo) plus placebo, nivolumab plus ipilimumab (Yervoy), or double placebo, with relapse-free survival as the primary outcome, Merrick I. Ross, MD, explained at a forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
“The patients who received adjuvant ipilimumab and nivolumab had amazing 24-month outcomes: a relapse-free survival of 70% versus 42% with nivolumab and 14% with placebo,” observed Dr. Ross, professor of surgical oncology and chief of the melanoma section at the University of Texas M.D. Anderson Cancer Center, Houston.
“It’s not a long-term survival outcome, but we’ll see what happens long term. This could be a very interesting approach to move forward with,” he commented.
By way of background, the cancer surgeon noted that nivolumab has achieved standard-of-care status as adjuvant immunotherapy in patients with resected stage IIIB-C and stage IV melanoma, largely on the strength of the CheckMate-238 trial, which randomized 906 such patients at 130 academic centers in 25 countries to 1 year of adjuvant therapy with either intravenous nivolumab or ipilimumab. In the study, nivolumab emerged as the clear winner, with a 4-year recurrence-free survival of 51.7%, compared with 41.2% for ipilimumab, for a 29% relative risk reduction. Ipilimumab was associated with greater toxicity.
The between-group difference in relapse-free survival in the overall study population also held true in the subgroup comprised of 169 CheckMate 238 participants with resected stage IV melanoma and no evidence of disease at enrollment, Dr. Ross noted.
In the IMMUNED trial, the superior outcome achieved with adjuvant nivolumab plus ipilimumab came at the cost of significantly greater toxicity than with nivolumab alone. Treatment-related adverse events led to medication discontinuation in 62% of the dual-adjuvant therapy group, compared with 13% of those on adjuvant nivolumab.
IMMUNED was funded by Bristol-Myers Squibb.
Dr. Ross reported having no financial conflicts regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
COVID-19 symptoms persist months after acute infection
, according to a follow-up study involving 1,733 patients.
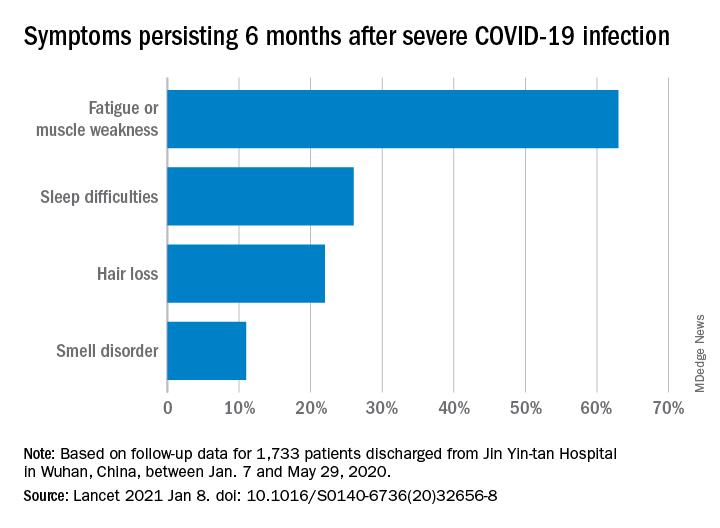
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
, according to a follow-up study involving 1,733 patients.
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
, according to a follow-up study involving 1,733 patients.
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
FROM THE LANCET
CVD deaths rose, imaging declined during pandemic
While the direct toll of the COVID-19 pandemic is being tallied and shared on the nightly news, the indirect effects will undoubtedly take years to fully measure.

In two papers published online Jan. 11 in the Journal of the American College of Cardiology, researchers have started the process of quantifying the impact of the pandemic on the care of patients with cardiovascular disease (CVD).
In the first study, Rishi Wadhera, MD, MPP, MPhil, and colleagues from the Beth Israel Deaconess Medical Center and Harvard Medical School in Boston examined population-level data to determine how deaths from cardiovascular causes changed in the United States in the early months of the pandemic relative to the same periods in 2019.
In a second paper, Andrew J. Einstein, MD, PhD, from Columbia University Irving Medical Center/New York–Presbyterian Hospital and colleagues looked at the pandemic’s international impact on the diagnosis of heart disease.
Using data from the National Center for Health Statistics, Dr. Wadhera and colleagues compared death rates from cardiovascular causes in the United States from March 18, 2020, to June 2, 2020, (the first wave of the pandemic) and from Jan. 1, 2020, to March 17, 2020, (the period just before the pandemic started) and compared them to the same periods in 2019. ICD codes were used to identify underlying causes of death.
Relative to 2019, they found a significant increase in deaths from ischemic heart disease nationally (1.11; 95% confidence interval, 1.04-1.18), as well as an increase in deaths caused by hypertensive disease (1.17; 95% CI, 1.09-1.26). There was no apparent increase in deaths from heart failure, cerebrovascular disease, or other diseases of the circulatory system.
When they looked just at New York City, the area hit hardest during the early part of the pandemic, the relative increases in deaths from ischemic heart disease were more pronounced.
Deaths from ischemic heart disease or hypertensive diseases jumped 139% and 164%, respectively, between March 18, 2020, and June 2, 2020.
More modest increases in deaths were seen in the remainder of New York state, New Jersey, Michigan and Illinois, while Massachusetts and Louisiana did not see a change in cardiovascular deaths.
Several studies from different parts of the world have indicated a 40%-50% drop in hospitalization for myocardial infarction in the initial months of the pandemic, said Dr. Wadhera in an interview.
“We wanted to understand where did all the heart attacks go? And we worried that patients with urgent heart conditions were not seeking the medical care they needed. I think our data suggest that this may have been the case,” reported Dr. Wadhera.
“This very much reflects the reality of what we’re seeing on the ground,” he told this news organization. “After the initial surge ended, when hospital volumes began to return to normal, we saw patients come into the hospital who clearly had a heart attack during the surge months – and were now experiencing complications of that event – because they had initially not come into the hospital due to concerns about exposure to the virus.”
A limitation of their data, he stressed, is whether some deaths coded as CVD deaths were really deaths from undiagnosed COVID-19. “It’s possible that some portion of the increased deaths we observed really reflect the cardiovascular complications of undiagnosed COVID-19, because we know that testing was quite limited during the early first surge of cases.”
“I think that basically three factors – patients avoiding the health care system because of fear of getting COVID, health care systems being strained and overwhelmed leading to the deferral of cardiovascular care and semi-elective procedures, and the cardiovascular complications of COVID-19 itself – all probably collectively contributed to the rise in cardiovascular deaths that we observed,” said Dr. Wadhera.
In an accompanying editorial, Michael N. Young, MD, Geisel School of Medicine at Dartmouth, Lebanon, N.H., and colleagues write that these data, taken together with an earlier study showing an increase in out-of-hospital cardiac arrests at the pandemic peak in New York City, “support the notion of excess fatalities due to unattended comorbid illnesses.” That said, attribution of death in the COVID era “remains problematic.”
In the second article, Andrew Einstein, MD, PhD, and the INCAPS COVID Investigators Group took a broader approach and looked at the impact of COVID-19 on cardiac diagnostic procedures in over 100 countries.
The INCAPS (International Atomic Energy Agency Noninvasive Cardiology Protocols Study) group has for the past decade conducted numerous studies addressing the use of best practices and worldwide practice variation in CVD diagnosis.
For this effort, they sent a survey link to INCAPS participants worldwide, ultimately including 909 survey responses from 108 countries in the final analysis.
Compared with March 2019, overall procedure volume decreased 42% in March 2020 and 64% in April 2020.
The greatest decreases were seen in stress testing (78%) and transesophageal echocardiography (76%), both procedures, noted Dr. Einstein, associated with a greater risk of aerosolization.
“Whether as we reset after COVID we return to the same place in terms of the use of cardiovascular diagnostic testing remains to be seen, but it certainly poses an opportunity to improve our utilization of various modes of testing,” said Dr. Einstein.
Using regression analysis, Dr. Einstein and colleagues were able to see that sites located in low-income and lower-middle-income countries saw an additional 22% reduction in cardiac procedures and less availability of personal protective equipment (PPE) and telehealth.
Fifty-two percent of survey respondents reported significant shortages of N95 masks early in the pandemic, with fewer issues in supplies of gloves, gowns, and face shields. Lower-income countries were more likely to face significant PPE shortages and less likely to be able to implement telehealth strategies to make up for reduced in-person care. PPE shortage itself, however, was not related to lower procedural volume on multivariable regression.
“It all really begs the question of whether there is more that the world can do to help out the developing world in terms of managing the pandemic in all its facets,” said Dr. Einstein in an interview, adding he was “shocked” to learn how difficult it was for some lower-income countries to get sufficient PPE.
Did shutdowns go too far?
Calling this a “remarkable study,” an editorial written by Darryl P. Leong, MBBS, PhD, John W. Eikelboom, MBBS, and Salim Yusuf, MBBS, DPhil, all from McMaster University, Hamilton, Ont., suggests that perhaps health systems in some places went too far in closing down during the first wave of the pandemic, naming specifically Canada, Eastern Europe, and Saudi Arabia as examples.
“Although these measures were taken to prepare for the worst, overwhelming numbers of patients with COVID-19 did not materialize during the first wave of the pandemic in these countries. It is possible that delaying so-called nonessential services may have been unnecessary and potentially harmful, because it likely led to delays in providing care for the treatment of serious non–COVID-19 illnesses.”
Since then, more experience and more data have largely allowed hospital systems to “tackle the ebb and flow” of COVID-19 cases in ways that limit shutdowns of important health services, they said.
Given the more pronounced effect in low- and middle-income countries, they stressed the need to focus resources on ways to promote prevention and treatment that do not rely on diagnostic procedures.
“This calls for more emphasis on developing efficient systems of telehealth, especially in poorer countries or in remote settings in all countries,” Dr. Leong and colleagues conclude.
Dr. Wadhera has reported research support from the National Heart, Lung, and Blood Institute, along with fellow senior author Robert W. Yeh, MD, MBA, who has also received personal fees and grants from several companies not related to the submitted work. Dr. Einstein, Dr. Leong, Dr. Eikelboom, and Dr. Yusuf have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
While the direct toll of the COVID-19 pandemic is being tallied and shared on the nightly news, the indirect effects will undoubtedly take years to fully measure.
In two papers published online Jan. 11 in the Journal of the American College of Cardiology, researchers have started the process of quantifying the impact of the pandemic on the care of patients with cardiovascular disease (CVD).
In the first study, Rishi Wadhera, MD, MPP, MPhil, and colleagues from the Beth Israel Deaconess Medical Center and Harvard Medical School in Boston examined population-level data to determine how deaths from cardiovascular causes changed in the United States in the early months of the pandemic relative to the same periods in 2019.
In a second paper, Andrew J. Einstein, MD, PhD, from Columbia University Irving Medical Center/New York–Presbyterian Hospital and colleagues looked at the pandemic’s international impact on the diagnosis of heart disease.
Using data from the National Center for Health Statistics, Dr. Wadhera and colleagues compared death rates from cardiovascular causes in the United States from March 18, 2020, to June 2, 2020, (the first wave of the pandemic) and from Jan. 1, 2020, to March 17, 2020, (the period just before the pandemic started) and compared them to the same periods in 2019. ICD codes were used to identify underlying causes of death.
Relative to 2019, they found a significant increase in deaths from ischemic heart disease nationally (1.11; 95% confidence interval, 1.04-1.18), as well as an increase in deaths caused by hypertensive disease (1.17; 95% CI, 1.09-1.26). There was no apparent increase in deaths from heart failure, cerebrovascular disease, or other diseases of the circulatory system.
When they looked just at New York City, the area hit hardest during the early part of the pandemic, the relative increases in deaths from ischemic heart disease were more pronounced.
Deaths from ischemic heart disease or hypertensive diseases jumped 139% and 164%, respectively, between March 18, 2020, and June 2, 2020.
More modest increases in deaths were seen in the remainder of New York state, New Jersey, Michigan and Illinois, while Massachusetts and Louisiana did not see a change in cardiovascular deaths.
Several studies from different parts of the world have indicated a 40%-50% drop in hospitalization for myocardial infarction in the initial months of the pandemic, said Dr. Wadhera in an interview.
“We wanted to understand where did all the heart attacks go? And we worried that patients with urgent heart conditions were not seeking the medical care they needed. I think our data suggest that this may have been the case,” reported Dr. Wadhera.
“This very much reflects the reality of what we’re seeing on the ground,” he told this news organization. “After the initial surge ended, when hospital volumes began to return to normal, we saw patients come into the hospital who clearly had a heart attack during the surge months – and were now experiencing complications of that event – because they had initially not come into the hospital due to concerns about exposure to the virus.”
A limitation of their data, he stressed, is whether some deaths coded as CVD deaths were really deaths from undiagnosed COVID-19. “It’s possible that some portion of the increased deaths we observed really reflect the cardiovascular complications of undiagnosed COVID-19, because we know that testing was quite limited during the early first surge of cases.”
“I think that basically three factors – patients avoiding the health care system because of fear of getting COVID, health care systems being strained and overwhelmed leading to the deferral of cardiovascular care and semi-elective procedures, and the cardiovascular complications of COVID-19 itself – all probably collectively contributed to the rise in cardiovascular deaths that we observed,” said Dr. Wadhera.
In an accompanying editorial, Michael N. Young, MD, Geisel School of Medicine at Dartmouth, Lebanon, N.H., and colleagues write that these data, taken together with an earlier study showing an increase in out-of-hospital cardiac arrests at the pandemic peak in New York City, “support the notion of excess fatalities due to unattended comorbid illnesses.” That said, attribution of death in the COVID era “remains problematic.”
In the second article, Andrew Einstein, MD, PhD, and the INCAPS COVID Investigators Group took a broader approach and looked at the impact of COVID-19 on cardiac diagnostic procedures in over 100 countries.
The INCAPS (International Atomic Energy Agency Noninvasive Cardiology Protocols Study) group has for the past decade conducted numerous studies addressing the use of best practices and worldwide practice variation in CVD diagnosis.
For this effort, they sent a survey link to INCAPS participants worldwide, ultimately including 909 survey responses from 108 countries in the final analysis.
Compared with March 2019, overall procedure volume decreased 42% in March 2020 and 64% in April 2020.
The greatest decreases were seen in stress testing (78%) and transesophageal echocardiography (76%), both procedures, noted Dr. Einstein, associated with a greater risk of aerosolization.
“Whether as we reset after COVID we return to the same place in terms of the use of cardiovascular diagnostic testing remains to be seen, but it certainly poses an opportunity to improve our utilization of various modes of testing,” said Dr. Einstein.
Using regression analysis, Dr. Einstein and colleagues were able to see that sites located in low-income and lower-middle-income countries saw an additional 22% reduction in cardiac procedures and less availability of personal protective equipment (PPE) and telehealth.
Fifty-two percent of survey respondents reported significant shortages of N95 masks early in the pandemic, with fewer issues in supplies of gloves, gowns, and face shields. Lower-income countries were more likely to face significant PPE shortages and less likely to be able to implement telehealth strategies to make up for reduced in-person care. PPE shortage itself, however, was not related to lower procedural volume on multivariable regression.
“It all really begs the question of whether there is more that the world can do to help out the developing world in terms of managing the pandemic in all its facets,” said Dr. Einstein in an interview, adding he was “shocked” to learn how difficult it was for some lower-income countries to get sufficient PPE.
Did shutdowns go too far?
Calling this a “remarkable study,” an editorial written by Darryl P. Leong, MBBS, PhD, John W. Eikelboom, MBBS, and Salim Yusuf, MBBS, DPhil, all from McMaster University, Hamilton, Ont., suggests that perhaps health systems in some places went too far in closing down during the first wave of the pandemic, naming specifically Canada, Eastern Europe, and Saudi Arabia as examples.
“Although these measures were taken to prepare for the worst, overwhelming numbers of patients with COVID-19 did not materialize during the first wave of the pandemic in these countries. It is possible that delaying so-called nonessential services may have been unnecessary and potentially harmful, because it likely led to delays in providing care for the treatment of serious non–COVID-19 illnesses.”
Since then, more experience and more data have largely allowed hospital systems to “tackle the ebb and flow” of COVID-19 cases in ways that limit shutdowns of important health services, they said.
Given the more pronounced effect in low- and middle-income countries, they stressed the need to focus resources on ways to promote prevention and treatment that do not rely on diagnostic procedures.
“This calls for more emphasis on developing efficient systems of telehealth, especially in poorer countries or in remote settings in all countries,” Dr. Leong and colleagues conclude.
Dr. Wadhera has reported research support from the National Heart, Lung, and Blood Institute, along with fellow senior author Robert W. Yeh, MD, MBA, who has also received personal fees and grants from several companies not related to the submitted work. Dr. Einstein, Dr. Leong, Dr. Eikelboom, and Dr. Yusuf have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
While the direct toll of the COVID-19 pandemic is being tallied and shared on the nightly news, the indirect effects will undoubtedly take years to fully measure.
In two papers published online Jan. 11 in the Journal of the American College of Cardiology, researchers have started the process of quantifying the impact of the pandemic on the care of patients with cardiovascular disease (CVD).
In the first study, Rishi Wadhera, MD, MPP, MPhil, and colleagues from the Beth Israel Deaconess Medical Center and Harvard Medical School in Boston examined population-level data to determine how deaths from cardiovascular causes changed in the United States in the early months of the pandemic relative to the same periods in 2019.
In a second paper, Andrew J. Einstein, MD, PhD, from Columbia University Irving Medical Center/New York–Presbyterian Hospital and colleagues looked at the pandemic’s international impact on the diagnosis of heart disease.
Using data from the National Center for Health Statistics, Dr. Wadhera and colleagues compared death rates from cardiovascular causes in the United States from March 18, 2020, to June 2, 2020, (the first wave of the pandemic) and from Jan. 1, 2020, to March 17, 2020, (the period just before the pandemic started) and compared them to the same periods in 2019. ICD codes were used to identify underlying causes of death.
Relative to 2019, they found a significant increase in deaths from ischemic heart disease nationally (1.11; 95% confidence interval, 1.04-1.18), as well as an increase in deaths caused by hypertensive disease (1.17; 95% CI, 1.09-1.26). There was no apparent increase in deaths from heart failure, cerebrovascular disease, or other diseases of the circulatory system.
When they looked just at New York City, the area hit hardest during the early part of the pandemic, the relative increases in deaths from ischemic heart disease were more pronounced.
Deaths from ischemic heart disease or hypertensive diseases jumped 139% and 164%, respectively, between March 18, 2020, and June 2, 2020.
More modest increases in deaths were seen in the remainder of New York state, New Jersey, Michigan and Illinois, while Massachusetts and Louisiana did not see a change in cardiovascular deaths.
Several studies from different parts of the world have indicated a 40%-50% drop in hospitalization for myocardial infarction in the initial months of the pandemic, said Dr. Wadhera in an interview.
“We wanted to understand where did all the heart attacks go? And we worried that patients with urgent heart conditions were not seeking the medical care they needed. I think our data suggest that this may have been the case,” reported Dr. Wadhera.
“This very much reflects the reality of what we’re seeing on the ground,” he told this news organization. “After the initial surge ended, when hospital volumes began to return to normal, we saw patients come into the hospital who clearly had a heart attack during the surge months – and were now experiencing complications of that event – because they had initially not come into the hospital due to concerns about exposure to the virus.”
A limitation of their data, he stressed, is whether some deaths coded as CVD deaths were really deaths from undiagnosed COVID-19. “It’s possible that some portion of the increased deaths we observed really reflect the cardiovascular complications of undiagnosed COVID-19, because we know that testing was quite limited during the early first surge of cases.”
“I think that basically three factors – patients avoiding the health care system because of fear of getting COVID, health care systems being strained and overwhelmed leading to the deferral of cardiovascular care and semi-elective procedures, and the cardiovascular complications of COVID-19 itself – all probably collectively contributed to the rise in cardiovascular deaths that we observed,” said Dr. Wadhera.
In an accompanying editorial, Michael N. Young, MD, Geisel School of Medicine at Dartmouth, Lebanon, N.H., and colleagues write that these data, taken together with an earlier study showing an increase in out-of-hospital cardiac arrests at the pandemic peak in New York City, “support the notion of excess fatalities due to unattended comorbid illnesses.” That said, attribution of death in the COVID era “remains problematic.”
In the second article, Andrew Einstein, MD, PhD, and the INCAPS COVID Investigators Group took a broader approach and looked at the impact of COVID-19 on cardiac diagnostic procedures in over 100 countries.
The INCAPS (International Atomic Energy Agency Noninvasive Cardiology Protocols Study) group has for the past decade conducted numerous studies addressing the use of best practices and worldwide practice variation in CVD diagnosis.
For this effort, they sent a survey link to INCAPS participants worldwide, ultimately including 909 survey responses from 108 countries in the final analysis.
Compared with March 2019, overall procedure volume decreased 42% in March 2020 and 64% in April 2020.
The greatest decreases were seen in stress testing (78%) and transesophageal echocardiography (76%), both procedures, noted Dr. Einstein, associated with a greater risk of aerosolization.
“Whether as we reset after COVID we return to the same place in terms of the use of cardiovascular diagnostic testing remains to be seen, but it certainly poses an opportunity to improve our utilization of various modes of testing,” said Dr. Einstein.
Using regression analysis, Dr. Einstein and colleagues were able to see that sites located in low-income and lower-middle-income countries saw an additional 22% reduction in cardiac procedures and less availability of personal protective equipment (PPE) and telehealth.
Fifty-two percent of survey respondents reported significant shortages of N95 masks early in the pandemic, with fewer issues in supplies of gloves, gowns, and face shields. Lower-income countries were more likely to face significant PPE shortages and less likely to be able to implement telehealth strategies to make up for reduced in-person care. PPE shortage itself, however, was not related to lower procedural volume on multivariable regression.
“It all really begs the question of whether there is more that the world can do to help out the developing world in terms of managing the pandemic in all its facets,” said Dr. Einstein in an interview, adding he was “shocked” to learn how difficult it was for some lower-income countries to get sufficient PPE.
Did shutdowns go too far?
Calling this a “remarkable study,” an editorial written by Darryl P. Leong, MBBS, PhD, John W. Eikelboom, MBBS, and Salim Yusuf, MBBS, DPhil, all from McMaster University, Hamilton, Ont., suggests that perhaps health systems in some places went too far in closing down during the first wave of the pandemic, naming specifically Canada, Eastern Europe, and Saudi Arabia as examples.
“Although these measures were taken to prepare for the worst, overwhelming numbers of patients with COVID-19 did not materialize during the first wave of the pandemic in these countries. It is possible that delaying so-called nonessential services may have been unnecessary and potentially harmful, because it likely led to delays in providing care for the treatment of serious non–COVID-19 illnesses.”
Since then, more experience and more data have largely allowed hospital systems to “tackle the ebb and flow” of COVID-19 cases in ways that limit shutdowns of important health services, they said.
Given the more pronounced effect in low- and middle-income countries, they stressed the need to focus resources on ways to promote prevention and treatment that do not rely on diagnostic procedures.
“This calls for more emphasis on developing efficient systems of telehealth, especially in poorer countries or in remote settings in all countries,” Dr. Leong and colleagues conclude.
Dr. Wadhera has reported research support from the National Heart, Lung, and Blood Institute, along with fellow senior author Robert W. Yeh, MD, MBA, who has also received personal fees and grants from several companies not related to the submitted work. Dr. Einstein, Dr. Leong, Dr. Eikelboom, and Dr. Yusuf have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Natural immunity from COVID-19 ‘may last months’
Infection with the SARS-CoV-2 virus may provide some immunity for at least 5 months, interim results from a study has found.
The first report from the Sarscov2 Immunity & Reinfection Evaluation (SIREN) study suggested that antibodies from people who had recovered from COVID-19 gave at least 83% protection against reinfection compared with people who had not had the disease before.
However, Public Health England (PHE) researchers said some people with antibodies may still be able to carry and transmit the SARS-CoV-2 virus.
‘Strongly encouraged’
Susan Hopkins, PhD, senior medical advisor at PHE, who is leading the study, said the overall findings were good news. She told a briefing hosted by the Science Media Centre: “I am strongly encouraged that people have immunity that is lasting much more than the few months that was speculated before the summer.”
She added: “It allows people to feel that their prior infection will protect them from future infections but at the same time it is not complete protection, and therefore they still need to be careful when they are out and about.”
PHE scientists said they would continue to assess whether protection might last longer than 5 months.
Eleanor Riley, PhD, professor of immunology and infectious disease at the University of Edinburgh, said the report suggested that “natural infection provides short-term protection against COVID-19 that is very similar to that conferred by vaccination.”
Simon Clarke, PhD, associate professor in cellular microbiology at the University of Reading, said: “The concerning finding is that some people who have COVID antibodies appear to still be able to carry the coronavirus and could spread it to others. This means that the vast majority of the population will either need to have natural immunity or have been immunised for us to fully lift restrictions on our lives.”
The analysis took place before the new variant of SARS-CoV-2 became widespread in the UK. The PHE scientists said that further work was underway to establish whether and to what extent antibodies also provide protection from the VOC202012/01 variant.
Healthcare Workers
The SIREN preprint analysed data from 20,787 health care workers from 102 NHS trusts who had undergone antibody and PCR testing from June 18 to November 9, 2020.
Of those, 6614 tested positive for COVID-19 antibodies.
Of the 44 potential reinfections identified, two were designated ‘probable’ and 42 ‘possible’, based on available evidence.
Both of the two individuals classified as probable reinfections reported having experienced COVID-19 symptoms during the first wave of the pandemic but were not tested at the time. Both reported that their symptoms were less severe the second time.
None of the 44 potential reinfection cases were PCR tested during the first wave, but all tested positive for COVID-19 antibodies at the time they were recruited to the study.
Tom Wingfield, PhD, senior clinical lecturer at the Liverpool School of Tropical Medicine, said that given the high risk of SARS-CoV-2 infection for frontline NHS staff, it was “vital that we do all that we can to understand, predict, and prevent risk of SARS-CoV-2 amongst healthcare workers”.
The study will continue to follow participants for 12 months to explore how long any immunity may last, the effectiveness of vaccines, and to what extent people with immunity are able to carry and transmit the virus.
A version of this article first appeared on Medscape.com.
Infection with the SARS-CoV-2 virus may provide some immunity for at least 5 months, interim results from a study has found.
The first report from the Sarscov2 Immunity & Reinfection Evaluation (SIREN) study suggested that antibodies from people who had recovered from COVID-19 gave at least 83% protection against reinfection compared with people who had not had the disease before.
However, Public Health England (PHE) researchers said some people with antibodies may still be able to carry and transmit the SARS-CoV-2 virus.
‘Strongly encouraged’
Susan Hopkins, PhD, senior medical advisor at PHE, who is leading the study, said the overall findings were good news. She told a briefing hosted by the Science Media Centre: “I am strongly encouraged that people have immunity that is lasting much more than the few months that was speculated before the summer.”
She added: “It allows people to feel that their prior infection will protect them from future infections but at the same time it is not complete protection, and therefore they still need to be careful when they are out and about.”
PHE scientists said they would continue to assess whether protection might last longer than 5 months.
Eleanor Riley, PhD, professor of immunology and infectious disease at the University of Edinburgh, said the report suggested that “natural infection provides short-term protection against COVID-19 that is very similar to that conferred by vaccination.”
Simon Clarke, PhD, associate professor in cellular microbiology at the University of Reading, said: “The concerning finding is that some people who have COVID antibodies appear to still be able to carry the coronavirus and could spread it to others. This means that the vast majority of the population will either need to have natural immunity or have been immunised for us to fully lift restrictions on our lives.”
The analysis took place before the new variant of SARS-CoV-2 became widespread in the UK. The PHE scientists said that further work was underway to establish whether and to what extent antibodies also provide protection from the VOC202012/01 variant.
Healthcare Workers
The SIREN preprint analysed data from 20,787 health care workers from 102 NHS trusts who had undergone antibody and PCR testing from June 18 to November 9, 2020.
Of those, 6614 tested positive for COVID-19 antibodies.
Of the 44 potential reinfections identified, two were designated ‘probable’ and 42 ‘possible’, based on available evidence.
Both of the two individuals classified as probable reinfections reported having experienced COVID-19 symptoms during the first wave of the pandemic but were not tested at the time. Both reported that their symptoms were less severe the second time.
None of the 44 potential reinfection cases were PCR tested during the first wave, but all tested positive for COVID-19 antibodies at the time they were recruited to the study.
Tom Wingfield, PhD, senior clinical lecturer at the Liverpool School of Tropical Medicine, said that given the high risk of SARS-CoV-2 infection for frontline NHS staff, it was “vital that we do all that we can to understand, predict, and prevent risk of SARS-CoV-2 amongst healthcare workers”.
The study will continue to follow participants for 12 months to explore how long any immunity may last, the effectiveness of vaccines, and to what extent people with immunity are able to carry and transmit the virus.
A version of this article first appeared on Medscape.com.
Infection with the SARS-CoV-2 virus may provide some immunity for at least 5 months, interim results from a study has found.
The first report from the Sarscov2 Immunity & Reinfection Evaluation (SIREN) study suggested that antibodies from people who had recovered from COVID-19 gave at least 83% protection against reinfection compared with people who had not had the disease before.
However, Public Health England (PHE) researchers said some people with antibodies may still be able to carry and transmit the SARS-CoV-2 virus.
‘Strongly encouraged’
Susan Hopkins, PhD, senior medical advisor at PHE, who is leading the study, said the overall findings were good news. She told a briefing hosted by the Science Media Centre: “I am strongly encouraged that people have immunity that is lasting much more than the few months that was speculated before the summer.”
She added: “It allows people to feel that their prior infection will protect them from future infections but at the same time it is not complete protection, and therefore they still need to be careful when they are out and about.”
PHE scientists said they would continue to assess whether protection might last longer than 5 months.
Eleanor Riley, PhD, professor of immunology and infectious disease at the University of Edinburgh, said the report suggested that “natural infection provides short-term protection against COVID-19 that is very similar to that conferred by vaccination.”
Simon Clarke, PhD, associate professor in cellular microbiology at the University of Reading, said: “The concerning finding is that some people who have COVID antibodies appear to still be able to carry the coronavirus and could spread it to others. This means that the vast majority of the population will either need to have natural immunity or have been immunised for us to fully lift restrictions on our lives.”
The analysis took place before the new variant of SARS-CoV-2 became widespread in the UK. The PHE scientists said that further work was underway to establish whether and to what extent antibodies also provide protection from the VOC202012/01 variant.
Healthcare Workers
The SIREN preprint analysed data from 20,787 health care workers from 102 NHS trusts who had undergone antibody and PCR testing from June 18 to November 9, 2020.
Of those, 6614 tested positive for COVID-19 antibodies.
Of the 44 potential reinfections identified, two were designated ‘probable’ and 42 ‘possible’, based on available evidence.
Both of the two individuals classified as probable reinfections reported having experienced COVID-19 symptoms during the first wave of the pandemic but were not tested at the time. Both reported that their symptoms were less severe the second time.
None of the 44 potential reinfection cases were PCR tested during the first wave, but all tested positive for COVID-19 antibodies at the time they were recruited to the study.
Tom Wingfield, PhD, senior clinical lecturer at the Liverpool School of Tropical Medicine, said that given the high risk of SARS-CoV-2 infection for frontline NHS staff, it was “vital that we do all that we can to understand, predict, and prevent risk of SARS-CoV-2 amongst healthcare workers”.
The study will continue to follow participants for 12 months to explore how long any immunity may last, the effectiveness of vaccines, and to what extent people with immunity are able to carry and transmit the virus.
A version of this article first appeared on Medscape.com.
COVID protections suppressed flu season in U.S.
Last fall, health experts said it was possible the United States could experience an easy 2020-21 flu season because health measures to fight COVID-19 would also thwart the spread of influenza.
It looks like that happened – and then some. Numbers are strikingly low for cases of the flu and other common respiratory and gastrointestinal viruses, health experts told the Washington Post.
“It’s crazy,” Lynnette Brammer, MPH, who leads the domestic influenza surveillance team at the Centers for Disease Control and Prevention, told the Washington Post. “This is my 30th flu season. I never would have expected to see flu activity this low.”
Influenza A, influenza B, parainfluenza, norovirus, respiratory syncytial virus, human metapneumovirus, and the bacteria that cause whooping cough and pneumonia are circulating at near-record-low levels.
As an example, the Washington Post said in the third week of December 2019, the CDC’s network of clinical labs reported 16.2% of almost 30,000 samples tested positive for influenza A. During the same period in 2020, only 0.3% tested positive.
But there’s a possible downside to this suppression of viruses, because flu and other viruses may rebound once the coronavirus is brought under control.
“The best analogy is to a forest fire,” Bryan Grenfell, PhD, an epidemiologist and population biologist at Princeton (N.J.) University, told the Washington Post. “For the fire to spread, it needs to have unburned wood. For epidemics to spread, they require people who haven’t previously been infected. So if people don’t get infected this year by these viruses, they likely will at some point later on.”
American health experts like Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Disease, said last fall that they noticed Australia and other nations in the southern hemisphere had easy flu seasons, apparently because of COVID protection measures. The flu season there runs March through August.
COVID-19 now has a very low presence in Australia, but in recent months the flu has been making a comeback. Flu cases among children aged 5 and younger rose sixfold by December, when such cases are usually at their lowest, the Washington Post said.
“That’s an important cautionary tale for us,” said Kevin Messacar, MD, an infectious disease doctor at Children’s Hospital Colorado, Aurora. “Just because we get through the winter and don’t see much RSV or influenza doesn’t mean we’ll be out of the woods.”
A version of this article first appeared on WebMD.com.
Last fall, health experts said it was possible the United States could experience an easy 2020-21 flu season because health measures to fight COVID-19 would also thwart the spread of influenza.
It looks like that happened – and then some. Numbers are strikingly low for cases of the flu and other common respiratory and gastrointestinal viruses, health experts told the Washington Post.
“It’s crazy,” Lynnette Brammer, MPH, who leads the domestic influenza surveillance team at the Centers for Disease Control and Prevention, told the Washington Post. “This is my 30th flu season. I never would have expected to see flu activity this low.”
Influenza A, influenza B, parainfluenza, norovirus, respiratory syncytial virus, human metapneumovirus, and the bacteria that cause whooping cough and pneumonia are circulating at near-record-low levels.
As an example, the Washington Post said in the third week of December 2019, the CDC’s network of clinical labs reported 16.2% of almost 30,000 samples tested positive for influenza A. During the same period in 2020, only 0.3% tested positive.
But there’s a possible downside to this suppression of viruses, because flu and other viruses may rebound once the coronavirus is brought under control.
“The best analogy is to a forest fire,” Bryan Grenfell, PhD, an epidemiologist and population biologist at Princeton (N.J.) University, told the Washington Post. “For the fire to spread, it needs to have unburned wood. For epidemics to spread, they require people who haven’t previously been infected. So if people don’t get infected this year by these viruses, they likely will at some point later on.”
American health experts like Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Disease, said last fall that they noticed Australia and other nations in the southern hemisphere had easy flu seasons, apparently because of COVID protection measures. The flu season there runs March through August.
COVID-19 now has a very low presence in Australia, but in recent months the flu has been making a comeback. Flu cases among children aged 5 and younger rose sixfold by December, when such cases are usually at their lowest, the Washington Post said.
“That’s an important cautionary tale for us,” said Kevin Messacar, MD, an infectious disease doctor at Children’s Hospital Colorado, Aurora. “Just because we get through the winter and don’t see much RSV or influenza doesn’t mean we’ll be out of the woods.”
A version of this article first appeared on WebMD.com.
Last fall, health experts said it was possible the United States could experience an easy 2020-21 flu season because health measures to fight COVID-19 would also thwart the spread of influenza.
It looks like that happened – and then some. Numbers are strikingly low for cases of the flu and other common respiratory and gastrointestinal viruses, health experts told the Washington Post.
“It’s crazy,” Lynnette Brammer, MPH, who leads the domestic influenza surveillance team at the Centers for Disease Control and Prevention, told the Washington Post. “This is my 30th flu season. I never would have expected to see flu activity this low.”
Influenza A, influenza B, parainfluenza, norovirus, respiratory syncytial virus, human metapneumovirus, and the bacteria that cause whooping cough and pneumonia are circulating at near-record-low levels.
As an example, the Washington Post said in the third week of December 2019, the CDC’s network of clinical labs reported 16.2% of almost 30,000 samples tested positive for influenza A. During the same period in 2020, only 0.3% tested positive.
But there’s a possible downside to this suppression of viruses, because flu and other viruses may rebound once the coronavirus is brought under control.
“The best analogy is to a forest fire,” Bryan Grenfell, PhD, an epidemiologist and population biologist at Princeton (N.J.) University, told the Washington Post. “For the fire to spread, it needs to have unburned wood. For epidemics to spread, they require people who haven’t previously been infected. So if people don’t get infected this year by these viruses, they likely will at some point later on.”
American health experts like Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Disease, said last fall that they noticed Australia and other nations in the southern hemisphere had easy flu seasons, apparently because of COVID protection measures. The flu season there runs March through August.
COVID-19 now has a very low presence in Australia, but in recent months the flu has been making a comeback. Flu cases among children aged 5 and younger rose sixfold by December, when such cases are usually at their lowest, the Washington Post said.
“That’s an important cautionary tale for us,” said Kevin Messacar, MD, an infectious disease doctor at Children’s Hospital Colorado, Aurora. “Just because we get through the winter and don’t see much RSV or influenza doesn’t mean we’ll be out of the woods.”
A version of this article first appeared on WebMD.com.
Diversification of dermatology workforce takes shape
Stephanie Florez-Pollack, MD, a dermatology resident at the University of Pennsylvania, Philadelphia, began considering the field of dermatology when, as part of the Latino Medical Students Association, she was invited by Amit Pandya, MD, to a pizza party and dermatology discussion during her first year of medical school at the University of Texas Southwestern Medical Center, Dallas.

There, she met three Latinx residents who were part of the University of Texas Southwestern dermatology program. “I was so excited to hear their stories, where they came from, and how they ended up in dermatology,” she said. Dermatology had not been on her radar screen. Now there was a spark.
Volunteering at the free Agape dermatology clinic in Dallas later that year sharpened her interest. “For the first time, I really saw myself working in the field. Hearing patients’ stories and what they went through with what many people might think are very simple skin diseases made me realize there was potential to make a big impact in a person’s life,” said Dr. Florez-Pollack, who immigrated from Colombia with her family when she was 15.
– one that reflects the ethnic and racial make-up of the population. It’s a movement that involves early outreach to medical students, stepped-up mentorship and sponsorship, implicit bias training, and holistic review of residency applicants.
There is no published study of all the changes being made – of how many dermatology programs have new outreach programs, for instance, or new approaches to resident application reviews. However, participation in the American Academy of Dermatology Diversity Champions program increased significantly between 2019 and 2020, and a sizable body of articles and editorials on diversity have been published in the dermatology literature in recent years, including at least several on holistic review of resident applications. Five years ago, there were few publications, sources said.
“The conversation is happening now at multiple levels, including in our peer-reviewed literature, where people are looking objectively at ... how we can make changes for the better,” said Nada Elbuluk, MD, director of the dermatology diversity and inclusion program at the University of Southern California, Los Angeles.
Unpublished findings also indicate that the number of UIM dermatology residents is inching upward. “Residency selection may not be on everyone’s mind, but an understanding of how we select people into our specialty is something every derm should know about and care about,” said Kanade Shinkai, MD, PhD, professor of dermatology at the University of California, San Francisco, and editor in chief of JAMA Dermatology.
The wake-up calls
The impetus for current changes first came in 2015, when Bruce Wintroub, MD, professor and chair of dermatology at UCSF, and interim dean of the medical school at the time, delivered a passionate plenary lecture at the annual AAD meeting about the lack of equity, diversity and inclusion in the specialty and the role of unconscious bias. Moved in part by a “White Coats for Black Lives” die-in by medical students on his campus following the killing of unarmed Black men, Dr. Wintroub called on his colleagues to recruit more UIM physicians into the specialty and to make the field more inclusive.
In 2016, Dr. Wintroub joined Dr. Pandya and two other academic dermatologists in authoring a commentary, published in the Journal of the American Academy of Dermatology, about the need to step up efforts and make diversity a priority. Dermatology was among the least ethnically and racially diverse specialties, second only to orthopedics, they wrote, with black dermatologists making up only 3% of all dermatologists and Hispanics only 4.2% in the United States, compared with 12.8% and 16.3% in the U.S. population, respectively.
For the next year or so, they and others from six academic institutions formed an incubator of sorts, actively tracking and sharing actions they were taking to improve diversity and the practice environment. “We wanted to learn from each other, then disseminate information to other programs,” said Dr. Pandya, who chaired the AAD diversity task force and led the self-branded “diversity champions.” (Dr. Pandya maintains his appointment at UTSW but now practices at the Palo Alto Foundation Medical Group in Sunnyvale, Calif.)
In 2017, at a President’s Conference on Diversity in Dermatology called for by then-AAD president Henry Lim, MD, leaders of the Association of Professors of Dermatology, the Society for Investigative Dermatology, and other dermatology organizations agreed on key action items, which they described in JAAD in 2018: Helping to increase the pipeline of UIM students applying to medical school, increasing UIM medical students’ early exposure to dermatology, and increasing the number of UIM students recruited into dermatology residency programs.
Diversity in the physician workforce has been shown to improve outcomes for all patients, and is important for ameliorating health care disparities and improving satisfaction and care for all patients, the authors of the 2018 paper wrote. “Multiple studies,” they noted, “have shown that UIM physicians are more likely to practice in areas where health care disparities exist.”
For specific proposed actions, the leaders attending the diversity conference drew largely upon the “diversity champions’” experiences, and agreed to fund and officially develop a diversity champions program. They also decided to invest in “bioskills” workshops for undergraduates and medical students at historically black colleges and universities, and other institutions at historically black colleges and universities at medical schools through a partnership with Nth Dimension – an organization founded in 2004 to bring more women and underrepresented minorities into orthopedic surgery.
In the last 2 years, more than 450 UIM students have attended these bioskills workshops, getting a taste of basic dermatology procedures and interacting with dermatologists.
And in September 2020, 157 dermatologists representing 80 programs throughout the country attended the second AAD Diversity Champions conference, up from 84 attendees and 30 programs in 2019. On the agenda: Discussions of holistic application review, mentorship, recruitment of UIM faculty, and a 2-hour session on microaggressions. Similar programs are being led by other dermatology organizations.
(UIM was coined by the American Association of Medical Colleges to describe racial and ethnic populations that are underrepresented in medicine relative to their numbers in the general population.)
Achievement of racial/ethnic diversity “won’t happen unless the field actively encourages people to look at it – which is not what we were doing,” Dr. Wintroub said in an interview. “I think that’s been the major change. We’re opening the door and saying: ‘We want you and we welcome you.’ ”
Rethinking traditional mentorship
For Dr. Florez-Pollack, the door almost shut when she began to hear from fellow medical students that dermatology is “too competitive ... a field for only the top people in the class.” She felt doubt settling in.
“I had peers who were throwing a lot of money toward prep materials ... peers who had siblings in medicine and had started studying from day one [for the step 1 exam],” she said. “I thought, was it really worth the effort? Do I really want to be perfect to get into the field when other fields would be happy to have me as I am right now?”
Her immense enjoyment of an “Art of Observation” elective course helped renew her interest in the field; it reinforced her visual abilities as well as the potential for her to address implicit bias as a dermatologist. She sought Dr. Pandya’s guidance and sponsorship to help her grow connections, polish her resume, and present herself to other faculty.
Doors were opened, she said, for her to secure a 1-year research experience before her final year of medical school with UTSW faculty, and then a 1-month rotation/mentorship with William D. James, MD, professor of dermatology at the University of Pennsylvania, an institution with a history of diversity initiatives and a longstanding skin of color program.
Dr. Florez-Pollack sees her experience reflected in the findings of a recently published study – a thematic content analysis of telephone interviews with applicants to the UTSW dermatology residency program during the 2013-14 and 2014-15 application cycles. Of the 44 applicants who participated in the study, 13 were UIM applicants.
Six of the seven UIM applicants who matched were involved in a pipeline or enrichment program – and were exposed to the field early – compared with one or two of the six UIM applicants who did not match. Underrepresented applicants were more often discouraged from applying (54%) – told, for instance, that they could better serve their communities through other specialties – than were non-UIM applicants (13%). They also were affected more often by a lack of equitable resources, according to comments made by 70% of applicants (UIM and non-UIM).
Also notably, the investigators said, all of the UIM applicants who matched (and the majority of non-UIMs who matched) reported having a mentor during the process of applying, compared with 44% of those who didn’t match.
Rebecca Vasquez, MD, assistant professor of dermatology at UTSW, who led the study, was herself a mentee of Dr. Pandya. “He believed in me and gave me the courage to consider dermatology,” she said. (Dr. Vasquez was one of the Latinx women who inspired Dr. Florez-Pollack, in turn, when they met at Dr. Pandya’s pizza party. Dr. Florez-Pollack assisted with the research and was a coauthor of the study.)
Amy McMichael, MD, professor and chair of dermatology at Wake Forest University, Winston-Salem, N.C., said that dermatology as a field has traditionally been “very good at mentoring.” Many of the dermatology societies have long had mentorship programs, for instance, that guide medical students, and sometimes residents, through defined experiences or through periods of time.
But she advocates going deeper. “When it comes to sponsorship, we fall a little short,” she said. “Sponsorship is about promoting that person to the next level, making sure they achieve what they want to achieve ... putting them up for opportunities they may not have known existed. It’s continuous and focused.”
Olabola Awosika, MD, a fourth-year dermatology resident at Henry Ford Health System, Detroit, said her interest in dermatology was solidified during her participation in the AAD’s month-long mentorship program after her second year of medical school at Howard University, Washington. However, it wasn’t until her fourth year, when she did an away rotation at Wake Forest, that she realized that “gaining access to the field” takes years of mentorship, research opportunities, and networking. It was too late.
After initially not matching, she did a rotation at Johns Hopkins in dermatology during an internship year, followed by a 2-year research fellowship at George Washington University, Washington. As does Dr. Florez-Pollack, who now mentors medical students. She also serves on the Women’s Dermatologic Society diversity committee, which is now developing initiatives to help UIM dermatologists “become upwardly mobile in dermatology [after residency], so they have a seat at the table in various settings.”
Holistic review for residency
Dr. Vasquez, who grew up in South Texas in an uninsured family that received most of its medical care across the border in Mexico, believes that the “biggest stride being made today” with respect to diversity in the dermatology workforce – and in the larger physician workforce – is increased understanding of the role of social and cultural capital.

“We’d never really talked about this concept ... about how, if you don’t have the same upbringing, education, and resources, you’re already behind … and you may not do as well on standardized tests,” she said. “Now people are listening to it and understand it. That’s why more programs are looking at how to practice a more holistic approach to selecting applicants to interview.”
Some dermatology programs – at Wake Forest, UCSF, USC, Vanderbilt, and George Washington University for instance – have eliminated the use of U.S. Medical Licensing Examination step 1 scores and Alpha Omega Alpha Medical Honor Society status as filtering/screening metrics. Some also take a “second look” at UIM applicants.
Overall, those making changes are looking “at everything the applicant brings to the table – their story, their experiences,” said Dr. Elbuluk. “We want to understand the full picture of who they are and their journey to becoming a physician.”
Implicit bias training for members of residency review committees is becoming more common, as is such training across the board in dermatology departments. “We have to bring it to the forefront so that we can create more inclusive environments,” said Sharon E. Albers, MD, a dermatologist at Vanderbilt University Medical Center, Nashville, Tenn., who serves as the dermatology department’s diversity liaison to the medical school, and who, as a former faculty member of Meharry Medical College, remains engaged with the historically black institution.
One of her recent efforts, inspired by participation in the diversity champions program, has been developing pipeline programs to speak to middle and high school students about medicine and dermatology. For now, however, she credits a holistic review process for change. Last year, three of the five matched dermatology residents at Vanderbilt were UIM physicians – unprecedented for the institution, Dr. Albers said, and “evidence that holistic review works if you’re very intentional about it.”
Dr. Vasquez has analyzed data from the Accreditation Council of Graduate Medical Education and says that UIM dermatology residents comprised 8.0% of the total in 2019, marking an improvement over the prior 7 years. “We’ve introduced so many changes at the same time,” making it difficult to discern what’s most impactful, she said. “But something is working.”
(The AAMC, which has invested in pipeline programs for more than a decade and has championed holistic medical school admissions, states in its 2019 diversity data report that efforts to improve diversity in medicine have made “only marginal differences” – and that Black males in particular continue to be significantly underrepresented in medical schools. Persistent, structural racism was a common theme in the association’s 2015 report on Black males in medicine.)
Efforts to diversify the workforce – particularly holistic review – haven’t been without detractors. “It brings reaction,” Dr. Wintroub said. “Some people think you’re lowering quality in the field ... but that’s just not true.”
Diversity in the dermatology workforce is important not only for the care of patients from diverse backgrounds, but “perhaps more importantly, it brings new ideas and views and experiences into the field,” he said. “It pushes us to think in new directions ... that can only make our field better and richer.”
“We need to make sure our workforce is representative of the patients we serve – but also that all derms can manage patients of all skin types and demographics,” Dr. Shinkai said. “And we need more diversity in the leadership of our departments and dermatology organizations ... inclusivity needs to extend all the way to the highest reaches of our specialty.”
Adam Friedman, MD, professor and interim chair of dermatology at George Washington University and director of the department’s diversity, equity, and inclusion committee, agreed. “We need to both make sure our workforce mirrors the patients we serve, and said workforce is prepared to manage patients of all skin types and demographics. We need to cover the spectrum, from revamping medical education and mentorship opportunities to advancing diversity in the leadership of our departments, institutions, and societies. Addressing only part of the puzzle will not and can not be enough.”
Correction, 3/3/21: An earlier version of this article misstated Dr. Stephanie Florez-Pollack's name.
Stephanie Florez-Pollack, MD, a dermatology resident at the University of Pennsylvania, Philadelphia, began considering the field of dermatology when, as part of the Latino Medical Students Association, she was invited by Amit Pandya, MD, to a pizza party and dermatology discussion during her first year of medical school at the University of Texas Southwestern Medical Center, Dallas.
There, she met three Latinx residents who were part of the University of Texas Southwestern dermatology program. “I was so excited to hear their stories, where they came from, and how they ended up in dermatology,” she said. Dermatology had not been on her radar screen. Now there was a spark.
Volunteering at the free Agape dermatology clinic in Dallas later that year sharpened her interest. “For the first time, I really saw myself working in the field. Hearing patients’ stories and what they went through with what many people might think are very simple skin diseases made me realize there was potential to make a big impact in a person’s life,” said Dr. Florez-Pollack, who immigrated from Colombia with her family when she was 15.
– one that reflects the ethnic and racial make-up of the population. It’s a movement that involves early outreach to medical students, stepped-up mentorship and sponsorship, implicit bias training, and holistic review of residency applicants.
There is no published study of all the changes being made – of how many dermatology programs have new outreach programs, for instance, or new approaches to resident application reviews. However, participation in the American Academy of Dermatology Diversity Champions program increased significantly between 2019 and 2020, and a sizable body of articles and editorials on diversity have been published in the dermatology literature in recent years, including at least several on holistic review of resident applications. Five years ago, there were few publications, sources said.
“The conversation is happening now at multiple levels, including in our peer-reviewed literature, where people are looking objectively at ... how we can make changes for the better,” said Nada Elbuluk, MD, director of the dermatology diversity and inclusion program at the University of Southern California, Los Angeles.
Unpublished findings also indicate that the number of UIM dermatology residents is inching upward. “Residency selection may not be on everyone’s mind, but an understanding of how we select people into our specialty is something every derm should know about and care about,” said Kanade Shinkai, MD, PhD, professor of dermatology at the University of California, San Francisco, and editor in chief of JAMA Dermatology.
The wake-up calls
The impetus for current changes first came in 2015, when Bruce Wintroub, MD, professor and chair of dermatology at UCSF, and interim dean of the medical school at the time, delivered a passionate plenary lecture at the annual AAD meeting about the lack of equity, diversity and inclusion in the specialty and the role of unconscious bias. Moved in part by a “White Coats for Black Lives” die-in by medical students on his campus following the killing of unarmed Black men, Dr. Wintroub called on his colleagues to recruit more UIM physicians into the specialty and to make the field more inclusive.
In 2016, Dr. Wintroub joined Dr. Pandya and two other academic dermatologists in authoring a commentary, published in the Journal of the American Academy of Dermatology, about the need to step up efforts and make diversity a priority. Dermatology was among the least ethnically and racially diverse specialties, second only to orthopedics, they wrote, with black dermatologists making up only 3% of all dermatologists and Hispanics only 4.2% in the United States, compared with 12.8% and 16.3% in the U.S. population, respectively.
For the next year or so, they and others from six academic institutions formed an incubator of sorts, actively tracking and sharing actions they were taking to improve diversity and the practice environment. “We wanted to learn from each other, then disseminate information to other programs,” said Dr. Pandya, who chaired the AAD diversity task force and led the self-branded “diversity champions.” (Dr. Pandya maintains his appointment at UTSW but now practices at the Palo Alto Foundation Medical Group in Sunnyvale, Calif.)
In 2017, at a President’s Conference on Diversity in Dermatology called for by then-AAD president Henry Lim, MD, leaders of the Association of Professors of Dermatology, the Society for Investigative Dermatology, and other dermatology organizations agreed on key action items, which they described in JAAD in 2018: Helping to increase the pipeline of UIM students applying to medical school, increasing UIM medical students’ early exposure to dermatology, and increasing the number of UIM students recruited into dermatology residency programs.
Diversity in the physician workforce has been shown to improve outcomes for all patients, and is important for ameliorating health care disparities and improving satisfaction and care for all patients, the authors of the 2018 paper wrote. “Multiple studies,” they noted, “have shown that UIM physicians are more likely to practice in areas where health care disparities exist.”
For specific proposed actions, the leaders attending the diversity conference drew largely upon the “diversity champions’” experiences, and agreed to fund and officially develop a diversity champions program. They also decided to invest in “bioskills” workshops for undergraduates and medical students at historically black colleges and universities, and other institutions at historically black colleges and universities at medical schools through a partnership with Nth Dimension – an organization founded in 2004 to bring more women and underrepresented minorities into orthopedic surgery.
In the last 2 years, more than 450 UIM students have attended these bioskills workshops, getting a taste of basic dermatology procedures and interacting with dermatologists.
And in September 2020, 157 dermatologists representing 80 programs throughout the country attended the second AAD Diversity Champions conference, up from 84 attendees and 30 programs in 2019. On the agenda: Discussions of holistic application review, mentorship, recruitment of UIM faculty, and a 2-hour session on microaggressions. Similar programs are being led by other dermatology organizations.
(UIM was coined by the American Association of Medical Colleges to describe racial and ethnic populations that are underrepresented in medicine relative to their numbers in the general population.)
Achievement of racial/ethnic diversity “won’t happen unless the field actively encourages people to look at it – which is not what we were doing,” Dr. Wintroub said in an interview. “I think that’s been the major change. We’re opening the door and saying: ‘We want you and we welcome you.’ ”
Rethinking traditional mentorship
For Dr. Florez-Pollack, the door almost shut when she began to hear from fellow medical students that dermatology is “too competitive ... a field for only the top people in the class.” She felt doubt settling in.
“I had peers who were throwing a lot of money toward prep materials ... peers who had siblings in medicine and had started studying from day one [for the step 1 exam],” she said. “I thought, was it really worth the effort? Do I really want to be perfect to get into the field when other fields would be happy to have me as I am right now?”
Her immense enjoyment of an “Art of Observation” elective course helped renew her interest in the field; it reinforced her visual abilities as well as the potential for her to address implicit bias as a dermatologist. She sought Dr. Pandya’s guidance and sponsorship to help her grow connections, polish her resume, and present herself to other faculty.
Doors were opened, she said, for her to secure a 1-year research experience before her final year of medical school with UTSW faculty, and then a 1-month rotation/mentorship with William D. James, MD, professor of dermatology at the University of Pennsylvania, an institution with a history of diversity initiatives and a longstanding skin of color program.
Dr. Florez-Pollack sees her experience reflected in the findings of a recently published study – a thematic content analysis of telephone interviews with applicants to the UTSW dermatology residency program during the 2013-14 and 2014-15 application cycles. Of the 44 applicants who participated in the study, 13 were UIM applicants.
Six of the seven UIM applicants who matched were involved in a pipeline or enrichment program – and were exposed to the field early – compared with one or two of the six UIM applicants who did not match. Underrepresented applicants were more often discouraged from applying (54%) – told, for instance, that they could better serve their communities through other specialties – than were non-UIM applicants (13%). They also were affected more often by a lack of equitable resources, according to comments made by 70% of applicants (UIM and non-UIM).
Also notably, the investigators said, all of the UIM applicants who matched (and the majority of non-UIMs who matched) reported having a mentor during the process of applying, compared with 44% of those who didn’t match.
Rebecca Vasquez, MD, assistant professor of dermatology at UTSW, who led the study, was herself a mentee of Dr. Pandya. “He believed in me and gave me the courage to consider dermatology,” she said. (Dr. Vasquez was one of the Latinx women who inspired Dr. Florez-Pollack, in turn, when they met at Dr. Pandya’s pizza party. Dr. Florez-Pollack assisted with the research and was a coauthor of the study.)
Amy McMichael, MD, professor and chair of dermatology at Wake Forest University, Winston-Salem, N.C., said that dermatology as a field has traditionally been “very good at mentoring.” Many of the dermatology societies have long had mentorship programs, for instance, that guide medical students, and sometimes residents, through defined experiences or through periods of time.
But she advocates going deeper. “When it comes to sponsorship, we fall a little short,” she said. “Sponsorship is about promoting that person to the next level, making sure they achieve what they want to achieve ... putting them up for opportunities they may not have known existed. It’s continuous and focused.”
Olabola Awosika, MD, a fourth-year dermatology resident at Henry Ford Health System, Detroit, said her interest in dermatology was solidified during her participation in the AAD’s month-long mentorship program after her second year of medical school at Howard University, Washington. However, it wasn’t until her fourth year, when she did an away rotation at Wake Forest, that she realized that “gaining access to the field” takes years of mentorship, research opportunities, and networking. It was too late.
After initially not matching, she did a rotation at Johns Hopkins in dermatology during an internship year, followed by a 2-year research fellowship at George Washington University, Washington. As does Dr. Florez-Pollack, who now mentors medical students. She also serves on the Women’s Dermatologic Society diversity committee, which is now developing initiatives to help UIM dermatologists “become upwardly mobile in dermatology [after residency], so they have a seat at the table in various settings.”
Holistic review for residency
Dr. Vasquez, who grew up in South Texas in an uninsured family that received most of its medical care across the border in Mexico, believes that the “biggest stride being made today” with respect to diversity in the dermatology workforce – and in the larger physician workforce – is increased understanding of the role of social and cultural capital.
“We’d never really talked about this concept ... about how, if you don’t have the same upbringing, education, and resources, you’re already behind … and you may not do as well on standardized tests,” she said. “Now people are listening to it and understand it. That’s why more programs are looking at how to practice a more holistic approach to selecting applicants to interview.”
Some dermatology programs – at Wake Forest, UCSF, USC, Vanderbilt, and George Washington University for instance – have eliminated the use of U.S. Medical Licensing Examination step 1 scores and Alpha Omega Alpha Medical Honor Society status as filtering/screening metrics. Some also take a “second look” at UIM applicants.
Overall, those making changes are looking “at everything the applicant brings to the table – their story, their experiences,” said Dr. Elbuluk. “We want to understand the full picture of who they are and their journey to becoming a physician.”
Implicit bias training for members of residency review committees is becoming more common, as is such training across the board in dermatology departments. “We have to bring it to the forefront so that we can create more inclusive environments,” said Sharon E. Albers, MD, a dermatologist at Vanderbilt University Medical Center, Nashville, Tenn., who serves as the dermatology department’s diversity liaison to the medical school, and who, as a former faculty member of Meharry Medical College, remains engaged with the historically black institution.
One of her recent efforts, inspired by participation in the diversity champions program, has been developing pipeline programs to speak to middle and high school students about medicine and dermatology. For now, however, she credits a holistic review process for change. Last year, three of the five matched dermatology residents at Vanderbilt were UIM physicians – unprecedented for the institution, Dr. Albers said, and “evidence that holistic review works if you’re very intentional about it.”
Dr. Vasquez has analyzed data from the Accreditation Council of Graduate Medical Education and says that UIM dermatology residents comprised 8.0% of the total in 2019, marking an improvement over the prior 7 years. “We’ve introduced so many changes at the same time,” making it difficult to discern what’s most impactful, she said. “But something is working.”
(The AAMC, which has invested in pipeline programs for more than a decade and has championed holistic medical school admissions, states in its 2019 diversity data report that efforts to improve diversity in medicine have made “only marginal differences” – and that Black males in particular continue to be significantly underrepresented in medical schools. Persistent, structural racism was a common theme in the association’s 2015 report on Black males in medicine.)
Efforts to diversify the workforce – particularly holistic review – haven’t been without detractors. “It brings reaction,” Dr. Wintroub said. “Some people think you’re lowering quality in the field ... but that’s just not true.”
Diversity in the dermatology workforce is important not only for the care of patients from diverse backgrounds, but “perhaps more importantly, it brings new ideas and views and experiences into the field,” he said. “It pushes us to think in new directions ... that can only make our field better and richer.”
“We need to make sure our workforce is representative of the patients we serve – but also that all derms can manage patients of all skin types and demographics,” Dr. Shinkai said. “And we need more diversity in the leadership of our departments and dermatology organizations ... inclusivity needs to extend all the way to the highest reaches of our specialty.”
Adam Friedman, MD, professor and interim chair of dermatology at George Washington University and director of the department’s diversity, equity, and inclusion committee, agreed. “We need to both make sure our workforce mirrors the patients we serve, and said workforce is prepared to manage patients of all skin types and demographics. We need to cover the spectrum, from revamping medical education and mentorship opportunities to advancing diversity in the leadership of our departments, institutions, and societies. Addressing only part of the puzzle will not and can not be enough.”
Correction, 3/3/21: An earlier version of this article misstated Dr. Stephanie Florez-Pollack's name.
Stephanie Florez-Pollack, MD, a dermatology resident at the University of Pennsylvania, Philadelphia, began considering the field of dermatology when, as part of the Latino Medical Students Association, she was invited by Amit Pandya, MD, to a pizza party and dermatology discussion during her first year of medical school at the University of Texas Southwestern Medical Center, Dallas.
There, she met three Latinx residents who were part of the University of Texas Southwestern dermatology program. “I was so excited to hear their stories, where they came from, and how they ended up in dermatology,” she said. Dermatology had not been on her radar screen. Now there was a spark.
Volunteering at the free Agape dermatology clinic in Dallas later that year sharpened her interest. “For the first time, I really saw myself working in the field. Hearing patients’ stories and what they went through with what many people might think are very simple skin diseases made me realize there was potential to make a big impact in a person’s life,” said Dr. Florez-Pollack, who immigrated from Colombia with her family when she was 15.
– one that reflects the ethnic and racial make-up of the population. It’s a movement that involves early outreach to medical students, stepped-up mentorship and sponsorship, implicit bias training, and holistic review of residency applicants.
There is no published study of all the changes being made – of how many dermatology programs have new outreach programs, for instance, or new approaches to resident application reviews. However, participation in the American Academy of Dermatology Diversity Champions program increased significantly between 2019 and 2020, and a sizable body of articles and editorials on diversity have been published in the dermatology literature in recent years, including at least several on holistic review of resident applications. Five years ago, there were few publications, sources said.
“The conversation is happening now at multiple levels, including in our peer-reviewed literature, where people are looking objectively at ... how we can make changes for the better,” said Nada Elbuluk, MD, director of the dermatology diversity and inclusion program at the University of Southern California, Los Angeles.
Unpublished findings also indicate that the number of UIM dermatology residents is inching upward. “Residency selection may not be on everyone’s mind, but an understanding of how we select people into our specialty is something every derm should know about and care about,” said Kanade Shinkai, MD, PhD, professor of dermatology at the University of California, San Francisco, and editor in chief of JAMA Dermatology.
The wake-up calls
The impetus for current changes first came in 2015, when Bruce Wintroub, MD, professor and chair of dermatology at UCSF, and interim dean of the medical school at the time, delivered a passionate plenary lecture at the annual AAD meeting about the lack of equity, diversity and inclusion in the specialty and the role of unconscious bias. Moved in part by a “White Coats for Black Lives” die-in by medical students on his campus following the killing of unarmed Black men, Dr. Wintroub called on his colleagues to recruit more UIM physicians into the specialty and to make the field more inclusive.
In 2016, Dr. Wintroub joined Dr. Pandya and two other academic dermatologists in authoring a commentary, published in the Journal of the American Academy of Dermatology, about the need to step up efforts and make diversity a priority. Dermatology was among the least ethnically and racially diverse specialties, second only to orthopedics, they wrote, with black dermatologists making up only 3% of all dermatologists and Hispanics only 4.2% in the United States, compared with 12.8% and 16.3% in the U.S. population, respectively.
For the next year or so, they and others from six academic institutions formed an incubator of sorts, actively tracking and sharing actions they were taking to improve diversity and the practice environment. “We wanted to learn from each other, then disseminate information to other programs,” said Dr. Pandya, who chaired the AAD diversity task force and led the self-branded “diversity champions.” (Dr. Pandya maintains his appointment at UTSW but now practices at the Palo Alto Foundation Medical Group in Sunnyvale, Calif.)
In 2017, at a President’s Conference on Diversity in Dermatology called for by then-AAD president Henry Lim, MD, leaders of the Association of Professors of Dermatology, the Society for Investigative Dermatology, and other dermatology organizations agreed on key action items, which they described in JAAD in 2018: Helping to increase the pipeline of UIM students applying to medical school, increasing UIM medical students’ early exposure to dermatology, and increasing the number of UIM students recruited into dermatology residency programs.
Diversity in the physician workforce has been shown to improve outcomes for all patients, and is important for ameliorating health care disparities and improving satisfaction and care for all patients, the authors of the 2018 paper wrote. “Multiple studies,” they noted, “have shown that UIM physicians are more likely to practice in areas where health care disparities exist.”
For specific proposed actions, the leaders attending the diversity conference drew largely upon the “diversity champions’” experiences, and agreed to fund and officially develop a diversity champions program. They also decided to invest in “bioskills” workshops for undergraduates and medical students at historically black colleges and universities, and other institutions at historically black colleges and universities at medical schools through a partnership with Nth Dimension – an organization founded in 2004 to bring more women and underrepresented minorities into orthopedic surgery.
In the last 2 years, more than 450 UIM students have attended these bioskills workshops, getting a taste of basic dermatology procedures and interacting with dermatologists.
And in September 2020, 157 dermatologists representing 80 programs throughout the country attended the second AAD Diversity Champions conference, up from 84 attendees and 30 programs in 2019. On the agenda: Discussions of holistic application review, mentorship, recruitment of UIM faculty, and a 2-hour session on microaggressions. Similar programs are being led by other dermatology organizations.
(UIM was coined by the American Association of Medical Colleges to describe racial and ethnic populations that are underrepresented in medicine relative to their numbers in the general population.)
Achievement of racial/ethnic diversity “won’t happen unless the field actively encourages people to look at it – which is not what we were doing,” Dr. Wintroub said in an interview. “I think that’s been the major change. We’re opening the door and saying: ‘We want you and we welcome you.’ ”
Rethinking traditional mentorship
For Dr. Florez-Pollack, the door almost shut when she began to hear from fellow medical students that dermatology is “too competitive ... a field for only the top people in the class.” She felt doubt settling in.
“I had peers who were throwing a lot of money toward prep materials ... peers who had siblings in medicine and had started studying from day one [for the step 1 exam],” she said. “I thought, was it really worth the effort? Do I really want to be perfect to get into the field when other fields would be happy to have me as I am right now?”
Her immense enjoyment of an “Art of Observation” elective course helped renew her interest in the field; it reinforced her visual abilities as well as the potential for her to address implicit bias as a dermatologist. She sought Dr. Pandya’s guidance and sponsorship to help her grow connections, polish her resume, and present herself to other faculty.
Doors were opened, she said, for her to secure a 1-year research experience before her final year of medical school with UTSW faculty, and then a 1-month rotation/mentorship with William D. James, MD, professor of dermatology at the University of Pennsylvania, an institution with a history of diversity initiatives and a longstanding skin of color program.
Dr. Florez-Pollack sees her experience reflected in the findings of a recently published study – a thematic content analysis of telephone interviews with applicants to the UTSW dermatology residency program during the 2013-14 and 2014-15 application cycles. Of the 44 applicants who participated in the study, 13 were UIM applicants.
Six of the seven UIM applicants who matched were involved in a pipeline or enrichment program – and were exposed to the field early – compared with one or two of the six UIM applicants who did not match. Underrepresented applicants were more often discouraged from applying (54%) – told, for instance, that they could better serve their communities through other specialties – than were non-UIM applicants (13%). They also were affected more often by a lack of equitable resources, according to comments made by 70% of applicants (UIM and non-UIM).
Also notably, the investigators said, all of the UIM applicants who matched (and the majority of non-UIMs who matched) reported having a mentor during the process of applying, compared with 44% of those who didn’t match.
Rebecca Vasquez, MD, assistant professor of dermatology at UTSW, who led the study, was herself a mentee of Dr. Pandya. “He believed in me and gave me the courage to consider dermatology,” she said. (Dr. Vasquez was one of the Latinx women who inspired Dr. Florez-Pollack, in turn, when they met at Dr. Pandya’s pizza party. Dr. Florez-Pollack assisted with the research and was a coauthor of the study.)
Amy McMichael, MD, professor and chair of dermatology at Wake Forest University, Winston-Salem, N.C., said that dermatology as a field has traditionally been “very good at mentoring.” Many of the dermatology societies have long had mentorship programs, for instance, that guide medical students, and sometimes residents, through defined experiences or through periods of time.
But she advocates going deeper. “When it comes to sponsorship, we fall a little short,” she said. “Sponsorship is about promoting that person to the next level, making sure they achieve what they want to achieve ... putting them up for opportunities they may not have known existed. It’s continuous and focused.”
Olabola Awosika, MD, a fourth-year dermatology resident at Henry Ford Health System, Detroit, said her interest in dermatology was solidified during her participation in the AAD’s month-long mentorship program after her second year of medical school at Howard University, Washington. However, it wasn’t until her fourth year, when she did an away rotation at Wake Forest, that she realized that “gaining access to the field” takes years of mentorship, research opportunities, and networking. It was too late.
After initially not matching, she did a rotation at Johns Hopkins in dermatology during an internship year, followed by a 2-year research fellowship at George Washington University, Washington. As does Dr. Florez-Pollack, who now mentors medical students. She also serves on the Women’s Dermatologic Society diversity committee, which is now developing initiatives to help UIM dermatologists “become upwardly mobile in dermatology [after residency], so they have a seat at the table in various settings.”
Holistic review for residency
Dr. Vasquez, who grew up in South Texas in an uninsured family that received most of its medical care across the border in Mexico, believes that the “biggest stride being made today” with respect to diversity in the dermatology workforce – and in the larger physician workforce – is increased understanding of the role of social and cultural capital.
“We’d never really talked about this concept ... about how, if you don’t have the same upbringing, education, and resources, you’re already behind … and you may not do as well on standardized tests,” she said. “Now people are listening to it and understand it. That’s why more programs are looking at how to practice a more holistic approach to selecting applicants to interview.”
Some dermatology programs – at Wake Forest, UCSF, USC, Vanderbilt, and George Washington University for instance – have eliminated the use of U.S. Medical Licensing Examination step 1 scores and Alpha Omega Alpha Medical Honor Society status as filtering/screening metrics. Some also take a “second look” at UIM applicants.
Overall, those making changes are looking “at everything the applicant brings to the table – their story, their experiences,” said Dr. Elbuluk. “We want to understand the full picture of who they are and their journey to becoming a physician.”
Implicit bias training for members of residency review committees is becoming more common, as is such training across the board in dermatology departments. “We have to bring it to the forefront so that we can create more inclusive environments,” said Sharon E. Albers, MD, a dermatologist at Vanderbilt University Medical Center, Nashville, Tenn., who serves as the dermatology department’s diversity liaison to the medical school, and who, as a former faculty member of Meharry Medical College, remains engaged with the historically black institution.
One of her recent efforts, inspired by participation in the diversity champions program, has been developing pipeline programs to speak to middle and high school students about medicine and dermatology. For now, however, she credits a holistic review process for change. Last year, three of the five matched dermatology residents at Vanderbilt were UIM physicians – unprecedented for the institution, Dr. Albers said, and “evidence that holistic review works if you’re very intentional about it.”
Dr. Vasquez has analyzed data from the Accreditation Council of Graduate Medical Education and says that UIM dermatology residents comprised 8.0% of the total in 2019, marking an improvement over the prior 7 years. “We’ve introduced so many changes at the same time,” making it difficult to discern what’s most impactful, she said. “But something is working.”
(The AAMC, which has invested in pipeline programs for more than a decade and has championed holistic medical school admissions, states in its 2019 diversity data report that efforts to improve diversity in medicine have made “only marginal differences” – and that Black males in particular continue to be significantly underrepresented in medical schools. Persistent, structural racism was a common theme in the association’s 2015 report on Black males in medicine.)
Efforts to diversify the workforce – particularly holistic review – haven’t been without detractors. “It brings reaction,” Dr. Wintroub said. “Some people think you’re lowering quality in the field ... but that’s just not true.”
Diversity in the dermatology workforce is important not only for the care of patients from diverse backgrounds, but “perhaps more importantly, it brings new ideas and views and experiences into the field,” he said. “It pushes us to think in new directions ... that can only make our field better and richer.”
“We need to make sure our workforce is representative of the patients we serve – but also that all derms can manage patients of all skin types and demographics,” Dr. Shinkai said. “And we need more diversity in the leadership of our departments and dermatology organizations ... inclusivity needs to extend all the way to the highest reaches of our specialty.”
Adam Friedman, MD, professor and interim chair of dermatology at George Washington University and director of the department’s diversity, equity, and inclusion committee, agreed. “We need to both make sure our workforce mirrors the patients we serve, and said workforce is prepared to manage patients of all skin types and demographics. We need to cover the spectrum, from revamping medical education and mentorship opportunities to advancing diversity in the leadership of our departments, institutions, and societies. Addressing only part of the puzzle will not and can not be enough.”
Correction, 3/3/21: An earlier version of this article misstated Dr. Stephanie Florez-Pollack's name.
Independent physicians finally get vaccine for selves, but not patients
Physicians unaffiliated with health care systems continue to have difficulties obtaining COVID-19 vaccinations for themselves and their staffs, but that challenge appears to be fading in some states. Yet, in many places, primary care physicians (PCPs) still aren’t being enlisted in the national vaccination effort, despite their numbers and their relationships with patients.
In the first few weeks after the Pfizer and Moderna vaccines received emergency-use authorizations from the Food and Drug Administration, they were distributed mostly to hospitals, pharmacies, and long-term care facilities. Naturally, the hospitals and health care systems vaccinated their own staffs and employed physicians first.
So, even though the guidelines from the Centers for Disease Control and Prevention specify that all frontline health care workers should be included in the first vaccination group, many non–hospital-affiliated private practices have been left out in the cold. Non–patient-facing hospital staff members in some facilities, as well as first responders such as police officers and firefighters, have taken precedence over independent primary care physicians.
In Florida, residents older than 65 years were invited to get vaccinated before some physicians had received shots, Anders Gilberg, senior vice president of government affairs for the Medical Group Management Association, said in an interview.
While the Department of Health & Human Services is now telling states to give vaccinations to everyone over 65, that wasn’t the case back then.
Community doctors in some areas are still finding it hard to get vaccinated or even find out how to get shots. Yul Ejnes, MD, an internist and partner in Coastal Medical, an independent medical group based in Cranston, R.I., said in an interview that he and his practice staff haven’t been vaccinated, while the staffs of local hospitals have received their shots.
In response to repeated inquiries from his group, he said, the state health department recently said independent practice staffs will start getting vaccinated the week of Jan. 25.
Dr. Ejnes said he understood why hospital personnel went first: Hospitals have the necessary infrastructure, “and the staff in the emergency department and the ICU are caring for the sickest of the sick.”
For primary care doctors like himself who don’t work for the hospital, he said, “I don’t think an infrastructure to get us the vaccine in a timely manner was developed – or if it was developed, it hasn’t been communicated to us.”
Nevertheless, Dr. Ejnes stressed that primary care physicians in the community are just as vulnerable to the coronavirus as hospital clinicians. “We’re seeing patients who have COVID but don’t know they have it. I’m seeing 15 patients a day, and we screen them – as everyone else does – for symptoms and contact and travel, and check their temp,” he said. “But not a day goes by that one of the clinicians in this office doesn’t get a phone call from a patient who was seen a day or 2 earlier to tell them it turns out they were COVID positive. I’m spending 15 minutes in a 100–sq ft room with a patient for a routine visit. And as much as we’re masking and gloving and wearing eye protection, I wouldn’t consider us to be at low risk, especially with the high prevalence of disease.”
In some other states, the situation seems to be improving. Ada Stewart, MD, president of the American Academy of Family Physicians, said that she and her colleagues in a community health center in Columbia, S.C., are in the process of being vaccinated. She got her own shot Jan. 6 at a local hospital.
Her clinic’s staff hadn’t been vaccinated earlier, she said, because nobody in the practice knew the contact person at the hospital who could help access the vaccine doses. Other independent practices in her state are now getting vaccinated, she said, after Gov. Henry McMaster of South Carolina ordered that all health care providers in the top priority category be inoculated by Jan. 15. “At this point, the issues have been diminished.”
However, Dr. Stewart added, independent doctors in some states are still unable to get their shots. AAFP state chapters, as well as the national organization, are trying to persuade governors to ensure all of these physicians are vaccinated. “We’re trying to make sure that the voices of physicians not affiliated with health systems are being heard,” she said.
Lucky shot for doctor
David Boles, DO, a family doctor in Clarksville, Tenn., was able to get his first dose of vaccine just before Christmas, he said in an interview, because he was medical director of a hospice that had received vaccine doses for first responders. When some firefighters and police officers failed to show up for their appointments, the hospice called him and said he had 45 minutes to get to the site if he wanted to be vaccinated.
In early January, his colleagues and staff were also vaccinated, he said, after they were notified of their eligibility as frontline health care workers.
Dr. Boles agreed with Dr. Ejnes that community physicians and nurses are as much at risk as hospital clinicians, except for those intubating patients in the ICU. They may be even more vulnerable, he added, because they have less personal protective equipment than hospital doctors and nurses.
Jennifer Brull, MD, a family physician in Plainville, Kan., said there have been plenty of COVID-19 cases in her small rural community, and the local critical access hospital nearly ran out of beds at one point. Through a collaborative relationship among her clinic (the lone one in the area), the hospital, and the county health department, nearly every frontline health care worker has been vaccinated, and most clinicians in her group have gotten their second doses.
Both the hospital and the health department received vaccine supplies, she said, and everyone in the high-priority category was offered shots. So far, about 170 health care workers have been vaccinated, and only a few declined. More than 300 other people – most of them essential non–health care workers and people older than 65 – have signed up for the next round of shots.
Expanding vaccination effort
Dr. Brull’s practice is the exception among private medical groups around the country. Mr. Gilberg said the MGMA is “concerned that independent practices are playing second fiddle because they’ve been left behind.” Physicians and patient-facing staff in private groups should be getting vaccinated before hospital information technology workers and other non–patient-facing staffers.
Medical practices also can and should play a much bigger role in the overall vaccination effort. Mr. Gilberg has spoken to leaders of several large primary care groups “that have the freezers [for vaccines] and the capacity but haven’t been folded into the distribution plan, especially if they’re not part of the hospital system.”
While hospitals have the storage, he said, they’re not set up to distribute vaccines throughout their communities. “Most health care in this country is delivered outside of the hospital setting. That’s how you’re going to get people vaccinated.”
Ironically, he added, “the same PCPs that are having trouble getting themselves and their staffs vaccinated would be the physicians who could help with vaccine distribution.”
Dr. Brull’s clinic stands ready to help the hospital and health department vaccinate the local population. When sufficient vaccine supplies arrive, she said, she envisioned the doctors and staff administering 200-400 shots per day on Saturdays or weekends.
Dr. Brull was the exception – the other physicians interviewed hadn’t been invited to participate in vaccination efforts.
Dr. Ejnes said his group is capable of vaccinating its patients if it uses the Moderna vaccine, which doesn’t require a super-cold freezer. There are logistical challenges, including social distancing and finding space to observe vaccinated patients for 15 minutes after their shots, he noted. “We’re ready and willing, but realistic about how much we’ll be able to do in this effort.”
The fact that doctors haven’t been enlisted yet in this campaign speaks volumes about “the neglect of the public health infrastructure,” Dr. Ejnes said. “We’re not mobilizing as quickly as we should.”
Alternative routes
Dr. Boles’ group has a refrigerator for pediatric vaccines, which could be used to store the Moderna vaccine, he noted. Shots could be administered to patients in their cars in the parking lot, and they could wait for a while afterward until a nurse came out to verify they were okay.
Mass vaccination sites might also be deployed, as Los Angeles is doing with Dodger Stadium, and physicians could take shifts there in their spare time, Dr. Boles said. But for right now, he views pharmacies as the primary venues for community vaccination.
Of course, the number of pharmacists and pharmacy-employed advanced practice nurses is tiny, compared with the number of primary care doctors, mid-level practitioners, and nurses in ambulatory care practices. Moreover, Mr. Gilberg said, practices know from their electronic health records which patients are most at risk and should be vaccinated first. “Walgreens and CVS don’t know that.”
Physicians should also take the lead in vaccinations because of their patient relationships, he noted. “They can help educate [vaccine-hesitant] patients on why it’s important and dispel some of the rumors and the misinformation that has been politicized. That’s why we should engage physicians in an outpatient setting. And we have to vaccinate them and their staffs. Otherwise, we’re never going to get this rollout underway.”
Dr. Stewart agreed. “We are really the foundation of how we’re going to accomplish this. Most folks are seen by a primary care physician. We touch millions of lives,” she said. “We’re part of the community. Our patients trust us. We’re out there doing it already. We’re doing prevention, giving flu shots, and we’re trying to encourage people to get the COVID vaccine.”
A version of this article first appeared on Medscape.com.
Physicians unaffiliated with health care systems continue to have difficulties obtaining COVID-19 vaccinations for themselves and their staffs, but that challenge appears to be fading in some states. Yet, in many places, primary care physicians (PCPs) still aren’t being enlisted in the national vaccination effort, despite their numbers and their relationships with patients.
In the first few weeks after the Pfizer and Moderna vaccines received emergency-use authorizations from the Food and Drug Administration, they were distributed mostly to hospitals, pharmacies, and long-term care facilities. Naturally, the hospitals and health care systems vaccinated their own staffs and employed physicians first.
So, even though the guidelines from the Centers for Disease Control and Prevention specify that all frontline health care workers should be included in the first vaccination group, many non–hospital-affiliated private practices have been left out in the cold. Non–patient-facing hospital staff members in some facilities, as well as first responders such as police officers and firefighters, have taken precedence over independent primary care physicians.
In Florida, residents older than 65 years were invited to get vaccinated before some physicians had received shots, Anders Gilberg, senior vice president of government affairs for the Medical Group Management Association, said in an interview.
While the Department of Health & Human Services is now telling states to give vaccinations to everyone over 65, that wasn’t the case back then.
Community doctors in some areas are still finding it hard to get vaccinated or even find out how to get shots. Yul Ejnes, MD, an internist and partner in Coastal Medical, an independent medical group based in Cranston, R.I., said in an interview that he and his practice staff haven’t been vaccinated, while the staffs of local hospitals have received their shots.
In response to repeated inquiries from his group, he said, the state health department recently said independent practice staffs will start getting vaccinated the week of Jan. 25.
Dr. Ejnes said he understood why hospital personnel went first: Hospitals have the necessary infrastructure, “and the staff in the emergency department and the ICU are caring for the sickest of the sick.”
For primary care doctors like himself who don’t work for the hospital, he said, “I don’t think an infrastructure to get us the vaccine in a timely manner was developed – or if it was developed, it hasn’t been communicated to us.”
Nevertheless, Dr. Ejnes stressed that primary care physicians in the community are just as vulnerable to the coronavirus as hospital clinicians. “We’re seeing patients who have COVID but don’t know they have it. I’m seeing 15 patients a day, and we screen them – as everyone else does – for symptoms and contact and travel, and check their temp,” he said. “But not a day goes by that one of the clinicians in this office doesn’t get a phone call from a patient who was seen a day or 2 earlier to tell them it turns out they were COVID positive. I’m spending 15 minutes in a 100–sq ft room with a patient for a routine visit. And as much as we’re masking and gloving and wearing eye protection, I wouldn’t consider us to be at low risk, especially with the high prevalence of disease.”
In some other states, the situation seems to be improving. Ada Stewart, MD, president of the American Academy of Family Physicians, said that she and her colleagues in a community health center in Columbia, S.C., are in the process of being vaccinated. She got her own shot Jan. 6 at a local hospital.
Her clinic’s staff hadn’t been vaccinated earlier, she said, because nobody in the practice knew the contact person at the hospital who could help access the vaccine doses. Other independent practices in her state are now getting vaccinated, she said, after Gov. Henry McMaster of South Carolina ordered that all health care providers in the top priority category be inoculated by Jan. 15. “At this point, the issues have been diminished.”
However, Dr. Stewart added, independent doctors in some states are still unable to get their shots. AAFP state chapters, as well as the national organization, are trying to persuade governors to ensure all of these physicians are vaccinated. “We’re trying to make sure that the voices of physicians not affiliated with health systems are being heard,” she said.
Lucky shot for doctor
David Boles, DO, a family doctor in Clarksville, Tenn., was able to get his first dose of vaccine just before Christmas, he said in an interview, because he was medical director of a hospice that had received vaccine doses for first responders. When some firefighters and police officers failed to show up for their appointments, the hospice called him and said he had 45 minutes to get to the site if he wanted to be vaccinated.
In early January, his colleagues and staff were also vaccinated, he said, after they were notified of their eligibility as frontline health care workers.
Dr. Boles agreed with Dr. Ejnes that community physicians and nurses are as much at risk as hospital clinicians, except for those intubating patients in the ICU. They may be even more vulnerable, he added, because they have less personal protective equipment than hospital doctors and nurses.
Jennifer Brull, MD, a family physician in Plainville, Kan., said there have been plenty of COVID-19 cases in her small rural community, and the local critical access hospital nearly ran out of beds at one point. Through a collaborative relationship among her clinic (the lone one in the area), the hospital, and the county health department, nearly every frontline health care worker has been vaccinated, and most clinicians in her group have gotten their second doses.
Both the hospital and the health department received vaccine supplies, she said, and everyone in the high-priority category was offered shots. So far, about 170 health care workers have been vaccinated, and only a few declined. More than 300 other people – most of them essential non–health care workers and people older than 65 – have signed up for the next round of shots.
Expanding vaccination effort
Dr. Brull’s practice is the exception among private medical groups around the country. Mr. Gilberg said the MGMA is “concerned that independent practices are playing second fiddle because they’ve been left behind.” Physicians and patient-facing staff in private groups should be getting vaccinated before hospital information technology workers and other non–patient-facing staffers.
Medical practices also can and should play a much bigger role in the overall vaccination effort. Mr. Gilberg has spoken to leaders of several large primary care groups “that have the freezers [for vaccines] and the capacity but haven’t been folded into the distribution plan, especially if they’re not part of the hospital system.”
While hospitals have the storage, he said, they’re not set up to distribute vaccines throughout their communities. “Most health care in this country is delivered outside of the hospital setting. That’s how you’re going to get people vaccinated.”
Ironically, he added, “the same PCPs that are having trouble getting themselves and their staffs vaccinated would be the physicians who could help with vaccine distribution.”
Dr. Brull’s clinic stands ready to help the hospital and health department vaccinate the local population. When sufficient vaccine supplies arrive, she said, she envisioned the doctors and staff administering 200-400 shots per day on Saturdays or weekends.
Dr. Brull was the exception – the other physicians interviewed hadn’t been invited to participate in vaccination efforts.
Dr. Ejnes said his group is capable of vaccinating its patients if it uses the Moderna vaccine, which doesn’t require a super-cold freezer. There are logistical challenges, including social distancing and finding space to observe vaccinated patients for 15 minutes after their shots, he noted. “We’re ready and willing, but realistic about how much we’ll be able to do in this effort.”
The fact that doctors haven’t been enlisted yet in this campaign speaks volumes about “the neglect of the public health infrastructure,” Dr. Ejnes said. “We’re not mobilizing as quickly as we should.”
Alternative routes
Dr. Boles’ group has a refrigerator for pediatric vaccines, which could be used to store the Moderna vaccine, he noted. Shots could be administered to patients in their cars in the parking lot, and they could wait for a while afterward until a nurse came out to verify they were okay.
Mass vaccination sites might also be deployed, as Los Angeles is doing with Dodger Stadium, and physicians could take shifts there in their spare time, Dr. Boles said. But for right now, he views pharmacies as the primary venues for community vaccination.
Of course, the number of pharmacists and pharmacy-employed advanced practice nurses is tiny, compared with the number of primary care doctors, mid-level practitioners, and nurses in ambulatory care practices. Moreover, Mr. Gilberg said, practices know from their electronic health records which patients are most at risk and should be vaccinated first. “Walgreens and CVS don’t know that.”
Physicians should also take the lead in vaccinations because of their patient relationships, he noted. “They can help educate [vaccine-hesitant] patients on why it’s important and dispel some of the rumors and the misinformation that has been politicized. That’s why we should engage physicians in an outpatient setting. And we have to vaccinate them and their staffs. Otherwise, we’re never going to get this rollout underway.”
Dr. Stewart agreed. “We are really the foundation of how we’re going to accomplish this. Most folks are seen by a primary care physician. We touch millions of lives,” she said. “We’re part of the community. Our patients trust us. We’re out there doing it already. We’re doing prevention, giving flu shots, and we’re trying to encourage people to get the COVID vaccine.”
A version of this article first appeared on Medscape.com.
Physicians unaffiliated with health care systems continue to have difficulties obtaining COVID-19 vaccinations for themselves and their staffs, but that challenge appears to be fading in some states. Yet, in many places, primary care physicians (PCPs) still aren’t being enlisted in the national vaccination effort, despite their numbers and their relationships with patients.
In the first few weeks after the Pfizer and Moderna vaccines received emergency-use authorizations from the Food and Drug Administration, they were distributed mostly to hospitals, pharmacies, and long-term care facilities. Naturally, the hospitals and health care systems vaccinated their own staffs and employed physicians first.
So, even though the guidelines from the Centers for Disease Control and Prevention specify that all frontline health care workers should be included in the first vaccination group, many non–hospital-affiliated private practices have been left out in the cold. Non–patient-facing hospital staff members in some facilities, as well as first responders such as police officers and firefighters, have taken precedence over independent primary care physicians.
In Florida, residents older than 65 years were invited to get vaccinated before some physicians had received shots, Anders Gilberg, senior vice president of government affairs for the Medical Group Management Association, said in an interview.
While the Department of Health & Human Services is now telling states to give vaccinations to everyone over 65, that wasn’t the case back then.
Community doctors in some areas are still finding it hard to get vaccinated or even find out how to get shots. Yul Ejnes, MD, an internist and partner in Coastal Medical, an independent medical group based in Cranston, R.I., said in an interview that he and his practice staff haven’t been vaccinated, while the staffs of local hospitals have received their shots.
In response to repeated inquiries from his group, he said, the state health department recently said independent practice staffs will start getting vaccinated the week of Jan. 25.
Dr. Ejnes said he understood why hospital personnel went first: Hospitals have the necessary infrastructure, “and the staff in the emergency department and the ICU are caring for the sickest of the sick.”
For primary care doctors like himself who don’t work for the hospital, he said, “I don’t think an infrastructure to get us the vaccine in a timely manner was developed – or if it was developed, it hasn’t been communicated to us.”
Nevertheless, Dr. Ejnes stressed that primary care physicians in the community are just as vulnerable to the coronavirus as hospital clinicians. “We’re seeing patients who have COVID but don’t know they have it. I’m seeing 15 patients a day, and we screen them – as everyone else does – for symptoms and contact and travel, and check their temp,” he said. “But not a day goes by that one of the clinicians in this office doesn’t get a phone call from a patient who was seen a day or 2 earlier to tell them it turns out they were COVID positive. I’m spending 15 minutes in a 100–sq ft room with a patient for a routine visit. And as much as we’re masking and gloving and wearing eye protection, I wouldn’t consider us to be at low risk, especially with the high prevalence of disease.”
In some other states, the situation seems to be improving. Ada Stewart, MD, president of the American Academy of Family Physicians, said that she and her colleagues in a community health center in Columbia, S.C., are in the process of being vaccinated. She got her own shot Jan. 6 at a local hospital.
Her clinic’s staff hadn’t been vaccinated earlier, she said, because nobody in the practice knew the contact person at the hospital who could help access the vaccine doses. Other independent practices in her state are now getting vaccinated, she said, after Gov. Henry McMaster of South Carolina ordered that all health care providers in the top priority category be inoculated by Jan. 15. “At this point, the issues have been diminished.”
However, Dr. Stewart added, independent doctors in some states are still unable to get their shots. AAFP state chapters, as well as the national organization, are trying to persuade governors to ensure all of these physicians are vaccinated. “We’re trying to make sure that the voices of physicians not affiliated with health systems are being heard,” she said.
Lucky shot for doctor
David Boles, DO, a family doctor in Clarksville, Tenn., was able to get his first dose of vaccine just before Christmas, he said in an interview, because he was medical director of a hospice that had received vaccine doses for first responders. When some firefighters and police officers failed to show up for their appointments, the hospice called him and said he had 45 minutes to get to the site if he wanted to be vaccinated.
In early January, his colleagues and staff were also vaccinated, he said, after they were notified of their eligibility as frontline health care workers.
Dr. Boles agreed with Dr. Ejnes that community physicians and nurses are as much at risk as hospital clinicians, except for those intubating patients in the ICU. They may be even more vulnerable, he added, because they have less personal protective equipment than hospital doctors and nurses.
Jennifer Brull, MD, a family physician in Plainville, Kan., said there have been plenty of COVID-19 cases in her small rural community, and the local critical access hospital nearly ran out of beds at one point. Through a collaborative relationship among her clinic (the lone one in the area), the hospital, and the county health department, nearly every frontline health care worker has been vaccinated, and most clinicians in her group have gotten their second doses.
Both the hospital and the health department received vaccine supplies, she said, and everyone in the high-priority category was offered shots. So far, about 170 health care workers have been vaccinated, and only a few declined. More than 300 other people – most of them essential non–health care workers and people older than 65 – have signed up for the next round of shots.
Expanding vaccination effort
Dr. Brull’s practice is the exception among private medical groups around the country. Mr. Gilberg said the MGMA is “concerned that independent practices are playing second fiddle because they’ve been left behind.” Physicians and patient-facing staff in private groups should be getting vaccinated before hospital information technology workers and other non–patient-facing staffers.
Medical practices also can and should play a much bigger role in the overall vaccination effort. Mr. Gilberg has spoken to leaders of several large primary care groups “that have the freezers [for vaccines] and the capacity but haven’t been folded into the distribution plan, especially if they’re not part of the hospital system.”
While hospitals have the storage, he said, they’re not set up to distribute vaccines throughout their communities. “Most health care in this country is delivered outside of the hospital setting. That’s how you’re going to get people vaccinated.”
Ironically, he added, “the same PCPs that are having trouble getting themselves and their staffs vaccinated would be the physicians who could help with vaccine distribution.”
Dr. Brull’s clinic stands ready to help the hospital and health department vaccinate the local population. When sufficient vaccine supplies arrive, she said, she envisioned the doctors and staff administering 200-400 shots per day on Saturdays or weekends.
Dr. Brull was the exception – the other physicians interviewed hadn’t been invited to participate in vaccination efforts.
Dr. Ejnes said his group is capable of vaccinating its patients if it uses the Moderna vaccine, which doesn’t require a super-cold freezer. There are logistical challenges, including social distancing and finding space to observe vaccinated patients for 15 minutes after their shots, he noted. “We’re ready and willing, but realistic about how much we’ll be able to do in this effort.”
The fact that doctors haven’t been enlisted yet in this campaign speaks volumes about “the neglect of the public health infrastructure,” Dr. Ejnes said. “We’re not mobilizing as quickly as we should.”
Alternative routes
Dr. Boles’ group has a refrigerator for pediatric vaccines, which could be used to store the Moderna vaccine, he noted. Shots could be administered to patients in their cars in the parking lot, and they could wait for a while afterward until a nurse came out to verify they were okay.
Mass vaccination sites might also be deployed, as Los Angeles is doing with Dodger Stadium, and physicians could take shifts there in their spare time, Dr. Boles said. But for right now, he views pharmacies as the primary venues for community vaccination.
Of course, the number of pharmacists and pharmacy-employed advanced practice nurses is tiny, compared with the number of primary care doctors, mid-level practitioners, and nurses in ambulatory care practices. Moreover, Mr. Gilberg said, practices know from their electronic health records which patients are most at risk and should be vaccinated first. “Walgreens and CVS don’t know that.”
Physicians should also take the lead in vaccinations because of their patient relationships, he noted. “They can help educate [vaccine-hesitant] patients on why it’s important and dispel some of the rumors and the misinformation that has been politicized. That’s why we should engage physicians in an outpatient setting. And we have to vaccinate them and their staffs. Otherwise, we’re never going to get this rollout underway.”
Dr. Stewart agreed. “We are really the foundation of how we’re going to accomplish this. Most folks are seen by a primary care physician. We touch millions of lives,” she said. “We’re part of the community. Our patients trust us. We’re out there doing it already. We’re doing prevention, giving flu shots, and we’re trying to encourage people to get the COVID vaccine.”
A version of this article first appeared on Medscape.com.
AMA president: Biden team must create national pandemic strategy
The incoming Biden administration must formulate an effective national strategy for the COVID-19 pandemic, Susan R. Bailey, MD, president of the American Medical Association (AMA), said in a speech delivered Jan. 12 at the National Press Club in Washington.
Dr. Bailey noted that America’s fight against the pandemic is in a critical phase, as evidenced by the escalation in cases, hospitalizations, and deaths in recent weeks. Emergency departments and ICUs are overwhelmed; many frontline clinicians are burned out; and the state- and local-level mechanisms for vaccine distribution have been slow and inconsistent, she said.
“The most important lesson for this moment, and for the year ahead, is that leaving state and local officials to shoulder this burden alone without adequate support from the federal government is not going to work,” Dr. Bailey emphasized.
She called on the Biden administration, which takes over on Jan. 20, to “provide states and local jurisdictions with additional resources, guidance, and support to enable rapid distribution and administration of vaccines.”
In addition, she said, the incoming administration needs to develop a more robust, national strategy for continued COVID-19 testing and PPE production “by tapping into the full powers of the Defense Production Act.”
Biden vaccine distribution policy
In a question-and-answer period following her speech, however, Dr. Bailey said she opposed the president-elect’s decision to release nearly all available vaccine supplies immediately, rather than hold back some doses for the second shots that the Pfizer and Moderna vaccines require. On Jan. 12, the Trump administration announced that it plans to do the same thing.
“We’re a little bit concerned about the announcement that [the Department of Health and Human Services] will not hold back vaccine doses to make sure that everyone who’s gotten their first dose will have a second dose in reserve,” Dr. Bailey said. “We don’t have adequate data to tell us that one dose is sufficient – we don’t think it is – and how long you can wait for the second dose without losing the benefits of the first dose.”
She added that it’s not recommended that people mix the two vaccines in the first and second doses. “Since the Pfizer vaccine has such rigid storage requirements, I want to make sure there’s plenty of vaccine for frontline health care workers who got the Pfizer vaccine because it was the first one to come out in December. I want to make sure they get their second dose on time and [do] not have to wait.”
Dr. Bailey said she hoped there will be plenty of vaccine supply. But she suggested that state and local health authorities be in communication with the federal government about whether there will be enough vaccine to guarantee people can get both doses.
Bolstering public health
In her speech, Dr. Bailey outlined five areas in which steps should be taken to improve the health system so that it isn’t overwhelmed the next time the United States has a public health crisis:
- Restore trust in science and science-based decision making. Make sure that scientific institutions such as the Centers for Disease Control and Prevention and the Food and Drug Administration are “free from political pressure, and that their actions are guided by the best available scientific evidence.”
- Ensure that the health system provides all Americans with affordable access to comprehensive health care. Dr. Bailey wasn’t talking about Medicare for All; she suggested that perhaps there be a second enrollment period for the Affordable Care Act’s individual insurance exchanges.
- Work to remove health care inequities that have hurt communities of color, who have been disproportionately impacted by the pandemic. She referred to a recent AMA that recognized racism as a public health threat.
- Improve public health domestically and globally. Among other things, she noted, the public health infrastructure needs to be revitalized after “decades of disinvestment and neglect,” which has contributed to the slow vaccine rollout.
- Recognize the global health community and restore America’s leadership in global efforts to combat disease, which are critical to preventing future threats. She praised President-Elect Biden for his promise that the United States will rejoin the World Health Organization.
At several points in her presentation, Dr. Bailey rejected political interference with science and health care. Among other things, she said public health could be improved by protecting the doctor-patient relationship from political interference.
Answering a question about how to separate politics from the pandemic, she replied, “The key is in sticking to the science and listening to our public health authorities. They all have to deliver the same message. Also, leaders at all levels, including in our communities, our schools, churches and college campuses, should wear masks and socially distance. This isn’t about anything other than the desire to get out of the pandemic and get our country on the right track again. Masks shouldn’t be political. Going back to school shouldn’t be political. Taking a certain medication or not shouldn’t be political. We need to stick to the science and listen to our public health authorities. That’s the quickest way out.”
Asked when she thought that life might get back to normal again in the United States, Dr. Bailey said a lot depends on the extent of vaccine uptake and how much self-discipline people exhibit in following public health advice. “I think we’re looking at the end of this year. I’m hopeful that by fall, things will have opened up quite a bit as the Venn diagrams of those who’ve gotten vaccines grow larger.”
A version of this article first appeared on Medscape.com.
The incoming Biden administration must formulate an effective national strategy for the COVID-19 pandemic, Susan R. Bailey, MD, president of the American Medical Association (AMA), said in a speech delivered Jan. 12 at the National Press Club in Washington.
Dr. Bailey noted that America’s fight against the pandemic is in a critical phase, as evidenced by the escalation in cases, hospitalizations, and deaths in recent weeks. Emergency departments and ICUs are overwhelmed; many frontline clinicians are burned out; and the state- and local-level mechanisms for vaccine distribution have been slow and inconsistent, she said.
“The most important lesson for this moment, and for the year ahead, is that leaving state and local officials to shoulder this burden alone without adequate support from the federal government is not going to work,” Dr. Bailey emphasized.
She called on the Biden administration, which takes over on Jan. 20, to “provide states and local jurisdictions with additional resources, guidance, and support to enable rapid distribution and administration of vaccines.”
In addition, she said, the incoming administration needs to develop a more robust, national strategy for continued COVID-19 testing and PPE production “by tapping into the full powers of the Defense Production Act.”
Biden vaccine distribution policy
In a question-and-answer period following her speech, however, Dr. Bailey said she opposed the president-elect’s decision to release nearly all available vaccine supplies immediately, rather than hold back some doses for the second shots that the Pfizer and Moderna vaccines require. On Jan. 12, the Trump administration announced that it plans to do the same thing.
“We’re a little bit concerned about the announcement that [the Department of Health and Human Services] will not hold back vaccine doses to make sure that everyone who’s gotten their first dose will have a second dose in reserve,” Dr. Bailey said. “We don’t have adequate data to tell us that one dose is sufficient – we don’t think it is – and how long you can wait for the second dose without losing the benefits of the first dose.”
She added that it’s not recommended that people mix the two vaccines in the first and second doses. “Since the Pfizer vaccine has such rigid storage requirements, I want to make sure there’s plenty of vaccine for frontline health care workers who got the Pfizer vaccine because it was the first one to come out in December. I want to make sure they get their second dose on time and [do] not have to wait.”
Dr. Bailey said she hoped there will be plenty of vaccine supply. But she suggested that state and local health authorities be in communication with the federal government about whether there will be enough vaccine to guarantee people can get both doses.
Bolstering public health
In her speech, Dr. Bailey outlined five areas in which steps should be taken to improve the health system so that it isn’t overwhelmed the next time the United States has a public health crisis:
- Restore trust in science and science-based decision making. Make sure that scientific institutions such as the Centers for Disease Control and Prevention and the Food and Drug Administration are “free from political pressure, and that their actions are guided by the best available scientific evidence.”
- Ensure that the health system provides all Americans with affordable access to comprehensive health care. Dr. Bailey wasn’t talking about Medicare for All; she suggested that perhaps there be a second enrollment period for the Affordable Care Act’s individual insurance exchanges.
- Work to remove health care inequities that have hurt communities of color, who have been disproportionately impacted by the pandemic. She referred to a recent AMA that recognized racism as a public health threat.
- Improve public health domestically and globally. Among other things, she noted, the public health infrastructure needs to be revitalized after “decades of disinvestment and neglect,” which has contributed to the slow vaccine rollout.
- Recognize the global health community and restore America’s leadership in global efforts to combat disease, which are critical to preventing future threats. She praised President-Elect Biden for his promise that the United States will rejoin the World Health Organization.
At several points in her presentation, Dr. Bailey rejected political interference with science and health care. Among other things, she said public health could be improved by protecting the doctor-patient relationship from political interference.
Answering a question about how to separate politics from the pandemic, she replied, “The key is in sticking to the science and listening to our public health authorities. They all have to deliver the same message. Also, leaders at all levels, including in our communities, our schools, churches and college campuses, should wear masks and socially distance. This isn’t about anything other than the desire to get out of the pandemic and get our country on the right track again. Masks shouldn’t be political. Going back to school shouldn’t be political. Taking a certain medication or not shouldn’t be political. We need to stick to the science and listen to our public health authorities. That’s the quickest way out.”
Asked when she thought that life might get back to normal again in the United States, Dr. Bailey said a lot depends on the extent of vaccine uptake and how much self-discipline people exhibit in following public health advice. “I think we’re looking at the end of this year. I’m hopeful that by fall, things will have opened up quite a bit as the Venn diagrams of those who’ve gotten vaccines grow larger.”
A version of this article first appeared on Medscape.com.
The incoming Biden administration must formulate an effective national strategy for the COVID-19 pandemic, Susan R. Bailey, MD, president of the American Medical Association (AMA), said in a speech delivered Jan. 12 at the National Press Club in Washington.
Dr. Bailey noted that America’s fight against the pandemic is in a critical phase, as evidenced by the escalation in cases, hospitalizations, and deaths in recent weeks. Emergency departments and ICUs are overwhelmed; many frontline clinicians are burned out; and the state- and local-level mechanisms for vaccine distribution have been slow and inconsistent, she said.
“The most important lesson for this moment, and for the year ahead, is that leaving state and local officials to shoulder this burden alone without adequate support from the federal government is not going to work,” Dr. Bailey emphasized.
She called on the Biden administration, which takes over on Jan. 20, to “provide states and local jurisdictions with additional resources, guidance, and support to enable rapid distribution and administration of vaccines.”
In addition, she said, the incoming administration needs to develop a more robust, national strategy for continued COVID-19 testing and PPE production “by tapping into the full powers of the Defense Production Act.”
Biden vaccine distribution policy
In a question-and-answer period following her speech, however, Dr. Bailey said she opposed the president-elect’s decision to release nearly all available vaccine supplies immediately, rather than hold back some doses for the second shots that the Pfizer and Moderna vaccines require. On Jan. 12, the Trump administration announced that it plans to do the same thing.
“We’re a little bit concerned about the announcement that [the Department of Health and Human Services] will not hold back vaccine doses to make sure that everyone who’s gotten their first dose will have a second dose in reserve,” Dr. Bailey said. “We don’t have adequate data to tell us that one dose is sufficient – we don’t think it is – and how long you can wait for the second dose without losing the benefits of the first dose.”
She added that it’s not recommended that people mix the two vaccines in the first and second doses. “Since the Pfizer vaccine has such rigid storage requirements, I want to make sure there’s plenty of vaccine for frontline health care workers who got the Pfizer vaccine because it was the first one to come out in December. I want to make sure they get their second dose on time and [do] not have to wait.”
Dr. Bailey said she hoped there will be plenty of vaccine supply. But she suggested that state and local health authorities be in communication with the federal government about whether there will be enough vaccine to guarantee people can get both doses.
Bolstering public health
In her speech, Dr. Bailey outlined five areas in which steps should be taken to improve the health system so that it isn’t overwhelmed the next time the United States has a public health crisis:
- Restore trust in science and science-based decision making. Make sure that scientific institutions such as the Centers for Disease Control and Prevention and the Food and Drug Administration are “free from political pressure, and that their actions are guided by the best available scientific evidence.”
- Ensure that the health system provides all Americans with affordable access to comprehensive health care. Dr. Bailey wasn’t talking about Medicare for All; she suggested that perhaps there be a second enrollment period for the Affordable Care Act’s individual insurance exchanges.
- Work to remove health care inequities that have hurt communities of color, who have been disproportionately impacted by the pandemic. She referred to a recent AMA that recognized racism as a public health threat.
- Improve public health domestically and globally. Among other things, she noted, the public health infrastructure needs to be revitalized after “decades of disinvestment and neglect,” which has contributed to the slow vaccine rollout.
- Recognize the global health community and restore America’s leadership in global efforts to combat disease, which are critical to preventing future threats. She praised President-Elect Biden for his promise that the United States will rejoin the World Health Organization.
At several points in her presentation, Dr. Bailey rejected political interference with science and health care. Among other things, she said public health could be improved by protecting the doctor-patient relationship from political interference.
Answering a question about how to separate politics from the pandemic, she replied, “The key is in sticking to the science and listening to our public health authorities. They all have to deliver the same message. Also, leaders at all levels, including in our communities, our schools, churches and college campuses, should wear masks and socially distance. This isn’t about anything other than the desire to get out of the pandemic and get our country on the right track again. Masks shouldn’t be political. Going back to school shouldn’t be political. Taking a certain medication or not shouldn’t be political. We need to stick to the science and listen to our public health authorities. That’s the quickest way out.”
Asked when she thought that life might get back to normal again in the United States, Dr. Bailey said a lot depends on the extent of vaccine uptake and how much self-discipline people exhibit in following public health advice. “I think we’re looking at the end of this year. I’m hopeful that by fall, things will have opened up quite a bit as the Venn diagrams of those who’ve gotten vaccines grow larger.”
A version of this article first appeared on Medscape.com.