User login
Meta-analysis: For large proximal polyps, clipping prevents bleeding
Prophylactically clipping large proximal colorectal lesions after resection may reduce risk of postprocedural bleeding, according to a meta-analysis involving nine randomized controlled trials.
Across all lesions, prophylactic clipping had no significant benefit, but when considering only large proximal lesions, clipping reduced bleeding risk by 63%, reported lead author Marco Spadaccini, MD, of Humanitas University, Rozzano, Italy, and colleagues.
According to the investigators, these findings emphasize the relevance of polyp size and location when assessing bleeding risk, which may influence future clinical guidance.
“Despite lack of high-quality evidence, prophylactic clipping has been advocated as a technique to reduce the risk of postprocedural bleeding,” the investigators wrote in Gastroenterology, referring to the European Society of Gastrointestinal Endoscopy recommendation that is based on patient risk factors.
Although previous meta-analyses reported that prophylactic clipping had no protective effect, these studies were “at high risk of bias” and predominantly evaluated lesions less than 20 mm in diameter, the investigators wrote.
Dr. Spadaccini and colleagues suggested that data from more recent, high-quality, randomized controlled trials could be used to identify subgroups that may benefit from clipping. This knowledge is particularly valuable considering the “costs and technical complexity” involved in the procedure, they noted.
The present meta-analysis comprised nine trials that included 7,197 colorectal lesions, of which 49.2% were proximally located and 22.5% were large (at least 20 mm in diameter).
Across all lesions, postprocedural bleeding occurred in 2.2% of clipped lesions and 3.3% of nonclipped lesions, a difference that was not statistically significant (P = .072). But for lesions 20 mm or larger, clipping was associated with a significantly lower rate of bleeding (4.3% vs. 7.6%; relative risk, 0.51; 95% CI, 0.33-0.78; P = .020). Similarly, clipping in the proximal location was independently associated with reduced bleeding risk (3.0% vs. 6.2%; RR, 0.53; 95% CI, 0.35-0.81; P less than .001). A multilevel meta-regression added further clarity by combining both size and location; it showed that clipping had a significant protective effect for large proximal lesions (RR, 0.37; 95% CI, 0.22-0.61; P = .021), but not for those that were small and proximal (RR, 0.88; 95% CI, 0.48-1.62; P = .581).
“According to our meta-analysis, routine practice of endoscopic clipping as a prophylactic intervention does not reduce the risk of postpolypectomy bleeding,” the investigators wrote. “However, clipping was effective in reducing the risk of postprocedural bleeding by nearly 50% for large lesions. If such lesions do not undergo endoscopic clipping, there was fourfold increase in the baseline risk of post-procedural bleeding as compared with those less than 20 mm.”
While the present analysis suggested that clipping was beneficial only for large lesions in the proximal colon, the investigators noted that the protective effect of clipping large lesions in the distal colon (RR, 0.70; 95% CI, 0.22-2.27) was “somewhat intermediate ... albeit not statistically significant” and driven by data from one trial.
“[T]his was not confirmed by other studies generating some uncertainty on the benefit of prophylactic clipping for large distal lesions,” the investigators wrote. “Thus, the decision for large and distal lesions should be tailored, especially taking into consideration other patient- and polyp-risk factors for postprocedural bleeding, such as the use of anti-thrombotic agents or intraprocedural bleeding.”
In contrast, the findings indicated that clipping is unnecessary for lesions less than 20 mm, the investigators wrote.
They went on to explain that clinical application of these findings could result in “significant cost savings” because one bleeding event would be prevented for every 23 large lesions clipped.
“Considering that clips are expensive and their placement might be technically demanding, prophylactic clipping tailored for a subgroup of higher-risk lesions/patients would decrease in parallel both adverse events and costs,” the investigators concluded.
The investigators reported no external funding or conflicts of interest.
ginews@gastro.org
SOURCE: Spadaccini M et al. Gastroenterology. 2020 Apr 1. doi: 10.1053/j.gastro.2020.03.051.
Prophylactically clipping large proximal colorectal lesions after resection may reduce risk of postprocedural bleeding, according to a meta-analysis involving nine randomized controlled trials.
Across all lesions, prophylactic clipping had no significant benefit, but when considering only large proximal lesions, clipping reduced bleeding risk by 63%, reported lead author Marco Spadaccini, MD, of Humanitas University, Rozzano, Italy, and colleagues.
According to the investigators, these findings emphasize the relevance of polyp size and location when assessing bleeding risk, which may influence future clinical guidance.
“Despite lack of high-quality evidence, prophylactic clipping has been advocated as a technique to reduce the risk of postprocedural bleeding,” the investigators wrote in Gastroenterology, referring to the European Society of Gastrointestinal Endoscopy recommendation that is based on patient risk factors.
Although previous meta-analyses reported that prophylactic clipping had no protective effect, these studies were “at high risk of bias” and predominantly evaluated lesions less than 20 mm in diameter, the investigators wrote.
Dr. Spadaccini and colleagues suggested that data from more recent, high-quality, randomized controlled trials could be used to identify subgroups that may benefit from clipping. This knowledge is particularly valuable considering the “costs and technical complexity” involved in the procedure, they noted.
The present meta-analysis comprised nine trials that included 7,197 colorectal lesions, of which 49.2% were proximally located and 22.5% were large (at least 20 mm in diameter).
Across all lesions, postprocedural bleeding occurred in 2.2% of clipped lesions and 3.3% of nonclipped lesions, a difference that was not statistically significant (P = .072). But for lesions 20 mm or larger, clipping was associated with a significantly lower rate of bleeding (4.3% vs. 7.6%; relative risk, 0.51; 95% CI, 0.33-0.78; P = .020). Similarly, clipping in the proximal location was independently associated with reduced bleeding risk (3.0% vs. 6.2%; RR, 0.53; 95% CI, 0.35-0.81; P less than .001). A multilevel meta-regression added further clarity by combining both size and location; it showed that clipping had a significant protective effect for large proximal lesions (RR, 0.37; 95% CI, 0.22-0.61; P = .021), but not for those that were small and proximal (RR, 0.88; 95% CI, 0.48-1.62; P = .581).
“According to our meta-analysis, routine practice of endoscopic clipping as a prophylactic intervention does not reduce the risk of postpolypectomy bleeding,” the investigators wrote. “However, clipping was effective in reducing the risk of postprocedural bleeding by nearly 50% for large lesions. If such lesions do not undergo endoscopic clipping, there was fourfold increase in the baseline risk of post-procedural bleeding as compared with those less than 20 mm.”
While the present analysis suggested that clipping was beneficial only for large lesions in the proximal colon, the investigators noted that the protective effect of clipping large lesions in the distal colon (RR, 0.70; 95% CI, 0.22-2.27) was “somewhat intermediate ... albeit not statistically significant” and driven by data from one trial.
“[T]his was not confirmed by other studies generating some uncertainty on the benefit of prophylactic clipping for large distal lesions,” the investigators wrote. “Thus, the decision for large and distal lesions should be tailored, especially taking into consideration other patient- and polyp-risk factors for postprocedural bleeding, such as the use of anti-thrombotic agents or intraprocedural bleeding.”
In contrast, the findings indicated that clipping is unnecessary for lesions less than 20 mm, the investigators wrote.
They went on to explain that clinical application of these findings could result in “significant cost savings” because one bleeding event would be prevented for every 23 large lesions clipped.
“Considering that clips are expensive and their placement might be technically demanding, prophylactic clipping tailored for a subgroup of higher-risk lesions/patients would decrease in parallel both adverse events and costs,” the investigators concluded.
The investigators reported no external funding or conflicts of interest.
ginews@gastro.org
SOURCE: Spadaccini M et al. Gastroenterology. 2020 Apr 1. doi: 10.1053/j.gastro.2020.03.051.
Prophylactically clipping large proximal colorectal lesions after resection may reduce risk of postprocedural bleeding, according to a meta-analysis involving nine randomized controlled trials.
Across all lesions, prophylactic clipping had no significant benefit, but when considering only large proximal lesions, clipping reduced bleeding risk by 63%, reported lead author Marco Spadaccini, MD, of Humanitas University, Rozzano, Italy, and colleagues.
According to the investigators, these findings emphasize the relevance of polyp size and location when assessing bleeding risk, which may influence future clinical guidance.
“Despite lack of high-quality evidence, prophylactic clipping has been advocated as a technique to reduce the risk of postprocedural bleeding,” the investigators wrote in Gastroenterology, referring to the European Society of Gastrointestinal Endoscopy recommendation that is based on patient risk factors.
Although previous meta-analyses reported that prophylactic clipping had no protective effect, these studies were “at high risk of bias” and predominantly evaluated lesions less than 20 mm in diameter, the investigators wrote.
Dr. Spadaccini and colleagues suggested that data from more recent, high-quality, randomized controlled trials could be used to identify subgroups that may benefit from clipping. This knowledge is particularly valuable considering the “costs and technical complexity” involved in the procedure, they noted.
The present meta-analysis comprised nine trials that included 7,197 colorectal lesions, of which 49.2% were proximally located and 22.5% were large (at least 20 mm in diameter).
Across all lesions, postprocedural bleeding occurred in 2.2% of clipped lesions and 3.3% of nonclipped lesions, a difference that was not statistically significant (P = .072). But for lesions 20 mm or larger, clipping was associated with a significantly lower rate of bleeding (4.3% vs. 7.6%; relative risk, 0.51; 95% CI, 0.33-0.78; P = .020). Similarly, clipping in the proximal location was independently associated with reduced bleeding risk (3.0% vs. 6.2%; RR, 0.53; 95% CI, 0.35-0.81; P less than .001). A multilevel meta-regression added further clarity by combining both size and location; it showed that clipping had a significant protective effect for large proximal lesions (RR, 0.37; 95% CI, 0.22-0.61; P = .021), but not for those that were small and proximal (RR, 0.88; 95% CI, 0.48-1.62; P = .581).
“According to our meta-analysis, routine practice of endoscopic clipping as a prophylactic intervention does not reduce the risk of postpolypectomy bleeding,” the investigators wrote. “However, clipping was effective in reducing the risk of postprocedural bleeding by nearly 50% for large lesions. If such lesions do not undergo endoscopic clipping, there was fourfold increase in the baseline risk of post-procedural bleeding as compared with those less than 20 mm.”
While the present analysis suggested that clipping was beneficial only for large lesions in the proximal colon, the investigators noted that the protective effect of clipping large lesions in the distal colon (RR, 0.70; 95% CI, 0.22-2.27) was “somewhat intermediate ... albeit not statistically significant” and driven by data from one trial.
“[T]his was not confirmed by other studies generating some uncertainty on the benefit of prophylactic clipping for large distal lesions,” the investigators wrote. “Thus, the decision for large and distal lesions should be tailored, especially taking into consideration other patient- and polyp-risk factors for postprocedural bleeding, such as the use of anti-thrombotic agents or intraprocedural bleeding.”
In contrast, the findings indicated that clipping is unnecessary for lesions less than 20 mm, the investigators wrote.
They went on to explain that clinical application of these findings could result in “significant cost savings” because one bleeding event would be prevented for every 23 large lesions clipped.
“Considering that clips are expensive and their placement might be technically demanding, prophylactic clipping tailored for a subgroup of higher-risk lesions/patients would decrease in parallel both adverse events and costs,” the investigators concluded.
The investigators reported no external funding or conflicts of interest.
ginews@gastro.org
SOURCE: Spadaccini M et al. Gastroenterology. 2020 Apr 1. doi: 10.1053/j.gastro.2020.03.051.
FROM GASTROENTEROLOGY
If you reopen it, will they come?
On April 16, the White House released federal guidelines for reopening American businesses – followed 3 days later by specific recommendations from the Centers for Medicare and Medicaid Services for .

Depending on where you live, you may have already reopened (or even never closed), or you may be awaiting the relaxation of restrictions in your state. (As I write this on June 10, the stay-at-home order in my state, New Jersey, is being rescinded.)
The big question, of course, is whether patients can be convinced that it is safe to leave their homes and come to your office. The answer may depend on how well you time your reopening and adhere to the appropriate federal, state, and independent guidelines.
The federal guidelines have three sections: criteria, which outline conditions each region or state should satisfy before reopening; preparedness, which lists how states should prepare for reopening; and phase guidelines, which detail responsibilities of individuals and employers during distinct reopening phases.
You should pay the most attention to the “criteria” section. The key question to ask: “Has my state or region satisfied the basic criteria for reopening?”
Those criteria are as follows:
- Symptoms reported within a 14-day period should be on a downward trajectory.
- Cases documented (or positive tests as a percentage of total tests) within a 14-day period should also be on a downward trajectory.
- Hospitals should be treating all patients without crisis care. They should also have a robust testing program in place for at-risk health care workers.
If your area meets these criteria, you can proceed to the CMS recommendations. They cover general advice related to personal protective equipment (PPE), workforce availability, facility considerations, sanitation protocols, supplies, and testing capacity.
The key takeaway: As long as your area has the resources to quickly respond to a surge of COVID-19 cases, you can start offering care to non-COVID patients. Keep seeing patients via telehealth as often as possible, and prioritize surgical/procedural care and high-complexity chronic disease management before moving on to preventive and cosmetic services.
The American Medical Association has issued its own checklist of criteria for reopening your practice to supplement the federal guidelines. Highlights include the following:
- Sit down with a calendar and pick an expected reopening day. Ideally, this should include a “soft reopening.” Make a plan to stock necessary PPE and write down plans for cleaning and staffing if an employee or patient is diagnosed with COVID-19 after visiting your office.
- Take a stepwise approach so you can identify challenges early and address them. It’s important to figure out which visits can continue via telehealth, and begin with just a few in-person visits each day. Plan out a schedule and clearly communicate it to patients, clinicians, and staff.
- Patient safety is your top concern. Encourage patients to visit without companions whenever possible, and of course, all individuals who visit the office should wear a cloth face covering.
- Screen employees for fevers and other symptoms of COVID-19; remember that those records are subject to HIPAA rules and must be kept confidential. Minimize contact between employees as much as possible.
- Do your best to screen patients before in-person visits, to verify they don’t have symptoms of COVID-19. Consider creating a script that office staff can use to contact patients 24 hours before they come in. Use this as a chance to ask about symptoms, and explain any reopening logistics they should know about.
- Contact your malpractice insurance carrier to discuss whether you need to make any changes to your coverage.
This would also be a great time to review your confidentiality, privacy, and data security protocols. COVID-19 presents new challenges for data privacy – for example, if you must inform coworkers or patients that they have come into contact with someone who tested positive. Make a plan that follows HIPAA guidelines during COVID-19. Also, make sure you have a plan for handling issues like paid sick leave or reporting COVID-19 cases to your local health department.
Another useful resource is the Medical Group Management Association’s COVID-19 Medical Practice Reopening Checklist. You can use it to confirm that you are addressing all the important items, and that you haven’t missed anything.
As for me, I am advising patients who are reluctant to seek treatment that many medical problems pose more risk than COVID-19, faster treatment means better outcomes, and because we maintain strict disinfection protocols, they are far less likely to be infected with COVID-19 in my office than, say, at a grocery store.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
On April 16, the White House released federal guidelines for reopening American businesses – followed 3 days later by specific recommendations from the Centers for Medicare and Medicaid Services for .
Depending on where you live, you may have already reopened (or even never closed), or you may be awaiting the relaxation of restrictions in your state. (As I write this on June 10, the stay-at-home order in my state, New Jersey, is being rescinded.)
The big question, of course, is whether patients can be convinced that it is safe to leave their homes and come to your office. The answer may depend on how well you time your reopening and adhere to the appropriate federal, state, and independent guidelines.
The federal guidelines have three sections: criteria, which outline conditions each region or state should satisfy before reopening; preparedness, which lists how states should prepare for reopening; and phase guidelines, which detail responsibilities of individuals and employers during distinct reopening phases.
You should pay the most attention to the “criteria” section. The key question to ask: “Has my state or region satisfied the basic criteria for reopening?”
Those criteria are as follows:
- Symptoms reported within a 14-day period should be on a downward trajectory.
- Cases documented (or positive tests as a percentage of total tests) within a 14-day period should also be on a downward trajectory.
- Hospitals should be treating all patients without crisis care. They should also have a robust testing program in place for at-risk health care workers.
If your area meets these criteria, you can proceed to the CMS recommendations. They cover general advice related to personal protective equipment (PPE), workforce availability, facility considerations, sanitation protocols, supplies, and testing capacity.
The key takeaway: As long as your area has the resources to quickly respond to a surge of COVID-19 cases, you can start offering care to non-COVID patients. Keep seeing patients via telehealth as often as possible, and prioritize surgical/procedural care and high-complexity chronic disease management before moving on to preventive and cosmetic services.
The American Medical Association has issued its own checklist of criteria for reopening your practice to supplement the federal guidelines. Highlights include the following:
- Sit down with a calendar and pick an expected reopening day. Ideally, this should include a “soft reopening.” Make a plan to stock necessary PPE and write down plans for cleaning and staffing if an employee or patient is diagnosed with COVID-19 after visiting your office.
- Take a stepwise approach so you can identify challenges early and address them. It’s important to figure out which visits can continue via telehealth, and begin with just a few in-person visits each day. Plan out a schedule and clearly communicate it to patients, clinicians, and staff.
- Patient safety is your top concern. Encourage patients to visit without companions whenever possible, and of course, all individuals who visit the office should wear a cloth face covering.
- Screen employees for fevers and other symptoms of COVID-19; remember that those records are subject to HIPAA rules and must be kept confidential. Minimize contact between employees as much as possible.
- Do your best to screen patients before in-person visits, to verify they don’t have symptoms of COVID-19. Consider creating a script that office staff can use to contact patients 24 hours before they come in. Use this as a chance to ask about symptoms, and explain any reopening logistics they should know about.
- Contact your malpractice insurance carrier to discuss whether you need to make any changes to your coverage.
This would also be a great time to review your confidentiality, privacy, and data security protocols. COVID-19 presents new challenges for data privacy – for example, if you must inform coworkers or patients that they have come into contact with someone who tested positive. Make a plan that follows HIPAA guidelines during COVID-19. Also, make sure you have a plan for handling issues like paid sick leave or reporting COVID-19 cases to your local health department.
Another useful resource is the Medical Group Management Association’s COVID-19 Medical Practice Reopening Checklist. You can use it to confirm that you are addressing all the important items, and that you haven’t missed anything.
As for me, I am advising patients who are reluctant to seek treatment that many medical problems pose more risk than COVID-19, faster treatment means better outcomes, and because we maintain strict disinfection protocols, they are far less likely to be infected with COVID-19 in my office than, say, at a grocery store.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
On April 16, the White House released federal guidelines for reopening American businesses – followed 3 days later by specific recommendations from the Centers for Medicare and Medicaid Services for .
Depending on where you live, you may have already reopened (or even never closed), or you may be awaiting the relaxation of restrictions in your state. (As I write this on June 10, the stay-at-home order in my state, New Jersey, is being rescinded.)
The big question, of course, is whether patients can be convinced that it is safe to leave their homes and come to your office. The answer may depend on how well you time your reopening and adhere to the appropriate federal, state, and independent guidelines.
The federal guidelines have three sections: criteria, which outline conditions each region or state should satisfy before reopening; preparedness, which lists how states should prepare for reopening; and phase guidelines, which detail responsibilities of individuals and employers during distinct reopening phases.
You should pay the most attention to the “criteria” section. The key question to ask: “Has my state or region satisfied the basic criteria for reopening?”
Those criteria are as follows:
- Symptoms reported within a 14-day period should be on a downward trajectory.
- Cases documented (or positive tests as a percentage of total tests) within a 14-day period should also be on a downward trajectory.
- Hospitals should be treating all patients without crisis care. They should also have a robust testing program in place for at-risk health care workers.
If your area meets these criteria, you can proceed to the CMS recommendations. They cover general advice related to personal protective equipment (PPE), workforce availability, facility considerations, sanitation protocols, supplies, and testing capacity.
The key takeaway: As long as your area has the resources to quickly respond to a surge of COVID-19 cases, you can start offering care to non-COVID patients. Keep seeing patients via telehealth as often as possible, and prioritize surgical/procedural care and high-complexity chronic disease management before moving on to preventive and cosmetic services.
The American Medical Association has issued its own checklist of criteria for reopening your practice to supplement the federal guidelines. Highlights include the following:
- Sit down with a calendar and pick an expected reopening day. Ideally, this should include a “soft reopening.” Make a plan to stock necessary PPE and write down plans for cleaning and staffing if an employee or patient is diagnosed with COVID-19 after visiting your office.
- Take a stepwise approach so you can identify challenges early and address them. It’s important to figure out which visits can continue via telehealth, and begin with just a few in-person visits each day. Plan out a schedule and clearly communicate it to patients, clinicians, and staff.
- Patient safety is your top concern. Encourage patients to visit without companions whenever possible, and of course, all individuals who visit the office should wear a cloth face covering.
- Screen employees for fevers and other symptoms of COVID-19; remember that those records are subject to HIPAA rules and must be kept confidential. Minimize contact between employees as much as possible.
- Do your best to screen patients before in-person visits, to verify they don’t have symptoms of COVID-19. Consider creating a script that office staff can use to contact patients 24 hours before they come in. Use this as a chance to ask about symptoms, and explain any reopening logistics they should know about.
- Contact your malpractice insurance carrier to discuss whether you need to make any changes to your coverage.
This would also be a great time to review your confidentiality, privacy, and data security protocols. COVID-19 presents new challenges for data privacy – for example, if you must inform coworkers or patients that they have come into contact with someone who tested positive. Make a plan that follows HIPAA guidelines during COVID-19. Also, make sure you have a plan for handling issues like paid sick leave or reporting COVID-19 cases to your local health department.
Another useful resource is the Medical Group Management Association’s COVID-19 Medical Practice Reopening Checklist. You can use it to confirm that you are addressing all the important items, and that you haven’t missed anything.
As for me, I am advising patients who are reluctant to seek treatment that many medical problems pose more risk than COVID-19, faster treatment means better outcomes, and because we maintain strict disinfection protocols, they are far less likely to be infected with COVID-19 in my office than, say, at a grocery store.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

Long-acting insulin analogue approved for type 1 and type 2 diabetes
the Food and Drug Administration announced June 11.

“Long-acting insulin products like insulin glargine play an important role in the treatment of types 1 and 2 diabetes mellitus,” Patrick Archdeacon, MD, acting associate director for therapeutics in the FDA’s Division of Diabetes, Lipid Disorders, and Obesity, said in a written statement via email.
Semglee will be marketed by Mylan Pharmaceuticals and will be available in a multidose 10-mL vial or a single-patient-use 3-mL prefilled pen.
The approval was based primarily on two randomized, confirmatory clinical trials called INSTRIDE1 and INSTRIDE 2, according to a release by Mylan and Biocon Biologic. They compared Semglee (MYL-1501D) to branded insulin glargine (Lantus) in adults and children for 1 year and found no treatment difference.
The FDA noted that, for patients with type 1 diabetes, Semglee must be used along with a short-acting insulin. The recommended starting dose is approximately one-third of the total daily insulin requirement. For those with type 2 diabetes, the starting dose is 0.2 units/kg or up to 10 units once daily, according to the prescribing information.
Semglee is not recommended for treating diabetic ketoacidosis and is contraindicated during episodes of hypoglycemia.
“Today’s approval provides patients with an additional safe and effective treatment option and also expands the number of products that are available to serve as a reference product for a proposed insulin glargine biosimilar or interchangeable biosimilar product now that the biosimilar pathway is available for insulin products following the statutory transition earlier this year,” Dr. Archdeacon said.
the Food and Drug Administration announced June 11.
“Long-acting insulin products like insulin glargine play an important role in the treatment of types 1 and 2 diabetes mellitus,” Patrick Archdeacon, MD, acting associate director for therapeutics in the FDA’s Division of Diabetes, Lipid Disorders, and Obesity, said in a written statement via email.
Semglee will be marketed by Mylan Pharmaceuticals and will be available in a multidose 10-mL vial or a single-patient-use 3-mL prefilled pen.
The approval was based primarily on two randomized, confirmatory clinical trials called INSTRIDE1 and INSTRIDE 2, according to a release by Mylan and Biocon Biologic. They compared Semglee (MYL-1501D) to branded insulin glargine (Lantus) in adults and children for 1 year and found no treatment difference.
The FDA noted that, for patients with type 1 diabetes, Semglee must be used along with a short-acting insulin. The recommended starting dose is approximately one-third of the total daily insulin requirement. For those with type 2 diabetes, the starting dose is 0.2 units/kg or up to 10 units once daily, according to the prescribing information.
Semglee is not recommended for treating diabetic ketoacidosis and is contraindicated during episodes of hypoglycemia.
“Today’s approval provides patients with an additional safe and effective treatment option and also expands the number of products that are available to serve as a reference product for a proposed insulin glargine biosimilar or interchangeable biosimilar product now that the biosimilar pathway is available for insulin products following the statutory transition earlier this year,” Dr. Archdeacon said.
the Food and Drug Administration announced June 11.
“Long-acting insulin products like insulin glargine play an important role in the treatment of types 1 and 2 diabetes mellitus,” Patrick Archdeacon, MD, acting associate director for therapeutics in the FDA’s Division of Diabetes, Lipid Disorders, and Obesity, said in a written statement via email.
Semglee will be marketed by Mylan Pharmaceuticals and will be available in a multidose 10-mL vial or a single-patient-use 3-mL prefilled pen.
The approval was based primarily on two randomized, confirmatory clinical trials called INSTRIDE1 and INSTRIDE 2, according to a release by Mylan and Biocon Biologic. They compared Semglee (MYL-1501D) to branded insulin glargine (Lantus) in adults and children for 1 year and found no treatment difference.
The FDA noted that, for patients with type 1 diabetes, Semglee must be used along with a short-acting insulin. The recommended starting dose is approximately one-third of the total daily insulin requirement. For those with type 2 diabetes, the starting dose is 0.2 units/kg or up to 10 units once daily, according to the prescribing information.
Semglee is not recommended for treating diabetic ketoacidosis and is contraindicated during episodes of hypoglycemia.
“Today’s approval provides patients with an additional safe and effective treatment option and also expands the number of products that are available to serve as a reference product for a proposed insulin glargine biosimilar or interchangeable biosimilar product now that the biosimilar pathway is available for insulin products following the statutory transition earlier this year,” Dr. Archdeacon said.
Perspectives of a black physician in the time of two pandemics
“Hey there – just checking on you and letting you know I’m thinking of you."
"I know words don't suffice right now. You are in my thoughts."
"If there's any way that I can be of support or if there's something you need, just let me know."
The texts and emails have come in waves. Pinging into my already distracted headspace when, like them, I’m supposed to be focused on a Zoom or WebEx department meeting. These somber reminders underscore what I have known for years but struggled to describe with each new “justice for” hashtag accompanying the name of the latest unarmed black person to die. This is grief.

With every headline in prior years, as black Americans we have usually found solace in our collective fellowship of suffering. Social media timelines become flooded with our own amen choirs and outrage along with words of comfort and inspiration. We remind ourselves of the prior atrocities survived by our people. And like them, we vow to rally; clinging to one other and praying to make it to shore. Though intermittently joined by a smattering of allies, our suffering has mostly been a private, repetitive mourning.
The two pandemics
The year 2020 ushered in a new decade along with the novel SARS-CoV2 (COVID-19) global pandemic. In addition to the thousands of lives that have been lost in the United States alone, COVID-19 brought with it a disruption of life in ways never seen by most generations. Schools and businesses were closed to mitigate spread. Mandatory shelter-in-place orders coupled with physical distancing recommendations limited human interactions and canceled everything from hospital visitations to graduations, intergenerational family gatherings, conferences, and weddings. As the data expanded, it quickly became apparent that minorities, particularly black Americans, shouldered a disproportionate burden of COVID-19. Known health disparities were amplified.
While caring for our patients as black physicians in the time of coronavirus, silently we mourned again. The connection and trust once found through racial concordance was now masked figuratively and literally by personal protective equipment (PPE). We ignored the sting of intimations that the staggering numbers of African Americans hospitalized and dying from COVID-19 could be explained by lack of discipline or, worse, genetic differences by race. Years of disenfranchisement and missed economic opportunities forced large numbers of our patients and loved ones out on the front lines to do essential jobs – but without the celebratory cheers or fanfare enjoyed by others. Frantic phone calls from family and acquaintances interrupted our quiet drives home from emotionally grueling shifts in the hospital – each conversation serving as our personal evidence of COVID-19 and her ruthless ravage of the black community. Add to this trying to serve as cultural bridges between the complexities of medical distrust and patient advocacy along with wrestling with our own vulnerability as potential COVID-19 patients, these have been overwhelming times to say the least.
Then came the acute decompensation of the chronic racism we’d always known in the form of three recent killings of more unarmed African Americans. On March 13, 2020, 26-year-old Breonna Taylor was shot after police forcibly entered her home after midnight on a “no knock” warrant. The story was buried in the news of COVID-19 – but we knew. Later we’d learn that 26-year-old Ahmaud Arbery was shot and killed by armed neighbors while running through a Brunswick, Georgia, neighborhood. His death on Feb. 23, 2020, initially yielded no criminal charges. Then, on May 25, 2020, George Floyd, a 46-year-old father arrested for suspected use of a counterfeit $20 bill, died after a law enforcement official kneeled with his full body weight upon Floyd’s neck for more than 8 minutes. The deaths of Arbery and Floyd were captured by cell phone cameras which, aided by social media, quickly reached the eyes of the entire world.
At first, it seemed plausible that this would be like it always has been. A black mother would stand before a podium filled with multiple microphones crying out in anguish. She would be flanked by community leaders and attorneys demanding justice. Hashtags would be formed. Our people would stand up or kneel down in solidarity – holding fast to our historic resilience. Evanescent allies would appear with signs on lawns and held high over heads. A few weeks would pass by and things would go back to normal. Black people would be left with what always remains: heads bowed and praying at dinner tables petitioning a higher power for protection followed by reaffirmations of what, if anything, could be done to keep our own mamas away from that podium. We’ve learned to treat the grief of racism as endemic to us alone, knowing that it has been a pandemic all along.
Dr. Manning is a professor of medicine and the associate vice chair of diversity, equity, and inclusion at Emory University in Atlanta, where she also is a hospitalist at Grady Memorial Hospital. To read the full version of this article, visit the Journal of Hospital Medicine, where it first appeared (doi: 10.12788/jhm.3481).
“Hey there – just checking on you and letting you know I’m thinking of you."
"I know words don't suffice right now. You are in my thoughts."
"If there's any way that I can be of support or if there's something you need, just let me know."
The texts and emails have come in waves. Pinging into my already distracted headspace when, like them, I’m supposed to be focused on a Zoom or WebEx department meeting. These somber reminders underscore what I have known for years but struggled to describe with each new “justice for” hashtag accompanying the name of the latest unarmed black person to die. This is grief.
With every headline in prior years, as black Americans we have usually found solace in our collective fellowship of suffering. Social media timelines become flooded with our own amen choirs and outrage along with words of comfort and inspiration. We remind ourselves of the prior atrocities survived by our people. And like them, we vow to rally; clinging to one other and praying to make it to shore. Though intermittently joined by a smattering of allies, our suffering has mostly been a private, repetitive mourning.
The two pandemics
The year 2020 ushered in a new decade along with the novel SARS-CoV2 (COVID-19) global pandemic. In addition to the thousands of lives that have been lost in the United States alone, COVID-19 brought with it a disruption of life in ways never seen by most generations. Schools and businesses were closed to mitigate spread. Mandatory shelter-in-place orders coupled with physical distancing recommendations limited human interactions and canceled everything from hospital visitations to graduations, intergenerational family gatherings, conferences, and weddings. As the data expanded, it quickly became apparent that minorities, particularly black Americans, shouldered a disproportionate burden of COVID-19. Known health disparities were amplified.
While caring for our patients as black physicians in the time of coronavirus, silently we mourned again. The connection and trust once found through racial concordance was now masked figuratively and literally by personal protective equipment (PPE). We ignored the sting of intimations that the staggering numbers of African Americans hospitalized and dying from COVID-19 could be explained by lack of discipline or, worse, genetic differences by race. Years of disenfranchisement and missed economic opportunities forced large numbers of our patients and loved ones out on the front lines to do essential jobs – but without the celebratory cheers or fanfare enjoyed by others. Frantic phone calls from family and acquaintances interrupted our quiet drives home from emotionally grueling shifts in the hospital – each conversation serving as our personal evidence of COVID-19 and her ruthless ravage of the black community. Add to this trying to serve as cultural bridges between the complexities of medical distrust and patient advocacy along with wrestling with our own vulnerability as potential COVID-19 patients, these have been overwhelming times to say the least.
Then came the acute decompensation of the chronic racism we’d always known in the form of three recent killings of more unarmed African Americans. On March 13, 2020, 26-year-old Breonna Taylor was shot after police forcibly entered her home after midnight on a “no knock” warrant. The story was buried in the news of COVID-19 – but we knew. Later we’d learn that 26-year-old Ahmaud Arbery was shot and killed by armed neighbors while running through a Brunswick, Georgia, neighborhood. His death on Feb. 23, 2020, initially yielded no criminal charges. Then, on May 25, 2020, George Floyd, a 46-year-old father arrested for suspected use of a counterfeit $20 bill, died after a law enforcement official kneeled with his full body weight upon Floyd’s neck for more than 8 minutes. The deaths of Arbery and Floyd were captured by cell phone cameras which, aided by social media, quickly reached the eyes of the entire world.
At first, it seemed plausible that this would be like it always has been. A black mother would stand before a podium filled with multiple microphones crying out in anguish. She would be flanked by community leaders and attorneys demanding justice. Hashtags would be formed. Our people would stand up or kneel down in solidarity – holding fast to our historic resilience. Evanescent allies would appear with signs on lawns and held high over heads. A few weeks would pass by and things would go back to normal. Black people would be left with what always remains: heads bowed and praying at dinner tables petitioning a higher power for protection followed by reaffirmations of what, if anything, could be done to keep our own mamas away from that podium. We’ve learned to treat the grief of racism as endemic to us alone, knowing that it has been a pandemic all along.
Dr. Manning is a professor of medicine and the associate vice chair of diversity, equity, and inclusion at Emory University in Atlanta, where she also is a hospitalist at Grady Memorial Hospital. To read the full version of this article, visit the Journal of Hospital Medicine, where it first appeared (doi: 10.12788/jhm.3481).
“Hey there – just checking on you and letting you know I’m thinking of you."
"I know words don't suffice right now. You are in my thoughts."
"If there's any way that I can be of support or if there's something you need, just let me know."
The texts and emails have come in waves. Pinging into my already distracted headspace when, like them, I’m supposed to be focused on a Zoom or WebEx department meeting. These somber reminders underscore what I have known for years but struggled to describe with each new “justice for” hashtag accompanying the name of the latest unarmed black person to die. This is grief.
With every headline in prior years, as black Americans we have usually found solace in our collective fellowship of suffering. Social media timelines become flooded with our own amen choirs and outrage along with words of comfort and inspiration. We remind ourselves of the prior atrocities survived by our people. And like them, we vow to rally; clinging to one other and praying to make it to shore. Though intermittently joined by a smattering of allies, our suffering has mostly been a private, repetitive mourning.
The two pandemics
The year 2020 ushered in a new decade along with the novel SARS-CoV2 (COVID-19) global pandemic. In addition to the thousands of lives that have been lost in the United States alone, COVID-19 brought with it a disruption of life in ways never seen by most generations. Schools and businesses were closed to mitigate spread. Mandatory shelter-in-place orders coupled with physical distancing recommendations limited human interactions and canceled everything from hospital visitations to graduations, intergenerational family gatherings, conferences, and weddings. As the data expanded, it quickly became apparent that minorities, particularly black Americans, shouldered a disproportionate burden of COVID-19. Known health disparities were amplified.
While caring for our patients as black physicians in the time of coronavirus, silently we mourned again. The connection and trust once found through racial concordance was now masked figuratively and literally by personal protective equipment (PPE). We ignored the sting of intimations that the staggering numbers of African Americans hospitalized and dying from COVID-19 could be explained by lack of discipline or, worse, genetic differences by race. Years of disenfranchisement and missed economic opportunities forced large numbers of our patients and loved ones out on the front lines to do essential jobs – but without the celebratory cheers or fanfare enjoyed by others. Frantic phone calls from family and acquaintances interrupted our quiet drives home from emotionally grueling shifts in the hospital – each conversation serving as our personal evidence of COVID-19 and her ruthless ravage of the black community. Add to this trying to serve as cultural bridges between the complexities of medical distrust and patient advocacy along with wrestling with our own vulnerability as potential COVID-19 patients, these have been overwhelming times to say the least.
Then came the acute decompensation of the chronic racism we’d always known in the form of three recent killings of more unarmed African Americans. On March 13, 2020, 26-year-old Breonna Taylor was shot after police forcibly entered her home after midnight on a “no knock” warrant. The story was buried in the news of COVID-19 – but we knew. Later we’d learn that 26-year-old Ahmaud Arbery was shot and killed by armed neighbors while running through a Brunswick, Georgia, neighborhood. His death on Feb. 23, 2020, initially yielded no criminal charges. Then, on May 25, 2020, George Floyd, a 46-year-old father arrested for suspected use of a counterfeit $20 bill, died after a law enforcement official kneeled with his full body weight upon Floyd’s neck for more than 8 minutes. The deaths of Arbery and Floyd were captured by cell phone cameras which, aided by social media, quickly reached the eyes of the entire world.
At first, it seemed plausible that this would be like it always has been. A black mother would stand before a podium filled with multiple microphones crying out in anguish. She would be flanked by community leaders and attorneys demanding justice. Hashtags would be formed. Our people would stand up or kneel down in solidarity – holding fast to our historic resilience. Evanescent allies would appear with signs on lawns and held high over heads. A few weeks would pass by and things would go back to normal. Black people would be left with what always remains: heads bowed and praying at dinner tables petitioning a higher power for protection followed by reaffirmations of what, if anything, could be done to keep our own mamas away from that podium. We’ve learned to treat the grief of racism as endemic to us alone, knowing that it has been a pandemic all along.
Dr. Manning is a professor of medicine and the associate vice chair of diversity, equity, and inclusion at Emory University in Atlanta, where she also is a hospitalist at Grady Memorial Hospital. To read the full version of this article, visit the Journal of Hospital Medicine, where it first appeared (doi: 10.12788/jhm.3481).
Subcutaneous hep A vaccination as effective as intramuscular for bleeding disorder patients
Subcutaneous hepatitis A vaccination is as effective and may be safer for patients with bleeding disorders, according to a study by Mayumi Nakasone, MD, and colleagues.

The large number of donor exposures in bleeding disorder patients who require routine use of clotting factor concentrates remains a concern with regard to the risk of virus infection. Therefore, vaccinations for viruses such as hepatitis A are recommended. Although the intramuscular (IM) route is recommended for hepatitis A vaccination, patients with bleeding disorders have been advised to avoid IM injections because of the risk of bleeding and bruising of muscles, requiring infusion of clotting factor concentrates or other blood products for its treatment, according to Dr. Nakasone of the University of São Paulo and colleagues. They assessed 78 adult and pediatric patients with blood disorders randomized to vaccination for hepatitis A either subcutaneously (SC) or IM, according their study published on Vaccine.
The study was conducted at a single hemophilia center between May 2006 and February 2017.
Among the 78 patients, 58 (74.4%) presented hemophilia A (34 of the SC group and 24 of the IM group), 13 (16.7%) hemophilia B (4 of the SC group and 9 of the IM group) and 7 (8.9%) other bleeding disorders. There were no statistically significant differences between the SC and the IM groups in patients diagnosis or sex.
A total of 38 patients had serology performed after the first vaccine dose, determining seroconversion rates of 83.3% and 90.0% for the SC and the IM group, respectively, a nonsignificant difference. After the second vaccine dose, the seroconversion rate for the SC group was 97.5% and for the IM group was 97.4%, also a nonsignificant difference.
At a median of 9 years after a second vaccine dose, antibody titers for the SC group were slightly greater than the IM group (7.6 vs. 7.4), but this was also not a significant difference. There were no serious adverse events in both groups, according to Dr. Nakasone and colleagues. And although twice as many patients of the IM group required clotting factor concentrates for adverse events, compared with the SC group (15.8% vs. 7.5%), the difference was not significant.
“Hepatitis A vaccine administered subcutaneously is as immunogenic, long-term protective, and even safer as the intramuscular route for both children and adults not only with hemophilia, but also with other bleeding disorders,” the researchers concluded.
The authors declared that they had no disclosures.
SOURCE: Nakasone M et al. Vaccine 2020;38:4162-6.
Subcutaneous hepatitis A vaccination is as effective and may be safer for patients with bleeding disorders, according to a study by Mayumi Nakasone, MD, and colleagues.
The large number of donor exposures in bleeding disorder patients who require routine use of clotting factor concentrates remains a concern with regard to the risk of virus infection. Therefore, vaccinations for viruses such as hepatitis A are recommended. Although the intramuscular (IM) route is recommended for hepatitis A vaccination, patients with bleeding disorders have been advised to avoid IM injections because of the risk of bleeding and bruising of muscles, requiring infusion of clotting factor concentrates or other blood products for its treatment, according to Dr. Nakasone of the University of São Paulo and colleagues. They assessed 78 adult and pediatric patients with blood disorders randomized to vaccination for hepatitis A either subcutaneously (SC) or IM, according their study published on Vaccine.
The study was conducted at a single hemophilia center between May 2006 and February 2017.
Among the 78 patients, 58 (74.4%) presented hemophilia A (34 of the SC group and 24 of the IM group), 13 (16.7%) hemophilia B (4 of the SC group and 9 of the IM group) and 7 (8.9%) other bleeding disorders. There were no statistically significant differences between the SC and the IM groups in patients diagnosis or sex.
A total of 38 patients had serology performed after the first vaccine dose, determining seroconversion rates of 83.3% and 90.0% for the SC and the IM group, respectively, a nonsignificant difference. After the second vaccine dose, the seroconversion rate for the SC group was 97.5% and for the IM group was 97.4%, also a nonsignificant difference.
At a median of 9 years after a second vaccine dose, antibody titers for the SC group were slightly greater than the IM group (7.6 vs. 7.4), but this was also not a significant difference. There were no serious adverse events in both groups, according to Dr. Nakasone and colleagues. And although twice as many patients of the IM group required clotting factor concentrates for adverse events, compared with the SC group (15.8% vs. 7.5%), the difference was not significant.
“Hepatitis A vaccine administered subcutaneously is as immunogenic, long-term protective, and even safer as the intramuscular route for both children and adults not only with hemophilia, but also with other bleeding disorders,” the researchers concluded.
The authors declared that they had no disclosures.
SOURCE: Nakasone M et al. Vaccine 2020;38:4162-6.
Subcutaneous hepatitis A vaccination is as effective and may be safer for patients with bleeding disorders, according to a study by Mayumi Nakasone, MD, and colleagues.
The large number of donor exposures in bleeding disorder patients who require routine use of clotting factor concentrates remains a concern with regard to the risk of virus infection. Therefore, vaccinations for viruses such as hepatitis A are recommended. Although the intramuscular (IM) route is recommended for hepatitis A vaccination, patients with bleeding disorders have been advised to avoid IM injections because of the risk of bleeding and bruising of muscles, requiring infusion of clotting factor concentrates or other blood products for its treatment, according to Dr. Nakasone of the University of São Paulo and colleagues. They assessed 78 adult and pediatric patients with blood disorders randomized to vaccination for hepatitis A either subcutaneously (SC) or IM, according their study published on Vaccine.
The study was conducted at a single hemophilia center between May 2006 and February 2017.
Among the 78 patients, 58 (74.4%) presented hemophilia A (34 of the SC group and 24 of the IM group), 13 (16.7%) hemophilia B (4 of the SC group and 9 of the IM group) and 7 (8.9%) other bleeding disorders. There were no statistically significant differences between the SC and the IM groups in patients diagnosis or sex.
A total of 38 patients had serology performed after the first vaccine dose, determining seroconversion rates of 83.3% and 90.0% for the SC and the IM group, respectively, a nonsignificant difference. After the second vaccine dose, the seroconversion rate for the SC group was 97.5% and for the IM group was 97.4%, also a nonsignificant difference.
At a median of 9 years after a second vaccine dose, antibody titers for the SC group were slightly greater than the IM group (7.6 vs. 7.4), but this was also not a significant difference. There were no serious adverse events in both groups, according to Dr. Nakasone and colleagues. And although twice as many patients of the IM group required clotting factor concentrates for adverse events, compared with the SC group (15.8% vs. 7.5%), the difference was not significant.
“Hepatitis A vaccine administered subcutaneously is as immunogenic, long-term protective, and even safer as the intramuscular route for both children and adults not only with hemophilia, but also with other bleeding disorders,” the researchers concluded.
The authors declared that they had no disclosures.
SOURCE: Nakasone M et al. Vaccine 2020;38:4162-6.
FROM VACCINE
Key clinical point: Subcutaneous hepatitis A vaccination is as immunogenic, but appeared safer than intramuscular injections for bleeding disorder patients.
Major finding: A total of 38 patients assessed after first vaccine dose showed seroconversion rates of 83.3% and 90.0% for the subcutaneous versus the intramuscular group, respectively.
Study details: A comparison of hepatitis A vaccination administered subcutaneously or intramuscularly in 78 children and adults with hemophilia and other bleeding disorders.
Disclosures: The authors declared that they had no disclosures.
Source: Nakasone M et al. Vaccine. 2020;38:4162-6.
Racism joins COVID-19 at the primary care table
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, two-thirds of the survey’s 586 respondents said that George Floyd’s death and related events had been the subject of practice conversations and 12% “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement.
One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being, and that connection was expressed even more strongly in a related survey of 1,111 patients that was conducted June 8.
In that survey, about 65% of patients said that racism affected emotional, psychological, and behavioral health, and 40% noted that George Floyd’s death had a negative impact on the well-being of friends, the Larry A. Green Center said in partnership with the Primary Care Collaborative and 3rd Conversation.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers.
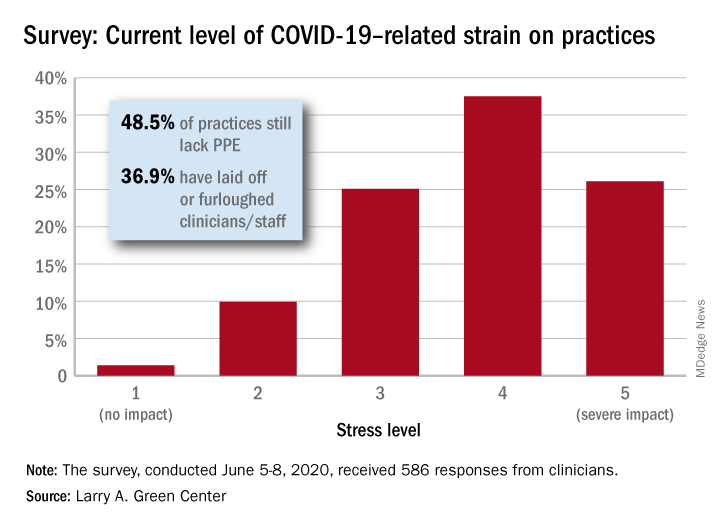
COVID-19, in the meantime, is still doing its thing. Almost two-thirds (63%) of respondents to the clinician survey said that stress levels at their practices had reached all-time-high levels in the last 4 weeks.
Just 1.4% of the primary care clinicians said that the pandemic had put no strain on their practices (see graph), and just 10% rated that strain as a 2 on a scale of 1-5, the center said. Among the stressors:
About 49% continue to lack PPE.
About 40% still have no or limited ability for testing.
About 37% of practice settings still report layoffs and furloughs.
About 31% report that clinician salaries are still being skipped or deferred.
“Both public and private policy makers must take immediate steps to stabilize primary care,” said Ann Greiner, president and CEO of the Primary Care Collaborative. “This financial support is necessary but not sufficient. Instead, we need wholesale reform of payment in order to achieve the kind of high-performing primary care that truly meets patient needs.”
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, two-thirds of the survey’s 586 respondents said that George Floyd’s death and related events had been the subject of practice conversations and 12% “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement.
One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being, and that connection was expressed even more strongly in a related survey of 1,111 patients that was conducted June 8.
In that survey, about 65% of patients said that racism affected emotional, psychological, and behavioral health, and 40% noted that George Floyd’s death had a negative impact on the well-being of friends, the Larry A. Green Center said in partnership with the Primary Care Collaborative and 3rd Conversation.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers.
COVID-19, in the meantime, is still doing its thing. Almost two-thirds (63%) of respondents to the clinician survey said that stress levels at their practices had reached all-time-high levels in the last 4 weeks.
Just 1.4% of the primary care clinicians said that the pandemic had put no strain on their practices (see graph), and just 10% rated that strain as a 2 on a scale of 1-5, the center said. Among the stressors:
About 49% continue to lack PPE.
About 40% still have no or limited ability for testing.
About 37% of practice settings still report layoffs and furloughs.
About 31% report that clinician salaries are still being skipped or deferred.
“Both public and private policy makers must take immediate steps to stabilize primary care,” said Ann Greiner, president and CEO of the Primary Care Collaborative. “This financial support is necessary but not sufficient. Instead, we need wholesale reform of payment in order to achieve the kind of high-performing primary care that truly meets patient needs.”
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, two-thirds of the survey’s 586 respondents said that George Floyd’s death and related events had been the subject of practice conversations and 12% “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement.
One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being, and that connection was expressed even more strongly in a related survey of 1,111 patients that was conducted June 8.
In that survey, about 65% of patients said that racism affected emotional, psychological, and behavioral health, and 40% noted that George Floyd’s death had a negative impact on the well-being of friends, the Larry A. Green Center said in partnership with the Primary Care Collaborative and 3rd Conversation.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers.
COVID-19, in the meantime, is still doing its thing. Almost two-thirds (63%) of respondents to the clinician survey said that stress levels at their practices had reached all-time-high levels in the last 4 weeks.
Just 1.4% of the primary care clinicians said that the pandemic had put no strain on their practices (see graph), and just 10% rated that strain as a 2 on a scale of 1-5, the center said. Among the stressors:
About 49% continue to lack PPE.
About 40% still have no or limited ability for testing.
About 37% of practice settings still report layoffs and furloughs.
About 31% report that clinician salaries are still being skipped or deferred.
“Both public and private policy makers must take immediate steps to stabilize primary care,” said Ann Greiner, president and CEO of the Primary Care Collaborative. “This financial support is necessary but not sufficient. Instead, we need wholesale reform of payment in order to achieve the kind of high-performing primary care that truly meets patient needs.”
New long-term data for antipsychotic in pediatric bipolar depression
The antipsychotic lurasidone (Latuda, Sunovion Pharmaceuticals) has long-term efficacy in the treatment of bipolar depression (BD) in children and adolescents, new research suggests.
In an open-label extension study involving patients aged 10-17 years, up to 2 years of treatment with lurasidone was associated with continued improvement in depressive symptoms. There were progressively higher rates of remission, recovery, and sustained remission.
Coinvestigator Manpreet K. Singh, MD, director of the Stanford Pediatric Mood Disorders Program, Stanford (Calif.) University, noted that early onset of BD is common. Although in pediatric populations, prevalence has been fairly stable at around 1.8%, these patients have “a very limited number of treatment options available for the depressed phases of BD,” which is often predominant and can be difficult to identify.
“A lot of youths who are experiencing depressive symptoms in the context of having had a manic episode will often have a relapsing and remitting course, even after the acute phase of treatment, so because kids can be on medications for long periods of time, a better understanding of what works ... is very important,” Dr. Singh said in an interview.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) 2020 annual meeting.
Long-term Efficacy
The Food and Drug Administration approved lurasidone as monotherapy for BD in children and adolescents in 2018. The aim of the current study was to evaluate the drug’s long-term efficacy in achieving response or remission in this population.
A total of 305 children who completed an initial 6-week double-blind study of lurasidone versus placebo entered the 2-year, open-label extension study. In the extension, they either continued taking lurasidone or were switched from placebo to lurasidone 20-80 mg/day. Of this group, 195 children completed 52 weeks of treatment, and 93 completed 104 weeks of treatment.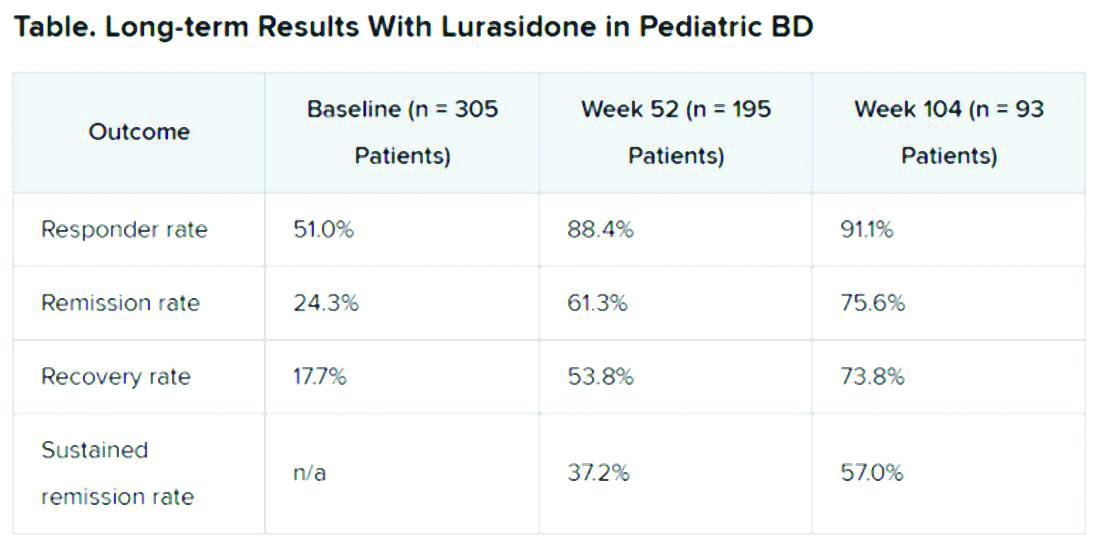
Efficacy was measured with the Children’s Depression Rating Scale, Revised (CDRS-R) and the Clinical Global Impression, Bipolar Depression Severity scale (CGI-BP-S). Functioning was evaluated with the clinician-rated Children’s Global Assessment Scale (CGAS); on that scale, a score of 70 or higher indicates no clinically meaningful functional impairment.
Remission criteria were met if a patient achieved a CDRS-R total score of 28 or less, a Young Mania Rating Scale (YMRS) total score of 8 or less, and a CGI-BP-S depression score of 3 or less.
Recovery criteria were met if a patient achieved remission and had a CGAS score of at least 70.
Sustained remission, a more stringent outcome, required that the patient meet remission criteria for at least 24 consecutive weeks.
In addition, there was a strong inverse correlation (r = –0.71) between depression severity, as measured by CDRS-R total score, and functioning, as measured by the CGAS.
“That’s the cool thing: As the depression symptoms and severity came down, the overall functioning in these kids improved,” Dr. Singh noted.
“This improvement in functioning ends up being much more clinically relevant and useful to clinicians than just showing an improvement in a set of symptoms because what brings a kid – or even an adult, for that matter – to see a clinician to get treatment is because something about their symptoms is causing significant functional impairment,” she said.
“So this is the take-home message: You can see that lurasidone ... demonstrates not just recovery from depressive symptoms but that this reduction in depressive symptoms corresponds to an improvement in functioning for these youths,” she added.
Potential Limitations
Commenting on the study, Christoph U. Correll, MD, professor of child and adolescent psychiatry, Charite Universitatsmedizin, Berlin, Germany, noted that BD is difficult to treat, especially for patients who are going through “a developmentally vulnerable phase of their lives.”
“Lurasidone is the only monotherapy approved for bipolar depression in youth and is fairly well tolerated,” said Dr. Correll, who was not part of the research. He added that the long-term effectiveness data on response and remission “add relevant information” to the field.
However, he noted that it is not clear whether the high and increasing rates of response and remission were based on the reporting of observed cases or on last-observation-carried-forward analyses. “Given the naturally high dropout rate in such a long-term study and the potential for a survival bias, this is a relevant methodological question that affects the interpretation of the data,” he said.
“Nevertheless, the very favorable results for cumulative response, remission, and sustained remission add to the evidence that lurasidone is an effective treatment for youth with bipolar depression. Since efficacy cannot be interpreted in isolation, data describing the tolerability, including long-term cardiometabolic effects, will be important complementary data to consider,” Dr. Correll said.
The study was funded by Sunovion Pharmaceuticals. Dr. Singh is on the advisory board for Sunovion, is a consultant for Google X and Limbix, and receives royalties from American Psychiatric Association Publishing. She has also received research support from Stanford’s Maternal Child Health Research Institute and Department of Psychiatry, the National Institute of Mental Health, the National Institute on Aging, Johnson and Johnson, Allergan, PCORI, and the Brain and Behavior Research Foundation. Dr. Correll has been a consultant or adviser to and has received honoraria from Sunovion, as well as Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, Gerson Lehrman Group, Intra-Cellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Sumitomo Dainippon, Supernus, Takeda, and Teva.
A version of this article originally appeared on Medscape.com.
The antipsychotic lurasidone (Latuda, Sunovion Pharmaceuticals) has long-term efficacy in the treatment of bipolar depression (BD) in children and adolescents, new research suggests.
In an open-label extension study involving patients aged 10-17 years, up to 2 years of treatment with lurasidone was associated with continued improvement in depressive symptoms. There were progressively higher rates of remission, recovery, and sustained remission.
Coinvestigator Manpreet K. Singh, MD, director of the Stanford Pediatric Mood Disorders Program, Stanford (Calif.) University, noted that early onset of BD is common. Although in pediatric populations, prevalence has been fairly stable at around 1.8%, these patients have “a very limited number of treatment options available for the depressed phases of BD,” which is often predominant and can be difficult to identify.
“A lot of youths who are experiencing depressive symptoms in the context of having had a manic episode will often have a relapsing and remitting course, even after the acute phase of treatment, so because kids can be on medications for long periods of time, a better understanding of what works ... is very important,” Dr. Singh said in an interview.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) 2020 annual meeting.
Long-term Efficacy
The Food and Drug Administration approved lurasidone as monotherapy for BD in children and adolescents in 2018. The aim of the current study was to evaluate the drug’s long-term efficacy in achieving response or remission in this population.
A total of 305 children who completed an initial 6-week double-blind study of lurasidone versus placebo entered the 2-year, open-label extension study. In the extension, they either continued taking lurasidone or were switched from placebo to lurasidone 20-80 mg/day. Of this group, 195 children completed 52 weeks of treatment, and 93 completed 104 weeks of treatment.
Efficacy was measured with the Children’s Depression Rating Scale, Revised (CDRS-R) and the Clinical Global Impression, Bipolar Depression Severity scale (CGI-BP-S). Functioning was evaluated with the clinician-rated Children’s Global Assessment Scale (CGAS); on that scale, a score of 70 or higher indicates no clinically meaningful functional impairment.
Remission criteria were met if a patient achieved a CDRS-R total score of 28 or less, a Young Mania Rating Scale (YMRS) total score of 8 or less, and a CGI-BP-S depression score of 3 or less.
Recovery criteria were met if a patient achieved remission and had a CGAS score of at least 70.
Sustained remission, a more stringent outcome, required that the patient meet remission criteria for at least 24 consecutive weeks.
In addition, there was a strong inverse correlation (r = –0.71) between depression severity, as measured by CDRS-R total score, and functioning, as measured by the CGAS.
“That’s the cool thing: As the depression symptoms and severity came down, the overall functioning in these kids improved,” Dr. Singh noted.
“This improvement in functioning ends up being much more clinically relevant and useful to clinicians than just showing an improvement in a set of symptoms because what brings a kid – or even an adult, for that matter – to see a clinician to get treatment is because something about their symptoms is causing significant functional impairment,” she said.
“So this is the take-home message: You can see that lurasidone ... demonstrates not just recovery from depressive symptoms but that this reduction in depressive symptoms corresponds to an improvement in functioning for these youths,” she added.
Potential Limitations
Commenting on the study, Christoph U. Correll, MD, professor of child and adolescent psychiatry, Charite Universitatsmedizin, Berlin, Germany, noted that BD is difficult to treat, especially for patients who are going through “a developmentally vulnerable phase of their lives.”
“Lurasidone is the only monotherapy approved for bipolar depression in youth and is fairly well tolerated,” said Dr. Correll, who was not part of the research. He added that the long-term effectiveness data on response and remission “add relevant information” to the field.
However, he noted that it is not clear whether the high and increasing rates of response and remission were based on the reporting of observed cases or on last-observation-carried-forward analyses. “Given the naturally high dropout rate in such a long-term study and the potential for a survival bias, this is a relevant methodological question that affects the interpretation of the data,” he said.
“Nevertheless, the very favorable results for cumulative response, remission, and sustained remission add to the evidence that lurasidone is an effective treatment for youth with bipolar depression. Since efficacy cannot be interpreted in isolation, data describing the tolerability, including long-term cardiometabolic effects, will be important complementary data to consider,” Dr. Correll said.
The study was funded by Sunovion Pharmaceuticals. Dr. Singh is on the advisory board for Sunovion, is a consultant for Google X and Limbix, and receives royalties from American Psychiatric Association Publishing. She has also received research support from Stanford’s Maternal Child Health Research Institute and Department of Psychiatry, the National Institute of Mental Health, the National Institute on Aging, Johnson and Johnson, Allergan, PCORI, and the Brain and Behavior Research Foundation. Dr. Correll has been a consultant or adviser to and has received honoraria from Sunovion, as well as Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, Gerson Lehrman Group, Intra-Cellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Sumitomo Dainippon, Supernus, Takeda, and Teva.
A version of this article originally appeared on Medscape.com.
The antipsychotic lurasidone (Latuda, Sunovion Pharmaceuticals) has long-term efficacy in the treatment of bipolar depression (BD) in children and adolescents, new research suggests.
In an open-label extension study involving patients aged 10-17 years, up to 2 years of treatment with lurasidone was associated with continued improvement in depressive symptoms. There were progressively higher rates of remission, recovery, and sustained remission.
Coinvestigator Manpreet K. Singh, MD, director of the Stanford Pediatric Mood Disorders Program, Stanford (Calif.) University, noted that early onset of BD is common. Although in pediatric populations, prevalence has been fairly stable at around 1.8%, these patients have “a very limited number of treatment options available for the depressed phases of BD,” which is often predominant and can be difficult to identify.
“A lot of youths who are experiencing depressive symptoms in the context of having had a manic episode will often have a relapsing and remitting course, even after the acute phase of treatment, so because kids can be on medications for long periods of time, a better understanding of what works ... is very important,” Dr. Singh said in an interview.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) 2020 annual meeting.
Long-term Efficacy
The Food and Drug Administration approved lurasidone as monotherapy for BD in children and adolescents in 2018. The aim of the current study was to evaluate the drug’s long-term efficacy in achieving response or remission in this population.
A total of 305 children who completed an initial 6-week double-blind study of lurasidone versus placebo entered the 2-year, open-label extension study. In the extension, they either continued taking lurasidone or were switched from placebo to lurasidone 20-80 mg/day. Of this group, 195 children completed 52 weeks of treatment, and 93 completed 104 weeks of treatment.
Efficacy was measured with the Children’s Depression Rating Scale, Revised (CDRS-R) and the Clinical Global Impression, Bipolar Depression Severity scale (CGI-BP-S). Functioning was evaluated with the clinician-rated Children’s Global Assessment Scale (CGAS); on that scale, a score of 70 or higher indicates no clinically meaningful functional impairment.
Remission criteria were met if a patient achieved a CDRS-R total score of 28 or less, a Young Mania Rating Scale (YMRS) total score of 8 or less, and a CGI-BP-S depression score of 3 or less.
Recovery criteria were met if a patient achieved remission and had a CGAS score of at least 70.
Sustained remission, a more stringent outcome, required that the patient meet remission criteria for at least 24 consecutive weeks.
In addition, there was a strong inverse correlation (r = –0.71) between depression severity, as measured by CDRS-R total score, and functioning, as measured by the CGAS.
“That’s the cool thing: As the depression symptoms and severity came down, the overall functioning in these kids improved,” Dr. Singh noted.
“This improvement in functioning ends up being much more clinically relevant and useful to clinicians than just showing an improvement in a set of symptoms because what brings a kid – or even an adult, for that matter – to see a clinician to get treatment is because something about their symptoms is causing significant functional impairment,” she said.
“So this is the take-home message: You can see that lurasidone ... demonstrates not just recovery from depressive symptoms but that this reduction in depressive symptoms corresponds to an improvement in functioning for these youths,” she added.
Potential Limitations
Commenting on the study, Christoph U. Correll, MD, professor of child and adolescent psychiatry, Charite Universitatsmedizin, Berlin, Germany, noted that BD is difficult to treat, especially for patients who are going through “a developmentally vulnerable phase of their lives.”
“Lurasidone is the only monotherapy approved for bipolar depression in youth and is fairly well tolerated,” said Dr. Correll, who was not part of the research. He added that the long-term effectiveness data on response and remission “add relevant information” to the field.
However, he noted that it is not clear whether the high and increasing rates of response and remission were based on the reporting of observed cases or on last-observation-carried-forward analyses. “Given the naturally high dropout rate in such a long-term study and the potential for a survival bias, this is a relevant methodological question that affects the interpretation of the data,” he said.
“Nevertheless, the very favorable results for cumulative response, remission, and sustained remission add to the evidence that lurasidone is an effective treatment for youth with bipolar depression. Since efficacy cannot be interpreted in isolation, data describing the tolerability, including long-term cardiometabolic effects, will be important complementary data to consider,” Dr. Correll said.
The study was funded by Sunovion Pharmaceuticals. Dr. Singh is on the advisory board for Sunovion, is a consultant for Google X and Limbix, and receives royalties from American Psychiatric Association Publishing. She has also received research support from Stanford’s Maternal Child Health Research Institute and Department of Psychiatry, the National Institute of Mental Health, the National Institute on Aging, Johnson and Johnson, Allergan, PCORI, and the Brain and Behavior Research Foundation. Dr. Correll has been a consultant or adviser to and has received honoraria from Sunovion, as well as Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, Gerson Lehrman Group, Intra-Cellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Sumitomo Dainippon, Supernus, Takeda, and Teva.
A version of this article originally appeared on Medscape.com.
FROM ASCP 2020
Surge in colonoscopies postponed by COVID-19 expected
An expected surge in the number of people seeking colonoscopy after the peak of the COVID-19 pandemic passes could cause physicians to rethink patient prioritization, could create a strain on endoscopy capacity, and might raise the specter of detecting colorectal cancer in more patients at a later stage of disease.

Furthermore, months of delay in diagnosis of colorectal cancer (CRC) could shorten survival, although more data is needed, according to expert analysis from a gastroenterologist, a medical oncologist, and a colorectal surgeon.
“It has been a big decrease in the number of colonoscopies performed at our hospital in Alicante, Spain,” Rodrigo Jover Martinez, MD, PhD, said during a COVID-19 and Digestive Health webinar presented by United European Gastroenterology (UEG). He estimated colonoscopy procedures are down 60%-90%, and the number of CRC surgeries has dropped by 60%. “As you know, the COVID-19 pandemic is hitting Europe hard.”
When patients do return, “the backlog will be huge ... in already exhausted endoscopy units,” predicted Dr. Martinez, a gastroenterologist at Hospital General Universitario in Alicante.
Multiple risks
Not knowing which patients with CRC will develop severe COVID-19 infection is another challenge, Bartomeu Massuti, MD, of the medical oncology service at the Hospital General Universitario de Alicante, said during the webinar.
Caution is warranted because “we know cancer patients have an increased risk of infection.” However, he added, most evidence supports an elevated risk for bacterial infections, not viral infections.
Therefore, physicians must continue to balance the risks associated with potential COVID-19 exposure against the risks associated with postponed treatment, Dr. Massuti said. “The goal of oncology care is to try to maintain the preplanned treatment and follow-up. We need mainly to avoid stopping or delaying treatment ... because we will lose efficacy in oncology disease outcomes.”
Imran Aslam, MD, PhD, a colorectal surgeon who moderated and presented during the webinar, agreed: “By delaying the treatment, we might do harm to our patients.”
Dr. Aslam cited data about clinical costs of delaying CRC surgery. A 2019 population-based study in PLOS ONE evaluated different times from diagnosis to treatment. The researchers found a delay of more than 150 days “significantly reduced survival, even during stage I, II, and III disease,” he said. The stage I hazard ratio was 2.66, compared with a reference HR of 1.00 for 90 days or fewer. They also reported elevated risk for people with stage II CRC (HR, 2.80), stage III CRC (HR, 2.70), and stage IV CRC (HR, 1.36).
“This could become more and more abysmal if the pandemic continues,” added Dr. Aslam, consultant colorectal surgeon at University Hospitals of Coventry and Warwickshire, England.
Prioritizing patients
Restarting endoscopy with prioritization strategies and increasing patient capacity are possible solutions. Dr. Martinez suggested a four-quadrant matrix in which physicians place patients into “now,” “next,” “delayed,” or “never” categories based on clinical indicators. The priority 1 “now” patients, for example, will be those with suspected CRC based on physical examination, imaging results, and/or an abnormal fecal immunochemical test result.
He suggested, furthermore, that more widespread CRC screening can resume once “endoscopy units have been alleviated of priority 1, symptomatic patients.”
Dr. Massuti concurred with Dr. Martinez’s call to prioritize patients carefully. He suggested a green, yellow, and red classification system based on treatment priority recommendations from the European Society for Medical Oncology. The green group, for example, should receive priority for intervention based on a condition that is immediately clinically unstable or life threatening.
“The main goal is to preserve the continuum of care,” he added.
Another concern – although data are limited – is that treatment might also increase risk of mortality among cancer patients with COVID-19, according to a cohort study of nearly 1,000 such patients reported May 2020 in The Lancet. Dr. Massuti, who was not affiliated with the research, noted that 12% of the patients had GI tumors. In addition to increased risk associated with male sex (odds ratio, 1.63), cytotoxic cancer treatment in the prior 4 weeks increased risk (OR, 1.47), as did surgery in the same time frame (OR, 1.52).
“This means patients on treatment have an increased risk of mortality,” Dr. Massuti said.
Moving forward
Implementing telehealth information and communication technologies will continue to grow in importance, Dr. Massuti said. Dr. Aslam noted that video consultation with patients before surgery is already replacing face-to-face interaction, and most follow-up care at his hospital is now done by telephone.
Postoperative care is just as essential in the COVID-19 era, if not more so. “We need to be very vigilant to manage postoperative complications – any symptoms of pyrexia or sepsis, or any sign of COVID,” Dr. Aslam said, including postoperative fever. “If there is any doubt, do a chest CT scan.”
Dr. Aslam predicted the time to perform endoscopy or surgery for each patient will be longer, “so the number of patients done in 1 day will be less than 4 months ago.” In addition, elective surgery patients at his institution undergo COVID-19 testing twice, 3 days apart, prior to intervention.
“This disease will continue in the community for a while, so we have to continue what we’ve done well, like social distancing,” Dr. Aslam said. “We’ve gone through a storm and we are awaiting a tsunami. That tsunami of patients will overwhelm us in the coming months.”
Dr. Martinez, Dr. Massuti, and Dr. Aslam had no relevant disclosures.
An expected surge in the number of people seeking colonoscopy after the peak of the COVID-19 pandemic passes could cause physicians to rethink patient prioritization, could create a strain on endoscopy capacity, and might raise the specter of detecting colorectal cancer in more patients at a later stage of disease.
Furthermore, months of delay in diagnosis of colorectal cancer (CRC) could shorten survival, although more data is needed, according to expert analysis from a gastroenterologist, a medical oncologist, and a colorectal surgeon.
“It has been a big decrease in the number of colonoscopies performed at our hospital in Alicante, Spain,” Rodrigo Jover Martinez, MD, PhD, said during a COVID-19 and Digestive Health webinar presented by United European Gastroenterology (UEG). He estimated colonoscopy procedures are down 60%-90%, and the number of CRC surgeries has dropped by 60%. “As you know, the COVID-19 pandemic is hitting Europe hard.”
When patients do return, “the backlog will be huge ... in already exhausted endoscopy units,” predicted Dr. Martinez, a gastroenterologist at Hospital General Universitario in Alicante.
Multiple risks
Not knowing which patients with CRC will develop severe COVID-19 infection is another challenge, Bartomeu Massuti, MD, of the medical oncology service at the Hospital General Universitario de Alicante, said during the webinar.
Caution is warranted because “we know cancer patients have an increased risk of infection.” However, he added, most evidence supports an elevated risk for bacterial infections, not viral infections.
Therefore, physicians must continue to balance the risks associated with potential COVID-19 exposure against the risks associated with postponed treatment, Dr. Massuti said. “The goal of oncology care is to try to maintain the preplanned treatment and follow-up. We need mainly to avoid stopping or delaying treatment ... because we will lose efficacy in oncology disease outcomes.”
Imran Aslam, MD, PhD, a colorectal surgeon who moderated and presented during the webinar, agreed: “By delaying the treatment, we might do harm to our patients.”
Dr. Aslam cited data about clinical costs of delaying CRC surgery. A 2019 population-based study in PLOS ONE evaluated different times from diagnosis to treatment. The researchers found a delay of more than 150 days “significantly reduced survival, even during stage I, II, and III disease,” he said. The stage I hazard ratio was 2.66, compared with a reference HR of 1.00 for 90 days or fewer. They also reported elevated risk for people with stage II CRC (HR, 2.80), stage III CRC (HR, 2.70), and stage IV CRC (HR, 1.36).
“This could become more and more abysmal if the pandemic continues,” added Dr. Aslam, consultant colorectal surgeon at University Hospitals of Coventry and Warwickshire, England.
Prioritizing patients
Restarting endoscopy with prioritization strategies and increasing patient capacity are possible solutions. Dr. Martinez suggested a four-quadrant matrix in which physicians place patients into “now,” “next,” “delayed,” or “never” categories based on clinical indicators. The priority 1 “now” patients, for example, will be those with suspected CRC based on physical examination, imaging results, and/or an abnormal fecal immunochemical test result.
He suggested, furthermore, that more widespread CRC screening can resume once “endoscopy units have been alleviated of priority 1, symptomatic patients.”
Dr. Massuti concurred with Dr. Martinez’s call to prioritize patients carefully. He suggested a green, yellow, and red classification system based on treatment priority recommendations from the European Society for Medical Oncology. The green group, for example, should receive priority for intervention based on a condition that is immediately clinically unstable or life threatening.
“The main goal is to preserve the continuum of care,” he added.
Another concern – although data are limited – is that treatment might also increase risk of mortality among cancer patients with COVID-19, according to a cohort study of nearly 1,000 such patients reported May 2020 in The Lancet. Dr. Massuti, who was not affiliated with the research, noted that 12% of the patients had GI tumors. In addition to increased risk associated with male sex (odds ratio, 1.63), cytotoxic cancer treatment in the prior 4 weeks increased risk (OR, 1.47), as did surgery in the same time frame (OR, 1.52).
“This means patients on treatment have an increased risk of mortality,” Dr. Massuti said.
Moving forward
Implementing telehealth information and communication technologies will continue to grow in importance, Dr. Massuti said. Dr. Aslam noted that video consultation with patients before surgery is already replacing face-to-face interaction, and most follow-up care at his hospital is now done by telephone.
Postoperative care is just as essential in the COVID-19 era, if not more so. “We need to be very vigilant to manage postoperative complications – any symptoms of pyrexia or sepsis, or any sign of COVID,” Dr. Aslam said, including postoperative fever. “If there is any doubt, do a chest CT scan.”
Dr. Aslam predicted the time to perform endoscopy or surgery for each patient will be longer, “so the number of patients done in 1 day will be less than 4 months ago.” In addition, elective surgery patients at his institution undergo COVID-19 testing twice, 3 days apart, prior to intervention.
“This disease will continue in the community for a while, so we have to continue what we’ve done well, like social distancing,” Dr. Aslam said. “We’ve gone through a storm and we are awaiting a tsunami. That tsunami of patients will overwhelm us in the coming months.”
Dr. Martinez, Dr. Massuti, and Dr. Aslam had no relevant disclosures.
An expected surge in the number of people seeking colonoscopy after the peak of the COVID-19 pandemic passes could cause physicians to rethink patient prioritization, could create a strain on endoscopy capacity, and might raise the specter of detecting colorectal cancer in more patients at a later stage of disease.
Furthermore, months of delay in diagnosis of colorectal cancer (CRC) could shorten survival, although more data is needed, according to expert analysis from a gastroenterologist, a medical oncologist, and a colorectal surgeon.
“It has been a big decrease in the number of colonoscopies performed at our hospital in Alicante, Spain,” Rodrigo Jover Martinez, MD, PhD, said during a COVID-19 and Digestive Health webinar presented by United European Gastroenterology (UEG). He estimated colonoscopy procedures are down 60%-90%, and the number of CRC surgeries has dropped by 60%. “As you know, the COVID-19 pandemic is hitting Europe hard.”
When patients do return, “the backlog will be huge ... in already exhausted endoscopy units,” predicted Dr. Martinez, a gastroenterologist at Hospital General Universitario in Alicante.
Multiple risks
Not knowing which patients with CRC will develop severe COVID-19 infection is another challenge, Bartomeu Massuti, MD, of the medical oncology service at the Hospital General Universitario de Alicante, said during the webinar.
Caution is warranted because “we know cancer patients have an increased risk of infection.” However, he added, most evidence supports an elevated risk for bacterial infections, not viral infections.
Therefore, physicians must continue to balance the risks associated with potential COVID-19 exposure against the risks associated with postponed treatment, Dr. Massuti said. “The goal of oncology care is to try to maintain the preplanned treatment and follow-up. We need mainly to avoid stopping or delaying treatment ... because we will lose efficacy in oncology disease outcomes.”
Imran Aslam, MD, PhD, a colorectal surgeon who moderated and presented during the webinar, agreed: “By delaying the treatment, we might do harm to our patients.”
Dr. Aslam cited data about clinical costs of delaying CRC surgery. A 2019 population-based study in PLOS ONE evaluated different times from diagnosis to treatment. The researchers found a delay of more than 150 days “significantly reduced survival, even during stage I, II, and III disease,” he said. The stage I hazard ratio was 2.66, compared with a reference HR of 1.00 for 90 days or fewer. They also reported elevated risk for people with stage II CRC (HR, 2.80), stage III CRC (HR, 2.70), and stage IV CRC (HR, 1.36).
“This could become more and more abysmal if the pandemic continues,” added Dr. Aslam, consultant colorectal surgeon at University Hospitals of Coventry and Warwickshire, England.
Prioritizing patients
Restarting endoscopy with prioritization strategies and increasing patient capacity are possible solutions. Dr. Martinez suggested a four-quadrant matrix in which physicians place patients into “now,” “next,” “delayed,” or “never” categories based on clinical indicators. The priority 1 “now” patients, for example, will be those with suspected CRC based on physical examination, imaging results, and/or an abnormal fecal immunochemical test result.
He suggested, furthermore, that more widespread CRC screening can resume once “endoscopy units have been alleviated of priority 1, symptomatic patients.”
Dr. Massuti concurred with Dr. Martinez’s call to prioritize patients carefully. He suggested a green, yellow, and red classification system based on treatment priority recommendations from the European Society for Medical Oncology. The green group, for example, should receive priority for intervention based on a condition that is immediately clinically unstable or life threatening.
“The main goal is to preserve the continuum of care,” he added.
Another concern – although data are limited – is that treatment might also increase risk of mortality among cancer patients with COVID-19, according to a cohort study of nearly 1,000 such patients reported May 2020 in The Lancet. Dr. Massuti, who was not affiliated with the research, noted that 12% of the patients had GI tumors. In addition to increased risk associated with male sex (odds ratio, 1.63), cytotoxic cancer treatment in the prior 4 weeks increased risk (OR, 1.47), as did surgery in the same time frame (OR, 1.52).
“This means patients on treatment have an increased risk of mortality,” Dr. Massuti said.
Moving forward
Implementing telehealth information and communication technologies will continue to grow in importance, Dr. Massuti said. Dr. Aslam noted that video consultation with patients before surgery is already replacing face-to-face interaction, and most follow-up care at his hospital is now done by telephone.
Postoperative care is just as essential in the COVID-19 era, if not more so. “We need to be very vigilant to manage postoperative complications – any symptoms of pyrexia or sepsis, or any sign of COVID,” Dr. Aslam said, including postoperative fever. “If there is any doubt, do a chest CT scan.”
Dr. Aslam predicted the time to perform endoscopy or surgery for each patient will be longer, “so the number of patients done in 1 day will be less than 4 months ago.” In addition, elective surgery patients at his institution undergo COVID-19 testing twice, 3 days apart, prior to intervention.
“This disease will continue in the community for a while, so we have to continue what we’ve done well, like social distancing,” Dr. Aslam said. “We’ve gone through a storm and we are awaiting a tsunami. That tsunami of patients will overwhelm us in the coming months.”
Dr. Martinez, Dr. Massuti, and Dr. Aslam had no relevant disclosures.
Mortality differs by LVEF between women and men
, Simon Stewart, PhD, reported at the European Society of Cardiology Heart Failure Discoveries virtual meeting.
This analysis from the ongoing National Echocardiography Database of Australia (NEDA) included 499,153 men and women who underwent echocardiography in routine clinical practice for a variety of indications, with more than 3 million person-years of follow-up.
This study broke new ground. There is surprisingly little information from routine clinical practice to describe the spectrum and prognostic importance of left ventricular ejection fraction (LVEF). Indeed, most data have come from clinical trials in patients with heart failure with reduced ejection fraction (HFrEF), in which women are traditionally underrepresented. By comparison, the NEDA analysis included 237,046 women in routine care, noted Dr. Stewart, a National Health and Medical Research Council of Australia Senior Principal Research Fellow at Torrens University in Adelaide.
Among the novel findings in the new NEDA analysis: an LVEF below 50% was more than twice as common in men than women, occurring in 17.6% and 8.3%, respectively. Also, women had a higher average LVEF: 64.2%, compared with 59.5% in men. The overall 1- and 5-year all-cause mortality rates in the half-million participants were 5.8% and 18.4%.
Cardiovascular-related mortality occurred in 7.1% of women in median of 5.6 years of follow-up and in 8.1% of men with 5.5 years of follow-up.
All-cause and cardiovascular mortality rates followed a J-shaped curve, with the clear nadir occurring at an LVEF of 65%-69.9% in both women and men. But for LVEF values outside the nadir, a striking sex-based difference was present. Cardiovascular mortality, when adjusted for body mass index, age, heart rate, valvular heart disease, E-wave velocity, and other potential confounders, wasn’t significantly different between men whose LVEF was 65%-69.9% and those with an LVEF of 45%-64.9%. It started climbing in earnest only at an LVEF below 45%. In contrast, women with an LVEF of 45%-54.9% had a statistically significant twofold increased cardiovascular mortality rate compared to those in the nadir. Moreover, women with an LVEF of 55%-59.9% showed a trend in the same unwanted direction.
High LVEF, higher mortality in women
Dr. Stewart drew attention to an inflection point in the mortality curve for women whereby mortality began climbing at LVEF values of 70% or more. Values in that high range were documented in 72,379 women and 51,317 men.
He noted that the NEDA finding of an increasing mortality risk at LVEFs of at least 70%, especially in women, is similar to a recent report from another big data study, this one involving more than 200,000 patients who underwent echocardiography in routine clinical practice in the Geisinger health system in Pennsylvania. The investigators found in this retrospective study that during a median of 4 years of follow-up after echocardiography, the adjusted risk for all-cause mortality followed a U-shaped curve. The nadir of risk occurred in patients with an LVEF of 60%-65%, with a 1.71-fold increased risk at an LVEF at 70% or more and a near-identical 1.73-fold increased risk at an LVEF of 35%-40%. In this study, however, which was less than half the size of the NEDA analysis, the U-shaped LVEF/mortality curve applied to both men and women. Similar findings were seen in a validation cohort of nearly 36,000 patients from New Zealand (Eur Heart J. 2020 Mar 21;41[12]:1249-57).
The investigators predicted that in addition to the existing categories of HFrEF, heart failure with preserved ejection fraction (HFpEF), and the more recently proposed heart failure with midrange ejection fraction (HFmrEF), their results “may herald the recognition of a new phenotype characterized by supranormal LVEF,” with a moniker of HFsnEF.
New treatment opportunity for women?
Discussant Lars Lund, MD, PhD, professor of cardiology at the Karolinska Institute, Stockholm, said that it’s not possible to make any statements about what constitutes a “normal” LVEF in men or women based on the NEDA study, since all participants underwent medically indicated echocardiography. He added that what he found most interesting about the NEDA analysis was the observation that women with mid-range or mildly reduced LVEF had increased mortality, while men didn’t. That’s a finding that helps explain the suggestion of possible benefit for sacubitril-valsartan in patients with lower ejection fraction and in women in the PARAGON-HF trial of angiotensin-neprilysin inhibition in patients with heart failure with preserved ejection fraction (N Engl J Med. 2019 Oct 24;381[17]:1609-20).
Dr. Lund expressed the hope that the NEDA investigators will do an analysis of the relationship between echocardiographic left atrial size and mortality. Dr. Stewart replied that, as a matter of fact,such a study is planned. The enormous and continuously growing NEDA database has already been used to provide new insights into aortic stenosis and pulmonary hypertension, he noted.
Session moderator Andrew Coats, MD, incoming president of the ESC Heart Failure Association, said that there are many different methods used for echocardiographic measurement of LVEF. He wondered about the validity of pooling them in a single analysis.
Dr. Stewart replied that NEDA software applies a hierarchical weighting of the various methods used to quantify LVEF. And the submitted data come from the top echocardiography laboratories throughout Australia.
“We’ve done some sensitivity analyses around the different methods of quantifying LVEF and we get the same patterns,” he said. “We’re comfortable with the validity of what we’ve done. The big data allows us to do that.”
Dr. Stewart reported receiving speakers fees and travel support from Novartis, a partial funder of NEDA.
SOURCE: Stewart S. ESC Heart Failure 2020.
, Simon Stewart, PhD, reported at the European Society of Cardiology Heart Failure Discoveries virtual meeting.
This analysis from the ongoing National Echocardiography Database of Australia (NEDA) included 499,153 men and women who underwent echocardiography in routine clinical practice for a variety of indications, with more than 3 million person-years of follow-up.
This study broke new ground. There is surprisingly little information from routine clinical practice to describe the spectrum and prognostic importance of left ventricular ejection fraction (LVEF). Indeed, most data have come from clinical trials in patients with heart failure with reduced ejection fraction (HFrEF), in which women are traditionally underrepresented. By comparison, the NEDA analysis included 237,046 women in routine care, noted Dr. Stewart, a National Health and Medical Research Council of Australia Senior Principal Research Fellow at Torrens University in Adelaide.
Among the novel findings in the new NEDA analysis: an LVEF below 50% was more than twice as common in men than women, occurring in 17.6% and 8.3%, respectively. Also, women had a higher average LVEF: 64.2%, compared with 59.5% in men. The overall 1- and 5-year all-cause mortality rates in the half-million participants were 5.8% and 18.4%.
Cardiovascular-related mortality occurred in 7.1% of women in median of 5.6 years of follow-up and in 8.1% of men with 5.5 years of follow-up.
All-cause and cardiovascular mortality rates followed a J-shaped curve, with the clear nadir occurring at an LVEF of 65%-69.9% in both women and men. But for LVEF values outside the nadir, a striking sex-based difference was present. Cardiovascular mortality, when adjusted for body mass index, age, heart rate, valvular heart disease, E-wave velocity, and other potential confounders, wasn’t significantly different between men whose LVEF was 65%-69.9% and those with an LVEF of 45%-64.9%. It started climbing in earnest only at an LVEF below 45%. In contrast, women with an LVEF of 45%-54.9% had a statistically significant twofold increased cardiovascular mortality rate compared to those in the nadir. Moreover, women with an LVEF of 55%-59.9% showed a trend in the same unwanted direction.
High LVEF, higher mortality in women
Dr. Stewart drew attention to an inflection point in the mortality curve for women whereby mortality began climbing at LVEF values of 70% or more. Values in that high range were documented in 72,379 women and 51,317 men.
He noted that the NEDA finding of an increasing mortality risk at LVEFs of at least 70%, especially in women, is similar to a recent report from another big data study, this one involving more than 200,000 patients who underwent echocardiography in routine clinical practice in the Geisinger health system in Pennsylvania. The investigators found in this retrospective study that during a median of 4 years of follow-up after echocardiography, the adjusted risk for all-cause mortality followed a U-shaped curve. The nadir of risk occurred in patients with an LVEF of 60%-65%, with a 1.71-fold increased risk at an LVEF at 70% or more and a near-identical 1.73-fold increased risk at an LVEF of 35%-40%. In this study, however, which was less than half the size of the NEDA analysis, the U-shaped LVEF/mortality curve applied to both men and women. Similar findings were seen in a validation cohort of nearly 36,000 patients from New Zealand (Eur Heart J. 2020 Mar 21;41[12]:1249-57).
The investigators predicted that in addition to the existing categories of HFrEF, heart failure with preserved ejection fraction (HFpEF), and the more recently proposed heart failure with midrange ejection fraction (HFmrEF), their results “may herald the recognition of a new phenotype characterized by supranormal LVEF,” with a moniker of HFsnEF.
New treatment opportunity for women?
Discussant Lars Lund, MD, PhD, professor of cardiology at the Karolinska Institute, Stockholm, said that it’s not possible to make any statements about what constitutes a “normal” LVEF in men or women based on the NEDA study, since all participants underwent medically indicated echocardiography. He added that what he found most interesting about the NEDA analysis was the observation that women with mid-range or mildly reduced LVEF had increased mortality, while men didn’t. That’s a finding that helps explain the suggestion of possible benefit for sacubitril-valsartan in patients with lower ejection fraction and in women in the PARAGON-HF trial of angiotensin-neprilysin inhibition in patients with heart failure with preserved ejection fraction (N Engl J Med. 2019 Oct 24;381[17]:1609-20).
Dr. Lund expressed the hope that the NEDA investigators will do an analysis of the relationship between echocardiographic left atrial size and mortality. Dr. Stewart replied that, as a matter of fact,such a study is planned. The enormous and continuously growing NEDA database has already been used to provide new insights into aortic stenosis and pulmonary hypertension, he noted.
Session moderator Andrew Coats, MD, incoming president of the ESC Heart Failure Association, said that there are many different methods used for echocardiographic measurement of LVEF. He wondered about the validity of pooling them in a single analysis.
Dr. Stewart replied that NEDA software applies a hierarchical weighting of the various methods used to quantify LVEF. And the submitted data come from the top echocardiography laboratories throughout Australia.
“We’ve done some sensitivity analyses around the different methods of quantifying LVEF and we get the same patterns,” he said. “We’re comfortable with the validity of what we’ve done. The big data allows us to do that.”
Dr. Stewart reported receiving speakers fees and travel support from Novartis, a partial funder of NEDA.
SOURCE: Stewart S. ESC Heart Failure 2020.
, Simon Stewart, PhD, reported at the European Society of Cardiology Heart Failure Discoveries virtual meeting.
This analysis from the ongoing National Echocardiography Database of Australia (NEDA) included 499,153 men and women who underwent echocardiography in routine clinical practice for a variety of indications, with more than 3 million person-years of follow-up.
This study broke new ground. There is surprisingly little information from routine clinical practice to describe the spectrum and prognostic importance of left ventricular ejection fraction (LVEF). Indeed, most data have come from clinical trials in patients with heart failure with reduced ejection fraction (HFrEF), in which women are traditionally underrepresented. By comparison, the NEDA analysis included 237,046 women in routine care, noted Dr. Stewart, a National Health and Medical Research Council of Australia Senior Principal Research Fellow at Torrens University in Adelaide.
Among the novel findings in the new NEDA analysis: an LVEF below 50% was more than twice as common in men than women, occurring in 17.6% and 8.3%, respectively. Also, women had a higher average LVEF: 64.2%, compared with 59.5% in men. The overall 1- and 5-year all-cause mortality rates in the half-million participants were 5.8% and 18.4%.
Cardiovascular-related mortality occurred in 7.1% of women in median of 5.6 years of follow-up and in 8.1% of men with 5.5 years of follow-up.
All-cause and cardiovascular mortality rates followed a J-shaped curve, with the clear nadir occurring at an LVEF of 65%-69.9% in both women and men. But for LVEF values outside the nadir, a striking sex-based difference was present. Cardiovascular mortality, when adjusted for body mass index, age, heart rate, valvular heart disease, E-wave velocity, and other potential confounders, wasn’t significantly different between men whose LVEF was 65%-69.9% and those with an LVEF of 45%-64.9%. It started climbing in earnest only at an LVEF below 45%. In contrast, women with an LVEF of 45%-54.9% had a statistically significant twofold increased cardiovascular mortality rate compared to those in the nadir. Moreover, women with an LVEF of 55%-59.9% showed a trend in the same unwanted direction.
High LVEF, higher mortality in women
Dr. Stewart drew attention to an inflection point in the mortality curve for women whereby mortality began climbing at LVEF values of 70% or more. Values in that high range were documented in 72,379 women and 51,317 men.
He noted that the NEDA finding of an increasing mortality risk at LVEFs of at least 70%, especially in women, is similar to a recent report from another big data study, this one involving more than 200,000 patients who underwent echocardiography in routine clinical practice in the Geisinger health system in Pennsylvania. The investigators found in this retrospective study that during a median of 4 years of follow-up after echocardiography, the adjusted risk for all-cause mortality followed a U-shaped curve. The nadir of risk occurred in patients with an LVEF of 60%-65%, with a 1.71-fold increased risk at an LVEF at 70% or more and a near-identical 1.73-fold increased risk at an LVEF of 35%-40%. In this study, however, which was less than half the size of the NEDA analysis, the U-shaped LVEF/mortality curve applied to both men and women. Similar findings were seen in a validation cohort of nearly 36,000 patients from New Zealand (Eur Heart J. 2020 Mar 21;41[12]:1249-57).
The investigators predicted that in addition to the existing categories of HFrEF, heart failure with preserved ejection fraction (HFpEF), and the more recently proposed heart failure with midrange ejection fraction (HFmrEF), their results “may herald the recognition of a new phenotype characterized by supranormal LVEF,” with a moniker of HFsnEF.
New treatment opportunity for women?
Discussant Lars Lund, MD, PhD, professor of cardiology at the Karolinska Institute, Stockholm, said that it’s not possible to make any statements about what constitutes a “normal” LVEF in men or women based on the NEDA study, since all participants underwent medically indicated echocardiography. He added that what he found most interesting about the NEDA analysis was the observation that women with mid-range or mildly reduced LVEF had increased mortality, while men didn’t. That’s a finding that helps explain the suggestion of possible benefit for sacubitril-valsartan in patients with lower ejection fraction and in women in the PARAGON-HF trial of angiotensin-neprilysin inhibition in patients with heart failure with preserved ejection fraction (N Engl J Med. 2019 Oct 24;381[17]:1609-20).
Dr. Lund expressed the hope that the NEDA investigators will do an analysis of the relationship between echocardiographic left atrial size and mortality. Dr. Stewart replied that, as a matter of fact,such a study is planned. The enormous and continuously growing NEDA database has already been used to provide new insights into aortic stenosis and pulmonary hypertension, he noted.
Session moderator Andrew Coats, MD, incoming president of the ESC Heart Failure Association, said that there are many different methods used for echocardiographic measurement of LVEF. He wondered about the validity of pooling them in a single analysis.
Dr. Stewart replied that NEDA software applies a hierarchical weighting of the various methods used to quantify LVEF. And the submitted data come from the top echocardiography laboratories throughout Australia.
“We’ve done some sensitivity analyses around the different methods of quantifying LVEF and we get the same patterns,” he said. “We’re comfortable with the validity of what we’ve done. The big data allows us to do that.”
Dr. Stewart reported receiving speakers fees and travel support from Novartis, a partial funder of NEDA.
SOURCE: Stewart S. ESC Heart Failure 2020.
FROM ESC HEART FAILURE 2020
Disparate study results on elective labor costs fuel debate
Cost concerns have circulated regarding elective induction of labor, a method that’s become increasingly popular in the United States. Two studies in Obstetrics & Gynecology, however, offer no consensus on the cost burden of this method.

A retrospective analysis of a large cohort in California reported higher costs for induction, compared with spontaneous labor, after accounting for variables such as parity, mode of delivery, and gestational age. A prospective study of five Utah hospitals found no significant cost differences between induction and expectant management.
The ARRIVE trial (A Randomized Trial of Induction versus Expectant Management), a multicenter study that compared elective labor induction at 39 weeks of gestation with spontaneous labor in low-risk nulliparous women, suggests that induction may have some benefits. While its researchers found no differences in perinatal outcomes, induction cases had fewer cesareans, fewer hypertensive disorders, and fewer newborns requiring respiratory support.
One key question that remains following ARRIVE is whether this practice should be implemented universally, Alyssa R. Hersh, MD, MPH, lead author of the California study, said in an interview. Quantifying the costs associated with elective labor is important because “health care in the United States is already much more expensive than in other countries, and [elective labor] could have a dramatic impact on annual health care costs.”
In a retrospective analysis, Dr. Hersh, of the Oregon Health & Science University, Portland, and her colleagues examined data from more than 1.2 million women in California with singleton, nonanomalous births. They excluded for multiple factors such as medically indicated induction of labor, placenta previa, breech presentation, or planned cesarean delivery.
Estimating cost differences between elective induction and spontaneous labor for mothers and neonates, they stratified results by vaginal or cesarean delivery, parity, gestational age at delivery, and geographic location. Elective induced labor represented 15% of the overall cohort of 1.2 million women.
Among vaginal deliveries, median maternal hospitalization costs were $10,175 in the induction group and $9,462 in the spontaneous labor group. For cesarean deliveries, the median costs were $20,294 with induction of labor and $18,812 with spontaneous labor.
Costs of maternal hospitalization with elective induction of labor were significantly higher than that of spontaneous labor, regardless of parity, mode of delivery, and gestational age at delivery, the authors reported. Comparing costs at rural and urban areas, the induction group saw higher maternal hospitalization costs and longer lengths of stay regardless of scenario.
Neonatal care was the one metric that incurred lower costs and lengths of stay in the induction group. Fewer adverse outcomes in this group could explain this outlier. “However, because this is observational data, we cannot elucidate what exactly contributed to these decreased costs,” Dr. Hersh and colleagues noted.
Timeliness was another limitation. “It is important to note that our study was conducted between 2007 and 2011, and the patients undergoing elective induction of labor during those years may differ from women undergoing elective induction of labor currently,” the authors acknowledged.
Another study by Brett D. Einerson, MD, MPH, of the University of Utah Health, Salt Lake City, and associates evaluated the actual hospital costs of patients undergoing elective induction and expectant management in a subset of patients from the ARRIVE trial.
“If, medically speaking, induction is equal to expectant management or has some benefit, as the larger ARRIVE trial suggests, we wanted to know: At what cost?” Dr. Einerson said in an interview.
Study participants hailed from five Utah hospitals within two health systems: the University of Utah Health and Intermountain Healthcare. Taking available data for 1,231 enrollees, investigators randomized 608 to labor induction and 623 to spontaneous labor. They measured actual hospital costs using advanced value-based analytics platforms at the Utah hospitals, comparing cost means and reporting the relative difference between induction and expectant management.
Overall, they found no significant differences between the mean total cost of elective induction and expectant management (adjusted mean difference, +4.7%). This was the case for other metrics: Costs did not vary among the five health systems or in most phases of care, including maternal inpatient postpartum care, maternal outpatient care after discharge, neonatal hospital care, and neonatal care after discharge.
The induction group did incur higher maternal inpatient intrapartum and delivery care costs (17%). However, these were offset by savings achieved during outpatient antenatal care (–47%). The assumption was additional costs of time spent on the labor ward might overwhelm cost savings elsewhere (reduced cesarean deliveries, fewer prenatal appointments and tests). “But this was not the case,” Dr. Einerson said.
Ultimately, the study was not large enough to find smaller differences in cost, he noted. It was only large enough to say that cost didn’t differentiate between arms with a margin of +/–7%. “A cost increase (or cost savings) with induction of 7% is meaningful over time and on a national scale,” Dr. Einerson explained.
Taken together, the two studies show that cost is not an insurmountable barrier to elective induced labor, Jeffrey L. Ecker, MD, and Mark A. Clapp, MD, MPH, wrote in an accompanying editorial (Obstet Gynecol. 2020;136[1]:6-7).
“This will be especially true if we are innovative and creatively adapt our facilities and spaces, thinking about where and how some of the required care can be appropriately and more economically offered,” they noted.
“Specifically, strategies to safely reduce labor and delivery time for inductions of labor, including considering and studying outpatient cervical ripening, may make elective induction of labor at 39 weeks of gestation even less costly and even more feasible to offer to all women,” suggested Dr. Ecker and Dr. Clapp, both at Massachusetts General Hospital and Harvard Medical School, both in Boston.
Dr. Hersh and coauthors had no relevant financial disclosures, and there was no external funding for their study. Dr. Einerson and most coauthors reported no relevant financial disclosures; one coauthor reported receiving funds from GestVision as a consultant, and another coauthor reported funds paid to her or her institution from some pharmaceutical companies when she was primary investigator on various trials or a consultant. This study was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Neither Dr. Ecker nor Dr Clapp had any relevant financial disclosures or received any funding.
SOURCES: Hersh AR et al. Obstet Gynecol. 2020. doi: 10.1097/AOG.0000000000003865; Einerson BD et al. Obstet Gynecol. 2020. doi: 10.1097/AOG.0000000000003930.
Cost concerns have circulated regarding elective induction of labor, a method that’s become increasingly popular in the United States. Two studies in Obstetrics & Gynecology, however, offer no consensus on the cost burden of this method.
A retrospective analysis of a large cohort in California reported higher costs for induction, compared with spontaneous labor, after accounting for variables such as parity, mode of delivery, and gestational age. A prospective study of five Utah hospitals found no significant cost differences between induction and expectant management.
The ARRIVE trial (A Randomized Trial of Induction versus Expectant Management), a multicenter study that compared elective labor induction at 39 weeks of gestation with spontaneous labor in low-risk nulliparous women, suggests that induction may have some benefits. While its researchers found no differences in perinatal outcomes, induction cases had fewer cesareans, fewer hypertensive disorders, and fewer newborns requiring respiratory support.
One key question that remains following ARRIVE is whether this practice should be implemented universally, Alyssa R. Hersh, MD, MPH, lead author of the California study, said in an interview. Quantifying the costs associated with elective labor is important because “health care in the United States is already much more expensive than in other countries, and [elective labor] could have a dramatic impact on annual health care costs.”
In a retrospective analysis, Dr. Hersh, of the Oregon Health & Science University, Portland, and her colleagues examined data from more than 1.2 million women in California with singleton, nonanomalous births. They excluded for multiple factors such as medically indicated induction of labor, placenta previa, breech presentation, or planned cesarean delivery.
Estimating cost differences between elective induction and spontaneous labor for mothers and neonates, they stratified results by vaginal or cesarean delivery, parity, gestational age at delivery, and geographic location. Elective induced labor represented 15% of the overall cohort of 1.2 million women.
Among vaginal deliveries, median maternal hospitalization costs were $10,175 in the induction group and $9,462 in the spontaneous labor group. For cesarean deliveries, the median costs were $20,294 with induction of labor and $18,812 with spontaneous labor.
Costs of maternal hospitalization with elective induction of labor were significantly higher than that of spontaneous labor, regardless of parity, mode of delivery, and gestational age at delivery, the authors reported. Comparing costs at rural and urban areas, the induction group saw higher maternal hospitalization costs and longer lengths of stay regardless of scenario.
Neonatal care was the one metric that incurred lower costs and lengths of stay in the induction group. Fewer adverse outcomes in this group could explain this outlier. “However, because this is observational data, we cannot elucidate what exactly contributed to these decreased costs,” Dr. Hersh and colleagues noted.
Timeliness was another limitation. “It is important to note that our study was conducted between 2007 and 2011, and the patients undergoing elective induction of labor during those years may differ from women undergoing elective induction of labor currently,” the authors acknowledged.
Another study by Brett D. Einerson, MD, MPH, of the University of Utah Health, Salt Lake City, and associates evaluated the actual hospital costs of patients undergoing elective induction and expectant management in a subset of patients from the ARRIVE trial.
“If, medically speaking, induction is equal to expectant management or has some benefit, as the larger ARRIVE trial suggests, we wanted to know: At what cost?” Dr. Einerson said in an interview.
Study participants hailed from five Utah hospitals within two health systems: the University of Utah Health and Intermountain Healthcare. Taking available data for 1,231 enrollees, investigators randomized 608 to labor induction and 623 to spontaneous labor. They measured actual hospital costs using advanced value-based analytics platforms at the Utah hospitals, comparing cost means and reporting the relative difference between induction and expectant management.
Overall, they found no significant differences between the mean total cost of elective induction and expectant management (adjusted mean difference, +4.7%). This was the case for other metrics: Costs did not vary among the five health systems or in most phases of care, including maternal inpatient postpartum care, maternal outpatient care after discharge, neonatal hospital care, and neonatal care after discharge.
The induction group did incur higher maternal inpatient intrapartum and delivery care costs (17%). However, these were offset by savings achieved during outpatient antenatal care (–47%). The assumption was additional costs of time spent on the labor ward might overwhelm cost savings elsewhere (reduced cesarean deliveries, fewer prenatal appointments and tests). “But this was not the case,” Dr. Einerson said.
Ultimately, the study was not large enough to find smaller differences in cost, he noted. It was only large enough to say that cost didn’t differentiate between arms with a margin of +/–7%. “A cost increase (or cost savings) with induction of 7% is meaningful over time and on a national scale,” Dr. Einerson explained.
Taken together, the two studies show that cost is not an insurmountable barrier to elective induced labor, Jeffrey L. Ecker, MD, and Mark A. Clapp, MD, MPH, wrote in an accompanying editorial (Obstet Gynecol. 2020;136[1]:6-7).
“This will be especially true if we are innovative and creatively adapt our facilities and spaces, thinking about where and how some of the required care can be appropriately and more economically offered,” they noted.
“Specifically, strategies to safely reduce labor and delivery time for inductions of labor, including considering and studying outpatient cervical ripening, may make elective induction of labor at 39 weeks of gestation even less costly and even more feasible to offer to all women,” suggested Dr. Ecker and Dr. Clapp, both at Massachusetts General Hospital and Harvard Medical School, both in Boston.
Dr. Hersh and coauthors had no relevant financial disclosures, and there was no external funding for their study. Dr. Einerson and most coauthors reported no relevant financial disclosures; one coauthor reported receiving funds from GestVision as a consultant, and another coauthor reported funds paid to her or her institution from some pharmaceutical companies when she was primary investigator on various trials or a consultant. This study was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Neither Dr. Ecker nor Dr Clapp had any relevant financial disclosures or received any funding.
SOURCES: Hersh AR et al. Obstet Gynecol. 2020. doi: 10.1097/AOG.0000000000003865; Einerson BD et al. Obstet Gynecol. 2020. doi: 10.1097/AOG.0000000000003930.
Cost concerns have circulated regarding elective induction of labor, a method that’s become increasingly popular in the United States. Two studies in Obstetrics & Gynecology, however, offer no consensus on the cost burden of this method.
A retrospective analysis of a large cohort in California reported higher costs for induction, compared with spontaneous labor, after accounting for variables such as parity, mode of delivery, and gestational age. A prospective study of five Utah hospitals found no significant cost differences between induction and expectant management.
The ARRIVE trial (A Randomized Trial of Induction versus Expectant Management), a multicenter study that compared elective labor induction at 39 weeks of gestation with spontaneous labor in low-risk nulliparous women, suggests that induction may have some benefits. While its researchers found no differences in perinatal outcomes, induction cases had fewer cesareans, fewer hypertensive disorders, and fewer newborns requiring respiratory support.
One key question that remains following ARRIVE is whether this practice should be implemented universally, Alyssa R. Hersh, MD, MPH, lead author of the California study, said in an interview. Quantifying the costs associated with elective labor is important because “health care in the United States is already much more expensive than in other countries, and [elective labor] could have a dramatic impact on annual health care costs.”
In a retrospective analysis, Dr. Hersh, of the Oregon Health & Science University, Portland, and her colleagues examined data from more than 1.2 million women in California with singleton, nonanomalous births. They excluded for multiple factors such as medically indicated induction of labor, placenta previa, breech presentation, or planned cesarean delivery.
Estimating cost differences between elective induction and spontaneous labor for mothers and neonates, they stratified results by vaginal or cesarean delivery, parity, gestational age at delivery, and geographic location. Elective induced labor represented 15% of the overall cohort of 1.2 million women.
Among vaginal deliveries, median maternal hospitalization costs were $10,175 in the induction group and $9,462 in the spontaneous labor group. For cesarean deliveries, the median costs were $20,294 with induction of labor and $18,812 with spontaneous labor.
Costs of maternal hospitalization with elective induction of labor were significantly higher than that of spontaneous labor, regardless of parity, mode of delivery, and gestational age at delivery, the authors reported. Comparing costs at rural and urban areas, the induction group saw higher maternal hospitalization costs and longer lengths of stay regardless of scenario.
Neonatal care was the one metric that incurred lower costs and lengths of stay in the induction group. Fewer adverse outcomes in this group could explain this outlier. “However, because this is observational data, we cannot elucidate what exactly contributed to these decreased costs,” Dr. Hersh and colleagues noted.
Timeliness was another limitation. “It is important to note that our study was conducted between 2007 and 2011, and the patients undergoing elective induction of labor during those years may differ from women undergoing elective induction of labor currently,” the authors acknowledged.
Another study by Brett D. Einerson, MD, MPH, of the University of Utah Health, Salt Lake City, and associates evaluated the actual hospital costs of patients undergoing elective induction and expectant management in a subset of patients from the ARRIVE trial.
“If, medically speaking, induction is equal to expectant management or has some benefit, as the larger ARRIVE trial suggests, we wanted to know: At what cost?” Dr. Einerson said in an interview.
Study participants hailed from five Utah hospitals within two health systems: the University of Utah Health and Intermountain Healthcare. Taking available data for 1,231 enrollees, investigators randomized 608 to labor induction and 623 to spontaneous labor. They measured actual hospital costs using advanced value-based analytics platforms at the Utah hospitals, comparing cost means and reporting the relative difference between induction and expectant management.
Overall, they found no significant differences between the mean total cost of elective induction and expectant management (adjusted mean difference, +4.7%). This was the case for other metrics: Costs did not vary among the five health systems or in most phases of care, including maternal inpatient postpartum care, maternal outpatient care after discharge, neonatal hospital care, and neonatal care after discharge.
The induction group did incur higher maternal inpatient intrapartum and delivery care costs (17%). However, these were offset by savings achieved during outpatient antenatal care (–47%). The assumption was additional costs of time spent on the labor ward might overwhelm cost savings elsewhere (reduced cesarean deliveries, fewer prenatal appointments and tests). “But this was not the case,” Dr. Einerson said.
Ultimately, the study was not large enough to find smaller differences in cost, he noted. It was only large enough to say that cost didn’t differentiate between arms with a margin of +/–7%. “A cost increase (or cost savings) with induction of 7% is meaningful over time and on a national scale,” Dr. Einerson explained.
Taken together, the two studies show that cost is not an insurmountable barrier to elective induced labor, Jeffrey L. Ecker, MD, and Mark A. Clapp, MD, MPH, wrote in an accompanying editorial (Obstet Gynecol. 2020;136[1]:6-7).
“This will be especially true if we are innovative and creatively adapt our facilities and spaces, thinking about where and how some of the required care can be appropriately and more economically offered,” they noted.
“Specifically, strategies to safely reduce labor and delivery time for inductions of labor, including considering and studying outpatient cervical ripening, may make elective induction of labor at 39 weeks of gestation even less costly and even more feasible to offer to all women,” suggested Dr. Ecker and Dr. Clapp, both at Massachusetts General Hospital and Harvard Medical School, both in Boston.
Dr. Hersh and coauthors had no relevant financial disclosures, and there was no external funding for their study. Dr. Einerson and most coauthors reported no relevant financial disclosures; one coauthor reported receiving funds from GestVision as a consultant, and another coauthor reported funds paid to her or her institution from some pharmaceutical companies when she was primary investigator on various trials or a consultant. This study was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Neither Dr. Ecker nor Dr Clapp had any relevant financial disclosures or received any funding.
SOURCES: Hersh AR et al. Obstet Gynecol. 2020. doi: 10.1097/AOG.0000000000003865; Einerson BD et al. Obstet Gynecol. 2020. doi: 10.1097/AOG.0000000000003930.
