User login
A New Treatment Target for PTSD?
Adults with posttraumatic stress disorder (PTSD) have smaller cerebellums than unaffected adults, suggesting that this part of the brain may be a potential therapeutic target.
According to recent research on more than 4000 adults, cerebellum volume was significantly smaller (by about 2%) in those with PTSD than in trauma-exposed and trauma-naive controls without PTSD.
“The differences were largely within the posterior lobe, where a lot of the more cognitive functions attributed to the cerebellum seem to localize, as well as the vermis, which is linked to a lot of emotional processing functions,” lead author Ashley Huggins, PhD, said in a news release.
“If we know what areas are implicated, then we can start to focus interventions like brain stimulation on the cerebellum and potentially improve treatment outcomes,” said Dr. Huggins, who worked on the study while a postdoctoral researcher in the lab of Rajendra A. Morey, MD, at Duke University, Durham, North Carolina, and is now at the University of Arizona, Tucson.
While the cerebellum is known for its role in coordinating movement and balance, it also plays a key role in emotions and memory, which are affected by PTSD.
Smaller cerebellar volume has been observed in some adult and pediatric populations with PTSD.
However, those studies have been limited by either small sample sizes, the failure to consider key neuroanatomical subdivisions of the cerebellum, or a focus on certain populations such as veterans of sexual assault victims with PTSD.
To overcome these limitations, the researchers conducted a mega-analysis of total and subregional cerebellar volumes in a large, multicohort dataset from the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA)-Psychiatric Genomics Consortium PTSD workgroup that was published online on January 10, 2024, in Molecular Psychiatry.
They employed a novel, standardized ENIGMA cerebellum parcellation protocol to quantify cerebellar lobule volumes using structural MRI data from 1642 adults with PTSD and 2573 healthy controls without PTSD (88% trauma-exposed and 12% trauma-naive).
After adjustment for age, gender, and total intracranial volume, PTSD was associated with significant gray and white matter reductions of the cerebellum.
People with PTSD demonstrated smaller total cerebellum volume as well as reduced volume in subregions primarily within the posterior cerebellum, vermis, and flocculonodular cerebellum than controls.
In general, PTSD severity was more robustly associated with cerebellar volume differences than PTSD diagnosis.
Focusing purely on a “yes-or-no” categorical diagnosis didn’t always provide the clearest picture. “When we looked at PTSD severity, people who had more severe forms of the disorder had an even smaller cerebellar volume,” Dr. Huggins explained in the news release.
Novel Treatment Target
These findings add to “an emerging literature that underscores the relevance of cerebellar structure in the pathophysiology of PTSD,” the researchers noted.
They caution that despite the significant findings suggesting associations between PTSD and smaller cerebellar volumes, effect sizes were small. “As such, it is unlikely that structural cerebellar volumes alone will provide a clinically useful biomarker (eg, for individual-level prediction).”
Nonetheless, the study highlights the cerebellum as a “novel treatment target that may be leveraged to improve treatment outcomes for PTSD,” they wrote.
They noted that prior work has shown that the cerebellum is sensitive to external modulation. For example, noninvasive brain stimulation of the cerebellum has been shown to modulate cognitive, emotional, and social processes commonly disrupted in PTSD.
Commenting on this research, Cyrus A. Raji, MD, PhD, associate professor of radiology and neurology at Washington University in St. Louis, noted that this “large neuroimaging study links PTSD to cerebellar volume loss.”
“However, PTSD and traumatic brain injury frequently co-occur, and PTSD also frequently arises after TBI. Additionally, TBI is strongly linked to cerebellar volume loss,” Dr. Raji pointed out.
“Future studies need to better delineate volume loss from these conditions, especially when they are comorbid, though the expectation is these effects would be additive with TBI being the initial and most severe driving force,” Dr. Raji added.
The research had no commercial funding. Author disclosures are listed with the original article. Dr. Raji is a consultant for Brainreader, Apollo Health, Pacific Neuroscience Foundation, and Neurevolution Medicine LLC.
A version of this article appears on Medscape.com.
Adults with posttraumatic stress disorder (PTSD) have smaller cerebellums than unaffected adults, suggesting that this part of the brain may be a potential therapeutic target.
According to recent research on more than 4000 adults, cerebellum volume was significantly smaller (by about 2%) in those with PTSD than in trauma-exposed and trauma-naive controls without PTSD.
“The differences were largely within the posterior lobe, where a lot of the more cognitive functions attributed to the cerebellum seem to localize, as well as the vermis, which is linked to a lot of emotional processing functions,” lead author Ashley Huggins, PhD, said in a news release.
“If we know what areas are implicated, then we can start to focus interventions like brain stimulation on the cerebellum and potentially improve treatment outcomes,” said Dr. Huggins, who worked on the study while a postdoctoral researcher in the lab of Rajendra A. Morey, MD, at Duke University, Durham, North Carolina, and is now at the University of Arizona, Tucson.
While the cerebellum is known for its role in coordinating movement and balance, it also plays a key role in emotions and memory, which are affected by PTSD.
Smaller cerebellar volume has been observed in some adult and pediatric populations with PTSD.
However, those studies have been limited by either small sample sizes, the failure to consider key neuroanatomical subdivisions of the cerebellum, or a focus on certain populations such as veterans of sexual assault victims with PTSD.
To overcome these limitations, the researchers conducted a mega-analysis of total and subregional cerebellar volumes in a large, multicohort dataset from the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA)-Psychiatric Genomics Consortium PTSD workgroup that was published online on January 10, 2024, in Molecular Psychiatry.
They employed a novel, standardized ENIGMA cerebellum parcellation protocol to quantify cerebellar lobule volumes using structural MRI data from 1642 adults with PTSD and 2573 healthy controls without PTSD (88% trauma-exposed and 12% trauma-naive).
After adjustment for age, gender, and total intracranial volume, PTSD was associated with significant gray and white matter reductions of the cerebellum.
People with PTSD demonstrated smaller total cerebellum volume as well as reduced volume in subregions primarily within the posterior cerebellum, vermis, and flocculonodular cerebellum than controls.
In general, PTSD severity was more robustly associated with cerebellar volume differences than PTSD diagnosis.
Focusing purely on a “yes-or-no” categorical diagnosis didn’t always provide the clearest picture. “When we looked at PTSD severity, people who had more severe forms of the disorder had an even smaller cerebellar volume,” Dr. Huggins explained in the news release.
Novel Treatment Target
These findings add to “an emerging literature that underscores the relevance of cerebellar structure in the pathophysiology of PTSD,” the researchers noted.
They caution that despite the significant findings suggesting associations between PTSD and smaller cerebellar volumes, effect sizes were small. “As such, it is unlikely that structural cerebellar volumes alone will provide a clinically useful biomarker (eg, for individual-level prediction).”
Nonetheless, the study highlights the cerebellum as a “novel treatment target that may be leveraged to improve treatment outcomes for PTSD,” they wrote.
They noted that prior work has shown that the cerebellum is sensitive to external modulation. For example, noninvasive brain stimulation of the cerebellum has been shown to modulate cognitive, emotional, and social processes commonly disrupted in PTSD.
Commenting on this research, Cyrus A. Raji, MD, PhD, associate professor of radiology and neurology at Washington University in St. Louis, noted that this “large neuroimaging study links PTSD to cerebellar volume loss.”
“However, PTSD and traumatic brain injury frequently co-occur, and PTSD also frequently arises after TBI. Additionally, TBI is strongly linked to cerebellar volume loss,” Dr. Raji pointed out.
“Future studies need to better delineate volume loss from these conditions, especially when they are comorbid, though the expectation is these effects would be additive with TBI being the initial and most severe driving force,” Dr. Raji added.
The research had no commercial funding. Author disclosures are listed with the original article. Dr. Raji is a consultant for Brainreader, Apollo Health, Pacific Neuroscience Foundation, and Neurevolution Medicine LLC.
A version of this article appears on Medscape.com.
Adults with posttraumatic stress disorder (PTSD) have smaller cerebellums than unaffected adults, suggesting that this part of the brain may be a potential therapeutic target.
According to recent research on more than 4000 adults, cerebellum volume was significantly smaller (by about 2%) in those with PTSD than in trauma-exposed and trauma-naive controls without PTSD.
“The differences were largely within the posterior lobe, where a lot of the more cognitive functions attributed to the cerebellum seem to localize, as well as the vermis, which is linked to a lot of emotional processing functions,” lead author Ashley Huggins, PhD, said in a news release.
“If we know what areas are implicated, then we can start to focus interventions like brain stimulation on the cerebellum and potentially improve treatment outcomes,” said Dr. Huggins, who worked on the study while a postdoctoral researcher in the lab of Rajendra A. Morey, MD, at Duke University, Durham, North Carolina, and is now at the University of Arizona, Tucson.
While the cerebellum is known for its role in coordinating movement and balance, it also plays a key role in emotions and memory, which are affected by PTSD.
Smaller cerebellar volume has been observed in some adult and pediatric populations with PTSD.
However, those studies have been limited by either small sample sizes, the failure to consider key neuroanatomical subdivisions of the cerebellum, or a focus on certain populations such as veterans of sexual assault victims with PTSD.
To overcome these limitations, the researchers conducted a mega-analysis of total and subregional cerebellar volumes in a large, multicohort dataset from the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA)-Psychiatric Genomics Consortium PTSD workgroup that was published online on January 10, 2024, in Molecular Psychiatry.
They employed a novel, standardized ENIGMA cerebellum parcellation protocol to quantify cerebellar lobule volumes using structural MRI data from 1642 adults with PTSD and 2573 healthy controls without PTSD (88% trauma-exposed and 12% trauma-naive).
After adjustment for age, gender, and total intracranial volume, PTSD was associated with significant gray and white matter reductions of the cerebellum.
People with PTSD demonstrated smaller total cerebellum volume as well as reduced volume in subregions primarily within the posterior cerebellum, vermis, and flocculonodular cerebellum than controls.
In general, PTSD severity was more robustly associated with cerebellar volume differences than PTSD diagnosis.
Focusing purely on a “yes-or-no” categorical diagnosis didn’t always provide the clearest picture. “When we looked at PTSD severity, people who had more severe forms of the disorder had an even smaller cerebellar volume,” Dr. Huggins explained in the news release.
Novel Treatment Target
These findings add to “an emerging literature that underscores the relevance of cerebellar structure in the pathophysiology of PTSD,” the researchers noted.
They caution that despite the significant findings suggesting associations between PTSD and smaller cerebellar volumes, effect sizes were small. “As such, it is unlikely that structural cerebellar volumes alone will provide a clinically useful biomarker (eg, for individual-level prediction).”
Nonetheless, the study highlights the cerebellum as a “novel treatment target that may be leveraged to improve treatment outcomes for PTSD,” they wrote.
They noted that prior work has shown that the cerebellum is sensitive to external modulation. For example, noninvasive brain stimulation of the cerebellum has been shown to modulate cognitive, emotional, and social processes commonly disrupted in PTSD.
Commenting on this research, Cyrus A. Raji, MD, PhD, associate professor of radiology and neurology at Washington University in St. Louis, noted that this “large neuroimaging study links PTSD to cerebellar volume loss.”
“However, PTSD and traumatic brain injury frequently co-occur, and PTSD also frequently arises after TBI. Additionally, TBI is strongly linked to cerebellar volume loss,” Dr. Raji pointed out.
“Future studies need to better delineate volume loss from these conditions, especially when they are comorbid, though the expectation is these effects would be additive with TBI being the initial and most severe driving force,” Dr. Raji added.
The research had no commercial funding. Author disclosures are listed with the original article. Dr. Raji is a consultant for Brainreader, Apollo Health, Pacific Neuroscience Foundation, and Neurevolution Medicine LLC.
A version of this article appears on Medscape.com.
Weight Loss Not Enough to Sustain Type 2 Diabetes Remission
Very few patients with type 2 diabetes (T2D) achieve and sustain diabetes remission via weight loss alone, new research suggests.
Among more than 37,000 people with T2D in Hong Kong, only 6% had achieved and sustained diabetes remission solely through weight loss up to 8 years after diagnosis. Among those who initially achieved remission, 67% had hyperglycemia at 3 years.
People who lost the most weight (10% of their body weight or more) in the first year after diagnosis were most likely to have sustained remission.
The study “helped to confirm the low rate of diabetes remission and high rate of returning to hyperglycemia in real-world practice,” Andrea Luk, MD, of the Chinese University of Hong Kong, told this news organization. “Over 80% of diabetes remission occurred within the first 5 years of a diabetes diagnosis. This is in line with our understanding that beta cell function will gradually decline over time, making diabetes remission increasingly difficult even with weight reduction.”
The study was published in PLOS Medicine.
Early Weight Management Works
Recent clinical trials have demonstrated that T2D remission can be achieved following sustained weight loss through bariatric surgery or lifestyle interventions, the authors noted. In this study, they investigated the association of weight change at 1 year after a diabetes diagnosis with the long-term incidence and sustainability of T2D remission in real-world settings, using data from the territory-wide Risk Assessment and Management Programme-Diabetes Mellitus (RAMP-DM).
A total of 37,326 people with newly diagnosed T2D who were enrolled in the RAMP-DM between 2000 and 2017 were included and followed until 2019.
At baseline, participants’ mean age was 56.6 years, mean body mass index (BMI) was 26.4 kg/m2, and mean A1c was 7.7%, and 65% were using glucose-lowering drugs (GLDs).
T2D remission was defined as two consecutive A1c < 6.5% measurements at least 6 months apart without GLDs currently or in the previous 3 months.
During a median follow-up of 7.9 years, 6.1% of people achieved remission, with an incidence rate of 7.8 per 1000 person-years. The proportion was higher among those with greater weight loss: 14.4% of people who lost 10% of their body weight or more achieved remission compared with 9.9% of those with 5%-9.9% weight loss, 6.5% of those with 0%-4.9% weight loss, and 4.5% of those who gained weight.
After adjustment for age at diagnosis, sex, assessment year, BMI, other metabolic indices, smoking, alcohol drinking, and medication use, the hazard ratio (HR) for diabetes remission was 3.28 for those with 10% or greater weight loss within 1 year of diagnosis, 2.29 for 5%-9.9% weight loss, and 1.34 for 0%-4.9% weight loss compared to weight gain.
The incidence of diabetes remission in the study was significantly lower than that in clinical trials, possibly because trial participants were in structured programs that included intensive lifestyle interventions, regular monitoring and feedback, and reinforcement of a holistic approach to managing diabetes, the authors noted. Real-world settings may or may not include such interventions.
Further analyses showed that within a median follow-up of 3.1 years, 67.2% of people who had achieved diabetes remission returned to hyperglycemia — an incidence rate of 184.8 per 1000 person-years.
The adjusted HR for returning to hyperglycemia was 0.52 for people with 10% or greater weight loss, 0.78 for those with 5%-9.9% weight loss, and 0.90 for those with 0%-4.9% weight loss compared to people with weight gain.
In addition, diabetes remission was associated with a 31% (HR, 0.69) decreased risk for all-cause mortality.
The study “provides evidence for policymakers to design and implement early weight management interventions” for people diagnosed with T2D, the authors concluded.
Clinicians also have a role to play, Dr. Luk said. “At the first encounter with an individual with newly diagnosed T2D, clinicians should emphasize the importance of weight reduction and guide the individual on how this can be achieved through making healthy lifestyle choices. Pharmacotherapy and metabolic surgery for weight management can be considered in appropriate individuals.”
Overall, she added, “clinicians should be informed that the likelihood of achieving and maintaining diabetes remission is low, and patients should be counseled accordingly.”
Similar to US Experience
Mona Mshayekhi, MD, PhD, an assistant professor of medicine in the division of Diabetes, Endocrinology and Metabolism at Vanderbilt University Medical Center, Nashville, Tennessee, commented on the study for this news organization.
“These findings mirror clinical experience in the US very well,” she said. “We know that sustained weight loss without the use of medications or surgery is extremely difficult in the real-world setting due to the hormonal drivers of obesity, in combination with socioeconomic challenges.”
The study was done before newer weight-management strategies such as glucagon-like peptide 1 receptor agonists were widely available, she noted. “This actually strengthens the finding that weight loss without the routine use of medications has a multitude of benefits, including diabetes remission and reduction of all-cause mortality.”
That said, she added, “I suspect that future studies with more modern cohorts will reveal much higher rates of diabetes remission with the use of newer medications.”
“Our ability to help our patients lose meaningful weight has been limited until recently,” she said. “With new tools in our armamentarium, clinicians need to take the lead in helping patients address and treat obesity and fight the stigma that prevents many from even discussing it with their providers.”
The study did not receive funding. Dr. Luk has received research grants or contracts from Amgen, AstraZeneca, Bayer, Biogen, Boehringer Ingelheim, Eli Lilly, Junshi, Lee Pharmaceutical, MSD, Novo Nordisk, Roche, Sanofi, Shanghai Junshi Biosciences, Sugardown, and Takeda and received travel grants and honoraria for speaking from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and MSD. Dr. Mshayekhi reported no conflicts of interest.
A version of this article appeared on Medscape.com.
Very few patients with type 2 diabetes (T2D) achieve and sustain diabetes remission via weight loss alone, new research suggests.
Among more than 37,000 people with T2D in Hong Kong, only 6% had achieved and sustained diabetes remission solely through weight loss up to 8 years after diagnosis. Among those who initially achieved remission, 67% had hyperglycemia at 3 years.
People who lost the most weight (10% of their body weight or more) in the first year after diagnosis were most likely to have sustained remission.
The study “helped to confirm the low rate of diabetes remission and high rate of returning to hyperglycemia in real-world practice,” Andrea Luk, MD, of the Chinese University of Hong Kong, told this news organization. “Over 80% of diabetes remission occurred within the first 5 years of a diabetes diagnosis. This is in line with our understanding that beta cell function will gradually decline over time, making diabetes remission increasingly difficult even with weight reduction.”
The study was published in PLOS Medicine.
Early Weight Management Works
Recent clinical trials have demonstrated that T2D remission can be achieved following sustained weight loss through bariatric surgery or lifestyle interventions, the authors noted. In this study, they investigated the association of weight change at 1 year after a diabetes diagnosis with the long-term incidence and sustainability of T2D remission in real-world settings, using data from the territory-wide Risk Assessment and Management Programme-Diabetes Mellitus (RAMP-DM).
A total of 37,326 people with newly diagnosed T2D who were enrolled in the RAMP-DM between 2000 and 2017 were included and followed until 2019.
At baseline, participants’ mean age was 56.6 years, mean body mass index (BMI) was 26.4 kg/m2, and mean A1c was 7.7%, and 65% were using glucose-lowering drugs (GLDs).
T2D remission was defined as two consecutive A1c < 6.5% measurements at least 6 months apart without GLDs currently or in the previous 3 months.
During a median follow-up of 7.9 years, 6.1% of people achieved remission, with an incidence rate of 7.8 per 1000 person-years. The proportion was higher among those with greater weight loss: 14.4% of people who lost 10% of their body weight or more achieved remission compared with 9.9% of those with 5%-9.9% weight loss, 6.5% of those with 0%-4.9% weight loss, and 4.5% of those who gained weight.
After adjustment for age at diagnosis, sex, assessment year, BMI, other metabolic indices, smoking, alcohol drinking, and medication use, the hazard ratio (HR) for diabetes remission was 3.28 for those with 10% or greater weight loss within 1 year of diagnosis, 2.29 for 5%-9.9% weight loss, and 1.34 for 0%-4.9% weight loss compared to weight gain.
The incidence of diabetes remission in the study was significantly lower than that in clinical trials, possibly because trial participants were in structured programs that included intensive lifestyle interventions, regular monitoring and feedback, and reinforcement of a holistic approach to managing diabetes, the authors noted. Real-world settings may or may not include such interventions.
Further analyses showed that within a median follow-up of 3.1 years, 67.2% of people who had achieved diabetes remission returned to hyperglycemia — an incidence rate of 184.8 per 1000 person-years.
The adjusted HR for returning to hyperglycemia was 0.52 for people with 10% or greater weight loss, 0.78 for those with 5%-9.9% weight loss, and 0.90 for those with 0%-4.9% weight loss compared to people with weight gain.
In addition, diabetes remission was associated with a 31% (HR, 0.69) decreased risk for all-cause mortality.
The study “provides evidence for policymakers to design and implement early weight management interventions” for people diagnosed with T2D, the authors concluded.
Clinicians also have a role to play, Dr. Luk said. “At the first encounter with an individual with newly diagnosed T2D, clinicians should emphasize the importance of weight reduction and guide the individual on how this can be achieved through making healthy lifestyle choices. Pharmacotherapy and metabolic surgery for weight management can be considered in appropriate individuals.”
Overall, she added, “clinicians should be informed that the likelihood of achieving and maintaining diabetes remission is low, and patients should be counseled accordingly.”
Similar to US Experience
Mona Mshayekhi, MD, PhD, an assistant professor of medicine in the division of Diabetes, Endocrinology and Metabolism at Vanderbilt University Medical Center, Nashville, Tennessee, commented on the study for this news organization.
“These findings mirror clinical experience in the US very well,” she said. “We know that sustained weight loss without the use of medications or surgery is extremely difficult in the real-world setting due to the hormonal drivers of obesity, in combination with socioeconomic challenges.”
The study was done before newer weight-management strategies such as glucagon-like peptide 1 receptor agonists were widely available, she noted. “This actually strengthens the finding that weight loss without the routine use of medications has a multitude of benefits, including diabetes remission and reduction of all-cause mortality.”
That said, she added, “I suspect that future studies with more modern cohorts will reveal much higher rates of diabetes remission with the use of newer medications.”
“Our ability to help our patients lose meaningful weight has been limited until recently,” she said. “With new tools in our armamentarium, clinicians need to take the lead in helping patients address and treat obesity and fight the stigma that prevents many from even discussing it with their providers.”
The study did not receive funding. Dr. Luk has received research grants or contracts from Amgen, AstraZeneca, Bayer, Biogen, Boehringer Ingelheim, Eli Lilly, Junshi, Lee Pharmaceutical, MSD, Novo Nordisk, Roche, Sanofi, Shanghai Junshi Biosciences, Sugardown, and Takeda and received travel grants and honoraria for speaking from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and MSD. Dr. Mshayekhi reported no conflicts of interest.
A version of this article appeared on Medscape.com.
Very few patients with type 2 diabetes (T2D) achieve and sustain diabetes remission via weight loss alone, new research suggests.
Among more than 37,000 people with T2D in Hong Kong, only 6% had achieved and sustained diabetes remission solely through weight loss up to 8 years after diagnosis. Among those who initially achieved remission, 67% had hyperglycemia at 3 years.
People who lost the most weight (10% of their body weight or more) in the first year after diagnosis were most likely to have sustained remission.
The study “helped to confirm the low rate of diabetes remission and high rate of returning to hyperglycemia in real-world practice,” Andrea Luk, MD, of the Chinese University of Hong Kong, told this news organization. “Over 80% of diabetes remission occurred within the first 5 years of a diabetes diagnosis. This is in line with our understanding that beta cell function will gradually decline over time, making diabetes remission increasingly difficult even with weight reduction.”
The study was published in PLOS Medicine.
Early Weight Management Works
Recent clinical trials have demonstrated that T2D remission can be achieved following sustained weight loss through bariatric surgery or lifestyle interventions, the authors noted. In this study, they investigated the association of weight change at 1 year after a diabetes diagnosis with the long-term incidence and sustainability of T2D remission in real-world settings, using data from the territory-wide Risk Assessment and Management Programme-Diabetes Mellitus (RAMP-DM).
A total of 37,326 people with newly diagnosed T2D who were enrolled in the RAMP-DM between 2000 and 2017 were included and followed until 2019.
At baseline, participants’ mean age was 56.6 years, mean body mass index (BMI) was 26.4 kg/m2, and mean A1c was 7.7%, and 65% were using glucose-lowering drugs (GLDs).
T2D remission was defined as two consecutive A1c < 6.5% measurements at least 6 months apart without GLDs currently or in the previous 3 months.
During a median follow-up of 7.9 years, 6.1% of people achieved remission, with an incidence rate of 7.8 per 1000 person-years. The proportion was higher among those with greater weight loss: 14.4% of people who lost 10% of their body weight or more achieved remission compared with 9.9% of those with 5%-9.9% weight loss, 6.5% of those with 0%-4.9% weight loss, and 4.5% of those who gained weight.
After adjustment for age at diagnosis, sex, assessment year, BMI, other metabolic indices, smoking, alcohol drinking, and medication use, the hazard ratio (HR) for diabetes remission was 3.28 for those with 10% or greater weight loss within 1 year of diagnosis, 2.29 for 5%-9.9% weight loss, and 1.34 for 0%-4.9% weight loss compared to weight gain.
The incidence of diabetes remission in the study was significantly lower than that in clinical trials, possibly because trial participants were in structured programs that included intensive lifestyle interventions, regular monitoring and feedback, and reinforcement of a holistic approach to managing diabetes, the authors noted. Real-world settings may or may not include such interventions.
Further analyses showed that within a median follow-up of 3.1 years, 67.2% of people who had achieved diabetes remission returned to hyperglycemia — an incidence rate of 184.8 per 1000 person-years.
The adjusted HR for returning to hyperglycemia was 0.52 for people with 10% or greater weight loss, 0.78 for those with 5%-9.9% weight loss, and 0.90 for those with 0%-4.9% weight loss compared to people with weight gain.
In addition, diabetes remission was associated with a 31% (HR, 0.69) decreased risk for all-cause mortality.
The study “provides evidence for policymakers to design and implement early weight management interventions” for people diagnosed with T2D, the authors concluded.
Clinicians also have a role to play, Dr. Luk said. “At the first encounter with an individual with newly diagnosed T2D, clinicians should emphasize the importance of weight reduction and guide the individual on how this can be achieved through making healthy lifestyle choices. Pharmacotherapy and metabolic surgery for weight management can be considered in appropriate individuals.”
Overall, she added, “clinicians should be informed that the likelihood of achieving and maintaining diabetes remission is low, and patients should be counseled accordingly.”
Similar to US Experience
Mona Mshayekhi, MD, PhD, an assistant professor of medicine in the division of Diabetes, Endocrinology and Metabolism at Vanderbilt University Medical Center, Nashville, Tennessee, commented on the study for this news organization.
“These findings mirror clinical experience in the US very well,” she said. “We know that sustained weight loss without the use of medications or surgery is extremely difficult in the real-world setting due to the hormonal drivers of obesity, in combination with socioeconomic challenges.”
The study was done before newer weight-management strategies such as glucagon-like peptide 1 receptor agonists were widely available, she noted. “This actually strengthens the finding that weight loss without the routine use of medications has a multitude of benefits, including diabetes remission and reduction of all-cause mortality.”
That said, she added, “I suspect that future studies with more modern cohorts will reveal much higher rates of diabetes remission with the use of newer medications.”
“Our ability to help our patients lose meaningful weight has been limited until recently,” she said. “With new tools in our armamentarium, clinicians need to take the lead in helping patients address and treat obesity and fight the stigma that prevents many from even discussing it with their providers.”
The study did not receive funding. Dr. Luk has received research grants or contracts from Amgen, AstraZeneca, Bayer, Biogen, Boehringer Ingelheim, Eli Lilly, Junshi, Lee Pharmaceutical, MSD, Novo Nordisk, Roche, Sanofi, Shanghai Junshi Biosciences, Sugardown, and Takeda and received travel grants and honoraria for speaking from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and MSD. Dr. Mshayekhi reported no conflicts of interest.
A version of this article appeared on Medscape.com.
FROM PLOS MEDICINE
Young Myeloma Specialist Forges Ahead, Gives Back
Ahead of the conference held in San Diego in December, Dr. Mohyuddin, a blood cancer specialist with a focus on multiple myeloma and medical education, put out a heartfelt appeal on X (formerly Twitter): “If you’re a trainee and interested in meeting me at #ASH23, please reach out … (especially if [international medical graduate]) I’d love to meet and offer support in whatever capacity I can! I can’t have a research project for each one of you, but happy to help/mentor in any other way possible,” he posted on X back in late November.
An international medical graduate himself, Dr. Mohyuddin recalls how overwhelmed he felt when he first attended an annual ASH conference as a trainee, so he aims to reassure others that they “don’t have to know everything.”
“It’s about networking and broadening horizons,” he said in an interview that took place between ASH sessions, his own research presentations, and meetings with the many trainees who took him up on the offer he made via X. “I’ve spent most of this ASH meeting trainees — it’s the most rewarding thing for me at these meetings.
“Reassurance is a lot of what we do in oncology,” he continued, drawing a connection between his affinity for helping trainees and providing compassionate care to patients. “For an oncologist, the single most important thing is having excellent communication skills and being able to express support and empathy. The ability to connect deeply with your patients during their time of need is profoundly important.
“You can compensate for lack of knowledge, because we have so many other sources of support for knowledge, but you simply cannot compensate for poor communication skills, and your patient suffers as a result,” he said.
Relationship Building
In addition to the guidance he received from mentors, Dr. Mohyuddin noted that it was the chance to build supportive, empathetic relationships that drew him to specialize in blood cancer and, in particular, to caring for patients with multiple myeloma and conducting research focused on improving the patient experience.
Dr. Mohyuddin attended medical school at the Aga Khan University in Pakistan, then completed his internal medicine residency and fellowship at the University of Kansas in Kansas City. As a chief resident there, he focused on novel approaches to education delivery and improving access to research for trainees. As a fellow, he developed clinical and research interests in multiple myeloma, which he describes as an “incredibly rewarding field” marked by “truly spectacular advances over the last two decades.”
“There are some cancers you can cure, which means you don’t get to see patients often, and there are some you can’t cure, where patients die early, and there’s not a lot of time to build a relationship,” he said. “But there are some where patients can do well even though they aren’t currently cured, and you get to form really amazing and meaningful relationships over a long period of time.
“Multiple myeloma occupies that space, and that’s why I’m drawn to it,” Dr. Mohyuddin added, noting that he doesn’t shy away from forging emotional connections with patients. “I recognize that makes me vulnerable, but I think that is essentially what your patients deserve from you — to be invested at an emotional level with them through their suffering.”
Improving value and the patient experience
“One thing, philosophically, that I research is value in multiple myeloma care: identifying areas where we are overtreating patients and where we can do less and get away with it,” he said.
Despite the major advances in multiple myeloma in recent years, which “represent a lot of what is going right with oncology,” this blood cancer still “also represents a lot of what is wrong with oncology,” he noted. As an example, he cited “the approval of low-value drugs, the sequencing of drugs, adding more and more drugs without responsibly addressing quality-of-life questions, and identifying more responsible ways to provide high-value efficacious care without bankrupting the economy.
“So my research and policy work apply to that,” he explained. “What can we do better? What sort of trials should we be doing? What populations do we enroll? Are we asking the right questions or looking at trivialities? Are we serving patients foremost?”
Sometimes, this means comparing multiple myeloma staging systems in a real-world cohort, or assessing whether a widely available, cheap, and safe drug like budesonide can help patients avoid diarrhea during chemotherapy, whether control arms in myeloma randomized trials are fair, whether drugs ever get approved in low- or middle-income countries after their approval in the United States, and whether smoldering myeloma, a multiple myeloma precursor, really requires treatment, as current guidelines suggest, or if patients would do just as well — or perhaps better — with a close surveillance protocol.
“Pharma won’t do those studies and many key opinion leaders feel the question [about whether smoldering myeloma needs to be treated] has already been answered, so we are launching a prospective study that will define the natural history of smoldering myeloma and allow for patients to stay off therapy while undergoing rigorous surveillance with imaging,” he said.
Another study Dr. Mohyuddin hopes to launch soon will look at a “start low, go slow” treatment approach for the frailest patients with newly diagnosed myeloma.
His upbringing in Pakistan, where there are “mind-boggling” differences in health care access, affordability, and outcomes when compared with the United States, provided a foundation for both his “enthusiasm for cost-effective care” and his desire to give back, he said.
Another aspect of life in Pakistan — an across-the-board sense of closeness and solidarity in families and communities that is sometimes lacking in the United States — contributed to his desire to build relationships.
“That is something I dearly miss,” he said. “I am very privileged and so thankful to be here in the US, but that is one thing I do deeply miss.”
Connecting and Making a Difference
Dr. Mohyuddin seeks connection through his relationships with patients, trainees, and his many followers on social media platforms like X, where he frequently shares his thoughts on research quality and findings, heme/onc trends, and treatment-related insight.
“How to treat myeloma after #ASH23,” he posted on X as the conference came to a close. His takeaways: Don’t treat smoldering myeloma, do quadruple therapy for transplant-eligible patients (but no cd38 maintenance therapy afterward), don’t do quads for carfilzomib in newly diagnosed frail or older patients, and don’t do a salvage autologous transplant, no matter how good the first transplant was.
Dr. Mohyuddin also works to make a difference through his research and involvement in helping to launch initiatives like Common Sense Oncology, an ambitious global effort to reform cancer clinical trials and care, and through a current project with colleagues in India and Pakistan to create a consortium for pooling data on hematologic malignancies from South Asian countries. The hope is that such a collaborative effort will lead to good prospective research relevant to the needs of participating countries, he explained.
“Those are things where I want to make a difference. Taking care of patients is number one, but more than research, the number two thing for me is teaching and hopefully inspiring trainees and others to think differently, to look at data differently,” he said, noting that despite the major advances in myeloma, the reality is that “a lot of what we offer in oncology is very marginal.”
The effect sizes of interventions are often very small, and outcomes can still be really bad, he explained, adding that “[i]t really hits you when you see a lot of death and suffering. It’s a huge wake-up call … we have so many advances, but the reality is very, very sobering.
“Critically understanding and interpreting data is something where education really fails us. I’m incredibly passionate about it. I’ve found great resources to help me interpret data better, and I want to make them more accessible and inspire others to understand better,” he said. “We need to know how to defend ourselves from the hype.”
His efforts have not gone unnoticed. Dr. Mohyuddin was the recipient of the 2023 Hematology and Medical Oncology Fellowship Faculty Teaching Award at the University of Utah, Salt Lake City, where he is currently a faculty member.
“The recognition means more than any publication or grant award,” he said. “It’s great to know that medical education is appreciated, because so often we are in a rat race of getting more papers and grants out, but teaching and inspiring people is what is really, really important to me.”
Ahead of the conference held in San Diego in December, Dr. Mohyuddin, a blood cancer specialist with a focus on multiple myeloma and medical education, put out a heartfelt appeal on X (formerly Twitter): “If you’re a trainee and interested in meeting me at #ASH23, please reach out … (especially if [international medical graduate]) I’d love to meet and offer support in whatever capacity I can! I can’t have a research project for each one of you, but happy to help/mentor in any other way possible,” he posted on X back in late November.
An international medical graduate himself, Dr. Mohyuddin recalls how overwhelmed he felt when he first attended an annual ASH conference as a trainee, so he aims to reassure others that they “don’t have to know everything.”
“It’s about networking and broadening horizons,” he said in an interview that took place between ASH sessions, his own research presentations, and meetings with the many trainees who took him up on the offer he made via X. “I’ve spent most of this ASH meeting trainees — it’s the most rewarding thing for me at these meetings.
“Reassurance is a lot of what we do in oncology,” he continued, drawing a connection between his affinity for helping trainees and providing compassionate care to patients. “For an oncologist, the single most important thing is having excellent communication skills and being able to express support and empathy. The ability to connect deeply with your patients during their time of need is profoundly important.
“You can compensate for lack of knowledge, because we have so many other sources of support for knowledge, but you simply cannot compensate for poor communication skills, and your patient suffers as a result,” he said.
Relationship Building
In addition to the guidance he received from mentors, Dr. Mohyuddin noted that it was the chance to build supportive, empathetic relationships that drew him to specialize in blood cancer and, in particular, to caring for patients with multiple myeloma and conducting research focused on improving the patient experience.
Dr. Mohyuddin attended medical school at the Aga Khan University in Pakistan, then completed his internal medicine residency and fellowship at the University of Kansas in Kansas City. As a chief resident there, he focused on novel approaches to education delivery and improving access to research for trainees. As a fellow, he developed clinical and research interests in multiple myeloma, which he describes as an “incredibly rewarding field” marked by “truly spectacular advances over the last two decades.”
“There are some cancers you can cure, which means you don’t get to see patients often, and there are some you can’t cure, where patients die early, and there’s not a lot of time to build a relationship,” he said. “But there are some where patients can do well even though they aren’t currently cured, and you get to form really amazing and meaningful relationships over a long period of time.
“Multiple myeloma occupies that space, and that’s why I’m drawn to it,” Dr. Mohyuddin added, noting that he doesn’t shy away from forging emotional connections with patients. “I recognize that makes me vulnerable, but I think that is essentially what your patients deserve from you — to be invested at an emotional level with them through their suffering.”
Improving value and the patient experience
“One thing, philosophically, that I research is value in multiple myeloma care: identifying areas where we are overtreating patients and where we can do less and get away with it,” he said.
Despite the major advances in multiple myeloma in recent years, which “represent a lot of what is going right with oncology,” this blood cancer still “also represents a lot of what is wrong with oncology,” he noted. As an example, he cited “the approval of low-value drugs, the sequencing of drugs, adding more and more drugs without responsibly addressing quality-of-life questions, and identifying more responsible ways to provide high-value efficacious care without bankrupting the economy.
“So my research and policy work apply to that,” he explained. “What can we do better? What sort of trials should we be doing? What populations do we enroll? Are we asking the right questions or looking at trivialities? Are we serving patients foremost?”
Sometimes, this means comparing multiple myeloma staging systems in a real-world cohort, or assessing whether a widely available, cheap, and safe drug like budesonide can help patients avoid diarrhea during chemotherapy, whether control arms in myeloma randomized trials are fair, whether drugs ever get approved in low- or middle-income countries after their approval in the United States, and whether smoldering myeloma, a multiple myeloma precursor, really requires treatment, as current guidelines suggest, or if patients would do just as well — or perhaps better — with a close surveillance protocol.
“Pharma won’t do those studies and many key opinion leaders feel the question [about whether smoldering myeloma needs to be treated] has already been answered, so we are launching a prospective study that will define the natural history of smoldering myeloma and allow for patients to stay off therapy while undergoing rigorous surveillance with imaging,” he said.
Another study Dr. Mohyuddin hopes to launch soon will look at a “start low, go slow” treatment approach for the frailest patients with newly diagnosed myeloma.
His upbringing in Pakistan, where there are “mind-boggling” differences in health care access, affordability, and outcomes when compared with the United States, provided a foundation for both his “enthusiasm for cost-effective care” and his desire to give back, he said.
Another aspect of life in Pakistan — an across-the-board sense of closeness and solidarity in families and communities that is sometimes lacking in the United States — contributed to his desire to build relationships.
“That is something I dearly miss,” he said. “I am very privileged and so thankful to be here in the US, but that is one thing I do deeply miss.”
Connecting and Making a Difference
Dr. Mohyuddin seeks connection through his relationships with patients, trainees, and his many followers on social media platforms like X, where he frequently shares his thoughts on research quality and findings, heme/onc trends, and treatment-related insight.
“How to treat myeloma after #ASH23,” he posted on X as the conference came to a close. His takeaways: Don’t treat smoldering myeloma, do quadruple therapy for transplant-eligible patients (but no cd38 maintenance therapy afterward), don’t do quads for carfilzomib in newly diagnosed frail or older patients, and don’t do a salvage autologous transplant, no matter how good the first transplant was.
Dr. Mohyuddin also works to make a difference through his research and involvement in helping to launch initiatives like Common Sense Oncology, an ambitious global effort to reform cancer clinical trials and care, and through a current project with colleagues in India and Pakistan to create a consortium for pooling data on hematologic malignancies from South Asian countries. The hope is that such a collaborative effort will lead to good prospective research relevant to the needs of participating countries, he explained.
“Those are things where I want to make a difference. Taking care of patients is number one, but more than research, the number two thing for me is teaching and hopefully inspiring trainees and others to think differently, to look at data differently,” he said, noting that despite the major advances in myeloma, the reality is that “a lot of what we offer in oncology is very marginal.”
The effect sizes of interventions are often very small, and outcomes can still be really bad, he explained, adding that “[i]t really hits you when you see a lot of death and suffering. It’s a huge wake-up call … we have so many advances, but the reality is very, very sobering.
“Critically understanding and interpreting data is something where education really fails us. I’m incredibly passionate about it. I’ve found great resources to help me interpret data better, and I want to make them more accessible and inspire others to understand better,” he said. “We need to know how to defend ourselves from the hype.”
His efforts have not gone unnoticed. Dr. Mohyuddin was the recipient of the 2023 Hematology and Medical Oncology Fellowship Faculty Teaching Award at the University of Utah, Salt Lake City, where he is currently a faculty member.
“The recognition means more than any publication or grant award,” he said. “It’s great to know that medical education is appreciated, because so often we are in a rat race of getting more papers and grants out, but teaching and inspiring people is what is really, really important to me.”
Ahead of the conference held in San Diego in December, Dr. Mohyuddin, a blood cancer specialist with a focus on multiple myeloma and medical education, put out a heartfelt appeal on X (formerly Twitter): “If you’re a trainee and interested in meeting me at #ASH23, please reach out … (especially if [international medical graduate]) I’d love to meet and offer support in whatever capacity I can! I can’t have a research project for each one of you, but happy to help/mentor in any other way possible,” he posted on X back in late November.
An international medical graduate himself, Dr. Mohyuddin recalls how overwhelmed he felt when he first attended an annual ASH conference as a trainee, so he aims to reassure others that they “don’t have to know everything.”
“It’s about networking and broadening horizons,” he said in an interview that took place between ASH sessions, his own research presentations, and meetings with the many trainees who took him up on the offer he made via X. “I’ve spent most of this ASH meeting trainees — it’s the most rewarding thing for me at these meetings.
“Reassurance is a lot of what we do in oncology,” he continued, drawing a connection between his affinity for helping trainees and providing compassionate care to patients. “For an oncologist, the single most important thing is having excellent communication skills and being able to express support and empathy. The ability to connect deeply with your patients during their time of need is profoundly important.
“You can compensate for lack of knowledge, because we have so many other sources of support for knowledge, but you simply cannot compensate for poor communication skills, and your patient suffers as a result,” he said.
Relationship Building
In addition to the guidance he received from mentors, Dr. Mohyuddin noted that it was the chance to build supportive, empathetic relationships that drew him to specialize in blood cancer and, in particular, to caring for patients with multiple myeloma and conducting research focused on improving the patient experience.
Dr. Mohyuddin attended medical school at the Aga Khan University in Pakistan, then completed his internal medicine residency and fellowship at the University of Kansas in Kansas City. As a chief resident there, he focused on novel approaches to education delivery and improving access to research for trainees. As a fellow, he developed clinical and research interests in multiple myeloma, which he describes as an “incredibly rewarding field” marked by “truly spectacular advances over the last two decades.”
“There are some cancers you can cure, which means you don’t get to see patients often, and there are some you can’t cure, where patients die early, and there’s not a lot of time to build a relationship,” he said. “But there are some where patients can do well even though they aren’t currently cured, and you get to form really amazing and meaningful relationships over a long period of time.
“Multiple myeloma occupies that space, and that’s why I’m drawn to it,” Dr. Mohyuddin added, noting that he doesn’t shy away from forging emotional connections with patients. “I recognize that makes me vulnerable, but I think that is essentially what your patients deserve from you — to be invested at an emotional level with them through their suffering.”
Improving value and the patient experience
“One thing, philosophically, that I research is value in multiple myeloma care: identifying areas where we are overtreating patients and where we can do less and get away with it,” he said.
Despite the major advances in multiple myeloma in recent years, which “represent a lot of what is going right with oncology,” this blood cancer still “also represents a lot of what is wrong with oncology,” he noted. As an example, he cited “the approval of low-value drugs, the sequencing of drugs, adding more and more drugs without responsibly addressing quality-of-life questions, and identifying more responsible ways to provide high-value efficacious care without bankrupting the economy.
“So my research and policy work apply to that,” he explained. “What can we do better? What sort of trials should we be doing? What populations do we enroll? Are we asking the right questions or looking at trivialities? Are we serving patients foremost?”
Sometimes, this means comparing multiple myeloma staging systems in a real-world cohort, or assessing whether a widely available, cheap, and safe drug like budesonide can help patients avoid diarrhea during chemotherapy, whether control arms in myeloma randomized trials are fair, whether drugs ever get approved in low- or middle-income countries after their approval in the United States, and whether smoldering myeloma, a multiple myeloma precursor, really requires treatment, as current guidelines suggest, or if patients would do just as well — or perhaps better — with a close surveillance protocol.
“Pharma won’t do those studies and many key opinion leaders feel the question [about whether smoldering myeloma needs to be treated] has already been answered, so we are launching a prospective study that will define the natural history of smoldering myeloma and allow for patients to stay off therapy while undergoing rigorous surveillance with imaging,” he said.
Another study Dr. Mohyuddin hopes to launch soon will look at a “start low, go slow” treatment approach for the frailest patients with newly diagnosed myeloma.
His upbringing in Pakistan, where there are “mind-boggling” differences in health care access, affordability, and outcomes when compared with the United States, provided a foundation for both his “enthusiasm for cost-effective care” and his desire to give back, he said.
Another aspect of life in Pakistan — an across-the-board sense of closeness and solidarity in families and communities that is sometimes lacking in the United States — contributed to his desire to build relationships.
“That is something I dearly miss,” he said. “I am very privileged and so thankful to be here in the US, but that is one thing I do deeply miss.”
Connecting and Making a Difference
Dr. Mohyuddin seeks connection through his relationships with patients, trainees, and his many followers on social media platforms like X, where he frequently shares his thoughts on research quality and findings, heme/onc trends, and treatment-related insight.
“How to treat myeloma after #ASH23,” he posted on X as the conference came to a close. His takeaways: Don’t treat smoldering myeloma, do quadruple therapy for transplant-eligible patients (but no cd38 maintenance therapy afterward), don’t do quads for carfilzomib in newly diagnosed frail or older patients, and don’t do a salvage autologous transplant, no matter how good the first transplant was.
Dr. Mohyuddin also works to make a difference through his research and involvement in helping to launch initiatives like Common Sense Oncology, an ambitious global effort to reform cancer clinical trials and care, and through a current project with colleagues in India and Pakistan to create a consortium for pooling data on hematologic malignancies from South Asian countries. The hope is that such a collaborative effort will lead to good prospective research relevant to the needs of participating countries, he explained.
“Those are things where I want to make a difference. Taking care of patients is number one, but more than research, the number two thing for me is teaching and hopefully inspiring trainees and others to think differently, to look at data differently,” he said, noting that despite the major advances in myeloma, the reality is that “a lot of what we offer in oncology is very marginal.”
The effect sizes of interventions are often very small, and outcomes can still be really bad, he explained, adding that “[i]t really hits you when you see a lot of death and suffering. It’s a huge wake-up call … we have so many advances, but the reality is very, very sobering.
“Critically understanding and interpreting data is something where education really fails us. I’m incredibly passionate about it. I’ve found great resources to help me interpret data better, and I want to make them more accessible and inspire others to understand better,” he said. “We need to know how to defend ourselves from the hype.”
His efforts have not gone unnoticed. Dr. Mohyuddin was the recipient of the 2023 Hematology and Medical Oncology Fellowship Faculty Teaching Award at the University of Utah, Salt Lake City, where he is currently a faculty member.
“The recognition means more than any publication or grant award,” he said. “It’s great to know that medical education is appreciated, because so often we are in a rat race of getting more papers and grants out, but teaching and inspiring people is what is really, really important to me.”
Bladder Cancer: Is Active Surveillance the Way Forward?
PARIS — Should clinicians promote active surveillance for non–muscle-invasive bladder tumors (NMIBT) and establish it as a comprehensive management approach, as with prostate and kidney cancers?
During the 117th congress of the French Association of Urology (AFU), Benjamin Pradère, MD, urologic surgeon at Croix du Sud Clinic in Quint-Fonsegrives, France, advocated for this approach, suggesting that the use of biomarkers could enhance its effectiveness.
However, it requires careful patient selection, proper information, and relevant follow-up,” said Dr. Pradère, who is a member of the AFU Cancer Committee (CCAFU).
Low-Grade Tumors
NMIBTs are precancerous lesions and constitute 70%-80% of diagnosed bladder tumors. The remaining tumors are more severe invasive tumors that infiltrate deep tissues. NMIBTs, however, entail a high risk for recurrence (reaching 80% after endoscopic resection), as well as a high risk for progression.
As a result, the diagnosis of NMIBT involves follow-up that significantly impacts patients’ quality of life due to repeated cystoscopies and endovesical treatments. “Tumors with the most impact are low-grade Ta tumors”, with longer-term monitoring required for these low-risk tumors.
Hematuria is the most frequent clinical sign. NMIBT diagnosis occurs after endoscopic tumor resection via transurethral resection, followed by an anatomopathological analysis to determine cell grade and tumor stage. Treatment depends on the risk of recurrence and progression, as well as the risk of therapeutic failure after the initial resection.
Risk stratification distinguishes the following four levels:
- Low-risk tumors: Low-grade pTa urothelial tumors, unifocal, < 3 cm, no history of bladder tumors. Low risk of recurrence and progression.
- Intermediate-risk tumors: Other low-grade pTa urothelial tumors with no high-risk criteria. Low risk of progression but high risk of recurrence.
- High-risk tumors: Tumors with at least one risk factor: Stage pT1, high grade, presence of carcinoma in situ. High risks of progression and recurrence.
- Very high-risk tumors: Tumors combining all risk factors (pT1 grade with carcinoma in situ). Very high and early risk of progression.
“We know that low-grade NMIBTs have no impact on survival,” said Dr. Pradère. For these tumors, which represent 60% of diagnosed NMIBTs, or approximately 250,000 new cases annually in France, specific survival is > 99%, meaning that most diagnosed patients will not die of bladder cancer.
The recurrence rate for low-grade tumors is 50%, but recurrences are “almost always low-grade and rarely invade the basement membrane,” said Pradère. Implementing active surveillance to limit surgical intervention to more advanced forms seems to be relevant for these tumors.
Cystoscopy Every 3 Months
According to CCAFU recommendations, “active surveillance is a therapeutic alternative that can be proposed for patients with recurrent low-risk NMIBT after the initial diagnosis.” Criteria include low-grade pTa, fewer than five tumors, size ≤ 15 mm, negative urinary cytology, asymptomatic nature, and the patient’s acceptance of closer monitoring.
While active surveillance has become the standard treatment for low-risk prostate cancer, this therapeutic option remains marginal in bladder cancer, as in kidney cancer. The goal is to defer or avoid surgical treatment by closely monitoring the natural progression of the disease.
For NMIBTs, follow-up modalities are not yet specifically recommended because of a lack of data, said Dr. Pradère. According to a consensus, cystoscopy should be repeated every 3 months for a year and then every 6 months. Unlike standard follow-up, it includes cytology “to not miss the transition to high grade.”
CCAFU recommends discontinuing active surveillance if any of the following criteria are present:
- More than 10 lesions
- Size > 30 mm
- Positive cytology
- Symptoms (hematuria, micturition disorders, and recurring infections).
Literature on the benefits of active surveillance in bladder tumors is still limited. Only seven studies are available. Overall, for nearly 600 included patients, tumors progressed in about 12% of cases. Progression to invasive tumors occurred in 0.8% of patients (n = 5).
13 Months’ Surveillance
According to a long-term study (median follow-up of 38 months), patients mostly exit active surveillance in the first year. The median duration of active surveillance is 13 months. Active surveillance is discontinued to surgically treat tumors that turn out to be low-grade Ta tumors in 70% of cases.
The following factors predicting recurrence and progression of tumors have been identified: Multiple tumors, early recurrence (within a year of initial diagnosis), frequent recurrence (more than one recurrence per year), tumors > 3 cm, and failure of previous endovesical treatment.
Recent studies have shown that with at least three of these recurrence and progression factors, the median duration under active surveillance is 15 months compared with 28 months in the absence of such factors. “Considering these factors, it is possible to assess the benefit of active surveillance for the patient,” said Dr. Pradère.
If active surveillance for bladder tumors is still not widely practiced, then the contribution of imaging (MRI and ultrasound) and biomarkers could promote its adoption. “The use of biomarkers should change the game and encourage active surveillance in patients with small polyps,” said Dr. Pradère.
ADXBladder Test Utility
A study highlighted the importance of evaluating minichromosome maintenance protein 5 expression during active surveillance using the ADXBladder ELISA test on a urine sample. This test is usually used in bladder cancer diagnosis.
“This study showed that a negative result in two consecutive tests during active surveillance is associated with an almost zero recurrence risk. After two negative tests, most patients do not exit active surveillance,” said Dr. Pradère. But the positive predictive value of biomarkers remains low for low-grade tumors.
The future of active surveillance in bladder cancer should involve better patient selection that relies on risk factors, enhanced modalities through imaging and biomarkers, and the advent of artificial intelligence to analyze cystoscopy results, concluded Dr. Pradère.
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
PARIS — Should clinicians promote active surveillance for non–muscle-invasive bladder tumors (NMIBT) and establish it as a comprehensive management approach, as with prostate and kidney cancers?
During the 117th congress of the French Association of Urology (AFU), Benjamin Pradère, MD, urologic surgeon at Croix du Sud Clinic in Quint-Fonsegrives, France, advocated for this approach, suggesting that the use of biomarkers could enhance its effectiveness.
However, it requires careful patient selection, proper information, and relevant follow-up,” said Dr. Pradère, who is a member of the AFU Cancer Committee (CCAFU).
Low-Grade Tumors
NMIBTs are precancerous lesions and constitute 70%-80% of diagnosed bladder tumors. The remaining tumors are more severe invasive tumors that infiltrate deep tissues. NMIBTs, however, entail a high risk for recurrence (reaching 80% after endoscopic resection), as well as a high risk for progression.
As a result, the diagnosis of NMIBT involves follow-up that significantly impacts patients’ quality of life due to repeated cystoscopies and endovesical treatments. “Tumors with the most impact are low-grade Ta tumors”, with longer-term monitoring required for these low-risk tumors.
Hematuria is the most frequent clinical sign. NMIBT diagnosis occurs after endoscopic tumor resection via transurethral resection, followed by an anatomopathological analysis to determine cell grade and tumor stage. Treatment depends on the risk of recurrence and progression, as well as the risk of therapeutic failure after the initial resection.
Risk stratification distinguishes the following four levels:
- Low-risk tumors: Low-grade pTa urothelial tumors, unifocal, < 3 cm, no history of bladder tumors. Low risk of recurrence and progression.
- Intermediate-risk tumors: Other low-grade pTa urothelial tumors with no high-risk criteria. Low risk of progression but high risk of recurrence.
- High-risk tumors: Tumors with at least one risk factor: Stage pT1, high grade, presence of carcinoma in situ. High risks of progression and recurrence.
- Very high-risk tumors: Tumors combining all risk factors (pT1 grade with carcinoma in situ). Very high and early risk of progression.
“We know that low-grade NMIBTs have no impact on survival,” said Dr. Pradère. For these tumors, which represent 60% of diagnosed NMIBTs, or approximately 250,000 new cases annually in France, specific survival is > 99%, meaning that most diagnosed patients will not die of bladder cancer.
The recurrence rate for low-grade tumors is 50%, but recurrences are “almost always low-grade and rarely invade the basement membrane,” said Pradère. Implementing active surveillance to limit surgical intervention to more advanced forms seems to be relevant for these tumors.
Cystoscopy Every 3 Months
According to CCAFU recommendations, “active surveillance is a therapeutic alternative that can be proposed for patients with recurrent low-risk NMIBT after the initial diagnosis.” Criteria include low-grade pTa, fewer than five tumors, size ≤ 15 mm, negative urinary cytology, asymptomatic nature, and the patient’s acceptance of closer monitoring.
While active surveillance has become the standard treatment for low-risk prostate cancer, this therapeutic option remains marginal in bladder cancer, as in kidney cancer. The goal is to defer or avoid surgical treatment by closely monitoring the natural progression of the disease.
For NMIBTs, follow-up modalities are not yet specifically recommended because of a lack of data, said Dr. Pradère. According to a consensus, cystoscopy should be repeated every 3 months for a year and then every 6 months. Unlike standard follow-up, it includes cytology “to not miss the transition to high grade.”
CCAFU recommends discontinuing active surveillance if any of the following criteria are present:
- More than 10 lesions
- Size > 30 mm
- Positive cytology
- Symptoms (hematuria, micturition disorders, and recurring infections).
Literature on the benefits of active surveillance in bladder tumors is still limited. Only seven studies are available. Overall, for nearly 600 included patients, tumors progressed in about 12% of cases. Progression to invasive tumors occurred in 0.8% of patients (n = 5).
13 Months’ Surveillance
According to a long-term study (median follow-up of 38 months), patients mostly exit active surveillance in the first year. The median duration of active surveillance is 13 months. Active surveillance is discontinued to surgically treat tumors that turn out to be low-grade Ta tumors in 70% of cases.
The following factors predicting recurrence and progression of tumors have been identified: Multiple tumors, early recurrence (within a year of initial diagnosis), frequent recurrence (more than one recurrence per year), tumors > 3 cm, and failure of previous endovesical treatment.
Recent studies have shown that with at least three of these recurrence and progression factors, the median duration under active surveillance is 15 months compared with 28 months in the absence of such factors. “Considering these factors, it is possible to assess the benefit of active surveillance for the patient,” said Dr. Pradère.
If active surveillance for bladder tumors is still not widely practiced, then the contribution of imaging (MRI and ultrasound) and biomarkers could promote its adoption. “The use of biomarkers should change the game and encourage active surveillance in patients with small polyps,” said Dr. Pradère.
ADXBladder Test Utility
A study highlighted the importance of evaluating minichromosome maintenance protein 5 expression during active surveillance using the ADXBladder ELISA test on a urine sample. This test is usually used in bladder cancer diagnosis.
“This study showed that a negative result in two consecutive tests during active surveillance is associated with an almost zero recurrence risk. After two negative tests, most patients do not exit active surveillance,” said Dr. Pradère. But the positive predictive value of biomarkers remains low for low-grade tumors.
The future of active surveillance in bladder cancer should involve better patient selection that relies on risk factors, enhanced modalities through imaging and biomarkers, and the advent of artificial intelligence to analyze cystoscopy results, concluded Dr. Pradère.
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
PARIS — Should clinicians promote active surveillance for non–muscle-invasive bladder tumors (NMIBT) and establish it as a comprehensive management approach, as with prostate and kidney cancers?
During the 117th congress of the French Association of Urology (AFU), Benjamin Pradère, MD, urologic surgeon at Croix du Sud Clinic in Quint-Fonsegrives, France, advocated for this approach, suggesting that the use of biomarkers could enhance its effectiveness.
However, it requires careful patient selection, proper information, and relevant follow-up,” said Dr. Pradère, who is a member of the AFU Cancer Committee (CCAFU).
Low-Grade Tumors
NMIBTs are precancerous lesions and constitute 70%-80% of diagnosed bladder tumors. The remaining tumors are more severe invasive tumors that infiltrate deep tissues. NMIBTs, however, entail a high risk for recurrence (reaching 80% after endoscopic resection), as well as a high risk for progression.
As a result, the diagnosis of NMIBT involves follow-up that significantly impacts patients’ quality of life due to repeated cystoscopies and endovesical treatments. “Tumors with the most impact are low-grade Ta tumors”, with longer-term monitoring required for these low-risk tumors.
Hematuria is the most frequent clinical sign. NMIBT diagnosis occurs after endoscopic tumor resection via transurethral resection, followed by an anatomopathological analysis to determine cell grade and tumor stage. Treatment depends on the risk of recurrence and progression, as well as the risk of therapeutic failure after the initial resection.
Risk stratification distinguishes the following four levels:
- Low-risk tumors: Low-grade pTa urothelial tumors, unifocal, < 3 cm, no history of bladder tumors. Low risk of recurrence and progression.
- Intermediate-risk tumors: Other low-grade pTa urothelial tumors with no high-risk criteria. Low risk of progression but high risk of recurrence.
- High-risk tumors: Tumors with at least one risk factor: Stage pT1, high grade, presence of carcinoma in situ. High risks of progression and recurrence.
- Very high-risk tumors: Tumors combining all risk factors (pT1 grade with carcinoma in situ). Very high and early risk of progression.
“We know that low-grade NMIBTs have no impact on survival,” said Dr. Pradère. For these tumors, which represent 60% of diagnosed NMIBTs, or approximately 250,000 new cases annually in France, specific survival is > 99%, meaning that most diagnosed patients will not die of bladder cancer.
The recurrence rate for low-grade tumors is 50%, but recurrences are “almost always low-grade and rarely invade the basement membrane,” said Pradère. Implementing active surveillance to limit surgical intervention to more advanced forms seems to be relevant for these tumors.
Cystoscopy Every 3 Months
According to CCAFU recommendations, “active surveillance is a therapeutic alternative that can be proposed for patients with recurrent low-risk NMIBT after the initial diagnosis.” Criteria include low-grade pTa, fewer than five tumors, size ≤ 15 mm, negative urinary cytology, asymptomatic nature, and the patient’s acceptance of closer monitoring.
While active surveillance has become the standard treatment for low-risk prostate cancer, this therapeutic option remains marginal in bladder cancer, as in kidney cancer. The goal is to defer or avoid surgical treatment by closely monitoring the natural progression of the disease.
For NMIBTs, follow-up modalities are not yet specifically recommended because of a lack of data, said Dr. Pradère. According to a consensus, cystoscopy should be repeated every 3 months for a year and then every 6 months. Unlike standard follow-up, it includes cytology “to not miss the transition to high grade.”
CCAFU recommends discontinuing active surveillance if any of the following criteria are present:
- More than 10 lesions
- Size > 30 mm
- Positive cytology
- Symptoms (hematuria, micturition disorders, and recurring infections).
Literature on the benefits of active surveillance in bladder tumors is still limited. Only seven studies are available. Overall, for nearly 600 included patients, tumors progressed in about 12% of cases. Progression to invasive tumors occurred in 0.8% of patients (n = 5).
13 Months’ Surveillance
According to a long-term study (median follow-up of 38 months), patients mostly exit active surveillance in the first year. The median duration of active surveillance is 13 months. Active surveillance is discontinued to surgically treat tumors that turn out to be low-grade Ta tumors in 70% of cases.
The following factors predicting recurrence and progression of tumors have been identified: Multiple tumors, early recurrence (within a year of initial diagnosis), frequent recurrence (more than one recurrence per year), tumors > 3 cm, and failure of previous endovesical treatment.
Recent studies have shown that with at least three of these recurrence and progression factors, the median duration under active surveillance is 15 months compared with 28 months in the absence of such factors. “Considering these factors, it is possible to assess the benefit of active surveillance for the patient,” said Dr. Pradère.
If active surveillance for bladder tumors is still not widely practiced, then the contribution of imaging (MRI and ultrasound) and biomarkers could promote its adoption. “The use of biomarkers should change the game and encourage active surveillance in patients with small polyps,” said Dr. Pradère.
ADXBladder Test Utility
A study highlighted the importance of evaluating minichromosome maintenance protein 5 expression during active surveillance using the ADXBladder ELISA test on a urine sample. This test is usually used in bladder cancer diagnosis.
“This study showed that a negative result in two consecutive tests during active surveillance is associated with an almost zero recurrence risk. After two negative tests, most patients do not exit active surveillance,” said Dr. Pradère. But the positive predictive value of biomarkers remains low for low-grade tumors.
The future of active surveillance in bladder cancer should involve better patient selection that relies on risk factors, enhanced modalities through imaging and biomarkers, and the advent of artificial intelligence to analyze cystoscopy results, concluded Dr. Pradère.
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
DoxyPEP: A New Option to Prevent Sexually Transmitted Infections
Sexually transmitted infections (STIs) continue to have a significant impact on the lives of adolescents and young adults. According to the Centers for Disease Control and Prevention’s (CDC) 2021 surveillance report, rates of gonorrhea and syphilis in the United States were at their highest since the early 1990s. Chlamydia, one of the most common STIs, had a peak rate in 2019, but more recent rates may have been impacted by the COVID-19 pandemic. In 2021, those 15-24 years of age accounted for 58.5% of all chlamydia infections, 40.4% of all gonorrhea infections, and 18.3% of all syphilis infections in the US.
While pediatricians should discuss sexual health and STI screening with all their adolescent and young adult patients, LGBTQ+ youth are disproportionately impacted by STIs. For example, cisgender men who have sex with men have significantly higher rates of HIV, gonorrhea, and syphilis. These disparities are likely related to unequal access to care, systemic homophobia/transphobia, stigma, and differences in sexual networks and are even more pronounced for those with intersectional minoritized identities such as LGBTQ+ youth of color.1

In the past 12 years, there have been significant advances in HIV prevention methods, including the approval and use of pre-exposure prophylaxis or “PrEP” (a medication regimen that is taken on an ongoing basis to provide highly effective protection against HIV infection) and more widespread use of post-exposure prophylaxis or “PEP” (a medication regimen taken for 1 month after a potential exposure to HIV to prevent HIV from establishing an ongoing infection) outside of the medical setting. While these interventions have the potential to decrease rates of HIV infection, they do not prevent any other STIs.2-3
The current strategies to prevent bacterial STIs include discussions of sexual practices, counseling on risk reduction strategies such as decreased number of partners and condom use, routine screening in those at risk every 3-12 months, and timely diagnosis and treatment of infections in patients and their partners to avoid further transmission.4 Given the increasing rates of bacterial STIs (gonorrhea, chlamydia, and syphilis), additional biomedical prevention methods are greatly needed.
Doxycycline as post-exposure prophylaxis
Doxycycline is a tetracycline antibiotic effective against a wide range of bacteria and is commonly used in the treatment of acne, skin infections, Lyme disease, and STIs, and can also be used in the treatment and prevention of malaria.5 For STIs, doxycycline is currently the recommended treatment for chlamydia and is also an alternate therapy for syphilis in nonpregnant patients when penicillin is not accessible or in those with severe penicillin allergy.4 This medication is often well tolerated with the most common side effects including gastrointestinal irritation and photosensitivity. Doxycycline is contraindicated in pregnancy due to its potential impact on tooth and bone development.5
Given its general tolerability and activity against bacterial STIs, new and emerging studies have examined doxycycline as post-exposure prophylaxis (DoxyPEP: one dose of doxycycline 200 mg PO within 72 hours after unprotected sex) in an attempt to decrease the incidence of new bacterial STIs in populations at risk. Three of the studies cited in the preliminary CDC DoxyPEP guidelines were conducted in cisgender men who have sex with men and transgender women either living with HIV or taking PrEP for HIV prevention. All three studies demonstrated significantly lower risk of chlamydia and syphilis, while two of the studies also showed a significantly lower risk of gonorrhea. One additional study was conducted in cisgender women in Kenya. This study did not show any statistically significant difference in the risk of chlamydia or gonorrhea in the intervention group, but may have been limited by low adherence to the DoxyPEP regimen. There were no serious adverse events reported in any of the studies attributed to doxycycline.6
Avoiding antibiotic resistance
With the increased use of antibiotics, attention must always be paid to the potential for increasing antibiotic resistance. The preliminary CDC DoxyPEP guidelines outline mixed results in the DoxyPEP studies that had limited follow-up timeframes, making it difficult to draw conclusions: “Current data suggest overall benefit of the use of doxycycline PEP, but potential risks related to the development of resistance and impacts on the microbiome will need to be closely monitored after implementation of these guidelines.” Official guideline recommendations from the CDC regarding DoxyPEP are currently pending after a period of public comment on the preliminary drafted guidelines.6 However, the New York State Department of Health AIDS Institute released guidelines for DoxyPEP in September 2023 and several large urban public health departments have also issued their own guidance that largely align with the preliminary CDC guidelines.7
Recommendations currently emphasize that the goal is to allow for implementation of DoxyPEP in those who would benefit the most from the intervention (i.e., cisgender men who have sex with men and transgender women with a history of at least one bacterial STI in the last 12 months with ongoing risk of infection), while also minimizing antibiotic use. It should also be considered for those without a recent infection who have increased likelihood of exposure to bacterial STIs. DoxyPEP is likely to be effective in other populations (e.g., cisgender women, cisgender men who have sex with women, transgender men), but data are currently limited, and the risk/benefit ratio may be different in these populations. The recommended dose for DoxyPEP is doxycycline 200 mg once as soon as possible (within 72 hours) of unprotected oral, vaginal, or anal sex with a maximum of one dose every 24 hours. For those being prescribed DoxyPEP, gonorrhea and chlamydia screening of all anatomic sites of exposure (urine sample or frontal swab, throat swab, and/or rectal swab) should be conducted at baseline and then every 3-6 months in addition to blood testing for syphilis and HIV if indicated.6-7
Another option in our toolkit
DoxyPEP should be viewed as one more option in our toolkit of sexual health services alongside risk reduction strategies (e.g., open discussions with partners, decreased number of partners, and condom use), routine STI screening and treatment, PrEP and PEP for HIV prevention, and pregnancy prevention. Not all of these tools will be relevant to each individual and discussions around sexual health should be patient-centered and focused on their own personal goals. As pediatricians, we should provide guidance to all adolescents and young adults on options to improve their sexual health and empower them to embrace their bodily autonomy.
Dr. Warus is in the division of adolescent and young adult medicine at Children’s Hospital of Los Angeles, where he specializes in care for transgender and gender-nonconforming youth, and LGBTQ health for youth. He is an assistant professor of pediatrics at USC.
Resources
CDC – Sexually Transmitted Infection Treatment Guidelines, 2021
CDC – [Preliminary] Guidelines for the Use of Doxycycline Post-Exposure Prophylaxis for Bacterial Sexually Transmitted Infection (STI) Prevention
New York State Department of Health AIDS Institute – Doxycycline Post-Exposure Prophylaxis to Prevent Bacterial Sexually Transmitted Infections
Los Angeles County Department of Public Health – DoxyPEP for STI Prevention
References
1. Division of STD Prevention, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2021: National Overview of STDs, 2021. Last Reviewed May 16, 2023.
2. Centers for Disease Control and Prevention: US Public Health Service: Preexposure Prophylaxis for the Prevention of HIV Infection in the United States – 2021 Update: A Clinical Practice Guideline. Published 2021.
3. Centers for Disease Control and Prevention: US Department of Health and Human Services: Updated Guidelines for Antiretroviral Postexposure Prophylaxis After Sexual, Injection Drug Use, or Other Nonoccupational Exposure to HIV – United States, 2016. Published 2016. .
4. Workowski KA et al. Sexually Transmitted Infection Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):2-10.
5. Patel RS and Parmar M. Doxycycline Hyclate. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Last Updated May 22, 2023.
6. Centers for Disease Control and Prevention. [Preliminary] Guidelines for the Use of Doxycycline Post-Exposure Prophylaxis for Bacterial Sexually Transmitted Infection (STI) Prevention. Published Oct 1, 2023.
7. DiMarco DE, et al. Doxycycline Post-Exposure Prophylaxis to Prevent Bacterial Sexually Transmitted Infections. New York State Department of Health AIDS Institute. Published September 25, 2023.
Sexually transmitted infections (STIs) continue to have a significant impact on the lives of adolescents and young adults. According to the Centers for Disease Control and Prevention’s (CDC) 2021 surveillance report, rates of gonorrhea and syphilis in the United States were at their highest since the early 1990s. Chlamydia, one of the most common STIs, had a peak rate in 2019, but more recent rates may have been impacted by the COVID-19 pandemic. In 2021, those 15-24 years of age accounted for 58.5% of all chlamydia infections, 40.4% of all gonorrhea infections, and 18.3% of all syphilis infections in the US.
While pediatricians should discuss sexual health and STI screening with all their adolescent and young adult patients, LGBTQ+ youth are disproportionately impacted by STIs. For example, cisgender men who have sex with men have significantly higher rates of HIV, gonorrhea, and syphilis. These disparities are likely related to unequal access to care, systemic homophobia/transphobia, stigma, and differences in sexual networks and are even more pronounced for those with intersectional minoritized identities such as LGBTQ+ youth of color.1
In the past 12 years, there have been significant advances in HIV prevention methods, including the approval and use of pre-exposure prophylaxis or “PrEP” (a medication regimen that is taken on an ongoing basis to provide highly effective protection against HIV infection) and more widespread use of post-exposure prophylaxis or “PEP” (a medication regimen taken for 1 month after a potential exposure to HIV to prevent HIV from establishing an ongoing infection) outside of the medical setting. While these interventions have the potential to decrease rates of HIV infection, they do not prevent any other STIs.2-3
The current strategies to prevent bacterial STIs include discussions of sexual practices, counseling on risk reduction strategies such as decreased number of partners and condom use, routine screening in those at risk every 3-12 months, and timely diagnosis and treatment of infections in patients and their partners to avoid further transmission.4 Given the increasing rates of bacterial STIs (gonorrhea, chlamydia, and syphilis), additional biomedical prevention methods are greatly needed.
Doxycycline as post-exposure prophylaxis
Doxycycline is a tetracycline antibiotic effective against a wide range of bacteria and is commonly used in the treatment of acne, skin infections, Lyme disease, and STIs, and can also be used in the treatment and prevention of malaria.5 For STIs, doxycycline is currently the recommended treatment for chlamydia and is also an alternate therapy for syphilis in nonpregnant patients when penicillin is not accessible or in those with severe penicillin allergy.4 This medication is often well tolerated with the most common side effects including gastrointestinal irritation and photosensitivity. Doxycycline is contraindicated in pregnancy due to its potential impact on tooth and bone development.5
Given its general tolerability and activity against bacterial STIs, new and emerging studies have examined doxycycline as post-exposure prophylaxis (DoxyPEP: one dose of doxycycline 200 mg PO within 72 hours after unprotected sex) in an attempt to decrease the incidence of new bacterial STIs in populations at risk. Three of the studies cited in the preliminary CDC DoxyPEP guidelines were conducted in cisgender men who have sex with men and transgender women either living with HIV or taking PrEP for HIV prevention. All three studies demonstrated significantly lower risk of chlamydia and syphilis, while two of the studies also showed a significantly lower risk of gonorrhea. One additional study was conducted in cisgender women in Kenya. This study did not show any statistically significant difference in the risk of chlamydia or gonorrhea in the intervention group, but may have been limited by low adherence to the DoxyPEP regimen. There were no serious adverse events reported in any of the studies attributed to doxycycline.6
Avoiding antibiotic resistance
With the increased use of antibiotics, attention must always be paid to the potential for increasing antibiotic resistance. The preliminary CDC DoxyPEP guidelines outline mixed results in the DoxyPEP studies that had limited follow-up timeframes, making it difficult to draw conclusions: “Current data suggest overall benefit of the use of doxycycline PEP, but potential risks related to the development of resistance and impacts on the microbiome will need to be closely monitored after implementation of these guidelines.” Official guideline recommendations from the CDC regarding DoxyPEP are currently pending after a period of public comment on the preliminary drafted guidelines.6 However, the New York State Department of Health AIDS Institute released guidelines for DoxyPEP in September 2023 and several large urban public health departments have also issued their own guidance that largely align with the preliminary CDC guidelines.7
Recommendations currently emphasize that the goal is to allow for implementation of DoxyPEP in those who would benefit the most from the intervention (i.e., cisgender men who have sex with men and transgender women with a history of at least one bacterial STI in the last 12 months with ongoing risk of infection), while also minimizing antibiotic use. It should also be considered for those without a recent infection who have increased likelihood of exposure to bacterial STIs. DoxyPEP is likely to be effective in other populations (e.g., cisgender women, cisgender men who have sex with women, transgender men), but data are currently limited, and the risk/benefit ratio may be different in these populations. The recommended dose for DoxyPEP is doxycycline 200 mg once as soon as possible (within 72 hours) of unprotected oral, vaginal, or anal sex with a maximum of one dose every 24 hours. For those being prescribed DoxyPEP, gonorrhea and chlamydia screening of all anatomic sites of exposure (urine sample or frontal swab, throat swab, and/or rectal swab) should be conducted at baseline and then every 3-6 months in addition to blood testing for syphilis and HIV if indicated.6-7
Another option in our toolkit
DoxyPEP should be viewed as one more option in our toolkit of sexual health services alongside risk reduction strategies (e.g., open discussions with partners, decreased number of partners, and condom use), routine STI screening and treatment, PrEP and PEP for HIV prevention, and pregnancy prevention. Not all of these tools will be relevant to each individual and discussions around sexual health should be patient-centered and focused on their own personal goals. As pediatricians, we should provide guidance to all adolescents and young adults on options to improve their sexual health and empower them to embrace their bodily autonomy.
Dr. Warus is in the division of adolescent and young adult medicine at Children’s Hospital of Los Angeles, where he specializes in care for transgender and gender-nonconforming youth, and LGBTQ health for youth. He is an assistant professor of pediatrics at USC.
Resources
CDC – Sexually Transmitted Infection Treatment Guidelines, 2021
CDC – [Preliminary] Guidelines for the Use of Doxycycline Post-Exposure Prophylaxis for Bacterial Sexually Transmitted Infection (STI) Prevention
New York State Department of Health AIDS Institute – Doxycycline Post-Exposure Prophylaxis to Prevent Bacterial Sexually Transmitted Infections
Los Angeles County Department of Public Health – DoxyPEP for STI Prevention
References
1. Division of STD Prevention, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2021: National Overview of STDs, 2021. Last Reviewed May 16, 2023.
2. Centers for Disease Control and Prevention: US Public Health Service: Preexposure Prophylaxis for the Prevention of HIV Infection in the United States – 2021 Update: A Clinical Practice Guideline. Published 2021.
3. Centers for Disease Control and Prevention: US Department of Health and Human Services: Updated Guidelines for Antiretroviral Postexposure Prophylaxis After Sexual, Injection Drug Use, or Other Nonoccupational Exposure to HIV – United States, 2016. Published 2016. .
4. Workowski KA et al. Sexually Transmitted Infection Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):2-10.
5. Patel RS and Parmar M. Doxycycline Hyclate. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Last Updated May 22, 2023.
6. Centers for Disease Control and Prevention. [Preliminary] Guidelines for the Use of Doxycycline Post-Exposure Prophylaxis for Bacterial Sexually Transmitted Infection (STI) Prevention. Published Oct 1, 2023.
7. DiMarco DE, et al. Doxycycline Post-Exposure Prophylaxis to Prevent Bacterial Sexually Transmitted Infections. New York State Department of Health AIDS Institute. Published September 25, 2023.
Sexually transmitted infections (STIs) continue to have a significant impact on the lives of adolescents and young adults. According to the Centers for Disease Control and Prevention’s (CDC) 2021 surveillance report, rates of gonorrhea and syphilis in the United States were at their highest since the early 1990s. Chlamydia, one of the most common STIs, had a peak rate in 2019, but more recent rates may have been impacted by the COVID-19 pandemic. In 2021, those 15-24 years of age accounted for 58.5% of all chlamydia infections, 40.4% of all gonorrhea infections, and 18.3% of all syphilis infections in the US.
While pediatricians should discuss sexual health and STI screening with all their adolescent and young adult patients, LGBTQ+ youth are disproportionately impacted by STIs. For example, cisgender men who have sex with men have significantly higher rates of HIV, gonorrhea, and syphilis. These disparities are likely related to unequal access to care, systemic homophobia/transphobia, stigma, and differences in sexual networks and are even more pronounced for those with intersectional minoritized identities such as LGBTQ+ youth of color.1
In the past 12 years, there have been significant advances in HIV prevention methods, including the approval and use of pre-exposure prophylaxis or “PrEP” (a medication regimen that is taken on an ongoing basis to provide highly effective protection against HIV infection) and more widespread use of post-exposure prophylaxis or “PEP” (a medication regimen taken for 1 month after a potential exposure to HIV to prevent HIV from establishing an ongoing infection) outside of the medical setting. While these interventions have the potential to decrease rates of HIV infection, they do not prevent any other STIs.2-3
The current strategies to prevent bacterial STIs include discussions of sexual practices, counseling on risk reduction strategies such as decreased number of partners and condom use, routine screening in those at risk every 3-12 months, and timely diagnosis and treatment of infections in patients and their partners to avoid further transmission.4 Given the increasing rates of bacterial STIs (gonorrhea, chlamydia, and syphilis), additional biomedical prevention methods are greatly needed.
Doxycycline as post-exposure prophylaxis
Doxycycline is a tetracycline antibiotic effective against a wide range of bacteria and is commonly used in the treatment of acne, skin infections, Lyme disease, and STIs, and can also be used in the treatment and prevention of malaria.5 For STIs, doxycycline is currently the recommended treatment for chlamydia and is also an alternate therapy for syphilis in nonpregnant patients when penicillin is not accessible or in those with severe penicillin allergy.4 This medication is often well tolerated with the most common side effects including gastrointestinal irritation and photosensitivity. Doxycycline is contraindicated in pregnancy due to its potential impact on tooth and bone development.5
Given its general tolerability and activity against bacterial STIs, new and emerging studies have examined doxycycline as post-exposure prophylaxis (DoxyPEP: one dose of doxycycline 200 mg PO within 72 hours after unprotected sex) in an attempt to decrease the incidence of new bacterial STIs in populations at risk. Three of the studies cited in the preliminary CDC DoxyPEP guidelines were conducted in cisgender men who have sex with men and transgender women either living with HIV or taking PrEP for HIV prevention. All three studies demonstrated significantly lower risk of chlamydia and syphilis, while two of the studies also showed a significantly lower risk of gonorrhea. One additional study was conducted in cisgender women in Kenya. This study did not show any statistically significant difference in the risk of chlamydia or gonorrhea in the intervention group, but may have been limited by low adherence to the DoxyPEP regimen. There were no serious adverse events reported in any of the studies attributed to doxycycline.6
Avoiding antibiotic resistance
With the increased use of antibiotics, attention must always be paid to the potential for increasing antibiotic resistance. The preliminary CDC DoxyPEP guidelines outline mixed results in the DoxyPEP studies that had limited follow-up timeframes, making it difficult to draw conclusions: “Current data suggest overall benefit of the use of doxycycline PEP, but potential risks related to the development of resistance and impacts on the microbiome will need to be closely monitored after implementation of these guidelines.” Official guideline recommendations from the CDC regarding DoxyPEP are currently pending after a period of public comment on the preliminary drafted guidelines.6 However, the New York State Department of Health AIDS Institute released guidelines for DoxyPEP in September 2023 and several large urban public health departments have also issued their own guidance that largely align with the preliminary CDC guidelines.7
Recommendations currently emphasize that the goal is to allow for implementation of DoxyPEP in those who would benefit the most from the intervention (i.e., cisgender men who have sex with men and transgender women with a history of at least one bacterial STI in the last 12 months with ongoing risk of infection), while also minimizing antibiotic use. It should also be considered for those without a recent infection who have increased likelihood of exposure to bacterial STIs. DoxyPEP is likely to be effective in other populations (e.g., cisgender women, cisgender men who have sex with women, transgender men), but data are currently limited, and the risk/benefit ratio may be different in these populations. The recommended dose for DoxyPEP is doxycycline 200 mg once as soon as possible (within 72 hours) of unprotected oral, vaginal, or anal sex with a maximum of one dose every 24 hours. For those being prescribed DoxyPEP, gonorrhea and chlamydia screening of all anatomic sites of exposure (urine sample or frontal swab, throat swab, and/or rectal swab) should be conducted at baseline and then every 3-6 months in addition to blood testing for syphilis and HIV if indicated.6-7
Another option in our toolkit
DoxyPEP should be viewed as one more option in our toolkit of sexual health services alongside risk reduction strategies (e.g., open discussions with partners, decreased number of partners, and condom use), routine STI screening and treatment, PrEP and PEP for HIV prevention, and pregnancy prevention. Not all of these tools will be relevant to each individual and discussions around sexual health should be patient-centered and focused on their own personal goals. As pediatricians, we should provide guidance to all adolescents and young adults on options to improve their sexual health and empower them to embrace their bodily autonomy.
Dr. Warus is in the division of adolescent and young adult medicine at Children’s Hospital of Los Angeles, where he specializes in care for transgender and gender-nonconforming youth, and LGBTQ health for youth. He is an assistant professor of pediatrics at USC.
Resources
CDC – Sexually Transmitted Infection Treatment Guidelines, 2021
CDC – [Preliminary] Guidelines for the Use of Doxycycline Post-Exposure Prophylaxis for Bacterial Sexually Transmitted Infection (STI) Prevention
New York State Department of Health AIDS Institute – Doxycycline Post-Exposure Prophylaxis to Prevent Bacterial Sexually Transmitted Infections
Los Angeles County Department of Public Health – DoxyPEP for STI Prevention
References
1. Division of STD Prevention, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2021: National Overview of STDs, 2021. Last Reviewed May 16, 2023.
2. Centers for Disease Control and Prevention: US Public Health Service: Preexposure Prophylaxis for the Prevention of HIV Infection in the United States – 2021 Update: A Clinical Practice Guideline. Published 2021.
3. Centers for Disease Control and Prevention: US Department of Health and Human Services: Updated Guidelines for Antiretroviral Postexposure Prophylaxis After Sexual, Injection Drug Use, or Other Nonoccupational Exposure to HIV – United States, 2016. Published 2016. .
4. Workowski KA et al. Sexually Transmitted Infection Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):2-10.
5. Patel RS and Parmar M. Doxycycline Hyclate. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Last Updated May 22, 2023.
6. Centers for Disease Control and Prevention. [Preliminary] Guidelines for the Use of Doxycycline Post-Exposure Prophylaxis for Bacterial Sexually Transmitted Infection (STI) Prevention. Published Oct 1, 2023.
7. DiMarco DE, et al. Doxycycline Post-Exposure Prophylaxis to Prevent Bacterial Sexually Transmitted Infections. New York State Department of Health AIDS Institute. Published September 25, 2023.
Commentary: Drug Comparisons and Contact Allergy in AD, February 2024

But here's the thing: We should not be making clinical judgments on the basis of differences in relative risk; clinical decisions should be based on absolute risks. Should we worry about VTE risk when treating patients with AD? This paper did not focus on absolute risk, but we can get an idea of the absolute risk by looking at the data presented in the figures in the paper. The risk for VTE in patients without AD was about 1 in 400, whereas with AD the risk was about 1 in 300, even before controlling for risk factors. This rate is sufficiently low for both groups that it doesn't seem like this risk would affect whether we would use a drug that might be associated with some minimal or theoretical increased risk for VTE.
The bottom line is that the findings of this study are reassuring, at least to me.
I'm already convinced that dupilumab is a very safe treatment for our patients with AD. The study by Simpson and colleagues looked at data from a registry of patients followed in real-life practice. The 2-year study showed no new concerns for dupilumab treatment of AD. The most common adverse event was conjunctivitis, and that was seen in only 2.4% of the patients. Perhaps the most interesting finding was that 83% of the patients who started in the study were still on dupilumab treatment at the end of 2 years. Dupilumab has a good level of efficacy and safety such that the great majority of patients who start on it seem to do well.
Dupilumab is a highly effective, very safe treatment for AD. Rademikibart Is another interleukin-4 receptor alpha-chain blocker. Not surprisingly, rademikibart also seems to be an effective, safe treatment for AD (Silverberg et al). Rademikibart may serve as another option for AD, and I imagine that it could be used if a patient on dupilumab were to develop an anti-drug antibody and lose effectiveness.
The very interesting analysis by Silverberg and colleagues looks at a new way to compare the effectiveness of different drugs for AD. They use this new approach to compare upadacitinib and dupilumab. What they found, not surprisingly, was that upadacitinib was generally more effective for AD than dupilumab. I used to think I would never see anything more effective for AD than dupilumab, but, clearly, based on head-to-head trials, upadacitinib is more effective for AD than is dupilumab. But does that greater efficacy mean that we should use upadacitinib first? We need to consider safety, too. Dupilumab works well enough for the great majority of patients and is extremely safe. I think upadacitinib is a great choice for patients who did not respond to dupilumab and could also be considered for those patients who want to take the most effective treatment option.
Trimeche and colleagues' study of contact allergens in patients with AD may change how I practice. In this study, 60% of the AD patients had positive patch test results of which 71% were considered relevant. The most frequent allergens included textile dye mix (25%), nickel (20%), cobalt (13%), isothiazolinone (9%), quanterium-15 (4%), and balsam of Peru (4%). Two patients were allergic to corticosteroids. Avoidance of relevant allergens resulted in improvement. I need to warn my AD patients to be on the lookout for contact allergens that may be causing or exacerbating their skin disease.
But here's the thing: We should not be making clinical judgments on the basis of differences in relative risk; clinical decisions should be based on absolute risks. Should we worry about VTE risk when treating patients with AD? This paper did not focus on absolute risk, but we can get an idea of the absolute risk by looking at the data presented in the figures in the paper. The risk for VTE in patients without AD was about 1 in 400, whereas with AD the risk was about 1 in 300, even before controlling for risk factors. This rate is sufficiently low for both groups that it doesn't seem like this risk would affect whether we would use a drug that might be associated with some minimal or theoretical increased risk for VTE.
The bottom line is that the findings of this study are reassuring, at least to me.
I'm already convinced that dupilumab is a very safe treatment for our patients with AD. The study by Simpson and colleagues looked at data from a registry of patients followed in real-life practice. The 2-year study showed no new concerns for dupilumab treatment of AD. The most common adverse event was conjunctivitis, and that was seen in only 2.4% of the patients. Perhaps the most interesting finding was that 83% of the patients who started in the study were still on dupilumab treatment at the end of 2 years. Dupilumab has a good level of efficacy and safety such that the great majority of patients who start on it seem to do well.
Dupilumab is a highly effective, very safe treatment for AD. Rademikibart Is another interleukin-4 receptor alpha-chain blocker. Not surprisingly, rademikibart also seems to be an effective, safe treatment for AD (Silverberg et al). Rademikibart may serve as another option for AD, and I imagine that it could be used if a patient on dupilumab were to develop an anti-drug antibody and lose effectiveness.
The very interesting analysis by Silverberg and colleagues looks at a new way to compare the effectiveness of different drugs for AD. They use this new approach to compare upadacitinib and dupilumab. What they found, not surprisingly, was that upadacitinib was generally more effective for AD than dupilumab. I used to think I would never see anything more effective for AD than dupilumab, but, clearly, based on head-to-head trials, upadacitinib is more effective for AD than is dupilumab. But does that greater efficacy mean that we should use upadacitinib first? We need to consider safety, too. Dupilumab works well enough for the great majority of patients and is extremely safe. I think upadacitinib is a great choice for patients who did not respond to dupilumab and could also be considered for those patients who want to take the most effective treatment option.
Trimeche and colleagues' study of contact allergens in patients with AD may change how I practice. In this study, 60% of the AD patients had positive patch test results of which 71% were considered relevant. The most frequent allergens included textile dye mix (25%), nickel (20%), cobalt (13%), isothiazolinone (9%), quanterium-15 (4%), and balsam of Peru (4%). Two patients were allergic to corticosteroids. Avoidance of relevant allergens resulted in improvement. I need to warn my AD patients to be on the lookout for contact allergens that may be causing or exacerbating their skin disease.
But here's the thing: We should not be making clinical judgments on the basis of differences in relative risk; clinical decisions should be based on absolute risks. Should we worry about VTE risk when treating patients with AD? This paper did not focus on absolute risk, but we can get an idea of the absolute risk by looking at the data presented in the figures in the paper. The risk for VTE in patients without AD was about 1 in 400, whereas with AD the risk was about 1 in 300, even before controlling for risk factors. This rate is sufficiently low for both groups that it doesn't seem like this risk would affect whether we would use a drug that might be associated with some minimal or theoretical increased risk for VTE.
The bottom line is that the findings of this study are reassuring, at least to me.
I'm already convinced that dupilumab is a very safe treatment for our patients with AD. The study by Simpson and colleagues looked at data from a registry of patients followed in real-life practice. The 2-year study showed no new concerns for dupilumab treatment of AD. The most common adverse event was conjunctivitis, and that was seen in only 2.4% of the patients. Perhaps the most interesting finding was that 83% of the patients who started in the study were still on dupilumab treatment at the end of 2 years. Dupilumab has a good level of efficacy and safety such that the great majority of patients who start on it seem to do well.
Dupilumab is a highly effective, very safe treatment for AD. Rademikibart Is another interleukin-4 receptor alpha-chain blocker. Not surprisingly, rademikibart also seems to be an effective, safe treatment for AD (Silverberg et al). Rademikibart may serve as another option for AD, and I imagine that it could be used if a patient on dupilumab were to develop an anti-drug antibody and lose effectiveness.
The very interesting analysis by Silverberg and colleagues looks at a new way to compare the effectiveness of different drugs for AD. They use this new approach to compare upadacitinib and dupilumab. What they found, not surprisingly, was that upadacitinib was generally more effective for AD than dupilumab. I used to think I would never see anything more effective for AD than dupilumab, but, clearly, based on head-to-head trials, upadacitinib is more effective for AD than is dupilumab. But does that greater efficacy mean that we should use upadacitinib first? We need to consider safety, too. Dupilumab works well enough for the great majority of patients and is extremely safe. I think upadacitinib is a great choice for patients who did not respond to dupilumab and could also be considered for those patients who want to take the most effective treatment option.
Trimeche and colleagues' study of contact allergens in patients with AD may change how I practice. In this study, 60% of the AD patients had positive patch test results of which 71% were considered relevant. The most frequent allergens included textile dye mix (25%), nickel (20%), cobalt (13%), isothiazolinone (9%), quanterium-15 (4%), and balsam of Peru (4%). Two patients were allergic to corticosteroids. Avoidance of relevant allergens resulted in improvement. I need to warn my AD patients to be on the lookout for contact allergens that may be causing or exacerbating their skin disease.
A Military Nurse Saves a Life After a Brutal Rollover Crash
Emergencies happen anywhere and anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a series telling these stories.
A week earlier I’d had a heart surgery and was heading out for a post-op appointment when I saw it: I had a flat tire. It didn’t make sense. The tire was brand new, and there was no puncture. But it was flat.
I swapped out the flat for the spare and went off base to a tire shop. While I was there, my surgeon’s office called and rescheduled my appointment for a couple of hours later. That was lucky because by the time the tire was fixed, I had just enough time to get there.
The hospital is right near I-35 in San Antonio, Texas. I got off the freeway and onto the access road and paused to turn into the parking lot. That’s when I heard an enormous crash.
I saw a big poof of white smoke, and a car barreled off the freeway and came rolling down the embankment.
When the car hit the access road, I saw a woman ejected through the windshield. She bounced and landed in the road about 25 feet in front of me.
I put my car in park, grabbed my face mask and gloves, and started running toward her. But another vehicle — a truck towing a trailer — came from behind to drive around me. The driver didn’t realize what had happened and couldn’t stop in time…
The trailer ran over her.
I didn’t know if anyone could’ve survived that, but I went to her. I saw several other bystanders, but they were frozen in shock. I was praying, dear God, if she’s alive, let me do whatever I need to do to save her life.
It was a horrible scene. This poor lady was in a bloody heap in the middle of the road. Her right arm was twisted up under her neck so tightly, she was choking herself. So, the first thing I did was straighten her arm out to protect her airway.
I started yelling at people, “Call 9-1-1! Run to the hospital! Let them know there’s an accident out here, and I need help!”
The woman had a pulse, but it was super rapid. On first glance, she clearly had multiple fractures and a bad head bleed. With the sheer number of times she’d been injured, I didn’t know what was going on internally, but it was bad. She was gargling on her own blood and spitting it up. She was drowning.
A couple of technicians from the hospital came and brought me a tiny emergency kit. It had a blood pressure cuff and an oral airway. All the vital signs indicated the lady was going into shock. She’d lost a lot of blood on the pavement.
I was able to get the oral airway in. A few minutes later, a fire chief showed up. By now, the traffic had backed up so badly, the emergency vehicles couldn’t get in. But he managed to get there another way and gave me a cervical collar (C collar) and an Ambu bag.
I was hyper-focused on what I could do at that moment and what I needed to do next. Her stats were going down, but she still had a pulse. If she lost the pulse or went into a lethal rhythm, I’d have to start cardiopulmonary resuscitation (CPR). I asked the other people, but nobody else knew CPR, so I wouldn’t have help.
I could tell the lady had a pelvic fracture, and we needed to stabilize her. I directed people how to hold her neck safely and log-roll her flat on the ground. I also needed to put pressure on the back of her head because of all the bleeding. I got people to give me their clothes and tried to do that as I was bagging her.
The windows of her vehicle had all been blown out. I asked somebody to go find her purse with her ID. Then I noticed something …
My heart jumped into my stomach.
A car seat. There was an empty child’s car seat in the back of the car.
I started yelling at everyone, “Look for a baby! Go up and down the embankment and across the road. There might have been a baby in the car!”
But there wasn’t. Thank God. She hadn’t been driving with her child.
At that point, a paramedic came running from behind all the traffic. We did life support together until the ambulance finally arrived.
Emergency medical services got an intravenous line in and used medical anti-shock trousers. Thankfully, I already had the C collar on, and we’d been bagging her, so they could load her very quickly.
I got rid of my bloody gloves. I told a police officer I would come back. And then I went to my doctor’s appointment.
The window at my doctor’s office faced the access road, so the people there had seen all the traffic. They asked me what happened, and I said, “It was me. I saw it happen. I tried to help.” I was a little frazzled.
When I got back to the scene, the police and the fire chief kept thanking me for stopping. Why wouldn’t I stop? It was astounding to realize that they imagined somebody wouldn’t stop in a situation like this.
They told me the lady was alive. She was in the intensive care unit in critical condition, but she had survived. At that moment, I had this overwhelming feeling: God had put me in this exact place at the exact time to save her life.
Looking back, I think about how God ordered my steps. Without the mysterious flat tire, I would’ve gone to the hospital earlier. If my appointment hadn’t been rescheduled, I wouldn’t have been on the access road. All those events brought me there.
Several months later, the woman’s family contacted me and asked if we could meet. I found out more about her injuries. She’d had multiple skull fractures, facial fractures, and a broken jaw. Her upper arm was broken in three places. Her clavicle was broken. She had internal bleeding, a pelvic fracture, and a broken leg. She was 28 years old.
She’d had multiple surgeries, spent 2 months in the ICU, and another 3 months in intensive rehab. But she survived. It was incredible.
We all met up at a McDonald’s. First, her little son — who was the baby I thought might have been in the car — ran up to me and said, “Thank you for saving my mommy’s life.”
Then I turned, and there she was — a beautiful lady looking at me with awe and crying, saying, “It’s me.”
She obviously had gone through a transformation from all the injuries and the medications. She had a little bit of a speech delay, but mentally, she was there. She could walk.
She said, “You’re my angel. God put you there to save my life.” Her family all came up and hugged me. It was so beautiful.
She told me about the accident. She’d been speeding that day, zigzagging through lanes to get around the traffic. And she didn’t have her seatbelt on. She’d driven onto the shoulder to try to pass everyone, but it started narrowing. She clipped somebody’s bumper, went into a tailspin, and collided with a second vehicle, which caused her to flip over and down the embankment.
“God’s given me a new lease on life,” she said, “a fresh start. I will forever wear my seatbelt. And I’m going to do whatever I can to give back to other people because I don’t even feel like I deserve this.”
I just cried.
I’ve been a nurse for 29 years, first on the civilian side and later in the military. I’ve led codes and responded to trauma in a hospital setting or a deployed environment. I was well prepared to do what I did. But doing it under such stress with adrenaline bombarding me ... I’m amazed. I just think God’s hand was on me.
At that time, I was personally going through some things. After my heart surgery, I was in an emotional place where I didn’t feel loved or valued. But when I had that realization — when I knew that I was meant to be there to save her life, I also got the very clear message that I was valued and loved so much.
I know I have a very strong purpose. That day changed my life.
US Air Force Lt. Col. Anne Staley is the officer in charge of the Military Training Network, a division of the Defense Health Agency Education and Training Directorate in San Antonio, Texas.
A version of this article appeared on Medscape.com.
Emergencies happen anywhere and anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a series telling these stories.
A week earlier I’d had a heart surgery and was heading out for a post-op appointment when I saw it: I had a flat tire. It didn’t make sense. The tire was brand new, and there was no puncture. But it was flat.
I swapped out the flat for the spare and went off base to a tire shop. While I was there, my surgeon’s office called and rescheduled my appointment for a couple of hours later. That was lucky because by the time the tire was fixed, I had just enough time to get there.
The hospital is right near I-35 in San Antonio, Texas. I got off the freeway and onto the access road and paused to turn into the parking lot. That’s when I heard an enormous crash.
I saw a big poof of white smoke, and a car barreled off the freeway and came rolling down the embankment.
When the car hit the access road, I saw a woman ejected through the windshield. She bounced and landed in the road about 25 feet in front of me.
I put my car in park, grabbed my face mask and gloves, and started running toward her. But another vehicle — a truck towing a trailer — came from behind to drive around me. The driver didn’t realize what had happened and couldn’t stop in time…
The trailer ran over her.
I didn’t know if anyone could’ve survived that, but I went to her. I saw several other bystanders, but they were frozen in shock. I was praying, dear God, if she’s alive, let me do whatever I need to do to save her life.
It was a horrible scene. This poor lady was in a bloody heap in the middle of the road. Her right arm was twisted up under her neck so tightly, she was choking herself. So, the first thing I did was straighten her arm out to protect her airway.
I started yelling at people, “Call 9-1-1! Run to the hospital! Let them know there’s an accident out here, and I need help!”
The woman had a pulse, but it was super rapid. On first glance, she clearly had multiple fractures and a bad head bleed. With the sheer number of times she’d been injured, I didn’t know what was going on internally, but it was bad. She was gargling on her own blood and spitting it up. She was drowning.
A couple of technicians from the hospital came and brought me a tiny emergency kit. It had a blood pressure cuff and an oral airway. All the vital signs indicated the lady was going into shock. She’d lost a lot of blood on the pavement.
I was able to get the oral airway in. A few minutes later, a fire chief showed up. By now, the traffic had backed up so badly, the emergency vehicles couldn’t get in. But he managed to get there another way and gave me a cervical collar (C collar) and an Ambu bag.
I was hyper-focused on what I could do at that moment and what I needed to do next. Her stats were going down, but she still had a pulse. If she lost the pulse or went into a lethal rhythm, I’d have to start cardiopulmonary resuscitation (CPR). I asked the other people, but nobody else knew CPR, so I wouldn’t have help.
I could tell the lady had a pelvic fracture, and we needed to stabilize her. I directed people how to hold her neck safely and log-roll her flat on the ground. I also needed to put pressure on the back of her head because of all the bleeding. I got people to give me their clothes and tried to do that as I was bagging her.
The windows of her vehicle had all been blown out. I asked somebody to go find her purse with her ID. Then I noticed something …
My heart jumped into my stomach.
A car seat. There was an empty child’s car seat in the back of the car.
I started yelling at everyone, “Look for a baby! Go up and down the embankment and across the road. There might have been a baby in the car!”
But there wasn’t. Thank God. She hadn’t been driving with her child.
At that point, a paramedic came running from behind all the traffic. We did life support together until the ambulance finally arrived.
Emergency medical services got an intravenous line in and used medical anti-shock trousers. Thankfully, I already had the C collar on, and we’d been bagging her, so they could load her very quickly.
I got rid of my bloody gloves. I told a police officer I would come back. And then I went to my doctor’s appointment.
The window at my doctor’s office faced the access road, so the people there had seen all the traffic. They asked me what happened, and I said, “It was me. I saw it happen. I tried to help.” I was a little frazzled.
When I got back to the scene, the police and the fire chief kept thanking me for stopping. Why wouldn’t I stop? It was astounding to realize that they imagined somebody wouldn’t stop in a situation like this.
They told me the lady was alive. She was in the intensive care unit in critical condition, but she had survived. At that moment, I had this overwhelming feeling: God had put me in this exact place at the exact time to save her life.
Looking back, I think about how God ordered my steps. Without the mysterious flat tire, I would’ve gone to the hospital earlier. If my appointment hadn’t been rescheduled, I wouldn’t have been on the access road. All those events brought me there.
Several months later, the woman’s family contacted me and asked if we could meet. I found out more about her injuries. She’d had multiple skull fractures, facial fractures, and a broken jaw. Her upper arm was broken in three places. Her clavicle was broken. She had internal bleeding, a pelvic fracture, and a broken leg. She was 28 years old.
She’d had multiple surgeries, spent 2 months in the ICU, and another 3 months in intensive rehab. But she survived. It was incredible.
We all met up at a McDonald’s. First, her little son — who was the baby I thought might have been in the car — ran up to me and said, “Thank you for saving my mommy’s life.”
Then I turned, and there she was — a beautiful lady looking at me with awe and crying, saying, “It’s me.”
She obviously had gone through a transformation from all the injuries and the medications. She had a little bit of a speech delay, but mentally, she was there. She could walk.
She said, “You’re my angel. God put you there to save my life.” Her family all came up and hugged me. It was so beautiful.
She told me about the accident. She’d been speeding that day, zigzagging through lanes to get around the traffic. And she didn’t have her seatbelt on. She’d driven onto the shoulder to try to pass everyone, but it started narrowing. She clipped somebody’s bumper, went into a tailspin, and collided with a second vehicle, which caused her to flip over and down the embankment.
“God’s given me a new lease on life,” she said, “a fresh start. I will forever wear my seatbelt. And I’m going to do whatever I can to give back to other people because I don’t even feel like I deserve this.”
I just cried.
I’ve been a nurse for 29 years, first on the civilian side and later in the military. I’ve led codes and responded to trauma in a hospital setting or a deployed environment. I was well prepared to do what I did. But doing it under such stress with adrenaline bombarding me ... I’m amazed. I just think God’s hand was on me.
At that time, I was personally going through some things. After my heart surgery, I was in an emotional place where I didn’t feel loved or valued. But when I had that realization — when I knew that I was meant to be there to save her life, I also got the very clear message that I was valued and loved so much.
I know I have a very strong purpose. That day changed my life.
US Air Force Lt. Col. Anne Staley is the officer in charge of the Military Training Network, a division of the Defense Health Agency Education and Training Directorate in San Antonio, Texas.
A version of this article appeared on Medscape.com.
Emergencies happen anywhere and anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a series telling these stories.
A week earlier I’d had a heart surgery and was heading out for a post-op appointment when I saw it: I had a flat tire. It didn’t make sense. The tire was brand new, and there was no puncture. But it was flat.
I swapped out the flat for the spare and went off base to a tire shop. While I was there, my surgeon’s office called and rescheduled my appointment for a couple of hours later. That was lucky because by the time the tire was fixed, I had just enough time to get there.
The hospital is right near I-35 in San Antonio, Texas. I got off the freeway and onto the access road and paused to turn into the parking lot. That’s when I heard an enormous crash.
I saw a big poof of white smoke, and a car barreled off the freeway and came rolling down the embankment.
When the car hit the access road, I saw a woman ejected through the windshield. She bounced and landed in the road about 25 feet in front of me.
I put my car in park, grabbed my face mask and gloves, and started running toward her. But another vehicle — a truck towing a trailer — came from behind to drive around me. The driver didn’t realize what had happened and couldn’t stop in time…
The trailer ran over her.
I didn’t know if anyone could’ve survived that, but I went to her. I saw several other bystanders, but they were frozen in shock. I was praying, dear God, if she’s alive, let me do whatever I need to do to save her life.
It was a horrible scene. This poor lady was in a bloody heap in the middle of the road. Her right arm was twisted up under her neck so tightly, she was choking herself. So, the first thing I did was straighten her arm out to protect her airway.
I started yelling at people, “Call 9-1-1! Run to the hospital! Let them know there’s an accident out here, and I need help!”
The woman had a pulse, but it was super rapid. On first glance, she clearly had multiple fractures and a bad head bleed. With the sheer number of times she’d been injured, I didn’t know what was going on internally, but it was bad. She was gargling on her own blood and spitting it up. She was drowning.
A couple of technicians from the hospital came and brought me a tiny emergency kit. It had a blood pressure cuff and an oral airway. All the vital signs indicated the lady was going into shock. She’d lost a lot of blood on the pavement.
I was able to get the oral airway in. A few minutes later, a fire chief showed up. By now, the traffic had backed up so badly, the emergency vehicles couldn’t get in. But he managed to get there another way and gave me a cervical collar (C collar) and an Ambu bag.
I was hyper-focused on what I could do at that moment and what I needed to do next. Her stats were going down, but she still had a pulse. If she lost the pulse or went into a lethal rhythm, I’d have to start cardiopulmonary resuscitation (CPR). I asked the other people, but nobody else knew CPR, so I wouldn’t have help.
I could tell the lady had a pelvic fracture, and we needed to stabilize her. I directed people how to hold her neck safely and log-roll her flat on the ground. I also needed to put pressure on the back of her head because of all the bleeding. I got people to give me their clothes and tried to do that as I was bagging her.
The windows of her vehicle had all been blown out. I asked somebody to go find her purse with her ID. Then I noticed something …
My heart jumped into my stomach.
A car seat. There was an empty child’s car seat in the back of the car.
I started yelling at everyone, “Look for a baby! Go up and down the embankment and across the road. There might have been a baby in the car!”
But there wasn’t. Thank God. She hadn’t been driving with her child.
At that point, a paramedic came running from behind all the traffic. We did life support together until the ambulance finally arrived.
Emergency medical services got an intravenous line in and used medical anti-shock trousers. Thankfully, I already had the C collar on, and we’d been bagging her, so they could load her very quickly.
I got rid of my bloody gloves. I told a police officer I would come back. And then I went to my doctor’s appointment.
The window at my doctor’s office faced the access road, so the people there had seen all the traffic. They asked me what happened, and I said, “It was me. I saw it happen. I tried to help.” I was a little frazzled.
When I got back to the scene, the police and the fire chief kept thanking me for stopping. Why wouldn’t I stop? It was astounding to realize that they imagined somebody wouldn’t stop in a situation like this.
They told me the lady was alive. She was in the intensive care unit in critical condition, but she had survived. At that moment, I had this overwhelming feeling: God had put me in this exact place at the exact time to save her life.
Looking back, I think about how God ordered my steps. Without the mysterious flat tire, I would’ve gone to the hospital earlier. If my appointment hadn’t been rescheduled, I wouldn’t have been on the access road. All those events brought me there.
Several months later, the woman’s family contacted me and asked if we could meet. I found out more about her injuries. She’d had multiple skull fractures, facial fractures, and a broken jaw. Her upper arm was broken in three places. Her clavicle was broken. She had internal bleeding, a pelvic fracture, and a broken leg. She was 28 years old.
She’d had multiple surgeries, spent 2 months in the ICU, and another 3 months in intensive rehab. But she survived. It was incredible.
We all met up at a McDonald’s. First, her little son — who was the baby I thought might have been in the car — ran up to me and said, “Thank you for saving my mommy’s life.”
Then I turned, and there she was — a beautiful lady looking at me with awe and crying, saying, “It’s me.”
She obviously had gone through a transformation from all the injuries and the medications. She had a little bit of a speech delay, but mentally, she was there. She could walk.
She said, “You’re my angel. God put you there to save my life.” Her family all came up and hugged me. It was so beautiful.
She told me about the accident. She’d been speeding that day, zigzagging through lanes to get around the traffic. And she didn’t have her seatbelt on. She’d driven onto the shoulder to try to pass everyone, but it started narrowing. She clipped somebody’s bumper, went into a tailspin, and collided with a second vehicle, which caused her to flip over and down the embankment.
“God’s given me a new lease on life,” she said, “a fresh start. I will forever wear my seatbelt. And I’m going to do whatever I can to give back to other people because I don’t even feel like I deserve this.”
I just cried.
I’ve been a nurse for 29 years, first on the civilian side and later in the military. I’ve led codes and responded to trauma in a hospital setting or a deployed environment. I was well prepared to do what I did. But doing it under such stress with adrenaline bombarding me ... I’m amazed. I just think God’s hand was on me.
At that time, I was personally going through some things. After my heart surgery, I was in an emotional place where I didn’t feel loved or valued. But when I had that realization — when I knew that I was meant to be there to save her life, I also got the very clear message that I was valued and loved so much.
I know I have a very strong purpose. That day changed my life.
US Air Force Lt. Col. Anne Staley is the officer in charge of the Military Training Network, a division of the Defense Health Agency Education and Training Directorate in San Antonio, Texas.
A version of this article appeared on Medscape.com.
Shelf Life for Opioid Overdose Drug Naloxone Extended
At the request of the US Food and Drug Administration (FDA), Emergent BioSolutions has extended the shelf life of the rapid opioid overdose reversal agent, naloxone (4 mg) nasal spray (Narcan), from 3 to 4 years.
Naloxone is “an important tool” in addressing opioid overdoses, and this extension supports the FDA’s “efforts to ensure more OTC naloxone products remain available to the public,” Marta Sokolowska, PhD, with the FDA Center for Drug Evaluation and Research, said in a statement.
Naloxone nasal spray was first approved by the FDA in 2015 as a prescription drug. Last spring, the agency approved the drug for over-the-counter use.
“The shelf life of products that were produced and distributed prior to this announcement is not affected and remains unchanged. Prescribers, patients, and caregivers are advised to continue to abide by the expiration date printed on each product’s packaging and within the product’s labeling,” the FDA advised.
“FDA’s request for this shelf-life extension is a testament to the agency’s continuing progress toward implementing the FDA Overdose Prevention Framework, which provides our vision to undertake impactful, creative actions to encourage harm reduction and innovation in reducing controlled substance-related overdoses and deaths,” the agency said.
According to the US Centers for Disease Control and Prevention, from 1999 to 2021, nearly 645,000 people died from an overdose involving any opioid, including prescription and illicit opioids.
A version of this article appeared on Medscape.com.
At the request of the US Food and Drug Administration (FDA), Emergent BioSolutions has extended the shelf life of the rapid opioid overdose reversal agent, naloxone (4 mg) nasal spray (Narcan), from 3 to 4 years.
Naloxone is “an important tool” in addressing opioid overdoses, and this extension supports the FDA’s “efforts to ensure more OTC naloxone products remain available to the public,” Marta Sokolowska, PhD, with the FDA Center for Drug Evaluation and Research, said in a statement.
Naloxone nasal spray was first approved by the FDA in 2015 as a prescription drug. Last spring, the agency approved the drug for over-the-counter use.
“The shelf life of products that were produced and distributed prior to this announcement is not affected and remains unchanged. Prescribers, patients, and caregivers are advised to continue to abide by the expiration date printed on each product’s packaging and within the product’s labeling,” the FDA advised.
“FDA’s request for this shelf-life extension is a testament to the agency’s continuing progress toward implementing the FDA Overdose Prevention Framework, which provides our vision to undertake impactful, creative actions to encourage harm reduction and innovation in reducing controlled substance-related overdoses and deaths,” the agency said.
According to the US Centers for Disease Control and Prevention, from 1999 to 2021, nearly 645,000 people died from an overdose involving any opioid, including prescription and illicit opioids.
A version of this article appeared on Medscape.com.
At the request of the US Food and Drug Administration (FDA), Emergent BioSolutions has extended the shelf life of the rapid opioid overdose reversal agent, naloxone (4 mg) nasal spray (Narcan), from 3 to 4 years.
Naloxone is “an important tool” in addressing opioid overdoses, and this extension supports the FDA’s “efforts to ensure more OTC naloxone products remain available to the public,” Marta Sokolowska, PhD, with the FDA Center for Drug Evaluation and Research, said in a statement.
Naloxone nasal spray was first approved by the FDA in 2015 as a prescription drug. Last spring, the agency approved the drug for over-the-counter use.
“The shelf life of products that were produced and distributed prior to this announcement is not affected and remains unchanged. Prescribers, patients, and caregivers are advised to continue to abide by the expiration date printed on each product’s packaging and within the product’s labeling,” the FDA advised.
“FDA’s request for this shelf-life extension is a testament to the agency’s continuing progress toward implementing the FDA Overdose Prevention Framework, which provides our vision to undertake impactful, creative actions to encourage harm reduction and innovation in reducing controlled substance-related overdoses and deaths,” the agency said.
According to the US Centers for Disease Control and Prevention, from 1999 to 2021, nearly 645,000 people died from an overdose involving any opioid, including prescription and illicit opioids.
A version of this article appeared on Medscape.com.
Even Intentional Weight Loss Linked With Cancer
This transcript has been edited for clarity.
As anyone who has been through medical training will tell you, some little scenes just stick with you. I had been seeing a patient in our resident clinic in West Philly for a couple of years. She was in her mid-60s with diabetes and hypertension and a distant smoking history. She was overweight and had been trying to improve her diet and lose weight since I started seeing her. One day she came in and was delighted to report that she had finally started shedding some pounds — about 15 in the past 2 months.
I enthusiastically told my preceptor that my careful dietary counseling had finally done the job. She looked through the chart for a moment and asked, “Is she up to date on her cancer screening?” A workup revealed adenocarcinoma of the lung. The patient did well, actually, but the story stuck with me.
The textbooks call it “unintentional weight loss,” often in big, scary letters, and every doctor will go just a bit pale if a patient tells them that, despite efforts not to, they are losing weight. But true unintentional weight loss is not that common. After all, most of us are at least half-heartedly trying to lose weight all the time. Should doctors be worried when we are successful?
A new study suggests that perhaps they should. We’re talking about this study, appearing in JAMA, which combined participants from two long-running observational cohorts: 120,000 women from the Nurses’ Health Study, and 50,000 men from the Health Professionals Follow-Up Study. (These cohorts started in the 1970s and 1980s, so we’ll give them a pass on the gender-specific study designs.)
The rationale of enrolling healthcare providers in these cohort studies is that they would be reliable witnesses of their own health status. If a nurse or doctor says they have pancreatic cancer, it’s likely that they truly have pancreatic cancer. Detailed health surveys were distributed to the participants every other year, and the average follow-up was more than a decade.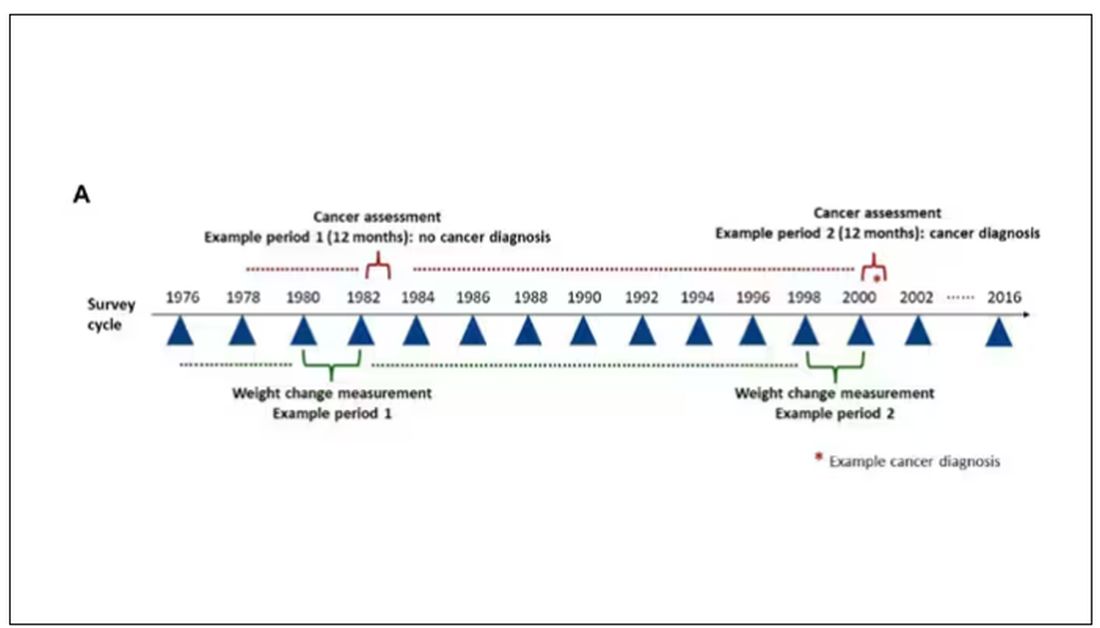
Participants recorded their weight — as an aside, a nested study found that self-reported rate was extremely well correlated with professionally measured weight — and whether they had received a cancer diagnosis since the last survey.
This allowed researchers to look at the phenomenon described above. Would weight loss precede a new diagnosis of cancer? And, more interestingly, would intentional weight loss precede a new diagnosis of cancer.
I don’t think it will surprise you to hear that individuals in the highest category of weight loss, those who lost more than 10% of their body weight over a 2-year period, had a larger risk of being diagnosed with cancer in the next year. That’s the yellow line in this graph. In fact, they had about a 40% higher risk than those who did not lose weight.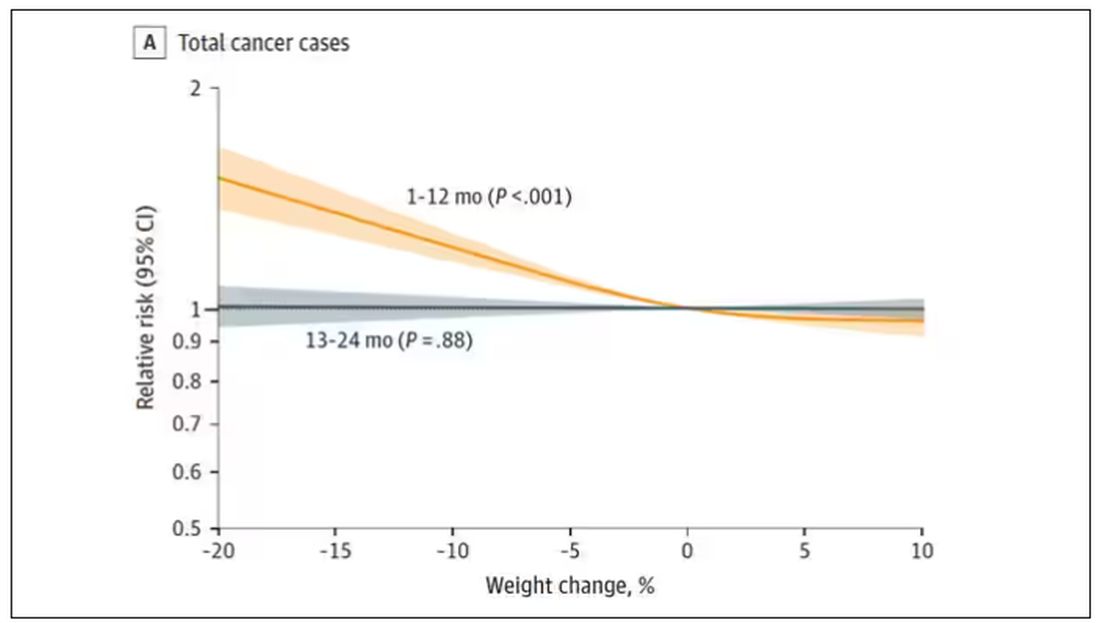
Increased risk was found across multiple cancer types, though cancers of the gastrointestinal tract, not surprisingly, were most strongly associated with antecedent weight loss.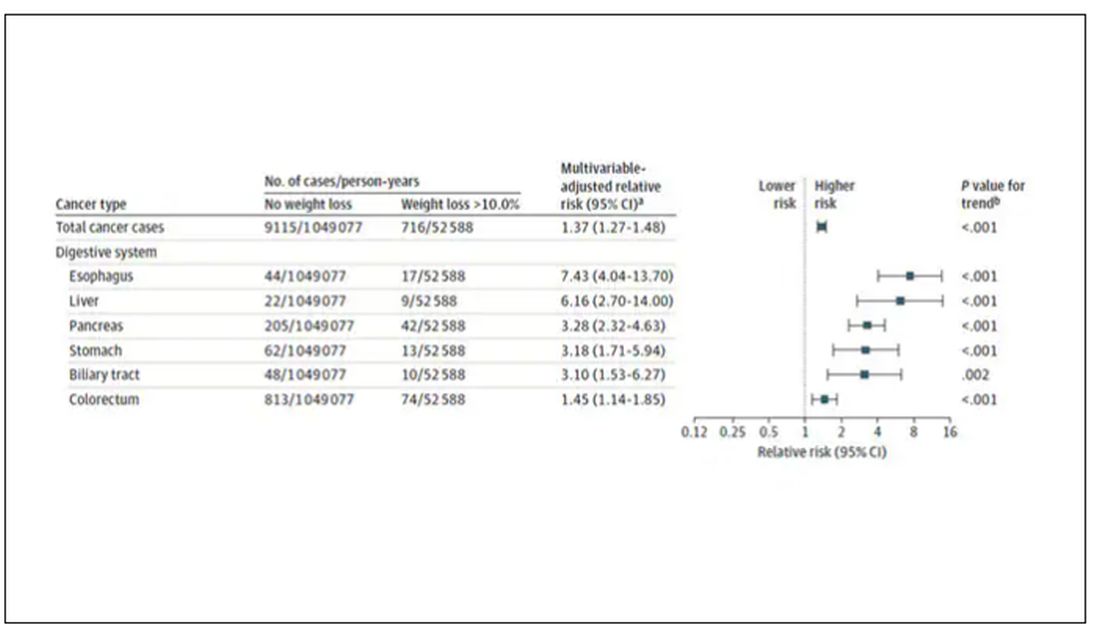
What about intentionality of weight loss? Unfortunately, the surveys did not ask participants whether they were trying to lose weight. Rather, the surveys asked about exercise and dietary habits. The researchers leveraged these responses to create three categories of participants: those who seemed to be trying to lose weight (defined as people who had increased their exercise and dietary quality); those who didn’t seem to be trying to lose weight (they changed neither exercise nor dietary behaviors); and a middle group, which changed one or the other of these behaviors but not both.
Let’s look at those who really seemed to be trying to lose weight. Over 2 years, they got more exercise and improved their diet.
If they succeeded in losing 10% or more of their body weight, they still had a higher risk for cancer than those who had not lost weight — about 30% higher, which is not that different from the 40% increased risk when you include those folks who weren’t changing their lifestyle.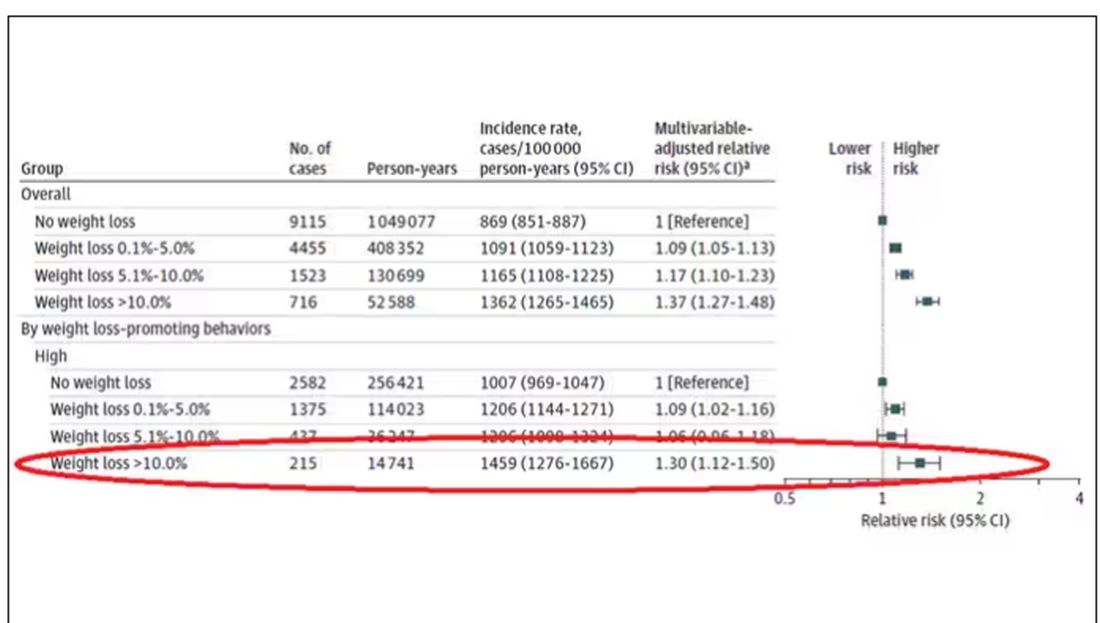
This is why this study is important. The classic teaching is that unintentional weight loss is a bad thing and needs a workup. That’s fine. But we live in a world where perhaps the majority of people are, at any given time, trying to lose weight.
We need to be careful here. I am not by any means trying to say that people who have successfully lost weight have cancer. Both of the following statements can be true:
Significant weight loss, whether intentional or not, is associated with a higher risk for cancer.
Most people with significant weight loss will not have cancer.
Both of these can be true because cancer is, fortunately, rare. Of people who lose weight, the vast majority will lose weight because they are engaging in healthier behaviors. A small number may lose weight because something else is wrong. It’s just hard to tell the two apart.
Out of the nearly 200,000 people in this study, only around 16,000 developed cancer during follow-up. Again, although the chance of having cancer is slightly higher if someone has experienced weight loss, the chance is still very low.
We also need to avoid suggesting that weight loss causes cancer. Some people lose weight because of an existing, as of yet undiagnosed cancer and its metabolic effects. This is borne out if you look at the risk of being diagnosed with cancer as you move further away from the interval of weight loss.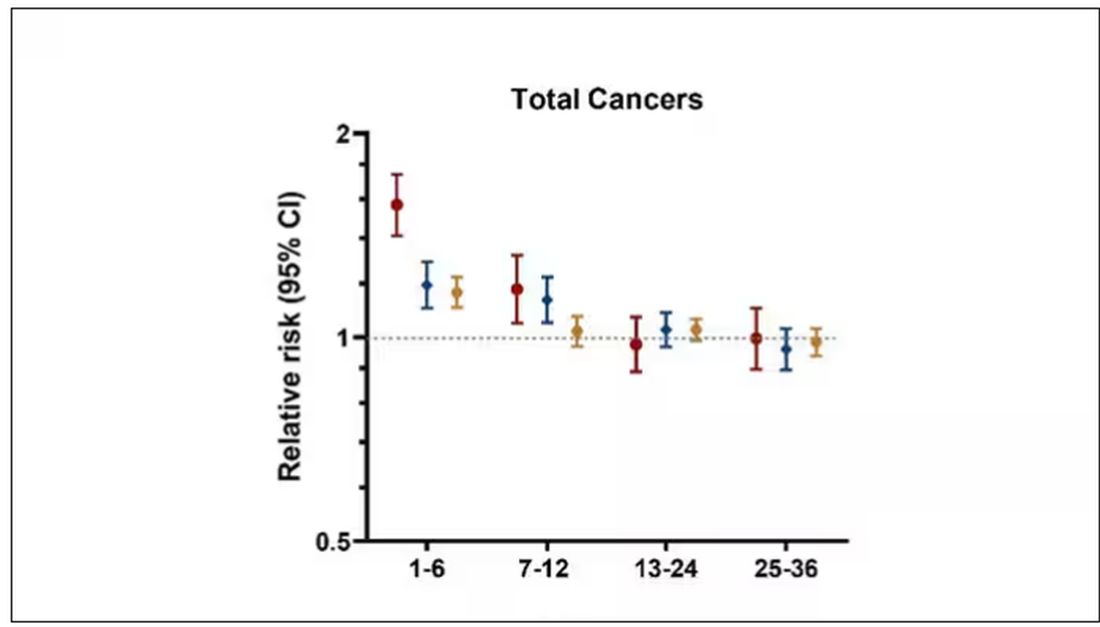
The further you get from the year of that 10% weight loss, the less likely you are to be diagnosed with cancer. Most of these cancers are diagnosed within a year of losing weight. In other words, if you’re reading this and getting worried that you lost weight 10 years ago, you’re probably out of the woods. That was, most likely, just you getting healthier.
Last thing: We have methods for weight loss now that are way more effective than diet or exercise. I’m looking at you, Ozempic. But aside from the weight loss wonder drugs, we have surgery and other interventions. This study did not capture any of that data. Ozempic wasn’t even on the market during this study, so we can’t say anything about the relationship between weight loss and cancer among people using nonlifestyle mechanisms to lose weight.
It’s a complicated system. But the clinically actionable point here is to notice if patients have lost weight. If they’ve lost it without trying, further workup is reasonable. If they’ve lost it but were trying to lose it, tell them “good job.” And consider a workup anyway.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
As anyone who has been through medical training will tell you, some little scenes just stick with you. I had been seeing a patient in our resident clinic in West Philly for a couple of years. She was in her mid-60s with diabetes and hypertension and a distant smoking history. She was overweight and had been trying to improve her diet and lose weight since I started seeing her. One day she came in and was delighted to report that she had finally started shedding some pounds — about 15 in the past 2 months.
I enthusiastically told my preceptor that my careful dietary counseling had finally done the job. She looked through the chart for a moment and asked, “Is she up to date on her cancer screening?” A workup revealed adenocarcinoma of the lung. The patient did well, actually, but the story stuck with me.
The textbooks call it “unintentional weight loss,” often in big, scary letters, and every doctor will go just a bit pale if a patient tells them that, despite efforts not to, they are losing weight. But true unintentional weight loss is not that common. After all, most of us are at least half-heartedly trying to lose weight all the time. Should doctors be worried when we are successful?
A new study suggests that perhaps they should. We’re talking about this study, appearing in JAMA, which combined participants from two long-running observational cohorts: 120,000 women from the Nurses’ Health Study, and 50,000 men from the Health Professionals Follow-Up Study. (These cohorts started in the 1970s and 1980s, so we’ll give them a pass on the gender-specific study designs.)
The rationale of enrolling healthcare providers in these cohort studies is that they would be reliable witnesses of their own health status. If a nurse or doctor says they have pancreatic cancer, it’s likely that they truly have pancreatic cancer. Detailed health surveys were distributed to the participants every other year, and the average follow-up was more than a decade.
Participants recorded their weight — as an aside, a nested study found that self-reported rate was extremely well correlated with professionally measured weight — and whether they had received a cancer diagnosis since the last survey.
This allowed researchers to look at the phenomenon described above. Would weight loss precede a new diagnosis of cancer? And, more interestingly, would intentional weight loss precede a new diagnosis of cancer.
I don’t think it will surprise you to hear that individuals in the highest category of weight loss, those who lost more than 10% of their body weight over a 2-year period, had a larger risk of being diagnosed with cancer in the next year. That’s the yellow line in this graph. In fact, they had about a 40% higher risk than those who did not lose weight.
Increased risk was found across multiple cancer types, though cancers of the gastrointestinal tract, not surprisingly, were most strongly associated with antecedent weight loss.
What about intentionality of weight loss? Unfortunately, the surveys did not ask participants whether they were trying to lose weight. Rather, the surveys asked about exercise and dietary habits. The researchers leveraged these responses to create three categories of participants: those who seemed to be trying to lose weight (defined as people who had increased their exercise and dietary quality); those who didn’t seem to be trying to lose weight (they changed neither exercise nor dietary behaviors); and a middle group, which changed one or the other of these behaviors but not both.
Let’s look at those who really seemed to be trying to lose weight. Over 2 years, they got more exercise and improved their diet.
If they succeeded in losing 10% or more of their body weight, they still had a higher risk for cancer than those who had not lost weight — about 30% higher, which is not that different from the 40% increased risk when you include those folks who weren’t changing their lifestyle.
This is why this study is important. The classic teaching is that unintentional weight loss is a bad thing and needs a workup. That’s fine. But we live in a world where perhaps the majority of people are, at any given time, trying to lose weight.
We need to be careful here. I am not by any means trying to say that people who have successfully lost weight have cancer. Both of the following statements can be true:
Significant weight loss, whether intentional or not, is associated with a higher risk for cancer.
Most people with significant weight loss will not have cancer.
Both of these can be true because cancer is, fortunately, rare. Of people who lose weight, the vast majority will lose weight because they are engaging in healthier behaviors. A small number may lose weight because something else is wrong. It’s just hard to tell the two apart.
Out of the nearly 200,000 people in this study, only around 16,000 developed cancer during follow-up. Again, although the chance of having cancer is slightly higher if someone has experienced weight loss, the chance is still very low.
We also need to avoid suggesting that weight loss causes cancer. Some people lose weight because of an existing, as of yet undiagnosed cancer and its metabolic effects. This is borne out if you look at the risk of being diagnosed with cancer as you move further away from the interval of weight loss.
The further you get from the year of that 10% weight loss, the less likely you are to be diagnosed with cancer. Most of these cancers are diagnosed within a year of losing weight. In other words, if you’re reading this and getting worried that you lost weight 10 years ago, you’re probably out of the woods. That was, most likely, just you getting healthier.
Last thing: We have methods for weight loss now that are way more effective than diet or exercise. I’m looking at you, Ozempic. But aside from the weight loss wonder drugs, we have surgery and other interventions. This study did not capture any of that data. Ozempic wasn’t even on the market during this study, so we can’t say anything about the relationship between weight loss and cancer among people using nonlifestyle mechanisms to lose weight.
It’s a complicated system. But the clinically actionable point here is to notice if patients have lost weight. If they’ve lost it without trying, further workup is reasonable. If they’ve lost it but were trying to lose it, tell them “good job.” And consider a workup anyway.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
As anyone who has been through medical training will tell you, some little scenes just stick with you. I had been seeing a patient in our resident clinic in West Philly for a couple of years. She was in her mid-60s with diabetes and hypertension and a distant smoking history. She was overweight and had been trying to improve her diet and lose weight since I started seeing her. One day she came in and was delighted to report that she had finally started shedding some pounds — about 15 in the past 2 months.
I enthusiastically told my preceptor that my careful dietary counseling had finally done the job. She looked through the chart for a moment and asked, “Is she up to date on her cancer screening?” A workup revealed adenocarcinoma of the lung. The patient did well, actually, but the story stuck with me.
The textbooks call it “unintentional weight loss,” often in big, scary letters, and every doctor will go just a bit pale if a patient tells them that, despite efforts not to, they are losing weight. But true unintentional weight loss is not that common. After all, most of us are at least half-heartedly trying to lose weight all the time. Should doctors be worried when we are successful?
A new study suggests that perhaps they should. We’re talking about this study, appearing in JAMA, which combined participants from two long-running observational cohorts: 120,000 women from the Nurses’ Health Study, and 50,000 men from the Health Professionals Follow-Up Study. (These cohorts started in the 1970s and 1980s, so we’ll give them a pass on the gender-specific study designs.)
The rationale of enrolling healthcare providers in these cohort studies is that they would be reliable witnesses of their own health status. If a nurse or doctor says they have pancreatic cancer, it’s likely that they truly have pancreatic cancer. Detailed health surveys were distributed to the participants every other year, and the average follow-up was more than a decade.
Participants recorded their weight — as an aside, a nested study found that self-reported rate was extremely well correlated with professionally measured weight — and whether they had received a cancer diagnosis since the last survey.
This allowed researchers to look at the phenomenon described above. Would weight loss precede a new diagnosis of cancer? And, more interestingly, would intentional weight loss precede a new diagnosis of cancer.
I don’t think it will surprise you to hear that individuals in the highest category of weight loss, those who lost more than 10% of their body weight over a 2-year period, had a larger risk of being diagnosed with cancer in the next year. That’s the yellow line in this graph. In fact, they had about a 40% higher risk than those who did not lose weight.
Increased risk was found across multiple cancer types, though cancers of the gastrointestinal tract, not surprisingly, were most strongly associated with antecedent weight loss.
What about intentionality of weight loss? Unfortunately, the surveys did not ask participants whether they were trying to lose weight. Rather, the surveys asked about exercise and dietary habits. The researchers leveraged these responses to create three categories of participants: those who seemed to be trying to lose weight (defined as people who had increased their exercise and dietary quality); those who didn’t seem to be trying to lose weight (they changed neither exercise nor dietary behaviors); and a middle group, which changed one or the other of these behaviors but not both.
Let’s look at those who really seemed to be trying to lose weight. Over 2 years, they got more exercise and improved their diet.
If they succeeded in losing 10% or more of their body weight, they still had a higher risk for cancer than those who had not lost weight — about 30% higher, which is not that different from the 40% increased risk when you include those folks who weren’t changing their lifestyle.
This is why this study is important. The classic teaching is that unintentional weight loss is a bad thing and needs a workup. That’s fine. But we live in a world where perhaps the majority of people are, at any given time, trying to lose weight.
We need to be careful here. I am not by any means trying to say that people who have successfully lost weight have cancer. Both of the following statements can be true:
Significant weight loss, whether intentional or not, is associated with a higher risk for cancer.
Most people with significant weight loss will not have cancer.
Both of these can be true because cancer is, fortunately, rare. Of people who lose weight, the vast majority will lose weight because they are engaging in healthier behaviors. A small number may lose weight because something else is wrong. It’s just hard to tell the two apart.
Out of the nearly 200,000 people in this study, only around 16,000 developed cancer during follow-up. Again, although the chance of having cancer is slightly higher if someone has experienced weight loss, the chance is still very low.
We also need to avoid suggesting that weight loss causes cancer. Some people lose weight because of an existing, as of yet undiagnosed cancer and its metabolic effects. This is borne out if you look at the risk of being diagnosed with cancer as you move further away from the interval of weight loss.
The further you get from the year of that 10% weight loss, the less likely you are to be diagnosed with cancer. Most of these cancers are diagnosed within a year of losing weight. In other words, if you’re reading this and getting worried that you lost weight 10 years ago, you’re probably out of the woods. That was, most likely, just you getting healthier.
Last thing: We have methods for weight loss now that are way more effective than diet or exercise. I’m looking at you, Ozempic. But aside from the weight loss wonder drugs, we have surgery and other interventions. This study did not capture any of that data. Ozempic wasn’t even on the market during this study, so we can’t say anything about the relationship between weight loss and cancer among people using nonlifestyle mechanisms to lose weight.
It’s a complicated system. But the clinically actionable point here is to notice if patients have lost weight. If they’ve lost it without trying, further workup is reasonable. If they’ve lost it but were trying to lose it, tell them “good job.” And consider a workup anyway.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
More Cardiologists Failing the Boards: Why and How to Fix?
Recent evidence suggests that more cardiologists are failing to pass their boards. , experts said.
Among the 1061 candidates who took their first American Board of Internal Medicine (ABIM) cardiovascular (CV) disease exam in 2022, about 80 fellows failed who might have passed had they trained in 2016-2019, according to Anis John Kadado, MD, University of Massachusetts Medical School–Baystate Campus, Springfield, Massachusetts, and colleagues, writing in a viewpoint article published in the Journal of the American College of Cardiology.
“The purpose of board examinations is to test the knowledge, core concepts, and fundamental principles of trainees as they deliver patient care,” said Dr. Kadado. “The decline in CV board pass rates reflects a potential gap in training, which may translate to suboptimal patient care.”
Why the Downturn?
Reasons for the increased failures are likely multifactorial, Dr. Kadado said. While some blame the ABIM, the exam has remained about the same over the past 6 years, so the test itself seems unlikely to explain the decline.
The main culprit, according to the viewpoint authors, is “the educational fallout from the disruptions caused by changes made in response to the COVID pandemic.” Changes that Dr. Kadado and colleagues said put the current class of graduating fellows at “high risk” of failing their boards in the fall.
The typical cardiology fellowship is 3 years or more for subspecialty training. Candidates who took the ABIM exam in 2021 had 18 months of training that overlapped with the pandemic response, and those who took the exam in 2022 had about 30 months of training disrupted by COVID. However, fellows who first took the exam in 2023 had essentially 36 months of training affected by COVID, potentially reducing their odds of passing.
“It is hard, if not impossible, to understand the driving forces for this recent decrease in performance on the initial ABIM certification examination, nor is it possible to forecast if there will be an end to this slide,” Jeffrey T. Kuvin, MD, chair of cardiology at the Zucker School of Medicine at Northwell Health, Manhasset, New York, and colleagues wrote in response to the viewpoint article.
The authors acknowledged that COVID disrupted graduate medical training and that the long-term effects of the disruption are now emerging. However, they also pinpoint other potential issues affecting fellows, including information/technology overload, a focus on patient volume over education, lack of attention to core concepts, and, as Dr. Kadado and colleagues noted, high burnout rates among fellows and knowledge gaps due to easy access to electronic resources rather than reading and studying to retain information.
COVID disruptions included limits on in-person learning, clinic exposure, research opportunities, and conference travel, according to the authors. From a 2020 viewpoint, Dr. Kuvin also noted the loss of bedside teaching and on-site grand rounds.
Furthermore, with deferrals of elective cardiac, endovascular, and structural catheterization procedures during the pandemic, elective cases normally done by fellows were postponed or canceled.
Restoring Education, Board Passing Rates
“Having recently passed the ABIM cardiovascular board exam myself, my take-home message at this point is for current fellows-in-training to remain organized, track training milestones, and foresee any training shortcomings,” Dr. Kadado said. Adding that fellows, graduates and leadership should “identify deficiencies and work on overcoming them.”
The viewpoint authors suggested strategies that fellowship leadership can use. These include:
- Regularly assessing faculty emotional well-being and burnout to ensure that they are engaged in meaningful teaching activities
- Emphasizing in-person learning, meaningful participation in conferences, and faculty oversight
- Encouraging fellows to pursue “self-directed learning” during off-hours
- Developing and implementing checklists, competency-based models, curricula, and rotations to ensure that training milestones are being met
- Returning to in-person imaging interpretation for imaging modalities such as echocardiography, cardiac CT, and cardiac MRI
- Ensuring that fellows take the American College of Cardiology in-training examination
- Providing practice question banks so that fellows can assess their knowledge gaps
“This might also be an opportune time to assess the assessment,” Dr. Kuvin and colleagues noted. “There are likely alternative or additional approaches that could provide a more comprehensive, modern tool to gauge clinical competence in a supportive manner.”
They suggested that these tools could include assessment by simulation for interventional cardiology and electrophysiology, oral case reviews, objective structured clinical exams, and evaluations of nonclinical competencies such as professionalism and health equity.
Implications for the New Cardiology Board
While the ABIM cardiology board exam days may be numbered, board certification via some type of exam process is not going away.
The American College of Cardiology and four other US CV societies — the American Heart Association, the Heart Failure Society of America, the Heart Rhythm Society, and the Society for Cardiovascular Angiography & Interventions — formally announced in September that they have joined forces to propose a new professional certification board called the American Board of Cardiovascular Medicine (ABCVM). The application to the ABMS for a separate cardiology board is still ongoing and will take time.
An initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured.
Preparing for the new board will likely be “largely the same” as for the ABIM board, Dr. Kadado said. “This includes access to practice question banks, faculty oversight, strong clinical exposure and practice, regular didactic sessions, and self-directed learning.”
“Passing the board exam is just one step in our ongoing journey as a cardiologist,” he added. “Our field is rapidly evolving, and continuous learning and adaptation are part of the very essence of being a healthcare professional.”
Dr. Kadado had no relevant relationships to disclose. Dr. Kuvin is an ACC trustee and has been heading up the working group to develop the ABCVM.
A version of this article appeared on Medscape.com.
Recent evidence suggests that more cardiologists are failing to pass their boards. , experts said.
Among the 1061 candidates who took their first American Board of Internal Medicine (ABIM) cardiovascular (CV) disease exam in 2022, about 80 fellows failed who might have passed had they trained in 2016-2019, according to Anis John Kadado, MD, University of Massachusetts Medical School–Baystate Campus, Springfield, Massachusetts, and colleagues, writing in a viewpoint article published in the Journal of the American College of Cardiology.
“The purpose of board examinations is to test the knowledge, core concepts, and fundamental principles of trainees as they deliver patient care,” said Dr. Kadado. “The decline in CV board pass rates reflects a potential gap in training, which may translate to suboptimal patient care.”
Why the Downturn?
Reasons for the increased failures are likely multifactorial, Dr. Kadado said. While some blame the ABIM, the exam has remained about the same over the past 6 years, so the test itself seems unlikely to explain the decline.
The main culprit, according to the viewpoint authors, is “the educational fallout from the disruptions caused by changes made in response to the COVID pandemic.” Changes that Dr. Kadado and colleagues said put the current class of graduating fellows at “high risk” of failing their boards in the fall.
The typical cardiology fellowship is 3 years or more for subspecialty training. Candidates who took the ABIM exam in 2021 had 18 months of training that overlapped with the pandemic response, and those who took the exam in 2022 had about 30 months of training disrupted by COVID. However, fellows who first took the exam in 2023 had essentially 36 months of training affected by COVID, potentially reducing their odds of passing.
“It is hard, if not impossible, to understand the driving forces for this recent decrease in performance on the initial ABIM certification examination, nor is it possible to forecast if there will be an end to this slide,” Jeffrey T. Kuvin, MD, chair of cardiology at the Zucker School of Medicine at Northwell Health, Manhasset, New York, and colleagues wrote in response to the viewpoint article.
The authors acknowledged that COVID disrupted graduate medical training and that the long-term effects of the disruption are now emerging. However, they also pinpoint other potential issues affecting fellows, including information/technology overload, a focus on patient volume over education, lack of attention to core concepts, and, as Dr. Kadado and colleagues noted, high burnout rates among fellows and knowledge gaps due to easy access to electronic resources rather than reading and studying to retain information.
COVID disruptions included limits on in-person learning, clinic exposure, research opportunities, and conference travel, according to the authors. From a 2020 viewpoint, Dr. Kuvin also noted the loss of bedside teaching and on-site grand rounds.
Furthermore, with deferrals of elective cardiac, endovascular, and structural catheterization procedures during the pandemic, elective cases normally done by fellows were postponed or canceled.
Restoring Education, Board Passing Rates
“Having recently passed the ABIM cardiovascular board exam myself, my take-home message at this point is for current fellows-in-training to remain organized, track training milestones, and foresee any training shortcomings,” Dr. Kadado said. Adding that fellows, graduates and leadership should “identify deficiencies and work on overcoming them.”
The viewpoint authors suggested strategies that fellowship leadership can use. These include:
- Regularly assessing faculty emotional well-being and burnout to ensure that they are engaged in meaningful teaching activities
- Emphasizing in-person learning, meaningful participation in conferences, and faculty oversight
- Encouraging fellows to pursue “self-directed learning” during off-hours
- Developing and implementing checklists, competency-based models, curricula, and rotations to ensure that training milestones are being met
- Returning to in-person imaging interpretation for imaging modalities such as echocardiography, cardiac CT, and cardiac MRI
- Ensuring that fellows take the American College of Cardiology in-training examination
- Providing practice question banks so that fellows can assess their knowledge gaps
“This might also be an opportune time to assess the assessment,” Dr. Kuvin and colleagues noted. “There are likely alternative or additional approaches that could provide a more comprehensive, modern tool to gauge clinical competence in a supportive manner.”
They suggested that these tools could include assessment by simulation for interventional cardiology and electrophysiology, oral case reviews, objective structured clinical exams, and evaluations of nonclinical competencies such as professionalism and health equity.
Implications for the New Cardiology Board
While the ABIM cardiology board exam days may be numbered, board certification via some type of exam process is not going away.
The American College of Cardiology and four other US CV societies — the American Heart Association, the Heart Failure Society of America, the Heart Rhythm Society, and the Society for Cardiovascular Angiography & Interventions — formally announced in September that they have joined forces to propose a new professional certification board called the American Board of Cardiovascular Medicine (ABCVM). The application to the ABMS for a separate cardiology board is still ongoing and will take time.
An initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured.
Preparing for the new board will likely be “largely the same” as for the ABIM board, Dr. Kadado said. “This includes access to practice question banks, faculty oversight, strong clinical exposure and practice, regular didactic sessions, and self-directed learning.”
“Passing the board exam is just one step in our ongoing journey as a cardiologist,” he added. “Our field is rapidly evolving, and continuous learning and adaptation are part of the very essence of being a healthcare professional.”
Dr. Kadado had no relevant relationships to disclose. Dr. Kuvin is an ACC trustee and has been heading up the working group to develop the ABCVM.
A version of this article appeared on Medscape.com.
Recent evidence suggests that more cardiologists are failing to pass their boards. , experts said.
Among the 1061 candidates who took their first American Board of Internal Medicine (ABIM) cardiovascular (CV) disease exam in 2022, about 80 fellows failed who might have passed had they trained in 2016-2019, according to Anis John Kadado, MD, University of Massachusetts Medical School–Baystate Campus, Springfield, Massachusetts, and colleagues, writing in a viewpoint article published in the Journal of the American College of Cardiology.
“The purpose of board examinations is to test the knowledge, core concepts, and fundamental principles of trainees as they deliver patient care,” said Dr. Kadado. “The decline in CV board pass rates reflects a potential gap in training, which may translate to suboptimal patient care.”
Why the Downturn?
Reasons for the increased failures are likely multifactorial, Dr. Kadado said. While some blame the ABIM, the exam has remained about the same over the past 6 years, so the test itself seems unlikely to explain the decline.
The main culprit, according to the viewpoint authors, is “the educational fallout from the disruptions caused by changes made in response to the COVID pandemic.” Changes that Dr. Kadado and colleagues said put the current class of graduating fellows at “high risk” of failing their boards in the fall.
The typical cardiology fellowship is 3 years or more for subspecialty training. Candidates who took the ABIM exam in 2021 had 18 months of training that overlapped with the pandemic response, and those who took the exam in 2022 had about 30 months of training disrupted by COVID. However, fellows who first took the exam in 2023 had essentially 36 months of training affected by COVID, potentially reducing their odds of passing.
“It is hard, if not impossible, to understand the driving forces for this recent decrease in performance on the initial ABIM certification examination, nor is it possible to forecast if there will be an end to this slide,” Jeffrey T. Kuvin, MD, chair of cardiology at the Zucker School of Medicine at Northwell Health, Manhasset, New York, and colleagues wrote in response to the viewpoint article.
The authors acknowledged that COVID disrupted graduate medical training and that the long-term effects of the disruption are now emerging. However, they also pinpoint other potential issues affecting fellows, including information/technology overload, a focus on patient volume over education, lack of attention to core concepts, and, as Dr. Kadado and colleagues noted, high burnout rates among fellows and knowledge gaps due to easy access to electronic resources rather than reading and studying to retain information.
COVID disruptions included limits on in-person learning, clinic exposure, research opportunities, and conference travel, according to the authors. From a 2020 viewpoint, Dr. Kuvin also noted the loss of bedside teaching and on-site grand rounds.
Furthermore, with deferrals of elective cardiac, endovascular, and structural catheterization procedures during the pandemic, elective cases normally done by fellows were postponed or canceled.
Restoring Education, Board Passing Rates
“Having recently passed the ABIM cardiovascular board exam myself, my take-home message at this point is for current fellows-in-training to remain organized, track training milestones, and foresee any training shortcomings,” Dr. Kadado said. Adding that fellows, graduates and leadership should “identify deficiencies and work on overcoming them.”
The viewpoint authors suggested strategies that fellowship leadership can use. These include:
- Regularly assessing faculty emotional well-being and burnout to ensure that they are engaged in meaningful teaching activities
- Emphasizing in-person learning, meaningful participation in conferences, and faculty oversight
- Encouraging fellows to pursue “self-directed learning” during off-hours
- Developing and implementing checklists, competency-based models, curricula, and rotations to ensure that training milestones are being met
- Returning to in-person imaging interpretation for imaging modalities such as echocardiography, cardiac CT, and cardiac MRI
- Ensuring that fellows take the American College of Cardiology in-training examination
- Providing practice question banks so that fellows can assess their knowledge gaps
“This might also be an opportune time to assess the assessment,” Dr. Kuvin and colleagues noted. “There are likely alternative or additional approaches that could provide a more comprehensive, modern tool to gauge clinical competence in a supportive manner.”
They suggested that these tools could include assessment by simulation for interventional cardiology and electrophysiology, oral case reviews, objective structured clinical exams, and evaluations of nonclinical competencies such as professionalism and health equity.
Implications for the New Cardiology Board
While the ABIM cardiology board exam days may be numbered, board certification via some type of exam process is not going away.
The American College of Cardiology and four other US CV societies — the American Heart Association, the Heart Failure Society of America, the Heart Rhythm Society, and the Society for Cardiovascular Angiography & Interventions — formally announced in September that they have joined forces to propose a new professional certification board called the American Board of Cardiovascular Medicine (ABCVM). The application to the ABMS for a separate cardiology board is still ongoing and will take time.
An initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured.
Preparing for the new board will likely be “largely the same” as for the ABIM board, Dr. Kadado said. “This includes access to practice question banks, faculty oversight, strong clinical exposure and practice, regular didactic sessions, and self-directed learning.”
“Passing the board exam is just one step in our ongoing journey as a cardiologist,” he added. “Our field is rapidly evolving, and continuous learning and adaptation are part of the very essence of being a healthcare professional.”
Dr. Kadado had no relevant relationships to disclose. Dr. Kuvin is an ACC trustee and has been heading up the working group to develop the ABCVM.
A version of this article appeared on Medscape.com.