User login
Zanubrutinib achieved high response rate in del(17p) CLL cohort
ORLANDO – Zanubrutinib has produced a high overall response rate in one the largest cohorts of patients with treatment-naive 17p-deletion chronic lymphocytic leukemia (CLL) studied to date.
An overall response rate of nearly 93% was seen in this 109-patient, high-risk cohort, enrolled as part of the phase 3 SEQUOIA study (BGB-3111-304), said Constantine S. Tam, MBBS, MD, of St. Vincent’s Hospital and Peter MacCallum Cancer Centre in Melbourne.
Tolerability of zanubrutinib was essentially consistent with previous reports of the agent as used in other B-cell malignancies, Dr. Tam said in an oral presentation of the results at the annual meeting of the American Society of Hematology.
Deletion of chromosome 17p13.1, or del(17p), is a marker of poor prognosis and poor response to chemotherapy in patients with CLL or small lymphocytic lymphoma (SLL). For patients with del(17p) CLL, the first-generation Bruton tyrosine kinase (BTK) inhibitor ibrutinib has become a standard of care, Dr. Tam said.
Zanubrutinib, a next-generation BTK inhibitor, was developed to improve BTK occupancy and minimize off-target inhibition of TEC and epidermal growth factor receptor kinases. “What this effectively means is that we are able to dose this drug at levels much higher than that achievable with ibrutinib, and not get intolerable side effects,” Dr. Tam said.
Zanubrutinib has been approved in the United States for previously treated mantle cell lymphoma, and generated durable responses among CLL/SLL patients with or without del(17p) in a phase 1/2 study, according to Dr. Tam.
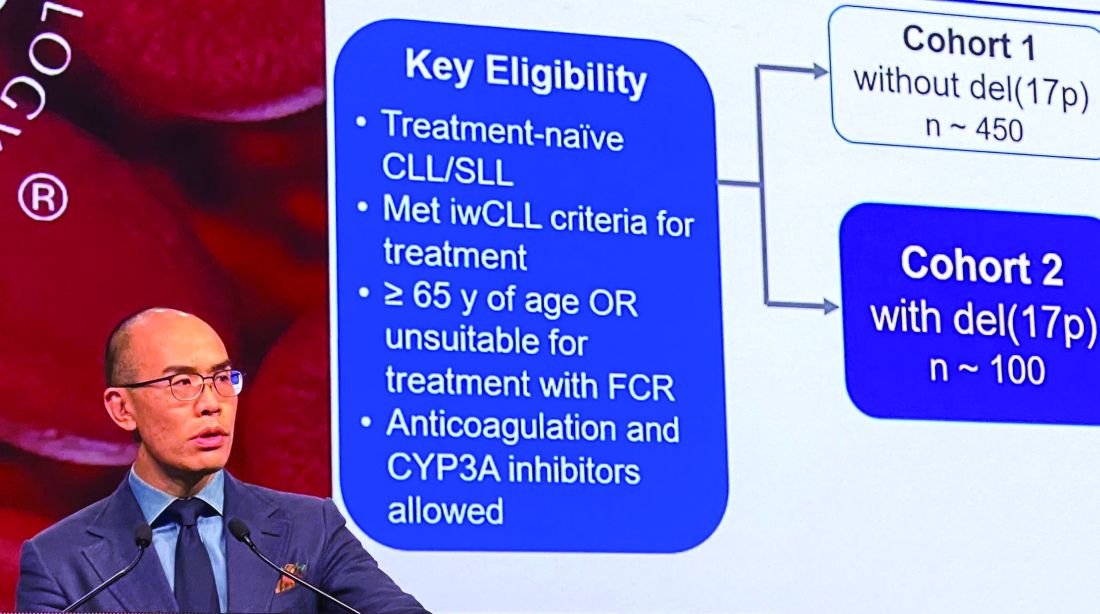
In the present study, which exclusively enrolled patients with del(17p) CLL/SLL, patients received 160 mg twice daily of zanubrutinib, Dr. Tam said. Out of 109 patients enrolled, 10 (9.2%) had SLL. All patients were aged at least 65 years or were deemed unsuitable for treatment with the combination of fludarabine, cyclophosphamide, and rituximab.
Of 109 patients enrolled, 104 received on-study treatment. The median age was 70 years, Dr. Tam reported, and a number of patients had other high-risk markers beyond del(17p), including unmutated IgVH status in 61.5% of patients.
With a median follow-up of 10 months, the overall response rate was 92.7%, including 1.9% complete responses and 78.9% partial responses. “Only one patient had primary progressive disease after starting this drug,” Dr. Tam said.
Time to response was rapid, according to the investigator, at about 2.8 months; after 6 months, 95% of responders remained in response.
Further analysis showed that the response rate was consistent across subgroups. “There was not a single group that did not respond with a high response rate, including poor prognostic groups,” Dr. Tam said.
Most adverse events were grade 1-2 in severity, and the most common events included confusion and upper respiratory tract infection. The only common grade 3 event, according to Dr. Tam, was neutropenia. Rates of grade 3 major bleeding were low, he said, and the rate of grade 3 atrial fibrillation was 0.9%. One patient died due to pneumonia.
The ongoing SEQUOIA study, designed to compare zanubrutinib to the combination of bendamustine and rituximab in patients with previously untreated CLL or SLL, is sponsored by BeiGene. Dr. Tam reported disclosures related to Novartis, Pharmacyclics, AbbVie, BeiGene, Janssen, and Roche.
SOURCE: Tam C et al. ASH 2019, Abstract 499.
ORLANDO – Zanubrutinib has produced a high overall response rate in one the largest cohorts of patients with treatment-naive 17p-deletion chronic lymphocytic leukemia (CLL) studied to date.
An overall response rate of nearly 93% was seen in this 109-patient, high-risk cohort, enrolled as part of the phase 3 SEQUOIA study (BGB-3111-304), said Constantine S. Tam, MBBS, MD, of St. Vincent’s Hospital and Peter MacCallum Cancer Centre in Melbourne.
Tolerability of zanubrutinib was essentially consistent with previous reports of the agent as used in other B-cell malignancies, Dr. Tam said in an oral presentation of the results at the annual meeting of the American Society of Hematology.
Deletion of chromosome 17p13.1, or del(17p), is a marker of poor prognosis and poor response to chemotherapy in patients with CLL or small lymphocytic lymphoma (SLL). For patients with del(17p) CLL, the first-generation Bruton tyrosine kinase (BTK) inhibitor ibrutinib has become a standard of care, Dr. Tam said.
Zanubrutinib, a next-generation BTK inhibitor, was developed to improve BTK occupancy and minimize off-target inhibition of TEC and epidermal growth factor receptor kinases. “What this effectively means is that we are able to dose this drug at levels much higher than that achievable with ibrutinib, and not get intolerable side effects,” Dr. Tam said.
Zanubrutinib has been approved in the United States for previously treated mantle cell lymphoma, and generated durable responses among CLL/SLL patients with or without del(17p) in a phase 1/2 study, according to Dr. Tam.
In the present study, which exclusively enrolled patients with del(17p) CLL/SLL, patients received 160 mg twice daily of zanubrutinib, Dr. Tam said. Out of 109 patients enrolled, 10 (9.2%) had SLL. All patients were aged at least 65 years or were deemed unsuitable for treatment with the combination of fludarabine, cyclophosphamide, and rituximab.
Of 109 patients enrolled, 104 received on-study treatment. The median age was 70 years, Dr. Tam reported, and a number of patients had other high-risk markers beyond del(17p), including unmutated IgVH status in 61.5% of patients.
With a median follow-up of 10 months, the overall response rate was 92.7%, including 1.9% complete responses and 78.9% partial responses. “Only one patient had primary progressive disease after starting this drug,” Dr. Tam said.
Time to response was rapid, according to the investigator, at about 2.8 months; after 6 months, 95% of responders remained in response.
Further analysis showed that the response rate was consistent across subgroups. “There was not a single group that did not respond with a high response rate, including poor prognostic groups,” Dr. Tam said.
Most adverse events were grade 1-2 in severity, and the most common events included confusion and upper respiratory tract infection. The only common grade 3 event, according to Dr. Tam, was neutropenia. Rates of grade 3 major bleeding were low, he said, and the rate of grade 3 atrial fibrillation was 0.9%. One patient died due to pneumonia.
The ongoing SEQUOIA study, designed to compare zanubrutinib to the combination of bendamustine and rituximab in patients with previously untreated CLL or SLL, is sponsored by BeiGene. Dr. Tam reported disclosures related to Novartis, Pharmacyclics, AbbVie, BeiGene, Janssen, and Roche.
SOURCE: Tam C et al. ASH 2019, Abstract 499.
ORLANDO – Zanubrutinib has produced a high overall response rate in one the largest cohorts of patients with treatment-naive 17p-deletion chronic lymphocytic leukemia (CLL) studied to date.
An overall response rate of nearly 93% was seen in this 109-patient, high-risk cohort, enrolled as part of the phase 3 SEQUOIA study (BGB-3111-304), said Constantine S. Tam, MBBS, MD, of St. Vincent’s Hospital and Peter MacCallum Cancer Centre in Melbourne.
Tolerability of zanubrutinib was essentially consistent with previous reports of the agent as used in other B-cell malignancies, Dr. Tam said in an oral presentation of the results at the annual meeting of the American Society of Hematology.
Deletion of chromosome 17p13.1, or del(17p), is a marker of poor prognosis and poor response to chemotherapy in patients with CLL or small lymphocytic lymphoma (SLL). For patients with del(17p) CLL, the first-generation Bruton tyrosine kinase (BTK) inhibitor ibrutinib has become a standard of care, Dr. Tam said.
Zanubrutinib, a next-generation BTK inhibitor, was developed to improve BTK occupancy and minimize off-target inhibition of TEC and epidermal growth factor receptor kinases. “What this effectively means is that we are able to dose this drug at levels much higher than that achievable with ibrutinib, and not get intolerable side effects,” Dr. Tam said.
Zanubrutinib has been approved in the United States for previously treated mantle cell lymphoma, and generated durable responses among CLL/SLL patients with or without del(17p) in a phase 1/2 study, according to Dr. Tam.
In the present study, which exclusively enrolled patients with del(17p) CLL/SLL, patients received 160 mg twice daily of zanubrutinib, Dr. Tam said. Out of 109 patients enrolled, 10 (9.2%) had SLL. All patients were aged at least 65 years or were deemed unsuitable for treatment with the combination of fludarabine, cyclophosphamide, and rituximab.
Of 109 patients enrolled, 104 received on-study treatment. The median age was 70 years, Dr. Tam reported, and a number of patients had other high-risk markers beyond del(17p), including unmutated IgVH status in 61.5% of patients.
With a median follow-up of 10 months, the overall response rate was 92.7%, including 1.9% complete responses and 78.9% partial responses. “Only one patient had primary progressive disease after starting this drug,” Dr. Tam said.
Time to response was rapid, according to the investigator, at about 2.8 months; after 6 months, 95% of responders remained in response.
Further analysis showed that the response rate was consistent across subgroups. “There was not a single group that did not respond with a high response rate, including poor prognostic groups,” Dr. Tam said.
Most adverse events were grade 1-2 in severity, and the most common events included confusion and upper respiratory tract infection. The only common grade 3 event, according to Dr. Tam, was neutropenia. Rates of grade 3 major bleeding were low, he said, and the rate of grade 3 atrial fibrillation was 0.9%. One patient died due to pneumonia.
The ongoing SEQUOIA study, designed to compare zanubrutinib to the combination of bendamustine and rituximab in patients with previously untreated CLL or SLL, is sponsored by BeiGene. Dr. Tam reported disclosures related to Novartis, Pharmacyclics, AbbVie, BeiGene, Janssen, and Roche.
SOURCE: Tam C et al. ASH 2019, Abstract 499.
REPORTING FROM ASH 2019
Cancer researchers win grants from DOD, GO2 Foundation
The GO2 Foundation for Lung Cancer has granted the 2019 Young Innovators Team Awards to two groups of investigators studying non-small cell lung cancer (NSCLC). Each group received $250,000 to support their work.
Yanxiang (Jessie) Guo, PhD, of Rutgers Cancer Institute of New Jersey, and Shawn Davidson, PhD, of Princeton University in New Jersey, won the award for their research on tumor metabolism and immunotherapy in KRAS-mutant NSCLC.
Dr. Guo and Dr. Davidson aim to prove that cancer cell metabolism affects the tumor microenvironment and leads to an impaired antitumor immune response. The pair’s ultimate goal is to overcome resistance to immunotherapy in KRAS-mutant NSCLC.
Matthew Bott, MD, of Memorial Sloan Kettering Cancer Center in New York, and Tuomas Tammela, MD, PhD, of Weill-Cornell Medical College in New York, won the award for their research on age-related differences in NSCLC.
Dr. Bott and Dr. Tammela aim to characterize differences in natural history and treatment response between younger and older patients with NSCLC. The main goal is to determine if different age groups require different approaches to treatment.
Two other researchers, both from Fox Chase Cancer Center in Philadelphia, received grants from the U.S. Department of Defense.
Jeffrey Peterson, PhD, was awarded a $1.4 million grant from the Department of Defense for his research on triple-negative breast cancer. Dr. Peterson will work with postdoctoral research fellows Alexander Beatty, PhD, and Tanu Singh, PhD, to determine if polyunsaturated fatty acids can be used to induce programmed cell death in triple-negative breast cancer.
Dr. Peterson theorizes that metastatic cells may be susceptible to preferential uptake of conjugated linoleic acid, which will trigger ferroptosis and destroy cancer cells without affecting normal cells. His ultimate goal is to set the stage for clinical trials of more effective, less toxic targeted therapies for triple-negative breast cancer.

Phillip Abbosh, MD, PhD, was awarded a $658,800 grant from the Department of Defense to investigate the role of the immune system and certain bacteria in mediating responses to therapy in bladder cancers.
Dr. Abbosh theorizes that a better understanding of the interaction between the immune system and bladder tumors could aid the development of new targeted therapies, and perhaps bacteria found in cancer patients’ bladders could be used to enhance treatment.
The GO2 Foundation for Lung Cancer has granted the 2019 Young Innovators Team Awards to two groups of investigators studying non-small cell lung cancer (NSCLC). Each group received $250,000 to support their work.
Yanxiang (Jessie) Guo, PhD, of Rutgers Cancer Institute of New Jersey, and Shawn Davidson, PhD, of Princeton University in New Jersey, won the award for their research on tumor metabolism and immunotherapy in KRAS-mutant NSCLC.
Dr. Guo and Dr. Davidson aim to prove that cancer cell metabolism affects the tumor microenvironment and leads to an impaired antitumor immune response. The pair’s ultimate goal is to overcome resistance to immunotherapy in KRAS-mutant NSCLC.
Matthew Bott, MD, of Memorial Sloan Kettering Cancer Center in New York, and Tuomas Tammela, MD, PhD, of Weill-Cornell Medical College in New York, won the award for their research on age-related differences in NSCLC.
Dr. Bott and Dr. Tammela aim to characterize differences in natural history and treatment response between younger and older patients with NSCLC. The main goal is to determine if different age groups require different approaches to treatment.
Two other researchers, both from Fox Chase Cancer Center in Philadelphia, received grants from the U.S. Department of Defense.
Jeffrey Peterson, PhD, was awarded a $1.4 million grant from the Department of Defense for his research on triple-negative breast cancer. Dr. Peterson will work with postdoctoral research fellows Alexander Beatty, PhD, and Tanu Singh, PhD, to determine if polyunsaturated fatty acids can be used to induce programmed cell death in triple-negative breast cancer.
Dr. Peterson theorizes that metastatic cells may be susceptible to preferential uptake of conjugated linoleic acid, which will trigger ferroptosis and destroy cancer cells without affecting normal cells. His ultimate goal is to set the stage for clinical trials of more effective, less toxic targeted therapies for triple-negative breast cancer.
Phillip Abbosh, MD, PhD, was awarded a $658,800 grant from the Department of Defense to investigate the role of the immune system and certain bacteria in mediating responses to therapy in bladder cancers.
Dr. Abbosh theorizes that a better understanding of the interaction between the immune system and bladder tumors could aid the development of new targeted therapies, and perhaps bacteria found in cancer patients’ bladders could be used to enhance treatment.
The GO2 Foundation for Lung Cancer has granted the 2019 Young Innovators Team Awards to two groups of investigators studying non-small cell lung cancer (NSCLC). Each group received $250,000 to support their work.
Yanxiang (Jessie) Guo, PhD, of Rutgers Cancer Institute of New Jersey, and Shawn Davidson, PhD, of Princeton University in New Jersey, won the award for their research on tumor metabolism and immunotherapy in KRAS-mutant NSCLC.
Dr. Guo and Dr. Davidson aim to prove that cancer cell metabolism affects the tumor microenvironment and leads to an impaired antitumor immune response. The pair’s ultimate goal is to overcome resistance to immunotherapy in KRAS-mutant NSCLC.
Matthew Bott, MD, of Memorial Sloan Kettering Cancer Center in New York, and Tuomas Tammela, MD, PhD, of Weill-Cornell Medical College in New York, won the award for their research on age-related differences in NSCLC.
Dr. Bott and Dr. Tammela aim to characterize differences in natural history and treatment response between younger and older patients with NSCLC. The main goal is to determine if different age groups require different approaches to treatment.
Two other researchers, both from Fox Chase Cancer Center in Philadelphia, received grants from the U.S. Department of Defense.
Jeffrey Peterson, PhD, was awarded a $1.4 million grant from the Department of Defense for his research on triple-negative breast cancer. Dr. Peterson will work with postdoctoral research fellows Alexander Beatty, PhD, and Tanu Singh, PhD, to determine if polyunsaturated fatty acids can be used to induce programmed cell death in triple-negative breast cancer.
Dr. Peterson theorizes that metastatic cells may be susceptible to preferential uptake of conjugated linoleic acid, which will trigger ferroptosis and destroy cancer cells without affecting normal cells. His ultimate goal is to set the stage for clinical trials of more effective, less toxic targeted therapies for triple-negative breast cancer.
Phillip Abbosh, MD, PhD, was awarded a $658,800 grant from the Department of Defense to investigate the role of the immune system and certain bacteria in mediating responses to therapy in bladder cancers.
Dr. Abbosh theorizes that a better understanding of the interaction between the immune system and bladder tumors could aid the development of new targeted therapies, and perhaps bacteria found in cancer patients’ bladders could be used to enhance treatment.
More than half of pediatric residents feel burned out
More than half of all pediatric residents report feeling burned out, in a trend that has now reached 3 years.

“The stable 54%-56% rate of burnout found during 2016-2018 in this study is similar to burnout rates previously reported in U.S. studies of pediatric residents,” Kathi Kemper, MD, Ohio State University, Columbus, and colleagues wrote (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-1030).
The “alarming rate of physician burnout is a call to action on behalf of current trainees and future generations of doctors,” Jeanine Ronan, MD, of Children’s Hospital of Philadelphia, said in an accompanying editorial (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-3210), adding that “although this concern was identified more than a decade ago, little progress has been made.”
The findings were based on the Pediatric Resident Burnout and Resilience Study Consortium surveys completed at 34 residency programs in 2016 (1,664 residents participated in the survey), 43 in 2017 (2,153 participated), and 49 in 2018 (2,241 participated). The 22-item Maslach Burnout Inventory Human Services Survey was used to assess burnout.
However, researchers noted that there were “no consistent significant differences between residents meeting criteria for burnout and those not meeting criteria for burnout in terms of any demographic characteristic,” the authors added.
For example, residency year and program size were associated with burnout in some years but not others.
There “were significant differences in burnout rates among postgraduate year 1 (PGY1), postgraduate year 2 (PGY2), and postgraduate year 3 (PGY3) in 2016 and 2017, but not in 2018,” the authors stated.
For 2016, burnout rates in PGY1, PGY2 and PGY3 were 36%, 34%, and 30%, respectively. In 2017, the rates changed to 33%, 36%, and 31%, respectively, while in 2018, the rates were reported to be 35% in the first postgraduate year and 33% each for the second and third postgraduate years.
Other findings from the survey revealed that residents who met the criteria for burnout reported worse mental health, more sleepiness, and greater stress, as well as lower mindfulness and self-compassion scores, less confidence in providing compassionate care, and lower levels of empathy and resilience.
“Residents who met the criteria for burnout were more likely to be on high-acuity rotations,” the Dr. Kemper and colleagues observed. “They were approximately twice as likely to report recently having made a medical error, more likely to report a work-life conflict, less likely to have had a vacation within the past month, and less likely to have had a recent weekend off than those who did not meet the criteria for burnout.
Additionally, residents reporting burnout “consistently reported significantly less satisfaction with support from family, spouse, friends, faculty, and colleagues,” the report states. “They also reported significantly lower quality of life, less satisfaction with their choice to go into pediatrics, and less satisfaction with their balance between personal and professional life.”
Dr. Ronan also noted that the survey “showed the negative impact of the environment on trainee performance and ability to cope with stress. Residency training programs should evaluate different scheduling and staffing models to determine if there are opportunities to enhance the learning environment.”
She also noted that given the link between electronic health record usage and administrative tasks and burnout, lessening administrative task burden on trainees may help decrease the rate of burnout.
Dr. Ronan added that mental health services also must be made readily available to trainees.
“The high burnout rate among pediatric residents must be addressed,” she said. “A comprehensive approach would include developing evidence-based training in mindfulness and coping techniques for the individual resident, an institutional approach to improve resident engagement and increase joy in the workplace, and the availability of mental health services when needed to address both urgent and chronic concerns.”
SOURCE: Kemper K et al. Pediatrics 2019 Dec 16. doi: 10.1542/peds.2019-1030.
More than half of all pediatric residents report feeling burned out, in a trend that has now reached 3 years.
“The stable 54%-56% rate of burnout found during 2016-2018 in this study is similar to burnout rates previously reported in U.S. studies of pediatric residents,” Kathi Kemper, MD, Ohio State University, Columbus, and colleagues wrote (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-1030).
The “alarming rate of physician burnout is a call to action on behalf of current trainees and future generations of doctors,” Jeanine Ronan, MD, of Children’s Hospital of Philadelphia, said in an accompanying editorial (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-3210), adding that “although this concern was identified more than a decade ago, little progress has been made.”
The findings were based on the Pediatric Resident Burnout and Resilience Study Consortium surveys completed at 34 residency programs in 2016 (1,664 residents participated in the survey), 43 in 2017 (2,153 participated), and 49 in 2018 (2,241 participated). The 22-item Maslach Burnout Inventory Human Services Survey was used to assess burnout.
However, researchers noted that there were “no consistent significant differences between residents meeting criteria for burnout and those not meeting criteria for burnout in terms of any demographic characteristic,” the authors added.
For example, residency year and program size were associated with burnout in some years but not others.
There “were significant differences in burnout rates among postgraduate year 1 (PGY1), postgraduate year 2 (PGY2), and postgraduate year 3 (PGY3) in 2016 and 2017, but not in 2018,” the authors stated.
For 2016, burnout rates in PGY1, PGY2 and PGY3 were 36%, 34%, and 30%, respectively. In 2017, the rates changed to 33%, 36%, and 31%, respectively, while in 2018, the rates were reported to be 35% in the first postgraduate year and 33% each for the second and third postgraduate years.
Other findings from the survey revealed that residents who met the criteria for burnout reported worse mental health, more sleepiness, and greater stress, as well as lower mindfulness and self-compassion scores, less confidence in providing compassionate care, and lower levels of empathy and resilience.
“Residents who met the criteria for burnout were more likely to be on high-acuity rotations,” the Dr. Kemper and colleagues observed. “They were approximately twice as likely to report recently having made a medical error, more likely to report a work-life conflict, less likely to have had a vacation within the past month, and less likely to have had a recent weekend off than those who did not meet the criteria for burnout.
Additionally, residents reporting burnout “consistently reported significantly less satisfaction with support from family, spouse, friends, faculty, and colleagues,” the report states. “They also reported significantly lower quality of life, less satisfaction with their choice to go into pediatrics, and less satisfaction with their balance between personal and professional life.”
Dr. Ronan also noted that the survey “showed the negative impact of the environment on trainee performance and ability to cope with stress. Residency training programs should evaluate different scheduling and staffing models to determine if there are opportunities to enhance the learning environment.”
She also noted that given the link between electronic health record usage and administrative tasks and burnout, lessening administrative task burden on trainees may help decrease the rate of burnout.
Dr. Ronan added that mental health services also must be made readily available to trainees.
“The high burnout rate among pediatric residents must be addressed,” she said. “A comprehensive approach would include developing evidence-based training in mindfulness and coping techniques for the individual resident, an institutional approach to improve resident engagement and increase joy in the workplace, and the availability of mental health services when needed to address both urgent and chronic concerns.”
SOURCE: Kemper K et al. Pediatrics 2019 Dec 16. doi: 10.1542/peds.2019-1030.
More than half of all pediatric residents report feeling burned out, in a trend that has now reached 3 years.
“The stable 54%-56% rate of burnout found during 2016-2018 in this study is similar to burnout rates previously reported in U.S. studies of pediatric residents,” Kathi Kemper, MD, Ohio State University, Columbus, and colleagues wrote (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-1030).
The “alarming rate of physician burnout is a call to action on behalf of current trainees and future generations of doctors,” Jeanine Ronan, MD, of Children’s Hospital of Philadelphia, said in an accompanying editorial (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-3210), adding that “although this concern was identified more than a decade ago, little progress has been made.”
The findings were based on the Pediatric Resident Burnout and Resilience Study Consortium surveys completed at 34 residency programs in 2016 (1,664 residents participated in the survey), 43 in 2017 (2,153 participated), and 49 in 2018 (2,241 participated). The 22-item Maslach Burnout Inventory Human Services Survey was used to assess burnout.
However, researchers noted that there were “no consistent significant differences between residents meeting criteria for burnout and those not meeting criteria for burnout in terms of any demographic characteristic,” the authors added.
For example, residency year and program size were associated with burnout in some years but not others.
There “were significant differences in burnout rates among postgraduate year 1 (PGY1), postgraduate year 2 (PGY2), and postgraduate year 3 (PGY3) in 2016 and 2017, but not in 2018,” the authors stated.
For 2016, burnout rates in PGY1, PGY2 and PGY3 were 36%, 34%, and 30%, respectively. In 2017, the rates changed to 33%, 36%, and 31%, respectively, while in 2018, the rates were reported to be 35% in the first postgraduate year and 33% each for the second and third postgraduate years.
Other findings from the survey revealed that residents who met the criteria for burnout reported worse mental health, more sleepiness, and greater stress, as well as lower mindfulness and self-compassion scores, less confidence in providing compassionate care, and lower levels of empathy and resilience.
“Residents who met the criteria for burnout were more likely to be on high-acuity rotations,” the Dr. Kemper and colleagues observed. “They were approximately twice as likely to report recently having made a medical error, more likely to report a work-life conflict, less likely to have had a vacation within the past month, and less likely to have had a recent weekend off than those who did not meet the criteria for burnout.
Additionally, residents reporting burnout “consistently reported significantly less satisfaction with support from family, spouse, friends, faculty, and colleagues,” the report states. “They also reported significantly lower quality of life, less satisfaction with their choice to go into pediatrics, and less satisfaction with their balance between personal and professional life.”
Dr. Ronan also noted that the survey “showed the negative impact of the environment on trainee performance and ability to cope with stress. Residency training programs should evaluate different scheduling and staffing models to determine if there are opportunities to enhance the learning environment.”
She also noted that given the link between electronic health record usage and administrative tasks and burnout, lessening administrative task burden on trainees may help decrease the rate of burnout.
Dr. Ronan added that mental health services also must be made readily available to trainees.
“The high burnout rate among pediatric residents must be addressed,” she said. “A comprehensive approach would include developing evidence-based training in mindfulness and coping techniques for the individual resident, an institutional approach to improve resident engagement and increase joy in the workplace, and the availability of mental health services when needed to address both urgent and chronic concerns.”
SOURCE: Kemper K et al. Pediatrics 2019 Dec 16. doi: 10.1542/peds.2019-1030.
FROM PEDIATRICS
Intersubject correlation analyses can be used to pinpoint neural patterns in ADHD
Functional MRI-based intersubject correlations (ISCs) hold promise for studying the neural bases of ADHD’s heterogeneous symptoms in situations that reflect real-world difficulties, new research shows.
“The present results provide the first evidence of a connection between symptom scales and brain activity recorded when the participants have been involved in a situation that is similar to the ones where their difficulties typically occur,” wrote Juha Salmi, of the department of neuroscience and biomedical engineering at Aalto University in Espoo, Finland, and associates. The study was published in NeuroImage.
Many imaging studies in ADHD are too narrow and fail to reflect real-world situations and distractions, the investigators wrote. For the current study, the investigators conducted fMRI scans of participants in “cocktail party” situations. During fMRI, the participants viewed excerpts from the 2008 Finnish film “Three Wise Men,” in which three men were talking.
“There were periods when no additional distractors were presented and periods when the film was embedded with irrelevant distractors that the participants were told to ignore. The three different distractors (white noise, green; jazz music, red; speech, magenta) and nondistracted periods (blue) were presented in a pseudo-randomized order so that all other distractor types had to occur before the same distractor type was presented again,” the authors wrote. Each distractor lasted for 15 seconds.
The ISC approach sought to gauge how much neural networks in each group, 51 with ADHD and 29 without, “ticked together” – that is, synchronized and coordinated in a feature-specific manner.
As expected, across the film, ISCs of those in the ADHD group were weaker than were those in the control group in multiple brain areas, including the left precuneus, bilateral medial occipital cortices, left lateral occipital cortex, left temporoparietal junction, and medial and posterior parts of the left superior temporal cortex. Likewise, when the other distractors occurred – with the exception of constant white noise – weaker ISCs were found among the ADHD group. In fact, there were no brain regions in which healthy controls had weaker ISCs than did those with ADHD.
“ the investigators wrote. “At least theoretically, this approach could be used to identify neural patterns reflecting specific symptoms in complex, dynamic situations.”
One limitation of naturalistic studies is that the inferences are by their nature more general than they might be in more conventional, discrete experiments. Bridging the gap between naturalistic studies such as this one and other more conventional designs are needed, the investigators wrote, because dove-tailing their findings could provide significant insights.
The study was supported by the Academy of Finland and the Åbo Akademi University Endowment for the BrainTrain project. None of the authors have any biomedical financial interests or potential conflicts of interest.
SOURCE: Salmi J et al. Neuroimage. 2019 Nov 12. doi: 10.1016/j.neuroimage.2019.116352.
Functional MRI-based intersubject correlations (ISCs) hold promise for studying the neural bases of ADHD’s heterogeneous symptoms in situations that reflect real-world difficulties, new research shows.
“The present results provide the first evidence of a connection between symptom scales and brain activity recorded when the participants have been involved in a situation that is similar to the ones where their difficulties typically occur,” wrote Juha Salmi, of the department of neuroscience and biomedical engineering at Aalto University in Espoo, Finland, and associates. The study was published in NeuroImage.
Many imaging studies in ADHD are too narrow and fail to reflect real-world situations and distractions, the investigators wrote. For the current study, the investigators conducted fMRI scans of participants in “cocktail party” situations. During fMRI, the participants viewed excerpts from the 2008 Finnish film “Three Wise Men,” in which three men were talking.
“There were periods when no additional distractors were presented and periods when the film was embedded with irrelevant distractors that the participants were told to ignore. The three different distractors (white noise, green; jazz music, red; speech, magenta) and nondistracted periods (blue) were presented in a pseudo-randomized order so that all other distractor types had to occur before the same distractor type was presented again,” the authors wrote. Each distractor lasted for 15 seconds.
The ISC approach sought to gauge how much neural networks in each group, 51 with ADHD and 29 without, “ticked together” – that is, synchronized and coordinated in a feature-specific manner.
As expected, across the film, ISCs of those in the ADHD group were weaker than were those in the control group in multiple brain areas, including the left precuneus, bilateral medial occipital cortices, left lateral occipital cortex, left temporoparietal junction, and medial and posterior parts of the left superior temporal cortex. Likewise, when the other distractors occurred – with the exception of constant white noise – weaker ISCs were found among the ADHD group. In fact, there were no brain regions in which healthy controls had weaker ISCs than did those with ADHD.
“ the investigators wrote. “At least theoretically, this approach could be used to identify neural patterns reflecting specific symptoms in complex, dynamic situations.”
One limitation of naturalistic studies is that the inferences are by their nature more general than they might be in more conventional, discrete experiments. Bridging the gap between naturalistic studies such as this one and other more conventional designs are needed, the investigators wrote, because dove-tailing their findings could provide significant insights.
The study was supported by the Academy of Finland and the Åbo Akademi University Endowment for the BrainTrain project. None of the authors have any biomedical financial interests or potential conflicts of interest.
SOURCE: Salmi J et al. Neuroimage. 2019 Nov 12. doi: 10.1016/j.neuroimage.2019.116352.
Functional MRI-based intersubject correlations (ISCs) hold promise for studying the neural bases of ADHD’s heterogeneous symptoms in situations that reflect real-world difficulties, new research shows.
“The present results provide the first evidence of a connection between symptom scales and brain activity recorded when the participants have been involved in a situation that is similar to the ones where their difficulties typically occur,” wrote Juha Salmi, of the department of neuroscience and biomedical engineering at Aalto University in Espoo, Finland, and associates. The study was published in NeuroImage.
Many imaging studies in ADHD are too narrow and fail to reflect real-world situations and distractions, the investigators wrote. For the current study, the investigators conducted fMRI scans of participants in “cocktail party” situations. During fMRI, the participants viewed excerpts from the 2008 Finnish film “Three Wise Men,” in which three men were talking.
“There were periods when no additional distractors were presented and periods when the film was embedded with irrelevant distractors that the participants were told to ignore. The three different distractors (white noise, green; jazz music, red; speech, magenta) and nondistracted periods (blue) were presented in a pseudo-randomized order so that all other distractor types had to occur before the same distractor type was presented again,” the authors wrote. Each distractor lasted for 15 seconds.
The ISC approach sought to gauge how much neural networks in each group, 51 with ADHD and 29 without, “ticked together” – that is, synchronized and coordinated in a feature-specific manner.
As expected, across the film, ISCs of those in the ADHD group were weaker than were those in the control group in multiple brain areas, including the left precuneus, bilateral medial occipital cortices, left lateral occipital cortex, left temporoparietal junction, and medial and posterior parts of the left superior temporal cortex. Likewise, when the other distractors occurred – with the exception of constant white noise – weaker ISCs were found among the ADHD group. In fact, there were no brain regions in which healthy controls had weaker ISCs than did those with ADHD.
“ the investigators wrote. “At least theoretically, this approach could be used to identify neural patterns reflecting specific symptoms in complex, dynamic situations.”
One limitation of naturalistic studies is that the inferences are by their nature more general than they might be in more conventional, discrete experiments. Bridging the gap between naturalistic studies such as this one and other more conventional designs are needed, the investigators wrote, because dove-tailing their findings could provide significant insights.
The study was supported by the Academy of Finland and the Åbo Akademi University Endowment for the BrainTrain project. None of the authors have any biomedical financial interests or potential conflicts of interest.
SOURCE: Salmi J et al. Neuroimage. 2019 Nov 12. doi: 10.1016/j.neuroimage.2019.116352.
FROM NEUROIMAGE
Heart rate changes during sleep may be diagnostic tool for depression
A heart rate–profiling algorithm shows promise at distinguishing differences in heart rate patterns during sleep between people with depression and healthy controls, research shows.
The algorithm was modeled using machine learning based on 1,203 polysomnograms from either people with depression or healthy controls, according to Mysa Saad, of the sleep research unit of the Royal’s Institute of Mental Health Research in Ottawa, and associates. That final algorithm was then tested on a new sample of 174 individuals (87 controls, 87 with depression) to categorize each person as either depressed or not depressed. This result was compared with medical record diagnoses. The study was published in BMC Psychiatry.
Compared with the control group, and in overall time. The algorithm incorrectly identified 15 patients with depression as being in the control group, and incorrectly identified 20 controls as having depression. The overall accuracy was 79.9%, with a sensitivity of 82.8% and a specificity of 77%.
“In addition to providing an improved biological underpinning for the diagnosis of depression, this [tool] could possibly offer supplemental information to psychiatric clinical assessment, and objective measures for early screening. Moreover, the use of distinct physiological variables as biomarkers of depression may help emphasize the interactions between mental and physical health. This may contribute to reducing the stigma associated with depression, lifting some social barriers to accessing psychiatric treatment, and allowing for more holistic patient care,” the investigators concluded.
Medibio provided partial funding for the salaries of research assistants; no other conflicts of interest were reported.
SOURCE: Saad M et al. BMC Psychiatry. 2019 Jun 7. doi: 10.1186/s12888-019-2152-1.
A heart rate–profiling algorithm shows promise at distinguishing differences in heart rate patterns during sleep between people with depression and healthy controls, research shows.
The algorithm was modeled using machine learning based on 1,203 polysomnograms from either people with depression or healthy controls, according to Mysa Saad, of the sleep research unit of the Royal’s Institute of Mental Health Research in Ottawa, and associates. That final algorithm was then tested on a new sample of 174 individuals (87 controls, 87 with depression) to categorize each person as either depressed or not depressed. This result was compared with medical record diagnoses. The study was published in BMC Psychiatry.
Compared with the control group, and in overall time. The algorithm incorrectly identified 15 patients with depression as being in the control group, and incorrectly identified 20 controls as having depression. The overall accuracy was 79.9%, with a sensitivity of 82.8% and a specificity of 77%.
“In addition to providing an improved biological underpinning for the diagnosis of depression, this [tool] could possibly offer supplemental information to psychiatric clinical assessment, and objective measures for early screening. Moreover, the use of distinct physiological variables as biomarkers of depression may help emphasize the interactions between mental and physical health. This may contribute to reducing the stigma associated with depression, lifting some social barriers to accessing psychiatric treatment, and allowing for more holistic patient care,” the investigators concluded.
Medibio provided partial funding for the salaries of research assistants; no other conflicts of interest were reported.
SOURCE: Saad M et al. BMC Psychiatry. 2019 Jun 7. doi: 10.1186/s12888-019-2152-1.
A heart rate–profiling algorithm shows promise at distinguishing differences in heart rate patterns during sleep between people with depression and healthy controls, research shows.
The algorithm was modeled using machine learning based on 1,203 polysomnograms from either people with depression or healthy controls, according to Mysa Saad, of the sleep research unit of the Royal’s Institute of Mental Health Research in Ottawa, and associates. That final algorithm was then tested on a new sample of 174 individuals (87 controls, 87 with depression) to categorize each person as either depressed or not depressed. This result was compared with medical record diagnoses. The study was published in BMC Psychiatry.
Compared with the control group, and in overall time. The algorithm incorrectly identified 15 patients with depression as being in the control group, and incorrectly identified 20 controls as having depression. The overall accuracy was 79.9%, with a sensitivity of 82.8% and a specificity of 77%.
“In addition to providing an improved biological underpinning for the diagnosis of depression, this [tool] could possibly offer supplemental information to psychiatric clinical assessment, and objective measures for early screening. Moreover, the use of distinct physiological variables as biomarkers of depression may help emphasize the interactions between mental and physical health. This may contribute to reducing the stigma associated with depression, lifting some social barriers to accessing psychiatric treatment, and allowing for more holistic patient care,” the investigators concluded.
Medibio provided partial funding for the salaries of research assistants; no other conflicts of interest were reported.
SOURCE: Saad M et al. BMC Psychiatry. 2019 Jun 7. doi: 10.1186/s12888-019-2152-1.
FROM BMC PSYCHIATRY
Frequent soaks ease pediatric atopic dermatitis
A regimen of twice-daily baths followed by occlusive moisturizer improved atopic dermatitis in children with moderate to severe disease more effectively than did a twice-weekly protocol, based on data from 42 children.
Guidelines for bathing frequency for children with atopic dermatitis are inconsistent and often confusing for parents, according to Ivan D. Cardona, MD, of Maine Medical Research Institute, Portland, and colleagues.
In a study published in the Journal of Allergy and Clinical Immunology: In Practice, the researchers randomized 42 children aged 6 months to 11 years with moderate to severe atopic dermatitis to a routine of twice-weekly “soak and seal” (SS) procedures consisting of soaking baths for 10 minutes or less, followed by an occlusive emollient, or to twice-daily SS with baths of 15-20 minutes followed by emollient. The groups were treated for 2 weeks, then switched protocols. The study included a total of four clinic visits over 5 weeks. All patients also received standard of care low-potency topical corticosteroids and moisturizer.
Overall, the frequent bathing (“wet method”) led to a decrease of 21.2 on the SCORing Atopic Dermatitis Index (SCORAD) compared with the less frequent bathing (“dry method”). Improvements in SCORAD (the primary outcome) correlated with a secondary outcome of improved scores on the parent-rated Atopic Dermatitis Quickscore.
The findings were limited by several factors including the small sample size, large rate of attrition prior to randomization among initially screened children, lack of data on environmental factors such as water temperature and quality, and the lack of a washout period between the treatment protocols, the researchers noted. They acknowledged that “twice-daily SS bathing in the real world can be time consuming, making adherence difficult for families.”
However, the results suggest that the frequent bathing protocol was safe and effective at improving symptoms of atopic dermatitis, and may reduce steroid use, they concluded.
The researchers had no financial conflicts to disclose.
SOURCE: Cardona ID et al. J Allergy Clin Immunol Pract. 2019 Nov 13. doi: 10.1016/j.jaip.2019.10.042.
A regimen of twice-daily baths followed by occlusive moisturizer improved atopic dermatitis in children with moderate to severe disease more effectively than did a twice-weekly protocol, based on data from 42 children.
Guidelines for bathing frequency for children with atopic dermatitis are inconsistent and often confusing for parents, according to Ivan D. Cardona, MD, of Maine Medical Research Institute, Portland, and colleagues.
In a study published in the Journal of Allergy and Clinical Immunology: In Practice, the researchers randomized 42 children aged 6 months to 11 years with moderate to severe atopic dermatitis to a routine of twice-weekly “soak and seal” (SS) procedures consisting of soaking baths for 10 minutes or less, followed by an occlusive emollient, or to twice-daily SS with baths of 15-20 minutes followed by emollient. The groups were treated for 2 weeks, then switched protocols. The study included a total of four clinic visits over 5 weeks. All patients also received standard of care low-potency topical corticosteroids and moisturizer.
Overall, the frequent bathing (“wet method”) led to a decrease of 21.2 on the SCORing Atopic Dermatitis Index (SCORAD) compared with the less frequent bathing (“dry method”). Improvements in SCORAD (the primary outcome) correlated with a secondary outcome of improved scores on the parent-rated Atopic Dermatitis Quickscore.
The findings were limited by several factors including the small sample size, large rate of attrition prior to randomization among initially screened children, lack of data on environmental factors such as water temperature and quality, and the lack of a washout period between the treatment protocols, the researchers noted. They acknowledged that “twice-daily SS bathing in the real world can be time consuming, making adherence difficult for families.”
However, the results suggest that the frequent bathing protocol was safe and effective at improving symptoms of atopic dermatitis, and may reduce steroid use, they concluded.
The researchers had no financial conflicts to disclose.
SOURCE: Cardona ID et al. J Allergy Clin Immunol Pract. 2019 Nov 13. doi: 10.1016/j.jaip.2019.10.042.
A regimen of twice-daily baths followed by occlusive moisturizer improved atopic dermatitis in children with moderate to severe disease more effectively than did a twice-weekly protocol, based on data from 42 children.
Guidelines for bathing frequency for children with atopic dermatitis are inconsistent and often confusing for parents, according to Ivan D. Cardona, MD, of Maine Medical Research Institute, Portland, and colleagues.
In a study published in the Journal of Allergy and Clinical Immunology: In Practice, the researchers randomized 42 children aged 6 months to 11 years with moderate to severe atopic dermatitis to a routine of twice-weekly “soak and seal” (SS) procedures consisting of soaking baths for 10 minutes or less, followed by an occlusive emollient, or to twice-daily SS with baths of 15-20 minutes followed by emollient. The groups were treated for 2 weeks, then switched protocols. The study included a total of four clinic visits over 5 weeks. All patients also received standard of care low-potency topical corticosteroids and moisturizer.
Overall, the frequent bathing (“wet method”) led to a decrease of 21.2 on the SCORing Atopic Dermatitis Index (SCORAD) compared with the less frequent bathing (“dry method”). Improvements in SCORAD (the primary outcome) correlated with a secondary outcome of improved scores on the parent-rated Atopic Dermatitis Quickscore.
The findings were limited by several factors including the small sample size, large rate of attrition prior to randomization among initially screened children, lack of data on environmental factors such as water temperature and quality, and the lack of a washout period between the treatment protocols, the researchers noted. They acknowledged that “twice-daily SS bathing in the real world can be time consuming, making adherence difficult for families.”
However, the results suggest that the frequent bathing protocol was safe and effective at improving symptoms of atopic dermatitis, and may reduce steroid use, they concluded.
The researchers had no financial conflicts to disclose.
SOURCE: Cardona ID et al. J Allergy Clin Immunol Pract. 2019 Nov 13. doi: 10.1016/j.jaip.2019.10.042.
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
SZC passes extension test for hyperkalemia
Treatment with sodium zirconium cyclosilicate (SZC) led to lasting improvement of hyperkalemia, according to results from an 11-month open-label extension study of the HARMONIZE randomized clinical trial.
SZC selectively binds potassium ions in the colon, reducing absorption and promoting excretion. In the original study, 248 patients with mild hyperkalemia were randomized to SZC or placebo. Within 48 hours, the drug returned potassium to normal and maintained those levels out to 4 weeks.
In the extension study, 123 patients with measured potassium levels of 3.5-6.2 mmol/L, 48 of whom had previously been assigned to placebo, received a 5- to 10-g dose of SZC once per day for up to 337 days. Median daily dose was 10 g, with a dose range of 2.5-15 g (Am J Nephrol. 2019;50[6]:473-480).
Just under 65% of patients completed the 11 months of the open-label extension study, with 88.3% of those achieving the primary endpoint of mean serum potassium levels of 5.1 mmol/L or lower, according to Simon D. Roger, MD, a nephrologist based in Gosford, Australia, and colleagues.
Most patients (83) were taking renin–angiotensin–aldosterone system inhibitors at baseline of the extension study; 78.3% continued a stable dose throughout the open-label phase, 8.4% increased the dose, and 3.6% discontinued.
Two-thirds of patients reported adverse events, most commonly gastrointestinal disorders (18.7%). Constipation was the most frequent (5.7%), followed by nausea, vomiting, and diarrhea (3.3% each).
Adverse events that occurred in 5% or more of participants included hypertension (12.2%), urinary tract infection (8.9%), and peripheral edema (8.1%). Hypertension severity was either mild (46.7%) or moderate (53.3%), and only one case was believed to be associated with the study medication. Thirteen percent of participants reported a total of 17 SMQ edema events. Eleven of the 16 patients had baseline risk factors for edema, leading the authors to conclude that causality between SZC and edema could not be established.
Serious adverse events occurred in 19.5% of participants, and 4.9% of participants discontinued SZC as a result.
SZC is approved for the treatment of hyperkalemia in the United States and Europe. The study was funded by AstraZeneca.
SOURCE: Roger S et al. Am J Nephrol;2019:50(6):473-80.
Treatment with sodium zirconium cyclosilicate (SZC) led to lasting improvement of hyperkalemia, according to results from an 11-month open-label extension study of the HARMONIZE randomized clinical trial.
SZC selectively binds potassium ions in the colon, reducing absorption and promoting excretion. In the original study, 248 patients with mild hyperkalemia were randomized to SZC or placebo. Within 48 hours, the drug returned potassium to normal and maintained those levels out to 4 weeks.
In the extension study, 123 patients with measured potassium levels of 3.5-6.2 mmol/L, 48 of whom had previously been assigned to placebo, received a 5- to 10-g dose of SZC once per day for up to 337 days. Median daily dose was 10 g, with a dose range of 2.5-15 g (Am J Nephrol. 2019;50[6]:473-480).
Just under 65% of patients completed the 11 months of the open-label extension study, with 88.3% of those achieving the primary endpoint of mean serum potassium levels of 5.1 mmol/L or lower, according to Simon D. Roger, MD, a nephrologist based in Gosford, Australia, and colleagues.
Most patients (83) were taking renin–angiotensin–aldosterone system inhibitors at baseline of the extension study; 78.3% continued a stable dose throughout the open-label phase, 8.4% increased the dose, and 3.6% discontinued.
Two-thirds of patients reported adverse events, most commonly gastrointestinal disorders (18.7%). Constipation was the most frequent (5.7%), followed by nausea, vomiting, and diarrhea (3.3% each).
Adverse events that occurred in 5% or more of participants included hypertension (12.2%), urinary tract infection (8.9%), and peripheral edema (8.1%). Hypertension severity was either mild (46.7%) or moderate (53.3%), and only one case was believed to be associated with the study medication. Thirteen percent of participants reported a total of 17 SMQ edema events. Eleven of the 16 patients had baseline risk factors for edema, leading the authors to conclude that causality between SZC and edema could not be established.
Serious adverse events occurred in 19.5% of participants, and 4.9% of participants discontinued SZC as a result.
SZC is approved for the treatment of hyperkalemia in the United States and Europe. The study was funded by AstraZeneca.
SOURCE: Roger S et al. Am J Nephrol;2019:50(6):473-80.
Treatment with sodium zirconium cyclosilicate (SZC) led to lasting improvement of hyperkalemia, according to results from an 11-month open-label extension study of the HARMONIZE randomized clinical trial.
SZC selectively binds potassium ions in the colon, reducing absorption and promoting excretion. In the original study, 248 patients with mild hyperkalemia were randomized to SZC or placebo. Within 48 hours, the drug returned potassium to normal and maintained those levels out to 4 weeks.
In the extension study, 123 patients with measured potassium levels of 3.5-6.2 mmol/L, 48 of whom had previously been assigned to placebo, received a 5- to 10-g dose of SZC once per day for up to 337 days. Median daily dose was 10 g, with a dose range of 2.5-15 g (Am J Nephrol. 2019;50[6]:473-480).
Just under 65% of patients completed the 11 months of the open-label extension study, with 88.3% of those achieving the primary endpoint of mean serum potassium levels of 5.1 mmol/L or lower, according to Simon D. Roger, MD, a nephrologist based in Gosford, Australia, and colleagues.
Most patients (83) were taking renin–angiotensin–aldosterone system inhibitors at baseline of the extension study; 78.3% continued a stable dose throughout the open-label phase, 8.4% increased the dose, and 3.6% discontinued.
Two-thirds of patients reported adverse events, most commonly gastrointestinal disorders (18.7%). Constipation was the most frequent (5.7%), followed by nausea, vomiting, and diarrhea (3.3% each).
Adverse events that occurred in 5% or more of participants included hypertension (12.2%), urinary tract infection (8.9%), and peripheral edema (8.1%). Hypertension severity was either mild (46.7%) or moderate (53.3%), and only one case was believed to be associated with the study medication. Thirteen percent of participants reported a total of 17 SMQ edema events. Eleven of the 16 patients had baseline risk factors for edema, leading the authors to conclude that causality between SZC and edema could not be established.
Serious adverse events occurred in 19.5% of participants, and 4.9% of participants discontinued SZC as a result.
SZC is approved for the treatment of hyperkalemia in the United States and Europe. The study was funded by AstraZeneca.
SOURCE: Roger S et al. Am J Nephrol;2019:50(6):473-80.
FROM AMERICAN JOURNAL OF NEPHROLOGY
Supreme Court weighs ACA back pay case
U.S. Supreme Court Justices heard oral arguments Dec. 10 in a case that centers on whether the federal government owes insurers billions based on an Affordable Care Act provision intended to help health plans mitigate risk under the law.

Maine Community Health Options v. United States, which consolidates several lawsuits against the government, involves the ACA’s risk corridor program, which required the U.S. Department of Health & Human Services to collect funds from profitable insurers that offered qualified health plans under the exchanges and distribute the funds to insurers with excessive losses.

Collections from profitable insurers under the program fell short in 2014, 2015, and 2016, while losses steadily grew, resulting in the HHS paying about 12 cents on the dollar in payments to insurers. More than 150 insurers now allege they were shortchanged and they want the Supreme Court to force the government to reimburse them $12 billion.
The U.S. Department of Justice counters that the government is not required to pay the plans because of appropriations measures passed by Congress in 2014 and later years that limited the funding available to compensate insurers for their losses. The federal government is not obligated to pay the insurers back for the losses and the suits should be dismissed, the DOJ attorneys argue.
The federal government and insurers have each experienced wins and losses at the lower court level. Most recently, the U.S. Court of Appeals for the Federal Circuit decided in favor of the government, ruling that while the ACA required the government to compensate the insurers for their losses, the appropriations measures repealed or suspended that requirement.
Insurers, economists, and state government led by both parties have weighed in on the case via court briefs.
The case could have important ramifications that have an impact on more than just insurers, said Timothy Jost, a health law expert and retired professor from Washington and Lee University in Lexington, Va.
“The insurers are left holding the bag, but a number of insurers went insolvent [due to the losses], so in those cases, the states are left holding the bag,” Mr. Jost said in an interview.
The outcome could influence future partnerships between the federal government and private entities, according to Katie Keith, an attorney and health law analyst who writes for the Health Affairs Blog. She noted that the U.S. Chamber of Commerce, which historically has not supported the ACA, sided with insurers in the case. In a court brief, attorneys for the chamber wrote that businesses make substantial financial investments to participate in federal programs, and their willingness to do so is based on having assurance that the government will honor its statutory commitments. If left uncorrected, the circuit’s decision “will have far-reaching consequences for myriad areas in which U.S. businesses partner with the federal government to provide vital goods and services,” chamber attorneys wrote.
“This is about more than the ACA. It’s about the fundamentals of public/private partnerships,” Ms. Keith said in an interview. “If you’re contracting with the government, can the government just break those promises or break those obligations after the fact? Folks at the chamber are making it about bigger, broader issues about what it means when the government partners with private organizations.”
Mr. Jost said it’s hard to say which way the Supreme Court will rule, but the fact that the court is reviewing the case speaks volumes.
“Its kind of hard to believe they’re going to order the federal government to pay $12 billion,” he said. “On the other hand, they didn’t have to take the case.”
A Supreme Court decision is expected in early 2020.
U.S. Supreme Court Justices heard oral arguments Dec. 10 in a case that centers on whether the federal government owes insurers billions based on an Affordable Care Act provision intended to help health plans mitigate risk under the law.
Maine Community Health Options v. United States, which consolidates several lawsuits against the government, involves the ACA’s risk corridor program, which required the U.S. Department of Health & Human Services to collect funds from profitable insurers that offered qualified health plans under the exchanges and distribute the funds to insurers with excessive losses.
Collections from profitable insurers under the program fell short in 2014, 2015, and 2016, while losses steadily grew, resulting in the HHS paying about 12 cents on the dollar in payments to insurers. More than 150 insurers now allege they were shortchanged and they want the Supreme Court to force the government to reimburse them $12 billion.
The U.S. Department of Justice counters that the government is not required to pay the plans because of appropriations measures passed by Congress in 2014 and later years that limited the funding available to compensate insurers for their losses. The federal government is not obligated to pay the insurers back for the losses and the suits should be dismissed, the DOJ attorneys argue.
The federal government and insurers have each experienced wins and losses at the lower court level. Most recently, the U.S. Court of Appeals for the Federal Circuit decided in favor of the government, ruling that while the ACA required the government to compensate the insurers for their losses, the appropriations measures repealed or suspended that requirement.
Insurers, economists, and state government led by both parties have weighed in on the case via court briefs.
The case could have important ramifications that have an impact on more than just insurers, said Timothy Jost, a health law expert and retired professor from Washington and Lee University in Lexington, Va.
“The insurers are left holding the bag, but a number of insurers went insolvent [due to the losses], so in those cases, the states are left holding the bag,” Mr. Jost said in an interview.
The outcome could influence future partnerships between the federal government and private entities, according to Katie Keith, an attorney and health law analyst who writes for the Health Affairs Blog. She noted that the U.S. Chamber of Commerce, which historically has not supported the ACA, sided with insurers in the case. In a court brief, attorneys for the chamber wrote that businesses make substantial financial investments to participate in federal programs, and their willingness to do so is based on having assurance that the government will honor its statutory commitments. If left uncorrected, the circuit’s decision “will have far-reaching consequences for myriad areas in which U.S. businesses partner with the federal government to provide vital goods and services,” chamber attorneys wrote.
“This is about more than the ACA. It’s about the fundamentals of public/private partnerships,” Ms. Keith said in an interview. “If you’re contracting with the government, can the government just break those promises or break those obligations after the fact? Folks at the chamber are making it about bigger, broader issues about what it means when the government partners with private organizations.”
Mr. Jost said it’s hard to say which way the Supreme Court will rule, but the fact that the court is reviewing the case speaks volumes.
“Its kind of hard to believe they’re going to order the federal government to pay $12 billion,” he said. “On the other hand, they didn’t have to take the case.”
A Supreme Court decision is expected in early 2020.
U.S. Supreme Court Justices heard oral arguments Dec. 10 in a case that centers on whether the federal government owes insurers billions based on an Affordable Care Act provision intended to help health plans mitigate risk under the law.
Maine Community Health Options v. United States, which consolidates several lawsuits against the government, involves the ACA’s risk corridor program, which required the U.S. Department of Health & Human Services to collect funds from profitable insurers that offered qualified health plans under the exchanges and distribute the funds to insurers with excessive losses.
Collections from profitable insurers under the program fell short in 2014, 2015, and 2016, while losses steadily grew, resulting in the HHS paying about 12 cents on the dollar in payments to insurers. More than 150 insurers now allege they were shortchanged and they want the Supreme Court to force the government to reimburse them $12 billion.
The U.S. Department of Justice counters that the government is not required to pay the plans because of appropriations measures passed by Congress in 2014 and later years that limited the funding available to compensate insurers for their losses. The federal government is not obligated to pay the insurers back for the losses and the suits should be dismissed, the DOJ attorneys argue.
The federal government and insurers have each experienced wins and losses at the lower court level. Most recently, the U.S. Court of Appeals for the Federal Circuit decided in favor of the government, ruling that while the ACA required the government to compensate the insurers for their losses, the appropriations measures repealed or suspended that requirement.
Insurers, economists, and state government led by both parties have weighed in on the case via court briefs.
The case could have important ramifications that have an impact on more than just insurers, said Timothy Jost, a health law expert and retired professor from Washington and Lee University in Lexington, Va.
“The insurers are left holding the bag, but a number of insurers went insolvent [due to the losses], so in those cases, the states are left holding the bag,” Mr. Jost said in an interview.
The outcome could influence future partnerships between the federal government and private entities, according to Katie Keith, an attorney and health law analyst who writes for the Health Affairs Blog. She noted that the U.S. Chamber of Commerce, which historically has not supported the ACA, sided with insurers in the case. In a court brief, attorneys for the chamber wrote that businesses make substantial financial investments to participate in federal programs, and their willingness to do so is based on having assurance that the government will honor its statutory commitments. If left uncorrected, the circuit’s decision “will have far-reaching consequences for myriad areas in which U.S. businesses partner with the federal government to provide vital goods and services,” chamber attorneys wrote.
“This is about more than the ACA. It’s about the fundamentals of public/private partnerships,” Ms. Keith said in an interview. “If you’re contracting with the government, can the government just break those promises or break those obligations after the fact? Folks at the chamber are making it about bigger, broader issues about what it means when the government partners with private organizations.”
Mr. Jost said it’s hard to say which way the Supreme Court will rule, but the fact that the court is reviewing the case speaks volumes.
“Its kind of hard to believe they’re going to order the federal government to pay $12 billion,” he said. “On the other hand, they didn’t have to take the case.”
A Supreme Court decision is expected in early 2020.
FDA clears first fully disposable duodenoscope
The Food and Drug Administration on Dec. 13 cleared Boston Scientific’s single-use duodenoscope, the Exalt Model D, for endoscopic retrograde cholangiopancreatography.

It’s the first disposable duodenoscope to hit the market in the wake of the agency’s August call for manufacturers and health care facilities to move to partially or fully disposable duodenoscopes. The goal is to eliminate the risk of spreading infections between patients from incomplete sterilization of traditional, multi-use scopes. The FDA also recently approved a Pentax duodenoscope with a disposable elevator, the most difficult part to clean.
The agency reported in April that 5.4% of samples from multi-use scopes test postive for Escherichia coli, Pseudomonas aeruginosa, or other “high-concern” organisms.
Boston Scientific spokesperson Kate Haranis said the Exalt Model D will be available in the first quarter of 2020, but the company is still working out how much it will charge.
Cost effectiveness will depend largely on the degree to which the price of the device is offset by the infections it prevents. It might prove particularly attractive to high-volume centers with higher than usual infection rates. It might also be of interest to smaller practices where the price of a multi-use scope doesn’t make sense for only a few procedures a year, said Gyanprakash Ketwaroo, MD, an interventional endoscopist and assistant professor of gastroenterology at Baylor University, Houston.
“The feel is a little different,” said Dr. Ketwaroo, who’s tried the new device, but “it’s pretty functional and probably okay to use in almost all endoscopic procedures that require ERCP.”
In a study funded by Boston Scientific, endoscopists reported a median overall satisfaction score of 9 out of 10 with the new scope (Clin Gastroenterol Hepatol. 2019 Nov 6. doi: 10.1016/j.cgh.2019.10.052).
As for using it at Baylor, Dr. Ketwaroo said, “we’re not sure yet; we are still evaluating it” and want to see if any problems emerge once it’s on the market. It’s also not clear if infection risks would be lower than with the disposable elevator model from Pentax, he added.
The Exalt Model D was granted breakthrough status by the FDA, and the agency worked closely with Boston Scientific to bring it to market.
“The availability of a fully disposable duodenoscope represents another major step forward for improving the safety of these devices, which are used in more than 500,000 procedures in the United States each year. The FDA continues to encourage innovative ways to improve the safety and effectiveness of these devices,” Jeff Shuren, MD, director of the FDA’s Center for Devices and Radiological Health, said in a statement.
Dr. Ketwaroo had no relevant financial disclosures.
The Food and Drug Administration on Dec. 13 cleared Boston Scientific’s single-use duodenoscope, the Exalt Model D, for endoscopic retrograde cholangiopancreatography.
It’s the first disposable duodenoscope to hit the market in the wake of the agency’s August call for manufacturers and health care facilities to move to partially or fully disposable duodenoscopes. The goal is to eliminate the risk of spreading infections between patients from incomplete sterilization of traditional, multi-use scopes. The FDA also recently approved a Pentax duodenoscope with a disposable elevator, the most difficult part to clean.
The agency reported in April that 5.4% of samples from multi-use scopes test postive for Escherichia coli, Pseudomonas aeruginosa, or other “high-concern” organisms.
Boston Scientific spokesperson Kate Haranis said the Exalt Model D will be available in the first quarter of 2020, but the company is still working out how much it will charge.
Cost effectiveness will depend largely on the degree to which the price of the device is offset by the infections it prevents. It might prove particularly attractive to high-volume centers with higher than usual infection rates. It might also be of interest to smaller practices where the price of a multi-use scope doesn’t make sense for only a few procedures a year, said Gyanprakash Ketwaroo, MD, an interventional endoscopist and assistant professor of gastroenterology at Baylor University, Houston.
“The feel is a little different,” said Dr. Ketwaroo, who’s tried the new device, but “it’s pretty functional and probably okay to use in almost all endoscopic procedures that require ERCP.”
In a study funded by Boston Scientific, endoscopists reported a median overall satisfaction score of 9 out of 10 with the new scope (Clin Gastroenterol Hepatol. 2019 Nov 6. doi: 10.1016/j.cgh.2019.10.052).
As for using it at Baylor, Dr. Ketwaroo said, “we’re not sure yet; we are still evaluating it” and want to see if any problems emerge once it’s on the market. It’s also not clear if infection risks would be lower than with the disposable elevator model from Pentax, he added.
The Exalt Model D was granted breakthrough status by the FDA, and the agency worked closely with Boston Scientific to bring it to market.
“The availability of a fully disposable duodenoscope represents another major step forward for improving the safety of these devices, which are used in more than 500,000 procedures in the United States each year. The FDA continues to encourage innovative ways to improve the safety and effectiveness of these devices,” Jeff Shuren, MD, director of the FDA’s Center for Devices and Radiological Health, said in a statement.
Dr. Ketwaroo had no relevant financial disclosures.
The Food and Drug Administration on Dec. 13 cleared Boston Scientific’s single-use duodenoscope, the Exalt Model D, for endoscopic retrograde cholangiopancreatography.
It’s the first disposable duodenoscope to hit the market in the wake of the agency’s August call for manufacturers and health care facilities to move to partially or fully disposable duodenoscopes. The goal is to eliminate the risk of spreading infections between patients from incomplete sterilization of traditional, multi-use scopes. The FDA also recently approved a Pentax duodenoscope with a disposable elevator, the most difficult part to clean.
The agency reported in April that 5.4% of samples from multi-use scopes test postive for Escherichia coli, Pseudomonas aeruginosa, or other “high-concern” organisms.
Boston Scientific spokesperson Kate Haranis said the Exalt Model D will be available in the first quarter of 2020, but the company is still working out how much it will charge.
Cost effectiveness will depend largely on the degree to which the price of the device is offset by the infections it prevents. It might prove particularly attractive to high-volume centers with higher than usual infection rates. It might also be of interest to smaller practices where the price of a multi-use scope doesn’t make sense for only a few procedures a year, said Gyanprakash Ketwaroo, MD, an interventional endoscopist and assistant professor of gastroenterology at Baylor University, Houston.
“The feel is a little different,” said Dr. Ketwaroo, who’s tried the new device, but “it’s pretty functional and probably okay to use in almost all endoscopic procedures that require ERCP.”
In a study funded by Boston Scientific, endoscopists reported a median overall satisfaction score of 9 out of 10 with the new scope (Clin Gastroenterol Hepatol. 2019 Nov 6. doi: 10.1016/j.cgh.2019.10.052).
As for using it at Baylor, Dr. Ketwaroo said, “we’re not sure yet; we are still evaluating it” and want to see if any problems emerge once it’s on the market. It’s also not clear if infection risks would be lower than with the disposable elevator model from Pentax, he added.
The Exalt Model D was granted breakthrough status by the FDA, and the agency worked closely with Boston Scientific to bring it to market.
“The availability of a fully disposable duodenoscope represents another major step forward for improving the safety of these devices, which are used in more than 500,000 procedures in the United States each year. The FDA continues to encourage innovative ways to improve the safety and effectiveness of these devices,” Jeff Shuren, MD, director of the FDA’s Center for Devices and Radiological Health, said in a statement.
Dr. Ketwaroo had no relevant financial disclosures.
FROM THE FDA

FDA clears first fully disposable duodenoscope
The Food and Drug Administration on Dec. 13 cleared Boston Scientific’s single-use duodenoscope, the Exalt Model D, for endoscopic retrograde cholangiopancreatography.
It’s the first disposable duodenoscope to hit the market in the wake of the agency’s August call for manufacturers and health care facilities to move to partially or fully disposable duodenoscopes. The goal is to eliminate the risk of spreading infections between patients from incomplete sterilization of traditional, multi-use scopes. The FDA also recently approved a Pentax duodenoscope with a disposable elevator, the most difficult part to clean.
The agency reported in April that 5.4% of samples from multi-use scopes test positive for Escherichia coli, Pseudomonas aeruginosa, or other “high-concern” organisms.
Boston Scientific spokesperson Kate Haranis said the Exalt Model D will be available in the first quarter of 2020, but the company is still working out how much it will charge.
Cost effectiveness will depend largely on the degree to which the price of the device is offset by the infections it prevents. It might prove particularly attractive to high-volume centers with higher than usual infection rates. It might also be of interest to smaller practices where the price of a multi-use scope doesn’t make sense for only a few procedures a year, said Gyanprakash Ketwaroo, MD, an interventional endoscopist and assistant professor of gastroenterology at Baylor University, Houston.
AGA is working with FDA to ensure physicians continue to have access to ERCP as new devices are introduced to the market and will continue to update members on the latest developments. The GI societies believe that device transitions can be incorporated over the life cycle of current instrumentation, to eliminate the potential for gaps in accessibility of care and to ensure that there is adequate efficacy and safety data to support the adoption of new technology. Review the GI societies’ guiding principles for continued scope evolution at https://www.gastro.org/news/gi-societies-advise-fda-on-duodenoscope-reprocessing.
Dr. Ketwaroo had no relevant financial disclosures.
The Food and Drug Administration on Dec. 13 cleared Boston Scientific’s single-use duodenoscope, the Exalt Model D, for endoscopic retrograde cholangiopancreatography.
It’s the first disposable duodenoscope to hit the market in the wake of the agency’s August call for manufacturers and health care facilities to move to partially or fully disposable duodenoscopes. The goal is to eliminate the risk of spreading infections between patients from incomplete sterilization of traditional, multi-use scopes. The FDA also recently approved a Pentax duodenoscope with a disposable elevator, the most difficult part to clean.
The agency reported in April that 5.4% of samples from multi-use scopes test positive for Escherichia coli, Pseudomonas aeruginosa, or other “high-concern” organisms.
Boston Scientific spokesperson Kate Haranis said the Exalt Model D will be available in the first quarter of 2020, but the company is still working out how much it will charge.
Cost effectiveness will depend largely on the degree to which the price of the device is offset by the infections it prevents. It might prove particularly attractive to high-volume centers with higher than usual infection rates. It might also be of interest to smaller practices where the price of a multi-use scope doesn’t make sense for only a few procedures a year, said Gyanprakash Ketwaroo, MD, an interventional endoscopist and assistant professor of gastroenterology at Baylor University, Houston.
AGA is working with FDA to ensure physicians continue to have access to ERCP as new devices are introduced to the market and will continue to update members on the latest developments. The GI societies believe that device transitions can be incorporated over the life cycle of current instrumentation, to eliminate the potential for gaps in accessibility of care and to ensure that there is adequate efficacy and safety data to support the adoption of new technology. Review the GI societies’ guiding principles for continued scope evolution at https://www.gastro.org/news/gi-societies-advise-fda-on-duodenoscope-reprocessing.
Dr. Ketwaroo had no relevant financial disclosures.
The Food and Drug Administration on Dec. 13 cleared Boston Scientific’s single-use duodenoscope, the Exalt Model D, for endoscopic retrograde cholangiopancreatography.
It’s the first disposable duodenoscope to hit the market in the wake of the agency’s August call for manufacturers and health care facilities to move to partially or fully disposable duodenoscopes. The goal is to eliminate the risk of spreading infections between patients from incomplete sterilization of traditional, multi-use scopes. The FDA also recently approved a Pentax duodenoscope with a disposable elevator, the most difficult part to clean.
The agency reported in April that 5.4% of samples from multi-use scopes test positive for Escherichia coli, Pseudomonas aeruginosa, or other “high-concern” organisms.
Boston Scientific spokesperson Kate Haranis said the Exalt Model D will be available in the first quarter of 2020, but the company is still working out how much it will charge.
Cost effectiveness will depend largely on the degree to which the price of the device is offset by the infections it prevents. It might prove particularly attractive to high-volume centers with higher than usual infection rates. It might also be of interest to smaller practices where the price of a multi-use scope doesn’t make sense for only a few procedures a year, said Gyanprakash Ketwaroo, MD, an interventional endoscopist and assistant professor of gastroenterology at Baylor University, Houston.
AGA is working with FDA to ensure physicians continue to have access to ERCP as new devices are introduced to the market and will continue to update members on the latest developments. The GI societies believe that device transitions can be incorporated over the life cycle of current instrumentation, to eliminate the potential for gaps in accessibility of care and to ensure that there is adequate efficacy and safety data to support the adoption of new technology. Review the GI societies’ guiding principles for continued scope evolution at https://www.gastro.org/news/gi-societies-advise-fda-on-duodenoscope-reprocessing.
Dr. Ketwaroo had no relevant financial disclosures.