User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

COVID-19 drives nursing homes to overhaul infection control efforts
The toll that COVID-19 has taken on nursing homes and their postacute and long-term care residents has a multilayered backstory involving underresourced organizational structures, inherent susceptibilities, minimally trained infection prevention staff, variable abilities to isolate and quarantine large numbers of patients and residents, and a lack of governmental support.
“Nursing homes have been trying their best to combat this pandemic using the best infection control procedures they have, but blindfolded and with their hands tied behind their backs,” said Joseph G. Ouslander, MD, professor of geriatric medicine at Florida Atlantic University, Boca Raton, which has teaching affiliations with three senior communities.
Nursing home leaders are debating how to best use testing to guide transmission-based precautions and isolation strategies and how to keep residents safe while allowing some socialization after months of conflicting guidance from public health officials (on testing and on sites of care for patients discharged from the hospital, for instance), with a lack of adequate personal protective equipment (PPE) and testing supplies, and with nursing home resident deaths estimated to account for at least one-quarter of the total COVID-19–related mortality in the United States.
“COVID is not going away [over the next couple of years],” said Michael Wasserman, MD, medical director of the Eisenberg Village at the Los Angeles Jewish Home and president of the California Association of Long-Term Care Medicine.
Dr. Wasserman and other experts in both long-term care and infectious disease said in interviews that, through the rest of the pandemic and beyond, nursing homes need the following:
- Full-time, well-trained “infection preventionists” – infection prevention managers, in essence – who can lead improvements in emergency preparedness and infection prevention and control (IPC)
- Medical directors who are well qualified and engaged
- A survey/inspection process that is educational and not solely punitive
- More resources and attention to structural reform
“If this pandemic doesn’t create significant change in the nursing home industry, nothing ever will,” Dr. Wasserman said.
Prepandemic experience
When Ghinwa Dumyati, MD, began working with nursing homes in early March to prevent and contain COVID-19 outbreaks, her focus was on PPE.
Nursing home staff were intimately familiar with standard precautions, and many had used contact precautions to prevent transmission of infections like Clostridioides difficile and Candida auris, as well as droplet precautions for influenza. With the threat of COVID-19, nursing homes “had a brand-new requirement to do both contact and droplet precautions – with a new need for eye protection – and in some situations, respiratory precautions with N95 masks,” said Dr. Dumyati, professor of medicine and director of communicable disease surveillance and prevention at the University of Rochester (N.Y.) Medical Center. “And on top of that, [staff] had to learn to conserve and reuse PPE.”
Staff had not been fit-tested for use of N95 respirators, she noted. “The only time an N95 was used in the nursing home prior to COVID-19,” she said, “was for a suspected tuberculosis patient [before hospital admission].”
Similarly, nursing homes had experience in quarantining units to prevent transmission of illnesses like influenza or norovirus – keeping residents in their rooms with no visitations or social activity, for instance – but never did they have to arrange “massive movements of residents to completely new units or parts of a unit,” said Dr. Dumyati, who also has led hospital and nursing home collaborative programs in Rochester to beat back C. difficile, and is now helping to formulate COVID-19 recommendations and guidance for members of AMDA – The Society for Post-Acute and Long-Term Care.
As the SARS-CoV-2 virus began its spread through the United States, efforts to strengthen IPC programs in nursing homes in Rochester and elsewhere had been focused largely on multidrug resistant organisms (MDROs) and antibiotic stewardship – not on pandemic preparedness.
Reducing antibiotic use had become a national priority, and a 2016 rule by the Centers for Medicare & Medicaid Services required nursing homes to develop, over a 3-year period, an IPC program that included an antibiotic stewardship component and employment of a trained infection preventionist on at least a half-time basis. Emergency preparedness (e.g., having alternate energy sources for a facility) was also included in the rule, but it was only in 2019 when CMS updated its “Requirements for Participation” rule to stipulate that emergency preparedness include planning for “emerging infectious diseases.”
“The 2016 regulations came about because infections were so problematic in nursing homes,” especially urinary tract infections, C. difficile, and drug-resistant infections, said Patricia Stone, PhD, RN, of the Center for Health Policy at the Columbia University School of Nursing, New York, who has published widely on infection prevention and control in nursing homes.
An analysis of IPC practices in 2014 and in 2018 suggests that the IPC-focused rules were helping, mainly with antibiotic stewardship programs but also with respect to some of the practices aimed at outbreak control, such as having policies in place for grouping infected residents together, instructing infected staff to stay home, and quarantining units on which outbreaks occur, Dr. Stone said. Policies for confining residents to rooms were reported by approximately 74% of nursing homes in 2014, and by approximately 87% in 2018, for instance. Overall, nursing homes were “getting better policies in place,” she said. The analysis compared data from two cross-sectional surveys of nursing homes conducted in 2014 and 2018 (945 and 888 facilities, respectively).
Nursing homes “have a long way to go,” however, with respect to the training of infection preventionists, Dr. Stone said. In 2014, her analysis shows, almost 65% of infection preventionists had no specific infection-control training and less than 3% were Certified in Infection Control (CIC) – a credential awarded by the Certification Board of Infection Control & Epidemiology. Of the 35% who had some form of official training, most completed state or local training courses.
The numbers improved slightly in 2018, with 7% of nursing homes reporting their infection preventionists had the highest-level certification, and 44% reporting that their infection preventionists had no specific infection-control training. Research has shown that infection-control training of any kind has a “strong effect” on IPC-related outcomes. While not demonstrated in research thus far, it seems plausible that “facilities with certified [infection preventionists] will have better processes in place,” said Dr. Stone, whose research has documented the need for more monitoring of staff compliance with hand-washing and other IPC procedures.
Infection preventionists in nursing homes typically have been directors of nursing or assistant directors of nursing who fold IPC responsibilities into a multitude of other responsibilities. Before the 2016 rules, some smaller facilities hired off-site consultants to do the job.
CMS upped the ante after several months of COVID-19, recommending in mid-May that nursing homes assign at least one individual with training in infection control “to provide on-site management of the IPC program.” The infection preventionists should be a “full-time role” in facilities that have more than 100 residents, the CMS guidance said. (Prior to the pandemic, CMS issued proposed regulations in 2019 that would modify the time an infection preventionist must devote to a facility from “part time” to “sufficient time.”)
However, neither the 2016 rule nor the most recent guidance on infection preventionists define the length or content of training.
Swati Gaur, MD, chair of the Infection Advisory Committee of AMDA and a certified medical director of two skilled nursing facilities in Gainesville, Ga., said that the pandemic “has really started to crystallize some of the limitations of having a very vague role, not just in terms of what an [infection preventionists] does [in the nursing home] but also the training,”
Fortunately, Dr. Gaur said, when SARS-CoV-2 struck, she had just transitioned her facilities’ designated infection preventionist to work full-time on the role. She had worked closely with her infection preventionist on IPC issues but wishes she had arranged for more rigorous independent training. “The role of the [infection preventionist] is huge and complicated,” now involving employee health, contract tracing, cohorting, isolation, and compliance with precautions and use of PPE, in addition to surveillance, data reporting, and communication with public health officials, she said.
“Facilities are finding out now that [the infection preventionist] cannot be an afterthought. And it won’t end with COVID. We have other respiratory illnesses like flu and other viruses that we struggle with all the time,” said Dr. Gaur, who is working alongside Dr. Dumyati and two other long-term care experts on AMDA’s COVID-19 guidance. The nursing homes that Dr. Gaur directs are part of the Northeast Georgia Health Care System and together include 271 beds.
Moving forward
IPC practices often collide with facilities’ role as a home, especially to those receiving long-term care. “We always have to measure what we do [to prevent and control infections] against patient autonomy and residents’ rights,” said Dr. Gaur. “We have struggled with these issues, prior to the pandemic. If patients are positive for multidrug resistant organisms [for instance], how long can they be isolated in their own rooms? You can’t for days and months put someone in a single room and create isolation. That’s where the science of infection prevention can collide with residents’ rights.”
Over the years, the Centers for Disease Control and Prevention has acknowledged this discordance, leaving it to facilities to decide, for instance, whether to actively screen for colonization with MDROs. In 2019, to help nursing homes prevent the transmission of MDROs from residents who are colonized but not actively infected, the CDC introduced new “enhanced barrier precautions” that require the use of gowns and gloves for specific resident activities identified as having a high risk of MDRO transmission. The new category of precautions is less restrictive than traditional contact precautions, which keep residents in their rooms.
Infection control in nursing homes “isn’t where it needs to be ... but we’re always going to have in nursing homes a situation where there’s a high potential for rapid transmission of infectious disease,” said Christopher Crnich, MD, PhD, an infectious disease specialist at the University of Wisconsin–Madison who chairs the long-term care special interest group of the Society of Healthcare Epidemiology of America and has offered COVID-19 advice to his state’s department of public health.
“Anytime you have a congregative community, particularly one that involves susceptible hosts, there will be an intrinsically susceptible environment ... I’m a bit disturbed by the emphasis on saying, ‘This nursing home had a COVID-19 outbreak, therefore this nursing home did something wrong,’ ” Dr. Crnich said.
“How we mitigate the size of the outbreaks is where we need to focus our attention,” he said. The goal with SARS-CoV-2, he said, is to recognize its introduction “as rapidly as possible” and stop its spread through empiric symptom- and exposure-based isolation, multiple waves of targeted testing, widespread use of contact and droplet precautions, and isolating staff as necessary.
As awareness grew this year among long-term care leaders that relying too heavily on symptom-based strategies may not be effective to prevent introduction and transmission of SARS-CoV-2, a study published in April in the New England Journal of Medicine cemented the need for a testing strategy not limited to symptomatic individuals.
The study documented that more than half of residents in a nursing home who had positive polymerase chain reaction (PCR) test results were asymptomatic at the time of testing, and that most went on to develop symptoms. The study was conducted after one case of COVID-19 had been identified.
Some states issued calls this spring for “universal testing” of all nursing home patients and staff, and the CMS recommendations issued to state and local officials in mid-May for phased nursing home “reopening” call for baseline testing of all residents and staff, followed by retesting all residents weekly until all residents test negative and by retesting all staff continuing every week.
However, the experts contacted for this story said that, without a highly accurate and accessible point-of-care test (and even with one, considering the virus’ incubation period), a universal approach that includes all nursing home residents may have more limited value than is being touted. In many scenarios, they said, it is most meaningful to focus still-limited testing supplies on the staff, many of whom work at more than one facility and are believed to be primary vectors of SARS-CoV-2.
Dr. Ouslander, Dr. Wasserman and other long-term care leaders have been discussing testing at length, trying to reach consensus on best policies. “I don’t think there’s any uniform approach or uniform agreement,” said Dr. Ouslander. “For me, under ideal circumstances what needs to be done to protect older people in nursing homes is to get access to as many accurate viral tests as possible and test staff at least once a week or every 10 days.”
In some facilities, there may be an unspoken barrier to the frequent testing of staff: Fear that staff who test positive will need to be quarantined, with no one to take their place on the front line. Dr. Ouslander said he knows of one county health department that has discouraged nursing homes from testing asymptomatic staff. “It’s insane and truly shocking,” he said.
At the University of Rochester Medical Center, Dr. Dumyati said, staffing agencies are running short of nurse aide substitutes, and staffing issues have become the “biggest challenge” facing a regional multidisciplinary group of medical directors, hospital leaders, and health department officials who are working to troubleshoot COVID-19 issues. “Some of our nursing homes have ended up sending some of their residents to other nursing homes or to the hospital [because of the loss of staff],” she said.
Currently in the state of New York, she noted, COVID-19 patients may not be discharged to nursing homes until they test negative for the virus through PCR testing. “And some people don’t clear by PCR for 4-6 weeks.”
The barriers
Staffing shortages – real in some locales, and anticipated in others as economic reopening grows – are reflective of underlying structural and financial factors that work against optimal IPC, experts said. It’s not uncommon for certified nurse assistants (CNAs) to be assigned to 10-15 residents. And according to AMDA, 30%-46% of CNAs are reported to receive some form of public assistance. Low wages force many CNAs to work other jobs, including shifts at other nursing homes.
Turnover of nursing home leadership also creates problems. Dr. Crnich calls it “one of the biggest barriers” to effective IPC in nursing homes. “Facilities can tolerate some turnover in their front line staff,” he said, “as long as their leadership structure remains relatively stable.” Dr. Stone and her coinvestigators have documented at least yearly turnover in top positions: They found that, in 2018, approximately one-quarter of facilities reported employing three or more infection preventionists, three or more administrators, and three or more directors of nursing during the prior 3 years.
Medical directors, moreover, are not uniformly qualified, engaged with their facilities, or supported by nursing home administrators. “It’s an open secret, I think, that a lot of facilities want a medical director who is a good referral source,” said Dr. Gaur. “A medical director needs to be completely engaged in [quality improvement and] infection control practices.”
Some nursing home chains, she noted, “have realized the value of the medical director, and have changed the way they’re paying them. They’re actually holding them accountable [for quality and outcomes].”
Medical directors such as Dr. Wasserman, who previously oversaw a 74-facility nursing home chain in California as chief medical officer and then chief executive officer and has worked on nursing home quality improvement processes for his state, said there is much that can be done clinically to prevent the spread of infections, such as more frequent use of telemedicine, more attention to “deprescribing” unnecessary medications (which reduces the number of medication passes and, thus, the number of “transmission opportunities”), and the use of continuous remote monitoring. He has been trying to secure Bluetooth-enabled pulse oximetry and temperature monitoring for the Los Angeles Jewish Home and other facilities.
Dr. Wasserman and other long-term care leaders believe that a more educational inspection process would also lead to improvements in IPC. “The punitive nature of the survey process is morally deflating to frontline staff [and] penalties take money away from operations,” Dr. Wasserman said. “It’s not a productive approach to quality improvement.”
Dr. Stone agreed. Infection control is now the primary focus of CMS’s inspection process, and she said that increased regulatory scrutiny of IPC beyond COVID-19 is a “good thing.” Her research has shown that most deficiencies identified by inspectors are infection control deficiencies, and that in 2014 and 2018, approximately one-third of nursing homes had infection control citations. (CMS recently increased penalties and fines for identified deficiencies.)
“But my hope would be that the survey process would be more educational [as it is for hospitals],” she said. “We need to be supporting nursing homes to do a better job.”
A silver lining of the COVID-19 pandemic, as Dr. Stone sees it, is that nursing homes may be more engaged with data reporting and infection surveillance going forward. Nursing homes are now required to report their COVID-19 cases to the CDC through its hospital-dominant National Healthcare Safety Network, and the CDC has made technical changes that now make it “easier [than it was in the past] for nursing homes to join and participate,” she said. “Now that all nursing homes are engaged, will they be engaged post-COVID, too? I hope so. Surveillance [of infections] is a first step toward better outcomes.”
For now, said Dr. Crnich, the intensive prevention and mitigation efforts that are being required of nursing homes to minimize COVID-19’s impact is “a big deal and will tax the resources of most nursing homes and exceed the resources of many” without outside support, Dr. Crnich said. “This has been the most illuminating part of all this, and will probably require us to reconsider how we’re resourcing our nursing homes moving forward into the future.”
The toll that COVID-19 has taken on nursing homes and their postacute and long-term care residents has a multilayered backstory involving underresourced organizational structures, inherent susceptibilities, minimally trained infection prevention staff, variable abilities to isolate and quarantine large numbers of patients and residents, and a lack of governmental support.
“Nursing homes have been trying their best to combat this pandemic using the best infection control procedures they have, but blindfolded and with their hands tied behind their backs,” said Joseph G. Ouslander, MD, professor of geriatric medicine at Florida Atlantic University, Boca Raton, which has teaching affiliations with three senior communities.
Nursing home leaders are debating how to best use testing to guide transmission-based precautions and isolation strategies and how to keep residents safe while allowing some socialization after months of conflicting guidance from public health officials (on testing and on sites of care for patients discharged from the hospital, for instance), with a lack of adequate personal protective equipment (PPE) and testing supplies, and with nursing home resident deaths estimated to account for at least one-quarter of the total COVID-19–related mortality in the United States.
“COVID is not going away [over the next couple of years],” said Michael Wasserman, MD, medical director of the Eisenberg Village at the Los Angeles Jewish Home and president of the California Association of Long-Term Care Medicine.
Dr. Wasserman and other experts in both long-term care and infectious disease said in interviews that, through the rest of the pandemic and beyond, nursing homes need the following:
- Full-time, well-trained “infection preventionists” – infection prevention managers, in essence – who can lead improvements in emergency preparedness and infection prevention and control (IPC)
- Medical directors who are well qualified and engaged
- A survey/inspection process that is educational and not solely punitive
- More resources and attention to structural reform
“If this pandemic doesn’t create significant change in the nursing home industry, nothing ever will,” Dr. Wasserman said.
Prepandemic experience
When Ghinwa Dumyati, MD, began working with nursing homes in early March to prevent and contain COVID-19 outbreaks, her focus was on PPE.
Nursing home staff were intimately familiar with standard precautions, and many had used contact precautions to prevent transmission of infections like Clostridioides difficile and Candida auris, as well as droplet precautions for influenza. With the threat of COVID-19, nursing homes “had a brand-new requirement to do both contact and droplet precautions – with a new need for eye protection – and in some situations, respiratory precautions with N95 masks,” said Dr. Dumyati, professor of medicine and director of communicable disease surveillance and prevention at the University of Rochester (N.Y.) Medical Center. “And on top of that, [staff] had to learn to conserve and reuse PPE.”
Staff had not been fit-tested for use of N95 respirators, she noted. “The only time an N95 was used in the nursing home prior to COVID-19,” she said, “was for a suspected tuberculosis patient [before hospital admission].”
Similarly, nursing homes had experience in quarantining units to prevent transmission of illnesses like influenza or norovirus – keeping residents in their rooms with no visitations or social activity, for instance – but never did they have to arrange “massive movements of residents to completely new units or parts of a unit,” said Dr. Dumyati, who also has led hospital and nursing home collaborative programs in Rochester to beat back C. difficile, and is now helping to formulate COVID-19 recommendations and guidance for members of AMDA – The Society for Post-Acute and Long-Term Care.
As the SARS-CoV-2 virus began its spread through the United States, efforts to strengthen IPC programs in nursing homes in Rochester and elsewhere had been focused largely on multidrug resistant organisms (MDROs) and antibiotic stewardship – not on pandemic preparedness.
Reducing antibiotic use had become a national priority, and a 2016 rule by the Centers for Medicare & Medicaid Services required nursing homes to develop, over a 3-year period, an IPC program that included an antibiotic stewardship component and employment of a trained infection preventionist on at least a half-time basis. Emergency preparedness (e.g., having alternate energy sources for a facility) was also included in the rule, but it was only in 2019 when CMS updated its “Requirements for Participation” rule to stipulate that emergency preparedness include planning for “emerging infectious diseases.”
“The 2016 regulations came about because infections were so problematic in nursing homes,” especially urinary tract infections, C. difficile, and drug-resistant infections, said Patricia Stone, PhD, RN, of the Center for Health Policy at the Columbia University School of Nursing, New York, who has published widely on infection prevention and control in nursing homes.
An analysis of IPC practices in 2014 and in 2018 suggests that the IPC-focused rules were helping, mainly with antibiotic stewardship programs but also with respect to some of the practices aimed at outbreak control, such as having policies in place for grouping infected residents together, instructing infected staff to stay home, and quarantining units on which outbreaks occur, Dr. Stone said. Policies for confining residents to rooms were reported by approximately 74% of nursing homes in 2014, and by approximately 87% in 2018, for instance. Overall, nursing homes were “getting better policies in place,” she said. The analysis compared data from two cross-sectional surveys of nursing homes conducted in 2014 and 2018 (945 and 888 facilities, respectively).
Nursing homes “have a long way to go,” however, with respect to the training of infection preventionists, Dr. Stone said. In 2014, her analysis shows, almost 65% of infection preventionists had no specific infection-control training and less than 3% were Certified in Infection Control (CIC) – a credential awarded by the Certification Board of Infection Control & Epidemiology. Of the 35% who had some form of official training, most completed state or local training courses.
The numbers improved slightly in 2018, with 7% of nursing homes reporting their infection preventionists had the highest-level certification, and 44% reporting that their infection preventionists had no specific infection-control training. Research has shown that infection-control training of any kind has a “strong effect” on IPC-related outcomes. While not demonstrated in research thus far, it seems plausible that “facilities with certified [infection preventionists] will have better processes in place,” said Dr. Stone, whose research has documented the need for more monitoring of staff compliance with hand-washing and other IPC procedures.
Infection preventionists in nursing homes typically have been directors of nursing or assistant directors of nursing who fold IPC responsibilities into a multitude of other responsibilities. Before the 2016 rules, some smaller facilities hired off-site consultants to do the job.
CMS upped the ante after several months of COVID-19, recommending in mid-May that nursing homes assign at least one individual with training in infection control “to provide on-site management of the IPC program.” The infection preventionists should be a “full-time role” in facilities that have more than 100 residents, the CMS guidance said. (Prior to the pandemic, CMS issued proposed regulations in 2019 that would modify the time an infection preventionist must devote to a facility from “part time” to “sufficient time.”)
However, neither the 2016 rule nor the most recent guidance on infection preventionists define the length or content of training.
Swati Gaur, MD, chair of the Infection Advisory Committee of AMDA and a certified medical director of two skilled nursing facilities in Gainesville, Ga., said that the pandemic “has really started to crystallize some of the limitations of having a very vague role, not just in terms of what an [infection preventionists] does [in the nursing home] but also the training,”
Fortunately, Dr. Gaur said, when SARS-CoV-2 struck, she had just transitioned her facilities’ designated infection preventionist to work full-time on the role. She had worked closely with her infection preventionist on IPC issues but wishes she had arranged for more rigorous independent training. “The role of the [infection preventionist] is huge and complicated,” now involving employee health, contract tracing, cohorting, isolation, and compliance with precautions and use of PPE, in addition to surveillance, data reporting, and communication with public health officials, she said.
“Facilities are finding out now that [the infection preventionist] cannot be an afterthought. And it won’t end with COVID. We have other respiratory illnesses like flu and other viruses that we struggle with all the time,” said Dr. Gaur, who is working alongside Dr. Dumyati and two other long-term care experts on AMDA’s COVID-19 guidance. The nursing homes that Dr. Gaur directs are part of the Northeast Georgia Health Care System and together include 271 beds.
Moving forward
IPC practices often collide with facilities’ role as a home, especially to those receiving long-term care. “We always have to measure what we do [to prevent and control infections] against patient autonomy and residents’ rights,” said Dr. Gaur. “We have struggled with these issues, prior to the pandemic. If patients are positive for multidrug resistant organisms [for instance], how long can they be isolated in their own rooms? You can’t for days and months put someone in a single room and create isolation. That’s where the science of infection prevention can collide with residents’ rights.”
Over the years, the Centers for Disease Control and Prevention has acknowledged this discordance, leaving it to facilities to decide, for instance, whether to actively screen for colonization with MDROs. In 2019, to help nursing homes prevent the transmission of MDROs from residents who are colonized but not actively infected, the CDC introduced new “enhanced barrier precautions” that require the use of gowns and gloves for specific resident activities identified as having a high risk of MDRO transmission. The new category of precautions is less restrictive than traditional contact precautions, which keep residents in their rooms.
Infection control in nursing homes “isn’t where it needs to be ... but we’re always going to have in nursing homes a situation where there’s a high potential for rapid transmission of infectious disease,” said Christopher Crnich, MD, PhD, an infectious disease specialist at the University of Wisconsin–Madison who chairs the long-term care special interest group of the Society of Healthcare Epidemiology of America and has offered COVID-19 advice to his state’s department of public health.
“Anytime you have a congregative community, particularly one that involves susceptible hosts, there will be an intrinsically susceptible environment ... I’m a bit disturbed by the emphasis on saying, ‘This nursing home had a COVID-19 outbreak, therefore this nursing home did something wrong,’ ” Dr. Crnich said.
“How we mitigate the size of the outbreaks is where we need to focus our attention,” he said. The goal with SARS-CoV-2, he said, is to recognize its introduction “as rapidly as possible” and stop its spread through empiric symptom- and exposure-based isolation, multiple waves of targeted testing, widespread use of contact and droplet precautions, and isolating staff as necessary.
As awareness grew this year among long-term care leaders that relying too heavily on symptom-based strategies may not be effective to prevent introduction and transmission of SARS-CoV-2, a study published in April in the New England Journal of Medicine cemented the need for a testing strategy not limited to symptomatic individuals.
The study documented that more than half of residents in a nursing home who had positive polymerase chain reaction (PCR) test results were asymptomatic at the time of testing, and that most went on to develop symptoms. The study was conducted after one case of COVID-19 had been identified.
Some states issued calls this spring for “universal testing” of all nursing home patients and staff, and the CMS recommendations issued to state and local officials in mid-May for phased nursing home “reopening” call for baseline testing of all residents and staff, followed by retesting all residents weekly until all residents test negative and by retesting all staff continuing every week.
However, the experts contacted for this story said that, without a highly accurate and accessible point-of-care test (and even with one, considering the virus’ incubation period), a universal approach that includes all nursing home residents may have more limited value than is being touted. In many scenarios, they said, it is most meaningful to focus still-limited testing supplies on the staff, many of whom work at more than one facility and are believed to be primary vectors of SARS-CoV-2.
Dr. Ouslander, Dr. Wasserman and other long-term care leaders have been discussing testing at length, trying to reach consensus on best policies. “I don’t think there’s any uniform approach or uniform agreement,” said Dr. Ouslander. “For me, under ideal circumstances what needs to be done to protect older people in nursing homes is to get access to as many accurate viral tests as possible and test staff at least once a week or every 10 days.”
In some facilities, there may be an unspoken barrier to the frequent testing of staff: Fear that staff who test positive will need to be quarantined, with no one to take their place on the front line. Dr. Ouslander said he knows of one county health department that has discouraged nursing homes from testing asymptomatic staff. “It’s insane and truly shocking,” he said.
At the University of Rochester Medical Center, Dr. Dumyati said, staffing agencies are running short of nurse aide substitutes, and staffing issues have become the “biggest challenge” facing a regional multidisciplinary group of medical directors, hospital leaders, and health department officials who are working to troubleshoot COVID-19 issues. “Some of our nursing homes have ended up sending some of their residents to other nursing homes or to the hospital [because of the loss of staff],” she said.
Currently in the state of New York, she noted, COVID-19 patients may not be discharged to nursing homes until they test negative for the virus through PCR testing. “And some people don’t clear by PCR for 4-6 weeks.”
The barriers
Staffing shortages – real in some locales, and anticipated in others as economic reopening grows – are reflective of underlying structural and financial factors that work against optimal IPC, experts said. It’s not uncommon for certified nurse assistants (CNAs) to be assigned to 10-15 residents. And according to AMDA, 30%-46% of CNAs are reported to receive some form of public assistance. Low wages force many CNAs to work other jobs, including shifts at other nursing homes.
Turnover of nursing home leadership also creates problems. Dr. Crnich calls it “one of the biggest barriers” to effective IPC in nursing homes. “Facilities can tolerate some turnover in their front line staff,” he said, “as long as their leadership structure remains relatively stable.” Dr. Stone and her coinvestigators have documented at least yearly turnover in top positions: They found that, in 2018, approximately one-quarter of facilities reported employing three or more infection preventionists, three or more administrators, and three or more directors of nursing during the prior 3 years.
Medical directors, moreover, are not uniformly qualified, engaged with their facilities, or supported by nursing home administrators. “It’s an open secret, I think, that a lot of facilities want a medical director who is a good referral source,” said Dr. Gaur. “A medical director needs to be completely engaged in [quality improvement and] infection control practices.”
Some nursing home chains, she noted, “have realized the value of the medical director, and have changed the way they’re paying them. They’re actually holding them accountable [for quality and outcomes].”
Medical directors such as Dr. Wasserman, who previously oversaw a 74-facility nursing home chain in California as chief medical officer and then chief executive officer and has worked on nursing home quality improvement processes for his state, said there is much that can be done clinically to prevent the spread of infections, such as more frequent use of telemedicine, more attention to “deprescribing” unnecessary medications (which reduces the number of medication passes and, thus, the number of “transmission opportunities”), and the use of continuous remote monitoring. He has been trying to secure Bluetooth-enabled pulse oximetry and temperature monitoring for the Los Angeles Jewish Home and other facilities.
Dr. Wasserman and other long-term care leaders believe that a more educational inspection process would also lead to improvements in IPC. “The punitive nature of the survey process is morally deflating to frontline staff [and] penalties take money away from operations,” Dr. Wasserman said. “It’s not a productive approach to quality improvement.”
Dr. Stone agreed. Infection control is now the primary focus of CMS’s inspection process, and she said that increased regulatory scrutiny of IPC beyond COVID-19 is a “good thing.” Her research has shown that most deficiencies identified by inspectors are infection control deficiencies, and that in 2014 and 2018, approximately one-third of nursing homes had infection control citations. (CMS recently increased penalties and fines for identified deficiencies.)
“But my hope would be that the survey process would be more educational [as it is for hospitals],” she said. “We need to be supporting nursing homes to do a better job.”
A silver lining of the COVID-19 pandemic, as Dr. Stone sees it, is that nursing homes may be more engaged with data reporting and infection surveillance going forward. Nursing homes are now required to report their COVID-19 cases to the CDC through its hospital-dominant National Healthcare Safety Network, and the CDC has made technical changes that now make it “easier [than it was in the past] for nursing homes to join and participate,” she said. “Now that all nursing homes are engaged, will they be engaged post-COVID, too? I hope so. Surveillance [of infections] is a first step toward better outcomes.”
For now, said Dr. Crnich, the intensive prevention and mitigation efforts that are being required of nursing homes to minimize COVID-19’s impact is “a big deal and will tax the resources of most nursing homes and exceed the resources of many” without outside support, Dr. Crnich said. “This has been the most illuminating part of all this, and will probably require us to reconsider how we’re resourcing our nursing homes moving forward into the future.”
The toll that COVID-19 has taken on nursing homes and their postacute and long-term care residents has a multilayered backstory involving underresourced organizational structures, inherent susceptibilities, minimally trained infection prevention staff, variable abilities to isolate and quarantine large numbers of patients and residents, and a lack of governmental support.
“Nursing homes have been trying their best to combat this pandemic using the best infection control procedures they have, but blindfolded and with their hands tied behind their backs,” said Joseph G. Ouslander, MD, professor of geriatric medicine at Florida Atlantic University, Boca Raton, which has teaching affiliations with three senior communities.
Nursing home leaders are debating how to best use testing to guide transmission-based precautions and isolation strategies and how to keep residents safe while allowing some socialization after months of conflicting guidance from public health officials (on testing and on sites of care for patients discharged from the hospital, for instance), with a lack of adequate personal protective equipment (PPE) and testing supplies, and with nursing home resident deaths estimated to account for at least one-quarter of the total COVID-19–related mortality in the United States.
“COVID is not going away [over the next couple of years],” said Michael Wasserman, MD, medical director of the Eisenberg Village at the Los Angeles Jewish Home and president of the California Association of Long-Term Care Medicine.
Dr. Wasserman and other experts in both long-term care and infectious disease said in interviews that, through the rest of the pandemic and beyond, nursing homes need the following:
- Full-time, well-trained “infection preventionists” – infection prevention managers, in essence – who can lead improvements in emergency preparedness and infection prevention and control (IPC)
- Medical directors who are well qualified and engaged
- A survey/inspection process that is educational and not solely punitive
- More resources and attention to structural reform
“If this pandemic doesn’t create significant change in the nursing home industry, nothing ever will,” Dr. Wasserman said.
Prepandemic experience
When Ghinwa Dumyati, MD, began working with nursing homes in early March to prevent and contain COVID-19 outbreaks, her focus was on PPE.
Nursing home staff were intimately familiar with standard precautions, and many had used contact precautions to prevent transmission of infections like Clostridioides difficile and Candida auris, as well as droplet precautions for influenza. With the threat of COVID-19, nursing homes “had a brand-new requirement to do both contact and droplet precautions – with a new need for eye protection – and in some situations, respiratory precautions with N95 masks,” said Dr. Dumyati, professor of medicine and director of communicable disease surveillance and prevention at the University of Rochester (N.Y.) Medical Center. “And on top of that, [staff] had to learn to conserve and reuse PPE.”
Staff had not been fit-tested for use of N95 respirators, she noted. “The only time an N95 was used in the nursing home prior to COVID-19,” she said, “was for a suspected tuberculosis patient [before hospital admission].”
Similarly, nursing homes had experience in quarantining units to prevent transmission of illnesses like influenza or norovirus – keeping residents in their rooms with no visitations or social activity, for instance – but never did they have to arrange “massive movements of residents to completely new units or parts of a unit,” said Dr. Dumyati, who also has led hospital and nursing home collaborative programs in Rochester to beat back C. difficile, and is now helping to formulate COVID-19 recommendations and guidance for members of AMDA – The Society for Post-Acute and Long-Term Care.
As the SARS-CoV-2 virus began its spread through the United States, efforts to strengthen IPC programs in nursing homes in Rochester and elsewhere had been focused largely on multidrug resistant organisms (MDROs) and antibiotic stewardship – not on pandemic preparedness.
Reducing antibiotic use had become a national priority, and a 2016 rule by the Centers for Medicare & Medicaid Services required nursing homes to develop, over a 3-year period, an IPC program that included an antibiotic stewardship component and employment of a trained infection preventionist on at least a half-time basis. Emergency preparedness (e.g., having alternate energy sources for a facility) was also included in the rule, but it was only in 2019 when CMS updated its “Requirements for Participation” rule to stipulate that emergency preparedness include planning for “emerging infectious diseases.”
“The 2016 regulations came about because infections were so problematic in nursing homes,” especially urinary tract infections, C. difficile, and drug-resistant infections, said Patricia Stone, PhD, RN, of the Center for Health Policy at the Columbia University School of Nursing, New York, who has published widely on infection prevention and control in nursing homes.
An analysis of IPC practices in 2014 and in 2018 suggests that the IPC-focused rules were helping, mainly with antibiotic stewardship programs but also with respect to some of the practices aimed at outbreak control, such as having policies in place for grouping infected residents together, instructing infected staff to stay home, and quarantining units on which outbreaks occur, Dr. Stone said. Policies for confining residents to rooms were reported by approximately 74% of nursing homes in 2014, and by approximately 87% in 2018, for instance. Overall, nursing homes were “getting better policies in place,” she said. The analysis compared data from two cross-sectional surveys of nursing homes conducted in 2014 and 2018 (945 and 888 facilities, respectively).
Nursing homes “have a long way to go,” however, with respect to the training of infection preventionists, Dr. Stone said. In 2014, her analysis shows, almost 65% of infection preventionists had no specific infection-control training and less than 3% were Certified in Infection Control (CIC) – a credential awarded by the Certification Board of Infection Control & Epidemiology. Of the 35% who had some form of official training, most completed state or local training courses.
The numbers improved slightly in 2018, with 7% of nursing homes reporting their infection preventionists had the highest-level certification, and 44% reporting that their infection preventionists had no specific infection-control training. Research has shown that infection-control training of any kind has a “strong effect” on IPC-related outcomes. While not demonstrated in research thus far, it seems plausible that “facilities with certified [infection preventionists] will have better processes in place,” said Dr. Stone, whose research has documented the need for more monitoring of staff compliance with hand-washing and other IPC procedures.
Infection preventionists in nursing homes typically have been directors of nursing or assistant directors of nursing who fold IPC responsibilities into a multitude of other responsibilities. Before the 2016 rules, some smaller facilities hired off-site consultants to do the job.
CMS upped the ante after several months of COVID-19, recommending in mid-May that nursing homes assign at least one individual with training in infection control “to provide on-site management of the IPC program.” The infection preventionists should be a “full-time role” in facilities that have more than 100 residents, the CMS guidance said. (Prior to the pandemic, CMS issued proposed regulations in 2019 that would modify the time an infection preventionist must devote to a facility from “part time” to “sufficient time.”)
However, neither the 2016 rule nor the most recent guidance on infection preventionists define the length or content of training.
Swati Gaur, MD, chair of the Infection Advisory Committee of AMDA and a certified medical director of two skilled nursing facilities in Gainesville, Ga., said that the pandemic “has really started to crystallize some of the limitations of having a very vague role, not just in terms of what an [infection preventionists] does [in the nursing home] but also the training,”
Fortunately, Dr. Gaur said, when SARS-CoV-2 struck, she had just transitioned her facilities’ designated infection preventionist to work full-time on the role. She had worked closely with her infection preventionist on IPC issues but wishes she had arranged for more rigorous independent training. “The role of the [infection preventionist] is huge and complicated,” now involving employee health, contract tracing, cohorting, isolation, and compliance with precautions and use of PPE, in addition to surveillance, data reporting, and communication with public health officials, she said.
“Facilities are finding out now that [the infection preventionist] cannot be an afterthought. And it won’t end with COVID. We have other respiratory illnesses like flu and other viruses that we struggle with all the time,” said Dr. Gaur, who is working alongside Dr. Dumyati and two other long-term care experts on AMDA’s COVID-19 guidance. The nursing homes that Dr. Gaur directs are part of the Northeast Georgia Health Care System and together include 271 beds.
Moving forward
IPC practices often collide with facilities’ role as a home, especially to those receiving long-term care. “We always have to measure what we do [to prevent and control infections] against patient autonomy and residents’ rights,” said Dr. Gaur. “We have struggled with these issues, prior to the pandemic. If patients are positive for multidrug resistant organisms [for instance], how long can they be isolated in their own rooms? You can’t for days and months put someone in a single room and create isolation. That’s where the science of infection prevention can collide with residents’ rights.”
Over the years, the Centers for Disease Control and Prevention has acknowledged this discordance, leaving it to facilities to decide, for instance, whether to actively screen for colonization with MDROs. In 2019, to help nursing homes prevent the transmission of MDROs from residents who are colonized but not actively infected, the CDC introduced new “enhanced barrier precautions” that require the use of gowns and gloves for specific resident activities identified as having a high risk of MDRO transmission. The new category of precautions is less restrictive than traditional contact precautions, which keep residents in their rooms.
Infection control in nursing homes “isn’t where it needs to be ... but we’re always going to have in nursing homes a situation where there’s a high potential for rapid transmission of infectious disease,” said Christopher Crnich, MD, PhD, an infectious disease specialist at the University of Wisconsin–Madison who chairs the long-term care special interest group of the Society of Healthcare Epidemiology of America and has offered COVID-19 advice to his state’s department of public health.
“Anytime you have a congregative community, particularly one that involves susceptible hosts, there will be an intrinsically susceptible environment ... I’m a bit disturbed by the emphasis on saying, ‘This nursing home had a COVID-19 outbreak, therefore this nursing home did something wrong,’ ” Dr. Crnich said.
“How we mitigate the size of the outbreaks is where we need to focus our attention,” he said. The goal with SARS-CoV-2, he said, is to recognize its introduction “as rapidly as possible” and stop its spread through empiric symptom- and exposure-based isolation, multiple waves of targeted testing, widespread use of contact and droplet precautions, and isolating staff as necessary.
As awareness grew this year among long-term care leaders that relying too heavily on symptom-based strategies may not be effective to prevent introduction and transmission of SARS-CoV-2, a study published in April in the New England Journal of Medicine cemented the need for a testing strategy not limited to symptomatic individuals.
The study documented that more than half of residents in a nursing home who had positive polymerase chain reaction (PCR) test results were asymptomatic at the time of testing, and that most went on to develop symptoms. The study was conducted after one case of COVID-19 had been identified.
Some states issued calls this spring for “universal testing” of all nursing home patients and staff, and the CMS recommendations issued to state and local officials in mid-May for phased nursing home “reopening” call for baseline testing of all residents and staff, followed by retesting all residents weekly until all residents test negative and by retesting all staff continuing every week.
However, the experts contacted for this story said that, without a highly accurate and accessible point-of-care test (and even with one, considering the virus’ incubation period), a universal approach that includes all nursing home residents may have more limited value than is being touted. In many scenarios, they said, it is most meaningful to focus still-limited testing supplies on the staff, many of whom work at more than one facility and are believed to be primary vectors of SARS-CoV-2.
Dr. Ouslander, Dr. Wasserman and other long-term care leaders have been discussing testing at length, trying to reach consensus on best policies. “I don’t think there’s any uniform approach or uniform agreement,” said Dr. Ouslander. “For me, under ideal circumstances what needs to be done to protect older people in nursing homes is to get access to as many accurate viral tests as possible and test staff at least once a week or every 10 days.”
In some facilities, there may be an unspoken barrier to the frequent testing of staff: Fear that staff who test positive will need to be quarantined, with no one to take their place on the front line. Dr. Ouslander said he knows of one county health department that has discouraged nursing homes from testing asymptomatic staff. “It’s insane and truly shocking,” he said.
At the University of Rochester Medical Center, Dr. Dumyati said, staffing agencies are running short of nurse aide substitutes, and staffing issues have become the “biggest challenge” facing a regional multidisciplinary group of medical directors, hospital leaders, and health department officials who are working to troubleshoot COVID-19 issues. “Some of our nursing homes have ended up sending some of their residents to other nursing homes or to the hospital [because of the loss of staff],” she said.
Currently in the state of New York, she noted, COVID-19 patients may not be discharged to nursing homes until they test negative for the virus through PCR testing. “And some people don’t clear by PCR for 4-6 weeks.”
The barriers
Staffing shortages – real in some locales, and anticipated in others as economic reopening grows – are reflective of underlying structural and financial factors that work against optimal IPC, experts said. It’s not uncommon for certified nurse assistants (CNAs) to be assigned to 10-15 residents. And according to AMDA, 30%-46% of CNAs are reported to receive some form of public assistance. Low wages force many CNAs to work other jobs, including shifts at other nursing homes.
Turnover of nursing home leadership also creates problems. Dr. Crnich calls it “one of the biggest barriers” to effective IPC in nursing homes. “Facilities can tolerate some turnover in their front line staff,” he said, “as long as their leadership structure remains relatively stable.” Dr. Stone and her coinvestigators have documented at least yearly turnover in top positions: They found that, in 2018, approximately one-quarter of facilities reported employing three or more infection preventionists, three or more administrators, and three or more directors of nursing during the prior 3 years.
Medical directors, moreover, are not uniformly qualified, engaged with their facilities, or supported by nursing home administrators. “It’s an open secret, I think, that a lot of facilities want a medical director who is a good referral source,” said Dr. Gaur. “A medical director needs to be completely engaged in [quality improvement and] infection control practices.”
Some nursing home chains, she noted, “have realized the value of the medical director, and have changed the way they’re paying them. They’re actually holding them accountable [for quality and outcomes].”
Medical directors such as Dr. Wasserman, who previously oversaw a 74-facility nursing home chain in California as chief medical officer and then chief executive officer and has worked on nursing home quality improvement processes for his state, said there is much that can be done clinically to prevent the spread of infections, such as more frequent use of telemedicine, more attention to “deprescribing” unnecessary medications (which reduces the number of medication passes and, thus, the number of “transmission opportunities”), and the use of continuous remote monitoring. He has been trying to secure Bluetooth-enabled pulse oximetry and temperature monitoring for the Los Angeles Jewish Home and other facilities.
Dr. Wasserman and other long-term care leaders believe that a more educational inspection process would also lead to improvements in IPC. “The punitive nature of the survey process is morally deflating to frontline staff [and] penalties take money away from operations,” Dr. Wasserman said. “It’s not a productive approach to quality improvement.”
Dr. Stone agreed. Infection control is now the primary focus of CMS’s inspection process, and she said that increased regulatory scrutiny of IPC beyond COVID-19 is a “good thing.” Her research has shown that most deficiencies identified by inspectors are infection control deficiencies, and that in 2014 and 2018, approximately one-third of nursing homes had infection control citations. (CMS recently increased penalties and fines for identified deficiencies.)
“But my hope would be that the survey process would be more educational [as it is for hospitals],” she said. “We need to be supporting nursing homes to do a better job.”
A silver lining of the COVID-19 pandemic, as Dr. Stone sees it, is that nursing homes may be more engaged with data reporting and infection surveillance going forward. Nursing homes are now required to report their COVID-19 cases to the CDC through its hospital-dominant National Healthcare Safety Network, and the CDC has made technical changes that now make it “easier [than it was in the past] for nursing homes to join and participate,” she said. “Now that all nursing homes are engaged, will they be engaged post-COVID, too? I hope so. Surveillance [of infections] is a first step toward better outcomes.”
For now, said Dr. Crnich, the intensive prevention and mitigation efforts that are being required of nursing homes to minimize COVID-19’s impact is “a big deal and will tax the resources of most nursing homes and exceed the resources of many” without outside support, Dr. Crnich said. “This has been the most illuminating part of all this, and will probably require us to reconsider how we’re resourcing our nursing homes moving forward into the future.”
Human sitters in the COVID era
Data collection needed for care of suicidal hospitalized patients
I am writing this commentary to bring to readers’ attention a medical and ethical complexity related to human sitters for presumably suicidal, COVID-19–positive hospitalized patients.

To shape and bundle the ethics issues addressed here into a single question, I offer the following: Should policies and practices requiring that patients in presumed need of a sitter because of assessed suicidality change when the patient is COVID-19–positive? Although the analysis might be similar when a sitter is monitoring a Patient Under Investigation (PUI), here I focus only on COVID-19–positive patients. Similarly, there are other reasons for sitters, of course, such as to prevent elopement, or, if a patient is in restraints, to prevent the patient from pulling out lines or tubes. Again, discussion of some of these ethical complications is beyond the scope of this piece. Just considering the matter of potential suicidality and sitters is complex enough. And so, to start, I sought out existing sources for guidance.
In looking for such sources, I first turned to the Centers for Medicare and Medicaid Services before COVID-19. CMS has required that there be a sitter for a patient who is suicidal and that the sitter remain in the room so that the sitter can intervene expeditiously if the patient tries to hurt himself or herself. There has been no change in this guidance since the COVID-19 pandemic in the United States. To the best of my knowledge, there is no substantive guidance for protecting sitters from contagion other than PPE. Given this, it begs the question:
In my hospital, I already have begun discussing the potential risks of harm and potential benefits to our suicidal patients of having a sitter directly outside the patient’s room. I also have considered whether to have one sitter watching several room cameras at once, commonly referred to as “telehealth strategies.”
To be sure, sitting for hours in the room of a COVID-19–positive patient is onerous. The sitter is required to be in full PPE (N-95 mask, gown, and gloves), which is hot and uncomfortable. Current practice is resource intensive in other ways. It requires changing out the sitter every 2 hours, which uses substantial amounts of PPE and multiple sitters.
Regardless, however, there are really no data upon which to base any sound ethics judgment about what should or should not be tried. We just have no information on how to attempt to balance potential risks and prospects for the benefit of whom and when. And, given that good clinical ethics always begin with the facts, I write this piece to see whether readers have thought about these issues before – and whether any of clinicians have started collecting the valuable data needed to begin making sound ethical judgments about how to care for our presumably suicidal COVID-19–positive patients and the sitters who watch over them.
Dr. Ritchie is chair of psychiatry at Medstar Washington Hospital Center and professor of psychiatry at Georgetown University, Washington. She has no disclosures and can be reached at cpnews@mdedge.com.
This column is an outcome of a discussion that occurred during Psych/Ethics rounds on June 5, and does not represent any official statements of Medstar Washington Hospital Center or any entity of the MedStar Corp. Dr. Ritchie would like to thank Evan G. DeRenzo, PhD, of the John J. Lynch Center for Ethics, for her thoughtful review of a previous draft of this commentary.
Data collection needed for care of suicidal hospitalized patients
Data collection needed for care of suicidal hospitalized patients
I am writing this commentary to bring to readers’ attention a medical and ethical complexity related to human sitters for presumably suicidal, COVID-19–positive hospitalized patients.
To shape and bundle the ethics issues addressed here into a single question, I offer the following: Should policies and practices requiring that patients in presumed need of a sitter because of assessed suicidality change when the patient is COVID-19–positive? Although the analysis might be similar when a sitter is monitoring a Patient Under Investigation (PUI), here I focus only on COVID-19–positive patients. Similarly, there are other reasons for sitters, of course, such as to prevent elopement, or, if a patient is in restraints, to prevent the patient from pulling out lines or tubes. Again, discussion of some of these ethical complications is beyond the scope of this piece. Just considering the matter of potential suicidality and sitters is complex enough. And so, to start, I sought out existing sources for guidance.
In looking for such sources, I first turned to the Centers for Medicare and Medicaid Services before COVID-19. CMS has required that there be a sitter for a patient who is suicidal and that the sitter remain in the room so that the sitter can intervene expeditiously if the patient tries to hurt himself or herself. There has been no change in this guidance since the COVID-19 pandemic in the United States. To the best of my knowledge, there is no substantive guidance for protecting sitters from contagion other than PPE. Given this, it begs the question:
In my hospital, I already have begun discussing the potential risks of harm and potential benefits to our suicidal patients of having a sitter directly outside the patient’s room. I also have considered whether to have one sitter watching several room cameras at once, commonly referred to as “telehealth strategies.”
To be sure, sitting for hours in the room of a COVID-19–positive patient is onerous. The sitter is required to be in full PPE (N-95 mask, gown, and gloves), which is hot and uncomfortable. Current practice is resource intensive in other ways. It requires changing out the sitter every 2 hours, which uses substantial amounts of PPE and multiple sitters.
Regardless, however, there are really no data upon which to base any sound ethics judgment about what should or should not be tried. We just have no information on how to attempt to balance potential risks and prospects for the benefit of whom and when. And, given that good clinical ethics always begin with the facts, I write this piece to see whether readers have thought about these issues before – and whether any of clinicians have started collecting the valuable data needed to begin making sound ethical judgments about how to care for our presumably suicidal COVID-19–positive patients and the sitters who watch over them.
Dr. Ritchie is chair of psychiatry at Medstar Washington Hospital Center and professor of psychiatry at Georgetown University, Washington. She has no disclosures and can be reached at cpnews@mdedge.com.
This column is an outcome of a discussion that occurred during Psych/Ethics rounds on June 5, and does not represent any official statements of Medstar Washington Hospital Center or any entity of the MedStar Corp. Dr. Ritchie would like to thank Evan G. DeRenzo, PhD, of the John J. Lynch Center for Ethics, for her thoughtful review of a previous draft of this commentary.
I am writing this commentary to bring to readers’ attention a medical and ethical complexity related to human sitters for presumably suicidal, COVID-19–positive hospitalized patients.
To shape and bundle the ethics issues addressed here into a single question, I offer the following: Should policies and practices requiring that patients in presumed need of a sitter because of assessed suicidality change when the patient is COVID-19–positive? Although the analysis might be similar when a sitter is monitoring a Patient Under Investigation (PUI), here I focus only on COVID-19–positive patients. Similarly, there are other reasons for sitters, of course, such as to prevent elopement, or, if a patient is in restraints, to prevent the patient from pulling out lines or tubes. Again, discussion of some of these ethical complications is beyond the scope of this piece. Just considering the matter of potential suicidality and sitters is complex enough. And so, to start, I sought out existing sources for guidance.
In looking for such sources, I first turned to the Centers for Medicare and Medicaid Services before COVID-19. CMS has required that there be a sitter for a patient who is suicidal and that the sitter remain in the room so that the sitter can intervene expeditiously if the patient tries to hurt himself or herself. There has been no change in this guidance since the COVID-19 pandemic in the United States. To the best of my knowledge, there is no substantive guidance for protecting sitters from contagion other than PPE. Given this, it begs the question:
In my hospital, I already have begun discussing the potential risks of harm and potential benefits to our suicidal patients of having a sitter directly outside the patient’s room. I also have considered whether to have one sitter watching several room cameras at once, commonly referred to as “telehealth strategies.”
To be sure, sitting for hours in the room of a COVID-19–positive patient is onerous. The sitter is required to be in full PPE (N-95 mask, gown, and gloves), which is hot and uncomfortable. Current practice is resource intensive in other ways. It requires changing out the sitter every 2 hours, which uses substantial amounts of PPE and multiple sitters.
Regardless, however, there are really no data upon which to base any sound ethics judgment about what should or should not be tried. We just have no information on how to attempt to balance potential risks and prospects for the benefit of whom and when. And, given that good clinical ethics always begin with the facts, I write this piece to see whether readers have thought about these issues before – and whether any of clinicians have started collecting the valuable data needed to begin making sound ethical judgments about how to care for our presumably suicidal COVID-19–positive patients and the sitters who watch over them.
Dr. Ritchie is chair of psychiatry at Medstar Washington Hospital Center and professor of psychiatry at Georgetown University, Washington. She has no disclosures and can be reached at cpnews@mdedge.com.
This column is an outcome of a discussion that occurred during Psych/Ethics rounds on June 5, and does not represent any official statements of Medstar Washington Hospital Center or any entity of the MedStar Corp. Dr. Ritchie would like to thank Evan G. DeRenzo, PhD, of the John J. Lynch Center for Ethics, for her thoughtful review of a previous draft of this commentary.
Elevated inflammation common in children’s severe COVID-19 disease
according to data from 50 patients at a single tertiary care center.

“Risk factors for severe disease in pediatric populations have not been clearly identified and the high prevalence of SARS-CoV-2 in NYC offers an opportunity to describe severe pediatric disease in more detail,” wrote Philip Zachariah, MD, of New York–Presbyterian Hospital, New York, and colleagues.
In a retrospective case series published in JAMA Pediatrics, the researchers reviewed data from 50 patients: 41 classified as severe and 9 classified as nonsevere. Among the patients, 27 were male and 25 were Hispanic. The patient population had a median of 2 days from symptom onset to hospital admission. The most common symptoms were fever (80%) and respiratory symptoms (64%). Seventy-six percent of patients had a median length of stay of 3 days (range 1-30 days).
At hospital admission, children with severe disease had significantly higher levels of several inflammatory markers compared with those without severe disease, notably C-reactive protein (median 8.978 mg/dL vs. 0.64 mg/dL) and procalcitonin (median 0.31 ng/mL vs. 0.17 ng/mL, (P < .001 for both). High mean peak levels of C-reactive protein, procalcitonin, interleukin 6, ferritin, and D-dimer were seen among the nine children (16%) who required mechanical ventilation, Dr. Zachariah and associates said.
None of the 14 infants and 1 of the 8 immunocompromised children in the study had severe disease, the researchers wrote.
Bacterial coinfections detected while patients were hospitalized were bacteremia in 6%, suspected bacterial pneumonia in 18%, urinary tract infections in 10%, skin and soft tissue infections in 6%, and streptococcus pharyngitis in 2%, Dr. Zachariah and associates reported.
Overall, 61% of the children had comorbidities identified in previous COVID-19 studies, of which obesity was the most common (22%); other comorbidities included asthma, sickle cell disease, cardiac disease, and diabetes. Obesity also was significantly associated with the need for mechanical ventilation in children aged 2 years and older (67%). A total of 16 patients required respiratory support, 9 of these were placed on mechanical ventilation; 6 of these 9 children were obese.
Fifteen patients (30%) who met criteria for increased oxygen requirements and respiratory distress received hydroxychloroquine, but the small sample size did not allow for assessment of treatment efficacy, the researchers said.
“Expanding our knowledge of COVID-19 [disease] in children will potentially permit early recognition of SARS-CoV-2 infection, understanding of the natural history of disease, and potential complications, said Stephen I. Pelton, MD, professor of pediatrics and epidemiology at Boston University and senior attending physician at Boston Medical Center. This review of 50 SARS-CoV-2 infected children (less than 21 years of age) “provides insight into the short period of symptoms prior to hospitalization, challenges the concept that infants less than 1 year are at greatest risk of severe disease (as from the experience in China), and suggests rapid recovery in many children, as median length of stay was 3 days.
“The review revealed two findings that were surprising to me. First, the median length of stay of 3 days. As nearly 20% of the children required mechanical ventilation, it suggests many of the children were discharged quickly after evaluation, suggesting that we need to identify markers of severity to predict those children likely to have progressive disease and require respiratory support,” Dr. Pelton noted.
“The second observation suggests high rates of bacterial infection (bacteremia, pneumonia, UTI, and skin and soft tissue infection). I do not think this has been widely reported in adults, and may represent a difference between child and adult disease. More studies such as this will be required to identify how common coinfection with bacteria is,” he said.
“The take-home message is that although most children with COVID-19 have a mild or even asymptomatic course, some become severely ill requiring ventilator support and potentially ECMO [extracorporeal membrane oxygenation]. Potential predictors of severity include high C-reactive protein, obesity, and older age [adolescence], said Dr. Pelton, who was not involved in the study.
What additional research is needed? Dr. Pelton said that better markers of severe disease are needed, as well as an understanding of why obesity is a risk factor for severe disease in both children and adults. Are these prediabetic patients? he asked.
The study findings were limited by the small sample size and high proportion of Hispanic patients, which may limit generalizability, and some symptoms and comorbidities may have been missed because of the retrospective nature of the study, the researchers noted. However, the results support the need for hospitals to remain vigilant to the variable presentations of COVID-19 infections in children.
“Therapeutic considerations need to [include] the risk of toxicity, control of antiviral replication, and early recognition and management of immune dysregulation,” they concluded.
The study received no outside funding. Dr. Zachariah had no financial conflicts to disclose. Two coauthors reported ties with various pharmaceutical companies and organizations. Dr. Pelton said he had no relevant financial disclosures.
SOURCE: Zachariah P et al. JAMA Pediatr. 2020 June 3. doi:10.1001/jamapediatrics.2020.2430.
according to data from 50 patients at a single tertiary care center.
“Risk factors for severe disease in pediatric populations have not been clearly identified and the high prevalence of SARS-CoV-2 in NYC offers an opportunity to describe severe pediatric disease in more detail,” wrote Philip Zachariah, MD, of New York–Presbyterian Hospital, New York, and colleagues.
In a retrospective case series published in JAMA Pediatrics, the researchers reviewed data from 50 patients: 41 classified as severe and 9 classified as nonsevere. Among the patients, 27 were male and 25 were Hispanic. The patient population had a median of 2 days from symptom onset to hospital admission. The most common symptoms were fever (80%) and respiratory symptoms (64%). Seventy-six percent of patients had a median length of stay of 3 days (range 1-30 days).
At hospital admission, children with severe disease had significantly higher levels of several inflammatory markers compared with those without severe disease, notably C-reactive protein (median 8.978 mg/dL vs. 0.64 mg/dL) and procalcitonin (median 0.31 ng/mL vs. 0.17 ng/mL, (P < .001 for both). High mean peak levels of C-reactive protein, procalcitonin, interleukin 6, ferritin, and D-dimer were seen among the nine children (16%) who required mechanical ventilation, Dr. Zachariah and associates said.
None of the 14 infants and 1 of the 8 immunocompromised children in the study had severe disease, the researchers wrote.
Bacterial coinfections detected while patients were hospitalized were bacteremia in 6%, suspected bacterial pneumonia in 18%, urinary tract infections in 10%, skin and soft tissue infections in 6%, and streptococcus pharyngitis in 2%, Dr. Zachariah and associates reported.
Overall, 61% of the children had comorbidities identified in previous COVID-19 studies, of which obesity was the most common (22%); other comorbidities included asthma, sickle cell disease, cardiac disease, and diabetes. Obesity also was significantly associated with the need for mechanical ventilation in children aged 2 years and older (67%). A total of 16 patients required respiratory support, 9 of these were placed on mechanical ventilation; 6 of these 9 children were obese.
Fifteen patients (30%) who met criteria for increased oxygen requirements and respiratory distress received hydroxychloroquine, but the small sample size did not allow for assessment of treatment efficacy, the researchers said.
“Expanding our knowledge of COVID-19 [disease] in children will potentially permit early recognition of SARS-CoV-2 infection, understanding of the natural history of disease, and potential complications, said Stephen I. Pelton, MD, professor of pediatrics and epidemiology at Boston University and senior attending physician at Boston Medical Center. This review of 50 SARS-CoV-2 infected children (less than 21 years of age) “provides insight into the short period of symptoms prior to hospitalization, challenges the concept that infants less than 1 year are at greatest risk of severe disease (as from the experience in China), and suggests rapid recovery in many children, as median length of stay was 3 days.
“The review revealed two findings that were surprising to me. First, the median length of stay of 3 days. As nearly 20% of the children required mechanical ventilation, it suggests many of the children were discharged quickly after evaluation, suggesting that we need to identify markers of severity to predict those children likely to have progressive disease and require respiratory support,” Dr. Pelton noted.
“The second observation suggests high rates of bacterial infection (bacteremia, pneumonia, UTI, and skin and soft tissue infection). I do not think this has been widely reported in adults, and may represent a difference between child and adult disease. More studies such as this will be required to identify how common coinfection with bacteria is,” he said.
“The take-home message is that although most children with COVID-19 have a mild or even asymptomatic course, some become severely ill requiring ventilator support and potentially ECMO [extracorporeal membrane oxygenation]. Potential predictors of severity include high C-reactive protein, obesity, and older age [adolescence], said Dr. Pelton, who was not involved in the study.
What additional research is needed? Dr. Pelton said that better markers of severe disease are needed, as well as an understanding of why obesity is a risk factor for severe disease in both children and adults. Are these prediabetic patients? he asked.
The study findings were limited by the small sample size and high proportion of Hispanic patients, which may limit generalizability, and some symptoms and comorbidities may have been missed because of the retrospective nature of the study, the researchers noted. However, the results support the need for hospitals to remain vigilant to the variable presentations of COVID-19 infections in children.
“Therapeutic considerations need to [include] the risk of toxicity, control of antiviral replication, and early recognition and management of immune dysregulation,” they concluded.
The study received no outside funding. Dr. Zachariah had no financial conflicts to disclose. Two coauthors reported ties with various pharmaceutical companies and organizations. Dr. Pelton said he had no relevant financial disclosures.
SOURCE: Zachariah P et al. JAMA Pediatr. 2020 June 3. doi:10.1001/jamapediatrics.2020.2430.
according to data from 50 patients at a single tertiary care center.
“Risk factors for severe disease in pediatric populations have not been clearly identified and the high prevalence of SARS-CoV-2 in NYC offers an opportunity to describe severe pediatric disease in more detail,” wrote Philip Zachariah, MD, of New York–Presbyterian Hospital, New York, and colleagues.
In a retrospective case series published in JAMA Pediatrics, the researchers reviewed data from 50 patients: 41 classified as severe and 9 classified as nonsevere. Among the patients, 27 were male and 25 were Hispanic. The patient population had a median of 2 days from symptom onset to hospital admission. The most common symptoms were fever (80%) and respiratory symptoms (64%). Seventy-six percent of patients had a median length of stay of 3 days (range 1-30 days).
At hospital admission, children with severe disease had significantly higher levels of several inflammatory markers compared with those without severe disease, notably C-reactive protein (median 8.978 mg/dL vs. 0.64 mg/dL) and procalcitonin (median 0.31 ng/mL vs. 0.17 ng/mL, (P < .001 for both). High mean peak levels of C-reactive protein, procalcitonin, interleukin 6, ferritin, and D-dimer were seen among the nine children (16%) who required mechanical ventilation, Dr. Zachariah and associates said.
None of the 14 infants and 1 of the 8 immunocompromised children in the study had severe disease, the researchers wrote.
Bacterial coinfections detected while patients were hospitalized were bacteremia in 6%, suspected bacterial pneumonia in 18%, urinary tract infections in 10%, skin and soft tissue infections in 6%, and streptococcus pharyngitis in 2%, Dr. Zachariah and associates reported.
Overall, 61% of the children had comorbidities identified in previous COVID-19 studies, of which obesity was the most common (22%); other comorbidities included asthma, sickle cell disease, cardiac disease, and diabetes. Obesity also was significantly associated with the need for mechanical ventilation in children aged 2 years and older (67%). A total of 16 patients required respiratory support, 9 of these were placed on mechanical ventilation; 6 of these 9 children were obese.
Fifteen patients (30%) who met criteria for increased oxygen requirements and respiratory distress received hydroxychloroquine, but the small sample size did not allow for assessment of treatment efficacy, the researchers said.
“Expanding our knowledge of COVID-19 [disease] in children will potentially permit early recognition of SARS-CoV-2 infection, understanding of the natural history of disease, and potential complications, said Stephen I. Pelton, MD, professor of pediatrics and epidemiology at Boston University and senior attending physician at Boston Medical Center. This review of 50 SARS-CoV-2 infected children (less than 21 years of age) “provides insight into the short period of symptoms prior to hospitalization, challenges the concept that infants less than 1 year are at greatest risk of severe disease (as from the experience in China), and suggests rapid recovery in many children, as median length of stay was 3 days.
“The review revealed two findings that were surprising to me. First, the median length of stay of 3 days. As nearly 20% of the children required mechanical ventilation, it suggests many of the children were discharged quickly after evaluation, suggesting that we need to identify markers of severity to predict those children likely to have progressive disease and require respiratory support,” Dr. Pelton noted.
“The second observation suggests high rates of bacterial infection (bacteremia, pneumonia, UTI, and skin and soft tissue infection). I do not think this has been widely reported in adults, and may represent a difference between child and adult disease. More studies such as this will be required to identify how common coinfection with bacteria is,” he said.
“The take-home message is that although most children with COVID-19 have a mild or even asymptomatic course, some become severely ill requiring ventilator support and potentially ECMO [extracorporeal membrane oxygenation]. Potential predictors of severity include high C-reactive protein, obesity, and older age [adolescence], said Dr. Pelton, who was not involved in the study.
What additional research is needed? Dr. Pelton said that better markers of severe disease are needed, as well as an understanding of why obesity is a risk factor for severe disease in both children and adults. Are these prediabetic patients? he asked.
The study findings were limited by the small sample size and high proportion of Hispanic patients, which may limit generalizability, and some symptoms and comorbidities may have been missed because of the retrospective nature of the study, the researchers noted. However, the results support the need for hospitals to remain vigilant to the variable presentations of COVID-19 infections in children.
“Therapeutic considerations need to [include] the risk of toxicity, control of antiviral replication, and early recognition and management of immune dysregulation,” they concluded.
The study received no outside funding. Dr. Zachariah had no financial conflicts to disclose. Two coauthors reported ties with various pharmaceutical companies and organizations. Dr. Pelton said he had no relevant financial disclosures.
SOURCE: Zachariah P et al. JAMA Pediatr. 2020 June 3. doi:10.1001/jamapediatrics.2020.2430.
FROM JAMA PEDIATRICS
By the numbers: Asthma-COPD overlap deaths
Death rates for combined asthma and chronic obstructive pulmonary disease declined during 1999-2016, but the risk remains higher among women, compared with men, and in certain occupations, according to a recent report from the Centers for Disease Control and Prevention.
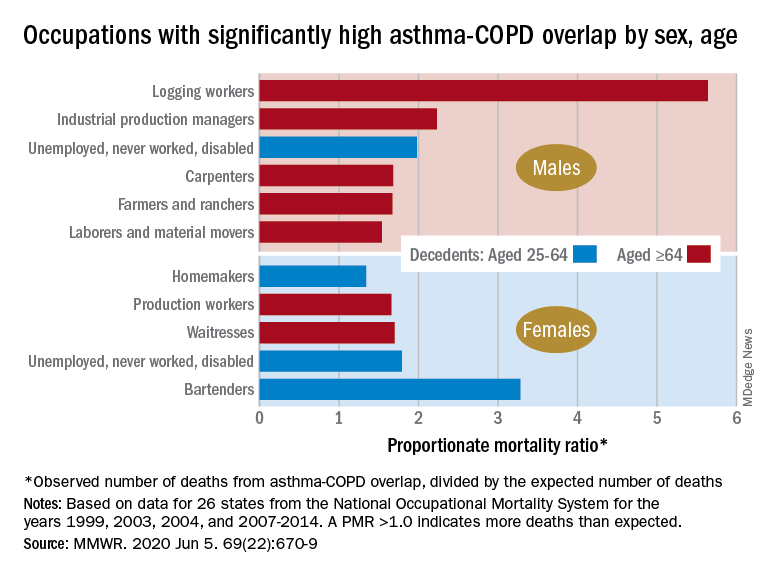
There is also an association between mortality and nonworking status among adults aged 25-64 years, which “suggests that asthma-COPD overlap might be associated with substantial morbidity,” Katelynn E. Dodd, MPH, and associates at the CDC’s National Institute for Occupational Safety and Health said in the Morbidity and Mortality Weekly Report. “These patients have been reported to have worse health outcomes than do those with asthma or COPD alone.”
For females with asthma-COPD overlap, the age-adjusted death rate among adults aged 25 years and older dropped from 7.71 per million in 1999 to 4.01 in 2016, with corresponding rates of 6.70 and 3.01 per million for males, they reported.
In 1999-2016, a total of 18,766 U.S. decedents aged ≥25 years had both asthma and COPD assigned as the underlying or contributing cause of death (12,028 women and 6,738 men), for an overall death rate of 5.03 per million persons (women, 5.59; men, 4.30), data from the National Vital Statistics System show.
Additional analysis, based on the calculation of proportionate mortality ratios (PMRs), also showed that mortality varied by occupational status and age for both males and females, the investigators said, noting that workplace exposures, such as dusts and secondhand smoke, are known to cause both asthma and COPD.
The PMR represents the observed number of deaths from asthma-COPD overlap in a specified industry or occupation, divided by the expected number of deaths, so a value over 1.0 indicates that there were more deaths associated with the condition than expected, Ms. Dodd and her associates explained.
Among female decedents, the occupation with the highest PMR that was statistically significant was bartending at 3.28. For men, the highest significant PMR, 5.64, occurred in logging workers. Those rates, however, only applied to one of the two age groups: 25-64 years in women and ≥65 in men, based on data from the National Occupational Mortality Surveillance, which included information from 26 states for the years 1999, 2003, 2004, and 2007-2014.
Occupationally speaking, the one area of common ground between males and females was lack of occupation. PMRs for those aged 25-64 years “were significantly elevated among men (1.98) and women (1.79) who were unemployed, never worked, or were disabled workers,” they said. PMRs were elevated for nonworking older males and females but were not significant.
The elevated PMRs suggest “that asthma-COPD overlap might be associated with substantial morbidity resulting in loss of employment [because] retired and unemployed persons might have left the workforce because of severe asthma or COPD,” the investigators wrote.
SOURCE: Dodd KE et al. MMWR. 2020 Jun 5. 69(22):670-9.
Death rates for combined asthma and chronic obstructive pulmonary disease declined during 1999-2016, but the risk remains higher among women, compared with men, and in certain occupations, according to a recent report from the Centers for Disease Control and Prevention.
There is also an association between mortality and nonworking status among adults aged 25-64 years, which “suggests that asthma-COPD overlap might be associated with substantial morbidity,” Katelynn E. Dodd, MPH, and associates at the CDC’s National Institute for Occupational Safety and Health said in the Morbidity and Mortality Weekly Report. “These patients have been reported to have worse health outcomes than do those with asthma or COPD alone.”
For females with asthma-COPD overlap, the age-adjusted death rate among adults aged 25 years and older dropped from 7.71 per million in 1999 to 4.01 in 2016, with corresponding rates of 6.70 and 3.01 per million for males, they reported.
In 1999-2016, a total of 18,766 U.S. decedents aged ≥25 years had both asthma and COPD assigned as the underlying or contributing cause of death (12,028 women and 6,738 men), for an overall death rate of 5.03 per million persons (women, 5.59; men, 4.30), data from the National Vital Statistics System show.
Additional analysis, based on the calculation of proportionate mortality ratios (PMRs), also showed that mortality varied by occupational status and age for both males and females, the investigators said, noting that workplace exposures, such as dusts and secondhand smoke, are known to cause both asthma and COPD.
The PMR represents the observed number of deaths from asthma-COPD overlap in a specified industry or occupation, divided by the expected number of deaths, so a value over 1.0 indicates that there were more deaths associated with the condition than expected, Ms. Dodd and her associates explained.
Among female decedents, the occupation with the highest PMR that was statistically significant was bartending at 3.28. For men, the highest significant PMR, 5.64, occurred in logging workers. Those rates, however, only applied to one of the two age groups: 25-64 years in women and ≥65 in men, based on data from the National Occupational Mortality Surveillance, which included information from 26 states for the years 1999, 2003, 2004, and 2007-2014.
Occupationally speaking, the one area of common ground between males and females was lack of occupation. PMRs for those aged 25-64 years “were significantly elevated among men (1.98) and women (1.79) who were unemployed, never worked, or were disabled workers,” they said. PMRs were elevated for nonworking older males and females but were not significant.
The elevated PMRs suggest “that asthma-COPD overlap might be associated with substantial morbidity resulting in loss of employment [because] retired and unemployed persons might have left the workforce because of severe asthma or COPD,” the investigators wrote.
SOURCE: Dodd KE et al. MMWR. 2020 Jun 5. 69(22):670-9.
Death rates for combined asthma and chronic obstructive pulmonary disease declined during 1999-2016, but the risk remains higher among women, compared with men, and in certain occupations, according to a recent report from the Centers for Disease Control and Prevention.
There is also an association between mortality and nonworking status among adults aged 25-64 years, which “suggests that asthma-COPD overlap might be associated with substantial morbidity,” Katelynn E. Dodd, MPH, and associates at the CDC’s National Institute for Occupational Safety and Health said in the Morbidity and Mortality Weekly Report. “These patients have been reported to have worse health outcomes than do those with asthma or COPD alone.”
For females with asthma-COPD overlap, the age-adjusted death rate among adults aged 25 years and older dropped from 7.71 per million in 1999 to 4.01 in 2016, with corresponding rates of 6.70 and 3.01 per million for males, they reported.
In 1999-2016, a total of 18,766 U.S. decedents aged ≥25 years had both asthma and COPD assigned as the underlying or contributing cause of death (12,028 women and 6,738 men), for an overall death rate of 5.03 per million persons (women, 5.59; men, 4.30), data from the National Vital Statistics System show.
Additional analysis, based on the calculation of proportionate mortality ratios (PMRs), also showed that mortality varied by occupational status and age for both males and females, the investigators said, noting that workplace exposures, such as dusts and secondhand smoke, are known to cause both asthma and COPD.
The PMR represents the observed number of deaths from asthma-COPD overlap in a specified industry or occupation, divided by the expected number of deaths, so a value over 1.0 indicates that there were more deaths associated with the condition than expected, Ms. Dodd and her associates explained.
Among female decedents, the occupation with the highest PMR that was statistically significant was bartending at 3.28. For men, the highest significant PMR, 5.64, occurred in logging workers. Those rates, however, only applied to one of the two age groups: 25-64 years in women and ≥65 in men, based on data from the National Occupational Mortality Surveillance, which included information from 26 states for the years 1999, 2003, 2004, and 2007-2014.
Occupationally speaking, the one area of common ground between males and females was lack of occupation. PMRs for those aged 25-64 years “were significantly elevated among men (1.98) and women (1.79) who were unemployed, never worked, or were disabled workers,” they said. PMRs were elevated for nonworking older males and females but were not significant.
The elevated PMRs suggest “that asthma-COPD overlap might be associated with substantial morbidity resulting in loss of employment [because] retired and unemployed persons might have left the workforce because of severe asthma or COPD,” the investigators wrote.
SOURCE: Dodd KE et al. MMWR. 2020 Jun 5. 69(22):670-9.
FROM MMWR
Rapid changes to health system spurred by COVID might be here to stay
The U.S. health care system is famously resistant to government-imposed change. It took decades to create Medicare and Medicaid, mostly because of opposition from the medical-industrial complex. Then it was nearly another half-century before the passage of the Affordable Care Act.
“Health care is never going back to the way it was before,” said Gail Wilensky, a health economist who ran the Medicare and Medicaid programs for President George H.W. Bush in the early 1990s.
Ms. Wilensky is far from the only longtime observer of the American health care system to marvel at the speed of some long-sought changes. But experts warn that the breakthroughs may not all make the health system work better or make it less expensive.
That said, here are three trends that seem likely to continue.
Telehealth for all
Telehealth is not new; medical professionals have used it to reach patients in rural or remote settings since the late 1980s.
But even while technology has made video visits easier, it has failed to reach critical mass, largely because of political fights. Licensing has been one main obstacle – determining how a doctor in one state can legally treat a patient in a state where the doctor is not licensed.
The other obstacle, not surprisingly, is payment. Should a video visit be reimbursed at the same rate as an in-person visit? Will making it easier for doctors and other medical professionals to use telehealth encourage unnecessary care, thus driving up the nation’s $3.6 trillion health tab even more? Or could it replace care once provided free by phone?
Still, the pandemic has pushed aside those sticking points. Almost overnight, by necessity, every health care provider who can is delivering telemedicine. A new survey from Gallup found the number of patients reporting “virtual” medical visits more than doubled, from 12% to 27%, from late March to mid-May. That is attributable, at least in part, to Medicare having made it easier for doctors to bill for virtual visits.
It’s easy to see why many patients like video visits – there’s no parking to find and pay for, and it takes far less time out of a workday than going to an office.
Doctors and other practitioners seem more ambivalent. On one hand, it can be harder to examine a patient over video and some services just can’t be done via a digital connection. On the other hand, they can see more patients in the same amount of time and may need less support staff and possibly smaller offices if more visits are conducted virtually.
Of course, telemedicine doesn’t work for everyone. Many areas and patients don’t have reliable or robust broadband connections that make video visits work. And some patients, particularly the oldest seniors, lack the technological skills needed to connect.
Primary care doctors in peril
Another trend that has suddenly accelerated is worry over the nation’s dwindling supply of primary care doctors. The exodus of practitioners performing primary care has been a concern over the past several years, as baby boomer doctors retire and others have grown weary of more and more bureaucracy from government and private payers. Having faced a difficult financial crisis during the pandemic, more family physicians may move into retirement or seek other professional options.
At the same time, fewer current medical students are choosing specialties in primary care.
“I’ve been trying to raise the alarm about the kind of perilous future of primary care,” said Farzad Mostashari, MD, a top Department of Health & Human Services official in the Obama administration. Dr. Mostashari runs Aledade, a company that helps primary care doctors make the transition from fee-for-service medicine to new payment models.
The American Academy of Family Physicians reports that 70% of primary care physicians are reporting declines in patient volume of 50% or more since March, and 40% have laid off or furloughed staff. The AAFP has joined other primary care and insurance groups in asking HHS for an infusion of cash.
“This is absolutely essential to effectively treat patients today and to maintain their ongoing operations until we overcome this public health emergency,” the groups wrote.
One easy way to help keep primary care doctors afloat would be to pay them not according to what they do, but in a lump sum to keep patients healthy. This move from fee-for-service to what’s known as capitation or value-based care has unfolded gradually and was championed in the Affordable Care Act.
But some experts argue it needs to happen more quickly and they predict that the coronavirus pandemic could finally mark the beginning of the end for doctors who still charge for each service individually. Dr. Mostashari, who spends his time helping doctors make the transition, said in times like these, it would make more sense for primary care doctors to have “a steady monthly revenue stream, and [the doctor] can decide the best way to deliver that care: unlimited texts, phone calls, video calls. The goal is to give you satisfactory outcomes and a great patient experience.”
Still, many physicians, particularly those in solo or small practices, worry about the potential financial risk – especially the possibility of getting paid less if they don’t meet certain benchmarks that the doctors may not be able to directly control.
But with many practices now ground to a halt, or just starting to reopen, those physicians who get paid per patient rather than per service are in a much better position to stay afloat. That model may gain traction as doctors ponder the next pandemic, or the next wave of this one.
Hospitals on the decline?
The pandemic also might lead to less emphasis on hospital-based care. While hospitals in many parts of the country have obviously been full of very sick COVID patients, they have closed down other nonemergency services to preserve supplies and resources to fight the pandemic. People with other ailments have stayed away in droves even when services were available, for fear of catching something worse than what they already have.
Many experts predict that care won’t just snap back when the current emergency wanes. Mark Smith, MD, former president of the California Health Care Foundation, said among consumers, a switch has been flipped. “Overnight it seems we’ve gone from high-touch to no-touch.”
Which is not great for hospitals that have spent millions trying to attract patients to their labor-and-delivery units, orthopedic centers, and other parts of the facility that once generated lots of income.
Even more concerning is that hospitals’ ability to weather the current financial shock varies widely. Those most in danger of closing are in rural and underserved areas, where patients could wind up with even less access to care that is scarce already.
All of which underscores the point that not all these changes will necessarily be good for the health system or society. Financial pressures could end up driving more consolidation, which could push up prices as large groups of hospitals and doctors gain more bargaining clout.
But the changes are definitely happening at a pace few have ever seen, said Ms. Wilensky, “When you’re forced to find different ways of doing things, and you find out they are easier and more efficient, it’s going to be hard to go back to the old way.”
A version of this article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The U.S. health care system is famously resistant to government-imposed change. It took decades to create Medicare and Medicaid, mostly because of opposition from the medical-industrial complex. Then it was nearly another half-century before the passage of the Affordable Care Act.
“Health care is never going back to the way it was before,” said Gail Wilensky, a health economist who ran the Medicare and Medicaid programs for President George H.W. Bush in the early 1990s.
Ms. Wilensky is far from the only longtime observer of the American health care system to marvel at the speed of some long-sought changes. But experts warn that the breakthroughs may not all make the health system work better or make it less expensive.
That said, here are three trends that seem likely to continue.
Telehealth for all
Telehealth is not new; medical professionals have used it to reach patients in rural or remote settings since the late 1980s.
But even while technology has made video visits easier, it has failed to reach critical mass, largely because of political fights. Licensing has been one main obstacle – determining how a doctor in one state can legally treat a patient in a state where the doctor is not licensed.
The other obstacle, not surprisingly, is payment. Should a video visit be reimbursed at the same rate as an in-person visit? Will making it easier for doctors and other medical professionals to use telehealth encourage unnecessary care, thus driving up the nation’s $3.6 trillion health tab even more? Or could it replace care once provided free by phone?
Still, the pandemic has pushed aside those sticking points. Almost overnight, by necessity, every health care provider who can is delivering telemedicine. A new survey from Gallup found the number of patients reporting “virtual” medical visits more than doubled, from 12% to 27%, from late March to mid-May. That is attributable, at least in part, to Medicare having made it easier for doctors to bill for virtual visits.
It’s easy to see why many patients like video visits – there’s no parking to find and pay for, and it takes far less time out of a workday than going to an office.
Doctors and other practitioners seem more ambivalent. On one hand, it can be harder to examine a patient over video and some services just can’t be done via a digital connection. On the other hand, they can see more patients in the same amount of time and may need less support staff and possibly smaller offices if more visits are conducted virtually.
Of course, telemedicine doesn’t work for everyone. Many areas and patients don’t have reliable or robust broadband connections that make video visits work. And some patients, particularly the oldest seniors, lack the technological skills needed to connect.
Primary care doctors in peril
Another trend that has suddenly accelerated is worry over the nation’s dwindling supply of primary care doctors. The exodus of practitioners performing primary care has been a concern over the past several years, as baby boomer doctors retire and others have grown weary of more and more bureaucracy from government and private payers. Having faced a difficult financial crisis during the pandemic, more family physicians may move into retirement or seek other professional options.
At the same time, fewer current medical students are choosing specialties in primary care.
“I’ve been trying to raise the alarm about the kind of perilous future of primary care,” said Farzad Mostashari, MD, a top Department of Health & Human Services official in the Obama administration. Dr. Mostashari runs Aledade, a company that helps primary care doctors make the transition from fee-for-service medicine to new payment models.
The American Academy of Family Physicians reports that 70% of primary care physicians are reporting declines in patient volume of 50% or more since March, and 40% have laid off or furloughed staff. The AAFP has joined other primary care and insurance groups in asking HHS for an infusion of cash.
“This is absolutely essential to effectively treat patients today and to maintain their ongoing operations until we overcome this public health emergency,” the groups wrote.
One easy way to help keep primary care doctors afloat would be to pay them not according to what they do, but in a lump sum to keep patients healthy. This move from fee-for-service to what’s known as capitation or value-based care has unfolded gradually and was championed in the Affordable Care Act.
But some experts argue it needs to happen more quickly and they predict that the coronavirus pandemic could finally mark the beginning of the end for doctors who still charge for each service individually. Dr. Mostashari, who spends his time helping doctors make the transition, said in times like these, it would make more sense for primary care doctors to have “a steady monthly revenue stream, and [the doctor] can decide the best way to deliver that care: unlimited texts, phone calls, video calls. The goal is to give you satisfactory outcomes and a great patient experience.”
Still, many physicians, particularly those in solo or small practices, worry about the potential financial risk – especially the possibility of getting paid less if they don’t meet certain benchmarks that the doctors may not be able to directly control.
But with many practices now ground to a halt, or just starting to reopen, those physicians who get paid per patient rather than per service are in a much better position to stay afloat. That model may gain traction as doctors ponder the next pandemic, or the next wave of this one.
Hospitals on the decline?
The pandemic also might lead to less emphasis on hospital-based care. While hospitals in many parts of the country have obviously been full of very sick COVID patients, they have closed down other nonemergency services to preserve supplies and resources to fight the pandemic. People with other ailments have stayed away in droves even when services were available, for fear of catching something worse than what they already have.
Many experts predict that care won’t just snap back when the current emergency wanes. Mark Smith, MD, former president of the California Health Care Foundation, said among consumers, a switch has been flipped. “Overnight it seems we’ve gone from high-touch to no-touch.”
Which is not great for hospitals that have spent millions trying to attract patients to their labor-and-delivery units, orthopedic centers, and other parts of the facility that once generated lots of income.
Even more concerning is that hospitals’ ability to weather the current financial shock varies widely. Those most in danger of closing are in rural and underserved areas, where patients could wind up with even less access to care that is scarce already.
All of which underscores the point that not all these changes will necessarily be good for the health system or society. Financial pressures could end up driving more consolidation, which could push up prices as large groups of hospitals and doctors gain more bargaining clout.
But the changes are definitely happening at a pace few have ever seen, said Ms. Wilensky, “When you’re forced to find different ways of doing things, and you find out they are easier and more efficient, it’s going to be hard to go back to the old way.”
A version of this article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The U.S. health care system is famously resistant to government-imposed change. It took decades to create Medicare and Medicaid, mostly because of opposition from the medical-industrial complex. Then it was nearly another half-century before the passage of the Affordable Care Act.
“Health care is never going back to the way it was before,” said Gail Wilensky, a health economist who ran the Medicare and Medicaid programs for President George H.W. Bush in the early 1990s.
Ms. Wilensky is far from the only longtime observer of the American health care system to marvel at the speed of some long-sought changes. But experts warn that the breakthroughs may not all make the health system work better or make it less expensive.
That said, here are three trends that seem likely to continue.
Telehealth for all
Telehealth is not new; medical professionals have used it to reach patients in rural or remote settings since the late 1980s.
But even while technology has made video visits easier, it has failed to reach critical mass, largely because of political fights. Licensing has been one main obstacle – determining how a doctor in one state can legally treat a patient in a state where the doctor is not licensed.
The other obstacle, not surprisingly, is payment. Should a video visit be reimbursed at the same rate as an in-person visit? Will making it easier for doctors and other medical professionals to use telehealth encourage unnecessary care, thus driving up the nation’s $3.6 trillion health tab even more? Or could it replace care once provided free by phone?
Still, the pandemic has pushed aside those sticking points. Almost overnight, by necessity, every health care provider who can is delivering telemedicine. A new survey from Gallup found the number of patients reporting “virtual” medical visits more than doubled, from 12% to 27%, from late March to mid-May. That is attributable, at least in part, to Medicare having made it easier for doctors to bill for virtual visits.
It’s easy to see why many patients like video visits – there’s no parking to find and pay for, and it takes far less time out of a workday than going to an office.
Doctors and other practitioners seem more ambivalent. On one hand, it can be harder to examine a patient over video and some services just can’t be done via a digital connection. On the other hand, they can see more patients in the same amount of time and may need less support staff and possibly smaller offices if more visits are conducted virtually.
Of course, telemedicine doesn’t work for everyone. Many areas and patients don’t have reliable or robust broadband connections that make video visits work. And some patients, particularly the oldest seniors, lack the technological skills needed to connect.
Primary care doctors in peril
Another trend that has suddenly accelerated is worry over the nation’s dwindling supply of primary care doctors. The exodus of practitioners performing primary care has been a concern over the past several years, as baby boomer doctors retire and others have grown weary of more and more bureaucracy from government and private payers. Having faced a difficult financial crisis during the pandemic, more family physicians may move into retirement or seek other professional options.
At the same time, fewer current medical students are choosing specialties in primary care.
“I’ve been trying to raise the alarm about the kind of perilous future of primary care,” said Farzad Mostashari, MD, a top Department of Health & Human Services official in the Obama administration. Dr. Mostashari runs Aledade, a company that helps primary care doctors make the transition from fee-for-service medicine to new payment models.
The American Academy of Family Physicians reports that 70% of primary care physicians are reporting declines in patient volume of 50% or more since March, and 40% have laid off or furloughed staff. The AAFP has joined other primary care and insurance groups in asking HHS for an infusion of cash.
“This is absolutely essential to effectively treat patients today and to maintain their ongoing operations until we overcome this public health emergency,” the groups wrote.
One easy way to help keep primary care doctors afloat would be to pay them not according to what they do, but in a lump sum to keep patients healthy. This move from fee-for-service to what’s known as capitation or value-based care has unfolded gradually and was championed in the Affordable Care Act.
But some experts argue it needs to happen more quickly and they predict that the coronavirus pandemic could finally mark the beginning of the end for doctors who still charge for each service individually. Dr. Mostashari, who spends his time helping doctors make the transition, said in times like these, it would make more sense for primary care doctors to have “a steady monthly revenue stream, and [the doctor] can decide the best way to deliver that care: unlimited texts, phone calls, video calls. The goal is to give you satisfactory outcomes and a great patient experience.”
Still, many physicians, particularly those in solo or small practices, worry about the potential financial risk – especially the possibility of getting paid less if they don’t meet certain benchmarks that the doctors may not be able to directly control.
But with many practices now ground to a halt, or just starting to reopen, those physicians who get paid per patient rather than per service are in a much better position to stay afloat. That model may gain traction as doctors ponder the next pandemic, or the next wave of this one.
Hospitals on the decline?
The pandemic also might lead to less emphasis on hospital-based care. While hospitals in many parts of the country have obviously been full of very sick COVID patients, they have closed down other nonemergency services to preserve supplies and resources to fight the pandemic. People with other ailments have stayed away in droves even when services were available, for fear of catching something worse than what they already have.
Many experts predict that care won’t just snap back when the current emergency wanes. Mark Smith, MD, former president of the California Health Care Foundation, said among consumers, a switch has been flipped. “Overnight it seems we’ve gone from high-touch to no-touch.”
Which is not great for hospitals that have spent millions trying to attract patients to their labor-and-delivery units, orthopedic centers, and other parts of the facility that once generated lots of income.
Even more concerning is that hospitals’ ability to weather the current financial shock varies widely. Those most in danger of closing are in rural and underserved areas, where patients could wind up with even less access to care that is scarce already.
All of which underscores the point that not all these changes will necessarily be good for the health system or society. Financial pressures could end up driving more consolidation, which could push up prices as large groups of hospitals and doctors gain more bargaining clout.
But the changes are definitely happening at a pace few have ever seen, said Ms. Wilensky, “When you’re forced to find different ways of doing things, and you find out they are easier and more efficient, it’s going to be hard to go back to the old way.”
A version of this article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Pandemic conditions can complicate care of patients with PAH
in these patients, according to a research article published in Pulmonary Circulation.
“The impetus for this manuscript was a recent discussion within the Pulmonary Hypertension Association (PHA) and [its] Scientific Leadership Council who expressed a need for guidelines from experts in the field,” wrote John J. Ryan, MD, of the University of Utah, Salt Lake City, and colleagues.
The authors highlight some of the unique challenges in caring for patients with pulmonary hypertension (PH), particularly pulmonary arterial hypertension (PAH), in the context of the COVID-19 pandemic.
Telemedicine and temporary visit schedules for new and returning PAH patients can help reduce risk of virus transmission, if patient accessibility to telemedicine is feasible. Protocols to reduce the risk of virus exposure or transmission in the office setting included less frequent echocardiography and 6-Minute Walk Tests (6MWTs) for patients in stable condition. In stable patients, “avoid pulmonary function of V/Q tests when possible,” the authors wrote.
New patients who have been referred for PAH present a challenge in conducting a thorough evaluation that would normally include measurement of invasive hemodynamics in keeping with current diagnostic guidelines. Clinicians will need to balance the potential risks of COVID-19 exposure during elective procedures against the benefits of full evaluations to plan PAH treatment, the authors noted.
For established patients who are clinically stable, remote visits may be an option, with a risk/benefit assessment of the need for in-person diagnostic tests at the current time, they said. However, telemedicine’s limitations include not only patient accessibility and understanding of audio and video technology, but also inability to accurately measure vital signs, they said.
As for routine testing such as echocardiograms, 6MWTs, and other laboratory testing, “it is important to consider the additive value of these sometimes comprehensive tests in the context of the risks associated with visiting the hospital or clinic to obtain them,” the authors said.
Patients who are unstable and experience worsening right heart failure (RHF) at home may have contracted a COVID-19 infection, but the differential diagnosis includes sepsis, ischemia, and PAH disease progression. “During the current pandemic, fever at home in a PAH patient should be assumed to represent a COVID-19 infection,” and patients with worsening respiratory symptoms that require hospitalization should be tested for COVID-19, the authors emphasized.
Use of ECMO or other intensive interventions should be considered in the context of risk assessment, the authors said. “As a general recommendation, practitioners should consider utilizing an established PAH-specific risk assessment tool to help identify patients who are more likely to survive heroic interventions during the COVID-19 outbreak,” they wrote.
Training and education of PH providers will continue to be limited by the pandemic, and many clinical trials and research programs have been suspended and will need to be restructured to minimize risk of transmission of the COVID-19 virus, the authors said. However, health care providers must continue to provide PAH patients and families with advice and updates in best practices, while “acknowledging that the situation changes rapidly,” they concluded.
Dr. Ryan disclosed participating on the speakers bureau, and provides consulting services for, Actelion and Bayer, as well as research support from the Reagan Corporation, the Gordon Family, and the Cushman Family.
SOURCE: Ryan JJ et al. Pulm Circ. 2020 Apr 29. doi: 10.1177/2045894020920153.
in these patients, according to a research article published in Pulmonary Circulation.
“The impetus for this manuscript was a recent discussion within the Pulmonary Hypertension Association (PHA) and [its] Scientific Leadership Council who expressed a need for guidelines from experts in the field,” wrote John J. Ryan, MD, of the University of Utah, Salt Lake City, and colleagues.
The authors highlight some of the unique challenges in caring for patients with pulmonary hypertension (PH), particularly pulmonary arterial hypertension (PAH), in the context of the COVID-19 pandemic.
Telemedicine and temporary visit schedules for new and returning PAH patients can help reduce risk of virus transmission, if patient accessibility to telemedicine is feasible. Protocols to reduce the risk of virus exposure or transmission in the office setting included less frequent echocardiography and 6-Minute Walk Tests (6MWTs) for patients in stable condition. In stable patients, “avoid pulmonary function of V/Q tests when possible,” the authors wrote.
New patients who have been referred for PAH present a challenge in conducting a thorough evaluation that would normally include measurement of invasive hemodynamics in keeping with current diagnostic guidelines. Clinicians will need to balance the potential risks of COVID-19 exposure during elective procedures against the benefits of full evaluations to plan PAH treatment, the authors noted.
For established patients who are clinically stable, remote visits may be an option, with a risk/benefit assessment of the need for in-person diagnostic tests at the current time, they said. However, telemedicine’s limitations include not only patient accessibility and understanding of audio and video technology, but also inability to accurately measure vital signs, they said.
As for routine testing such as echocardiograms, 6MWTs, and other laboratory testing, “it is important to consider the additive value of these sometimes comprehensive tests in the context of the risks associated with visiting the hospital or clinic to obtain them,” the authors said.
Patients who are unstable and experience worsening right heart failure (RHF) at home may have contracted a COVID-19 infection, but the differential diagnosis includes sepsis, ischemia, and PAH disease progression. “During the current pandemic, fever at home in a PAH patient should be assumed to represent a COVID-19 infection,” and patients with worsening respiratory symptoms that require hospitalization should be tested for COVID-19, the authors emphasized.
Use of ECMO or other intensive interventions should be considered in the context of risk assessment, the authors said. “As a general recommendation, practitioners should consider utilizing an established PAH-specific risk assessment tool to help identify patients who are more likely to survive heroic interventions during the COVID-19 outbreak,” they wrote.
Training and education of PH providers will continue to be limited by the pandemic, and many clinical trials and research programs have been suspended and will need to be restructured to minimize risk of transmission of the COVID-19 virus, the authors said. However, health care providers must continue to provide PAH patients and families with advice and updates in best practices, while “acknowledging that the situation changes rapidly,” they concluded.
Dr. Ryan disclosed participating on the speakers bureau, and provides consulting services for, Actelion and Bayer, as well as research support from the Reagan Corporation, the Gordon Family, and the Cushman Family.
SOURCE: Ryan JJ et al. Pulm Circ. 2020 Apr 29. doi: 10.1177/2045894020920153.
in these patients, according to a research article published in Pulmonary Circulation.
“The impetus for this manuscript was a recent discussion within the Pulmonary Hypertension Association (PHA) and [its] Scientific Leadership Council who expressed a need for guidelines from experts in the field,” wrote John J. Ryan, MD, of the University of Utah, Salt Lake City, and colleagues.
The authors highlight some of the unique challenges in caring for patients with pulmonary hypertension (PH), particularly pulmonary arterial hypertension (PAH), in the context of the COVID-19 pandemic.
Telemedicine and temporary visit schedules for new and returning PAH patients can help reduce risk of virus transmission, if patient accessibility to telemedicine is feasible. Protocols to reduce the risk of virus exposure or transmission in the office setting included less frequent echocardiography and 6-Minute Walk Tests (6MWTs) for patients in stable condition. In stable patients, “avoid pulmonary function of V/Q tests when possible,” the authors wrote.
New patients who have been referred for PAH present a challenge in conducting a thorough evaluation that would normally include measurement of invasive hemodynamics in keeping with current diagnostic guidelines. Clinicians will need to balance the potential risks of COVID-19 exposure during elective procedures against the benefits of full evaluations to plan PAH treatment, the authors noted.
For established patients who are clinically stable, remote visits may be an option, with a risk/benefit assessment of the need for in-person diagnostic tests at the current time, they said. However, telemedicine’s limitations include not only patient accessibility and understanding of audio and video technology, but also inability to accurately measure vital signs, they said.
As for routine testing such as echocardiograms, 6MWTs, and other laboratory testing, “it is important to consider the additive value of these sometimes comprehensive tests in the context of the risks associated with visiting the hospital or clinic to obtain them,” the authors said.
Patients who are unstable and experience worsening right heart failure (RHF) at home may have contracted a COVID-19 infection, but the differential diagnosis includes sepsis, ischemia, and PAH disease progression. “During the current pandemic, fever at home in a PAH patient should be assumed to represent a COVID-19 infection,” and patients with worsening respiratory symptoms that require hospitalization should be tested for COVID-19, the authors emphasized.
Use of ECMO or other intensive interventions should be considered in the context of risk assessment, the authors said. “As a general recommendation, practitioners should consider utilizing an established PAH-specific risk assessment tool to help identify patients who are more likely to survive heroic interventions during the COVID-19 outbreak,” they wrote.
Training and education of PH providers will continue to be limited by the pandemic, and many clinical trials and research programs have been suspended and will need to be restructured to minimize risk of transmission of the COVID-19 virus, the authors said. However, health care providers must continue to provide PAH patients and families with advice and updates in best practices, while “acknowledging that the situation changes rapidly,” they concluded.
Dr. Ryan disclosed participating on the speakers bureau, and provides consulting services for, Actelion and Bayer, as well as research support from the Reagan Corporation, the Gordon Family, and the Cushman Family.
SOURCE: Ryan JJ et al. Pulm Circ. 2020 Apr 29. doi: 10.1177/2045894020920153.
FROM PULMONARY CIRCULATION
Aspirin and warfarin together leads to increased bleeding without reducing thrombotic events
Background: Current guidelines recommend against using aspirin in combination with warfarin for patients with AFib, unless the patient has another indication for aspirin such as recent percutaneous coronary intervention (PCI) or a mechanical heart valve. These recommendations are based on limited clinical trial data that showed an increased risk of adverse events with combination therapy without clinical benefit. Despite these recommendations, recent studies have shown that aspirin use without a clinical indication remains common in patients taking warfarin for AFib. The prevalence of aspirin use without a clinical indication in patients taking warfarin for VTE is less well studied.

Study design: Registry-based cohort study.
Setting: Six anticoagulation clinics in Michigan.
Synopsis: Of the 6,539 patients included in the study, 2,453 patients (37.5%) were taking both warfarin and aspirin without an indication for aspirin therapy; 3,688 propensity score–matched patients (1,844 in each group) were compared to assess rates of bleeding and rates of observed thrombosis at 1 year in patients taking warfarin alone versus warfarin plus aspirin. Patients treated with warfarin plus aspirin experienced more bleeding events than did patients on warfarin monotherapy (95% confidence interval, 23.8%-28.3% vs. 95% CI, 18.3%-22.3%; P less than .001). Rates of observed thrombosis were similar between the two groups (95% CI, 1.6%-3.1% vs. 95% CI, 2.0%-3.6%; P = .40). This study demonstrates that aspirin use without a clinical indication remains common in patients taking warfarin for AFib or VTE, and that reducing inappropriate aspirin use in this patient population may help prevent adverse outcomes.
Bottom line: Use of aspirin without a clinical indication in patients taking warfarin is common and is associated with an increased risk of bleeding without significant clinical benefit.
Citation: Schaefer JK et al. Association of adding aspirin to warfarin therapy without an apparent indication with bleeding and other adverse events. JAMA Intern Med. 2019 Mar 4;179(4):533-41.
Dr. Wachter is an associate medical director at Duke Regional Hospital and an assistant professor of medicine at Duke University.
Background: Current guidelines recommend against using aspirin in combination with warfarin for patients with AFib, unless the patient has another indication for aspirin such as recent percutaneous coronary intervention (PCI) or a mechanical heart valve. These recommendations are based on limited clinical trial data that showed an increased risk of adverse events with combination therapy without clinical benefit. Despite these recommendations, recent studies have shown that aspirin use without a clinical indication remains common in patients taking warfarin for AFib. The prevalence of aspirin use without a clinical indication in patients taking warfarin for VTE is less well studied.
Study design: Registry-based cohort study.
Setting: Six anticoagulation clinics in Michigan.
Synopsis: Of the 6,539 patients included in the study, 2,453 patients (37.5%) were taking both warfarin and aspirin without an indication for aspirin therapy; 3,688 propensity score–matched patients (1,844 in each group) were compared to assess rates of bleeding and rates of observed thrombosis at 1 year in patients taking warfarin alone versus warfarin plus aspirin. Patients treated with warfarin plus aspirin experienced more bleeding events than did patients on warfarin monotherapy (95% confidence interval, 23.8%-28.3% vs. 95% CI, 18.3%-22.3%; P less than .001). Rates of observed thrombosis were similar between the two groups (95% CI, 1.6%-3.1% vs. 95% CI, 2.0%-3.6%; P = .40). This study demonstrates that aspirin use without a clinical indication remains common in patients taking warfarin for AFib or VTE, and that reducing inappropriate aspirin use in this patient population may help prevent adverse outcomes.
Bottom line: Use of aspirin without a clinical indication in patients taking warfarin is common and is associated with an increased risk of bleeding without significant clinical benefit.
Citation: Schaefer JK et al. Association of adding aspirin to warfarin therapy without an apparent indication with bleeding and other adverse events. JAMA Intern Med. 2019 Mar 4;179(4):533-41.
Dr. Wachter is an associate medical director at Duke Regional Hospital and an assistant professor of medicine at Duke University.
Background: Current guidelines recommend against using aspirin in combination with warfarin for patients with AFib, unless the patient has another indication for aspirin such as recent percutaneous coronary intervention (PCI) or a mechanical heart valve. These recommendations are based on limited clinical trial data that showed an increased risk of adverse events with combination therapy without clinical benefit. Despite these recommendations, recent studies have shown that aspirin use without a clinical indication remains common in patients taking warfarin for AFib. The prevalence of aspirin use without a clinical indication in patients taking warfarin for VTE is less well studied.
Study design: Registry-based cohort study.
Setting: Six anticoagulation clinics in Michigan.
Synopsis: Of the 6,539 patients included in the study, 2,453 patients (37.5%) were taking both warfarin and aspirin without an indication for aspirin therapy; 3,688 propensity score–matched patients (1,844 in each group) were compared to assess rates of bleeding and rates of observed thrombosis at 1 year in patients taking warfarin alone versus warfarin plus aspirin. Patients treated with warfarin plus aspirin experienced more bleeding events than did patients on warfarin monotherapy (95% confidence interval, 23.8%-28.3% vs. 95% CI, 18.3%-22.3%; P less than .001). Rates of observed thrombosis were similar between the two groups (95% CI, 1.6%-3.1% vs. 95% CI, 2.0%-3.6%; P = .40). This study demonstrates that aspirin use without a clinical indication remains common in patients taking warfarin for AFib or VTE, and that reducing inappropriate aspirin use in this patient population may help prevent adverse outcomes.
Bottom line: Use of aspirin without a clinical indication in patients taking warfarin is common and is associated with an increased risk of bleeding without significant clinical benefit.
Citation: Schaefer JK et al. Association of adding aspirin to warfarin therapy without an apparent indication with bleeding and other adverse events. JAMA Intern Med. 2019 Mar 4;179(4):533-41.
Dr. Wachter is an associate medical director at Duke Regional Hospital and an assistant professor of medicine at Duke University.
Preliminary evidence indicates famotidine might improve COVID-19 symptoms
High-dose oral famotidine might improve cardinal symptoms of COVID-19 infection, according to the findings of a small outpatient case series and a subsequent retrospective study.
After developing COVID-19 symptoms, the 10 patients in the case series began self-medicating with 60-240 mg famotidine daily over a median of 11 days. “All patients reported marked improvements of disease-related symptoms after starting famotidine,” first author Tobias Janowitz, MD, PhD, of Cold Spring Harbor Laboratory, N.Y., and associates wrote in Gut.
Improvements began within 24-48 hours of starting on the histamine-2 receptor antagonist. By 14 days after treatment initiation, all patients reported near-normalization of both respiratory and systemic symptoms, the researchers reported.
The patients were 23-71 years old. Seven tested positive for COVID-19, two had antibodies to COVID-19, and one had a clinical diagnosis of COVID-19 without laboratory confirmation. Over a median of 11 days (range, 5-21 days), six patients self-administered 80 mg famotidine three times daily and four self-administered lower amounts – from 60 to 150 mg of famotidine daily, divided into two or three doses. Patients started on famotidine between 2 and 26 days after symptom onset.
Through phone interviews and questionnaires, the researchers ascertained changes in cough, dyspnea, fatigue, headache, anosmia, and general unwellness by using a modified four-point Eastern Cooperative Oncology Group (ECOG) performance status scale. Improvements were seen across all symptom categories, and respiratory symptoms improved faster than systemic symptoms. Apart from two cases of persistent anosmia, symptoms resolved completely within 14 days of starting famotidine.
Seven patients reported no side effects of famotidine; one reported grade 1 dizziness and infrequent perceptions of tachycardia; one reported grade 1 dizziness, dry skin, and insomnia; and one reported grade 1 gastrointestinal symptoms and temporary forgetfulness. “Other than forgetfulness, all of these side effects are listed in the prescription information for famotidine, and all side effects resolved on discontinuation of famotidine,” the investigators wrote.
While the findings are intriguing, Dr. Janowitz and associates cautioned against overinterpretation of them. Another expert agreed: “This is a preliminary study based on a hypothesized antiviral effect. It’s important to know that it doesn’t really prove it works,” said Amesh Adalja, MD, senior scholar at the Johns Hopkins University Center for Health Security, Baltimore, and a spokesperson for the Infectious Diseases Society of America, during an interview with MDedge.
These patients might have improved anyway, without self-administering famotidine, said Dr. Adalja, who was not involved in the study.
Furthermore, the mechanism by which famotidine might act on COVID-19 remains unclear. The drug “could have a viral target, for example, one of the viral proteases, or a host target, resulting, for example, in modulation of the immunological response to the virus,” Dr. Janowitz and associates wrote.
Dr. Adalja noted that many compounds show effects against COVID-19 that are not well understood. He called for randomized trials to evaluate the biological plausibility of famotidine use, and its potential efficacy.
“This is a cheap, over-the-counter drug, but no drug is without side effects,” he added. “We need to know whether it works.”
Based on the case series findings, researchers conducted another retrospective study of patients hospitalized with COVID-19 infection. Those who were incidentally taking famotidine before or at hospitalization had a significantly reduced risk of intubation or death, with a hazard ratio of 0.43 (Gastroenterology. 2020 May 22. doi: 10.1053/j.gastro.2020.05.053)
The National Institutes of Health provided partial support. The investigators reported having no conflicts of interest.
SOURCE: Janowitz T et al. Gut. 2020 Jun 4. doi: 10.1136/gutjnl-2020-321852.
High-dose oral famotidine might improve cardinal symptoms of COVID-19 infection, according to the findings of a small outpatient case series and a subsequent retrospective study.
After developing COVID-19 symptoms, the 10 patients in the case series began self-medicating with 60-240 mg famotidine daily over a median of 11 days. “All patients reported marked improvements of disease-related symptoms after starting famotidine,” first author Tobias Janowitz, MD, PhD, of Cold Spring Harbor Laboratory, N.Y., and associates wrote in Gut.
Improvements began within 24-48 hours of starting on the histamine-2 receptor antagonist. By 14 days after treatment initiation, all patients reported near-normalization of both respiratory and systemic symptoms, the researchers reported.
The patients were 23-71 years old. Seven tested positive for COVID-19, two had antibodies to COVID-19, and one had a clinical diagnosis of COVID-19 without laboratory confirmation. Over a median of 11 days (range, 5-21 days), six patients self-administered 80 mg famotidine three times daily and four self-administered lower amounts – from 60 to 150 mg of famotidine daily, divided into two or three doses. Patients started on famotidine between 2 and 26 days after symptom onset.
Through phone interviews and questionnaires, the researchers ascertained changes in cough, dyspnea, fatigue, headache, anosmia, and general unwellness by using a modified four-point Eastern Cooperative Oncology Group (ECOG) performance status scale. Improvements were seen across all symptom categories, and respiratory symptoms improved faster than systemic symptoms. Apart from two cases of persistent anosmia, symptoms resolved completely within 14 days of starting famotidine.
Seven patients reported no side effects of famotidine; one reported grade 1 dizziness and infrequent perceptions of tachycardia; one reported grade 1 dizziness, dry skin, and insomnia; and one reported grade 1 gastrointestinal symptoms and temporary forgetfulness. “Other than forgetfulness, all of these side effects are listed in the prescription information for famotidine, and all side effects resolved on discontinuation of famotidine,” the investigators wrote.
While the findings are intriguing, Dr. Janowitz and associates cautioned against overinterpretation of them. Another expert agreed: “This is a preliminary study based on a hypothesized antiviral effect. It’s important to know that it doesn’t really prove it works,” said Amesh Adalja, MD, senior scholar at the Johns Hopkins University Center for Health Security, Baltimore, and a spokesperson for the Infectious Diseases Society of America, during an interview with MDedge.
These patients might have improved anyway, without self-administering famotidine, said Dr. Adalja, who was not involved in the study.
Furthermore, the mechanism by which famotidine might act on COVID-19 remains unclear. The drug “could have a viral target, for example, one of the viral proteases, or a host target, resulting, for example, in modulation of the immunological response to the virus,” Dr. Janowitz and associates wrote.
Dr. Adalja noted that many compounds show effects against COVID-19 that are not well understood. He called for randomized trials to evaluate the biological plausibility of famotidine use, and its potential efficacy.
“This is a cheap, over-the-counter drug, but no drug is without side effects,” he added. “We need to know whether it works.”
Based on the case series findings, researchers conducted another retrospective study of patients hospitalized with COVID-19 infection. Those who were incidentally taking famotidine before or at hospitalization had a significantly reduced risk of intubation or death, with a hazard ratio of 0.43 (Gastroenterology. 2020 May 22. doi: 10.1053/j.gastro.2020.05.053)
The National Institutes of Health provided partial support. The investigators reported having no conflicts of interest.
SOURCE: Janowitz T et al. Gut. 2020 Jun 4. doi: 10.1136/gutjnl-2020-321852.
High-dose oral famotidine might improve cardinal symptoms of COVID-19 infection, according to the findings of a small outpatient case series and a subsequent retrospective study.
After developing COVID-19 symptoms, the 10 patients in the case series began self-medicating with 60-240 mg famotidine daily over a median of 11 days. “All patients reported marked improvements of disease-related symptoms after starting famotidine,” first author Tobias Janowitz, MD, PhD, of Cold Spring Harbor Laboratory, N.Y., and associates wrote in Gut.
Improvements began within 24-48 hours of starting on the histamine-2 receptor antagonist. By 14 days after treatment initiation, all patients reported near-normalization of both respiratory and systemic symptoms, the researchers reported.
The patients were 23-71 years old. Seven tested positive for COVID-19, two had antibodies to COVID-19, and one had a clinical diagnosis of COVID-19 without laboratory confirmation. Over a median of 11 days (range, 5-21 days), six patients self-administered 80 mg famotidine three times daily and four self-administered lower amounts – from 60 to 150 mg of famotidine daily, divided into two or three doses. Patients started on famotidine between 2 and 26 days after symptom onset.
Through phone interviews and questionnaires, the researchers ascertained changes in cough, dyspnea, fatigue, headache, anosmia, and general unwellness by using a modified four-point Eastern Cooperative Oncology Group (ECOG) performance status scale. Improvements were seen across all symptom categories, and respiratory symptoms improved faster than systemic symptoms. Apart from two cases of persistent anosmia, symptoms resolved completely within 14 days of starting famotidine.
Seven patients reported no side effects of famotidine; one reported grade 1 dizziness and infrequent perceptions of tachycardia; one reported grade 1 dizziness, dry skin, and insomnia; and one reported grade 1 gastrointestinal symptoms and temporary forgetfulness. “Other than forgetfulness, all of these side effects are listed in the prescription information for famotidine, and all side effects resolved on discontinuation of famotidine,” the investigators wrote.
While the findings are intriguing, Dr. Janowitz and associates cautioned against overinterpretation of them. Another expert agreed: “This is a preliminary study based on a hypothesized antiviral effect. It’s important to know that it doesn’t really prove it works,” said Amesh Adalja, MD, senior scholar at the Johns Hopkins University Center for Health Security, Baltimore, and a spokesperson for the Infectious Diseases Society of America, during an interview with MDedge.
These patients might have improved anyway, without self-administering famotidine, said Dr. Adalja, who was not involved in the study.
Furthermore, the mechanism by which famotidine might act on COVID-19 remains unclear. The drug “could have a viral target, for example, one of the viral proteases, or a host target, resulting, for example, in modulation of the immunological response to the virus,” Dr. Janowitz and associates wrote.
Dr. Adalja noted that many compounds show effects against COVID-19 that are not well understood. He called for randomized trials to evaluate the biological plausibility of famotidine use, and its potential efficacy.
“This is a cheap, over-the-counter drug, but no drug is without side effects,” he added. “We need to know whether it works.”
Based on the case series findings, researchers conducted another retrospective study of patients hospitalized with COVID-19 infection. Those who were incidentally taking famotidine before or at hospitalization had a significantly reduced risk of intubation or death, with a hazard ratio of 0.43 (Gastroenterology. 2020 May 22. doi: 10.1053/j.gastro.2020.05.053)
The National Institutes of Health provided partial support. The investigators reported having no conflicts of interest.
SOURCE: Janowitz T et al. Gut. 2020 Jun 4. doi: 10.1136/gutjnl-2020-321852.
FROM GUT
Catheter ablation of AFib improves quality of life more than medications do
Background: Catheter ablation of AFib (primarily pulmonary vein isolation) has been shown to result in better maintenance of sinus rhythm than medications. Small studies of QOL have shown mixed results. Larger trials were needed.
Study design: Open-label randomized multisite clinical trial of catheter ablation (pulmonary vein isolation with additional ablation procedure at the treating physician discretion) versus standard rate and/or rhythm control medications (chosen by clinician discretion). Patients were included for paroxysmal or persistent AFib and either age 65 years or older or age younger than 65 years with one additional stroke risk factor. Quality of life surveys – the Atrial Fibrillation Effect on Quality of Life (AFEQT) questionnaire and the Mayo AF-Specific Symptom Inventory (MAFSI) – were completed at baseline, and at 3, 12, 24, 36, 48, and 60 months.
Setting: 126 centers in 10 countries.
Synopsis: The study included 2,204 patients with median age of 68 years, diagnosed with AFib a median of 1.1 years prior, who were followed for a median of 48 months. The median CHA2DS2-VASc score was 3.0.
Self-reported AFib dropped from 86.0% to 21.1% in the ablation group and from 83.7% to 39.8% in the medication group at 12 months. The AFEQT score (range 0-100, higher score indicating better QOL) increased from 62.9 to 86.4 in the ablation group and increased from 63.1 to 80.9 in the medication group (for a mean difference of 5.3 points [95% confidence interval, 3.7-6.9; P less than .001] favoring ablation). MAFSI symptom frequency score and symptom severity score also showed improvement in symptoms favoring ablation. Post hoc subgroup analysis showed that those with the most severe symptoms had the largest benefit from ablation.
The primary limitation is the lack of patient blinding (may bias self-reported symptoms).
While the CABANA trial efficacy study (published separately) showed that catheter ablation results in no significant difference in the combined outcome of death, disabling stroke, serious bleeding, or cardiac arrest, the CABANA QOL study, reviewed here, shows that ablation does result in improved QOL and reduced symptoms, compared with medical therapy.
Bottom line: Catheter ablation of AFib can be done safely and successfully at experienced centers. In patients with AFib-related symptoms, ablation reduces symptoms and improves QOL somewhat more than medications do. The most severely symptomatic patients appear to obtain the most benefit.
Citation: Packer DL et al. Effect of catheter ablation vs. antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: The CABANA Randomized Clinical Trial. JAMA. 2019 Mar 15. doi: 10.1001/jama.2019.0693.
Dr. Stafford is a hospitalist at Duke University Health System.
Background: Catheter ablation of AFib (primarily pulmonary vein isolation) has been shown to result in better maintenance of sinus rhythm than medications. Small studies of QOL have shown mixed results. Larger trials were needed.
Study design: Open-label randomized multisite clinical trial of catheter ablation (pulmonary vein isolation with additional ablation procedure at the treating physician discretion) versus standard rate and/or rhythm control medications (chosen by clinician discretion). Patients were included for paroxysmal or persistent AFib and either age 65 years or older or age younger than 65 years with one additional stroke risk factor. Quality of life surveys – the Atrial Fibrillation Effect on Quality of Life (AFEQT) questionnaire and the Mayo AF-Specific Symptom Inventory (MAFSI) – were completed at baseline, and at 3, 12, 24, 36, 48, and 60 months.
Setting: 126 centers in 10 countries.
Synopsis: The study included 2,204 patients with median age of 68 years, diagnosed with AFib a median of 1.1 years prior, who were followed for a median of 48 months. The median CHA2DS2-VASc score was 3.0.
Self-reported AFib dropped from 86.0% to 21.1% in the ablation group and from 83.7% to 39.8% in the medication group at 12 months. The AFEQT score (range 0-100, higher score indicating better QOL) increased from 62.9 to 86.4 in the ablation group and increased from 63.1 to 80.9 in the medication group (for a mean difference of 5.3 points [95% confidence interval, 3.7-6.9; P less than .001] favoring ablation). MAFSI symptom frequency score and symptom severity score also showed improvement in symptoms favoring ablation. Post hoc subgroup analysis showed that those with the most severe symptoms had the largest benefit from ablation.
The primary limitation is the lack of patient blinding (may bias self-reported symptoms).
While the CABANA trial efficacy study (published separately) showed that catheter ablation results in no significant difference in the combined outcome of death, disabling stroke, serious bleeding, or cardiac arrest, the CABANA QOL study, reviewed here, shows that ablation does result in improved QOL and reduced symptoms, compared with medical therapy.
Bottom line: Catheter ablation of AFib can be done safely and successfully at experienced centers. In patients with AFib-related symptoms, ablation reduces symptoms and improves QOL somewhat more than medications do. The most severely symptomatic patients appear to obtain the most benefit.
Citation: Packer DL et al. Effect of catheter ablation vs. antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: The CABANA Randomized Clinical Trial. JAMA. 2019 Mar 15. doi: 10.1001/jama.2019.0693.
Dr. Stafford is a hospitalist at Duke University Health System.
Background: Catheter ablation of AFib (primarily pulmonary vein isolation) has been shown to result in better maintenance of sinus rhythm than medications. Small studies of QOL have shown mixed results. Larger trials were needed.
Study design: Open-label randomized multisite clinical trial of catheter ablation (pulmonary vein isolation with additional ablation procedure at the treating physician discretion) versus standard rate and/or rhythm control medications (chosen by clinician discretion). Patients were included for paroxysmal or persistent AFib and either age 65 years or older or age younger than 65 years with one additional stroke risk factor. Quality of life surveys – the Atrial Fibrillation Effect on Quality of Life (AFEQT) questionnaire and the Mayo AF-Specific Symptom Inventory (MAFSI) – were completed at baseline, and at 3, 12, 24, 36, 48, and 60 months.
Setting: 126 centers in 10 countries.
Synopsis: The study included 2,204 patients with median age of 68 years, diagnosed with AFib a median of 1.1 years prior, who were followed for a median of 48 months. The median CHA2DS2-VASc score was 3.0.
Self-reported AFib dropped from 86.0% to 21.1% in the ablation group and from 83.7% to 39.8% in the medication group at 12 months. The AFEQT score (range 0-100, higher score indicating better QOL) increased from 62.9 to 86.4 in the ablation group and increased from 63.1 to 80.9 in the medication group (for a mean difference of 5.3 points [95% confidence interval, 3.7-6.9; P less than .001] favoring ablation). MAFSI symptom frequency score and symptom severity score also showed improvement in symptoms favoring ablation. Post hoc subgroup analysis showed that those with the most severe symptoms had the largest benefit from ablation.
The primary limitation is the lack of patient blinding (may bias self-reported symptoms).
While the CABANA trial efficacy study (published separately) showed that catheter ablation results in no significant difference in the combined outcome of death, disabling stroke, serious bleeding, or cardiac arrest, the CABANA QOL study, reviewed here, shows that ablation does result in improved QOL and reduced symptoms, compared with medical therapy.
Bottom line: Catheter ablation of AFib can be done safely and successfully at experienced centers. In patients with AFib-related symptoms, ablation reduces symptoms and improves QOL somewhat more than medications do. The most severely symptomatic patients appear to obtain the most benefit.
Citation: Packer DL et al. Effect of catheter ablation vs. antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: The CABANA Randomized Clinical Trial. JAMA. 2019 Mar 15. doi: 10.1001/jama.2019.0693.
Dr. Stafford is a hospitalist at Duke University Health System.
Restriction of Foley catheters in older trauma patients improved outcomes
and led to earlier discharge, findings from a study revealed. The results of the study were reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled because of COVID-19.
“We reduced the use of Foley catheters in our target population by more than 50%, which led to a decrease in the rate of hospital-acquired UTI and positively affected other perioperative outcomes,” reported Sanjit R. Konda, MD, an orthopedic surgeon with New York University Langone Health.
The quality initiative was introduced about 2 years ago specifically to reduce the risk of UTI in older patients admitted for femur or hip fractures. Previously at the level 1 trauma center where this quality initiative was introduced, placement of Foley catheters in these types of patients had been routine.
After the policy change, Foley catheters were only offered to these trauma patients 55 years of age or older when more than three episodes or urinary retention had been documented with a bladder scan. Urinary retention was defined as a volume of at least 600 mL.
When outcomes in 184 patients treated in the 15 months after the policy change were compared with 393 treated in the prior 38 months, Foley catheter use was substantially and significantly reduced (43.5% vs. 95.5%; P < .001), Dr. Konda said in an interview.
Although the lower rate of UTI following the policy change fell short of statistical significance (10.33% vs. 14.5%; P = .167), the policy change was associated with a decreased time to surgery (33.27 vs. 38.54 hours; P = .001), shorter length of stay (6.89 vs. 8.34 days; P < .001), and higher rate of home discharge (22.8% vs. 15.6%; P = .038).
When those who avoided a Foley catheter were compared with those who did not after the policy change, there was a significant reduction in UTI (4.81% vs. 17.4%; P = .014). In addition, patients who avoided a Foley catheter had a decreased time to surgery (P = .014), shorter length of stay (P < .001) and an almost 900% greater likelihood of home discharge (odds ratio, 9.9; P < .001).
“This quality initiative does increase the number of bladder scans required, meaning more work for nurses, but the program was developed in collaboration with our nursing staff, who were supportive of the goals,” Dr. Konda reported.
Reducing the incidence of UTI is an important initiative because the Centers for Medicare & Medicaid Services and other third-party payers employ this as a quality metric, according to Dr. Konda. This explains why hospital administrators generally embrace effective strategies to reduce UTI rates.
The improvement in outcomes, including the reduction in UTIs and length of stay, has cost implications, which will be evaluated in a future analysis, according to Dr. Konda.
Although this quality initiative was undertaken in a level 1 trauma center, Dr. Konda believes the same principles can be applied to other settings.
Jennifer A. Meddings, MD, an associate professor of medicine at the University of Michigan, Ann Arbor, agreed. Active in the evaluation of strategies to reduce hospital-acquired complications, Dr. Meddings published a study of procedural appropriateness ratings to guide strategies for improving the likelihood that catheters are employed only when needed (BMJ Qual Saf. 2019;28:56-66).
“In addition to avoiding UTI, reducing unnecessary placement of Foley catheters also eliminates the risk of trauma to the urinary tract,” Dr. Meddings said. This is a complication that is not well appreciated because the trauma is not always documented, according to Dr. Meddings, who believes increased risk of both UTI and urinary tract trauma should discourage use of Foley catheters when there is not a specific indication.
Although there are criteria other than excess bladder volume to determine when to consider a Foley catheter, Dr. Meddings encourages any systematic approach that increases the likelihood that catheters are not placed unnecessarily. She emphasized that a hip fracture by itself “is not a criterion for catheterization.”
Dr. Konda reported a financial relationship with Stryker.
and led to earlier discharge, findings from a study revealed. The results of the study were reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled because of COVID-19.
“We reduced the use of Foley catheters in our target population by more than 50%, which led to a decrease in the rate of hospital-acquired UTI and positively affected other perioperative outcomes,” reported Sanjit R. Konda, MD, an orthopedic surgeon with New York University Langone Health.
The quality initiative was introduced about 2 years ago specifically to reduce the risk of UTI in older patients admitted for femur or hip fractures. Previously at the level 1 trauma center where this quality initiative was introduced, placement of Foley catheters in these types of patients had been routine.
After the policy change, Foley catheters were only offered to these trauma patients 55 years of age or older when more than three episodes or urinary retention had been documented with a bladder scan. Urinary retention was defined as a volume of at least 600 mL.
When outcomes in 184 patients treated in the 15 months after the policy change were compared with 393 treated in the prior 38 months, Foley catheter use was substantially and significantly reduced (43.5% vs. 95.5%; P < .001), Dr. Konda said in an interview.
Although the lower rate of UTI following the policy change fell short of statistical significance (10.33% vs. 14.5%; P = .167), the policy change was associated with a decreased time to surgery (33.27 vs. 38.54 hours; P = .001), shorter length of stay (6.89 vs. 8.34 days; P < .001), and higher rate of home discharge (22.8% vs. 15.6%; P = .038).
When those who avoided a Foley catheter were compared with those who did not after the policy change, there was a significant reduction in UTI (4.81% vs. 17.4%; P = .014). In addition, patients who avoided a Foley catheter had a decreased time to surgery (P = .014), shorter length of stay (P < .001) and an almost 900% greater likelihood of home discharge (odds ratio, 9.9; P < .001).
“This quality initiative does increase the number of bladder scans required, meaning more work for nurses, but the program was developed in collaboration with our nursing staff, who were supportive of the goals,” Dr. Konda reported.
Reducing the incidence of UTI is an important initiative because the Centers for Medicare & Medicaid Services and other third-party payers employ this as a quality metric, according to Dr. Konda. This explains why hospital administrators generally embrace effective strategies to reduce UTI rates.
The improvement in outcomes, including the reduction in UTIs and length of stay, has cost implications, which will be evaluated in a future analysis, according to Dr. Konda.
Although this quality initiative was undertaken in a level 1 trauma center, Dr. Konda believes the same principles can be applied to other settings.
Jennifer A. Meddings, MD, an associate professor of medicine at the University of Michigan, Ann Arbor, agreed. Active in the evaluation of strategies to reduce hospital-acquired complications, Dr. Meddings published a study of procedural appropriateness ratings to guide strategies for improving the likelihood that catheters are employed only when needed (BMJ Qual Saf. 2019;28:56-66).
“In addition to avoiding UTI, reducing unnecessary placement of Foley catheters also eliminates the risk of trauma to the urinary tract,” Dr. Meddings said. This is a complication that is not well appreciated because the trauma is not always documented, according to Dr. Meddings, who believes increased risk of both UTI and urinary tract trauma should discourage use of Foley catheters when there is not a specific indication.
Although there are criteria other than excess bladder volume to determine when to consider a Foley catheter, Dr. Meddings encourages any systematic approach that increases the likelihood that catheters are not placed unnecessarily. She emphasized that a hip fracture by itself “is not a criterion for catheterization.”
Dr. Konda reported a financial relationship with Stryker.
and led to earlier discharge, findings from a study revealed. The results of the study were reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled because of COVID-19.
“We reduced the use of Foley catheters in our target population by more than 50%, which led to a decrease in the rate of hospital-acquired UTI and positively affected other perioperative outcomes,” reported Sanjit R. Konda, MD, an orthopedic surgeon with New York University Langone Health.
The quality initiative was introduced about 2 years ago specifically to reduce the risk of UTI in older patients admitted for femur or hip fractures. Previously at the level 1 trauma center where this quality initiative was introduced, placement of Foley catheters in these types of patients had been routine.
After the policy change, Foley catheters were only offered to these trauma patients 55 years of age or older when more than three episodes or urinary retention had been documented with a bladder scan. Urinary retention was defined as a volume of at least 600 mL.
When outcomes in 184 patients treated in the 15 months after the policy change were compared with 393 treated in the prior 38 months, Foley catheter use was substantially and significantly reduced (43.5% vs. 95.5%; P < .001), Dr. Konda said in an interview.
Although the lower rate of UTI following the policy change fell short of statistical significance (10.33% vs. 14.5%; P = .167), the policy change was associated with a decreased time to surgery (33.27 vs. 38.54 hours; P = .001), shorter length of stay (6.89 vs. 8.34 days; P < .001), and higher rate of home discharge (22.8% vs. 15.6%; P = .038).
When those who avoided a Foley catheter were compared with those who did not after the policy change, there was a significant reduction in UTI (4.81% vs. 17.4%; P = .014). In addition, patients who avoided a Foley catheter had a decreased time to surgery (P = .014), shorter length of stay (P < .001) and an almost 900% greater likelihood of home discharge (odds ratio, 9.9; P < .001).
“This quality initiative does increase the number of bladder scans required, meaning more work for nurses, but the program was developed in collaboration with our nursing staff, who were supportive of the goals,” Dr. Konda reported.
Reducing the incidence of UTI is an important initiative because the Centers for Medicare & Medicaid Services and other third-party payers employ this as a quality metric, according to Dr. Konda. This explains why hospital administrators generally embrace effective strategies to reduce UTI rates.
The improvement in outcomes, including the reduction in UTIs and length of stay, has cost implications, which will be evaluated in a future analysis, according to Dr. Konda.
Although this quality initiative was undertaken in a level 1 trauma center, Dr. Konda believes the same principles can be applied to other settings.
Jennifer A. Meddings, MD, an associate professor of medicine at the University of Michigan, Ann Arbor, agreed. Active in the evaluation of strategies to reduce hospital-acquired complications, Dr. Meddings published a study of procedural appropriateness ratings to guide strategies for improving the likelihood that catheters are employed only when needed (BMJ Qual Saf. 2019;28:56-66).
“In addition to avoiding UTI, reducing unnecessary placement of Foley catheters also eliminates the risk of trauma to the urinary tract,” Dr. Meddings said. This is a complication that is not well appreciated because the trauma is not always documented, according to Dr. Meddings, who believes increased risk of both UTI and urinary tract trauma should discourage use of Foley catheters when there is not a specific indication.
Although there are criteria other than excess bladder volume to determine when to consider a Foley catheter, Dr. Meddings encourages any systematic approach that increases the likelihood that catheters are not placed unnecessarily. She emphasized that a hip fracture by itself “is not a criterion for catheterization.”
Dr. Konda reported a financial relationship with Stryker.
FROM AAOS 2020