User login
VIDEO: HeartMate 3 LVAD solves pump thrombosis
NEW ORLEANS – HeartMate 3, the latest left ventricular assist device in the HeartMate line, appears to have solved the problem of pump thrombosis, a complication that has dogged ventricular pumps since the issue leapt into medical awareness about 3 years ago (New Engl J Med. 2014 Jan 2;370:33-40).
During 6 months of follow-up, none of 152 heart failure patients assigned to receive a HeartMate 3 left ventricular assist device (LVAD) developed suspected or confirmed pump thrombosis, compared with 14 patients (10%) having pump thrombosis out of 138 recipients of the prior-generation HeartMate II LVAD who served as the control group for the study.
“Three years ago, when the issue of pump thrombosis was first revealed, there was a lot of consternation and some drop in LVAD use, especially as destination therapy. We think that seeing no pump thrombosis whatsoever will give people renewed confidence in this technology,” said Dr. Mehra, professor of medicine at Harvard Medical School and medical director of the Heart and Vascular Center of Brigham and Women’s Hospital, both in Boston.
Pump thrombosis has also been a problem for the patients who have received a competitor LVAD, the HeartWare HVAD device (Circulation. 2015 Nov 10;132[suppl 3]:A19675), approved for U.S. use as bridge to transplant. HeartMate II is approved for both bridge to transplant and for destination therapy.
In addition to apparently eliminating pump thrombosis, HeartMate 3’s size and potential implantation approach should make its placement during routine use as quick and minimally invasive as the HeartWare device, features that should further help broader use of HeartMate 3, commented Mark Slaughter, MD, professor and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). But Dr. Slaughter and others were also quick to highlight the shortcomings that remain with both devices that will continue to hamper a broader role for LVAD treatment of patients with advanced heart failure.
“We thought that if there was less pump thrombosis we’d see less stroke, but that is not what the data suggest. It’s the big puzzle we need to figure out before we see widespread acceptance of this treatment,” Dr. Sweitzer said.
“This will not shift LVAD use substantially,” commented Christopher B. Granger, MD, a professor of medicine and a heart failure specialist at Duke University, Durham, N.C. “Reducing the need for reoperation is good for the field, and is an incremental advance, but it is not transformational,” he said in an interview.
The MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HeartMate 3) trial randomized 294 patients at 69 U.S. centers. The study’s primary endpoint of 6-month survival free from disabling stroke or reoperation to repair or replace the LVAD occurred in 86% of 152 patients who received a HeartMate 3 and 77% of 142 patients randomized to HeartMate II, a statistical difference that met the prespecified criteria for both noninferiority and superiority. Concurrently with Dr. Mehra’s report at the meeting, a journal article appeared online (New Engl J Med. 2016 Nov 16. doi: 10.1056/NEJMoa1610426). He stated that as far as he understood, St. Jude would submit the 6-month data he reported to the Food and Drug Administration in an application for marketing approval for HeartMate 3.
“I agree that there are still morbid evens [with HeartMate 3] that need to be surmounted, but this is a confidence-building step in the right direction,” Dr. Mehra said.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
By eliminating all episodes of pump thrombosis during 6-month follow-up, the HeartMate 3 appeared to resolve one of the major issues that has stood in the way of patients and physicians feeling comfortable with left ventricular assist devices. The smaller size of the HeartMate 3 pump and its ability to be placed with minimally invasive and fairly rapid surgery is another big advance, putting this device on par with the rival pump, the HeartWare HVAD.
But the performance of the HeartMate 3 left ventricular assist device (LVAD) in MOMENTUM 3 also highlighted the shortcomings that still remain for these devices: the unchanged rates of stroke, gastrointestinal bleeds, and infections with HeartMate 3, compared with HeartMate II in this trial, and similar 6-month survival rates in the two arms of the study.
The HeartMate 3 can be implanted without sternotomy, using an 8 cm incision on the lateral chest wall, resulting in a shorter postoperative stay and fewer perisurgical adverse events. Despite the less invasive surgery and absence of pump thrombosis, some patients and physicians will remain hesitant to use an LVAD unless it is unavoidable because of concern about strokes. Until further design and procedural refinements change the rate of serious strokes and other adverse events, LVADs will not be fully competitive with heart transplantation.
The competition between HeartMate and the HeartWare devices will help drive this field forward, leading to further improvements in outcomes and expanded LVAD use.
Mark Slaughter, MD, is professor of surgery and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). He was an investigator in MOMENTUM 3, he has been a consultant to EvaHeart and Oregon Heart, and he has received research support from Carmat and HeartWare. He made these comments as designated discussant for the report and in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
By eliminating all episodes of pump thrombosis during 6-month follow-up, the HeartMate 3 appeared to resolve one of the major issues that has stood in the way of patients and physicians feeling comfortable with left ventricular assist devices. The smaller size of the HeartMate 3 pump and its ability to be placed with minimally invasive and fairly rapid surgery is another big advance, putting this device on par with the rival pump, the HeartWare HVAD.
But the performance of the HeartMate 3 left ventricular assist device (LVAD) in MOMENTUM 3 also highlighted the shortcomings that still remain for these devices: the unchanged rates of stroke, gastrointestinal bleeds, and infections with HeartMate 3, compared with HeartMate II in this trial, and similar 6-month survival rates in the two arms of the study.
The HeartMate 3 can be implanted without sternotomy, using an 8 cm incision on the lateral chest wall, resulting in a shorter postoperative stay and fewer perisurgical adverse events. Despite the less invasive surgery and absence of pump thrombosis, some patients and physicians will remain hesitant to use an LVAD unless it is unavoidable because of concern about strokes. Until further design and procedural refinements change the rate of serious strokes and other adverse events, LVADs will not be fully competitive with heart transplantation.
The competition between HeartMate and the HeartWare devices will help drive this field forward, leading to further improvements in outcomes and expanded LVAD use.
Mark Slaughter, MD, is professor of surgery and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). He was an investigator in MOMENTUM 3, he has been a consultant to EvaHeart and Oregon Heart, and he has received research support from Carmat and HeartWare. He made these comments as designated discussant for the report and in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
By eliminating all episodes of pump thrombosis during 6-month follow-up, the HeartMate 3 appeared to resolve one of the major issues that has stood in the way of patients and physicians feeling comfortable with left ventricular assist devices. The smaller size of the HeartMate 3 pump and its ability to be placed with minimally invasive and fairly rapid surgery is another big advance, putting this device on par with the rival pump, the HeartWare HVAD.
But the performance of the HeartMate 3 left ventricular assist device (LVAD) in MOMENTUM 3 also highlighted the shortcomings that still remain for these devices: the unchanged rates of stroke, gastrointestinal bleeds, and infections with HeartMate 3, compared with HeartMate II in this trial, and similar 6-month survival rates in the two arms of the study.
The HeartMate 3 can be implanted without sternotomy, using an 8 cm incision on the lateral chest wall, resulting in a shorter postoperative stay and fewer perisurgical adverse events. Despite the less invasive surgery and absence of pump thrombosis, some patients and physicians will remain hesitant to use an LVAD unless it is unavoidable because of concern about strokes. Until further design and procedural refinements change the rate of serious strokes and other adverse events, LVADs will not be fully competitive with heart transplantation.
The competition between HeartMate and the HeartWare devices will help drive this field forward, leading to further improvements in outcomes and expanded LVAD use.
Mark Slaughter, MD, is professor of surgery and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). He was an investigator in MOMENTUM 3, he has been a consultant to EvaHeart and Oregon Heart, and he has received research support from Carmat and HeartWare. He made these comments as designated discussant for the report and in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW ORLEANS – HeartMate 3, the latest left ventricular assist device in the HeartMate line, appears to have solved the problem of pump thrombosis, a complication that has dogged ventricular pumps since the issue leapt into medical awareness about 3 years ago (New Engl J Med. 2014 Jan 2;370:33-40).
During 6 months of follow-up, none of 152 heart failure patients assigned to receive a HeartMate 3 left ventricular assist device (LVAD) developed suspected or confirmed pump thrombosis, compared with 14 patients (10%) having pump thrombosis out of 138 recipients of the prior-generation HeartMate II LVAD who served as the control group for the study.
“Three years ago, when the issue of pump thrombosis was first revealed, there was a lot of consternation and some drop in LVAD use, especially as destination therapy. We think that seeing no pump thrombosis whatsoever will give people renewed confidence in this technology,” said Dr. Mehra, professor of medicine at Harvard Medical School and medical director of the Heart and Vascular Center of Brigham and Women’s Hospital, both in Boston.
Pump thrombosis has also been a problem for the patients who have received a competitor LVAD, the HeartWare HVAD device (Circulation. 2015 Nov 10;132[suppl 3]:A19675), approved for U.S. use as bridge to transplant. HeartMate II is approved for both bridge to transplant and for destination therapy.
In addition to apparently eliminating pump thrombosis, HeartMate 3’s size and potential implantation approach should make its placement during routine use as quick and minimally invasive as the HeartWare device, features that should further help broader use of HeartMate 3, commented Mark Slaughter, MD, professor and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). But Dr. Slaughter and others were also quick to highlight the shortcomings that remain with both devices that will continue to hamper a broader role for LVAD treatment of patients with advanced heart failure.
“We thought that if there was less pump thrombosis we’d see less stroke, but that is not what the data suggest. It’s the big puzzle we need to figure out before we see widespread acceptance of this treatment,” Dr. Sweitzer said.
“This will not shift LVAD use substantially,” commented Christopher B. Granger, MD, a professor of medicine and a heart failure specialist at Duke University, Durham, N.C. “Reducing the need for reoperation is good for the field, and is an incremental advance, but it is not transformational,” he said in an interview.
The MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HeartMate 3) trial randomized 294 patients at 69 U.S. centers. The study’s primary endpoint of 6-month survival free from disabling stroke or reoperation to repair or replace the LVAD occurred in 86% of 152 patients who received a HeartMate 3 and 77% of 142 patients randomized to HeartMate II, a statistical difference that met the prespecified criteria for both noninferiority and superiority. Concurrently with Dr. Mehra’s report at the meeting, a journal article appeared online (New Engl J Med. 2016 Nov 16. doi: 10.1056/NEJMoa1610426). He stated that as far as he understood, St. Jude would submit the 6-month data he reported to the Food and Drug Administration in an application for marketing approval for HeartMate 3.
“I agree that there are still morbid evens [with HeartMate 3] that need to be surmounted, but this is a confidence-building step in the right direction,” Dr. Mehra said.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
NEW ORLEANS – HeartMate 3, the latest left ventricular assist device in the HeartMate line, appears to have solved the problem of pump thrombosis, a complication that has dogged ventricular pumps since the issue leapt into medical awareness about 3 years ago (New Engl J Med. 2014 Jan 2;370:33-40).
During 6 months of follow-up, none of 152 heart failure patients assigned to receive a HeartMate 3 left ventricular assist device (LVAD) developed suspected or confirmed pump thrombosis, compared with 14 patients (10%) having pump thrombosis out of 138 recipients of the prior-generation HeartMate II LVAD who served as the control group for the study.
“Three years ago, when the issue of pump thrombosis was first revealed, there was a lot of consternation and some drop in LVAD use, especially as destination therapy. We think that seeing no pump thrombosis whatsoever will give people renewed confidence in this technology,” said Dr. Mehra, professor of medicine at Harvard Medical School and medical director of the Heart and Vascular Center of Brigham and Women’s Hospital, both in Boston.
Pump thrombosis has also been a problem for the patients who have received a competitor LVAD, the HeartWare HVAD device (Circulation. 2015 Nov 10;132[suppl 3]:A19675), approved for U.S. use as bridge to transplant. HeartMate II is approved for both bridge to transplant and for destination therapy.
In addition to apparently eliminating pump thrombosis, HeartMate 3’s size and potential implantation approach should make its placement during routine use as quick and minimally invasive as the HeartWare device, features that should further help broader use of HeartMate 3, commented Mark Slaughter, MD, professor and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). But Dr. Slaughter and others were also quick to highlight the shortcomings that remain with both devices that will continue to hamper a broader role for LVAD treatment of patients with advanced heart failure.
“We thought that if there was less pump thrombosis we’d see less stroke, but that is not what the data suggest. It’s the big puzzle we need to figure out before we see widespread acceptance of this treatment,” Dr. Sweitzer said.
“This will not shift LVAD use substantially,” commented Christopher B. Granger, MD, a professor of medicine and a heart failure specialist at Duke University, Durham, N.C. “Reducing the need for reoperation is good for the field, and is an incremental advance, but it is not transformational,” he said in an interview.
The MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HeartMate 3) trial randomized 294 patients at 69 U.S. centers. The study’s primary endpoint of 6-month survival free from disabling stroke or reoperation to repair or replace the LVAD occurred in 86% of 152 patients who received a HeartMate 3 and 77% of 142 patients randomized to HeartMate II, a statistical difference that met the prespecified criteria for both noninferiority and superiority. Concurrently with Dr. Mehra’s report at the meeting, a journal article appeared online (New Engl J Med. 2016 Nov 16. doi: 10.1056/NEJMoa1610426). He stated that as far as he understood, St. Jude would submit the 6-month data he reported to the Food and Drug Administration in an application for marketing approval for HeartMate 3.
“I agree that there are still morbid evens [with HeartMate 3] that need to be surmounted, but this is a confidence-building step in the right direction,” Dr. Mehra said.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: During 6 months, suspected or confirmed pump thrombosis occurred in no HeartMate 3 patients and in 10% of HeartMate II recipients.
Data source: The MOMENTUM 3 trial, which randomized 294 patients at 69 U.S. centers.
Disclosures: MOMENTUM 3 was sponsored by St. Jude, the company developing the HeartMate 3 LVAD. Dr. Mehra has received travel reimbursements from St. Jude and has been a consultant to Medtronic, Stealth, and Teva. Dr. Sweitzer was an investigator in MOMENTUM 3 and has been a consultant to Acorda and Medtronic and received research support from Bayer, Corvia, and Novartis. Dr. Granger has been a consultant to Boehringer Ingelheim, and received research support from Medtronic and several other drug and device companies. Dr. Slaughter was an investigator in MOMENTUM 3, has been a consultant to EvaHeart and Oregon Heart, and has received research support from Carmat and HeartWare.

Tips for Living With Myasthenia Gravis
Click here to download the PDF. 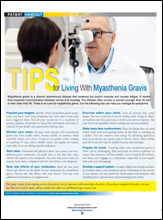
Click here to download the PDF.
Click here to download the PDF.

Time to consider cirrhosis medical homes
BOSTON – As part of the push to create value-based care across the specialties, hepatologists should consider medical homes for their patients, such as those with cirrhosis, according to experts.
“Cirrhosis is a chronic condition, highly symptomatic, and occurs in highly comorbid individuals. Treating them in a medical home scenario means we can offer services that we don’t otherwise do, but which are associated with better outcomes for our patients,” Fasiha Kanwal, MD, of the department of medicine at Baylor College of Medicine, Houston, said in a panel presentation at the annual meeting of the American Association for the Study of Liver Diseases.
Essentially, value-based care is the evolution of evidence-based medicine, according to Zobair M. Younossi, MD, AGAF, FAASLD, chair of the department of medicine at Inova Fairfax (Va.) Hospital. With value-based care, aligned incentives across all the specialties will lead to more precise accounting and efficiencies of care, said Dr. Younossi, who was also on the panel. “It would be very difficult right now to ask a hospital to tell you exactly what the cost of their liver care would be,” he said.

However, at present there are no true value-based models for hepatology in the United States, according to Dr. Kanwal, so clinicians should start by defining what will “truly constitute value for our patients.”
Because psychosocial support is essential to improved outcomes in patients with cirrhosis, she suggested adding case managers in practice, as they can help coordinate with services in the community at large. Other suggestions she offered included extending office hours, operating an after-hours hotline, and building teams that include general internists, additional nursing staff, and nutritionists.
Even though such changes in clinical practice models now are inevitable, Dr. Kanwal said there are few data at present that support how to innovate care in hospitalized patients with cirrhosis. This matters, as how patients present for outpatient follow-up care will impact reimbursements to the clinicians who treat them.
Some possible ways to improve hospital outcomes for patients with cirrhosis include creating a “best practice alert” that prompts a hepatology consult and triggers the implementation of a standardized set of guidelines for addressing ascites, bleeding, acute kidney injury, encephalopathy, and hepatorenal syndrome. For those with decompensated cirrhosis or for those who need transplants, a similar standardized checklist can be systematized between the hospital and clinic, emphasizing inpatient rifaximin and prophylactic antibiotics in case of spontaneous bacterial peritonitis.
With an overt emphasis on the needs of patients and payers, clinicians now must compete with one another to offer the most comprehensive, cost-effective care supported by information technology structures that can assess real time costs and outcomes, said Dr. Younossi. “Hepatology is lagging behind other fields in all this,” he added.
This worries Dr. Kanwal: “We should be the ones to determine what the value should be. We should be the ones to decide what the model will be and to engage with other fields, and the payers. Otherwise we will not have a seat at the table.”
Dr. Kanwal and Dr. Younossi did not have any relevant financial disclosures.
On Twitter @whitneymcknight
BOSTON – As part of the push to create value-based care across the specialties, hepatologists should consider medical homes for their patients, such as those with cirrhosis, according to experts.
“Cirrhosis is a chronic condition, highly symptomatic, and occurs in highly comorbid individuals. Treating them in a medical home scenario means we can offer services that we don’t otherwise do, but which are associated with better outcomes for our patients,” Fasiha Kanwal, MD, of the department of medicine at Baylor College of Medicine, Houston, said in a panel presentation at the annual meeting of the American Association for the Study of Liver Diseases.
Essentially, value-based care is the evolution of evidence-based medicine, according to Zobair M. Younossi, MD, AGAF, FAASLD, chair of the department of medicine at Inova Fairfax (Va.) Hospital. With value-based care, aligned incentives across all the specialties will lead to more precise accounting and efficiencies of care, said Dr. Younossi, who was also on the panel. “It would be very difficult right now to ask a hospital to tell you exactly what the cost of their liver care would be,” he said.
However, at present there are no true value-based models for hepatology in the United States, according to Dr. Kanwal, so clinicians should start by defining what will “truly constitute value for our patients.”
Because psychosocial support is essential to improved outcomes in patients with cirrhosis, she suggested adding case managers in practice, as they can help coordinate with services in the community at large. Other suggestions she offered included extending office hours, operating an after-hours hotline, and building teams that include general internists, additional nursing staff, and nutritionists.
Even though such changes in clinical practice models now are inevitable, Dr. Kanwal said there are few data at present that support how to innovate care in hospitalized patients with cirrhosis. This matters, as how patients present for outpatient follow-up care will impact reimbursements to the clinicians who treat them.
Some possible ways to improve hospital outcomes for patients with cirrhosis include creating a “best practice alert” that prompts a hepatology consult and triggers the implementation of a standardized set of guidelines for addressing ascites, bleeding, acute kidney injury, encephalopathy, and hepatorenal syndrome. For those with decompensated cirrhosis or for those who need transplants, a similar standardized checklist can be systematized between the hospital and clinic, emphasizing inpatient rifaximin and prophylactic antibiotics in case of spontaneous bacterial peritonitis.
With an overt emphasis on the needs of patients and payers, clinicians now must compete with one another to offer the most comprehensive, cost-effective care supported by information technology structures that can assess real time costs and outcomes, said Dr. Younossi. “Hepatology is lagging behind other fields in all this,” he added.
This worries Dr. Kanwal: “We should be the ones to determine what the value should be. We should be the ones to decide what the model will be and to engage with other fields, and the payers. Otherwise we will not have a seat at the table.”
Dr. Kanwal and Dr. Younossi did not have any relevant financial disclosures.
On Twitter @whitneymcknight
BOSTON – As part of the push to create value-based care across the specialties, hepatologists should consider medical homes for their patients, such as those with cirrhosis, according to experts.
“Cirrhosis is a chronic condition, highly symptomatic, and occurs in highly comorbid individuals. Treating them in a medical home scenario means we can offer services that we don’t otherwise do, but which are associated with better outcomes for our patients,” Fasiha Kanwal, MD, of the department of medicine at Baylor College of Medicine, Houston, said in a panel presentation at the annual meeting of the American Association for the Study of Liver Diseases.
Essentially, value-based care is the evolution of evidence-based medicine, according to Zobair M. Younossi, MD, AGAF, FAASLD, chair of the department of medicine at Inova Fairfax (Va.) Hospital. With value-based care, aligned incentives across all the specialties will lead to more precise accounting and efficiencies of care, said Dr. Younossi, who was also on the panel. “It would be very difficult right now to ask a hospital to tell you exactly what the cost of their liver care would be,” he said.
However, at present there are no true value-based models for hepatology in the United States, according to Dr. Kanwal, so clinicians should start by defining what will “truly constitute value for our patients.”
Because psychosocial support is essential to improved outcomes in patients with cirrhosis, she suggested adding case managers in practice, as they can help coordinate with services in the community at large. Other suggestions she offered included extending office hours, operating an after-hours hotline, and building teams that include general internists, additional nursing staff, and nutritionists.
Even though such changes in clinical practice models now are inevitable, Dr. Kanwal said there are few data at present that support how to innovate care in hospitalized patients with cirrhosis. This matters, as how patients present for outpatient follow-up care will impact reimbursements to the clinicians who treat them.
Some possible ways to improve hospital outcomes for patients with cirrhosis include creating a “best practice alert” that prompts a hepatology consult and triggers the implementation of a standardized set of guidelines for addressing ascites, bleeding, acute kidney injury, encephalopathy, and hepatorenal syndrome. For those with decompensated cirrhosis or for those who need transplants, a similar standardized checklist can be systematized between the hospital and clinic, emphasizing inpatient rifaximin and prophylactic antibiotics in case of spontaneous bacterial peritonitis.
With an overt emphasis on the needs of patients and payers, clinicians now must compete with one another to offer the most comprehensive, cost-effective care supported by information technology structures that can assess real time costs and outcomes, said Dr. Younossi. “Hepatology is lagging behind other fields in all this,” he added.
This worries Dr. Kanwal: “We should be the ones to determine what the value should be. We should be the ones to decide what the model will be and to engage with other fields, and the payers. Otherwise we will not have a seat at the table.”
Dr. Kanwal and Dr. Younossi did not have any relevant financial disclosures.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE LIVER MEETING 2016
Recognizing, addressing giftedness can be challenging
SAN FRANCISCO – Gifted children are far too commonly misunderstood, mislabeled, and misdiagnosed, leading to a mismatch between their needs and others’ perceptions of their needs, Dan Peters, PhD, a licensed psychologist and executive director of the Summit Center in the greater San Francisco and Los Angeles areas, explained at the annual meeting of the American Academy of Pediatrics.
Too often, one or more of these children’s health, developmental, social-emotional or learning needs are overlooked, or they receive an inappropriate mental health, developmental and/or learning disorder diagnosis. In fact, many of the risk factors for giftedness resemble those of other conditions: underachievement, difficulties with peers, social isolation, power struggles, perfectionism, anxiety, and depression.
Further, those who are culturally or linguistically diverse may not be recognized if a non-English first language obscures their performance ability or their socioeconomic status or lack of resources and enrichment opportunities leads them to be overlooked. It’s therefore important that practitioners understand what giftedness actually is and the characteristics gifted children might exhibit.
Understanding giftedness
A simple definition of giftedness is demonstrating a performance or the capacity for performance that significantly exceeds age or grade-level expectations, according to one school district’s gifted and talented education program.
A more involved description provided by the Columbus Group in 1991 defines giftedness as an “asynchronous development in which advanced cognitive abilities and heightened intensity combine to create inner experiences and awareness that are qualitatively different from the norm.” This asynchrony increases with higher intellectual capacity, they wrote. “The uniqueness of the gifted renders them vulnerable and requires modifications in parenting, teaching, and counseling in order for them to develop optimally.”
The level of a child’s giftedness makes a difference in their needs as well; these levels include advanced learners (IQ of 120-129), moderately gifted (130-144), highly gifted (145-159), exceptionally gifted (160-179), and profoundly gifted (180 and greater). Different spheres of giftedness can include intellectual ability, creative or productive thinking, leadership ability, and visual or performing arts. Consider the list of common characteristics of gifted children that Dr. Peters provided:
- Rapid learners.
- Strong memory.
- Large vocabulary.
- Advanced comprehension of nuances.
- Largely self-taught.
- Unusual emotional depth.
- Abstract/complex/logical/insightful thinking.
- Idealism and a sense of justice.
- Intense feelings and reactions.
- Highly sensitive.
- Long attention span and persistence.
- Preoccupied with own thoughts.
- Impatient with self and others’ inabilities and slowness.
- Asks probing questions (able to go beyond what is taught).
- Wide range of interests.
- Highly developed curiosity.
- Interest in experimenting and doing things differently.
- Divergent thinking.
- Keen and unusual sense of humor.
Dr. Peters cited Kazimierz Dabrowski, MD, PhD, a Polish psychiatrist of the mid-20th century, as explaining the sensitivity and intensity experienced by many gifted individuals in terms of overexcitabilities – a “greater capacity to be stimulated by and respond to external and internal stimuli.”
“Overexcitability permeates a gifted person’s existence and gives energy to their intelligence, talents, and personality,” Dr. Peters explained of Dabrowski’s ideas. This enhancement manifests in psychomotor terms as a strong drive, a lot of energy or movement, or extended bouts of activity. Intellectually, gifted children have an “insatiable curiosity, and voracious appetite and capacity for intellectual effort and stimulation,” Dr. Peters said. They may have heightened sensual experience in seeing, smelling, tasting, touching, or hearing, and they have an active imaginary and fantasy life. They also exhibit a capacity for great emotional depth and empathy – they deeply feel their own and others’ emotions.
How giftedness can be misdiagnosed
It is the combination of these very characteristics that can lead gifted children to receive an inappropriate mental or developmental diagnosis instead of being recognized as gifted.
“By current estimates, at any given time, approximately 11%-20% of children in the United States have a behavioral or emotional disorder as defined in the DSM-5,” Dr. Peters cited. Further, one study found that diagnoses of attention-deficit/hyperactivity disorder have increased 66% between 2000 and 2010, with 90% of those children taking psychostimulant medications – yet a study in the Journal of Health Economics estimated that one in five children diagnosed with ADHD are probably misdiagnosed and are receiving those medications.
Other incorrect diagnoses besides ADHD that gifted youth may commonly receive include anger diagnoses, ideational or anxiety disorders, developmental and personality disorders, mood disorders, and learning disorders.
Twice exceptionalism (2e)
Even more challenging are twice exceptional children, or 2e, those who are both gifted and have a learning or emotional disability or challenge. Common dual diagnoses in gifted children include anxiety disorders, depression (or existential depression), sleep disorders (such as nightmares, night terrors, or sleep walking), allergies, asthma, ADHD, oppositional-defiant disorder, obsessive-compulsive personality disorder, autism spectrum disorder, nonverbal learning disability, social/pragmatic communication disorder, and learning disorders such as dyslexia, dyscalculia, central auditory processing disorder, or sensory-motor integration disorder.
“It’s very complex. What happens is, a lot of people think you’re either gifted or not,” Dr. Peters said. “In the classroom, sometimes the advanced ability overshadows the weakness and so we get a lot of readers with an IQ of 130-150 and reading at the 50% percentile, and everyone says they’re fine, but they’re dyslexic.”
Other times, the weakness overshadows the strength, and sometimes they’re right in the middle where neither their giftedness nor their disability is recognized or addressed, Peters said. 2e children are very difficult to diagnose but also at higher risk for difficulties if one or both (or more) of their diagnoses are missed.
Maximizing gifted children’s developmental potential
Pediatricians have an opportunity to support gifted children by recognizing and accepting them for who they are, while also acknowledging that they want to feel “normal,” and therefore need extra reassurance and support from adults. Pediatricians should seek information about giftedness and 2e children from state and national gifted organizations, and, in the office, frame conversations with families and children’s differential diagnoses in terms of a child’s giftedness. If a pediatrician is themself gifted, they may be “a supportive and kindred spirit” to the child, Dr. Peters said.
In daily life, as well, gifted children need to be accepted for who they are, provided opportunities to be with their intellectual and academic peers, and provided challenges in their areas of strength, interests, or passions. Parents and teachers should follow their lead in learning: Keep up the pace for those who want to learn fast, and go deeper for those who want slower, more in-depth learning. Adults also need to understand their intensities and sensitivities and lead with their strengths in discussions.
Dr. Peters reported no disclosures.
SAN FRANCISCO – Gifted children are far too commonly misunderstood, mislabeled, and misdiagnosed, leading to a mismatch between their needs and others’ perceptions of their needs, Dan Peters, PhD, a licensed psychologist and executive director of the Summit Center in the greater San Francisco and Los Angeles areas, explained at the annual meeting of the American Academy of Pediatrics.
Too often, one or more of these children’s health, developmental, social-emotional or learning needs are overlooked, or they receive an inappropriate mental health, developmental and/or learning disorder diagnosis. In fact, many of the risk factors for giftedness resemble those of other conditions: underachievement, difficulties with peers, social isolation, power struggles, perfectionism, anxiety, and depression.
Further, those who are culturally or linguistically diverse may not be recognized if a non-English first language obscures their performance ability or their socioeconomic status or lack of resources and enrichment opportunities leads them to be overlooked. It’s therefore important that practitioners understand what giftedness actually is and the characteristics gifted children might exhibit.
Understanding giftedness
A simple definition of giftedness is demonstrating a performance or the capacity for performance that significantly exceeds age or grade-level expectations, according to one school district’s gifted and talented education program.
A more involved description provided by the Columbus Group in 1991 defines giftedness as an “asynchronous development in which advanced cognitive abilities and heightened intensity combine to create inner experiences and awareness that are qualitatively different from the norm.” This asynchrony increases with higher intellectual capacity, they wrote. “The uniqueness of the gifted renders them vulnerable and requires modifications in parenting, teaching, and counseling in order for them to develop optimally.”
The level of a child’s giftedness makes a difference in their needs as well; these levels include advanced learners (IQ of 120-129), moderately gifted (130-144), highly gifted (145-159), exceptionally gifted (160-179), and profoundly gifted (180 and greater). Different spheres of giftedness can include intellectual ability, creative or productive thinking, leadership ability, and visual or performing arts. Consider the list of common characteristics of gifted children that Dr. Peters provided:
- Rapid learners.
- Strong memory.
- Large vocabulary.
- Advanced comprehension of nuances.
- Largely self-taught.
- Unusual emotional depth.
- Abstract/complex/logical/insightful thinking.
- Idealism and a sense of justice.
- Intense feelings and reactions.
- Highly sensitive.
- Long attention span and persistence.
- Preoccupied with own thoughts.
- Impatient with self and others’ inabilities and slowness.
- Asks probing questions (able to go beyond what is taught).
- Wide range of interests.
- Highly developed curiosity.
- Interest in experimenting and doing things differently.
- Divergent thinking.
- Keen and unusual sense of humor.
Dr. Peters cited Kazimierz Dabrowski, MD, PhD, a Polish psychiatrist of the mid-20th century, as explaining the sensitivity and intensity experienced by many gifted individuals in terms of overexcitabilities – a “greater capacity to be stimulated by and respond to external and internal stimuli.”
“Overexcitability permeates a gifted person’s existence and gives energy to their intelligence, talents, and personality,” Dr. Peters explained of Dabrowski’s ideas. This enhancement manifests in psychomotor terms as a strong drive, a lot of energy or movement, or extended bouts of activity. Intellectually, gifted children have an “insatiable curiosity, and voracious appetite and capacity for intellectual effort and stimulation,” Dr. Peters said. They may have heightened sensual experience in seeing, smelling, tasting, touching, or hearing, and they have an active imaginary and fantasy life. They also exhibit a capacity for great emotional depth and empathy – they deeply feel their own and others’ emotions.
How giftedness can be misdiagnosed
It is the combination of these very characteristics that can lead gifted children to receive an inappropriate mental or developmental diagnosis instead of being recognized as gifted.
“By current estimates, at any given time, approximately 11%-20% of children in the United States have a behavioral or emotional disorder as defined in the DSM-5,” Dr. Peters cited. Further, one study found that diagnoses of attention-deficit/hyperactivity disorder have increased 66% between 2000 and 2010, with 90% of those children taking psychostimulant medications – yet a study in the Journal of Health Economics estimated that one in five children diagnosed with ADHD are probably misdiagnosed and are receiving those medications.
Other incorrect diagnoses besides ADHD that gifted youth may commonly receive include anger diagnoses, ideational or anxiety disorders, developmental and personality disorders, mood disorders, and learning disorders.
Twice exceptionalism (2e)
Even more challenging are twice exceptional children, or 2e, those who are both gifted and have a learning or emotional disability or challenge. Common dual diagnoses in gifted children include anxiety disorders, depression (or existential depression), sleep disorders (such as nightmares, night terrors, or sleep walking), allergies, asthma, ADHD, oppositional-defiant disorder, obsessive-compulsive personality disorder, autism spectrum disorder, nonverbal learning disability, social/pragmatic communication disorder, and learning disorders such as dyslexia, dyscalculia, central auditory processing disorder, or sensory-motor integration disorder.
“It’s very complex. What happens is, a lot of people think you’re either gifted or not,” Dr. Peters said. “In the classroom, sometimes the advanced ability overshadows the weakness and so we get a lot of readers with an IQ of 130-150 and reading at the 50% percentile, and everyone says they’re fine, but they’re dyslexic.”
Other times, the weakness overshadows the strength, and sometimes they’re right in the middle where neither their giftedness nor their disability is recognized or addressed, Peters said. 2e children are very difficult to diagnose but also at higher risk for difficulties if one or both (or more) of their diagnoses are missed.
Maximizing gifted children’s developmental potential
Pediatricians have an opportunity to support gifted children by recognizing and accepting them for who they are, while also acknowledging that they want to feel “normal,” and therefore need extra reassurance and support from adults. Pediatricians should seek information about giftedness and 2e children from state and national gifted organizations, and, in the office, frame conversations with families and children’s differential diagnoses in terms of a child’s giftedness. If a pediatrician is themself gifted, they may be “a supportive and kindred spirit” to the child, Dr. Peters said.
In daily life, as well, gifted children need to be accepted for who they are, provided opportunities to be with their intellectual and academic peers, and provided challenges in their areas of strength, interests, or passions. Parents and teachers should follow their lead in learning: Keep up the pace for those who want to learn fast, and go deeper for those who want slower, more in-depth learning. Adults also need to understand their intensities and sensitivities and lead with their strengths in discussions.
Dr. Peters reported no disclosures.
SAN FRANCISCO – Gifted children are far too commonly misunderstood, mislabeled, and misdiagnosed, leading to a mismatch between their needs and others’ perceptions of their needs, Dan Peters, PhD, a licensed psychologist and executive director of the Summit Center in the greater San Francisco and Los Angeles areas, explained at the annual meeting of the American Academy of Pediatrics.
Too often, one or more of these children’s health, developmental, social-emotional or learning needs are overlooked, or they receive an inappropriate mental health, developmental and/or learning disorder diagnosis. In fact, many of the risk factors for giftedness resemble those of other conditions: underachievement, difficulties with peers, social isolation, power struggles, perfectionism, anxiety, and depression.
Further, those who are culturally or linguistically diverse may not be recognized if a non-English first language obscures their performance ability or their socioeconomic status or lack of resources and enrichment opportunities leads them to be overlooked. It’s therefore important that practitioners understand what giftedness actually is and the characteristics gifted children might exhibit.
Understanding giftedness
A simple definition of giftedness is demonstrating a performance or the capacity for performance that significantly exceeds age or grade-level expectations, according to one school district’s gifted and talented education program.
A more involved description provided by the Columbus Group in 1991 defines giftedness as an “asynchronous development in which advanced cognitive abilities and heightened intensity combine to create inner experiences and awareness that are qualitatively different from the norm.” This asynchrony increases with higher intellectual capacity, they wrote. “The uniqueness of the gifted renders them vulnerable and requires modifications in parenting, teaching, and counseling in order for them to develop optimally.”
The level of a child’s giftedness makes a difference in their needs as well; these levels include advanced learners (IQ of 120-129), moderately gifted (130-144), highly gifted (145-159), exceptionally gifted (160-179), and profoundly gifted (180 and greater). Different spheres of giftedness can include intellectual ability, creative or productive thinking, leadership ability, and visual or performing arts. Consider the list of common characteristics of gifted children that Dr. Peters provided:
- Rapid learners.
- Strong memory.
- Large vocabulary.
- Advanced comprehension of nuances.
- Largely self-taught.
- Unusual emotional depth.
- Abstract/complex/logical/insightful thinking.
- Idealism and a sense of justice.
- Intense feelings and reactions.
- Highly sensitive.
- Long attention span and persistence.
- Preoccupied with own thoughts.
- Impatient with self and others’ inabilities and slowness.
- Asks probing questions (able to go beyond what is taught).
- Wide range of interests.
- Highly developed curiosity.
- Interest in experimenting and doing things differently.
- Divergent thinking.
- Keen and unusual sense of humor.
Dr. Peters cited Kazimierz Dabrowski, MD, PhD, a Polish psychiatrist of the mid-20th century, as explaining the sensitivity and intensity experienced by many gifted individuals in terms of overexcitabilities – a “greater capacity to be stimulated by and respond to external and internal stimuli.”
“Overexcitability permeates a gifted person’s existence and gives energy to their intelligence, talents, and personality,” Dr. Peters explained of Dabrowski’s ideas. This enhancement manifests in psychomotor terms as a strong drive, a lot of energy or movement, or extended bouts of activity. Intellectually, gifted children have an “insatiable curiosity, and voracious appetite and capacity for intellectual effort and stimulation,” Dr. Peters said. They may have heightened sensual experience in seeing, smelling, tasting, touching, or hearing, and they have an active imaginary and fantasy life. They also exhibit a capacity for great emotional depth and empathy – they deeply feel their own and others’ emotions.
How giftedness can be misdiagnosed
It is the combination of these very characteristics that can lead gifted children to receive an inappropriate mental or developmental diagnosis instead of being recognized as gifted.
“By current estimates, at any given time, approximately 11%-20% of children in the United States have a behavioral or emotional disorder as defined in the DSM-5,” Dr. Peters cited. Further, one study found that diagnoses of attention-deficit/hyperactivity disorder have increased 66% between 2000 and 2010, with 90% of those children taking psychostimulant medications – yet a study in the Journal of Health Economics estimated that one in five children diagnosed with ADHD are probably misdiagnosed and are receiving those medications.
Other incorrect diagnoses besides ADHD that gifted youth may commonly receive include anger diagnoses, ideational or anxiety disorders, developmental and personality disorders, mood disorders, and learning disorders.
Twice exceptionalism (2e)
Even more challenging are twice exceptional children, or 2e, those who are both gifted and have a learning or emotional disability or challenge. Common dual diagnoses in gifted children include anxiety disorders, depression (or existential depression), sleep disorders (such as nightmares, night terrors, or sleep walking), allergies, asthma, ADHD, oppositional-defiant disorder, obsessive-compulsive personality disorder, autism spectrum disorder, nonverbal learning disability, social/pragmatic communication disorder, and learning disorders such as dyslexia, dyscalculia, central auditory processing disorder, or sensory-motor integration disorder.
“It’s very complex. What happens is, a lot of people think you’re either gifted or not,” Dr. Peters said. “In the classroom, sometimes the advanced ability overshadows the weakness and so we get a lot of readers with an IQ of 130-150 and reading at the 50% percentile, and everyone says they’re fine, but they’re dyslexic.”
Other times, the weakness overshadows the strength, and sometimes they’re right in the middle where neither their giftedness nor their disability is recognized or addressed, Peters said. 2e children are very difficult to diagnose but also at higher risk for difficulties if one or both (or more) of their diagnoses are missed.
Maximizing gifted children’s developmental potential
Pediatricians have an opportunity to support gifted children by recognizing and accepting them for who they are, while also acknowledging that they want to feel “normal,” and therefore need extra reassurance and support from adults. Pediatricians should seek information about giftedness and 2e children from state and national gifted organizations, and, in the office, frame conversations with families and children’s differential diagnoses in terms of a child’s giftedness. If a pediatrician is themself gifted, they may be “a supportive and kindred spirit” to the child, Dr. Peters said.
In daily life, as well, gifted children need to be accepted for who they are, provided opportunities to be with their intellectual and academic peers, and provided challenges in their areas of strength, interests, or passions. Parents and teachers should follow their lead in learning: Keep up the pace for those who want to learn fast, and go deeper for those who want slower, more in-depth learning. Adults also need to understand their intensities and sensitivities and lead with their strengths in discussions.
Dr. Peters reported no disclosures.
EXPERT ANALYSIS FROM AAP 16
Mixed findings on iron repletion in HF
NEW ORLEANS – Oral iron supplementation was declared ineffective for the treatment of iron deficiency in patients with heart failure with reduced ejection fraction in one major randomized trial while intravenous ferric carboxymaltose improved exercise capacity and quality of life in another study presented at the American Heart Association scientific sessions.
Iron deficiency is present in roughly half of patients with heart failure with reduced ejection fraction (HFrEF). In affected patients it’s associated with diminished functional capacity and poor quality of life, and is an independent predictor of mortality. Thus, it has emerged as a potential therapeutic target in HFrEF.

The IRONOUT HF (Oral Iron Repletion Effects on Oxygen UpTake in Heart Failure) trial was a multicenter, randomized, double-blind, placebo-controlled clinical trial conducted by the National Heart, Lung, and Blood Institute’s Clinical Heart Failure Network investigators. It included 225 patients with HFrEF and iron deficiency who were randomized to 16 weeks of oral iron polysaccharide at 150 mg b.i.d. or matching placebo.
The primary endpoint was change from baseline to 16 weeks in exercise capacity, as measured via peak oxygen uptake during cardiopulmonary exercise testing. The results were no better in the iron-supplemented group than in placebo-treated controls. Nor was there any benefit for oral iron therapy in terms of quality of life, as assessed by the Kansas City Cardiomyopathy Questionnaire or any of numerous other secondary endpoints, according to Dr. Lewis, head of the heart failure section and director of the cardiopulmonary exercise testing laboratory at Massachusetts General Hospital, Boston.
Participants’ mean baseline hemoglobin level was 12.6 g/dL, but whether patients were anemic at baseline or not made no difference in terms of outcomes. Rates of venous congestion and bleeding were low during the trial.
The problem, the investigators found, was that high-dose oral iron only minimally repleted iron stores. Transferrin saturation increased by a paltry absolute 3% after 16 weeks of twice-daily therapy. Serum ferritin levels increased only 1/20th as much as after intravenous iron ferric carboxymaltose therapy in the earlier positive FAIR-HF (Ferinject Assessment in Patients With Iron Deficiency and Chronic Heart Failure) trial (N Engl J Med. 2009 Dec 17;361:2436-48).
Levels of hepcidin were elevated in study participants. And the higher the level of hepcidin – which Dr. Lewis called “a massive regulator of iron bioavailability and absorption” – the more refractory patients were to oral iron repletion.
“Hepcidin was invented by nature to protect against iron from stimulating growth of bacteria. And when it’s elevated, taking iron orally just has no chance of success,” explained Dr. Anker, professor of cardiology at the University of Gottingen (Germany).
Dr. Anker, who chaired the positive FAIR-HF trial of intravenous iron, said IRONOUT HF was a very well-conducted and definitive clinical trial of oral iron supplementation in HFrEF.
“It’s very simple: Oral iron does not work in patients with chronic heart failure. That’s the take home message. It’s true for peak VO2 [oxygen consumption], for 6-minute walk distance, for symptoms, for quality of life, and even for surrogate markers like NT-proBNP [N-terminal pro b-type natriuretic peptide]. If iron doesn’t get into the body, it’s really difficult to [imagine] that the iron that doesn’t get into the body can exert an effect,” he said.
The primary endpoint in EFFECT-HF was assessor-blinded change in peak VO2 from baseline to week 24. The control group experienced a decrease in peak VO2 over time such that there was a significant difference of 1.0 mL/kg per minute between the two groups.
The ferric carboxymaltose recipients also did significantly better in terms of secondary endpoints including improvement in New York Heart Association functional class, self-reported Patient Global Assessment score, and quality-of-life measures, reported Dr. van Veldhuisen, professor and chairman of cardiology at University Medical Center Groningen (the Netherlands).
Session moderator Clyde Yancy, MD, commented that intravenous iron is not ready for prime time use in clinical practice for several reasons. The open-label EFFECT-HF trial, like the earlier positive double-blind FAIR-HF and CONFIRM-HF IV ferric carboxymaltose trials, was too modest in size to be convincing, especially since this is an expensive and intrusive therapy.
“The endpoint of peak VO2, although a very powerful endpoint, is still one for which there may be some subjectivity, and so we need a more definitive endpoint to be absolutely certain about the potential benefit of the administration of ferric carboxymaltose,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
Discussant Adrian Hernandez, MD, of the Duke Clinical Research Institute in Durham, N.C., said he considers peak VO2 an important endpoint.
“When you talk to patients, exercise capacity is an outcome that matters to them,” he said. “They often comment that what matters to them is living longer with a better quality of life, free of worsening heart failure, and having improvement in everyday functional status. So the cardiopulmonary exercise test is not just a surrogate endpoint; it’s a measure of functional outcome that matters to patients,” he said.
Still, like Dr. Yancy, Dr. Hernandez said he thinks it’s time to have larger, longer, definitive trials with clinical endpoints in order to understand the role of intravenous iron. Both cardiologists applauded Dr. Anker’s announcement that such a trial, known as FAIR-HF2, is now getting started.
The IRONOUT HF trial was funded by the National Institutes of Health. Dr. Lewis reported receiving research support from a handful of pharmaceutical and medical device companies. Dr. van Velduisen reported serving as a scientific adviser to Vifor Pharma, which sponsored the EFFECT-HF trial. Dr. Anker, who was an EFFECT-HF investigator, serves as a consultant to Vifor and several other companies. Dr. Hernandez was an IRONOUT HF investigator and reported receiving research grants from a handful of pharmaceutical companies.
NEW ORLEANS – Oral iron supplementation was declared ineffective for the treatment of iron deficiency in patients with heart failure with reduced ejection fraction in one major randomized trial while intravenous ferric carboxymaltose improved exercise capacity and quality of life in another study presented at the American Heart Association scientific sessions.
Iron deficiency is present in roughly half of patients with heart failure with reduced ejection fraction (HFrEF). In affected patients it’s associated with diminished functional capacity and poor quality of life, and is an independent predictor of mortality. Thus, it has emerged as a potential therapeutic target in HFrEF.
The IRONOUT HF (Oral Iron Repletion Effects on Oxygen UpTake in Heart Failure) trial was a multicenter, randomized, double-blind, placebo-controlled clinical trial conducted by the National Heart, Lung, and Blood Institute’s Clinical Heart Failure Network investigators. It included 225 patients with HFrEF and iron deficiency who were randomized to 16 weeks of oral iron polysaccharide at 150 mg b.i.d. or matching placebo.
The primary endpoint was change from baseline to 16 weeks in exercise capacity, as measured via peak oxygen uptake during cardiopulmonary exercise testing. The results were no better in the iron-supplemented group than in placebo-treated controls. Nor was there any benefit for oral iron therapy in terms of quality of life, as assessed by the Kansas City Cardiomyopathy Questionnaire or any of numerous other secondary endpoints, according to Dr. Lewis, head of the heart failure section and director of the cardiopulmonary exercise testing laboratory at Massachusetts General Hospital, Boston.
Participants’ mean baseline hemoglobin level was 12.6 g/dL, but whether patients were anemic at baseline or not made no difference in terms of outcomes. Rates of venous congestion and bleeding were low during the trial.
The problem, the investigators found, was that high-dose oral iron only minimally repleted iron stores. Transferrin saturation increased by a paltry absolute 3% after 16 weeks of twice-daily therapy. Serum ferritin levels increased only 1/20th as much as after intravenous iron ferric carboxymaltose therapy in the earlier positive FAIR-HF (Ferinject Assessment in Patients With Iron Deficiency and Chronic Heart Failure) trial (N Engl J Med. 2009 Dec 17;361:2436-48).
Levels of hepcidin were elevated in study participants. And the higher the level of hepcidin – which Dr. Lewis called “a massive regulator of iron bioavailability and absorption” – the more refractory patients were to oral iron repletion.
“Hepcidin was invented by nature to protect against iron from stimulating growth of bacteria. And when it’s elevated, taking iron orally just has no chance of success,” explained Dr. Anker, professor of cardiology at the University of Gottingen (Germany).
Dr. Anker, who chaired the positive FAIR-HF trial of intravenous iron, said IRONOUT HF was a very well-conducted and definitive clinical trial of oral iron supplementation in HFrEF.
“It’s very simple: Oral iron does not work in patients with chronic heart failure. That’s the take home message. It’s true for peak VO2 [oxygen consumption], for 6-minute walk distance, for symptoms, for quality of life, and even for surrogate markers like NT-proBNP [N-terminal pro b-type natriuretic peptide]. If iron doesn’t get into the body, it’s really difficult to [imagine] that the iron that doesn’t get into the body can exert an effect,” he said.
The primary endpoint in EFFECT-HF was assessor-blinded change in peak VO2 from baseline to week 24. The control group experienced a decrease in peak VO2 over time such that there was a significant difference of 1.0 mL/kg per minute between the two groups.
The ferric carboxymaltose recipients also did significantly better in terms of secondary endpoints including improvement in New York Heart Association functional class, self-reported Patient Global Assessment score, and quality-of-life measures, reported Dr. van Veldhuisen, professor and chairman of cardiology at University Medical Center Groningen (the Netherlands).
Session moderator Clyde Yancy, MD, commented that intravenous iron is not ready for prime time use in clinical practice for several reasons. The open-label EFFECT-HF trial, like the earlier positive double-blind FAIR-HF and CONFIRM-HF IV ferric carboxymaltose trials, was too modest in size to be convincing, especially since this is an expensive and intrusive therapy.
“The endpoint of peak VO2, although a very powerful endpoint, is still one for which there may be some subjectivity, and so we need a more definitive endpoint to be absolutely certain about the potential benefit of the administration of ferric carboxymaltose,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
Discussant Adrian Hernandez, MD, of the Duke Clinical Research Institute in Durham, N.C., said he considers peak VO2 an important endpoint.
“When you talk to patients, exercise capacity is an outcome that matters to them,” he said. “They often comment that what matters to them is living longer with a better quality of life, free of worsening heart failure, and having improvement in everyday functional status. So the cardiopulmonary exercise test is not just a surrogate endpoint; it’s a measure of functional outcome that matters to patients,” he said.
Still, like Dr. Yancy, Dr. Hernandez said he thinks it’s time to have larger, longer, definitive trials with clinical endpoints in order to understand the role of intravenous iron. Both cardiologists applauded Dr. Anker’s announcement that such a trial, known as FAIR-HF2, is now getting started.
The IRONOUT HF trial was funded by the National Institutes of Health. Dr. Lewis reported receiving research support from a handful of pharmaceutical and medical device companies. Dr. van Velduisen reported serving as a scientific adviser to Vifor Pharma, which sponsored the EFFECT-HF trial. Dr. Anker, who was an EFFECT-HF investigator, serves as a consultant to Vifor and several other companies. Dr. Hernandez was an IRONOUT HF investigator and reported receiving research grants from a handful of pharmaceutical companies.
NEW ORLEANS – Oral iron supplementation was declared ineffective for the treatment of iron deficiency in patients with heart failure with reduced ejection fraction in one major randomized trial while intravenous ferric carboxymaltose improved exercise capacity and quality of life in another study presented at the American Heart Association scientific sessions.
Iron deficiency is present in roughly half of patients with heart failure with reduced ejection fraction (HFrEF). In affected patients it’s associated with diminished functional capacity and poor quality of life, and is an independent predictor of mortality. Thus, it has emerged as a potential therapeutic target in HFrEF.
The IRONOUT HF (Oral Iron Repletion Effects on Oxygen UpTake in Heart Failure) trial was a multicenter, randomized, double-blind, placebo-controlled clinical trial conducted by the National Heart, Lung, and Blood Institute’s Clinical Heart Failure Network investigators. It included 225 patients with HFrEF and iron deficiency who were randomized to 16 weeks of oral iron polysaccharide at 150 mg b.i.d. or matching placebo.
The primary endpoint was change from baseline to 16 weeks in exercise capacity, as measured via peak oxygen uptake during cardiopulmonary exercise testing. The results were no better in the iron-supplemented group than in placebo-treated controls. Nor was there any benefit for oral iron therapy in terms of quality of life, as assessed by the Kansas City Cardiomyopathy Questionnaire or any of numerous other secondary endpoints, according to Dr. Lewis, head of the heart failure section and director of the cardiopulmonary exercise testing laboratory at Massachusetts General Hospital, Boston.
Participants’ mean baseline hemoglobin level was 12.6 g/dL, but whether patients were anemic at baseline or not made no difference in terms of outcomes. Rates of venous congestion and bleeding were low during the trial.
The problem, the investigators found, was that high-dose oral iron only minimally repleted iron stores. Transferrin saturation increased by a paltry absolute 3% after 16 weeks of twice-daily therapy. Serum ferritin levels increased only 1/20th as much as after intravenous iron ferric carboxymaltose therapy in the earlier positive FAIR-HF (Ferinject Assessment in Patients With Iron Deficiency and Chronic Heart Failure) trial (N Engl J Med. 2009 Dec 17;361:2436-48).
Levels of hepcidin were elevated in study participants. And the higher the level of hepcidin – which Dr. Lewis called “a massive regulator of iron bioavailability and absorption” – the more refractory patients were to oral iron repletion.
“Hepcidin was invented by nature to protect against iron from stimulating growth of bacteria. And when it’s elevated, taking iron orally just has no chance of success,” explained Dr. Anker, professor of cardiology at the University of Gottingen (Germany).
Dr. Anker, who chaired the positive FAIR-HF trial of intravenous iron, said IRONOUT HF was a very well-conducted and definitive clinical trial of oral iron supplementation in HFrEF.
“It’s very simple: Oral iron does not work in patients with chronic heart failure. That’s the take home message. It’s true for peak VO2 [oxygen consumption], for 6-minute walk distance, for symptoms, for quality of life, and even for surrogate markers like NT-proBNP [N-terminal pro b-type natriuretic peptide]. If iron doesn’t get into the body, it’s really difficult to [imagine] that the iron that doesn’t get into the body can exert an effect,” he said.
The primary endpoint in EFFECT-HF was assessor-blinded change in peak VO2 from baseline to week 24. The control group experienced a decrease in peak VO2 over time such that there was a significant difference of 1.0 mL/kg per minute between the two groups.
The ferric carboxymaltose recipients also did significantly better in terms of secondary endpoints including improvement in New York Heart Association functional class, self-reported Patient Global Assessment score, and quality-of-life measures, reported Dr. van Veldhuisen, professor and chairman of cardiology at University Medical Center Groningen (the Netherlands).
Session moderator Clyde Yancy, MD, commented that intravenous iron is not ready for prime time use in clinical practice for several reasons. The open-label EFFECT-HF trial, like the earlier positive double-blind FAIR-HF and CONFIRM-HF IV ferric carboxymaltose trials, was too modest in size to be convincing, especially since this is an expensive and intrusive therapy.
“The endpoint of peak VO2, although a very powerful endpoint, is still one for which there may be some subjectivity, and so we need a more definitive endpoint to be absolutely certain about the potential benefit of the administration of ferric carboxymaltose,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
Discussant Adrian Hernandez, MD, of the Duke Clinical Research Institute in Durham, N.C., said he considers peak VO2 an important endpoint.
“When you talk to patients, exercise capacity is an outcome that matters to them,” he said. “They often comment that what matters to them is living longer with a better quality of life, free of worsening heart failure, and having improvement in everyday functional status. So the cardiopulmonary exercise test is not just a surrogate endpoint; it’s a measure of functional outcome that matters to patients,” he said.
Still, like Dr. Yancy, Dr. Hernandez said he thinks it’s time to have larger, longer, definitive trials with clinical endpoints in order to understand the role of intravenous iron. Both cardiologists applauded Dr. Anker’s announcement that such a trial, known as FAIR-HF2, is now getting started.
The IRONOUT HF trial was funded by the National Institutes of Health. Dr. Lewis reported receiving research support from a handful of pharmaceutical and medical device companies. Dr. van Velduisen reported serving as a scientific adviser to Vifor Pharma, which sponsored the EFFECT-HF trial. Dr. Anker, who was an EFFECT-HF investigator, serves as a consultant to Vifor and several other companies. Dr. Hernandez was an IRONOUT HF investigator and reported receiving research grants from a handful of pharmaceutical companies.
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
VIDEO: Appealing DAA denials is worth it for hepatitis C patients
BOSTON – Though criteria for insurance approval for direct-acting antivirals (DAAs) for hepatitis C virus (HCV) are loosening, many patients are still denied by both public and private carriers. Providers and patients should know that it’s worthwhile to appeal these denials; 78.1% (115 of 145) of initial DAA denials were approved on appeal, according to a recent study.
Jane Giang, PharmD, a clinical pharmacist at the University of North Carolina Health System, Chapel Hill, worked with colleagues to conduct a retrospective study of patients at her facility who were prescribed a DAA for HCV between October 2014 and April 2016.
Dr. Giang, in a video interview at the annual meeting of the American Association for the Study of Liver Diseases, said that she works alongside physicians in her clinic to craft appeals, tailoring appeal letters to individual patients’ circumstances.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In a poster presentation, Dr. Giang and her colleagues presented results from a total of 1,017 patients who were prescribed DAAs for HCV during the study time frame. Of these, three-quarters (n = 794, 78.1%) received initial approval for their medication, while one in five patients (n = 206, 20.2%) had their initial applications denied. The remaining patients either had their cases closed for a variety of reasons, or had pending applications at the time of data analysis.
About half of the patients (n = 496, 48.8%) had commercial insurance. Medicare was the primary insurance for another 207 (n = 20.4%), and Medicaid for 140 (13.8%).
Of the patients whose DAAs were initially denied, 65 (31.6%) of the denials were for fibrosis less than stage F2. Another quarter of patients (n = 57, 27.7%) did not meet approval criteria, and 41 (19.9%) of denials said that the DAA was nonformulary or excluded by the plan. The remaining denials were for missing information or a variety of other reasons.
Half of the patients (n = 504, 49.6%) had F4 fibrosis at the time of application for DAA treatment; 241 (23.7%) had F0 or F1 fibrosis, and the remainder were approximately evenly split between F3 and F4 fibrosis.
When a subset of these denials went through an appeals process, most were eventually approved. Of the 42 denials for less than F2 fibrosis that were appealed, 20 (47.6%) were eventually approved. Of the 40 patients whose applications for DAAs were based on not meeting criteria, 37 (92.5%) were approved on appeal, and of the 32 denials based on plan exclusions or DAAs being nonformulary, 29 (90.6%) were approved on appeal.
When Dr. Giang and her colleagues broke down the numbers by type of insurance, they found that of the 496 patients who had commercial insurance, only 44 (8.9%) eventually received a final denial. Medicare patients had a 3.9% final denial rate, while just one of the 172 patients (0.6%) without insurance who received medication through programs directly from the manufacturer had a final denial.
The largest number of final denials occurred in the group of patients with Medicaid. Of these 140 patients, 25 (17.9%) had a final denial. Dr. Giang said that in North Carolina, providers cannot file appeals for DAA approval on behalf of patients; the paperwork is sent directly to the patient’s home, and patients have to complete and file the forms. She said that she and her colleagues learned to alert these patients to be on the lookout for paperwork, and counseled them to bring the appeal forms into the clinic so that staff could assist them in completing the appeal.
Though Dr. Giang said that her study showed that payer type matters when it comes to reimbursement for HCV care, the “impact of payer type on access to care remains incompletely explored, especially among noninsured patients,” she said.
Dr. Giang reported no outside sources of funding, and no conflicts of interest.
koakes@frontlinemedcom.com
On Twitter@karioakes
BOSTON – Though criteria for insurance approval for direct-acting antivirals (DAAs) for hepatitis C virus (HCV) are loosening, many patients are still denied by both public and private carriers. Providers and patients should know that it’s worthwhile to appeal these denials; 78.1% (115 of 145) of initial DAA denials were approved on appeal, according to a recent study.
Jane Giang, PharmD, a clinical pharmacist at the University of North Carolina Health System, Chapel Hill, worked with colleagues to conduct a retrospective study of patients at her facility who were prescribed a DAA for HCV between October 2014 and April 2016.
Dr. Giang, in a video interview at the annual meeting of the American Association for the Study of Liver Diseases, said that she works alongside physicians in her clinic to craft appeals, tailoring appeal letters to individual patients’ circumstances.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In a poster presentation, Dr. Giang and her colleagues presented results from a total of 1,017 patients who were prescribed DAAs for HCV during the study time frame. Of these, three-quarters (n = 794, 78.1%) received initial approval for their medication, while one in five patients (n = 206, 20.2%) had their initial applications denied. The remaining patients either had their cases closed for a variety of reasons, or had pending applications at the time of data analysis.
About half of the patients (n = 496, 48.8%) had commercial insurance. Medicare was the primary insurance for another 207 (n = 20.4%), and Medicaid for 140 (13.8%).
Of the patients whose DAAs were initially denied, 65 (31.6%) of the denials were for fibrosis less than stage F2. Another quarter of patients (n = 57, 27.7%) did not meet approval criteria, and 41 (19.9%) of denials said that the DAA was nonformulary or excluded by the plan. The remaining denials were for missing information or a variety of other reasons.
Half of the patients (n = 504, 49.6%) had F4 fibrosis at the time of application for DAA treatment; 241 (23.7%) had F0 or F1 fibrosis, and the remainder were approximately evenly split between F3 and F4 fibrosis.
When a subset of these denials went through an appeals process, most were eventually approved. Of the 42 denials for less than F2 fibrosis that were appealed, 20 (47.6%) were eventually approved. Of the 40 patients whose applications for DAAs were based on not meeting criteria, 37 (92.5%) were approved on appeal, and of the 32 denials based on plan exclusions or DAAs being nonformulary, 29 (90.6%) were approved on appeal.
When Dr. Giang and her colleagues broke down the numbers by type of insurance, they found that of the 496 patients who had commercial insurance, only 44 (8.9%) eventually received a final denial. Medicare patients had a 3.9% final denial rate, while just one of the 172 patients (0.6%) without insurance who received medication through programs directly from the manufacturer had a final denial.
The largest number of final denials occurred in the group of patients with Medicaid. Of these 140 patients, 25 (17.9%) had a final denial. Dr. Giang said that in North Carolina, providers cannot file appeals for DAA approval on behalf of patients; the paperwork is sent directly to the patient’s home, and patients have to complete and file the forms. She said that she and her colleagues learned to alert these patients to be on the lookout for paperwork, and counseled them to bring the appeal forms into the clinic so that staff could assist them in completing the appeal.
Though Dr. Giang said that her study showed that payer type matters when it comes to reimbursement for HCV care, the “impact of payer type on access to care remains incompletely explored, especially among noninsured patients,” she said.
Dr. Giang reported no outside sources of funding, and no conflicts of interest.
koakes@frontlinemedcom.com
On Twitter@karioakes
BOSTON – Though criteria for insurance approval for direct-acting antivirals (DAAs) for hepatitis C virus (HCV) are loosening, many patients are still denied by both public and private carriers. Providers and patients should know that it’s worthwhile to appeal these denials; 78.1% (115 of 145) of initial DAA denials were approved on appeal, according to a recent study.
Jane Giang, PharmD, a clinical pharmacist at the University of North Carolina Health System, Chapel Hill, worked with colleagues to conduct a retrospective study of patients at her facility who were prescribed a DAA for HCV between October 2014 and April 2016.
Dr. Giang, in a video interview at the annual meeting of the American Association for the Study of Liver Diseases, said that she works alongside physicians in her clinic to craft appeals, tailoring appeal letters to individual patients’ circumstances.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In a poster presentation, Dr. Giang and her colleagues presented results from a total of 1,017 patients who were prescribed DAAs for HCV during the study time frame. Of these, three-quarters (n = 794, 78.1%) received initial approval for their medication, while one in five patients (n = 206, 20.2%) had their initial applications denied. The remaining patients either had their cases closed for a variety of reasons, or had pending applications at the time of data analysis.
About half of the patients (n = 496, 48.8%) had commercial insurance. Medicare was the primary insurance for another 207 (n = 20.4%), and Medicaid for 140 (13.8%).
Of the patients whose DAAs were initially denied, 65 (31.6%) of the denials were for fibrosis less than stage F2. Another quarter of patients (n = 57, 27.7%) did not meet approval criteria, and 41 (19.9%) of denials said that the DAA was nonformulary or excluded by the plan. The remaining denials were for missing information or a variety of other reasons.
Half of the patients (n = 504, 49.6%) had F4 fibrosis at the time of application for DAA treatment; 241 (23.7%) had F0 or F1 fibrosis, and the remainder were approximately evenly split between F3 and F4 fibrosis.
When a subset of these denials went through an appeals process, most were eventually approved. Of the 42 denials for less than F2 fibrosis that were appealed, 20 (47.6%) were eventually approved. Of the 40 patients whose applications for DAAs were based on not meeting criteria, 37 (92.5%) were approved on appeal, and of the 32 denials based on plan exclusions or DAAs being nonformulary, 29 (90.6%) were approved on appeal.
When Dr. Giang and her colleagues broke down the numbers by type of insurance, they found that of the 496 patients who had commercial insurance, only 44 (8.9%) eventually received a final denial. Medicare patients had a 3.9% final denial rate, while just one of the 172 patients (0.6%) without insurance who received medication through programs directly from the manufacturer had a final denial.
The largest number of final denials occurred in the group of patients with Medicaid. Of these 140 patients, 25 (17.9%) had a final denial. Dr. Giang said that in North Carolina, providers cannot file appeals for DAA approval on behalf of patients; the paperwork is sent directly to the patient’s home, and patients have to complete and file the forms. She said that she and her colleagues learned to alert these patients to be on the lookout for paperwork, and counseled them to bring the appeal forms into the clinic so that staff could assist them in completing the appeal.
Though Dr. Giang said that her study showed that payer type matters when it comes to reimbursement for HCV care, the “impact of payer type on access to care remains incompletely explored, especially among noninsured patients,” she said.
Dr. Giang reported no outside sources of funding, and no conflicts of interest.
koakes@frontlinemedcom.com
On Twitter@karioakes
AT THE LIVER MEETING 2016
Surgery for bowel obstruction in cancer patients didn’t increase 90-day mortality
CORONADO, CALIF. – Among advanced cancer patients with bowel obstruction, surgery was not an independent predictor of the ability to eat at discharge or survival within 90 days of consultation, results from a long-term retrospective study showed.
“I think this represents the complexity in treating these patients,” lead study author Brian D. Badgwell, MD, said at the annual meeting of the Western Surgical Association. “We need future studies to identify the optimal outcome measures.”
For the current study, the researchers retrospectively reviewed the medical records of 490 patients who required surgical consultation for bowel obstruction at MD Anderson Cancer Center between January 2000 and May 2014. They set out to determine the incidence of obstruction due to intra-abdominal tumor and to identify variables associated with the ability to eat at hospital discharge and 90-day survival. They excluded patients without clinical or radiologic features of mechanical bowel obstruction. Clinical variables of interest included obstruction site, tumor vs. non-tumor cause, laboratory parameters, radiologic extent of malignancy, and the type of treatment performed (surgical, medical, or interventional, defined as interventional radiology or endoscopy). Overall survival was calculated from the date of first surgical evaluation for bowel obstruction to any cause mortality or last follow-up. Univariate and multivariate analyses were performed for ability to eat and a Cox proportional hazards model for 90-day survival.
Dr. Badgwell reported that the most common obstruction site in the 490 patients was the small bowel (64%), followed by large bowel (20%) and gastric outlet (16%). Obstruction etiology was identified as tumor-related in 68% of cases, followed by adhesion-related (20%) and unclear (12%). Nearly half of patients (46%) received chemotherapy within 6 weeks of their surgical consultation, but only 4% were neutropenic. More than half of patients (52%) had an albumin level of less than 3.5 g/dL, 52% had a hemoglobin of 10 g/dL or greater, 36% had lymphadenopathy, 35% had ascites, 34% had peritoneal disease, and 31% had a primary or recurrent tumor in place. In addition, 53% had an abdominal visceral malignancy, 9% had bone metastases, and 14% had lung metastases.
About half of patients (49%) received medical management as their treatment, followed by surgical and procedural treatment (32% and 17%, respectively). Fifteen percent were discharged to in-home hospice or to an inpatient hospice facility. More than two-thirds (68%) were able to eat at the time of discharge, and 43% died within 90 days of surgical consultation.
Multivariate analysis revealed that the following factors were negatively associated with eating at discharge: an intact/primary local recurrence (odds ratio, 0.46), carcinomatosis (OR, 0.34), and albumin level of less than 3.5 g/dL (OR, 0.55). At the same time, variables associated with death within 90 days of consultation included having an intact primary/local recurrence (hazard ratio, 1.75), carcinomatosis (HR, 1.98), and abdominal visceral metastasis (HR, 1.75). Finally, compared with procedural treatment, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
“There is a high rate of non-mechanical bowel dysfunction in patients undergoing surgical consultation for bowel obstruction,” Dr. Badgwell concluded. “It’s very difficult to categorize these cases preoperatively. They do require a selective approach. Variables associated with outcome measures support caution in patients with carcinomatosis, hypoalbuminemia, and multiple sites of disease on imaging.”
Dr. Badgwell reported having no financial disclosures.
CORONADO, CALIF. – Among advanced cancer patients with bowel obstruction, surgery was not an independent predictor of the ability to eat at discharge or survival within 90 days of consultation, results from a long-term retrospective study showed.
“I think this represents the complexity in treating these patients,” lead study author Brian D. Badgwell, MD, said at the annual meeting of the Western Surgical Association. “We need future studies to identify the optimal outcome measures.”
For the current study, the researchers retrospectively reviewed the medical records of 490 patients who required surgical consultation for bowel obstruction at MD Anderson Cancer Center between January 2000 and May 2014. They set out to determine the incidence of obstruction due to intra-abdominal tumor and to identify variables associated with the ability to eat at hospital discharge and 90-day survival. They excluded patients without clinical or radiologic features of mechanical bowel obstruction. Clinical variables of interest included obstruction site, tumor vs. non-tumor cause, laboratory parameters, radiologic extent of malignancy, and the type of treatment performed (surgical, medical, or interventional, defined as interventional radiology or endoscopy). Overall survival was calculated from the date of first surgical evaluation for bowel obstruction to any cause mortality or last follow-up. Univariate and multivariate analyses were performed for ability to eat and a Cox proportional hazards model for 90-day survival.
Dr. Badgwell reported that the most common obstruction site in the 490 patients was the small bowel (64%), followed by large bowel (20%) and gastric outlet (16%). Obstruction etiology was identified as tumor-related in 68% of cases, followed by adhesion-related (20%) and unclear (12%). Nearly half of patients (46%) received chemotherapy within 6 weeks of their surgical consultation, but only 4% were neutropenic. More than half of patients (52%) had an albumin level of less than 3.5 g/dL, 52% had a hemoglobin of 10 g/dL or greater, 36% had lymphadenopathy, 35% had ascites, 34% had peritoneal disease, and 31% had a primary or recurrent tumor in place. In addition, 53% had an abdominal visceral malignancy, 9% had bone metastases, and 14% had lung metastases.
About half of patients (49%) received medical management as their treatment, followed by surgical and procedural treatment (32% and 17%, respectively). Fifteen percent were discharged to in-home hospice or to an inpatient hospice facility. More than two-thirds (68%) were able to eat at the time of discharge, and 43% died within 90 days of surgical consultation.
Multivariate analysis revealed that the following factors were negatively associated with eating at discharge: an intact/primary local recurrence (odds ratio, 0.46), carcinomatosis (OR, 0.34), and albumin level of less than 3.5 g/dL (OR, 0.55). At the same time, variables associated with death within 90 days of consultation included having an intact primary/local recurrence (hazard ratio, 1.75), carcinomatosis (HR, 1.98), and abdominal visceral metastasis (HR, 1.75). Finally, compared with procedural treatment, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
“There is a high rate of non-mechanical bowel dysfunction in patients undergoing surgical consultation for bowel obstruction,” Dr. Badgwell concluded. “It’s very difficult to categorize these cases preoperatively. They do require a selective approach. Variables associated with outcome measures support caution in patients with carcinomatosis, hypoalbuminemia, and multiple sites of disease on imaging.”
Dr. Badgwell reported having no financial disclosures.
CORONADO, CALIF. – Among advanced cancer patients with bowel obstruction, surgery was not an independent predictor of the ability to eat at discharge or survival within 90 days of consultation, results from a long-term retrospective study showed.
“I think this represents the complexity in treating these patients,” lead study author Brian D. Badgwell, MD, said at the annual meeting of the Western Surgical Association. “We need future studies to identify the optimal outcome measures.”
For the current study, the researchers retrospectively reviewed the medical records of 490 patients who required surgical consultation for bowel obstruction at MD Anderson Cancer Center between January 2000 and May 2014. They set out to determine the incidence of obstruction due to intra-abdominal tumor and to identify variables associated with the ability to eat at hospital discharge and 90-day survival. They excluded patients without clinical or radiologic features of mechanical bowel obstruction. Clinical variables of interest included obstruction site, tumor vs. non-tumor cause, laboratory parameters, radiologic extent of malignancy, and the type of treatment performed (surgical, medical, or interventional, defined as interventional radiology or endoscopy). Overall survival was calculated from the date of first surgical evaluation for bowel obstruction to any cause mortality or last follow-up. Univariate and multivariate analyses were performed for ability to eat and a Cox proportional hazards model for 90-day survival.
Dr. Badgwell reported that the most common obstruction site in the 490 patients was the small bowel (64%), followed by large bowel (20%) and gastric outlet (16%). Obstruction etiology was identified as tumor-related in 68% of cases, followed by adhesion-related (20%) and unclear (12%). Nearly half of patients (46%) received chemotherapy within 6 weeks of their surgical consultation, but only 4% were neutropenic. More than half of patients (52%) had an albumin level of less than 3.5 g/dL, 52% had a hemoglobin of 10 g/dL or greater, 36% had lymphadenopathy, 35% had ascites, 34% had peritoneal disease, and 31% had a primary or recurrent tumor in place. In addition, 53% had an abdominal visceral malignancy, 9% had bone metastases, and 14% had lung metastases.
About half of patients (49%) received medical management as their treatment, followed by surgical and procedural treatment (32% and 17%, respectively). Fifteen percent were discharged to in-home hospice or to an inpatient hospice facility. More than two-thirds (68%) were able to eat at the time of discharge, and 43% died within 90 days of surgical consultation.
Multivariate analysis revealed that the following factors were negatively associated with eating at discharge: an intact/primary local recurrence (odds ratio, 0.46), carcinomatosis (OR, 0.34), and albumin level of less than 3.5 g/dL (OR, 0.55). At the same time, variables associated with death within 90 days of consultation included having an intact primary/local recurrence (hazard ratio, 1.75), carcinomatosis (HR, 1.98), and abdominal visceral metastasis (HR, 1.75). Finally, compared with procedural treatment, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
“There is a high rate of non-mechanical bowel dysfunction in patients undergoing surgical consultation for bowel obstruction,” Dr. Badgwell concluded. “It’s very difficult to categorize these cases preoperatively. They do require a selective approach. Variables associated with outcome measures support caution in patients with carcinomatosis, hypoalbuminemia, and multiple sites of disease on imaging.”
Dr. Badgwell reported having no financial disclosures.
AT WSA 2016
Key clinical point:
Major finding: Compared with procedural treatment of bowel obstruction, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
Data source: A retrospective review of 490 patients with advanced cancer who required surgical consultation for bowel obstruction at MD Anderson Cancer Center, Houston, between January 2000 and May 2014.
Disclosures: Dr. Badgwell reported having no financial disclosures.
Helping patients heal after a bruising election campaign
One of us practices in the “new south” community of Charlotte, N.C., “a red state”; the other is in the “blue bubble” of Washington. In our respective polarized zones, the divergent reactions we heard about the presidential candidates were akin to projective responses to Rorschach tests.
As mental health clinicians, we knew that the country was wounded and in need of healing long before the outcome of the unconventional and acrimonious 2016 American presidential race. So, we were concerned about how patients, clinicians, and divergent communities would go about healing after an 18-month pre-election slugfest that revealed bigotry that persists more than 150 years after the Civil War.
Background of ‘two sides’
None of the nasty rhetoric delivered by our now president-elect or the clearly defensive responses we heard from our former secretary of state were going to be easily forgotten after Nov. 8, 2016. As the process unfolded, however, the voice of psychiatry, with some notable exceptions (the blog of Justin Frank, MD, for example), was absent from the public dialogue. 
Nevertheless, writing in June of this year, Bill Moyers and Michael Winship summed up the private assessment of many professionals and the fears for many of a Trump presidency:
There is a virus infecting our politics and right now it’s flourishing with a scarlet fever. It feeds on fear, paranoia and bigotry. All that was required for it to spread was a timely opportunity – and an opportunist with no scruples. ... There have been stretches of history when this virus lay dormant. ... Today its carrier is Donald Trump, but others came before him: narcissistic demagogues who lie and distort in pursuit of power and self-promotion. Bullies all, swaggering across the landscape with fistfuls of false promises, smears, innuendo and hatred for others, spite and spittle for anyone of a different race, faith, gender, or nationality.1
Alternatively, some had a smoldering fear of the progressive agenda to bring “others” – more women, African Americans, Latinos, the LGBTQ community, Muslims, and the disabled – securely under the tent of American democracy. Others, especially the underemployed cohort in neglected and struggling communities in Middle America, were simply opposed to a continuation of “politics as usual,” a.k.a. Hillary Clinton, and were desperate for change. 
The opposition views were summed up in the innuendo of the slogan: “Make America Great Again.” By the election, the tensions had begun to resemble the aggressive spirit of a sporting event: It’s “us” versus “them.”
Causes of concern
In the months leading up to the election, violent events strained the societal divisions. The police use of force2 resulted in the near-daily deaths of African American men and women and other people of color at the hands of police officers. The events built on a long and growing list of violent acts – the racially motivated shootings of nine men and women in a Charleston, S.C., church, the bombing injuries and deaths at the Boston Marathon, the shooting deaths of 20 children and 6 adults at Sandy Hook Elementary School, the homophobia-motivated shootings in a Florida nightclub – that have heightened levels of fear, anxiety, and concern for personal and family safety. For many, life has felt fragile and out of control, the perfect setup to motivate the electorate to cast their votes for the person they imagined had the most power and most interest in restoring their sense of control over their lives and, ultimately, their sense of safety.
Why the fear? A psychodynamic analysis
As psychiatrists trained in psychodynamic theory, we are quite familiar with the concept of identifying with the aggressor as a means of coping. The classic example is when a child watches his or her parents in an abusive relationship and identifies with the abusive parent in an attempt to avoid identifying with the victimized parent.
This dynamic is one that seems to have played out during this presidential election. By October 2016, Donald J. Trump already reportedly had insulted more than 280 people, places, and things on Twitter.3 Despite the evidence that Mr. Trump verbally bullied not only his opponents, but also the media, Latinos, women, the LGBTQ community, the Republican Party (his claimed party), and Muslims, people came out in numbers high enough to make him America’s president-elect. In the classic process of bullying his perceived enemies, those considered “the other,” he assigned names such as “crooked Hillary,” “little Marco,” and “lyin’ Ted” – just as a bully at school assigns names to the kid he’s decided does not have enough worth to be called by his given name.
He depicted women who accused him of sexual assault as either not being pretty enough to be worthy of assault or self-serving in their public accusations. Mexicans entering this country were referred to as “rapists and thugs.” African Americans were told that their lives are so bad that they “have nothing to lose” if they voted for a candidate who talked about erecting a wall to block out other people of color, and changing immigration laws that would banish an entire religion from entering our country.
The ‘blue bubble’ – Those who voted for Mrs. Clinton
So … this happened. And, in our consulting rooms, we are seeing a stark increase in the numbers of individuals, couples, and families reporting overwhelming anxiety, sadness, and a sense of de-realization (“it’s surreal”). At the core of their anxiety is concern for self, family, and friends as well as concern for the country as a whole.
The post-election notions that families would be immediately broken up, parents deported, the Affordable Care Act immediately dismantled, and countries bombed immediately after Election Day did not become realities. However, there is valid reason to be concerned. The Southern Poverty Law Center has noted a significant increase in post-election hate crimes throughout the nation.4
The new South ‘red states’ – those who voted for Mr. Trump
Trump supporters are feeling victorious because their “underdog” candidate ran an unconventional presidential campaign and won. However, some who voted for Mr. Trump will at some point experience anxiety when the excitement of “winning” wears off. Psychoanalyst Justin Frank speaks to this and more in his Nov. 9, 2016, blog in which he concludes: “While we mourn and blame others and ourselves for our American tragedy, Trump voters must eventually look at themselves in the mirror and exclaim, ‘what have we done?’ ”5
In his Oct. 25, 2016, New York Times article, Michael Barbaro summarized the behaviors that will become increasingly of concern to all as Mr. Trump accepts the oath of office:
The intense ambitions and undisciplined behaviors of Mr. Trump have confounded even those close to him.... In interviews, Mr. Trump makes clear just how difficult it is for him to imagine – let alone accept – defeat....
“I never had a failure,” Mr. Trump said in one of the interviews, despite his repeated corporate bankruptcies and business setbacks, “because I always turned a failure into a success.”6
This fundamental inability to accept responsibility and the attempt to distort reality is something that must concern each of us, regardless of our ideological differences.
Distress tolerance as a model for healing
Even before the outcome of the election, we were hearing from patients who did not feel safe and who reported being “terrified” about what our country might become. This is where a focus on processing the pain and decreasing anxiety is necessary. This is not an anxiety we can medicate with anxiolytics or rationalize by telling ourselves and our patients that the best man won “fair and square.” We have each – by this time – experienced patients who are quite shaken by this turn of events.
Although it has not received much press, many consider Mr. Trump’s victory to be, in part, a “white backlash.” Many supporters of Mr. Trump have felt too ashamed to publicly admit their support for a candidate who at least by innuendo incited fear, anger, and violence. This failure has created an anxiety reminiscent of the daytime anxiety experienced by people who survived nighttime lynchings in small Southern towns. The day after the lynching, it was not unusual for African American men, women, and children to wonder if their grocer, banker, postal carrier, or sheriff had donned a white hood the night before and lynched someone in their community.
The question of survival, how to survive the unimaginable, is what most distresses people. They’ve wondered out loud whether they, their family, and friends would be attacked and/or killed by those who now feel emboldened and authorized to act on their latent aggressive impulses. And, our patients’ fears are legitimate because, unfortunately, studies show that verbal aggression is correlated with increased risk of physical violence and even murder.7
In the dialectical behavioral therapy (DBT) construct developed by Marsha M. Linehan, PhD, the goals of distress tolerance are crisis survival, reality acceptance, and then freedom.8
As we apply our skills, we are uniquely positioned to help our patients and their families survive this crisis, accept that this is our president-elect, and ultimately be free from the anxiety created by the behavior that we all witnessed. We can aid in the navigation through this storm.
Acceptance
We’re already on to reality acceptance. The reality that so many African Americans and people of color have been living is now known and experienced by many who had felt immune to being marginalized. They now understand the loss of security that accompanies overwhelming fear of being the object of verbal, emotional, and physical aggression and violence.
Some are coping by entertaining fantasies that this election outcome will be undone, that the Electoral College will not approve our president-elect when it meets on Dec. 19 or that Mr. Trump will be impeached early in this upcoming term. The results of the presidential election are unlikely to be undone, so having more than 2 months between Election Day and the inauguration to work on acceptance will be helpful. The goal here is to accept the past, be hopeful about the future, and be vigilant in the present.
Freedom
Now, on to freedom. Our goal is to have all of our patients, families, colleagues, and communities able to live without fear that our leaders are not able to apply humanitarian principles to keep all of us safe. The next few months are crucial. Americans must speak out and debride the wound that bullying intentionally causes. Just as with a school bully, Mr. Trump’s behavior has to be called what it is, not sugarcoated or normalized.
History is full of critical moments in time in which, even in our fear, we said nothing. Even the most empathic of us watched the bully at school and felt relief that his behavior was not directed toward us. But we must not avert our gaze.
Bill Moyers and Michael Winship compared Mr. Trump to Sen. Joseph McCarthy, whose reign of terror was ended when journalist Edward R. Murrow courageously spoke out in defiance of the senator. At the end of one of his segments on “See It Now,” Mr. Murrow concluded as he signed off:
We will not walk in fear, one of another. We will not be driven by fear into an age of unreason, if we dig deep in our history and our doctrine, and remember that we are not descended from fearful men — not from men who feared to write, to speak, to associate and to defend causes that were, for the moment, unpopular.9
And, so, how do we cope?
Fortunately, we understand bullying. The bully doesn’t take over the entire school and won’t have the power to take over one’s entire life if the behavior is brought out in the open and openly discussed. But bullies need to accept responsibility, which is what Sen. Harry Reid of Nevada and other legislators urged President-elect Trump to do in days immediately following the election.10 They have called on him to discourage the fear, anger, and violence leading up to and following the election. This action on Mr. Trump’s part would promote a vitally needed national healing process.
Ultimately, this is “the land of the free, the home of the brave …” and we will do what we have always done as psychiatrists and mental health professionals who help to heal wounds. Not all of us will participate in social justice initiatives. However, each of us can listen with intense compassion and interest to those with whom we identify politically and to those whose views diverge from our own. This is our most potent tool in a conflict where we don’t understand the motives of unpredictable leaders or their followers. It is only with this skilled listening that a space is created in which each “other” hears the “other.” This is where real healing begins.
The views expressed in this article are solely those of the authors, and are not meant to represent the views of the American Psychiatric Association, Novant Health, Clinical Psychiatry News, or any other organization.
References
1. http://billposters/story/trump-virus-dark-age-unreason
2. http://blackdoctor.org/495036/national-medical-association-statement-on-police-use-of-force
3. http://www.nytimes.com/interactive/2016/01/28/upshot/donald-trump-twitter-insults.html?_r=0
4. https://www.splcenter.org/hatewatch/2016/11/11/over-200-incidents-hateful-harassment-and-intimidation-election-day
5. http://www.obamaonthecouch.com
6. http://www.nytimes.com/2016/10/26/us/politics/donald-trump-interviews.html
7. “The Nature of Prejudice,” (New York: Perseus Books Publishing, 1979).
8. DBT® Skills Training Handouts and Worksheets, Second Edition (New York: The Guilford Press, 2014).
9. http://billmoyers.com/story/trump-virus-dark-age-unreason
10. http://www.reid.senate.gov/press_releases/2016-11-11-reid-statement-on-the-election-of-donald-trump#.WC0iA6IrKgR
Dr. Dunlap, a psychiatrist and psychoanalyst who practices in Washington, is the immediate past president of the Washington Psychiatric Society, and associate clinical professor of psychiatry and behavioral sciences at George Washington University, Washington. She is interested in the role “difference” – race, culture, and ethnicity – plays in interpersonal relationships and group dynamics. Dr. Ifill-Taylor, a child, adolescent, and adult psychiatrist, is in practice as a medical director in Charlotte, N.C. Previously, she was in private practice in the Washington area and worked as a staff psychiatrist for the Department of Veterans Affairs. She is particularly interested in the effect of our social, political, and occupational environment on mental and physical health.
One of us practices in the “new south” community of Charlotte, N.C., “a red state”; the other is in the “blue bubble” of Washington. In our respective polarized zones, the divergent reactions we heard about the presidential candidates were akin to projective responses to Rorschach tests.
As mental health clinicians, we knew that the country was wounded and in need of healing long before the outcome of the unconventional and acrimonious 2016 American presidential race. So, we were concerned about how patients, clinicians, and divergent communities would go about healing after an 18-month pre-election slugfest that revealed bigotry that persists more than 150 years after the Civil War.
Background of ‘two sides’
None of the nasty rhetoric delivered by our now president-elect or the clearly defensive responses we heard from our former secretary of state were going to be easily forgotten after Nov. 8, 2016. As the process unfolded, however, the voice of psychiatry, with some notable exceptions (the blog of Justin Frank, MD, for example), was absent from the public dialogue.
Nevertheless, writing in June of this year, Bill Moyers and Michael Winship summed up the private assessment of many professionals and the fears for many of a Trump presidency:
There is a virus infecting our politics and right now it’s flourishing with a scarlet fever. It feeds on fear, paranoia and bigotry. All that was required for it to spread was a timely opportunity – and an opportunist with no scruples. ... There have been stretches of history when this virus lay dormant. ... Today its carrier is Donald Trump, but others came before him: narcissistic demagogues who lie and distort in pursuit of power and self-promotion. Bullies all, swaggering across the landscape with fistfuls of false promises, smears, innuendo and hatred for others, spite and spittle for anyone of a different race, faith, gender, or nationality.1
Alternatively, some had a smoldering fear of the progressive agenda to bring “others” – more women, African Americans, Latinos, the LGBTQ community, Muslims, and the disabled – securely under the tent of American democracy. Others, especially the underemployed cohort in neglected and struggling communities in Middle America, were simply opposed to a continuation of “politics as usual,” a.k.a. Hillary Clinton, and were desperate for change.
The opposition views were summed up in the innuendo of the slogan: “Make America Great Again.” By the election, the tensions had begun to resemble the aggressive spirit of a sporting event: It’s “us” versus “them.”
Causes of concern
In the months leading up to the election, violent events strained the societal divisions. The police use of force2 resulted in the near-daily deaths of African American men and women and other people of color at the hands of police officers. The events built on a long and growing list of violent acts – the racially motivated shootings of nine men and women in a Charleston, S.C., church, the bombing injuries and deaths at the Boston Marathon, the shooting deaths of 20 children and 6 adults at Sandy Hook Elementary School, the homophobia-motivated shootings in a Florida nightclub – that have heightened levels of fear, anxiety, and concern for personal and family safety. For many, life has felt fragile and out of control, the perfect setup to motivate the electorate to cast their votes for the person they imagined had the most power and most interest in restoring their sense of control over their lives and, ultimately, their sense of safety.
Why the fear? A psychodynamic analysis
As psychiatrists trained in psychodynamic theory, we are quite familiar with the concept of identifying with the aggressor as a means of coping. The classic example is when a child watches his or her parents in an abusive relationship and identifies with the abusive parent in an attempt to avoid identifying with the victimized parent.
This dynamic is one that seems to have played out during this presidential election. By October 2016, Donald J. Trump already reportedly had insulted more than 280 people, places, and things on Twitter.3 Despite the evidence that Mr. Trump verbally bullied not only his opponents, but also the media, Latinos, women, the LGBTQ community, the Republican Party (his claimed party), and Muslims, people came out in numbers high enough to make him America’s president-elect. In the classic process of bullying his perceived enemies, those considered “the other,” he assigned names such as “crooked Hillary,” “little Marco,” and “lyin’ Ted” – just as a bully at school assigns names to the kid he’s decided does not have enough worth to be called by his given name.
He depicted women who accused him of sexual assault as either not being pretty enough to be worthy of assault or self-serving in their public accusations. Mexicans entering this country were referred to as “rapists and thugs.” African Americans were told that their lives are so bad that they “have nothing to lose” if they voted for a candidate who talked about erecting a wall to block out other people of color, and changing immigration laws that would banish an entire religion from entering our country.
The ‘blue bubble’ – Those who voted for Mrs. Clinton
So … this happened. And, in our consulting rooms, we are seeing a stark increase in the numbers of individuals, couples, and families reporting overwhelming anxiety, sadness, and a sense of de-realization (“it’s surreal”). At the core of their anxiety is concern for self, family, and friends as well as concern for the country as a whole.
The post-election notions that families would be immediately broken up, parents deported, the Affordable Care Act immediately dismantled, and countries bombed immediately after Election Day did not become realities. However, there is valid reason to be concerned. The Southern Poverty Law Center has noted a significant increase in post-election hate crimes throughout the nation.4
The new South ‘red states’ – those who voted for Mr. Trump
Trump supporters are feeling victorious because their “underdog” candidate ran an unconventional presidential campaign and won. However, some who voted for Mr. Trump will at some point experience anxiety when the excitement of “winning” wears off. Psychoanalyst Justin Frank speaks to this and more in his Nov. 9, 2016, blog in which he concludes: “While we mourn and blame others and ourselves for our American tragedy, Trump voters must eventually look at themselves in the mirror and exclaim, ‘what have we done?’ ”5
In his Oct. 25, 2016, New York Times article, Michael Barbaro summarized the behaviors that will become increasingly of concern to all as Mr. Trump accepts the oath of office:
The intense ambitions and undisciplined behaviors of Mr. Trump have confounded even those close to him.... In interviews, Mr. Trump makes clear just how difficult it is for him to imagine – let alone accept – defeat....
“I never had a failure,” Mr. Trump said in one of the interviews, despite his repeated corporate bankruptcies and business setbacks, “because I always turned a failure into a success.”6
This fundamental inability to accept responsibility and the attempt to distort reality is something that must concern each of us, regardless of our ideological differences.
Distress tolerance as a model for healing
Even before the outcome of the election, we were hearing from patients who did not feel safe and who reported being “terrified” about what our country might become. This is where a focus on processing the pain and decreasing anxiety is necessary. This is not an anxiety we can medicate with anxiolytics or rationalize by telling ourselves and our patients that the best man won “fair and square.” We have each – by this time – experienced patients who are quite shaken by this turn of events.
Although it has not received much press, many consider Mr. Trump’s victory to be, in part, a “white backlash.” Many supporters of Mr. Trump have felt too ashamed to publicly admit their support for a candidate who at least by innuendo incited fear, anger, and violence. This failure has created an anxiety reminiscent of the daytime anxiety experienced by people who survived nighttime lynchings in small Southern towns. The day after the lynching, it was not unusual for African American men, women, and children to wonder if their grocer, banker, postal carrier, or sheriff had donned a white hood the night before and lynched someone in their community.
The question of survival, how to survive the unimaginable, is what most distresses people. They’ve wondered out loud whether they, their family, and friends would be attacked and/or killed by those who now feel emboldened and authorized to act on their latent aggressive impulses. And, our patients’ fears are legitimate because, unfortunately, studies show that verbal aggression is correlated with increased risk of physical violence and even murder.7
In the dialectical behavioral therapy (DBT) construct developed by Marsha M. Linehan, PhD, the goals of distress tolerance are crisis survival, reality acceptance, and then freedom.8
As we apply our skills, we are uniquely positioned to help our patients and their families survive this crisis, accept that this is our president-elect, and ultimately be free from the anxiety created by the behavior that we all witnessed. We can aid in the navigation through this storm.
Acceptance
We’re already on to reality acceptance. The reality that so many African Americans and people of color have been living is now known and experienced by many who had felt immune to being marginalized. They now understand the loss of security that accompanies overwhelming fear of being the object of verbal, emotional, and physical aggression and violence.
Some are coping by entertaining fantasies that this election outcome will be undone, that the Electoral College will not approve our president-elect when it meets on Dec. 19 or that Mr. Trump will be impeached early in this upcoming term. The results of the presidential election are unlikely to be undone, so having more than 2 months between Election Day and the inauguration to work on acceptance will be helpful. The goal here is to accept the past, be hopeful about the future, and be vigilant in the present.
Freedom
Now, on to freedom. Our goal is to have all of our patients, families, colleagues, and communities able to live without fear that our leaders are not able to apply humanitarian principles to keep all of us safe. The next few months are crucial. Americans must speak out and debride the wound that bullying intentionally causes. Just as with a school bully, Mr. Trump’s behavior has to be called what it is, not sugarcoated or normalized.
History is full of critical moments in time in which, even in our fear, we said nothing. Even the most empathic of us watched the bully at school and felt relief that his behavior was not directed toward us. But we must not avert our gaze.
Bill Moyers and Michael Winship compared Mr. Trump to Sen. Joseph McCarthy, whose reign of terror was ended when journalist Edward R. Murrow courageously spoke out in defiance of the senator. At the end of one of his segments on “See It Now,” Mr. Murrow concluded as he signed off:
We will not walk in fear, one of another. We will not be driven by fear into an age of unreason, if we dig deep in our history and our doctrine, and remember that we are not descended from fearful men — not from men who feared to write, to speak, to associate and to defend causes that were, for the moment, unpopular.9
And, so, how do we cope?
Fortunately, we understand bullying. The bully doesn’t take over the entire school and won’t have the power to take over one’s entire life if the behavior is brought out in the open and openly discussed. But bullies need to accept responsibility, which is what Sen. Harry Reid of Nevada and other legislators urged President-elect Trump to do in days immediately following the election.10 They have called on him to discourage the fear, anger, and violence leading up to and following the election. This action on Mr. Trump’s part would promote a vitally needed national healing process.
Ultimately, this is “the land of the free, the home of the brave …” and we will do what we have always done as psychiatrists and mental health professionals who help to heal wounds. Not all of us will participate in social justice initiatives. However, each of us can listen with intense compassion and interest to those with whom we identify politically and to those whose views diverge from our own. This is our most potent tool in a conflict where we don’t understand the motives of unpredictable leaders or their followers. It is only with this skilled listening that a space is created in which each “other” hears the “other.” This is where real healing begins.
The views expressed in this article are solely those of the authors, and are not meant to represent the views of the American Psychiatric Association, Novant Health, Clinical Psychiatry News, or any other organization.
References
1. http://billposters/story/trump-virus-dark-age-unreason
2. http://blackdoctor.org/495036/national-medical-association-statement-on-police-use-of-force
3. http://www.nytimes.com/interactive/2016/01/28/upshot/donald-trump-twitter-insults.html?_r=0
4. https://www.splcenter.org/hatewatch/2016/11/11/over-200-incidents-hateful-harassment-and-intimidation-election-day
5. http://www.obamaonthecouch.com
6. http://www.nytimes.com/2016/10/26/us/politics/donald-trump-interviews.html
7. “The Nature of Prejudice,” (New York: Perseus Books Publishing, 1979).
8. DBT® Skills Training Handouts and Worksheets, Second Edition (New York: The Guilford Press, 2014).
9. http://billmoyers.com/story/trump-virus-dark-age-unreason
10. http://www.reid.senate.gov/press_releases/2016-11-11-reid-statement-on-the-election-of-donald-trump#.WC0iA6IrKgR
Dr. Dunlap, a psychiatrist and psychoanalyst who practices in Washington, is the immediate past president of the Washington Psychiatric Society, and associate clinical professor of psychiatry and behavioral sciences at George Washington University, Washington. She is interested in the role “difference” – race, culture, and ethnicity – plays in interpersonal relationships and group dynamics. Dr. Ifill-Taylor, a child, adolescent, and adult psychiatrist, is in practice as a medical director in Charlotte, N.C. Previously, she was in private practice in the Washington area and worked as a staff psychiatrist for the Department of Veterans Affairs. She is particularly interested in the effect of our social, political, and occupational environment on mental and physical health.
One of us practices in the “new south” community of Charlotte, N.C., “a red state”; the other is in the “blue bubble” of Washington. In our respective polarized zones, the divergent reactions we heard about the presidential candidates were akin to projective responses to Rorschach tests.
As mental health clinicians, we knew that the country was wounded and in need of healing long before the outcome of the unconventional and acrimonious 2016 American presidential race. So, we were concerned about how patients, clinicians, and divergent communities would go about healing after an 18-month pre-election slugfest that revealed bigotry that persists more than 150 years after the Civil War.
Background of ‘two sides’
None of the nasty rhetoric delivered by our now president-elect or the clearly defensive responses we heard from our former secretary of state were going to be easily forgotten after Nov. 8, 2016. As the process unfolded, however, the voice of psychiatry, with some notable exceptions (the blog of Justin Frank, MD, for example), was absent from the public dialogue.
Nevertheless, writing in June of this year, Bill Moyers and Michael Winship summed up the private assessment of many professionals and the fears for many of a Trump presidency:
There is a virus infecting our politics and right now it’s flourishing with a scarlet fever. It feeds on fear, paranoia and bigotry. All that was required for it to spread was a timely opportunity – and an opportunist with no scruples. ... There have been stretches of history when this virus lay dormant. ... Today its carrier is Donald Trump, but others came before him: narcissistic demagogues who lie and distort in pursuit of power and self-promotion. Bullies all, swaggering across the landscape with fistfuls of false promises, smears, innuendo and hatred for others, spite and spittle for anyone of a different race, faith, gender, or nationality.1
Alternatively, some had a smoldering fear of the progressive agenda to bring “others” – more women, African Americans, Latinos, the LGBTQ community, Muslims, and the disabled – securely under the tent of American democracy. Others, especially the underemployed cohort in neglected and struggling communities in Middle America, were simply opposed to a continuation of “politics as usual,” a.k.a. Hillary Clinton, and were desperate for change.
The opposition views were summed up in the innuendo of the slogan: “Make America Great Again.” By the election, the tensions had begun to resemble the aggressive spirit of a sporting event: It’s “us” versus “them.”
Causes of concern
In the months leading up to the election, violent events strained the societal divisions. The police use of force2 resulted in the near-daily deaths of African American men and women and other people of color at the hands of police officers. The events built on a long and growing list of violent acts – the racially motivated shootings of nine men and women in a Charleston, S.C., church, the bombing injuries and deaths at the Boston Marathon, the shooting deaths of 20 children and 6 adults at Sandy Hook Elementary School, the homophobia-motivated shootings in a Florida nightclub – that have heightened levels of fear, anxiety, and concern for personal and family safety. For many, life has felt fragile and out of control, the perfect setup to motivate the electorate to cast their votes for the person they imagined had the most power and most interest in restoring their sense of control over their lives and, ultimately, their sense of safety.
Why the fear? A psychodynamic analysis
As psychiatrists trained in psychodynamic theory, we are quite familiar with the concept of identifying with the aggressor as a means of coping. The classic example is when a child watches his or her parents in an abusive relationship and identifies with the abusive parent in an attempt to avoid identifying with the victimized parent.
This dynamic is one that seems to have played out during this presidential election. By October 2016, Donald J. Trump already reportedly had insulted more than 280 people, places, and things on Twitter.3 Despite the evidence that Mr. Trump verbally bullied not only his opponents, but also the media, Latinos, women, the LGBTQ community, the Republican Party (his claimed party), and Muslims, people came out in numbers high enough to make him America’s president-elect. In the classic process of bullying his perceived enemies, those considered “the other,” he assigned names such as “crooked Hillary,” “little Marco,” and “lyin’ Ted” – just as a bully at school assigns names to the kid he’s decided does not have enough worth to be called by his given name.
He depicted women who accused him of sexual assault as either not being pretty enough to be worthy of assault or self-serving in their public accusations. Mexicans entering this country were referred to as “rapists and thugs.” African Americans were told that their lives are so bad that they “have nothing to lose” if they voted for a candidate who talked about erecting a wall to block out other people of color, and changing immigration laws that would banish an entire religion from entering our country.
The ‘blue bubble’ – Those who voted for Mrs. Clinton
So … this happened. And, in our consulting rooms, we are seeing a stark increase in the numbers of individuals, couples, and families reporting overwhelming anxiety, sadness, and a sense of de-realization (“it’s surreal”). At the core of their anxiety is concern for self, family, and friends as well as concern for the country as a whole.
The post-election notions that families would be immediately broken up, parents deported, the Affordable Care Act immediately dismantled, and countries bombed immediately after Election Day did not become realities. However, there is valid reason to be concerned. The Southern Poverty Law Center has noted a significant increase in post-election hate crimes throughout the nation.4
The new South ‘red states’ – those who voted for Mr. Trump
Trump supporters are feeling victorious because their “underdog” candidate ran an unconventional presidential campaign and won. However, some who voted for Mr. Trump will at some point experience anxiety when the excitement of “winning” wears off. Psychoanalyst Justin Frank speaks to this and more in his Nov. 9, 2016, blog in which he concludes: “While we mourn and blame others and ourselves for our American tragedy, Trump voters must eventually look at themselves in the mirror and exclaim, ‘what have we done?’ ”5
In his Oct. 25, 2016, New York Times article, Michael Barbaro summarized the behaviors that will become increasingly of concern to all as Mr. Trump accepts the oath of office:
The intense ambitions and undisciplined behaviors of Mr. Trump have confounded even those close to him.... In interviews, Mr. Trump makes clear just how difficult it is for him to imagine – let alone accept – defeat....
“I never had a failure,” Mr. Trump said in one of the interviews, despite his repeated corporate bankruptcies and business setbacks, “because I always turned a failure into a success.”6
This fundamental inability to accept responsibility and the attempt to distort reality is something that must concern each of us, regardless of our ideological differences.
Distress tolerance as a model for healing
Even before the outcome of the election, we were hearing from patients who did not feel safe and who reported being “terrified” about what our country might become. This is where a focus on processing the pain and decreasing anxiety is necessary. This is not an anxiety we can medicate with anxiolytics or rationalize by telling ourselves and our patients that the best man won “fair and square.” We have each – by this time – experienced patients who are quite shaken by this turn of events.
Although it has not received much press, many consider Mr. Trump’s victory to be, in part, a “white backlash.” Many supporters of Mr. Trump have felt too ashamed to publicly admit their support for a candidate who at least by innuendo incited fear, anger, and violence. This failure has created an anxiety reminiscent of the daytime anxiety experienced by people who survived nighttime lynchings in small Southern towns. The day after the lynching, it was not unusual for African American men, women, and children to wonder if their grocer, banker, postal carrier, or sheriff had donned a white hood the night before and lynched someone in their community.
The question of survival, how to survive the unimaginable, is what most distresses people. They’ve wondered out loud whether they, their family, and friends would be attacked and/or killed by those who now feel emboldened and authorized to act on their latent aggressive impulses. And, our patients’ fears are legitimate because, unfortunately, studies show that verbal aggression is correlated with increased risk of physical violence and even murder.7
In the dialectical behavioral therapy (DBT) construct developed by Marsha M. Linehan, PhD, the goals of distress tolerance are crisis survival, reality acceptance, and then freedom.8
As we apply our skills, we are uniquely positioned to help our patients and their families survive this crisis, accept that this is our president-elect, and ultimately be free from the anxiety created by the behavior that we all witnessed. We can aid in the navigation through this storm.
Acceptance
We’re already on to reality acceptance. The reality that so many African Americans and people of color have been living is now known and experienced by many who had felt immune to being marginalized. They now understand the loss of security that accompanies overwhelming fear of being the object of verbal, emotional, and physical aggression and violence.
Some are coping by entertaining fantasies that this election outcome will be undone, that the Electoral College will not approve our president-elect when it meets on Dec. 19 or that Mr. Trump will be impeached early in this upcoming term. The results of the presidential election are unlikely to be undone, so having more than 2 months between Election Day and the inauguration to work on acceptance will be helpful. The goal here is to accept the past, be hopeful about the future, and be vigilant in the present.
Freedom
Now, on to freedom. Our goal is to have all of our patients, families, colleagues, and communities able to live without fear that our leaders are not able to apply humanitarian principles to keep all of us safe. The next few months are crucial. Americans must speak out and debride the wound that bullying intentionally causes. Just as with a school bully, Mr. Trump’s behavior has to be called what it is, not sugarcoated or normalized.
History is full of critical moments in time in which, even in our fear, we said nothing. Even the most empathic of us watched the bully at school and felt relief that his behavior was not directed toward us. But we must not avert our gaze.
Bill Moyers and Michael Winship compared Mr. Trump to Sen. Joseph McCarthy, whose reign of terror was ended when journalist Edward R. Murrow courageously spoke out in defiance of the senator. At the end of one of his segments on “See It Now,” Mr. Murrow concluded as he signed off:
We will not walk in fear, one of another. We will not be driven by fear into an age of unreason, if we dig deep in our history and our doctrine, and remember that we are not descended from fearful men — not from men who feared to write, to speak, to associate and to defend causes that were, for the moment, unpopular.9
And, so, how do we cope?
Fortunately, we understand bullying. The bully doesn’t take over the entire school and won’t have the power to take over one’s entire life if the behavior is brought out in the open and openly discussed. But bullies need to accept responsibility, which is what Sen. Harry Reid of Nevada and other legislators urged President-elect Trump to do in days immediately following the election.10 They have called on him to discourage the fear, anger, and violence leading up to and following the election. This action on Mr. Trump’s part would promote a vitally needed national healing process.
Ultimately, this is “the land of the free, the home of the brave …” and we will do what we have always done as psychiatrists and mental health professionals who help to heal wounds. Not all of us will participate in social justice initiatives. However, each of us can listen with intense compassion and interest to those with whom we identify politically and to those whose views diverge from our own. This is our most potent tool in a conflict where we don’t understand the motives of unpredictable leaders or their followers. It is only with this skilled listening that a space is created in which each “other” hears the “other.” This is where real healing begins.
The views expressed in this article are solely those of the authors, and are not meant to represent the views of the American Psychiatric Association, Novant Health, Clinical Psychiatry News, or any other organization.
References
1. http://billposters/story/trump-virus-dark-age-unreason
2. http://blackdoctor.org/495036/national-medical-association-statement-on-police-use-of-force
3. http://www.nytimes.com/interactive/2016/01/28/upshot/donald-trump-twitter-insults.html?_r=0
4. https://www.splcenter.org/hatewatch/2016/11/11/over-200-incidents-hateful-harassment-and-intimidation-election-day
5. http://www.obamaonthecouch.com
6. http://www.nytimes.com/2016/10/26/us/politics/donald-trump-interviews.html
7. “The Nature of Prejudice,” (New York: Perseus Books Publishing, 1979).
8. DBT® Skills Training Handouts and Worksheets, Second Edition (New York: The Guilford Press, 2014).
9. http://billmoyers.com/story/trump-virus-dark-age-unreason
10. http://www.reid.senate.gov/press_releases/2016-11-11-reid-statement-on-the-election-of-donald-trump#.WC0iA6IrKgR
Dr. Dunlap, a psychiatrist and psychoanalyst who practices in Washington, is the immediate past president of the Washington Psychiatric Society, and associate clinical professor of psychiatry and behavioral sciences at George Washington University, Washington. She is interested in the role “difference” – race, culture, and ethnicity – plays in interpersonal relationships and group dynamics. Dr. Ifill-Taylor, a child, adolescent, and adult psychiatrist, is in practice as a medical director in Charlotte, N.C. Previously, she was in private practice in the Washington area and worked as a staff psychiatrist for the Department of Veterans Affairs. She is particularly interested in the effect of our social, political, and occupational environment on mental and physical health.

Hospital factors play key role in readmission risk after surgery
CORONADO, CALIF. – Variation in readmission risk across hospitals following certain surgical procedures is more attributable to hospital factors than to patient characteristics, results from a large analysis demonstrated.
Such is the impact of the care delivery macro environment (CDM), which Sarah A. Brownlee and coauthors defined as a series of complex interactions between patient characteristics and imposed hospital attributes than can impact patient outcomes postoperatively.
The purpose of the current study was to determine the relative contribution of various aspects of the CDM to 1-year readmission risk after surgery. Working with colleagues Anai Kothari, MD, and Paul Kuo MD, in the One:MAP Section of Clinical informatics and Analytics in the department of surgery at Loyola University Medical Center, Ms. Brownlee analyzed the Healthcare Cost and Utilization Project State Inpatient Databases from Florida, New York, and Washington between 2009 and 2013, which were linked to the American Hospital Association Annual Survey from that same time period.
The researchers used smoothed hazard estimates to determine all-cause readmission in the year after surgery, and multilevel survival models with shared frailty to determine the relative impact of hospital versus patient characteristics on the heterogeneity of readmission risk between hospitals. They limited the analysis to patients aged 18 years and older who underwent one the following procedures: abdominal aortic aneurysm repair, pancreatectomy, colectomy, coronary artery bypass graft, and total hip arthroplasty.
Ms. Brownlee reported results from 502,157 patients who underwent surgical procedures at 347 hospitals. The 1-year readmission rate was 23.5%, and ranged from 12% to 36% across procedures. After controlling for procedure, the researchers observed a 7.9% variation in readmission risk between hospitals. Staffing accounted for 9.8% of variance, followed by hospital structural characteristics such as teaching status and clinical programs (7.5%), patient ZIP code (3.8%), hospital perioperative resources such as inpatient rehab (2.9%), hospital volume (2.8%), and patient clinical characteristics (2.1%). The following hospital characteristics were significantly associated with a lower risk of 1-year readmission: high physician/bed ratio (hazard ratio 0.85; P = .00017); transplant status (HR 0.87; P = .022); high-income ZIP code (HR 0.89; P less than .001); high nurse bed/bed ratio (HR 0.90; P = .047), and cancer center designation (HR 0.93; P = .021).
“Compared to patient clinical characteristics, hospital factors such as staffing ratios, perioperative resources, and structural elements account for more variation in postoperative outcomes,” Ms. Brownlee concluded. “However, it’s important to note that in the present study, over 70% of variation in readmission rates is not explained by the covariates that we analyzed. It’s possible that there are other factors we need to consider. That’s where the direction of this research is going. Much of the variation in readmission risk across hospitals cannot be characterized with currently utilized administrative data.”
The National Institutes of Health provided funding for the study. Ms. Brownlee reported having no financial disclosures.
CORONADO, CALIF. – Variation in readmission risk across hospitals following certain surgical procedures is more attributable to hospital factors than to patient characteristics, results from a large analysis demonstrated.
Such is the impact of the care delivery macro environment (CDM), which Sarah A. Brownlee and coauthors defined as a series of complex interactions between patient characteristics and imposed hospital attributes than can impact patient outcomes postoperatively.
The purpose of the current study was to determine the relative contribution of various aspects of the CDM to 1-year readmission risk after surgery. Working with colleagues Anai Kothari, MD, and Paul Kuo MD, in the One:MAP Section of Clinical informatics and Analytics in the department of surgery at Loyola University Medical Center, Ms. Brownlee analyzed the Healthcare Cost and Utilization Project State Inpatient Databases from Florida, New York, and Washington between 2009 and 2013, which were linked to the American Hospital Association Annual Survey from that same time period.
The researchers used smoothed hazard estimates to determine all-cause readmission in the year after surgery, and multilevel survival models with shared frailty to determine the relative impact of hospital versus patient characteristics on the heterogeneity of readmission risk between hospitals. They limited the analysis to patients aged 18 years and older who underwent one the following procedures: abdominal aortic aneurysm repair, pancreatectomy, colectomy, coronary artery bypass graft, and total hip arthroplasty.
Ms. Brownlee reported results from 502,157 patients who underwent surgical procedures at 347 hospitals. The 1-year readmission rate was 23.5%, and ranged from 12% to 36% across procedures. After controlling for procedure, the researchers observed a 7.9% variation in readmission risk between hospitals. Staffing accounted for 9.8% of variance, followed by hospital structural characteristics such as teaching status and clinical programs (7.5%), patient ZIP code (3.8%), hospital perioperative resources such as inpatient rehab (2.9%), hospital volume (2.8%), and patient clinical characteristics (2.1%). The following hospital characteristics were significantly associated with a lower risk of 1-year readmission: high physician/bed ratio (hazard ratio 0.85; P = .00017); transplant status (HR 0.87; P = .022); high-income ZIP code (HR 0.89; P less than .001); high nurse bed/bed ratio (HR 0.90; P = .047), and cancer center designation (HR 0.93; P = .021).
“Compared to patient clinical characteristics, hospital factors such as staffing ratios, perioperative resources, and structural elements account for more variation in postoperative outcomes,” Ms. Brownlee concluded. “However, it’s important to note that in the present study, over 70% of variation in readmission rates is not explained by the covariates that we analyzed. It’s possible that there are other factors we need to consider. That’s where the direction of this research is going. Much of the variation in readmission risk across hospitals cannot be characterized with currently utilized administrative data.”
The National Institutes of Health provided funding for the study. Ms. Brownlee reported having no financial disclosures.
CORONADO, CALIF. – Variation in readmission risk across hospitals following certain surgical procedures is more attributable to hospital factors than to patient characteristics, results from a large analysis demonstrated.
Such is the impact of the care delivery macro environment (CDM), which Sarah A. Brownlee and coauthors defined as a series of complex interactions between patient characteristics and imposed hospital attributes than can impact patient outcomes postoperatively.
The purpose of the current study was to determine the relative contribution of various aspects of the CDM to 1-year readmission risk after surgery. Working with colleagues Anai Kothari, MD, and Paul Kuo MD, in the One:MAP Section of Clinical informatics and Analytics in the department of surgery at Loyola University Medical Center, Ms. Brownlee analyzed the Healthcare Cost and Utilization Project State Inpatient Databases from Florida, New York, and Washington between 2009 and 2013, which were linked to the American Hospital Association Annual Survey from that same time period.
The researchers used smoothed hazard estimates to determine all-cause readmission in the year after surgery, and multilevel survival models with shared frailty to determine the relative impact of hospital versus patient characteristics on the heterogeneity of readmission risk between hospitals. They limited the analysis to patients aged 18 years and older who underwent one the following procedures: abdominal aortic aneurysm repair, pancreatectomy, colectomy, coronary artery bypass graft, and total hip arthroplasty.
Ms. Brownlee reported results from 502,157 patients who underwent surgical procedures at 347 hospitals. The 1-year readmission rate was 23.5%, and ranged from 12% to 36% across procedures. After controlling for procedure, the researchers observed a 7.9% variation in readmission risk between hospitals. Staffing accounted for 9.8% of variance, followed by hospital structural characteristics such as teaching status and clinical programs (7.5%), patient ZIP code (3.8%), hospital perioperative resources such as inpatient rehab (2.9%), hospital volume (2.8%), and patient clinical characteristics (2.1%). The following hospital characteristics were significantly associated with a lower risk of 1-year readmission: high physician/bed ratio (hazard ratio 0.85; P = .00017); transplant status (HR 0.87; P = .022); high-income ZIP code (HR 0.89; P less than .001); high nurse bed/bed ratio (HR 0.90; P = .047), and cancer center designation (HR 0.93; P = .021).
“Compared to patient clinical characteristics, hospital factors such as staffing ratios, perioperative resources, and structural elements account for more variation in postoperative outcomes,” Ms. Brownlee concluded. “However, it’s important to note that in the present study, over 70% of variation in readmission rates is not explained by the covariates that we analyzed. It’s possible that there are other factors we need to consider. That’s where the direction of this research is going. Much of the variation in readmission risk across hospitals cannot be characterized with currently utilized administrative data.”
The National Institutes of Health provided funding for the study. Ms. Brownlee reported having no financial disclosures.
AT WSA 2016
Key clinical point:
Major finding: Staffing accounted for 9.8% of variance in readmission risk between hospitals, followed by hospital structural characteristics such as teaching status and clinical programs (7.5%).
Data source: Results from 502,157 patients who underwent surgical procedures at 347 hospitals in three states.
Disclosures: The National Institutes of Health provided funding for the study. Ms. Brownlee reported having no financial disclosures.
Recovery path complicated for trauma patients with VTE
CORONADO, CALIF. – Patients who develop a venous thromboembolism (VTE) following severe hemorrhage are more susceptible to complications, compared with their counterparts who do not; they also exhibit hypercoagulability and enhanced platelet function at admission, and have delayed recovery of coagulation and platelet function following injury.
Those are the key findings from a secondary analysis of data from the Pragmatic Randomized Optimal Platelet and Plasma Ratio (PROPPR) trial, which randomized 680 severely injured trauma patients from 12 level I trauma centers to receive 1:1:1 or 1:1:2 ratios of plasma to platelets to red blood cells (JAMA 2015;313[5]:471-82). “The prevention of VTE following traumatic injury is an ongoing challenge,” Belinda H. McCully, PhD, said at the annual meeting of the Western Surgical Association. “Despite prophylaxis, about 25% of patients present with VTE, which is associated with higher complications and an increased risk for mortality. Common risk factors for mortality include age, body mass index, extremity injury, and immobility, but the precise mechanisms that contribute to VTE development are not well understood. We do know that the three main factors contributing to thrombosis include static flow, endothelial injury, and hypercoagulability. Clinically, coagulation is the most feasible factor to assess, mainly through the use of conventional coagulation tests, thromboelastography, platelet levels, and platelet function assays.” 
Dr. McCully of the division of trauma, critical care, and acute care surgery in the department of surgery at Oregon Health & Science University, Portland, and her associates hypothesized that enhanced, earlier recovery of coagulation function is associated with increased VTE risk in severely injured trauma patients. To test this hypothesis, they conducted a secondary analysis of the PROPPR database, excluding patients who received anticoagulants, to rule out any bias against VTE development, as well as patients who died within 24 hours, to reduce the survival bias. This left 558 patients: 475 who did not develop a VTE, and 83 who did (defined as those who developed deep vein thrombosis or pulmonary embolism). Patient characteristics of interest included age, sex, BMI, mechanism of injury, and injury severity, as well as the transfusion group, the type of blood products given, and the percentage of patients given procoagulants. The investigators also assessed length of stay and complication incidence previously defined by the trial. During the trial, blood samples were taken from admission up to 72 hours and were used to asses both whole blood coagulation using thromboelastography and platelet function using the Multiplate assay.
Dr. McCully reported that VTE patients and non-VTE patients demonstrated similar admission platelet function activity and inhibition of all platelet function parameters at 24 hours (P less than .05). The onset of platelet function recovery was delayed in VTE patients, specifically for arachidonic acid, adenosine-5’-diphosphate, and collagen. Changes in thromboelastography, clot time to initiation, formation, rate of formation, and strength and index of platelet function from admission to 2 hours indicated increasing hypocoagulability (P less than .05) but suppressed clot lysis in both groups. Compared with patients in the non-VTE group, the VTE group had lower mortality (4% vs. 13%) but increased total hospital days (a mean of 30 vs. 16; P less than .05).
Adverse outcomes were also more prevalent in the VTE group, compared with the non-VTE group, and included systemic inflammatory response syndrome (82% vs. 72%), acute kidney injury (36% vs. 26%), infection (61% vs. 31%), sepsis (60% vs. 28%), and pneumonia (34% vs. 19%; P less than 0.05 for all associations). Conversely, regression analysis showed that VTE was associated only with total hospital days (odds ratio, 1.12), while adverse events were similar between the two groups. “From this we can conclude that VTE development following trauma may be attributed to hypercoagulable thromboelastography parameters and enhanced platelet function at admission, and compensatory mechanisms in response to a delayed recovery of coagulation and platelet function,” Dr. McCully said.
She acknowledged certain limitations of the study, including the fact that it was a secondary analysis of prospectively collected data. “We also plan to assess plasma markers of clot strength and fibrinolysis, which is an ongoing process,” she said. “Despite excluding patients that died within 24 hours, there was still a survival bias in the VTE group.”
The PROPPR study was supported by the National Heart, Lung, and Blood Institute and by the Department of Defense. Dr. McCully reported having no relevant financial disclosures.
CORONADO, CALIF. – Patients who develop a venous thromboembolism (VTE) following severe hemorrhage are more susceptible to complications, compared with their counterparts who do not; they also exhibit hypercoagulability and enhanced platelet function at admission, and have delayed recovery of coagulation and platelet function following injury.
Those are the key findings from a secondary analysis of data from the Pragmatic Randomized Optimal Platelet and Plasma Ratio (PROPPR) trial, which randomized 680 severely injured trauma patients from 12 level I trauma centers to receive 1:1:1 or 1:1:2 ratios of plasma to platelets to red blood cells (JAMA 2015;313[5]:471-82). “The prevention of VTE following traumatic injury is an ongoing challenge,” Belinda H. McCully, PhD, said at the annual meeting of the Western Surgical Association. “Despite prophylaxis, about 25% of patients present with VTE, which is associated with higher complications and an increased risk for mortality. Common risk factors for mortality include age, body mass index, extremity injury, and immobility, but the precise mechanisms that contribute to VTE development are not well understood. We do know that the three main factors contributing to thrombosis include static flow, endothelial injury, and hypercoagulability. Clinically, coagulation is the most feasible factor to assess, mainly through the use of conventional coagulation tests, thromboelastography, platelet levels, and platelet function assays.”
Dr. McCully of the division of trauma, critical care, and acute care surgery in the department of surgery at Oregon Health & Science University, Portland, and her associates hypothesized that enhanced, earlier recovery of coagulation function is associated with increased VTE risk in severely injured trauma patients. To test this hypothesis, they conducted a secondary analysis of the PROPPR database, excluding patients who received anticoagulants, to rule out any bias against VTE development, as well as patients who died within 24 hours, to reduce the survival bias. This left 558 patients: 475 who did not develop a VTE, and 83 who did (defined as those who developed deep vein thrombosis or pulmonary embolism). Patient characteristics of interest included age, sex, BMI, mechanism of injury, and injury severity, as well as the transfusion group, the type of blood products given, and the percentage of patients given procoagulants. The investigators also assessed length of stay and complication incidence previously defined by the trial. During the trial, blood samples were taken from admission up to 72 hours and were used to asses both whole blood coagulation using thromboelastography and platelet function using the Multiplate assay.
Dr. McCully reported that VTE patients and non-VTE patients demonstrated similar admission platelet function activity and inhibition of all platelet function parameters at 24 hours (P less than .05). The onset of platelet function recovery was delayed in VTE patients, specifically for arachidonic acid, adenosine-5’-diphosphate, and collagen. Changes in thromboelastography, clot time to initiation, formation, rate of formation, and strength and index of platelet function from admission to 2 hours indicated increasing hypocoagulability (P less than .05) but suppressed clot lysis in both groups. Compared with patients in the non-VTE group, the VTE group had lower mortality (4% vs. 13%) but increased total hospital days (a mean of 30 vs. 16; P less than .05).
Adverse outcomes were also more prevalent in the VTE group, compared with the non-VTE group, and included systemic inflammatory response syndrome (82% vs. 72%), acute kidney injury (36% vs. 26%), infection (61% vs. 31%), sepsis (60% vs. 28%), and pneumonia (34% vs. 19%; P less than 0.05 for all associations). Conversely, regression analysis showed that VTE was associated only with total hospital days (odds ratio, 1.12), while adverse events were similar between the two groups. “From this we can conclude that VTE development following trauma may be attributed to hypercoagulable thromboelastography parameters and enhanced platelet function at admission, and compensatory mechanisms in response to a delayed recovery of coagulation and platelet function,” Dr. McCully said.
She acknowledged certain limitations of the study, including the fact that it was a secondary analysis of prospectively collected data. “We also plan to assess plasma markers of clot strength and fibrinolysis, which is an ongoing process,” she said. “Despite excluding patients that died within 24 hours, there was still a survival bias in the VTE group.”
The PROPPR study was supported by the National Heart, Lung, and Blood Institute and by the Department of Defense. Dr. McCully reported having no relevant financial disclosures.
CORONADO, CALIF. – Patients who develop a venous thromboembolism (VTE) following severe hemorrhage are more susceptible to complications, compared with their counterparts who do not; they also exhibit hypercoagulability and enhanced platelet function at admission, and have delayed recovery of coagulation and platelet function following injury.
Those are the key findings from a secondary analysis of data from the Pragmatic Randomized Optimal Platelet and Plasma Ratio (PROPPR) trial, which randomized 680 severely injured trauma patients from 12 level I trauma centers to receive 1:1:1 or 1:1:2 ratios of plasma to platelets to red blood cells (JAMA 2015;313[5]:471-82). “The prevention of VTE following traumatic injury is an ongoing challenge,” Belinda H. McCully, PhD, said at the annual meeting of the Western Surgical Association. “Despite prophylaxis, about 25% of patients present with VTE, which is associated with higher complications and an increased risk for mortality. Common risk factors for mortality include age, body mass index, extremity injury, and immobility, but the precise mechanisms that contribute to VTE development are not well understood. We do know that the three main factors contributing to thrombosis include static flow, endothelial injury, and hypercoagulability. Clinically, coagulation is the most feasible factor to assess, mainly through the use of conventional coagulation tests, thromboelastography, platelet levels, and platelet function assays.”
Dr. McCully of the division of trauma, critical care, and acute care surgery in the department of surgery at Oregon Health & Science University, Portland, and her associates hypothesized that enhanced, earlier recovery of coagulation function is associated with increased VTE risk in severely injured trauma patients. To test this hypothesis, they conducted a secondary analysis of the PROPPR database, excluding patients who received anticoagulants, to rule out any bias against VTE development, as well as patients who died within 24 hours, to reduce the survival bias. This left 558 patients: 475 who did not develop a VTE, and 83 who did (defined as those who developed deep vein thrombosis or pulmonary embolism). Patient characteristics of interest included age, sex, BMI, mechanism of injury, and injury severity, as well as the transfusion group, the type of blood products given, and the percentage of patients given procoagulants. The investigators also assessed length of stay and complication incidence previously defined by the trial. During the trial, blood samples were taken from admission up to 72 hours and were used to asses both whole blood coagulation using thromboelastography and platelet function using the Multiplate assay.
Dr. McCully reported that VTE patients and non-VTE patients demonstrated similar admission platelet function activity and inhibition of all platelet function parameters at 24 hours (P less than .05). The onset of platelet function recovery was delayed in VTE patients, specifically for arachidonic acid, adenosine-5’-diphosphate, and collagen. Changes in thromboelastography, clot time to initiation, formation, rate of formation, and strength and index of platelet function from admission to 2 hours indicated increasing hypocoagulability (P less than .05) but suppressed clot lysis in both groups. Compared with patients in the non-VTE group, the VTE group had lower mortality (4% vs. 13%) but increased total hospital days (a mean of 30 vs. 16; P less than .05).
Adverse outcomes were also more prevalent in the VTE group, compared with the non-VTE group, and included systemic inflammatory response syndrome (82% vs. 72%), acute kidney injury (36% vs. 26%), infection (61% vs. 31%), sepsis (60% vs. 28%), and pneumonia (34% vs. 19%; P less than 0.05 for all associations). Conversely, regression analysis showed that VTE was associated only with total hospital days (odds ratio, 1.12), while adverse events were similar between the two groups. “From this we can conclude that VTE development following trauma may be attributed to hypercoagulable thromboelastography parameters and enhanced platelet function at admission, and compensatory mechanisms in response to a delayed recovery of coagulation and platelet function,” Dr. McCully said.
She acknowledged certain limitations of the study, including the fact that it was a secondary analysis of prospectively collected data. “We also plan to assess plasma markers of clot strength and fibrinolysis, which is an ongoing process,” she said. “Despite excluding patients that died within 24 hours, there was still a survival bias in the VTE group.”
The PROPPR study was supported by the National Heart, Lung, and Blood Institute and by the Department of Defense. Dr. McCully reported having no relevant financial disclosures.
AT WSA 2016
Key clinical point:
Major finding: Compared with patients in the non-VTE group, the VTE group had lower mortality (4% vs. 13%) but increased total hospital days (a mean of 30 vs. 16; P less than .05).
Data source: A secondary analysis of 558 patients from the Pragmatic Randomized Optimal Platelet and Plasma Ratio (PROPPR) trial, which randomized severely injured trauma patients from 12 level I trauma centers to receive 1:1:1 or 1:1:2 ratios of plasma to platelets to red blood cells.
Disclosures: The PROPPR study was supported by the National Heart, Lung, and Blood Institute and by the Department of Defense. Dr. McCully reported having no relevant financial disclosures.