User login
Doc’s lawsuit tests new crackdown on noncompete clauses
In a test of one of the nation’s most restrictive laws limiting noncompete clauses in medicine, an Indiana pediatric critical-care physician is suing to stop his former hospital employer from controlling his future employment prospects.
David Lankford, DO, acknowledges that he signed a contract with the Lutheran Health Network that included a noncompete clause. However,
Indiana’s law is notable among states because if a physician terminates his/her job for cause, the noncompete may be considered unenforceable.
“When you have physicians who are unable to work in their community, it creates a barrier for access to care for patients,” Dr. Lankford said in an interview. “I’m fighting to decrease barriers and continue to have patients be able to see their doctors in their own hometown or their own county.”
Lutheran Health’s media relations department did not respond to requests for comment.
Noncompete clauses ‘extremely common’
Non-compete clauses – which typically restrict when and where employees can take future jobs – are common in physician contracts, Anu Murthy, JD, who reviews employee contracts for a firm called Contract Diagnostics, said in an interview.
However, the tide has been turning against them.
About a dozen states and the District of Columbia have enacted legislation to limit the use of noncompetes in employment contracts, and about half of states have pending legislation that could dilute noncompete clauses, Ms. Murthy said. In June, the state of New York sent a noncompete ban bill to the governor’s desk.
For more about state-by-state restrictions on noncompete clauses, check this chart.
In his lawsuit, Dr. Lankford said he was hired in 2017 to work at Lutheran Hospital in Fort Wayne.
Dr. Lankford signed an employee renewal contract in 2020 that included a noncompete clause; his attorneys declined to provide details about the clause because of confidentiality restrictions.
In 2022, the lawsuit says, Lutheran Hospital told Dr. Lankford that he’d need to take on more work due to layoffs of pediatric hospitalists. His patient load subsequently grew by 4-5 times, and he quit as of Jan. 7, 2023.
Dr. Lankford wrote that he found a new job at Parkview Regional Medical Center in Fort Wayne, but his former employer threatened to take action under the noncompete clause, and Parkview withdrew its offer.
Among other things, the new Indiana law says that the clauses are not enforceable “if physician terminates the physician’s employment for cause.”
The lawsuit asks for a judge to prevent Lutheran Health Network from enforcing the clause.
Impact on patients
The new Indiana law also bans noncompete clauses for primary care physicians. Kathleen A. DeLaney, JD, one of Dr. Lankford’s attorneys, said in an interview that this provision came about because rural legislators didn’t want to add to the challenges of attracting primary care doctors to move to their communities.
State legislators have become less friendly to noncompete clauses in medicine because they’re wary of the negative effects on patients, Evan Starr, PhD, said in an interview. The clauses prevent doctors from taking new jobs where they could continue to treat their previous patients, said Dr. Starr, associate professor in the department of management and organization at the University of Maryland.
However, he said, hospitals are fighting to preserve the clauses, arguing that they provide a base of patients to physicians in return for their agreement not to go work for a competitor.
The legal landscape may change even more. The Federal Trade Commission has proposed banning the clauses nationally, and a decision is expected in 2024. However, it’s an election year, which may delay a decision, attorney Ms. Murthy said, “and there is also language in the proposed rule that could exempt nonprofit hospitals, which further complicates the issues.”
For now, Ms. Murthy said, “we are still seeing noncompetes and other restrictive covenants in almost every contract we review in all 50 states and across all specialties. We explicitly explain to every client that they should only sign the agreement with the expectation that their specific noncompete will be enforced as written. Large employer groups, including hospital systems, will likely fight any kind of restriction or dilution of noncompetes, and these types of legal challenges could be tied up in court for many years.”
A version of this article first appeared on Medscape.com.
In a test of one of the nation’s most restrictive laws limiting noncompete clauses in medicine, an Indiana pediatric critical-care physician is suing to stop his former hospital employer from controlling his future employment prospects.
David Lankford, DO, acknowledges that he signed a contract with the Lutheran Health Network that included a noncompete clause. However,
Indiana’s law is notable among states because if a physician terminates his/her job for cause, the noncompete may be considered unenforceable.
“When you have physicians who are unable to work in their community, it creates a barrier for access to care for patients,” Dr. Lankford said in an interview. “I’m fighting to decrease barriers and continue to have patients be able to see their doctors in their own hometown or their own county.”
Lutheran Health’s media relations department did not respond to requests for comment.
Noncompete clauses ‘extremely common’
Non-compete clauses – which typically restrict when and where employees can take future jobs – are common in physician contracts, Anu Murthy, JD, who reviews employee contracts for a firm called Contract Diagnostics, said in an interview.
However, the tide has been turning against them.
About a dozen states and the District of Columbia have enacted legislation to limit the use of noncompetes in employment contracts, and about half of states have pending legislation that could dilute noncompete clauses, Ms. Murthy said. In June, the state of New York sent a noncompete ban bill to the governor’s desk.
For more about state-by-state restrictions on noncompete clauses, check this chart.
In his lawsuit, Dr. Lankford said he was hired in 2017 to work at Lutheran Hospital in Fort Wayne.
Dr. Lankford signed an employee renewal contract in 2020 that included a noncompete clause; his attorneys declined to provide details about the clause because of confidentiality restrictions.
In 2022, the lawsuit says, Lutheran Hospital told Dr. Lankford that he’d need to take on more work due to layoffs of pediatric hospitalists. His patient load subsequently grew by 4-5 times, and he quit as of Jan. 7, 2023.
Dr. Lankford wrote that he found a new job at Parkview Regional Medical Center in Fort Wayne, but his former employer threatened to take action under the noncompete clause, and Parkview withdrew its offer.
Among other things, the new Indiana law says that the clauses are not enforceable “if physician terminates the physician’s employment for cause.”
The lawsuit asks for a judge to prevent Lutheran Health Network from enforcing the clause.
Impact on patients
The new Indiana law also bans noncompete clauses for primary care physicians. Kathleen A. DeLaney, JD, one of Dr. Lankford’s attorneys, said in an interview that this provision came about because rural legislators didn’t want to add to the challenges of attracting primary care doctors to move to their communities.
State legislators have become less friendly to noncompete clauses in medicine because they’re wary of the negative effects on patients, Evan Starr, PhD, said in an interview. The clauses prevent doctors from taking new jobs where they could continue to treat their previous patients, said Dr. Starr, associate professor in the department of management and organization at the University of Maryland.
However, he said, hospitals are fighting to preserve the clauses, arguing that they provide a base of patients to physicians in return for their agreement not to go work for a competitor.
The legal landscape may change even more. The Federal Trade Commission has proposed banning the clauses nationally, and a decision is expected in 2024. However, it’s an election year, which may delay a decision, attorney Ms. Murthy said, “and there is also language in the proposed rule that could exempt nonprofit hospitals, which further complicates the issues.”
For now, Ms. Murthy said, “we are still seeing noncompetes and other restrictive covenants in almost every contract we review in all 50 states and across all specialties. We explicitly explain to every client that they should only sign the agreement with the expectation that their specific noncompete will be enforced as written. Large employer groups, including hospital systems, will likely fight any kind of restriction or dilution of noncompetes, and these types of legal challenges could be tied up in court for many years.”
A version of this article first appeared on Medscape.com.
In a test of one of the nation’s most restrictive laws limiting noncompete clauses in medicine, an Indiana pediatric critical-care physician is suing to stop his former hospital employer from controlling his future employment prospects.
David Lankford, DO, acknowledges that he signed a contract with the Lutheran Health Network that included a noncompete clause. However,
Indiana’s law is notable among states because if a physician terminates his/her job for cause, the noncompete may be considered unenforceable.
“When you have physicians who are unable to work in their community, it creates a barrier for access to care for patients,” Dr. Lankford said in an interview. “I’m fighting to decrease barriers and continue to have patients be able to see their doctors in their own hometown or their own county.”
Lutheran Health’s media relations department did not respond to requests for comment.
Noncompete clauses ‘extremely common’
Non-compete clauses – which typically restrict when and where employees can take future jobs – are common in physician contracts, Anu Murthy, JD, who reviews employee contracts for a firm called Contract Diagnostics, said in an interview.
However, the tide has been turning against them.
About a dozen states and the District of Columbia have enacted legislation to limit the use of noncompetes in employment contracts, and about half of states have pending legislation that could dilute noncompete clauses, Ms. Murthy said. In June, the state of New York sent a noncompete ban bill to the governor’s desk.
For more about state-by-state restrictions on noncompete clauses, check this chart.
In his lawsuit, Dr. Lankford said he was hired in 2017 to work at Lutheran Hospital in Fort Wayne.
Dr. Lankford signed an employee renewal contract in 2020 that included a noncompete clause; his attorneys declined to provide details about the clause because of confidentiality restrictions.
In 2022, the lawsuit says, Lutheran Hospital told Dr. Lankford that he’d need to take on more work due to layoffs of pediatric hospitalists. His patient load subsequently grew by 4-5 times, and he quit as of Jan. 7, 2023.
Dr. Lankford wrote that he found a new job at Parkview Regional Medical Center in Fort Wayne, but his former employer threatened to take action under the noncompete clause, and Parkview withdrew its offer.
Among other things, the new Indiana law says that the clauses are not enforceable “if physician terminates the physician’s employment for cause.”
The lawsuit asks for a judge to prevent Lutheran Health Network from enforcing the clause.
Impact on patients
The new Indiana law also bans noncompete clauses for primary care physicians. Kathleen A. DeLaney, JD, one of Dr. Lankford’s attorneys, said in an interview that this provision came about because rural legislators didn’t want to add to the challenges of attracting primary care doctors to move to their communities.
State legislators have become less friendly to noncompete clauses in medicine because they’re wary of the negative effects on patients, Evan Starr, PhD, said in an interview. The clauses prevent doctors from taking new jobs where they could continue to treat their previous patients, said Dr. Starr, associate professor in the department of management and organization at the University of Maryland.
However, he said, hospitals are fighting to preserve the clauses, arguing that they provide a base of patients to physicians in return for their agreement not to go work for a competitor.
The legal landscape may change even more. The Federal Trade Commission has proposed banning the clauses nationally, and a decision is expected in 2024. However, it’s an election year, which may delay a decision, attorney Ms. Murthy said, “and there is also language in the proposed rule that could exempt nonprofit hospitals, which further complicates the issues.”
For now, Ms. Murthy said, “we are still seeing noncompetes and other restrictive covenants in almost every contract we review in all 50 states and across all specialties. We explicitly explain to every client that they should only sign the agreement with the expectation that their specific noncompete will be enforced as written. Large employer groups, including hospital systems, will likely fight any kind of restriction or dilution of noncompetes, and these types of legal challenges could be tied up in court for many years.”
A version of this article first appeared on Medscape.com.
Intensely pruritic rash
The history and findings in this case are consistent with atopic dermatitis (AD).
AD is a chronic inflammatory skin condition that affects more than 200 million people worldwide, including as many as 30% of children and 10% of adults. Although it is more common in children (and may persist into adulthood), approximately 1 in 4 adults with AD have adult-onset disease.
The etiology of AD is complex and includes both genetic and environmental factors, including a weakened skin barrier, immune dysregulation, and abnormalities of the skin microbiome. AD is a member of the atopic triad (ie, AD, allergic rhinoconjunctivitis, and asthma), which may commence concurrently or in succession in what is referred to as the "atopic march."
The presentation of adult-onset AD may differ from that seen in children. For example, the most commonly reported body regions affected in adult-onset AD are the hands, eyelids, neck, and flexural surfaces of the upper limbs. In contrast, childhood-onset AD is less specific to body regions other than flexural areas. Xerosis is a prominent feature, and lichenification may be present. Some patients may have a rippled, brown macular ring around the neck, simulating the pigmentations seen in macular amyloid but due instead to postinflammatory melanin deposition. Pruritus is the most common and bothersome symptom associated with AD; patients may also experience anxiety, depression, and sleep disturbances.
Diminished quality of life, reduced productivity at work and school, and increased healthcare costs (hospitalizations, emergency visits, outpatient visits, and medications) have all been reported in patients with AD. Triggers for flare-ups vary among individuals; commonly reported triggers include physical or emotional stress, changes in temperature or humidity, sweating, allergens, and irritants.
AD is typically diagnosed clinically given the characteristic distribution of lesions in various age groups (infancy, childhood, and adult). Associated findings such as keratosis pilaris may help to facilitate the diagnosis. No biomarker for the diagnosis of AD has been found and laboratory testing is rarely necessary. However, a swab of infected skin may help to isolate a specific involved organism (eg, Staphylococcus or Streptococcus) and antibiotic sensitivity. Allergy and radioallergosorbent testing are not necessary to make the diagnosis. A swab for viral polymerase chain reaction may be beneficial to help identify superinfection with herpes simplex virus and identify a diagnosis of eczema herpeticum. Testing for serum IgE level can also be helpful for supporting the diagnosis of AD.
The management of AD includes trigger avoidance, daily skin care with application of emollients, anti-inflammatory therapy, and other complementary modalities. For mild or moderate AD, first-line treatment consists of topical anti-inflammatory ointments and creams, including topical corticosteroids, which are available in a broad range of potencies. Other topical medications include topical calcineurin inhibitors (tacrolimus and pimecrolimus for patients aged ≥ 2 years), which may be particularly appropriate when there is concern for adverse events secondary to corticosteroid use; topical phosphodiesterase 4 inhibitor (crisaborole ointment for patients aged ≥ 3 months); and topical Janus kinase inhibitor (ruxolitinib cream for patients aged ≥ 12 years).
For patients with moderate to severe AD, or for those who are refractory to topical medications, treatment may include biologic therapy (dupilumab and tralokinumab for patients aged ≥ 6 months and ≥ 18 years, respectively), oral Janus kinase inhibitors (upadacitinib and abrocitinib for patients ages ≥ 12 and ≥ 18 years, respectively), phototherapy (commonly narrow-band ultraviolet light type B treatment), and oral immunomodulators (including methotrexate, mycophenolate, and azathioprine). Combination therapy may be required for the long-term management of more severe AD.
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are consistent with atopic dermatitis (AD).
AD is a chronic inflammatory skin condition that affects more than 200 million people worldwide, including as many as 30% of children and 10% of adults. Although it is more common in children (and may persist into adulthood), approximately 1 in 4 adults with AD have adult-onset disease.
The etiology of AD is complex and includes both genetic and environmental factors, including a weakened skin barrier, immune dysregulation, and abnormalities of the skin microbiome. AD is a member of the atopic triad (ie, AD, allergic rhinoconjunctivitis, and asthma), which may commence concurrently or in succession in what is referred to as the "atopic march."
The presentation of adult-onset AD may differ from that seen in children. For example, the most commonly reported body regions affected in adult-onset AD are the hands, eyelids, neck, and flexural surfaces of the upper limbs. In contrast, childhood-onset AD is less specific to body regions other than flexural areas. Xerosis is a prominent feature, and lichenification may be present. Some patients may have a rippled, brown macular ring around the neck, simulating the pigmentations seen in macular amyloid but due instead to postinflammatory melanin deposition. Pruritus is the most common and bothersome symptom associated with AD; patients may also experience anxiety, depression, and sleep disturbances.
Diminished quality of life, reduced productivity at work and school, and increased healthcare costs (hospitalizations, emergency visits, outpatient visits, and medications) have all been reported in patients with AD. Triggers for flare-ups vary among individuals; commonly reported triggers include physical or emotional stress, changes in temperature or humidity, sweating, allergens, and irritants.
AD is typically diagnosed clinically given the characteristic distribution of lesions in various age groups (infancy, childhood, and adult). Associated findings such as keratosis pilaris may help to facilitate the diagnosis. No biomarker for the diagnosis of AD has been found and laboratory testing is rarely necessary. However, a swab of infected skin may help to isolate a specific involved organism (eg, Staphylococcus or Streptococcus) and antibiotic sensitivity. Allergy and radioallergosorbent testing are not necessary to make the diagnosis. A swab for viral polymerase chain reaction may be beneficial to help identify superinfection with herpes simplex virus and identify a diagnosis of eczema herpeticum. Testing for serum IgE level can also be helpful for supporting the diagnosis of AD.
The management of AD includes trigger avoidance, daily skin care with application of emollients, anti-inflammatory therapy, and other complementary modalities. For mild or moderate AD, first-line treatment consists of topical anti-inflammatory ointments and creams, including topical corticosteroids, which are available in a broad range of potencies. Other topical medications include topical calcineurin inhibitors (tacrolimus and pimecrolimus for patients aged ≥ 2 years), which may be particularly appropriate when there is concern for adverse events secondary to corticosteroid use; topical phosphodiesterase 4 inhibitor (crisaborole ointment for patients aged ≥ 3 months); and topical Janus kinase inhibitor (ruxolitinib cream for patients aged ≥ 12 years).
For patients with moderate to severe AD, or for those who are refractory to topical medications, treatment may include biologic therapy (dupilumab and tralokinumab for patients aged ≥ 6 months and ≥ 18 years, respectively), oral Janus kinase inhibitors (upadacitinib and abrocitinib for patients ages ≥ 12 and ≥ 18 years, respectively), phototherapy (commonly narrow-band ultraviolet light type B treatment), and oral immunomodulators (including methotrexate, mycophenolate, and azathioprine). Combination therapy may be required for the long-term management of more severe AD.
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are consistent with atopic dermatitis (AD).
AD is a chronic inflammatory skin condition that affects more than 200 million people worldwide, including as many as 30% of children and 10% of adults. Although it is more common in children (and may persist into adulthood), approximately 1 in 4 adults with AD have adult-onset disease.
The etiology of AD is complex and includes both genetic and environmental factors, including a weakened skin barrier, immune dysregulation, and abnormalities of the skin microbiome. AD is a member of the atopic triad (ie, AD, allergic rhinoconjunctivitis, and asthma), which may commence concurrently or in succession in what is referred to as the "atopic march."
The presentation of adult-onset AD may differ from that seen in children. For example, the most commonly reported body regions affected in adult-onset AD are the hands, eyelids, neck, and flexural surfaces of the upper limbs. In contrast, childhood-onset AD is less specific to body regions other than flexural areas. Xerosis is a prominent feature, and lichenification may be present. Some patients may have a rippled, brown macular ring around the neck, simulating the pigmentations seen in macular amyloid but due instead to postinflammatory melanin deposition. Pruritus is the most common and bothersome symptom associated with AD; patients may also experience anxiety, depression, and sleep disturbances.
Diminished quality of life, reduced productivity at work and school, and increased healthcare costs (hospitalizations, emergency visits, outpatient visits, and medications) have all been reported in patients with AD. Triggers for flare-ups vary among individuals; commonly reported triggers include physical or emotional stress, changes in temperature or humidity, sweating, allergens, and irritants.
AD is typically diagnosed clinically given the characteristic distribution of lesions in various age groups (infancy, childhood, and adult). Associated findings such as keratosis pilaris may help to facilitate the diagnosis. No biomarker for the diagnosis of AD has been found and laboratory testing is rarely necessary. However, a swab of infected skin may help to isolate a specific involved organism (eg, Staphylococcus or Streptococcus) and antibiotic sensitivity. Allergy and radioallergosorbent testing are not necessary to make the diagnosis. A swab for viral polymerase chain reaction may be beneficial to help identify superinfection with herpes simplex virus and identify a diagnosis of eczema herpeticum. Testing for serum IgE level can also be helpful for supporting the diagnosis of AD.
The management of AD includes trigger avoidance, daily skin care with application of emollients, anti-inflammatory therapy, and other complementary modalities. For mild or moderate AD, first-line treatment consists of topical anti-inflammatory ointments and creams, including topical corticosteroids, which are available in a broad range of potencies. Other topical medications include topical calcineurin inhibitors (tacrolimus and pimecrolimus for patients aged ≥ 2 years), which may be particularly appropriate when there is concern for adverse events secondary to corticosteroid use; topical phosphodiesterase 4 inhibitor (crisaborole ointment for patients aged ≥ 3 months); and topical Janus kinase inhibitor (ruxolitinib cream for patients aged ≥ 12 years).
For patients with moderate to severe AD, or for those who are refractory to topical medications, treatment may include biologic therapy (dupilumab and tralokinumab for patients aged ≥ 6 months and ≥ 18 years, respectively), oral Janus kinase inhibitors (upadacitinib and abrocitinib for patients ages ≥ 12 and ≥ 18 years, respectively), phototherapy (commonly narrow-band ultraviolet light type B treatment), and oral immunomodulators (including methotrexate, mycophenolate, and azathioprine). Combination therapy may be required for the long-term management of more severe AD.
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.

A 52-year-old woman presents with complaints of an itchy rash on her arms, legs, neck, and eyelids. She reports having flares with a similar eruption on her arms and legs over the past 2 years, but on previous occasions she was able to manage it with topical emollients. Over the past 6 months, however, it has worsened both in intensity and spread. She describes the rash as intensely pruritic, and now that it has become more visible, she reports feeling embarrassed by it at work and during social outings. The itch is also disrupting her sleep. The patient states that she is undergoing an extremely stressful period in her life because of her parents' declining health and a recent separation from her husband.
Approximately 3 months ago, she visited her primary care provider, who diagnosed her with an allergic rash and prescribed a course of an oral glucocorticoid. Initially, she thought the treatment worked, but the rash soon recurred after she finished her treatment.
Physical examination reveals scaly, crusted hyperpigmented lesions involving the arms, flexural areas of the elbows and knees, neck, and eyelids. Lichenification and xerosis are observed. There is no evidence of conjunctivitis or scalp involvement. The turbinates are not inflamed. Complete blood count findings are within normal range. The patient is 5 ft 3 in and weighs 125 lb (BMI 22.1) and is a nonsmoker.

USPSTF maintains ‘insufficient evidence’ for lipid disorder screenings in kids and teens
The group’s final recommendation and corresponding evidence report were published in the Journal of the American Medical Association, following a draft recommendation in January.
The organization reached a similar conclusion following its evaluation in 2016.
“There’s just not enough evidence to determine whether or not screening all children for high cholesterol improves their heart health into adulthood,” said Katrina Donahue, MD, MPH, a USPSTF member and a professor in the department of family medicine at the University of North Carolina at Chapel Hill. “We’re calling for additional research on the effectiveness of screening for and treatment of high cholesterol in children and adolescents to prevent heart attacks, strokes, and death in adulthood.”
The task force recommended other evidence-based strategies to promote heart health, such as screening for obesity and interventions to prevent tobacco use.
The recommendation was the result of a review of 43 studies from MEDLINE and the Cochrane Central Register of Controlled Trials through May 16, 2022. No randomized controlled trial directly addressed the effectiveness or harms of lipid screening for children and adolescents. The task force continued to use article alerts and targeted journal searches through March 24, 2023.
Conditions such as familial hypercholesterolemia and multifactorial dyslipidemia can cause abnormally high lipid levels in children, potentially leading to premature cardiovascular events such as myocardial infarction, stroke, and death in adulthood. According to the USPSTF, the prevalence of FH in U.S. children and adolescents ranges from 0.2% to 0.4% (one in every 250-500 youth). Multifactorial dyslipidemia is more common – the prevalence in children and adolescents ranges from 7.1% to 9.4%.
In an editorial response to the task force’s statement, the authors, including Sarah D. de Ferranti, MD, department of pediatrics at Harvard Medical School, Boston, question the impact of not screening children to identify FH and other conditions and caution against the subsequent delay in treatment.
“Treating FH during childhood slows the progression of vascular finding in atherosclerosis,” the authors write.
They note that the recommendation “leaves a void for clinicians seeking to provide care for patients today” while additional research is conducted.
Sarah Nosal, MD, a member of the board of directors of the American Academy of Family Physicians, said that despite the lack of a recommendation, primary care clinicians can still encourage proper nutrition and physical activity for patients.
Dr. Nosal said that even without clear recommendations from the USPSTF, in the rare case of a patient with a family history of FH, she would order a lipid test and discuss treatment plans with the patient and family, if needed.
“We really don’t want to do tests that we don’t know what to do with the information,” she said.
One USPSTF member reported receiving grants from Healthwise, a nonprofit organization, outside the submitted work.
A version of this article first appeared on Medscape.com.
The group’s final recommendation and corresponding evidence report were published in the Journal of the American Medical Association, following a draft recommendation in January.
The organization reached a similar conclusion following its evaluation in 2016.
“There’s just not enough evidence to determine whether or not screening all children for high cholesterol improves their heart health into adulthood,” said Katrina Donahue, MD, MPH, a USPSTF member and a professor in the department of family medicine at the University of North Carolina at Chapel Hill. “We’re calling for additional research on the effectiveness of screening for and treatment of high cholesterol in children and adolescents to prevent heart attacks, strokes, and death in adulthood.”
The task force recommended other evidence-based strategies to promote heart health, such as screening for obesity and interventions to prevent tobacco use.
The recommendation was the result of a review of 43 studies from MEDLINE and the Cochrane Central Register of Controlled Trials through May 16, 2022. No randomized controlled trial directly addressed the effectiveness or harms of lipid screening for children and adolescents. The task force continued to use article alerts and targeted journal searches through March 24, 2023.
Conditions such as familial hypercholesterolemia and multifactorial dyslipidemia can cause abnormally high lipid levels in children, potentially leading to premature cardiovascular events such as myocardial infarction, stroke, and death in adulthood. According to the USPSTF, the prevalence of FH in U.S. children and adolescents ranges from 0.2% to 0.4% (one in every 250-500 youth). Multifactorial dyslipidemia is more common – the prevalence in children and adolescents ranges from 7.1% to 9.4%.
In an editorial response to the task force’s statement, the authors, including Sarah D. de Ferranti, MD, department of pediatrics at Harvard Medical School, Boston, question the impact of not screening children to identify FH and other conditions and caution against the subsequent delay in treatment.
“Treating FH during childhood slows the progression of vascular finding in atherosclerosis,” the authors write.
They note that the recommendation “leaves a void for clinicians seeking to provide care for patients today” while additional research is conducted.
Sarah Nosal, MD, a member of the board of directors of the American Academy of Family Physicians, said that despite the lack of a recommendation, primary care clinicians can still encourage proper nutrition and physical activity for patients.
Dr. Nosal said that even without clear recommendations from the USPSTF, in the rare case of a patient with a family history of FH, she would order a lipid test and discuss treatment plans with the patient and family, if needed.
“We really don’t want to do tests that we don’t know what to do with the information,” she said.
One USPSTF member reported receiving grants from Healthwise, a nonprofit organization, outside the submitted work.
A version of this article first appeared on Medscape.com.
The group’s final recommendation and corresponding evidence report were published in the Journal of the American Medical Association, following a draft recommendation in January.
The organization reached a similar conclusion following its evaluation in 2016.
“There’s just not enough evidence to determine whether or not screening all children for high cholesterol improves their heart health into adulthood,” said Katrina Donahue, MD, MPH, a USPSTF member and a professor in the department of family medicine at the University of North Carolina at Chapel Hill. “We’re calling for additional research on the effectiveness of screening for and treatment of high cholesterol in children and adolescents to prevent heart attacks, strokes, and death in adulthood.”
The task force recommended other evidence-based strategies to promote heart health, such as screening for obesity and interventions to prevent tobacco use.
The recommendation was the result of a review of 43 studies from MEDLINE and the Cochrane Central Register of Controlled Trials through May 16, 2022. No randomized controlled trial directly addressed the effectiveness or harms of lipid screening for children and adolescents. The task force continued to use article alerts and targeted journal searches through March 24, 2023.
Conditions such as familial hypercholesterolemia and multifactorial dyslipidemia can cause abnormally high lipid levels in children, potentially leading to premature cardiovascular events such as myocardial infarction, stroke, and death in adulthood. According to the USPSTF, the prevalence of FH in U.S. children and adolescents ranges from 0.2% to 0.4% (one in every 250-500 youth). Multifactorial dyslipidemia is more common – the prevalence in children and adolescents ranges from 7.1% to 9.4%.
In an editorial response to the task force’s statement, the authors, including Sarah D. de Ferranti, MD, department of pediatrics at Harvard Medical School, Boston, question the impact of not screening children to identify FH and other conditions and caution against the subsequent delay in treatment.
“Treating FH during childhood slows the progression of vascular finding in atherosclerosis,” the authors write.
They note that the recommendation “leaves a void for clinicians seeking to provide care for patients today” while additional research is conducted.
Sarah Nosal, MD, a member of the board of directors of the American Academy of Family Physicians, said that despite the lack of a recommendation, primary care clinicians can still encourage proper nutrition and physical activity for patients.
Dr. Nosal said that even without clear recommendations from the USPSTF, in the rare case of a patient with a family history of FH, she would order a lipid test and discuss treatment plans with the patient and family, if needed.
“We really don’t want to do tests that we don’t know what to do with the information,” she said.
One USPSTF member reported receiving grants from Healthwise, a nonprofit organization, outside the submitted work.
A version of this article first appeared on Medscape.com.
Quizartinib boosts AML survival, regardless of SCT
The research shows that “FLT3 inhibitors are most effective in patients who are minimal residual disease (MRD) positive before allo-HCT,” first author Richard Schlenk, MD, of Heidelberg (Germany) University Hospital and the German Cancer Research Center, Heidelberg, said in an interview.
The findings are from a post-hoc analysis of the phase 3, multicenter QuANTUM-First trial, which involved patients with the FLT3-ITD mutation, who make up about a quarter of those with AML and who can have shorter survival and increased risk of relapse, compared with patients without the mutation. The current post-hoc analysis of the trial was presented at the European Hematology Association 2023 Congress.
The trial, published in April in The Lancet, showed significant benefits in newly diagnosed patients with FLT3-ITD AML who were treated with quizartinib and standard induction and consolidation therapy and then continued on quizartinib as monotherapy for up to 3 years.
In the trial, quizartinib, combined with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, and continued as monotherapy following consolidation, was associated with a significant improvement in overall survival versus placebo (median 31.9 months versus 15.1 months, respectively; hazard ratio, 0.776; P = .0324).
For the post hoc analysis of the trial, the authors sought to evaluate if the effects were observed regardless of whether or not allo-HCT was received – which may not be recommended when patients go into remission after the first round of chemotherapy. The issue is important, as efficacy of other targeted therapy with the FLT3 inhibitors has been associated with allo-HCT treatment.
“Midostaurin, for example is mostly effective if [the drug] is followed by allo-HCT, and much less effective [no significant improvement] without allo-HCT,” Dr. Schlenk said.
The authors also sought to evaluate the relationship between minimal residual disease (MRD) prior to allo-HCT in FLT3-ITD and overall survival.
For the trial, 539 patients, with a median age of 56 were randomized to quizartinib (n = 268) or placebo (n = 271), and 147 patients (54.9%) in the quizartinib arm and 150 (55.4%) in the placebo arm achieved complete remission after induction. The rates of incomplete hematologic recovery (CRi) were 16.8% and 9.6%, respectively.
Of those achieving complete remission, 57.1% of patients on quizartinib and 48.7% of those receiving placebo underwent allo-HCT in the first complete remission. The median time to allo-HCT in the two groups was 3.5 months with quizartinib and 3.3 months for placebo.
Following the completion of allo-HCT, 61 patients (72.6%) receiving quizartinib and 36 (49.3%) receiving placebo started 3 years of continuation monotherapy.
In addition, 115 patients received allo-HCT outside of CR1, including 60 on quizartinib and 55 on placebo.
After adjustment for factors including region, age, and white blood count, patients treated with quizartinib treatment had a significantly higher overall survival (HR, 0.770; P = .0284), as did those receiving allo-HCT in CR1 (HR, 0.424; P < .0001).
Furthermore, patients receiving quizartinib had a longer overall survival regardless of whether they received allo-HCT in CR1 or not.
Of note, quizartinib-treated patients who were MRD positive prior to their allo-HCT transplant had a longer overall survival versus placebo (HR, 0.471); as did those who were MRD negative (HR, 0.717), to a lesser degree.
There were no new safety signals identified among patients undergoing allo-HCT.
Of note, cytomegalovirus infection was more common in the quizartinib group (11.8%) versus placebo (5.5%), while decreased appetite was less common with quizartinib (2.9%) versus placebo (12.1%).
Asked by an audience member about any risk of graft-versus-host disease (GVHD), Dr. Schlenk noted that “no difference between the quizartinib and placebo arms has been observed in GVHD acute and chronic.”
He added that patients “appear to benefit more from quizartinib if they have higher allelic frequency versus lower, overall,” and that younger patients, in general, showed greater benefit from quizartinib versus those over 60.
In general, “we see that for patients receiving allo-HCT transplantation, it’s beneficial to be randomized in the quizartinib arm [while] patients who did not undergo allo-HCT in first complete remission benefit equally when treated with quizartinib versus placebo,” he said in presenting the findings at the EHA meeting.
“And irrespective of pre–allo-HCT MRD status, longer survival was observed in those treated with quizartinib versus placebo, but most benefit was observed in those who were MRD positive.”
Quizartinib was approved in Japan this year in combination with chemotherapy for patients with newly diagnosed AML whose tumors harbor FLT3-ITD mutations.
The drug was granted a priority review by the U.S. Food and Drug Administration in October 2022. While the target action date was in April, a new decision date of July 21, 2023, is expected.
The study was sponsored by Daiichi Sankyo. Dr. Schlenk reported relationships with Daiichi Sankyo and other companies.
The research shows that “FLT3 inhibitors are most effective in patients who are minimal residual disease (MRD) positive before allo-HCT,” first author Richard Schlenk, MD, of Heidelberg (Germany) University Hospital and the German Cancer Research Center, Heidelberg, said in an interview.
The findings are from a post-hoc analysis of the phase 3, multicenter QuANTUM-First trial, which involved patients with the FLT3-ITD mutation, who make up about a quarter of those with AML and who can have shorter survival and increased risk of relapse, compared with patients without the mutation. The current post-hoc analysis of the trial was presented at the European Hematology Association 2023 Congress.
The trial, published in April in The Lancet, showed significant benefits in newly diagnosed patients with FLT3-ITD AML who were treated with quizartinib and standard induction and consolidation therapy and then continued on quizartinib as monotherapy for up to 3 years.
In the trial, quizartinib, combined with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, and continued as monotherapy following consolidation, was associated with a significant improvement in overall survival versus placebo (median 31.9 months versus 15.1 months, respectively; hazard ratio, 0.776; P = .0324).
For the post hoc analysis of the trial, the authors sought to evaluate if the effects were observed regardless of whether or not allo-HCT was received – which may not be recommended when patients go into remission after the first round of chemotherapy. The issue is important, as efficacy of other targeted therapy with the FLT3 inhibitors has been associated with allo-HCT treatment.
“Midostaurin, for example is mostly effective if [the drug] is followed by allo-HCT, and much less effective [no significant improvement] without allo-HCT,” Dr. Schlenk said.
The authors also sought to evaluate the relationship between minimal residual disease (MRD) prior to allo-HCT in FLT3-ITD and overall survival.
For the trial, 539 patients, with a median age of 56 were randomized to quizartinib (n = 268) or placebo (n = 271), and 147 patients (54.9%) in the quizartinib arm and 150 (55.4%) in the placebo arm achieved complete remission after induction. The rates of incomplete hematologic recovery (CRi) were 16.8% and 9.6%, respectively.
Of those achieving complete remission, 57.1% of patients on quizartinib and 48.7% of those receiving placebo underwent allo-HCT in the first complete remission. The median time to allo-HCT in the two groups was 3.5 months with quizartinib and 3.3 months for placebo.
Following the completion of allo-HCT, 61 patients (72.6%) receiving quizartinib and 36 (49.3%) receiving placebo started 3 years of continuation monotherapy.
In addition, 115 patients received allo-HCT outside of CR1, including 60 on quizartinib and 55 on placebo.
After adjustment for factors including region, age, and white blood count, patients treated with quizartinib treatment had a significantly higher overall survival (HR, 0.770; P = .0284), as did those receiving allo-HCT in CR1 (HR, 0.424; P < .0001).
Furthermore, patients receiving quizartinib had a longer overall survival regardless of whether they received allo-HCT in CR1 or not.
Of note, quizartinib-treated patients who were MRD positive prior to their allo-HCT transplant had a longer overall survival versus placebo (HR, 0.471); as did those who were MRD negative (HR, 0.717), to a lesser degree.
There were no new safety signals identified among patients undergoing allo-HCT.
Of note, cytomegalovirus infection was more common in the quizartinib group (11.8%) versus placebo (5.5%), while decreased appetite was less common with quizartinib (2.9%) versus placebo (12.1%).
Asked by an audience member about any risk of graft-versus-host disease (GVHD), Dr. Schlenk noted that “no difference between the quizartinib and placebo arms has been observed in GVHD acute and chronic.”
He added that patients “appear to benefit more from quizartinib if they have higher allelic frequency versus lower, overall,” and that younger patients, in general, showed greater benefit from quizartinib versus those over 60.
In general, “we see that for patients receiving allo-HCT transplantation, it’s beneficial to be randomized in the quizartinib arm [while] patients who did not undergo allo-HCT in first complete remission benefit equally when treated with quizartinib versus placebo,” he said in presenting the findings at the EHA meeting.
“And irrespective of pre–allo-HCT MRD status, longer survival was observed in those treated with quizartinib versus placebo, but most benefit was observed in those who were MRD positive.”
Quizartinib was approved in Japan this year in combination with chemotherapy for patients with newly diagnosed AML whose tumors harbor FLT3-ITD mutations.
The drug was granted a priority review by the U.S. Food and Drug Administration in October 2022. While the target action date was in April, a new decision date of July 21, 2023, is expected.
The study was sponsored by Daiichi Sankyo. Dr. Schlenk reported relationships with Daiichi Sankyo and other companies.
The research shows that “FLT3 inhibitors are most effective in patients who are minimal residual disease (MRD) positive before allo-HCT,” first author Richard Schlenk, MD, of Heidelberg (Germany) University Hospital and the German Cancer Research Center, Heidelberg, said in an interview.
The findings are from a post-hoc analysis of the phase 3, multicenter QuANTUM-First trial, which involved patients with the FLT3-ITD mutation, who make up about a quarter of those with AML and who can have shorter survival and increased risk of relapse, compared with patients without the mutation. The current post-hoc analysis of the trial was presented at the European Hematology Association 2023 Congress.
The trial, published in April in The Lancet, showed significant benefits in newly diagnosed patients with FLT3-ITD AML who were treated with quizartinib and standard induction and consolidation therapy and then continued on quizartinib as monotherapy for up to 3 years.
In the trial, quizartinib, combined with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, and continued as monotherapy following consolidation, was associated with a significant improvement in overall survival versus placebo (median 31.9 months versus 15.1 months, respectively; hazard ratio, 0.776; P = .0324).
For the post hoc analysis of the trial, the authors sought to evaluate if the effects were observed regardless of whether or not allo-HCT was received – which may not be recommended when patients go into remission after the first round of chemotherapy. The issue is important, as efficacy of other targeted therapy with the FLT3 inhibitors has been associated with allo-HCT treatment.
“Midostaurin, for example is mostly effective if [the drug] is followed by allo-HCT, and much less effective [no significant improvement] without allo-HCT,” Dr. Schlenk said.
The authors also sought to evaluate the relationship between minimal residual disease (MRD) prior to allo-HCT in FLT3-ITD and overall survival.
For the trial, 539 patients, with a median age of 56 were randomized to quizartinib (n = 268) or placebo (n = 271), and 147 patients (54.9%) in the quizartinib arm and 150 (55.4%) in the placebo arm achieved complete remission after induction. The rates of incomplete hematologic recovery (CRi) were 16.8% and 9.6%, respectively.
Of those achieving complete remission, 57.1% of patients on quizartinib and 48.7% of those receiving placebo underwent allo-HCT in the first complete remission. The median time to allo-HCT in the two groups was 3.5 months with quizartinib and 3.3 months for placebo.
Following the completion of allo-HCT, 61 patients (72.6%) receiving quizartinib and 36 (49.3%) receiving placebo started 3 years of continuation monotherapy.
In addition, 115 patients received allo-HCT outside of CR1, including 60 on quizartinib and 55 on placebo.
After adjustment for factors including region, age, and white blood count, patients treated with quizartinib treatment had a significantly higher overall survival (HR, 0.770; P = .0284), as did those receiving allo-HCT in CR1 (HR, 0.424; P < .0001).
Furthermore, patients receiving quizartinib had a longer overall survival regardless of whether they received allo-HCT in CR1 or not.
Of note, quizartinib-treated patients who were MRD positive prior to their allo-HCT transplant had a longer overall survival versus placebo (HR, 0.471); as did those who were MRD negative (HR, 0.717), to a lesser degree.
There were no new safety signals identified among patients undergoing allo-HCT.
Of note, cytomegalovirus infection was more common in the quizartinib group (11.8%) versus placebo (5.5%), while decreased appetite was less common with quizartinib (2.9%) versus placebo (12.1%).
Asked by an audience member about any risk of graft-versus-host disease (GVHD), Dr. Schlenk noted that “no difference between the quizartinib and placebo arms has been observed in GVHD acute and chronic.”
He added that patients “appear to benefit more from quizartinib if they have higher allelic frequency versus lower, overall,” and that younger patients, in general, showed greater benefit from quizartinib versus those over 60.
In general, “we see that for patients receiving allo-HCT transplantation, it’s beneficial to be randomized in the quizartinib arm [while] patients who did not undergo allo-HCT in first complete remission benefit equally when treated with quizartinib versus placebo,” he said in presenting the findings at the EHA meeting.
“And irrespective of pre–allo-HCT MRD status, longer survival was observed in those treated with quizartinib versus placebo, but most benefit was observed in those who were MRD positive.”
Quizartinib was approved in Japan this year in combination with chemotherapy for patients with newly diagnosed AML whose tumors harbor FLT3-ITD mutations.
The drug was granted a priority review by the U.S. Food and Drug Administration in October 2022. While the target action date was in April, a new decision date of July 21, 2023, is expected.
The study was sponsored by Daiichi Sankyo. Dr. Schlenk reported relationships with Daiichi Sankyo and other companies.
FROM THE EHA 2023 CONGRESS
Creating a fair time-off policy
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?

First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?
First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?
First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

Promising phase 3 results for Alzheimer’s drug donanemab
results of a phase 3 study showed.
“This trial demonstrates that an antiamyloid drug significantly slows the disease and provides meaningful benefit to patients, and we’re hoping that with approval, we will be able to make that drug available,” said Mark Mintun, MD, VP, pain and neurodegeneration research, Eli Lilly.
At a press briefing highlighting the new results, Maria Carrillo, PhD, chief science officer, Alzheimer’s Association, noted the “palpable excitement” surrounding this new study, which follows on the heels of other promising antiamyloid research. “This is the decade of Alzheimer’s disease, and it will get better from here,” she said.
The findings were presented at the Alzheimer’s Association International Conference and were published online in JAMA.
Primary, secondary endpoints met
The TRAILBLAZER-ALZ 2 study included 1,736 patients with mild cognitive impairment (MCI) or mild dementia for whom PET showed evidence of amyloid and tau pathology. The mean age of the participants was 73 years, and most of the participants were White.
Participants were randomly assigned to receive either placebo or donanemab, an investigational IgG1 monoclonal antibody directed against an insoluble, modified, N-terminal, truncated form of beta-amyloid. Donanemab was administered at a dose of 700 mg for the first three doses and 1,400 mg thereafter. The drug was administered intravenously every 4 weeks for up to 72 weeks.
Researchers stratified patients on the basis of the amount of tau, a biomarker for Alzheimer’s disease progression, into a low/medium tau group and a combined tau group (low/medium and high tau).
The primary endpoint was change from baseline to 76 weeks on the integrated Alzheimer’s Disease Rating Scale (iADRS), which measures cognition and activities of daily living.
In those with low/medium tau levels, the least squares mean (LSM) change in iADRS score was −6.02 (95% confidence interval, −7.01 to −5.03) in the donanemab group and −9.27 (95% CI, −10.23 to −8.31) in the placebo group (difference, 3.25; 95% CI, 1.88 – 4.62; P < .001), representing a 35.1% slowing of disease progression.
In the combined (tau) population, LSM change in iADRS was −10.19 (95% CI, −11.22 to −9.16) in the donanemab group and −13.11 (95% CI, −14.10 to −12.13) in the placebo group (difference, 2.92; 95% CI, 1.51 – 4.33; P < .001), representing a 22.3% slowing of disease progression.
The study also met all secondary endpoints regarding measurements of cognitive and functional decline, including the Clinical Dementia Rating–Sum of Boxes (CDR-SB), which showed 36% slowing of decline (P < .0001) over 18 months.
The authors noted that the changes on these scales were clinically meaningful (considered to be > 20% slowing of clinical progression) for both the low/medium tau and combined populations.
Greater benefit with lower tau
However, patients with low/medium tau generally demonstrated effect size estimates that were larger than those of the overall population, which suggests there’s greater benefit when amyloid-lowering therapies are initiated at an earlier disease stage, the investigators noted.
Additional support for clinical relevance was a 38.6% risk reduction of disease progression, as measured on the CDR–Global Score.
In addition, participants who received the active drug benefited in terms of activities of daily living, as demonstrated by 40% less decline (P < .0001) on the Alzheimer’s Disease Cooperative Study–Instrumental Activities of Daily Living Inventory.
Donanemab significantly reduced brain amyloid plaque: 80% (low/medium tau population) and 76% (combined population) of participants achieved amyloid clearance at 76 weeks. The intervention was also associated with a greater decrease in whole-brain volume.
The treatment effect continued to widen after patients were switched to placebo, as evidenced on PET scan at 6 or 12 months, said Dr. Mintun.
The effects of the drug were similar among men and women but were especially pronounced among younger participants, with a 48% slowing on iADRS and a 45% slowing on CDR-SB in those younger than 75 years.
Safety issues
However, the drug is not without some safety concerns. Amyloid-related imaging abnormalities (ARIAs) occurred in 36.8% of the treatment group versus 14.9% of the placebo group, and in 40.6% of patients who were homozygous for apo E4 and received the drug. Microhemorrhage occurred in 26.8% in the donanemab group versus 12.5% in the placebo group.
Most ARIA cases were mild to moderate and resolved or stabilized with appropriate management. However, three deaths were determined to be drug related among participants who developed serious ARIAs or brain bleeding and swelling.
An important study limitation was that it enrolled primarily White patients (91.5%), which may limit generalizability to other populations, and the age limit was 85 years, which some believe is an inadequate representation of older adults. In addition, the 18-month treatment window limits the long-term understanding of donanemab’s benefits and side effects.
Eli Lilly has filed a submission to the Food and Drug Administration. If approved, donanemab will be the third antiamyloid monoclonal antibody to receive this status, following aducanumab (Aduhelm) and lecanemab (Leqembi).
Strongest data yet
Commenting on the study findings, Percy Griffin, PhD, director of scientific engagement, Alzheimer’s Association, said these new results are “very, very exciting” and represent “the strongest data to-date” for antiamyloid monoclonal antibodies in Alzheimer’s disease.
“A good percentage of individuals on the drug actually saw a complete clearance of amyloid, and some had to be taken off the drug, because if you’re on an antiamyloid drug and there’s no amyloid, what are you going for?”
He noted that the study had some unique aspects, including using tau-PET “to see whether or not the drug is more effective in subpopulations.”
Access to this and other antiamyloid therapies should be a priority, said Dr. Griffin. “We have to make sure people who have the potential to benefit from these treatments do.”
The Alzheimer’s Association is calling for Medicare beneficiaries who are living with the disease to receive the same coverage afforded to those with other diseases.
“The Centers for Medicare & Medicaid Services policy to block Medicare access to FDA-approved Alzheimer’s disease treatments is in stark contrast to scientific evidence, is unprecedented and must be reversed immediately,” Joanne Pike, DrPH, president and CEO of the Alzheimer’s Association, said in a press release.
Also important is tracking the longitudinal performance of these drugs outside of clinical trials, said Dr. Griffin. “Not everyone is going to be in that Goldilocks zone of being able to see a doctor whenever they want and have access to these PET and MRI tools and other things used in clinical trials.”
He noted that the Alzheimer’s Association is leading a network for diagnostics and therapeutics (ALZ-NET) that will track the performance of novel FDA-approved Alzheimer’s disease therapies “in the real world.”
While these are exciting findings for antiamyloid therapy, “we can’t take our foot off the gas, we need more therapies that target different aspects of the disease biology,” said Dr. Griffin.
A version of this article appeared on Medscape.com.
results of a phase 3 study showed.
“This trial demonstrates that an antiamyloid drug significantly slows the disease and provides meaningful benefit to patients, and we’re hoping that with approval, we will be able to make that drug available,” said Mark Mintun, MD, VP, pain and neurodegeneration research, Eli Lilly.
At a press briefing highlighting the new results, Maria Carrillo, PhD, chief science officer, Alzheimer’s Association, noted the “palpable excitement” surrounding this new study, which follows on the heels of other promising antiamyloid research. “This is the decade of Alzheimer’s disease, and it will get better from here,” she said.
The findings were presented at the Alzheimer’s Association International Conference and were published online in JAMA.
Primary, secondary endpoints met
The TRAILBLAZER-ALZ 2 study included 1,736 patients with mild cognitive impairment (MCI) or mild dementia for whom PET showed evidence of amyloid and tau pathology. The mean age of the participants was 73 years, and most of the participants were White.
Participants were randomly assigned to receive either placebo or donanemab, an investigational IgG1 monoclonal antibody directed against an insoluble, modified, N-terminal, truncated form of beta-amyloid. Donanemab was administered at a dose of 700 mg for the first three doses and 1,400 mg thereafter. The drug was administered intravenously every 4 weeks for up to 72 weeks.
Researchers stratified patients on the basis of the amount of tau, a biomarker for Alzheimer’s disease progression, into a low/medium tau group and a combined tau group (low/medium and high tau).
The primary endpoint was change from baseline to 76 weeks on the integrated Alzheimer’s Disease Rating Scale (iADRS), which measures cognition and activities of daily living.
In those with low/medium tau levels, the least squares mean (LSM) change in iADRS score was −6.02 (95% confidence interval, −7.01 to −5.03) in the donanemab group and −9.27 (95% CI, −10.23 to −8.31) in the placebo group (difference, 3.25; 95% CI, 1.88 – 4.62; P < .001), representing a 35.1% slowing of disease progression.
In the combined (tau) population, LSM change in iADRS was −10.19 (95% CI, −11.22 to −9.16) in the donanemab group and −13.11 (95% CI, −14.10 to −12.13) in the placebo group (difference, 2.92; 95% CI, 1.51 – 4.33; P < .001), representing a 22.3% slowing of disease progression.
The study also met all secondary endpoints regarding measurements of cognitive and functional decline, including the Clinical Dementia Rating–Sum of Boxes (CDR-SB), which showed 36% slowing of decline (P < .0001) over 18 months.
The authors noted that the changes on these scales were clinically meaningful (considered to be > 20% slowing of clinical progression) for both the low/medium tau and combined populations.
Greater benefit with lower tau
However, patients with low/medium tau generally demonstrated effect size estimates that were larger than those of the overall population, which suggests there’s greater benefit when amyloid-lowering therapies are initiated at an earlier disease stage, the investigators noted.
Additional support for clinical relevance was a 38.6% risk reduction of disease progression, as measured on the CDR–Global Score.
In addition, participants who received the active drug benefited in terms of activities of daily living, as demonstrated by 40% less decline (P < .0001) on the Alzheimer’s Disease Cooperative Study–Instrumental Activities of Daily Living Inventory.
Donanemab significantly reduced brain amyloid plaque: 80% (low/medium tau population) and 76% (combined population) of participants achieved amyloid clearance at 76 weeks. The intervention was also associated with a greater decrease in whole-brain volume.
The treatment effect continued to widen after patients were switched to placebo, as evidenced on PET scan at 6 or 12 months, said Dr. Mintun.
The effects of the drug were similar among men and women but were especially pronounced among younger participants, with a 48% slowing on iADRS and a 45% slowing on CDR-SB in those younger than 75 years.
Safety issues
However, the drug is not without some safety concerns. Amyloid-related imaging abnormalities (ARIAs) occurred in 36.8% of the treatment group versus 14.9% of the placebo group, and in 40.6% of patients who were homozygous for apo E4 and received the drug. Microhemorrhage occurred in 26.8% in the donanemab group versus 12.5% in the placebo group.
Most ARIA cases were mild to moderate and resolved or stabilized with appropriate management. However, three deaths were determined to be drug related among participants who developed serious ARIAs or brain bleeding and swelling.
An important study limitation was that it enrolled primarily White patients (91.5%), which may limit generalizability to other populations, and the age limit was 85 years, which some believe is an inadequate representation of older adults. In addition, the 18-month treatment window limits the long-term understanding of donanemab’s benefits and side effects.
Eli Lilly has filed a submission to the Food and Drug Administration. If approved, donanemab will be the third antiamyloid monoclonal antibody to receive this status, following aducanumab (Aduhelm) and lecanemab (Leqembi).
Strongest data yet
Commenting on the study findings, Percy Griffin, PhD, director of scientific engagement, Alzheimer’s Association, said these new results are “very, very exciting” and represent “the strongest data to-date” for antiamyloid monoclonal antibodies in Alzheimer’s disease.
“A good percentage of individuals on the drug actually saw a complete clearance of amyloid, and some had to be taken off the drug, because if you’re on an antiamyloid drug and there’s no amyloid, what are you going for?”
He noted that the study had some unique aspects, including using tau-PET “to see whether or not the drug is more effective in subpopulations.”
Access to this and other antiamyloid therapies should be a priority, said Dr. Griffin. “We have to make sure people who have the potential to benefit from these treatments do.”
The Alzheimer’s Association is calling for Medicare beneficiaries who are living with the disease to receive the same coverage afforded to those with other diseases.
“The Centers for Medicare & Medicaid Services policy to block Medicare access to FDA-approved Alzheimer’s disease treatments is in stark contrast to scientific evidence, is unprecedented and must be reversed immediately,” Joanne Pike, DrPH, president and CEO of the Alzheimer’s Association, said in a press release.
Also important is tracking the longitudinal performance of these drugs outside of clinical trials, said Dr. Griffin. “Not everyone is going to be in that Goldilocks zone of being able to see a doctor whenever they want and have access to these PET and MRI tools and other things used in clinical trials.”
He noted that the Alzheimer’s Association is leading a network for diagnostics and therapeutics (ALZ-NET) that will track the performance of novel FDA-approved Alzheimer’s disease therapies “in the real world.”
While these are exciting findings for antiamyloid therapy, “we can’t take our foot off the gas, we need more therapies that target different aspects of the disease biology,” said Dr. Griffin.
A version of this article appeared on Medscape.com.
results of a phase 3 study showed.
“This trial demonstrates that an antiamyloid drug significantly slows the disease and provides meaningful benefit to patients, and we’re hoping that with approval, we will be able to make that drug available,” said Mark Mintun, MD, VP, pain and neurodegeneration research, Eli Lilly.
At a press briefing highlighting the new results, Maria Carrillo, PhD, chief science officer, Alzheimer’s Association, noted the “palpable excitement” surrounding this new study, which follows on the heels of other promising antiamyloid research. “This is the decade of Alzheimer’s disease, and it will get better from here,” she said.
The findings were presented at the Alzheimer’s Association International Conference and were published online in JAMA.
Primary, secondary endpoints met
The TRAILBLAZER-ALZ 2 study included 1,736 patients with mild cognitive impairment (MCI) or mild dementia for whom PET showed evidence of amyloid and tau pathology. The mean age of the participants was 73 years, and most of the participants were White.
Participants were randomly assigned to receive either placebo or donanemab, an investigational IgG1 monoclonal antibody directed against an insoluble, modified, N-terminal, truncated form of beta-amyloid. Donanemab was administered at a dose of 700 mg for the first three doses and 1,400 mg thereafter. The drug was administered intravenously every 4 weeks for up to 72 weeks.
Researchers stratified patients on the basis of the amount of tau, a biomarker for Alzheimer’s disease progression, into a low/medium tau group and a combined tau group (low/medium and high tau).
The primary endpoint was change from baseline to 76 weeks on the integrated Alzheimer’s Disease Rating Scale (iADRS), which measures cognition and activities of daily living.
In those with low/medium tau levels, the least squares mean (LSM) change in iADRS score was −6.02 (95% confidence interval, −7.01 to −5.03) in the donanemab group and −9.27 (95% CI, −10.23 to −8.31) in the placebo group (difference, 3.25; 95% CI, 1.88 – 4.62; P < .001), representing a 35.1% slowing of disease progression.
In the combined (tau) population, LSM change in iADRS was −10.19 (95% CI, −11.22 to −9.16) in the donanemab group and −13.11 (95% CI, −14.10 to −12.13) in the placebo group (difference, 2.92; 95% CI, 1.51 – 4.33; P < .001), representing a 22.3% slowing of disease progression.
The study also met all secondary endpoints regarding measurements of cognitive and functional decline, including the Clinical Dementia Rating–Sum of Boxes (CDR-SB), which showed 36% slowing of decline (P < .0001) over 18 months.
The authors noted that the changes on these scales were clinically meaningful (considered to be > 20% slowing of clinical progression) for both the low/medium tau and combined populations.
Greater benefit with lower tau
However, patients with low/medium tau generally demonstrated effect size estimates that were larger than those of the overall population, which suggests there’s greater benefit when amyloid-lowering therapies are initiated at an earlier disease stage, the investigators noted.
Additional support for clinical relevance was a 38.6% risk reduction of disease progression, as measured on the CDR–Global Score.
In addition, participants who received the active drug benefited in terms of activities of daily living, as demonstrated by 40% less decline (P < .0001) on the Alzheimer’s Disease Cooperative Study–Instrumental Activities of Daily Living Inventory.
Donanemab significantly reduced brain amyloid plaque: 80% (low/medium tau population) and 76% (combined population) of participants achieved amyloid clearance at 76 weeks. The intervention was also associated with a greater decrease in whole-brain volume.
The treatment effect continued to widen after patients were switched to placebo, as evidenced on PET scan at 6 or 12 months, said Dr. Mintun.
The effects of the drug were similar among men and women but were especially pronounced among younger participants, with a 48% slowing on iADRS and a 45% slowing on CDR-SB in those younger than 75 years.
Safety issues
However, the drug is not without some safety concerns. Amyloid-related imaging abnormalities (ARIAs) occurred in 36.8% of the treatment group versus 14.9% of the placebo group, and in 40.6% of patients who were homozygous for apo E4 and received the drug. Microhemorrhage occurred in 26.8% in the donanemab group versus 12.5% in the placebo group.
Most ARIA cases were mild to moderate and resolved or stabilized with appropriate management. However, three deaths were determined to be drug related among participants who developed serious ARIAs or brain bleeding and swelling.
An important study limitation was that it enrolled primarily White patients (91.5%), which may limit generalizability to other populations, and the age limit was 85 years, which some believe is an inadequate representation of older adults. In addition, the 18-month treatment window limits the long-term understanding of donanemab’s benefits and side effects.
Eli Lilly has filed a submission to the Food and Drug Administration. If approved, donanemab will be the third antiamyloid monoclonal antibody to receive this status, following aducanumab (Aduhelm) and lecanemab (Leqembi).
Strongest data yet
Commenting on the study findings, Percy Griffin, PhD, director of scientific engagement, Alzheimer’s Association, said these new results are “very, very exciting” and represent “the strongest data to-date” for antiamyloid monoclonal antibodies in Alzheimer’s disease.
“A good percentage of individuals on the drug actually saw a complete clearance of amyloid, and some had to be taken off the drug, because if you’re on an antiamyloid drug and there’s no amyloid, what are you going for?”
He noted that the study had some unique aspects, including using tau-PET “to see whether or not the drug is more effective in subpopulations.”
Access to this and other antiamyloid therapies should be a priority, said Dr. Griffin. “We have to make sure people who have the potential to benefit from these treatments do.”
The Alzheimer’s Association is calling for Medicare beneficiaries who are living with the disease to receive the same coverage afforded to those with other diseases.
“The Centers for Medicare & Medicaid Services policy to block Medicare access to FDA-approved Alzheimer’s disease treatments is in stark contrast to scientific evidence, is unprecedented and must be reversed immediately,” Joanne Pike, DrPH, president and CEO of the Alzheimer’s Association, said in a press release.
Also important is tracking the longitudinal performance of these drugs outside of clinical trials, said Dr. Griffin. “Not everyone is going to be in that Goldilocks zone of being able to see a doctor whenever they want and have access to these PET and MRI tools and other things used in clinical trials.”
He noted that the Alzheimer’s Association is leading a network for diagnostics and therapeutics (ALZ-NET) that will track the performance of novel FDA-approved Alzheimer’s disease therapies “in the real world.”
While these are exciting findings for antiamyloid therapy, “we can’t take our foot off the gas, we need more therapies that target different aspects of the disease biology,” said Dr. Griffin.
A version of this article appeared on Medscape.com.
FROM AAIC 2023
New global initiative aims to reform cancer trials and care
After 15 years of researching what works well in oncology – and where the field has gone awry – Christopher Booth, MD, had a career moment.
“As I approached mid-career, I realized publishing and describing problems wasn’t fulfilling. It wasn’t doing enough,” recalled Dr. Booth, an oncologist and professor at Queen’s University, Kingston, Ont. “I wanted to change mindsets and change systems so that things actually improved for the better for patients.”
His colleague, Bishal Gyawali, MD, PhD, described a similar epiphany. As a trainee, he noticed that the real-world effects of some so-called blockbuster cancer drugs too often failed to measure up to the hype.
“I realized we were lacking common sense in oncology,” said Dr. Gyawali, a medical oncologist and assistant professor at Queen’s University.
In 2019, Dr. Gyawali launched a Medscape column addressing what he considers to be that lack of common sense, and in 2022, he and Dr. Booth published a similarly titled opinion piece in Nature Medicine. The core idea: The cancer community needs to prioritize cancer treatments that benefit patients, treatments that meaningfully improve survival and quality of life.
Aaron Goodman, MD, a hematologist and associate professor at UC San Diego Health, was on the same page. He’d been interested in the evidence-based medicine movement since his time as a hematology fellow when that movement was “a bit of a counterculture,” he explained.
Dr. Goodman and Dr. Booth connected through their common interests and collaborated on a 2021 paper exploring the discomfort clinicians might feel when a patient’s needs fall on the “edge of oncology”: that is, when the guideline-recommended standard of care offers marginal benefit, at best, and could, at worst, cause patient harm.
“We said, ‘Now is the time to make change,’ ” he recalled. It was time to stop talking and do something.
Common sense and a common purpose
Dr. Booth, Dr. Gyawali, and Dr. Goodman joined forces and, with the backing of a philanthropist who had experience as a patient with cancer, convened an organizing committee of more than 30 like-minded oncologists and patient advocates from across the globe.
The group convened for a 3-day “meeting of the minds” in Kingston in April and laid out their intentions in a position paper published online in The Lancet Oncology.
In their paper, the committee outline the vision for Common Sense Oncology. The mission: prioritize patient-centered and equitable care by focusing on treatments that improve survival and quality of life, communication that promotes informed decision-making, and systems that ensure access to all patients.
However, increasingly, the cancer community faces a “troubling paradox,” the team wrote in The Lancet. In some instance, treatments that bring minimal benefit are overused while those that can make a meaningful difference in patients’ lives are not accessible to most worldwide.
One reason for this shift: Commercial interests, rather than patient interests, appear to be driving cancer research and care. The team explained, for instance, that over the past few decades, clinical trials have largely pivoted from publicly funded efforts to industry funded ones “designed to achieve regulatory approval or commercial advantage, [often] at the expense of investigating new approaches to surgery, radiotherapy, palliative care, and prevention.”
But “patients deserve better,” the group wrote.
The team outlined three pillars for the initiative: evidence generation, evidence interpretation, and evidence communication.
The evidence generation pillar will aim to improve trial design and reporting to prioritize outcomes that matter to patients.
“One concern is that over the last 10 years or so, most of our new treatments have had very, very small benefits, and we think the bar has dropped too low,” Dr. Booth said, explaining that many trials have moved away from focusing on improving survival and quality of life and toward detecting small differences between treatments on other endpoints – namely progression-free survival. “Those small benefits need to be balanced against the very real risks to our patients.”
The evidence interpretation pillar will aim to foster critical thinking so that clinicians can better identify poorly designed or reported trials and help patients make more informed decisions.
Lastly, the evidence communication pillar will focus on fostering better communication about treatment options among patients, the public, and policymakers. Without clear and thoughtful communication, patients may have unrealistic expectations about the effectiveness of treatments that offer only marginal clinical benefits.
The team also emphasized a need to focus on improving global equity and access to affordable treatments so all patients can benefit from care that extends survival or quality of life.
It’s an ambitious undertaking, especially for a group of full-time clinicians, researchers, and patient advocates “volunteering their time for societal good,” said Dr. Gyawali, but the project teams intend to hit the ground running.
The team has established short-term targets, such as identifying deficiencies in data interpretation within education programs within 6 months and developing educational materials that begin to correct those deficiencies within 12 months, Dr. Booth explained. In the longer term, the team will also aim to design clinical trials that focus on patient outcomes, such as overall survival and quality of life.
Breast cancer survivor and patient advocate Michelle Tregear, PhD, who was recruited to help with Common Sense Oncology, also hopes the initiative will lead to better regulatory control that requires trial sponsors to “focus on what matters to patients, not on surrogate endpoints.”
When it comes to clinical trials, “more, more, more is not always better,” said Dr. Tregear, director of Education and Training Programs for patient advocates at the National Breast Cancer Coalition, Washington, D.C. “Industry interests are not always aligned with patient interests,” and “the system, by and large, is not addressing questions that really matter to patients and their families.”
Although “it’s a tall order to change the direction that we’re going in,” Dr. Tregear is up to the challenge of helping raise awareness, which will hopefully spur patients to demand change.
When Dr. Goodman announced the Common Sense Oncology initiative on Twitter, the news brought excitement, with many oncologists asking to join.
With its sweeping, ambitious goals, the Common Sense Oncology initiative has a long road ahead. Figuring out how to implement some of its aims in practice will take time, Dr. Booth acknowledges, and the initial launch marks the first steps, which will continue to evolve over time.
“We’re not proposing we have all the answers or that we know what every patient would want – we’re saying we’ve not done a good job of communicating to patients the relative benefits and risks of different treatments,” Dr. Booth explained. “We want to celebrate and promote what helps and speak out about what’s not in the best interest of patients.”
Dr. Goodman reported consulting fees from Seattle Genetics and speaking honoraria from Curio. Dr. Booth, Dr. Gyawali, and Dr. Tregear reported having no financial conflicts of interest.
A version of this article appeared on Medscape.com.
After 15 years of researching what works well in oncology – and where the field has gone awry – Christopher Booth, MD, had a career moment.
“As I approached mid-career, I realized publishing and describing problems wasn’t fulfilling. It wasn’t doing enough,” recalled Dr. Booth, an oncologist and professor at Queen’s University, Kingston, Ont. “I wanted to change mindsets and change systems so that things actually improved for the better for patients.”
His colleague, Bishal Gyawali, MD, PhD, described a similar epiphany. As a trainee, he noticed that the real-world effects of some so-called blockbuster cancer drugs too often failed to measure up to the hype.
“I realized we were lacking common sense in oncology,” said Dr. Gyawali, a medical oncologist and assistant professor at Queen’s University.
In 2019, Dr. Gyawali launched a Medscape column addressing what he considers to be that lack of common sense, and in 2022, he and Dr. Booth published a similarly titled opinion piece in Nature Medicine. The core idea: The cancer community needs to prioritize cancer treatments that benefit patients, treatments that meaningfully improve survival and quality of life.
Aaron Goodman, MD, a hematologist and associate professor at UC San Diego Health, was on the same page. He’d been interested in the evidence-based medicine movement since his time as a hematology fellow when that movement was “a bit of a counterculture,” he explained.
Dr. Goodman and Dr. Booth connected through their common interests and collaborated on a 2021 paper exploring the discomfort clinicians might feel when a patient’s needs fall on the “edge of oncology”: that is, when the guideline-recommended standard of care offers marginal benefit, at best, and could, at worst, cause patient harm.
“We said, ‘Now is the time to make change,’ ” he recalled. It was time to stop talking and do something.
Common sense and a common purpose
Dr. Booth, Dr. Gyawali, and Dr. Goodman joined forces and, with the backing of a philanthropist who had experience as a patient with cancer, convened an organizing committee of more than 30 like-minded oncologists and patient advocates from across the globe.
The group convened for a 3-day “meeting of the minds” in Kingston in April and laid out their intentions in a position paper published online in The Lancet Oncology.
In their paper, the committee outline the vision for Common Sense Oncology. The mission: prioritize patient-centered and equitable care by focusing on treatments that improve survival and quality of life, communication that promotes informed decision-making, and systems that ensure access to all patients.
However, increasingly, the cancer community faces a “troubling paradox,” the team wrote in The Lancet. In some instance, treatments that bring minimal benefit are overused while those that can make a meaningful difference in patients’ lives are not accessible to most worldwide.
One reason for this shift: Commercial interests, rather than patient interests, appear to be driving cancer research and care. The team explained, for instance, that over the past few decades, clinical trials have largely pivoted from publicly funded efforts to industry funded ones “designed to achieve regulatory approval or commercial advantage, [often] at the expense of investigating new approaches to surgery, radiotherapy, palliative care, and prevention.”
But “patients deserve better,” the group wrote.
The team outlined three pillars for the initiative: evidence generation, evidence interpretation, and evidence communication.
The evidence generation pillar will aim to improve trial design and reporting to prioritize outcomes that matter to patients.
“One concern is that over the last 10 years or so, most of our new treatments have had very, very small benefits, and we think the bar has dropped too low,” Dr. Booth said, explaining that many trials have moved away from focusing on improving survival and quality of life and toward detecting small differences between treatments on other endpoints – namely progression-free survival. “Those small benefits need to be balanced against the very real risks to our patients.”
The evidence interpretation pillar will aim to foster critical thinking so that clinicians can better identify poorly designed or reported trials and help patients make more informed decisions.
Lastly, the evidence communication pillar will focus on fostering better communication about treatment options among patients, the public, and policymakers. Without clear and thoughtful communication, patients may have unrealistic expectations about the effectiveness of treatments that offer only marginal clinical benefits.
The team also emphasized a need to focus on improving global equity and access to affordable treatments so all patients can benefit from care that extends survival or quality of life.
It’s an ambitious undertaking, especially for a group of full-time clinicians, researchers, and patient advocates “volunteering their time for societal good,” said Dr. Gyawali, but the project teams intend to hit the ground running.
The team has established short-term targets, such as identifying deficiencies in data interpretation within education programs within 6 months and developing educational materials that begin to correct those deficiencies within 12 months, Dr. Booth explained. In the longer term, the team will also aim to design clinical trials that focus on patient outcomes, such as overall survival and quality of life.
Breast cancer survivor and patient advocate Michelle Tregear, PhD, who was recruited to help with Common Sense Oncology, also hopes the initiative will lead to better regulatory control that requires trial sponsors to “focus on what matters to patients, not on surrogate endpoints.”
When it comes to clinical trials, “more, more, more is not always better,” said Dr. Tregear, director of Education and Training Programs for patient advocates at the National Breast Cancer Coalition, Washington, D.C. “Industry interests are not always aligned with patient interests,” and “the system, by and large, is not addressing questions that really matter to patients and their families.”
Although “it’s a tall order to change the direction that we’re going in,” Dr. Tregear is up to the challenge of helping raise awareness, which will hopefully spur patients to demand change.
When Dr. Goodman announced the Common Sense Oncology initiative on Twitter, the news brought excitement, with many oncologists asking to join.
With its sweeping, ambitious goals, the Common Sense Oncology initiative has a long road ahead. Figuring out how to implement some of its aims in practice will take time, Dr. Booth acknowledges, and the initial launch marks the first steps, which will continue to evolve over time.
“We’re not proposing we have all the answers or that we know what every patient would want – we’re saying we’ve not done a good job of communicating to patients the relative benefits and risks of different treatments,” Dr. Booth explained. “We want to celebrate and promote what helps and speak out about what’s not in the best interest of patients.”
Dr. Goodman reported consulting fees from Seattle Genetics and speaking honoraria from Curio. Dr. Booth, Dr. Gyawali, and Dr. Tregear reported having no financial conflicts of interest.
A version of this article appeared on Medscape.com.
After 15 years of researching what works well in oncology – and where the field has gone awry – Christopher Booth, MD, had a career moment.
“As I approached mid-career, I realized publishing and describing problems wasn’t fulfilling. It wasn’t doing enough,” recalled Dr. Booth, an oncologist and professor at Queen’s University, Kingston, Ont. “I wanted to change mindsets and change systems so that things actually improved for the better for patients.”
His colleague, Bishal Gyawali, MD, PhD, described a similar epiphany. As a trainee, he noticed that the real-world effects of some so-called blockbuster cancer drugs too often failed to measure up to the hype.
“I realized we were lacking common sense in oncology,” said Dr. Gyawali, a medical oncologist and assistant professor at Queen’s University.
In 2019, Dr. Gyawali launched a Medscape column addressing what he considers to be that lack of common sense, and in 2022, he and Dr. Booth published a similarly titled opinion piece in Nature Medicine. The core idea: The cancer community needs to prioritize cancer treatments that benefit patients, treatments that meaningfully improve survival and quality of life.
Aaron Goodman, MD, a hematologist and associate professor at UC San Diego Health, was on the same page. He’d been interested in the evidence-based medicine movement since his time as a hematology fellow when that movement was “a bit of a counterculture,” he explained.
Dr. Goodman and Dr. Booth connected through their common interests and collaborated on a 2021 paper exploring the discomfort clinicians might feel when a patient’s needs fall on the “edge of oncology”: that is, when the guideline-recommended standard of care offers marginal benefit, at best, and could, at worst, cause patient harm.
“We said, ‘Now is the time to make change,’ ” he recalled. It was time to stop talking and do something.
Common sense and a common purpose
Dr. Booth, Dr. Gyawali, and Dr. Goodman joined forces and, with the backing of a philanthropist who had experience as a patient with cancer, convened an organizing committee of more than 30 like-minded oncologists and patient advocates from across the globe.
The group convened for a 3-day “meeting of the minds” in Kingston in April and laid out their intentions in a position paper published online in The Lancet Oncology.
In their paper, the committee outline the vision for Common Sense Oncology. The mission: prioritize patient-centered and equitable care by focusing on treatments that improve survival and quality of life, communication that promotes informed decision-making, and systems that ensure access to all patients.
However, increasingly, the cancer community faces a “troubling paradox,” the team wrote in The Lancet. In some instance, treatments that bring minimal benefit are overused while those that can make a meaningful difference in patients’ lives are not accessible to most worldwide.
One reason for this shift: Commercial interests, rather than patient interests, appear to be driving cancer research and care. The team explained, for instance, that over the past few decades, clinical trials have largely pivoted from publicly funded efforts to industry funded ones “designed to achieve regulatory approval or commercial advantage, [often] at the expense of investigating new approaches to surgery, radiotherapy, palliative care, and prevention.”
But “patients deserve better,” the group wrote.
The team outlined three pillars for the initiative: evidence generation, evidence interpretation, and evidence communication.
The evidence generation pillar will aim to improve trial design and reporting to prioritize outcomes that matter to patients.
“One concern is that over the last 10 years or so, most of our new treatments have had very, very small benefits, and we think the bar has dropped too low,” Dr. Booth said, explaining that many trials have moved away from focusing on improving survival and quality of life and toward detecting small differences between treatments on other endpoints – namely progression-free survival. “Those small benefits need to be balanced against the very real risks to our patients.”
The evidence interpretation pillar will aim to foster critical thinking so that clinicians can better identify poorly designed or reported trials and help patients make more informed decisions.
Lastly, the evidence communication pillar will focus on fostering better communication about treatment options among patients, the public, and policymakers. Without clear and thoughtful communication, patients may have unrealistic expectations about the effectiveness of treatments that offer only marginal clinical benefits.
The team also emphasized a need to focus on improving global equity and access to affordable treatments so all patients can benefit from care that extends survival or quality of life.
It’s an ambitious undertaking, especially for a group of full-time clinicians, researchers, and patient advocates “volunteering their time for societal good,” said Dr. Gyawali, but the project teams intend to hit the ground running.
The team has established short-term targets, such as identifying deficiencies in data interpretation within education programs within 6 months and developing educational materials that begin to correct those deficiencies within 12 months, Dr. Booth explained. In the longer term, the team will also aim to design clinical trials that focus on patient outcomes, such as overall survival and quality of life.
Breast cancer survivor and patient advocate Michelle Tregear, PhD, who was recruited to help with Common Sense Oncology, also hopes the initiative will lead to better regulatory control that requires trial sponsors to “focus on what matters to patients, not on surrogate endpoints.”
When it comes to clinical trials, “more, more, more is not always better,” said Dr. Tregear, director of Education and Training Programs for patient advocates at the National Breast Cancer Coalition, Washington, D.C. “Industry interests are not always aligned with patient interests,” and “the system, by and large, is not addressing questions that really matter to patients and their families.”
Although “it’s a tall order to change the direction that we’re going in,” Dr. Tregear is up to the challenge of helping raise awareness, which will hopefully spur patients to demand change.
When Dr. Goodman announced the Common Sense Oncology initiative on Twitter, the news brought excitement, with many oncologists asking to join.
With its sweeping, ambitious goals, the Common Sense Oncology initiative has a long road ahead. Figuring out how to implement some of its aims in practice will take time, Dr. Booth acknowledges, and the initial launch marks the first steps, which will continue to evolve over time.
“We’re not proposing we have all the answers or that we know what every patient would want – we’re saying we’ve not done a good job of communicating to patients the relative benefits and risks of different treatments,” Dr. Booth explained. “We want to celebrate and promote what helps and speak out about what’s not in the best interest of patients.”
Dr. Goodman reported consulting fees from Seattle Genetics and speaking honoraria from Curio. Dr. Booth, Dr. Gyawali, and Dr. Tregear reported having no financial conflicts of interest.
A version of this article appeared on Medscape.com.
Remote teams offer chance to improve difficult-to-treat PsA
DUBLIN – according to presenters at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
In the same session at the meeting, GRAPPA also announced a new initiative to define difficult-to-treat PsA.
Deepak Jadon, MBBCh, PhD, a rheumatologist with Cambridge (England) University Hospitals NHS Foundation Trust, described his experience of running a clinic for patients with difficult-to-treat PsA in eastern England, covering a catchment area of approximately 6 million people between six and seven hospitals. He discussed how the MDT in his region operates to discuss the management of such patients, whose treatment options may also have indications for comorbidities such as inflammatory bowel disease or uveitis, or have complicating factors such as metabolic syndrome.
“You have to have an interested and engaged colleague to form that collaboration,” Dr. Jadon said. “If you are working in isolation, without your colleagues in the same building, that becomes harder. We have been running remote multispecialty meetings without the patient being present, and I have had the good fortune of having medical students brought into our practice. We discussed approximately 220 patients, initially in our psoriasis-spondyloarthritis MDT and subsequently in our inflammatory bowel disease–spondyloarthritis MDT.”
There are also MDTs with hepatologist colleagues carried out on an ad hoc basis to discuss patients with nonalcoholic fatty liver disease, as well as patients with hepatitis or a transplanted liver, who have psoriatic disease.
This difficult-to-treat cohort is discussed in MDT meetings conducted on Zoom. At MDT meetings, carried out with frequencies ranging from monthly to bimonthly, Dr. Jadon said there would be two dermatologists, two rheumatologists, one to four dermatology and rheumatology trainees and fellows, one to four specialist nurses, one to three research nurses, and one biologics pharmacist. They record the meetings and discuss anywhere from 4 to 18 patients, reviewing items in their electronic medical record, calling or writing patients and/or their primary care clinician as needed. They take about an hour to meet, with a half hour of prep time and another 1.5 hours to undertake necessary actions.
“Generally, the question is, how can we change treatment to best cover the domains of disease?” Dr. Jadon said. “Progressively, more patients are being put onto biologics as a result of these conversations, and I do feel that it has helped our patients and us to consolidate their management plan. Naturally, as all clinicians do, we doubt ourselves and wonder if we are missing something. Is there an aspect of the disease [being missed]? Is there a treatment that I haven’t been using? [The meetings have] been reassuring in that regard. I also learn from my colleagues who have earlier access to treatments, especially in dermatology.”
In a small number of patients, some combinations of advanced therapies, such as combining a Janus kinase inhibitor with a biologic, have been used as a result of these collaborations, “and to discuss this in an MDT has been reassuring, including from a medico-legal perspective,” Dr. Jadon said. “One of the main things we found to be useful is having a brief referral pro forma. Usually, by the time patients reach this forum, they have used a lot of treatments, and it can be difficult to remember that on the spot. It is also important to focus on what the actual question is. Naturally, in these discussions, where you talk about the complexities and various facets of disease, you can get a bit lost and sometimes you actually don’t address the original question.”
He also said it has been very beneficial to use screen sharing in the remote MDTs so that different disciplines can review images together, such as with radiology colleagues. “There are varying skill sets among our colleagues, especially in radiology, and it has been quite nice to review their peripheral imaging, their axial imaging, laboratory markers, and skin lesions together.”
New GRAPPA project to provide clarity
A new GRAPPA project has been devised to help physicians identify and define difficult-to-treat and difficult-to-manage PsA in order to help physicians to categorize and treat these patients.
“We have a growing treatment armamentarium ... but we still do not reach all the patients that we would like to,” said Fabian Proft, MD, of Charité University Medicine, Berlin. “We set our targets, but we see in the real world that we are only reaching them in 40% or 50% of our patients. So, we need to do better, and in order to do better, we need to understand better.”
“We should not only make a definition of difficult-to-treat PsA, which is nonresponse to treatment with objective signs of inflammation, but also we need to address and acknowledge difficult-to-manage [patients],” Dr. Proft said. “We should not stop as soon as we come up with a definition. This will be a working definition and will need to be validated.”
The speakers reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
DUBLIN – according to presenters at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
In the same session at the meeting, GRAPPA also announced a new initiative to define difficult-to-treat PsA.
Deepak Jadon, MBBCh, PhD, a rheumatologist with Cambridge (England) University Hospitals NHS Foundation Trust, described his experience of running a clinic for patients with difficult-to-treat PsA in eastern England, covering a catchment area of approximately 6 million people between six and seven hospitals. He discussed how the MDT in his region operates to discuss the management of such patients, whose treatment options may also have indications for comorbidities such as inflammatory bowel disease or uveitis, or have complicating factors such as metabolic syndrome.
“You have to have an interested and engaged colleague to form that collaboration,” Dr. Jadon said. “If you are working in isolation, without your colleagues in the same building, that becomes harder. We have been running remote multispecialty meetings without the patient being present, and I have had the good fortune of having medical students brought into our practice. We discussed approximately 220 patients, initially in our psoriasis-spondyloarthritis MDT and subsequently in our inflammatory bowel disease–spondyloarthritis MDT.”
There are also MDTs with hepatologist colleagues carried out on an ad hoc basis to discuss patients with nonalcoholic fatty liver disease, as well as patients with hepatitis or a transplanted liver, who have psoriatic disease.
This difficult-to-treat cohort is discussed in MDT meetings conducted on Zoom. At MDT meetings, carried out with frequencies ranging from monthly to bimonthly, Dr. Jadon said there would be two dermatologists, two rheumatologists, one to four dermatology and rheumatology trainees and fellows, one to four specialist nurses, one to three research nurses, and one biologics pharmacist. They record the meetings and discuss anywhere from 4 to 18 patients, reviewing items in their electronic medical record, calling or writing patients and/or their primary care clinician as needed. They take about an hour to meet, with a half hour of prep time and another 1.5 hours to undertake necessary actions.
“Generally, the question is, how can we change treatment to best cover the domains of disease?” Dr. Jadon said. “Progressively, more patients are being put onto biologics as a result of these conversations, and I do feel that it has helped our patients and us to consolidate their management plan. Naturally, as all clinicians do, we doubt ourselves and wonder if we are missing something. Is there an aspect of the disease [being missed]? Is there a treatment that I haven’t been using? [The meetings have] been reassuring in that regard. I also learn from my colleagues who have earlier access to treatments, especially in dermatology.”
In a small number of patients, some combinations of advanced therapies, such as combining a Janus kinase inhibitor with a biologic, have been used as a result of these collaborations, “and to discuss this in an MDT has been reassuring, including from a medico-legal perspective,” Dr. Jadon said. “One of the main things we found to be useful is having a brief referral pro forma. Usually, by the time patients reach this forum, they have used a lot of treatments, and it can be difficult to remember that on the spot. It is also important to focus on what the actual question is. Naturally, in these discussions, where you talk about the complexities and various facets of disease, you can get a bit lost and sometimes you actually don’t address the original question.”
He also said it has been very beneficial to use screen sharing in the remote MDTs so that different disciplines can review images together, such as with radiology colleagues. “There are varying skill sets among our colleagues, especially in radiology, and it has been quite nice to review their peripheral imaging, their axial imaging, laboratory markers, and skin lesions together.”
New GRAPPA project to provide clarity
A new GRAPPA project has been devised to help physicians identify and define difficult-to-treat and difficult-to-manage PsA in order to help physicians to categorize and treat these patients.
“We have a growing treatment armamentarium ... but we still do not reach all the patients that we would like to,” said Fabian Proft, MD, of Charité University Medicine, Berlin. “We set our targets, but we see in the real world that we are only reaching them in 40% or 50% of our patients. So, we need to do better, and in order to do better, we need to understand better.”
“We should not only make a definition of difficult-to-treat PsA, which is nonresponse to treatment with objective signs of inflammation, but also we need to address and acknowledge difficult-to-manage [patients],” Dr. Proft said. “We should not stop as soon as we come up with a definition. This will be a working definition and will need to be validated.”
The speakers reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
DUBLIN – according to presenters at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
In the same session at the meeting, GRAPPA also announced a new initiative to define difficult-to-treat PsA.
Deepak Jadon, MBBCh, PhD, a rheumatologist with Cambridge (England) University Hospitals NHS Foundation Trust, described his experience of running a clinic for patients with difficult-to-treat PsA in eastern England, covering a catchment area of approximately 6 million people between six and seven hospitals. He discussed how the MDT in his region operates to discuss the management of such patients, whose treatment options may also have indications for comorbidities such as inflammatory bowel disease or uveitis, or have complicating factors such as metabolic syndrome.
“You have to have an interested and engaged colleague to form that collaboration,” Dr. Jadon said. “If you are working in isolation, without your colleagues in the same building, that becomes harder. We have been running remote multispecialty meetings without the patient being present, and I have had the good fortune of having medical students brought into our practice. We discussed approximately 220 patients, initially in our psoriasis-spondyloarthritis MDT and subsequently in our inflammatory bowel disease–spondyloarthritis MDT.”
There are also MDTs with hepatologist colleagues carried out on an ad hoc basis to discuss patients with nonalcoholic fatty liver disease, as well as patients with hepatitis or a transplanted liver, who have psoriatic disease.
This difficult-to-treat cohort is discussed in MDT meetings conducted on Zoom. At MDT meetings, carried out with frequencies ranging from monthly to bimonthly, Dr. Jadon said there would be two dermatologists, two rheumatologists, one to four dermatology and rheumatology trainees and fellows, one to four specialist nurses, one to three research nurses, and one biologics pharmacist. They record the meetings and discuss anywhere from 4 to 18 patients, reviewing items in their electronic medical record, calling or writing patients and/or their primary care clinician as needed. They take about an hour to meet, with a half hour of prep time and another 1.5 hours to undertake necessary actions.
“Generally, the question is, how can we change treatment to best cover the domains of disease?” Dr. Jadon said. “Progressively, more patients are being put onto biologics as a result of these conversations, and I do feel that it has helped our patients and us to consolidate their management plan. Naturally, as all clinicians do, we doubt ourselves and wonder if we are missing something. Is there an aspect of the disease [being missed]? Is there a treatment that I haven’t been using? [The meetings have] been reassuring in that regard. I also learn from my colleagues who have earlier access to treatments, especially in dermatology.”
In a small number of patients, some combinations of advanced therapies, such as combining a Janus kinase inhibitor with a biologic, have been used as a result of these collaborations, “and to discuss this in an MDT has been reassuring, including from a medico-legal perspective,” Dr. Jadon said. “One of the main things we found to be useful is having a brief referral pro forma. Usually, by the time patients reach this forum, they have used a lot of treatments, and it can be difficult to remember that on the spot. It is also important to focus on what the actual question is. Naturally, in these discussions, where you talk about the complexities and various facets of disease, you can get a bit lost and sometimes you actually don’t address the original question.”
He also said it has been very beneficial to use screen sharing in the remote MDTs so that different disciplines can review images together, such as with radiology colleagues. “There are varying skill sets among our colleagues, especially in radiology, and it has been quite nice to review their peripheral imaging, their axial imaging, laboratory markers, and skin lesions together.”
New GRAPPA project to provide clarity
A new GRAPPA project has been devised to help physicians identify and define difficult-to-treat and difficult-to-manage PsA in order to help physicians to categorize and treat these patients.
“We have a growing treatment armamentarium ... but we still do not reach all the patients that we would like to,” said Fabian Proft, MD, of Charité University Medicine, Berlin. “We set our targets, but we see in the real world that we are only reaching them in 40% or 50% of our patients. So, we need to do better, and in order to do better, we need to understand better.”
“We should not only make a definition of difficult-to-treat PsA, which is nonresponse to treatment with objective signs of inflammation, but also we need to address and acknowledge difficult-to-manage [patients],” Dr. Proft said. “We should not stop as soon as we come up with a definition. This will be a working definition and will need to be validated.”
The speakers reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
AT GRAPPA 2023
Keep depression, anxiety screening top of mind in patients with psoriatic disease
DUBLIN – , warranting routine screening and having community contacts for mental health professional referrals, Elizabeth Wallace, MD, said at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
Dr. Wallace, of Cherry Hills Dermatology, Englewood, Colo., discussed the complex interactions between mental illness and psoriatic disease and the potential pitfalls of this comorbidity for these patients.
The topic of mental health is “consistently at the top of our patients’ minds, and certainly our minds too,” said session comoderator and GRAPPA president-elect Joseph F. Merola, MD, MMSc.
“In the U.S., around 17% of people with psoriasis have depression vs. 9% in those without psoriasis,” Dr. Wallace explained. “Psoriasis patients are twice as likely to have depression, compared to those without psoriasis, and psoriasis patients are 33% more likely to attempt suicide and 20% more likely to complete suicide, compared to those without psoriasis.” More severe psoriasis and younger age of onset are also associated with a greater likelihood of suicidality, she added.
Mediators of depression
“The inflammatory mechanisms driving PsD can drive depression and anxiety, and vice-versa,” she said. “There are often also genetic links, for example genetic variations in serotonin receptors, and psychological issues in psoriatic disease are predictably worsened by feelings of stigmatization, embarrassment, and social isolation.”
There are also efforts underway in clinics to “normalize” screening for anxiety and depression among this patient cohort, Dr. Wallace said. “We know that our psoriasis patients face social stigma from the visibility of their disease, and that stress can lead to flares of their condition,” she told the attendees. “We also know that patients who experience stigma also have an increased risk of depressive symptoms. We all know now that psoriasis has well-established pathways with upregulated proinflammatory cytokines.
“Increased cytokines stimulate indoleamine 2,3-dioxygenase, which converts tryptophan to kynurenine. Kynurenine is metabolized to quinolinic acid, which is neurotoxic.” She explained that because serotonin derives from tryptophan, decreases in tryptophan lead to reduced serotonin, and therefore increased risk of depression.
Interleukin-6 is known to be upregulated in depression and downregulated with the use of antidepressant medications, Dr. Wallace said. Mouse models in research have shown that deletion of the IL-6 gene produces antidepressant effects, and studies in humans have shown that IL-6, more than any other serum cytokine, is found at higher levels in humans with depression and psoriatic disease.
IL-17 is also implicated in psoriatic disease and mental health problems, Dr. Wallace said. “With stress, you get upregulation of the Tc17 cells, which produce IL-17,” she explained. “IL-17, along with other inflammatory markers, can actually make the blood-brain barrier more permeable, and when you get more permeability to the blood-brain barrier, you get these cytokines that can cross from the periphery and into the brain.
“With this crossing into the brain, you get further activation of more Th17 [cells] and that, on neurons, leads to increased potassium production, which is directly neurotoxic, so you get neuron destruction.”
Talking about depression
“So, what can we share with our patients?” Dr. Wallace asked. “We can discuss with them that psoriatic patients in general are more likely to be depressed or to have higher rates of suicide. The literature consistently shows that patients whose psoriasis is successfully treated experience reduced depression, and we can provide an understandable review of systemic medications, with warnings on depression and/or suicidality.”
Dr. Wallace advised to screen for depression with the Patient Health Questionnaire-2 (PHQ-2), a validated, two-item tool that asks, “Over the past 2 weeks, how often have you been bothered by having little interest or pleasure in doing things?” and “Over the past 2 weeks, how often have you been bothered by feeling down, depressed, or hopeless?”
She presented a case study illustrative of the type of presentation she sees in her clinic. It involved a 32-year-old man with plaque psoriasis and a high degree of body surface affected. “It’s now July in Colorado, it’s getting warm, people want to wear their shorts and T-shirts, but he said he could no longer hide his psoriasis,” said Dr. Wallace. “Further, it’s in areas that he cannot hide, such as his scalp, his beard, and he also has nail disease. Often, these patients don’t want to shake hands with their bosses or their colleagues and that’s very embarrassing for them.”
Dr. Wallace explained that this patient had seen advertisements for biologic drugs and requested to commence a treatment course. “During the exam, and now that you are developing some rapport with him, you discover that he is feeling down, is embarrassed at work, and has started to avoid social situations.” This is illustrative of a patient who should be screened for mental health conditions, specifically using PHQ-2, she said.
“You can be the person at the front line to screen these patients for mental health conditions, and, specifically for depression, with PHQ-2,” she said. PHQ-2 scores range from 0 to 6, and a score of 3 or higher is considered a positive screen.
“This is where your relationship with another health provider who is most qualified to care for these patients and validate them for their mental health condition can be absolutely critical,” Dr. Wallace said.
Successful PsD treatment lessens the risk for mental health comorbidities, and this is also seen in psoriatic arthritis, Dr. Wallace pointed out. Patient education is critical regarding their increased risk for depression and potential suicidal ideation, she added.
“It’s our job as clinicians to provide patients with an understandable, easy-to-digest review of systemic medications and warnings on depression and suicidality so that they can be aware of these factors.”
Perspective from Dr. Merola
In an interview, Dr. Merola, a double board-certified dermatologist and rheumatologist at Brigham and Women’s Hospital, Boston, discussed the interactions between mental and physical illness.
“One of the things we are learning is that it’s very much a multifactorial issue, in that skin and joints contribute, in some obvious ways, to anxiety and depression, like the fact that somebody doesn’t feel good about their appearance, or they can’t complete daily activities,” he said. “Those are the more obvious ones. But there is data and evidence that there is a biology behind that as well – inflammatory cytokines that drive skin disease probably also have a direct impact on the CNS and probably also drive anxiety and depression.
“We know that disordered sleep contributes to anxiety – think about how we feel if we get a horrible night’s sleep ... it’s hard to pick apart: ‘Am I depressed, am I anxious because I am having too much coffee? Because I am fatigued?’ So, we get into these circles, but the point is, we have to break these cycles, and we have to do it in multiple places. Yes, we have to fix the skin and the joints, but we also have to have interventions and think about how to screen for anxiety and depression. We also have to think about identifying disordered sleep, and how we intervene there as well.”
These challenges require a collaborative approach among physicians. “We can help patients to build their team that gets them help for their skin, for their joints, for their anxiety or depression, their disordered sleep, for their nutritional disorders, their obesity, and so on. So, we are trying to pick apart and unpack those complexities,” he said.
In regard to the potential impacts of this holistic strategy on physician workloads, Dr. Merola acknowledged it is important to consider physician wellness. “There’s no question that we want to be doing the best we can for our colleagues, but we don’t want to overload our colleagues by saying, ‘By the way, not only should we be treating their skin and joints,’ which of course we should be doing, but ‘could you also manage their diabetes, their obesity, their disordered sleep, their anxiety, their depression, difficulties with insurance, getting access to treatments, etc.’
“This is where effective collaboration between physicians becomes important,” he stressed. “We can’t manage every single piece, but we can make sure our patients are informed, are aware, and assist them to get the help that they need.”
In the United States, there “is a real issue” with access to mental health care and greater awareness needs to be created around this issue, he added.
Dr. Wallace and Dr. Merola report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DUBLIN – , warranting routine screening and having community contacts for mental health professional referrals, Elizabeth Wallace, MD, said at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
Dr. Wallace, of Cherry Hills Dermatology, Englewood, Colo., discussed the complex interactions between mental illness and psoriatic disease and the potential pitfalls of this comorbidity for these patients.
The topic of mental health is “consistently at the top of our patients’ minds, and certainly our minds too,” said session comoderator and GRAPPA president-elect Joseph F. Merola, MD, MMSc.
“In the U.S., around 17% of people with psoriasis have depression vs. 9% in those without psoriasis,” Dr. Wallace explained. “Psoriasis patients are twice as likely to have depression, compared to those without psoriasis, and psoriasis patients are 33% more likely to attempt suicide and 20% more likely to complete suicide, compared to those without psoriasis.” More severe psoriasis and younger age of onset are also associated with a greater likelihood of suicidality, she added.
Mediators of depression
“The inflammatory mechanisms driving PsD can drive depression and anxiety, and vice-versa,” she said. “There are often also genetic links, for example genetic variations in serotonin receptors, and psychological issues in psoriatic disease are predictably worsened by feelings of stigmatization, embarrassment, and social isolation.”
There are also efforts underway in clinics to “normalize” screening for anxiety and depression among this patient cohort, Dr. Wallace said. “We know that our psoriasis patients face social stigma from the visibility of their disease, and that stress can lead to flares of their condition,” she told the attendees. “We also know that patients who experience stigma also have an increased risk of depressive symptoms. We all know now that psoriasis has well-established pathways with upregulated proinflammatory cytokines.
“Increased cytokines stimulate indoleamine 2,3-dioxygenase, which converts tryptophan to kynurenine. Kynurenine is metabolized to quinolinic acid, which is neurotoxic.” She explained that because serotonin derives from tryptophan, decreases in tryptophan lead to reduced serotonin, and therefore increased risk of depression.
Interleukin-6 is known to be upregulated in depression and downregulated with the use of antidepressant medications, Dr. Wallace said. Mouse models in research have shown that deletion of the IL-6 gene produces antidepressant effects, and studies in humans have shown that IL-6, more than any other serum cytokine, is found at higher levels in humans with depression and psoriatic disease.
IL-17 is also implicated in psoriatic disease and mental health problems, Dr. Wallace said. “With stress, you get upregulation of the Tc17 cells, which produce IL-17,” she explained. “IL-17, along with other inflammatory markers, can actually make the blood-brain barrier more permeable, and when you get more permeability to the blood-brain barrier, you get these cytokines that can cross from the periphery and into the brain.
“With this crossing into the brain, you get further activation of more Th17 [cells] and that, on neurons, leads to increased potassium production, which is directly neurotoxic, so you get neuron destruction.”
Talking about depression
“So, what can we share with our patients?” Dr. Wallace asked. “We can discuss with them that psoriatic patients in general are more likely to be depressed or to have higher rates of suicide. The literature consistently shows that patients whose psoriasis is successfully treated experience reduced depression, and we can provide an understandable review of systemic medications, with warnings on depression and/or suicidality.”
Dr. Wallace advised to screen for depression with the Patient Health Questionnaire-2 (PHQ-2), a validated, two-item tool that asks, “Over the past 2 weeks, how often have you been bothered by having little interest or pleasure in doing things?” and “Over the past 2 weeks, how often have you been bothered by feeling down, depressed, or hopeless?”
She presented a case study illustrative of the type of presentation she sees in her clinic. It involved a 32-year-old man with plaque psoriasis and a high degree of body surface affected. “It’s now July in Colorado, it’s getting warm, people want to wear their shorts and T-shirts, but he said he could no longer hide his psoriasis,” said Dr. Wallace. “Further, it’s in areas that he cannot hide, such as his scalp, his beard, and he also has nail disease. Often, these patients don’t want to shake hands with their bosses or their colleagues and that’s very embarrassing for them.”
Dr. Wallace explained that this patient had seen advertisements for biologic drugs and requested to commence a treatment course. “During the exam, and now that you are developing some rapport with him, you discover that he is feeling down, is embarrassed at work, and has started to avoid social situations.” This is illustrative of a patient who should be screened for mental health conditions, specifically using PHQ-2, she said.
“You can be the person at the front line to screen these patients for mental health conditions, and, specifically for depression, with PHQ-2,” she said. PHQ-2 scores range from 0 to 6, and a score of 3 or higher is considered a positive screen.
“This is where your relationship with another health provider who is most qualified to care for these patients and validate them for their mental health condition can be absolutely critical,” Dr. Wallace said.
Successful PsD treatment lessens the risk for mental health comorbidities, and this is also seen in psoriatic arthritis, Dr. Wallace pointed out. Patient education is critical regarding their increased risk for depression and potential suicidal ideation, she added.
“It’s our job as clinicians to provide patients with an understandable, easy-to-digest review of systemic medications and warnings on depression and suicidality so that they can be aware of these factors.”
Perspective from Dr. Merola
In an interview, Dr. Merola, a double board-certified dermatologist and rheumatologist at Brigham and Women’s Hospital, Boston, discussed the interactions between mental and physical illness.
“One of the things we are learning is that it’s very much a multifactorial issue, in that skin and joints contribute, in some obvious ways, to anxiety and depression, like the fact that somebody doesn’t feel good about their appearance, or they can’t complete daily activities,” he said. “Those are the more obvious ones. But there is data and evidence that there is a biology behind that as well – inflammatory cytokines that drive skin disease probably also have a direct impact on the CNS and probably also drive anxiety and depression.
“We know that disordered sleep contributes to anxiety – think about how we feel if we get a horrible night’s sleep ... it’s hard to pick apart: ‘Am I depressed, am I anxious because I am having too much coffee? Because I am fatigued?’ So, we get into these circles, but the point is, we have to break these cycles, and we have to do it in multiple places. Yes, we have to fix the skin and the joints, but we also have to have interventions and think about how to screen for anxiety and depression. We also have to think about identifying disordered sleep, and how we intervene there as well.”
These challenges require a collaborative approach among physicians. “We can help patients to build their team that gets them help for their skin, for their joints, for their anxiety or depression, their disordered sleep, for their nutritional disorders, their obesity, and so on. So, we are trying to pick apart and unpack those complexities,” he said.
In regard to the potential impacts of this holistic strategy on physician workloads, Dr. Merola acknowledged it is important to consider physician wellness. “There’s no question that we want to be doing the best we can for our colleagues, but we don’t want to overload our colleagues by saying, ‘By the way, not only should we be treating their skin and joints,’ which of course we should be doing, but ‘could you also manage their diabetes, their obesity, their disordered sleep, their anxiety, their depression, difficulties with insurance, getting access to treatments, etc.’
“This is where effective collaboration between physicians becomes important,” he stressed. “We can’t manage every single piece, but we can make sure our patients are informed, are aware, and assist them to get the help that they need.”
In the United States, there “is a real issue” with access to mental health care and greater awareness needs to be created around this issue, he added.
Dr. Wallace and Dr. Merola report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DUBLIN – , warranting routine screening and having community contacts for mental health professional referrals, Elizabeth Wallace, MD, said at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
Dr. Wallace, of Cherry Hills Dermatology, Englewood, Colo., discussed the complex interactions between mental illness and psoriatic disease and the potential pitfalls of this comorbidity for these patients.
The topic of mental health is “consistently at the top of our patients’ minds, and certainly our minds too,” said session comoderator and GRAPPA president-elect Joseph F. Merola, MD, MMSc.
“In the U.S., around 17% of people with psoriasis have depression vs. 9% in those without psoriasis,” Dr. Wallace explained. “Psoriasis patients are twice as likely to have depression, compared to those without psoriasis, and psoriasis patients are 33% more likely to attempt suicide and 20% more likely to complete suicide, compared to those without psoriasis.” More severe psoriasis and younger age of onset are also associated with a greater likelihood of suicidality, she added.
Mediators of depression
“The inflammatory mechanisms driving PsD can drive depression and anxiety, and vice-versa,” she said. “There are often also genetic links, for example genetic variations in serotonin receptors, and psychological issues in psoriatic disease are predictably worsened by feelings of stigmatization, embarrassment, and social isolation.”
There are also efforts underway in clinics to “normalize” screening for anxiety and depression among this patient cohort, Dr. Wallace said. “We know that our psoriasis patients face social stigma from the visibility of their disease, and that stress can lead to flares of their condition,” she told the attendees. “We also know that patients who experience stigma also have an increased risk of depressive symptoms. We all know now that psoriasis has well-established pathways with upregulated proinflammatory cytokines.
“Increased cytokines stimulate indoleamine 2,3-dioxygenase, which converts tryptophan to kynurenine. Kynurenine is metabolized to quinolinic acid, which is neurotoxic.” She explained that because serotonin derives from tryptophan, decreases in tryptophan lead to reduced serotonin, and therefore increased risk of depression.
Interleukin-6 is known to be upregulated in depression and downregulated with the use of antidepressant medications, Dr. Wallace said. Mouse models in research have shown that deletion of the IL-6 gene produces antidepressant effects, and studies in humans have shown that IL-6, more than any other serum cytokine, is found at higher levels in humans with depression and psoriatic disease.
IL-17 is also implicated in psoriatic disease and mental health problems, Dr. Wallace said. “With stress, you get upregulation of the Tc17 cells, which produce IL-17,” she explained. “IL-17, along with other inflammatory markers, can actually make the blood-brain barrier more permeable, and when you get more permeability to the blood-brain barrier, you get these cytokines that can cross from the periphery and into the brain.
“With this crossing into the brain, you get further activation of more Th17 [cells] and that, on neurons, leads to increased potassium production, which is directly neurotoxic, so you get neuron destruction.”
Talking about depression
“So, what can we share with our patients?” Dr. Wallace asked. “We can discuss with them that psoriatic patients in general are more likely to be depressed or to have higher rates of suicide. The literature consistently shows that patients whose psoriasis is successfully treated experience reduced depression, and we can provide an understandable review of systemic medications, with warnings on depression and/or suicidality.”
Dr. Wallace advised to screen for depression with the Patient Health Questionnaire-2 (PHQ-2), a validated, two-item tool that asks, “Over the past 2 weeks, how often have you been bothered by having little interest or pleasure in doing things?” and “Over the past 2 weeks, how often have you been bothered by feeling down, depressed, or hopeless?”
She presented a case study illustrative of the type of presentation she sees in her clinic. It involved a 32-year-old man with plaque psoriasis and a high degree of body surface affected. “It’s now July in Colorado, it’s getting warm, people want to wear their shorts and T-shirts, but he said he could no longer hide his psoriasis,” said Dr. Wallace. “Further, it’s in areas that he cannot hide, such as his scalp, his beard, and he also has nail disease. Often, these patients don’t want to shake hands with their bosses or their colleagues and that’s very embarrassing for them.”
Dr. Wallace explained that this patient had seen advertisements for biologic drugs and requested to commence a treatment course. “During the exam, and now that you are developing some rapport with him, you discover that he is feeling down, is embarrassed at work, and has started to avoid social situations.” This is illustrative of a patient who should be screened for mental health conditions, specifically using PHQ-2, she said.
“You can be the person at the front line to screen these patients for mental health conditions, and, specifically for depression, with PHQ-2,” she said. PHQ-2 scores range from 0 to 6, and a score of 3 or higher is considered a positive screen.
“This is where your relationship with another health provider who is most qualified to care for these patients and validate them for their mental health condition can be absolutely critical,” Dr. Wallace said.
Successful PsD treatment lessens the risk for mental health comorbidities, and this is also seen in psoriatic arthritis, Dr. Wallace pointed out. Patient education is critical regarding their increased risk for depression and potential suicidal ideation, she added.
“It’s our job as clinicians to provide patients with an understandable, easy-to-digest review of systemic medications and warnings on depression and suicidality so that they can be aware of these factors.”
Perspective from Dr. Merola
In an interview, Dr. Merola, a double board-certified dermatologist and rheumatologist at Brigham and Women’s Hospital, Boston, discussed the interactions between mental and physical illness.
“One of the things we are learning is that it’s very much a multifactorial issue, in that skin and joints contribute, in some obvious ways, to anxiety and depression, like the fact that somebody doesn’t feel good about their appearance, or they can’t complete daily activities,” he said. “Those are the more obvious ones. But there is data and evidence that there is a biology behind that as well – inflammatory cytokines that drive skin disease probably also have a direct impact on the CNS and probably also drive anxiety and depression.
“We know that disordered sleep contributes to anxiety – think about how we feel if we get a horrible night’s sleep ... it’s hard to pick apart: ‘Am I depressed, am I anxious because I am having too much coffee? Because I am fatigued?’ So, we get into these circles, but the point is, we have to break these cycles, and we have to do it in multiple places. Yes, we have to fix the skin and the joints, but we also have to have interventions and think about how to screen for anxiety and depression. We also have to think about identifying disordered sleep, and how we intervene there as well.”
These challenges require a collaborative approach among physicians. “We can help patients to build their team that gets them help for their skin, for their joints, for their anxiety or depression, their disordered sleep, for their nutritional disorders, their obesity, and so on. So, we are trying to pick apart and unpack those complexities,” he said.
In regard to the potential impacts of this holistic strategy on physician workloads, Dr. Merola acknowledged it is important to consider physician wellness. “There’s no question that we want to be doing the best we can for our colleagues, but we don’t want to overload our colleagues by saying, ‘By the way, not only should we be treating their skin and joints,’ which of course we should be doing, but ‘could you also manage their diabetes, their obesity, their disordered sleep, their anxiety, their depression, difficulties with insurance, getting access to treatments, etc.’
“This is where effective collaboration between physicians becomes important,” he stressed. “We can’t manage every single piece, but we can make sure our patients are informed, are aware, and assist them to get the help that they need.”
In the United States, there “is a real issue” with access to mental health care and greater awareness needs to be created around this issue, he added.
Dr. Wallace and Dr. Merola report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT GRAPPA 2023
Summer diarrhea – Time to think outside the box
It’s “summertime and the livin’ is easy” according to the lyric from an old George Gershwin song. But sometimes, summer activities can lead to illnesses that can disrupt a child’s easy living.
Case: An otherwise healthy 11-year-old presents with four to five loose stools per day, mild nausea, excess flatulence, and cramps for 12 days with a 5-pound weight loss. His loose-to-mushy stools have no blood or mucous but smell worse than usual. He has had no fever, vomiting, rashes, or joint symptoms. A month ago, he went hiking/camping on the Appalachian Trail, drank boiled stream water. and slept in a common-use semi-enclosed shelter. He waded through streams and shared “Trail Magic” (soft drinks being cooled in a fresh mountain stream). Two other campers report similar symptoms.

Differential diagnosis: Broadly, we should consider bacteria, viruses, and parasites. But generally, bacteria are likely to produce more systemic symptoms and usually do not last 12 days. That said, this could be Clostridioides difficile, yet that seems unlikely because he is otherwise healthy and has no apparent risk factors. Salmonella spp., Campylobacter spp. and some Escherichia coli infections may drag on for more than a week but the lack of systemic symptoms or blood/mucous lowers the likelihood. Viral agents (rotavirus, norovirus, adenovirus, astrovirus, calicivirus, or sapovirus) seem unlikely because of the long symptom duration and the child’s preteen age.
The history and presentation seem more likely attributable to a parasite. Uncommonly detected protozoa include Microsporidium (mostly Enterocytozoon bieneusi) and amoeba. Microsporidium is very rare and seen mostly in immune compromised hosts, for example, those living with HIV. Amebiasis occurs mostly after travel to endemic areas, and stools usually contain blood or mucous. Some roundworm or tapeworm infestations cause abdominal pain and abnormal stools, but the usual exposures are absent. Giardia spp., Cryptosporidium spp., Cyclospora cayetanensis, and/or Cystoisospora belli best fit this presentation given his hiking/camping trip.
Workup. Laboratory testing of stool is warranted (because of weight loss and persistent diarrhea) despite a lack of systemic signs. Initially, bacterial culture, C. difficile testing, and viral testing seem unwarranted. The best initial approach, given our most likely suspects, is protozoan/parasite testing.
The Centers for Disease Control and Prevention recommends testing up to three stools collected on separate days.1 Initially, stool testing for giardia and cryptosporidium antigens by EIA assays could be done as a point-of-care test. Such antigen tests are often the first step because of their ease of use, relatively low expense, reasonably high sensitivity and specificity, and rapid turnaround (as little as 1 hour). Alternatively, direct examination of three stools for ova and parasites (O&P) and acid-fast stain or direct fluorescent antibody testing can usually detect our main suspects (giardia, cryptosporidium, cyclospora, and cystoisospora) along with other less likely parasites.
Some laboratories, however, use syndromic stool testing approaches (multiplex nucleic acid panels) that detect over 20 different bacteria, viruses, and select parasites. Multiplex testing has yielded increased detection rates, compared with microscopic examination alone in some settings. Further, they also share ease-of-use and rapid turnaround times with parasite antigen assays while requiring less hands-on time by laboratory personnel, compared with direct microscopic examination. However, multiplex assays are expensive and more readily detect commensal organisms, so they are not necessarily the ideal test in all diarrheal illnesses.
Diagnosis. You decide to first order giardia and cryptosporidium antigen testing because you are highly suspicious that giardia is the cause, based on wild-water exposure, the presentation, and symptom duration. You also order full microscopic O&P examination because you know that parasites can “run in packs.” Results of testing the first stool are positive for giardia. Microscopic examination on each of three stools is negative except for giardia trophozoites (the noninfectious form) in stools two and three.
Giardia overview. Giardia is the most common protozoan causing diarrhea in the United States, is fecal-oral spread, and like Shigella spp., is a low-inoculum infection (ingestion of as few as 10-100 cysts). Acquisition in the United States has been estimated as being 75% from contaminated water (streams are a classic source.2 Other sources are contaminated food (fresh produce is classic) and in some cases sexual encounters (mostly in men who have sex with men). Most detections are sporadic, but outbreaks can occur with case numbers usually below 20; 40% of outbreaks are attributable to contaminated water or food.3 Evaluating symptomatic household members can be important as transmission in families can occur.
After ingestion, the cysts uncoat and form trophozoites, which reside mostly in the small bowel (Figure), causing inflammation and altering gut membrane permeability, thereby reducing nutrient absorption and circulating amino acids. Along with decreased food intake, altered absorption can lead to weight loss and potentially reduce growth in young children. Some trophozoites replicate while others encyst, eventually passing into stool. The cysts can survive for months in water or the environment (lakes, swimming pools, and clear mountain streams). Giardia has been linked to beavers’ feces contaminating wild-water sources, hence the moniker “Beaver fever” and warnings about stream water related to wilderness hiking.4
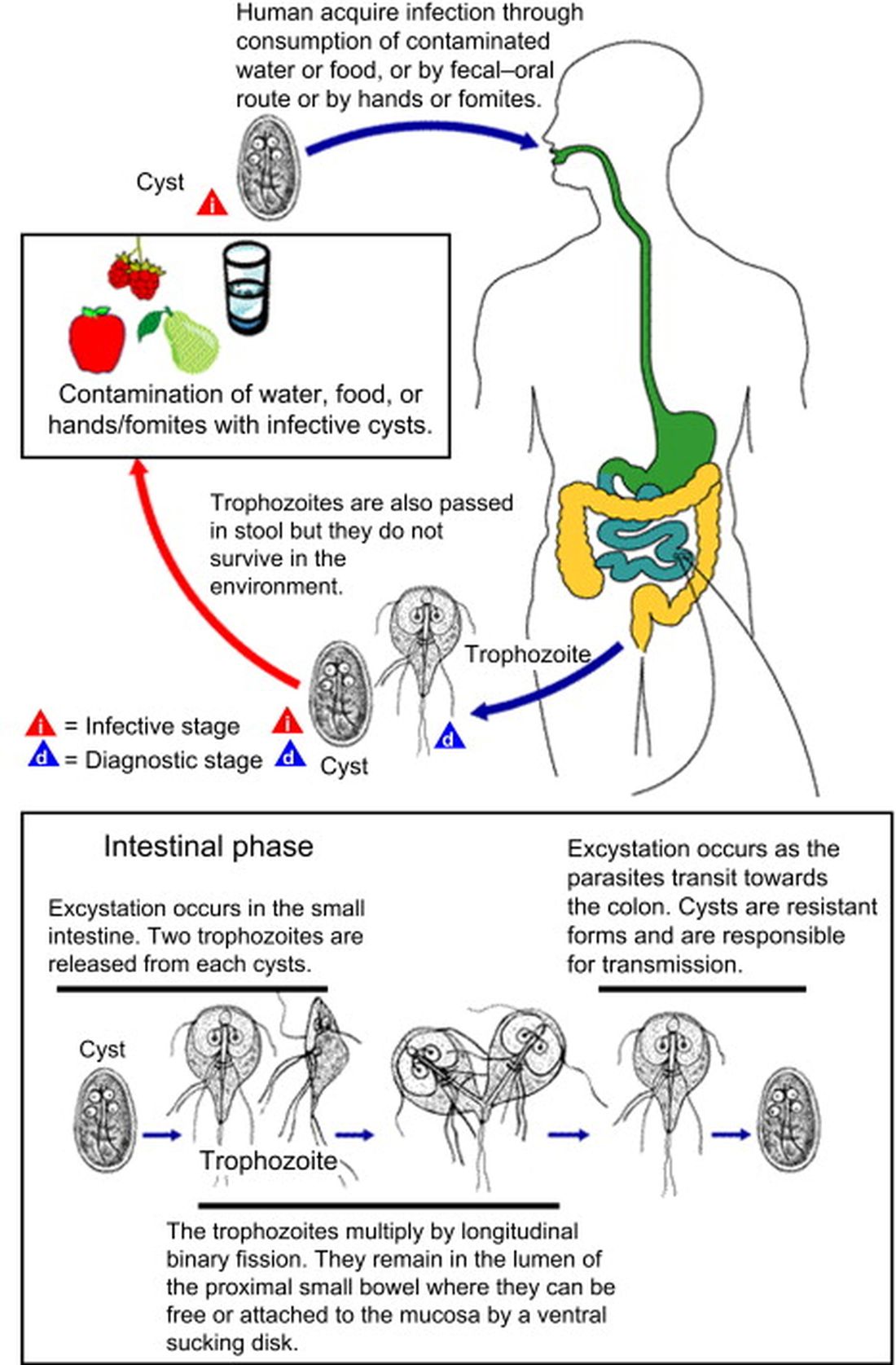
Management. Supportive therapy as with any diarrheal illness is the cornerstone of management. Specific antiparasitic treatment has traditionally been with metronidazole compounded into a liquid for young children, but the awful taste and frequent dosing often result in poor adherence. Nevertheless, published cure rates range from 80% to 100%. The taste issue, known adverse effects, and lack of FDA approval for giardia, have led to use of other drugs.5 One dose of tinidazole is as effective as metronidazole and can be prescribed for children 3 years old or older. But the drug nitazoxanide is becoming more standard. It is as effective as either alternative, and is FDA approved for children 1 year old and older. Nitazoxanide also is effective against other intestinal parasites (e.g., cryptosporidium). Nitazoxanide’s 3-day course involves every-12-hour dosing with food with each dose being 5 mL (100 mg) for 1- to 3-year-olds, 10 mL (200 mg) for 4- to 11-year-olds, and one tablet (500 mg) or 25 mL (500 mg) for children 12 years old or older.6
Key elements in this subacute nonsystemic diarrheal presentation were primitive camping history, multiple stream water contacts, nearly 2 weeks of symptoms, weight loss, and flatulence/cramping, but no fever or stool blood/mucous. Two friends also appear to be similarly symptomatic, so a common exposure seemed likely This is typical for several summertime activity–related parasites. So,
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital–Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines. The hospital also receives CDC funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus. Email Dr. Harrison at pdnews@mdedge.com.
References
1. Diagnosis and Treatment Information for Medical Professionals, Giardia, Parasites. CDC.
2. Krumrie S et al. Curr Res Parasitol Vector Borne Dis. 2022;2:100084. doi: 10.1016/j.crpvbd.2022.100084.
3. Baldursson S and Karanis P. Water Res. 2011 Dec 15. doi: 10.1016/j.watres.2011.10.013.
4. “Water on the Appalachian Trail” AppalachianTrail.com.
5. Giardiasis: Treatment and prevention. UpToDate.
6. Kimberlin D et al. Red Book: 2021-2024 Report of the Committee on Infectious Diseases (Itasca, Ill.: American Academy of Pediatrics, 2021. 32nd ed.) Giardia duodenalis infections. pp. 335-8; and p. 961 (Table 4.11).
It’s “summertime and the livin’ is easy” according to the lyric from an old George Gershwin song. But sometimes, summer activities can lead to illnesses that can disrupt a child’s easy living.
Case: An otherwise healthy 11-year-old presents with four to five loose stools per day, mild nausea, excess flatulence, and cramps for 12 days with a 5-pound weight loss. His loose-to-mushy stools have no blood or mucous but smell worse than usual. He has had no fever, vomiting, rashes, or joint symptoms. A month ago, he went hiking/camping on the Appalachian Trail, drank boiled stream water. and slept in a common-use semi-enclosed shelter. He waded through streams and shared “Trail Magic” (soft drinks being cooled in a fresh mountain stream). Two other campers report similar symptoms.
Differential diagnosis: Broadly, we should consider bacteria, viruses, and parasites. But generally, bacteria are likely to produce more systemic symptoms and usually do not last 12 days. That said, this could be Clostridioides difficile, yet that seems unlikely because he is otherwise healthy and has no apparent risk factors. Salmonella spp., Campylobacter spp. and some Escherichia coli infections may drag on for more than a week but the lack of systemic symptoms or blood/mucous lowers the likelihood. Viral agents (rotavirus, norovirus, adenovirus, astrovirus, calicivirus, or sapovirus) seem unlikely because of the long symptom duration and the child’s preteen age.
The history and presentation seem more likely attributable to a parasite. Uncommonly detected protozoa include Microsporidium (mostly Enterocytozoon bieneusi) and amoeba. Microsporidium is very rare and seen mostly in immune compromised hosts, for example, those living with HIV. Amebiasis occurs mostly after travel to endemic areas, and stools usually contain blood or mucous. Some roundworm or tapeworm infestations cause abdominal pain and abnormal stools, but the usual exposures are absent. Giardia spp., Cryptosporidium spp., Cyclospora cayetanensis, and/or Cystoisospora belli best fit this presentation given his hiking/camping trip.
Workup. Laboratory testing of stool is warranted (because of weight loss and persistent diarrhea) despite a lack of systemic signs. Initially, bacterial culture, C. difficile testing, and viral testing seem unwarranted. The best initial approach, given our most likely suspects, is protozoan/parasite testing.
The Centers for Disease Control and Prevention recommends testing up to three stools collected on separate days.1 Initially, stool testing for giardia and cryptosporidium antigens by EIA assays could be done as a point-of-care test. Such antigen tests are often the first step because of their ease of use, relatively low expense, reasonably high sensitivity and specificity, and rapid turnaround (as little as 1 hour). Alternatively, direct examination of three stools for ova and parasites (O&P) and acid-fast stain or direct fluorescent antibody testing can usually detect our main suspects (giardia, cryptosporidium, cyclospora, and cystoisospora) along with other less likely parasites.
Some laboratories, however, use syndromic stool testing approaches (multiplex nucleic acid panels) that detect over 20 different bacteria, viruses, and select parasites. Multiplex testing has yielded increased detection rates, compared with microscopic examination alone in some settings. Further, they also share ease-of-use and rapid turnaround times with parasite antigen assays while requiring less hands-on time by laboratory personnel, compared with direct microscopic examination. However, multiplex assays are expensive and more readily detect commensal organisms, so they are not necessarily the ideal test in all diarrheal illnesses.
Diagnosis. You decide to first order giardia and cryptosporidium antigen testing because you are highly suspicious that giardia is the cause, based on wild-water exposure, the presentation, and symptom duration. You also order full microscopic O&P examination because you know that parasites can “run in packs.” Results of testing the first stool are positive for giardia. Microscopic examination on each of three stools is negative except for giardia trophozoites (the noninfectious form) in stools two and three.
Giardia overview. Giardia is the most common protozoan causing diarrhea in the United States, is fecal-oral spread, and like Shigella spp., is a low-inoculum infection (ingestion of as few as 10-100 cysts). Acquisition in the United States has been estimated as being 75% from contaminated water (streams are a classic source.2 Other sources are contaminated food (fresh produce is classic) and in some cases sexual encounters (mostly in men who have sex with men). Most detections are sporadic, but outbreaks can occur with case numbers usually below 20; 40% of outbreaks are attributable to contaminated water or food.3 Evaluating symptomatic household members can be important as transmission in families can occur.
After ingestion, the cysts uncoat and form trophozoites, which reside mostly in the small bowel (Figure), causing inflammation and altering gut membrane permeability, thereby reducing nutrient absorption and circulating amino acids. Along with decreased food intake, altered absorption can lead to weight loss and potentially reduce growth in young children. Some trophozoites replicate while others encyst, eventually passing into stool. The cysts can survive for months in water or the environment (lakes, swimming pools, and clear mountain streams). Giardia has been linked to beavers’ feces contaminating wild-water sources, hence the moniker “Beaver fever” and warnings about stream water related to wilderness hiking.4
Management. Supportive therapy as with any diarrheal illness is the cornerstone of management. Specific antiparasitic treatment has traditionally been with metronidazole compounded into a liquid for young children, but the awful taste and frequent dosing often result in poor adherence. Nevertheless, published cure rates range from 80% to 100%. The taste issue, known adverse effects, and lack of FDA approval for giardia, have led to use of other drugs.5 One dose of tinidazole is as effective as metronidazole and can be prescribed for children 3 years old or older. But the drug nitazoxanide is becoming more standard. It is as effective as either alternative, and is FDA approved for children 1 year old and older. Nitazoxanide also is effective against other intestinal parasites (e.g., cryptosporidium). Nitazoxanide’s 3-day course involves every-12-hour dosing with food with each dose being 5 mL (100 mg) for 1- to 3-year-olds, 10 mL (200 mg) for 4- to 11-year-olds, and one tablet (500 mg) or 25 mL (500 mg) for children 12 years old or older.6
Key elements in this subacute nonsystemic diarrheal presentation were primitive camping history, multiple stream water contacts, nearly 2 weeks of symptoms, weight loss, and flatulence/cramping, but no fever or stool blood/mucous. Two friends also appear to be similarly symptomatic, so a common exposure seemed likely This is typical for several summertime activity–related parasites. So,
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital–Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines. The hospital also receives CDC funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus. Email Dr. Harrison at pdnews@mdedge.com.
References
1. Diagnosis and Treatment Information for Medical Professionals, Giardia, Parasites. CDC.
2. Krumrie S et al. Curr Res Parasitol Vector Borne Dis. 2022;2:100084. doi: 10.1016/j.crpvbd.2022.100084.
3. Baldursson S and Karanis P. Water Res. 2011 Dec 15. doi: 10.1016/j.watres.2011.10.013.
4. “Water on the Appalachian Trail” AppalachianTrail.com.
5. Giardiasis: Treatment and prevention. UpToDate.
6. Kimberlin D et al. Red Book: 2021-2024 Report of the Committee on Infectious Diseases (Itasca, Ill.: American Academy of Pediatrics, 2021. 32nd ed.) Giardia duodenalis infections. pp. 335-8; and p. 961 (Table 4.11).
It’s “summertime and the livin’ is easy” according to the lyric from an old George Gershwin song. But sometimes, summer activities can lead to illnesses that can disrupt a child’s easy living.
Case: An otherwise healthy 11-year-old presents with four to five loose stools per day, mild nausea, excess flatulence, and cramps for 12 days with a 5-pound weight loss. His loose-to-mushy stools have no blood or mucous but smell worse than usual. He has had no fever, vomiting, rashes, or joint symptoms. A month ago, he went hiking/camping on the Appalachian Trail, drank boiled stream water. and slept in a common-use semi-enclosed shelter. He waded through streams and shared “Trail Magic” (soft drinks being cooled in a fresh mountain stream). Two other campers report similar symptoms.
Differential diagnosis: Broadly, we should consider bacteria, viruses, and parasites. But generally, bacteria are likely to produce more systemic symptoms and usually do not last 12 days. That said, this could be Clostridioides difficile, yet that seems unlikely because he is otherwise healthy and has no apparent risk factors. Salmonella spp., Campylobacter spp. and some Escherichia coli infections may drag on for more than a week but the lack of systemic symptoms or blood/mucous lowers the likelihood. Viral agents (rotavirus, norovirus, adenovirus, astrovirus, calicivirus, or sapovirus) seem unlikely because of the long symptom duration and the child’s preteen age.
The history and presentation seem more likely attributable to a parasite. Uncommonly detected protozoa include Microsporidium (mostly Enterocytozoon bieneusi) and amoeba. Microsporidium is very rare and seen mostly in immune compromised hosts, for example, those living with HIV. Amebiasis occurs mostly after travel to endemic areas, and stools usually contain blood or mucous. Some roundworm or tapeworm infestations cause abdominal pain and abnormal stools, but the usual exposures are absent. Giardia spp., Cryptosporidium spp., Cyclospora cayetanensis, and/or Cystoisospora belli best fit this presentation given his hiking/camping trip.
Workup. Laboratory testing of stool is warranted (because of weight loss and persistent diarrhea) despite a lack of systemic signs. Initially, bacterial culture, C. difficile testing, and viral testing seem unwarranted. The best initial approach, given our most likely suspects, is protozoan/parasite testing.
The Centers for Disease Control and Prevention recommends testing up to three stools collected on separate days.1 Initially, stool testing for giardia and cryptosporidium antigens by EIA assays could be done as a point-of-care test. Such antigen tests are often the first step because of their ease of use, relatively low expense, reasonably high sensitivity and specificity, and rapid turnaround (as little as 1 hour). Alternatively, direct examination of three stools for ova and parasites (O&P) and acid-fast stain or direct fluorescent antibody testing can usually detect our main suspects (giardia, cryptosporidium, cyclospora, and cystoisospora) along with other less likely parasites.
Some laboratories, however, use syndromic stool testing approaches (multiplex nucleic acid panels) that detect over 20 different bacteria, viruses, and select parasites. Multiplex testing has yielded increased detection rates, compared with microscopic examination alone in some settings. Further, they also share ease-of-use and rapid turnaround times with parasite antigen assays while requiring less hands-on time by laboratory personnel, compared with direct microscopic examination. However, multiplex assays are expensive and more readily detect commensal organisms, so they are not necessarily the ideal test in all diarrheal illnesses.
Diagnosis. You decide to first order giardia and cryptosporidium antigen testing because you are highly suspicious that giardia is the cause, based on wild-water exposure, the presentation, and symptom duration. You also order full microscopic O&P examination because you know that parasites can “run in packs.” Results of testing the first stool are positive for giardia. Microscopic examination on each of three stools is negative except for giardia trophozoites (the noninfectious form) in stools two and three.
Giardia overview. Giardia is the most common protozoan causing diarrhea in the United States, is fecal-oral spread, and like Shigella spp., is a low-inoculum infection (ingestion of as few as 10-100 cysts). Acquisition in the United States has been estimated as being 75% from contaminated water (streams are a classic source.2 Other sources are contaminated food (fresh produce is classic) and in some cases sexual encounters (mostly in men who have sex with men). Most detections are sporadic, but outbreaks can occur with case numbers usually below 20; 40% of outbreaks are attributable to contaminated water or food.3 Evaluating symptomatic household members can be important as transmission in families can occur.
After ingestion, the cysts uncoat and form trophozoites, which reside mostly in the small bowel (Figure), causing inflammation and altering gut membrane permeability, thereby reducing nutrient absorption and circulating amino acids. Along with decreased food intake, altered absorption can lead to weight loss and potentially reduce growth in young children. Some trophozoites replicate while others encyst, eventually passing into stool. The cysts can survive for months in water or the environment (lakes, swimming pools, and clear mountain streams). Giardia has been linked to beavers’ feces contaminating wild-water sources, hence the moniker “Beaver fever” and warnings about stream water related to wilderness hiking.4
Management. Supportive therapy as with any diarrheal illness is the cornerstone of management. Specific antiparasitic treatment has traditionally been with metronidazole compounded into a liquid for young children, but the awful taste and frequent dosing often result in poor adherence. Nevertheless, published cure rates range from 80% to 100%. The taste issue, known adverse effects, and lack of FDA approval for giardia, have led to use of other drugs.5 One dose of tinidazole is as effective as metronidazole and can be prescribed for children 3 years old or older. But the drug nitazoxanide is becoming more standard. It is as effective as either alternative, and is FDA approved for children 1 year old and older. Nitazoxanide also is effective against other intestinal parasites (e.g., cryptosporidium). Nitazoxanide’s 3-day course involves every-12-hour dosing with food with each dose being 5 mL (100 mg) for 1- to 3-year-olds, 10 mL (200 mg) for 4- to 11-year-olds, and one tablet (500 mg) or 25 mL (500 mg) for children 12 years old or older.6
Key elements in this subacute nonsystemic diarrheal presentation were primitive camping history, multiple stream water contacts, nearly 2 weeks of symptoms, weight loss, and flatulence/cramping, but no fever or stool blood/mucous. Two friends also appear to be similarly symptomatic, so a common exposure seemed likely This is typical for several summertime activity–related parasites. So,
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital–Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines. The hospital also receives CDC funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus. Email Dr. Harrison at pdnews@mdedge.com.
References
1. Diagnosis and Treatment Information for Medical Professionals, Giardia, Parasites. CDC.
2. Krumrie S et al. Curr Res Parasitol Vector Borne Dis. 2022;2:100084. doi: 10.1016/j.crpvbd.2022.100084.
3. Baldursson S and Karanis P. Water Res. 2011 Dec 15. doi: 10.1016/j.watres.2011.10.013.
4. “Water on the Appalachian Trail” AppalachianTrail.com.
5. Giardiasis: Treatment and prevention. UpToDate.
6. Kimberlin D et al. Red Book: 2021-2024 Report of the Committee on Infectious Diseases (Itasca, Ill.: American Academy of Pediatrics, 2021. 32nd ed.) Giardia duodenalis infections. pp. 335-8; and p. 961 (Table 4.11).