User login
Big data breaks down Sjögren’s syndrome
The severity of Sjögren’s syndrome and its organ involvement has direct links to clinical characteristics that include age, gender, ethnicity, and geographical location, according to new research findings from a large, worldwide database of primary Sjögren’s syndrome patients.
Risk factors for more severe disease included male sex, earlier age at diagnosis, black/African-American (BAA) ethnicity, and living in more southerly countries, including below the equator. The authors hailed these factors as potentially helping to predict the presence of systemic disease in newly-diagnosed patients, as well as helping to determine the optimum follow-up strategy.
But not everyone agrees. In interviews, other experts suggested that the data were interesting and valuable, but were not ready to make reliable clinical predictions. “The predictive value of these data are limited when it comes to an individual patient sitting in front of you in the office,” said Tomas Mustelin, MD, professor of medicine at the University of Washington, Seattle.
“It would be an important clinical thing if you can figure out who’s at risk for systemic complications and who isn’t. This is a nice step in that direction,” said Hal Scofield, MD, professor of medicine and pathology at the University of Oklahoma, Oklahoma City, agreeing that the data were too preliminary to be broadly useful because there is too much overlap between different patient groups.
If there is one clinical message, it is that physicians should be looking beyond dry eyes and dry mouth in newly diagnosed Sjögren’s syndrome, according to Sarah Chung, MD, who is an acting instructor of rheumatology at the University of Washington. “It’s a reminder to investigate these extra-glandular manifestations, and a reminder that it is a heterogeneous presentation, so we have to keep an open mind and investigate thoroughly,” she said.
In the research published online in Rheumatology, first author Pilar Brito-Zerón, MD, PhD, of the University of Barcelona Hospital Clínic, and colleagues in the Sjögren Big Data Consortium used European League Against Rheumatism Sjögren’s syndrome disease activity index (ESSDAI) scores to examine phenotype and patient characteristics among 10,007 subjects drawn from the international consortium.

Overall, 93.5% of subjects were women, and the mean age at diagnosis was 53 (standard deviation [SD], 14.1 years). The mean total ESSDAI score was 6.1 (SD, 7.5).
Men had higher mean ESSDAI (8.1 vs. 6.0; P less than .001) and clinical ESSDAI (8.4 vs. 6.1; P less than .001) scores and were more likely to have a high disease activity state (22.5% vs. 11.7%; P less than .001). Domains that scored higher in men included lymphadenopathy (P less than .001), glandular (P less than .001), pulmonary (P = .001), peripheral nervous system (PNS) (P less than .001), and CNS (P less than .001).
The highest global ESSDAI scores were reported in patients younger than 35, but organ dominance differed by age group: The constitutional, lymphadenopathy, glandular, cutaneous, renal, hematologic, and biologic domains were highest in this age group, but pulmonary and peripheral nervous system were highest in patients over 65.
By ethnicity, the highest ESSDAI scores occurred in black/African-American patients (6.7), followed by white (6.5), Asian (5.4), and Hispanic (4.8; P less than .001). The organ-specific domains also tracked by ethnicity, with BAA patients experiencing the highest frequencies of activity in the lymphadenopathy, articular, neurologic, and biologic domains. White patients were more often affected in the glandular, cutaneous, and muscular domains, whereas Asians most often experienced the pulmonary, renal, and hematologic domains, and Hispanics the constitutional domain.
The survey included Europe, America, and Asia, and global ESSDAI scores were higher in the southern countries of Asia and Europe, and higher in countries below the equator in the Americas. The organ-by-organ activity scores had a differentiated pattern between northern and southern locales. Worldwide, the gradient of patients with moderate systemic activity (global ESSDAI score of 5 or higher) at diagnosis followed a north-south gradient.
The study had no specific funding, and the authors have no relevant financial disclosures. Dr. Mustelin, Dr. Scofield, and Dr. Chung have no relevant financial disclosures.
SOURCE: Brito-Zerón P et al. Rheumatology. 2019 Dec 24. doi: 10.1093/rheumatology/kez578.
The severity of Sjögren’s syndrome and its organ involvement has direct links to clinical characteristics that include age, gender, ethnicity, and geographical location, according to new research findings from a large, worldwide database of primary Sjögren’s syndrome patients.
Risk factors for more severe disease included male sex, earlier age at diagnosis, black/African-American (BAA) ethnicity, and living in more southerly countries, including below the equator. The authors hailed these factors as potentially helping to predict the presence of systemic disease in newly-diagnosed patients, as well as helping to determine the optimum follow-up strategy.
But not everyone agrees. In interviews, other experts suggested that the data were interesting and valuable, but were not ready to make reliable clinical predictions. “The predictive value of these data are limited when it comes to an individual patient sitting in front of you in the office,” said Tomas Mustelin, MD, professor of medicine at the University of Washington, Seattle.
“It would be an important clinical thing if you can figure out who’s at risk for systemic complications and who isn’t. This is a nice step in that direction,” said Hal Scofield, MD, professor of medicine and pathology at the University of Oklahoma, Oklahoma City, agreeing that the data were too preliminary to be broadly useful because there is too much overlap between different patient groups.
If there is one clinical message, it is that physicians should be looking beyond dry eyes and dry mouth in newly diagnosed Sjögren’s syndrome, according to Sarah Chung, MD, who is an acting instructor of rheumatology at the University of Washington. “It’s a reminder to investigate these extra-glandular manifestations, and a reminder that it is a heterogeneous presentation, so we have to keep an open mind and investigate thoroughly,” she said.
In the research published online in Rheumatology, first author Pilar Brito-Zerón, MD, PhD, of the University of Barcelona Hospital Clínic, and colleagues in the Sjögren Big Data Consortium used European League Against Rheumatism Sjögren’s syndrome disease activity index (ESSDAI) scores to examine phenotype and patient characteristics among 10,007 subjects drawn from the international consortium.
Overall, 93.5% of subjects were women, and the mean age at diagnosis was 53 (standard deviation [SD], 14.1 years). The mean total ESSDAI score was 6.1 (SD, 7.5).
Men had higher mean ESSDAI (8.1 vs. 6.0; P less than .001) and clinical ESSDAI (8.4 vs. 6.1; P less than .001) scores and were more likely to have a high disease activity state (22.5% vs. 11.7%; P less than .001). Domains that scored higher in men included lymphadenopathy (P less than .001), glandular (P less than .001), pulmonary (P = .001), peripheral nervous system (PNS) (P less than .001), and CNS (P less than .001).
The highest global ESSDAI scores were reported in patients younger than 35, but organ dominance differed by age group: The constitutional, lymphadenopathy, glandular, cutaneous, renal, hematologic, and biologic domains were highest in this age group, but pulmonary and peripheral nervous system were highest in patients over 65.
By ethnicity, the highest ESSDAI scores occurred in black/African-American patients (6.7), followed by white (6.5), Asian (5.4), and Hispanic (4.8; P less than .001). The organ-specific domains also tracked by ethnicity, with BAA patients experiencing the highest frequencies of activity in the lymphadenopathy, articular, neurologic, and biologic domains. White patients were more often affected in the glandular, cutaneous, and muscular domains, whereas Asians most often experienced the pulmonary, renal, and hematologic domains, and Hispanics the constitutional domain.
The survey included Europe, America, and Asia, and global ESSDAI scores were higher in the southern countries of Asia and Europe, and higher in countries below the equator in the Americas. The organ-by-organ activity scores had a differentiated pattern between northern and southern locales. Worldwide, the gradient of patients with moderate systemic activity (global ESSDAI score of 5 or higher) at diagnosis followed a north-south gradient.
The study had no specific funding, and the authors have no relevant financial disclosures. Dr. Mustelin, Dr. Scofield, and Dr. Chung have no relevant financial disclosures.
SOURCE: Brito-Zerón P et al. Rheumatology. 2019 Dec 24. doi: 10.1093/rheumatology/kez578.
The severity of Sjögren’s syndrome and its organ involvement has direct links to clinical characteristics that include age, gender, ethnicity, and geographical location, according to new research findings from a large, worldwide database of primary Sjögren’s syndrome patients.
Risk factors for more severe disease included male sex, earlier age at diagnosis, black/African-American (BAA) ethnicity, and living in more southerly countries, including below the equator. The authors hailed these factors as potentially helping to predict the presence of systemic disease in newly-diagnosed patients, as well as helping to determine the optimum follow-up strategy.
But not everyone agrees. In interviews, other experts suggested that the data were interesting and valuable, but were not ready to make reliable clinical predictions. “The predictive value of these data are limited when it comes to an individual patient sitting in front of you in the office,” said Tomas Mustelin, MD, professor of medicine at the University of Washington, Seattle.
“It would be an important clinical thing if you can figure out who’s at risk for systemic complications and who isn’t. This is a nice step in that direction,” said Hal Scofield, MD, professor of medicine and pathology at the University of Oklahoma, Oklahoma City, agreeing that the data were too preliminary to be broadly useful because there is too much overlap between different patient groups.
If there is one clinical message, it is that physicians should be looking beyond dry eyes and dry mouth in newly diagnosed Sjögren’s syndrome, according to Sarah Chung, MD, who is an acting instructor of rheumatology at the University of Washington. “It’s a reminder to investigate these extra-glandular manifestations, and a reminder that it is a heterogeneous presentation, so we have to keep an open mind and investigate thoroughly,” she said.
In the research published online in Rheumatology, first author Pilar Brito-Zerón, MD, PhD, of the University of Barcelona Hospital Clínic, and colleagues in the Sjögren Big Data Consortium used European League Against Rheumatism Sjögren’s syndrome disease activity index (ESSDAI) scores to examine phenotype and patient characteristics among 10,007 subjects drawn from the international consortium.
Overall, 93.5% of subjects were women, and the mean age at diagnosis was 53 (standard deviation [SD], 14.1 years). The mean total ESSDAI score was 6.1 (SD, 7.5).
Men had higher mean ESSDAI (8.1 vs. 6.0; P less than .001) and clinical ESSDAI (8.4 vs. 6.1; P less than .001) scores and were more likely to have a high disease activity state (22.5% vs. 11.7%; P less than .001). Domains that scored higher in men included lymphadenopathy (P less than .001), glandular (P less than .001), pulmonary (P = .001), peripheral nervous system (PNS) (P less than .001), and CNS (P less than .001).
The highest global ESSDAI scores were reported in patients younger than 35, but organ dominance differed by age group: The constitutional, lymphadenopathy, glandular, cutaneous, renal, hematologic, and biologic domains were highest in this age group, but pulmonary and peripheral nervous system were highest in patients over 65.
By ethnicity, the highest ESSDAI scores occurred in black/African-American patients (6.7), followed by white (6.5), Asian (5.4), and Hispanic (4.8; P less than .001). The organ-specific domains also tracked by ethnicity, with BAA patients experiencing the highest frequencies of activity in the lymphadenopathy, articular, neurologic, and biologic domains. White patients were more often affected in the glandular, cutaneous, and muscular domains, whereas Asians most often experienced the pulmonary, renal, and hematologic domains, and Hispanics the constitutional domain.
The survey included Europe, America, and Asia, and global ESSDAI scores were higher in the southern countries of Asia and Europe, and higher in countries below the equator in the Americas. The organ-by-organ activity scores had a differentiated pattern between northern and southern locales. Worldwide, the gradient of patients with moderate systemic activity (global ESSDAI score of 5 or higher) at diagnosis followed a north-south gradient.
The study had no specific funding, and the authors have no relevant financial disclosures. Dr. Mustelin, Dr. Scofield, and Dr. Chung have no relevant financial disclosures.
SOURCE: Brito-Zerón P et al. Rheumatology. 2019 Dec 24. doi: 10.1093/rheumatology/kez578.
FROM RHEUMATOLOGY
Children with resistant UTIs unexpectedly may respond to discordant antibiotics
Children with urinary tract infections (UTIs) may improve clinically, and pyuria may resolve, during empiric treatment with an antibiotic that turns out to be discordant, according a retrospective study in Pediatrics.

“The low rate of care escalation and high rate of clinical improvement while on discordant antibiotics suggests that, for most patients, it would be reasonable to continue current empiric antibiotic practices until urine culture sensitivities return,” said first author Marie E. Wang, MD, a pediatric hospitalist at Stanford (Calif.) University, and colleagues.
The researchers examined the initial clinical response and escalation of care for 316 children with UTIs who received therapy to which the infecting isolate was not susceptible. The study included patients who had infections that were resistant to third-generation cephalosporins – that is, urinalysis found that the infections were not susceptible to ceftriaxone or cefotaxime in vitro. Before the resistant organisms were identified, however, the patients were started on discordant antibiotics.
Escalation of care was uncommon
The patients had a median age of 2.4 years, and 78% were girls. Approximately 90% were started on a cephalosporin, and about 65% received a first-generation cephalosporin. Patients presented during 2012-2017 to one of five children’s hospitals or to a large managed care organization with 10 hospitals in the United States. The investigators defined care escalation as a visit to the emergency department, hospitalization, or transfer to the ICU.
In all, seven patients (2%) had escalation of care on discordant antibiotics. Four children visited an emergency department without hospitalization, and three children were hospitalized because of persistent symptoms.
Among 230 cases for which the researchers had data about clinical response at a median follow-up of 3 days, 84% “had overall clinical improvement while on discordant antibiotics,” the authors said.
For 22 children who had repeat urine testing while on discordant antibiotics, 53% had resolution of pyuria, and 32% had improvement of pyuria, whereas 16% did not have improvement. Of the three patients without improvement, one had no change, and two had worsening.
Of 17 patients who had a repeat urine culture on discordant therapy, 65% had a negative repeat culture, and 18% grew the same pathogen with a decreased colony count. Two patients had a colony count that remained unchanged, and one patient had an increased colony count.
Small studies outside the United States have reported similar results, the researchers noted. Spontaneous resolution of UTIs or antibiotics reaching a sufficient concentration in the urine and renal parenchyma to achieve a clinical response are possible explanations for the findings, they wrote.
“Few children required escalation of care and most experienced initial clinical improvement,” noted Dr. Wang and colleagues. “Furthermore, in the small group of children that underwent repeat urine testing while on discordant therapy, most had resolution or improvement in pyuria and sterilization of their urine cultures. Our findings suggest that Additionally, given that these patients initially received what would generally be considered inadequate treatment, our findings may provide some insight into the natural history of UTIs and/or trigger further investigation into the relationship between in vitro urine culture susceptibilities and in vivo clinical response to treatment.”
‘Caution is needed’
The study “highlights an intriguing observation about children with UTIs unexpectedly responding to discordant antibiotic therapy,” Tej K. Mattoo, MD, and Basim I. Asmar, MD, wrote in an accompanying commentary.(doi: 10.1542/peds.2019-3512). Dr. Mattoo and Dr. Asmar, a pediatric nephrologist and a specialist in pediatric infectious diseases, respectively, at Wayne State University and affiliated with Children’s Hospital of Michigan, both in Detroit.
In an inpatient setting, it may be easy for physicians to reassess patients “once urine culture results reveal resistance to the treating antibiotic,” they noted. In an ambulatory setting, however, “it is likely that some patients will receive a full course of an antibiotic that does not have in vitro activity against the urinary pathogen.”
Physicians have a responsibility to use antibiotics judiciously, they said. Widely accepted principles include avoiding repeated courses of antibiotics, diagnosing UTIs appropriately, and not treating asymptomatic bacteriuria.
The study had no external funding. The authors had no relevant financial disclosures.
SOURCE: Wang ME et al. Pediatrics. 2020 Jan 17. doi: 10.1542/peds.2019-1608.
This article was updated 2/4/2020.
Children with urinary tract infections (UTIs) may improve clinically, and pyuria may resolve, during empiric treatment with an antibiotic that turns out to be discordant, according a retrospective study in Pediatrics.
“The low rate of care escalation and high rate of clinical improvement while on discordant antibiotics suggests that, for most patients, it would be reasonable to continue current empiric antibiotic practices until urine culture sensitivities return,” said first author Marie E. Wang, MD, a pediatric hospitalist at Stanford (Calif.) University, and colleagues.
The researchers examined the initial clinical response and escalation of care for 316 children with UTIs who received therapy to which the infecting isolate was not susceptible. The study included patients who had infections that were resistant to third-generation cephalosporins – that is, urinalysis found that the infections were not susceptible to ceftriaxone or cefotaxime in vitro. Before the resistant organisms were identified, however, the patients were started on discordant antibiotics.
Escalation of care was uncommon
The patients had a median age of 2.4 years, and 78% were girls. Approximately 90% were started on a cephalosporin, and about 65% received a first-generation cephalosporin. Patients presented during 2012-2017 to one of five children’s hospitals or to a large managed care organization with 10 hospitals in the United States. The investigators defined care escalation as a visit to the emergency department, hospitalization, or transfer to the ICU.
In all, seven patients (2%) had escalation of care on discordant antibiotics. Four children visited an emergency department without hospitalization, and three children were hospitalized because of persistent symptoms.
Among 230 cases for which the researchers had data about clinical response at a median follow-up of 3 days, 84% “had overall clinical improvement while on discordant antibiotics,” the authors said.
For 22 children who had repeat urine testing while on discordant antibiotics, 53% had resolution of pyuria, and 32% had improvement of pyuria, whereas 16% did not have improvement. Of the three patients without improvement, one had no change, and two had worsening.
Of 17 patients who had a repeat urine culture on discordant therapy, 65% had a negative repeat culture, and 18% grew the same pathogen with a decreased colony count. Two patients had a colony count that remained unchanged, and one patient had an increased colony count.
Small studies outside the United States have reported similar results, the researchers noted. Spontaneous resolution of UTIs or antibiotics reaching a sufficient concentration in the urine and renal parenchyma to achieve a clinical response are possible explanations for the findings, they wrote.
“Few children required escalation of care and most experienced initial clinical improvement,” noted Dr. Wang and colleagues. “Furthermore, in the small group of children that underwent repeat urine testing while on discordant therapy, most had resolution or improvement in pyuria and sterilization of their urine cultures. Our findings suggest that Additionally, given that these patients initially received what would generally be considered inadequate treatment, our findings may provide some insight into the natural history of UTIs and/or trigger further investigation into the relationship between in vitro urine culture susceptibilities and in vivo clinical response to treatment.”
‘Caution is needed’
The study “highlights an intriguing observation about children with UTIs unexpectedly responding to discordant antibiotic therapy,” Tej K. Mattoo, MD, and Basim I. Asmar, MD, wrote in an accompanying commentary.(doi: 10.1542/peds.2019-3512). Dr. Mattoo and Dr. Asmar, a pediatric nephrologist and a specialist in pediatric infectious diseases, respectively, at Wayne State University and affiliated with Children’s Hospital of Michigan, both in Detroit.
In an inpatient setting, it may be easy for physicians to reassess patients “once urine culture results reveal resistance to the treating antibiotic,” they noted. In an ambulatory setting, however, “it is likely that some patients will receive a full course of an antibiotic that does not have in vitro activity against the urinary pathogen.”
Physicians have a responsibility to use antibiotics judiciously, they said. Widely accepted principles include avoiding repeated courses of antibiotics, diagnosing UTIs appropriately, and not treating asymptomatic bacteriuria.
The study had no external funding. The authors had no relevant financial disclosures.
SOURCE: Wang ME et al. Pediatrics. 2020 Jan 17. doi: 10.1542/peds.2019-1608.
This article was updated 2/4/2020.
Children with urinary tract infections (UTIs) may improve clinically, and pyuria may resolve, during empiric treatment with an antibiotic that turns out to be discordant, according a retrospective study in Pediatrics.
“The low rate of care escalation and high rate of clinical improvement while on discordant antibiotics suggests that, for most patients, it would be reasonable to continue current empiric antibiotic practices until urine culture sensitivities return,” said first author Marie E. Wang, MD, a pediatric hospitalist at Stanford (Calif.) University, and colleagues.
The researchers examined the initial clinical response and escalation of care for 316 children with UTIs who received therapy to which the infecting isolate was not susceptible. The study included patients who had infections that were resistant to third-generation cephalosporins – that is, urinalysis found that the infections were not susceptible to ceftriaxone or cefotaxime in vitro. Before the resistant organisms were identified, however, the patients were started on discordant antibiotics.
Escalation of care was uncommon
The patients had a median age of 2.4 years, and 78% were girls. Approximately 90% were started on a cephalosporin, and about 65% received a first-generation cephalosporin. Patients presented during 2012-2017 to one of five children’s hospitals or to a large managed care organization with 10 hospitals in the United States. The investigators defined care escalation as a visit to the emergency department, hospitalization, or transfer to the ICU.
In all, seven patients (2%) had escalation of care on discordant antibiotics. Four children visited an emergency department without hospitalization, and three children were hospitalized because of persistent symptoms.
Among 230 cases for which the researchers had data about clinical response at a median follow-up of 3 days, 84% “had overall clinical improvement while on discordant antibiotics,” the authors said.
For 22 children who had repeat urine testing while on discordant antibiotics, 53% had resolution of pyuria, and 32% had improvement of pyuria, whereas 16% did not have improvement. Of the three patients without improvement, one had no change, and two had worsening.
Of 17 patients who had a repeat urine culture on discordant therapy, 65% had a negative repeat culture, and 18% grew the same pathogen with a decreased colony count. Two patients had a colony count that remained unchanged, and one patient had an increased colony count.
Small studies outside the United States have reported similar results, the researchers noted. Spontaneous resolution of UTIs or antibiotics reaching a sufficient concentration in the urine and renal parenchyma to achieve a clinical response are possible explanations for the findings, they wrote.
“Few children required escalation of care and most experienced initial clinical improvement,” noted Dr. Wang and colleagues. “Furthermore, in the small group of children that underwent repeat urine testing while on discordant therapy, most had resolution or improvement in pyuria and sterilization of their urine cultures. Our findings suggest that Additionally, given that these patients initially received what would generally be considered inadequate treatment, our findings may provide some insight into the natural history of UTIs and/or trigger further investigation into the relationship between in vitro urine culture susceptibilities and in vivo clinical response to treatment.”
‘Caution is needed’
The study “highlights an intriguing observation about children with UTIs unexpectedly responding to discordant antibiotic therapy,” Tej K. Mattoo, MD, and Basim I. Asmar, MD, wrote in an accompanying commentary.(doi: 10.1542/peds.2019-3512). Dr. Mattoo and Dr. Asmar, a pediatric nephrologist and a specialist in pediatric infectious diseases, respectively, at Wayne State University and affiliated with Children’s Hospital of Michigan, both in Detroit.
In an inpatient setting, it may be easy for physicians to reassess patients “once urine culture results reveal resistance to the treating antibiotic,” they noted. In an ambulatory setting, however, “it is likely that some patients will receive a full course of an antibiotic that does not have in vitro activity against the urinary pathogen.”
Physicians have a responsibility to use antibiotics judiciously, they said. Widely accepted principles include avoiding repeated courses of antibiotics, diagnosing UTIs appropriately, and not treating asymptomatic bacteriuria.
The study had no external funding. The authors had no relevant financial disclosures.
SOURCE: Wang ME et al. Pediatrics. 2020 Jan 17. doi: 10.1542/peds.2019-1608.
This article was updated 2/4/2020.
FROM PEDIATRICS
FDA approves CV disease benefit for once-weekly semaglutide
(Ozempic, Novo Nordisk) in the treatment of type 2 diabetes and has added new trial data information to the label of the oral version (Rybelsus, Novo Nordisk) pertaining to CV safety.
The agency expanded the once-weekly injectable semaglutide’s label to include an indication for reducing the risk for major adverse cardiovascular events (MACE), including CV death, nonfatal myocardial infarction (MI), or nonfatal stroke, in adults with type 2 diabetes who have established CV disease.
Initially approved for the treatment of type 2 diabetes in adults in December 2017, once-weekly subcutaneously injectable semaglutide comes in 0.5-mg and 1.0-mg doses in a dedicated prefilled pen device.
The approval for the new indication was based on data from the 2-year randomized Trial to Evaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Subjects With Type 2 Diabetes (SUSTAIN 6), in which injectable semaglutide or placebo was added to standard of care in 3,297 adults with type 2 diabetes and established CV disease.
As reported by Medscape Medical News in September 2016, patients who underwent treatment with one of the two doses of semaglutide had a significant 26% lower risk for the primary composite outcome of first occurrence of CV death, nonfatal MI, or nonfatal stroke, compared with those who received placebo.
The reduced CV risk was driven primarily by significant reductions in nonfatal stroke and nonfatal MI (39% and 26%, respectively). There was no difference in CV death between drug and placebo groups. Gastrointestinal adverse events were more frequent with semaglutide than placebo, with the majority occurring during the first 30 weeks.
The oral semaglutide formulation, taken daily in 7-mg or 14-mg doses, was approved for the treatment of type 2 diabetes in September 2019, the first orally available GLP-1 agonist.
Now, the FDA has updated the prescribing information in the clinical studies section (section 14) to include results from the randomized, placebo-controlled, 3,183-subject Trial Investigating the Cardiovascular Safety of Oral Semaglutide in Subjects With Type 2 Diabetes (PIONEER 6), reported in June 2019, which found a nonsignificant 21% reduction in three-component MACE with oral semaglutide. The addition to the label for Rybelsus is with regard to CV safety, not benefit.
SOUL: Large ongoing CV outcomes trial for oral semaglutide
In June 2019, Novo Nordisk initiated a larger CV outcomes trial of oral semaglutide, A Heart Disease Study of Semaglutide in Patients With Type 2 Diabetes (SOUL). The trial, which includes 9,642 adults with type 2 diabetes and established CV disease, is further investigating the drug’s effects on the incidence of MACE. The estimated completion date is July 2024.
Semaglutide joins a growing list of drugs approved for treating type 2 diabetes that have been granted additional label indications for benefits beyond the lowering of glucose.
These include Novo Nordisk’s other injectable GLP-1 agonist, liraglutide (Victoza), additionally approved for reducing CV events in high-risk patients with type 2 diabetes, and the sodium-glucose transport 2 inhibitors empagliflozin (Jardiance, Boehringer Ingelheim/Lilly), for reducing CV death; canagliflozin (Invokana, Janssen), for reducing major adverse CV events,; kidney disease, CV death, and heart failure hospitalization; and dapagliflozin (Farxiga, AstraZeneca), for reducing heart failure hospitalization.
Recently, in an exclusive Medscape Medical News article, some experts questioned the design of these CV outcomes trials, suggesting that imbalances in glycemic control, blood pressure, and diuretic use between treatment and placebo arms could have biased the CV and renal outcomes of the trials in favor of the study drugs
A version of this story originally appeared on Medscape.com.
(Ozempic, Novo Nordisk) in the treatment of type 2 diabetes and has added new trial data information to the label of the oral version (Rybelsus, Novo Nordisk) pertaining to CV safety.
The agency expanded the once-weekly injectable semaglutide’s label to include an indication for reducing the risk for major adverse cardiovascular events (MACE), including CV death, nonfatal myocardial infarction (MI), or nonfatal stroke, in adults with type 2 diabetes who have established CV disease.
Initially approved for the treatment of type 2 diabetes in adults in December 2017, once-weekly subcutaneously injectable semaglutide comes in 0.5-mg and 1.0-mg doses in a dedicated prefilled pen device.
The approval for the new indication was based on data from the 2-year randomized Trial to Evaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Subjects With Type 2 Diabetes (SUSTAIN 6), in which injectable semaglutide or placebo was added to standard of care in 3,297 adults with type 2 diabetes and established CV disease.
As reported by Medscape Medical News in September 2016, patients who underwent treatment with one of the two doses of semaglutide had a significant 26% lower risk for the primary composite outcome of first occurrence of CV death, nonfatal MI, or nonfatal stroke, compared with those who received placebo.
The reduced CV risk was driven primarily by significant reductions in nonfatal stroke and nonfatal MI (39% and 26%, respectively). There was no difference in CV death between drug and placebo groups. Gastrointestinal adverse events were more frequent with semaglutide than placebo, with the majority occurring during the first 30 weeks.
The oral semaglutide formulation, taken daily in 7-mg or 14-mg doses, was approved for the treatment of type 2 diabetes in September 2019, the first orally available GLP-1 agonist.
Now, the FDA has updated the prescribing information in the clinical studies section (section 14) to include results from the randomized, placebo-controlled, 3,183-subject Trial Investigating the Cardiovascular Safety of Oral Semaglutide in Subjects With Type 2 Diabetes (PIONEER 6), reported in June 2019, which found a nonsignificant 21% reduction in three-component MACE with oral semaglutide. The addition to the label for Rybelsus is with regard to CV safety, not benefit.
SOUL: Large ongoing CV outcomes trial for oral semaglutide
In June 2019, Novo Nordisk initiated a larger CV outcomes trial of oral semaglutide, A Heart Disease Study of Semaglutide in Patients With Type 2 Diabetes (SOUL). The trial, which includes 9,642 adults with type 2 diabetes and established CV disease, is further investigating the drug’s effects on the incidence of MACE. The estimated completion date is July 2024.
Semaglutide joins a growing list of drugs approved for treating type 2 diabetes that have been granted additional label indications for benefits beyond the lowering of glucose.
These include Novo Nordisk’s other injectable GLP-1 agonist, liraglutide (Victoza), additionally approved for reducing CV events in high-risk patients with type 2 diabetes, and the sodium-glucose transport 2 inhibitors empagliflozin (Jardiance, Boehringer Ingelheim/Lilly), for reducing CV death; canagliflozin (Invokana, Janssen), for reducing major adverse CV events,; kidney disease, CV death, and heart failure hospitalization; and dapagliflozin (Farxiga, AstraZeneca), for reducing heart failure hospitalization.
Recently, in an exclusive Medscape Medical News article, some experts questioned the design of these CV outcomes trials, suggesting that imbalances in glycemic control, blood pressure, and diuretic use between treatment and placebo arms could have biased the CV and renal outcomes of the trials in favor of the study drugs
A version of this story originally appeared on Medscape.com.
(Ozempic, Novo Nordisk) in the treatment of type 2 diabetes and has added new trial data information to the label of the oral version (Rybelsus, Novo Nordisk) pertaining to CV safety.
The agency expanded the once-weekly injectable semaglutide’s label to include an indication for reducing the risk for major adverse cardiovascular events (MACE), including CV death, nonfatal myocardial infarction (MI), or nonfatal stroke, in adults with type 2 diabetes who have established CV disease.
Initially approved for the treatment of type 2 diabetes in adults in December 2017, once-weekly subcutaneously injectable semaglutide comes in 0.5-mg and 1.0-mg doses in a dedicated prefilled pen device.
The approval for the new indication was based on data from the 2-year randomized Trial to Evaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Subjects With Type 2 Diabetes (SUSTAIN 6), in which injectable semaglutide or placebo was added to standard of care in 3,297 adults with type 2 diabetes and established CV disease.
As reported by Medscape Medical News in September 2016, patients who underwent treatment with one of the two doses of semaglutide had a significant 26% lower risk for the primary composite outcome of first occurrence of CV death, nonfatal MI, or nonfatal stroke, compared with those who received placebo.
The reduced CV risk was driven primarily by significant reductions in nonfatal stroke and nonfatal MI (39% and 26%, respectively). There was no difference in CV death between drug and placebo groups. Gastrointestinal adverse events were more frequent with semaglutide than placebo, with the majority occurring during the first 30 weeks.
The oral semaglutide formulation, taken daily in 7-mg or 14-mg doses, was approved for the treatment of type 2 diabetes in September 2019, the first orally available GLP-1 agonist.
Now, the FDA has updated the prescribing information in the clinical studies section (section 14) to include results from the randomized, placebo-controlled, 3,183-subject Trial Investigating the Cardiovascular Safety of Oral Semaglutide in Subjects With Type 2 Diabetes (PIONEER 6), reported in June 2019, which found a nonsignificant 21% reduction in three-component MACE with oral semaglutide. The addition to the label for Rybelsus is with regard to CV safety, not benefit.
SOUL: Large ongoing CV outcomes trial for oral semaglutide
In June 2019, Novo Nordisk initiated a larger CV outcomes trial of oral semaglutide, A Heart Disease Study of Semaglutide in Patients With Type 2 Diabetes (SOUL). The trial, which includes 9,642 adults with type 2 diabetes and established CV disease, is further investigating the drug’s effects on the incidence of MACE. The estimated completion date is July 2024.
Semaglutide joins a growing list of drugs approved for treating type 2 diabetes that have been granted additional label indications for benefits beyond the lowering of glucose.
These include Novo Nordisk’s other injectable GLP-1 agonist, liraglutide (Victoza), additionally approved for reducing CV events in high-risk patients with type 2 diabetes, and the sodium-glucose transport 2 inhibitors empagliflozin (Jardiance, Boehringer Ingelheim/Lilly), for reducing CV death; canagliflozin (Invokana, Janssen), for reducing major adverse CV events,; kidney disease, CV death, and heart failure hospitalization; and dapagliflozin (Farxiga, AstraZeneca), for reducing heart failure hospitalization.
Recently, in an exclusive Medscape Medical News article, some experts questioned the design of these CV outcomes trials, suggesting that imbalances in glycemic control, blood pressure, and diuretic use between treatment and placebo arms could have biased the CV and renal outcomes of the trials in favor of the study drugs
A version of this story originally appeared on Medscape.com.
Pyrrolidone carboxylic acid may be a key cutaneous biomarker
Pyrrolidone carboxylic acid (PCA), the primary constituent of the natural moisturizing factor (NMF),1 including its derivatives – such as simple2 and novel3 esters as well as sugar complexes4 – is the subject of great interest and research regarding its capacity to moisturize the stratum corneum via topical application.

Creams and lotions containing the sodium salt of PCA are widely reported to aid in hydrating the skin and ameliorating dry flaky skin conditions.5,6 In addition, the zinc salt of L-pyrrolidone carboxylate is a longtime cosmetic ingredient due to antimicrobial and astringent qualities. This column briefly addresses the role of PCA in skin health.7
Dry skin
In a comprehensive literature review from 1981, Clar and Fourtanier reported conclusive evidence that PCA acts as a hydrating agent and that all the cosmetic formulations with a minimum of 2% PCA and PCA salt that they tested in their own 8-year study enhanced dry skin in short- and long-term conditions given suitable vehicles (no aqueous solutions).6
In a 2014 clinical study of 64 healthy white women with either normal or cosmetic dry skin, Feng et al. noted that tape stripped samples of stratum corneum revealed significantly lower ratios of free amino acids to protein and PCA to protein. This was associated with decreased hydration levels compared with normal skin. The investigators concluded that lower NMF levels across the depth of the stratum corneum and reduced cohesivity characterize cosmetic dry skin and that these clinical endpoints merit attention in evaluating the usefulness of treatments for dry skin.8
In 2016, Wei et al. reported on their assessment of the barrier function, hydration, and dryness of the lower leg skin of 25 female patients during the winter and then in the subsequent summer. They found that PCA levels were significantly greater during the summer, as were keratins. Hydration was also higher during the summer, while transepidermal water loss and visual dryness grades were substantially lower.9
Atopic dermatitis
A 2014 clinical study by Brandt et al. in patients with skin prone to developing atopic dermatitis (AD) revealed that a body wash composed of the filaggrin metabolites arginine and PCA was well tolerated and diminished pruritus. Patients reported liking the product and suggested that it improved their quality of life.10
Later that year, Jung et al. characterized the relationship of PCA levels, and other factors, with the clinical severity of AD. Specifically, in a study of 73 subjects (21 with mild AD, 21 with moderate to severe AD, 13 with X-linked ichthyosis as a negative control for filaggrin gene mutation, and 18 healthy controls), the investigators assessed transepidermal water loss, stratum corneum hydration, and skin surface pH. They found that PCA levels and caspase-14 were lower in inflammatory lesions compared with nonlesional skin in subjects with AD. These levels also were associated with clinical AD severity as measured by eczema area and severity index scores as well as skin barrier function.11
PCA as a biomarker
In 2009, Kezic et al. determined that the use of tape stripping to cull PCA in the stratum corneum was effective in revealing that PCA concentration in the outermost skin layer is a viable biomarker of filaggrin genotype.12
Raj et al. conducted an interesting study in 2016 in which they set out to describe the various markers for total NMF levels and link them to the activities of plasmin and corneocyte maturation in the photoexposed cheek and photoprotected postauricular regions of healthy white, black African, and albino African women in South Africa. PCA levels were highest among the albino African group, followed by black African and then white participants. The investigators also found that bleomycin hydrolase was linked to PCA synthesis, as suggested by higher bleomycin levels in albino African participants. In this group, corneocyte maturation was also observed to be impeded.13
The next year, the same team studied stratum corneum physiology and biochemistry of the cheeks in 48 white women with sensitive skin. The goal was to ascertain the connections between bleomycin hydrolase and calpain-1, PCA levels, corneocyte maturation, and transglutaminase and plasmin activities. Capsaicin sensitivity was observed in 52% of subjects, with PCA levels and bleomycin hydrolase activity found to be lower in the capsaicin-sensitive panel and correlated in subjects not sensitive to capsaicin. The researchers concluded that reduced levels of PCA, bleomycin hydrolase, and transglutaminase combined with a larger volume of immature corneocytes suggest comparatively poor stratum corneum maturation in individuals with sensitive skin.14
Other uses
In 2012, Takino et al. used cultured normal human dermal fibroblasts to show that zinc l-pyrrolidone carboxylate blocked UVA induction of activator protein-1, diminished matrix metalloproteinase-1 synthesis, and spurred type I collagen production. The researchers suggested that such results suggest the potential of zinc PCA for further investigation as an agent to combat photoaging.7
Conclusion
. Recent research suggests that it may serve as an important biomarker of filaggrin, NMF levels, and skin hydration. In addition, new data point to its usefulness as a gauge for ADs. More investigations are necessary to ascertain the feasibility of adjusting PCA levels through topical administration and what effects topically applied PCA may have on various skin parameters.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014), as well as a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC. Write to her at dermnews@mdedge.com.
References
1. Björklund S et al. Soft Matter. 2014 Jul 7;10(25):4535-46.
2. Hall KJ, Hill JC. J Soc Cosmet Chem. 1986;37(6):397-407.
3. Tezuka T et al. Dermatology. 1994;188(1):21-4.
4. Kwoya Hakko Kogyo Co. Pyrrolidone carboxylic acid esters containing composition used to prevent loss of moisture from the skin. Patent JA 48 82 046 (1982).
5. Org Santerre. l-pyrrolidone carboxylic acid-sugar compounds as rehydrating ingredients in cosmetics. Patent Fr 2 277 823 (1977).
6. Clar EJ, Fourtanier A. Int J Cosmet Sci. 1981 Jun;3(3):101-13.
7. Takino Y et al. Int J Cosmet Sci. 2012 Feb;34(1):23-8.
8. Feng L et al. Int J Cosmet Sci. 2014 Jun;36(3):231-8.
9. Wei KS et al. J Cosmet Sci. 2016 May-Jun;67(3):185-203.
10. Brandt S et al. J Drugs Dermatol. 2014 Sep;13(9):1108-11.
11. Jung M et al. J Dermatol Sci. 2014 Dec;76(3):231-9.
12. Kezic S et al. Br J Dermatol. 2009 Nov;161(5):1098-104.
13. Raj N et al. Int J Cosmet Sci. 2016 Dec;38(6):567-75.
14. Raj N et al. Int J Cosmet Sci. 2017 Feb;39(1):2-10.
Pyrrolidone carboxylic acid (PCA), the primary constituent of the natural moisturizing factor (NMF),1 including its derivatives – such as simple2 and novel3 esters as well as sugar complexes4 – is the subject of great interest and research regarding its capacity to moisturize the stratum corneum via topical application.
Creams and lotions containing the sodium salt of PCA are widely reported to aid in hydrating the skin and ameliorating dry flaky skin conditions.5,6 In addition, the zinc salt of L-pyrrolidone carboxylate is a longtime cosmetic ingredient due to antimicrobial and astringent qualities. This column briefly addresses the role of PCA in skin health.7
Dry skin
In a comprehensive literature review from 1981, Clar and Fourtanier reported conclusive evidence that PCA acts as a hydrating agent and that all the cosmetic formulations with a minimum of 2% PCA and PCA salt that they tested in their own 8-year study enhanced dry skin in short- and long-term conditions given suitable vehicles (no aqueous solutions).6
In a 2014 clinical study of 64 healthy white women with either normal or cosmetic dry skin, Feng et al. noted that tape stripped samples of stratum corneum revealed significantly lower ratios of free amino acids to protein and PCA to protein. This was associated with decreased hydration levels compared with normal skin. The investigators concluded that lower NMF levels across the depth of the stratum corneum and reduced cohesivity characterize cosmetic dry skin and that these clinical endpoints merit attention in evaluating the usefulness of treatments for dry skin.8
In 2016, Wei et al. reported on their assessment of the barrier function, hydration, and dryness of the lower leg skin of 25 female patients during the winter and then in the subsequent summer. They found that PCA levels were significantly greater during the summer, as were keratins. Hydration was also higher during the summer, while transepidermal water loss and visual dryness grades were substantially lower.9
Atopic dermatitis
A 2014 clinical study by Brandt et al. in patients with skin prone to developing atopic dermatitis (AD) revealed that a body wash composed of the filaggrin metabolites arginine and PCA was well tolerated and diminished pruritus. Patients reported liking the product and suggested that it improved their quality of life.10
Later that year, Jung et al. characterized the relationship of PCA levels, and other factors, with the clinical severity of AD. Specifically, in a study of 73 subjects (21 with mild AD, 21 with moderate to severe AD, 13 with X-linked ichthyosis as a negative control for filaggrin gene mutation, and 18 healthy controls), the investigators assessed transepidermal water loss, stratum corneum hydration, and skin surface pH. They found that PCA levels and caspase-14 were lower in inflammatory lesions compared with nonlesional skin in subjects with AD. These levels also were associated with clinical AD severity as measured by eczema area and severity index scores as well as skin barrier function.11
PCA as a biomarker
In 2009, Kezic et al. determined that the use of tape stripping to cull PCA in the stratum corneum was effective in revealing that PCA concentration in the outermost skin layer is a viable biomarker of filaggrin genotype.12
Raj et al. conducted an interesting study in 2016 in which they set out to describe the various markers for total NMF levels and link them to the activities of plasmin and corneocyte maturation in the photoexposed cheek and photoprotected postauricular regions of healthy white, black African, and albino African women in South Africa. PCA levels were highest among the albino African group, followed by black African and then white participants. The investigators also found that bleomycin hydrolase was linked to PCA synthesis, as suggested by higher bleomycin levels in albino African participants. In this group, corneocyte maturation was also observed to be impeded.13
The next year, the same team studied stratum corneum physiology and biochemistry of the cheeks in 48 white women with sensitive skin. The goal was to ascertain the connections between bleomycin hydrolase and calpain-1, PCA levels, corneocyte maturation, and transglutaminase and plasmin activities. Capsaicin sensitivity was observed in 52% of subjects, with PCA levels and bleomycin hydrolase activity found to be lower in the capsaicin-sensitive panel and correlated in subjects not sensitive to capsaicin. The researchers concluded that reduced levels of PCA, bleomycin hydrolase, and transglutaminase combined with a larger volume of immature corneocytes suggest comparatively poor stratum corneum maturation in individuals with sensitive skin.14
Other uses
In 2012, Takino et al. used cultured normal human dermal fibroblasts to show that zinc l-pyrrolidone carboxylate blocked UVA induction of activator protein-1, diminished matrix metalloproteinase-1 synthesis, and spurred type I collagen production. The researchers suggested that such results suggest the potential of zinc PCA for further investigation as an agent to combat photoaging.7
Conclusion
. Recent research suggests that it may serve as an important biomarker of filaggrin, NMF levels, and skin hydration. In addition, new data point to its usefulness as a gauge for ADs. More investigations are necessary to ascertain the feasibility of adjusting PCA levels through topical administration and what effects topically applied PCA may have on various skin parameters.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014), as well as a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC. Write to her at dermnews@mdedge.com.
References
1. Björklund S et al. Soft Matter. 2014 Jul 7;10(25):4535-46.
2. Hall KJ, Hill JC. J Soc Cosmet Chem. 1986;37(6):397-407.
3. Tezuka T et al. Dermatology. 1994;188(1):21-4.
4. Kwoya Hakko Kogyo Co. Pyrrolidone carboxylic acid esters containing composition used to prevent loss of moisture from the skin. Patent JA 48 82 046 (1982).
5. Org Santerre. l-pyrrolidone carboxylic acid-sugar compounds as rehydrating ingredients in cosmetics. Patent Fr 2 277 823 (1977).
6. Clar EJ, Fourtanier A. Int J Cosmet Sci. 1981 Jun;3(3):101-13.
7. Takino Y et al. Int J Cosmet Sci. 2012 Feb;34(1):23-8.
8. Feng L et al. Int J Cosmet Sci. 2014 Jun;36(3):231-8.
9. Wei KS et al. J Cosmet Sci. 2016 May-Jun;67(3):185-203.
10. Brandt S et al. J Drugs Dermatol. 2014 Sep;13(9):1108-11.
11. Jung M et al. J Dermatol Sci. 2014 Dec;76(3):231-9.
12. Kezic S et al. Br J Dermatol. 2009 Nov;161(5):1098-104.
13. Raj N et al. Int J Cosmet Sci. 2016 Dec;38(6):567-75.
14. Raj N et al. Int J Cosmet Sci. 2017 Feb;39(1):2-10.
Pyrrolidone carboxylic acid (PCA), the primary constituent of the natural moisturizing factor (NMF),1 including its derivatives – such as simple2 and novel3 esters as well as sugar complexes4 – is the subject of great interest and research regarding its capacity to moisturize the stratum corneum via topical application.
Creams and lotions containing the sodium salt of PCA are widely reported to aid in hydrating the skin and ameliorating dry flaky skin conditions.5,6 In addition, the zinc salt of L-pyrrolidone carboxylate is a longtime cosmetic ingredient due to antimicrobial and astringent qualities. This column briefly addresses the role of PCA in skin health.7
Dry skin
In a comprehensive literature review from 1981, Clar and Fourtanier reported conclusive evidence that PCA acts as a hydrating agent and that all the cosmetic formulations with a minimum of 2% PCA and PCA salt that they tested in their own 8-year study enhanced dry skin in short- and long-term conditions given suitable vehicles (no aqueous solutions).6
In a 2014 clinical study of 64 healthy white women with either normal or cosmetic dry skin, Feng et al. noted that tape stripped samples of stratum corneum revealed significantly lower ratios of free amino acids to protein and PCA to protein. This was associated with decreased hydration levels compared with normal skin. The investigators concluded that lower NMF levels across the depth of the stratum corneum and reduced cohesivity characterize cosmetic dry skin and that these clinical endpoints merit attention in evaluating the usefulness of treatments for dry skin.8
In 2016, Wei et al. reported on their assessment of the barrier function, hydration, and dryness of the lower leg skin of 25 female patients during the winter and then in the subsequent summer. They found that PCA levels were significantly greater during the summer, as were keratins. Hydration was also higher during the summer, while transepidermal water loss and visual dryness grades were substantially lower.9
Atopic dermatitis
A 2014 clinical study by Brandt et al. in patients with skin prone to developing atopic dermatitis (AD) revealed that a body wash composed of the filaggrin metabolites arginine and PCA was well tolerated and diminished pruritus. Patients reported liking the product and suggested that it improved their quality of life.10
Later that year, Jung et al. characterized the relationship of PCA levels, and other factors, with the clinical severity of AD. Specifically, in a study of 73 subjects (21 with mild AD, 21 with moderate to severe AD, 13 with X-linked ichthyosis as a negative control for filaggrin gene mutation, and 18 healthy controls), the investigators assessed transepidermal water loss, stratum corneum hydration, and skin surface pH. They found that PCA levels and caspase-14 were lower in inflammatory lesions compared with nonlesional skin in subjects with AD. These levels also were associated with clinical AD severity as measured by eczema area and severity index scores as well as skin barrier function.11
PCA as a biomarker
In 2009, Kezic et al. determined that the use of tape stripping to cull PCA in the stratum corneum was effective in revealing that PCA concentration in the outermost skin layer is a viable biomarker of filaggrin genotype.12
Raj et al. conducted an interesting study in 2016 in which they set out to describe the various markers for total NMF levels and link them to the activities of plasmin and corneocyte maturation in the photoexposed cheek and photoprotected postauricular regions of healthy white, black African, and albino African women in South Africa. PCA levels were highest among the albino African group, followed by black African and then white participants. The investigators also found that bleomycin hydrolase was linked to PCA synthesis, as suggested by higher bleomycin levels in albino African participants. In this group, corneocyte maturation was also observed to be impeded.13
The next year, the same team studied stratum corneum physiology and biochemistry of the cheeks in 48 white women with sensitive skin. The goal was to ascertain the connections between bleomycin hydrolase and calpain-1, PCA levels, corneocyte maturation, and transglutaminase and plasmin activities. Capsaicin sensitivity was observed in 52% of subjects, with PCA levels and bleomycin hydrolase activity found to be lower in the capsaicin-sensitive panel and correlated in subjects not sensitive to capsaicin. The researchers concluded that reduced levels of PCA, bleomycin hydrolase, and transglutaminase combined with a larger volume of immature corneocytes suggest comparatively poor stratum corneum maturation in individuals with sensitive skin.14
Other uses
In 2012, Takino et al. used cultured normal human dermal fibroblasts to show that zinc l-pyrrolidone carboxylate blocked UVA induction of activator protein-1, diminished matrix metalloproteinase-1 synthesis, and spurred type I collagen production. The researchers suggested that such results suggest the potential of zinc PCA for further investigation as an agent to combat photoaging.7
Conclusion
. Recent research suggests that it may serve as an important biomarker of filaggrin, NMF levels, and skin hydration. In addition, new data point to its usefulness as a gauge for ADs. More investigations are necessary to ascertain the feasibility of adjusting PCA levels through topical administration and what effects topically applied PCA may have on various skin parameters.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014), as well as a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC. Write to her at dermnews@mdedge.com.
References
1. Björklund S et al. Soft Matter. 2014 Jul 7;10(25):4535-46.
2. Hall KJ, Hill JC. J Soc Cosmet Chem. 1986;37(6):397-407.
3. Tezuka T et al. Dermatology. 1994;188(1):21-4.
4. Kwoya Hakko Kogyo Co. Pyrrolidone carboxylic acid esters containing composition used to prevent loss of moisture from the skin. Patent JA 48 82 046 (1982).
5. Org Santerre. l-pyrrolidone carboxylic acid-sugar compounds as rehydrating ingredients in cosmetics. Patent Fr 2 277 823 (1977).
6. Clar EJ, Fourtanier A. Int J Cosmet Sci. 1981 Jun;3(3):101-13.
7. Takino Y et al. Int J Cosmet Sci. 2012 Feb;34(1):23-8.
8. Feng L et al. Int J Cosmet Sci. 2014 Jun;36(3):231-8.
9. Wei KS et al. J Cosmet Sci. 2016 May-Jun;67(3):185-203.
10. Brandt S et al. J Drugs Dermatol. 2014 Sep;13(9):1108-11.
11. Jung M et al. J Dermatol Sci. 2014 Dec;76(3):231-9.
12. Kezic S et al. Br J Dermatol. 2009 Nov;161(5):1098-104.
13. Raj N et al. Int J Cosmet Sci. 2016 Dec;38(6):567-75.
14. Raj N et al. Int J Cosmet Sci. 2017 Feb;39(1):2-10.
Scleromyxedema in a Patient With Thyroid Disease: An Atypical Case or a Case for Revised Criteria?
Scleromyxedema (SM) is a generalized papular and sclerodermoid form of lichen myxedematosus (LM), commonly referred to as papular mucinosis. It is a rare progressive disease of unknown etiology with systemic manifestations that cause serious morbidity and mortality. Diagnostic criteria were initially created by Montgomery and Underwood1 in 1953 and revised by Rongioletti and Rebora2 in 2001 as follows: (1) generalized papular and sclerodermoid eruption; (2) histologic triad of mucin deposition, fibroblast proliferation, and fibrosis; (3) monoclonal gammopathy; and (4) absence of thyroid disease. There are several reports of LM in association with hypothyroidism, most of which can be characterized as atypical.3-8 We present a case of SM in a patient with Hashimoto thyroiditis and propose that the presence of thyroid disease should not preclude the diagnosis of SM.
Case Report
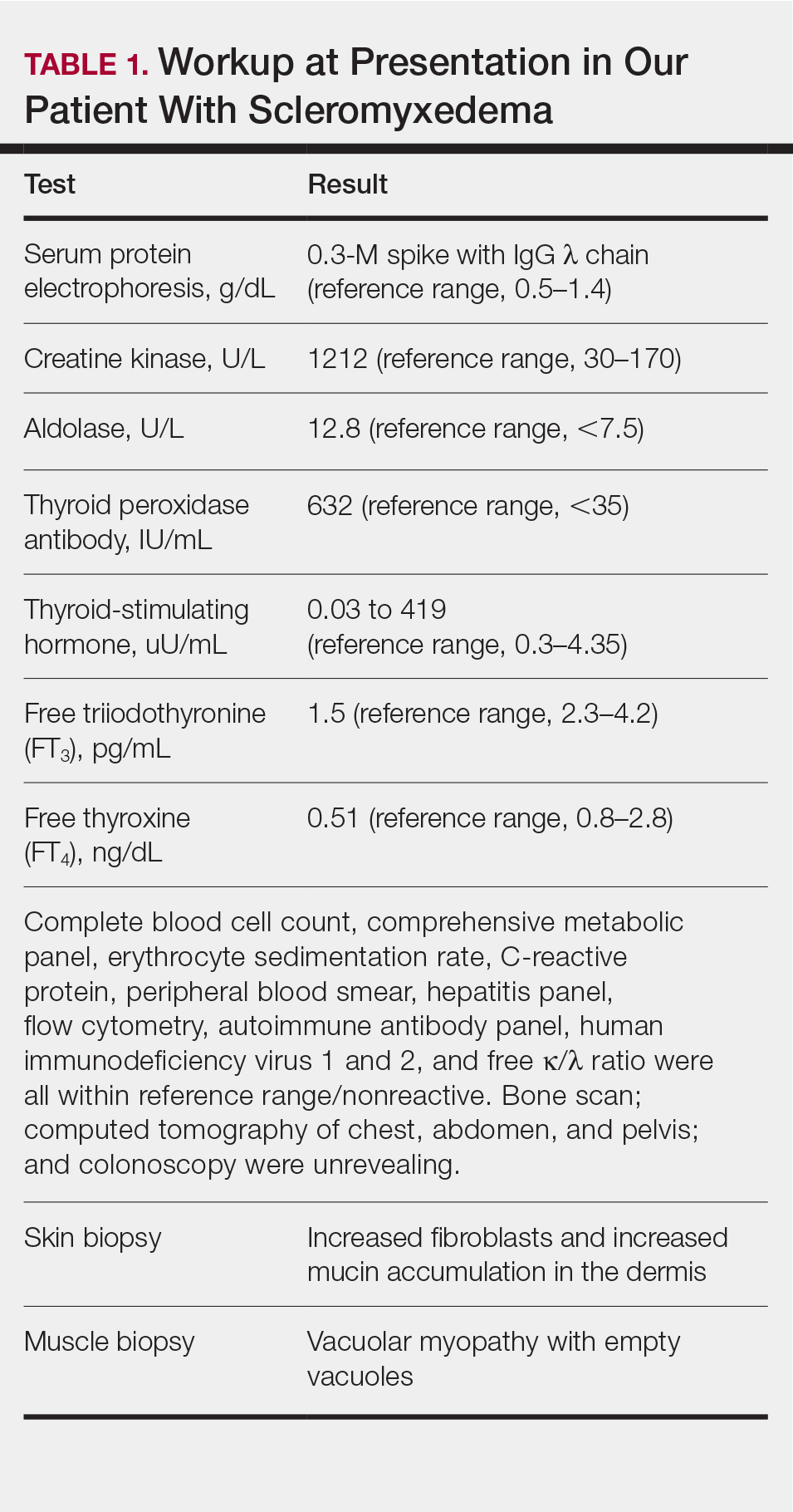
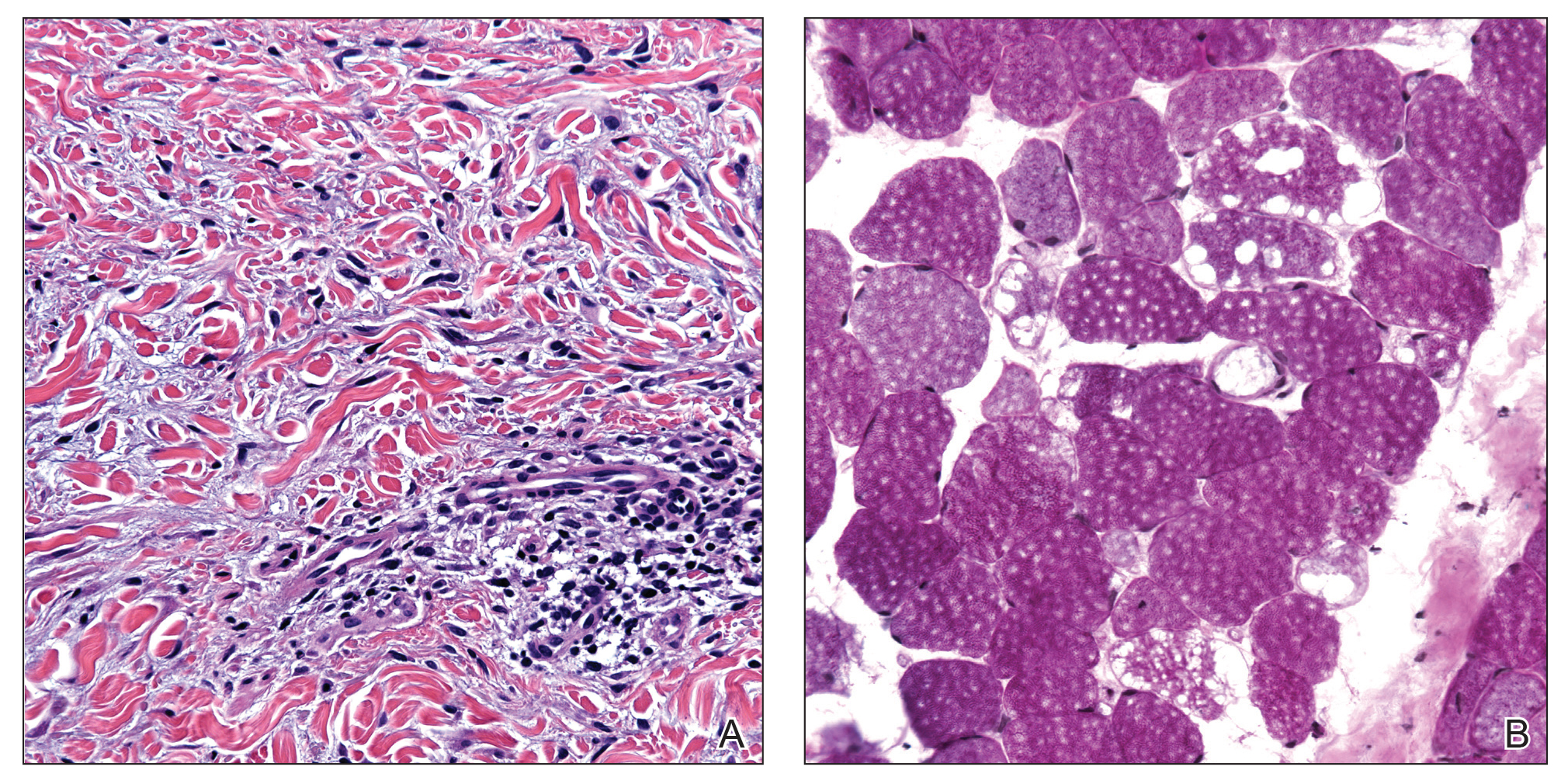
A 44-year-old woman presented with a progressive eruption of thickened skin and papules spanning many months. The papules ranged from flesh colored to erythematous and covered more than 80% of the body surface area, most notably involving the face, neck, ears, arms, chest, abdomen, and thighs (Figures 1A and 2A). Review of systems was notable for pruritus, muscle pain but no weakness, dysphagia, and constipation. Her medical history included childhood atopic dermatitis and Hashimoto thyroiditis. Hypothyroidism was diagnosed with support of a thyroid ultrasound and thyroid peroxidase antibodies. It was treated with oral levothyroxine for 2 years prior to the skin eruption. Thyroid biopsy was not performed. Her thyroid-stimulating hormone levels notably fluctuated in the year prior to presentation despite close clinical and laboratory monitoring by an endocrinologist. Laboratory results are summarized in Table 1. Both skin and muscle9 biopsies were consistent with SM (Figure 3) and are summarized in Table 1.
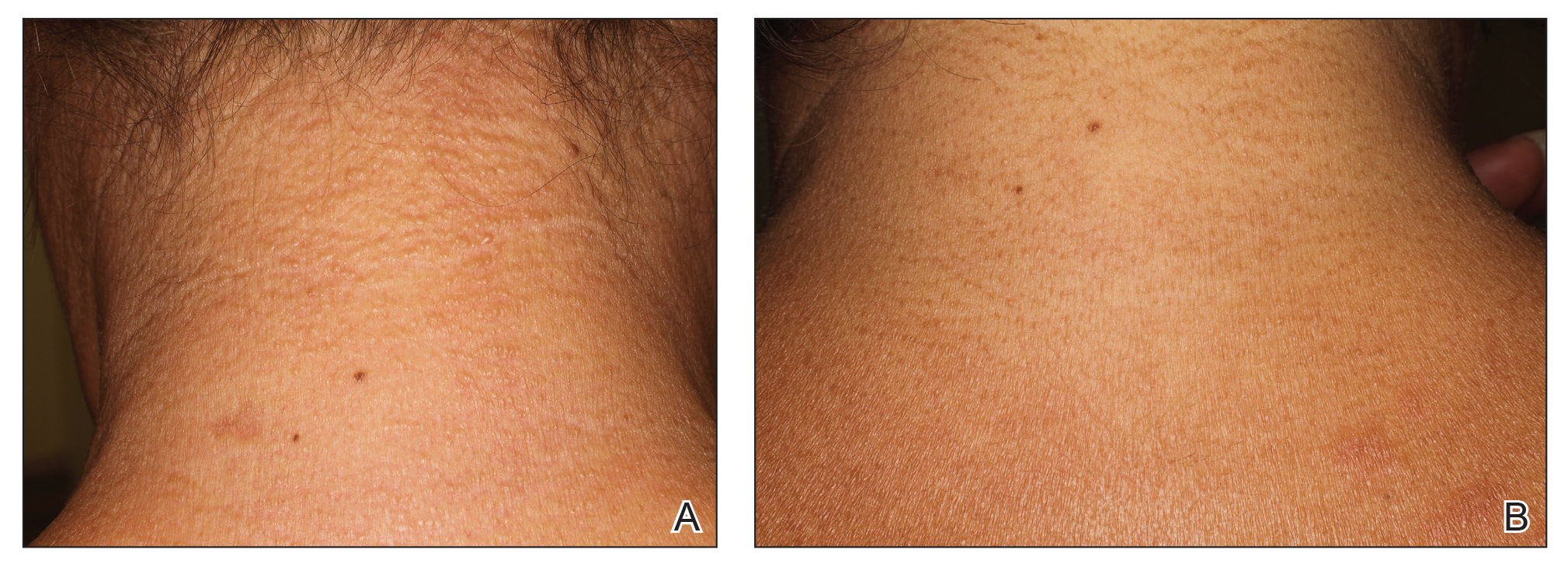

Shortly after presentation to our clinic the patient developed acute concerns of confusion and muscle weakness. She was admitted for further inpatient management due to concern for dermato-neuro syndrome, a rare but potentially fatal decline in neurological status that can progress to coma and death, rather than myxedema coma. On admission, a thyroid function test showed subclinical hypothyroidism with a thyroid-stimulating hormone level of 6.35 uU/mL (reference range, 0.3–4.35 uU/mL) and free thyroxine (FT4) level of 1.5 ng/dL (reference range, 0.8–2.8 ng/dL). While hospitalized she was started on intravenous levothyroxine, systemic steroids, and a course of intravenous immunoglobulin (IVIg) treatment consisting of 2 g/kg divided over 5 days. On this regimen, her mental status quickly returned to baseline and other symptoms improved, including the skin eruption (Figures 1B and 2B). She has been maintained on lenalidomide 25 mg/d for the first 3 weeks of each month as well as monthly IVIg infusions. Her thyroid levels have persistently fluctuated despite intramuscular levothyroxine dosing, but her skin has remained clear with continued SM-directed therapy.
Comment
Classification
Lichen myxedematosus is differentiated into localized and generalized forms. The former is limited to the skin and lacks monoclonal gammopathy. The latter, also known as SM, is associated with monoclonal gammopathy and systemic symptoms. Atypical LM is an umbrella term for intermediate cases.
Clinical Presentation
Skin manifestations of SM are described as 1- to 3-mm, firm, waxy, dome-shaped papules that commonly affect the hands, forearms, face, neck, trunk, and thighs. The surrounding skin may be reddish brown and edematous with evidence of skin thickening. Extracutaneous manifestations in SM are numerous and unpredictable. Any organ system can be involved, but gastrointestinal, rheumatologic, pulmonary, and cardiovascular complications are most common.10 A comprehensive multidisciplinary evaluation is necessary based on clinical symptoms and laboratory findings.
Management
Many treatments have been proposed for SM in case reports and case series. Prior treatments have had little success. Most recently, in one of the largest case series on SM, Rongioletti et al10 demonstrated IVIg to be a safe and effective treatment modality.
Differential Diagnosis
An important differential diagnosis is generalized myxedema, which is seen in long-standing hypothyroidism and may present with cutaneous mucinosis and systemic symptoms that resemble SM. Hypothyroid myxedema is associated with a widespread slowing of the body’s metabolic processes and deposition of mucin in various organs, including the skin, creating a generalized nonpitting edema. Classic clinical signs include macroglossia, periorbital puffiness, thick lips, and acral swelling. The skin tends to be cold, dry, and pale. Hair is characterized as being coarse, dry, and brittle with diffuse partial alopecia. Histologically, there is hyperkeratosis with follicular plugging and diffuse mucin and edema splaying between collagen fibers spanning the entire dermis.11 In contradistinction with SM, there is no fibroblast proliferation. The treatment is thyroid replacement therapy. Hyperthyroidism has distinct clinical and histologic changes. Clinically, there is moist and smooth skin with soft, fine, and sometimes alopecic hair. Graves disease, the most common cause of hyperthyroidism, is further characterized by Graves ophthalmopathy and pretibial myxedema, or pink to brown, raised, firm, indurated, asymmetric plaques most commonly affecting the shins. Histologically there is increased mucin in the lower to mid dermis without fibroblast proliferation. The epidermis can be hyperkeratotic, which will clinically correlate with verrucous lesions.12
Hypothyroid encephalopathy is a rare disorder that can cause a change in mental status. It is a steroid-responsive autoimmune process characterized by encephalopathy that is associated with cognitive impairment and psychiatric features. It is a diagnosis of exclusion and should be suspected in women with a history of autoimmune disease, especially antithyroid peroxidase antibodies, a negative infectious workup, and encephalitis with behavioral changes. Although typically highly responsive to systemic steroids, IVIg also has shown efficacy.13
Presence of Thyroid Disease
According to a PubMed search of articles indexed for MEDLINE using the terms scleromyxedema and lichen myxedematosus, there are 7 cases in the literature that potentially describe LM associated with hypothyroidism (Table 2).3-8 The majority of these cases lack monoclonal gammopathy; improved with thyroid replacement therapy; or had severely atypical clinical presentations, rendering them cases of atypical LM or atypical thyroid dermopathy.3-6 Macnab and Kenny7 presented a case of subclinical hypothyroidism with a generalized papular eruption, monoclonal gammopathy, and consistent histologic changes that responded to IVIg therapy. These findings are suggestive of SM, but limited to the current diagnostic criteria, the patient was diagnosed with atypical LM.7 Shenoy et al8 described 2 cases of LM with hypothyroidism. One patient had biopsy-proven SM that was responsive to IVIg as well as Hashimoto thyroiditis with delayed onset of monoclonal gammopathy. The second patient had a medical history of hypothyroidism and Hodgkin lymphoma with active rheumatoid arthritis and biopsy-proven LM that was responsive to systemic steroids.8
Current literature states that thyroid disorder precludes the diagnosis of SM. However, historic literature would suggest otherwise. Because of inconsistent reports and theories regarding the pathogenesis of various sclerodermoid and mucin deposition diseases, in 1953 Montgomery and Underwood1 sought to differentiate LM from scleroderma and generalized myxedema. They stressed clinical appearance and proposed diagnostic criteria for LM as generalized papular mucinosis in which “[n]o relation to disturbance of the thyroid or other endocrine glands is apparent,” whereas generalized myxedema was defined as a “[t]rue cutaneous myxedema, with diffuse edema and the usual commonly recognized changes” in patients with endocrine abnormalities.1 With this classification, the authors made a clear distinction between mucinosis caused by thyroid abnormalities and LM, which is not caused by a thyroid disorder. Since this original description was published, associations with monoclonal gammopathy and fibroblast proliferation have been made, ultimately culminating into the current 2001 criteria that incorporate the absence of thyroid disease.2

Conclusion
We believe our case is consistent with the classification initially proposed by Montgomery and Underwood1 and is strengthened with the more recent associations with monoclonal gammopathy and specific histopathologic findings. Although there is no definitive way to rule out myxedema coma or Hashimoto encephalopathy to describe our patient’s transient neurologic decline, her clinical symptoms, laboratory findings, and biopsy results all supported the diagnosis of SM. Furthermore, her response to SM-directed therapy, despite fluctuating thyroid function test results, also supported the diagnosis. In the setting of cutaneous mucinosis with conflicting findings for hypothyroid myxedema, LM should be ruled out. Given the features presented in this report and others, diagnostic criteria should allow for SM and thyroid dysfunction to be concurrent diagnoses. Most importantly, we believe it is essential to identify and diagnose SM in a timely manner to facilitate SM-directed therapy, namely IVIg, to potentially minimize the disease’s notable morbidity and mortality.
- Montgomery H, Underwood LJ. Lichen myxedematosus; differentiation from cutaneous myxedemas or mucoid states. J Invest Dermatol. 1953;20:213-236.
- Rongioletti F, Rebora A. Updated classification of papular mucinosis, lichen myxedematosus and scleromyxedema. J Am Acad Dermatol. 2001;44:273-281.
- Archibald GC, Calvert HT. Hypothyroidsm and lichen myxedematosus. Arch Dermatol. 1977;113:684.
- Schaeffer D, Bruce S, Rosen T. Cutaneous mucinosis associated with thyroid dysfunction. Cutis. 1983;11:449-456.
- Martin-Ezquerra G, Sanchez-Regaña M, Massana-Gil J, et al. Papular mucinosis associated with subclinical hypothyroidism: improvement with thyroxine therapy. J Eur Acad Dermatol Venereol. 2006;20:1340-1341.
- Volpato MB, Jaime TJ, Proença MP, et al. Papular mucinosis associated with hypothyroidism. An Bras Dermatol. 2010;85:89-92.
- Macnab M, Kenny P. Successful intravenous immunoglobulin treatment of atypical lichen myxedematosus associated with hypothyroidism and central nervous system. involvement: case report and discussion of the literature. J Cutan Med Surg. 2013;17:69-73.
- Shenoy A, Steixner J, Beltrani V, et al. Discrete papular lichen myxedematosus and scleromyxedema with hypothyroidism: a report of two cases. Case Rep Dermatol. 2019;11:64-70.
- Helfrich DJ, Walker ER, Martinez AJ, et al. Scleromyxedema myopathy: case report and review of the literature. Arthritis Rheum. 1988;31:1437-1441.
- Rongioletti F, Merlo G, Cinotti E, et al. Scleromyxedema: a multicenter study of characteristics, comorbidities, course, and therapy in 30 patients. J Am Acad Dermatol. 2013;69:66-72.
- Jackson EM, English JC 3rd. Diffuse cutaneous mucinoses. Dermatol Clin. 2002;20:493-501.
- Leonhardt JM, Heymann WR. Thyroid disease and the skin. Dermatol Clin. 2002;20:473-481.
- Zhou JY, Xu B, Lopes J, et al. Hashimoto encephalopathy: literature review. Acta Neurol Scand. 2017;135:285-290.
Scleromyxedema (SM) is a generalized papular and sclerodermoid form of lichen myxedematosus (LM), commonly referred to as papular mucinosis. It is a rare progressive disease of unknown etiology with systemic manifestations that cause serious morbidity and mortality. Diagnostic criteria were initially created by Montgomery and Underwood1 in 1953 and revised by Rongioletti and Rebora2 in 2001 as follows: (1) generalized papular and sclerodermoid eruption; (2) histologic triad of mucin deposition, fibroblast proliferation, and fibrosis; (3) monoclonal gammopathy; and (4) absence of thyroid disease. There are several reports of LM in association with hypothyroidism, most of which can be characterized as atypical.3-8 We present a case of SM in a patient with Hashimoto thyroiditis and propose that the presence of thyroid disease should not preclude the diagnosis of SM.
Case Report
A 44-year-old woman presented with a progressive eruption of thickened skin and papules spanning many months. The papules ranged from flesh colored to erythematous and covered more than 80% of the body surface area, most notably involving the face, neck, ears, arms, chest, abdomen, and thighs (Figures 1A and 2A). Review of systems was notable for pruritus, muscle pain but no weakness, dysphagia, and constipation. Her medical history included childhood atopic dermatitis and Hashimoto thyroiditis. Hypothyroidism was diagnosed with support of a thyroid ultrasound and thyroid peroxidase antibodies. It was treated with oral levothyroxine for 2 years prior to the skin eruption. Thyroid biopsy was not performed. Her thyroid-stimulating hormone levels notably fluctuated in the year prior to presentation despite close clinical and laboratory monitoring by an endocrinologist. Laboratory results are summarized in Table 1. Both skin and muscle9 biopsies were consistent with SM (Figure 3) and are summarized in Table 1.
Shortly after presentation to our clinic the patient developed acute concerns of confusion and muscle weakness. She was admitted for further inpatient management due to concern for dermato-neuro syndrome, a rare but potentially fatal decline in neurological status that can progress to coma and death, rather than myxedema coma. On admission, a thyroid function test showed subclinical hypothyroidism with a thyroid-stimulating hormone level of 6.35 uU/mL (reference range, 0.3–4.35 uU/mL) and free thyroxine (FT4) level of 1.5 ng/dL (reference range, 0.8–2.8 ng/dL). While hospitalized she was started on intravenous levothyroxine, systemic steroids, and a course of intravenous immunoglobulin (IVIg) treatment consisting of 2 g/kg divided over 5 days. On this regimen, her mental status quickly returned to baseline and other symptoms improved, including the skin eruption (Figures 1B and 2B). She has been maintained on lenalidomide 25 mg/d for the first 3 weeks of each month as well as monthly IVIg infusions. Her thyroid levels have persistently fluctuated despite intramuscular levothyroxine dosing, but her skin has remained clear with continued SM-directed therapy.
Comment
Classification
Lichen myxedematosus is differentiated into localized and generalized forms. The former is limited to the skin and lacks monoclonal gammopathy. The latter, also known as SM, is associated with monoclonal gammopathy and systemic symptoms. Atypical LM is an umbrella term for intermediate cases.
Clinical Presentation
Skin manifestations of SM are described as 1- to 3-mm, firm, waxy, dome-shaped papules that commonly affect the hands, forearms, face, neck, trunk, and thighs. The surrounding skin may be reddish brown and edematous with evidence of skin thickening. Extracutaneous manifestations in SM are numerous and unpredictable. Any organ system can be involved, but gastrointestinal, rheumatologic, pulmonary, and cardiovascular complications are most common.10 A comprehensive multidisciplinary evaluation is necessary based on clinical symptoms and laboratory findings.
Management
Many treatments have been proposed for SM in case reports and case series. Prior treatments have had little success. Most recently, in one of the largest case series on SM, Rongioletti et al10 demonstrated IVIg to be a safe and effective treatment modality.
Differential Diagnosis
An important differential diagnosis is generalized myxedema, which is seen in long-standing hypothyroidism and may present with cutaneous mucinosis and systemic symptoms that resemble SM. Hypothyroid myxedema is associated with a widespread slowing of the body’s metabolic processes and deposition of mucin in various organs, including the skin, creating a generalized nonpitting edema. Classic clinical signs include macroglossia, periorbital puffiness, thick lips, and acral swelling. The skin tends to be cold, dry, and pale. Hair is characterized as being coarse, dry, and brittle with diffuse partial alopecia. Histologically, there is hyperkeratosis with follicular plugging and diffuse mucin and edema splaying between collagen fibers spanning the entire dermis.11 In contradistinction with SM, there is no fibroblast proliferation. The treatment is thyroid replacement therapy. Hyperthyroidism has distinct clinical and histologic changes. Clinically, there is moist and smooth skin with soft, fine, and sometimes alopecic hair. Graves disease, the most common cause of hyperthyroidism, is further characterized by Graves ophthalmopathy and pretibial myxedema, or pink to brown, raised, firm, indurated, asymmetric plaques most commonly affecting the shins. Histologically there is increased mucin in the lower to mid dermis without fibroblast proliferation. The epidermis can be hyperkeratotic, which will clinically correlate with verrucous lesions.12
Hypothyroid encephalopathy is a rare disorder that can cause a change in mental status. It is a steroid-responsive autoimmune process characterized by encephalopathy that is associated with cognitive impairment and psychiatric features. It is a diagnosis of exclusion and should be suspected in women with a history of autoimmune disease, especially antithyroid peroxidase antibodies, a negative infectious workup, and encephalitis with behavioral changes. Although typically highly responsive to systemic steroids, IVIg also has shown efficacy.13
Presence of Thyroid Disease
According to a PubMed search of articles indexed for MEDLINE using the terms scleromyxedema and lichen myxedematosus, there are 7 cases in the literature that potentially describe LM associated with hypothyroidism (Table 2).3-8 The majority of these cases lack monoclonal gammopathy; improved with thyroid replacement therapy; or had severely atypical clinical presentations, rendering them cases of atypical LM or atypical thyroid dermopathy.3-6 Macnab and Kenny7 presented a case of subclinical hypothyroidism with a generalized papular eruption, monoclonal gammopathy, and consistent histologic changes that responded to IVIg therapy. These findings are suggestive of SM, but limited to the current diagnostic criteria, the patient was diagnosed with atypical LM.7 Shenoy et al8 described 2 cases of LM with hypothyroidism. One patient had biopsy-proven SM that was responsive to IVIg as well as Hashimoto thyroiditis with delayed onset of monoclonal gammopathy. The second patient had a medical history of hypothyroidism and Hodgkin lymphoma with active rheumatoid arthritis and biopsy-proven LM that was responsive to systemic steroids.8
Current literature states that thyroid disorder precludes the diagnosis of SM. However, historic literature would suggest otherwise. Because of inconsistent reports and theories regarding the pathogenesis of various sclerodermoid and mucin deposition diseases, in 1953 Montgomery and Underwood1 sought to differentiate LM from scleroderma and generalized myxedema. They stressed clinical appearance and proposed diagnostic criteria for LM as generalized papular mucinosis in which “[n]o relation to disturbance of the thyroid or other endocrine glands is apparent,” whereas generalized myxedema was defined as a “[t]rue cutaneous myxedema, with diffuse edema and the usual commonly recognized changes” in patients with endocrine abnormalities.1 With this classification, the authors made a clear distinction between mucinosis caused by thyroid abnormalities and LM, which is not caused by a thyroid disorder. Since this original description was published, associations with monoclonal gammopathy and fibroblast proliferation have been made, ultimately culminating into the current 2001 criteria that incorporate the absence of thyroid disease.2
Conclusion
We believe our case is consistent with the classification initially proposed by Montgomery and Underwood1 and is strengthened with the more recent associations with monoclonal gammopathy and specific histopathologic findings. Although there is no definitive way to rule out myxedema coma or Hashimoto encephalopathy to describe our patient’s transient neurologic decline, her clinical symptoms, laboratory findings, and biopsy results all supported the diagnosis of SM. Furthermore, her response to SM-directed therapy, despite fluctuating thyroid function test results, also supported the diagnosis. In the setting of cutaneous mucinosis with conflicting findings for hypothyroid myxedema, LM should be ruled out. Given the features presented in this report and others, diagnostic criteria should allow for SM and thyroid dysfunction to be concurrent diagnoses. Most importantly, we believe it is essential to identify and diagnose SM in a timely manner to facilitate SM-directed therapy, namely IVIg, to potentially minimize the disease’s notable morbidity and mortality.
Scleromyxedema (SM) is a generalized papular and sclerodermoid form of lichen myxedematosus (LM), commonly referred to as papular mucinosis. It is a rare progressive disease of unknown etiology with systemic manifestations that cause serious morbidity and mortality. Diagnostic criteria were initially created by Montgomery and Underwood1 in 1953 and revised by Rongioletti and Rebora2 in 2001 as follows: (1) generalized papular and sclerodermoid eruption; (2) histologic triad of mucin deposition, fibroblast proliferation, and fibrosis; (3) monoclonal gammopathy; and (4) absence of thyroid disease. There are several reports of LM in association with hypothyroidism, most of which can be characterized as atypical.3-8 We present a case of SM in a patient with Hashimoto thyroiditis and propose that the presence of thyroid disease should not preclude the diagnosis of SM.
Case Report
A 44-year-old woman presented with a progressive eruption of thickened skin and papules spanning many months. The papules ranged from flesh colored to erythematous and covered more than 80% of the body surface area, most notably involving the face, neck, ears, arms, chest, abdomen, and thighs (Figures 1A and 2A). Review of systems was notable for pruritus, muscle pain but no weakness, dysphagia, and constipation. Her medical history included childhood atopic dermatitis and Hashimoto thyroiditis. Hypothyroidism was diagnosed with support of a thyroid ultrasound and thyroid peroxidase antibodies. It was treated with oral levothyroxine for 2 years prior to the skin eruption. Thyroid biopsy was not performed. Her thyroid-stimulating hormone levels notably fluctuated in the year prior to presentation despite close clinical and laboratory monitoring by an endocrinologist. Laboratory results are summarized in Table 1. Both skin and muscle9 biopsies were consistent with SM (Figure 3) and are summarized in Table 1.
Shortly after presentation to our clinic the patient developed acute concerns of confusion and muscle weakness. She was admitted for further inpatient management due to concern for dermato-neuro syndrome, a rare but potentially fatal decline in neurological status that can progress to coma and death, rather than myxedema coma. On admission, a thyroid function test showed subclinical hypothyroidism with a thyroid-stimulating hormone level of 6.35 uU/mL (reference range, 0.3–4.35 uU/mL) and free thyroxine (FT4) level of 1.5 ng/dL (reference range, 0.8–2.8 ng/dL). While hospitalized she was started on intravenous levothyroxine, systemic steroids, and a course of intravenous immunoglobulin (IVIg) treatment consisting of 2 g/kg divided over 5 days. On this regimen, her mental status quickly returned to baseline and other symptoms improved, including the skin eruption (Figures 1B and 2B). She has been maintained on lenalidomide 25 mg/d for the first 3 weeks of each month as well as monthly IVIg infusions. Her thyroid levels have persistently fluctuated despite intramuscular levothyroxine dosing, but her skin has remained clear with continued SM-directed therapy.
Comment
Classification
Lichen myxedematosus is differentiated into localized and generalized forms. The former is limited to the skin and lacks monoclonal gammopathy. The latter, also known as SM, is associated with monoclonal gammopathy and systemic symptoms. Atypical LM is an umbrella term for intermediate cases.
Clinical Presentation
Skin manifestations of SM are described as 1- to 3-mm, firm, waxy, dome-shaped papules that commonly affect the hands, forearms, face, neck, trunk, and thighs. The surrounding skin may be reddish brown and edematous with evidence of skin thickening. Extracutaneous manifestations in SM are numerous and unpredictable. Any organ system can be involved, but gastrointestinal, rheumatologic, pulmonary, and cardiovascular complications are most common.10 A comprehensive multidisciplinary evaluation is necessary based on clinical symptoms and laboratory findings.
Management
Many treatments have been proposed for SM in case reports and case series. Prior treatments have had little success. Most recently, in one of the largest case series on SM, Rongioletti et al10 demonstrated IVIg to be a safe and effective treatment modality.
Differential Diagnosis
An important differential diagnosis is generalized myxedema, which is seen in long-standing hypothyroidism and may present with cutaneous mucinosis and systemic symptoms that resemble SM. Hypothyroid myxedema is associated with a widespread slowing of the body’s metabolic processes and deposition of mucin in various organs, including the skin, creating a generalized nonpitting edema. Classic clinical signs include macroglossia, periorbital puffiness, thick lips, and acral swelling. The skin tends to be cold, dry, and pale. Hair is characterized as being coarse, dry, and brittle with diffuse partial alopecia. Histologically, there is hyperkeratosis with follicular plugging and diffuse mucin and edema splaying between collagen fibers spanning the entire dermis.11 In contradistinction with SM, there is no fibroblast proliferation. The treatment is thyroid replacement therapy. Hyperthyroidism has distinct clinical and histologic changes. Clinically, there is moist and smooth skin with soft, fine, and sometimes alopecic hair. Graves disease, the most common cause of hyperthyroidism, is further characterized by Graves ophthalmopathy and pretibial myxedema, or pink to brown, raised, firm, indurated, asymmetric plaques most commonly affecting the shins. Histologically there is increased mucin in the lower to mid dermis without fibroblast proliferation. The epidermis can be hyperkeratotic, which will clinically correlate with verrucous lesions.12
Hypothyroid encephalopathy is a rare disorder that can cause a change in mental status. It is a steroid-responsive autoimmune process characterized by encephalopathy that is associated with cognitive impairment and psychiatric features. It is a diagnosis of exclusion and should be suspected in women with a history of autoimmune disease, especially antithyroid peroxidase antibodies, a negative infectious workup, and encephalitis with behavioral changes. Although typically highly responsive to systemic steroids, IVIg also has shown efficacy.13
Presence of Thyroid Disease
According to a PubMed search of articles indexed for MEDLINE using the terms scleromyxedema and lichen myxedematosus, there are 7 cases in the literature that potentially describe LM associated with hypothyroidism (Table 2).3-8 The majority of these cases lack monoclonal gammopathy; improved with thyroid replacement therapy; or had severely atypical clinical presentations, rendering them cases of atypical LM or atypical thyroid dermopathy.3-6 Macnab and Kenny7 presented a case of subclinical hypothyroidism with a generalized papular eruption, monoclonal gammopathy, and consistent histologic changes that responded to IVIg therapy. These findings are suggestive of SM, but limited to the current diagnostic criteria, the patient was diagnosed with atypical LM.7 Shenoy et al8 described 2 cases of LM with hypothyroidism. One patient had biopsy-proven SM that was responsive to IVIg as well as Hashimoto thyroiditis with delayed onset of monoclonal gammopathy. The second patient had a medical history of hypothyroidism and Hodgkin lymphoma with active rheumatoid arthritis and biopsy-proven LM that was responsive to systemic steroids.8
Current literature states that thyroid disorder precludes the diagnosis of SM. However, historic literature would suggest otherwise. Because of inconsistent reports and theories regarding the pathogenesis of various sclerodermoid and mucin deposition diseases, in 1953 Montgomery and Underwood1 sought to differentiate LM from scleroderma and generalized myxedema. They stressed clinical appearance and proposed diagnostic criteria for LM as generalized papular mucinosis in which “[n]o relation to disturbance of the thyroid or other endocrine glands is apparent,” whereas generalized myxedema was defined as a “[t]rue cutaneous myxedema, with diffuse edema and the usual commonly recognized changes” in patients with endocrine abnormalities.1 With this classification, the authors made a clear distinction between mucinosis caused by thyroid abnormalities and LM, which is not caused by a thyroid disorder. Since this original description was published, associations with monoclonal gammopathy and fibroblast proliferation have been made, ultimately culminating into the current 2001 criteria that incorporate the absence of thyroid disease.2
Conclusion
We believe our case is consistent with the classification initially proposed by Montgomery and Underwood1 and is strengthened with the more recent associations with monoclonal gammopathy and specific histopathologic findings. Although there is no definitive way to rule out myxedema coma or Hashimoto encephalopathy to describe our patient’s transient neurologic decline, her clinical symptoms, laboratory findings, and biopsy results all supported the diagnosis of SM. Furthermore, her response to SM-directed therapy, despite fluctuating thyroid function test results, also supported the diagnosis. In the setting of cutaneous mucinosis with conflicting findings for hypothyroid myxedema, LM should be ruled out. Given the features presented in this report and others, diagnostic criteria should allow for SM and thyroid dysfunction to be concurrent diagnoses. Most importantly, we believe it is essential to identify and diagnose SM in a timely manner to facilitate SM-directed therapy, namely IVIg, to potentially minimize the disease’s notable morbidity and mortality.
- Montgomery H, Underwood LJ. Lichen myxedematosus; differentiation from cutaneous myxedemas or mucoid states. J Invest Dermatol. 1953;20:213-236.
- Rongioletti F, Rebora A. Updated classification of papular mucinosis, lichen myxedematosus and scleromyxedema. J Am Acad Dermatol. 2001;44:273-281.
- Archibald GC, Calvert HT. Hypothyroidsm and lichen myxedematosus. Arch Dermatol. 1977;113:684.
- Schaeffer D, Bruce S, Rosen T. Cutaneous mucinosis associated with thyroid dysfunction. Cutis. 1983;11:449-456.
- Martin-Ezquerra G, Sanchez-Regaña M, Massana-Gil J, et al. Papular mucinosis associated with subclinical hypothyroidism: improvement with thyroxine therapy. J Eur Acad Dermatol Venereol. 2006;20:1340-1341.
- Volpato MB, Jaime TJ, Proença MP, et al. Papular mucinosis associated with hypothyroidism. An Bras Dermatol. 2010;85:89-92.
- Macnab M, Kenny P. Successful intravenous immunoglobulin treatment of atypical lichen myxedematosus associated with hypothyroidism and central nervous system. involvement: case report and discussion of the literature. J Cutan Med Surg. 2013;17:69-73.
- Shenoy A, Steixner J, Beltrani V, et al. Discrete papular lichen myxedematosus and scleromyxedema with hypothyroidism: a report of two cases. Case Rep Dermatol. 2019;11:64-70.
- Helfrich DJ, Walker ER, Martinez AJ, et al. Scleromyxedema myopathy: case report and review of the literature. Arthritis Rheum. 1988;31:1437-1441.
- Rongioletti F, Merlo G, Cinotti E, et al. Scleromyxedema: a multicenter study of characteristics, comorbidities, course, and therapy in 30 patients. J Am Acad Dermatol. 2013;69:66-72.
- Jackson EM, English JC 3rd. Diffuse cutaneous mucinoses. Dermatol Clin. 2002;20:493-501.
- Leonhardt JM, Heymann WR. Thyroid disease and the skin. Dermatol Clin. 2002;20:473-481.
- Zhou JY, Xu B, Lopes J, et al. Hashimoto encephalopathy: literature review. Acta Neurol Scand. 2017;135:285-290.
- Montgomery H, Underwood LJ. Lichen myxedematosus; differentiation from cutaneous myxedemas or mucoid states. J Invest Dermatol. 1953;20:213-236.
- Rongioletti F, Rebora A. Updated classification of papular mucinosis, lichen myxedematosus and scleromyxedema. J Am Acad Dermatol. 2001;44:273-281.
- Archibald GC, Calvert HT. Hypothyroidsm and lichen myxedematosus. Arch Dermatol. 1977;113:684.
- Schaeffer D, Bruce S, Rosen T. Cutaneous mucinosis associated with thyroid dysfunction. Cutis. 1983;11:449-456.
- Martin-Ezquerra G, Sanchez-Regaña M, Massana-Gil J, et al. Papular mucinosis associated with subclinical hypothyroidism: improvement with thyroxine therapy. J Eur Acad Dermatol Venereol. 2006;20:1340-1341.
- Volpato MB, Jaime TJ, Proença MP, et al. Papular mucinosis associated with hypothyroidism. An Bras Dermatol. 2010;85:89-92.
- Macnab M, Kenny P. Successful intravenous immunoglobulin treatment of atypical lichen myxedematosus associated with hypothyroidism and central nervous system. involvement: case report and discussion of the literature. J Cutan Med Surg. 2013;17:69-73.
- Shenoy A, Steixner J, Beltrani V, et al. Discrete papular lichen myxedematosus and scleromyxedema with hypothyroidism: a report of two cases. Case Rep Dermatol. 2019;11:64-70.
- Helfrich DJ, Walker ER, Martinez AJ, et al. Scleromyxedema myopathy: case report and review of the literature. Arthritis Rheum. 1988;31:1437-1441.
- Rongioletti F, Merlo G, Cinotti E, et al. Scleromyxedema: a multicenter study of characteristics, comorbidities, course, and therapy in 30 patients. J Am Acad Dermatol. 2013;69:66-72.
- Jackson EM, English JC 3rd. Diffuse cutaneous mucinoses. Dermatol Clin. 2002;20:493-501.
- Leonhardt JM, Heymann WR. Thyroid disease and the skin. Dermatol Clin. 2002;20:473-481.
- Zhou JY, Xu B, Lopes J, et al. Hashimoto encephalopathy: literature review. Acta Neurol Scand. 2017;135:285-290.
Practice Points
- Scleromyxedema (SM) is progressive disease of unknown etiology with unpredictable behavior.
- Systemic manifestations associated with SM can cause serious morbidity and mortality.
- Intravenous immunoglobulin is the most effective treatment modality in SM.
- The presence of thyroid disease should not preclude the diagnosis of SM.

Cutaneous Pemphigus Vegetans Co-occurring With Oral Pemphigus Vulgaris
To the Editor:
A 74-year-old man with a history of colon cancer and no history of sexually transmitted diseases presented with tender, moist, vegetating, and verrucous plaques localized to the inguinal creases and behind the scrotum of 3 weeks’ duration (Figure 1). The patient recently had taken lisinopril prescribed by his primary care physician for a couple of years for hypertension before switching to losartan prior to the current presentation. He later noticed the groin eruptions. He also noticed white tongue plaques temporally associated with the groin plaques and a long history of recurrent oral ulcerations. Prior to being seen in our clinic, outside physicians cultured methicillin-sensitive Staphylococcus aureus from the groin plaques and treated him with oral clindamycin, cephalexin, and topical mupirocin without a clinical response.

Our differential diagnosis included condyloma acuminata, condyloma lata, and cutaneous pemphigus vegetans. Laboratory testing revealed a nonreactive rapid plasma reagin test and peripheral eosinophilia of 14.9% (reference range, 0%–6%). Biopsy of a left groin plaque revealed epidermal hyperplasia with spongiosis and an eosinophilic-rich infiltrate on hematoxylin and eosin staining (Figure 2A), and direct immunofluorescence revealed diffuse epidermal intercellular IgG deposits (Figure 2B). The patient’s clinical and histologic presentation was consistent with cutaneous pemphigus vegetans. Biopsy of an oral ulcer revealed denuded acantholytic mucositis with eosinophilic-rich submucosal infiltrate and fibrosis (Figure 3A). Direct immunofluorescence was positive for lacelike intercellular staining for IgG and C3 within the squamous epithelium (Figure 3B). Together the clinical and histologic findings were consistent with oral pemphigus vulgaris.
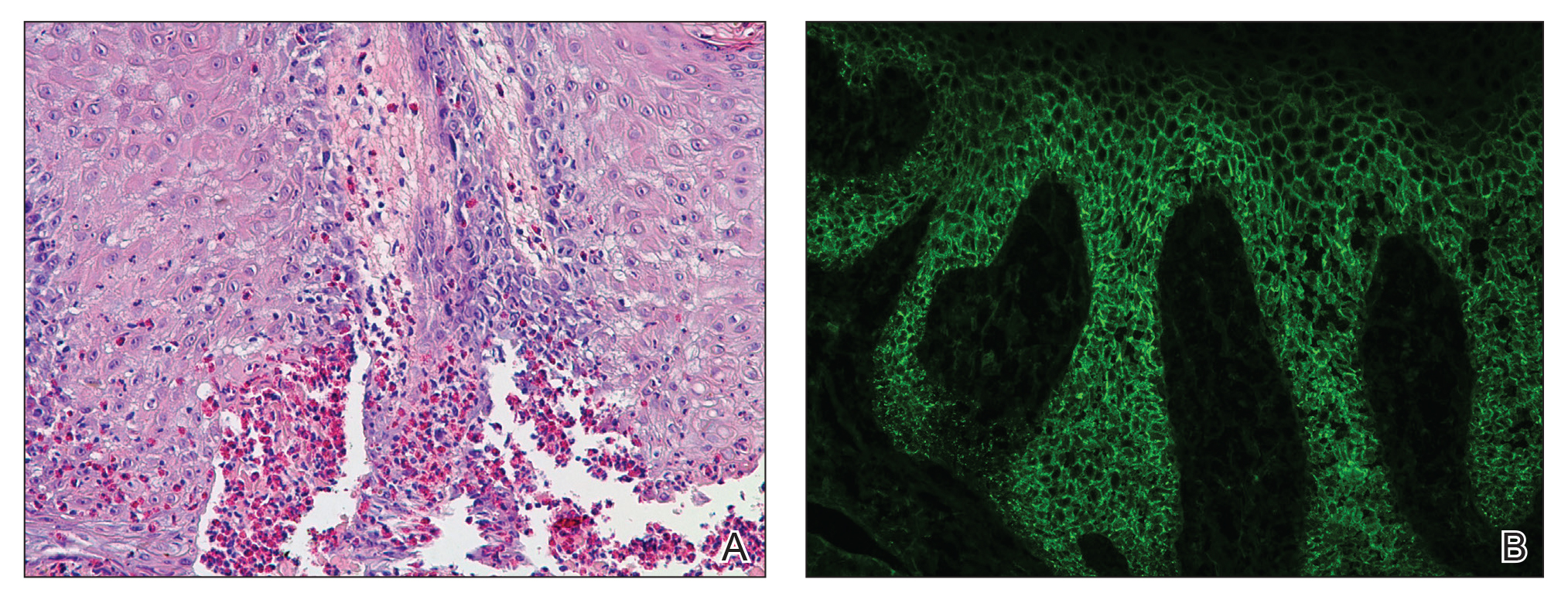
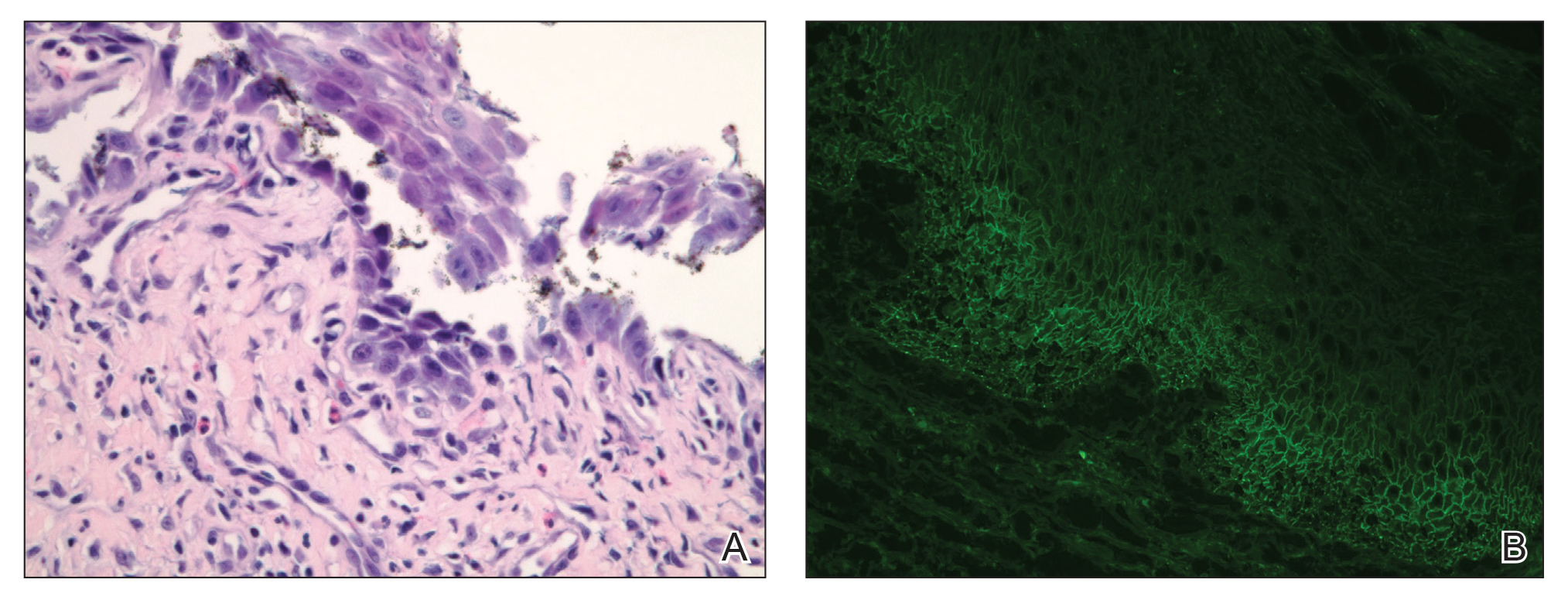
The patient initially was started on oral minocycline 100 mg twice daily and mometasone furoate cream 0.1% twice daily to affected groin areas. With these interventions, the groin plaques almost completely resolved after several months, leaving only residual hyperpigmentation (Figure 4). The oral pemphigus vulgaris initially was treated with dexamethasone 0.5 mg/5 mL solution 2 to 3 times daily, but the lesions were refractory to this approach and also did not improve after the losartan was discontinued for several months. As such, mycophenolate mofetil was started. He was titrated to the lowest effective dose and showed near-complete resolution with 500 mg 3 times daily.

Cutaneous pemphigus vegetans, a rare variant of pemphigus vulgaris, is characterized by vegetating plaques commonly localized to the skin folds, scalp, face, and mucous membranes.1 Involvement of the oral mucosa occurs in a majority of cases. Although our patient had oral ulcerations, he did not have characteristic cerebriform changes of the dorsal tongue or associated verrucous hyperkeratotic lesions involving the buccal mucosa, hard and soft palate, or vermilion border of the lips that typically are seen in pemphigus vegetans.2-5 Subsequent biopsy of the oral mucosa confirmed oral pemphigus vulgaris in our patient.
This case presentation of co-occurring cutaneous pemphigus vegetans and oral pemphigus vulgaris is uncommonly reported in the literature. Although the etiology of this co-occurrence is not clear, it could represent a form of epitope spread, with the mechanism similar to that proposed for the progression of pemphigus vulgaris from the mucosal to the mucocutaneous stage by Chan et al,6 who suggested that an autoimmune reaction against specific desmoglein 3 epitopes (an important protein component for desmosomes and the autoantigen in pemphigus vulgaris) on mucosal membranes could induce local damage. These injuries could then expose the autoreactive immune cells to a secondary desmoglein 3 epitope present in the skin, leading to the development of cutaneous lesions.6 Salato et al7 also supported this idea of intramolecular epitope spread in pemphigus vulgaris, explaining that at various stages of the disease (mucosal and mucocutaneous), the antibodies have “different tissue-binding patterns and pathogenic activities, suggesting that they may recognize distinct epitopes.” This concept of epitope spread from the oral mucosal form to the cutaneous form of pemphigus vulgaris also could help explain our patient’s presentation, as he had a long history of recurrent oral ulcerations prior to developing the vegetating cutaneous plaques of cutaneous pemphigus vegetans.
We also appreciate that either the cutaneous pemphigus vegetans or oral pemphigus vulgaris could have been drug induced in our case. Captopril has been reported to cause pemphigus vulgaris,8 so it is conceivable that the related medication lisinopril was the culprit in our case. A prior case report described an elderly man who developed lisinopril-induced pemphigus foliaceus; however, there was no oral involvement in this case and no further blister formation within 48 hours of discontinuing lisinopril.9 An additional case report implicated lisinopril in the development of a bullous eruption on the oral mucosa in a female patient, though direct and indirect immunofluorescence did not reveal the autoantibodies that typically are seen in pemphigus vulgaris.10 Our patient’s blood eosinophilia also could support an adverse drug reaction. Our patient’s losartan was discontinued for several months without respite of the oral ulcerations and thus was restarted. The cutaneous pemphigus vegetans continues to be in remission and was unaffected by restarting the losartan, making it a less likely culprit for his presentation.
We identified another case in the literature in which an individual with a history of colon cancer was diagnosed with cutaneous pemphigus vegetans.11 As such, we considered a possible link between the 2 diagnoses; however, the temporal disconnect between both conditions in our patient makes this less likely, unlike the other reported case in which the internal neoplasm and pemphigus vegetans appeared nearly simultaneously.11
Finally, our case supports a combination of topical steroids and minocycline for treatment of cutaneous pemphigus vegetans.
Our case demonstrates the importance of considering cutaneous pemphigus vegetans in the differential diagnosis, despite its rarity, when patients present with vegetating plaques. In addition, although oral involvement is common with this condition, if the patient’s oral lesions do not fit the characteristic oral findings seen in pemphigus vegetans, alternative diagnoses should be considered.
- de Almeida HL Jr, Neugebauer MG, Guarenti IM, et al. Pemphigus vegetans associated with verrucous lesions: expanding a phenotype. Clinics (Sao Paulo). 2006;61:279-282.
- Danopoulou I, Stavropoulos P, Stratigos A, et al. Pemphigus vegetans confined to the scalp. Int J Dermatol. 2006;45:1008-1009.
- Markopoulos AK, Antoniades DZ, Zaraboukas T. Pemphigus vegetans of the oral cavity. Int J Dermatol. 2006;45:425-428.
- Woo TY, Solomon AR, Fairley JA. Pemphigus vegetans limited to the lips and oral mucosa. Arch Dermatol. 1985;121:271-272.
- Yuen KL, Yau KC. An old gentleman with vegetative plaques and erosions: a case of pemphigus vegetans. Hong Kong J Dermatol Venereol. 2012;20:179-182.
- Chan LS, Vanderlugt CJ, Hashimoto T, et al. Epitope spreading: lessons from autoimmune skin diseases. J Invest Dermatol. 1998;110:103-109.
- Salato VK, Hacker-Foegen MK, Lazarova Z, et al. Role of intramolecular epitope spreading in pemphigus vulgaris. Clin Immunol. 2005;116:54-64.
- Dashore A, Choudhary SD. Captopril induced pemphigus vulgaris. Indian J Dermatol Venereol Leprol. 1987;53:293-294.
- Patterson CR, Davies MG. Pemphigus foliaceus: an adverse reaction to lisinopril. J Dermatolog Treat. 2004;15:60-62.
- Baričević M, Mravak Stipeti´c M, Situm M, et al. Oral bullous eruption after taking lisinopril—case report and literature review. Wien Klin Wochenschr. 2013;125:408-411.
- Torres T, Ferreira M, Sanches M, et al. Pemphigus vegetans in a patient with colonic cancer. Indian J Dermatol Venereol Leprol. 2009;75:603-605.
To the Editor:
A 74-year-old man with a history of colon cancer and no history of sexually transmitted diseases presented with tender, moist, vegetating, and verrucous plaques localized to the inguinal creases and behind the scrotum of 3 weeks’ duration (Figure 1). The patient recently had taken lisinopril prescribed by his primary care physician for a couple of years for hypertension before switching to losartan prior to the current presentation. He later noticed the groin eruptions. He also noticed white tongue plaques temporally associated with the groin plaques and a long history of recurrent oral ulcerations. Prior to being seen in our clinic, outside physicians cultured methicillin-sensitive Staphylococcus aureus from the groin plaques and treated him with oral clindamycin, cephalexin, and topical mupirocin without a clinical response.
Our differential diagnosis included condyloma acuminata, condyloma lata, and cutaneous pemphigus vegetans. Laboratory testing revealed a nonreactive rapid plasma reagin test and peripheral eosinophilia of 14.9% (reference range, 0%–6%). Biopsy of a left groin plaque revealed epidermal hyperplasia with spongiosis and an eosinophilic-rich infiltrate on hematoxylin and eosin staining (Figure 2A), and direct immunofluorescence revealed diffuse epidermal intercellular IgG deposits (Figure 2B). The patient’s clinical and histologic presentation was consistent with cutaneous pemphigus vegetans. Biopsy of an oral ulcer revealed denuded acantholytic mucositis with eosinophilic-rich submucosal infiltrate and fibrosis (Figure 3A). Direct immunofluorescence was positive for lacelike intercellular staining for IgG and C3 within the squamous epithelium (Figure 3B). Together the clinical and histologic findings were consistent with oral pemphigus vulgaris.
The patient initially was started on oral minocycline 100 mg twice daily and mometasone furoate cream 0.1% twice daily to affected groin areas. With these interventions, the groin plaques almost completely resolved after several months, leaving only residual hyperpigmentation (Figure 4). The oral pemphigus vulgaris initially was treated with dexamethasone 0.5 mg/5 mL solution 2 to 3 times daily, but the lesions were refractory to this approach and also did not improve after the losartan was discontinued for several months. As such, mycophenolate mofetil was started. He was titrated to the lowest effective dose and showed near-complete resolution with 500 mg 3 times daily.
Cutaneous pemphigus vegetans, a rare variant of pemphigus vulgaris, is characterized by vegetating plaques commonly localized to the skin folds, scalp, face, and mucous membranes.1 Involvement of the oral mucosa occurs in a majority of cases. Although our patient had oral ulcerations, he did not have characteristic cerebriform changes of the dorsal tongue or associated verrucous hyperkeratotic lesions involving the buccal mucosa, hard and soft palate, or vermilion border of the lips that typically are seen in pemphigus vegetans.2-5 Subsequent biopsy of the oral mucosa confirmed oral pemphigus vulgaris in our patient.
This case presentation of co-occurring cutaneous pemphigus vegetans and oral pemphigus vulgaris is uncommonly reported in the literature. Although the etiology of this co-occurrence is not clear, it could represent a form of epitope spread, with the mechanism similar to that proposed for the progression of pemphigus vulgaris from the mucosal to the mucocutaneous stage by Chan et al,6 who suggested that an autoimmune reaction against specific desmoglein 3 epitopes (an important protein component for desmosomes and the autoantigen in pemphigus vulgaris) on mucosal membranes could induce local damage. These injuries could then expose the autoreactive immune cells to a secondary desmoglein 3 epitope present in the skin, leading to the development of cutaneous lesions.6 Salato et al7 also supported this idea of intramolecular epitope spread in pemphigus vulgaris, explaining that at various stages of the disease (mucosal and mucocutaneous), the antibodies have “different tissue-binding patterns and pathogenic activities, suggesting that they may recognize distinct epitopes.” This concept of epitope spread from the oral mucosal form to the cutaneous form of pemphigus vulgaris also could help explain our patient’s presentation, as he had a long history of recurrent oral ulcerations prior to developing the vegetating cutaneous plaques of cutaneous pemphigus vegetans.
We also appreciate that either the cutaneous pemphigus vegetans or oral pemphigus vulgaris could have been drug induced in our case. Captopril has been reported to cause pemphigus vulgaris,8 so it is conceivable that the related medication lisinopril was the culprit in our case. A prior case report described an elderly man who developed lisinopril-induced pemphigus foliaceus; however, there was no oral involvement in this case and no further blister formation within 48 hours of discontinuing lisinopril.9 An additional case report implicated lisinopril in the development of a bullous eruption on the oral mucosa in a female patient, though direct and indirect immunofluorescence did not reveal the autoantibodies that typically are seen in pemphigus vulgaris.10 Our patient’s blood eosinophilia also could support an adverse drug reaction. Our patient’s losartan was discontinued for several months without respite of the oral ulcerations and thus was restarted. The cutaneous pemphigus vegetans continues to be in remission and was unaffected by restarting the losartan, making it a less likely culprit for his presentation.
We identified another case in the literature in which an individual with a history of colon cancer was diagnosed with cutaneous pemphigus vegetans.11 As such, we considered a possible link between the 2 diagnoses; however, the temporal disconnect between both conditions in our patient makes this less likely, unlike the other reported case in which the internal neoplasm and pemphigus vegetans appeared nearly simultaneously.11
Finally, our case supports a combination of topical steroids and minocycline for treatment of cutaneous pemphigus vegetans.
Our case demonstrates the importance of considering cutaneous pemphigus vegetans in the differential diagnosis, despite its rarity, when patients present with vegetating plaques. In addition, although oral involvement is common with this condition, if the patient’s oral lesions do not fit the characteristic oral findings seen in pemphigus vegetans, alternative diagnoses should be considered.
To the Editor:
A 74-year-old man with a history of colon cancer and no history of sexually transmitted diseases presented with tender, moist, vegetating, and verrucous plaques localized to the inguinal creases and behind the scrotum of 3 weeks’ duration (Figure 1). The patient recently had taken lisinopril prescribed by his primary care physician for a couple of years for hypertension before switching to losartan prior to the current presentation. He later noticed the groin eruptions. He also noticed white tongue plaques temporally associated with the groin plaques and a long history of recurrent oral ulcerations. Prior to being seen in our clinic, outside physicians cultured methicillin-sensitive Staphylococcus aureus from the groin plaques and treated him with oral clindamycin, cephalexin, and topical mupirocin without a clinical response.
Our differential diagnosis included condyloma acuminata, condyloma lata, and cutaneous pemphigus vegetans. Laboratory testing revealed a nonreactive rapid plasma reagin test and peripheral eosinophilia of 14.9% (reference range, 0%–6%). Biopsy of a left groin plaque revealed epidermal hyperplasia with spongiosis and an eosinophilic-rich infiltrate on hematoxylin and eosin staining (Figure 2A), and direct immunofluorescence revealed diffuse epidermal intercellular IgG deposits (Figure 2B). The patient’s clinical and histologic presentation was consistent with cutaneous pemphigus vegetans. Biopsy of an oral ulcer revealed denuded acantholytic mucositis with eosinophilic-rich submucosal infiltrate and fibrosis (Figure 3A). Direct immunofluorescence was positive for lacelike intercellular staining for IgG and C3 within the squamous epithelium (Figure 3B). Together the clinical and histologic findings were consistent with oral pemphigus vulgaris.
The patient initially was started on oral minocycline 100 mg twice daily and mometasone furoate cream 0.1% twice daily to affected groin areas. With these interventions, the groin plaques almost completely resolved after several months, leaving only residual hyperpigmentation (Figure 4). The oral pemphigus vulgaris initially was treated with dexamethasone 0.5 mg/5 mL solution 2 to 3 times daily, but the lesions were refractory to this approach and also did not improve after the losartan was discontinued for several months. As such, mycophenolate mofetil was started. He was titrated to the lowest effective dose and showed near-complete resolution with 500 mg 3 times daily.
Cutaneous pemphigus vegetans, a rare variant of pemphigus vulgaris, is characterized by vegetating plaques commonly localized to the skin folds, scalp, face, and mucous membranes.1 Involvement of the oral mucosa occurs in a majority of cases. Although our patient had oral ulcerations, he did not have characteristic cerebriform changes of the dorsal tongue or associated verrucous hyperkeratotic lesions involving the buccal mucosa, hard and soft palate, or vermilion border of the lips that typically are seen in pemphigus vegetans.2-5 Subsequent biopsy of the oral mucosa confirmed oral pemphigus vulgaris in our patient.
This case presentation of co-occurring cutaneous pemphigus vegetans and oral pemphigus vulgaris is uncommonly reported in the literature. Although the etiology of this co-occurrence is not clear, it could represent a form of epitope spread, with the mechanism similar to that proposed for the progression of pemphigus vulgaris from the mucosal to the mucocutaneous stage by Chan et al,6 who suggested that an autoimmune reaction against specific desmoglein 3 epitopes (an important protein component for desmosomes and the autoantigen in pemphigus vulgaris) on mucosal membranes could induce local damage. These injuries could then expose the autoreactive immune cells to a secondary desmoglein 3 epitope present in the skin, leading to the development of cutaneous lesions.6 Salato et al7 also supported this idea of intramolecular epitope spread in pemphigus vulgaris, explaining that at various stages of the disease (mucosal and mucocutaneous), the antibodies have “different tissue-binding patterns and pathogenic activities, suggesting that they may recognize distinct epitopes.” This concept of epitope spread from the oral mucosal form to the cutaneous form of pemphigus vulgaris also could help explain our patient’s presentation, as he had a long history of recurrent oral ulcerations prior to developing the vegetating cutaneous plaques of cutaneous pemphigus vegetans.
We also appreciate that either the cutaneous pemphigus vegetans or oral pemphigus vulgaris could have been drug induced in our case. Captopril has been reported to cause pemphigus vulgaris,8 so it is conceivable that the related medication lisinopril was the culprit in our case. A prior case report described an elderly man who developed lisinopril-induced pemphigus foliaceus; however, there was no oral involvement in this case and no further blister formation within 48 hours of discontinuing lisinopril.9 An additional case report implicated lisinopril in the development of a bullous eruption on the oral mucosa in a female patient, though direct and indirect immunofluorescence did not reveal the autoantibodies that typically are seen in pemphigus vulgaris.10 Our patient’s blood eosinophilia also could support an adverse drug reaction. Our patient’s losartan was discontinued for several months without respite of the oral ulcerations and thus was restarted. The cutaneous pemphigus vegetans continues to be in remission and was unaffected by restarting the losartan, making it a less likely culprit for his presentation.
We identified another case in the literature in which an individual with a history of colon cancer was diagnosed with cutaneous pemphigus vegetans.11 As such, we considered a possible link between the 2 diagnoses; however, the temporal disconnect between both conditions in our patient makes this less likely, unlike the other reported case in which the internal neoplasm and pemphigus vegetans appeared nearly simultaneously.11
Finally, our case supports a combination of topical steroids and minocycline for treatment of cutaneous pemphigus vegetans.
Our case demonstrates the importance of considering cutaneous pemphigus vegetans in the differential diagnosis, despite its rarity, when patients present with vegetating plaques. In addition, although oral involvement is common with this condition, if the patient’s oral lesions do not fit the characteristic oral findings seen in pemphigus vegetans, alternative diagnoses should be considered.
- de Almeida HL Jr, Neugebauer MG, Guarenti IM, et al. Pemphigus vegetans associated with verrucous lesions: expanding a phenotype. Clinics (Sao Paulo). 2006;61:279-282.
- Danopoulou I, Stavropoulos P, Stratigos A, et al. Pemphigus vegetans confined to the scalp. Int J Dermatol. 2006;45:1008-1009.
- Markopoulos AK, Antoniades DZ, Zaraboukas T. Pemphigus vegetans of the oral cavity. Int J Dermatol. 2006;45:425-428.
- Woo TY, Solomon AR, Fairley JA. Pemphigus vegetans limited to the lips and oral mucosa. Arch Dermatol. 1985;121:271-272.
- Yuen KL, Yau KC. An old gentleman with vegetative plaques and erosions: a case of pemphigus vegetans. Hong Kong J Dermatol Venereol. 2012;20:179-182.
- Chan LS, Vanderlugt CJ, Hashimoto T, et al. Epitope spreading: lessons from autoimmune skin diseases. J Invest Dermatol. 1998;110:103-109.
- Salato VK, Hacker-Foegen MK, Lazarova Z, et al. Role of intramolecular epitope spreading in pemphigus vulgaris. Clin Immunol. 2005;116:54-64.
- Dashore A, Choudhary SD. Captopril induced pemphigus vulgaris. Indian J Dermatol Venereol Leprol. 1987;53:293-294.
- Patterson CR, Davies MG. Pemphigus foliaceus: an adverse reaction to lisinopril. J Dermatolog Treat. 2004;15:60-62.
- Baričević M, Mravak Stipeti´c M, Situm M, et al. Oral bullous eruption after taking lisinopril—case report and literature review. Wien Klin Wochenschr. 2013;125:408-411.
- Torres T, Ferreira M, Sanches M, et al. Pemphigus vegetans in a patient with colonic cancer. Indian J Dermatol Venereol Leprol. 2009;75:603-605.
- de Almeida HL Jr, Neugebauer MG, Guarenti IM, et al. Pemphigus vegetans associated with verrucous lesions: expanding a phenotype. Clinics (Sao Paulo). 2006;61:279-282.
- Danopoulou I, Stavropoulos P, Stratigos A, et al. Pemphigus vegetans confined to the scalp. Int J Dermatol. 2006;45:1008-1009.
- Markopoulos AK, Antoniades DZ, Zaraboukas T. Pemphigus vegetans of the oral cavity. Int J Dermatol. 2006;45:425-428.
- Woo TY, Solomon AR, Fairley JA. Pemphigus vegetans limited to the lips and oral mucosa. Arch Dermatol. 1985;121:271-272.
- Yuen KL, Yau KC. An old gentleman with vegetative plaques and erosions: a case of pemphigus vegetans. Hong Kong J Dermatol Venereol. 2012;20:179-182.
- Chan LS, Vanderlugt CJ, Hashimoto T, et al. Epitope spreading: lessons from autoimmune skin diseases. J Invest Dermatol. 1998;110:103-109.
- Salato VK, Hacker-Foegen MK, Lazarova Z, et al. Role of intramolecular epitope spreading in pemphigus vulgaris. Clin Immunol. 2005;116:54-64.
- Dashore A, Choudhary SD. Captopril induced pemphigus vulgaris. Indian J Dermatol Venereol Leprol. 1987;53:293-294.
- Patterson CR, Davies MG. Pemphigus foliaceus: an adverse reaction to lisinopril. J Dermatolog Treat. 2004;15:60-62.
- Baričević M, Mravak Stipeti´c M, Situm M, et al. Oral bullous eruption after taking lisinopril—case report and literature review. Wien Klin Wochenschr. 2013;125:408-411.
- Torres T, Ferreira M, Sanches M, et al. Pemphigus vegetans in a patient with colonic cancer. Indian J Dermatol Venereol Leprol. 2009;75:603-605.
Practice Points
- Recognize the clinical and histologic features of pemphigus vegetans, a rare variant of pemphigus vulgaris.
- Consider mechanisms of co-occurring cutaneous pemphigus vegetans and oral pemphigus vulgaris.

Cardiovascular Medicine and Surgery NetWork
Evolution of point of care ultrasound (POCUS) education: cardiovascular, pulmonary, and beyond
A recent CHEST Physician article noted the ubiquity of POCUS employment but lamented inconsistencies and possible inadequacies of POCUS education amongst ACGME specialty fellowships (Satterwhite L. An update on the current standard for ultrasound education in fellowship. CHEST Physician. 2019 Dec. 9). POCUS education/training is no longer limited to physician fellowships but has percolated into the undergraduate medical education curricula of first-year medical students and physician assistant (PA) programs (Hoppmann RA, et al. Crit Ultrasound J. 2011;[3]:1; Rizzolo D, et al. J Physician Assist Educ. 2019;30[2]:103). Some PA residencies have long-incorporated POCUS training to varying degrees, providing emergency/critical care/cardiovascular ultrasound training comparable to that of physician residencies (Daymude ML, et al. J Physician Assist Educ. 2007;18[1]:29). A 12-month POCUS fellowship, which mirrors physician POCUS fellowship curricula, is also available for PAs at Madigan and Brooke Army Medical Centers and allows graduates the opportunity to earn RDMS/RDCS credentials (Monti J. J Physician Assist Educ. 2017;28[1]:27). POCUS employment is not limited to physicians and PAs, however. Respiratory therapists and other allied health professionals are also exploring the value of pulmonary, cardiovascular, and other critical care POCUS applications in their respective practices (Karthika M, et al. Respir Care. 2019;64[2]:217). Meanwhile, POCUS devices continue to evolve toward inexpensive handheld machines that incorporate machine learning/artificial intelligence, further mitigating barriers to integration of POCUS into routine clinical practice (Tsay D, et al. Circulation. 2018;138[22]:2569). With the expansion of POCUS across the full spectrum of health care, leadership from multiprofessional organizations, such as CHEST and the Society of Point-of-Care Ultrasound (SPOCUS), are well-positioned to leverage their diverse leadership to govern the training and safe employment of POCUS.

Robert Baeten II, DmSc, FCCP Steering Committee Member
Chest infections
New laboratory testing guidelines for diagnosing fungal infections
Secondary to a growing number of immunosuppressed individuals, the incidence of invasive fungal infections (IFI) is increasing. IFIs can be difficult to treat and are associated with a high mortality rate. Effective treatment is predicated on early recognition and accurate diagnosis (Limper AH, et al. Am J Respir Crit Care Med. 2011;183[1]:96). Therefore, the American Thoracic Society created a clinical practice guideline on laboratory diagnosis of the most common fungal infections (Hage CA, et al. Am J Respir Crit Care Med. 2019;200[5]:535). The most important diagnostic considerations for clinicians are summarized below:
1. Serum galactomannan and serum aspergillus PCR are recommended in severely immunocompromised patients suspected of having invasive pulmonary aspergillosis (IPA).
2. Galactomannan and aspergillus PCR in bronchoalveolar lavage (BAL) are recommended for patients who are strongly suspected of having IPA, especially if serum is negative. In less severe immunocompromised patients, the BAL sensitivity of galactomannan is better compared with serum, without reducing specificity.
3. Due to low specificity/high false-positive rate, 1,3-B-D-glucan should not be used in isolation to diagnose invasive candidiasis.
4. No single best test exists for the diagnosis of blastomycosis or coccidioidomycosis; rather, more than one diagnostic test including fungal smear, culture, serum antibody, and antigen testing should be used for suspected blastomycosis or coccidioidomycosis.
5. Urine or serum antigen testing is recommended for patients with suspected disseminated or acute histoplasmosis. For immunocompetent patients suspected of pulmonary histoplasmosis, serologic testing is recommended; antigen testing may increase the diagnostic yield.

While these recommendations provide a basis for laboratory testing for the most common IFIs, they must be integrated into the clinical context to ensure accurate diagnosis.
Kelly Pennington, MD, Steering Committee MemberEva M. Carmona, MD, PhD, NetWork Member
Clinical pulmonary medicine
Definitive pleural interventions in malignant pleural effusions
Malignant pleural effusions (MPEs) contribute significantly to symptom burden, and an emphasis on patient-centered outcomes prioritizes palliation of symptoms and definitive management with pleurodesis. Clinical guidelines (Feller-Kopman DJ, et al. Am J Respir Crit Care Med. 2018;198[7]:839) for MPE recommend an indwelling pleural catheter (IPC) or chemical pleurodesis as first-line definitive pleural intervention. In a recent prospective study, Bhatnagar and colleagues (Bhatnagar R, et al. JAMA. 2019 Dec 5. doi: 10.1001/jama.2019.19997) evaluated the effectiveness of thoracoscopy with talc poudrage compared with chest tube placement with talc slurry. The authors randomized 330 patients with MPE and expandable lung, and the primary outcome was pleurodesis failure at 90 days after randomization. There was no significant difference in primary outcome, and pleurodesis failure at 90 days was 22% with talc poudrage and 24% with talc slurry. Similar results for pleurodesis failure at 30 and 180 days were noted.

Secondary outcomes for all-cause mortality, quality of life measures, symptom (chest pain, dyspnea) scores, hospital days, and radiographic opacification also showed no difference. This supports an earlier study by Dresler and associates (Dresler CM, et al. Chest. 2005 Mar;127[3]:909) that reported similar efficacy of talc poudrage and talc slurry. Interestingly, Bhatnagar’s group (Bhatnagar R, et al. N Engl J Med. 2018 Apr 5;378[14]:1313) previously demonstrated administration of talc slurry via IPC was safe and effective in the outpatient setting, but no direct comparison of IPC combined with talc poudrage or talc slurry is available.
These studies provide support for flexibility in MPE management, and selection of definitive pleural intervention can be tailored for each individual patient.
Saadia Faiz, MD, FCCP, Steering Committee Member
Mark Warner, MD, FCCP, NetWork Member
Interprofessional team
Interprofessional team and noninvasive ventilation in COPD exacerbation
Noninvasive ventilation (NIV) is a standard of care for treatment of COPD exacerbations, resulting in reduced need for mechanical ventilation, length of hospital stay, and mortality. Patient selection is as important to success as is choice of an appropriate interface, maintenance of synchrony, and a dedicated interprofessional team. Prior studies have identified that necessary factors for successful implementation of NIV in exacerbations of severe COPD include adequate equipment, sufficient numbers of qualified respiratory therapists, flexibility in staffing, provider buy-in, respiratory therapist autonomy, interdisciplinary teamwork, and staff education (Fisher et al. Ann Am Thorac Soc. 2017;14[11]:1674). These studies also suggest that efforts to increase the use of NIV in COPD need to account for the complex and interdisciplinary nature of NIV delivery and the need for team coordination. The authors further point out that although NIV is a cornerstone of treatment for patients with severe exacerbations of COPD with proven reduced need for intubation, hospital length of stay, and mortality and despite high-quality evidence and strong recommendations in clinical guidelines, use of NIV varies widely across hospitals.

Since interdisciplinary teamwork, respiratory therapy autonomy, and staff education have been identified as important factors in appropriate implementation of NIV, investigators are currently studying the effectiveness, acceptability, and feasibility of interprofessional education for physicians, respiratory therapists, and nurses vs online education for increasing the delivery of NIV in patients hospitalized with COPD exacerbation (R01 HL 146615 – 01 Implementation of interprofessional training to improve uptake of noninvasive ventilation in patients hospitalized with severe COPD exacerbation).

More importantly, this work will further elucidate the interdisciplinary nature of NIV therapy and the benefit of an interprofessional approach to team education.
Mary Jo Farmer, MD, PhD, FCCP, Steering Committee Member Munish Luthra, MD, FCCP, Steering Committee Member
Evolution of point of care ultrasound (POCUS) education: cardiovascular, pulmonary, and beyond
A recent CHEST Physician article noted the ubiquity of POCUS employment but lamented inconsistencies and possible inadequacies of POCUS education amongst ACGME specialty fellowships (Satterwhite L. An update on the current standard for ultrasound education in fellowship. CHEST Physician. 2019 Dec. 9). POCUS education/training is no longer limited to physician fellowships but has percolated into the undergraduate medical education curricula of first-year medical students and physician assistant (PA) programs (Hoppmann RA, et al. Crit Ultrasound J. 2011;[3]:1; Rizzolo D, et al. J Physician Assist Educ. 2019;30[2]:103). Some PA residencies have long-incorporated POCUS training to varying degrees, providing emergency/critical care/cardiovascular ultrasound training comparable to that of physician residencies (Daymude ML, et al. J Physician Assist Educ. 2007;18[1]:29). A 12-month POCUS fellowship, which mirrors physician POCUS fellowship curricula, is also available for PAs at Madigan and Brooke Army Medical Centers and allows graduates the opportunity to earn RDMS/RDCS credentials (Monti J. J Physician Assist Educ. 2017;28[1]:27). POCUS employment is not limited to physicians and PAs, however. Respiratory therapists and other allied health professionals are also exploring the value of pulmonary, cardiovascular, and other critical care POCUS applications in their respective practices (Karthika M, et al. Respir Care. 2019;64[2]:217). Meanwhile, POCUS devices continue to evolve toward inexpensive handheld machines that incorporate machine learning/artificial intelligence, further mitigating barriers to integration of POCUS into routine clinical practice (Tsay D, et al. Circulation. 2018;138[22]:2569). With the expansion of POCUS across the full spectrum of health care, leadership from multiprofessional organizations, such as CHEST and the Society of Point-of-Care Ultrasound (SPOCUS), are well-positioned to leverage their diverse leadership to govern the training and safe employment of POCUS.
Robert Baeten II, DmSc, FCCP Steering Committee Member
Chest infections
New laboratory testing guidelines for diagnosing fungal infections
Secondary to a growing number of immunosuppressed individuals, the incidence of invasive fungal infections (IFI) is increasing. IFIs can be difficult to treat and are associated with a high mortality rate. Effective treatment is predicated on early recognition and accurate diagnosis (Limper AH, et al. Am J Respir Crit Care Med. 2011;183[1]:96). Therefore, the American Thoracic Society created a clinical practice guideline on laboratory diagnosis of the most common fungal infections (Hage CA, et al. Am J Respir Crit Care Med. 2019;200[5]:535). The most important diagnostic considerations for clinicians are summarized below:
1. Serum galactomannan and serum aspergillus PCR are recommended in severely immunocompromised patients suspected of having invasive pulmonary aspergillosis (IPA).
2. Galactomannan and aspergillus PCR in bronchoalveolar lavage (BAL) are recommended for patients who are strongly suspected of having IPA, especially if serum is negative. In less severe immunocompromised patients, the BAL sensitivity of galactomannan is better compared with serum, without reducing specificity.
3. Due to low specificity/high false-positive rate, 1,3-B-D-glucan should not be used in isolation to diagnose invasive candidiasis.
4. No single best test exists for the diagnosis of blastomycosis or coccidioidomycosis; rather, more than one diagnostic test including fungal smear, culture, serum antibody, and antigen testing should be used for suspected blastomycosis or coccidioidomycosis.
5. Urine or serum antigen testing is recommended for patients with suspected disseminated or acute histoplasmosis. For immunocompetent patients suspected of pulmonary histoplasmosis, serologic testing is recommended; antigen testing may increase the diagnostic yield.
While these recommendations provide a basis for laboratory testing for the most common IFIs, they must be integrated into the clinical context to ensure accurate diagnosis.
Kelly Pennington, MD, Steering Committee MemberEva M. Carmona, MD, PhD, NetWork Member
Clinical pulmonary medicine
Definitive pleural interventions in malignant pleural effusions
Malignant pleural effusions (MPEs) contribute significantly to symptom burden, and an emphasis on patient-centered outcomes prioritizes palliation of symptoms and definitive management with pleurodesis. Clinical guidelines (Feller-Kopman DJ, et al. Am J Respir Crit Care Med. 2018;198[7]:839) for MPE recommend an indwelling pleural catheter (IPC) or chemical pleurodesis as first-line definitive pleural intervention. In a recent prospective study, Bhatnagar and colleagues (Bhatnagar R, et al. JAMA. 2019 Dec 5. doi: 10.1001/jama.2019.19997) evaluated the effectiveness of thoracoscopy with talc poudrage compared with chest tube placement with talc slurry. The authors randomized 330 patients with MPE and expandable lung, and the primary outcome was pleurodesis failure at 90 days after randomization. There was no significant difference in primary outcome, and pleurodesis failure at 90 days was 22% with talc poudrage and 24% with talc slurry. Similar results for pleurodesis failure at 30 and 180 days were noted.
Secondary outcomes for all-cause mortality, quality of life measures, symptom (chest pain, dyspnea) scores, hospital days, and radiographic opacification also showed no difference. This supports an earlier study by Dresler and associates (Dresler CM, et al. Chest. 2005 Mar;127[3]:909) that reported similar efficacy of talc poudrage and talc slurry. Interestingly, Bhatnagar’s group (Bhatnagar R, et al. N Engl J Med. 2018 Apr 5;378[14]:1313) previously demonstrated administration of talc slurry via IPC was safe and effective in the outpatient setting, but no direct comparison of IPC combined with talc poudrage or talc slurry is available.
These studies provide support for flexibility in MPE management, and selection of definitive pleural intervention can be tailored for each individual patient.
Saadia Faiz, MD, FCCP, Steering Committee Member
Mark Warner, MD, FCCP, NetWork Member
Interprofessional team
Interprofessional team and noninvasive ventilation in COPD exacerbation
Noninvasive ventilation (NIV) is a standard of care for treatment of COPD exacerbations, resulting in reduced need for mechanical ventilation, length of hospital stay, and mortality. Patient selection is as important to success as is choice of an appropriate interface, maintenance of synchrony, and a dedicated interprofessional team. Prior studies have identified that necessary factors for successful implementation of NIV in exacerbations of severe COPD include adequate equipment, sufficient numbers of qualified respiratory therapists, flexibility in staffing, provider buy-in, respiratory therapist autonomy, interdisciplinary teamwork, and staff education (Fisher et al. Ann Am Thorac Soc. 2017;14[11]:1674). These studies also suggest that efforts to increase the use of NIV in COPD need to account for the complex and interdisciplinary nature of NIV delivery and the need for team coordination. The authors further point out that although NIV is a cornerstone of treatment for patients with severe exacerbations of COPD with proven reduced need for intubation, hospital length of stay, and mortality and despite high-quality evidence and strong recommendations in clinical guidelines, use of NIV varies widely across hospitals.
Since interdisciplinary teamwork, respiratory therapy autonomy, and staff education have been identified as important factors in appropriate implementation of NIV, investigators are currently studying the effectiveness, acceptability, and feasibility of interprofessional education for physicians, respiratory therapists, and nurses vs online education for increasing the delivery of NIV in patients hospitalized with COPD exacerbation (R01 HL 146615 – 01 Implementation of interprofessional training to improve uptake of noninvasive ventilation in patients hospitalized with severe COPD exacerbation).
More importantly, this work will further elucidate the interdisciplinary nature of NIV therapy and the benefit of an interprofessional approach to team education.
Mary Jo Farmer, MD, PhD, FCCP, Steering Committee Member Munish Luthra, MD, FCCP, Steering Committee Member
Evolution of point of care ultrasound (POCUS) education: cardiovascular, pulmonary, and beyond
A recent CHEST Physician article noted the ubiquity of POCUS employment but lamented inconsistencies and possible inadequacies of POCUS education amongst ACGME specialty fellowships (Satterwhite L. An update on the current standard for ultrasound education in fellowship. CHEST Physician. 2019 Dec. 9). POCUS education/training is no longer limited to physician fellowships but has percolated into the undergraduate medical education curricula of first-year medical students and physician assistant (PA) programs (Hoppmann RA, et al. Crit Ultrasound J. 2011;[3]:1; Rizzolo D, et al. J Physician Assist Educ. 2019;30[2]:103). Some PA residencies have long-incorporated POCUS training to varying degrees, providing emergency/critical care/cardiovascular ultrasound training comparable to that of physician residencies (Daymude ML, et al. J Physician Assist Educ. 2007;18[1]:29). A 12-month POCUS fellowship, which mirrors physician POCUS fellowship curricula, is also available for PAs at Madigan and Brooke Army Medical Centers and allows graduates the opportunity to earn RDMS/RDCS credentials (Monti J. J Physician Assist Educ. 2017;28[1]:27). POCUS employment is not limited to physicians and PAs, however. Respiratory therapists and other allied health professionals are also exploring the value of pulmonary, cardiovascular, and other critical care POCUS applications in their respective practices (Karthika M, et al. Respir Care. 2019;64[2]:217). Meanwhile, POCUS devices continue to evolve toward inexpensive handheld machines that incorporate machine learning/artificial intelligence, further mitigating barriers to integration of POCUS into routine clinical practice (Tsay D, et al. Circulation. 2018;138[22]:2569). With the expansion of POCUS across the full spectrum of health care, leadership from multiprofessional organizations, such as CHEST and the Society of Point-of-Care Ultrasound (SPOCUS), are well-positioned to leverage their diverse leadership to govern the training and safe employment of POCUS.
Robert Baeten II, DmSc, FCCP Steering Committee Member
Chest infections
New laboratory testing guidelines for diagnosing fungal infections
Secondary to a growing number of immunosuppressed individuals, the incidence of invasive fungal infections (IFI) is increasing. IFIs can be difficult to treat and are associated with a high mortality rate. Effective treatment is predicated on early recognition and accurate diagnosis (Limper AH, et al. Am J Respir Crit Care Med. 2011;183[1]:96). Therefore, the American Thoracic Society created a clinical practice guideline on laboratory diagnosis of the most common fungal infections (Hage CA, et al. Am J Respir Crit Care Med. 2019;200[5]:535). The most important diagnostic considerations for clinicians are summarized below:
1. Serum galactomannan and serum aspergillus PCR are recommended in severely immunocompromised patients suspected of having invasive pulmonary aspergillosis (IPA).
2. Galactomannan and aspergillus PCR in bronchoalveolar lavage (BAL) are recommended for patients who are strongly suspected of having IPA, especially if serum is negative. In less severe immunocompromised patients, the BAL sensitivity of galactomannan is better compared with serum, without reducing specificity.
3. Due to low specificity/high false-positive rate, 1,3-B-D-glucan should not be used in isolation to diagnose invasive candidiasis.
4. No single best test exists for the diagnosis of blastomycosis or coccidioidomycosis; rather, more than one diagnostic test including fungal smear, culture, serum antibody, and antigen testing should be used for suspected blastomycosis or coccidioidomycosis.
5. Urine or serum antigen testing is recommended for patients with suspected disseminated or acute histoplasmosis. For immunocompetent patients suspected of pulmonary histoplasmosis, serologic testing is recommended; antigen testing may increase the diagnostic yield.
While these recommendations provide a basis for laboratory testing for the most common IFIs, they must be integrated into the clinical context to ensure accurate diagnosis.
Kelly Pennington, MD, Steering Committee MemberEva M. Carmona, MD, PhD, NetWork Member
Clinical pulmonary medicine
Definitive pleural interventions in malignant pleural effusions
Malignant pleural effusions (MPEs) contribute significantly to symptom burden, and an emphasis on patient-centered outcomes prioritizes palliation of symptoms and definitive management with pleurodesis. Clinical guidelines (Feller-Kopman DJ, et al. Am J Respir Crit Care Med. 2018;198[7]:839) for MPE recommend an indwelling pleural catheter (IPC) or chemical pleurodesis as first-line definitive pleural intervention. In a recent prospective study, Bhatnagar and colleagues (Bhatnagar R, et al. JAMA. 2019 Dec 5. doi: 10.1001/jama.2019.19997) evaluated the effectiveness of thoracoscopy with talc poudrage compared with chest tube placement with talc slurry. The authors randomized 330 patients with MPE and expandable lung, and the primary outcome was pleurodesis failure at 90 days after randomization. There was no significant difference in primary outcome, and pleurodesis failure at 90 days was 22% with talc poudrage and 24% with talc slurry. Similar results for pleurodesis failure at 30 and 180 days were noted.
Secondary outcomes for all-cause mortality, quality of life measures, symptom (chest pain, dyspnea) scores, hospital days, and radiographic opacification also showed no difference. This supports an earlier study by Dresler and associates (Dresler CM, et al. Chest. 2005 Mar;127[3]:909) that reported similar efficacy of talc poudrage and talc slurry. Interestingly, Bhatnagar’s group (Bhatnagar R, et al. N Engl J Med. 2018 Apr 5;378[14]:1313) previously demonstrated administration of talc slurry via IPC was safe and effective in the outpatient setting, but no direct comparison of IPC combined with talc poudrage or talc slurry is available.
These studies provide support for flexibility in MPE management, and selection of definitive pleural intervention can be tailored for each individual patient.
Saadia Faiz, MD, FCCP, Steering Committee Member
Mark Warner, MD, FCCP, NetWork Member
Interprofessional team
Interprofessional team and noninvasive ventilation in COPD exacerbation
Noninvasive ventilation (NIV) is a standard of care for treatment of COPD exacerbations, resulting in reduced need for mechanical ventilation, length of hospital stay, and mortality. Patient selection is as important to success as is choice of an appropriate interface, maintenance of synchrony, and a dedicated interprofessional team. Prior studies have identified that necessary factors for successful implementation of NIV in exacerbations of severe COPD include adequate equipment, sufficient numbers of qualified respiratory therapists, flexibility in staffing, provider buy-in, respiratory therapist autonomy, interdisciplinary teamwork, and staff education (Fisher et al. Ann Am Thorac Soc. 2017;14[11]:1674). These studies also suggest that efforts to increase the use of NIV in COPD need to account for the complex and interdisciplinary nature of NIV delivery and the need for team coordination. The authors further point out that although NIV is a cornerstone of treatment for patients with severe exacerbations of COPD with proven reduced need for intubation, hospital length of stay, and mortality and despite high-quality evidence and strong recommendations in clinical guidelines, use of NIV varies widely across hospitals.
Since interdisciplinary teamwork, respiratory therapy autonomy, and staff education have been identified as important factors in appropriate implementation of NIV, investigators are currently studying the effectiveness, acceptability, and feasibility of interprofessional education for physicians, respiratory therapists, and nurses vs online education for increasing the delivery of NIV in patients hospitalized with COPD exacerbation (R01 HL 146615 – 01 Implementation of interprofessional training to improve uptake of noninvasive ventilation in patients hospitalized with severe COPD exacerbation).
More importantly, this work will further elucidate the interdisciplinary nature of NIV therapy and the benefit of an interprofessional approach to team education.
Mary Jo Farmer, MD, PhD, FCCP, Steering Committee Member Munish Luthra, MD, FCCP, Steering Committee Member
Welcome New CHEST Physician Editorial Board Members
A. Christine Argento, MD, FCCP

Dr. Argento is an Assistant Professor of Medicine and Thoracic Surgery, is the Director of Interventional Pulmonary and the Interventional Pulmonary Fellowship Program Director at Northwestern University, Feinberg School of Medicine. She has been very involved in simulation training and education, particularly with respect to bronchoscopy, interventional pulmonary, and pleural procedures. She is the current Secretary-Treasurer of the Association of Interventional Pulmonary Program Directors (AIPPD) and a member of the CHEST Bronchoscopy Domain Task Force.
David L. Bowton, MD, FCCP

Dr. Bowton is Professor Emeritus in the Department of Anesthesiology, Section on Critical Care at Wake Forest University Baptist Medical Center in Winston Salem, North Carolina. He was formerly Head of the Section on Critical Care in the Department of Anesthesiology and the Medical Director of Respiratory Care, the Neurocritical Care ICU, and the Cardiovascular Surgical ICU. His current interests are in critical care education, especially with respect to simulation education in the areas of mechanical ventilation and airway management. He is the current Chair of the CHEST Cardiovascular Medicine and Surgery NetWork.
Mary Cataletto, MD, FCCP

Dr. Cataletto is a pulmonologist in the Department of Pediatrics at NYU Health and the current chair of the Pediatric NetWork at the American College of Chest Physicians. She completed her fellowship training in Pulmonary Physiology and Critical Care Pediatrics at the Albert Einstein College of Medicine at Yeshiva University and her Masters in Medical Management at the H. John Heinz III School of Public Policy and Management at Carnegie Mellon University in Pittsburgh. Dr. Cataletto is Professor of Clinical Pediatrics at both the NYU Grossman School of Medicine and the Renaissance School of Medicine at Stony Brook University. She has a long standing interest in medical education and medical publishing - serving as Editor in chief of Pediatric Allergy, Immunology and Pulmonology, as well as on the editorial boards of multiple subspecialty texts and review books. Her research interests include sleep and breathing in children with craniofacial abnormalities, including those with Trisomy 21 and Prader-Willi syndrome.
Megan Conroy, MD

Dr. Conroy is Chief Pulmonary and Critical Care Fellow at The Ohio State University in Columbus, Ohio. Upon completion of her training, she will join The Ohio State University Division of Pulmonary, Critical Care, and Sleep Medicine as an Assistant Professor of Clinical Medicine. Her clinical expertise is in severe asthma and critical care medicine. She serves as the CHEST Fellow-In-Training member of the Airways Disorders NetWork Steering Committee and as a member of the Trainee Work Group. Her other interests include medical education.
Sachin Gupta, MD, FCCP

Dr. Gupta is a Pulmonary and Critical Care physician in group private practice in the San Francisco, Bay Area. His clinical expertise is in the fields of pulmonary hypertension, interstitial lung diseases, and non-tuberculous mycobacterial infections. He is actively participating in several societies, including the Pulmonary Hypertension Association, California Thoracic Society, and CHEST. In addition to his clinical interests, he has been an international medical volunteer and highly involved in the Bay Area in digital health tech consulting.
Mangala Narasimhan, DO, FCCP

Dr. Narasimhan works for Northwell Health as the Regional Director of Critical Care Services and is an attending in the Division of Pulmonary, Critical Care, and Sleep Medicine. She is the Medical Director of the Northwell Acute Lung Injury Center/VV ECMO program and ICU Director of the Medical ICU at Long Island Jewish Medical Center. She is a Professor of Medicine at the Zucker School of Medicine at Hofstra/Northwell. She has been teaching ultrasound and advanced echo nationally and internationally for 15 years. Her research interests include point of care ultrasound in the critically ill, ECMO for acute lung injury, and outcomes research in the ICU.
Brandon M. Seay, MD, MPH

Dr. Seay is a Pediatric Pulmonologist and Sleep Specialist for the Children’s Physician Group Pulmonology in Atlanta, Georgia. HIs clinical interests include asthma, cystic fibrosis, sleep apnea, and behavioral insomnia of childhood. His interests include medical education through social media and health advocacy via legislative and social media efforts. He is currently a member of the CHEST Social Media Work Group as a lead on video efforts.
A. Christine Argento, MD, FCCP
Dr. Argento is an Assistant Professor of Medicine and Thoracic Surgery, is the Director of Interventional Pulmonary and the Interventional Pulmonary Fellowship Program Director at Northwestern University, Feinberg School of Medicine. She has been very involved in simulation training and education, particularly with respect to bronchoscopy, interventional pulmonary, and pleural procedures. She is the current Secretary-Treasurer of the Association of Interventional Pulmonary Program Directors (AIPPD) and a member of the CHEST Bronchoscopy Domain Task Force.
David L. Bowton, MD, FCCP
Dr. Bowton is Professor Emeritus in the Department of Anesthesiology, Section on Critical Care at Wake Forest University Baptist Medical Center in Winston Salem, North Carolina. He was formerly Head of the Section on Critical Care in the Department of Anesthesiology and the Medical Director of Respiratory Care, the Neurocritical Care ICU, and the Cardiovascular Surgical ICU. His current interests are in critical care education, especially with respect to simulation education in the areas of mechanical ventilation and airway management. He is the current Chair of the CHEST Cardiovascular Medicine and Surgery NetWork.
Mary Cataletto, MD, FCCP
Dr. Cataletto is a pulmonologist in the Department of Pediatrics at NYU Health and the current chair of the Pediatric NetWork at the American College of Chest Physicians. She completed her fellowship training in Pulmonary Physiology and Critical Care Pediatrics at the Albert Einstein College of Medicine at Yeshiva University and her Masters in Medical Management at the H. John Heinz III School of Public Policy and Management at Carnegie Mellon University in Pittsburgh. Dr. Cataletto is Professor of Clinical Pediatrics at both the NYU Grossman School of Medicine and the Renaissance School of Medicine at Stony Brook University. She has a long standing interest in medical education and medical publishing - serving as Editor in chief of Pediatric Allergy, Immunology and Pulmonology, as well as on the editorial boards of multiple subspecialty texts and review books. Her research interests include sleep and breathing in children with craniofacial abnormalities, including those with Trisomy 21 and Prader-Willi syndrome.
Megan Conroy, MD
Dr. Conroy is Chief Pulmonary and Critical Care Fellow at The Ohio State University in Columbus, Ohio. Upon completion of her training, she will join The Ohio State University Division of Pulmonary, Critical Care, and Sleep Medicine as an Assistant Professor of Clinical Medicine. Her clinical expertise is in severe asthma and critical care medicine. She serves as the CHEST Fellow-In-Training member of the Airways Disorders NetWork Steering Committee and as a member of the Trainee Work Group. Her other interests include medical education.
Sachin Gupta, MD, FCCP
Dr. Gupta is a Pulmonary and Critical Care physician in group private practice in the San Francisco, Bay Area. His clinical expertise is in the fields of pulmonary hypertension, interstitial lung diseases, and non-tuberculous mycobacterial infections. He is actively participating in several societies, including the Pulmonary Hypertension Association, California Thoracic Society, and CHEST. In addition to his clinical interests, he has been an international medical volunteer and highly involved in the Bay Area in digital health tech consulting.
Mangala Narasimhan, DO, FCCP
Dr. Narasimhan works for Northwell Health as the Regional Director of Critical Care Services and is an attending in the Division of Pulmonary, Critical Care, and Sleep Medicine. She is the Medical Director of the Northwell Acute Lung Injury Center/VV ECMO program and ICU Director of the Medical ICU at Long Island Jewish Medical Center. She is a Professor of Medicine at the Zucker School of Medicine at Hofstra/Northwell. She has been teaching ultrasound and advanced echo nationally and internationally for 15 years. Her research interests include point of care ultrasound in the critically ill, ECMO for acute lung injury, and outcomes research in the ICU.
Brandon M. Seay, MD, MPH
Dr. Seay is a Pediatric Pulmonologist and Sleep Specialist for the Children’s Physician Group Pulmonology in Atlanta, Georgia. HIs clinical interests include asthma, cystic fibrosis, sleep apnea, and behavioral insomnia of childhood. His interests include medical education through social media and health advocacy via legislative and social media efforts. He is currently a member of the CHEST Social Media Work Group as a lead on video efforts.
A. Christine Argento, MD, FCCP
Dr. Argento is an Assistant Professor of Medicine and Thoracic Surgery, is the Director of Interventional Pulmonary and the Interventional Pulmonary Fellowship Program Director at Northwestern University, Feinberg School of Medicine. She has been very involved in simulation training and education, particularly with respect to bronchoscopy, interventional pulmonary, and pleural procedures. She is the current Secretary-Treasurer of the Association of Interventional Pulmonary Program Directors (AIPPD) and a member of the CHEST Bronchoscopy Domain Task Force.
David L. Bowton, MD, FCCP
Dr. Bowton is Professor Emeritus in the Department of Anesthesiology, Section on Critical Care at Wake Forest University Baptist Medical Center in Winston Salem, North Carolina. He was formerly Head of the Section on Critical Care in the Department of Anesthesiology and the Medical Director of Respiratory Care, the Neurocritical Care ICU, and the Cardiovascular Surgical ICU. His current interests are in critical care education, especially with respect to simulation education in the areas of mechanical ventilation and airway management. He is the current Chair of the CHEST Cardiovascular Medicine and Surgery NetWork.
Mary Cataletto, MD, FCCP
Dr. Cataletto is a pulmonologist in the Department of Pediatrics at NYU Health and the current chair of the Pediatric NetWork at the American College of Chest Physicians. She completed her fellowship training in Pulmonary Physiology and Critical Care Pediatrics at the Albert Einstein College of Medicine at Yeshiva University and her Masters in Medical Management at the H. John Heinz III School of Public Policy and Management at Carnegie Mellon University in Pittsburgh. Dr. Cataletto is Professor of Clinical Pediatrics at both the NYU Grossman School of Medicine and the Renaissance School of Medicine at Stony Brook University. She has a long standing interest in medical education and medical publishing - serving as Editor in chief of Pediatric Allergy, Immunology and Pulmonology, as well as on the editorial boards of multiple subspecialty texts and review books. Her research interests include sleep and breathing in children with craniofacial abnormalities, including those with Trisomy 21 and Prader-Willi syndrome.
Megan Conroy, MD
Dr. Conroy is Chief Pulmonary and Critical Care Fellow at The Ohio State University in Columbus, Ohio. Upon completion of her training, she will join The Ohio State University Division of Pulmonary, Critical Care, and Sleep Medicine as an Assistant Professor of Clinical Medicine. Her clinical expertise is in severe asthma and critical care medicine. She serves as the CHEST Fellow-In-Training member of the Airways Disorders NetWork Steering Committee and as a member of the Trainee Work Group. Her other interests include medical education.
Sachin Gupta, MD, FCCP
Dr. Gupta is a Pulmonary and Critical Care physician in group private practice in the San Francisco, Bay Area. His clinical expertise is in the fields of pulmonary hypertension, interstitial lung diseases, and non-tuberculous mycobacterial infections. He is actively participating in several societies, including the Pulmonary Hypertension Association, California Thoracic Society, and CHEST. In addition to his clinical interests, he has been an international medical volunteer and highly involved in the Bay Area in digital health tech consulting.
Mangala Narasimhan, DO, FCCP
Dr. Narasimhan works for Northwell Health as the Regional Director of Critical Care Services and is an attending in the Division of Pulmonary, Critical Care, and Sleep Medicine. She is the Medical Director of the Northwell Acute Lung Injury Center/VV ECMO program and ICU Director of the Medical ICU at Long Island Jewish Medical Center. She is a Professor of Medicine at the Zucker School of Medicine at Hofstra/Northwell. She has been teaching ultrasound and advanced echo nationally and internationally for 15 years. Her research interests include point of care ultrasound in the critically ill, ECMO for acute lung injury, and outcomes research in the ICU.
Brandon M. Seay, MD, MPH
Dr. Seay is a Pediatric Pulmonologist and Sleep Specialist for the Children’s Physician Group Pulmonology in Atlanta, Georgia. HIs clinical interests include asthma, cystic fibrosis, sleep apnea, and behavioral insomnia of childhood. His interests include medical education through social media and health advocacy via legislative and social media efforts. He is currently a member of the CHEST Social Media Work Group as a lead on video efforts.
ABIM’s longitudinal assessment option anticipated to launch in 2022
Physicians have asked for more flexible and convenient ways to maintain their ABIM Board certification and the recently announced longitudinal assessment option is being designed to accomplish these requests. It is anticipated to launch in 2022 in as many specialties as possible, allowing time prior to launch for engagement with the medical community to produce the best possible experience.

How will the new longitudinal assessment option be different? Question delivery will be structured to allow physicians greater ease of use and mobility, enabling access from virtually anywhere. Answer feedback will be immediate, and physicians will see the rationale behind the answer, along with links to educational material. The preferred pace for answering questions during each administration window will be determined by the examinee, and access to all the resources you use in practice, such as journals or websites, will also be allowed.
Engaging the community
As a Council member, I can attest to the fact that the ABIM has spent a lot of time thinking through key features that are “must haves” in the new option, but there are details that are still being defined. ABIM has prioritized engaging the community, and the suggestions, insights, and questions coming out of these efforts are being used to guide the development of the new longitudinal assessment option.
Following the initial announcement in August, nearly 1,400 physicians submitted comments about the new option. ABIM conducted 69 one-on-one interviews with board-certified physicians and ran user-testing on existing longitudinal assessment platforms from other Boards. ABIM staff attended society meetings throughout the fall and also assembled a Physician Advisory Panel of 11 physicians from members of our Community Insights Network. We want to ensure the features we are considering work well for physicians and provide the high quality experience they deserve.
How can you get involved?
Physicians interested in giving ABIM feedback are invited to connect with us through our Community Insights Network. By joining the Network, you’ll have an opportunity to share your ideas through surveys, interviews, and user tests and be a member of our online community “ABIM Engage.”
ABIM staff will also be in attendance at society meetings to provide individualized guidance and answer your questions. We had a booth at CHEST this past October, and you can find upcoming society meetings staff who will be attending on their website.
What Should You Do Now?
All current ABIM MOC program requirements and policies remain in effect, and ABIM will communicate any program changes well in advance of implementation. If you have an assessment due in 2020 or 2021, you can choose from the options currently available in your discipline.
Registration for all 2020 MOC assessments opened December 1, and physicians may have several pathways to choose from, including taking the Knowledge Check-In at home, office, or testing center or the traditional point-in-time assessment taken at a PearsonVUE center.
The next Knowledge Check-In in Pulmonary Disease will be offered in 2021. ABIM’s website lists the full schedule of available assessment options (https://tinyurl.com/t5bfg55). You can find all of your MOC program requirements and deadlines by signing into your Physician Portal at abim.org.
To keep up to date with developments in ABIM’s longitudinal assessment program, visit the new longitudinal FAQ webpage (https://tinyurl.com/u5bbdgw) that is updated as information becomes available.
Physicians have asked for more flexible and convenient ways to maintain their ABIM Board certification and the recently announced longitudinal assessment option is being designed to accomplish these requests. It is anticipated to launch in 2022 in as many specialties as possible, allowing time prior to launch for engagement with the medical community to produce the best possible experience.
How will the new longitudinal assessment option be different? Question delivery will be structured to allow physicians greater ease of use and mobility, enabling access from virtually anywhere. Answer feedback will be immediate, and physicians will see the rationale behind the answer, along with links to educational material. The preferred pace for answering questions during each administration window will be determined by the examinee, and access to all the resources you use in practice, such as journals or websites, will also be allowed.
Engaging the community
As a Council member, I can attest to the fact that the ABIM has spent a lot of time thinking through key features that are “must haves” in the new option, but there are details that are still being defined. ABIM has prioritized engaging the community, and the suggestions, insights, and questions coming out of these efforts are being used to guide the development of the new longitudinal assessment option.
Following the initial announcement in August, nearly 1,400 physicians submitted comments about the new option. ABIM conducted 69 one-on-one interviews with board-certified physicians and ran user-testing on existing longitudinal assessment platforms from other Boards. ABIM staff attended society meetings throughout the fall and also assembled a Physician Advisory Panel of 11 physicians from members of our Community Insights Network. We want to ensure the features we are considering work well for physicians and provide the high quality experience they deserve.
How can you get involved?
Physicians interested in giving ABIM feedback are invited to connect with us through our Community Insights Network. By joining the Network, you’ll have an opportunity to share your ideas through surveys, interviews, and user tests and be a member of our online community “ABIM Engage.”
ABIM staff will also be in attendance at society meetings to provide individualized guidance and answer your questions. We had a booth at CHEST this past October, and you can find upcoming society meetings staff who will be attending on their website.
What Should You Do Now?
All current ABIM MOC program requirements and policies remain in effect, and ABIM will communicate any program changes well in advance of implementation. If you have an assessment due in 2020 or 2021, you can choose from the options currently available in your discipline.
Registration for all 2020 MOC assessments opened December 1, and physicians may have several pathways to choose from, including taking the Knowledge Check-In at home, office, or testing center or the traditional point-in-time assessment taken at a PearsonVUE center.
The next Knowledge Check-In in Pulmonary Disease will be offered in 2021. ABIM’s website lists the full schedule of available assessment options (https://tinyurl.com/t5bfg55). You can find all of your MOC program requirements and deadlines by signing into your Physician Portal at abim.org.
To keep up to date with developments in ABIM’s longitudinal assessment program, visit the new longitudinal FAQ webpage (https://tinyurl.com/u5bbdgw) that is updated as information becomes available.
Physicians have asked for more flexible and convenient ways to maintain their ABIM Board certification and the recently announced longitudinal assessment option is being designed to accomplish these requests. It is anticipated to launch in 2022 in as many specialties as possible, allowing time prior to launch for engagement with the medical community to produce the best possible experience.
How will the new longitudinal assessment option be different? Question delivery will be structured to allow physicians greater ease of use and mobility, enabling access from virtually anywhere. Answer feedback will be immediate, and physicians will see the rationale behind the answer, along with links to educational material. The preferred pace for answering questions during each administration window will be determined by the examinee, and access to all the resources you use in practice, such as journals or websites, will also be allowed.
Engaging the community
As a Council member, I can attest to the fact that the ABIM has spent a lot of time thinking through key features that are “must haves” in the new option, but there are details that are still being defined. ABIM has prioritized engaging the community, and the suggestions, insights, and questions coming out of these efforts are being used to guide the development of the new longitudinal assessment option.
Following the initial announcement in August, nearly 1,400 physicians submitted comments about the new option. ABIM conducted 69 one-on-one interviews with board-certified physicians and ran user-testing on existing longitudinal assessment platforms from other Boards. ABIM staff attended society meetings throughout the fall and also assembled a Physician Advisory Panel of 11 physicians from members of our Community Insights Network. We want to ensure the features we are considering work well for physicians and provide the high quality experience they deserve.
How can you get involved?
Physicians interested in giving ABIM feedback are invited to connect with us through our Community Insights Network. By joining the Network, you’ll have an opportunity to share your ideas through surveys, interviews, and user tests and be a member of our online community “ABIM Engage.”
ABIM staff will also be in attendance at society meetings to provide individualized guidance and answer your questions. We had a booth at CHEST this past October, and you can find upcoming society meetings staff who will be attending on their website.
What Should You Do Now?
All current ABIM MOC program requirements and policies remain in effect, and ABIM will communicate any program changes well in advance of implementation. If you have an assessment due in 2020 or 2021, you can choose from the options currently available in your discipline.
Registration for all 2020 MOC assessments opened December 1, and physicians may have several pathways to choose from, including taking the Knowledge Check-In at home, office, or testing center or the traditional point-in-time assessment taken at a PearsonVUE center.
The next Knowledge Check-In in Pulmonary Disease will be offered in 2021. ABIM’s website lists the full schedule of available assessment options (https://tinyurl.com/t5bfg55). You can find all of your MOC program requirements and deadlines by signing into your Physician Portal at abim.org.
To keep up to date with developments in ABIM’s longitudinal assessment program, visit the new longitudinal FAQ webpage (https://tinyurl.com/u5bbdgw) that is updated as information becomes available.
Winners: CHEST Challenge Championship 2019
1st Place
Ohio State University
Elie Homsy, MD
Rachel Quaney, MD
Ryan Story, MD
Program Director: Jennifer McCallister, MD, FCCP
2nd Place
Walter Reed National Military Medical Center
Jeannette Collins, MD
Ian Grasso, MD
Arthur Holtzcalw, MD
Program Director: Aaron Holley, MD, FCCP
3rd Place
Maimonides Medical Center
Sushil Gupta, MBBS
Ankur Sinha, MD
Vignesh Ponnusamy, MD
Program Directors: Yizhek Kupfer, MD, and Stephan Kamholz, MD, FCCP
1st Place
Ohio State University
Elie Homsy, MD
Rachel Quaney, MD
Ryan Story, MD
Program Director: Jennifer McCallister, MD, FCCP
2nd Place
Walter Reed National Military Medical Center
Jeannette Collins, MD
Ian Grasso, MD
Arthur Holtzcalw, MD
Program Director: Aaron Holley, MD, FCCP
3rd Place
Maimonides Medical Center
Sushil Gupta, MBBS
Ankur Sinha, MD
Vignesh Ponnusamy, MD
Program Directors: Yizhek Kupfer, MD, and Stephan Kamholz, MD, FCCP
1st Place
Ohio State University
Elie Homsy, MD
Rachel Quaney, MD
Ryan Story, MD
Program Director: Jennifer McCallister, MD, FCCP
2nd Place
Walter Reed National Military Medical Center
Jeannette Collins, MD
Ian Grasso, MD
Arthur Holtzcalw, MD
Program Director: Aaron Holley, MD, FCCP
3rd Place
Maimonides Medical Center
Sushil Gupta, MBBS
Ankur Sinha, MD
Vignesh Ponnusamy, MD
Program Directors: Yizhek Kupfer, MD, and Stephan Kamholz, MD, FCCP